User login
CBT, Exercise Reduce Fibromyalgia Symptoms
ROME – A tailored combination of cognitive-behavioral therapy and physical exercise training has achieved the largest treatment benefit ever reported for fibromyalgia in a randomized, placebo-controlled trial.
The durability of the results was particularly impressive. The large improvements in psychological and physical functioning that were documented at the end of the 8-week treatment program were maintained at the 6-month follow-up, Saskia van Koulil said.
The success of this customized treatment approach hinged upon a two-stage screening process. First, patients who have had their fibromyalgia for fewer than 5 years and were at high risk of long-term dysfunction were selected because prior studies indicated that such individuals tend to have better treatment outcomes in general.
Within this group of high-risk patients, specific cognitive-behavioral patterns seemed to drive their fibromyalgia pain and disability. It is possible to screen for these patterns of thought and behavior. One school of thought among clinical psychologists, including Ms. van Koulil, holds that there are two main patterns: pain avoidance and pain persistence. The treatment programs for the two are quite different, explained Ms. van Koulil of St. Radboud University Medical Center in Nijmegen, the Netherlands.
The high treatment success rate in this randomized trial validated this concept of the pain-avoidance and pain-persistence fibromyalgia subtypes, she continued.
In her experience, close to two-thirds of patients with fibromyalgia of fewer than 5 years' duration have a high-risk profile. This is characterized by high levels of anxiety and/or negative mood on standard measures of distress, along with worse physical functioning, greater impact of fibromyalgia on daily life, and obvious maladaptive cognitive-behavioral patterns such as high levels of helplessness and worrying. This high-level psychological distress is an indicator of treatment motivation, according to Ms. van Koulil.
In the randomized trial, 158 high-risk fibromyalgia patients (95% of whom were women) were evaluated with a brief screening instrument for pain-avoidance behavior. Those with a high score were assigned to the pain-avoidance treatment group or a wait-list control arm, whereas patients with a low score were randomized to the pain-persistence group or the control arm.
The pain-avoidance subtype of fibromyalgia is characterized by fear of pain, hypervigilance, catastrophizing, and zealous avoidance of pain. In contrast, the pain-persistence subtype is characterized by an overactive lifestyle and low levels of pain avoidance. In fact, these highly self-demanding patients tend to ignore pain, ignore their physical limits, and display high levels of task persistence. Both subtypes end up via different routes at the same place, which is marked by functional disability, psychologic distress, fatigue, and chronic pain. The pain-persistence group, however, tends to be more physically fit. Of study participants, 53% were categorized as pain avoidant, whereas 47% were classified in the pain-persistence group.
Patients in both active-treatment arms received 16 twice-weekly treatment sessions in eight-patient groups, each session 4 hours in length, plus homework assignments. The first half of each session was devoted to cognitive-behavioral therapy (CBT), the second half to exercise training. Each exercise session included aerobic exercises, either strength or flexibility training, and relaxation techniques. The patient's significant other attended the 3rd, 9th, and 15th sessions. Also, a booster session was held 3 months after completion of the 8-week program.
The CBT was delivered by therapists with experience in CBT for fibromyalgia and other rheumatologic conditions. Therapy was guided by a written manual. The exercise training was provided by physical therapists.
The pain-avoidance treatment regimen was tailored toward achieving increased daily activities, reduced fear of pain and pain-avoidance behaviors through titrated exposure, and a gradual gain in physical condition. The emphasis in the pain-persistence group was on learning to improve pacing and regulation of activities of daily life and physical exercise, along with altering pain-persistence cognitions.
Five of the six primary outcome end points in the study were changes from baseline in pain, fatigue, functional disability, negative mood, and anxiety as measured on the Impact of Rheumatic Diseases on General Health and Lifestyle scale, which is derived from the Arthritis Impact Measurement Scales (The sixth outcome measure was change in the impact of fibromyalgia on daily life, as assessed by the 10-item Fibromyalgia Impact Questionnaire (FIQ).
The results were striking: In all, 60% of patients in the tailored-therapy arms experienced a clinically significant reduction in the impact of fibromyalgia on daily life, compared with 24% of controls. Of the tailored-therapy patients, 67% had a clinically significant improvement in the physical function domain combining pain, fatigue, and functional disability, compared with 33% of controls. And 62% of tailored-therapy patients demonstrated a clinically significant improvement in psychological function as reflected in reduced scores for negative mood and anxiety, compared with 33% of controls.
The size of the improvements in the various end points was consistently numerically greater in the pain-avoidance group than in the pain-persistence arm, but not statistically significantly so.
The study was financially supported by the Dutch Arthritis Association and the Netherlands Organization for Health Research. Ms. van Koulil reported having no conflicts of interest.
{kind=link}
Patients in the exercise session participated in aerobic exercises and relaxation techniques.
Source ©BRANDXPICTURES
ROME – A tailored combination of cognitive-behavioral therapy and physical exercise training has achieved the largest treatment benefit ever reported for fibromyalgia in a randomized, placebo-controlled trial.
The durability of the results was particularly impressive. The large improvements in psychological and physical functioning that were documented at the end of the 8-week treatment program were maintained at the 6-month follow-up, Saskia van Koulil said.
The success of this customized treatment approach hinged upon a two-stage screening process. First, patients who have had their fibromyalgia for fewer than 5 years and were at high risk of long-term dysfunction were selected because prior studies indicated that such individuals tend to have better treatment outcomes in general.
Within this group of high-risk patients, specific cognitive-behavioral patterns seemed to drive their fibromyalgia pain and disability. It is possible to screen for these patterns of thought and behavior. One school of thought among clinical psychologists, including Ms. van Koulil, holds that there are two main patterns: pain avoidance and pain persistence. The treatment programs for the two are quite different, explained Ms. van Koulil of St. Radboud University Medical Center in Nijmegen, the Netherlands.
The high treatment success rate in this randomized trial validated this concept of the pain-avoidance and pain-persistence fibromyalgia subtypes, she continued.
In her experience, close to two-thirds of patients with fibromyalgia of fewer than 5 years' duration have a high-risk profile. This is characterized by high levels of anxiety and/or negative mood on standard measures of distress, along with worse physical functioning, greater impact of fibromyalgia on daily life, and obvious maladaptive cognitive-behavioral patterns such as high levels of helplessness and worrying. This high-level psychological distress is an indicator of treatment motivation, according to Ms. van Koulil.
In the randomized trial, 158 high-risk fibromyalgia patients (95% of whom were women) were evaluated with a brief screening instrument for pain-avoidance behavior. Those with a high score were assigned to the pain-avoidance treatment group or a wait-list control arm, whereas patients with a low score were randomized to the pain-persistence group or the control arm.
The pain-avoidance subtype of fibromyalgia is characterized by fear of pain, hypervigilance, catastrophizing, and zealous avoidance of pain. In contrast, the pain-persistence subtype is characterized by an overactive lifestyle and low levels of pain avoidance. In fact, these highly self-demanding patients tend to ignore pain, ignore their physical limits, and display high levels of task persistence. Both subtypes end up via different routes at the same place, which is marked by functional disability, psychologic distress, fatigue, and chronic pain. The pain-persistence group, however, tends to be more physically fit. Of study participants, 53% were categorized as pain avoidant, whereas 47% were classified in the pain-persistence group.
Patients in both active-treatment arms received 16 twice-weekly treatment sessions in eight-patient groups, each session 4 hours in length, plus homework assignments. The first half of each session was devoted to cognitive-behavioral therapy (CBT), the second half to exercise training. Each exercise session included aerobic exercises, either strength or flexibility training, and relaxation techniques. The patient's significant other attended the 3rd, 9th, and 15th sessions. Also, a booster session was held 3 months after completion of the 8-week program.
The CBT was delivered by therapists with experience in CBT for fibromyalgia and other rheumatologic conditions. Therapy was guided by a written manual. The exercise training was provided by physical therapists.
The pain-avoidance treatment regimen was tailored toward achieving increased daily activities, reduced fear of pain and pain-avoidance behaviors through titrated exposure, and a gradual gain in physical condition. The emphasis in the pain-persistence group was on learning to improve pacing and regulation of activities of daily life and physical exercise, along with altering pain-persistence cognitions.
Five of the six primary outcome end points in the study were changes from baseline in pain, fatigue, functional disability, negative mood, and anxiety as measured on the Impact of Rheumatic Diseases on General Health and Lifestyle scale, which is derived from the Arthritis Impact Measurement Scales (The sixth outcome measure was change in the impact of fibromyalgia on daily life, as assessed by the 10-item Fibromyalgia Impact Questionnaire (FIQ).
The results were striking: In all, 60% of patients in the tailored-therapy arms experienced a clinically significant reduction in the impact of fibromyalgia on daily life, compared with 24% of controls. Of the tailored-therapy patients, 67% had a clinically significant improvement in the physical function domain combining pain, fatigue, and functional disability, compared with 33% of controls. And 62% of tailored-therapy patients demonstrated a clinically significant improvement in psychological function as reflected in reduced scores for negative mood and anxiety, compared with 33% of controls.
The size of the improvements in the various end points was consistently numerically greater in the pain-avoidance group than in the pain-persistence arm, but not statistically significantly so.
The study was financially supported by the Dutch Arthritis Association and the Netherlands Organization for Health Research. Ms. van Koulil reported having no conflicts of interest.
Patients in the exercise session participated in aerobic exercises and relaxation techniques.
Source ©BRANDXPICTURES
ROME – A tailored combination of cognitive-behavioral therapy and physical exercise training has achieved the largest treatment benefit ever reported for fibromyalgia in a randomized, placebo-controlled trial.
The durability of the results was particularly impressive. The large improvements in psychological and physical functioning that were documented at the end of the 8-week treatment program were maintained at the 6-month follow-up, Saskia van Koulil said.
The success of this customized treatment approach hinged upon a two-stage screening process. First, patients who have had their fibromyalgia for fewer than 5 years and were at high risk of long-term dysfunction were selected because prior studies indicated that such individuals tend to have better treatment outcomes in general.
Within this group of high-risk patients, specific cognitive-behavioral patterns seemed to drive their fibromyalgia pain and disability. It is possible to screen for these patterns of thought and behavior. One school of thought among clinical psychologists, including Ms. van Koulil, holds that there are two main patterns: pain avoidance and pain persistence. The treatment programs for the two are quite different, explained Ms. van Koulil of St. Radboud University Medical Center in Nijmegen, the Netherlands.
The high treatment success rate in this randomized trial validated this concept of the pain-avoidance and pain-persistence fibromyalgia subtypes, she continued.
In her experience, close to two-thirds of patients with fibromyalgia of fewer than 5 years' duration have a high-risk profile. This is characterized by high levels of anxiety and/or negative mood on standard measures of distress, along with worse physical functioning, greater impact of fibromyalgia on daily life, and obvious maladaptive cognitive-behavioral patterns such as high levels of helplessness and worrying. This high-level psychological distress is an indicator of treatment motivation, according to Ms. van Koulil.
In the randomized trial, 158 high-risk fibromyalgia patients (95% of whom were women) were evaluated with a brief screening instrument for pain-avoidance behavior. Those with a high score were assigned to the pain-avoidance treatment group or a wait-list control arm, whereas patients with a low score were randomized to the pain-persistence group or the control arm.
The pain-avoidance subtype of fibromyalgia is characterized by fear of pain, hypervigilance, catastrophizing, and zealous avoidance of pain. In contrast, the pain-persistence subtype is characterized by an overactive lifestyle and low levels of pain avoidance. In fact, these highly self-demanding patients tend to ignore pain, ignore their physical limits, and display high levels of task persistence. Both subtypes end up via different routes at the same place, which is marked by functional disability, psychologic distress, fatigue, and chronic pain. The pain-persistence group, however, tends to be more physically fit. Of study participants, 53% were categorized as pain avoidant, whereas 47% were classified in the pain-persistence group.
Patients in both active-treatment arms received 16 twice-weekly treatment sessions in eight-patient groups, each session 4 hours in length, plus homework assignments. The first half of each session was devoted to cognitive-behavioral therapy (CBT), the second half to exercise training. Each exercise session included aerobic exercises, either strength or flexibility training, and relaxation techniques. The patient's significant other attended the 3rd, 9th, and 15th sessions. Also, a booster session was held 3 months after completion of the 8-week program.
The CBT was delivered by therapists with experience in CBT for fibromyalgia and other rheumatologic conditions. Therapy was guided by a written manual. The exercise training was provided by physical therapists.
The pain-avoidance treatment regimen was tailored toward achieving increased daily activities, reduced fear of pain and pain-avoidance behaviors through titrated exposure, and a gradual gain in physical condition. The emphasis in the pain-persistence group was on learning to improve pacing and regulation of activities of daily life and physical exercise, along with altering pain-persistence cognitions.
Five of the six primary outcome end points in the study were changes from baseline in pain, fatigue, functional disability, negative mood, and anxiety as measured on the Impact of Rheumatic Diseases on General Health and Lifestyle scale, which is derived from the Arthritis Impact Measurement Scales (The sixth outcome measure was change in the impact of fibromyalgia on daily life, as assessed by the 10-item Fibromyalgia Impact Questionnaire (FIQ).
The results were striking: In all, 60% of patients in the tailored-therapy arms experienced a clinically significant reduction in the impact of fibromyalgia on daily life, compared with 24% of controls. Of the tailored-therapy patients, 67% had a clinically significant improvement in the physical function domain combining pain, fatigue, and functional disability, compared with 33% of controls. And 62% of tailored-therapy patients demonstrated a clinically significant improvement in psychological function as reflected in reduced scores for negative mood and anxiety, compared with 33% of controls.
