User login
International survey sheds new light on adult atopic dermatitis
GENEVA – The prevalence of atopic dermatitis (AD) among adults ages 18-65 years varies across countries in North America, Europe, and Asia, and regionally within those countries as well, according to an unprecedented eight-country survey of roughly 90,000 subjects.
The industry-supported web-based survey included roughly 20,000 U.S. respondents along with 10,000 from each of seven other countries: Italy, Spain, France, Germany, United Kingdom, Canada, and Japan. Most prior studies have focused on pediatric AD, Laurent Eckert, PhD, observed at the annual congress of the European Academy of Dermatology and Venereology.
The prevalence of adult AD was highest in Italy (8.1%) and Spain (7.2%), followed by the United States (4.9%), France (3.6%), Canada (3.5%), United Kingdom (2.5%), Germany (2.2%), and Japan (2.1%). Other investigators had previously reported a lower figure for the United States: 3.2% versus the 4.9% found in the new international survey, noted Dr. Eckert, an epidemiologist at Sanofi in Chilly-Mazarin, France.
The United States was the only country in which the prevalence of AD was higher in men than women, albeit by the narrow margin of 5.1% versus 4.9%. The rate was similar in men and women in the United Kingdom, and significantly greater in women in the other six participating countries. For example, the male:female prevalence ratio in Canada was 3.0%:4:0%, while in Italy it was 6.0%:10.0%.
Some degree of regional variability in the prevalence of AD was seen within each country. The biggest regional differences were seen within Italy and France. “The regional variability within Italy was in accord with a previous study that showed higher rates in Mediterranean regions relative to those in a more northern, continental climate,” Dr. Eckert said.
Two-stage criteria had to be met to label a respondent as having AD in this web-based survey. The participant had to be positive on the basis of the U.K. Working Party’s diagnostic criteria for AD (Br J Dermatol. 1994 Sep;131[3]:406-16), the key element of which is an affirmative answer to the question, “In the past 12 months, did you ever have an itchy rash that was coming and going for at least 6 months?” And the subject also had to self-report having received a physician diagnosis of AD.
Dr. Eckert and his coinvestigators employed three different validated methods of assessing AD severity: Physician Global Assessment, the Patient-Oriented Eczema Measure, and the Patient-Oriented Scoring AD. These three methods yielded wide variability in the distribution of individuals labeled as having severe AD. The Physician Global Assessment categorized 3%-8% of adult AD patients as having severe disease, depending upon the country, while the Patient-Oriented Eczema Measure yielded a 9%-17% prevalence of severe disease, and Patient-Oriented Scoring AD rated 12%-21% of adults with AD as having severe disease.
“The variability is severity distribution based on the outcome measure used suggests a need for standardization of severity assessment,” Dr. Eckert said.
In most countries, the peak prevalence of adult AD occurred in the 35- to 44-year-old age group, then fell steadily. In the United States, however, the peak came a decade earlier: The prevalence was 4.5% among 18- to 24-year-olds, it was 7.2% in the 25-34 age bracket, and it declined to 6.0% at age 35-44, 3.8% at 45-54, and 2.7% among 55- to 65-year-olds.
Dr. Eckert was also first author of a new study of the burden of adult AD in the United States. The study, which analyzed health care resource utilization data from the 2013 National Health and Wellness Survey, showed that the cost burden of adult AD was comparable to that of psoriasis, although adults with AD had more emergency department visits and higher rates of asthma and other atopic comorbidities (J Am Acad Dermatol. 2017 Oct 7. pii: S0190-9622[17]32181-3. doi: 10.1016/j.jaad.2017.08.002. [Epub ahead of print]).
The international survey was supported by Sanofi, which markets dupilumab with Regeneron.
GENEVA – The prevalence of atopic dermatitis (AD) among adults ages 18-65 years varies across countries in North America, Europe, and Asia, and regionally within those countries as well, according to an unprecedented eight-country survey of roughly 90,000 subjects.
The industry-supported web-based survey included roughly 20,000 U.S. respondents along with 10,000 from each of seven other countries: Italy, Spain, France, Germany, United Kingdom, Canada, and Japan. Most prior studies have focused on pediatric AD, Laurent Eckert, PhD, observed at the annual congress of the European Academy of Dermatology and Venereology.
The prevalence of adult AD was highest in Italy (8.1%) and Spain (7.2%), followed by the United States (4.9%), France (3.6%), Canada (3.5%), United Kingdom (2.5%), Germany (2.2%), and Japan (2.1%). Other investigators had previously reported a lower figure for the United States: 3.2% versus the 4.9% found in the new international survey, noted Dr. Eckert, an epidemiologist at Sanofi in Chilly-Mazarin, France.
The United States was the only country in which the prevalence of AD was higher in men than women, albeit by the narrow margin of 5.1% versus 4.9%. The rate was similar in men and women in the United Kingdom, and significantly greater in women in the other six participating countries. For example, the male:female prevalence ratio in Canada was 3.0%:4:0%, while in Italy it was 6.0%:10.0%.
Some degree of regional variability in the prevalence of AD was seen within each country. The biggest regional differences were seen within Italy and France. “The regional variability within Italy was in accord with a previous study that showed higher rates in Mediterranean regions relative to those in a more northern, continental climate,” Dr. Eckert said.
Two-stage criteria had to be met to label a respondent as having AD in this web-based survey. The participant had to be positive on the basis of the U.K. Working Party’s diagnostic criteria for AD (Br J Dermatol. 1994 Sep;131[3]:406-16), the key element of which is an affirmative answer to the question, “In the past 12 months, did you ever have an itchy rash that was coming and going for at least 6 months?” And the subject also had to self-report having received a physician diagnosis of AD.
Dr. Eckert and his coinvestigators employed three different validated methods of assessing AD severity: Physician Global Assessment, the Patient-Oriented Eczema Measure, and the Patient-Oriented Scoring AD. These three methods yielded wide variability in the distribution of individuals labeled as having severe AD. The Physician Global Assessment categorized 3%-8% of adult AD patients as having severe disease, depending upon the country, while the Patient-Oriented Eczema Measure yielded a 9%-17% prevalence of severe disease, and Patient-Oriented Scoring AD rated 12%-21% of adults with AD as having severe disease.
“The variability is severity distribution based on the outcome measure used suggests a need for standardization of severity assessment,” Dr. Eckert said.
In most countries, the peak prevalence of adult AD occurred in the 35- to 44-year-old age group, then fell steadily. In the United States, however, the peak came a decade earlier: The prevalence was 4.5% among 18- to 24-year-olds, it was 7.2% in the 25-34 age bracket, and it declined to 6.0% at age 35-44, 3.8% at 45-54, and 2.7% among 55- to 65-year-olds.
Dr. Eckert was also first author of a new study of the burden of adult AD in the United States. The study, which analyzed health care resource utilization data from the 2013 National Health and Wellness Survey, showed that the cost burden of adult AD was comparable to that of psoriasis, although adults with AD had more emergency department visits and higher rates of asthma and other atopic comorbidities (J Am Acad Dermatol. 2017 Oct 7. pii: S0190-9622[17]32181-3. doi: 10.1016/j.jaad.2017.08.002. [Epub ahead of print]).
The international survey was supported by Sanofi, which markets dupilumab with Regeneron.
GENEVA – The prevalence of atopic dermatitis (AD) among adults ages 18-65 years varies across countries in North America, Europe, and Asia, and regionally within those countries as well, according to an unprecedented eight-country survey of roughly 90,000 subjects.
The industry-supported web-based survey included roughly 20,000 U.S. respondents along with 10,000 from each of seven other countries: Italy, Spain, France, Germany, United Kingdom, Canada, and Japan. Most prior studies have focused on pediatric AD, Laurent Eckert, PhD, observed at the annual congress of the European Academy of Dermatology and Venereology.
The prevalence of adult AD was highest in Italy (8.1%) and Spain (7.2%), followed by the United States (4.9%), France (3.6%), Canada (3.5%), United Kingdom (2.5%), Germany (2.2%), and Japan (2.1%). Other investigators had previously reported a lower figure for the United States: 3.2% versus the 4.9% found in the new international survey, noted Dr. Eckert, an epidemiologist at Sanofi in Chilly-Mazarin, France.
The United States was the only country in which the prevalence of AD was higher in men than women, albeit by the narrow margin of 5.1% versus 4.9%. The rate was similar in men and women in the United Kingdom, and significantly greater in women in the other six participating countries. For example, the male:female prevalence ratio in Canada was 3.0%:4:0%, while in Italy it was 6.0%:10.0%.
Some degree of regional variability in the prevalence of AD was seen within each country. The biggest regional differences were seen within Italy and France. “The regional variability within Italy was in accord with a previous study that showed higher rates in Mediterranean regions relative to those in a more northern, continental climate,” Dr. Eckert said.
Two-stage criteria had to be met to label a respondent as having AD in this web-based survey. The participant had to be positive on the basis of the U.K. Working Party’s diagnostic criteria for AD (Br J Dermatol. 1994 Sep;131[3]:406-16), the key element of which is an affirmative answer to the question, “In the past 12 months, did you ever have an itchy rash that was coming and going for at least 6 months?” And the subject also had to self-report having received a physician diagnosis of AD.
Dr. Eckert and his coinvestigators employed three different validated methods of assessing AD severity: Physician Global Assessment, the Patient-Oriented Eczema Measure, and the Patient-Oriented Scoring AD. These three methods yielded wide variability in the distribution of individuals labeled as having severe AD. The Physician Global Assessment categorized 3%-8% of adult AD patients as having severe disease, depending upon the country, while the Patient-Oriented Eczema Measure yielded a 9%-17% prevalence of severe disease, and Patient-Oriented Scoring AD rated 12%-21% of adults with AD as having severe disease.
“The variability is severity distribution based on the outcome measure used suggests a need for standardization of severity assessment,” Dr. Eckert said.
In most countries, the peak prevalence of adult AD occurred in the 35- to 44-year-old age group, then fell steadily. In the United States, however, the peak came a decade earlier: The prevalence was 4.5% among 18- to 24-year-olds, it was 7.2% in the 25-34 age bracket, and it declined to 6.0% at age 35-44, 3.8% at 45-54, and 2.7% among 55- to 65-year-olds.
Dr. Eckert was also first author of a new study of the burden of adult AD in the United States. The study, which analyzed health care resource utilization data from the 2013 National Health and Wellness Survey, showed that the cost burden of adult AD was comparable to that of psoriasis, although adults with AD had more emergency department visits and higher rates of asthma and other atopic comorbidities (J Am Acad Dermatol. 2017 Oct 7. pii: S0190-9622[17]32181-3. doi: 10.1016/j.jaad.2017.08.002. [Epub ahead of print]).
The international survey was supported by Sanofi, which markets dupilumab with Regeneron.
AT THE EADV CONGRESS
Key clinical point:
Major finding: The prevalence of atopic dermatitis among adults ages 18-65 ranged from a high of 8.1% in Italy to 2.1% in Japan.
Data source: A web-based survey of roughly 90,000 adults in the United States and seven other countries in North America, Europe, and Asia.
Disclosures: The survey was supported by Sanofi and presented by a company employee.
ACC survey: Burnout pervasive in cardiologists
ANAHEIM, CALIF. – A disturbingly high 27% of U.S. cardiologists reported currently feeling burnout in the American College of Cardiology’s third Professional Life Survey, Laxmi S. Mehta, MD, said at the American Heart Association scientific sessions.
A gender gap existed: The prevalence of burnout was 29% greater among female cardiologists than their male counterparts, by a margin of 31%-24%.

“These are the doctors who are taking care of people’s hearts, and we know that when you’re burned out, there are higher rates of medical errors and the quality of care is poorer. So this is problematic,” she said in an interview.
Burnout had a negative effect on career satisfaction: While 94% of cardiologists in the nonburnout group professed they were satisfied with their career, that was the case for only 74% of cardiologists who felt burnout. Just 56% percent of the burnout group said they would recommend cardiology as a career, compared with 80% of the practitioners who felt no burnout.
The 2015 ACC survey was completed by 2,313 U.S. cardiologists, 964 of whom were women. The first round of results, which focused on career satisfaction and racial and gender discrimination in the workplace, have been published (J Am Coll Cardiol. 2017 Jan 31;69[4]:452-62). The survey included the validated 10-question Mini Z burnout assessment, the results of which were the focus of the new analysis.
The 27% of cardiologists in the burnout group fell into three subcategories, the largest of which comprised those who reported feeling at least one burnout symptom of physical or mental exhaustion. Those who said their burnout symptoms don’t go away and that they think about their work frustrations frequently made up a smaller group. Just a few percent of survey participants fell into the completely burned out category.
Only 51% of the burnout group were satisfied with their financial compensation, compared with 68% of the nonburnout group. Sixty-one percent of the burnout group felt they were treated fairly at their job, as did 86% of the cardiologists who felt burnout. Half of the cardiologists with burnout reported experiencing past discrimination, compared with 37% of the nonburnout group. And 40% of the burnout group felt their family responsibilities hindered career advancement, a sentiment expressed by 22% of the nonburnout group.
EMR “pajama time” cited as a major burden
Two-thirds of cardiologists with constant burnout symptoms or complete burnout cited excessive time spent completing their electronic medical records as a significant contributing factor.
“The electronic medical record ends up taking over our personal time,” according to Dr. Mehta. “We call it ‘pajama time’ because many of us are doing the charts or responding to patients at midnight, on vacation, at meetings like this. There is no separation, and that’s a problem.”
What can be done to reduce burnout
The 2015 Professional Life Survey was the third one in 20 years. Compared with the earlier two, the most recent survey painted a picture of an aging workforce that is less likely to be in private practice. The survey – the first one to assess burnout within the specialty – was carried out by the ACC Women in Cardiology Leadership Council. Armed with the survey results, the ACC leadership is now in the process of redefining the organization’s mission statement to incorporate a new emphasis on providing for physician health and well-being in addition to the more traditional goals of improving the quality and reducing the cost of care.
“Many cardiologists are working a lot harder than they used to, with less personal time. We need to work on mechanisms to reduce burnout by reducing the burdens put on them. The survey data help because they show the cardiology profession, and hopefully hospital administrators, the importance of making a better work environment. That’s the hope,” Dr. Mehta said.
She reported having no financial conflicts of interest regarding the survey.
ANAHEIM, CALIF. – A disturbingly high 27% of U.S. cardiologists reported currently feeling burnout in the American College of Cardiology’s third Professional Life Survey, Laxmi S. Mehta, MD, said at the American Heart Association scientific sessions.
A gender gap existed: The prevalence of burnout was 29% greater among female cardiologists than their male counterparts, by a margin of 31%-24%.
“These are the doctors who are taking care of people’s hearts, and we know that when you’re burned out, there are higher rates of medical errors and the quality of care is poorer. So this is problematic,” she said in an interview.
Burnout had a negative effect on career satisfaction: While 94% of cardiologists in the nonburnout group professed they were satisfied with their career, that was the case for only 74% of cardiologists who felt burnout. Just 56% percent of the burnout group said they would recommend cardiology as a career, compared with 80% of the practitioners who felt no burnout.
The 2015 ACC survey was completed by 2,313 U.S. cardiologists, 964 of whom were women. The first round of results, which focused on career satisfaction and racial and gender discrimination in the workplace, have been published (J Am Coll Cardiol. 2017 Jan 31;69[4]:452-62). The survey included the validated 10-question Mini Z burnout assessment, the results of which were the focus of the new analysis.
The 27% of cardiologists in the burnout group fell into three subcategories, the largest of which comprised those who reported feeling at least one burnout symptom of physical or mental exhaustion. Those who said their burnout symptoms don’t go away and that they think about their work frustrations frequently made up a smaller group. Just a few percent of survey participants fell into the completely burned out category.
Only 51% of the burnout group were satisfied with their financial compensation, compared with 68% of the nonburnout group. Sixty-one percent of the burnout group felt they were treated fairly at their job, as did 86% of the cardiologists who felt burnout. Half of the cardiologists with burnout reported experiencing past discrimination, compared with 37% of the nonburnout group. And 40% of the burnout group felt their family responsibilities hindered career advancement, a sentiment expressed by 22% of the nonburnout group.
