User login
Rifaximin May Relieve Symptoms in Some Patients With IBS
A 2-week course of rifaximin was associated with adequate relief of irritable bowel syndrome symptoms for the first 4 weeks after completion of therapy in 41% of patients who had IBS without constipation.
The results of two identical phase III placebo-controlled studies, TARGET 1 and TARGET 2, were similar overall, Dr. Mark Pimentel and his colleagues wrote in the Jan. 6 issue of the New England Journal of Medicine (2011;364:22-32).
TARGET 1 found that 41% of those taking rifaximin reported adequate relief of their global IBS symptoms, compared with 31% of those taking placebo (P = .01), for at least 2 of the first 4 weeks after treatment ended. In TARGET 2, those numbers were 41% vs. 32% (P = .03), and for the two studies combined the results were also 41% vs. 32%, respectively (P less than .001).
Rifaximin, a poorly absorbed broad-spectrum antibiotic, may work by controlling bacterial overgrowth in the gut, wrote Dr. Pimentel of the Cedars–Sinai Medical Center, Los Angeles, and his colleagues. However, the authors explained, "Some patients in both of our studies did not have a response to treatment, a finding that is consistent with the results of other placebo-controlled clinical trials involving patients with IBS and that may reflect differences in the underlying cause of the symptoms."
Both studies were funded by Salix Pharmaceuticals, the drug’s manufacturer. They included a total of 1,260 patients (623 in TARGET 1 and 637 in TARGET 2). All patients were randomized to 14 days of either placebo or 550 mg rifaximin three times daily and were followed weekly for 10 additional weeks. Study retention was high, with 90% completing the entire trial. Last-results carried forward were used in a secondary analysis.
The patients’ average age was 46 years in each group. Overall, most patients (about 72%) were female, and 91% were white. All had IBS without constipation, with an average duration of 11-12 years.
Patients eligible for the study rated their IBS symptoms of abdominal pain and bloating as a 2-4.5 on a 7-point Likert scale (where 0 = not at all, and 6 = a very great deal). Most patients (82%) reported daily stool urgency.
The primary end point was adequate relief of global IBS symptoms, which patients answered with "yes" or "no." The authors prospectively determined the threshold of "adequate relief" as a score of 0 or 1 for at least 50% of days in a given week and 1 or 2 for 100% of the days in a given week. Additionally, patients were asked to rate relief of bloating, abdominal pain and discomfort, and daily stool consistency.
Overall, significantly more patients in the active group than the placebo group met the primary end point (41% vs. 32%). The secondary analysis with last observation carried forward yielded similar results.
In the two studies combined, significantly more patients in the active group than the placebo group reported adequate relief of bloating for at least 2 of the first 4 weeks after treatment (40% vs. 30%; P less than .001). For the composite end point of abdominal pain or discomfort and loose or watery stools during this time period, significantly more patients treated with rifaximin had relief, compared with placebo-group patients (TARGET 1: 47% vs. 39%, P = .04; TARGET 2: 47% vs. 36%, P = .008).
In an analysis of durability of response based on a weekly assessment, "more patients in the rifaximin group than in the placebo group in both studies had adequate relief of global IBS symptoms within the first month, with continued relief during the first 2 months and during all 3 months in both studies," the authors wrote, noting that the difference was significant at P less than .001 for both studies combined, for relief during all 3 months.
The authors provided a supplementary appendix containing graphs showing that the percentage of patients with adequate relief of global IBS symptoms declined in both groups, in both studies, during the 10 weeks after treatment.
Two patients in the rifaximin group and five in the placebo group had serious adverse events. The incidence of infections was similar in the two groups. There were no cases of ischemic colitis and no deaths.
Regarding the mechanism of action, the authors noted several possible pathways. Besides altering the balance of the gut flora, the drug might also decrease gas associated with bacterial activity, reduce local inflammatory response to bacteria, or alter both the bacteria and host response.
"Whatever the final pathway, the durable effects suggest that rifaximin is affecting an underlying cause of IBS that is linked to an alteration in the intestinal microbiota," they said.
In an accompanying editorial, Dr. Jan Tack of the University of Leuven, Belgium, noted the declining durability of rifaximin’s effect and the relatively small difference between the active and placebo responses. "The therapeutic gain, with the rates of response to treatment (i.e., adequate relief) ranging between 9 and 12% more with rifaximin than with placebo, is in the lower spectrum of what is considered to be clinically relevant," he wrote. Dr. Tack also noted that since IBS is a chronic disorder, the follow-up period was relatively short (N. Eng. J. Med. 2011;364:81-2).
Despite the studies’ positive findings, including the favorable safety profile, he wrote that, "clinicians should proceed with caution." Although "rifaximin has the potential to provide a welcome addition to the limited armamentarium of agents that are available to treat IBS," he also wrote that, "taking into account the high prevalence of IBS in the general population, the effect that larger-scale use of poorly absorbed antibiotics may have on antibiotic-resistance profiles should be taken into account."
Until researchers are able to identify a subgroup of patients that might respond well to the drug, "It seems prudent to restrict the use of nonabsorbable antibiotics to patients in whom small-intestine bacterial overgrowth has been confirmed, or to single treatment cycles in patients who have IBS without constipation and who have not had a response to currently available symptom-directed therapies," Dr. Tack wrote.
