User login
Carcinoma of the colon in a child
Colon cancer is not common in childhood even though cases have been reported in children and adolescents.1,2 Although it is sporadic, it can arise in the setting of predisposing illnesses such as familial polyposis syndrome or inflammatory bowel disease.2-5 Only 1 or 2 cases per million children are reported globally each year, but the incidence has been noted to be on the rise.2 The nonspecific gastrointestinal symptoms and anemia as features of the disease could also be seen in other common childhood ailments, such as helminthiasis in our region in West Africa. As a result, unless there is a high index of suspicion at the outset, there is a risk that colon cancer will be diagnosed at a late stage, especially in children with no apparent predisposing factor.
In this case, an 11-year-old girl presented to our institution with abdominal pain, melena, abdominal swelling, and iron deficiency anemia. A positive family history of colon cancer in the mother and a brain tumor in an elder sibling prompted a search for and subsequent diagnosis of colon cancer. Her case highlights the importance of a high index of suspicion in making an early diagnosis to achieve the best possible outcomes. This case is being reported in line with the SCARE guidelines.6
Case summary and presentation
An 11-year-old girl presented to our facilty with recurrent abdominal pain of 8 months duration, a 4-month history of progressive paleness of the palms, and a month-long fever. There was an associated change in bowel habit to about 2-3 times per day, weight loss despite a preserved appetite, and black, tarry stools. A month before she presented, she developed low-grade pyrexia, dysuria, and pica. She was treated for iron deficiency anemia at a peripheral hospital where she first sought for care with oral iron, folic acid, and vitamin C, but with no improvement in symptoms.
She was the youngest of 8 children born to parents who were first cousins. Her father had died in a car accident when she was a year old, and her mother had died 6 years later after being diagnosed with and treated for colon cancer. An elder sibling died of a brain tumor at the age of 9 years.
On admission to our institution, the girl looked acutely ill. She was severely pale, but afebrile and anicteric. She had no petechial or purpuric skin rashes, but had glossitis with areas of papules on the anterior two-thirds of the dorsum of the tongue. She had no gingival hypertrophy, but had significant peripheral lymphadenopathy and weighed 67% of the weight for her age. In addition, she had generalized abdominal pain and a soft, well-circumscribed tender mass located at the right iliac fossa was palpated and estimated to be 8 cm x 6 cm.
A full blood count showed severe hypochromic microcytic anemia, with a red blood cell count of 2.53 x 1012/L, packed cell volume of 9%, white blood cell count 9.4 x109/L, platelet cell count of 453 x 109/L, mean corpuscular volume of 48.6 fl, and a red cell distribution width of 23.7%. Iron studies could not be done because we lacked the facilities, but a bone marrow aspiration biopsy showed reduced bone marrow iron stores. A fecal occult blood test was positive for blood, but negative for culture, ova, or cysts. An abdominopelvic ultrasound showed the well-circumscribed mass at the right iliac fossa, and that was confirmed by a computed-tomographic scan (Figure 1).
An upper endoscopy revealed fundal and prepyloric erosions and reflux eosophagitis. Although findings from a sigmoidoscopy were normal, a histology of biopsied tissues showed features of chronic inflammation.
There was a delay in arriving at the final diagnosis because the patient’s family faced financial difficulties and some of the imaging procedures were not available at our institution. Other diagnoses that were entertained and managed in this case were iron deficiency anemia from peptic ulcer disease. Six weeks after her initial presentation to our institution, the patient had an exploratory laparotomy. The findings intra-operatively were those of a huge tumor involving the ascending colon measuring 16 x14 cm and extending to involve the cecum and mesenteric lymph nodes (Figure 2).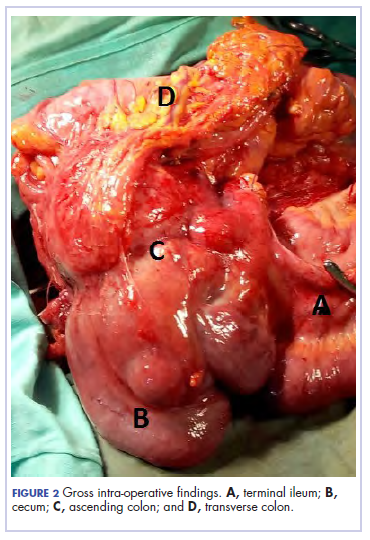
Kidneys, liver and spleen were macroscopically normal. An assessment of Duke’s stage 3C colon cancer was made and she had an extended radical hemicolectomy with anastomosis.
A 44.5-cm long right hemicolectomy segment comprising a 17-cm ileal segment, a 6-cm cecum, 21.5-cm ascending colon, and an 8-cm appendix was removed. The tumor was located in the ascending colon at 7.5 cm from the distal resection margin and extending 1 cm into the cecum. It had a circumference of 27 cm with fibrinous exudates on its peritoneal surface. Dissection revealed uneven circumferential thickening of the bowel wall, luminal dilatation, marked mucosal ulcerations, and liquid content made up of fecal material and necrotic debris. The tumor cut surface was solid white. We also removed 4 lymph nodes. Other uninvolved areas showed focal mucosal hyperemia, but no polyps were observed. Histology showed moderately differentiated adenocarcinoma (pT4) with ¼ nodal involvement (Figure 3).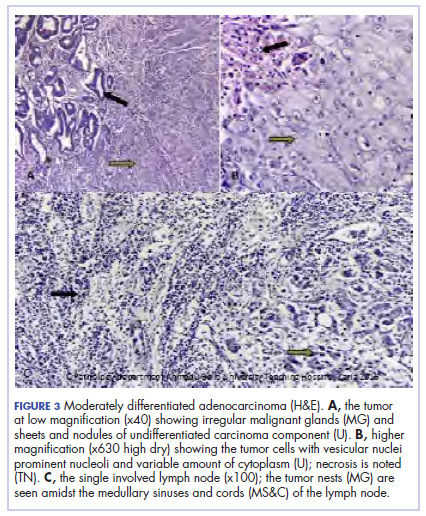
The patient’s postoperative course was uneventful, and she had adjuvant chemotherapy with oral capecitabine and intravenous oxaliplatin. She completed the 8-cycle protocol with excellent clinical response and minimal adverse events were recorded. A repeat abdominal CT scan showed no residual tumor (Figure 4), and her full blood count showed normal hematological profile with no evidence of iron deficiency.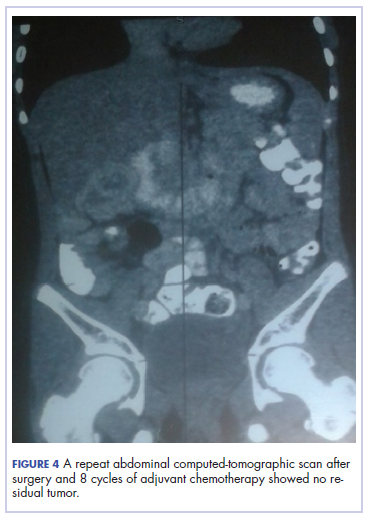
She is presently on follow up 2 years after confirmation of the diagnosis. (Her histological diagnosis was made June 2016, and her last clinic follow-up was March 2018.
Discussion
Our patient presented with symptoms of abdominal pain, dysuria, melena, and pallor as in other case reports.7-10 A diagnosis of iron deficiency anemia was initially entertained in view of the hematologic profile, and for which management was instituted. The findings of gastric and duodenal erosions on endoscopy further supported the assumption for and treatment of peptic ulcer disease. Iron deficiency in this patient was owing to chronic blood loss from a tumour located at the upper parts of the. Vague and nonspecific symptoms are associated with delayed diagnosis and poor prognosis.1-5,11 Nonspecificity of symptoms is typical feature of colon cancer as reported in other studies.1,11-13 However, the strong family history of colon cancer heightened suspicion in this case, otherwise the diagnosis of an ascending colon tumor could have been delayed until much later and with graver consequences.
The diagnosis of colon cancer in this child was made about a year after her initial symptoms, and 3 months after her presentation to us. Ascending and transverse colon cancers are usually diagnosed late because the symptoms of intestinal obstruction – frank bleeding – will not present until the illness is substantially advanced. Ameh and Nmadu reported a case series of 8 patients from our facility with rectosigmoid tumor, of whom 6 had mucinous adenocarcinaoma and 5 of those 6 had stage 3C disease. Although the patient in the present case had an advanced disease at diagnosis, she had a moderately differentiated histology in contrast to the 6 previously reported cases, who had mucinous histology.14
Previous studies have shown that colorectal carcinoma is a rare disease worldwide, with an annual age-adjusted incidence of 0.38 people/million.1,2 When it occurs in the young, familial or hereditary predisposition should be highly suspected.1-3 To date, there is scant literature on children younger than 16 years in Nigeria.15 Various studies have found a relationship between patients with early-stage colon cancer and inherited genetic predisposition to the disease.2,5 Familial adenomatous polyposis syndrome is an autosomal dominant disorder characterized by the development of polyps during the first decade of life, extensive polyposis in the second decade, and transformation into frank carcinoma in early adulthood.1-5
Although our patient’s mother was diagnosed with and died of colon cancer, the type of which could not be ascertained because her records could not be traced. However, the operative and histological findings in this patient did not suggest the presence of polyposis. The clinical phenotype for the autosomal recessive mismatch repair deficiency includes susceptibity to glioma, leukemia, lymphoma, and colorectal carcinoma in children and young adults.1,5 Screening for genetic markers in the child in the present case might have identified the genetic abnormalities involved and would have been invaluable in the evaluation of her 6 surviving siblings and further management of this family. In conclusion. A high index of suspicion should prompt inclusion of colon cancer in the differential diagnosis of nonspecific gastrointestinal symptoms associated with colon cancer in children.
Acknowledg
The authors obtained written informed consent from the patient and her elder sibling before writing this report. In addition, the authors thank all the staff involved in the management of this child in the pediatric medical and surgical wards.
1. Sultan I, Rodriguez-Galindo C, El-Taani H, Pastore G, Casanova M, Gallino G, Ferrari A. Distinct features of colorectal cancer in children and adolescents. A population-based study of 159 cases. Cancer. 2010;1;116(3):758-65.
2. Ferrari A. Intestinal carcinomas. In: Schneider DT, Brecht IB, Olson TA, Ferrari A (eds). Rare tumors in children and adolescents. 1st ed. Copyright, Springer-Verlag Berlin Heidelberg; 2012; chap 32.
3. Hill DA, Furman WL, Bilups CA, Riedly SE, Cain AM, Rao BN. Colorectal carcinoma in childhood and adolescence: a clinicopathological review. J Clin Oncol. 2007;25(36):5808-5814.
4. Saab OKR, Furman WL. Epidemiology and management options for colorectal cancer in children. Paediatr Drugs. 2008;10(3):177-192.
5. Bertario L, Signoroni S. Gastrointestinal cancer predisposition syndromes. In: Schneider DT, Brecht IB, Olson TA, Ferrari A (eds). Rare tumors in children and adolescents. Copyright, Springer-Verlag Berlin Heidelberg; 2012; chap 30.
6. Agha RA, Fowler AJ, Saetta A, et al, for the SCARE Group. The SCARE Statement: consensus-based surgical case report guidelines. Int J Surg. 2016;34:180-186.
7. Tricoli JV, Seibel NL, Blair DG, Albritton K, Hayes-Lattin B. Unique characteristics of adolescent and young adult acute lymphoblastic leukemia, breast cancer, and colon cancer. J Natl Cancer Inst. 2011;103(8):628-635.
8. Begum M, Khan ZJ, Hassan K, Karim S. Carcinoma colon of a child presenting with abdominal pain. Bangaladesh J Child Health. 2014;38(1):44-47.
9. Woods R, Larkin JO, Muldoon C, Kennedy MJ, Mehigan B, McCormick P. Metastatic paediatric colorectal carcinoma. Ir Med J. 2012;105(3):88-89.
10. Bjoernsen LP, Lindsay MB. An unusual case of pediatric abdominal pain. CJEM. 2011;13(2):133-138.
11. Takalkar UV, Asegaonkar SB, Kulkarni U, Jadhav A, Advani S, Reddy DN. Carcinoma of colon in an adolescent: a case report with review of literature. Int J Sci Rep 2015;1(2):151-3.
12. Zamir N, Ahmad S, Akhtar J. Mucinous adenocarcinoma of colon. APSP J Case Rep. 2010;1(2):20.
13. Al-Tonbary Y, Darwish A, El-Hussein A, Fouda A. Adenocarcinoma of the colon in children: case series and mini-review of the literature. Hematol Oncol Stem Cell Ther. 2013;6(1):29-33.
14. Ameh EA, Nmadu PT. Colorectal adenocarcinoma in children and adolescents: a report of 8 patients from Zaria, Nigeria. West Afr J Med. 2000;19(4):273-276.
15. Ibrahim, AE, Afolayan KA, Adeniji OM, Buhari KB. Colorectal carcinoma in children and young adults in Ilorin, Nigeria. West Afr J Med. 2011;30(3):202-205.
Colon cancer is not common in childhood even though cases have been reported in children and adolescents.1,2 Although it is sporadic, it can arise in the setting of predisposing illnesses such as familial polyposis syndrome or inflammatory bowel disease.2-5 Only 1 or 2 cases per million children are reported globally each year, but the incidence has been noted to be on the rise.2 The nonspecific gastrointestinal symptoms and anemia as features of the disease could also be seen in other common childhood ailments, such as helminthiasis in our region in West Africa. As a result, unless there is a high index of suspicion at the outset, there is a risk that colon cancer will be diagnosed at a late stage, especially in children with no apparent predisposing factor.
In this case, an 11-year-old girl presented to our institution with abdominal pain, melena, abdominal swelling, and iron deficiency anemia. A positive family history of colon cancer in the mother and a brain tumor in an elder sibling prompted a search for and subsequent diagnosis of colon cancer. Her case highlights the importance of a high index of suspicion in making an early diagnosis to achieve the best possible outcomes. This case is being reported in line with the SCARE guidelines.6
Case summary and presentation
An 11-year-old girl presented to our facilty with recurrent abdominal pain of 8 months duration, a 4-month history of progressive paleness of the palms, and a month-long fever. There was an associated change in bowel habit to about 2-3 times per day, weight loss despite a preserved appetite, and black, tarry stools. A month before she presented, she developed low-grade pyrexia, dysuria, and pica. She was treated for iron deficiency anemia at a peripheral hospital where she first sought for care with oral iron, folic acid, and vitamin C, but with no improvement in symptoms.
She was the youngest of 8 children born to parents who were first cousins. Her father had died in a car accident when she was a year old, and her mother had died 6 years later after being diagnosed with and treated for colon cancer. An elder sibling died of a brain tumor at the age of 9 years.
On admission to our institution, the girl looked acutely ill. She was severely pale, but afebrile and anicteric. She had no petechial or purpuric skin rashes, but had glossitis with areas of papules on the anterior two-thirds of the dorsum of the tongue. She had no gingival hypertrophy, but had significant peripheral lymphadenopathy and weighed 67% of the weight for her age. In addition, she had generalized abdominal pain and a soft, well-circumscribed tender mass located at the right iliac fossa was palpated and estimated to be 8 cm x 6 cm.
A full blood count showed severe hypochromic microcytic anemia, with a red blood cell count of 2.53 x 1012/L, packed cell volume of 9%, white blood cell count 9.4 x109/L, platelet cell count of 453 x 109/L, mean corpuscular volume of 48.6 fl, and a red cell distribution width of 23.7%. Iron studies could not be done because we lacked the facilities, but a bone marrow aspiration biopsy showed reduced bone marrow iron stores. A fecal occult blood test was positive for blood, but negative for culture, ova, or cysts. An abdominopelvic ultrasound showed the well-circumscribed mass at the right iliac fossa, and that was confirmed by a computed-tomographic scan (Figure 1).
An upper endoscopy revealed fundal and prepyloric erosions and reflux eosophagitis. Although findings from a sigmoidoscopy were normal, a histology of biopsied tissues showed features of chronic inflammation.
There was a delay in arriving at the final diagnosis because the patient’s family faced financial difficulties and some of the imaging procedures were not available at our institution. Other diagnoses that were entertained and managed in this case were iron deficiency anemia from peptic ulcer disease. Six weeks after her initial presentation to our institution, the patient had an exploratory laparotomy. The findings intra-operatively were those of a huge tumor involving the ascending colon measuring 16 x14 cm and extending to involve the cecum and mesenteric lymph nodes (Figure 2).
Kidneys, liver and spleen were macroscopically normal. An assessment of Duke’s stage 3C colon cancer was made and she had an extended radical hemicolectomy with anastomosis.
