User login
PAS: Flu shots increasing among children with asthma
SAN DIEGO – The proportion of children with asthma receiving the influenza vaccine has continued to increase in the past decade or so, though not as quickly as for children without asthma, results from national survey data found.
While the influenza vaccine is recommended for all children aged 6 months and older, trends in influenza vaccination for early (August-October) versus late (November-May) vaccination in children with asthma have not been examined, lead study author Dr. Alan E. Simon said during a poster session at the annual meeting of the Pediatric Academic Societies.
Dr. Simon, a medical officer with the office of analysis and epidemiology at the National Center for Health Statistics, Hyattsville, Md., and his associates evaluated National Health Interview Survey (NHIS) sample child files for 2005-2013. They limited the analysis to children aged 2-17 years and defined current asthma as a “yes” response to two questions: “Has your doctor ever told you that your child has asthma?” and “Does your child still have asthma?” A total of 31,668 NHIS interviews conducted between April and July 2005-2013 were assessed for vaccine receipt between August and May of the previous flu season. The researchers conducted logistic regression with predictive margins with receipt of flu shot as the dependent variable, and year, current asthma, and the interaction between year and asthma as dependent variables.
Dr. Simon reported that the percentage of children with asthma who received a flu shot increased an average of 3.2 percentage points per year during the time period, reaching 55% in 2012-2013. At the same time, the percentage of children without asthma who received a flu shot increased an average of 4.2 percentage points per year, reaching 45% in 2012-2013. Meanwhile, the percentage of children in both groups who received early vaccination increased about 1.5% per year, reaching 32% in children with asthma and 27% among children without asthma in 2012-2013.
The researchers also found that over the last three flu seasons, the following characteristics were predictive of children with asthma having a longer time to vaccination or a lower probability of vaccination: being aged 12-17 years vs. 2-5 years (adjusted hazard ratio of 0.75; P less than .01); being uninsured vs. privately insured (aHR 0.52; P less than .01), and living in the South or the West vs. the Northeast (aHR 0.79; P less than .05).
Dr. Simon said that similar overall results were observed when he and his associates conducted a separate analysis that assessed 85,087 NHIS interviews from 2005 to 2013 and used Kaplan-Meier survival statistics to estimate yearly vaccination estimates and early vaccination estimates.
The study was funded by the Centers for Disease Control and Prevention. Dr. Simon reported having no relevant financial conflicts.
On Twitter @dougbrunk
SAN DIEGO – The proportion of children with asthma receiving the influenza vaccine has continued to increase in the past decade or so, though not as quickly as for children without asthma, results from national survey data found.
While the influenza vaccine is recommended for all children aged 6 months and older, trends in influenza vaccination for early (August-October) versus late (November-May) vaccination in children with asthma have not been examined, lead study author Dr. Alan E. Simon said during a poster session at the annual meeting of the Pediatric Academic Societies.
Dr. Simon, a medical officer with the office of analysis and epidemiology at the National Center for Health Statistics, Hyattsville, Md., and his associates evaluated National Health Interview Survey (NHIS) sample child files for 2005-2013. They limited the analysis to children aged 2-17 years and defined current asthma as a “yes” response to two questions: “Has your doctor ever told you that your child has asthma?” and “Does your child still have asthma?” A total of 31,668 NHIS interviews conducted between April and July 2005-2013 were assessed for vaccine receipt between August and May of the previous flu season. The researchers conducted logistic regression with predictive margins with receipt of flu shot as the dependent variable, and year, current asthma, and the interaction between year and asthma as dependent variables.
Dr. Simon reported that the percentage of children with asthma who received a flu shot increased an average of 3.2 percentage points per year during the time period, reaching 55% in 2012-2013. At the same time, the percentage of children without asthma who received a flu shot increased an average of 4.2 percentage points per year, reaching 45% in 2012-2013. Meanwhile, the percentage of children in both groups who received early vaccination increased about 1.5% per year, reaching 32% in children with asthma and 27% among children without asthma in 2012-2013.
The researchers also found that over the last three flu seasons, the following characteristics were predictive of children with asthma having a longer time to vaccination or a lower probability of vaccination: being aged 12-17 years vs. 2-5 years (adjusted hazard ratio of 0.75; P less than .01); being uninsured vs. privately insured (aHR 0.52; P less than .01), and living in the South or the West vs. the Northeast (aHR 0.79; P less than .05).
Dr. Simon said that similar overall results were observed when he and his associates conducted a separate analysis that assessed 85,087 NHIS interviews from 2005 to 2013 and used Kaplan-Meier survival statistics to estimate yearly vaccination estimates and early vaccination estimates.
The study was funded by the Centers for Disease Control and Prevention. Dr. Simon reported having no relevant financial conflicts.
On Twitter @dougbrunk
SAN DIEGO – The proportion of children with asthma receiving the influenza vaccine has continued to increase in the past decade or so, though not as quickly as for children without asthma, results from national survey data found.
While the influenza vaccine is recommended for all children aged 6 months and older, trends in influenza vaccination for early (August-October) versus late (November-May) vaccination in children with asthma have not been examined, lead study author Dr. Alan E. Simon said during a poster session at the annual meeting of the Pediatric Academic Societies.
Dr. Simon, a medical officer with the office of analysis and epidemiology at the National Center for Health Statistics, Hyattsville, Md., and his associates evaluated National Health Interview Survey (NHIS) sample child files for 2005-2013. They limited the analysis to children aged 2-17 years and defined current asthma as a “yes” response to two questions: “Has your doctor ever told you that your child has asthma?” and “Does your child still have asthma?” A total of 31,668 NHIS interviews conducted between April and July 2005-2013 were assessed for vaccine receipt between August and May of the previous flu season. The researchers conducted logistic regression with predictive margins with receipt of flu shot as the dependent variable, and year, current asthma, and the interaction between year and asthma as dependent variables.
Dr. Simon reported that the percentage of children with asthma who received a flu shot increased an average of 3.2 percentage points per year during the time period, reaching 55% in 2012-2013. At the same time, the percentage of children without asthma who received a flu shot increased an average of 4.2 percentage points per year, reaching 45% in 2012-2013. Meanwhile, the percentage of children in both groups who received early vaccination increased about 1.5% per year, reaching 32% in children with asthma and 27% among children without asthma in 2012-2013.
The researchers also found that over the last three flu seasons, the following characteristics were predictive of children with asthma having a longer time to vaccination or a lower probability of vaccination: being aged 12-17 years vs. 2-5 years (adjusted hazard ratio of 0.75; P less than .01); being uninsured vs. privately insured (aHR 0.52; P less than .01), and living in the South or the West vs. the Northeast (aHR 0.79; P less than .05).
Dr. Simon said that similar overall results were observed when he and his associates conducted a separate analysis that assessed 85,087 NHIS interviews from 2005 to 2013 and used Kaplan-Meier survival statistics to estimate yearly vaccination estimates and early vaccination estimates.
The study was funded by the Centers for Disease Control and Prevention. Dr. Simon reported having no relevant financial conflicts.
On Twitter @dougbrunk
AT THE PAS ANNUAL MEETING
Key clinical point: Influenza vaccination among children with asthma has continued to increase in recent years.
Major finding: The percentage of children with asthma who received a flu shot increased an average of 3.2 percentage points per year from 2005 to 2013, reaching 55% in 2012-2013.
Data source: An analysis of 31,668 National Health Interview Survey sample child files for 2005-2013.
Disclosures: The study was funded by the Centers for Disease Control and Prevention. Dr. Simon reported having no relevant financial conflicts.
Teens’ Tdap Booster Dose Begins to Wane After 2 Years
A sixth dose of Tdap is initially effective in preventing pertussis in teens, but its effectiveness declines by half within 4 years after the booster, a recent study found.
“This waning is likely contributing to the increase in pertussis among adolescents,” reported Dr. Anna M. Acosta of the Centers for Disease Control and Prevention, Atlanta, and her associates (Pediatrics 2015 [doi: 10.1542/peds.2014-3358]).
“Advances in our understanding of the immunology and bacteriology of Bordetella pertussis are essential to optimize future prevention and control measures,” they wrote. “However, novel pertussis vaccines that effectively limit infection and transmission are also likely needed to reduce the burden of pertussis disease in the United States.”

The researchers matched three controls by birth year and primary provider practice (total 2,322 controls) to each of 836 cases of pertussis in seven counties of Washington during the 2012 pertussis epidemic. Cases were more likely than were controls to be non-Hispanic and white, but there was a lack of race/ethnicity data.
Receipt of the five childhood series doses was similar among cases (74%) and controls (75%), but a smaller proportion of both (60% cases, 58% controls) were on schedule. Among more than 84% of participants who received Tdap between ages 11 and 12, 81% of the cases and 90% of the controls received the sixth dose.
Among the 450 cases and 1,246 controls who received all acellular vaccines for the primary series, Tdap effectiveness was 63.9% overall. Stratified by time since Tdap vaccination, however, it was 73.1% within 12 months, 54.9% within 12-23 months, and 34.2% within 24-47 months.