All of the paper’s authors reported financial relationships with Salix, either in the form of grants, payment for producing educational materials, travel expenses, speakers fees, company stock, or company employment. Cedars–Sinai Medical Center, employer of Dr. Pimentel, holds patents licensed by Salix Pharmaceuticals. Dr. Tack reported no financial relationship with Salix.
A 2-week course of rifaximin was associated with adequate relief of irritable bowel syndrome symptoms for the first 4 weeks after completion of therapy in 41% of patients who had IBS without constipation.
The results of two identical phase III placebo-controlled studies, TARGET 1 and TARGET 2, were similar overall, Dr. Mark Pimentel and his colleagues wrote in the Jan. 6 issue of the New England Journal of Medicine (2011;364:22-32).
TARGET 1 found that 41% of those taking rifaximin reported adequate relief of their global IBS symptoms, compared with 31% of those taking placebo (P = .01), for at least 2 of the first 4 weeks after treatment ended. In TARGET 2, those numbers were 41% vs. 32% (P = .03), and for the two studies combined the results were also 41% vs. 32%, respectively (P less than .001).
Rifaximin, a poorly absorbed broad-spectrum antibiotic, may work by controlling bacterial overgrowth in the gut, wrote Dr. Pimentel of the Cedars–Sinai Medical Center, Los Angeles, and his colleagues. However, the authors explained, "Some patients in both of our studies did not have a response to treatment, a finding that is consistent with the results of other placebo-controlled clinical trials involving patients with IBS and that may reflect differences in the underlying cause of the symptoms."
Both studies were funded by Salix Pharmaceuticals, the drug’s manufacturer. They included a total of 1,260 patients (623 in TARGET 1 and 637 in TARGET 2). All patients were randomized to 14 days of either placebo or 550 mg rifaximin three times daily and were followed weekly for 10 additional weeks. Study retention was high, with 90% completing the entire trial. Last-results carried forward were used in a secondary analysis.
The patients’ average age was 46 years in each group. Overall, most patients (about 72%) were female, and 91% were white. All had IBS without constipation, with an average duration of 11-12 years.
Patients eligible for the study rated their IBS symptoms of abdominal pain and bloating as a 2-4.5 on a 7-point Likert scale (where 0 = not at all, and 6 = a very great deal). Most patients (82%) reported daily stool urgency.
The primary end point was adequate relief of global IBS symptoms, which patients answered with "yes" or "no." The authors prospectively determined the threshold of "adequate relief" as a score of 0 or 1 for at least 50% of days in a given week and 1 or 2 for 100% of the days in a given week. Additionally, patients were asked to rate relief of bloating, abdominal pain and discomfort, and daily stool consistency.
Overall, significantly more patients in the active group than the placebo group met the primary end point (41% vs. 32%). The secondary analysis with last observation carried forward yielded similar results.
In the two studies combined, significantly more patients in the active group than the placebo group reported adequate relief of bloating for at least 2 of the first 4 weeks after treatment (40% vs. 30%; P less than .001). For the composite end point of abdominal pain or discomfort and loose or watery stools during this time period, significantly more patients treated with rifaximin had relief, compared with placebo-group patients (TARGET 1: 47% vs. 39%, P = .04; TARGET 2: 47% vs. 36%, P = .008).
In an analysis of durability of response based on a weekly assessment, "more patients in the rifaximin group than in the placebo group in both studies had adequate relief of global IBS symptoms within the first month, with continued relief during the first 2 months and during all 3 months in both studies," the authors wrote, noting that the difference was significant at P less than .001 for both studies combined, for relief during all 3 months.
The authors provided a supplementary appendix containing graphs showing that the percentage of patients with adequate relief of global IBS symptoms declined in both groups, in both studies, during the 10 weeks after treatment.
Two patients in the rifaximin group and five in the placebo group had serious adverse events. The incidence of infections was similar in the two groups. There were no cases of ischemic colitis and no deaths.
Regarding the mechanism of action, the authors noted several possible pathways. Besides altering the balance of the gut flora, the drug might also decrease gas associated with bacterial activity, reduce local inflammatory response to bacteria, or alter both the bacteria and host response.
"Whatever the final pathway, the durable effects suggest that rifaximin is affecting an underlying cause of IBS that is linked to an alteration in the intestinal microbiota," they said.
In an accompanying editorial, Dr. Jan Tack of the University of Leuven, Belgium, noted the declining durability of rifaximin’s effect and the relatively small difference between the active and placebo responses. "The therapeutic gain, with the rates of response to treatment (i.e., adequate relief) ranging between 9 and 12% more with rifaximin than with placebo, is in the lower spectrum of what is considered to be clinically relevant," he wrote. Dr. Tack also noted that since IBS is a chronic disorder, the follow-up period was relatively short (N. Eng. J. Med. 2011;364:81-2).
Despite the studies’ positive findings, including the favorable safety profile, he wrote that, "clinicians should proceed with caution." Although "rifaximin has the potential to provide a welcome addition to the limited armamentarium of agents that are available to treat IBS," he also wrote that, "taking into account the high prevalence of IBS in the general population, the effect that larger-scale use of poorly absorbed antibiotics may have on antibiotic-resistance profiles should be taken into account."
Until researchers are able to identify a subgroup of patients that might respond well to the drug, "It seems prudent to restrict the use of nonabsorbable antibiotics to patients in whom small-intestine bacterial overgrowth has been confirmed, or to single treatment cycles in patients who have IBS without constipation and who have not had a response to currently available symptom-directed therapies," Dr. Tack wrote.
