User login
For MD-IQ use only
Artificial sweeteners: A modifiable cancer risk?
People with higher (above the median) consumption of artificial sweeteners – especially aspartame and acesulfame-potassium (acesulfame-K) – had a 13% higher risk of overall cancer over 8 years than those who did not consume these sweeteners.
Higher consumption of aspartame was associated with a 22% increased risk of breast cancer and a 15% increased risk of obesity-related cancer, compared with not consuming any of these sweeteners.*
These findings from the Nutri-Santé population-based observational study in France were published online March 24, 2022, in PLoS Medicine.
“Our findings do not support the use of artificial sweeteners as safe alternatives for sugar in foods or beverages and provide important and novel information to address the controversies about their potential adverse health effect,” Charlotte Debras, of the French National Institute for Health and Medical Research (Inserm) and Sorbonne Paris Nord University, and colleagues wrote.
“Results from the NutriNet-Santé cohort (n = 102,865) suggest that artificial sweeteners found in many food and beverage brands worldwide may be associated with increased cancer risk, in line with several experimental in vivo/in vitro studies. These findings provide novel information for the re-evaluation of these food additives by health agencies,” they wrote.
Commenting to the U.K. Science Media Center, Duane Mellor, PhD, registered dietitian and senior teaching fellow, Aston (England) University, said: “This study does not prove or even suggest that we should go back to sugar and turn our backs on artificial sweeteners or diet drinks.
“It does, however, suggest that artificial sweeteners are not a perfect replacement for sugar, they come with their own potential risks, as does sugar. The ideal answer is probably to move away from both, however, that may be unappealing to many who like a little sweetness in their life, so ditching the regular or diet soft drink (soda) for water may not be a well-received health message.”
Important analysis, interpret with caution
“I think that this is an important analysis, but the results need to be interpreted with caution,” another expert, John L. Sievenpiper, MD, PhD, associate professor, departments of nutritional sciences and medicine, University of Toronto, said in an interview.
“Large observational studies like this one that assess the exposure to low and no calorie sweeteners with obesity-related chronic diseases are at risk of reverse causality,” he explained. This is “a caveat that is well recognized by investigators in this field ... and guideline and policy makers.”
Reverse causality is a possibility because “it is likely that many high consumers of low- and no-calorie sweeteners (of which aspartame and acesulfame-K are the most common) will be consuming these sweeteners as a weight-loss strategy,” he added, “as opposed to these sweeteners causing obesity and its complications (including cancers).”
His team recently published a Diabetes and Nutrition Study Group–commissioned systematic review and meta-analysis of 17 randomized controlled trials (JAMA Netw Open. 2022;5[3]:e222092). Their findings “suggest that over the moderate term [low- and no-calorie sweetened beverages] are a viable alternative to water as a replacement strategy in adults with overweight or obesity who are at risk for or have diabetes,” states one of two syntheses (the other is in press in Diabetes Care) for the update of the European Association for the Study of Diabetes guidelines coming in the fall of 2022.
“The bottom line” for the current study, according to Dr. Sievenpiper, “is that it is difficult to disentangle the signals for low- and no-calorie sweeteners from obesity itself and the signals for the sugars and calories that they are replacing/displacing in this analysis. Substitution analyses would be useful to address some of these concerns.”
Conflicting results
Recent epidemiologic and animal studies about a possible link between artificial sweeteners and risk of cancer have had conflicting results, and information about specific types of sweeteners and consumption of artificially sweetened foods as well as beverages is lacking, Ms. Debras and colleagues wrote.
They aimed to investigate the associations between intakes of artificial sweeteners (total and the most common ones – aspartame, acesulfame-K, and sucralose) and cancer risk (overall risk and most frequent types – breast, prostate, and obesity-related cancers) in the ongoing NutriNet-Santé study.
“Obesity-related cancers are cancers for which obesity is involved in their etiology as one of the risk (or protective) factors, as recognized by the World Cancer Research Fund (independently of participant BMI [body mass index] status): colorectal, stomach, liver, mouth, pharynx, larynx, esophageal, breast (with opposite associations pre- and post menopause), ovarian, endometrial, and prostate cancers,” the researchers explained.
According to a recent study , “obesity increases the risk of breast cancer in postmenopausal women but, conversely, it appears to be protective in premenopausal women,” Dr. Sievenpiper noted.
The ongoing NutriNet-Santé study was initiated in 2009 to investigate associations between nutrition and health in the French population. Participants aged 18 and older with Internet access enroll voluntarily and self-report medical history and sociodemographic, diet, lifestyle, and health data.
The current cohort included 102,865 adults who enrolled in 2009-2021.
Consumption of artificial sweeteners was determined from repeated 24-hour dietary records that included brand names of processed foods.
At enrollment, participants were an average age of 42 years and 79% were women. They had a mean BMI of 24 kg/m2. On average, they had 5.6 dietary records.
Most participants did not consume artificial sweeteners (63%); those who did were classified as lower consumers (18.5%) or higher consumers (18.5%).
Aspartame was the most common artificial sweetener (58% of intake), followed by acesulfame-K (29%) and sucralose (10%), and these were mostly in soft drinks (53%), table-top sweeteners (29%), and yogurt/cottage cheese (8%).
During a median 7.7-year follow-up, 3,358 incident cancers – 982 breast, 403 prostate, and 2023 obesity-related cancers – were diagnosed in participants who were a mean age of 60.
Compared with nonconsumers, higher consumers of artificial sweeteners had a higher risk of overall cancer (hazard ratio, 1.13; 95% confidence interval, 1.03-1.25; P-trend = .002), after adjusting for age, sex, education, physical activity, smoking, BMI, height, weight gain during follow-up, diabetes, family history of cancer, number of 24-hour dietary records, baseline caloric intake, and consumption of alcohol, sodium, saturated fatty acids, fiber, sugar, fruit and vegetables, whole-grain foods, and dairy products.
Participants who were higher consumers of aspartame had an increased risk of overall cancer (HR, 1.15; 95% CI, 1.03-1.28; P = .002), as did higher consumers of acesulfame-K (HR, 1.13; 95% CI, 1.01-1.26; P = .007), compared with nonconsumers, after adjusting for the multiple variables.
Higher consumers of aspartame had a higher risk of breast cancer (HR, 1.22; 95% CI, 1.01-1.48; P = .036) and obesity-related cancers (HR, 1.15; 95% CI, 1.01-1.32; P = .026) than nonconsumers.
Higher consumers of total artificial sweeteners had a higher risk of obesity-related cancers than nonconsumers (HR, 1.13; 95% CI, 1.00-1.28; P = .036).
The researchers acknowledged that study limitations include potential selection bias, residual confounding, and reverse causality, though sensitivity analyses were performed to address these concerns.
The NutriNet-Santé study was supported by several French public institutions. Ms. Debras was supported by a grant from the French National Cancer Institute. This project has received funding from the European Research Council, the French National Cancer Institute, the French Ministry of Health, and the IdEx Université de Paris. Dr. Sievenpiper has reported receiving funding from the Tate and Lyle Nutritional Research Fund at the University of Toronto, the Nutrition Trialists Fund at the University of Toronto, and the International Sweeteners Association.
Correction, 3/31: An earlier version of this article erroneously stated that there was a 22% increased risk of overall cancer, rather than breast cancer.
A version of this article first appeared on Medscape.com.
People with higher (above the median) consumption of artificial sweeteners – especially aspartame and acesulfame-potassium (acesulfame-K) – had a 13% higher risk of overall cancer over 8 years than those who did not consume these sweeteners.
Higher consumption of aspartame was associated with a 22% increased risk of breast cancer and a 15% increased risk of obesity-related cancer, compared with not consuming any of these sweeteners.*
These findings from the Nutri-Santé population-based observational study in France were published online March 24, 2022, in PLoS Medicine.
“Our findings do not support the use of artificial sweeteners as safe alternatives for sugar in foods or beverages and provide important and novel information to address the controversies about their potential adverse health effect,” Charlotte Debras, of the French National Institute for Health and Medical Research (Inserm) and Sorbonne Paris Nord University, and colleagues wrote.
“Results from the NutriNet-Santé cohort (n = 102,865) suggest that artificial sweeteners found in many food and beverage brands worldwide may be associated with increased cancer risk, in line with several experimental in vivo/in vitro studies. These findings provide novel information for the re-evaluation of these food additives by health agencies,” they wrote.
Commenting to the U.K. Science Media Center, Duane Mellor, PhD, registered dietitian and senior teaching fellow, Aston (England) University, said: “This study does not prove or even suggest that we should go back to sugar and turn our backs on artificial sweeteners or diet drinks.
“It does, however, suggest that artificial sweeteners are not a perfect replacement for sugar, they come with their own potential risks, as does sugar. The ideal answer is probably to move away from both, however, that may be unappealing to many who like a little sweetness in their life, so ditching the regular or diet soft drink (soda) for water may not be a well-received health message.”
Important analysis, interpret with caution
“I think that this is an important analysis, but the results need to be interpreted with caution,” another expert, John L. Sievenpiper, MD, PhD, associate professor, departments of nutritional sciences and medicine, University of Toronto, said in an interview.
“Large observational studies like this one that assess the exposure to low and no calorie sweeteners with obesity-related chronic diseases are at risk of reverse causality,” he explained. This is “a caveat that is well recognized by investigators in this field ... and guideline and policy makers.”
Reverse causality is a possibility because “it is likely that many high consumers of low- and no-calorie sweeteners (of which aspartame and acesulfame-K are the most common) will be consuming these sweeteners as a weight-loss strategy,” he added, “as opposed to these sweeteners causing obesity and its complications (including cancers).”
His team recently published a Diabetes and Nutrition Study Group–commissioned systematic review and meta-analysis of 17 randomized controlled trials (JAMA Netw Open. 2022;5[3]:e222092). Their findings “suggest that over the moderate term [low- and no-calorie sweetened beverages] are a viable alternative to water as a replacement strategy in adults with overweight or obesity who are at risk for or have diabetes,” states one of two syntheses (the other is in press in Diabetes Care) for the update of the European Association for the Study of Diabetes guidelines coming in the fall of 2022.
“The bottom line” for the current study, according to Dr. Sievenpiper, “is that it is difficult to disentangle the signals for low- and no-calorie sweeteners from obesity itself and the signals for the sugars and calories that they are replacing/displacing in this analysis. Substitution analyses would be useful to address some of these concerns.”
Conflicting results
Recent epidemiologic and animal studies about a possible link between artificial sweeteners and risk of cancer have had conflicting results, and information about specific types of sweeteners and consumption of artificially sweetened foods as well as beverages is lacking, Ms. Debras and colleagues wrote.
They aimed to investigate the associations between intakes of artificial sweeteners (total and the most common ones – aspartame, acesulfame-K, and sucralose) and cancer risk (overall risk and most frequent types – breast, prostate, and obesity-related cancers) in the ongoing NutriNet-Santé study.
“Obesity-related cancers are cancers for which obesity is involved in their etiology as one of the risk (or protective) factors, as recognized by the World Cancer Research Fund (independently of participant BMI [body mass index] status): colorectal, stomach, liver, mouth, pharynx, larynx, esophageal, breast (with opposite associations pre- and post menopause), ovarian, endometrial, and prostate cancers,” the researchers explained.
According to a recent study , “obesity increases the risk of breast cancer in postmenopausal women but, conversely, it appears to be protective in premenopausal women,” Dr. Sievenpiper noted.
The ongoing NutriNet-Santé study was initiated in 2009 to investigate associations between nutrition and health in the French population. Participants aged 18 and older with Internet access enroll voluntarily and self-report medical history and sociodemographic, diet, lifestyle, and health data.
The current cohort included 102,865 adults who enrolled in 2009-2021.
Consumption of artificial sweeteners was determined from repeated 24-hour dietary records that included brand names of processed foods.
At enrollment, participants were an average age of 42 years and 79% were women. They had a mean BMI of 24 kg/m2. On average, they had 5.6 dietary records.
Most participants did not consume artificial sweeteners (63%); those who did were classified as lower consumers (18.5%) or higher consumers (18.5%).
Aspartame was the most common artificial sweetener (58% of intake), followed by acesulfame-K (29%) and sucralose (10%), and these were mostly in soft drinks (53%), table-top sweeteners (29%), and yogurt/cottage cheese (8%).
During a median 7.7-year follow-up, 3,358 incident cancers – 982 breast, 403 prostate, and 2023 obesity-related cancers – were diagnosed in participants who were a mean age of 60.
Compared with nonconsumers, higher consumers of artificial sweeteners had a higher risk of overall cancer (hazard ratio, 1.13; 95% confidence interval, 1.03-1.25; P-trend = .002), after adjusting for age, sex, education, physical activity, smoking, BMI, height, weight gain during follow-up, diabetes, family history of cancer, number of 24-hour dietary records, baseline caloric intake, and consumption of alcohol, sodium, saturated fatty acids, fiber, sugar, fruit and vegetables, whole-grain foods, and dairy products.
Participants who were higher consumers of aspartame had an increased risk of overall cancer (HR, 1.15; 95% CI, 1.03-1.28; P = .002), as did higher consumers of acesulfame-K (HR, 1.13; 95% CI, 1.01-1.26; P = .007), compared with nonconsumers, after adjusting for the multiple variables.
Higher consumers of aspartame had a higher risk of breast cancer (HR, 1.22; 95% CI, 1.01-1.48; P = .036) and obesity-related cancers (HR, 1.15; 95% CI, 1.01-1.32; P = .026) than nonconsumers.
Higher consumers of total artificial sweeteners had a higher risk of obesity-related cancers than nonconsumers (HR, 1.13; 95% CI, 1.00-1.28; P = .036).
The researchers acknowledged that study limitations include potential selection bias, residual confounding, and reverse causality, though sensitivity analyses were performed to address these concerns.
The NutriNet-Santé study was supported by several French public institutions. Ms. Debras was supported by a grant from the French National Cancer Institute. This project has received funding from the European Research Council, the French National Cancer Institute, the French Ministry of Health, and the IdEx Université de Paris. Dr. Sievenpiper has reported receiving funding from the Tate and Lyle Nutritional Research Fund at the University of Toronto, the Nutrition Trialists Fund at the University of Toronto, and the International Sweeteners Association.
Correction, 3/31: An earlier version of this article erroneously stated that there was a 22% increased risk of overall cancer, rather than breast cancer.
A version of this article first appeared on Medscape.com.
People with higher (above the median) consumption of artificial sweeteners – especially aspartame and acesulfame-potassium (acesulfame-K) – had a 13% higher risk of overall cancer over 8 years than those who did not consume these sweeteners.
Higher consumption of aspartame was associated with a 22% increased risk of breast cancer and a 15% increased risk of obesity-related cancer, compared with not consuming any of these sweeteners.*
These findings from the Nutri-Santé population-based observational study in France were published online March 24, 2022, in PLoS Medicine.
“Our findings do not support the use of artificial sweeteners as safe alternatives for sugar in foods or beverages and provide important and novel information to address the controversies about their potential adverse health effect,” Charlotte Debras, of the French National Institute for Health and Medical Research (Inserm) and Sorbonne Paris Nord University, and colleagues wrote.
“Results from the NutriNet-Santé cohort (n = 102,865) suggest that artificial sweeteners found in many food and beverage brands worldwide may be associated with increased cancer risk, in line with several experimental in vivo/in vitro studies. These findings provide novel information for the re-evaluation of these food additives by health agencies,” they wrote.
Commenting to the U.K. Science Media Center, Duane Mellor, PhD, registered dietitian and senior teaching fellow, Aston (England) University, said: “This study does not prove or even suggest that we should go back to sugar and turn our backs on artificial sweeteners or diet drinks.
“It does, however, suggest that artificial sweeteners are not a perfect replacement for sugar, they come with their own potential risks, as does sugar. The ideal answer is probably to move away from both, however, that may be unappealing to many who like a little sweetness in their life, so ditching the regular or diet soft drink (soda) for water may not be a well-received health message.”
Important analysis, interpret with caution
“I think that this is an important analysis, but the results need to be interpreted with caution,” another expert, John L. Sievenpiper, MD, PhD, associate professor, departments of nutritional sciences and medicine, University of Toronto, said in an interview.
“Large observational studies like this one that assess the exposure to low and no calorie sweeteners with obesity-related chronic diseases are at risk of reverse causality,” he explained. This is “a caveat that is well recognized by investigators in this field ... and guideline and policy makers.”
Reverse causality is a possibility because “it is likely that many high consumers of low- and no-calorie sweeteners (of which aspartame and acesulfame-K are the most common) will be consuming these sweeteners as a weight-loss strategy,” he added, “as opposed to these sweeteners causing obesity and its complications (including cancers).”
His team recently published a Diabetes and Nutrition Study Group–commissioned systematic review and meta-analysis of 17 randomized controlled trials (JAMA Netw Open. 2022;5[3]:e222092). Their findings “suggest that over the moderate term [low- and no-calorie sweetened beverages] are a viable alternative to water as a replacement strategy in adults with overweight or obesity who are at risk for or have diabetes,” states one of two syntheses (the other is in press in Diabetes Care) for the update of the European Association for the Study of Diabetes guidelines coming in the fall of 2022.
“The bottom line” for the current study, according to Dr. Sievenpiper, “is that it is difficult to disentangle the signals for low- and no-calorie sweeteners from obesity itself and the signals for the sugars and calories that they are replacing/displacing in this analysis. Substitution analyses would be useful to address some of these concerns.”
Conflicting results
Recent epidemiologic and animal studies about a possible link between artificial sweeteners and risk of cancer have had conflicting results, and information about specific types of sweeteners and consumption of artificially sweetened foods as well as beverages is lacking, Ms. Debras and colleagues wrote.
They aimed to investigate the associations between intakes of artificial sweeteners (total and the most common ones – aspartame, acesulfame-K, and sucralose) and cancer risk (overall risk and most frequent types – breast, prostate, and obesity-related cancers) in the ongoing NutriNet-Santé study.
“Obesity-related cancers are cancers for which obesity is involved in their etiology as one of the risk (or protective) factors, as recognized by the World Cancer Research Fund (independently of participant BMI [body mass index] status): colorectal, stomach, liver, mouth, pharynx, larynx, esophageal, breast (with opposite associations pre- and post menopause), ovarian, endometrial, and prostate cancers,” the researchers explained.
According to a recent study , “obesity increases the risk of breast cancer in postmenopausal women but, conversely, it appears to be protective in premenopausal women,” Dr. Sievenpiper noted.
The ongoing NutriNet-Santé study was initiated in 2009 to investigate associations between nutrition and health in the French population. Participants aged 18 and older with Internet access enroll voluntarily and self-report medical history and sociodemographic, diet, lifestyle, and health data.
The current cohort included 102,865 adults who enrolled in 2009-2021.
Consumption of artificial sweeteners was determined from repeated 24-hour dietary records that included brand names of processed foods.
At enrollment, participants were an average age of 42 years and 79% were women. They had a mean BMI of 24 kg/m2. On average, they had 5.6 dietary records.
Most participants did not consume artificial sweeteners (63%); those who did were classified as lower consumers (18.5%) or higher consumers (18.5%).
Aspartame was the most common artificial sweetener (58% of intake), followed by acesulfame-K (29%) and sucralose (10%), and these were mostly in soft drinks (53%), table-top sweeteners (29%), and yogurt/cottage cheese (8%).
During a median 7.7-year follow-up, 3,358 incident cancers – 982 breast, 403 prostate, and 2023 obesity-related cancers – were diagnosed in participants who were a mean age of 60.
Compared with nonconsumers, higher consumers of artificial sweeteners had a higher risk of overall cancer (hazard ratio, 1.13; 95% confidence interval, 1.03-1.25; P-trend = .002), after adjusting for age, sex, education, physical activity, smoking, BMI, height, weight gain during follow-up, diabetes, family history of cancer, number of 24-hour dietary records, baseline caloric intake, and consumption of alcohol, sodium, saturated fatty acids, fiber, sugar, fruit and vegetables, whole-grain foods, and dairy products.
Participants who were higher consumers of aspartame had an increased risk of overall cancer (HR, 1.15; 95% CI, 1.03-1.28; P = .002), as did higher consumers of acesulfame-K (HR, 1.13; 95% CI, 1.01-1.26; P = .007), compared with nonconsumers, after adjusting for the multiple variables.
Higher consumers of aspartame had a higher risk of breast cancer (HR, 1.22; 95% CI, 1.01-1.48; P = .036) and obesity-related cancers (HR, 1.15; 95% CI, 1.01-1.32; P = .026) than nonconsumers.
Higher consumers of total artificial sweeteners had a higher risk of obesity-related cancers than nonconsumers (HR, 1.13; 95% CI, 1.00-1.28; P = .036).
The researchers acknowledged that study limitations include potential selection bias, residual confounding, and reverse causality, though sensitivity analyses were performed to address these concerns.
The NutriNet-Santé study was supported by several French public institutions. Ms. Debras was supported by a grant from the French National Cancer Institute. This project has received funding from the European Research Council, the French National Cancer Institute, the French Ministry of Health, and the IdEx Université de Paris. Dr. Sievenpiper has reported receiving funding from the Tate and Lyle Nutritional Research Fund at the University of Toronto, the Nutrition Trialists Fund at the University of Toronto, and the International Sweeteners Association.
Correction, 3/31: An earlier version of this article erroneously stated that there was a 22% increased risk of overall cancer, rather than breast cancer.
A version of this article first appeared on Medscape.com.
FROM PLOS MEDICINE
Infectious disease pop quiz: Clinical challenge #20 for the ObGyn
What are the principal microorganisms that cause puerperal mastitis?
Continue to the answer...
Staphylococci and Streptococcus viridans are the 2 dominant microorganisms that cause puerperal mastitis. For the initial treatment of mastitis, the drug of choice is dicloxacillin sodium (500 mg orally every 6 to 8 hours for 7 to 10 days). If the patient has a mild allergy to penicillin, cephalexin (500 mg orally every 6 to 8 hours for 7 to 10 days) is an appropriate alternative. If the allergy to penicillin is severe or if methicillin-resistant Staphylococcus aureus (MRSA) infection is suspected, either clindamycin (300 mg orally twice daily for 7 to 10 days) or trimethoprim-sulfamethoxazole double strength orally twice daily for 7 to 10 days should be used.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.

Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.

Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
What are the principal microorganisms that cause puerperal mastitis?
Continue to the answer...
Staphylococci and Streptococcus viridans are the 2 dominant microorganisms that cause puerperal mastitis. For the initial treatment of mastitis, the drug of choice is dicloxacillin sodium (500 mg orally every 6 to 8 hours for 7 to 10 days). If the patient has a mild allergy to penicillin, cephalexin (500 mg orally every 6 to 8 hours for 7 to 10 days) is an appropriate alternative. If the allergy to penicillin is severe or if methicillin-resistant Staphylococcus aureus (MRSA) infection is suspected, either clindamycin (300 mg orally twice daily for 7 to 10 days) or trimethoprim-sulfamethoxazole double strength orally twice daily for 7 to 10 days should be used.
What are the principal microorganisms that cause puerperal mastitis?
Continue to the answer...
