User login
M. Alexander Otto began his reporting career early in 1999 covering the pharmaceutical industry for a national pharmacists' magazine and freelancing for the Washington Post and other newspapers. He then joined BNA, now part of Bloomberg News, covering health law and the protection of people and animals in medical research. Alex next worked for the McClatchy Company. Based on his work, Alex won a year-long Knight Science Journalism Fellowship to MIT in 2008-2009. He joined the company shortly thereafter. Alex has a newspaper journalism degree from Syracuse (N.Y.) University and a master's degree in medical science -- a physician assistant degree -- from George Washington University. Alex is based in Seattle.
One prenatal steroid dose is better than none
VANCOUVER, B.C. – When there isn’t time for a full course of prenatal steroids before early preterm birth, a partial course is better than nothing, according to investigators at the National Institute of Child Health and Human Development’s Neonatal Research Network.
In a study of 5,248 infants born between 24 and 27 weeks’ gestational age who were alive at 18-22 months, 17.6% (120/683) whose mothers got no prenatal steroids (PNS) before delivery had cerebral palsy, a statistically significant difference from the 13% (178/1,369) whose mothers got one dose of PNS – betamethasone in almost all cases – and the 10.5% (336/3,196) whose mothers got the full course of two betamethasone doses, 24 hours apart.

Similarly, intact survival at follow-up – survival free of hearing loss, blindness, and cerebral palsy, plus scores greater than 85 points on the Bayley Scales of Infant and Toddler Development III – was 55% in the no-PNS infants, 65% in the partial-PNS infants, and 69% in the PNS infants who got a full course, all statistically significant differences.
Compared with full-course PNS infants, those who got no PNS (odds ratio, 1.4; 95% confidence interval, 1.2-1.7) or partial PNS (OR, 1.2; 95% CI, 1.1-1.4) were more likely to have died or have neurodevelopmental impairment at 18-22 months.
Earlier results of the study, at discharge, were largely the same, with greater survival and fewer neurodevelopmental impairments when mothers got at least one dose of PNS before delivery.
The reason was that even one dose before delivery helped prevent both brain hemorrhages and cystic periventricular leucomalacia, the investigators found.
Prenatal steroids have long been known to help prevent both problems. What’s new in the findings is confirmation that even one dose helps.
"The intention is always to give a complete course," but when imminent delivery makes that impossible, even "one dose is better than no dose. The results help us counsel parents when we know" what dose children got before delivery. Also, "for research, the question shouldn’t be [prenatal] steroids, yes or no," but the completeness of the course, said lead investigator and neonatologist Sanjay Chawla of the department of pediatrics at the Children’s Hospital of Michigan, Detroit.
"Some people say, ‘She’s going to C-section in an hour, so it doesn’t matter’" That’s wrong. "One shot [of betamethasone] is still better than nothing. It makes a difference," said Dr. Nathalie Maitre, a neonatologist at Vanderbilt University in Nashville, Tenn., who helped moderate Dr. Chawla’s presentation at the Pediatric Academic Societies annual meeting.
There were some significant differences between the groups. No-PNS infants were born a bit earlier, at a mean of 24 weeks instead of about 25 weeks, and were a bit lighter at birth, 690 g instead of almost 800 g in the partial and full PNS groups. They were also a bit more likely to be black and on Medicaid.
Also, partial and full PNS infants were a bit more likely to be born by C-section. Boys and girls were split 50-50 in all three groups.
Dr. Chawla and Dr. Maitre said they had no relevant financial disclosures. The National Institutes of Health funded the work.
The findings of this study are not surprising, but confirm what physicians have intuitively believed to be true: that a partial dose of antenatal steroids is better than no steroids for infants delivered preterm, commented Dr. James Cummings.
Two small retrospective studies done about 10 years ago suggested a dose-dependent effect of antenatal steroids on several neonatal outcomes, including intracranial hemorrhage and death, but neither study reported long-term follow-up data, as the current study does.
"We don't really know how much antenatal steroid to give the mother, because we have limited knowledge regarding the optimal fetal levels to improve outcome. But the data are irrefutable that maternal administration of steroids does reduce the risk of respiratory distress syndrome and intracranial hemorrhage. This study is reassuring and consistent with what we know," he said.
What is missing, and the researchers may have this information, is whether the proximity of steroid dosing to delivery affected outcomes. This is important, since we know that the physiologic effects of steroids generally accrue over several hours. This suggests that when threatened with a preterm delivery, the obstetrician shouldn't hesitate about giving steroids, but should administer them as soon as possible, Dr. Cummings said.
Dr. Cummings is vice chair of pediatrics at Albany (N.Y.) Medical College and a member of the American Academy of Pediatrics Committee on the Fetus and Newborn. Dr. Cummings, who was asked to comment on the study, said he had no relevant financial disclosures.
The findings of this study are not surprising, but confirm what physicians have intuitively believed to be true: that a partial dose of antenatal steroids is better than no steroids for infants delivered preterm, commented Dr. James Cummings.
Two small retrospective studies done about 10 years ago suggested a dose-dependent effect of antenatal steroids on several neonatal outcomes, including intracranial hemorrhage and death, but neither study reported long-term follow-up data, as the current study does.
"We don't really know how much antenatal steroid to give the mother, because we have limited knowledge regarding the optimal fetal levels to improve outcome. But the data are irrefutable that maternal administration of steroids does reduce the risk of respiratory distress syndrome and intracranial hemorrhage. This study is reassuring and consistent with what we know," he said.
What is missing, and the researchers may have this information, is whether the proximity of steroid dosing to delivery affected outcomes. This is important, since we know that the physiologic effects of steroids generally accrue over several hours. This suggests that when threatened with a preterm delivery, the obstetrician shouldn't hesitate about giving steroids, but should administer them as soon as possible, Dr. Cummings said.
Dr. Cummings is vice chair of pediatrics at Albany (N.Y.) Medical College and a member of the American Academy of Pediatrics Committee on the Fetus and Newborn. Dr. Cummings, who was asked to comment on the study, said he had no relevant financial disclosures.
The findings of this study are not surprising, but confirm what physicians have intuitively believed to be true: that a partial dose of antenatal steroids is better than no steroids for infants delivered preterm, commented Dr. James Cummings.
Two small retrospective studies done about 10 years ago suggested a dose-dependent effect of antenatal steroids on several neonatal outcomes, including intracranial hemorrhage and death, but neither study reported long-term follow-up data, as the current study does.
"We don't really know how much antenatal steroid to give the mother, because we have limited knowledge regarding the optimal fetal levels to improve outcome. But the data are irrefutable that maternal administration of steroids does reduce the risk of respiratory distress syndrome and intracranial hemorrhage. This study is reassuring and consistent with what we know," he said.
What is missing, and the researchers may have this information, is whether the proximity of steroid dosing to delivery affected outcomes. This is important, since we know that the physiologic effects of steroids generally accrue over several hours. This suggests that when threatened with a preterm delivery, the obstetrician shouldn't hesitate about giving steroids, but should administer them as soon as possible, Dr. Cummings said.
Dr. Cummings is vice chair of pediatrics at Albany (N.Y.) Medical College and a member of the American Academy of Pediatrics Committee on the Fetus and Newborn. Dr. Cummings, who was asked to comment on the study, said he had no relevant financial disclosures.
VANCOUVER, B.C. – When there isn’t time for a full course of prenatal steroids before early preterm birth, a partial course is better than nothing, according to investigators at the National Institute of Child Health and Human Development’s Neonatal Research Network.
In a study of 5,248 infants born between 24 and 27 weeks’ gestational age who were alive at 18-22 months, 17.6% (120/683) whose mothers got no prenatal steroids (PNS) before delivery had cerebral palsy, a statistically significant difference from the 13% (178/1,369) whose mothers got one dose of PNS – betamethasone in almost all cases – and the 10.5% (336/3,196) whose mothers got the full course of two betamethasone doses, 24 hours apart.
Similarly, intact survival at follow-up – survival free of hearing loss, blindness, and cerebral palsy, plus scores greater than 85 points on the Bayley Scales of Infant and Toddler Development III – was 55% in the no-PNS infants, 65% in the partial-PNS infants, and 69% in the PNS infants who got a full course, all statistically significant differences.
Compared with full-course PNS infants, those who got no PNS (odds ratio, 1.4; 95% confidence interval, 1.2-1.7) or partial PNS (OR, 1.2; 95% CI, 1.1-1.4) were more likely to have died or have neurodevelopmental impairment at 18-22 months.
Earlier results of the study, at discharge, were largely the same, with greater survival and fewer neurodevelopmental impairments when mothers got at least one dose of PNS before delivery.
The reason was that even one dose before delivery helped prevent both brain hemorrhages and cystic periventricular leucomalacia, the investigators found.
Prenatal steroids have long been known to help prevent both problems. What’s new in the findings is confirmation that even one dose helps.
"The intention is always to give a complete course," but when imminent delivery makes that impossible, even "one dose is better than no dose. The results help us counsel parents when we know" what dose children got before delivery. Also, "for research, the question shouldn’t be [prenatal] steroids, yes or no," but the completeness of the course, said lead investigator and neonatologist Sanjay Chawla of the department of pediatrics at the Children’s Hospital of Michigan, Detroit.
"Some people say, ‘She’s going to C-section in an hour, so it doesn’t matter’" That’s wrong. "One shot [of betamethasone] is still better than nothing. It makes a difference," said Dr. Nathalie Maitre, a neonatologist at Vanderbilt University in Nashville, Tenn., who helped moderate Dr. Chawla’s presentation at the Pediatric Academic Societies annual meeting.
There were some significant differences between the groups. No-PNS infants were born a bit earlier, at a mean of 24 weeks instead of about 25 weeks, and were a bit lighter at birth, 690 g instead of almost 800 g in the partial and full PNS groups. They were also a bit more likely to be black and on Medicaid.
Also, partial and full PNS infants were a bit more likely to be born by C-section. Boys and girls were split 50-50 in all three groups.
Dr. Chawla and Dr. Maitre said they had no relevant financial disclosures. The National Institutes of Health funded the work.
VANCOUVER, B.C. – When there isn’t time for a full course of prenatal steroids before early preterm birth, a partial course is better than nothing, according to investigators at the National Institute of Child Health and Human Development’s Neonatal Research Network.
In a study of 5,248 infants born between 24 and 27 weeks’ gestational age who were alive at 18-22 months, 17.6% (120/683) whose mothers got no prenatal steroids (PNS) before delivery had cerebral palsy, a statistically significant difference from the 13% (178/1,369) whose mothers got one dose of PNS – betamethasone in almost all cases – and the 10.5% (336/3,196) whose mothers got the full course of two betamethasone doses, 24 hours apart.
Similarly, intact survival at follow-up – survival free of hearing loss, blindness, and cerebral palsy, plus scores greater than 85 points on the Bayley Scales of Infant and Toddler Development III – was 55% in the no-PNS infants, 65% in the partial-PNS infants, and 69% in the PNS infants who got a full course, all statistically significant differences.
Compared with full-course PNS infants, those who got no PNS (odds ratio, 1.4; 95% confidence interval, 1.2-1.7) or partial PNS (OR, 1.2; 95% CI, 1.1-1.4) were more likely to have died or have neurodevelopmental impairment at 18-22 months.
Earlier results of the study, at discharge, were largely the same, with greater survival and fewer neurodevelopmental impairments when mothers got at least one dose of PNS before delivery.
The reason was that even one dose before delivery helped prevent both brain hemorrhages and cystic periventricular leucomalacia, the investigators found.
Prenatal steroids have long been known to help prevent both problems. What’s new in the findings is confirmation that even one dose helps.
"The intention is always to give a complete course," but when imminent delivery makes that impossible, even "one dose is better than no dose. The results help us counsel parents when we know" what dose children got before delivery. Also, "for research, the question shouldn’t be [prenatal] steroids, yes or no," but the completeness of the course, said lead investigator and neonatologist Sanjay Chawla of the department of pediatrics at the Children’s Hospital of Michigan, Detroit.
"Some people say, ‘She’s going to C-section in an hour, so it doesn’t matter’" That’s wrong. "One shot [of betamethasone] is still better than nothing. It makes a difference," said Dr. Nathalie Maitre, a neonatologist at Vanderbilt University in Nashville, Tenn., who helped moderate Dr. Chawla’s presentation at the Pediatric Academic Societies annual meeting.
