User login
For MD-IQ use only
Infectious disease pop quiz: Clinical challenge #10 for the ObGyn
What are the characteristic mucocutaneous lesions of primary, secondary, and tertiary syphilis?
Continue to answer...
The characteristic mucosal lesion of primary syphilis is the painless chancre. The usual mucocutaneous manifestations of secondary syphilis are maculopapular lesions (red or violet in color) on the palms and soles, mucous patches on the oral membranes, and condyloma lata on the genitalia. The classic mucocutaneous lesion of tertiary syphilis is the gumma.
Other serious manifestations of advanced syphilis include central nervous system abnormalities, such as tabes dorsalis, the Argyll Robertson pupil, and dementia, and cardiac abnormalities, such as aortitis, which can lead to a dissecting aneurysm of the aortic root. (Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64[RR3]:1-137.)
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.

Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
What are the characteristic mucocutaneous lesions of primary, secondary, and tertiary syphilis?
Continue to answer...
The characteristic mucosal lesion of primary syphilis is the painless chancre. The usual mucocutaneous manifestations of secondary syphilis are maculopapular lesions (red or violet in color) on the palms and soles, mucous patches on the oral membranes, and condyloma lata on the genitalia. The classic mucocutaneous lesion of tertiary syphilis is the gumma.
Other serious manifestations of advanced syphilis include central nervous system abnormalities, such as tabes dorsalis, the Argyll Robertson pupil, and dementia, and cardiac abnormalities, such as aortitis, which can lead to a dissecting aneurysm of the aortic root. (Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64[RR3]:1-137.)
What are the characteristic mucocutaneous lesions of primary, secondary, and tertiary syphilis?
Continue to answer...
The characteristic mucosal lesion of primary syphilis is the painless chancre. The usual mucocutaneous manifestations of secondary syphilis are maculopapular lesions (red or violet in color) on the palms and soles, mucous patches on the oral membranes, and condyloma lata on the genitalia. The classic mucocutaneous lesion of tertiary syphilis is the gumma.
Other serious manifestations of advanced syphilis include central nervous system abnormalities, such as tabes dorsalis, the Argyll Robertson pupil, and dementia, and cardiac abnormalities, such as aortitis, which can lead to a dissecting aneurysm of the aortic root. (Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64[RR3]:1-137.)
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
Wilderness Medical Society issues clinical guidelines for tick-borne illness
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM WILDERNESS ENVIRONMENTAL MEDICINE
More vitamin D not better for reducing cancer or CVD incidence
according to a new randomized controlled study.
In the cohort of nearly 2,500 healthy individuals, the researchers found no differences in cancer or CVD incidence over 5 years between the groups randomly assigned to vitamin D supplementation and to placebo.
The findings, published online Jan. 4, 2022, in the American Journal of Clinical Nutrition, may be influenced by the fact that most participants had sufficient vitamin D levels at baseline, and thus received higher than recommended doses of vitamin D during the study.
“Vitamin D3 supplementation with 1600 or 3200 IU/day for 5 years did not reduce the incidence of major CVD events, any invasive cancer, or mortality among generally healthy and mostly vitamin D sufficient older adults in Finland,” write the authors, led by Jyrki Virtanen, RD, PhD, associate professor of nutrition and public health at University of Eastern Finland, Kuopio.
“The low number of subjects with low vitamin D concentrations was a bit of a surprise for us also, but it likely reflects the quite successful food fortification policy in Finland,” Dr. Virtanen told this news organization.
Prior research has found that vitamin D insufficiency is associated with a higher risk of nearly all diseases. Although the evidence on the benefits of vitamin D supplementation remains more limited, a meta-analysis reported a consistent and significant 13% reduction in cancer mortality in those who received vitamin D supplements.
In this study, Dr. Virtanen and colleagues investigated the effects of vitamin D3 supplementation on cancer and CVD incidence in a cohort of 2,495 healthy participants.
Men 60 years or older and women 65 years or older were randomly assigned to one of three groups: placebo, 40 mcg (1,600 IU) of daily vitamin D3, or 80 mcg (3,200 IU) of daily vitamin D3.
Data collected at baseline and throughout the trial included serum 25(OH)D concentrations, nutrition, sun exposure, medication use, mental health, and other factors that could affect the risk of disease.
The study’s primary endpoints were incident of major CVD and invasive cancer. Secondary endpoints included incidence of myocardial infarction, stroke, and CVD mortality as well as site-specific cancers and cancer death.
Follow-up occurred via annual study questionnaires and national registry data. A representative subcohort of 551 participants had more detailed in-person evaluations. In the sub-cohort, mean serum 25(OH)D concentration was 75 nmol/L (30 ng/mL) at baseline; 9.1% had concentrations less than 50 nmol/L (20 ng/mL) and 50.0% had concentrations of at least 75 nmol/L (30 ng/mL).
The authors identified no major differences between the three arms at baseline, but noted that, compared with the overall study population, those in the subcohort were younger, more likely to use their own vitamin D supplements, and more likely to rate their health as good or excellent.
Among 503 participants that had complete data from baseline, the mean increase in serum 25(OH)D in participants receiving 1,600 IU/day vitamin D3 was 23.4 nmol/L (9.4 ng/mL) and 43.6 nmol/L (17.4 ng/mL) in the arm receiving 3,200 IU/day between baseline and 6 months. The authors observed a small additional increase in levels between the 6-month and 12-month visits, but few changes in vitamin D3 levels in the placebo arm.
At the 5-year follow-up, major CVD events occurred in 4.9% of participants in the placebo arm, 5% in those in the 1,600 IU/d arm (hazard ratio, 0.97), and 4.3% of those in the 3,200 IU/d arm (HR, 0.84; P = .44). Invasive cancer at follow-up was diagnosed in 4.9% of placebo recipients, 5.8% of those on 1,600 IU/d supplementation (HR, 1.14; P = .55), and 4.8% in the 3,200 IU/d group (HR, 0.95; P = .81). No significant differences were observed in the secondary endpoints or in total mortality.
The authors did not conduct a subanalysis in participants who had low 25(OH)D concentrations levels at baseline because “there were too few participants to do any meaningful analyses,” said Dr. Virtanen, who noted that blood samples were available for a representative subgroup of 550 subjects, and only 9% of them had low 25(OH)D concentrations at baseline.
Dr. Virtanen noted that future vitamin D supplementation trials should focus on recruiting participants with low vitamin D status.
The study was supported by funding from the Academy of Finland, University of Eastern Finland, Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and Finnish Cultural Foundation. Dr. Virtanen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new randomized controlled study.
In the cohort of nearly 2,500 healthy individuals, the researchers found no differences in cancer or CVD incidence over 5 years between the groups randomly assigned to vitamin D supplementation and to placebo.
The findings, published online Jan. 4, 2022, in the American Journal of Clinical Nutrition, may be influenced by the fact that most participants had sufficient vitamin D levels at baseline, and thus received higher than recommended doses of vitamin D during the study.
“Vitamin D3 supplementation with 1600 or 3200 IU/day for 5 years did not reduce the incidence of major CVD events, any invasive cancer, or mortality among generally healthy and mostly vitamin D sufficient older adults in Finland,” write the authors, led by Jyrki Virtanen, RD, PhD, associate professor of nutrition and public health at University of Eastern Finland, Kuopio.
“The low number of subjects with low vitamin D concentrations was a bit of a surprise for us also, but it likely reflects the quite successful food fortification policy in Finland,” Dr. Virtanen told this news organization.
Prior research has found that vitamin D insufficiency is associated with a higher risk of nearly all diseases. Although the evidence on the benefits of vitamin D supplementation remains more limited, a meta-analysis reported a consistent and significant 13% reduction in cancer mortality in those who received vitamin D supplements.
In this study, Dr. Virtanen and colleagues investigated the effects of vitamin D3 supplementation on cancer and CVD incidence in a cohort of 2,495 healthy participants.
Men 60 years or older and women 65 years or older were randomly assigned to one of three groups: placebo, 40 mcg (1,600 IU) of daily vitamin D3, or 80 mcg (3,200 IU) of daily vitamin D3.
Data collected at baseline and throughout the trial included serum 25(OH)D concentrations, nutrition, sun exposure, medication use, mental health, and other factors that could affect the risk of disease.
The study’s primary endpoints were incident of major CVD and invasive cancer. Secondary endpoints included incidence of myocardial infarction, stroke, and CVD mortality as well as site-specific cancers and cancer death.
Follow-up occurred via annual study questionnaires and national registry data. A representative subcohort of 551 participants had more detailed in-person evaluations. In the sub-cohort, mean serum 25(OH)D concentration was 75 nmol/L (30 ng/mL) at baseline; 9.1% had concentrations less than 50 nmol/L (20 ng/mL) and 50.0% had concentrations of at least 75 nmol/L (30 ng/mL).
The authors identified no major differences between the three arms at baseline, but noted that, compared with the overall study population, those in the subcohort were younger, more likely to use their own vitamin D supplements, and more likely to rate their health as good or excellent.
Among 503 participants that had complete data from baseline, the mean increase in serum 25(OH)D in participants receiving 1,600 IU/day vitamin D3 was 23.4 nmol/L (9.4 ng/mL) and 43.6 nmol/L (17.4 ng/mL) in the arm receiving 3,200 IU/day between baseline and 6 months. The authors observed a small additional increase in levels between the 6-month and 12-month visits, but few changes in vitamin D3 levels in the placebo arm.
At the 5-year follow-up, major CVD events occurred in 4.9% of participants in the placebo arm, 5% in those in the 1,600 IU/d arm (hazard ratio, 0.97), and 4.3% of those in the 3,200 IU/d arm (HR, 0.84; P = .44). Invasive cancer at follow-up was diagnosed in 4.9% of placebo recipients, 5.8% of those on 1,600 IU/d supplementation (HR, 1.14; P = .55), and 4.8% in the 3,200 IU/d group (HR, 0.95; P = .81). No significant differences were observed in the secondary endpoints or in total mortality.
The authors did not conduct a subanalysis in participants who had low 25(OH)D concentrations levels at baseline because “there were too few participants to do any meaningful analyses,” said Dr. Virtanen, who noted that blood samples were available for a representative subgroup of 550 subjects, and only 9% of them had low 25(OH)D concentrations at baseline.
Dr. Virtanen noted that future vitamin D supplementation trials should focus on recruiting participants with low vitamin D status.
The study was supported by funding from the Academy of Finland, University of Eastern Finland, Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and Finnish Cultural Foundation. Dr. Virtanen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new randomized controlled study.
In the cohort of nearly 2,500 healthy individuals, the researchers found no differences in cancer or CVD incidence over 5 years between the groups randomly assigned to vitamin D supplementation and to placebo.
The findings, published online Jan. 4, 2022, in the American Journal of Clinical Nutrition, may be influenced by the fact that most participants had sufficient vitamin D levels at baseline, and thus received higher than recommended doses of vitamin D during the study.
“Vitamin D3 supplementation with 1600 or 3200 IU/day for 5 years did not reduce the incidence of major CVD events, any invasive cancer, or mortality among generally healthy and mostly vitamin D sufficient older adults in Finland,” write the authors, led by Jyrki Virtanen, RD, PhD, associate professor of nutrition and public health at University of Eastern Finland, Kuopio.
“The low number of subjects with low vitamin D concentrations was a bit of a surprise for us also, but it likely reflects the quite successful food fortification policy in Finland,” Dr. Virtanen told this news organization.
Prior research has found that vitamin D insufficiency is associated with a higher risk of nearly all diseases. Although the evidence on the benefits of vitamin D supplementation remains more limited, a meta-analysis reported a consistent and significant 13% reduction in cancer mortality in those who received vitamin D supplements.
In this study, Dr. Virtanen and colleagues investigated the effects of vitamin D3 supplementation on cancer and CVD incidence in a cohort of 2,495 healthy participants.
Men 60 years or older and women 65 years or older were randomly assigned to one of three groups: placebo, 40 mcg (1,600 IU) of daily vitamin D3, or 80 mcg (3,200 IU) of daily vitamin D3.
Data collected at baseline and throughout the trial included serum 25(OH)D concentrations, nutrition, sun exposure, medication use, mental health, and other factors that could affect the risk of disease.
The study’s primary endpoints were incident of major CVD and invasive cancer. Secondary endpoints included incidence of myocardial infarction, stroke, and CVD mortality as well as site-specific cancers and cancer death.
Follow-up occurred via annual study questionnaires and national registry data. A representative subcohort of 551 participants had more detailed in-person evaluations. In the sub-cohort, mean serum 25(OH)D concentration was 75 nmol/L (30 ng/mL) at baseline; 9.1% had concentrations less than 50 nmol/L (20 ng/mL) and 50.0% had concentrations of at least 75 nmol/L (30 ng/mL).
The authors identified no major differences between the three arms at baseline, but noted that, compared with the overall study population, those in the subcohort were younger, more likely to use their own vitamin D supplements, and more likely to rate their health as good or excellent.
Among 503 participants that had complete data from baseline, the mean increase in serum 25(OH)D in participants receiving 1,600 IU/day vitamin D3 was 23.4 nmol/L (9.4 ng/mL) and 43.6 nmol/L (17.4 ng/mL) in the arm receiving 3,200 IU/day between baseline and 6 months. The authors observed a small additional increase in levels between the 6-month and 12-month visits, but few changes in vitamin D3 levels in the placebo arm.
At the 5-year follow-up, major CVD events occurred in 4.9% of participants in the placebo arm, 5% in those in the 1,600 IU/d arm (hazard ratio, 0.97), and 4.3% of those in the 3,200 IU/d arm (HR, 0.84; P = .44). Invasive cancer at follow-up was diagnosed in 4.9% of placebo recipients, 5.8% of those on 1,600 IU/d supplementation (HR, 1.14; P = .55), and 4.8% in the 3,200 IU/d group (HR, 0.95; P = .81). No significant differences were observed in the secondary endpoints or in total mortality.
The authors did not conduct a subanalysis in participants who had low 25(OH)D concentrations levels at baseline because “there were too few participants to do any meaningful analyses,” said Dr. Virtanen, who noted that blood samples were available for a representative subgroup of 550 subjects, and only 9% of them had low 25(OH)D concentrations at baseline.
Dr. Virtanen noted that future vitamin D supplementation trials should focus on recruiting participants with low vitamin D status.
The study was supported by funding from the Academy of Finland, University of Eastern Finland, Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and Finnish Cultural Foundation. Dr. Virtanen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF CLINICAL NUTRITION
Docs react: Crowd crush survival guide, more dewormer, sizzling earwax
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
What does a pig-to-human heart transplant mean for medicine?
Scientific achievements usually raise big new questions, and the remarkable surgery that took place on Jan. 7, when Maryland resident David Bennett was transplanted with a genetically modified heart from a pig, has been no different.
The 57-year-old with end-stage heart failure had been repeatedly turned down for a standard transplant and was judged a poor candidate for a ventricular assist device. Now his new heart is beating soundly and apparently accepted by his immune system as Mr. Bennett, his physicians at the University of Maryland where the procedure took place, and indeed the world set out on a journey with far more unknowns than knowns.

“I think even just a couple of years ago, people felt that xenotransplantation for the heart and other organs was still a long way off. And it seems like it’s started to move very quickly,” Larry A. Allen, MD, University of Colorado, Aurora, said in an interview.