Those born from 1999 to 2000 were presumed to have received the DTaP in infancy, and those born from 1993 to 1997 were presumed to have received a mixture of the acellular and whole-cell (DTwP) vaccines. Among those with vaccine lot numbers recorded, all vaccines administered after 1998 were acellular. A direct comparison of Tdap effectiveness between those vaccinated with the acellular primary series and those vaccinated with a mixed primary series was not possible because of time differences in vaccination between the two groups.
The research did not receive external funding, and the authors reported no relevant financial disclosures.
In the study by Acosta et al., the duration of Tdap effectiveness is disappointing, particularly because case-control studies tend to inflate efficacy. The resurgence of pertussis is often attributed to the switch from whole-cell pertussis vaccines to acellular products. However, the increase in reported pertussis began 14 years before the universal use of diphtheria-tetanus-acellular pertussis (DTaP) vaccines in childhood commenced. The two greatest contributors to the resurgence of pertussis are greater awareness and more sensitive diagnosis (routine use of polymerase chain reaction).
In the pre-DTaP and pre-Tdap eras, the pertussis attack rate in nonepidemic periods in largely whole-cell pertussis vaccine–primed adolescents and adults was 370 to 500 per 100,000 per year. These rates are underestimates because of clear evidence of “observer bias” in both studies. In this present Washington State study, the attack rate during the epidemic was only 182.3 per 100,000 for the one-half-year study period.
Factors that I think are most important relating to DTaP vaccine failure are as follows: decay in antibody over time; a T helper (Th) 1/Th2 versus a Th1, Th17 cellular response; incomplete antigen package; incorrect balance of antigens in the vaccine; linked-epitope suppression; and the occurrence of pertactin-deficient B. pertussis strains. Some, but not all, of these factors also may relate to Tdap failure over time.
Although adequate data are not available, it can be assumed that adolescents and adults who were primed in infancy by infection or DTP will have a Th1, Th17 response to Tdap. In contrast, those who were primed by DTaP will have a Th1/Th2 response. In line with the results of these two recent Tdap effectiveness studies, we should examine our present Tdap immunization recommendations. It is my opinion that we should continue with our present Tdap schedules. Of most importance is to see that all pregnant women receive Tdap with each pregnancy. This alone can prevent virtually all pertussis deaths in young infants.
James D. Cherry, M.D., is professor of pediatrics at the University of California, Los Angeles. These comments are excerpted from an editorial (Pediatrics 2015 [doi:10.1542/peds.2014-4118]) accompanying Dr. Acosta’s study. Dr. Cherry is a member of the Sanofi Pasteur speakers bureau and of the Global Pertussis Initiative, supported by Sanofi Pastuer. He receives royalties from Elsevier for “Feigin and Cherry’s Textbook of Pediatric Infectious Diseases.”
In the study by Acosta et al., the duration of Tdap effectiveness is disappointing, particularly because case-control studies tend to inflate efficacy. The resurgence of pertussis is often attributed to the switch from whole-cell pertussis vaccines to acellular products. However, the increase in reported pertussis began 14 years before the universal use of diphtheria-tetanus-acellular pertussis (DTaP) vaccines in childhood commenced. The two greatest contributors to the resurgence of pertussis are greater awareness and more sensitive diagnosis (routine use of polymerase chain reaction).
In the pre-DTaP and pre-Tdap eras, the pertussis attack rate in nonepidemic periods in largely whole-cell pertussis vaccine–primed adolescents and adults was 370 to 500 per 100,000 per year. These rates are underestimates because of clear evidence of “observer bias” in both studies. In this present Washington State study, the attack rate during the epidemic was only 182.3 per 100,000 for the one-half-year study period.
Factors that I think are most important relating to DTaP vaccine failure are as follows: decay in antibody over time; a T helper (Th) 1/Th2 versus a Th1, Th17 cellular response; incomplete antigen package; incorrect balance of antigens in the vaccine; linked-epitope suppression; and the occurrence of pertactin-deficient B. pertussis strains. Some, but not all, of these factors also may relate to Tdap failure over time.
Although adequate data are not available, it can be assumed that adolescents and adults who were primed in infancy by infection or DTP will have a Th1, Th17 response to Tdap. In contrast, those who were primed by DTaP will have a Th1/Th2 response. In line with the results of these two recent Tdap effectiveness studies, we should examine our present Tdap immunization recommendations. It is my opinion that we should continue with our present Tdap schedules. Of most importance is to see that all pregnant women receive Tdap with each pregnancy. This alone can prevent virtually all pertussis deaths in young infants.
James D. Cherry, M.D., is professor of pediatrics at the University of California, Los Angeles. These comments are excerpted from an editorial (Pediatrics 2015 [doi:10.1542/peds.2014-4118]) accompanying Dr. Acosta’s study. Dr. Cherry is a member of the Sanofi Pasteur speakers bureau and of the Global Pertussis Initiative, supported by Sanofi Pastuer. He receives royalties from Elsevier for “Feigin and Cherry’s Textbook of Pediatric Infectious Diseases.”
In the study by Acosta et al., the duration of Tdap effectiveness is disappointing, particularly because case-control studies tend to inflate efficacy. The resurgence of pertussis is often attributed to the switch from whole-cell pertussis vaccines to acellular products. However, the increase in reported pertussis began 14 years before the universal use of diphtheria-tetanus-acellular pertussis (DTaP) vaccines in childhood commenced. The two greatest contributors to the resurgence of pertussis are greater awareness and more sensitive diagnosis (routine use of polymerase chain reaction).
In the pre-DTaP and pre-Tdap eras, the pertussis attack rate in nonepidemic periods in largely whole-cell pertussis vaccine–primed adolescents and adults was 370 to 500 per 100,000 per year. These rates are underestimates because of clear evidence of “observer bias” in both studies. In this present Washington State study, the attack rate during the epidemic was only 182.3 per 100,000 for the one-half-year study period.
Factors that I think are most important relating to DTaP vaccine failure are as follows: decay in antibody over time; a T helper (Th) 1/Th2 versus a Th1, Th17 cellular response; incomplete antigen package; incorrect balance of antigens in the vaccine; linked-epitope suppression; and the occurrence of pertactin-deficient B. pertussis strains. Some, but not all, of these factors also may relate to Tdap failure over time.
Although adequate data are not available, it can be assumed that adolescents and adults who were primed in infancy by infection or DTP will have a Th1, Th17 response to Tdap. In contrast, those who were primed by DTaP will have a Th1/Th2 response. In line with the results of these two recent Tdap effectiveness studies, we should examine our present Tdap immunization recommendations. It is my opinion that we should continue with our present Tdap schedules. Of most importance is to see that all pregnant women receive Tdap with each pregnancy. This alone can prevent virtually all pertussis deaths in young infants.
James D. Cherry, M.D., is professor of pediatrics at the University of California, Los Angeles. These comments are excerpted from an editorial (Pediatrics 2015 [doi:10.1542/peds.2014-4118]) accompanying Dr. Acosta’s study. Dr. Cherry is a member of the Sanofi Pasteur speakers bureau and of the Global Pertussis Initiative, supported by Sanofi Pastuer. He receives royalties from Elsevier for “Feigin and Cherry’s Textbook of Pediatric Infectious Diseases.”
A sixth dose of Tdap is initially effective in preventing pertussis in teens, but its effectiveness declines by half within 4 years after the booster, a recent study found.
“This waning is likely contributing to the increase in pertussis among adolescents,” reported Dr. Anna M. Acosta of the Centers for Disease Control and Prevention, Atlanta, and her associates (Pediatrics 2015 [doi: 10.1542/peds.2014-3358]).
“Advances in our understanding of the immunology and bacteriology of Bordetella pertussis are essential to optimize future prevention and control measures,” they wrote. “However, novel pertussis vaccines that effectively limit infection and transmission are also likely needed to reduce the burden of pertussis disease in the United States.”
The researchers matched three controls by birth year and primary provider practice (total 2,322 controls) to each of 836 cases of pertussis in seven counties of Washington during the 2012 pertussis epidemic. Cases were more likely than were controls to be non-Hispanic and white, but there was a lack of race/ethnicity data.
Receipt of the five childhood series doses was similar among cases (74%) and controls (75%), but a smaller proportion of both (60% cases, 58% controls) were on schedule. Among more than 84% of participants who received Tdap between ages 11 and 12, 81% of the cases and 90% of the controls received the sixth dose.
Among the 450 cases and 1,246 controls who received all acellular vaccines for the primary series, Tdap effectiveness was 63.9% overall. Stratified by time since Tdap vaccination, however, it was 73.1% within 12 months, 54.9% within 12-23 months, and 34.2% within 24-47 months.
