User login
ED to Wards: Beating the Boarding Problem
Boarding has been a growing problem over the last decade and may worsen – at least in the short term – with the fuller implementation of the Affordable Care Act, according to experts who are calling for hospitals to implement proven remedies.
Hospital efficiency has suffered as institutions seek to cut costs while coping with a rising influx of uninsured and Medicaid patients. That financial pressure will not improve under health care reform, at least not initially, as millions more Medicaid patients are likely to seek care in the ED when they cannot access primary care, Dr. Jody Crane, emergency department faculty for the Institute for Healthcare Improvement, Cambridge, Mass., said in an interview.

Medicaid pay is already low, and an estimated 8 million more Medicaid patients will visit EDs annually after reform. In addition, as Medicare dials back its reimbursement to hospitals and physicians to help fund the Affordable Care Act, Va. That will put a squeeze on already tight hospital margins, he said.
"Every hospital is going to have to do the same or more with less," said Dr. Crane. Boarding – holding patients in the ED while they wait for admission to inpatient services – can be costly, reduces patient satisfaction, and has been shown to ultimately increase length of stay and mortality.
"Boarding in some hospitals is a capacity issue, but in others it’s also a management issue," Dr. Crane pointed out. Technical issues, including matching resources to the demand coming through the door, are also factors, he said.
"Ultimately, a coordinated effort is needed between the ED and the hospitalist to ensure quality transitions of care that maximize both health and financial outcomes," said Dr. Franklin A. Michota, director of academic affairs in the department of hospital medicine at the Cleveland Clinic. "Each hospital does need to analyze where their bottlenecks exist and whether a staffing solution is part of the answer. But the ED also needs to look at the accuracy and quality of their triage and their ability to adequately prepare the patient for the trip upstairs."
"For example," Dr. Michota continued, "sending a patient upstairs with sickle cell crisis and inadequate pain control just ties up the hospitalist unnecessarily and will delay the hospitalist in getting to the next new admission. Or failing to order a CT scan that would have sent a patient to the operating room and bypass the medical hospitalist altogether will again just delay getting to the next admission.
"Everything relies on everything else....the chain is only as strong as its weakest link."
Indeed, "the primary reason it’s a hard problem to fix is because it’s so multifactorial," said Dr. Jesse Pines, associate professor of emergency medicine and health policy at George Washington University in Washington, D.C.
What Works?
A recent study in Health Affairs showed that many hospitals still are not taking advantage of proven strategies to reduce boarding – among them, so-called smoothing of elective surgical schedules, active bed management by hospitalists, and the "full capacity protocol" that was developed by Dr. Peter Viccellio and his colleagues at the State University of New York at Stony Brook.
"This paper is another in a long series of wake-up calls about the dangerous practice of ‘boarding’ admitted patients in [emergency departments]," ACEP President Dr. David Seaberg said in a statement. "I just hope that hospital administrators and legislators smell the coffee. Their leadership is critical to changing the flow of patients from the front door of the emergency department to the inpatient floors of the hospital."
Emergency departments and hospitals can work together to find ways to improve efficiency, but several important ingredients are needed, Dr. Pines said. The Health Affairs article (2012;31:1757-66 [doi: 10.1377/hlthaff.2011.0786]) cites certain protocols that work, "but you need people to make them work," he said. "You need a strong leader in the ED who can get buy-in from the emergency group. ... You also need a supportive administration and medical staff to make it happen."
It is important to have a local quality improvement group whose members can look at the overall process by which patients get moved from the ED to inpatient services, and examine how patients are managed in the ED after they are admitted, Dr. Pines said. After the existing process is analyzed, hospital staff can identify and address the inefficiencies causing the delays.

The inefficiencies are highly particular to each facility, and often to each day and each shift in the ED and on inpatient wards, he said.
Staffing shortfalls – especially inpatient nursing staff – can be a major contributor to bottlenecks, Dr. Crane said. In response to financial pressures, many hospitals are reducing nursing staff, resulting in increased nurse-to-bed ratios. "That prolongs the inpatient length of stay," he said, because it leads to more work per nurse and more delays in admitting and discharging patients.
There has been a recent administrative trend toward real-time capacity management,which can be an effective way to accommodate the variation in admissions over time.. With this approach, if there is not an identified demand for nurses, they can be sent home or told not to come to work.This ability to change staffing levels according to real-time needs can be an effective way to accommodate the variation in admissions over time
Handoffs and Beds
Dr. Crane contends there are three specific elements to improving patient flow: the physician handoff, the nursing handoff, and bed efficiency.
The physician handoff can be made more efficient by optimizing the coordination between hospitalists and emergency physicians. Due to the high variation in arrival of admissions from the ED and the low numbers of admitting hospitalists at certain times, patients can queue in the ED awaiting admission orders, Dr. Crane noted.
So now, many emergency physicians write holding orders – which have an expiration time – until the patient can be admitted. Holding orders allow the patient to be moved out of the ED, Dr. Crane said. Until recently, emergency physicians have been reluctant to write holding orders, but this trend has reversed because it can be dramatically effective.ACEP now endorses the practice and notes that any associated risk is limited.
The unpredictability of admissions "creates all kinds of logistical nightmares handing off from the emergency department to the floor nurse," Dr. Crane said. Just adding more nurses is not necessarily the answer, and, in general, hospitals don’t have the money to add staff. Instead, hospitals need to better align existing resources and staff. For instance, nurses should probably not be transporting patients or cleaning rooms. That can be done with lower-priced and less-resource-intensive staff, Dr. Crane said.
Bed capacity is the third major element that hospitals should address to reduce boarding, according to Dr. Crane. Demand from the ED cannot be controlled, but on the inpatient side, hospitals can "smooth" the elective surgery schedule by moving more procedures to the middle and end of the week so that all the beds aren’t occupied early in the week. And that is not necessarily easy: "When you change block schedules, you get into cultural issues" with surgeons who do not want to have to see patients on the weekends, Dr. Crane said.
There are also practical issues limiting weekend care. Namely, the typical services such as physical therapy and case management are not routinely present on the weekends. As such, patients who could otherwise be discharged stay in their beds until Monday, when bed demands from the ED and OR increase dramatically. Bed capacity could be improved if hospitals can find ways to make services like testing and therapy available on weekends, and find surgeons and other consultants who will round on Saturdays and Sundays. That might mean hiring a physician’s assistant or other midlevel provider to cover.
Observation Units
Hospitals have also started making use of "observation" status for patients or adding observation units.
At Mary Washington Hospital, where Dr. Crane practices, a team of physicians, nurses, and administrators is designing a streamlined protocol for observation patients. Instead of the standard admission history and physical, an abbreviated assessment has been designed, incorporating use of the ED record and a brief assessment format. Consultations are reduced, and evidence-based pathways are being created for a variety of admitting diagnoses. Patients are treated as outpatients unless test results indicate they need to be moved to the inpatient side, and due to the reduced workload, nurses may be able to work comfortably with higher bed-to-nurse ratios.
The target is to hold patients for observation for 24 hours or less, Dr. Crane said.
Because observation patients are considered outpatients, insurers will pay the hospital less for the visit than if the patient is admitted, Dr. Pines noted, and it leaves the patient vulnerable to higher expenses than just an ED copay.
Another recent study in Health Affairs found that observation stays have been rapidly increasing – from 86.9 observation stays per 1,000 inpatient admissions in 2007 for Medicare beneficiaries to 116.6 in 2009 (Health Affairs 2012;31:1251-9). Of every 1,000 Medicare beneficiaries, 2 were under observation each month in 2007 and almost 3 were under observation each month in 2009. Meanwhile, inpatient admissions per 1,000 declined.
The Sharp Stick of Regulation
Voluntary efforts by hospitals may not be enough, said Dr. Sandra Schneider, former president of the American College of Emergency Physicians. Because hospitals are still paid for the patients who are boarded, they might not see the hidden costs of boarding, she said.

"We have to change that playing field if we want to get serious about [boarding]," Dr. Schneider said.
Among the game changers she cited are the increasing requirements for public reporting on quality measures, including those related to boarding.
Currently, hospitals get paid more by Medicare if they report certain inpatient quality measures. On the outpatient side, emergency departments report on the median time from ED arrival to ED departure for discharged patients and on patients who leave without being seen. In addition, it is now voluntary for hospitals to report on the average time patients spend in the ED before being admitted as an inpatient, and the average time patients spend in the ED after admission but before leaving the ED for their inpatient room.
Data from hospitals that have reported on these measures can be found on the Hospital Compare website.
The Joint Commission is also revisiting its standard on patient flow in the ED, which will go into effect in January 2013. Among other things, the commission is considering defining an episode of boarding as any case in which a patient remains in the ED 4 hours or more after a decision has been made to admit or transfer that patient.
Dr. Pines said that hospital administrators will be motivated both by public reporting imperatives and by Joint Commission standards. Dr. Crane, however, said that "until there are some significant incentives to moving patients upstairs in a timely manner, what’s going to drive senior executives is finance." He thinks that these new standards may help, but more incentives may be needed, such as penalties imposed if boarding limits are exceeded.
Australia, Canada, the United Kingdom, and other developed countries impose such limits and levy penalties.
Hospital Compare data – which will be more fully reported at the end of the first quarter of 2013 – “is going to show us once and for all where the median is and who are the outliers,” Dr. Schneider said. It’s hoped that the outliers will "realize they don’t just have a boarding problem – they have a serious boarding problem," she said.
"If not, then we may have to do what the rest of the world is doing."
For hospitals that are full (above 95% occupied) and have high surgical and critical care volume, boarding in the ED does not lose money – in fact, it does the opposite. Surgery and critical care are well reimbursed and most hospitals would be well served financially to eliminate medical admissions altogether and simply take care of surgery and critical care patients. Of course, not- for-profit hospitals (like the Cleveland Clinic) have a duty and obligation to serve the community at large, and we must maintain an open ED and provide inpatient medical care as part of our mission (and tax status).
The vast majority of ED admissions today are medical patients who are Medicare or Medicare plus Medicaid, Even if the hospital takes care of these patients efficiently and matches the DRG reimbursement with the length of stay, the opportunity cost of having a nursing home patient with the flu tie up a bed that could have been used for an open heart surgery or lap chole, etc., is huge.
It is often said that from a financial perspective, a medical patient is only slightly better than an empty bed. One of the major operational drivers for hospitalist groups is to maximize efficiency on the medical patient so that there are always beds available for an elective surgical patient. Of course, if a hospital is not full there would be a financial loss for putting aa medical patient in an empty bed that would otherwise go unfilled altogether.
Emergency departments everywhere need to recognize and understand that no one “wins” by replacing an ED problem with an inpatient ward problem. Boarding in either location is dangerous and leads to poor patient satisfaction. The notion that the patient is better off upstairs in the hallway is misguided and not well proven.
Geographical units (i.e., similar patients with specific nurse competencies or service assignments in close proximity) have been shown in the hospital medicine literature to improve efficiency and outcomes. As such, we do not want patients strewn about the hospital for the sake of eliminating an ED boarder if it will lead to a longer length of stay and further inefficiency upstairs. Then, a hospital that should be at 85% capacity will find itself at 90% and once again, and the ED will suffer soon enough too.
Franklin A. Michota, M.D. is medical editor of Hospitalist News and director of academic affairs in the department of hospital medicine at the Cleveland Clinic.
For hospitals that are full (above 95% occupied) and have high surgical and critical care volume, boarding in the ED does not lose money – in fact, it does the opposite. Surgery and critical care are well reimbursed and most hospitals would be well served financially to eliminate medical admissions altogether and simply take care of surgery and critical care patients. Of course, not- for-profit hospitals (like the Cleveland Clinic) have a duty and obligation to serve the community at large, and we must maintain an open ED and provide inpatient medical care as part of our mission (and tax status).
The vast majority of ED admissions today are medical patients who are Medicare or Medicare plus Medicaid, Even if the hospital takes care of these patients efficiently and matches the DRG reimbursement with the length of stay, the opportunity cost of having a nursing home patient with the flu tie up a bed that could have been used for an open heart surgery or lap chole, etc., is huge.
It is often said that from a financial perspective, a medical patient is only slightly better than an empty bed. One of the major operational drivers for hospitalist groups is to maximize efficiency on the medical patient so that there are always beds available for an elective surgical patient. Of course, if a hospital is not full there would be a financial loss for putting aa medical patient in an empty bed that would otherwise go unfilled altogether.
Emergency departments everywhere need to recognize and understand that no one “wins” by replacing an ED problem with an inpatient ward problem. Boarding in either location is dangerous and leads to poor patient satisfaction. The notion that the patient is better off upstairs in the hallway is misguided and not well proven.
Geographical units (i.e., similar patients with specific nurse competencies or service assignments in close proximity) have been shown in the hospital medicine literature to improve efficiency and outcomes. As such, we do not want patients strewn about the hospital for the sake of eliminating an ED boarder if it will lead to a longer length of stay and further inefficiency upstairs. Then, a hospital that should be at 85% capacity will find itself at 90% and once again, and the ED will suffer soon enough too.
Franklin A. Michota, M.D. is medical editor of Hospitalist News and director of academic affairs in the department of hospital medicine at the Cleveland Clinic.
For hospitals that are full (above 95% occupied) and have high surgical and critical care volume, boarding in the ED does not lose money – in fact, it does the opposite. Surgery and critical care are well reimbursed and most hospitals would be well served financially to eliminate medical admissions altogether and simply take care of surgery and critical care patients. Of course, not- for-profit hospitals (like the Cleveland Clinic) have a duty and obligation to serve the community at large, and we must maintain an open ED and provide inpatient medical care as part of our mission (and tax status).
The vast majority of ED admissions today are medical patients who are Medicare or Medicare plus Medicaid, Even if the hospital takes care of these patients efficiently and matches the DRG reimbursement with the length of stay, the opportunity cost of having a nursing home patient with the flu tie up a bed that could have been used for an open heart surgery or lap chole, etc., is huge.
It is often said that from a financial perspective, a medical patient is only slightly better than an empty bed. One of the major operational drivers for hospitalist groups is to maximize efficiency on the medical patient so that there are always beds available for an elective surgical patient. Of course, if a hospital is not full there would be a financial loss for putting aa medical patient in an empty bed that would otherwise go unfilled altogether.
Emergency departments everywhere need to recognize and understand that no one “wins” by replacing an ED problem with an inpatient ward problem. Boarding in either location is dangerous and leads to poor patient satisfaction. The notion that the patient is better off upstairs in the hallway is misguided and not well proven.
Geographical units (i.e., similar patients with specific nurse competencies or service assignments in close proximity) have been shown in the hospital medicine literature to improve efficiency and outcomes. As such, we do not want patients strewn about the hospital for the sake of eliminating an ED boarder if it will lead to a longer length of stay and further inefficiency upstairs. Then, a hospital that should be at 85% capacity will find itself at 90% and once again, and the ED will suffer soon enough too.