The size of the improvements in the various end points was consistently numerically greater in the pain-avoidance group than in the pain-persistence arm, but not statistically significantly so.
The study was financially supported by the Dutch Arthritis Association and the Netherlands Organization for Health Research. Ms. van Koulil reported having no conflicts of interest.
Patients in the exercise session participated in aerobic exercises and relaxation techniques.
Source ©BRANDXPICTURES
Light Marijuana Use Appears Protective Against Diabetes
Major Finding: The age-adjusted prevalence of diabetes was 4% in nonusers and significantly lower at 3% in marijuana users. In a multiple logistic regression analysis adjusted for socio-demographic factors, comorbid conditions, laboratory values, and inflammatory markers, marijuana users had a 66% lower likelihood of having diabetes.
Data Source: A cross-sectional study involving 10,896 NHANES III participants aged 20–59 years.
Disclosures: The study was funded by Omics Biotechnology, which is pursuing potential medical applications for nonpsychotropic cannabinoid receptor agonists. Dr. Shaheen declared she has no relevant financial relationships.
DENVER – Marijuana use may be associated with a markedly decreased risk of diabetes.
A provocative new analysis of data from the Third National Health and Nutrition Examination Survey (NHANES III) indicates marijuana users had 66% lower odds of having diabetes after adjustment for numerous potential confounding factors, Dr. Magda Shaheen reported at the meeting.
This robust observed benefit has a biologically plausible mechanism, she noted.
In addition to defects in pancreatic beta-cell function and insulin sensitivity, the pathogenesis of diabetes is thought to involve systemic inflammation. Marijuana contains bioactive cannabinoids that have been shown to have an anti-inflammatory effect. This was borne out in the NHANES III analysis, where the prevalence of an elevated C-reactive protein level in excess of 0.5 mg/dL was significantly higher in nonusers of marijuana, at 18.9%, than in past users, with a 13% prevalence of elevated CRP, current light users (16%), or current heavy users of the illicit drug (9%), according to Dr. Shaheen of Charles R. Drew University of Medicine and Science, Los Angeles.
The study population consisted of 10,896 NHANES III participants aged 20–59 years; they constituted a statistically representative sample of the broader U.S. civilian population in 1988–1994, when the survey was conducted. The majority of subjects – 55% – reported never having used marijuana. Another 37% were past users, meaning they hadn't used marijuana during the previous month. The 6% of subjects who reported currently using the drug 1–4 days per month were categorized as current light users, while 3.3% of subjects were current heavier users.
The age-adjusted prevalence of diabetes in this cross-sectional study was 4% in nonusers and significantly lower at 3% in marijuana users. Current and past users were significantly younger, had a lower body mass index, were more physically active, and were more likely to smoke cigarettes, drink alcohol, and use cocaine than were nonusers. They were more likely to have an HDL level greater than 40 mg/dL and had lower mean total cholesterol, LDL, and triglyceride levels.
In a multiple logistic regression analysis adjusted for sociodemographic factors, comorbid conditions, laboratory values, and inflammatory markers, marijuana users had a 66% lower likelihood of having diabetes. This benefit was confined to the 41- to 59-year-old age group, where the reduction in diabetes risk associated with marijuana use was 67%. In contrast, the 7% reduction in risk among 20- to 40-year-olds was not statistically significant. These findings could be the result of the markedly higher occurrence of diabetes in middle age.
Unlike in diabetes, marijuana use was not associated with a lower prevalence of the other chronic diseases that Dr. Shaheen and colleagues looked at in which systemic inflammation also plays a role: myocardial infarction, heart failure, stroke, and hypertension. “This was probably due to the lower prevalence of these diseases in this age group,” she commented.
Dr. Shaheen noted that the lowest prevalence of diabetes was found in current light users of marijuana, although past users and current heavy users also had lower rates than did nonusers. “This finding in light marijuana users is similar to the effect of alcohol on diabetes mellitus and the metabolic syndrome. Studies have shown that mild alcohol use was associated with a lower prevalence of diabetes and metabolic syndrome, and higher use was associated with a higher prevalence.”
Dr. Shaheen said this was a cross-sectional study that can't establish causality. “Prospective studies need to be performed in rodents and humans to determine a causal relationship between cannabinoid receptor activation and diabetes. Until those studies are performed, we do not advocate the use of marijuana in patients at risk for diabetes mellitus,” the investigator stressed.
Major Finding: The age-adjusted prevalence of diabetes was 4% in nonusers and significantly lower at 3% in marijuana users. In a multiple logistic regression analysis adjusted for socio-demographic factors, comorbid conditions, laboratory values, and inflammatory markers, marijuana users had a 66% lower likelihood of having diabetes.
Data Source: A cross-sectional study involving 10,896 NHANES III participants aged 20–59 years.
Disclosures: The study was funded by Omics Biotechnology, which is pursuing potential medical applications for nonpsychotropic cannabinoid receptor agonists. Dr. Shaheen declared she has no relevant financial relationships.
DENVER – Marijuana use may be associated with a markedly decreased risk of diabetes.
A provocative new analysis of data from the Third National Health and Nutrition Examination Survey (NHANES III) indicates marijuana users had 66% lower odds of having diabetes after adjustment for numerous potential confounding factors, Dr. Magda Shaheen reported at the meeting.
This robust observed benefit has a biologically plausible mechanism, she noted.
In addition to defects in pancreatic beta-cell function and insulin sensitivity, the pathogenesis of diabetes is thought to involve systemic inflammation. Marijuana contains bioactive cannabinoids that have been shown to have an anti-inflammatory effect. This was borne out in the NHANES III analysis, where the prevalence of an elevated C-reactive protein level in excess of 0.5 mg/dL was significantly higher in nonusers of marijuana, at 18.9%, than in past users, with a 13% prevalence of elevated CRP, current light users (16%), or current heavy users of the illicit drug (9%), according to Dr. Shaheen of Charles R. Drew University of Medicine and Science, Los Angeles.
The study population consisted of 10,896 NHANES III participants aged 20–59 years; they constituted a statistically representative sample of the broader U.S. civilian population in 1988–1994, when the survey was conducted. The majority of subjects – 55% – reported never having used marijuana. Another 37% were past users, meaning they hadn't used marijuana during the previous month. The 6% of subjects who reported currently using the drug 1–4 days per month were categorized as current light users, while 3.3% of subjects were current heavier users.
The age-adjusted prevalence of diabetes in this cross-sectional study was 4% in nonusers and significantly lower at 3% in marijuana users. Current and past users were significantly younger, had a lower body mass index, were more physically active, and were more likely to smoke cigarettes, drink alcohol, and use cocaine than were nonusers. They were more likely to have an HDL level greater than 40 mg/dL and had lower mean total cholesterol, LDL, and triglyceride levels.
In a multiple logistic regression analysis adjusted for sociodemographic factors, comorbid conditions, laboratory values, and inflammatory markers, marijuana users had a 66% lower likelihood of having diabetes. This benefit was confined to the 41- to 59-year-old age group, where the reduction in diabetes risk associated with marijuana use was 67%. In contrast, the 7% reduction in risk among 20- to 40-year-olds was not statistically significant. These findings could be the result of the markedly higher occurrence of diabetes in middle age.
Unlike in diabetes, marijuana use was not associated with a lower prevalence of the other chronic diseases that Dr. Shaheen and colleagues looked at in which systemic inflammation also plays a role: myocardial infarction, heart failure, stroke, and hypertension. “This was probably due to the lower prevalence of these diseases in this age group,” she commented.
Dr. Shaheen noted that the lowest prevalence of diabetes was found in current light users of marijuana, although past users and current heavy users also had lower rates than did nonusers. “This finding in light marijuana users is similar to the effect of alcohol on diabetes mellitus and the metabolic syndrome. Studies have shown that mild alcohol use was associated with a lower prevalence of diabetes and metabolic syndrome, and higher use was associated with a higher prevalence.”
Dr. Shaheen said this was a cross-sectional study that can't establish causality. “Prospective studies need to be performed in rodents and humans to determine a causal relationship between cannabinoid receptor activation and diabetes. Until those studies are performed, we do not advocate the use of marijuana in patients at risk for diabetes mellitus,” the investigator stressed.
Major Finding: The age-adjusted prevalence of diabetes was 4% in nonusers and significantly lower at 3% in marijuana users. In a multiple logistic regression analysis adjusted for socio-demographic factors, comorbid conditions, laboratory values, and inflammatory markers, marijuana users had a 66% lower likelihood of having diabetes.
Data Source: A cross-sectional study involving 10,896 NHANES III participants aged 20–59 years.
Disclosures: The study was funded by Omics Biotechnology, which is pursuing potential medical applications for nonpsychotropic cannabinoid receptor agonists. Dr. Shaheen declared she has no relevant financial relationships.
DENVER – Marijuana use may be associated with a markedly decreased risk of diabetes.
A provocative new analysis of data from the Third National Health and Nutrition Examination Survey (NHANES III) indicates marijuana users had 66% lower odds of having diabetes after adjustment for numerous potential confounding factors, Dr. Magda Shaheen reported at the meeting.
This robust observed benefit has a biologically plausible mechanism, she noted.
In addition to defects in pancreatic beta-cell function and insulin sensitivity, the pathogenesis of diabetes is thought to involve systemic inflammation. Marijuana contains bioactive cannabinoids that have been shown to have an anti-inflammatory effect. This was borne out in the NHANES III analysis, where the prevalence of an elevated C-reactive protein level in excess of 0.5 mg/dL was significantly higher in nonusers of marijuana, at 18.9%, than in past users, with a 13% prevalence of elevated CRP, current light users (16%), or current heavy users of the illicit drug (9%), according to Dr. Shaheen of Charles R. Drew University of Medicine and Science, Los Angeles.
The study population consisted of 10,896 NHANES III participants aged 20–59 years; they constituted a statistically representative sample of the broader U.S. civilian population in 1988–1994, when the survey was conducted. The majority of subjects – 55% – reported never having used marijuana. Another 37% were past users, meaning they hadn't used marijuana during the previous month. The 6% of subjects who reported currently using the drug 1–4 days per month were categorized as current light users, while 3.3% of subjects were current heavier users.
The age-adjusted prevalence of diabetes in this cross-sectional study was 4% in nonusers and significantly lower at 3% in marijuana users. Current and past users were significantly younger, had a lower body mass index, were more physically active, and were more likely to smoke cigarettes, drink alcohol, and use cocaine than were nonusers. They were more likely to have an HDL level greater than 40 mg/dL and had lower mean total cholesterol, LDL, and triglyceride levels.
In a multiple logistic regression analysis adjusted for sociodemographic factors, comorbid conditions, laboratory values, and inflammatory markers, marijuana users had a 66% lower likelihood of having diabetes. This benefit was confined to the 41- to 59-year-old age group, where the reduction in diabetes risk associated with marijuana use was 67%. In contrast, the 7% reduction in risk among 20- to 40-year-olds was not statistically significant. These findings could be the result of the markedly higher occurrence of diabetes in middle age.
Unlike in diabetes, marijuana use was not associated with a lower prevalence of the other chronic diseases that Dr. Shaheen and colleagues looked at in which systemic inflammation also plays a role: myocardial infarction, heart failure, stroke, and hypertension. “This was probably due to the lower prevalence of these diseases in this age group,” she commented.
Dr. Shaheen noted that the lowest prevalence of diabetes was found in current light users of marijuana, although past users and current heavy users also had lower rates than did nonusers. “This finding in light marijuana users is similar to the effect of alcohol on diabetes mellitus and the metabolic syndrome. Studies have shown that mild alcohol use was associated with a lower prevalence of diabetes and metabolic syndrome, and higher use was associated with a higher prevalence.”
Dr. Shaheen said this was a cross-sectional study that can't establish causality. “Prospective studies need to be performed in rodents and humans to determine a causal relationship between cannabinoid receptor activation and diabetes. Until those studies are performed, we do not advocate the use of marijuana in patients at risk for diabetes mellitus,” the investigator stressed.
One in Five College Football Tailgaters Is Intoxicated
DENVER – During last year’s college football season, one in five fans tailgating on the campus of a large Midwestern university before games was intoxicated. But more than half of the tailgaters thought they were, according to a season-long Breathalyzer survey.

The highest average game-day blood alcohol concentrations among randomly sampled University of Toledo tailgaters occurred before the nationally televised opening game and again at the homecoming game (0.061 and 0.067 mL/L, respectively), Robert E. Braun reported at the annual meeting of the American Public Health Association.
The average blood alcohol level among tailgaters over the course of the season of parking-lot partying was 0.054 mL/L, but the fans significantly overestimated their levels, which they guessed were on average 0.072 mL/L.
In all, 20% of the tailgating fans – students, alumni, and partying visitors – were inebriated based upon a Breathalyzer reading of 0.08 mL/L or more, which is over the legal threshold for driving a motor vehicle. But 53% of the 466 tailgaters who took the Breathalyzer test and completed a 19-item questionnaire perceived themselves to be intoxicated. This suggests a need for social norm campaigns addressing game-day drinking, noted Mr. Braun of the university.
Results of this study underscore the point that alcohol abuse in conjunction with sporting events is a serious public health issue. University officials around the country need to design interventions to curb game-day drinking. One possibility would be to restrict pregame tailgating to, say, 3.5 hours to reduce excessive alcohol consumption, he argued.
Banning alcohol altogether on campus is seen as unrealistic at many universities. Of the surveyed tailgaters, 85% expressed support for designating selected tailgating locations on campus where alcohol consumption would be legal.
Mr. Braun declared having no financial conflicts regarding this university-funded study.