Those born from 1999 to 2000 were presumed to have received the DTaP in infancy, and those born from 1993 to 1997 were presumed to have received a mixture of the acellular and whole-cell (DTwP) vaccines. Among those with vaccine lot numbers recorded, all vaccines administered after 1998 were acellular. A direct comparison of Tdap effectiveness between those vaccinated with the acellular primary series and those vaccinated with a mixed primary series was not possible because of time differences in vaccination between the two groups.
The research did not receive external funding, and the authors reported no relevant financial disclosures.
A sixth dose of Tdap is initially effective in preventing pertussis in teens, but its effectiveness declines by half within 4 years after the booster, a recent study found.
“This waning is likely contributing to the increase in pertussis among adolescents,” reported Dr. Anna M. Acosta of the Centers for Disease Control and Prevention, Atlanta, and her associates (Pediatrics 2015 [doi: 10.1542/peds.2014-3358]).
“Advances in our understanding of the immunology and bacteriology of Bordetella pertussis are essential to optimize future prevention and control measures,” they wrote. “However, novel pertussis vaccines that effectively limit infection and transmission are also likely needed to reduce the burden of pertussis disease in the United States.”
The researchers matched three controls by birth year and primary provider practice (total 2,322 controls) to each of 836 cases of pertussis in seven counties of Washington during the 2012 pertussis epidemic. Cases were more likely than were controls to be non-Hispanic and white, but there was a lack of race/ethnicity data.
Receipt of the five childhood series doses was similar among cases (74%) and controls (75%), but a smaller proportion of both (60% cases, 58% controls) were on schedule. Among more than 84% of participants who received Tdap between ages 11 and 12, 81% of the cases and 90% of the controls received the sixth dose.
Among the 450 cases and 1,246 controls who received all acellular vaccines for the primary series, Tdap effectiveness was 63.9% overall. Stratified by time since Tdap vaccination, however, it was 73.1% within 12 months, 54.9% within 12-23 months, and 34.2% within 24-47 months.
Those born from 1999 to 2000 were presumed to have received the DTaP in infancy, and those born from 1993 to 1997 were presumed to have received a mixture of the acellular and whole-cell (DTwP) vaccines. Among those with vaccine lot numbers recorded, all vaccines administered after 1998 were acellular. A direct comparison of Tdap effectiveness between those vaccinated with the acellular primary series and those vaccinated with a mixed primary series was not possible because of time differences in vaccination between the two groups.
The research did not receive external funding, and the authors reported no relevant financial disclosures.
FROM PEDIATRICS

AAAAI: Grass allergy tablets show favorable NNT
HOUSTON – The number needed to treat with Timothy grass sublingual immunotherapy tablets for allergic rhinitis to achieve a clinically meaningful response is 7.9, Dr. Stephen R. Durham reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
What the low number needed to treat (NNT) means in this instance is that, on average, 7.9 children or adults with Timothy grass–induced allergic rhinitis with or without conjunctivitis would need to be treated with Merck’s sublingual immunotherapy tablet (SLIT) rather than placebo daily for 3 years in order for 1 additional patient to obtain sustained benefit. Sustained benefit was defined as at least 50% well days for the entire grass pollen season during each of the 3 treatment years plus the subsequent 2 years of no treatment, explained Dr. Durham of Royal Brompton and Harefield Hospitals and Imperial College, London.

A ‘well day’ was considered as a day with no use of open-label rescue medication and in which the worst score recorded was ‘none’ or ‘mild’ for each of the four nasal and two ocular symptoms measured. This NNT analysis was based upon pooled data from six pivotal randomized, double-blind, phase III, placebo-controlled clinical trials totaling 3,094 patients, Dr. Durham added.
A separate analysis of the same pooled data using a different definition of favorable response – that is, a total combined daily symptom and daily medication score of 3 or less during the entire grass pollen season during the 3 treatment years, plus the following 2 no-treatment years – yielded an NNT of 9.4. The maximum total daily symptom score during any given year was 18, while the maximum daily medication score per year was 30-36, depending upon whether the participant was a child or adult, and whether the study was conducted in Europe or the United States.
The risk-benefit ratio of SLIT for allergic rhinitis in the pooled analysis was favorable as reflected in a number needed to harm of 303, with harm defined as a treatment-related systemic allergic reaction. When the NNH was recalculated using epinephrine usage as the harmful endpoint, the NNH was closely similar at 305.
Merck’s Timothy grass SLIT, marketed as Grastek, is FDA-approved for treatment of allergic rhinitis in adults and children as young as 5 years of age.
Dr. Durham reported receiving research grants and serving as a consultant to Merck, ALK, and Stallergenes. The NNT analysis was funded by Merck, and the phase III clinical trials on which the analysis was based were supported by ALK and Merck.
HOUSTON – The number needed to treat with Timothy grass sublingual immunotherapy tablets for allergic rhinitis to achieve a clinically meaningful response is 7.9, Dr. Stephen R. Durham reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
What the low number needed to treat (NNT) means in this instance is that, on average, 7.9 children or adults with Timothy grass–induced allergic rhinitis with or without conjunctivitis would need to be treated with Merck’s sublingual immunotherapy tablet (SLIT) rather than placebo daily for 3 years in order for 1 additional patient to obtain sustained benefit. Sustained benefit was defined as at least 50% well days for the entire grass pollen season during each of the 3 treatment years plus the subsequent 2 years of no treatment, explained Dr. Durham of Royal Brompton and Harefield Hospitals and Imperial College, London.
A ‘well day’ was considered as a day with no use of open-label rescue medication and in which the worst score recorded was ‘none’ or ‘mild’ for each of the four nasal and two ocular symptoms measured. This NNT analysis was based upon pooled data from six pivotal randomized, double-blind, phase III, placebo-controlled clinical trials totaling 3,094 patients, Dr. Durham added.
A separate analysis of the same pooled data using a different definition of favorable response – that is, a total combined daily symptom and daily medication score of 3 or less during the entire grass pollen season during the 3 treatment years, plus the following 2 no-treatment years – yielded an NNT of 9.4. The maximum total daily symptom score during any given year was 18, while the maximum daily medication score per year was 30-36, depending upon whether the participant was a child or adult, and whether the study was conducted in Europe or the United States.
The risk-benefit ratio of SLIT for allergic rhinitis in the pooled analysis was favorable as reflected in a number needed to harm of 303, with harm defined as a treatment-related systemic allergic reaction. When the NNH was recalculated using epinephrine usage as the harmful endpoint, the NNH was closely similar at 305.
Merck’s Timothy grass SLIT, marketed as Grastek, is FDA-approved for treatment of allergic rhinitis in adults and children as young as 5 years of age.
Dr. Durham reported receiving research grants and serving as a consultant to Merck, ALK, and Stallergenes. The NNT analysis was funded by Merck, and the phase III clinical trials on which the analysis was based were supported by ALK and Merck.
HOUSTON – The number needed to treat with Timothy grass sublingual immunotherapy tablets for allergic rhinitis to achieve a clinically meaningful response is 7.9, Dr. Stephen R. Durham reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
What the low number needed to treat (NNT) means in this instance is that, on average, 7.9 children or adults with Timothy grass–induced allergic rhinitis with or without conjunctivitis would need to be treated with Merck’s sublingual immunotherapy tablet (SLIT) rather than placebo daily for 3 years in order for 1 additional patient to obtain sustained benefit. Sustained benefit was defined as at least 50% well days for the entire grass pollen season during each of the 3 treatment years plus the subsequent 2 years of no treatment, explained Dr. Durham of Royal Brompton and Harefield Hospitals and Imperial College, London.
A ‘well day’ was considered as a day with no use of open-label rescue medication and in which the worst score recorded was ‘none’ or ‘mild’ for each of the four nasal and two ocular symptoms measured. This NNT analysis was based upon pooled data from six pivotal randomized, double-blind, phase III, placebo-controlled clinical trials totaling 3,094 patients, Dr. Durham added.
A separate analysis of the same pooled data using a different definition of favorable response – that is, a total combined daily symptom and daily medication score of 3 or less during the entire grass pollen season during the 3 treatment years, plus the following 2 no-treatment years – yielded an NNT of 9.4. The maximum total daily symptom score during any given year was 18, while the maximum daily medication score per year was 30-36, depending upon whether the participant was a child or adult, and whether the study was conducted in Europe or the United States.
The risk-benefit ratio of SLIT for allergic rhinitis in the pooled analysis was favorable as reflected in a number needed to harm of 303, with harm defined as a treatment-related systemic allergic reaction. When the NNH was recalculated using epinephrine usage as the harmful endpoint, the NNH was closely similar at 305.
Merck’s Timothy grass SLIT, marketed as Grastek, is FDA-approved for treatment of allergic rhinitis in adults and children as young as 5 years of age.
Dr. Durham reported receiving research grants and serving as a consultant to Merck, ALK, and Stallergenes. The NNT analysis was funded by Merck, and the phase III clinical trials on which the analysis was based were supported by ALK and Merck.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: The number of allergic rhinitis patients who need to be treated with Timothy grass immunotherapy tablets to obtain a sustained clinically important response is 7.9.