All of the paper’s authors reported financial relationships with Salix, either in the form of grants, payment for producing educational materials, travel expenses, speakers fees, company stock, or company employment. Cedars–Sinai Medical Center, employer of Dr. Pimentel, holds patents licensed by Salix Pharmaceuticals. Dr. Tack reported no financial relationship with Salix.
A 2-week course of rifaximin was associated with adequate relief of irritable bowel syndrome symptoms for the first 4 weeks after completion of therapy in 41% of patients who had IBS without constipation.
The results of two identical phase III placebo-controlled studies, TARGET 1 and TARGET 2, were similar overall, Dr. Mark Pimentel and his colleagues wrote in the Jan. 6 issue of the New England Journal of Medicine (2011;364:22-32).
TARGET 1 found that 41% of those taking rifaximin reported adequate relief of their global IBS symptoms, compared with 31% of those taking placebo (P = .01), for at least 2 of the first 4 weeks after treatment ended. In TARGET 2, those numbers were 41% vs. 32% (P = .03), and for the two studies combined the results were also 41% vs. 32%, respectively (P less than .001).
Rifaximin, a poorly absorbed broad-spectrum antibiotic, may work by controlling bacterial overgrowth in the gut, wrote Dr. Pimentel of the Cedars–Sinai Medical Center, Los Angeles, and his colleagues. However, the authors explained, "Some patients in both of our studies did not have a response to treatment, a finding that is consistent with the results of other placebo-controlled clinical trials involving patients with IBS and that may reflect differences in the underlying cause of the symptoms."
Both studies were funded by Salix Pharmaceuticals, the drug’s manufacturer. They included a total of 1,260 patients (623 in TARGET 1 and 637 in TARGET 2). All patients were randomized to 14 days of either placebo or 550 mg rifaximin three times daily and were followed weekly for 10 additional weeks. Study retention was high, with 90% completing the entire trial. Last-results carried forward were used in a secondary analysis.
The patients’ average age was 46 years in each group. Overall, most patients (about 72%) were female, and 91% were white. All had IBS without constipation, with an average duration of 11-12 years.
Patients eligible for the study rated their IBS symptoms of abdominal pain and bloating as a 2-4.5 on a 7-point Likert scale (where 0 = not at all, and 6 = a very great deal). Most patients (82%) reported daily stool urgency.
The primary end point was adequate relief of global IBS symptoms, which patients answered with "yes" or "no." The authors prospectively determined the threshold of "adequate relief" as a score of 0 or 1 for at least 50% of days in a given week and 1 or 2 for 100% of the days in a given week. Additionally, patients were asked to rate relief of bloating, abdominal pain and discomfort, and daily stool consistency.
Overall, significantly more patients in the active group than the placebo group met the primary end point (41% vs. 32%). The secondary analysis with last observation carried forward yielded similar results.
In the two studies combined, significantly more patients in the active group than the placebo group reported adequate relief of bloating for at least 2 of the first 4 weeks after treatment (40% vs. 30%; P less than .001). For the composite end point of abdominal pain or discomfort and loose or watery stools during this time period, significantly more patients treated with rifaximin had relief, compared with placebo-group patients (TARGET 1: 47% vs. 39%, P = .04; TARGET 2: 47% vs. 36%, P = .008).
In an analysis of durability of response based on a weekly assessment, "more patients in the rifaximin group than in the placebo group in both studies had adequate relief of global IBS symptoms within the first month, with continued relief during the first 2 months and during all 3 months in both studies," the authors wrote, noting that the difference was significant at P less than .001 for both studies combined, for relief during all 3 months.
The authors provided a supplementary appendix containing graphs showing that the percentage of patients with adequate relief of global IBS symptoms declined in both groups, in both studies, during the 10 weeks after treatment.
Two patients in the rifaximin group and five in the placebo group had serious adverse events. The incidence of infections was similar in the two groups. There were no cases of ischemic colitis and no deaths.
Regarding the mechanism of action, the authors noted several possible pathways. Besides altering the balance of the gut flora, the drug might also decrease gas associated with bacterial activity, reduce local inflammatory response to bacteria, or alter both the bacteria and host response.
"Whatever the final pathway, the durable effects suggest that rifaximin is affecting an underlying cause of IBS that is linked to an alteration in the intestinal microbiota," they said.
In an accompanying editorial, Dr. Jan Tack of the University of Leuven, Belgium, noted the declining durability of rifaximin’s effect and the relatively small difference between the active and placebo responses. "The therapeutic gain, with the rates of response to treatment (i.e., adequate relief) ranging between 9 and 12% more with rifaximin than with placebo, is in the lower spectrum of what is considered to be clinically relevant," he wrote. Dr. Tack also noted that since IBS is a chronic disorder, the follow-up period was relatively short (N. Eng. J. Med. 2011;364:81-2).
Despite the studies’ positive findings, including the favorable safety profile, he wrote that, "clinicians should proceed with caution." Although "rifaximin has the potential to provide a welcome addition to the limited armamentarium of agents that are available to treat IBS," he also wrote that, "taking into account the high prevalence of IBS in the general population, the effect that larger-scale use of poorly absorbed antibiotics may have on antibiotic-resistance profiles should be taken into account."
Until researchers are able to identify a subgroup of patients that might respond well to the drug, "It seems prudent to restrict the use of nonabsorbable antibiotics to patients in whom small-intestine bacterial overgrowth has been confirmed, or to single treatment cycles in patients who have IBS without constipation and who have not had a response to currently available symptom-directed therapies," Dr. Tack wrote.