Staphylococci and Streptococcus viridans are the 2 dominant microorganisms that cause puerperal mastitis. For the initial treatment of mastitis, the drug of choice is dicloxacillin sodium (500 mg orally every 6 to 8 hours for 7 to 10 days). If the patient has a mild allergy to penicillin, cephalexin (500 mg orally every 6 to 8 hours for 7 to 10 days) is an appropriate alternative. If the allergy to penicillin is severe or if methicillin-resistant Staphylococcus aureus (MRSA) infection is suspected, either clindamycin (300 mg orally twice daily for 7 to 10 days) or trimethoprim-sulfamethoxazole double strength orally twice daily for 7 to 10 days should be used.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
Few new cancer drugs replace current standards of care
, a new analysis shows.
Of more than 200 agents evaluated, most (42%) received approval as second-, third-, or later-line therapies.
“While there is justified enthusiasm for the high volume of new cancer drug approvals in oncology and malignant hematology, these approvals must be evaluated in the context of their use,” the authors note in a report published online March 15 in JAMA Network Open. Later-line drugs may, for instance, “benefit patients with few alternatives but also add to cost of care and further delay palliative and comfort services” compared to first-line therapies, which may alter “the treatment paradigm for a certain indication.”
The U.S. Food and Drug Administration approves several new cancer drugs each month, but it’s not clear how many transform the treatment landscape.
To investigate, David Benjamin, MD, with the Division of Hematology and Oncology, University of California, Irvine, and colleagues evaluated all 207 cancer drugs approved in the U.S. between May 1, 2016 and May 31, 2021.
The researchers found that only 28 drugs (14%) displaced the prior first-line standard of care for an indication.
Examples of these cancer drugs include alectinib for anaplastic lymphoma kinase rearrangement–positive metastatic non–small cell lung cancer (NSCLC), osimertinib for epidermal growth factor receptor exon 19 deletion or exon 21 L858R substitution NSCLC, atezolizumab plus bevacizumab for unresectable or metastatic hepatocellular carcinoma, and cabozantinib for advanced kidney cancer.
A total of 32 drugs (15%) were approved as first-line alternatives or new drugs. These drugs were approved for use in the first-line setting but did not necessarily replace the standard of care at the time of approval or were first-of-their-class therapies.
Examples of these drug approvals include apalutamide for nonmetastatic castrate-resistant prostate cancer, tepotinib for metastatic MET exon 14-skipping NSCLC, and avapritinib for unresectable or metastatic gastrointestinal stromal tumor with platelet-derived growth factor receptor alpha exon 18 variant, including D842V variant.
A total of 61 drugs (29%) were approved as add-on therapies for use in combination with a previously approved therapy or in the adjuvant or maintenance settings. These drugs “can only increase the cost of care,” the study team says.
Most new approvals (n = 86) were for use in second-, third- or later-line settings, often for patients for whom other treatment options had been exhausted.
The authors highlight disparities among approvals based on tumor type. Lung-related tumors received the most approvals (n = 37), followed by genitourinary tumors (n = 28), leukemia (n = 25), lymphoma (n = 22), breast cancer (n = 19), and gastrointestinal cancers (n = 14).
The authors note that cancer drugs considered new standards of care or approved as first-line setting alternatives could “provide market competition and work to lower cancer drug prices.”
The study was funded by a grant from Arnold Ventures.
A version of this article first appeared on Medscape.com.
, a new analysis shows.
Of more than 200 agents evaluated, most (42%) received approval as second-, third-, or later-line therapies.
“While there is justified enthusiasm for the high volume of new cancer drug approvals in oncology and malignant hematology, these approvals must be evaluated in the context of their use,” the authors note in a report published online March 15 in JAMA Network Open. Later-line drugs may, for instance, “benefit patients with few alternatives but also add to cost of care and further delay palliative and comfort services” compared to first-line therapies, which may alter “the treatment paradigm for a certain indication.”
The U.S. Food and Drug Administration approves several new cancer drugs each month, but it’s not clear how many transform the treatment landscape.
To investigate, David Benjamin, MD, with the Division of Hematology and Oncology, University of California, Irvine, and colleagues evaluated all 207 cancer drugs approved in the U.S. between May 1, 2016 and May 31, 2021.
The researchers found that only 28 drugs (14%) displaced the prior first-line standard of care for an indication.
Examples of these cancer drugs include alectinib for anaplastic lymphoma kinase rearrangement–positive metastatic non–small cell lung cancer (NSCLC), osimertinib for epidermal growth factor receptor exon 19 deletion or exon 21 L858R substitution NSCLC, atezolizumab plus bevacizumab for unresectable or metastatic hepatocellular carcinoma, and cabozantinib for advanced kidney cancer.
A total of 32 drugs (15%) were approved as first-line alternatives or new drugs. These drugs were approved for use in the first-line setting but did not necessarily replace the standard of care at the time of approval or were first-of-their-class therapies.
Examples of these drug approvals include apalutamide for nonmetastatic castrate-resistant prostate cancer, tepotinib for metastatic MET exon 14-skipping NSCLC, and avapritinib for unresectable or metastatic gastrointestinal stromal tumor with platelet-derived growth factor receptor alpha exon 18 variant, including D842V variant.
A total of 61 drugs (29%) were approved as add-on therapies for use in combination with a previously approved therapy or in the adjuvant or maintenance settings. These drugs “can only increase the cost of care,” the study team says.
Most new approvals (n = 86) were for use in second-, third- or later-line settings, often for patients for whom other treatment options had been exhausted.
The authors highlight disparities among approvals based on tumor type. Lung-related tumors received the most approvals (n = 37), followed by genitourinary tumors (n = 28), leukemia (n = 25), lymphoma (n = 22), breast cancer (n = 19), and gastrointestinal cancers (n = 14).
The authors note that cancer drugs considered new standards of care or approved as first-line setting alternatives could “provide market competition and work to lower cancer drug prices.”
The study was funded by a grant from Arnold Ventures.
A version of this article first appeared on Medscape.com.
, a new analysis shows.
Of more than 200 agents evaluated, most (42%) received approval as second-, third-, or later-line therapies.
“While there is justified enthusiasm for the high volume of new cancer drug approvals in oncology and malignant hematology, these approvals must be evaluated in the context of their use,” the authors note in a report published online March 15 in JAMA Network Open. Later-line drugs may, for instance, “benefit patients with few alternatives but also add to cost of care and further delay palliative and comfort services” compared to first-line therapies, which may alter “the treatment paradigm for a certain indication.”
The U.S. Food and Drug Administration approves several new cancer drugs each month, but it’s not clear how many transform the treatment landscape.
To investigate, David Benjamin, MD, with the Division of Hematology and Oncology, University of California, Irvine, and colleagues evaluated all 207 cancer drugs approved in the U.S. between May 1, 2016 and May 31, 2021.
The researchers found that only 28 drugs (14%) displaced the prior first-line standard of care for an indication.
Examples of these cancer drugs include alectinib for anaplastic lymphoma kinase rearrangement–positive metastatic non–small cell lung cancer (NSCLC), osimertinib for epidermal growth factor receptor exon 19 deletion or exon 21 L858R substitution NSCLC, atezolizumab plus bevacizumab for unresectable or metastatic hepatocellular carcinoma, and cabozantinib for advanced kidney cancer.
A total of 32 drugs (15%) were approved as first-line alternatives or new drugs. These drugs were approved for use in the first-line setting but did not necessarily replace the standard of care at the time of approval or were first-of-their-class therapies.
Examples of these drug approvals include apalutamide for nonmetastatic castrate-resistant prostate cancer, tepotinib for metastatic MET exon 14-skipping NSCLC, and avapritinib for unresectable or metastatic gastrointestinal stromal tumor with platelet-derived growth factor receptor alpha exon 18 variant, including D842V variant.
A total of 61 drugs (29%) were approved as add-on therapies for use in combination with a previously approved therapy or in the adjuvant or maintenance settings. These drugs “can only increase the cost of care,” the study team says.
Most new approvals (n = 86) were for use in second-, third- or later-line settings, often for patients for whom other treatment options had been exhausted.
The authors highlight disparities among approvals based on tumor type. Lung-related tumors received the most approvals (n = 37), followed by genitourinary tumors (n = 28), leukemia (n = 25), lymphoma (n = 22), breast cancer (n = 19), and gastrointestinal cancers (n = 14).
The authors note that cancer drugs considered new standards of care or approved as first-line setting alternatives could “provide market competition and work to lower cancer drug prices.”
The study was funded by a grant from Arnold Ventures.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Boring is good. Boring is right. Boring is … interesting
Can you keep it down? I’m trying to be boring
He chides his friends for not looking both ways before crossing the road. He is never questioned by the police because they fall asleep listening to him talk. He has won the office’s coveted perfect attendance award 10 years running. Look out, Dos Equis guy, you’ve got some new competition. That’s right, it’s the most boring man in the world.
For this boring study (sorry, study on boredom) conducted by English researchers and published in Personality and Social Psychology Bulletin, people were surveyed on various jobs and hobbies, ranking them by how exciting or boring they are, as well as how competent someone with those jobs/hobbies would be, their willingness to avoid someone with those jobs/hobbies, and how much they’d need to be paid to spend time with someone who had an undesirable job/hobby.
According to the British public, the most boring person in the world is a religious data analyst who likes to sleep and lives in a small town. In fact, spending time with this person is almost a full-time job on its own: To make it worth their while, survey subjects wanted 35 pounds a day. The boring person also was viewed as less competent, as is anyone with a boring job.
Now, there probably aren’t a lot of religious data analysts out there, but don’t worry, there are plenty of other boring jobs – accounting, tax/insurance, cleaning, and banking rounded out the top five (apparently people don’t like finances) – and hobbies – watching TV, observing animals, and mathematics filled out the top five. In case you’re curious, performing artists, scientists, journalists, health professionals, and teachers were viewed as having exciting jobs; exciting hobbies included gaming, reading, domestic tasks (really?), gardening, and writing.
Lead researcher Wijnand Van Tilburg, PhD, made an excellent point about people with boring jobs: They “have power in society – perhaps we should try not to upset them and stereotype them as boring!”
We think they should lean into it and make The Most Boring Man in the World ads: “When I drive a car off the lot, its value increases because I used the correct lending association. Batman trusts me with his Batmobile insurance. I can make those Cuban cigars tax exempt. Stay financially solvent, my friends.”
Fungi, but make it fashion
Fashion is an expensive and costly industry to sustain. Cotton production takes a toll on the environment, leather production comes with environmental and ethical/moral conundrums, and thanks to fast fashion, about 85% of textiles are being thrown away in the United States.
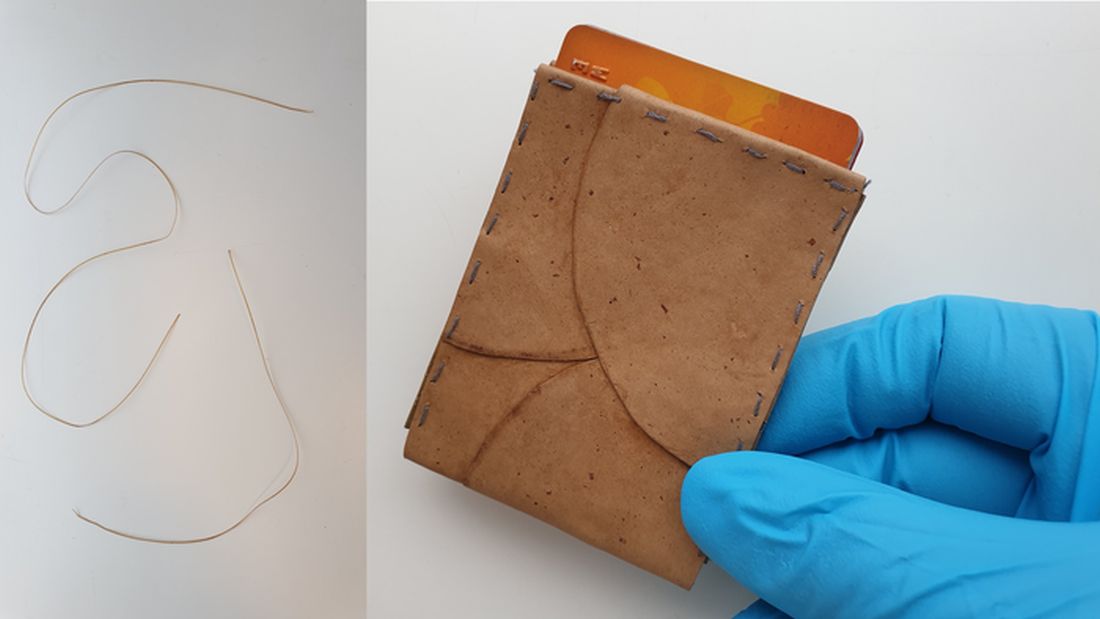
Researchers at the University of Borås in Sweden, however, have found a newish solution to create leather, cotton, and other textiles. And as with so many of the finer things, it starts with unsold bread from the grocery store.
Akram Zamani, PhD, and her team take that bread and turn it into breadcrumbs, then combine it with water and Rhizopus delemar, a fungus typically found in decaying food. After a couple of days of feasting on the bread, the fungus produces natural fibers made of chitin and chitosan that accumulate in the cell walls. After proteins, lipids, and other byproducts are removed, the team is left with a jelly-like substance made of those fibrous cell walls that can be spun into a fabric.
The researchers started small with very thin nonpliable sheets, but with a little layering by using tree tannins for softness and alkali for strength, their fungal leather is more like real leather than competing fungal leathers. Not to mention its being able to be produced in a fraction of the time.
This new fungal leather is fast to produce, it’s biodegradable, and it uses only natural ingredients to treat the materials. It’s the ultimate environmental fashion statement.
Who’s afraid of cancer? Not C. elegans
And now, we bring you part 2 of our ongoing series: Creatures that can diagnose cancer. Last week, we discovered that ants are well on their way to replacing dogs in our medical labs and in our hearts. This week, we present the even-more-lovable nematode.
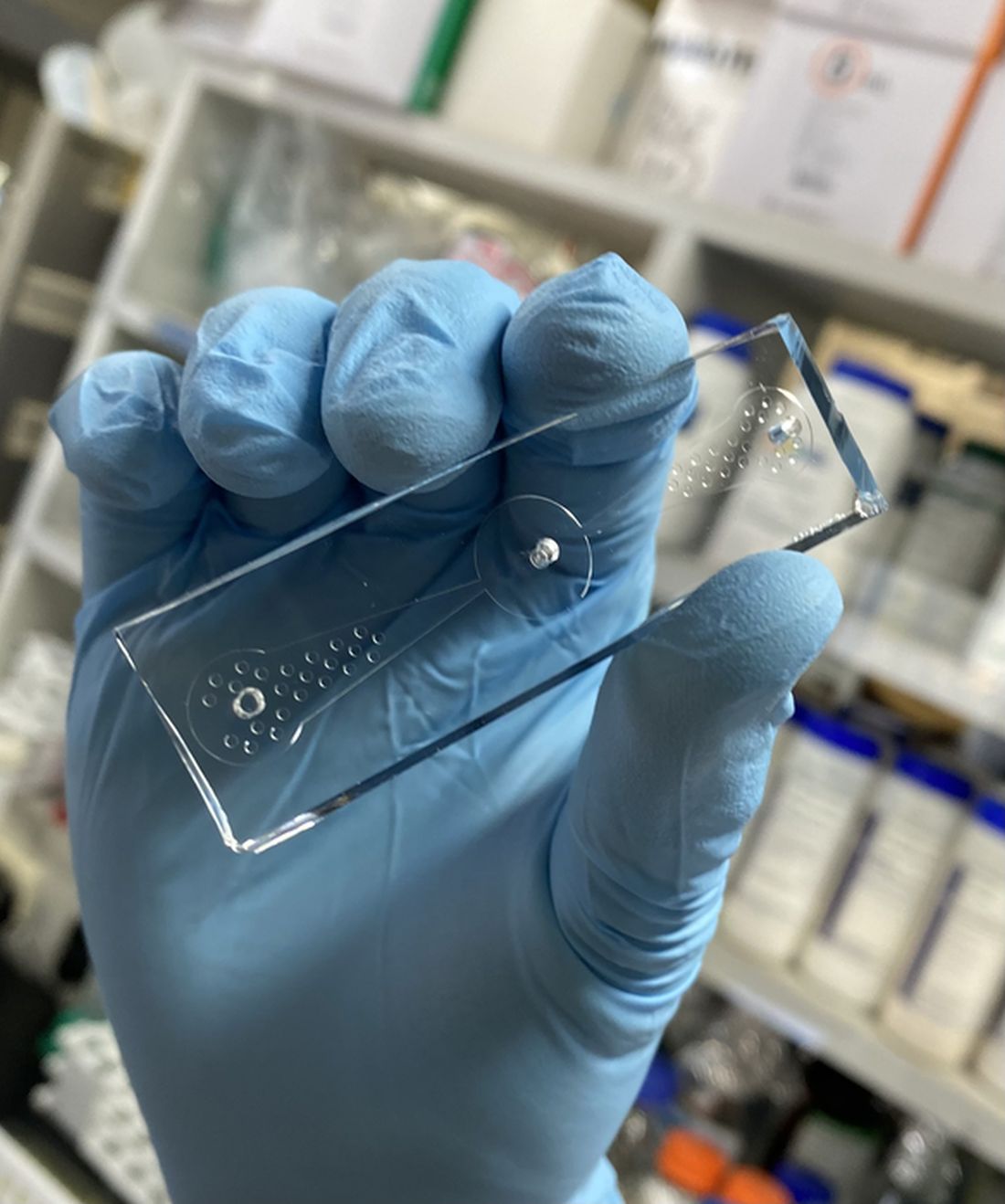
The soil-dwelling nematode Caenorhabditis elegans, which is less than 1 mm long, is known to be “attracted or repelled by certain odors, so we came up with an idea that the roundworm could be used to detect lung cancer,” Shin Sik Choi, PhD, of Myongji University in South Korea, who is the project’s principal investigator, said in a statement on Eurekalert.
Dr. Choi’s team created a “worm-on-a-chip” that allowed the nematodes to choose between a drop of culture media from lung cancer cells and media from normal lung fibroblasts. An hour after being placed in the chip’s central chamber, more nematodes had crawled toward the lung cancer media than the normal-cell sample.
The investigators estimate that the device is about 70% effective at detecting cancer cells, but “they hope to increase both the accuracy and sensitivity of the method by using worms that were previously exposed to cancer cell media and therefore have a ‘memory’ of cancer-specific odor molecules,” according to the statement from the American Chemical Society.
Since C. elegans is easy to grow in a lab and, apparently, easy to train, the researchers hope that the worm-on-a-chip can become a quick, easy, economical, and noninvasive cancer screen.
So watch out cancer, because we never bet against the creepy crawlies.
Mosquitoes have us figured out
We are nearing mosquito season; quite possibly the most annoying and itchy time of the year. We stock up on bottles of bug spray, but somehow we still get bite after bite. It appears that mosquitoes are basically able to ignore our bug sprays, which explains why we’re still covered in bites after the Fourth of July fireworks. It turns out mosquitoes are more complex than we thought for such tiny creatures.

There’s plenty of research on the best ways to keep mosquitoes away, because not only are they incredibly annoying, but they also carry potentially harmful diseases. In a recent experiment, researchers used mosquitoes that were genetically modified to have an excessive amount of an odor receptor called AgOR2, which responds to the smell of humans.
“AgOR2 overexpression threw a wrench in the whole system by inactivating olfactory receptors in these mosquitoes,” Christopher Potter, PhD, associate professor of neuroscience at Johns Hopkins University, said in a written statement.
After testing how these genetically modified mosquitoes reacted to some of the common smells of bug spray such as lemongrass, they discovered that it’s easy for the mosquitoes to ignore the smell. We wish it were that easy for us to ignore that chemically fruity smell.
Researchers continue to work hard to figure out how to repel mosquitoes and we’re rooting for them as summer approaches, despite the mosquito’s status as a creepy crawly.
Can you keep it down? I’m trying to be boring
He chides his friends for not looking both ways before crossing the road. He is never questioned by the police because they fall asleep listening to him talk. He has won the office’s coveted perfect attendance award 10 years running. Look out, Dos Equis guy, you’ve got some new competition. That’s right, it’s the most boring man in the world.
For this boring study (sorry, study on boredom) conducted by English researchers and published in Personality and Social Psychology Bulletin, people were surveyed on various jobs and hobbies, ranking them by how exciting or boring they are, as well as how competent someone with those jobs/hobbies would be, their willingness to avoid someone with those jobs/hobbies, and how much they’d need to be paid to spend time with someone who had an undesirable job/hobby.
According to the British public, the most boring person in the world is a religious data analyst who likes to sleep and lives in a small town. In fact, spending time with this person is almost a full-time job on its own: To make it worth their while, survey subjects wanted 35 pounds a day. The boring person also was viewed as less competent, as is anyone with a boring job.
Now, there probably aren’t a lot of religious data analysts out there, but don’t worry, there are plenty of other boring jobs – accounting, tax/insurance, cleaning, and banking rounded out the top five (apparently people don’t like finances) – and hobbies – watching TV, observing animals, and mathematics filled out the top five. In case you’re curious, performing artists, scientists, journalists, health professionals, and teachers were viewed as having exciting jobs; exciting hobbies included gaming, reading, domestic tasks (really?), gardening, and writing.
Lead researcher Wijnand Van Tilburg, PhD, made an excellent point about people with boring jobs: They “have power in society – perhaps we should try not to upset them and stereotype them as boring!”
We think they should lean into it and make The Most Boring Man in the World ads: “When I drive a car off the lot, its value increases because I used the correct lending association. Batman trusts me with his Batmobile insurance. I can make those Cuban cigars tax exempt. Stay financially solvent, my friends.”
Fungi, but make it fashion
Fashion is an expensive and costly industry to sustain. Cotton production takes a toll on the environment, leather production comes with environmental and ethical/moral conundrums, and thanks to fast fashion, about 85% of textiles are being thrown away in the United States.
Researchers at the University of Borås in Sweden, however, have found a newish solution to create leather, cotton, and other textiles. And as with so many of the finer things, it starts with unsold bread from the grocery store.
Akram Zamani, PhD, and her team take that bread and turn it into breadcrumbs, then combine it with water and Rhizopus delemar, a fungus typically found in decaying food. After a couple of days of feasting on the bread, the fungus produces natural fibers made of chitin and chitosan that accumulate in the cell walls. After proteins, lipids, and other byproducts are removed, the team is left with a jelly-like substance made of those fibrous cell walls that can be spun into a fabric.
The researchers started small with very thin nonpliable sheets, but with a little layering by using tree tannins for softness and alkali for strength, their fungal leather is more like real leather than competing fungal leathers. Not to mention its being able to be produced in a fraction of the time.
This new fungal leather is fast to produce, it’s biodegradable, and it uses only natural ingredients to treat the materials. It’s the ultimate environmental fashion statement.
Who’s afraid of cancer? Not C. elegans
And now, we bring you part 2 of our ongoing series: Creatures that can diagnose cancer. Last week, we discovered that ants are well on their way to replacing dogs in our medical labs and in our hearts. This week, we present the even-more-lovable nematode.
