User login
When the tail wags the dog: Clinical skills in the age of technology
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
- Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
- Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
- Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
- Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
- Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
- Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
- Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
- Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
- Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
- Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
- Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
- Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
- Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
- Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
- Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
- Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
- Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
- Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
- Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
- Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
- Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
- Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
- Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
- Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
- Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
- Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
- Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
- Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
- Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
- Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
- Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
- Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
- Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
- Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
- Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
- Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
- Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
- Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
- Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
- Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.
- Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
- Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
- Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
- Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
- Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
- Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
- Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
- Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
- Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
- Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
- Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
- Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
- Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
- Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
- Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
- Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
- Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
- Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
- Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
- Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.

Bedbugs: Awareness is key
In 2004, knowing of my medical interest in arthropods, a resident came to my office to discuss an “unusual case” of pubic louse infestation seen at another hospital: a middle-aged woman had been afflicted for months with a skin eruption with excoriation and impetigo that involved the arms and legs but not the pubic area.
In a bag, the resident had a dead insect, 5 mm in length, with a brown, lens-shaped body and short hairs on the pronotum that were visible with a hand lens. An attending dermatologist at the other hospital had identified the insect—incorrectly—as a pubic louse.
With deference, I informed the resident that I did not share the opinion that this was a pubic louse, unless the insect represented a new “Cleveland variant” of the species (a reference to the 1975 Bruce Maness sci-fi film, The Tomato That Ate Cleveland). Rather, I stated, “I believe this is a bedbug, but I have not seen many specimens.”
In hindsight, these words were prophetic, for since 2004, the incidence of bedbug infestations has remarkably surged.1 The trend has not abated, making the review by Ibrahim et al in this issue of the Cleveland Clinic Journal of Medicine timely for all practitioners.2
BEDBUGS ARE BACK…
Bedbugs have plagued man for millennia. In 1939, it was estimated that 4 million Londoners (in a city of 8.5 million) were bitten by bedbugs each night.3 However, as Ibrahim et al describe, long-acting pesticides introduced during World War II dramatically reduced infestation rates. By 1997, some college entomology programs reported difficulty in locating a single teaching specimen.4
The modern resurgence of bedbugs is multifactorial, including a ban on long-acting pesticides such as dichlorodiphenyltrichloroethane (DDT), as well as population growth and increased travel. In days past, bedbug infestations may have pertained to hygiene and social status. But today, travel is a major factor in the resurgence, and bedbugs now affect a broader segment of the population, including the affluent—something that must be kept in mind in the clinical setting.5
…AND THEY’RE EVERYWHERE
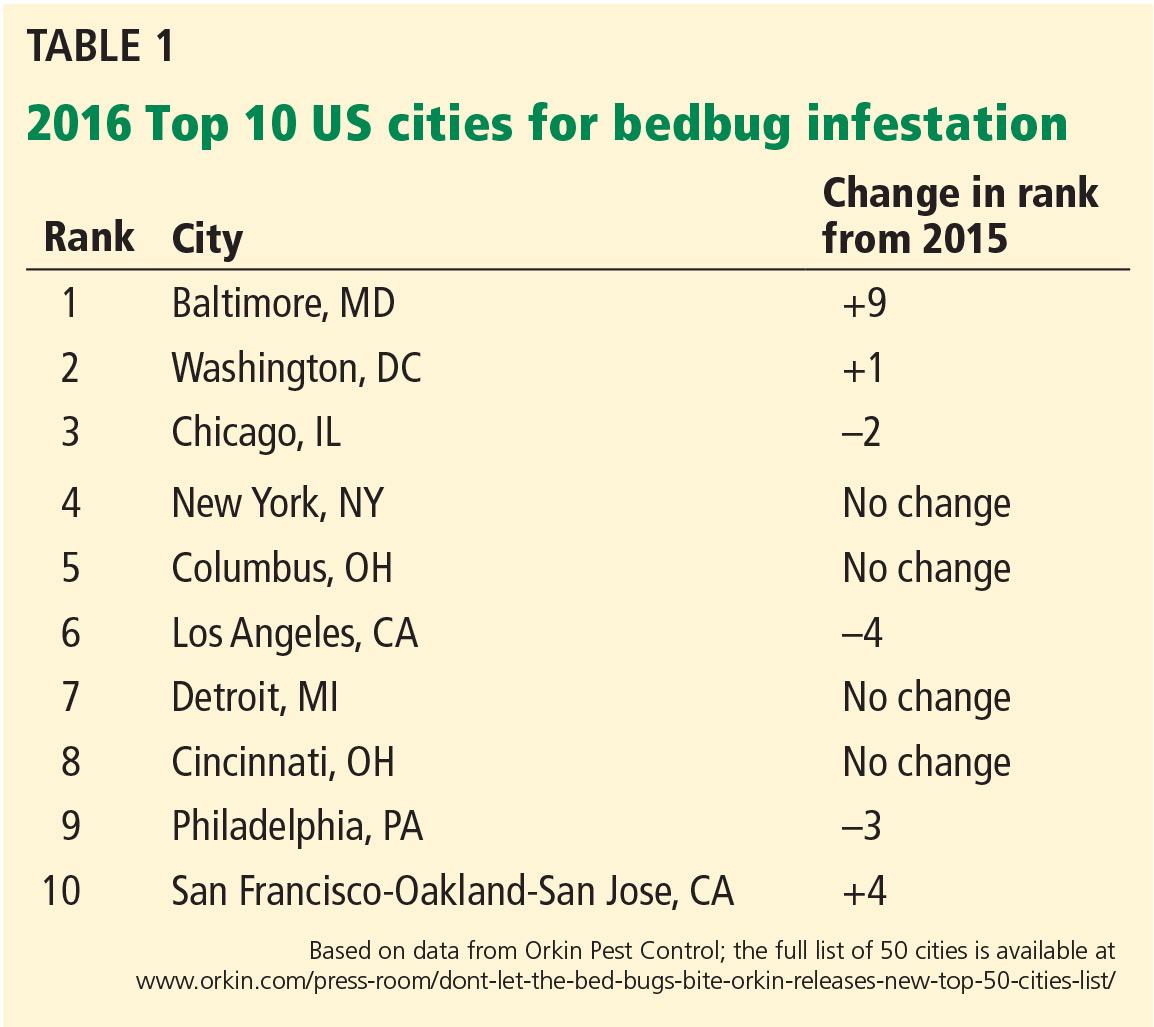
Many prominent US cities are experiencing near-epidemic numbers of bedbug infestations (Table 1). Bedbug infestations occur not only in homes and hotel rooms, but also in hospitals,6 office buildings,7 movie theaters,8 schools,9 and even on subways and trains,10 expanding the number of people potentially exposed.
Understanding that bedbugs affect more than people who are in bed, or with hygiene challenges, Ibrahim et al describe the presentation of bedbug bites—useful information for all practitioners, regardless of medical specialty.
Bedbugs bite skin that is exposed during sleep (ie, the distal extremities and the head, face, and neck). Quasilinear bites, in groups of three (the notorious “breakfast, lunch, and dinner” sign) are a good clue to remember. Unusually exuberant reactions to bedbug bites may be confused with autoimmune bullous conditions or primary vasculitides.11
NOT ALL WHO ARE BITTEN HAVE REACTIONS
Intricate entomologic studies have shown that substances in bedbug saliva drive bite reactions.12,13 However, as Ibrahim et al mention, not all bites provoke a reaction in all persons.
This fact cannot be overstated, for providers in primary care and urgent and emergency care settings may have learned to ask questions about scabies such as, “Are other persons in the household similarly affected?” While it is uncommon for a person with scabies not to present with visible skin lesions, one does not want to misinterpret this historical detail in the setting of bedbug bites. If one person in a household has lesions and another does not, this does not exclude a bedbug infestation!
Ibrahim et al emphasize that treatment of bedbug bites is supportive in nature. Most often, extermination in the home or any other setting should be conducted by professionals. During travel, prevention by inspection is widely advocated.5 There has been interest in using oral ivermectin in affected patients to adversely affect the bedbug colony, but to date, early experiments have encountered daunting pharmacokinetic concerns.14
PSYCHOLOGICAL AND OTHER SEQUELAE
A final consideration in bedbug infestations is any lasting sequelae beyond the bites themselves. Bedbug infestations severe enough to cause anemia and exacerbate or trigger adverse cardiac events have been reported.15 While bedbugs carry human pathogens such as methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus faecium, hepatitis B virus, Bartonella quintana, and Trypanosoma cruzi, Ibrahim et al correctly inform the reader that there are no compelling reports of transmission of these diseases via bedbug bites.16
However, there may be lasting psychological sequelae. Anxiety, hypervigilance, insomnia, avoidance behaviors, and personal dysfunction can persist, even long after the infestation has been eradicated.
Bedbugs are a national and even global health problem worthy of familiarity by all healthcare providers, regardless of specialty. In this regard, Ibrahim et al succinctly and accurately provide a functional and clinically useful guide.
- Alalawi AH. Bed bugs epidemic in the United States. Entomol Ornithol Herpetol 2015; 4:143–148.
- Ibrahim O, Syed UM, Tomecki KJ. Bedbugs: a practical review. Clev Clin J Med 2017; 84:207–211.
- Velten H. Beastly London—A History of Animals in the City. London: Reaktion Books. November 15, 2013. p. 221.
- Snetsinger R. Bed bugs and other bugs. In: Moreland D, editor. Mallis Handbook of Pest Control: The Behavior, Life History, and Control of House Pests, 8th edition. Cleveland, OH: GIE Publishers, 1997:392–424.
- Kolb A, Needham GR, Neyman KM, High WA. Bedbugs. Dermatol Ther 2009; 22:347–352.
- Totten V, Charbonneau H, Hoch W, Shah C, Sheele J. The cost of decontaminating an ED after finding a bed bug: results from a single academic medical center. Am J Emerg Med 2016; 34:649.
- Baumblatt JA, Dunn JR, Schaffner W, Moncayo AC, Stull-Lane A, Jones TF. An outbreak of bed bug infestation in an office building. J Environ Health 2014; 76:16–18.
- Chalupka S. Preventing bedbug infestation. AAOHN J 2010; 58:500.
- Scisicione P. Bed bugs: they are back! The role of the school nurse in bed bug management. NASN Sch Nurse 2012; 27:268–273.
- Anders D, Brocker EB, Hamm H. Cimex lectularius—an unwelcome train attendant. Eur J Dermatol 2010; 20:239–240.
- deShazo RD, Feldlaufer MF, Mihm MC Jr, Goddard J. Bullous reactions to bedbug bites reflect cutaneous vasculitis. Am J Med 2012; 125:688–694.
- Potter MF, Haynes KF, Deutsch M, et al. The sensitivity spectrum: human reactions to bed bug bites. Pest Control Technology Magazine 2010; 70–75.
- Reinhardt K, Kempke D, Naylor RA, Siva-Jothy MT. Sensitivity to bites by the bedbug, Cimex lectularius. Med Vet Entomol 2009; 23:163–166.
- Sheele JM, Anderson JF, Tran TD, et al. Ivermectin causes Cimex lectularius (bedbug) morbidity and mortality. J Emerg Med 2013; 45:433–440.
- Paulke-Korinek M, Széll M, Laferl H, Auer H, Wenisch C. Bed bugs can cause severe anaemia in adults. Parasitol Res 2012; 110:2577–2579.
- Ho D, Lai O, Glick S, Jagdeo J. Lack of evidence that bedbugs transmit pathogens to humans. J Am Acad Dermatol 2016; 74:1261.
In 2004, knowing of my medical interest in arthropods, a resident came to my office to discuss an “unusual case” of pubic louse infestation seen at another hospital: a middle-aged woman had been afflicted for months with a skin eruption with excoriation and impetigo that involved the arms and legs but not the pubic area.
In a bag, the resident had a dead insect, 5 mm in length, with a brown, lens-shaped body and short hairs on the pronotum that were visible with a hand lens. An attending dermatologist at the other hospital had identified the insect—incorrectly—as a pubic louse.
With deference, I informed the resident that I did not share the opinion that this was a pubic louse, unless the insect represented a new “Cleveland variant” of the species (a reference to the 1975 Bruce Maness sci-fi film, The Tomato That Ate Cleveland). Rather, I stated, “I believe this is a bedbug, but I have not seen many specimens.”
In hindsight, these words were prophetic, for since 2004, the incidence of bedbug infestations has remarkably surged.1 The trend has not abated, making the review by Ibrahim et al in this issue of the Cleveland Clinic Journal of Medicine timely for all practitioners.2
BEDBUGS ARE BACK…
Bedbugs have plagued man for millennia. In 1939, it was estimated that 4 million Londoners (in a city of 8.5 million) were bitten by bedbugs each night.3 However, as Ibrahim et al describe, long-acting pesticides introduced during World War II dramatically reduced infestation rates. By 1997, some college entomology programs reported difficulty in locating a single teaching specimen.4
The modern resurgence of bedbugs is multifactorial, including a ban on long-acting pesticides such as dichlorodiphenyltrichloroethane (DDT), as well as population growth and increased travel. In days past, bedbug infestations may have pertained to hygiene and social status. But today, travel is a major factor in the resurgence, and bedbugs now affect a broader segment of the population, including the affluent—something that must be kept in mind in the clinical setting.5
…AND THEY’RE EVERYWHERE
Many prominent US cities are experiencing near-epidemic numbers of bedbug infestations (Table 1). Bedbug infestations occur not only in homes and hotel rooms, but also in hospitals,6 office buildings,7 movie theaters,8 schools,9 and even on subways and trains,10 expanding the number of people potentially exposed.
Understanding that bedbugs affect more than people who are in bed, or with hygiene challenges, Ibrahim et al describe the presentation of bedbug bites—useful information for all practitioners, regardless of medical specialty.
Bedbugs bite skin that is exposed during sleep (ie, the distal extremities and the head, face, and neck). Quasilinear bites, in groups of three (the notorious “breakfast, lunch, and dinner” sign) are a good clue to remember. Unusually exuberant reactions to bedbug bites may be confused with autoimmune bullous conditions or primary vasculitides.11
NOT ALL WHO ARE BITTEN HAVE REACTIONS
Intricate entomologic studies have shown that substances in bedbug saliva drive bite reactions.12,13 However, as Ibrahim et al mention, not all bites provoke a reaction in all persons.
This fact cannot be overstated, for providers in primary care and urgent and emergency care settings may have learned to ask questions about scabies such as, “Are other persons in the household similarly affected?” While it is uncommon for a person with scabies not to present with visible skin lesions, one does not want to misinterpret this historical detail in the setting of bedbug bites. If one person in a household has lesions and another does not, this does not exclude a bedbug infestation!
Ibrahim et al emphasize that treatment of bedbug bites is supportive in nature. Most often, extermination in the home or any other setting should be conducted by professionals. During travel, prevention by inspection is widely advocated.5 There has been interest in using oral ivermectin in affected patients to adversely affect the bedbug colony, but to date, early experiments have encountered daunting pharmacokinetic concerns.14
PSYCHOLOGICAL AND OTHER SEQUELAE
A final consideration in bedbug infestations is any lasting sequelae beyond the bites themselves. Bedbug infestations severe enough to cause anemia and exacerbate or trigger adverse cardiac events have been reported.15 While bedbugs carry human pathogens such as methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus faecium, hepatitis B virus, Bartonella quintana, and Trypanosoma cruzi, Ibrahim et al correctly inform the reader that there are no compelling reports of transmission of these diseases via bedbug bites.16
However, there may be lasting psychological sequelae. Anxiety, hypervigilance, insomnia, avoidance behaviors, and personal dysfunction can persist, even long after the infestation has been eradicated.
Bedbugs are a national and even global health problem worthy of familiarity by all healthcare providers, regardless of specialty. In this regard, Ibrahim et al succinctly and accurately provide a functional and clinically useful guide.
In 2004, knowing of my medical interest in arthropods, a resident came to my office to discuss an “unusual case” of pubic louse infestation seen at another hospital: a middle-aged woman had been afflicted for months with a skin eruption with excoriation and impetigo that involved the arms and legs but not the pubic area.
In a bag, the resident had a dead insect, 5 mm in length, with a brown, lens-shaped body and short hairs on the pronotum that were visible with a hand lens. An attending dermatologist at the other hospital had identified the insect—incorrectly—as a pubic louse.
With deference, I informed the resident that I did not share the opinion that this was a pubic louse, unless the insect represented a new “Cleveland variant” of the species (a reference to the 1975 Bruce Maness sci-fi film, The Tomato That Ate Cleveland). Rather, I stated, “I believe this is a bedbug, but I have not seen many specimens.”
In hindsight, these words were prophetic, for since 2004, the incidence of bedbug infestations has remarkably surged.1 The trend has not abated, making the review by Ibrahim et al in this issue of the Cleveland Clinic Journal of Medicine timely for all practitioners.2
BEDBUGS ARE BACK…
Bedbugs have plagued man for millennia. In 1939, it was estimated that 4 million Londoners (in a city of 8.5 million) were bitten by bedbugs each night.3 However, as Ibrahim et al describe, long-acting pesticides introduced during World War II dramatically reduced infestation rates. By 1997, some college entomology programs reported difficulty in locating a single teaching specimen.4
The modern resurgence of bedbugs is multifactorial, including a ban on long-acting pesticides such as dichlorodiphenyltrichloroethane (DDT), as well as population growth and increased travel. In days past, bedbug infestations may have pertained to hygiene and social status. But today, travel is a major factor in the resurgence, and bedbugs now affect a broader segment of the population, including the affluent—something that must be kept in mind in the clinical setting.5
…AND THEY’RE EVERYWHERE
Many prominent US cities are experiencing near-epidemic numbers of bedbug infestations (Table 1). Bedbug infestations occur not only in homes and hotel rooms, but also in hospitals,6 office buildings,7 movie theaters,8 schools,9 and even on subways and trains,10 expanding the number of people potentially exposed.
Understanding that bedbugs affect more than people who are in bed, or with hygiene challenges, Ibrahim et al describe the presentation of bedbug bites—useful information for all practitioners, regardless of medical specialty.
