User login
For MD-IQ use only
Crohn’s disease research goes to the dogs
Why it might be better to be a dog person
Here’s that old debate again: Dogs or cats? You probably have your own opinion, but research presented at this year’s Digestive Disease Week may have tipped the scale by showing that children who lived with dogs may be less likely to have Crohn’s disease as adults.
The research was done by having approximately 4,300 people closely related to patients with Crohn’s disease fill out an environmental questionnaire. Using these data, the research team looked into environmental factors such as size of the families, where the home was, how many bathrooms the homes had, and quality of drinking water.
The researchers found that those who had or were exposed to dogs between the ages of 5 and 15 years were more likely to have healthy gut permeability and balanced microbes, which increased their protection against Crohn’s disease.
“Our study seems to add to others that have explored the ‘hygiene hypothesis’ which suggests that the lack of exposure to microbes early in life may lead to lack of immune regulation toward environmental microbes,” senior author Williams Turpin, PhD, said in the written statement.
The researchers aren’t sure why they didn’t get the same findings with cats, but Dr. Turpin theorized that dog owners tend to be outside more with their dogs or live in places with more green space, which are good protectors against Crohn’s disease.
It’s all good for dog owners, but do their pets’ parasites make you more attractive? Just more fuel for the ongoing debate.
Come for the history, stay for the fossilized parasites
Another week, another analysis of old British poop. LOTME really is your one-stop shop for all the important, hard-hitting news about historic parasites. You’re welcome, Internet.

The news this week is from Stonehenge, which is apparently kind of a big deal. Rocks in a circle, celestial calendar, cultural significance, whatever. We’re not here to talk about rocks. We’re here to talk about, uh, rocks. Smaller rocks. Specifically, coprolites, which are essentially poop turned into a rock. (Though now we’re imagining Stonehenge made out of fossilized poop rocks. Would it still be a big tourist destination? We can see both sides of the argument on that one.)
Archaeologists from the University of Cambridge have conducted an analysis of coprolites from Durrington Walls, a Neolithic settlement just a few kilometers from Stonehenge. The town dates to the same time that Stonehenge was constructed, and it’s believed that the residents were responsible for building the landmark. These coprolites, depending on what’s inside, can tell us a lot about how the builders of Stonehenge lived and, more specifically, how they ate.
In this case, the coprolites of one human and three dogs contained capillariid worm eggs. These worms come from cows, and when a human is typically infected, the eggs embed in the liver and do not pass through the body. Finding them in excrement indicates that the people were eating raw cow organs and feeding leftovers to their dogs. This is interesting, because a preponderance of pottery and cooking implements also found at the site indicates that the residents of Durrington Walls were spit-roasting or boiling their beef and pork. So the meat was cooked, but not the organs. That is an interesting dietary decision, ancient British people. Then again, modern British cuisine exists. At least now we know where they got it from.
This new research raises one other very important question: When are we going to get a full-on guided tour of all the important coprolite sites in Britain? They’ve clearly got plenty of them, and the tourist demand for ancient parasites must be sky-high. Come on, capitalism, follow through on this. We’d go.
Everyone lies: Food intake edition
Do you have any patients on special diets? Do you ask them if they are following those diets? Don’t bother, because they’re lying. Everyone lies about the food they eat. Everyone. Obese people lie, and nonobese people lie.

Investigators at the University of Essex in England asked 221 adults to keep food diaries, and then they checked on energy consumption by analyzing radioactive water levels in the participants’ urine over a 10-day period.
Underreporting of food consumption was rampant, even among those who were not obese. The obese subjects did underreport by a greater extent (1,200 calories per day) than did those who were not obese, who were off by only 800 calories, but the obese participants burned about 400 calories more each day than did the nonobese, so the difference was a wash.
Everyone ended up underreporting their calorie consumption by an average of about 900 calories, and the investigators were good enough to provide some food equivalents, tops on the list being three MacDonald’s cheeseburgers.
“Public health recommendations have historically relied heavily on self-reported energy intake values,” senior author Gavin Sandercock, PhD, said in a EurekAlert statement, and “recognising that the measures of energy intake are incorrect might result in the setting of more realistic targets.”
Maybe you can be more realistic with your patients, too. Go ahead and ask Mr. Smith about the burger sticking out of his coat pocket, because there are probably two more you can’t see. We’ve each got 900 calories hiding on us somewhere. Ours is usually pizza.
The art of the gallbladder
Ever thought you would see a portrait of a gallbladder hanging up in a gallery? Not just an artist’s rendition, but an actual photo from an actual patient? Well, you can at the Soloway Gallery in Brooklyn, N.Y., at least until June 12.

The artist? K.C. Joseph, MD, a general surgeon from St. Marie, Pa., who died in 2015. His daughter Melissa is the curator of the show and told ARTnews about the interesting connection her father had with art and surgery.
In 2010, Dr. Joseph gave his daughter a box of photos and said “Make me a famous artist,” she recalled. At first, “I was like, ‘These are weird,’ and then I put them under my bed for 10 years.”
Apparently he had been making art with his patients’ organs for about 15 years and had a system in which he put each one together. Before a surgery Dr. Joseph would make a note card with the patient’s name handwritten in calligraphy with a couple of pages taken out of the magazine from the waiting room as the backdrop. Afterward, when the patient was in recovery, the removed organ would be placed among the pages and the name card. A photo was taken with the same endoscope that was used for the procedure.
After the show’s debut, people reached out expressing their love for their photos. “I wish, before he died, I had asked him more questions about it,” Ms. Joseph told ARTnews. “I’m regretting it so much now, kicking myself.”
Who gets to take home an artsy photo of their gallbladder after getting it removed? Not us, that’s who. Each collage is a one-of-a-kind piece. They definitely should be framed and shown in an art gallery. Oh, right. Never mind.
Why it might be better to be a dog person
Here’s that old debate again: Dogs or cats? You probably have your own opinion, but research presented at this year’s Digestive Disease Week may have tipped the scale by showing that children who lived with dogs may be less likely to have Crohn’s disease as adults.
The research was done by having approximately 4,300 people closely related to patients with Crohn’s disease fill out an environmental questionnaire. Using these data, the research team looked into environmental factors such as size of the families, where the home was, how many bathrooms the homes had, and quality of drinking water.
The researchers found that those who had or were exposed to dogs between the ages of 5 and 15 years were more likely to have healthy gut permeability and balanced microbes, which increased their protection against Crohn’s disease.
“Our study seems to add to others that have explored the ‘hygiene hypothesis’ which suggests that the lack of exposure to microbes early in life may lead to lack of immune regulation toward environmental microbes,” senior author Williams Turpin, PhD, said in the written statement.
The researchers aren’t sure why they didn’t get the same findings with cats, but Dr. Turpin theorized that dog owners tend to be outside more with their dogs or live in places with more green space, which are good protectors against Crohn’s disease.
It’s all good for dog owners, but do their pets’ parasites make you more attractive? Just more fuel for the ongoing debate.
Come for the history, stay for the fossilized parasites
Another week, another analysis of old British poop. LOTME really is your one-stop shop for all the important, hard-hitting news about historic parasites. You’re welcome, Internet.
The news this week is from Stonehenge, which is apparently kind of a big deal. Rocks in a circle, celestial calendar, cultural significance, whatever. We’re not here to talk about rocks. We’re here to talk about, uh, rocks. Smaller rocks. Specifically, coprolites, which are essentially poop turned into a rock. (Though now we’re imagining Stonehenge made out of fossilized poop rocks. Would it still be a big tourist destination? We can see both sides of the argument on that one.)
Archaeologists from the University of Cambridge have conducted an analysis of coprolites from Durrington Walls, a Neolithic settlement just a few kilometers from Stonehenge. The town dates to the same time that Stonehenge was constructed, and it’s believed that the residents were responsible for building the landmark. These coprolites, depending on what’s inside, can tell us a lot about how the builders of Stonehenge lived and, more specifically, how they ate.
In this case, the coprolites of one human and three dogs contained capillariid worm eggs. These worms come from cows, and when a human is typically infected, the eggs embed in the liver and do not pass through the body. Finding them in excrement indicates that the people were eating raw cow organs and feeding leftovers to their dogs. This is interesting, because a preponderance of pottery and cooking implements also found at the site indicates that the residents of Durrington Walls were spit-roasting or boiling their beef and pork. So the meat was cooked, but not the organs. That is an interesting dietary decision, ancient British people. Then again, modern British cuisine exists. At least now we know where they got it from.
This new research raises one other very important question: When are we going to get a full-on guided tour of all the important coprolite sites in Britain? They’ve clearly got plenty of them, and the tourist demand for ancient parasites must be sky-high. Come on, capitalism, follow through on this. We’d go.
Everyone lies: Food intake edition
Do you have any patients on special diets? Do you ask them if they are following those diets? Don’t bother, because they’re lying. Everyone lies about the food they eat. Everyone. Obese people lie, and nonobese people lie.
Investigators at the University of Essex in England asked 221 adults to keep food diaries, and then they checked on energy consumption by analyzing radioactive water levels in the participants’ urine over a 10-day period.
Underreporting of food consumption was rampant, even among those who were not obese. The obese subjects did underreport by a greater extent (1,200 calories per day) than did those who were not obese, who were off by only 800 calories, but the obese participants burned about 400 calories more each day than did the nonobese, so the difference was a wash.
Everyone ended up underreporting their calorie consumption by an average of about 900 calories, and the investigators were good enough to provide some food equivalents, tops on the list being three MacDonald’s cheeseburgers.
“Public health recommendations have historically relied heavily on self-reported energy intake values,” senior author Gavin Sandercock, PhD, said in a EurekAlert statement, and “recognising that the measures of energy intake are incorrect might result in the setting of more realistic targets.”
Maybe you can be more realistic with your patients, too. Go ahead and ask Mr. Smith about the burger sticking out of his coat pocket, because there are probably two more you can’t see. We’ve each got 900 calories hiding on us somewhere. Ours is usually pizza.
The art of the gallbladder
Ever thought you would see a portrait of a gallbladder hanging up in a gallery? Not just an artist’s rendition, but an actual photo from an actual patient? Well, you can at the Soloway Gallery in Brooklyn, N.Y., at least until June 12.
The artist? K.C. Joseph, MD, a general surgeon from St. Marie, Pa., who died in 2015. His daughter Melissa is the curator of the show and told ARTnews about the interesting connection her father had with art and surgery.
In 2010, Dr. Joseph gave his daughter a box of photos and said “Make me a famous artist,” she recalled. At first, “I was like, ‘These are weird,’ and then I put them under my bed for 10 years.”
Apparently he had been making art with his patients’ organs for about 15 years and had a system in which he put each one together. Before a surgery Dr. Joseph would make a note card with the patient’s name handwritten in calligraphy with a couple of pages taken out of the magazine from the waiting room as the backdrop. Afterward, when the patient was in recovery, the removed organ would be placed among the pages and the name card. A photo was taken with the same endoscope that was used for the procedure.
After the show’s debut, people reached out expressing their love for their photos. “I wish, before he died, I had asked him more questions about it,” Ms. Joseph told ARTnews. “I’m regretting it so much now, kicking myself.”
Who gets to take home an artsy photo of their gallbladder after getting it removed? Not us, that’s who. Each collage is a one-of-a-kind piece. They definitely should be framed and shown in an art gallery. Oh, right. Never mind.