EMR “pajama time” cited as a major burden
Two-thirds of cardiologists with constant burnout symptoms or complete burnout cited excessive time spent completing their electronic medical records as a significant contributing factor.
“The electronic medical record ends up taking over our personal time,” according to Dr. Mehta. “We call it ‘pajama time’ because many of us are doing the charts or responding to patients at midnight, on vacation, at meetings like this. There is no separation, and that’s a problem.”
What can be done to reduce burnout
The 2015 Professional Life Survey was the third one in 20 years. Compared with the earlier two, the most recent survey painted a picture of an aging workforce that is less likely to be in private practice. The survey – the first one to assess burnout within the specialty – was carried out by the ACC Women in Cardiology Leadership Council. Armed with the survey results, the ACC leadership is now in the process of redefining the organization’s mission statement to incorporate a new emphasis on providing for physician health and well-being in addition to the more traditional goals of improving the quality and reducing the cost of care.
“Many cardiologists are working a lot harder than they used to, with less personal time. We need to work on mechanisms to reduce burnout by reducing the burdens put on them. The survey data help because they show the cardiology profession, and hopefully hospital administrators, the importance of making a better work environment. That’s the hope,” Dr. Mehta said.
She reported having no financial conflicts of interest regarding the survey.
ANAHEIM, CALIF. – A disturbingly high 27% of U.S. cardiologists reported currently feeling burnout in the American College of Cardiology’s third Professional Life Survey, Laxmi S. Mehta, MD, said at the American Heart Association scientific sessions.
A gender gap existed: The prevalence of burnout was 29% greater among female cardiologists than their male counterparts, by a margin of 31%-24%.
“These are the doctors who are taking care of people’s hearts, and we know that when you’re burned out, there are higher rates of medical errors and the quality of care is poorer. So this is problematic,” she said in an interview.
Burnout had a negative effect on career satisfaction: While 94% of cardiologists in the nonburnout group professed they were satisfied with their career, that was the case for only 74% of cardiologists who felt burnout. Just 56% percent of the burnout group said they would recommend cardiology as a career, compared with 80% of the practitioners who felt no burnout.
The 2015 ACC survey was completed by 2,313 U.S. cardiologists, 964 of whom were women. The first round of results, which focused on career satisfaction and racial and gender discrimination in the workplace, have been published (J Am Coll Cardiol. 2017 Jan 31;69[4]:452-62). The survey included the validated 10-question Mini Z burnout assessment, the results of which were the focus of the new analysis.
The 27% of cardiologists in the burnout group fell into three subcategories, the largest of which comprised those who reported feeling at least one burnout symptom of physical or mental exhaustion. Those who said their burnout symptoms don’t go away and that they think about their work frustrations frequently made up a smaller group. Just a few percent of survey participants fell into the completely burned out category.
Only 51% of the burnout group were satisfied with their financial compensation, compared with 68% of the nonburnout group. Sixty-one percent of the burnout group felt they were treated fairly at their job, as did 86% of the cardiologists who felt burnout. Half of the cardiologists with burnout reported experiencing past discrimination, compared with 37% of the nonburnout group. And 40% of the burnout group felt their family responsibilities hindered career advancement, a sentiment expressed by 22% of the nonburnout group.
EMR “pajama time” cited as a major burden
Two-thirds of cardiologists with constant burnout symptoms or complete burnout cited excessive time spent completing their electronic medical records as a significant contributing factor.
“The electronic medical record ends up taking over our personal time,” according to Dr. Mehta. “We call it ‘pajama time’ because many of us are doing the charts or responding to patients at midnight, on vacation, at meetings like this. There is no separation, and that’s a problem.”
What can be done to reduce burnout
The 2015 Professional Life Survey was the third one in 20 years. Compared with the earlier two, the most recent survey painted a picture of an aging workforce that is less likely to be in private practice. The survey – the first one to assess burnout within the specialty – was carried out by the ACC Women in Cardiology Leadership Council. Armed with the survey results, the ACC leadership is now in the process of redefining the organization’s mission statement to incorporate a new emphasis on providing for physician health and well-being in addition to the more traditional goals of improving the quality and reducing the cost of care.
“Many cardiologists are working a lot harder than they used to, with less personal time. We need to work on mechanisms to reduce burnout by reducing the burdens put on them. The survey data help because they show the cardiology profession, and hopefully hospital administrators, the importance of making a better work environment. That’s the hope,” Dr. Mehta said.
She reported having no financial conflicts of interest regarding the survey.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: There is a noticeable gender gap in U.S. cardiologist burnout.
Data source: This survey of 2,313 U.S. cardiologists addressed burnout and career satisfaction within the profession.
Disclosures: The presenter reported having no financial conflicts of interest regarding the survey, conducted by the American College of Cardiology.
Schizophrenia’s silent epidemic: Iatrogenic sexual dysfunction
PARIS – Many psychiatrists have no inkling of how often the antipsychotic agents they prescribe cause hyperprolactinemia-related sexual dysfunction, or the serious negative consequences these common side effects have on quality of life and treatment adherence, Ángel L. Montejo, MD, PhD, declared at the annual congress of the European College of Neuropsychopharmacology.
Psychiatrists are largely uninformed about these matters, because for the most part, they avoid talking with their schizophrenia patients about their sexual activity or inquiring about sexual dysfunction. And they don’t perform the physical examinations that might reveal tell-tale stigmatizing gynecomastia or galactorrhea, according to Dr. Montejo, professor of psychiatry at the University of Salamanca (Spain).

The consensus report includes recommendations for the detection and management of the full range of manifestations of iatrogenic hyperprolactinemia, including osteoporosis and hip fracture, hypogonadism, premature menopause, cardiovascular disease, breast and endometrial cancer, and immunologic disorders.
However, the most common expression of antipsychotic-related hyperprolactinemia is sexual dysfunction, and that’s what Dr. Montejo focused on. This is an issue that directly relates to clinical outcomes. The literature shows that roughly 36% of male and 19% of female schizophrenia patients either stop taking their medication because of its sexual side effects, which include decreased libido, erectile difficulty, vaginal dryness, and anorgasmia, or are thinking about doing so. At least two in three schizophrenia patients engage in some sort of sexual activity. Sixty percent of patients say that having a sexual life is important to them. Yet 73% of psychiatrists in one survey indicated that they don’t interview their patients about their sexual relations.
“If sexual activity is good for you, why isn’t it good for your patients? We’re talking about love, about human relationships. Having a sexual and emotional life can help patients get the best outcomes,” said Dr. Montejo.
“If you don’t ask about sexual dysfunction, your patients won’t tell. Therefore, you may not see it, but your patients will experience it. They know the difference between their sexual life before treatment and during treatment,” he continued.
The incidence of sexual dysfunction in patients on antipsychotic therapy is a function of the agent they are on. Iatrogenic hyperprolactinemia is a consequence of intense blockade of dopamine D2 receptors. The most potent antipsychotic dopamine D2 receptor antagonists are risperidone and paliperidone, followed by haloperidol and most other first-generation antipsychotics.
A normal prolactin level is less than 25 ng/mL in women and less than 20 ng/mL in men. Endocrinologists divide hyperprolactinemia into three categories: mild hyperprolactinemia is a level of 25-50 ng/mL, moderate is 51-100 ng/mL, and severe is anything over 100 ng/mL.
In one study, 44% of patients on oral risperidone at a mean dose of 4.9 mg/day had moderate and 23% had severe hyperprolactinemia; in patients on the injectable long-acting formulation of the drug at a mean dose of 46.2 mg/month, 23% of patients had moderate and 31% had severe hyperprolactinemia. Patients on oral paliperidone at a mean dose of 8.5 mg/day had a 45% prevalence of moderate and an 18% rate of severe hyperprolactinemia, while 40% of those on long-acting injectable paliperidone at a mean of 104 mg/month had moderate and another 40% had severe hyperprolactinemia.
Sixty to 80% of patients on risperidone or paliperidone experience hyperprolactinemia-induced sexual dysfunction. At the other end of the spectrum is the prolactin-sparing antipsychotic aripiprazole, which is associated with sexual dysfunction in about 5% of treated patients. In a meta-analysis, the other prolactin-sparing antipsychotics included ziprasidone, with a 10% rate, quetiapine at 12%, and olanzapine with a 20% rate.
Screening tests for sexual dysfunction
Psychiatrists who are uncomfortable asking patients about sexual dysfunction or don’t want to take the time to do so have other good options. Four easy-to-use, validated instruments are available for free online: the four-question Arizona Sexual Experiences Scale; the Change in Sexual Function Questionnaire, or CSFQ; the Sex Effects Scale, or SexFX; and the Psychotropic-Related Sexual Dysfunction Questionnaire (PRSexDQ-SALSEX).
Managing antipsychotic-induced hyperprolactinemia
The Spanish consensus panel recommended that before psychiatrists prescribe an antipsychotic, they should always explain to patients their risk of antipsychotic-related hyperprolactinemia and make an assessment of personal and family history of risk factors for its possible downstream consequences, including osteoporosis and cancer. And Dr. Montejo stressed that clinicians must “always, always, always” get a baseline serum prolactin measurement, to be repeated after increasing the drug dosage, changing antipsychotics, or upon development of symptoms of hyperprolactinemia.
When a patient’s prolactin level climbs above 50 ng/mL or symptoms of hyperprolactinemia arise, the preferred strategy is to switch to a prolactin-sparing antipsychotic. Most of the alternative options are unsatisfactory. For example, waiting for a sexual side effect to pass is pointless, because it won’t happen spontaneously. A drug holiday undermines compliance. Reducing the antipsychotic dose increases the risk of relapse.
And as for prescribing adjunctive dopamine agonist therapy, well: “Adding a dopamine agonist is not the first step. It should be one of the last steps, because it greatly increases the odds of worsening psychosis,” Dr. Montejo said.
If switching to a different antipsychotic is not possible, the expert panel recommended add-on aripiprazole, accompanied if possible by a downward dose adjustment of the offending antipsychotic. This is an effective way to lower elevated serum prolactin levels.
It’s appropriate to order a lumbar spine and proximal femur bone mineral density measurement in patients on antipsychotic agents if they are older than age 65, have had amenorrhea for at least 6 months, experienced menopause before age 35, have a body mass index below 19 kg/m2, or are experiencing any symptoms of hyperprolactinemia, including sexual dysfunction, according to the Spanish consensus algorithm.
Dr. Montejo reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies.
PARIS – Many psychiatrists have no inkling of how often the antipsychotic agents they prescribe cause hyperprolactinemia-related sexual dysfunction, or the serious negative consequences these common side effects have on quality of life and treatment adherence, Ángel L. Montejo, MD, PhD, declared at the annual congress of the European College of Neuropsychopharmacology.
Psychiatrists are largely uninformed about these matters, because for the most part, they avoid talking with their schizophrenia patients about their sexual activity or inquiring about sexual dysfunction. And they don’t perform the physical examinations that might reveal tell-tale stigmatizing gynecomastia or galactorrhea, according to Dr. Montejo, professor of psychiatry at the University of Salamanca (Spain).
The consensus report includes recommendations for the detection and management of the full range of manifestations of iatrogenic hyperprolactinemia, including osteoporosis and hip fracture, hypogonadism, premature menopause, cardiovascular disease, breast and endometrial cancer, and immunologic disorders.
However, the most common expression of antipsychotic-related hyperprolactinemia is sexual dysfunction, and that’s what Dr. Montejo focused on. This is an issue that directly relates to clinical outcomes. The literature shows that roughly 36% of male and 19% of female schizophrenia patients either stop taking their medication because of its sexual side effects, which include decreased libido, erectile difficulty, vaginal dryness, and anorgasmia, or are thinking about doing so. At least two in three schizophrenia patients engage in some sort of sexual activity. Sixty percent of patients say that having a sexual life is important to them. Yet 73% of psychiatrists in one survey indicated that they don’t interview their patients about their sexual relations.
“If sexual activity is good for you, why isn’t it good for your patients? We’re talking about love, about human relationships. Having a sexual and emotional life can help patients get the best outcomes,” said Dr. Montejo.
“If you don’t ask about sexual dysfunction, your patients won’t tell. Therefore, you may not see it, but your patients will experience it. They know the difference between their sexual life before treatment and during treatment,” he continued.
The incidence of sexual dysfunction in patients on antipsychotic therapy is a function of the agent they are on. Iatrogenic hyperprolactinemia is a consequence of intense blockade of dopamine D2 receptors. The most potent antipsychotic dopamine D2 receptor antagonists are risperidone and paliperidone, followed by haloperidol and most other first-generation antipsychotics.
A normal prolactin level is less than 25 ng/mL in women and less than 20 ng/mL in men. Endocrinologists divide hyperprolactinemia into three categories: mild hyperprolactinemia is a level of 25-50 ng/mL, moderate is 51-100 ng/mL, and severe is anything over 100 ng/mL.
In one study, 44% of patients on oral risperidone at a mean dose of 4.9 mg/day had moderate and 23% had severe hyperprolactinemia; in patients on the injectable long-acting formulation of the drug at a mean dose of 46.2 mg/month, 23% of patients had moderate and 31% had severe hyperprolactinemia. Patients on oral paliperidone at a mean dose of 8.5 mg/day had a 45% prevalence of moderate and an 18% rate of severe hyperprolactinemia, while 40% of those on long-acting injectable paliperidone at a mean of 104 mg/month had moderate and another 40% had severe hyperprolactinemia.
Sixty to 80% of patients on risperidone or paliperidone experience hyperprolactinemia-induced sexual dysfunction. At the other end of the spectrum is the prolactin-sparing antipsychotic aripiprazole, which is associated with sexual dysfunction in about 5% of treated patients. In a meta-analysis, the other prolactin-sparing antipsychotics included ziprasidone, with a 10% rate, quetiapine at 12%, and olanzapine with a 20% rate.
Screening tests for sexual dysfunction
Psychiatrists who are uncomfortable asking patients about sexual dysfunction or don’t want to take the time to do so have other good options. Four easy-to-use, validated instruments are available for free online: the four-question Arizona Sexual Experiences Scale; the Change in Sexual Function Questionnaire, or CSFQ; the Sex Effects Scale, or SexFX; and the Psychotropic-Related Sexual Dysfunction Questionnaire (PRSexDQ-SALSEX).
Managing antipsychotic-induced hyperprolactinemia
The Spanish consensus panel recommended that before psychiatrists prescribe an antipsychotic, they should always explain to patients their risk of antipsychotic-related hyperprolactinemia and make an assessment of personal and family history of risk factors for its possible downstream consequences, including osteoporosis and cancer. And Dr. Montejo stressed that clinicians must “always, always, always” get a baseline serum prolactin measurement, to be repeated after increasing the drug dosage, changing antipsychotics, or upon development of symptoms of hyperprolactinemia.
When a patient’s prolactin level climbs above 50 ng/mL or symptoms of hyperprolactinemia arise, the preferred strategy is to switch to a prolactin-sparing antipsychotic. Most of the alternative options are unsatisfactory. For example, waiting for a sexual side effect to pass is pointless, because it won’t happen spontaneously. A drug holiday undermines compliance. Reducing the antipsychotic dose increases the risk of relapse.
And as for prescribing adjunctive dopamine agonist therapy, well: “Adding a dopamine agonist is not the first step. It should be one of the last steps, because it greatly increases the odds of worsening psychosis,” Dr. Montejo said.
If switching to a different antipsychotic is not possible, the expert panel recommended add-on aripiprazole, accompanied if possible by a downward dose adjustment of the offending antipsychotic. This is an effective way to lower elevated serum prolactin levels.
It’s appropriate to order a lumbar spine and proximal femur bone mineral density measurement in patients on antipsychotic agents if they are older than age 65, have had amenorrhea for at least 6 months, experienced menopause before age 35, have a body mass index below 19 kg/m2, or are experiencing any symptoms of hyperprolactinemia, including sexual dysfunction, according to the Spanish consensus algorithm.
