User login
For NSCLC, neoadjuvant, adjuvant, or both?
This transcript has been edited for clarity.
Dr. West: Here at ASCO 2023 [American Society of Clinical Oncology] in Chicago, we’ve seen some blockbuster presentations in thoracic oncology. Many of these have brought up some important questions about the clinical implications that we need to discuss further.
At ASCO, as well as in the couple or 3 months preceding ASCO, we’ve gotten more and more data on perioperative approaches. Of course, over the past couple of years, we’ve had some new options of postoperative immunotherapy for a year, say, after chemotherapy or possibly after chemotherapy.
We have also had very influential data, such as the CheckMate 816 trial that gave three cycles of chemotherapy with nivolumab vs. chemotherapy alone to patients with stage IB to IIIA disease, but largely, nearly two thirds, with IIIA disease. That showed a very clear improvement in the pathologic complete response (pCR) rate with nivolumab added to chemotherapy and also a highly significant improvement in event-free survival and a strong trend toward improved overall survival. This is FDA approved and has been increasingly adopted, I would say, maybe with some variability by geography and center, but really a good amount of enthusiasm.
Now, we have a bunch of trials that give chemotherapy with immunotherapy. We’ve got the AEGEAN trial with durvalumab. We have Neotorch with chemotherapy and toripalimab. At ASCO 2023, we had a highly prominent presentation of KEYNOTE-671, giving four cycles of chemotherapy with pembrolizumab vs. chemotherapy and placebo.
Then there’s the built-in postoperative component of a year of immunotherapy as well, in all these trials. The data for KEYNOTE-671 look quite good. Of course, the other trials also were significant. I would say the comparator now is not nothing or chemotherapy alone anymore; it’s really against what is the best current standard of care.
It certainly adds some cost, it adds some risk for toxicity, and it adds a year of a patient coming into the clinic and getting IV infusions all this time to get a treatment that the patient has already had for four cycles in most of these trials.
If your cancer is resistant, is there going to be an incremental benefit to giving more of it? What are your thoughts about the risk and benefit? Going to a patient in your own clinic, how are you going to counsel your patients? Will anything change after the presentation of all these data and how you approach preoperatively?
Dr. Rotow: I agree. In some sense, it’s an embarrassment of riches, right?
Dr. West: Yes.
Dr. Rotow: We have so many positive studies looking at perioperative immunotherapy for our patients. They all show improved outcomes, but of course, they all compare with the old control arm of chemotherapy alone in some form, and this is no longer a useful control in this space. The open question is, do you use neoadjuvant, do you use adjuvant, or do you use both?
My high-level takeaway from these data is that the neoadjuvant component appears to be important. I think the overall trend, comparing across studies, of course, is that outcomes seem to be better with the neoadjuvant component. You also get the advantage of potential downstaging and potential greater ease of surgical resection. We know they have lower morbidity resection and shorter surgeries. You can comment on that. You also get your pathologic response data.
Dr. West: You get the feedback.
Dr. Rotow: Exactly.
Dr. West: The deliverability is also a big issue. You know you can much more reliably deliver your intended treatment by doing neoadjuvant followed by surgery.
Dr. Rotow: Exactly.
Dr. West: We know there’s major drop-off if patients have surgery, and in the recovery room they hear you got it all, and then they need to come back and maybe get chemotherapy and immunotherapy for a year. They’d ask, “What for? I can’t see anything.”
Dr. Rotow: Exactly. I think there are many advantages to that neoadjuvant component. I think all or many of us now have integrated this into our routine practice. Now the question is, do you need the adjuvant element or not on top? That is challenging because no trial has compared adjuvant to nonadjuvant. I think we all advocate for the need for this trial to answer this in a more randomized, prospective fashion. Of course, that doesn’t help our clinic practice tomorrow when we see a patient.
Dr. West: Or for the next 4 years.
Dr. Rotow: Or for the next 4 years – exactly. There’s going to be the open question of who really needs this? In some sense, we may be guided by the path response during the surgery itself. I think there may be those who claim that if you have a pCR, do you really need additional therapy? We don’t know the answer, but it’s tempting to say we know the outcomes in event-free survival are extremely good with a pCR.
Dr. West: Which is only 20% or 25% of patients, so it’s not most.
Dr. Rotow: It’s not most, but it’s better than the 2% or so with chemotherapy alone. That’s real progress, and it’s nice to have that readout. For that 80% without a pCR, what to do? I suspect there will be variation from provider to provider and from patient to patient, depending on tolerability to prior therapy, the patient’s wishes around the goals of care, and the patient’s risk for autoimmune toxicities.
Maybe there’s a patient with underlying autoimmune disease who’s gotten their neoadjuvant therapy and done well. You don’t want to risk that ongoing risk of exposure. Perhaps a patient with no risk factors who desires very aggressive treatment might be interested in more treatment.
In KEYNOTE-671, I was interested in the PD-L1 subgroups. These did trend the way you expect, with better responses in PD-L1 high, but there were also good outcomes and benefit to immunotherapy with the perioperative strategy in PD-L1–negative patients.
Dr. West: That didn’t really exclude anybody.
Dr. Rotow: It didn’t exclude anybody. In CheckMate 816, everyone benefited, but the benefit was less with those PD-L1–negative patients.
Dr. West: True.
Dr. Rotow: Absent further data to guide me or any prospective data here comparing these strategies, I might lean toward a longer course of immunotherapy in that population in hopes of triggering a response. I suspect that there will be variation from clinician to clinician in that space.
Dr. West: This is a setting where I feel like I have equipoise. I really feel that the incremental benefit is pretty small.
Dr. Rotow: Small. I agree.
Dr. West: It’s, frankly, somewhat dubious. On the other hand, you’re in a situation where if you know that three of four patients will experience a relapse and less-than-amazing outcomes, it’s hard to leave something that’s FDA approved and studied and a well-sanctioned option on the table if this patient may have relapse later.
In the end, I feel like I’d like to offer this and discuss it with all my patients. I think it’s a great place for shared decision-making because if a patient hears about that and decides they’re not interested, I’ll be fine with that. I think that’s a very sensible approach, but I don’t want to make it unilaterally. Other patients may say they want every opportunity, and if it comes back, at least I’ll know I did everything we could.
Dr. Rotow: Exactly. I agree with your statement about equipoise. I truly think that this is present here in the situation, and that there’s room for discussion in both directions with patients.
Now, one caveat I’d like to add to all these data is that the data should not apply to patients with some of our classic nonsmoking-associated driver mutations. This is another piece to the neoadjuvant data that I think is worth commenting on – the need to get appropriate testing before initiation of therapy and the pitfalls of starting this kind of treatment without knowing full biomarker testing. I think that’s something we have to watch for in our clinical practice as well.
Dr. West: Perhaps especially if we’re talking about doing a year of postoperative and someone has an ALK rearrangement or an EGFR mutation and we didn’t know it. That is a group where we’re worried about a rapid transition and potentially prohibitive, even life-threatening, toxicities from not planning in advance for this. This is something you don’t want to give concurrently or one right on top of the other. You don’t want to give immunotherapy and then transition right to targeted therapy. It’s dangerous.
Dr. Rotow: Exactly. The stakes were already high with neoadjuvant alone, but at least you had that gap of the presurgical period, surgical recovery, and then initiation of adjuvant therapy, if needed, or at relapse. With a postoperative long adjuvant period, those stakes are elevated because the immunotherapy exposure continues, so it’s something to be mindful of.
Dr. West: We have a general sense that many, but not all, of the targets that we’re talking about are associated with low benefit from immunotherapy. It’s not that well studied. I think this is another place for individualized discussion of the pros and cons. They were included in the trial, but they probably benefit less.
Dr. Rotow: Exactly. I think with the best established, EGFR and ALK probably are not benefiting much. They were actually included in the trial. Many of the neoadjuvant studies do not allow them to enroll if they’re known. On the other end of that spectrum, I think KRAS is just fine to treat with immunotherapy.
Dr. West: Sure.
Dr. Rotow: It’s an actionable driver. It’s not a traditional nonsmoking-associated driver, and those do just fine.
Dr. West: The studies show that these patients benefit just as much, at least, as the other patients.
Dr. Rotow: Exactly. I would never withhold this form of therapy for a KRAS driver mutation. The others, I think, are still in a gray zone. Depending on the patient demographics and tobacco use, I may elicit more or less caution in that space.
Dr. West: Well, I think we’re going to have much to still tease apart, with room for judgment here without a strong sense of the data telling us exactly what to do.
Dr. Rotow: Exactly.
Dr. West: There’s a large amount of excitement and interest in these new data, but there are still many open questions. I hope we continue to mull it over as we get more data and more insight to shape our plans.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. Rotow is the clinical director of the Lowe Center for Thoracic Oncology at the Dana-Farber Cancer Institute in Boston. Dr. West reported conflicts of interest with Ariad/Takeda, Bristol Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly. Dr. Rotow reported conflicts of interest with Genentech, AstraZeneca,Guardant, and Janssen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Dr. West: Here at ASCO 2023 [American Society of Clinical Oncology] in Chicago, we’ve seen some blockbuster presentations in thoracic oncology. Many of these have brought up some important questions about the clinical implications that we need to discuss further.
At ASCO, as well as in the couple or 3 months preceding ASCO, we’ve gotten more and more data on perioperative approaches. Of course, over the past couple of years, we’ve had some new options of postoperative immunotherapy for a year, say, after chemotherapy or possibly after chemotherapy.
We have also had very influential data, such as the CheckMate 816 trial that gave three cycles of chemotherapy with nivolumab vs. chemotherapy alone to patients with stage IB to IIIA disease, but largely, nearly two thirds, with IIIA disease. That showed a very clear improvement in the pathologic complete response (pCR) rate with nivolumab added to chemotherapy and also a highly significant improvement in event-free survival and a strong trend toward improved overall survival. This is FDA approved and has been increasingly adopted, I would say, maybe with some variability by geography and center, but really a good amount of enthusiasm.
Now, we have a bunch of trials that give chemotherapy with immunotherapy. We’ve got the AEGEAN trial with durvalumab. We have Neotorch with chemotherapy and toripalimab. At ASCO 2023, we had a highly prominent presentation of KEYNOTE-671, giving four cycles of chemotherapy with pembrolizumab vs. chemotherapy and placebo.