A 44.5-cm long right hemicolectomy segment comprising a 17-cm ileal segment, a 6-cm cecum, 21.5-cm ascending colon, and an 8-cm appendix was removed. The tumor was located in the ascending colon at 7.5 cm from the distal resection margin and extending 1 cm into the cecum. It had a circumference of 27 cm with fibrinous exudates on its peritoneal surface. Dissection revealed uneven circumferential thickening of the bowel wall, luminal dilatation, marked mucosal ulcerations, and liquid content made up of fecal material and necrotic debris. The tumor cut surface was solid white. We also removed 4 lymph nodes. Other uninvolved areas showed focal mucosal hyperemia, but no polyps were observed. Histology showed moderately differentiated adenocarcinoma (pT4) with ¼ nodal involvement (Figure 3).
The patient’s postoperative course was uneventful, and she had adjuvant chemotherapy with oral capecitabine and intravenous oxaliplatin. She completed the 8-cycle protocol with excellent clinical response and minimal adverse events were recorded. A repeat abdominal CT scan showed no residual tumor (Figure 4), and her full blood count showed normal hematological profile with no evidence of iron deficiency.
She is presently on follow up 2 years after confirmation of the diagnosis. (Her histological diagnosis was made June 2016, and her last clinic follow-up was March 2018.
Discussion
Our patient presented with symptoms of abdominal pain, dysuria, melena, and pallor as in other case reports.7-10 A diagnosis of iron deficiency anemia was initially entertained in view of the hematologic profile, and for which management was instituted. The findings of gastric and duodenal erosions on endoscopy further supported the assumption for and treatment of peptic ulcer disease. Iron deficiency in this patient was owing to chronic blood loss from a tumour located at the upper parts of the. Vague and nonspecific symptoms are associated with delayed diagnosis and poor prognosis.1-5,11 Nonspecificity of symptoms is typical feature of colon cancer as reported in other studies.1,11-13 However, the strong family history of colon cancer heightened suspicion in this case, otherwise the diagnosis of an ascending colon tumor could have been delayed until much later and with graver consequences.
The diagnosis of colon cancer in this child was made about a year after her initial symptoms, and 3 months after her presentation to us. Ascending and transverse colon cancers are usually diagnosed late because the symptoms of intestinal obstruction – frank bleeding – will not present until the illness is substantially advanced. Ameh and Nmadu reported a case series of 8 patients from our facility with rectosigmoid tumor, of whom 6 had mucinous adenocarcinaoma and 5 of those 6 had stage 3C disease. Although the patient in the present case had an advanced disease at diagnosis, she had a moderately differentiated histology in contrast to the 6 previously reported cases, who had mucinous histology.14
Previous studies have shown that colorectal carcinoma is a rare disease worldwide, with an annual age-adjusted incidence of 0.38 people/million.1,2 When it occurs in the young, familial or hereditary predisposition should be highly suspected.1-3 To date, there is scant literature on children younger than 16 years in Nigeria.15 Various studies have found a relationship between patients with early-stage colon cancer and inherited genetic predisposition to the disease.2,5 Familial adenomatous polyposis syndrome is an autosomal dominant disorder characterized by the development of polyps during the first decade of life, extensive polyposis in the second decade, and transformation into frank carcinoma in early adulthood.1-5
Although our patient’s mother was diagnosed with and died of colon cancer, the type of which could not be ascertained because her records could not be traced. However, the operative and histological findings in this patient did not suggest the presence of polyposis. The clinical phenotype for the autosomal recessive mismatch repair deficiency includes susceptibity to glioma, leukemia, lymphoma, and colorectal carcinoma in children and young adults.1,5 Screening for genetic markers in the child in the present case might have identified the genetic abnormalities involved and would have been invaluable in the evaluation of her 6 surviving siblings and further management of this family. In conclusion. A high index of suspicion should prompt inclusion of colon cancer in the differential diagnosis of nonspecific gastrointestinal symptoms associated with colon cancer in children.
Acknowledg
The authors obtained written informed consent from the patient and her elder sibling before writing this report. In addition, the authors thank all the staff involved in the management of this child in the pediatric medical and surgical wards.
Colon cancer is not common in childhood even though cases have been reported in children and adolescents.1,2 Although it is sporadic, it can arise in the setting of predisposing illnesses such as familial polyposis syndrome or inflammatory bowel disease.2-5 Only 1 or 2 cases per million children are reported globally each year, but the incidence has been noted to be on the rise.2 The nonspecific gastrointestinal symptoms and anemia as features of the disease could also be seen in other common childhood ailments, such as helminthiasis in our region in West Africa. As a result, unless there is a high index of suspicion at the outset, there is a risk that colon cancer will be diagnosed at a late stage, especially in children with no apparent predisposing factor.
In this case, an 11-year-old girl presented to our institution with abdominal pain, melena, abdominal swelling, and iron deficiency anemia. A positive family history of colon cancer in the mother and a brain tumor in an elder sibling prompted a search for and subsequent diagnosis of colon cancer. Her case highlights the importance of a high index of suspicion in making an early diagnosis to achieve the best possible outcomes. This case is being reported in line with the SCARE guidelines.6
Case summary and presentation
An 11-year-old girl presented to our facilty with recurrent abdominal pain of 8 months duration, a 4-month history of progressive paleness of the palms, and a month-long fever. There was an associated change in bowel habit to about 2-3 times per day, weight loss despite a preserved appetite, and black, tarry stools. A month before she presented, she developed low-grade pyrexia, dysuria, and pica. She was treated for iron deficiency anemia at a peripheral hospital where she first sought for care with oral iron, folic acid, and vitamin C, but with no improvement in symptoms.
She was the youngest of 8 children born to parents who were first cousins. Her father had died in a car accident when she was a year old, and her mother had died 6 years later after being diagnosed with and treated for colon cancer. An elder sibling died of a brain tumor at the age of 9 years.
On admission to our institution, the girl looked acutely ill. She was severely pale, but afebrile and anicteric. She had no petechial or purpuric skin rashes, but had glossitis with areas of papules on the anterior two-thirds of the dorsum of the tongue. She had no gingival hypertrophy, but had significant peripheral lymphadenopathy and weighed 67% of the weight for her age. In addition, she had generalized abdominal pain and a soft, well-circumscribed tender mass located at the right iliac fossa was palpated and estimated to be 8 cm x 6 cm.
A full blood count showed severe hypochromic microcytic anemia, with a red blood cell count of 2.53 x 1012/L, packed cell volume of 9%, white blood cell count 9.4 x109/L, platelet cell count of 453 x 109/L, mean corpuscular volume of 48.6 fl, and a red cell distribution width of 23.7%. Iron studies could not be done because we lacked the facilities, but a bone marrow aspiration biopsy showed reduced bone marrow iron stores. A fecal occult blood test was positive for blood, but negative for culture, ova, or cysts. An abdominopelvic ultrasound showed the well-circumscribed mass at the right iliac fossa, and that was confirmed by a computed-tomographic scan (Figure 1).
An upper endoscopy revealed fundal and prepyloric erosions and reflux eosophagitis. Although findings from a sigmoidoscopy were normal, a histology of biopsied tissues showed features of chronic inflammation.
There was a delay in arriving at the final diagnosis because the patient’s family faced financial difficulties and some of the imaging procedures were not available at our institution. Other diagnoses that were entertained and managed in this case were iron deficiency anemia from peptic ulcer disease. Six weeks after her initial presentation to our institution, the patient had an exploratory laparotomy. The findings intra-operatively were those of a huge tumor involving the ascending colon measuring 16 x14 cm and extending to involve the cecum and mesenteric lymph nodes (Figure 2).
Kidneys, liver and spleen were macroscopically normal. An assessment of Duke’s stage 3C colon cancer was made and she had an extended radical hemicolectomy with anastomosis.
A 44.5-cm long right hemicolectomy segment comprising a 17-cm ileal segment, a 6-cm cecum, 21.5-cm ascending colon, and an 8-cm appendix was removed. The tumor was located in the ascending colon at 7.5 cm from the distal resection margin and extending 1 cm into the cecum. It had a circumference of 27 cm with fibrinous exudates on its peritoneal surface. Dissection revealed uneven circumferential thickening of the bowel wall, luminal dilatation, marked mucosal ulcerations, and liquid content made up of fecal material and necrotic debris. The tumor cut surface was solid white. We also removed 4 lymph nodes. Other uninvolved areas showed focal mucosal hyperemia, but no polyps were observed. Histology showed moderately differentiated adenocarcinoma (pT4) with ¼ nodal involvement (Figure 3).
The patient’s postoperative course was uneventful, and she had adjuvant chemotherapy with oral capecitabine and intravenous oxaliplatin. She completed the 8-cycle protocol with excellent clinical response and minimal adverse events were recorded. A repeat abdominal CT scan showed no residual tumor (Figure 4), and her full blood count showed normal hematological profile with no evidence of iron deficiency.
She is presently on follow up 2 years after confirmation of the diagnosis. (Her histological diagnosis was made June 2016, and her last clinic follow-up was March 2018.
Discussion
Our patient presented with symptoms of abdominal pain, dysuria, melena, and pallor as in other case reports.7-10 A diagnosis of iron deficiency anemia was initially entertained in view of the hematologic profile, and for which management was instituted. The findings of gastric and duodenal erosions on endoscopy further supported the assumption for and treatment of peptic ulcer disease. Iron deficiency in this patient was owing to chronic blood loss from a tumour located at the upper parts of the. Vague and nonspecific symptoms are associated with delayed diagnosis and poor prognosis.1-5,11 Nonspecificity of symptoms is typical feature of colon cancer as reported in other studies.1,11-13 However, the strong family history of colon cancer heightened suspicion in this case, otherwise the diagnosis of an ascending colon tumor could have been delayed until much later and with graver consequences.
The diagnosis of colon cancer in this child was made about a year after her initial symptoms, and 3 months after her presentation to us. Ascending and transverse colon cancers are usually diagnosed late because the symptoms of intestinal obstruction – frank bleeding – will not present until the illness is substantially advanced. Ameh and Nmadu reported a case series of 8 patients from our facility with rectosigmoid tumor, of whom 6 had mucinous adenocarcinaoma and 5 of those 6 had stage 3C disease. Although the patient in the present case had an advanced disease at diagnosis, she had a moderately differentiated histology in contrast to the 6 previously reported cases, who had mucinous histology.14
Previous studies have shown that colorectal carcinoma is a rare disease worldwide, with an annual age-adjusted incidence of 0.38 people/million.1,2 When it occurs in the young, familial or hereditary predisposition should be highly suspected.1-3 To date, there is scant literature on children younger than 16 years in Nigeria.15 Various studies have found a relationship between patients with early-stage colon cancer and inherited genetic predisposition to the disease.2,5 Familial adenomatous polyposis syndrome is an autosomal dominant disorder characterized by the development of polyps during the first decade of life, extensive polyposis in the second decade, and transformation into frank carcinoma in early adulthood.1-5
Although our patient’s mother was diagnosed with and died of colon cancer, the type of which could not be ascertained because her records could not be traced. However, the operative and histological findings in this patient did not suggest the presence of polyposis. The clinical phenotype for the autosomal recessive mismatch repair deficiency includes susceptibity to glioma, leukemia, lymphoma, and colorectal carcinoma in children and young adults.1,5 Screening for genetic markers in the child in the present case might have identified the genetic abnormalities involved and would have been invaluable in the evaluation of her 6 surviving siblings and further management of this family. In conclusion. A high index of suspicion should prompt inclusion of colon cancer in the differential diagnosis of nonspecific gastrointestinal symptoms associated with colon cancer in children.
Acknowledg
The authors obtained written informed consent from the patient and her elder sibling before writing this report. In addition, the authors thank all the staff involved in the management of this child in the pediatric medical and surgical wards.
1. Sultan I, Rodriguez-Galindo C, El-Taani H, Pastore G, Casanova M, Gallino G, Ferrari A. Distinct features of colorectal cancer in children and adolescents. A population-based study of 159 cases. Cancer. 2010;1;116(3):758-65.
2. Ferrari A. Intestinal carcinomas. In: Schneider DT, Brecht IB, Olson TA, Ferrari A (eds). Rare tumors in children and adolescents. 1st ed. Copyright, Springer-Verlag Berlin Heidelberg; 2012; chap 32.
3. Hill DA, Furman WL, Bilups CA, Riedly SE, Cain AM, Rao BN. Colorectal carcinoma in childhood and adolescence: a clinicopathological review. J Clin Oncol. 2007;25(36):5808-5814.
4. Saab OKR, Furman WL. Epidemiology and management options for colorectal cancer in children. Paediatr Drugs. 2008;10(3):177-192.
5. Bertario L, Signoroni S. Gastrointestinal cancer predisposition syndromes. In: Schneider DT, Brecht IB, Olson TA, Ferrari A (eds). Rare tumors in children and adolescents. Copyright, Springer-Verlag Berlin Heidelberg; 2012; chap 30.
6. Agha RA, Fowler AJ, Saetta A, et al, for the SCARE Group. The SCARE Statement: consensus-based surgical case report guidelines. Int J Surg. 2016;34:180-186.
7. Tricoli JV, Seibel NL, Blair DG, Albritton K, Hayes-Lattin B. Unique characteristics of adolescent and young adult acute lymphoblastic leukemia, breast cancer, and colon cancer. J Natl Cancer Inst. 2011;103(8):628-635.
8. Begum M, Khan ZJ, Hassan K, Karim S. Carcinoma colon of a child presenting with abdominal pain. Bangaladesh J Child Health. 2014;38(1):44-47.
9. Woods R, Larkin JO, Muldoon C, Kennedy MJ, Mehigan B, McCormick P. Metastatic paediatric colorectal carcinoma. Ir Med J. 2012;105(3):88-89.
10. Bjoernsen LP, Lindsay MB. An unusual case of pediatric abdominal pain. CJEM. 2011;13(2):133-138.
11. Takalkar UV, Asegaonkar SB, Kulkarni U, Jadhav A, Advani S, Reddy DN. Carcinoma of colon in an adolescent: a case report with review of literature. Int J Sci Rep 2015;1(2):151-3.
12. Zamir N, Ahmad S, Akhtar J. Mucinous adenocarcinoma of colon. APSP J Case Rep. 2010;1(2):20.
13. Al-Tonbary Y, Darwish A, El-Hussein A, Fouda A. Adenocarcinoma of the colon in children: case series and mini-review of the literature. Hematol Oncol Stem Cell Ther. 2013;6(1):29-33.
14. Ameh EA, Nmadu PT. Colorectal adenocarcinoma in children and adolescents: a report of 8 patients from Zaria, Nigeria. West Afr J Med. 2000;19(4):273-276.
15. Ibrahim, AE, Afolayan KA, Adeniji OM, Buhari KB. Colorectal carcinoma in children and young adults in Ilorin, Nigeria. West Afr J Med. 2011;30(3):202-205.
1. Sultan I, Rodriguez-Galindo C, El-Taani H, Pastore G, Casanova M, Gallino G, Ferrari A. Distinct features of colorectal cancer in children and adolescents. A population-based study of 159 cases. Cancer. 2010;1;116(3):758-65.
2. Ferrari A. Intestinal carcinomas. In: Schneider DT, Brecht IB, Olson TA, Ferrari A (eds). Rare tumors in children and adolescents. 1st ed. Copyright, Springer-Verlag Berlin Heidelberg; 2012; chap 32.
3. Hill DA, Furman WL, Bilups CA, Riedly SE, Cain AM, Rao BN. Colorectal carcinoma in childhood and adolescence: a clinicopathological review. J Clin Oncol. 2007;25(36):5808-5814.
4. Saab OKR, Furman WL. Epidemiology and management options for colorectal cancer in children. Paediatr Drugs. 2008;10(3):177-192.
5. Bertario L, Signoroni S. Gastrointestinal cancer predisposition syndromes. In: Schneider DT, Brecht IB, Olson TA, Ferrari A (eds). Rare tumors in children and adolescents. Copyright, Springer-Verlag Berlin Heidelberg; 2012; chap 30.
6. Agha RA, Fowler AJ, Saetta A, et al, for the SCARE Group. The SCARE Statement: consensus-based surgical case report guidelines. Int J Surg. 2016;34:180-186.
7. Tricoli JV, Seibel NL, Blair DG, Albritton K, Hayes-Lattin B. Unique characteristics of adolescent and young adult acute lymphoblastic leukemia, breast cancer, and colon cancer. J Natl Cancer Inst. 2011;103(8):628-635.
8. Begum M, Khan ZJ, Hassan K, Karim S. Carcinoma colon of a child presenting with abdominal pain. Bangaladesh J Child Health. 2014;38(1):44-47.
9. Woods R, Larkin JO, Muldoon C, Kennedy MJ, Mehigan B, McCormick P. Metastatic paediatric colorectal carcinoma. Ir Med J. 2012;105(3):88-89.
10. Bjoernsen LP, Lindsay MB. An unusual case of pediatric abdominal pain. CJEM. 2011;13(2):133-138.
11. Takalkar UV, Asegaonkar SB, Kulkarni U, Jadhav A, Advani S, Reddy DN. Carcinoma of colon in an adolescent: a case report with review of literature. Int J Sci Rep 2015;1(2):151-3.
