User login
Challenge of Personality Disorders
All practicing hospitalists encounter challenging patient situations that stem from issues beyond medical illness. Those situations include the patient who demands to talk with the doctor repeatedly disregarding the lack of urgency, or the patient who, despite seeing multiple well‐regarded specialists, attempts to split the healthcare team by generating unwarranted praise or criticism toward individual caregivers.
Although these patients may be labeled difficult, hateful, or simply a unique patient‐management opportunity, effective care requires a more nuanced understanding of a possible underlying personality disorder that adversely affects the patientphysician relationship. In this issue of the Journal of Hospital Medicine, Riddle et al. provide an important review that outlines a framework for identifying the likely presence of a personality disorder along with practical advice for how to manage these patients.[1] As the authors point out, personality disorders are relatively common among patients seeking medical care but are challenging to diagnose, particularly in the setting of superimposed medical illness. Common to all personality disorders are difficulties forming and maintaining positive relationships with others such that care providers find themselves feeling frustrated, fearful, or inadequate. Inpatient providers typically receive very little training in how to care for patients with personality disorders.
The approach of avoiding collaborative teaching rounds, driven perhaps by a need for time efficiency, deprives learners of the chance to reflect on effective interactions with these patients.
Personality disorders result from genetic predisposition, complex brain dysfunction, and environmental influences. Social determinants also play a role, although limited social networks may simultaneously be a result of a personality disorder and a contributing factor.[2] Although there is a temptation to view personality disorders separate from medical conditions such as diabetes mellitus, diagnosing a personality disorder is far more complicated than simply checking a glycosylated hemoglobin. As Riddle et al. suggest, making a specific diagnosis from the list of 10 personality disorders is challenging in the hospital setting, even for experienced psychiatrists. Given the danger of propagating a diagnosis unabated and unquestioned through the electronic medical record, the attending hospitalist should be reluctant to include a diagnosis such as borderline personality disorder or histrionic personality disorder in the patient problem list without input from experts. Instead, it is useful to document the specific behaviors that are impacting patient care during this episode of illness.
We are concerned about the impact of personality disorders on a number of aspects of patient care, and these are areas that are potentially fertile ground for scholarship and research.
EFFECT ON THE PATIENT EXPERIENCE
Patients with personality disorders may have difficulty assessing the severity of their own medical illnesses. Educating patients on the meaning and value of recovery may be helpful in establishing appropriate expectations of care,[3] although it is equally important to assess the value of illness from the patient's perspective. As Riddle et al. point out, the goal for the hospitalist team is to mitigate the negative impact of adverse behavior on overall care. A recent pilot study of smartphone applications for use by patients with borderline personality disorder might have utility in the inpatient setting.[4] These types of innovations provide opportunities for hospitalist research in the care of patients with personality disorders.
EFFECT OF PERSONALITY DISORDERS ON TEAM‐BASED CLINICAL CARE
A recent observational study published in the Journal of Hospital Medicine identified several important attributes of a high‐functioning inpatient care team.[5] The findings reinforced the concept that patient care is a social activity. To provide high‐quality care, a high‐functioning partnership between team members is required. Riddle et al. point out that patients with personality traits and disorders can negatively impact the relationship among care team members. The hospitalist may be tempted to leave the nursing staff to handle the unwanted communication with the patient. This strategy is maladaptive and creates friction between the hospitalist and the nursing staff. In addition, it reduces an opportunity to recognize important real‐time changes in patients' clinical status that may adversely affect patient outcomes.
EFFECT ON DIAGNOSTIC REASONING
Clinical and diagnostic reasoning plays a central role in patient care. Hospitalists must identify key elements from empirical data and formulate their problem representation to assist in planning the next diagnostic and treatment plans. The medical literature regarding the effect of providing care to patients with maladaptive personality structures is limited. Recent literature investigating the effect of negative patient attributes on diagnostic reasoning suggests that caring for disruptive patients, such as those with maladaptive personality structures, adversely impacts the diagnostic reasoning process. In other words, we are more likely to make cognitive errors when faced with patients who foster a negative feeling. When given vignettes of the same diagnosis but prefaced with patient characteristics that would affect their likeability, trainees of both family practice and internal medicine made significantly fewer correct diagnoses in patients who were given negative connotation, such as overly demanding, a trait not uncommonly seen in patients with personality disorders/traits.[6] The diagnosis rate was more pronounced with complex cases. It is theorized that our cognitive reasoning and use of illness scripts can overcome maladaptive behavior when it comes to common presentations of common illness. However, more complex or atypical presentations require a higher level of diagnostic reasoning that may be impacted by patients who have maladaptive behaviors. The authors hypothesize a resource depletion of mental energy as a result of managing these patients.