Then there’s the built-in postoperative component of a year of immunotherapy as well, in all these trials. The data for KEYNOTE-671 look quite good. Of course, the other trials also were significant. I would say the comparator now is not nothing or chemotherapy alone anymore; it’s really against what is the best current standard of care.
It certainly adds some cost, it adds some risk for toxicity, and it adds a year of a patient coming into the clinic and getting IV infusions all this time to get a treatment that the patient has already had for four cycles in most of these trials.
If your cancer is resistant, is there going to be an incremental benefit to giving more of it? What are your thoughts about the risk and benefit? Going to a patient in your own clinic, how are you going to counsel your patients? Will anything change after the presentation of all these data and how you approach preoperatively?
Dr. Rotow: I agree. In some sense, it’s an embarrassment of riches, right?
Dr. West: Yes.
Dr. Rotow: We have so many positive studies looking at perioperative immunotherapy for our patients. They all show improved outcomes, but of course, they all compare with the old control arm of chemotherapy alone in some form, and this is no longer a useful control in this space. The open question is, do you use neoadjuvant, do you use adjuvant, or do you use both?
My high-level takeaway from these data is that the neoadjuvant component appears to be important. I think the overall trend, comparing across studies, of course, is that outcomes seem to be better with the neoadjuvant component. You also get the advantage of potential downstaging and potential greater ease of surgical resection. We know they have lower morbidity resection and shorter surgeries. You can comment on that. You also get your pathologic response data.
Dr. West: You get the feedback.
Dr. Rotow: Exactly.
Dr. West: The deliverability is also a big issue. You know you can much more reliably deliver your intended treatment by doing neoadjuvant followed by surgery.
Dr. Rotow: Exactly.
Dr. West: We know there’s major drop-off if patients have surgery, and in the recovery room they hear you got it all, and then they need to come back and maybe get chemotherapy and immunotherapy for a year. They’d ask, “What for? I can’t see anything.”
Dr. Rotow: Exactly. I think there are many advantages to that neoadjuvant component. I think all or many of us now have integrated this into our routine practice. Now the question is, do you need the adjuvant element or not on top? That is challenging because no trial has compared adjuvant to nonadjuvant. I think we all advocate for the need for this trial to answer this in a more randomized, prospective fashion. Of course, that doesn’t help our clinic practice tomorrow when we see a patient.
Dr. West: Or for the next 4 years.
Dr. Rotow: Or for the next 4 years – exactly. There’s going to be the open question of who really needs this? In some sense, we may be guided by the path response during the surgery itself. I think there may be those who claim that if you have a pCR, do you really need additional therapy? We don’t know the answer, but it’s tempting to say we know the outcomes in event-free survival are extremely good with a pCR.
Dr. West: Which is only 20% or 25% of patients, so it’s not most.
Dr. Rotow: It’s not most, but it’s better than the 2% or so with chemotherapy alone. That’s real progress, and it’s nice to have that readout. For that 80% without a pCR, what to do? I suspect there will be variation from provider to provider and from patient to patient, depending on tolerability to prior therapy, the patient’s wishes around the goals of care, and the patient’s risk for autoimmune toxicities.
Maybe there’s a patient with underlying autoimmune disease who’s gotten their neoadjuvant therapy and done well. You don’t want to risk that ongoing risk of exposure. Perhaps a patient with no risk factors who desires very aggressive treatment might be interested in more treatment.
In KEYNOTE-671, I was interested in the PD-L1 subgroups. These did trend the way you expect, with better responses in PD-L1 high, but there were also good outcomes and benefit to immunotherapy with the perioperative strategy in PD-L1–negative patients.
Dr. West: That didn’t really exclude anybody.
Dr. Rotow: It didn’t exclude anybody. In CheckMate 816, everyone benefited, but the benefit was less with those PD-L1–negative patients.
Dr. West: True.
Dr. Rotow: Absent further data to guide me or any prospective data here comparing these strategies, I might lean toward a longer course of immunotherapy in that population in hopes of triggering a response. I suspect that there will be variation from clinician to clinician in that space.
Dr. West: This is a setting where I feel like I have equipoise. I really feel that the incremental benefit is pretty small.
Dr. Rotow: Small. I agree.
Dr. West: It’s, frankly, somewhat dubious. On the other hand, you’re in a situation where if you know that three of four patients will experience a relapse and less-than-amazing outcomes, it’s hard to leave something that’s FDA approved and studied and a well-sanctioned option on the table if this patient may have relapse later.
In the end, I feel like I’d like to offer this and discuss it with all my patients. I think it’s a great place for shared decision-making because if a patient hears about that and decides they’re not interested, I’ll be fine with that. I think that’s a very sensible approach, but I don’t want to make it unilaterally. Other patients may say they want every opportunity, and if it comes back, at least I’ll know I did everything we could.
Dr. Rotow: Exactly. I agree with your statement about equipoise. I truly think that this is present here in the situation, and that there’s room for discussion in both directions with patients.
Now, one caveat I’d like to add to all these data is that the data should not apply to patients with some of our classic nonsmoking-associated driver mutations. This is another piece to the neoadjuvant data that I think is worth commenting on – the need to get appropriate testing before initiation of therapy and the pitfalls of starting this kind of treatment without knowing full biomarker testing. I think that’s something we have to watch for in our clinical practice as well.
Dr. West: Perhaps especially if we’re talking about doing a year of postoperative and someone has an ALK rearrangement or an EGFR mutation and we didn’t know it. That is a group where we’re worried about a rapid transition and potentially prohibitive, even life-threatening, toxicities from not planning in advance for this. This is something you don’t want to give concurrently or one right on top of the other. You don’t want to give immunotherapy and then transition right to targeted therapy. It’s dangerous.
Dr. Rotow: Exactly. The stakes were already high with neoadjuvant alone, but at least you had that gap of the presurgical period, surgical recovery, and then initiation of adjuvant therapy, if needed, or at relapse. With a postoperative long adjuvant period, those stakes are elevated because the immunotherapy exposure continues, so it’s something to be mindful of.
Dr. West: We have a general sense that many, but not all, of the targets that we’re talking about are associated with low benefit from immunotherapy. It’s not that well studied. I think this is another place for individualized discussion of the pros and cons. They were included in the trial, but they probably benefit less.
Dr. Rotow: Exactly. I think with the best established, EGFR and ALK probably are not benefiting much. They were actually included in the trial. Many of the neoadjuvant studies do not allow them to enroll if they’re known. On the other end of that spectrum, I think KRAS is just fine to treat with immunotherapy.
Dr. West: Sure.
Dr. Rotow: It’s an actionable driver. It’s not a traditional nonsmoking-associated driver, and those do just fine.
Dr. West: The studies show that these patients benefit just as much, at least, as the other patients.
Dr. Rotow: Exactly. I would never withhold this form of therapy for a KRAS driver mutation. The others, I think, are still in a gray zone. Depending on the patient demographics and tobacco use, I may elicit more or less caution in that space.
Dr. West: Well, I think we’re going to have much to still tease apart, with room for judgment here without a strong sense of the data telling us exactly what to do.
Dr. Rotow: Exactly.
Dr. West: There’s a large amount of excitement and interest in these new data, but there are still many open questions. I hope we continue to mull it over as we get more data and more insight to shape our plans.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. Rotow is the clinical director of the Lowe Center for Thoracic Oncology at the Dana-Farber Cancer Institute in Boston. Dr. West reported conflicts of interest with Ariad/Takeda, Bristol Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly. Dr. Rotow reported conflicts of interest with Genentech, AstraZeneca,Guardant, and Janssen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Dr. West: Here at ASCO 2023 [American Society of Clinical Oncology] in Chicago, we’ve seen some blockbuster presentations in thoracic oncology. Many of these have brought up some important questions about the clinical implications that we need to discuss further.
At ASCO, as well as in the couple or 3 months preceding ASCO, we’ve gotten more and more data on perioperative approaches. Of course, over the past couple of years, we’ve had some new options of postoperative immunotherapy for a year, say, after chemotherapy or possibly after chemotherapy.
We have also had very influential data, such as the CheckMate 816 trial that gave three cycles of chemotherapy with nivolumab vs. chemotherapy alone to patients with stage IB to IIIA disease, but largely, nearly two thirds, with IIIA disease. That showed a very clear improvement in the pathologic complete response (pCR) rate with nivolumab added to chemotherapy and also a highly significant improvement in event-free survival and a strong trend toward improved overall survival. This is FDA approved and has been increasingly adopted, I would say, maybe with some variability by geography and center, but really a good amount of enthusiasm.
Now, we have a bunch of trials that give chemotherapy with immunotherapy. We’ve got the AEGEAN trial with durvalumab. We have Neotorch with chemotherapy and toripalimab. At ASCO 2023, we had a highly prominent presentation of KEYNOTE-671, giving four cycles of chemotherapy with pembrolizumab vs. chemotherapy and placebo.
Then there’s the built-in postoperative component of a year of immunotherapy as well, in all these trials. The data for KEYNOTE-671 look quite good. Of course, the other trials also were significant. I would say the comparator now is not nothing or chemotherapy alone anymore; it’s really against what is the best current standard of care.
It certainly adds some cost, it adds some risk for toxicity, and it adds a year of a patient coming into the clinic and getting IV infusions all this time to get a treatment that the patient has already had for four cycles in most of these trials.
If your cancer is resistant, is there going to be an incremental benefit to giving more of it? What are your thoughts about the risk and benefit? Going to a patient in your own clinic, how are you going to counsel your patients? Will anything change after the presentation of all these data and how you approach preoperatively?
Dr. Rotow: I agree. In some sense, it’s an embarrassment of riches, right?
Dr. West: Yes.
Dr. Rotow: We have so many positive studies looking at perioperative immunotherapy for our patients. They all show improved outcomes, but of course, they all compare with the old control arm of chemotherapy alone in some form, and this is no longer a useful control in this space. The open question is, do you use neoadjuvant, do you use adjuvant, or do you use both?