Franklin A. Michota, M.D. is medical editor of Hospitalist News and director of academic affairs in the department of hospital medicine at the Cleveland Clinic.
Boarding has been a growing problem over the last decade and may worsen – at least in the short term – with the fuller implementation of the Affordable Care Act, according to experts who are calling for hospitals to implement proven remedies.
Hospital efficiency has suffered as institutions seek to cut costs while coping with a rising influx of uninsured and Medicaid patients. That financial pressure will not improve under health care reform, at least not initially, as millions more Medicaid patients are likely to seek care in the ED when they cannot access primary care, Dr. Jody Crane, emergency department faculty for the Institute for Healthcare Improvement, Cambridge, Mass., said in an interview.
Medicaid pay is already low, and an estimated 8 million more Medicaid patients will visit EDs annually after reform. In addition, as Medicare dials back its reimbursement to hospitals and physicians to help fund the Affordable Care Act, Va. That will put a squeeze on already tight hospital margins, he said.
"Every hospital is going to have to do the same or more with less," said Dr. Crane. Boarding – holding patients in the ED while they wait for admission to inpatient services – can be costly, reduces patient satisfaction, and has been shown to ultimately increase length of stay and mortality.
"Boarding in some hospitals is a capacity issue, but in others it’s also a management issue," Dr. Crane pointed out. Technical issues, including matching resources to the demand coming through the door, are also factors, he said.
"Ultimately, a coordinated effort is needed between the ED and the hospitalist to ensure quality transitions of care that maximize both health and financial outcomes," said Dr. Franklin A. Michota, director of academic affairs in the department of hospital medicine at the Cleveland Clinic. "Each hospital does need to analyze where their bottlenecks exist and whether a staffing solution is part of the answer. But the ED also needs to look at the accuracy and quality of their triage and their ability to adequately prepare the patient for the trip upstairs."
"For example," Dr. Michota continued, "sending a patient upstairs with sickle cell crisis and inadequate pain control just ties up the hospitalist unnecessarily and will delay the hospitalist in getting to the next new admission. Or failing to order a CT scan that would have sent a patient to the operating room and bypass the medical hospitalist altogether will again just delay getting to the next admission.
"Everything relies on everything else....the chain is only as strong as its weakest link."
Indeed, "the primary reason it’s a hard problem to fix is because it’s so multifactorial," said Dr. Jesse Pines, associate professor of emergency medicine and health policy at George Washington University in Washington, D.C.
What Works?
A recent study in Health Affairs showed that many hospitals still are not taking advantage of proven strategies to reduce boarding – among them, so-called smoothing of elective surgical schedules, active bed management by hospitalists, and the "full capacity protocol" that was developed by Dr. Peter Viccellio and his colleagues at the State University of New York at Stony Brook.
"This paper is another in a long series of wake-up calls about the dangerous practice of ‘boarding’ admitted patients in [emergency departments]," ACEP President Dr. David Seaberg said in a statement. "I just hope that hospital administrators and legislators smell the coffee. Their leadership is critical to changing the flow of patients from the front door of the emergency department to the inpatient floors of the hospital."
Emergency departments and hospitals can work together to find ways to improve efficiency, but several important ingredients are needed, Dr. Pines said. The Health Affairs article (2012;31:1757-66 [doi: 10.1377/hlthaff.2011.0786]) cites certain protocols that work, "but you need people to make them work," he said. "You need a strong leader in the ED who can get buy-in from the emergency group. ... You also need a supportive administration and medical staff to make it happen."
It is important to have a local quality improvement group whose members can look at the overall process by which patients get moved from the ED to inpatient services, and examine how patients are managed in the ED after they are admitted, Dr. Pines said. After the existing process is analyzed, hospital staff can identify and address the inefficiencies causing the delays.
The inefficiencies are highly particular to each facility, and often to each day and each shift in the ED and on inpatient wards, he said.
Staffing shortfalls – especially inpatient nursing staff – can be a major contributor to bottlenecks, Dr. Crane said. In response to financial pressures, many hospitals are reducing nursing staff, resulting in increased nurse-to-bed ratios. "That prolongs the inpatient length of stay," he said, because it leads to more work per nurse and more delays in admitting and discharging patients.
There has been a recent administrative trend toward real-time capacity management,which can be an effective way to accommodate the variation in admissions over time.. With this approach, if there is not an identified demand for nurses, they can be sent home or told not to come to work.This ability to change staffing levels according to real-time needs can be an effective way to accommodate the variation in admissions over time
Handoffs and Beds
Dr. Crane contends there are three specific elements to improving patient flow: the physician handoff, the nursing handoff, and bed efficiency.
The physician handoff can be made more efficient by optimizing the coordination between hospitalists and emergency physicians. Due to the high variation in arrival of admissions from the ED and the low numbers of admitting hospitalists at certain times, patients can queue in the ED awaiting admission orders, Dr. Crane noted.
So now, many emergency physicians write holding orders – which have an expiration time – until the patient can be admitted. Holding orders allow the patient to be moved out of the ED, Dr. Crane said. Until recently, emergency physicians have been reluctant to write holding orders, but this trend has reversed because it can be dramatically effective.ACEP now endorses the practice and notes that any associated risk is limited.
The unpredictability of admissions "creates all kinds of logistical nightmares handing off from the emergency department to the floor nurse," Dr. Crane said. Just adding more nurses is not necessarily the answer, and, in general, hospitals don’t have the money to add staff. Instead, hospitals need to better align existing resources and staff. For instance, nurses should probably not be transporting patients or cleaning rooms. That can be done with lower-priced and less-resource-intensive staff, Dr. Crane said.
Bed capacity is the third major element that hospitals should address to reduce boarding, according to Dr. Crane. Demand from the ED cannot be controlled, but on the inpatient side, hospitals can "smooth" the elective surgery schedule by moving more procedures to the middle and end of the week so that all the beds aren’t occupied early in the week. And that is not necessarily easy: "When you change block schedules, you get into cultural issues" with surgeons who do not want to have to see patients on the weekends, Dr. Crane said.
There are also practical issues limiting weekend care. Namely, the typical services such as physical therapy and case management are not routinely present on the weekends. As such, patients who could otherwise be discharged stay in their beds until Monday, when bed demands from the ED and OR increase dramatically. Bed capacity could be improved if hospitals can find ways to make services like testing and therapy available on weekends, and find surgeons and other consultants who will round on Saturdays and Sundays. That might mean hiring a physician’s assistant or other midlevel provider to cover.
Observation Units
Hospitals have also started making use of "observation" status for patients or adding observation units.
At Mary Washington Hospital, where Dr. Crane practices, a team of physicians, nurses, and administrators is designing a streamlined protocol for observation patients. Instead of the standard admission history and physical, an abbreviated assessment has been designed, incorporating use of the ED record and a brief assessment format. Consultations are reduced, and evidence-based pathways are being created for a variety of admitting diagnoses. Patients are treated as outpatients unless test results indicate they need to be moved to the inpatient side, and due to the reduced workload, nurses may be able to work comfortably with higher bed-to-nurse ratios.
The target is to hold patients for observation for 24 hours or less, Dr. Crane said.
Because observation patients are considered outpatients, insurers will pay the hospital less for the visit than if the patient is admitted, Dr. Pines noted, and it leaves the patient vulnerable to higher expenses than just an ED copay.
Another recent study in Health Affairs found that observation stays have been rapidly increasing – from 86.9 observation stays per 1,000 inpatient admissions in 2007 for Medicare beneficiaries to 116.6 in 2009 (Health Affairs 2012;31:1251-9). Of every 1,000 Medicare beneficiaries, 2 were under observation each month in 2007 and almost 3 were under observation each month in 2009. Meanwhile, inpatient admissions per 1,000 declined.
The Sharp Stick of Regulation
Voluntary efforts by hospitals may not be enough, said Dr. Sandra Schneider, former president of the American College of Emergency Physicians. Because hospitals are still paid for the patients who are boarded, they might not see the hidden costs of boarding, she said.
"We have to change that playing field if we want to get serious about [boarding]," Dr. Schneider said.
Among the game changers she cited are the increasing requirements for public reporting on quality measures, including those related to boarding.
Currently, hospitals get paid more by Medicare if they report certain inpatient quality measures. On the outpatient side, emergency departments report on the median time from ED arrival to ED departure for discharged patients and on patients who leave without being seen. In addition, it is now voluntary for hospitals to report on the average time patients spend in the ED before being admitted as an inpatient, and the average time patients spend in the ED after admission but before leaving the ED for their inpatient room.
Data from hospitals that have reported on these measures can be found on the Hospital Compare website.
The Joint Commission is also revisiting its standard on patient flow in the ED, which will go into effect in January 2013. Among other things, the commission is considering defining an episode of boarding as any case in which a patient remains in the ED 4 hours or more after a decision has been made to admit or transfer that patient.
Dr. Pines said that hospital administrators will be motivated both by public reporting imperatives and by Joint Commission standards. Dr. Crane, however, said that "until there are some significant incentives to moving patients upstairs in a timely manner, what’s going to drive senior executives is finance." He thinks that these new standards may help, but more incentives may be needed, such as penalties imposed if boarding limits are exceeded.
Australia, Canada, the United Kingdom, and other developed countries impose such limits and levy penalties.
Hospital Compare data – which will be more fully reported at the end of the first quarter of 2013 – “is going to show us once and for all where the median is and who are the outliers,” Dr. Schneider said. It’s hoped that the outliers will "realize they don’t just have a boarding problem – they have a serious boarding problem," she said.
"If not, then we may have to do what the rest of the world is doing."
Boarding has been a growing problem over the last decade and may worsen – at least in the short term – with the fuller implementation of the Affordable Care Act, according to experts who are calling for hospitals to implement proven remedies.
Hospital efficiency has suffered as institutions seek to cut costs while coping with a rising influx of uninsured and Medicaid patients. That financial pressure will not improve under health care reform, at least not initially, as millions more Medicaid patients are likely to seek care in the ED when they cannot access primary care, Dr. Jody Crane, emergency department faculty for the Institute for Healthcare Improvement, Cambridge, Mass., said in an interview.
Medicaid pay is already low, and an estimated 8 million more Medicaid patients will visit EDs annually after reform. In addition, as Medicare dials back its reimbursement to hospitals and physicians to help fund the Affordable Care Act, Va. That will put a squeeze on already tight hospital margins, he said.
"Every hospital is going to have to do the same or more with less," said Dr. Crane. Boarding – holding patients in the ED while they wait for admission to inpatient services – can be costly, reduces patient satisfaction, and has been shown to ultimately increase length of stay and mortality.
"Boarding in some hospitals is a capacity issue, but in others it’s also a management issue," Dr. Crane pointed out. Technical issues, including matching resources to the demand coming through the door, are also factors, he said.
"Ultimately, a coordinated effort is needed between the ED and the hospitalist to ensure quality transitions of care that maximize both health and financial outcomes," said Dr. Franklin A. Michota, director of academic affairs in the department of hospital medicine at the Cleveland Clinic. "Each hospital does need to analyze where their bottlenecks exist and whether a staffing solution is part of the answer. But the ED also needs to look at the accuracy and quality of their triage and their ability to adequately prepare the patient for the trip upstairs."
"For example," Dr. Michota continued, "sending a patient upstairs with sickle cell crisis and inadequate pain control just ties up the hospitalist unnecessarily and will delay the hospitalist in getting to the next new admission. Or failing to order a CT scan that would have sent a patient to the operating room and bypass the medical hospitalist altogether will again just delay getting to the next admission.
"Everything relies on everything else....the chain is only as strong as its weakest link."
Indeed, "the primary reason it’s a hard problem to fix is because it’s so multifactorial," said Dr. Jesse Pines, associate professor of emergency medicine and health policy at George Washington University in Washington, D.C.
What Works?
A recent study in Health Affairs showed that many hospitals still are not taking advantage of proven strategies to reduce boarding – among them, so-called smoothing of elective surgical schedules, active bed management by hospitalists, and the "full capacity protocol" that was developed by Dr. Peter Viccellio and his colleagues at the State University of New York at Stony Brook.
"This paper is another in a long series of wake-up calls about the dangerous practice of ‘boarding’ admitted patients in [emergency departments]," ACEP President Dr. David Seaberg said in a statement. "I just hope that hospital administrators and legislators smell the coffee. Their leadership is critical to changing the flow of patients from the front door of the emergency department to the inpatient floors of the hospital."
Emergency departments and hospitals can work together to find ways to improve efficiency, but several important ingredients are needed, Dr. Pines said. The Health Affairs article (2012;31:1757-66 [doi: 10.1377/hlthaff.2011.0786]) cites certain protocols that work, "but you need people to make them work," he said. "You need a strong leader in the ED who can get buy-in from the emergency group. ... You also need a supportive administration and medical staff to make it happen."
It is important to have a local quality improvement group whose members can look at the overall process by which patients get moved from the ED to inpatient services, and examine how patients are managed in the ED after they are admitted, Dr. Pines said. After the existing process is analyzed, hospital staff can identify and address the inefficiencies causing the delays.
The inefficiencies are highly particular to each facility, and often to each day and each shift in the ED and on inpatient wards, he said.
Staffing shortfalls – especially inpatient nursing staff – can be a major contributor to bottlenecks, Dr. Crane said. In response to financial pressures, many hospitals are reducing nursing staff, resulting in increased nurse-to-bed ratios. "That prolongs the inpatient length of stay," he said, because it leads to more work per nurse and more delays in admitting and discharging patients.
There has been a recent administrative trend toward real-time capacity management,which can be an effective way to accommodate the variation in admissions over time.. With this approach, if there is not an identified demand for nurses, they can be sent home or told not to come to work.This ability to change staffing levels according to real-time needs can be an effective way to accommodate the variation in admissions over time
Handoffs and Beds
Dr. Crane contends there are three specific elements to improving patient flow: the physician handoff, the nursing handoff, and bed efficiency.
The physician handoff can be made more efficient by optimizing the coordination between hospitalists and emergency physicians. Due to the high variation in arrival of admissions from the ED and the low numbers of admitting hospitalists at certain times, patients can queue in the ED awaiting admission orders, Dr. Crane noted.
So now, many emergency physicians write holding orders – which have an expiration time – until the patient can be admitted. Holding orders allow the patient to be moved out of the ED, Dr. Crane said. Until recently, emergency physicians have been reluctant to write holding orders, but this trend has reversed because it can be dramatically effective.ACEP now endorses the practice and notes that any associated risk is limited.
The unpredictability of admissions "creates all kinds of logistical nightmares handing off from the emergency department to the floor nurse," Dr. Crane said. Just adding more nurses is not necessarily the answer, and, in general, hospitals don’t have the money to add staff. Instead, hospitals need to better align existing resources and staff. For instance, nurses should probably not be transporting patients or cleaning rooms. That can be done with lower-priced and less-resource-intensive staff, Dr. Crane said.