The soil-dwelling nematode Caenorhabditis elegans, which is less than 1 mm long, is known to be “attracted or repelled by certain odors, so we came up with an idea that the roundworm could be used to detect lung cancer,” Shin Sik Choi, PhD, of Myongji University in South Korea, who is the project’s principal investigator, said in a statement on Eurekalert.
Dr. Choi’s team created a “worm-on-a-chip” that allowed the nematodes to choose between a drop of culture media from lung cancer cells and media from normal lung fibroblasts. An hour after being placed in the chip’s central chamber, more nematodes had crawled toward the lung cancer media than the normal-cell sample.
The investigators estimate that the device is about 70% effective at detecting cancer cells, but “they hope to increase both the accuracy and sensitivity of the method by using worms that were previously exposed to cancer cell media and therefore have a ‘memory’ of cancer-specific odor molecules,” according to the statement from the American Chemical Society.
Since C. elegans is easy to grow in a lab and, apparently, easy to train, the researchers hope that the worm-on-a-chip can become a quick, easy, economical, and noninvasive cancer screen.
So watch out cancer, because we never bet against the creepy crawlies.
Mosquitoes have us figured out
We are nearing mosquito season; quite possibly the most annoying and itchy time of the year. We stock up on bottles of bug spray, but somehow we still get bite after bite. It appears that mosquitoes are basically able to ignore our bug sprays, which explains why we’re still covered in bites after the Fourth of July fireworks. It turns out mosquitoes are more complex than we thought for such tiny creatures.
There’s plenty of research on the best ways to keep mosquitoes away, because not only are they incredibly annoying, but they also carry potentially harmful diseases. In a recent experiment, researchers used mosquitoes that were genetically modified to have an excessive amount of an odor receptor called AgOR2, which responds to the smell of humans.
“AgOR2 overexpression threw a wrench in the whole system by inactivating olfactory receptors in these mosquitoes,” Christopher Potter, PhD, associate professor of neuroscience at Johns Hopkins University, said in a written statement.
After testing how these genetically modified mosquitoes reacted to some of the common smells of bug spray such as lemongrass, they discovered that it’s easy for the mosquitoes to ignore the smell. We wish it were that easy for us to ignore that chemically fruity smell.
Researchers continue to work hard to figure out how to repel mosquitoes and we’re rooting for them as summer approaches, despite the mosquito’s status as a creepy crawly.
Can you keep it down? I’m trying to be boring
He chides his friends for not looking both ways before crossing the road. He is never questioned by the police because they fall asleep listening to him talk. He has won the office’s coveted perfect attendance award 10 years running. Look out, Dos Equis guy, you’ve got some new competition. That’s right, it’s the most boring man in the world.
For this boring study (sorry, study on boredom) conducted by English researchers and published in Personality and Social Psychology Bulletin, people were surveyed on various jobs and hobbies, ranking them by how exciting or boring they are, as well as how competent someone with those jobs/hobbies would be, their willingness to avoid someone with those jobs/hobbies, and how much they’d need to be paid to spend time with someone who had an undesirable job/hobby.
According to the British public, the most boring person in the world is a religious data analyst who likes to sleep and lives in a small town. In fact, spending time with this person is almost a full-time job on its own: To make it worth their while, survey subjects wanted 35 pounds a day. The boring person also was viewed as less competent, as is anyone with a boring job.
Now, there probably aren’t a lot of religious data analysts out there, but don’t worry, there are plenty of other boring jobs – accounting, tax/insurance, cleaning, and banking rounded out the top five (apparently people don’t like finances) – and hobbies – watching TV, observing animals, and mathematics filled out the top five. In case you’re curious, performing artists, scientists, journalists, health professionals, and teachers were viewed as having exciting jobs; exciting hobbies included gaming, reading, domestic tasks (really?), gardening, and writing.
Lead researcher Wijnand Van Tilburg, PhD, made an excellent point about people with boring jobs: They “have power in society – perhaps we should try not to upset them and stereotype them as boring!”
We think they should lean into it and make The Most Boring Man in the World ads: “When I drive a car off the lot, its value increases because I used the correct lending association. Batman trusts me with his Batmobile insurance. I can make those Cuban cigars tax exempt. Stay financially solvent, my friends.”
Fungi, but make it fashion
Fashion is an expensive and costly industry to sustain. Cotton production takes a toll on the environment, leather production comes with environmental and ethical/moral conundrums, and thanks to fast fashion, about 85% of textiles are being thrown away in the United States.
Researchers at the University of Borås in Sweden, however, have found a newish solution to create leather, cotton, and other textiles. And as with so many of the finer things, it starts with unsold bread from the grocery store.
Akram Zamani, PhD, and her team take that bread and turn it into breadcrumbs, then combine it with water and Rhizopus delemar, a fungus typically found in decaying food. After a couple of days of feasting on the bread, the fungus produces natural fibers made of chitin and chitosan that accumulate in the cell walls. After proteins, lipids, and other byproducts are removed, the team is left with a jelly-like substance made of those fibrous cell walls that can be spun into a fabric.
The researchers started small with very thin nonpliable sheets, but with a little layering by using tree tannins for softness and alkali for strength, their fungal leather is more like real leather than competing fungal leathers. Not to mention its being able to be produced in a fraction of the time.
This new fungal leather is fast to produce, it’s biodegradable, and it uses only natural ingredients to treat the materials. It’s the ultimate environmental fashion statement.
Who’s afraid of cancer? Not C. elegans
And now, we bring you part 2 of our ongoing series: Creatures that can diagnose cancer. Last week, we discovered that ants are well on their way to replacing dogs in our medical labs and in our hearts. This week, we present the even-more-lovable nematode.
The soil-dwelling nematode Caenorhabditis elegans, which is less than 1 mm long, is known to be “attracted or repelled by certain odors, so we came up with an idea that the roundworm could be used to detect lung cancer,” Shin Sik Choi, PhD, of Myongji University in South Korea, who is the project’s principal investigator, said in a statement on Eurekalert.
Dr. Choi’s team created a “worm-on-a-chip” that allowed the nematodes to choose between a drop of culture media from lung cancer cells and media from normal lung fibroblasts. An hour after being placed in the chip’s central chamber, more nematodes had crawled toward the lung cancer media than the normal-cell sample.
The investigators estimate that the device is about 70% effective at detecting cancer cells, but “they hope to increase both the accuracy and sensitivity of the method by using worms that were previously exposed to cancer cell media and therefore have a ‘memory’ of cancer-specific odor molecules,” according to the statement from the American Chemical Society.
Since C. elegans is easy to grow in a lab and, apparently, easy to train, the researchers hope that the worm-on-a-chip can become a quick, easy, economical, and noninvasive cancer screen.
So watch out cancer, because we never bet against the creepy crawlies.
Mosquitoes have us figured out
We are nearing mosquito season; quite possibly the most annoying and itchy time of the year. We stock up on bottles of bug spray, but somehow we still get bite after bite. It appears that mosquitoes are basically able to ignore our bug sprays, which explains why we’re still covered in bites after the Fourth of July fireworks. It turns out mosquitoes are more complex than we thought for such tiny creatures.
There’s plenty of research on the best ways to keep mosquitoes away, because not only are they incredibly annoying, but they also carry potentially harmful diseases. In a recent experiment, researchers used mosquitoes that were genetically modified to have an excessive amount of an odor receptor called AgOR2, which responds to the smell of humans.
“AgOR2 overexpression threw a wrench in the whole system by inactivating olfactory receptors in these mosquitoes,” Christopher Potter, PhD, associate professor of neuroscience at Johns Hopkins University, said in a written statement.
After testing how these genetically modified mosquitoes reacted to some of the common smells of bug spray such as lemongrass, they discovered that it’s easy for the mosquitoes to ignore the smell. We wish it were that easy for us to ignore that chemically fruity smell.
Researchers continue to work hard to figure out how to repel mosquitoes and we’re rooting for them as summer approaches, despite the mosquito’s status as a creepy crawly.
Coordinating cancer care for patients displaced by war
across the border into neighboring countries, which makes the role of oncology groups vitally important.
“They’re trying to deal with an extremely vulnerable and traumatized population – children who’ve lost their families, elderly who are confused and potentially abandoned,” commented Richard Sullivan, MD, PhD.
“The triage that’s happening on the border is not focusing on noncommunicable diseases,” he continued. “We know from previous crises that many cancer patients are lost; they simply do not present with their symptoms once they become refugees, and that’s going to become a really big issue.”
Oncology groups are needed to “provide the navigation, the treatment, and also the intelligence to ensure we deliver excellent cancer care where it’s needed for our Ukrainian friends,” he added. Dr. Sullivan is a member of the World Health Organization’s Emergency Committee and is director of the Institute of Cancer Policy at King’s College London.
He was speaking at a virtual briefing organized by the American Society of Clinical Oncology (ASCO) and the European Cancer Organisation (ECO), which have joined forces to centralize cancer care efforts.
With an estimated 3.3 million refugees having already crossed Ukraine’s borders, neighboring countries are experiencing an approximately 5% increase in their overall populations, making increased demand for cancer care inevitable, said Dr. Sullivan.
“Suggestions are that with 4 million refugees, you’re going to be looking at an increase of 13,000-16,000 cancer patients per month. ... But it will take time for the issue to evolve. At the moment, people are not being overwhelmed ... but there’s no doubt cancer care capacity for host countries is going to be an issue in the future.”
So far, about 2 million refugees are in Poland, where cancer centers have experienced a 10% increase in new patients since the war started, said Piotr Rutkowski, MD, PhD, professor of surgical oncology at the Maria Sklodowska-Curie Memorial Cancer Center and Institute of Oncology in Warsaw.
“Of course, our resources are limited,” he said, adding that efforts are underway to accredit Ukrainian health care workers to work in Poland. “It’s unpredictable how the health care system in Europe can overcome these difficulties.”
“Until now, I don’t think any cancer patients have not received care, so still, we are in a positive situation, but the waiting list can enlarge in the near future,” Dr. Rutkowsli commented.
Indeed, the anticipated increase will “likely exceed the possibilities of the Polish health system” soon, warned Jacek Jassem, MD, PhD, professor of clinical oncology and radiotherapy and the head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
Although there is an EU international agreement for a more widespread allocation of cancer patients, “when they come to Poland, many of them want to be treated in Poland, because they have family here, the language is more familiar.”
Dr. Jassem suggests the best way to avoid overwhelming host cancer centers is to triage patients directly from Ukraine. “Some therapies shouldn’t be interrupted. So, for example, radiotherapy started in Ukraine should be continued there, but otherwise, chemotherapy can be continued elsewhere, surgery may be postponed and done elsewhere. These are the decisions that should be considered in Ukraine, and then patients who are selected for particular therapies should be reallocated to other countries,” he suggested.
Romania has seen an influx of about 400,000 refugees, including cancer patients seeking systemic therapy, radiotherapy, or follow-up, said Nicoleta Antone, MD, a medical oncologist at the Cancer Institute of Ion Chiricuta in Cluj-Napoca, Romania. “We have seen patients mainly with breast cancer because most of the refugees [with cancer] are women looking for systemic therapy, but also all the other tumor types, both solid and hematologic tumors.”
Dr. Sullivan says attempts by EU member states to address cancer needs are complicated by the fact that many refugees are still on the move. They have been passing through their initial host countries and moving on to Greece, Slovenia, Austria, Germany, Italy, and Turkey, “making the therapeutic geographies at any potential time quite challenging to keep an eye on.” Other countries, such as Moldova, are not part of the EU, “so we dealing with some really quite complex political and financial issues.”
The situation calls for a broader approach to refugees generally, he added. “We’re talking free cancer care for Ukrainian patients, but there’s also, of course, this dialogue of ensuring there’s free care for all refugees. Europe already has a large refugee contingent from other countries, so there’s no doubt this is an opportunity to talk more broadly about cancer care for refugees and also progressive universalism.
“You can’t have rules for one set of patients and a different set of rules for another set of patients, so there’s going to be a real issue around fairness and equity which Europe is going to have to address,” he said.
In an attempt, ASCO and ECO have joined forces in a special network, noted Julie Gralow, MD, chief medical officer at ASCO.
“The ECO/ASCO Special Network is all about collaboration and coordination across professional societies, across cancer patient groups, across academic and other clinical centers. We’re providing information in the various national languages and trying to amplify the work that each of us is doing. ... We’re sharing intelligence, regular reports from the field, information, experience, and most of all, contacts. We’re all being approached individually about people who need help or people who want to help, and we’re trying to bring this all together in a focused way.”
Separately, there is also an ASCO resource page, as well as an ECO resource page.
The American Cancer Society also has patient resources on their site, including a 24-hour international call center in multiple languages and a Volunteer Corp of Clinicians, which currently has 123 active volunteers (and another 300 applicants) available to answer questions.
Europe and other countries must consider both a medium and a long-term commitment to refugees with cancer, said Dr. Sullivan. “Because even if the war stopped tomorrow, it’s going to take between a year and a year and a half to rebuild cancer care in Ukraine.”
A version of this article first appeared on Medscape.com.
across the border into neighboring countries, which makes the role of oncology groups vitally important.
“They’re trying to deal with an extremely vulnerable and traumatized population – children who’ve lost their families, elderly who are confused and potentially abandoned,” commented Richard Sullivan, MD, PhD.
“The triage that’s happening on the border is not focusing on noncommunicable diseases,” he continued. “We know from previous crises that many cancer patients are lost; they simply do not present with their symptoms once they become refugees, and that’s going to become a really big issue.”
Oncology groups are needed to “provide the navigation, the treatment, and also the intelligence to ensure we deliver excellent cancer care where it’s needed for our Ukrainian friends,” he added. Dr. Sullivan is a member of the World Health Organization’s Emergency Committee and is director of the Institute of Cancer Policy at King’s College London.
He was speaking at a virtual briefing organized by the American Society of Clinical Oncology (ASCO) and the European Cancer Organisation (ECO), which have joined forces to centralize cancer care efforts.
With an estimated 3.3 million refugees having already crossed Ukraine’s borders, neighboring countries are experiencing an approximately 5% increase in their overall populations, making increased demand for cancer care inevitable, said Dr. Sullivan.
“Suggestions are that with 4 million refugees, you’re going to be looking at an increase of 13,000-16,000 cancer patients per month. ... But it will take time for the issue to evolve. At the moment, people are not being overwhelmed ... but there’s no doubt cancer care capacity for host countries is going to be an issue in the future.”
So far, about 2 million refugees are in Poland, where cancer centers have experienced a 10% increase in new patients since the war started, said Piotr Rutkowski, MD, PhD, professor of surgical oncology at the Maria Sklodowska-Curie Memorial Cancer Center and Institute of Oncology in Warsaw.
“Of course, our resources are limited,” he said, adding that efforts are underway to accredit Ukrainian health care workers to work in Poland. “It’s unpredictable how the health care system in Europe can overcome these difficulties.”
“Until now, I don’t think any cancer patients have not received care, so still, we are in a positive situation, but the waiting list can enlarge in the near future,” Dr. Rutkowsli commented.
Indeed, the anticipated increase will “likely exceed the possibilities of the Polish health system” soon, warned Jacek Jassem, MD, PhD, professor of clinical oncology and radiotherapy and the head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
Although there is an EU international agreement for a more widespread allocation of cancer patients, “when they come to Poland, many of them want to be treated in Poland, because they have family here, the language is more familiar.”
Dr. Jassem suggests the best way to avoid overwhelming host cancer centers is to triage patients directly from Ukraine. “Some therapies shouldn’t be interrupted. So, for example, radiotherapy started in Ukraine should be continued there, but otherwise, chemotherapy can be continued elsewhere, surgery may be postponed and done elsewhere. These are the decisions that should be considered in Ukraine, and then patients who are selected for particular therapies should be reallocated to other countries,” he suggested.
Romania has seen an influx of about 400,000 refugees, including cancer patients seeking systemic therapy, radiotherapy, or follow-up, said Nicoleta Antone, MD, a medical oncologist at the Cancer Institute of Ion Chiricuta in Cluj-Napoca, Romania. “We have seen patients mainly with breast cancer because most of the refugees [with cancer] are women looking for systemic therapy, but also all the other tumor types, both solid and hematologic tumors.”
Dr. Sullivan says attempts by EU member states to address cancer needs are complicated by the fact that many refugees are still on the move. They have been passing through their initial host countries and moving on to Greece, Slovenia, Austria, Germany, Italy, and Turkey, “making the therapeutic geographies at any potential time quite challenging to keep an eye on.” Other countries, such as Moldova, are not part of the EU, “so we dealing with some really quite complex political and financial issues.”
The situation calls for a broader approach to refugees generally, he added. “We’re talking free cancer care for Ukrainian patients, but there’s also, of course, this dialogue of ensuring there’s free care for all refugees. Europe already has a large refugee contingent from other countries, so there’s no doubt this is an opportunity to talk more broadly about cancer care for refugees and also progressive universalism.
“You can’t have rules for one set of patients and a different set of rules for another set of patients, so there’s going to be a real issue around fairness and equity which Europe is going to have to address,” he said.
In an attempt, ASCO and ECO have joined forces in a special network, noted Julie Gralow, MD, chief medical officer at ASCO.
“The ECO/ASCO Special Network is all about collaboration and coordination across professional societies, across cancer patient groups, across academic and other clinical centers. We’re providing information in the various national languages and trying to amplify the work that each of us is doing. ... We’re sharing intelligence, regular reports from the field, information, experience, and most of all, contacts. We’re all being approached individually about people who need help or people who want to help, and we’re trying to bring this all together in a focused way.”
Separately, there is also an ASCO resource page, as well as an ECO resource page.
The American Cancer Society also has patient resources on their site, including a 24-hour international call center in multiple languages and a Volunteer Corp of Clinicians, which currently has 123 active volunteers (and another 300 applicants) available to answer questions.
Europe and other countries must consider both a medium and a long-term commitment to refugees with cancer, said Dr. Sullivan. “Because even if the war stopped tomorrow, it’s going to take between a year and a year and a half to rebuild cancer care in Ukraine.”
A version of this article first appeared on Medscape.com.
across the border into neighboring countries, which makes the role of oncology groups vitally important.
“They’re trying to deal with an extremely vulnerable and traumatized population – children who’ve lost their families, elderly who are confused and potentially abandoned,” commented Richard Sullivan, MD, PhD.
“The triage that’s happening on the border is not focusing on noncommunicable diseases,” he continued. “We know from previous crises that many cancer patients are lost; they simply do not present with their symptoms once they become refugees, and that’s going to become a really big issue.”
Oncology groups are needed to “provide the navigation, the treatment, and also the intelligence to ensure we deliver excellent cancer care where it’s needed for our Ukrainian friends,” he added. Dr. Sullivan is a member of the World Health Organization’s Emergency Committee and is director of the Institute of Cancer Policy at King’s College London.
He was speaking at a virtual briefing organized by the American Society of Clinical Oncology (ASCO) and the European Cancer Organisation (ECO), which have joined forces to centralize cancer care efforts.
With an estimated 3.3 million refugees having already crossed Ukraine’s borders, neighboring countries are experiencing an approximately 5% increase in their overall populations, making increased demand for cancer care inevitable, said Dr. Sullivan.
“Suggestions are that with 4 million refugees, you’re going to be looking at an increase of 13,000-16,000 cancer patients per month. ... But it will take time for the issue to evolve. At the moment, people are not being overwhelmed ... but there’s no doubt cancer care capacity for host countries is going to be an issue in the future.”
So far, about 2 million refugees are in Poland, where cancer centers have experienced a 10% increase in new patients since the war started, said Piotr Rutkowski, MD, PhD, professor of surgical oncology at the Maria Sklodowska-Curie Memorial Cancer Center and Institute of Oncology in Warsaw.
“Of course, our resources are limited,” he said, adding that efforts are underway to accredit Ukrainian health care workers to work in Poland. “It’s unpredictable how the health care system in Europe can overcome these difficulties.”
“Until now, I don’t think any cancer patients have not received care, so still, we are in a positive situation, but the waiting list can enlarge in the near future,” Dr. Rutkowsli commented.
Indeed, the anticipated increase will “likely exceed the possibilities of the Polish health system” soon, warned Jacek Jassem, MD, PhD, professor of clinical oncology and radiotherapy and the head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
Although there is an EU international agreement for a more widespread allocation of cancer patients, “when they come to Poland, many of them want to be treated in Poland, because they have family here, the language is more familiar.”
Dr. Jassem suggests the best way to avoid overwhelming host cancer centers is to triage patients directly from Ukraine. “Some therapies shouldn’t be interrupted. So, for example, radiotherapy started in Ukraine should be continued there, but otherwise, chemotherapy can be continued elsewhere, surgery may be postponed and done elsewhere. These are the decisions that should be considered in Ukraine, and then patients who are selected for particular therapies should be reallocated to other countries,” he suggested.
Romania has seen an influx of about 400,000 refugees, including cancer patients seeking systemic therapy, radiotherapy, or follow-up, said Nicoleta Antone, MD, a medical oncologist at the Cancer Institute of Ion Chiricuta in Cluj-Napoca, Romania. “We have seen patients mainly with breast cancer because most of the refugees [with cancer] are women looking for systemic therapy, but also all the other tumor types, both solid and hematologic tumors.”
Dr. Sullivan says attempts by EU member states to address cancer needs are complicated by the fact that many refugees are still on the move. They have been passing through their initial host countries and moving on to Greece, Slovenia, Austria, Germany, Italy, and Turkey, “making the therapeutic geographies at any potential time quite challenging to keep an eye on.” Other countries, such as Moldova, are not part of the EU, “so we dealing with some really quite complex political and financial issues.”
The situation calls for a broader approach to refugees generally, he added. “We’re talking free cancer care for Ukrainian patients, but there’s also, of course, this dialogue of ensuring there’s free care for all refugees. Europe already has a large refugee contingent from other countries, so there’s no doubt this is an opportunity to talk more broadly about cancer care for refugees and also progressive universalism.
“You can’t have rules for one set of patients and a different set of rules for another set of patients, so there’s going to be a real issue around fairness and equity which Europe is going to have to address,” he said.
In an attempt, ASCO and ECO have joined forces in a special network, noted Julie Gralow, MD, chief medical officer at ASCO.
“The ECO/ASCO Special Network is all about collaboration and coordination across professional societies, across cancer patient groups, across academic and other clinical centers. We’re providing information in the various national languages and trying to amplify the work that each of us is doing. ... We’re sharing intelligence, regular reports from the field, information, experience, and most of all, contacts. We’re all being approached individually about people who need help or people who want to help, and we’re trying to bring this all together in a focused way.”
Separately, there is also an ASCO resource page, as well as an ECO resource page.
The American Cancer Society also has patient resources on their site, including a 24-hour international call center in multiple languages and a Volunteer Corp of Clinicians, which currently has 123 active volunteers (and another 300 applicants) available to answer questions.
Europe and other countries must consider both a medium and a long-term commitment to refugees with cancer, said Dr. Sullivan. “Because even if the war stopped tomorrow, it’s going to take between a year and a year and a half to rebuild cancer care in Ukraine.”
A version of this article first appeared on Medscape.com.
Are ‘antibiotic diets’ good practice?