My high-level takeaway from these data is that the neoadjuvant component appears to be important. I think the overall trend, comparing across studies, of course, is that outcomes seem to be better with the neoadjuvant component. You also get the advantage of potential downstaging and potential greater ease of surgical resection. We know they have lower morbidity resection and shorter surgeries. You can comment on that. You also get your pathologic response data.
Dr. West: You get the feedback.
Dr. Rotow: Exactly.
Dr. West: The deliverability is also a big issue. You know you can much more reliably deliver your intended treatment by doing neoadjuvant followed by surgery.
Dr. Rotow: Exactly.
Dr. West: We know there’s major drop-off if patients have surgery, and in the recovery room they hear you got it all, and then they need to come back and maybe get chemotherapy and immunotherapy for a year. They’d ask, “What for? I can’t see anything.”
Dr. Rotow: Exactly. I think there are many advantages to that neoadjuvant component. I think all or many of us now have integrated this into our routine practice. Now the question is, do you need the adjuvant element or not on top? That is challenging because no trial has compared adjuvant to nonadjuvant. I think we all advocate for the need for this trial to answer this in a more randomized, prospective fashion. Of course, that doesn’t help our clinic practice tomorrow when we see a patient.
Dr. West: Or for the next 4 years.
Dr. Rotow: Or for the next 4 years – exactly. There’s going to be the open question of who really needs this? In some sense, we may be guided by the path response during the surgery itself. I think there may be those who claim that if you have a pCR, do you really need additional therapy? We don’t know the answer, but it’s tempting to say we know the outcomes in event-free survival are extremely good with a pCR.
Dr. West: Which is only 20% or 25% of patients, so it’s not most.
Dr. Rotow: It’s not most, but it’s better than the 2% or so with chemotherapy alone. That’s real progress, and it’s nice to have that readout. For that 80% without a pCR, what to do? I suspect there will be variation from provider to provider and from patient to patient, depending on tolerability to prior therapy, the patient’s wishes around the goals of care, and the patient’s risk for autoimmune toxicities.
Maybe there’s a patient with underlying autoimmune disease who’s gotten their neoadjuvant therapy and done well. You don’t want to risk that ongoing risk of exposure. Perhaps a patient with no risk factors who desires very aggressive treatment might be interested in more treatment.
In KEYNOTE-671, I was interested in the PD-L1 subgroups. These did trend the way you expect, with better responses in PD-L1 high, but there were also good outcomes and benefit to immunotherapy with the perioperative strategy in PD-L1–negative patients.
Dr. West: That didn’t really exclude anybody.
Dr. Rotow: It didn’t exclude anybody. In CheckMate 816, everyone benefited, but the benefit was less with those PD-L1–negative patients.
Dr. West: True.
Dr. Rotow: Absent further data to guide me or any prospective data here comparing these strategies, I might lean toward a longer course of immunotherapy in that population in hopes of triggering a response. I suspect that there will be variation from clinician to clinician in that space.
Dr. West: This is a setting where I feel like I have equipoise. I really feel that the incremental benefit is pretty small.
Dr. Rotow: Small. I agree.
Dr. West: It’s, frankly, somewhat dubious. On the other hand, you’re in a situation where if you know that three of four patients will experience a relapse and less-than-amazing outcomes, it’s hard to leave something that’s FDA approved and studied and a well-sanctioned option on the table if this patient may have relapse later.
In the end, I feel like I’d like to offer this and discuss it with all my patients. I think it’s a great place for shared decision-making because if a patient hears about that and decides they’re not interested, I’ll be fine with that. I think that’s a very sensible approach, but I don’t want to make it unilaterally. Other patients may say they want every opportunity, and if it comes back, at least I’ll know I did everything we could.
Dr. Rotow: Exactly. I agree with your statement about equipoise. I truly think that this is present here in the situation, and that there’s room for discussion in both directions with patients.
Now, one caveat I’d like to add to all these data is that the data should not apply to patients with some of our classic nonsmoking-associated driver mutations. This is another piece to the neoadjuvant data that I think is worth commenting on – the need to get appropriate testing before initiation of therapy and the pitfalls of starting this kind of treatment without knowing full biomarker testing. I think that’s something we have to watch for in our clinical practice as well.
Dr. West: Perhaps especially if we’re talking about doing a year of postoperative and someone has an ALK rearrangement or an EGFR mutation and we didn’t know it. That is a group where we’re worried about a rapid transition and potentially prohibitive, even life-threatening, toxicities from not planning in advance for this. This is something you don’t want to give concurrently or one right on top of the other. You don’t want to give immunotherapy and then transition right to targeted therapy. It’s dangerous.
Dr. Rotow: Exactly. The stakes were already high with neoadjuvant alone, but at least you had that gap of the presurgical period, surgical recovery, and then initiation of adjuvant therapy, if needed, or at relapse. With a postoperative long adjuvant period, those stakes are elevated because the immunotherapy exposure continues, so it’s something to be mindful of.
Dr. West: We have a general sense that many, but not all, of the targets that we’re talking about are associated with low benefit from immunotherapy. It’s not that well studied. I think this is another place for individualized discussion of the pros and cons. They were included in the trial, but they probably benefit less.
Dr. Rotow: Exactly. I think with the best established, EGFR and ALK probably are not benefiting much. They were actually included in the trial. Many of the neoadjuvant studies do not allow them to enroll if they’re known. On the other end of that spectrum, I think KRAS is just fine to treat with immunotherapy.
Dr. West: Sure.
Dr. Rotow: It’s an actionable driver. It’s not a traditional nonsmoking-associated driver, and those do just fine.
Dr. West: The studies show that these patients benefit just as much, at least, as the other patients.
Dr. Rotow: Exactly. I would never withhold this form of therapy for a KRAS driver mutation. The others, I think, are still in a gray zone. Depending on the patient demographics and tobacco use, I may elicit more or less caution in that space.
Dr. West: Well, I think we’re going to have much to still tease apart, with room for judgment here without a strong sense of the data telling us exactly what to do.
Dr. Rotow: Exactly.
Dr. West: There’s a large amount of excitement and interest in these new data, but there are still many open questions. I hope we continue to mull it over as we get more data and more insight to shape our plans.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. Rotow is the clinical director of the Lowe Center for Thoracic Oncology at the Dana-Farber Cancer Institute in Boston. Dr. West reported conflicts of interest with Ariad/Takeda, Bristol Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly. Dr. Rotow reported conflicts of interest with Genentech, AstraZeneca,Guardant, and Janssen.
A version of this article first appeared on Medscape.com.
FROM ASCO 2023
RFS failed as endpoint in adjuvant immunotherapy trials
TOPLINE:
METHODOLOGY:
- FDA approvals in the adjuvant setting for cancer immunotherapy are increasingly based on trials that use RFS as a surrogate endpoint for overall survival, largely because such a design allows for smaller, speedier trials.
- To test the validity of using RFS as a surrogate for overall survival in this setting, investigators conducted a meta-analysis of 15 phase 2 and 3 randomized controlled trials (RCTs) of adjuvant CTLA4 and anti–PD-1/PD-L1 blockers for melanoma, non–small cell lung cancer, renal cell cancer, and other tumors.
- The team used weighted regression at the arm and trial levels to assess the efficacy of RFS as a surrogate for overall survival.
- The strength of the association was quantified by weighted coefficients of determination (R2)12Dante MT Stdplz make sure all mentions of R’2’ are superscript, with a strong correlation considered to be R2 of 0.7 or higher.
- If there were strong correlations at both the arm and trial levels, RFS would be considered a robust surrogate endpoint for overall survival; however, if one of the correlations at the arm or trial level was not strong, RFS would not be considered a surrogate endpoint for overall survival.
TAKEAWAY:
- At the arm level, moderate and strong associations were observed between 2-year RFS and 3-year overall survival (R2, 0.58) and between 3-year RFS and 5-year overall survival (R2, 0.72; 95% confidence interval, 0.38-.00).
- At the trial level, a moderate association was observed between effect of treatment on RFS and overall survival (R2, 0.63).
- The findings were confirmed in several sensitivity analyses that were based on different trial phases, experimental arms, cancer types, and treatment strategies.
IN PRACTICE:
“Our meta-analysis failed to find a significantly strong association between RFS and OS in RCTs of adjuvant immunotherapy,” the authors concluded. “RFS should not be used as a surrogate endpoint for OS in this clinical context.” Instead, the finding indicates that overall survival is “the ideal primary endpoint” in this setting.
SOURCE:
The study, led by Yuanfang Li, PhD, of Sun Yat-sen University Cancer Center in Guangzhou, China, was published in the Journal of the National Cancer Institute.
LIMITATIONS:
- Correlations were calculated from a relatively limited number of RCTs that involved different types of cancer, and overall survival data were not fully mature in some of the trials.
- The analysis did not include patient-level data.
DISCLOSURES:
- The work was funded by the National Natural Science Foundation of China and others.
- The investigators had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- FDA approvals in the adjuvant setting for cancer immunotherapy are increasingly based on trials that use RFS as a surrogate endpoint for overall survival, largely because such a design allows for smaller, speedier trials.
- To test the validity of using RFS as a surrogate for overall survival in this setting, investigators conducted a meta-analysis of 15 phase 2 and 3 randomized controlled trials (RCTs) of adjuvant CTLA4 and anti–PD-1/PD-L1 blockers for melanoma, non–small cell lung cancer, renal cell cancer, and other tumors.
- The team used weighted regression at the arm and trial levels to assess the efficacy of RFS as a surrogate for overall survival.
- The strength of the association was quantified by weighted coefficients of determination (R2)12Dante MT Stdplz make sure all mentions of R’2’ are superscript, with a strong correlation considered to be R2 of 0.7 or higher.
- If there were strong correlations at both the arm and trial levels, RFS would be considered a robust surrogate endpoint for overall survival; however, if one of the correlations at the arm or trial level was not strong, RFS would not be considered a surrogate endpoint for overall survival.
TAKEAWAY:
- At the arm level, moderate and strong associations were observed between 2-year RFS and 3-year overall survival (R2, 0.58) and between 3-year RFS and 5-year overall survival (R2, 0.72; 95% confidence interval, 0.38-.00).
- At the trial level, a moderate association was observed between effect of treatment on RFS and overall survival (R2, 0.63).