Bedbugs bite skin that is exposed during sleep (ie, the distal extremities and the head, face, and neck). Quasilinear bites, in groups of three (the notorious “breakfast, lunch, and dinner” sign) are a good clue to remember. Unusually exuberant reactions to bedbug bites may be confused with autoimmune bullous conditions or primary vasculitides.11
NOT ALL WHO ARE BITTEN HAVE REACTIONS
Intricate entomologic studies have shown that substances in bedbug saliva drive bite reactions.12,13 However, as Ibrahim et al mention, not all bites provoke a reaction in all persons.
This fact cannot be overstated, for providers in primary care and urgent and emergency care settings may have learned to ask questions about scabies such as, “Are other persons in the household similarly affected?” While it is uncommon for a person with scabies not to present with visible skin lesions, one does not want to misinterpret this historical detail in the setting of bedbug bites. If one person in a household has lesions and another does not, this does not exclude a bedbug infestation!
Ibrahim et al emphasize that treatment of bedbug bites is supportive in nature. Most often, extermination in the home or any other setting should be conducted by professionals. During travel, prevention by inspection is widely advocated.5 There has been interest in using oral ivermectin in affected patients to adversely affect the bedbug colony, but to date, early experiments have encountered daunting pharmacokinetic concerns.14
PSYCHOLOGICAL AND OTHER SEQUELAE
A final consideration in bedbug infestations is any lasting sequelae beyond the bites themselves. Bedbug infestations severe enough to cause anemia and exacerbate or trigger adverse cardiac events have been reported.15 While bedbugs carry human pathogens such as methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus faecium, hepatitis B virus, Bartonella quintana, and Trypanosoma cruzi, Ibrahim et al correctly inform the reader that there are no compelling reports of transmission of these diseases via bedbug bites.16
However, there may be lasting psychological sequelae. Anxiety, hypervigilance, insomnia, avoidance behaviors, and personal dysfunction can persist, even long after the infestation has been eradicated.
Bedbugs are a national and even global health problem worthy of familiarity by all healthcare providers, regardless of specialty. In this regard, Ibrahim et al succinctly and accurately provide a functional and clinically useful guide.
- Alalawi AH. Bed bugs epidemic in the United States. Entomol Ornithol Herpetol 2015; 4:143–148.
- Ibrahim O, Syed UM, Tomecki KJ. Bedbugs: a practical review. Clev Clin J Med 2017; 84:207–211.
- Velten H. Beastly London—A History of Animals in the City. London: Reaktion Books. November 15, 2013. p. 221.
- Snetsinger R. Bed bugs and other bugs. In: Moreland D, editor. Mallis Handbook of Pest Control: The Behavior, Life History, and Control of House Pests, 8th edition. Cleveland, OH: GIE Publishers, 1997:392–424.
- Kolb A, Needham GR, Neyman KM, High WA. Bedbugs. Dermatol Ther 2009; 22:347–352.
- Totten V, Charbonneau H, Hoch W, Shah C, Sheele J. The cost of decontaminating an ED after finding a bed bug: results from a single academic medical center. Am J Emerg Med 2016; 34:649.
- Baumblatt JA, Dunn JR, Schaffner W, Moncayo AC, Stull-Lane A, Jones TF. An outbreak of bed bug infestation in an office building. J Environ Health 2014; 76:16–18.
- Chalupka S. Preventing bedbug infestation. AAOHN J 2010; 58:500.
- Scisicione P. Bed bugs: they are back! The role of the school nurse in bed bug management. NASN Sch Nurse 2012; 27:268–273.
- Anders D, Brocker EB, Hamm H. Cimex lectularius—an unwelcome train attendant. Eur J Dermatol 2010; 20:239–240.
- deShazo RD, Feldlaufer MF, Mihm MC Jr, Goddard J. Bullous reactions to bedbug bites reflect cutaneous vasculitis. Am J Med 2012; 125:688–694.
- Potter MF, Haynes KF, Deutsch M, et al. The sensitivity spectrum: human reactions to bed bug bites. Pest Control Technology Magazine 2010; 70–75.
- Reinhardt K, Kempke D, Naylor RA, Siva-Jothy MT. Sensitivity to bites by the bedbug, Cimex lectularius. Med Vet Entomol 2009; 23:163–166.
- Sheele JM, Anderson JF, Tran TD, et al. Ivermectin causes Cimex lectularius (bedbug) morbidity and mortality. J Emerg Med 2013; 45:433–440.
- Paulke-Korinek M, Széll M, Laferl H, Auer H, Wenisch C. Bed bugs can cause severe anaemia in adults. Parasitol Res 2012; 110:2577–2579.
- Ho D, Lai O, Glick S, Jagdeo J. Lack of evidence that bedbugs transmit pathogens to humans. J Am Acad Dermatol 2016; 74:1261.
- Alalawi AH. Bed bugs epidemic in the United States. Entomol Ornithol Herpetol 2015; 4:143–148.
- Ibrahim O, Syed UM, Tomecki KJ. Bedbugs: a practical review. Clev Clin J Med 2017; 84:207–211.
- Velten H. Beastly London—A History of Animals in the City. London: Reaktion Books. November 15, 2013. p. 221.
- Snetsinger R. Bed bugs and other bugs. In: Moreland D, editor. Mallis Handbook of Pest Control: The Behavior, Life History, and Control of House Pests, 8th edition. Cleveland, OH: GIE Publishers, 1997:392–424.
- Kolb A, Needham GR, Neyman KM, High WA. Bedbugs. Dermatol Ther 2009; 22:347–352.
- Totten V, Charbonneau H, Hoch W, Shah C, Sheele J. The cost of decontaminating an ED after finding a bed bug: results from a single academic medical center. Am J Emerg Med 2016; 34:649.
- Baumblatt JA, Dunn JR, Schaffner W, Moncayo AC, Stull-Lane A, Jones TF. An outbreak of bed bug infestation in an office building. J Environ Health 2014; 76:16–18.
- Chalupka S. Preventing bedbug infestation. AAOHN J 2010; 58:500.
- Scisicione P. Bed bugs: they are back! The role of the school nurse in bed bug management. NASN Sch Nurse 2012; 27:268–273.
- Anders D, Brocker EB, Hamm H. Cimex lectularius—an unwelcome train attendant. Eur J Dermatol 2010; 20:239–240.
- deShazo RD, Feldlaufer MF, Mihm MC Jr, Goddard J. Bullous reactions to bedbug bites reflect cutaneous vasculitis. Am J Med 2012; 125:688–694.
- Potter MF, Haynes KF, Deutsch M, et al. The sensitivity spectrum: human reactions to bed bug bites. Pest Control Technology Magazine 2010; 70–75.
- Reinhardt K, Kempke D, Naylor RA, Siva-Jothy MT. Sensitivity to bites by the bedbug, Cimex lectularius. Med Vet Entomol 2009; 23:163–166.
- Sheele JM, Anderson JF, Tran TD, et al. Ivermectin causes Cimex lectularius (bedbug) morbidity and mortality. J Emerg Med 2013; 45:433–440.
- Paulke-Korinek M, Széll M, Laferl H, Auer H, Wenisch C. Bed bugs can cause severe anaemia in adults. Parasitol Res 2012; 110:2577–2579.
- Ho D, Lai O, Glick S, Jagdeo J. Lack of evidence that bedbugs transmit pathogens to humans. J Am Acad Dermatol 2016; 74:1261.
Medicare and the 3-inpatient midnight requirement: A statute in need of modernization
On July 30, 1965, Lyndon B. Johnson signed H.R. 6675 into law, establishing Medicare and Medicaid as Title XVIII and Title XIX of the Social Security Act.1 Shortly after, Medicare’s “extended care benefit” began, offering Medicare beneficiaries skilled nursing facility (SNF) care after a qualifying stay of 3 or more consecutive inpatient midnights.2 Fifty years later, the word “inpatient” remains embedded in statute, limiting SNF coverage for Medicare beneficiaries hospitalized as outpatients under observation for part or all of a 3-midnight stay.3
At the individual Medicare beneficiary level, the financial impact of this policy is clear. The Office of Inspector General (OIG) reported a $10,503 beneficiary out-of-pocket cost per uncovered SNF stay following an observation hospitalization in 2012.4 But the actual number of Medicare beneficiaries impacted by this coverage gap is unknown. Using 2009 claims data, Feng et al.5 estimated that 0.75% of previously community dwelling Medicare beneficiaries are discharged to a SNF following an observation hospitalization, and the OIG reported 617,702 beneficiary hospital stays of 3 or more midnights not meeting the 3-midnight inpatient requirement in 2012, with 4% of these beneficiaries discharging to SNFs.4 Yet these studies based on Medicare claims data only capture actual SNF utilization, failing to answer the critical question: How many Medicare beneficiaries need, but forgo, SNF care following a non-qualifying observation hospital stay? In this issue of the Journal of Hospital Medicine, Goldstein et al.6 provide insight to that question. Using chart review of physical therapy and case management recommendations for post-acute SNF care, Goldstein et al.6 compare actual discharge rate to SNF or acute inpatient rehabilitation following an observation stay when such disposition is recommended. In their two-hospital system, fewer than 20% of previously community-dwelling hospitalist patients followed recommendation for post-acute facility stay after observation hospitalization, and more than 40% cited financial concerns as the reason for declining. Patients recommended for SNF also were more likely to be rehospitalized in the subsequent 30 days after discharge, confirming this as a vulnerable patient population. Given Medicare’s original intent to improve health care access for seniors, the case for change seems clear, and the repercussions of not addressing the plight of patients hospitalized under observation is having negative financial and overall detrimental health impacts.
But there are other compelling reasons why this 50-year-old law needs to be improved. Hospital care today is vastly different than when Medicare became law. Average hospital length of stay for patients 65 years and older was 14.2 days in 19657 compared to 5.2 days today,8 clearly a shift in what 3 days of hospital care means. Most importantly, observation stays have become a major part of hospital care. Between 2006 and 2014, per-beneficiary outpatient visits (which include all observation stays) increased 44.2% nationally, while inpatient discharges decreased 19.9%.9 In 2012, the Centers for Medicare & Medicaid Services (CMS) received 1.7 million outpatient observation claims and an additional 700,000 inpatient claims that started with observation days.10 CMS also expected the 2-midnight rule to reduce outpatient observation stays,4 but a recent OIG report11 found that outpatient stays increased 8.1% in the first year (FY 2014) under the new rule, and there were still 748,337 long observation stays (those lasting 2 midnights or longer) in 2014, only a small (2.8%) decrease from the prior year. These factors limit Medicare beneficiary post–acute SNF eligibility in ways that could not have been anticipated when the extended care benefit was created to help seniors access needed health care.
Policymakers must consider cost when considering statutory change. Waiver programs in the 1980s suspending the 3-midnight requirement raised concerns over potential increase in both SNF utilization and associated costs.12 However, more recent data suggest that altering the 3-midnight requirement may not increase post-acute SNF utilization. From 2006 to 2010, Medicare Advantage programs that waived the 3-midnight requirement saw a decrease in hospital length of stay without increased SNF utilization or SNF length of stay, indicating that access to the right level of care at the right time could be cost-saving.13 Recent data from the Bundled Payments for Care Improvement (BPCI) program found savings were largely related to decreased SNF utilization when payments were episode-based,14 a trend that may continue as Medicare moves away from fee-for-service towards bundled payments for more conditions. And although neither example directly tests changing the 3-midnight requirement to include observation midnights, both studies suggest that innovative health care delivery and modification of SNF access did not result in increased SNF utilization or greater post-acute costs. In fact, as Goldstein et al.6 showed, patients recommended for post-acute SNF following observation stay were more likely to be rehospitalized within 30 days, an additional cost that could potentially be avoided if these patients had SNF access. We believe that these correlations strongly support rescinding the 3-
That being said, what can be done? In 2015, the Medicare Payment Advisory Commission (MedPAC) recommended changing the 3-night requirement to require just one of 3 midnights to be inpatient to make a qualifying stay.10 Although an improvement over current law, this proposal would not help the majority of beneficiaries who are exclusively hospitalized under observation status. The “Improving Access to Medicare Coverage Act of 2015”, to be reintroduced in Congress in the coming weeks, would count any midnight spent in the hospital towards the 3-midnight stay requirement, and has bipartisan, bicameral support and cosponsorship.15 In 2015, through unanimous bipartisan, bicameral support, Congress passed the NOTICE Act (PL 114-42), which requires hospitals to inform Medicare beneficiaries hospitalized under observation.16 We believe that the data are clear to both sides of the aisle that Congress should now work together using scientifically-supported research to improve the exact observation policies they felt patients should be informed of. Passing the Improving Access to Medicare Coverage Act is the logical next step in this arena.
Medicare was intended to give seniors access to the healthcare they need. Growth in hospital-based observation care begs for modernization of the statutory 3-inpatient midnight rule. Counting all midnights towards the 3-midnight requirement, whether those midnights are outpatient observation or inpatient, is the right first step.
Disclosures
Representative Courtney is the bill sponsor of the Improving Access to Medicare Coverage Act. The authors report no other conflicts.
1. Medicare & Medicaid Milestones 1937-2015. https://www.cms.gov/About-CMS/Agency-Information/History/Downloads/Medicare-and-Medicaid-Milestones-1937-2015.pdf . Accessed September 25, 2016.
2. Loewenstein R. Early effects of Medicare on the health care of the aged. https://www.ssa.gov/policy/docs/ssb/v34n4/v34n4p3.pdf. Accessed September 25, 2016.
3. US Social Security Act, Sec. 1861 (i). [42 U.S.C. 1395x]. https://www.ssa.gov/OP_Home/ssact/title18/1861.htm. Accessed September 25, 2016.
4. Department of Health and Human Services Office of Inspector General. Hospitals’ use of observation stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. Available at: https://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed September 25, 2016.
5. Feng Z, Jung H-Y, Wright B, Mor V. The origin and disposition of Medicare observation stays. Med Care 2014;52:796-800. PubMed
6. Goldstein JN, Schwartz JS, McGraw P, Banks TL, Hicks LS. The unmet need for postacute rehabilitation among medicare observation patients: a single-center study. J Hosp Med. 2017;12(3):168-172.
7. Vital and Health Statistics. Trends in hospital utilization: United States, 1965-1986. https://www.cdc.gov/nchs/data/series/sr_13/sr13_101.pdf. Accessed September 25, 2016.
8. Healthcare Cost and Utilization Project (HCUP). Statistical brief #180. Overview of hospital stays in the United States, 2012. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.pdf. Accessed September 25, 2016.
9. MedPAC March 2016 Report to the Congress. Chapter 3. Hospital inpatient and outpatient services. http://www.medpac.gov/docs/default-source/reports/march-2016-report-to-the-congress-medicare-payment-policy.pdf?sfvrsn=0. Accessed September 25, 2016.
10. MedPAC. June 2015 Report to the Congress. Chapter 7: Hospital short-stay policy issues. http://www.medpac.gov/docs/default-source/reports/chapter-7-hospital-short-stay-policy-issues-june-2015-report-.pdf?sfvrsn=0 Accessed September 25, 2016.
11. Department of Health and Human Services Office of Inspector General. Vulnerabilities remain under Medicare’s 2-midnight hospital policy, OEI-02-15-00020. https://oig.hhs.gov/oei/reports/oei-02-15-00020.pdf. Accessed February 19, 2017.
12. Lipsitz L. The 3-night hospital stay and Medicare coverage for skilled nursing care. JAMA. 2013;310: 1441-1442. PubMed
13. Grebela R, Keohane L Lee Y, Lipsitz L, Rahman M, Trevedi A. Waiving the three-day rule: admissions and length-of-stay at hospitals and skilled nursing facilities did not increase. Health Affairs. 2015;34:1324-1330. PubMed
14. Dummit L, Kahvecioglu D, Marrufo G, et al. Association between hospital participation in a Medicare bundled payment initiative and payments and quality outcomes for lower extremity joint replacement episodes. JAMA. 2016;316(12):1267-1278. PubMed
15. HR. 1571 Improving Access to Medicare Coverage Act of 2015. https://www.govtrack.us/congress/bills/114/hr1571/text. Accessed September 25, 2016.
16. PL 114-42. The NOTICE Act. https://www.govtrack.us/congress/bills/114/hr876. Accessed September 25, 2016.
On July 30, 1965, Lyndon B. Johnson signed H.R. 6675 into law, establishing Medicare and Medicaid as Title XVIII and Title XIX of the Social Security Act.1 Shortly after, Medicare’s “extended care benefit” began, offering Medicare beneficiaries skilled nursing facility (SNF) care after a qualifying stay of 3 or more consecutive inpatient midnights.2 Fifty years later, the word “inpatient” remains embedded in statute, limiting SNF coverage for Medicare beneficiaries hospitalized as outpatients under observation for part or all of a 3-midnight stay.3
At the individual Medicare beneficiary level, the financial impact of this policy is clear. The Office of Inspector General (OIG) reported a $10,503 beneficiary out-of-pocket cost per uncovered SNF stay following an observation hospitalization in 2012.4 But the actual number of Medicare beneficiaries impacted by this coverage gap is unknown. Using 2009 claims data, Feng et al.5 estimated that 0.75% of previously community dwelling Medicare beneficiaries are discharged to a SNF following an observation hospitalization, and the OIG reported 617,702 beneficiary hospital stays of 3 or more midnights not meeting the 3-midnight inpatient requirement in 2012, with 4% of these beneficiaries discharging to SNFs.4 Yet these studies based on Medicare claims data only capture actual SNF utilization, failing to answer the critical question: How many Medicare beneficiaries need, but forgo, SNF care following a non-qualifying observation hospital stay? In this issue of the Journal of Hospital Medicine, Goldstein et al.6 provide insight to that question. Using chart review of physical therapy and case management recommendations for post-acute SNF care, Goldstein et al.6 compare actual discharge rate to SNF or acute inpatient rehabilitation following an observation stay when such disposition is recommended. In their two-hospital system, fewer than 20% of previously community-dwelling hospitalist patients followed recommendation for post-acute facility stay after observation hospitalization, and more than 40% cited financial concerns as the reason for declining. Patients recommended for SNF also were more likely to be rehospitalized in the subsequent 30 days after discharge, confirming this as a vulnerable patient population. Given Medicare’s original intent to improve health care access for seniors, the case for change seems clear, and the repercussions of not addressing the plight of patients hospitalized under observation is having negative financial and overall detrimental health impacts.
