User login
Registration now open for the Crohn’s & Colitis Congress
Registration for the Crohn’s & Colitis Congress,® the premier conference on inflammatory bowel disease (IBD), is open. The Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association, will take place Feb. 7-9, 2019, at the Bellagio, in Las Vegas.
Led by committee chair Brent Polk, MD, AGAF, and co-chairs Maria T. Abreu, MD, AGAF, and David T. Rubin, MD, AGAF, invited faculty include IBD thought-leaders in the fields of GI, research investigation, surgery, pediatrics, advanced practice, IBD nursing, diet and nutrition, mental health, radiology, and pathology.
The 2019 Congress’ agenda includes main sessions that will emphasize case studies and panel discussions. There will also be parallel sessions on basic and translational science for senior and junior investigators.
In addition, several pre-Congress workshops, taking place Feb. 7, will be available for selection.
There will also be plenty of social events and plenty of time to enjoy Las Vegas; including a Friday night Welcome Reception that should not be missed. It’s a great opportunity to network and celebrate.
Abstract submissions for basic, translational, and clinical research will be accepted beginning Aug. 1 and ending Oct. 24.
To learn more and register, visit www.crohnscolitiscongress.org.
Registration for the Crohn’s & Colitis Congress,® the premier conference on inflammatory bowel disease (IBD), is open. The Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association, will take place Feb. 7-9, 2019, at the Bellagio, in Las Vegas.
Led by committee chair Brent Polk, MD, AGAF, and co-chairs Maria T. Abreu, MD, AGAF, and David T. Rubin, MD, AGAF, invited faculty include IBD thought-leaders in the fields of GI, research investigation, surgery, pediatrics, advanced practice, IBD nursing, diet and nutrition, mental health, radiology, and pathology.
The 2019 Congress’ agenda includes main sessions that will emphasize case studies and panel discussions. There will also be parallel sessions on basic and translational science for senior and junior investigators.
In addition, several pre-Congress workshops, taking place Feb. 7, will be available for selection.
There will also be plenty of social events and plenty of time to enjoy Las Vegas; including a Friday night Welcome Reception that should not be missed. It’s a great opportunity to network and celebrate.
Abstract submissions for basic, translational, and clinical research will be accepted beginning Aug. 1 and ending Oct. 24.
To learn more and register, visit www.crohnscolitiscongress.org.
Registration for the Crohn’s & Colitis Congress,® the premier conference on inflammatory bowel disease (IBD), is open. The Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association, will take place Feb. 7-9, 2019, at the Bellagio, in Las Vegas.
Led by committee chair Brent Polk, MD, AGAF, and co-chairs Maria T. Abreu, MD, AGAF, and David T. Rubin, MD, AGAF, invited faculty include IBD thought-leaders in the fields of GI, research investigation, surgery, pediatrics, advanced practice, IBD nursing, diet and nutrition, mental health, radiology, and pathology.
The 2019 Congress’ agenda includes main sessions that will emphasize case studies and panel discussions. There will also be parallel sessions on basic and translational science for senior and junior investigators.
In addition, several pre-Congress workshops, taking place Feb. 7, will be available for selection.
There will also be plenty of social events and plenty of time to enjoy Las Vegas; including a Friday night Welcome Reception that should not be missed. It’s a great opportunity to network and celebrate.
Abstract submissions for basic, translational, and clinical research will be accepted beginning Aug. 1 and ending Oct. 24.
To learn more and register, visit www.crohnscolitiscongress.org.
Meet our 2018 AGA Research Scholar Award recipients
The six investigators awarded AGA’s flagship research grant are working on impressive research projects that address important unmet needs for GI patients.
In partnership with generous supporters, the AGA Research Foundation provided more than $2 million in research funding to 41 investigators in 2018. The AGA Research Scholar Award was given to 6 exceptional early-career investigators who represent the future of GI research. Read about their research projects below.
Sarah Andres, PhD
University of Pennsylvania, Philadelphia
Project title: The mRNA binding protein IMP1 regulates intestinal epithelial exosome biology during homeostasis and metastasis
Dr. Andres will use this award to delve more deeply into understanding how RNA binding proteins regulate exosomes within the intestinal and colonic epithelium and how this plays a part in health and disease. RNA binding proteins provide an exquisite layer of biological regulation to gene expression and downstream cellular processes, which is only beginning to be appreciated. Dr. Andres’s long-term hope is that her work will improve the diagnosis, treatment, and ultimately survival of patients with colon cancer.
Swathi Eluri, MD, MSCR
University of North Carolina at Chapel Hill
Project title: Improving Barrett’s esophagus screening practices in primary care
Dr. Eluri’s AGA-funded project will gather data to develop and test a multi-level screening intervention for Barrett’s esophagus to be implemented in primary care. The ultimate goal of her work is to improve esophageal adenocarcinoma detection. Given our highly effective endoscopic therapies for early neoplasia in Barrett’s esophagus, early detection has the potential to yield substantial benefits for patients.
Jill Hoffman, PhD
University of California, Los Angeles
AGA-Takeda Pharmaceuticals Research Scholar Award in IBD
Project title: Characterization of CRHR2-mediated enteric glial cell function during colitis
Dr. Hoffman will use her AGA-Takeda funding to define a role for corticotropin-releasing hormone (CRH) signaling in enteric glial cell function, and determine CRHR2-dependent crosstalk between enteric glial cells and the intestinal epithelium during inflammation. Through research aiming to understand the basic mechanisms of cell-to-cell signaling during intestinal inflammation, Dr. Hoffman hopes to determine how to harness these pathways to limit inflammation and promote repair in patients with IBD.
Elizabeth Jensen, MPH, PhD
Wake Forest University, Winston-Salem, NC
Project title: Early life factors, gene-environment interaction, and eosinophilic esophagitis (EoE)
With this funding, Dr. Jensen will conduct the largest study to date on early life factors and EoE, using data that have been collected prospectively through population-based registries in Denmark. Ultimately, Dr. Jensen hopes her research will lead to advancements in our understanding of etiologic factors for development of immune-mediated GI diseases, such as EoE, and will lead to the identification of modifiable factors for disease prevention.
Sumera Rizvi, MD
Mayo Clinic, Rochester, MN
Project title: Necrosis enhances tumor immunogenicity and augments cholangiocarcinoma tumor suppression in combination with PD-L1 blockade
Dr. Rizvi’s research is focused on elucidating immunogenic cell death mechanisms and exploring novel, immune-mediated therapeutic approaches in cholangiocarcinoma. This work has the potential to open novel therapeutic avenues for treatment of cholangiocarcinoma, which will ultimately improve the outcomes of patients with this devastating malignancy.
Niels Vande Casteele, PhD
University of California, San Diego
Project title: Identifying optimal thresholds and personalized dosing regimens of infliximab to maximize endoscopic remission rates in patients with ulcerative colitis
Dr. Vande Casteele’s research project is all about determining the right drug for the right patient at the right time using the right dose. By studying optimal thresholds and personalized dosing regimens of infliximab, Dr. Vande Casteele will build the basis for exposure-based dosing regimens that can be applied to other anti-TNF antibodies and antibodies with other targets used in the treatment of patients with IBD, as well as other chronic inflammatory diseases and/or oncology. Dr. Vande Casteele’s goal is for his work to have a direct impact on patients by allowing us to achieve better treatment outcomes with minimal side effects.
Learn more about the AGA Research Foundation at www.gastro.org/foundation.
The six investigators awarded AGA’s flagship research grant are working on impressive research projects that address important unmet needs for GI patients.
In partnership with generous supporters, the AGA Research Foundation provided more than $2 million in research funding to 41 investigators in 2018. The AGA Research Scholar Award was given to 6 exceptional early-career investigators who represent the future of GI research. Read about their research projects below.
Sarah Andres, PhD
University of Pennsylvania, Philadelphia
Project title: The mRNA binding protein IMP1 regulates intestinal epithelial exosome biology during homeostasis and metastasis
Dr. Andres will use this award to delve more deeply into understanding how RNA binding proteins regulate exosomes within the intestinal and colonic epithelium and how this plays a part in health and disease. RNA binding proteins provide an exquisite layer of biological regulation to gene expression and downstream cellular processes, which is only beginning to be appreciated. Dr. Andres’s long-term hope is that her work will improve the diagnosis, treatment, and ultimately survival of patients with colon cancer.
Swathi Eluri, MD, MSCR
University of North Carolina at Chapel Hill
Project title: Improving Barrett’s esophagus screening practices in primary care
Dr. Eluri’s AGA-funded project will gather data to develop and test a multi-level screening intervention for Barrett’s esophagus to be implemented in primary care. The ultimate goal of her work is to improve esophageal adenocarcinoma detection. Given our highly effective endoscopic therapies for early neoplasia in Barrett’s esophagus, early detection has the potential to yield substantial benefits for patients.
Jill Hoffman, PhD
University of California, Los Angeles
AGA-Takeda Pharmaceuticals Research Scholar Award in IBD
Project title: Characterization of CRHR2-mediated enteric glial cell function during colitis
Dr. Hoffman will use her AGA-Takeda funding to define a role for corticotropin-releasing hormone (CRH) signaling in enteric glial cell function, and determine CRHR2-dependent crosstalk between enteric glial cells and the intestinal epithelium during inflammation. Through research aiming to understand the basic mechanisms of cell-to-cell signaling during intestinal inflammation, Dr. Hoffman hopes to determine how to harness these pathways to limit inflammation and promote repair in patients with IBD.
Elizabeth Jensen, MPH, PhD
Wake Forest University, Winston-Salem, NC
Project title: Early life factors, gene-environment interaction, and eosinophilic esophagitis (EoE)
With this funding, Dr. Jensen will conduct the largest study to date on early life factors and EoE, using data that have been collected prospectively through population-based registries in Denmark. Ultimately, Dr. Jensen hopes her research will lead to advancements in our understanding of etiologic factors for development of immune-mediated GI diseases, such as EoE, and will lead to the identification of modifiable factors for disease prevention.
Sumera Rizvi, MD
Mayo Clinic, Rochester, MN
Project title: Necrosis enhances tumor immunogenicity and augments cholangiocarcinoma tumor suppression in combination with PD-L1 blockade
Dr. Rizvi’s research is focused on elucidating immunogenic cell death mechanisms and exploring novel, immune-mediated therapeutic approaches in cholangiocarcinoma. This work has the potential to open novel therapeutic avenues for treatment of cholangiocarcinoma, which will ultimately improve the outcomes of patients with this devastating malignancy.
Niels Vande Casteele, PhD
University of California, San Diego
Project title: Identifying optimal thresholds and personalized dosing regimens of infliximab to maximize endoscopic remission rates in patients with ulcerative colitis
Dr. Vande Casteele’s research project is all about determining the right drug for the right patient at the right time using the right dose. By studying optimal thresholds and personalized dosing regimens of infliximab, Dr. Vande Casteele will build the basis for exposure-based dosing regimens that can be applied to other anti-TNF antibodies and antibodies with other targets used in the treatment of patients with IBD, as well as other chronic inflammatory diseases and/or oncology. Dr. Vande Casteele’s goal is for his work to have a direct impact on patients by allowing us to achieve better treatment outcomes with minimal side effects.
Learn more about the AGA Research Foundation at www.gastro.org/foundation.
The six investigators awarded AGA’s flagship research grant are working on impressive research projects that address important unmet needs for GI patients.
In partnership with generous supporters, the AGA Research Foundation provided more than $2 million in research funding to 41 investigators in 2018. The AGA Research Scholar Award was given to 6 exceptional early-career investigators who represent the future of GI research. Read about their research projects below.
Sarah Andres, PhD
University of Pennsylvania, Philadelphia
Project title: The mRNA binding protein IMP1 regulates intestinal epithelial exosome biology during homeostasis and metastasis
Dr. Andres will use this award to delve more deeply into understanding how RNA binding proteins regulate exosomes within the intestinal and colonic epithelium and how this plays a part in health and disease. RNA binding proteins provide an exquisite layer of biological regulation to gene expression and downstream cellular processes, which is only beginning to be appreciated. Dr. Andres’s long-term hope is that her work will improve the diagnosis, treatment, and ultimately survival of patients with colon cancer.