Demand for donor hearts far outstrips supply, and despite advances in the development of ventricular assist pumps and artificial hearts, “there are still significant limitations to them in terms of clotting, stroke, and infection. We’ve seen the use of those devices plateau,” Dr. Allen said. “So, the concept of a nonhuman source of organs is exciting and very much in need, if people can get it to work.”
“I really credit the surgeons at the University of Maryland for courageous clinical work and a brilliant scientific innovation,” Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, said in an interview. “But it’s always in the implementation that we have to hold our breath.” Heart xenotransplantation is an old idea that “has never before been successful,” he said. And standard heart transplantation has set a high bar, with a 1-year survival of about 90% and low 1-year risk for rejection. Whether the new procedure can meet that standard is unknown, as is its potential for complications, such as chronic rejection or cancers due to long-term immunosuppression. Those are “major questions requiring more time and careful follow-up.”

‘Still a nascent technology’
“This is an exciting and courageous step forward in heart transplantation, and kudos to the team at the University of Maryland,” said Mandeep R. Mehra, MD, Brigham and Woman’s Hospital, Boston. But “there are many challenges here.”
The procedure’s 10 gene modifications were reportedly aimed at preventing hyperacute rejection of the heart and its excessive growth after transplantation, and making the organ less immunogenic, Dr. Mehra said in an interview. But even if those goals are met, could the same changes potentially impede the heart’s adaptation to human physiology, such as during ambulation or stress?
That kind of adaptation may become important. For example, Dr. Mehra observed, normally a pig heart “provides flow in a four-footed configuration, and pig temperature is inherently higher than humans by several degrees, so it will be functioning in a relatively hypothermic environment.”
Transplantation remains the gold standard for patients with advanced heart failure despite modern medical and device therapy, Dr. Allen agreed. But “if we can raise pig hearts that provide the organ, and it can be implanted with a surgery that’s been done for 50 years, and rejection can be managed with gene editing and tailored immunosuppression, then it’s not hard to think about this very rapidly replacing a lot of what we do in the advanced heart failure and transplantation world.”
Certainly, it would be a major advance if the gene editing technique successfully improves the heart’s immunologic compatibility, Dr. Yancy noted. But do we have enough genomic knowledge to select gene deletions and insertions in the safest way for a successful outcome? “We have to appreciate that this is still a nascent technology, and we should be careful that there might be consequences that we haven’t anticipated.”
For example, he said, the xenotransplantation and gene-modifying techniques should be explored in a range of patients, including older and younger people, women and men, and people of different ethnicities and races.
“There may be some differences based on ancestry, based on gender, based on aging, that will influence the way in which these engineered donor hearts are experienced clinically,” Dr. Yancy said.
The xenotransplantation technique’s potential impact on health equity should also be considered, as it “almost assuredly will be a very expensive technology that will be utilized in a very select population,” he noted. “We need to have a really wide lens to think about all of the potential ramifications.”
‘This field needs to evolve’
Dr. Mehra also flagged the procedure’s potential cost should it become mainstream. Perhaps that would promote dialogue on how to primarily use it “after legitimately exhausting all available options, such as total artificial heart support.”
It might also teach the field to take greater advantage of the many donated hearts discarded as suboptimal. “The general usage rate for offered organs is around a third,” despite opportunities to expand use of those that are “less than perfect,” Dr. Mehra said. “I think that the field will grow with the community focusing on reduced discards of current available heart organs, and not necessarily grow because of the availability of ‘xeno-organs.’ ”
“This field needs to evolve because we’re actively transplanting patients today. But in my mind, the real future is to have such a sufficient understanding of the biology of left ventricular dysfunction that transplantation is a rare event,” Dr. Yancy proposed.
“I’m not certain that heart transplantation per se is the endgame. I think the avoidance of transplantation is the real endgame,” he said. “This may be controversial, but my vision of the future is not one where we have a supply of animals that we can use for transplantation. My vision of the future is that heart transplantation becomes obsolete.”
A version of this article first appeared on Medscape.com.
Scientific achievements usually raise big new questions, and the remarkable surgery that took place on Jan. 7, when Maryland resident David Bennett was transplanted with a genetically modified heart from a pig, has been no different.
The 57-year-old with end-stage heart failure had been repeatedly turned down for a standard transplant and was judged a poor candidate for a ventricular assist device. Now his new heart is beating soundly and apparently accepted by his immune system as Mr. Bennett, his physicians at the University of Maryland where the procedure took place, and indeed the world set out on a journey with far more unknowns than knowns.
“I think even just a couple of years ago, people felt that xenotransplantation for the heart and other organs was still a long way off. And it seems like it’s started to move very quickly,” Larry A. Allen, MD, University of Colorado, Aurora, said in an interview.
Demand for donor hearts far outstrips supply, and despite advances in the development of ventricular assist pumps and artificial hearts, “there are still significant limitations to them in terms of clotting, stroke, and infection. We’ve seen the use of those devices plateau,” Dr. Allen said. “So, the concept of a nonhuman source of organs is exciting and very much in need, if people can get it to work.”
“I really credit the surgeons at the University of Maryland for courageous clinical work and a brilliant scientific innovation,” Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, said in an interview. “But it’s always in the implementation that we have to hold our breath.” Heart xenotransplantation is an old idea that “has never before been successful,” he said. And standard heart transplantation has set a high bar, with a 1-year survival of about 90% and low 1-year risk for rejection. Whether the new procedure can meet that standard is unknown, as is its potential for complications, such as chronic rejection or cancers due to long-term immunosuppression. Those are “major questions requiring more time and careful follow-up.”
‘Still a nascent technology’
“This is an exciting and courageous step forward in heart transplantation, and kudos to the team at the University of Maryland,” said Mandeep R. Mehra, MD, Brigham and Woman’s Hospital, Boston. But “there are many challenges here.”
The procedure’s 10 gene modifications were reportedly aimed at preventing hyperacute rejection of the heart and its excessive growth after transplantation, and making the organ less immunogenic, Dr. Mehra said in an interview. But even if those goals are met, could the same changes potentially impede the heart’s adaptation to human physiology, such as during ambulation or stress?
That kind of adaptation may become important. For example, Dr. Mehra observed, normally a pig heart “provides flow in a four-footed configuration, and pig temperature is inherently higher than humans by several degrees, so it will be functioning in a relatively hypothermic environment.”
Transplantation remains the gold standard for patients with advanced heart failure despite modern medical and device therapy, Dr. Allen agreed. But “if we can raise pig hearts that provide the organ, and it can be implanted with a surgery that’s been done for 50 years, and rejection can be managed with gene editing and tailored immunosuppression, then it’s not hard to think about this very rapidly replacing a lot of what we do in the advanced heart failure and transplantation world.”
Certainly, it would be a major advance if the gene editing technique successfully improves the heart’s immunologic compatibility, Dr. Yancy noted. But do we have enough genomic knowledge to select gene deletions and insertions in the safest way for a successful outcome? “We have to appreciate that this is still a nascent technology, and we should be careful that there might be consequences that we haven’t anticipated.”
For example, he said, the xenotransplantation and gene-modifying techniques should be explored in a range of patients, including older and younger people, women and men, and people of different ethnicities and races.
“There may be some differences based on ancestry, based on gender, based on aging, that will influence the way in which these engineered donor hearts are experienced clinically,” Dr. Yancy said.
The xenotransplantation technique’s potential impact on health equity should also be considered, as it “almost assuredly will be a very expensive technology that will be utilized in a very select population,” he noted. “We need to have a really wide lens to think about all of the potential ramifications.”
‘This field needs to evolve’
Dr. Mehra also flagged the procedure’s potential cost should it become mainstream. Perhaps that would promote dialogue on how to primarily use it “after legitimately exhausting all available options, such as total artificial heart support.”
It might also teach the field to take greater advantage of the many donated hearts discarded as suboptimal. “The general usage rate for offered organs is around a third,” despite opportunities to expand use of those that are “less than perfect,” Dr. Mehra said. “I think that the field will grow with the community focusing on reduced discards of current available heart organs, and not necessarily grow because of the availability of ‘xeno-organs.’ ”
“This field needs to evolve because we’re actively transplanting patients today. But in my mind, the real future is to have such a sufficient understanding of the biology of left ventricular dysfunction that transplantation is a rare event,” Dr. Yancy proposed.
“I’m not certain that heart transplantation per se is the endgame. I think the avoidance of transplantation is the real endgame,” he said. “This may be controversial, but my vision of the future is not one where we have a supply of animals that we can use for transplantation. My vision of the future is that heart transplantation becomes obsolete.”
A version of this article first appeared on Medscape.com.
Scientific achievements usually raise big new questions, and the remarkable surgery that took place on Jan. 7, when Maryland resident David Bennett was transplanted with a genetically modified heart from a pig, has been no different.
The 57-year-old with end-stage heart failure had been repeatedly turned down for a standard transplant and was judged a poor candidate for a ventricular assist device. Now his new heart is beating soundly and apparently accepted by his immune system as Mr. Bennett, his physicians at the University of Maryland where the procedure took place, and indeed the world set out on a journey with far more unknowns than knowns.
“I think even just a couple of years ago, people felt that xenotransplantation for the heart and other organs was still a long way off. And it seems like it’s started to move very quickly,” Larry A. Allen, MD, University of Colorado, Aurora, said in an interview.
Demand for donor hearts far outstrips supply, and despite advances in the development of ventricular assist pumps and artificial hearts, “there are still significant limitations to them in terms of clotting, stroke, and infection. We’ve seen the use of those devices plateau,” Dr. Allen said. “So, the concept of a nonhuman source of organs is exciting and very much in need, if people can get it to work.”
“I really credit the surgeons at the University of Maryland for courageous clinical work and a brilliant scientific innovation,” Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, said in an interview. “But it’s always in the implementation that we have to hold our breath.” Heart xenotransplantation is an old idea that “has never before been successful,” he said. And standard heart transplantation has set a high bar, with a 1-year survival of about 90% and low 1-year risk for rejection. Whether the new procedure can meet that standard is unknown, as is its potential for complications, such as chronic rejection or cancers due to long-term immunosuppression. Those are “major questions requiring more time and careful follow-up.”
‘Still a nascent technology’
“This is an exciting and courageous step forward in heart transplantation, and kudos to the team at the University of Maryland,” said Mandeep R. Mehra, MD, Brigham and Woman’s Hospital, Boston. But “there are many challenges here.”
The procedure’s 10 gene modifications were reportedly aimed at preventing hyperacute rejection of the heart and its excessive growth after transplantation, and making the organ less immunogenic, Dr. Mehra said in an interview. But even if those goals are met, could the same changes potentially impede the heart’s adaptation to human physiology, such as during ambulation or stress?
That kind of adaptation may become important. For example, Dr. Mehra observed, normally a pig heart “provides flow in a four-footed configuration, and pig temperature is inherently higher than humans by several degrees, so it will be functioning in a relatively hypothermic environment.”
Transplantation remains the gold standard for patients with advanced heart failure despite modern medical and device therapy, Dr. Allen agreed. But “if we can raise pig hearts that provide the organ, and it can be implanted with a surgery that’s been done for 50 years, and rejection can be managed with gene editing and tailored immunosuppression, then it’s not hard to think about this very rapidly replacing a lot of what we do in the advanced heart failure and transplantation world.”
Certainly, it would be a major advance if the gene editing technique successfully improves the heart’s immunologic compatibility, Dr. Yancy noted. But do we have enough genomic knowledge to select gene deletions and insertions in the safest way for a successful outcome? “We have to appreciate that this is still a nascent technology, and we should be careful that there might be consequences that we haven’t anticipated.”
For example, he said, the xenotransplantation and gene-modifying techniques should be explored in a range of patients, including older and younger people, women and men, and people of different ethnicities and races.
“There may be some differences based on ancestry, based on gender, based on aging, that will influence the way in which these engineered donor hearts are experienced clinically,” Dr. Yancy said.
The xenotransplantation technique’s potential impact on health equity should also be considered, as it “almost assuredly will be a very expensive technology that will be utilized in a very select population,” he noted. “We need to have a really wide lens to think about all of the potential ramifications.”
‘This field needs to evolve’
Dr. Mehra also flagged the procedure’s potential cost should it become mainstream. Perhaps that would promote dialogue on how to primarily use it “after legitimately exhausting all available options, such as total artificial heart support.”
It might also teach the field to take greater advantage of the many donated hearts discarded as suboptimal. “The general usage rate for offered organs is around a third,” despite opportunities to expand use of those that are “less than perfect,” Dr. Mehra said. “I think that the field will grow with the community focusing on reduced discards of current available heart organs, and not necessarily grow because of the availability of ‘xeno-organs.’ ”
“This field needs to evolve because we’re actively transplanting patients today. But in my mind, the real future is to have such a sufficient understanding of the biology of left ventricular dysfunction that transplantation is a rare event,” Dr. Yancy proposed.
“I’m not certain that heart transplantation per se is the endgame. I think the avoidance of transplantation is the real endgame,” he said. “This may be controversial, but my vision of the future is not one where we have a supply of animals that we can use for transplantation. My vision of the future is that heart transplantation becomes obsolete.”
A version of this article first appeared on Medscape.com.
Progress still needed for pregnant and postpartum gastroenterologists
Despite increasing numbers joining the field, women remain a minority group in gastroenterology, where they constitute only 18% of these physicians.1 Additionally, women continue to be underrepresented among senior faculty and in leadership roles in both academic and private practice settings.2 While women now make up a majority of medical school matriculants3,4 women trainees are frequently dissuaded from pursuing specialty fellowships following residency, particularly in procedurally based fields like gastroenterology, because of perceived incompatibility with childbearing and child-rearing.5-8 For many who choose to enter the field despite these challenges, gastroenterology training and early practice often coincide with childbearing years.910 These structural impediments may contribute to the “leaky pipeline” and female physician attrition during the first decade of independent practice after fellowship.11-13 Urgent changes are needed in order to retain and support clinicians and physician-scientists through this period so that they, their offspring, their patients, and the field are able to thrive.

Fertility and pregnancy
The decision to have a child is a major milestone for many physicians and often occurs during gastroenterology training or early practice.10 Medical-training and early-career environments are not yet optimized to support women who become pregnant. At baseline, the formative years of a career are challenging ones, punctuated by long hours and both intellectually and emotionally demanding work. They are also often physically grueling, particularly while one is learning and becoming efficient in endoscopy. The ergonomics in the endoscopy suite (as in other areas of medicine) are not optimized for physicians of shorter stature, smaller hand sizes, and those who may have difficulty pushing a several-hundred-pound endoscopy cart bedside, all of which contribute to increased injury risk for female proceduralists.7,14-16 Methods to reduce endoscopic injuries in pregnant endoscopists have not yet been studied. Additionally, the existence of maternity and gender bias has been well-documented, in our field and beyond.17-20 Not surprisingly, women in gastroenterology commonly report delayed childbearing, with expected consequences, including increased infertility rates, compared with nonphysician peers.21 After 5 and 10 years as attendings, female gastroenterologists continue to report fewer children than male colleagues.22,23 Once pregnant, there are a number of field-specific challenges to navigate. These include decisions about the safety of performing procedures involving fluoroscopy or high infectious risk, particularly early in pregnancy when organogenesis occurs.7,24 Additionally, engaging in appropriate obstetric care can be challenging given the need for regular physician and ultrasound appointments.

