User login
Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
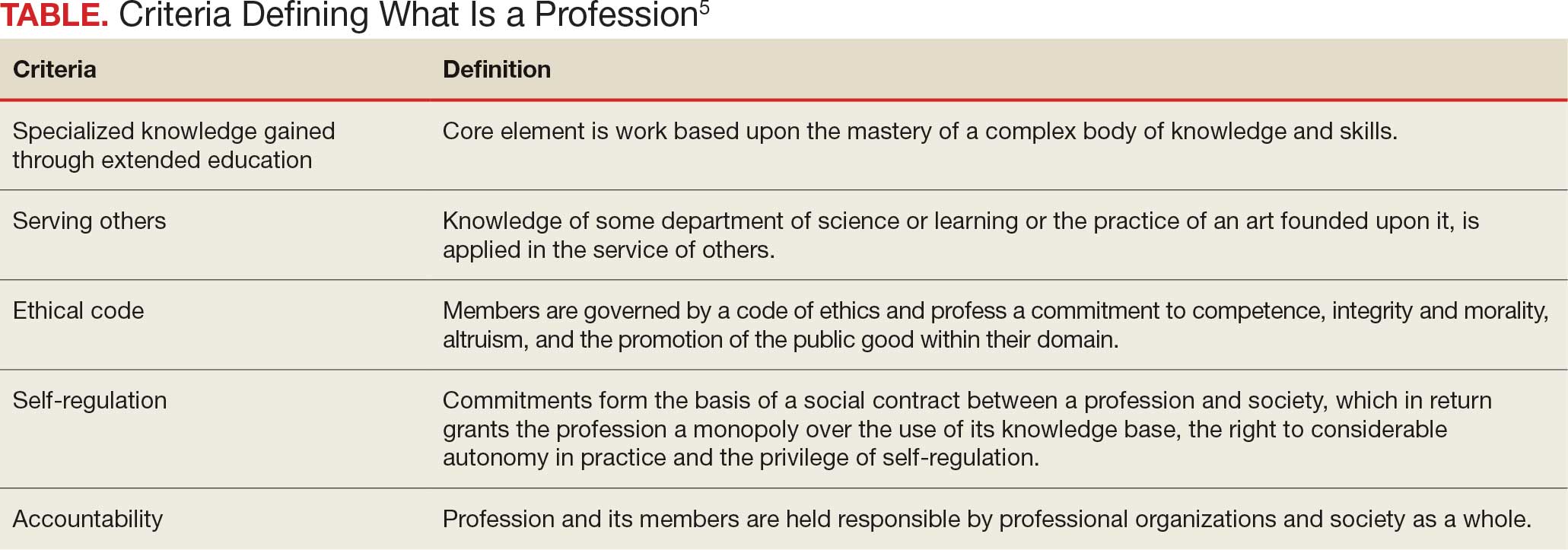
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?

The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
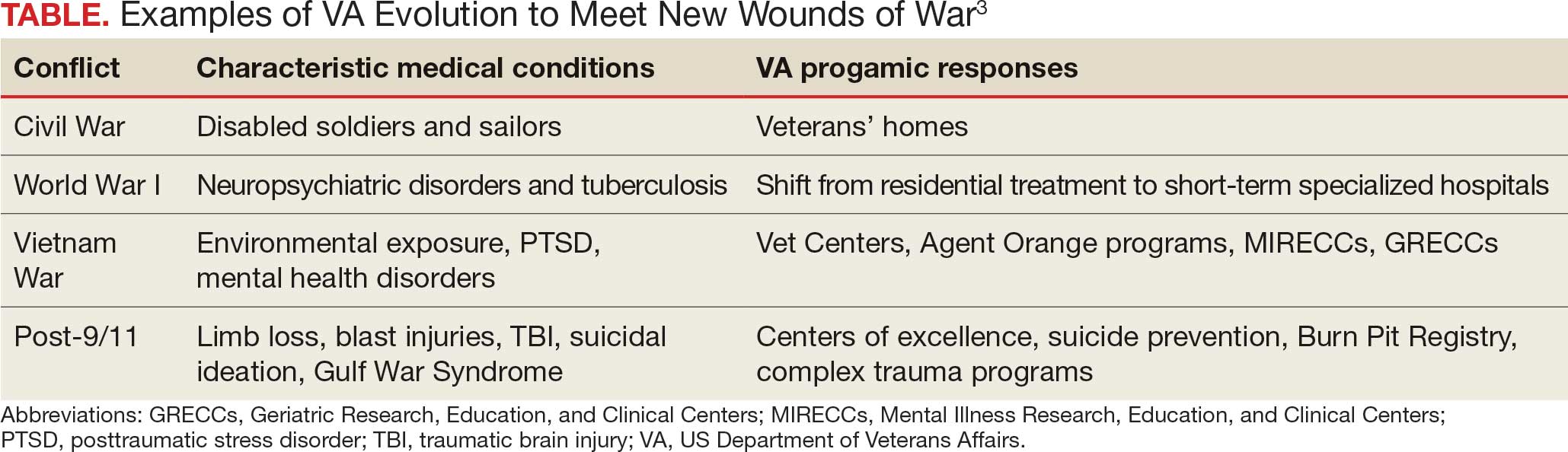
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration

Divine Calling and Human Rank: The Locus of Authority for Military Chaplains
Divine Calling and Human Rank: The Locus of Authority for Military Chaplains
Render unto Caesar the things that are Caesar’s, and to God the things that are God’s.
Matthew 22:21
While in my 20s, I taught religious education at a church on the Army base where I was born and had the honor of working with military chaplains. During my US Department of Veterans Affairs career, I closely collaborated with chaplains—many of whom were veterans—on patient care and ethics consultations. Some were quite proud of their rank and interested in climbing the ladder of promotion. A few made sure you knew what they wore or had worn on their uniform, while most were incredibly humble and sheepish when soldiers saluted them. Those visible responses to rank may be hidden if chaplains will no longer be permitted to wear insignia indicating their grade.
Department of War Secretary Peter Hegseth, a combat veteran who has championed a “combative” form of Christianity, announced in April 2026 that chaplains would no longer wear their rank on their uniform.1 Details of how this shift will be translated into regulation, policy, and actions were not provided. Secretary Hegseth did not remove the actual rank of members of the chaplain corps and they would retain their rank, attendant pay, benefits, responsibilities, and privileges. However, instead of bearing the insignia of their military station, under this new policy only the symbol of their religious profession would identify them. Currently, both a military officer’s rank and religious symbol are displayed.2
Useful insight can be gained from an historical perspective, which demonstrates that the concerns and contention about the issue of chaplain’s wearing rank are not new. There have been chaplains in the US Army since 1775.3 Army chaplains initially wore only a religious symbol on their clothing. In April 1914, chaplain leaders successful argued that chaplains deserved the privileges, respect, and prospect for promotion that rank symbolized and where authorized to display their position. Four years later, General Jack Pershing cabled the then Secretary of War opposing the new policy: “Believe the work of chaplains would be facilitated if they were not given military rank ... Many of our principal ministers believe that their relations would be closer if they did not have military titles and did not wear insignia.”4 Interestingly, Secretary Hegseth articulated the same concern: “A chaplain is first and foremost a chaplain and an officer second. This change is a visual representation of that fact.”5
Hegseth has stated that in recent years the military chaplain corps had drifted too far in the direction of providing spiritual counseling and psychological support. This contravenes the current competencies especially for company-grade military chaplains who primarily minister to the moral distress and spiritual needs of service members.4 The removal of rank is thus best understood as part of Secretary Hegseth’s broader plan to remake the chaplain corps into his vision of religious ministry in the military.5
Secretary Hegseth proffered several arguments for the necessity of removing rank in part to reorient the chaplain corps to what he calls a more fundamental mission. The first was theological: chaplains need to prioritize their “divine calling” rather than any human distinction. Chaplain theologians and ethicists have expressed similar concerns that in wearing rank, military chaplains become servants of the state and not of God. Adam Tietje articulates the corruptive influence this shift in the source of legitimacy has on the military chaplain’s spiritual mission:
This undermines the ability of chaplains to provide care and counsel to both soldiers and leaders that is not muddied with the interests of the military. Chaplains without rank are better positioned to hear and advocate for their soldier’s matters of conscience as well as bear witness to the moral claims of their respective religious communities especially about war itself.3
The second argument is pastoral. Hegseth contends that service members of lower rank would feel more comfortable and secure approaching chaplains with no outward sign of their higher position. Chaplain interactions with military personnel carry a degree of confidentiality higher than that of either doctors or lawyers. Chaplains, as they were in the past, remain divided on this important consideration.4,5
The third argument is ethical in nature. Secretary Hegseth contends that excluding any manifestation of military rank, “speaks to the difficult balance of the duality” of the role.6 It seems he is proposing that chaplains displaying only the image of their faith commitment symbolically resolves the inherent moral conflict between serving human masters as a military officer, and the divine as a minister.7 Military chaplains and health care professionals are all too familiar with the dilemma of having 2 masters and the challenge of negotiating legally and ethically overlapping roles.8-10
This may seem to some like a minor change in chaplain etiquette to some, but to others it signals a significant ethical and political change with potential import beyond chaplaincy. One military commentator has suggested the move sets a dangerous precedent that could eventually be applied to both health care professionals and the judge advocate corps.11 At this point this is only speculation and its slippery slope arguments are logically suspect without evidence. Yet at least 1 study suggests that the influence of military physician’s rank on patient care may lead to inequities in the care delivered to patients with lower grade.12
It is commanders who are the decision-makers in the military. Chaplains who are field grade officers serve as trusted staff advisors in moral, ethical, and spiritual matters.4 Some chaplains fear that without rank leaders at all levels will not have adequate trust and sufficient respect to heed their crucial counsel especially regarding high-stakes strategic decisions in wartime.8 The more serious concern is with a major shift in the locus of authority to determine the professional identity of chaplains, that could in theory be expanded to impact military health care practitioners, and attorneys. The independent expert judgment of these professionals regarding what is necessary to fulfil their respective roles in providing spiritual ministry, medical care, and legal is critical to uphold the highest values of the US military.11 Chaplains have long struggled with what they owe to the Caesar and to God: how the Secretary’s recent decision will shape that rendering is uncertain. What is certain is that military chaplains of all faiths and in every branch of the armed services will continue to minister to their brothers and sisters in arms with courage and compassion.
- Baker R, Graham R. Pete Hegseth and his ‘battle cry’ for a new christian crusade. The New York Times. December 6, 2024. Accessed April 24, 2026. https://www.nytimes.com/2024/12/05/us/hegseth-church-crusades.html
- Sampson E. Hegseth removes rank insignia from military chaplains. Military Times. March 25, 2026. Accessed April 24, 2026. https://www.militarytimes.com/news/pentagon-congress/2026/03/25/hegseth-removes-rank-insignia-from-military-chaplains/
- Tietje A. A seductive confusion of authority: military chaplains and the wearing of rank. J Church State. 2020;62:506-524.
- Morris JT. Military chaplaincy in the USA: an unfolding of roles and functions. In: Weiss H, Federschmidt KH, Louw DJ, et al, eds. Care, Healing, and Human Well-Being Within Interreligious Discourses. African Sun Media; 2021:319-333.
- Cox M. Hegseth’s push for chaplain’s to shed remove rank sparks debate. Air and Space Forces Magazine. March 27, 2026. Accessed April 29, 2026. https://www.airandspaceforces.com/chaplains-ordered-to-shed-rank-ret-af-leaders-question-move/
- Mitchell E. Hegseth: Military chaplains will no longer display rank. The Hill. March 25, 2026. Accessed April 24, 2026. https://thehill.com/policy/defense/5800026-pete-hegseth-military-chaplains-faith-insignia/
- Banks AM. Hegseth’s removal of the top Army chaplain raises ‘troubling questions’ from Black denomination. Religious News Service. April 9, 2026. Accessed April 24, 2026. https://religionnews.com/2026/04/09/army-chaplains-chiefs-firing-prompts-serious-concern-from-black-baptist-denomination/
- Burchard WW. Role conflicts of military chaplains. Amer Sociolog Rev. 1954;19:528-535 https://www.jstor.org/stable/2087790
- Sturtz DL. Commitment. Mil Med. 2001;166:741-744.
- Carver D. New Department of War policy: military chaplains no longer wear rank insignia. North American Mission Board. April 8, 2026. Accessed April 24, 2026. https://www.namb.net/resource/new-department-of-war-policy-military-chaplains-no-longer-wear-rank-insignia/
- Petri D. If chaplains are ‘officers second,’ which staff corps officers are next? Military Times. April 1, 2026. Accessed April 24, 2026. https://www.militarytimes.com/opinion/2026/04/01/if-chaplains-are-officers-second-which-staff-corps-officers-are-next/
- Schwab SD, Singh M. How power shapes behavior: evidence from physicians. Science. 2024; 384:802-807.
Render unto Caesar the things that are Caesar’s, and to God the things that are God’s.
Matthew 22:21
While in my 20s, I taught religious education at a church on the Army base where I was born and had the honor of working with military chaplains. During my US Department of Veterans Affairs career, I closely collaborated with chaplains—many of whom were veterans—on patient care and ethics consultations. Some were quite proud of their rank and interested in climbing the ladder of promotion. A few made sure you knew what they wore or had worn on their uniform, while most were incredibly humble and sheepish when soldiers saluted them. Those visible responses to rank may be hidden if chaplains will no longer be permitted to wear insignia indicating their grade.
Department of War Secretary Peter Hegseth, a combat veteran who has championed a “combative” form of Christianity, announced in April 2026 that chaplains would no longer wear their rank on their uniform.1 Details of how this shift will be translated into regulation, policy, and actions were not provided. Secretary Hegseth did not remove the actual rank of members of the chaplain corps and they would retain their rank, attendant pay, benefits, responsibilities, and privileges. However, instead of bearing the insignia of their military station, under this new policy only the symbol of their religious profession would identify them. Currently, both a military officer’s rank and religious symbol are displayed.2
Useful insight can be gained from an historical perspective, which demonstrates that the concerns and contention about the issue of chaplain’s wearing rank are not new. There have been chaplains in the US Army since 1775.3 Army chaplains initially wore only a religious symbol on their clothing. In April 1914, chaplain leaders successful argued that chaplains deserved the privileges, respect, and prospect for promotion that rank symbolized and where authorized to display their position. Four years later, General Jack Pershing cabled the then Secretary of War opposing the new policy: “Believe the work of chaplains would be facilitated if they were not given military rank ... Many of our principal ministers believe that their relations would be closer if they did not have military titles and did not wear insignia.”4 Interestingly, Secretary Hegseth articulated the same concern: “A chaplain is first and foremost a chaplain and an officer second. This change is a visual representation of that fact.”5
Hegseth has stated that in recent years the military chaplain corps had drifted too far in the direction of providing spiritual counseling and psychological support. This contravenes the current competencies especially for company-grade military chaplains who primarily minister to the moral distress and spiritual needs of service members.4 The removal of rank is thus best understood as part of Secretary Hegseth’s broader plan to remake the chaplain corps into his vision of religious ministry in the military.5
Secretary Hegseth proffered several arguments for the necessity of removing rank in part to reorient the chaplain corps to what he calls a more fundamental mission. The first was theological: chaplains need to prioritize their “divine calling” rather than any human distinction. Chaplain theologians and ethicists have expressed similar concerns that in wearing rank, military chaplains become servants of the state and not of God. Adam Tietje articulates the corruptive influence this shift in the source of legitimacy has on the military chaplain’s spiritual mission:
This undermines the ability of chaplains to provide care and counsel to both soldiers and leaders that is not muddied with the interests of the military. Chaplains without rank are better positioned to hear and advocate for their soldier’s matters of conscience as well as bear witness to the moral claims of their respective religious communities especially about war itself.3
The second argument is pastoral. Hegseth contends that service members of lower rank would feel more comfortable and secure approaching chaplains with no outward sign of their higher position. Chaplain interactions with military personnel carry a degree of confidentiality higher than that of either doctors or lawyers. Chaplains, as they were in the past, remain divided on this important consideration.4,5
The third argument is ethical in nature. Secretary Hegseth contends that excluding any manifestation of military rank, “speaks to the difficult balance of the duality” of the role.6 It seems he is proposing that chaplains displaying only the image of their faith commitment symbolically resolves the inherent moral conflict between serving human masters as a military officer, and the divine as a minister.7 Military chaplains and health care professionals are all too familiar with the dilemma of having 2 masters and the challenge of negotiating legally and ethically overlapping roles.8-10
This may seem to some like a minor change in chaplain etiquette to some, but to others it signals a significant ethical and political change with potential import beyond chaplaincy. One military commentator has suggested the move sets a dangerous precedent that could eventually be applied to both health care professionals and the judge advocate corps.11 At this point this is only speculation and its slippery slope arguments are logically suspect without evidence. Yet at least 1 study suggests that the influence of military physician’s rank on patient care may lead to inequities in the care delivered to patients with lower grade.12
It is commanders who are the decision-makers in the military. Chaplains who are field grade officers serve as trusted staff advisors in moral, ethical, and spiritual matters.4 Some chaplains fear that without rank leaders at all levels will not have adequate trust and sufficient respect to heed their crucial counsel especially regarding high-stakes strategic decisions in wartime.8 The more serious concern is with a major shift in the locus of authority to determine the professional identity of chaplains, that could in theory be expanded to impact military health care practitioners, and attorneys. The independent expert judgment of these professionals regarding what is necessary to fulfil their respective roles in providing spiritual ministry, medical care, and legal is critical to uphold the highest values of the US military.11 Chaplains have long struggled with what they owe to the Caesar and to God: how the Secretary’s recent decision will shape that rendering is uncertain. What is certain is that military chaplains of all faiths and in every branch of the armed services will continue to minister to their brothers and sisters in arms with courage and compassion.