DENVER – During last year’s college football season, one in five fans tailgating on the campus of a large Midwestern university before games was intoxicated. But more than half of the tailgaters thought they were, according to a season-long Breathalyzer survey.
The highest average game-day blood alcohol concentrations among randomly sampled University of Toledo tailgaters occurred before the nationally televised opening game and again at the homecoming game (0.061 and 0.067 mL/L, respectively), Robert E. Braun reported at the annual meeting of the American Public Health Association.
The average blood alcohol level among tailgaters over the course of the season of parking-lot partying was 0.054 mL/L, but the fans significantly overestimated their levels, which they guessed were on average 0.072 mL/L.
In all, 20% of the tailgating fans – students, alumni, and partying visitors – were inebriated based upon a Breathalyzer reading of 0.08 mL/L or more, which is over the legal threshold for driving a motor vehicle. But 53% of the 466 tailgaters who took the Breathalyzer test and completed a 19-item questionnaire perceived themselves to be intoxicated. This suggests a need for social norm campaigns addressing game-day drinking, noted Mr. Braun of the university.
Results of this study underscore the point that alcohol abuse in conjunction with sporting events is a serious public health issue. University officials around the country need to design interventions to curb game-day drinking. One possibility would be to restrict pregame tailgating to, say, 3.5 hours to reduce excessive alcohol consumption, he argued.
Banning alcohol altogether on campus is seen as unrealistic at many universities. Of the surveyed tailgaters, 85% expressed support for designating selected tailgating locations on campus where alcohol consumption would be legal.
Mr. Braun declared having no financial conflicts regarding this university-funded study.
DENVER – During last year’s college football season, one in five fans tailgating on the campus of a large Midwestern university before games was intoxicated. But more than half of the tailgaters thought they were, according to a season-long Breathalyzer survey.
The highest average game-day blood alcohol concentrations among randomly sampled University of Toledo tailgaters occurred before the nationally televised opening game and again at the homecoming game (0.061 and 0.067 mL/L, respectively), Robert E. Braun reported at the annual meeting of the American Public Health Association.
The average blood alcohol level among tailgaters over the course of the season of parking-lot partying was 0.054 mL/L, but the fans significantly overestimated their levels, which they guessed were on average 0.072 mL/L.
In all, 20% of the tailgating fans – students, alumni, and partying visitors – were inebriated based upon a Breathalyzer reading of 0.08 mL/L or more, which is over the legal threshold for driving a motor vehicle. But 53% of the 466 tailgaters who took the Breathalyzer test and completed a 19-item questionnaire perceived themselves to be intoxicated. This suggests a need for social norm campaigns addressing game-day drinking, noted Mr. Braun of the university.
Results of this study underscore the point that alcohol abuse in conjunction with sporting events is a serious public health issue. University officials around the country need to design interventions to curb game-day drinking. One possibility would be to restrict pregame tailgating to, say, 3.5 hours to reduce excessive alcohol consumption, he argued.
Banning alcohol altogether on campus is seen as unrealistic at many universities. Of the surveyed tailgaters, 85% expressed support for designating selected tailgating locations on campus where alcohol consumption would be legal.
Mr. Braun declared having no financial conflicts regarding this university-funded study.
Blood Type Linked to Diminished Ovarian Reserve
DENVER – Infertile women with blood type O have an increased prevalence of diminished ovarian reserve, according to Dr. Edward J. Nejat.
In contrast, the A blood group antigen, comprised of blood types A and AB, appears to be protective against diminished ovarian reserve, he reported at the annual meeting of the American Society for Reproductive Medicine.
These are novel findings whose clinical implications must await further study, added Dr. Nejat of Albert Einstein College of Medicine, New York.
He presented a cross-sectional observational study involving 563 women under age 45 years seeking treatment for infertility at Montefiore Medical Center in New York or at the Yale University in vitro fertilization program in New Haven, Conn. Diminished ovarian reserve, defined by a baseline serum follicle-stimulating hormone level greater than 10 mIU/mL, was present in 70 subjects.
Ovarian reserve reflects the quantity of gametes available for procreation. Dr. Nejat and his coworkers decided to look for a possible association between blood type and ovarian reserve because other than advancing age, the determinants of ovarian reserve are unclear. Other investigators have previously described a link between blood type A and ovarian hyperstimulation syndrome.
A total of 61% of women with diminished ovarian reserve were blood type O, as were 43% of those with a baseline follicle-stimulation hormone level of 10 mIU/mL. After adjusting the results for age and site, women with blood type O were at twofold greater risk of having diminished ovarian reserve than were women with other blood types.
The A blood group antigen was present in 26% of women with diminished ovarian reserve and 41% of those with adequate ovarian reserve. The adjusted risk of diminished ovarian reserve in women possessing the A blood group antigen was half that in women with blood types O or B.
The relationship between blood type and diminished ovarian reserve was independent of age.
Dr. Nejat said he had no relevant financial conflicts.
DENVER – Infertile women with blood type O have an increased prevalence of diminished ovarian reserve, according to Dr. Edward J. Nejat.
In contrast, the A blood group antigen, comprised of blood types A and AB, appears to be protective against diminished ovarian reserve, he reported at the annual meeting of the American Society for Reproductive Medicine.
These are novel findings whose clinical implications must await further study, added Dr. Nejat of Albert Einstein College of Medicine, New York.
He presented a cross-sectional observational study involving 563 women under age 45 years seeking treatment for infertility at Montefiore Medical Center in New York or at the Yale University in vitro fertilization program in New Haven, Conn. Diminished ovarian reserve, defined by a baseline serum follicle-stimulating hormone level greater than 10 mIU/mL, was present in 70 subjects.
Ovarian reserve reflects the quantity of gametes available for procreation. Dr. Nejat and his coworkers decided to look for a possible association between blood type and ovarian reserve because other than advancing age, the determinants of ovarian reserve are unclear. Other investigators have previously described a link between blood type A and ovarian hyperstimulation syndrome.
A total of 61% of women with diminished ovarian reserve were blood type O, as were 43% of those with a baseline follicle-stimulation hormone level of 10 mIU/mL. After adjusting the results for age and site, women with blood type O were at twofold greater risk of having diminished ovarian reserve than were women with other blood types.
The A blood group antigen was present in 26% of women with diminished ovarian reserve and 41% of those with adequate ovarian reserve. The adjusted risk of diminished ovarian reserve in women possessing the A blood group antigen was half that in women with blood types O or B.
The relationship between blood type and diminished ovarian reserve was independent of age.
Dr. Nejat said he had no relevant financial conflicts.
DENVER – Infertile women with blood type O have an increased prevalence of diminished ovarian reserve, according to Dr. Edward J. Nejat.
In contrast, the A blood group antigen, comprised of blood types A and AB, appears to be protective against diminished ovarian reserve, he reported at the annual meeting of the American Society for Reproductive Medicine.
These are novel findings whose clinical implications must await further study, added Dr. Nejat of Albert Einstein College of Medicine, New York.
He presented a cross-sectional observational study involving 563 women under age 45 years seeking treatment for infertility at Montefiore Medical Center in New York or at the Yale University in vitro fertilization program in New Haven, Conn. Diminished ovarian reserve, defined by a baseline serum follicle-stimulating hormone level greater than 10 mIU/mL, was present in 70 subjects.
Ovarian reserve reflects the quantity of gametes available for procreation. Dr. Nejat and his coworkers decided to look for a possible association between blood type and ovarian reserve because other than advancing age, the determinants of ovarian reserve are unclear. Other investigators have previously described a link between blood type A and ovarian hyperstimulation syndrome.
A total of 61% of women with diminished ovarian reserve were blood type O, as were 43% of those with a baseline follicle-stimulation hormone level of 10 mIU/mL. After adjusting the results for age and site, women with blood type O were at twofold greater risk of having diminished ovarian reserve than were women with other blood types.
The A blood group antigen was present in 26% of women with diminished ovarian reserve and 41% of those with adequate ovarian reserve. The adjusted risk of diminished ovarian reserve in women possessing the A blood group antigen was half that in women with blood types O or B.
The relationship between blood type and diminished ovarian reserve was independent of age.
Dr. Nejat said he had no relevant financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE
Oral Tranexamic Acid Has Quality of Life Benefits in Menorrhagia
DENVER – A novel oral formulation of tranexamic acid provided immediate and enduring improvement in two quality of life measures among women with menorrhagia in a large open-label study.
The improved quality of life benefits were noted during the first menstrual cycle after initiating treatment. Also, the benefits were maintained throughout the 15-cycle study, Dr. Ken Muse reported at the annual meeting of the American Society for Reproductive Medicine.
Tranexamic acid is a lysine analogue that acts as a competitive plasmin inhibitor and an antifibrinolytic agent. The oral formulation was approved by the Food and Drug Administration late last year for the treatment of cyclic heavy menstrual bleeding and is marketed under the trade name Lysteda. It’s a valuable alternative to surgical or hormonal treatments for this disorder, which affects up to 22 million Americans, said Dr. Muse of the University of Kentucky, Lexington.
Oral tranexamic acid won marketing approval on the strength of studies showing it reduced menstrual flow by nearly 40%. The quality of life study was conducted because what drives many women to consult a physician regarding menorrhagia is the disorder’s negative impact on their daily activities.
The study involved 723 women who took oral tranexamic acid at 1.3 g three times per day for a maximum of 5 days per menstrual cycle, starting with the onset of heavy menstrual bleeding. General quality of life was assessed using the 36-Item Short Form Health Survey. The Aberdeen Menorrhagia Clinical Outcome Questionnaire (AMCOQ) was used as a disease-specific measure of the impact of treatment.
Significant improvements were noted in six of eight SF-36 categories and domains at cycle 15, compared with baseline. The greatest improvements were in vitality, with a 13.5% gain, and social functioning, with an 8.3% gain. Patients also showed significant long-term improvements in bodily pain, mental health, role-physical, and role-emotional items. Only physical functioning and general health weren’t significantly different at cycle 15, compared with baseline.
Women on oral tranexamic acid had a mean 5.4% long-term improvement in the mental health component of the SF-36, and a less robust but nonetheless significant 1.7% gain in the physical functioning component, according to Dr. Muse.
Oral tranexamic acid was well tolerated. Adverse events deemed by investigators to be probably or definitely treatment related occurred in 7.3% of subjects; these were mild to moderate in nature and most often consisted of headache, menstrual discomfort, or back pain. There were few gastrointestinal side effects, and no thrombotic or thromboembolic events.
Scores on the AMCOQ indicated patients had a consistent improvement in daily activities that are affected by cyclic heavy menstrual bleeding.
The study was funded by Xanodyne Pharmaceuticals Inc. and Ferring Pharmaceuticals, which acquired global marketing rights to Lysteda last May. Dr. Muse disclosed that he has received research grants and served as an adviser to Xanodyne.
DENVER – A novel oral formulation of tranexamic acid provided immediate and enduring improvement in two quality of life measures among women with menorrhagia in a large open-label study.
The improved quality of life benefits were noted during the first menstrual cycle after initiating treatment. Also, the benefits were maintained throughout the 15-cycle study, Dr. Ken Muse reported at the annual meeting of the American Society for Reproductive Medicine.
Tranexamic acid is a lysine analogue that acts as a competitive plasmin inhibitor and an antifibrinolytic agent. The oral formulation was approved by the Food and Drug Administration late last year for the treatment of cyclic heavy menstrual bleeding and is marketed under the trade name Lysteda. It’s a valuable alternative to surgical or hormonal treatments for this disorder, which affects up to 22 million Americans, said Dr. Muse of the University of Kentucky, Lexington.
Oral tranexamic acid won marketing approval on the strength of studies showing it reduced menstrual flow by nearly 40%. The quality of life study was conducted because what drives many women to consult a physician regarding menorrhagia is the disorder’s negative impact on their daily activities.
The study involved 723 women who took oral tranexamic acid at 1.3 g three times per day for a maximum of 5 days per menstrual cycle, starting with the onset of heavy menstrual bleeding. General quality of life was assessed using the 36-Item Short Form Health Survey. The Aberdeen Menorrhagia Clinical Outcome Questionnaire (AMCOQ) was used as a disease-specific measure of the impact of treatment.
Significant improvements were noted in six of eight SF-36 categories and domains at cycle 15, compared with baseline. The greatest improvements were in vitality, with a 13.5% gain, and social functioning, with an 8.3% gain. Patients also showed significant long-term improvements in bodily pain, mental health, role-physical, and role-emotional items. Only physical functioning and general health weren’t significantly different at cycle 15, compared with baseline.
Women on oral tranexamic acid had a mean 5.4% long-term improvement in the mental health component of the SF-36, and a less robust but nonetheless significant 1.7% gain in the physical functioning component, according to Dr. Muse.
Oral tranexamic acid was well tolerated. Adverse events deemed by investigators to be probably or definitely treatment related occurred in 7.3% of subjects; these were mild to moderate in nature and most often consisted of headache, menstrual discomfort, or back pain. There were few gastrointestinal side effects, and no thrombotic or thromboembolic events.
Scores on the AMCOQ indicated patients had a consistent improvement in daily activities that are affected by cyclic heavy menstrual bleeding.
The study was funded by Xanodyne Pharmaceuticals Inc. and Ferring Pharmaceuticals, which acquired global marketing rights to Lysteda last May. Dr. Muse disclosed that he has received research grants and served as an adviser to Xanodyne.
DENVER – A novel oral formulation of tranexamic acid provided immediate and enduring improvement in two quality of life measures among women with menorrhagia in a large open-label study.
