User login
How to manage school failure
The start of the school year brings excitement and some expected anxiety, around seeing friends and undertaking new challenges. While setbacks, small failures, and disappointments are an essential part of a child’s mastery of new challenges, academic and otherwise, occasionally a child will experience school failure in many areas. When this happens, the school usually will engage parents to help understand and address what might be interfering with the child’s performance at school. Parents may turn to their trusted pediatricians for guidance in sorting out school failure, as the list of possible causes is very long. By asking the right questions and knowing your patient, you can efficiently investigate this problem so that your patient may quickly get back on track, both academically and in overall development.

Are their academic problems a striking change from prior years? If your patients previously had managed coursework with ease, then there is a new problem interfering with their performance, unless they are young enough that earlier years were not as challenging. Possibly a previous school was not as demanding or new academic expectations such as writing an essay or a dramatic increase in reading expectations have exposed a learning disability or attentional issue that is interfering with performance. This can be sorted out by asking more specific questions about their function. Do they struggle more with reading, essay writing, or math? Do they struggle with sustained attention on assignments or handing in completed work? Your patients can help answer these questions, as can as parents and teachers. Neuropsychological testing can elucidate specific learning disabilities or indicate marked problems with attention, working memory, or processing speed that may be improved with cognitive coaching, in-class strategies, and even medications. With older patients, a new problem is less likely to be the first presentation of an underlying learning or attentional issue and will need further investigation.
Do your patients still enjoy school or are they resisting attending? Students who are avoiding school may be struggling with anxiety. This may be a consequence of their academic struggles, as they try to avoid the shame, embarrassment, or discomfort of their failure to understand material, keep up, or perform. Alternately, the anxiety may have come first, leading to an inability to manage the challenges of school and then failure academically. Similarly, a mood disorder such as depression can create problems with attention, energy, interest, and motivation that make it difficult to attend and participate in school.

Ask about any family history of school problems and psychiatric disorders as these issues often run in families. Ask if there is anxiety around academic or social performance or more generalized anxiety. Are they experiencing trouble with sleep, energy, appetite? Have they withdrawn from other interests? Are they more tearful or irritable in all settings? When these symptoms are universal (i.e., occurring across settings and affecting school), there is likely an underlying psychiatric disorder driving them, and they require a full psychiatric assessment. It is worth noting that often children or adolescents with mood or anxiety disorders will experience somatic symptoms such as stomach aches or headaches alongside the loss of energy and motivation. They may come to the pediatrician first, and it is important to investigate the likely psychiatric illnesses (anxiety in prepubertal children and anxiety or depression in adolescents) as well as the more esoteric medical problems that could be causing such universal impairment in a child or teenager. Stigma still exists around psychiatric illness and it is powerful when a pediatrician can tell a family that these illnesses are common in young people (affecting nearly 20% of children by the age of 18) and very treatable.
Drug and alcohol abuse may be associated with another psychiatric illness or can be independent problems that interfere with the healthy development and school performance of young people, including middle school students. Find out if your patients are drinking alcohol, using marijuana, vaping, utilizing prescription medications that are not their own, or using other illegal drugs. Substance use that has led to problems at school is by definition a problem (in addition to being illegal) and will not improve without treatment. These young people need a full psychiatric evaluation, and they and their parents require specialized treatment and support to address the substance abuse problem.

Of course, school failure may represent other sources of stress. It is critical to find out from your patients if they feel safe at school. Are they being bullied or threatened? Do they have a safe way to get to and from school? Has something else occurred at the school that has left them feeling vigilant and unable to concentrate on classwork? While bullying or living in a neighborhood plagued by violence may not be easy problems to fix, it is critical to find out about them so the adults – parents, teachers, and others – can provide the students with support while directly addressing the safety issue. Do not fail to find out if the fear is at home. Children who are managing physical or sexual abuse may be too stressed to complete homework or even attend school. A caring, curious pediatrician will be a lifeline to a safer future for these children.
Similarly, it is important to find out if your patient is managing less dramatic stresses at home. Perhaps a parent has been seriously ill, working two jobs, or managing a problem with drugs or alcohol, and your patient is caring for that person, or for siblings, instead of keeping up with schoolwork. Perhaps there has been a stressful loss or transition, such as the death of a grandparent or pet, the loss of a job, or a big move, or family discord/violence that has made it difficult for your patient to focus on homework or interfered with parental supervision or homework help. Perhaps your patient has gotten a job to help the family financially and has no time for homework. Bringing such a challenge out into the open and rallying support for your patient and the family in these circumstances is often enough to foster adaptation to these stresses and a return to healthy function in school.
Finally, it is possible that school failure is a function of milder imbalances in a young person’s life. Some children may respond to the expanded independence of adolescence by making poor choices. When do they go to bed at night? Are they staying up late playing video games or surfing the web? Not all insomnia represents illness. Find out how much independence your patients have and how they are managing their time and responsibilities. Help them to think about how to protect time for both responsibilities and relaxation. You also may help the parents of these young people think about how to set expectations and basic rules while stepping back appropriately to allow for expanding independence in ways that will help their children to flourish.
Once defined, Setting reasonable expectations, curriculum adjustments, any needed psychiatric treatment, building on a child’s strengths, and paying attention to self-esteem are the hallmarks of effective interventions.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
The start of the school year brings excitement and some expected anxiety, around seeing friends and undertaking new challenges. While setbacks, small failures, and disappointments are an essential part of a child’s mastery of new challenges, academic and otherwise, occasionally a child will experience school failure in many areas. When this happens, the school usually will engage parents to help understand and address what might be interfering with the child’s performance at school. Parents may turn to their trusted pediatricians for guidance in sorting out school failure, as the list of possible causes is very long. By asking the right questions and knowing your patient, you can efficiently investigate this problem so that your patient may quickly get back on track, both academically and in overall development.
Are their academic problems a striking change from prior years? If your patients previously had managed coursework with ease, then there is a new problem interfering with their performance, unless they are young enough that earlier years were not as challenging. Possibly a previous school was not as demanding or new academic expectations such as writing an essay or a dramatic increase in reading expectations have exposed a learning disability or attentional issue that is interfering with performance. This can be sorted out by asking more specific questions about their function. Do they struggle more with reading, essay writing, or math? Do they struggle with sustained attention on assignments or handing in completed work? Your patients can help answer these questions, as can as parents and teachers. Neuropsychological testing can elucidate specific learning disabilities or indicate marked problems with attention, working memory, or processing speed that may be improved with cognitive coaching, in-class strategies, and even medications. With older patients, a new problem is less likely to be the first presentation of an underlying learning or attentional issue and will need further investigation.
Do your patients still enjoy school or are they resisting attending? Students who are avoiding school may be struggling with anxiety. This may be a consequence of their academic struggles, as they try to avoid the shame, embarrassment, or discomfort of their failure to understand material, keep up, or perform. Alternately, the anxiety may have come first, leading to an inability to manage the challenges of school and then failure academically. Similarly, a mood disorder such as depression can create problems with attention, energy, interest, and motivation that make it difficult to attend and participate in school.
Ask about any family history of school problems and psychiatric disorders as these issues often run in families. Ask if there is anxiety around academic or social performance or more generalized anxiety. Are they experiencing trouble with sleep, energy, appetite? Have they withdrawn from other interests? Are they more tearful or irritable in all settings? When these symptoms are universal (i.e., occurring across settings and affecting school), there is likely an underlying psychiatric disorder driving them, and they require a full psychiatric assessment. It is worth noting that often children or adolescents with mood or anxiety disorders will experience somatic symptoms such as stomach aches or headaches alongside the loss of energy and motivation. They may come to the pediatrician first, and it is important to investigate the likely psychiatric illnesses (anxiety in prepubertal children and anxiety or depression in adolescents) as well as the more esoteric medical problems that could be causing such universal impairment in a child or teenager. Stigma still exists around psychiatric illness and it is powerful when a pediatrician can tell a family that these illnesses are common in young people (affecting nearly 20% of children by the age of 18) and very treatable.
Drug and alcohol abuse may be associated with another psychiatric illness or can be independent problems that interfere with the healthy development and school performance of young people, including middle school students. Find out if your patients are drinking alcohol, using marijuana, vaping, utilizing prescription medications that are not their own, or using other illegal drugs. Substance use that has led to problems at school is by definition a problem (in addition to being illegal) and will not improve without treatment. These young people need a full psychiatric evaluation, and they and their parents require specialized treatment and support to address the substance abuse problem.
Of course, school failure may represent other sources of stress. It is critical to find out from your patients if they feel safe at school. Are they being bullied or threatened? Do they have a safe way to get to and from school? Has something else occurred at the school that has left them feeling vigilant and unable to concentrate on classwork? While bullying or living in a neighborhood plagued by violence may not be easy problems to fix, it is critical to find out about them so the adults – parents, teachers, and others – can provide the students with support while directly addressing the safety issue. Do not fail to find out if the fear is at home. Children who are managing physical or sexual abuse may be too stressed to complete homework or even attend school. A caring, curious pediatrician will be a lifeline to a safer future for these children.
Similarly, it is important to find out if your patient is managing less dramatic stresses at home. Perhaps a parent has been seriously ill, working two jobs, or managing a problem with drugs or alcohol, and your patient is caring for that person, or for siblings, instead of keeping up with schoolwork. Perhaps there has been a stressful loss or transition, such as the death of a grandparent or pet, the loss of a job, or a big move, or family discord/violence that has made it difficult for your patient to focus on homework or interfered with parental supervision or homework help. Perhaps your patient has gotten a job to help the family financially and has no time for homework. Bringing such a challenge out into the open and rallying support for your patient and the family in these circumstances is often enough to foster adaptation to these stresses and a return to healthy function in school.
Finally, it is possible that school failure is a function of milder imbalances in a young person’s life. Some children may respond to the expanded independence of adolescence by making poor choices. When do they go to bed at night? Are they staying up late playing video games or surfing the web? Not all insomnia represents illness. Find out how much independence your patients have and how they are managing their time and responsibilities. Help them to think about how to protect time for both responsibilities and relaxation. You also may help the parents of these young people think about how to set expectations and basic rules while stepping back appropriately to allow for expanding independence in ways that will help their children to flourish.
Once defined, Setting reasonable expectations, curriculum adjustments, any needed psychiatric treatment, building on a child’s strengths, and paying attention to self-esteem are the hallmarks of effective interventions.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
The start of the school year brings excitement and some expected anxiety, around seeing friends and undertaking new challenges. While setbacks, small failures, and disappointments are an essential part of a child’s mastery of new challenges, academic and otherwise, occasionally a child will experience school failure in many areas. When this happens, the school usually will engage parents to help understand and address what might be interfering with the child’s performance at school. Parents may turn to their trusted pediatricians for guidance in sorting out school failure, as the list of possible causes is very long. By asking the right questions and knowing your patient, you can efficiently investigate this problem so that your patient may quickly get back on track, both academically and in overall development.
Are their academic problems a striking change from prior years? If your patients previously had managed coursework with ease, then there is a new problem interfering with their performance, unless they are young enough that earlier years were not as challenging. Possibly a previous school was not as demanding or new academic expectations such as writing an essay or a dramatic increase in reading expectations have exposed a learning disability or attentional issue that is interfering with performance. This can be sorted out by asking more specific questions about their function. Do they struggle more with reading, essay writing, or math? Do they struggle with sustained attention on assignments or handing in completed work? Your patients can help answer these questions, as can as parents and teachers. Neuropsychological testing can elucidate specific learning disabilities or indicate marked problems with attention, working memory, or processing speed that may be improved with cognitive coaching, in-class strategies, and even medications. With older patients, a new problem is less likely to be the first presentation of an underlying learning or attentional issue and will need further investigation.
Do your patients still enjoy school or are they resisting attending? Students who are avoiding school may be struggling with anxiety. This may be a consequence of their academic struggles, as they try to avoid the shame, embarrassment, or discomfort of their failure to understand material, keep up, or perform. Alternately, the anxiety may have come first, leading to an inability to manage the challenges of school and then failure academically. Similarly, a mood disorder such as depression can create problems with attention, energy, interest, and motivation that make it difficult to attend and participate in school.
Ask about any family history of school problems and psychiatric disorders as these issues often run in families. Ask if there is anxiety around academic or social performance or more generalized anxiety. Are they experiencing trouble with sleep, energy, appetite? Have they withdrawn from other interests? Are they more tearful or irritable in all settings? When these symptoms are universal (i.e., occurring across settings and affecting school), there is likely an underlying psychiatric disorder driving them, and they require a full psychiatric assessment. It is worth noting that often children or adolescents with mood or anxiety disorders will experience somatic symptoms such as stomach aches or headaches alongside the loss of energy and motivation. They may come to the pediatrician first, and it is important to investigate the likely psychiatric illnesses (anxiety in prepubertal children and anxiety or depression in adolescents) as well as the more esoteric medical problems that could be causing such universal impairment in a child or teenager. Stigma still exists around psychiatric illness and it is powerful when a pediatrician can tell a family that these illnesses are common in young people (affecting nearly 20% of children by the age of 18) and very treatable.