Render unto Caesar the things that are Caesar’s, and to God the things that are God’s.
Matthew 22:21
While in my 20s, I taught religious education at a church on the Army base where I was born and had the honor of working with military chaplains. During my US Department of Veterans Affairs career, I closely collaborated with chaplains—many of whom were veterans—on patient care and ethics consultations. Some were quite proud of their rank and interested in climbing the ladder of promotion. A few made sure you knew what they wore or had worn on their uniform, while most were incredibly humble and sheepish when soldiers saluted them. Those visible responses to rank may be hidden if chaplains will no longer be permitted to wear insignia indicating their grade.
Department of War Secretary Peter Hegseth, a combat veteran who has championed a “combative” form of Christianity, announced in April 2026 that chaplains would no longer wear their rank on their uniform.1 Details of how this shift will be translated into regulation, policy, and actions were not provided. Secretary Hegseth did not remove the actual rank of members of the chaplain corps and they would retain their rank, attendant pay, benefits, responsibilities, and privileges. However, instead of bearing the insignia of their military station, under this new policy only the symbol of their religious profession would identify them. Currently, both a military officer’s rank and religious symbol are displayed.2
Useful insight can be gained from an historical perspective, which demonstrates that the concerns and contention about the issue of chaplain’s wearing rank are not new. There have been chaplains in the US Army since 1775.3 Army chaplains initially wore only a religious symbol on their clothing. In April 1914, chaplain leaders successful argued that chaplains deserved the privileges, respect, and prospect for promotion that rank symbolized and where authorized to display their position. Four years later, General Jack Pershing cabled the then Secretary of War opposing the new policy: “Believe the work of chaplains would be facilitated if they were not given military rank ... Many of our principal ministers believe that their relations would be closer if they did not have military titles and did not wear insignia.”4 Interestingly, Secretary Hegseth articulated the same concern: “A chaplain is first and foremost a chaplain and an officer second. This change is a visual representation of that fact.”5
Hegseth has stated that in recent years the military chaplain corps had drifted too far in the direction of providing spiritual counseling and psychological support. This contravenes the current competencies especially for company-grade military chaplains who primarily minister to the moral distress and spiritual needs of service members.4 The removal of rank is thus best understood as part of Secretary Hegseth’s broader plan to remake the chaplain corps into his vision of religious ministry in the military.5
Secretary Hegseth proffered several arguments for the necessity of removing rank in part to reorient the chaplain corps to what he calls a more fundamental mission. The first was theological: chaplains need to prioritize their “divine calling” rather than any human distinction. Chaplain theologians and ethicists have expressed similar concerns that in wearing rank, military chaplains become servants of the state and not of God. Adam Tietje articulates the corruptive influence this shift in the source of legitimacy has on the military chaplain’s spiritual mission:
This undermines the ability of chaplains to provide care and counsel to both soldiers and leaders that is not muddied with the interests of the military. Chaplains without rank are better positioned to hear and advocate for their soldier’s matters of conscience as well as bear witness to the moral claims of their respective religious communities especially about war itself.3
The second argument is pastoral. Hegseth contends that service members of lower rank would feel more comfortable and secure approaching chaplains with no outward sign of their higher position. Chaplain interactions with military personnel carry a degree of confidentiality higher than that of either doctors or lawyers. Chaplains, as they were in the past, remain divided on this important consideration.4,5
The third argument is ethical in nature. Secretary Hegseth contends that excluding any manifestation of military rank, “speaks to the difficult balance of the duality” of the role.6 It seems he is proposing that chaplains displaying only the image of their faith commitment symbolically resolves the inherent moral conflict between serving human masters as a military officer, and the divine as a minister.7 Military chaplains and health care professionals are all too familiar with the dilemma of having 2 masters and the challenge of negotiating legally and ethically overlapping roles.8-10
This may seem to some like a minor change in chaplain etiquette to some, but to others it signals a significant ethical and political change with potential import beyond chaplaincy. One military commentator has suggested the move sets a dangerous precedent that could eventually be applied to both health care professionals and the judge advocate corps.11 At this point this is only speculation and its slippery slope arguments are logically suspect without evidence. Yet at least 1 study suggests that the influence of military physician’s rank on patient care may lead to inequities in the care delivered to patients with lower grade.12
It is commanders who are the decision-makers in the military. Chaplains who are field grade officers serve as trusted staff advisors in moral, ethical, and spiritual matters.4 Some chaplains fear that without rank leaders at all levels will not have adequate trust and sufficient respect to heed their crucial counsel especially regarding high-stakes strategic decisions in wartime.8 The more serious concern is with a major shift in the locus of authority to determine the professional identity of chaplains, that could in theory be expanded to impact military health care practitioners, and attorneys. The independent expert judgment of these professionals regarding what is necessary to fulfil their respective roles in providing spiritual ministry, medical care, and legal is critical to uphold the highest values of the US military.11 Chaplains have long struggled with what they owe to the Caesar and to God: how the Secretary’s recent decision will shape that rendering is uncertain. What is certain is that military chaplains of all faiths and in every branch of the armed services will continue to minister to their brothers and sisters in arms with courage and compassion.
- Baker R, Graham R. Pete Hegseth and his ‘battle cry’ for a new christian crusade. The New York Times. December 6, 2024. Accessed April 24, 2026. https://www.nytimes.com/2024/12/05/us/hegseth-church-crusades.html
- Sampson E. Hegseth removes rank insignia from military chaplains. Military Times. March 25, 2026. Accessed April 24, 2026. https://www.militarytimes.com/news/pentagon-congress/2026/03/25/hegseth-removes-rank-insignia-from-military-chaplains/
- Tietje A. A seductive confusion of authority: military chaplains and the wearing of rank. J Church State. 2020;62:506-524.
- Morris JT. Military chaplaincy in the USA: an unfolding of roles and functions. In: Weiss H, Federschmidt KH, Louw DJ, et al, eds. Care, Healing, and Human Well-Being Within Interreligious Discourses. African Sun Media; 2021:319-333.
- Cox M. Hegseth’s push for chaplain’s to shed remove rank sparks debate. Air and Space Forces Magazine. March 27, 2026. Accessed April 29, 2026. https://www.airandspaceforces.com/chaplains-ordered-to-shed-rank-ret-af-leaders-question-move/
- Mitchell E. Hegseth: Military chaplains will no longer display rank. The Hill. March 25, 2026. Accessed April 24, 2026. https://thehill.com/policy/defense/5800026-pete-hegseth-military-chaplains-faith-insignia/
- Banks AM. Hegseth’s removal of the top Army chaplain raises ‘troubling questions’ from Black denomination. Religious News Service. April 9, 2026. Accessed April 24, 2026. https://religionnews.com/2026/04/09/army-chaplains-chiefs-firing-prompts-serious-concern-from-black-baptist-denomination/
- Burchard WW. Role conflicts of military chaplains. Amer Sociolog Rev. 1954;19:528-535 https://www.jstor.org/stable/2087790
- Sturtz DL. Commitment. Mil Med. 2001;166:741-744.
- Carver D. New Department of War policy: military chaplains no longer wear rank insignia. North American Mission Board. April 8, 2026. Accessed April 24, 2026. https://www.namb.net/resource/new-department-of-war-policy-military-chaplains-no-longer-wear-rank-insignia/
- Petri D. If chaplains are ‘officers second,’ which staff corps officers are next? Military Times. April 1, 2026. Accessed April 24, 2026. https://www.militarytimes.com/opinion/2026/04/01/if-chaplains-are-officers-second-which-staff-corps-officers-are-next/
- Schwab SD, Singh M. How power shapes behavior: evidence from physicians. Science. 2024; 384:802-807.
- Baker R, Graham R. Pete Hegseth and his ‘battle cry’ for a new christian crusade. The New York Times. December 6, 2024. Accessed April 24, 2026. https://www.nytimes.com/2024/12/05/us/hegseth-church-crusades.html
- Sampson E. Hegseth removes rank insignia from military chaplains. Military Times. March 25, 2026. Accessed April 24, 2026. https://www.militarytimes.com/news/pentagon-congress/2026/03/25/hegseth-removes-rank-insignia-from-military-chaplains/
- Tietje A. A seductive confusion of authority: military chaplains and the wearing of rank. J Church State. 2020;62:506-524.
- Morris JT. Military chaplaincy in the USA: an unfolding of roles and functions. In: Weiss H, Federschmidt KH, Louw DJ, et al, eds. Care, Healing, and Human Well-Being Within Interreligious Discourses. African Sun Media; 2021:319-333.
- Cox M. Hegseth’s push for chaplain’s to shed remove rank sparks debate. Air and Space Forces Magazine. March 27, 2026. Accessed April 29, 2026. https://www.airandspaceforces.com/chaplains-ordered-to-shed-rank-ret-af-leaders-question-move/
- Mitchell E. Hegseth: Military chaplains will no longer display rank. The Hill. March 25, 2026. Accessed April 24, 2026. https://thehill.com/policy/defense/5800026-pete-hegseth-military-chaplains-faith-insignia/
- Banks AM. Hegseth’s removal of the top Army chaplain raises ‘troubling questions’ from Black denomination. Religious News Service. April 9, 2026. Accessed April 24, 2026. https://religionnews.com/2026/04/09/army-chaplains-chiefs-firing-prompts-serious-concern-from-black-baptist-denomination/
- Burchard WW. Role conflicts of military chaplains. Amer Sociolog Rev. 1954;19:528-535 https://www.jstor.org/stable/2087790
- Sturtz DL. Commitment. Mil Med. 2001;166:741-744.
- Carver D. New Department of War policy: military chaplains no longer wear rank insignia. North American Mission Board. April 8, 2026. Accessed April 24, 2026. https://www.namb.net/resource/new-department-of-war-policy-military-chaplains-no-longer-wear-rank-insignia/
- Petri D. If chaplains are ‘officers second,’ which staff corps officers are next? Military Times. April 1, 2026. Accessed April 24, 2026. https://www.militarytimes.com/opinion/2026/04/01/if-chaplains-are-officers-second-which-staff-corps-officers-are-next/
- Schwab SD, Singh M. How power shapes behavior: evidence from physicians. Science. 2024; 384:802-807.
Divine Calling and Human Rank: The Locus of Authority for Military Chaplains
Divine Calling and Human Rank: The Locus of Authority for Military Chaplains

Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
The Gap in VA Dental Care is Nothing to Smile About
The Gap in VA Dental Care is Nothing to Smile About
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
The Gap in VA Dental Care is Nothing to Smile About
The Gap in VA Dental Care is Nothing to Smile About
American Hunger Games: Food Insecurity Among the Military and Veterans
American Hunger Games: Food Insecurity Among the Military and Veterans
The requisites of government are that there be sufficiency of food, sufficiency of military equipment, and the confidence of the people in their ruler.
Analects by Confucius1
From ancient festivals to modern holidays, autumn has long been associated with the gathering of the harvest. Friends and families come together around tables laden with delicious food to enjoy the pleasures of peace and plenty. During these celebrations, we must never forget that without the strength of the nation’s military and the service of its veterans, this freedom and abundance would not be possible. Our debt of gratitude to the current and former members of the armed services makes the fact that a substantial minority experiences food insecurity not only a human tragedy, but a travesty of the nation’s promise to support those who wear or have worn the uniform.
The National Defense Authorization Act for Fiscal Year 2020 charged the Secretary of Defense to investigate food insecurity among active-duty service members and their dependents.2 The RAND Corporation conducted the assessment and, based on the results of its analysis, made recommendations to reduce hunger among armed forces members and their families.3
The RAND study found that 10% of active-duty military met US Department of Agriculture (USDA) criteria for very low food security; another 15% were classified as having low food security. The USDA defines food insecurity with hunger as “reports of multiple indications of disrupted eating patterns and reduced food intake.” USDA defines low food security as “reports of reduced quality, variety, or desirability of diet. Little or no indication of reduced food intake.”4
As someone who grew up on an Army base with the commissary a short trip from military housing, I was unpleasantly surprised that food insecurity was more common among in-service members living on post. I was even more dismayed to read that a variety of factors constrained 14% of active-duty military experiencing food insecurity to seek public assistance to feed themselves and their families. As with so many health care and social services, (eg, mental health care), those wearing the uniform were concerned that participating in a food assistance program would damage their career or stigmatize them. Others did not seek help, perhaps because they believed they were not eligible, and in many cases were correct: they did not qualify for food banks or food stamps due to receiving other benefits. A variety of factors contribute to periods of food insecurity among military families, including remote or rural bases that lack access to grocery stores or jobs for partners or other family members, and low base military pay.5
Food insecurity is an even more serious concern among veterans who are frequently older and have more comorbidities, often leading to unemployment and homelessness. Feeding America, the nation’s largest organization of community food banks, estimates that 1 in 9 working-age veterans are food insecure.5 US Department of Veterans Affairs (VA) statistics indicate that veterans are 7% more likely to experience food insecurity than other sectors of the population.6 The Veterans Health Administration has recognized that food insecurity is directly related to medical problems already common among veterans, including diabetes, obesity, and depression. Women and minority veterans are the most at risk of food insecurity.7
Recognizing that many veterans are at risk of food insecurity, the US Department of Defense and VA have taken steps to try and reduce hunger among those who serve. In response to the shocking statistic that food insecurity was found in 27% of Iraq and Afghanistan veterans, the VA and Rockefeller Foundation are partnering on the Food as Medicine initiative to improve veteran nutrition as a means of improving nutrition-related health consequences of food insecurity.8
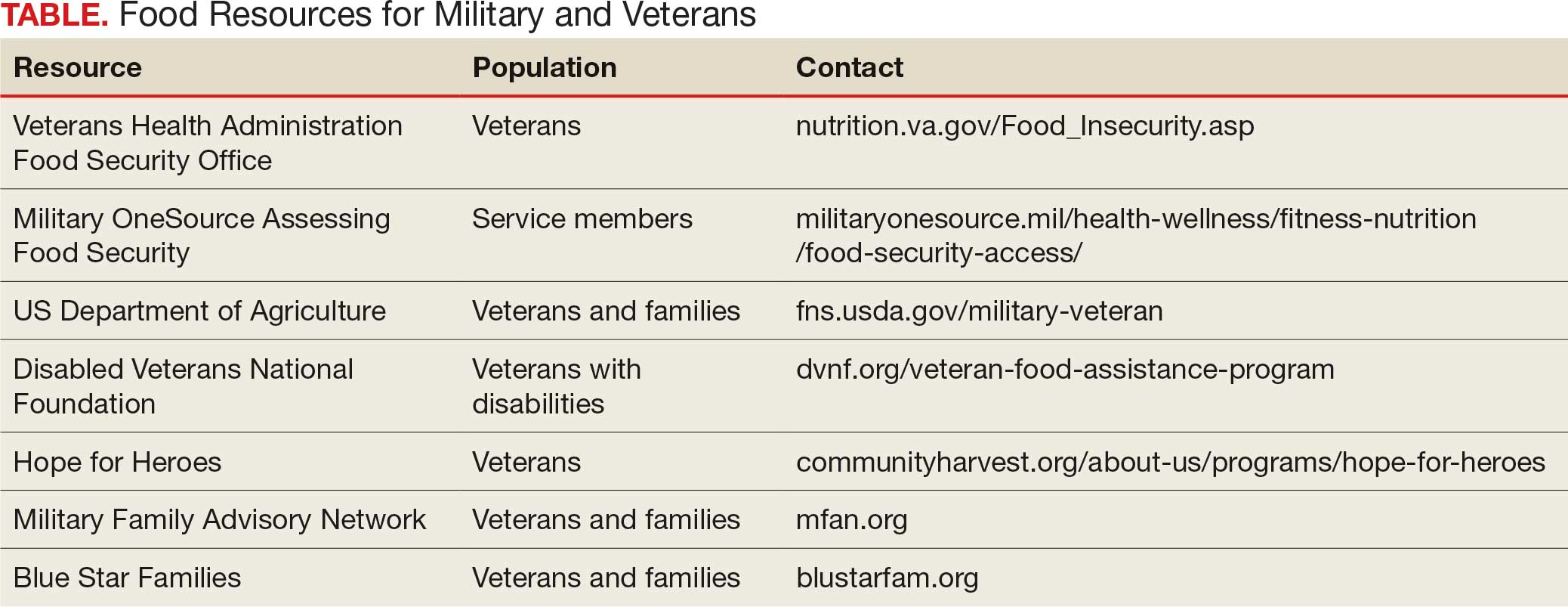
Like many federal practitioners, I was unaware of the food insecurity assistance available to active-duty service members or veterans, or how to help individuals access it. In addition to the resources outlined in the Table, there are many community-based options open to anyone, including veterans and service members.