The improved quality of life benefits were noted during the first menstrual cycle after initiating treatment. Also, the benefits were maintained throughout the 15-cycle study, Dr. Ken Muse reported at the annual meeting of the American Society for Reproductive Medicine.
Tranexamic acid is a lysine analogue that acts as a competitive plasmin inhibitor and an antifibrinolytic agent. The oral formulation was approved by the Food and Drug Administration late last year for the treatment of cyclic heavy menstrual bleeding and is marketed under the trade name Lysteda. It’s a valuable alternative to surgical or hormonal treatments for this disorder, which affects up to 22 million Americans, said Dr. Muse of the University of Kentucky, Lexington.
Oral tranexamic acid won marketing approval on the strength of studies showing it reduced menstrual flow by nearly 40%. The quality of life study was conducted because what drives many women to consult a physician regarding menorrhagia is the disorder’s negative impact on their daily activities.
The study involved 723 women who took oral tranexamic acid at 1.3 g three times per day for a maximum of 5 days per menstrual cycle, starting with the onset of heavy menstrual bleeding. General quality of life was assessed using the 36-Item Short Form Health Survey. The Aberdeen Menorrhagia Clinical Outcome Questionnaire (AMCOQ) was used as a disease-specific measure of the impact of treatment.
Significant improvements were noted in six of eight SF-36 categories and domains at cycle 15, compared with baseline. The greatest improvements were in vitality, with a 13.5% gain, and social functioning, with an 8.3% gain. Patients also showed significant long-term improvements in bodily pain, mental health, role-physical, and role-emotional items. Only physical functioning and general health weren’t significantly different at cycle 15, compared with baseline.
Women on oral tranexamic acid had a mean 5.4% long-term improvement in the mental health component of the SF-36, and a less robust but nonetheless significant 1.7% gain in the physical functioning component, according to Dr. Muse.
Oral tranexamic acid was well tolerated. Adverse events deemed by investigators to be probably or definitely treatment related occurred in 7.3% of subjects; these were mild to moderate in nature and most often consisted of headache, menstrual discomfort, or back pain. There were few gastrointestinal side effects, and no thrombotic or thromboembolic events.
Scores on the AMCOQ indicated patients had a consistent improvement in daily activities that are affected by cyclic heavy menstrual bleeding.
The study was funded by Xanodyne Pharmaceuticals Inc. and Ferring Pharmaceuticals, which acquired global marketing rights to Lysteda last May. Dr. Muse disclosed that he has received research grants and served as an adviser to Xanodyne.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE
Major Finding: Six of eight SF-36 categories and domains improved significantly at cycle 15 compared with baseline. Scores on the AMCOQ indicated patients experienced a consistent improvement in daily activities that are impacted by cyclic heavy menstrual bleeding.
Data Source: An open label study of quality of life in 723 women who took oral tranexamic acid at 1.3 g three times per day for a maximum of 5 days per menstrual cycle, starting with the onset of heavy menstrual bleeding.
Disclosures: The study was funded by Xanodyne Pharmaceuticals and Ferring Pharmaceuticals, which acquired global marketing rights to Lysteda last May. Dr. Muse disclosed that he has received research grants and served as an adviser to Xanodyne.
ASCOT: CRP Does Not Improve Upon Standard Framingham Score
CHICAGO – Measurement of high-sensitivity C-reactive protein had little to no utility in refining cardiovascular risk assessment beyond that provided by the classic risk factors in a new secondary analysis of the ASCOT trial, throwing into question the biomarker’s appropriate role in clinical practice.
"In the ASCOT–Lipid Lowering Arm, neither baseline nor on-treatment CRP provided any useful information about the efficacy of statin treatment to reduce cardiovascular events beyond LDL cholesterol reduction. These results do not support current proposals to measure CRP in the clinical setting, either to assign statins to individuals on the basis of an elevated CRP alone or to monitor CRP levels as an indicator of the efficacy of statin treatment," Dr. Peter S. Sever said at the annual scientific sessions of the American Heart Association. In ASCOT (the Anglo-Scandinavian Cardiac Outcomes Trial), combining a baseline determination of CRP with a standard Framingham Risk Score did not significantly enhance the ability to predict future cardiovascular disease events beyond that provided by Framingham score alone. And while once patients were on statin therapy, the resultant reduction in LDL was associated with an impressive 55% reduction in cardiovascular events, compared with placebo, the decrease in CRP was not linked to a significant decrease in such events, according to Dr. Sever, professor of clinical pharmacology and therapeutics at Imperial College, London.
ASCOT was a landmark primary prevention trial in which nearly 20,000 hypertensive patients were randomized to one of two antihypertensive regimens, then the 10,305 participants with a total cholesterol level of 250 mg/dL or less were re-randomized to 10 mg/day of atorvastatin (Lipitor) or placebo. Although this was a primary prevention trial, these were high-risk patients with three other cardiovascular risk factors in addition to hypertension and a mean 28% risk of developing cardiovascular disease within the next 10 years based upon their Framingham Risk Score.
The new retrospective ASCOT analysis involved 485 patients who experienced a coronary event or stroke during 3.3 years of follow-up and 1,367 controls who did not. Analyzing the data with use of four different statistical methods, neither baseline CRP nor change in CRP level after 6 months of statin therapy provided any practical information.
"I think our conclusion is fairly clear: In patients with hypertension, they’re on statins. In patients with diabetes, they’re on statins. In patients with stable coronary artery disease, they’re on statins. There’s no additional benefit to be gained from measuring CRP," Dr. Sever said.
Discussant Dr. Donald Lloyd-Jones concurred.
"The ASCOT data are the latest adding to a large body of literature suggesting minimal clinical utility for CRP in risk assessment and decision making for lipid-lowering therapy, and a small, growing, and frankly mixed literature examining the utility of on-treatment CRP levels," observed Dr. Lloyd-Jones, professor of preventive medicine at Northwestern University, Chicago.
In ASCOT, patients with an on-treatment LDL below the median had a reduced cardiovascular event risk regardless of their CRP level, while those with a higher LDL had a higher risk regardless of their CRP level. And among patients with a low on-treatment LDL, having a low CRP was not associated with additional benefit, he noted.
Factoring in baseline CRP resulted in a net reclassification improvement score, or NRI, of 0.005 in ASCOT participants at intermediate risk on the basis of their Framingham score. The NRI is a recently developed statistical measure that has been embraced by preventive medicine specialists because it expresses how useful a novel cardiovascular risk factor is in further defining Framingham intermediate-risk patients as either high- or low-risk. The NRI for baseline CRP in ASCOT was weak and nonsignificant. By contrast, the NRI for coronary artery calcium score in Framingham intermediate-risk patients in the Multi-Ethnic Study of Atherosclerosis (MESA) was a robust 0.55, more than two orders of magnitude greater than for CRP in ASCOT, the cardiologist said.
ASCOT is just the latest in a growing number of studies that raise a central question, he added: "Is CRP something we need to be spending our time on?"
So how often does Dr. Lloyd-Jones obtain a CRP measurement in his own clinical practice? "Never," he said in an interview.
Asked to comment, Dr. Christopher Cannon of Brigham and Women’s Hospital, Boston, said his interpretation of the ASCOT results is that in patients who already have a good indication for statin therapy, knowing the baseline CRP level does not provide additional useful information.
"Once you get into places where you should be treating anyway, then CRP isn’t helpful. But in the JUPITER trial they had patients largely without other risk factors, and in that lower-risk group a high baseline CRP picked out those who would benefit from statin therapy," Dr. Cannon explained.
He agreed with Dr. Sever and Dr. Lloyd-Jones that the message from ASCOT regarding the use of on-treatment CRP to titrate statin therapy is that it doesn’t make sense.
Dr. Sever declared that he is a consultant to and is on the speakers bureau for Pfizer, which sponsored the ASCOT trial. Dr. Cannon is also on the speakers bureau for Pfizer. Dr. Lloyd-Jones reported no relevant financial interests.
CHICAGO – Measurement of high-sensitivity C-reactive protein had little to no utility in refining cardiovascular risk assessment beyond that provided by the classic risk factors in a new secondary analysis of the ASCOT trial, throwing into question the biomarker’s appropriate role in clinical practice.
"In the ASCOT–Lipid Lowering Arm, neither baseline nor on-treatment CRP provided any useful information about the efficacy of statin treatment to reduce cardiovascular events beyond LDL cholesterol reduction. These results do not support current proposals to measure CRP in the clinical setting, either to assign statins to individuals on the basis of an elevated CRP alone or to monitor CRP levels as an indicator of the efficacy of statin treatment," Dr. Peter S. Sever said at the annual scientific sessions of the American Heart Association. In ASCOT (the Anglo-Scandinavian Cardiac Outcomes Trial), combining a baseline determination of CRP with a standard Framingham Risk Score did not significantly enhance the ability to predict future cardiovascular disease events beyond that provided by Framingham score alone. And while once patients were on statin therapy, the resultant reduction in LDL was associated with an impressive 55% reduction in cardiovascular events, compared with placebo, the decrease in CRP was not linked to a significant decrease in such events, according to Dr. Sever, professor of clinical pharmacology and therapeutics at Imperial College, London.
ASCOT was a landmark primary prevention trial in which nearly 20,000 hypertensive patients were randomized to one of two antihypertensive regimens, then the 10,305 participants with a total cholesterol level of 250 mg/dL or less were re-randomized to 10 mg/day of atorvastatin (Lipitor) or placebo. Although this was a primary prevention trial, these were high-risk patients with three other cardiovascular risk factors in addition to hypertension and a mean 28% risk of developing cardiovascular disease within the next 10 years based upon their Framingham Risk Score.
The new retrospective ASCOT analysis involved 485 patients who experienced a coronary event or stroke during 3.3 years of follow-up and 1,367 controls who did not. Analyzing the data with use of four different statistical methods, neither baseline CRP nor change in CRP level after 6 months of statin therapy provided any practical information.
"I think our conclusion is fairly clear: In patients with hypertension, they’re on statins. In patients with diabetes, they’re on statins. In patients with stable coronary artery disease, they’re on statins. There’s no additional benefit to be gained from measuring CRP," Dr. Sever said.
Discussant Dr. Donald Lloyd-Jones concurred.
"The ASCOT data are the latest adding to a large body of literature suggesting minimal clinical utility for CRP in risk assessment and decision making for lipid-lowering therapy, and a small, growing, and frankly mixed literature examining the utility of on-treatment CRP levels," observed Dr. Lloyd-Jones, professor of preventive medicine at Northwestern University, Chicago.
In ASCOT, patients with an on-treatment LDL below the median had a reduced cardiovascular event risk regardless of their CRP level, while those with a higher LDL had a higher risk regardless of their CRP level. And among patients with a low on-treatment LDL, having a low CRP was not associated with additional benefit, he noted.
Factoring in baseline CRP resulted in a net reclassification improvement score, or NRI, of 0.005 in ASCOT participants at intermediate risk on the basis of their Framingham score. The NRI is a recently developed statistical measure that has been embraced by preventive medicine specialists because it expresses how useful a novel cardiovascular risk factor is in further defining Framingham intermediate-risk patients as either high- or low-risk. The NRI for baseline CRP in ASCOT was weak and nonsignificant. By contrast, the NRI for coronary artery calcium score in Framingham intermediate-risk patients in the Multi-Ethnic Study of Atherosclerosis (MESA) was a robust 0.55, more than two orders of magnitude greater than for CRP in ASCOT, the cardiologist said.
ASCOT is just the latest in a growing number of studies that raise a central question, he added: "Is CRP something we need to be spending our time on?"
So how often does Dr. Lloyd-Jones obtain a CRP measurement in his own clinical practice? "Never," he said in an interview.
Asked to comment, Dr. Christopher Cannon of Brigham and Women’s Hospital, Boston, said his interpretation of the ASCOT results is that in patients who already have a good indication for statin therapy, knowing the baseline CRP level does not provide additional useful information.
"Once you get into places where you should be treating anyway, then CRP isn’t helpful. But in the JUPITER trial they had patients largely without other risk factors, and in that lower-risk group a high baseline CRP picked out those who would benefit from statin therapy," Dr. Cannon explained.
He agreed with Dr. Sever and Dr. Lloyd-Jones that the message from ASCOT regarding the use of on-treatment CRP to titrate statin therapy is that it doesn’t make sense.
Dr. Sever declared that he is a consultant to and is on the speakers bureau for Pfizer, which sponsored the ASCOT trial. Dr. Cannon is also on the speakers bureau for Pfizer. Dr. Lloyd-Jones reported no relevant financial interests.
CHICAGO – Measurement of high-sensitivity C-reactive protein had little to no utility in refining cardiovascular risk assessment beyond that provided by the classic risk factors in a new secondary analysis of the ASCOT trial, throwing into question the biomarker’s appropriate role in clinical practice.
"In the ASCOT–Lipid Lowering Arm, neither baseline nor on-treatment CRP provided any useful information about the efficacy of statin treatment to reduce cardiovascular events beyond LDL cholesterol reduction. These results do not support current proposals to measure CRP in the clinical setting, either to assign statins to individuals on the basis of an elevated CRP alone or to monitor CRP levels as an indicator of the efficacy of statin treatment," Dr. Peter S. Sever said at the annual scientific sessions of the American Heart Association. In ASCOT (the Anglo-Scandinavian Cardiac Outcomes Trial), combining a baseline determination of CRP with a standard Framingham Risk Score did not significantly enhance the ability to predict future cardiovascular disease events beyond that provided by Framingham score alone. And while once patients were on statin therapy, the resultant reduction in LDL was associated with an impressive 55% reduction in cardiovascular events, compared with placebo, the decrease in CRP was not linked to a significant decrease in such events, according to Dr. Sever, professor of clinical pharmacology and therapeutics at Imperial College, London.