Dr. Montejo reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies.
PARIS – Many psychiatrists have no inkling of how often the antipsychotic agents they prescribe cause hyperprolactinemia-related sexual dysfunction, or the serious negative consequences these common side effects have on quality of life and treatment adherence, Ángel L. Montejo, MD, PhD, declared at the annual congress of the European College of Neuropsychopharmacology.
Psychiatrists are largely uninformed about these matters, because for the most part, they avoid talking with their schizophrenia patients about their sexual activity or inquiring about sexual dysfunction. And they don’t perform the physical examinations that might reveal tell-tale stigmatizing gynecomastia or galactorrhea, according to Dr. Montejo, professor of psychiatry at the University of Salamanca (Spain).
The consensus report includes recommendations for the detection and management of the full range of manifestations of iatrogenic hyperprolactinemia, including osteoporosis and hip fracture, hypogonadism, premature menopause, cardiovascular disease, breast and endometrial cancer, and immunologic disorders.
However, the most common expression of antipsychotic-related hyperprolactinemia is sexual dysfunction, and that’s what Dr. Montejo focused on. This is an issue that directly relates to clinical outcomes. The literature shows that roughly 36% of male and 19% of female schizophrenia patients either stop taking their medication because of its sexual side effects, which include decreased libido, erectile difficulty, vaginal dryness, and anorgasmia, or are thinking about doing so. At least two in three schizophrenia patients engage in some sort of sexual activity. Sixty percent of patients say that having a sexual life is important to them. Yet 73% of psychiatrists in one survey indicated that they don’t interview their patients about their sexual relations.
“If sexual activity is good for you, why isn’t it good for your patients? We’re talking about love, about human relationships. Having a sexual and emotional life can help patients get the best outcomes,” said Dr. Montejo.
“If you don’t ask about sexual dysfunction, your patients won’t tell. Therefore, you may not see it, but your patients will experience it. They know the difference between their sexual life before treatment and during treatment,” he continued.
The incidence of sexual dysfunction in patients on antipsychotic therapy is a function of the agent they are on. Iatrogenic hyperprolactinemia is a consequence of intense blockade of dopamine D2 receptors. The most potent antipsychotic dopamine D2 receptor antagonists are risperidone and paliperidone, followed by haloperidol and most other first-generation antipsychotics.
A normal prolactin level is less than 25 ng/mL in women and less than 20 ng/mL in men. Endocrinologists divide hyperprolactinemia into three categories: mild hyperprolactinemia is a level of 25-50 ng/mL, moderate is 51-100 ng/mL, and severe is anything over 100 ng/mL.
In one study, 44% of patients on oral risperidone at a mean dose of 4.9 mg/day had moderate and 23% had severe hyperprolactinemia; in patients on the injectable long-acting formulation of the drug at a mean dose of 46.2 mg/month, 23% of patients had moderate and 31% had severe hyperprolactinemia. Patients on oral paliperidone at a mean dose of 8.5 mg/day had a 45% prevalence of moderate and an 18% rate of severe hyperprolactinemia, while 40% of those on long-acting injectable paliperidone at a mean of 104 mg/month had moderate and another 40% had severe hyperprolactinemia.
Sixty to 80% of patients on risperidone or paliperidone experience hyperprolactinemia-induced sexual dysfunction. At the other end of the spectrum is the prolactin-sparing antipsychotic aripiprazole, which is associated with sexual dysfunction in about 5% of treated patients. In a meta-analysis, the other prolactin-sparing antipsychotics included ziprasidone, with a 10% rate, quetiapine at 12%, and olanzapine with a 20% rate.
Screening tests for sexual dysfunction
Psychiatrists who are uncomfortable asking patients about sexual dysfunction or don’t want to take the time to do so have other good options. Four easy-to-use, validated instruments are available for free online: the four-question Arizona Sexual Experiences Scale; the Change in Sexual Function Questionnaire, or CSFQ; the Sex Effects Scale, or SexFX; and the Psychotropic-Related Sexual Dysfunction Questionnaire (PRSexDQ-SALSEX).
Managing antipsychotic-induced hyperprolactinemia
The Spanish consensus panel recommended that before psychiatrists prescribe an antipsychotic, they should always explain to patients their risk of antipsychotic-related hyperprolactinemia and make an assessment of personal and family history of risk factors for its possible downstream consequences, including osteoporosis and cancer. And Dr. Montejo stressed that clinicians must “always, always, always” get a baseline serum prolactin measurement, to be repeated after increasing the drug dosage, changing antipsychotics, or upon development of symptoms of hyperprolactinemia.
When a patient’s prolactin level climbs above 50 ng/mL or symptoms of hyperprolactinemia arise, the preferred strategy is to switch to a prolactin-sparing antipsychotic. Most of the alternative options are unsatisfactory. For example, waiting for a sexual side effect to pass is pointless, because it won’t happen spontaneously. A drug holiday undermines compliance. Reducing the antipsychotic dose increases the risk of relapse.
And as for prescribing adjunctive dopamine agonist therapy, well: “Adding a dopamine agonist is not the first step. It should be one of the last steps, because it greatly increases the odds of worsening psychosis,” Dr. Montejo said.
If switching to a different antipsychotic is not possible, the expert panel recommended add-on aripiprazole, accompanied if possible by a downward dose adjustment of the offending antipsychotic. This is an effective way to lower elevated serum prolactin levels.
It’s appropriate to order a lumbar spine and proximal femur bone mineral density measurement in patients on antipsychotic agents if they are older than age 65, have had amenorrhea for at least 6 months, experienced menopause before age 35, have a body mass index below 19 kg/m2, or are experiencing any symptoms of hyperprolactinemia, including sexual dysfunction, according to the Spanish consensus algorithm.
Dr. Montejo reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies.
EXPERT ANALYSIS FROM THE ECNP CONGRESS
Scandinavian registries answer key questions about ADHD
PARIS – Huge longitudinal Scandinavian population registries constitute a unique data source that, in recent years, has provided new insights into attention-deficit/hyperactivity disorder and its associated risks of suicidal behavior, accidents, and early mortality, Henrik Larsson, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
“Randomized, controlled trials have provided little information about real-world effectiveness of ADHD medications, such as their potential effects on adverse health outcomes,” said Dr. Larsson of the Karolinska Institute in Stockholm.

Suicidality
Dr. Larsson was senior author of a Swedish national registry study that identified 51,707 patients with ADHD matched by sex and birth year to 258,535 controls. The ADHD patients had significantly higher rates of both attempted and completed suicide.
After adjustment for socioeconomic status, these individuals were at 8.46-fold increased risk for attempted suicide. However, after further adjustment for comorbid psychiatric disorders, this dropped substantially to a 3.62-fold increased risk.
The same pattern pertained to completed suicide: The risk after adjustment for socioeconomic status was increased 12.3-fold in individuals with ADHD, compared with controls, but the risk dropped to 5.91-fold after further adjustment for comorbid psychiatric disorders (JAMA Psychiatry. 2014 Aug;71[8]:958-64).
The clinical take home point: “Detection and treatment of comorbid conditions probably will help reduce suicidal behavior in ADHD,” Dr. Larsson said.
This study also showed that increased familial risk also is a key factor in the increased risk of suicidal behavior in the ADHD population. Parents of individuals with ADHD were at 2.42-fold increased risk of attempted suicide, compared with controls, and full siblings were at 2.28-fold increased risk. In contrast, the risk in half-siblings, while significantly greater than in controls, was lower than in the genetically closer first-degree relatives: Maternal half-siblings were at 1.57-fold increased risk, and paternal half-siblings were at 1.57-fold greater risk. Cousins were at 1.39-fold increased risk.
The same held true for completed suicide risk. And the familial associations remained significant even after excluding relatives with ADHD.
“Regarding the shared familial factors, I’m tempted to hypothesize that this might involve pleiotropic effects reflecting genetic variants associated with impulsivity,” said Dr. Larsson. To further understand the biological mechanisms underlying ADHD and associated adverse health outcomes requires multiple disciplines to work together. For such work, Dr. Larsson collaborates with international colleagues in several consortia.
ADHD medications and suicidality
Concerns regarding this question were raised by a meta-analysis based on clinical trials data that suggested patients’ increased suicidality might be caused by the effects of ADHD medications. But the meta-analysis was seriously flawed by what epidemiologists call confounding by indication, which is the potential for bias to be introduced when a group of patients on medication is compared with another group off medication. The confounding results from the fact that ADHD patients on medication are different from those who aren’t: They are likely to be more symptomatic and have more comorbidities.
To bypass the confounding issue, Dr. Larsson and his coinvestigators turned to the Swedish registries and identified 37,936 patients with ADHD with a total of 7,019 suicide-related events during nearly 151,000 person-years of follow-up. When they compared patients on drug treatment with those who were not, they found – as in the other investigators’ meta-analysis – that drug treatment was associated with a statistically significant 1.31-fold increased risk of suicide-related events. However, when they performed a more appropriate between-individual analysis, Dr. Larsson and his colleagues found that, when patients with ADHD were using stimulant medications, they had a significant 19% lower risk of suicide-related events than when they were off medication. While on nonstimulant ADHD medications, their suicidality risk was no different from when off medication (BMJ. 2014 Jun 18;348:g3769. doi: 10.1136/bmj.g3769).
ADHD and early mortality risk
Prior studies have established that ADHD is associated with a proclivity to engage in risk-taking behaviors, including substance abuse, criminality, risky sexual behavior, and accidents, which are themselves associated with early mortality.
Sure enough, when Danish investigators turned to their national registries, identified 32,061 individuals with ADHD born during 1981-2011, and followed them through 2013, they found that, during nearly 25 million person-years of follow-up, the mortality rate was 5.85 deaths per 10,000 person-years in individuals with ADHD, compared with 2.21 deaths per 10,000 person-years in controls, resulting in a fully adjusted mortality rate ratio of 2.07. The rate ratio was 1.86 for ADHD patients under age 6 years, 1.58 in those aged 6-17 years, and 4.25 for patients aged 18 years and older (Lancet. 2015 May 30;385[9983]:2190-6).
Accidents were the most common cause of death. Could ADHD medications modify this risk of fatal accidents?
Serious motor vehicle accidents
Dr. Larsson and his coinvestigators used registry data to follow 17,408 Swedish adults with ADHD for serious transport accidents involving a trip to the emergency room or death during 2006-2009. The risk was increased by an adjusted 1.47-fold in men with ADHD and by 1.45-fold in women with the disorder. However, in the within-individual analysis, men were 58% less likely to have a serious transport accident when they were on ADHD medication than when off medication. There was no statistically significant effect of ADHD medications on the risk in women with ADHD.
The investigators estimated that 41%-49% of transport accidents in men with ADHD could have been avoided had they been on drug therapy continuously throughout the follow-up period (JAMA Psychiatry. 2014 Mar;71[3]:319-25).
Similar results – that is, data showing that being on ADHD medication reduces the elevated risk of serious accidents – have been reported in four other independent studies conducted in Denmark, Germany, Hong Kong, and most recently in a U.S. analysis by Dr. Larsson and coinvestigators of more than 2.3 million patients with ADHD in a U.S. commercial health insurance claims database (JAMA Psychiatry. 2017 Jun 1;74[6]:597-603).
These findings collectively highlight the public health importance of diagnosing and treating ADHD.
But Dr. Larsson wanted his audience to take home another key lesson: “ADHD is a disorder that can be associated with serious outcomes, including suicide and accidents. It’s nevertheless important to remember that the absolute risks here are very low for any of these outcomes, so the majority of individuals with ADHD will never suffer from any of these outcomes. It’s important to keep that in mind.”
Dr. Larsson’s research is funded by the Swedish Research Council, the National Institute of Mental Health, FORTE, Horizon 2020, and Shire.
bjancin@frontlinemedcom.com
PARIS – Huge longitudinal Scandinavian population registries constitute a unique data source that, in recent years, has provided new insights into attention-deficit/hyperactivity disorder and its associated risks of suicidal behavior, accidents, and early mortality, Henrik Larsson, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
“Randomized, controlled trials have provided little information about real-world effectiveness of ADHD medications, such as their potential effects on adverse health outcomes,” said Dr. Larsson of the Karolinska Institute in Stockholm.
Suicidality
Dr. Larsson was senior author of a Swedish national registry study that identified 51,707 patients with ADHD matched by sex and birth year to 258,535 controls. The ADHD patients had significantly higher rates of both attempted and completed suicide.
After adjustment for socioeconomic status, these individuals were at 8.46-fold increased risk for attempted suicide. However, after further adjustment for comorbid psychiatric disorders, this dropped substantially to a 3.62-fold increased risk.
The same pattern pertained to completed suicide: The risk after adjustment for socioeconomic status was increased 12.3-fold in individuals with ADHD, compared with controls, but the risk dropped to 5.91-fold after further adjustment for comorbid psychiatric disorders (JAMA Psychiatry. 2014 Aug;71[8]:958-64).
The clinical take home point: “Detection and treatment of comorbid conditions probably will help reduce suicidal behavior in ADHD,” Dr. Larsson said.
This study also showed that increased familial risk also is a key factor in the increased risk of suicidal behavior in the ADHD population. Parents of individuals with ADHD were at 2.42-fold increased risk of attempted suicide, compared with controls, and full siblings were at 2.28-fold increased risk. In contrast, the risk in half-siblings, while significantly greater than in controls, was lower than in the genetically closer first-degree relatives: Maternal half-siblings were at 1.57-fold increased risk, and paternal half-siblings were at 1.57-fold greater risk. Cousins were at 1.39-fold increased risk.
The same held true for completed suicide risk. And the familial associations remained significant even after excluding relatives with ADHD.
“Regarding the shared familial factors, I’m tempted to hypothesize that this might involve pleiotropic effects reflecting genetic variants associated with impulsivity,” said Dr. Larsson. To further understand the biological mechanisms underlying ADHD and associated adverse health outcomes requires multiple disciplines to work together. For such work, Dr. Larsson collaborates with international colleagues in several consortia.
ADHD medications and suicidality
Concerns regarding this question were raised by a meta-analysis based on clinical trials data that suggested patients’ increased suicidality might be caused by the effects of ADHD medications. But the meta-analysis was seriously flawed by what epidemiologists call confounding by indication, which is the potential for bias to be introduced when a group of patients on medication is compared with another group off medication. The confounding results from the fact that ADHD patients on medication are different from those who aren’t: They are likely to be more symptomatic and have more comorbidities.
To bypass the confounding issue, Dr. Larsson and his coinvestigators turned to the Swedish registries and identified 37,936 patients with ADHD with a total of 7,019 suicide-related events during nearly 151,000 person-years of follow-up. When they compared patients on drug treatment with those who were not, they found – as in the other investigators’ meta-analysis – that drug treatment was associated with a statistically significant 1.31-fold increased risk of suicide-related events. However, when they performed a more appropriate between-individual analysis, Dr. Larsson and his colleagues found that, when patients with ADHD were using stimulant medications, they had a significant 19% lower risk of suicide-related events than when they were off medication. While on nonstimulant ADHD medications, their suicidality risk was no different from when off medication (BMJ. 2014 Jun 18;348:g3769. doi: 10.1136/bmj.g3769).
ADHD and early mortality risk
Prior studies have established that ADHD is associated with a proclivity to engage in risk-taking behaviors, including substance abuse, criminality, risky sexual behavior, and accidents, which are themselves associated with early mortality.
Sure enough, when Danish investigators turned to their national registries, identified 32,061 individuals with ADHD born during 1981-2011, and followed them through 2013, they found that, during nearly 25 million person-years of follow-up, the mortality rate was 5.85 deaths per 10,000 person-years in individuals with ADHD, compared with 2.21 deaths per 10,000 person-years in controls, resulting in a fully adjusted mortality rate ratio of 2.07. The rate ratio was 1.86 for ADHD patients under age 6 years, 1.58 in those aged 6-17 years, and 4.25 for patients aged 18 years and older (Lancet. 2015 May 30;385[9983]:2190-6).