Drug and alcohol abuse may be associated with another psychiatric illness or can be independent problems that interfere with the healthy development and school performance of young people, including middle school students. Find out if your patients are drinking alcohol, using marijuana, vaping, utilizing prescription medications that are not their own, or using other illegal drugs. Substance use that has led to problems at school is by definition a problem (in addition to being illegal) and will not improve without treatment. These young people need a full psychiatric evaluation, and they and their parents require specialized treatment and support to address the substance abuse problem.
Of course, school failure may represent other sources of stress. It is critical to find out from your patients if they feel safe at school. Are they being bullied or threatened? Do they have a safe way to get to and from school? Has something else occurred at the school that has left them feeling vigilant and unable to concentrate on classwork? While bullying or living in a neighborhood plagued by violence may not be easy problems to fix, it is critical to find out about them so the adults – parents, teachers, and others – can provide the students with support while directly addressing the safety issue. Do not fail to find out if the fear is at home. Children who are managing physical or sexual abuse may be too stressed to complete homework or even attend school. A caring, curious pediatrician will be a lifeline to a safer future for these children.
Similarly, it is important to find out if your patient is managing less dramatic stresses at home. Perhaps a parent has been seriously ill, working two jobs, or managing a problem with drugs or alcohol, and your patient is caring for that person, or for siblings, instead of keeping up with schoolwork. Perhaps there has been a stressful loss or transition, such as the death of a grandparent or pet, the loss of a job, or a big move, or family discord/violence that has made it difficult for your patient to focus on homework or interfered with parental supervision or homework help. Perhaps your patient has gotten a job to help the family financially and has no time for homework. Bringing such a challenge out into the open and rallying support for your patient and the family in these circumstances is often enough to foster adaptation to these stresses and a return to healthy function in school.
Finally, it is possible that school failure is a function of milder imbalances in a young person’s life. Some children may respond to the expanded independence of adolescence by making poor choices. When do they go to bed at night? Are they staying up late playing video games or surfing the web? Not all insomnia represents illness. Find out how much independence your patients have and how they are managing their time and responsibilities. Help them to think about how to protect time for both responsibilities and relaxation. You also may help the parents of these young people think about how to set expectations and basic rules while stepping back appropriately to allow for expanding independence in ways that will help their children to flourish.
Once defined, Setting reasonable expectations, curriculum adjustments, any needed psychiatric treatment, building on a child’s strengths, and paying attention to self-esteem are the hallmarks of effective interventions.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.

Five-year follow-up confirms safety of antibiotics for uncomplicated appendicitis
Longer-term outcomes of treating uncomplicated acute appendicitis with antibiotics suggest it is a feasible alternative to appendectomy.

Researchers have presented the 5-year follow-up data from the Appendicitis Acuta (APPAC) multicenter randomized clinical trial comparing appendectomy with antibiotic therapy in 530 patients.
They found that 39.1% (100) of the 257 patients randomized to antibiotic therapy – 3 days of intravenous ertapenem followed by 7 days of oral levofloxacin and metronidazole – experienced a recurrence of appendicitis within 5 years and subsequently had surgery.
However the authors noted that seven of these patients were later found not to have appendicitis, so the true success rate for antibiotic treatment was actually 63.7%.
Seventy of the patients who experienced a recurrence underwent surgery in the first year after randomization, 17 in the second year, 3 in the third year, 5 in the fourth year, and the remaining 5 patients in the fifth year, the authors wrote in an article published in JAMA.
However the overall complication rate was similar in patients who were randomized to undergo appendectomy and in those who were initially randomized to the antibiotic group but later experienced a recurrence and underwent surgery.
“No patient initially treated with antibiotics, who ultimately developed recurrent appendicitis, had any complications related to the delay in surgery,” wrote Paulina Salminen, MD, from Turku (Finland) University Hospital and coauthors. “Nearly two-thirds of all patients who initially presented with uncomplicated appendicitis were successfully treated with antibiotics alone, and those who ultimately developed recurrent disease did not experience any adverse outcomes related to the delay in appendectomy.”
Of the 100 patients randomized to antibiotics who underwent appendectomy after a recurrence, 15 were operated on when they were first hospitalized at study admission.
The authors commented that the study design allowed for surgeons to exercise their clinical judgment in choosing when to perform an appendectomy on patients in the antibiotic group, because antibiotics alone was not considered acceptable treatment for appendicitis.
“This led to some patients undergoing appendectomy who did not have appendicitis or who might have been successfully treated with antibiotics or an another course of antibiotics,” they wrote. “Future studies should investigate protocols for further imaging or antibiotic treatment for patients who develop recurrent appendicitis after they were initially treated with antibiotics.”
In the recurrence group, the majority were found to have uncomplicated appendicitis, but complicated appendicitis was seen in two patients between 2 and 5 years after the index admission.
There was a significant 17.9% higher complication rate in the appendectomy group, compared with the antibiotic group – 24.4% versus 6.5% – at 5 years and two patients in the appendectomy group had severe complications requiring reoperation.
They suggested that the higher complication rate with surgery, which was mostly attributable to infections, could be reduced by the use of laparoscopic appendectomy, which is also associated with faster recovery.
The median length of hospital stay was 3 days for both the appendectomy group and the antibiotics-only group, but patients randomized to appendectomy took a median of 22 days of sick leave, compared with 11 days for those randomized to antibiotics (P less than .001).
In the absence of standard protocol on treating appendicitis with antibiotics, the authors noted that they took a conservative approach, using broad-spectrum antibiotics and keeping patients in hospital for 3 days for observation.
“The success of antibiotic treatment for appendicitis calls into question prior beliefs that appendicitis inevitably results in serious intra-abdominal infection if appendectomy is not performed.”
The study was supported by the Mary and Georg C. Ehrnrooth Foundation, the EVO Foundation, and Turku University. One author declared lecture fees from three pharmaceutical companies but no other conflicts of interest were declared.
SOURCE: Salminen P et al. JAMA 2018;320:1259-65. doi: 10.1001/jama.2018.13201.
“When the earlier results of the APPAC trial were published, showing that 73% of patients with uncomplicated acute appendicitis did not require surgery at 1 year of follow-up, critics raised concerns that many more of these patients would eventually require surgery,” wrote Edward H. Livingston, MD, deputy editor of JAMA in an accompanying editorial (JAMA 2018;320:1245-46).Surgeons have since been waiting until longer-term outcomes were known. These 5-year results are supportive of the antibiotics approach. “They show no increase in major complications in patients who experienced a recurrence and underwent appendectomy after initially being randomized to antibiotic therapy. They challenge the notion that uncomplicated acute appendicitis is a surgical emergency and show that nonsurgical treatment is a reasonable option,” Dr Livingston wrote.
He declared no conflicts of interest.
“When the earlier results of the APPAC trial were published, showing that 73% of patients with uncomplicated acute appendicitis did not require surgery at 1 year of follow-up, critics raised concerns that many more of these patients would eventually require surgery,” wrote Edward H. Livingston, MD, deputy editor of JAMA in an accompanying editorial (JAMA 2018;320:1245-46).Surgeons have since been waiting until longer-term outcomes were known. These 5-year results are supportive of the antibiotics approach. “They show no increase in major complications in patients who experienced a recurrence and underwent appendectomy after initially being randomized to antibiotic therapy. They challenge the notion that uncomplicated acute appendicitis is a surgical emergency and show that nonsurgical treatment is a reasonable option,” Dr Livingston wrote.
He declared no conflicts of interest.
“When the earlier results of the APPAC trial were published, showing that 73% of patients with uncomplicated acute appendicitis did not require surgery at 1 year of follow-up, critics raised concerns that many more of these patients would eventually require surgery,” wrote Edward H. Livingston, MD, deputy editor of JAMA in an accompanying editorial (JAMA 2018;320:1245-46).Surgeons have since been waiting until longer-term outcomes were known. These 5-year results are supportive of the antibiotics approach. “They show no increase in major complications in patients who experienced a recurrence and underwent appendectomy after initially being randomized to antibiotic therapy. They challenge the notion that uncomplicated acute appendicitis is a surgical emergency and show that nonsurgical treatment is a reasonable option,” Dr Livingston wrote.
He declared no conflicts of interest.
Longer-term outcomes of treating uncomplicated acute appendicitis with antibiotics suggest it is a feasible alternative to appendectomy.
Researchers have presented the 5-year follow-up data from the Appendicitis Acuta (APPAC) multicenter randomized clinical trial comparing appendectomy with antibiotic therapy in 530 patients.
They found that 39.1% (100) of the 257 patients randomized to antibiotic therapy – 3 days of intravenous ertapenem followed by 7 days of oral levofloxacin and metronidazole – experienced a recurrence of appendicitis within 5 years and subsequently had surgery.
However the authors noted that seven of these patients were later found not to have appendicitis, so the true success rate for antibiotic treatment was actually 63.7%.
Seventy of the patients who experienced a recurrence underwent surgery in the first year after randomization, 17 in the second year, 3 in the third year, 5 in the fourth year, and the remaining 5 patients in the fifth year, the authors wrote in an article published in JAMA.
However the overall complication rate was similar in patients who were randomized to undergo appendectomy and in those who were initially randomized to the antibiotic group but later experienced a recurrence and underwent surgery.
“No patient initially treated with antibiotics, who ultimately developed recurrent appendicitis, had any complications related to the delay in surgery,” wrote Paulina Salminen, MD, from Turku (Finland) University Hospital and coauthors. “Nearly two-thirds of all patients who initially presented with uncomplicated appendicitis were successfully treated with antibiotics alone, and those who ultimately developed recurrent disease did not experience any adverse outcomes related to the delay in appendectomy.”
Of the 100 patients randomized to antibiotics who underwent appendectomy after a recurrence, 15 were operated on when they were first hospitalized at study admission.
The authors commented that the study design allowed for surgeons to exercise their clinical judgment in choosing when to perform an appendectomy on patients in the antibiotic group, because antibiotics alone was not considered acceptable treatment for appendicitis.
“This led to some patients undergoing appendectomy who did not have appendicitis or who might have been successfully treated with antibiotics or an another course of antibiotics,” they wrote. “Future studies should investigate protocols for further imaging or antibiotic treatment for patients who develop recurrent appendicitis after they were initially treated with antibiotics.”
In the recurrence group, the majority were found to have uncomplicated appendicitis, but complicated appendicitis was seen in two patients between 2 and 5 years after the index admission.
There was a significant 17.9% higher complication rate in the appendectomy group, compared with the antibiotic group – 24.4% versus 6.5% – at 5 years and two patients in the appendectomy group had severe complications requiring reoperation.
They suggested that the higher complication rate with surgery, which was mostly attributable to infections, could be reduced by the use of laparoscopic appendectomy, which is also associated with faster recovery.
The median length of hospital stay was 3 days for both the appendectomy group and the antibiotics-only group, but patients randomized to appendectomy took a median of 22 days of sick leave, compared with 11 days for those randomized to antibiotics (P less than .001).
In the absence of standard protocol on treating appendicitis with antibiotics, the authors noted that they took a conservative approach, using broad-spectrum antibiotics and keeping patients in hospital for 3 days for observation.
“The success of antibiotic treatment for appendicitis calls into question prior beliefs that appendicitis inevitably results in serious intra-abdominal infection if appendectomy is not performed.”
The study was supported by the Mary and Georg C. Ehrnrooth Foundation, the EVO Foundation, and Turku University. One author declared lecture fees from three pharmaceutical companies but no other conflicts of interest were declared.
SOURCE: Salminen P et al. JAMA 2018;320:1259-65. doi: 10.1001/jama.2018.13201.
Longer-term outcomes of treating uncomplicated acute appendicitis with antibiotics suggest it is a feasible alternative to appendectomy.
Researchers have presented the 5-year follow-up data from the Appendicitis Acuta (APPAC) multicenter randomized clinical trial comparing appendectomy with antibiotic therapy in 530 patients.
They found that 39.1% (100) of the 257 patients randomized to antibiotic therapy – 3 days of intravenous ertapenem followed by 7 days of oral levofloxacin and metronidazole – experienced a recurrence of appendicitis within 5 years and subsequently had surgery.
However the authors noted that seven of these patients were later found not to have appendicitis, so the true success rate for antibiotic treatment was actually 63.7%.
Seventy of the patients who experienced a recurrence underwent surgery in the first year after randomization, 17 in the second year, 3 in the third year, 5 in the fourth year, and the remaining 5 patients in the fifth year, the authors wrote in an article published in JAMA.
However the overall complication rate was similar in patients who were randomized to undergo appendectomy and in those who were initially randomized to the antibiotic group but later experienced a recurrence and underwent surgery.