Bed capacity is the third major element that hospitals should address to reduce boarding, according to Dr. Crane. Demand from the ED cannot be controlled, but on the inpatient side, hospitals can "smooth" the elective surgery schedule by moving more procedures to the middle and end of the week so that all the beds aren’t occupied early in the week. And that is not necessarily easy: "When you change block schedules, you get into cultural issues" with surgeons who do not want to have to see patients on the weekends, Dr. Crane said.
There are also practical issues limiting weekend care. Namely, the typical services such as physical therapy and case management are not routinely present on the weekends. As such, patients who could otherwise be discharged stay in their beds until Monday, when bed demands from the ED and OR increase dramatically. Bed capacity could be improved if hospitals can find ways to make services like testing and therapy available on weekends, and find surgeons and other consultants who will round on Saturdays and Sundays. That might mean hiring a physician’s assistant or other midlevel provider to cover.
Observation Units
Hospitals have also started making use of "observation" status for patients or adding observation units.
At Mary Washington Hospital, where Dr. Crane practices, a team of physicians, nurses, and administrators is designing a streamlined protocol for observation patients. Instead of the standard admission history and physical, an abbreviated assessment has been designed, incorporating use of the ED record and a brief assessment format. Consultations are reduced, and evidence-based pathways are being created for a variety of admitting diagnoses. Patients are treated as outpatients unless test results indicate they need to be moved to the inpatient side, and due to the reduced workload, nurses may be able to work comfortably with higher bed-to-nurse ratios.
The target is to hold patients for observation for 24 hours or less, Dr. Crane said.
Because observation patients are considered outpatients, insurers will pay the hospital less for the visit than if the patient is admitted, Dr. Pines noted, and it leaves the patient vulnerable to higher expenses than just an ED copay.
Another recent study in Health Affairs found that observation stays have been rapidly increasing – from 86.9 observation stays per 1,000 inpatient admissions in 2007 for Medicare beneficiaries to 116.6 in 2009 (Health Affairs 2012;31:1251-9). Of every 1,000 Medicare beneficiaries, 2 were under observation each month in 2007 and almost 3 were under observation each month in 2009. Meanwhile, inpatient admissions per 1,000 declined.
The Sharp Stick of Regulation
Voluntary efforts by hospitals may not be enough, said Dr. Sandra Schneider, former president of the American College of Emergency Physicians. Because hospitals are still paid for the patients who are boarded, they might not see the hidden costs of boarding, she said.
"We have to change that playing field if we want to get serious about [boarding]," Dr. Schneider said.
Among the game changers she cited are the increasing requirements for public reporting on quality measures, including those related to boarding.
Currently, hospitals get paid more by Medicare if they report certain inpatient quality measures. On the outpatient side, emergency departments report on the median time from ED arrival to ED departure for discharged patients and on patients who leave without being seen. In addition, it is now voluntary for hospitals to report on the average time patients spend in the ED before being admitted as an inpatient, and the average time patients spend in the ED after admission but before leaving the ED for their inpatient room.
Data from hospitals that have reported on these measures can be found on the Hospital Compare website.
The Joint Commission is also revisiting its standard on patient flow in the ED, which will go into effect in January 2013. Among other things, the commission is considering defining an episode of boarding as any case in which a patient remains in the ED 4 hours or more after a decision has been made to admit or transfer that patient.
Dr. Pines said that hospital administrators will be motivated both by public reporting imperatives and by Joint Commission standards. Dr. Crane, however, said that "until there are some significant incentives to moving patients upstairs in a timely manner, what’s going to drive senior executives is finance." He thinks that these new standards may help, but more incentives may be needed, such as penalties imposed if boarding limits are exceeded.
Australia, Canada, the United Kingdom, and other developed countries impose such limits and levy penalties.
Hospital Compare data – which will be more fully reported at the end of the first quarter of 2013 – “is going to show us once and for all where the median is and who are the outliers,” Dr. Schneider said. It’s hoped that the outliers will "realize they don’t just have a boarding problem – they have a serious boarding problem," she said.
"If not, then we may have to do what the rest of the world is doing."

Family Physicians Endorse Same-Sex Civil Marriage
PHILADELPHIA – The American Academy of Family Physicians Congress of Delegates has approved a new policy to support civil marriage for same-sex couples, making it one of the few medical societies to explicitly endorse gay marriage.
AAFP policy now states that the organization supports "civil marriage for same-gender couples to contribute to overall health and longevity, improved family stability, and to benefit children of gay, lesbian, bisexual, transgender (GLBT) families."

The congress voted 75-44 to approve that language, which was crafted from two resolutions brought forward by the resident and student sections. This was the third year in a row that the congress had weighed whether the organization should give its backing to same-sex marriage. And, as in past years, debate was lengthy and impassioned.
Many supporters testified that their own same-sex partnerships had suffered as a result of being denied the ability to marry.
Dr. Mark Dressner, president-elect of the California chapter, said that he felt that he and his partner had been treated as second-class citizens. Others spoke of the emotional and physical damage they had witnessed in patients and family members as a result of discrimination against homosexuals.
Dr. Lloyd Van Winkle of Castroville, Tex., who was just elected to the AAFP board, said that a young relation* committed suicide at age 19 because he felt persecuted about his homosexuality.
Dr. Paul W. Davis, a delegate from Alaska, spoke about his long journey from "the extreme conservative religious right wing on this debate to a committed solidarity with the opposite pole."
Dr. Davis said that he had watched patients struggle with major depression over their sexual and gender identity. "I am not proud of the fact that I am a late adopter on this important issue," he said, urging his fellow delegates that "we need to boldly make a decision and move forward."
But opponents said that AAFP should not be wading so deeply into what they considered largely treacherous political waters.
Dr. Justin V. Bartos, a delegate from Texas, said that his state’s chapter opposed the resolution because it was too much of a political statement and diverged from the AAFP’s mission.
Members of the Texas Academy of Family Physicians "do not want us to endorse such a politically polarizing issue," Dr. Bartos said. He noted that family doctors in Texas are struggling to get their state legislature to restore funding for community-based residencies, and that lawmakers in the largely conservative state would note the AAFP’s support of gay marriage.
The Tennessee delegation also opposed the policy change for the same reasons – that it would politicize the AAFP.
Another Texas delegate, Dr. Erica Swegler*, said that current AAFP policy was enough to indicate the organization’s support for equal access to health care for all Americans.
During testimony before the reference committee charged with weighing the policy change, an Arkansas delegate said that more than 300 members might leave the AAFP if it gave its approval to gay marriage.
The AAFP joins the American Psychiatric Association and the American Psychological Association in supporting same sex marriage. The psychiatrists approved a resolution of support in 2005, and the psychology association made it official policy in 2011.
The American Medical Association has not backed gay marriage specifically, but has a host of policies supporting equality for same-sex households.
The American College of Obstetricians and Gynecologists in 2009 issued a policy statement that same-sex couples should get same legal rights as married heterosexuals.
*Correction, 11/8/12: An earlier version of this story misidentified Dr. Van Winkle's relation and misspelled Dr. Swegler's name.
PHILADELPHIA – The American Academy of Family Physicians Congress of Delegates has approved a new policy to support civil marriage for same-sex couples, making it one of the few medical societies to explicitly endorse gay marriage.
AAFP policy now states that the organization supports "civil marriage for same-gender couples to contribute to overall health and longevity, improved family stability, and to benefit children of gay, lesbian, bisexual, transgender (GLBT) families."
The congress voted 75-44 to approve that language, which was crafted from two resolutions brought forward by the resident and student sections. This was the third year in a row that the congress had weighed whether the organization should give its backing to same-sex marriage. And, as in past years, debate was lengthy and impassioned.
Many supporters testified that their own same-sex partnerships had suffered as a result of being denied the ability to marry.
Dr. Mark Dressner, president-elect of the California chapter, said that he felt that he and his partner had been treated as second-class citizens. Others spoke of the emotional and physical damage they had witnessed in patients and family members as a result of discrimination against homosexuals.
Dr. Lloyd Van Winkle of Castroville, Tex., who was just elected to the AAFP board, said that a young relation* committed suicide at age 19 because he felt persecuted about his homosexuality.
Dr. Paul W. Davis, a delegate from Alaska, spoke about his long journey from "the extreme conservative religious right wing on this debate to a committed solidarity with the opposite pole."
Dr. Davis said that he had watched patients struggle with major depression over their sexual and gender identity. "I am not proud of the fact that I am a late adopter on this important issue," he said, urging his fellow delegates that "we need to boldly make a decision and move forward."
But opponents said that AAFP should not be wading so deeply into what they considered largely treacherous political waters.
Dr. Justin V. Bartos, a delegate from Texas, said that his state’s chapter opposed the resolution because it was too much of a political statement and diverged from the AAFP’s mission.
Members of the Texas Academy of Family Physicians "do not want us to endorse such a politically polarizing issue," Dr. Bartos said. He noted that family doctors in Texas are struggling to get their state legislature to restore funding for community-based residencies, and that lawmakers in the largely conservative state would note the AAFP’s support of gay marriage.
The Tennessee delegation also opposed the policy change for the same reasons – that it would politicize the AAFP.
Another Texas delegate, Dr. Erica Swegler*, said that current AAFP policy was enough to indicate the organization’s support for equal access to health care for all Americans.
During testimony before the reference committee charged with weighing the policy change, an Arkansas delegate said that more than 300 members might leave the AAFP if it gave its approval to gay marriage.
The AAFP joins the American Psychiatric Association and the American Psychological Association in supporting same sex marriage. The psychiatrists approved a resolution of support in 2005, and the psychology association made it official policy in 2011.
The American Medical Association has not backed gay marriage specifically, but has a host of policies supporting equality for same-sex households.
The American College of Obstetricians and Gynecologists in 2009 issued a policy statement that same-sex couples should get same legal rights as married heterosexuals.
*Correction, 11/8/12: An earlier version of this story misidentified Dr. Van Winkle's relation and misspelled Dr. Swegler's name.
PHILADELPHIA – The American Academy of Family Physicians Congress of Delegates has approved a new policy to support civil marriage for same-sex couples, making it one of the few medical societies to explicitly endorse gay marriage.
AAFP policy now states that the organization supports "civil marriage for same-gender couples to contribute to overall health and longevity, improved family stability, and to benefit children of gay, lesbian, bisexual, transgender (GLBT) families."
The congress voted 75-44 to approve that language, which was crafted from two resolutions brought forward by the resident and student sections. This was the third year in a row that the congress had weighed whether the organization should give its backing to same-sex marriage. And, as in past years, debate was lengthy and impassioned.
Many supporters testified that their own same-sex partnerships had suffered as a result of being denied the ability to marry.
Dr. Mark Dressner, president-elect of the California chapter, said that he felt that he and his partner had been treated as second-class citizens. Others spoke of the emotional and physical damage they had witnessed in patients and family members as a result of discrimination against homosexuals.
Dr. Lloyd Van Winkle of Castroville, Tex., who was just elected to the AAFP board, said that a young relation* committed suicide at age 19 because he felt persecuted about his homosexuality.
Dr. Paul W. Davis, a delegate from Alaska, spoke about his long journey from "the extreme conservative religious right wing on this debate to a committed solidarity with the opposite pole."
Dr. Davis said that he had watched patients struggle with major depression over their sexual and gender identity. "I am not proud of the fact that I am a late adopter on this important issue," he said, urging his fellow delegates that "we need to boldly make a decision and move forward."
But opponents said that AAFP should not be wading so deeply into what they considered largely treacherous political waters.
Dr. Justin V. Bartos, a delegate from Texas, said that his state’s chapter opposed the resolution because it was too much of a political statement and diverged from the AAFP’s mission.
Members of the Texas Academy of Family Physicians "do not want us to endorse such a politically polarizing issue," Dr. Bartos said. He noted that family doctors in Texas are struggling to get their state legislature to restore funding for community-based residencies, and that lawmakers in the largely conservative state would note the AAFP’s support of gay marriage.
The Tennessee delegation also opposed the policy change for the same reasons – that it would politicize the AAFP.
Another Texas delegate, Dr. Erica Swegler*, said that current AAFP policy was enough to indicate the organization’s support for equal access to health care for all Americans.
During testimony before the reference committee charged with weighing the policy change, an Arkansas delegate said that more than 300 members might leave the AAFP if it gave its approval to gay marriage.
The AAFP joins the American Psychiatric Association and the American Psychological Association in supporting same sex marriage. The psychiatrists approved a resolution of support in 2005, and the psychology association made it official policy in 2011.
The American Medical Association has not backed gay marriage specifically, but has a host of policies supporting equality for same-sex households.
The American College of Obstetricians and Gynecologists in 2009 issued a policy statement that same-sex couples should get same legal rights as married heterosexuals.
*Correction, 11/8/12: An earlier version of this story misidentified Dr. Van Winkle's relation and misspelled Dr. Swegler's name.
AT THE AAFP CONGRESS OF DELEGATES

AAFP Vows to Continue Fight for Better Pay
PHILADELPHIA – The American Academy of Family Physicians opened its Congress of Delegates meeting here with a vow to press forward with efforts to have government and private payers reimburse the specialty at a higher rate.
At a Town Hall forum on the evening of Oct. 14 and the first general session on Oct. 15, the academy’s leadership said that it would continue to fight for a higher valuation for family medicine through its representation on the American Medical Association’s Relative Value Scale Update Committee (RUC). In the fall of 2011, the AAFP threatened to pull out of the RUC if the payment concerns of family physicians were not addressed.

In March, however, the academy said it would consider alternate ways to support a revaluation of family medicine.
Many AAFP members have not been happy with that approach and have floated several resolutions to keep hammering at the issue. Among them: a resolution to create a set of family medicine–specific codes. Testimony at the AAFP’s Reference Committee on Practice Enhancement seemed to lean largely against that proposal, but there was consensus that family medicine is consistently undervalued.
"This congress is very familiar with family medicine’s frustration with the RUC," AAFP President Glen Stream said at the meeting. He noted, however, that for the moment, "remaining in the RUC allows the opportunity to advocate and press for [the] changes."
The full congress will probably take up the RUC-related resolutions and put them to a vote on Oct. 16 or Oct. 17.
The same committee also heard cautionary testimony on a resolution that would make it AAFP policy to oppose telemedicine that is provided in the absence of a pre-existing physician-patient relationship. The resolution emerged from concerns about the rise of for-profit entities – such as pharmacy chains – that bypass physicians in the community.
Impassioned and lengthy testimony at the Reference Committee on Advocacy addressed two resolutions seeking the AAFP’s backing of same-sex civil marriage. An overwhelming number of speakers said that such marriages would help improve public and individual health. More than a handful gave personal anecdotes about their own same-sex relationships, but several of the opposing delegates said that they would leave AAFP if gave its support to the resolution.