There were some significant differences between the groups. No-PNS infants were born a bit earlier, at a mean of 24 weeks instead of about 25 weeks, and were a bit lighter at birth, 690 g instead of almost 800 g in the partial and full PNS groups. They were also a bit more likely to be black and on Medicaid.
Also, partial and full PNS infants were a bit more likely to be born by C-section. Boys and girls were split 50-50 in all three groups.
Dr. Chawla and Dr. Maitre said they had no relevant financial disclosures. The National Institutes of Health funded the work.
AT THE PAS ANNUAL MEETING
Key clinical point: It is important to give at least a partial course of prenatal steroids before early preterm delivery.
Major finding: Compared with complete prenatal steroid courses, no PNS (OR, 1.4; 95% CI, 1.2-1.7) and partial PNS (OR, 1.2; 95% CI, 1.1-1.4) are both associated with neurodevelopmental impairment and mortality at 18-22 months.
Data source: A Neonatal Research Network study of infants born from 24 to 27 weeks’ gestational age
Disclosures: The lead investigator had no disclosures. The National Institutes of Health funded the work.

Automated screening system might detect suicidality after trauma
LOS ANGELES – About half of trauma patients report suicidal ideation within a year of their injury, and about 20% do so at any given time during that year, according to an investigation of 206 patients at Harborview Medical Center, the University of Washington’s Level I trauma center in Seattle.
A patient’s ties to assault and some of the other risk factors identified in the study could be spotted automatically by electronic medical records (EMR) systems. With a few programming tweaks, records systems can alert clinicians to those most likely to be considering suicide so preventive steps can be taken, said lead investigator Stephen S. O’Connor, Ph.D., formerly of the University of Washington, but now with the department of psychological sciences at Western Kentucky University, in Bowling Green.

"We feel that this is a really pressing need. Suicidality is endemic within the trauma population, and a lot of it is under the radar." An automated screening system might prevent suicidal people from falling through the cracks amid the tumult of trauma and follow-up care, he said at the annual conference of the American Association of Suicidology.
At some point during the 12-month investigation, 101 (49%) patients acknowledged that they had thought they’d be better off dead or had thought about hurting themselves, as assessed by the Patient Health Questionnaire-9.
About 26% admitted to those feelings while in the hospital, and the number dipped only moderately during regular, semimonthly reassessments, with 18% of the sample acknowledging suicidal thoughts at month 12.
While in the hospital, suicidal ideation was predicted by a previous mental health visit (relative risk,1.89; 95% confidence interval, 1.02-3.5; P = .04); total score on the Personal Health Questionnaire Depression Scale-8 (RR ,1.12; 95% CI 1.07-1.19; P less than .001); and general mental health function on the Short Form Health Survey-12 (RR, 0.98; 95% CI 0.97-1.00; P = .04). There was also a nonsignificant trend for injury severity.
Having children was protective (RR, 0.55; 95% CI 0.35-0.85; P = .01).
After discharge, patients who had been assaulted were most likely to be considering suicide (RR 2.03; 95% CI 1.28-3.20; P less than 0.01), as were patients who had injury-related legal proceedings (RR, 4.32; 95% CI 2.24-8.33; P less than .001), thoughts of suicide while in the hospital (RR, 3.34; 95% CI 2.28-4.89; P less than .001), and histories of PTSD (posttraumatic stress disorder) (RR, 1.72; 95% CI 1.09-2.71; P = .02).
Being older (RR, 1.03; 95% CI 1.01-1.04; P less than .001) and in pain (RR, 1.11; 95% CI 1.00-1.22; P = .05) also increased the risk. Once again, a nonsignificant trend was found for injury severity.
"Many of these are the kinds of risk factors that you could pick up from sweeping the EMR. Being assaulted by someone quickly gets an ICD code," for instance, Dr. O’Connor said.
Harborview "already has an automated screening system for PTSD; you could do the same thing with suicidal ideation. We’re moving in that direction," he said, noting that the efforts, besides saving lives, would help meet the Joint Commission’s call for better identification of suicidal patients.
Data for the analysis came from a previous PTSD intervention trial at Harborview. All of the subjects had screened positive for PTSD at 1 month, as part of the earlier work. They were about 38 years old on average, about half were women, and about half had completed high school. About a quarter of the subjects reported annual incomes of $30,000 or more.
Dr. O’Connor has no relevant disclosures. The work was funded by the National Institutes of Health.
LOS ANGELES – About half of trauma patients report suicidal ideation within a year of their injury, and about 20% do so at any given time during that year, according to an investigation of 206 patients at Harborview Medical Center, the University of Washington’s Level I trauma center in Seattle.
A patient’s ties to assault and some of the other risk factors identified in the study could be spotted automatically by electronic medical records (EMR) systems. With a few programming tweaks, records systems can alert clinicians to those most likely to be considering suicide so preventive steps can be taken, said lead investigator Stephen S. O’Connor, Ph.D., formerly of the University of Washington, but now with the department of psychological sciences at Western Kentucky University, in Bowling Green.
"We feel that this is a really pressing need. Suicidality is endemic within the trauma population, and a lot of it is under the radar." An automated screening system might prevent suicidal people from falling through the cracks amid the tumult of trauma and follow-up care, he said at the annual conference of the American Association of Suicidology.
At some point during the 12-month investigation, 101 (49%) patients acknowledged that they had thought they’d be better off dead or had thought about hurting themselves, as assessed by the Patient Health Questionnaire-9.
About 26% admitted to those feelings while in the hospital, and the number dipped only moderately during regular, semimonthly reassessments, with 18% of the sample acknowledging suicidal thoughts at month 12.
While in the hospital, suicidal ideation was predicted by a previous mental health visit (relative risk,1.89; 95% confidence interval, 1.02-3.5; P = .04); total score on the Personal Health Questionnaire Depression Scale-8 (RR ,1.12; 95% CI 1.07-1.19; P less than .001); and general mental health function on the Short Form Health Survey-12 (RR, 0.98; 95% CI 0.97-1.00; P = .04). There was also a nonsignificant trend for injury severity.
Having children was protective (RR, 0.55; 95% CI 0.35-0.85; P = .01).
After discharge, patients who had been assaulted were most likely to be considering suicide (RR 2.03; 95% CI 1.28-3.20; P less than 0.01), as were patients who had injury-related legal proceedings (RR, 4.32; 95% CI 2.24-8.33; P less than .001), thoughts of suicide while in the hospital (RR, 3.34; 95% CI 2.28-4.89; P less than .001), and histories of PTSD (posttraumatic stress disorder) (RR, 1.72; 95% CI 1.09-2.71; P = .02).
Being older (RR, 1.03; 95% CI 1.01-1.04; P less than .001) and in pain (RR, 1.11; 95% CI 1.00-1.22; P = .05) also increased the risk. Once again, a nonsignificant trend was found for injury severity.
"Many of these are the kinds of risk factors that you could pick up from sweeping the EMR. Being assaulted by someone quickly gets an ICD code," for instance, Dr. O’Connor said.
Harborview "already has an automated screening system for PTSD; you could do the same thing with suicidal ideation. We’re moving in that direction," he said, noting that the efforts, besides saving lives, would help meet the Joint Commission’s call for better identification of suicidal patients.
Data for the analysis came from a previous PTSD intervention trial at Harborview. All of the subjects had screened positive for PTSD at 1 month, as part of the earlier work. They were about 38 years old on average, about half were women, and about half had completed high school. About a quarter of the subjects reported annual incomes of $30,000 or more.
Dr. O’Connor has no relevant disclosures. The work was funded by the National Institutes of Health.
LOS ANGELES – About half of trauma patients report suicidal ideation within a year of their injury, and about 20% do so at any given time during that year, according to an investigation of 206 patients at Harborview Medical Center, the University of Washington’s Level I trauma center in Seattle.
A patient’s ties to assault and some of the other risk factors identified in the study could be spotted automatically by electronic medical records (EMR) systems. With a few programming tweaks, records systems can alert clinicians to those most likely to be considering suicide so preventive steps can be taken, said lead investigator Stephen S. O’Connor, Ph.D., formerly of the University of Washington, but now with the department of psychological sciences at Western Kentucky University, in Bowling Green.
"We feel that this is a really pressing need. Suicidality is endemic within the trauma population, and a lot of it is under the radar." An automated screening system might prevent suicidal people from falling through the cracks amid the tumult of trauma and follow-up care, he said at the annual conference of the American Association of Suicidology.
At some point during the 12-month investigation, 101 (49%) patients acknowledged that they had thought they’d be better off dead or had thought about hurting themselves, as assessed by the Patient Health Questionnaire-9.
About 26% admitted to those feelings while in the hospital, and the number dipped only moderately during regular, semimonthly reassessments, with 18% of the sample acknowledging suicidal thoughts at month 12.
While in the hospital, suicidal ideation was predicted by a previous mental health visit (relative risk,1.89; 95% confidence interval, 1.02-3.5; P = .04); total score on the Personal Health Questionnaire Depression Scale-8 (RR ,1.12; 95% CI 1.07-1.19; P less than .001); and general mental health function on the Short Form Health Survey-12 (RR, 0.98; 95% CI 0.97-1.00; P = .04). There was also a nonsignificant trend for injury severity.
Having children was protective (RR, 0.55; 95% CI 0.35-0.85; P = .01).
After discharge, patients who had been assaulted were most likely to be considering suicide (RR 2.03; 95% CI 1.28-3.20; P less than 0.01), as were patients who had injury-related legal proceedings (RR, 4.32; 95% CI 2.24-8.33; P less than .001), thoughts of suicide while in the hospital (RR, 3.34; 95% CI 2.28-4.89; P less than .001), and histories of PTSD (posttraumatic stress disorder) (RR, 1.72; 95% CI 1.09-2.71; P = .02).
Being older (RR, 1.03; 95% CI 1.01-1.04; P less than .001) and in pain (RR, 1.11; 95% CI 1.00-1.22; P = .05) also increased the risk. Once again, a nonsignificant trend was found for injury severity.
"Many of these are the kinds of risk factors that you could pick up from sweeping the EMR. Being assaulted by someone quickly gets an ICD code," for instance, Dr. O’Connor said.
Harborview "already has an automated screening system for PTSD; you could do the same thing with suicidal ideation. We’re moving in that direction," he said, noting that the efforts, besides saving lives, would help meet the Joint Commission’s call for better identification of suicidal patients.
Data for the analysis came from a previous PTSD intervention trial at Harborview. All of the subjects had screened positive for PTSD at 1 month, as part of the earlier work. They were about 38 years old on average, about half were women, and about half had completed high school. About a quarter of the subjects reported annual incomes of $30,000 or more.
Dr. O’Connor has no relevant disclosures. The work was funded by the National Institutes of Health.
AT THE ANNUAL AAS CONFERENCE
Key clinical point: ‘Suicidality is endemic within the trauma population, and a lot of it is under the radar.’
Major finding: Victims of assault are more than twice as likely as other trauma patients to consider suicide (RR, 2.03; 95% CI 1.28-3.20; P less than .01); patients involved in legal proceedings because of their injuries are more than four times as likely (RR, 4.32; 95% CI 2.24-8.33; P less than.001).
Data source: 206 patients treated at a Level I trauma center.
Disclosures: Dr. O’Connor has no relevant disclosures. The work was funded by the National Institutes of Health.

Antimicrobial prophylaxis halves UTI risk in pediatric vesicoureteral reflux
VANCOUVER – Two years of low-dose trimethoprim-sulfamethoxazole prophylaxis halved the risk of recurrent urinary tract infections, but did not prevent renal scarring in a trial of 607 children with vesicoureteral reflux that was published online May 4 in the New England Journal of Medicine, and presented concurrently at the annual meeting of the Pediatric Academic Societies.
Within 112 days of their first or second febrile or symptomatic urinary tract infection (UTI), 302 young children diagnosed with vesicoureteral reflux (VUR) by voiding cystourethrogram were randomized to 3 mg of trimethoprim plus 15 mg of sulfamethoxazole per kilogram; and 305 other VUR children were randomized to placebo.