“No patient initially treated with antibiotics, who ultimately developed recurrent appendicitis, had any complications related to the delay in surgery,” wrote Paulina Salminen, MD, from Turku (Finland) University Hospital and coauthors. “Nearly two-thirds of all patients who initially presented with uncomplicated appendicitis were successfully treated with antibiotics alone, and those who ultimately developed recurrent disease did not experience any adverse outcomes related to the delay in appendectomy.”
Of the 100 patients randomized to antibiotics who underwent appendectomy after a recurrence, 15 were operated on when they were first hospitalized at study admission.
The authors commented that the study design allowed for surgeons to exercise their clinical judgment in choosing when to perform an appendectomy on patients in the antibiotic group, because antibiotics alone was not considered acceptable treatment for appendicitis.
“This led to some patients undergoing appendectomy who did not have appendicitis or who might have been successfully treated with antibiotics or an another course of antibiotics,” they wrote. “Future studies should investigate protocols for further imaging or antibiotic treatment for patients who develop recurrent appendicitis after they were initially treated with antibiotics.”
In the recurrence group, the majority were found to have uncomplicated appendicitis, but complicated appendicitis was seen in two patients between 2 and 5 years after the index admission.
There was a significant 17.9% higher complication rate in the appendectomy group, compared with the antibiotic group – 24.4% versus 6.5% – at 5 years and two patients in the appendectomy group had severe complications requiring reoperation.
They suggested that the higher complication rate with surgery, which was mostly attributable to infections, could be reduced by the use of laparoscopic appendectomy, which is also associated with faster recovery.
The median length of hospital stay was 3 days for both the appendectomy group and the antibiotics-only group, but patients randomized to appendectomy took a median of 22 days of sick leave, compared with 11 days for those randomized to antibiotics (P less than .001).
In the absence of standard protocol on treating appendicitis with antibiotics, the authors noted that they took a conservative approach, using broad-spectrum antibiotics and keeping patients in hospital for 3 days for observation.
“The success of antibiotic treatment for appendicitis calls into question prior beliefs that appendicitis inevitably results in serious intra-abdominal infection if appendectomy is not performed.”
The study was supported by the Mary and Georg C. Ehrnrooth Foundation, the EVO Foundation, and Turku University. One author declared lecture fees from three pharmaceutical companies but no other conflicts of interest were declared.
SOURCE: Salminen P et al. JAMA 2018;320:1259-65. doi: 10.1001/jama.2018.13201.
FROM JAMA
Key clinical point: Antibiotics could be used as an alternative to surgery for uncomplicated acute appendicitis.
Major finding: Around two-thirds of patients with acute appendicitis treated with antibiotics only did not experience a recurrence in 5 years.
Study details: Randomized controlled study in 530 patients with uncomplicated acute appendicitis.
Disclosures: The study was supported by the Mary and Georg C. Ehrnrooth Foundation, the EVO Foundation, and Turku University. One author declared lecture fees from three pharmaceutical companies but no other conflicts of interest were declared.
Source: Salminen P et al. JAMA 2018;320:1259-65. doi: 10.1001/jama.2018.13201.
ADHD in the long term
Parents whose kids are diagnosed with ADHD face important questions about what to expect in the long term and how that might inform treatment. Studies find that ADHD diagnosed in childhood tends to persist in up to 65% of adolescents (some estimates are lower depending on criteria used),1 and about 50% of people are estimated to continue to meet criteria for ADHD as adults.2 Many studies have attempted to understand what long-term risks are associated with ADHD, as well as the factors that help better predict which characteristics in childhood might predict those risks. A recent article was published on a cohort of boys followed over 33 years.3 This, as well as other large prospective studies, such as the Multimodal Treatment of ADHD (MTA) provide us with helpful long-range data that inform this article.4-6 This article reviews risks in adolescence and adulthood and the factors thought to be associated with them.

What predicts persistence of ADHD symptoms in adolescence?
Several factors emerge consistently, including higher symptom severity, comorbid conduct disorder, and lower childhood IQ; other findings include family-related factors, such as lower parental mental health, less-positive parenting, and lower rates of parental education. In general, hyperactivity and impulsivity wanes, while inattention symptoms remain more stable.
What does ADHD predict for adolescents?
Adolescents with ADHD are more than twice as likely to be involved in pregnancies under the age of 18 years, true for both male and female genders.7 This finding also is associated with increased substance use and low academic achievement but not completely explained by it. Adolescents with persistent ADHD symptoms experience poorer educational success than do kids without ADHD symptoms, according to teacher reports of performance and measurements of grade point average. They are more likely to repeat a grade.8 Related but independent is the relationship of substance use disorders in kids with ADHD. Adolescents with ADHD are more likely to use nicotine or marijuana or meet criteria for any substance use disorder than adolescents without ADHD. Finally, adolescents aged 12-18 years with ADHD are at higher risk for motor vehicle accidents and all types of accidental injuries.9
What predicts persistence of ADHD symptoms in adulthood?
A follow-up study of the MTA trial 16 years later looked at ADHD diagnosed before age 12 years and the association with symptom persistence in adulthood, defined by the DSM-5 cutoff criteria of five symptoms. The following factors related to symptom persistence: childhood psychiatric comorbidity, higher ADHD symptom severity, and parental mental health problems. Notably, family socioeconomic status, child IQ, and parental education were not associated. In addition to looking at symptom persistence, other studies have looked at predictors of functional impairment in adulthood following a childhood ADHD diagnosis (independent of whether people continue to meet criteria for the disorder). The main findings that seem consistently related to all functional outcomes, including social, occupational, and educational, are lower childhood IQ and history of conduct problems (in the absence of meeting criteria for full childhood conduct disorder). Educational family-related factors, such as socioeconomic status and lower parental education, were related to lower educational functioning only.
What does ADHD predict for adults?
It appears that overall, adults who were diagnosed with ADHD as children show poorer functional outcomes than did those who weren’t, and there is a step-wise relationship when considering adults whose symptoms persist, with more severe outcomes compared with adults whose symptoms have desisted, who in turn have worse outcomes than adults who were never diagnosed with ADHD. Educational attainments follow this pattern with the highest average levels of education in the non-ADHD group and the lowest average years in the group with persistent symptoms. Occupational success and percent receiving public assistance again separated between each group, with the symptom persisters faring the worst, the symptom desisters better, and those never affected by ADHD, the best. In terms of emotional disorders, it was only the symptom persisters who suffered from higher rates of mood and anxiety disorders. Similarly, only the symptom persisters had significantly more marijuana use disorders. No other substance use disorders or legal outcomes were significant.
How does this affect how we approach treatment?
Clinicians and researchers who specialize in ADHD have been arguing for ADHD to be treated as more of a chronic disease and for impairment to be the focus of treatment, rather than simply symptom control.10 With what we know about long-term functional impairment, there is reason to consider a more holistic picture of a child or an adolescent and how they are functioning in their academic, emotional, and social domains. A meta-analysis of treatment and long-term outcomes suggests that psychostimulant treatment, psychotherapy treatment, and combined treatment all improve long-term functioning, especially self-esteem, social functioning, and academic functioning, with combined psychotherapeutic and pharmacologic treatments associated with the highest effect sizes.11

For those who treat ADHD, it is our job to provide education to families about the chronic risks associated with the diagnosis, and the importance of offering multimodal therapy that can address family factors that might be contributing to risks, as well as the child’s overall well-being. If we are to make sense of how adults may experience impairment even in the absence of ongoing symptoms, we might look at how their overall wellness was interrupted during development. Maybe they fell into a different crowd of kids? Maybe they stopped achieving at school in a way that changed the achievement trajectory they were on? Maybe they impulsively picked up substances or got in trouble with the law? These events can have lasting impacts on well-being. We must use medicine and psychotherapy to help with symptoms, but we must look beyond treating illness and use evidence-based strategies to promote wellness at the level of the entire family.
Dr. Guth is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and the University of Vermont, both in Burlington. She works with children and adolescents as well as women in the perinatal period. She has no relevant financial disclosures.
References
1. Psychol Med. 2006 Feb;36(2):159-65.
2. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):937-44.e4.
3. J Am Acad Child Adolesc Psychiatry. 2018 Aug;57(8):571-82.e1.
4. J Am Acad Child Adolesc Psychiatry. 2017 Aug;56(8):687-95.e7.
5. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):945-52.e2.
6. J Am Acad Child Adolesc Psychiatry. 2009 May;48(5):484-500.
7. J Atten Disord. 2017 Sep 1:1087054717730610. doi: 10.1177/1087054717730610.
8. J Atten Disord. 2016 May;20(5):383-9.
9. Eur Child Adolesc Psychiatry. 2014 Feb;23(2):95-102.
10. JAMA Pediatr. 2018 Aug 13. doi: 10.1001/jamapediatrics.2018.1642.
11. PLoS One. 2015 Feb 25;10(2):e0116407.
Parents whose kids are diagnosed with ADHD face important questions about what to expect in the long term and how that might inform treatment. Studies find that ADHD diagnosed in childhood tends to persist in up to 65% of adolescents (some estimates are lower depending on criteria used),1 and about 50% of people are estimated to continue to meet criteria for ADHD as adults.2 Many studies have attempted to understand what long-term risks are associated with ADHD, as well as the factors that help better predict which characteristics in childhood might predict those risks. A recent article was published on a cohort of boys followed over 33 years.3 This, as well as other large prospective studies, such as the Multimodal Treatment of ADHD (MTA) provide us with helpful long-range data that inform this article.4-6 This article reviews risks in adolescence and adulthood and the factors thought to be associated with them.
What predicts persistence of ADHD symptoms in adolescence?
Several factors emerge consistently, including higher symptom severity, comorbid conduct disorder, and lower childhood IQ; other findings include family-related factors, such as lower parental mental health, less-positive parenting, and lower rates of parental education. In general, hyperactivity and impulsivity wanes, while inattention symptoms remain more stable.
What does ADHD predict for adolescents?
Adolescents with ADHD are more than twice as likely to be involved in pregnancies under the age of 18 years, true for both male and female genders.7 This finding also is associated with increased substance use and low academic achievement but not completely explained by it. Adolescents with persistent ADHD symptoms experience poorer educational success than do kids without ADHD symptoms, according to teacher reports of performance and measurements of grade point average. They are more likely to repeat a grade.8 Related but independent is the relationship of substance use disorders in kids with ADHD. Adolescents with ADHD are more likely to use nicotine or marijuana or meet criteria for any substance use disorder than adolescents without ADHD. Finally, adolescents aged 12-18 years with ADHD are at higher risk for motor vehicle accidents and all types of accidental injuries.9
What predicts persistence of ADHD symptoms in adulthood?
A follow-up study of the MTA trial 16 years later looked at ADHD diagnosed before age 12 years and the association with symptom persistence in adulthood, defined by the DSM-5 cutoff criteria of five symptoms. The following factors related to symptom persistence: childhood psychiatric comorbidity, higher ADHD symptom severity, and parental mental health problems. Notably, family socioeconomic status, child IQ, and parental education were not associated. In addition to looking at symptom persistence, other studies have looked at predictors of functional impairment in adulthood following a childhood ADHD diagnosis (independent of whether people continue to meet criteria for the disorder). The main findings that seem consistently related to all functional outcomes, including social, occupational, and educational, are lower childhood IQ and history of conduct problems (in the absence of meeting criteria for full childhood conduct disorder). Educational family-related factors, such as socioeconomic status and lower parental education, were related to lower educational functioning only.
What does ADHD predict for adults?
It appears that overall, adults who were diagnosed with ADHD as children show poorer functional outcomes than did those who weren’t, and there is a step-wise relationship when considering adults whose symptoms persist, with more severe outcomes compared with adults whose symptoms have desisted, who in turn have worse outcomes than adults who were never diagnosed with ADHD. Educational attainments follow this pattern with the highest average levels of education in the non-ADHD group and the lowest average years in the group with persistent symptoms. Occupational success and percent receiving public assistance again separated between each group, with the symptom persisters faring the worst, the symptom desisters better, and those never affected by ADHD, the best. In terms of emotional disorders, it was only the symptom persisters who suffered from higher rates of mood and anxiety disorders. Similarly, only the symptom persisters had significantly more marijuana use disorders. No other substance use disorders or legal outcomes were significant.
How does this affect how we approach treatment?
Clinicians and researchers who specialize in ADHD have been arguing for ADHD to be treated as more of a chronic disease and for impairment to be the focus of treatment, rather than simply symptom control.10 With what we know about long-term functional impairment, there is reason to consider a more holistic picture of a child or an adolescent and how they are functioning in their academic, emotional, and social domains. A meta-analysis of treatment and long-term outcomes suggests that psychostimulant treatment, psychotherapy treatment, and combined treatment all improve long-term functioning, especially self-esteem, social functioning, and academic functioning, with combined psychotherapeutic and pharmacologic treatments associated with the highest effect sizes.11
For those who treat ADHD, it is our job to provide education to families about the chronic risks associated with the diagnosis, and the importance of offering multimodal therapy that can address family factors that might be contributing to risks, as well as the child’s overall well-being. If we are to make sense of how adults may experience impairment even in the absence of ongoing symptoms, we might look at how their overall wellness was interrupted during development. Maybe they fell into a different crowd of kids? Maybe they stopped achieving at school in a way that changed the achievement trajectory they were on? Maybe they impulsively picked up substances or got in trouble with the law? These events can have lasting impacts on well-being. We must use medicine and psychotherapy to help with symptoms, but we must look beyond treating illness and use evidence-based strategies to promote wellness at the level of the entire family.