But there are other compelling reasons why this 50-year-old law needs to be improved. Hospital care today is vastly different than when Medicare became law. Average hospital length of stay for patients 65 years and older was 14.2 days in 19657 compared to 5.2 days today,8 clearly a shift in what 3 days of hospital care means. Most importantly, observation stays have become a major part of hospital care. Between 2006 and 2014, per-beneficiary outpatient visits (which include all observation stays) increased 44.2% nationally, while inpatient discharges decreased 19.9%.9 In 2012, the Centers for Medicare & Medicaid Services (CMS) received 1.7 million outpatient observation claims and an additional 700,000 inpatient claims that started with observation days.10 CMS also expected the 2-midnight rule to reduce outpatient observation stays,4 but a recent OIG report11 found that outpatient stays increased 8.1% in the first year (FY 2014) under the new rule, and there were still 748,337 long observation stays (those lasting 2 midnights or longer) in 2014, only a small (2.8%) decrease from the prior year. These factors limit Medicare beneficiary post–acute SNF eligibility in ways that could not have been anticipated when the extended care benefit was created to help seniors access needed health care.
Policymakers must consider cost when considering statutory change. Waiver programs in the 1980s suspending the 3-midnight requirement raised concerns over potential increase in both SNF utilization and associated costs.12 However, more recent data suggest that altering the 3-midnight requirement may not increase post-acute SNF utilization. From 2006 to 2010, Medicare Advantage programs that waived the 3-midnight requirement saw a decrease in hospital length of stay without increased SNF utilization or SNF length of stay, indicating that access to the right level of care at the right time could be cost-saving.13 Recent data from the Bundled Payments for Care Improvement (BPCI) program found savings were largely related to decreased SNF utilization when payments were episode-based,14 a trend that may continue as Medicare moves away from fee-for-service towards bundled payments for more conditions. And although neither example directly tests changing the 3-midnight requirement to include observation midnights, both studies suggest that innovative health care delivery and modification of SNF access did not result in increased SNF utilization or greater post-acute costs. In fact, as Goldstein et al.6 showed, patients recommended for post-acute SNF following observation stay were more likely to be rehospitalized within 30 days, an additional cost that could potentially be avoided if these patients had SNF access. We believe that these correlations strongly support rescinding the 3-
That being said, what can be done? In 2015, the Medicare Payment Advisory Commission (MedPAC) recommended changing the 3-night requirement to require just one of 3 midnights to be inpatient to make a qualifying stay.10 Although an improvement over current law, this proposal would not help the majority of beneficiaries who are exclusively hospitalized under observation status. The “Improving Access to Medicare Coverage Act of 2015”, to be reintroduced in Congress in the coming weeks, would count any midnight spent in the hospital towards the 3-midnight stay requirement, and has bipartisan, bicameral support and cosponsorship.15 In 2015, through unanimous bipartisan, bicameral support, Congress passed the NOTICE Act (PL 114-42), which requires hospitals to inform Medicare beneficiaries hospitalized under observation.16 We believe that the data are clear to both sides of the aisle that Congress should now work together using scientifically-supported research to improve the exact observation policies they felt patients should be informed of. Passing the Improving Access to Medicare Coverage Act is the logical next step in this arena.
Medicare was intended to give seniors access to the healthcare they need. Growth in hospital-based observation care begs for modernization of the statutory 3-inpatient midnight rule. Counting all midnights towards the 3-midnight requirement, whether those midnights are outpatient observation or inpatient, is the right first step.
Disclosures
Representative Courtney is the bill sponsor of the Improving Access to Medicare Coverage Act. The authors report no other conflicts.
On July 30, 1965, Lyndon B. Johnson signed H.R. 6675 into law, establishing Medicare and Medicaid as Title XVIII and Title XIX of the Social Security Act.1 Shortly after, Medicare’s “extended care benefit” began, offering Medicare beneficiaries skilled nursing facility (SNF) care after a qualifying stay of 3 or more consecutive inpatient midnights.2 Fifty years later, the word “inpatient” remains embedded in statute, limiting SNF coverage for Medicare beneficiaries hospitalized as outpatients under observation for part or all of a 3-midnight stay.3
At the individual Medicare beneficiary level, the financial impact of this policy is clear. The Office of Inspector General (OIG) reported a $10,503 beneficiary out-of-pocket cost per uncovered SNF stay following an observation hospitalization in 2012.4 But the actual number of Medicare beneficiaries impacted by this coverage gap is unknown. Using 2009 claims data, Feng et al.5 estimated that 0.75% of previously community dwelling Medicare beneficiaries are discharged to a SNF following an observation hospitalization, and the OIG reported 617,702 beneficiary hospital stays of 3 or more midnights not meeting the 3-midnight inpatient requirement in 2012, with 4% of these beneficiaries discharging to SNFs.4 Yet these studies based on Medicare claims data only capture actual SNF utilization, failing to answer the critical question: How many Medicare beneficiaries need, but forgo, SNF care following a non-qualifying observation hospital stay? In this issue of the Journal of Hospital Medicine, Goldstein et al.6 provide insight to that question. Using chart review of physical therapy and case management recommendations for post-acute SNF care, Goldstein et al.6 compare actual discharge rate to SNF or acute inpatient rehabilitation following an observation stay when such disposition is recommended. In their two-hospital system, fewer than 20% of previously community-dwelling hospitalist patients followed recommendation for post-acute facility stay after observation hospitalization, and more than 40% cited financial concerns as the reason for declining. Patients recommended for SNF also were more likely to be rehospitalized in the subsequent 30 days after discharge, confirming this as a vulnerable patient population. Given Medicare’s original intent to improve health care access for seniors, the case for change seems clear, and the repercussions of not addressing the plight of patients hospitalized under observation is having negative financial and overall detrimental health impacts.
But there are other compelling reasons why this 50-year-old law needs to be improved. Hospital care today is vastly different than when Medicare became law. Average hospital length of stay for patients 65 years and older was 14.2 days in 19657 compared to 5.2 days today,8 clearly a shift in what 3 days of hospital care means. Most importantly, observation stays have become a major part of hospital care. Between 2006 and 2014, per-beneficiary outpatient visits (which include all observation stays) increased 44.2% nationally, while inpatient discharges decreased 19.9%.9 In 2012, the Centers for Medicare & Medicaid Services (CMS) received 1.7 million outpatient observation claims and an additional 700,000 inpatient claims that started with observation days.10 CMS also expected the 2-midnight rule to reduce outpatient observation stays,4 but a recent OIG report11 found that outpatient stays increased 8.1% in the first year (FY 2014) under the new rule, and there were still 748,337 long observation stays (those lasting 2 midnights or longer) in 2014, only a small (2.8%) decrease from the prior year. These factors limit Medicare beneficiary post–acute SNF eligibility in ways that could not have been anticipated when the extended care benefit was created to help seniors access needed health care.
Policymakers must consider cost when considering statutory change. Waiver programs in the 1980s suspending the 3-midnight requirement raised concerns over potential increase in both SNF utilization and associated costs.12 However, more recent data suggest that altering the 3-midnight requirement may not increase post-acute SNF utilization. From 2006 to 2010, Medicare Advantage programs that waived the 3-midnight requirement saw a decrease in hospital length of stay without increased SNF utilization or SNF length of stay, indicating that access to the right level of care at the right time could be cost-saving.13 Recent data from the Bundled Payments for Care Improvement (BPCI) program found savings were largely related to decreased SNF utilization when payments were episode-based,14 a trend that may continue as Medicare moves away from fee-for-service towards bundled payments for more conditions. And although neither example directly tests changing the 3-midnight requirement to include observation midnights, both studies suggest that innovative health care delivery and modification of SNF access did not result in increased SNF utilization or greater post-acute costs. In fact, as Goldstein et al.6 showed, patients recommended for post-acute SNF following observation stay were more likely to be rehospitalized within 30 days, an additional cost that could potentially be avoided if these patients had SNF access. We believe that these correlations strongly support rescinding the 3-
That being said, what can be done? In 2015, the Medicare Payment Advisory Commission (MedPAC) recommended changing the 3-night requirement to require just one of 3 midnights to be inpatient to make a qualifying stay.10 Although an improvement over current law, this proposal would not help the majority of beneficiaries who are exclusively hospitalized under observation status. The “Improving Access to Medicare Coverage Act of 2015”, to be reintroduced in Congress in the coming weeks, would count any midnight spent in the hospital towards the 3-midnight stay requirement, and has bipartisan, bicameral support and cosponsorship.15 In 2015, through unanimous bipartisan, bicameral support, Congress passed the NOTICE Act (PL 114-42), which requires hospitals to inform Medicare beneficiaries hospitalized under observation.16 We believe that the data are clear to both sides of the aisle that Congress should now work together using scientifically-supported research to improve the exact observation policies they felt patients should be informed of. Passing the Improving Access to Medicare Coverage Act is the logical next step in this arena.
Medicare was intended to give seniors access to the healthcare they need. Growth in hospital-based observation care begs for modernization of the statutory 3-inpatient midnight rule. Counting all midnights towards the 3-midnight requirement, whether those midnights are outpatient observation or inpatient, is the right first step.
Disclosures
Representative Courtney is the bill sponsor of the Improving Access to Medicare Coverage Act. The authors report no other conflicts.
1. Medicare & Medicaid Milestones 1937-2015. https://www.cms.gov/About-CMS/Agency-Information/History/Downloads/Medicare-and-Medicaid-Milestones-1937-2015.pdf . Accessed September 25, 2016.
2. Loewenstein R. Early effects of Medicare on the health care of the aged. https://www.ssa.gov/policy/docs/ssb/v34n4/v34n4p3.pdf. Accessed September 25, 2016.
3. US Social Security Act, Sec. 1861 (i). [42 U.S.C. 1395x]. https://www.ssa.gov/OP_Home/ssact/title18/1861.htm. Accessed September 25, 2016.
4. Department of Health and Human Services Office of Inspector General. Hospitals’ use of observation stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. Available at: https://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed September 25, 2016.
5. Feng Z, Jung H-Y, Wright B, Mor V. The origin and disposition of Medicare observation stays. Med Care 2014;52:796-800. PubMed
6. Goldstein JN, Schwartz JS, McGraw P, Banks TL, Hicks LS. The unmet need for postacute rehabilitation among medicare observation patients: a single-center study. J Hosp Med. 2017;12(3):168-172.
7. Vital and Health Statistics. Trends in hospital utilization: United States, 1965-1986. https://www.cdc.gov/nchs/data/series/sr_13/sr13_101.pdf. Accessed September 25, 2016.
8. Healthcare Cost and Utilization Project (HCUP). Statistical brief #180. Overview of hospital stays in the United States, 2012. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.pdf. Accessed September 25, 2016.
9. MedPAC March 2016 Report to the Congress. Chapter 3. Hospital inpatient and outpatient services. http://www.medpac.gov/docs/default-source/reports/march-2016-report-to-the-congress-medicare-payment-policy.pdf?sfvrsn=0. Accessed September 25, 2016.
10. MedPAC. June 2015 Report to the Congress. Chapter 7: Hospital short-stay policy issues. http://www.medpac.gov/docs/default-source/reports/chapter-7-hospital-short-stay-policy-issues-june-2015-report-.pdf?sfvrsn=0 Accessed September 25, 2016.
11. Department of Health and Human Services Office of Inspector General. Vulnerabilities remain under Medicare’s 2-midnight hospital policy, OEI-02-15-00020. https://oig.hhs.gov/oei/reports/oei-02-15-00020.pdf. Accessed February 19, 2017.
12. Lipsitz L. The 3-night hospital stay and Medicare coverage for skilled nursing care. JAMA. 2013;310: 1441-1442. PubMed
13. Grebela R, Keohane L Lee Y, Lipsitz L, Rahman M, Trevedi A. Waiving the three-day rule: admissions and length-of-stay at hospitals and skilled nursing facilities did not increase. Health Affairs. 2015;34:1324-1330. PubMed
14. Dummit L, Kahvecioglu D, Marrufo G, et al. Association between hospital participation in a Medicare bundled payment initiative and payments and quality outcomes for lower extremity joint replacement episodes. JAMA. 2016;316(12):1267-1278. PubMed
15. HR. 1571 Improving Access to Medicare Coverage Act of 2015. https://www.govtrack.us/congress/bills/114/hr1571/text. Accessed September 25, 2016.
16. PL 114-42. The NOTICE Act. https://www.govtrack.us/congress/bills/114/hr876. Accessed September 25, 2016.
1. Medicare & Medicaid Milestones 1937-2015. https://www.cms.gov/About-CMS/Agency-Information/History/Downloads/Medicare-and-Medicaid-Milestones-1937-2015.pdf . Accessed September 25, 2016.
2. Loewenstein R. Early effects of Medicare on the health care of the aged. https://www.ssa.gov/policy/docs/ssb/v34n4/v34n4p3.pdf. Accessed September 25, 2016.
3. US Social Security Act, Sec. 1861 (i). [42 U.S.C. 1395x]. https://www.ssa.gov/OP_Home/ssact/title18/1861.htm. Accessed September 25, 2016.
4. Department of Health and Human Services Office of Inspector General. Hospitals’ use of observation stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. Available at: https://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed September 25, 2016.
5. Feng Z, Jung H-Y, Wright B, Mor V. The origin and disposition of Medicare observation stays. Med Care 2014;52:796-800. PubMed
6. Goldstein JN, Schwartz JS, McGraw P, Banks TL, Hicks LS. The unmet need for postacute rehabilitation among medicare observation patients: a single-center study. J Hosp Med. 2017;12(3):168-172.
7. Vital and Health Statistics. Trends in hospital utilization: United States, 1965-1986. https://www.cdc.gov/nchs/data/series/sr_13/sr13_101.pdf. Accessed September 25, 2016.
8. Healthcare Cost and Utilization Project (HCUP). Statistical brief #180. Overview of hospital stays in the United States, 2012. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.pdf. Accessed September 25, 2016.
9. MedPAC March 2016 Report to the Congress. Chapter 3. Hospital inpatient and outpatient services. http://www.medpac.gov/docs/default-source/reports/march-2016-report-to-the-congress-medicare-payment-policy.pdf?sfvrsn=0. Accessed September 25, 2016.
10. MedPAC. June 2015 Report to the Congress. Chapter 7: Hospital short-stay policy issues. http://www.medpac.gov/docs/default-source/reports/chapter-7-hospital-short-stay-policy-issues-june-2015-report-.pdf?sfvrsn=0 Accessed September 25, 2016.
11. Department of Health and Human Services Office of Inspector General. Vulnerabilities remain under Medicare’s 2-midnight hospital policy, OEI-02-15-00020. https://oig.hhs.gov/oei/reports/oei-02-15-00020.pdf. Accessed February 19, 2017.
12. Lipsitz L. The 3-night hospital stay and Medicare coverage for skilled nursing care. JAMA. 2013;310: 1441-1442. PubMed
13. Grebela R, Keohane L Lee Y, Lipsitz L, Rahman M, Trevedi A. Waiving the three-day rule: admissions and length-of-stay at hospitals and skilled nursing facilities did not increase. Health Affairs. 2015;34:1324-1330. PubMed
14. Dummit L, Kahvecioglu D, Marrufo G, et al. Association between hospital participation in a Medicare bundled payment initiative and payments and quality outcomes for lower extremity joint replacement episodes. JAMA. 2016;316(12):1267-1278. PubMed
15. HR. 1571 Improving Access to Medicare Coverage Act of 2015. https://www.govtrack.us/congress/bills/114/hr1571/text. Accessed September 25, 2016.
16. PL 114-42. The NOTICE Act. https://www.govtrack.us/congress/bills/114/hr876. Accessed September 25, 2016.
© 2017 Society of Hospital Medicine
Acute kidney injury is important in the hospital and afterward
Acute kidney injury (AKI) is a major contributor to morbidity and mortality in hospitalized patients across the world.1 Affecting up to 20% of all admissions (depending on which definition of AKI is used),2 AKI is the most common reason for new-inpatient nephrology consultation. Recent data suggest that AKI incidence has risen rapidly, by up to 10% per year.3,4
AKI is associated with a variety of serious short- and long-term complications. Approximately 33% to 60% of critically ill patients who develop dialysis-requiring AKI do not survive to hospital discharge, and mortality associated with dialysis-requiring AKI is greater than that associated with other serious conditions such as myocardial infarction or acute respiratory distress syndrome.5 Even relatively mild AKI in the acute inpatient setting appears to be an independent risk factor for mortality.6
For several decades, many physicians believed that AKI was a self-limited process followed by complete recovery of renal function to pre-AKI levels among survivors. (Numerous trainees have been taught some variant of the old adage: “If the patients survive, so will their kidneys.”) But studies linking AKI with the development of new-onset chronic kidney disease (CKD) or the accelerated progression of pre-existing CKD have changed this view.7 One important reason the long-term impact of AKI hasn’t been appreciated is that, traditionally, clinical studies of AKI examined inhospital outcomes such as short-term mortality and resource usage and did not consider what transpired months to years after discharge. More recently, epidemiologic studies linking inpatient events with outpatient outcomes have filled this knowledge gap.8 Contemporary animal models of AKI have shed light on potential mechanisms of maladaptive repair after AKI, characterized by fibrosis, vascular rarefaction, tubular loss, glomerulosclerosis, and chronic interstitial inflammation, all of which result in renal function decline. So over the last decade there has been a paradigm shift in how we think about AKI and CKD. Rather than distinct entities, AKI and CKD are now viewed as interconnected syndromes since AKI is a risk factor for CKD progression and CKD is a risk factor for new episodes of AKI.9
Two studies published in this issue of the Journal of Hospital Medicine augment our understanding of AKI and its clinical impact in hospitalized patients. Analyzing data from the National Inpatient Sample, Silver et al.10 found that hospitalizations that include AKI are substantially costlier and associated with longer lengths of stay than hospitalizations without AKI. The authors also highlight that the additional economic costs of AKI exceeded those of many other higher-profile yet less-common acute medical conditions, such as myocardial infarction and gastrointestinal bleeding. These results re-emphasize the important economic burden of AKI at a national level and expand on prior literature by confirming findings previously limited to single-center and regional studies. Better defining the impact AKI has on our healthcare system could help ensure that adequate resources are invested to combat AKI.