I have written columns on many difficult issues in my years as the Editor-in-Chief of Federal Practitioner, but personally this is one of the most distressing editorials I have ever published. That individuals dedicated to defending our rights and protecting our safety should be compelled to go hungry or not know if they have enough money at the end of the month to buy food is manifestly unjust. It is challenging when faced with such a large-scale injustice to think we cannot make a difference, but that resignation or abdication only magnifies this inequity. I have a friend who kept giving back even after they retired from federal service: they volunteered at a community garden and brought produce to the local food bank and helped distribute it. That may seem too much for those still working yet almost anyone can pick up a few items on their weekly shopping trip and donate them to a food drive.
As we approach Veterans Day, let’s not just express our gratitude to our military and veterans in words but in deeds like feeding the hungry and urging elected representatives to fulfill their commitment to ensure that service members and veterans and their families do not experience food insecurity. Confucian wisdom written in a very distant time and vastly dissimilar context still rings true: there are direct and critical links between food and trust and between hunger and the military.1
Dawson MM. The Wisdom of Confucius: A Collection of the Ethical Sayings of Confucius and of his disciples. International Pocket Library; 1932.
National Defense Authorization Act for Fiscal Year 2020. 116th Cong (2019), Public Law 116-92. U.S. Government Printing Office. https://www.govinfo.gov/content/pkg/PLAW-116publ92/html/PLAW-116publ92.htm
Asch BJ, Rennane S, Trail TE, et al. Food insecurity among members of the armed forces and their dependents. RAND Corporation. January 3, 2023. Accessed September 22, 2025. https://www.rand.org/pubs/research_reports/RRA1230-1.html
US Department of Agriculture Economic Research Service. Food Security in the U.S.—Definitions of Food Security. US Department of Agriculture Economic Research Service. January 10, 2025. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security
Active military and veteran food insecurity. Feeding America. Accessed September 22, 2025. https://www.feedingamerica.org/hunger-in-america/food-insecurity-in-veterans
Pradun S. Find access to stop food insecurity in your community. VA News. September 19, 2025. Accessed September 22, 2025. https://news.va.gov/142733/find-access-stop-food-insecurity-your-community/
Cohen AJ, Dosa DM, Rudolph JL, et al. Risk factors for veteran food insecurity: findings from a National US Department of Veterans Affairs Food Insecurity Screener. Public Health Nutr. 2022;25:819-828. doi:10.1017/S1368980021004584
Chen C. VA and Rockefeller Foundation collaborate to access food for Veterans. VA News. September 5, 2023. Accessed September 22, 2025. https://news.va.gov/123228/va-rockefeller-foundation-expand-access-to-food/
The requisites of government are that there be sufficiency of food, sufficiency of military equipment, and the confidence of the people in their ruler.
Analects by Confucius1
From ancient festivals to modern holidays, autumn has long been associated with the gathering of the harvest. Friends and families come together around tables laden with delicious food to enjoy the pleasures of peace and plenty. During these celebrations, we must never forget that without the strength of the nation’s military and the service of its veterans, this freedom and abundance would not be possible. Our debt of gratitude to the current and former members of the armed services makes the fact that a substantial minority experiences food insecurity not only a human tragedy, but a travesty of the nation’s promise to support those who wear or have worn the uniform.
The National Defense Authorization Act for Fiscal Year 2020 charged the Secretary of Defense to investigate food insecurity among active-duty service members and their dependents.2 The RAND Corporation conducted the assessment and, based on the results of its analysis, made recommendations to reduce hunger among armed forces members and their families.3
The RAND study found that 10% of active-duty military met US Department of Agriculture (USDA) criteria for very low food security; another 15% were classified as having low food security. The USDA defines food insecurity with hunger as “reports of multiple indications of disrupted eating patterns and reduced food intake.” USDA defines low food security as “reports of reduced quality, variety, or desirability of diet. Little or no indication of reduced food intake.”4
As someone who grew up on an Army base with the commissary a short trip from military housing, I was unpleasantly surprised that food insecurity was more common among in-service members living on post. I was even more dismayed to read that a variety of factors constrained 14% of active-duty military experiencing food insecurity to seek public assistance to feed themselves and their families. As with so many health care and social services, (eg, mental health care), those wearing the uniform were concerned that participating in a food assistance program would damage their career or stigmatize them. Others did not seek help, perhaps because they believed they were not eligible, and in many cases were correct: they did not qualify for food banks or food stamps due to receiving other benefits. A variety of factors contribute to periods of food insecurity among military families, including remote or rural bases that lack access to grocery stores or jobs for partners or other family members, and low base military pay.5
Food insecurity is an even more serious concern among veterans who are frequently older and have more comorbidities, often leading to unemployment and homelessness. Feeding America, the nation’s largest organization of community food banks, estimates that 1 in 9 working-age veterans are food insecure.5 US Department of Veterans Affairs (VA) statistics indicate that veterans are 7% more likely to experience food insecurity than other sectors of the population.6 The Veterans Health Administration has recognized that food insecurity is directly related to medical problems already common among veterans, including diabetes, obesity, and depression. Women and minority veterans are the most at risk of food insecurity.7
Recognizing that many veterans are at risk of food insecurity, the US Department of Defense and VA have taken steps to try and reduce hunger among those who serve. In response to the shocking statistic that food insecurity was found in 27% of Iraq and Afghanistan veterans, the VA and Rockefeller Foundation are partnering on the Food as Medicine initiative to improve veteran nutrition as a means of improving nutrition-related health consequences of food insecurity.8
Like many federal practitioners, I was unaware of the food insecurity assistance available to active-duty service members or veterans, or how to help individuals access it. In addition to the resources outlined in the Table, there are many community-based options open to anyone, including veterans and service members.
I have written columns on many difficult issues in my years as the Editor-in-Chief of Federal Practitioner, but personally this is one of the most distressing editorials I have ever published. That individuals dedicated to defending our rights and protecting our safety should be compelled to go hungry or not know if they have enough money at the end of the month to buy food is manifestly unjust. It is challenging when faced with such a large-scale injustice to think we cannot make a difference, but that resignation or abdication only magnifies this inequity. I have a friend who kept giving back even after they retired from federal service: they volunteered at a community garden and brought produce to the local food bank and helped distribute it. That may seem too much for those still working yet almost anyone can pick up a few items on their weekly shopping trip and donate them to a food drive.
As we approach Veterans Day, let’s not just express our gratitude to our military and veterans in words but in deeds like feeding the hungry and urging elected representatives to fulfill their commitment to ensure that service members and veterans and their families do not experience food insecurity. Confucian wisdom written in a very distant time and vastly dissimilar context still rings true: there are direct and critical links between food and trust and between hunger and the military.1
The requisites of government are that there be sufficiency of food, sufficiency of military equipment, and the confidence of the people in their ruler.
Analects by Confucius1
From ancient festivals to modern holidays, autumn has long been associated with the gathering of the harvest. Friends and families come together around tables laden with delicious food to enjoy the pleasures of peace and plenty. During these celebrations, we must never forget that without the strength of the nation’s military and the service of its veterans, this freedom and abundance would not be possible. Our debt of gratitude to the current and former members of the armed services makes the fact that a substantial minority experiences food insecurity not only a human tragedy, but a travesty of the nation’s promise to support those who wear or have worn the uniform.
The National Defense Authorization Act for Fiscal Year 2020 charged the Secretary of Defense to investigate food insecurity among active-duty service members and their dependents.2 The RAND Corporation conducted the assessment and, based on the results of its analysis, made recommendations to reduce hunger among armed forces members and their families.3
The RAND study found that 10% of active-duty military met US Department of Agriculture (USDA) criteria for very low food security; another 15% were classified as having low food security. The USDA defines food insecurity with hunger as “reports of multiple indications of disrupted eating patterns and reduced food intake.” USDA defines low food security as “reports of reduced quality, variety, or desirability of diet. Little or no indication of reduced food intake.”4
As someone who grew up on an Army base with the commissary a short trip from military housing, I was unpleasantly surprised that food insecurity was more common among in-service members living on post. I was even more dismayed to read that a variety of factors constrained 14% of active-duty military experiencing food insecurity to seek public assistance to feed themselves and their families. As with so many health care and social services, (eg, mental health care), those wearing the uniform were concerned that participating in a food assistance program would damage their career or stigmatize them. Others did not seek help, perhaps because they believed they were not eligible, and in many cases were correct: they did not qualify for food banks or food stamps due to receiving other benefits. A variety of factors contribute to periods of food insecurity among military families, including remote or rural bases that lack access to grocery stores or jobs for partners or other family members, and low base military pay.5
Food insecurity is an even more serious concern among veterans who are frequently older and have more comorbidities, often leading to unemployment and homelessness. Feeding America, the nation’s largest organization of community food banks, estimates that 1 in 9 working-age veterans are food insecure.5 US Department of Veterans Affairs (VA) statistics indicate that veterans are 7% more likely to experience food insecurity than other sectors of the population.6 The Veterans Health Administration has recognized that food insecurity is directly related to medical problems already common among veterans, including diabetes, obesity, and depression. Women and minority veterans are the most at risk of food insecurity.7
Recognizing that many veterans are at risk of food insecurity, the US Department of Defense and VA have taken steps to try and reduce hunger among those who serve. In response to the shocking statistic that food insecurity was found in 27% of Iraq and Afghanistan veterans, the VA and Rockefeller Foundation are partnering on the Food as Medicine initiative to improve veteran nutrition as a means of improving nutrition-related health consequences of food insecurity.8
Like many federal practitioners, I was unaware of the food insecurity assistance available to active-duty service members or veterans, or how to help individuals access it. In addition to the resources outlined in the Table, there are many community-based options open to anyone, including veterans and service members.
I have written columns on many difficult issues in my years as the Editor-in-Chief of Federal Practitioner, but personally this is one of the most distressing editorials I have ever published. That individuals dedicated to defending our rights and protecting our safety should be compelled to go hungry or not know if they have enough money at the end of the month to buy food is manifestly unjust. It is challenging when faced with such a large-scale injustice to think we cannot make a difference, but that resignation or abdication only magnifies this inequity. I have a friend who kept giving back even after they retired from federal service: they volunteered at a community garden and brought produce to the local food bank and helped distribute it. That may seem too much for those still working yet almost anyone can pick up a few items on their weekly shopping trip and donate them to a food drive.
As we approach Veterans Day, let’s not just express our gratitude to our military and veterans in words but in deeds like feeding the hungry and urging elected representatives to fulfill their commitment to ensure that service members and veterans and their families do not experience food insecurity. Confucian wisdom written in a very distant time and vastly dissimilar context still rings true: there are direct and critical links between food and trust and between hunger and the military.1
Dawson MM. The Wisdom of Confucius: A Collection of the Ethical Sayings of Confucius and of his disciples. International Pocket Library; 1932.
National Defense Authorization Act for Fiscal Year 2020. 116th Cong (2019), Public Law 116-92. U.S. Government Printing Office. https://www.govinfo.gov/content/pkg/PLAW-116publ92/html/PLAW-116publ92.htm
Asch BJ, Rennane S, Trail TE, et al. Food insecurity among members of the armed forces and their dependents. RAND Corporation. January 3, 2023. Accessed September 22, 2025. https://www.rand.org/pubs/research_reports/RRA1230-1.html
US Department of Agriculture Economic Research Service. Food Security in the U.S.—Definitions of Food Security. US Department of Agriculture Economic Research Service. January 10, 2025. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security
Active military and veteran food insecurity. Feeding America. Accessed September 22, 2025. https://www.feedingamerica.org/hunger-in-america/food-insecurity-in-veterans
Pradun S. Find access to stop food insecurity in your community. VA News. September 19, 2025. Accessed September 22, 2025. https://news.va.gov/142733/find-access-stop-food-insecurity-your-community/
Cohen AJ, Dosa DM, Rudolph JL, et al. Risk factors for veteran food insecurity: findings from a National US Department of Veterans Affairs Food Insecurity Screener. Public Health Nutr. 2022;25:819-828. doi:10.1017/S1368980021004584
Chen C. VA and Rockefeller Foundation collaborate to access food for Veterans. VA News. September 5, 2023. Accessed September 22, 2025. https://news.va.gov/123228/va-rockefeller-foundation-expand-access-to-food/
Dawson MM. The Wisdom of Confucius: A Collection of the Ethical Sayings of Confucius and of his disciples. International Pocket Library; 1932.
National Defense Authorization Act for Fiscal Year 2020. 116th Cong (2019), Public Law 116-92. U.S. Government Printing Office. https://www.govinfo.gov/content/pkg/PLAW-116publ92/html/PLAW-116publ92.htm
Asch BJ, Rennane S, Trail TE, et al. Food insecurity among members of the armed forces and their dependents. RAND Corporation. January 3, 2023. Accessed September 22, 2025. https://www.rand.org/pubs/research_reports/RRA1230-1.html
US Department of Agriculture Economic Research Service. Food Security in the U.S.—Definitions of Food Security. US Department of Agriculture Economic Research Service. January 10, 2025. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security
Active military and veteran food insecurity. Feeding America. Accessed September 22, 2025. https://www.feedingamerica.org/hunger-in-america/food-insecurity-in-veterans
Pradun S. Find access to stop food insecurity in your community. VA News. September 19, 2025. Accessed September 22, 2025. https://news.va.gov/142733/find-access-stop-food-insecurity-your-community/
Cohen AJ, Dosa DM, Rudolph JL, et al. Risk factors for veteran food insecurity: findings from a National US Department of Veterans Affairs Food Insecurity Screener. Public Health Nutr. 2022;25:819-828. doi:10.1017/S1368980021004584
Chen C. VA and Rockefeller Foundation collaborate to access food for Veterans. VA News. September 5, 2023. Accessed September 22, 2025. https://news.va.gov/123228/va-rockefeller-foundation-expand-access-to-food/
American Hunger Games: Food Insecurity Among the Military and Veterans
American Hunger Games: Food Insecurity Among the Military and Veterans

When The Giants and Those Who Stand on Their Shoulders Are Gone: The Loss of VA Institutional Memory
When The Giants and Those Who Stand on Their Shoulders Are Gone: The Loss of VA Institutional Memory
If I have seen further, it is by standing on the shoulders of giants.
Sir Isaac Newton (1642-1727) 1
Early in residency, I decided I only wanted to work at the US Department of Veterans Affairs (VA). It was a way to follow the example of service that my parents, an Army doctor and nurse, had set. I spent much of my residency, including all of my last year of training, at a VA medical center, hoping a vacancy would open in the psychiatry service. In those days, VA jobs were hard to come by; doctors spent their entire careers in the system, only retiring after decades of commitment to its unique mission. Finally, close to graduation, one of my favorite attending physicians left his post. After mountains of paperwork and running the human resources obstacle course with the usual stumbles, I arrived at my dream job as a VA psychiatrist.
So, it is with immense sadness and even shock that I read a recent ProPublica article reporting that from January to March 2025 almost 40% of the physicians who received employment offers from the Veterans Health Administration (VHA) declined the positions.2 Medical media rapidly picked up the story, likely further discouraging potential applicants.3
There have always been health care professionals (HCPs) who had zero interest in working for the VA. Medical students and residents often have a love/hate relationship with the VA, with some trainees not having the patience for the behemoth pace of the bureaucracy or finding the old-style physical environment and more relaxed pace antiquated and inefficient.