Accidents were the most common cause of death. Could ADHD medications modify this risk of fatal accidents?
Serious motor vehicle accidents
Dr. Larsson and his coinvestigators used registry data to follow 17,408 Swedish adults with ADHD for serious transport accidents involving a trip to the emergency room or death during 2006-2009. The risk was increased by an adjusted 1.47-fold in men with ADHD and by 1.45-fold in women with the disorder. However, in the within-individual analysis, men were 58% less likely to have a serious transport accident when they were on ADHD medication than when off medication. There was no statistically significant effect of ADHD medications on the risk in women with ADHD.
The investigators estimated that 41%-49% of transport accidents in men with ADHD could have been avoided had they been on drug therapy continuously throughout the follow-up period (JAMA Psychiatry. 2014 Mar;71[3]:319-25).
Similar results – that is, data showing that being on ADHD medication reduces the elevated risk of serious accidents – have been reported in four other independent studies conducted in Denmark, Germany, Hong Kong, and most recently in a U.S. analysis by Dr. Larsson and coinvestigators of more than 2.3 million patients with ADHD in a U.S. commercial health insurance claims database (JAMA Psychiatry. 2017 Jun 1;74[6]:597-603).
These findings collectively highlight the public health importance of diagnosing and treating ADHD.
But Dr. Larsson wanted his audience to take home another key lesson: “ADHD is a disorder that can be associated with serious outcomes, including suicide and accidents. It’s nevertheless important to remember that the absolute risks here are very low for any of these outcomes, so the majority of individuals with ADHD will never suffer from any of these outcomes. It’s important to keep that in mind.”
Dr. Larsson’s research is funded by the Swedish Research Council, the National Institute of Mental Health, FORTE, Horizon 2020, and Shire.
bjancin@frontlinemedcom.com
PARIS – Huge longitudinal Scandinavian population registries constitute a unique data source that, in recent years, has provided new insights into attention-deficit/hyperactivity disorder and its associated risks of suicidal behavior, accidents, and early mortality, Henrik Larsson, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
“Randomized, controlled trials have provided little information about real-world effectiveness of ADHD medications, such as their potential effects on adverse health outcomes,” said Dr. Larsson of the Karolinska Institute in Stockholm.
Suicidality
Dr. Larsson was senior author of a Swedish national registry study that identified 51,707 patients with ADHD matched by sex and birth year to 258,535 controls. The ADHD patients had significantly higher rates of both attempted and completed suicide.
After adjustment for socioeconomic status, these individuals were at 8.46-fold increased risk for attempted suicide. However, after further adjustment for comorbid psychiatric disorders, this dropped substantially to a 3.62-fold increased risk.
The same pattern pertained to completed suicide: The risk after adjustment for socioeconomic status was increased 12.3-fold in individuals with ADHD, compared with controls, but the risk dropped to 5.91-fold after further adjustment for comorbid psychiatric disorders (JAMA Psychiatry. 2014 Aug;71[8]:958-64).
The clinical take home point: “Detection and treatment of comorbid conditions probably will help reduce suicidal behavior in ADHD,” Dr. Larsson said.
This study also showed that increased familial risk also is a key factor in the increased risk of suicidal behavior in the ADHD population. Parents of individuals with ADHD were at 2.42-fold increased risk of attempted suicide, compared with controls, and full siblings were at 2.28-fold increased risk. In contrast, the risk in half-siblings, while significantly greater than in controls, was lower than in the genetically closer first-degree relatives: Maternal half-siblings were at 1.57-fold increased risk, and paternal half-siblings were at 1.57-fold greater risk. Cousins were at 1.39-fold increased risk.
The same held true for completed suicide risk. And the familial associations remained significant even after excluding relatives with ADHD.
“Regarding the shared familial factors, I’m tempted to hypothesize that this might involve pleiotropic effects reflecting genetic variants associated with impulsivity,” said Dr. Larsson. To further understand the biological mechanisms underlying ADHD and associated adverse health outcomes requires multiple disciplines to work together. For such work, Dr. Larsson collaborates with international colleagues in several consortia.
ADHD medications and suicidality
Concerns regarding this question were raised by a meta-analysis based on clinical trials data that suggested patients’ increased suicidality might be caused by the effects of ADHD medications. But the meta-analysis was seriously flawed by what epidemiologists call confounding by indication, which is the potential for bias to be introduced when a group of patients on medication is compared with another group off medication. The confounding results from the fact that ADHD patients on medication are different from those who aren’t: They are likely to be more symptomatic and have more comorbidities.
To bypass the confounding issue, Dr. Larsson and his coinvestigators turned to the Swedish registries and identified 37,936 patients with ADHD with a total of 7,019 suicide-related events during nearly 151,000 person-years of follow-up. When they compared patients on drug treatment with those who were not, they found – as in the other investigators’ meta-analysis – that drug treatment was associated with a statistically significant 1.31-fold increased risk of suicide-related events. However, when they performed a more appropriate between-individual analysis, Dr. Larsson and his colleagues found that, when patients with ADHD were using stimulant medications, they had a significant 19% lower risk of suicide-related events than when they were off medication. While on nonstimulant ADHD medications, their suicidality risk was no different from when off medication (BMJ. 2014 Jun 18;348:g3769. doi: 10.1136/bmj.g3769).
ADHD and early mortality risk
Prior studies have established that ADHD is associated with a proclivity to engage in risk-taking behaviors, including substance abuse, criminality, risky sexual behavior, and accidents, which are themselves associated with early mortality.
Sure enough, when Danish investigators turned to their national registries, identified 32,061 individuals with ADHD born during 1981-2011, and followed them through 2013, they found that, during nearly 25 million person-years of follow-up, the mortality rate was 5.85 deaths per 10,000 person-years in individuals with ADHD, compared with 2.21 deaths per 10,000 person-years in controls, resulting in a fully adjusted mortality rate ratio of 2.07. The rate ratio was 1.86 for ADHD patients under age 6 years, 1.58 in those aged 6-17 years, and 4.25 for patients aged 18 years and older (Lancet. 2015 May 30;385[9983]:2190-6).
Accidents were the most common cause of death. Could ADHD medications modify this risk of fatal accidents?
Serious motor vehicle accidents
Dr. Larsson and his coinvestigators used registry data to follow 17,408 Swedish adults with ADHD for serious transport accidents involving a trip to the emergency room or death during 2006-2009. The risk was increased by an adjusted 1.47-fold in men with ADHD and by 1.45-fold in women with the disorder. However, in the within-individual analysis, men were 58% less likely to have a serious transport accident when they were on ADHD medication than when off medication. There was no statistically significant effect of ADHD medications on the risk in women with ADHD.
The investigators estimated that 41%-49% of transport accidents in men with ADHD could have been avoided had they been on drug therapy continuously throughout the follow-up period (JAMA Psychiatry. 2014 Mar;71[3]:319-25).
Similar results – that is, data showing that being on ADHD medication reduces the elevated risk of serious accidents – have been reported in four other independent studies conducted in Denmark, Germany, Hong Kong, and most recently in a U.S. analysis by Dr. Larsson and coinvestigators of more than 2.3 million patients with ADHD in a U.S. commercial health insurance claims database (JAMA Psychiatry. 2017 Jun 1;74[6]:597-603).
These findings collectively highlight the public health importance of diagnosing and treating ADHD.
But Dr. Larsson wanted his audience to take home another key lesson: “ADHD is a disorder that can be associated with serious outcomes, including suicide and accidents. It’s nevertheless important to remember that the absolute risks here are very low for any of these outcomes, so the majority of individuals with ADHD will never suffer from any of these outcomes. It’s important to keep that in mind.”
Dr. Larsson’s research is funded by the Swedish Research Council, the National Institute of Mental Health, FORTE, Horizon 2020, and Shire.
bjancin@frontlinemedcom.com
expert analysis from THE ECNP CONGRESS
Serlopitant is itching to quell chronic pruritus
GENEVA – Serlopitant, a novel once-daily oral neurokinin-1 receptor antagonist, brought significant improvement for patients with treatment-resistant chronic pruritus as early as day 2, in a phase 2 randomized trial, Paul Kwon, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
In a separate phase 2 study presented at the congress, serlopitant showed strong efficacy in patients with prurigo nodularis.
Serlopitant is an oral small molecule with high selectivity for the neurokinin-1 receptor (NK1R). At the 5-mg dose, the drug occupies more than 90% of CNS NK1Rs. The NK1R is the primary receptor for substance P, and thus plays an important role in pruritus signaling.

Chronic pruritus is an often-debilitating condition that can have a multitude of causes. It’s associated with increased rates of anxiety, depression, and sleep deprivation. Existing treatments often fail to provide adequate relief from the severe chronic itching, or they are associated with safety or tolerability issues.
“Chronic pruritus can disrupt quality of life to a level comparable to chronic pain,” the dermatologist observed. “I think we in the medical community are hearing more and more about treatment for chronic pruritus as being a major unmet medical need.”
Dr. Kwon noted that investigators at Emory University in Atlanta have found that the quality of life disruption imposed by chronic pruritus is comparable to that of chronic pain (Arch Dermatol. 2011 Oct;147[10]:1153-6).
The phase 2, randomized, double-blind, placebo-controlled, 6-week trial comprised 257 patients with chronic pruritus at 25 U.S. centers. All were non- or inadequate responders to topical corticosteroids or oral antihistamines. This was essentially an all-comers study that was not restricted to patients with any particular specific cause of their chronic itch. They had to have severe chronic pruritus, as defined by a baseline self-rated pruritus visual analogue score of at least 7 on a 0-10 scale. Patients were randomized to once-daily oral serlopitant at 0.25 mg, 1 mg, or 5 mg, or to placebo.
The primary endpoint was change in mean visual analogue score from baseline to week 6. The serlopitant 1-mg and 5-mg groups reported mean 41.4% and 42.5% reductions, respectively, which were significantly better than the 28.3% reduction in controls.
“It seems that the drug is working in a broad set of subjects,” Dr. Kwon said. “It is not entirely shutting off itch in significant numbers, but the majority of patients appear to be deriving benefit from serlopitant.”
He highlighted the rapidity with which chronic pruritus responded to serlopitant. The first dose was taken on the evening of day 1. The next day, the 1-mg serlopitant group already showed a significantly greater improvement than did placebo-treated controls. The day after that, so did the 5-mg group. Those between-group differences grew steadily larger throughout the 6-week study period.
That rapid response is clinically highly relevant, because numerous studies have demonstrated that fast onset of therapeutic effect improves patient satisfaction, quality of life, and compliance with treatment for a variety of medical conditions, he said.
Dr. Kwon characterized the safety profile of serlopitant in the trial as “fairly robust,” with only mild or moderate treatment-emergent adverse events being seen. Diarrhea and somnolence were the only adverse events more common with serlopitant than placebo, and their incidence was in the mid single digits.
“We have not uncovered any significant safety signal in this study,” Dr. Kwon declared.
Also at the EADV Congress, Sonja Ständer, MD, presented a phase 2 study of serlopitant in patients with prurigo nodularis. The randomized, double-blind, 8-week, 127-patient trial was conducted at 15 sites in Germany, where patients were randomized to once-daily serlopitant at 5 mg or placebo. All participants had a baseline pruritus VAS of 7 or more. Thirty percent of patients had more than a 10-year history of prurigo nodularis, and 24% had the condition for 5-10 years.
The primary endpoint was the difference from baseline to weeks 4 and 8 in the average pruritus VAS over the previous 24 hours. The baseline score was 7.9. The serlopitant group averaged a 1.0-point greater reduction, compared with controls, at week 4, and a 1.7-point greater decrease at week 8.
Multiple other measures of pruritus serving as secondary endpoints consistently showed significantly greater improvement in the serlopitant group. For example, at the week 8 assessment, 54% of serlopitant-treated patients reported no or only mild itch, compared with 29% of controls. And two-thirds of the serlopitant group reported some degree of improvement in the severity of their eruptive papulonodular lesions at week 8, versus 40% of controls, according to Dr. Ständer, professor of dermatology and neurodermatology and head of the Center for Chronic Pruritus at the University of Münster (Germany).
Of note, nasopharyngitis occurred in 17.2% of the serlopitant group and in 3.2% of controls. Diarrhea was also more common in the serlopitant group, by a margin of 10.9% versus 4.8%.
Dr. Kwon said additional phase 2 as well as phase 3 randomized trials of serlopitant are in the works for both chronic pruritus and prurigo nodularis. The drug is also under study for chronic itch due to other specific etiologies, as well as for refractory chronic cough.
Menlo Therapeutics sponsored the study. Dr. Kwon is a Menlo Therapeutics officer. Dr. Ständer, who was also principal investigator in the chronic pruritus trial, reported having no financial conflicts of interest.
GENEVA – Serlopitant, a novel once-daily oral neurokinin-1 receptor antagonist, brought significant improvement for patients with treatment-resistant chronic pruritus as early as day 2, in a phase 2 randomized trial, Paul Kwon, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
In a separate phase 2 study presented at the congress, serlopitant showed strong efficacy in patients with prurigo nodularis.
Serlopitant is an oral small molecule with high selectivity for the neurokinin-1 receptor (NK1R). At the 5-mg dose, the drug occupies more than 90% of CNS NK1Rs. The NK1R is the primary receptor for substance P, and thus plays an important role in pruritus signaling.
Chronic pruritus is an often-debilitating condition that can have a multitude of causes. It’s associated with increased rates of anxiety, depression, and sleep deprivation. Existing treatments often fail to provide adequate relief from the severe chronic itching, or they are associated with safety or tolerability issues.
“Chronic pruritus can disrupt quality of life to a level comparable to chronic pain,” the dermatologist observed. “I think we in the medical community are hearing more and more about treatment for chronic pruritus as being a major unmet medical need.”
Dr. Kwon noted that investigators at Emory University in Atlanta have found that the quality of life disruption imposed by chronic pruritus is comparable to that of chronic pain (Arch Dermatol. 2011 Oct;147[10]:1153-6).
The phase 2, randomized, double-blind, placebo-controlled, 6-week trial comprised 257 patients with chronic pruritus at 25 U.S. centers. All were non- or inadequate responders to topical corticosteroids or oral antihistamines. This was essentially an all-comers study that was not restricted to patients with any particular specific cause of their chronic itch. They had to have severe chronic pruritus, as defined by a baseline self-rated pruritus visual analogue score of at least 7 on a 0-10 scale. Patients were randomized to once-daily oral serlopitant at 0.25 mg, 1 mg, or 5 mg, or to placebo.
The primary endpoint was change in mean visual analogue score from baseline to week 6. The serlopitant 1-mg and 5-mg groups reported mean 41.4% and 42.5% reductions, respectively, which were significantly better than the 28.3% reduction in controls.
“It seems that the drug is working in a broad set of subjects,” Dr. Kwon said. “It is not entirely shutting off itch in significant numbers, but the majority of patients appear to be deriving benefit from serlopitant.”
He highlighted the rapidity with which chronic pruritus responded to serlopitant. The first dose was taken on the evening of day 1. The next day, the 1-mg serlopitant group already showed a significantly greater improvement than did placebo-treated controls. The day after that, so did the 5-mg group. Those between-group differences grew steadily larger throughout the 6-week study period.
That rapid response is clinically highly relevant, because numerous studies have demonstrated that fast onset of therapeutic effect improves patient satisfaction, quality of life, and compliance with treatment for a variety of medical conditions, he said.
Dr. Kwon characterized the safety profile of serlopitant in the trial as “fairly robust,” with only mild or moderate treatment-emergent adverse events being seen. Diarrhea and somnolence were the only adverse events more common with serlopitant than placebo, and their incidence was in the mid single digits.
“We have not uncovered any significant safety signal in this study,” Dr. Kwon declared.
Also at the EADV Congress, Sonja Ständer, MD, presented a phase 2 study of serlopitant in patients with prurigo nodularis. The randomized, double-blind, 8-week, 127-patient trial was conducted at 15 sites in Germany, where patients were randomized to once-daily serlopitant at 5 mg or placebo. All participants had a baseline pruritus VAS of 7 or more. Thirty percent of patients had more than a 10-year history of prurigo nodularis, and 24% had the condition for 5-10 years.