The second study, by Rutter et al.,11 found that among hospitalized patients with normal baseline renal function, use of vancomycin in combination with piperacillin-tazobactam is associated with a higher incidence of AKI after antibiotic exposure than use of either agent as monotherapy. This association persisted even after adjusting for potential confounders such as underlying comorbidities, exposure to nephrotoxic agents, documented hypotension, and baseline renal impairment. This study adds to a growing body of literature that suggests synergistic nephrotoxicity between vancomycin and piperacillin-tazobactam. It underscores that any medical intervention—even treatments typically envisioned as non-hazardous and frequently life-saving—involve inherent risks and should prompt the medical community to promote proper antimicrobial stewardship. Whether such exposures to vancomycin or beta-lactam derivatives cause AKI via direct tubular damage, interstitial nephritis, or some other novel mechanism remains to be elucidated. Better delineation of the contemporary causes of AKI, including increased antibiotic exposure, is the first step toward identifying ways to reduce AKI incidence.
Both of these papers serve to highlight the clinical importance of AKI among hospitalized patients. Their findings re-emphasize the need for vigilance in detecting AKI and intervening early to achieve the best clinical outcomes.
Given recent understanding that survivors of AKI are at greater risk for more rapid loss of renal function long after hospital discharge, one goal the US Department of Health and Human Services put forth for Healthy People 2020 is to “increase the proportion of hospital patients who incurred AKI who have follow-up renal evaluation in 6 months post-discharge” (10% improvement targeted).12 Transitions of care after hospitalizations complicated by AKI require special attention to ensure that patients’ needs are optimally monitored and managed during the critical post-discharge period. One recent study analyzing discharge documentation for hospitalizations including AKI found that fewer than half of the discharge summaries and patient instructions commented on the presence, cause, or course of AKI, indicating clear room for improvement.13 And currently, it appears that only a minority of patients with AKI—even AKI severe enough to require dialysis—are seen by a nephrologist within 90 days of discharge.14
Hospitalists play a crucial role in coordinating care as vulnerable patients transition from the inpatient to outpatient setting. We suggest that AKI should be properly documented in the discharge summary. In addition, patients should be informed that they experienced AKI so they can discuss with future caregivers potential strategies to avoid additional renal insults. Discharge referrals to nephrology should be arranged for high-risk patients, including those whose renal function remains decreased at discharge or those who had recurrent AKI episodes during prior hospitalizations. For patients with pre-hospitalization baseline CKD, nephrology should be consulted before indefinitely discontinuing medications like angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. These medications are indispensable in retarding the progression of proteinuric CKD, even though they may predispose patients to AKI under certain circumstances (eg, in states of decreased renal perfusion). Adopting these simple steps may substantially improve the long-term outcomes of patients who experience AKI during hospitalization.
Acknowledgments
The authors are supported by NIH-NIDDK Grants T32DK007219 (BJL) and K24DK92291 (CYH).
Disclosure
Nothing to report.
1. Lameire NH, Bagga A, Cruz D, et al. Acute kidney injury: an increasing global concern. Lancet. 2013;382(9887):170-179. PubMed
2. Zeng X, McMahon GM, Brunelli SM, Bates DW, Waikar SS. Incidence, outcomes, and comparisons across definitions of AKI in hospitalized individuals. Clin J Am Soc Nephrol. 2014;9(1):12-20. PubMed
3. Hsu RK, McCulloch CE, Dudley RA, Lo LJ, Hsu CY. Temporal changes in incidence of dialysis-requiring AKI. J Am Soc Nephrol. 2013;24(1):37-42. PubMed
4. Siew ED, Davenport A. The growth of acute kidney injury: a rising tide or just closer attention to detail? Kidney Int. 2015;87(1):46-61. PubMed
5. Cerdá J, Liu KD, Cruz DN, et al. Promoting kidney function recovery in patients with AKI requiring RRT. Clin J Am Soc Nephrol. 2015;10(10):1859-1867. PubMed
6. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-3370. PubMed
7. Hsu CY. Yes, AKI truly leads to CKD. J Am Soc Nephrol. 2012;23(6):967-969. PubMed
8. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442-448. PubMed
9. Chawla LS, Eggers PW, Star RA, Kimmel PL. Acute kidney injury and chronic kidney disease as interconnected syndromes. New Engl J Med. 2014;371(1):58-66. PubMed
10. Silver SA, Long J, Zheng Y, Chertow GM. Cost of acute kidney injury in hospitalized patients. J Hosp Med. 2017;12(2):70-76. Full Text
11. Rutter WC, Burgess DR, Talbert JC, Burgess DS. Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: a retrospective cohort analysis. J Hosp Med. 2017;12(2):77-82. Full Text
12. US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020. Available at: https://www.healthypeople.gov/node/4093/data_details. Accessed September 2, 2016.
13. Greer RC, Liu Y, Crews DC, Jaar BG, Rabb H, Boulware LE. Hospital discharge communications during care transitions for patients with acute kidney injury: a cross-sectional study. BMC Health Serv Res. 2016;16:449. PubMed
14. Siew ED, Peterson JF, Eden SK, et al. Outpatient nephrology referral rates after acute kidney injury. J Am Soc Nephrol. 2012;23(2):305-312. PubMed
Acute kidney injury (AKI) is a major contributor to morbidity and mortality in hospitalized patients across the world.1 Affecting up to 20% of all admissions (depending on which definition of AKI is used),2 AKI is the most common reason for new-inpatient nephrology consultation. Recent data suggest that AKI incidence has risen rapidly, by up to 10% per year.3,4
AKI is associated with a variety of serious short- and long-term complications. Approximately 33% to 60% of critically ill patients who develop dialysis-requiring AKI do not survive to hospital discharge, and mortality associated with dialysis-requiring AKI is greater than that associated with other serious conditions such as myocardial infarction or acute respiratory distress syndrome.5 Even relatively mild AKI in the acute inpatient setting appears to be an independent risk factor for mortality.6
For several decades, many physicians believed that AKI was a self-limited process followed by complete recovery of renal function to pre-AKI levels among survivors. (Numerous trainees have been taught some variant of the old adage: “If the patients survive, so will their kidneys.”) But studies linking AKI with the development of new-onset chronic kidney disease (CKD) or the accelerated progression of pre-existing CKD have changed this view.7 One important reason the long-term impact of AKI hasn’t been appreciated is that, traditionally, clinical studies of AKI examined inhospital outcomes such as short-term mortality and resource usage and did not consider what transpired months to years after discharge. More recently, epidemiologic studies linking inpatient events with outpatient outcomes have filled this knowledge gap.8 Contemporary animal models of AKI have shed light on potential mechanisms of maladaptive repair after AKI, characterized by fibrosis, vascular rarefaction, tubular loss, glomerulosclerosis, and chronic interstitial inflammation, all of which result in renal function decline. So over the last decade there has been a paradigm shift in how we think about AKI and CKD. Rather than distinct entities, AKI and CKD are now viewed as interconnected syndromes since AKI is a risk factor for CKD progression and CKD is a risk factor for new episodes of AKI.9
Two studies published in this issue of the Journal of Hospital Medicine augment our understanding of AKI and its clinical impact in hospitalized patients. Analyzing data from the National Inpatient Sample, Silver et al.10 found that hospitalizations that include AKI are substantially costlier and associated with longer lengths of stay than hospitalizations without AKI. The authors also highlight that the additional economic costs of AKI exceeded those of many other higher-profile yet less-common acute medical conditions, such as myocardial infarction and gastrointestinal bleeding. These results re-emphasize the important economic burden of AKI at a national level and expand on prior literature by confirming findings previously limited to single-center and regional studies. Better defining the impact AKI has on our healthcare system could help ensure that adequate resources are invested to combat AKI.
The second study, by Rutter et al.,11 found that among hospitalized patients with normal baseline renal function, use of vancomycin in combination with piperacillin-tazobactam is associated with a higher incidence of AKI after antibiotic exposure than use of either agent as monotherapy. This association persisted even after adjusting for potential confounders such as underlying comorbidities, exposure to nephrotoxic agents, documented hypotension, and baseline renal impairment. This study adds to a growing body of literature that suggests synergistic nephrotoxicity between vancomycin and piperacillin-tazobactam. It underscores that any medical intervention—even treatments typically envisioned as non-hazardous and frequently life-saving—involve inherent risks and should prompt the medical community to promote proper antimicrobial stewardship. Whether such exposures to vancomycin or beta-lactam derivatives cause AKI via direct tubular damage, interstitial nephritis, or some other novel mechanism remains to be elucidated. Better delineation of the contemporary causes of AKI, including increased antibiotic exposure, is the first step toward identifying ways to reduce AKI incidence.
Both of these papers serve to highlight the clinical importance of AKI among hospitalized patients. Their findings re-emphasize the need for vigilance in detecting AKI and intervening early to achieve the best clinical outcomes.
Given recent understanding that survivors of AKI are at greater risk for more rapid loss of renal function long after hospital discharge, one goal the US Department of Health and Human Services put forth for Healthy People 2020 is to “increase the proportion of hospital patients who incurred AKI who have follow-up renal evaluation in 6 months post-discharge” (10% improvement targeted).12 Transitions of care after hospitalizations complicated by AKI require special attention to ensure that patients’ needs are optimally monitored and managed during the critical post-discharge period. One recent study analyzing discharge documentation for hospitalizations including AKI found that fewer than half of the discharge summaries and patient instructions commented on the presence, cause, or course of AKI, indicating clear room for improvement.13 And currently, it appears that only a minority of patients with AKI—even AKI severe enough to require dialysis—are seen by a nephrologist within 90 days of discharge.14
Hospitalists play a crucial role in coordinating care as vulnerable patients transition from the inpatient to outpatient setting. We suggest that AKI should be properly documented in the discharge summary. In addition, patients should be informed that they experienced AKI so they can discuss with future caregivers potential strategies to avoid additional renal insults. Discharge referrals to nephrology should be arranged for high-risk patients, including those whose renal function remains decreased at discharge or those who had recurrent AKI episodes during prior hospitalizations. For patients with pre-hospitalization baseline CKD, nephrology should be consulted before indefinitely discontinuing medications like angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. These medications are indispensable in retarding the progression of proteinuric CKD, even though they may predispose patients to AKI under certain circumstances (eg, in states of decreased renal perfusion). Adopting these simple steps may substantially improve the long-term outcomes of patients who experience AKI during hospitalization.
Acknowledgments
The authors are supported by NIH-NIDDK Grants T32DK007219 (BJL) and K24DK92291 (CYH).
Disclosure
Nothing to report.
Acute kidney injury (AKI) is a major contributor to morbidity and mortality in hospitalized patients across the world.1 Affecting up to 20% of all admissions (depending on which definition of AKI is used),2 AKI is the most common reason for new-inpatient nephrology consultation. Recent data suggest that AKI incidence has risen rapidly, by up to 10% per year.3,4
AKI is associated with a variety of serious short- and long-term complications. Approximately 33% to 60% of critically ill patients who develop dialysis-requiring AKI do not survive to hospital discharge, and mortality associated with dialysis-requiring AKI is greater than that associated with other serious conditions such as myocardial infarction or acute respiratory distress syndrome.5 Even relatively mild AKI in the acute inpatient setting appears to be an independent risk factor for mortality.6
For several decades, many physicians believed that AKI was a self-limited process followed by complete recovery of renal function to pre-AKI levels among survivors. (Numerous trainees have been taught some variant of the old adage: “If the patients survive, so will their kidneys.”) But studies linking AKI with the development of new-onset chronic kidney disease (CKD) or the accelerated progression of pre-existing CKD have changed this view.7 One important reason the long-term impact of AKI hasn’t been appreciated is that, traditionally, clinical studies of AKI examined inhospital outcomes such as short-term mortality and resource usage and did not consider what transpired months to years after discharge. More recently, epidemiologic studies linking inpatient events with outpatient outcomes have filled this knowledge gap.8 Contemporary animal models of AKI have shed light on potential mechanisms of maladaptive repair after AKI, characterized by fibrosis, vascular rarefaction, tubular loss, glomerulosclerosis, and chronic interstitial inflammation, all of which result in renal function decline. So over the last decade there has been a paradigm shift in how we think about AKI and CKD. Rather than distinct entities, AKI and CKD are now viewed as interconnected syndromes since AKI is a risk factor for CKD progression and CKD is a risk factor for new episodes of AKI.9
Two studies published in this issue of the Journal of Hospital Medicine augment our understanding of AKI and its clinical impact in hospitalized patients. Analyzing data from the National Inpatient Sample, Silver et al.10 found that hospitalizations that include AKI are substantially costlier and associated with longer lengths of stay than hospitalizations without AKI. The authors also highlight that the additional economic costs of AKI exceeded those of many other higher-profile yet less-common acute medical conditions, such as myocardial infarction and gastrointestinal bleeding. These results re-emphasize the important economic burden of AKI at a national level and expand on prior literature by confirming findings previously limited to single-center and regional studies. Better defining the impact AKI has on our healthcare system could help ensure that adequate resources are invested to combat AKI.
The second study, by Rutter et al.,11 found that among hospitalized patients with normal baseline renal function, use of vancomycin in combination with piperacillin-tazobactam is associated with a higher incidence of AKI after antibiotic exposure than use of either agent as monotherapy. This association persisted even after adjusting for potential confounders such as underlying comorbidities, exposure to nephrotoxic agents, documented hypotension, and baseline renal impairment. This study adds to a growing body of literature that suggests synergistic nephrotoxicity between vancomycin and piperacillin-tazobactam. It underscores that any medical intervention—even treatments typically envisioned as non-hazardous and frequently life-saving—involve inherent risks and should prompt the medical community to promote proper antimicrobial stewardship. Whether such exposures to vancomycin or beta-lactam derivatives cause AKI via direct tubular damage, interstitial nephritis, or some other novel mechanism remains to be elucidated. Better delineation of the contemporary causes of AKI, including increased antibiotic exposure, is the first step toward identifying ways to reduce AKI incidence.
Both of these papers serve to highlight the clinical importance of AKI among hospitalized patients. Their findings re-emphasize the need for vigilance in detecting AKI and intervening early to achieve the best clinical outcomes.
Given recent understanding that survivors of AKI are at greater risk for more rapid loss of renal function long after hospital discharge, one goal the US Department of Health and Human Services put forth for Healthy People 2020 is to “increase the proportion of hospital patients who incurred AKI who have follow-up renal evaluation in 6 months post-discharge” (10% improvement targeted).12 Transitions of care after hospitalizations complicated by AKI require special attention to ensure that patients’ needs are optimally monitored and managed during the critical post-discharge period. One recent study analyzing discharge documentation for hospitalizations including AKI found that fewer than half of the discharge summaries and patient instructions commented on the presence, cause, or course of AKI, indicating clear room for improvement.13 And currently, it appears that only a minority of patients with AKI—even AKI severe enough to require dialysis—are seen by a nephrologist within 90 days of discharge.14
Hospitalists play a crucial role in coordinating care as vulnerable patients transition from the inpatient to outpatient setting. We suggest that AKI should be properly documented in the discharge summary. In addition, patients should be informed that they experienced AKI so they can discuss with future caregivers potential strategies to avoid additional renal insults. Discharge referrals to nephrology should be arranged for high-risk patients, including those whose renal function remains decreased at discharge or those who had recurrent AKI episodes during prior hospitalizations. For patients with pre-hospitalization baseline CKD, nephrology should be consulted before indefinitely discontinuing medications like angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. These medications are indispensable in retarding the progression of proteinuric CKD, even though they may predispose patients to AKI under certain circumstances (eg, in states of decreased renal perfusion). Adopting these simple steps may substantially improve the long-term outcomes of patients who experience AKI during hospitalization.
Acknowledgments
The authors are supported by NIH-NIDDK Grants T32DK007219 (BJL) and K24DK92291 (CYH).
Disclosure
Nothing to report.
1. Lameire NH, Bagga A, Cruz D, et al. Acute kidney injury: an increasing global concern. Lancet. 2013;382(9887):170-179. PubMed
2. Zeng X, McMahon GM, Brunelli SM, Bates DW, Waikar SS. Incidence, outcomes, and comparisons across definitions of AKI in hospitalized individuals. Clin J Am Soc Nephrol. 2014;9(1):12-20. PubMed
3. Hsu RK, McCulloch CE, Dudley RA, Lo LJ, Hsu CY. Temporal changes in incidence of dialysis-requiring AKI. J Am Soc Nephrol. 2013;24(1):37-42. PubMed
4. Siew ED, Davenport A. The growth of acute kidney injury: a rising tide or just closer attention to detail? Kidney Int. 2015;87(1):46-61. PubMed
5. Cerdá J, Liu KD, Cruz DN, et al. Promoting kidney function recovery in patients with AKI requiring RRT. Clin J Am Soc Nephrol. 2015;10(10):1859-1867. PubMed
6. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-3370. PubMed
7. Hsu CY. Yes, AKI truly leads to CKD. J Am Soc Nephrol. 2012;23(6):967-969. PubMed
8. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442-448. PubMed
9. Chawla LS, Eggers PW, Star RA, Kimmel PL. Acute kidney injury and chronic kidney disease as interconnected syndromes. New Engl J Med. 2014;371(1):58-66. PubMed
10. Silver SA, Long J, Zheng Y, Chertow GM. Cost of acute kidney injury in hospitalized patients. J Hosp Med. 2017;12(2):70-76. Full Text
11. Rutter WC, Burgess DR, Talbert JC, Burgess DS. Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: a retrospective cohort analysis. J Hosp Med. 2017;12(2):77-82. Full Text
12. US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020. Available at: https://www.healthypeople.gov/node/4093/data_details. Accessed September 2, 2016.