Swathi Eluri, MD, MSCR
University of North Carolina at Chapel Hill
Project title: Improving Barrett’s esophagus screening practices in primary care
Dr. Eluri’s AGA-funded project will gather data to develop and test a multi-level screening intervention for Barrett’s esophagus to be implemented in primary care. The ultimate goal of her work is to improve esophageal adenocarcinoma detection. Given our highly effective endoscopic therapies for early neoplasia in Barrett’s esophagus, early detection has the potential to yield substantial benefits for patients.
Jill Hoffman, PhD
University of California, Los Angeles
AGA-Takeda Pharmaceuticals Research Scholar Award in IBD
Project title: Characterization of CRHR2-mediated enteric glial cell function during colitis
Dr. Hoffman will use her AGA-Takeda funding to define a role for corticotropin-releasing hormone (CRH) signaling in enteric glial cell function, and determine CRHR2-dependent crosstalk between enteric glial cells and the intestinal epithelium during inflammation. Through research aiming to understand the basic mechanisms of cell-to-cell signaling during intestinal inflammation, Dr. Hoffman hopes to determine how to harness these pathways to limit inflammation and promote repair in patients with IBD.
Elizabeth Jensen, MPH, PhD
Wake Forest University, Winston-Salem, NC
Project title: Early life factors, gene-environment interaction, and eosinophilic esophagitis (EoE)
With this funding, Dr. Jensen will conduct the largest study to date on early life factors and EoE, using data that have been collected prospectively through population-based registries in Denmark. Ultimately, Dr. Jensen hopes her research will lead to advancements in our understanding of etiologic factors for development of immune-mediated GI diseases, such as EoE, and will lead to the identification of modifiable factors for disease prevention.
Sumera Rizvi, MD
Mayo Clinic, Rochester, MN
Project title: Necrosis enhances tumor immunogenicity and augments cholangiocarcinoma tumor suppression in combination with PD-L1 blockade
Dr. Rizvi’s research is focused on elucidating immunogenic cell death mechanisms and exploring novel, immune-mediated therapeutic approaches in cholangiocarcinoma. This work has the potential to open novel therapeutic avenues for treatment of cholangiocarcinoma, which will ultimately improve the outcomes of patients with this devastating malignancy.
Niels Vande Casteele, PhD
University of California, San Diego
Project title: Identifying optimal thresholds and personalized dosing regimens of infliximab to maximize endoscopic remission rates in patients with ulcerative colitis
Dr. Vande Casteele’s research project is all about determining the right drug for the right patient at the right time using the right dose. By studying optimal thresholds and personalized dosing regimens of infliximab, Dr. Vande Casteele will build the basis for exposure-based dosing regimens that can be applied to other anti-TNF antibodies and antibodies with other targets used in the treatment of patients with IBD, as well as other chronic inflammatory diseases and/or oncology. Dr. Vande Casteele’s goal is for his work to have a direct impact on patients by allowing us to achieve better treatment outcomes with minimal side effects.
Learn more about the AGA Research Foundation at www.gastro.org/foundation.

AGA continues to ‘push the envelope,’ President says
“AGA is pushing the envelope in a number of areas,” said outgoing AGA President Sheila E. Crowe MD, AGAF, during the AGA Presidential Plenary at Digestive Disease Week® (DDW). “And in a changing world, there are battlefronts where we must continue to work toward innovative solutions.”
The association continues to push reform in maintenance of certification (MOC). The Gastroenterologist-accountable Professionalism in Practice (G-APP) alternative certification pathway introduced 2 years ago created a strong platform to continue guiding the American Board of Internal Medicine (ABIM) to adapt its own MOC process to be more flexible, less costly, and more reflective of the realities of clinical practice.
“ABIM has responded to our pressure by unveiling the 2-year check-in,” Dr. Crowe said. “This is progress, but it still fails to address all the concerns we have expressed to ABIM. AGA will continue to work collaboratively, but forcefully, to make sure that recertification is convenient, relevant, and meaningful.”
AGA has successfully pushed for improvements to the Medicare Quality Payments program. Dr. Crowe said the association remains committed to reducing the regulatory hoops, red tape, and associated costs that practices must navigate.
The continuing push to ease regulatory burdens of practice is buoyed by successes in other areas.
AGA built a new partnership with the Crohn’s and Colitis Foundation and launched the first annual Crohn’s & Colitis Congress™ earlier this year. Registration for the 2019 Congress opens later this month.
The AGA Community (community.gastro.org) became a vibrant hub for clinicians to discuss their most difficult cases. Most recently, AGA made its patient education materials freely available online through the AGA GI Patient Center (patient.gastro.org). All educational pieces are available in both English and Spanish.
Research has been a top priority since AGA was founded 121 years ago, Dr. Crowe added.
“We are proud to be part of a coalition that aggressively advocated for increases at NIH and were pleased that a $3 billion increase was secured in the budget,” she said. “It was a big win in a tough environment.”
To help bridge the continuing shortfall in federal funding, the AGA Research Foundation launched an active year of fundraising and funding. The Foundation provided $2 million in research funding to 41 young investigators in the past year. An expanded awards program provided more pilot awards and more research scholar awards (RSA).
The past year also saw the launch of the AGA Fecal Microbiota Transplantation (FMT) National Registry. The new registry will assess the short- and long-term patient outcomes associated with FMT. In addition, AGA created a clinical research registry for endoscopic suturing procedures. The annual AGA Tech Summit continues to push for innovation in all areas of GI. The ultimate goal, Dr. Crowe said, is to put the most effective innovations into the hands of clinicians as quickly as possible.
During the plenary, Dr. Crowe presented the annual Julius Friedenwald Medal to Loren Laine, MD, AGAF. In addition to a distinguished academic career, Dr. Laine helped create the AGA Center for Gut Microbiome Research and Education while he was AGA president and helped establish AGA’s guideline development process.
“AGA is pushing the envelope in a number of areas,” said outgoing AGA President Sheila E. Crowe MD, AGAF, during the AGA Presidential Plenary at Digestive Disease Week® (DDW). “And in a changing world, there are battlefronts where we must continue to work toward innovative solutions.”
The association continues to push reform in maintenance of certification (MOC). The Gastroenterologist-accountable Professionalism in Practice (G-APP) alternative certification pathway introduced 2 years ago created a strong platform to continue guiding the American Board of Internal Medicine (ABIM) to adapt its own MOC process to be more flexible, less costly, and more reflective of the realities of clinical practice.
“ABIM has responded to our pressure by unveiling the 2-year check-in,” Dr. Crowe said. “This is progress, but it still fails to address all the concerns we have expressed to ABIM. AGA will continue to work collaboratively, but forcefully, to make sure that recertification is convenient, relevant, and meaningful.”
AGA has successfully pushed for improvements to the Medicare Quality Payments program. Dr. Crowe said the association remains committed to reducing the regulatory hoops, red tape, and associated costs that practices must navigate.
The continuing push to ease regulatory burdens of practice is buoyed by successes in other areas.
AGA built a new partnership with the Crohn’s and Colitis Foundation and launched the first annual Crohn’s & Colitis Congress™ earlier this year. Registration for the 2019 Congress opens later this month.
The AGA Community (community.gastro.org) became a vibrant hub for clinicians to discuss their most difficult cases. Most recently, AGA made its patient education materials freely available online through the AGA GI Patient Center (patient.gastro.org). All educational pieces are available in both English and Spanish.
Research has been a top priority since AGA was founded 121 years ago, Dr. Crowe added.
“We are proud to be part of a coalition that aggressively advocated for increases at NIH and were pleased that a $3 billion increase was secured in the budget,” she said. “It was a big win in a tough environment.”
To help bridge the continuing shortfall in federal funding, the AGA Research Foundation launched an active year of fundraising and funding. The Foundation provided $2 million in research funding to 41 young investigators in the past year. An expanded awards program provided more pilot awards and more research scholar awards (RSA).
The past year also saw the launch of the AGA Fecal Microbiota Transplantation (FMT) National Registry. The new registry will assess the short- and long-term patient outcomes associated with FMT. In addition, AGA created a clinical research registry for endoscopic suturing procedures. The annual AGA Tech Summit continues to push for innovation in all areas of GI. The ultimate goal, Dr. Crowe said, is to put the most effective innovations into the hands of clinicians as quickly as possible.
During the plenary, Dr. Crowe presented the annual Julius Friedenwald Medal to Loren Laine, MD, AGAF. In addition to a distinguished academic career, Dr. Laine helped create the AGA Center for Gut Microbiome Research and Education while he was AGA president and helped establish AGA’s guideline development process.
“AGA is pushing the envelope in a number of areas,” said outgoing AGA President Sheila E. Crowe MD, AGAF, during the AGA Presidential Plenary at Digestive Disease Week® (DDW). “And in a changing world, there are battlefronts where we must continue to work toward innovative solutions.”
The association continues to push reform in maintenance of certification (MOC). The Gastroenterologist-accountable Professionalism in Practice (G-APP) alternative certification pathway introduced 2 years ago created a strong platform to continue guiding the American Board of Internal Medicine (ABIM) to adapt its own MOC process to be more flexible, less costly, and more reflective of the realities of clinical practice.
“ABIM has responded to our pressure by unveiling the 2-year check-in,” Dr. Crowe said. “This is progress, but it still fails to address all the concerns we have expressed to ABIM. AGA will continue to work collaboratively, but forcefully, to make sure that recertification is convenient, relevant, and meaningful.”
AGA has successfully pushed for improvements to the Medicare Quality Payments program. Dr. Crowe said the association remains committed to reducing the regulatory hoops, red tape, and associated costs that practices must navigate.
The continuing push to ease regulatory burdens of practice is buoyed by successes in other areas.
AGA built a new partnership with the Crohn’s and Colitis Foundation and launched the first annual Crohn’s & Colitis Congress™ earlier this year. Registration for the 2019 Congress opens later this month.
The AGA Community (community.gastro.org) became a vibrant hub for clinicians to discuss their most difficult cases. Most recently, AGA made its patient education materials freely available online through the AGA GI Patient Center (patient.gastro.org). All educational pieces are available in both English and Spanish.
Research has been a top priority since AGA was founded 121 years ago, Dr. Crowe added.
“We are proud to be part of a coalition that aggressively advocated for increases at NIH and were pleased that a $3 billion increase was secured in the budget,” she said. “It was a big win in a tough environment.”
To help bridge the continuing shortfall in federal funding, the AGA Research Foundation launched an active year of fundraising and funding. The Foundation provided $2 million in research funding to 41 young investigators in the past year. An expanded awards program provided more pilot awards and more research scholar awards (RSA).
The past year also saw the launch of the AGA Fecal Microbiota Transplantation (FMT) National Registry. The new registry will assess the short- and long-term patient outcomes associated with FMT. In addition, AGA created a clinical research registry for endoscopic suturing procedures. The annual AGA Tech Summit continues to push for innovation in all areas of GI. The ultimate goal, Dr. Crowe said, is to put the most effective innovations into the hands of clinicians as quickly as possible.
During the plenary, Dr. Crowe presented the annual Julius Friedenwald Medal to Loren Laine, MD, AGAF. In addition to a distinguished academic career, Dr. Laine helped create the AGA Center for Gut Microbiome Research and Education while he was AGA president and helped establish AGA’s guideline development process.
Meet our 2018 AGA Research Scholar Award Recipients
In 2018, the AGA Research Foundation was proud to provide more than $2 million in research funding to 41 investigators.
AGA’s flagship award, the AGA Research Scholar Award, was given to five exceptional early-career investigators who represent the future of GI research. In addition, one researcher was awarded the AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease. Read about the 2018 awardees’ research projects below.