Antibiotics are among the most commonly prescribed medications in both outpatient and hospital settings. Global efforts at curbing antibiotic-resistant strains have prompted clinicians to pursue better stewardship, whereby they limit their prescribing of such medications to those who truly need them.
Yet there’s another possible means of addressing antibiotic resistance – using dietary interventions to reduce the gastrointestinal complaints that so often accompany the use of antibiotics: vomiting, nausea, diarrhea, bloating/indigestion, abdominal pain, and loss of appetite. Far from being a mere nuisance, these complications can have major ramifications.
“Often [these side effects] will result in people stopping an antibiotic they need or taking a second- or third-generation one, which potentially causes even more problems with resistance,” explained Daniel J. Merenstein, MD, a professor of family medicine at Georgetown University, Washington, who has conducted multiple trials on antibiotic stewardship and probiotics.
And it’s not just clinicians who would like to find a way around these common complaints. On lifestyle blogs such as Livestrong and Goop, medical news websites, and via academic institutions, patients can learn how the right probiotic supplement or certain fermented or high-fiber foods, for example, might spare them the upset stomach that often accompanies a course of antibiotics.
Yet according to experts in the field, there are notable questions to be answered about whether there’s evidence to support this approach.
The cost of GI discomfort
Pinpointing the exact manner by which antibiotics upend GI tracts is a complex task, according to Gail Cresci, PhD, RD, a microbiome researcher in the department of pediatric gastroenterology, hepatology, and nutrition and director of nutrition research at the Cleveland Clinic.
“A lot of different mechanisms can go awry,” Dr. Cresci said. “But normally, the good microbes are there to help keep the balance, so when that balance is gone, the pathogens can take over and lead to this disruption.”
According to Lynne V. McFarland, PhD, a recently retired infectious disease epidemiologist who now serves as a private consultant, such complications can have substantial ramifications for patients and health care systems.
“If you’re an inpatient and develop antibiotic-associated diarrhea, it usually increases the length of stay from 8 to 20 days. It also increases the cost of care. And small children who have this can get severely dehydrated, which can become life threatening.”
Proponents of probiotics
Several of the researchers who were interviewed believe there’s convincing evidence supporting probiotics for the treatment of common antibiotic-related GI complaints. In many instances, they were involved in the studies themselves.
During Dr. McFarland’s 4-decade career in probiotics research, she has participated in early animal studies with strains such as Saccharomyces boulardii and was involved in meta-analyses of their role in Clostridioides difficile infection and associated diarrhea and even as a potential GI intervention for COVID-19 patients (Antibiotics (Basel). 2021 Apr 9;10(4):408).
In mouse model studies from 2013 and 2018, Dr. Cresci and colleagues showed that the probiotic strains Lactobacillus GG and Faecalibacterium prausnitzii reduced the structural gut changes that lead to antibiotic-associated diarrhea and minimized the risk of C. difficile infection.
In a 2021 randomized controlled trial led by Merenstein, healthy participants were given a trial of amoxicillin/clavulanate (days 1-7) in conjunction with either yogurt containing the probiotic Bifidobacterium animalis subsp lactis BB-12 or control yogurt (days 1-14). After assessing feces samples over a 30-day period, they found that those who received the probiotic yogurt had a significantly smaller decrease in short-chain fatty acid levels and a more stable taxonomic microbiota profile than control persons.
Dr. Merenstein said that, on the basis of results such as these and others, he’s comfortable being relatively definitive about the value of probiotics.
“I believe it’s close to standard of care that if you’re prescribing antibiotics, especially for more than 7 days, you really need to put people on probiotics that have been studied, simply because the evidence is robust enough now,” he said.
Even for proponents, there are caveats
However, all the researchers recommending the use of probiotics did so with caveats. First and foremost, they advise clinicians that the term “probiotics” is an imprecise catchall and is essentially meaningless.
“A lot of products label themselves as probiotic. It’s a great marketing scheme, but many of the products out there aren’t really probiotics; they’re not proven with randomized control trials and don’t have the scientific background,” said Dr. McFarland. “We’ve found that the efficacy is extremely strain specific and disease specific. A strain may work for one disease and not work for another.”
In 2018, Dr. McFarland coauthored an evidence-based practical guide to help clinicians and patients identify the specific strain that works in certain indications. Dr. Cresci recommends that clinicians consult websites such as Probiotics.org or the National Institutes of Health’s database to find the strains that have been proven to work in well-designed clinical trials.
There was also agreement that, to date, the most robust data support probiotics for the treatment of antibiotic-associated diarrhea.
Although the optimal timing of probiotics is a subject of debate, most proponents agreed that the general rule is “the sooner the better.”
Dr. McFarland recommended incorporating probiotics within 24 hours of starting an antibiotic “because the damage done to your GI tract microbiome is pretty quick, and the probiotics work best if they’re established before major disruption occurs.” She added that patients should continue taking probiotics for 2-8 weeks after stopping antibiotics.
“It takes a long time for your normal flora to get restored,” she said. “It’s best to cover your bases.”
For others, the evidence is not definitive
Opinions on the value of probiotics to combat antibiotic-related GI side effects are divergent, though.
“I would not recommend the routine use of probiotics, and certainly not in the prevention of C. difficile or antibiotic-related diarrhea,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk. “I think the evidence does not support that, and I stand strongly on that recommendation.”
Dr. Johnson cited the 2020 guidelines from the American Gastroenterological Association, which offer only a conditional recommendation for the use of specific probiotics and only in preventing antibiotic-associated C. difficile infection.
Geoffrey A. Preidis, MD, PhD, an assistant professor of pediatrics in the section of gastroenterology, hepatology, and nutrition at Baylor College of Medicine, Houston, served as a coauthor of the AGA’s guidelines. He noted that after reviewing 39 published trials of approximately 10,000 patients given probiotics while receiving antibiotics, the authors “did find some evidence that specific probiotics might decrease the risk of C. difficile diarrhea, but the quality of that evidence was low.”
Dr. Preidis attributed this to the lack of well-designed multicenter trials that can isolate the effects of certain strains and determine their benefit in this application.
“The majority of published trials have not reported safety data as rigorously as these data are reported in pharmaceutical trials, so the risk of side effects could be higher than we think,” said Dr. Preidis. “As living microbes, probiotics can move from the intestines into the bloodstream, causing sepsis. Contamination in the manufacturing process has been reported. There might be other long-term effects that we are not yet aware of.”
When asked to characterize the available data on probiotics, Dr. Johnson replied, “I’d generally label it, ‘caveat emptor.’ ”
Dr. McFarland agreed that the field would benefit from better-designed studies and called out meta-analyses that pool outcomes with various strains for particular criticism.
“When researchers do that, it’s no longer valid and shouldn’t have been published, in my opinion,” she told this news organization.
‘Antibiotic diets’ as a possible approach
A compromise between the two sides may be the so-called antibiotic diet. The theory behind such diets is that foods and beverages with biome-boosting properties may be a risk-free intervention that patients can adopt to alleviate antibiotic-related side effects.
“You want your diet to include more soluble fibers to help support the good bacteria, particularly when you’re taking antibiotics,” said Dr. Cresci. “You can get this through eating fresh fruits and vegetables, whole grains, and foods that have more prebiotic, like potatoes. You can also eat fermented food, such as kefir, kombucha, kimchi, and yogurt, so you’re adding more beneficial bacteria into your intestinal tract.”
There is ample published evidence that such foods can boost microbiome diversity and decrease inflammation, including a July 2021 study in Cell. However, the protection this may confer while taking antibiotics isn’t known. Establishing a clear role for the efficacy of such interventions is made additionally difficult by the well-established limitations of conducting dietary clinical trials.
Dr. Merenstein said that there is no compelling evidence that antibiotic-related complications can be offset by changing what goes onto our dinner plates. He joked: “We can’t say, ‘Here’s amoxicillin for your ear infection, now make sure you increase your fermented food, fiber, and water.’ ”
Dr. Johnson said he’s intrigued by studies of prebiotics – fibers that boost beneficial bacteria in the GI system.
“I would love to have more findings about prebiotic identification; that is, things we could do in a healthy way to keep the gut balanced while it’s subject to a change with antibiotics,” he said. “We’re just not there yet.”
Dr. Johnson added that he generally recommends that patients taking antibiotics eat “a bland diet, avoiding things that may have been provocative in the past.”
If patients are already enjoying foods with microbiome-boosting reputations, Dr. Johnson sees “very little downside to continuing that [while on antibiotics].” However, he noted that the period in which you’re taking antibiotics isn’t ideal for trying new foods, given the lack of experience with how the gut bacteria will react.
There are data about foods to avoid while taking antibiotics, which generally fall in line with common dietary knowledge. Many patients may know not to drink grapefruit juice with certain medications, but it’s worth a reminder. Certain antibiotics may also require delaying or avoiding dairy products, although this does not apply to yogurt.
A fiber-deficient diet can aggravate microbiota collapse following antibiotics. In a 2020 study, researchers showed that people on a high-fat diet who were using antibiotics were 8.6 times more likely to have preinflammatory bowel disease than those eating low-fat foods and who had no recent history of antibiotic use. Mouse model data from the same study indicated that poor diet and antibiotics may have worked in conjunction to reduce oxygen in the gut.
Dr. McFarland noted that building a healthy microbiome is a lifelong pursuit and that several factors (for example, environmental or genetic) are out of individuals’ hands. The general public might want a quick fix – ironically, one of the main drivers behind their requesting and receiving antibiotics when they’re not indicated – but it’s likely not available to them.
“You can’t eat one salad and suddenly have a healthy gut, unfortunately.”
A version of this article first appeared on Medscape.com.
Antibiotics are among the most commonly prescribed medications in both outpatient and hospital settings. Global efforts at curbing antibiotic-resistant strains have prompted clinicians to pursue better stewardship, whereby they limit their prescribing of such medications to those who truly need them.
Yet there’s another possible means of addressing antibiotic resistance – using dietary interventions to reduce the gastrointestinal complaints that so often accompany the use of antibiotics: vomiting, nausea, diarrhea, bloating/indigestion, abdominal pain, and loss of appetite. Far from being a mere nuisance, these complications can have major ramifications.
“Often [these side effects] will result in people stopping an antibiotic they need or taking a second- or third-generation one, which potentially causes even more problems with resistance,” explained Daniel J. Merenstein, MD, a professor of family medicine at Georgetown University, Washington, who has conducted multiple trials on antibiotic stewardship and probiotics.
And it’s not just clinicians who would like to find a way around these common complaints. On lifestyle blogs such as Livestrong and Goop, medical news websites, and via academic institutions, patients can learn how the right probiotic supplement or certain fermented or high-fiber foods, for example, might spare them the upset stomach that often accompanies a course of antibiotics.
Yet according to experts in the field, there are notable questions to be answered about whether there’s evidence to support this approach.
The cost of GI discomfort
Pinpointing the exact manner by which antibiotics upend GI tracts is a complex task, according to Gail Cresci, PhD, RD, a microbiome researcher in the department of pediatric gastroenterology, hepatology, and nutrition and director of nutrition research at the Cleveland Clinic.
“A lot of different mechanisms can go awry,” Dr. Cresci said. “But normally, the good microbes are there to help keep the balance, so when that balance is gone, the pathogens can take over and lead to this disruption.”
According to Lynne V. McFarland, PhD, a recently retired infectious disease epidemiologist who now serves as a private consultant, such complications can have substantial ramifications for patients and health care systems.
“If you’re an inpatient and develop antibiotic-associated diarrhea, it usually increases the length of stay from 8 to 20 days. It also increases the cost of care. And small children who have this can get severely dehydrated, which can become life threatening.”
Proponents of probiotics
Several of the researchers who were interviewed believe there’s convincing evidence supporting probiotics for the treatment of common antibiotic-related GI complaints. In many instances, they were involved in the studies themselves.
During Dr. McFarland’s 4-decade career in probiotics research, she has participated in early animal studies with strains such as Saccharomyces boulardii and was involved in meta-analyses of their role in Clostridioides difficile infection and associated diarrhea and even as a potential GI intervention for COVID-19 patients (Antibiotics (Basel). 2021 Apr 9;10(4):408).
In mouse model studies from 2013 and 2018, Dr. Cresci and colleagues showed that the probiotic strains Lactobacillus GG and Faecalibacterium prausnitzii reduced the structural gut changes that lead to antibiotic-associated diarrhea and minimized the risk of C. difficile infection.
In a 2021 randomized controlled trial led by Merenstein, healthy participants were given a trial of amoxicillin/clavulanate (days 1-7) in conjunction with either yogurt containing the probiotic Bifidobacterium animalis subsp lactis BB-12 or control yogurt (days 1-14). After assessing feces samples over a 30-day period, they found that those who received the probiotic yogurt had a significantly smaller decrease in short-chain fatty acid levels and a more stable taxonomic microbiota profile than control persons.
Dr. Merenstein said that, on the basis of results such as these and others, he’s comfortable being relatively definitive about the value of probiotics.
“I believe it’s close to standard of care that if you’re prescribing antibiotics, especially for more than 7 days, you really need to put people on probiotics that have been studied, simply because the evidence is robust enough now,” he said.
Even for proponents, there are caveats
However, all the researchers recommending the use of probiotics did so with caveats. First and foremost, they advise clinicians that the term “probiotics” is an imprecise catchall and is essentially meaningless.
“A lot of products label themselves as probiotic. It’s a great marketing scheme, but many of the products out there aren’t really probiotics; they’re not proven with randomized control trials and don’t have the scientific background,” said Dr. McFarland. “We’ve found that the efficacy is extremely strain specific and disease specific. A strain may work for one disease and not work for another.”
In 2018, Dr. McFarland coauthored an evidence-based practical guide to help clinicians and patients identify the specific strain that works in certain indications. Dr. Cresci recommends that clinicians consult websites such as Probiotics.org or the National Institutes of Health’s database to find the strains that have been proven to work in well-designed clinical trials.
There was also agreement that, to date, the most robust data support probiotics for the treatment of antibiotic-associated diarrhea.
Although the optimal timing of probiotics is a subject of debate, most proponents agreed that the general rule is “the sooner the better.”
Dr. McFarland recommended incorporating probiotics within 24 hours of starting an antibiotic “because the damage done to your GI tract microbiome is pretty quick, and the probiotics work best if they’re established before major disruption occurs.” She added that patients should continue taking probiotics for 2-8 weeks after stopping antibiotics.
“It takes a long time for your normal flora to get restored,” she said. “It’s best to cover your bases.”
For others, the evidence is not definitive
Opinions on the value of probiotics to combat antibiotic-related GI side effects are divergent, though.
“I would not recommend the routine use of probiotics, and certainly not in the prevention of C. difficile or antibiotic-related diarrhea,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk. “I think the evidence does not support that, and I stand strongly on that recommendation.”
Dr. Johnson cited the 2020 guidelines from the American Gastroenterological Association, which offer only a conditional recommendation for the use of specific probiotics and only in preventing antibiotic-associated C. difficile infection.
Geoffrey A. Preidis, MD, PhD, an assistant professor of pediatrics in the section of gastroenterology, hepatology, and nutrition at Baylor College of Medicine, Houston, served as a coauthor of the AGA’s guidelines. He noted that after reviewing 39 published trials of approximately 10,000 patients given probiotics while receiving antibiotics, the authors “did find some evidence that specific probiotics might decrease the risk of C. difficile diarrhea, but the quality of that evidence was low.”
Dr. Preidis attributed this to the lack of well-designed multicenter trials that can isolate the effects of certain strains and determine their benefit in this application.
“The majority of published trials have not reported safety data as rigorously as these data are reported in pharmaceutical trials, so the risk of side effects could be higher than we think,” said Dr. Preidis. “As living microbes, probiotics can move from the intestines into the bloodstream, causing sepsis. Contamination in the manufacturing process has been reported. There might be other long-term effects that we are not yet aware of.”
When asked to characterize the available data on probiotics, Dr. Johnson replied, “I’d generally label it, ‘caveat emptor.’ ”
Dr. McFarland agreed that the field would benefit from better-designed studies and called out meta-analyses that pool outcomes with various strains for particular criticism.
“When researchers do that, it’s no longer valid and shouldn’t have been published, in my opinion,” she told this news organization.
‘Antibiotic diets’ as a possible approach
A compromise between the two sides may be the so-called antibiotic diet. The theory behind such diets is that foods and beverages with biome-boosting properties may be a risk-free intervention that patients can adopt to alleviate antibiotic-related side effects.
“You want your diet to include more soluble fibers to help support the good bacteria, particularly when you’re taking antibiotics,” said Dr. Cresci. “You can get this through eating fresh fruits and vegetables, whole grains, and foods that have more prebiotic, like potatoes. You can also eat fermented food, such as kefir, kombucha, kimchi, and yogurt, so you’re adding more beneficial bacteria into your intestinal tract.”
There is ample published evidence that such foods can boost microbiome diversity and decrease inflammation, including a July 2021 study in Cell. However, the protection this may confer while taking antibiotics isn’t known. Establishing a clear role for the efficacy of such interventions is made additionally difficult by the well-established limitations of conducting dietary clinical trials.
Dr. Merenstein said that there is no compelling evidence that antibiotic-related complications can be offset by changing what goes onto our dinner plates. He joked: “We can’t say, ‘Here’s amoxicillin for your ear infection, now make sure you increase your fermented food, fiber, and water.’ ”
Dr. Johnson said he’s intrigued by studies of prebiotics – fibers that boost beneficial bacteria in the GI system.
“I would love to have more findings about prebiotic identification; that is, things we could do in a healthy way to keep the gut balanced while it’s subject to a change with antibiotics,” he said. “We’re just not there yet.”
Dr. Johnson added that he generally recommends that patients taking antibiotics eat “a bland diet, avoiding things that may have been provocative in the past.”
If patients are already enjoying foods with microbiome-boosting reputations, Dr. Johnson sees “very little downside to continuing that [while on antibiotics].” However, he noted that the period in which you’re taking antibiotics isn’t ideal for trying new foods, given the lack of experience with how the gut bacteria will react.
There are data about foods to avoid while taking antibiotics, which generally fall in line with common dietary knowledge. Many patients may know not to drink grapefruit juice with certain medications, but it’s worth a reminder. Certain antibiotics may also require delaying or avoiding dairy products, although this does not apply to yogurt.
A fiber-deficient diet can aggravate microbiota collapse following antibiotics. In a 2020 study, researchers showed that people on a high-fat diet who were using antibiotics were 8.6 times more likely to have preinflammatory bowel disease than those eating low-fat foods and who had no recent history of antibiotic use. Mouse model data from the same study indicated that poor diet and antibiotics may have worked in conjunction to reduce oxygen in the gut.
Dr. McFarland noted that building a healthy microbiome is a lifelong pursuit and that several factors (for example, environmental or genetic) are out of individuals’ hands. The general public might want a quick fix – ironically, one of the main drivers behind their requesting and receiving antibiotics when they’re not indicated – but it’s likely not available to them.
“You can’t eat one salad and suddenly have a healthy gut, unfortunately.”
A version of this article first appeared on Medscape.com.
Antibiotics are among the most commonly prescribed medications in both outpatient and hospital settings. Global efforts at curbing antibiotic-resistant strains have prompted clinicians to pursue better stewardship, whereby they limit their prescribing of such medications to those who truly need them.
Yet there’s another possible means of addressing antibiotic resistance – using dietary interventions to reduce the gastrointestinal complaints that so often accompany the use of antibiotics: vomiting, nausea, diarrhea, bloating/indigestion, abdominal pain, and loss of appetite. Far from being a mere nuisance, these complications can have major ramifications.
“Often [these side effects] will result in people stopping an antibiotic they need or taking a second- or third-generation one, which potentially causes even more problems with resistance,” explained Daniel J. Merenstein, MD, a professor of family medicine at Georgetown University, Washington, who has conducted multiple trials on antibiotic stewardship and probiotics.
And it’s not just clinicians who would like to find a way around these common complaints. On lifestyle blogs such as Livestrong and Goop, medical news websites, and via academic institutions, patients can learn how the right probiotic supplement or certain fermented or high-fiber foods, for example, might spare them the upset stomach that often accompanies a course of antibiotics.
Yet according to experts in the field, there are notable questions to be answered about whether there’s evidence to support this approach.
The cost of GI discomfort
Pinpointing the exact manner by which antibiotics upend GI tracts is a complex task, according to Gail Cresci, PhD, RD, a microbiome researcher in the department of pediatric gastroenterology, hepatology, and nutrition and director of nutrition research at the Cleveland Clinic.
“A lot of different mechanisms can go awry,” Dr. Cresci said. “But normally, the good microbes are there to help keep the balance, so when that balance is gone, the pathogens can take over and lead to this disruption.”
According to Lynne V. McFarland, PhD, a recently retired infectious disease epidemiologist who now serves as a private consultant, such complications can have substantial ramifications for patients and health care systems.
“If you’re an inpatient and develop antibiotic-associated diarrhea, it usually increases the length of stay from 8 to 20 days. It also increases the cost of care. And small children who have this can get severely dehydrated, which can become life threatening.”
Proponents of probiotics
Several of the researchers who were interviewed believe there’s convincing evidence supporting probiotics for the treatment of common antibiotic-related GI complaints. In many instances, they were involved in the studies themselves.
During Dr. McFarland’s 4-decade career in probiotics research, she has participated in early animal studies with strains such as Saccharomyces boulardii and was involved in meta-analyses of their role in Clostridioides difficile infection and associated diarrhea and even as a potential GI intervention for COVID-19 patients (Antibiotics (Basel). 2021 Apr 9;10(4):408).
In mouse model studies from 2013 and 2018, Dr. Cresci and colleagues showed that the probiotic strains Lactobacillus GG and Faecalibacterium prausnitzii reduced the structural gut changes that lead to antibiotic-associated diarrhea and minimized the risk of C. difficile infection.
In a 2021 randomized controlled trial led by Merenstein, healthy participants were given a trial of amoxicillin/clavulanate (days 1-7) in conjunction with either yogurt containing the probiotic Bifidobacterium animalis subsp lactis BB-12 or control yogurt (days 1-14). After assessing feces samples over a 30-day period, they found that those who received the probiotic yogurt had a significantly smaller decrease in short-chain fatty acid levels and a more stable taxonomic microbiota profile than control persons.
Dr. Merenstein said that, on the basis of results such as these and others, he’s comfortable being relatively definitive about the value of probiotics.
“I believe it’s close to standard of care that if you’re prescribing antibiotics, especially for more than 7 days, you really need to put people on probiotics that have been studied, simply because the evidence is robust enough now,” he said.
Even for proponents, there are caveats
However, all the researchers recommending the use of probiotics did so with caveats. First and foremost, they advise clinicians that the term “probiotics” is an imprecise catchall and is essentially meaningless.
“A lot of products label themselves as probiotic. It’s a great marketing scheme, but many of the products out there aren’t really probiotics; they’re not proven with randomized control trials and don’t have the scientific background,” said Dr. McFarland. “We’ve found that the efficacy is extremely strain specific and disease specific. A strain may work for one disease and not work for another.”