EFFECT ON PHYSICIAN WELL‐BEING
Patients with personality disorders require increased time from healthcare providers. Burnout is a major issue for internists.[7] Any provider who has cared for patients with personality disorders can attest to the effects on emotional energy, although this effect deserves study. Without adequate coping strategies by care providers, we run the risk of depleting both our empathy and our mental resources, all of which can negatively affect patient experience and outcomes. The coping strategies that are described by Riddle et al. should be helpful in mitigating the anticipated challenges of caring for these patients and improve both our diagnostic reasoning and care‐provider resiliency.
There is still much to be learned about the long‐term effects of maladaptive personality structures on patient outcomes. We believe that is imperative to have the skills to recognize our patients with maladaptive personality traits and how the care of these patients poses challenges on the functioning of the interdisciplinary care team. Without the advanced training to make the challenging diagnosis of a personality disorder during an acute inpatient stay, it is recommended that hospitalists document the specific behaviors that are impacting patient care and the care team. It is our hope that effective coping strategies can lead to reduced risk of diagnostic errors and bolster the resiliency of the hospitalist.
Disclosure
Nothing to report.
- , , , . When personality is the problem: managing patients with difficulty personalities on the acute care unit. J Hosp Med. 2016;11(12):873–878.
- , . An examination of social network quality and composition in women with and without borderline personality disorder [published online June 27, 2016]. Personal Disord. doi:10.1037/per0000201.
- , , , et al. Values as determinant of meaning among patients with psychiatric disorders in the perspective of recovery [published online June 8, 2016]. Sci Rep. doi:10.1038/srep27617.
- , , , et al. EMOTEO: a smartphone application for monitoring and reducing aversive tension in borderline personality disorder patients, a pilot study [published online July 21, 2016]. Perspect Psychiatr Care. doi:10.1111/ppc12178.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- , , , et al. Why patients' disruptive behaviours impair diagnostic reasoning: a randomised experiment [published online March 7, 2016]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-005065.
- , , , . A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
All practicing hospitalists encounter challenging patient situations that stem from issues beyond medical illness. Those situations include the patient who demands to talk with the doctor repeatedly disregarding the lack of urgency, or the patient who, despite seeing multiple well‐regarded specialists, attempts to split the healthcare team by generating unwarranted praise or criticism toward individual caregivers.
Although these patients may be labeled difficult, hateful, or simply a unique patient‐management opportunity, effective care requires a more nuanced understanding of a possible underlying personality disorder that adversely affects the patientphysician relationship. In this issue of the Journal of Hospital Medicine, Riddle et al. provide an important review that outlines a framework for identifying the likely presence of a personality disorder along with practical advice for how to manage these patients.[1] As the authors point out, personality disorders are relatively common among patients seeking medical care but are challenging to diagnose, particularly in the setting of superimposed medical illness. Common to all personality disorders are difficulties forming and maintaining positive relationships with others such that care providers find themselves feeling frustrated, fearful, or inadequate. Inpatient providers typically receive very little training in how to care for patients with personality disorders.
The approach of avoiding collaborative teaching rounds, driven perhaps by a need for time efficiency, deprives learners of the chance to reflect on effective interactions with these patients.
Personality disorders result from genetic predisposition, complex brain dysfunction, and environmental influences. Social determinants also play a role, although limited social networks may simultaneously be a result of a personality disorder and a contributing factor.[2] Although there is a temptation to view personality disorders separate from medical conditions such as diabetes mellitus, diagnosing a personality disorder is far more complicated than simply checking a glycosylated hemoglobin. As Riddle et al. suggest, making a specific diagnosis from the list of 10 personality disorders is challenging in the hospital setting, even for experienced psychiatrists. Given the danger of propagating a diagnosis unabated and unquestioned through the electronic medical record, the attending hospitalist should be reluctant to include a diagnosis such as borderline personality disorder or histrionic personality disorder in the patient problem list without input from experts. Instead, it is useful to document the specific behaviors that are impacting patient care during this episode of illness.
We are concerned about the impact of personality disorders on a number of aspects of patient care, and these are areas that are potentially fertile ground for scholarship and research.
EFFECT ON THE PATIENT EXPERIENCE
Patients with personality disorders may have difficulty assessing the severity of their own medical illnesses. Educating patients on the meaning and value of recovery may be helpful in establishing appropriate expectations of care,[3] although it is equally important to assess the value of illness from the patient's perspective. As Riddle et al. point out, the goal for the hospitalist team is to mitigate the negative impact of adverse behavior on overall care. A recent pilot study of smartphone applications for use by patients with borderline personality disorder might have utility in the inpatient setting.[4] These types of innovations provide opportunities for hospitalist research in the care of patients with personality disorders.