Sarah Andres, PhD
University of Pennsylvania, Philadelphia
Project title: The mRNA-binding protein IMP1 regulates intestinal epithelial exosome biology during homeostasis and metastasis

Dr. Andres will use this award to delve more deeply into understanding how RNA-binding proteins regulate exosomes within the intestinal and colonic epithelium and how this plays a part in health and disease. RNA-binding proteins provide an exquisite layer of biological regulation to gene expression and downstream cellular processes, which is only beginning to be appreciated. Dr. Andres’ long-term hope is that her work will improve the diagnosis, treatment and ultimately survival of patients with colon cancer.
Swathi Eluri, MD, MSCR
University North Carolina at Chapel Hill
Project title: Improving Barrett’s esophagus screening practices in primary care

Dr. Eluri’s AGA-funded project will gather data to develop and test a multilevel screening intervention for Barrett’s esophagus to be implemented in primary care. The ultimate goal of her work is to improve esophageal adenocarcinoma detection. Given our highly effective endoscopic therapies for early neoplasia in Barrett’s esophagus, early detection has the potential to yield substantial benefits for patients.
Jill Hoffman, PhD
University of California, Los Angeles
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
Project title: Characterization of CRHR2-mediated enteric glial cell function during colitis

Dr. Hoffman will use her AGA-Takeda funding to define a role for corticotropin-releasing hormone (CRH) signaling in enteric glial cell function and determine CRHR2-dependent crosstalk between enteric glial cells and the intestinal epithelium during inflammation. Through research aimed at understanding the basic mechanisms of cell-to-cell signaling during intestinal inflammation, Dr. Hoffman hopes to determine how to harness these pathways to limit inflammation and promote repair in patients with IBD.
Elizabeth Jensen, MPH, PhD
Wake Forest University, Winston-Salem, N.C.
Project title: Early-life factors, gene-environment interaction and eosinophilic esophagitis (EoE)

With this funding, Dr. Jensen will conduct the largest study to date on early-life factors and EoE, using data that have been collected prospectively through population-based registries in Denmark. Ultimately, Dr. Jensen hopes her research will lead to advancements in our understanding of etiologic factors for development of immune-mediated GI diseases, such as EoE, and will lead to the identification of modifiable factors for disease prevention.
Sumera Rizvi, MD
Mayo Clinic, Rochester, Minn.
Project title: Necrosis enhances tumor immunogenicity and augments cholangiocarcinoma tumor suppression in combination with PD-L1 blockade

Dr. Rizvi’s research is focused on elucidating immunogenic cell death mechanisms and exploring novel, immune-mediated therapeutic approaches in cholangiocarcinoma. This work has the potential to open novel therapeutic avenues for treatment of cholangiocarcinoma, which will ultimately improve the outcomes of patients with this devastating malignancy.
Niels Vande Casteele, PhD
University of California, San Diego
Project title: Identifying optimal thresholds & personalized dosing regimens of infliximab to maximize endoscopic remission rates in patients with ulcerative colitis

Dr. Vande Casteele’s research project is all about determining the right drug for the right patient at the right time using the right dose. By studying optimal thresholds and personalized dosing regimens of infliximab, Dr. Vande Casteele will build the basis for exposure-based dosing regimens that can be applied to other anti-TNF antibodies and antibodies with other targets used in the treatment of patients with IBD, as well as other chronic inflammatory diseases and/or oncology. Dr. Vande Casteele’s goal is for his work to have a direct impact on patients by allowing us to achieve better treatment outcomes with minimal side effects.
View the 2019 AGA research funding opportunities. Please review the deadlines as application deadlines have shifted. Research Scholar Award applications open Sept. 7, 2018.
In 2018, the AGA Research Foundation was proud to provide more than $2 million in research funding to 41 investigators.
AGA’s flagship award, the AGA Research Scholar Award, was given to five exceptional early-career investigators who represent the future of GI research. In addition, one researcher was awarded the AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease. Read about the 2018 awardees’ research projects below.
Sarah Andres, PhD
University of Pennsylvania, Philadelphia
Project title: The mRNA-binding protein IMP1 regulates intestinal epithelial exosome biology during homeostasis and metastasis
Dr. Andres will use this award to delve more deeply into understanding how RNA-binding proteins regulate exosomes within the intestinal and colonic epithelium and how this plays a part in health and disease. RNA-binding proteins provide an exquisite layer of biological regulation to gene expression and downstream cellular processes, which is only beginning to be appreciated. Dr. Andres’ long-term hope is that her work will improve the diagnosis, treatment and ultimately survival of patients with colon cancer.
Swathi Eluri, MD, MSCR
University North Carolina at Chapel Hill
Project title: Improving Barrett’s esophagus screening practices in primary care
Dr. Eluri’s AGA-funded project will gather data to develop and test a multilevel screening intervention for Barrett’s esophagus to be implemented in primary care. The ultimate goal of her work is to improve esophageal adenocarcinoma detection. Given our highly effective endoscopic therapies for early neoplasia in Barrett’s esophagus, early detection has the potential to yield substantial benefits for patients.
Jill Hoffman, PhD
University of California, Los Angeles
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
Project title: Characterization of CRHR2-mediated enteric glial cell function during colitis
Dr. Hoffman will use her AGA-Takeda funding to define a role for corticotropin-releasing hormone (CRH) signaling in enteric glial cell function and determine CRHR2-dependent crosstalk between enteric glial cells and the intestinal epithelium during inflammation. Through research aimed at understanding the basic mechanisms of cell-to-cell signaling during intestinal inflammation, Dr. Hoffman hopes to determine how to harness these pathways to limit inflammation and promote repair in patients with IBD.
Elizabeth Jensen, MPH, PhD
Wake Forest University, Winston-Salem, N.C.
Project title: Early-life factors, gene-environment interaction and eosinophilic esophagitis (EoE)
With this funding, Dr. Jensen will conduct the largest study to date on early-life factors and EoE, using data that have been collected prospectively through population-based registries in Denmark. Ultimately, Dr. Jensen hopes her research will lead to advancements in our understanding of etiologic factors for development of immune-mediated GI diseases, such as EoE, and will lead to the identification of modifiable factors for disease prevention.
Sumera Rizvi, MD
Mayo Clinic, Rochester, Minn.
Project title: Necrosis enhances tumor immunogenicity and augments cholangiocarcinoma tumor suppression in combination with PD-L1 blockade
Dr. Rizvi’s research is focused on elucidating immunogenic cell death mechanisms and exploring novel, immune-mediated therapeutic approaches in cholangiocarcinoma. This work has the potential to open novel therapeutic avenues for treatment of cholangiocarcinoma, which will ultimately improve the outcomes of patients with this devastating malignancy.
Niels Vande Casteele, PhD
University of California, San Diego
Project title: Identifying optimal thresholds & personalized dosing regimens of infliximab to maximize endoscopic remission rates in patients with ulcerative colitis
Dr. Vande Casteele’s research project is all about determining the right drug for the right patient at the right time using the right dose. By studying optimal thresholds and personalized dosing regimens of infliximab, Dr. Vande Casteele will build the basis for exposure-based dosing regimens that can be applied to other anti-TNF antibodies and antibodies with other targets used in the treatment of patients with IBD, as well as other chronic inflammatory diseases and/or oncology. Dr. Vande Casteele’s goal is for his work to have a direct impact on patients by allowing us to achieve better treatment outcomes with minimal side effects.
View the 2019 AGA research funding opportunities. Please review the deadlines as application deadlines have shifted. Research Scholar Award applications open Sept. 7, 2018.
In 2018, the AGA Research Foundation was proud to provide more than $2 million in research funding to 41 investigators.
AGA’s flagship award, the AGA Research Scholar Award, was given to five exceptional early-career investigators who represent the future of GI research. In addition, one researcher was awarded the AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease. Read about the 2018 awardees’ research projects below.
Sarah Andres, PhD
University of Pennsylvania, Philadelphia
Project title: The mRNA-binding protein IMP1 regulates intestinal epithelial exosome biology during homeostasis and metastasis
Dr. Andres will use this award to delve more deeply into understanding how RNA-binding proteins regulate exosomes within the intestinal and colonic epithelium and how this plays a part in health and disease. RNA-binding proteins provide an exquisite layer of biological regulation to gene expression and downstream cellular processes, which is only beginning to be appreciated. Dr. Andres’ long-term hope is that her work will improve the diagnosis, treatment and ultimately survival of patients with colon cancer.
Swathi Eluri, MD, MSCR
University North Carolina at Chapel Hill
Project title: Improving Barrett’s esophagus screening practices in primary care
Dr. Eluri’s AGA-funded project will gather data to develop and test a multilevel screening intervention for Barrett’s esophagus to be implemented in primary care. The ultimate goal of her work is to improve esophageal adenocarcinoma detection. Given our highly effective endoscopic therapies for early neoplasia in Barrett’s esophagus, early detection has the potential to yield substantial benefits for patients.
Jill Hoffman, PhD
University of California, Los Angeles
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
Project title: Characterization of CRHR2-mediated enteric glial cell function during colitis
Dr. Hoffman will use her AGA-Takeda funding to define a role for corticotropin-releasing hormone (CRH) signaling in enteric glial cell function and determine CRHR2-dependent crosstalk between enteric glial cells and the intestinal epithelium during inflammation. Through research aimed at understanding the basic mechanisms of cell-to-cell signaling during intestinal inflammation, Dr. Hoffman hopes to determine how to harness these pathways to limit inflammation and promote repair in patients with IBD.
Elizabeth Jensen, MPH, PhD
Wake Forest University, Winston-Salem, N.C.
Project title: Early-life factors, gene-environment interaction and eosinophilic esophagitis (EoE)
With this funding, Dr. Jensen will conduct the largest study to date on early-life factors and EoE, using data that have been collected prospectively through population-based registries in Denmark. Ultimately, Dr. Jensen hopes her research will lead to advancements in our understanding of etiologic factors for development of immune-mediated GI diseases, such as EoE, and will lead to the identification of modifiable factors for disease prevention.
Sumera Rizvi, MD
Mayo Clinic, Rochester, Minn.
Project title: Necrosis enhances tumor immunogenicity and augments cholangiocarcinoma tumor suppression in combination with PD-L1 blockade
Dr. Rizvi’s research is focused on elucidating immunogenic cell death mechanisms and exploring novel, immune-mediated therapeutic approaches in cholangiocarcinoma. This work has the potential to open novel therapeutic avenues for treatment of cholangiocarcinoma, which will ultimately improve the outcomes of patients with this devastating malignancy.
Niels Vande Casteele, PhD
University of California, San Diego
Project title: Identifying optimal thresholds & personalized dosing regimens of infliximab to maximize endoscopic remission rates in patients with ulcerative colitis
Dr. Vande Casteele’s research project is all about determining the right drug for the right patient at the right time using the right dose. By studying optimal thresholds and personalized dosing regimens of infliximab, Dr. Vande Casteele will build the basis for exposure-based dosing regimens that can be applied to other anti-TNF antibodies and antibodies with other targets used in the treatment of patients with IBD, as well as other chronic inflammatory diseases and/or oncology. Dr. Vande Casteele’s goal is for his work to have a direct impact on patients by allowing us to achieve better treatment outcomes with minimal side effects.
View the 2019 AGA research funding opportunities. Please review the deadlines as application deadlines have shifted. Research Scholar Award applications open Sept. 7, 2018.
Don’t lose your access to essential resources
If you are a current AGA trainee, medical resident, or student member, please renew your membership today to ensure the continuation of your career-enhancing benefits for the upcoming membership year. Prepare for your next chapter with the latest news and breakthroughs in the field, as well as access to educational programs, events and much more.
While renewing, please update your member profile at My AGA for news and resources tailored to your professional interests. The deadline to renew is Aug. 31, 2018.
If you have any questions, please contact AGA Member Relations at member@gastro.org or 301-941-2651.
If you are a current AGA trainee, medical resident, or student member, please renew your membership today to ensure the continuation of your career-enhancing benefits for the upcoming membership year. Prepare for your next chapter with the latest news and breakthroughs in the field, as well as access to educational programs, events and much more.
While renewing, please update your member profile at My AGA for news and resources tailored to your professional interests. The deadline to renew is Aug. 31, 2018.
If you have any questions, please contact AGA Member Relations at member@gastro.org or 301-941-2651.