- The findings were confirmed in several sensitivity analyses that were based on different trial phases, experimental arms, cancer types, and treatment strategies.
IN PRACTICE:
“Our meta-analysis failed to find a significantly strong association between RFS and OS in RCTs of adjuvant immunotherapy,” the authors concluded. “RFS should not be used as a surrogate endpoint for OS in this clinical context.” Instead, the finding indicates that overall survival is “the ideal primary endpoint” in this setting.
SOURCE:
The study, led by Yuanfang Li, PhD, of Sun Yat-sen University Cancer Center in Guangzhou, China, was published in the Journal of the National Cancer Institute.
LIMITATIONS:
- Correlations were calculated from a relatively limited number of RCTs that involved different types of cancer, and overall survival data were not fully mature in some of the trials.
- The analysis did not include patient-level data.
DISCLOSURES:
- The work was funded by the National Natural Science Foundation of China and others.
- The investigators had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- FDA approvals in the adjuvant setting for cancer immunotherapy are increasingly based on trials that use RFS as a surrogate endpoint for overall survival, largely because such a design allows for smaller, speedier trials.
- To test the validity of using RFS as a surrogate for overall survival in this setting, investigators conducted a meta-analysis of 15 phase 2 and 3 randomized controlled trials (RCTs) of adjuvant CTLA4 and anti–PD-1/PD-L1 blockers for melanoma, non–small cell lung cancer, renal cell cancer, and other tumors.
- The team used weighted regression at the arm and trial levels to assess the efficacy of RFS as a surrogate for overall survival.
- The strength of the association was quantified by weighted coefficients of determination (R2)12Dante MT Stdplz make sure all mentions of R’2’ are superscript, with a strong correlation considered to be R2 of 0.7 or higher.
- If there were strong correlations at both the arm and trial levels, RFS would be considered a robust surrogate endpoint for overall survival; however, if one of the correlations at the arm or trial level was not strong, RFS would not be considered a surrogate endpoint for overall survival.
TAKEAWAY:
- At the arm level, moderate and strong associations were observed between 2-year RFS and 3-year overall survival (R2, 0.58) and between 3-year RFS and 5-year overall survival (R2, 0.72; 95% confidence interval, 0.38-.00).
- At the trial level, a moderate association was observed between effect of treatment on RFS and overall survival (R2, 0.63).
- The findings were confirmed in several sensitivity analyses that were based on different trial phases, experimental arms, cancer types, and treatment strategies.
IN PRACTICE:
“Our meta-analysis failed to find a significantly strong association between RFS and OS in RCTs of adjuvant immunotherapy,” the authors concluded. “RFS should not be used as a surrogate endpoint for OS in this clinical context.” Instead, the finding indicates that overall survival is “the ideal primary endpoint” in this setting.
SOURCE:
The study, led by Yuanfang Li, PhD, of Sun Yat-sen University Cancer Center in Guangzhou, China, was published in the Journal of the National Cancer Institute.
LIMITATIONS:
- Correlations were calculated from a relatively limited number of RCTs that involved different types of cancer, and overall survival data were not fully mature in some of the trials.
- The analysis did not include patient-level data.
DISCLOSURES:
- The work was funded by the National Natural Science Foundation of China and others.
- The investigators had no disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Short bursts of activity may cut cancer risk
, a new study published in JAMA Oncology says.
Researchers at the University of Sydney studied data from wearable fitness devices worn by more than 22,000 “non-exercisers,” then examined their health records for 6 or 7 years.
The scientists found that people who did 4-5 minutes of “vigorous intermittent lifestyle physical activity” (VILPA) had a “substantially” lower cancer risk than people who did no VILPA.
Examples of VILPA are vigorous housework, carrying heavy shopping bags around the grocery store, bursts of power walking, and playing high-energy games with children. The activities could occur in 1-minute bursts, instead of all at once.

The study found that a minimum of around 3.5 minutes of daily VILPA was linked to an 18% reduction in cancer rates, compared with no VILPA. The study said 4.5 minutes of daily VILPA was linked to a 32% reduction in cancers related to physical activity, including lung, kidney, bladder, and stomach cancers.
“We know the majority of middle-aged people don’t regularly exercise, which puts them at increased cancer risk, but it’s only through the advent of wearable technology like activity trackers that we are able to look at the impact of short bursts of incidental physical activity done as part of daily living,” Emmanuel Stamatakis, PhD, the lead author of the study and a professor at the University of Sydney’s Charles Perkins Centre, said in a news release.
Study participants had an average age of 62 and reported that they didn’t exercise in their spare time. VILPA, a concept coined by researchers at the university, was measured by wrist accelerometers that people in the study wore over 7 days at the start of the study, the news release said.
“We are just starting to glimpse the potential of wearable technology to track physical activity and understand how unexplored aspects of our lives affect our long-term health – the potential impact on cancer prevention and a host of other health outcomes is enormous,” Dr. Stamatakis said.
A version of this article first appeared on WebMD.com.
, a new study published in JAMA Oncology says.
Researchers at the University of Sydney studied data from wearable fitness devices worn by more than 22,000 “non-exercisers,” then examined their health records for 6 or 7 years.
The scientists found that people who did 4-5 minutes of “vigorous intermittent lifestyle physical activity” (VILPA) had a “substantially” lower cancer risk than people who did no VILPA.
Examples of VILPA are vigorous housework, carrying heavy shopping bags around the grocery store, bursts of power walking, and playing high-energy games with children. The activities could occur in 1-minute bursts, instead of all at once.
The study found that a minimum of around 3.5 minutes of daily VILPA was linked to an 18% reduction in cancer rates, compared with no VILPA. The study said 4.5 minutes of daily VILPA was linked to a 32% reduction in cancers related to physical activity, including lung, kidney, bladder, and stomach cancers.
“We know the majority of middle-aged people don’t regularly exercise, which puts them at increased cancer risk, but it’s only through the advent of wearable technology like activity trackers that we are able to look at the impact of short bursts of incidental physical activity done as part of daily living,” Emmanuel Stamatakis, PhD, the lead author of the study and a professor at the University of Sydney’s Charles Perkins Centre, said in a news release.
Study participants had an average age of 62 and reported that they didn’t exercise in their spare time. VILPA, a concept coined by researchers at the university, was measured by wrist accelerometers that people in the study wore over 7 days at the start of the study, the news release said.
“We are just starting to glimpse the potential of wearable technology to track physical activity and understand how unexplored aspects of our lives affect our long-term health – the potential impact on cancer prevention and a host of other health outcomes is enormous,” Dr. Stamatakis said.
A version of this article first appeared on WebMD.com.
, a new study published in JAMA Oncology says.
Researchers at the University of Sydney studied data from wearable fitness devices worn by more than 22,000 “non-exercisers,” then examined their health records for 6 or 7 years.
The scientists found that people who did 4-5 minutes of “vigorous intermittent lifestyle physical activity” (VILPA) had a “substantially” lower cancer risk than people who did no VILPA.
Examples of VILPA are vigorous housework, carrying heavy shopping bags around the grocery store, bursts of power walking, and playing high-energy games with children. The activities could occur in 1-minute bursts, instead of all at once.
The study found that a minimum of around 3.5 minutes of daily VILPA was linked to an 18% reduction in cancer rates, compared with no VILPA. The study said 4.5 minutes of daily VILPA was linked to a 32% reduction in cancers related to physical activity, including lung, kidney, bladder, and stomach cancers.
“We know the majority of middle-aged people don’t regularly exercise, which puts them at increased cancer risk, but it’s only through the advent of wearable technology like activity trackers that we are able to look at the impact of short bursts of incidental physical activity done as part of daily living,” Emmanuel Stamatakis, PhD, the lead author of the study and a professor at the University of Sydney’s Charles Perkins Centre, said in a news release.
Study participants had an average age of 62 and reported that they didn’t exercise in their spare time. VILPA, a concept coined by researchers at the university, was measured by wrist accelerometers that people in the study wore over 7 days at the start of the study, the news release said.
“We are just starting to glimpse the potential of wearable technology to track physical activity and understand how unexplored aspects of our lives affect our long-term health – the potential impact on cancer prevention and a host of other health outcomes is enormous,” Dr. Stamatakis said.
A version of this article first appeared on WebMD.com.
FROM JAMA ONCOLOGY
Do some randomized controlled trials stack the deck?
Randomized controlled trials in oncology can make or break an investigational drug, with both patient lives and pharmaceutical company profits at stake.
These trials typically pit two options against each other, an investigational therapy and a control therapy – often a standard of care – to see which has greater benefit.
But These biases may result in substandard care for trial participants, even harm, and can invalidate or dilute scientific findings.
One major issue is whether participants in the control arm of a trial receive the standard of care or active therapy after disease progression. In clinical trial parlance, this practice is called crossover.
Patients who do not receive standard-of-care therapy after disease progression may be “unfairly disadvantaged,” experts wrote in a commentary published in late June.What’s worse, optimal crossover does not always happen, commentary author Edward R. Scheffer Cliff, MBBS, MPH, from Brigham and Women’s Hospital in Boston said in an interview.
A recent example comes from the ADAURA trial comparing adjuvant therapy with osimertinib (Tagrisso) to placebo following complete resection of localized or locally advanced stage IB-IIIA non–small cell lung cancer (NSCLC) harboring EGFR mutations.
The trial, which began in November 2015, was unblinded early and halted on the recommendation of the independent data-monitoring committee because osimertinib was associated with a nearly 80% reduction in the risk of disease recurrence or death. These data led to the Food and Drug Administration’s 2018 approval of osimertinib as first-line treatment in this setting.
The recent overall survival data from ADAURA, presented at the 2023 American Society of Clinical Oncology annual meeting, helped confirm the drug’s benefit: Osimertinib was associated with a 51% reduced risk for death, compared with placebo.
But critics of this report were troubled by the fact that, despite the reported benefits of osimertinib, only 79 of 205 patients (38.5%) in the control arm who relapsed received the drug – now considered standard of care in this setting.
The low rate of osimertinib crossover represents a serious flaw in the trial design and potentially an ethical problem.