13. Greer RC, Liu Y, Crews DC, Jaar BG, Rabb H, Boulware LE. Hospital discharge communications during care transitions for patients with acute kidney injury: a cross-sectional study. BMC Health Serv Res. 2016;16:449. PubMed
14. Siew ED, Peterson JF, Eden SK, et al. Outpatient nephrology referral rates after acute kidney injury. J Am Soc Nephrol. 2012;23(2):305-312. PubMed
1. Lameire NH, Bagga A, Cruz D, et al. Acute kidney injury: an increasing global concern. Lancet. 2013;382(9887):170-179. PubMed
2. Zeng X, McMahon GM, Brunelli SM, Bates DW, Waikar SS. Incidence, outcomes, and comparisons across definitions of AKI in hospitalized individuals. Clin J Am Soc Nephrol. 2014;9(1):12-20. PubMed
3. Hsu RK, McCulloch CE, Dudley RA, Lo LJ, Hsu CY. Temporal changes in incidence of dialysis-requiring AKI. J Am Soc Nephrol. 2013;24(1):37-42. PubMed
4. Siew ED, Davenport A. The growth of acute kidney injury: a rising tide or just closer attention to detail? Kidney Int. 2015;87(1):46-61. PubMed
5. Cerdá J, Liu KD, Cruz DN, et al. Promoting kidney function recovery in patients with AKI requiring RRT. Clin J Am Soc Nephrol. 2015;10(10):1859-1867. PubMed
6. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-3370. PubMed
7. Hsu CY. Yes, AKI truly leads to CKD. J Am Soc Nephrol. 2012;23(6):967-969. PubMed
8. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442-448. PubMed
9. Chawla LS, Eggers PW, Star RA, Kimmel PL. Acute kidney injury and chronic kidney disease as interconnected syndromes. New Engl J Med. 2014;371(1):58-66. PubMed
10. Silver SA, Long J, Zheng Y, Chertow GM. Cost of acute kidney injury in hospitalized patients. J Hosp Med. 2017;12(2):70-76. Full Text
11. Rutter WC, Burgess DR, Talbert JC, Burgess DS. Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: a retrospective cohort analysis. J Hosp Med. 2017;12(2):77-82. Full Text
12. US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020. Available at: https://www.healthypeople.gov/node/4093/data_details. Accessed September 2, 2016.
13. Greer RC, Liu Y, Crews DC, Jaar BG, Rabb H, Boulware LE. Hospital discharge communications during care transitions for patients with acute kidney injury: a cross-sectional study. BMC Health Serv Res. 2016;16:449. PubMed
14. Siew ED, Peterson JF, Eden SK, et al. Outpatient nephrology referral rates after acute kidney injury. J Am Soc Nephrol. 2012;23(2):305-312. PubMed
© 2017 Society of Hospital Medicine
Statin therapy in the frail elderly: A nuanced decision
The growing elderly population varies widely in functional capacity and mental agility. Age by itself is not a reliable indicator of physiologic performance in patients with cardiovascular disease.1
The concept of frailty helps to identify elderly patients most susceptible to adverse outcomes. Frailty is a powerful indicator of disability, loss of independence, hospitalization, and death. In a patient whose health is declining, frailty is an appropriate impetus for the clinician and patient to reevaluate the goals of care.
In this issue of the Journal, Mallery et al2 address an important topic: the use of preventive lipid-lowering therapies in frail patients with limited life expectancy. For these patients, they recommend against lipid-lowering therapy for primary prevention, and only in extenuating circumstances for secondary prevention.
No trials have evaluated lipid-lowering therapy specifically in frail older adults, and therefore, these recommendations are based on an evidence-informed appraisal of the literature. Mallery et al2 suggest that in the frail elderly, improvement in function and quality of life are more relevant end points than traditional cardiovascular outcomes. They conclude that available evidence does not support lipid-lowering therapy for most patients with advanced frailty.
POINTS TO CONSIDER
Mallery et al2 effectively articulate the need for frailty-specific care. Multimorbidity, polypharmacy, and increased adverse drug effects require special attention in the frail elderly. The authors make a sound argument against lipid-lowering therapy for primary prevention in the severely frail elderly, in whom the evidence for short-term benefit is not compelling. They also recommend against nonstatin lipid-lowering medications, and against statin therapy for heart failure, which is consistent with major guidelines. In the modern era of reflexive testing and prescribing, the authors’ “less is more” approach provides needed encouragement for thoughtful care in these vulnerable patients.
However, certain points of contention deserve additional consideration, including the imprecise definition of frailty, potential benefits and harms of statin therapy in high-risk patients, and the importance of shared decision-making.
How should frailty be defined?
Frailty biology is a field of ongoing research, and there is a lack of consensus on how best to define the condition.3 Estimates of the prevalence of frailty among older adults with cardiovascular disease range from 10% to 60%, owing to considerable variability in the tools used for frailty assessment.4
Mallery et al2 consider an individual to be severely frail if he or she requires assistance with basic activities of daily living as the result of any physical or cognitive deficit (derived from the Clinical Frailty Scale or Frailty Assessment for Care Planning Tool). While functional dependence may be a consequence of frailty, this generalized definition does not characterize the clinical phenotype, which includes slowness, weakness, low physical activity, exhaustion, and unintentional weight loss.
Furthermore, this definition offers no insight into the unique characteristics, causes, and clinical course related to frailty. Significant heterogeneity among “frail” patients precludes a uniform treatment approach in this population.
Do statins benefit frail patients at high risk?
Regarding secondary prevention, the authors highlight a meta-analysis by Afilalo et al,5 the most comprehensive assessment to date of statin therapy in elderly patients with documented coronary heart disease. This study included nearly 20,000 elderly patients in nine secondary prevention trials, including the secondary prevention subgroup of the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) trial.6
Afilalo et al5 calculated that statin therapy reduced the rates of all-cause mortality by 22% and coronary death by 30%, with even greater reductions in the rates of nonfatal myocardial infarction, stroke, and revascularization. Furthermore, the absolute risk reduction was higher and the number needed to treat was lower in those over age 80. Overall, these data convincingly showed that high-risk patients ages 65 to 82 enrolled in clinical trials derive substantial benefit from statin therapy.
Mallery et al2 contend that many of the secondary prevention statin trials evaluated composite outcomes over many years of follow-up and therefore are not generalizable to the frail elderly. However, the Afilalo meta-analysis5 does not provide patient-level data, and therefore the benefit for different clinical and demographic subgroups is unknown. It is only speculative to infer that those with frailty are unlikely to benefit. In fact, the improved outcomes observed with increasing age would argue against this notion.
Given the compelling data supporting statin therapy in the high-risk elderly population, some patients and clinicians may reasonably feel there is value in statin therapy—even in those with advanced frailty.
What about symptoms, disability, quality of life, and short-term benefits? Asymptomatic or “silent” myocardial infarction is associated with angina, congestive heart failure, and subsequent symptomatic myocardial infarction.7,8 Dismissing the importance of these end points in clinical trials fails to recognize potential downstream effects that are directly relevant to a patient’s overall health status.
The Study Assessing Goals in the Elderly (SAGE) trial9 assessed the effect of statin therapy on ischemia burden in patients ages 65 to 85 with stable coronary disease. The results showed that both moderate and intensive statin dosing significantly reduced myocardial ischemia at 3 and 12 months, as detected by continuous electrocardiographic monitoring.
More research is needed to determine the effect of statin therapy on functional capacity and quality of life. Currently, it is premature to conclude that statins have no relevance to these important patient-centered outcomes.
What are the potential harms?
Mallery et al2 cite numerous articles that emphasize the potential adverse effects of statin therapy in the elderly. Unfortunately, data supporting the safety of statin therapy in the elderly were not included. This should be stressed, given that older statin-eligible patients are often undertreated in contemporary practice.10
A 2015 systematic review and meta-analysis indicated that statin-related events are relatively rare in the elderly.11 Another study showed elderly patients who started statin therapy after a myocardial infarction had no change in short-term cognitive or physical function.12
Older age and low body mass index are risk factors for statin myopathy, underscoring the need for close monitoring in frail patients. However, it is important to maintain an objective and balanced approach when considering potential harms.
Need for shared decision-making
Mallery et al2 make no mention of shared decision-making. Best practice guidelines for the management of frailty support a holistic medical review to establish an individualized care plan for each patient.13 Firm recommendations based on indeterminate evidence undermine the patient-physician relationship and do not allow for personal preferences of care. In an environment of uncertain benefit and harm, the patient’s priorities and values should serve as the cornerstone for clinical decisions.
- Barakat K, Wilkinson P, Deaner A, Fluck D, Ranjadayalan K, Timmis A. How should age affect management of acute myocardial infarction? A prospective cohort study. Lancet 1999; 353:955–959.
- Mallery L, Moorhouse P, McLea Veysey P, Allen M, Fleming I. Frail elderly patients do not need lipid-lowering drugs. Cleve Clin J Med 2016; 83:131–142.
- Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm—issues and controversies. J Gerontol A Biol Sci Med Sci 2007; 62:731–737.
- Afilalo J, Alexander KP, Mack MJ, et al. Frailty assessment in the cardiovascular care of older adults. J Am Coll Cardiol 2014; 63:747–762.
- Afilalo J, Duque G, Steele R, Jukema JW, de Craen AJ, Eisenberg MJ. Statins for secondary prevention in elderly patients: a hierarchical bayesian meta-analysis. J Am Coll Cardiol 2008; 51:37–45.
- Shepherd J, Blauw GJ, Murphy MB, et al; PROSPER study group. PROspective Study of Pravastatin in the Elderly at Risk. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet 2002; 360:1623–1630.
- Nadelmann J, Frishman WH, Ooi WL, et al. Prevalence, incidence and prognosis of recognized and unrecognized myocardial infarction in persons aged 75 years or older: The Bronx Aging Study. Am J Cardiol 1990; 66:533–537.
- Sheifer SE, Gersh BJ, Yanez ND 3rd, Ades PA, Burke GL, Manolio TA. Prevalence, predisposing factors, and prognosis of clinically unrecognized myocardial infarction in the elderly. J Am Coll Cardiol 2000; 35:119–126.
- Deedwania P, Stone PH, Bairey Merz CN, et al. Effects of intensive versus moderate lipid-lowering therapy on myocardial ischemia in older patients with coronary heart disease: results of the Study Assessing Goals in the Elderly (SAGE). Circulation 2007; 115:700–707.
- Maddox TM, Borden WB, Tang F, et al. Implications of the 2013 ACC/AHA cholesterol guidelines for adults in contemporary cardiovascular practice: insights from the NCDR PINNACLE registry. J Am Coll Cardiol 2014; 64:2183–2192.
- Iwere RB, Hewitt J. Myopathy in older people receiving statin therapy: a systematic review and meta-analysis. Br J Clin Pharmacol 2015; 80:363–371.
- Swiger KJ, Martin SS, Tang F, et al. Cognitive and physical function by statin exposure in elderly individuals following acute myocardial infarction. Clin Cardiol 2015; 38:455–461.
- Turner G, Clegg A; British Geriatrics Society; Age UK; Royal College of General Practioners. Best practice guidelines for the management of frailty: a British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing 2014; 43:744–747.
The growing elderly population varies widely in functional capacity and mental agility. Age by itself is not a reliable indicator of physiologic performance in patients with cardiovascular disease.1
The concept of frailty helps to identify elderly patients most susceptible to adverse outcomes. Frailty is a powerful indicator of disability, loss of independence, hospitalization, and death. In a patient whose health is declining, frailty is an appropriate impetus for the clinician and patient to reevaluate the goals of care.
In this issue of the Journal, Mallery et al2 address an important topic: the use of preventive lipid-lowering therapies in frail patients with limited life expectancy. For these patients, they recommend against lipid-lowering therapy for primary prevention, and only in extenuating circumstances for secondary prevention.
No trials have evaluated lipid-lowering therapy specifically in frail older adults, and therefore, these recommendations are based on an evidence-informed appraisal of the literature. Mallery et al2 suggest that in the frail elderly, improvement in function and quality of life are more relevant end points than traditional cardiovascular outcomes. They conclude that available evidence does not support lipid-lowering therapy for most patients with advanced frailty.
POINTS TO CONSIDER
Mallery et al2 effectively articulate the need for frailty-specific care. Multimorbidity, polypharmacy, and increased adverse drug effects require special attention in the frail elderly. The authors make a sound argument against lipid-lowering therapy for primary prevention in the severely frail elderly, in whom the evidence for short-term benefit is not compelling. They also recommend against nonstatin lipid-lowering medications, and against statin therapy for heart failure, which is consistent with major guidelines. In the modern era of reflexive testing and prescribing, the authors’ “less is more” approach provides needed encouragement for thoughtful care in these vulnerable patients.
However, certain points of contention deserve additional consideration, including the imprecise definition of frailty, potential benefits and harms of statin therapy in high-risk patients, and the importance of shared decision-making.
How should frailty be defined?
Frailty biology is a field of ongoing research, and there is a lack of consensus on how best to define the condition.3 Estimates of the prevalence of frailty among older adults with cardiovascular disease range from 10% to 60%, owing to considerable variability in the tools used for frailty assessment.4
Mallery et al2 consider an individual to be severely frail if he or she requires assistance with basic activities of daily living as the result of any physical or cognitive deficit (derived from the Clinical Frailty Scale or Frailty Assessment for Care Planning Tool). While functional dependence may be a consequence of frailty, this generalized definition does not characterize the clinical phenotype, which includes slowness, weakness, low physical activity, exhaustion, and unintentional weight loss.
Furthermore, this definition offers no insight into the unique characteristics, causes, and clinical course related to frailty. Significant heterogeneity among “frail” patients precludes a uniform treatment approach in this population.
Do statins benefit frail patients at high risk?
Regarding secondary prevention, the authors highlight a meta-analysis by Afilalo et al,5 the most comprehensive assessment to date of statin therapy in elderly patients with documented coronary heart disease. This study included nearly 20,000 elderly patients in nine secondary prevention trials, including the secondary prevention subgroup of the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) trial.6
Afilalo et al5 calculated that statin therapy reduced the rates of all-cause mortality by 22% and coronary death by 30%, with even greater reductions in the rates of nonfatal myocardial infarction, stroke, and revascularization. Furthermore, the absolute risk reduction was higher and the number needed to treat was lower in those over age 80. Overall, these data convincingly showed that high-risk patients ages 65 to 82 enrolled in clinical trials derive substantial benefit from statin therapy.
Mallery et al2 contend that many of the secondary prevention statin trials evaluated composite outcomes over many years of follow-up and therefore are not generalizable to the frail elderly. However, the Afilalo meta-analysis5 does not provide patient-level data, and therefore the benefit for different clinical and demographic subgroups is unknown. It is only speculative to infer that those with frailty are unlikely to benefit. In fact, the improved outcomes observed with increasing age would argue against this notion.
Given the compelling data supporting statin therapy in the high-risk elderly population, some patients and clinicians may reasonably feel there is value in statin therapy—even in those with advanced frailty.
What about symptoms, disability, quality of life, and short-term benefits? Asymptomatic or “silent” myocardial infarction is associated with angina, congestive heart failure, and subsequent symptomatic myocardial infarction.7,8 Dismissing the importance of these end points in clinical trials fails to recognize potential downstream effects that are directly relevant to a patient’s overall health status.
The Study Assessing Goals in the Elderly (SAGE) trial9 assessed the effect of statin therapy on ischemia burden in patients ages 65 to 85 with stable coronary disease. The results showed that both moderate and intensive statin dosing significantly reduced myocardial ischemia at 3 and 12 months, as detected by continuous electrocardiographic monitoring.
More research is needed to determine the effect of statin therapy on functional capacity and quality of life. Currently, it is premature to conclude that statins have no relevance to these important patient-centered outcomes.
What are the potential harms?
Mallery et al2 cite numerous articles that emphasize the potential adverse effects of statin therapy in the elderly. Unfortunately, data supporting the safety of statin therapy in the elderly were not included. This should be stressed, given that older statin-eligible patients are often undertreated in contemporary practice.10
A 2015 systematic review and meta-analysis indicated that statin-related events are relatively rare in the elderly.11 Another study showed elderly patients who started statin therapy after a myocardial infarction had no change in short-term cognitive or physical function.12
Older age and low body mass index are risk factors for statin myopathy, underscoring the need for close monitoring in frail patients. However, it is important to maintain an objective and balanced approach when considering potential harms.
Need for shared decision-making
Mallery et al2 make no mention of shared decision-making. Best practice guidelines for the management of frailty support a holistic medical review to establish an individualized care plan for each patient.13 Firm recommendations based on indeterminate evidence undermine the patient-physician relationship and do not allow for personal preferences of care. In an environment of uncertain benefit and harm, the patient’s priorities and values should serve as the cornerstone for clinical decisions.
The growing elderly population varies widely in functional capacity and mental agility. Age by itself is not a reliable indicator of physiologic performance in patients with cardiovascular disease.1
The concept of frailty helps to identify elderly patients most susceptible to adverse outcomes. Frailty is a powerful indicator of disability, loss of independence, hospitalization, and death. In a patient whose health is declining, frailty is an appropriate impetus for the clinician and patient to reevaluate the goals of care.
In this issue of the Journal, Mallery et al2 address an important topic: the use of preventive lipid-lowering therapies in frail patients with limited life expectancy. For these patients, they recommend against lipid-lowering therapy for primary prevention, and only in extenuating circumstances for secondary prevention.
No trials have evaluated lipid-lowering therapy specifically in frail older adults, and therefore, these recommendations are based on an evidence-informed appraisal of the literature. Mallery et al2 suggest that in the frail elderly, improvement in function and quality of life are more relevant end points than traditional cardiovascular outcomes. They conclude that available evidence does not support lipid-lowering therapy for most patients with advanced frailty.