All of the paper’s authors reported financial relationships with Salix, either in the form of grants, payment for producing educational materials, travel expenses, speakers fees, company stock, or company employment. Cedars–Sinai Medical Center, employer of Dr. Pimentel, holds patents licensed by Salix Pharmaceuticals. Dr. Tack reported no financial relationship with Salix.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
New Imaging Agent Correlates Amyloid With Alzheimer Autopsy Findings
Positron emission tomography in combination with the radiolabeled compound florbetapir F-18 detected beta-amyloid plaques with 93% sensitivity and 100% specificity in the brains of 35 elderly patients, most of whom had some form of dementia.
Lead investigator Dr. Christopher Clark and his colleagues wrote that florbetapir-PET imaging could be an important diagnostic tool for Alzheimer’s disease – perhaps with the ability to detect brain plaques early in a prodromal stage of the disease – and to measure plaque changes in relation to therapeutic response in future drug studies, according to Dr. Clark, medical director of Avid Radiopharmaceuticals, the company testing the compound (JAMA 2011;305:275-83).
The study also represents the first time an amyloid imaging agent has been tested against autopsy results, said coinvestigator Dr. Marwan N. Sabbagh, founding director of the Cleo Roberts Center for Clinical Research in Sun City, Ariz. "It’s really exciting to be able to correlate imaging so strongly with autopsy findings."
But Dr. Clark and his coinvestigators cautioned that the study does not make it clear what specific clinical applications the imaging procedure could have, be it the clinical diagnosis of Alzheimer’s disease or the prediction of progression to dementia.
The Food and Drug Administration’s Peripheral and Central Nervous System Drugs Advisory Committee will meet on Jan. 20 to discuss the compound and the study’s findings.
Like Pittsburgh imaging compound B (PiB), florbetapir binds to beta-amyloid plaques in the living brain. PiB’s use, however, has been limited by its short half-life of 20 minutes. Florbetapir achieves maximum uptake at 30 minutes and remains unchanged for the next 60 minutes, "providing a wide time window to obtain a 10-minute image," the authors noted.
The prospective study involved 35 patients in hospice or long-term care facilities who were expected to die within 6 months. Six of the patients were used to validate the imaging procedure while the remaining 29 were used in the primary validation study.
Among the 29 in the validation analysis, the mean age was 80 years. This group included 13 with a clinical diagnosis of Alzheimer’s, 5 with other dementias, 9 with normal cognition, and the rest with mild cognitive impairment. Their mean Mini-Mental State Examination (MMSE) score was 3.8.
The control group comprised 74 young, healthy subjects, 27 of whom were positive for the APOE e4 allele, which greatly increases the risk of developing Alzheimer’s in later life.
The control subjects had a mean age of 27 years and a mean MMSE score of 29.7. Florbetapir imaging was negative for all 74 subjects, including those with the APOE e4 allele.
Florbetapir-PET imaging in the 35 patients was significantly correlated with both immunohistochemistry and silver stain for beta-amyloid plaques in each of the six brain regions that the investigators examined (frontal, temporal, parietal, anterior and posterior cingulate, precuneus, and cerebellum).
At autopsy, 15 patients in the validation group met pathologic criteria for Alzheimer’s disease. Of these, 14 had positive florbetapir-PET scans, leading to a sensitivity of 93%.
The other 14 patients had low levels of beta-amyloid plaque on autopsy, and thus did not meet the diagnostic criteria for Alzheimer’s. All 14 also had negative florbetapir-PET scans, giving 100% specificity.
"The neuropathological diagnosis in the participants who did not meet pathological criteria for AD included dementia with Lewy bodies, hippocampal sclerosis, Parkinson’s disease, subcortical microscopic infarct, mesial temporal lobe neurofibrillary tangles, neurofibrillary tangles with argyrophilic grains and glial tauopathy, and no neuropathology," the authors wrote.
Of the 15 patients in the validation cohort who had a clinical diagnosis of dementia during life, 3 did not have the same diagnosis on autopsy. One of these patients had a clinical diagnosis of probable Alzheimer’s but did not have it on autopsy, whereas one with a clinical diagnosis of Parkinson’s disease dementia and one with a clinical diagnosis of Lewy body dementia actually had Alzheimer’s. Florbetapir-PET correctly predicted the presence or absence of Alzheimer’s disease in these patients.
The authors noted that the patient sample used in the study did not represent a typical clinical population, most of whom would be referred for initial signs of cognitive impairment. Rather, the cohort was selected "for their unique ability to provide information about the ability of florbetapir-PET imaging to accurately identify and quantify beta-amyloid with the shortest interval between imaging and definitive pathological evaluation possible."
The study was funded primarily by Avid Radiopharmaceuticals, which Eli Lilly acquired last November. Dr. Clark and eight of the coauthors are stockholders and/or employees of Avid. All of the other coauthors are financially related to the company, either as educators, paid investigators, or members of the speakers bureau for Avid or Lilly. Dr. Sabbagh said he had no financial ties with either company, other than a research grant from Avid for this study.
While a valid Alzheimer’s biomarker is clearly a clinical necessity, it is too early to jump on the florbetapir bandwagon, Dr. Monique Breteler cautioned in an accompanying editorial (JAMA 2011;305:304-5).
"A biomarker must be validated in the population and clinical setting for which the biomarker is intended," wrote Dr. Breteler. "A diagnostic marker for Alzheimer’s would typically be used to distinguish between individuals with cognitive problems who have AD-type pathology and those who do not, or, in the case of early diagnosis, to predict which of the cognitively healthy persons might develop cognitive decline over time."