Thirty-nine (13%) children who received antimicrobial prophylaxis developed a recurrent febrile or symptomatic UTI, compared with 72 (24%) who received a placebo (hazard ratio for risk of recurrence, 0.50; 95% confidence interval, 0.34-0.74). Prophylaxis was particularly effective in children whose index UTI was febrile (HR, 0.41; 95% CI, 0.26-0.64) and in those with baseline bladder and bowel dysfunction (HR, 0.21; 95% CI, 0.08-0.58).
Nuclear imaging showed no significant between-group differences in the incidence of renal scarring (11.9% in the treated group vs. 10.2% in the placebo group; P = 0.55), severe renal scars (4.0% vs. 2.6%; P = 0.37), or new renal scars since baseline (8.2% vs. 8.4%; P = 0.94) at trial completion (N. Eng. J. Med. 2014 May 4 [doi: 10.1056/NEJMoa1401811]).
"This study showed unequivocal evidence that antimicrobial prophylaxis reduced at least in half the likelihood of children having recurrent UTIs. Rates of renal scarring ... were low and not reduced by prophylaxis, perhaps because most children were enrolled after their first infection and because parents, instructed to be vigilant, sought early medical attention," said Dr. Alejandro Hoberman, a professor of pediatrics at the University of Pittsburgh and lead investigator in the multicenter study, dubbed the RIVUR (Randomized Intervention for Children with Vesicoureteral Reflux) trial.
"As long as evidence supporting the benefit of prophylaxis was dubious, the recommendation of a watchful-waiting approach, without performance of a voiding cystourethrographic study, seemed reasonable, because the imaging findings would not affect the nature of treatment. However, our finding that antimicrobial prophylaxis was associated with a reduced risk of recurrence may warrant reconsideration of that recommendation," the investigators said.
Eight children would have had to be treated for 2 years to prevent one case of febrile or symptomatic UTI. Several audience members, after hearing the results, wondered if the benefits of prophylaxis outweighed the costs, given that there was no effect on the incidence of renal scarring in the short term, and the difficulty and expense of performing voiding cystourethrographic studies, among other concerns.
Dr. Hoberman plans to investigate the cost-effectiveness implications of the findings, and, in the meantime, he noted that the study offers proof that prophylaxis helps prevent recurrent UTIs, something that was uncertain in the past. Also, he noted, the study was not powered to detect a difference in renal scarring as a primary outcome.
The children were aged 2-71 months (median age, 12 months), and 92% were girls. Eighty percent had grade II or III vesicoureteral reflux, and 48% had bilateral reflux.
Among 87 children with a first recurrence caused by Escherichia coli, the proportion of isolates that were resistant to trimethoprim-sulfamethoxazole was 63% in the prophylaxis group and 19% in the placebo group. "Not unexpectedly, recurrences that did occur in children who received prophylaxis were more likely to have been caused by a resistant pathogen," the investigators said.
Parents of 77% of the children reported that they had given the study medication at least 75% of the time, and parents of 85% reported administering it at least 50% of the time. There was no significant difference in reported adherence between the study groups.
Dr. Hoberman had no disclosures. The work was funded by the National Institute of Diabetes and Digestive and Kidney Diseases.
"As in most studies of complex conditions, unresolved questions remain. Only one form of antibiotic prophylaxis was used [in the study]; therefore, the effectiveness of other prophylactic antibiotic strategies remains untested. The evaluation of scarring was determined after only 2 years, leaving the long-term degree of renal injury unknown.
Sadly, the decision to use antibiotic prophylaxis in children with reflux remains a clinical dilemma, despite this well-done study. In the face of the emergence of antibiotic resistance, the lack of a significant between-group difference in renal parenchymal scarring, and questions about generalizability, the RIVUR study results would imply that the general recommendation of prophylactic antibiotics for vesicoureteral reflux in young children awaits more evidence before universal adoption."
Dr. Julie Ingelfinger is the senior consultant in pediatric nephrology at the Massachusetts General Hospital in Boston. Dr. F. Bruder Stapleton is a professor and chair of pediatrics at the University of Washington in Seattle. They made their comments in an editorial that accompanied the study (N. Eng. J. Med. 2014 May 4 [doi: 10.1056/NEJMe1404774]), and they had no relevant disclosures.
"As in most studies of complex conditions, unresolved questions remain. Only one form of antibiotic prophylaxis was used [in the study]; therefore, the effectiveness of other prophylactic antibiotic strategies remains untested. The evaluation of scarring was determined after only 2 years, leaving the long-term degree of renal injury unknown.
Sadly, the decision to use antibiotic prophylaxis in children with reflux remains a clinical dilemma, despite this well-done study. In the face of the emergence of antibiotic resistance, the lack of a significant between-group difference in renal parenchymal scarring, and questions about generalizability, the RIVUR study results would imply that the general recommendation of prophylactic antibiotics for vesicoureteral reflux in young children awaits more evidence before universal adoption."
Dr. Julie Ingelfinger is the senior consultant in pediatric nephrology at the Massachusetts General Hospital in Boston. Dr. F. Bruder Stapleton is a professor and chair of pediatrics at the University of Washington in Seattle. They made their comments in an editorial that accompanied the study (N. Eng. J. Med. 2014 May 4 [doi: 10.1056/NEJMe1404774]), and they had no relevant disclosures.
"As in most studies of complex conditions, unresolved questions remain. Only one form of antibiotic prophylaxis was used [in the study]; therefore, the effectiveness of other prophylactic antibiotic strategies remains untested. The evaluation of scarring was determined after only 2 years, leaving the long-term degree of renal injury unknown.
Sadly, the decision to use antibiotic prophylaxis in children with reflux remains a clinical dilemma, despite this well-done study. In the face of the emergence of antibiotic resistance, the lack of a significant between-group difference in renal parenchymal scarring, and questions about generalizability, the RIVUR study results would imply that the general recommendation of prophylactic antibiotics for vesicoureteral reflux in young children awaits more evidence before universal adoption."
Dr. Julie Ingelfinger is the senior consultant in pediatric nephrology at the Massachusetts General Hospital in Boston. Dr. F. Bruder Stapleton is a professor and chair of pediatrics at the University of Washington in Seattle. They made their comments in an editorial that accompanied the study (N. Eng. J. Med. 2014 May 4 [doi: 10.1056/NEJMe1404774]), and they had no relevant disclosures.
VANCOUVER – Two years of low-dose trimethoprim-sulfamethoxazole prophylaxis halved the risk of recurrent urinary tract infections, but did not prevent renal scarring in a trial of 607 children with vesicoureteral reflux that was published online May 4 in the New England Journal of Medicine, and presented concurrently at the annual meeting of the Pediatric Academic Societies.
Within 112 days of their first or second febrile or symptomatic urinary tract infection (UTI), 302 young children diagnosed with vesicoureteral reflux (VUR) by voiding cystourethrogram were randomized to 3 mg of trimethoprim plus 15 mg of sulfamethoxazole per kilogram; and 305 other VUR children were randomized to placebo.
Thirty-nine (13%) children who received antimicrobial prophylaxis developed a recurrent febrile or symptomatic UTI, compared with 72 (24%) who received a placebo (hazard ratio for risk of recurrence, 0.50; 95% confidence interval, 0.34-0.74). Prophylaxis was particularly effective in children whose index UTI was febrile (HR, 0.41; 95% CI, 0.26-0.64) and in those with baseline bladder and bowel dysfunction (HR, 0.21; 95% CI, 0.08-0.58).
Nuclear imaging showed no significant between-group differences in the incidence of renal scarring (11.9% in the treated group vs. 10.2% in the placebo group; P = 0.55), severe renal scars (4.0% vs. 2.6%; P = 0.37), or new renal scars since baseline (8.2% vs. 8.4%; P = 0.94) at trial completion (N. Eng. J. Med. 2014 May 4 [doi: 10.1056/NEJMoa1401811]).
"This study showed unequivocal evidence that antimicrobial prophylaxis reduced at least in half the likelihood of children having recurrent UTIs. Rates of renal scarring ... were low and not reduced by prophylaxis, perhaps because most children were enrolled after their first infection and because parents, instructed to be vigilant, sought early medical attention," said Dr. Alejandro Hoberman, a professor of pediatrics at the University of Pittsburgh and lead investigator in the multicenter study, dubbed the RIVUR (Randomized Intervention for Children with Vesicoureteral Reflux) trial.
"As long as evidence supporting the benefit of prophylaxis was dubious, the recommendation of a watchful-waiting approach, without performance of a voiding cystourethrographic study, seemed reasonable, because the imaging findings would not affect the nature of treatment. However, our finding that antimicrobial prophylaxis was associated with a reduced risk of recurrence may warrant reconsideration of that recommendation," the investigators said.
Eight children would have had to be treated for 2 years to prevent one case of febrile or symptomatic UTI. Several audience members, after hearing the results, wondered if the benefits of prophylaxis outweighed the costs, given that there was no effect on the incidence of renal scarring in the short term, and the difficulty and expense of performing voiding cystourethrographic studies, among other concerns.
Dr. Hoberman plans to investigate the cost-effectiveness implications of the findings, and, in the meantime, he noted that the study offers proof that prophylaxis helps prevent recurrent UTIs, something that was uncertain in the past. Also, he noted, the study was not powered to detect a difference in renal scarring as a primary outcome.
The children were aged 2-71 months (median age, 12 months), and 92% were girls. Eighty percent had grade II or III vesicoureteral reflux, and 48% had bilateral reflux.
Among 87 children with a first recurrence caused by Escherichia coli, the proportion of isolates that were resistant to trimethoprim-sulfamethoxazole was 63% in the prophylaxis group and 19% in the placebo group. "Not unexpectedly, recurrences that did occur in children who received prophylaxis were more likely to have been caused by a resistant pathogen," the investigators said.
Parents of 77% of the children reported that they had given the study medication at least 75% of the time, and parents of 85% reported administering it at least 50% of the time. There was no significant difference in reported adherence between the study groups.
Dr. Hoberman had no disclosures. The work was funded by the National Institute of Diabetes and Digestive and Kidney Diseases.
VANCOUVER – Two years of low-dose trimethoprim-sulfamethoxazole prophylaxis halved the risk of recurrent urinary tract infections, but did not prevent renal scarring in a trial of 607 children with vesicoureteral reflux that was published online May 4 in the New England Journal of Medicine, and presented concurrently at the annual meeting of the Pediatric Academic Societies.
Within 112 days of their first or second febrile or symptomatic urinary tract infection (UTI), 302 young children diagnosed with vesicoureteral reflux (VUR) by voiding cystourethrogram were randomized to 3 mg of trimethoprim plus 15 mg of sulfamethoxazole per kilogram; and 305 other VUR children were randomized to placebo.
Thirty-nine (13%) children who received antimicrobial prophylaxis developed a recurrent febrile or symptomatic UTI, compared with 72 (24%) who received a placebo (hazard ratio for risk of recurrence, 0.50; 95% confidence interval, 0.34-0.74). Prophylaxis was particularly effective in children whose index UTI was febrile (HR, 0.41; 95% CI, 0.26-0.64) and in those with baseline bladder and bowel dysfunction (HR, 0.21; 95% CI, 0.08-0.58).
Nuclear imaging showed no significant between-group differences in the incidence of renal scarring (11.9% in the treated group vs. 10.2% in the placebo group; P = 0.55), severe renal scars (4.0% vs. 2.6%; P = 0.37), or new renal scars since baseline (8.2% vs. 8.4%; P = 0.94) at trial completion (N. Eng. J. Med. 2014 May 4 [doi: 10.1056/NEJMoa1401811]).
"This study showed unequivocal evidence that antimicrobial prophylaxis reduced at least in half the likelihood of children having recurrent UTIs. Rates of renal scarring ... were low and not reduced by prophylaxis, perhaps because most children were enrolled after their first infection and because parents, instructed to be vigilant, sought early medical attention," said Dr. Alejandro Hoberman, a professor of pediatrics at the University of Pittsburgh and lead investigator in the multicenter study, dubbed the RIVUR (Randomized Intervention for Children with Vesicoureteral Reflux) trial.
"As long as evidence supporting the benefit of prophylaxis was dubious, the recommendation of a watchful-waiting approach, without performance of a voiding cystourethrographic study, seemed reasonable, because the imaging findings would not affect the nature of treatment. However, our finding that antimicrobial prophylaxis was associated with a reduced risk of recurrence may warrant reconsideration of that recommendation," the investigators said.