The reasons doctors are saying no to VA employment at 4 times the previous rate are different and more disturbing. According to ProPublica, VA officials in Texas reported in a June internal presentation that about 90 people had turned down job offers due to the “uncertainty of reorganization.”2 They reported that low morale was causing existing employees to recommend against working at the VA. My own anecdotal experience is similar: contrary to prior years, few residents, if any, are interested in working at the VA because of concerns about the stability of employment and the direction of its organizational culture.
It is fair to question the objectivity of the ProPublica report. However, the latest VA Office of the Inspector General (OIG) analysis of staffing had similar findings. “Despite the ability to make noncompetitive appointments for such occupations, VHA continues to experience severe occupational staffing shortages for these occupations that are fundamental to the delivery of health care.” The 4434 severe occupational shortage figures in fiscal year (FY) 2025 were 50% higher than in FY 2024.4 OIG reported that 57% of facilities noted severe occupational staffing shortages for psychology, making it the most frequently reported clinical shortage.
At this critical juncture, when new health care professional energy is not flowing into the VHA, there is an unprecedented drain of the lifeblood of any system—the departure of the bearers of institutional memory. Early and scheduled retirements, the deferred resignation program, and severance have decimated the ranks of senior HCPs, experienced leaders, and career clinicians. ProPublica noted the loss of 600 doctors and 1900 nurses at the VHA so far in 2025.2 Internal VA data from exit interviews suggest similar motivations. Many cited lack of trust and confidence in senior leaders and job stress/pressure.5
It should be noted the VA has an alternative and plausible explanation for the expected departure of 30,000 employees. They argue that the VHA was overstaffed and the increased workforce decreased the efficiency of service. Voluntary separation from employment, VA contends, has avoided the need for a far more disruptive reduction in force. VA leaders avow that downsizing has not adversely impacted its ability to deliver high-quality health care and benefits and they assert that a reduction in red tape will enable VA to provide easier access to care. VA Secretary Doug Collins has concluded that because of these difficult but necessary changes, “VA is headed in the right direction.”6
What is institutional memory, and why is it important? “The core of institutional memory is collective awareness and understanding of a collective set of facts, concepts, experiences, and know-how,” Bhugra and Ventriglio explain. “These are all held collectively at various levels in any given institution. Thus, collective memory or history can be utilized to build on what has gone before and how we take things forward.”7
The authors of this quote offer a modern twist on what Sir Isaac Newton described in more metaphorical language in the epigraph: to survive, and even more to thrive, an enterprise must have those who have accumulated technical knowledge and professional wisdom as well as those who assume responsibility for appropriating and adding to this storehouse of operational skill, expertise, unique cultural values, and ethical commitments. The VHA is losing its instructors and students of institutional memory which deals a serious blow to the stability and vitality of any learning health system.6 As Bhugra and Ventriglio put it, institutional memory identifies “what has worked in delivering the aims in the past and what has not, thereby ensuring the lessons learnt are remembered and passed on to the next generation.”7
Nearly every week, at all levels of the agency, I have encountered this exodus of builders and bearers of institutional memory. Those who have left did so for many of the same reasons cited by those who declined to come, leaving incalculable gaps at both ends of the career spectrum. Both the old and new are essential for organizational resilience: fresh ideas enable an institution to be agile in responding to challenges, while operational savvy ensures responses are ecologically aligned with the organizational mission.8
The dire shortage of HCPs—especially in mental health and primary care—has opened up unprecedented opportunities.9 Colleagues have noted that with only a little searching they found multiple lucrative positions. Once, HCPs picked the VA because they valued the commitment to public service and being part of a community of education and research more than fame or fortune. Having the best benefits packages in the industry only reinforced its value.
Even so, surpassing a genius such as Sir Isaac Newton, writing to a scientific competitor, Robert Hooke, recognized that progress and discovery in science and medicine are nigh well impossible without the collective achievements housed in institutional memory.1 It was inspiring teachers and attending physicians—Newton’s giants—who attracted the best and brightest in medicine and nursing, other HCPs, and research, to the VA, where they could participate in a transactive organizational learning process from their seniors, and then grow that fund of knowledge to improve patient care, educate their learners, and innovate. What will happen when there are no longer shoulders of giants or anyone to stand on them?
- Chen C. Mapping Scientific Frontiers: The Quest for Knowledge Visualization. Springer; 2013:135.
- Armstrong D, Umansky E, Coleman V. Veterans’ care at risk under Trump as hundreds of doctors and nurses reject working at VA hospitals. ProPublica. August 8, 2025. Accessed August 25, 2025. https://www.propublica.org/article/veterans-affairs-hospital-shortages-trump
- Kuchno K. VA physician job offers rejections up fourfold in 2025: report. Becker’s Hospital Review. August 12, 2025. Accessed August 26, 2025. https://www.beckershospitalreview.com/workforce/va-physician-job-offer-rejections-up-fourfold-in-2025-report/
- US Department of Veterans Affairs, Office of Inspector General. OIG determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2025. August 12, 2025. Accessed August 25, 2025. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-1
- US Department of Veterans Affairs. VA workforce dashboard. July 25, 2025. Accessed August 25, 2025. https://www.va.gov/EMPLOYEE/docs/workforce/VA-Workforce-Dashboard-Issue-27.pdf
- VA to reduce staff by nearly 30K by end of FY2025. News release. Veterans Affairs News. July 7, 2025. Accessed August 25, 2025. https://news.va.gov/press-room/va-to-reduce-staff-by-nearly-30k-by-end-of-fy2025/
- Bhugra D, Ventriglio A. Institutions, institutional memory, healthcare and research. Int J Soc Psychiatry. 2023;69(8):1843-1844. doi:10.1177/00207640231213905
- Jain A. Is organizational memory a useful capability? An analysis of its effects on productivity, absorptive capacity adaptation. In Argote L, Levine JM. The Oxford Handbook of Group and Organizational Learning. Oxford; 2020.
- Broder J. Ready to pick a specialty? These may have the brightest futures. Medscape. April 21, 2025. Accessed August 25, 2025. https://www.medscape.com/viewarticle/ready-pick-specialty-these-may-have-brightest-futures-2025a10009if
If I have seen further, it is by standing on the shoulders of giants.
Sir Isaac Newton (1642-1727) 1
Early in residency, I decided I only wanted to work at the US Department of Veterans Affairs (VA). It was a way to follow the example of service that my parents, an Army doctor and nurse, had set. I spent much of my residency, including all of my last year of training, at a VA medical center, hoping a vacancy would open in the psychiatry service. In those days, VA jobs were hard to come by; doctors spent their entire careers in the system, only retiring after decades of commitment to its unique mission. Finally, close to graduation, one of my favorite attending physicians left his post. After mountains of paperwork and running the human resources obstacle course with the usual stumbles, I arrived at my dream job as a VA psychiatrist.
So, it is with immense sadness and even shock that I read a recent ProPublica article reporting that from January to March 2025 almost 40% of the physicians who received employment offers from the Veterans Health Administration (VHA) declined the positions.2 Medical media rapidly picked up the story, likely further discouraging potential applicants.3
There have always been health care professionals (HCPs) who had zero interest in working for the VA. Medical students and residents often have a love/hate relationship with the VA, with some trainees not having the patience for the behemoth pace of the bureaucracy or finding the old-style physical environment and more relaxed pace antiquated and inefficient.
The reasons doctors are saying no to VA employment at 4 times the previous rate are different and more disturbing. According to ProPublica, VA officials in Texas reported in a June internal presentation that about 90 people had turned down job offers due to the “uncertainty of reorganization.”2 They reported that low morale was causing existing employees to recommend against working at the VA. My own anecdotal experience is similar: contrary to prior years, few residents, if any, are interested in working at the VA because of concerns about the stability of employment and the direction of its organizational culture.
It is fair to question the objectivity of the ProPublica report. However, the latest VA Office of the Inspector General (OIG) analysis of staffing had similar findings. “Despite the ability to make noncompetitive appointments for such occupations, VHA continues to experience severe occupational staffing shortages for these occupations that are fundamental to the delivery of health care.” The 4434 severe occupational shortage figures in fiscal year (FY) 2025 were 50% higher than in FY 2024.4 OIG reported that 57% of facilities noted severe occupational staffing shortages for psychology, making it the most frequently reported clinical shortage.
At this critical juncture, when new health care professional energy is not flowing into the VHA, there is an unprecedented drain of the lifeblood of any system—the departure of the bearers of institutional memory. Early and scheduled retirements, the deferred resignation program, and severance have decimated the ranks of senior HCPs, experienced leaders, and career clinicians. ProPublica noted the loss of 600 doctors and 1900 nurses at the VHA so far in 2025.2 Internal VA data from exit interviews suggest similar motivations. Many cited lack of trust and confidence in senior leaders and job stress/pressure.5
It should be noted the VA has an alternative and plausible explanation for the expected departure of 30,000 employees. They argue that the VHA was overstaffed and the increased workforce decreased the efficiency of service. Voluntary separation from employment, VA contends, has avoided the need for a far more disruptive reduction in force. VA leaders avow that downsizing has not adversely impacted its ability to deliver high-quality health care and benefits and they assert that a reduction in red tape will enable VA to provide easier access to care. VA Secretary Doug Collins has concluded that because of these difficult but necessary changes, “VA is headed in the right direction.”6
What is institutional memory, and why is it important? “The core of institutional memory is collective awareness and understanding of a collective set of facts, concepts, experiences, and know-how,” Bhugra and Ventriglio explain. “These are all held collectively at various levels in any given institution. Thus, collective memory or history can be utilized to build on what has gone before and how we take things forward.”7
The authors of this quote offer a modern twist on what Sir Isaac Newton described in more metaphorical language in the epigraph: to survive, and even more to thrive, an enterprise must have those who have accumulated technical knowledge and professional wisdom as well as those who assume responsibility for appropriating and adding to this storehouse of operational skill, expertise, unique cultural values, and ethical commitments. The VHA is losing its instructors and students of institutional memory which deals a serious blow to the stability and vitality of any learning health system.6 As Bhugra and Ventriglio put it, institutional memory identifies “what has worked in delivering the aims in the past and what has not, thereby ensuring the lessons learnt are remembered and passed on to the next generation.”7
Nearly every week, at all levels of the agency, I have encountered this exodus of builders and bearers of institutional memory. Those who have left did so for many of the same reasons cited by those who declined to come, leaving incalculable gaps at both ends of the career spectrum. Both the old and new are essential for organizational resilience: fresh ideas enable an institution to be agile in responding to challenges, while operational savvy ensures responses are ecologically aligned with the organizational mission.8
The dire shortage of HCPs—especially in mental health and primary care—has opened up unprecedented opportunities.9 Colleagues have noted that with only a little searching they found multiple lucrative positions. Once, HCPs picked the VA because they valued the commitment to public service and being part of a community of education and research more than fame or fortune. Having the best benefits packages in the industry only reinforced its value.
Even so, surpassing a genius such as Sir Isaac Newton, writing to a scientific competitor, Robert Hooke, recognized that progress and discovery in science and medicine are nigh well impossible without the collective achievements housed in institutional memory.1 It was inspiring teachers and attending physicians—Newton’s giants—who attracted the best and brightest in medicine and nursing, other HCPs, and research, to the VA, where they could participate in a transactive organizational learning process from their seniors, and then grow that fund of knowledge to improve patient care, educate their learners, and innovate. What will happen when there are no longer shoulders of giants or anyone to stand on them?
If I have seen further, it is by standing on the shoulders of giants.
Sir Isaac Newton (1642-1727) 1
Early in residency, I decided I only wanted to work at the US Department of Veterans Affairs (VA). It was a way to follow the example of service that my parents, an Army doctor and nurse, had set. I spent much of my residency, including all of my last year of training, at a VA medical center, hoping a vacancy would open in the psychiatry service. In those days, VA jobs were hard to come by; doctors spent their entire careers in the system, only retiring after decades of commitment to its unique mission. Finally, close to graduation, one of my favorite attending physicians left his post. After mountains of paperwork and running the human resources obstacle course with the usual stumbles, I arrived at my dream job as a VA psychiatrist.
So, it is with immense sadness and even shock that I read a recent ProPublica article reporting that from January to March 2025 almost 40% of the physicians who received employment offers from the Veterans Health Administration (VHA) declined the positions.2 Medical media rapidly picked up the story, likely further discouraging potential applicants.3
There have always been health care professionals (HCPs) who had zero interest in working for the VA. Medical students and residents often have a love/hate relationship with the VA, with some trainees not having the patience for the behemoth pace of the bureaucracy or finding the old-style physical environment and more relaxed pace antiquated and inefficient.
The reasons doctors are saying no to VA employment at 4 times the previous rate are different and more disturbing. According to ProPublica, VA officials in Texas reported in a June internal presentation that about 90 people had turned down job offers due to the “uncertainty of reorganization.”2 They reported that low morale was causing existing employees to recommend against working at the VA. My own anecdotal experience is similar: contrary to prior years, few residents, if any, are interested in working at the VA because of concerns about the stability of employment and the direction of its organizational culture.
It is fair to question the objectivity of the ProPublica report. However, the latest VA Office of the Inspector General (OIG) analysis of staffing had similar findings. “Despite the ability to make noncompetitive appointments for such occupations, VHA continues to experience severe occupational staffing shortages for these occupations that are fundamental to the delivery of health care.” The 4434 severe occupational shortage figures in fiscal year (FY) 2025 were 50% higher than in FY 2024.4 OIG reported that 57% of facilities noted severe occupational staffing shortages for psychology, making it the most frequently reported clinical shortage.
At this critical juncture, when new health care professional energy is not flowing into the VHA, there is an unprecedented drain of the lifeblood of any system—the departure of the bearers of institutional memory. Early and scheduled retirements, the deferred resignation program, and severance have decimated the ranks of senior HCPs, experienced leaders, and career clinicians. ProPublica noted the loss of 600 doctors and 1900 nurses at the VHA so far in 2025.2 Internal VA data from exit interviews suggest similar motivations. Many cited lack of trust and confidence in senior leaders and job stress/pressure.5
It should be noted the VA has an alternative and plausible explanation for the expected departure of 30,000 employees. They argue that the VHA was overstaffed and the increased workforce decreased the efficiency of service. Voluntary separation from employment, VA contends, has avoided the need for a far more disruptive reduction in force. VA leaders avow that downsizing has not adversely impacted its ability to deliver high-quality health care and benefits and they assert that a reduction in red tape will enable VA to provide easier access to care. VA Secretary Doug Collins has concluded that because of these difficult but necessary changes, “VA is headed in the right direction.”6
What is institutional memory, and why is it important? “The core of institutional memory is collective awareness and understanding of a collective set of facts, concepts, experiences, and know-how,” Bhugra and Ventriglio explain. “These are all held collectively at various levels in any given institution. Thus, collective memory or history can be utilized to build on what has gone before and how we take things forward.”7
The authors of this quote offer a modern twist on what Sir Isaac Newton described in more metaphorical language in the epigraph: to survive, and even more to thrive, an enterprise must have those who have accumulated technical knowledge and professional wisdom as well as those who assume responsibility for appropriating and adding to this storehouse of operational skill, expertise, unique cultural values, and ethical commitments. The VHA is losing its instructors and students of institutional memory which deals a serious blow to the stability and vitality of any learning health system.6 As Bhugra and Ventriglio put it, institutional memory identifies “what has worked in delivering the aims in the past and what has not, thereby ensuring the lessons learnt are remembered and passed on to the next generation.”7
Nearly every week, at all levels of the agency, I have encountered this exodus of builders and bearers of institutional memory. Those who have left did so for many of the same reasons cited by those who declined to come, leaving incalculable gaps at both ends of the career spectrum. Both the old and new are essential for organizational resilience: fresh ideas enable an institution to be agile in responding to challenges, while operational savvy ensures responses are ecologically aligned with the organizational mission.8
The dire shortage of HCPs—especially in mental health and primary care—has opened up unprecedented opportunities.9 Colleagues have noted that with only a little searching they found multiple lucrative positions. Once, HCPs picked the VA because they valued the commitment to public service and being part of a community of education and research more than fame or fortune. Having the best benefits packages in the industry only reinforced its value.
Even so, surpassing a genius such as Sir Isaac Newton, writing to a scientific competitor, Robert Hooke, recognized that progress and discovery in science and medicine are nigh well impossible without the collective achievements housed in institutional memory.1 It was inspiring teachers and attending physicians—Newton’s giants—who attracted the best and brightest in medicine and nursing, other HCPs, and research, to the VA, where they could participate in a transactive organizational learning process from their seniors, and then grow that fund of knowledge to improve patient care, educate their learners, and innovate. What will happen when there are no longer shoulders of giants or anyone to stand on them?