Major finding: For every 7.9 patients who took the sublingual immunotherapy tablets rather than placebo daily for 3 years, one additional patient experienced ‘well days’ for the entire grass pollen season during those 3 years, along with the next 2 years of no treatment.
Data source: This analysis was based upon six pivotal phase III, randomized, double-blind, placebo-controlled clinical trials totaling 3,094 adults and children with allergic rhinitis.
Disclosures: This NNT analysis was sponsored by Merck. The presenter reported receiving a research grant from the company.

Send kids home 2 hours after food challenge testing
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: Food-allergic children who don’t experience a severe immediate reaction following double-blind, placebo-controlled food challenges can safely be discharged home 2 hours post-testing.
Major finding: No severe late reactions occurred in a large cohort of children who underwent double-blind, placebo-controlled food challenges with cow’s milk, cashew, peanut, egg, and hazelnut.
Data source: This retrospective study included 1,142 Dutch children who underwent double-blind, placebo-controlled food challenges at a university clinic.
Disclosures: The presenter reported no conflicts of interest with regard to this university-supported study.

Aspirin desensitization making headway in U.S.
HOUSTON – About 63% of allergists and fellows in training perform aspirin desensitization for aspirin-exacerbated respiratory disease, according to a national survey.
That figure is lower than it should be, given the wealth of published evidence that aspirin desensitization is a safe and effective component of the treatment of aspirin-exacerbated respiratory disease (AERD), Dr. Jeremy D. Waldram asserted in presenting the survey findings at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Moreover, the figure likely overcalls the true rate, since participation in the survey was voluntary and fans of aspirin desensitization were probably more inclined to complete the 16-item questionnaire, added Dr. Waldram, a fellow in allergy and immunology at the Scripps Clinic in San Diego.

Was he surprised to find that aspirin desensitization isn’t more widely utilized?
“I think the number that surprised me more was that among the 37.5% of allergists who don’t do aspirin desensitization, almost 30% of them don’t even refer their patients to others who do the procedure. We don’t know why they don’t refer out; it wasn’t a question included in the survey. Perhaps they see patients who are of a less severe phenotype,” he said in an interview.
The 684 survey responses represented a 15% response rate. While 37.5% of respondents indicated they don’t perform aspirin desensitization, 73% of those who reported doing the procedure said they do an average of 1-5 cases annually.
Among allergists who don’t perform aspirin desensitization, safety concerns were the leading reason cited. Indeed, 70% of those who don’t do aspirin desensitization indicated safety risks were the main reason. More than one reason could be given, however, and 30% of allergists cited poor compensation for the procedure as a deterrent, nearly 60% said the logistics of monitoring care were too onerous, and one-third said they didn’t perform aspirin desensitization because they hadn’t been trained to do it.
Of allergists who reported doing aspirin desensitization, 52% perform the procedure in an outpatient setting unattached to a hospital. Another 21% do so in an outpatient clinic that’s physically attached to a hospital.
Within the past 5 years, 9% of respondents said that they’ve had a patient react severely to aspirin desensitization, requiring an unanticipated transfer to a higher level of care. That’s contrary to the experience among allergists at the Scripps Clinic, which is widely credited with pioneering the outpatient approach.
“We essentially do all our aspirin desensitizations for AERD in the outpatient setting. In 1,500 treated patients we’ve never had one that we had to transfer to a higher level of care. We don’t have any special setup. It’s a typical outpatient clinic. We usually don’t start IVs or do anything above and beyond,” Dr. Waldram said.
While 26% of respondents reported they generally recommend aspirin desensitization immediately upon identifying a patient history that supports the diagnosis of AERD, another 54% said they usually recommend the procedure to patients only after they’ve failed to improve on typical medical therapy.
Twenty percent of physicians rated aspirin desensitization as “extremely helpful for the majority of patients,” another 49% said they find it most beneficial as an adjuvant to ongoing medical therapy.
Forty-four percent of allergists who perform aspirin desensitization reported that they learned to do the procedure during fellowship training. Fourteen percent said they learned to the procedure at an annual meeting, and 36% picked it up by reviewing the relevant literature.
Several allergists commented that had Dr. Waldram’s survey been conducted even a couple of years ago the rate of utilization of aspirin desensitization would have been far lower. They interpreted his reported 62.5% rate as a sign of progress. Dr. Waldram said he believes the key to further boosting utilization of aspirin desensitization lies in increasing exposure to the procedure during fellowship training. He noted that internal medicine-trained fellows who responded to the survey had a significantly higher aspirin desensitization utilization rate than those who came to their allergy fellowship with a background in pediatrics.
The hallmarks of AERD are difficult-to-treat nasal polyps, chronic eosinophilic sinusitis, and asthma in a patient with sensitivity to aspirin and other COX-1 inhibitors.
Dr. Waldram reported having no financial conflicts with regard to his study, which was conducted free of commercial support.
HOUSTON – About 63% of allergists and fellows in training perform aspirin desensitization for aspirin-exacerbated respiratory disease, according to a national survey.
That figure is lower than it should be, given the wealth of published evidence that aspirin desensitization is a safe and effective component of the treatment of aspirin-exacerbated respiratory disease (AERD), Dr. Jeremy D. Waldram asserted in presenting the survey findings at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Moreover, the figure likely overcalls the true rate, since participation in the survey was voluntary and fans of aspirin desensitization were probably more inclined to complete the 16-item questionnaire, added Dr. Waldram, a fellow in allergy and immunology at the Scripps Clinic in San Diego.
Was he surprised to find that aspirin desensitization isn’t more widely utilized?
“I think the number that surprised me more was that among the 37.5% of allergists who don’t do aspirin desensitization, almost 30% of them don’t even refer their patients to others who do the procedure. We don’t know why they don’t refer out; it wasn’t a question included in the survey. Perhaps they see patients who are of a less severe phenotype,” he said in an interview.
The 684 survey responses represented a 15% response rate. While 37.5% of respondents indicated they don’t perform aspirin desensitization, 73% of those who reported doing the procedure said they do an average of 1-5 cases annually.
Among allergists who don’t perform aspirin desensitization, safety concerns were the leading reason cited. Indeed, 70% of those who don’t do aspirin desensitization indicated safety risks were the main reason. More than one reason could be given, however, and 30% of allergists cited poor compensation for the procedure as a deterrent, nearly 60% said the logistics of monitoring care were too onerous, and one-third said they didn’t perform aspirin desensitization because they hadn’t been trained to do it.
Of allergists who reported doing aspirin desensitization, 52% perform the procedure in an outpatient setting unattached to a hospital. Another 21% do so in an outpatient clinic that’s physically attached to a hospital.
Within the past 5 years, 9% of respondents said that they’ve had a patient react severely to aspirin desensitization, requiring an unanticipated transfer to a higher level of care. That’s contrary to the experience among allergists at the Scripps Clinic, which is widely credited with pioneering the outpatient approach.
“We essentially do all our aspirin desensitizations for AERD in the outpatient setting. In 1,500 treated patients we’ve never had one that we had to transfer to a higher level of care. We don’t have any special setup. It’s a typical outpatient clinic. We usually don’t start IVs or do anything above and beyond,” Dr. Waldram said.
While 26% of respondents reported they generally recommend aspirin desensitization immediately upon identifying a patient history that supports the diagnosis of AERD, another 54% said they usually recommend the procedure to patients only after they’ve failed to improve on typical medical therapy.
Twenty percent of physicians rated aspirin desensitization as “extremely helpful for the majority of patients,” another 49% said they find it most beneficial as an adjuvant to ongoing medical therapy.
Forty-four percent of allergists who perform aspirin desensitization reported that they learned to do the procedure during fellowship training. Fourteen percent said they learned to the procedure at an annual meeting, and 36% picked it up by reviewing the relevant literature.
Several allergists commented that had Dr. Waldram’s survey been conducted even a couple of years ago the rate of utilization of aspirin desensitization would have been far lower. They interpreted his reported 62.5% rate as a sign of progress. Dr. Waldram said he believes the key to further boosting utilization of aspirin desensitization lies in increasing exposure to the procedure during fellowship training. He noted that internal medicine-trained fellows who responded to the survey had a significantly higher aspirin desensitization utilization rate than those who came to their allergy fellowship with a background in pediatrics.
The hallmarks of AERD are difficult-to-treat nasal polyps, chronic eosinophilic sinusitis, and asthma in a patient with sensitivity to aspirin and other COX-1 inhibitors.
Dr. Waldram reported having no financial conflicts with regard to his study, which was conducted free of commercial support.
HOUSTON – About 63% of allergists and fellows in training perform aspirin desensitization for aspirin-exacerbated respiratory disease, according to a national survey.