12. Zamir N, Ahmad S, Akhtar J. Mucinous adenocarcinoma of colon. APSP J Case Rep. 2010;1(2):20.
13. Al-Tonbary Y, Darwish A, El-Hussein A, Fouda A. Adenocarcinoma of the colon in children: case series and mini-review of the literature. Hematol Oncol Stem Cell Ther. 2013;6(1):29-33.
14. Ameh EA, Nmadu PT. Colorectal adenocarcinoma in children and adolescents: a report of 8 patients from Zaria, Nigeria. West Afr J Med. 2000;19(4):273-276.
15. Ibrahim, AE, Afolayan KA, Adeniji OM, Buhari KB. Colorectal carcinoma in children and young adults in Ilorin, Nigeria. West Afr J Med. 2011;30(3):202-205.
Role of SES in childhood cancer survival disparities

Socioeconomic status (SES) may explain some racial/ethnic disparities in childhood cancer survival, according to new research.
The study showed that whites had a significant survival advantage over blacks and Hispanics for several childhood cancers.
SES significantly mediated the association between race/ethnicity and survival for acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), neuroblastoma, and non-Hodgkin lymphoma (NHL).
Rebecca Kehm, PhD, of Columbia University in New York, New York, and her colleagues reported these findings in Cancer alongside a related editorial.
The researchers examined population-based cancer survival data from the Surveillance, Epidemiology, and End Results database.
The team collected information on 31,866 patients, ages 0 to 19, who were diagnosed with cancer between 2000 and 2011.
Survival differences by race/ethnicity
The researchers found that whites had a significant survival advantage over blacks for the cancers listed in the following table.
| Survival—black vs white | |||
| Cancer | Mortality hazard ratio | 95% confidence interval | P value |
| ALL | 1.43 | 1.15-1.77 | <0.01 |
| AML | 1.68 | 1.36-2.07 | <0.001 |
| Neuroblastoma | 1.38 | 1.08-1.75 | 0.01 |
| NHL | 1.53 | 1.14-2.07 | 0.01 |
| Hodgkin lymphoma | 1.66 | 1.06-2.60 | 0.03 |
| Astrocytoma | 1.95 | 1.57-2.43 | <0.001 |
| Non-astrocytoma CNS tumor | 1.53 | 1.25-1.88 | <0.001 |
| Non-rhabdomyosarcoma STS | 1.40 | 1.06-1.84 | 0.02 |
| Rhabdomyosarcoma | 1.44 | 1.10-1.88 | 0.01 |
In addition, whites had a significant survival advantage over Hispanics for the following cancers.
| Survival—Hispanic vs white | |||
| Cancer | Mortality hazard ratio | 95% confidence interval | P value |
| ALL | 1.63 | 1.43-1.86 | <0.001 |
| Neuroblastoma | 1.31 | 1.04-1.65 | 0.02 |
| NHL | 1.65 | 1.29-2.12 | <0.001 |
| Astrocytoma | 1.34 | 1.10-1.64 | <0.01 |
| Wilms tumor | 1.60 | 1.04-2.45 | 0.03 |
| Germ cell tumor | 1.63 | 1.19-2.24 | <0.01 |
Impact of SES
SES significantly mediated the association between race/ethnicity and survival for ALL, AML, neuroblastoma, and NHL but not for Hodgkin lymphoma or other cancers.
For black versus white patients, SES reduced the original association between race/ethnicity and survival by:
- 44% for ALL
- 28% for AML
- 49% for neuroblastoma
- 34% for NHL.
For Hispanics versus whites, SES reduced the original association between race/ethnicity and survival by:
- 31% for ALL
- 73% for AML
- 48% for neuroblastoma
- 28% for NHL.
“These findings provide insight for future intervention efforts aimed at closing the survival gap,” Dr Kehm said.
“For cancers in which socioeconomic status is a key factor in explaining racial and ethnic survival disparities, behavioral and supportive interventions that address social and economic barriers to effective care are warranted. However, for cancers in which survival is less influenced by socioeconomic status, more research is needed on underlying differences in tumor biology and drug processing.”
This research was supported by a grant from the National Institutes of Health, and the study’s authors made no disclosures.
Socioeconomic status (SES) may explain some racial/ethnic disparities in childhood cancer survival, according to new research.
The study showed that whites had a significant survival advantage over blacks and Hispanics for several childhood cancers.
SES significantly mediated the association between race/ethnicity and survival for acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), neuroblastoma, and non-Hodgkin lymphoma (NHL).
Rebecca Kehm, PhD, of Columbia University in New York, New York, and her colleagues reported these findings in Cancer alongside a related editorial.
The researchers examined population-based cancer survival data from the Surveillance, Epidemiology, and End Results database.
The team collected information on 31,866 patients, ages 0 to 19, who were diagnosed with cancer between 2000 and 2011.
Survival differences by race/ethnicity
The researchers found that whites had a significant survival advantage over blacks for the cancers listed in the following table.
| Survival—black vs white | |||
| Cancer | Mortality hazard ratio | 95% confidence interval | P value |
| ALL | 1.43 | 1.15-1.77 | <0.01 |
| AML | 1.68 | 1.36-2.07 | <0.001 |
| Neuroblastoma | 1.38 | 1.08-1.75 | 0.01 |
| NHL | 1.53 | 1.14-2.07 | 0.01 |
| Hodgkin lymphoma | 1.66 | 1.06-2.60 | 0.03 |
| Astrocytoma | 1.95 | 1.57-2.43 | <0.001 |
| Non-astrocytoma CNS tumor | 1.53 | 1.25-1.88 | <0.001 |
| Non-rhabdomyosarcoma STS | 1.40 | 1.06-1.84 | 0.02 |
| Rhabdomyosarcoma | 1.44 | 1.10-1.88 | 0.01 |
In addition, whites had a significant survival advantage over Hispanics for the following cancers.
| Survival—Hispanic vs white | |||
| Cancer | Mortality hazard ratio | 95% confidence interval | P value |
| ALL | 1.63 | 1.43-1.86 | <0.001 |
| Neuroblastoma | 1.31 | 1.04-1.65 | 0.02 |
| NHL | 1.65 | 1.29-2.12 | <0.001 |
| Astrocytoma | 1.34 | 1.10-1.64 | <0.01 |
| Wilms tumor | 1.60 | 1.04-2.45 | 0.03 |
| Germ cell tumor | 1.63 | 1.19-2.24 | <0.01 |
Impact of SES
SES significantly mediated the association between race/ethnicity and survival for ALL, AML, neuroblastoma, and NHL but not for Hodgkin lymphoma or other cancers.
For black versus white patients, SES reduced the original association between race/ethnicity and survival by:
- 44% for ALL
- 28% for AML
- 49% for neuroblastoma
- 34% for NHL.
For Hispanics versus whites, SES reduced the original association between race/ethnicity and survival by:
- 31% for ALL
- 73% for AML
- 48% for neuroblastoma
- 28% for NHL.
“These findings provide insight for future intervention efforts aimed at closing the survival gap,” Dr Kehm said.
“For cancers in which socioeconomic status is a key factor in explaining racial and ethnic survival disparities, behavioral and supportive interventions that address social and economic barriers to effective care are warranted. However, for cancers in which survival is less influenced by socioeconomic status, more research is needed on underlying differences in tumor biology and drug processing.”
This research was supported by a grant from the National Institutes of Health, and the study’s authors made no disclosures.
Socioeconomic status (SES) may explain some racial/ethnic disparities in childhood cancer survival, according to new research.
The study showed that whites had a significant survival advantage over blacks and Hispanics for several childhood cancers.
SES significantly mediated the association between race/ethnicity and survival for acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), neuroblastoma, and non-Hodgkin lymphoma (NHL).
Rebecca Kehm, PhD, of Columbia University in New York, New York, and her colleagues reported these findings in Cancer alongside a related editorial.
The researchers examined population-based cancer survival data from the Surveillance, Epidemiology, and End Results database.
The team collected information on 31,866 patients, ages 0 to 19, who were diagnosed with cancer between 2000 and 2011.
Survival differences by race/ethnicity
The researchers found that whites had a significant survival advantage over blacks for the cancers listed in the following table.
| Survival—black vs white | |||
| Cancer | Mortality hazard ratio | 95% confidence interval | P value |
| ALL | 1.43 | 1.15-1.77 | <0.01 |
| AML | 1.68 | 1.36-2.07 | <0.001 |
| Neuroblastoma | 1.38 | 1.08-1.75 | 0.01 |
| NHL | 1.53 | 1.14-2.07 | 0.01 |
| Hodgkin lymphoma | 1.66 | 1.06-2.60 | 0.03 |
| Astrocytoma | 1.95 | 1.57-2.43 | <0.001 |
| Non-astrocytoma CNS tumor | 1.53 | 1.25-1.88 | <0.001 |
| Non-rhabdomyosarcoma STS | 1.40 | 1.06-1.84 | 0.02 |
| Rhabdomyosarcoma | 1.44 | 1.10-1.88 | 0.01 |
In addition, whites had a significant survival advantage over Hispanics for the following cancers.
| Survival—Hispanic vs white | |||
| Cancer | Mortality hazard ratio | 95% confidence interval | P value |
| ALL | 1.63 | 1.43-1.86 | <0.001 |
| Neuroblastoma | 1.31 | 1.04-1.65 | 0.02 |
| NHL | 1.65 | 1.29-2.12 | <0.001 |
| Astrocytoma | 1.34 | 1.10-1.64 | <0.01 |
| Wilms tumor | 1.60 | 1.04-2.45 | 0.03 |
| Germ cell tumor | 1.63 | 1.19-2.24 | <0.01 |
Impact of SES
SES significantly mediated the association between race/ethnicity and survival for ALL, AML, neuroblastoma, and NHL but not for Hodgkin lymphoma or other cancers.
For black versus white patients, SES reduced the original association between race/ethnicity and survival by:
- 44% for ALL
- 28% for AML
- 49% for neuroblastoma
- 34% for NHL.
For Hispanics versus whites, SES reduced the original association between race/ethnicity and survival by:
- 31% for ALL
- 73% for AML
- 48% for neuroblastoma
- 28% for NHL.
“These findings provide insight for future intervention efforts aimed at closing the survival gap,” Dr Kehm said.
“For cancers in which socioeconomic status is a key factor in explaining racial and ethnic survival disparities, behavioral and supportive interventions that address social and economic barriers to effective care are warranted. However, for cancers in which survival is less influenced by socioeconomic status, more research is needed on underlying differences in tumor biology and drug processing.”
This research was supported by a grant from the National Institutes of Health, and the study’s authors made no disclosures.
No increase in primary ovarian insufficiency with HPV vaccine
The human papillomavirus vaccine does not appear to be associated with an increased risk of ovarian insufficiency, according to researchers.

Allison L. Naleway, PhD, of the Center for Health Research at Kaiser Permanente Northwest, Portland, Ore., and her coauthors wrote that a previous case series had raised concerns about a possible link between the human papillomavirus (HPV) vaccine and primary ovarian insufficiency (POI) in six young women who developed the condition within 12 months of vaccination.
Using EHR data, researchers identified 46 women aged 11-34 years with idiopathic POI – 33 probable cases and 13 possible cases – after excluding cases with known causes. Eighteen of these cases also were excluded because they were diagnosed before the HPV vaccine was available.
They found that only 1 of the remaining 28 patients had been vaccinated against HPV before the symptom onset: a 16-year-old girl who was vaccinated about 23 months before the first clinical evaluation for delayed menarche. Their report was published in Pediatrics.
The adjusted hazard ratio for POI was therefore 0.30 after HPV vaccine, compared with 0.88 after Tdap, 1.42 after inactivated influenza vaccine, and 0.94 after meningococcal conjugate vaccine.
More than one-half of the 46 confirmed POI cases were diagnosed at age 27 years or older, and only one patient was diagnosed under 15 years of age.
“If POI is triggered by HPV or other adolescent vaccine exposure, we would have expected to see elevated incidence in the younger women who were most likely to be vaccinated, but instead we observed higher incidence in older women (greater than 26 years of age), which is consistent with 1 other population-based study of POI prevalence,” the authors wrote.
They acknowledged that studying POI as a vaccine-related adverse event was challenging because the time from symptom onset to diagnosis was variable. However, they said that 81% of their cohort was followed up for more than 2 years, and a mean of 5.14 years, so the potential for misclassification was “minimal.”
Dr. Naleway and her associates also noted that diagnoses of POI can be difficult to accurately identify, and symptoms may be masked by oral contraceptive use.
“Despite the challenges and limitations discussed above, we believe this study should lessen concern surrounding potential impact on fertility from HPV or other adolescent vaccination,” they wrote.
The Centers for Disease Control and Prevention supported the study. Three authors declared funding from pharmaceutical companies for unrelated studies. No other conflicts of interest were declared.
SOURCE: Naleway A et al. Pediatrics 2018;42(3):e20180943.
The human papillomavirus vaccine does not appear to be associated with an increased risk of ovarian insufficiency, according to researchers.
Allison L. Naleway, PhD, of the Center for Health Research at Kaiser Permanente Northwest, Portland, Ore., and her coauthors wrote that a previous case series had raised concerns about a possible link between the human papillomavirus (HPV) vaccine and primary ovarian insufficiency (POI) in six young women who developed the condition within 12 months of vaccination.
Using EHR data, researchers identified 46 women aged 11-34 years with idiopathic POI – 33 probable cases and 13 possible cases – after excluding cases with known causes. Eighteen of these cases also were excluded because they were diagnosed before the HPV vaccine was available.
They found that only 1 of the remaining 28 patients had been vaccinated against HPV before the symptom onset: a 16-year-old girl who was vaccinated about 23 months before the first clinical evaluation for delayed menarche. Their report was published in Pediatrics.
The adjusted hazard ratio for POI was therefore 0.30 after HPV vaccine, compared with 0.88 after Tdap, 1.42 after inactivated influenza vaccine, and 0.94 after meningococcal conjugate vaccine.
More than one-half of the 46 confirmed POI cases were diagnosed at age 27 years or older, and only one patient was diagnosed under 15 years of age.
“If POI is triggered by HPV or other adolescent vaccine exposure, we would have expected to see elevated incidence in the younger women who were most likely to be vaccinated, but instead we observed higher incidence in older women (greater than 26 years of age), which is consistent with 1 other population-based study of POI prevalence,” the authors wrote.
They acknowledged that studying POI as a vaccine-related adverse event was challenging because the time from symptom onset to diagnosis was variable. However, they said that 81% of their cohort was followed up for more than 2 years, and a mean of 5.14 years, so the potential for misclassification was “minimal.”
Dr. Naleway and her associates also noted that diagnoses of POI can be difficult to accurately identify, and symptoms may be masked by oral contraceptive use.
“Despite the challenges and limitations discussed above, we believe this study should lessen concern surrounding potential impact on fertility from HPV or other adolescent vaccination,” they wrote.
The Centers for Disease Control and Prevention supported the study. Three authors declared funding from pharmaceutical companies for unrelated studies. No other conflicts of interest were declared.
SOURCE: Naleway A et al. Pediatrics 2018;42(3):e20180943.
The human papillomavirus vaccine does not appear to be associated with an increased risk of ovarian insufficiency, according to researchers.
Allison L. Naleway, PhD, of the Center for Health Research at Kaiser Permanente Northwest, Portland, Ore., and her coauthors wrote that a previous case series had raised concerns about a possible link between the human papillomavirus (HPV) vaccine and primary ovarian insufficiency (POI) in six young women who developed the condition within 12 months of vaccination.
Using EHR data, researchers identified 46 women aged 11-34 years with idiopathic POI – 33 probable cases and 13 possible cases – after excluding cases with known causes. Eighteen of these cases also were excluded because they were diagnosed before the HPV vaccine was available.
They found that only 1 of the remaining 28 patients had been vaccinated against HPV before the symptom onset: a 16-year-old girl who was vaccinated about 23 months before the first clinical evaluation for delayed menarche. Their report was published in Pediatrics.
The adjusted hazard ratio for POI was therefore 0.30 after HPV vaccine, compared with 0.88 after Tdap, 1.42 after inactivated influenza vaccine, and 0.94 after meningococcal conjugate vaccine.
More than one-half of the 46 confirmed POI cases were diagnosed at age 27 years or older, and only one patient was diagnosed under 15 years of age.
“If POI is triggered by HPV or other adolescent vaccine exposure, we would have expected to see elevated incidence in the younger women who were most likely to be vaccinated, but instead we observed higher incidence in older women (greater than 26 years of age), which is consistent with 1 other population-based study of POI prevalence,” the authors wrote.