Dr. Guth is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and the University of Vermont, both in Burlington. She works with children and adolescents as well as women in the perinatal period. She has no relevant financial disclosures.
References
1. Psychol Med. 2006 Feb;36(2):159-65.
2. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):937-44.e4.
3. J Am Acad Child Adolesc Psychiatry. 2018 Aug;57(8):571-82.e1.
4. J Am Acad Child Adolesc Psychiatry. 2017 Aug;56(8):687-95.e7.
5. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):945-52.e2.
6. J Am Acad Child Adolesc Psychiatry. 2009 May;48(5):484-500.
7. J Atten Disord. 2017 Sep 1:1087054717730610. doi: 10.1177/1087054717730610.
8. J Atten Disord. 2016 May;20(5):383-9.
9. Eur Child Adolesc Psychiatry. 2014 Feb;23(2):95-102.
10. JAMA Pediatr. 2018 Aug 13. doi: 10.1001/jamapediatrics.2018.1642.
11. PLoS One. 2015 Feb 25;10(2):e0116407.
Parents whose kids are diagnosed with ADHD face important questions about what to expect in the long term and how that might inform treatment. Studies find that ADHD diagnosed in childhood tends to persist in up to 65% of adolescents (some estimates are lower depending on criteria used),1 and about 50% of people are estimated to continue to meet criteria for ADHD as adults.2 Many studies have attempted to understand what long-term risks are associated with ADHD, as well as the factors that help better predict which characteristics in childhood might predict those risks. A recent article was published on a cohort of boys followed over 33 years.3 This, as well as other large prospective studies, such as the Multimodal Treatment of ADHD (MTA) provide us with helpful long-range data that inform this article.4-6 This article reviews risks in adolescence and adulthood and the factors thought to be associated with them.
What predicts persistence of ADHD symptoms in adolescence?
Several factors emerge consistently, including higher symptom severity, comorbid conduct disorder, and lower childhood IQ; other findings include family-related factors, such as lower parental mental health, less-positive parenting, and lower rates of parental education. In general, hyperactivity and impulsivity wanes, while inattention symptoms remain more stable.
What does ADHD predict for adolescents?
Adolescents with ADHD are more than twice as likely to be involved in pregnancies under the age of 18 years, true for both male and female genders.7 This finding also is associated with increased substance use and low academic achievement but not completely explained by it. Adolescents with persistent ADHD symptoms experience poorer educational success than do kids without ADHD symptoms, according to teacher reports of performance and measurements of grade point average. They are more likely to repeat a grade.8 Related but independent is the relationship of substance use disorders in kids with ADHD. Adolescents with ADHD are more likely to use nicotine or marijuana or meet criteria for any substance use disorder than adolescents without ADHD. Finally, adolescents aged 12-18 years with ADHD are at higher risk for motor vehicle accidents and all types of accidental injuries.9
What predicts persistence of ADHD symptoms in adulthood?
A follow-up study of the MTA trial 16 years later looked at ADHD diagnosed before age 12 years and the association with symptom persistence in adulthood, defined by the DSM-5 cutoff criteria of five symptoms. The following factors related to symptom persistence: childhood psychiatric comorbidity, higher ADHD symptom severity, and parental mental health problems. Notably, family socioeconomic status, child IQ, and parental education were not associated. In addition to looking at symptom persistence, other studies have looked at predictors of functional impairment in adulthood following a childhood ADHD diagnosis (independent of whether people continue to meet criteria for the disorder). The main findings that seem consistently related to all functional outcomes, including social, occupational, and educational, are lower childhood IQ and history of conduct problems (in the absence of meeting criteria for full childhood conduct disorder). Educational family-related factors, such as socioeconomic status and lower parental education, were related to lower educational functioning only.
What does ADHD predict for adults?
It appears that overall, adults who were diagnosed with ADHD as children show poorer functional outcomes than did those who weren’t, and there is a step-wise relationship when considering adults whose symptoms persist, with more severe outcomes compared with adults whose symptoms have desisted, who in turn have worse outcomes than adults who were never diagnosed with ADHD. Educational attainments follow this pattern with the highest average levels of education in the non-ADHD group and the lowest average years in the group with persistent symptoms. Occupational success and percent receiving public assistance again separated between each group, with the symptom persisters faring the worst, the symptom desisters better, and those never affected by ADHD, the best. In terms of emotional disorders, it was only the symptom persisters who suffered from higher rates of mood and anxiety disorders. Similarly, only the symptom persisters had significantly more marijuana use disorders. No other substance use disorders or legal outcomes were significant.
How does this affect how we approach treatment?
Clinicians and researchers who specialize in ADHD have been arguing for ADHD to be treated as more of a chronic disease and for impairment to be the focus of treatment, rather than simply symptom control.10 With what we know about long-term functional impairment, there is reason to consider a more holistic picture of a child or an adolescent and how they are functioning in their academic, emotional, and social domains. A meta-analysis of treatment and long-term outcomes suggests that psychostimulant treatment, psychotherapy treatment, and combined treatment all improve long-term functioning, especially self-esteem, social functioning, and academic functioning, with combined psychotherapeutic and pharmacologic treatments associated with the highest effect sizes.11
For those who treat ADHD, it is our job to provide education to families about the chronic risks associated with the diagnosis, and the importance of offering multimodal therapy that can address family factors that might be contributing to risks, as well as the child’s overall well-being. If we are to make sense of how adults may experience impairment even in the absence of ongoing symptoms, we might look at how their overall wellness was interrupted during development. Maybe they fell into a different crowd of kids? Maybe they stopped achieving at school in a way that changed the achievement trajectory they were on? Maybe they impulsively picked up substances or got in trouble with the law? These events can have lasting impacts on well-being. We must use medicine and psychotherapy to help with symptoms, but we must look beyond treating illness and use evidence-based strategies to promote wellness at the level of the entire family.
Dr. Guth is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and the University of Vermont, both in Burlington. She works with children and adolescents as well as women in the perinatal period. She has no relevant financial disclosures.
References
1. Psychol Med. 2006 Feb;36(2):159-65.
2. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):937-44.e4.
3. J Am Acad Child Adolesc Psychiatry. 2018 Aug;57(8):571-82.e1.
4. J Am Acad Child Adolesc Psychiatry. 2017 Aug;56(8):687-95.e7.
5. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):945-52.e2.
6. J Am Acad Child Adolesc Psychiatry. 2009 May;48(5):484-500.
7. J Atten Disord. 2017 Sep 1:1087054717730610. doi: 10.1177/1087054717730610.
8. J Atten Disord. 2016 May;20(5):383-9.
9. Eur Child Adolesc Psychiatry. 2014 Feb;23(2):95-102.
10. JAMA Pediatr. 2018 Aug 13. doi: 10.1001/jamapediatrics.2018.1642.
11. PLoS One. 2015 Feb 25;10(2):e0116407.
New AAP policy statement addresses teen driver risks
The American Academy of Pediatric has issued a policy statement regarding teen drivers because, although becoming a driver is a rite of passage for many, there are unique risks associated with teen drivers – and important ways to address them.

“In 2015, among 15- to 20-year-old individuals, 1,886 young drivers died in MVCs [motor vehicle crashes], which is an increase of 9% from 2014,” the statement explains. “Another 195,000 young drivers were in MVCs, which is up 14% from 2014.”
Risk factors associated with crashes in teenage drivers include their inexperience, the presence of other teens in the car, high-speed and risky driving, distraction, lack of sleep, nighttime driving, and alcohol, marijuana, and medication use. Mobile phones and other electronic devices pose a major threat to driver safety because they contribute opportunities for three different kinds of distraction – visual, manual, and cognitive. Drug and alcohol use poses another threat; for example, tetrahydrocannabinol, found in marijuana, is associated with a 1.25 higher risk of crash, according Elizabeth M. Alderman, MD, and her associates on the Committee on Adolescence and the Council on Injury, Violence, and Poison Prevention who crafted the policy statement.
The policy statement also outlined several interventions to help mitigate these risks. Graduated driver licensing, which has been adopted in all 50 states, has helped reduce teen crashes by promoting skills development and reducing exposure to risky-driving situations. Parents can help model safer-driving practices and set expectations, as well as monitor and affect their teens’ driving behaviors during the supervised-driving phase. Driver education programs, on the other hand, counterintuitively have little effect on teen driving safety, which the authors suggested is because “the knowledge required to pass licensing exams is seldom related to an evidence-based understanding of the behaviors and skills associated with novice driver crash risk.” There also have been technological advances that can help improve driving safety among teenage drivers, such as automatic braking and lane-maintenance alerts.
“Policies, programs, and technologies exist to mitigate these risks but, in most cases, depend on active participation by the teenager and parents,” the authors concluded. “Pediatricians, communities, and governments need to take action to better educate teen drivers and their parents around these risks and strategies to reduce them.”
The full policy statement includes specific recommendations for anticipatory guidance, professional practice, community advocacy, and legislative advocacy. It also includes many resources and links to further information.
SOURCE: Alderman EM et al. Pediatrics. 2018 Oct;142(4):e20182163.
The American Academy of Pediatric has issued a policy statement regarding teen drivers because, although becoming a driver is a rite of passage for many, there are unique risks associated with teen drivers – and important ways to address them.
“In 2015, among 15- to 20-year-old individuals, 1,886 young drivers died in MVCs [motor vehicle crashes], which is an increase of 9% from 2014,” the statement explains. “Another 195,000 young drivers were in MVCs, which is up 14% from 2014.”
Risk factors associated with crashes in teenage drivers include their inexperience, the presence of other teens in the car, high-speed and risky driving, distraction, lack of sleep, nighttime driving, and alcohol, marijuana, and medication use. Mobile phones and other electronic devices pose a major threat to driver safety because they contribute opportunities for three different kinds of distraction – visual, manual, and cognitive. Drug and alcohol use poses another threat; for example, tetrahydrocannabinol, found in marijuana, is associated with a 1.25 higher risk of crash, according Elizabeth M. Alderman, MD, and her associates on the Committee on Adolescence and the Council on Injury, Violence, and Poison Prevention who crafted the policy statement.
The policy statement also outlined several interventions to help mitigate these risks. Graduated driver licensing, which has been adopted in all 50 states, has helped reduce teen crashes by promoting skills development and reducing exposure to risky-driving situations. Parents can help model safer-driving practices and set expectations, as well as monitor and affect their teens’ driving behaviors during the supervised-driving phase. Driver education programs, on the other hand, counterintuitively have little effect on teen driving safety, which the authors suggested is because “the knowledge required to pass licensing exams is seldom related to an evidence-based understanding of the behaviors and skills associated with novice driver crash risk.” There also have been technological advances that can help improve driving safety among teenage drivers, such as automatic braking and lane-maintenance alerts.
“Policies, programs, and technologies exist to mitigate these risks but, in most cases, depend on active participation by the teenager and parents,” the authors concluded. “Pediatricians, communities, and governments need to take action to better educate teen drivers and their parents around these risks and strategies to reduce them.”
The full policy statement includes specific recommendations for anticipatory guidance, professional practice, community advocacy, and legislative advocacy. It also includes many resources and links to further information.
SOURCE: Alderman EM et al. Pediatrics. 2018 Oct;142(4):e20182163.
The American Academy of Pediatric has issued a policy statement regarding teen drivers because, although becoming a driver is a rite of passage for many, there are unique risks associated with teen drivers – and important ways to address them.
“In 2015, among 15- to 20-year-old individuals, 1,886 young drivers died in MVCs [motor vehicle crashes], which is an increase of 9% from 2014,” the statement explains. “Another 195,000 young drivers were in MVCs, which is up 14% from 2014.”
Risk factors associated with crashes in teenage drivers include their inexperience, the presence of other teens in the car, high-speed and risky driving, distraction, lack of sleep, nighttime driving, and alcohol, marijuana, and medication use. Mobile phones and other electronic devices pose a major threat to driver safety because they contribute opportunities for three different kinds of distraction – visual, manual, and cognitive. Drug and alcohol use poses another threat; for example, tetrahydrocannabinol, found in marijuana, is associated with a 1.25 higher risk of crash, according Elizabeth M. Alderman, MD, and her associates on the Committee on Adolescence and the Council on Injury, Violence, and Poison Prevention who crafted the policy statement.