Eight children would have had to be treated for 2 years to prevent one case of febrile or symptomatic UTI. Several audience members, after hearing the results, wondered if the benefits of prophylaxis outweighed the costs, given that there was no effect on the incidence of renal scarring in the short term, and the difficulty and expense of performing voiding cystourethrographic studies, among other concerns.
Dr. Hoberman plans to investigate the cost-effectiveness implications of the findings, and, in the meantime, he noted that the study offers proof that prophylaxis helps prevent recurrent UTIs, something that was uncertain in the past. Also, he noted, the study was not powered to detect a difference in renal scarring as a primary outcome.
The children were aged 2-71 months (median age, 12 months), and 92% were girls. Eighty percent had grade II or III vesicoureteral reflux, and 48% had bilateral reflux.
Among 87 children with a first recurrence caused by Escherichia coli, the proportion of isolates that were resistant to trimethoprim-sulfamethoxazole was 63% in the prophylaxis group and 19% in the placebo group. "Not unexpectedly, recurrences that did occur in children who received prophylaxis were more likely to have been caused by a resistant pathogen," the investigators said.
Parents of 77% of the children reported that they had given the study medication at least 75% of the time, and parents of 85% reported administering it at least 50% of the time. There was no significant difference in reported adherence between the study groups.
Dr. Hoberman had no disclosures. The work was funded by the National Institute of Diabetes and Digestive and Kidney Diseases.
AT THE PAS ANNUAL MEETING
Major finding: Over 2 years, 13% of children with vesicoureteral reflux who received antimicrobial prophylaxis developed a recurrent febrile or symptomatic UTI, compared with 24% who received a placebo (HR for risk of recurrence, 0.50; 95% CI, 0.34-0.74).
Data Source: Randomized, placebo-controlled trial in 607 children aged 2-71 months.
Disclosures: The lead investigator had no disclosures. The work was funded by the National Institute of Diabetes and Digestive and Kidney Diseases.

Laparoscopic-assisted colonoscopic polypectomy means shorter hospital stays
Laparoscopic-assisted colonoscopic polypectomy works as well as standard laparoscopic hemicolectomy to remove difficult to reach polyps in the right colon, with fewer complications and shorter hospital stays, according to data from a recent trial.
Instead of taking out a section of the ascending colon to remove the polyp, a surgeon uses a laparoscope to mobilize and position the right colon during laparoscopic-assisted colonoscopic polypectomy (LACP) so that an endoscopist can reach, snare, and remove it.
The team randomized 14 patients to LACP and 14 to laparoscopic hemicolectomy (LHC). The LACP group had shorter mean operating times (95 vs. 179 min.), less blood loss (13 vs. 63 mL), and required less intravenous fluid (2.1 vs. 3.1 L). LACP patients were also quicker to pass flatus (1.44 vs. 2.88 days), resume solid food (1.69 vs. 3.94 days), and leave the hospital (2.63 vs. 4.94 days), all statistically significant differences.
One LACP patient required conversion to LHC, while four LHC patients required conversion to laparotomy. There were no significant between-group differences in postoperative complications, readmissions, or second operations.
"That ability to remove polyps with LACP was as effective and safe as the standard laparoscopic hemicolectomy ... and patients were discharged from the hospital earlier. We think this is a very exciting change in how we deal with these difficult to remove colon polyps," said Dr. Jonathan Buscaglia, director of advanced endoscopy at Stony Brook (N.Y.) University.
There are a few case series in the literature about the technique, but uptake seems to have been slow so far. "I think the biggest roadblock is the ability of a surgeon to coordinate with a gastroenterologist. You need good working relationships, and schedules able to accommodate [both]. That’s not always easy, depending on where one works," Dr. Buscaglia said at a teleconference in advance of the annual Digestive Disease Week.
The patients in the trial had benign polyps with lift signs and generally tubular or tubulovillous adenomas. The groups were evenly matched for age, sex, body mass index, American Society of Anesthesiologists physical status, and previous abdominal surgery, plus polyp morphology, location, size, and histology.
It’s too soon after the procedures for serial surveillance colonoscopies and to know if any of the patients went on to develop cancer after their operations.
The right side is technically an easier place for laparoscopic surgeons to operate; with the left colon, operators have to worry more about diverticulitis, scarring, and tight anatomy. Even so, LACP may still be useful. "We are looking forward to conducting" a larger, possibly multicenter study on its application to polyps "in all areas of the colon," Dr. Buscaglia said.
The investigators have no disclosures.
Laparoscopic-assisted colonoscopic polypectomy works as well as standard laparoscopic hemicolectomy to remove difficult to reach polyps in the right colon, with fewer complications and shorter hospital stays, according to data from a recent trial.
Instead of taking out a section of the ascending colon to remove the polyp, a surgeon uses a laparoscope to mobilize and position the right colon during laparoscopic-assisted colonoscopic polypectomy (LACP) so that an endoscopist can reach, snare, and remove it.
The team randomized 14 patients to LACP and 14 to laparoscopic hemicolectomy (LHC). The LACP group had shorter mean operating times (95 vs. 179 min.), less blood loss (13 vs. 63 mL), and required less intravenous fluid (2.1 vs. 3.1 L). LACP patients were also quicker to pass flatus (1.44 vs. 2.88 days), resume solid food (1.69 vs. 3.94 days), and leave the hospital (2.63 vs. 4.94 days), all statistically significant differences.
One LACP patient required conversion to LHC, while four LHC patients required conversion to laparotomy. There were no significant between-group differences in postoperative complications, readmissions, or second operations.
"That ability to remove polyps with LACP was as effective and safe as the standard laparoscopic hemicolectomy ... and patients were discharged from the hospital earlier. We think this is a very exciting change in how we deal with these difficult to remove colon polyps," said Dr. Jonathan Buscaglia, director of advanced endoscopy at Stony Brook (N.Y.) University.
There are a few case series in the literature about the technique, but uptake seems to have been slow so far. "I think the biggest roadblock is the ability of a surgeon to coordinate with a gastroenterologist. You need good working relationships, and schedules able to accommodate [both]. That’s not always easy, depending on where one works," Dr. Buscaglia said at a teleconference in advance of the annual Digestive Disease Week.
The patients in the trial had benign polyps with lift signs and generally tubular or tubulovillous adenomas. The groups were evenly matched for age, sex, body mass index, American Society of Anesthesiologists physical status, and previous abdominal surgery, plus polyp morphology, location, size, and histology.
It’s too soon after the procedures for serial surveillance colonoscopies and to know if any of the patients went on to develop cancer after their operations.
The right side is technically an easier place for laparoscopic surgeons to operate; with the left colon, operators have to worry more about diverticulitis, scarring, and tight anatomy. Even so, LACP may still be useful. "We are looking forward to conducting" a larger, possibly multicenter study on its application to polyps "in all areas of the colon," Dr. Buscaglia said.
The investigators have no disclosures.
Laparoscopic-assisted colonoscopic polypectomy works as well as standard laparoscopic hemicolectomy to remove difficult to reach polyps in the right colon, with fewer complications and shorter hospital stays, according to data from a recent trial.
Instead of taking out a section of the ascending colon to remove the polyp, a surgeon uses a laparoscope to mobilize and position the right colon during laparoscopic-assisted colonoscopic polypectomy (LACP) so that an endoscopist can reach, snare, and remove it.
The team randomized 14 patients to LACP and 14 to laparoscopic hemicolectomy (LHC). The LACP group had shorter mean operating times (95 vs. 179 min.), less blood loss (13 vs. 63 mL), and required less intravenous fluid (2.1 vs. 3.1 L). LACP patients were also quicker to pass flatus (1.44 vs. 2.88 days), resume solid food (1.69 vs. 3.94 days), and leave the hospital (2.63 vs. 4.94 days), all statistically significant differences.
One LACP patient required conversion to LHC, while four LHC patients required conversion to laparotomy. There were no significant between-group differences in postoperative complications, readmissions, or second operations.
"That ability to remove polyps with LACP was as effective and safe as the standard laparoscopic hemicolectomy ... and patients were discharged from the hospital earlier. We think this is a very exciting change in how we deal with these difficult to remove colon polyps," said Dr. Jonathan Buscaglia, director of advanced endoscopy at Stony Brook (N.Y.) University.
There are a few case series in the literature about the technique, but uptake seems to have been slow so far. "I think the biggest roadblock is the ability of a surgeon to coordinate with a gastroenterologist. You need good working relationships, and schedules able to accommodate [both]. That’s not always easy, depending on where one works," Dr. Buscaglia said at a teleconference in advance of the annual Digestive Disease Week.
The patients in the trial had benign polyps with lift signs and generally tubular or tubulovillous adenomas. The groups were evenly matched for age, sex, body mass index, American Society of Anesthesiologists physical status, and previous abdominal surgery, plus polyp morphology, location, size, and histology.
It’s too soon after the procedures for serial surveillance colonoscopies and to know if any of the patients went on to develop cancer after their operations.
The right side is technically an easier place for laparoscopic surgeons to operate; with the left colon, operators have to worry more about diverticulitis, scarring, and tight anatomy. Even so, LACP may still be useful. "We are looking forward to conducting" a larger, possibly multicenter study on its application to polyps "in all areas of the colon," Dr. Buscaglia said.
The investigators have no disclosures.
FROM DDW 2014
Major finding: Compared with those undergoing laparoscopic hemicolectomy, patients whose right-colon polyps are removed by laparoscopic-assisted colonoscopic polypectomy have shorter mean operating times (95 min. vs. 179 min.), lose less blood (13 vs. 63 mL), and require less intravenous fluid (2.1 vs. 3.1 L). LACP patients are also quicker to pass flatus (1.44 vs. 2.88 days), resume solid food (1.69 vs. 3.94 days), and leave the hospital (2.63 vs. 4.94 days).
Data source: Randomized, unblinded trial in 28 patients with benign right-colon polyps.
Disclosures: The investigators have no disclosures.
NAFLD Mortality Higher in Normal Weight Patients
Lean patients with nonalcoholic fatty liver disease had a higher overall mortality than did overweight or obese patients with NAFLD, according to a review of 1,090 biopsy-confirmed patients in the United States, Australia, Thailand, and Europe.
Reviewing blood and other samples taken at the time of liver biopsy, the investigators found that the 125 (11.5%) patients with a body mass index (BMI) below 25 kg/m2 (average 23 kg/m2) had less insulin resistance and less advanced fibrosis than did the 965 (88.5%) who presented with higher BMIs (average 33 kg/m2).
But among the 483 patients biopsied before 2005, 9 of the 32 (28%) lean patients died, compared with 62 of the 451 (14%) who were overweight or obese.
The cumulative survival was significantly shorter in lean patients, as well; only lean NAFLD (hazard ratio, 11.8; 95% confidence interval, 2.8-50.1; P = .001) and age (HR, 1.05; 95% CI, 1.008-1.1; P =.02) remained significant when the findings were adjusted for sex, degree of fibrosis, and other confounding factors.
Cardiovascular disease, malignancy, and liver problems were the main causes of death in both lean and overweight patients; there were no significant differences between the groups, and the reason is unclear. Perhaps lean patients have greater central fat distribution; the team plans to investigate the matter further.
"I thought patients with lean fatty liver would have lower mortality; it was exactly the opposite. The risk factors for fatty liver go beyond a person’s body weight, and signs of liver disease secondary to NAFLD in lean patients should be taken very seriously. We must not assume that patients of relatively healthy weight can’t have fatty liver disease," said senior investigator Dr. Paul Angulo, chief of hepatology at the University of Kentucky Medical Center in Lexington.
"We need to be more aggressive in patients with lean fatty liver in terms of biopsy to see how much liver injury they have, and really make a concerted effort to increase their physical activity and change their diet. They don’t need to lose weight, but they need less fat and carbohydrates and more exercise to increase insulin sensitivity, especially in the muscle mass and liver," he said at a teleconference in advance of the annual Digestive Disease Week.
Lean NAFLD patients were more likely to be men; nonwhite, especially Asian and Hispanic; and to have fewer chronic conditions, such as diabetes, hypertension, and dyslipidemia. They also had lower levels of alanine aminotransferase, fewer fatty liver deposits, and less advanced fibrosis, but more severe lobular inflammation. There was no significant difference between the two groups in age (average, 46 years), hepatocyte ballooning, or incidence of nonalcoholic steatohepatitis.