The primary endpoint was the difference from baseline to weeks 4 and 8 in the average pruritus VAS over the previous 24 hours. The baseline score was 7.9. The serlopitant group averaged a 1.0-point greater reduction, compared with controls, at week 4, and a 1.7-point greater decrease at week 8.
Multiple other measures of pruritus serving as secondary endpoints consistently showed significantly greater improvement in the serlopitant group. For example, at the week 8 assessment, 54% of serlopitant-treated patients reported no or only mild itch, compared with 29% of controls. And two-thirds of the serlopitant group reported some degree of improvement in the severity of their eruptive papulonodular lesions at week 8, versus 40% of controls, according to Dr. Ständer, professor of dermatology and neurodermatology and head of the Center for Chronic Pruritus at the University of Münster (Germany).
Of note, nasopharyngitis occurred in 17.2% of the serlopitant group and in 3.2% of controls. Diarrhea was also more common in the serlopitant group, by a margin of 10.9% versus 4.8%.
Dr. Kwon said additional phase 2 as well as phase 3 randomized trials of serlopitant are in the works for both chronic pruritus and prurigo nodularis. The drug is also under study for chronic itch due to other specific etiologies, as well as for refractory chronic cough.
Menlo Therapeutics sponsored the study. Dr. Kwon is a Menlo Therapeutics officer. Dr. Ständer, who was also principal investigator in the chronic pruritus trial, reported having no financial conflicts of interest.
GENEVA – Serlopitant, a novel once-daily oral neurokinin-1 receptor antagonist, brought significant improvement for patients with treatment-resistant chronic pruritus as early as day 2, in a phase 2 randomized trial, Paul Kwon, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
In a separate phase 2 study presented at the congress, serlopitant showed strong efficacy in patients with prurigo nodularis.
Serlopitant is an oral small molecule with high selectivity for the neurokinin-1 receptor (NK1R). At the 5-mg dose, the drug occupies more than 90% of CNS NK1Rs. The NK1R is the primary receptor for substance P, and thus plays an important role in pruritus signaling.
Chronic pruritus is an often-debilitating condition that can have a multitude of causes. It’s associated with increased rates of anxiety, depression, and sleep deprivation. Existing treatments often fail to provide adequate relief from the severe chronic itching, or they are associated with safety or tolerability issues.
“Chronic pruritus can disrupt quality of life to a level comparable to chronic pain,” the dermatologist observed. “I think we in the medical community are hearing more and more about treatment for chronic pruritus as being a major unmet medical need.”
Dr. Kwon noted that investigators at Emory University in Atlanta have found that the quality of life disruption imposed by chronic pruritus is comparable to that of chronic pain (Arch Dermatol. 2011 Oct;147[10]:1153-6).
The phase 2, randomized, double-blind, placebo-controlled, 6-week trial comprised 257 patients with chronic pruritus at 25 U.S. centers. All were non- or inadequate responders to topical corticosteroids or oral antihistamines. This was essentially an all-comers study that was not restricted to patients with any particular specific cause of their chronic itch. They had to have severe chronic pruritus, as defined by a baseline self-rated pruritus visual analogue score of at least 7 on a 0-10 scale. Patients were randomized to once-daily oral serlopitant at 0.25 mg, 1 mg, or 5 mg, or to placebo.
The primary endpoint was change in mean visual analogue score from baseline to week 6. The serlopitant 1-mg and 5-mg groups reported mean 41.4% and 42.5% reductions, respectively, which were significantly better than the 28.3% reduction in controls.
“It seems that the drug is working in a broad set of subjects,” Dr. Kwon said. “It is not entirely shutting off itch in significant numbers, but the majority of patients appear to be deriving benefit from serlopitant.”
He highlighted the rapidity with which chronic pruritus responded to serlopitant. The first dose was taken on the evening of day 1. The next day, the 1-mg serlopitant group already showed a significantly greater improvement than did placebo-treated controls. The day after that, so did the 5-mg group. Those between-group differences grew steadily larger throughout the 6-week study period.
That rapid response is clinically highly relevant, because numerous studies have demonstrated that fast onset of therapeutic effect improves patient satisfaction, quality of life, and compliance with treatment for a variety of medical conditions, he said.
Dr. Kwon characterized the safety profile of serlopitant in the trial as “fairly robust,” with only mild or moderate treatment-emergent adverse events being seen. Diarrhea and somnolence were the only adverse events more common with serlopitant than placebo, and their incidence was in the mid single digits.
“We have not uncovered any significant safety signal in this study,” Dr. Kwon declared.
Also at the EADV Congress, Sonja Ständer, MD, presented a phase 2 study of serlopitant in patients with prurigo nodularis. The randomized, double-blind, 8-week, 127-patient trial was conducted at 15 sites in Germany, where patients were randomized to once-daily serlopitant at 5 mg or placebo. All participants had a baseline pruritus VAS of 7 or more. Thirty percent of patients had more than a 10-year history of prurigo nodularis, and 24% had the condition for 5-10 years.
The primary endpoint was the difference from baseline to weeks 4 and 8 in the average pruritus VAS over the previous 24 hours. The baseline score was 7.9. The serlopitant group averaged a 1.0-point greater reduction, compared with controls, at week 4, and a 1.7-point greater decrease at week 8.
Multiple other measures of pruritus serving as secondary endpoints consistently showed significantly greater improvement in the serlopitant group. For example, at the week 8 assessment, 54% of serlopitant-treated patients reported no or only mild itch, compared with 29% of controls. And two-thirds of the serlopitant group reported some degree of improvement in the severity of their eruptive papulonodular lesions at week 8, versus 40% of controls, according to Dr. Ständer, professor of dermatology and neurodermatology and head of the Center for Chronic Pruritus at the University of Münster (Germany).
Of note, nasopharyngitis occurred in 17.2% of the serlopitant group and in 3.2% of controls. Diarrhea was also more common in the serlopitant group, by a margin of 10.9% versus 4.8%.
Dr. Kwon said additional phase 2 as well as phase 3 randomized trials of serlopitant are in the works for both chronic pruritus and prurigo nodularis. The drug is also under study for chronic itch due to other specific etiologies, as well as for refractory chronic cough.
Menlo Therapeutics sponsored the study. Dr. Kwon is a Menlo Therapeutics officer. Dr. Ständer, who was also principal investigator in the chronic pruritus trial, reported having no financial conflicts of interest.
AT THE EADV CONGRESS
Key clinical point:
Major finding: Mean self-rated pruritus scores fell by 41% and 43% from baseline to week 6 in patients on serlopitant at 1 mg/day and 5 mg/day, compared with 28% in placebo-treated controls.
Data source: A randomized, double-blind, multicenter, placebo-controlled, 6-week, phase 2 clinical trial comprising 257 patients with treatment-resistant chronic pruritus.
Disclosures: Menlo Therapeutics sponsored the study. Dr. Kwon is a Menlo Therapeutics officer. Dr. Ständer reported having no financial conflicts of interest.
Heart transplantation: Preop LVAD erases adverse impact of pulmonary hypertension
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.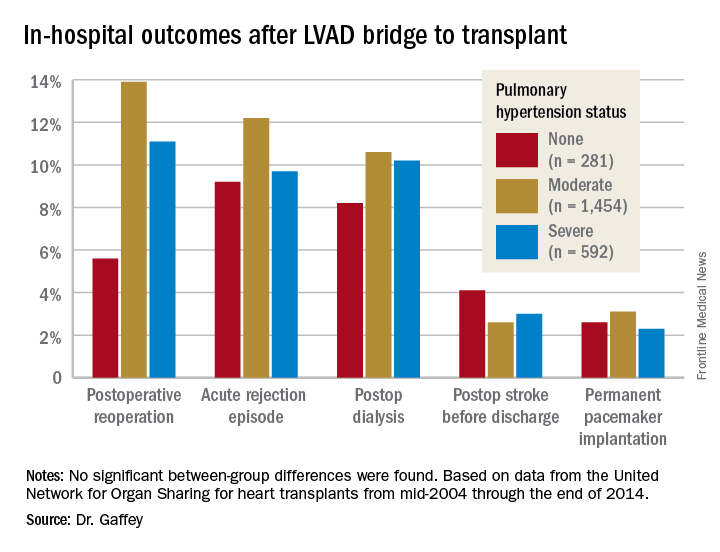
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: It’s time to reconsider the practice of excluding patients with pulmonary hypertension from consideration for a donor heart.
Data source: A retrospective analysis of the United Network for Organ Sharing database including outcomes out to 5 years on 3,951 heart transplant recipients who had been bridged to transplant with an LVAD, most of whom had moderate or severe pulmonary hypertension before transplant.
Disclosures: This study was conducted free of commercial support. The presenter reported having no relevant financial conflicts of interest.
VIDEO: Regionalized STEMI care slashes in-hospital mortality
ANAHEIM, CALIF. – An American Heart Association program aimed at streamlining care of patients with ST-elevation MI resulted in a dramatic near-halving of in-hospital mortality, compared with STEMI patients treated in hospitals not participating in the project, James G. Jollis, MD, reported at the American Heart Association scientific sessions.
He presented the results of the STEMI ACCELERATOR 2 study, which involved 12 participating metropolitan regions across the United States, 132 percutaneous coronary intervention–capable hospitals, and 946 emergency medical services agencies. The ACCELERATOR 2 program entailed regional implementation of a structured STEMI care plan in which EMS personnel were trained to obtain prehospital ECGs and to activate cardiac catheterization labs prior to hospital arrival, bypassing the emergency department when appropriate.
Key elements of the project, which was part of the AHA’s Mission: Lifeline program, included having participating hospitals measure their performance of key processes and send that information as well as patient outcome data to the National Cardiovascular Data Registry’s ACTION–Get With The Guidelines registry. The hospitals in turn received quarterly feedback reports containing blinded hospital comparisons.

Dr. Jollis and his coinvestigators worked to obtain buy-in from local stakeholders, organize regional leadership, and help in drafting a central regional STEMI plan featuring prespecified treatment protocols.
The STEMI ACCELERATOR 2 study was carried out in 2015-2017, during which 10,730 patients with STEMI were transported directly to participating hospitals with PCI capability.
The primary study outcome was the change from the first to the final quarter of the study in the proportion of EMS-transported patients with a time from first medical contact to treatment in the cath lab of 90 minutes or less. This improved significantly, from 67% at baseline to 74% in the final quarter. Nine of the 12 participating regions reduced their time from first medical contact to treatment in the cath lab, and eight reached the national of goal of having 75% of STEMI patients treated within 90 minutes.
The other key time-to-care measures improved, too: At baseline, only 38% of patients had a time from first medical contact to cath lab activation of 20 minutes or less; by the final quarter, this figure had climbed to 56%. That’s an important metric, as evidenced by the study finding that in-hospital mortality occurred in 4.5% of patients with a time from first medical contact to cath lab activation of more than 20 minutes, compared with 2.2% in those with a time of 20 minutes or less.
Also, the proportion of patients who spent 20 minutes or less in the emergency department improved from 33% to 43%.
In-hospital mortality improved from 4.4% in the baseline quarter to 2.3% in the final quarter. No similar improvement in in-hospital mortality occurred in a comparison group of 22,651 STEMI patients treated at hospitals not involved in ACCELERATOR 2.
A significant reduction in the rate of in-hospital congestive heart failure occurred in the ACCELERATOR 2 centers, from 7.4% at baseline to 5.0%. In contrast, stroke, cardiogenic shock, and major bleeding rates were unchanged over time.
The ACCELERATOR 2 model of emergency cardiovascular care is designed to be highly generalizable, according to Dr. Jollis.
“This study supports the implementation of regionally coordinated systems across the United States to abort heart attacks, save lives, and enable heart attack victims to return to their families and productive lives,” he said.
The ACCELERATOR 2 operations manual – essentially a blueprint for organizing a regional STEMI system of care – is available gratis.

Dr. Allen, a cardiologist at the University of Colorado, Denver, said the ACCELERATOR 2 model has been successful because it is consistent with a fundamental principle of implementation science as described by Carolyn Clancy, MD, Executive in Charge at the Veterans Health Affairs Administration, who has said it’s a matter of making the right thing to do the easy thing to do.
Gregg C. Fonarow, MD, founder of the Get With the Guidelines program, predicted that the success of this program will lead to a ramping up of efforts to regionalize and coordinate STEMI care across the country. “I hope and anticipate that the AHA will take and run with the ACCELERATOR 2 model and adopt this into Mission: Lifeline, hoping to make this the standard approach to further improving care and outcomes in these patients,” said Dr. Fonarow, professor and cochief of cardiology at the University of California, Los Angeles, in a video interview.
Simultaneous with his presentation at the AHA conference, the results of STEMI ACCELERATOR 2 were published online in Circulation (2017 Nov 14; doi: 0.1161/CIRCULATIONAHA.117.032446).
The trial was sponsored by research and educational grants from AstraZeneca and The Medicines Company. Dr. Jollis reported having no financial conflicts of interest.
ANAHEIM, CALIF. – An American Heart Association program aimed at streamlining care of patients with ST-elevation MI resulted in a dramatic near-halving of in-hospital mortality, compared with STEMI patients treated in hospitals not participating in the project, James G. Jollis, MD, reported at the American Heart Association scientific sessions.
He presented the results of the STEMI ACCELERATOR 2 study, which involved 12 participating metropolitan regions across the United States, 132 percutaneous coronary intervention–capable hospitals, and 946 emergency medical services agencies. The ACCELERATOR 2 program entailed regional implementation of a structured STEMI care plan in which EMS personnel were trained to obtain prehospital ECGs and to activate cardiac catheterization labs prior to hospital arrival, bypassing the emergency department when appropriate.
Key elements of the project, which was part of the AHA’s Mission: Lifeline program, included having participating hospitals measure their performance of key processes and send that information as well as patient outcome data to the National Cardiovascular Data Registry’s ACTION–Get With The Guidelines registry. The hospitals in turn received quarterly feedback reports containing blinded hospital comparisons.
Dr. Jollis and his coinvestigators worked to obtain buy-in from local stakeholders, organize regional leadership, and help in drafting a central regional STEMI plan featuring prespecified treatment protocols.
The STEMI ACCELERATOR 2 study was carried out in 2015-2017, during which 10,730 patients with STEMI were transported directly to participating hospitals with PCI capability.
The primary study outcome was the change from the first to the final quarter of the study in the proportion of EMS-transported patients with a time from first medical contact to treatment in the cath lab of 90 minutes or less. This improved significantly, from 67% at baseline to 74% in the final quarter. Nine of the 12 participating regions reduced their time from first medical contact to treatment in the cath lab, and eight reached the national of goal of having 75% of STEMI patients treated within 90 minutes.
The other key time-to-care measures improved, too: At baseline, only 38% of patients had a time from first medical contact to cath lab activation of 20 minutes or less; by the final quarter, this figure had climbed to 56%. That’s an important metric, as evidenced by the study finding that in-hospital mortality occurred in 4.5% of patients with a time from first medical contact to cath lab activation of more than 20 minutes, compared with 2.2% in those with a time of 20 minutes or less.
Also, the proportion of patients who spent 20 minutes or less in the emergency department improved from 33% to 43%.
In-hospital mortality improved from 4.4% in the baseline quarter to 2.3% in the final quarter. No similar improvement in in-hospital mortality occurred in a comparison group of 22,651 STEMI patients treated at hospitals not involved in ACCELERATOR 2.
A significant reduction in the rate of in-hospital congestive heart failure occurred in the ACCELERATOR 2 centers, from 7.4% at baseline to 5.0%. In contrast, stroke, cardiogenic shock, and major bleeding rates were unchanged over time.
The ACCELERATOR 2 model of emergency cardiovascular care is designed to be highly generalizable, according to Dr. Jollis.
“This study supports the implementation of regionally coordinated systems across the United States to abort heart attacks, save lives, and enable heart attack victims to return to their families and productive lives,” he said.