The policy statement also outlined several interventions to help mitigate these risks. Graduated driver licensing, which has been adopted in all 50 states, has helped reduce teen crashes by promoting skills development and reducing exposure to risky-driving situations. Parents can help model safer-driving practices and set expectations, as well as monitor and affect their teens’ driving behaviors during the supervised-driving phase. Driver education programs, on the other hand, counterintuitively have little effect on teen driving safety, which the authors suggested is because “the knowledge required to pass licensing exams is seldom related to an evidence-based understanding of the behaviors and skills associated with novice driver crash risk.” There also have been technological advances that can help improve driving safety among teenage drivers, such as automatic braking and lane-maintenance alerts.
“Policies, programs, and technologies exist to mitigate these risks but, in most cases, depend on active participation by the teenager and parents,” the authors concluded. “Pediatricians, communities, and governments need to take action to better educate teen drivers and their parents around these risks and strategies to reduce them.”
The full policy statement includes specific recommendations for anticipatory guidance, professional practice, community advocacy, and legislative advocacy. It also includes many resources and links to further information.
SOURCE: Alderman EM et al. Pediatrics. 2018 Oct;142(4):e20182163.
FROM PEDIATRICS
Residents curb IV antibiotic overuse in children
ATLANTA – It took less than a year to curb overuse of intravenous antibiotics at the Cincinnati Children’s Hospital, according to a report given at the Pediatric Hospital Medicine meeting.

Overuse of IV antibiotics – continuing IV formulations when oral formulations would work just as well – is a widespread concern in hospital medicine. Patients can often be switched to an oral antibiotic after an initial IV course. It lowers costs, lessens the risk of antimicrobial resistance, and reduces IV complications, but timely transitions don’t always happen.
They certainly weren’t happening at Cincinnati Children’s. “Despite a strong antimicrobial stewardship program, we identified a problem with overuse of IV antibiotics. The majority of pediatric patients admitted to an in-hospital service were started on IV antibiotics regardless of diagnosis or condition. Conversion to enteral antibiotics was often not considered until the day of discharge, even if patients were taking other enteral medications earlier in the admission,” said project leader Sonya Girdwood, MD, a research fellow at the hospital.
To get a handle on the problem, her team focused on two common IV antibiotics, ampicillin and clindamycin, that have oral equivalents with equal bioavailability: amoxicillin in the case of ampicillin, and oral clindamycin. To further define the project, they zeroed in on two common indications: clindamycin for uncomplicated skin and soft-tissue infections, and ampicillin for community-acquired pneumonia, in children over 2 months old.
The team figured that, if patients were able to take other oral medications, they should also be able to take oral antibiotics, so the goal of the project was to increase the rate of antibiotics given orally in children who were taking other enteral medications.
That percentage was 44% at baseline, and increased to 80% by month 8, saving an estimated $30,000 annually. There was no increase in 30-day readmissions. Length of stay held steady overall at about a day and half, but Dr. Girdwood suspected it might have been reduced for cellulitis.
Improvement efforts focused on residents and started in January 2017. Among the first lessons was that IV ampicillin is about 21 times more expensive than amoxicillin and that IV clindamycin is about twice as expensive as its oral formulation.
Residents were tasked with forming a plan at admission to transition children to oral antibiotics as soon as possible and to discuss those plans with attending physicians in preround huddles. Often, “this led to [transition] orders being placed even before rounds started,” Dr. Girdwood said.
A time was set up during evening huddles – 10 p.m. – for residents working overnight to discuss transition timing with attending. Failures – patients still on IV clindamycin or ampicillin when they were taking oral meds – were identified and shared with resident teams.
The gains have been maintained for almost a year with little backsliding; residents are reminded weekly of transition goals.
Children with skin and soft-tissue infections with bone or eye involvement were excluded from the project, along with pneumonia patients with chest tubes or complex or loculated effusions requiring a surgery consult.
There was no external funding, and the investigators had no disclosures.
ATLANTA – It took less than a year to curb overuse of intravenous antibiotics at the Cincinnati Children’s Hospital, according to a report given at the Pediatric Hospital Medicine meeting.
Overuse of IV antibiotics – continuing IV formulations when oral formulations would work just as well – is a widespread concern in hospital medicine. Patients can often be switched to an oral antibiotic after an initial IV course. It lowers costs, lessens the risk of antimicrobial resistance, and reduces IV complications, but timely transitions don’t always happen.
They certainly weren’t happening at Cincinnati Children’s. “Despite a strong antimicrobial stewardship program, we identified a problem with overuse of IV antibiotics. The majority of pediatric patients admitted to an in-hospital service were started on IV antibiotics regardless of diagnosis or condition. Conversion to enteral antibiotics was often not considered until the day of discharge, even if patients were taking other enteral medications earlier in the admission,” said project leader Sonya Girdwood, MD, a research fellow at the hospital.
To get a handle on the problem, her team focused on two common IV antibiotics, ampicillin and clindamycin, that have oral equivalents with equal bioavailability: amoxicillin in the case of ampicillin, and oral clindamycin. To further define the project, they zeroed in on two common indications: clindamycin for uncomplicated skin and soft-tissue infections, and ampicillin for community-acquired pneumonia, in children over 2 months old.
The team figured that, if patients were able to take other oral medications, they should also be able to take oral antibiotics, so the goal of the project was to increase the rate of antibiotics given orally in children who were taking other enteral medications.
That percentage was 44% at baseline, and increased to 80% by month 8, saving an estimated $30,000 annually. There was no increase in 30-day readmissions. Length of stay held steady overall at about a day and half, but Dr. Girdwood suspected it might have been reduced for cellulitis.
Improvement efforts focused on residents and started in January 2017. Among the first lessons was that IV ampicillin is about 21 times more expensive than amoxicillin and that IV clindamycin is about twice as expensive as its oral formulation.
Residents were tasked with forming a plan at admission to transition children to oral antibiotics as soon as possible and to discuss those plans with attending physicians in preround huddles. Often, “this led to [transition] orders being placed even before rounds started,” Dr. Girdwood said.
A time was set up during evening huddles – 10 p.m. – for residents working overnight to discuss transition timing with attending. Failures – patients still on IV clindamycin or ampicillin when they were taking oral meds – were identified and shared with resident teams.
The gains have been maintained for almost a year with little backsliding; residents are reminded weekly of transition goals.
Children with skin and soft-tissue infections with bone or eye involvement were excluded from the project, along with pneumonia patients with chest tubes or complex or loculated effusions requiring a surgery consult.
There was no external funding, and the investigators had no disclosures.
ATLANTA – It took less than a year to curb overuse of intravenous antibiotics at the Cincinnati Children’s Hospital, according to a report given at the Pediatric Hospital Medicine meeting.
Overuse of IV antibiotics – continuing IV formulations when oral formulations would work just as well – is a widespread concern in hospital medicine. Patients can often be switched to an oral antibiotic after an initial IV course. It lowers costs, lessens the risk of antimicrobial resistance, and reduces IV complications, but timely transitions don’t always happen.
They certainly weren’t happening at Cincinnati Children’s. “Despite a strong antimicrobial stewardship program, we identified a problem with overuse of IV antibiotics. The majority of pediatric patients admitted to an in-hospital service were started on IV antibiotics regardless of diagnosis or condition. Conversion to enteral antibiotics was often not considered until the day of discharge, even if patients were taking other enteral medications earlier in the admission,” said project leader Sonya Girdwood, MD, a research fellow at the hospital.
To get a handle on the problem, her team focused on two common IV antibiotics, ampicillin and clindamycin, that have oral equivalents with equal bioavailability: amoxicillin in the case of ampicillin, and oral clindamycin. To further define the project, they zeroed in on two common indications: clindamycin for uncomplicated skin and soft-tissue infections, and ampicillin for community-acquired pneumonia, in children over 2 months old.
The team figured that, if patients were able to take other oral medications, they should also be able to take oral antibiotics, so the goal of the project was to increase the rate of antibiotics given orally in children who were taking other enteral medications.
That percentage was 44% at baseline, and increased to 80% by month 8, saving an estimated $30,000 annually. There was no increase in 30-day readmissions. Length of stay held steady overall at about a day and half, but Dr. Girdwood suspected it might have been reduced for cellulitis.
Improvement efforts focused on residents and started in January 2017. Among the first lessons was that IV ampicillin is about 21 times more expensive than amoxicillin and that IV clindamycin is about twice as expensive as its oral formulation.
Residents were tasked with forming a plan at admission to transition children to oral antibiotics as soon as possible and to discuss those plans with attending physicians in preround huddles. Often, “this led to [transition] orders being placed even before rounds started,” Dr. Girdwood said.
A time was set up during evening huddles – 10 p.m. – for residents working overnight to discuss transition timing with attending. Failures – patients still on IV clindamycin or ampicillin when they were taking oral meds – were identified and shared with resident teams.
The gains have been maintained for almost a year with little backsliding; residents are reminded weekly of transition goals.
Children with skin and soft-tissue infections with bone or eye involvement were excluded from the project, along with pneumonia patients with chest tubes or complex or loculated effusions requiring a surgery consult.
There was no external funding, and the investigators had no disclosures.
REPORTING FROM PHM 2018
Key clinical point:
Major finding: The percentage of antibiotics given orally to children who were taking other enteral medications rose from 44% to 80% over 8 months, saving an estimated $30,000 annually.
Study details: Quality improvement project
Disclosures: There was no external funding, and the investigators didn’t have any disclosures.
Trifarotene cream for acne meets all endpoints in twin phase 3 trials
PARIS – A novel kinder, gentler topical retinoid met all of its primary and secondary endpoints in two identical phase 3 randomized trials totaling 2,420 patients with moderate acne vulgaris on both the face and trunk.

Trifarotene cream 50 mcg/g selectively targets the gamma retinoic acid receptor. This unique selectivity for just one of the three retinoic acid receptors results in less of the classic retinoid side effects – redness, scaling, dryness, stinging, burning – that can limit the clinical utility of existing retinoids. This was borne out by the high completion rates in trifarotene-treated participants in the two 12-week trials: 88.2% in the PERFECT 1 trial and 92.7% in PERFECT 2, compared with rates of 89.8% and 93.9% in vehicle-treated controls, Jerry K.L. Tan, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
“Most adverse events involved local intolerance occurring at application sites and were mild and transient,” Dr. Tan, a dermatologist at the University of Western Ontario, Windsor, and head of Windsor Clinical Research, reported.
PERFECT 1 and 2 were multicenter, double-blind, randomized, vehicle-controlled, 12-week phase 3 trials. Of note, these were the first-ever large-scale randomized trials to simultaneously evaluate a topical therapy for treatment of both facial and truncal acne. This ambitious goal created some unique challenges, which Dr. Tan described.
Participants, all of whom had moderate acne vulgaris on the face and trunk, ranged in age from 9 to 58 years, with a mean age of 19 years. They were randomized to once-daily application of trifarotene cream 50 mcg/g or its vehicle in the evening.
Primary and secondary outcomes
One major efficacy endpoint on the face was achievement of Investigator Global Assessment success as defined by a score of 0 or 1, meaning clear or almost clear, coupled with at least a 2-grade improvement from baseline to week 12. In PERFECT 1 and 2 this was achieved by 29.7% and 42.8% of trifarotene cream-treated patients, response rates significantly better than the 20% and 25.8% in vehicle-treated controls.
Another endpoint for facial therapy were the absolute reductions from baseline in facial inflammatory and noninflammatory acne lesions. The mean reduction in inflammatory lesion count in trifarotene-treated patients was 19.6% in PERFECT 1 and 24.6% in PERFECT 2, both significantly better than the mean 15.8% and 19.6% decreases in controls. Noninflammatory facial lesion counts dropped by 26.7% and 30.4% with trifarotene, versus 18.9% and 22.3% with vehicle.
The efficacy yardsticks utilized on the trunk were the same as on the face except that Physician Global Assessment was the terminology utilized in lieu of Investigator Global Assessment. Physician Global Assessment success on the trunk was achieved by 35.8% and 41.1% of trifarotene-treated patients in the two trials, as compared with 25.7% and 30.1% of controls.
The mean reductions in truncal inflammatory lesion count obtained with trifarotene cream were 22% and 26.1%, both significantly better than the 18.8% and 20.3% rates with vehicle.
Treatment-emergent adverse events leading to study discontinuation occurred in 1.9% of trifarotene-treated patients in one trial and 1% in the other.
One audience member commented that the vehicle response rates looked too strong for that compound to be inert. Dr. Tan agreed. “The vehicle looks really good. One of the issues with vehicles is that many of them have to contain products to prevent decay, fermentation, and proliferation of yeast and bacteria. So I quite agree: I think many of our vehicles do have active ingredients,” he replied. “If you look at the topical dapsone trials, the vehicles look amazing.”
“The other possibility is that there’s what we call ‘investigator creep,’” the dermatologist continued. “It’s the notion that you have no idea what the patients are getting, but they look like maybe they’re getting better, so you grade it as better.”
Dr. Tan reported serving as an advisor and consultant to, speaker for, and recipient of research grants from Galderma, which sponsored the two phase 3 trials. The company is also developing trifarotene for the treatment of lamellar ichthyosis.