The advocacy committee also heard pro and con on a resolution to back over-the-counter emergency contraception for all women of childbearing age.
Finally, the AAFP leadership said that the board had given approval to generate a new report on what family medicine should look like going forward. The AAFP developed just such a blueprint 8 years ago, but the research that supported that paper has become dated, said Dr. Douglas Henley, AAFP executive vice president.
"Now is a critical time to begin a discussion and perhaps revisit research or even initiate new research about what comprehensive primary care means in 2012 and into the future," Dr. Henley said.
The process has begun, he noted, adding that AAFP members should expect to hear more in January.
PHILADELPHIA – The American Academy of Family Physicians opened its Congress of Delegates meeting here with a vow to press forward with efforts to have government and private payers reimburse the specialty at a higher rate.
At a Town Hall forum on the evening of Oct. 14 and the first general session on Oct. 15, the academy’s leadership said that it would continue to fight for a higher valuation for family medicine through its representation on the American Medical Association’s Relative Value Scale Update Committee (RUC). In the fall of 2011, the AAFP threatened to pull out of the RUC if the payment concerns of family physicians were not addressed.
In March, however, the academy said it would consider alternate ways to support a revaluation of family medicine.
Many AAFP members have not been happy with that approach and have floated several resolutions to keep hammering at the issue. Among them: a resolution to create a set of family medicine–specific codes. Testimony at the AAFP’s Reference Committee on Practice Enhancement seemed to lean largely against that proposal, but there was consensus that family medicine is consistently undervalued.
"This congress is very familiar with family medicine’s frustration with the RUC," AAFP President Glen Stream said at the meeting. He noted, however, that for the moment, "remaining in the RUC allows the opportunity to advocate and press for [the] changes."
The full congress will probably take up the RUC-related resolutions and put them to a vote on Oct. 16 or Oct. 17.
The same committee also heard cautionary testimony on a resolution that would make it AAFP policy to oppose telemedicine that is provided in the absence of a pre-existing physician-patient relationship. The resolution emerged from concerns about the rise of for-profit entities – such as pharmacy chains – that bypass physicians in the community.
Impassioned and lengthy testimony at the Reference Committee on Advocacy addressed two resolutions seeking the AAFP’s backing of same-sex civil marriage. An overwhelming number of speakers said that such marriages would help improve public and individual health. More than a handful gave personal anecdotes about their own same-sex relationships, but several of the opposing delegates said that they would leave AAFP if gave its support to the resolution.
The advocacy committee also heard pro and con on a resolution to back over-the-counter emergency contraception for all women of childbearing age.
Finally, the AAFP leadership said that the board had given approval to generate a new report on what family medicine should look like going forward. The AAFP developed just such a blueprint 8 years ago, but the research that supported that paper has become dated, said Dr. Douglas Henley, AAFP executive vice president.
"Now is a critical time to begin a discussion and perhaps revisit research or even initiate new research about what comprehensive primary care means in 2012 and into the future," Dr. Henley said.
The process has begun, he noted, adding that AAFP members should expect to hear more in January.
PHILADELPHIA – The American Academy of Family Physicians opened its Congress of Delegates meeting here with a vow to press forward with efforts to have government and private payers reimburse the specialty at a higher rate.
At a Town Hall forum on the evening of Oct. 14 and the first general session on Oct. 15, the academy’s leadership said that it would continue to fight for a higher valuation for family medicine through its representation on the American Medical Association’s Relative Value Scale Update Committee (RUC). In the fall of 2011, the AAFP threatened to pull out of the RUC if the payment concerns of family physicians were not addressed.
In March, however, the academy said it would consider alternate ways to support a revaluation of family medicine.
Many AAFP members have not been happy with that approach and have floated several resolutions to keep hammering at the issue. Among them: a resolution to create a set of family medicine–specific codes. Testimony at the AAFP’s Reference Committee on Practice Enhancement seemed to lean largely against that proposal, but there was consensus that family medicine is consistently undervalued.
"This congress is very familiar with family medicine’s frustration with the RUC," AAFP President Glen Stream said at the meeting. He noted, however, that for the moment, "remaining in the RUC allows the opportunity to advocate and press for [the] changes."
The full congress will probably take up the RUC-related resolutions and put them to a vote on Oct. 16 or Oct. 17.
The same committee also heard cautionary testimony on a resolution that would make it AAFP policy to oppose telemedicine that is provided in the absence of a pre-existing physician-patient relationship. The resolution emerged from concerns about the rise of for-profit entities – such as pharmacy chains – that bypass physicians in the community.
Impassioned and lengthy testimony at the Reference Committee on Advocacy addressed two resolutions seeking the AAFP’s backing of same-sex civil marriage. An overwhelming number of speakers said that such marriages would help improve public and individual health. More than a handful gave personal anecdotes about their own same-sex relationships, but several of the opposing delegates said that they would leave AAFP if gave its support to the resolution.
The advocacy committee also heard pro and con on a resolution to back over-the-counter emergency contraception for all women of childbearing age.
Finally, the AAFP leadership said that the board had given approval to generate a new report on what family medicine should look like going forward. The AAFP developed just such a blueprint 8 years ago, but the research that supported that paper has become dated, said Dr. Douglas Henley, AAFP executive vice president.
"Now is a critical time to begin a discussion and perhaps revisit research or even initiate new research about what comprehensive primary care means in 2012 and into the future," Dr. Henley said.
The process has begun, he noted, adding that AAFP members should expect to hear more in January.
AT THE AAFP CONGRESS OF DELEGATES

Alzheimer's Imaging Agent Considered for Medicare Coverage
The imaging agent florbetapir F 18 injection (Amyvid), used to exclude a diagnosis of Alzheimer’s disease, is being evaluated for Medicare reimbursement, the Centers for Medicare and Medicaid Services has announced.
The agency stated on Oct. 9 that it expected a preliminary decision by July 2013, and a final decision by October 2013.

The CMS is accepting public comments on its proposed coverage of florbetapir until Nov. 8.
Florbetapir, approved by the Food and Drug Administration in April, is used in conjunction with positron emission tomography (PET). Eli Lilly, which owns florbetapir maker Avid Radiopharmaceuticals, requested the coverage determination. The company laid out its case for reimbursement in a 47-page letter to the CMS in June.
In the request, Lilly noted that the CMS approved coverage of FDG-PET for patients who had a recent dementia diagnosis and cognitive decline over 6 months and who met diagnostic criteria for Alzheimer’s disease and frontotemporal dementia.
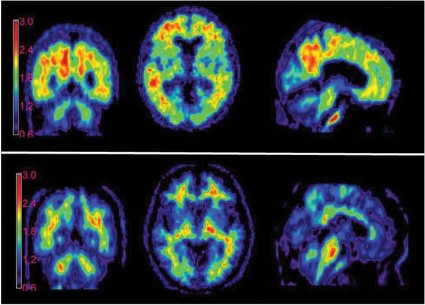
According to Avid, florbetapir binds to beta-amyloid plaques in the brain, which are considered markers for Alzheimer’s. Without the ability to see those plaques in real time, diagnosis has been based on symptoms and cognitive testing. But that is imperfect, missing perhaps a fifth of cases.
At the time of florbetapir’s approval, the Alzheimer's Association said the imaging agent would be useful in diagnosis and in tracking of treatment response, but also expressed concern about potentially unscrupulous uses of the technology.
The organization has convened a task force with the Society of Nuclear Medicine to develop guidelines on florbetapir use.
An estimated 5 million Americans have Alzheimer’s, and the incidence is rising with the aging of the U.S. population. Only 4% of those with the disease are under the Medicare age of 65, according to Lilly; 40%-45% of Americans over age 75 are estimated to have the disease.
The imaging agent florbetapir F 18 injection (Amyvid), used to exclude a diagnosis of Alzheimer’s disease, is being evaluated for Medicare reimbursement, the Centers for Medicare and Medicaid Services has announced.
The agency stated on Oct. 9 that it expected a preliminary decision by July 2013, and a final decision by October 2013.
The CMS is accepting public comments on its proposed coverage of florbetapir until Nov. 8.
Florbetapir, approved by the Food and Drug Administration in April, is used in conjunction with positron emission tomography (PET). Eli Lilly, which owns florbetapir maker Avid Radiopharmaceuticals, requested the coverage determination. The company laid out its case for reimbursement in a 47-page letter to the CMS in June.
In the request, Lilly noted that the CMS approved coverage of FDG-PET for patients who had a recent dementia diagnosis and cognitive decline over 6 months and who met diagnostic criteria for Alzheimer’s disease and frontotemporal dementia.
According to Avid, florbetapir binds to beta-amyloid plaques in the brain, which are considered markers for Alzheimer’s. Without the ability to see those plaques in real time, diagnosis has been based on symptoms and cognitive testing. But that is imperfect, missing perhaps a fifth of cases.
At the time of florbetapir’s approval, the Alzheimer's Association said the imaging agent would be useful in diagnosis and in tracking of treatment response, but also expressed concern about potentially unscrupulous uses of the technology.
The organization has convened a task force with the Society of Nuclear Medicine to develop guidelines on florbetapir use.
An estimated 5 million Americans have Alzheimer’s, and the incidence is rising with the aging of the U.S. population. Only 4% of those with the disease are under the Medicare age of 65, according to Lilly; 40%-45% of Americans over age 75 are estimated to have the disease.
The imaging agent florbetapir F 18 injection (Amyvid), used to exclude a diagnosis of Alzheimer’s disease, is being evaluated for Medicare reimbursement, the Centers for Medicare and Medicaid Services has announced.
The agency stated on Oct. 9 that it expected a preliminary decision by July 2013, and a final decision by October 2013.
The CMS is accepting public comments on its proposed coverage of florbetapir until Nov. 8.
Florbetapir, approved by the Food and Drug Administration in April, is used in conjunction with positron emission tomography (PET). Eli Lilly, which owns florbetapir maker Avid Radiopharmaceuticals, requested the coverage determination. The company laid out its case for reimbursement in a 47-page letter to the CMS in June.
In the request, Lilly noted that the CMS approved coverage of FDG-PET for patients who had a recent dementia diagnosis and cognitive decline over 6 months and who met diagnostic criteria for Alzheimer’s disease and frontotemporal dementia.
According to Avid, florbetapir binds to beta-amyloid plaques in the brain, which are considered markers for Alzheimer’s. Without the ability to see those plaques in real time, diagnosis has been based on symptoms and cognitive testing. But that is imperfect, missing perhaps a fifth of cases.
At the time of florbetapir’s approval, the Alzheimer's Association said the imaging agent would be useful in diagnosis and in tracking of treatment response, but also expressed concern about potentially unscrupulous uses of the technology.
The organization has convened a task force with the Society of Nuclear Medicine to develop guidelines on florbetapir use.
An estimated 5 million Americans have Alzheimer’s, and the incidence is rising with the aging of the U.S. population. Only 4% of those with the disease are under the Medicare age of 65, according to Lilly; 40%-45% of Americans over age 75 are estimated to have the disease.
FDA Targets Thousands of Illegal Online Pharmacies
The Food and Drug Administration took action this week against 4,100 Internet pharmacies selling counterfeit and illegal medicines, part of a coordinated international crackdown on the $75 billion counterfeit drug market.
The larger worldwide initiative, known as Operation Pangea V, shut down more than 18,000 illegal pharmacy websites and seized $10.5 million in pharmaceuticals worldwide during the week of Sept. 25-Oct. 2.
"Because these criminals do not respect international borders, the international coordinated law enforcement response represented by Operation Pangea demonstrates that international cooperation is the best way to protect the American public from the risk of unsafe drugs," said John Roth, director of the FDA’s Office of Criminal Investigations, in a statement.
Counterfeit drug sales hit $75 billion worldwide in 2010, a 90% increase from the previous year, according to the Center for Safe Internet Pharmacies (CSIP).
INTERPOL, the World Customs Organization, the Permanent Forum of International Pharmaceutical Crime, the Heads of Medicines Agencies Working Group of Enforcement Officers, Pharmaceutical Security Institute, and Europol directed the Pangea V, with participation from more than 100 countries.
The operation also received support from CSIP, as well as a group of Internet and e-commerce companies that includes Visa, American Express, MasterCard, Yahoo, Facebook, and PayPal.
The FDA said it targeted websites selling "unapproved and potentially dangerous medicines." The agency sent warning letters to the operators of more than 4,100 identified websites and then notified registries, Internet service providers, and domain name registrars that these websites were selling products in violation of U.S. law.
During the week-long crackdown, the FDA screened all drug products received through the international mail facilities. The screenings found antibiotics, antidepressants, and other drugs for high cholesterol, diabetes, and high blood pressure headed for American consumers. Many of those drugs could be risky to take without the supervision of a physician, the agency warned.
Some of the drugs intercepted also had been removed from the U.S. market, including domperidone, which was taken off the U.S. market in 1998 because of its potential to cause severe cardiac effects, including sudden death.
Also found in the mail were the acne drug isotretinoin, which is available in the United States only through a risk management distribution program; sildenafil citrate (Viagra); and the antiviral oseltamivir (Tamiflu), which is often sold as a "generic," though there is no such approved U.S. generic. Tests by the FDA have shown that fraudulent generic versions of Tamiflu contained the wrong active ingredient, which would not be effective in treating flu.
Seventy-nine people have been arrested or are under investigation, according to INTERPOL.
The FDA launched a consumer-oriented campaign in late September, called BeSafeRx–Know Your Online Pharmacy. The website gives consumers tips on how to understand who they are buying from and when it might not be a good idea to purchase through a website.
The agency said one-quarter of consumers buy prescription drugs online, according to a survey it conducted, but that one-third of respondents said they did not have confidence in how to make safe online purchases.
"Fraudulent and illegal online pharmacies often offer deeply discounted products," said FDA Commissioner Margaret Hamburg in a statement. "If the low prices seem too good to be true, they probably are," she said.
The FDA urged patients to only buy online through pharmacies that require a valid prescription from a doctor or other health care professional; are located in the United States; have a licensed pharmacist available for consultation; and are licensed by the patient’s state board of pharmacy.
The Food and Drug Administration took action this week against 4,100 Internet pharmacies selling counterfeit and illegal medicines, part of a coordinated international crackdown on the $75 billion counterfeit drug market.
The larger worldwide initiative, known as Operation Pangea V, shut down more than 18,000 illegal pharmacy websites and seized $10.5 million in pharmaceuticals worldwide during the week of Sept. 25-Oct. 2.
"Because these criminals do not respect international borders, the international coordinated law enforcement response represented by Operation Pangea demonstrates that international cooperation is the best way to protect the American public from the risk of unsafe drugs," said John Roth, director of the FDA’s Office of Criminal Investigations, in a statement.