In the commentary, Dr. Cliff, alongside colleagues Aaron S. Kesselheim, MD, JD, MPH, and William B. Feldman, MD, DPhil, MPH, detailed the ethical issues associated with substandard crossover in clinical trials.
“In the ethical design of clinical trials, patients make important sacrifices to participate, and in exchange, the academic and clinical communities owe them optimal treatment both during the intervention part of the trial and, if they progress, after progression, especially when it is directly in the control of the trial sponsor as to whether a drug that they produce is made available to a clinical trial participant,” Dr. Cliff and colleagues wrote.
The authors highlighted 10 clinical trials – including SHINE, ZUMA-7, CLL14, ALCYONE, and JAVELIN 100 – that had problematic crossover. In the SHINE trial, for instance, 39% of control arm patients with mantle cell lymphoma received BTKi therapy post progression, while in the ALCYONE trial of multiple myeloma, only 10% of control patients received daratumumab at first progression. The VISION trial had the lowest crossover rate, with only one control arm patient (0.5%) with metastatic castration-resistant prostate cancer receiving lutetium-PSMA-617 after progression.
“Depriving control arm patients access to standard-of-care post-RCT therapy also has important scientific implications,” Dr. Cliff and colleagues wrote. In oncology, “if patients in the control arm do not receive standard-of-care therapy after disease progression, then they are unfairly disadvantaged, and it becomes difficult to assess whether the intervention has indeed improved quality of life or survival.”
Clinical trials should be designed with both ethical behavior and scientific integrity in mind, Dr. Cliff told this news organization. It’s incumbent on everyone directly or peripherally involved in randomized trials to ensure that they are designed with mandatory unblinding at the time of disease progression, and that crossover is both allowed and funded by the trial sponsor and mandated by the trial investigators and FDA.
When it comes to clinical trials and the sacrifices patients make to participate, “I think everyone needs to lift their game,” Dr. Cliff said.
The commentary by Dr. Cliff and colleagues was supported by Arnold Ventures. Dr. Cliff disclosed institutional funding from the firm. Dr. Kesselheim reported reimbursement for expert testimony. Dr. Feldman reported consulting for Alosa Health and Aetion, and expert testimony on litigation.
A version of this article appeared on Medscape.com.
Randomized controlled trials in oncology can make or break an investigational drug, with both patient lives and pharmaceutical company profits at stake.
These trials typically pit two options against each other, an investigational therapy and a control therapy – often a standard of care – to see which has greater benefit.
But These biases may result in substandard care for trial participants, even harm, and can invalidate or dilute scientific findings.
One major issue is whether participants in the control arm of a trial receive the standard of care or active therapy after disease progression. In clinical trial parlance, this practice is called crossover.
Patients who do not receive standard-of-care therapy after disease progression may be “unfairly disadvantaged,” experts wrote in a commentary published in late June.What’s worse, optimal crossover does not always happen, commentary author Edward R. Scheffer Cliff, MBBS, MPH, from Brigham and Women’s Hospital in Boston said in an interview.
A recent example comes from the ADAURA trial comparing adjuvant therapy with osimertinib (Tagrisso) to placebo following complete resection of localized or locally advanced stage IB-IIIA non–small cell lung cancer (NSCLC) harboring EGFR mutations.
The trial, which began in November 2015, was unblinded early and halted on the recommendation of the independent data-monitoring committee because osimertinib was associated with a nearly 80% reduction in the risk of disease recurrence or death. These data led to the Food and Drug Administration’s 2018 approval of osimertinib as first-line treatment in this setting.
The recent overall survival data from ADAURA, presented at the 2023 American Society of Clinical Oncology annual meeting, helped confirm the drug’s benefit: Osimertinib was associated with a 51% reduced risk for death, compared with placebo.
But critics of this report were troubled by the fact that, despite the reported benefits of osimertinib, only 79 of 205 patients (38.5%) in the control arm who relapsed received the drug – now considered standard of care in this setting.
The low rate of osimertinib crossover represents a serious flaw in the trial design and potentially an ethical problem.
In the commentary, Dr. Cliff, alongside colleagues Aaron S. Kesselheim, MD, JD, MPH, and William B. Feldman, MD, DPhil, MPH, detailed the ethical issues associated with substandard crossover in clinical trials.
“In the ethical design of clinical trials, patients make important sacrifices to participate, and in exchange, the academic and clinical communities owe them optimal treatment both during the intervention part of the trial and, if they progress, after progression, especially when it is directly in the control of the trial sponsor as to whether a drug that they produce is made available to a clinical trial participant,” Dr. Cliff and colleagues wrote.
The authors highlighted 10 clinical trials – including SHINE, ZUMA-7, CLL14, ALCYONE, and JAVELIN 100 – that had problematic crossover. In the SHINE trial, for instance, 39% of control arm patients with mantle cell lymphoma received BTKi therapy post progression, while in the ALCYONE trial of multiple myeloma, only 10% of control patients received daratumumab at first progression. The VISION trial had the lowest crossover rate, with only one control arm patient (0.5%) with metastatic castration-resistant prostate cancer receiving lutetium-PSMA-617 after progression.
“Depriving control arm patients access to standard-of-care post-RCT therapy also has important scientific implications,” Dr. Cliff and colleagues wrote. In oncology, “if patients in the control arm do not receive standard-of-care therapy after disease progression, then they are unfairly disadvantaged, and it becomes difficult to assess whether the intervention has indeed improved quality of life or survival.”
Clinical trials should be designed with both ethical behavior and scientific integrity in mind, Dr. Cliff told this news organization. It’s incumbent on everyone directly or peripherally involved in randomized trials to ensure that they are designed with mandatory unblinding at the time of disease progression, and that crossover is both allowed and funded by the trial sponsor and mandated by the trial investigators and FDA.
When it comes to clinical trials and the sacrifices patients make to participate, “I think everyone needs to lift their game,” Dr. Cliff said.
The commentary by Dr. Cliff and colleagues was supported by Arnold Ventures. Dr. Cliff disclosed institutional funding from the firm. Dr. Kesselheim reported reimbursement for expert testimony. Dr. Feldman reported consulting for Alosa Health and Aetion, and expert testimony on litigation.
A version of this article appeared on Medscape.com.
Randomized controlled trials in oncology can make or break an investigational drug, with both patient lives and pharmaceutical company profits at stake.
These trials typically pit two options against each other, an investigational therapy and a control therapy – often a standard of care – to see which has greater benefit.
But These biases may result in substandard care for trial participants, even harm, and can invalidate or dilute scientific findings.
One major issue is whether participants in the control arm of a trial receive the standard of care or active therapy after disease progression. In clinical trial parlance, this practice is called crossover.
Patients who do not receive standard-of-care therapy after disease progression may be “unfairly disadvantaged,” experts wrote in a commentary published in late June.What’s worse, optimal crossover does not always happen, commentary author Edward R. Scheffer Cliff, MBBS, MPH, from Brigham and Women’s Hospital in Boston said in an interview.
A recent example comes from the ADAURA trial comparing adjuvant therapy with osimertinib (Tagrisso) to placebo following complete resection of localized or locally advanced stage IB-IIIA non–small cell lung cancer (NSCLC) harboring EGFR mutations.
The trial, which began in November 2015, was unblinded early and halted on the recommendation of the independent data-monitoring committee because osimertinib was associated with a nearly 80% reduction in the risk of disease recurrence or death. These data led to the Food and Drug Administration’s 2018 approval of osimertinib as first-line treatment in this setting.
The recent overall survival data from ADAURA, presented at the 2023 American Society of Clinical Oncology annual meeting, helped confirm the drug’s benefit: Osimertinib was associated with a 51% reduced risk for death, compared with placebo.
But critics of this report were troubled by the fact that, despite the reported benefits of osimertinib, only 79 of 205 patients (38.5%) in the control arm who relapsed received the drug – now considered standard of care in this setting.
The low rate of osimertinib crossover represents a serious flaw in the trial design and potentially an ethical problem.
In the commentary, Dr. Cliff, alongside colleagues Aaron S. Kesselheim, MD, JD, MPH, and William B. Feldman, MD, DPhil, MPH, detailed the ethical issues associated with substandard crossover in clinical trials.
“In the ethical design of clinical trials, patients make important sacrifices to participate, and in exchange, the academic and clinical communities owe them optimal treatment both during the intervention part of the trial and, if they progress, after progression, especially when it is directly in the control of the trial sponsor as to whether a drug that they produce is made available to a clinical trial participant,” Dr. Cliff and colleagues wrote.
The authors highlighted 10 clinical trials – including SHINE, ZUMA-7, CLL14, ALCYONE, and JAVELIN 100 – that had problematic crossover. In the SHINE trial, for instance, 39% of control arm patients with mantle cell lymphoma received BTKi therapy post progression, while in the ALCYONE trial of multiple myeloma, only 10% of control patients received daratumumab at first progression. The VISION trial had the lowest crossover rate, with only one control arm patient (0.5%) with metastatic castration-resistant prostate cancer receiving lutetium-PSMA-617 after progression.
“Depriving control arm patients access to standard-of-care post-RCT therapy also has important scientific implications,” Dr. Cliff and colleagues wrote. In oncology, “if patients in the control arm do not receive standard-of-care therapy after disease progression, then they are unfairly disadvantaged, and it becomes difficult to assess whether the intervention has indeed improved quality of life or survival.”
Clinical trials should be designed with both ethical behavior and scientific integrity in mind, Dr. Cliff told this news organization. It’s incumbent on everyone directly or peripherally involved in randomized trials to ensure that they are designed with mandatory unblinding at the time of disease progression, and that crossover is both allowed and funded by the trial sponsor and mandated by the trial investigators and FDA.
When it comes to clinical trials and the sacrifices patients make to participate, “I think everyone needs to lift their game,” Dr. Cliff said.
The commentary by Dr. Cliff and colleagues was supported by Arnold Ventures. Dr. Cliff disclosed institutional funding from the firm. Dr. Kesselheim reported reimbursement for expert testimony. Dr. Feldman reported consulting for Alosa Health and Aetion, and expert testimony on litigation.
A version of this article appeared on Medscape.com.
FROM ASCO 2023
Atezolizumab in NSCLC: Push the positive, bury the negative?
Recently published
Here’s why.