The study by Dr. Clark and her colleagues "was not a random sample of individuals with cognitive problems who might be tested for presence and extent of amyloid pathology, nor were they a random selection of asymptomatic persons who might be evaluated to determine whether some of them already had amyloid pathology developing."
Instead, she pointed out, the study presented a convenience sample of terminally ill patients, most of whom had a confirmed dementia. "A priori, one would expect a very large contrast in brain amyloid load, as well as in more generalized brain pathology, between the participants with and without dementia. The reported agreement (97%) between florbetapir-PET and the postmortem pathologic diagnosis is likely inflated because of the selection of participants in the study."
Furthermore, she noted that amyloid brain plaques may or may not be the relevant pathologic marker of Alzheimer’s, and this question is beyond the scope of the current study. Many cognitively normal elderly patients show amyloid pathology, while many with dementia whose additional pathology besides the plaques and tangles generally associated with the disease. "The toxic species are the soluble beta-amyloid oligomers, which can become safely sequestered and deposited as amyloid plaques, she said. "This may explain why immunization against beta-amyloid 42 can lead to amyloid plaque clearance but not diminish further neurodegeneration and the clinical symptoms of dementia."
Dr. Breteler is an epidemiologist and biostatistician at the Erasmus University Medical Center, Rotterdam, the Netherlands. She had no relevant disclosures.
While a valid Alzheimer’s biomarker is clearly a clinical necessity, it is too early to jump on the florbetapir bandwagon, Dr. Monique Breteler cautioned in an accompanying editorial (JAMA 2011;305:304-5).
"A biomarker must be validated in the population and clinical setting for which the biomarker is intended," wrote Dr. Breteler. "A diagnostic marker for Alzheimer’s would typically be used to distinguish between individuals with cognitive problems who have AD-type pathology and those who do not, or, in the case of early diagnosis, to predict which of the cognitively healthy persons might develop cognitive decline over time."
The study by Dr. Clark and her colleagues "was not a random sample of individuals with cognitive problems who might be tested for presence and extent of amyloid pathology, nor were they a random selection of asymptomatic persons who might be evaluated to determine whether some of them already had amyloid pathology developing."
Instead, she pointed out, the study presented a convenience sample of terminally ill patients, most of whom had a confirmed dementia. "A priori, one would expect a very large contrast in brain amyloid load, as well as in more generalized brain pathology, between the participants with and without dementia. The reported agreement (97%) between florbetapir-PET and the postmortem pathologic diagnosis is likely inflated because of the selection of participants in the study."
Furthermore, she noted that amyloid brain plaques may or may not be the relevant pathologic marker of Alzheimer’s, and this question is beyond the scope of the current study. Many cognitively normal elderly patients show amyloid pathology, while many with dementia whose additional pathology besides the plaques and tangles generally associated with the disease. "The toxic species are the soluble beta-amyloid oligomers, which can become safely sequestered and deposited as amyloid plaques, she said. "This may explain why immunization against beta-amyloid 42 can lead to amyloid plaque clearance but not diminish further neurodegeneration and the clinical symptoms of dementia."
Dr. Breteler is an epidemiologist and biostatistician at the Erasmus University Medical Center, Rotterdam, the Netherlands. She had no relevant disclosures.
While a valid Alzheimer’s biomarker is clearly a clinical necessity, it is too early to jump on the florbetapir bandwagon, Dr. Monique Breteler cautioned in an accompanying editorial (JAMA 2011;305:304-5).
"A biomarker must be validated in the population and clinical setting for which the biomarker is intended," wrote Dr. Breteler. "A diagnostic marker for Alzheimer’s would typically be used to distinguish between individuals with cognitive problems who have AD-type pathology and those who do not, or, in the case of early diagnosis, to predict which of the cognitively healthy persons might develop cognitive decline over time."
The study by Dr. Clark and her colleagues "was not a random sample of individuals with cognitive problems who might be tested for presence and extent of amyloid pathology, nor were they a random selection of asymptomatic persons who might be evaluated to determine whether some of them already had amyloid pathology developing."
Instead, she pointed out, the study presented a convenience sample of terminally ill patients, most of whom had a confirmed dementia. "A priori, one would expect a very large contrast in brain amyloid load, as well as in more generalized brain pathology, between the participants with and without dementia. The reported agreement (97%) between florbetapir-PET and the postmortem pathologic diagnosis is likely inflated because of the selection of participants in the study."
Furthermore, she noted that amyloid brain plaques may or may not be the relevant pathologic marker of Alzheimer’s, and this question is beyond the scope of the current study. Many cognitively normal elderly patients show amyloid pathology, while many with dementia whose additional pathology besides the plaques and tangles generally associated with the disease. "The toxic species are the soluble beta-amyloid oligomers, which can become safely sequestered and deposited as amyloid plaques, she said. "This may explain why immunization against beta-amyloid 42 can lead to amyloid plaque clearance but not diminish further neurodegeneration and the clinical symptoms of dementia."
Dr. Breteler is an epidemiologist and biostatistician at the Erasmus University Medical Center, Rotterdam, the Netherlands. She had no relevant disclosures.
Positron emission tomography in combination with the radiolabeled compound florbetapir F-18 detected beta-amyloid plaques with 93% sensitivity and 100% specificity in the brains of 35 elderly patients, most of whom had some form of dementia.