If you are a current AGA trainee, medical resident, or student member, please renew your membership today to ensure the continuation of your career-enhancing benefits for the upcoming membership year. Prepare for your next chapter with the latest news and breakthroughs in the field, as well as access to educational programs, events and much more.
While renewing, please update your member profile at My AGA for news and resources tailored to your professional interests. The deadline to renew is Aug. 31, 2018.
If you have any questions, please contact AGA Member Relations at member@gastro.org or 301-941-2651.
A successful career starts with taking charge
Successful careers don’t just happen. They are made by individuals who take charge and build their own success. The alternative is burnout.
“Part of burnout is feeling overburdened, overworked, and out of control,” said Barbara Jung, MD, AGAF, professor and chief of gastroenterology and hepatology at the University of Illinois at Chicago, during Strategies for a Successful Career: Wellness, Empowerment, Leadership and Resilience at Digestive Disease Week® (DDW) 2018. “If somebody is staying until 9 or 10 o’clock [at night] to finish notes, I have a discussion with them. It is good to be done at 5 p.m. and go home. It is all about setting your own priorities and not letting the job take over your life.”
Associations have a role to play, too. The ASGE Technology Committee reported in 2010 that up to 89% of GIs suffer musculoskeletal injuries from manipulating scopes. Colonoscopist’s thumb (left thumb tendonitis) and metacarpophalangeal joint strain were the most common injuries.
“Risk factors are part of our work,” said Mehnaz Shafi, MD, AGAF, professor of gastroenterology, hepatology and nutrition at the University of Texas MD Anderson Cancer Center, Houston. “Pinching, pushing, pulling, and awkward positions are part of what we do. This is an injury with consequences.”
Dr. Shafi chairs the AGA Task Force on Ergonomics. The group has recommended changes to endoscopic work stations that minimize injury. The most important changes include mounting monitors on flexible stands to accommodate GIs of all heights, adding straps to the control head to allow the fingers to relax, providing ergonomic training to all GIs and using patient beds that can be raised and lowered to accommodate both tall and short GIs.
“Shaping your career is one of the key principles in preventing burnout,” said Arthur DeCross, MD, AGAF, professor of medicine, gastroenterology and hepatology at the University of Rochester Medical Center, N.Y. “We know that more than half of gastroenterologists self-identify as being burned out. And one of the major contributors to burnout is lack of control over your work environment, your career, your colleagues. Taking control of your career can make a difference.”
Taking control can be particularly important for women. An AGA burnout survey in 2015 found that 51% of male GIs reported burnout versus 62% of female GIs.
One reason is women’s tendency to negotiate poorly on their own behalf, said Marie-Pier Tétreault, PhD, assistant professor of gastroenterology and hepatology at Northwestern University Feinberg School of Medicine, Chicago.
“It’s a matter of attitude,” she explained. “Men tend to believe they can and should make life happen. Women tend to believe that what you see is what you get. Even when women do negotiate, they tend to ask for 15%-30% less than their male colleagues. If you don’t ask, you won’t get.”
Simply taking the lead in negotiations can improve the outcome, she continued. Network with colleagues and mentors to find the appropriate ranges for salaries, benefits, and perks such as parking, spousal job opportunities, facilities and space, teaching expectations, administrative support, and more.
Successful careers don’t just happen. They are made by individuals who take charge and build their own success. The alternative is burnout.
“Part of burnout is feeling overburdened, overworked, and out of control,” said Barbara Jung, MD, AGAF, professor and chief of gastroenterology and hepatology at the University of Illinois at Chicago, during Strategies for a Successful Career: Wellness, Empowerment, Leadership and Resilience at Digestive Disease Week® (DDW) 2018. “If somebody is staying until 9 or 10 o’clock [at night] to finish notes, I have a discussion with them. It is good to be done at 5 p.m. and go home. It is all about setting your own priorities and not letting the job take over your life.”
Associations have a role to play, too. The ASGE Technology Committee reported in 2010 that up to 89% of GIs suffer musculoskeletal injuries from manipulating scopes. Colonoscopist’s thumb (left thumb tendonitis) and metacarpophalangeal joint strain were the most common injuries.
“Risk factors are part of our work,” said Mehnaz Shafi, MD, AGAF, professor of gastroenterology, hepatology and nutrition at the University of Texas MD Anderson Cancer Center, Houston. “Pinching, pushing, pulling, and awkward positions are part of what we do. This is an injury with consequences.”
Dr. Shafi chairs the AGA Task Force on Ergonomics. The group has recommended changes to endoscopic work stations that minimize injury. The most important changes include mounting monitors on flexible stands to accommodate GIs of all heights, adding straps to the control head to allow the fingers to relax, providing ergonomic training to all GIs and using patient beds that can be raised and lowered to accommodate both tall and short GIs.
“Shaping your career is one of the key principles in preventing burnout,” said Arthur DeCross, MD, AGAF, professor of medicine, gastroenterology and hepatology at the University of Rochester Medical Center, N.Y. “We know that more than half of gastroenterologists self-identify as being burned out. And one of the major contributors to burnout is lack of control over your work environment, your career, your colleagues. Taking control of your career can make a difference.”
Taking control can be particularly important for women. An AGA burnout survey in 2015 found that 51% of male GIs reported burnout versus 62% of female GIs.
One reason is women’s tendency to negotiate poorly on their own behalf, said Marie-Pier Tétreault, PhD, assistant professor of gastroenterology and hepatology at Northwestern University Feinberg School of Medicine, Chicago.
“It’s a matter of attitude,” she explained. “Men tend to believe they can and should make life happen. Women tend to believe that what you see is what you get. Even when women do negotiate, they tend to ask for 15%-30% less than their male colleagues. If you don’t ask, you won’t get.”
Simply taking the lead in negotiations can improve the outcome, she continued. Network with colleagues and mentors to find the appropriate ranges for salaries, benefits, and perks such as parking, spousal job opportunities, facilities and space, teaching expectations, administrative support, and more.
Successful careers don’t just happen. They are made by individuals who take charge and build their own success. The alternative is burnout.
“Part of burnout is feeling overburdened, overworked, and out of control,” said Barbara Jung, MD, AGAF, professor and chief of gastroenterology and hepatology at the University of Illinois at Chicago, during Strategies for a Successful Career: Wellness, Empowerment, Leadership and Resilience at Digestive Disease Week® (DDW) 2018. “If somebody is staying until 9 or 10 o’clock [at night] to finish notes, I have a discussion with them. It is good to be done at 5 p.m. and go home. It is all about setting your own priorities and not letting the job take over your life.”
Associations have a role to play, too. The ASGE Technology Committee reported in 2010 that up to 89% of GIs suffer musculoskeletal injuries from manipulating scopes. Colonoscopist’s thumb (left thumb tendonitis) and metacarpophalangeal joint strain were the most common injuries.
“Risk factors are part of our work,” said Mehnaz Shafi, MD, AGAF, professor of gastroenterology, hepatology and nutrition at the University of Texas MD Anderson Cancer Center, Houston. “Pinching, pushing, pulling, and awkward positions are part of what we do. This is an injury with consequences.”
Dr. Shafi chairs the AGA Task Force on Ergonomics. The group has recommended changes to endoscopic work stations that minimize injury. The most important changes include mounting monitors on flexible stands to accommodate GIs of all heights, adding straps to the control head to allow the fingers to relax, providing ergonomic training to all GIs and using patient beds that can be raised and lowered to accommodate both tall and short GIs.
“Shaping your career is one of the key principles in preventing burnout,” said Arthur DeCross, MD, AGAF, professor of medicine, gastroenterology and hepatology at the University of Rochester Medical Center, N.Y. “We know that more than half of gastroenterologists self-identify as being burned out. And one of the major contributors to burnout is lack of control over your work environment, your career, your colleagues. Taking control of your career can make a difference.”
Taking control can be particularly important for women. An AGA burnout survey in 2015 found that 51% of male GIs reported burnout versus 62% of female GIs.
One reason is women’s tendency to negotiate poorly on their own behalf, said Marie-Pier Tétreault, PhD, assistant professor of gastroenterology and hepatology at Northwestern University Feinberg School of Medicine, Chicago.
“It’s a matter of attitude,” she explained. “Men tend to believe they can and should make life happen. Women tend to believe that what you see is what you get. Even when women do negotiate, they tend to ask for 15%-30% less than their male colleagues. If you don’t ask, you won’t get.”
Simply taking the lead in negotiations can improve the outcome, she continued. Network with colleagues and mentors to find the appropriate ranges for salaries, benefits, and perks such as parking, spousal job opportunities, facilities and space, teaching expectations, administrative support, and more.
AGA honors GI Congressional champions Sen. Bill Cassidy and Rep. Mike Thompson
During Digestive Disease Week® (DDW) this year the AGA Political Action Committee (PAC) honored Sen. Bill Cassidy, R-La., and Rep. Mike Thompson, D-Calif., for their support over the years in advancing the science and practice of gastroenterology on Capitol Hill.
Cassidy has been instrumental in passing legislation that reformed the broken sustainable growth rate (SGR) formula and transitioned physicians to more value-based payments in the Medicare Access and Chip Reauthorization Act (MACRA). Cassidy was particularly helpful in creating a pathway for specialty physician–focused payment models and was helpful to AGA in communicating with the Centers for Medicare & Medicaid Services (CMS) about the need for specialty-driven health care models. Cassidy also championed our transparency campaign when the GI codes were being reevaluated and because of his help, CMS reformed the way they announce changes to the fee schedule and now provide notice so that stakeholders are able to participate in the process. Cassidy has also been a strong proponent in providing more transparency across our health care system and helping to provide regulatory relief to physicians, especially in the area of electronic health records.
Thompson has been a champion for GIs and our patients by supporting efforts to increase access to colorectal cancer screenings. He is a cosponsor of Removing Barriers to the Colorectal Cancer Screening Act, legislation that would correct the problem of requiring patients to pay a copay when a screening colonoscopy turns therapeutic. He also played a key role in AGA’s efforts to require CMS to change its fee setting system to one that is more transparent and provides stakeholders such as AGA the opportunity to participate more meaningfully in the process. Thompson signed onto two key letters to CMS calling on the agency to change its system to a more transparent one and to heed stakeholder input into the process. He has also been a strong supporter of meaningful funding increases for the National Institutes of Health.
During Digestive Disease Week® (DDW) this year the AGA Political Action Committee (PAC) honored Sen. Bill Cassidy, R-La., and Rep. Mike Thompson, D-Calif., for their support over the years in advancing the science and practice of gastroenterology on Capitol Hill.
Cassidy has been instrumental in passing legislation that reformed the broken sustainable growth rate (SGR) formula and transitioned physicians to more value-based payments in the Medicare Access and Chip Reauthorization Act (MACRA). Cassidy was particularly helpful in creating a pathway for specialty physician–focused payment models and was helpful to AGA in communicating with the Centers for Medicare & Medicaid Services (CMS) about the need for specialty-driven health care models. Cassidy also championed our transparency campaign when the GI codes were being reevaluated and because of his help, CMS reformed the way they announce changes to the fee schedule and now provide notice so that stakeholders are able to participate in the process. Cassidy has also been a strong proponent in providing more transparency across our health care system and helping to provide regulatory relief to physicians, especially in the area of electronic health records.
Thompson has been a champion for GIs and our patients by supporting efforts to increase access to colorectal cancer screenings. He is a cosponsor of Removing Barriers to the Colorectal Cancer Screening Act, legislation that would correct the problem of requiring patients to pay a copay when a screening colonoscopy turns therapeutic. He also played a key role in AGA’s efforts to require CMS to change its fee setting system to one that is more transparent and provides stakeholders such as AGA the opportunity to participate more meaningfully in the process. Thompson signed onto two key letters to CMS calling on the agency to change its system to a more transparent one and to heed stakeholder input into the process. He has also been a strong supporter of meaningful funding increases for the National Institutes of Health.
During Digestive Disease Week® (DDW) this year the AGA Political Action Committee (PAC) honored Sen. Bill Cassidy, R-La., and Rep. Mike Thompson, D-Calif., for their support over the years in advancing the science and practice of gastroenterology on Capitol Hill.