EFFECT OF PERSONALITY DISORDERS ON TEAM‐BASED CLINICAL CARE
A recent observational study published in the Journal of Hospital Medicine identified several important attributes of a high‐functioning inpatient care team.[5] The findings reinforced the concept that patient care is a social activity. To provide high‐quality care, a high‐functioning partnership between team members is required. Riddle et al. point out that patients with personality traits and disorders can negatively impact the relationship among care team members. The hospitalist may be tempted to leave the nursing staff to handle the unwanted communication with the patient. This strategy is maladaptive and creates friction between the hospitalist and the nursing staff. In addition, it reduces an opportunity to recognize important real‐time changes in patients' clinical status that may adversely affect patient outcomes.
EFFECT ON DIAGNOSTIC REASONING
Clinical and diagnostic reasoning plays a central role in patient care. Hospitalists must identify key elements from empirical data and formulate their problem representation to assist in planning the next diagnostic and treatment plans. The medical literature regarding the effect of providing care to patients with maladaptive personality structures is limited. Recent literature investigating the effect of negative patient attributes on diagnostic reasoning suggests that caring for disruptive patients, such as those with maladaptive personality structures, adversely impacts the diagnostic reasoning process. In other words, we are more likely to make cognitive errors when faced with patients who foster a negative feeling. When given vignettes of the same diagnosis but prefaced with patient characteristics that would affect their likeability, trainees of both family practice and internal medicine made significantly fewer correct diagnoses in patients who were given negative connotation, such as overly demanding, a trait not uncommonly seen in patients with personality disorders/traits.[6] The diagnosis rate was more pronounced with complex cases. It is theorized that our cognitive reasoning and use of illness scripts can overcome maladaptive behavior when it comes to common presentations of common illness. However, more complex or atypical presentations require a higher level of diagnostic reasoning that may be impacted by patients who have maladaptive behaviors. The authors hypothesize a resource depletion of mental energy as a result of managing these patients.
EFFECT ON PHYSICIAN WELL‐BEING
Patients with personality disorders require increased time from healthcare providers. Burnout is a major issue for internists.[7] Any provider who has cared for patients with personality disorders can attest to the effects on emotional energy, although this effect deserves study. Without adequate coping strategies by care providers, we run the risk of depleting both our empathy and our mental resources, all of which can negatively affect patient experience and outcomes. The coping strategies that are described by Riddle et al. should be helpful in mitigating the anticipated challenges of caring for these patients and improve both our diagnostic reasoning and care‐provider resiliency.
There is still much to be learned about the long‐term effects of maladaptive personality structures on patient outcomes. We believe that is imperative to have the skills to recognize our patients with maladaptive personality traits and how the care of these patients poses challenges on the functioning of the interdisciplinary care team. Without the advanced training to make the challenging diagnosis of a personality disorder during an acute inpatient stay, it is recommended that hospitalists document the specific behaviors that are impacting patient care and the care team. It is our hope that effective coping strategies can lead to reduced risk of diagnostic errors and bolster the resiliency of the hospitalist.
Disclosure
Nothing to report.
All practicing hospitalists encounter challenging patient situations that stem from issues beyond medical illness. Those situations include the patient who demands to talk with the doctor repeatedly disregarding the lack of urgency, or the patient who, despite seeing multiple well‐regarded specialists, attempts to split the healthcare team by generating unwarranted praise or criticism toward individual caregivers.
Although these patients may be labeled difficult, hateful, or simply a unique patient‐management opportunity, effective care requires a more nuanced understanding of a possible underlying personality disorder that adversely affects the patientphysician relationship. In this issue of the Journal of Hospital Medicine, Riddle et al. provide an important review that outlines a framework for identifying the likely presence of a personality disorder along with practical advice for how to manage these patients.[1] As the authors point out, personality disorders are relatively common among patients seeking medical care but are challenging to diagnose, particularly in the setting of superimposed medical illness. Common to all personality disorders are difficulties forming and maintaining positive relationships with others such that care providers find themselves feeling frustrated, fearful, or inadequate. Inpatient providers typically receive very little training in how to care for patients with personality disorders.
The approach of avoiding collaborative teaching rounds, driven perhaps by a need for time efficiency, deprives learners of the chance to reflect on effective interactions with these patients.