- Chen C. Mapping Scientific Frontiers: The Quest for Knowledge Visualization. Springer; 2013:135.
- Armstrong D, Umansky E, Coleman V. Veterans’ care at risk under Trump as hundreds of doctors and nurses reject working at VA hospitals. ProPublica. August 8, 2025. Accessed August 25, 2025. https://www.propublica.org/article/veterans-affairs-hospital-shortages-trump
- Kuchno K. VA physician job offers rejections up fourfold in 2025: report. Becker’s Hospital Review. August 12, 2025. Accessed August 26, 2025. https://www.beckershospitalreview.com/workforce/va-physician-job-offer-rejections-up-fourfold-in-2025-report/
- US Department of Veterans Affairs, Office of Inspector General. OIG determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2025. August 12, 2025. Accessed August 25, 2025. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-1
- US Department of Veterans Affairs. VA workforce dashboard. July 25, 2025. Accessed August 25, 2025. https://www.va.gov/EMPLOYEE/docs/workforce/VA-Workforce-Dashboard-Issue-27.pdf
- VA to reduce staff by nearly 30K by end of FY2025. News release. Veterans Affairs News. July 7, 2025. Accessed August 25, 2025. https://news.va.gov/press-room/va-to-reduce-staff-by-nearly-30k-by-end-of-fy2025/
- Bhugra D, Ventriglio A. Institutions, institutional memory, healthcare and research. Int J Soc Psychiatry. 2023;69(8):1843-1844. doi:10.1177/00207640231213905
- Jain A. Is organizational memory a useful capability? An analysis of its effects on productivity, absorptive capacity adaptation. In Argote L, Levine JM. The Oxford Handbook of Group and Organizational Learning. Oxford; 2020.
- Broder J. Ready to pick a specialty? These may have the brightest futures. Medscape. April 21, 2025. Accessed August 25, 2025. https://www.medscape.com/viewarticle/ready-pick-specialty-these-may-have-brightest-futures-2025a10009if
- Chen C. Mapping Scientific Frontiers: The Quest for Knowledge Visualization. Springer; 2013:135.
- Armstrong D, Umansky E, Coleman V. Veterans’ care at risk under Trump as hundreds of doctors and nurses reject working at VA hospitals. ProPublica. August 8, 2025. Accessed August 25, 2025. https://www.propublica.org/article/veterans-affairs-hospital-shortages-trump
- Kuchno K. VA physician job offers rejections up fourfold in 2025: report. Becker’s Hospital Review. August 12, 2025. Accessed August 26, 2025. https://www.beckershospitalreview.com/workforce/va-physician-job-offer-rejections-up-fourfold-in-2025-report/
- US Department of Veterans Affairs, Office of Inspector General. OIG determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2025. August 12, 2025. Accessed August 25, 2025. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-1
- US Department of Veterans Affairs. VA workforce dashboard. July 25, 2025. Accessed August 25, 2025. https://www.va.gov/EMPLOYEE/docs/workforce/VA-Workforce-Dashboard-Issue-27.pdf
- VA to reduce staff by nearly 30K by end of FY2025. News release. Veterans Affairs News. July 7, 2025. Accessed August 25, 2025. https://news.va.gov/press-room/va-to-reduce-staff-by-nearly-30k-by-end-of-fy2025/
- Bhugra D, Ventriglio A. Institutions, institutional memory, healthcare and research. Int J Soc Psychiatry. 2023;69(8):1843-1844. doi:10.1177/00207640231213905
- Jain A. Is organizational memory a useful capability? An analysis of its effects on productivity, absorptive capacity adaptation. In Argote L, Levine JM. The Oxford Handbook of Group and Organizational Learning. Oxford; 2020.
- Broder J. Ready to pick a specialty? These may have the brightest futures. Medscape. April 21, 2025. Accessed August 25, 2025. https://www.medscape.com/viewarticle/ready-pick-specialty-these-may-have-brightest-futures-2025a10009if
When The Giants and Those Who Stand on Their Shoulders Are Gone: The Loss of VA Institutional Memory
When The Giants and Those Who Stand on Their Shoulders Are Gone: The Loss of VA Institutional Memory

Military Imposters: What Drives Them and How They Damage Us All
Military Imposters: What Drives Them and How They Damage Us All
The better part of valor is discretion.
Henry IV, Part 1 by William Shakespeare1
This is the second part of an exploration of the phenomenon of stolen valor, where individuals claim military exploits or acts of heroism that are either fabricated or exaggerated, and/or awards and medals they did not earn.2 In June, I focused on the unsettling story of Sarah Cavanaugh, a young US Department of Veterans Affairs (VA) social worker who posed as a decorated, heroic, and seriously wounded Marine veteran for years. Cavanaugh’s manipulative masquerade allowed her to receive coveted spots in veteran recovery programs, thousands of dollars in fraudulent donations, the leadership of a local Veterans of Foreign Wars post, and eventually a federal conviction and prison sentence.3 The first column focused on the legal history of stolen valor; this editorial analyzes the clinical import and ethical impact of the behavior of military imposters. Military imposters are the culprits who steal valor.
It would be easy and perhaps reassuring to assume that stolen valor has emerged as another deplorable example of a national culture in which the betrayal of trust in human beings and loss of faith in institutions and aspirations has reached a nadir. Ironically, stolen valor is inextricably linked to the founding of the United States. When General George Washington inaugurated the American military tradition of awarding decorations to honor the bravery and sacrifices of the patriot Army, he anticipated military imposters. He tried to deter stolen valor through the threat of chastisement: “Should any who are not entitled to these honors have the insolence to assume the badges of them, they shall be severely punished,” Washington warned.4
It is plausible to think such despicable conduct occurs only as the ugly side of the beauty of our unparalleled national freedom, but this is a mistake. Cases of stolen valor have been reported in many countries around the world, with some of the most infamous found in the United Kingdom.5
While many brazen military imposters like Cavanaugh never serve, there is a small subset who honorably wore a uniform yet embellish their service record with secret missions and meritorious gallantry that purportedly earned them high rank and even higher awards. A most puzzling and disturbing example of this group is an allegation that surfaced when celebrated Navy SEAL Chris Kyle declared in American Sniper that he had won 3 additional combat awards for combat valor in addition to the Silver Star and 3 Bronze Stars actually listed in his service record.6
The fact that for centuries stolen valor has plagued multiple nations suggests, at least to this psychiatrically trained mind, that something deeper and darker in human nature than profit alone drives military imposters. Philosopher Verna Gehring has distilled these less tangible motivations into the concept of virtue imposters. According to Gehring, military phonies are a notorious exemplar: “The military phony adopts a past not her own, acts of courage she did not perform—she impersonates the heroic character and virtues she does not possess.”7 There could be no more apposite depiction of Cavanaugh, other military imposters, or a legion of other offenders of honor. 8
As with Cavanaugh, financial gain is a byproduct of the machinations of military imposters and is usually secondary to the pursuit of nonmaterial rewards such as power, influence, admiration, emulation, empathy, and charity. Gehring contends, and I agree, that virtue imposters are more pernicious and culpable than the plethora of more prosaic scammers and swindlers who use deceit primarily as a means of economic exploitation: “The virtue impostor by contrast plays on people’s better natures—their generosity, humility, and their need for heroes.”7
Military imposters cause real and lasting harm. Every veteran who exaggerates claims or scams the VA unjustly steals human and monetary resources from other deserving veterans whose integrity would not permit them to break the rules.9 Yet, even more harmful is the potential damage to therapeutic relationships: federal practitioners may become skeptical of a veteran’s history even when there is little to no grounds for suspicion. Veterans, in turn, may experience a breach of trust and betrayal not only from health care professionals and VA leaders but from their brothers and sisters in arms. On an ever-wider scale, every military impostor who is exposed may diminish the respect and honor all veterans have earned.
It is clear, then, why a small group of former service members has adopted the cause of uncovering military imposters and adroitly using the media to identify signs of stolen valor.10 Yet deception mars even these mostly well-intentioned campaigns, as some more zealous stolen valor hunters may make allegations that turn out to be false.11 Nevertheless, 500 years ago and in a very different context Shakespeare was, right on the mark: the better part of valor is discretion in describing one’s achievements, in relying on the veracity of our veteran’s narratives, and when there are sound reasons to do so verifying the truth of what our patients, friends, and even family tell us about their time in the military.1
- Shakespeare W. Introduction in: Henry IV, Part 1. Folger Sharespeare Library. Accessed July 24, 2025. https://www.folger.edu/explore/shakespeares-works/henry-iv-part-1/
- Geppert CM. What about stolen valor actually is illegal? Fed Pract. 2025;42(6):218-219. doi:10.12788/fp.0599
- Lehrfeld J. Woman who faked being cancer-stricken Marine gets 6 years in prison. Military Times. March 15, 2023. Accessed July 24, 2025. https://www.militarytimes.com/news/your-military/2023/03/15/woman-who-faked-being-sick-marine-purple-heart-gets-6-years-in-prison/
- Washington G. General Orders, 7 August 1782 in: Papers of George Washington. Founders Online. August 7, 1782. Accessed July 24, 2025. https://founders.archives.gov/documents/Washington/99-01-02-09056 5. Simpson LK. The men who impersonate military personnel for stolen glory. The Conversation. Updated November 17, 2016. Accessed July 24, 2025. https://theconversation.com/the-men-who-impersonate-military-personnel-for-stolen-glory-62233
- Larter DB. New questions cast doubt on ‘American Sniper‘ Chris Kyle‘s combat record. Navy Times. May 25, 2016. Accessed July 24, 2025. https://www.navytimes.com/news/your-navy/2016/05/25/new-questions-cast-doubt-on-american-sniper-chris-kyle-s-combat-record
- Gehring VV. Phonies, fakes, and frauds—and the social harms they cause. Philos Public Policy Q. 2003;23:14-20.
- Liem, E. The 6 most shocking military imposters ever. Military.com. July 7, 2015. Accessed July 29, 2025. https://www.military.com/undertheradar/2015/07/the-6-most-shocking-military-impostors-ever 9. Sisk R. Some vets with PTSD are scamming the VA: testimony. Military.com. June 8, 2017. Accessed July 24, 2025. https://www.military.com/daily-news/2017/06/08/some-vets-with-ptsd-are-scamming-va-testimony.html
- Bushatz A. How to spot a veteran. Military.com. October 3, 2022. Updated September 16, 2024. Accessed July 24, 2025. https://www.military.com/veterans-day/how-spot-veteran.html
- Monroe R. How to spot a military imposter. The New Yorker. October 19, 2020. Accessed July 24, 2025. https://www.newyorker.com/magazine/2020/10/26/how-to-spot-a-military-impostor
The better part of valor is discretion.
Henry IV, Part 1 by William Shakespeare1
This is the second part of an exploration of the phenomenon of stolen valor, where individuals claim military exploits or acts of heroism that are either fabricated or exaggerated, and/or awards and medals they did not earn.2 In June, I focused on the unsettling story of Sarah Cavanaugh, a young US Department of Veterans Affairs (VA) social worker who posed as a decorated, heroic, and seriously wounded Marine veteran for years. Cavanaugh’s manipulative masquerade allowed her to receive coveted spots in veteran recovery programs, thousands of dollars in fraudulent donations, the leadership of a local Veterans of Foreign Wars post, and eventually a federal conviction and prison sentence.3 The first column focused on the legal history of stolen valor; this editorial analyzes the clinical import and ethical impact of the behavior of military imposters. Military imposters are the culprits who steal valor.
It would be easy and perhaps reassuring to assume that stolen valor has emerged as another deplorable example of a national culture in which the betrayal of trust in human beings and loss of faith in institutions and aspirations has reached a nadir. Ironically, stolen valor is inextricably linked to the founding of the United States. When General George Washington inaugurated the American military tradition of awarding decorations to honor the bravery and sacrifices of the patriot Army, he anticipated military imposters. He tried to deter stolen valor through the threat of chastisement: “Should any who are not entitled to these honors have the insolence to assume the badges of them, they shall be severely punished,” Washington warned.4
It is plausible to think such despicable conduct occurs only as the ugly side of the beauty of our unparalleled national freedom, but this is a mistake. Cases of stolen valor have been reported in many countries around the world, with some of the most infamous found in the United Kingdom.5
While many brazen military imposters like Cavanaugh never serve, there is a small subset who honorably wore a uniform yet embellish their service record with secret missions and meritorious gallantry that purportedly earned them high rank and even higher awards. A most puzzling and disturbing example of this group is an allegation that surfaced when celebrated Navy SEAL Chris Kyle declared in American Sniper that he had won 3 additional combat awards for combat valor in addition to the Silver Star and 3 Bronze Stars actually listed in his service record.6
The fact that for centuries stolen valor has plagued multiple nations suggests, at least to this psychiatrically trained mind, that something deeper and darker in human nature than profit alone drives military imposters. Philosopher Verna Gehring has distilled these less tangible motivations into the concept of virtue imposters. According to Gehring, military phonies are a notorious exemplar: “The military phony adopts a past not her own, acts of courage she did not perform—she impersonates the heroic character and virtues she does not possess.”7 There could be no more apposite depiction of Cavanaugh, other military imposters, or a legion of other offenders of honor. 8
As with Cavanaugh, financial gain is a byproduct of the machinations of military imposters and is usually secondary to the pursuit of nonmaterial rewards such as power, influence, admiration, emulation, empathy, and charity. Gehring contends, and I agree, that virtue imposters are more pernicious and culpable than the plethora of more prosaic scammers and swindlers who use deceit primarily as a means of economic exploitation: “The virtue impostor by contrast plays on people’s better natures—their generosity, humility, and their need for heroes.”7
Military imposters cause real and lasting harm. Every veteran who exaggerates claims or scams the VA unjustly steals human and monetary resources from other deserving veterans whose integrity would not permit them to break the rules.9 Yet, even more harmful is the potential damage to therapeutic relationships: federal practitioners may become skeptical of a veteran’s history even when there is little to no grounds for suspicion. Veterans, in turn, may experience a breach of trust and betrayal not only from health care professionals and VA leaders but from their brothers and sisters in arms. On an ever-wider scale, every military impostor who is exposed may diminish the respect and honor all veterans have earned.
It is clear, then, why a small group of former service members has adopted the cause of uncovering military imposters and adroitly using the media to identify signs of stolen valor.10 Yet deception mars even these mostly well-intentioned campaigns, as some more zealous stolen valor hunters may make allegations that turn out to be false.11 Nevertheless, 500 years ago and in a very different context Shakespeare was, right on the mark: the better part of valor is discretion in describing one’s achievements, in relying on the veracity of our veteran’s narratives, and when there are sound reasons to do so verifying the truth of what our patients, friends, and even family tell us about their time in the military.1
The better part of valor is discretion.
Henry IV, Part 1 by William Shakespeare1
This is the second part of an exploration of the phenomenon of stolen valor, where individuals claim military exploits or acts of heroism that are either fabricated or exaggerated, and/or awards and medals they did not earn.2 In June, I focused on the unsettling story of Sarah Cavanaugh, a young US Department of Veterans Affairs (VA) social worker who posed as a decorated, heroic, and seriously wounded Marine veteran for years. Cavanaugh’s manipulative masquerade allowed her to receive coveted spots in veteran recovery programs, thousands of dollars in fraudulent donations, the leadership of a local Veterans of Foreign Wars post, and eventually a federal conviction and prison sentence.3 The first column focused on the legal history of stolen valor; this editorial analyzes the clinical import and ethical impact of the behavior of military imposters. Military imposters are the culprits who steal valor.