Cassidy has been instrumental in passing legislation that reformed the broken sustainable growth rate (SGR) formula and transitioned physicians to more value-based payments in the Medicare Access and Chip Reauthorization Act (MACRA). Cassidy was particularly helpful in creating a pathway for specialty physician–focused payment models and was helpful to AGA in communicating with the Centers for Medicare & Medicaid Services (CMS) about the need for specialty-driven health care models. Cassidy also championed our transparency campaign when the GI codes were being reevaluated and because of his help, CMS reformed the way they announce changes to the fee schedule and now provide notice so that stakeholders are able to participate in the process. Cassidy has also been a strong proponent in providing more transparency across our health care system and helping to provide regulatory relief to physicians, especially in the area of electronic health records.
Thompson has been a champion for GIs and our patients by supporting efforts to increase access to colorectal cancer screenings. He is a cosponsor of Removing Barriers to the Colorectal Cancer Screening Act, legislation that would correct the problem of requiring patients to pay a copay when a screening colonoscopy turns therapeutic. He also played a key role in AGA’s efforts to require CMS to change its fee setting system to one that is more transparent and provides stakeholders such as AGA the opportunity to participate more meaningfully in the process. Thompson signed onto two key letters to CMS calling on the agency to change its system to a more transparent one and to heed stakeholder input into the process. He has also been a strong supporter of meaningful funding increases for the National Institutes of Health.
Current and future applications of telemedicine to optimize the delivery of care in chronic liver disease
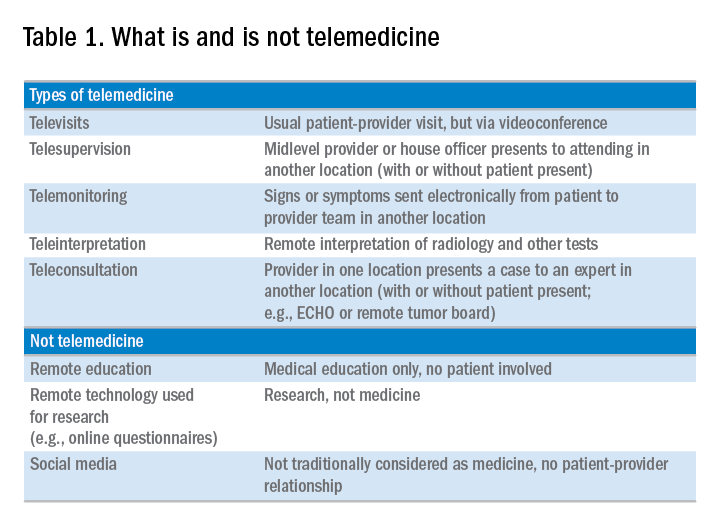
Telemedicine is defined broadly by the World Health Organization as the delivery of health care services at a distance using electronic means for “the diagnosis of treatment, and prevention of disease and injuries, research and evaluation, education of health care providers”1 to improve health. Although no single accepted definition exists, telehealth often is used as the umbrella term to encompass telemedicine (health care delivery) in addition to other activities such as education, research, health surveillance, and public health promotion.2 These various terms often are used interchangeably throughout the literature, leading to confusion.1,3 For the purpose of this review, we will use the term telemedicine to describe any care delivery model whereby patient care is provided at a distance using information technology such as cellphones, computers, or other electronic devices.
In the United States, the use of telemedicine is increasing. According to a 2017 survey of 184 health care executives conducted by the American Telemedicine Association, 88% believed that they would invest in telehealth in the near future, 98% believed that it offered a competitive advantage, with the caveat that 71% believed that lack of coverage and payments were barriers to implementation. Recent studies have shown that telehealth interventions are effective at improving clinical outcomes and decreasing inpatient utilization, with good patient satisfaction in the areas of mental health and chronic disease management. The Veterans Administration has emerged as an early telehealth adopter in chronic disease settings such as mental health, dermatology, hypertension, heart failure, and, as of 2016, has provided care to nearly 700,000 (12%) veterans since its inception.4-6 Despite the increased uptake, significant infrastructure and legal barriers to telemedicine remain and the literature regarding its utility in clinical practice continues to emerge.
Compared with other chronic diseases (e.g., heart failure, diabetes, mental illness) there is a dearth of literature on the use of telemedicine in liver disease. The first portion of this review synthesizes currently published literature of telemedicine/telehealth interventions to improve health care delivery and health outcomes in chronic liver disease including published peer-reviewed articles, abstracts, and ongoing clinical trials. The second portion discusses a framework for the future development of telemedicine and its integration into clinical practice by citing examples currently used throughout the country as well as ways to overcome implementation barriers.
Use of telemedicine in chronic liver disease: A literature review
We performed a systematic review of telemedicine in chronic liver disease. In consultation with a biomedical librarian, we searched for English-language articles for relevant studies with adult participants from July 1984 to May 2017 in PubMed, OVID Medline, American Association for the Study of Liver Disease, EMBASE, Web of Science, ClinicalTrials.gov, Elsevier/Science Direct, and the Cochrane Library (the search strategy is shown in the Supplementary Material at https://doi.org/10.1016/j.cgh.2017.10.004). The references of original publications and of review articles additionally were screened for potentially relevant studies. Abstracts that later resulted in no publications and studies in which telemedicine was used to deliver care, but was neither an exposure nor outcome, were excluded. Social media studies were not considered telemedicine if no patient care was involved. Studies of purely medical education interventions or those that evaluated the accuracy of technology to aid in diagnosis also were excluded.
Supplementary Table 1 (https://doi.org/10.1016/j.cgh.2017.10.004) shows the 20 published articles of telemedicine studies. Among these, there were 9 prospective trials, 3 retrospective studies, 2 case reports, and 6 small case series. One of the studies was randomized prospectively and 10 were uncontrolled.
Telemedicine in hepatitis C treatment

Telemedicine to aid in procedural/surgical management
A few reports have been published in the use of synchronous video and digital technology to aid in periprocedural management in liver disease. A case report highlighted a successful example of gastroenterologist-led teleproctoring using basic video technology to enable a surgeon to perform sclerotherapy for hemostasis in the setting of a variceal bleed.9 Another case report described the transmission of smart phone images from surgical trainees to an attending physician to make a real-time decision regarding a possibly questionable liver procurement, which took place 545 km away from the university hospital.10 A retrospective case series described the feasibility and successful use of high-resolution digital macroscopic photography and electronic transmission between liver transplant centers in the United Kingdom to increase the utilization of split liver transplantation, a setting in which detailed knowledge of vessel anatomy is needed for advanced surgical planning.11 Similarly, an uncontrolled case series from Greece reported on the feasibility and reliability of macroscopic image transmission to aid in the evaluation of liver grafts for transplantation.12
Telemedicine to support evaluation and management of hepatocellular carcinoma
One recent abstract reported on the use of asynchronous store-and-forward telemedicine for screening and management of hepatocellular carcinoma and evaluated process outcomes of specialty care access for newly diagnosed patients.13 A multifaceted approach included live video teleconferencing and centralized radiology review, which was conducted by a multidisciplinary tumor board at an expert hub site, which provided expert opinion and subsequent care (e.g., locoregional therapy, liver transplant evaluation) to spoke sites. As a result of the initiative, the time to specialty evaluation and receipt of hepatocellular carcinoma therapy decreased by 23 and 25 days, respectively.
Remote monitoring interventions

Proposed framework for advancing telemedicine in liver disease: The case for more research and policy changes
Telemedicine can serve two main goals in liver disease: improve access to specialty care, and improve care between visits. For the first goal, the technology is straightforward and limited research is required; the main barriers are regulatory and reimbursement. As an example, one of the authors (M.L.V.) uses telemedicine to perform liver transplant evaluations in Las Vegas, N.V., a state without a liver transplant program. Patients are seen initially by a nurse practitioner who resides in Las Vegas, and those patients needing transplant evaluation are scheduled for a video visit with the attending physician who is physically in California. This works well and patients love it; however, the business model is dependent on the downstream financial incentive of transplantation. In addition, various regulatory requirements must be satisfied such as monthly in-person visits. For the second goal, a number of exciting possibilities exist such as remote monitoring and patient disease management, but more research is needed.
Research
According to the Pew Research Center, 95% of American adults own a cellphone and 77% own a smartphone. These devices passively gather an extraordinary amount of data that could be harnessed to identify early warning signs of complications (remote monitoring). Another potentially fruitful area of research is patient disease management. This includes using technology (e.g., reminder texts) to effect behavior change such as with medication adherence, lifestyle modification, education, or peer mentoring. As an example, the coauthor (M.S.) is leading a study to promote physical activity among liver transplant recipients by using an online web portal developed by researchers at the University of Pennsylvania (Way to Health), which interfaces with patient cell phones and digital accelerometer devices. Participants receive daily feedback through text messages with their step counts, and small financial incentives are provided for adequate levels of physical activity. Technology also can facilitate the development of disease management platforms, which could improve both access and in-between visit monitoring, especially in remote areas. One of the authors (M.L.V.) currently is leading the development of a remote disease management program with funding from the American Association for the Study of Liver Diseases.
Despite the tremendous promise, traditional research methods in telemedicine may be challenging given the rapid and increasing uptake of health technology among patients and health systems. As such, the classic paradigm of randomized controlled trials to evaluate the success of an intervention or change in care delivery often is not feasible. We believe there is a need to recalibrate the definition of what constitutes a high-quality telemedicine study. For example, pragmatic trials and those designed within an implementation science framework that evaluate feasibility, scalability, and cost, in parallel with traditional clinical outcomes, may be better suited and should be accepted more widely.17
Policy
Even when the technology is available and research shows efficacy, the implementation of telemedicine in clinical practice faces regulatory and reimbursement barriers. The first regulatory question is whether a patient–provider relationship is being established (with the exception of limited provider–provider curbside consultation, the answer usually is yes). If so, the practice then is subject to all the usual regulatory concerns. The provider needs to be licensed at the site of origin (where the patient is located) and hold malpractice coverage for that location, and the video and medical record transmission should be compliant with the Health Insurance Portability and Accountability Act. The next challenge is reimbursement. Medicare only pays for video consultation if the patient lives in a designated rural Health Professional Shortage Area (www.cms.gov), and reimbursement by private payers varies. Even this is dependent on ever-changing state laws. Reimbursement for remote patient monitoring is even more limited (the National Telehealth Policy Research Center publishes a useful handbook: http://www.cchpca.org/sites/default/files/resources/50%20State%20FINAL%20April%202016.pdf). Absent a bipartisan Congressional effort to remedy this situation, the best hope for removing reimbursement barriers lies with payment reform. The Medicare Access and CHIP Reauthorization Act of 2015 mandates that the Centers for Medicare and Medicaid Services shift from fee-for-service to alternative payment models in the coming years. In these alternate payment models, providers are responsible for the overall quality and total cost of care for a population of patients. In this scenario, there may be a financial incentive for telemedicine, especially remote monitoring, to keep patients out of the hospital. Until then, under current payment models, reimbursement is limited and the barriers to widespread implementation are high.
Conclusions
Telemedicine has continued to increase in uptake and shows tremendous promise in expanding access to health care, promoting patient disease management, and facilitating in-between health care visit monitoring. Although the future is bright, more research is needed to determine optimal ways to integrate telemedicine — especially remote monitoring — into routine clinical care. We call on our specialty societies to send a clear political advocacy message that policy changes are needed to overcome regulatory and reimbursement challenges.
Acknowledgments
The authors would like to thank Lauren Jones and Mackenzie McDougal for their assistance with the literature review.
Supplementary materials and methods
The telemedicine interventions PubMed literature search strategy was as follows: ((“liver diseases”[MeSH Terms] OR (“liver”[All Fields] AND “diseases”[All Fields]) OR “liver diseases”[All Fields] OR (“liver”[All Fields] AND “disease”[All Fields]) OR “liver disease”[All Fields] OR liver dysfunction OR liver dysfunctions)) OR “liver transplantation”[MeSH Terms] OR “liver transplantation” [All Fields] AND (((“telemedicine”[MeSH Terms] OR “telemedicine”[All Fields] OR mobile health OR mhealth OR telehealth OR mhealth)) OR (videoconferencing OR videoconference)).