At a median follow-up of 45.3 months, 127 of 507 patients (25%) in the atezolizumab group and 124 of 498 (24.9%) in the best supportive care group had died.
Among all 882 patients with stage II-IIIA disease, the investigators found no significant improvement in overall survival with atezolizumab, compared with best supportive care (hazard ratio, 0.95; 95% confidence interval, 0.74-1.24).
The researchers, however, concluded that the trial showed a “positive” trend favoring atezolizumab in PD-L1 subgroup analyses.
In a subgroup of 476 patients with tumor PD-L1 expression ≥ 1%, patients who received atezolizumab exhibited a nonsignificant 29% improvement in overall survival (HR, 0.71; 95% CI, 0.49-1.03). The best results were in the subgroup of 229 patients with tumor PD-L1 expression ≥ 50% – these patients exhibited a 57% improvement in overall survival with atezolizumab (HR, 0.43; 95% CI, 0.24-0.78). Those with PD-L1 expression 1%-49%, however, demonstrated no improvement in overall survival (HR, 0.95).
In a Twitter post, H. Jack West, MD, City of Hope Comprehensive Cancer Center, Duarte, Calif., urged caution in interpreting the study data: “Let’s be clear: OS results are neg for OS benefit in PD-L1+ NSCLC. If we’re going to rely on smaller subgroups to highlight HR of 0.43 for those w/high PD-L1, we should also note HR for OS was 0.95 (i.e., NO trend for OS benefit) for those w/PD-L1 1-49%.”
The tweet continued: “With favorable results driven entirely by a 30% subgroup, it’s understandable that Roche would want to also promote benefit in broader population. But we shouldn’t perpetuate misinformation that there’s a benefit for broad group of PD-L1+, even if the effort is to market it this way.”
In an interview, Dr. West elaborated on his tweet, explaining that the way the overall survival data are presented in the paper is “disingenuous and misleading.”
The paper clearly highlights that the drug was significantly beneficial for the narrower population who had high PD-L1 expression. But the hazard ratio of 0.95 for the entire population is like “where’s Waldo in this paper. It’s almost impossible to find, but it should have been prominently included in the figure of results by subgroup,” Dr. West said.
“This is something that should have been objected to by the oncologists on the paper and by the reviews and the editors,” Dr. West said.
Two other oncologists agreed.
Joel Grossman, MD, tweeted: “Bingo. I’m not sure we need cancer ground shots or lengthy treatises on common sense, but I am damn sure we need honest interpretation of clinical trial data as Jack shows here. We can’t tolerate over-broad borderline deception that leads to poor and wasteful decision-making.”
Jeff Ryckman, MD, tweeted: “Problem is, this is a routine FDA #CarteBlanche approval regardless of no benefit in PD-L1 1%-49%. This will be Rx’d to everyone.”
Regulatory ‘gamesmanship’
The results of the IMpower010 analysis were published online in Annals of Oncology. The interim overall survival data were first reported last year at the World Conference on Lung Cancer.
IMpower010 was a global, randomized, open-label trial of 1,280 patients with completely resected stage IB (tumors ≥ 4 cm) through stage IIIA NSCLC for whom tissue samples were available for PD-L1 analysis.
All patients received four cycles of chemotherapy with cisplatin plus either pemetrexed, gemcitabine, docetaxel, or vinorelbine and were randomly assigned in a 1:1 ratio to receive either 16 cycles of atezolizumab or best supportive care.
Interim disease-free survival (DFS) results from IMpower010, presented at ASCO 2021, showed that patients with PD-L1 expression ≥ 1% experienced a 34% improvement in DFS, equating to a 21% improvement across all randomly assigned patients with stage II-IIIA disease.
On the basis of DFS findings, in 2021, the U.S. Food and Drug Administration granted atezolizumab a new indication – the adjuvant treatment following resection and platinum-based chemotherapy for patients with stage II-IIIA NSCLC whose tumors have PD-L1 expression ≥ 1%.
Looking at the big picture, Dr. West noted that regulatory approval for a drug allows for a certain amount of “gamesmanship.”
“It behooves a company to work with FDA to get approval for a broader population than it should be, relative to where the true clinical benefit lies,” he explained.
To this end, Dr. West noted that progression-free survival is increasingly being used as a primary endpoint in trials, but long-term data indicate that this surrogate endpoint is often not tethered to an overall survival benefit. However, drugs are often being approved now on the basis of a progression-free survival benefit.
“Unfortunately, that’s the system we live in today, with a bias toward, ‘If it could plausibly be interpreted as beneficial, we’ll wave it through for the broadest population possible,” Dr. West said.
The IMpower010 study and Annals of Oncology manuscript were funded by F. Hoffmann-La Roche. Several authors have disclosed relationships with the company. Dr. West has a regular column on Medscape.com and reported personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article appeared on Medscape.com.
Recently published
Here’s why.
At a median follow-up of 45.3 months, 127 of 507 patients (25%) in the atezolizumab group and 124 of 498 (24.9%) in the best supportive care group had died.
Among all 882 patients with stage II-IIIA disease, the investigators found no significant improvement in overall survival with atezolizumab, compared with best supportive care (hazard ratio, 0.95; 95% confidence interval, 0.74-1.24).
The researchers, however, concluded that the trial showed a “positive” trend favoring atezolizumab in PD-L1 subgroup analyses.
In a subgroup of 476 patients with tumor PD-L1 expression ≥ 1%, patients who received atezolizumab exhibited a nonsignificant 29% improvement in overall survival (HR, 0.71; 95% CI, 0.49-1.03). The best results were in the subgroup of 229 patients with tumor PD-L1 expression ≥ 50% – these patients exhibited a 57% improvement in overall survival with atezolizumab (HR, 0.43; 95% CI, 0.24-0.78). Those with PD-L1 expression 1%-49%, however, demonstrated no improvement in overall survival (HR, 0.95).
In a Twitter post, H. Jack West, MD, City of Hope Comprehensive Cancer Center, Duarte, Calif., urged caution in interpreting the study data: “Let’s be clear: OS results are neg for OS benefit in PD-L1+ NSCLC. If we’re going to rely on smaller subgroups to highlight HR of 0.43 for those w/high PD-L1, we should also note HR for OS was 0.95 (i.e., NO trend for OS benefit) for those w/PD-L1 1-49%.”
The tweet continued: “With favorable results driven entirely by a 30% subgroup, it’s understandable that Roche would want to also promote benefit in broader population. But we shouldn’t perpetuate misinformation that there’s a benefit for broad group of PD-L1+, even if the effort is to market it this way.”
In an interview, Dr. West elaborated on his tweet, explaining that the way the overall survival data are presented in the paper is “disingenuous and misleading.”
The paper clearly highlights that the drug was significantly beneficial for the narrower population who had high PD-L1 expression. But the hazard ratio of 0.95 for the entire population is like “where’s Waldo in this paper. It’s almost impossible to find, but it should have been prominently included in the figure of results by subgroup,” Dr. West said.
“This is something that should have been objected to by the oncologists on the paper and by the reviews and the editors,” Dr. West said.
Two other oncologists agreed.
Joel Grossman, MD, tweeted: “Bingo. I’m not sure we need cancer ground shots or lengthy treatises on common sense, but I am damn sure we need honest interpretation of clinical trial data as Jack shows here. We can’t tolerate over-broad borderline deception that leads to poor and wasteful decision-making.”
Jeff Ryckman, MD, tweeted: “Problem is, this is a routine FDA #CarteBlanche approval regardless of no benefit in PD-L1 1%-49%. This will be Rx’d to everyone.”
Regulatory ‘gamesmanship’
The results of the IMpower010 analysis were published online in Annals of Oncology. The interim overall survival data were first reported last year at the World Conference on Lung Cancer.
IMpower010 was a global, randomized, open-label trial of 1,280 patients with completely resected stage IB (tumors ≥ 4 cm) through stage IIIA NSCLC for whom tissue samples were available for PD-L1 analysis.
All patients received four cycles of chemotherapy with cisplatin plus either pemetrexed, gemcitabine, docetaxel, or vinorelbine and were randomly assigned in a 1:1 ratio to receive either 16 cycles of atezolizumab or best supportive care.
Interim disease-free survival (DFS) results from IMpower010, presented at ASCO 2021, showed that patients with PD-L1 expression ≥ 1% experienced a 34% improvement in DFS, equating to a 21% improvement across all randomly assigned patients with stage II-IIIA disease.
On the basis of DFS findings, in 2021, the U.S. Food and Drug Administration granted atezolizumab a new indication – the adjuvant treatment following resection and platinum-based chemotherapy for patients with stage II-IIIA NSCLC whose tumors have PD-L1 expression ≥ 1%.
Looking at the big picture, Dr. West noted that regulatory approval for a drug allows for a certain amount of “gamesmanship.”
“It behooves a company to work with FDA to get approval for a broader population than it should be, relative to where the true clinical benefit lies,” he explained.
To this end, Dr. West noted that progression-free survival is increasingly being used as a primary endpoint in trials, but long-term data indicate that this surrogate endpoint is often not tethered to an overall survival benefit. However, drugs are often being approved now on the basis of a progression-free survival benefit.
“Unfortunately, that’s the system we live in today, with a bias toward, ‘If it could plausibly be interpreted as beneficial, we’ll wave it through for the broadest population possible,” Dr. West said.
The IMpower010 study and Annals of Oncology manuscript were funded by F. Hoffmann-La Roche. Several authors have disclosed relationships with the company. Dr. West has a regular column on Medscape.com and reported personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article appeared on Medscape.com.
Recently published
Here’s why.
At a median follow-up of 45.3 months, 127 of 507 patients (25%) in the atezolizumab group and 124 of 498 (24.9%) in the best supportive care group had died.
Among all 882 patients with stage II-IIIA disease, the investigators found no significant improvement in overall survival with atezolizumab, compared with best supportive care (hazard ratio, 0.95; 95% confidence interval, 0.74-1.24).
The researchers, however, concluded that the trial showed a “positive” trend favoring atezolizumab in PD-L1 subgroup analyses.