They acknowledged that studying POI as a vaccine-related adverse event was challenging because the time from symptom onset to diagnosis was variable. However, they said that 81% of their cohort was followed up for more than 2 years, and a mean of 5.14 years, so the potential for misclassification was “minimal.”
Dr. Naleway and her associates also noted that diagnoses of POI can be difficult to accurately identify, and symptoms may be masked by oral contraceptive use.
“Despite the challenges and limitations discussed above, we believe this study should lessen concern surrounding potential impact on fertility from HPV or other adolescent vaccination,” they wrote.
The Centers for Disease Control and Prevention supported the study. Three authors declared funding from pharmaceutical companies for unrelated studies. No other conflicts of interest were declared.
SOURCE: Naleway A et al. Pediatrics 2018;42(3):e20180943.
FROM PEDIATRICS
Key clinical point:
Major finding: The adjusted hazard ratio for POI was 0.30 after HPV vaccine, compared with 0.88 after Tdap, 1.42 after inactivated influenza vaccine, and 0.94 after meningococcal conjugate vaccine.
Study details: Analysis of medical records data for 46 women with confirmed iatrogenic primary ovarian failure.
Disclosures: The study was supported by the Centers for Disease Control and Prevention. Three authors declared funding from pharmaceutical companies for unrelated studies. No other conflicts of interest were declared.
Source: Naleway A et al. Pediatrics 2018;142(3):e20180943.
AAP report: Prioritize play for young children
Pediatricians, parents, and teachers should prioritize play for children under their care because of its significant benefits, such as encouraging learning, building social bonds, and regulating stress, according to a clinical report from the American Academy of Pediatrics.

“We’re recommending that doctors write a prescription for play because it’s so important,” Michael Yogman, MD, of the department of pediatrics at Harvard Medical School, Boston, and Mount Auburn Hospital in Cambridge, Mass., said in a press release.
“Play with parents and peers is fundamentally important for developing a suite of 21st century skills, including social, emotional, language, and cognitive skills, all needed by the next generation in an economically competitive world that requires collaboration and innovation,” he continued. “The benefits of play cannot really be overstated in terms of mitigating stress, improving academic skills, and helping to build the safe, stable, and nurturing relationships that buffer against toxic stress and build social-emotional resilience.”
The report, published in the journal Pediatrics, is an update to a 2007 report that adds new research about the importance of play for children even as society has shifted its focus to “academic readiness” rather than “playful learning.” In the report, the authors cited the numerous benefits of active play for both children and adults. They noted a study of children who were aged 3-4 years that showed a twofold decrease in their anxiety after playing with toys or with their peers for 15 minutes, compared with listening to a teacher read a story. In another study, preschool children who played with blocks at home with minimal adult supervision and guidance had better language acquisition skills after 6 months. Results from studies also have shown that children who had 1 hour each day of active playtime had better creative and multitasking skills. For adults, the authors said playtime is an opportunity for them to “reawaken the joy of childhood and rejuvenate themselves,” as well as a chance to bond and become more effective communicators with their children.
However, Dr. Yogman and his associates noted there are many modern barriers to play. They cited how overscheduling of enrichment programs leaves little time for free play, an increased focus on academic achievement and test scores, the ways that economically challenged families may have less time to play with their children, and safety concerns about playing outdoors as some of the reasons for a decrease in active play among children. Between 1981 and 1997, there was a 25% decrease in the number of children who went outdoors to play once per day, and there is now a 30% decrease in kindergarten children who have access to recess because of an increased focus on academics, they wrote. In addition, the average child of preschool age spends 4.5 hours each day watching television.
“Media use, such as television, video games, smartphone, and tablet apps, [is] increasingly distracting children from play. It’s concerning when immersion in electronic media takes away time for real play, either outdoors or indoors,” Jeffrey Hutchinson, MD, a study coauthor, said in a press release.
“Although active engagement with age-appropriate media can be beneficial for older children, especially if supported by co-watching or co-play with peers or parents, real time social interactions and play are superior to digital media for learning,” said Dr. Hutchinson of the Uniformed Services University, Bethesda, Md.
The AAP made the following recommendations, among many others, to parents, pediatricians, and teachers for encouraging play in children aged 6 years and younger:
- During the first year, parents should place children in different positions so they can crawl, explore, and see their environment from different perspectives.
- Parents should talk to their children so they learn their parents’ voices and answer their children when they babble or coo.
- When children are aged 1-3 years, parents should read to them often and encourage pretend play based on the stories.
- When children are aged 1-3 years, their parents should be encouraged to provide blocks, plastic containers, wooden spoons, and puzzles for play.
- Pediatricians should check in with new parents during the first 2 years and write a “prescription for play” at well visits.
- Educators should promote and encourage unstructured playtime and playful learning, rather than didactic learning, at preschool and school.
- All adult caregivers of children should schedule some form of active play or recess each day.
“The next time your child wants to play with you, say yes. It’s one of the best parts of being a parent and one of the best things you can do for your child,” Dr. Yogman said. “Play helps children learn language, math, and social skills and lowers stress. Play is important both for children and their parents since sharing joyful moments together during play can only enhance their relationship.”
The authors reported no relevant conflicts of interest.
SOURCE: Yogman M et al. Pediatrics. 2018 Aug 20. doi: 10.1542/peds.2018-2058.
I wholeheartedly agree with the new American Academy of Pediatrics clinical report, “The power of play: A pediatric role in enhancing development in young children.” We should not be surprised that play – and not play structured by predetermined rules such as those in sports or those that are part of lessons such as piano – has such a meaningful role in development. For thousands of years, humans grew up without schools, electricity, and sports leagues and with only apprentice-level training in survival skills. As a result, thousands of hours of children’s activities were self-generated, and these activities, by their nature, encouraged the development of physical, social, and cognitive abilities.
And we still see elements of natural play, especially as we observe babies and toddlers playing – before our culture begins to channel this play activity into more structured, less spontaneous, and less social forms. As Jean Piaget, PhD, observed, play stems from a child’s “need to function” – to move, explore, learn, understand, and integrate the world around them. Watch a 9-month-old drop a toy and learn that it still exists and that dropping it is an interpersonal, fun game. Or watch how a toddler figures out how to stack and knock over some metal pots and pans on the kitchen floor or how 5-year-olds climb all over rocks or jungle gyms in a local park.
Of course, in a complex society like ours, these evolving activities have to be channeled into school, specific skills, and even homework. What the AAP clinical report suggests is that we may be pushing the structure, expectations, and isolation of learning too far, too rigidly, and too prematurely. We may be decreasing natural play below some threshold essential to necessary for skill development, especially that of self-esteem and social skills.
Children have a wide range of developmental paths and adaptability, but too much structure, too much isolation, too much screen time, overly high expectations, and now too little play all can have unanticipated and unhappy consequences.
Michael S. Jellinek, MD, is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. He was asked to comment on the AAP clinical report (http://pediatrics.aappublications.org/content/early/2018/08/16/peds.2018-2058).
I wholeheartedly agree with the new American Academy of Pediatrics clinical report, “The power of play: A pediatric role in enhancing development in young children.” We should not be surprised that play – and not play structured by predetermined rules such as those in sports or those that are part of lessons such as piano – has such a meaningful role in development. For thousands of years, humans grew up without schools, electricity, and sports leagues and with only apprentice-level training in survival skills. As a result, thousands of hours of children’s activities were self-generated, and these activities, by their nature, encouraged the development of physical, social, and cognitive abilities.
And we still see elements of natural play, especially as we observe babies and toddlers playing – before our culture begins to channel this play activity into more structured, less spontaneous, and less social forms. As Jean Piaget, PhD, observed, play stems from a child’s “need to function” – to move, explore, learn, understand, and integrate the world around them. Watch a 9-month-old drop a toy and learn that it still exists and that dropping it is an interpersonal, fun game. Or watch how a toddler figures out how to stack and knock over some metal pots and pans on the kitchen floor or how 5-year-olds climb all over rocks or jungle gyms in a local park.
Of course, in a complex society like ours, these evolving activities have to be channeled into school, specific skills, and even homework. What the AAP clinical report suggests is that we may be pushing the structure, expectations, and isolation of learning too far, too rigidly, and too prematurely. We may be decreasing natural play below some threshold essential to necessary for skill development, especially that of self-esteem and social skills.
Children have a wide range of developmental paths and adaptability, but too much structure, too much isolation, too much screen time, overly high expectations, and now too little play all can have unanticipated and unhappy consequences.
Michael S. Jellinek, MD, is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. He was asked to comment on the AAP clinical report (http://pediatrics.aappublications.org/content/early/2018/08/16/peds.2018-2058).
I wholeheartedly agree with the new American Academy of Pediatrics clinical report, “The power of play: A pediatric role in enhancing development in young children.” We should not be surprised that play – and not play structured by predetermined rules such as those in sports or those that are part of lessons such as piano – has such a meaningful role in development. For thousands of years, humans grew up without schools, electricity, and sports leagues and with only apprentice-level training in survival skills. As a result, thousands of hours of children’s activities were self-generated, and these activities, by their nature, encouraged the development of physical, social, and cognitive abilities.
And we still see elements of natural play, especially as we observe babies and toddlers playing – before our culture begins to channel this play activity into more structured, less spontaneous, and less social forms. As Jean Piaget, PhD, observed, play stems from a child’s “need to function” – to move, explore, learn, understand, and integrate the world around them. Watch a 9-month-old drop a toy and learn that it still exists and that dropping it is an interpersonal, fun game. Or watch how a toddler figures out how to stack and knock over some metal pots and pans on the kitchen floor or how 5-year-olds climb all over rocks or jungle gyms in a local park.
Of course, in a complex society like ours, these evolving activities have to be channeled into school, specific skills, and even homework. What the AAP clinical report suggests is that we may be pushing the structure, expectations, and isolation of learning too far, too rigidly, and too prematurely. We may be decreasing natural play below some threshold essential to necessary for skill development, especially that of self-esteem and social skills.
Children have a wide range of developmental paths and adaptability, but too much structure, too much isolation, too much screen time, overly high expectations, and now too little play all can have unanticipated and unhappy consequences.
Michael S. Jellinek, MD, is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. He was asked to comment on the AAP clinical report (http://pediatrics.aappublications.org/content/early/2018/08/16/peds.2018-2058).
Pediatricians, parents, and teachers should prioritize play for children under their care because of its significant benefits, such as encouraging learning, building social bonds, and regulating stress, according to a clinical report from the American Academy of Pediatrics.
“We’re recommending that doctors write a prescription for play because it’s so important,” Michael Yogman, MD, of the department of pediatrics at Harvard Medical School, Boston, and Mount Auburn Hospital in Cambridge, Mass., said in a press release.
“Play with parents and peers is fundamentally important for developing a suite of 21st century skills, including social, emotional, language, and cognitive skills, all needed by the next generation in an economically competitive world that requires collaboration and innovation,” he continued. “The benefits of play cannot really be overstated in terms of mitigating stress, improving academic skills, and helping to build the safe, stable, and nurturing relationships that buffer against toxic stress and build social-emotional resilience.”
The report, published in the journal Pediatrics, is an update to a 2007 report that adds new research about the importance of play for children even as society has shifted its focus to “academic readiness” rather than “playful learning.” In the report, the authors cited the numerous benefits of active play for both children and adults. They noted a study of children who were aged 3-4 years that showed a twofold decrease in their anxiety after playing with toys or with their peers for 15 minutes, compared with listening to a teacher read a story. In another study, preschool children who played with blocks at home with minimal adult supervision and guidance had better language acquisition skills after 6 months. Results from studies also have shown that children who had 1 hour each day of active playtime had better creative and multitasking skills. For adults, the authors said playtime is an opportunity for them to “reawaken the joy of childhood and rejuvenate themselves,” as well as a chance to bond and become more effective communicators with their children.
However, Dr. Yogman and his associates noted there are many modern barriers to play. They cited how overscheduling of enrichment programs leaves little time for free play, an increased focus on academic achievement and test scores, the ways that economically challenged families may have less time to play with their children, and safety concerns about playing outdoors as some of the reasons for a decrease in active play among children. Between 1981 and 1997, there was a 25% decrease in the number of children who went outdoors to play once per day, and there is now a 30% decrease in kindergarten children who have access to recess because of an increased focus on academics, they wrote. In addition, the average child of preschool age spends 4.5 hours each day watching television.
“Media use, such as television, video games, smartphone, and tablet apps, [is] increasingly distracting children from play. It’s concerning when immersion in electronic media takes away time for real play, either outdoors or indoors,” Jeffrey Hutchinson, MD, a study coauthor, said in a press release.
“Although active engagement with age-appropriate media can be beneficial for older children, especially if supported by co-watching or co-play with peers or parents, real time social interactions and play are superior to digital media for learning,” said Dr. Hutchinson of the Uniformed Services University, Bethesda, Md.
The AAP made the following recommendations, among many others, to parents, pediatricians, and teachers for encouraging play in children aged 6 years and younger:
- During the first year, parents should place children in different positions so they can crawl, explore, and see their environment from different perspectives.
- Parents should talk to their children so they learn their parents’ voices and answer their children when they babble or coo.
- When children are aged 1-3 years, parents should read to them often and encourage pretend play based on the stories.
- When children are aged 1-3 years, their parents should be encouraged to provide blocks, plastic containers, wooden spoons, and puzzles for play.
- Pediatricians should check in with new parents during the first 2 years and write a “prescription for play” at well visits.
- Educators should promote and encourage unstructured playtime and playful learning, rather than didactic learning, at preschool and school.
- All adult caregivers of children should schedule some form of active play or recess each day.
“The next time your child wants to play with you, say yes. It’s one of the best parts of being a parent and one of the best things you can do for your child,” Dr. Yogman said. “Play helps children learn language, math, and social skills and lowers stress. Play is important both for children and their parents since sharing joyful moments together during play can only enhance their relationship.”
The authors reported no relevant conflicts of interest.
SOURCE: Yogman M et al. Pediatrics. 2018 Aug 20. doi: 10.1542/peds.2018-2058.
Pediatricians, parents, and teachers should prioritize play for children under their care because of its significant benefits, such as encouraging learning, building social bonds, and regulating stress, according to a clinical report from the American Academy of Pediatrics.
“We’re recommending that doctors write a prescription for play because it’s so important,” Michael Yogman, MD, of the department of pediatrics at Harvard Medical School, Boston, and Mount Auburn Hospital in Cambridge, Mass., said in a press release.
“Play with parents and peers is fundamentally important for developing a suite of 21st century skills, including social, emotional, language, and cognitive skills, all needed by the next generation in an economically competitive world that requires collaboration and innovation,” he continued. “The benefits of play cannot really be overstated in terms of mitigating stress, improving academic skills, and helping to build the safe, stable, and nurturing relationships that buffer against toxic stress and build social-emotional resilience.”
The report, published in the journal Pediatrics, is an update to a 2007 report that adds new research about the importance of play for children even as society has shifted its focus to “academic readiness” rather than “playful learning.” In the report, the authors cited the numerous benefits of active play for both children and adults. They noted a study of children who were aged 3-4 years that showed a twofold decrease in their anxiety after playing with toys or with their peers for 15 minutes, compared with listening to a teacher read a story. In another study, preschool children who played with blocks at home with minimal adult supervision and guidance had better language acquisition skills after 6 months. Results from studies also have shown that children who had 1 hour each day of active playtime had better creative and multitasking skills. For adults, the authors said playtime is an opportunity for them to “reawaken the joy of childhood and rejuvenate themselves,” as well as a chance to bond and become more effective communicators with their children.
However, Dr. Yogman and his associates noted there are many modern barriers to play. They cited how overscheduling of enrichment programs leaves little time for free play, an increased focus on academic achievement and test scores, the ways that economically challenged families may have less time to play with their children, and safety concerns about playing outdoors as some of the reasons for a decrease in active play among children. Between 1981 and 1997, there was a 25% decrease in the number of children who went outdoors to play once per day, and there is now a 30% decrease in kindergarten children who have access to recess because of an increased focus on academics, they wrote. In addition, the average child of preschool age spends 4.5 hours each day watching television.
“Media use, such as television, video games, smartphone, and tablet apps, [is] increasingly distracting children from play. It’s concerning when immersion in electronic media takes away time for real play, either outdoors or indoors,” Jeffrey Hutchinson, MD, a study coauthor, said in a press release.
“Although active engagement with age-appropriate media can be beneficial for older children, especially if supported by co-watching or co-play with peers or parents, real time social interactions and play are superior to digital media for learning,” said Dr. Hutchinson of the Uniformed Services University, Bethesda, Md.
The AAP made the following recommendations, among many others, to parents, pediatricians, and teachers for encouraging play in children aged 6 years and younger:
- During the first year, parents should place children in different positions so they can crawl, explore, and see their environment from different perspectives.
- Parents should talk to their children so they learn their parents’ voices and answer their children when they babble or coo.
- When children are aged 1-3 years, parents should read to them often and encourage pretend play based on the stories.