References
1. Kirsh S., Su G.L., Sales A., et al. Access to outpatient specialty care: solutions from an integrated health care system. Am J Med Qual. 2015;30:88-90.
2. Wilson L.S., Maeder A.J. recent directions in telemedicine: review of trends in research and practice. Healthc Inform Res. 2015;21:213-22.
3. Cross R.K., Kane, S. Integration of telemedicine into clinical gastroenterology and hepatology practice. Clin Gastroenterol Hepatol. 2017;15:175-81.
4. Darkins A., Ryan P., Kobb R., et al. Care coordination/home telehealth: the systematic implementation of health informatics, home telehealth, and disease management to support the care of veteran patients with chronic conditions. Telemed J E Health. 2008;14:1118-26.
5. Tuerk P.W., Fortney J., Bosworth H.B., et al. Toward the development of national telehealth services: the role of Veterans Health Administration and future directions for research. Telemed J E Health. 2010;16:115-7.
6. VA Press Release. Available: https://www.va.gov/opa/pressrel/includes/viewPDF.cfm?id=2789. Accessed: July 27, 2017.
7. Arora S., Kalishman S., Thornton K., et al. Expanding access to hepatitis C virus treatment-extension for Community Healthcare Outcomes (ECHO) project: disruptive innovation in specialty care. Hepatology. 2010;52:1124-33.
8. Mitruka K., Thornton K., Cusick S., et al. Expanding primary care capacity to treat hepatitis C virus infection through an evidence-based care model–Arizona and Utah, 2012-2014. MMWR Morb Mortal Wkly Rep. 2014;63:393-8.
9. Ahmed A., Slosberg E., Prasad P., et al. The successful use of telemedicine in acute variceal hemorrhage. J Clin Gastroenterol. 1999;29:212-3.
10. Croome K.P., Shum J., Al-Basheer M.A., et al. The benefit of smart phone usage in liver organ procurement. J Telemed Telecare. 2011;17:158-60.
11. Bhati C.S., Wigmore S.J., Reddy S., et al. Web-based image transmission: a novel approach to aid communication in split liver transplantation. Clin Transplant. 2010;24:98-103.
12. Mammas C.S., Geropoulos S., Saatsakis G., et al. Telepathology as a method to optimize quality in organ transplantation: a feasibility and reliability study of the virtual benching of liver graft. Stud Health Technol Inform. 2013;190:276-8.
13. Egert E.M., et al. A regional multidisciplinary liver tumor board improves access to hepatocellular carcinoma treatment for patients geographically distant from tertiary medical center. Hepatology. 2015;62:469A
14. Thomson M., Volk M., Kim H.M., et al. An automated telephone monitoring system to identify patients with cirrhosis at risk of re-hospitalization. Dig Dis Sci. 2015;60:3563-9.
15. Ertel A.E., Kaiser T.E., Abbott D.E., et al. Use of video-based education and tele-health home monitoring after liver transplantation: results of a novel pilot study. Surgery. 2016;160:869-76.
16. Thygesen G.B., Andersen H., Damsgaard B.S. et al. The effect of nurse performed telemedical video consultations for patients suffering from alcohol-related liver cirrhosis. J Hepatol. 2017;66:S349
17. Proctor E., Silmere H., Raghavan R. et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38:65-76.
Dr. Serper is in the division of gastroenterology, University of Pennsylvania Perelman School of Medicine, Philadelphia, and the department of medicine, Corporal Michael J. Crescenz VA Medical Center, Philadelphia; Dr. Volk is in the division of gastroenterology and Transplantation Institute, Loma Linda University, Loma Linda, Calif. The authors disclose no conflicts.
Telemedicine is defined broadly by the World Health Organization as the delivery of health care services at a distance using electronic means for “the diagnosis of treatment, and prevention of disease and injuries, research and evaluation, education of health care providers”1 to improve health. Although no single accepted definition exists, telehealth often is used as the umbrella term to encompass telemedicine (health care delivery) in addition to other activities such as education, research, health surveillance, and public health promotion.2 These various terms often are used interchangeably throughout the literature, leading to confusion.1,3 For the purpose of this review, we will use the term telemedicine to describe any care delivery model whereby patient care is provided at a distance using information technology such as cellphones, computers, or other electronic devices.
In the United States, the use of telemedicine is increasing. According to a 2017 survey of 184 health care executives conducted by the American Telemedicine Association, 88% believed that they would invest in telehealth in the near future, 98% believed that it offered a competitive advantage, with the caveat that 71% believed that lack of coverage and payments were barriers to implementation. Recent studies have shown that telehealth interventions are effective at improving clinical outcomes and decreasing inpatient utilization, with good patient satisfaction in the areas of mental health and chronic disease management. The Veterans Administration has emerged as an early telehealth adopter in chronic disease settings such as mental health, dermatology, hypertension, heart failure, and, as of 2016, has provided care to nearly 700,000 (12%) veterans since its inception.4-6 Despite the increased uptake, significant infrastructure and legal barriers to telemedicine remain and the literature regarding its utility in clinical practice continues to emerge.
Compared with other chronic diseases (e.g., heart failure, diabetes, mental illness) there is a dearth of literature on the use of telemedicine in liver disease. The first portion of this review synthesizes currently published literature of telemedicine/telehealth interventions to improve health care delivery and health outcomes in chronic liver disease including published peer-reviewed articles, abstracts, and ongoing clinical trials. The second portion discusses a framework for the future development of telemedicine and its integration into clinical practice by citing examples currently used throughout the country as well as ways to overcome implementation barriers.
Use of telemedicine in chronic liver disease: A literature review
We performed a systematic review of telemedicine in chronic liver disease. In consultation with a biomedical librarian, we searched for English-language articles for relevant studies with adult participants from July 1984 to May 2017 in PubMed, OVID Medline, American Association for the Study of Liver Disease, EMBASE, Web of Science, ClinicalTrials.gov, Elsevier/Science Direct, and the Cochrane Library (the search strategy is shown in the Supplementary Material at https://doi.org/10.1016/j.cgh.2017.10.004). The references of original publications and of review articles additionally were screened for potentially relevant studies. Abstracts that later resulted in no publications and studies in which telemedicine was used to deliver care, but was neither an exposure nor outcome, were excluded. Social media studies were not considered telemedicine if no patient care was involved. Studies of purely medical education interventions or those that evaluated the accuracy of technology to aid in diagnosis also were excluded.
Supplementary Table 1 (https://doi.org/10.1016/j.cgh.2017.10.004) shows the 20 published articles of telemedicine studies. Among these, there were 9 prospective trials, 3 retrospective studies, 2 case reports, and 6 small case series. One of the studies was randomized prospectively and 10 were uncontrolled.
Telemedicine in hepatitis C treatment
Telemedicine to aid in procedural/surgical management
A few reports have been published in the use of synchronous video and digital technology to aid in periprocedural management in liver disease. A case report highlighted a successful example of gastroenterologist-led teleproctoring using basic video technology to enable a surgeon to perform sclerotherapy for hemostasis in the setting of a variceal bleed.9 Another case report described the transmission of smart phone images from surgical trainees to an attending physician to make a real-time decision regarding a possibly questionable liver procurement, which took place 545 km away from the university hospital.10 A retrospective case series described the feasibility and successful use of high-resolution digital macroscopic photography and electronic transmission between liver transplant centers in the United Kingdom to increase the utilization of split liver transplantation, a setting in which detailed knowledge of vessel anatomy is needed for advanced surgical planning.11 Similarly, an uncontrolled case series from Greece reported on the feasibility and reliability of macroscopic image transmission to aid in the evaluation of liver grafts for transplantation.12
Telemedicine to support evaluation and management of hepatocellular carcinoma
One recent abstract reported on the use of asynchronous store-and-forward telemedicine for screening and management of hepatocellular carcinoma and evaluated process outcomes of specialty care access for newly diagnosed patients.13 A multifaceted approach included live video teleconferencing and centralized radiology review, which was conducted by a multidisciplinary tumor board at an expert hub site, which provided expert opinion and subsequent care (e.g., locoregional therapy, liver transplant evaluation) to spoke sites. As a result of the initiative, the time to specialty evaluation and receipt of hepatocellular carcinoma therapy decreased by 23 and 25 days, respectively.
Remote monitoring interventions
Proposed framework for advancing telemedicine in liver disease: The case for more research and policy changes
Telemedicine can serve two main goals in liver disease: improve access to specialty care, and improve care between visits. For the first goal, the technology is straightforward and limited research is required; the main barriers are regulatory and reimbursement. As an example, one of the authors (M.L.V.) uses telemedicine to perform liver transplant evaluations in Las Vegas, N.V., a state without a liver transplant program. Patients are seen initially by a nurse practitioner who resides in Las Vegas, and those patients needing transplant evaluation are scheduled for a video visit with the attending physician who is physically in California. This works well and patients love it; however, the business model is dependent on the downstream financial incentive of transplantation. In addition, various regulatory requirements must be satisfied such as monthly in-person visits. For the second goal, a number of exciting possibilities exist such as remote monitoring and patient disease management, but more research is needed.
Research
According to the Pew Research Center, 95% of American adults own a cellphone and 77% own a smartphone. These devices passively gather an extraordinary amount of data that could be harnessed to identify early warning signs of complications (remote monitoring). Another potentially fruitful area of research is patient disease management. This includes using technology (e.g., reminder texts) to effect behavior change such as with medication adherence, lifestyle modification, education, or peer mentoring. As an example, the coauthor (M.S.) is leading a study to promote physical activity among liver transplant recipients by using an online web portal developed by researchers at the University of Pennsylvania (Way to Health), which interfaces with patient cell phones and digital accelerometer devices. Participants receive daily feedback through text messages with their step counts, and small financial incentives are provided for adequate levels of physical activity. Technology also can facilitate the development of disease management platforms, which could improve both access and in-between visit monitoring, especially in remote areas. One of the authors (M.L.V.) currently is leading the development of a remote disease management program with funding from the American Association for the Study of Liver Diseases.
Despite the tremendous promise, traditional research methods in telemedicine may be challenging given the rapid and increasing uptake of health technology among patients and health systems. As such, the classic paradigm of randomized controlled trials to evaluate the success of an intervention or change in care delivery often is not feasible. We believe there is a need to recalibrate the definition of what constitutes a high-quality telemedicine study. For example, pragmatic trials and those designed within an implementation science framework that evaluate feasibility, scalability, and cost, in parallel with traditional clinical outcomes, may be better suited and should be accepted more widely.17
Policy
Even when the technology is available and research shows efficacy, the implementation of telemedicine in clinical practice faces regulatory and reimbursement barriers. The first regulatory question is whether a patient–provider relationship is being established (with the exception of limited provider–provider curbside consultation, the answer usually is yes). If so, the practice then is subject to all the usual regulatory concerns. The provider needs to be licensed at the site of origin (where the patient is located) and hold malpractice coverage for that location, and the video and medical record transmission should be compliant with the Health Insurance Portability and Accountability Act. The next challenge is reimbursement. Medicare only pays for video consultation if the patient lives in a designated rural Health Professional Shortage Area (www.cms.gov), and reimbursement by private payers varies. Even this is dependent on ever-changing state laws. Reimbursement for remote patient monitoring is even more limited (the National Telehealth Policy Research Center publishes a useful handbook: http://www.cchpca.org/sites/default/files/resources/50%20State%20FINAL%20April%202016.pdf). Absent a bipartisan Congressional effort to remedy this situation, the best hope for removing reimbursement barriers lies with payment reform. The Medicare Access and CHIP Reauthorization Act of 2015 mandates that the Centers for Medicare and Medicaid Services shift from fee-for-service to alternative payment models in the coming years. In these alternate payment models, providers are responsible for the overall quality and total cost of care for a population of patients. In this scenario, there may be a financial incentive for telemedicine, especially remote monitoring, to keep patients out of the hospital. Until then, under current payment models, reimbursement is limited and the barriers to widespread implementation are high.