Personality disorders result from genetic predisposition, complex brain dysfunction, and environmental influences. Social determinants also play a role, although limited social networks may simultaneously be a result of a personality disorder and a contributing factor.[2] Although there is a temptation to view personality disorders separate from medical conditions such as diabetes mellitus, diagnosing a personality disorder is far more complicated than simply checking a glycosylated hemoglobin. As Riddle et al. suggest, making a specific diagnosis from the list of 10 personality disorders is challenging in the hospital setting, even for experienced psychiatrists. Given the danger of propagating a diagnosis unabated and unquestioned through the electronic medical record, the attending hospitalist should be reluctant to include a diagnosis such as borderline personality disorder or histrionic personality disorder in the patient problem list without input from experts. Instead, it is useful to document the specific behaviors that are impacting patient care during this episode of illness.
We are concerned about the impact of personality disorders on a number of aspects of patient care, and these are areas that are potentially fertile ground for scholarship and research.
EFFECT ON THE PATIENT EXPERIENCE
Patients with personality disorders may have difficulty assessing the severity of their own medical illnesses. Educating patients on the meaning and value of recovery may be helpful in establishing appropriate expectations of care,[3] although it is equally important to assess the value of illness from the patient's perspective. As Riddle et al. point out, the goal for the hospitalist team is to mitigate the negative impact of adverse behavior on overall care. A recent pilot study of smartphone applications for use by patients with borderline personality disorder might have utility in the inpatient setting.[4] These types of innovations provide opportunities for hospitalist research in the care of patients with personality disorders.
EFFECT OF PERSONALITY DISORDERS ON TEAM‐BASED CLINICAL CARE
A recent observational study published in the Journal of Hospital Medicine identified several important attributes of a high‐functioning inpatient care team.[5] The findings reinforced the concept that patient care is a social activity. To provide high‐quality care, a high‐functioning partnership between team members is required. Riddle et al. point out that patients with personality traits and disorders can negatively impact the relationship among care team members. The hospitalist may be tempted to leave the nursing staff to handle the unwanted communication with the patient. This strategy is maladaptive and creates friction between the hospitalist and the nursing staff. In addition, it reduces an opportunity to recognize important real‐time changes in patients' clinical status that may adversely affect patient outcomes.
EFFECT ON DIAGNOSTIC REASONING
Clinical and diagnostic reasoning plays a central role in patient care. Hospitalists must identify key elements from empirical data and formulate their problem representation to assist in planning the next diagnostic and treatment plans. The medical literature regarding the effect of providing care to patients with maladaptive personality structures is limited. Recent literature investigating the effect of negative patient attributes on diagnostic reasoning suggests that caring for disruptive patients, such as those with maladaptive personality structures, adversely impacts the diagnostic reasoning process. In other words, we are more likely to make cognitive errors when faced with patients who foster a negative feeling. When given vignettes of the same diagnosis but prefaced with patient characteristics that would affect their likeability, trainees of both family practice and internal medicine made significantly fewer correct diagnoses in patients who were given negative connotation, such as overly demanding, a trait not uncommonly seen in patients with personality disorders/traits.[6] The diagnosis rate was more pronounced with complex cases. It is theorized that our cognitive reasoning and use of illness scripts can overcome maladaptive behavior when it comes to common presentations of common illness. However, more complex or atypical presentations require a higher level of diagnostic reasoning that may be impacted by patients who have maladaptive behaviors. The authors hypothesize a resource depletion of mental energy as a result of managing these patients.
EFFECT ON PHYSICIAN WELL‐BEING
Patients with personality disorders require increased time from healthcare providers. Burnout is a major issue for internists.[7] Any provider who has cared for patients with personality disorders can attest to the effects on emotional energy, although this effect deserves study. Without adequate coping strategies by care providers, we run the risk of depleting both our empathy and our mental resources, all of which can negatively affect patient experience and outcomes. The coping strategies that are described by Riddle et al. should be helpful in mitigating the anticipated challenges of caring for these patients and improve both our diagnostic reasoning and care‐provider resiliency.
There is still much to be learned about the long‐term effects of maladaptive personality structures on patient outcomes. We believe that is imperative to have the skills to recognize our patients with maladaptive personality traits and how the care of these patients poses challenges on the functioning of the interdisciplinary care team. Without the advanced training to make the challenging diagnosis of a personality disorder during an acute inpatient stay, it is recommended that hospitalists document the specific behaviors that are impacting patient care and the care team. It is our hope that effective coping strategies can lead to reduced risk of diagnostic errors and bolster the resiliency of the hospitalist.
Disclosure
Nothing to report.