Counterfeit drug sales hit $75 billion worldwide in 2010, a 90% increase from the previous year, according to the Center for Safe Internet Pharmacies (CSIP).
INTERPOL, the World Customs Organization, the Permanent Forum of International Pharmaceutical Crime, the Heads of Medicines Agencies Working Group of Enforcement Officers, Pharmaceutical Security Institute, and Europol directed the Pangea V, with participation from more than 100 countries.
The operation also received support from CSIP, as well as a group of Internet and e-commerce companies that includes Visa, American Express, MasterCard, Yahoo, Facebook, and PayPal.
The FDA said it targeted websites selling "unapproved and potentially dangerous medicines." The agency sent warning letters to the operators of more than 4,100 identified websites and then notified registries, Internet service providers, and domain name registrars that these websites were selling products in violation of U.S. law.
During the week-long crackdown, the FDA screened all drug products received through the international mail facilities. The screenings found antibiotics, antidepressants, and other drugs for high cholesterol, diabetes, and high blood pressure headed for American consumers. Many of those drugs could be risky to take without the supervision of a physician, the agency warned.
Some of the drugs intercepted also had been removed from the U.S. market, including domperidone, which was taken off the U.S. market in 1998 because of its potential to cause severe cardiac effects, including sudden death.
Also found in the mail were the acne drug isotretinoin, which is available in the United States only through a risk management distribution program; sildenafil citrate (Viagra); and the antiviral oseltamivir (Tamiflu), which is often sold as a "generic," though there is no such approved U.S. generic. Tests by the FDA have shown that fraudulent generic versions of Tamiflu contained the wrong active ingredient, which would not be effective in treating flu.
Seventy-nine people have been arrested or are under investigation, according to INTERPOL.
The FDA launched a consumer-oriented campaign in late September, called BeSafeRx–Know Your Online Pharmacy. The website gives consumers tips on how to understand who they are buying from and when it might not be a good idea to purchase through a website.
The agency said one-quarter of consumers buy prescription drugs online, according to a survey it conducted, but that one-third of respondents said they did not have confidence in how to make safe online purchases.
"Fraudulent and illegal online pharmacies often offer deeply discounted products," said FDA Commissioner Margaret Hamburg in a statement. "If the low prices seem too good to be true, they probably are," she said.
The FDA urged patients to only buy online through pharmacies that require a valid prescription from a doctor or other health care professional; are located in the United States; have a licensed pharmacist available for consultation; and are licensed by the patient’s state board of pharmacy.
The Food and Drug Administration took action this week against 4,100 Internet pharmacies selling counterfeit and illegal medicines, part of a coordinated international crackdown on the $75 billion counterfeit drug market.
The larger worldwide initiative, known as Operation Pangea V, shut down more than 18,000 illegal pharmacy websites and seized $10.5 million in pharmaceuticals worldwide during the week of Sept. 25-Oct. 2.
"Because these criminals do not respect international borders, the international coordinated law enforcement response represented by Operation Pangea demonstrates that international cooperation is the best way to protect the American public from the risk of unsafe drugs," said John Roth, director of the FDA’s Office of Criminal Investigations, in a statement.
Counterfeit drug sales hit $75 billion worldwide in 2010, a 90% increase from the previous year, according to the Center for Safe Internet Pharmacies (CSIP).
INTERPOL, the World Customs Organization, the Permanent Forum of International Pharmaceutical Crime, the Heads of Medicines Agencies Working Group of Enforcement Officers, Pharmaceutical Security Institute, and Europol directed the Pangea V, with participation from more than 100 countries.
The operation also received support from CSIP, as well as a group of Internet and e-commerce companies that includes Visa, American Express, MasterCard, Yahoo, Facebook, and PayPal.
The FDA said it targeted websites selling "unapproved and potentially dangerous medicines." The agency sent warning letters to the operators of more than 4,100 identified websites and then notified registries, Internet service providers, and domain name registrars that these websites were selling products in violation of U.S. law.
During the week-long crackdown, the FDA screened all drug products received through the international mail facilities. The screenings found antibiotics, antidepressants, and other drugs for high cholesterol, diabetes, and high blood pressure headed for American consumers. Many of those drugs could be risky to take without the supervision of a physician, the agency warned.
Some of the drugs intercepted also had been removed from the U.S. market, including domperidone, which was taken off the U.S. market in 1998 because of its potential to cause severe cardiac effects, including sudden death.
Also found in the mail were the acne drug isotretinoin, which is available in the United States only through a risk management distribution program; sildenafil citrate (Viagra); and the antiviral oseltamivir (Tamiflu), which is often sold as a "generic," though there is no such approved U.S. generic. Tests by the FDA have shown that fraudulent generic versions of Tamiflu contained the wrong active ingredient, which would not be effective in treating flu.
Seventy-nine people have been arrested or are under investigation, according to INTERPOL.
The FDA launched a consumer-oriented campaign in late September, called BeSafeRx–Know Your Online Pharmacy. The website gives consumers tips on how to understand who they are buying from and when it might not be a good idea to purchase through a website.
The agency said one-quarter of consumers buy prescription drugs online, according to a survey it conducted, but that one-third of respondents said they did not have confidence in how to make safe online purchases.
"Fraudulent and illegal online pharmacies often offer deeply discounted products," said FDA Commissioner Margaret Hamburg in a statement. "If the low prices seem too good to be true, they probably are," she said.
The FDA urged patients to only buy online through pharmacies that require a valid prescription from a doctor or other health care professional; are located in the United States; have a licensed pharmacist available for consultation; and are licensed by the patient’s state board of pharmacy.
FDA Approves First Subcutaneous ICD
The Food and Drug Administration has approved a new implantable cardioverter defibrillator that is implanted subcutaneously as a treatment for ventricular tachyarrhythmias.
The agency approved the Subcutaneous Implantable Defibrillator (S-ICD) System only for patients who do not require a pacemaker or pacing therapy.

The S-ICD System, made by Cameron Health of San Clemente, Calif., is the first such device that can be placed without transvenous leads. Instead, the leads are placed under the skin and then connected to the heart.
"The S-ICD System provides an alternative for treating patients with life-threatening heart arrhythmias for whom the routine ICD placement procedure is not ideal," said Christy Foreman, director of the Office of Device Evaluation at FDA’s Center for Devices and Radiological Health, in a statement. "Some patients with anatomy that makes it challenging to place one of the implantable defibrillators currently on the market may especially benefit from this device."
The device won near-unanimous backing of the FDA’s Circulatory System Devices Panel in April. The panel voted 7-1 that the benefits of the S-ICD system outweighed its risks in patients who meet the criteria in the indication proposed by Cameron Health: to provide "defibrillation therapy for the treatment of life-threatening ventricular tachyarrhythmias in patients who do not have symptomatic bradycardia; incessant ventricular tachycardia; or spontaneous, frequently recurring ventricular tachycardia that is reliably terminated with antitachycardia pacing."
Safety and efficacy data for the approval came from a 321-patient study, which was reported at the Heart Rhythm Society in May. In that trial, 304 patients were successfully implanted and the device converted all abnormal heart rhythms that it detected back to normal rhythms, according to the FDA. In the 6 months postimplantation, the S-ICD detected and recorded 78 spontaneous arrhythmias in 21 patients that were either all converted or resolved on their own.
The FDA said that the most common complications included inappropriate shocks, discomfort, system infection, and electrode movement. Eight patients died during the study, but the S-ICD was not definitively seen as the cause. There were 11 explants. Six months after implantation, 90% of the device recipients had no complications.
Cameron Health reported in May that the S-ICD is distributed in 10 other countries and that more than 1,200 patients have been implanted worldwide.
The company proposed a postmarketing study when it submitted its application for approval. The FDA will require that study, seeking assessment of how it performs over the long term, and across genders. The study will follow 1,616 patients for 5 years, according to the agency.
The Food and Drug Administration has approved a new implantable cardioverter defibrillator that is implanted subcutaneously as a treatment for ventricular tachyarrhythmias.
The agency approved the Subcutaneous Implantable Defibrillator (S-ICD) System only for patients who do not require a pacemaker or pacing therapy.
The S-ICD System, made by Cameron Health of San Clemente, Calif., is the first such device that can be placed without transvenous leads. Instead, the leads are placed under the skin and then connected to the heart.
"The S-ICD System provides an alternative for treating patients with life-threatening heart arrhythmias for whom the routine ICD placement procedure is not ideal," said Christy Foreman, director of the Office of Device Evaluation at FDA’s Center for Devices and Radiological Health, in a statement. "Some patients with anatomy that makes it challenging to place one of the implantable defibrillators currently on the market may especially benefit from this device."
The device won near-unanimous backing of the FDA’s Circulatory System Devices Panel in April. The panel voted 7-1 that the benefits of the S-ICD system outweighed its risks in patients who meet the criteria in the indication proposed by Cameron Health: to provide "defibrillation therapy for the treatment of life-threatening ventricular tachyarrhythmias in patients who do not have symptomatic bradycardia; incessant ventricular tachycardia; or spontaneous, frequently recurring ventricular tachycardia that is reliably terminated with antitachycardia pacing."
Safety and efficacy data for the approval came from a 321-patient study, which was reported at the Heart Rhythm Society in May. In that trial, 304 patients were successfully implanted and the device converted all abnormal heart rhythms that it detected back to normal rhythms, according to the FDA. In the 6 months postimplantation, the S-ICD detected and recorded 78 spontaneous arrhythmias in 21 patients that were either all converted or resolved on their own.
The FDA said that the most common complications included inappropriate shocks, discomfort, system infection, and electrode movement. Eight patients died during the study, but the S-ICD was not definitively seen as the cause. There were 11 explants. Six months after implantation, 90% of the device recipients had no complications.
Cameron Health reported in May that the S-ICD is distributed in 10 other countries and that more than 1,200 patients have been implanted worldwide.
The company proposed a postmarketing study when it submitted its application for approval. The FDA will require that study, seeking assessment of how it performs over the long term, and across genders. The study will follow 1,616 patients for 5 years, according to the agency.
The Food and Drug Administration has approved a new implantable cardioverter defibrillator that is implanted subcutaneously as a treatment for ventricular tachyarrhythmias.
The agency approved the Subcutaneous Implantable Defibrillator (S-ICD) System only for patients who do not require a pacemaker or pacing therapy.
The S-ICD System, made by Cameron Health of San Clemente, Calif., is the first such device that can be placed without transvenous leads. Instead, the leads are placed under the skin and then connected to the heart.
"The S-ICD System provides an alternative for treating patients with life-threatening heart arrhythmias for whom the routine ICD placement procedure is not ideal," said Christy Foreman, director of the Office of Device Evaluation at FDA’s Center for Devices and Radiological Health, in a statement. "Some patients with anatomy that makes it challenging to place one of the implantable defibrillators currently on the market may especially benefit from this device."
The device won near-unanimous backing of the FDA’s Circulatory System Devices Panel in April. The panel voted 7-1 that the benefits of the S-ICD system outweighed its risks in patients who meet the criteria in the indication proposed by Cameron Health: to provide "defibrillation therapy for the treatment of life-threatening ventricular tachyarrhythmias in patients who do not have symptomatic bradycardia; incessant ventricular tachycardia; or spontaneous, frequently recurring ventricular tachycardia that is reliably terminated with antitachycardia pacing."
Safety and efficacy data for the approval came from a 321-patient study, which was reported at the Heart Rhythm Society in May. In that trial, 304 patients were successfully implanted and the device converted all abnormal heart rhythms that it detected back to normal rhythms, according to the FDA. In the 6 months postimplantation, the S-ICD detected and recorded 78 spontaneous arrhythmias in 21 patients that were either all converted or resolved on their own.
The FDA said that the most common complications included inappropriate shocks, discomfort, system infection, and electrode movement. Eight patients died during the study, but the S-ICD was not definitively seen as the cause. There were 11 explants. Six months after implantation, 90% of the device recipients had no complications.
Cameron Health reported in May that the S-ICD is distributed in 10 other countries and that more than 1,200 patients have been implanted worldwide.
The company proposed a postmarketing study when it submitted its application for approval. The FDA will require that study, seeking assessment of how it performs over the long term, and across genders. The study will follow 1,616 patients for 5 years, according to the agency.
Health Care More Expensive Under Romney, Wonks Say
WASHINGTON – The projected cost of private, non-group health insurance would be twice as high for American families in 2016 if the Affordable Care Act is repealed and replaced with Republican proposals, according to an analysis by three prominent health care economists.
Families would pay $11,481 per year for private, non–group health insurance under the policies advocated by Republican presidential candidate Mitt Romney, compared with $5,985 a year under the Affordable Care Act.
The advocacy group Families USA issued the analysis at a Sept. 27 briefing as both candidates were heating up their campaign rhetoric.
The analysis was conducted with the help of three health policy experts, all of whom advised then-Gov. Romney as he developed the Massachusetts health insurance law. The Massachusetts law, enacted in 2006, is widely considered a model for the ACA.

"There is no doubt, it was the model for the [ACA]," Jonathan Gruber, a professor of economics at the Massachusetts Institute of Technology, Cambridge, said at the briefing. He helped with the Families USA analysis and was a principal adviser to Mr. Romney, as well as to the Obama Administration on the ACA.
While the Massachusetts health law, dubbed "RomneyCare" by the Families USA report, is very similar to the ACA, "RomneyCandidateCare" – what the report terms policies espoused by the Romney campaign – is not the same, said Ron Pollack, executive director of Families USA. They are "as different as day and night."
Under "ObamaCare" (the report’s term for the ACA), depending on income, families would receive tax credits to help pay for premiums and in some cases, for other out-of-pocket costs. Under "RomneyCandidateCare," families would receive tax deductions.
Mr. Gruber and two other analysts – Stuart Altman of Brandeis University, Waltham, Mass., and John McDonough of Harvard School of Public Health, Boston – determined that the average size of the credit under the ACA would be $4,231 in 2016, while the Romney tax deduction would be around $2,490.
Some 20.3 million people would receive subsidies under the ACA, while only 10.1 million people would under Mr. Romney’s plan.
The year 2016 was selected because it is the end of the next presidential term.
The economists also projected a huge increase in the number of uninsured under a Romney administration. Using Census Department and Congressional Budget Office estimates, they project that without any health reform at all, the number of uninsured Americans would hit 56 million in 2016.
As enacted, the ACA is slated to reduce the number of uninsured to 25.3 million at that time. Conversely, the Romney plan would increase the number of uninsured to 67.2 million, the analysis found.
When looking at the three plans, the economists made certain assumptions regarding how "RomneyCandidateCare" would be implemented, should Mr. Romney be elected:
• The ACA would be repealed.
• Medicaid would be funded through block grants to the states.
• End tax discrimination against the individual purchase of insurance (per the Romney campaign website).
• Protections would be included for those with preexisting conditions.