Why it might be better to be a dog person
Here’s that old debate again: Dogs or cats? You probably have your own opinion, but research presented at this year’s Digestive Disease Week may have tipped the scale by showing that children who lived with dogs may be less likely to have Crohn’s disease as adults.
The research was done by having approximately 4,300 people closely related to patients with Crohn’s disease fill out an environmental questionnaire. Using these data, the research team looked into environmental factors such as size of the families, where the home was, how many bathrooms the homes had, and quality of drinking water.
The researchers found that those who had or were exposed to dogs between the ages of 5 and 15 years were more likely to have healthy gut permeability and balanced microbes, which increased their protection against Crohn’s disease.
“Our study seems to add to others that have explored the ‘hygiene hypothesis’ which suggests that the lack of exposure to microbes early in life may lead to lack of immune regulation toward environmental microbes,” senior author Williams Turpin, PhD, said in the written statement.
The researchers aren’t sure why they didn’t get the same findings with cats, but Dr. Turpin theorized that dog owners tend to be outside more with their dogs or live in places with more green space, which are good protectors against Crohn’s disease.
It’s all good for dog owners, but do their pets’ parasites make you more attractive? Just more fuel for the ongoing debate.
Come for the history, stay for the fossilized parasites
Another week, another analysis of old British poop. LOTME really is your one-stop shop for all the important, hard-hitting news about historic parasites. You’re welcome, Internet.
The news this week is from Stonehenge, which is apparently kind of a big deal. Rocks in a circle, celestial calendar, cultural significance, whatever. We’re not here to talk about rocks. We’re here to talk about, uh, rocks. Smaller rocks. Specifically, coprolites, which are essentially poop turned into a rock. (Though now we’re imagining Stonehenge made out of fossilized poop rocks. Would it still be a big tourist destination? We can see both sides of the argument on that one.)
Archaeologists from the University of Cambridge have conducted an analysis of coprolites from Durrington Walls, a Neolithic settlement just a few kilometers from Stonehenge. The town dates to the same time that Stonehenge was constructed, and it’s believed that the residents were responsible for building the landmark. These coprolites, depending on what’s inside, can tell us a lot about how the builders of Stonehenge lived and, more specifically, how they ate.
In this case, the coprolites of one human and three dogs contained capillariid worm eggs. These worms come from cows, and when a human is typically infected, the eggs embed in the liver and do not pass through the body. Finding them in excrement indicates that the people were eating raw cow organs and feeding leftovers to their dogs. This is interesting, because a preponderance of pottery and cooking implements also found at the site indicates that the residents of Durrington Walls were spit-roasting or boiling their beef and pork. So the meat was cooked, but not the organs. That is an interesting dietary decision, ancient British people. Then again, modern British cuisine exists. At least now we know where they got it from.
This new research raises one other very important question: When are we going to get a full-on guided tour of all the important coprolite sites in Britain? They’ve clearly got plenty of them, and the tourist demand for ancient parasites must be sky-high. Come on, capitalism, follow through on this. We’d go.
Everyone lies: Food intake edition
Do you have any patients on special diets? Do you ask them if they are following those diets? Don’t bother, because they’re lying. Everyone lies about the food they eat. Everyone. Obese people lie, and nonobese people lie.
Investigators at the University of Essex in England asked 221 adults to keep food diaries, and then they checked on energy consumption by analyzing radioactive water levels in the participants’ urine over a 10-day period.
Underreporting of food consumption was rampant, even among those who were not obese. The obese subjects did underreport by a greater extent (1,200 calories per day) than did those who were not obese, who were off by only 800 calories, but the obese participants burned about 400 calories more each day than did the nonobese, so the difference was a wash.
Everyone ended up underreporting their calorie consumption by an average of about 900 calories, and the investigators were good enough to provide some food equivalents, tops on the list being three MacDonald’s cheeseburgers.
“Public health recommendations have historically relied heavily on self-reported energy intake values,” senior author Gavin Sandercock, PhD, said in a EurekAlert statement, and “recognising that the measures of energy intake are incorrect might result in the setting of more realistic targets.”
Maybe you can be more realistic with your patients, too. Go ahead and ask Mr. Smith about the burger sticking out of his coat pocket, because there are probably two more you can’t see. We’ve each got 900 calories hiding on us somewhere. Ours is usually pizza.
The art of the gallbladder
Ever thought you would see a portrait of a gallbladder hanging up in a gallery? Not just an artist’s rendition, but an actual photo from an actual patient? Well, you can at the Soloway Gallery in Brooklyn, N.Y., at least until June 12.
The artist? K.C. Joseph, MD, a general surgeon from St. Marie, Pa., who died in 2015. His daughter Melissa is the curator of the show and told ARTnews about the interesting connection her father had with art and surgery.
In 2010, Dr. Joseph gave his daughter a box of photos and said “Make me a famous artist,” she recalled. At first, “I was like, ‘These are weird,’ and then I put them under my bed for 10 years.”
Apparently he had been making art with his patients’ organs for about 15 years and had a system in which he put each one together. Before a surgery Dr. Joseph would make a note card with the patient’s name handwritten in calligraphy with a couple of pages taken out of the magazine from the waiting room as the backdrop. Afterward, when the patient was in recovery, the removed organ would be placed among the pages and the name card. A photo was taken with the same endoscope that was used for the procedure.
After the show’s debut, people reached out expressing their love for their photos. “I wish, before he died, I had asked him more questions about it,” Ms. Joseph told ARTnews. “I’m regretting it so much now, kicking myself.”
Who gets to take home an artsy photo of their gallbladder after getting it removed? Not us, that’s who. Each collage is a one-of-a-kind piece. They definitely should be framed and shown in an art gallery. Oh, right. Never mind.
Topical tranexamic acid reduces postop bleeding following Mohs surgery
The use of adjunctive , in a double-blind, randomized, controlled trial.
The findings suggest that “topical TXA application is an inexpensive and easy topical preventative measure to consider adding to the wound care of granulating defects in the setting of Mohs micrographic surgery,” first author Brianna Castillo, MD, chief dermatology resident at the University of Missouri, Columbia, told this news organization.

The study results were presented at the annual meeting of the American College of Mohs Surgery.
In wound healing by second intent after Mohs micrographic surgery, postoperative bleeding is common and can lead to patient distress, as well as return visits or emergency care, resulting in additional health care costs, Dr. Castillo said.
Topical TXA, an antifibrinolytic, synthetic lysine analogue that prevents blood clots from breaking down, is commonly used in surgical settings including cardiothoracic, orthopedic, gynecologic, oral, and trauma surgery, showing no increased risk of thrombotic events. However, its use is relatively new in dermatology.
TXA is approved by the Food and Drug Administration only as an oral formulation for menorrhagia in women and as a short-term preventative measure for hemophilia; however, other formulations are available for topical and subcutaneous uses, Dr. Castillo noted.
To evaluate the potential benefits of the treatment in postsurgical Mohs microsurgery bleeding, Dr. Castillo and colleagues enrolled 124 patients undergoing the surgery between October 2020 and December 2021 who had surgical defects deemed appropriate for second intention healing.
The patients were randomized to groups of 62 patients each to receive normal saline-soaked Telfa pads applied to the wound bed upon completion of surgery or TXA 25 mg/mL at a volume of 1 mL/cm2-soaked Telfa pads to the wound bed upon completion of the surgery.
In both groups, a standard pressure dressing was placed on top of the Telfa pads.
Most participants were men (90 vs. 34 patients), 45 were taking antiplatelet therapy, and 20 were taking anticoagulants, and in all cases, patients were similarly randomized in the two groups. Most of the surgical defects were on the head and neck or an extremity, and most (74) were under 2 cm.
All patients were provided with instructions to apply pressure to their wounds and to report bleeding complications. They were interviewed by phone 3 days following their surgeries regarding postoperative bleeding and any potential issues relating to the TXA treatment.
In follow-up interviews, six patients in the placebo group (9.7%) reported active bleeding from their wounds within 48 hours of surgery, with one patient requiring an intervention, while there were no reports of bleeding in the TXA group (P = .028). No side effects were reported in either group.
In the setting of Mohs micrographic surgery, subcutaneous TXA has previously been studied as an intraoperative hemostatic agent, with bleeding measured prior to the second layer or closure, Dr. Castillo explained. However, “no studies have evaluated topical TXA with the aim to reduce postoperative bleeding in the setting of Mohs micrographic surgery,” she said.
Dr. Castillo noted that topical TXA is relatively inexpensive and typically available in hospital pharmacies. “It’s only about $7 per vial of 10 ccs and we do dilute it,” she noted during the session. “It has a pretty good shelf-life and does not have to be refrigerated.”
“We have implemented this into our practice at the University of Missouri,” she added.
Commenting on the study, M. Laurin Council, MD, associate professor of dermatology in the division of dermatology, department of internal medicine, Washington University, St. Louis, noted that second intention healing is “an excellent option for certain patients after skin cancer removal.
“One problem with this method, however, is that postsurgical wounds may bleed in the hours after a procedure, [and] this can be incredibly distressing to patients and their families,” she told this news organization.
“The study presented here shows great promise for the drug TXA for preventing postsurgical bleeding in this subset of patients,” said Dr. Council, director of dermatologic surgery and director of micrographic surgery and the dermatologic oncology fellowship at Washington University.
Commenting that “the results are impressive,” she noted the study had some limitations. “This is a small pilot study, and we don’t know about confounding factors in each group, such as the proportion of patients who are on blood thinners or who have low platelets, and therefore trouble clotting, for example.”
The authors have reported no relevant financial relationships. Dr. Council has consulted for AbbVie, Castle Biosciences, and Sanofi-Genzyme/Regeneron; however, the consulting was not relevant to the current study.
A version of this article first appeared on Medscape.com.
The use of adjunctive , in a double-blind, randomized, controlled trial.
The findings suggest that “topical TXA application is an inexpensive and easy topical preventative measure to consider adding to the wound care of granulating defects in the setting of Mohs micrographic surgery,” first author Brianna Castillo, MD, chief dermatology resident at the University of Missouri, Columbia, told this news organization.
The study results were presented at the annual meeting of the American College of Mohs Surgery.
In wound healing by second intent after Mohs micrographic surgery, postoperative bleeding is common and can lead to patient distress, as well as return visits or emergency care, resulting in additional health care costs, Dr. Castillo said.
Topical TXA, an antifibrinolytic, synthetic lysine analogue that prevents blood clots from breaking down, is commonly used in surgical settings including cardiothoracic, orthopedic, gynecologic, oral, and trauma surgery, showing no increased risk of thrombotic events. However, its use is relatively new in dermatology.
TXA is approved by the Food and Drug Administration only as an oral formulation for menorrhagia in women and as a short-term preventative measure for hemophilia; however, other formulations are available for topical and subcutaneous uses, Dr. Castillo noted.
To evaluate the potential benefits of the treatment in postsurgical Mohs microsurgery bleeding, Dr. Castillo and colleagues enrolled 124 patients undergoing the surgery between October 2020 and December 2021 who had surgical defects deemed appropriate for second intention healing.
The patients were randomized to groups of 62 patients each to receive normal saline-soaked Telfa pads applied to the wound bed upon completion of surgery or TXA 25 mg/mL at a volume of 1 mL/cm2-soaked Telfa pads to the wound bed upon completion of the surgery.
In both groups, a standard pressure dressing was placed on top of the Telfa pads.