- , , , . When personality is the problem: managing patients with difficulty personalities on the acute care unit. J Hosp Med. 2016;11(12):873–878.
- , . An examination of social network quality and composition in women with and without borderline personality disorder [published online June 27, 2016]. Personal Disord. doi:10.1037/per0000201.
- , , , et al. Values as determinant of meaning among patients with psychiatric disorders in the perspective of recovery [published online June 8, 2016]. Sci Rep. doi:10.1038/srep27617.
- , , , et al. EMOTEO: a smartphone application for monitoring and reducing aversive tension in borderline personality disorder patients, a pilot study [published online July 21, 2016]. Perspect Psychiatr Care. doi:10.1111/ppc12178.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- , , , et al. Why patients' disruptive behaviours impair diagnostic reasoning: a randomised experiment [published online March 7, 2016]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-005065.
- , , , . A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
- , , , . When personality is the problem: managing patients with difficulty personalities on the acute care unit. J Hosp Med. 2016;11(12):873–878.
- , . An examination of social network quality and composition in women with and without borderline personality disorder [published online June 27, 2016]. Personal Disord. doi:10.1037/per0000201.
- , , , et al. Values as determinant of meaning among patients with psychiatric disorders in the perspective of recovery [published online June 8, 2016]. Sci Rep. doi:10.1038/srep27617.
- , , , et al. EMOTEO: a smartphone application for monitoring and reducing aversive tension in borderline personality disorder patients, a pilot study [published online July 21, 2016]. Perspect Psychiatr Care. doi:10.1111/ppc12178.
- , , , et al. Relationships within inpatient physician housestaff teams and their association with hospitalized patient outcomes. J Hosp Med. 2014;9(12):764–771.
- , , , et al. Why patients' disruptive behaviours impair diagnostic reasoning: a randomised experiment [published online March 7, 2016]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-005065.
- , , , . A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
Diet in the pathophysiology and management of irritable bowel syndrome
Diet plays an important role in the pathophysiology of irritable bowel syndrome (IBS) and is an effective tool in managing this disorder. This includes a diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs).
These indigestible and poorly absorbed short-chain carbohydrates trigger IBS symptoms and are thought to exert their effects by increasing osmotic pressure in the lumen of the intestine and by providing a substrate for bacterial fermentation with consequent gas production.1 The gas causes abdominal distention, and the change in pressure in the lumen of the large intestine affects the release of serotonin, causing abdominal pain and discomfort.
THE MECHANISMS ARE COMPLICATED
Recent studies have shown that the mechanisms by which FODMAPs exert their effects are more complicated than originally thought.1
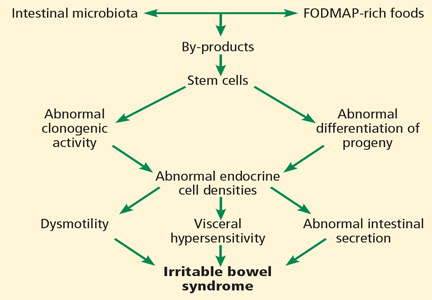
All segments of the gastrointestinal tract contain endocrine cells scattered between the mucosal epithelial cells facing the intestinal lumen.1,2 There are at least 10 types of endocrine cell, and they regulate gastrointestinal motility, secretion, absorption, visceral sensitivity, local immune defense, cell proliferation, and appetite.2–4 Abnormal densities of gastrointestinal endocrine cells have been reported in patients with IBS, which may explain the dysmotility, visceral hypersensitivity, and abnormal intestinal secretion seen in these patients.5
But other factors such as diet, intestinal microbiota, genetics, and low-grade inflammation also play pivotal roles in the pathophysiology of IBS by exerting effects on gastrointestinal endocrine cells. The abnormalities in the gastrointestinal endocrine cells in IBS are thought to be brought about by aberrant differentiation of stem cells into endocrine cells (Figure 1).6
A diet low in FODMAPs appears to induce changes in the intestinal microbiota and gastrointestinal endocrine cells and to reduce IBS symptoms.6
GLUTEN IS IMPLICATED
Another dietary factor in IBS is gluten. Symptoms of IBS and celiac disease overlap: most studies have found that fewer than 5% of patients with celiac disease are misdiagnosed as having IBS based on the symptom criteria for IBS, but some studies report a rate as high as 32%.7 In addition, 38% of patients with celiac disease who consume a gluten-free diet fulfill the symptom-based Rome criteria for IBS.7
The contribution of gluten to IBS does not end with the coexistence of IBS and celiac disease, but also includes the newly debated diagnosis of nonceliac gluten sensitivity, characterized by gastrointestinal symptoms (abdominal pain, diarrhea, constipation, nausea, and vomiting) and other symptoms (headache, musculoskeletal pain, “brain fog,” fatigue, and depression) that are similar to those of IBS. Symptoms are triggered by the ingestion of wheat products, are improved after wheat products are removed from the diet, and relapse after a wheat challenge.7
Nonceliac gluten sensitivity is often perceivable by patients, resulting in self-diagnosis and self-treatment.4 However, it is not clear whether it is gluten or the fructans and galactans in wheat that are responsible for triggering their symptoms.7
DIETARY GUIDANCE IS NEEDED
A low-FODMAP diet with small amounts of insoluble dietary fiber improves symptoms and quality of life in patients with IBS, but dietary guidance is critical and should be personalized because patients differ in how they tolerate foods rich in FODMAPs, probably owing to differing intestinal microbiota among individuals.3,8 Intake of probiotics increases tolerance of FODMAP-rich foods and should also be recommended.3,8,9 Because of the rigorous restrictions of the low-FODMAP diet, patients who receive personalized guidance are more inclined to adhere to the diet and to avoid vitamin and mineral deficiencies.9
- El-Salhy M, Gundersen D. Diet in irritable bowel syndrome. Nutr J 2015; 14:36–46.