Lead investigator Dr. Christopher Clark and his colleagues wrote that florbetapir-PET imaging could be an important diagnostic tool for Alzheimer’s disease – perhaps with the ability to detect brain plaques early in a prodromal stage of the disease – and to measure plaque changes in relation to therapeutic response in future drug studies, according to Dr. Clark, medical director of Avid Radiopharmaceuticals, the company testing the compound (JAMA 2011;305:275-83).
The study also represents the first time an amyloid imaging agent has been tested against autopsy results, said coinvestigator Dr. Marwan N. Sabbagh, founding director of the Cleo Roberts Center for Clinical Research in Sun City, Ariz. "It’s really exciting to be able to correlate imaging so strongly with autopsy findings."
But Dr. Clark and his coinvestigators cautioned that the study does not make it clear what specific clinical applications the imaging procedure could have, be it the clinical diagnosis of Alzheimer’s disease or the prediction of progression to dementia.
The Food and Drug Administration’s Peripheral and Central Nervous System Drugs Advisory Committee will meet on Jan. 20 to discuss the compound and the study’s findings.
Like Pittsburgh imaging compound B (PiB), florbetapir binds to beta-amyloid plaques in the living brain. PiB’s use, however, has been limited by its short half-life of 20 minutes. Florbetapir achieves maximum uptake at 30 minutes and remains unchanged for the next 60 minutes, "providing a wide time window to obtain a 10-minute image," the authors noted.
The prospective study involved 35 patients in hospice or long-term care facilities who were expected to die within 6 months. Six of the patients were used to validate the imaging procedure while the remaining 29 were used in the primary validation study.
Among the 29 in the validation analysis, the mean age was 80 years. This group included 13 with a clinical diagnosis of Alzheimer’s, 5 with other dementias, 9 with normal cognition, and the rest with mild cognitive impairment. Their mean Mini-Mental State Examination (MMSE) score was 3.8.
The control group comprised 74 young, healthy subjects, 27 of whom were positive for the APOE e4 allele, which greatly increases the risk of developing Alzheimer’s in later life.
The control subjects had a mean age of 27 years and a mean MMSE score of 29.7. Florbetapir imaging was negative for all 74 subjects, including those with the APOE e4 allele.
Florbetapir-PET imaging in the 35 patients was significantly correlated with both immunohistochemistry and silver stain for beta-amyloid plaques in each of the six brain regions that the investigators examined (frontal, temporal, parietal, anterior and posterior cingulate, precuneus, and cerebellum).
At autopsy, 15 patients in the validation group met pathologic criteria for Alzheimer’s disease. Of these, 14 had positive florbetapir-PET scans, leading to a sensitivity of 93%.
The other 14 patients had low levels of beta-amyloid plaque on autopsy, and thus did not meet the diagnostic criteria for Alzheimer’s. All 14 also had negative florbetapir-PET scans, giving 100% specificity.
"The neuropathological diagnosis in the participants who did not meet pathological criteria for AD included dementia with Lewy bodies, hippocampal sclerosis, Parkinson’s disease, subcortical microscopic infarct, mesial temporal lobe neurofibrillary tangles, neurofibrillary tangles with argyrophilic grains and glial tauopathy, and no neuropathology," the authors wrote.
Of the 15 patients in the validation cohort who had a clinical diagnosis of dementia during life, 3 did not have the same diagnosis on autopsy. One of these patients had a clinical diagnosis of probable Alzheimer’s but did not have it on autopsy, whereas one with a clinical diagnosis of Parkinson’s disease dementia and one with a clinical diagnosis of Lewy body dementia actually had Alzheimer’s. Florbetapir-PET correctly predicted the presence or absence of Alzheimer’s disease in these patients.
The authors noted that the patient sample used in the study did not represent a typical clinical population, most of whom would be referred for initial signs of cognitive impairment. Rather, the cohort was selected "for their unique ability to provide information about the ability of florbetapir-PET imaging to accurately identify and quantify beta-amyloid with the shortest interval between imaging and definitive pathological evaluation possible."
The study was funded primarily by Avid Radiopharmaceuticals, which Eli Lilly acquired last November. Dr. Clark and eight of the coauthors are stockholders and/or employees of Avid. All of the other coauthors are financially related to the company, either as educators, paid investigators, or members of the speakers bureau for Avid or Lilly. Dr. Sabbagh said he had no financial ties with either company, other than a research grant from Avid for this study.
Positron emission tomography in combination with the radiolabeled compound florbetapir F-18 detected beta-amyloid plaques with 93% sensitivity and 100% specificity in the brains of 35 elderly patients, most of whom had some form of dementia.
Lead investigator Dr. Christopher Clark and his colleagues wrote that florbetapir-PET imaging could be an important diagnostic tool for Alzheimer’s disease – perhaps with the ability to detect brain plaques early in a prodromal stage of the disease – and to measure plaque changes in relation to therapeutic response in future drug studies, according to Dr. Clark, medical director of Avid Radiopharmaceuticals, the company testing the compound (JAMA 2011;305:275-83).
The study also represents the first time an amyloid imaging agent has been tested against autopsy results, said coinvestigator Dr. Marwan N. Sabbagh, founding director of the Cleo Roberts Center for Clinical Research in Sun City, Ariz. "It’s really exciting to be able to correlate imaging so strongly with autopsy findings."