Simple, cost-efficient interventions may be effective in decreasing infertility rates, pregnancy loss, and poor physician experiences during pregnancy. For one, all gastroenterology divisions could craft written policies that include a no-tolerance approach to expressions of maternity bias against pregnant or postpartum trainees and faculty.12,25 Additionally, ergonomic improvements, such as standing pads, dial extenders, and adjusted screen heights may decrease injury rates and increase comfort for female endoscopists.26,27 There should also be a no-penalty, no-questions-asked approach for any female endoscopist who defers performance of an obstetrically high-risk procedure to a nonpregnant colleague. Additionally, pregnant gastroenterologists should be supported in obtaining high-quality obstetric care. At an individual level, nonpregnant gastroenterologists, and particularly male allies, can support pregnant colleagues by agreeing to perform higher-risk procedures, stepping in if a fellow is unable to perform endoscopy because of pregnancy, and by offering to push the endoscopy cart on behalf of a pregnant colleague to bedside, if necessary.10,28
Parental leave
Following delivery, parental leave presents an additional challenge for the physician parent. Paid maternal leave has been associated with improved child and maternal outcomes and is widely available to physicians outside the United States.29,30 At present, duration of leave varies significantly by career stage (fellows versus attending), practice setting (academic center versus private practice), and geographic location. The American Academy of Pediatrics recommends a minimum of 12 weeks of leave.31 This length has been associated with lower rates of postpartum depression and higher rates of sustained breastfeeding, with subsequent improved health outcomes for mother and child.32-34 An increasing number of states have passed laws mandating minimum paid and unpaid parental leave time (for example, in Massachusetts, gastroenterology trainees and faculty are afforded 12 weeks of leave, in accordance with state law).35 Recent changes to board eligibility and training requirements via the American Board of Medical Specialties and the American Council for Graduate Medical Education now provide 6 weeks for parental leave. This is an improvement over prior policies which rendered many physician-parents board-ineligible if they took more than 4 weeks of leave, although it must be noted that even the revised policies allow for less time than either that of Obstetricians and Gynecologists or than the American Academy of Pediatrics recommends.
Our data, presented at the 2021 ACG conference, suggest that many trainees report receiving 4 weeks or less of parental leave, despite the ACGME and ABMS policies described above. We also found that physicians were frequently not aware of their institution or division leave policies.10 Ideally, all gastroenterology divisions in the United States would follow the recommended leave duration set forth by the medical societies of specialties that care for pregnant and postpartum mothers and their infants. Additionally, the impact of leave time on graduation and board eligibility, as well as academic and practice promotion, should be made clear at the time of leave and should minimize adverse consequences for the careers of pregnant and postpartum gastroenterologists. Gastroenterology trainees and faculty should be educated in the existence and details of their institution or practice policies, and these policies should be made readily available to all physicians and administrators.
Postpartum period
The transition back to work is a challenging one for mothers in all fields of medicine, particularly for those returning to procedurally based subspecialties such as gastroenterology. This is especially true for trainees and faculty who have returned to work sooner than the recommended 12 weeks and for those who are post cesarean section, for whom physical healing may not be complete. Long days performing endoscopy may be physically challenging or impossible for some women during the postpartum period. Additionally, expressing breast milk, a metabolically intensive activity, also necessitates time, space, and privacy to perform and is frequently made more difficult by insufficient lactation accommodations. The COVID-19 pandemic has increased logistic challenges for lactating mothers, because of the need for well-ventilated lactation spaces to minimize infectious risk.19 Our colleagues have reported pumping in their vehicles, in supply closets, and in spaces that require so much travel time (in addition to time required to express milk, store milk, and clean pump equipment) that the practice was unsustainable, and the physician stopped breastfeeding prematurely.36
The benefits of breastfeeding for mother and infant are well-established, and exclusive breastfeeding for the first 6 months of life is supported by the American College of Obstetricians and Gynecologists, whose position statement reads as follows: “Policies that protect the right of a woman and her child to breastfeed ... and that accommodate milk expression, such as ... paid maternity leave, on-site childcare, break time for expressing milk, and a clean, private location for expressing milk, are essential to sustaining breastfeeding.”37 We would add to these recommendations provision of dedicated milk storage space and establishment of clear, supportive policies that allow lactating physicians to breastfeed and express breast milk if they choose without career penalty. Several institutions offer scheduled protected clinical time and modified work relative value units (RVU) for lactating physicians, such that returning parents can have protected time for expressing breast milk and still meet RVU targets.38 Additionally, many academic institutions offer productivity adjustments for tenure-track faculty who have recently had children.
Creating a more supportive environment for women gastroenterologists who desire children allows the field to be more representative of our patient population and has been shown to positively impact outcomes from improved colorectal cancer screening rates to more guideline-directed informed consent conversations.39-41 Gastroenterology should comprise a physician workforce predicated on clinical and research excellence alone and should not require its practitioners to delay or abstain from pregnancy and child rearing. Robust, clear, and generous parental leave and postpartum accommodations will allow the field to retain and promote talented physicians, who will then contribute to the betterment of patients and the field over decades.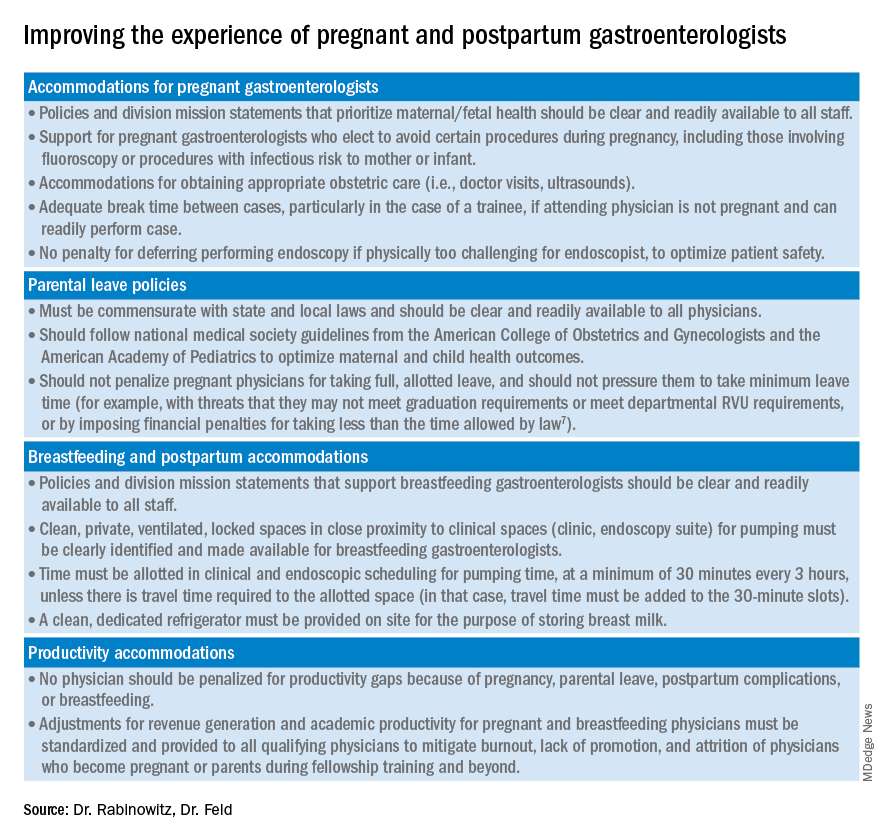
Dr. Rabinowitz is a faculty member in the department of medicine and division of gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston. Dr. Feld is a transplant hepatology fellow, division of gastroenterology, department of medicine, University of Washington, Seattle. Dr. Rabinowitz and Dr. Feld have no conflicts of interest to disclose.
References
1. AAMC. Diversity in Medicine: Facts and Figures 2019. 2018.
2. Colleges AoAM. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2015-2016. 2016. www.aamc.org/download/481206/data/2015table11.pdf.
3. AAMC. Table B-3: Total U.S. Medical School Enrollment by Race/Ethnicity and Sex, 2014-2015 through 2018-2019, 2019.
4. Rabinowitz LG. Recognizing blind spots – a remedy for gender bias in medicine? (N Engl. J Med. 2018; 378[24]: 2253-5).
5. Douglas PS et al. Career preferences and perceptions of cardiology among US internal medicine trainees: Factors influencing cardiology career choice. JAMA Cardiol 2018; 3(8):682-91.
6. Stack SW et al. Childbearing decisions in residency: A multicenter survey of female residents. Acad Med 2020;95(10):1550-7.
7. David YN et al. Pregnancy and the working gastroenterologist: Perceptions, realities, and systemic challenges. Gastroenterology 2021;161(3):756-60.
8. Rembacken BJ et al. Barriers and bias standing in the way of female trainees wanting to learn advanced endoscopy. United European Gastroenterol J. 2019;7(8):1141-5.
9. Arlow FL et al. Gastroenterology training and career choices: A prospective longitudinal study of the impact of gender and of managed care. Am J Gastroenterol. 2002;97(2):459-69.
10. Feld L et al. Parental leave for gastroenterology fellows: A national survey of current fellows. Am J Gastroenterol. 2021;116:S611-2.
11. Rabinowitz LG et al. Addressing gender in gastroenterology: opportunities for change. Gastrointest Endosc. 2020;91(1):155-61.
12. Feld LD. Baby steps in the right direction: Toward a parental leave policy for gastroenterology fellows. Am J Gastroenterol. 2021;116(3):505-8.
13. Feld LD. Interviewing for two. Am J Gastroenterol. 2020;116(3):445-6
14. Rabinowitz LG et al. Gender dynamics in education and practice of gastroenterology. Gastrointest Endosc. 2021;93(5):1047-56.e5.
15. Harvin G. Review of musculoskeletal injuries and prevention in the endoscopy practitioner. J Clin Gastroenterol. 2014;48(7):590-4.
16. LabX Oecs. www.labx.com/product/endoscopy-cart (accessed 2021 Nov 19.
17. Heilman ME and Okimoto TG. Motherhood: A potential source of bias in employment decisions. J Appl Psychol. 2008;93(1):189-98.
18. Robinson K et al. Racism, bias, and discrimination as modifiable barriers to breastfeeding for African American women: A scoping review of the literature. J Midwifery Womens Health. 2019;64(6):734-42.
19. Rabinowitz LG and Rabinowitz DG. Women on the Frontline: A Changed Workforce and the Fight Against COVID-19. Acad Med. 2021 Jun 1;96(6):808-12.
20. Rabinowitz LG et al. Gender in the endoscopy suite. Lancet Gastroenterol Hepatol. 2020 Dec;5(12):1032-4.
21. Stentz NC et al. Fertility and childbearing among American female physicians. J Womens Health. 2016; 25(10):1059-65.
22. Burke CA et al. Gender disparity in the practice of gastroenterology: The first 5 years of a career. Am J Gastroenterol. 2005;100(2):259-64.
23. Singh A et al. Women in gastroenterology committee of American College of G. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008;103(7):1589-95.
24. Krueger KJ and Hoffman BJ. Radiation exposure during gastroenterologic fluoroscopy: Risk assessment for pregnant workers. Am J Gastroenterol. 1992;87(4):429-31.
25. Krause ML et al. Impact of pregnancy and gender on internal medicine resident evaluations: A retrospective cohort study. J Gen Intern Med. 2017;32(6):648-53.
26. Pawa S et al. Are all endoscopy-related musculoskeletal injuries created equal? Results of a national gender-based survey. Am J Gastroenterol. 2021;116(3):530-8.
27. David YN et al. Gender-specific factors influencing gastroenterologists to pursue careers in advanced endoscopy: perceptions vs reality. Am J Gastroenterol. 2021;116(3):539-50.
28. Bilal M et al. The need for allyship in achieving gender equity in gastroenterology. Am J Gastroenterol. 2021 Oct 19. doi: 10.14309/ajg.0000000000001508. Online ahead of print.
29. Jou J et al. Paid maternity leave in the United States: Associations with maternal and infant health. Matern Child Health J. 2018;22(2):216-25.
30. Aitken Z et al. The maternal health outcomes of paid maternity leave: A systematic review. Soc Sci Med. 2015;130:32-41.
31. Dodson NA and Talib HJ. Paid parental leave for mothers and fathers can improve physician wellness. AAP News. 2020 Jul 1. https://publications.aap.org/aapnews/news/12432.
32. Kornfeind KR and Sipsma HL. Exploring the link between maternity leave and postpartum depression. Womens Health Issues 2018;28(4):321-6.
33. Navarro-Rosenblatt D and Garmendia ML. Maternity leave and its impact on breastfeeding: A review of the literature. Breastfeed Med 2018;13(9):589-97.
34. Stack SW et al. Maternity leave in residency: A multicenter study of determinants and wellness outcomes. Acad Med. 2019;94(11):1738-45.
35. Mass.gov. Paid Family and Medical Leave Information for Massachusetts Employers. 2020.
36. Ares Segura S et al. en representacion del Comite de Lactancia Materna de la Asociacion Espanola de P. [The importance of maternal nutrition during breastfeeding: Do breastfeeding mothers need nutritional supplements?]. An Pediatr. (Barc) 2016;84(6):347 e1-7.
37. American College of Obstetricians and Gynecologists, Committee on Obstetric Practice. Committee Opinion No. 658: Optimizing Support for Breastfeeding as Part of Obstetric Practice. Obstet Gynecol. 2016;127(2):e86-92.
38. Porter KK et al. A lactation credit model to support breastfeeding in radiology: The new gold standard to support “liquid gold.” Clin Imaging 2021;80:16-8.
39. Davis J et al. Clinical practice patterns suggest female patients prefer female endoscopists. Dig Dis Sci. 2015;60(10):3149-50.
40. Menees SB et al. Women patients’ preference for women physicians is a barrier to colon cancer screening. Gastrointest Endosc. 2005;62(2):219-23.
41. Feld LD et al. Management of code status in the periendoscopic period: A national survey of current practices and beliefs of U.S. gastroenterologists. Gastrointest Endosc. 2021;94(1):172-7.e2.
Despite increasing numbers joining the field, women remain a minority group in gastroenterology, where they constitute only 18% of these physicians.1 Additionally, women continue to be underrepresented among senior faculty and in leadership roles in both academic and private practice settings.2 While women now make up a majority of medical school matriculants3,4 women trainees are frequently dissuaded from pursuing specialty fellowships following residency, particularly in procedurally based fields like gastroenterology, because of perceived incompatibility with childbearing and child-rearing.5-8 For many who choose to enter the field despite these challenges, gastroenterology training and early practice often coincide with childbearing years.910 These structural impediments may contribute to the “leaky pipeline” and female physician attrition during the first decade of independent practice after fellowship.11-13 Urgent changes are needed in order to retain and support clinicians and physician-scientists through this period so that they, their offspring, their patients, and the field are able to thrive.
Fertility and pregnancy
The decision to have a child is a major milestone for many physicians and often occurs during gastroenterology training or early practice.10 Medical-training and early-career environments are not yet optimized to support women who become pregnant. At baseline, the formative years of a career are challenging ones, punctuated by long hours and both intellectually and emotionally demanding work. They are also often physically grueling, particularly while one is learning and becoming efficient in endoscopy. The ergonomics in the endoscopy suite (as in other areas of medicine) are not optimized for physicians of shorter stature, smaller hand sizes, and those who may have difficulty pushing a several-hundred-pound endoscopy cart bedside, all of which contribute to increased injury risk for female proceduralists.7,14-16 Methods to reduce endoscopic injuries in pregnant endoscopists have not yet been studied. Additionally, the existence of maternity and gender bias has been well-documented, in our field and beyond.17-20 Not surprisingly, women in gastroenterology commonly report delayed childbearing, with expected consequences, including increased infertility rates, compared with nonphysician peers.21 After 5 and 10 years as attendings, female gastroenterologists continue to report fewer children than male colleagues.22,23 Once pregnant, there are a number of field-specific challenges to navigate. These include decisions about the safety of performing procedures involving fluoroscopy or high infectious risk, particularly early in pregnancy when organogenesis occurs.7,24 Additionally, engaging in appropriate obstetric care can be challenging given the need for regular physician and ultrasound appointments.
Simple, cost-efficient interventions may be effective in decreasing infertility rates, pregnancy loss, and poor physician experiences during pregnancy. For one, all gastroenterology divisions could craft written policies that include a no-tolerance approach to expressions of maternity bias against pregnant or postpartum trainees and faculty.12,25 Additionally, ergonomic improvements, such as standing pads, dial extenders, and adjusted screen heights may decrease injury rates and increase comfort for female endoscopists.26,27 There should also be a no-penalty, no-questions-asked approach for any female endoscopist who defers performance of an obstetrically high-risk procedure to a nonpregnant colleague. Additionally, pregnant gastroenterologists should be supported in obtaining high-quality obstetric care. At an individual level, nonpregnant gastroenterologists, and particularly male allies, can support pregnant colleagues by agreeing to perform higher-risk procedures, stepping in if a fellow is unable to perform endoscopy because of pregnancy, and by offering to push the endoscopy cart on behalf of a pregnant colleague to bedside, if necessary.10,28
Parental leave
Following delivery, parental leave presents an additional challenge for the physician parent. Paid maternal leave has been associated with improved child and maternal outcomes and is widely available to physicians outside the United States.29,30 At present, duration of leave varies significantly by career stage (fellows versus attending), practice setting (academic center versus private practice), and geographic location. The American Academy of Pediatrics recommends a minimum of 12 weeks of leave.31 This length has been associated with lower rates of postpartum depression and higher rates of sustained breastfeeding, with subsequent improved health outcomes for mother and child.32-34 An increasing number of states have passed laws mandating minimum paid and unpaid parental leave time (for example, in Massachusetts, gastroenterology trainees and faculty are afforded 12 weeks of leave, in accordance with state law).35 Recent changes to board eligibility and training requirements via the American Board of Medical Specialties and the American Council for Graduate Medical Education now provide 6 weeks for parental leave. This is an improvement over prior policies which rendered many physician-parents board-ineligible if they took more than 4 weeks of leave, although it must be noted that even the revised policies allow for less time than either that of Obstetricians and Gynecologists or than the American Academy of Pediatrics recommends.
Our data, presented at the 2021 ACG conference, suggest that many trainees report receiving 4 weeks or less of parental leave, despite the ACGME and ABMS policies described above. We also found that physicians were frequently not aware of their institution or division leave policies.10 Ideally, all gastroenterology divisions in the United States would follow the recommended leave duration set forth by the medical societies of specialties that care for pregnant and postpartum mothers and their infants. Additionally, the impact of leave time on graduation and board eligibility, as well as academic and practice promotion, should be made clear at the time of leave and should minimize adverse consequences for the careers of pregnant and postpartum gastroenterologists. Gastroenterology trainees and faculty should be educated in the existence and details of their institution or practice policies, and these policies should be made readily available to all physicians and administrators.
Postpartum period
The transition back to work is a challenging one for mothers in all fields of medicine, particularly for those returning to procedurally based subspecialties such as gastroenterology. This is especially true for trainees and faculty who have returned to work sooner than the recommended 12 weeks and for those who are post cesarean section, for whom physical healing may not be complete. Long days performing endoscopy may be physically challenging or impossible for some women during the postpartum period. Additionally, expressing breast milk, a metabolically intensive activity, also necessitates time, space, and privacy to perform and is frequently made more difficult by insufficient lactation accommodations. The COVID-19 pandemic has increased logistic challenges for lactating mothers, because of the need for well-ventilated lactation spaces to minimize infectious risk.19 Our colleagues have reported pumping in their vehicles, in supply closets, and in spaces that require so much travel time (in addition to time required to express milk, store milk, and clean pump equipment) that the practice was unsustainable, and the physician stopped breastfeeding prematurely.36
The benefits of breastfeeding for mother and infant are well-established, and exclusive breastfeeding for the first 6 months of life is supported by the American College of Obstetricians and Gynecologists, whose position statement reads as follows: “Policies that protect the right of a woman and her child to breastfeed ... and that accommodate milk expression, such as ... paid maternity leave, on-site childcare, break time for expressing milk, and a clean, private location for expressing milk, are essential to sustaining breastfeeding.”37 We would add to these recommendations provision of dedicated milk storage space and establishment of clear, supportive policies that allow lactating physicians to breastfeed and express breast milk if they choose without career penalty. Several institutions offer scheduled protected clinical time and modified work relative value units (RVU) for lactating physicians, such that returning parents can have protected time for expressing breast milk and still meet RVU targets.38 Additionally, many academic institutions offer productivity adjustments for tenure-track faculty who have recently had children.
Creating a more supportive environment for women gastroenterologists who desire children allows the field to be more representative of our patient population and has been shown to positively impact outcomes from improved colorectal cancer screening rates to more guideline-directed informed consent conversations.39-41 Gastroenterology should comprise a physician workforce predicated on clinical and research excellence alone and should not require its practitioners to delay or abstain from pregnancy and child rearing. Robust, clear, and generous parental leave and postpartum accommodations will allow the field to retain and promote talented physicians, who will then contribute to the betterment of patients and the field over decades.
Dr. Rabinowitz is a faculty member in the department of medicine and division of gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston. Dr. Feld is a transplant hepatology fellow, division of gastroenterology, department of medicine, University of Washington, Seattle. Dr. Rabinowitz and Dr. Feld have no conflicts of interest to disclose.
References
1. AAMC. Diversity in Medicine: Facts and Figures 2019. 2018.
2. Colleges AoAM. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2015-2016. 2016. www.aamc.org/download/481206/data/2015table11.pdf.
3. AAMC. Table B-3: Total U.S. Medical School Enrollment by Race/Ethnicity and Sex, 2014-2015 through 2018-2019, 2019.
4. Rabinowitz LG. Recognizing blind spots – a remedy for gender bias in medicine? (N Engl. J Med. 2018; 378[24]: 2253-5).
5. Douglas PS et al. Career preferences and perceptions of cardiology among US internal medicine trainees: Factors influencing cardiology career choice. JAMA Cardiol 2018; 3(8):682-91.
6. Stack SW et al. Childbearing decisions in residency: A multicenter survey of female residents. Acad Med 2020;95(10):1550-7.
7. David YN et al. Pregnancy and the working gastroenterologist: Perceptions, realities, and systemic challenges. Gastroenterology 2021;161(3):756-60.
8. Rembacken BJ et al. Barriers and bias standing in the way of female trainees wanting to learn advanced endoscopy. United European Gastroenterol J. 2019;7(8):1141-5.
9. Arlow FL et al. Gastroenterology training and career choices: A prospective longitudinal study of the impact of gender and of managed care. Am J Gastroenterol. 2002;97(2):459-69.
10. Feld L et al. Parental leave for gastroenterology fellows: A national survey of current fellows. Am J Gastroenterol. 2021;116:S611-2.
11. Rabinowitz LG et al. Addressing gender in gastroenterology: opportunities for change. Gastrointest Endosc. 2020;91(1):155-61.
12. Feld LD. Baby steps in the right direction: Toward a parental leave policy for gastroenterology fellows. Am J Gastroenterol. 2021;116(3):505-8.
13. Feld LD. Interviewing for two. Am J Gastroenterol. 2020;116(3):445-6
14. Rabinowitz LG et al. Gender dynamics in education and practice of gastroenterology. Gastrointest Endosc. 2021;93(5):1047-56.e5.
15. Harvin G. Review of musculoskeletal injuries and prevention in the endoscopy practitioner. J Clin Gastroenterol. 2014;48(7):590-4.
16. LabX Oecs. www.labx.com/product/endoscopy-cart (accessed 2021 Nov 19.
17. Heilman ME and Okimoto TG. Motherhood: A potential source of bias in employment decisions. J Appl Psychol. 2008;93(1):189-98.
18. Robinson K et al. Racism, bias, and discrimination as modifiable barriers to breastfeeding for African American women: A scoping review of the literature. J Midwifery Womens Health. 2019;64(6):734-42.
19. Rabinowitz LG and Rabinowitz DG. Women on the Frontline: A Changed Workforce and the Fight Against COVID-19. Acad Med. 2021 Jun 1;96(6):808-12.
20. Rabinowitz LG et al. Gender in the endoscopy suite. Lancet Gastroenterol Hepatol. 2020 Dec;5(12):1032-4.
21. Stentz NC et al. Fertility and childbearing among American female physicians. J Womens Health. 2016; 25(10):1059-65.
22. Burke CA et al. Gender disparity in the practice of gastroenterology: The first 5 years of a career. Am J Gastroenterol. 2005;100(2):259-64.
23. Singh A et al. Women in gastroenterology committee of American College of G. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008;103(7):1589-95.
24. Krueger KJ and Hoffman BJ. Radiation exposure during gastroenterologic fluoroscopy: Risk assessment for pregnant workers. Am J Gastroenterol. 1992;87(4):429-31.
25. Krause ML et al. Impact of pregnancy and gender on internal medicine resident evaluations: A retrospective cohort study. J Gen Intern Med. 2017;32(6):648-53.
26. Pawa S et al. Are all endoscopy-related musculoskeletal injuries created equal? Results of a national gender-based survey. Am J Gastroenterol. 2021;116(3):530-8.
27. David YN et al. Gender-specific factors influencing gastroenterologists to pursue careers in advanced endoscopy: perceptions vs reality. Am J Gastroenterol. 2021;116(3):539-50.
28. Bilal M et al. The need for allyship in achieving gender equity in gastroenterology. Am J Gastroenterol. 2021 Oct 19. doi: 10.14309/ajg.0000000000001508. Online ahead of print.
29. Jou J et al. Paid maternity leave in the United States: Associations with maternal and infant health. Matern Child Health J. 2018;22(2):216-25.
30. Aitken Z et al. The maternal health outcomes of paid maternity leave: A systematic review. Soc Sci Med. 2015;130:32-41.
31. Dodson NA and Talib HJ. Paid parental leave for mothers and fathers can improve physician wellness. AAP News. 2020 Jul 1. https://publications.aap.org/aapnews/news/12432.
32. Kornfeind KR and Sipsma HL. Exploring the link between maternity leave and postpartum depression. Womens Health Issues 2018;28(4):321-6.
33. Navarro-Rosenblatt D and Garmendia ML. Maternity leave and its impact on breastfeeding: A review of the literature. Breastfeed Med 2018;13(9):589-97.
34. Stack SW et al. Maternity leave in residency: A multicenter study of determinants and wellness outcomes. Acad Med. 2019;94(11):1738-45.
35. Mass.gov. Paid Family and Medical Leave Information for Massachusetts Employers. 2020.
36. Ares Segura S et al. en representacion del Comite de Lactancia Materna de la Asociacion Espanola de P. [The importance of maternal nutrition during breastfeeding: Do breastfeeding mothers need nutritional supplements?]. An Pediatr. (Barc) 2016;84(6):347 e1-7.
37. American College of Obstetricians and Gynecologists, Committee on Obstetric Practice. Committee Opinion No. 658: Optimizing Support for Breastfeeding as Part of Obstetric Practice. Obstet Gynecol. 2016;127(2):e86-92.
38. Porter KK et al. A lactation credit model to support breastfeeding in radiology: The new gold standard to support “liquid gold.” Clin Imaging 2021;80:16-8.
39. Davis J et al. Clinical practice patterns suggest female patients prefer female endoscopists. Dig Dis Sci. 2015;60(10):3149-50.
40. Menees SB et al. Women patients’ preference for women physicians is a barrier to colon cancer screening. Gastrointest Endosc. 2005;62(2):219-23.
41. Feld LD et al. Management of code status in the periendoscopic period: A national survey of current practices and beliefs of U.S. gastroenterologists. Gastrointest Endosc. 2021;94(1):172-7.e2.
Despite increasing numbers joining the field, women remain a minority group in gastroenterology, where they constitute only 18% of these physicians.1 Additionally, women continue to be underrepresented among senior faculty and in leadership roles in both academic and private practice settings.2 While women now make up a majority of medical school matriculants3,4 women trainees are frequently dissuaded from pursuing specialty fellowships following residency, particularly in procedurally based fields like gastroenterology, because of perceived incompatibility with childbearing and child-rearing.5-8 For many who choose to enter the field despite these challenges, gastroenterology training and early practice often coincide with childbearing years.910 These structural impediments may contribute to the “leaky pipeline” and female physician attrition during the first decade of independent practice after fellowship.11-13 Urgent changes are needed in order to retain and support clinicians and physician-scientists through this period so that they, their offspring, their patients, and the field are able to thrive.
Fertility and pregnancy
The decision to have a child is a major milestone for many physicians and often occurs during gastroenterology training or early practice.10 Medical-training and early-career environments are not yet optimized to support women who become pregnant. At baseline, the formative years of a career are challenging ones, punctuated by long hours and both intellectually and emotionally demanding work. They are also often physically grueling, particularly while one is learning and becoming efficient in endoscopy. The ergonomics in the endoscopy suite (as in other areas of medicine) are not optimized for physicians of shorter stature, smaller hand sizes, and those who may have difficulty pushing a several-hundred-pound endoscopy cart bedside, all of which contribute to increased injury risk for female proceduralists.7,14-16 Methods to reduce endoscopic injuries in pregnant endoscopists have not yet been studied. Additionally, the existence of maternity and gender bias has been well-documented, in our field and beyond.17-20 Not surprisingly, women in gastroenterology commonly report delayed childbearing, with expected consequences, including increased infertility rates, compared with nonphysician peers.21 After 5 and 10 years as attendings, female gastroenterologists continue to report fewer children than male colleagues.22,23 Once pregnant, there are a number of field-specific challenges to navigate. These include decisions about the safety of performing procedures involving fluoroscopy or high infectious risk, particularly early in pregnancy when organogenesis occurs.7,24 Additionally, engaging in appropriate obstetric care can be challenging given the need for regular physician and ultrasound appointments.
Simple, cost-efficient interventions may be effective in decreasing infertility rates, pregnancy loss, and poor physician experiences during pregnancy. For one, all gastroenterology divisions could craft written policies that include a no-tolerance approach to expressions of maternity bias against pregnant or postpartum trainees and faculty.12,25 Additionally, ergonomic improvements, such as standing pads, dial extenders, and adjusted screen heights may decrease injury rates and increase comfort for female endoscopists.26,27 There should also be a no-penalty, no-questions-asked approach for any female endoscopist who defers performance of an obstetrically high-risk procedure to a nonpregnant colleague. Additionally, pregnant gastroenterologists should be supported in obtaining high-quality obstetric care. At an individual level, nonpregnant gastroenterologists, and particularly male allies, can support pregnant colleagues by agreeing to perform higher-risk procedures, stepping in if a fellow is unable to perform endoscopy because of pregnancy, and by offering to push the endoscopy cart on behalf of a pregnant colleague to bedside, if necessary.10,28
Parental leave
Following delivery, parental leave presents an additional challenge for the physician parent. Paid maternal leave has been associated with improved child and maternal outcomes and is widely available to physicians outside the United States.29,30 At present, duration of leave varies significantly by career stage (fellows versus attending), practice setting (academic center versus private practice), and geographic location. The American Academy of Pediatrics recommends a minimum of 12 weeks of leave.31 This length has been associated with lower rates of postpartum depression and higher rates of sustained breastfeeding, with subsequent improved health outcomes for mother and child.32-34 An increasing number of states have passed laws mandating minimum paid and unpaid parental leave time (for example, in Massachusetts, gastroenterology trainees and faculty are afforded 12 weeks of leave, in accordance with state law).35 Recent changes to board eligibility and training requirements via the American Board of Medical Specialties and the American Council for Graduate Medical Education now provide 6 weeks for parental leave. This is an improvement over prior policies which rendered many physician-parents board-ineligible if they took more than 4 weeks of leave, although it must be noted that even the revised policies allow for less time than either that of Obstetricians and Gynecologists or than the American Academy of Pediatrics recommends.
Our data, presented at the 2021 ACG conference, suggest that many trainees report receiving 4 weeks or less of parental leave, despite the ACGME and ABMS policies described above. We also found that physicians were frequently not aware of their institution or division leave policies.10 Ideally, all gastroenterology divisions in the United States would follow the recommended leave duration set forth by the medical societies of specialties that care for pregnant and postpartum mothers and their infants. Additionally, the impact of leave time on graduation and board eligibility, as well as academic and practice promotion, should be made clear at the time of leave and should minimize adverse consequences for the careers of pregnant and postpartum gastroenterologists. Gastroenterology trainees and faculty should be educated in the existence and details of their institution or practice policies, and these policies should be made readily available to all physicians and administrators.
Postpartum period
The transition back to work is a challenging one for mothers in all fields of medicine, particularly for those returning to procedurally based subspecialties such as gastroenterology. This is especially true for trainees and faculty who have returned to work sooner than the recommended 12 weeks and for those who are post cesarean section, for whom physical healing may not be complete. Long days performing endoscopy may be physically challenging or impossible for some women during the postpartum period. Additionally, expressing breast milk, a metabolically intensive activity, also necessitates time, space, and privacy to perform and is frequently made more difficult by insufficient lactation accommodations. The COVID-19 pandemic has increased logistic challenges for lactating mothers, because of the need for well-ventilated lactation spaces to minimize infectious risk.19 Our colleagues have reported pumping in their vehicles, in supply closets, and in spaces that require so much travel time (in addition to time required to express milk, store milk, and clean pump equipment) that the practice was unsustainable, and the physician stopped breastfeeding prematurely.36
The benefits of breastfeeding for mother and infant are well-established, and exclusive breastfeeding for the first 6 months of life is supported by the American College of Obstetricians and Gynecologists, whose position statement reads as follows: “Policies that protect the right of a woman and her child to breastfeed ... and that accommodate milk expression, such as ... paid maternity leave, on-site childcare, break time for expressing milk, and a clean, private location for expressing milk, are essential to sustaining breastfeeding.”37 We would add to these recommendations provision of dedicated milk storage space and establishment of clear, supportive policies that allow lactating physicians to breastfeed and express breast milk if they choose without career penalty. Several institutions offer scheduled protected clinical time and modified work relative value units (RVU) for lactating physicians, such that returning parents can have protected time for expressing breast milk and still meet RVU targets.38 Additionally, many academic institutions offer productivity adjustments for tenure-track faculty who have recently had children.
Creating a more supportive environment for women gastroenterologists who desire children allows the field to be more representative of our patient population and has been shown to positively impact outcomes from improved colorectal cancer screening rates to more guideline-directed informed consent conversations.39-41 Gastroenterology should comprise a physician workforce predicated on clinical and research excellence alone and should not require its practitioners to delay or abstain from pregnancy and child rearing. Robust, clear, and generous parental leave and postpartum accommodations will allow the field to retain and promote talented physicians, who will then contribute to the betterment of patients and the field over decades.
Dr. Rabinowitz is a faculty member in the department of medicine and division of gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston. Dr. Feld is a transplant hepatology fellow, division of gastroenterology, department of medicine, University of Washington, Seattle. Dr. Rabinowitz and Dr. Feld have no conflicts of interest to disclose.
References
1. AAMC. Diversity in Medicine: Facts and Figures 2019. 2018.
2. Colleges AoAM. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2015-2016. 2016. www.aamc.org/download/481206/data/2015table11.pdf.
3. AAMC. Table B-3: Total U.S. Medical School Enrollment by Race/Ethnicity and Sex, 2014-2015 through 2018-2019, 2019.
4. Rabinowitz LG. Recognizing blind spots – a remedy for gender bias in medicine? (N Engl. J Med. 2018; 378[24]: 2253-5).
5. Douglas PS et al. Career preferences and perceptions of cardiology among US internal medicine trainees: Factors influencing cardiology career choice. JAMA Cardiol 2018; 3(8):682-91.
6. Stack SW et al. Childbearing decisions in residency: A multicenter survey of female residents. Acad Med 2020;95(10):1550-7.
7. David YN et al. Pregnancy and the working gastroenterologist: Perceptions, realities, and systemic challenges. Gastroenterology 2021;161(3):756-60.
8. Rembacken BJ et al. Barriers and bias standing in the way of female trainees wanting to learn advanced endoscopy. United European Gastroenterol J. 2019;7(8):1141-5.
9. Arlow FL et al. Gastroenterology training and career choices: A prospective longitudinal study of the impact of gender and of managed care. Am J Gastroenterol. 2002;97(2):459-69.
10. Feld L et al. Parental leave for gastroenterology fellows: A national survey of current fellows. Am J Gastroenterol. 2021;116:S611-2.
11. Rabinowitz LG et al. Addressing gender in gastroenterology: opportunities for change. Gastrointest Endosc. 2020;91(1):155-61.
12. Feld LD. Baby steps in the right direction: Toward a parental leave policy for gastroenterology fellows. Am J Gastroenterol. 2021;116(3):505-8.
13. Feld LD. Interviewing for two. Am J Gastroenterol. 2020;116(3):445-6
14. Rabinowitz LG et al. Gender dynamics in education and practice of gastroenterology. Gastrointest Endosc. 2021;93(5):1047-56.e5.
15. Harvin G. Review of musculoskeletal injuries and prevention in the endoscopy practitioner. J Clin Gastroenterol. 2014;48(7):590-4.
16. LabX Oecs. www.labx.com/product/endoscopy-cart (accessed 2021 Nov 19.
17. Heilman ME and Okimoto TG. Motherhood: A potential source of bias in employment decisions. J Appl Psychol. 2008;93(1):189-98.
18. Robinson K et al. Racism, bias, and discrimination as modifiable barriers to breastfeeding for African American women: A scoping review of the literature. J Midwifery Womens Health. 2019;64(6):734-42.
19. Rabinowitz LG and Rabinowitz DG. Women on the Frontline: A Changed Workforce and the Fight Against COVID-19. Acad Med. 2021 Jun 1;96(6):808-12.
20. Rabinowitz LG et al. Gender in the endoscopy suite. Lancet Gastroenterol Hepatol. 2020 Dec;5(12):1032-4.
21. Stentz NC et al. Fertility and childbearing among American female physicians. J Womens Health. 2016; 25(10):1059-65.
22. Burke CA et al. Gender disparity in the practice of gastroenterology: The first 5 years of a career. Am J Gastroenterol. 2005;100(2):259-64.
23. Singh A et al. Women in gastroenterology committee of American College of G. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008;103(7):1589-95.
24. Krueger KJ and Hoffman BJ. Radiation exposure during gastroenterologic fluoroscopy: Risk assessment for pregnant workers. Am J Gastroenterol. 1992;87(4):429-31.
25. Krause ML et al. Impact of pregnancy and gender on internal medicine resident evaluations: A retrospective cohort study. J Gen Intern Med. 2017;32(6):648-53.
26. Pawa S et al. Are all endoscopy-related musculoskeletal injuries created equal? Results of a national gender-based survey. Am J Gastroenterol. 2021;116(3):530-8.
27. David YN et al. Gender-specific factors influencing gastroenterologists to pursue careers in advanced endoscopy: perceptions vs reality. Am J Gastroenterol. 2021;116(3):539-50.
28. Bilal M et al. The need for allyship in achieving gender equity in gastroenterology. Am J Gastroenterol. 2021 Oct 19. doi: 10.14309/ajg.0000000000001508. Online ahead of print.
29. Jou J et al. Paid maternity leave in the United States: Associations with maternal and infant health. Matern Child Health J. 2018;22(2):216-25.
30. Aitken Z et al. The maternal health outcomes of paid maternity leave: A systematic review. Soc Sci Med. 2015;130:32-41.
31. Dodson NA and Talib HJ. Paid parental leave for mothers and fathers can improve physician wellness. AAP News. 2020 Jul 1. https://publications.aap.org/aapnews/news/12432.
32. Kornfeind KR and Sipsma HL. Exploring the link between maternity leave and postpartum depression. Womens Health Issues 2018;28(4):321-6.
33. Navarro-Rosenblatt D and Garmendia ML. Maternity leave and its impact on breastfeeding: A review of the literature. Breastfeed Med 2018;13(9):589-97.
34. Stack SW et al. Maternity leave in residency: A multicenter study of determinants and wellness outcomes. Acad Med. 2019;94(11):1738-45.
35. Mass.gov. Paid Family and Medical Leave Information for Massachusetts Employers. 2020.
36. Ares Segura S et al. en representacion del Comite de Lactancia Materna de la Asociacion Espanola de P. [The importance of maternal nutrition during breastfeeding: Do breastfeeding mothers need nutritional supplements?]. An Pediatr. (Barc) 2016;84(6):347 e1-7.
37. American College of Obstetricians and Gynecologists, Committee on Obstetric Practice. Committee Opinion No. 658: Optimizing Support for Breastfeeding as Part of Obstetric Practice. Obstet Gynecol. 2016;127(2):e86-92.
38. Porter KK et al. A lactation credit model to support breastfeeding in radiology: The new gold standard to support “liquid gold.” Clin Imaging 2021;80:16-8.
39. Davis J et al. Clinical practice patterns suggest female patients prefer female endoscopists. Dig Dis Sci. 2015;60(10):3149-50.
40. Menees SB et al. Women patients’ preference for women physicians is a barrier to colon cancer screening. Gastrointest Endosc. 2005;62(2):219-23.
41. Feld LD et al. Management of code status in the periendoscopic period: A national survey of current practices and beliefs of U.S. gastroenterologists. Gastrointest Endosc. 2021;94(1):172-7.e2.
Olive oil intake tied to reduced mortality
Compared with men and women who rarely or never consumed olive oil (the lowest intake), those who consumed greater than 0.5 tablespoon/day or more than 7 g/day (the highest intake) had a 19% lower mortality risk over a 28-year follow-up, starting from an average age of 56 years.
Moreover, compared with those with the lowest olive oil intake, those with the highest intake had a 19% lower cardiovascular disease (CVD) mortality, a 17% lower risk of dying from cancer, a 29% lower risk of dying from neurodegenerative disease, and an 18% lower risk of dying from respiratory disease during follow-up.
The researchers estimate that replacing 10 g/day of margarine, butter, mayonnaise, or dairy fat with the same amount of olive oil is associated with an 8%-34% lower risk of death from various causes.
The study by Marta Guasch-Ferré, PhD, and colleagues was published online Jan. 10 in the Journal of the American College of Cardiology.
Results support plant-based dietary fat recommendations
“Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity,” the researchers summarize.
However, “I wouldn’t say that olive oil is the only way to help you live longer,” Dr. Guasch-Ferré, a senior research scientist in the department of nutrition, Harvard T.H. Chan School of Public Health, Boston, cautioned in an interview with this news organization.
“Other things are very important, such as not smoking, doing physical activity, etc., but one recommendation could be to try to eat more plant-based food including olive oil and healthy fat,” she added, and to use it for cooking, salad dressing, and baking, and substitute it for saturated fat or animal fat, especially for cooking.
The study suggests that people should “consume a more plant-based diet and prioritize fatty acids such as olive oil because they have a better nutritional composition (high in phenols and antioxidants), instead of using butter or margarines or other animal fats that have been shown to have detrimental effects for health,” she added, which is consistent with recommendations in the Dietary Guidelines for Americans.
“That said,” Dr. Guasch-Ferré summarized, “replication is needed in other cohorts and populations to see if the results are similar.”
In an accompanying editorial, Susanna C. Larsson, PhD, writes that “this was a well-designed study, with long-term follow-up and repeated measurements of dietary intake and other risk factors for diseases.”
“However, the difference in olive oil consumption between those with the highest and those with the lowest/no olive oil consumption was very low (0.5 tablespoon) and a [12%] reduced mortality risk was observed already at a much lower intake (0.5 teaspoon, about 1.5 g/day) of olive oil,” she noted in an email to this news organization.
“It’s a bit hard to believe that such a small amount could have an independent effect on mortality risk,” Dr. Larsson, associate professor of epidemiology at the Karolinska Institutet, Stockholm, cautioned.
Like Dr. Guasch-Ferré, she noted that “just adding one or two teaspoons of olive oil to the diet each day will likely not change the risk of mortality.”
Rather, “people may need to make larger changes in the whole diet, not focus on fat only. An overall healthier diet, rich in nonrefined plant-based foods (vegetables, whole grains, nuts), low/no intake of processed foods, and a switch to healthier fat (eg, olive oil) is needed.”
Importantly, “this study cannot say anything about causality, that is, whether it’s olive oil specifically that reduces mortality risk or if there are many other beneficial factors that act together to reduce mortality rate among those with high olive oil consumption.”
The researchers acknowledge this observational study limitation and that the findings may not be generalizable to other populations.
Novel findings regarding Alzheimer’s and respiratory disease
Dr. Larsson highlights two novel findings of this study.
First, it showed a 27% reduction in risk of dementia-related mortality for those in the highest versus lowest category of olive oil consumption. “Considering the lack of preventive strategies for Alzheimer’s disease and the high morbidity and mortality related to this disease, this finding, if confirmed, is of great public health importance,” she said.
Second, the study reported an inverse association of olive oil consumption with risk of respiratory disease mortality. “Because residual confounding from smoking cannot be ruled out,” Dr. Larsson said, “this finding is tentative and requires confirmation in a study that is less susceptible to confounding, such as a randomized trial.”
And although the current study and previous studies have found that consumption of olive oil may have health benefits, she identified several remaining questions.
“Are the associations causal or spurious?” she noted. Is olive oil consumption protective for certain cardiovascular diseases like stroke or atrial fibrillation only, as has been shown in other studies, or also for other major diseases and causes of death, she added. What is the amount of olive oil required for a protective effect?
Further, is the potential effect related to monounsaturated fatty acids (MUFAs) or phenolic compounds; that is, “is the protective effect confined to polyphenol-rich extra-virgin olive oil or are refined olive oil and other vegetable oils as beneficial? More research is needed to address these questions,” she concludes.
“Further studies are needed,” the researchers agree, “to confirm the association of olive oil consumption with reduced mortality, clarify the mechanisms responsible, and quantify the dose/volume boundaries around this effect.”
Virgin olive oil has more polyphenols
Olive oil, a key component of the Mediterranean diet, is high in MUFAs, especially oleic acid, as well as vitamin E and polyphenols, which contribute to its anti-inflammatory and antioxidant properties, the researchers explain.
Virgin olive oil, produced by mechanically pressing ripe olives, contains multiple bioactive and antioxidant components and has an acidity of less than 1.5%. And extra-virgin olive oil is produced the same way but has a higher quality, more intense taste, and lower acidity (less than 1%).
Refined or processed olive oil contains less phytochemicals, as some are lost during processing; it usually contains more than 80% refined oil, plus virgin oil added back to enhance flavor, and may also be labeled “pure” or “light.” However, refined olive oil “still has a good amount of healthy fatty acids but less bioactive compounds,” Dr. Guasch-Ferré noted.
Until now, no large prospective study has examined the link between olive oil intake and all-cause and cause-specific mortality in a U.S. population, where olive oil consumption is limited, compared with Mediterranean countries.
The researchers identified 60,582 women in the Nurses’ Health Study and 31,801 men in the Health Professionals Follow-up Study who were free of CVD or cancer in 1990, the first year that food frequency questionnaires in these studies asked about olive oil.
Participants replied to questionnaires every 4 years that asked about use of olive oil (for salad dressing, baking, frying, sautéing, and spreading on bread), other vegetable oils (for example, corn, safflower, soybean, canola oil), margarine, butter, and dairy fat. The researchers averaged the consumption of these fats during the follow-up years.
From 1990 to 2019, the average consumption of olive oil increased from 1.6 g/day to 4 g/day. Margarine in the 1990s contained saturated fat and trans fats, whereas more recently margarine contains beneficial olive oil or vegetable fat, Dr. Guasch-Ferré noted.
Baseline olive oil consumption in this U.S. population “differed remarkably” from that in the Spanish population in the PREDIMED (Prevención con Dieta Mediterránea) trial, which was, on average, 20-22 g/day of extra-virgin olive oil and 16-18 g/day of refined/mixed olive oil, Larsson pointed out.
Because olive oil consumption was so low in this U.S. study, the researchers did not distinguish between virgin/extra-virgin olive oil and refined/processed olive oil.
The participants were almost all White (99%) and were generally healthier than the average U.S. population; on average, they had a body mass index of 25.3-25.8 kg/m2 and ate 4.8-7.2 fruits and vegetables/day.
Those with the highest olive oil consumption were more physically active, had a healthier diet, were more likely to have Southern European or Mediterranean ancestry, and were less likely to smoke.
During 28 years of follow-up, 36,856 participants died. The researchers classified the deaths into five categories: CVD, cancer, neurodegenerative disease (including Alzheimer’s disease, Parkinson’s disease, multiple sclerosis), respiratory disease (such as chronic obstructive pulmonary disease), and all other causes (including suicide, injury, infections, diabetes, and kidney disease).
After adjusting for multiple confounders, compared with participants who rarely or never consumed olive oil, those in the highest quartile for olive oil consumption had a decreased risk of death from all causes (hazard ratio, 0.81; 95% confidence interval, 0.78 - 0.84) and from CVD (HR, 0.81; 95% CI, 0.75-0.87), cancer (HR, 0.83; 95% CI, 0.78-0.89), neurodegenerative disease (HR, 0.71; 95% CI, 0.64-0.78), and respiratory disease (HR, 0.82; 95% CI, 0.72-0.93).
There was no decrease in mortality in models where the researchers substituted olive oil for vegetable oil, suggesting that vegetable oils may provide similar health benefits as olive oil.
The research was supported by grants from the National Institutes of Health. Dr. Guasch-Ferré was supported by the American Diabetes Association. Coauthor Salas-Salvadó is partially supported by the Catalan Institution for Research and Advanced Studies and received the virgin olive oil that was used in the PREDIMED and PREDIMED-Plus studies from the Patrimonio Communal Olivalero and Hojiblanca (Málaga, Spain). The other study authors and Dr. Larsson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with men and women who rarely or never consumed olive oil (the lowest intake), those who consumed greater than 0.5 tablespoon/day or more than 7 g/day (the highest intake) had a 19% lower mortality risk over a 28-year follow-up, starting from an average age of 56 years.
Moreover, compared with those with the lowest olive oil intake, those with the highest intake had a 19% lower cardiovascular disease (CVD) mortality, a 17% lower risk of dying from cancer, a 29% lower risk of dying from neurodegenerative disease, and an 18% lower risk of dying from respiratory disease during follow-up.
The researchers estimate that replacing 10 g/day of margarine, butter, mayonnaise, or dairy fat with the same amount of olive oil is associated with an 8%-34% lower risk of death from various causes.
The study by Marta Guasch-Ferré, PhD, and colleagues was published online Jan. 10 in the Journal of the American College of Cardiology.
Results support plant-based dietary fat recommendations
“Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity,” the researchers summarize.
However, “I wouldn’t say that olive oil is the only way to help you live longer,” Dr. Guasch-Ferré, a senior research scientist in the department of nutrition, Harvard T.H. Chan School of Public Health, Boston, cautioned in an interview with this news organization.
“Other things are very important, such as not smoking, doing physical activity, etc., but one recommendation could be to try to eat more plant-based food including olive oil and healthy fat,” she added, and to use it for cooking, salad dressing, and baking, and substitute it for saturated fat or animal fat, especially for cooking.
The study suggests that people should “consume a more plant-based diet and prioritize fatty acids such as olive oil because they have a better nutritional composition (high in phenols and antioxidants), instead of using butter or margarines or other animal fats that have been shown to have detrimental effects for health,” she added, which is consistent with recommendations in the Dietary Guidelines for Americans.
“That said,” Dr. Guasch-Ferré summarized, “replication is needed in other cohorts and populations to see if the results are similar.”
In an accompanying editorial, Susanna C. Larsson, PhD, writes that “this was a well-designed study, with long-term follow-up and repeated measurements of dietary intake and other risk factors for diseases.”
“However, the difference in olive oil consumption between those with the highest and those with the lowest/no olive oil consumption was very low (0.5 tablespoon) and a [12%] reduced mortality risk was observed already at a much lower intake (0.5 teaspoon, about 1.5 g/day) of olive oil,” she noted in an email to this news organization.
“It’s a bit hard to believe that such a small amount could have an independent effect on mortality risk,” Dr. Larsson, associate professor of epidemiology at the Karolinska Institutet, Stockholm, cautioned.
Like Dr. Guasch-Ferré, she noted that “just adding one or two teaspoons of olive oil to the diet each day will likely not change the risk of mortality.”
Rather, “people may need to make larger changes in the whole diet, not focus on fat only. An overall healthier diet, rich in nonrefined plant-based foods (vegetables, whole grains, nuts), low/no intake of processed foods, and a switch to healthier fat (eg, olive oil) is needed.”
Importantly, “this study cannot say anything about causality, that is, whether it’s olive oil specifically that reduces mortality risk or if there are many other beneficial factors that act together to reduce mortality rate among those with high olive oil consumption.”
The researchers acknowledge this observational study limitation and that the findings may not be generalizable to other populations.
Novel findings regarding Alzheimer’s and respiratory disease
Dr. Larsson highlights two novel findings of this study.
First, it showed a 27% reduction in risk of dementia-related mortality for those in the highest versus lowest category of olive oil consumption. “Considering the lack of preventive strategies for Alzheimer’s disease and the high morbidity and mortality related to this disease, this finding, if confirmed, is of great public health importance,” she said.
Second, the study reported an inverse association of olive oil consumption with risk of respiratory disease mortality. “Because residual confounding from smoking cannot be ruled out,” Dr. Larsson said, “this finding is tentative and requires confirmation in a study that is less susceptible to confounding, such as a randomized trial.”
And although the current study and previous studies have found that consumption of olive oil may have health benefits, she identified several remaining questions.
“Are the associations causal or spurious?” she noted. Is olive oil consumption protective for certain cardiovascular diseases like stroke or atrial fibrillation only, as has been shown in other studies, or also for other major diseases and causes of death, she added. What is the amount of olive oil required for a protective effect?
Further, is the potential effect related to monounsaturated fatty acids (MUFAs) or phenolic compounds; that is, “is the protective effect confined to polyphenol-rich extra-virgin olive oil or are refined olive oil and other vegetable oils as beneficial? More research is needed to address these questions,” she concludes.
“Further studies are needed,” the researchers agree, “to confirm the association of olive oil consumption with reduced mortality, clarify the mechanisms responsible, and quantify the dose/volume boundaries around this effect.”
Virgin olive oil has more polyphenols
Olive oil, a key component of the Mediterranean diet, is high in MUFAs, especially oleic acid, as well as vitamin E and polyphenols, which contribute to its anti-inflammatory and antioxidant properties, the researchers explain.
Virgin olive oil, produced by mechanically pressing ripe olives, contains multiple bioactive and antioxidant components and has an acidity of less than 1.5%. And extra-virgin olive oil is produced the same way but has a higher quality, more intense taste, and lower acidity (less than 1%).
Refined or processed olive oil contains less phytochemicals, as some are lost during processing; it usually contains more than 80% refined oil, plus virgin oil added back to enhance flavor, and may also be labeled “pure” or “light.” However, refined olive oil “still has a good amount of healthy fatty acids but less bioactive compounds,” Dr. Guasch-Ferré noted.
Until now, no large prospective study has examined the link between olive oil intake and all-cause and cause-specific mortality in a U.S. population, where olive oil consumption is limited, compared with Mediterranean countries.
The researchers identified 60,582 women in the Nurses’ Health Study and 31,801 men in the Health Professionals Follow-up Study who were free of CVD or cancer in 1990, the first year that food frequency questionnaires in these studies asked about olive oil.
Participants replied to questionnaires every 4 years that asked about use of olive oil (for salad dressing, baking, frying, sautéing, and spreading on bread), other vegetable oils (for example, corn, safflower, soybean, canola oil), margarine, butter, and dairy fat. The researchers averaged the consumption of these fats during the follow-up years.
From 1990 to 2019, the average consumption of olive oil increased from 1.6 g/day to 4 g/day. Margarine in the 1990s contained saturated fat and trans fats, whereas more recently margarine contains beneficial olive oil or vegetable fat, Dr. Guasch-Ferré noted.
Baseline olive oil consumption in this U.S. population “differed remarkably” from that in the Spanish population in the PREDIMED (Prevención con Dieta Mediterránea) trial, which was, on average, 20-22 g/day of extra-virgin olive oil and 16-18 g/day of refined/mixed olive oil, Larsson pointed out.
Because olive oil consumption was so low in this U.S. study, the researchers did not distinguish between virgin/extra-virgin olive oil and refined/processed olive oil.
The participants were almost all White (99%) and were generally healthier than the average U.S. population; on average, they had a body mass index of 25.3-25.8 kg/m2 and ate 4.8-7.2 fruits and vegetables/day.
Those with the highest olive oil consumption were more physically active, had a healthier diet, were more likely to have Southern European or Mediterranean ancestry, and were less likely to smoke.
During 28 years of follow-up, 36,856 participants died. The researchers classified the deaths into five categories: CVD, cancer, neurodegenerative disease (including Alzheimer’s disease, Parkinson’s disease, multiple sclerosis), respiratory disease (such as chronic obstructive pulmonary disease), and all other causes (including suicide, injury, infections, diabetes, and kidney disease).
After adjusting for multiple confounders, compared with participants who rarely or never consumed olive oil, those in the highest quartile for olive oil consumption had a decreased risk of death from all causes (hazard ratio, 0.81; 95% confidence interval, 0.78 - 0.84) and from CVD (HR, 0.81; 95% CI, 0.75-0.87), cancer (HR, 0.83; 95% CI, 0.78-0.89), neurodegenerative disease (HR, 0.71; 95% CI, 0.64-0.78), and respiratory disease (HR, 0.82; 95% CI, 0.72-0.93).
There was no decrease in mortality in models where the researchers substituted olive oil for vegetable oil, suggesting that vegetable oils may provide similar health benefits as olive oil.
The research was supported by grants from the National Institutes of Health. Dr. Guasch-Ferré was supported by the American Diabetes Association. Coauthor Salas-Salvadó is partially supported by the Catalan Institution for Research and Advanced Studies and received the virgin olive oil that was used in the PREDIMED and PREDIMED-Plus studies from the Patrimonio Communal Olivalero and Hojiblanca (Málaga, Spain). The other study authors and Dr. Larsson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with men and women who rarely or never consumed olive oil (the lowest intake), those who consumed greater than 0.5 tablespoon/day or more than 7 g/day (the highest intake) had a 19% lower mortality risk over a 28-year follow-up, starting from an average age of 56 years.
Moreover, compared with those with the lowest olive oil intake, those with the highest intake had a 19% lower cardiovascular disease (CVD) mortality, a 17% lower risk of dying from cancer, a 29% lower risk of dying from neurodegenerative disease, and an 18% lower risk of dying from respiratory disease during follow-up.
The researchers estimate that replacing 10 g/day of margarine, butter, mayonnaise, or dairy fat with the same amount of olive oil is associated with an 8%-34% lower risk of death from various causes.
The study by Marta Guasch-Ferré, PhD, and colleagues was published online Jan. 10 in the Journal of the American College of Cardiology.
Results support plant-based dietary fat recommendations
“Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity,” the researchers summarize.
However, “I wouldn’t say that olive oil is the only way to help you live longer,” Dr. Guasch-Ferré, a senior research scientist in the department of nutrition, Harvard T.H. Chan School of Public Health, Boston, cautioned in an interview with this news organization.
“Other things are very important, such as not smoking, doing physical activity, etc., but one recommendation could be to try to eat more plant-based food including olive oil and healthy fat,” she added, and to use it for cooking, salad dressing, and baking, and substitute it for saturated fat or animal fat, especially for cooking.
The study suggests that people should “consume a more plant-based diet and prioritize fatty acids such as olive oil because they have a better nutritional composition (high in phenols and antioxidants), instead of using butter or margarines or other animal fats that have been shown to have detrimental effects for health,” she added, which is consistent with recommendations in the Dietary Guidelines for Americans.
“That said,” Dr. Guasch-Ferré summarized, “replication is needed in other cohorts and populations to see if the results are similar.”
In an accompanying editorial, Susanna C. Larsson, PhD, writes that “this was a well-designed study, with long-term follow-up and repeated measurements of dietary intake and other risk factors for diseases.”
“However, the difference in olive oil consumption between those with the highest and those with the lowest/no olive oil consumption was very low (0.5 tablespoon) and a [12%] reduced mortality risk was observed already at a much lower intake (0.5 teaspoon, about 1.5 g/day) of olive oil,” she noted in an email to this news organization.
“It’s a bit hard to believe that such a small amount could have an independent effect on mortality risk,” Dr. Larsson, associate professor of epidemiology at the Karolinska Institutet, Stockholm, cautioned.
Like Dr. Guasch-Ferré, she noted that “just adding one or two teaspoons of olive oil to the diet each day will likely not change the risk of mortality.”
Rather, “people may need to make larger changes in the whole diet, not focus on fat only. An overall healthier diet, rich in nonrefined plant-based foods (vegetables, whole grains, nuts), low/no intake of processed foods, and a switch to healthier fat (eg, olive oil) is needed.”
Importantly, “this study cannot say anything about causality, that is, whether it’s olive oil specifically that reduces mortality risk or if there are many other beneficial factors that act together to reduce mortality rate among those with high olive oil consumption.”
The researchers acknowledge this observational study limitation and that the findings may not be generalizable to other populations.
Novel findings regarding Alzheimer’s and respiratory disease
Dr. Larsson highlights two novel findings of this study.
First, it showed a 27% reduction in risk of dementia-related mortality for those in the highest versus lowest category of olive oil consumption. “Considering the lack of preventive strategies for Alzheimer’s disease and the high morbidity and mortality related to this disease, this finding, if confirmed, is of great public health importance,” she said.
Second, the study reported an inverse association of olive oil consumption with risk of respiratory disease mortality. “Because residual confounding from smoking cannot be ruled out,” Dr. Larsson said, “this finding is tentative and requires confirmation in a study that is less susceptible to confounding, such as a randomized trial.”
And although the current study and previous studies have found that consumption of olive oil may have health benefits, she identified several remaining questions.
“Are the associations causal or spurious?” she noted. Is olive oil consumption protective for certain cardiovascular diseases like stroke or atrial fibrillation only, as has been shown in other studies, or also for other major diseases and causes of death, she added. What is the amount of olive oil required for a protective effect?
Further, is the potential effect related to monounsaturated fatty acids (MUFAs) or phenolic compounds; that is, “is the protective effect confined to polyphenol-rich extra-virgin olive oil or are refined olive oil and other vegetable oils as beneficial? More research is needed to address these questions,” she concludes.
“Further studies are needed,” the researchers agree, “to confirm the association of olive oil consumption with reduced mortality, clarify the mechanisms responsible, and quantify the dose/volume boundaries around this effect.”
Virgin olive oil has more polyphenols
Olive oil, a key component of the Mediterranean diet, is high in MUFAs, especially oleic acid, as well as vitamin E and polyphenols, which contribute to its anti-inflammatory and antioxidant properties, the researchers explain.
Virgin olive oil, produced by mechanically pressing ripe olives, contains multiple bioactive and antioxidant components and has an acidity of less than 1.5%. And extra-virgin olive oil is produced the same way but has a higher quality, more intense taste, and lower acidity (less than 1%).
Refined or processed olive oil contains less phytochemicals, as some are lost during processing; it usually contains more than 80% refined oil, plus virgin oil added back to enhance flavor, and may also be labeled “pure” or “light.” However, refined olive oil “still has a good amount of healthy fatty acids but less bioactive compounds,” Dr. Guasch-Ferré noted.
Until now, no large prospective study has examined the link between olive oil intake and all-cause and cause-specific mortality in a U.S. population, where olive oil consumption is limited, compared with Mediterranean countries.
The researchers identified 60,582 women in the Nurses’ Health Study and 31,801 men in the Health Professionals Follow-up Study who were free of CVD or cancer in 1990, the first year that food frequency questionnaires in these studies asked about olive oil.
Participants replied to questionnaires every 4 years that asked about use of olive oil (for salad dressing, baking, frying, sautéing, and spreading on bread), other vegetable oils (for example, corn, safflower, soybean, canola oil), margarine, butter, and dairy fat. The researchers averaged the consumption of these fats during the follow-up years.
From 1990 to 2019, the average consumption of olive oil increased from 1.6 g/day to 4 g/day. Margarine in the 1990s contained saturated fat and trans fats, whereas more recently margarine contains beneficial olive oil or vegetable fat, Dr. Guasch-Ferré noted.
Baseline olive oil consumption in this U.S. population “differed remarkably” from that in the Spanish population in the PREDIMED (Prevención con Dieta Mediterránea) trial, which was, on average, 20-22 g/day of extra-virgin olive oil and 16-18 g/day of refined/mixed olive oil, Larsson pointed out.
Because olive oil consumption was so low in this U.S. study, the researchers did not distinguish between virgin/extra-virgin olive oil and refined/processed olive oil.
The participants were almost all White (99%) and were generally healthier than the average U.S. population; on average, they had a body mass index of 25.3-25.8 kg/m2 and ate 4.8-7.2 fruits and vegetables/day.
Those with the highest olive oil consumption were more physically active, had a healthier diet, were more likely to have Southern European or Mediterranean ancestry, and were less likely to smoke.
During 28 years of follow-up, 36,856 participants died. The researchers classified the deaths into five categories: CVD, cancer, neurodegenerative disease (including Alzheimer’s disease, Parkinson’s disease, multiple sclerosis), respiratory disease (such as chronic obstructive pulmonary disease), and all other causes (including suicide, injury, infections, diabetes, and kidney disease).
After adjusting for multiple confounders, compared with participants who rarely or never consumed olive oil, those in the highest quartile for olive oil consumption had a decreased risk of death from all causes (hazard ratio, 0.81; 95% confidence interval, 0.78 - 0.84) and from CVD (HR, 0.81; 95% CI, 0.75-0.87), cancer (HR, 0.83; 95% CI, 0.78-0.89), neurodegenerative disease (HR, 0.71; 95% CI, 0.64-0.78), and respiratory disease (HR, 0.82; 95% CI, 0.72-0.93).
There was no decrease in mortality in models where the researchers substituted olive oil for vegetable oil, suggesting that vegetable oils may provide similar health benefits as olive oil.
The research was supported by grants from the National Institutes of Health. Dr. Guasch-Ferré was supported by the American Diabetes Association. Coauthor Salas-Salvadó is partially supported by the Catalan Institution for Research and Advanced Studies and received the virgin olive oil that was used in the PREDIMED and PREDIMED-Plus studies from the Patrimonio Communal Olivalero and Hojiblanca (Málaga, Spain). The other study authors and Dr. Larsson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AGA News - February 2022
Registration now open: Gut Microbiota for Health World Summit 2022
Registration is now open for the Gut Microbiota for Health (GMFH) World Summit 2022, taking place March 12-13 in Washington, D.C., and virtually.
Organized by AGA and the European Society of Neurogastroenterology and Motility (ESNM), the GMFH World Summit is the preeminent international meeting on the gut microbiome for clinicians, dietitians, and researchers.
Now in its tenth year, this year’s program will focus on “The Gut Microbiome in Precision Nutrition and Medicine.” Join us to gain a deeper understanding of the role of the gut microbiome in precision medicine and discover personalized approaches to modulating the gut microbiome that may promote health and improve patient outcomes for a variety of disorders and diseases.
https://www.gutmicrobiotaforhealth.com/summit
See Gastroenterology’s curated Equity in GI journal collection
Gastroenterology is proud to announce the release of a special collection of articles focused on the intersection of diversity, equity, and inclusion (DEI) and gastroenterology and hepatology. This curated collection, under the guidance of the journal’s new DEI section editor Dr. Chyke Doubeni, includes original research, reviews, commentaries and editorials on matters of health disparities, socioeconomic determinants of health outcomes, and population-based studies on disease incidence among races and ethnicities, among other topics. New articles are added to the collection as they are published.
View the special collection on Gastroenterology’s website, which is designed to help you quickly and easily look over the latest DEI articles and content of interest. Recent articles include:
- How to incorporate health equity training into GI/hepatology fellowships by Jannel Lee-Allen and Brijen J. Shah
- Disparities in preventable mortality from colorectal cancer: are they the result of structural racism? By Chyke A. Doubeni, Kevin Selby and Theodore R. Levin
- COVID-19 pediatric patients: GI symptoms, presentations and disparities by race/ethnicity in a large, multicenter U.S. study by Yusuf Ashktorab, Anas Brim, Antonio Pizuorno, Vijay Gayam, Sahar Nikdel and Hassan Brim
View all of Gastroenterology’s curated article collections.
Registration now open: Gut Microbiota for Health World Summit 2022
Registration is now open for the Gut Microbiota for Health (GMFH) World Summit 2022, taking place March 12-13 in Washington, D.C., and virtually.
Organized by AGA and the European Society of Neurogastroenterology and Motility (ESNM), the GMFH World Summit is the preeminent international meeting on the gut microbiome for clinicians, dietitians, and researchers.
Now in its tenth year, this year’s program will focus on “The Gut Microbiome in Precision Nutrition and Medicine.” Join us to gain a deeper understanding of the role of the gut microbiome in precision medicine and discover personalized approaches to modulating the gut microbiome that may promote health and improve patient outcomes for a variety of disorders and diseases.
https://www.gutmicrobiotaforhealth.com/summit
See Gastroenterology’s curated Equity in GI journal collection
Gastroenterology is proud to announce the release of a special collection of articles focused on the intersection of diversity, equity, and inclusion (DEI) and gastroenterology and hepatology. This curated collection, under the guidance of the journal’s new DEI section editor Dr. Chyke Doubeni, includes original research, reviews, commentaries and editorials on matters of health disparities, socioeconomic determinants of health outcomes, and population-based studies on disease incidence among races and ethnicities, among other topics. New articles are added to the collection as they are published.
View the special collection on Gastroenterology’s website, which is designed to help you quickly and easily look over the latest DEI articles and content of interest. Recent articles include:
- How to incorporate health equity training into GI/hepatology fellowships by Jannel Lee-Allen and Brijen J. Shah
- Disparities in preventable mortality from colorectal cancer: are they the result of structural racism? By Chyke A. Doubeni, Kevin Selby and Theodore R. Levin
- COVID-19 pediatric patients: GI symptoms, presentations and disparities by race/ethnicity in a large, multicenter U.S. study by Yusuf Ashktorab, Anas Brim, Antonio Pizuorno, Vijay Gayam, Sahar Nikdel and Hassan Brim
View all of Gastroenterology’s curated article collections.
Registration now open: Gut Microbiota for Health World Summit 2022
Registration is now open for the Gut Microbiota for Health (GMFH) World Summit 2022, taking place March 12-13 in Washington, D.C., and virtually.
Organized by AGA and the European Society of Neurogastroenterology and Motility (ESNM), the GMFH World Summit is the preeminent international meeting on the gut microbiome for clinicians, dietitians, and researchers.
Now in its tenth year, this year’s program will focus on “The Gut Microbiome in Precision Nutrition and Medicine.” Join us to gain a deeper understanding of the role of the gut microbiome in precision medicine and discover personalized approaches to modulating the gut microbiome that may promote health and improve patient outcomes for a variety of disorders and diseases.
https://www.gutmicrobiotaforhealth.com/summit
See Gastroenterology’s curated Equity in GI journal collection
Gastroenterology is proud to announce the release of a special collection of articles focused on the intersection of diversity, equity, and inclusion (DEI) and gastroenterology and hepatology. This curated collection, under the guidance of the journal’s new DEI section editor Dr. Chyke Doubeni, includes original research, reviews, commentaries and editorials on matters of health disparities, socioeconomic determinants of health outcomes, and population-based studies on disease incidence among races and ethnicities, among other topics. New articles are added to the collection as they are published.
View the special collection on Gastroenterology’s website, which is designed to help you quickly and easily look over the latest DEI articles and content of interest. Recent articles include:
- How to incorporate health equity training into GI/hepatology fellowships by Jannel Lee-Allen and Brijen J. Shah
- Disparities in preventable mortality from colorectal cancer: are they the result of structural racism? By Chyke A. Doubeni, Kevin Selby and Theodore R. Levin
- COVID-19 pediatric patients: GI symptoms, presentations and disparities by race/ethnicity in a large, multicenter U.S. study by Yusuf Ashktorab, Anas Brim, Antonio Pizuorno, Vijay Gayam, Sahar Nikdel and Hassan Brim
View all of Gastroenterology’s curated article collections.
February 2022 – ICYMI
Gastroenterology
November 2021
How to navigate national societal organizations for leadership development and academic promotion: A guide for trainees and young faculty
Aby ES et al. Gastroenterology. 2021 Nov;161(5):1361-1365. doi: 10.1053/j.gastro.2021.08.044.
Value of pH impedance monitoring while on twice-daily proton pump inhibitor therapy to identify need for escalation of reflux management
Gyawali CG et al. Gastroenterology. 2021 Nov;161(5):1412-1422. doi: 10.1053/j.gastro.2021.07.004.
The sulfur microbial diet is associated with increased risk of early-onset colorectal cancer precursors
Nguyen LH et al. Gastroenterology. 2021 Nov;161(5):1423-1432.e4. doi: 10.1053/j.gastro.2021.07.008.
Underwater vs conventional endoscopic mucosal resection of large sessile or flat colorectal polyps: A prospective randomized controlled trial
Nagl S et al. Gastroenterology. 2021 Nov;161(5):1460-1474.e1. doi: 10.1053/j.gastro.2021.07.044.
December 2021
How to approach long-term enteral and parenteral nutrition
Hadefi A, Arvanitakis M. Gastroenterology. 2021 Dec;161(6):1780-1786. doi: 10.1053/j.gastro.2021.09.030.
Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: Pooled analysis of 3 prospective cohorts
Xia B et al. Gastroenterology. 2021 Dec;161(6):1842-1852.e10. doi: 10.1053/j.gastro.2021.08.005.
January 2022
Serologic response to Coronavirus Disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: A systematic review and meta-analysis
Sakuraba A et al. Gastroenterology. 2022 Jan;162(1):88-108.e9. doi: 10.1053/j.gastro.2021.09.055.
Advancing diversity, equity, and inclusion in scientific publishing
Doubeni CA et al. Gastroenterology. 2022 Jan;162(1):59-62.e1. doi: 10.1053/j.gastro.2021.10.043.
How we approach difficult to eradicate Helicobacter pylori
Argueta EA, Moss SF. Gastroenterology. 2022 Jan;162(1):32-37. doi: 10.1053/j.gastro.2021.10.048.
Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis
Iannuzzi JP et al. Gastroenterology. 2022 Jan;162(1):122-134. doi: 10.1053/j.gastro.2021.09.043.
Epidemiology, etiology, and treatment of gastroparesis: Real-world evidence from a large US national claims database
Ye Y et al. Gastroenterology. 2022 Jan;162(1):109-121.e5. doi: 10.1053/j.gastro.2021.09.064.
Clinical Gastroenterology and Hepatology
November 2021
AGA Clinical Practice Update on endoscopic management of perforations in gastrointestinal tract: Expert Review
Lee JH et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2252-2261.e2. doi: 10.1016/j.cgh.2021.06.045.
Food allergies and intolerances: A clinical approach to the diagnosis and management of adverse reactions to food
Onyimba F et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2230-2240.e1. doi: 10.1016/j.cgh.2021.01.025.
Management of gastrointestinal side effects of immune checkpoint inhibitors
Lui RN et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2262-2265. doi: 10.1016/j.cgh.2021.06.038.
December 2021
Optimizing the endoscopic examination in eosinophilic esophagitis
Dellon ES. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2489-2492.e1. doi: 10.1016/j.cgh.2021.07.011.
Diagnostic accuracy of fecal calprotectin concentration in evaluating therapeutic outcomes of patients with ulcerative colitis
Stevens TW et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2333-2342. doi: 10.1016/j.cgh.2020.08.019.
Factors associated with inpatient endoscopy delay and its impact on hospital length-of-stay and 30-day readmission
Jacobs CC et al. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2648-2655. doi: 10.1016/j.cgh.2021.06.009.
January 2022
Comparing costs and outcomes of treatments for irritable bowel syndrome with diarrhea: Cost-benefit analysis
Shah ED et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):136-144.e31. doi: 10.1016/j.cgh.2020.09.043.
Next generation academic gastroenterology
Allen JI, Berry S. Clin Gastroenterol Hepatol. 2022 Jan;20(1):5-8. doi: 10.1016/j.cgh.2021.09.038.
Beyond metoclopramide for gastroparesis
Camilleri M. Clin Gastroenterol Hepatol. 2022 Jan;20(1):19-24. doi: 10.1016/j.cgh.2021.08.052.
Comparative safety and effectiveness of vedolizumab to tumor necrosis factor antagonist therapy for ulcerative colitis
Lukin D et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):126-135. doi: 10.1016/j.cgh.2020.10.003.
Techniques and Innovations in Gastrointestinal Endoscopy
Impact of the COVID-19 pandemic on utilization of EGD and colonoscopy in the United States: An analysis of the GIQuIC registry
Calderwood AH et al. Tech Innov Gastrointest Endosc. 2021;23(4):313-321. doi: 10.1016/j.tige.2021.07.003.
How to approach small polyps in colon: Tips and tricks
Mahmood S et al. Tech Inov Gastroinest Endosc. 2021;23(4):238-335. doi: 10.1016/j.tige.2021.06.007
Gastroenterology
November 2021
How to navigate national societal organizations for leadership development and academic promotion: A guide for trainees and young faculty
Aby ES et al. Gastroenterology. 2021 Nov;161(5):1361-1365. doi: 10.1053/j.gastro.2021.08.044.
Value of pH impedance monitoring while on twice-daily proton pump inhibitor therapy to identify need for escalation of reflux management
Gyawali CG et al. Gastroenterology. 2021 Nov;161(5):1412-1422. doi: 10.1053/j.gastro.2021.07.004.
The sulfur microbial diet is associated with increased risk of early-onset colorectal cancer precursors
Nguyen LH et al. Gastroenterology. 2021 Nov;161(5):1423-1432.e4. doi: 10.1053/j.gastro.2021.07.008.
Underwater vs conventional endoscopic mucosal resection of large sessile or flat colorectal polyps: A prospective randomized controlled trial
Nagl S et al. Gastroenterology. 2021 Nov;161(5):1460-1474.e1. doi: 10.1053/j.gastro.2021.07.044.
December 2021
How to approach long-term enteral and parenteral nutrition
Hadefi A, Arvanitakis M. Gastroenterology. 2021 Dec;161(6):1780-1786. doi: 10.1053/j.gastro.2021.09.030.
Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: Pooled analysis of 3 prospective cohorts
Xia B et al. Gastroenterology. 2021 Dec;161(6):1842-1852.e10. doi: 10.1053/j.gastro.2021.08.005.
January 2022
Serologic response to Coronavirus Disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: A systematic review and meta-analysis
Sakuraba A et al. Gastroenterology. 2022 Jan;162(1):88-108.e9. doi: 10.1053/j.gastro.2021.09.055.
Advancing diversity, equity, and inclusion in scientific publishing
Doubeni CA et al. Gastroenterology. 2022 Jan;162(1):59-62.e1. doi: 10.1053/j.gastro.2021.10.043.
How we approach difficult to eradicate Helicobacter pylori
Argueta EA, Moss SF. Gastroenterology. 2022 Jan;162(1):32-37. doi: 10.1053/j.gastro.2021.10.048.
Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis
Iannuzzi JP et al. Gastroenterology. 2022 Jan;162(1):122-134. doi: 10.1053/j.gastro.2021.09.043.
Epidemiology, etiology, and treatment of gastroparesis: Real-world evidence from a large US national claims database
Ye Y et al. Gastroenterology. 2022 Jan;162(1):109-121.e5. doi: 10.1053/j.gastro.2021.09.064.
Clinical Gastroenterology and Hepatology
November 2021
AGA Clinical Practice Update on endoscopic management of perforations in gastrointestinal tract: Expert Review
Lee JH et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2252-2261.e2. doi: 10.1016/j.cgh.2021.06.045.
Food allergies and intolerances: A clinical approach to the diagnosis and management of adverse reactions to food
Onyimba F et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2230-2240.e1. doi: 10.1016/j.cgh.2021.01.025.
Management of gastrointestinal side effects of immune checkpoint inhibitors
Lui RN et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2262-2265. doi: 10.1016/j.cgh.2021.06.038.
December 2021
Optimizing the endoscopic examination in eosinophilic esophagitis
Dellon ES. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2489-2492.e1. doi: 10.1016/j.cgh.2021.07.011.
Diagnostic accuracy of fecal calprotectin concentration in evaluating therapeutic outcomes of patients with ulcerative colitis
Stevens TW et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2333-2342. doi: 10.1016/j.cgh.2020.08.019.
Factors associated with inpatient endoscopy delay and its impact on hospital length-of-stay and 30-day readmission
Jacobs CC et al. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2648-2655. doi: 10.1016/j.cgh.2021.06.009.
January 2022
Comparing costs and outcomes of treatments for irritable bowel syndrome with diarrhea: Cost-benefit analysis
Shah ED et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):136-144.e31. doi: 10.1016/j.cgh.2020.09.043.
Next generation academic gastroenterology
Allen JI, Berry S. Clin Gastroenterol Hepatol. 2022 Jan;20(1):5-8. doi: 10.1016/j.cgh.2021.09.038.
Beyond metoclopramide for gastroparesis
Camilleri M. Clin Gastroenterol Hepatol. 2022 Jan;20(1):19-24. doi: 10.1016/j.cgh.2021.08.052.
Comparative safety and effectiveness of vedolizumab to tumor necrosis factor antagonist therapy for ulcerative colitis
Lukin D et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):126-135. doi: 10.1016/j.cgh.2020.10.003.
Techniques and Innovations in Gastrointestinal Endoscopy
Impact of the COVID-19 pandemic on utilization of EGD and colonoscopy in the United States: An analysis of the GIQuIC registry
Calderwood AH et al. Tech Innov Gastrointest Endosc. 2021;23(4):313-321. doi: 10.1016/j.tige.2021.07.003.
How to approach small polyps in colon: Tips and tricks
Mahmood S et al. Tech Inov Gastroinest Endosc. 2021;23(4):238-335. doi: 10.1016/j.tige.2021.06.007
Gastroenterology
November 2021
How to navigate national societal organizations for leadership development and academic promotion: A guide for trainees and young faculty
Aby ES et al. Gastroenterology. 2021 Nov;161(5):1361-1365. doi: 10.1053/j.gastro.2021.08.044.
Value of pH impedance monitoring while on twice-daily proton pump inhibitor therapy to identify need for escalation of reflux management
Gyawali CG et al. Gastroenterology. 2021 Nov;161(5):1412-1422. doi: 10.1053/j.gastro.2021.07.004.
The sulfur microbial diet is associated with increased risk of early-onset colorectal cancer precursors
Nguyen LH et al. Gastroenterology. 2021 Nov;161(5):1423-1432.e4. doi: 10.1053/j.gastro.2021.07.008.
Underwater vs conventional endoscopic mucosal resection of large sessile or flat colorectal polyps: A prospective randomized controlled trial
Nagl S et al. Gastroenterology. 2021 Nov;161(5):1460-1474.e1. doi: 10.1053/j.gastro.2021.07.044.
December 2021
How to approach long-term enteral and parenteral nutrition
Hadefi A, Arvanitakis M. Gastroenterology. 2021 Dec;161(6):1780-1786. doi: 10.1053/j.gastro.2021.09.030.
Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: Pooled analysis of 3 prospective cohorts
Xia B et al. Gastroenterology. 2021 Dec;161(6):1842-1852.e10. doi: 10.1053/j.gastro.2021.08.005.
January 2022
Serologic response to Coronavirus Disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: A systematic review and meta-analysis
Sakuraba A et al. Gastroenterology. 2022 Jan;162(1):88-108.e9. doi: 10.1053/j.gastro.2021.09.055.
Advancing diversity, equity, and inclusion in scientific publishing
Doubeni CA et al. Gastroenterology. 2022 Jan;162(1):59-62.e1. doi: 10.1053/j.gastro.2021.10.043.
How we approach difficult to eradicate Helicobacter pylori
Argueta EA, Moss SF. Gastroenterology. 2022 Jan;162(1):32-37. doi: 10.1053/j.gastro.2021.10.048.
Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis
Iannuzzi JP et al. Gastroenterology. 2022 Jan;162(1):122-134. doi: 10.1053/j.gastro.2021.09.043.
Epidemiology, etiology, and treatment of gastroparesis: Real-world evidence from a large US national claims database
Ye Y et al. Gastroenterology. 2022 Jan;162(1):109-121.e5. doi: 10.1053/j.gastro.2021.09.064.
Clinical Gastroenterology and Hepatology
November 2021
AGA Clinical Practice Update on endoscopic management of perforations in gastrointestinal tract: Expert Review
Lee JH et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2252-2261.e2. doi: 10.1016/j.cgh.2021.06.045.
Food allergies and intolerances: A clinical approach to the diagnosis and management of adverse reactions to food
Onyimba F et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2230-2240.e1. doi: 10.1016/j.cgh.2021.01.025.
Management of gastrointestinal side effects of immune checkpoint inhibitors
Lui RN et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2262-2265. doi: 10.1016/j.cgh.2021.06.038.
December 2021
Optimizing the endoscopic examination in eosinophilic esophagitis
Dellon ES. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2489-2492.e1. doi: 10.1016/j.cgh.2021.07.011.
Diagnostic accuracy of fecal calprotectin concentration in evaluating therapeutic outcomes of patients with ulcerative colitis
Stevens TW et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2333-2342. doi: 10.1016/j.cgh.2020.08.019.
Factors associated with inpatient endoscopy delay and its impact on hospital length-of-stay and 30-day readmission
Jacobs CC et al. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2648-2655. doi: 10.1016/j.cgh.2021.06.009.
January 2022
Comparing costs and outcomes of treatments for irritable bowel syndrome with diarrhea: Cost-benefit analysis
Shah ED et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):136-144.e31. doi: 10.1016/j.cgh.2020.09.043.
Next generation academic gastroenterology
Allen JI, Berry S. Clin Gastroenterol Hepatol. 2022 Jan;20(1):5-8. doi: 10.1016/j.cgh.2021.09.038.
Beyond metoclopramide for gastroparesis
Camilleri M. Clin Gastroenterol Hepatol. 2022 Jan;20(1):19-24. doi: 10.1016/j.cgh.2021.08.052.
Comparative safety and effectiveness of vedolizumab to tumor necrosis factor antagonist therapy for ulcerative colitis
Lukin D et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):126-135. doi: 10.1016/j.cgh.2020.10.003.
Techniques and Innovations in Gastrointestinal Endoscopy
Impact of the COVID-19 pandemic on utilization of EGD and colonoscopy in the United States: An analysis of the GIQuIC registry
Calderwood AH et al. Tech Innov Gastrointest Endosc. 2021;23(4):313-321. doi: 10.1016/j.tige.2021.07.003.
How to approach small polyps in colon: Tips and tricks
Mahmood S et al. Tech Inov Gastroinest Endosc. 2021;23(4):238-335. doi: 10.1016/j.tige.2021.06.007
Pig heart successfully transplanted to man
A genetically modified pig heart has been successfully transplanted into a 57-year-old man who had no other treatment options but is “doing well” 3 days after the procedure, officials at the University of Maryland Medical Center (UMMC), Baltimore, announced Jan. 10.
“This organ transplant demonstrated for the first time that a genetically modified animal heart can function like a human heart without immediate rejection by the body,” they said.
Three genes associated with antibody-mediated rejection had been knocked out in the pig supplying the transplanted heart, and six human genes associated with immune acceptance of the organ had been inserted into the pig’s genome, notes a UMMC press release.
“Lastly, one additional gene in the pig was knocked out to prevent excessive growth of the pig heart tissue, which totaled 10 unique gene edits made in the donor pig,” the release states.
The patient, Maryland resident David Bennett, had required mechanical circulatory support to stay alive but was rejected for standard heart transplantation at UMMC and other centers. He was ineligible for an implanted ventricular assist device due to ventricular arrhythmias.
Mr. Bennett “is being carefully monitored over the next days and weeks to determine whether the transplant provides lifesaving benefits,” the announcement says.
“We are proceeding cautiously, but we are also optimistic that this first-in-the-world surgery will provide an important new option for patients in the future,” notes a quote from Bartley P. Griffith, MD, the UMMC surgeon who performed the procedure.
The pig supplying the heart was provided to the center by Revivicor (Blacksburg, Virginia), a regenerative medicine company. An experimental antirejection medication (Kiniksa Pharmaceuticals; Lexington, Massachusetts) was also used, in addition to standard immunosuppressants.
A version of this article first appeared on Medscape.com.
A genetically modified pig heart has been successfully transplanted into a 57-year-old man who had no other treatment options but is “doing well” 3 days after the procedure, officials at the University of Maryland Medical Center (UMMC), Baltimore, announced Jan. 10.
“This organ transplant demonstrated for the first time that a genetically modified animal heart can function like a human heart without immediate rejection by the body,” they said.
Three genes associated with antibody-mediated rejection had been knocked out in the pig supplying the transplanted heart, and six human genes associated with immune acceptance of the organ had been inserted into the pig’s genome, notes a UMMC press release.
“Lastly, one additional gene in the pig was knocked out to prevent excessive growth of the pig heart tissue, which totaled 10 unique gene edits made in the donor pig,” the release states.
The patient, Maryland resident David Bennett, had required mechanical circulatory support to stay alive but was rejected for standard heart transplantation at UMMC and other centers. He was ineligible for an implanted ventricular assist device due to ventricular arrhythmias.
Mr. Bennett “is being carefully monitored over the next days and weeks to determine whether the transplant provides lifesaving benefits,” the announcement says.
“We are proceeding cautiously, but we are also optimistic that this first-in-the-world surgery will provide an important new option for patients in the future,” notes a quote from Bartley P. Griffith, MD, the UMMC surgeon who performed the procedure.
The pig supplying the heart was provided to the center by Revivicor (Blacksburg, Virginia), a regenerative medicine company. An experimental antirejection medication (Kiniksa Pharmaceuticals; Lexington, Massachusetts) was also used, in addition to standard immunosuppressants.
A version of this article first appeared on Medscape.com.
A genetically modified pig heart has been successfully transplanted into a 57-year-old man who had no other treatment options but is “doing well” 3 days after the procedure, officials at the University of Maryland Medical Center (UMMC), Baltimore, announced Jan. 10.
“This organ transplant demonstrated for the first time that a genetically modified animal heart can function like a human heart without immediate rejection by the body,” they said.
Three genes associated with antibody-mediated rejection had been knocked out in the pig supplying the transplanted heart, and six human genes associated with immune acceptance of the organ had been inserted into the pig’s genome, notes a UMMC press release.
“Lastly, one additional gene in the pig was knocked out to prevent excessive growth of the pig heart tissue, which totaled 10 unique gene edits made in the donor pig,” the release states.
The patient, Maryland resident David Bennett, had required mechanical circulatory support to stay alive but was rejected for standard heart transplantation at UMMC and other centers. He was ineligible for an implanted ventricular assist device due to ventricular arrhythmias.
Mr. Bennett “is being carefully monitored over the next days and weeks to determine whether the transplant provides lifesaving benefits,” the announcement says.
“We are proceeding cautiously, but we are also optimistic that this first-in-the-world surgery will provide an important new option for patients in the future,” notes a quote from Bartley P. Griffith, MD, the UMMC surgeon who performed the procedure.
The pig supplying the heart was provided to the center by Revivicor (Blacksburg, Virginia), a regenerative medicine company. An experimental antirejection medication (Kiniksa Pharmaceuticals; Lexington, Massachusetts) was also used, in addition to standard immunosuppressants.
A version of this article first appeared on Medscape.com.