Most participants were men (90 vs. 34 patients), 45 were taking antiplatelet therapy, and 20 were taking anticoagulants, and in all cases, patients were similarly randomized in the two groups. Most of the surgical defects were on the head and neck or an extremity, and most (74) were under 2 cm.
All patients were provided with instructions to apply pressure to their wounds and to report bleeding complications. They were interviewed by phone 3 days following their surgeries regarding postoperative bleeding and any potential issues relating to the TXA treatment.
In follow-up interviews, six patients in the placebo group (9.7%) reported active bleeding from their wounds within 48 hours of surgery, with one patient requiring an intervention, while there were no reports of bleeding in the TXA group (P = .028). No side effects were reported in either group.
In the setting of Mohs micrographic surgery, subcutaneous TXA has previously been studied as an intraoperative hemostatic agent, with bleeding measured prior to the second layer or closure, Dr. Castillo explained. However, “no studies have evaluated topical TXA with the aim to reduce postoperative bleeding in the setting of Mohs micrographic surgery,” she said.
Dr. Castillo noted that topical TXA is relatively inexpensive and typically available in hospital pharmacies. “It’s only about $7 per vial of 10 ccs and we do dilute it,” she noted during the session. “It has a pretty good shelf-life and does not have to be refrigerated.”
“We have implemented this into our practice at the University of Missouri,” she added.
Commenting on the study, M. Laurin Council, MD, associate professor of dermatology in the division of dermatology, department of internal medicine, Washington University, St. Louis, noted that second intention healing is “an excellent option for certain patients after skin cancer removal.
“One problem with this method, however, is that postsurgical wounds may bleed in the hours after a procedure, [and] this can be incredibly distressing to patients and their families,” she told this news organization.
“The study presented here shows great promise for the drug TXA for preventing postsurgical bleeding in this subset of patients,” said Dr. Council, director of dermatologic surgery and director of micrographic surgery and the dermatologic oncology fellowship at Washington University.
Commenting that “the results are impressive,” she noted the study had some limitations. “This is a small pilot study, and we don’t know about confounding factors in each group, such as the proportion of patients who are on blood thinners or who have low platelets, and therefore trouble clotting, for example.”
The authors have reported no relevant financial relationships. Dr. Council has consulted for AbbVie, Castle Biosciences, and Sanofi-Genzyme/Regeneron; however, the consulting was not relevant to the current study.
A version of this article first appeared on Medscape.com.
The use of adjunctive , in a double-blind, randomized, controlled trial.
The findings suggest that “topical TXA application is an inexpensive and easy topical preventative measure to consider adding to the wound care of granulating defects in the setting of Mohs micrographic surgery,” first author Brianna Castillo, MD, chief dermatology resident at the University of Missouri, Columbia, told this news organization.
The study results were presented at the annual meeting of the American College of Mohs Surgery.
In wound healing by second intent after Mohs micrographic surgery, postoperative bleeding is common and can lead to patient distress, as well as return visits or emergency care, resulting in additional health care costs, Dr. Castillo said.
Topical TXA, an antifibrinolytic, synthetic lysine analogue that prevents blood clots from breaking down, is commonly used in surgical settings including cardiothoracic, orthopedic, gynecologic, oral, and trauma surgery, showing no increased risk of thrombotic events. However, its use is relatively new in dermatology.
TXA is approved by the Food and Drug Administration only as an oral formulation for menorrhagia in women and as a short-term preventative measure for hemophilia; however, other formulations are available for topical and subcutaneous uses, Dr. Castillo noted.
To evaluate the potential benefits of the treatment in postsurgical Mohs microsurgery bleeding, Dr. Castillo and colleagues enrolled 124 patients undergoing the surgery between October 2020 and December 2021 who had surgical defects deemed appropriate for second intention healing.
The patients were randomized to groups of 62 patients each to receive normal saline-soaked Telfa pads applied to the wound bed upon completion of surgery or TXA 25 mg/mL at a volume of 1 mL/cm2-soaked Telfa pads to the wound bed upon completion of the surgery.
In both groups, a standard pressure dressing was placed on top of the Telfa pads.
Most participants were men (90 vs. 34 patients), 45 were taking antiplatelet therapy, and 20 were taking anticoagulants, and in all cases, patients were similarly randomized in the two groups. Most of the surgical defects were on the head and neck or an extremity, and most (74) were under 2 cm.
All patients were provided with instructions to apply pressure to their wounds and to report bleeding complications. They were interviewed by phone 3 days following their surgeries regarding postoperative bleeding and any potential issues relating to the TXA treatment.
In follow-up interviews, six patients in the placebo group (9.7%) reported active bleeding from their wounds within 48 hours of surgery, with one patient requiring an intervention, while there were no reports of bleeding in the TXA group (P = .028). No side effects were reported in either group.
In the setting of Mohs micrographic surgery, subcutaneous TXA has previously been studied as an intraoperative hemostatic agent, with bleeding measured prior to the second layer or closure, Dr. Castillo explained. However, “no studies have evaluated topical TXA with the aim to reduce postoperative bleeding in the setting of Mohs micrographic surgery,” she said.
Dr. Castillo noted that topical TXA is relatively inexpensive and typically available in hospital pharmacies. “It’s only about $7 per vial of 10 ccs and we do dilute it,” she noted during the session. “It has a pretty good shelf-life and does not have to be refrigerated.”
“We have implemented this into our practice at the University of Missouri,” she added.
Commenting on the study, M. Laurin Council, MD, associate professor of dermatology in the division of dermatology, department of internal medicine, Washington University, St. Louis, noted that second intention healing is “an excellent option for certain patients after skin cancer removal.
“One problem with this method, however, is that postsurgical wounds may bleed in the hours after a procedure, [and] this can be incredibly distressing to patients and their families,” she told this news organization.
“The study presented here shows great promise for the drug TXA for preventing postsurgical bleeding in this subset of patients,” said Dr. Council, director of dermatologic surgery and director of micrographic surgery and the dermatologic oncology fellowship at Washington University.
Commenting that “the results are impressive,” she noted the study had some limitations. “This is a small pilot study, and we don’t know about confounding factors in each group, such as the proportion of patients who are on blood thinners or who have low platelets, and therefore trouble clotting, for example.”
The authors have reported no relevant financial relationships. Dr. Council has consulted for AbbVie, Castle Biosciences, and Sanofi-Genzyme/Regeneron; however, the consulting was not relevant to the current study.
A version of this article first appeared on Medscape.com.
FROM THE ACMS ANNUAL MEETING
APA targets structural racism, offers solutions
, released to coincide with the annual meeting of the American Psychiatric Association.
The hope is this special issue will “motivate clinicians, educators, and researchers to take actions that will make a difference,” Ned H. Kalin, MD, AJP editor-in-chief, wrotes in an editor’s note.
“We cannot overestimate the impact of structural racism from the standpoint of its consequences related to mental health issues and mental health care,” Dr. Kalin said during an APA press briefing.
“This is one of our highest priorities, if not our highest priority,” he noted. The journal is the “voice of American and international psychiatry” and is a “great vehicle” for moving the field forward, he added.
Articles in the issue highlight “new directions to understand and eliminate mental health disparities [through a] multidimensional lens,” wrote Crystal L. Barksdale, PhD, health scientist administrator and program director with the National Institute on Minority Health and Health Disparities. Dr. Barksdale was guest editor for the issue.
A new agenda for change
In one article, Margarita Alegría, PhD, chief of the disparities research unit at Massachusetts General Hospital, Boston, and colleagues, wrote that the Biden Administration’s new budget offers the opportunity to redesign mental health research and service delivery in marginalized communities.
Given the rising mental health crisis in the U.S., the FY22 budget includes $1.6 billion for the community mental health services block grant program, which is more than double the money allocated in FY21.
Dr. Alegría and colleagues describe several interventions that have “sound evidence” of improving mental health or related outcomes among people of color in the U.S. within 5 years – by addressing social determinants of health.
They include universal school meal programs, community-based interventions delivered by paraprofessionals in after-school recreational programs, individual placement and support for employment, mental health literacy programs, senior centers offering health promotion activities, and a chronic disease self-management program.
Dr. Alegría noted that reducing structural racism and mental health disparities requires multilevel structural solutions and action by multiple stakeholders. In essence, “it takes a village,” she said.
A national conversation
Another article highlighted at the press briefing focuses on structural racism as it relates to youth suicide prevention.
Studies have shown the risk for suicide is higher earlier in life for youth of color. Suicide rates peak in adolescence and young adulthood for youth of color; for White populations, the peak happens in middle age and later life, noted lead author Kiara Alvarez, PhD, research scientist with Mass General’s disparities research unit.
However, there are well documented mental health service disparities where youth of color experiencing suicidal thoughts and behaviors have lower rates of access to needed services. They also have delays in access compared with their White peers, Dr. Alvarez said.
The authors propose a framework to address structural racism and mental health disparities as it relates to youth suicide prevention, with a focus on systems that are “preventive, rather than reactive; restorative, rather than punitive; and community-driven, rather than externally imposed.
“Ultimately, only structural solutions can dismantle structural racism,” they wrote.
The special issue of AJP aligns with the theme of this year’s APA meeting, which is the social determinants of mental health.
“Mental health has clearly become part of the national conversation. This has given us the opportunity to discuss how factors outside of the office and hospitals can impact the lives of many with mental illness and substance use disorder,” APA President Vivian B. Pender, MD, said during a preconference press briefing.
“These factors may include where you live, the air you breathe, how you’re educated, exposure to violence, and the impact of racism. These social determinants have become especially relevant to good mental health,” Dr. Pender said.
The research was supported by grants from the National Institute of Mental Health, the National Institute on Minority Health and Health Disparities, the National Institute of Drug Abuse, the National Institute of Alcohol Abuse and Alcoholism, and the National Institute of Child Health and Human Development. Dr. Kalin, Dr. Barksdale, Dr. Alegría, Dr. Alvarez, and Dr. Pender have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, released to coincide with the annual meeting of the American Psychiatric Association.
The hope is this special issue will “motivate clinicians, educators, and researchers to take actions that will make a difference,” Ned H. Kalin, MD, AJP editor-in-chief, wrotes in an editor’s note.
“We cannot overestimate the impact of structural racism from the standpoint of its consequences related to mental health issues and mental health care,” Dr. Kalin said during an APA press briefing.
“This is one of our highest priorities, if not our highest priority,” he noted. The journal is the “voice of American and international psychiatry” and is a “great vehicle” for moving the field forward, he added.
Articles in the issue highlight “new directions to understand and eliminate mental health disparities [through a] multidimensional lens,” wrote Crystal L. Barksdale, PhD, health scientist administrator and program director with the National Institute on Minority Health and Health Disparities. Dr. Barksdale was guest editor for the issue.
A new agenda for change
In one article, Margarita Alegría, PhD, chief of the disparities research unit at Massachusetts General Hospital, Boston, and colleagues, wrote that the Biden Administration’s new budget offers the opportunity to redesign mental health research and service delivery in marginalized communities.
Given the rising mental health crisis in the U.S., the FY22 budget includes $1.6 billion for the community mental health services block grant program, which is more than double the money allocated in FY21.
Dr. Alegría and colleagues describe several interventions that have “sound evidence” of improving mental health or related outcomes among people of color in the U.S. within 5 years – by addressing social determinants of health.
They include universal school meal programs, community-based interventions delivered by paraprofessionals in after-school recreational programs, individual placement and support for employment, mental health literacy programs, senior centers offering health promotion activities, and a chronic disease self-management program.