In 2018, Dr. McFarland coauthored an evidence-based practical guide to help clinicians and patients identify the specific strain that works in certain indications. Dr. Cresci recommends that clinicians consult websites such as Probiotics.org or the National Institutes of Health’s database to find the strains that have been proven to work in well-designed clinical trials.
There was also agreement that, to date, the most robust data support probiotics for the treatment of antibiotic-associated diarrhea.
Although the optimal timing of probiotics is a subject of debate, most proponents agreed that the general rule is “the sooner the better.”
Dr. McFarland recommended incorporating probiotics within 24 hours of starting an antibiotic “because the damage done to your GI tract microbiome is pretty quick, and the probiotics work best if they’re established before major disruption occurs.” She added that patients should continue taking probiotics for 2-8 weeks after stopping antibiotics.
“It takes a long time for your normal flora to get restored,” she said. “It’s best to cover your bases.”
For others, the evidence is not definitive
Opinions on the value of probiotics to combat antibiotic-related GI side effects are divergent, though.
“I would not recommend the routine use of probiotics, and certainly not in the prevention of C. difficile or antibiotic-related diarrhea,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk. “I think the evidence does not support that, and I stand strongly on that recommendation.”
Dr. Johnson cited the 2020 guidelines from the American Gastroenterological Association, which offer only a conditional recommendation for the use of specific probiotics and only in preventing antibiotic-associated C. difficile infection.
Geoffrey A. Preidis, MD, PhD, an assistant professor of pediatrics in the section of gastroenterology, hepatology, and nutrition at Baylor College of Medicine, Houston, served as a coauthor of the AGA’s guidelines. He noted that after reviewing 39 published trials of approximately 10,000 patients given probiotics while receiving antibiotics, the authors “did find some evidence that specific probiotics might decrease the risk of C. difficile diarrhea, but the quality of that evidence was low.”
Dr. Preidis attributed this to the lack of well-designed multicenter trials that can isolate the effects of certain strains and determine their benefit in this application.
“The majority of published trials have not reported safety data as rigorously as these data are reported in pharmaceutical trials, so the risk of side effects could be higher than we think,” said Dr. Preidis. “As living microbes, probiotics can move from the intestines into the bloodstream, causing sepsis. Contamination in the manufacturing process has been reported. There might be other long-term effects that we are not yet aware of.”
When asked to characterize the available data on probiotics, Dr. Johnson replied, “I’d generally label it, ‘caveat emptor.’ ”
Dr. McFarland agreed that the field would benefit from better-designed studies and called out meta-analyses that pool outcomes with various strains for particular criticism.
“When researchers do that, it’s no longer valid and shouldn’t have been published, in my opinion,” she told this news organization.
‘Antibiotic diets’ as a possible approach
A compromise between the two sides may be the so-called antibiotic diet. The theory behind such diets is that foods and beverages with biome-boosting properties may be a risk-free intervention that patients can adopt to alleviate antibiotic-related side effects.
“You want your diet to include more soluble fibers to help support the good bacteria, particularly when you’re taking antibiotics,” said Dr. Cresci. “You can get this through eating fresh fruits and vegetables, whole grains, and foods that have more prebiotic, like potatoes. You can also eat fermented food, such as kefir, kombucha, kimchi, and yogurt, so you’re adding more beneficial bacteria into your intestinal tract.”
There is ample published evidence that such foods can boost microbiome diversity and decrease inflammation, including a July 2021 study in Cell. However, the protection this may confer while taking antibiotics isn’t known. Establishing a clear role for the efficacy of such interventions is made additionally difficult by the well-established limitations of conducting dietary clinical trials.
Dr. Merenstein said that there is no compelling evidence that antibiotic-related complications can be offset by changing what goes onto our dinner plates. He joked: “We can’t say, ‘Here’s amoxicillin for your ear infection, now make sure you increase your fermented food, fiber, and water.’ ”
Dr. Johnson said he’s intrigued by studies of prebiotics – fibers that boost beneficial bacteria in the GI system.
“I would love to have more findings about prebiotic identification; that is, things we could do in a healthy way to keep the gut balanced while it’s subject to a change with antibiotics,” he said. “We’re just not there yet.”
Dr. Johnson added that he generally recommends that patients taking antibiotics eat “a bland diet, avoiding things that may have been provocative in the past.”
If patients are already enjoying foods with microbiome-boosting reputations, Dr. Johnson sees “very little downside to continuing that [while on antibiotics].” However, he noted that the period in which you’re taking antibiotics isn’t ideal for trying new foods, given the lack of experience with how the gut bacteria will react.
There are data about foods to avoid while taking antibiotics, which generally fall in line with common dietary knowledge. Many patients may know not to drink grapefruit juice with certain medications, but it’s worth a reminder. Certain antibiotics may also require delaying or avoiding dairy products, although this does not apply to yogurt.
A fiber-deficient diet can aggravate microbiota collapse following antibiotics. In a 2020 study, researchers showed that people on a high-fat diet who were using antibiotics were 8.6 times more likely to have preinflammatory bowel disease than those eating low-fat foods and who had no recent history of antibiotic use. Mouse model data from the same study indicated that poor diet and antibiotics may have worked in conjunction to reduce oxygen in the gut.
Dr. McFarland noted that building a healthy microbiome is a lifelong pursuit and that several factors (for example, environmental or genetic) are out of individuals’ hands. The general public might want a quick fix – ironically, one of the main drivers behind their requesting and receiving antibiotics when they’re not indicated – but it’s likely not available to them.
“You can’t eat one salad and suddenly have a healthy gut, unfortunately.”
A version of this article first appeared on Medscape.com.
Hands trained for surgery now on machine gun: Kyiv oncologist
The pediatric oncology unit in Kyiv’s National Cancer Institute is empty, with all the children evacuated to safer hospitals in Western Ukraine or further, making it a good place to talk on Zoom.
Against a backdrop of colorful animals painted on the wall, Oleksandr Stakhovskyi, MD, PhD, speaks optimistically about the future of his city, his country, and even his patients, despite acknowledging that his surgical hands are now trained to use a machine gun.
“It’s not as bad as last week,” he laughs, explaining that residents of Kyiv are more relaxed now, despite the air raid sirens, because the city’s anti-missile system has thus far kept them safe.
Even still, missiles have continued hitting civilian residences and Dr. Stakhovskyi, a urologic-oncology surgeon, has evacuated his wife and children out of the country, as have 70% of his colleagues. But for those who stayed in Kyiv, there is a strong resolve.
“People working in IT, in law, in other professions — they just took the guns and stayed in Kyiv,” he said in an interview. “They are just civilians, armed, trying to protect and fortify Kyiv — to make it unbreakable.”
Dr. Stakhovskyi doesn’t have a background in the military, but he now knows how to use a machine gun. “I am a super-specialized oncologist, [but] I realize if I leave right now it will give the Russians momentum to come in. The longer it takes, the weaker the opponent army will become, and we are more and more optimistic,” he said.
In Kyiv, Dr. Stakhovskyi is working half the time at the cancer hospital and the other half at the nearby military hospital, but he said so far war casualties are minimal within the city, and even the flow of patients with cancer has reduced.
“I had my surgeries planned up until the end of March, but when the war started, they were all postponed,” he said. Emergency cancer surgeries have continued, and now there is talk of resuming some others. “We will stratify patients into categories based on need,” he said. “For those patients whose surgery can basically stop the disease and they don’t need neoadjuvant chemo, we’ll probably be doing those.”
Medical oncology clinics have also resumed, said Dr. Stakhovskyi, but the volume of patients is low, because many have left the city. An estimated 3.3 million people have left Ukraine since the Russian invasion on February 24.
Across the country, in Lviv near the Polish border, another surgical oncologist tells a different story. Andriy Hrynkiv, MD, from Lviv Regional Cancer Center, says his hospital has seen a dramatic increase in patients, displaced internally from areas where the medical infrastructure has collapsed.
“Russian forces have destroyed more than 117 hospitals, 43 ambulances have been shot at, 6 doctors have been killed, and 13 wounded,” Dr. Hrynkiv said. In the city of Mariupol, “doctors and patients have been taken hostage,” he said, used by Russian forces as a human shield. In Kharkiv, with approximately 1.5 million residents, the only oncologic hospital has been destroyed.
There is a shortage and instability of medical supplies including all iodine-containing medications that citizens are stocking up on in the face of a potential nuclear attack, he said.
Dr. Hrynkiv was speaking on a webcast organized by the American Society of Clinical Oncology (ASCO) and European Cancer Organisation (ECO).
The two organizations are collaborating with each other and the World Health Organization to create a special network that is aiming to connect professionals, academic and clinical centers, and patient groups.
Additionally, the Ukranian Society of Clinical Oncology (USCO), cofounded by Dr. Stakhovskyi, is trying to keep patients connected with nongovernment organizations.
“These patient organizations moved west when the war started, but they still use us to help them make contact with foreign doctors,” he said. “We have tried to centralize this process but it’s very difficult because patients and organizations are also calling doctors and centers directly looking for treatment options.”
He says USCO is also coordinating the distribution of a donation of immunotherapy pembrolizumab (Keytruda) from pharmaceutical company Merck Sharp & Dohme. “It’s a huge influx of this drug,” he says. “They’ve promised something like 2,000 doses to cover 230 patients for 3 months at least. Usually this is not an easy drug to access for people in Ukraine because it’s really expensive.”
Dr. Stakhovskyi said the optimism he feels is fueled by the support that Ukrainians feel from the rest of the world.
“We see the reaction of our international colleagues. It is so impressive and touching — lots of my ex-professors are texting me and sending me messages from all over the place, from Germany, from Canada, from France, from the United States,” he said. “And if we can be optimistic for ourselves, definitely that translates to our patients.”
A version of this article first appeared on Medscape.com.
The pediatric oncology unit in Kyiv’s National Cancer Institute is empty, with all the children evacuated to safer hospitals in Western Ukraine or further, making it a good place to talk on Zoom.
Against a backdrop of colorful animals painted on the wall, Oleksandr Stakhovskyi, MD, PhD, speaks optimistically about the future of his city, his country, and even his patients, despite acknowledging that his surgical hands are now trained to use a machine gun.
“It’s not as bad as last week,” he laughs, explaining that residents of Kyiv are more relaxed now, despite the air raid sirens, because the city’s anti-missile system has thus far kept them safe.
Even still, missiles have continued hitting civilian residences and Dr. Stakhovskyi, a urologic-oncology surgeon, has evacuated his wife and children out of the country, as have 70% of his colleagues. But for those who stayed in Kyiv, there is a strong resolve.
“People working in IT, in law, in other professions — they just took the guns and stayed in Kyiv,” he said in an interview. “They are just civilians, armed, trying to protect and fortify Kyiv — to make it unbreakable.”
Dr. Stakhovskyi doesn’t have a background in the military, but he now knows how to use a machine gun. “I am a super-specialized oncologist, [but] I realize if I leave right now it will give the Russians momentum to come in. The longer it takes, the weaker the opponent army will become, and we are more and more optimistic,” he said.
In Kyiv, Dr. Stakhovskyi is working half the time at the cancer hospital and the other half at the nearby military hospital, but he said so far war casualties are minimal within the city, and even the flow of patients with cancer has reduced.
“I had my surgeries planned up until the end of March, but when the war started, they were all postponed,” he said. Emergency cancer surgeries have continued, and now there is talk of resuming some others. “We will stratify patients into categories based on need,” he said. “For those patients whose surgery can basically stop the disease and they don’t need neoadjuvant chemo, we’ll probably be doing those.”
Medical oncology clinics have also resumed, said Dr. Stakhovskyi, but the volume of patients is low, because many have left the city. An estimated 3.3 million people have left Ukraine since the Russian invasion on February 24.
Across the country, in Lviv near the Polish border, another surgical oncologist tells a different story. Andriy Hrynkiv, MD, from Lviv Regional Cancer Center, says his hospital has seen a dramatic increase in patients, displaced internally from areas where the medical infrastructure has collapsed.
“Russian forces have destroyed more than 117 hospitals, 43 ambulances have been shot at, 6 doctors have been killed, and 13 wounded,” Dr. Hrynkiv said. In the city of Mariupol, “doctors and patients have been taken hostage,” he said, used by Russian forces as a human shield. In Kharkiv, with approximately 1.5 million residents, the only oncologic hospital has been destroyed.
There is a shortage and instability of medical supplies including all iodine-containing medications that citizens are stocking up on in the face of a potential nuclear attack, he said.
Dr. Hrynkiv was speaking on a webcast organized by the American Society of Clinical Oncology (ASCO) and European Cancer Organisation (ECO).
The two organizations are collaborating with each other and the World Health Organization to create a special network that is aiming to connect professionals, academic and clinical centers, and patient groups.
Additionally, the Ukranian Society of Clinical Oncology (USCO), cofounded by Dr. Stakhovskyi, is trying to keep patients connected with nongovernment organizations.
“These patient organizations moved west when the war started, but they still use us to help them make contact with foreign doctors,” he said. “We have tried to centralize this process but it’s very difficult because patients and organizations are also calling doctors and centers directly looking for treatment options.”
He says USCO is also coordinating the distribution of a donation of immunotherapy pembrolizumab (Keytruda) from pharmaceutical company Merck Sharp & Dohme. “It’s a huge influx of this drug,” he says. “They’ve promised something like 2,000 doses to cover 230 patients for 3 months at least. Usually this is not an easy drug to access for people in Ukraine because it’s really expensive.”
Dr. Stakhovskyi said the optimism he feels is fueled by the support that Ukrainians feel from the rest of the world.
“We see the reaction of our international colleagues. It is so impressive and touching — lots of my ex-professors are texting me and sending me messages from all over the place, from Germany, from Canada, from France, from the United States,” he said. “And if we can be optimistic for ourselves, definitely that translates to our patients.”
A version of this article first appeared on Medscape.com.
The pediatric oncology unit in Kyiv’s National Cancer Institute is empty, with all the children evacuated to safer hospitals in Western Ukraine or further, making it a good place to talk on Zoom.
Against a backdrop of colorful animals painted on the wall, Oleksandr Stakhovskyi, MD, PhD, speaks optimistically about the future of his city, his country, and even his patients, despite acknowledging that his surgical hands are now trained to use a machine gun.
“It’s not as bad as last week,” he laughs, explaining that residents of Kyiv are more relaxed now, despite the air raid sirens, because the city’s anti-missile system has thus far kept them safe.
Even still, missiles have continued hitting civilian residences and Dr. Stakhovskyi, a urologic-oncology surgeon, has evacuated his wife and children out of the country, as have 70% of his colleagues. But for those who stayed in Kyiv, there is a strong resolve.
“People working in IT, in law, in other professions — they just took the guns and stayed in Kyiv,” he said in an interview. “They are just civilians, armed, trying to protect and fortify Kyiv — to make it unbreakable.”
Dr. Stakhovskyi doesn’t have a background in the military, but he now knows how to use a machine gun. “I am a super-specialized oncologist, [but] I realize if I leave right now it will give the Russians momentum to come in. The longer it takes, the weaker the opponent army will become, and we are more and more optimistic,” he said.
In Kyiv, Dr. Stakhovskyi is working half the time at the cancer hospital and the other half at the nearby military hospital, but he said so far war casualties are minimal within the city, and even the flow of patients with cancer has reduced.
“I had my surgeries planned up until the end of March, but when the war started, they were all postponed,” he said. Emergency cancer surgeries have continued, and now there is talk of resuming some others. “We will stratify patients into categories based on need,” he said. “For those patients whose surgery can basically stop the disease and they don’t need neoadjuvant chemo, we’ll probably be doing those.”
Medical oncology clinics have also resumed, said Dr. Stakhovskyi, but the volume of patients is low, because many have left the city. An estimated 3.3 million people have left Ukraine since the Russian invasion on February 24.
Across the country, in Lviv near the Polish border, another surgical oncologist tells a different story. Andriy Hrynkiv, MD, from Lviv Regional Cancer Center, says his hospital has seen a dramatic increase in patients, displaced internally from areas where the medical infrastructure has collapsed.
“Russian forces have destroyed more than 117 hospitals, 43 ambulances have been shot at, 6 doctors have been killed, and 13 wounded,” Dr. Hrynkiv said. In the city of Mariupol, “doctors and patients have been taken hostage,” he said, used by Russian forces as a human shield. In Kharkiv, with approximately 1.5 million residents, the only oncologic hospital has been destroyed.
There is a shortage and instability of medical supplies including all iodine-containing medications that citizens are stocking up on in the face of a potential nuclear attack, he said.
Dr. Hrynkiv was speaking on a webcast organized by the American Society of Clinical Oncology (ASCO) and European Cancer Organisation (ECO).
The two organizations are collaborating with each other and the World Health Organization to create a special network that is aiming to connect professionals, academic and clinical centers, and patient groups.
Additionally, the Ukranian Society of Clinical Oncology (USCO), cofounded by Dr. Stakhovskyi, is trying to keep patients connected with nongovernment organizations.
“These patient organizations moved west when the war started, but they still use us to help them make contact with foreign doctors,” he said. “We have tried to centralize this process but it’s very difficult because patients and organizations are also calling doctors and centers directly looking for treatment options.”
He says USCO is also coordinating the distribution of a donation of immunotherapy pembrolizumab (Keytruda) from pharmaceutical company Merck Sharp & Dohme. “It’s a huge influx of this drug,” he says. “They’ve promised something like 2,000 doses to cover 230 patients for 3 months at least. Usually this is not an easy drug to access for people in Ukraine because it’s really expensive.”
Dr. Stakhovskyi said the optimism he feels is fueled by the support that Ukrainians feel from the rest of the world.
“We see the reaction of our international colleagues. It is so impressive and touching — lots of my ex-professors are texting me and sending me messages from all over the place, from Germany, from Canada, from France, from the United States,” he said. “And if we can be optimistic for ourselves, definitely that translates to our patients.”
A version of this article first appeared on Medscape.com.
Yes, Russian docs should be shut out of medical associations, says ethicist
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at the NYU Grossman School of Medicine.
There are many difficult moral issues that are being fueled by the terrible war that Russia is waging against Ukraine. I think there is no way to justify anything that the Russians are doing. Ukraine did not do anything to violate Russian integrity, Russian territorial integrity, or anything by way of being aggressive toward Russia.
Russia decided at some point it wanted the Ukraine back. Putin has a dream, as the long-standing leader of Russia, to restore the Soviet empire, and Ukraine is top of the list of the places that he wants back for a variety of reasons.
We’re not here to debate the merits and demerits of this terrible act of war.
The European Society of Cardiology made a decision very recently to drop, as members, both Russia and Belarus, Russia’s ally in this aggressive war against Ukraine. They basically found it intolerable to have business as usual with these subsidiary cardiology societies as part of the ongoing activities of the European group.
The sole goal of this overarching European group is to reduce the health burden of cardiovascular disease. It doesn’t have political goals. It doesn’t have much to say about anything other than, “Let’s get evidence-based medicine used to try and prevent heart disease or treat heart disease.” So there’s noble intent.
Many of its members asked, “What are we doing in politics? Why are we punishing Russian and Belarussian cardiologists, acting as if somehow they are responsible for what the Russian army is doing or for what Putin has decided to do? Why are we acting against them? They are just trying to fight heart disease. That’s a legitimate goal for any doctor, public health official, or scientist.” They didn’t see, as members, why this exclusion had taken place.
I believe the exclusion is appropriate and some of the membership, obviously, in the European Society of Cardiology, agrees. It’s not because they’re holding doctors or scientists directly accountable for Putin’s war crimes, ethnic cleansing assault, or bombing and shelling of hospitals, maternity hospitals, and civilians.
They understand that these scientists and doctors have little to do with such things, but we are in a new form of warfare, and that warfare is basically economic and sociologic: turning Russia, as an inexcusably aggressive state, into a pariah.
The reason to break the ties is that that is the way to bring pressure upon Putin and his kleptocratic, oligarchic advisers to stop the attack, to try and bring down their economy, to say, “Business is not going to go on as usual. You will be excluded from normal scientific and medical commerce. We’re not going to be holding conferences or exchanging ideas,” and in my view, extending it to say, “We’re not taking your papers, we’re not publishing anything you do. We’re not even having you speak at our meetings until this war, this aggressive invasion, and these war crimes come to a halt.”
There is actually a basis for this action. It isn’t in the organization’s own bylaws, which as I said, are very simple — reduce cardiovascular disease burden — but they are a member of a broader group, the Biomedical Alliance in Europe, which does have a very explicit code of ethics.
I’m going to read you a little bit from that code. It says healthcare organizations should uphold and promote equality, diversity and inclusion, accountability, transparency, and equality. They also say that all members, including the European Society of Cardiology, should be committed both to the Declaration of Helsinki, a fundamental medical ethics document, and the Declaration of Geneva. These rules refer to the highest respect of human beings, responsible resource allocation, and preservation of the environment, among other things.
What the organization is doing is consistent with the code of ethics that the broader organization of all the medical societies of Europe say that these individual groups should be doing. You can’t collaborate with war criminals. You can’t act as if business as usual is going on. That’s not inclusive. That’s not respect for diversity.
I think the Ukrainian medical societies of cardiology and other specialties would find it grimly ironic to say that keeping Russian and Belarus members makes sense, given what’s going on in their country and what is happening to them. They’re under attack. They’re being killed. Their healthcare institutions are being indiscriminately shelled and bombed.
It’s very hard — and I understand that — to say we’re going to punish scientists. We’re going to, perhaps, even cause public health problems in Russia because we’re not going to collaborate right now with doctors and scientists in cardiology or any other medical specialty. I think it’s what has to be done.
We’re in a new era of trying to combat what is basically organized, international ethnic terrorism, complete with war crimes. We fight financially. We fight by isolating. We fight by excluding. It’s painful. It’s difficult. It’s somewhat unfair to individuals.
Only through that kind of pain are we going to get the kind of pressure that will achieve justice. I think that is a goal that we have to commend the European Society of Cardiology for honoring.
Dr. Caplan is director of the division of medical ethics at New York University. He is the author or editor of 35 books and 750 peer-reviewed articles as well as a frequent commentator in the media on bioethical issues. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (an unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at the NYU Grossman School of Medicine.
There are many difficult moral issues that are being fueled by the terrible war that Russia is waging against Ukraine. I think there is no way to justify anything that the Russians are doing. Ukraine did not do anything to violate Russian integrity, Russian territorial integrity, or anything by way of being aggressive toward Russia.
Russia decided at some point it wanted the Ukraine back. Putin has a dream, as the long-standing leader of Russia, to restore the Soviet empire, and Ukraine is top of the list of the places that he wants back for a variety of reasons.
We’re not here to debate the merits and demerits of this terrible act of war.
The European Society of Cardiology made a decision very recently to drop, as members, both Russia and Belarus, Russia’s ally in this aggressive war against Ukraine. They basically found it intolerable to have business as usual with these subsidiary cardiology societies as part of the ongoing activities of the European group.
The sole goal of this overarching European group is to reduce the health burden of cardiovascular disease. It doesn’t have political goals. It doesn’t have much to say about anything other than, “Let’s get evidence-based medicine used to try and prevent heart disease or treat heart disease.” So there’s noble intent.