PARIS – A novel kinder, gentler topical retinoid met all of its primary and secondary endpoints in two identical phase 3 randomized trials totaling 2,420 patients with moderate acne vulgaris on both the face and trunk.
Trifarotene cream 50 mcg/g selectively targets the gamma retinoic acid receptor. This unique selectivity for just one of the three retinoic acid receptors results in less of the classic retinoid side effects – redness, scaling, dryness, stinging, burning – that can limit the clinical utility of existing retinoids. This was borne out by the high completion rates in trifarotene-treated participants in the two 12-week trials: 88.2% in the PERFECT 1 trial and 92.7% in PERFECT 2, compared with rates of 89.8% and 93.9% in vehicle-treated controls, Jerry K.L. Tan, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
“Most adverse events involved local intolerance occurring at application sites and were mild and transient,” Dr. Tan, a dermatologist at the University of Western Ontario, Windsor, and head of Windsor Clinical Research, reported.
PERFECT 1 and 2 were multicenter, double-blind, randomized, vehicle-controlled, 12-week phase 3 trials. Of note, these were the first-ever large-scale randomized trials to simultaneously evaluate a topical therapy for treatment of both facial and truncal acne. This ambitious goal created some unique challenges, which Dr. Tan described.
Participants, all of whom had moderate acne vulgaris on the face and trunk, ranged in age from 9 to 58 years, with a mean age of 19 years. They were randomized to once-daily application of trifarotene cream 50 mcg/g or its vehicle in the evening.
Primary and secondary outcomes
One major efficacy endpoint on the face was achievement of Investigator Global Assessment success as defined by a score of 0 or 1, meaning clear or almost clear, coupled with at least a 2-grade improvement from baseline to week 12. In PERFECT 1 and 2 this was achieved by 29.7% and 42.8% of trifarotene cream-treated patients, response rates significantly better than the 20% and 25.8% in vehicle-treated controls.
Another endpoint for facial therapy were the absolute reductions from baseline in facial inflammatory and noninflammatory acne lesions. The mean reduction in inflammatory lesion count in trifarotene-treated patients was 19.6% in PERFECT 1 and 24.6% in PERFECT 2, both significantly better than the mean 15.8% and 19.6% decreases in controls. Noninflammatory facial lesion counts dropped by 26.7% and 30.4% with trifarotene, versus 18.9% and 22.3% with vehicle.
The efficacy yardsticks utilized on the trunk were the same as on the face except that Physician Global Assessment was the terminology utilized in lieu of Investigator Global Assessment. Physician Global Assessment success on the trunk was achieved by 35.8% and 41.1% of trifarotene-treated patients in the two trials, as compared with 25.7% and 30.1% of controls.
The mean reductions in truncal inflammatory lesion count obtained with trifarotene cream were 22% and 26.1%, both significantly better than the 18.8% and 20.3% rates with vehicle.
Treatment-emergent adverse events leading to study discontinuation occurred in 1.9% of trifarotene-treated patients in one trial and 1% in the other.
One audience member commented that the vehicle response rates looked too strong for that compound to be inert. Dr. Tan agreed. “The vehicle looks really good. One of the issues with vehicles is that many of them have to contain products to prevent decay, fermentation, and proliferation of yeast and bacteria. So I quite agree: I think many of our vehicles do have active ingredients,” he replied. “If you look at the topical dapsone trials, the vehicles look amazing.”
“The other possibility is that there’s what we call ‘investigator creep,’” the dermatologist continued. “It’s the notion that you have no idea what the patients are getting, but they look like maybe they’re getting better, so you grade it as better.”
Dr. Tan reported serving as an advisor and consultant to, speaker for, and recipient of research grants from Galderma, which sponsored the two phase 3 trials. The company is also developing trifarotene for the treatment of lamellar ichthyosis.
PARIS – A novel kinder, gentler topical retinoid met all of its primary and secondary endpoints in two identical phase 3 randomized trials totaling 2,420 patients with moderate acne vulgaris on both the face and trunk.
Trifarotene cream 50 mcg/g selectively targets the gamma retinoic acid receptor. This unique selectivity for just one of the three retinoic acid receptors results in less of the classic retinoid side effects – redness, scaling, dryness, stinging, burning – that can limit the clinical utility of existing retinoids. This was borne out by the high completion rates in trifarotene-treated participants in the two 12-week trials: 88.2% in the PERFECT 1 trial and 92.7% in PERFECT 2, compared with rates of 89.8% and 93.9% in vehicle-treated controls, Jerry K.L. Tan, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
“Most adverse events involved local intolerance occurring at application sites and were mild and transient,” Dr. Tan, a dermatologist at the University of Western Ontario, Windsor, and head of Windsor Clinical Research, reported.
PERFECT 1 and 2 were multicenter, double-blind, randomized, vehicle-controlled, 12-week phase 3 trials. Of note, these were the first-ever large-scale randomized trials to simultaneously evaluate a topical therapy for treatment of both facial and truncal acne. This ambitious goal created some unique challenges, which Dr. Tan described.
Participants, all of whom had moderate acne vulgaris on the face and trunk, ranged in age from 9 to 58 years, with a mean age of 19 years. They were randomized to once-daily application of trifarotene cream 50 mcg/g or its vehicle in the evening.
Primary and secondary outcomes
One major efficacy endpoint on the face was achievement of Investigator Global Assessment success as defined by a score of 0 or 1, meaning clear or almost clear, coupled with at least a 2-grade improvement from baseline to week 12. In PERFECT 1 and 2 this was achieved by 29.7% and 42.8% of trifarotene cream-treated patients, response rates significantly better than the 20% and 25.8% in vehicle-treated controls.
Another endpoint for facial therapy were the absolute reductions from baseline in facial inflammatory and noninflammatory acne lesions. The mean reduction in inflammatory lesion count in trifarotene-treated patients was 19.6% in PERFECT 1 and 24.6% in PERFECT 2, both significantly better than the mean 15.8% and 19.6% decreases in controls. Noninflammatory facial lesion counts dropped by 26.7% and 30.4% with trifarotene, versus 18.9% and 22.3% with vehicle.
The efficacy yardsticks utilized on the trunk were the same as on the face except that Physician Global Assessment was the terminology utilized in lieu of Investigator Global Assessment. Physician Global Assessment success on the trunk was achieved by 35.8% and 41.1% of trifarotene-treated patients in the two trials, as compared with 25.7% and 30.1% of controls.
The mean reductions in truncal inflammatory lesion count obtained with trifarotene cream were 22% and 26.1%, both significantly better than the 18.8% and 20.3% rates with vehicle.
Treatment-emergent adverse events leading to study discontinuation occurred in 1.9% of trifarotene-treated patients in one trial and 1% in the other.
One audience member commented that the vehicle response rates looked too strong for that compound to be inert. Dr. Tan agreed. “The vehicle looks really good. One of the issues with vehicles is that many of them have to contain products to prevent decay, fermentation, and proliferation of yeast and bacteria. So I quite agree: I think many of our vehicles do have active ingredients,” he replied. “If you look at the topical dapsone trials, the vehicles look amazing.”
“The other possibility is that there’s what we call ‘investigator creep,’” the dermatologist continued. “It’s the notion that you have no idea what the patients are getting, but they look like maybe they’re getting better, so you grade it as better.”
Dr. Tan reported serving as an advisor and consultant to, speaker for, and recipient of research grants from Galderma, which sponsored the two phase 3 trials. The company is also developing trifarotene for the treatment of lamellar ichthyosis.
REPORTING FROM THE EADV CONGRESS
Key clinical point:
Major finding: Treatment-emergent adverse events leading to study discontinuation occurred in 1.9% of trifarotene cream–treated patients in one trial and 1% in the other.
Study details: PERFECT 1 and PERFECT 2 were identically designed 12-week phase 3 randomized trials including 2,420 patients with moderate facial and truncal acne.
Disclosures: The study presenter reported serving as an advisor, consultant to, speaker for, and recipient of research grants from Galderma, which sponsored the two phase 3 trials.
Amantadine-Induced Livedo Reticularis in a Child Treated Off Label for Neurobehavioral Disorders
Livedo reticularis (LR) is a common dermatologic finding consisting of diffuse, reticulated, violaceous patches. It often is a benign physical finding known as cutis marmorata; however, LR can be associated with other medical conditions as well as with the use of some medications.1,2 Amantadine is a common cause of LR in Parkinson disease patients.3,4 We present a rare case of amantadine-induced LR in a pediatric patient and highlight the off-label use of this medication in children.
Case Report
An 8-year-old boy presented with a diffuse rash on the trunk, arms, and legs of 9 months’ duration. The patient denied any associated symptoms as well as alleviating or exacerbating factors. He also denied any changes with temperature. He had no recent international travel and no prior drug allergies. His medical history was remarkable for attention deficit hyperactivity disorder (ADHD), bipolar disorder, and autism spectrum disorder. His previously prescribed medications included atomoxetine, quetiapine, and valproic acid. The only new medication that had been started within the last year was amantadine. Physical examination revealed a diffuse, reticulated, erythematous to violaceous, blanching rash that was most notable on the legs (Figure 1A) but also was present on the trunk (Figure 1B) and arms (Figure 1C). The clinical examination was consistent with LR, which was presumed to be secondary to amantadine use. Given the multiple psychiatric diagnoses and medication history in this young patient, a consultation with child psychiatry was facilitated. His medications and diagnosis were reviewed, and amantadine was discontinued. At a follow-up visit 5 months later, the patient’s LR had improved (Figure 2).
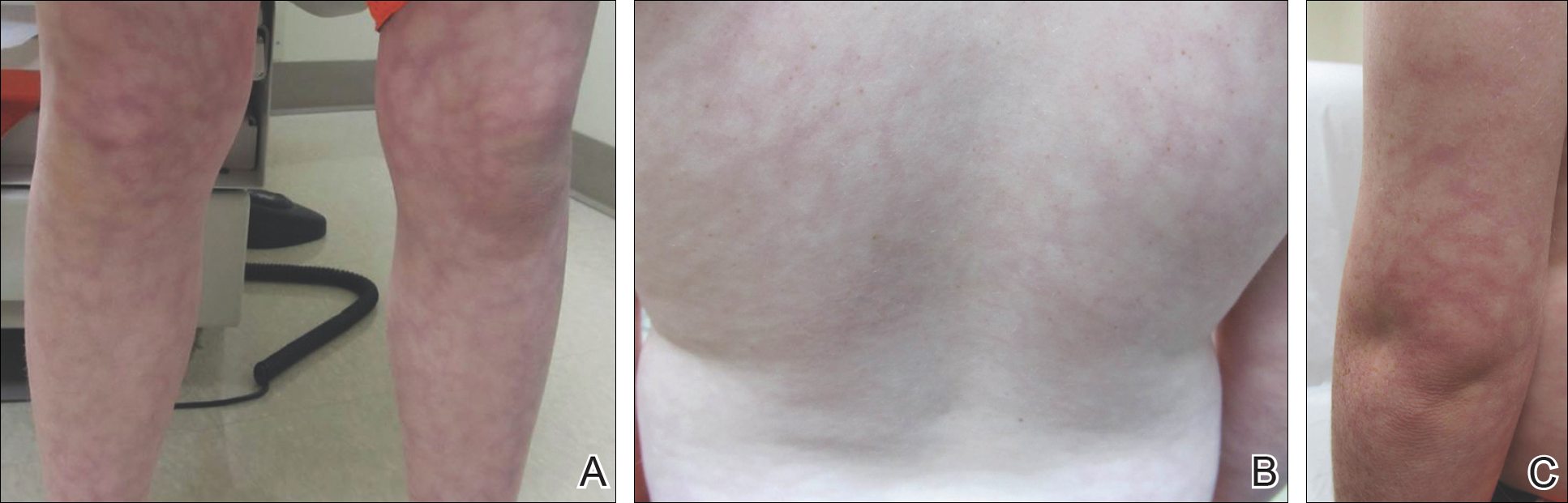
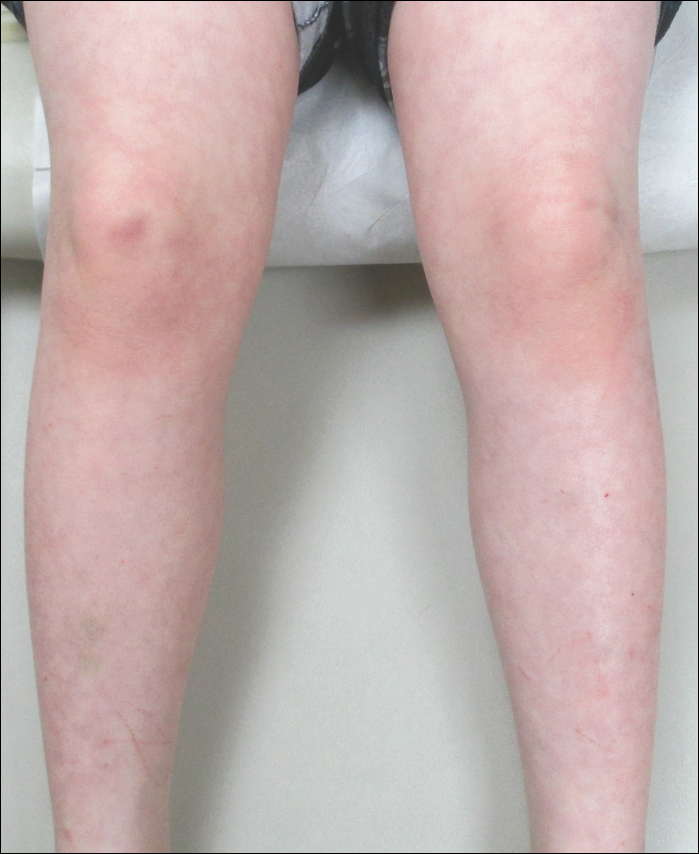
Comment
Amantadine has a well-documented association with LR in patients with Parkinson disease,3,4 which has been reported in up to 40% of those taking amantadine.2 More recently, amantadine has been used off label to treat neurobehavioral disorders in children due to beneficial effects including improvement in attention and concentration, distractibility, and fatigue.5 Our patient was being treated off label with amantadine for ADHD and bipolar disorder. Amantadine acts as a noncompetitive antagonist of the N-methyl-D-aspartate receptor, enhancing dopamine release to reduce symptoms of ADHD.5,6 Additionally, amantadine can cause a depletion of catecholamines in the peripheral nerve terminals, which may lead to dilatation of dermal vessels.4,6 This sequence of events has been proposed as a possible mechanism contributing to amantadine-induced LR, though the pathophysiology is not fully understood.1,3,4
Our case of LR likely was induced by amantadine given the temporal relationship between initiation of the medication, onset of the rash, and the considerable improvement of the rash upon discontinuation of amantadine. Barrera and Browning6 reported another case of amantadine-induced LR in a pediatric patient. Because amantadine is increasingly being used off label to treat childhood neurobehavioral disorders, amantadine-induced LR may become more prevalent in patients who do not have Parkinson disease; therefore, physicians who treat pediatric patients must be aware of this side effect.5
- Quaresma MV, Gomes-Dias AC, Serruya A, et al. Amantadine-induced livedo reticularis: a case report. An Bras Dermatol. 2015;90:745-747.