The senior investigator has no disclosures. One of the other dozen investigators is on the board of Abbott, and another advises Bristol-Myers Squibb, Gilead, Merck, Novartis, and Roche.
I have patients like this in my practice, and I am certainly going to pay attention to them now. In the past, I had assumed that the absence of risk factors was a good thing, but now I’ve learned it may not be. Pending study that demonstrates a benefit for specific interventions, I am going to follow Dr. Angulo’s advice and encourage these patients to exercise more robustly. We need to find out the optimal approach for them.
Dr. Lawrence Friedman is chair of the department of medicine at Newton-Wellesley (Mass.) Hospital. He moderated Dr. Angulo’s presentation but was not involved in the project.
I have patients like this in my practice, and I am certainly going to pay attention to them now. In the past, I had assumed that the absence of risk factors was a good thing, but now I’ve learned it may not be. Pending study that demonstrates a benefit for specific interventions, I am going to follow Dr. Angulo’s advice and encourage these patients to exercise more robustly. We need to find out the optimal approach for them.
Dr. Lawrence Friedman is chair of the department of medicine at Newton-Wellesley (Mass.) Hospital. He moderated Dr. Angulo’s presentation but was not involved in the project.
I have patients like this in my practice, and I am certainly going to pay attention to them now. In the past, I had assumed that the absence of risk factors was a good thing, but now I’ve learned it may not be. Pending study that demonstrates a benefit for specific interventions, I am going to follow Dr. Angulo’s advice and encourage these patients to exercise more robustly. We need to find out the optimal approach for them.
Dr. Lawrence Friedman is chair of the department of medicine at Newton-Wellesley (Mass.) Hospital. He moderated Dr. Angulo’s presentation but was not involved in the project.
Lean patients with nonalcoholic fatty liver disease had a higher overall mortality than did overweight or obese patients with NAFLD, according to a review of 1,090 biopsy-confirmed patients in the United States, Australia, Thailand, and Europe.
Reviewing blood and other samples taken at the time of liver biopsy, the investigators found that the 125 (11.5%) patients with a body mass index (BMI) below 25 kg/m2 (average 23 kg/m2) had less insulin resistance and less advanced fibrosis than did the 965 (88.5%) who presented with higher BMIs (average 33 kg/m2).
But among the 483 patients biopsied before 2005, 9 of the 32 (28%) lean patients died, compared with 62 of the 451 (14%) who were overweight or obese.
The cumulative survival was significantly shorter in lean patients, as well; only lean NAFLD (hazard ratio, 11.8; 95% confidence interval, 2.8-50.1; P = .001) and age (HR, 1.05; 95% CI, 1.008-1.1; P =.02) remained significant when the findings were adjusted for sex, degree of fibrosis, and other confounding factors.
Cardiovascular disease, malignancy, and liver problems were the main causes of death in both lean and overweight patients; there were no significant differences between the groups, and the reason is unclear. Perhaps lean patients have greater central fat distribution; the team plans to investigate the matter further.
"I thought patients with lean fatty liver would have lower mortality; it was exactly the opposite. The risk factors for fatty liver go beyond a person’s body weight, and signs of liver disease secondary to NAFLD in lean patients should be taken very seriously. We must not assume that patients of relatively healthy weight can’t have fatty liver disease," said senior investigator Dr. Paul Angulo, chief of hepatology at the University of Kentucky Medical Center in Lexington.
"We need to be more aggressive in patients with lean fatty liver in terms of biopsy to see how much liver injury they have, and really make a concerted effort to increase their physical activity and change their diet. They don’t need to lose weight, but they need less fat and carbohydrates and more exercise to increase insulin sensitivity, especially in the muscle mass and liver," he said at a teleconference in advance of the annual Digestive Disease Week.
Lean NAFLD patients were more likely to be men; nonwhite, especially Asian and Hispanic; and to have fewer chronic conditions, such as diabetes, hypertension, and dyslipidemia. They also had lower levels of alanine aminotransferase, fewer fatty liver deposits, and less advanced fibrosis, but more severe lobular inflammation. There was no significant difference between the two groups in age (average, 46 years), hepatocyte ballooning, or incidence of nonalcoholic steatohepatitis.
The senior investigator has no disclosures. One of the other dozen investigators is on the board of Abbott, and another advises Bristol-Myers Squibb, Gilead, Merck, Novartis, and Roche.
Lean patients with nonalcoholic fatty liver disease had a higher overall mortality than did overweight or obese patients with NAFLD, according to a review of 1,090 biopsy-confirmed patients in the United States, Australia, Thailand, and Europe.
Reviewing blood and other samples taken at the time of liver biopsy, the investigators found that the 125 (11.5%) patients with a body mass index (BMI) below 25 kg/m2 (average 23 kg/m2) had less insulin resistance and less advanced fibrosis than did the 965 (88.5%) who presented with higher BMIs (average 33 kg/m2).
But among the 483 patients biopsied before 2005, 9 of the 32 (28%) lean patients died, compared with 62 of the 451 (14%) who were overweight or obese.
The cumulative survival was significantly shorter in lean patients, as well; only lean NAFLD (hazard ratio, 11.8; 95% confidence interval, 2.8-50.1; P = .001) and age (HR, 1.05; 95% CI, 1.008-1.1; P =.02) remained significant when the findings were adjusted for sex, degree of fibrosis, and other confounding factors.
Cardiovascular disease, malignancy, and liver problems were the main causes of death in both lean and overweight patients; there were no significant differences between the groups, and the reason is unclear. Perhaps lean patients have greater central fat distribution; the team plans to investigate the matter further.
"I thought patients with lean fatty liver would have lower mortality; it was exactly the opposite. The risk factors for fatty liver go beyond a person’s body weight, and signs of liver disease secondary to NAFLD in lean patients should be taken very seriously. We must not assume that patients of relatively healthy weight can’t have fatty liver disease," said senior investigator Dr. Paul Angulo, chief of hepatology at the University of Kentucky Medical Center in Lexington.
"We need to be more aggressive in patients with lean fatty liver in terms of biopsy to see how much liver injury they have, and really make a concerted effort to increase their physical activity and change their diet. They don’t need to lose weight, but they need less fat and carbohydrates and more exercise to increase insulin sensitivity, especially in the muscle mass and liver," he said at a teleconference in advance of the annual Digestive Disease Week.
Lean NAFLD patients were more likely to be men; nonwhite, especially Asian and Hispanic; and to have fewer chronic conditions, such as diabetes, hypertension, and dyslipidemia. They also had lower levels of alanine aminotransferase, fewer fatty liver deposits, and less advanced fibrosis, but more severe lobular inflammation. There was no significant difference between the two groups in age (average, 46 years), hepatocyte ballooning, or incidence of nonalcoholic steatohepatitis.
The senior investigator has no disclosures. One of the other dozen investigators is on the board of Abbott, and another advises Bristol-Myers Squibb, Gilead, Merck, Novartis, and Roche.
FROM DDW 2014
NAFLD mortality higher in normal weight patients
Lean patients with nonalcoholic fatty liver disease had a higher overall mortality than did overweight or obese patients with NAFLD, according to a review of 1,090 biopsy-confirmed patients in the United States, Australia, Thailand, and Europe.
Reviewing blood and other samples taken at the time of liver biopsy, the investigators found that the 125 (11.5%) patients with a body mass index (BMI) below 25 kg/m2 (average 23 kg/m2) had less insulin resistance and less advanced fibrosis than did the 965 (88.5%) who presented with higher BMIs (average 33 kg/m2).
But among the 483 patients biopsied before 2005, 9 of the 32 (28%) lean patients died, compared with 62 of the 451 (14%) who were overweight or obese.
The cumulative survival was significantly shorter in lean patients, as well; only lean NAFLD (hazard ratio, 11.8; 95% confidence interval, 2.8-50.1; P = .001) and age (HR, 1.05; 95% CI, 1.008-1.1; P =.02) remained significant when the findings were adjusted for sex, degree of fibrosis, and other confounding factors.
Cardiovascular disease, malignancy, and liver problems were the main causes of death in both lean and overweight patients; there were no significant differences between the groups, and the reason is unclear. Perhaps lean patients have greater central fat distribution; the team plans to investigate the matter further.
"I thought patients with lean fatty liver would have lower mortality; it was exactly the opposite. The risk factors for fatty liver go beyond a person’s body weight, and signs of liver disease secondary to NAFLD in lean patients should be taken very seriously. We must not assume that patients of relatively healthy weight can’t have fatty liver disease," said senior investigator Dr. Paul Angulo, chief of hepatology at the University of Kentucky Medical Center in Lexington.
"We need to be more aggressive in patients with lean fatty liver in terms of biopsy to see how much liver injury they have, and really make a concerted effort to increase their physical activity and change their diet. They don’t need to lose weight, but they need less fat and carbohydrates and more exercise to increase insulin sensitivity, especially in the muscle mass and liver," he said at a teleconference in advance of the annual Digestive Disease Week.
Lean NAFLD patients were more likely to be men; nonwhite, especially Asian and Hispanic; and to have fewer chronic conditions, such as diabetes, hypertension, and dyslipidemia. They also had lower levels of alanine aminotransferase, fewer fatty liver deposits, and less advanced fibrosis, but more severe lobular inflammation. There was no significant difference between the two groups in age (average, 46 years), hepatocyte ballooning, or incidence of nonalcoholic steatohepatitis.
The senior investigator has no disclosures. One of the other dozen investigators is on the board of Abbott, and another advises Bristol-Myers Squibb, Gilead, Merck, Novartis, and Roche.
I have patients like this in my practice, and I am certainly going to pay attention to them now. In the past, I had assumed that the absence of risk factors was a good thing, but now I’ve learned it may not be. Pending study that demonstrates a benefit for specific interventions, I am going to follow Dr. Angulo’s advice and encourage these patients to exercise more robustly. We need to find out the optimal approach for them.
Dr. Lawrence Friedman is chair of the department of medicine at Newton-Wellesley (Mass.) Hospital. He moderated Dr. Angulo’s presentation but was not involved in the project.
I have patients like this in my practice, and I am certainly going to pay attention to them now. In the past, I had assumed that the absence of risk factors was a good thing, but now I’ve learned it may not be. Pending study that demonstrates a benefit for specific interventions, I am going to follow Dr. Angulo’s advice and encourage these patients to exercise more robustly. We need to find out the optimal approach for them.
Dr. Lawrence Friedman is chair of the department of medicine at Newton-Wellesley (Mass.) Hospital. He moderated Dr. Angulo’s presentation but was not involved in the project.
I have patients like this in my practice, and I am certainly going to pay attention to them now. In the past, I had assumed that the absence of risk factors was a good thing, but now I’ve learned it may not be. Pending study that demonstrates a benefit for specific interventions, I am going to follow Dr. Angulo’s advice and encourage these patients to exercise more robustly. We need to find out the optimal approach for them.
Dr. Lawrence Friedman is chair of the department of medicine at Newton-Wellesley (Mass.) Hospital. He moderated Dr. Angulo’s presentation but was not involved in the project.
Lean patients with nonalcoholic fatty liver disease had a higher overall mortality than did overweight or obese patients with NAFLD, according to a review of 1,090 biopsy-confirmed patients in the United States, Australia, Thailand, and Europe.
Reviewing blood and other samples taken at the time of liver biopsy, the investigators found that the 125 (11.5%) patients with a body mass index (BMI) below 25 kg/m2 (average 23 kg/m2) had less insulin resistance and less advanced fibrosis than did the 965 (88.5%) who presented with higher BMIs (average 33 kg/m2).
But among the 483 patients biopsied before 2005, 9 of the 32 (28%) lean patients died, compared with 62 of the 451 (14%) who were overweight or obese.
The cumulative survival was significantly shorter in lean patients, as well; only lean NAFLD (hazard ratio, 11.8; 95% confidence interval, 2.8-50.1; P = .001) and age (HR, 1.05; 95% CI, 1.008-1.1; P =.02) remained significant when the findings were adjusted for sex, degree of fibrosis, and other confounding factors.