Dr. Alegría noted that reducing structural racism and mental health disparities requires multilevel structural solutions and action by multiple stakeholders. In essence, “it takes a village,” she said.
A national conversation
Another article highlighted at the press briefing focuses on structural racism as it relates to youth suicide prevention.
Studies have shown the risk for suicide is higher earlier in life for youth of color. Suicide rates peak in adolescence and young adulthood for youth of color; for White populations, the peak happens in middle age and later life, noted lead author Kiara Alvarez, PhD, research scientist with Mass General’s disparities research unit.
However, there are well documented mental health service disparities where youth of color experiencing suicidal thoughts and behaviors have lower rates of access to needed services. They also have delays in access compared with their White peers, Dr. Alvarez said.
The authors propose a framework to address structural racism and mental health disparities as it relates to youth suicide prevention, with a focus on systems that are “preventive, rather than reactive; restorative, rather than punitive; and community-driven, rather than externally imposed.
“Ultimately, only structural solutions can dismantle structural racism,” they wrote.
The special issue of AJP aligns with the theme of this year’s APA meeting, which is the social determinants of mental health.
“Mental health has clearly become part of the national conversation. This has given us the opportunity to discuss how factors outside of the office and hospitals can impact the lives of many with mental illness and substance use disorder,” APA President Vivian B. Pender, MD, said during a preconference press briefing.
“These factors may include where you live, the air you breathe, how you’re educated, exposure to violence, and the impact of racism. These social determinants have become especially relevant to good mental health,” Dr. Pender said.
The research was supported by grants from the National Institute of Mental Health, the National Institute on Minority Health and Health Disparities, the National Institute of Drug Abuse, the National Institute of Alcohol Abuse and Alcoholism, and the National Institute of Child Health and Human Development. Dr. Kalin, Dr. Barksdale, Dr. Alegría, Dr. Alvarez, and Dr. Pender have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, released to coincide with the annual meeting of the American Psychiatric Association.
The hope is this special issue will “motivate clinicians, educators, and researchers to take actions that will make a difference,” Ned H. Kalin, MD, AJP editor-in-chief, wrotes in an editor’s note.
“We cannot overestimate the impact of structural racism from the standpoint of its consequences related to mental health issues and mental health care,” Dr. Kalin said during an APA press briefing.
“This is one of our highest priorities, if not our highest priority,” he noted. The journal is the “voice of American and international psychiatry” and is a “great vehicle” for moving the field forward, he added.
Articles in the issue highlight “new directions to understand and eliminate mental health disparities [through a] multidimensional lens,” wrote Crystal L. Barksdale, PhD, health scientist administrator and program director with the National Institute on Minority Health and Health Disparities. Dr. Barksdale was guest editor for the issue.
A new agenda for change
In one article, Margarita Alegría, PhD, chief of the disparities research unit at Massachusetts General Hospital, Boston, and colleagues, wrote that the Biden Administration’s new budget offers the opportunity to redesign mental health research and service delivery in marginalized communities.
Given the rising mental health crisis in the U.S., the FY22 budget includes $1.6 billion for the community mental health services block grant program, which is more than double the money allocated in FY21.
Dr. Alegría and colleagues describe several interventions that have “sound evidence” of improving mental health or related outcomes among people of color in the U.S. within 5 years – by addressing social determinants of health.
They include universal school meal programs, community-based interventions delivered by paraprofessionals in after-school recreational programs, individual placement and support for employment, mental health literacy programs, senior centers offering health promotion activities, and a chronic disease self-management program.
Dr. Alegría noted that reducing structural racism and mental health disparities requires multilevel structural solutions and action by multiple stakeholders. In essence, “it takes a village,” she said.
A national conversation
Another article highlighted at the press briefing focuses on structural racism as it relates to youth suicide prevention.
Studies have shown the risk for suicide is higher earlier in life for youth of color. Suicide rates peak in adolescence and young adulthood for youth of color; for White populations, the peak happens in middle age and later life, noted lead author Kiara Alvarez, PhD, research scientist with Mass General’s disparities research unit.
However, there are well documented mental health service disparities where youth of color experiencing suicidal thoughts and behaviors have lower rates of access to needed services. They also have delays in access compared with their White peers, Dr. Alvarez said.
The authors propose a framework to address structural racism and mental health disparities as it relates to youth suicide prevention, with a focus on systems that are “preventive, rather than reactive; restorative, rather than punitive; and community-driven, rather than externally imposed.
“Ultimately, only structural solutions can dismantle structural racism,” they wrote.
The special issue of AJP aligns with the theme of this year’s APA meeting, which is the social determinants of mental health.
“Mental health has clearly become part of the national conversation. This has given us the opportunity to discuss how factors outside of the office and hospitals can impact the lives of many with mental illness and substance use disorder,” APA President Vivian B. Pender, MD, said during a preconference press briefing.
“These factors may include where you live, the air you breathe, how you’re educated, exposure to violence, and the impact of racism. These social determinants have become especially relevant to good mental health,” Dr. Pender said.
The research was supported by grants from the National Institute of Mental Health, the National Institute on Minority Health and Health Disparities, the National Institute of Drug Abuse, the National Institute of Alcohol Abuse and Alcoholism, and the National Institute of Child Health and Human Development. Dr. Kalin, Dr. Barksdale, Dr. Alegría, Dr. Alvarez, and Dr. Pender have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
PA convicted of distributing more than 1.2 million opioid pills
A federal sting operation led to the recent conviction of a Texas physician assistant on charges of illegally prescribing a total of $3 million in drugs to patients at two “pill mill” clinics in Houston and helping others do the same.
The May 20 conviction of Charles Thompson, 76, of Houston, was based on charges of distributing more than 1.2 million opioid pills to thousands of individuals posing as patients at two pain management clinics, according to the U.S. Department of Justice.
Thompson’s conviction was the latest legal action in a string of cases involving the operation, including a doctor convicted in March who worked with Thompson at the West Parker Medical Clinic. Internist James Pierre, MD, 52, faces charges of unlawfully prescribing more than $1 million worth of opioid hydrocodone, according to federal officials.
Thompson also worked at Priority Wellness Clinic. Six people have pled guilty in connection with their conduct at West Parker or Priority Wellness, the justice department reported.
From June 2015 through July 2016, while Thompson was at West Parker, he helped Dr. Pierre unlawfully prescribe hydrocodone and the muscle relaxant carisoprodol, a combination of controlled substances for pain management known as the “Las Vegas cocktail,” to people in the sting operations pretending to be patients, authorities stated.
Thompson also distributed unlawful prescriptions for carisoprodol. So-called “runners” brought numerous people to pose as patients at West Parker and paid the clinic about $220 to $500 in cash for each visit that resulted in prescriptions for dangerous drugs. Throughout the scheme, West Parker pocketed about $1.75 million from prescriptions; Thompson was paid more than $208,000.
According to authorities, Thompson also helped others illegally prescribe controlled substances, including hydrocodone and oxycodone, from May to July 2017 at Priority Wellness, which opened in December 2016 after West Parker closed.
Priority Wellness reportedly operated as a pill mill similar to West Parker’s. Runners brought people posing as patients to Priority Wellness and paid the clinic between $300 and $600. The cost depended on whether the purported patient received a prescription for hydrocodone or oxycodone, almost always prescribed in combination with carisoprodol, authorities said. Throughout the scheme, Priority Wellness made about $1.1 million, and Thompson made between $700 and $900 a day.
He was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and seven counts of unlawfully distributing and dispensing controlled substances in connection with his conduct at West Parker. For his conduct at Priority Wellness, he was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and one count of unlawfully distributing and dispensing controlled substances.
He faces up to 20 years in prison for each count of conviction with sentencing scheduled for Oct. 3.
A version of this article first appeared on Medscape.com.
A federal sting operation led to the recent conviction of a Texas physician assistant on charges of illegally prescribing a total of $3 million in drugs to patients at two “pill mill” clinics in Houston and helping others do the same.
The May 20 conviction of Charles Thompson, 76, of Houston, was based on charges of distributing more than 1.2 million opioid pills to thousands of individuals posing as patients at two pain management clinics, according to the U.S. Department of Justice.
Thompson’s conviction was the latest legal action in a string of cases involving the operation, including a doctor convicted in March who worked with Thompson at the West Parker Medical Clinic. Internist James Pierre, MD, 52, faces charges of unlawfully prescribing more than $1 million worth of opioid hydrocodone, according to federal officials.
Thompson also worked at Priority Wellness Clinic. Six people have pled guilty in connection with their conduct at West Parker or Priority Wellness, the justice department reported.
From June 2015 through July 2016, while Thompson was at West Parker, he helped Dr. Pierre unlawfully prescribe hydrocodone and the muscle relaxant carisoprodol, a combination of controlled substances for pain management known as the “Las Vegas cocktail,” to people in the sting operations pretending to be patients, authorities stated.
Thompson also distributed unlawful prescriptions for carisoprodol. So-called “runners” brought numerous people to pose as patients at West Parker and paid the clinic about $220 to $500 in cash for each visit that resulted in prescriptions for dangerous drugs. Throughout the scheme, West Parker pocketed about $1.75 million from prescriptions; Thompson was paid more than $208,000.
According to authorities, Thompson also helped others illegally prescribe controlled substances, including hydrocodone and oxycodone, from May to July 2017 at Priority Wellness, which opened in December 2016 after West Parker closed.
Priority Wellness reportedly operated as a pill mill similar to West Parker’s. Runners brought people posing as patients to Priority Wellness and paid the clinic between $300 and $600. The cost depended on whether the purported patient received a prescription for hydrocodone or oxycodone, almost always prescribed in combination with carisoprodol, authorities said. Throughout the scheme, Priority Wellness made about $1.1 million, and Thompson made between $700 and $900 a day.
He was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and seven counts of unlawfully distributing and dispensing controlled substances in connection with his conduct at West Parker. For his conduct at Priority Wellness, he was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and one count of unlawfully distributing and dispensing controlled substances.
He faces up to 20 years in prison for each count of conviction with sentencing scheduled for Oct. 3.
A version of this article first appeared on Medscape.com.
A federal sting operation led to the recent conviction of a Texas physician assistant on charges of illegally prescribing a total of $3 million in drugs to patients at two “pill mill” clinics in Houston and helping others do the same.
The May 20 conviction of Charles Thompson, 76, of Houston, was based on charges of distributing more than 1.2 million opioid pills to thousands of individuals posing as patients at two pain management clinics, according to the U.S. Department of Justice.
Thompson’s conviction was the latest legal action in a string of cases involving the operation, including a doctor convicted in March who worked with Thompson at the West Parker Medical Clinic. Internist James Pierre, MD, 52, faces charges of unlawfully prescribing more than $1 million worth of opioid hydrocodone, according to federal officials.
Thompson also worked at Priority Wellness Clinic. Six people have pled guilty in connection with their conduct at West Parker or Priority Wellness, the justice department reported.
From June 2015 through July 2016, while Thompson was at West Parker, he helped Dr. Pierre unlawfully prescribe hydrocodone and the muscle relaxant carisoprodol, a combination of controlled substances for pain management known as the “Las Vegas cocktail,” to people in the sting operations pretending to be patients, authorities stated.