POINTS TO CONSIDER
Mallery et al2 effectively articulate the need for frailty-specific care. Multimorbidity, polypharmacy, and increased adverse drug effects require special attention in the frail elderly. The authors make a sound argument against lipid-lowering therapy for primary prevention in the severely frail elderly, in whom the evidence for short-term benefit is not compelling. They also recommend against nonstatin lipid-lowering medications, and against statin therapy for heart failure, which is consistent with major guidelines. In the modern era of reflexive testing and prescribing, the authors’ “less is more” approach provides needed encouragement for thoughtful care in these vulnerable patients.
However, certain points of contention deserve additional consideration, including the imprecise definition of frailty, potential benefits and harms of statin therapy in high-risk patients, and the importance of shared decision-making.
How should frailty be defined?
Frailty biology is a field of ongoing research, and there is a lack of consensus on how best to define the condition.3 Estimates of the prevalence of frailty among older adults with cardiovascular disease range from 10% to 60%, owing to considerable variability in the tools used for frailty assessment.4
Mallery et al2 consider an individual to be severely frail if he or she requires assistance with basic activities of daily living as the result of any physical or cognitive deficit (derived from the Clinical Frailty Scale or Frailty Assessment for Care Planning Tool). While functional dependence may be a consequence of frailty, this generalized definition does not characterize the clinical phenotype, which includes slowness, weakness, low physical activity, exhaustion, and unintentional weight loss.
Furthermore, this definition offers no insight into the unique characteristics, causes, and clinical course related to frailty. Significant heterogeneity among “frail” patients precludes a uniform treatment approach in this population.
Do statins benefit frail patients at high risk?
Regarding secondary prevention, the authors highlight a meta-analysis by Afilalo et al,5 the most comprehensive assessment to date of statin therapy in elderly patients with documented coronary heart disease. This study included nearly 20,000 elderly patients in nine secondary prevention trials, including the secondary prevention subgroup of the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) trial.6
Afilalo et al5 calculated that statin therapy reduced the rates of all-cause mortality by 22% and coronary death by 30%, with even greater reductions in the rates of nonfatal myocardial infarction, stroke, and revascularization. Furthermore, the absolute risk reduction was higher and the number needed to treat was lower in those over age 80. Overall, these data convincingly showed that high-risk patients ages 65 to 82 enrolled in clinical trials derive substantial benefit from statin therapy.
Mallery et al2 contend that many of the secondary prevention statin trials evaluated composite outcomes over many years of follow-up and therefore are not generalizable to the frail elderly. However, the Afilalo meta-analysis5 does not provide patient-level data, and therefore the benefit for different clinical and demographic subgroups is unknown. It is only speculative to infer that those with frailty are unlikely to benefit. In fact, the improved outcomes observed with increasing age would argue against this notion.
Given the compelling data supporting statin therapy in the high-risk elderly population, some patients and clinicians may reasonably feel there is value in statin therapy—even in those with advanced frailty.
What about symptoms, disability, quality of life, and short-term benefits? Asymptomatic or “silent” myocardial infarction is associated with angina, congestive heart failure, and subsequent symptomatic myocardial infarction.7,8 Dismissing the importance of these end points in clinical trials fails to recognize potential downstream effects that are directly relevant to a patient’s overall health status.
The Study Assessing Goals in the Elderly (SAGE) trial9 assessed the effect of statin therapy on ischemia burden in patients ages 65 to 85 with stable coronary disease. The results showed that both moderate and intensive statin dosing significantly reduced myocardial ischemia at 3 and 12 months, as detected by continuous electrocardiographic monitoring.
More research is needed to determine the effect of statin therapy on functional capacity and quality of life. Currently, it is premature to conclude that statins have no relevance to these important patient-centered outcomes.
What are the potential harms?
Mallery et al2 cite numerous articles that emphasize the potential adverse effects of statin therapy in the elderly. Unfortunately, data supporting the safety of statin therapy in the elderly were not included. This should be stressed, given that older statin-eligible patients are often undertreated in contemporary practice.10
A 2015 systematic review and meta-analysis indicated that statin-related events are relatively rare in the elderly.11 Another study showed elderly patients who started statin therapy after a myocardial infarction had no change in short-term cognitive or physical function.12
Older age and low body mass index are risk factors for statin myopathy, underscoring the need for close monitoring in frail patients. However, it is important to maintain an objective and balanced approach when considering potential harms.
Need for shared decision-making
Mallery et al2 make no mention of shared decision-making. Best practice guidelines for the management of frailty support a holistic medical review to establish an individualized care plan for each patient.13 Firm recommendations based on indeterminate evidence undermine the patient-physician relationship and do not allow for personal preferences of care. In an environment of uncertain benefit and harm, the patient’s priorities and values should serve as the cornerstone for clinical decisions.
- Barakat K, Wilkinson P, Deaner A, Fluck D, Ranjadayalan K, Timmis A. How should age affect management of acute myocardial infarction? A prospective cohort study. Lancet 1999; 353:955–959.
- Mallery L, Moorhouse P, McLea Veysey P, Allen M, Fleming I. Frail elderly patients do not need lipid-lowering drugs. Cleve Clin J Med 2016; 83:131–142.
- Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm—issues and controversies. J Gerontol A Biol Sci Med Sci 2007; 62:731–737.
- Afilalo J, Alexander KP, Mack MJ, et al. Frailty assessment in the cardiovascular care of older adults. J Am Coll Cardiol 2014; 63:747–762.
- Afilalo J, Duque G, Steele R, Jukema JW, de Craen AJ, Eisenberg MJ. Statins for secondary prevention in elderly patients: a hierarchical bayesian meta-analysis. J Am Coll Cardiol 2008; 51:37–45.
- Shepherd J, Blauw GJ, Murphy MB, et al; PROSPER study group. PROspective Study of Pravastatin in the Elderly at Risk. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet 2002; 360:1623–1630.
- Nadelmann J, Frishman WH, Ooi WL, et al. Prevalence, incidence and prognosis of recognized and unrecognized myocardial infarction in persons aged 75 years or older: The Bronx Aging Study. Am J Cardiol 1990; 66:533–537.
- Sheifer SE, Gersh BJ, Yanez ND 3rd, Ades PA, Burke GL, Manolio TA. Prevalence, predisposing factors, and prognosis of clinically unrecognized myocardial infarction in the elderly. J Am Coll Cardiol 2000; 35:119–126.
- Deedwania P, Stone PH, Bairey Merz CN, et al. Effects of intensive versus moderate lipid-lowering therapy on myocardial ischemia in older patients with coronary heart disease: results of the Study Assessing Goals in the Elderly (SAGE). Circulation 2007; 115:700–707.
- Maddox TM, Borden WB, Tang F, et al. Implications of the 2013 ACC/AHA cholesterol guidelines for adults in contemporary cardiovascular practice: insights from the NCDR PINNACLE registry. J Am Coll Cardiol 2014; 64:2183–2192.
- Iwere RB, Hewitt J. Myopathy in older people receiving statin therapy: a systematic review and meta-analysis. Br J Clin Pharmacol 2015; 80:363–371.
- Swiger KJ, Martin SS, Tang F, et al. Cognitive and physical function by statin exposure in elderly individuals following acute myocardial infarction. Clin Cardiol 2015; 38:455–461.
- Turner G, Clegg A; British Geriatrics Society; Age UK; Royal College of General Practioners. Best practice guidelines for the management of frailty: a British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing 2014; 43:744–747.
- Barakat K, Wilkinson P, Deaner A, Fluck D, Ranjadayalan K, Timmis A. How should age affect management of acute myocardial infarction? A prospective cohort study. Lancet 1999; 353:955–959.
- Mallery L, Moorhouse P, McLea Veysey P, Allen M, Fleming I. Frail elderly patients do not need lipid-lowering drugs. Cleve Clin J Med 2016; 83:131–142.
- Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm—issues and controversies. J Gerontol A Biol Sci Med Sci 2007; 62:731–737.
- Afilalo J, Alexander KP, Mack MJ, et al. Frailty assessment in the cardiovascular care of older adults. J Am Coll Cardiol 2014; 63:747–762.
- Afilalo J, Duque G, Steele R, Jukema JW, de Craen AJ, Eisenberg MJ. Statins for secondary prevention in elderly patients: a hierarchical bayesian meta-analysis. J Am Coll Cardiol 2008; 51:37–45.
- Shepherd J, Blauw GJ, Murphy MB, et al; PROSPER study group. PROspective Study of Pravastatin in the Elderly at Risk. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet 2002; 360:1623–1630.
- Nadelmann J, Frishman WH, Ooi WL, et al. Prevalence, incidence and prognosis of recognized and unrecognized myocardial infarction in persons aged 75 years or older: The Bronx Aging Study. Am J Cardiol 1990; 66:533–537.
- Sheifer SE, Gersh BJ, Yanez ND 3rd, Ades PA, Burke GL, Manolio TA. Prevalence, predisposing factors, and prognosis of clinically unrecognized myocardial infarction in the elderly. J Am Coll Cardiol 2000; 35:119–126.
- Deedwania P, Stone PH, Bairey Merz CN, et al. Effects of intensive versus moderate lipid-lowering therapy on myocardial ischemia in older patients with coronary heart disease: results of the Study Assessing Goals in the Elderly (SAGE). Circulation 2007; 115:700–707.
- Maddox TM, Borden WB, Tang F, et al. Implications of the 2013 ACC/AHA cholesterol guidelines for adults in contemporary cardiovascular practice: insights from the NCDR PINNACLE registry. J Am Coll Cardiol 2014; 64:2183–2192.
- Iwere RB, Hewitt J. Myopathy in older people receiving statin therapy: a systematic review and meta-analysis. Br J Clin Pharmacol 2015; 80:363–371.
- Swiger KJ, Martin SS, Tang F, et al. Cognitive and physical function by statin exposure in elderly individuals following acute myocardial infarction. Clin Cardiol 2015; 38:455–461.
- Turner G, Clegg A; British Geriatrics Society; Age UK; Royal College of General Practioners. Best practice guidelines for the management of frailty: a British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing 2014; 43:744–747.

A Problem of Capacity
For a number of years, those challenged with improving discharge transitions and preventing readmissions have suggested more—more case managers, more checklists and systems, more discharge pharmacists; and better—better communication, better medication reconciliation, better discharge documentation, better follow-up. In a study by Chan Carusone et al.,1 high-need, high-complexity patients receiving treatment at Casey House, a specialized urban hospital providing inpatient and community programs, were afforded a full complement of discharge planning and posthospitalization services. Despite these services, the patients achieved little success in maintaining their health and following their discharge plans after hospitalization.
This longitudinal qualitative study detailing the lived experience of discharge extends our knowledge of challenges faced by patients during the posthospital transition,2 and further elucidates the differences between patients’ expectations and assessments of their resources and goals, and their actual abilities and priorities on discharge. Despite substantial assistance, including housing, food assistance, and case management, Chan Carusone et al. found that the exigencies of day-to-day existence exceeded the patients’ capacities to sustain themselves outside the hospital. This failure implies a question: If the interventions alluded to in this study were not enough, then how much more, and how much better, is needed?
Attention to this question of how to best serve high-need patients continues to increase,3 and success in intervening to improve care transitions for this population is limited,4 in part because providing more care and more coordination requires more resources. Observing the challenges that remain for patients treated in the highly-resourced setting that is Casey House, the authors propose a previously described theoretical construct, minimally disruptive medicine (MDM),5 as a framework to guide patients and providers in creating a discharge plan that relies on the patient’s capacity to integrate disease self-management into his or her daily circumstances. MDM hinges on the concept of balancing workload and capacity: the burden of managing disease with the resources and abilities to do so. On first consideration, this seems an attractive approach to operationalizing patient-centered care by tailoring a discharge plan to a patient’s goals and capacities. On closer examination, however, MDM, applied to a single transition episode, raises some important concerns.
As Chan Carusone et al. describe, patients may poorly judge their future resources and capacity when making decisions in the hospital setting. Likewise, physicians and other team members may lack insight, perspective, and detailed knowledge of resources and barriers in the outpatient setting. From their vantage point, they may not see the fragile contingencies of the discharge plan that is reflected in the patients’ spoken words. At any moment, a well-meant, seemingly well-crafted discharge plan could fall apart.
Within the walls of the hospital, we tend to perform what might be termed maximally disruptive medicine—the treatments provided are exactly those that can’t be delivered in a nonhospital setting. For many patients, these interventions are not curative, but rather stabilizing;6 we assuage chronic conditions that had become exacerbated by new illness, disease progression, or conditions outside the hospital. To return the patient to his or her home situation, especially one that is under-resourced, with minimized workload can feel counterproductive and demoralizing at best. What prevents one from worrying that, where capacity can’t be improved, planning for MDM is, in essence, planning for minimal care?
Viewed in the broader context of a life course health development framework,7 which integrates biological, psychological, cultural, and historical experience to explain the development of health trajectories over an individual’s lifetime, a minimally disruptive approach might be viewed as amplifying disparities. The patients contributing to the study by Chan Carusone et al. may have arrived in their respective situations through a life course marked by poverty, violence, inadequate housing, poor nutrition, discrimination, and other disadvantages that may have resulted from accident, malfeasance, or choice. Their limited personal capacity and the ongoing chaos that is reflected in many of their comments requires that discharge planning uses imagination and dialogue, with careful, compassionate listening by providers, and close partnering and decision-making by patient and providers. Approaches to building the capacity for such compassion, as well as structural interventions to provide care that is necessary and just for these most vulnerable patients by considering their experiences and beliefs,8 remain to be articulated.
In a sense, the narrative unfolded by Chan Carusone et al. appropriately emphasizes that care transitions contain both complex problems and “wicked” problems.9 While aspects of transitions are complex and can be reasonably addressed with complex solutions, these same complex solutions are inadequate to mitigate the seemingly intractable socioeconomic challenges that drive hospital dependence for many high-need patients. Addressing these likely requires a reexamination of what we expect from hospitals, what systems we are able to design and are willing to support to keep people from returning to them, and what it means that for some people returning is the best, and sometimes only, thing to do.
As we continue to seek new models for healthcare in high-need, high-risk populations, we may do well to focus further longitudinal qualitative study on building a deep understanding of when and how patients achieve success following discharge. What characterizes patients, caregivers, service networks, and communities in healthcare settings with the highest rates of effective transitions? Maintaining equilibrium outside an institutional setting is convoluted, time-consuming, nuanced, and taxing; that those who have not experienced doing so as a patient or caregiver might struggle to help others should not surprise us. The concepts of capacity and workload lend themselves to structuring discovery of the resources that patients, not providers and policy-makers, have found through their lived experience to be most crucial to their enduring well-being. Learning from these experiences may shift the balance by increasing our own capacity to understand what constitutes success.
Disclosures
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs. The authors report no conflicts of interest.
References
1. Chan Carusone S, O’Leary B, McWatt S, Stewart S, Craig S, Brennan D. The lived experience of the hospital discharge “plan”: a longitudinal qualitative study of complex patients. J Hosp Med. 2017;12(1):5-10. PubMed
2. Kangovi S, Barg FK, Carter T, et al. Challenges faced by patients with low socioeconomic status during the post-hospital transition. J Gen Intern Med. 2014;29:283-289. PubMed
3. Blumenthal D, Chernof B, Fulmer T, Lumpkin J, Selberg J. Caring for high-need, high-cost patients - an urgent priority. N Engl J Med. 2016;375:909-911. PubMed
4. Powers BW, Milstein A, Jain SH. Delivery models for high-risk older patients: back to the future? JAMA. 2016;315:23-24. PubMed
5. Abu Dabrh AM, Gallacher K, Boehmer KR, Hargraves IG, Mair FS. Minimally disruptive medicine: the evidence and conceptual progress supporting a new era of healthcare. J R Coll Physicians Edinb. 2015;45:114-117. PubMed
6. Pannick S, Wachter RM, Vincent C, Sevdalis N. Rethinking medical ward quality. BMJ. 2016;355:i5417. PubMed
7. Kressin NR, Chapman SE, Magnani JW. A tale of two patients: patient-centered approaches to adherence as a gateway to reducing disparities. Circulation. 2016;133:2583-2592. PubMed
8. Thiel de Bocanegra H, Gany F. Good provider, good patient: changing behaviors to eliminate disparities in healthcare. Am J Manag Care. 2004;10:SP20-28. PubMed
9. Churchman CW. Wicked problems. Manage Sci. 1967;14(4):B141-B142.
For a number of years, those challenged with improving discharge transitions and preventing readmissions have suggested more—more case managers, more checklists and systems, more discharge pharmacists; and better—better communication, better medication reconciliation, better discharge documentation, better follow-up. In a study by Chan Carusone et al.,1 high-need, high-complexity patients receiving treatment at Casey House, a specialized urban hospital providing inpatient and community programs, were afforded a full complement of discharge planning and posthospitalization services. Despite these services, the patients achieved little success in maintaining their health and following their discharge plans after hospitalization.
This longitudinal qualitative study detailing the lived experience of discharge extends our knowledge of challenges faced by patients during the posthospital transition,2 and further elucidates the differences between patients’ expectations and assessments of their resources and goals, and their actual abilities and priorities on discharge. Despite substantial assistance, including housing, food assistance, and case management, Chan Carusone et al. found that the exigencies of day-to-day existence exceeded the patients’ capacities to sustain themselves outside the hospital. This failure implies a question: If the interventions alluded to in this study were not enough, then how much more, and how much better, is needed?
Attention to this question of how to best serve high-need patients continues to increase,3 and success in intervening to improve care transitions for this population is limited,4 in part because providing more care and more coordination requires more resources. Observing the challenges that remain for patients treated in the highly-resourced setting that is Casey House, the authors propose a previously described theoretical construct, minimally disruptive medicine (MDM),5 as a framework to guide patients and providers in creating a discharge plan that relies on the patient’s capacity to integrate disease self-management into his or her daily circumstances. MDM hinges on the concept of balancing workload and capacity: the burden of managing disease with the resources and abilities to do so. On first consideration, this seems an attractive approach to operationalizing patient-centered care by tailoring a discharge plan to a patient’s goals and capacities. On closer examination, however, MDM, applied to a single transition episode, raises some important concerns.