- Gibbs MB, English JC, Zirwas MJ. Livedo reticularis: an update. J Am Acad Dermatol. 2005;52:1009-1019.
- Silva SB, Miot HA. Case for diagnosis. amantadine-induced livedo reticularis. An Bras Dermatol. 2012;87:319-321.
- Vollum DI, Parkes JD, Doyle D. Livedo reticularis during amantadine treatment. Br Med J. 1971;2:627-628.
- Hosenbocus S, Chahal R. Amantadine: a review of use in child and adolescent psychiatry. J Can Acad Child Adolesc Psychiatry. 2013;22:55-60.
- Barrera F, Browning JC. Likely amantadine-induced livedo reticularis in a child. Pediatr Dermatol. 2012;29:329-330.
Livedo reticularis (LR) is a common dermatologic finding consisting of diffuse, reticulated, violaceous patches. It often is a benign physical finding known as cutis marmorata; however, LR can be associated with other medical conditions as well as with the use of some medications.1,2 Amantadine is a common cause of LR in Parkinson disease patients.3,4 We present a rare case of amantadine-induced LR in a pediatric patient and highlight the off-label use of this medication in children.
Case Report
An 8-year-old boy presented with a diffuse rash on the trunk, arms, and legs of 9 months’ duration. The patient denied any associated symptoms as well as alleviating or exacerbating factors. He also denied any changes with temperature. He had no recent international travel and no prior drug allergies. His medical history was remarkable for attention deficit hyperactivity disorder (ADHD), bipolar disorder, and autism spectrum disorder. His previously prescribed medications included atomoxetine, quetiapine, and valproic acid. The only new medication that had been started within the last year was amantadine. Physical examination revealed a diffuse, reticulated, erythematous to violaceous, blanching rash that was most notable on the legs (Figure 1A) but also was present on the trunk (Figure 1B) and arms (Figure 1C). The clinical examination was consistent with LR, which was presumed to be secondary to amantadine use. Given the multiple psychiatric diagnoses and medication history in this young patient, a consultation with child psychiatry was facilitated. His medications and diagnosis were reviewed, and amantadine was discontinued. At a follow-up visit 5 months later, the patient’s LR had improved (Figure 2).
Comment
Amantadine has a well-documented association with LR in patients with Parkinson disease,3,4 which has been reported in up to 40% of those taking amantadine.2 More recently, amantadine has been used off label to treat neurobehavioral disorders in children due to beneficial effects including improvement in attention and concentration, distractibility, and fatigue.5 Our patient was being treated off label with amantadine for ADHD and bipolar disorder. Amantadine acts as a noncompetitive antagonist of the N-methyl-D-aspartate receptor, enhancing dopamine release to reduce symptoms of ADHD.5,6 Additionally, amantadine can cause a depletion of catecholamines in the peripheral nerve terminals, which may lead to dilatation of dermal vessels.4,6 This sequence of events has been proposed as a possible mechanism contributing to amantadine-induced LR, though the pathophysiology is not fully understood.1,3,4
Our case of LR likely was induced by amantadine given the temporal relationship between initiation of the medication, onset of the rash, and the considerable improvement of the rash upon discontinuation of amantadine. Barrera and Browning6 reported another case of amantadine-induced LR in a pediatric patient. Because amantadine is increasingly being used off label to treat childhood neurobehavioral disorders, amantadine-induced LR may become more prevalent in patients who do not have Parkinson disease; therefore, physicians who treat pediatric patients must be aware of this side effect.5
Livedo reticularis (LR) is a common dermatologic finding consisting of diffuse, reticulated, violaceous patches. It often is a benign physical finding known as cutis marmorata; however, LR can be associated with other medical conditions as well as with the use of some medications.1,2 Amantadine is a common cause of LR in Parkinson disease patients.3,4 We present a rare case of amantadine-induced LR in a pediatric patient and highlight the off-label use of this medication in children.
Case Report
An 8-year-old boy presented with a diffuse rash on the trunk, arms, and legs of 9 months’ duration. The patient denied any associated symptoms as well as alleviating or exacerbating factors. He also denied any changes with temperature. He had no recent international travel and no prior drug allergies. His medical history was remarkable for attention deficit hyperactivity disorder (ADHD), bipolar disorder, and autism spectrum disorder. His previously prescribed medications included atomoxetine, quetiapine, and valproic acid. The only new medication that had been started within the last year was amantadine. Physical examination revealed a diffuse, reticulated, erythematous to violaceous, blanching rash that was most notable on the legs (Figure 1A) but also was present on the trunk (Figure 1B) and arms (Figure 1C). The clinical examination was consistent with LR, which was presumed to be secondary to amantadine use. Given the multiple psychiatric diagnoses and medication history in this young patient, a consultation with child psychiatry was facilitated. His medications and diagnosis were reviewed, and amantadine was discontinued. At a follow-up visit 5 months later, the patient’s LR had improved (Figure 2).
Comment
Amantadine has a well-documented association with LR in patients with Parkinson disease,3,4 which has been reported in up to 40% of those taking amantadine.2 More recently, amantadine has been used off label to treat neurobehavioral disorders in children due to beneficial effects including improvement in attention and concentration, distractibility, and fatigue.5 Our patient was being treated off label with amantadine for ADHD and bipolar disorder. Amantadine acts as a noncompetitive antagonist of the N-methyl-D-aspartate receptor, enhancing dopamine release to reduce symptoms of ADHD.5,6 Additionally, amantadine can cause a depletion of catecholamines in the peripheral nerve terminals, which may lead to dilatation of dermal vessels.4,6 This sequence of events has been proposed as a possible mechanism contributing to amantadine-induced LR, though the pathophysiology is not fully understood.1,3,4
Our case of LR likely was induced by amantadine given the temporal relationship between initiation of the medication, onset of the rash, and the considerable improvement of the rash upon discontinuation of amantadine. Barrera and Browning6 reported another case of amantadine-induced LR in a pediatric patient. Because amantadine is increasingly being used off label to treat childhood neurobehavioral disorders, amantadine-induced LR may become more prevalent in patients who do not have Parkinson disease; therefore, physicians who treat pediatric patients must be aware of this side effect.5
- Quaresma MV, Gomes-Dias AC, Serruya A, et al. Amantadine-induced livedo reticularis: a case report. An Bras Dermatol. 2015;90:745-747.
- Gibbs MB, English JC, Zirwas MJ. Livedo reticularis: an update. J Am Acad Dermatol. 2005;52:1009-1019.
- Silva SB, Miot HA. Case for diagnosis. amantadine-induced livedo reticularis. An Bras Dermatol. 2012;87:319-321.
- Vollum DI, Parkes JD, Doyle D. Livedo reticularis during amantadine treatment. Br Med J. 1971;2:627-628.
- Hosenbocus S, Chahal R. Amantadine: a review of use in child and adolescent psychiatry. J Can Acad Child Adolesc Psychiatry. 2013;22:55-60.
- Barrera F, Browning JC. Likely amantadine-induced livedo reticularis in a child. Pediatr Dermatol. 2012;29:329-330.
- Quaresma MV, Gomes-Dias AC, Serruya A, et al. Amantadine-induced livedo reticularis: a case report. An Bras Dermatol. 2015;90:745-747.
- Gibbs MB, English JC, Zirwas MJ. Livedo reticularis: an update. J Am Acad Dermatol. 2005;52:1009-1019.
- Silva SB, Miot HA. Case for diagnosis. amantadine-induced livedo reticularis. An Bras Dermatol. 2012;87:319-321.
- Vollum DI, Parkes JD, Doyle D. Livedo reticularis during amantadine treatment. Br Med J. 1971;2:627-628.
- Hosenbocus S, Chahal R. Amantadine: a review of use in child and adolescent psychiatry. J Can Acad Child Adolesc Psychiatry. 2013;22:55-60.
- Barrera F, Browning JC. Likely amantadine-induced livedo reticularis in a child. Pediatr Dermatol. 2012;29:329-330.
Practice Points
- Amantadine is a generally well-tolerated medication that is more commonly used for off-label treatment of several pediatric neurobehavioral conditions such as attention deficit hyperactivity disorder, autism spectrum disorders, obsessive compulsive disorder, depression, and others.
- Livedo reticularis has known associations with several medications and diseases; however, the most common presentation is cutis marmorata, a benign condition that typically affects newborns.

AAP guidelines emphasize gender-affirmative care
according to an American Academy of Pediatrics policy statement published in Pediatrics.

The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.

Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.
Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.
Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
according to an American Academy of Pediatrics policy statement published in Pediatrics.
The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
according to an American Academy of Pediatrics policy statement published in Pediatrics.
The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
FROM PEDATRICS

Decline of infant walker–related injuries continues
but most of that drop occurred before the federal mandatory safety standard went into effect in 2010, according to an analysis of a federal injury database.
In 1990, there were 20,650 walker-related injuries among children younger than 15 months, and by 2003 that number was down to 3,201 – a significant decline of 85%. In 2014, the last year for which data were available, there were 1,995 such injuries, which translates to a nonsignificant decrease of 38% from 2003 to 2014, Ariel Sims, MS, and her associates at the Center for Injury Research and Policy at Nationwide Children’s Hospital, Columbus, Ohio, wrote in Pediatrics.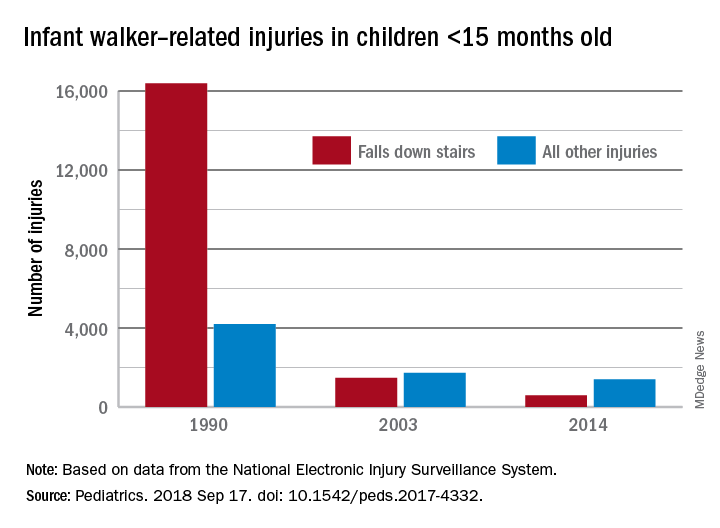
During the study period from 1990 to 2014, a total of 230,676 children aged less than 15 months received treatment in emergency departments after walker-related injuries, with the majority (74%) caused by falls down stairs. That percentage did go down over time, though, with falls down stairs representing more than 80% of all such injuries during 1990-1996, 66% during 1997-2009, and 41% during 2010-2014, Ms. Sims and her associates reported based on data from the National Electronic Injury Surveillance System.