ASCOT was a landmark primary prevention trial in which nearly 20,000 hypertensive patients were randomized to one of two antihypertensive regimens, then the 10,305 participants with a total cholesterol level of 250 mg/dL or less were re-randomized to 10 mg/day of atorvastatin (Lipitor) or placebo. Although this was a primary prevention trial, these were high-risk patients with three other cardiovascular risk factors in addition to hypertension and a mean 28% risk of developing cardiovascular disease within the next 10 years based upon their Framingham Risk Score.
The new retrospective ASCOT analysis involved 485 patients who experienced a coronary event or stroke during 3.3 years of follow-up and 1,367 controls who did not. Analyzing the data with use of four different statistical methods, neither baseline CRP nor change in CRP level after 6 months of statin therapy provided any practical information.
"I think our conclusion is fairly clear: In patients with hypertension, they’re on statins. In patients with diabetes, they’re on statins. In patients with stable coronary artery disease, they’re on statins. There’s no additional benefit to be gained from measuring CRP," Dr. Sever said.
Discussant Dr. Donald Lloyd-Jones concurred.
"The ASCOT data are the latest adding to a large body of literature suggesting minimal clinical utility for CRP in risk assessment and decision making for lipid-lowering therapy, and a small, growing, and frankly mixed literature examining the utility of on-treatment CRP levels," observed Dr. Lloyd-Jones, professor of preventive medicine at Northwestern University, Chicago.
In ASCOT, patients with an on-treatment LDL below the median had a reduced cardiovascular event risk regardless of their CRP level, while those with a higher LDL had a higher risk regardless of their CRP level. And among patients with a low on-treatment LDL, having a low CRP was not associated with additional benefit, he noted.
Factoring in baseline CRP resulted in a net reclassification improvement score, or NRI, of 0.005 in ASCOT participants at intermediate risk on the basis of their Framingham score. The NRI is a recently developed statistical measure that has been embraced by preventive medicine specialists because it expresses how useful a novel cardiovascular risk factor is in further defining Framingham intermediate-risk patients as either high- or low-risk. The NRI for baseline CRP in ASCOT was weak and nonsignificant. By contrast, the NRI for coronary artery calcium score in Framingham intermediate-risk patients in the Multi-Ethnic Study of Atherosclerosis (MESA) was a robust 0.55, more than two orders of magnitude greater than for CRP in ASCOT, the cardiologist said.
ASCOT is just the latest in a growing number of studies that raise a central question, he added: "Is CRP something we need to be spending our time on?"
So how often does Dr. Lloyd-Jones obtain a CRP measurement in his own clinical practice? "Never," he said in an interview.
Asked to comment, Dr. Christopher Cannon of Brigham and Women’s Hospital, Boston, said his interpretation of the ASCOT results is that in patients who already have a good indication for statin therapy, knowing the baseline CRP level does not provide additional useful information.
"Once you get into places where you should be treating anyway, then CRP isn’t helpful. But in the JUPITER trial they had patients largely without other risk factors, and in that lower-risk group a high baseline CRP picked out those who would benefit from statin therapy," Dr. Cannon explained.
He agreed with Dr. Sever and Dr. Lloyd-Jones that the message from ASCOT regarding the use of on-treatment CRP to titrate statin therapy is that it doesn’t make sense.
Dr. Sever declared that he is a consultant to and is on the speakers bureau for Pfizer, which sponsored the ASCOT trial. Dr. Cannon is also on the speakers bureau for Pfizer. Dr. Lloyd-Jones reported no relevant financial interests.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
ASCOT: CRP Does Not Improve Upon Standard Framingham Score
CHICAGO – Measurement of high-sensitivity C-reactive protein had little to no utility in refining cardiovascular risk assessment beyond that provided by the classic risk factors in a new secondary analysis of the ASCOT trial, throwing into question the biomarker’s appropriate role in clinical practice.
"In the ASCOT–Lipid Lowering Arm, neither baseline nor on-treatment CRP provided any useful information about the efficacy of statin treatment to reduce cardiovascular events beyond LDL cholesterol reduction. These results do not support current proposals to measure CRP in the clinical setting, either to assign statins to individuals on the basis of an elevated CRP alone or to monitor CRP levels as an indicator of the efficacy of statin treatment," Dr. Peter S. Sever said at the annual scientific sessions of the American Heart Association. In ASCOT (the Anglo-Scandinavian Cardiac Outcomes Trial), combining a baseline determination of CRP with a standard Framingham Risk Score did not significantly enhance the ability to predict future cardiovascular disease events beyond that provided by Framingham score alone. And while once patients were on statin therapy, the resultant reduction in LDL was associated with an impressive 55% reduction in cardiovascular events, compared with placebo, the decrease in CRP was not linked to a significant decrease in such events, according to Dr. Sever, professor of clinical pharmacology and therapeutics at Imperial College, London.
ASCOT was a landmark primary prevention trial in which nearly 20,000 hypertensive patients were randomized to one of two antihypertensive regimens, then the 10,305 participants with a total cholesterol level of 250 mg/dL or less were re-randomized to 10 mg/day of atorvastatin (Lipitor) or placebo. Although this was a primary prevention trial, these were high-risk patients with three other cardiovascular risk factors in addition to hypertension and a mean 28% risk of developing cardiovascular disease within the next 10 years based upon their Framingham Risk Score.
The new retrospective ASCOT analysis involved 485 patients who experienced a coronary event or stroke during 3.3 years of follow-up and 1,367 controls who did not. Analyzing the data with use of four different statistical methods, neither baseline CRP nor change in CRP level after 6 months of statin therapy provided any practical information.
"I think our conclusion is fairly clear: In patients with hypertension, they’re on statins. In patients with diabetes, they’re on statins. In patients with stable coronary artery disease, they’re on statins. There’s no additional benefit to be gained from measuring CRP," Dr. Sever said.
Discussant Dr. Donald Lloyd-Jones concurred.
"The ASCOT data are the latest adding to a large body of literature suggesting minimal clinical utility for CRP in risk assessment and decision making for lipid-lowering therapy, and a small, growing, and frankly mixed literature examining the utility of on-treatment CRP levels," observed Dr. Lloyd-Jones, professor of preventive medicine at Northwestern University, Chicago.
In ASCOT, patients with an on-treatment LDL below the median had a reduced cardiovascular event risk regardless of their CRP level, while those with a higher LDL had a higher risk regardless of their CRP level. And among patients with a low on-treatment LDL, having a low CRP was not associated with additional benefit, he noted.
Factoring in baseline CRP resulted in a net reclassification improvement score, or NRI, of 0.005 in ASCOT participants at intermediate risk on the basis of their Framingham score. The NRI is a recently developed statistical measure that has been embraced by preventive medicine specialists because it expresses how useful a novel cardiovascular risk factor is in further defining Framingham intermediate-risk patients as either high- or low-risk. The NRI for baseline CRP in ASCOT was weak and nonsignificant. By contrast, the NRI for coronary artery calcium score in Framingham intermediate-risk patients in the Multi-Ethnic Study of Atherosclerosis (MESA) was a robust 0.55, more than two orders of magnitude greater than for CRP in ASCOT, the cardiologist said.
ASCOT is just the latest in a growing number of studies that raise a central question, he added: "Is CRP something we need to be spending our time on?"
So how often does Dr. Lloyd-Jones obtain a CRP measurement in his own clinical practice? "Never," he said in an interview.
Asked to comment, Dr. Christopher Cannon of Brigham and Women’s Hospital, Boston, said his interpretation of the ASCOT results is that in patients who already have a good indication for statin therapy, knowing the baseline CRP level does not provide additional useful information.
"Once you get into places where you should be treating anyway, then CRP isn’t helpful. But in the JUPITER trial they had patients largely without other risk factors, and in that lower-risk group a high baseline CRP picked out those who would benefit from statin therapy," Dr. Cannon explained.
He agreed with Dr. Sever and Dr. Lloyd-Jones that the message from ASCOT regarding the use of on-treatment CRP to titrate statin therapy is that it doesn’t make sense.
Dr. Sever declared that he is a consultant to and is on the speakers bureau for Pfizer, which sponsored the ASCOT trial. Dr. Cannon is also on the speakers bureau for Pfizer. Dr. Lloyd-Jones reported no relevant financial interests.
CHICAGO – Measurement of high-sensitivity C-reactive protein had little to no utility in refining cardiovascular risk assessment beyond that provided by the classic risk factors in a new secondary analysis of the ASCOT trial, throwing into question the biomarker’s appropriate role in clinical practice.
"In the ASCOT–Lipid Lowering Arm, neither baseline nor on-treatment CRP provided any useful information about the efficacy of statin treatment to reduce cardiovascular events beyond LDL cholesterol reduction. These results do not support current proposals to measure CRP in the clinical setting, either to assign statins to individuals on the basis of an elevated CRP alone or to monitor CRP levels as an indicator of the efficacy of statin treatment," Dr. Peter S. Sever said at the annual scientific sessions of the American Heart Association. In ASCOT (the Anglo-Scandinavian Cardiac Outcomes Trial), combining a baseline determination of CRP with a standard Framingham Risk Score did not significantly enhance the ability to predict future cardiovascular disease events beyond that provided by Framingham score alone. And while once patients were on statin therapy, the resultant reduction in LDL was associated with an impressive 55% reduction in cardiovascular events, compared with placebo, the decrease in CRP was not linked to a significant decrease in such events, according to Dr. Sever, professor of clinical pharmacology and therapeutics at Imperial College, London.
ASCOT was a landmark primary prevention trial in which nearly 20,000 hypertensive patients were randomized to one of two antihypertensive regimens, then the 10,305 participants with a total cholesterol level of 250 mg/dL or less were re-randomized to 10 mg/day of atorvastatin (Lipitor) or placebo. Although this was a primary prevention trial, these were high-risk patients with three other cardiovascular risk factors in addition to hypertension and a mean 28% risk of developing cardiovascular disease within the next 10 years based upon their Framingham Risk Score.
The new retrospective ASCOT analysis involved 485 patients who experienced a coronary event or stroke during 3.3 years of follow-up and 1,367 controls who did not. Analyzing the data with use of four different statistical methods, neither baseline CRP nor change in CRP level after 6 months of statin therapy provided any practical information.
"I think our conclusion is fairly clear: In patients with hypertension, they’re on statins. In patients with diabetes, they’re on statins. In patients with stable coronary artery disease, they’re on statins. There’s no additional benefit to be gained from measuring CRP," Dr. Sever said.
Discussant Dr. Donald Lloyd-Jones concurred.
"The ASCOT data are the latest adding to a large body of literature suggesting minimal clinical utility for CRP in risk assessment and decision making for lipid-lowering therapy, and a small, growing, and frankly mixed literature examining the utility of on-treatment CRP levels," observed Dr. Lloyd-Jones, professor of preventive medicine at Northwestern University, Chicago.
In ASCOT, patients with an on-treatment LDL below the median had a reduced cardiovascular event risk regardless of their CRP level, while those with a higher LDL had a higher risk regardless of their CRP level. And among patients with a low on-treatment LDL, having a low CRP was not associated with additional benefit, he noted.
Factoring in baseline CRP resulted in a net reclassification improvement score, or NRI, of 0.005 in ASCOT participants at intermediate risk on the basis of their Framingham score. The NRI is a recently developed statistical measure that has been embraced by preventive medicine specialists because it expresses how useful a novel cardiovascular risk factor is in further defining Framingham intermediate-risk patients as either high- or low-risk. The NRI for baseline CRP in ASCOT was weak and nonsignificant. By contrast, the NRI for coronary artery calcium score in Framingham intermediate-risk patients in the Multi-Ethnic Study of Atherosclerosis (MESA) was a robust 0.55, more than two orders of magnitude greater than for CRP in ASCOT, the cardiologist said.
ASCOT is just the latest in a growing number of studies that raise a central question, he added: "Is CRP something we need to be spending our time on?"
So how often does Dr. Lloyd-Jones obtain a CRP measurement in his own clinical practice? "Never," he said in an interview.
Asked to comment, Dr. Christopher Cannon of Brigham and Women’s Hospital, Boston, said his interpretation of the ASCOT results is that in patients who already have a good indication for statin therapy, knowing the baseline CRP level does not provide additional useful information.
"Once you get into places where you should be treating anyway, then CRP isn’t helpful. But in the JUPITER trial they had patients largely without other risk factors, and in that lower-risk group a high baseline CRP picked out those who would benefit from statin therapy," Dr. Cannon explained.
He agreed with Dr. Sever and Dr. Lloyd-Jones that the message from ASCOT regarding the use of on-treatment CRP to titrate statin therapy is that it doesn’t make sense.
Dr. Sever declared that he is a consultant to and is on the speakers bureau for Pfizer, which sponsored the ASCOT trial. Dr. Cannon is also on the speakers bureau for Pfizer. Dr. Lloyd-Jones reported no relevant financial interests.
CHICAGO – Measurement of high-sensitivity C-reactive protein had little to no utility in refining cardiovascular risk assessment beyond that provided by the classic risk factors in a new secondary analysis of the ASCOT trial, throwing into question the biomarker’s appropriate role in clinical practice.