Many of its members asked, “What are we doing in politics? Why are we punishing Russian and Belarussian cardiologists, acting as if somehow they are responsible for what the Russian army is doing or for what Putin has decided to do? Why are we acting against them? They are just trying to fight heart disease. That’s a legitimate goal for any doctor, public health official, or scientist.” They didn’t see, as members, why this exclusion had taken place.
I believe the exclusion is appropriate and some of the membership, obviously, in the European Society of Cardiology, agrees. It’s not because they’re holding doctors or scientists directly accountable for Putin’s war crimes, ethnic cleansing assault, or bombing and shelling of hospitals, maternity hospitals, and civilians.
They understand that these scientists and doctors have little to do with such things, but we are in a new form of warfare, and that warfare is basically economic and sociologic: turning Russia, as an inexcusably aggressive state, into a pariah.
The reason to break the ties is that that is the way to bring pressure upon Putin and his kleptocratic, oligarchic advisers to stop the attack, to try and bring down their economy, to say, “Business is not going to go on as usual. You will be excluded from normal scientific and medical commerce. We’re not going to be holding conferences or exchanging ideas,” and in my view, extending it to say, “We’re not taking your papers, we’re not publishing anything you do. We’re not even having you speak at our meetings until this war, this aggressive invasion, and these war crimes come to a halt.”
There is actually a basis for this action. It isn’t in the organization’s own bylaws, which as I said, are very simple — reduce cardiovascular disease burden — but they are a member of a broader group, the Biomedical Alliance in Europe, which does have a very explicit code of ethics.
I’m going to read you a little bit from that code. It says healthcare organizations should uphold and promote equality, diversity and inclusion, accountability, transparency, and equality. They also say that all members, including the European Society of Cardiology, should be committed both to the Declaration of Helsinki, a fundamental medical ethics document, and the Declaration of Geneva. These rules refer to the highest respect of human beings, responsible resource allocation, and preservation of the environment, among other things.
What the organization is doing is consistent with the code of ethics that the broader organization of all the medical societies of Europe say that these individual groups should be doing. You can’t collaborate with war criminals. You can’t act as if business as usual is going on. That’s not inclusive. That’s not respect for diversity.
I think the Ukrainian medical societies of cardiology and other specialties would find it grimly ironic to say that keeping Russian and Belarus members makes sense, given what’s going on in their country and what is happening to them. They’re under attack. They’re being killed. Their healthcare institutions are being indiscriminately shelled and bombed.
It’s very hard — and I understand that — to say we’re going to punish scientists. We’re going to, perhaps, even cause public health problems in Russia because we’re not going to collaborate right now with doctors and scientists in cardiology or any other medical specialty. I think it’s what has to be done.
We’re in a new era of trying to combat what is basically organized, international ethnic terrorism, complete with war crimes. We fight financially. We fight by isolating. We fight by excluding. It’s painful. It’s difficult. It’s somewhat unfair to individuals.
Only through that kind of pain are we going to get the kind of pressure that will achieve justice. I think that is a goal that we have to commend the European Society of Cardiology for honoring.
Dr. Caplan is director of the division of medical ethics at New York University. He is the author or editor of 35 books and 750 peer-reviewed articles as well as a frequent commentator in the media on bioethical issues. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (an unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at the NYU Grossman School of Medicine.
There are many difficult moral issues that are being fueled by the terrible war that Russia is waging against Ukraine. I think there is no way to justify anything that the Russians are doing. Ukraine did not do anything to violate Russian integrity, Russian territorial integrity, or anything by way of being aggressive toward Russia.
Russia decided at some point it wanted the Ukraine back. Putin has a dream, as the long-standing leader of Russia, to restore the Soviet empire, and Ukraine is top of the list of the places that he wants back for a variety of reasons.
We’re not here to debate the merits and demerits of this terrible act of war.
The European Society of Cardiology made a decision very recently to drop, as members, both Russia and Belarus, Russia’s ally in this aggressive war against Ukraine. They basically found it intolerable to have business as usual with these subsidiary cardiology societies as part of the ongoing activities of the European group.
The sole goal of this overarching European group is to reduce the health burden of cardiovascular disease. It doesn’t have political goals. It doesn’t have much to say about anything other than, “Let’s get evidence-based medicine used to try and prevent heart disease or treat heart disease.” So there’s noble intent.
Many of its members asked, “What are we doing in politics? Why are we punishing Russian and Belarussian cardiologists, acting as if somehow they are responsible for what the Russian army is doing or for what Putin has decided to do? Why are we acting against them? They are just trying to fight heart disease. That’s a legitimate goal for any doctor, public health official, or scientist.” They didn’t see, as members, why this exclusion had taken place.
I believe the exclusion is appropriate and some of the membership, obviously, in the European Society of Cardiology, agrees. It’s not because they’re holding doctors or scientists directly accountable for Putin’s war crimes, ethnic cleansing assault, or bombing and shelling of hospitals, maternity hospitals, and civilians.
They understand that these scientists and doctors have little to do with such things, but we are in a new form of warfare, and that warfare is basically economic and sociologic: turning Russia, as an inexcusably aggressive state, into a pariah.
The reason to break the ties is that that is the way to bring pressure upon Putin and his kleptocratic, oligarchic advisers to stop the attack, to try and bring down their economy, to say, “Business is not going to go on as usual. You will be excluded from normal scientific and medical commerce. We’re not going to be holding conferences or exchanging ideas,” and in my view, extending it to say, “We’re not taking your papers, we’re not publishing anything you do. We’re not even having you speak at our meetings until this war, this aggressive invasion, and these war crimes come to a halt.”
There is actually a basis for this action. It isn’t in the organization’s own bylaws, which as I said, are very simple — reduce cardiovascular disease burden — but they are a member of a broader group, the Biomedical Alliance in Europe, which does have a very explicit code of ethics.
I’m going to read you a little bit from that code. It says healthcare organizations should uphold and promote equality, diversity and inclusion, accountability, transparency, and equality. They also say that all members, including the European Society of Cardiology, should be committed both to the Declaration of Helsinki, a fundamental medical ethics document, and the Declaration of Geneva. These rules refer to the highest respect of human beings, responsible resource allocation, and preservation of the environment, among other things.
What the organization is doing is consistent with the code of ethics that the broader organization of all the medical societies of Europe say that these individual groups should be doing. You can’t collaborate with war criminals. You can’t act as if business as usual is going on. That’s not inclusive. That’s not respect for diversity.
I think the Ukrainian medical societies of cardiology and other specialties would find it grimly ironic to say that keeping Russian and Belarus members makes sense, given what’s going on in their country and what is happening to them. They’re under attack. They’re being killed. Their healthcare institutions are being indiscriminately shelled and bombed.
It’s very hard — and I understand that — to say we’re going to punish scientists. We’re going to, perhaps, even cause public health problems in Russia because we’re not going to collaborate right now with doctors and scientists in cardiology or any other medical specialty. I think it’s what has to be done.
We’re in a new era of trying to combat what is basically organized, international ethnic terrorism, complete with war crimes. We fight financially. We fight by isolating. We fight by excluding. It’s painful. It’s difficult. It’s somewhat unfair to individuals.
Only through that kind of pain are we going to get the kind of pressure that will achieve justice. I think that is a goal that we have to commend the European Society of Cardiology for honoring.
Dr. Caplan is director of the division of medical ethics at New York University. He is the author or editor of 35 books and 750 peer-reviewed articles as well as a frequent commentator in the media on bioethical issues. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (an unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
Lancet Commission reexamines the current approach to death
“The story of dying in the 21st century is a story of paradox.” This is the opening line of a report recently published in the Lancet, in which the Lancet Commission experts tackle what is, for many, a very sensitive topic: the end of life. The recommendations they present aim at “bringing death back into life.”
What makes the story a paradox is that, in end-of-life situations, many people are overtreated, and on the other hand, many people are undertreated.
In short, when all is said and done, “people die bad deaths.” A natural event, a natural part of life, has turned into something that people fear or, in some cases, refuse to even acknowledge or talk about.
This was the motivating factor for the Lancet Commission, a group of experts from various disciplines, to come together to try to better understand this complex concept. , as well as a balance between life and death.
This sensitive topic was explored by Marina Sozzi, PhD. She is the director of the Association for the Support and Assistance of People With Chronic and Oncological Diseases, a nonprofit organization that for more than 30 years has been dedicated to “providing palliative care and supporting individuals with oncological or other chronic and degenerative diseases.”
Call for rebalancing
To give people an idea of a better system in which life and death are in balance, the Lancet Commission experts described a realistic utopia, which they summarized in the following five principles:
- The social determinants of death, dying, and grieving are confronted.
- Dying is understood to be a relational and spiritual process rather than simply a physiological event.
- Networks of care provide support for people who are dying, those caring for them, and those grieving.
- Conversations and stories about everyday death, dying, and grief become common.
- Death is recognized as having value.
Achieving this utopia will not be easy, especially considering the current systems that are in place. “There have been tremendous medical advances over the last hundred years, particularly in increasing life expectancy and curing diseases that were once considered death sentences,” Dr. Sozzi explained. “Indeed, over the course of that time period, medical science acquired an enormous degree of social power, and matters of death – which in previous centuries had been within the purview of religions and houses of worship – were handed over to be handled by doctors and nurses.”
The COVID-19 pandemic has made the medical field’s role in matters of death more prominent: every day, people saw footage of dying people in hospital beds being cared for by health care professionals in masks and gowns. These patients were otherwise alone, their only contact with loved ones being over the phone or online. They died the ultimate medicalized deaths, stripped of almost all opportunities to get emotional support from family and friends.
New perspective needed
The Lancet Commission experts were certain about one point: The need to move away from the reductionist approach to death in order to integrate a more holistic approach, one that takes into account all of the dimensions of death without limiting itself only to the medical aspects.
“Medicine has its own take on the death phenomenon and on disease, which is a reductionist take,” said Dr. Sozzi, noting that, thanks to processes that make it possible to reduce phenomena to the measurable, medicine has managed to make tremendous progress. The same approach has been applied to the view of death, which has by and large become a biologic event.
“The problem is that, in reality, death is a much more complex phenomenon: cultural, social, involving families and society,” she explained. “Not all of these aspects are taken into consideration by medicine, and therefore, our culture has diminished its view of the death phenomenon.” Dr. Sozzi pointed out that, if looked upon more closely, the very question: “What did the person die of?” presupposes, in a certain sense, that it might have been possible to prevent that death – if only medicine had the right technology. So, death comes to be seen as something that could have been avoided.
Power of palliative care
Changing the approach to death requires a profound culture shift and, therefore, a lot of time. The good news is that, although there is still a long way to go, a few steps have been taken in this direction. “Talking about death, and even organizing courses aimed at health care professionals, is definitely easier these days than it was even just 10 years ago,” said Dr. Sozzi, citing, as an example, a project she developed for training nursing home operators in palliative care.
It is in palliative care where the greatest progress has been made in end-of-life matters. “The culture of palliative care allows us to think about death in very different terms and to recognize that moment when we should stop looking at curative care and direct our efforts at ‘comfort care.’ And this care of the dying has to be holistic,” Dr. Sozzi explained. She adds that we are increasingly talking about simultaneous palliative care – care that is not limited to the final days of a person’s life but that rather starts early on, when active treatments are still in place.
Dr. Sozzi mentioned Italy’s Law 38, which took effect in 2010. It regulates access to palliative care and pain management, expanding the right to receive these treatments to patients “in any health care setting, at any stage of life, and for any chronic or progressive condition which has no treatment or has a treatment that is not sufficient to stabilize it.”
A culture shift is also needed in this area; there has already been a movement away from general practitioners to health care professionals who can and must direct a patient to palliative care.
“We need to provide these doctors with more training and make them more aware of what a difference this kind of care can make throughout a patient’s life, not only during the final stages,” said Dr. Sozzi. Concerning training, she mentioned that Italy had recently introduced a specialization in palliative care for medical school graduates. This is another small step and one that adds a sense of dignity to this new approach to life and to death.
The experts’ recommendations
In attempting to find a balance between life and death, we must not look at the period prior to the 1900s as some kind of golden age. Dr. Sozzi explained that back then there was almost none of the medical technology now available to treat people at the end of life. “Palliative care has also set forth original technical aspects for eliminating pain. Without having eliminated a patient’s pain, I can hardly begin a discussion with them about spiritual aspects,” she said, emphasizing the importance of always contextualizing approaches to death.
The Lancet Commission experts assessed the approach to death in many different contexts. They recommended that, to best handle end-of-life matters in all their complexity, one should keep in mind the importance of relationships and networks across society.
They recommended that health care and social care professionals improve their skills and their capacity for taking care of dying patients and their families. When the patient has a life-limiting illness, a caring and compassionate approach should be taken when providing clear information about all interventions involved in palliative care, as well as when having conversations about death.
Governments and policy makers are advised to implement actions to allow all citizens to have the same access to necessary palliative care. In addition, all strategies and reports on social care and well-being more broadly should always include consideration of death, dying, and grieving. It’s an uphill climb, but one that must be made if we’re to build a new culture aimed at bringing death back into life. “As we continue stepping toward this new culture, let us each put a stone in place,” Dr. Sozzi concluded.
A version of this article first appeared on Medscape.com.
“The story of dying in the 21st century is a story of paradox.” This is the opening line of a report recently published in the Lancet, in which the Lancet Commission experts tackle what is, for many, a very sensitive topic: the end of life. The recommendations they present aim at “bringing death back into life.”
What makes the story a paradox is that, in end-of-life situations, many people are overtreated, and on the other hand, many people are undertreated.
In short, when all is said and done, “people die bad deaths.” A natural event, a natural part of life, has turned into something that people fear or, in some cases, refuse to even acknowledge or talk about.
This was the motivating factor for the Lancet Commission, a group of experts from various disciplines, to come together to try to better understand this complex concept. , as well as a balance between life and death.
This sensitive topic was explored by Marina Sozzi, PhD. She is the director of the Association for the Support and Assistance of People With Chronic and Oncological Diseases, a nonprofit organization that for more than 30 years has been dedicated to “providing palliative care and supporting individuals with oncological or other chronic and degenerative diseases.”
Call for rebalancing
To give people an idea of a better system in which life and death are in balance, the Lancet Commission experts described a realistic utopia, which they summarized in the following five principles:
- The social determinants of death, dying, and grieving are confronted.
- Dying is understood to be a relational and spiritual process rather than simply a physiological event.
- Networks of care provide support for people who are dying, those caring for them, and those grieving.
- Conversations and stories about everyday death, dying, and grief become common.
- Death is recognized as having value.
Achieving this utopia will not be easy, especially considering the current systems that are in place. “There have been tremendous medical advances over the last hundred years, particularly in increasing life expectancy and curing diseases that were once considered death sentences,” Dr. Sozzi explained. “Indeed, over the course of that time period, medical science acquired an enormous degree of social power, and matters of death – which in previous centuries had been within the purview of religions and houses of worship – were handed over to be handled by doctors and nurses.”
The COVID-19 pandemic has made the medical field’s role in matters of death more prominent: every day, people saw footage of dying people in hospital beds being cared for by health care professionals in masks and gowns. These patients were otherwise alone, their only contact with loved ones being over the phone or online. They died the ultimate medicalized deaths, stripped of almost all opportunities to get emotional support from family and friends.
New perspective needed
The Lancet Commission experts were certain about one point: The need to move away from the reductionist approach to death in order to integrate a more holistic approach, one that takes into account all of the dimensions of death without limiting itself only to the medical aspects.
“Medicine has its own take on the death phenomenon and on disease, which is a reductionist take,” said Dr. Sozzi, noting that, thanks to processes that make it possible to reduce phenomena to the measurable, medicine has managed to make tremendous progress. The same approach has been applied to the view of death, which has by and large become a biologic event.
“The problem is that, in reality, death is a much more complex phenomenon: cultural, social, involving families and society,” she explained. “Not all of these aspects are taken into consideration by medicine, and therefore, our culture has diminished its view of the death phenomenon.” Dr. Sozzi pointed out that, if looked upon more closely, the very question: “What did the person die of?” presupposes, in a certain sense, that it might have been possible to prevent that death – if only medicine had the right technology. So, death comes to be seen as something that could have been avoided.
Power of palliative care
Changing the approach to death requires a profound culture shift and, therefore, a lot of time. The good news is that, although there is still a long way to go, a few steps have been taken in this direction. “Talking about death, and even organizing courses aimed at health care professionals, is definitely easier these days than it was even just 10 years ago,” said Dr. Sozzi, citing, as an example, a project she developed for training nursing home operators in palliative care.
It is in palliative care where the greatest progress has been made in end-of-life matters. “The culture of palliative care allows us to think about death in very different terms and to recognize that moment when we should stop looking at curative care and direct our efforts at ‘comfort care.’ And this care of the dying has to be holistic,” Dr. Sozzi explained. She adds that we are increasingly talking about simultaneous palliative care – care that is not limited to the final days of a person’s life but that rather starts early on, when active treatments are still in place.
Dr. Sozzi mentioned Italy’s Law 38, which took effect in 2010. It regulates access to palliative care and pain management, expanding the right to receive these treatments to patients “in any health care setting, at any stage of life, and for any chronic or progressive condition which has no treatment or has a treatment that is not sufficient to stabilize it.”
A culture shift is also needed in this area; there has already been a movement away from general practitioners to health care professionals who can and must direct a patient to palliative care.
“We need to provide these doctors with more training and make them more aware of what a difference this kind of care can make throughout a patient’s life, not only during the final stages,” said Dr. Sozzi. Concerning training, she mentioned that Italy had recently introduced a specialization in palliative care for medical school graduates. This is another small step and one that adds a sense of dignity to this new approach to life and to death.
The experts’ recommendations
In attempting to find a balance between life and death, we must not look at the period prior to the 1900s as some kind of golden age. Dr. Sozzi explained that back then there was almost none of the medical technology now available to treat people at the end of life. “Palliative care has also set forth original technical aspects for eliminating pain. Without having eliminated a patient’s pain, I can hardly begin a discussion with them about spiritual aspects,” she said, emphasizing the importance of always contextualizing approaches to death.
The Lancet Commission experts assessed the approach to death in many different contexts. They recommended that, to best handle end-of-life matters in all their complexity, one should keep in mind the importance of relationships and networks across society.
They recommended that health care and social care professionals improve their skills and their capacity for taking care of dying patients and their families. When the patient has a life-limiting illness, a caring and compassionate approach should be taken when providing clear information about all interventions involved in palliative care, as well as when having conversations about death.
Governments and policy makers are advised to implement actions to allow all citizens to have the same access to necessary palliative care. In addition, all strategies and reports on social care and well-being more broadly should always include consideration of death, dying, and grieving. It’s an uphill climb, but one that must be made if we’re to build a new culture aimed at bringing death back into life. “As we continue stepping toward this new culture, let us each put a stone in place,” Dr. Sozzi concluded.
A version of this article first appeared on Medscape.com.
“The story of dying in the 21st century is a story of paradox.” This is the opening line of a report recently published in the Lancet, in which the Lancet Commission experts tackle what is, for many, a very sensitive topic: the end of life. The recommendations they present aim at “bringing death back into life.”
What makes the story a paradox is that, in end-of-life situations, many people are overtreated, and on the other hand, many people are undertreated.
In short, when all is said and done, “people die bad deaths.” A natural event, a natural part of life, has turned into something that people fear or, in some cases, refuse to even acknowledge or talk about.
This was the motivating factor for the Lancet Commission, a group of experts from various disciplines, to come together to try to better understand this complex concept. , as well as a balance between life and death.
This sensitive topic was explored by Marina Sozzi, PhD. She is the director of the Association for the Support and Assistance of People With Chronic and Oncological Diseases, a nonprofit organization that for more than 30 years has been dedicated to “providing palliative care and supporting individuals with oncological or other chronic and degenerative diseases.”
Call for rebalancing
To give people an idea of a better system in which life and death are in balance, the Lancet Commission experts described a realistic utopia, which they summarized in the following five principles:
- The social determinants of death, dying, and grieving are confronted.
- Dying is understood to be a relational and spiritual process rather than simply a physiological event.
- Networks of care provide support for people who are dying, those caring for them, and those grieving.
- Conversations and stories about everyday death, dying, and grief become common.
- Death is recognized as having value.
Achieving this utopia will not be easy, especially considering the current systems that are in place. “There have been tremendous medical advances over the last hundred years, particularly in increasing life expectancy and curing diseases that were once considered death sentences,” Dr. Sozzi explained. “Indeed, over the course of that time period, medical science acquired an enormous degree of social power, and matters of death – which in previous centuries had been within the purview of religions and houses of worship – were handed over to be handled by doctors and nurses.”
The COVID-19 pandemic has made the medical field’s role in matters of death more prominent: every day, people saw footage of dying people in hospital beds being cared for by health care professionals in masks and gowns. These patients were otherwise alone, their only contact with loved ones being over the phone or online. They died the ultimate medicalized deaths, stripped of almost all opportunities to get emotional support from family and friends.
New perspective needed
The Lancet Commission experts were certain about one point: The need to move away from the reductionist approach to death in order to integrate a more holistic approach, one that takes into account all of the dimensions of death without limiting itself only to the medical aspects.
“Medicine has its own take on the death phenomenon and on disease, which is a reductionist take,” said Dr. Sozzi, noting that, thanks to processes that make it possible to reduce phenomena to the measurable, medicine has managed to make tremendous progress. The same approach has been applied to the view of death, which has by and large become a biologic event.
“The problem is that, in reality, death is a much more complex phenomenon: cultural, social, involving families and society,” she explained. “Not all of these aspects are taken into consideration by medicine, and therefore, our culture has diminished its view of the death phenomenon.” Dr. Sozzi pointed out that, if looked upon more closely, the very question: “What did the person die of?” presupposes, in a certain sense, that it might have been possible to prevent that death – if only medicine had the right technology. So, death comes to be seen as something that could have been avoided.
Power of palliative care
Changing the approach to death requires a profound culture shift and, therefore, a lot of time. The good news is that, although there is still a long way to go, a few steps have been taken in this direction. “Talking about death, and even organizing courses aimed at health care professionals, is definitely easier these days than it was even just 10 years ago,” said Dr. Sozzi, citing, as an example, a project she developed for training nursing home operators in palliative care.
It is in palliative care where the greatest progress has been made in end-of-life matters. “The culture of palliative care allows us to think about death in very different terms and to recognize that moment when we should stop looking at curative care and direct our efforts at ‘comfort care.’ And this care of the dying has to be holistic,” Dr. Sozzi explained. She adds that we are increasingly talking about simultaneous palliative care – care that is not limited to the final days of a person’s life but that rather starts early on, when active treatments are still in place.
Dr. Sozzi mentioned Italy’s Law 38, which took effect in 2010. It regulates access to palliative care and pain management, expanding the right to receive these treatments to patients “in any health care setting, at any stage of life, and for any chronic or progressive condition which has no treatment or has a treatment that is not sufficient to stabilize it.”
A culture shift is also needed in this area; there has already been a movement away from general practitioners to health care professionals who can and must direct a patient to palliative care.
“We need to provide these doctors with more training and make them more aware of what a difference this kind of care can make throughout a patient’s life, not only during the final stages,” said Dr. Sozzi. Concerning training, she mentioned that Italy had recently introduced a specialization in palliative care for medical school graduates. This is another small step and one that adds a sense of dignity to this new approach to life and to death.