The ACCELERATOR 2 operations manual – essentially a blueprint for organizing a regional STEMI system of care – is available gratis.
Dr. Allen, a cardiologist at the University of Colorado, Denver, said the ACCELERATOR 2 model has been successful because it is consistent with a fundamental principle of implementation science as described by Carolyn Clancy, MD, Executive in Charge at the Veterans Health Affairs Administration, who has said it’s a matter of making the right thing to do the easy thing to do.
Gregg C. Fonarow, MD, founder of the Get With the Guidelines program, predicted that the success of this program will lead to a ramping up of efforts to regionalize and coordinate STEMI care across the country. “I hope and anticipate that the AHA will take and run with the ACCELERATOR 2 model and adopt this into Mission: Lifeline, hoping to make this the standard approach to further improving care and outcomes in these patients,” said Dr. Fonarow, professor and cochief of cardiology at the University of California, Los Angeles, in a video interview.
Simultaneous with his presentation at the AHA conference, the results of STEMI ACCELERATOR 2 were published online in Circulation (2017 Nov 14; doi: 0.1161/CIRCULATIONAHA.117.032446).
The trial was sponsored by research and educational grants from AstraZeneca and The Medicines Company. Dr. Jollis reported having no financial conflicts of interest.
ANAHEIM, CALIF. – An American Heart Association program aimed at streamlining care of patients with ST-elevation MI resulted in a dramatic near-halving of in-hospital mortality, compared with STEMI patients treated in hospitals not participating in the project, James G. Jollis, MD, reported at the American Heart Association scientific sessions.
He presented the results of the STEMI ACCELERATOR 2 study, which involved 12 participating metropolitan regions across the United States, 132 percutaneous coronary intervention–capable hospitals, and 946 emergency medical services agencies. The ACCELERATOR 2 program entailed regional implementation of a structured STEMI care plan in which EMS personnel were trained to obtain prehospital ECGs and to activate cardiac catheterization labs prior to hospital arrival, bypassing the emergency department when appropriate.
Key elements of the project, which was part of the AHA’s Mission: Lifeline program, included having participating hospitals measure their performance of key processes and send that information as well as patient outcome data to the National Cardiovascular Data Registry’s ACTION–Get With The Guidelines registry. The hospitals in turn received quarterly feedback reports containing blinded hospital comparisons.
Dr. Jollis and his coinvestigators worked to obtain buy-in from local stakeholders, organize regional leadership, and help in drafting a central regional STEMI plan featuring prespecified treatment protocols.
The STEMI ACCELERATOR 2 study was carried out in 2015-2017, during which 10,730 patients with STEMI were transported directly to participating hospitals with PCI capability.
The primary study outcome was the change from the first to the final quarter of the study in the proportion of EMS-transported patients with a time from first medical contact to treatment in the cath lab of 90 minutes or less. This improved significantly, from 67% at baseline to 74% in the final quarter. Nine of the 12 participating regions reduced their time from first medical contact to treatment in the cath lab, and eight reached the national of goal of having 75% of STEMI patients treated within 90 minutes.
The other key time-to-care measures improved, too: At baseline, only 38% of patients had a time from first medical contact to cath lab activation of 20 minutes or less; by the final quarter, this figure had climbed to 56%. That’s an important metric, as evidenced by the study finding that in-hospital mortality occurred in 4.5% of patients with a time from first medical contact to cath lab activation of more than 20 minutes, compared with 2.2% in those with a time of 20 minutes or less.
Also, the proportion of patients who spent 20 minutes or less in the emergency department improved from 33% to 43%.
In-hospital mortality improved from 4.4% in the baseline quarter to 2.3% in the final quarter. No similar improvement in in-hospital mortality occurred in a comparison group of 22,651 STEMI patients treated at hospitals not involved in ACCELERATOR 2.
A significant reduction in the rate of in-hospital congestive heart failure occurred in the ACCELERATOR 2 centers, from 7.4% at baseline to 5.0%. In contrast, stroke, cardiogenic shock, and major bleeding rates were unchanged over time.
The ACCELERATOR 2 model of emergency cardiovascular care is designed to be highly generalizable, according to Dr. Jollis.
“This study supports the implementation of regionally coordinated systems across the United States to abort heart attacks, save lives, and enable heart attack victims to return to their families and productive lives,” he said.
The ACCELERATOR 2 operations manual – essentially a blueprint for organizing a regional STEMI system of care – is available gratis.
Dr. Allen, a cardiologist at the University of Colorado, Denver, said the ACCELERATOR 2 model has been successful because it is consistent with a fundamental principle of implementation science as described by Carolyn Clancy, MD, Executive in Charge at the Veterans Health Affairs Administration, who has said it’s a matter of making the right thing to do the easy thing to do.
Gregg C. Fonarow, MD, founder of the Get With the Guidelines program, predicted that the success of this program will lead to a ramping up of efforts to regionalize and coordinate STEMI care across the country. “I hope and anticipate that the AHA will take and run with the ACCELERATOR 2 model and adopt this into Mission: Lifeline, hoping to make this the standard approach to further improving care and outcomes in these patients,” said Dr. Fonarow, professor and cochief of cardiology at the University of California, Los Angeles, in a video interview.
Simultaneous with his presentation at the AHA conference, the results of STEMI ACCELERATOR 2 were published online in Circulation (2017 Nov 14; doi: 0.1161/CIRCULATIONAHA.117.032446).
The trial was sponsored by research and educational grants from AstraZeneca and The Medicines Company. Dr. Jollis reported having no financial conflicts of interest.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The in-hospital mortality rate of STEMI patients dropped from 4.4% in the baseline quarter to 2.3% in the final quarter of a study that examined the impact of introducing regionalized STEMI care.
Data source: This was a prospective study of an intervention that involved implementation of regionalized STEMI care in a dozen U.S. metropolitan areas.
Disclosures: The study was sponsored by research and educational grants from AstraZeneca and The Medicines Company. The presenter reported having no financial conflicts of interest.
Healing chronic venous ulcers? Compression, compression, compression
ESTES PARK, COLO. – Meg A. Lemon, MD, said at a conference on internal medicine sponsored by the University of Colorado at Denver, Aurora.
“The top nine ways of treating venous leg ulcers are compression,” explained Dr. Lemon, a Denver-area dermatologist in private practice. “You generally don’t have an active patient who’s moving around [and] allowing the calf to squeeze venous blood back into the circulation, so you have to compress externally. I spend a lot of time with patients saying, ‘If we don’t wear the compression stockings and we don’t elevate the legs, the wound will never heal.’ ”

Compression stockings are no longer frumpy – they have gotten hip. Endurance athletes have embraced them as a recovery aid, and they now come in a multitude of colorful styles. It’s best to start patients off at 15-20 mm Hg of compression so they don’t get discouraged by the initial challenges of getting the stockings on and off, Dr. Lemon explained, then work up to at least 30 mm Hg. Application devices that function much like a shoehorn can assist patients in getting the stockings on if they report difficulties.
As soon as patients get out of bed in the morning, their venous pressure skyrockets, and inflammatory compounds start accumulating in their legs: “I tell patients they need to put the stockings on before getting out of bed to pee in the morning,” the dermatologist said.
A meta-analysis has shown that adequate compression, coupled with wound debridement when indicated, resulted in the healing of 57% of longstanding chronic venous lower-extremity ulcers within 10 weeks and of 75% within 16 weeks, she reported.
Elevating the legs has therapeutic benefit as well, but it has to be done right. The legs must be above the heart for hours at a time, such as while sleeping or while laying on a couch to read or watch television. Putting three bed pillows under the entire calf – rather than under the feet – does the job. Simply sticking the pillows under the feet can result in painful knee hyperextension, which can lead to poor compliance.
“We’re all basically large columns of fluid,” Dr. Lemon said. “We stand around or sit all the time, and the fluid pools in our legs because the valves in the veins stop closing properly as we age. The increased pressure in the vein causes the vein to leak inflammatory compounds into the surrounding tissue, producing edema and chronic inflammation. The chronicity of the disease leads to really profound changes in the skin that are extraordinarily helpful diagnostically.”
Diagnostic tips
These cutaneous changes include a dark brown discoloration – reminiscent of rust – because of deposition of hemosiderin in tissues. The skin becomes fibrous, hard, and ulcerated. The end stage of chronic venous insufficiency is lipodermatosclerosis, in which the skin becomes almost immobile and the lower leg takes on a champagne bottle shape because of hardening of the skin close to the ankle.
Venography, long preferred in definitively diagnosing venous lower-extremity ulcers, is giving way to venous duplex ultrasound, which is not quite as accurate but spares patients the pain associated with the older procedure.
Roughly 70% of chronic lower-extremity ulcers are of venous origin, Dr. Lemon noted.
She encounters quite a few patients who are hospitalized for what is mistakenly diagnosed as bilateral cellulitis, when their true problem is chronic venous insufficiency. The patient’s response to two questions makes it easy to differentiate the two disorders. One is, “Do your legs hurt more or itch more?”
“If the legs itch more, the patient doesn’t have cellulitis,” Dr. Lemon explained. “Cellulitis doesn’t itch. Also, ask the patient, ‘When did your legs last look normal?’ They usually say it was years ago. That’s not bilateral cellulitis – an acute problem requiring hospitalization. It’s a chronic problem requiring extensive chronic wound care.”
If the lower leg wound site looks like cellulitis, with redness, swelling, and warmth to touch, but it itches rather than hurts, she noted, it’s probably stasis dermatitis, which is very common in patients with venous lower-extremity ulcers. The treatment is a potent topical steroid.
“Don’t be afraid of potent steroids,” Dr. Lemon said. “There is so much inflammation in those tissues, they need a potent steroid on the leg. I usually prescribe fluocinonide 0.05% because it’s reliably beneficial.”
An exudative venous wound should receive a moist dressing.
“Forget what your granny told you, and stop telling patients their wounds need to breathe,” she cautioned. “Wounds generally need to be suffocated and covered with an ointment like Vaseline. A dry wound heals about six times slower than a moist one; that’s been extensively studied in the dermatology, surgery, and burn literature.”
If, after 5-6 months of Dr. Lemon’s efforts, a patient’s wound still isn’t healing, the dermatologist will obtain a venous surgical consultation. In some reported series, surgical treatment of insufficiency – venous stripping – has resulted in improved healing time and fewer recurrent ulcers.
Dr. Lemon reported having no financial conflicts regarding her presentation.
ESTES PARK, COLO. – Meg A. Lemon, MD, said at a conference on internal medicine sponsored by the University of Colorado at Denver, Aurora.
“The top nine ways of treating venous leg ulcers are compression,” explained Dr. Lemon, a Denver-area dermatologist in private practice. “You generally don’t have an active patient who’s moving around [and] allowing the calf to squeeze venous blood back into the circulation, so you have to compress externally. I spend a lot of time with patients saying, ‘If we don’t wear the compression stockings and we don’t elevate the legs, the wound will never heal.’ ”
Compression stockings are no longer frumpy – they have gotten hip. Endurance athletes have embraced them as a recovery aid, and they now come in a multitude of colorful styles. It’s best to start patients off at 15-20 mm Hg of compression so they don’t get discouraged by the initial challenges of getting the stockings on and off, Dr. Lemon explained, then work up to at least 30 mm Hg. Application devices that function much like a shoehorn can assist patients in getting the stockings on if they report difficulties.
As soon as patients get out of bed in the morning, their venous pressure skyrockets, and inflammatory compounds start accumulating in their legs: “I tell patients they need to put the stockings on before getting out of bed to pee in the morning,” the dermatologist said.
A meta-analysis has shown that adequate compression, coupled with wound debridement when indicated, resulted in the healing of 57% of longstanding chronic venous lower-extremity ulcers within 10 weeks and of 75% within 16 weeks, she reported.
Elevating the legs has therapeutic benefit as well, but it has to be done right. The legs must be above the heart for hours at a time, such as while sleeping or while laying on a couch to read or watch television. Putting three bed pillows under the entire calf – rather than under the feet – does the job. Simply sticking the pillows under the feet can result in painful knee hyperextension, which can lead to poor compliance.
“We’re all basically large columns of fluid,” Dr. Lemon said. “We stand around or sit all the time, and the fluid pools in our legs because the valves in the veins stop closing properly as we age. The increased pressure in the vein causes the vein to leak inflammatory compounds into the surrounding tissue, producing edema and chronic inflammation. The chronicity of the disease leads to really profound changes in the skin that are extraordinarily helpful diagnostically.”
Diagnostic tips
These cutaneous changes include a dark brown discoloration – reminiscent of rust – because of deposition of hemosiderin in tissues. The skin becomes fibrous, hard, and ulcerated. The end stage of chronic venous insufficiency is lipodermatosclerosis, in which the skin becomes almost immobile and the lower leg takes on a champagne bottle shape because of hardening of the skin close to the ankle.
Venography, long preferred in definitively diagnosing venous lower-extremity ulcers, is giving way to venous duplex ultrasound, which is not quite as accurate but spares patients the pain associated with the older procedure.
Roughly 70% of chronic lower-extremity ulcers are of venous origin, Dr. Lemon noted.
She encounters quite a few patients who are hospitalized for what is mistakenly diagnosed as bilateral cellulitis, when their true problem is chronic venous insufficiency. The patient’s response to two questions makes it easy to differentiate the two disorders. One is, “Do your legs hurt more or itch more?”
“If the legs itch more, the patient doesn’t have cellulitis,” Dr. Lemon explained. “Cellulitis doesn’t itch. Also, ask the patient, ‘When did your legs last look normal?’ They usually say it was years ago. That’s not bilateral cellulitis – an acute problem requiring hospitalization. It’s a chronic problem requiring extensive chronic wound care.”
If the lower leg wound site looks like cellulitis, with redness, swelling, and warmth to touch, but it itches rather than hurts, she noted, it’s probably stasis dermatitis, which is very common in patients with venous lower-extremity ulcers. The treatment is a potent topical steroid.
“Don’t be afraid of potent steroids,” Dr. Lemon said. “There is so much inflammation in those tissues, they need a potent steroid on the leg. I usually prescribe fluocinonide 0.05% because it’s reliably beneficial.”
An exudative venous wound should receive a moist dressing.
“Forget what your granny told you, and stop telling patients their wounds need to breathe,” she cautioned. “Wounds generally need to be suffocated and covered with an ointment like Vaseline. A dry wound heals about six times slower than a moist one; that’s been extensively studied in the dermatology, surgery, and burn literature.”
If, after 5-6 months of Dr. Lemon’s efforts, a patient’s wound still isn’t healing, the dermatologist will obtain a venous surgical consultation. In some reported series, surgical treatment of insufficiency – venous stripping – has resulted in improved healing time and fewer recurrent ulcers.
Dr. Lemon reported having no financial conflicts regarding her presentation.
ESTES PARK, COLO. – Meg A. Lemon, MD, said at a conference on internal medicine sponsored by the University of Colorado at Denver, Aurora.
“The top nine ways of treating venous leg ulcers are compression,” explained Dr. Lemon, a Denver-area dermatologist in private practice. “You generally don’t have an active patient who’s moving around [and] allowing the calf to squeeze venous blood back into the circulation, so you have to compress externally. I spend a lot of time with patients saying, ‘If we don’t wear the compression stockings and we don’t elevate the legs, the wound will never heal.’ ”
Compression stockings are no longer frumpy – they have gotten hip. Endurance athletes have embraced them as a recovery aid, and they now come in a multitude of colorful styles. It’s best to start patients off at 15-20 mm Hg of compression so they don’t get discouraged by the initial challenges of getting the stockings on and off, Dr. Lemon explained, then work up to at least 30 mm Hg. Application devices that function much like a shoehorn can assist patients in getting the stockings on if they report difficulties.
As soon as patients get out of bed in the morning, their venous pressure skyrockets, and inflammatory compounds start accumulating in their legs: “I tell patients they need to put the stockings on before getting out of bed to pee in the morning,” the dermatologist said.
A meta-analysis has shown that adequate compression, coupled with wound debridement when indicated, resulted in the healing of 57% of longstanding chronic venous lower-extremity ulcers within 10 weeks and of 75% within 16 weeks, she reported.