That figure is lower than it should be, given the wealth of published evidence that aspirin desensitization is a safe and effective component of the treatment of aspirin-exacerbated respiratory disease (AERD), Dr. Jeremy D. Waldram asserted in presenting the survey findings at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Moreover, the figure likely overcalls the true rate, since participation in the survey was voluntary and fans of aspirin desensitization were probably more inclined to complete the 16-item questionnaire, added Dr. Waldram, a fellow in allergy and immunology at the Scripps Clinic in San Diego.
Was he surprised to find that aspirin desensitization isn’t more widely utilized?
“I think the number that surprised me more was that among the 37.5% of allergists who don’t do aspirin desensitization, almost 30% of them don’t even refer their patients to others who do the procedure. We don’t know why they don’t refer out; it wasn’t a question included in the survey. Perhaps they see patients who are of a less severe phenotype,” he said in an interview.
The 684 survey responses represented a 15% response rate. While 37.5% of respondents indicated they don’t perform aspirin desensitization, 73% of those who reported doing the procedure said they do an average of 1-5 cases annually.
Among allergists who don’t perform aspirin desensitization, safety concerns were the leading reason cited. Indeed, 70% of those who don’t do aspirin desensitization indicated safety risks were the main reason. More than one reason could be given, however, and 30% of allergists cited poor compensation for the procedure as a deterrent, nearly 60% said the logistics of monitoring care were too onerous, and one-third said they didn’t perform aspirin desensitization because they hadn’t been trained to do it.
Of allergists who reported doing aspirin desensitization, 52% perform the procedure in an outpatient setting unattached to a hospital. Another 21% do so in an outpatient clinic that’s physically attached to a hospital.
Within the past 5 years, 9% of respondents said that they’ve had a patient react severely to aspirin desensitization, requiring an unanticipated transfer to a higher level of care. That’s contrary to the experience among allergists at the Scripps Clinic, which is widely credited with pioneering the outpatient approach.
“We essentially do all our aspirin desensitizations for AERD in the outpatient setting. In 1,500 treated patients we’ve never had one that we had to transfer to a higher level of care. We don’t have any special setup. It’s a typical outpatient clinic. We usually don’t start IVs or do anything above and beyond,” Dr. Waldram said.
While 26% of respondents reported they generally recommend aspirin desensitization immediately upon identifying a patient history that supports the diagnosis of AERD, another 54% said they usually recommend the procedure to patients only after they’ve failed to improve on typical medical therapy.
Twenty percent of physicians rated aspirin desensitization as “extremely helpful for the majority of patients,” another 49% said they find it most beneficial as an adjuvant to ongoing medical therapy.
Forty-four percent of allergists who perform aspirin desensitization reported that they learned to do the procedure during fellowship training. Fourteen percent said they learned to the procedure at an annual meeting, and 36% picked it up by reviewing the relevant literature.
Several allergists commented that had Dr. Waldram’s survey been conducted even a couple of years ago the rate of utilization of aspirin desensitization would have been far lower. They interpreted his reported 62.5% rate as a sign of progress. Dr. Waldram said he believes the key to further boosting utilization of aspirin desensitization lies in increasing exposure to the procedure during fellowship training. He noted that internal medicine-trained fellows who responded to the survey had a significantly higher aspirin desensitization utilization rate than those who came to their allergy fellowship with a background in pediatrics.
The hallmarks of AERD are difficult-to-treat nasal polyps, chronic eosinophilic sinusitis, and asthma in a patient with sensitivity to aspirin and other COX-1 inhibitors.
Dr. Waldram reported having no financial conflicts with regard to his study, which was conducted free of commercial support.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: Aspirin desensitization for patients with aspirin-exacerbated respiratory disease is catching on among U.S. allergists.
Major finding: Roughly 63% of allergists and allergy fellows who responded to a national survey indicated they perform aspirin desensitization for aspirin-exacerbated respiratory disease.
Data source: This was a 16-question survey of aspirin desensitization practices among U.S. allergists and allergy fellows. The national survey drew 684 responses.
Disclosures: The presenter reported having no financial conflicts with regard to his study, which was funded without commercial support.
Risk factors identified for gestational eczema
HOUSTON– New-onset eczema during pregnancy is a common phenomenon with several newly identified risk factors.
This disease entity deserves a proper name: gestational eczema, Dr. Wilfried J.J. Karmaus asserted at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In contrast, the likelihood of new-onset asthma arising during pregnancy isn’t significantly more common than in an affected woman’s male partner during the same time frame.
“There was no large difference in wheezing between the women and men. Therefore, we cannot propose the term ‘gestational asthma,’” said Dr. Karmaus, professor of epidemiology at the University of Memphis. “Investigations into how to prevent eczema and asthma in pregnancy are really important, because eczema and asthma in pregnancy can increase the risk of these diseases in the offspring. This is a totally undeveloped field.”
He presented new findings from the Isle of Wight study, a prospective study in which a cohort of women has been followed from birth through pregnancy across three generations.
Eczema and asthma are common atopic diseases, and they are particularly common during pregnancy. Indeed, eczema is the most common skin disease seen in pregnancy, accounting for 35%-50% of all dermatoses in previous studies by other investigators. In those studies, only 20%-40% of women with eczema during pregnancy had a prepregnancy history of the disease.
In the Isle of Wight cohort, women were evaluated for asthma and eczema symptoms at ages 1, 2, 4, 10, and 18 years and again during pregnancy at gestational weeks 20 and 28. A total of 26 of 116 women developed eczema during pregnancy, with eight of them (31%) experiencing the skin disease for the first time in their lives. In contrast, only six of their male partners had eczema during the pregnancy time frame, and just one of them had new-onset eczema.
A history of maternal eczema in the preceding generation was associated with a 52% increased relative risk of having eczema by age 18 and a 3.1-fold increased likelihood of eczema during pregnancy. Also, methylation of the filaggrin gene at the cytosine-phosphate-guanine site cg13447818 when assessed at age 18 was associated with a significantly increased likelihood of eczema in a subject’s mother as well as increased risk of gestational eczema 1-7 years later, Dr. Karmaus continued.
Eighteen percent of women in the Isle of Wight cohort had asthma during pregnancy, as did a similar proportion of their male partners. Twenty-seven percent of women with asthma during pregnancy had no previous history of the respiratory disease, a rate which was again comparable in their male partners with asthma.
DNA methylation of the IL1RL1 gene at cg17738684 was significantly associated with asthma heritability across three generations in the Isle of Wight study. The IL1RL1 gene at cg17738684 is a candidate gene for asthma that encodes for interleukin-33. This finding raises the possibility that addressing this DNA methylation could prove fruitful as a transgenerational asthma prevention strategy.
The Isle of Wight birth cohort study is funded by the National Institutes of Health, Asthma UK, and the Isle of Wight Trust. Dr. Karmaus reported having no financial conflicts of interest.
HOUSTON– New-onset eczema during pregnancy is a common phenomenon with several newly identified risk factors.
This disease entity deserves a proper name: gestational eczema, Dr. Wilfried J.J. Karmaus asserted at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In contrast, the likelihood of new-onset asthma arising during pregnancy isn’t significantly more common than in an affected woman’s male partner during the same time frame.
“There was no large difference in wheezing between the women and men. Therefore, we cannot propose the term ‘gestational asthma,’” said Dr. Karmaus, professor of epidemiology at the University of Memphis. “Investigations into how to prevent eczema and asthma in pregnancy are really important, because eczema and asthma in pregnancy can increase the risk of these diseases in the offspring. This is a totally undeveloped field.”
He presented new findings from the Isle of Wight study, a prospective study in which a cohort of women has been followed from birth through pregnancy across three generations.
Eczema and asthma are common atopic diseases, and they are particularly common during pregnancy. Indeed, eczema is the most common skin disease seen in pregnancy, accounting for 35%-50% of all dermatoses in previous studies by other investigators. In those studies, only 20%-40% of women with eczema during pregnancy had a prepregnancy history of the disease.
In the Isle of Wight cohort, women were evaluated for asthma and eczema symptoms at ages 1, 2, 4, 10, and 18 years and again during pregnancy at gestational weeks 20 and 28. A total of 26 of 116 women developed eczema during pregnancy, with eight of them (31%) experiencing the skin disease for the first time in their lives. In contrast, only six of their male partners had eczema during the pregnancy time frame, and just one of them had new-onset eczema.
A history of maternal eczema in the preceding generation was associated with a 52% increased relative risk of having eczema by age 18 and a 3.1-fold increased likelihood of eczema during pregnancy. Also, methylation of the filaggrin gene at the cytosine-phosphate-guanine site cg13447818 when assessed at age 18 was associated with a significantly increased likelihood of eczema in a subject’s mother as well as increased risk of gestational eczema 1-7 years later, Dr. Karmaus continued.
Eighteen percent of women in the Isle of Wight cohort had asthma during pregnancy, as did a similar proportion of their male partners. Twenty-seven percent of women with asthma during pregnancy had no previous history of the respiratory disease, a rate which was again comparable in their male partners with asthma.