In a subgroup of 476 patients with tumor PD-L1 expression ≥ 1%, patients who received atezolizumab exhibited a nonsignificant 29% improvement in overall survival (HR, 0.71; 95% CI, 0.49-1.03). The best results were in the subgroup of 229 patients with tumor PD-L1 expression ≥ 50% – these patients exhibited a 57% improvement in overall survival with atezolizumab (HR, 0.43; 95% CI, 0.24-0.78). Those with PD-L1 expression 1%-49%, however, demonstrated no improvement in overall survival (HR, 0.95).
In a Twitter post, H. Jack West, MD, City of Hope Comprehensive Cancer Center, Duarte, Calif., urged caution in interpreting the study data: “Let’s be clear: OS results are neg for OS benefit in PD-L1+ NSCLC. If we’re going to rely on smaller subgroups to highlight HR of 0.43 for those w/high PD-L1, we should also note HR for OS was 0.95 (i.e., NO trend for OS benefit) for those w/PD-L1 1-49%.”
The tweet continued: “With favorable results driven entirely by a 30% subgroup, it’s understandable that Roche would want to also promote benefit in broader population. But we shouldn’t perpetuate misinformation that there’s a benefit for broad group of PD-L1+, even if the effort is to market it this way.”
In an interview, Dr. West elaborated on his tweet, explaining that the way the overall survival data are presented in the paper is “disingenuous and misleading.”
The paper clearly highlights that the drug was significantly beneficial for the narrower population who had high PD-L1 expression. But the hazard ratio of 0.95 for the entire population is like “where’s Waldo in this paper. It’s almost impossible to find, but it should have been prominently included in the figure of results by subgroup,” Dr. West said.
“This is something that should have been objected to by the oncologists on the paper and by the reviews and the editors,” Dr. West said.
Two other oncologists agreed.
Joel Grossman, MD, tweeted: “Bingo. I’m not sure we need cancer ground shots or lengthy treatises on common sense, but I am damn sure we need honest interpretation of clinical trial data as Jack shows here. We can’t tolerate over-broad borderline deception that leads to poor and wasteful decision-making.”
Jeff Ryckman, MD, tweeted: “Problem is, this is a routine FDA #CarteBlanche approval regardless of no benefit in PD-L1 1%-49%. This will be Rx’d to everyone.”
Regulatory ‘gamesmanship’
The results of the IMpower010 analysis were published online in Annals of Oncology. The interim overall survival data were first reported last year at the World Conference on Lung Cancer.
IMpower010 was a global, randomized, open-label trial of 1,280 patients with completely resected stage IB (tumors ≥ 4 cm) through stage IIIA NSCLC for whom tissue samples were available for PD-L1 analysis.
All patients received four cycles of chemotherapy with cisplatin plus either pemetrexed, gemcitabine, docetaxel, or vinorelbine and were randomly assigned in a 1:1 ratio to receive either 16 cycles of atezolizumab or best supportive care.
Interim disease-free survival (DFS) results from IMpower010, presented at ASCO 2021, showed that patients with PD-L1 expression ≥ 1% experienced a 34% improvement in DFS, equating to a 21% improvement across all randomly assigned patients with stage II-IIIA disease.
On the basis of DFS findings, in 2021, the U.S. Food and Drug Administration granted atezolizumab a new indication – the adjuvant treatment following resection and platinum-based chemotherapy for patients with stage II-IIIA NSCLC whose tumors have PD-L1 expression ≥ 1%.
Looking at the big picture, Dr. West noted that regulatory approval for a drug allows for a certain amount of “gamesmanship.”
“It behooves a company to work with FDA to get approval for a broader population than it should be, relative to where the true clinical benefit lies,” he explained.
To this end, Dr. West noted that progression-free survival is increasingly being used as a primary endpoint in trials, but long-term data indicate that this surrogate endpoint is often not tethered to an overall survival benefit. However, drugs are often being approved now on the basis of a progression-free survival benefit.
“Unfortunately, that’s the system we live in today, with a bias toward, ‘If it could plausibly be interpreted as beneficial, we’ll wave it through for the broadest population possible,” Dr. West said.
The IMpower010 study and Annals of Oncology manuscript were funded by F. Hoffmann-La Roche. Several authors have disclosed relationships with the company. Dr. West has a regular column on Medscape.com and reported personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article appeared on Medscape.com.
FROM ANNALS OF ONCOLOGY
No benefit to adding limited radiation in advanced cancer
TOPLINE:
METHODOLOGY:
- In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
- Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
- Most patients had more than three lesions.
- Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
- Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
- Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
- However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
- The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
- There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
- More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
- Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
- Most patients had more than three lesions.
- Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
- Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
- Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
- However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
- The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
- There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
- More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
- Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
- Most patients had more than three lesions.
- Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
- Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
- Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
- However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
- The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
- There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
- More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
Diabetes may short circuit pembrolizumab benefits in NSCLC
TOPLINE:
METHODOLOGY:
- Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
- Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
- Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
- Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
- Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
- After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
- In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
- Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
- The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
- No funding source was reported.
- Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
- Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
- Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
- Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
- Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
- After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
- In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
- Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
- The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
- No funding source was reported.
- Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
- Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
- Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
- Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
- Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
- After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
- In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
- Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
- The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
- No funding source was reported.
- Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
Cancer Data Trends 2023
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.

In this issue:
- COVID-19 Outcomes in Veterans With Hematologic Cancers
- Promising New Approaches for Testicular and Prostate Cancer
- Screening Guideline Updates and New Treatments in Colon Cancer
- Exposure-Related Cancers: A Look at the PACT Act
- New Classifications and Emerging Treatments in Brain Cancer
- Gender Disparity in Breast Cancer Among US Veterans
- Lung Cancer Screening in Veterans
- Necessary Updates to Skin Cancer Risk Stratification
- Innovation in Cancer Treatment