"In the ASCOT–Lipid Lowering Arm, neither baseline nor on-treatment CRP provided any useful information about the efficacy of statin treatment to reduce cardiovascular events beyond LDL cholesterol reduction. These results do not support current proposals to measure CRP in the clinical setting, either to assign statins to individuals on the basis of an elevated CRP alone or to monitor CRP levels as an indicator of the efficacy of statin treatment," Dr. Peter S. Sever said at the annual scientific sessions of the American Heart Association. In ASCOT (the Anglo-Scandinavian Cardiac Outcomes Trial), combining a baseline determination of CRP with a standard Framingham Risk Score did not significantly enhance the ability to predict future cardiovascular disease events beyond that provided by Framingham score alone. And while once patients were on statin therapy, the resultant reduction in LDL was associated with an impressive 55% reduction in cardiovascular events, compared with placebo, the decrease in CRP was not linked to a significant decrease in such events, according to Dr. Sever, professor of clinical pharmacology and therapeutics at Imperial College, London.
ASCOT was a landmark primary prevention trial in which nearly 20,000 hypertensive patients were randomized to one of two antihypertensive regimens, then the 10,305 participants with a total cholesterol level of 250 mg/dL or less were re-randomized to 10 mg/day of atorvastatin (Lipitor) or placebo. Although this was a primary prevention trial, these were high-risk patients with three other cardiovascular risk factors in addition to hypertension and a mean 28% risk of developing cardiovascular disease within the next 10 years based upon their Framingham Risk Score.
The new retrospective ASCOT analysis involved 485 patients who experienced a coronary event or stroke during 3.3 years of follow-up and 1,367 controls who did not. Analyzing the data with use of four different statistical methods, neither baseline CRP nor change in CRP level after 6 months of statin therapy provided any practical information.
"I think our conclusion is fairly clear: In patients with hypertension, they’re on statins. In patients with diabetes, they’re on statins. In patients with stable coronary artery disease, they’re on statins. There’s no additional benefit to be gained from measuring CRP," Dr. Sever said.
Discussant Dr. Donald Lloyd-Jones concurred.
"The ASCOT data are the latest adding to a large body of literature suggesting minimal clinical utility for CRP in risk assessment and decision making for lipid-lowering therapy, and a small, growing, and frankly mixed literature examining the utility of on-treatment CRP levels," observed Dr. Lloyd-Jones, professor of preventive medicine at Northwestern University, Chicago.
In ASCOT, patients with an on-treatment LDL below the median had a reduced cardiovascular event risk regardless of their CRP level, while those with a higher LDL had a higher risk regardless of their CRP level. And among patients with a low on-treatment LDL, having a low CRP was not associated with additional benefit, he noted.
Factoring in baseline CRP resulted in a net reclassification improvement score, or NRI, of 0.005 in ASCOT participants at intermediate risk on the basis of their Framingham score. The NRI is a recently developed statistical measure that has been embraced by preventive medicine specialists because it expresses how useful a novel cardiovascular risk factor is in further defining Framingham intermediate-risk patients as either high- or low-risk. The NRI for baseline CRP in ASCOT was weak and nonsignificant. By contrast, the NRI for coronary artery calcium score in Framingham intermediate-risk patients in the Multi-Ethnic Study of Atherosclerosis (MESA) was a robust 0.55, more than two orders of magnitude greater than for CRP in ASCOT, the cardiologist said.
ASCOT is just the latest in a growing number of studies that raise a central question, he added: "Is CRP something we need to be spending our time on?"
So how often does Dr. Lloyd-Jones obtain a CRP measurement in his own clinical practice? "Never," he said in an interview.
Asked to comment, Dr. Christopher Cannon of Brigham and Women’s Hospital, Boston, said his interpretation of the ASCOT results is that in patients who already have a good indication for statin therapy, knowing the baseline CRP level does not provide additional useful information.
"Once you get into places where you should be treating anyway, then CRP isn’t helpful. But in the JUPITER trial they had patients largely without other risk factors, and in that lower-risk group a high baseline CRP picked out those who would benefit from statin therapy," Dr. Cannon explained.
He agreed with Dr. Sever and Dr. Lloyd-Jones that the message from ASCOT regarding the use of on-treatment CRP to titrate statin therapy is that it doesn’t make sense.
Dr. Sever declared that he is a consultant to and is on the speakers bureau for Pfizer, which sponsored the ASCOT trial. Dr. Cannon is also on the speakers bureau for Pfizer. Dr. Lloyd-Jones reported no relevant financial interests.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Briakinumab for Psoriasis Impresses in Phase III Trial
GOTHENBURG, SWEDEN – Phase III clinical trial results for briakinumab show high treatment response levels with the passage of time.
In the 52-week M10-255 trial, for example, 317 psoriasis patients were randomized to an investigational interleukin-12 and interleukin-23 inhibitor or to oral methotrexate for a year. The PASI 75 rate (the proportion of patients who showed at least a 75% improvement in scores on the Psoriasis Area and Severity Index), compared with baseline, was 82% at week 24 and 66% at week 52 in the briakinumab arm.
More interestingly, the PASI 90 rate was 64% at week 24 and 60% at week 52. That means that almost everyone who achieved a PASI 75 also had a PASI 90 response. And the PASI 100 rate was also impressive, at 42% by week 24 and 45.5% by week 52, Dr. Kristian Reich reported at a satellite symposium sponsored by Abbott at the congress.
"It appears we have a new pattern of clinical response here. If you are a responding patient, with time there is a tendency to achieve a very high level of response. For me personally, these PASI 90 and 100 rates are a different level of efficacy that I have not seen ... with any other therapy in psoriasis," said Dr. Reich, professor of dermatology at Georg-August University in Göttingen, Germany.
No head-to-head comparative studies have been done pitting briakinumab against other biologic agents for psoriasis. Nevertheless, the 42% PASI 100 rate seen with briakinumab in the M10-255 trial exceeds the week-24 or -28 PASI 100s reported in published trials involving other biologics: a high of 29% with ustekinumab at 90 mg, 26% with infliximab, 22% with adalimumab, and a low of 19% with ustekinumab at 45 mg, Dr. Reich said.
Psoriasis patients in the M10-255 trial had a mean baseline PASI score of 18, and a 19-year history of the disease. They were randomized to briakinumab at 200 mg at weeks 0 and 4, then 100 mg once every 4 weeks, or to oral methotrexate with folic acid.
In all, 72% of patients in the methotrexate arm discontinued the drug by week 52, with lack of efficacy the reason for 80% of dropouts. Only 6% of subjects discontinued methotrexate because of adverse events. This was the same percentage of patients who dropped out of briakinumab therapy because of adverse events; another 14% did so because of lack of efficacy.
NAPSI (Nail Psoriasis Severity Index) scores decreased by 58% and 78% at 24 and 52 weeks, respectively, in the briakinumab group, compared with 37% and 39% with methotrexate.
Through 1 year of follow-up, the safety profile was quite similar in the two study arms, with the exception of a higher rate of diarrhea with briakinumab – 9.7% compared with 3.7% with methotrexate – and a twofold higher rate of nausea in the methotrexate arm, he noted.
An interim safety analysis from the open-label extensions of all phase III trials in the briakinumab development program, involving 2,298 treated patients, indicated that the incidence of malignancy was 1.4 cases per 100 patient-years, whereas any serious infection occurred at a rate of 1.0 per 100 patient-years. The rates of these and other adverse events are what one would expect from an anti-interleukin-12/23 drug, and are on balance quite acceptable, said Dr. Reich.
He disclosed that he has served as a consultant and speaker for and/or participated in clinical trials sponsored by Abbott (which funded the M10-255 trial), Biogen Idec, Bristol-Myers Squibb Co., Centocor, Merck Serono, Schering-Plough, UCB, and Wyeth.
GOTHENBURG, SWEDEN – Phase III clinical trial results for briakinumab show high treatment response levels with the passage of time.
In the 52-week M10-255 trial, for example, 317 psoriasis patients were randomized to an investigational interleukin-12 and interleukin-23 inhibitor or to oral methotrexate for a year. The PASI 75 rate (the proportion of patients who showed at least a 75% improvement in scores on the Psoriasis Area and Severity Index), compared with baseline, was 82% at week 24 and 66% at week 52 in the briakinumab arm.
More interestingly, the PASI 90 rate was 64% at week 24 and 60% at week 52. That means that almost everyone who achieved a PASI 75 also had a PASI 90 response. And the PASI 100 rate was also impressive, at 42% by week 24 and 45.5% by week 52, Dr. Kristian Reich reported at a satellite symposium sponsored by Abbott at the congress.
"It appears we have a new pattern of clinical response here. If you are a responding patient, with time there is a tendency to achieve a very high level of response. For me personally, these PASI 90 and 100 rates are a different level of efficacy that I have not seen ... with any other therapy in psoriasis," said Dr. Reich, professor of dermatology at Georg-August University in Göttingen, Germany.
No head-to-head comparative studies have been done pitting briakinumab against other biologic agents for psoriasis. Nevertheless, the 42% PASI 100 rate seen with briakinumab in the M10-255 trial exceeds the week-24 or -28 PASI 100s reported in published trials involving other biologics: a high of 29% with ustekinumab at 90 mg, 26% with infliximab, 22% with adalimumab, and a low of 19% with ustekinumab at 45 mg, Dr. Reich said.
Psoriasis patients in the M10-255 trial had a mean baseline PASI score of 18, and a 19-year history of the disease. They were randomized to briakinumab at 200 mg at weeks 0 and 4, then 100 mg once every 4 weeks, or to oral methotrexate with folic acid.
In all, 72% of patients in the methotrexate arm discontinued the drug by week 52, with lack of efficacy the reason for 80% of dropouts. Only 6% of subjects discontinued methotrexate because of adverse events. This was the same percentage of patients who dropped out of briakinumab therapy because of adverse events; another 14% did so because of lack of efficacy.
NAPSI (Nail Psoriasis Severity Index) scores decreased by 58% and 78% at 24 and 52 weeks, respectively, in the briakinumab group, compared with 37% and 39% with methotrexate.
Through 1 year of follow-up, the safety profile was quite similar in the two study arms, with the exception of a higher rate of diarrhea with briakinumab – 9.7% compared with 3.7% with methotrexate – and a twofold higher rate of nausea in the methotrexate arm, he noted.
An interim safety analysis from the open-label extensions of all phase III trials in the briakinumab development program, involving 2,298 treated patients, indicated that the incidence of malignancy was 1.4 cases per 100 patient-years, whereas any serious infection occurred at a rate of 1.0 per 100 patient-years. The rates of these and other adverse events are what one would expect from an anti-interleukin-12/23 drug, and are on balance quite acceptable, said Dr. Reich.
He disclosed that he has served as a consultant and speaker for and/or participated in clinical trials sponsored by Abbott (which funded the M10-255 trial), Biogen Idec, Bristol-Myers Squibb Co., Centocor, Merck Serono, Schering-Plough, UCB, and Wyeth.
GOTHENBURG, SWEDEN – Phase III clinical trial results for briakinumab show high treatment response levels with the passage of time.
In the 52-week M10-255 trial, for example, 317 psoriasis patients were randomized to an investigational interleukin-12 and interleukin-23 inhibitor or to oral methotrexate for a year. The PASI 75 rate (the proportion of patients who showed at least a 75% improvement in scores on the Psoriasis Area and Severity Index), compared with baseline, was 82% at week 24 and 66% at week 52 in the briakinumab arm.
More interestingly, the PASI 90 rate was 64% at week 24 and 60% at week 52. That means that almost everyone who achieved a PASI 75 also had a PASI 90 response. And the PASI 100 rate was also impressive, at 42% by week 24 and 45.5% by week 52, Dr. Kristian Reich reported at a satellite symposium sponsored by Abbott at the congress.
"It appears we have a new pattern of clinical response here. If you are a responding patient, with time there is a tendency to achieve a very high level of response. For me personally, these PASI 90 and 100 rates are a different level of efficacy that I have not seen ... with any other therapy in psoriasis," said Dr. Reich, professor of dermatology at Georg-August University in Göttingen, Germany.
No head-to-head comparative studies have been done pitting briakinumab against other biologic agents for psoriasis. Nevertheless, the 42% PASI 100 rate seen with briakinumab in the M10-255 trial exceeds the week-24 or -28 PASI 100s reported in published trials involving other biologics: a high of 29% with ustekinumab at 90 mg, 26% with infliximab, 22% with adalimumab, and a low of 19% with ustekinumab at 45 mg, Dr. Reich said.
Psoriasis patients in the M10-255 trial had a mean baseline PASI score of 18, and a 19-year history of the disease. They were randomized to briakinumab at 200 mg at weeks 0 and 4, then 100 mg once every 4 weeks, or to oral methotrexate with folic acid.
In all, 72% of patients in the methotrexate arm discontinued the drug by week 52, with lack of efficacy the reason for 80% of dropouts. Only 6% of subjects discontinued methotrexate because of adverse events. This was the same percentage of patients who dropped out of briakinumab therapy because of adverse events; another 14% did so because of lack of efficacy.
NAPSI (Nail Psoriasis Severity Index) scores decreased by 58% and 78% at 24 and 52 weeks, respectively, in the briakinumab group, compared with 37% and 39% with methotrexate.
Through 1 year of follow-up, the safety profile was quite similar in the two study arms, with the exception of a higher rate of diarrhea with briakinumab – 9.7% compared with 3.7% with methotrexate – and a twofold higher rate of nausea in the methotrexate arm, he noted.
An interim safety analysis from the open-label extensions of all phase III trials in the briakinumab development program, involving 2,298 treated patients, indicated that the incidence of malignancy was 1.4 cases per 100 patient-years, whereas any serious infection occurred at a rate of 1.0 per 100 patient-years. The rates of these and other adverse events are what one would expect from an anti-interleukin-12/23 drug, and are on balance quite acceptable, said Dr. Reich.