Thompson also distributed unlawful prescriptions for carisoprodol. So-called “runners” brought numerous people to pose as patients at West Parker and paid the clinic about $220 to $500 in cash for each visit that resulted in prescriptions for dangerous drugs. Throughout the scheme, West Parker pocketed about $1.75 million from prescriptions; Thompson was paid more than $208,000.
According to authorities, Thompson also helped others illegally prescribe controlled substances, including hydrocodone and oxycodone, from May to July 2017 at Priority Wellness, which opened in December 2016 after West Parker closed.
Priority Wellness reportedly operated as a pill mill similar to West Parker’s. Runners brought people posing as patients to Priority Wellness and paid the clinic between $300 and $600. The cost depended on whether the purported patient received a prescription for hydrocodone or oxycodone, almost always prescribed in combination with carisoprodol, authorities said. Throughout the scheme, Priority Wellness made about $1.1 million, and Thompson made between $700 and $900 a day.
He was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and seven counts of unlawfully distributing and dispensing controlled substances in connection with his conduct at West Parker. For his conduct at Priority Wellness, he was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and one count of unlawfully distributing and dispensing controlled substances.
He faces up to 20 years in prison for each count of conviction with sentencing scheduled for Oct. 3.
A version of this article first appeared on Medscape.com.
Third-generation Black woman physician makes cancer research history
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
A psychiatric patient confesses to murder: Now what?
NEW ORLEANS – The patient, a 60-year-old woman who’d just tried to kill herself by overdosing on gabapentin, felt the need to make a confession. As she told a resident psychiatrist late one night at a Philadelphia crisis response center, she’d just murdered two people and buried them in her backyard. More details kept coming, including who was dead and where their bodies were.
It didn’t take long for the attending physician’s phone to ring as the resident sought guidance. This wasn’t a typical “duty to warn” case since there was no one to warn of a threat of violence. But then what kind of case was it? As Meghan Musselman, MD, and colleagues noted in a report presented at the annual meeting of the American Psychiatric Association, the law and medical ethics didn’t present a clear-cut solution to whether the patient’s claim should be reported to the authorities.

“This was much more of a gray zone case than we typically see,” said Dr. Musselman, of the department of psychiatry at Temple University in Philadelphia, in an interview. “If someone is threatening to harm someone, most states have statutes about what to do in that situation. The same doesn’t really exist for when the crime has already happened.”
Even so, might the existing “duty to warn/protect” laws be helpful as a guide to what to do? Maybe, but it’s complicated. The laws, which address the waiving of therapist-patient confidentiality when violence is threatened, are widely variable. Some don’t specifically cover psychiatrists, according to the National Conference of State Legislatures. Some simply allow – but don’t require – certain mental-health professionals to take action regarding threats of violence without getting in trouble themselves.
There are no duty to warn/protect laws in Nevada, North Dakota, North Carolina, and Maine. Pennsylvania requires “mental-health professionals” to act when there’s a “clear and immediate danger to others or to society.”
In an interview, Columbia University, New York, psychiatrist and medical law/ethics specialist Paul S. Appelbaum, MD, said that “with the exception of situations like child abuse or elder abuse, for which psychiatrists are mandatory reporters, psychiatrists generally have the same responsibilities for reporting crimes as other citizens.”

He added that there is a crime in English common law known as “misprision” that refers to failing to report a felony. “A few states still have misprision statutes, but courts have tended to interpret them to require an affirmative act to conceal a crime, not just failure to report,” he said. “Unless the patient’s confession indicates a continuing threat to other people – e.g., a serial rapist or murderer – there is probably no obligation to report a previous crime.”
In this case, Dr. Musselman said, the physicians thought they might be able to waive confidentiality because it was possible that the alleged murder victims were still alive and in need of help.
However, the patient ultimately took the decision out of the hands of the psychiatrists and agreed to confess to the police. There’s a happy ending: The patient later recanted the story, Dr. Musselman said, and there was no follow-up by the authorities.
What should psychiatrists do in a similar situation? Besides the law, Dr. Musselman said, it’s important to consider medical ethics, confidentiality, and the greater good. “Doctors may have to ask themselves: Would I rather be sued because I’m breaking confidentiality or potentially play a part in someone’s suffering?”
She recommended reaching out to attorneys for legal guidance. “There’s a saying in forensic psychiatry by [Harvard University psychiatrist] Thomas Gutheil: Never worry alone.”
Dr. Applebaum agreed, and added: “Psychiatrists should consider the credibility of the patient’s confession: Could it represent a delusion? Is it being proffered as a way of manipulating the therapist? What is the extent to which, if valid, it indicates an ongoing threat to others? Is the patient is willing to contact the police and admit to the crime or authorize the psychiatrist to do so? Only in the case of a credible confession, an ongoing threat, and a patient unwilling to contact the police themselves should the psychiatrist seriously consider breaching confidentiality to report.”
No study funding or disclosures were reported.
NEW ORLEANS – The patient, a 60-year-old woman who’d just tried to kill herself by overdosing on gabapentin, felt the need to make a confession. As she told a resident psychiatrist late one night at a Philadelphia crisis response center, she’d just murdered two people and buried them in her backyard. More details kept coming, including who was dead and where their bodies were.
It didn’t take long for the attending physician’s phone to ring as the resident sought guidance. This wasn’t a typical “duty to warn” case since there was no one to warn of a threat of violence. But then what kind of case was it? As Meghan Musselman, MD, and colleagues noted in a report presented at the annual meeting of the American Psychiatric Association, the law and medical ethics didn’t present a clear-cut solution to whether the patient’s claim should be reported to the authorities.
“This was much more of a gray zone case than we typically see,” said Dr. Musselman, of the department of psychiatry at Temple University in Philadelphia, in an interview. “If someone is threatening to harm someone, most states have statutes about what to do in that situation. The same doesn’t really exist for when the crime has already happened.”
Even so, might the existing “duty to warn/protect” laws be helpful as a guide to what to do? Maybe, but it’s complicated. The laws, which address the waiving of therapist-patient confidentiality when violence is threatened, are widely variable. Some don’t specifically cover psychiatrists, according to the National Conference of State Legislatures. Some simply allow – but don’t require – certain mental-health professionals to take action regarding threats of violence without getting in trouble themselves.
There are no duty to warn/protect laws in Nevada, North Dakota, North Carolina, and Maine. Pennsylvania requires “mental-health professionals” to act when there’s a “clear and immediate danger to others or to society.”
In an interview, Columbia University, New York, psychiatrist and medical law/ethics specialist Paul S. Appelbaum, MD, said that “with the exception of situations like child abuse or elder abuse, for which psychiatrists are mandatory reporters, psychiatrists generally have the same responsibilities for reporting crimes as other citizens.”
He added that there is a crime in English common law known as “misprision” that refers to failing to report a felony. “A few states still have misprision statutes, but courts have tended to interpret them to require an affirmative act to conceal a crime, not just failure to report,” he said. “Unless the patient’s confession indicates a continuing threat to other people – e.g., a serial rapist or murderer – there is probably no obligation to report a previous crime.”
In this case, Dr. Musselman said, the physicians thought they might be able to waive confidentiality because it was possible that the alleged murder victims were still alive and in need of help.
However, the patient ultimately took the decision out of the hands of the psychiatrists and agreed to confess to the police. There’s a happy ending: The patient later recanted the story, Dr. Musselman said, and there was no follow-up by the authorities.
What should psychiatrists do in a similar situation? Besides the law, Dr. Musselman said, it’s important to consider medical ethics, confidentiality, and the greater good. “Doctors may have to ask themselves: Would I rather be sued because I’m breaking confidentiality or potentially play a part in someone’s suffering?”
She recommended reaching out to attorneys for legal guidance. “There’s a saying in forensic psychiatry by [Harvard University psychiatrist] Thomas Gutheil: Never worry alone.”
Dr. Applebaum agreed, and added: “Psychiatrists should consider the credibility of the patient’s confession: Could it represent a delusion? Is it being proffered as a way of manipulating the therapist? What is the extent to which, if valid, it indicates an ongoing threat to others? Is the patient is willing to contact the police and admit to the crime or authorize the psychiatrist to do so? Only in the case of a credible confession, an ongoing threat, and a patient unwilling to contact the police themselves should the psychiatrist seriously consider breaching confidentiality to report.”
No study funding or disclosures were reported.
NEW ORLEANS – The patient, a 60-year-old woman who’d just tried to kill herself by overdosing on gabapentin, felt the need to make a confession. As she told a resident psychiatrist late one night at a Philadelphia crisis response center, she’d just murdered two people and buried them in her backyard. More details kept coming, including who was dead and where their bodies were.
It didn’t take long for the attending physician’s phone to ring as the resident sought guidance. This wasn’t a typical “duty to warn” case since there was no one to warn of a threat of violence. But then what kind of case was it? As Meghan Musselman, MD, and colleagues noted in a report presented at the annual meeting of the American Psychiatric Association, the law and medical ethics didn’t present a clear-cut solution to whether the patient’s claim should be reported to the authorities.
“This was much more of a gray zone case than we typically see,” said Dr. Musselman, of the department of psychiatry at Temple University in Philadelphia, in an interview. “If someone is threatening to harm someone, most states have statutes about what to do in that situation. The same doesn’t really exist for when the crime has already happened.”
Even so, might the existing “duty to warn/protect” laws be helpful as a guide to what to do? Maybe, but it’s complicated. The laws, which address the waiving of therapist-patient confidentiality when violence is threatened, are widely variable. Some don’t specifically cover psychiatrists, according to the National Conference of State Legislatures. Some simply allow – but don’t require – certain mental-health professionals to take action regarding threats of violence without getting in trouble themselves.
There are no duty to warn/protect laws in Nevada, North Dakota, North Carolina, and Maine. Pennsylvania requires “mental-health professionals” to act when there’s a “clear and immediate danger to others or to society.”
In an interview, Columbia University, New York, psychiatrist and medical law/ethics specialist Paul S. Appelbaum, MD, said that “with the exception of situations like child abuse or elder abuse, for which psychiatrists are mandatory reporters, psychiatrists generally have the same responsibilities for reporting crimes as other citizens.”
He added that there is a crime in English common law known as “misprision” that refers to failing to report a felony. “A few states still have misprision statutes, but courts have tended to interpret them to require an affirmative act to conceal a crime, not just failure to report,” he said. “Unless the patient’s confession indicates a continuing threat to other people – e.g., a serial rapist or murderer – there is probably no obligation to report a previous crime.”
In this case, Dr. Musselman said, the physicians thought they might be able to waive confidentiality because it was possible that the alleged murder victims were still alive and in need of help.
However, the patient ultimately took the decision out of the hands of the psychiatrists and agreed to confess to the police. There’s a happy ending: The patient later recanted the story, Dr. Musselman said, and there was no follow-up by the authorities.
What should psychiatrists do in a similar situation? Besides the law, Dr. Musselman said, it’s important to consider medical ethics, confidentiality, and the greater good. “Doctors may have to ask themselves: Would I rather be sued because I’m breaking confidentiality or potentially play a part in someone’s suffering?”
She recommended reaching out to attorneys for legal guidance. “There’s a saying in forensic psychiatry by [Harvard University psychiatrist] Thomas Gutheil: Never worry alone.”
Dr. Applebaum agreed, and added: “Psychiatrists should consider the credibility of the patient’s confession: Could it represent a delusion? Is it being proffered as a way of manipulating the therapist? What is the extent to which, if valid, it indicates an ongoing threat to others? Is the patient is willing to contact the police and admit to the crime or authorize the psychiatrist to do so? Only in the case of a credible confession, an ongoing threat, and a patient unwilling to contact the police themselves should the psychiatrist seriously consider breaching confidentiality to report.”