- When children are aged 1-3 years, their parents should be encouraged to provide blocks, plastic containers, wooden spoons, and puzzles for play.
- Pediatricians should check in with new parents during the first 2 years and write a “prescription for play” at well visits.
- Educators should promote and encourage unstructured playtime and playful learning, rather than didactic learning, at preschool and school.
- All adult caregivers of children should schedule some form of active play or recess each day.
“The next time your child wants to play with you, say yes. It’s one of the best parts of being a parent and one of the best things you can do for your child,” Dr. Yogman said. “Play helps children learn language, math, and social skills and lowers stress. Play is important both for children and their parents since sharing joyful moments together during play can only enhance their relationship.”
The authors reported no relevant conflicts of interest.
SOURCE: Yogman M et al. Pediatrics. 2018 Aug 20. doi: 10.1542/peds.2018-2058.
FROM PEDIATRICS
In the U.S., breastfeeding starts out strong, but drops off fast
More than half the infants born in the United States in 2015 (57.6%) were still breastfeeding at 6 months old – an improvement over 2014 survey results, and another step toward the 61% goal set forth in Healthy People 2020.

The CDC Breastfeeding Report Card for 2018 found that about 83% of infants born in 2015 started to breastfeed at birth. Further, five of eight Healthy People 2020 breastfeeding goals were met in 2015.
Yet, the numbers also paint a picture familiar to many clinicians and families: By 1 year, only 36% of infants were still breastfeeding, and just 25% of infants were exclusively breastfed through 6 months, as the American Academy of Pediatrics recommends. This puts the U.S. on the lower end of the global breastfeeding scale, with most countries reporting rates of 30% and higher, according to World Health Organization data. Globally, 41% of mothers breastfeed exclusively through 6 months, according to the latest UNICEF data.
The report concludes that U.S. mothers may not be getting the support they need from health care providers, family members, and employers to meet their breastfeeding goals.
“High breastfeeding initiation rates show that most mothers in the United States want to breastfeed and start out doing so,” the report states. “However, despite the recommendation to breastfeed exclusively for about the first 6 months, less than 50% of infants were exclusively breastfed through 3 months and about 25% were exclusively breastfed through 6 months.”
The CDC Breastfeeding Report Card provides national- and state-level data to help clinicians, child care providers, and families promote breastfeeding and support the women who choose it. In addition to providing an in-depth look at the numbers, the report compares current findings to the breastfeeding goals outlined in Healthy People 2020. This year, it looked at data on breastfeeding practices and support in all 50 states, the District of Columbia, Puerto Rico, the Virgin Islands, and – for the first time – Guam.
The report is published every 2 years, but the data comprising it are updated annually. The latest rates reflect breastfeeding practices among U.S. infants born in 2015 and are based on results of the 2016 and 2017 U.S. National Immunization Surveys.
Since the first report card in 2007, rates of exclusive breastfeeding at 3 and 6 months have increased. However, although rates for any breastfeeding at 6 and 12 months increased in 2015 from 2014 rates, there was no appreciable increase in exclusive breastfeeding at 3 and 6 months, the report noted. And about 17% of infants who were breastfed at birth still got some formula supplementation in the first 2 days of life.
Recognizing that breastfeeding support at the birth facility is a key driver of success, Healthy People 2020 tracks the proportion of live births in facilities that provided the recommended support. These “baby-friendly hospitals” receive a special designation from the WHO/UNICEF Baby-Friendly Hospital Initiative, and their numbers are increasing, the report noted. In 12 states, more than 40% of births occurred in such facilities, comprising more than 1 million infants in 2015 (26%), and far exceeding the HP2020 8% goal.
In a nation in which many new mothers must return to employment outside the home, breastfeeding support at work is crucial. Just 49% of employers provide breastfeeding facilities for these women, the report found. While this may seem less than optimal, it still exceeds the HP2020 goal of 38%.
“All sectors of society – family and friends, hospitals, health care offices/clinics, childcare facilities, community-based organizations, and workplaces – can play a role in improving the health of families by supporting breastfeeding,” the report said. “To reach their breastfeeding goals, mothers need continuity of care, which is achieved by consistent, collaborative, and high-quality breastfeeding services and support.”
SOURCE: CDC Breastfeeding Report Card
More than half the infants born in the United States in 2015 (57.6%) were still breastfeeding at 6 months old – an improvement over 2014 survey results, and another step toward the 61% goal set forth in Healthy People 2020.
The CDC Breastfeeding Report Card for 2018 found that about 83% of infants born in 2015 started to breastfeed at birth. Further, five of eight Healthy People 2020 breastfeeding goals were met in 2015.
Yet, the numbers also paint a picture familiar to many clinicians and families: By 1 year, only 36% of infants were still breastfeeding, and just 25% of infants were exclusively breastfed through 6 months, as the American Academy of Pediatrics recommends. This puts the U.S. on the lower end of the global breastfeeding scale, with most countries reporting rates of 30% and higher, according to World Health Organization data. Globally, 41% of mothers breastfeed exclusively through 6 months, according to the latest UNICEF data.
The report concludes that U.S. mothers may not be getting the support they need from health care providers, family members, and employers to meet their breastfeeding goals.
“High breastfeeding initiation rates show that most mothers in the United States want to breastfeed and start out doing so,” the report states. “However, despite the recommendation to breastfeed exclusively for about the first 6 months, less than 50% of infants were exclusively breastfed through 3 months and about 25% were exclusively breastfed through 6 months.”
The CDC Breastfeeding Report Card provides national- and state-level data to help clinicians, child care providers, and families promote breastfeeding and support the women who choose it. In addition to providing an in-depth look at the numbers, the report compares current findings to the breastfeeding goals outlined in Healthy People 2020. This year, it looked at data on breastfeeding practices and support in all 50 states, the District of Columbia, Puerto Rico, the Virgin Islands, and – for the first time – Guam.
The report is published every 2 years, but the data comprising it are updated annually. The latest rates reflect breastfeeding practices among U.S. infants born in 2015 and are based on results of the 2016 and 2017 U.S. National Immunization Surveys.
Since the first report card in 2007, rates of exclusive breastfeeding at 3 and 6 months have increased. However, although rates for any breastfeeding at 6 and 12 months increased in 2015 from 2014 rates, there was no appreciable increase in exclusive breastfeeding at 3 and 6 months, the report noted. And about 17% of infants who were breastfed at birth still got some formula supplementation in the first 2 days of life.
Recognizing that breastfeeding support at the birth facility is a key driver of success, Healthy People 2020 tracks the proportion of live births in facilities that provided the recommended support. These “baby-friendly hospitals” receive a special designation from the WHO/UNICEF Baby-Friendly Hospital Initiative, and their numbers are increasing, the report noted. In 12 states, more than 40% of births occurred in such facilities, comprising more than 1 million infants in 2015 (26%), and far exceeding the HP2020 8% goal.
In a nation in which many new mothers must return to employment outside the home, breastfeeding support at work is crucial. Just 49% of employers provide breastfeeding facilities for these women, the report found. While this may seem less than optimal, it still exceeds the HP2020 goal of 38%.
“All sectors of society – family and friends, hospitals, health care offices/clinics, childcare facilities, community-based organizations, and workplaces – can play a role in improving the health of families by supporting breastfeeding,” the report said. “To reach their breastfeeding goals, mothers need continuity of care, which is achieved by consistent, collaborative, and high-quality breastfeeding services and support.”
SOURCE: CDC Breastfeeding Report Card
More than half the infants born in the United States in 2015 (57.6%) were still breastfeeding at 6 months old – an improvement over 2014 survey results, and another step toward the 61% goal set forth in Healthy People 2020.
The CDC Breastfeeding Report Card for 2018 found that about 83% of infants born in 2015 started to breastfeed at birth. Further, five of eight Healthy People 2020 breastfeeding goals were met in 2015.
Yet, the numbers also paint a picture familiar to many clinicians and families: By 1 year, only 36% of infants were still breastfeeding, and just 25% of infants were exclusively breastfed through 6 months, as the American Academy of Pediatrics recommends. This puts the U.S. on the lower end of the global breastfeeding scale, with most countries reporting rates of 30% and higher, according to World Health Organization data. Globally, 41% of mothers breastfeed exclusively through 6 months, according to the latest UNICEF data.
The report concludes that U.S. mothers may not be getting the support they need from health care providers, family members, and employers to meet their breastfeeding goals.
“High breastfeeding initiation rates show that most mothers in the United States want to breastfeed and start out doing so,” the report states. “However, despite the recommendation to breastfeed exclusively for about the first 6 months, less than 50% of infants were exclusively breastfed through 3 months and about 25% were exclusively breastfed through 6 months.”
The CDC Breastfeeding Report Card provides national- and state-level data to help clinicians, child care providers, and families promote breastfeeding and support the women who choose it. In addition to providing an in-depth look at the numbers, the report compares current findings to the breastfeeding goals outlined in Healthy People 2020. This year, it looked at data on breastfeeding practices and support in all 50 states, the District of Columbia, Puerto Rico, the Virgin Islands, and – for the first time – Guam.
The report is published every 2 years, but the data comprising it are updated annually. The latest rates reflect breastfeeding practices among U.S. infants born in 2015 and are based on results of the 2016 and 2017 U.S. National Immunization Surveys.
Since the first report card in 2007, rates of exclusive breastfeeding at 3 and 6 months have increased. However, although rates for any breastfeeding at 6 and 12 months increased in 2015 from 2014 rates, there was no appreciable increase in exclusive breastfeeding at 3 and 6 months, the report noted. And about 17% of infants who were breastfed at birth still got some formula supplementation in the first 2 days of life.
Recognizing that breastfeeding support at the birth facility is a key driver of success, Healthy People 2020 tracks the proportion of live births in facilities that provided the recommended support. These “baby-friendly hospitals” receive a special designation from the WHO/UNICEF Baby-Friendly Hospital Initiative, and their numbers are increasing, the report noted. In 12 states, more than 40% of births occurred in such facilities, comprising more than 1 million infants in 2015 (26%), and far exceeding the HP2020 8% goal.
In a nation in which many new mothers must return to employment outside the home, breastfeeding support at work is crucial. Just 49% of employers provide breastfeeding facilities for these women, the report found. While this may seem less than optimal, it still exceeds the HP2020 goal of 38%.
“All sectors of society – family and friends, hospitals, health care offices/clinics, childcare facilities, community-based organizations, and workplaces – can play a role in improving the health of families by supporting breastfeeding,” the report said. “To reach their breastfeeding goals, mothers need continuity of care, which is achieved by consistent, collaborative, and high-quality breastfeeding services and support.”
SOURCE: CDC Breastfeeding Report Card
Nighttime media use threatens teen sleep
Nighttime media use was associated with less sleep, as well as self-reported anxiety and depression, in teens with attention-deficit/hyperactivity disorder, based on data from 81 adolescents.
“This is the first study to document an association between nighttime media use and more sleep problems and internalizing symptoms in adolescents diagnosed with ADHD,” wrote Stephen P. Becker, PhD, of the University of Cincinnati and colleagues.
Although previous research has addressed the impact of screen time on sleep, anxiety, and depression in children and teens, the impact on adolescents with conditions such as ADHD has not been well studied, the researchers noted.
In a study published in Sleep Medicine, the researchers conducted a study of 81 adolescents aged 13-17 years who met diagnostic criteria for ADHD. The School Sleep Habits Survey (SSHS) was used to measure sleep patterns based on self-reports, and parents reported on teens’ sleep using the Sleep Disturbance Scale for Children. In addition, several other tools that measured ADHD symptoms, daytime sleepiness, anxiety, and depression were administered to both the teens and their parents.
The researchers assessed the number of technologies in each participant’s bedroom and the total hours of electronic media use at night, defined as after 9:00 p.m.
Overall, approximately 60% of the teens in the sample reported more than 4 hours of nighttime media use; 63% reported less than 8 hours of sleep on school nights, but this figure reached 76% when parent reports of teens’ sleep was used. When the teens’ self-reports were used, media use was not significantly different between those who had less than 8 hours of sleep vs. those who had 8 hours or more (5.85 vs. 4.39 hours of nighttime media use). But their parents’ reports told another story. In the parent reports, media use was significantly higher in the short sleepers vs. long sleepers (6.12 vs. 2.65 hours of nighttime media use).
After controlling for factors including age, sex, pubertal stage, use of stimulant medication, and severity of ADHD symptoms, nighttime media use was significantly associated with shorter sleep duration, the researchers said.
Nighttime media use also was significantly associated with greater adolescent-reported depressive symptoms, total anxiety symptoms overall, and panic symptoms in particular, as well as with parent-reported generalized anxiety symptoms.
The study findings were limited by several factors including the cross-sectional design, the lack of an objective sleep measure, and the lack of non-ADHD controls, the researchers noted. Also, the researchers were unable to measure parental control over teen media use or to examine different types of media use, including media multitasking (such as texting while video gaming).
However, the findings “suggest that it is important for clinicians to consider nighttime media use when assessing and treating adolescent ADHD, specifically regarding sleep issues and co-occurring depression and anxiety,” they said.
The researchers had no financial conflicts to disclose. The study was funded by grants from the National Institutes of Mental Health.
SOURCE: Becker S et al. Sleep Med. 2018. doi: 10.1016/ j.sleep.2018.06.021.
Nighttime media use was associated with less sleep, as well as self-reported anxiety and depression, in teens with attention-deficit/hyperactivity disorder, based on data from 81 adolescents.
“This is the first study to document an association between nighttime media use and more sleep problems and internalizing symptoms in adolescents diagnosed with ADHD,” wrote Stephen P. Becker, PhD, of the University of Cincinnati and colleagues.
Although previous research has addressed the impact of screen time on sleep, anxiety, and depression in children and teens, the impact on adolescents with conditions such as ADHD has not been well studied, the researchers noted.
In a study published in Sleep Medicine, the researchers conducted a study of 81 adolescents aged 13-17 years who met diagnostic criteria for ADHD. The School Sleep Habits Survey (SSHS) was used to measure sleep patterns based on self-reports, and parents reported on teens’ sleep using the Sleep Disturbance Scale for Children. In addition, several other tools that measured ADHD symptoms, daytime sleepiness, anxiety, and depression were administered to both the teens and their parents.
The researchers assessed the number of technologies in each participant’s bedroom and the total hours of electronic media use at night, defined as after 9:00 p.m.
Overall, approximately 60% of the teens in the sample reported more than 4 hours of nighttime media use; 63% reported less than 8 hours of sleep on school nights, but this figure reached 76% when parent reports of teens’ sleep was used. When the teens’ self-reports were used, media use was not significantly different between those who had less than 8 hours of sleep vs. those who had 8 hours or more (5.85 vs. 4.39 hours of nighttime media use). But their parents’ reports told another story. In the parent reports, media use was significantly higher in the short sleepers vs. long sleepers (6.12 vs. 2.65 hours of nighttime media use).
After controlling for factors including age, sex, pubertal stage, use of stimulant medication, and severity of ADHD symptoms, nighttime media use was significantly associated with shorter sleep duration, the researchers said.
Nighttime media use also was significantly associated with greater adolescent-reported depressive symptoms, total anxiety symptoms overall, and panic symptoms in particular, as well as with parent-reported generalized anxiety symptoms.
The study findings were limited by several factors including the cross-sectional design, the lack of an objective sleep measure, and the lack of non-ADHD controls, the researchers noted. Also, the researchers were unable to measure parental control over teen media use or to examine different types of media use, including media multitasking (such as texting while video gaming).
However, the findings “suggest that it is important for clinicians to consider nighttime media use when assessing and treating adolescent ADHD, specifically regarding sleep issues and co-occurring depression and anxiety,” they said.
The researchers had no financial conflicts to disclose. The study was funded by grants from the National Institutes of Mental Health.
SOURCE: Becker S et al. Sleep Med. 2018. doi: 10.1016/ j.sleep.2018.06.021.
Nighttime media use was associated with less sleep, as well as self-reported anxiety and depression, in teens with attention-deficit/hyperactivity disorder, based on data from 81 adolescents.
“This is the first study to document an association between nighttime media use and more sleep problems and internalizing symptoms in adolescents diagnosed with ADHD,” wrote Stephen P. Becker, PhD, of the University of Cincinnati and colleagues.
Although previous research has addressed the impact of screen time on sleep, anxiety, and depression in children and teens, the impact on adolescents with conditions such as ADHD has not been well studied, the researchers noted.
In a study published in Sleep Medicine, the researchers conducted a study of 81 adolescents aged 13-17 years who met diagnostic criteria for ADHD. The School Sleep Habits Survey (SSHS) was used to measure sleep patterns based on self-reports, and parents reported on teens’ sleep using the Sleep Disturbance Scale for Children. In addition, several other tools that measured ADHD symptoms, daytime sleepiness, anxiety, and depression were administered to both the teens and their parents.