The experts’ recommendations
In attempting to find a balance between life and death, we must not look at the period prior to the 1900s as some kind of golden age. Dr. Sozzi explained that back then there was almost none of the medical technology now available to treat people at the end of life. “Palliative care has also set forth original technical aspects for eliminating pain. Without having eliminated a patient’s pain, I can hardly begin a discussion with them about spiritual aspects,” she said, emphasizing the importance of always contextualizing approaches to death.
The Lancet Commission experts assessed the approach to death in many different contexts. They recommended that, to best handle end-of-life matters in all their complexity, one should keep in mind the importance of relationships and networks across society.
They recommended that health care and social care professionals improve their skills and their capacity for taking care of dying patients and their families. When the patient has a life-limiting illness, a caring and compassionate approach should be taken when providing clear information about all interventions involved in palliative care, as well as when having conversations about death.
Governments and policy makers are advised to implement actions to allow all citizens to have the same access to necessary palliative care. In addition, all strategies and reports on social care and well-being more broadly should always include consideration of death, dying, and grieving. It’s an uphill climb, but one that must be made if we’re to build a new culture aimed at bringing death back into life. “As we continue stepping toward this new culture, let us each put a stone in place,” Dr. Sozzi concluded.
A version of this article first appeared on Medscape.com.
FROM THE LANCET
First-year fellows guide to gastroenterology
After the excitement and the well-deserved celebrations of matching in a gastroenterology fellowship program, a whole new set of unanswered questions and worries can start forming in a first-year fellow’s mind. “I made it, but now what? How do I learn a whole new career skill like endoscopy? Is my GI knowledge solid and wide enough to manage patients and answer the medical team consult? How will I keep up with my reading and learning with a busy fellowship schedule? How do I balance growth in clinical knowledge, endoscopy, and research? Can I integrate ‘life’ alongside a busy fellowship?” All of these questions and more can be overwhelming to answer in the beginning. The following guide is designed to help you through this transition and navigate the various aspects of first-year fellowship.
First-year goals
It is important to keep in mind that you have 3 full years to become a well-rounded, highly skilled, and knowledgeable gastroenterologist and endoscopist. So, set realistic goals and expectations for your first year, but be mindful that this year also lays the solid foundations of who you will become as a clinician, educator, or researcher.

One of the main goals of fellowship is to learn and implement evidence-based medicine in the diagnosis and management of GI conditions, as well as to learn endoscopic skills and ethics, all while keeping the patient (as a whole person) at the center of what you do. According to a recently published article by Bollipo and colleagues,1 the overall growth as a gastroenterologist not only depends on acquisition of knowledge but also involves cultivating teamwork, communication, situational awareness, compassion, leadership, and situational awareness. Beyond your medical education, your professional growth is also dependent on intentionally working towards acquiring the following skills:
1. Manage your time efficiently and prioritize your daily tasks
2. Become a consultant: effectively communicate with others, teach, lead, and delegate as appropriate
3. Work as a team with colleagues, faculty, and endoscopy staff
4. Develop critical thinking, give and receive constructive feedback, and understand your skills, limitations, and growth potential
5. Identify mentors and potential niche area
6. Start building your professional network and your reputation
7. Get involved in national GI societies
Consults
Mindset
Shifting gear from residency to fellowship involves a shifting of your clinical mindset too, going from being part of a primary care team responsible for all aspects of a patient’s medical care, to that of a consulting team focused on a patient’s GI condition. It is important to find the right balance of refraining from micromanaging non-GI comorbidities while being fully aware of their impact on your diagnostic and therapeutic approach to the GI condition.

Let’s face it, you will not always get “exciting and interesting GI cases” consults, and on a busy day some consultations might feel unnecessary and frustrating to you. Remember that what seems obvious to you, based on your focused GI knowledge, might not be so simple to the primary team. In addition, every consult is an opportunity to improve your approach to patient care, as well as an opportunity to learn and teach others, from medical students to residents. So, always be professional and respectful when you pick up the phone, and build positive collaborative bridges between you and the medical or surgical consulting teams. Be the GI fellow others are not reluctant to call for help, and better, be the one who communicates GI pearls along the way, inspires others to join the field of gastroenterology, and positively represent the GI division.
Triage
When you answer your consult page, ask the primary team what specific question they have for you and/or what is the main GI complaint or test abnormality the patient has. This will help you assess the urgency and the complexity of the consult, and hence allow you to prioritize each consult (which one you need to see first and give the attending a heads-up), assign (or not) a rotating medical resident or student to the consult, tailor your preliminary recommendations to the primary team, and anticipate the need for a procedure. When you anticipate a procedure, assess its (semi-)urgency to get the process ready for same day or a bedside procedure by getting information on the patient’s vitals, basic labs, significant acute comorbidities, and supportive therapies in place. In other words, by judiciously obtaining key information from the primary team, you can efficiently triage the consults and keep your day organized and manageable (for the most part). Learn to divide and conquer the tasks of the day: split inpatient endoscopy and consults with your cofellows, assign appropriate consults and follow-ups to residents or students rotating on the GI service, and properly communicate with the primary team a plan of care (even a preliminary one) to avoid recurrent pages and interruptions. Some days the number or urgency of the consults and the required multitasking can be overwhelming: stop, breathe, and ask for help from your co-fellows and your attending. Remember, this is a fellowship, not a solo-ship and your program is here to support your work and growth.
Communication
Timely and efficient communication, between you and the different stakeholders, is crucial to provide optimal patient care and minimize the risk of “things falling through the cracks”. Convey to the primary team your recommendations and plan of care clearly, and use direct verbal communication (not just a note in the chart) when managing complex or urgent situations. Obtain information regarding current patient level of care (i.e., ICU), isolation precautions, and cardiac devices (i.e., left ventricular assist device). Keep the dialogue open with your attending about acutely ill patients and potentially urgent procedures. Inform the endoscopy suite early that you are adding a procedure on the same day, and communicate anticipated needs (such as intubation, fluoroscopy room, pediatric scope, stent). Using a “closed-loop” communication structure can ensure that your recommendations are received and implemented appropriately.2
Time management and structure

Having a structured routine to your day, in what seems to be a chaotic process of juggling different duties and being in different locations at once, will ensure that you efficiently complete your tasks in a timely manner. Find what works best for you, taking into account the challenges and resources available to you, such as the number of fellows and other trainees on the GI consult service, the average number of consults per day and their acuity, the availability of inpatient protocols for specific clinical situations (GI bleed, acute severe ulcerative colitis, etc.), and the time and style preferences of the rounding attending. We suggest the following schedule on a consult day: Round early in the morning and leave a note in the chart and/or communicate with the team key information, then review with the rotating trainees the patients they are following and personally reassess some patients as needed. Inform the endoscopy suite of the same day procedures and let your attending know of any issues that require immediate attention. Take your team and head to radiology and review the imaging studies on your patients. Learn and teach key points in diagnosis and therapeutic approach as you move through your day from the inpatient floors to the hallways. Divide consults during the day with your team and agree on a time to touch base. Review your patient list at the end of the day and assess which patients the GI service no longer need to follow and communicate that clearly to the primary team along with the appropriate outpatient GI care follow-up. Let the endoscopy suite know of any procedures you are adding for the next day along with their degree of urgency to allow the charge nurse to prioritize cases. When you leave the hospital, be intentional with your free time: Read about the GI conditions you have encountered, enjoy some fun relaxing time, and rest!
Call
Know your call environment and your emergency cart
Familiarize yourself with the locations where you could potentially perform an emergent case (i.e., the ICU, ED, operating room) and the relevant points of contact (such as the charge nurse, the anesthesia team, the on-call tech team) for overnight or weekend cases. Whether or not you have an endoscopy support team on call, learn to set up the emergency cart, find and check your equipment, and troubleshoot technical issues by soliciting an “in-service” from senior fellows or the endoscopy technical support staff. Before heading to an urgent case, double check that you have your “bleeder” or “food impaction” tools. For food impaction, consider obtaining rat tooth forceps, snares, Roth nets, and an overtube. For bleeding cases, obtain a therapeutic upper endoscope, hemostatic clips, clear caps, injection needles, epinephrine, HemosprayTM, banding kits, and the appropriate electrocautery/thermal set up.
What is an emergency?
Consults that require your immediate attention include food impactions, acute biliary conditions leading to septic shock, and hemodynamically unstable GI bleeds, especially variceal bleeds. Remember that patients who are hemodynamically unstable require adequate resuscitation before proceeding with any endoscopic intervention. Assess the need for intubation, the timing of the procedure, and the most optimal location to perform the procedure, depending on the time and acuity of the patients’ presentation, how they respond to resuscitation measures, and the resources and preferences of your institution.
The overnight ‘nonemergent’ call
Non-emergent consults can be addressed the next day, after reviewing the clinical information provided by the consulting team and the patient’s EMR to ensure no urgent measures are needed. Overnight call may include patient phone calls, from inquiries about colon prep (so familiarize yourself with the different prep instructions and how to troubleshoot prep difficulties) to GI symptoms that you will need to triage to either the ED or to an outpatient follow-up. Document all phone encounters in the EMR and route your note to the appropriate clinician and nurse or administrative assistant for follow-up.
The five E’s of endoscopy
Endoscopy training is a large component of a GI fellowship and can create achievement anxiety in many first-year fellows seeking the cecum! But there is more to endoscopy than technical skills: It is as important to adequately evaluate clinical situations, understand the indications and potential limitations and complications of the procedure, and assess how it will impact the management of the patient. And no, you don’t have to be a video gamer to be a good endoscopist; and yes, you will be able to regularly complete a colonoscopy before the end of your first year!
Evaluation
In order to improve your endoscopic skills, it is important to honestly assess your areas of proficiency and improvement and to welcome real-time constructive feedback from your teaching attending about your endoscopic skills range. Consider meeting regularly with your attending to discuss your short-term and long-term endoscopic goals and how to enhance your skills. This practice demonstrates responsibility, credibility, and accountability amongst your peers as well as a genuine commitment to your growth as an endoscopist.
Efficiency
In addition to focusing on the quality of your endoscopy, learn to be efficient in the pre- and postprocedure time flow. This entails any step from properly explaining the procedure to patients before they come to the endoscopy suite, making sure the needed endoscopy equipment and tools are available in your room, completing your personal setup (i.e., gowning up, setting up your bed/monitor height, testing your endoscope) even before time out, to discharging the patient and communicating key findings and plan of care to the primary team. Depending on the acuity of the procedure and patient’s comorbidities, certain procedures may need to be performed or completed by a more efficient and experienced senior fellow or attending; don’t let this situation trigger passive frustration in you, but rather use it as an active and engaging opportunity to learn.
Expectations
You (and all the other neighborhood kids) didn’t learn to ride a bike without falling, struggling, needing help, and practicing over and over again, and it goes the same when learning to scope as a first-year fellow. Keep this in mind to lessen frustration, set realistic expectations, and be patient with yourself and celebrate all the small victories. Set tangible goals with your attending prior to procedural days/rotations so they can help you hone in and perfect the desired endoscopy skills.
Ergonomics
In a recent study, endoscopy-related injury (ERI) was reported to occur in up to 75% of gastroenterologists.3 While your primary focus might be reaching the cecum, it is as crucial for you to learn how to prevent ERI to ensure your long term health and continued success in procedures.
Excellence over quantity
Your main focus as a trainee is to learn how to provide effective, efficient, and safe care to patients, including in endoscopy. The quality of the endoscopy you perform is much more important than the total number of procedures you do. Thus, it is key to take each procedure as a complete learning opportunity to perform a thorough evaluation, improve your technical skills, interpret the findings, and develop a therapeutic plan.
Work-life balance and burnout
Fellowship is a marathon and not a sprint, so you need to slow down after a busy workday and care for yourself and enjoy time with loved ones. The cognitive, physical, mental, and emotional demands for first-year fellows are arguably the highest during GI training and can lead to burnout. Signs of burnout include emotional exhaustion, loss of empathy, fatigue, depersonalization and detachment, and feelings of personal inadequacy.4 Antiburnout measures include respecting basic healthy life hygiene (eat and sleep well, regular physical activity), having a hobby, practicing meditation, avoiding taking work home, and having a healthy social network.5 Remember that your cofellows whom you share common experiences with are not only your colleagues but can also be your friends and your social support. If you are a parent juggling work and family, remember to ask for help from your peers if you need it and have an open discussion with your attending to find practical solutions to your schedule.
Professional growth in the field of gastroenterology
Becoming a successful gastroenterologist and endoscopist involves going above the “I” and into the inclusive “we.” Building collegial and professional relationships early on with different stakeholders will set you up for success during and beyond your fellowship.
Building relationships
Developing genuine collegial and collaborative relationships with cofellows and faculty will positively impact your wellness during fellowship but also build the foundation of your professional network necessary to your career growth. Be inclusive of your cofellows in your research projects and publications, and support and amplify their work as much as you amplify your own. Your cofellows or attendings are likely to be the ones to help you find the right job, invite you to speak at grand rounds, or sit on a GI committee and promote your postfellowship professional growth.
Mentorship, being an educator and role model
It is important to identify and seek out mentors, within or outside your fellowship program or institution, who can not only guide you in your career choices but also open doors for you and sponsor you to advance your career. On the other hand, you too can be a role model, mentor, and sponsor to medical residents and students interested in the field of GI. Teach others in didactic settings or on the consult service, include trainees in quality improvement projects and publications, and lead by example.
Research
Most academic GI programs have a baseline requirement of research. Choose and devise a project you can realistically complete despite your busy first-year schedule: expand on a residency research project, focus on a specific simple question triggered by a clinical situation you encountered, proceed with a retrospective chart review or quality improvement project, and include other fellows and trainees to divide tasks. Alternatively, devise a specific timeline with a research mentor to complete a larger research project during your three years of fellowship.
Involvement in GI societies/committees
Become a member of one (or all) of the national GI societies that align with your interests. Membership gives you access not only to peer-reviewed scientific articles and guidelines but also to fellow-focused programs, committees’ opportunities, early career research grants, and mentorship.6-10
Summary
The first year of a GI fellowship lays the foundation for your next 3 years: Be mindful of how you can optimize the opportunities at hand to learn, teach, build a solid reputation, and grow your professional network. But also remember you have 3 full years to accomplish all your goals, so be patient, pace yourself, and include others in your journey. Judiciously use the many resources within your program and GI societies to help you achieve your goals, reach out to others to overcome difficulties and barriers, and dedicate time to care for your personal health and growth. This is what a true comprehensive and healthy fellowship is all about!
Dr. Advani is with the division of gastroenterology and hepatology, Stony Brook (N.Y.) University Hospital. Dr. Saeed is with the division of gastroenterology and hepatology, University of Kentucky, Lexington. Dr. Charabaty is with the division of gastroenterology, Johns Hopkins University, Baltimore, and Johns Hopkins–Sibley Memorial Hospital, Washington. Dr. Advani and Dr. Saeed have no conflicts to disclose. Dr. Charabaty disclosed ties to AbbVie, Janssen, Takeda, Pfizer, and Bristol-Myers Squibb and is founder of @MondayNightIBD, and cofounder of Scrubs & Heels.
References
1. Bollipo S. Gastroenterology. 2020 Nov;159(5):1648-52.
2. Adams MA et al. Gastroenterology. 2014 Jan 1;146(1):5-9.
3. Pawa S et al. Am J Gastroenterol. 2021 Mar 1;116(3):530-8.
4. DeCross AJ. Gastroenterology. 2020 Jan 1;158(1):32-5.
5. Burke C et al. Am J Gastroenterol. 2017 Oct 1;112:S593-4.
6. Fellows Resources under Fellows & Early Career. American Gastroenterological Association. https://gastro.org/fellows-and-early-career/training-resources/fellows-resources/.
7. Trainee Courses and Events. American College of Gastroenterology. https://gi.org/trainees/trainee-courses-and-events/.
8. Trainee Resources. American Association for the Study of Liver Diseases. https://www.aasld.org/membership/hepatology-associates/trainee-resources.
9. First Year Fellows Courses under Education. American Society of Gastrointestinal Endoscopy. https://www.asge.org/home/education/advanced-education-training/first-year-fellow-(fyf)-courses.
10. Annual GI Fellow Summer Course Presentations. New York Society for Gastrointestinal Endoscopy. https://www.nysge.org/annual%20gi%20fellows%20summer%20course.
After the excitement and the well-deserved celebrations of matching in a gastroenterology fellowship program, a whole new set of unanswered questions and worries can start forming in a first-year fellow’s mind. “I made it, but now what? How do I learn a whole new career skill like endoscopy? Is my GI knowledge solid and wide enough to manage patients and answer the medical team consult? How will I keep up with my reading and learning with a busy fellowship schedule? How do I balance growth in clinical knowledge, endoscopy, and research? Can I integrate ‘life’ alongside a busy fellowship?” All of these questions and more can be overwhelming to answer in the beginning. The following guide is designed to help you through this transition and navigate the various aspects of first-year fellowship.
First-year goals
It is important to keep in mind that you have 3 full years to become a well-rounded, highly skilled, and knowledgeable gastroenterologist and endoscopist. So, set realistic goals and expectations for your first year, but be mindful that this year also lays the solid foundations of who you will become as a clinician, educator, or researcher.
One of the main goals of fellowship is to learn and implement evidence-based medicine in the diagnosis and management of GI conditions, as well as to learn endoscopic skills and ethics, all while keeping the patient (as a whole person) at the center of what you do. According to a recently published article by Bollipo and colleagues,1 the overall growth as a gastroenterologist not only depends on acquisition of knowledge but also involves cultivating teamwork, communication, situational awareness, compassion, leadership, and situational awareness. Beyond your medical education, your professional growth is also dependent on intentionally working towards acquiring the following skills:
1. Manage your time efficiently and prioritize your daily tasks
2. Become a consultant: effectively communicate with others, teach, lead, and delegate as appropriate
3. Work as a team with colleagues, faculty, and endoscopy staff
4. Develop critical thinking, give and receive constructive feedback, and understand your skills, limitations, and growth potential
5. Identify mentors and potential niche area
6. Start building your professional network and your reputation
7. Get involved in national GI societies
Consults
Mindset
Shifting gear from residency to fellowship involves a shifting of your clinical mindset too, going from being part of a primary care team responsible for all aspects of a patient’s medical care, to that of a consulting team focused on a patient’s GI condition. It is important to find the right balance of refraining from micromanaging non-GI comorbidities while being fully aware of their impact on your diagnostic and therapeutic approach to the GI condition.
Let’s face it, you will not always get “exciting and interesting GI cases” consults, and on a busy day some consultations might feel unnecessary and frustrating to you. Remember that what seems obvious to you, based on your focused GI knowledge, might not be so simple to the primary team. In addition, every consult is an opportunity to improve your approach to patient care, as well as an opportunity to learn and teach others, from medical students to residents. So, always be professional and respectful when you pick up the phone, and build positive collaborative bridges between you and the medical or surgical consulting teams. Be the GI fellow others are not reluctant to call for help, and better, be the one who communicates GI pearls along the way, inspires others to join the field of gastroenterology, and positively represent the GI division.
Triage
When you answer your consult page, ask the primary team what specific question they have for you and/or what is the main GI complaint or test abnormality the patient has. This will help you assess the urgency and the complexity of the consult, and hence allow you to prioritize each consult (which one you need to see first and give the attending a heads-up), assign (or not) a rotating medical resident or student to the consult, tailor your preliminary recommendations to the primary team, and anticipate the need for a procedure. When you anticipate a procedure, assess its (semi-)urgency to get the process ready for same day or a bedside procedure by getting information on the patient’s vitals, basic labs, significant acute comorbidities, and supportive therapies in place. In other words, by judiciously obtaining key information from the primary team, you can efficiently triage the consults and keep your day organized and manageable (for the most part). Learn to divide and conquer the tasks of the day: split inpatient endoscopy and consults with your cofellows, assign appropriate consults and follow-ups to residents or students rotating on the GI service, and properly communicate with the primary team a plan of care (even a preliminary one) to avoid recurrent pages and interruptions. Some days the number or urgency of the consults and the required multitasking can be overwhelming: stop, breathe, and ask for help from your co-fellows and your attending. Remember, this is a fellowship, not a solo-ship and your program is here to support your work and growth.
Communication
Timely and efficient communication, between you and the different stakeholders, is crucial to provide optimal patient care and minimize the risk of “things falling through the cracks”. Convey to the primary team your recommendations and plan of care clearly, and use direct verbal communication (not just a note in the chart) when managing complex or urgent situations. Obtain information regarding current patient level of care (i.e., ICU), isolation precautions, and cardiac devices (i.e., left ventricular assist device). Keep the dialogue open with your attending about acutely ill patients and potentially urgent procedures. Inform the endoscopy suite early that you are adding a procedure on the same day, and communicate anticipated needs (such as intubation, fluoroscopy room, pediatric scope, stent). Using a “closed-loop” communication structure can ensure that your recommendations are received and implemented appropriately.2
Time management and structure
Having a structured routine to your day, in what seems to be a chaotic process of juggling different duties and being in different locations at once, will ensure that you efficiently complete your tasks in a timely manner. Find what works best for you, taking into account the challenges and resources available to you, such as the number of fellows and other trainees on the GI consult service, the average number of consults per day and their acuity, the availability of inpatient protocols for specific clinical situations (GI bleed, acute severe ulcerative colitis, etc.), and the time and style preferences of the rounding attending. We suggest the following schedule on a consult day: Round early in the morning and leave a note in the chart and/or communicate with the team key information, then review with the rotating trainees the patients they are following and personally reassess some patients as needed. Inform the endoscopy suite of the same day procedures and let your attending know of any issues that require immediate attention. Take your team and head to radiology and review the imaging studies on your patients. Learn and teach key points in diagnosis and therapeutic approach as you move through your day from the inpatient floors to the hallways. Divide consults during the day with your team and agree on a time to touch base. Review your patient list at the end of the day and assess which patients the GI service no longer need to follow and communicate that clearly to the primary team along with the appropriate outpatient GI care follow-up. Let the endoscopy suite know of any procedures you are adding for the next day along with their degree of urgency to allow the charge nurse to prioritize cases. When you leave the hospital, be intentional with your free time: Read about the GI conditions you have encountered, enjoy some fun relaxing time, and rest!
Call
Know your call environment and your emergency cart
Familiarize yourself with the locations where you could potentially perform an emergent case (i.e., the ICU, ED, operating room) and the relevant points of contact (such as the charge nurse, the anesthesia team, the on-call tech team) for overnight or weekend cases. Whether or not you have an endoscopy support team on call, learn to set up the emergency cart, find and check your equipment, and troubleshoot technical issues by soliciting an “in-service” from senior fellows or the endoscopy technical support staff. Before heading to an urgent case, double check that you have your “bleeder” or “food impaction” tools. For food impaction, consider obtaining rat tooth forceps, snares, Roth nets, and an overtube. For bleeding cases, obtain a therapeutic upper endoscope, hemostatic clips, clear caps, injection needles, epinephrine, HemosprayTM, banding kits, and the appropriate electrocautery/thermal set up.