It would be easy and perhaps reassuring to assume that stolen valor has emerged as another deplorable example of a national culture in which the betrayal of trust in human beings and loss of faith in institutions and aspirations has reached a nadir. Ironically, stolen valor is inextricably linked to the founding of the United States. When General George Washington inaugurated the American military tradition of awarding decorations to honor the bravery and sacrifices of the patriot Army, he anticipated military imposters. He tried to deter stolen valor through the threat of chastisement: “Should any who are not entitled to these honors have the insolence to assume the badges of them, they shall be severely punished,” Washington warned.4
It is plausible to think such despicable conduct occurs only as the ugly side of the beauty of our unparalleled national freedom, but this is a mistake. Cases of stolen valor have been reported in many countries around the world, with some of the most infamous found in the United Kingdom.5
While many brazen military imposters like Cavanaugh never serve, there is a small subset who honorably wore a uniform yet embellish their service record with secret missions and meritorious gallantry that purportedly earned them high rank and even higher awards. A most puzzling and disturbing example of this group is an allegation that surfaced when celebrated Navy SEAL Chris Kyle declared in American Sniper that he had won 3 additional combat awards for combat valor in addition to the Silver Star and 3 Bronze Stars actually listed in his service record.6
The fact that for centuries stolen valor has plagued multiple nations suggests, at least to this psychiatrically trained mind, that something deeper and darker in human nature than profit alone drives military imposters. Philosopher Verna Gehring has distilled these less tangible motivations into the concept of virtue imposters. According to Gehring, military phonies are a notorious exemplar: “The military phony adopts a past not her own, acts of courage she did not perform—she impersonates the heroic character and virtues she does not possess.”7 There could be no more apposite depiction of Cavanaugh, other military imposters, or a legion of other offenders of honor. 8
As with Cavanaugh, financial gain is a byproduct of the machinations of military imposters and is usually secondary to the pursuit of nonmaterial rewards such as power, influence, admiration, emulation, empathy, and charity. Gehring contends, and I agree, that virtue imposters are more pernicious and culpable than the plethora of more prosaic scammers and swindlers who use deceit primarily as a means of economic exploitation: “The virtue impostor by contrast plays on people’s better natures—their generosity, humility, and their need for heroes.”7
Military imposters cause real and lasting harm. Every veteran who exaggerates claims or scams the VA unjustly steals human and monetary resources from other deserving veterans whose integrity would not permit them to break the rules.9 Yet, even more harmful is the potential damage to therapeutic relationships: federal practitioners may become skeptical of a veteran’s history even when there is little to no grounds for suspicion. Veterans, in turn, may experience a breach of trust and betrayal not only from health care professionals and VA leaders but from their brothers and sisters in arms. On an ever-wider scale, every military impostor who is exposed may diminish the respect and honor all veterans have earned.
It is clear, then, why a small group of former service members has adopted the cause of uncovering military imposters and adroitly using the media to identify signs of stolen valor.10 Yet deception mars even these mostly well-intentioned campaigns, as some more zealous stolen valor hunters may make allegations that turn out to be false.11 Nevertheless, 500 years ago and in a very different context Shakespeare was, right on the mark: the better part of valor is discretion in describing one’s achievements, in relying on the veracity of our veteran’s narratives, and when there are sound reasons to do so verifying the truth of what our patients, friends, and even family tell us about their time in the military.1
- Shakespeare W. Introduction in: Henry IV, Part 1. Folger Sharespeare Library. Accessed July 24, 2025. https://www.folger.edu/explore/shakespeares-works/henry-iv-part-1/
- Geppert CM. What about stolen valor actually is illegal? Fed Pract. 2025;42(6):218-219. doi:10.12788/fp.0599
- Lehrfeld J. Woman who faked being cancer-stricken Marine gets 6 years in prison. Military Times. March 15, 2023. Accessed July 24, 2025. https://www.militarytimes.com/news/your-military/2023/03/15/woman-who-faked-being-sick-marine-purple-heart-gets-6-years-in-prison/
- Washington G. General Orders, 7 August 1782 in: Papers of George Washington. Founders Online. August 7, 1782. Accessed July 24, 2025. https://founders.archives.gov/documents/Washington/99-01-02-09056 5. Simpson LK. The men who impersonate military personnel for stolen glory. The Conversation. Updated November 17, 2016. Accessed July 24, 2025. https://theconversation.com/the-men-who-impersonate-military-personnel-for-stolen-glory-62233
- Larter DB. New questions cast doubt on ‘American Sniper‘ Chris Kyle‘s combat record. Navy Times. May 25, 2016. Accessed July 24, 2025. https://www.navytimes.com/news/your-navy/2016/05/25/new-questions-cast-doubt-on-american-sniper-chris-kyle-s-combat-record
- Gehring VV. Phonies, fakes, and frauds—and the social harms they cause. Philos Public Policy Q. 2003;23:14-20.
- Liem, E. The 6 most shocking military imposters ever. Military.com. July 7, 2015. Accessed July 29, 2025. https://www.military.com/undertheradar/2015/07/the-6-most-shocking-military-impostors-ever 9. Sisk R. Some vets with PTSD are scamming the VA: testimony. Military.com. June 8, 2017. Accessed July 24, 2025. https://www.military.com/daily-news/2017/06/08/some-vets-with-ptsd-are-scamming-va-testimony.html
- Bushatz A. How to spot a veteran. Military.com. October 3, 2022. Updated September 16, 2024. Accessed July 24, 2025. https://www.military.com/veterans-day/how-spot-veteran.html
- Monroe R. How to spot a military imposter. The New Yorker. October 19, 2020. Accessed July 24, 2025. https://www.newyorker.com/magazine/2020/10/26/how-to-spot-a-military-impostor
- Shakespeare W. Introduction in: Henry IV, Part 1. Folger Sharespeare Library. Accessed July 24, 2025. https://www.folger.edu/explore/shakespeares-works/henry-iv-part-1/
- Geppert CM. What about stolen valor actually is illegal? Fed Pract. 2025;42(6):218-219. doi:10.12788/fp.0599
- Lehrfeld J. Woman who faked being cancer-stricken Marine gets 6 years in prison. Military Times. March 15, 2023. Accessed July 24, 2025. https://www.militarytimes.com/news/your-military/2023/03/15/woman-who-faked-being-sick-marine-purple-heart-gets-6-years-in-prison/
- Washington G. General Orders, 7 August 1782 in: Papers of George Washington. Founders Online. August 7, 1782. Accessed July 24, 2025. https://founders.archives.gov/documents/Washington/99-01-02-09056 5. Simpson LK. The men who impersonate military personnel for stolen glory. The Conversation. Updated November 17, 2016. Accessed July 24, 2025. https://theconversation.com/the-men-who-impersonate-military-personnel-for-stolen-glory-62233
- Larter DB. New questions cast doubt on ‘American Sniper‘ Chris Kyle‘s combat record. Navy Times. May 25, 2016. Accessed July 24, 2025. https://www.navytimes.com/news/your-navy/2016/05/25/new-questions-cast-doubt-on-american-sniper-chris-kyle-s-combat-record
- Gehring VV. Phonies, fakes, and frauds—and the social harms they cause. Philos Public Policy Q. 2003;23:14-20.
- Liem, E. The 6 most shocking military imposters ever. Military.com. July 7, 2015. Accessed July 29, 2025. https://www.military.com/undertheradar/2015/07/the-6-most-shocking-military-impostors-ever 9. Sisk R. Some vets with PTSD are scamming the VA: testimony. Military.com. June 8, 2017. Accessed July 24, 2025. https://www.military.com/daily-news/2017/06/08/some-vets-with-ptsd-are-scamming-va-testimony.html
- Bushatz A. How to spot a veteran. Military.com. October 3, 2022. Updated September 16, 2024. Accessed July 24, 2025. https://www.military.com/veterans-day/how-spot-veteran.html
- Monroe R. How to spot a military imposter. The New Yorker. October 19, 2020. Accessed July 24, 2025. https://www.newyorker.com/magazine/2020/10/26/how-to-spot-a-military-impostor
Military Imposters: What Drives Them and How They Damage Us All
Military Imposters: What Drives Them and How They Damage Us All

What About Stolen Valor is Actually Illegal?
What About Stolen Valor is Actually Illegal?
Memorial Day is the most solemn of all American military commemorations. It is the day when we honor those who sacrificed their lives so that their fellow citizens could flourish in freedom. At 3 PM, a grateful nation is called to observe 2 minutes of silence in remembrance of the heroes who died in battle or of the wounds they sustained in combat. Communities across the country will carry out ceremonies, lining national cemeteries with flags, holding patriotic parades, and conducting spiritual observances.1
Sadly, almost as long as there has been a United States, there has been a parallel practice dishonoring the uniform and deceiving veterans and the public alike known as stolen valor. Stolen valor is a persistent, yet strange, psychological behavior: individuals who never served in the US Armed Forces claim they have done heroic deeds for which they often sustained serious injuries in the line of duty and almost always won medals for their heroism.2 This editorial will trace the US legal history of stolen valor cases to provide the background for next month’s editorial examining its clinical and ethical aspects.
While many cases of stolen valor do not receive media attention, the experience of Sarah Cavanaugh, a former VA social worker who claimed to be a marine veteran who served in Iraq and Afghanistan, was the subject of the Deep Cover podcast series.3 Cavanaugh had claimed that an improvised explosive device blew up her Humvee, crushing her hip. Still she somehow was able to help her fellow Marines and earned the Bronze Star among other decorations for her heroism. That was not the only lie Cavanaugh told: she also told her friends and wife that she had advanced lung cancer due to burn pit exposure. In line with the best-worst of those who have stolen valor, her mastery of manipulation enabled her to become the commander of a local Veterans of Foreign Wars post. Using stolen identities and fraudulent documents, Cavanaugh was able to purloin veteran benefits, donated leave from other VA employees and money, and stole goods and services from various charitable organizations whose mission was to help wounded veterans and those struggling to adjust to civilian life. Before law enforcement unraveled her sordid tale, she misappropriated hundreds of thousands of dollars in VA benefits and donations and exploited dozens of generous veterans and compassionate civilians.4
Cavanaugh’s story was so sordidly compelling that I kept saying out loud to myself (and my spouse), “This has to be illegal.” The truth about stolen valor law is far more ambivalent and frustrating than I had anticipated or wanted. The first insult to my sense of justice was that lying about military service is not in itself illegal: you can pad your military resume with unearned decorations or impress a future partner or employer with your combat exploits without much fear of legal repercussions. The legal history of attempting to make stealing valor a crime has almost as many twists and turns as the fallacious narratives of military imposters and illustrates the uniquely American experiment in balancing freedom and fairness.
The Stolen Valor Act of 2005 made it a federal misdemeanor to wear, manufacture, or sell military decorations, or medals (Cavanaugh bought her medals online) without legal authorization. It also made it a crime to falsely represent oneself as having been the recipient of a decoration, medical, or service badge that Congress or the Armed Forces authorized. There were even stiffer penalties if the medal was a Silver Star, Distinguished Service Cross, US Air Force or US Navy Cross, or Purple Heart. Punishments include fines and imprisonment. The stated legislative purpose was to prohibit fraud that devalued military awards and the dignity of those who legitimately earned them.5
Next comes a distinctly American reaction to the initial Congressional attempt to protect the legacy of those who served—a lawsuit. Xavier Alvarez was an official on a California district water board claimed to be a 25-year veteran of the US Marine Corps wounded in combat and received the Congressional Medal of Honor. The Federal Bureau of Investigation exposed the lie and instead of the nation’s highest honor, Alvarez was the first to be convicted under the Stolen Valor Act of 2005. Alvarez appealed the decision, ironically claiming the law violated his free speech rights. The case landed in the Supreme Court, which ruled that the Stolen Valor Act did indeed violate the Free Speech Clause of the First Amendment. The majority opinion found the Act as passed was too encompassing of all speech and needed to target only cases in which false statements resulted in actual harm.6
The Stolen Valor Act of 2013 amends the criminal code regarding fraudulent claims about military service to include those who don’t only lie but also profit from it, as Cavanaugh did. The revised act specifically focuses on individuals who claim to have earned military honors for the intended purpose of obtaining money, property, or any other tangible benefit.7
Despite the complicated nature of Stolen Valor Law, it did prevail in Cavanaugh’s case. A US District Court Judge in Rhode Island found her guilty of stolen valor in all its permutations, along with identity theft of other veterans’ military and medical records and fraud in obtaining benefits and services intended for real veterans. Cavanaugh was sentenced to 70 months in federal prison, 3 years of supervised release, ordered to pay $284,796.82 in restitution, and to restore 261 hours of donated leave to the federal government, charitable organizations, and good Samaritans she duped and swindled.8
The revised law under which Cavanaugh was punished lasted 10 years until another classically American ethical concern—privacy—motivated additional legislative effort. A 2023/2024 US House of Representatives proposal to amend the Stolen Valor Act would have strengthened the privacy protections afforded military records. It would have required the information to only be accessed with the permission of the individual who served or their family or through a Freedom of Information Act request. This would make the kind of journalistic and law enforcement investigations that eventually caught Cavanaugh in her lies far more laborious for false valor hunters while at the same time preventing unscrupulous inquiries into service members’ personal information. Advocates for free speech and defenders of military honor are both lobbying Congress; as of this writing the legislation has not been passed.9
As we close part 1 of this review of stolen valor, we return to Memorial Day. This day provides the somber recognition that without the brave men and women of integrity who died in defense of a democracy that promotes the political activity of its citizens, we would not even be able to have this debate over justice, freedom, and truth.
- US Department of Veterans Affairs. The difference between Veterans Day and Memorial Day. October 30, 2023. Accessed May 27, 2025. https://news.va.gov/125549/difference-between-veterans-day-memorial-day/
- Home of Heroes. Stolen valor. Accessed May 27, 2025. https://homeofheroes.com/stolen-valor
- Halpern J. Deep cover: the truth about Sarah. May 2025. Accessed May 27, 2025. https://www.pushkin.fm/podcasts/deep-cover
- Stillwell B. The latest season of the ‘deep cover’ podcast dives into one of the biggest stolen valor cases ever. Military. com. May 22, 2025. Accessed May 27, 2025. https:// www.military.com/off-duty/2025/05/22/latest-season-of-deep-cover-podcast-dives-one-of-biggest-stolen-valor-cases-ever.html
- The Stolen Valor Act of 2005. Pub L No: 109-437. 120 Stat 3266
- Alvarez v United States. 567 US 2012.
- The Stolen Valor Act of 2013. 18 USC § 704(b)
- US Attorney’s Office, District of Rhode Island. Rhode Island woman sentenced to federal prison for falsifying military service; false use of military medals; identify theft, and fraudulently collecting more than $250,000, in veteran benefits and charitable contributions. March 14, 2023. Accessed May 27, 2025. https://www.justice.gov/usao-ri/pr/rhode-island-woman-sentenced-federal-prison-falsifying-military-service-false-use
- Armed Forces Benefit Association. Stolen Valor Act: all you need to know. February 21, 2024. Accessed May 27, 2025. https://www.afba.com/military-life/active-duty-and-veterans/stolen-valor-act-all-you-need-to-know/
Memorial Day is the most solemn of all American military commemorations. It is the day when we honor those who sacrificed their lives so that their fellow citizens could flourish in freedom. At 3 PM, a grateful nation is called to observe 2 minutes of silence in remembrance of the heroes who died in battle or of the wounds they sustained in combat. Communities across the country will carry out ceremonies, lining national cemeteries with flags, holding patriotic parades, and conducting spiritual observances.1
Sadly, almost as long as there has been a United States, there has been a parallel practice dishonoring the uniform and deceiving veterans and the public alike known as stolen valor. Stolen valor is a persistent, yet strange, psychological behavior: individuals who never served in the US Armed Forces claim they have done heroic deeds for which they often sustained serious injuries in the line of duty and almost always won medals for their heroism.2 This editorial will trace the US legal history of stolen valor cases to provide the background for next month’s editorial examining its clinical and ethical aspects.
While many cases of stolen valor do not receive media attention, the experience of Sarah Cavanaugh, a former VA social worker who claimed to be a marine veteran who served in Iraq and Afghanistan, was the subject of the Deep Cover podcast series.3 Cavanaugh had claimed that an improvised explosive device blew up her Humvee, crushing her hip. Still she somehow was able to help her fellow Marines and earned the Bronze Star among other decorations for her heroism. That was not the only lie Cavanaugh told: she also told her friends and wife that she had advanced lung cancer due to burn pit exposure. In line with the best-worst of those who have stolen valor, her mastery of manipulation enabled her to become the commander of a local Veterans of Foreign Wars post. Using stolen identities and fraudulent documents, Cavanaugh was able to purloin veteran benefits, donated leave from other VA employees and money, and stole goods and services from various charitable organizations whose mission was to help wounded veterans and those struggling to adjust to civilian life. Before law enforcement unraveled her sordid tale, she misappropriated hundreds of thousands of dollars in VA benefits and donations and exploited dozens of generous veterans and compassionate civilians.4
Cavanaugh’s story was so sordidly compelling that I kept saying out loud to myself (and my spouse), “This has to be illegal.” The truth about stolen valor law is far more ambivalent and frustrating than I had anticipated or wanted. The first insult to my sense of justice was that lying about military service is not in itself illegal: you can pad your military resume with unearned decorations or impress a future partner or employer with your combat exploits without much fear of legal repercussions. The legal history of attempting to make stealing valor a crime has almost as many twists and turns as the fallacious narratives of military imposters and illustrates the uniquely American experiment in balancing freedom and fairness.