The researchers assessed the number of technologies in each participant’s bedroom and the total hours of electronic media use at night, defined as after 9:00 p.m.
Overall, approximately 60% of the teens in the sample reported more than 4 hours of nighttime media use; 63% reported less than 8 hours of sleep on school nights, but this figure reached 76% when parent reports of teens’ sleep was used. When the teens’ self-reports were used, media use was not significantly different between those who had less than 8 hours of sleep vs. those who had 8 hours or more (5.85 vs. 4.39 hours of nighttime media use). But their parents’ reports told another story. In the parent reports, media use was significantly higher in the short sleepers vs. long sleepers (6.12 vs. 2.65 hours of nighttime media use).
After controlling for factors including age, sex, pubertal stage, use of stimulant medication, and severity of ADHD symptoms, nighttime media use was significantly associated with shorter sleep duration, the researchers said.
Nighttime media use also was significantly associated with greater adolescent-reported depressive symptoms, total anxiety symptoms overall, and panic symptoms in particular, as well as with parent-reported generalized anxiety symptoms.
The study findings were limited by several factors including the cross-sectional design, the lack of an objective sleep measure, and the lack of non-ADHD controls, the researchers noted. Also, the researchers were unable to measure parental control over teen media use or to examine different types of media use, including media multitasking (such as texting while video gaming).
However, the findings “suggest that it is important for clinicians to consider nighttime media use when assessing and treating adolescent ADHD, specifically regarding sleep issues and co-occurring depression and anxiety,” they said.
The researchers had no financial conflicts to disclose. The study was funded by grants from the National Institutes of Mental Health.
SOURCE: Becker S et al. Sleep Med. 2018. doi: 10.1016/ j.sleep.2018.06.021.
FROM SLEEP MEDICINE
Key clinical point: Among teens with ADHD, those who had significantly more nighttime media use tended to get less than 8 hours of sleep at night.
Major finding: About 60% of the teens reported more than 4 hours of nighttime media use; 63% reported less than 8 hours of sleep on school nights.
Study details: The data come from a range of research tools used to gather sleep and media use data on 81 adolescents with ADHD, aged 13-17 years.
Disclosures: The researchers had no financial conflicts to disclose. The study was funded by grants from the National Institutes of Mental Health.
Source: Becker S et al. Sleep Med. 2018. doi: 10.1016/ j.sleep.2018.06.021.
What is your treatment plan?
The treatment choice is oral terbinafine for tinea capitis with kerion, a scalp dermatophyte infection with a concurrent inflammatory process. Tinea capitis is a very common infection with the peak occurrence at age 3-7 years. Tinea capitis is caused by a variety of dermatophyte species, most commonly by Trichophyton tonsurans or Microsporum canis. T. tonsurans is an endothrix infection, invading the hair shaft and superficial hair while M. canis is an ectothrix infection. T. tonsurans has a person to person transmission; in contrast, M. canis is a zoonotic infection most commonly acquired from infected pets.1 The epidemiology of tinea capitis is affected by multiple factors, including immigration patterns. For example, in Montreal, a study showed a sixfold increase of African dermatophyte species, M. audouinii and T. soudanense.2 Similarly, global variation has increased prevalence of T. violaceum, more commonly found in Europe and Africa, which has been seen in immigrant populations in the United States.1 Kerion is thought to be a hypersensitivity reaction to dermatophytes. Often, misdiagnosis of kerion can result in unnecessary antibiotic prescription and delays in initiation of antifungal therapy.3,4
Tinea capitis can present with focal, “patchy,” well-demarcated hair loss and overlying scale, broken-off hairs at the scalp, and often with pustules. It may be associated with occipital or posterior cervical lymphadenopathy. which presents as a painful boggy scalp mass with or without purulent drainage. Kerions can have associated fever. It is important to differentiate tinea capitis with kerion from processes requiring a different treatment course.3,5 Bacterial folliculitis may have erythema and pustules but only rarely causes hair loss. Similarly, alopecia areata can present with focal alopecia but lacks the scalp inflammation and pustules. Scalp psoriasis is quite scaly, but is more thickened, and usually does not have pustules, nor would purulent drainage be evident. There is a broader differential for other inflammatory focal alopecias including discoid lupus, lichen planopilaris, and dissecting cellulitis of the scalp, which can have similar pus-filled lumps, and cause permanent hair loss, but may be differentiated by associated conditions such as acne conglobata, hidradenitis suppurativa, and pilonidal sinus.

While some clinicians advocate clinical diagnosis of tinea capitis, we advocate confirmation of infection by fungal culture, which can identify the causative organism and influence therapy selection.1 The presence of a fungal infection can be confirmed on potassium hydroxide wet mount prep if hyphae and small spores are seen.6,7 Wood lamp examination will fluoresce if there are ectothrix species, however a negative fluorescence does not differentiate between an endothrix species or lack of infection.
It is important that tinea capitis with kerion is treated with systemic antifungal treatments to allow resolution of the infection, recovery of hair growth, and to prevent or minimize scarring. Systemic antifungal options include terbinafine, griseofulvin, and azoles. Terbinafine is becoming the treatment of choice given shorter duration of treatment with similar efficacy.1T. tonsurans also is thought to respond better to terbinafine than to griseofulvin.8 Griseofulvin is the historical treatment of choice because of its history of clinical safety and no need for laboratory testing. It is important to note that higher doses of griseofulvin (20-25 mg/kg) are recommended, as older lower dose regimens have high rates of failure. Griseofulvin may be more effective for treatment of Microsporum spp than is terbinafine.8 Fluconazole is the only oral antifungal agent that is approved for patients younger than 2 years of age, however it has lower cure rates, compared with terbinafine and griseofulvin.1 Tinea capitis with kerion does not generally require antibiotics unless there is superimposed bacterial infection. Kerion also do not require incision or drainage, which may increase scarring and complicate the clinical course.
Management of tinea capitis should include evaluation of any other household members for coinfection. Depending on the dermatophyte involved there can be risk of person-to-person transmission.5 Families should be educated about fomite transmission via shared combs or hats. Additionally, if a zoophilic dermatophyte is suspected, pets also should be appropriately examined and treated. Topical antifungals are insufficient to eradicate tinea capitis but can be used as adjunctive therapy. Kerion can be treated with oral prednisone in addition to oral antifungals if the lesions are very painful, however there is limited data on this treatment option.9

Ms. Kaushik is a research fellow and Dr. Eichenfield is professor of dermatology and pediatrics in the division of pediatric and adolescent dermatology at Rady Children’s Hospital and the University of California, both in San Diego. They have no conflicts of interest or relevant financial disclosures.
References
1. “Red Book: Report of the Committee on Infectious Diseases,” 31st Edition, (Elk Grove Village, Ill.: American Academy of Pediatrics, 2018, p. 1264).
2. Pediatr Dermatol. 2018 May;35(3):323-8
3. Arch Dis Child. 2016 May;101(5):503.
4. IDCases. 2018 Jun 28;14:e00418.
5. Int J Dermatol. 2018 Jan;57(1):3-9.
6. Pediatr Rev. 2007 May;28(5):164-74.
7. Clin Cosmet Investig Dermatol. 2010;3:89-98.
8. Cochrane Database Syst Rev. 2016 May 12;(5):CD004685.
9. Med Mycol. 1999 Apr;37(2):97-9.
The treatment choice is oral terbinafine for tinea capitis with kerion, a scalp dermatophyte infection with a concurrent inflammatory process. Tinea capitis is a very common infection with the peak occurrence at age 3-7 years. Tinea capitis is caused by a variety of dermatophyte species, most commonly by Trichophyton tonsurans or Microsporum canis. T. tonsurans is an endothrix infection, invading the hair shaft and superficial hair while M. canis is an ectothrix infection. T. tonsurans has a person to person transmission; in contrast, M. canis is a zoonotic infection most commonly acquired from infected pets.1 The epidemiology of tinea capitis is affected by multiple factors, including immigration patterns. For example, in Montreal, a study showed a sixfold increase of African dermatophyte species, M. audouinii and T. soudanense.2 Similarly, global variation has increased prevalence of T. violaceum, more commonly found in Europe and Africa, which has been seen in immigrant populations in the United States.1 Kerion is thought to be a hypersensitivity reaction to dermatophytes. Often, misdiagnosis of kerion can result in unnecessary antibiotic prescription and delays in initiation of antifungal therapy.3,4
Tinea capitis can present with focal, “patchy,” well-demarcated hair loss and overlying scale, broken-off hairs at the scalp, and often with pustules. It may be associated with occipital or posterior cervical lymphadenopathy. which presents as a painful boggy scalp mass with or without purulent drainage. Kerions can have associated fever. It is important to differentiate tinea capitis with kerion from processes requiring a different treatment course.3,5 Bacterial folliculitis may have erythema and pustules but only rarely causes hair loss. Similarly, alopecia areata can present with focal alopecia but lacks the scalp inflammation and pustules. Scalp psoriasis is quite scaly, but is more thickened, and usually does not have pustules, nor would purulent drainage be evident. There is a broader differential for other inflammatory focal alopecias including discoid lupus, lichen planopilaris, and dissecting cellulitis of the scalp, which can have similar pus-filled lumps, and cause permanent hair loss, but may be differentiated by associated conditions such as acne conglobata, hidradenitis suppurativa, and pilonidal sinus.
While some clinicians advocate clinical diagnosis of tinea capitis, we advocate confirmation of infection by fungal culture, which can identify the causative organism and influence therapy selection.1 The presence of a fungal infection can be confirmed on potassium hydroxide wet mount prep if hyphae and small spores are seen.6,7 Wood lamp examination will fluoresce if there are ectothrix species, however a negative fluorescence does not differentiate between an endothrix species or lack of infection.
It is important that tinea capitis with kerion is treated with systemic antifungal treatments to allow resolution of the infection, recovery of hair growth, and to prevent or minimize scarring. Systemic antifungal options include terbinafine, griseofulvin, and azoles. Terbinafine is becoming the treatment of choice given shorter duration of treatment with similar efficacy.1T. tonsurans also is thought to respond better to terbinafine than to griseofulvin.8 Griseofulvin is the historical treatment of choice because of its history of clinical safety and no need for laboratory testing. It is important to note that higher doses of griseofulvin (20-25 mg/kg) are recommended, as older lower dose regimens have high rates of failure. Griseofulvin may be more effective for treatment of Microsporum spp than is terbinafine.8 Fluconazole is the only oral antifungal agent that is approved for patients younger than 2 years of age, however it has lower cure rates, compared with terbinafine and griseofulvin.1 Tinea capitis with kerion does not generally require antibiotics unless there is superimposed bacterial infection. Kerion also do not require incision or drainage, which may increase scarring and complicate the clinical course.
Management of tinea capitis should include evaluation of any other household members for coinfection. Depending on the dermatophyte involved there can be risk of person-to-person transmission.5 Families should be educated about fomite transmission via shared combs or hats. Additionally, if a zoophilic dermatophyte is suspected, pets also should be appropriately examined and treated. Topical antifungals are insufficient to eradicate tinea capitis but can be used as adjunctive therapy. Kerion can be treated with oral prednisone in addition to oral antifungals if the lesions are very painful, however there is limited data on this treatment option.9
Ms. Kaushik is a research fellow and Dr. Eichenfield is professor of dermatology and pediatrics in the division of pediatric and adolescent dermatology at Rady Children’s Hospital and the University of California, both in San Diego. They have no conflicts of interest or relevant financial disclosures.
References
1. “Red Book: Report of the Committee on Infectious Diseases,” 31st Edition, (Elk Grove Village, Ill.: American Academy of Pediatrics, 2018, p. 1264).
2. Pediatr Dermatol. 2018 May;35(3):323-8
3. Arch Dis Child. 2016 May;101(5):503.
4. IDCases. 2018 Jun 28;14:e00418.
5. Int J Dermatol. 2018 Jan;57(1):3-9.
6. Pediatr Rev. 2007 May;28(5):164-74.
7. Clin Cosmet Investig Dermatol. 2010;3:89-98.
8. Cochrane Database Syst Rev. 2016 May 12;(5):CD004685.
9. Med Mycol. 1999 Apr;37(2):97-9.
The treatment choice is oral terbinafine for tinea capitis with kerion, a scalp dermatophyte infection with a concurrent inflammatory process. Tinea capitis is a very common infection with the peak occurrence at age 3-7 years. Tinea capitis is caused by a variety of dermatophyte species, most commonly by Trichophyton tonsurans or Microsporum canis. T. tonsurans is an endothrix infection, invading the hair shaft and superficial hair while M. canis is an ectothrix infection. T. tonsurans has a person to person transmission; in contrast, M. canis is a zoonotic infection most commonly acquired from infected pets.1 The epidemiology of tinea capitis is affected by multiple factors, including immigration patterns. For example, in Montreal, a study showed a sixfold increase of African dermatophyte species, M. audouinii and T. soudanense.2 Similarly, global variation has increased prevalence of T. violaceum, more commonly found in Europe and Africa, which has been seen in immigrant populations in the United States.1 Kerion is thought to be a hypersensitivity reaction to dermatophytes. Often, misdiagnosis of kerion can result in unnecessary antibiotic prescription and delays in initiation of antifungal therapy.3,4
Tinea capitis can present with focal, “patchy,” well-demarcated hair loss and overlying scale, broken-off hairs at the scalp, and often with pustules. It may be associated with occipital or posterior cervical lymphadenopathy. which presents as a painful boggy scalp mass with or without purulent drainage. Kerions can have associated fever. It is important to differentiate tinea capitis with kerion from processes requiring a different treatment course.3,5 Bacterial folliculitis may have erythema and pustules but only rarely causes hair loss. Similarly, alopecia areata can present with focal alopecia but lacks the scalp inflammation and pustules. Scalp psoriasis is quite scaly, but is more thickened, and usually does not have pustules, nor would purulent drainage be evident. There is a broader differential for other inflammatory focal alopecias including discoid lupus, lichen planopilaris, and dissecting cellulitis of the scalp, which can have similar pus-filled lumps, and cause permanent hair loss, but may be differentiated by associated conditions such as acne conglobata, hidradenitis suppurativa, and pilonidal sinus.
While some clinicians advocate clinical diagnosis of tinea capitis, we advocate confirmation of infection by fungal culture, which can identify the causative organism and influence therapy selection.1 The presence of a fungal infection can be confirmed on potassium hydroxide wet mount prep if hyphae and small spores are seen.6,7 Wood lamp examination will fluoresce if there are ectothrix species, however a negative fluorescence does not differentiate between an endothrix species or lack of infection.
It is important that tinea capitis with kerion is treated with systemic antifungal treatments to allow resolution of the infection, recovery of hair growth, and to prevent or minimize scarring. Systemic antifungal options include terbinafine, griseofulvin, and azoles. Terbinafine is becoming the treatment of choice given shorter duration of treatment with similar efficacy.1T. tonsurans also is thought to respond better to terbinafine than to griseofulvin.8 Griseofulvin is the historical treatment of choice because of its history of clinical safety and no need for laboratory testing. It is important to note that higher doses of griseofulvin (20-25 mg/kg) are recommended, as older lower dose regimens have high rates of failure. Griseofulvin may be more effective for treatment of Microsporum spp than is terbinafine.8 Fluconazole is the only oral antifungal agent that is approved for patients younger than 2 years of age, however it has lower cure rates, compared with terbinafine and griseofulvin.1 Tinea capitis with kerion does not generally require antibiotics unless there is superimposed bacterial infection. Kerion also do not require incision or drainage, which may increase scarring and complicate the clinical course.
Management of tinea capitis should include evaluation of any other household members for coinfection. Depending on the dermatophyte involved there can be risk of person-to-person transmission.5 Families should be educated about fomite transmission via shared combs or hats. Additionally, if a zoophilic dermatophyte is suspected, pets also should be appropriately examined and treated. Topical antifungals are insufficient to eradicate tinea capitis but can be used as adjunctive therapy. Kerion can be treated with oral prednisone in addition to oral antifungals if the lesions are very painful, however there is limited data on this treatment option.9
Ms. Kaushik is a research fellow and Dr. Eichenfield is professor of dermatology and pediatrics in the division of pediatric and adolescent dermatology at Rady Children’s Hospital and the University of California, both in San Diego. They have no conflicts of interest or relevant financial disclosures.
References
1. “Red Book: Report of the Committee on Infectious Diseases,” 31st Edition, (Elk Grove Village, Ill.: American Academy of Pediatrics, 2018, p. 1264).