But Dr. Clark and his coinvestigators cautioned that the study does not make it clear what specific clinical applications the imaging procedure could have, be it the clinical diagnosis of Alzheimer’s disease or the prediction of progression to dementia.
The Food and Drug Administration’s Peripheral and Central Nervous System Drugs Advisory Committee will meet on Jan. 20 to discuss the compound and the study’s findings.
Like Pittsburgh imaging compound B (PiB), florbetapir binds to beta-amyloid plaques in the living brain. PiB’s use, however, has been limited by its short half-life of 20 minutes. Florbetapir achieves maximum uptake at 30 minutes and remains unchanged for the next 60 minutes, "providing a wide time window to obtain a 10-minute image," the authors noted.
The prospective study involved 35 patients in hospice or long-term care facilities who were expected to die within 6 months. Six of the patients were used to validate the imaging procedure while the remaining 29 were used in the primary validation study.
Among the 29 in the validation analysis, the mean age was 80 years. This group included 13 with a clinical diagnosis of Alzheimer’s, 5 with other dementias, 9 with normal cognition, and the rest with mild cognitive impairment. Their mean Mini-Mental State Examination (MMSE) score was 3.8.
The control group comprised 74 young, healthy subjects, 27 of whom were positive for the APOE e4 allele, which greatly increases the risk of developing Alzheimer’s in later life.
The control subjects had a mean age of 27 years and a mean MMSE score of 29.7. Florbetapir imaging was negative for all 74 subjects, including those with the APOE e4 allele.
Florbetapir-PET imaging in the 35 patients was significantly correlated with both immunohistochemistry and silver stain for beta-amyloid plaques in each of the six brain regions that the investigators examined (frontal, temporal, parietal, anterior and posterior cingulate, precuneus, and cerebellum).
At autopsy, 15 patients in the validation group met pathologic criteria for Alzheimer’s disease. Of these, 14 had positive florbetapir-PET scans, leading to a sensitivity of 93%.
The other 14 patients had low levels of beta-amyloid plaque on autopsy, and thus did not meet the diagnostic criteria for Alzheimer’s. All 14 also had negative florbetapir-PET scans, giving 100% specificity.
"The neuropathological diagnosis in the participants who did not meet pathological criteria for AD included dementia with Lewy bodies, hippocampal sclerosis, Parkinson’s disease, subcortical microscopic infarct, mesial temporal lobe neurofibrillary tangles, neurofibrillary tangles with argyrophilic grains and glial tauopathy, and no neuropathology," the authors wrote.
Of the 15 patients in the validation cohort who had a clinical diagnosis of dementia during life, 3 did not have the same diagnosis on autopsy. One of these patients had a clinical diagnosis of probable Alzheimer’s but did not have it on autopsy, whereas one with a clinical diagnosis of Parkinson’s disease dementia and one with a clinical diagnosis of Lewy body dementia actually had Alzheimer’s. Florbetapir-PET correctly predicted the presence or absence of Alzheimer’s disease in these patients.
The authors noted that the patient sample used in the study did not represent a typical clinical population, most of whom would be referred for initial signs of cognitive impairment. Rather, the cohort was selected "for their unique ability to provide information about the ability of florbetapir-PET imaging to accurately identify and quantify beta-amyloid with the shortest interval between imaging and definitive pathological evaluation possible."
The study was funded primarily by Avid Radiopharmaceuticals, which Eli Lilly acquired last November. Dr. Clark and eight of the coauthors are stockholders and/or employees of Avid. All of the other coauthors are financially related to the company, either as educators, paid investigators, or members of the speakers bureau for Avid or Lilly. Dr. Sabbagh said he had no financial ties with either company, other than a research grant from Avid for this study.
FROM JAMA
Major Finding: PET brain imaging with florbetapir was 93% sensitive and 100% specific in identifying beta-amyloid plaques in 35 elderly patients, most of whom had a clinical diagnosis of some form of dementia.
Data Source: A prospective study of 35 elderly patients in hospice or long-term care facilities, and a control group of 74 young, healthy volunteers.
Disclosures: The study was funded primarily by Avid Radiopharmaceuticals. Dr. Clark and eight of the coauthors are stockholders and/or employees of the company. All of the other coauthors received research grants, and most are educators, paid investigators, or members of the speakers bureau for Avid or for Eli Lilly, which acquired the company last November.
Type 1 Genetic Variants Also Tied to Juvenile Arthritis
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, England, and colleagues.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2169-72).
The researchers compared DNA from 1,054 patients with juvenile idiopathic arthritis with that of 3,129 healthy controls. All the subjects were white. The study focused on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease.
One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with juvenile idiopathic arthritis. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease. LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. It also has been linked to Ras signaling, a process important in cell growth, differentiation, and survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype.
The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T cell–independent induction of interferon gamma, the authors noted.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, England, and colleagues.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2169-72).
The researchers compared DNA from 1,054 patients with juvenile idiopathic arthritis with that of 3,129 healthy controls. All the subjects were white. The study focused on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease.
One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with juvenile idiopathic arthritis. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease. LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. It also has been linked to Ras signaling, a process important in cell growth, differentiation, and survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype.
The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T cell–independent induction of interferon gamma, the authors noted.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, England, and colleagues.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2169-72).
The researchers compared DNA from 1,054 patients with juvenile idiopathic arthritis with that of 3,129 healthy controls. All the subjects were white. The study focused on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease.
One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with juvenile idiopathic arthritis. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease. LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. It also has been linked to Ras signaling, a process important in cell growth, differentiation, and survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype.