Cardiovascular disease, malignancy, and liver problems were the main causes of death in both lean and overweight patients; there were no significant differences between the groups, and the reason is unclear. Perhaps lean patients have greater central fat distribution; the team plans to investigate the matter further.
"I thought patients with lean fatty liver would have lower mortality; it was exactly the opposite. The risk factors for fatty liver go beyond a person’s body weight, and signs of liver disease secondary to NAFLD in lean patients should be taken very seriously. We must not assume that patients of relatively healthy weight can’t have fatty liver disease," said senior investigator Dr. Paul Angulo, chief of hepatology at the University of Kentucky Medical Center in Lexington.
"We need to be more aggressive in patients with lean fatty liver in terms of biopsy to see how much liver injury they have, and really make a concerted effort to increase their physical activity and change their diet. They don’t need to lose weight, but they need less fat and carbohydrates and more exercise to increase insulin sensitivity, especially in the muscle mass and liver," he said at a teleconference in advance of the annual Digestive Disease Week.
Lean NAFLD patients were more likely to be men; nonwhite, especially Asian and Hispanic; and to have fewer chronic conditions, such as diabetes, hypertension, and dyslipidemia. They also had lower levels of alanine aminotransferase, fewer fatty liver deposits, and less advanced fibrosis, but more severe lobular inflammation. There was no significant difference between the two groups in age (average, 46 years), hepatocyte ballooning, or incidence of nonalcoholic steatohepatitis.
The senior investigator has no disclosures. One of the other dozen investigators is on the board of Abbott, and another advises Bristol-Myers Squibb, Gilead, Merck, Novartis, and Roche.
Lean patients with nonalcoholic fatty liver disease had a higher overall mortality than did overweight or obese patients with NAFLD, according to a review of 1,090 biopsy-confirmed patients in the United States, Australia, Thailand, and Europe.
Reviewing blood and other samples taken at the time of liver biopsy, the investigators found that the 125 (11.5%) patients with a body mass index (BMI) below 25 kg/m2 (average 23 kg/m2) had less insulin resistance and less advanced fibrosis than did the 965 (88.5%) who presented with higher BMIs (average 33 kg/m2).
But among the 483 patients biopsied before 2005, 9 of the 32 (28%) lean patients died, compared with 62 of the 451 (14%) who were overweight or obese.
The cumulative survival was significantly shorter in lean patients, as well; only lean NAFLD (hazard ratio, 11.8; 95% confidence interval, 2.8-50.1; P = .001) and age (HR, 1.05; 95% CI, 1.008-1.1; P =.02) remained significant when the findings were adjusted for sex, degree of fibrosis, and other confounding factors.
Cardiovascular disease, malignancy, and liver problems were the main causes of death in both lean and overweight patients; there were no significant differences between the groups, and the reason is unclear. Perhaps lean patients have greater central fat distribution; the team plans to investigate the matter further.
"I thought patients with lean fatty liver would have lower mortality; it was exactly the opposite. The risk factors for fatty liver go beyond a person’s body weight, and signs of liver disease secondary to NAFLD in lean patients should be taken very seriously. We must not assume that patients of relatively healthy weight can’t have fatty liver disease," said senior investigator Dr. Paul Angulo, chief of hepatology at the University of Kentucky Medical Center in Lexington.
"We need to be more aggressive in patients with lean fatty liver in terms of biopsy to see how much liver injury they have, and really make a concerted effort to increase their physical activity and change their diet. They don’t need to lose weight, but they need less fat and carbohydrates and more exercise to increase insulin sensitivity, especially in the muscle mass and liver," he said at a teleconference in advance of the annual Digestive Disease Week.
Lean NAFLD patients were more likely to be men; nonwhite, especially Asian and Hispanic; and to have fewer chronic conditions, such as diabetes, hypertension, and dyslipidemia. They also had lower levels of alanine aminotransferase, fewer fatty liver deposits, and less advanced fibrosis, but more severe lobular inflammation. There was no significant difference between the two groups in age (average, 46 years), hepatocyte ballooning, or incidence of nonalcoholic steatohepatitis.
The senior investigator has no disclosures. One of the other dozen investigators is on the board of Abbott, and another advises Bristol-Myers Squibb, Gilead, Merck, Novartis, and Roche.
FROM DDW 2014
Major finding: Among 483 patients with liver biopsies before 2005, 9 of the 32 (28%) lean patients died, compared with 62 of the 451 (14%) who were overweight or obese.
Data source: Retrospective, international review of 1,090 NAFLD cases.
Disclosures: The senior investigator has no disclosures. One of the other dozen investigators is on the board of Abbott, and another advises Bristol-Myers Squibb, Gilead, Merck, Novartis, and Roche.
VIDEO: After suicide, survivors need help
LOS ANGELES – In some ways, those left behind after a suicide are the forgotten victims. They suffer posttraumatic stress disorder and are at high risk for taking their own lives – but often have a hard time finding help.
That’s why Ronnie S. Walker, a licensed clinical mental health counselor in the Chicago area, founded the Alliance of Hope for Suicide Survivors, an online resource with a clinically moderated forum where survivors can share their stories and get help from one another and from professionals. About 20,000 people visit the website each month, and a few new survivors join the forum just about every day.
In this video, Ms. Walker, a survivor herself, shared her insights about what those left behind go through and the help that they need at the annual conference of the American Association of Suicidology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LOS ANGELES – In some ways, those left behind after a suicide are the forgotten victims. They suffer posttraumatic stress disorder and are at high risk for taking their own lives – but often have a hard time finding help.
That’s why Ronnie S. Walker, a licensed clinical mental health counselor in the Chicago area, founded the Alliance of Hope for Suicide Survivors, an online resource with a clinically moderated forum where survivors can share their stories and get help from one another and from professionals. About 20,000 people visit the website each month, and a few new survivors join the forum just about every day.
In this video, Ms. Walker, a survivor herself, shared her insights about what those left behind go through and the help that they need at the annual conference of the American Association of Suicidology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LOS ANGELES – In some ways, those left behind after a suicide are the forgotten victims. They suffer posttraumatic stress disorder and are at high risk for taking their own lives – but often have a hard time finding help.
That’s why Ronnie S. Walker, a licensed clinical mental health counselor in the Chicago area, founded the Alliance of Hope for Suicide Survivors, an online resource with a clinically moderated forum where survivors can share their stories and get help from one another and from professionals. About 20,000 people visit the website each month, and a few new survivors join the forum just about every day.
In this video, Ms. Walker, a survivor herself, shared her insights about what those left behind go through and the help that they need at the annual conference of the American Association of Suicidology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ANNUAL AAS CONFERENCE

Air pollution linked to suicide risk
LOS ANGELES – Exposure to air pollution might be linked to suicide risk, investigators in Salt Lake County, Utah, suggest.
Using the Environmental Protection Agency’s air data Web site, Amanda V. Bakian, Ph.D., and her associates checked air quality in the 3 days leading up to each of the 1,546 suicides in the county from 2000 to 2010, dividing the concentration of pollution into quartiles. They found a 20% increase in suicide risk between the lowest and highest quartiles of nitrogen dioxide (adjusted odds ratio, 1.20; 95% CI, 1.04-1.39), and a 5% interquartile risk increase for fine particulate matter (AOR, 1.05; 95% CI, 1.01-1.10).
The finding was not surprising; suicide risk has been linked to particulate matter in both Taiwan and South Korea, but "it’s interesting that we see consistent findings for areas that are vastly different culturally, meteorologically, and geographically," said Dr. Bakian of the department of psychiatry at the University of Utah, Salt Lake City, lead investigator of the study.

What was surprising was that the risk was not worst in the winter, when temperature inversions are most likely to trap air pollution in the area’s valleys. Instead, suicide risk was greatest in the spring after exposure to high levels of fine particles (AOR, 1.28; 95% CI, 1.00-1.61), and in the spring/fall transition after exposure to high levels of nitrogen dioxide (AOR, 1.34; 95% CI, 1.09-1.66).
"I was surprised we didn’t find peak association in winter. [Perhaps,] air pollution is interacting with other springtime risk factors for suicide, such as pollen and maybe mood disorders; we see suicide peaks in the spring for individuals with mood disorders," Dr. Bakian said.
"We didn’t design the study to test cause and effect, so we cannot say that air pollution causes suicide. The study was only designed to look for a relationship between the two," she said. Next up, the team plans to review patient-level data, including psychiatric histories and socioeconomic status.
Air pollution exposures are tied to cognitive deficits, oxidative stress, neuroinflammation, and neurodegeneration (Exp. Toxicol. Pathol. 2013;65:503-11). Fossil fuels are the primary source of both fine particulate matter and nitrogen dioxide. Indoor sources of fine particles include tobacco smoke, fuel-burning space heaters, and cooking.
If the link to suicide proves real, Dr. Bakian suggested oxidative stress or hypoxia as two possible explanations. In the meantime, "air pollution is a modifiable risk factor; people can reduce their exposure." Besides environmental clean-up, face masks and indoor air filters might help, she said.
The team found no suicide link for atmospheric concentrations of coarse particulate matter and sulfur dioxide.
Dr. Bakian has no relevant disclosures. The work had no outside funding.
LOS ANGELES – Exposure to air pollution might be linked to suicide risk, investigators in Salt Lake County, Utah, suggest.
Using the Environmental Protection Agency’s air data Web site, Amanda V. Bakian, Ph.D., and her associates checked air quality in the 3 days leading up to each of the 1,546 suicides in the county from 2000 to 2010, dividing the concentration of pollution into quartiles. They found a 20% increase in suicide risk between the lowest and highest quartiles of nitrogen dioxide (adjusted odds ratio, 1.20; 95% CI, 1.04-1.39), and a 5% interquartile risk increase for fine particulate matter (AOR, 1.05; 95% CI, 1.01-1.10).
The finding was not surprising; suicide risk has been linked to particulate matter in both Taiwan and South Korea, but "it’s interesting that we see consistent findings for areas that are vastly different culturally, meteorologically, and geographically," said Dr. Bakian of the department of psychiatry at the University of Utah, Salt Lake City, lead investigator of the study.
What was surprising was that the risk was not worst in the winter, when temperature inversions are most likely to trap air pollution in the area’s valleys. Instead, suicide risk was greatest in the spring after exposure to high levels of fine particles (AOR, 1.28; 95% CI, 1.00-1.61), and in the spring/fall transition after exposure to high levels of nitrogen dioxide (AOR, 1.34; 95% CI, 1.09-1.66).
"I was surprised we didn’t find peak association in winter. [Perhaps,] air pollution is interacting with other springtime risk factors for suicide, such as pollen and maybe mood disorders; we see suicide peaks in the spring for individuals with mood disorders," Dr. Bakian said.
"We didn’t design the study to test cause and effect, so we cannot say that air pollution causes suicide. The study was only designed to look for a relationship between the two," she said. Next up, the team plans to review patient-level data, including psychiatric histories and socioeconomic status.
Air pollution exposures are tied to cognitive deficits, oxidative stress, neuroinflammation, and neurodegeneration (Exp. Toxicol. Pathol. 2013;65:503-11). Fossil fuels are the primary source of both fine particulate matter and nitrogen dioxide. Indoor sources of fine particles include tobacco smoke, fuel-burning space heaters, and cooking.
If the link to suicide proves real, Dr. Bakian suggested oxidative stress or hypoxia as two possible explanations. In the meantime, "air pollution is a modifiable risk factor; people can reduce their exposure." Besides environmental clean-up, face masks and indoor air filters might help, she said.
The team found no suicide link for atmospheric concentrations of coarse particulate matter and sulfur dioxide.
Dr. Bakian has no relevant disclosures. The work had no outside funding.
LOS ANGELES – Exposure to air pollution might be linked to suicide risk, investigators in Salt Lake County, Utah, suggest.
Using the Environmental Protection Agency’s air data Web site, Amanda V. Bakian, Ph.D., and her associates checked air quality in the 3 days leading up to each of the 1,546 suicides in the county from 2000 to 2010, dividing the concentration of pollution into quartiles. They found a 20% increase in suicide risk between the lowest and highest quartiles of nitrogen dioxide (adjusted odds ratio, 1.20; 95% CI, 1.04-1.39), and a 5% interquartile risk increase for fine particulate matter (AOR, 1.05; 95% CI, 1.01-1.10).