DNA methylation of the IL1RL1 gene at cg17738684 was significantly associated with asthma heritability across three generations in the Isle of Wight study. The IL1RL1 gene at cg17738684 is a candidate gene for asthma that encodes for interleukin-33. This finding raises the possibility that addressing this DNA methylation could prove fruitful as a transgenerational asthma prevention strategy.
The Isle of Wight birth cohort study is funded by the National Institutes of Health, Asthma UK, and the Isle of Wight Trust. Dr. Karmaus reported having no financial conflicts of interest.
HOUSTON– New-onset eczema during pregnancy is a common phenomenon with several newly identified risk factors.
This disease entity deserves a proper name: gestational eczema, Dr. Wilfried J.J. Karmaus asserted at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In contrast, the likelihood of new-onset asthma arising during pregnancy isn’t significantly more common than in an affected woman’s male partner during the same time frame.
“There was no large difference in wheezing between the women and men. Therefore, we cannot propose the term ‘gestational asthma,’” said Dr. Karmaus, professor of epidemiology at the University of Memphis. “Investigations into how to prevent eczema and asthma in pregnancy are really important, because eczema and asthma in pregnancy can increase the risk of these diseases in the offspring. This is a totally undeveloped field.”
He presented new findings from the Isle of Wight study, a prospective study in which a cohort of women has been followed from birth through pregnancy across three generations.
Eczema and asthma are common atopic diseases, and they are particularly common during pregnancy. Indeed, eczema is the most common skin disease seen in pregnancy, accounting for 35%-50% of all dermatoses in previous studies by other investigators. In those studies, only 20%-40% of women with eczema during pregnancy had a prepregnancy history of the disease.
In the Isle of Wight cohort, women were evaluated for asthma and eczema symptoms at ages 1, 2, 4, 10, and 18 years and again during pregnancy at gestational weeks 20 and 28. A total of 26 of 116 women developed eczema during pregnancy, with eight of them (31%) experiencing the skin disease for the first time in their lives. In contrast, only six of their male partners had eczema during the pregnancy time frame, and just one of them had new-onset eczema.
A history of maternal eczema in the preceding generation was associated with a 52% increased relative risk of having eczema by age 18 and a 3.1-fold increased likelihood of eczema during pregnancy. Also, methylation of the filaggrin gene at the cytosine-phosphate-guanine site cg13447818 when assessed at age 18 was associated with a significantly increased likelihood of eczema in a subject’s mother as well as increased risk of gestational eczema 1-7 years later, Dr. Karmaus continued.
Eighteen percent of women in the Isle of Wight cohort had asthma during pregnancy, as did a similar proportion of their male partners. Twenty-seven percent of women with asthma during pregnancy had no previous history of the respiratory disease, a rate which was again comparable in their male partners with asthma.
DNA methylation of the IL1RL1 gene at cg17738684 was significantly associated with asthma heritability across three generations in the Isle of Wight study. The IL1RL1 gene at cg17738684 is a candidate gene for asthma that encodes for interleukin-33. This finding raises the possibility that addressing this DNA methylation could prove fruitful as a transgenerational asthma prevention strategy.
The Isle of Wight birth cohort study is funded by the National Institutes of Health, Asthma UK, and the Isle of Wight Trust. Dr. Karmaus reported having no financial conflicts of interest.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: Thirty-one percent of cases of eczema and 27% of asthma in a group of pregnant women occurred for the first time in the woman’s life.
Major finding: A history of maternal eczema was associated with a 3.1-fold increased likelihood of eczema during the offspring’s pregnancy.
Data source: The Isle of Wight birth cohort study is a prospective study following three generations from birth through pregnancy.
Disclosures: The study is funded by the National Institutes of Health, Asthma UK, and the Isle of Wight Trust. The presenter reported having no financial conflicts of interest.
Aerosolized Measles Vaccine Inferior to Subcutaneous
An aerosolized measles vaccine proved to be immunogenic but inferior to the subcutaneous vaccine in inducing seropositivity among infants in rural India, according to a report published online April 16 in the New England Journal of Medicine.
Aerosolized delivery of a measles vaccine could prove especially helpful in resource-poor countries where major measles outbreaks continue to occur because of poor health service infrastructure, but data concerning the efficacy of this form of delivery have been inconsistent. “Given the established record of injectable measles vaccine, alternative delivery methods should show noninferiority,” wrote Dr. Nicola Low of the Institute of Social and Preventive Medicine, University of Bern (Switzerland), and her associates.
They performed a randomized, open-label noninferiority trial comparing a primary dose of aerosolized measles vaccine (1,001 children) against subcutaneous measles vaccine (1,003 children) among babies aged 9-11.9 months living in villages in rural India. The primary endpoint – seropositivity for serum antibodies against measles at 91 days after vaccination – was 85.4% for aerosolized vaccine and 94.6% for subcutaneous vaccine. This difference of 9.2 percentage points did not reach the threshold for noninferiority, which was 5.0 percentage points, the investigators said (N. Engl. J. Med. 2015;372:1519-29 [doi:10.1056/NEJMoa1407417]).
Among the children who did achieve seropositivity, however, the geometric mean concentrations of measles antibodies were similar between the two study groups.
Adverse-event profiles were similar between aerosolized and subcutaneous vaccine, and adverse events were rare. The most common effects judged likely to be related to the vaccines were rash, coryza, cough, diarrhea, and fever.
After this study was designed, experts recommended providing a second dose of measles vaccine to protect children who did not respond to the first dose. Using this two-dose strategy, the aerosolized formulation induced higher and more sustained levels of seropositivity than the subcutaneous formulation in studies of school-aged children in South Africa. So it is possible that the aerosolized measles vaccine may prove to be noninferior in future studies involving a different dosing schedule and an older pediatric patient population, Dr. Low and her associates noted.
This study was funded by the Bill and Melinda Gates Foundation. The Serum Institute of India provided vaccines free of charge and Aerogen provided the delivery devices free of charge. Dr. Low reported several grants plus monies paid to her institution from the World Health Organization for projects about vaccines and sexually transmitted infections; her associates reported ties to the Serum Institute of India, Aerogen, and Dance Biopharm. One associate has a patent pending on an aerosol device licensed to Novartis and another has a patent pending related to vaccine nebulizers.
An aerosolized measles vaccine proved to be immunogenic but inferior to the subcutaneous vaccine in inducing seropositivity among infants in rural India, according to a report published online April 16 in the New England Journal of Medicine.
Aerosolized delivery of a measles vaccine could prove especially helpful in resource-poor countries where major measles outbreaks continue to occur because of poor health service infrastructure, but data concerning the efficacy of this form of delivery have been inconsistent. “Given the established record of injectable measles vaccine, alternative delivery methods should show noninferiority,” wrote Dr. Nicola Low of the Institute of Social and Preventive Medicine, University of Bern (Switzerland), and her associates.
They performed a randomized, open-label noninferiority trial comparing a primary dose of aerosolized measles vaccine (1,001 children) against subcutaneous measles vaccine (1,003 children) among babies aged 9-11.9 months living in villages in rural India. The primary endpoint – seropositivity for serum antibodies against measles at 91 days after vaccination – was 85.4% for aerosolized vaccine and 94.6% for subcutaneous vaccine. This difference of 9.2 percentage points did not reach the threshold for noninferiority, which was 5.0 percentage points, the investigators said (N. Engl. J. Med. 2015;372:1519-29 [doi:10.1056/NEJMoa1407417]).
Among the children who did achieve seropositivity, however, the geometric mean concentrations of measles antibodies were similar between the two study groups.
Adverse-event profiles were similar between aerosolized and subcutaneous vaccine, and adverse events were rare. The most common effects judged likely to be related to the vaccines were rash, coryza, cough, diarrhea, and fever.
After this study was designed, experts recommended providing a second dose of measles vaccine to protect children who did not respond to the first dose. Using this two-dose strategy, the aerosolized formulation induced higher and more sustained levels of seropositivity than the subcutaneous formulation in studies of school-aged children in South Africa. So it is possible that the aerosolized measles vaccine may prove to be noninferior in future studies involving a different dosing schedule and an older pediatric patient population, Dr. Low and her associates noted.
This study was funded by the Bill and Melinda Gates Foundation. The Serum Institute of India provided vaccines free of charge and Aerogen provided the delivery devices free of charge. Dr. Low reported several grants plus monies paid to her institution from the World Health Organization for projects about vaccines and sexually transmitted infections; her associates reported ties to the Serum Institute of India, Aerogen, and Dance Biopharm. One associate has a patent pending on an aerosol device licensed to Novartis and another has a patent pending related to vaccine nebulizers.
An aerosolized measles vaccine proved to be immunogenic but inferior to the subcutaneous vaccine in inducing seropositivity among infants in rural India, according to a report published online April 16 in the New England Journal of Medicine.