Elevating the legs has therapeutic benefit as well, but it has to be done right. The legs must be above the heart for hours at a time, such as while sleeping or while laying on a couch to read or watch television. Putting three bed pillows under the entire calf – rather than under the feet – does the job. Simply sticking the pillows under the feet can result in painful knee hyperextension, which can lead to poor compliance.
“We’re all basically large columns of fluid,” Dr. Lemon said. “We stand around or sit all the time, and the fluid pools in our legs because the valves in the veins stop closing properly as we age. The increased pressure in the vein causes the vein to leak inflammatory compounds into the surrounding tissue, producing edema and chronic inflammation. The chronicity of the disease leads to really profound changes in the skin that are extraordinarily helpful diagnostically.”
Diagnostic tips
These cutaneous changes include a dark brown discoloration – reminiscent of rust – because of deposition of hemosiderin in tissues. The skin becomes fibrous, hard, and ulcerated. The end stage of chronic venous insufficiency is lipodermatosclerosis, in which the skin becomes almost immobile and the lower leg takes on a champagne bottle shape because of hardening of the skin close to the ankle.
Venography, long preferred in definitively diagnosing venous lower-extremity ulcers, is giving way to venous duplex ultrasound, which is not quite as accurate but spares patients the pain associated with the older procedure.
Roughly 70% of chronic lower-extremity ulcers are of venous origin, Dr. Lemon noted.
She encounters quite a few patients who are hospitalized for what is mistakenly diagnosed as bilateral cellulitis, when their true problem is chronic venous insufficiency. The patient’s response to two questions makes it easy to differentiate the two disorders. One is, “Do your legs hurt more or itch more?”
“If the legs itch more, the patient doesn’t have cellulitis,” Dr. Lemon explained. “Cellulitis doesn’t itch. Also, ask the patient, ‘When did your legs last look normal?’ They usually say it was years ago. That’s not bilateral cellulitis – an acute problem requiring hospitalization. It’s a chronic problem requiring extensive chronic wound care.”
If the lower leg wound site looks like cellulitis, with redness, swelling, and warmth to touch, but it itches rather than hurts, she noted, it’s probably stasis dermatitis, which is very common in patients with venous lower-extremity ulcers. The treatment is a potent topical steroid.
“Don’t be afraid of potent steroids,” Dr. Lemon said. “There is so much inflammation in those tissues, they need a potent steroid on the leg. I usually prescribe fluocinonide 0.05% because it’s reliably beneficial.”
An exudative venous wound should receive a moist dressing.
“Forget what your granny told you, and stop telling patients their wounds need to breathe,” she cautioned. “Wounds generally need to be suffocated and covered with an ointment like Vaseline. A dry wound heals about six times slower than a moist one; that’s been extensively studied in the dermatology, surgery, and burn literature.”
If, after 5-6 months of Dr. Lemon’s efforts, a patient’s wound still isn’t healing, the dermatologist will obtain a venous surgical consultation. In some reported series, surgical treatment of insufficiency – venous stripping – has resulted in improved healing time and fewer recurrent ulcers.
Dr. Lemon reported having no financial conflicts regarding her presentation.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
Prenatal maternal anxiety linked to hyperactivity in offspring as teenagers
PARIS – Maternal somatic anxiety during pregnancy and early childhood is associated in dose-response fashion with increased hyperactivity symptoms in mothers’ teenage children, according to an update from the landmark Avon Longitudinal Study of Parents and Offspring.
Perhaps the most intriguing finding in the new analysis was that the dose-response effect did not apply to the offspring of mothers in the highest quintile of somatic anxiety as measured during pregnancy and early childhood.
“It’s possible that a ceiling effect exists for those children that are exposed to continuous high levels of anxiety from pregnancy up to 5 years old,” Blanca Bolea-Alamanac, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Dr. Bolea-Alamanac of the department of psychiatry at the University of Toronto offered a couple possible explanations for this apparent ceiling effect. One is that children continuously exposed to high levels of maternal stress hormones in utero and through breast feeding become desensitized to the effects of those hormones in ways that affect their future behavior.
Another possibility is that children exposed to very high levels of anxiety in early life later develop internalizing-type symptoms rather than externalizing hyperactivity-type symptoms, she continued.
The Avon Longitudinal Study of Parents and Children is a birth cohort study conducted in Southwest England, where women who were pregnant in 1990 and their 14,062 offspring have been followed prospectively for 26 years.
Dr. Bolea-Alamanac’s analysis included the 8,725 women with maternal anxiety assessments obtained at 18 and 32 weeks of pregnancy, as well as at 8 weeks, 8 months, 2.67 years, and 5 years post partum. Maternal anxiety was measured using the Crown-Crisp Experiential Index, which provided a specific indicator of somatic anxiety via responses to questions including, “Are you troubled by dizziness or shortness of breath?” “Do you experience a tingling or prickling sensation in your body, arms, or legs?” “Have you felt that you may faint, feel sick, or have indigestion?” and “Do you experience extra sweating?” The response options to each question were “never,” “sometimes,” “often,” or “very often.”
All women understandably experienced increased anxiety during pregnancy, peaking in the weeks shortly prior to delivery. But by examining the totality of data obtained at two time points in pregnancy and four points post pregnancy, the psychiatrist was able to construct a model with five distinct quintiles of maternal anxiety.
Hyperactivity symptoms were assessed in 3,417 of their offspring using the Strengths and Difficulties Questionnaire hyperactivity subscale.
Class 1, the reference class, was comprised of women with low anxiety during pregnancy and after delivery. In a logistic regression analysis adjusted for maternal age, alcohol intake, and education, life events during pregnancy, socioeconomic status, and the child’s sex, the women in class 2 were at 1.44-fold increased risk of having a hyperactive teenager. Those who were more anxious, in class 3, were at 1.87-fold increased risk, and those in class 4 were at 2.5-fold greater risk than those in class 1. All those increased risks were statistically significant.
In contrast, women in class 5 – those who scored highest for somatic anxiety both in pregnancy and during the next 5 years – had only a nonsignificant trend toward an increased risk of having a hyperactive teenager.
The association between prenatal and postnatal maternal somatic anxiety and hyperactivity symptoms in their children seen in the Avon study is consistent with Barker’s theory, according to Dr. Bolea-Alamanac. Barker’s theory, developed by the prominent late British epidemiologist David Barker, MD, PhD, holds that intrauterine influences interact with the environment at birth to produce specific disease risks for the child. Dr. Barker’s theory has gained considerable traction over the years, as evidenced by the creation of the multidisciplinary International Society for Developmental Origins of Health and Disease.
Dr. Bolea-Alamanac reported having no relevant financial conflicts of interest.
PARIS – Maternal somatic anxiety during pregnancy and early childhood is associated in dose-response fashion with increased hyperactivity symptoms in mothers’ teenage children, according to an update from the landmark Avon Longitudinal Study of Parents and Offspring.
Perhaps the most intriguing finding in the new analysis was that the dose-response effect did not apply to the offspring of mothers in the highest quintile of somatic anxiety as measured during pregnancy and early childhood.
“It’s possible that a ceiling effect exists for those children that are exposed to continuous high levels of anxiety from pregnancy up to 5 years old,” Blanca Bolea-Alamanac, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Dr. Bolea-Alamanac of the department of psychiatry at the University of Toronto offered a couple possible explanations for this apparent ceiling effect. One is that children continuously exposed to high levels of maternal stress hormones in utero and through breast feeding become desensitized to the effects of those hormones in ways that affect their future behavior.
Another possibility is that children exposed to very high levels of anxiety in early life later develop internalizing-type symptoms rather than externalizing hyperactivity-type symptoms, she continued.
The Avon Longitudinal Study of Parents and Children is a birth cohort study conducted in Southwest England, where women who were pregnant in 1990 and their 14,062 offspring have been followed prospectively for 26 years.
Dr. Bolea-Alamanac’s analysis included the 8,725 women with maternal anxiety assessments obtained at 18 and 32 weeks of pregnancy, as well as at 8 weeks, 8 months, 2.67 years, and 5 years post partum. Maternal anxiety was measured using the Crown-Crisp Experiential Index, which provided a specific indicator of somatic anxiety via responses to questions including, “Are you troubled by dizziness or shortness of breath?” “Do you experience a tingling or prickling sensation in your body, arms, or legs?” “Have you felt that you may faint, feel sick, or have indigestion?” and “Do you experience extra sweating?” The response options to each question were “never,” “sometimes,” “often,” or “very often.”
All women understandably experienced increased anxiety during pregnancy, peaking in the weeks shortly prior to delivery. But by examining the totality of data obtained at two time points in pregnancy and four points post pregnancy, the psychiatrist was able to construct a model with five distinct quintiles of maternal anxiety.
Hyperactivity symptoms were assessed in 3,417 of their offspring using the Strengths and Difficulties Questionnaire hyperactivity subscale.
Class 1, the reference class, was comprised of women with low anxiety during pregnancy and after delivery. In a logistic regression analysis adjusted for maternal age, alcohol intake, and education, life events during pregnancy, socioeconomic status, and the child’s sex, the women in class 2 were at 1.44-fold increased risk of having a hyperactive teenager. Those who were more anxious, in class 3, were at 1.87-fold increased risk, and those in class 4 were at 2.5-fold greater risk than those in class 1. All those increased risks were statistically significant.
In contrast, women in class 5 – those who scored highest for somatic anxiety both in pregnancy and during the next 5 years – had only a nonsignificant trend toward an increased risk of having a hyperactive teenager.
The association between prenatal and postnatal maternal somatic anxiety and hyperactivity symptoms in their children seen in the Avon study is consistent with Barker’s theory, according to Dr. Bolea-Alamanac. Barker’s theory, developed by the prominent late British epidemiologist David Barker, MD, PhD, holds that intrauterine influences interact with the environment at birth to produce specific disease risks for the child. Dr. Barker’s theory has gained considerable traction over the years, as evidenced by the creation of the multidisciplinary International Society for Developmental Origins of Health and Disease.
Dr. Bolea-Alamanac reported having no relevant financial conflicts of interest.
PARIS – Maternal somatic anxiety during pregnancy and early childhood is associated in dose-response fashion with increased hyperactivity symptoms in mothers’ teenage children, according to an update from the landmark Avon Longitudinal Study of Parents and Offspring.
Perhaps the most intriguing finding in the new analysis was that the dose-response effect did not apply to the offspring of mothers in the highest quintile of somatic anxiety as measured during pregnancy and early childhood.
“It’s possible that a ceiling effect exists for those children that are exposed to continuous high levels of anxiety from pregnancy up to 5 years old,” Blanca Bolea-Alamanac, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Dr. Bolea-Alamanac of the department of psychiatry at the University of Toronto offered a couple possible explanations for this apparent ceiling effect. One is that children continuously exposed to high levels of maternal stress hormones in utero and through breast feeding become desensitized to the effects of those hormones in ways that affect their future behavior.
Another possibility is that children exposed to very high levels of anxiety in early life later develop internalizing-type symptoms rather than externalizing hyperactivity-type symptoms, she continued.
The Avon Longitudinal Study of Parents and Children is a birth cohort study conducted in Southwest England, where women who were pregnant in 1990 and their 14,062 offspring have been followed prospectively for 26 years.
Dr. Bolea-Alamanac’s analysis included the 8,725 women with maternal anxiety assessments obtained at 18 and 32 weeks of pregnancy, as well as at 8 weeks, 8 months, 2.67 years, and 5 years post partum. Maternal anxiety was measured using the Crown-Crisp Experiential Index, which provided a specific indicator of somatic anxiety via responses to questions including, “Are you troubled by dizziness or shortness of breath?” “Do you experience a tingling or prickling sensation in your body, arms, or legs?” “Have you felt that you may faint, feel sick, or have indigestion?” and “Do you experience extra sweating?” The response options to each question were “never,” “sometimes,” “often,” or “very often.”
All women understandably experienced increased anxiety during pregnancy, peaking in the weeks shortly prior to delivery. But by examining the totality of data obtained at two time points in pregnancy and four points post pregnancy, the psychiatrist was able to construct a model with five distinct quintiles of maternal anxiety.
Hyperactivity symptoms were assessed in 3,417 of their offspring using the Strengths and Difficulties Questionnaire hyperactivity subscale.
Class 1, the reference class, was comprised of women with low anxiety during pregnancy and after delivery. In a logistic regression analysis adjusted for maternal age, alcohol intake, and education, life events during pregnancy, socioeconomic status, and the child’s sex, the women in class 2 were at 1.44-fold increased risk of having a hyperactive teenager. Those who were more anxious, in class 3, were at 1.87-fold increased risk, and those in class 4 were at 2.5-fold greater risk than those in class 1. All those increased risks were statistically significant.
In contrast, women in class 5 – those who scored highest for somatic anxiety both in pregnancy and during the next 5 years – had only a nonsignificant trend toward an increased risk of having a hyperactive teenager.
The association between prenatal and postnatal maternal somatic anxiety and hyperactivity symptoms in their children seen in the Avon study is consistent with Barker’s theory, according to Dr. Bolea-Alamanac. Barker’s theory, developed by the prominent late British epidemiologist David Barker, MD, PhD, holds that intrauterine influences interact with the environment at birth to produce specific disease risks for the child. Dr. Barker’s theory has gained considerable traction over the years, as evidenced by the creation of the multidisciplinary International Society for Developmental Origins of Health and Disease.
Dr. Bolea-Alamanac reported having no relevant financial conflicts of interest.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: Women in the fourth quintile of somatic anxiety level during pregnancy and early childhood were at 2.5-fold increased risk of later having a hyperactive 16-year-old, compared with women in the lowest quintile of somatic anxiety.
Data source: Data gathered prospectively in the landmark Avon Longitudinal Study of Parents and Offspring.
Disclosures: The study presenter reported having no relevant financial conflicts of interest.
Targeting PCSK9 inhibitors to reap most benefit
ANAHEIM, CALIF. – Patients with symptomatic peripheral artery disease or a high-risk history of MI got the biggest bang for the buck from aggressive LDL cholesterol lowering with evolocumab in two new prespecified subgroup analyses from the landmark FOURIER trial presented at the American Heart Association scientific sessions.
“At the end of the day, not all of our patients with ASCVD [atherosclerotic cardiovascular disease] can have these expensive medications. These subgroup analyses will help clinicians to target use of PCSK9 inhibitors to the patients who will benefit the most,” Lynne T. Braun, PhD, commented in her role as discussant of the two secondary analyses, presented back to back in a late-breaking science session. Dr. Braun is a professor in the department of internal medicine at Rush University, Chicago.
The FOURIER trial included 27,564 high-risk patients with prior MI, stroke, and/or symptomatic peripheral arterial disease (PAD) who had an LDL cholesterol level of 70 mg/dL or more on high- or moderate-intensity statin therapy. They were randomized in double-blind fashion to add-on subcutaneous evolocumab (Repatha) at either 140 mg every 2 weeks or 420 mg/month or to placebo, for a median of 2.5 years of follow-up. The evolocumab group experienced a 59% reduction in LDL cholesterol, compared with the controls on background statin therapy plus placebo, down to a mean LDL cholesterol level of just 30 mg/dL.
As previously reported, the risk of the primary composite endpoint – comprising cardiovascular death, MI, stroke, unstable angina, or coronary revascularization – was reduced by 15% in the evolocumab group at 3 years. The secondary endpoint of cardiovascular death, MI, or stroke was reduced by 20%, from 9.9% to 7.9% (N Engl J Med. 2017;376:1713-22).
Evolocumab tamed PAD
At the AHA scientific sessions, Marc P. Bonaca, MD, presented a secondary analysis restricted to the 3,642 FOURIER participants with symptomatic PAD. The goal was to answer two unresolved questions: Does LDL cholesterol lowering beyond what’s achievable with a statin further reduce PAD patients’ cardiovascular risk? And does it reduce their risk of major adverse leg events (MALE), defined as a composite of acute limb ischemia, major amputation, and urgent revascularization?