As for the 2010 federal safety standard, the annual average injury total went from 2,801 for the previous 4 years (2006-2009) to 2,165 for the 4 years after (2010-2014) – a decline of 23% (P = .019), they noted.
The federal standard may have contributed to the overall decline, Ms. Sims and her associates suggested, but the “reduction is most likely attributable to … an increase in public awareness of infant walker–related injury risks when advocacy groups petitioned the [Consumer Product Safety Commission] in 1992 to ban infant walker sales in the United States, the increasing use of stationary activity centers as an alternative to infant walkers, and improvements in the voluntary infant walker safety standard.”
In a September 2001 policy statement, the American Academy of Pediatrics recommended a ban on the manufacture and sale of mobile infant walkers (Pediatrics. 2001 Sep. doi: 10.1542/peds.108.3.790). This policy has been reaffirmed every 5 years in accordance with AAP policy.
Ms. Sims received a research stipend from the Research Institute at Nationwide Children’s Hospital and was funded by the Centers for Disease Control and Prevention and the Child Injury Prevention Alliance. The other investigators said that they have no relevant financial disclosures.
SOURCE: Sims A et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2017-4332.
but most of that drop occurred before the federal mandatory safety standard went into effect in 2010, according to an analysis of a federal injury database.
In 1990, there were 20,650 walker-related injuries among children younger than 15 months, and by 2003 that number was down to 3,201 – a significant decline of 85%. In 2014, the last year for which data were available, there were 1,995 such injuries, which translates to a nonsignificant decrease of 38% from 2003 to 2014, Ariel Sims, MS, and her associates at the Center for Injury Research and Policy at Nationwide Children’s Hospital, Columbus, Ohio, wrote in Pediatrics.
During the study period from 1990 to 2014, a total of 230,676 children aged less than 15 months received treatment in emergency departments after walker-related injuries, with the majority (74%) caused by falls down stairs. That percentage did go down over time, though, with falls down stairs representing more than 80% of all such injuries during 1990-1996, 66% during 1997-2009, and 41% during 2010-2014, Ms. Sims and her associates reported based on data from the National Electronic Injury Surveillance System.
As for the 2010 federal safety standard, the annual average injury total went from 2,801 for the previous 4 years (2006-2009) to 2,165 for the 4 years after (2010-2014) – a decline of 23% (P = .019), they noted.
The federal standard may have contributed to the overall decline, Ms. Sims and her associates suggested, but the “reduction is most likely attributable to … an increase in public awareness of infant walker–related injury risks when advocacy groups petitioned the [Consumer Product Safety Commission] in 1992 to ban infant walker sales in the United States, the increasing use of stationary activity centers as an alternative to infant walkers, and improvements in the voluntary infant walker safety standard.”
In a September 2001 policy statement, the American Academy of Pediatrics recommended a ban on the manufacture and sale of mobile infant walkers (Pediatrics. 2001 Sep. doi: 10.1542/peds.108.3.790). This policy has been reaffirmed every 5 years in accordance with AAP policy.
Ms. Sims received a research stipend from the Research Institute at Nationwide Children’s Hospital and was funded by the Centers for Disease Control and Prevention and the Child Injury Prevention Alliance. The other investigators said that they have no relevant financial disclosures.
SOURCE: Sims A et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2017-4332.
but most of that drop occurred before the federal mandatory safety standard went into effect in 2010, according to an analysis of a federal injury database.
In 1990, there were 20,650 walker-related injuries among children younger than 15 months, and by 2003 that number was down to 3,201 – a significant decline of 85%. In 2014, the last year for which data were available, there were 1,995 such injuries, which translates to a nonsignificant decrease of 38% from 2003 to 2014, Ariel Sims, MS, and her associates at the Center for Injury Research and Policy at Nationwide Children’s Hospital, Columbus, Ohio, wrote in Pediatrics.
During the study period from 1990 to 2014, a total of 230,676 children aged less than 15 months received treatment in emergency departments after walker-related injuries, with the majority (74%) caused by falls down stairs. That percentage did go down over time, though, with falls down stairs representing more than 80% of all such injuries during 1990-1996, 66% during 1997-2009, and 41% during 2010-2014, Ms. Sims and her associates reported based on data from the National Electronic Injury Surveillance System.
As for the 2010 federal safety standard, the annual average injury total went from 2,801 for the previous 4 years (2006-2009) to 2,165 for the 4 years after (2010-2014) – a decline of 23% (P = .019), they noted.
The federal standard may have contributed to the overall decline, Ms. Sims and her associates suggested, but the “reduction is most likely attributable to … an increase in public awareness of infant walker–related injury risks when advocacy groups petitioned the [Consumer Product Safety Commission] in 1992 to ban infant walker sales in the United States, the increasing use of stationary activity centers as an alternative to infant walkers, and improvements in the voluntary infant walker safety standard.”
In a September 2001 policy statement, the American Academy of Pediatrics recommended a ban on the manufacture and sale of mobile infant walkers (Pediatrics. 2001 Sep. doi: 10.1542/peds.108.3.790). This policy has been reaffirmed every 5 years in accordance with AAP policy.
Ms. Sims received a research stipend from the Research Institute at Nationwide Children’s Hospital and was funded by the Centers for Disease Control and Prevention and the Child Injury Prevention Alliance. The other investigators said that they have no relevant financial disclosures.
SOURCE: Sims A et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2017-4332.
FROM PEDIATRICS
Natural history is comparable for astrovirus, sapovirus, norovirus
ATLANTA – Astrovirus and sapovirus in children visiting the ED with acute gastroenteritis have a similar natural history, which is also similar to that of norovirus, according to findings from a prospective cohort study.
Thanks to the increased use of molecular diagnostic testing, astrovirus and sapovirus (AsV and SaV) recently gained new appreciation as a cause of gastroenteritis, but little is known about their natural history.
The current findings from the Alberta Provincial Pediatric Enteric Infection Team (APPETITE) study provide some longitudinal insight regarding that history, Gillian A. M. Tarr, PhD, of the University of Calgary (Alta.), and her colleagues noted in a poster presentation at the International Conference on Emerging Infectious Diseases.
The investigators tested rectal swabs and stool samples from 2,590 children under age 18 years who had experienced at least three episodes of diarrhea and/or vomiting in 24 hours. AsV was detected in 84 children (3.2%), SaV was detected in 229 (8.8%), and norovirus (NoV) was detected in 655 (25%). After excluding those with coinfection, a total of 54, 144, and 478 children with AsV, SaV, and NoV, respectively, were included.
Vomiting occurred in 83%, 92%, and 98%; diarrhea occurred in 94%, 79% and 75%; and blood was present in the stool in 4.0%, 7.0%, and 3.5%, of those with AsV, SaV, and NoV, respectively, they reported.
The median maximal vomiting episodes per day was slightly lower for AsV versus SaV and NoV (about 3 vs. 5 and 7, respectively); the median maximal diarrhea episodes was slightly higher for AsV (about 5 vs. 4 for both SaV and NoV).
Vomiting duration was similar for AsV and SaV (about 3 days) and slightly longer than for NoV (about 2 days); median diarrhea duration was about 5 days for all three viruses.
“Most AsV cases present with both vomiting and diarrhea; most SaV cases present with vomiting and only approximately half with diarrhea,” the investigators wrote.
APPETITE study participants were enrolled from the EDs of two large children’s hospitals from December 2014 to May 2018. All were tested for 18 enteric pathogens and information on patient symptoms, medications, and potential exposures at enrollment and at 14 days was provided by patients and parents/guardians.
“We compared the natural histories of AsV and SaV to that of NoV, and found that all are comparable. These data provide a clearer picture than previously available of the duration and intensity of cardinal gastroenteritis symptoms associated with AsV and SaV infections,” they concluded.
Dr. Tarr reported having no financial disclosures.
ATLANTA – Astrovirus and sapovirus in children visiting the ED with acute gastroenteritis have a similar natural history, which is also similar to that of norovirus, according to findings from a prospective cohort study.
Thanks to the increased use of molecular diagnostic testing, astrovirus and sapovirus (AsV and SaV) recently gained new appreciation as a cause of gastroenteritis, but little is known about their natural history.
The current findings from the Alberta Provincial Pediatric Enteric Infection Team (APPETITE) study provide some longitudinal insight regarding that history, Gillian A. M. Tarr, PhD, of the University of Calgary (Alta.), and her colleagues noted in a poster presentation at the International Conference on Emerging Infectious Diseases.
The investigators tested rectal swabs and stool samples from 2,590 children under age 18 years who had experienced at least three episodes of diarrhea and/or vomiting in 24 hours. AsV was detected in 84 children (3.2%), SaV was detected in 229 (8.8%), and norovirus (NoV) was detected in 655 (25%). After excluding those with coinfection, a total of 54, 144, and 478 children with AsV, SaV, and NoV, respectively, were included.
Vomiting occurred in 83%, 92%, and 98%; diarrhea occurred in 94%, 79% and 75%; and blood was present in the stool in 4.0%, 7.0%, and 3.5%, of those with AsV, SaV, and NoV, respectively, they reported.
The median maximal vomiting episodes per day was slightly lower for AsV versus SaV and NoV (about 3 vs. 5 and 7, respectively); the median maximal diarrhea episodes was slightly higher for AsV (about 5 vs. 4 for both SaV and NoV).
Vomiting duration was similar for AsV and SaV (about 3 days) and slightly longer than for NoV (about 2 days); median diarrhea duration was about 5 days for all three viruses.
“Most AsV cases present with both vomiting and diarrhea; most SaV cases present with vomiting and only approximately half with diarrhea,” the investigators wrote.
APPETITE study participants were enrolled from the EDs of two large children’s hospitals from December 2014 to May 2018. All were tested for 18 enteric pathogens and information on patient symptoms, medications, and potential exposures at enrollment and at 14 days was provided by patients and parents/guardians.
“We compared the natural histories of AsV and SaV to that of NoV, and found that all are comparable. These data provide a clearer picture than previously available of the duration and intensity of cardinal gastroenteritis symptoms associated with AsV and SaV infections,” they concluded.
Dr. Tarr reported having no financial disclosures.
ATLANTA – Astrovirus and sapovirus in children visiting the ED with acute gastroenteritis have a similar natural history, which is also similar to that of norovirus, according to findings from a prospective cohort study.
Thanks to the increased use of molecular diagnostic testing, astrovirus and sapovirus (AsV and SaV) recently gained new appreciation as a cause of gastroenteritis, but little is known about their natural history.
The current findings from the Alberta Provincial Pediatric Enteric Infection Team (APPETITE) study provide some longitudinal insight regarding that history, Gillian A. M. Tarr, PhD, of the University of Calgary (Alta.), and her colleagues noted in a poster presentation at the International Conference on Emerging Infectious Diseases.
The investigators tested rectal swabs and stool samples from 2,590 children under age 18 years who had experienced at least three episodes of diarrhea and/or vomiting in 24 hours. AsV was detected in 84 children (3.2%), SaV was detected in 229 (8.8%), and norovirus (NoV) was detected in 655 (25%). After excluding those with coinfection, a total of 54, 144, and 478 children with AsV, SaV, and NoV, respectively, were included.
Vomiting occurred in 83%, 92%, and 98%; diarrhea occurred in 94%, 79% and 75%; and blood was present in the stool in 4.0%, 7.0%, and 3.5%, of those with AsV, SaV, and NoV, respectively, they reported.
The median maximal vomiting episodes per day was slightly lower for AsV versus SaV and NoV (about 3 vs. 5 and 7, respectively); the median maximal diarrhea episodes was slightly higher for AsV (about 5 vs. 4 for both SaV and NoV).
Vomiting duration was similar for AsV and SaV (about 3 days) and slightly longer than for NoV (about 2 days); median diarrhea duration was about 5 days for all three viruses.
“Most AsV cases present with both vomiting and diarrhea; most SaV cases present with vomiting and only approximately half with diarrhea,” the investigators wrote.
APPETITE study participants were enrolled from the EDs of two large children’s hospitals from December 2014 to May 2018. All were tested for 18 enteric pathogens and information on patient symptoms, medications, and potential exposures at enrollment and at 14 days was provided by patients and parents/guardians.
“We compared the natural histories of AsV and SaV to that of NoV, and found that all are comparable. These data provide a clearer picture than previously available of the duration and intensity of cardinal gastroenteritis symptoms associated with AsV and SaV infections,” they concluded.
Dr. Tarr reported having no financial disclosures.
REPORTING FROM ICEID 2018
Key clinical point:
Major finding: Vomiting lasted about 3 days for astrovirus and sapovirus and 2 days for norovirus; diarrhea lasted about 5 days for all three viruses.
Study details: A prospective cohort study of 2,590 children.
Disclosures: Dr. Tarr reported having no financial disclosures.