- El-Salhy M, Seim I, Chopin L, Gundersen D, Hatlebakk JG, Hausken T. Irritable bowel syndrome: the role of gut neuroendocrine peptides. Front Biosci (Elite Ed) 2012; 4:2783–2800.
- El-Salhy M, Gundersen D, Hatlebakk JG, Hausken T. Irritable bowel syndrome: diagnosis, pathogenesis and treatment options. 1st ed. New York, NY: Nova Science Publishers, Inc.; 2014.
- El-Salhy M, Ostgaard H, Gundersen D, Hatlebakk JG, Hausken T. The role of diet in the pathogenesis and management of irritable bowel syndrome (review). Int J Mol Med 2012; 29:723–731.
- El-Salhy M, Gundersen D, Gilja OH, Hatlebakk JG, Hausken T. Is irritable bowel syndrome an organic disorder? World J Gastroenterol 2014; 20:384–400.
- El-Salhy M. Recent developments in the pathophysiology of irritable bowel syndrome. World J Gastroenterol 2015; 21:7621–7636.
- El-Salhy M, Hatlebakk JG, Gilja OH, Hausken T. The relation between celiac disease, nonceliac gluten sensitivity and irritable bowel syndrome. Nutr J 2015; 14:92–99.
- El-Salhy M, Lillebo E, Reinemo A, Salmelid L, Hausken T. Effects of a health program comprising reassurance, diet management, probiotic administration and regular exercise on symptoms and quality of life in patients with irritable bowel syndrome. Gastroenterology Insights 2010; 2:21–26. doi: http://dx.doi.org/10.4081/gi.2010.e6.
- Ostgaard H, Hausken T, Gundersen D, El-Salhy M. Diet and effects of diet management on quality of life and symptoms in patients with irritable bowel syndrome. Mol Med Rep 2012; 5:1382–1390.
Diet plays an important role in the pathophysiology of irritable bowel syndrome (IBS) and is an effective tool in managing this disorder. This includes a diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs).
These indigestible and poorly absorbed short-chain carbohydrates trigger IBS symptoms and are thought to exert their effects by increasing osmotic pressure in the lumen of the intestine and by providing a substrate for bacterial fermentation with consequent gas production.1 The gas causes abdominal distention, and the change in pressure in the lumen of the large intestine affects the release of serotonin, causing abdominal pain and discomfort.