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
In this issue:
- COVID-19 Outcomes in Veterans With Hematologic Cancers
- Promising New Approaches for Testicular and Prostate Cancer
- Screening Guideline Updates and New Treatments in Colon Cancer
- Exposure-Related Cancers: A Look at the PACT Act
- New Classifications and Emerging Treatments in Brain Cancer
- Gender Disparity in Breast Cancer Among US Veterans
- Lung Cancer Screening in Veterans
- Necessary Updates to Skin Cancer Risk Stratification
- Innovation in Cancer Treatment
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
In this issue:
- COVID-19 Outcomes in Veterans With Hematologic Cancers
- Promising New Approaches for Testicular and Prostate Cancer
- Screening Guideline Updates and New Treatments in Colon Cancer
- Exposure-Related Cancers: A Look at the PACT Act
- New Classifications and Emerging Treatments in Brain Cancer
- Gender Disparity in Breast Cancer Among US Veterans
- Lung Cancer Screening in Veterans
- Necessary Updates to Skin Cancer Risk Stratification
- Innovation in Cancer Treatment
Lung Cancer Screening in Veterans
- Spalluto LB et al. J Am Coll Radiol. 2021;18(6):809-819. doi:10.1016/j.jacr.2020.12.010
- Lewis JA et al. JNCI Cancer Spectr. 2020;4(5):pkaa053. doi:10.1093/jncics/pkaa053
- Wallace C. Largest-ever lung cancer screening study reveals ways to increase screening outreach. Medical University of South Carolina. November 22, 2022. Accessed January 4, 202 https://hollingscancercenter.musc.edu/news/archive/2022/11/22/largest-ever-lung-cancer-screening-study-reveals-ways-to-increase-screening-outreach
- Screening facts & figures. Go2 For Lung Cancer. 2022. Accessed January 4, 2023. https://go2.org/risk-early-detection/screening-facts-figures/
- Dyer O. BMJ. 2021;372:n698. doi:10.1136/bmj.n698
- Boudreau JH et al. Chest. 2021;160(1):358-367. doi:10.1016/j.chest.2021.02.016
- Maurice NM, Tanner NT. Semin Oncol. 2022;S0093-7754(22)00041-0. doi:10.1053/j.seminoncol.2022.06.001
- Rusher TN et al. Fed Pract. 2022;39(suppl 2):S48-S51. doi:10.12788/fp.0269
- Núñez ER et al. JAMA Netw Open. 2021;4(7):e2116233. doi:10.1001/jamanetworkopen.2021.16233
- Lake M et al. BMC Cancer. 2020;20(1):561. doi:1186/s12885-020-06923-0
- Spalluto LB et al. J Am Coll Radiol. 2021;18(6):809-819. doi:10.1016/j.jacr.2020.12.010
- Lewis JA et al. JNCI Cancer Spectr. 2020;4(5):pkaa053. doi:10.1093/jncics/pkaa053
- Wallace C. Largest-ever lung cancer screening study reveals ways to increase screening outreach. Medical University of South Carolina. November 22, 2022. Accessed January 4, 202 https://hollingscancercenter.musc.edu/news/archive/2022/11/22/largest-ever-lung-cancer-screening-study-reveals-ways-to-increase-screening-outreach
- Screening facts & figures. Go2 For Lung Cancer. 2022. Accessed January 4, 2023. https://go2.org/risk-early-detection/screening-facts-figures/
- Dyer O. BMJ. 2021;372:n698. doi:10.1136/bmj.n698
- Boudreau JH et al. Chest. 2021;160(1):358-367. doi:10.1016/j.chest.2021.02.016
- Maurice NM, Tanner NT. Semin Oncol. 2022;S0093-7754(22)00041-0. doi:10.1053/j.seminoncol.2022.06.001
- Rusher TN et al. Fed Pract. 2022;39(suppl 2):S48-S51. doi:10.12788/fp.0269
- Núñez ER et al. JAMA Netw Open. 2021;4(7):e2116233. doi:10.1001/jamanetworkopen.2021.16233
- Lake M et al. BMC Cancer. 2020;20(1):561. doi:1186/s12885-020-06923-0
- Spalluto LB et al. J Am Coll Radiol. 2021;18(6):809-819. doi:10.1016/j.jacr.2020.12.010
- Lewis JA et al. JNCI Cancer Spectr. 2020;4(5):pkaa053. doi:10.1093/jncics/pkaa053
- Wallace C. Largest-ever lung cancer screening study reveals ways to increase screening outreach. Medical University of South Carolina. November 22, 2022. Accessed January 4, 202 https://hollingscancercenter.musc.edu/news/archive/2022/11/22/largest-ever-lung-cancer-screening-study-reveals-ways-to-increase-screening-outreach
- Screening facts & figures. Go2 For Lung Cancer. 2022. Accessed January 4, 2023. https://go2.org/risk-early-detection/screening-facts-figures/
- Dyer O. BMJ. 2021;372:n698. doi:10.1136/bmj.n698
- Boudreau JH et al. Chest. 2021;160(1):358-367. doi:10.1016/j.chest.2021.02.016
- Maurice NM, Tanner NT. Semin Oncol. 2022;S0093-7754(22)00041-0. doi:10.1053/j.seminoncol.2022.06.001
- Rusher TN et al. Fed Pract. 2022;39(suppl 2):S48-S51. doi:10.12788/fp.0269
- Núñez ER et al. JAMA Netw Open. 2021;4(7):e2116233. doi:10.1001/jamanetworkopen.2021.16233
- Lake M et al. BMC Cancer. 2020;20(1):561. doi:1186/s12885-020-06923-0
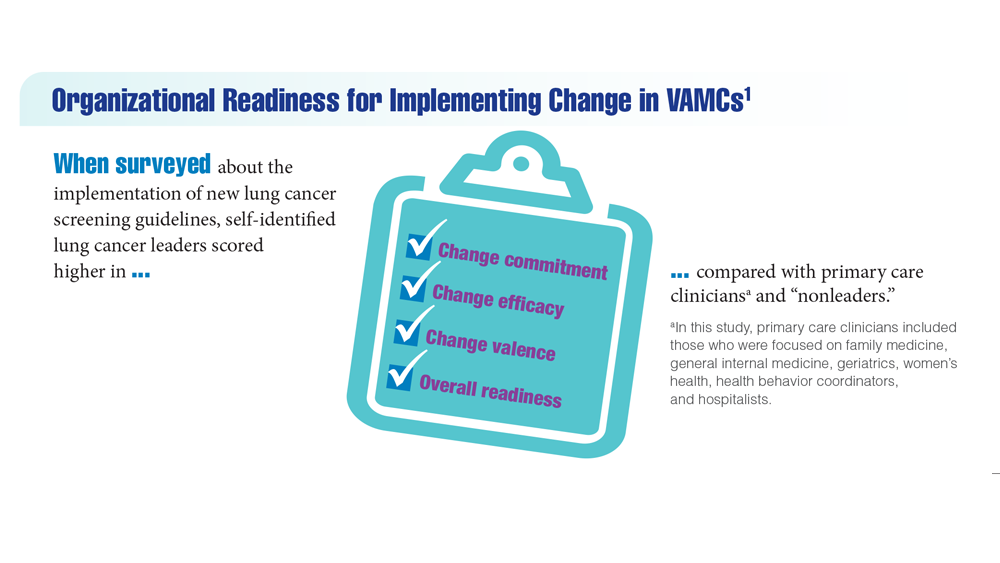
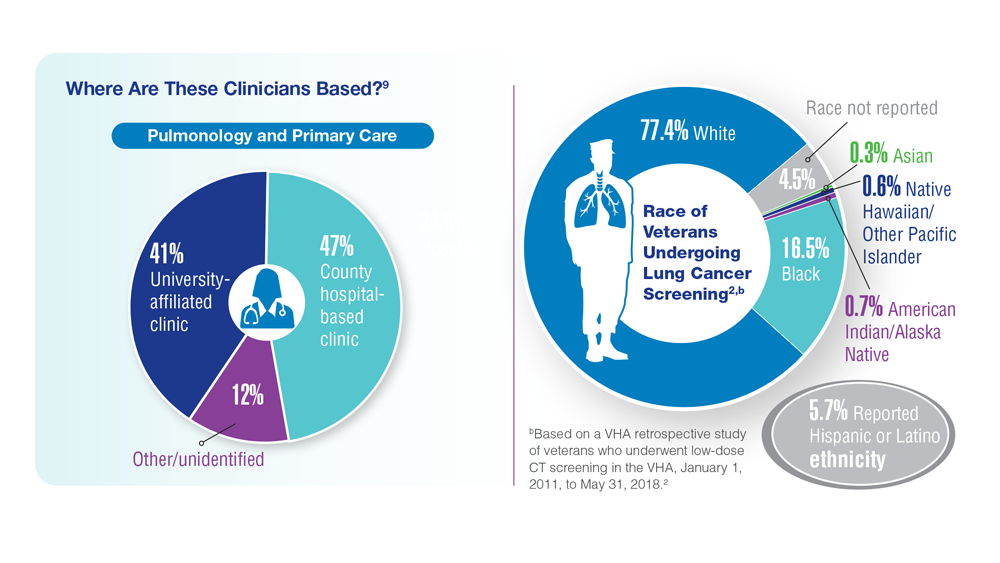


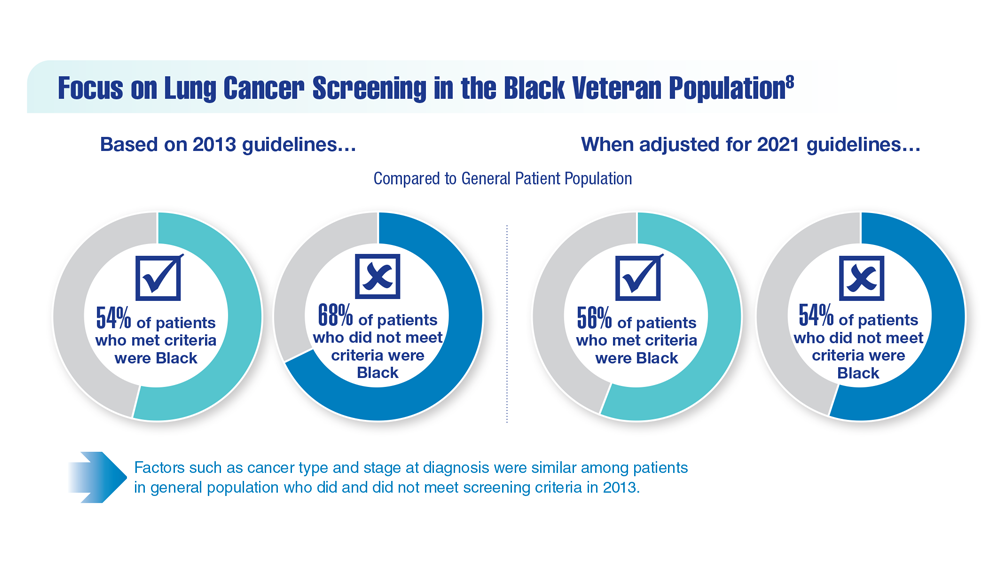

Treating Veterans With Small-Cell Lung Cancer
Small-cell lung cancer (SCLC) occurs almost exclusively in cigarette smokers. Veterans are particularly vulnerable to SCLC because of their prevalent smoking history and exposures to carcinogens, including Agent Orange.
SCLC is characterized by the early development of widespread metastases, including liver, bone, and brain.
Unlike, non–-small cell lung cancer, which has seen great improvement in survival from the introduction of immunotherapy and targeted agents, there has been relatively little improvement in SCLC.
Patients generally are classified into limited- and extensive-stage disease, but platinum-based chemotherapy is almost always the standard first-line treatment. Unfortunately, most patients relapse within a year.
In this ReCAP, Dr Shadia Jalal, of Indiana University Melvin and Bren Simon Comprehensive Cancer Center, discusses second-line treatment options for SCLC patients who relapse after chemotherapy. She also discusses four subtypes of SCLC categorized on the basis of specific transcription regulators, which may offer the potential of targeted therapies for this patient population.
--
Shadia Jalal, MD, Associate Professor of Medicine, Physician, Indiana University Melvin and Bren Simon Comprehensive Cancer Center, Indianapolis, Indiana
Shadia Jalal, MD, has disclosed no relevant financial relationships.
Small-cell lung cancer (SCLC) occurs almost exclusively in cigarette smokers. Veterans are particularly vulnerable to SCLC because of their prevalent smoking history and exposures to carcinogens, including Agent Orange.
SCLC is characterized by the early development of widespread metastases, including liver, bone, and brain.
Unlike, non–-small cell lung cancer, which has seen great improvement in survival from the introduction of immunotherapy and targeted agents, there has been relatively little improvement in SCLC.
Patients generally are classified into limited- and extensive-stage disease, but platinum-based chemotherapy is almost always the standard first-line treatment. Unfortunately, most patients relapse within a year.
In this ReCAP, Dr Shadia Jalal, of Indiana University Melvin and Bren Simon Comprehensive Cancer Center, discusses second-line treatment options for SCLC patients who relapse after chemotherapy. She also discusses four subtypes of SCLC categorized on the basis of specific transcription regulators, which may offer the potential of targeted therapies for this patient population.
--
Shadia Jalal, MD, Associate Professor of Medicine, Physician, Indiana University Melvin and Bren Simon Comprehensive Cancer Center, Indianapolis, Indiana
Shadia Jalal, MD, has disclosed no relevant financial relationships.
Small-cell lung cancer (SCLC) occurs almost exclusively in cigarette smokers. Veterans are particularly vulnerable to SCLC because of their prevalent smoking history and exposures to carcinogens, including Agent Orange.
SCLC is characterized by the early development of widespread metastases, including liver, bone, and brain.
Unlike, non–-small cell lung cancer, which has seen great improvement in survival from the introduction of immunotherapy and targeted agents, there has been relatively little improvement in SCLC.
Patients generally are classified into limited- and extensive-stage disease, but platinum-based chemotherapy is almost always the standard first-line treatment. Unfortunately, most patients relapse within a year.
In this ReCAP, Dr Shadia Jalal, of Indiana University Melvin and Bren Simon Comprehensive Cancer Center, discusses second-line treatment options for SCLC patients who relapse after chemotherapy. She also discusses four subtypes of SCLC categorized on the basis of specific transcription regulators, which may offer the potential of targeted therapies for this patient population.
--
Shadia Jalal, MD, Associate Professor of Medicine, Physician, Indiana University Melvin and Bren Simon Comprehensive Cancer Center, Indianapolis, Indiana
Shadia Jalal, MD, has disclosed no relevant financial relationships.