The report homed in on potential effects of a Romney presidency on Medicare. The aim was in part to dispute the Romney campaign’s allegation that the ACA will cut Medicare benefits by $716 billion.

"Nothing could be further from the truth," said Mr. Altman, who added that the reduction came from a rejiggering of Medicare payments to private insurance plans for beneficiaries enrolled in Medicare Advantage.
Further, should the ACA be repealed, Medicare would no longer provide many free preventive care services and efforts to reduce beneficiaries out-of-pocket costs under Part D would be rolled back.
Finally, the report noted that the ACA would extend the life of the Medicare Trust Fund, in part by requiring higher income workers to pay in slightly more, and by reducing the Medicare Advantage payments. "RomneyCandidateCare" would not do so, and would also threaten Medicare by converting it to a voucher program, according to the analysis.
That’s because over time, the program would reduce the value of the Medicare subsidy, while costs would continue to rise. "By the time people born in 1983 reach Medicare eligibility age, their coverage would be worth 42% less than it would be under ObamaCare," the report said.
WASHINGTON – The projected cost of private, non-group health insurance would be twice as high for American families in 2016 if the Affordable Care Act is repealed and replaced with Republican proposals, according to an analysis by three prominent health care economists.
Families would pay $11,481 per year for private, non–group health insurance under the policies advocated by Republican presidential candidate Mitt Romney, compared with $5,985 a year under the Affordable Care Act.
The advocacy group Families USA issued the analysis at a Sept. 27 briefing as both candidates were heating up their campaign rhetoric.
The analysis was conducted with the help of three health policy experts, all of whom advised then-Gov. Romney as he developed the Massachusetts health insurance law. The Massachusetts law, enacted in 2006, is widely considered a model for the ACA.
"There is no doubt, it was the model for the [ACA]," Jonathan Gruber, a professor of economics at the Massachusetts Institute of Technology, Cambridge, said at the briefing. He helped with the Families USA analysis and was a principal adviser to Mr. Romney, as well as to the Obama Administration on the ACA.
While the Massachusetts health law, dubbed "RomneyCare" by the Families USA report, is very similar to the ACA, "RomneyCandidateCare" – what the report terms policies espoused by the Romney campaign – is not the same, said Ron Pollack, executive director of Families USA. They are "as different as day and night."
Under "ObamaCare" (the report’s term for the ACA), depending on income, families would receive tax credits to help pay for premiums and in some cases, for other out-of-pocket costs. Under "RomneyCandidateCare," families would receive tax deductions.
Mr. Gruber and two other analysts – Stuart Altman of Brandeis University, Waltham, Mass., and John McDonough of Harvard School of Public Health, Boston – determined that the average size of the credit under the ACA would be $4,231 in 2016, while the Romney tax deduction would be around $2,490.
Some 20.3 million people would receive subsidies under the ACA, while only 10.1 million people would under Mr. Romney’s plan.
The year 2016 was selected because it is the end of the next presidential term.
The economists also projected a huge increase in the number of uninsured under a Romney administration. Using Census Department and Congressional Budget Office estimates, they project that without any health reform at all, the number of uninsured Americans would hit 56 million in 2016.
As enacted, the ACA is slated to reduce the number of uninsured to 25.3 million at that time. Conversely, the Romney plan would increase the number of uninsured to 67.2 million, the analysis found.
When looking at the three plans, the economists made certain assumptions regarding how "RomneyCandidateCare" would be implemented, should Mr. Romney be elected:
• The ACA would be repealed.
• Medicaid would be funded through block grants to the states.
• End tax discrimination against the individual purchase of insurance (per the Romney campaign website).
• Protections would be included for those with preexisting conditions.
The report homed in on potential effects of a Romney presidency on Medicare. The aim was in part to dispute the Romney campaign’s allegation that the ACA will cut Medicare benefits by $716 billion.
"Nothing could be further from the truth," said Mr. Altman, who added that the reduction came from a rejiggering of Medicare payments to private insurance plans for beneficiaries enrolled in Medicare Advantage.
Further, should the ACA be repealed, Medicare would no longer provide many free preventive care services and efforts to reduce beneficiaries out-of-pocket costs under Part D would be rolled back.
Finally, the report noted that the ACA would extend the life of the Medicare Trust Fund, in part by requiring higher income workers to pay in slightly more, and by reducing the Medicare Advantage payments. "RomneyCandidateCare" would not do so, and would also threaten Medicare by converting it to a voucher program, according to the analysis.
That’s because over time, the program would reduce the value of the Medicare subsidy, while costs would continue to rise. "By the time people born in 1983 reach Medicare eligibility age, their coverage would be worth 42% less than it would be under ObamaCare," the report said.
WASHINGTON – The projected cost of private, non-group health insurance would be twice as high for American families in 2016 if the Affordable Care Act is repealed and replaced with Republican proposals, according to an analysis by three prominent health care economists.
Families would pay $11,481 per year for private, non–group health insurance under the policies advocated by Republican presidential candidate Mitt Romney, compared with $5,985 a year under the Affordable Care Act.
The advocacy group Families USA issued the analysis at a Sept. 27 briefing as both candidates were heating up their campaign rhetoric.
The analysis was conducted with the help of three health policy experts, all of whom advised then-Gov. Romney as he developed the Massachusetts health insurance law. The Massachusetts law, enacted in 2006, is widely considered a model for the ACA.
"There is no doubt, it was the model for the [ACA]," Jonathan Gruber, a professor of economics at the Massachusetts Institute of Technology, Cambridge, said at the briefing. He helped with the Families USA analysis and was a principal adviser to Mr. Romney, as well as to the Obama Administration on the ACA.
While the Massachusetts health law, dubbed "RomneyCare" by the Families USA report, is very similar to the ACA, "RomneyCandidateCare" – what the report terms policies espoused by the Romney campaign – is not the same, said Ron Pollack, executive director of Families USA. They are "as different as day and night."
Under "ObamaCare" (the report’s term for the ACA), depending on income, families would receive tax credits to help pay for premiums and in some cases, for other out-of-pocket costs. Under "RomneyCandidateCare," families would receive tax deductions.
Mr. Gruber and two other analysts – Stuart Altman of Brandeis University, Waltham, Mass., and John McDonough of Harvard School of Public Health, Boston – determined that the average size of the credit under the ACA would be $4,231 in 2016, while the Romney tax deduction would be around $2,490.
Some 20.3 million people would receive subsidies under the ACA, while only 10.1 million people would under Mr. Romney’s plan.
The year 2016 was selected because it is the end of the next presidential term.
The economists also projected a huge increase in the number of uninsured under a Romney administration. Using Census Department and Congressional Budget Office estimates, they project that without any health reform at all, the number of uninsured Americans would hit 56 million in 2016.
As enacted, the ACA is slated to reduce the number of uninsured to 25.3 million at that time. Conversely, the Romney plan would increase the number of uninsured to 67.2 million, the analysis found.
When looking at the three plans, the economists made certain assumptions regarding how "RomneyCandidateCare" would be implemented, should Mr. Romney be elected:
• The ACA would be repealed.
• Medicaid would be funded through block grants to the states.
• End tax discrimination against the individual purchase of insurance (per the Romney campaign website).
• Protections would be included for those with preexisting conditions.
The report homed in on potential effects of a Romney presidency on Medicare. The aim was in part to dispute the Romney campaign’s allegation that the ACA will cut Medicare benefits by $716 billion.
"Nothing could be further from the truth," said Mr. Altman, who added that the reduction came from a rejiggering of Medicare payments to private insurance plans for beneficiaries enrolled in Medicare Advantage.
Further, should the ACA be repealed, Medicare would no longer provide many free preventive care services and efforts to reduce beneficiaries out-of-pocket costs under Part D would be rolled back.
Finally, the report noted that the ACA would extend the life of the Medicare Trust Fund, in part by requiring higher income workers to pay in slightly more, and by reducing the Medicare Advantage payments. "RomneyCandidateCare" would not do so, and would also threaten Medicare by converting it to a voucher program, according to the analysis.
That’s because over time, the program would reduce the value of the Medicare subsidy, while costs would continue to rise. "By the time people born in 1983 reach Medicare eligibility age, their coverage would be worth 42% less than it would be under ObamaCare," the report said.
FROM A BRIEFING HELD BY FAMILIES USA

Cosmetic Derm Society Disbands
*This story was updated on 10/3/2012.
The American Society of Cosmetic Dermatology and Aesthetic Surgery has permanently disbanded, according to an announcement on its website.
In an open letter to members, ASCDAS president Ellen Marmur wrote, "This difficult decision was made after careful analysis of the current economic conditions and in the context of what the Society might accomplish for its membership and for dermatologic and aesthetic surgery."
The organization was founded in 2000 by a group of dermatologists that included Dr. Cherie M. Ditre. However, Dr. Ditre left the organization in 2007 after new leadership asked her and several other board members to step down, she told Skin & Allergy News.
In 2009, the American Society for Dermatologic Surgery and the ASCDAS combined their annual meetings, citing among other reasons the down economy. Officials from both societies said at the time that holding the meetings together would make it more financially feasible for dermatologists to attend. Dr. Phil Werschler, ASCDAS president at the time, also noted that many dermatologists were members of both societies
The disbanding of the ASCDAS brings into question the fate of the group’s annual meeting, slated for Nov. 29-Dec. 2 in Las Vegas.
*Dr. Joel Schlessinger, a past president of the ASCDAS, said that he was surprised that the society disbanded. He also said that it has caused confusion about whether Cosmetic Surgery Forum (Nov. 29-Dec. 1) is still being held in Las Vegas.
"I will still be having Cosmetic Surgery Forum this year at the Venetian/Palazzo. ... We have had quite a few vendors who were going to exhibit at the ASCDAS meeting who are now interested" in exhibiting at Cosmetic Surgery Forum, he said. Dr. Schlessinger also noted that his meeting has always been completely separate from the ASCDAS meeting that has been held around the same time in Las Vegas for the past 4 years.
The ASCDAS’s mission, according to a statement on the website, was in part "to promote the advancement of ethical aesthetic dermatology as a medical and surgical discipline."
The ASCDAS was one of several societies dedicated to cosmetic and aesthetic dermatology.
Calls to ASCDAS officials had not been returned as of press time.
*This story was updated on 10/3/2012.
The American Society of Cosmetic Dermatology and Aesthetic Surgery has permanently disbanded, according to an announcement on its website.
In an open letter to members, ASCDAS president Ellen Marmur wrote, "This difficult decision was made after careful analysis of the current economic conditions and in the context of what the Society might accomplish for its membership and for dermatologic and aesthetic surgery."
The organization was founded in 2000 by a group of dermatologists that included Dr. Cherie M. Ditre. However, Dr. Ditre left the organization in 2007 after new leadership asked her and several other board members to step down, she told Skin & Allergy News.
In 2009, the American Society for Dermatologic Surgery and the ASCDAS combined their annual meetings, citing among other reasons the down economy. Officials from both societies said at the time that holding the meetings together would make it more financially feasible for dermatologists to attend. Dr. Phil Werschler, ASCDAS president at the time, also noted that many dermatologists were members of both societies
The disbanding of the ASCDAS brings into question the fate of the group’s annual meeting, slated for Nov. 29-Dec. 2 in Las Vegas.
*Dr. Joel Schlessinger, a past president of the ASCDAS, said that he was surprised that the society disbanded. He also said that it has caused confusion about whether Cosmetic Surgery Forum (Nov. 29-Dec. 1) is still being held in Las Vegas.
"I will still be having Cosmetic Surgery Forum this year at the Venetian/Palazzo. ... We have had quite a few vendors who were going to exhibit at the ASCDAS meeting who are now interested" in exhibiting at Cosmetic Surgery Forum, he said. Dr. Schlessinger also noted that his meeting has always been completely separate from the ASCDAS meeting that has been held around the same time in Las Vegas for the past 4 years.
The ASCDAS’s mission, according to a statement on the website, was in part "to promote the advancement of ethical aesthetic dermatology as a medical and surgical discipline."
The ASCDAS was one of several societies dedicated to cosmetic and aesthetic dermatology.
Calls to ASCDAS officials had not been returned as of press time.
*This story was updated on 10/3/2012.
The American Society of Cosmetic Dermatology and Aesthetic Surgery has permanently disbanded, according to an announcement on its website.
In an open letter to members, ASCDAS president Ellen Marmur wrote, "This difficult decision was made after careful analysis of the current economic conditions and in the context of what the Society might accomplish for its membership and for dermatologic and aesthetic surgery."
The organization was founded in 2000 by a group of dermatologists that included Dr. Cherie M. Ditre. However, Dr. Ditre left the organization in 2007 after new leadership asked her and several other board members to step down, she told Skin & Allergy News.
In 2009, the American Society for Dermatologic Surgery and the ASCDAS combined their annual meetings, citing among other reasons the down economy. Officials from both societies said at the time that holding the meetings together would make it more financially feasible for dermatologists to attend. Dr. Phil Werschler, ASCDAS president at the time, also noted that many dermatologists were members of both societies
The disbanding of the ASCDAS brings into question the fate of the group’s annual meeting, slated for Nov. 29-Dec. 2 in Las Vegas.
*Dr. Joel Schlessinger, a past president of the ASCDAS, said that he was surprised that the society disbanded. He also said that it has caused confusion about whether Cosmetic Surgery Forum (Nov. 29-Dec. 1) is still being held in Las Vegas.
"I will still be having Cosmetic Surgery Forum this year at the Venetian/Palazzo. ... We have had quite a few vendors who were going to exhibit at the ASCDAS meeting who are now interested" in exhibiting at Cosmetic Surgery Forum, he said. Dr. Schlessinger also noted that his meeting has always been completely separate from the ASCDAS meeting that has been held around the same time in Las Vegas for the past 4 years.
The ASCDAS’s mission, according to a statement on the website, was in part "to promote the advancement of ethical aesthetic dermatology as a medical and surgical discipline."
The ASCDAS was one of several societies dedicated to cosmetic and aesthetic dermatology.
Calls to ASCDAS officials had not been returned as of press time.
Sequestration Will Hit Pay But Spare Incentives
Medicare physician pay would be cut by at least 2% in 2013 while some Affordable Care Act programs would be spared the automatic cuts called for under the Budget Control Act of 2011, according to a report from the federal Office of Management and Budget.
The report provides details on how to cut $1.2 trillion from the federal budget by 2021 and was mandated after the Joint Select Committee on Deficit Reduction failed to do the same. The process – known as sequestration – would cut funding for most federal agencies across the board.
The Office of Management and Budget (OMB) report noted that the estimates are preliminary; the true magnitude of the cuts won’t be known until sequestration actually occurs.
The report also notes that the White House firmly opposes the automatic cuts.