2. Pediatr Dermatol. 2018 May;35(3):323-8
3. Arch Dis Child. 2016 May;101(5):503.
4. IDCases. 2018 Jun 28;14:e00418.
5. Int J Dermatol. 2018 Jan;57(1):3-9.
6. Pediatr Rev. 2007 May;28(5):164-74.
7. Clin Cosmet Investig Dermatol. 2010;3:89-98.
8. Cochrane Database Syst Rev. 2016 May 12;(5):CD004685.
9. Med Mycol. 1999 Apr;37(2):97-9.
A 10-year-old otherwise-healthy male presents for a progressing lesion on his scalp. One month prior to coming in, he developed some peeling and itch followed by loss of hair. This had worsened, becoming a painful and boggy mass on the back of his head with focal alopecia. He went to the local ED, where he had plain films of his skull, which were normal and was prescribed cephalexin. He has not shown any improvement after starting the antibiotics. He has had no fevers in this time, but the pain persists.

On physical exam, he is noted to have a hairless patch on a boggy left occipital mass, which is tender to palpation. There is a small amount of overlying honey-colored crusting. He has associated posterior occipital nontender lymphadenopathy.
The patient's older sister has a small area of scalp hair loss.
Comparison of analgesia methods for neonatal circumcision
Multiple pain management interventions exist
Clinical question
What is the optimal way to manage analgesia during neonatal circumcision?
Background
Neonatal circumcision is one of the most commonly performed surgical procedures. The American Academy of Pediatrics in 2012 noted that the health benefits outweigh the minor risks of the procedure, but that parents should make the decision to circumcise based on their own cultural, ethical, and religious beliefs.
One of the primary risks of neonatal circumcision is pain during and after the procedure. Multiple methods for managing analgesia exist, but it is unknown what combination of methods is optimal. Usual analgesia techniques include: local anesthetic cream composed of lidocaine and prilocaine (EMLA) applied to the skin prior to the procedure; oral sucrose solution given throughout the procedure; dorsal penile nerve block (DPNB); and penile ring block (RB).
Study design
Single-center, double-blinded, randomized, controlled trial.
Setting
Multispecialty freestanding hospital.
Synopsis
Parents of infant boys born at 36-41 weeks’ gestation who chose to have their children circumcised were offered participation in the study. Of 83 eligible participants, 70 were randomized, with 10 in the control group (EMLA only) and 20 in each intervention (EMLA + sucrose, EMLA + sucrose + RB, EMLA + sucrose + DPNB). A single pediatric urologist performed all circumcisions using the Gomco clamp technique.
A video camera recorded the infant’s face and upper torso during the procedure. Two researchers, who were blinded to the analgesia plan, scored these videos using a modified Neonatal Infant Pain Scale (NIPS). The NIPS used ranged from 0 to 6, with 6 considered severe pain. For rating purposes, the procedure was divided into 6 stages with a NIPS score assigned at each stage. There were no significant differences in baseline characteristics among the groups; no significant differences in the duration of the procedure by intervention; and there were no complications. Interrater reliability for the NIPS was good (kappa, 0.84). All interventions were superior to EMLA alone, with significantly decreased NIPS for all stages of the procedure. No significant differences in NIPS were found among the following:
EMLA + sucrose.
EMLA + sucrose + RB.
EMLA + sucrose + DPNB (for any stage of the procedure).
The one exception was that following lysis of foreskin adhesions, EMLA + sucrose + RB was superior (NIPS 2.25 for EMLA + sucrose + RB vs. NIPS 4.4 for EMLA + sucrose + DPNB vs. NIPS 4.3 for EMLA + sucrose vs. NIPS 5.8 for EMLA alone). In terms of crying time during the procedure, all interventions were significantly superior to EMLA alone. Of the interventions, crying time was statistically and clinically significantly shorter with EMLA + sucrose + RB (5.78 seconds vs. 11.5 for EMLA + sucrose + DPNB vs. 16.5 for EMLA + sucrose vs. 45.4 for EMLA alone). This was a single-center study and the procedures were performed by a pediatric urologist rather than by a general pediatrician, which potentially limits applicability.
Bottom line
All tested analgesia modalities for neonatal circumcision were superior to EMLA alone. The most effective analgesia of those tested was EMLA + sucrose + penile ring block.
Citation
Sharara-Chami R et al. Combination analgesia for neonatal circumcision: a randomized controlled trial. Pediatrics. 2017. doi: 10.1542/peds.2017-1935.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and a clinical assistant professor of pediatrics at Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia.
Multiple pain management interventions exist
Multiple pain management interventions exist
Clinical question
What is the optimal way to manage analgesia during neonatal circumcision?
Background
Neonatal circumcision is one of the most commonly performed surgical procedures. The American Academy of Pediatrics in 2012 noted that the health benefits outweigh the minor risks of the procedure, but that parents should make the decision to circumcise based on their own cultural, ethical, and religious beliefs.
One of the primary risks of neonatal circumcision is pain during and after the procedure. Multiple methods for managing analgesia exist, but it is unknown what combination of methods is optimal. Usual analgesia techniques include: local anesthetic cream composed of lidocaine and prilocaine (EMLA) applied to the skin prior to the procedure; oral sucrose solution given throughout the procedure; dorsal penile nerve block (DPNB); and penile ring block (RB).
Study design
Single-center, double-blinded, randomized, controlled trial.
Setting
Multispecialty freestanding hospital.
Synopsis
Parents of infant boys born at 36-41 weeks’ gestation who chose to have their children circumcised were offered participation in the study. Of 83 eligible participants, 70 were randomized, with 10 in the control group (EMLA only) and 20 in each intervention (EMLA + sucrose, EMLA + sucrose + RB, EMLA + sucrose + DPNB). A single pediatric urologist performed all circumcisions using the Gomco clamp technique.
A video camera recorded the infant’s face and upper torso during the procedure. Two researchers, who were blinded to the analgesia plan, scored these videos using a modified Neonatal Infant Pain Scale (NIPS). The NIPS used ranged from 0 to 6, with 6 considered severe pain. For rating purposes, the procedure was divided into 6 stages with a NIPS score assigned at each stage. There were no significant differences in baseline characteristics among the groups; no significant differences in the duration of the procedure by intervention; and there were no complications. Interrater reliability for the NIPS was good (kappa, 0.84). All interventions were superior to EMLA alone, with significantly decreased NIPS for all stages of the procedure. No significant differences in NIPS were found among the following:
EMLA + sucrose.
EMLA + sucrose + RB.
EMLA + sucrose + DPNB (for any stage of the procedure).
The one exception was that following lysis of foreskin adhesions, EMLA + sucrose + RB was superior (NIPS 2.25 for EMLA + sucrose + RB vs. NIPS 4.4 for EMLA + sucrose + DPNB vs. NIPS 4.3 for EMLA + sucrose vs. NIPS 5.8 for EMLA alone). In terms of crying time during the procedure, all interventions were significantly superior to EMLA alone. Of the interventions, crying time was statistically and clinically significantly shorter with EMLA + sucrose + RB (5.78 seconds vs. 11.5 for EMLA + sucrose + DPNB vs. 16.5 for EMLA + sucrose vs. 45.4 for EMLA alone). This was a single-center study and the procedures were performed by a pediatric urologist rather than by a general pediatrician, which potentially limits applicability.
Bottom line
All tested analgesia modalities for neonatal circumcision were superior to EMLA alone. The most effective analgesia of those tested was EMLA + sucrose + penile ring block.
Citation
Sharara-Chami R et al. Combination analgesia for neonatal circumcision: a randomized controlled trial. Pediatrics. 2017. doi: 10.1542/peds.2017-1935.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and a clinical assistant professor of pediatrics at Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia.
Clinical question
What is the optimal way to manage analgesia during neonatal circumcision?
Background
Neonatal circumcision is one of the most commonly performed surgical procedures. The American Academy of Pediatrics in 2012 noted that the health benefits outweigh the minor risks of the procedure, but that parents should make the decision to circumcise based on their own cultural, ethical, and religious beliefs.
One of the primary risks of neonatal circumcision is pain during and after the procedure. Multiple methods for managing analgesia exist, but it is unknown what combination of methods is optimal. Usual analgesia techniques include: local anesthetic cream composed of lidocaine and prilocaine (EMLA) applied to the skin prior to the procedure; oral sucrose solution given throughout the procedure; dorsal penile nerve block (DPNB); and penile ring block (RB).
Study design
Single-center, double-blinded, randomized, controlled trial.
Setting
Multispecialty freestanding hospital.
Synopsis
Parents of infant boys born at 36-41 weeks’ gestation who chose to have their children circumcised were offered participation in the study. Of 83 eligible participants, 70 were randomized, with 10 in the control group (EMLA only) and 20 in each intervention (EMLA + sucrose, EMLA + sucrose + RB, EMLA + sucrose + DPNB). A single pediatric urologist performed all circumcisions using the Gomco clamp technique.
A video camera recorded the infant’s face and upper torso during the procedure. Two researchers, who were blinded to the analgesia plan, scored these videos using a modified Neonatal Infant Pain Scale (NIPS). The NIPS used ranged from 0 to 6, with 6 considered severe pain. For rating purposes, the procedure was divided into 6 stages with a NIPS score assigned at each stage. There were no significant differences in baseline characteristics among the groups; no significant differences in the duration of the procedure by intervention; and there were no complications. Interrater reliability for the NIPS was good (kappa, 0.84). All interventions were superior to EMLA alone, with significantly decreased NIPS for all stages of the procedure. No significant differences in NIPS were found among the following:
EMLA + sucrose.
EMLA + sucrose + RB.
EMLA + sucrose + DPNB (for any stage of the procedure).
The one exception was that following lysis of foreskin adhesions, EMLA + sucrose + RB was superior (NIPS 2.25 for EMLA + sucrose + RB vs. NIPS 4.4 for EMLA + sucrose + DPNB vs. NIPS 4.3 for EMLA + sucrose vs. NIPS 5.8 for EMLA alone). In terms of crying time during the procedure, all interventions were significantly superior to EMLA alone. Of the interventions, crying time was statistically and clinically significantly shorter with EMLA + sucrose + RB (5.78 seconds vs. 11.5 for EMLA + sucrose + DPNB vs. 16.5 for EMLA + sucrose vs. 45.4 for EMLA alone). This was a single-center study and the procedures were performed by a pediatric urologist rather than by a general pediatrician, which potentially limits applicability.
Bottom line
All tested analgesia modalities for neonatal circumcision were superior to EMLA alone. The most effective analgesia of those tested was EMLA + sucrose + penile ring block.
Citation
Sharara-Chami R et al. Combination analgesia for neonatal circumcision: a randomized controlled trial. Pediatrics. 2017. doi: 10.1542/peds.2017-1935.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and a clinical assistant professor of pediatrics at Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia.
When your patients are your neighbors
“We’ll have one strawberry sugar cone, two chocolate swirls, and a mocha almond.”

“Dr. Wilkoff, I haven’t seen you in ... must be 5 years. You look great! How’s retirement going?”
“You look great too, Kim. The neighborhood has needed an ice cream parlor like yours for a long time. How’s the family?”
Alerted by the commotion of our catching up, Kim’s husband came outside to see what was going on. Looking at my wife, he said, “You know he saved our daughter’s life?”
Well, not exactly. A timely referral to a psychologist I knew was good with eating disorders had started the slow process of returning their anorectic daughter to health. I thanked him and tried to put a more historically correct spin on his story.
Most of my encounters with former patients and their parents aren’t as dramatic as this one at Kim’s Ice Cream Shack, but they always leave me with a warm, positive feeling that stays with me all day. Every now and then they include a compliment or a thank you, but most of the time the conversations are dominated by questions about how the other are doing and what our families are up to.
One of the perks of living in the town where you practice is that your patients also are your neighbors. Not every physician views this proximity as a positive, but for me, it was a gift that has kept on giving after I retired.
Our house phone number was always listed in the phone book, and I can count on the fingers of two hands how many times in 40 years that I received what I would consider an inappropriate or invasive call. Our office offered evening and weekend hours and a generous schedule of phone-in call times. But I’m convinced that it was the neighbor-to-neighbor relationship that kept the work/home balance intact. Even though I may have helped a plumber and his wife with their sick children, that professional arrangement didn’t include a free pass to call him after hours if I knew my leaking faucet could wait until the weekend was over.

By the same token, when a patient or a customer is also your neighbor there is an unspoken ethic that the service you provide must be your best effort. That’s not an admission that I was in the habit of offering substandard care to “folks from away,” but there is special motivation when your work is being scrutinized by people you’re likely to see next week at the grocery store checkout.
Office visits with neighbors often tended to take longer because there was a tendency to drift off topic and ask about a sibling’s baseball game I had read about in the paper or how the lobster catch was running that season. On the other hand, I must admit that I did my share of reporting (really it was bragging) on my own children’s accomplishments.
But now I’m reaping the benefits of those extra minutes invested in the office, because I suspect former patients and their families are more likely to want to reminisce when we meet in a restaurant or at the farmers’ market.
If you are a young physician and worrying about finding a good work/life balance, I urge you to consider living and working and then staying on in a place in which your patients also will be your neighbors. It will enrich your work experience and repay you many times over when it’s time to retire.
If you can’t find that place, at least treat your patients as though they were your neighbors.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
“We’ll have one strawberry sugar cone, two chocolate swirls, and a mocha almond.”
“Dr. Wilkoff, I haven’t seen you in ... must be 5 years. You look great! How’s retirement going?”
“You look great too, Kim. The neighborhood has needed an ice cream parlor like yours for a long time. How’s the family?”
Alerted by the commotion of our catching up, Kim’s husband came outside to see what was going on. Looking at my wife, he said, “You know he saved our daughter’s life?”
Well, not exactly. A timely referral to a psychologist I knew was good with eating disorders had started the slow process of returning their anorectic daughter to health. I thanked him and tried to put a more historically correct spin on his story.
Most of my encounters with former patients and their parents aren’t as dramatic as this one at Kim’s Ice Cream Shack, but they always leave me with a warm, positive feeling that stays with me all day. Every now and then they include a compliment or a thank you, but most of the time the conversations are dominated by questions about how the other are doing and what our families are up to.
One of the perks of living in the town where you practice is that your patients also are your neighbors. Not every physician views this proximity as a positive, but for me, it was a gift that has kept on giving after I retired.
Our house phone number was always listed in the phone book, and I can count on the fingers of two hands how many times in 40 years that I received what I would consider an inappropriate or invasive call. Our office offered evening and weekend hours and a generous schedule of phone-in call times. But I’m convinced that it was the neighbor-to-neighbor relationship that kept the work/home balance intact. Even though I may have helped a plumber and his wife with their sick children, that professional arrangement didn’t include a free pass to call him after hours if I knew my leaking faucet could wait until the weekend was over.
By the same token, when a patient or a customer is also your neighbor there is an unspoken ethic that the service you provide must be your best effort. That’s not an admission that I was in the habit of offering substandard care to “folks from away,” but there is special motivation when your work is being scrutinized by people you’re likely to see next week at the grocery store checkout.
Office visits with neighbors often tended to take longer because there was a tendency to drift off topic and ask about a sibling’s baseball game I had read about in the paper or how the lobster catch was running that season. On the other hand, I must admit that I did my share of reporting (really it was bragging) on my own children’s accomplishments.
But now I’m reaping the benefits of those extra minutes invested in the office, because I suspect former patients and their families are more likely to want to reminisce when we meet in a restaurant or at the farmers’ market.
If you are a young physician and worrying about finding a good work/life balance, I urge you to consider living and working and then staying on in a place in which your patients also will be your neighbors. It will enrich your work experience and repay you many times over when it’s time to retire.
If you can’t find that place, at least treat your patients as though they were your neighbors.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
“We’ll have one strawberry sugar cone, two chocolate swirls, and a mocha almond.”
“Dr. Wilkoff, I haven’t seen you in ... must be 5 years. You look great! How’s retirement going?”
“You look great too, Kim. The neighborhood has needed an ice cream parlor like yours for a long time. How’s the family?”
Alerted by the commotion of our catching up, Kim’s husband came outside to see what was going on. Looking at my wife, he said, “You know he saved our daughter’s life?”
Well, not exactly. A timely referral to a psychologist I knew was good with eating disorders had started the slow process of returning their anorectic daughter to health. I thanked him and tried to put a more historically correct spin on his story.
Most of my encounters with former patients and their parents aren’t as dramatic as this one at Kim’s Ice Cream Shack, but they always leave me with a warm, positive feeling that stays with me all day. Every now and then they include a compliment or a thank you, but most of the time the conversations are dominated by questions about how the other are doing and what our families are up to.
One of the perks of living in the town where you practice is that your patients also are your neighbors. Not every physician views this proximity as a positive, but for me, it was a gift that has kept on giving after I retired.
Our house phone number was always listed in the phone book, and I can count on the fingers of two hands how many times in 40 years that I received what I would consider an inappropriate or invasive call. Our office offered evening and weekend hours and a generous schedule of phone-in call times. But I’m convinced that it was the neighbor-to-neighbor relationship that kept the work/home balance intact. Even though I may have helped a plumber and his wife with their sick children, that professional arrangement didn’t include a free pass to call him after hours if I knew my leaking faucet could wait until the weekend was over.