No study funding or disclosures were reported.
AT APA 2022
Fever after a tropical trip: A guide to differential diagnosis
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.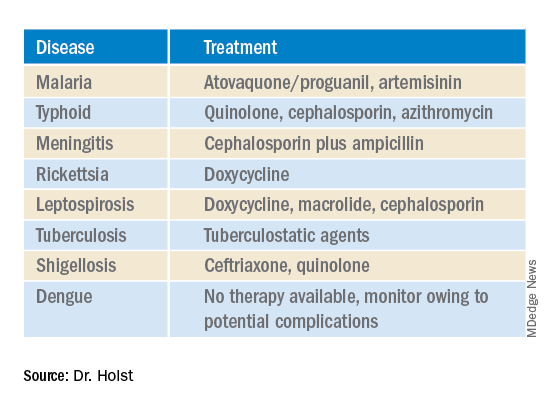
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
Bacterial cocktail, spores counter recurrent C. diff
SAN DIEGO – A novel combination of eight human commensal bacteria has shown efficacy in preventing recurrent Clostridioides difficile infections in high-risk populations. The cocktail of bacterial strains (VE303), produced under tightly-controlled conditions, is delivered in powdered form over a period of 14 days.
The approach, sponsored by Vedanta Biosciences, is one of several efforts to use carefully defined microbial populations instead of fecal microbiota transplantation (FMT) to treat or prevent C. diff infections.
The key issue is that not all of the bacteria found in FMTs are needed to provide a therapeutic effect, according to Thomas Louie, MD, professor of medicine at the University of Calgary (Alta.). “You don’t need all the bugs. You don’t need raw [stool]. You can take only the good parts,” said Dr. Louie, who presented the results of the phase 2 study at the annual Digestive Disease Week® (DDW). In fact, FMT carries the risk of infection of pathogenic bacteria.
The strains found in VE303 were consistently identified in patients’ microbiota following successful FMTs, though they were absent before the transplant. Animal and human studies then showed that the microbes could repopulate microbiota.
Among 78 patients included in the efficacy analysis of the study, after 8 weeks, 13.8% of the VE303 group experienced a recurrent C. diff infection, versus 45.5% of the placebo group, amounting to more than an 80% reduction in risk (odds ratio, 0.192; P = .0077). Adverse events were mild and similar across both groups, with no treatment-related serious adverse events reported.
The same session included a post hoc analysis of a phase 3 study sponsored by Seres Therapeutics, which showed that the company’s oral product SER-109, composed of purified Firmicutes spores, reduced the risk of recurrent C. diff infection after 8 weeks compared to placebo (12.4% versus 39.8%; P < .001).
The new analysis examined short-, medium-, and branch-chained fatty acids in patient stools. After just 1 week of treatment, there was an increase in the short-chain fatty acid butyrate and medium-chain fatty acids valerate and hexanoate. They continued to be higher in weeks 2 and 8 in the treatment arm. The results suggest that increased fatty acid production might boost clinical outcomes, according to Kevin Litcofsky of Seres, who presented the results.
Both approaches have potential, according to Melinda Engevik, PhD, who comoderated the session where the study was presented. “I think that they’re both interesting ideas. The spores [from Seres], I think, are going to be better at passing through the stomach and a little bit more resistant, but then they have to germinate and engraft, whereas if you give the lyophilized bacteria [from Vedanta], you might lose some more, but they’re already primed and ready to go. So I think they’re both very different approaches, but the data from both seem to support that they worked and probably in different ways,” said Dr. Engevik, assistant professor at the Medical University of South Carolina, Charleston.
“Patients that have recurrent [C. diff], they are desperate to be able to break the cycle of recurrence. I think that they’ve shown a lot of safety with this, which is an issue for FMT. Both of the talks seemed like there is a path moving forward to help those patients. I was encouraged,” said Dr. Engevik.
Comoderator Anoop Kumar, PhD, assistant professor of gastroenterology and hepatology at University of Illinois, Chicago, agreed and noted the advantage of such treatments over FMT during the COVID-19 pandemic, which has disrupted FMT delivery.
Previous studies have looked at probiotics, but results so far have been mixed, said Dr. Engevik. She suspects these two approaches, containing more bacterial strains, are likely to have better success. “I think you really have to have a complex gut microbiota community, at least minimally complex, to be able to get the effects. I think it’s the wave of the future,” she said.
Dr. Engevik also suggested that the benefits might not stop at C. diff. She highlighted research in other gastrointestinal diseases such as inflammatory bowel disease, and even efforts underway to enhance responses to checkpoint inhibitors in the treatment of cancer. “Gut microbes are master regulators, so they have these wide-reaching effects. I think that a lot of human health will be started to be targeted by looking at the gut microbiota,” she said.
Dr. Louie also highlighted the potential for more applications. “C. diff is low-hanging fruit. I think these bugs will have some usefulness for [irritable bowel syndrome]. I’ve transplanted some patients with IBS and it seemed to work. I haven’t had time to design and do an IBS trial, but the future is these bugs.”
Dr. Louie also participated in the Seres study. He has been on the advisory board for Vedanta, Seres, Finch Therapeutics, and Artugen Therapeutics. Dr. Engevik and Dr. Kumar have no relevant financial disclosures.
SAN DIEGO – A novel combination of eight human commensal bacteria has shown efficacy in preventing recurrent Clostridioides difficile infections in high-risk populations. The cocktail of bacterial strains (VE303), produced under tightly-controlled conditions, is delivered in powdered form over a period of 14 days.
The approach, sponsored by Vedanta Biosciences, is one of several efforts to use carefully defined microbial populations instead of fecal microbiota transplantation (FMT) to treat or prevent C. diff infections.
The key issue is that not all of the bacteria found in FMTs are needed to provide a therapeutic effect, according to Thomas Louie, MD, professor of medicine at the University of Calgary (Alta.). “You don’t need all the bugs. You don’t need raw [stool]. You can take only the good parts,” said Dr. Louie, who presented the results of the phase 2 study at the annual Digestive Disease Week® (DDW). In fact, FMT carries the risk of infection of pathogenic bacteria.
The strains found in VE303 were consistently identified in patients’ microbiota following successful FMTs, though they were absent before the transplant. Animal and human studies then showed that the microbes could repopulate microbiota.
Among 78 patients included in the efficacy analysis of the study, after 8 weeks, 13.8% of the VE303 group experienced a recurrent C. diff infection, versus 45.5% of the placebo group, amounting to more than an 80% reduction in risk (odds ratio, 0.192; P = .0077). Adverse events were mild and similar across both groups, with no treatment-related serious adverse events reported.
The same session included a post hoc analysis of a phase 3 study sponsored by Seres Therapeutics, which showed that the company’s oral product SER-109, composed of purified Firmicutes spores, reduced the risk of recurrent C. diff infection after 8 weeks compared to placebo (12.4% versus 39.8%; P < .001).
The new analysis examined short-, medium-, and branch-chained fatty acids in patient stools. After just 1 week of treatment, there was an increase in the short-chain fatty acid butyrate and medium-chain fatty acids valerate and hexanoate. They continued to be higher in weeks 2 and 8 in the treatment arm. The results suggest that increased fatty acid production might boost clinical outcomes, according to Kevin Litcofsky of Seres, who presented the results.
Both approaches have potential, according to Melinda Engevik, PhD, who comoderated the session where the study was presented. “I think that they’re both interesting ideas. The spores [from Seres], I think, are going to be better at passing through the stomach and a little bit more resistant, but then they have to germinate and engraft, whereas if you give the lyophilized bacteria [from Vedanta], you might lose some more, but they’re already primed and ready to go. So I think they’re both very different approaches, but the data from both seem to support that they worked and probably in different ways,” said Dr. Engevik, assistant professor at the Medical University of South Carolina, Charleston.
“Patients that have recurrent [C. diff], they are desperate to be able to break the cycle of recurrence. I think that they’ve shown a lot of safety with this, which is an issue for FMT. Both of the talks seemed like there is a path moving forward to help those patients. I was encouraged,” said Dr. Engevik.
Comoderator Anoop Kumar, PhD, assistant professor of gastroenterology and hepatology at University of Illinois, Chicago, agreed and noted the advantage of such treatments over FMT during the COVID-19 pandemic, which has disrupted FMT delivery.
Previous studies have looked at probiotics, but results so far have been mixed, said Dr. Engevik. She suspects these two approaches, containing more bacterial strains, are likely to have better success. “I think you really have to have a complex gut microbiota community, at least minimally complex, to be able to get the effects. I think it’s the wave of the future,” she said.
Dr. Engevik also suggested that the benefits might not stop at C. diff. She highlighted research in other gastrointestinal diseases such as inflammatory bowel disease, and even efforts underway to enhance responses to checkpoint inhibitors in the treatment of cancer. “Gut microbes are master regulators, so they have these wide-reaching effects. I think that a lot of human health will be started to be targeted by looking at the gut microbiota,” she said.
Dr. Louie also highlighted the potential for more applications. “C. diff is low-hanging fruit. I think these bugs will have some usefulness for [irritable bowel syndrome]. I’ve transplanted some patients with IBS and it seemed to work. I haven’t had time to design and do an IBS trial, but the future is these bugs.”
Dr. Louie also participated in the Seres study. He has been on the advisory board for Vedanta, Seres, Finch Therapeutics, and Artugen Therapeutics. Dr. Engevik and Dr. Kumar have no relevant financial disclosures.
SAN DIEGO – A novel combination of eight human commensal bacteria has shown efficacy in preventing recurrent Clostridioides difficile infections in high-risk populations. The cocktail of bacterial strains (VE303), produced under tightly-controlled conditions, is delivered in powdered form over a period of 14 days.
The approach, sponsored by Vedanta Biosciences, is one of several efforts to use carefully defined microbial populations instead of fecal microbiota transplantation (FMT) to treat or prevent C. diff infections.
The key issue is that not all of the bacteria found in FMTs are needed to provide a therapeutic effect, according to Thomas Louie, MD, professor of medicine at the University of Calgary (Alta.). “You don’t need all the bugs. You don’t need raw [stool]. You can take only the good parts,” said Dr. Louie, who presented the results of the phase 2 study at the annual Digestive Disease Week® (DDW). In fact, FMT carries the risk of infection of pathogenic bacteria.
The strains found in VE303 were consistently identified in patients’ microbiota following successful FMTs, though they were absent before the transplant. Animal and human studies then showed that the microbes could repopulate microbiota.
Among 78 patients included in the efficacy analysis of the study, after 8 weeks, 13.8% of the VE303 group experienced a recurrent C. diff infection, versus 45.5% of the placebo group, amounting to more than an 80% reduction in risk (odds ratio, 0.192; P = .0077). Adverse events were mild and similar across both groups, with no treatment-related serious adverse events reported.
The same session included a post hoc analysis of a phase 3 study sponsored by Seres Therapeutics, which showed that the company’s oral product SER-109, composed of purified Firmicutes spores, reduced the risk of recurrent C. diff infection after 8 weeks compared to placebo (12.4% versus 39.8%; P < .001).