The Stolen Valor Act of 2005 made it a federal misdemeanor to wear, manufacture, or sell military decorations, or medals (Cavanaugh bought her medals online) without legal authorization. It also made it a crime to falsely represent oneself as having been the recipient of a decoration, medical, or service badge that Congress or the Armed Forces authorized. There were even stiffer penalties if the medal was a Silver Star, Distinguished Service Cross, US Air Force or US Navy Cross, or Purple Heart. Punishments include fines and imprisonment. The stated legislative purpose was to prohibit fraud that devalued military awards and the dignity of those who legitimately earned them.5
Next comes a distinctly American reaction to the initial Congressional attempt to protect the legacy of those who served—a lawsuit. Xavier Alvarez was an official on a California district water board claimed to be a 25-year veteran of the US Marine Corps wounded in combat and received the Congressional Medal of Honor. The Federal Bureau of Investigation exposed the lie and instead of the nation’s highest honor, Alvarez was the first to be convicted under the Stolen Valor Act of 2005. Alvarez appealed the decision, ironically claiming the law violated his free speech rights. The case landed in the Supreme Court, which ruled that the Stolen Valor Act did indeed violate the Free Speech Clause of the First Amendment. The majority opinion found the Act as passed was too encompassing of all speech and needed to target only cases in which false statements resulted in actual harm.6
The Stolen Valor Act of 2013 amends the criminal code regarding fraudulent claims about military service to include those who don’t only lie but also profit from it, as Cavanaugh did. The revised act specifically focuses on individuals who claim to have earned military honors for the intended purpose of obtaining money, property, or any other tangible benefit.7
Despite the complicated nature of Stolen Valor Law, it did prevail in Cavanaugh’s case. A US District Court Judge in Rhode Island found her guilty of stolen valor in all its permutations, along with identity theft of other veterans’ military and medical records and fraud in obtaining benefits and services intended for real veterans. Cavanaugh was sentenced to 70 months in federal prison, 3 years of supervised release, ordered to pay $284,796.82 in restitution, and to restore 261 hours of donated leave to the federal government, charitable organizations, and good Samaritans she duped and swindled.8
The revised law under which Cavanaugh was punished lasted 10 years until another classically American ethical concern—privacy—motivated additional legislative effort. A 2023/2024 US House of Representatives proposal to amend the Stolen Valor Act would have strengthened the privacy protections afforded military records. It would have required the information to only be accessed with the permission of the individual who served or their family or through a Freedom of Information Act request. This would make the kind of journalistic and law enforcement investigations that eventually caught Cavanaugh in her lies far more laborious for false valor hunters while at the same time preventing unscrupulous inquiries into service members’ personal information. Advocates for free speech and defenders of military honor are both lobbying Congress; as of this writing the legislation has not been passed.9
As we close part 1 of this review of stolen valor, we return to Memorial Day. This day provides the somber recognition that without the brave men and women of integrity who died in defense of a democracy that promotes the political activity of its citizens, we would not even be able to have this debate over justice, freedom, and truth.
Memorial Day is the most solemn of all American military commemorations. It is the day when we honor those who sacrificed their lives so that their fellow citizens could flourish in freedom. At 3 PM, a grateful nation is called to observe 2 minutes of silence in remembrance of the heroes who died in battle or of the wounds they sustained in combat. Communities across the country will carry out ceremonies, lining national cemeteries with flags, holding patriotic parades, and conducting spiritual observances.1
Sadly, almost as long as there has been a United States, there has been a parallel practice dishonoring the uniform and deceiving veterans and the public alike known as stolen valor. Stolen valor is a persistent, yet strange, psychological behavior: individuals who never served in the US Armed Forces claim they have done heroic deeds for which they often sustained serious injuries in the line of duty and almost always won medals for their heroism.2 This editorial will trace the US legal history of stolen valor cases to provide the background for next month’s editorial examining its clinical and ethical aspects.
While many cases of stolen valor do not receive media attention, the experience of Sarah Cavanaugh, a former VA social worker who claimed to be a marine veteran who served in Iraq and Afghanistan, was the subject of the Deep Cover podcast series.3 Cavanaugh had claimed that an improvised explosive device blew up her Humvee, crushing her hip. Still she somehow was able to help her fellow Marines and earned the Bronze Star among other decorations for her heroism. That was not the only lie Cavanaugh told: she also told her friends and wife that she had advanced lung cancer due to burn pit exposure. In line with the best-worst of those who have stolen valor, her mastery of manipulation enabled her to become the commander of a local Veterans of Foreign Wars post. Using stolen identities and fraudulent documents, Cavanaugh was able to purloin veteran benefits, donated leave from other VA employees and money, and stole goods and services from various charitable organizations whose mission was to help wounded veterans and those struggling to adjust to civilian life. Before law enforcement unraveled her sordid tale, she misappropriated hundreds of thousands of dollars in VA benefits and donations and exploited dozens of generous veterans and compassionate civilians.4
Cavanaugh’s story was so sordidly compelling that I kept saying out loud to myself (and my spouse), “This has to be illegal.” The truth about stolen valor law is far more ambivalent and frustrating than I had anticipated or wanted. The first insult to my sense of justice was that lying about military service is not in itself illegal: you can pad your military resume with unearned decorations or impress a future partner or employer with your combat exploits without much fear of legal repercussions. The legal history of attempting to make stealing valor a crime has almost as many twists and turns as the fallacious narratives of military imposters and illustrates the uniquely American experiment in balancing freedom and fairness.
The Stolen Valor Act of 2005 made it a federal misdemeanor to wear, manufacture, or sell military decorations, or medals (Cavanaugh bought her medals online) without legal authorization. It also made it a crime to falsely represent oneself as having been the recipient of a decoration, medical, or service badge that Congress or the Armed Forces authorized. There were even stiffer penalties if the medal was a Silver Star, Distinguished Service Cross, US Air Force or US Navy Cross, or Purple Heart. Punishments include fines and imprisonment. The stated legislative purpose was to prohibit fraud that devalued military awards and the dignity of those who legitimately earned them.5
Next comes a distinctly American reaction to the initial Congressional attempt to protect the legacy of those who served—a lawsuit. Xavier Alvarez was an official on a California district water board claimed to be a 25-year veteran of the US Marine Corps wounded in combat and received the Congressional Medal of Honor. The Federal Bureau of Investigation exposed the lie and instead of the nation’s highest honor, Alvarez was the first to be convicted under the Stolen Valor Act of 2005. Alvarez appealed the decision, ironically claiming the law violated his free speech rights. The case landed in the Supreme Court, which ruled that the Stolen Valor Act did indeed violate the Free Speech Clause of the First Amendment. The majority opinion found the Act as passed was too encompassing of all speech and needed to target only cases in which false statements resulted in actual harm.6
The Stolen Valor Act of 2013 amends the criminal code regarding fraudulent claims about military service to include those who don’t only lie but also profit from it, as Cavanaugh did. The revised act specifically focuses on individuals who claim to have earned military honors for the intended purpose of obtaining money, property, or any other tangible benefit.7
Despite the complicated nature of Stolen Valor Law, it did prevail in Cavanaugh’s case. A US District Court Judge in Rhode Island found her guilty of stolen valor in all its permutations, along with identity theft of other veterans’ military and medical records and fraud in obtaining benefits and services intended for real veterans. Cavanaugh was sentenced to 70 months in federal prison, 3 years of supervised release, ordered to pay $284,796.82 in restitution, and to restore 261 hours of donated leave to the federal government, charitable organizations, and good Samaritans she duped and swindled.8
The revised law under which Cavanaugh was punished lasted 10 years until another classically American ethical concern—privacy—motivated additional legislative effort. A 2023/2024 US House of Representatives proposal to amend the Stolen Valor Act would have strengthened the privacy protections afforded military records. It would have required the information to only be accessed with the permission of the individual who served or their family or through a Freedom of Information Act request. This would make the kind of journalistic and law enforcement investigations that eventually caught Cavanaugh in her lies far more laborious for false valor hunters while at the same time preventing unscrupulous inquiries into service members’ personal information. Advocates for free speech and defenders of military honor are both lobbying Congress; as of this writing the legislation has not been passed.9
As we close part 1 of this review of stolen valor, we return to Memorial Day. This day provides the somber recognition that without the brave men and women of integrity who died in defense of a democracy that promotes the political activity of its citizens, we would not even be able to have this debate over justice, freedom, and truth.
- US Department of Veterans Affairs. The difference between Veterans Day and Memorial Day. October 30, 2023. Accessed May 27, 2025. https://news.va.gov/125549/difference-between-veterans-day-memorial-day/
- Home of Heroes. Stolen valor. Accessed May 27, 2025. https://homeofheroes.com/stolen-valor
- Halpern J. Deep cover: the truth about Sarah. May 2025. Accessed May 27, 2025. https://www.pushkin.fm/podcasts/deep-cover
- Stillwell B. The latest season of the ‘deep cover’ podcast dives into one of the biggest stolen valor cases ever. Military. com. May 22, 2025. Accessed May 27, 2025. https:// www.military.com/off-duty/2025/05/22/latest-season-of-deep-cover-podcast-dives-one-of-biggest-stolen-valor-cases-ever.html
- The Stolen Valor Act of 2005. Pub L No: 109-437. 120 Stat 3266
- Alvarez v United States. 567 US 2012.
- The Stolen Valor Act of 2013. 18 USC § 704(b)
- US Attorney’s Office, District of Rhode Island. Rhode Island woman sentenced to federal prison for falsifying military service; false use of military medals; identify theft, and fraudulently collecting more than $250,000, in veteran benefits and charitable contributions. March 14, 2023. Accessed May 27, 2025. https://www.justice.gov/usao-ri/pr/rhode-island-woman-sentenced-federal-prison-falsifying-military-service-false-use
- Armed Forces Benefit Association. Stolen Valor Act: all you need to know. February 21, 2024. Accessed May 27, 2025. https://www.afba.com/military-life/active-duty-and-veterans/stolen-valor-act-all-you-need-to-know/
- US Department of Veterans Affairs. The difference between Veterans Day and Memorial Day. October 30, 2023. Accessed May 27, 2025. https://news.va.gov/125549/difference-between-veterans-day-memorial-day/
- Home of Heroes. Stolen valor. Accessed May 27, 2025. https://homeofheroes.com/stolen-valor
- Halpern J. Deep cover: the truth about Sarah. May 2025. Accessed May 27, 2025. https://www.pushkin.fm/podcasts/deep-cover
- Stillwell B. The latest season of the ‘deep cover’ podcast dives into one of the biggest stolen valor cases ever. Military. com. May 22, 2025. Accessed May 27, 2025. https:// www.military.com/off-duty/2025/05/22/latest-season-of-deep-cover-podcast-dives-one-of-biggest-stolen-valor-cases-ever.html
- The Stolen Valor Act of 2005. Pub L No: 109-437. 120 Stat 3266
- Alvarez v United States. 567 US 2012.
- The Stolen Valor Act of 2013. 18 USC § 704(b)
- US Attorney’s Office, District of Rhode Island. Rhode Island woman sentenced to federal prison for falsifying military service; false use of military medals; identify theft, and fraudulently collecting more than $250,000, in veteran benefits and charitable contributions. March 14, 2023. Accessed May 27, 2025. https://www.justice.gov/usao-ri/pr/rhode-island-woman-sentenced-federal-prison-falsifying-military-service-false-use
- Armed Forces Benefit Association. Stolen Valor Act: all you need to know. February 21, 2024. Accessed May 27, 2025. https://www.afba.com/military-life/active-duty-and-veterans/stolen-valor-act-all-you-need-to-know/
What About Stolen Valor is Actually Illegal?
What About Stolen Valor is Actually Illegal?

Should I Stay or Should I Go? Federal Health Care Professional Retirement Dilemmas
Should I Stay or Should I Go? Federal Health Care Professional Retirement Dilemmas
The uselessness of men above sixty years of age and the incalculable benefit it would be in commercial, in political, and in professional life, if as a matter of course, men stopped working at this age.
Sir William Osler1
The first time I remember hearing the word retirement was when I was 5 or 6 years old. My mother told me that my father had been given new orders: either be promoted to general and move to oversee a hospital somewhere far away, or retire from the Army. He was a scholar, teacher, and physician with no interest or aptitude for military politics and health care administration. Reluctantly, he resigned himself to retirement before he had planned. I recall being angry with him, because in my solipsistic child mind he was depriving me of the opportunity to live in a big house across from the parade field, where the generals lived or having a reserved parking spot in front of the post exchange. As a psychiatrist, I suspect that the anger was a primitive defense against the fear of leaving the only home I had ever known on an Army base.
I recently finished reading Michael Bliss’s seminal biography of Sir William Osler (1848-1919), the great Anglo-American physician and medical educator.2 Bliss found few blemishes on Osler’s character or missteps in his stellar career, but one of the few may be his views on retirement. The epigraph is from an address Osler gave before leaving Johns Hopkins for semiretirement in Oxford, England. The farewell speech caused a media controversy with his comments reflecting attitudes that seem ageist today, when many people are active, productive, and happy long past the age of 60 years.3 I do not endorse Osler’s philosophy of aging, nor his exclusion of women (if I did, I would not be around to write this editorial). Not even Osler himself followed his advice: he was active in medicine almost until his death at 70 years old.2
Yet like many of my fellow federal health care practitioners (HCPs), I have been thinking about and planning for retirement earlier than expected, given the memos and directives about voluntary early retirement, deferred resignation, and reductions in force.4,5 The COVID-19 pandemic sadly compelled many burned-out and traumatized HCPs to cross the retirement Rubicon far sooner than they imagined.6
A Google search for information about HCP retirement, particularly among physicians, produces a cascade of advisory articles. They primarily focus on finances, with many pushing their own commercial agenda for retirement planning.7 Although money is a necessary piece of the retirement puzzle, for HCPs it may not be sufficient to ensure a healthy and satisfying retirement. Two other considerations may be even more important to weigh in making the retirement decision, namely timing and meaning.8
For earlier generations of HCPs, work was almost their sole identity. Although younger practitioners are more likely to embrace a better work-life balance, it is still a driving factor for many in the decision to retire.9 It is not just about the cliché of being a workaholic, rather many clinicians continue to enjoy lifelong learning, the rewards of helping people in need, and professional satisfaction. HCPs also spend a longer time training than many other professions; perhaps since we waited so long to practice, we want to stay a little longer.10 For those whose motivation for federal practice was a commitment to service, these may be even more powerful incentives to continue working.
When a nurse, physician, pharmacist, or social worker no longer finds the same gratification and stimulation in their work, whether due to unwelcome changes in the clinical setting or the profession at large, declining health or emotional exhaustion, or the very human need to move onto another phase of life (what Osler likely really meant), then that may be a signal to think hard about retiring. Of course, there have always been—and will continue to be—professionals of all stripes who, even in the most agreeable situation, just cannot wait to retire. Simply because there are so many other ways they want to spend their remaining energy and time: travel, grandchildren, hobbies, even a second career. Because none of us knows how far out our life extends, it is prudent to periodically ask what is the optimal path that combines both purpose and well-being.
All of us as HCPs, and even more as human beings with desires and duties far beyond our respective professions, face a dilemma: a choice between 2 goods that cannot both be fulfilled simultaneously. This is likely why HCPs frequently do what is technically called a phased retirement, a fancy name for working part-time, or retiring from 1 position and taking up another. This temporizes the decision and tempers the bittersweet emotional experience of leaving the profession in one way, and in another, it delays the inevitable.
Over the last few years, I have learned 2 important lessons while watching many of my closest friends retire. First, for those who are still working and those who are retired may seem to inhabit a separate country; hence, special efforts must be made to both appreciate them while they are in our immediate circle of concern and to make efforts to stay in contact once they are emeriti. It is almost as if after being a daily integral aspect of the workplace they have passed into a different dimension of existence. In terms of priorities and mindsets, many of them have. Second, what makes retirement a reality with peace and growth rather than regret and stagnation is owning the decision to retire. There are always constraints: financial, medical, and familial. However, those who retire on their own terms and not primarily in response to fear or uncertainty appear to fare better than those feeling the same pressures who give away their power.11 Having read about retirement in the last months, the best advice I have seen is from Harry Emerson Fosdick, a Protestant minister in the early 20th century: “Don’t simply retire from something; have something to retire to.”12
I have not yet decided about my retirement. Whatever decision you make, remember it is solely yours. After a lifetime of caring for others, retirement is all about caring for yourself.
- Osler W. The Fixed Period. In: Osler W, ed. Aequanimitas With Other Addresses to Medical Students, Nurses and Practitioners of Medicine. 3rd ed. The Blakiston Company; 1932:373-393.
- Bliss M. William Osler: A Life in Medicine. Oxford University Press; 1999.