Conclusions
Telemedicine has continued to increase in uptake and shows tremendous promise in expanding access to health care, promoting patient disease management, and facilitating in-between health care visit monitoring. Although the future is bright, more research is needed to determine optimal ways to integrate telemedicine — especially remote monitoring — into routine clinical care. We call on our specialty societies to send a clear political advocacy message that policy changes are needed to overcome regulatory and reimbursement challenges.
Acknowledgments
The authors would like to thank Lauren Jones and Mackenzie McDougal for their assistance with the literature review.
Supplementary materials and methods
The telemedicine interventions PubMed literature search strategy was as follows: ((“liver diseases”[MeSH Terms] OR (“liver”[All Fields] AND “diseases”[All Fields]) OR “liver diseases”[All Fields] OR (“liver”[All Fields] AND “disease”[All Fields]) OR “liver disease”[All Fields] OR liver dysfunction OR liver dysfunctions)) OR “liver transplantation”[MeSH Terms] OR “liver transplantation” [All Fields] AND (((“telemedicine”[MeSH Terms] OR “telemedicine”[All Fields] OR mobile health OR mhealth OR telehealth OR mhealth)) OR (videoconferencing OR videoconference)).
References
1. Kirsh S., Su G.L., Sales A., et al. Access to outpatient specialty care: solutions from an integrated health care system. Am J Med Qual. 2015;30:88-90.
2. Wilson L.S., Maeder A.J. recent directions in telemedicine: review of trends in research and practice. Healthc Inform Res. 2015;21:213-22.
3. Cross R.K., Kane, S. Integration of telemedicine into clinical gastroenterology and hepatology practice. Clin Gastroenterol Hepatol. 2017;15:175-81.
4. Darkins A., Ryan P., Kobb R., et al. Care coordination/home telehealth: the systematic implementation of health informatics, home telehealth, and disease management to support the care of veteran patients with chronic conditions. Telemed J E Health. 2008;14:1118-26.
5. Tuerk P.W., Fortney J., Bosworth H.B., et al. Toward the development of national telehealth services: the role of Veterans Health Administration and future directions for research. Telemed J E Health. 2010;16:115-7.
6. VA Press Release. Available: https://www.va.gov/opa/pressrel/includes/viewPDF.cfm?id=2789. Accessed: July 27, 2017.
7. Arora S., Kalishman S., Thornton K., et al. Expanding access to hepatitis C virus treatment-extension for Community Healthcare Outcomes (ECHO) project: disruptive innovation in specialty care. Hepatology. 2010;52:1124-33.
8. Mitruka K., Thornton K., Cusick S., et al. Expanding primary care capacity to treat hepatitis C virus infection through an evidence-based care model–Arizona and Utah, 2012-2014. MMWR Morb Mortal Wkly Rep. 2014;63:393-8.
9. Ahmed A., Slosberg E., Prasad P., et al. The successful use of telemedicine in acute variceal hemorrhage. J Clin Gastroenterol. 1999;29:212-3.
10. Croome K.P., Shum J., Al-Basheer M.A., et al. The benefit of smart phone usage in liver organ procurement. J Telemed Telecare. 2011;17:158-60.
11. Bhati C.S., Wigmore S.J., Reddy S., et al. Web-based image transmission: a novel approach to aid communication in split liver transplantation. Clin Transplant. 2010;24:98-103.
12. Mammas C.S., Geropoulos S., Saatsakis G., et al. Telepathology as a method to optimize quality in organ transplantation: a feasibility and reliability study of the virtual benching of liver graft. Stud Health Technol Inform. 2013;190:276-8.
13. Egert E.M., et al. A regional multidisciplinary liver tumor board improves access to hepatocellular carcinoma treatment for patients geographically distant from tertiary medical center. Hepatology. 2015;62:469A
14. Thomson M., Volk M., Kim H.M., et al. An automated telephone monitoring system to identify patients with cirrhosis at risk of re-hospitalization. Dig Dis Sci. 2015;60:3563-9.
15. Ertel A.E., Kaiser T.E., Abbott D.E., et al. Use of video-based education and tele-health home monitoring after liver transplantation: results of a novel pilot study. Surgery. 2016;160:869-76.
16. Thygesen G.B., Andersen H., Damsgaard B.S. et al. The effect of nurse performed telemedical video consultations for patients suffering from alcohol-related liver cirrhosis. J Hepatol. 2017;66:S349
17. Proctor E., Silmere H., Raghavan R. et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38:65-76.
Dr. Serper is in the division of gastroenterology, University of Pennsylvania Perelman School of Medicine, Philadelphia, and the department of medicine, Corporal Michael J. Crescenz VA Medical Center, Philadelphia; Dr. Volk is in the division of gastroenterology and Transplantation Institute, Loma Linda University, Loma Linda, Calif. The authors disclose no conflicts.
Telemedicine is defined broadly by the World Health Organization as the delivery of health care services at a distance using electronic means for “the diagnosis of treatment, and prevention of disease and injuries, research and evaluation, education of health care providers”1 to improve health. Although no single accepted definition exists, telehealth often is used as the umbrella term to encompass telemedicine (health care delivery) in addition to other activities such as education, research, health surveillance, and public health promotion.2 These various terms often are used interchangeably throughout the literature, leading to confusion.1,3 For the purpose of this review, we will use the term telemedicine to describe any care delivery model whereby patient care is provided at a distance using information technology such as cellphones, computers, or other electronic devices.
In the United States, the use of telemedicine is increasing. According to a 2017 survey of 184 health care executives conducted by the American Telemedicine Association, 88% believed that they would invest in telehealth in the near future, 98% believed that it offered a competitive advantage, with the caveat that 71% believed that lack of coverage and payments were barriers to implementation. Recent studies have shown that telehealth interventions are effective at improving clinical outcomes and decreasing inpatient utilization, with good patient satisfaction in the areas of mental health and chronic disease management. The Veterans Administration has emerged as an early telehealth adopter in chronic disease settings such as mental health, dermatology, hypertension, heart failure, and, as of 2016, has provided care to nearly 700,000 (12%) veterans since its inception.4-6 Despite the increased uptake, significant infrastructure and legal barriers to telemedicine remain and the literature regarding its utility in clinical practice continues to emerge.
Compared with other chronic diseases (e.g., heart failure, diabetes, mental illness) there is a dearth of literature on the use of telemedicine in liver disease. The first portion of this review synthesizes currently published literature of telemedicine/telehealth interventions to improve health care delivery and health outcomes in chronic liver disease including published peer-reviewed articles, abstracts, and ongoing clinical trials. The second portion discusses a framework for the future development of telemedicine and its integration into clinical practice by citing examples currently used throughout the country as well as ways to overcome implementation barriers.
Use of telemedicine in chronic liver disease: A literature review
We performed a systematic review of telemedicine in chronic liver disease. In consultation with a biomedical librarian, we searched for English-language articles for relevant studies with adult participants from July 1984 to May 2017 in PubMed, OVID Medline, American Association for the Study of Liver Disease, EMBASE, Web of Science, ClinicalTrials.gov, Elsevier/Science Direct, and the Cochrane Library (the search strategy is shown in the Supplementary Material at https://doi.org/10.1016/j.cgh.2017.10.004). The references of original publications and of review articles additionally were screened for potentially relevant studies. Abstracts that later resulted in no publications and studies in which telemedicine was used to deliver care, but was neither an exposure nor outcome, were excluded. Social media studies were not considered telemedicine if no patient care was involved. Studies of purely medical education interventions or those that evaluated the accuracy of technology to aid in diagnosis also were excluded.
Supplementary Table 1 (https://doi.org/10.1016/j.cgh.2017.10.004) shows the 20 published articles of telemedicine studies. Among these, there were 9 prospective trials, 3 retrospective studies, 2 case reports, and 6 small case series. One of the studies was randomized prospectively and 10 were uncontrolled.
Telemedicine in hepatitis C treatment
Telemedicine to aid in procedural/surgical management
A few reports have been published in the use of synchronous video and digital technology to aid in periprocedural management in liver disease. A case report highlighted a successful example of gastroenterologist-led teleproctoring using basic video technology to enable a surgeon to perform sclerotherapy for hemostasis in the setting of a variceal bleed.9 Another case report described the transmission of smart phone images from surgical trainees to an attending physician to make a real-time decision regarding a possibly questionable liver procurement, which took place 545 km away from the university hospital.10 A retrospective case series described the feasibility and successful use of high-resolution digital macroscopic photography and electronic transmission between liver transplant centers in the United Kingdom to increase the utilization of split liver transplantation, a setting in which detailed knowledge of vessel anatomy is needed for advanced surgical planning.11 Similarly, an uncontrolled case series from Greece reported on the feasibility and reliability of macroscopic image transmission to aid in the evaluation of liver grafts for transplantation.12
Telemedicine to support evaluation and management of hepatocellular carcinoma
One recent abstract reported on the use of asynchronous store-and-forward telemedicine for screening and management of hepatocellular carcinoma and evaluated process outcomes of specialty care access for newly diagnosed patients.13 A multifaceted approach included live video teleconferencing and centralized radiology review, which was conducted by a multidisciplinary tumor board at an expert hub site, which provided expert opinion and subsequent care (e.g., locoregional therapy, liver transplant evaluation) to spoke sites. As a result of the initiative, the time to specialty evaluation and receipt of hepatocellular carcinoma therapy decreased by 23 and 25 days, respectively.
Remote monitoring interventions
Proposed framework for advancing telemedicine in liver disease: The case for more research and policy changes
Telemedicine can serve two main goals in liver disease: improve access to specialty care, and improve care between visits. For the first goal, the technology is straightforward and limited research is required; the main barriers are regulatory and reimbursement. As an example, one of the authors (M.L.V.) uses telemedicine to perform liver transplant evaluations in Las Vegas, N.V., a state without a liver transplant program. Patients are seen initially by a nurse practitioner who resides in Las Vegas, and those patients needing transplant evaluation are scheduled for a video visit with the attending physician who is physically in California. This works well and patients love it; however, the business model is dependent on the downstream financial incentive of transplantation. In addition, various regulatory requirements must be satisfied such as monthly in-person visits. For the second goal, a number of exciting possibilities exist such as remote monitoring and patient disease management, but more research is needed.
Research
According to the Pew Research Center, 95% of American adults own a cellphone and 77% own a smartphone. These devices passively gather an extraordinary amount of data that could be harnessed to identify early warning signs of complications (remote monitoring). Another potentially fruitful area of research is patient disease management. This includes using technology (e.g., reminder texts) to effect behavior change such as with medication adherence, lifestyle modification, education, or peer mentoring. As an example, the coauthor (M.S.) is leading a study to promote physical activity among liver transplant recipients by using an online web portal developed by researchers at the University of Pennsylvania (Way to Health), which interfaces with patient cell phones and digital accelerometer devices. Participants receive daily feedback through text messages with their step counts, and small financial incentives are provided for adequate levels of physical activity. Technology also can facilitate the development of disease management platforms, which could improve both access and in-between visit monitoring, especially in remote areas. One of the authors (M.L.V.) currently is leading the development of a remote disease management program with funding from the American Association for the Study of Liver Diseases.