THE MECHANISMS ARE COMPLICATED
Recent studies have shown that the mechanisms by which FODMAPs exert their effects are more complicated than originally thought.1
All segments of the gastrointestinal tract contain endocrine cells scattered between the mucosal epithelial cells facing the intestinal lumen.1,2 There are at least 10 types of endocrine cell, and they regulate gastrointestinal motility, secretion, absorption, visceral sensitivity, local immune defense, cell proliferation, and appetite.2–4 Abnormal densities of gastrointestinal endocrine cells have been reported in patients with IBS, which may explain the dysmotility, visceral hypersensitivity, and abnormal intestinal secretion seen in these patients.5
But other factors such as diet, intestinal microbiota, genetics, and low-grade inflammation also play pivotal roles in the pathophysiology of IBS by exerting effects on gastrointestinal endocrine cells. The abnormalities in the gastrointestinal endocrine cells in IBS are thought to be brought about by aberrant differentiation of stem cells into endocrine cells (Figure 1).6
A diet low in FODMAPs appears to induce changes in the intestinal microbiota and gastrointestinal endocrine cells and to reduce IBS symptoms.6
GLUTEN IS IMPLICATED
Another dietary factor in IBS is gluten. Symptoms of IBS and celiac disease overlap: most studies have found that fewer than 5% of patients with celiac disease are misdiagnosed as having IBS based on the symptom criteria for IBS, but some studies report a rate as high as 32%.7 In addition, 38% of patients with celiac disease who consume a gluten-free diet fulfill the symptom-based Rome criteria for IBS.7
The contribution of gluten to IBS does not end with the coexistence of IBS and celiac disease, but also includes the newly debated diagnosis of nonceliac gluten sensitivity, characterized by gastrointestinal symptoms (abdominal pain, diarrhea, constipation, nausea, and vomiting) and other symptoms (headache, musculoskeletal pain, “brain fog,” fatigue, and depression) that are similar to those of IBS. Symptoms are triggered by the ingestion of wheat products, are improved after wheat products are removed from the diet, and relapse after a wheat challenge.7
Nonceliac gluten sensitivity is often perceivable by patients, resulting in self-diagnosis and self-treatment.4 However, it is not clear whether it is gluten or the fructans and galactans in wheat that are responsible for triggering their symptoms.7
DIETARY GUIDANCE IS NEEDED
A low-FODMAP diet with small amounts of insoluble dietary fiber improves symptoms and quality of life in patients with IBS, but dietary guidance is critical and should be personalized because patients differ in how they tolerate foods rich in FODMAPs, probably owing to differing intestinal microbiota among individuals.3,8 Intake of probiotics increases tolerance of FODMAP-rich foods and should also be recommended.3,8,9 Because of the rigorous restrictions of the low-FODMAP diet, patients who receive personalized guidance are more inclined to adhere to the diet and to avoid vitamin and mineral deficiencies.9
Diet plays an important role in the pathophysiology of irritable bowel syndrome (IBS) and is an effective tool in managing this disorder. This includes a diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs).
These indigestible and poorly absorbed short-chain carbohydrates trigger IBS symptoms and are thought to exert their effects by increasing osmotic pressure in the lumen of the intestine and by providing a substrate for bacterial fermentation with consequent gas production.1 The gas causes abdominal distention, and the change in pressure in the lumen of the large intestine affects the release of serotonin, causing abdominal pain and discomfort.
THE MECHANISMS ARE COMPLICATED
Recent studies have shown that the mechanisms by which FODMAPs exert their effects are more complicated than originally thought.1
All segments of the gastrointestinal tract contain endocrine cells scattered between the mucosal epithelial cells facing the intestinal lumen.1,2 There are at least 10 types of endocrine cell, and they regulate gastrointestinal motility, secretion, absorption, visceral sensitivity, local immune defense, cell proliferation, and appetite.2–4 Abnormal densities of gastrointestinal endocrine cells have been reported in patients with IBS, which may explain the dysmotility, visceral hypersensitivity, and abnormal intestinal secretion seen in these patients.5
But other factors such as diet, intestinal microbiota, genetics, and low-grade inflammation also play pivotal roles in the pathophysiology of IBS by exerting effects on gastrointestinal endocrine cells. The abnormalities in the gastrointestinal endocrine cells in IBS are thought to be brought about by aberrant differentiation of stem cells into endocrine cells (Figure 1).6
A diet low in FODMAPs appears to induce changes in the intestinal microbiota and gastrointestinal endocrine cells and to reduce IBS symptoms.6
GLUTEN IS IMPLICATED
Another dietary factor in IBS is gluten. Symptoms of IBS and celiac disease overlap: most studies have found that fewer than 5% of patients with celiac disease are misdiagnosed as having IBS based on the symptom criteria for IBS, but some studies report a rate as high as 32%.7 In addition, 38% of patients with celiac disease who consume a gluten-free diet fulfill the symptom-based Rome criteria for IBS.7
The contribution of gluten to IBS does not end with the coexistence of IBS and celiac disease, but also includes the newly debated diagnosis of nonceliac gluten sensitivity, characterized by gastrointestinal symptoms (abdominal pain, diarrhea, constipation, nausea, and vomiting) and other symptoms (headache, musculoskeletal pain, “brain fog,” fatigue, and depression) that are similar to those of IBS. Symptoms are triggered by the ingestion of wheat products, are improved after wheat products are removed from the diet, and relapse after a wheat challenge.7
Nonceliac gluten sensitivity is often perceivable by patients, resulting in self-diagnosis and self-treatment.4 However, it is not clear whether it is gluten or the fructans and galactans in wheat that are responsible for triggering their symptoms.7
DIETARY GUIDANCE IS NEEDED
A low-FODMAP diet with small amounts of insoluble dietary fiber improves symptoms and quality of life in patients with IBS, but dietary guidance is critical and should be personalized because patients differ in how they tolerate foods rich in FODMAPs, probably owing to differing intestinal microbiota among individuals.3,8 Intake of probiotics increases tolerance of FODMAP-rich foods and should also be recommended.3,8,9 Because of the rigorous restrictions of the low-FODMAP diet, patients who receive personalized guidance are more inclined to adhere to the diet and to avoid vitamin and mineral deficiencies.9
- El-Salhy M, Gundersen D. Diet in irritable bowel syndrome. Nutr J 2015; 14:36–46.