Aerosolized delivery of a measles vaccine could prove especially helpful in resource-poor countries where major measles outbreaks continue to occur because of poor health service infrastructure, but data concerning the efficacy of this form of delivery have been inconsistent. “Given the established record of injectable measles vaccine, alternative delivery methods should show noninferiority,” wrote Dr. Nicola Low of the Institute of Social and Preventive Medicine, University of Bern (Switzerland), and her associates.
They performed a randomized, open-label noninferiority trial comparing a primary dose of aerosolized measles vaccine (1,001 children) against subcutaneous measles vaccine (1,003 children) among babies aged 9-11.9 months living in villages in rural India. The primary endpoint – seropositivity for serum antibodies against measles at 91 days after vaccination – was 85.4% for aerosolized vaccine and 94.6% for subcutaneous vaccine. This difference of 9.2 percentage points did not reach the threshold for noninferiority, which was 5.0 percentage points, the investigators said (N. Engl. J. Med. 2015;372:1519-29 [doi:10.1056/NEJMoa1407417]).
Among the children who did achieve seropositivity, however, the geometric mean concentrations of measles antibodies were similar between the two study groups.
Adverse-event profiles were similar between aerosolized and subcutaneous vaccine, and adverse events were rare. The most common effects judged likely to be related to the vaccines were rash, coryza, cough, diarrhea, and fever.
After this study was designed, experts recommended providing a second dose of measles vaccine to protect children who did not respond to the first dose. Using this two-dose strategy, the aerosolized formulation induced higher and more sustained levels of seropositivity than the subcutaneous formulation in studies of school-aged children in South Africa. So it is possible that the aerosolized measles vaccine may prove to be noninferior in future studies involving a different dosing schedule and an older pediatric patient population, Dr. Low and her associates noted.
This study was funded by the Bill and Melinda Gates Foundation. The Serum Institute of India provided vaccines free of charge and Aerogen provided the delivery devices free of charge. Dr. Low reported several grants plus monies paid to her institution from the World Health Organization for projects about vaccines and sexually transmitted infections; her associates reported ties to the Serum Institute of India, Aerogen, and Dance Biopharm. One associate has a patent pending on an aerosol device licensed to Novartis and another has a patent pending related to vaccine nebulizers.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Respiratory disorders most common cause of childhood hospitalization
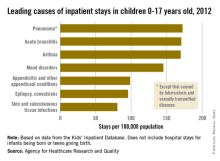
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
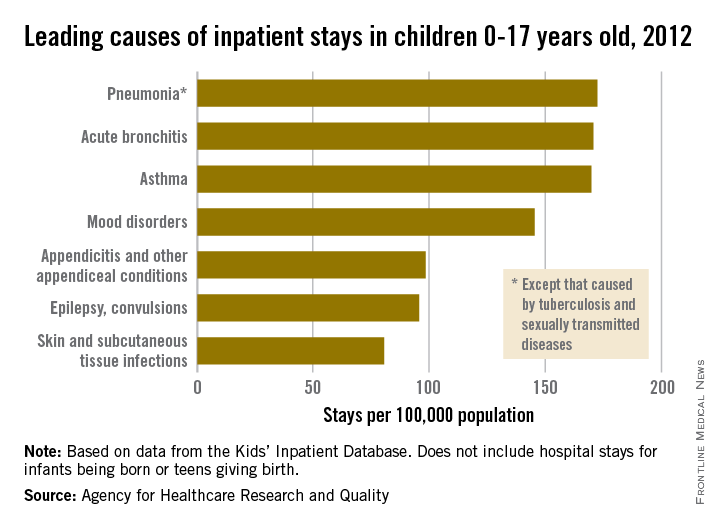
CDC Ebola Vaccine Trial Underway in Sierra Leone
The Centers for Disease Control and Prevention is looking to enroll 6,000 people in an Ebola vaccine trial now underway in Sierra Leone.
Frontline workers are being randomized to the experimental vaccine rVSV-ZEBOV either up front or 6 months after enrollment. Subjects then will be followed for 6 months to see how well the vaccine protects them from infection. The trial will cost about $25 million, funded mostly by the U.S. government.

“The Ebola epidemic has been devastating for West Africa. I really hope that this is the beginning of a new positive chapter for Sierra Leone and the story of battling this virus,” said Dr. Anne Schuchat, director of CDC’s National Center for Immunization and Respiratory Diseases.
So far, about 200 people have enrolled in the study, and more than 90 have gotten the shot. Foreign aid workers are eligible for the trial, but because subjects need to be in country long enough for follow-up, most will be from Sierra Leone. To cover time and transportation costs, participants are paid $10 for enrollment and $30 after they get the vaccine, Dr. Schuchat said in an April 14 teleconference.
Subjects include doctors, nurses, janitors, lab technicians, security guards, pharmacists, administrators, burial workers, and those who wash the bodies of the newly dead. The study is being conducted in hard-hit areas of Sierra Leone, including the capital of Freetown. Similar studies are underway in Liberia and Guinea.
Ebola cases “are way down” in West Africa lately, “but people are continuing to get” the disease, “and some of the Ebola outbreaks in the past have had long tails,” so health care workers remain at risk, according to Dr. Schuchat.
With infection rates down, it’s unclear whether or not the study will have enough cases to demonstrate efficacy for rVSV-ZEBOV. Even so, “we plan to collect information on safety and immune response that could contribute to licensure pathways even if we are not able to estimate efficacy,” she said.
About 800 people have gotten rVSV-ZEBOV in other trials. Common side effects include fatigue, fever, headaches, and muscle aches. There have also been reports of mild, self-limited joint pain and swelling.
CDC is working with the Sierra Leone College of Medicine and Allied Health Sciences and the Sierra Leone Ministry of Health and Sanitation to conduct the trial, dubbed The Sierra Leone Trial to Introduce a Vaccine against Ebola (STRIVE). About 350 local people have been hired and trained to help with the study.
The vaccine uses a vesicular stomatitis virus carrying a noninfectious Ebola virus gene, and has been shown to produce an immune response against the virus. It was developed by the Public Health Agency of Canada’s National Microbiology Laboratory and is licensed to NewLink Genetics. In 2014, NewLink entered into a licensing and collaboration agreement with Merck to develop rVSV-ZEBOV.
Until it is known whether or not the vaccine works, and how well, CDC cautioned that vaccinated people still need to take full protective measures against Ebola.
The Centers for Disease Control and Prevention is looking to enroll 6,000 people in an Ebola vaccine trial now underway in Sierra Leone.
Frontline workers are being randomized to the experimental vaccine rVSV-ZEBOV either up front or 6 months after enrollment. Subjects then will be followed for 6 months to see how well the vaccine protects them from infection. The trial will cost about $25 million, funded mostly by the U.S. government.
“The Ebola epidemic has been devastating for West Africa. I really hope that this is the beginning of a new positive chapter for Sierra Leone and the story of battling this virus,” said Dr. Anne Schuchat, director of CDC’s National Center for Immunization and Respiratory Diseases.
So far, about 200 people have enrolled in the study, and more than 90 have gotten the shot. Foreign aid workers are eligible for the trial, but because subjects need to be in country long enough for follow-up, most will be from Sierra Leone. To cover time and transportation costs, participants are paid $10 for enrollment and $30 after they get the vaccine, Dr. Schuchat said in an April 14 teleconference.
Subjects include doctors, nurses, janitors, lab technicians, security guards, pharmacists, administrators, burial workers, and those who wash the bodies of the newly dead. The study is being conducted in hard-hit areas of Sierra Leone, including the capital of Freetown. Similar studies are underway in Liberia and Guinea.
Ebola cases “are way down” in West Africa lately, “but people are continuing to get” the disease, “and some of the Ebola outbreaks in the past have had long tails,” so health care workers remain at risk, according to Dr. Schuchat.
With infection rates down, it’s unclear whether or not the study will have enough cases to demonstrate efficacy for rVSV-ZEBOV. Even so, “we plan to collect information on safety and immune response that could contribute to licensure pathways even if we are not able to estimate efficacy,” she said.
About 800 people have gotten rVSV-ZEBOV in other trials. Common side effects include fatigue, fever, headaches, and muscle aches. There have also been reports of mild, self-limited joint pain and swelling.
CDC is working with the Sierra Leone College of Medicine and Allied Health Sciences and the Sierra Leone Ministry of Health and Sanitation to conduct the trial, dubbed The Sierra Leone Trial to Introduce a Vaccine against Ebola (STRIVE). About 350 local people have been hired and trained to help with the study.
The vaccine uses a vesicular stomatitis virus carrying a noninfectious Ebola virus gene, and has been shown to produce an immune response against the virus. It was developed by the Public Health Agency of Canada’s National Microbiology Laboratory and is licensed to NewLink Genetics. In 2014, NewLink entered into a licensing and collaboration agreement with Merck to develop rVSV-ZEBOV.
Until it is known whether or not the vaccine works, and how well, CDC cautioned that vaccinated people still need to take full protective measures against Ebola.