He disclosed that he has served as a consultant and speaker for and/or participated in clinical trials sponsored by Abbott (which funded the M10-255 trial), Biogen Idec, Bristol-Myers Squibb Co., Centocor, Merck Serono, Schering-Plough, UCB, and Wyeth.
FROM THE ANNUAL CONGRESS OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
Major Finding: The PASI 90 rate was 64% at week 24 and 60% at week 52 with briakinumab.
Data Source: Psoriasis patients (n = 317) in the M10-255 trial had a mean baseline PASI score of 18, and a 19-year history of the disease.
Disclosures: Dr. Reich disclosed that he has served as a consultant and speaker for and/or participated in clinical trials sponsored by Abbott (which funded the M10-255 trial), Biogen Idec, Bristol-Myers Squibb, Centocor, Merck Serono, Schering-Plough, UCB, and Wyeth.
Risk of First-Ever Depression Rises During Perimenopause
DENVER – Women with no history of depression are at sharply increased risk of first-ever, clinically significant depressive symptoms during the menopausal transition, three major prospective longitudinal studies have shown.
It’s a situation that requires clinicians to have their depression-detection radar fully powered up, according to Dr. Nanette F. Santoro.

"A very important thing to remember is that this type of depression is new to these women. This is their first episode. They may come into our offices clearly in distress, but they don’t have the vocabulary to tell you they’re depressed because they don’t know what that feels like," she said in a plenary lecture at the annual meeting of the American Society for Reproductive Medicine.
Dr. Santoro presented highlights from the ongoing observational Study of Women’s Health Across the Nation (SWAN), in which 3,302 African American, white, Hispanic, Japanese, and Chinese women at seven U.S. sites have been evaluated annually since their enrollment during 1996-1997 at age 42-52.
"We’re now in our 14th year of SWAN, and we’re still cranking out data," noted Dr. Santoro, professor and chair of the department of obstetrics and gynecology at the University of Colorado, Denver.
At baseline, when the women were premenopausal, 23% had clinically relevant depressive symptoms, as defined by a score of 16 or more on the Center for Epidemiologic Studies Depression Scale (CES-D).
The other 77% of women, those with low baseline CES-D scores and no lifetime history of depression, were hit particularly hard by depressed mood symptoms in the menopausal transition. In a multivariate analysis, a woman with a CES-D of less than 16 at baseline had a 30% higher odds of having a CES-D score of 16 or greater when she was in the early perimenopausal period, which is marked by increased menstrual irregularity but at least one menses within the past 3 months.
Women in the late perimenopausal period, as defined by 3-11 months of amenorrhea, had an adjusted 73% increased odds of significant depressive symptoms, compared with those who were still premenopausal. The risk was elevated even more in women with significant vasomotor symptoms (J. Affect. Disord. 2007;103:267-72).
"That late perimenopause is just a bummer. It almost doubles the risk," Dr. Santoro observed.
The risk declines slightly to a 63% increased odds of significant depressive symptoms during the postmenopausal period.
Hormone therapy, which was used by 20% of the SWAN women, may have conferred modest relief from depressive symptoms, as HT users had a peak 64% increase in the odds of a CES-D of 16 or more during the menopausal transition.
The risk of new-onset depressive symptoms during menopause was independent of demographic, psychosocial, and behavioral factors, as well as comorbid conditions, all of which were factored into the multivariate regression analysis. Chinese women had half the risk of depressive symptoms compared with white women, but the risk in the other ethnic groups didn’t vary significantly from that in the white women.
Similar results have been reported from the Harvard Study of Moods and Cycles, in which Dr. Lee S. Cohen and his coworkers studied a cohort of premenopausal women with no lifetime history of major depression. The investigators found that for these women, who were less racially diverse than the SWAN women, entry into perimenopause was associated with a doubled likelihood of developing significant depressive symptoms compared with similar-age women who remained premenopausal.
As in SWAN, the risk of depression was even greater in women with self-reported significant hot flashes and night sweats. In the Harvard longitudinal study, the use of HT didn’t affect the risk of developing depressive symptoms; there was a suggestion that it might have lessened the risk of severe depression arising during the menopausal transition, although the patient numbers were too small to draw firm conclusions (Arch. Gen. Psychiatry 2006;63:385-90).
Investigators at the University of Pennsylvania, Philadelphia, reported that women with no history of depression at enrollment in their longitudinal study were 4.3-fold more likely to post high CES-D scores during the menopausal transition than when they were premenopausal. Formal diagnosis of a depressive disorder was 2.5 times more likely to occur in the menopausal transition (Arch. Gen. Psychiatry 2006;63:375-82).
The Harvard group speculated that the increased risk for developing a first episode of depression when entering the perimenopause could be due in part to the marked sleep disruption caused by hot flashes, and/or to sensitivity to abrupt changes in the reproductive hormone milieu.
In line with that hypothesis, the SWAN investigators recently reported that higher testosterone levels appear to contribute to depressive symptoms arising during the menopausal transition. No other hormones were associated with a CES-D score of 16 or more (Arch. Gen. Psychiatry 2010;67:598-607).
The SWAN study is funded by the National Institutes of Health. Dr. Santoro said he had no relevant financial conflicts of interest.
DENVER – Women with no history of depression are at sharply increased risk of first-ever, clinically significant depressive symptoms during the menopausal transition, three major prospective longitudinal studies have shown.
It’s a situation that requires clinicians to have their depression-detection radar fully powered up, according to Dr. Nanette F. Santoro.
"A very important thing to remember is that this type of depression is new to these women. This is their first episode. They may come into our offices clearly in distress, but they don’t have the vocabulary to tell you they’re depressed because they don’t know what that feels like," she said in a plenary lecture at the annual meeting of the American Society for Reproductive Medicine.
Dr. Santoro presented highlights from the ongoing observational Study of Women’s Health Across the Nation (SWAN), in which 3,302 African American, white, Hispanic, Japanese, and Chinese women at seven U.S. sites have been evaluated annually since their enrollment during 1996-1997 at age 42-52.
"We’re now in our 14th year of SWAN, and we’re still cranking out data," noted Dr. Santoro, professor and chair of the department of obstetrics and gynecology at the University of Colorado, Denver.
At baseline, when the women were premenopausal, 23% had clinically relevant depressive symptoms, as defined by a score of 16 or more on the Center for Epidemiologic Studies Depression Scale (CES-D).
The other 77% of women, those with low baseline CES-D scores and no lifetime history of depression, were hit particularly hard by depressed mood symptoms in the menopausal transition. In a multivariate analysis, a woman with a CES-D of less than 16 at baseline had a 30% higher odds of having a CES-D score of 16 or greater when she was in the early perimenopausal period, which is marked by increased menstrual irregularity but at least one menses within the past 3 months.
Women in the late perimenopausal period, as defined by 3-11 months of amenorrhea, had an adjusted 73% increased odds of significant depressive symptoms, compared with those who were still premenopausal. The risk was elevated even more in women with significant vasomotor symptoms (J. Affect. Disord. 2007;103:267-72).
"That late perimenopause is just a bummer. It almost doubles the risk," Dr. Santoro observed.
The risk declines slightly to a 63% increased odds of significant depressive symptoms during the postmenopausal period.
Hormone therapy, which was used by 20% of the SWAN women, may have conferred modest relief from depressive symptoms, as HT users had a peak 64% increase in the odds of a CES-D of 16 or more during the menopausal transition.
The risk of new-onset depressive symptoms during menopause was independent of demographic, psychosocial, and behavioral factors, as well as comorbid conditions, all of which were factored into the multivariate regression analysis. Chinese women had half the risk of depressive symptoms compared with white women, but the risk in the other ethnic groups didn’t vary significantly from that in the white women.
Similar results have been reported from the Harvard Study of Moods and Cycles, in which Dr. Lee S. Cohen and his coworkers studied a cohort of premenopausal women with no lifetime history of major depression. The investigators found that for these women, who were less racially diverse than the SWAN women, entry into perimenopause was associated with a doubled likelihood of developing significant depressive symptoms compared with similar-age women who remained premenopausal.
As in SWAN, the risk of depression was even greater in women with self-reported significant hot flashes and night sweats. In the Harvard longitudinal study, the use of HT didn’t affect the risk of developing depressive symptoms; there was a suggestion that it might have lessened the risk of severe depression arising during the menopausal transition, although the patient numbers were too small to draw firm conclusions (Arch. Gen. Psychiatry 2006;63:385-90).
Investigators at the University of Pennsylvania, Philadelphia, reported that women with no history of depression at enrollment in their longitudinal study were 4.3-fold more likely to post high CES-D scores during the menopausal transition than when they were premenopausal. Formal diagnosis of a depressive disorder was 2.5 times more likely to occur in the menopausal transition (Arch. Gen. Psychiatry 2006;63:375-82).
The Harvard group speculated that the increased risk for developing a first episode of depression when entering the perimenopause could be due in part to the marked sleep disruption caused by hot flashes, and/or to sensitivity to abrupt changes in the reproductive hormone milieu.
In line with that hypothesis, the SWAN investigators recently reported that higher testosterone levels appear to contribute to depressive symptoms arising during the menopausal transition. No other hormones were associated with a CES-D score of 16 or more (Arch. Gen. Psychiatry 2010;67:598-607).
The SWAN study is funded by the National Institutes of Health. Dr. Santoro said he had no relevant financial conflicts of interest.
DENVER – Women with no history of depression are at sharply increased risk of first-ever, clinically significant depressive symptoms during the menopausal transition, three major prospective longitudinal studies have shown.
It’s a situation that requires clinicians to have their depression-detection radar fully powered up, according to Dr. Nanette F. Santoro.
"A very important thing to remember is that this type of depression is new to these women. This is their first episode. They may come into our offices clearly in distress, but they don’t have the vocabulary to tell you they’re depressed because they don’t know what that feels like," she said in a plenary lecture at the annual meeting of the American Society for Reproductive Medicine.
Dr. Santoro presented highlights from the ongoing observational Study of Women’s Health Across the Nation (SWAN), in which 3,302 African American, white, Hispanic, Japanese, and Chinese women at seven U.S. sites have been evaluated annually since their enrollment during 1996-1997 at age 42-52.
"We’re now in our 14th year of SWAN, and we’re still cranking out data," noted Dr. Santoro, professor and chair of the department of obstetrics and gynecology at the University of Colorado, Denver.
At baseline, when the women were premenopausal, 23% had clinically relevant depressive symptoms, as defined by a score of 16 or more on the Center for Epidemiologic Studies Depression Scale (CES-D).
The other 77% of women, those with low baseline CES-D scores and no lifetime history of depression, were hit particularly hard by depressed mood symptoms in the menopausal transition. In a multivariate analysis, a woman with a CES-D of less than 16 at baseline had a 30% higher odds of having a CES-D score of 16 or greater when she was in the early perimenopausal period, which is marked by increased menstrual irregularity but at least one menses within the past 3 months.
Women in the late perimenopausal period, as defined by 3-11 months of amenorrhea, had an adjusted 73% increased odds of significant depressive symptoms, compared with those who were still premenopausal. The risk was elevated even more in women with significant vasomotor symptoms (J. Affect. Disord. 2007;103:267-72).
"That late perimenopause is just a bummer. It almost doubles the risk," Dr. Santoro observed.
The risk declines slightly to a 63% increased odds of significant depressive symptoms during the postmenopausal period.
Hormone therapy, which was used by 20% of the SWAN women, may have conferred modest relief from depressive symptoms, as HT users had a peak 64% increase in the odds of a CES-D of 16 or more during the menopausal transition.
The risk of new-onset depressive symptoms during menopause was independent of demographic, psychosocial, and behavioral factors, as well as comorbid conditions, all of which were factored into the multivariate regression analysis. Chinese women had half the risk of depressive symptoms compared with white women, but the risk in the other ethnic groups didn’t vary significantly from that in the white women.
Similar results have been reported from the Harvard Study of Moods and Cycles, in which Dr. Lee S. Cohen and his coworkers studied a cohort of premenopausal women with no lifetime history of major depression. The investigators found that for these women, who were less racially diverse than the SWAN women, entry into perimenopause was associated with a doubled likelihood of developing significant depressive symptoms compared with similar-age women who remained premenopausal.
As in SWAN, the risk of depression was even greater in women with self-reported significant hot flashes and night sweats. In the Harvard longitudinal study, the use of HT didn’t affect the risk of developing depressive symptoms; there was a suggestion that it might have lessened the risk of severe depression arising during the menopausal transition, although the patient numbers were too small to draw firm conclusions (Arch. Gen. Psychiatry 2006;63:385-90).
Investigators at the University of Pennsylvania, Philadelphia, reported that women with no history of depression at enrollment in their longitudinal study were 4.3-fold more likely to post high CES-D scores during the menopausal transition than when they were premenopausal. Formal diagnosis of a depressive disorder was 2.5 times more likely to occur in the menopausal transition (Arch. Gen. Psychiatry 2006;63:375-82).
The Harvard group speculated that the increased risk for developing a first episode of depression when entering the perimenopause could be due in part to the marked sleep disruption caused by hot flashes, and/or to sensitivity to abrupt changes in the reproductive hormone milieu.
In line with that hypothesis, the SWAN investigators recently reported that higher testosterone levels appear to contribute to depressive symptoms arising during the menopausal transition. No other hormones were associated with a CES-D score of 16 or more (Arch. Gen. Psychiatry 2010;67:598-607).
The SWAN study is funded by the National Institutes of Health. Dr. Santoro said he had no relevant financial conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE
Renal Denervation Slashed Blood Pressure in Drug-Resistant Hypertensives
CHICAGO – Deactivating the renal sympathetic nerves via a catheter-based procedure achieved impressively large and durable reductions in blood pressure in the first randomized, multicenter trial of the novel therapy in patients with resistant hypertension.
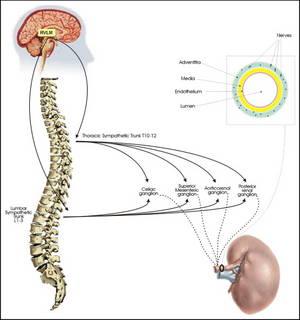
The renal sympathetic denervation procedure was straightforward and safe, and the sizeable reduction in blood pressure was maintained throughout the scheduled 6 months of follow-up. In patients treated earlier outside of the clinical trial, blood pressures have continued to drift slightly lower through 2.5 years of follow-up, raising the possibility that this procedure provides once-and-for-all treatment, Dr. Murray D. Esler said at the annual scientific sessions of the American Heart Association.
The primary endpoint in the 106-patient Symplicity HTN-2 trial was office-based blood pressure at 6 months. There was a mean 32/12 mm Hg reduction from a baseline of 178/96 mm Hg in patients in the renal denervation arm, all of whom remained on multidrug therapy. Home and ambulatory blood pressure readings followed suit, although the measured reductions were less robust.
In contrast, blood pressure was unchanged over time in patients in the control arm, even though they remained on optimally dosed multidrug antihypertensive therapy, according to Dr. Esler, associate director of the Baker IDI Heart and Diabetes Institute in Melbourne, Australia.
The encouraging results of Symplicity HTN-2 open the door to an entirely new approach to resistant hypertension, one that sidesteps the expense of lifelong therapy with multiple antihypertensive agents, the inherent limited efficacy of the drugs currently available, and compliance issues that commonly arise with multidrug therapy for a silent disease, he added.
Renal denervation therapy could be widely applicable. Roughly 15%-20% of hypertensive patients have resistant hypertension as defined by blood pressures remaining above target in spite of optimal doses of at least three antihypertensive agents, one of which should be a diuretic. This was the population enrolled in Symplicity HTN-2; in fact, nearly two-thirds of participants were on at least five antihypertensive drugs.
Future trials will evaluate renal denervation in milder forms of essential hypertension, as well as in other diseases involving activation of renal sympathetic outflow, including heart failure, cirrhosis with ascites, and chronic kidney disease.
The denervation procedure entails using standard endovascular technique to pass a proprietary radiofrequency catheter via femoral access into the renal artery lumen. The operator then delivers four to six bursts of low-power radiofrequency energy along the length of each renal artery to ablate the renal nerves, located in the adventitia of the renal artery. This results in decreased whole-body noradrenaline spillover, increased renal blood flow, and reduced plasma renin activity, the investigators noted in a published report released online simultaneously with Dr. Elser’s presentation (Lancet Nov. 17, 2010 [doi: 10.1016/S0140-6736(10)62039-9]).
No serious procedure-related complications occurred. Renal function remained unchanged during follow-up, even in patients who had mild to moderate renal impairment at baseline.
Blood pressure reductions of the magnitude achieved in Symplicity HTN-2 could, in theory, be expected to result in roughly 60% decreases in stroke and MI rates in these sorts of very-high-risk patients, according to Dr. Elser and others.
He said that the inspiration for the development of catheter-based renal denervation came from the earlier success of nonselective surgical sympathetectomy as a means of lowering blood pressure in severe hypertension in the days before modern antihypertensive drugs.
"In the current era, drugs blocking the renin-angiotensin system have moved to the fore and the sympathetic nervous system has kind of been swept into the shadows," he noted.
A U.S. clinical trial of the device therapy will begin early next year. Meanwhile, the therapy is being introduced into clinical practice in Australia and Europe. Dr. Elser said he would not be surprised to see a turf battle between interventional cardiologists and interventional radiologists over who performs the procedure.
Discussant Dr. Suzanne Oparil said, "This is an extremely important study. It has a number of great strengths and the potential to really revolutionize the way we deal with treatment-resistant hypertension."
The absence of adverse events, given the fact that 24 centers were involved in the trial, is a remarkable finding that speaks to the procedure’s safety and ease, observed Dr. Oparil, professor of medicine, physiology, and biophysics and director of the vascular biology and hypertension program at the University of Alabama, Birmingham. However, several limitations of the study were of concern, particularly the fact that only 17% of patients were being treated with aldosterone antagonists, which could be an indication that the patient population was not truly drug resistant.
Dr. Esler disclosed that he has received consulting fees and travel expenses from Ardian, which sponsored the Symplicity HTN-2 trial. Dr. Oparil is a consultant to Amylin, Boehringer-Ingelheim, Daiichi Sankyo, Forest Laboratories, Merck, NicOx, Novartis, and VIVUS.
CHICAGO – Deactivating the renal sympathetic nerves via a catheter-based procedure achieved impressively large and durable reductions in blood pressure in the first randomized, multicenter trial of the novel therapy in patients with resistant hypertension.
The renal sympathetic denervation procedure was straightforward and safe, and the sizeable reduction in blood pressure was maintained throughout the scheduled 6 months of follow-up. In patients treated earlier outside of the clinical trial, blood pressures have continued to drift slightly lower through 2.5 years of follow-up, raising the possibility that this procedure provides once-and-for-all treatment, Dr. Murray D. Esler said at the annual scientific sessions of the American Heart Association.
The primary endpoint in the 106-patient Symplicity HTN-2 trial was office-based blood pressure at 6 months. There was a mean 32/12 mm Hg reduction from a baseline of 178/96 mm Hg in patients in the renal denervation arm, all of whom remained on multidrug therapy. Home and ambulatory blood pressure readings followed suit, although the measured reductions were less robust.
In contrast, blood pressure was unchanged over time in patients in the control arm, even though they remained on optimally dosed multidrug antihypertensive therapy, according to Dr. Esler, associate director of the Baker IDI Heart and Diabetes Institute in Melbourne, Australia.
The encouraging results of Symplicity HTN-2 open the door to an entirely new approach to resistant hypertension, one that sidesteps the expense of lifelong therapy with multiple antihypertensive agents, the inherent limited efficacy of the drugs currently available, and compliance issues that commonly arise with multidrug therapy for a silent disease, he added.
Renal denervation therapy could be widely applicable. Roughly 15%-20% of hypertensive patients have resistant hypertension as defined by blood pressures remaining above target in spite of optimal doses of at least three antihypertensive agents, one of which should be a diuretic. This was the population enrolled in Symplicity HTN-2; in fact, nearly two-thirds of participants were on at least five antihypertensive drugs.
Future trials will evaluate renal denervation in milder forms of essential hypertension, as well as in other diseases involving activation of renal sympathetic outflow, including heart failure, cirrhosis with ascites, and chronic kidney disease.
The denervation procedure entails using standard endovascular technique to pass a proprietary radiofrequency catheter via femoral access into the renal artery lumen. The operator then delivers four to six bursts of low-power radiofrequency energy along the length of each renal artery to ablate the renal nerves, located in the adventitia of the renal artery. This results in decreased whole-body noradrenaline spillover, increased renal blood flow, and reduced plasma renin activity, the investigators noted in a published report released online simultaneously with Dr. Elser’s presentation (Lancet Nov. 17, 2010 [doi: 10.1016/S0140-6736(10)62039-9]).
No serious procedure-related complications occurred. Renal function remained unchanged during follow-up, even in patients who had mild to moderate renal impairment at baseline.
Blood pressure reductions of the magnitude achieved in Symplicity HTN-2 could, in theory, be expected to result in roughly 60% decreases in stroke and MI rates in these sorts of very-high-risk patients, according to Dr. Elser and others.
He said that the inspiration for the development of catheter-based renal denervation came from the earlier success of nonselective surgical sympathetectomy as a means of lowering blood pressure in severe hypertension in the days before modern antihypertensive drugs.
"In the current era, drugs blocking the renin-angiotensin system have moved to the fore and the sympathetic nervous system has kind of been swept into the shadows," he noted.
A U.S. clinical trial of the device therapy will begin early next year. Meanwhile, the therapy is being introduced into clinical practice in Australia and Europe. Dr. Elser said he would not be surprised to see a turf battle between interventional cardiologists and interventional radiologists over who performs the procedure.
Discussant Dr. Suzanne Oparil said, "This is an extremely important study. It has a number of great strengths and the potential to really revolutionize the way we deal with treatment-resistant hypertension."
The absence of adverse events, given the fact that 24 centers were involved in the trial, is a remarkable finding that speaks to the procedure’s safety and ease, observed Dr. Oparil, professor of medicine, physiology, and biophysics and director of the vascular biology and hypertension program at the University of Alabama, Birmingham. However, several limitations of the study were of concern, particularly the fact that only 17% of patients were being treated with aldosterone antagonists, which could be an indication that the patient population was not truly drug resistant.
Dr. Esler disclosed that he has received consulting fees and travel expenses from Ardian, which sponsored the Symplicity HTN-2 trial. Dr. Oparil is a consultant to Amylin, Boehringer-Ingelheim, Daiichi Sankyo, Forest Laboratories, Merck, NicOx, Novartis, and VIVUS.
CHICAGO – Deactivating the renal sympathetic nerves via a catheter-based procedure achieved impressively large and durable reductions in blood pressure in the first randomized, multicenter trial of the novel therapy in patients with resistant hypertension.
The renal sympathetic denervation procedure was straightforward and safe, and the sizeable reduction in blood pressure was maintained throughout the scheduled 6 months of follow-up. In patients treated earlier outside of the clinical trial, blood pressures have continued to drift slightly lower through 2.5 years of follow-up, raising the possibility that this procedure provides once-and-for-all treatment, Dr. Murray D. Esler said at the annual scientific sessions of the American Heart Association.
The primary endpoint in the 106-patient Symplicity HTN-2 trial was office-based blood pressure at 6 months. There was a mean 32/12 mm Hg reduction from a baseline of 178/96 mm Hg in patients in the renal denervation arm, all of whom remained on multidrug therapy. Home and ambulatory blood pressure readings followed suit, although the measured reductions were less robust.
In contrast, blood pressure was unchanged over time in patients in the control arm, even though they remained on optimally dosed multidrug antihypertensive therapy, according to Dr. Esler, associate director of the Baker IDI Heart and Diabetes Institute in Melbourne, Australia.
The encouraging results of Symplicity HTN-2 open the door to an entirely new approach to resistant hypertension, one that sidesteps the expense of lifelong therapy with multiple antihypertensive agents, the inherent limited efficacy of the drugs currently available, and compliance issues that commonly arise with multidrug therapy for a silent disease, he added.
Renal denervation therapy could be widely applicable. Roughly 15%-20% of hypertensive patients have resistant hypertension as defined by blood pressures remaining above target in spite of optimal doses of at least three antihypertensive agents, one of which should be a diuretic. This was the population enrolled in Symplicity HTN-2; in fact, nearly two-thirds of participants were on at least five antihypertensive drugs.
Future trials will evaluate renal denervation in milder forms of essential hypertension, as well as in other diseases involving activation of renal sympathetic outflow, including heart failure, cirrhosis with ascites, and chronic kidney disease.
The denervation procedure entails using standard endovascular technique to pass a proprietary radiofrequency catheter via femoral access into the renal artery lumen. The operator then delivers four to six bursts of low-power radiofrequency energy along the length of each renal artery to ablate the renal nerves, located in the adventitia of the renal artery. This results in decreased whole-body noradrenaline spillover, increased renal blood flow, and reduced plasma renin activity, the investigators noted in a published report released online simultaneously with Dr. Elser’s presentation (Lancet Nov. 17, 2010 [doi: 10.1016/S0140-6736(10)62039-9]).
No serious procedure-related complications occurred. Renal function remained unchanged during follow-up, even in patients who had mild to moderate renal impairment at baseline.
Blood pressure reductions of the magnitude achieved in Symplicity HTN-2 could, in theory, be expected to result in roughly 60% decreases in stroke and MI rates in these sorts of very-high-risk patients, according to Dr. Elser and others.
He said that the inspiration for the development of catheter-based renal denervation came from the earlier success of nonselective surgical sympathetectomy as a means of lowering blood pressure in severe hypertension in the days before modern antihypertensive drugs.
"In the current era, drugs blocking the renin-angiotensin system have moved to the fore and the sympathetic nervous system has kind of been swept into the shadows," he noted.
A U.S. clinical trial of the device therapy will begin early next year. Meanwhile, the therapy is being introduced into clinical practice in Australia and Europe. Dr. Elser said he would not be surprised to see a turf battle between interventional cardiologists and interventional radiologists over who performs the procedure.
Discussant Dr. Suzanne Oparil said, "This is an extremely important study. It has a number of great strengths and the potential to really revolutionize the way we deal with treatment-resistant hypertension."
The absence of adverse events, given the fact that 24 centers were involved in the trial, is a remarkable finding that speaks to the procedure’s safety and ease, observed Dr. Oparil, professor of medicine, physiology, and biophysics and director of the vascular biology and hypertension program at the University of Alabama, Birmingham. However, several limitations of the study were of concern, particularly the fact that only 17% of patients were being treated with aldosterone antagonists, which could be an indication that the patient population was not truly drug resistant.
Dr. Esler disclosed that he has received consulting fees and travel expenses from Ardian, which sponsored the Symplicity HTN-2 trial. Dr. Oparil is a consultant to Amylin, Boehringer-Ingelheim, Daiichi Sankyo, Forest Laboratories, Merck, NicOx, Novartis, and VIVUS.