The new analysis examined short-, medium-, and branch-chained fatty acids in patient stools. After just 1 week of treatment, there was an increase in the short-chain fatty acid butyrate and medium-chain fatty acids valerate and hexanoate. They continued to be higher in weeks 2 and 8 in the treatment arm. The results suggest that increased fatty acid production might boost clinical outcomes, according to Kevin Litcofsky of Seres, who presented the results.
Both approaches have potential, according to Melinda Engevik, PhD, who comoderated the session where the study was presented. “I think that they’re both interesting ideas. The spores [from Seres], I think, are going to be better at passing through the stomach and a little bit more resistant, but then they have to germinate and engraft, whereas if you give the lyophilized bacteria [from Vedanta], you might lose some more, but they’re already primed and ready to go. So I think they’re both very different approaches, but the data from both seem to support that they worked and probably in different ways,” said Dr. Engevik, assistant professor at the Medical University of South Carolina, Charleston.
“Patients that have recurrent [C. diff], they are desperate to be able to break the cycle of recurrence. I think that they’ve shown a lot of safety with this, which is an issue for FMT. Both of the talks seemed like there is a path moving forward to help those patients. I was encouraged,” said Dr. Engevik.
Comoderator Anoop Kumar, PhD, assistant professor of gastroenterology and hepatology at University of Illinois, Chicago, agreed and noted the advantage of such treatments over FMT during the COVID-19 pandemic, which has disrupted FMT delivery.
Previous studies have looked at probiotics, but results so far have been mixed, said Dr. Engevik. She suspects these two approaches, containing more bacterial strains, are likely to have better success. “I think you really have to have a complex gut microbiota community, at least minimally complex, to be able to get the effects. I think it’s the wave of the future,” she said.
Dr. Engevik also suggested that the benefits might not stop at C. diff. She highlighted research in other gastrointestinal diseases such as inflammatory bowel disease, and even efforts underway to enhance responses to checkpoint inhibitors in the treatment of cancer. “Gut microbes are master regulators, so they have these wide-reaching effects. I think that a lot of human health will be started to be targeted by looking at the gut microbiota,” she said.
Dr. Louie also highlighted the potential for more applications. “C. diff is low-hanging fruit. I think these bugs will have some usefulness for [irritable bowel syndrome]. I’ve transplanted some patients with IBS and it seemed to work. I haven’t had time to design and do an IBS trial, but the future is these bugs.”
Dr. Louie also participated in the Seres study. He has been on the advisory board for Vedanta, Seres, Finch Therapeutics, and Artugen Therapeutics. Dr. Engevik and Dr. Kumar have no relevant financial disclosures.
AT DDW 2022
Treatment for alcohol abuse reduces hepatitis readmission
SAN DIEGO – Treating people with alcoholic hepatitis for alcohol abuse may reduce their risk of hospital readmission, researchers reported.
In a retrospective analysis of nationwide data, 7.83% of those patients who received psychotherapy, counseling, or drug treatment for alcohol abuse were readmitted within 30 days, versus 11.67% of those who did not receive these kinds of treatment.
The finding lends support to the argument that hospitals should invest more in the treatments, despite the complexities involved.
“It takes a multidisciplinary approach, starting from the physician or the health care provider along with the pharmacists, the behavioral health specialists, or a psychiatrist or psychologist, along with case management as well,” said Harleen Chela, MD, a third-year resident at the University of Missouri in Columbia. She presented the findings at the annual Digestive Disease Week® (DDW).
The researchers started with the premise that patients with alcoholic hepatitis can prevent the condition from worsening by abstaining from alcohol. To see whether interventions aimed at encouraging that abstention could prevent readmissions, Dr. Chela and colleagues analyzed data on readmissions for the first 11 months of the year 2018.
They included patients who were at least 18 years of age and who had a nonelective admission with a principal diagnosis of alcohol abuse.
Using procedure codes, they compared those patients given psychotherapy (including cognitive behavioral therapy), formal inpatient counseling, and drug treatment for alcohol abuse to those who didn’t. Then they counted how many patients were readmitted within 30 days.
They found records of 45,617 patients admitted for alcoholic hepatitis of whom 1,552 received treatment for alcohol abuse and 44,065 did not.
They did not find any significant difference between the two groups in demographics, income, or insurance status.
Adjusting for such factors, the researchers found that people who received alcohol abuse treatment were 64% as likely to be readmitted as were those who did not (hazard ratio, 0.64; 95% confidence interval, 0.46-0.91; P = 0.01).
If alcohol abuse treatment is so effective, why isn’t it routine? “It’s not always feasible to implement this, on the inpatient side, because it takes more than a day or two just to get some of these things put in place,” Dr. Chela told this news organization.
They did find that people were more likely to get treatment for alcohol abuse if they were admitted to a hospital in a big city rather than a small town and if their hospital was owned by private investors rather than by a not-for-profit organization or the government.
“Larger hospitals and private sector institutions have more access to resources and money to have those kinds of systems in place for the patients,” said Dr. Chela.
She became interested in the issue at her hospital when she noticed that patients with alcoholic hepatitis were not getting behavioral counseling. “The inpatient load in the behavioral health side is so much that they don’t have time for these kinds of consults,” she said. “That’s one of the challenges: A shortage of behavioral specialists like psychiatrists.”
And hospitals tend to focus on treating conditions that threaten their patients’ lives in the short term. “Someone who has a heart attack or a gastrointestinal bleed – there’s more focus on resources for those kinds of patients,” she said.
Virginia Commonwealth University in Richmond provides alcohol abuse treatment to patients with alcoholic hepatitis partly using telehealth, said Richard Sterling, MD, MSc, chief of hepatology, who was not involved in the study. “For people who live too far away, don’t have transportation, or have other health disparities, we now have technology and mechanisms to keep them engaged in care,” he told this news organization. “We’re doing a lot of Zoom visits.”
Dr. Chela and colleagues also found that those who got alcohol abuse treatment were less likely to be discharged to a skilled nursing facility or to home health. The data couldn’t give the researchers a definitive reason for this, but Dr. Chela speculated that the patients who received treatment for alcohol abuse stayed longer in the hospital and may have been in better shape when they were discharged.
The U.S. health care system doesn’t necessarily provide incentives to keep patients healthy, Dr. Sterling said. “Hospital systems make money off of filling beds, and providing a lot of inpatient care and hospital days,” he said. “That may be not necessarily congruent with a health system that is supposed to provide health for these covered lives.”
Neither Dr. Chela nor Dr. Sterling reported any relevant financial relationships.
SAN DIEGO – Treating people with alcoholic hepatitis for alcohol abuse may reduce their risk of hospital readmission, researchers reported.
In a retrospective analysis of nationwide data, 7.83% of those patients who received psychotherapy, counseling, or drug treatment for alcohol abuse were readmitted within 30 days, versus 11.67% of those who did not receive these kinds of treatment.
The finding lends support to the argument that hospitals should invest more in the treatments, despite the complexities involved.
“It takes a multidisciplinary approach, starting from the physician or the health care provider along with the pharmacists, the behavioral health specialists, or a psychiatrist or psychologist, along with case management as well,” said Harleen Chela, MD, a third-year resident at the University of Missouri in Columbia. She presented the findings at the annual Digestive Disease Week® (DDW).
The researchers started with the premise that patients with alcoholic hepatitis can prevent the condition from worsening by abstaining from alcohol. To see whether interventions aimed at encouraging that abstention could prevent readmissions, Dr. Chela and colleagues analyzed data on readmissions for the first 11 months of the year 2018.
They included patients who were at least 18 years of age and who had a nonelective admission with a principal diagnosis of alcohol abuse.
Using procedure codes, they compared those patients given psychotherapy (including cognitive behavioral therapy), formal inpatient counseling, and drug treatment for alcohol abuse to those who didn’t. Then they counted how many patients were readmitted within 30 days.
They found records of 45,617 patients admitted for alcoholic hepatitis of whom 1,552 received treatment for alcohol abuse and 44,065 did not.
They did not find any significant difference between the two groups in demographics, income, or insurance status.
Adjusting for such factors, the researchers found that people who received alcohol abuse treatment were 64% as likely to be readmitted as were those who did not (hazard ratio, 0.64; 95% confidence interval, 0.46-0.91; P = 0.01).
If alcohol abuse treatment is so effective, why isn’t it routine? “It’s not always feasible to implement this, on the inpatient side, because it takes more than a day or two just to get some of these things put in place,” Dr. Chela told this news organization.
They did find that people were more likely to get treatment for alcohol abuse if they were admitted to a hospital in a big city rather than a small town and if their hospital was owned by private investors rather than by a not-for-profit organization or the government.
“Larger hospitals and private sector institutions have more access to resources and money to have those kinds of systems in place for the patients,” said Dr. Chela.
She became interested in the issue at her hospital when she noticed that patients with alcoholic hepatitis were not getting behavioral counseling. “The inpatient load in the behavioral health side is so much that they don’t have time for these kinds of consults,” she said. “That’s one of the challenges: A shortage of behavioral specialists like psychiatrists.”
And hospitals tend to focus on treating conditions that threaten their patients’ lives in the short term. “Someone who has a heart attack or a gastrointestinal bleed – there’s more focus on resources for those kinds of patients,” she said.
Virginia Commonwealth University in Richmond provides alcohol abuse treatment to patients with alcoholic hepatitis partly using telehealth, said Richard Sterling, MD, MSc, chief of hepatology, who was not involved in the study. “For people who live too far away, don’t have transportation, or have other health disparities, we now have technology and mechanisms to keep them engaged in care,” he told this news organization. “We’re doing a lot of Zoom visits.”
Dr. Chela and colleagues also found that those who got alcohol abuse treatment were less likely to be discharged to a skilled nursing facility or to home health. The data couldn’t give the researchers a definitive reason for this, but Dr. Chela speculated that the patients who received treatment for alcohol abuse stayed longer in the hospital and may have been in better shape when they were discharged.
The U.S. health care system doesn’t necessarily provide incentives to keep patients healthy, Dr. Sterling said. “Hospital systems make money off of filling beds, and providing a lot of inpatient care and hospital days,” he said. “That may be not necessarily congruent with a health system that is supposed to provide health for these covered lives.”
Neither Dr. Chela nor Dr. Sterling reported any relevant financial relationships.
SAN DIEGO – Treating people with alcoholic hepatitis for alcohol abuse may reduce their risk of hospital readmission, researchers reported.
In a retrospective analysis of nationwide data, 7.83% of those patients who received psychotherapy, counseling, or drug treatment for alcohol abuse were readmitted within 30 days, versus 11.67% of those who did not receive these kinds of treatment.
The finding lends support to the argument that hospitals should invest more in the treatments, despite the complexities involved.
“It takes a multidisciplinary approach, starting from the physician or the health care provider along with the pharmacists, the behavioral health specialists, or a psychiatrist or psychologist, along with case management as well,” said Harleen Chela, MD, a third-year resident at the University of Missouri in Columbia. She presented the findings at the annual Digestive Disease Week® (DDW).
The researchers started with the premise that patients with alcoholic hepatitis can prevent the condition from worsening by abstaining from alcohol. To see whether interventions aimed at encouraging that abstention could prevent readmissions, Dr. Chela and colleagues analyzed data on readmissions for the first 11 months of the year 2018.
They included patients who were at least 18 years of age and who had a nonelective admission with a principal diagnosis of alcohol abuse.
Using procedure codes, they compared those patients given psychotherapy (including cognitive behavioral therapy), formal inpatient counseling, and drug treatment for alcohol abuse to those who didn’t. Then they counted how many patients were readmitted within 30 days.