As Chan Carusone et al. describe, patients may poorly judge their future resources and capacity when making decisions in the hospital setting. Likewise, physicians and other team members may lack insight, perspective, and detailed knowledge of resources and barriers in the outpatient setting. From their vantage point, they may not see the fragile contingencies of the discharge plan that is reflected in the patients’ spoken words. At any moment, a well-meant, seemingly well-crafted discharge plan could fall apart.
Within the walls of the hospital, we tend to perform what might be termed maximally disruptive medicine—the treatments provided are exactly those that can’t be delivered in a nonhospital setting. For many patients, these interventions are not curative, but rather stabilizing;6 we assuage chronic conditions that had become exacerbated by new illness, disease progression, or conditions outside the hospital. To return the patient to his or her home situation, especially one that is under-resourced, with minimized workload can feel counterproductive and demoralizing at best. What prevents one from worrying that, where capacity can’t be improved, planning for MDM is, in essence, planning for minimal care?
Viewed in the broader context of a life course health development framework,7 which integrates biological, psychological, cultural, and historical experience to explain the development of health trajectories over an individual’s lifetime, a minimally disruptive approach might be viewed as amplifying disparities. The patients contributing to the study by Chan Carusone et al. may have arrived in their respective situations through a life course marked by poverty, violence, inadequate housing, poor nutrition, discrimination, and other disadvantages that may have resulted from accident, malfeasance, or choice. Their limited personal capacity and the ongoing chaos that is reflected in many of their comments requires that discharge planning uses imagination and dialogue, with careful, compassionate listening by providers, and close partnering and decision-making by patient and providers. Approaches to building the capacity for such compassion, as well as structural interventions to provide care that is necessary and just for these most vulnerable patients by considering their experiences and beliefs,8 remain to be articulated.
In a sense, the narrative unfolded by Chan Carusone et al. appropriately emphasizes that care transitions contain both complex problems and “wicked” problems.9 While aspects of transitions are complex and can be reasonably addressed with complex solutions, these same complex solutions are inadequate to mitigate the seemingly intractable socioeconomic challenges that drive hospital dependence for many high-need patients. Addressing these likely requires a reexamination of what we expect from hospitals, what systems we are able to design and are willing to support to keep people from returning to them, and what it means that for some people returning is the best, and sometimes only, thing to do.
As we continue to seek new models for healthcare in high-need, high-risk populations, we may do well to focus further longitudinal qualitative study on building a deep understanding of when and how patients achieve success following discharge. What characterizes patients, caregivers, service networks, and communities in healthcare settings with the highest rates of effective transitions? Maintaining equilibrium outside an institutional setting is convoluted, time-consuming, nuanced, and taxing; that those who have not experienced doing so as a patient or caregiver might struggle to help others should not surprise us. The concepts of capacity and workload lend themselves to structuring discovery of the resources that patients, not providers and policy-makers, have found through their lived experience to be most crucial to their enduring well-being. Learning from these experiences may shift the balance by increasing our own capacity to understand what constitutes success.
Disclosures
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs. The authors report no conflicts of interest.
For a number of years, those challenged with improving discharge transitions and preventing readmissions have suggested more—more case managers, more checklists and systems, more discharge pharmacists; and better—better communication, better medication reconciliation, better discharge documentation, better follow-up. In a study by Chan Carusone et al.,1 high-need, high-complexity patients receiving treatment at Casey House, a specialized urban hospital providing inpatient and community programs, were afforded a full complement of discharge planning and posthospitalization services. Despite these services, the patients achieved little success in maintaining their health and following their discharge plans after hospitalization.
This longitudinal qualitative study detailing the lived experience of discharge extends our knowledge of challenges faced by patients during the posthospital transition,2 and further elucidates the differences between patients’ expectations and assessments of their resources and goals, and their actual abilities and priorities on discharge. Despite substantial assistance, including housing, food assistance, and case management, Chan Carusone et al. found that the exigencies of day-to-day existence exceeded the patients’ capacities to sustain themselves outside the hospital. This failure implies a question: If the interventions alluded to in this study were not enough, then how much more, and how much better, is needed?
Attention to this question of how to best serve high-need patients continues to increase,3 and success in intervening to improve care transitions for this population is limited,4 in part because providing more care and more coordination requires more resources. Observing the challenges that remain for patients treated in the highly-resourced setting that is Casey House, the authors propose a previously described theoretical construct, minimally disruptive medicine (MDM),5 as a framework to guide patients and providers in creating a discharge plan that relies on the patient’s capacity to integrate disease self-management into his or her daily circumstances. MDM hinges on the concept of balancing workload and capacity: the burden of managing disease with the resources and abilities to do so. On first consideration, this seems an attractive approach to operationalizing patient-centered care by tailoring a discharge plan to a patient’s goals and capacities. On closer examination, however, MDM, applied to a single transition episode, raises some important concerns.
As Chan Carusone et al. describe, patients may poorly judge their future resources and capacity when making decisions in the hospital setting. Likewise, physicians and other team members may lack insight, perspective, and detailed knowledge of resources and barriers in the outpatient setting. From their vantage point, they may not see the fragile contingencies of the discharge plan that is reflected in the patients’ spoken words. At any moment, a well-meant, seemingly well-crafted discharge plan could fall apart.
Within the walls of the hospital, we tend to perform what might be termed maximally disruptive medicine—the treatments provided are exactly those that can’t be delivered in a nonhospital setting. For many patients, these interventions are not curative, but rather stabilizing;6 we assuage chronic conditions that had become exacerbated by new illness, disease progression, or conditions outside the hospital. To return the patient to his or her home situation, especially one that is under-resourced, with minimized workload can feel counterproductive and demoralizing at best. What prevents one from worrying that, where capacity can’t be improved, planning for MDM is, in essence, planning for minimal care?
Viewed in the broader context of a life course health development framework,7 which integrates biological, psychological, cultural, and historical experience to explain the development of health trajectories over an individual’s lifetime, a minimally disruptive approach might be viewed as amplifying disparities. The patients contributing to the study by Chan Carusone et al. may have arrived in their respective situations through a life course marked by poverty, violence, inadequate housing, poor nutrition, discrimination, and other disadvantages that may have resulted from accident, malfeasance, or choice. Their limited personal capacity and the ongoing chaos that is reflected in many of their comments requires that discharge planning uses imagination and dialogue, with careful, compassionate listening by providers, and close partnering and decision-making by patient and providers. Approaches to building the capacity for such compassion, as well as structural interventions to provide care that is necessary and just for these most vulnerable patients by considering their experiences and beliefs,8 remain to be articulated.
In a sense, the narrative unfolded by Chan Carusone et al. appropriately emphasizes that care transitions contain both complex problems and “wicked” problems.9 While aspects of transitions are complex and can be reasonably addressed with complex solutions, these same complex solutions are inadequate to mitigate the seemingly intractable socioeconomic challenges that drive hospital dependence for many high-need patients. Addressing these likely requires a reexamination of what we expect from hospitals, what systems we are able to design and are willing to support to keep people from returning to them, and what it means that for some people returning is the best, and sometimes only, thing to do.
As we continue to seek new models for healthcare in high-need, high-risk populations, we may do well to focus further longitudinal qualitative study on building a deep understanding of when and how patients achieve success following discharge. What characterizes patients, caregivers, service networks, and communities in healthcare settings with the highest rates of effective transitions? Maintaining equilibrium outside an institutional setting is convoluted, time-consuming, nuanced, and taxing; that those who have not experienced doing so as a patient or caregiver might struggle to help others should not surprise us. The concepts of capacity and workload lend themselves to structuring discovery of the resources that patients, not providers and policy-makers, have found through their lived experience to be most crucial to their enduring well-being. Learning from these experiences may shift the balance by increasing our own capacity to understand what constitutes success.
Disclosures
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs. The authors report no conflicts of interest.
References
1. Chan Carusone S, O’Leary B, McWatt S, Stewart S, Craig S, Brennan D. The lived experience of the hospital discharge “plan”: a longitudinal qualitative study of complex patients. J Hosp Med. 2017;12(1):5-10. PubMed
2. Kangovi S, Barg FK, Carter T, et al. Challenges faced by patients with low socioeconomic status during the post-hospital transition. J Gen Intern Med. 2014;29:283-289. PubMed
3. Blumenthal D, Chernof B, Fulmer T, Lumpkin J, Selberg J. Caring for high-need, high-cost patients - an urgent priority. N Engl J Med. 2016;375:909-911. PubMed
4. Powers BW, Milstein A, Jain SH. Delivery models for high-risk older patients: back to the future? JAMA. 2016;315:23-24. PubMed
5. Abu Dabrh AM, Gallacher K, Boehmer KR, Hargraves IG, Mair FS. Minimally disruptive medicine: the evidence and conceptual progress supporting a new era of healthcare. J R Coll Physicians Edinb. 2015;45:114-117. PubMed
6. Pannick S, Wachter RM, Vincent C, Sevdalis N. Rethinking medical ward quality. BMJ. 2016;355:i5417. PubMed
7. Kressin NR, Chapman SE, Magnani JW. A tale of two patients: patient-centered approaches to adherence as a gateway to reducing disparities. Circulation. 2016;133:2583-2592. PubMed
8. Thiel de Bocanegra H, Gany F. Good provider, good patient: changing behaviors to eliminate disparities in healthcare. Am J Manag Care. 2004;10:SP20-28. PubMed
9. Churchman CW. Wicked problems. Manage Sci. 1967;14(4):B141-B142.
References
1. Chan Carusone S, O’Leary B, McWatt S, Stewart S, Craig S, Brennan D. The lived experience of the hospital discharge “plan”: a longitudinal qualitative study of complex patients. J Hosp Med. 2017;12(1):5-10. PubMed
2. Kangovi S, Barg FK, Carter T, et al. Challenges faced by patients with low socioeconomic status during the post-hospital transition. J Gen Intern Med. 2014;29:283-289. PubMed
3. Blumenthal D, Chernof B, Fulmer T, Lumpkin J, Selberg J. Caring for high-need, high-cost patients - an urgent priority. N Engl J Med. 2016;375:909-911. PubMed
4. Powers BW, Milstein A, Jain SH. Delivery models for high-risk older patients: back to the future? JAMA. 2016;315:23-24. PubMed
5. Abu Dabrh AM, Gallacher K, Boehmer KR, Hargraves IG, Mair FS. Minimally disruptive medicine: the evidence and conceptual progress supporting a new era of healthcare. J R Coll Physicians Edinb. 2015;45:114-117. PubMed
6. Pannick S, Wachter RM, Vincent C, Sevdalis N. Rethinking medical ward quality. BMJ. 2016;355:i5417. PubMed
7. Kressin NR, Chapman SE, Magnani JW. A tale of two patients: patient-centered approaches to adherence as a gateway to reducing disparities. Circulation. 2016;133:2583-2592. PubMed
8. Thiel de Bocanegra H, Gany F. Good provider, good patient: changing behaviors to eliminate disparities in healthcare. Am J Manag Care. 2004;10:SP20-28. PubMed
9. Churchman CW. Wicked problems. Manage Sci. 1967;14(4):B141-B142.
© 2017 Society of Hospital Medicine
Improving Quality in Against Medical Advice Discharges
Against Medical Advice (AMA) discharges, when a patient chooses to leave the hospital prior to a clinically specified and physician recommended endpoint, remain a healthcare quality problem. Patients who leave the hospital AMA challenge the healthcare professionals entrusted to care for them as well as the institutions that work to promote continuity and improved quality. AMA discharges account for up to 2% of all hospital discharges and, compared with conventional discharges, are associated with worse health and health services outcomes. Patients discharged AMA have higher rates of 30-day readmission, morbidity, and 30-day mortality.1,2 Additionally, the burden of worse health outcomes is disproportionate among disadvantaged patient populations. Patients with human immunodeficiency virus,3 substance use disorders,4 and psychiatric illness5 are more likely to be discharged AMA, as are patients with low socioeconomic status, without insurance, or with Medicaid insurance.
In this issue of the Journal of Hospital Medicine, Stearns and colleagues6 provide an important contribution to this area of medicine in need of more high quality empiric studies. The study reviewed all AMA discharges from a single year in an urban community hospital in order to assess provider perceptions and knowledge about AMA discharges. The study reconfirmed both the patient-level predictors of AMA discharges that have been demonstrated consistently (ie, male gender, younger age, Medicare or no insurance, and injection drug use) as well as the low rates of documentation of patient capacity, medication prescribed, and follow-up plans in AMA discharges.7
The authors’ investigation has also advanced the study of AMA discharges in two important directions. First, by characterizing patients with multiple AMA discharges, the authors focus on a more vulnerable population. These patients, who may have particular difficulty in consistently engaging in care, could help provide insight into the general phenomenon of AMA discharges. Second, the authors broadened their attention to include the study of nurses, a group of healthcare professionals who may play an important but not well recognized role in the AMA discharge process. In further characterizing nurses’ attitudes toward AMA discharges, medication prescriptions, and outpatient follow-up, the authors highlight nurses’ role in gathering critical patient information and promoting ethical practices in discharge planning. To better understand this dynamic and its potential role in mediating adverse health outcomes, further studies should also examine the attitudes of other central members of the treatment team (eg, pharmacists, social workers, etc.) who participate in discharge planning.
Inadequate documentation of AMA discharges remains a problem. In an attempt to address this, some institutions use AMA discharge forms to facilitate documentation of the informed consent process, the patient’s signed declination of care, medico-legal considerations, and the resulting treatment plan. Although systematic efforts to improve documentation should be encouraged, significant uncertainty about the optimal use of AMA discharge forms remains. Specifically, the use of a patient-signed AMA discharge form has not been demonstrated to advance patient care and may promote harm by stigmatizing patients8 and reducing the likelihood that they will pursue follow-up care.9 Furthermore, given that these forms may be written using institution-centered legalistic language or at an inappropriate reading level, this common hospital practice should be evaluated to assess whether patients comprehend and benefit from the forms, and how the forms influence healthcare decision making.10
Finally, the authors’ finding that 38% of nurses, 22% of physician trainees, and 6% of attendings believe patients discharged AMA lose the “right” to follow-up is noteworthy. The practice would suggest a significant lapse in understanding the professional obligation to acknowledge and communicate that the informed consent process is voluntary and patients have the right to decline recommended treatment without forfeiting future access to care. Harm reduction principles indicate that simply choosing to decline an episode of inpatient care does not make a patient ineligible for other medically indicated treatments and services. Previous studies have demonstrated that physicians may incorrectly inform patients that insurance will not pay for their care if they leave AMA, in order to persuade them to remain hospitalized.11 The current study suggests similar and potentially well-meaning but coercive attitudes about AMA discharge that can undermine a patient’s voluntary choice to accept medical care.
Stearns and colleagues6 rightly point to educational and policy interventions to improve the quality of care for patients discharged AMA. Additionally, setting patients’ expectations early in the hospitalization,12 empathically addressing their concerns,13 and sharing clinical decisions with patients by providing a medically reasonable range of clinical options rather than a single choice14 are practical bedside interventions that all clinicians can implement. System changes like developing clear policies and electronic medical records templates are particularly important, as they are more likely to lead to durable institutional change that is systematic, transparent, and fair. Moreover, research that expands the object of study beyond the physician-patient relationship could significantly improve outcomes in this vulnerable population of patients. Recent studies have begun to elucidate the deficiencies that may underlie communication failures with patients before they choose to leave AMA,15 how providers decide to designate a discharge as AMA,16 and how changing the structure and environment of care for patients who use injection drugs can reduce AMA discharges and improve health outcomes.17
AMA discharges are a persistent, complicated healthcare quality problem that defies an easy solution. Improving the quality of care for these patients will require building upon the empirical research base, providing enhanced education and guidance to healthcare professionals in the ethical and clinical management of AMA discharges, and making systems changes that promote enduring institutional change. We are moving in the right direction, but we have further to go.
Disclosures
The views expressed in this article are those of the author and do not necessarily reflect the position or policy of the US Department of Veterans Affairs or the National Center for Ethics in Health Care. The author has no conflicts of interest to disclose.
References
1. Alfandre DJ. “I’m going home”: discharges against medical advice. Mayo Clin Proc. 2009;84(3):255-260. PubMed
2. Southern WN, Nahvi S, Arnsten JH. Increased risk of mortality and readmission among patients discharged against medical advice. Am J Med. 2012;125(6):
594-602. PubMed
3. Anis AH, Sun H, Guh DP, Palepu A, Schechter MT, O’Shaughnessy MV. Leaving hospital against medical advice among HIV-positive patients. CMAJ. 2002;167(6):633-637. PubMed
4. Chan AC, Palepu A, Guh DP, et al. HIV-positive injection drug users who leave the hospital against medical advice: the mitigating role of methadone and social support. J Acquir Immune Defic Syndr. 2004;35(1):56-59. PubMed
5. Kuo CJ, Tsai SY, Liao YT, Lee WC, Sung XW, Chen CC. Psychiatric discharge against medical advice is a risk factor for suicide but not for other causes of death. J Clin Psychiatry. 2010;71(6):808-809. PubMed
6. Edwards J, Markert R, Bricker D. Discharge against medical advice: how often do we intervene? J Hosp Med. 2013;8(10):574-577. PubMed
7. Stearns CR, Bakamjian A, Sattar S, Ritterman Weintraub M. Discharges against medical advice at a county hospital: provider perceptions and practice. J Hosp Med. 2017;12(1):11-17. PubMed
8. Windish DM, Ratanawongsa N. Providers’ perceptions of relationships and professional roles when caring for patients who leave the hospital against medical advice. J Gen Intern Med. 2008;23(10):1698-1707. PubMed
9. Jerrard DA, Chasm RM. Patients leaving against medical advice (AMA) from the emergency department—disease prevalence and willingness to return. J Emerg Med. 2011;41(4):412-417. PubMed
10. Alfandre D. Reconsidering against medical advice discharges: embracing patient-centeredness to promote high quality care and a renewed research agenda.