The finding was not surprising; suicide risk has been linked to particulate matter in both Taiwan and South Korea, but "it’s interesting that we see consistent findings for areas that are vastly different culturally, meteorologically, and geographically," said Dr. Bakian of the department of psychiatry at the University of Utah, Salt Lake City, lead investigator of the study.
What was surprising was that the risk was not worst in the winter, when temperature inversions are most likely to trap air pollution in the area’s valleys. Instead, suicide risk was greatest in the spring after exposure to high levels of fine particles (AOR, 1.28; 95% CI, 1.00-1.61), and in the spring/fall transition after exposure to high levels of nitrogen dioxide (AOR, 1.34; 95% CI, 1.09-1.66).
"I was surprised we didn’t find peak association in winter. [Perhaps,] air pollution is interacting with other springtime risk factors for suicide, such as pollen and maybe mood disorders; we see suicide peaks in the spring for individuals with mood disorders," Dr. Bakian said.
"We didn’t design the study to test cause and effect, so we cannot say that air pollution causes suicide. The study was only designed to look for a relationship between the two," she said. Next up, the team plans to review patient-level data, including psychiatric histories and socioeconomic status.
Air pollution exposures are tied to cognitive deficits, oxidative stress, neuroinflammation, and neurodegeneration (Exp. Toxicol. Pathol. 2013;65:503-11). Fossil fuels are the primary source of both fine particulate matter and nitrogen dioxide. Indoor sources of fine particles include tobacco smoke, fuel-burning space heaters, and cooking.
If the link to suicide proves real, Dr. Bakian suggested oxidative stress or hypoxia as two possible explanations. In the meantime, "air pollution is a modifiable risk factor; people can reduce their exposure." Besides environmental clean-up, face masks and indoor air filters might help, she said.
The team found no suicide link for atmospheric concentrations of coarse particulate matter and sulfur dioxide.
Dr. Bakian has no relevant disclosures. The work had no outside funding.
AT THE AMERICAN ASSOCIATION OF SUICIDOLOGY ANNUAL MEETING
Major finding: A 20% increase in suicide risk was found when levels of atmospheric nitrogen dioxide are at their highest and a 5% increase when fine particles are at their peak.
Data source: The findings are based on a coupling of air-quality data and the timing of 1,546 suicides from 2000 to 2010.
Disclosures: The lead investigator has no relevant disclosures, and the work received no outside funding.

Despite VTE prophylaxis, more bleeds, no benefit in medical inpatients
LAS VEGAS – Venous thromboembolism prophylaxis does not seem to prevent symptomatic deep vein thrombosis or pulmonary embolism in nonsurgical, non-ICU hospital patients, but it does seem to increase the risk of major bleeding, according to a series of large, observational studies from the Michigan Hospital Medicine Safety Consortium, a quality improvement program involving 40 Michigan hospitals.
Spurred by the Joint Commission and others, hospitalists across the United States have "put their foot on the gas to increase pharmacologic prophylaxis, and we’re using it in patients we think really should get it, but also in some patients who probably shouldn’t. We need more research to" distinguish between the two groups. "Many of us feel that the pendulum has swung too far, and that we need to bring it back to the middle," said investigator Dr. Scott Kaatz, chief quality officer and leader of the hospitalist program at Hurley Medical Center in Flint, Mich.
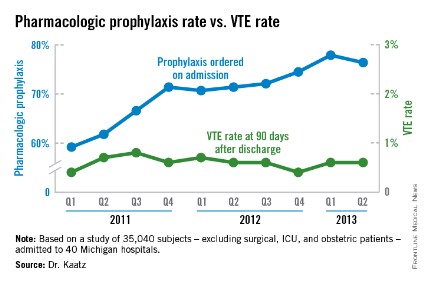
Among the Consortium’s findings, venous thromboembolism (VTE) prophylaxis – generally a subcutaneous shot with a heparin product – was ordered at admission for 59.2% of general adult inpatients in the first quarter of 2011, excluding surgical, ICU, and obstetric patients. By the second quarter of 2013, that had risen to 76.4%. Even so, among the 35,040 subjects included in the analysis, the rate of symptomatic VTEs averaged 0.56% throughout the observation period, and did not decrease as more patients were prophylaxed (P for trend = .114). The investigators followed their subjects in the hospital, and for 3 months afterward.
"We have not shown a good correlation between increasing prophylaxis and decreasing hospital-associated VTE," Dr. Kaatz said at the Society of Hospital Medicine annual meeting.
Meanwhile, in a second analysis of 26,205 prophylaxed medical inpatients, the rates of major bleeding tripled from 0.2% to 0.6% over the 2-plus years that prophylaxis was becoming more common (P = .052). Prophylaxis rates also climbed from 8.7% to 25.8% among a subset of 1,165 patients contraindicated because of their bleeding risks. The relationship between contraindications and the increased bleeding rate isn’t clear; some who bled had contraindications, but others did not.

"Five years ago, I was an advocate: prophylaxis everybody. [Now,] I’m really worried that I might be causing some bleeding. VTE rates are pretty low," and lower than once thought among general medical inpatients, may be caused by early mobilization and shorter hospital stays. "We are really spending a lot of effort to prophylaxis something that’s" uncommon, without clear benefit and possible harm. "I think several of us will take [these findings] back to our hospitals to change our prophylaxis protocols," Dr. Kaatz said.
Consortium members came up with their own list of contraindications because "there’s not a lot of literature, unfortunately," to help, he noted. The list included brain metastases; intracranial monitoring devices; severe head or spine trauma within 24 hours; gastrointestinal, genitourinary or other hemorrhages within 6 months; intracranial hemorrhage within a year; and platelet counts below 50,000/mm3.
The Caprini score is one of several proposed to distinguish high-risk VTE patients from others, but in a third study, investigators found that it "did not effectively discriminate populations for which pharmacologic prophylaxis was useful." Scores of 5 or higher did predict risk, but among high-scorers, 0.72% who received prophylaxis – and 0.86% who did not – developed VTEs, an insignificant difference (P = .26). Michigan researchers have found other scoring systems to be problematic, as well.
"The mantra for years now has been to prophylaxis for VTEs, so a lot of us are treating to prophylaxis everybody," even low Caprini-score patients. "Now, we’re taking a step back. There’s a movement toward weighing VTE and bleeding risks. If we can find the population that doesn’t warrant prophylaxis, that would be a big step," said investigator Dr. Paul Grant, a hospitalist who is with the internal medicine department at the University of Michigan in Ann Arbor.
The consortium is funded by Blue Cross/Blue Shield of Michigan and the Blue Care Network. Dr. Grant has no disclosures. Dr. Kaatz is a speaker for Boehringer Ingelheim, Janssen, Daiichi Sankyo, and Bristol-Myers Squibb.
It may be worth looking again at prophylaxis in the general medical inpatient who’s at low risk for VTE, and who’s going to be in the hospital for a short period of time. It’s been generally believed that hospitalized patients are at moderate risk, but as we are getting more data like these, we are realizing that there may be a population of hospitalized patients who are at lower risk than we thought. That raises a question: Do they really need prophylaxis?
In general, we need to be more thoughtful about VTE prophylaxis. It costs money, and may have adverse outcomes.
Dr. Eduard E. Vasilevskis is a hospitalist and is in the department of medicine at Vanderbilt University in Nashville, Tenn. He has no relevant disclosures.
It may be worth looking again at prophylaxis in the general medical inpatient who’s at low risk for VTE, and who’s going to be in the hospital for a short period of time. It’s been generally believed that hospitalized patients are at moderate risk, but as we are getting more data like these, we are realizing that there may be a population of hospitalized patients who are at lower risk than we thought. That raises a question: Do they really need prophylaxis?
In general, we need to be more thoughtful about VTE prophylaxis. It costs money, and may have adverse outcomes.
Dr. Eduard E. Vasilevskis is a hospitalist and is in the department of medicine at Vanderbilt University in Nashville, Tenn. He has no relevant disclosures.
It may be worth looking again at prophylaxis in the general medical inpatient who’s at low risk for VTE, and who’s going to be in the hospital for a short period of time. It’s been generally believed that hospitalized patients are at moderate risk, but as we are getting more data like these, we are realizing that there may be a population of hospitalized patients who are at lower risk than we thought. That raises a question: Do they really need prophylaxis?
In general, we need to be more thoughtful about VTE prophylaxis. It costs money, and may have adverse outcomes.
Dr. Eduard E. Vasilevskis is a hospitalist and is in the department of medicine at Vanderbilt University in Nashville, Tenn. He has no relevant disclosures.
LAS VEGAS – Venous thromboembolism prophylaxis does not seem to prevent symptomatic deep vein thrombosis or pulmonary embolism in nonsurgical, non-ICU hospital patients, but it does seem to increase the risk of major bleeding, according to a series of large, observational studies from the Michigan Hospital Medicine Safety Consortium, a quality improvement program involving 40 Michigan hospitals.
Spurred by the Joint Commission and others, hospitalists across the United States have "put their foot on the gas to increase pharmacologic prophylaxis, and we’re using it in patients we think really should get it, but also in some patients who probably shouldn’t. We need more research to" distinguish between the two groups. "Many of us feel that the pendulum has swung too far, and that we need to bring it back to the middle," said investigator Dr. Scott Kaatz, chief quality officer and leader of the hospitalist program at Hurley Medical Center in Flint, Mich.
Among the Consortium’s findings, venous thromboembolism (VTE) prophylaxis – generally a subcutaneous shot with a heparin product – was ordered at admission for 59.2% of general adult inpatients in the first quarter of 2011, excluding surgical, ICU, and obstetric patients. By the second quarter of 2013, that had risen to 76.4%. Even so, among the 35,040 subjects included in the analysis, the rate of symptomatic VTEs averaged 0.56% throughout the observation period, and did not decrease as more patients were prophylaxed (P for trend = .114). The investigators followed their subjects in the hospital, and for 3 months afterward.
"We have not shown a good correlation between increasing prophylaxis and decreasing hospital-associated VTE," Dr. Kaatz said at the Society of Hospital Medicine annual meeting.
Meanwhile, in a second analysis of 26,205 prophylaxed medical inpatients, the rates of major bleeding tripled from 0.2% to 0.6% over the 2-plus years that prophylaxis was becoming more common (P = .052). Prophylaxis rates also climbed from 8.7% to 25.8% among a subset of 1,165 patients contraindicated because of their bleeding risks. The relationship between contraindications and the increased bleeding rate isn’t clear; some who bled had contraindications, but others did not.
"Five years ago, I was an advocate: prophylaxis everybody. [Now,] I’m really worried that I might be causing some bleeding. VTE rates are pretty low," and lower than once thought among general medical inpatients, may be caused by early mobilization and shorter hospital stays. "We are really spending a lot of effort to prophylaxis something that’s" uncommon, without clear benefit and possible harm. "I think several of us will take [these findings] back to our hospitals to change our prophylaxis protocols," Dr. Kaatz said.
Consortium members came up with their own list of contraindications because "there’s not a lot of literature, unfortunately," to help, he noted. The list included brain metastases; intracranial monitoring devices; severe head or spine trauma within 24 hours; gastrointestinal, genitourinary or other hemorrhages within 6 months; intracranial hemorrhage within a year; and platelet counts below 50,000/mm3.
The Caprini score is one of several proposed to distinguish high-risk VTE patients from others, but in a third study, investigators found that it "did not effectively discriminate populations for which pharmacologic prophylaxis was useful." Scores of 5 or higher did predict risk, but among high-scorers, 0.72% who received prophylaxis – and 0.86% who did not – developed VTEs, an insignificant difference (P = .26). Michigan researchers have found other scoring systems to be problematic, as well.
"The mantra for years now has been to prophylaxis for VTEs, so a lot of us are treating to prophylaxis everybody," even low Caprini-score patients. "Now, we’re taking a step back. There’s a movement toward weighing VTE and bleeding risks. If we can find the population that doesn’t warrant prophylaxis, that would be a big step," said investigator Dr. Paul Grant, a hospitalist who is with the internal medicine department at the University of Michigan in Ann Arbor.
The consortium is funded by Blue Cross/Blue Shield of Michigan and the Blue Care Network. Dr. Grant has no disclosures. Dr. Kaatz is a speaker for Boehringer Ingelheim, Janssen, Daiichi Sankyo, and Bristol-Myers Squibb.