"Sequestration is a blunt and indiscriminate instrument. It is not the responsible way for our nation to achieve deficit reduction," according to the report. OMB called on Congress to avoid sequestration either by passing the President’s budget proposals or otherwise approving "a comprehensive and balanced deficit reduction package."
Under sequestration, there would be a 9.4% cut to defense discretionary funding, 10% to mandatory defense programs, 8.2% reduction to nondefense discretionary funding, and 7.6% to nondefense mandatory programs.
Medicare – including physician and hospital payment – is slated for a 2%, or $11 billion, cut in 2013 alone. The 2% reduction will continue each year through 2021.
The American Hospital Association, American Medical Association, and American Nurses Association in a joint statement said that as many as 766,000 health care and related jobs could be lost by 2021 if the Medicare cuts are allowed to stand, in part because of the reduction in payments to physicians and hospitals. They also predicted a ripple effect, including reduced spending on goods and services by health care providers and organizations, as well as reduced household purchases by health care workers who lose their jobs.
"Hospitals’ ability to maintain the kind of access to services that their communities need is being threatened," AHA President and CEO Rich Umbdenstock said in a statement. "Cuts to hospital services could create devastating job losses in communities where hospitals have long been an economic mainstay."
Dr. Jeremy A. Lazarus, president of the AMA, said, "Coupled with the looming 27% Medicare physician payment cut, this 2% sequester will hurt patient access to care and will inject more uncertainty into our Medicare system. We need stability in Medicare physician payment as we work to improve our nation’s Medicare payment and delivery system to promote high-quality, high-value, better-coordinated care to our patients."
Among other programs at the Center for Medicare and Medicaid Services that would take a hit under sequestration: health insurance exchange grants ($66 million); state demonstration grants ($40 million); fraud and abuse ($78 million); the prevention and public health fund ($76 million); the Office of the National Coordinator for Health Information Technology ($1 million); the Office of Inspector General ($5 million); and the Hospital Insurance Trust Fund ($5.6 billion).
Many programs would be exempt from sequestration, however, including the Children’s Health Insurance Program, Medicare and Medicaid incentive payments for participating in health IT programs, and the consumer operated and oriented plan and the pre-existing condition insurance plan, both of which were created by the ACA.
Food and Drug Administration funding would be cut $319 million, and the Centers for Disease Control and Prevention would see at least a $490 million budget reduction, with $14 million of that coming out of the World Trade Center Health Program Fund. Funding for the National Institutes of Health would be cut $2.6 billion.
Medicare physician pay would be cut by at least 2% in 2013 while some Affordable Care Act programs would be spared the automatic cuts called for under the Budget Control Act of 2011, according to a report from the federal Office of Management and Budget.
The report provides details on how to cut $1.2 trillion from the federal budget by 2021 and was mandated after the Joint Select Committee on Deficit Reduction failed to do the same. The process – known as sequestration – would cut funding for most federal agencies across the board.
The Office of Management and Budget (OMB) report noted that the estimates are preliminary; the true magnitude of the cuts won’t be known until sequestration actually occurs.
The report also notes that the White House firmly opposes the automatic cuts.
"Sequestration is a blunt and indiscriminate instrument. It is not the responsible way for our nation to achieve deficit reduction," according to the report. OMB called on Congress to avoid sequestration either by passing the President’s budget proposals or otherwise approving "a comprehensive and balanced deficit reduction package."
Under sequestration, there would be a 9.4% cut to defense discretionary funding, 10% to mandatory defense programs, 8.2% reduction to nondefense discretionary funding, and 7.6% to nondefense mandatory programs.
Medicare – including physician and hospital payment – is slated for a 2%, or $11 billion, cut in 2013 alone. The 2% reduction will continue each year through 2021.
The American Hospital Association, American Medical Association, and American Nurses Association in a joint statement said that as many as 766,000 health care and related jobs could be lost by 2021 if the Medicare cuts are allowed to stand, in part because of the reduction in payments to physicians and hospitals. They also predicted a ripple effect, including reduced spending on goods and services by health care providers and organizations, as well as reduced household purchases by health care workers who lose their jobs.
"Hospitals’ ability to maintain the kind of access to services that their communities need is being threatened," AHA President and CEO Rich Umbdenstock said in a statement. "Cuts to hospital services could create devastating job losses in communities where hospitals have long been an economic mainstay."
Dr. Jeremy A. Lazarus, president of the AMA, said, "Coupled with the looming 27% Medicare physician payment cut, this 2% sequester will hurt patient access to care and will inject more uncertainty into our Medicare system. We need stability in Medicare physician payment as we work to improve our nation’s Medicare payment and delivery system to promote high-quality, high-value, better-coordinated care to our patients."
Among other programs at the Center for Medicare and Medicaid Services that would take a hit under sequestration: health insurance exchange grants ($66 million); state demonstration grants ($40 million); fraud and abuse ($78 million); the prevention and public health fund ($76 million); the Office of the National Coordinator for Health Information Technology ($1 million); the Office of Inspector General ($5 million); and the Hospital Insurance Trust Fund ($5.6 billion).
Many programs would be exempt from sequestration, however, including the Children’s Health Insurance Program, Medicare and Medicaid incentive payments for participating in health IT programs, and the consumer operated and oriented plan and the pre-existing condition insurance plan, both of which were created by the ACA.
Food and Drug Administration funding would be cut $319 million, and the Centers for Disease Control and Prevention would see at least a $490 million budget reduction, with $14 million of that coming out of the World Trade Center Health Program Fund. Funding for the National Institutes of Health would be cut $2.6 billion.
Medicare physician pay would be cut by at least 2% in 2013 while some Affordable Care Act programs would be spared the automatic cuts called for under the Budget Control Act of 2011, according to a report from the federal Office of Management and Budget.
The report provides details on how to cut $1.2 trillion from the federal budget by 2021 and was mandated after the Joint Select Committee on Deficit Reduction failed to do the same. The process – known as sequestration – would cut funding for most federal agencies across the board.
The Office of Management and Budget (OMB) report noted that the estimates are preliminary; the true magnitude of the cuts won’t be known until sequestration actually occurs.
The report also notes that the White House firmly opposes the automatic cuts.
"Sequestration is a blunt and indiscriminate instrument. It is not the responsible way for our nation to achieve deficit reduction," according to the report. OMB called on Congress to avoid sequestration either by passing the President’s budget proposals or otherwise approving "a comprehensive and balanced deficit reduction package."
Under sequestration, there would be a 9.4% cut to defense discretionary funding, 10% to mandatory defense programs, 8.2% reduction to nondefense discretionary funding, and 7.6% to nondefense mandatory programs.
Medicare – including physician and hospital payment – is slated for a 2%, or $11 billion, cut in 2013 alone. The 2% reduction will continue each year through 2021.
The American Hospital Association, American Medical Association, and American Nurses Association in a joint statement said that as many as 766,000 health care and related jobs could be lost by 2021 if the Medicare cuts are allowed to stand, in part because of the reduction in payments to physicians and hospitals. They also predicted a ripple effect, including reduced spending on goods and services by health care providers and organizations, as well as reduced household purchases by health care workers who lose their jobs.
"Hospitals’ ability to maintain the kind of access to services that their communities need is being threatened," AHA President and CEO Rich Umbdenstock said in a statement. "Cuts to hospital services could create devastating job losses in communities where hospitals have long been an economic mainstay."
Dr. Jeremy A. Lazarus, president of the AMA, said, "Coupled with the looming 27% Medicare physician payment cut, this 2% sequester will hurt patient access to care and will inject more uncertainty into our Medicare system. We need stability in Medicare physician payment as we work to improve our nation’s Medicare payment and delivery system to promote high-quality, high-value, better-coordinated care to our patients."
Among other programs at the Center for Medicare and Medicaid Services that would take a hit under sequestration: health insurance exchange grants ($66 million); state demonstration grants ($40 million); fraud and abuse ($78 million); the prevention and public health fund ($76 million); the Office of the National Coordinator for Health Information Technology ($1 million); the Office of Inspector General ($5 million); and the Hospital Insurance Trust Fund ($5.6 billion).
Many programs would be exempt from sequestration, however, including the Children’s Health Insurance Program, Medicare and Medicaid incentive payments for participating in health IT programs, and the consumer operated and oriented plan and the pre-existing condition insurance plan, both of which were created by the ACA.
Food and Drug Administration funding would be cut $319 million, and the Centers for Disease Control and Prevention would see at least a $490 million budget reduction, with $14 million of that coming out of the World Trade Center Health Program Fund. Funding for the National Institutes of Health would be cut $2.6 billion.
Comprehensive Primary Care Initiative a Potentially Worthwhile Gamble
The federal government’s Comprehensive Primary Care Initiative could initially be a boon for physicians who participate, but may prove to be a more difficult proposition for them in the program’s later years, say some participants.
For the first 2 years, the 500 physician practices in seven regions selected for the program – sponsored by the Center for Medicare and Medicaid Innovation – will receive from Medicare a per member, monthly payment averaging $20, in addition to their normal fee-for-service payments.
Doctors are being given the fee in exchange for meeting certain goals and criteria, all with the aim of providing comprehensive primary care. CMS wants practices to better and more intensively manage patients with multiple conditions; ensure better access to care by keeping longer hours and via tools such as e-mail and patient portals; increase preventive care; and better coordinate care with specialists.
A handful of additional payers are participating in each state. Those payers – private insurers and in some states, Medicaid – also will give physicians a per patient/per month fee. The additional payers were selected in April, so that doctors would know how many of their patients might be covered by the added month payments when deciding to apply for the program.
But, by the third and fourth year of the program, the Medicare monthly fee will be reduced to an average of $15, and it’s not clear what private payers will do. Physicians will have an opportunity to share in savings, but it still represents a gamble, say some.
Dr. Stacey Zimmerman, an internist in Clinton, Ark., is looking forward to the revenue stream that will be provided by the primary care initiative, but says she is concerned about how she will manage once the payments drop. With better care coordination, patients will not need as many services, which means practice revenues will drop, she said in an interview. Meanwhile, expenses are not likely to moderate. "So how do we meet our overhead?" she asked.

"I think that is a bit of a concern for everyone," agreed Dr. Gregory Reicks, with Foresight Family Physicians in Grand Junction, Colo. Doctors will be building new practice models that are dependent on the per patient/per month fees. The challenge is to find a way to keep funding the new model, he said in an interview.
"Our hope is that the private payers will see the value of it, based on better overall patient satisfaction and lower costs, and that they’ll hopefully want to fund it going forward," he said.
Improving Revenue, Adding Services
Overall, both Dr. Zimmerman and Dr. Reicks said they were very happy to have been chosen for the program.
According to CMS, the practices were selected through a competitive application process. The practices, representing 2,144 providers caring for 313,000 Medicare beneficiaries, are in Arkansas; Colorado; New Jersey; the Capital District/Hudson Valley, N.Y., region; the Cincinnati/Dayton region of Ohio and Kentucky; the greater Tulsa (Okla.) area, and Oregon.
To be selected, practices had to demonstrate that they already had an electronic health record system, that they were already delivering advanced primary care, or that they were engaged in transforming their practices. They also had to have enough patients covered by Medicare and participating private payers to make it worthwhile.
The idea is to provide money to help practices fully transform, said Dr. Robert A. Gluckman, Chair of the American College of Physicians Medical Practice and Quality Committee.
In a traditional model, physicians are only paid for face-to-face encounters. Under this initiative, the monthly fee will help cover services delivered by e-mail, phone, group visits, or by allied health professionals like nutrition and behavioral counselors, said Dr. Gluckman, who also is the chief medical officer for Providence Health Plans. Providence is one of the participating payers in Oregon.
"This is going to be a tremendous opportunity for primary care practices to have the revenue to practice medicine differently," he said.
From a payer point of view, it was worth participating to help "facilitate a more robust primary care network," Dr. Gluckman said. "Payers are increasingly recognizing that we need a more robust primary care delivery system to deliver care more effectively," he said, noting that effective primary care can decrease emergency department visits and curb hospitalizations. "If no one ever tries to deliver care differently, we’re going to keep getting what we’re getting – high cost and some variation in quality."
Dr. Zimmerman said that she has already seen the benefits of creating a better primary care delivery model: happier and somewhat healthier patients. But it was all done without the additional revenue, which meant it was not sustainable, she said.
For the last 2 years, her practice, comprised of herself and two nurse practitioners, participated in a patient-centered medical home pilot program with Arkansas Blue Cross Blue Shield. It is ending in December. No additional payments were given for doing things like creating a patient portal and offering consultations by phone after hours. And not all of her 5,800 patients were covered by the pilot.
The current initiative, with four participating payers in Arkansas – Blue Cross Blue Shield, QualChoice, Humana, and Medicare – will cover 92% of her patients. It’s not clear yet what the monthly payment will be from Medicare or those insurers, but payments are due to start Oct. 1, Dr. Zimmerman said.
The additional funds will let her invest in areas that she couldn’t before, like diabetes education, and to perhaps hire a care coordinator. It also eill help her maintain her EHR and improve her patient portal. Only about a third of patients are using it – to make appointments, request prescription refills, and access lab results or e-mail Dr. Zimmerman. She uses it to send patients a visit summary and lab results and to share educational materials.
The portal makes her work a lot easier, she said. For instance, the system tracks whether a patient has accessed those educational materials or lab results and notifies the physician that the materials have been – or have not been – read. It also allows relatives – say a daughter of an elderly patient – to see medical records and communicate directly with her. That’s especially important if the daughter lives elsewhere.
She also uses her website and a clinic Facebook page to stay in touch with patients. In rural Arkansas, a large number of people have smartphones because so many use Facebook as entertainment, said Dr. Zimmerman. "I would rather them get on my Facebook page and read about something I posted from the Mayo Clinic than surf the web and look up something that’s not good educational information," she said.
Dr. Reicks also says that his patients have been enthusiastic about his patient portal, though only about a third have signed up for access. Initially, the practice’s providers – three physicians, a nurse practitioner, and a physician assistant – were worried that inviting patients to e-mail would open up a flood that would take away from actual practice time.
But uptake has been slow, and "we’ve found it to be convenient and effective," saving time, money on postage, and miscommunications, Dr. Reicks said.
His practice has had an EHR since 2007, and it participated in the Colorado Beacon Consortium, a CMS-funded practice-improvement program in western Colorado. Though the practice underwent a huge transformation, it was looking to move to the next level, said Dr. Reicks.
The per patient/per month fee under the primary care initiative will help the practice "pull in additional human resources," he said. That would include case managers, health coaches, and behavioral health specialists. The idea is to offer truly comprehensive care, Dr. Reicks said.