They found records of 45,617 patients admitted for alcoholic hepatitis of whom 1,552 received treatment for alcohol abuse and 44,065 did not.
They did not find any significant difference between the two groups in demographics, income, or insurance status.
Adjusting for such factors, the researchers found that people who received alcohol abuse treatment were 64% as likely to be readmitted as were those who did not (hazard ratio, 0.64; 95% confidence interval, 0.46-0.91; P = 0.01).
If alcohol abuse treatment is so effective, why isn’t it routine? “It’s not always feasible to implement this, on the inpatient side, because it takes more than a day or two just to get some of these things put in place,” Dr. Chela told this news organization.
They did find that people were more likely to get treatment for alcohol abuse if they were admitted to a hospital in a big city rather than a small town and if their hospital was owned by private investors rather than by a not-for-profit organization or the government.
“Larger hospitals and private sector institutions have more access to resources and money to have those kinds of systems in place for the patients,” said Dr. Chela.
She became interested in the issue at her hospital when she noticed that patients with alcoholic hepatitis were not getting behavioral counseling. “The inpatient load in the behavioral health side is so much that they don’t have time for these kinds of consults,” she said. “That’s one of the challenges: A shortage of behavioral specialists like psychiatrists.”
And hospitals tend to focus on treating conditions that threaten their patients’ lives in the short term. “Someone who has a heart attack or a gastrointestinal bleed – there’s more focus on resources for those kinds of patients,” she said.
Virginia Commonwealth University in Richmond provides alcohol abuse treatment to patients with alcoholic hepatitis partly using telehealth, said Richard Sterling, MD, MSc, chief of hepatology, who was not involved in the study. “For people who live too far away, don’t have transportation, or have other health disparities, we now have technology and mechanisms to keep them engaged in care,” he told this news organization. “We’re doing a lot of Zoom visits.”
Dr. Chela and colleagues also found that those who got alcohol abuse treatment were less likely to be discharged to a skilled nursing facility or to home health. The data couldn’t give the researchers a definitive reason for this, but Dr. Chela speculated that the patients who received treatment for alcohol abuse stayed longer in the hospital and may have been in better shape when they were discharged.
The U.S. health care system doesn’t necessarily provide incentives to keep patients healthy, Dr. Sterling said. “Hospital systems make money off of filling beds, and providing a lot of inpatient care and hospital days,” he said. “That may be not necessarily congruent with a health system that is supposed to provide health for these covered lives.”
Neither Dr. Chela nor Dr. Sterling reported any relevant financial relationships.
AT DDW 2022
Climate change, medical education, and dermatology
The recent article on including the impact of climate on health in medical education programs shines an important light on the challenge – and urgent need – of integrating climate change training into medical education. These nascent efforts are just getting underway across the country, with some programs – notably Harvard’s C-CHANGE (Center for Climate, Health, and the Global Environment) program, mentioned in the article, and others, such as the University of Colorado’s Climate Medicine diploma course – leading the way. A number of publications, such as the editorial titled “A planetary health curriculum for medicine” published in 2021 in the BMJ, offer a roadmap to do so.

Medical schools, residency programs, and other medical specialty programs – including those for advanced practice providers, dentists, nurses, and more – should be incorporating climate change and its myriad of health impacts into their training pathways. The medical student group, Medical Students for a Sustainable Future, has put forth a planetary health report card that evaluates training programs on the strength of their focus on the intersections between climate and health.
While the article did not specifically focus on dermatology, these impacts are true in our field as well. The article notes that “at least one medical journal has recently ramped up its efforts to educate physicians on the links between health issues and climate change.” Notably in dermatology, the International Journal of Women’s Dermatology devoted an entire 124-page themed issue to climate change and dermatology in January, 2021, while JAMA Dermatology editor Kanade Shinkai, MD, PhD, called out climate change as one of the journal’s priorities in her annual editorial, stating, “Another priority for the journal is to better understand the effect of climate change on human health, specifically skin disease.”
The impacts of climate change in dermatology range from heat-related illness (a major cause of climate-associated mortality, with the skin serving as an essential thermoregulatory organ) to changing patterns of vector-borne illnesses to pollution and wildfire smoke flaring inflammatory skin diseases, to an increase in skin cancer, and more. While incorporation of health issues relating to climate change is important at a medical school level, it is also critical at the residency training – and board exam/certification – level as well.
Beyond the importance of building climate education into undergraduate and graduate medical education, it is also important that practicing physicians, post-residency training, remain up to date and keep abreast of changing patterns of disease in our rapidly changing climate. Lyme disease now occurs in Canada – and both earlier and later in the year even in places that are geographically used to seeing it. Early recognition is essential, but unprepared physicians may miss the early erythema migrans rash, and patients may suffer more severe sequelae as a result.
Finally, it’s important that medical organizations are aware of not just the health implications of climate change, but also potential policy impacts. Health care is a major emitter of CO2, and assistant secretary for health for the U.S. Department of Health and Human Services, Admiral Rachel L. Levine, MD, with the National Academy of Medicine, has appropriately pledged to reduce health care carbon emissions as part of the necessary steps that we must all take to avert the worst impacts of a warming world. The field of medicine and individual providers should educate themselves and actively work toward sustainability in health care, to improve the health of their patients, populations, and future generations.
Dr. Rosenbach is associate professor of dermatology and medicine at the University of Pennsylvania, Philadelphia, and is the founder and cochair of the American Academy of Dermatology Expert Resource Group for Climate Change and Environmental Issues. Dr. Rosenbach is speaking on behalf of himself and not the AAD.
The recent article on including the impact of climate on health in medical education programs shines an important light on the challenge – and urgent need – of integrating climate change training into medical education. These nascent efforts are just getting underway across the country, with some programs – notably Harvard’s C-CHANGE (Center for Climate, Health, and the Global Environment) program, mentioned in the article, and others, such as the University of Colorado’s Climate Medicine diploma course – leading the way. A number of publications, such as the editorial titled “A planetary health curriculum for medicine” published in 2021 in the BMJ, offer a roadmap to do so.
Medical schools, residency programs, and other medical specialty programs – including those for advanced practice providers, dentists, nurses, and more – should be incorporating climate change and its myriad of health impacts into their training pathways. The medical student group, Medical Students for a Sustainable Future, has put forth a planetary health report card that evaluates training programs on the strength of their focus on the intersections between climate and health.
While the article did not specifically focus on dermatology, these impacts are true in our field as well. The article notes that “at least one medical journal has recently ramped up its efforts to educate physicians on the links between health issues and climate change.” Notably in dermatology, the International Journal of Women’s Dermatology devoted an entire 124-page themed issue to climate change and dermatology in January, 2021, while JAMA Dermatology editor Kanade Shinkai, MD, PhD, called out climate change as one of the journal’s priorities in her annual editorial, stating, “Another priority for the journal is to better understand the effect of climate change on human health, specifically skin disease.”
The impacts of climate change in dermatology range from heat-related illness (a major cause of climate-associated mortality, with the skin serving as an essential thermoregulatory organ) to changing patterns of vector-borne illnesses to pollution and wildfire smoke flaring inflammatory skin diseases, to an increase in skin cancer, and more. While incorporation of health issues relating to climate change is important at a medical school level, it is also critical at the residency training – and board exam/certification – level as well.
Beyond the importance of building climate education into undergraduate and graduate medical education, it is also important that practicing physicians, post-residency training, remain up to date and keep abreast of changing patterns of disease in our rapidly changing climate. Lyme disease now occurs in Canada – and both earlier and later in the year even in places that are geographically used to seeing it. Early recognition is essential, but unprepared physicians may miss the early erythema migrans rash, and patients may suffer more severe sequelae as a result.
Finally, it’s important that medical organizations are aware of not just the health implications of climate change, but also potential policy impacts. Health care is a major emitter of CO2, and assistant secretary for health for the U.S. Department of Health and Human Services, Admiral Rachel L. Levine, MD, with the National Academy of Medicine, has appropriately pledged to reduce health care carbon emissions as part of the necessary steps that we must all take to avert the worst impacts of a warming world. The field of medicine and individual providers should educate themselves and actively work toward sustainability in health care, to improve the health of their patients, populations, and future generations.
Dr. Rosenbach is associate professor of dermatology and medicine at the University of Pennsylvania, Philadelphia, and is the founder and cochair of the American Academy of Dermatology Expert Resource Group for Climate Change and Environmental Issues. Dr. Rosenbach is speaking on behalf of himself and not the AAD.
The recent article on including the impact of climate on health in medical education programs shines an important light on the challenge – and urgent need – of integrating climate change training into medical education. These nascent efforts are just getting underway across the country, with some programs – notably Harvard’s C-CHANGE (Center for Climate, Health, and the Global Environment) program, mentioned in the article, and others, such as the University of Colorado’s Climate Medicine diploma course – leading the way. A number of publications, such as the editorial titled “A planetary health curriculum for medicine” published in 2021 in the BMJ, offer a roadmap to do so.
Medical schools, residency programs, and other medical specialty programs – including those for advanced practice providers, dentists, nurses, and more – should be incorporating climate change and its myriad of health impacts into their training pathways. The medical student group, Medical Students for a Sustainable Future, has put forth a planetary health report card that evaluates training programs on the strength of their focus on the intersections between climate and health.
While the article did not specifically focus on dermatology, these impacts are true in our field as well. The article notes that “at least one medical journal has recently ramped up its efforts to educate physicians on the links between health issues and climate change.” Notably in dermatology, the International Journal of Women’s Dermatology devoted an entire 124-page themed issue to climate change and dermatology in January, 2021, while JAMA Dermatology editor Kanade Shinkai, MD, PhD, called out climate change as one of the journal’s priorities in her annual editorial, stating, “Another priority for the journal is to better understand the effect of climate change on human health, specifically skin disease.”
The impacts of climate change in dermatology range from heat-related illness (a major cause of climate-associated mortality, with the skin serving as an essential thermoregulatory organ) to changing patterns of vector-borne illnesses to pollution and wildfire smoke flaring inflammatory skin diseases, to an increase in skin cancer, and more. While incorporation of health issues relating to climate change is important at a medical school level, it is also critical at the residency training – and board exam/certification – level as well.
Beyond the importance of building climate education into undergraduate and graduate medical education, it is also important that practicing physicians, post-residency training, remain up to date and keep abreast of changing patterns of disease in our rapidly changing climate. Lyme disease now occurs in Canada – and both earlier and later in the year even in places that are geographically used to seeing it. Early recognition is essential, but unprepared physicians may miss the early erythema migrans rash, and patients may suffer more severe sequelae as a result.
Finally, it’s important that medical organizations are aware of not just the health implications of climate change, but also potential policy impacts. Health care is a major emitter of CO2, and assistant secretary for health for the U.S. Department of Health and Human Services, Admiral Rachel L. Levine, MD, with the National Academy of Medicine, has appropriately pledged to reduce health care carbon emissions as part of the necessary steps that we must all take to avert the worst impacts of a warming world. The field of medicine and individual providers should educate themselves and actively work toward sustainability in health care, to improve the health of their patients, populations, and future generations.
Dr. Rosenbach is associate professor of dermatology and medicine at the University of Pennsylvania, Philadelphia, and is the founder and cochair of the American Academy of Dermatology Expert Resource Group for Climate Change and Environmental Issues. Dr. Rosenbach is speaking on behalf of himself and not the AAD.