LAS VEGAS – Venous thromboembolism prophylaxis does not seem to prevent symptomatic deep vein thrombosis or pulmonary embolism in nonsurgical, non-ICU hospital patients, but it does seem to increase the risk of major bleeding, according to a series of large, observational studies from the Michigan Hospital Medicine Safety Consortium, a quality improvement program involving 40 Michigan hospitals.
Spurred by the Joint Commission and others, hospitalists across the United States have "put their foot on the gas to increase pharmacologic prophylaxis, and we’re using it in patients we think really should get it, but also in some patients who probably shouldn’t. We need more research to" distinguish between the two groups. "Many of us feel that the pendulum has swung too far, and that we need to bring it back to the middle," said investigator Dr. Scott Kaatz, chief quality officer and leader of the hospitalist program at Hurley Medical Center in Flint, Mich.
Among the Consortium’s findings, venous thromboembolism (VTE) prophylaxis – generally a subcutaneous shot with a heparin product – was ordered at admission for 59.2% of general adult inpatients in the first quarter of 2011, excluding surgical, ICU, and obstetric patients. By the second quarter of 2013, that had risen to 76.4%. Even so, among the 35,040 subjects included in the analysis, the rate of symptomatic VTEs averaged 0.56% throughout the observation period, and did not decrease as more patients were prophylaxed (P for trend = .114). The investigators followed their subjects in the hospital, and for 3 months afterward.
"We have not shown a good correlation between increasing prophylaxis and decreasing hospital-associated VTE," Dr. Kaatz said at the Society of Hospital Medicine annual meeting.
Meanwhile, in a second analysis of 26,205 prophylaxed medical inpatients, the rates of major bleeding tripled from 0.2% to 0.6% over the 2-plus years that prophylaxis was becoming more common (P = .052). Prophylaxis rates also climbed from 8.7% to 25.8% among a subset of 1,165 patients contraindicated because of their bleeding risks. The relationship between contraindications and the increased bleeding rate isn’t clear; some who bled had contraindications, but others did not.
"Five years ago, I was an advocate: prophylaxis everybody. [Now,] I’m really worried that I might be causing some bleeding. VTE rates are pretty low," and lower than once thought among general medical inpatients, may be caused by early mobilization and shorter hospital stays. "We are really spending a lot of effort to prophylaxis something that’s" uncommon, without clear benefit and possible harm. "I think several of us will take [these findings] back to our hospitals to change our prophylaxis protocols," Dr. Kaatz said.
Consortium members came up with their own list of contraindications because "there’s not a lot of literature, unfortunately," to help, he noted. The list included brain metastases; intracranial monitoring devices; severe head or spine trauma within 24 hours; gastrointestinal, genitourinary or other hemorrhages within 6 months; intracranial hemorrhage within a year; and platelet counts below 50,000/mm3.
The Caprini score is one of several proposed to distinguish high-risk VTE patients from others, but in a third study, investigators found that it "did not effectively discriminate populations for which pharmacologic prophylaxis was useful." Scores of 5 or higher did predict risk, but among high-scorers, 0.72% who received prophylaxis – and 0.86% who did not – developed VTEs, an insignificant difference (P = .26). Michigan researchers have found other scoring systems to be problematic, as well.
"The mantra for years now has been to prophylaxis for VTEs, so a lot of us are treating to prophylaxis everybody," even low Caprini-score patients. "Now, we’re taking a step back. There’s a movement toward weighing VTE and bleeding risks. If we can find the population that doesn’t warrant prophylaxis, that would be a big step," said investigator Dr. Paul Grant, a hospitalist who is with the internal medicine department at the University of Michigan in Ann Arbor.
The consortium is funded by Blue Cross/Blue Shield of Michigan and the Blue Care Network. Dr. Grant has no disclosures. Dr. Kaatz is a speaker for Boehringer Ingelheim, Janssen, Daiichi Sankyo, and Bristol-Myers Squibb.
AT HOSPITAL MEDICINE 2014
Major finding: As VTE prophylaxis climbed from 59.2% to 77.9% over 2-plus years, the rate of symptomatic VTEs held steady at 0.56%, but major bleeds associated with prophylaxis increased from 0.2% to 0.6%.
Data Source: Observational studies involving tens of thousands of nonsurgical, non-ICU adult inpatients in Michigan hospitals.
Disclosures: The work was funded by Blue Cross Blue Shield of Michigan and the Blue Care Network. A principal investigator reports ties to Boehringer Ingelheim, Janssen, Daiichi Sankyo, and Pfizer-Bristol-Myers Squibb.
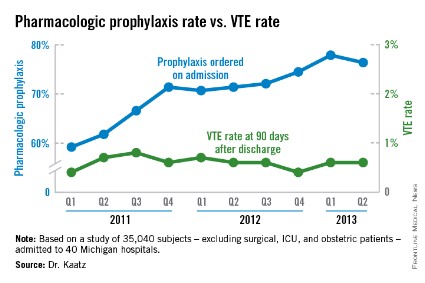
Don’t discount suicide attempts in borderline patients
LOS ANGELES – No matter how many times borderline personality disorder patients seem to cry wolf, the threat of suicide is real and needs to be taken seriously, according to investigators at the University of Mississippi Medical Center in Jackson.
"A common clinical assumption" about borderline patients "is that their suicide attempts are not ... medically serious. The assumption ... is not supported by our findings," they said.

The team surveyed patients admitted to the university’s level 1 trauma center in Jackson within 24 hours of a suicide attempt and found no statistical difference in demographics, medical lethality, suicide intent, or problematic alcohol use between 62 patients with borderline features and 28 without them.
Meanwhile, patients with borderline features – defined as a score of at least 38 points on the Personality Assessment Inventory-Borderline Features Scale – were significantly more depressed and had higher problematic drug use (43.55% vs. 10.71%) and more previous attempts (70.97% vs. 46.43%).
"It’s very common to hear medical providers say attempts" by borderline patients "are just a gesture." In fact, "people presenting with these features need to be helped in the same way as people who present without them," and might need more help with depression and drug use in particular, lead investigator Jalessa Perez said at the annual conference of the American Association of Suicidology.
"If you are writing off their attempts, you are not really treating what needs to be treated," said Ms. Perez, a research assistant at the medical center.
The mean score on the Center for Epidemiologic Studies Depression Scale was 22.93 points in the borderline group, suggesting possible clinical depression, but 15.43 points among other patients, indicating milder symptoms.
Borderline patients scored a mean of 14.51 points and nonborderline patients a mean of 12.96 on the Beck Suicide Intent Scale, a nonsignificant difference indicating moderate intent. Borderline patients scored a mean of 2.25 points and nonborderline patient a mean of 2.39 on the 8-point Medical Lethality Rating Scale, indicating physical harm in both cases; with a score of 8 indicating death.
The mean age in both groups was about 35 years. About 70% were white in the borderline group, and about 61% women. In the nonborderline group, 54% were women and about 60% white.
Up to one in 10 patients with borderline personality disorder commit suicide, far more than in the general population.
Ms. Perez has no disclosures. The senior investigator, Courtney L. Bagge, Ph.D., of the medical center, has funding from the National Institute on Alcohol Abuse and Alcoholism and the Military Suicide Research Consortium.
LOS ANGELES – No matter how many times borderline personality disorder patients seem to cry wolf, the threat of suicide is real and needs to be taken seriously, according to investigators at the University of Mississippi Medical Center in Jackson.
"A common clinical assumption" about borderline patients "is that their suicide attempts are not ... medically serious. The assumption ... is not supported by our findings," they said.
The team surveyed patients admitted to the university’s level 1 trauma center in Jackson within 24 hours of a suicide attempt and found no statistical difference in demographics, medical lethality, suicide intent, or problematic alcohol use between 62 patients with borderline features and 28 without them.
Meanwhile, patients with borderline features – defined as a score of at least 38 points on the Personality Assessment Inventory-Borderline Features Scale – were significantly more depressed and had higher problematic drug use (43.55% vs. 10.71%) and more previous attempts (70.97% vs. 46.43%).
"It’s very common to hear medical providers say attempts" by borderline patients "are just a gesture." In fact, "people presenting with these features need to be helped in the same way as people who present without them," and might need more help with depression and drug use in particular, lead investigator Jalessa Perez said at the annual conference of the American Association of Suicidology.
"If you are writing off their attempts, you are not really treating what needs to be treated," said Ms. Perez, a research assistant at the medical center.
The mean score on the Center for Epidemiologic Studies Depression Scale was 22.93 points in the borderline group, suggesting possible clinical depression, but 15.43 points among other patients, indicating milder symptoms.
Borderline patients scored a mean of 14.51 points and nonborderline patients a mean of 12.96 on the Beck Suicide Intent Scale, a nonsignificant difference indicating moderate intent. Borderline patients scored a mean of 2.25 points and nonborderline patient a mean of 2.39 on the 8-point Medical Lethality Rating Scale, indicating physical harm in both cases; with a score of 8 indicating death.
The mean age in both groups was about 35 years. About 70% were white in the borderline group, and about 61% women. In the nonborderline group, 54% were women and about 60% white.
Up to one in 10 patients with borderline personality disorder commit suicide, far more than in the general population.
Ms. Perez has no disclosures. The senior investigator, Courtney L. Bagge, Ph.D., of the medical center, has funding from the National Institute on Alcohol Abuse and Alcoholism and the Military Suicide Research Consortium.
LOS ANGELES – No matter how many times borderline personality disorder patients seem to cry wolf, the threat of suicide is real and needs to be taken seriously, according to investigators at the University of Mississippi Medical Center in Jackson.
"A common clinical assumption" about borderline patients "is that their suicide attempts are not ... medically serious. The assumption ... is not supported by our findings," they said.
The team surveyed patients admitted to the university’s level 1 trauma center in Jackson within 24 hours of a suicide attempt and found no statistical difference in demographics, medical lethality, suicide intent, or problematic alcohol use between 62 patients with borderline features and 28 without them.
Meanwhile, patients with borderline features – defined as a score of at least 38 points on the Personality Assessment Inventory-Borderline Features Scale – were significantly more depressed and had higher problematic drug use (43.55% vs. 10.71%) and more previous attempts (70.97% vs. 46.43%).
"It’s very common to hear medical providers say attempts" by borderline patients "are just a gesture." In fact, "people presenting with these features need to be helped in the same way as people who present without them," and might need more help with depression and drug use in particular, lead investigator Jalessa Perez said at the annual conference of the American Association of Suicidology.
"If you are writing off their attempts, you are not really treating what needs to be treated," said Ms. Perez, a research assistant at the medical center.
The mean score on the Center for Epidemiologic Studies Depression Scale was 22.93 points in the borderline group, suggesting possible clinical depression, but 15.43 points among other patients, indicating milder symptoms.
Borderline patients scored a mean of 14.51 points and nonborderline patients a mean of 12.96 on the Beck Suicide Intent Scale, a nonsignificant difference indicating moderate intent. Borderline patients scored a mean of 2.25 points and nonborderline patient a mean of 2.39 on the 8-point Medical Lethality Rating Scale, indicating physical harm in both cases; with a score of 8 indicating death.
The mean age in both groups was about 35 years. About 70% were white in the borderline group, and about 61% women. In the nonborderline group, 54% were women and about 60% white.
Up to one in 10 patients with borderline personality disorder commit suicide, far more than in the general population.
Ms. Perez has no disclosures. The senior investigator, Courtney L. Bagge, Ph.D., of the medical center, has funding from the National Institute on Alcohol Abuse and Alcoholism and the Military Suicide Research Consortium.
AT THE ANNUAL AAS CONFERENCE
Major finding: Following suicide attempts, patients with borderline personality features scored a mean of 14.51 points and nonborderline patients a mean of 12.96 on the Beck Suicide Intent Scale. Borderline patients scored a mean of 2.25 points and nonborderline patients a mean of 2.39 on the Medical Lethality Rating Scale. The differences were not significant.
Data Source: Surveys of 90 patients admitted within 24 hours of a suicide attempt.
Disclosures: The lead investigator has no disclosures. The senior investigator has funding from the National Institute on Alcohol Abuse and Alcoholism and the Military Suicide Research Consortium.