J Gen Intern Med. 2013;28(12):1657-1662. PubMed
11. Schaefer GR, Matus H, Schumann JH, et al. Financial responsibility of hospitalized patients who left against medical advice: Medical urban legend? J Gen Intern Med. 2012;27(7):825-830. PubMed
12. Steinglass P, Grantham CE, Hertzman M. Predicting which patients will be discharged against medical advice: a pilot study. Am J Psychiatry. 1980;137(11):
1385-1389. PubMed
13. Clark MA, Abbott JT, Adyanthaya T. Ethics seminars: a best-practice approach to navigating the against-medical-advice discharge. Acad Emerg Med. 2014;21(9):1050-1057. PubMed
14. Alfandre D. Clinical recommendations in medical practice: a proposed framework to reduce bias and improve the quality of medical decisions. J Clin Ethics. 2016;27(1):21-27. PubMed
15. Lekas HM, Alfandre D, Gordon P, Harwood K, Yin MT. The role of patient-provider interactions: Using an accounts framework to explain hospital discharges against medical advice. Soc Sci Med. 2016;156:106-113. PubMed
16. Brenner J, Joslin J, Goulette A, Grant WD, Wojcik SM. Against medical advice: A survey of ED clinicians’ rationale for use. J Emerg Nurs. 2016;42(5):408-411. PubMed
17. McNeil R, Small W, Wood E, Kerr T. Hospitals as a ‘risk environment’: an ethno-epidemiological study of voluntary and involuntary discharge from hospital against medical advice among people who inject drugs. Soc Sci Med. 2014;105:59-66. PubMed
Against Medical Advice (AMA) discharges, when a patient chooses to leave the hospital prior to a clinically specified and physician recommended endpoint, remain a healthcare quality problem. Patients who leave the hospital AMA challenge the healthcare professionals entrusted to care for them as well as the institutions that work to promote continuity and improved quality. AMA discharges account for up to 2% of all hospital discharges and, compared with conventional discharges, are associated with worse health and health services outcomes. Patients discharged AMA have higher rates of 30-day readmission, morbidity, and 30-day mortality.1,2 Additionally, the burden of worse health outcomes is disproportionate among disadvantaged patient populations. Patients with human immunodeficiency virus,3 substance use disorders,4 and psychiatric illness5 are more likely to be discharged AMA, as are patients with low socioeconomic status, without insurance, or with Medicaid insurance.
In this issue of the Journal of Hospital Medicine, Stearns and colleagues6 provide an important contribution to this area of medicine in need of more high quality empiric studies. The study reviewed all AMA discharges from a single year in an urban community hospital in order to assess provider perceptions and knowledge about AMA discharges. The study reconfirmed both the patient-level predictors of AMA discharges that have been demonstrated consistently (ie, male gender, younger age, Medicare or no insurance, and injection drug use) as well as the low rates of documentation of patient capacity, medication prescribed, and follow-up plans in AMA discharges.7
The authors’ investigation has also advanced the study of AMA discharges in two important directions. First, by characterizing patients with multiple AMA discharges, the authors focus on a more vulnerable population. These patients, who may have particular difficulty in consistently engaging in care, could help provide insight into the general phenomenon of AMA discharges. Second, the authors broadened their attention to include the study of nurses, a group of healthcare professionals who may play an important but not well recognized role in the AMA discharge process. In further characterizing nurses’ attitudes toward AMA discharges, medication prescriptions, and outpatient follow-up, the authors highlight nurses’ role in gathering critical patient information and promoting ethical practices in discharge planning. To better understand this dynamic and its potential role in mediating adverse health outcomes, further studies should also examine the attitudes of other central members of the treatment team (eg, pharmacists, social workers, etc.) who participate in discharge planning.
Inadequate documentation of AMA discharges remains a problem. In an attempt to address this, some institutions use AMA discharge forms to facilitate documentation of the informed consent process, the patient’s signed declination of care, medico-legal considerations, and the resulting treatment plan. Although systematic efforts to improve documentation should be encouraged, significant uncertainty about the optimal use of AMA discharge forms remains. Specifically, the use of a patient-signed AMA discharge form has not been demonstrated to advance patient care and may promote harm by stigmatizing patients8 and reducing the likelihood that they will pursue follow-up care.9 Furthermore, given that these forms may be written using institution-centered legalistic language or at an inappropriate reading level, this common hospital practice should be evaluated to assess whether patients comprehend and benefit from the forms, and how the forms influence healthcare decision making.10
Finally, the authors’ finding that 38% of nurses, 22% of physician trainees, and 6% of attendings believe patients discharged AMA lose the “right” to follow-up is noteworthy. The practice would suggest a significant lapse in understanding the professional obligation to acknowledge and communicate that the informed consent process is voluntary and patients have the right to decline recommended treatment without forfeiting future access to care. Harm reduction principles indicate that simply choosing to decline an episode of inpatient care does not make a patient ineligible for other medically indicated treatments and services. Previous studies have demonstrated that physicians may incorrectly inform patients that insurance will not pay for their care if they leave AMA, in order to persuade them to remain hospitalized.11 The current study suggests similar and potentially well-meaning but coercive attitudes about AMA discharge that can undermine a patient’s voluntary choice to accept medical care.
Stearns and colleagues6 rightly point to educational and policy interventions to improve the quality of care for patients discharged AMA. Additionally, setting patients’ expectations early in the hospitalization,12 empathically addressing their concerns,13 and sharing clinical decisions with patients by providing a medically reasonable range of clinical options rather than a single choice14 are practical bedside interventions that all clinicians can implement. System changes like developing clear policies and electronic medical records templates are particularly important, as they are more likely to lead to durable institutional change that is systematic, transparent, and fair. Moreover, research that expands the object of study beyond the physician-patient relationship could significantly improve outcomes in this vulnerable population of patients. Recent studies have begun to elucidate the deficiencies that may underlie communication failures with patients before they choose to leave AMA,15 how providers decide to designate a discharge as AMA,16 and how changing the structure and environment of care for patients who use injection drugs can reduce AMA discharges and improve health outcomes.17
AMA discharges are a persistent, complicated healthcare quality problem that defies an easy solution. Improving the quality of care for these patients will require building upon the empirical research base, providing enhanced education and guidance to healthcare professionals in the ethical and clinical management of AMA discharges, and making systems changes that promote enduring institutional change. We are moving in the right direction, but we have further to go.
Disclosures
The views expressed in this article are those of the author and do not necessarily reflect the position or policy of the US Department of Veterans Affairs or the National Center for Ethics in Health Care. The author has no conflicts of interest to disclose.
Against Medical Advice (AMA) discharges, when a patient chooses to leave the hospital prior to a clinically specified and physician recommended endpoint, remain a healthcare quality problem. Patients who leave the hospital AMA challenge the healthcare professionals entrusted to care for them as well as the institutions that work to promote continuity and improved quality. AMA discharges account for up to 2% of all hospital discharges and, compared with conventional discharges, are associated with worse health and health services outcomes. Patients discharged AMA have higher rates of 30-day readmission, morbidity, and 30-day mortality.1,2 Additionally, the burden of worse health outcomes is disproportionate among disadvantaged patient populations. Patients with human immunodeficiency virus,3 substance use disorders,4 and psychiatric illness5 are more likely to be discharged AMA, as are patients with low socioeconomic status, without insurance, or with Medicaid insurance.
In this issue of the Journal of Hospital Medicine, Stearns and colleagues6 provide an important contribution to this area of medicine in need of more high quality empiric studies. The study reviewed all AMA discharges from a single year in an urban community hospital in order to assess provider perceptions and knowledge about AMA discharges. The study reconfirmed both the patient-level predictors of AMA discharges that have been demonstrated consistently (ie, male gender, younger age, Medicare or no insurance, and injection drug use) as well as the low rates of documentation of patient capacity, medication prescribed, and follow-up plans in AMA discharges.7
The authors’ investigation has also advanced the study of AMA discharges in two important directions. First, by characterizing patients with multiple AMA discharges, the authors focus on a more vulnerable population. These patients, who may have particular difficulty in consistently engaging in care, could help provide insight into the general phenomenon of AMA discharges. Second, the authors broadened their attention to include the study of nurses, a group of healthcare professionals who may play an important but not well recognized role in the AMA discharge process. In further characterizing nurses’ attitudes toward AMA discharges, medication prescriptions, and outpatient follow-up, the authors highlight nurses’ role in gathering critical patient information and promoting ethical practices in discharge planning. To better understand this dynamic and its potential role in mediating adverse health outcomes, further studies should also examine the attitudes of other central members of the treatment team (eg, pharmacists, social workers, etc.) who participate in discharge planning.
Inadequate documentation of AMA discharges remains a problem. In an attempt to address this, some institutions use AMA discharge forms to facilitate documentation of the informed consent process, the patient’s signed declination of care, medico-legal considerations, and the resulting treatment plan. Although systematic efforts to improve documentation should be encouraged, significant uncertainty about the optimal use of AMA discharge forms remains. Specifically, the use of a patient-signed AMA discharge form has not been demonstrated to advance patient care and may promote harm by stigmatizing patients8 and reducing the likelihood that they will pursue follow-up care.9 Furthermore, given that these forms may be written using institution-centered legalistic language or at an inappropriate reading level, this common hospital practice should be evaluated to assess whether patients comprehend and benefit from the forms, and how the forms influence healthcare decision making.10
Finally, the authors’ finding that 38% of nurses, 22% of physician trainees, and 6% of attendings believe patients discharged AMA lose the “right” to follow-up is noteworthy. The practice would suggest a significant lapse in understanding the professional obligation to acknowledge and communicate that the informed consent process is voluntary and patients have the right to decline recommended treatment without forfeiting future access to care. Harm reduction principles indicate that simply choosing to decline an episode of inpatient care does not make a patient ineligible for other medically indicated treatments and services. Previous studies have demonstrated that physicians may incorrectly inform patients that insurance will not pay for their care if they leave AMA, in order to persuade them to remain hospitalized.11 The current study suggests similar and potentially well-meaning but coercive attitudes about AMA discharge that can undermine a patient’s voluntary choice to accept medical care.
Stearns and colleagues6 rightly point to educational and policy interventions to improve the quality of care for patients discharged AMA. Additionally, setting patients’ expectations early in the hospitalization,12 empathically addressing their concerns,13 and sharing clinical decisions with patients by providing a medically reasonable range of clinical options rather than a single choice14 are practical bedside interventions that all clinicians can implement. System changes like developing clear policies and electronic medical records templates are particularly important, as they are more likely to lead to durable institutional change that is systematic, transparent, and fair. Moreover, research that expands the object of study beyond the physician-patient relationship could significantly improve outcomes in this vulnerable population of patients. Recent studies have begun to elucidate the deficiencies that may underlie communication failures with patients before they choose to leave AMA,15 how providers decide to designate a discharge as AMA,16 and how changing the structure and environment of care for patients who use injection drugs can reduce AMA discharges and improve health outcomes.17
AMA discharges are a persistent, complicated healthcare quality problem that defies an easy solution. Improving the quality of care for these patients will require building upon the empirical research base, providing enhanced education and guidance to healthcare professionals in the ethical and clinical management of AMA discharges, and making systems changes that promote enduring institutional change. We are moving in the right direction, but we have further to go.
Disclosures
The views expressed in this article are those of the author and do not necessarily reflect the position or policy of the US Department of Veterans Affairs or the National Center for Ethics in Health Care. The author has no conflicts of interest to disclose.
References
1. Alfandre DJ. “I’m going home”: discharges against medical advice. Mayo Clin Proc. 2009;84(3):255-260. PubMed
2. Southern WN, Nahvi S, Arnsten JH. Increased risk of mortality and readmission among patients discharged against medical advice. Am J Med. 2012;125(6):
594-602. PubMed
3. Anis AH, Sun H, Guh DP, Palepu A, Schechter MT, O’Shaughnessy MV. Leaving hospital against medical advice among HIV-positive patients. CMAJ. 2002;167(6):633-637. PubMed
4. Chan AC, Palepu A, Guh DP, et al. HIV-positive injection drug users who leave the hospital against medical advice: the mitigating role of methadone and social support. J Acquir Immune Defic Syndr. 2004;35(1):56-59. PubMed
5. Kuo CJ, Tsai SY, Liao YT, Lee WC, Sung XW, Chen CC. Psychiatric discharge against medical advice is a risk factor for suicide but not for other causes of death. J Clin Psychiatry. 2010;71(6):808-809. PubMed
6. Edwards J, Markert R, Bricker D. Discharge against medical advice: how often do we intervene? J Hosp Med. 2013;8(10):574-577. PubMed
7. Stearns CR, Bakamjian A, Sattar S, Ritterman Weintraub M. Discharges against medical advice at a county hospital: provider perceptions and practice. J Hosp Med. 2017;12(1):11-17. PubMed
8. Windish DM, Ratanawongsa N. Providers’ perceptions of relationships and professional roles when caring for patients who leave the hospital against medical advice. J Gen Intern Med. 2008;23(10):1698-1707. PubMed
9. Jerrard DA, Chasm RM. Patients leaving against medical advice (AMA) from the emergency department—disease prevalence and willingness to return. J Emerg Med. 2011;41(4):412-417. PubMed
10. Alfandre D. Reconsidering against medical advice discharges: embracing patient-centeredness to promote high quality care and a renewed research agenda.
J Gen Intern Med. 2013;28(12):1657-1662. PubMed
11. Schaefer GR, Matus H, Schumann JH, et al. Financial responsibility of hospitalized patients who left against medical advice: Medical urban legend? J Gen Intern Med. 2012;27(7):825-830. PubMed
12. Steinglass P, Grantham CE, Hertzman M. Predicting which patients will be discharged against medical advice: a pilot study. Am J Psychiatry. 1980;137(11):
1385-1389. PubMed
13. Clark MA, Abbott JT, Adyanthaya T. Ethics seminars: a best-practice approach to navigating the against-medical-advice discharge. Acad Emerg Med. 2014;21(9):1050-1057. PubMed
14. Alfandre D. Clinical recommendations in medical practice: a proposed framework to reduce bias and improve the quality of medical decisions. J Clin Ethics. 2016;27(1):21-27. PubMed
15. Lekas HM, Alfandre D, Gordon P, Harwood K, Yin MT. The role of patient-provider interactions: Using an accounts framework to explain hospital discharges against medical advice. Soc Sci Med. 2016;156:106-113. PubMed
16. Brenner J, Joslin J, Goulette A, Grant WD, Wojcik SM. Against medical advice: A survey of ED clinicians’ rationale for use. J Emerg Nurs. 2016;42(5):408-411. PubMed
17. McNeil R, Small W, Wood E, Kerr T. Hospitals as a ‘risk environment’: an ethno-epidemiological study of voluntary and involuntary discharge from hospital against medical advice among people who inject drugs. Soc Sci Med. 2014;105:59-66. PubMed
References
1. Alfandre DJ. “I’m going home”: discharges against medical advice. Mayo Clin Proc. 2009;84(3):255-260. PubMed
2. Southern WN, Nahvi S, Arnsten JH. Increased risk of mortality and readmission among patients discharged against medical advice. Am J Med. 2012;125(6):
594-602. PubMed
3. Anis AH, Sun H, Guh DP, Palepu A, Schechter MT, O’Shaughnessy MV. Leaving hospital against medical advice among HIV-positive patients. CMAJ. 2002;167(6):633-637. PubMed
4. Chan AC, Palepu A, Guh DP, et al. HIV-positive injection drug users who leave the hospital against medical advice: the mitigating role of methadone and social support. J Acquir Immune Defic Syndr. 2004;35(1):56-59. PubMed
5. Kuo CJ, Tsai SY, Liao YT, Lee WC, Sung XW, Chen CC. Psychiatric discharge against medical advice is a risk factor for suicide but not for other causes of death. J Clin Psychiatry. 2010;71(6):808-809. PubMed
6. Edwards J, Markert R, Bricker D. Discharge against medical advice: how often do we intervene? J Hosp Med. 2013;8(10):574-577. PubMed
7. Stearns CR, Bakamjian A, Sattar S, Ritterman Weintraub M. Discharges against medical advice at a county hospital: provider perceptions and practice. J Hosp Med. 2017;12(1):11-17. PubMed
8. Windish DM, Ratanawongsa N. Providers’ perceptions of relationships and professional roles when caring for patients who leave the hospital against medical advice. J Gen Intern Med. 2008;23(10):1698-1707. PubMed
9. Jerrard DA, Chasm RM. Patients leaving against medical advice (AMA) from the emergency department—disease prevalence and willingness to return. J Emerg Med. 2011;41(4):412-417. PubMed
10. Alfandre D. Reconsidering against medical advice discharges: embracing patient-centeredness to promote high quality care and a renewed research agenda.
J Gen Intern Med. 2013;28(12):1657-1662. PubMed
11. Schaefer GR, Matus H, Schumann JH, et al. Financial responsibility of hospitalized patients who left against medical advice: Medical urban legend? J Gen Intern Med. 2012;27(7):825-830. PubMed
12. Steinglass P, Grantham CE, Hertzman M. Predicting which patients will be discharged against medical advice: a pilot study. Am J Psychiatry. 1980;137(11):
1385-1389. PubMed
13. Clark MA, Abbott JT, Adyanthaya T. Ethics seminars: a best-practice approach to navigating the against-medical-advice discharge. Acad Emerg Med. 2014;21(9):1050-1057. PubMed
14. Alfandre D. Clinical recommendations in medical practice: a proposed framework to reduce bias and improve the quality of medical decisions. J Clin Ethics. 2016;27(1):21-27. PubMed
15. Lekas HM, Alfandre D, Gordon P, Harwood K, Yin MT. The role of patient-provider interactions: Using an accounts framework to explain hospital discharges against medical advice. Soc Sci Med. 2016;156:106-113. PubMed
16. Brenner J, Joslin J, Goulette A, Grant WD, Wojcik SM. Against medical advice: A survey of ED clinicians’ rationale for use. J Emerg Nurs. 2016;42(5):408-411. PubMed
17. McNeil R, Small W, Wood E, Kerr T. Hospitals as a ‘risk environment’: an ethno-epidemiological study of voluntary and involuntary discharge from hospital against medical advice among people who inject drugs. Soc Sci Med. 2014;105:59-66. PubMed
© 2017 Society of Hospital Medicine