What is an emergency?
Consults that require your immediate attention include food impactions, acute biliary conditions leading to septic shock, and hemodynamically unstable GI bleeds, especially variceal bleeds. Remember that patients who are hemodynamically unstable require adequate resuscitation before proceeding with any endoscopic intervention. Assess the need for intubation, the timing of the procedure, and the most optimal location to perform the procedure, depending on the time and acuity of the patients’ presentation, how they respond to resuscitation measures, and the resources and preferences of your institution.
The overnight ‘nonemergent’ call
Non-emergent consults can be addressed the next day, after reviewing the clinical information provided by the consulting team and the patient’s EMR to ensure no urgent measures are needed. Overnight call may include patient phone calls, from inquiries about colon prep (so familiarize yourself with the different prep instructions and how to troubleshoot prep difficulties) to GI symptoms that you will need to triage to either the ED or to an outpatient follow-up. Document all phone encounters in the EMR and route your note to the appropriate clinician and nurse or administrative assistant for follow-up.
The five E’s of endoscopy
Endoscopy training is a large component of a GI fellowship and can create achievement anxiety in many first-year fellows seeking the cecum! But there is more to endoscopy than technical skills: It is as important to adequately evaluate clinical situations, understand the indications and potential limitations and complications of the procedure, and assess how it will impact the management of the patient. And no, you don’t have to be a video gamer to be a good endoscopist; and yes, you will be able to regularly complete a colonoscopy before the end of your first year!
Evaluation
In order to improve your endoscopic skills, it is important to honestly assess your areas of proficiency and improvement and to welcome real-time constructive feedback from your teaching attending about your endoscopic skills range. Consider meeting regularly with your attending to discuss your short-term and long-term endoscopic goals and how to enhance your skills. This practice demonstrates responsibility, credibility, and accountability amongst your peers as well as a genuine commitment to your growth as an endoscopist.
Efficiency
In addition to focusing on the quality of your endoscopy, learn to be efficient in the pre- and postprocedure time flow. This entails any step from properly explaining the procedure to patients before they come to the endoscopy suite, making sure the needed endoscopy equipment and tools are available in your room, completing your personal setup (i.e., gowning up, setting up your bed/monitor height, testing your endoscope) even before time out, to discharging the patient and communicating key findings and plan of care to the primary team. Depending on the acuity of the procedure and patient’s comorbidities, certain procedures may need to be performed or completed by a more efficient and experienced senior fellow or attending; don’t let this situation trigger passive frustration in you, but rather use it as an active and engaging opportunity to learn.
Expectations
You (and all the other neighborhood kids) didn’t learn to ride a bike without falling, struggling, needing help, and practicing over and over again, and it goes the same when learning to scope as a first-year fellow. Keep this in mind to lessen frustration, set realistic expectations, and be patient with yourself and celebrate all the small victories. Set tangible goals with your attending prior to procedural days/rotations so they can help you hone in and perfect the desired endoscopy skills.
Ergonomics
In a recent study, endoscopy-related injury (ERI) was reported to occur in up to 75% of gastroenterologists.3 While your primary focus might be reaching the cecum, it is as crucial for you to learn how to prevent ERI to ensure your long term health and continued success in procedures.
Excellence over quantity
Your main focus as a trainee is to learn how to provide effective, efficient, and safe care to patients, including in endoscopy. The quality of the endoscopy you perform is much more important than the total number of procedures you do. Thus, it is key to take each procedure as a complete learning opportunity to perform a thorough evaluation, improve your technical skills, interpret the findings, and develop a therapeutic plan.
Work-life balance and burnout
Fellowship is a marathon and not a sprint, so you need to slow down after a busy workday and care for yourself and enjoy time with loved ones. The cognitive, physical, mental, and emotional demands for first-year fellows are arguably the highest during GI training and can lead to burnout. Signs of burnout include emotional exhaustion, loss of empathy, fatigue, depersonalization and detachment, and feelings of personal inadequacy.4 Antiburnout measures include respecting basic healthy life hygiene (eat and sleep well, regular physical activity), having a hobby, practicing meditation, avoiding taking work home, and having a healthy social network.5 Remember that your cofellows whom you share common experiences with are not only your colleagues but can also be your friends and your social support. If you are a parent juggling work and family, remember to ask for help from your peers if you need it and have an open discussion with your attending to find practical solutions to your schedule.
Professional growth in the field of gastroenterology
Becoming a successful gastroenterologist and endoscopist involves going above the “I” and into the inclusive “we.” Building collegial and professional relationships early on with different stakeholders will set you up for success during and beyond your fellowship.
Building relationships
Developing genuine collegial and collaborative relationships with cofellows and faculty will positively impact your wellness during fellowship but also build the foundation of your professional network necessary to your career growth. Be inclusive of your cofellows in your research projects and publications, and support and amplify their work as much as you amplify your own. Your cofellows or attendings are likely to be the ones to help you find the right job, invite you to speak at grand rounds, or sit on a GI committee and promote your postfellowship professional growth.
Mentorship, being an educator and role model
It is important to identify and seek out mentors, within or outside your fellowship program or institution, who can not only guide you in your career choices but also open doors for you and sponsor you to advance your career. On the other hand, you too can be a role model, mentor, and sponsor to medical residents and students interested in the field of GI. Teach others in didactic settings or on the consult service, include trainees in quality improvement projects and publications, and lead by example.
Research
Most academic GI programs have a baseline requirement of research. Choose and devise a project you can realistically complete despite your busy first-year schedule: expand on a residency research project, focus on a specific simple question triggered by a clinical situation you encountered, proceed with a retrospective chart review or quality improvement project, and include other fellows and trainees to divide tasks. Alternatively, devise a specific timeline with a research mentor to complete a larger research project during your three years of fellowship.
Involvement in GI societies/committees
Become a member of one (or all) of the national GI societies that align with your interests. Membership gives you access not only to peer-reviewed scientific articles and guidelines but also to fellow-focused programs, committees’ opportunities, early career research grants, and mentorship.6-10
Summary
The first year of a GI fellowship lays the foundation for your next 3 years: Be mindful of how you can optimize the opportunities at hand to learn, teach, build a solid reputation, and grow your professional network. But also remember you have 3 full years to accomplish all your goals, so be patient, pace yourself, and include others in your journey. Judiciously use the many resources within your program and GI societies to help you achieve your goals, reach out to others to overcome difficulties and barriers, and dedicate time to care for your personal health and growth. This is what a true comprehensive and healthy fellowship is all about!
Dr. Advani is with the division of gastroenterology and hepatology, Stony Brook (N.Y.) University Hospital. Dr. Saeed is with the division of gastroenterology and hepatology, University of Kentucky, Lexington. Dr. Charabaty is with the division of gastroenterology, Johns Hopkins University, Baltimore, and Johns Hopkins–Sibley Memorial Hospital, Washington. Dr. Advani and Dr. Saeed have no conflicts to disclose. Dr. Charabaty disclosed ties to AbbVie, Janssen, Takeda, Pfizer, and Bristol-Myers Squibb and is founder of @MondayNightIBD, and cofounder of Scrubs & Heels.
References
1. Bollipo S. Gastroenterology. 2020 Nov;159(5):1648-52.
2. Adams MA et al. Gastroenterology. 2014 Jan 1;146(1):5-9.
3. Pawa S et al. Am J Gastroenterol. 2021 Mar 1;116(3):530-8.
4. DeCross AJ. Gastroenterology. 2020 Jan 1;158(1):32-5.
5. Burke C et al. Am J Gastroenterol. 2017 Oct 1;112:S593-4.
6. Fellows Resources under Fellows & Early Career. American Gastroenterological Association. https://gastro.org/fellows-and-early-career/training-resources/fellows-resources/.
7. Trainee Courses and Events. American College of Gastroenterology. https://gi.org/trainees/trainee-courses-and-events/.
8. Trainee Resources. American Association for the Study of Liver Diseases. https://www.aasld.org/membership/hepatology-associates/trainee-resources.
9. First Year Fellows Courses under Education. American Society of Gastrointestinal Endoscopy. https://www.asge.org/home/education/advanced-education-training/first-year-fellow-(fyf)-courses.
10. Annual GI Fellow Summer Course Presentations. New York Society for Gastrointestinal Endoscopy. https://www.nysge.org/annual%20gi%20fellows%20summer%20course.
After the excitement and the well-deserved celebrations of matching in a gastroenterology fellowship program, a whole new set of unanswered questions and worries can start forming in a first-year fellow’s mind. “I made it, but now what? How do I learn a whole new career skill like endoscopy? Is my GI knowledge solid and wide enough to manage patients and answer the medical team consult? How will I keep up with my reading and learning with a busy fellowship schedule? How do I balance growth in clinical knowledge, endoscopy, and research? Can I integrate ‘life’ alongside a busy fellowship?” All of these questions and more can be overwhelming to answer in the beginning. The following guide is designed to help you through this transition and navigate the various aspects of first-year fellowship.
First-year goals
It is important to keep in mind that you have 3 full years to become a well-rounded, highly skilled, and knowledgeable gastroenterologist and endoscopist. So, set realistic goals and expectations for your first year, but be mindful that this year also lays the solid foundations of who you will become as a clinician, educator, or researcher.
One of the main goals of fellowship is to learn and implement evidence-based medicine in the diagnosis and management of GI conditions, as well as to learn endoscopic skills and ethics, all while keeping the patient (as a whole person) at the center of what you do. According to a recently published article by Bollipo and colleagues,1 the overall growth as a gastroenterologist not only depends on acquisition of knowledge but also involves cultivating teamwork, communication, situational awareness, compassion, leadership, and situational awareness. Beyond your medical education, your professional growth is also dependent on intentionally working towards acquiring the following skills:
1. Manage your time efficiently and prioritize your daily tasks
2. Become a consultant: effectively communicate with others, teach, lead, and delegate as appropriate
3. Work as a team with colleagues, faculty, and endoscopy staff
4. Develop critical thinking, give and receive constructive feedback, and understand your skills, limitations, and growth potential
5. Identify mentors and potential niche area
6. Start building your professional network and your reputation
7. Get involved in national GI societies
Consults
Mindset
Shifting gear from residency to fellowship involves a shifting of your clinical mindset too, going from being part of a primary care team responsible for all aspects of a patient’s medical care, to that of a consulting team focused on a patient’s GI condition. It is important to find the right balance of refraining from micromanaging non-GI comorbidities while being fully aware of their impact on your diagnostic and therapeutic approach to the GI condition.
Let’s face it, you will not always get “exciting and interesting GI cases” consults, and on a busy day some consultations might feel unnecessary and frustrating to you. Remember that what seems obvious to you, based on your focused GI knowledge, might not be so simple to the primary team. In addition, every consult is an opportunity to improve your approach to patient care, as well as an opportunity to learn and teach others, from medical students to residents. So, always be professional and respectful when you pick up the phone, and build positive collaborative bridges between you and the medical or surgical consulting teams. Be the GI fellow others are not reluctant to call for help, and better, be the one who communicates GI pearls along the way, inspires others to join the field of gastroenterology, and positively represent the GI division.
Triage
When you answer your consult page, ask the primary team what specific question they have for you and/or what is the main GI complaint or test abnormality the patient has. This will help you assess the urgency and the complexity of the consult, and hence allow you to prioritize each consult (which one you need to see first and give the attending a heads-up), assign (or not) a rotating medical resident or student to the consult, tailor your preliminary recommendations to the primary team, and anticipate the need for a procedure. When you anticipate a procedure, assess its (semi-)urgency to get the process ready for same day or a bedside procedure by getting information on the patient’s vitals, basic labs, significant acute comorbidities, and supportive therapies in place. In other words, by judiciously obtaining key information from the primary team, you can efficiently triage the consults and keep your day organized and manageable (for the most part). Learn to divide and conquer the tasks of the day: split inpatient endoscopy and consults with your cofellows, assign appropriate consults and follow-ups to residents or students rotating on the GI service, and properly communicate with the primary team a plan of care (even a preliminary one) to avoid recurrent pages and interruptions. Some days the number or urgency of the consults and the required multitasking can be overwhelming: stop, breathe, and ask for help from your co-fellows and your attending. Remember, this is a fellowship, not a solo-ship and your program is here to support your work and growth.
Communication
Timely and efficient communication, between you and the different stakeholders, is crucial to provide optimal patient care and minimize the risk of “things falling through the cracks”. Convey to the primary team your recommendations and plan of care clearly, and use direct verbal communication (not just a note in the chart) when managing complex or urgent situations. Obtain information regarding current patient level of care (i.e., ICU), isolation precautions, and cardiac devices (i.e., left ventricular assist device). Keep the dialogue open with your attending about acutely ill patients and potentially urgent procedures. Inform the endoscopy suite early that you are adding a procedure on the same day, and communicate anticipated needs (such as intubation, fluoroscopy room, pediatric scope, stent). Using a “closed-loop” communication structure can ensure that your recommendations are received and implemented appropriately.2
Time management and structure
Having a structured routine to your day, in what seems to be a chaotic process of juggling different duties and being in different locations at once, will ensure that you efficiently complete your tasks in a timely manner. Find what works best for you, taking into account the challenges and resources available to you, such as the number of fellows and other trainees on the GI consult service, the average number of consults per day and their acuity, the availability of inpatient protocols for specific clinical situations (GI bleed, acute severe ulcerative colitis, etc.), and the time and style preferences of the rounding attending. We suggest the following schedule on a consult day: Round early in the morning and leave a note in the chart and/or communicate with the team key information, then review with the rotating trainees the patients they are following and personally reassess some patients as needed. Inform the endoscopy suite of the same day procedures and let your attending know of any issues that require immediate attention. Take your team and head to radiology and review the imaging studies on your patients. Learn and teach key points in diagnosis and therapeutic approach as you move through your day from the inpatient floors to the hallways. Divide consults during the day with your team and agree on a time to touch base. Review your patient list at the end of the day and assess which patients the GI service no longer need to follow and communicate that clearly to the primary team along with the appropriate outpatient GI care follow-up. Let the endoscopy suite know of any procedures you are adding for the next day along with their degree of urgency to allow the charge nurse to prioritize cases. When you leave the hospital, be intentional with your free time: Read about the GI conditions you have encountered, enjoy some fun relaxing time, and rest!
Call
Know your call environment and your emergency cart
Familiarize yourself with the locations where you could potentially perform an emergent case (i.e., the ICU, ED, operating room) and the relevant points of contact (such as the charge nurse, the anesthesia team, the on-call tech team) for overnight or weekend cases. Whether or not you have an endoscopy support team on call, learn to set up the emergency cart, find and check your equipment, and troubleshoot technical issues by soliciting an “in-service” from senior fellows or the endoscopy technical support staff. Before heading to an urgent case, double check that you have your “bleeder” or “food impaction” tools. For food impaction, consider obtaining rat tooth forceps, snares, Roth nets, and an overtube. For bleeding cases, obtain a therapeutic upper endoscope, hemostatic clips, clear caps, injection needles, epinephrine, HemosprayTM, banding kits, and the appropriate electrocautery/thermal set up.
What is an emergency?
Consults that require your immediate attention include food impactions, acute biliary conditions leading to septic shock, and hemodynamically unstable GI bleeds, especially variceal bleeds. Remember that patients who are hemodynamically unstable require adequate resuscitation before proceeding with any endoscopic intervention. Assess the need for intubation, the timing of the procedure, and the most optimal location to perform the procedure, depending on the time and acuity of the patients’ presentation, how they respond to resuscitation measures, and the resources and preferences of your institution.
The overnight ‘nonemergent’ call
Non-emergent consults can be addressed the next day, after reviewing the clinical information provided by the consulting team and the patient’s EMR to ensure no urgent measures are needed. Overnight call may include patient phone calls, from inquiries about colon prep (so familiarize yourself with the different prep instructions and how to troubleshoot prep difficulties) to GI symptoms that you will need to triage to either the ED or to an outpatient follow-up. Document all phone encounters in the EMR and route your note to the appropriate clinician and nurse or administrative assistant for follow-up.
The five E’s of endoscopy
Endoscopy training is a large component of a GI fellowship and can create achievement anxiety in many first-year fellows seeking the cecum! But there is more to endoscopy than technical skills: It is as important to adequately evaluate clinical situations, understand the indications and potential limitations and complications of the procedure, and assess how it will impact the management of the patient. And no, you don’t have to be a video gamer to be a good endoscopist; and yes, you will be able to regularly complete a colonoscopy before the end of your first year!
Evaluation
In order to improve your endoscopic skills, it is important to honestly assess your areas of proficiency and improvement and to welcome real-time constructive feedback from your teaching attending about your endoscopic skills range. Consider meeting regularly with your attending to discuss your short-term and long-term endoscopic goals and how to enhance your skills. This practice demonstrates responsibility, credibility, and accountability amongst your peers as well as a genuine commitment to your growth as an endoscopist.
Efficiency
In addition to focusing on the quality of your endoscopy, learn to be efficient in the pre- and postprocedure time flow. This entails any step from properly explaining the procedure to patients before they come to the endoscopy suite, making sure the needed endoscopy equipment and tools are available in your room, completing your personal setup (i.e., gowning up, setting up your bed/monitor height, testing your endoscope) even before time out, to discharging the patient and communicating key findings and plan of care to the primary team. Depending on the acuity of the procedure and patient’s comorbidities, certain procedures may need to be performed or completed by a more efficient and experienced senior fellow or attending; don’t let this situation trigger passive frustration in you, but rather use it as an active and engaging opportunity to learn.
Expectations
You (and all the other neighborhood kids) didn’t learn to ride a bike without falling, struggling, needing help, and practicing over and over again, and it goes the same when learning to scope as a first-year fellow. Keep this in mind to lessen frustration, set realistic expectations, and be patient with yourself and celebrate all the small victories. Set tangible goals with your attending prior to procedural days/rotations so they can help you hone in and perfect the desired endoscopy skills.
Ergonomics
In a recent study, endoscopy-related injury (ERI) was reported to occur in up to 75% of gastroenterologists.3 While your primary focus might be reaching the cecum, it is as crucial for you to learn how to prevent ERI to ensure your long term health and continued success in procedures.
Excellence over quantity
Your main focus as a trainee is to learn how to provide effective, efficient, and safe care to patients, including in endoscopy. The quality of the endoscopy you perform is much more important than the total number of procedures you do. Thus, it is key to take each procedure as a complete learning opportunity to perform a thorough evaluation, improve your technical skills, interpret the findings, and develop a therapeutic plan.
Work-life balance and burnout
Fellowship is a marathon and not a sprint, so you need to slow down after a busy workday and care for yourself and enjoy time with loved ones. The cognitive, physical, mental, and emotional demands for first-year fellows are arguably the highest during GI training and can lead to burnout. Signs of burnout include emotional exhaustion, loss of empathy, fatigue, depersonalization and detachment, and feelings of personal inadequacy.4 Antiburnout measures include respecting basic healthy life hygiene (eat and sleep well, regular physical activity), having a hobby, practicing meditation, avoiding taking work home, and having a healthy social network.5 Remember that your cofellows whom you share common experiences with are not only your colleagues but can also be your friends and your social support. If you are a parent juggling work and family, remember to ask for help from your peers if you need it and have an open discussion with your attending to find practical solutions to your schedule.
Professional growth in the field of gastroenterology
Becoming a successful gastroenterologist and endoscopist involves going above the “I” and into the inclusive “we.” Building collegial and professional relationships early on with different stakeholders will set you up for success during and beyond your fellowship.
Building relationships
Developing genuine collegial and collaborative relationships with cofellows and faculty will positively impact your wellness during fellowship but also build the foundation of your professional network necessary to your career growth. Be inclusive of your cofellows in your research projects and publications, and support and amplify their work as much as you amplify your own. Your cofellows or attendings are likely to be the ones to help you find the right job, invite you to speak at grand rounds, or sit on a GI committee and promote your postfellowship professional growth.
Mentorship, being an educator and role model
It is important to identify and seek out mentors, within or outside your fellowship program or institution, who can not only guide you in your career choices but also open doors for you and sponsor you to advance your career. On the other hand, you too can be a role model, mentor, and sponsor to medical residents and students interested in the field of GI. Teach others in didactic settings or on the consult service, include trainees in quality improvement projects and publications, and lead by example.
Research
Most academic GI programs have a baseline requirement of research. Choose and devise a project you can realistically complete despite your busy first-year schedule: expand on a residency research project, focus on a specific simple question triggered by a clinical situation you encountered, proceed with a retrospective chart review or quality improvement project, and include other fellows and trainees to divide tasks. Alternatively, devise a specific timeline with a research mentor to complete a larger research project during your three years of fellowship.
Involvement in GI societies/committees
Become a member of one (or all) of the national GI societies that align with your interests. Membership gives you access not only to peer-reviewed scientific articles and guidelines but also to fellow-focused programs, committees’ opportunities, early career research grants, and mentorship.6-10
Summary
The first year of a GI fellowship lays the foundation for your next 3 years: Be mindful of how you can optimize the opportunities at hand to learn, teach, build a solid reputation, and grow your professional network. But also remember you have 3 full years to accomplish all your goals, so be patient, pace yourself, and include others in your journey. Judiciously use the many resources within your program and GI societies to help you achieve your goals, reach out to others to overcome difficulties and barriers, and dedicate time to care for your personal health and growth. This is what a true comprehensive and healthy fellowship is all about!
Dr. Advani is with the division of gastroenterology and hepatology, Stony Brook (N.Y.) University Hospital. Dr. Saeed is with the division of gastroenterology and hepatology, University of Kentucky, Lexington. Dr. Charabaty is with the division of gastroenterology, Johns Hopkins University, Baltimore, and Johns Hopkins–Sibley Memorial Hospital, Washington. Dr. Advani and Dr. Saeed have no conflicts to disclose. Dr. Charabaty disclosed ties to AbbVie, Janssen, Takeda, Pfizer, and Bristol-Myers Squibb and is founder of @MondayNightIBD, and cofounder of Scrubs & Heels.
References
1. Bollipo S. Gastroenterology. 2020 Nov;159(5):1648-52.
2. Adams MA et al. Gastroenterology. 2014 Jan 1;146(1):5-9.
3. Pawa S et al. Am J Gastroenterol. 2021 Mar 1;116(3):530-8.
4. DeCross AJ. Gastroenterology. 2020 Jan 1;158(1):32-5.
5. Burke C et al. Am J Gastroenterol. 2017 Oct 1;112:S593-4.
6. Fellows Resources under Fellows & Early Career. American Gastroenterological Association. https://gastro.org/fellows-and-early-career/training-resources/fellows-resources/.
7. Trainee Courses and Events. American College of Gastroenterology. https://gi.org/trainees/trainee-courses-and-events/.
8. Trainee Resources. American Association for the Study of Liver Diseases. https://www.aasld.org/membership/hepatology-associates/trainee-resources.
9. First Year Fellows Courses under Education. American Society of Gastrointestinal Endoscopy. https://www.asge.org/home/education/advanced-education-training/first-year-fellow-(fyf)-courses.
10. Annual GI Fellow Summer Course Presentations. New York Society for Gastrointestinal Endoscopy. https://www.nysge.org/annual%20gi%20fellows%20summer%20course.