The rate of the composite endpoint comprising cardiovascular death, MI, or stroke was 13% over 3 years in PAD patients randomized to placebo, which was 81% greater than the 7.6% rate in placebo-treated participants with a baseline history of stroke or MI but no PAD, in an analysis adjusted for demographics, cardiovascular risk factors, kidney function, body mass index, and prior revascularization.
The event rate was even higher in patients with PAD plus a history of MI or stroke, at 14.9%. Evolocumab reduced that risk by 27%, compared with placebo in patients with PAD, for an absolute risk reduction of 3.5% and a number-needed-to-treat (NNT) of 29 for 2.5 years.
The benefit of evolocumab was even more pronounced in the subgroup of 1,505 patients with baseline PAD but no prior MI or stroke: a 43% relative risk reduction, from 10.3% to 5.5%, for an absolute risk reduction of 4.8% and a NNT of 21.
A linear relationship was seen between the MALE rate during follow-up and LDL cholesterol level after 1 month of therapy, down to an LDL cholesterol level of less than 10 mg/dL. The clinically relevant composite endpoint of MACE (major adverse cardiovascular events – a composite of cardiovascular death, MI, and stroke) or MALE in patients with baseline PAD but no history of MI or stroke occurred in 12.8% of controls and 6.5% of the evolocumab group. This translated to a 48% relative risk reduction, a 6.3% absolute risk reduction, and a NNT of 16. The event curves in the evolocumab and control arms separated quite early, within the first 90 days of treatment.
The take home message: “LDL reduction to very low levels should be considered in patients with PAD, regardless of their history of MI or stroke, to reduce the risk of MACE [major adverse cardiovascular event] and MALE,” declared Dr. Bonaca of Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Spotting the patients with a history of MI who’re at highest risk
Marc S. Sabatine, MD, presented the subanalysis involving the 22,351 FOURIER patients with a prior MI. He and his coinvestigators identified three high-risk features within this group: an MI within the past 2 years, a history of two or more MIs, and residual multivessel CAD. Each of these three features was individually associated with a 34%-90% increased risk of MACE during follow-up. All told, 63% of FOURIER participants with prior MI had one or more of the high-risk features.

The use of evolocumab in patients with at least one of the three high-risk features was associated with a 22% relative risk reduction and an absolute 2.5% risk reduction, compared with placebo. The event curves diverged at about 6 months, and the gap between them steadily widened during follow-up. Extrapolating from this pattern, it’s likely that evolocumab would achieve an absolute 5% risk reduction in MACE, compared with placebo over 5 years, with an NNT of 20, according to Dr. Sabatine, professor of medicine at Harvard Medical School and chairman of the Thrombolysis in Myocardial Infarction (TIMI) Study Group.
Lingering questions
Dr. Braun was particularly impressed that the absolute risk reduction in MACE was even larger in patients with baseline PAD but no history of stroke or MI than in PAD patients with such a history. She added that, while she recognizes the value of selecting objectively assessable hard clinical MACE as the primary endpoint in FOURIER, her own patients care even more about other outcomes.
“What my patients with PAD care most about is whether profound LDL lowering translates to less claudication, improved quality of life, and greater physical activity tolerance. These were prespecified secondary outcomes in FOURIER, and I look forward to future reports addressing those issues,” she said.
Another unanswered question involves the mechanism by which intensive LDL cholesterol lowering results in fewer MACE and MALE events in high-risk subgroups. The possibilities include the plaque regression that was documented in the GLAGOV trial, an anti-inflammatory plaque-stabilizing effect being exerted through PCSK9 inhibition, or perhaps the PCSK9 inhibitors’ ability to moderately lower lipoprotein(a) cholesterol levels.
Simultaneous with Dr. Bonaca’s presentation at the AHA, the FOURIER PAD analysis was published online in Circulation (2017 Nov 13; doi: 10.1161/CIRCULATIONAHA.117.032235).
The FOURIER trial was sponsored by Amgen. Dr. Bonaca and Dr. Sabatine reported receiving research grants from and serving as consultants to Amgen and other companies.
ANAHEIM, CALIF. – Patients with symptomatic peripheral artery disease or a high-risk history of MI got the biggest bang for the buck from aggressive LDL cholesterol lowering with evolocumab in two new prespecified subgroup analyses from the landmark FOURIER trial presented at the American Heart Association scientific sessions.
“At the end of the day, not all of our patients with ASCVD [atherosclerotic cardiovascular disease] can have these expensive medications. These subgroup analyses will help clinicians to target use of PCSK9 inhibitors to the patients who will benefit the most,” Lynne T. Braun, PhD, commented in her role as discussant of the two secondary analyses, presented back to back in a late-breaking science session. Dr. Braun is a professor in the department of internal medicine at Rush University, Chicago.
The FOURIER trial included 27,564 high-risk patients with prior MI, stroke, and/or symptomatic peripheral arterial disease (PAD) who had an LDL cholesterol level of 70 mg/dL or more on high- or moderate-intensity statin therapy. They were randomized in double-blind fashion to add-on subcutaneous evolocumab (Repatha) at either 140 mg every 2 weeks or 420 mg/month or to placebo, for a median of 2.5 years of follow-up. The evolocumab group experienced a 59% reduction in LDL cholesterol, compared with the controls on background statin therapy plus placebo, down to a mean LDL cholesterol level of just 30 mg/dL.
As previously reported, the risk of the primary composite endpoint – comprising cardiovascular death, MI, stroke, unstable angina, or coronary revascularization – was reduced by 15% in the evolocumab group at 3 years. The secondary endpoint of cardiovascular death, MI, or stroke was reduced by 20%, from 9.9% to 7.9% (N Engl J Med. 2017;376:1713-22).
Evolocumab tamed PAD
At the AHA scientific sessions, Marc P. Bonaca, MD, presented a secondary analysis restricted to the 3,642 FOURIER participants with symptomatic PAD. The goal was to answer two unresolved questions: Does LDL cholesterol lowering beyond what’s achievable with a statin further reduce PAD patients’ cardiovascular risk? And does it reduce their risk of major adverse leg events (MALE), defined as a composite of acute limb ischemia, major amputation, and urgent revascularization?
The rate of the composite endpoint comprising cardiovascular death, MI, or stroke was 13% over 3 years in PAD patients randomized to placebo, which was 81% greater than the 7.6% rate in placebo-treated participants with a baseline history of stroke or MI but no PAD, in an analysis adjusted for demographics, cardiovascular risk factors, kidney function, body mass index, and prior revascularization.
The event rate was even higher in patients with PAD plus a history of MI or stroke, at 14.9%. Evolocumab reduced that risk by 27%, compared with placebo in patients with PAD, for an absolute risk reduction of 3.5% and a number-needed-to-treat (NNT) of 29 for 2.5 years.
The benefit of evolocumab was even more pronounced in the subgroup of 1,505 patients with baseline PAD but no prior MI or stroke: a 43% relative risk reduction, from 10.3% to 5.5%, for an absolute risk reduction of 4.8% and a NNT of 21.
A linear relationship was seen between the MALE rate during follow-up and LDL cholesterol level after 1 month of therapy, down to an LDL cholesterol level of less than 10 mg/dL. The clinically relevant composite endpoint of MACE (major adverse cardiovascular events – a composite of cardiovascular death, MI, and stroke) or MALE in patients with baseline PAD but no history of MI or stroke occurred in 12.8% of controls and 6.5% of the evolocumab group. This translated to a 48% relative risk reduction, a 6.3% absolute risk reduction, and a NNT of 16. The event curves in the evolocumab and control arms separated quite early, within the first 90 days of treatment.
The take home message: “LDL reduction to very low levels should be considered in patients with PAD, regardless of their history of MI or stroke, to reduce the risk of MACE [major adverse cardiovascular event] and MALE,” declared Dr. Bonaca of Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Spotting the patients with a history of MI who’re at highest risk
Marc S. Sabatine, MD, presented the subanalysis involving the 22,351 FOURIER patients with a prior MI. He and his coinvestigators identified three high-risk features within this group: an MI within the past 2 years, a history of two or more MIs, and residual multivessel CAD. Each of these three features was individually associated with a 34%-90% increased risk of MACE during follow-up. All told, 63% of FOURIER participants with prior MI had one or more of the high-risk features.
The use of evolocumab in patients with at least one of the three high-risk features was associated with a 22% relative risk reduction and an absolute 2.5% risk reduction, compared with placebo. The event curves diverged at about 6 months, and the gap between them steadily widened during follow-up. Extrapolating from this pattern, it’s likely that evolocumab would achieve an absolute 5% risk reduction in MACE, compared with placebo over 5 years, with an NNT of 20, according to Dr. Sabatine, professor of medicine at Harvard Medical School and chairman of the Thrombolysis in Myocardial Infarction (TIMI) Study Group.
Lingering questions
Dr. Braun was particularly impressed that the absolute risk reduction in MACE was even larger in patients with baseline PAD but no history of stroke or MI than in PAD patients with such a history. She added that, while she recognizes the value of selecting objectively assessable hard clinical MACE as the primary endpoint in FOURIER, her own patients care even more about other outcomes.
“What my patients with PAD care most about is whether profound LDL lowering translates to less claudication, improved quality of life, and greater physical activity tolerance. These were prespecified secondary outcomes in FOURIER, and I look forward to future reports addressing those issues,” she said.
Another unanswered question involves the mechanism by which intensive LDL cholesterol lowering results in fewer MACE and MALE events in high-risk subgroups. The possibilities include the plaque regression that was documented in the GLAGOV trial, an anti-inflammatory plaque-stabilizing effect being exerted through PCSK9 inhibition, or perhaps the PCSK9 inhibitors’ ability to moderately lower lipoprotein(a) cholesterol levels.
Simultaneous with Dr. Bonaca’s presentation at the AHA, the FOURIER PAD analysis was published online in Circulation (2017 Nov 13; doi: 10.1161/CIRCULATIONAHA.117.032235).
The FOURIER trial was sponsored by Amgen. Dr. Bonaca and Dr. Sabatine reported receiving research grants from and serving as consultants to Amgen and other companies.
ANAHEIM, CALIF. – Patients with symptomatic peripheral artery disease or a high-risk history of MI got the biggest bang for the buck from aggressive LDL cholesterol lowering with evolocumab in two new prespecified subgroup analyses from the landmark FOURIER trial presented at the American Heart Association scientific sessions.
“At the end of the day, not all of our patients with ASCVD [atherosclerotic cardiovascular disease] can have these expensive medications. These subgroup analyses will help clinicians to target use of PCSK9 inhibitors to the patients who will benefit the most,” Lynne T. Braun, PhD, commented in her role as discussant of the two secondary analyses, presented back to back in a late-breaking science session. Dr. Braun is a professor in the department of internal medicine at Rush University, Chicago.
The FOURIER trial included 27,564 high-risk patients with prior MI, stroke, and/or symptomatic peripheral arterial disease (PAD) who had an LDL cholesterol level of 70 mg/dL or more on high- or moderate-intensity statin therapy. They were randomized in double-blind fashion to add-on subcutaneous evolocumab (Repatha) at either 140 mg every 2 weeks or 420 mg/month or to placebo, for a median of 2.5 years of follow-up. The evolocumab group experienced a 59% reduction in LDL cholesterol, compared with the controls on background statin therapy plus placebo, down to a mean LDL cholesterol level of just 30 mg/dL.
As previously reported, the risk of the primary composite endpoint – comprising cardiovascular death, MI, stroke, unstable angina, or coronary revascularization – was reduced by 15% in the evolocumab group at 3 years. The secondary endpoint of cardiovascular death, MI, or stroke was reduced by 20%, from 9.9% to 7.9% (N Engl J Med. 2017;376:1713-22).
Evolocumab tamed PAD
At the AHA scientific sessions, Marc P. Bonaca, MD, presented a secondary analysis restricted to the 3,642 FOURIER participants with symptomatic PAD. The goal was to answer two unresolved questions: Does LDL cholesterol lowering beyond what’s achievable with a statin further reduce PAD patients’ cardiovascular risk? And does it reduce their risk of major adverse leg events (MALE), defined as a composite of acute limb ischemia, major amputation, and urgent revascularization?
The rate of the composite endpoint comprising cardiovascular death, MI, or stroke was 13% over 3 years in PAD patients randomized to placebo, which was 81% greater than the 7.6% rate in placebo-treated participants with a baseline history of stroke or MI but no PAD, in an analysis adjusted for demographics, cardiovascular risk factors, kidney function, body mass index, and prior revascularization.
The event rate was even higher in patients with PAD plus a history of MI or stroke, at 14.9%. Evolocumab reduced that risk by 27%, compared with placebo in patients with PAD, for an absolute risk reduction of 3.5% and a number-needed-to-treat (NNT) of 29 for 2.5 years.
The benefit of evolocumab was even more pronounced in the subgroup of 1,505 patients with baseline PAD but no prior MI or stroke: a 43% relative risk reduction, from 10.3% to 5.5%, for an absolute risk reduction of 4.8% and a NNT of 21.
A linear relationship was seen between the MALE rate during follow-up and LDL cholesterol level after 1 month of therapy, down to an LDL cholesterol level of less than 10 mg/dL. The clinically relevant composite endpoint of MACE (major adverse cardiovascular events – a composite of cardiovascular death, MI, and stroke) or MALE in patients with baseline PAD but no history of MI or stroke occurred in 12.8% of controls and 6.5% of the evolocumab group. This translated to a 48% relative risk reduction, a 6.3% absolute risk reduction, and a NNT of 16. The event curves in the evolocumab and control arms separated quite early, within the first 90 days of treatment.
The take home message: “LDL reduction to very low levels should be considered in patients with PAD, regardless of their history of MI or stroke, to reduce the risk of MACE [major adverse cardiovascular event] and MALE,” declared Dr. Bonaca of Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Spotting the patients with a history of MI who’re at highest risk
Marc S. Sabatine, MD, presented the subanalysis involving the 22,351 FOURIER patients with a prior MI. He and his coinvestigators identified three high-risk features within this group: an MI within the past 2 years, a history of two or more MIs, and residual multivessel CAD. Each of these three features was individually associated with a 34%-90% increased risk of MACE during follow-up. All told, 63% of FOURIER participants with prior MI had one or more of the high-risk features.
The use of evolocumab in patients with at least one of the three high-risk features was associated with a 22% relative risk reduction and an absolute 2.5% risk reduction, compared with placebo. The event curves diverged at about 6 months, and the gap between them steadily widened during follow-up. Extrapolating from this pattern, it’s likely that evolocumab would achieve an absolute 5% risk reduction in MACE, compared with placebo over 5 years, with an NNT of 20, according to Dr. Sabatine, professor of medicine at Harvard Medical School and chairman of the Thrombolysis in Myocardial Infarction (TIMI) Study Group.
Lingering questions
Dr. Braun was particularly impressed that the absolute risk reduction in MACE was even larger in patients with baseline PAD but no history of stroke or MI than in PAD patients with such a history. She added that, while she recognizes the value of selecting objectively assessable hard clinical MACE as the primary endpoint in FOURIER, her own patients care even more about other outcomes.
“What my patients with PAD care most about is whether profound LDL lowering translates to less claudication, improved quality of life, and greater physical activity tolerance. These were prespecified secondary outcomes in FOURIER, and I look forward to future reports addressing those issues,” she said.
Another unanswered question involves the mechanism by which intensive LDL cholesterol lowering results in fewer MACE and MALE events in high-risk subgroups. The possibilities include the plaque regression that was documented in the GLAGOV trial, an anti-inflammatory plaque-stabilizing effect being exerted through PCSK9 inhibition, or perhaps the PCSK9 inhibitors’ ability to moderately lower lipoprotein(a) cholesterol levels.
Simultaneous with Dr. Bonaca’s presentation at the AHA, the FOURIER PAD analysis was published online in Circulation (2017 Nov 13; doi: 10.1161/CIRCULATIONAHA.117.032235).
The FOURIER trial was sponsored by Amgen. Dr. Bonaca and Dr. Sabatine reported receiving research grants from and serving as consultants to Amgen and other companies.
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS