User login
Pneumonia in infancy predicts respiratory problems in early childhood
Preschoolers who experienced community-acquired pneumonia in infancy were significantly more likely than were those with no history of pneumonia to develop chronic respiratory disorders, based on data from approximately 7,000 individuals.
“Lower respiratory tract infections (LRTI) during the first years of life cause injury to the rapidly developing lung at its most critical stage,” wrote Rotem Lapidot, MD, of Boston University, and colleagues. Previous research has linked pneumonia with subsequent chronic cough, bronchitis, and recurrent pneumonia in children, but data are needed to assess the impact of early community-acquired pneumonia (CAP) on respiratory health in otherwise healthy infants, the researchers said.
In a retrospective matched cohort study published in Respiratory Medicine , the researchers identified 1,343 infants who had CAP in the first 2 years of life, and 6,715 controls, using a large electronic health records dataset (Optum EHR dataset) for the period from Jan. 2011 through June 2018.
The primary outcomes were the development of any chronic respiratory disorders, reactive airway disease, and CAP hospitalizations between ages 2 and 5 years. Infants in the CAP group were otherwise healthy; those with congenital or other conditions that might predispose them to pneumonia were excluded. Baseline characteristics were similar between the CAP patients and controls.
Future risk
Overall, the rates per 100 patient-years for any chronic respiratory disorder were 11.6 for CAP patients versus 4.9 for controls (relative risk, 2.4). Rates for reactive airway disease and CAP hospitalization were 6.1 versus 1.9 per 100 patient-years (RR, 3.2) and 1.0 versus 0.2 per 100 patient-years (RR, 6.3) for the CAP patients and controls, respectively.
The distribution of CAP etiology of CAP in infants at the first hospitalization was 20% bacterial, 27% viral, and 53% unspecified. The relative rates of later respiratory illness were similar across etiologies of the initial hospitalization for CAP, which support the association between infant CAP and later respiratory disease, the researchers said.
Nearly all (97%) of the CAP patients had only one qualifying hospitalization for CAP before 2 years of age, and the mean age at the first hospitalization was 8.9 months. “Rates and relative rates of any chronic respiratory disorder, and our composite for reactive airway disease, increased with age at which the initial CAP hospitalization occurred,” and were highest for children hospitalized at close to 2 years of age, the researchers noted.
Persistent inflammation?
“Our findings add to the evolving hypothesis that persistent inflammation following pneumonia creates an increased risk for subsequent respiratory disease and exacerbations of underlying disease,” the researchers wrote.
The study findings were limited by several factors, including the potential for misclassification of some infants with and without underlying conditions, reliance on discharge information for etiology, and possible lack of generalizability to other populations, the researchers noted.
However, the results indicate an increased risk for respiratory illness in early childhood among infants with CAP, and support the need for greater attention to CAP prevention and for strategies to reduce inflammation after pneumonia, they said. “Further study is needed to confirm the long-term consequences of infant CAP and the underlying mechanisms that lead to such long-term sequelae,” they concluded.
Dr. Lapidot and several coauthors disclosed ties with Pfizer, the study sponsor.
A version of this article first appeared on Medscape.com.
Preschoolers who experienced community-acquired pneumonia in infancy were significantly more likely than were those with no history of pneumonia to develop chronic respiratory disorders, based on data from approximately 7,000 individuals.
“Lower respiratory tract infections (LRTI) during the first years of life cause injury to the rapidly developing lung at its most critical stage,” wrote Rotem Lapidot, MD, of Boston University, and colleagues. Previous research has linked pneumonia with subsequent chronic cough, bronchitis, and recurrent pneumonia in children, but data are needed to assess the impact of early community-acquired pneumonia (CAP) on respiratory health in otherwise healthy infants, the researchers said.
In a retrospective matched cohort study published in Respiratory Medicine , the researchers identified 1,343 infants who had CAP in the first 2 years of life, and 6,715 controls, using a large electronic health records dataset (Optum EHR dataset) for the period from Jan. 2011 through June 2018.
The primary outcomes were the development of any chronic respiratory disorders, reactive airway disease, and CAP hospitalizations between ages 2 and 5 years. Infants in the CAP group were otherwise healthy; those with congenital or other conditions that might predispose them to pneumonia were excluded. Baseline characteristics were similar between the CAP patients and controls.
Future risk
Overall, the rates per 100 patient-years for any chronic respiratory disorder were 11.6 for CAP patients versus 4.9 for controls (relative risk, 2.4). Rates for reactive airway disease and CAP hospitalization were 6.1 versus 1.9 per 100 patient-years (RR, 3.2) and 1.0 versus 0.2 per 100 patient-years (RR, 6.3) for the CAP patients and controls, respectively.
The distribution of CAP etiology of CAP in infants at the first hospitalization was 20% bacterial, 27% viral, and 53% unspecified. The relative rates of later respiratory illness were similar across etiologies of the initial hospitalization for CAP, which support the association between infant CAP and later respiratory disease, the researchers said.
Nearly all (97%) of the CAP patients had only one qualifying hospitalization for CAP before 2 years of age, and the mean age at the first hospitalization was 8.9 months. “Rates and relative rates of any chronic respiratory disorder, and our composite for reactive airway disease, increased with age at which the initial CAP hospitalization occurred,” and were highest for children hospitalized at close to 2 years of age, the researchers noted.
Persistent inflammation?
“Our findings add to the evolving hypothesis that persistent inflammation following pneumonia creates an increased risk for subsequent respiratory disease and exacerbations of underlying disease,” the researchers wrote.
The study findings were limited by several factors, including the potential for misclassification of some infants with and without underlying conditions, reliance on discharge information for etiology, and possible lack of generalizability to other populations, the researchers noted.
However, the results indicate an increased risk for respiratory illness in early childhood among infants with CAP, and support the need for greater attention to CAP prevention and for strategies to reduce inflammation after pneumonia, they said. “Further study is needed to confirm the long-term consequences of infant CAP and the underlying mechanisms that lead to such long-term sequelae,” they concluded.
Dr. Lapidot and several coauthors disclosed ties with Pfizer, the study sponsor.
A version of this article first appeared on Medscape.com.
Preschoolers who experienced community-acquired pneumonia in infancy were significantly more likely than were those with no history of pneumonia to develop chronic respiratory disorders, based on data from approximately 7,000 individuals.
“Lower respiratory tract infections (LRTI) during the first years of life cause injury to the rapidly developing lung at its most critical stage,” wrote Rotem Lapidot, MD, of Boston University, and colleagues. Previous research has linked pneumonia with subsequent chronic cough, bronchitis, and recurrent pneumonia in children, but data are needed to assess the impact of early community-acquired pneumonia (CAP) on respiratory health in otherwise healthy infants, the researchers said.
In a retrospective matched cohort study published in Respiratory Medicine , the researchers identified 1,343 infants who had CAP in the first 2 years of life, and 6,715 controls, using a large electronic health records dataset (Optum EHR dataset) for the period from Jan. 2011 through June 2018.
The primary outcomes were the development of any chronic respiratory disorders, reactive airway disease, and CAP hospitalizations between ages 2 and 5 years. Infants in the CAP group were otherwise healthy; those with congenital or other conditions that might predispose them to pneumonia were excluded. Baseline characteristics were similar between the CAP patients and controls.
Future risk
Overall, the rates per 100 patient-years for any chronic respiratory disorder were 11.6 for CAP patients versus 4.9 for controls (relative risk, 2.4). Rates for reactive airway disease and CAP hospitalization were 6.1 versus 1.9 per 100 patient-years (RR, 3.2) and 1.0 versus 0.2 per 100 patient-years (RR, 6.3) for the CAP patients and controls, respectively.
The distribution of CAP etiology of CAP in infants at the first hospitalization was 20% bacterial, 27% viral, and 53% unspecified. The relative rates of later respiratory illness were similar across etiologies of the initial hospitalization for CAP, which support the association between infant CAP and later respiratory disease, the researchers said.
Nearly all (97%) of the CAP patients had only one qualifying hospitalization for CAP before 2 years of age, and the mean age at the first hospitalization was 8.9 months. “Rates and relative rates of any chronic respiratory disorder, and our composite for reactive airway disease, increased with age at which the initial CAP hospitalization occurred,” and were highest for children hospitalized at close to 2 years of age, the researchers noted.
Persistent inflammation?
“Our findings add to the evolving hypothesis that persistent inflammation following pneumonia creates an increased risk for subsequent respiratory disease and exacerbations of underlying disease,” the researchers wrote.
The study findings were limited by several factors, including the potential for misclassification of some infants with and without underlying conditions, reliance on discharge information for etiology, and possible lack of generalizability to other populations, the researchers noted.
However, the results indicate an increased risk for respiratory illness in early childhood among infants with CAP, and support the need for greater attention to CAP prevention and for strategies to reduce inflammation after pneumonia, they said. “Further study is needed to confirm the long-term consequences of infant CAP and the underlying mechanisms that lead to such long-term sequelae,” they concluded.
Dr. Lapidot and several coauthors disclosed ties with Pfizer, the study sponsor.
A version of this article first appeared on Medscape.com.
FROM RESPIRATORY MEDICINE
Longitudinal course of atopic dermatitis often overlooked, expert says
In the opinion of Raj Chovatiya, MD, PhD, the longitudinal course of atopic dermatitis (AD) is an important yet overlooked clinical domain of the disease.
“We know that AD is associated with fluctuating severity, disease flares, long-term persistence, and periods of quiescence, but its longitudinal course is not routinely incorporated into guidelines or clinical trials,” Dr. Chovatiya, assistant professor in the department of dermatology at Northwestern University, Chicago, said during the Revolutionizing Atopic Dermatitis virtual symposium. “Understanding the long-term course may improve our ability to phenotype, prognosticate, and personalize our care.”

The classic view of AD is that it starts in early childhood, follows a waxing and waning course for a few years, and burns out by adulthood. “I think we all know that this is generally false,” he said. “This was largely based on anecdotal clinical experience and large cross-sectional studies, not ones that consider the heterogeneity of AD.”
Results from a large-scale, prospective study of 7,157 children enrolled in the Pediatric Eczema Elective Registry (PEER), suggests that AD commonly persists beyond adulthood. PEER was a phase IV postmarketing safety study of children aged 12-17 with moderate to severe AD who were exposed to topical pimecrolimus and who were surveyed every 6 months (JAMA Dermatol. 2014;150[6]:593-600). The researchers found that more persistent disease was associated with self-reported disease activity, many environmental exposures, White race, history of AD, and an annual household income of less than $50,000. By age 20, 50% reported at least one 6-month symptom- and medication-free period. “The important takeaway was that at every age, greater than 80% reported active AD as defined by symptoms or medication use, meaning that persistence was extremely high – much higher than what was originally thought,” Dr. Chovatiya said. “If you take a look at the literature before this study, many were retrospective analyses, and persistence was estimated to be in the 40%-60% range.”
International prospective studies have provided a more conservative estimate of persistence. For example, the German Multicenter Allergy Study followed 1,314 from birth through age 7 (J Allergy Clin Immunol. 2004;113[5]:925-31). Of these, 22% had AD within the first 2 years of life. Of these, 43% were in remission by age 3, while 38% had intermittent AD, and 19% had symptoms every year of the study. “Studies of other birth cohorts in the world came out suggesting that the rates of AD persistence ranges in the single digits to the teens,” Dr. Chovatiya said.
To reconcile these heterogeneous estimates of AD persistence, researchers conducted a systematic review and meta-analysis of 45 studies that included 110,651 subjects from 15 countries and spanned 434,992 patient-years (J Am Acad Dermatol. 2016;75:681-7.e11). They found that 80% of childhood AD had at least one observed period of disease clearance by 8 years of age. “Most importantly, less than 5% of childhood AD was persistent 20 years after diagnosis,” Dr. Chovatiya said. “However, interestingly, increased persistence was associated with later onset AD, more years of persistence, and more patient/caregiver-assessed disease.” He pointed out inherent limitations to all studies of AD persistence, including nonuniform methods of data collection, differing cohorts, different ways of diagnosing AD, different disease severity scales, and the fact that most don’t assess flares or recurrence beyond the initial period of disease clearance. “This can lead to a potential underestimation of longer-term persistence,” he said.
Childhood AD features unique predictors of persistence that may define AD trajectories. For example, in several existing studies, more persistent disease was associated with higher baseline severity, earlier-onset AD, personal history of atopy, family history of AD, AD genetic risk score (heritability, including common Filaggrin mutations), urban environment, non-White race, Hispanic ethnicity, female sex, lower household income, and overall poorer health status.
Dr. Chovatiya said. “I think that AD classification can take a lesson from asthma. When we think about how our allergy colleagues think about asthma, it is commonly classified as intermittent, mild persistent, moderate persistent, and severe persistent. Those that have intermittent disease get reactive treatment, while those with persistent disease get proactive treatment. Similarly, AD could be classified as mild intermittent, mild persistent, moderate to severe intermittent and moderate to severe persistent.”
He concluded his presentation by recommending that the fluctuating course of AD be better captured in clinical trials. “Current randomized, controlled trials use validated measures of AD signs and symptoms as inclusion criteria and measures of efficacy,” he said. “Static assessments may confound treatment effects, and assessment of prespecified time points are somewhat arbitrary in the context of disease subsets.” He proposes studies that examine aggregate measures of long-term disease control, such as number of itch-free days, weeks with clear skin, and flares experienced. “Long-term control assessment in RCTs should include signs, symptoms, health-related quality of life, and a patient global domain over time to better understand how AD is doing in the long run,” he said.
Dr. Chovatiya disclosed that he is a consultant to, a speaker for, and/or a member of the advisory board for AbbVie, Arcutis, Arena, Incyte, Pfizer, Regeneron, and Sanofi Genzyme.
In the opinion of Raj Chovatiya, MD, PhD, the longitudinal course of atopic dermatitis (AD) is an important yet overlooked clinical domain of the disease.
“We know that AD is associated with fluctuating severity, disease flares, long-term persistence, and periods of quiescence, but its longitudinal course is not routinely incorporated into guidelines or clinical trials,” Dr. Chovatiya, assistant professor in the department of dermatology at Northwestern University, Chicago, said during the Revolutionizing Atopic Dermatitis virtual symposium. “Understanding the long-term course may improve our ability to phenotype, prognosticate, and personalize our care.”
The classic view of AD is that it starts in early childhood, follows a waxing and waning course for a few years, and burns out by adulthood. “I think we all know that this is generally false,” he said. “This was largely based on anecdotal clinical experience and large cross-sectional studies, not ones that consider the heterogeneity of AD.”
Results from a large-scale, prospective study of 7,157 children enrolled in the Pediatric Eczema Elective Registry (PEER), suggests that AD commonly persists beyond adulthood. PEER was a phase IV postmarketing safety study of children aged 12-17 with moderate to severe AD who were exposed to topical pimecrolimus and who were surveyed every 6 months (JAMA Dermatol. 2014;150[6]:593-600). The researchers found that more persistent disease was associated with self-reported disease activity, many environmental exposures, White race, history of AD, and an annual household income of less than $50,000. By age 20, 50% reported at least one 6-month symptom- and medication-free period. “The important takeaway was that at every age, greater than 80% reported active AD as defined by symptoms or medication use, meaning that persistence was extremely high – much higher than what was originally thought,” Dr. Chovatiya said. “If you take a look at the literature before this study, many were retrospective analyses, and persistence was estimated to be in the 40%-60% range.”
International prospective studies have provided a more conservative estimate of persistence. For example, the German Multicenter Allergy Study followed 1,314 from birth through age 7 (J Allergy Clin Immunol. 2004;113[5]:925-31). Of these, 22% had AD within the first 2 years of life. Of these, 43% were in remission by age 3, while 38% had intermittent AD, and 19% had symptoms every year of the study. “Studies of other birth cohorts in the world came out suggesting that the rates of AD persistence ranges in the single digits to the teens,” Dr. Chovatiya said.
To reconcile these heterogeneous estimates of AD persistence, researchers conducted a systematic review and meta-analysis of 45 studies that included 110,651 subjects from 15 countries and spanned 434,992 patient-years (J Am Acad Dermatol. 2016;75:681-7.e11). They found that 80% of childhood AD had at least one observed period of disease clearance by 8 years of age. “Most importantly, less than 5% of childhood AD was persistent 20 years after diagnosis,” Dr. Chovatiya said. “However, interestingly, increased persistence was associated with later onset AD, more years of persistence, and more patient/caregiver-assessed disease.” He pointed out inherent limitations to all studies of AD persistence, including nonuniform methods of data collection, differing cohorts, different ways of diagnosing AD, different disease severity scales, and the fact that most don’t assess flares or recurrence beyond the initial period of disease clearance. “This can lead to a potential underestimation of longer-term persistence,” he said.
Childhood AD features unique predictors of persistence that may define AD trajectories. For example, in several existing studies, more persistent disease was associated with higher baseline severity, earlier-onset AD, personal history of atopy, family history of AD, AD genetic risk score (heritability, including common Filaggrin mutations), urban environment, non-White race, Hispanic ethnicity, female sex, lower household income, and overall poorer health status.
Dr. Chovatiya said. “I think that AD classification can take a lesson from asthma. When we think about how our allergy colleagues think about asthma, it is commonly classified as intermittent, mild persistent, moderate persistent, and severe persistent. Those that have intermittent disease get reactive treatment, while those with persistent disease get proactive treatment. Similarly, AD could be classified as mild intermittent, mild persistent, moderate to severe intermittent and moderate to severe persistent.”
He concluded his presentation by recommending that the fluctuating course of AD be better captured in clinical trials. “Current randomized, controlled trials use validated measures of AD signs and symptoms as inclusion criteria and measures of efficacy,” he said. “Static assessments may confound treatment effects, and assessment of prespecified time points are somewhat arbitrary in the context of disease subsets.” He proposes studies that examine aggregate measures of long-term disease control, such as number of itch-free days, weeks with clear skin, and flares experienced. “Long-term control assessment in RCTs should include signs, symptoms, health-related quality of life, and a patient global domain over time to better understand how AD is doing in the long run,” he said.
Dr. Chovatiya disclosed that he is a consultant to, a speaker for, and/or a member of the advisory board for AbbVie, Arcutis, Arena, Incyte, Pfizer, Regeneron, and Sanofi Genzyme.
In the opinion of Raj Chovatiya, MD, PhD, the longitudinal course of atopic dermatitis (AD) is an important yet overlooked clinical domain of the disease.
“We know that AD is associated with fluctuating severity, disease flares, long-term persistence, and periods of quiescence, but its longitudinal course is not routinely incorporated into guidelines or clinical trials,” Dr. Chovatiya, assistant professor in the department of dermatology at Northwestern University, Chicago, said during the Revolutionizing Atopic Dermatitis virtual symposium. “Understanding the long-term course may improve our ability to phenotype, prognosticate, and personalize our care.”
The classic view of AD is that it starts in early childhood, follows a waxing and waning course for a few years, and burns out by adulthood. “I think we all know that this is generally false,” he said. “This was largely based on anecdotal clinical experience and large cross-sectional studies, not ones that consider the heterogeneity of AD.”
Results from a large-scale, prospective study of 7,157 children enrolled in the Pediatric Eczema Elective Registry (PEER), suggests that AD commonly persists beyond adulthood. PEER was a phase IV postmarketing safety study of children aged 12-17 with moderate to severe AD who were exposed to topical pimecrolimus and who were surveyed every 6 months (JAMA Dermatol. 2014;150[6]:593-600). The researchers found that more persistent disease was associated with self-reported disease activity, many environmental exposures, White race, history of AD, and an annual household income of less than $50,000. By age 20, 50% reported at least one 6-month symptom- and medication-free period. “The important takeaway was that at every age, greater than 80% reported active AD as defined by symptoms or medication use, meaning that persistence was extremely high – much higher than what was originally thought,” Dr. Chovatiya said. “If you take a look at the literature before this study, many were retrospective analyses, and persistence was estimated to be in the 40%-60% range.”
International prospective studies have provided a more conservative estimate of persistence. For example, the German Multicenter Allergy Study followed 1,314 from birth through age 7 (J Allergy Clin Immunol. 2004;113[5]:925-31). Of these, 22% had AD within the first 2 years of life. Of these, 43% were in remission by age 3, while 38% had intermittent AD, and 19% had symptoms every year of the study. “Studies of other birth cohorts in the world came out suggesting that the rates of AD persistence ranges in the single digits to the teens,” Dr. Chovatiya said.
To reconcile these heterogeneous estimates of AD persistence, researchers conducted a systematic review and meta-analysis of 45 studies that included 110,651 subjects from 15 countries and spanned 434,992 patient-years (J Am Acad Dermatol. 2016;75:681-7.e11). They found that 80% of childhood AD had at least one observed period of disease clearance by 8 years of age. “Most importantly, less than 5% of childhood AD was persistent 20 years after diagnosis,” Dr. Chovatiya said. “However, interestingly, increased persistence was associated with later onset AD, more years of persistence, and more patient/caregiver-assessed disease.” He pointed out inherent limitations to all studies of AD persistence, including nonuniform methods of data collection, differing cohorts, different ways of diagnosing AD, different disease severity scales, and the fact that most don’t assess flares or recurrence beyond the initial period of disease clearance. “This can lead to a potential underestimation of longer-term persistence,” he said.
Childhood AD features unique predictors of persistence that may define AD trajectories. For example, in several existing studies, more persistent disease was associated with higher baseline severity, earlier-onset AD, personal history of atopy, family history of AD, AD genetic risk score (heritability, including common Filaggrin mutations), urban environment, non-White race, Hispanic ethnicity, female sex, lower household income, and overall poorer health status.
Dr. Chovatiya said. “I think that AD classification can take a lesson from asthma. When we think about how our allergy colleagues think about asthma, it is commonly classified as intermittent, mild persistent, moderate persistent, and severe persistent. Those that have intermittent disease get reactive treatment, while those with persistent disease get proactive treatment. Similarly, AD could be classified as mild intermittent, mild persistent, moderate to severe intermittent and moderate to severe persistent.”
He concluded his presentation by recommending that the fluctuating course of AD be better captured in clinical trials. “Current randomized, controlled trials use validated measures of AD signs and symptoms as inclusion criteria and measures of efficacy,” he said. “Static assessments may confound treatment effects, and assessment of prespecified time points are somewhat arbitrary in the context of disease subsets.” He proposes studies that examine aggregate measures of long-term disease control, such as number of itch-free days, weeks with clear skin, and flares experienced. “Long-term control assessment in RCTs should include signs, symptoms, health-related quality of life, and a patient global domain over time to better understand how AD is doing in the long run,” he said.
Dr. Chovatiya disclosed that he is a consultant to, a speaker for, and/or a member of the advisory board for AbbVie, Arcutis, Arena, Incyte, Pfizer, Regeneron, and Sanofi Genzyme.
FROM REVOLUTIONIZING AD 2021
Gene mutations may drive sudden unexplained deaths in children
, researchers have found.
Previous studies have found de novo genetic variants – those not found in either parent but which occur for the first time in their offspring – that increase the risk of cardiac and seizure disorders, but research on sudden unexplained deaths in children (SUDC) is limited, according to Matthew Halvorsen, PhD, of the University of North Carolina at Chapel Hill, and colleagues. Most cases of SUDC occur in children aged 1-4 years, and a lack of standardized investigation systems likely leads to misclassification of these deaths, they said.
Compared with sudden infant death syndrome (SIDS), which occurs in approximately 1,400 children in the United States each year, approximately 400 children aged 1 year and older die from SUDC annually. A major obstacle to studying these cases is that so-called molecular autopsies – which incorporate genetic analysis into the postmortem examination – typically do not assess the parents’ genetic information and thus limit the ability to identify de novo mutations, they added.
In a study published in the Proceedings of the National Academy of Sciences, Dr. Halvorsen’s group obtained whole exome sequence data from 124 “trios,” meaning a dead child and two living parents. They tested for excessive de novo mutations for different genes involved in conditions that included cardiac arrhythmias and epilepsy. The average age at the time of death for the children was 34.2 months; 54% were male, and 82% were White.
Children who died of SUDC were nearly 10 times as likely to have de novo mutations in genes associated with cardiac and seizure disorders as were unrelated healthy controls (odds ratio, 9.76). Most pathogenic variants were de novo, which highlights the importance of trio studies, the researchers noted.
The researchers identified 11 variants associated with increased risk of SUDC, 7 of which were de novo. Three of the 124 cases carried mutations (two for RYR2 and 1 for TNNI3) affecting genes in the CardiacEpilepsy dataset proposed by the American College of Medical Genetics and Genomics, strengthening the connection to seizure disorders.
Another notable finding was the identification of six de novo mutations involved in altering calcium-related regulation, which suggests a cardiac susceptibility to sudden death.
The data support “novel genetic causes of pediatric sudden deaths that could be discovered with larger cohorts,” the researchers noted. Taken together, they say, the gene mutations could play a role in approximately 9% of SUDC cases.
The study findings were limited by several factors, including lack of population-based case ascertainment, exclusive focus on unexplained deaths, potentially missed mutations, and use of DNA from blood as opposed to organs, the researchers noted.
However, they concluded, “the data indicate that deleterious de novo mutations are significant genetic risk factors for childhood sudden unexplained death, and that their identification may lead to medical intervention that ultimately saves lives.”
Findings highlight impact of SUDC
“This study is important because SUDC is a much more pressing medical need than most people realize,” said Richard Tsien, PhD, of New York University Langone Medical Center, and the corresponding author of the study.
Although SUDC is less common than SIDS, SUDC has essentially no targeted research funding, Dr. Tsien said. Study coauthor Laura Gould, MA, a researcher and mother who lost a young child to SUDC, worked with Orrin Devinsky, MD, to create a registry for families with cases of SUDC. This registry was instrumental in allowing the researchers to “do the molecular detective work we need to do” to see whether a genetic basis exists for SUDC, Dr. Tsien said.
“The detective work comes up with a consistent story,” he said. “More than half of the genes that we found are involved in the normal function of the heart and brain,” performing such functions as delivering calcium ions to the inside of the heart cells and nerve cells.
The study “is the first of its kind,” given the difficulty of acquiring DNA from the child and two parents in SUDC cases, Dr. Tsien said.
Overall, approximately 10% of the cases have a compelling explanation based on the coding of DNA, Dr. Tsien said. From a clinical standpoint, that information might affect what a clinician says to a parent.
A key takeaway is that most of the genetic mutations are spontaneous and are not inherited from the parents, Dr. Tsien said. The study findings indicate that parents who suffer an SUDC loss need not be discouraged from having children, he added.
For the long term, “the more we understand about these disorders, the more information we can offer to families,” he said. Eventually, clinicians might be able to use genetics to identify signs of when SUDC might be more likely. “For example, if a child shows a very mild seizure, this would alert them that there might be potential for a more drastic outcome.”
Meanwhile, families with SUDC cases may find support and benefit in signing up for the registry and knowing that other families have been through a similar experience, Dr. Tsien said.
Genetic studies create opportunities
A significant portion of pediatric mortality remains unexplained, according to Richard D. Goldstein, MD, of Boston Children’s Hospital. One reason is the lack of a formal diagnostic code to identify these deaths.
Research to date has suggested links between SUDC and a family history of febrile seizures, as well as differences in brain structure associated with epilepsy, Dr. Goldstein said.
“An important hypothesis is that these deaths are part of a continuum that also includes stillbirths, SIDS, and sudden unexpected death in epilepsy [SUDEP],” Dr. Goldstein said. “By mandate, investigations of these deaths occur under the jurisdiction of medical examiners and coroners and have, for the most part, been insulated from developments in modern medicine like genomics and proteomics, elements of what are referred to as the molecular autopsy, and studies such as the current study bring attention to what is being missed.”
Dr. Goldstein said the new study buttresses the “conventional clinical suspicion” about the likely causes of SUDC, “but also strengthens the association between sudden unexpected death in pediatrics (SUDP) and SUDEP that we and others have been positing. I think the researchers very nicely make the point that epilepsy and cardiac arrhythmia genes are not as separated in their effects as many would believe.”
As for the clinical applicability of the findings, Dr. Goldstein said medicine needs to offer parents more: “Pediatric deaths without explanation deserve more than a forensic investigation that concerns itself mostly with whether there has been foul play,” he said. “We need to figure out how to engage families, at an incredibly vulnerable time, in helping find the cause of the child’s death and also contributing to needed research. Most of the reported variants were de novo, which means that parent participation is needed to figure out these genetic factors but also that we can offer reassurance to families that other children are not at risk.”
The study was supported by the SUDC Foundation and Finding a Cure for Epilepsy and Seizures (New York University). Dr. Tsien disclosed support from the National Institutes of Health and a grant from FACES. Dr. Goldstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, researchers have found.
Previous studies have found de novo genetic variants – those not found in either parent but which occur for the first time in their offspring – that increase the risk of cardiac and seizure disorders, but research on sudden unexplained deaths in children (SUDC) is limited, according to Matthew Halvorsen, PhD, of the University of North Carolina at Chapel Hill, and colleagues. Most cases of SUDC occur in children aged 1-4 years, and a lack of standardized investigation systems likely leads to misclassification of these deaths, they said.
Compared with sudden infant death syndrome (SIDS), which occurs in approximately 1,400 children in the United States each year, approximately 400 children aged 1 year and older die from SUDC annually. A major obstacle to studying these cases is that so-called molecular autopsies – which incorporate genetic analysis into the postmortem examination – typically do not assess the parents’ genetic information and thus limit the ability to identify de novo mutations, they added.
In a study published in the Proceedings of the National Academy of Sciences, Dr. Halvorsen’s group obtained whole exome sequence data from 124 “trios,” meaning a dead child and two living parents. They tested for excessive de novo mutations for different genes involved in conditions that included cardiac arrhythmias and epilepsy. The average age at the time of death for the children was 34.2 months; 54% were male, and 82% were White.
Children who died of SUDC were nearly 10 times as likely to have de novo mutations in genes associated with cardiac and seizure disorders as were unrelated healthy controls (odds ratio, 9.76). Most pathogenic variants were de novo, which highlights the importance of trio studies, the researchers noted.
The researchers identified 11 variants associated with increased risk of SUDC, 7 of which were de novo. Three of the 124 cases carried mutations (two for RYR2 and 1 for TNNI3) affecting genes in the CardiacEpilepsy dataset proposed by the American College of Medical Genetics and Genomics, strengthening the connection to seizure disorders.
Another notable finding was the identification of six de novo mutations involved in altering calcium-related regulation, which suggests a cardiac susceptibility to sudden death.
The data support “novel genetic causes of pediatric sudden deaths that could be discovered with larger cohorts,” the researchers noted. Taken together, they say, the gene mutations could play a role in approximately 9% of SUDC cases.
The study findings were limited by several factors, including lack of population-based case ascertainment, exclusive focus on unexplained deaths, potentially missed mutations, and use of DNA from blood as opposed to organs, the researchers noted.
However, they concluded, “the data indicate that deleterious de novo mutations are significant genetic risk factors for childhood sudden unexplained death, and that their identification may lead to medical intervention that ultimately saves lives.”
Findings highlight impact of SUDC
“This study is important because SUDC is a much more pressing medical need than most people realize,” said Richard Tsien, PhD, of New York University Langone Medical Center, and the corresponding author of the study.
Although SUDC is less common than SIDS, SUDC has essentially no targeted research funding, Dr. Tsien said. Study coauthor Laura Gould, MA, a researcher and mother who lost a young child to SUDC, worked with Orrin Devinsky, MD, to create a registry for families with cases of SUDC. This registry was instrumental in allowing the researchers to “do the molecular detective work we need to do” to see whether a genetic basis exists for SUDC, Dr. Tsien said.
“The detective work comes up with a consistent story,” he said. “More than half of the genes that we found are involved in the normal function of the heart and brain,” performing such functions as delivering calcium ions to the inside of the heart cells and nerve cells.
The study “is the first of its kind,” given the difficulty of acquiring DNA from the child and two parents in SUDC cases, Dr. Tsien said.
Overall, approximately 10% of the cases have a compelling explanation based on the coding of DNA, Dr. Tsien said. From a clinical standpoint, that information might affect what a clinician says to a parent.
A key takeaway is that most of the genetic mutations are spontaneous and are not inherited from the parents, Dr. Tsien said. The study findings indicate that parents who suffer an SUDC loss need not be discouraged from having children, he added.
For the long term, “the more we understand about these disorders, the more information we can offer to families,” he said. Eventually, clinicians might be able to use genetics to identify signs of when SUDC might be more likely. “For example, if a child shows a very mild seizure, this would alert them that there might be potential for a more drastic outcome.”
Meanwhile, families with SUDC cases may find support and benefit in signing up for the registry and knowing that other families have been through a similar experience, Dr. Tsien said.
Genetic studies create opportunities
A significant portion of pediatric mortality remains unexplained, according to Richard D. Goldstein, MD, of Boston Children’s Hospital. One reason is the lack of a formal diagnostic code to identify these deaths.
Research to date has suggested links between SUDC and a family history of febrile seizures, as well as differences in brain structure associated with epilepsy, Dr. Goldstein said.
“An important hypothesis is that these deaths are part of a continuum that also includes stillbirths, SIDS, and sudden unexpected death in epilepsy [SUDEP],” Dr. Goldstein said. “By mandate, investigations of these deaths occur under the jurisdiction of medical examiners and coroners and have, for the most part, been insulated from developments in modern medicine like genomics and proteomics, elements of what are referred to as the molecular autopsy, and studies such as the current study bring attention to what is being missed.”
Dr. Goldstein said the new study buttresses the “conventional clinical suspicion” about the likely causes of SUDC, “but also strengthens the association between sudden unexpected death in pediatrics (SUDP) and SUDEP that we and others have been positing. I think the researchers very nicely make the point that epilepsy and cardiac arrhythmia genes are not as separated in their effects as many would believe.”
As for the clinical applicability of the findings, Dr. Goldstein said medicine needs to offer parents more: “Pediatric deaths without explanation deserve more than a forensic investigation that concerns itself mostly with whether there has been foul play,” he said. “We need to figure out how to engage families, at an incredibly vulnerable time, in helping find the cause of the child’s death and also contributing to needed research. Most of the reported variants were de novo, which means that parent participation is needed to figure out these genetic factors but also that we can offer reassurance to families that other children are not at risk.”
The study was supported by the SUDC Foundation and Finding a Cure for Epilepsy and Seizures (New York University). Dr. Tsien disclosed support from the National Institutes of Health and a grant from FACES. Dr. Goldstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, researchers have found.
Previous studies have found de novo genetic variants – those not found in either parent but which occur for the first time in their offspring – that increase the risk of cardiac and seizure disorders, but research on sudden unexplained deaths in children (SUDC) is limited, according to Matthew Halvorsen, PhD, of the University of North Carolina at Chapel Hill, and colleagues. Most cases of SUDC occur in children aged 1-4 years, and a lack of standardized investigation systems likely leads to misclassification of these deaths, they said.
Compared with sudden infant death syndrome (SIDS), which occurs in approximately 1,400 children in the United States each year, approximately 400 children aged 1 year and older die from SUDC annually. A major obstacle to studying these cases is that so-called molecular autopsies – which incorporate genetic analysis into the postmortem examination – typically do not assess the parents’ genetic information and thus limit the ability to identify de novo mutations, they added.
In a study published in the Proceedings of the National Academy of Sciences, Dr. Halvorsen’s group obtained whole exome sequence data from 124 “trios,” meaning a dead child and two living parents. They tested for excessive de novo mutations for different genes involved in conditions that included cardiac arrhythmias and epilepsy. The average age at the time of death for the children was 34.2 months; 54% were male, and 82% were White.
Children who died of SUDC were nearly 10 times as likely to have de novo mutations in genes associated with cardiac and seizure disorders as were unrelated healthy controls (odds ratio, 9.76). Most pathogenic variants were de novo, which highlights the importance of trio studies, the researchers noted.
The researchers identified 11 variants associated with increased risk of SUDC, 7 of which were de novo. Three of the 124 cases carried mutations (two for RYR2 and 1 for TNNI3) affecting genes in the CardiacEpilepsy dataset proposed by the American College of Medical Genetics and Genomics, strengthening the connection to seizure disorders.
Another notable finding was the identification of six de novo mutations involved in altering calcium-related regulation, which suggests a cardiac susceptibility to sudden death.
The data support “novel genetic causes of pediatric sudden deaths that could be discovered with larger cohorts,” the researchers noted. Taken together, they say, the gene mutations could play a role in approximately 9% of SUDC cases.
The study findings were limited by several factors, including lack of population-based case ascertainment, exclusive focus on unexplained deaths, potentially missed mutations, and use of DNA from blood as opposed to organs, the researchers noted.
However, they concluded, “the data indicate that deleterious de novo mutations are significant genetic risk factors for childhood sudden unexplained death, and that their identification may lead to medical intervention that ultimately saves lives.”
Findings highlight impact of SUDC
“This study is important because SUDC is a much more pressing medical need than most people realize,” said Richard Tsien, PhD, of New York University Langone Medical Center, and the corresponding author of the study.
Although SUDC is less common than SIDS, SUDC has essentially no targeted research funding, Dr. Tsien said. Study coauthor Laura Gould, MA, a researcher and mother who lost a young child to SUDC, worked with Orrin Devinsky, MD, to create a registry for families with cases of SUDC. This registry was instrumental in allowing the researchers to “do the molecular detective work we need to do” to see whether a genetic basis exists for SUDC, Dr. Tsien said.
“The detective work comes up with a consistent story,” he said. “More than half of the genes that we found are involved in the normal function of the heart and brain,” performing such functions as delivering calcium ions to the inside of the heart cells and nerve cells.
The study “is the first of its kind,” given the difficulty of acquiring DNA from the child and two parents in SUDC cases, Dr. Tsien said.
Overall, approximately 10% of the cases have a compelling explanation based on the coding of DNA, Dr. Tsien said. From a clinical standpoint, that information might affect what a clinician says to a parent.
A key takeaway is that most of the genetic mutations are spontaneous and are not inherited from the parents, Dr. Tsien said. The study findings indicate that parents who suffer an SUDC loss need not be discouraged from having children, he added.
For the long term, “the more we understand about these disorders, the more information we can offer to families,” he said. Eventually, clinicians might be able to use genetics to identify signs of when SUDC might be more likely. “For example, if a child shows a very mild seizure, this would alert them that there might be potential for a more drastic outcome.”
Meanwhile, families with SUDC cases may find support and benefit in signing up for the registry and knowing that other families have been through a similar experience, Dr. Tsien said.
Genetic studies create opportunities
A significant portion of pediatric mortality remains unexplained, according to Richard D. Goldstein, MD, of Boston Children’s Hospital. One reason is the lack of a formal diagnostic code to identify these deaths.
Research to date has suggested links between SUDC and a family history of febrile seizures, as well as differences in brain structure associated with epilepsy, Dr. Goldstein said.
“An important hypothesis is that these deaths are part of a continuum that also includes stillbirths, SIDS, and sudden unexpected death in epilepsy [SUDEP],” Dr. Goldstein said. “By mandate, investigations of these deaths occur under the jurisdiction of medical examiners and coroners and have, for the most part, been insulated from developments in modern medicine like genomics and proteomics, elements of what are referred to as the molecular autopsy, and studies such as the current study bring attention to what is being missed.”
Dr. Goldstein said the new study buttresses the “conventional clinical suspicion” about the likely causes of SUDC, “but also strengthens the association between sudden unexpected death in pediatrics (SUDP) and SUDEP that we and others have been positing. I think the researchers very nicely make the point that epilepsy and cardiac arrhythmia genes are not as separated in their effects as many would believe.”
As for the clinical applicability of the findings, Dr. Goldstein said medicine needs to offer parents more: “Pediatric deaths without explanation deserve more than a forensic investigation that concerns itself mostly with whether there has been foul play,” he said. “We need to figure out how to engage families, at an incredibly vulnerable time, in helping find the cause of the child’s death and also contributing to needed research. Most of the reported variants were de novo, which means that parent participation is needed to figure out these genetic factors but also that we can offer reassurance to families that other children are not at risk.”
The study was supported by the SUDC Foundation and Finding a Cure for Epilepsy and Seizures (New York University). Dr. Tsien disclosed support from the National Institutes of Health and a grant from FACES. Dr. Goldstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Obesity prevention in infants benefits second-born too
According to a statement from the National Institutes of Health, who funded the study, it is the first such infant obesity intervention to show the spillover effect. Findings were published online Dec. 21, 2021, in Obesity.
The program is called Infants Growing on Healthy Trajectories (INSIGHT) responsive parenting (RP) intervention, and it included guidance on feeding, sleep, interactive play, and regulating emotion.
Parents were given guidance by nurses who came to their homes on how to respond when their child is drowsy, sleeping, fussy, and alert. They also learned how to put infants to bed drowsy, but awake, and avoid feeding infants to get them to sleep; how to respond to infants waking up at night; when to start solid foods; how to limit inactive time; and how to use growth charts.
The control group program focused on safety and matched the guidance categories. For example, early visits included information on prevention of sudden infant death syndrome for sleep, breast milk storage and formula for feeding, and safe bathing.
Jennifer S. Savage, Center for Childhood Obesity Research, Penn State University, University Park, led the study that enrolled 117 infants in a randomized controlled trial. Mother and firstborn children were randomized to the RP or home safety intervention (control) group 10-14 days after delivery. Their second-born siblings were enrolled in an observation-only ancillary study.
Second-born children were delivered 2.5 (standard deviation, 0.9) years after firstborns. Anthropometrics were measured in both siblings at ages 3, 16, 28, and 52 weeks.
Firstborn children at 1 year had a body mass index (BMI) that was 0.44 kg/m2 lower than the control group (95% confidence interval, −0.82 to −0.06), and second-born children whose parents received the RP intervention with their first child had BMI that was 0.36 kg/m2 lower.
“What we saw here is that it worked again,” coauthor Ian Paul, MD, MSc, professor of pediatrics and public health sciences at Penn State University, Hershey, said in an interview.
“Once we imprint them with a certain approach to parenting with the first child, they’re doing the same thing with the second child, which is wonderful to see,” he said.
He noted that this happened with second children without any reinforcements or booster information.
Dr. Paul said it’s still not clear which of the interventions – whether related to feeding techniques or sleeping or activity – helps most. And for each family the problematic behaviors may be different.
Responsive parenting programs have shown success previously among firstborns, the authors wrote, but 80% of those children grow up with younger siblings, so an intervention that also benefits them is important.
Weighing the costs of the intervention
The intervention was extensive. It involved four hour-plus nurse visits a year, often by the same nurse who built a relationship with the family.
But Ms. Savage said that it is possible to replicate INSIGHT on a larger scale in the United States with the dozens of home visitation models.
“Currently, 21 home visitation models meet the U.S. Department of Health & Human Services criteria for evidence of effectiveness, such as Nurse Family Partnership, Family Check-up, and Early Head Start Home Based Option. There is an opportunity to use home visitation models at the national scale to potentially interrupt the cycle of poor multigenerational outcomes such as obesity,” she said.
Dr. Paul said the initial investment “can save money in the long term,” given what’s at stake. “We know that 20%-25% of 2- to 5-year-olds are already overweight or obese and if they are already overweight or obese at that age, that;’s likely to persist.”
However, he acknowledged that staff shortages and costs are a challenge.
“Other countries have made that investment in their health care system,” he said. “In the U.S. only a fraction of new mothers and babies get home visitation. The kind of work that we did for obesity prevention has not yet been incorporated into evidence-based models of home visitation, though it certainly could be.”
Dr. Paul said his team is hoping to collaborate with others in the near future on expanding this program to such models of home visitation.
Telehealth, though a less desirable option, compared with in-home visits, could also be utilized, he said.
Short of the comprehensive intervention, he said, many of the concepts can be put into practice by pediatricians and parents.
Dr. Paul noted that the Robert Wood Johnson Foundation has endorsed “responsive feeding” as the preferred approach to feeding infants and toddlers. Responsive feeding – helping parents recognize hunger and satiety cues as opposed to other distress cues – is a big part of the intervention.
“Feeding to soothe is not the preferred approach,” he said. “Food and milk and formula should be used for hunger.” That’s something pediatricians may not be stressing to parents, he said.
Pediatricians can also counsel parents on not using food as a reward. “We shouldn’t be giving kids M&Ms to teach them how to potty train,” he said.
‘Promising’ findings
Charles Wood, MD, a childhood obesity specialist at Duke University, Durham, N.C., who was not part of the study, called the findings “very promising.”
It also makes sense that the “aha moments” of first-time parents learning from the INSIGHT intervention would carry over to the second sibling, he said.
Dr. Wood agreed costs are a big factor. However, he said, the potential downstream costs of not preventing obesity are worse. And this study indicates the benefits may keep spreading with future siblings.
Dr. Wood said accessing obesity interventions outside the pediatrician visit can also help. Connecting patients with support groups or dietitians or with a counselor from Women, Infants, and Children can help. However, consistent messaging among the providers is key, he noted.
Dr. Wood’s research group is investigating text messaging platforms so parents can get answer to real-time questions, such as those about feeding behaviors.
He pointed to a limitation the authors mention, which is that the study was done in mostly White, highly educated, higher-income families.
“There’s a big problem with racial disparities and obesity,” Dr. Wood noted. “We definitely need solutions that address disparities as well.”
Mothers included in the study had given birth for the first time and their infants were enrolled after birth from a single maternity ward between January 2012 and March 2014. Major eligibility criteria were that the babies were full term (at least 37 weeks’ gestation), single births, and delivered to English-speaking mothers at least 20 years of age. Infants who weighed less than 2,500 g at birth were excluded.
The paper’s authors and Dr. Wood declared no relevant financial relationships.
This research was supported by the National Institutes of Health, the National Institute of Diabetes and Digestive and Kidney Diseases; and the Department of Agriculture.
According to a statement from the National Institutes of Health, who funded the study, it is the first such infant obesity intervention to show the spillover effect. Findings were published online Dec. 21, 2021, in Obesity.
The program is called Infants Growing on Healthy Trajectories (INSIGHT) responsive parenting (RP) intervention, and it included guidance on feeding, sleep, interactive play, and regulating emotion.
Parents were given guidance by nurses who came to their homes on how to respond when their child is drowsy, sleeping, fussy, and alert. They also learned how to put infants to bed drowsy, but awake, and avoid feeding infants to get them to sleep; how to respond to infants waking up at night; when to start solid foods; how to limit inactive time; and how to use growth charts.
The control group program focused on safety and matched the guidance categories. For example, early visits included information on prevention of sudden infant death syndrome for sleep, breast milk storage and formula for feeding, and safe bathing.
Jennifer S. Savage, Center for Childhood Obesity Research, Penn State University, University Park, led the study that enrolled 117 infants in a randomized controlled trial. Mother and firstborn children were randomized to the RP or home safety intervention (control) group 10-14 days after delivery. Their second-born siblings were enrolled in an observation-only ancillary study.
Second-born children were delivered 2.5 (standard deviation, 0.9) years after firstborns. Anthropometrics were measured in both siblings at ages 3, 16, 28, and 52 weeks.
Firstborn children at 1 year had a body mass index (BMI) that was 0.44 kg/m2 lower than the control group (95% confidence interval, −0.82 to −0.06), and second-born children whose parents received the RP intervention with their first child had BMI that was 0.36 kg/m2 lower.
“What we saw here is that it worked again,” coauthor Ian Paul, MD, MSc, professor of pediatrics and public health sciences at Penn State University, Hershey, said in an interview.
“Once we imprint them with a certain approach to parenting with the first child, they’re doing the same thing with the second child, which is wonderful to see,” he said.
He noted that this happened with second children without any reinforcements or booster information.
Dr. Paul said it’s still not clear which of the interventions – whether related to feeding techniques or sleeping or activity – helps most. And for each family the problematic behaviors may be different.
Responsive parenting programs have shown success previously among firstborns, the authors wrote, but 80% of those children grow up with younger siblings, so an intervention that also benefits them is important.
Weighing the costs of the intervention
The intervention was extensive. It involved four hour-plus nurse visits a year, often by the same nurse who built a relationship with the family.
But Ms. Savage said that it is possible to replicate INSIGHT on a larger scale in the United States with the dozens of home visitation models.
“Currently, 21 home visitation models meet the U.S. Department of Health & Human Services criteria for evidence of effectiveness, such as Nurse Family Partnership, Family Check-up, and Early Head Start Home Based Option. There is an opportunity to use home visitation models at the national scale to potentially interrupt the cycle of poor multigenerational outcomes such as obesity,” she said.
Dr. Paul said the initial investment “can save money in the long term,” given what’s at stake. “We know that 20%-25% of 2- to 5-year-olds are already overweight or obese and if they are already overweight or obese at that age, that;’s likely to persist.”
However, he acknowledged that staff shortages and costs are a challenge.
“Other countries have made that investment in their health care system,” he said. “In the U.S. only a fraction of new mothers and babies get home visitation. The kind of work that we did for obesity prevention has not yet been incorporated into evidence-based models of home visitation, though it certainly could be.”
Dr. Paul said his team is hoping to collaborate with others in the near future on expanding this program to such models of home visitation.
Telehealth, though a less desirable option, compared with in-home visits, could also be utilized, he said.
Short of the comprehensive intervention, he said, many of the concepts can be put into practice by pediatricians and parents.
Dr. Paul noted that the Robert Wood Johnson Foundation has endorsed “responsive feeding” as the preferred approach to feeding infants and toddlers. Responsive feeding – helping parents recognize hunger and satiety cues as opposed to other distress cues – is a big part of the intervention.
“Feeding to soothe is not the preferred approach,” he said. “Food and milk and formula should be used for hunger.” That’s something pediatricians may not be stressing to parents, he said.
Pediatricians can also counsel parents on not using food as a reward. “We shouldn’t be giving kids M&Ms to teach them how to potty train,” he said.
‘Promising’ findings
Charles Wood, MD, a childhood obesity specialist at Duke University, Durham, N.C., who was not part of the study, called the findings “very promising.”
It also makes sense that the “aha moments” of first-time parents learning from the INSIGHT intervention would carry over to the second sibling, he said.
Dr. Wood agreed costs are a big factor. However, he said, the potential downstream costs of not preventing obesity are worse. And this study indicates the benefits may keep spreading with future siblings.
Dr. Wood said accessing obesity interventions outside the pediatrician visit can also help. Connecting patients with support groups or dietitians or with a counselor from Women, Infants, and Children can help. However, consistent messaging among the providers is key, he noted.
Dr. Wood’s research group is investigating text messaging platforms so parents can get answer to real-time questions, such as those about feeding behaviors.
He pointed to a limitation the authors mention, which is that the study was done in mostly White, highly educated, higher-income families.
“There’s a big problem with racial disparities and obesity,” Dr. Wood noted. “We definitely need solutions that address disparities as well.”
Mothers included in the study had given birth for the first time and their infants were enrolled after birth from a single maternity ward between January 2012 and March 2014. Major eligibility criteria were that the babies were full term (at least 37 weeks’ gestation), single births, and delivered to English-speaking mothers at least 20 years of age. Infants who weighed less than 2,500 g at birth were excluded.
The paper’s authors and Dr. Wood declared no relevant financial relationships.
This research was supported by the National Institutes of Health, the National Institute of Diabetes and Digestive and Kidney Diseases; and the Department of Agriculture.
According to a statement from the National Institutes of Health, who funded the study, it is the first such infant obesity intervention to show the spillover effect. Findings were published online Dec. 21, 2021, in Obesity.
The program is called Infants Growing on Healthy Trajectories (INSIGHT) responsive parenting (RP) intervention, and it included guidance on feeding, sleep, interactive play, and regulating emotion.
Parents were given guidance by nurses who came to their homes on how to respond when their child is drowsy, sleeping, fussy, and alert. They also learned how to put infants to bed drowsy, but awake, and avoid feeding infants to get them to sleep; how to respond to infants waking up at night; when to start solid foods; how to limit inactive time; and how to use growth charts.
The control group program focused on safety and matched the guidance categories. For example, early visits included information on prevention of sudden infant death syndrome for sleep, breast milk storage and formula for feeding, and safe bathing.
Jennifer S. Savage, Center for Childhood Obesity Research, Penn State University, University Park, led the study that enrolled 117 infants in a randomized controlled trial. Mother and firstborn children were randomized to the RP or home safety intervention (control) group 10-14 days after delivery. Their second-born siblings were enrolled in an observation-only ancillary study.
Second-born children were delivered 2.5 (standard deviation, 0.9) years after firstborns. Anthropometrics were measured in both siblings at ages 3, 16, 28, and 52 weeks.
Firstborn children at 1 year had a body mass index (BMI) that was 0.44 kg/m2 lower than the control group (95% confidence interval, −0.82 to −0.06), and second-born children whose parents received the RP intervention with their first child had BMI that was 0.36 kg/m2 lower.
“What we saw here is that it worked again,” coauthor Ian Paul, MD, MSc, professor of pediatrics and public health sciences at Penn State University, Hershey, said in an interview.
“Once we imprint them with a certain approach to parenting with the first child, they’re doing the same thing with the second child, which is wonderful to see,” he said.
He noted that this happened with second children without any reinforcements or booster information.
Dr. Paul said it’s still not clear which of the interventions – whether related to feeding techniques or sleeping or activity – helps most. And for each family the problematic behaviors may be different.
Responsive parenting programs have shown success previously among firstborns, the authors wrote, but 80% of those children grow up with younger siblings, so an intervention that also benefits them is important.
Weighing the costs of the intervention
The intervention was extensive. It involved four hour-plus nurse visits a year, often by the same nurse who built a relationship with the family.
But Ms. Savage said that it is possible to replicate INSIGHT on a larger scale in the United States with the dozens of home visitation models.
“Currently, 21 home visitation models meet the U.S. Department of Health & Human Services criteria for evidence of effectiveness, such as Nurse Family Partnership, Family Check-up, and Early Head Start Home Based Option. There is an opportunity to use home visitation models at the national scale to potentially interrupt the cycle of poor multigenerational outcomes such as obesity,” she said.
Dr. Paul said the initial investment “can save money in the long term,” given what’s at stake. “We know that 20%-25% of 2- to 5-year-olds are already overweight or obese and if they are already overweight or obese at that age, that;’s likely to persist.”
However, he acknowledged that staff shortages and costs are a challenge.
“Other countries have made that investment in their health care system,” he said. “In the U.S. only a fraction of new mothers and babies get home visitation. The kind of work that we did for obesity prevention has not yet been incorporated into evidence-based models of home visitation, though it certainly could be.”
Dr. Paul said his team is hoping to collaborate with others in the near future on expanding this program to such models of home visitation.
Telehealth, though a less desirable option, compared with in-home visits, could also be utilized, he said.
Short of the comprehensive intervention, he said, many of the concepts can be put into practice by pediatricians and parents.
Dr. Paul noted that the Robert Wood Johnson Foundation has endorsed “responsive feeding” as the preferred approach to feeding infants and toddlers. Responsive feeding – helping parents recognize hunger and satiety cues as opposed to other distress cues – is a big part of the intervention.
“Feeding to soothe is not the preferred approach,” he said. “Food and milk and formula should be used for hunger.” That’s something pediatricians may not be stressing to parents, he said.
Pediatricians can also counsel parents on not using food as a reward. “We shouldn’t be giving kids M&Ms to teach them how to potty train,” he said.
‘Promising’ findings
Charles Wood, MD, a childhood obesity specialist at Duke University, Durham, N.C., who was not part of the study, called the findings “very promising.”
It also makes sense that the “aha moments” of first-time parents learning from the INSIGHT intervention would carry over to the second sibling, he said.
Dr. Wood agreed costs are a big factor. However, he said, the potential downstream costs of not preventing obesity are worse. And this study indicates the benefits may keep spreading with future siblings.
Dr. Wood said accessing obesity interventions outside the pediatrician visit can also help. Connecting patients with support groups or dietitians or with a counselor from Women, Infants, and Children can help. However, consistent messaging among the providers is key, he noted.
Dr. Wood’s research group is investigating text messaging platforms so parents can get answer to real-time questions, such as those about feeding behaviors.
He pointed to a limitation the authors mention, which is that the study was done in mostly White, highly educated, higher-income families.
“There’s a big problem with racial disparities and obesity,” Dr. Wood noted. “We definitely need solutions that address disparities as well.”
Mothers included in the study had given birth for the first time and their infants were enrolled after birth from a single maternity ward between January 2012 and March 2014. Major eligibility criteria were that the babies were full term (at least 37 weeks’ gestation), single births, and delivered to English-speaking mothers at least 20 years of age. Infants who weighed less than 2,500 g at birth were excluded.
The paper’s authors and Dr. Wood declared no relevant financial relationships.
This research was supported by the National Institutes of Health, the National Institute of Diabetes and Digestive and Kidney Diseases; and the Department of Agriculture.
FROM OBESITY
Helping teens make the switch from pediatrics to gynecology
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Surgeon General releases child mental health call to action
The nation’s Surgeon General, Vice Admiral Vivek H. Murthy, MD, MBA, recently released an advisory report on the current state of youth mental health and recommendations to improve well-being. This action follows a number of emergency declarations that have been made by professional organizations such as the American Academy of Child and Adolescent Psychiatry (AACAP), the American Academy of Pediatrics (AAP), and other health care groups to raise awareness about the alarming increase of depression, suicide, anxiety, and other mental health problems in youth.
These reports can be helpful in focusing attention and resources for important public health problems. Many still reference the 1999 report from former Surgeon General David Satcher, MD, PhD, which offered a number of eye-opening statistics regarding the prevalence of mental health conditions and the amount of disability associated with them.

Sadly, the present report indicates that many of these indices have grown worse in the past 20 years. For example, the advisory notes that, even before COVID-19, fully half of female high school students reported persistent feelings of sadness or hopelessness (up 40% from 2009). The report then goes on to cite a number of studies documenting even further rises in youth mental health problems associated with the pandemic.
Most of the advisory, however, is devoted to actions that can be taken by different groups, including young people themselves, parents, educators, the government, and even social media and video game companies, to support mental health and well-being. Multiple online resources are provided at the end of each of these sections.
One of the segments is aimed at health care organizations and professionals. While first making a fairly sweeping statement that “our health care system today is not set up optimally to support the mental health and well-being of children and youth,” this part then outlines five broad recommendations that might help improve the fit. These include the following.
- Increase prevention efforts, such as coordination to enrichment programs and referrals for economic and legal supports for families in need.
- Screen routinely for mental health conditions and link those who screen in with appropriate care.
- Identify mental health needs in parents and caregivers such as depression and substance use that can have negative effects on children.
- Increase partnerships between health care groups and community organizations.
- Build multidisciplinary teams that are culturally appropriate and maximally engage children and caretakers in the decision-making process.
The current report is downloadable for free (see reference below) and it is certainly worthwhile for pediatricians to take a look. Dr. Murthy writes, regarding the current state of mental health, that “it would be a tragedy if we beat back one public health crisis only to allow another to grow in its place.”
The report also outlines specific areas where additional research is needed, such as data on racial and sexual minorities and research on innovative and scalable therapies. In addition to the online resources that are provided, the report is backed by over 250 references.
Since its release, the report has generally been well received, and, indeed, there is much to support. The well-known Child Mind Institute in New York tweeted that “this document is a wake-up call for the country and a long-overdue statement of leadership from the federal government.”
Many of the recommendations are admittedly somewhat commons sense, but there are some that are much less so. For example, one recommendation to youth themselves is to serve others – something that may first come across as counterintuitive but can indeed help children and adolescents develop a sense of purpose and self-worth. The call for pediatric health care professionals to screen parents in addition to the patients themselves will likely result in some debate as well. The recommendation to reduce access to lethal means, including the specific naming of firearms, is also a welcome addition. This report also rightly puts a spotlight on the role of societal factors such as racism and poverty in the development of mental health problems and in getting access to quality treatment.
Also worth noting is how much of the advisory examined the role of media in both the problem and the solution. While recognizing that technology, smartphones, and social media are here to stay, a number of suggestions were given to parents, media organizations, journalists, and entertainment companies to reduce the negative impacts these mediums can have. Explicitly recognized in the report is that “there can be tension between what’s best for the technology company and what’s best for the individual user or society.” Also acknowledged was that the link between media of various types and mental health is complex and inconsistent with there being a strong need for additional work in this area when it comes to academic research as well as product development within these companies themselves.
Yet while there is much to like about the advisory, there remain some areas that seem lacking. For example, the text about what causes mental health conditions gets a little dualistic in mentioning biological and environmental factors without much appreciation that these are hardly independent domains. Perhaps more substantially, there was surprisingly little airtime devoted to an enormous issue that underlies so many other challenges related to mental health care – namely an inadequate workforce that gets smaller by the minute. The topic was treated much too superficially with lots of vague calls to “expand” the workforce that lacked substance or detail.
Overall, however, the new Surgeon General’s Advisory is a welcome document that offers updated knowledge of our current challenges and provides practical responses that truly could make a difference. Now all we have to do is put these recommendations into action.
Dr. Rettew is a child and adolescent psychiatrist and medical director of Lane County Behavioral Health in Eugene, Ore. His latest book is “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
“Protecting Youth Mental Health – The U.S. Surgeon General’s Advisory,” U.S. Department of Health & Human Services (2021).
The nation’s Surgeon General, Vice Admiral Vivek H. Murthy, MD, MBA, recently released an advisory report on the current state of youth mental health and recommendations to improve well-being. This action follows a number of emergency declarations that have been made by professional organizations such as the American Academy of Child and Adolescent Psychiatry (AACAP), the American Academy of Pediatrics (AAP), and other health care groups to raise awareness about the alarming increase of depression, suicide, anxiety, and other mental health problems in youth.
These reports can be helpful in focusing attention and resources for important public health problems. Many still reference the 1999 report from former Surgeon General David Satcher, MD, PhD, which offered a number of eye-opening statistics regarding the prevalence of mental health conditions and the amount of disability associated with them.
Sadly, the present report indicates that many of these indices have grown worse in the past 20 years. For example, the advisory notes that, even before COVID-19, fully half of female high school students reported persistent feelings of sadness or hopelessness (up 40% from 2009). The report then goes on to cite a number of studies documenting even further rises in youth mental health problems associated with the pandemic.
Most of the advisory, however, is devoted to actions that can be taken by different groups, including young people themselves, parents, educators, the government, and even social media and video game companies, to support mental health and well-being. Multiple online resources are provided at the end of each of these sections.
One of the segments is aimed at health care organizations and professionals. While first making a fairly sweeping statement that “our health care system today is not set up optimally to support the mental health and well-being of children and youth,” this part then outlines five broad recommendations that might help improve the fit. These include the following.
- Increase prevention efforts, such as coordination to enrichment programs and referrals for economic and legal supports for families in need.
- Screen routinely for mental health conditions and link those who screen in with appropriate care.
- Identify mental health needs in parents and caregivers such as depression and substance use that can have negative effects on children.
- Increase partnerships between health care groups and community organizations.
- Build multidisciplinary teams that are culturally appropriate and maximally engage children and caretakers in the decision-making process.
The current report is downloadable for free (see reference below) and it is certainly worthwhile for pediatricians to take a look. Dr. Murthy writes, regarding the current state of mental health, that “it would be a tragedy if we beat back one public health crisis only to allow another to grow in its place.”
The report also outlines specific areas where additional research is needed, such as data on racial and sexual minorities and research on innovative and scalable therapies. In addition to the online resources that are provided, the report is backed by over 250 references.
Since its release, the report has generally been well received, and, indeed, there is much to support. The well-known Child Mind Institute in New York tweeted that “this document is a wake-up call for the country and a long-overdue statement of leadership from the federal government.”
Many of the recommendations are admittedly somewhat commons sense, but there are some that are much less so. For example, one recommendation to youth themselves is to serve others – something that may first come across as counterintuitive but can indeed help children and adolescents develop a sense of purpose and self-worth. The call for pediatric health care professionals to screen parents in addition to the patients themselves will likely result in some debate as well. The recommendation to reduce access to lethal means, including the specific naming of firearms, is also a welcome addition. This report also rightly puts a spotlight on the role of societal factors such as racism and poverty in the development of mental health problems and in getting access to quality treatment.
Also worth noting is how much of the advisory examined the role of media in both the problem and the solution. While recognizing that technology, smartphones, and social media are here to stay, a number of suggestions were given to parents, media organizations, journalists, and entertainment companies to reduce the negative impacts these mediums can have. Explicitly recognized in the report is that “there can be tension between what’s best for the technology company and what’s best for the individual user or society.” Also acknowledged was that the link between media of various types and mental health is complex and inconsistent with there being a strong need for additional work in this area when it comes to academic research as well as product development within these companies themselves.
Yet while there is much to like about the advisory, there remain some areas that seem lacking. For example, the text about what causes mental health conditions gets a little dualistic in mentioning biological and environmental factors without much appreciation that these are hardly independent domains. Perhaps more substantially, there was surprisingly little airtime devoted to an enormous issue that underlies so many other challenges related to mental health care – namely an inadequate workforce that gets smaller by the minute. The topic was treated much too superficially with lots of vague calls to “expand” the workforce that lacked substance or detail.
Overall, however, the new Surgeon General’s Advisory is a welcome document that offers updated knowledge of our current challenges and provides practical responses that truly could make a difference. Now all we have to do is put these recommendations into action.
Dr. Rettew is a child and adolescent psychiatrist and medical director of Lane County Behavioral Health in Eugene, Ore. His latest book is “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
“Protecting Youth Mental Health – The U.S. Surgeon General’s Advisory,” U.S. Department of Health & Human Services (2021).
The nation’s Surgeon General, Vice Admiral Vivek H. Murthy, MD, MBA, recently released an advisory report on the current state of youth mental health and recommendations to improve well-being. This action follows a number of emergency declarations that have been made by professional organizations such as the American Academy of Child and Adolescent Psychiatry (AACAP), the American Academy of Pediatrics (AAP), and other health care groups to raise awareness about the alarming increase of depression, suicide, anxiety, and other mental health problems in youth.
These reports can be helpful in focusing attention and resources for important public health problems. Many still reference the 1999 report from former Surgeon General David Satcher, MD, PhD, which offered a number of eye-opening statistics regarding the prevalence of mental health conditions and the amount of disability associated with them.
Sadly, the present report indicates that many of these indices have grown worse in the past 20 years. For example, the advisory notes that, even before COVID-19, fully half of female high school students reported persistent feelings of sadness or hopelessness (up 40% from 2009). The report then goes on to cite a number of studies documenting even further rises in youth mental health problems associated with the pandemic.
Most of the advisory, however, is devoted to actions that can be taken by different groups, including young people themselves, parents, educators, the government, and even social media and video game companies, to support mental health and well-being. Multiple online resources are provided at the end of each of these sections.
One of the segments is aimed at health care organizations and professionals. While first making a fairly sweeping statement that “our health care system today is not set up optimally to support the mental health and well-being of children and youth,” this part then outlines five broad recommendations that might help improve the fit. These include the following.
- Increase prevention efforts, such as coordination to enrichment programs and referrals for economic and legal supports for families in need.
- Screen routinely for mental health conditions and link those who screen in with appropriate care.
- Identify mental health needs in parents and caregivers such as depression and substance use that can have negative effects on children.
- Increase partnerships between health care groups and community organizations.
- Build multidisciplinary teams that are culturally appropriate and maximally engage children and caretakers in the decision-making process.
The current report is downloadable for free (see reference below) and it is certainly worthwhile for pediatricians to take a look. Dr. Murthy writes, regarding the current state of mental health, that “it would be a tragedy if we beat back one public health crisis only to allow another to grow in its place.”
The report also outlines specific areas where additional research is needed, such as data on racial and sexual minorities and research on innovative and scalable therapies. In addition to the online resources that are provided, the report is backed by over 250 references.
Since its release, the report has generally been well received, and, indeed, there is much to support. The well-known Child Mind Institute in New York tweeted that “this document is a wake-up call for the country and a long-overdue statement of leadership from the federal government.”
Many of the recommendations are admittedly somewhat commons sense, but there are some that are much less so. For example, one recommendation to youth themselves is to serve others – something that may first come across as counterintuitive but can indeed help children and adolescents develop a sense of purpose and self-worth. The call for pediatric health care professionals to screen parents in addition to the patients themselves will likely result in some debate as well. The recommendation to reduce access to lethal means, including the specific naming of firearms, is also a welcome addition. This report also rightly puts a spotlight on the role of societal factors such as racism and poverty in the development of mental health problems and in getting access to quality treatment.
Also worth noting is how much of the advisory examined the role of media in both the problem and the solution. While recognizing that technology, smartphones, and social media are here to stay, a number of suggestions were given to parents, media organizations, journalists, and entertainment companies to reduce the negative impacts these mediums can have. Explicitly recognized in the report is that “there can be tension between what’s best for the technology company and what’s best for the individual user or society.” Also acknowledged was that the link between media of various types and mental health is complex and inconsistent with there being a strong need for additional work in this area when it comes to academic research as well as product development within these companies themselves.
Yet while there is much to like about the advisory, there remain some areas that seem lacking. For example, the text about what causes mental health conditions gets a little dualistic in mentioning biological and environmental factors without much appreciation that these are hardly independent domains. Perhaps more substantially, there was surprisingly little airtime devoted to an enormous issue that underlies so many other challenges related to mental health care – namely an inadequate workforce that gets smaller by the minute. The topic was treated much too superficially with lots of vague calls to “expand” the workforce that lacked substance or detail.
Overall, however, the new Surgeon General’s Advisory is a welcome document that offers updated knowledge of our current challenges and provides practical responses that truly could make a difference. Now all we have to do is put these recommendations into action.
Dr. Rettew is a child and adolescent psychiatrist and medical director of Lane County Behavioral Health in Eugene, Ore. His latest book is “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
“Protecting Youth Mental Health – The U.S. Surgeon General’s Advisory,” U.S. Department of Health & Human Services (2021).
Children and COVID: New cases, admissions are higher than ever
Weekly COVID-19 cases in children passed 300,000 for the first time since the pandemic started, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The rate of new COVID-related hospital admissions also reached a new high of 0.74 per 100,000 children as of Dec. 31. The highest rate seen before the current Omicron-fueled surge was 0.47 per 100,000 in early September, data from the Centers for Disease Control and Prevention show.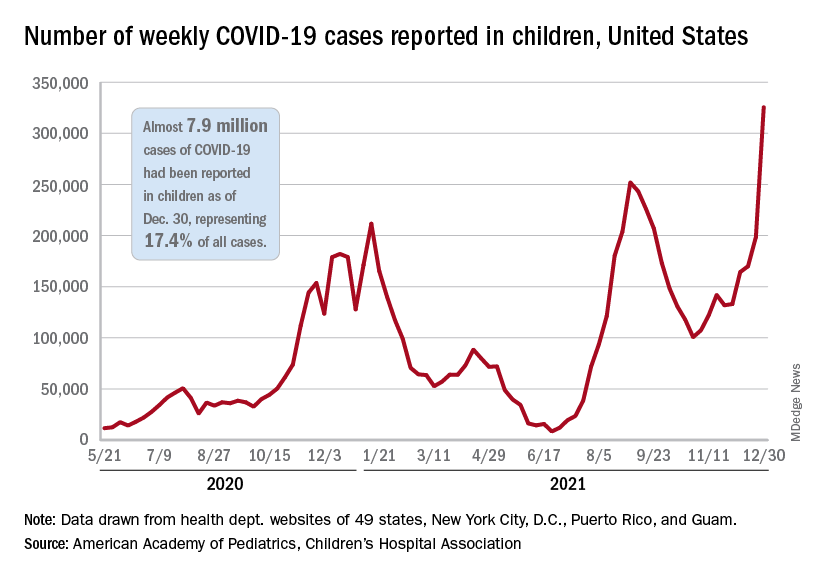
and exceeding the previous week’s count by almost 64%, the AAP and CHA said in their weekly COVID report.
New cases were up in all four regions of the United States, with the Northeast adding the most newly infected children while setting a new high for the fifth consecutive week. The South was just behind for the week but still well off the record it reached in September, the Midwest was third but recorded its busiest week ever, and the West was fourth and nowhere near its previous high, the AAP/CHA report indicated.
The total number of child cases since the pandemic began is almost 7.9 million, they said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. That figure represents 17.4% of all cases reported in the United States, and the cumulative rate of COVID infection is up to almost 10,500 per 100,000 children, meaning that 1 in 10 children have been infected.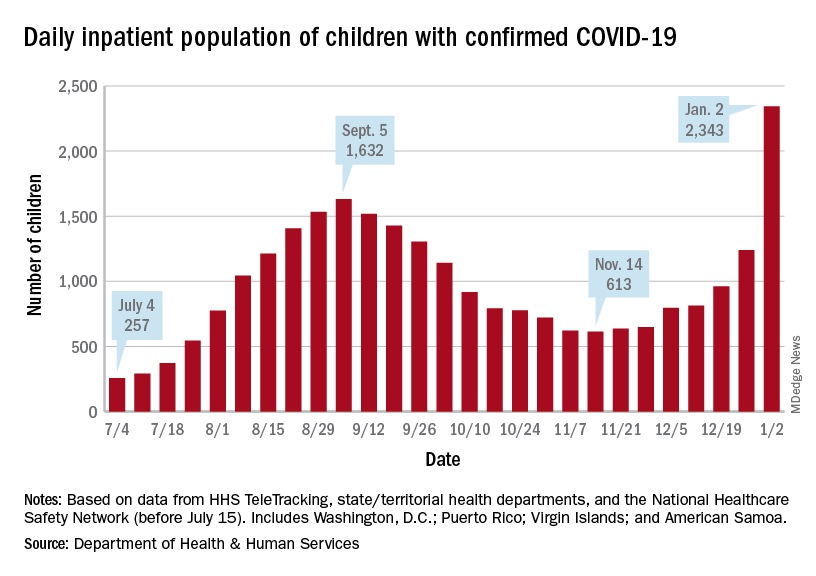
Children are still less likely to be hospitalized than adults, but the gap appears to be closing. On Jan. 2 there were 2,343 children and 87,690 adults in the hospital with confirmed COVID, a ratio of 37 adults for each child, but on Sept. 5, at the height of the previous surge, the ratio of hospitalized adults (93,647) to children (1,632) was 57:1, according to data from the Department of Health & Human Services.
New admissions show a similar pattern: The 0.74 admissions per 100,000 children recorded on Dec. 31 was lower than, for example, adults aged 30-39 years (2.7 per 100,000) or 50-59 years (4.25 per 100,000), but on Sept. 5 the corresponding figures were 0.46 (children), 2.74 (ages 30-39), and 5.03 (aged 50-59), based on the HHS data.
A look at vaccinations
The vaccination response to Omicron, however, has been more subdued and somewhat inconsistent. Vaccine initiation, not surprisingly, was down among eligible children for the week of Dec. 23-29. Before that, both the 5- to 11-year-olds and 12- to 15-year-olds were down for the second week of December and then up a bit (5.6% and 14.3%, respectively) during the third week, while the 16- to 17-year-olds, increased initiation by 63.2%, CDC’s COVID Data Tracker shows.
Less than a quarter (23.5%) of children aged 5-11 received at least one dose of the vaccine in the first 2 months of their eligibility, and only 14.7% are fully vaccinated. Among the older children, coverage looks like this: at least one dose for 61.2% of 12- to 15-year-olds and 67.4% of 16- to 17-year-olds and full vaccination for 51.3% and 57.6%, respectively, the CDC said.
At the state level, Massachusetts and Hawaii have the highest rates for children aged 12-17 years, with 86% having received a least one dose, and Vermont is highest for children aged 5-11 at 56%. The lowest rates can be found in Wyoming (38%) for 12- to 17-year-olds and in Mississippi (6%) for 5- to 11-year-olds, the AAP said in a separate report.
Weekly COVID-19 cases in children passed 300,000 for the first time since the pandemic started, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The rate of new COVID-related hospital admissions also reached a new high of 0.74 per 100,000 children as of Dec. 31. The highest rate seen before the current Omicron-fueled surge was 0.47 per 100,000 in early September, data from the Centers for Disease Control and Prevention show.
and exceeding the previous week’s count by almost 64%, the AAP and CHA said in their weekly COVID report.
New cases were up in all four regions of the United States, with the Northeast adding the most newly infected children while setting a new high for the fifth consecutive week. The South was just behind for the week but still well off the record it reached in September, the Midwest was third but recorded its busiest week ever, and the West was fourth and nowhere near its previous high, the AAP/CHA report indicated.
The total number of child cases since the pandemic began is almost 7.9 million, they said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. That figure represents 17.4% of all cases reported in the United States, and the cumulative rate of COVID infection is up to almost 10,500 per 100,000 children, meaning that 1 in 10 children have been infected.
Children are still less likely to be hospitalized than adults, but the gap appears to be closing. On Jan. 2 there were 2,343 children and 87,690 adults in the hospital with confirmed COVID, a ratio of 37 adults for each child, but on Sept. 5, at the height of the previous surge, the ratio of hospitalized adults (93,647) to children (1,632) was 57:1, according to data from the Department of Health & Human Services.
New admissions show a similar pattern: The 0.74 admissions per 100,000 children recorded on Dec. 31 was lower than, for example, adults aged 30-39 years (2.7 per 100,000) or 50-59 years (4.25 per 100,000), but on Sept. 5 the corresponding figures were 0.46 (children), 2.74 (ages 30-39), and 5.03 (aged 50-59), based on the HHS data.
A look at vaccinations
The vaccination response to Omicron, however, has been more subdued and somewhat inconsistent. Vaccine initiation, not surprisingly, was down among eligible children for the week of Dec. 23-29. Before that, both the 5- to 11-year-olds and 12- to 15-year-olds were down for the second week of December and then up a bit (5.6% and 14.3%, respectively) during the third week, while the 16- to 17-year-olds, increased initiation by 63.2%, CDC’s COVID Data Tracker shows.
Less than a quarter (23.5%) of children aged 5-11 received at least one dose of the vaccine in the first 2 months of their eligibility, and only 14.7% are fully vaccinated. Among the older children, coverage looks like this: at least one dose for 61.2% of 12- to 15-year-olds and 67.4% of 16- to 17-year-olds and full vaccination for 51.3% and 57.6%, respectively, the CDC said.
At the state level, Massachusetts and Hawaii have the highest rates for children aged 12-17 years, with 86% having received a least one dose, and Vermont is highest for children aged 5-11 at 56%. The lowest rates can be found in Wyoming (38%) for 12- to 17-year-olds and in Mississippi (6%) for 5- to 11-year-olds, the AAP said in a separate report.
Weekly COVID-19 cases in children passed 300,000 for the first time since the pandemic started, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The rate of new COVID-related hospital admissions also reached a new high of 0.74 per 100,000 children as of Dec. 31. The highest rate seen before the current Omicron-fueled surge was 0.47 per 100,000 in early September, data from the Centers for Disease Control and Prevention show.
and exceeding the previous week’s count by almost 64%, the AAP and CHA said in their weekly COVID report.
New cases were up in all four regions of the United States, with the Northeast adding the most newly infected children while setting a new high for the fifth consecutive week. The South was just behind for the week but still well off the record it reached in September, the Midwest was third but recorded its busiest week ever, and the West was fourth and nowhere near its previous high, the AAP/CHA report indicated.
The total number of child cases since the pandemic began is almost 7.9 million, they said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. That figure represents 17.4% of all cases reported in the United States, and the cumulative rate of COVID infection is up to almost 10,500 per 100,000 children, meaning that 1 in 10 children have been infected.
Children are still less likely to be hospitalized than adults, but the gap appears to be closing. On Jan. 2 there were 2,343 children and 87,690 adults in the hospital with confirmed COVID, a ratio of 37 adults for each child, but on Sept. 5, at the height of the previous surge, the ratio of hospitalized adults (93,647) to children (1,632) was 57:1, according to data from the Department of Health & Human Services.
New admissions show a similar pattern: The 0.74 admissions per 100,000 children recorded on Dec. 31 was lower than, for example, adults aged 30-39 years (2.7 per 100,000) or 50-59 years (4.25 per 100,000), but on Sept. 5 the corresponding figures were 0.46 (children), 2.74 (ages 30-39), and 5.03 (aged 50-59), based on the HHS data.
A look at vaccinations
The vaccination response to Omicron, however, has been more subdued and somewhat inconsistent. Vaccine initiation, not surprisingly, was down among eligible children for the week of Dec. 23-29. Before that, both the 5- to 11-year-olds and 12- to 15-year-olds were down for the second week of December and then up a bit (5.6% and 14.3%, respectively) during the third week, while the 16- to 17-year-olds, increased initiation by 63.2%, CDC’s COVID Data Tracker shows.
Less than a quarter (23.5%) of children aged 5-11 received at least one dose of the vaccine in the first 2 months of their eligibility, and only 14.7% are fully vaccinated. Among the older children, coverage looks like this: at least one dose for 61.2% of 12- to 15-year-olds and 67.4% of 16- to 17-year-olds and full vaccination for 51.3% and 57.6%, respectively, the CDC said.
At the state level, Massachusetts and Hawaii have the highest rates for children aged 12-17 years, with 86% having received a least one dose, and Vermont is highest for children aged 5-11 at 56%. The lowest rates can be found in Wyoming (38%) for 12- to 17-year-olds and in Mississippi (6%) for 5- to 11-year-olds, the AAP said in a separate report.
Peanut desensitization plummets 1 month after avoiding exposure
Children with peanut allergies treated with peanut oral immunotherapy for 3 years can tolerate increasingly higher exposures to peanuts. But avoidance of peanut-protein exposure for just a single month after the treatment leads to rapid and substantial decreases in tolerance, findings from a small study show.
The findings “underscore the fact that the desensitization achieved with peanut oral immunotherapy is a transient immune state,” report the authors of the study, published in December in The Journal of Allergy and Clinical Immunology: In Practice.
Therefore, “adherence to dosing [in peanut immunotherapy] is very important, and clinicians should expect a decline in tolerance with lapse in dosing,” first author Carla M. Davis, MD, director of the Texas Children’s Hospital Food Allergy Program at Baylor College of Medicine, Houston, told this news organization.
Oral immunotherapy, involving small exposures to peanut protein to build up desensitization, has been shown to mitigate allergic reactions, and, as reported by this news organization, the first peanut oral immunotherapy drug recently received approval from the U.S. Food and Drug Administration.
However, current approaches involve very low daily exposure of about 300 mg of peanut protein, equivalent to only about one to two peanuts, and research is lacking regarding the maximum tolerated doses, as well as on how long the tolerance is sustained if maintenance therapy is discontinued. “For the peanut-allergic population that would like to eat more than 1-2 peanuts, an achievable dose is currently unknown,” the study authors write. “The critical question, of the maximum tolerated dose achieved after POIT, has not been answered.”
To evaluate those issues in their phase 2 study, Dr. Davis and her colleagues enrolled 28 subjects between the ages of 5 and 13 with a diagnosis of eosinophilic esophagitis and peanut allergy.
The treatment protocol included a 1-year buildup phase of oral immunotherapy, followed by a 2-year daily maintenance phase with a dose of 3,900 mg of peanut protein.
After consenting, 11 patients dropped out of the study due to a lack of interest, and two more withdrew after failing to tolerate their first dose, leaving 15 who started treatment in the study, with a mean age of 8.7 years (range, 5.2-12.5 years), and 47% female.
Twelve patients reached the maintenance dose of 3,900 mg over a median of 13 months, and double-blind, placebo-controlled peanut challenges showed that, on average, their mean maximum cumulative tolerated dose after 12 months increased by 12,063 mg (P < .001), and the mean dose triggering a reaction increased by 15,667 mg.
Of the 12 patients, 11 (91.7%) were able to successfully tolerate at least 10,725 mg after 12 months of treatment, and six patients (50.0%) successfully tolerated at least 15,225 mg.
Two patients were able to tolerate up to the maximum cumulative target dose of 26,225 mg, equivalent to more than 105 peanuts.
“The ability to tolerate [greater than] 100 peanuts following peanut oral immunotherapy has never before been demonstrated and gives insight into the potential for food oral immunotherapy to be utilized in a subset of patients who have an immunologic phenotype accepting of this therapy,” the authors write.
“Understanding the risk of ingestion of peanut protein higher than the prescribed peanut oral immunotherapy maintenance dose will improve the safe, practical use of [the therapy],” they add.
Tolerance plummets with avoidance
In the protocol’s third phase, after the 3-year buildup and maintenance therapy, daily peanut exposure was avoided for 30 days, and among the six patients who participated, the mean maximum cumulative tolerated dose declined to just 2,783 mg, and the reaction dose dropped to 4,614 mg (P = .03).
“This was a disappointing finding, because we thought the desensitization would last longer after such a long period of treatment,” Dr. Davis said.
While the avoidance period was only a month, Dr. Davis said she expects the rebound in sensitivity would continue if avoidance was prolonged. “Other studies indicate the decline in tolerance would continue over time, [and] we believe it would continue to decline,” she said.
Further analysis of peanut allergy biomarkers showed significant decreases in skin prick test wheal size and cytokine expression within the first 6 weeks of initiation of the peanut oral immunotherapy. The patterns were reversed during the 1-month avoidance, with both measures increasing.
Of note, the changes in biomarkers varied significantly among the participants.
In terms of adverse events, eight patients (53%) required one or two doses of epinephrine during the study, with all but two patients receiving the epinephrine during the 12-month buildup phase, consistent with previous studies.
In commenting on the study, Richard L. Wasserman, MD, PhD, medical director of pediatric allergy and immunology at Medical City Children’s Hospital, Dallas, noted that the findings pertain to the subset of peanut oral immunotherapy patients (about 30%) who want to be able to eat peanuts.
“Most families just want protection against accidental ingestion, and these observations don’t relate to those patients,” he said in an interview.
Dr. Wasserman noted that his approach with patients is to wait until 3 years of daily maintenance after buildup (as opposed to 2 years in the study) before considering an avoidance challenge.
“When our patients pass a sustained unresponsiveness challenge, we recommend continued exposure of 2,000 mg at least weekly,” he explained.
Dr. Wasserman added that the study’s findings on biomarker changes were notable.
“The eventual reduction in peanut serum IgE in all of their patients is very interesting,” he said. “Many of our patients’ peanut serum IgE plateaus after 2 or 3 years.”
And he added, “This report suggests that we should be making patients aware that they may further decrease their peanut serum IgE by increasing their maintenance dose.”
The study was funded by the Scurlock Foundation/Waring Family Foundation and the Texas Children’s Hospital food allergy program. Dr. Davis is a consultant for Aimmune, DBV, and Moonlight Therapeutics. Dr. Wasserman is a consultant for Aimmune and DBV.
A version of this article first appeared on Medscape.com.
Children with peanut allergies treated with peanut oral immunotherapy for 3 years can tolerate increasingly higher exposures to peanuts. But avoidance of peanut-protein exposure for just a single month after the treatment leads to rapid and substantial decreases in tolerance, findings from a small study show.
The findings “underscore the fact that the desensitization achieved with peanut oral immunotherapy is a transient immune state,” report the authors of the study, published in December in The Journal of Allergy and Clinical Immunology: In Practice.
Therefore, “adherence to dosing [in peanut immunotherapy] is very important, and clinicians should expect a decline in tolerance with lapse in dosing,” first author Carla M. Davis, MD, director of the Texas Children’s Hospital Food Allergy Program at Baylor College of Medicine, Houston, told this news organization.
Oral immunotherapy, involving small exposures to peanut protein to build up desensitization, has been shown to mitigate allergic reactions, and, as reported by this news organization, the first peanut oral immunotherapy drug recently received approval from the U.S. Food and Drug Administration.
However, current approaches involve very low daily exposure of about 300 mg of peanut protein, equivalent to only about one to two peanuts, and research is lacking regarding the maximum tolerated doses, as well as on how long the tolerance is sustained if maintenance therapy is discontinued. “For the peanut-allergic population that would like to eat more than 1-2 peanuts, an achievable dose is currently unknown,” the study authors write. “The critical question, of the maximum tolerated dose achieved after POIT, has not been answered.”
To evaluate those issues in their phase 2 study, Dr. Davis and her colleagues enrolled 28 subjects between the ages of 5 and 13 with a diagnosis of eosinophilic esophagitis and peanut allergy.
The treatment protocol included a 1-year buildup phase of oral immunotherapy, followed by a 2-year daily maintenance phase with a dose of 3,900 mg of peanut protein.
After consenting, 11 patients dropped out of the study due to a lack of interest, and two more withdrew after failing to tolerate their first dose, leaving 15 who started treatment in the study, with a mean age of 8.7 years (range, 5.2-12.5 years), and 47% female.
Twelve patients reached the maintenance dose of 3,900 mg over a median of 13 months, and double-blind, placebo-controlled peanut challenges showed that, on average, their mean maximum cumulative tolerated dose after 12 months increased by 12,063 mg (P < .001), and the mean dose triggering a reaction increased by 15,667 mg.
Of the 12 patients, 11 (91.7%) were able to successfully tolerate at least 10,725 mg after 12 months of treatment, and six patients (50.0%) successfully tolerated at least 15,225 mg.
Two patients were able to tolerate up to the maximum cumulative target dose of 26,225 mg, equivalent to more than 105 peanuts.
“The ability to tolerate [greater than] 100 peanuts following peanut oral immunotherapy has never before been demonstrated and gives insight into the potential for food oral immunotherapy to be utilized in a subset of patients who have an immunologic phenotype accepting of this therapy,” the authors write.
“Understanding the risk of ingestion of peanut protein higher than the prescribed peanut oral immunotherapy maintenance dose will improve the safe, practical use of [the therapy],” they add.
Tolerance plummets with avoidance
In the protocol’s third phase, after the 3-year buildup and maintenance therapy, daily peanut exposure was avoided for 30 days, and among the six patients who participated, the mean maximum cumulative tolerated dose declined to just 2,783 mg, and the reaction dose dropped to 4,614 mg (P = .03).
“This was a disappointing finding, because we thought the desensitization would last longer after such a long period of treatment,” Dr. Davis said.
While the avoidance period was only a month, Dr. Davis said she expects the rebound in sensitivity would continue if avoidance was prolonged. “Other studies indicate the decline in tolerance would continue over time, [and] we believe it would continue to decline,” she said.
Further analysis of peanut allergy biomarkers showed significant decreases in skin prick test wheal size and cytokine expression within the first 6 weeks of initiation of the peanut oral immunotherapy. The patterns were reversed during the 1-month avoidance, with both measures increasing.
Of note, the changes in biomarkers varied significantly among the participants.
In terms of adverse events, eight patients (53%) required one or two doses of epinephrine during the study, with all but two patients receiving the epinephrine during the 12-month buildup phase, consistent with previous studies.
In commenting on the study, Richard L. Wasserman, MD, PhD, medical director of pediatric allergy and immunology at Medical City Children’s Hospital, Dallas, noted that the findings pertain to the subset of peanut oral immunotherapy patients (about 30%) who want to be able to eat peanuts.
“Most families just want protection against accidental ingestion, and these observations don’t relate to those patients,” he said in an interview.
Dr. Wasserman noted that his approach with patients is to wait until 3 years of daily maintenance after buildup (as opposed to 2 years in the study) before considering an avoidance challenge.
“When our patients pass a sustained unresponsiveness challenge, we recommend continued exposure of 2,000 mg at least weekly,” he explained.
Dr. Wasserman added that the study’s findings on biomarker changes were notable.
“The eventual reduction in peanut serum IgE in all of their patients is very interesting,” he said. “Many of our patients’ peanut serum IgE plateaus after 2 or 3 years.”
And he added, “This report suggests that we should be making patients aware that they may further decrease their peanut serum IgE by increasing their maintenance dose.”
The study was funded by the Scurlock Foundation/Waring Family Foundation and the Texas Children’s Hospital food allergy program. Dr. Davis is a consultant for Aimmune, DBV, and Moonlight Therapeutics. Dr. Wasserman is a consultant for Aimmune and DBV.
A version of this article first appeared on Medscape.com.
Children with peanut allergies treated with peanut oral immunotherapy for 3 years can tolerate increasingly higher exposures to peanuts. But avoidance of peanut-protein exposure for just a single month after the treatment leads to rapid and substantial decreases in tolerance, findings from a small study show.
The findings “underscore the fact that the desensitization achieved with peanut oral immunotherapy is a transient immune state,” report the authors of the study, published in December in The Journal of Allergy and Clinical Immunology: In Practice.
Therefore, “adherence to dosing [in peanut immunotherapy] is very important, and clinicians should expect a decline in tolerance with lapse in dosing,” first author Carla M. Davis, MD, director of the Texas Children’s Hospital Food Allergy Program at Baylor College of Medicine, Houston, told this news organization.
Oral immunotherapy, involving small exposures to peanut protein to build up desensitization, has been shown to mitigate allergic reactions, and, as reported by this news organization, the first peanut oral immunotherapy drug recently received approval from the U.S. Food and Drug Administration.
However, current approaches involve very low daily exposure of about 300 mg of peanut protein, equivalent to only about one to two peanuts, and research is lacking regarding the maximum tolerated doses, as well as on how long the tolerance is sustained if maintenance therapy is discontinued. “For the peanut-allergic population that would like to eat more than 1-2 peanuts, an achievable dose is currently unknown,” the study authors write. “The critical question, of the maximum tolerated dose achieved after POIT, has not been answered.”
To evaluate those issues in their phase 2 study, Dr. Davis and her colleagues enrolled 28 subjects between the ages of 5 and 13 with a diagnosis of eosinophilic esophagitis and peanut allergy.
The treatment protocol included a 1-year buildup phase of oral immunotherapy, followed by a 2-year daily maintenance phase with a dose of 3,900 mg of peanut protein.
After consenting, 11 patients dropped out of the study due to a lack of interest, and two more withdrew after failing to tolerate their first dose, leaving 15 who started treatment in the study, with a mean age of 8.7 years (range, 5.2-12.5 years), and 47% female.
Twelve patients reached the maintenance dose of 3,900 mg over a median of 13 months, and double-blind, placebo-controlled peanut challenges showed that, on average, their mean maximum cumulative tolerated dose after 12 months increased by 12,063 mg (P < .001), and the mean dose triggering a reaction increased by 15,667 mg.
Of the 12 patients, 11 (91.7%) were able to successfully tolerate at least 10,725 mg after 12 months of treatment, and six patients (50.0%) successfully tolerated at least 15,225 mg.
Two patients were able to tolerate up to the maximum cumulative target dose of 26,225 mg, equivalent to more than 105 peanuts.
“The ability to tolerate [greater than] 100 peanuts following peanut oral immunotherapy has never before been demonstrated and gives insight into the potential for food oral immunotherapy to be utilized in a subset of patients who have an immunologic phenotype accepting of this therapy,” the authors write.
“Understanding the risk of ingestion of peanut protein higher than the prescribed peanut oral immunotherapy maintenance dose will improve the safe, practical use of [the therapy],” they add.
Tolerance plummets with avoidance
In the protocol’s third phase, after the 3-year buildup and maintenance therapy, daily peanut exposure was avoided for 30 days, and among the six patients who participated, the mean maximum cumulative tolerated dose declined to just 2,783 mg, and the reaction dose dropped to 4,614 mg (P = .03).
“This was a disappointing finding, because we thought the desensitization would last longer after such a long period of treatment,” Dr. Davis said.
While the avoidance period was only a month, Dr. Davis said she expects the rebound in sensitivity would continue if avoidance was prolonged. “Other studies indicate the decline in tolerance would continue over time, [and] we believe it would continue to decline,” she said.
Further analysis of peanut allergy biomarkers showed significant decreases in skin prick test wheal size and cytokine expression within the first 6 weeks of initiation of the peanut oral immunotherapy. The patterns were reversed during the 1-month avoidance, with both measures increasing.
Of note, the changes in biomarkers varied significantly among the participants.
In terms of adverse events, eight patients (53%) required one or two doses of epinephrine during the study, with all but two patients receiving the epinephrine during the 12-month buildup phase, consistent with previous studies.
In commenting on the study, Richard L. Wasserman, MD, PhD, medical director of pediatric allergy and immunology at Medical City Children’s Hospital, Dallas, noted that the findings pertain to the subset of peanut oral immunotherapy patients (about 30%) who want to be able to eat peanuts.
“Most families just want protection against accidental ingestion, and these observations don’t relate to those patients,” he said in an interview.
Dr. Wasserman noted that his approach with patients is to wait until 3 years of daily maintenance after buildup (as opposed to 2 years in the study) before considering an avoidance challenge.
“When our patients pass a sustained unresponsiveness challenge, we recommend continued exposure of 2,000 mg at least weekly,” he explained.
Dr. Wasserman added that the study’s findings on biomarker changes were notable.
“The eventual reduction in peanut serum IgE in all of their patients is very interesting,” he said. “Many of our patients’ peanut serum IgE plateaus after 2 or 3 years.”
And he added, “This report suggests that we should be making patients aware that they may further decrease their peanut serum IgE by increasing their maintenance dose.”
The study was funded by the Scurlock Foundation/Waring Family Foundation and the Texas Children’s Hospital food allergy program. Dr. Davis is a consultant for Aimmune, DBV, and Moonlight Therapeutics. Dr. Wasserman is a consultant for Aimmune and DBV.
A version of this article first appeared on Medscape.com.
Tech can help teens connect with docs about sexual health
Maria Trent, MD, MPH, was studying ways clinicians can leverage technology to care for adolescents years before COVID-19 exposed the challenges and advantages of telehealth.
Dr. Trent, a pediatrician and adolescent medicine specialist and professor of pediatrics at Johns Hopkins University, Baltimore, has long believed that the phones in her patients’ pockets have the potential to improve the sexual health of youth. The pandemic has only made that view stronger.
“They’re a generation that’s really wired and online,” Dr. Trent told this news organization. “I think that we can meet them in that space.”
Her research has incorporated texting, apps, and videos. Out of necessity, technology increasingly became part of patient care during the pandemic. “We had to stretch our ability to do some basic triage and assessments of patients online,” Dr. Trent said.
Even when clinics are closed, doctors might be able to provide initial care remotely, such as writing prescriptions to manage symptoms or directing patients to a lab for testing.
Telemedicine could allow a clinician to guide a teenager who thinks they might be pregnant to take a store-bought test and avoid possible exposure to COVID-19 in the ED, for instance.
But doctors have concerns about the legal and practical limits of privacy and confidentiality. Who else is at home listening to a phone conversation? Are parents accessing the patient’s online portal? Will parents receive an explanation of benefits that lists testing for a sexually transmitted infection, or see a testing kit that is delivered to their home?
When a young patient needs in-person care, transportation can be a barrier. And then there’s the matter of clinicians being able to bill for telehealth services.
Practices are learning how to navigate these issues, and relevant laws vary by state.
“I think this is going to become part of standard practice,” Dr. Trent said. “I think we have to do the hard work to make sure that it’s safe, that it’s accessible, and that it is actually improving care.”
Texts, apps, videos
In one early study, Dr. Trent and colleagues found that showing adolescents with pelvic inflammatory disease a 6-minute video may improve treatment rates for their sexual partners.
Another study provided preliminary evidence that text messaging support might improve clinic attendance for moderately long-acting reversible contraception.
A third trial showed that adolescents and young adults with pelvic inflammatory disease who were randomly assigned to receive text-message prompts to take their medications and provide information about the doses they consumed had greater decreases in Neisseria gonorrhoeae and Chlamydia trachomatis infections, compared with patients who received standard care.
Dr. Trent and coinvestigators are assessing a technology-based intervention for youth with HIV, in which patients can use an app to submit videos of themselves taking antiretroviral therapy and report any side effects. The technology provides a way to monitor patients remotely and support them between visits, she said.
Will pandemic-driven options remain?
In 2020, Laura D. Lindberg, PhD, principal research scientist at the Guttmacher Institute in New York, and coauthors discussed the possible ramifications of the pandemic on the sexual and reproductive health of adolescents and young adults.
If telemedicine options driven by COVID-19 are here to stay, adolescents and young adults could be “the age group most likely to continue that approach rather than returning to traditional in-person visits,” the researchers wrote. “Innovations in health care service provision, such as use of telemedicine and obtaining contraceptives and STI testing by mail, will help expand access to [sexual and reproductive health] care for young people.”
At the 2021 annual conference of the American Academy of Pediatrics, Dr. Trent described telehealth as a viable way to provide sexual and reproductive health care to adolescents and young adults, including anticipatory guidance, contraception counseling, coordination of follow-up care and testing, and connecting patients to resources.
Her presentation cited several websites that can help patients receive testing for STIs, including Yes Means Test, the Centers for Disease Control and Prevention’s GetTested page, and I Want the Kit. Planned Parenthood has telehealth options, and the Kaiser Family Foundation compiled information about 26 online platforms that were providing contraception or STI services.
Who else is in the room?
“There’s only so much time in the day and so many patients you can see, regardless of whether you have telehealth or not,” said David L. Bell, MD, MPH, president of the Society for Adolescent Health and Medicine and a coauthor of the Perspectives on Sexual and Reproductive Health paper. In addition, “you never know who else is in the room” with the patient on the other end, added Dr. Bell, a professor of population and family health and pediatrics at the Columbia University Medical Center and medical director of the Young Men’s Clinic, both in New York.
In some respects, young patients may not be able to participate in telehealth visits the same way they would in a medical office, Dr. Trent acknowledged. Encouraging the use of headphones is one way to help protect confidentiality when talking with patients who are at home and might not be alone.
But if patients are able to find a private space for remote visits, they might be more open than usual. In that way, telemedicine could provide additional opportunities to address issues like substance use disorders and mental health, as well, she said.
“Then, if they need something, we have to problem solve,” Dr. Trent said. Next steps may involve engaging a parent or getting the patient to a lab or the clinic.
Sex ed may be lacking
The Perspectives article also raised concerns that the pandemic might exacerbate shortcomings in sex education, which already may have been lacking.
“Before the pandemic, schools were a key source of formal sex education for young people,” the authors wrote. “Sex education, which was already limited in many areas of the country, has likely not been included in the national shift to online learning. Even when in-person schooling resumes, missed sex education instruction is unlikely to be made up, given the modest attention it received prior to the pandemic.”
A recently published study in the Journal of Adolescent Health indicates that American teenagers currently receive less formal sex education than they did 25 years ago, with “troubling” inequities by race.
Researchers surveyed adolescents about what they had learned about topics such as how to say no to sex, methods of birth control and where to get them, and STIs.
Dr. Lindberg and Leslie M. Kantor, PhD, MPH, professor and chair of the department of urban-global public health at Rutgers University, Newark, N.J., conducted the analysis.
“Pediatricians and other health care providers that work with children and adolescents have a critical role to play in providing information about sexuality to both the patients and to the parents,” said Dr. Kantor, who also coauthored the Perspectives article with Dr. Lindberg and Dr. Bell. The new research “shows that doctors play an even more critical role, because they can’t assume that their patients are going to get the information that they need in a timely way from schools.”
By age 15, 21% of girls and 20% of boys have had sexual intercourse at least once, according to data from the 2015-2017 National Survey of Family Growth. By age 17, the percentages were 53% of girls and 48% of boys. By age 20, the percentages were 79% of women and 77% of men. The CDC’s 2021 guidelines on treatment and screening for STIs note that prevalence rates of certain infections – such as chlamydia and gonorrhea in females – are highest among adolescents and young adults.
Those trends underscore the importance of counseling on sexual health that clinicians can provide, but time constraints may limit how much they can discuss in a single session with a patient. To cover all topics that are important to parents and patients, doctors may need to discuss sexual and reproductive health sooner and more frequently.
Young people are getting more and more explicit information from their phones and media, yet educators are giving them less information to navigate these topics and learn what’s real, Dr. Kantor said. That mismatch can be toxic. In a December 2021 interview with Howard Stern, the pop star Billie Eilish said she started watching pornography at about age 11 and frequently watched videos that were violent. “I think it really destroyed my brain and I feel incredibly devastated that I was exposed to so much porn,” Ms. Eilish told Mr. Stern.
Researchers and a psychologist told CNN that the singer’s story may be typical. It also highlights a need to be aware of kids’ online activities and to have conversations about how pornography may not depict healthy interactions, they said.
Beyond discussing a plan for preventing pregnancy and STIs, Dr. Kantor encouraged discussions about what constitutes healthy relationships, as well as check-ins about intimate partner violence and how romantic relationships are going.
“I think for pediatricians and for parents, it’s a muscle,” she said. “As you bring up these topics more, listen, and respond, you get more comfortable with it.”
Dr. Trent has served as an advisory board member on a sexual health council for Trojan (Church & Dwight Company) and has received research funding from Hologic and research supplies from SpeeDx. Dr. Bell has received funds from the Merck Foundation, Merck, and Gilead. Dr. Kantor had no disclosures.
A version of this article first appeared on Medscape.com.
Maria Trent, MD, MPH, was studying ways clinicians can leverage technology to care for adolescents years before COVID-19 exposed the challenges and advantages of telehealth.
Dr. Trent, a pediatrician and adolescent medicine specialist and professor of pediatrics at Johns Hopkins University, Baltimore, has long believed that the phones in her patients’ pockets have the potential to improve the sexual health of youth. The pandemic has only made that view stronger.
“They’re a generation that’s really wired and online,” Dr. Trent told this news organization. “I think that we can meet them in that space.”
Her research has incorporated texting, apps, and videos. Out of necessity, technology increasingly became part of patient care during the pandemic. “We had to stretch our ability to do some basic triage and assessments of patients online,” Dr. Trent said.
Even when clinics are closed, doctors might be able to provide initial care remotely, such as writing prescriptions to manage symptoms or directing patients to a lab for testing.
Telemedicine could allow a clinician to guide a teenager who thinks they might be pregnant to take a store-bought test and avoid possible exposure to COVID-19 in the ED, for instance.
But doctors have concerns about the legal and practical limits of privacy and confidentiality. Who else is at home listening to a phone conversation? Are parents accessing the patient’s online portal? Will parents receive an explanation of benefits that lists testing for a sexually transmitted infection, or see a testing kit that is delivered to their home?
When a young patient needs in-person care, transportation can be a barrier. And then there’s the matter of clinicians being able to bill for telehealth services.
Practices are learning how to navigate these issues, and relevant laws vary by state.
“I think this is going to become part of standard practice,” Dr. Trent said. “I think we have to do the hard work to make sure that it’s safe, that it’s accessible, and that it is actually improving care.”
Texts, apps, videos
In one early study, Dr. Trent and colleagues found that showing adolescents with pelvic inflammatory disease a 6-minute video may improve treatment rates for their sexual partners.
Another study provided preliminary evidence that text messaging support might improve clinic attendance for moderately long-acting reversible contraception.
A third trial showed that adolescents and young adults with pelvic inflammatory disease who were randomly assigned to receive text-message prompts to take their medications and provide information about the doses they consumed had greater decreases in Neisseria gonorrhoeae and Chlamydia trachomatis infections, compared with patients who received standard care.
Dr. Trent and coinvestigators are assessing a technology-based intervention for youth with HIV, in which patients can use an app to submit videos of themselves taking antiretroviral therapy and report any side effects. The technology provides a way to monitor patients remotely and support them between visits, she said.
Will pandemic-driven options remain?
In 2020, Laura D. Lindberg, PhD, principal research scientist at the Guttmacher Institute in New York, and coauthors discussed the possible ramifications of the pandemic on the sexual and reproductive health of adolescents and young adults.
If telemedicine options driven by COVID-19 are here to stay, adolescents and young adults could be “the age group most likely to continue that approach rather than returning to traditional in-person visits,” the researchers wrote. “Innovations in health care service provision, such as use of telemedicine and obtaining contraceptives and STI testing by mail, will help expand access to [sexual and reproductive health] care for young people.”
At the 2021 annual conference of the American Academy of Pediatrics, Dr. Trent described telehealth as a viable way to provide sexual and reproductive health care to adolescents and young adults, including anticipatory guidance, contraception counseling, coordination of follow-up care and testing, and connecting patients to resources.
Her presentation cited several websites that can help patients receive testing for STIs, including Yes Means Test, the Centers for Disease Control and Prevention’s GetTested page, and I Want the Kit. Planned Parenthood has telehealth options, and the Kaiser Family Foundation compiled information about 26 online platforms that were providing contraception or STI services.
Who else is in the room?
“There’s only so much time in the day and so many patients you can see, regardless of whether you have telehealth or not,” said David L. Bell, MD, MPH, president of the Society for Adolescent Health and Medicine and a coauthor of the Perspectives on Sexual and Reproductive Health paper. In addition, “you never know who else is in the room” with the patient on the other end, added Dr. Bell, a professor of population and family health and pediatrics at the Columbia University Medical Center and medical director of the Young Men’s Clinic, both in New York.
In some respects, young patients may not be able to participate in telehealth visits the same way they would in a medical office, Dr. Trent acknowledged. Encouraging the use of headphones is one way to help protect confidentiality when talking with patients who are at home and might not be alone.
But if patients are able to find a private space for remote visits, they might be more open than usual. In that way, telemedicine could provide additional opportunities to address issues like substance use disorders and mental health, as well, she said.
“Then, if they need something, we have to problem solve,” Dr. Trent said. Next steps may involve engaging a parent or getting the patient to a lab or the clinic.
Sex ed may be lacking
The Perspectives article also raised concerns that the pandemic might exacerbate shortcomings in sex education, which already may have been lacking.
“Before the pandemic, schools were a key source of formal sex education for young people,” the authors wrote. “Sex education, which was already limited in many areas of the country, has likely not been included in the national shift to online learning. Even when in-person schooling resumes, missed sex education instruction is unlikely to be made up, given the modest attention it received prior to the pandemic.”
A recently published study in the Journal of Adolescent Health indicates that American teenagers currently receive less formal sex education than they did 25 years ago, with “troubling” inequities by race.
Researchers surveyed adolescents about what they had learned about topics such as how to say no to sex, methods of birth control and where to get them, and STIs.
Dr. Lindberg and Leslie M. Kantor, PhD, MPH, professor and chair of the department of urban-global public health at Rutgers University, Newark, N.J., conducted the analysis.
“Pediatricians and other health care providers that work with children and adolescents have a critical role to play in providing information about sexuality to both the patients and to the parents,” said Dr. Kantor, who also coauthored the Perspectives article with Dr. Lindberg and Dr. Bell. The new research “shows that doctors play an even more critical role, because they can’t assume that their patients are going to get the information that they need in a timely way from schools.”
By age 15, 21% of girls and 20% of boys have had sexual intercourse at least once, according to data from the 2015-2017 National Survey of Family Growth. By age 17, the percentages were 53% of girls and 48% of boys. By age 20, the percentages were 79% of women and 77% of men. The CDC’s 2021 guidelines on treatment and screening for STIs note that prevalence rates of certain infections – such as chlamydia and gonorrhea in females – are highest among adolescents and young adults.
Those trends underscore the importance of counseling on sexual health that clinicians can provide, but time constraints may limit how much they can discuss in a single session with a patient. To cover all topics that are important to parents and patients, doctors may need to discuss sexual and reproductive health sooner and more frequently.
Young people are getting more and more explicit information from their phones and media, yet educators are giving them less information to navigate these topics and learn what’s real, Dr. Kantor said. That mismatch can be toxic. In a December 2021 interview with Howard Stern, the pop star Billie Eilish said she started watching pornography at about age 11 and frequently watched videos that were violent. “I think it really destroyed my brain and I feel incredibly devastated that I was exposed to so much porn,” Ms. Eilish told Mr. Stern.
Researchers and a psychologist told CNN that the singer’s story may be typical. It also highlights a need to be aware of kids’ online activities and to have conversations about how pornography may not depict healthy interactions, they said.
Beyond discussing a plan for preventing pregnancy and STIs, Dr. Kantor encouraged discussions about what constitutes healthy relationships, as well as check-ins about intimate partner violence and how romantic relationships are going.
“I think for pediatricians and for parents, it’s a muscle,” she said. “As you bring up these topics more, listen, and respond, you get more comfortable with it.”
Dr. Trent has served as an advisory board member on a sexual health council for Trojan (Church & Dwight Company) and has received research funding from Hologic and research supplies from SpeeDx. Dr. Bell has received funds from the Merck Foundation, Merck, and Gilead. Dr. Kantor had no disclosures.
A version of this article first appeared on Medscape.com.
Maria Trent, MD, MPH, was studying ways clinicians can leverage technology to care for adolescents years before COVID-19 exposed the challenges and advantages of telehealth.
Dr. Trent, a pediatrician and adolescent medicine specialist and professor of pediatrics at Johns Hopkins University, Baltimore, has long believed that the phones in her patients’ pockets have the potential to improve the sexual health of youth. The pandemic has only made that view stronger.
“They’re a generation that’s really wired and online,” Dr. Trent told this news organization. “I think that we can meet them in that space.”
Her research has incorporated texting, apps, and videos. Out of necessity, technology increasingly became part of patient care during the pandemic. “We had to stretch our ability to do some basic triage and assessments of patients online,” Dr. Trent said.
Even when clinics are closed, doctors might be able to provide initial care remotely, such as writing prescriptions to manage symptoms or directing patients to a lab for testing.
Telemedicine could allow a clinician to guide a teenager who thinks they might be pregnant to take a store-bought test and avoid possible exposure to COVID-19 in the ED, for instance.
But doctors have concerns about the legal and practical limits of privacy and confidentiality. Who else is at home listening to a phone conversation? Are parents accessing the patient’s online portal? Will parents receive an explanation of benefits that lists testing for a sexually transmitted infection, or see a testing kit that is delivered to their home?
When a young patient needs in-person care, transportation can be a barrier. And then there’s the matter of clinicians being able to bill for telehealth services.
Practices are learning how to navigate these issues, and relevant laws vary by state.
“I think this is going to become part of standard practice,” Dr. Trent said. “I think we have to do the hard work to make sure that it’s safe, that it’s accessible, and that it is actually improving care.”
Texts, apps, videos
In one early study, Dr. Trent and colleagues found that showing adolescents with pelvic inflammatory disease a 6-minute video may improve treatment rates for their sexual partners.
Another study provided preliminary evidence that text messaging support might improve clinic attendance for moderately long-acting reversible contraception.
A third trial showed that adolescents and young adults with pelvic inflammatory disease who were randomly assigned to receive text-message prompts to take their medications and provide information about the doses they consumed had greater decreases in Neisseria gonorrhoeae and Chlamydia trachomatis infections, compared with patients who received standard care.
Dr. Trent and coinvestigators are assessing a technology-based intervention for youth with HIV, in which patients can use an app to submit videos of themselves taking antiretroviral therapy and report any side effects. The technology provides a way to monitor patients remotely and support them between visits, she said.
Will pandemic-driven options remain?
In 2020, Laura D. Lindberg, PhD, principal research scientist at the Guttmacher Institute in New York, and coauthors discussed the possible ramifications of the pandemic on the sexual and reproductive health of adolescents and young adults.
If telemedicine options driven by COVID-19 are here to stay, adolescents and young adults could be “the age group most likely to continue that approach rather than returning to traditional in-person visits,” the researchers wrote. “Innovations in health care service provision, such as use of telemedicine and obtaining contraceptives and STI testing by mail, will help expand access to [sexual and reproductive health] care for young people.”
At the 2021 annual conference of the American Academy of Pediatrics, Dr. Trent described telehealth as a viable way to provide sexual and reproductive health care to adolescents and young adults, including anticipatory guidance, contraception counseling, coordination of follow-up care and testing, and connecting patients to resources.
Her presentation cited several websites that can help patients receive testing for STIs, including Yes Means Test, the Centers for Disease Control and Prevention’s GetTested page, and I Want the Kit. Planned Parenthood has telehealth options, and the Kaiser Family Foundation compiled information about 26 online platforms that were providing contraception or STI services.
Who else is in the room?
“There’s only so much time in the day and so many patients you can see, regardless of whether you have telehealth or not,” said David L. Bell, MD, MPH, president of the Society for Adolescent Health and Medicine and a coauthor of the Perspectives on Sexual and Reproductive Health paper. In addition, “you never know who else is in the room” with the patient on the other end, added Dr. Bell, a professor of population and family health and pediatrics at the Columbia University Medical Center and medical director of the Young Men’s Clinic, both in New York.
In some respects, young patients may not be able to participate in telehealth visits the same way they would in a medical office, Dr. Trent acknowledged. Encouraging the use of headphones is one way to help protect confidentiality when talking with patients who are at home and might not be alone.
But if patients are able to find a private space for remote visits, they might be more open than usual. In that way, telemedicine could provide additional opportunities to address issues like substance use disorders and mental health, as well, she said.
“Then, if they need something, we have to problem solve,” Dr. Trent said. Next steps may involve engaging a parent or getting the patient to a lab or the clinic.
Sex ed may be lacking
The Perspectives article also raised concerns that the pandemic might exacerbate shortcomings in sex education, which already may have been lacking.
“Before the pandemic, schools were a key source of formal sex education for young people,” the authors wrote. “Sex education, which was already limited in many areas of the country, has likely not been included in the national shift to online learning. Even when in-person schooling resumes, missed sex education instruction is unlikely to be made up, given the modest attention it received prior to the pandemic.”
A recently published study in the Journal of Adolescent Health indicates that American teenagers currently receive less formal sex education than they did 25 years ago, with “troubling” inequities by race.
Researchers surveyed adolescents about what they had learned about topics such as how to say no to sex, methods of birth control and where to get them, and STIs.
Dr. Lindberg and Leslie M. Kantor, PhD, MPH, professor and chair of the department of urban-global public health at Rutgers University, Newark, N.J., conducted the analysis.
“Pediatricians and other health care providers that work with children and adolescents have a critical role to play in providing information about sexuality to both the patients and to the parents,” said Dr. Kantor, who also coauthored the Perspectives article with Dr. Lindberg and Dr. Bell. The new research “shows that doctors play an even more critical role, because they can’t assume that their patients are going to get the information that they need in a timely way from schools.”
By age 15, 21% of girls and 20% of boys have had sexual intercourse at least once, according to data from the 2015-2017 National Survey of Family Growth. By age 17, the percentages were 53% of girls and 48% of boys. By age 20, the percentages were 79% of women and 77% of men. The CDC’s 2021 guidelines on treatment and screening for STIs note that prevalence rates of certain infections – such as chlamydia and gonorrhea in females – are highest among adolescents and young adults.
Those trends underscore the importance of counseling on sexual health that clinicians can provide, but time constraints may limit how much they can discuss in a single session with a patient. To cover all topics that are important to parents and patients, doctors may need to discuss sexual and reproductive health sooner and more frequently.
Young people are getting more and more explicit information from their phones and media, yet educators are giving them less information to navigate these topics and learn what’s real, Dr. Kantor said. That mismatch can be toxic. In a December 2021 interview with Howard Stern, the pop star Billie Eilish said she started watching pornography at about age 11 and frequently watched videos that were violent. “I think it really destroyed my brain and I feel incredibly devastated that I was exposed to so much porn,” Ms. Eilish told Mr. Stern.
Researchers and a psychologist told CNN that the singer’s story may be typical. It also highlights a need to be aware of kids’ online activities and to have conversations about how pornography may not depict healthy interactions, they said.
Beyond discussing a plan for preventing pregnancy and STIs, Dr. Kantor encouraged discussions about what constitutes healthy relationships, as well as check-ins about intimate partner violence and how romantic relationships are going.
“I think for pediatricians and for parents, it’s a muscle,” she said. “As you bring up these topics more, listen, and respond, you get more comfortable with it.”
Dr. Trent has served as an advisory board member on a sexual health council for Trojan (Church & Dwight Company) and has received research funding from Hologic and research supplies from SpeeDx. Dr. Bell has received funds from the Merck Foundation, Merck, and Gilead. Dr. Kantor had no disclosures.
A version of this article first appeared on Medscape.com.
Serious problems rare in ages 5-11 from COVID vaccine
The CDC has released two studies that showed vaccine safety for ages 5-11 and emphasized the importance of vaccinating children against the coronavirus to prevent serious illness and hospitalization.
In one study published in the Morbidity and Mortality Weekly Report, researchers found that serious problems were rare among children who had received the Pfizer vaccine.
In another study, researchers looked at hundreds of pediatric hospitalizations from the summer and found that nearly all of children who developed severe COVID-19 weren’t fully vaccinated.
“This study demonstrates that unvaccinated children hospitalized for COVID-19 could experience severe disease and reinforces the importance of vaccination of all eligible children to provide individual protection and to protect those who are not yet eligible to be vaccinated,” the authors of the second study wrote.
Nearly 9 million doses of the Pfizer vaccine have been given to children aged 5-11 in the United States so far, according to The New York Times. By mid-December, or about 6 weeks after the age group became eligible for vaccination in October, the CDC said it had received very few reports of serious problems.
CDC researchers evaluated reports received from doctors and the public, including survey responses from parents and guardians of about 43,000 children between ages 5 and 11. Many children reported nonserious events such as pain at the injection site, fatigue, or a headache, especially after the second dose.
Among more than 4,100 adverse event reports received in November and December, 100 were for serious events, with the most common being fever or vomiting.
The CDC had received 11 verified reports of myocarditis, or inflammation of the heart muscle, which has been noted as a rare side effect of the vaccine among boys and men between ages 12 and 29. Among those, seven children had already recovered and four were still recovering at the time of the report.
The CDC received reports of two deaths – girls who were aged 5 and 6 – who had chronic medical conditions and were in “fragile health” before their shots. The agency said that no data suggested a “causal association between death and vaccination.”
The CDC also received some reports that children between ages 5 and 11 received the larger vaccine dose meant for older children and adults. Most reports said that the children didn’t experience any problems after an incorrect dose.
In a separate study about pediatric hospitalizations, CDC researchers looked at more than 700 children under age 18 who were hospitalized for COVID-19 in July and August at six children’s hospitals in Arkansas, Florida, Illinois, Louisiana, Texas, and Washington, D.C.
Researchers found that only one of the 272 vaccine-eligible patients between ages 12 and 17 had been fully vaccinated, and 12 were partially vaccinated.
In addition, about two-thirds of the hospitalized children between ages 12 and 17 had an underlying condition, with obesity being the most common. About one-third of children under age 5 had more than one viral infection.
Overall, about 30% of the children had to be treated in intensive care units, and 15% needed invasive medical ventilation, CDC researchers found. Nearly 3% had multisystem inflammatory syndrome in children, or MIS-C, which is a rare but serious inflammatory condition associated with COVID-19.
Among all the children hospitalized with COVID-19, about 1.5% died.
“Few vaccine-eligible patients hospitalized for COVID-19 were vaccinated, highlighting the importance of vaccination for those aged ≥5 years and other prevention strategies to protect children and adolescents from COVID-19, particularly those with underlying medical conditions,” study authors wrote.
A version of this article first appeared on WebMD.com.
The CDC has released two studies that showed vaccine safety for ages 5-11 and emphasized the importance of vaccinating children against the coronavirus to prevent serious illness and hospitalization.
In one study published in the Morbidity and Mortality Weekly Report, researchers found that serious problems were rare among children who had received the Pfizer vaccine.
In another study, researchers looked at hundreds of pediatric hospitalizations from the summer and found that nearly all of children who developed severe COVID-19 weren’t fully vaccinated.
“This study demonstrates that unvaccinated children hospitalized for COVID-19 could experience severe disease and reinforces the importance of vaccination of all eligible children to provide individual protection and to protect those who are not yet eligible to be vaccinated,” the authors of the second study wrote.
Nearly 9 million doses of the Pfizer vaccine have been given to children aged 5-11 in the United States so far, according to The New York Times. By mid-December, or about 6 weeks after the age group became eligible for vaccination in October, the CDC said it had received very few reports of serious problems.
CDC researchers evaluated reports received from doctors and the public, including survey responses from parents and guardians of about 43,000 children between ages 5 and 11. Many children reported nonserious events such as pain at the injection site, fatigue, or a headache, especially after the second dose.
Among more than 4,100 adverse event reports received in November and December, 100 were for serious events, with the most common being fever or vomiting.
The CDC had received 11 verified reports of myocarditis, or inflammation of the heart muscle, which has been noted as a rare side effect of the vaccine among boys and men between ages 12 and 29. Among those, seven children had already recovered and four were still recovering at the time of the report.
The CDC received reports of two deaths – girls who were aged 5 and 6 – who had chronic medical conditions and were in “fragile health” before their shots. The agency said that no data suggested a “causal association between death and vaccination.”
The CDC also received some reports that children between ages 5 and 11 received the larger vaccine dose meant for older children and adults. Most reports said that the children didn’t experience any problems after an incorrect dose.
In a separate study about pediatric hospitalizations, CDC researchers looked at more than 700 children under age 18 who were hospitalized for COVID-19 in July and August at six children’s hospitals in Arkansas, Florida, Illinois, Louisiana, Texas, and Washington, D.C.
Researchers found that only one of the 272 vaccine-eligible patients between ages 12 and 17 had been fully vaccinated, and 12 were partially vaccinated.
In addition, about two-thirds of the hospitalized children between ages 12 and 17 had an underlying condition, with obesity being the most common. About one-third of children under age 5 had more than one viral infection.
Overall, about 30% of the children had to be treated in intensive care units, and 15% needed invasive medical ventilation, CDC researchers found. Nearly 3% had multisystem inflammatory syndrome in children, or MIS-C, which is a rare but serious inflammatory condition associated with COVID-19.
Among all the children hospitalized with COVID-19, about 1.5% died.
“Few vaccine-eligible patients hospitalized for COVID-19 were vaccinated, highlighting the importance of vaccination for those aged ≥5 years and other prevention strategies to protect children and adolescents from COVID-19, particularly those with underlying medical conditions,” study authors wrote.
A version of this article first appeared on WebMD.com.
The CDC has released two studies that showed vaccine safety for ages 5-11 and emphasized the importance of vaccinating children against the coronavirus to prevent serious illness and hospitalization.
In one study published in the Morbidity and Mortality Weekly Report, researchers found that serious problems were rare among children who had received the Pfizer vaccine.
In another study, researchers looked at hundreds of pediatric hospitalizations from the summer and found that nearly all of children who developed severe COVID-19 weren’t fully vaccinated.
“This study demonstrates that unvaccinated children hospitalized for COVID-19 could experience severe disease and reinforces the importance of vaccination of all eligible children to provide individual protection and to protect those who are not yet eligible to be vaccinated,” the authors of the second study wrote.
Nearly 9 million doses of the Pfizer vaccine have been given to children aged 5-11 in the United States so far, according to The New York Times. By mid-December, or about 6 weeks after the age group became eligible for vaccination in October, the CDC said it had received very few reports of serious problems.
CDC researchers evaluated reports received from doctors and the public, including survey responses from parents and guardians of about 43,000 children between ages 5 and 11. Many children reported nonserious events such as pain at the injection site, fatigue, or a headache, especially after the second dose.
Among more than 4,100 adverse event reports received in November and December, 100 were for serious events, with the most common being fever or vomiting.
The CDC had received 11 verified reports of myocarditis, or inflammation of the heart muscle, which has been noted as a rare side effect of the vaccine among boys and men between ages 12 and 29. Among those, seven children had already recovered and four were still recovering at the time of the report.
The CDC received reports of two deaths – girls who were aged 5 and 6 – who had chronic medical conditions and were in “fragile health” before their shots. The agency said that no data suggested a “causal association between death and vaccination.”
The CDC also received some reports that children between ages 5 and 11 received the larger vaccine dose meant for older children and adults. Most reports said that the children didn’t experience any problems after an incorrect dose.
In a separate study about pediatric hospitalizations, CDC researchers looked at more than 700 children under age 18 who were hospitalized for COVID-19 in July and August at six children’s hospitals in Arkansas, Florida, Illinois, Louisiana, Texas, and Washington, D.C.
Researchers found that only one of the 272 vaccine-eligible patients between ages 12 and 17 had been fully vaccinated, and 12 were partially vaccinated.
In addition, about two-thirds of the hospitalized children between ages 12 and 17 had an underlying condition, with obesity being the most common. About one-third of children under age 5 had more than one viral infection.
Overall, about 30% of the children had to be treated in intensive care units, and 15% needed invasive medical ventilation, CDC researchers found. Nearly 3% had multisystem inflammatory syndrome in children, or MIS-C, which is a rare but serious inflammatory condition associated with COVID-19.
Among all the children hospitalized with COVID-19, about 1.5% died.
“Few vaccine-eligible patients hospitalized for COVID-19 were vaccinated, highlighting the importance of vaccination for those aged ≥5 years and other prevention strategies to protect children and adolescents from COVID-19, particularly those with underlying medical conditions,” study authors wrote.
A version of this article first appeared on WebMD.com.