Despite the tremendous promise, traditional research methods in telemedicine may be challenging given the rapid and increasing uptake of health technology among patients and health systems. As such, the classic paradigm of randomized controlled trials to evaluate the success of an intervention or change in care delivery often is not feasible. We believe there is a need to recalibrate the definition of what constitutes a high-quality telemedicine study. For example, pragmatic trials and those designed within an implementation science framework that evaluate feasibility, scalability, and cost, in parallel with traditional clinical outcomes, may be better suited and should be accepted more widely.17
Policy
Even when the technology is available and research shows efficacy, the implementation of telemedicine in clinical practice faces regulatory and reimbursement barriers. The first regulatory question is whether a patient–provider relationship is being established (with the exception of limited provider–provider curbside consultation, the answer usually is yes). If so, the practice then is subject to all the usual regulatory concerns. The provider needs to be licensed at the site of origin (where the patient is located) and hold malpractice coverage for that location, and the video and medical record transmission should be compliant with the Health Insurance Portability and Accountability Act. The next challenge is reimbursement. Medicare only pays for video consultation if the patient lives in a designated rural Health Professional Shortage Area (www.cms.gov), and reimbursement by private payers varies. Even this is dependent on ever-changing state laws. Reimbursement for remote patient monitoring is even more limited (the National Telehealth Policy Research Center publishes a useful handbook: http://www.cchpca.org/sites/default/files/resources/50%20State%20FINAL%20April%202016.pdf). Absent a bipartisan Congressional effort to remedy this situation, the best hope for removing reimbursement barriers lies with payment reform. The Medicare Access and CHIP Reauthorization Act of 2015 mandates that the Centers for Medicare and Medicaid Services shift from fee-for-service to alternative payment models in the coming years. In these alternate payment models, providers are responsible for the overall quality and total cost of care for a population of patients. In this scenario, there may be a financial incentive for telemedicine, especially remote monitoring, to keep patients out of the hospital. Until then, under current payment models, reimbursement is limited and the barriers to widespread implementation are high.
Conclusions
Telemedicine has continued to increase in uptake and shows tremendous promise in expanding access to health care, promoting patient disease management, and facilitating in-between health care visit monitoring. Although the future is bright, more research is needed to determine optimal ways to integrate telemedicine — especially remote monitoring — into routine clinical care. We call on our specialty societies to send a clear political advocacy message that policy changes are needed to overcome regulatory and reimbursement challenges.
Acknowledgments
The authors would like to thank Lauren Jones and Mackenzie McDougal for their assistance with the literature review.
Supplementary materials and methods
The telemedicine interventions PubMed literature search strategy was as follows: ((“liver diseases”[MeSH Terms] OR (“liver”[All Fields] AND “diseases”[All Fields]) OR “liver diseases”[All Fields] OR (“liver”[All Fields] AND “disease”[All Fields]) OR “liver disease”[All Fields] OR liver dysfunction OR liver dysfunctions)) OR “liver transplantation”[MeSH Terms] OR “liver transplantation” [All Fields] AND (((“telemedicine”[MeSH Terms] OR “telemedicine”[All Fields] OR mobile health OR mhealth OR telehealth OR mhealth)) OR (videoconferencing OR videoconference)).
References
1. Kirsh S., Su G.L., Sales A., et al. Access to outpatient specialty care: solutions from an integrated health care system. Am J Med Qual. 2015;30:88-90.
2. Wilson L.S., Maeder A.J. recent directions in telemedicine: review of trends in research and practice. Healthc Inform Res. 2015;21:213-22.
3. Cross R.K., Kane, S. Integration of telemedicine into clinical gastroenterology and hepatology practice. Clin Gastroenterol Hepatol. 2017;15:175-81.
4. Darkins A., Ryan P., Kobb R., et al. Care coordination/home telehealth: the systematic implementation of health informatics, home telehealth, and disease management to support the care of veteran patients with chronic conditions. Telemed J E Health. 2008;14:1118-26.
5. Tuerk P.W., Fortney J., Bosworth H.B., et al. Toward the development of national telehealth services: the role of Veterans Health Administration and future directions for research. Telemed J E Health. 2010;16:115-7.
6. VA Press Release. Available: https://www.va.gov/opa/pressrel/includes/viewPDF.cfm?id=2789. Accessed: July 27, 2017.
7. Arora S., Kalishman S., Thornton K., et al. Expanding access to hepatitis C virus treatment-extension for Community Healthcare Outcomes (ECHO) project: disruptive innovation in specialty care. Hepatology. 2010;52:1124-33.
8. Mitruka K., Thornton K., Cusick S., et al. Expanding primary care capacity to treat hepatitis C virus infection through an evidence-based care model–Arizona and Utah, 2012-2014. MMWR Morb Mortal Wkly Rep. 2014;63:393-8.
9. Ahmed A., Slosberg E., Prasad P., et al. The successful use of telemedicine in acute variceal hemorrhage. J Clin Gastroenterol. 1999;29:212-3.
10. Croome K.P., Shum J., Al-Basheer M.A., et al. The benefit of smart phone usage in liver organ procurement. J Telemed Telecare. 2011;17:158-60.
11. Bhati C.S., Wigmore S.J., Reddy S., et al. Web-based image transmission: a novel approach to aid communication in split liver transplantation. Clin Transplant. 2010;24:98-103.
12. Mammas C.S., Geropoulos S., Saatsakis G., et al. Telepathology as a method to optimize quality in organ transplantation: a feasibility and reliability study of the virtual benching of liver graft. Stud Health Technol Inform. 2013;190:276-8.
13. Egert E.M., et al. A regional multidisciplinary liver tumor board improves access to hepatocellular carcinoma treatment for patients geographically distant from tertiary medical center. Hepatology. 2015;62:469A
14. Thomson M., Volk M., Kim H.M., et al. An automated telephone monitoring system to identify patients with cirrhosis at risk of re-hospitalization. Dig Dis Sci. 2015;60:3563-9.
15. Ertel A.E., Kaiser T.E., Abbott D.E., et al. Use of video-based education and tele-health home monitoring after liver transplantation: results of a novel pilot study. Surgery. 2016;160:869-76.
16. Thygesen G.B., Andersen H., Damsgaard B.S. et al. The effect of nurse performed telemedical video consultations for patients suffering from alcohol-related liver cirrhosis. J Hepatol. 2017;66:S349
17. Proctor E., Silmere H., Raghavan R. et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38:65-76.
Dr. Serper is in the division of gastroenterology, University of Pennsylvania Perelman School of Medicine, Philadelphia, and the department of medicine, Corporal Michael J. Crescenz VA Medical Center, Philadelphia; Dr. Volk is in the division of gastroenterology and Transplantation Institute, Loma Linda University, Loma Linda, Calif. The authors disclose no conflicts.
Introducing the 2018 class of AGA Research Foundation awardees
The American Gastroenterological Association (AGA) and the AGA Research Foundation are pleased to award 41 investigators with more than $2 million in research funding in the 2018 award year.
“We were impressed by the quality of applications received in 2018,” said Robert S. Sandler, MD, MPH, AGAF, chair, AGA Research Foundation. “The AGA Research Foundation is excited to add 41 investigators into the AGA Research Foundation awards family and we look forward to seeing the results of their research. Based on the proposals, we are confident that the newest class of awardees will continue to push gastroenterology and hepatology research forward and contribute to the next big discoveries in our field.”
The AGA Research Foundation Awards Program recruits, retains, and supports the most promising investigators in gastroenterology and hepatology. With AGA Research Foundation funding, recipients have protected time to continue their fundamental research into causes and treatments for digestive disorders. AGA grants have launched the careers of investigators doing important work that translates to new patient care tools for clinicians and better outcomes for patients. To view the list of recipients go to https://www.gastro.org/press-release/introducing-the-2018-class-of-aga-research-foundation-awardees.
The awards program is made possible thanks to generous donors and funders contributing to the AGA Research Foundation. Learn more about the AGA Research Foundation at www.gastro.org/foundation.
The American Gastroenterological Association (AGA) and the AGA Research Foundation are pleased to award 41 investigators with more than $2 million in research funding in the 2018 award year.
“We were impressed by the quality of applications received in 2018,” said Robert S. Sandler, MD, MPH, AGAF, chair, AGA Research Foundation. “The AGA Research Foundation is excited to add 41 investigators into the AGA Research Foundation awards family and we look forward to seeing the results of their research. Based on the proposals, we are confident that the newest class of awardees will continue to push gastroenterology and hepatology research forward and contribute to the next big discoveries in our field.”
The AGA Research Foundation Awards Program recruits, retains, and supports the most promising investigators in gastroenterology and hepatology. With AGA Research Foundation funding, recipients have protected time to continue their fundamental research into causes and treatments for digestive disorders. AGA grants have launched the careers of investigators doing important work that translates to new patient care tools for clinicians and better outcomes for patients. To view the list of recipients go to https://www.gastro.org/press-release/introducing-the-2018-class-of-aga-research-foundation-awardees.
The awards program is made possible thanks to generous donors and funders contributing to the AGA Research Foundation. Learn more about the AGA Research Foundation at www.gastro.org/foundation.
The American Gastroenterological Association (AGA) and the AGA Research Foundation are pleased to award 41 investigators with more than $2 million in research funding in the 2018 award year.
“We were impressed by the quality of applications received in 2018,” said Robert S. Sandler, MD, MPH, AGAF, chair, AGA Research Foundation. “The AGA Research Foundation is excited to add 41 investigators into the AGA Research Foundation awards family and we look forward to seeing the results of their research. Based on the proposals, we are confident that the newest class of awardees will continue to push gastroenterology and hepatology research forward and contribute to the next big discoveries in our field.”
The AGA Research Foundation Awards Program recruits, retains, and supports the most promising investigators in gastroenterology and hepatology. With AGA Research Foundation funding, recipients have protected time to continue their fundamental research into causes and treatments for digestive disorders. AGA grants have launched the careers of investigators doing important work that translates to new patient care tools for clinicians and better outcomes for patients. To view the list of recipients go to https://www.gastro.org/press-release/introducing-the-2018-class-of-aga-research-foundation-awardees.
The awards program is made possible thanks to generous donors and funders contributing to the AGA Research Foundation. Learn more about the AGA Research Foundation at www.gastro.org/foundation.
AGA announces its newest class of Fellows
AGA Fellowship status is an honor awarded to members who demonstrate a personal commitment to the field of gastroenterology, as well as professional achievement in clinical private or academic practice and in basic or clinical research.
The most recent inductees into the AGA Fellows Program were recognized at Digestive Disease Week® (DDW) 2018 and received a digital ribbon in their AGA Community profile. The 2018 class of AGA Fellows includes 112 members, who added the designation “AGAF” in their professional activities.
Join the AGA Fellowship Recognition Panel in congratulating these distinguished members and view the 2018 class of AGA Fellows in the AGA Community forum, community.gastro.org
Learn more about joining this international community of excellence. Applications for the 2019 cohort are now being accepted. Those in clinical private or academic practice and in basic or clinical research who meet the AGAF criteria are invited to apply. Applications are due Aug. 27, 2018. Learn more at gastro.org/fellowship.
AGA Fellowship status is an honor awarded to members who demonstrate a personal commitment to the field of gastroenterology, as well as professional achievement in clinical private or academic practice and in basic or clinical research.
The most recent inductees into the AGA Fellows Program were recognized at Digestive Disease Week® (DDW) 2018 and received a digital ribbon in their AGA Community profile. The 2018 class of AGA Fellows includes 112 members, who added the designation “AGAF” in their professional activities.
Join the AGA Fellowship Recognition Panel in congratulating these distinguished members and view the 2018 class of AGA Fellows in the AGA Community forum, community.gastro.org
Learn more about joining this international community of excellence. Applications for the 2019 cohort are now being accepted. Those in clinical private or academic practice and in basic or clinical research who meet the AGAF criteria are invited to apply. Applications are due Aug. 27, 2018. Learn more at gastro.org/fellowship.
AGA Fellowship status is an honor awarded to members who demonstrate a personal commitment to the field of gastroenterology, as well as professional achievement in clinical private or academic practice and in basic or clinical research.
The most recent inductees into the AGA Fellows Program were recognized at Digestive Disease Week® (DDW) 2018 and received a digital ribbon in their AGA Community profile. The 2018 class of AGA Fellows includes 112 members, who added the designation “AGAF” in their professional activities.
Join the AGA Fellowship Recognition Panel in congratulating these distinguished members and view the 2018 class of AGA Fellows in the AGA Community forum, community.gastro.org
Learn more about joining this international community of excellence. Applications for the 2019 cohort are now being accepted. Those in clinical private or academic practice and in basic or clinical research who meet the AGAF criteria are invited to apply. Applications are due Aug. 27, 2018. Learn more at gastro.org/fellowship.