The Centers for Disease Control and Prevention is looking to enroll 6,000 people in an Ebola vaccine trial now underway in Sierra Leone.
Frontline workers are being randomized to the experimental vaccine rVSV-ZEBOV either up front or 6 months after enrollment. Subjects then will be followed for 6 months to see how well the vaccine protects them from infection. The trial will cost about $25 million, funded mostly by the U.S. government.
“The Ebola epidemic has been devastating for West Africa. I really hope that this is the beginning of a new positive chapter for Sierra Leone and the story of battling this virus,” said Dr. Anne Schuchat, director of CDC’s National Center for Immunization and Respiratory Diseases.
So far, about 200 people have enrolled in the study, and more than 90 have gotten the shot. Foreign aid workers are eligible for the trial, but because subjects need to be in country long enough for follow-up, most will be from Sierra Leone. To cover time and transportation costs, participants are paid $10 for enrollment and $30 after they get the vaccine, Dr. Schuchat said in an April 14 teleconference.
Subjects include doctors, nurses, janitors, lab technicians, security guards, pharmacists, administrators, burial workers, and those who wash the bodies of the newly dead. The study is being conducted in hard-hit areas of Sierra Leone, including the capital of Freetown. Similar studies are underway in Liberia and Guinea.
Ebola cases “are way down” in West Africa lately, “but people are continuing to get” the disease, “and some of the Ebola outbreaks in the past have had long tails,” so health care workers remain at risk, according to Dr. Schuchat.
With infection rates down, it’s unclear whether or not the study will have enough cases to demonstrate efficacy for rVSV-ZEBOV. Even so, “we plan to collect information on safety and immune response that could contribute to licensure pathways even if we are not able to estimate efficacy,” she said.
About 800 people have gotten rVSV-ZEBOV in other trials. Common side effects include fatigue, fever, headaches, and muscle aches. There have also been reports of mild, self-limited joint pain and swelling.
CDC is working with the Sierra Leone College of Medicine and Allied Health Sciences and the Sierra Leone Ministry of Health and Sanitation to conduct the trial, dubbed The Sierra Leone Trial to Introduce a Vaccine against Ebola (STRIVE). About 350 local people have been hired and trained to help with the study.
The vaccine uses a vesicular stomatitis virus carrying a noninfectious Ebola virus gene, and has been shown to produce an immune response against the virus. It was developed by the Public Health Agency of Canada’s National Microbiology Laboratory and is licensed to NewLink Genetics. In 2014, NewLink entered into a licensing and collaboration agreement with Merck to develop rVSV-ZEBOV.
Until it is known whether or not the vaccine works, and how well, CDC cautioned that vaccinated people still need to take full protective measures against Ebola.
FROM A CDC TELECONFERENCE

Mast cells predict hypersensitive reactions in rituximab desensitization
HOUSTON – For rituximab patients undergoing desensitization, mast cell degranulation is a more effective predictor of hypersensitive reactions (HSR) than are the traditionally employed skin tests, according to a study presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“In this particular study, we were interested in investigating the roles of immunoglobulin E (IgE) in the mast cells in rituximab hypersensitivity,” said Dr. Johnson T. Wong of Massachusetts General Hospital, Boston, who presented the findings during a session dedicated to “Novel Insights in Drug Allergy.”
The study comprised 25 patients with persistent or severe rituximab sensitivity (RITS) who were treated at Massachusetts General between 2008 and 2013. Dr. Wong and his coinvestigators performed skin testing on 18 subjects, of which 7 (39%) reacted positively at least once during the course of testing.
HSR reactions occurred at similar rates in subjects who reacted positively and negatively to skin testing. Tryptase levels were taken in 18 subjects (72%), during 67% of the HSR desensitizations and 21% of the asymptomatic desensitizations.
Overall, elevated levels were noted in 21% of the HSR desensitizations.
The elevated tryptase levels in patients experiencing HSR indicates that mast cell degranulation is likely a major contributing factor in causing HSR, with cytokine release and tumor lysis also playing an important role, Dr. Wong said. Mast cell degranulations also points to an association with IgE mechanisms as a reliable indicator of HSR likelihood.
Dr. Wong and his coauthors concluded via tryptase level testing that asymptomatic mast cell degranulation happened very rarely, as only 1 out of 27 assessments (3%) indicated that result. One patient was excluded from the HSR desensitization cohort’s results because of probable mast cell activation syndrome, which caused abnormally elevated tryptase levels throughout the study period.
“In both positive and negative skin test patients, our desensitization protocol was able to reduce the reaction rate to less than 30%, so around 70% of patients had no reaction at all during desensitization,” said Dr. Wong, adding that nearly all desensitizations were completed successfully.
Dr. Wong had no disclosures.
HOUSTON – For rituximab patients undergoing desensitization, mast cell degranulation is a more effective predictor of hypersensitive reactions (HSR) than are the traditionally employed skin tests, according to a study presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“In this particular study, we were interested in investigating the roles of immunoglobulin E (IgE) in the mast cells in rituximab hypersensitivity,” said Dr. Johnson T. Wong of Massachusetts General Hospital, Boston, who presented the findings during a session dedicated to “Novel Insights in Drug Allergy.”
The study comprised 25 patients with persistent or severe rituximab sensitivity (RITS) who were treated at Massachusetts General between 2008 and 2013. Dr. Wong and his coinvestigators performed skin testing on 18 subjects, of which 7 (39%) reacted positively at least once during the course of testing.
HSR reactions occurred at similar rates in subjects who reacted positively and negatively to skin testing. Tryptase levels were taken in 18 subjects (72%), during 67% of the HSR desensitizations and 21% of the asymptomatic desensitizations.
Overall, elevated levels were noted in 21% of the HSR desensitizations.
The elevated tryptase levels in patients experiencing HSR indicates that mast cell degranulation is likely a major contributing factor in causing HSR, with cytokine release and tumor lysis also playing an important role, Dr. Wong said. Mast cell degranulations also points to an association with IgE mechanisms as a reliable indicator of HSR likelihood.
Dr. Wong and his coauthors concluded via tryptase level testing that asymptomatic mast cell degranulation happened very rarely, as only 1 out of 27 assessments (3%) indicated that result. One patient was excluded from the HSR desensitization cohort’s results because of probable mast cell activation syndrome, which caused abnormally elevated tryptase levels throughout the study period.
“In both positive and negative skin test patients, our desensitization protocol was able to reduce the reaction rate to less than 30%, so around 70% of patients had no reaction at all during desensitization,” said Dr. Wong, adding that nearly all desensitizations were completed successfully.
Dr. Wong had no disclosures.
HOUSTON – For rituximab patients undergoing desensitization, mast cell degranulation is a more effective predictor of hypersensitive reactions (HSR) than are the traditionally employed skin tests, according to a study presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“In this particular study, we were interested in investigating the roles of immunoglobulin E (IgE) in the mast cells in rituximab hypersensitivity,” said Dr. Johnson T. Wong of Massachusetts General Hospital, Boston, who presented the findings during a session dedicated to “Novel Insights in Drug Allergy.”
The study comprised 25 patients with persistent or severe rituximab sensitivity (RITS) who were treated at Massachusetts General between 2008 and 2013. Dr. Wong and his coinvestigators performed skin testing on 18 subjects, of which 7 (39%) reacted positively at least once during the course of testing.
HSR reactions occurred at similar rates in subjects who reacted positively and negatively to skin testing. Tryptase levels were taken in 18 subjects (72%), during 67% of the HSR desensitizations and 21% of the asymptomatic desensitizations.
Overall, elevated levels were noted in 21% of the HSR desensitizations.
The elevated tryptase levels in patients experiencing HSR indicates that mast cell degranulation is likely a major contributing factor in causing HSR, with cytokine release and tumor lysis also playing an important role, Dr. Wong said. Mast cell degranulations also points to an association with IgE mechanisms as a reliable indicator of HSR likelihood.
Dr. Wong and his coauthors concluded via tryptase level testing that asymptomatic mast cell degranulation happened very rarely, as only 1 out of 27 assessments (3%) indicated that result. One patient was excluded from the HSR desensitization cohort’s results because of probable mast cell activation syndrome, which caused abnormally elevated tryptase levels throughout the study period.
“In both positive and negative skin test patients, our desensitization protocol was able to reduce the reaction rate to less than 30%, so around 70% of patients had no reaction at all during desensitization,” said Dr. Wong, adding that nearly all desensitizations were completed successfully.
Dr. Wong had no disclosures.
AT THE 2015 AAAAI ANNUAL MEETING
Key clinical point: Look to mast cell degranulation, not skin tests, for accurate information regarding the likelihood of hypersensitive reactions in rituximab patients undergoing desensitization.
Major finding: Tryptase levels were elevated in 21% of patients who experienced hypersensitive reactions during desensitization.
Data source: Study of 25 patients with rituximab sensitivity at Massachusetts General Hospital.
Disclosures: Dr. Wong reported no relevant financial disclosures.