About 4,500 of the practice’s 10,000 patients will be covered under the initiative, including some 3,000 Medicare patients and 800 Medicaid patients. The practice anticipates an average $10 per patient monthly fee, but it could be more after Medicare payment is risk-adjusted. Like Dr. Zimmerman, Dr. Reicks is waiting on getting word from the private payers – which include Rocky Mountain Health Plans, Anthem Blue Cross Blue Shield, UnitedHealthcare and Cigna – on their monthly payment. But at least one payer – Rocky Mountain Health Plans – has suggested that it will offer in-kind resources such as health coaches instead of an actual payment, Dr. Reicks said.
The uncertainty over the revenue stream is a familiar, but vexing problem, he said. CMS is requiring the participating practices to submit a plan detailing how the monthly fees will be spent. "And we don’t know how much will be coming in," Dr. Reicks said.
It begs the question of why a practice would seek out participation in this initiative.
Besides improving patient satisfaction and health outcomes, "we’re hoping this will somehow restore the joy of practicing medicine again," he said.
The federal government’s Comprehensive Primary Care Initiative could initially be a boon for physicians who participate, but may prove to be a more difficult proposition for them in the program’s later years, say some participants.
For the first 2 years, the 500 physician practices in seven regions selected for the program – sponsored by the Center for Medicare and Medicaid Innovation – will receive from Medicare a per member, monthly payment averaging $20, in addition to their normal fee-for-service payments.
Doctors are being given the fee in exchange for meeting certain goals and criteria, all with the aim of providing comprehensive primary care. CMS wants practices to better and more intensively manage patients with multiple conditions; ensure better access to care by keeping longer hours and via tools such as e-mail and patient portals; increase preventive care; and better coordinate care with specialists.
A handful of additional payers are participating in each state. Those payers – private insurers and in some states, Medicaid – also will give physicians a per patient/per month fee. The additional payers were selected in April, so that doctors would know how many of their patients might be covered by the added month payments when deciding to apply for the program.
But, by the third and fourth year of the program, the Medicare monthly fee will be reduced to an average of $15, and it’s not clear what private payers will do. Physicians will have an opportunity to share in savings, but it still represents a gamble, say some.
Dr. Stacey Zimmerman, an internist in Clinton, Ark., is looking forward to the revenue stream that will be provided by the primary care initiative, but says she is concerned about how she will manage once the payments drop. With better care coordination, patients will not need as many services, which means practice revenues will drop, she said in an interview. Meanwhile, expenses are not likely to moderate. "So how do we meet our overhead?" she asked.
"I think that is a bit of a concern for everyone," agreed Dr. Gregory Reicks, with Foresight Family Physicians in Grand Junction, Colo. Doctors will be building new practice models that are dependent on the per patient/per month fees. The challenge is to find a way to keep funding the new model, he said in an interview.
"Our hope is that the private payers will see the value of it, based on better overall patient satisfaction and lower costs, and that they’ll hopefully want to fund it going forward," he said.
Improving Revenue, Adding Services
Overall, both Dr. Zimmerman and Dr. Reicks said they were very happy to have been chosen for the program.
According to CMS, the practices were selected through a competitive application process. The practices, representing 2,144 providers caring for 313,000 Medicare beneficiaries, are in Arkansas; Colorado; New Jersey; the Capital District/Hudson Valley, N.Y., region; the Cincinnati/Dayton region of Ohio and Kentucky; the greater Tulsa (Okla.) area, and Oregon.
To be selected, practices had to demonstrate that they already had an electronic health record system, that they were already delivering advanced primary care, or that they were engaged in transforming their practices. They also had to have enough patients covered by Medicare and participating private payers to make it worthwhile.
The idea is to provide money to help practices fully transform, said Dr. Robert A. Gluckman, Chair of the American College of Physicians Medical Practice and Quality Committee.
In a traditional model, physicians are only paid for face-to-face encounters. Under this initiative, the monthly fee will help cover services delivered by e-mail, phone, group visits, or by allied health professionals like nutrition and behavioral counselors, said Dr. Gluckman, who also is the chief medical officer for Providence Health Plans. Providence is one of the participating payers in Oregon.
"This is going to be a tremendous opportunity for primary care practices to have the revenue to practice medicine differently," he said.
From a payer point of view, it was worth participating to help "facilitate a more robust primary care network," Dr. Gluckman said. "Payers are increasingly recognizing that we need a more robust primary care delivery system to deliver care more effectively," he said, noting that effective primary care can decrease emergency department visits and curb hospitalizations. "If no one ever tries to deliver care differently, we’re going to keep getting what we’re getting – high cost and some variation in quality."
Dr. Zimmerman said that she has already seen the benefits of creating a better primary care delivery model: happier and somewhat healthier patients. But it was all done without the additional revenue, which meant it was not sustainable, she said.
For the last 2 years, her practice, comprised of herself and two nurse practitioners, participated in a patient-centered medical home pilot program with Arkansas Blue Cross Blue Shield. It is ending in December. No additional payments were given for doing things like creating a patient portal and offering consultations by phone after hours. And not all of her 5,800 patients were covered by the pilot.
The current initiative, with four participating payers in Arkansas – Blue Cross Blue Shield, QualChoice, Humana, and Medicare – will cover 92% of her patients. It’s not clear yet what the monthly payment will be from Medicare or those insurers, but payments are due to start Oct. 1, Dr. Zimmerman said.
The additional funds will let her invest in areas that she couldn’t before, like diabetes education, and to perhaps hire a care coordinator. It also eill help her maintain her EHR and improve her patient portal. Only about a third of patients are using it – to make appointments, request prescription refills, and access lab results or e-mail Dr. Zimmerman. She uses it to send patients a visit summary and lab results and to share educational materials.
The portal makes her work a lot easier, she said. For instance, the system tracks whether a patient has accessed those educational materials or lab results and notifies the physician that the materials have been – or have not been – read. It also allows relatives – say a daughter of an elderly patient – to see medical records and communicate directly with her. That’s especially important if the daughter lives elsewhere.
She also uses her website and a clinic Facebook page to stay in touch with patients. In rural Arkansas, a large number of people have smartphones because so many use Facebook as entertainment, said Dr. Zimmerman. "I would rather them get on my Facebook page and read about something I posted from the Mayo Clinic than surf the web and look up something that’s not good educational information," she said.
Dr. Reicks also says that his patients have been enthusiastic about his patient portal, though only about a third have signed up for access. Initially, the practice’s providers – three physicians, a nurse practitioner, and a physician assistant – were worried that inviting patients to e-mail would open up a flood that would take away from actual practice time.
But uptake has been slow, and "we’ve found it to be convenient and effective," saving time, money on postage, and miscommunications, Dr. Reicks said.
His practice has had an EHR since 2007, and it participated in the Colorado Beacon Consortium, a CMS-funded practice-improvement program in western Colorado. Though the practice underwent a huge transformation, it was looking to move to the next level, said Dr. Reicks.
The per patient/per month fee under the primary care initiative will help the practice "pull in additional human resources," he said. That would include case managers, health coaches, and behavioral health specialists. The idea is to offer truly comprehensive care, Dr. Reicks said.
About 4,500 of the practice’s 10,000 patients will be covered under the initiative, including some 3,000 Medicare patients and 800 Medicaid patients. The practice anticipates an average $10 per patient monthly fee, but it could be more after Medicare payment is risk-adjusted. Like Dr. Zimmerman, Dr. Reicks is waiting on getting word from the private payers – which include Rocky Mountain Health Plans, Anthem Blue Cross Blue Shield, UnitedHealthcare and Cigna – on their monthly payment. But at least one payer – Rocky Mountain Health Plans – has suggested that it will offer in-kind resources such as health coaches instead of an actual payment, Dr. Reicks said.
The uncertainty over the revenue stream is a familiar, but vexing problem, he said. CMS is requiring the participating practices to submit a plan detailing how the monthly fees will be spent. "And we don’t know how much will be coming in," Dr. Reicks said.
It begs the question of why a practice would seek out participation in this initiative.
Besides improving patient satisfaction and health outcomes, "we’re hoping this will somehow restore the joy of practicing medicine again," he said.
The federal government’s Comprehensive Primary Care Initiative could initially be a boon for physicians who participate, but may prove to be a more difficult proposition for them in the program’s later years, say some participants.
For the first 2 years, the 500 physician practices in seven regions selected for the program – sponsored by the Center for Medicare and Medicaid Innovation – will receive from Medicare a per member, monthly payment averaging $20, in addition to their normal fee-for-service payments.
Doctors are being given the fee in exchange for meeting certain goals and criteria, all with the aim of providing comprehensive primary care. CMS wants practices to better and more intensively manage patients with multiple conditions; ensure better access to care by keeping longer hours and via tools such as e-mail and patient portals; increase preventive care; and better coordinate care with specialists.
A handful of additional payers are participating in each state. Those payers – private insurers and in some states, Medicaid – also will give physicians a per patient/per month fee. The additional payers were selected in April, so that doctors would know how many of their patients might be covered by the added month payments when deciding to apply for the program.
But, by the third and fourth year of the program, the Medicare monthly fee will be reduced to an average of $15, and it’s not clear what private payers will do. Physicians will have an opportunity to share in savings, but it still represents a gamble, say some.
Dr. Stacey Zimmerman, an internist in Clinton, Ark., is looking forward to the revenue stream that will be provided by the primary care initiative, but says she is concerned about how she will manage once the payments drop. With better care coordination, patients will not need as many services, which means practice revenues will drop, she said in an interview. Meanwhile, expenses are not likely to moderate. "So how do we meet our overhead?" she asked.
"I think that is a bit of a concern for everyone," agreed Dr. Gregory Reicks, with Foresight Family Physicians in Grand Junction, Colo. Doctors will be building new practice models that are dependent on the per patient/per month fees. The challenge is to find a way to keep funding the new model, he said in an interview.
"Our hope is that the private payers will see the value of it, based on better overall patient satisfaction and lower costs, and that they’ll hopefully want to fund it going forward," he said.
Improving Revenue, Adding Services
Overall, both Dr. Zimmerman and Dr. Reicks said they were very happy to have been chosen for the program.
According to CMS, the practices were selected through a competitive application process. The practices, representing 2,144 providers caring for 313,000 Medicare beneficiaries, are in Arkansas; Colorado; New Jersey; the Capital District/Hudson Valley, N.Y., region; the Cincinnati/Dayton region of Ohio and Kentucky; the greater Tulsa (Okla.) area, and Oregon.
To be selected, practices had to demonstrate that they already had an electronic health record system, that they were already delivering advanced primary care, or that they were engaged in transforming their practices. They also had to have enough patients covered by Medicare and participating private payers to make it worthwhile.
The idea is to provide money to help practices fully transform, said Dr. Robert A. Gluckman, Chair of the American College of Physicians Medical Practice and Quality Committee.
In a traditional model, physicians are only paid for face-to-face encounters. Under this initiative, the monthly fee will help cover services delivered by e-mail, phone, group visits, or by allied health professionals like nutrition and behavioral counselors, said Dr. Gluckman, who also is the chief medical officer for Providence Health Plans. Providence is one of the participating payers in Oregon.
"This is going to be a tremendous opportunity for primary care practices to have the revenue to practice medicine differently," he said.
From a payer point of view, it was worth participating to help "facilitate a more robust primary care network," Dr. Gluckman said. "Payers are increasingly recognizing that we need a more robust primary care delivery system to deliver care more effectively," he said, noting that effective primary care can decrease emergency department visits and curb hospitalizations. "If no one ever tries to deliver care differently, we’re going to keep getting what we’re getting – high cost and some variation in quality."
Dr. Zimmerman said that she has already seen the benefits of creating a better primary care delivery model: happier and somewhat healthier patients. But it was all done without the additional revenue, which meant it was not sustainable, she said.
For the last 2 years, her practice, comprised of herself and two nurse practitioners, participated in a patient-centered medical home pilot program with Arkansas Blue Cross Blue Shield. It is ending in December. No additional payments were given for doing things like creating a patient portal and offering consultations by phone after hours. And not all of her 5,800 patients were covered by the pilot.
The current initiative, with four participating payers in Arkansas – Blue Cross Blue Shield, QualChoice, Humana, and Medicare – will cover 92% of her patients. It’s not clear yet what the monthly payment will be from Medicare or those insurers, but payments are due to start Oct. 1, Dr. Zimmerman said.
The additional funds will let her invest in areas that she couldn’t before, like diabetes education, and to perhaps hire a care coordinator. It also eill help her maintain her EHR and improve her patient portal. Only about a third of patients are using it – to make appointments, request prescription refills, and access lab results or e-mail Dr. Zimmerman. She uses it to send patients a visit summary and lab results and to share educational materials.
The portal makes her work a lot easier, she said. For instance, the system tracks whether a patient has accessed those educational materials or lab results and notifies the physician that the materials have been – or have not been – read. It also allows relatives – say a daughter of an elderly patient – to see medical records and communicate directly with her. That’s especially important if the daughter lives elsewhere.
She also uses her website and a clinic Facebook page to stay in touch with patients. In rural Arkansas, a large number of people have smartphones because so many use Facebook as entertainment, said Dr. Zimmerman. "I would rather them get on my Facebook page and read about something I posted from the Mayo Clinic than surf the web and look up something that’s not good educational information," she said.
Dr. Reicks also says that his patients have been enthusiastic about his patient portal, though only about a third have signed up for access. Initially, the practice’s providers – three physicians, a nurse practitioner, and a physician assistant – were worried that inviting patients to e-mail would open up a flood that would take away from actual practice time.
But uptake has been slow, and "we’ve found it to be convenient and effective," saving time, money on postage, and miscommunications, Dr. Reicks said.
His practice has had an EHR since 2007, and it participated in the Colorado Beacon Consortium, a CMS-funded practice-improvement program in western Colorado. Though the practice underwent a huge transformation, it was looking to move to the next level, said Dr. Reicks.
The per patient/per month fee under the primary care initiative will help the practice "pull in additional human resources," he said. That would include case managers, health coaches, and behavioral health specialists. The idea is to offer truly comprehensive care, Dr. Reicks said.
About 4,500 of the practice’s 10,000 patients will be covered under the initiative, including some 3,000 Medicare patients and 800 Medicaid patients. The practice anticipates an average $10 per patient monthly fee, but it could be more after Medicare payment is risk-adjusted. Like Dr. Zimmerman, Dr. Reicks is waiting on getting word from the private payers – which include Rocky Mountain Health Plans, Anthem Blue Cross Blue Shield, UnitedHealthcare and Cigna – on their monthly payment. But at least one payer – Rocky Mountain Health Plans – has suggested that it will offer in-kind resources such as health coaches instead of an actual payment, Dr. Reicks said.
The uncertainty over the revenue stream is a familiar, but vexing problem, he said. CMS is requiring the participating practices to submit a plan detailing how the monthly fees will be spent. "And we don’t know how much will be coming in," Dr. Reicks said.
It begs the question of why a practice would seek out participation in this initiative.
Besides improving patient satisfaction and health outcomes, "we’re hoping this will somehow restore the joy of practicing medicine again," he said.