- Anderson M, Scofield RH. The “Fixed period,” the wildfire news, and an unpublished manuscript: Osler’s farewell speech revisited in geographical breadth and emotional depth. Am J Med Sci. Published online February 11, 2025. doi:10.1016/j.amjms.2025.02.005
- Obis A. What federal workers should consider before accepting deferred resignation. Federal News Network. April 8, 2025. Accessed April 25, 2025. https://federalnewsnetwork.com/workforce/2025/04/what-federal-workers-should-consider-before-accepting-deferred-resignation/
- Dyer J. VA exempts clinical staff from OPM deferred resignation program. Federal Practitioner. February 11, 2025. Accessed April 28, 2025. https://www.mdedge.com/content/va-exempts-clinical-staff-opm-deferred-resignation-program
- Shyrock T. Retirement planning secrets for physicians. Medical Economics. 2024;101(8). Accessed April 28, 2025. https:// www.medicaleconomics.com/view/retirement-planningsecrets-for-physicians
- Sinsky CA, Brown RL, Stillman MJ, Linzer M. COVID-related stress and work intentions in a sample of US health care workers. Mayo Clin Proc Innov Qual Outcomes. 2021;5(6):1165-1173. doi:10.1016/j.mayocpiqo.2021.08.007
- Tabloski PA. Life after retirement. American Nurse. March 3, 2022. Accessed April 25, 2025. https://www.myamericannurse.com/life-after-retirement/
- Chen T-P. Young doctors want work-life balance. Older doctors say that’s not the job. The Wall Street Journal. November 3, 2024. Accessed April 25, 2025. https://www.wsj.com/lifestyle/careers/young-doctors-want-work-life-balance-older-doctors-say-thats-not-the-job-6cb37d48
- Sweeny JF. Physician retirement: Why it’s hard for doctors to retire. Medical Economics. 2019;96(4). Accessed April 25, 2025. https://www.medicaleconomics.com/view/physician-retirement-why-its-hard-doctors-retire
- Nelson J. Wisdom for Our Time. W.W. Norton; 1961.
- Silver MP, Hamilton AD, Biswas A, Williams SA. Life after medicine: a systematic review of studies physician’s adjustment to retirement. Arch Community Med Public Health. 2016;2(1):001-007. doi:10.17352/2455-5479.000006
The uselessness of men above sixty years of age and the incalculable benefit it would be in commercial, in political, and in professional life, if as a matter of course, men stopped working at this age.
Sir William Osler1
The first time I remember hearing the word retirement was when I was 5 or 6 years old. My mother told me that my father had been given new orders: either be promoted to general and move to oversee a hospital somewhere far away, or retire from the Army. He was a scholar, teacher, and physician with no interest or aptitude for military politics and health care administration. Reluctantly, he resigned himself to retirement before he had planned. I recall being angry with him, because in my solipsistic child mind he was depriving me of the opportunity to live in a big house across from the parade field, where the generals lived or having a reserved parking spot in front of the post exchange. As a psychiatrist, I suspect that the anger was a primitive defense against the fear of leaving the only home I had ever known on an Army base.
I recently finished reading Michael Bliss’s seminal biography of Sir William Osler (1848-1919), the great Anglo-American physician and medical educator.2 Bliss found few blemishes on Osler’s character or missteps in his stellar career, but one of the few may be his views on retirement. The epigraph is from an address Osler gave before leaving Johns Hopkins for semiretirement in Oxford, England. The farewell speech caused a media controversy with his comments reflecting attitudes that seem ageist today, when many people are active, productive, and happy long past the age of 60 years.3 I do not endorse Osler’s philosophy of aging, nor his exclusion of women (if I did, I would not be around to write this editorial). Not even Osler himself followed his advice: he was active in medicine almost until his death at 70 years old.2
Yet like many of my fellow federal health care practitioners (HCPs), I have been thinking about and planning for retirement earlier than expected, given the memos and directives about voluntary early retirement, deferred resignation, and reductions in force.4,5 The COVID-19 pandemic sadly compelled many burned-out and traumatized HCPs to cross the retirement Rubicon far sooner than they imagined.6
A Google search for information about HCP retirement, particularly among physicians, produces a cascade of advisory articles. They primarily focus on finances, with many pushing their own commercial agenda for retirement planning.7 Although money is a necessary piece of the retirement puzzle, for HCPs it may not be sufficient to ensure a healthy and satisfying retirement. Two other considerations may be even more important to weigh in making the retirement decision, namely timing and meaning.8
For earlier generations of HCPs, work was almost their sole identity. Although younger practitioners are more likely to embrace a better work-life balance, it is still a driving factor for many in the decision to retire.9 It is not just about the cliché of being a workaholic, rather many clinicians continue to enjoy lifelong learning, the rewards of helping people in need, and professional satisfaction. HCPs also spend a longer time training than many other professions; perhaps since we waited so long to practice, we want to stay a little longer.10 For those whose motivation for federal practice was a commitment to service, these may be even more powerful incentives to continue working.
When a nurse, physician, pharmacist, or social worker no longer finds the same gratification and stimulation in their work, whether due to unwelcome changes in the clinical setting or the profession at large, declining health or emotional exhaustion, or the very human need to move onto another phase of life (what Osler likely really meant), then that may be a signal to think hard about retiring. Of course, there have always been—and will continue to be—professionals of all stripes who, even in the most agreeable situation, just cannot wait to retire. Simply because there are so many other ways they want to spend their remaining energy and time: travel, grandchildren, hobbies, even a second career. Because none of us knows how far out our life extends, it is prudent to periodically ask what is the optimal path that combines both purpose and well-being.
All of us as HCPs, and even more as human beings with desires and duties far beyond our respective professions, face a dilemma: a choice between 2 goods that cannot both be fulfilled simultaneously. This is likely why HCPs frequently do what is technically called a phased retirement, a fancy name for working part-time, or retiring from 1 position and taking up another. This temporizes the decision and tempers the bittersweet emotional experience of leaving the profession in one way, and in another, it delays the inevitable.
Over the last few years, I have learned 2 important lessons while watching many of my closest friends retire. First, for those who are still working and those who are retired may seem to inhabit a separate country; hence, special efforts must be made to both appreciate them while they are in our immediate circle of concern and to make efforts to stay in contact once they are emeriti. It is almost as if after being a daily integral aspect of the workplace they have passed into a different dimension of existence. In terms of priorities and mindsets, many of them have. Second, what makes retirement a reality with peace and growth rather than regret and stagnation is owning the decision to retire. There are always constraints: financial, medical, and familial. However, those who retire on their own terms and not primarily in response to fear or uncertainty appear to fare better than those feeling the same pressures who give away their power.11 Having read about retirement in the last months, the best advice I have seen is from Harry Emerson Fosdick, a Protestant minister in the early 20th century: “Don’t simply retire from something; have something to retire to.”12
I have not yet decided about my retirement. Whatever decision you make, remember it is solely yours. After a lifetime of caring for others, retirement is all about caring for yourself.
The uselessness of men above sixty years of age and the incalculable benefit it would be in commercial, in political, and in professional life, if as a matter of course, men stopped working at this age.
Sir William Osler1
The first time I remember hearing the word retirement was when I was 5 or 6 years old. My mother told me that my father had been given new orders: either be promoted to general and move to oversee a hospital somewhere far away, or retire from the Army. He was a scholar, teacher, and physician with no interest or aptitude for military politics and health care administration. Reluctantly, he resigned himself to retirement before he had planned. I recall being angry with him, because in my solipsistic child mind he was depriving me of the opportunity to live in a big house across from the parade field, where the generals lived or having a reserved parking spot in front of the post exchange. As a psychiatrist, I suspect that the anger was a primitive defense against the fear of leaving the only home I had ever known on an Army base.
I recently finished reading Michael Bliss’s seminal biography of Sir William Osler (1848-1919), the great Anglo-American physician and medical educator.2 Bliss found few blemishes on Osler’s character or missteps in his stellar career, but one of the few may be his views on retirement. The epigraph is from an address Osler gave before leaving Johns Hopkins for semiretirement in Oxford, England. The farewell speech caused a media controversy with his comments reflecting attitudes that seem ageist today, when many people are active, productive, and happy long past the age of 60 years.3 I do not endorse Osler’s philosophy of aging, nor his exclusion of women (if I did, I would not be around to write this editorial). Not even Osler himself followed his advice: he was active in medicine almost until his death at 70 years old.2
Yet like many of my fellow federal health care practitioners (HCPs), I have been thinking about and planning for retirement earlier than expected, given the memos and directives about voluntary early retirement, deferred resignation, and reductions in force.4,5 The COVID-19 pandemic sadly compelled many burned-out and traumatized HCPs to cross the retirement Rubicon far sooner than they imagined.6
A Google search for information about HCP retirement, particularly among physicians, produces a cascade of advisory articles. They primarily focus on finances, with many pushing their own commercial agenda for retirement planning.7 Although money is a necessary piece of the retirement puzzle, for HCPs it may not be sufficient to ensure a healthy and satisfying retirement. Two other considerations may be even more important to weigh in making the retirement decision, namely timing and meaning.8
For earlier generations of HCPs, work was almost their sole identity. Although younger practitioners are more likely to embrace a better work-life balance, it is still a driving factor for many in the decision to retire.9 It is not just about the cliché of being a workaholic, rather many clinicians continue to enjoy lifelong learning, the rewards of helping people in need, and professional satisfaction. HCPs also spend a longer time training than many other professions; perhaps since we waited so long to practice, we want to stay a little longer.10 For those whose motivation for federal practice was a commitment to service, these may be even more powerful incentives to continue working.
When a nurse, physician, pharmacist, or social worker no longer finds the same gratification and stimulation in their work, whether due to unwelcome changes in the clinical setting or the profession at large, declining health or emotional exhaustion, or the very human need to move onto another phase of life (what Osler likely really meant), then that may be a signal to think hard about retiring. Of course, there have always been—and will continue to be—professionals of all stripes who, even in the most agreeable situation, just cannot wait to retire. Simply because there are so many other ways they want to spend their remaining energy and time: travel, grandchildren, hobbies, even a second career. Because none of us knows how far out our life extends, it is prudent to periodically ask what is the optimal path that combines both purpose and well-being.
All of us as HCPs, and even more as human beings with desires and duties far beyond our respective professions, face a dilemma: a choice between 2 goods that cannot both be fulfilled simultaneously. This is likely why HCPs frequently do what is technically called a phased retirement, a fancy name for working part-time, or retiring from 1 position and taking up another. This temporizes the decision and tempers the bittersweet emotional experience of leaving the profession in one way, and in another, it delays the inevitable.
Over the last few years, I have learned 2 important lessons while watching many of my closest friends retire. First, for those who are still working and those who are retired may seem to inhabit a separate country; hence, special efforts must be made to both appreciate them while they are in our immediate circle of concern and to make efforts to stay in contact once they are emeriti. It is almost as if after being a daily integral aspect of the workplace they have passed into a different dimension of existence. In terms of priorities and mindsets, many of them have. Second, what makes retirement a reality with peace and growth rather than regret and stagnation is owning the decision to retire. There are always constraints: financial, medical, and familial. However, those who retire on their own terms and not primarily in response to fear or uncertainty appear to fare better than those feeling the same pressures who give away their power.11 Having read about retirement in the last months, the best advice I have seen is from Harry Emerson Fosdick, a Protestant minister in the early 20th century: “Don’t simply retire from something; have something to retire to.”12
I have not yet decided about my retirement. Whatever decision you make, remember it is solely yours. After a lifetime of caring for others, retirement is all about caring for yourself.
- Osler W. The Fixed Period. In: Osler W, ed. Aequanimitas With Other Addresses to Medical Students, Nurses and Practitioners of Medicine. 3rd ed. The Blakiston Company; 1932:373-393.
- Bliss M. William Osler: A Life in Medicine. Oxford University Press; 1999.
- Anderson M, Scofield RH. The “Fixed period,” the wildfire news, and an unpublished manuscript: Osler’s farewell speech revisited in geographical breadth and emotional depth. Am J Med Sci. Published online February 11, 2025. doi:10.1016/j.amjms.2025.02.005
- Obis A. What federal workers should consider before accepting deferred resignation. Federal News Network. April 8, 2025. Accessed April 25, 2025. https://federalnewsnetwork.com/workforce/2025/04/what-federal-workers-should-consider-before-accepting-deferred-resignation/
- Dyer J. VA exempts clinical staff from OPM deferred resignation program. Federal Practitioner. February 11, 2025. Accessed April 28, 2025. https://www.mdedge.com/content/va-exempts-clinical-staff-opm-deferred-resignation-program
- Shyrock T. Retirement planning secrets for physicians. Medical Economics. 2024;101(8). Accessed April 28, 2025. https:// www.medicaleconomics.com/view/retirement-planningsecrets-for-physicians
- Sinsky CA, Brown RL, Stillman MJ, Linzer M. COVID-related stress and work intentions in a sample of US health care workers. Mayo Clin Proc Innov Qual Outcomes. 2021;5(6):1165-1173. doi:10.1016/j.mayocpiqo.2021.08.007
- Tabloski PA. Life after retirement. American Nurse. March 3, 2022. Accessed April 25, 2025. https://www.myamericannurse.com/life-after-retirement/
- Chen T-P. Young doctors want work-life balance. Older doctors say that’s not the job. The Wall Street Journal. November 3, 2024. Accessed April 25, 2025. https://www.wsj.com/lifestyle/careers/young-doctors-want-work-life-balance-older-doctors-say-thats-not-the-job-6cb37d48
- Sweeny JF. Physician retirement: Why it’s hard for doctors to retire. Medical Economics. 2019;96(4). Accessed April 25, 2025. https://www.medicaleconomics.com/view/physician-retirement-why-its-hard-doctors-retire
- Nelson J. Wisdom for Our Time. W.W. Norton; 1961.
- Silver MP, Hamilton AD, Biswas A, Williams SA. Life after medicine: a systematic review of studies physician’s adjustment to retirement. Arch Community Med Public Health. 2016;2(1):001-007. doi:10.17352/2455-5479.000006
- Osler W. The Fixed Period. In: Osler W, ed. Aequanimitas With Other Addresses to Medical Students, Nurses and Practitioners of Medicine. 3rd ed. The Blakiston Company; 1932:373-393.
- Bliss M. William Osler: A Life in Medicine. Oxford University Press; 1999.
- Anderson M, Scofield RH. The “Fixed period,” the wildfire news, and an unpublished manuscript: Osler’s farewell speech revisited in geographical breadth and emotional depth. Am J Med Sci. Published online February 11, 2025. doi:10.1016/j.amjms.2025.02.005
- Obis A. What federal workers should consider before accepting deferred resignation. Federal News Network. April 8, 2025. Accessed April 25, 2025. https://federalnewsnetwork.com/workforce/2025/04/what-federal-workers-should-consider-before-accepting-deferred-resignation/
- Dyer J. VA exempts clinical staff from OPM deferred resignation program. Federal Practitioner. February 11, 2025. Accessed April 28, 2025. https://www.mdedge.com/content/va-exempts-clinical-staff-opm-deferred-resignation-program
- Shyrock T. Retirement planning secrets for physicians. Medical Economics. 2024;101(8). Accessed April 28, 2025. https:// www.medicaleconomics.com/view/retirement-planningsecrets-for-physicians
- Sinsky CA, Brown RL, Stillman MJ, Linzer M. COVID-related stress and work intentions in a sample of US health care workers. Mayo Clin Proc Innov Qual Outcomes. 2021;5(6):1165-1173. doi:10.1016/j.mayocpiqo.2021.08.007
- Tabloski PA. Life after retirement. American Nurse. March 3, 2022. Accessed April 25, 2025. https://www.myamericannurse.com/life-after-retirement/
- Chen T-P. Young doctors want work-life balance. Older doctors say that’s not the job. The Wall Street Journal. November 3, 2024. Accessed April 25, 2025. https://www.wsj.com/lifestyle/careers/young-doctors-want-work-life-balance-older-doctors-say-thats-not-the-job-6cb37d48
- Sweeny JF. Physician retirement: Why it’s hard for doctors to retire. Medical Economics. 2019;96(4). Accessed April 25, 2025. https://www.medicaleconomics.com/view/physician-retirement-why-its-hard-doctors-retire
- Nelson J. Wisdom for Our Time. W.W. Norton; 1961.
- Silver MP, Hamilton AD, Biswas A, Williams SA. Life after medicine: a systematic review of studies physician’s adjustment to retirement. Arch Community Med Public Health. 2016;2(1):001-007. doi:10.17352/2455-5479.000006
Should I Stay or Should I Go? Federal Health Care Professional Retirement Dilemmas
Should I Stay or Should I Go? Federal Health Care Professional Retirement Dilemmas