- El-Salhy M, Seim I, Chopin L, Gundersen D, Hatlebakk JG, Hausken T. Irritable bowel syndrome: the role of gut neuroendocrine peptides. Front Biosci (Elite Ed) 2012; 4:2783–2800.
- El-Salhy M, Gundersen D, Hatlebakk JG, Hausken T. Irritable bowel syndrome: diagnosis, pathogenesis and treatment options. 1st ed. New York, NY: Nova Science Publishers, Inc.; 2014.
- El-Salhy M, Ostgaard H, Gundersen D, Hatlebakk JG, Hausken T. The role of diet in the pathogenesis and management of irritable bowel syndrome (review). Int J Mol Med 2012; 29:723–731.
- El-Salhy M, Gundersen D, Gilja OH, Hatlebakk JG, Hausken T. Is irritable bowel syndrome an organic disorder? World J Gastroenterol 2014; 20:384–400.
- El-Salhy M. Recent developments in the pathophysiology of irritable bowel syndrome. World J Gastroenterol 2015; 21:7621–7636.
- El-Salhy M, Hatlebakk JG, Gilja OH, Hausken T. The relation between celiac disease, nonceliac gluten sensitivity and irritable bowel syndrome. Nutr J 2015; 14:92–99.
- El-Salhy M, Lillebo E, Reinemo A, Salmelid L, Hausken T. Effects of a health program comprising reassurance, diet management, probiotic administration and regular exercise on symptoms and quality of life in patients with irritable bowel syndrome. Gastroenterology Insights 2010; 2:21–26. doi: http://dx.doi.org/10.4081/gi.2010.e6.
- Ostgaard H, Hausken T, Gundersen D, El-Salhy M. Diet and effects of diet management on quality of life and symptoms in patients with irritable bowel syndrome. Mol Med Rep 2012; 5:1382–1390.
- El-Salhy M, Gundersen D. Diet in irritable bowel syndrome. Nutr J 2015; 14:36–46.
- El-Salhy M, Seim I, Chopin L, Gundersen D, Hatlebakk JG, Hausken T. Irritable bowel syndrome: the role of gut neuroendocrine peptides. Front Biosci (Elite Ed) 2012; 4:2783–2800.
- El-Salhy M, Gundersen D, Hatlebakk JG, Hausken T. Irritable bowel syndrome: diagnosis, pathogenesis and treatment options. 1st ed. New York, NY: Nova Science Publishers, Inc.; 2014.
- El-Salhy M, Ostgaard H, Gundersen D, Hatlebakk JG, Hausken T. The role of diet in the pathogenesis and management of irritable bowel syndrome (review). Int J Mol Med 2012; 29:723–731.
- El-Salhy M, Gundersen D, Gilja OH, Hatlebakk JG, Hausken T. Is irritable bowel syndrome an organic disorder? World J Gastroenterol 2014; 20:384–400.
- El-Salhy M. Recent developments in the pathophysiology of irritable bowel syndrome. World J Gastroenterol 2015; 21:7621–7636.
- El-Salhy M, Hatlebakk JG, Gilja OH, Hausken T. The relation between celiac disease, nonceliac gluten sensitivity and irritable bowel syndrome. Nutr J 2015; 14:92–99.
- El-Salhy M, Lillebo E, Reinemo A, Salmelid L, Hausken T. Effects of a health program comprising reassurance, diet management, probiotic administration and regular exercise on symptoms and quality of life in patients with irritable bowel syndrome. Gastroenterology Insights 2010; 2:21–26. doi: http://dx.doi.org/10.4081/gi.2010.e6.
- Ostgaard H, Hausken T, Gundersen D, El-Salhy M. Diet and effects of diet management on quality of life and symptoms in patients with irritable bowel syndrome. Mol Med Rep 2012; 5:1382–1390.