By the same token, when a patient or a customer is also your neighbor there is an unspoken ethic that the service you provide must be your best effort. That’s not an admission that I was in the habit of offering substandard care to “folks from away,” but there is special motivation when your work is being scrutinized by people you’re likely to see next week at the grocery store checkout.
Office visits with neighbors often tended to take longer because there was a tendency to drift off topic and ask about a sibling’s baseball game I had read about in the paper or how the lobster catch was running that season. On the other hand, I must admit that I did my share of reporting (really it was bragging) on my own children’s accomplishments.
But now I’m reaping the benefits of those extra minutes invested in the office, because I suspect former patients and their families are more likely to want to reminisce when we meet in a restaurant or at the farmers’ market.
If you are a young physician and worrying about finding a good work/life balance, I urge you to consider living and working and then staying on in a place in which your patients also will be your neighbors. It will enrich your work experience and repay you many times over when it’s time to retire.
If you can’t find that place, at least treat your patients as though they were your neighbors.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Many physicians don’t discuss MenB vaccine in teen well visits
survey results showed.

About half of pediatricians and one-third of family physicians said they always or often initiate discussion of MenB vaccines for adolescents aged 16- 18 year, according to a report on the survey published in Pediatrics.
However, it is challenging to say whether or not that level of discussion is on track with ideal clinical practice, according to Allison Kempe, MD, MPH, of the University of Colorado at Denver and Children’s Hospital Colorado, Aurora, and her coauthors. While MenB vaccines are recommended in this setting, the new Category B designation used for the recommendation indicates that the vaccines “may be administered” in the context of individual clinical decision making.
While some interpret the new Category B recommendation to mean that a discussion should always occur, others may interpret the recommendation as applicable to their own assessment of risks and benefits, without the need to involve patients and parents.
“Providers not initiating a discussion may not think the time required to discuss the MenB vaccine is justified by the risks posed by the disease or the benefits offered by these vaccines,” wrote Dr. Kempe and her associates. “Alternatively, they may have a low level of awareness regarding the disease or the MenB vaccine and feel insufficiently knowledgeable to have an informed discussion about the pros and cons of vaccination. They also may have been entirely unaware of the ACIP [Advisory Committee on Immunization Practices] recommendation for MenB vaccination.”
Dr. Kempe and her colleagues invited a nationally representative sample of primary care physicians to complete the survey, which was administered via Internet or mail between October and December 2016. They heard back from 374 of 475 (79%) pediatricians and 286 of 441 (65%) family physicians.
A total of 50% of pediatricians and 31% of family physicians said they always or often discussed MenB vaccines during routine visits with adolescents aged 16-18 years, with slightly higher percentages saying they initiated discussions during precollege physical exams, according to the report. Of the pediatricians, 58% recommended the MenB vaccine to those in this age group, compared with 50% of family physicians. Not all physicians who recommended the vaccine reported consistently initiating a discussion about it.
Nearly three-fourths of pediatricians and 41% of family physicians reported currently administering the MenB vaccine in their practices, the authors said, adding that greater awareness of disease outbreaks was linked to higher likelihood of discussing the vaccine, while working in an HMO setting was linked to lower likelihood of initiating that discussion.
Recommending MenB vaccination was closely tied to discussing the vaccine. Physicians who said they initiated discussion almost always reported making a recommendation to vaccinate, and conversely, those who rarely initiated discussions were unlikely to recommend it, according to Dr. Kempe and her colleagues.
Factors that made physicians more likely to recommend vaccine included awareness of outbreaks, effectiveness and safety data, and duration of vaccine protection.
The Category B recommendation, on the other hand, was one of the key factors that made physicians less likely to recommend MenB vaccine, according to this survey. ACIP made the Category B recommendation in October 2015, stating that those aged 16- 23 years may be vaccinated, with a preferred age of 16-18 years for administration. The accompanying rationale for the Category B designation referenced the low disease prevalence and insufficient data on effectiveness and safety for the two vaccines, which were both licensed under an accelerated approval mechanism following the outbreaks that have occurred on college campuses.
The Centers for Disease Control and Prevention did not provide additional guidance on how that Category B recommendation should be implemented, Dr. Kempe and her coauthors noted in their report.
“With our data, we highlight the challenges providers face with implementing recommendations for vaccination based on individual clinical decision making when they have limited experience with a disease and limited knowledge of a new vaccine,” they wrote.
The research was funded by the CDC. Dr. Kempe and her coauthors reported no relevant financial relationships or potential conflicts of interest.
SOURCE: Kempe A et al. Pediatrics. 2018 Aug 20. doi: 10.1542/peds.2018-0344.
These survey results suggest primary care physicians’ zeal for discussing meningococcal serogroup B (MenB) vaccines during adolescent well visits is affected by the recommendation that they “may be administered” in this setting, according to Michael T. Brady, MD.
“When pediatricians are fortunate to have 16- to 18-year-old patients come to a routine visit, there are many important issues to discuss, such as sexual activity, tobacco, alcohol and illicit drug use, contraception, and mental health,” Dr. Brady wrote in an editorial discussing the survey results.
The new Category B designation, used by the Advisory Committee on Immunization Practices to recommend MenB vaccines for adolescents and young adults not at increased risk for meningococcal B disease, puts the recommendation in the realm of individual clinical decision making, Dr. Brady noted. “Without specific and clear guidance as to how to quantify benefits, risks, and costs for their individual patients, it is easy to understand why providers would have disparate responses reflecting the challenge associated with a new vaccine and a new vaccine recommendation classification.”
Pediatricians can achieve “exceptional rates of immunization” when recommendations are “evidence based, clear, and unequivocal,” but by contrast, they will remain challenged by Category B or permissive recommendations when clear guidance on how to implement the recommendation is not provided, he concluded.
Dr. Brad is a pediatric infectious diseases specialist at Nationwide Children’s Hospital and the Ohio State University, Columbus. These comments are from his editorial in Pediatrics (2018 Aug 20. doi: 10.1542/peds.2018-1633) . Dr. Brady reported receiving royalties from Up-To-Date for a chapter on human herpesvirus 6, but received no external funding for this editorial. He reported no potential conflicts of interest.
These survey results suggest primary care physicians’ zeal for discussing meningococcal serogroup B (MenB) vaccines during adolescent well visits is affected by the recommendation that they “may be administered” in this setting, according to Michael T. Brady, MD.
“When pediatricians are fortunate to have 16- to 18-year-old patients come to a routine visit, there are many important issues to discuss, such as sexual activity, tobacco, alcohol and illicit drug use, contraception, and mental health,” Dr. Brady wrote in an editorial discussing the survey results.
The new Category B designation, used by the Advisory Committee on Immunization Practices to recommend MenB vaccines for adolescents and young adults not at increased risk for meningococcal B disease, puts the recommendation in the realm of individual clinical decision making, Dr. Brady noted. “Without specific and clear guidance as to how to quantify benefits, risks, and costs for their individual patients, it is easy to understand why providers would have disparate responses reflecting the challenge associated with a new vaccine and a new vaccine recommendation classification.”
Pediatricians can achieve “exceptional rates of immunization” when recommendations are “evidence based, clear, and unequivocal,” but by contrast, they will remain challenged by Category B or permissive recommendations when clear guidance on how to implement the recommendation is not provided, he concluded.
Dr. Brad is a pediatric infectious diseases specialist at Nationwide Children’s Hospital and the Ohio State University, Columbus. These comments are from his editorial in Pediatrics (2018 Aug 20. doi: 10.1542/peds.2018-1633) . Dr. Brady reported receiving royalties from Up-To-Date for a chapter on human herpesvirus 6, but received no external funding for this editorial. He reported no potential conflicts of interest.
These survey results suggest primary care physicians’ zeal for discussing meningococcal serogroup B (MenB) vaccines during adolescent well visits is affected by the recommendation that they “may be administered” in this setting, according to Michael T. Brady, MD.
“When pediatricians are fortunate to have 16- to 18-year-old patients come to a routine visit, there are many important issues to discuss, such as sexual activity, tobacco, alcohol and illicit drug use, contraception, and mental health,” Dr. Brady wrote in an editorial discussing the survey results.
The new Category B designation, used by the Advisory Committee on Immunization Practices to recommend MenB vaccines for adolescents and young adults not at increased risk for meningococcal B disease, puts the recommendation in the realm of individual clinical decision making, Dr. Brady noted. “Without specific and clear guidance as to how to quantify benefits, risks, and costs for their individual patients, it is easy to understand why providers would have disparate responses reflecting the challenge associated with a new vaccine and a new vaccine recommendation classification.”
Pediatricians can achieve “exceptional rates of immunization” when recommendations are “evidence based, clear, and unequivocal,” but by contrast, they will remain challenged by Category B or permissive recommendations when clear guidance on how to implement the recommendation is not provided, he concluded.
Dr. Brad is a pediatric infectious diseases specialist at Nationwide Children’s Hospital and the Ohio State University, Columbus. These comments are from his editorial in Pediatrics (2018 Aug 20. doi: 10.1542/peds.2018-1633) . Dr. Brady reported receiving royalties from Up-To-Date for a chapter on human herpesvirus 6, but received no external funding for this editorial. He reported no potential conflicts of interest.
survey results showed.
About half of pediatricians and one-third of family physicians said they always or often initiate discussion of MenB vaccines for adolescents aged 16- 18 year, according to a report on the survey published in Pediatrics.
However, it is challenging to say whether or not that level of discussion is on track with ideal clinical practice, according to Allison Kempe, MD, MPH, of the University of Colorado at Denver and Children’s Hospital Colorado, Aurora, and her coauthors. While MenB vaccines are recommended in this setting, the new Category B designation used for the recommendation indicates that the vaccines “may be administered” in the context of individual clinical decision making.
While some interpret the new Category B recommendation to mean that a discussion should always occur, others may interpret the recommendation as applicable to their own assessment of risks and benefits, without the need to involve patients and parents.
“Providers not initiating a discussion may not think the time required to discuss the MenB vaccine is justified by the risks posed by the disease or the benefits offered by these vaccines,” wrote Dr. Kempe and her associates. “Alternatively, they may have a low level of awareness regarding the disease or the MenB vaccine and feel insufficiently knowledgeable to have an informed discussion about the pros and cons of vaccination. They also may have been entirely unaware of the ACIP [Advisory Committee on Immunization Practices] recommendation for MenB vaccination.”
Dr. Kempe and her colleagues invited a nationally representative sample of primary care physicians to complete the survey, which was administered via Internet or mail between October and December 2016. They heard back from 374 of 475 (79%) pediatricians and 286 of 441 (65%) family physicians.
A total of 50% of pediatricians and 31% of family physicians said they always or often discussed MenB vaccines during routine visits with adolescents aged 16-18 years, with slightly higher percentages saying they initiated discussions during precollege physical exams, according to the report. Of the pediatricians, 58% recommended the MenB vaccine to those in this age group, compared with 50% of family physicians. Not all physicians who recommended the vaccine reported consistently initiating a discussion about it.
Nearly three-fourths of pediatricians and 41% of family physicians reported currently administering the MenB vaccine in their practices, the authors said, adding that greater awareness of disease outbreaks was linked to higher likelihood of discussing the vaccine, while working in an HMO setting was linked to lower likelihood of initiating that discussion.
Recommending MenB vaccination was closely tied to discussing the vaccine. Physicians who said they initiated discussion almost always reported making a recommendation to vaccinate, and conversely, those who rarely initiated discussions were unlikely to recommend it, according to Dr. Kempe and her colleagues.
Factors that made physicians more likely to recommend vaccine included awareness of outbreaks, effectiveness and safety data, and duration of vaccine protection.
The Category B recommendation, on the other hand, was one of the key factors that made physicians less likely to recommend MenB vaccine, according to this survey. ACIP made the Category B recommendation in October 2015, stating that those aged 16- 23 years may be vaccinated, with a preferred age of 16-18 years for administration. The accompanying rationale for the Category B designation referenced the low disease prevalence and insufficient data on effectiveness and safety for the two vaccines, which were both licensed under an accelerated approval mechanism following the outbreaks that have occurred on college campuses.
The Centers for Disease Control and Prevention did not provide additional guidance on how that Category B recommendation should be implemented, Dr. Kempe and her coauthors noted in their report.
“With our data, we highlight the challenges providers face with implementing recommendations for vaccination based on individual clinical decision making when they have limited experience with a disease and limited knowledge of a new vaccine,” they wrote.
The research was funded by the CDC. Dr. Kempe and her coauthors reported no relevant financial relationships or potential conflicts of interest.
SOURCE: Kempe A et al. Pediatrics. 2018 Aug 20. doi: 10.1542/peds.2018-0344.
survey results showed.
About half of pediatricians and one-third of family physicians said they always or often initiate discussion of MenB vaccines for adolescents aged 16- 18 year, according to a report on the survey published in Pediatrics.
However, it is challenging to say whether or not that level of discussion is on track with ideal clinical practice, according to Allison Kempe, MD, MPH, of the University of Colorado at Denver and Children’s Hospital Colorado, Aurora, and her coauthors. While MenB vaccines are recommended in this setting, the new Category B designation used for the recommendation indicates that the vaccines “may be administered” in the context of individual clinical decision making.
While some interpret the new Category B recommendation to mean that a discussion should always occur, others may interpret the recommendation as applicable to their own assessment of risks and benefits, without the need to involve patients and parents.
“Providers not initiating a discussion may not think the time required to discuss the MenB vaccine is justified by the risks posed by the disease or the benefits offered by these vaccines,” wrote Dr. Kempe and her associates. “Alternatively, they may have a low level of awareness regarding the disease or the MenB vaccine and feel insufficiently knowledgeable to have an informed discussion about the pros and cons of vaccination. They also may have been entirely unaware of the ACIP [Advisory Committee on Immunization Practices] recommendation for MenB vaccination.”
Dr. Kempe and her colleagues invited a nationally representative sample of primary care physicians to complete the survey, which was administered via Internet or mail between October and December 2016. They heard back from 374 of 475 (79%) pediatricians and 286 of 441 (65%) family physicians.
A total of 50% of pediatricians and 31% of family physicians said they always or often discussed MenB vaccines during routine visits with adolescents aged 16-18 years, with slightly higher percentages saying they initiated discussions during precollege physical exams, according to the report. Of the pediatricians, 58% recommended the MenB vaccine to those in this age group, compared with 50% of family physicians. Not all physicians who recommended the vaccine reported consistently initiating a discussion about it.
Nearly three-fourths of pediatricians and 41% of family physicians reported currently administering the MenB vaccine in their practices, the authors said, adding that greater awareness of disease outbreaks was linked to higher likelihood of discussing the vaccine, while working in an HMO setting was linked to lower likelihood of initiating that discussion.
Recommending MenB vaccination was closely tied to discussing the vaccine. Physicians who said they initiated discussion almost always reported making a recommendation to vaccinate, and conversely, those who rarely initiated discussions were unlikely to recommend it, according to Dr. Kempe and her colleagues.
Factors that made physicians more likely to recommend vaccine included awareness of outbreaks, effectiveness and safety data, and duration of vaccine protection.
The Category B recommendation, on the other hand, was one of the key factors that made physicians less likely to recommend MenB vaccine, according to this survey. ACIP made the Category B recommendation in October 2015, stating that those aged 16- 23 years may be vaccinated, with a preferred age of 16-18 years for administration. The accompanying rationale for the Category B designation referenced the low disease prevalence and insufficient data on effectiveness and safety for the two vaccines, which were both licensed under an accelerated approval mechanism following the outbreaks that have occurred on college campuses.
The Centers for Disease Control and Prevention did not provide additional guidance on how that Category B recommendation should be implemented, Dr. Kempe and her coauthors noted in their report.
“With our data, we highlight the challenges providers face with implementing recommendations for vaccination based on individual clinical decision making when they have limited experience with a disease and limited knowledge of a new vaccine,” they wrote.
The research was funded by the CDC. Dr. Kempe and her coauthors reported no relevant financial relationships or potential conflicts of interest.
SOURCE: Kempe A et al. Pediatrics. 2018 Aug 20. doi: 10.1542/peds.2018-0344.
FROM PEDIATRICS
Key clinical point: Many primary care physicians are not discussing serogroup B meningococcal (MenB) vaccines during routine adolescent visits, possibly because of uncertainty about how current recommendations should be implemented.
Major finding: Half of pediatricians and 31% of family physicians said they always or often discussed MenB during routine visits with those aged 16- 18 years. Of the pediatricians, 58% recommended the MenB vaccine to adolescents in this age group, compared with 50% of family physicians.
Study details: A late 2016 survey of a nationally representative sample of 374 pediatricians and 286 family physicians.
Disclosures: The research was funded by the Centers for Disease Control and Prevention. Dr. Kempe and her coauthors reported no relevant financial relationships or potential conflicts of interest.
Source: Kempe A et al. Pediatrics. 2018 Aug 20. doi: 10.1542/peds.2018-0344.