The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T cell–independent induction of interferon gamma, the authors noted.
FROM THE ANNALS OF THE RHEUMATIC DISEASES
Major Finding: Two genetic variants with known associations to
type 1 diabetes or celiac disease also predispose to juvenile
idiopathic arthritis.
Data Source: DNA from 1,054 patients
with juvenile idiopathic arthritis was compared with that of 3,129
healthy controls. Thirteen single nucleotide polymorphisms (SNPs) that
already had confirmed associations with type 1 diabetes or celiac
disease were investigated.
Disclosures: The study was
sponsored by Arthritis Research U.K. and supported by the NIHR
Manchester Biomedical Research Council. Genotype data used was funded by
grants from the Medical Research Council and the Wellcome Trust. The
authors said they had no relevant financial disclosures.
Healthy People 2020 Reflects Graying of America
Healthy People 2010 is growing up. The Department of Health and Human Services has announced the birth of Healthy People 2020, a new generation of the nation's 10-year plan for health promotion and disease prevention.
“The launch of Healthy People 2020 comes at a critical time,” HHS Secretary Kathleen Sebelius said in a press statement. “Our challenge and opportunity is to avoid preventable disease from occurring in the first place.”
Because chronic diseases – like diabetes, heart disease, and cancer – account for 70% of deaths and consume 75% of national health spending, Healthy People 2020 stresses incorporating lifestyle changes that have repeatedly been proved to protect against those disorders. “Many of the risk factors that contribute to the development of these diseases are preventable,” said Dr. Howard Koh, assistant secretary for health. “Too many people are not reaching their full potential for health because of preventable conditions. Healthy People is the nation's road map and compass for better health, providing our society a vision for improving both the quantity and quality of life for all Americans.”
The team behind Healthy People 2020 began putting their plan together in 2007. The panel drew on input from public and private health officials, including experts in preventive medicine, representatives of more than 2,000 health organizations, and more than 8,000 public comments.
Healthy People 2020 isn't just intended for individuals, though, Dr. Jonathan Fielding said during a press briefing on the program's launch. Researchers, clinicians, educators and members of both public and private health care agencies need to band together to make the program a success, said Dr. Fielding, chairman of the Secretary's Advisory Committee on Health Promotion and Disease Prevention Objectives for 2020.
In response to the growing elderly segment of the American population, the new program includes a topic area for dementias, including Alzheimer's disease. Other new areas in the initiative are early and middle childhood and adolescent health; blood disorders and blood safety; genomics; global health; and health-related quality of life and well-being.
Like all children growing up in a technology-based society, Healthy People 2020 will incorporate the Internet and other technology media in both its message and its method. The newly designed Web site allows users to tailor information to their individual needs and look for evidence-based ways to put the program's recommendations to work in their lives.
Developers are also issuing a challenge to encourage the tech-savvy to create easy-to-use applications for those who are working with Healthy People 2020 objectives and community health data. Winning ideas will reap financial rewards – $4,000 in prize money is available.
“This milestone in disease prevention and health promotion creates an opportunity to leverage information technology to make Healthy People come alive for all Americans in their communities and work places,” said HHS Chief Technology Officer Todd Park.
“The 'my HealthyPeople' applications challenge will help spur innovative approaches to helping communities track their progress using Health People objectives and targets as well as develop an agenda for health improvement.”
Healthy People 2010 is growing up. The Department of Health and Human Services has announced the birth of Healthy People 2020, a new generation of the nation's 10-year plan for health promotion and disease prevention.
“The launch of Healthy People 2020 comes at a critical time,” HHS Secretary Kathleen Sebelius said in a press statement. “Our challenge and opportunity is to avoid preventable disease from occurring in the first place.”
Because chronic diseases – like diabetes, heart disease, and cancer – account for 70% of deaths and consume 75% of national health spending, Healthy People 2020 stresses incorporating lifestyle changes that have repeatedly been proved to protect against those disorders. “Many of the risk factors that contribute to the development of these diseases are preventable,” said Dr. Howard Koh, assistant secretary for health. “Too many people are not reaching their full potential for health because of preventable conditions. Healthy People is the nation's road map and compass for better health, providing our society a vision for improving both the quantity and quality of life for all Americans.”
The team behind Healthy People 2020 began putting their plan together in 2007. The panel drew on input from public and private health officials, including experts in preventive medicine, representatives of more than 2,000 health organizations, and more than 8,000 public comments.
Healthy People 2020 isn't just intended for individuals, though, Dr. Jonathan Fielding said during a press briefing on the program's launch. Researchers, clinicians, educators and members of both public and private health care agencies need to band together to make the program a success, said Dr. Fielding, chairman of the Secretary's Advisory Committee on Health Promotion and Disease Prevention Objectives for 2020.
In response to the growing elderly segment of the American population, the new program includes a topic area for dementias, including Alzheimer's disease. Other new areas in the initiative are early and middle childhood and adolescent health; blood disorders and blood safety; genomics; global health; and health-related quality of life and well-being.
Like all children growing up in a technology-based society, Healthy People 2020 will incorporate the Internet and other technology media in both its message and its method. The newly designed Web site allows users to tailor information to their individual needs and look for evidence-based ways to put the program's recommendations to work in their lives.
Developers are also issuing a challenge to encourage the tech-savvy to create easy-to-use applications for those who are working with Healthy People 2020 objectives and community health data. Winning ideas will reap financial rewards – $4,000 in prize money is available.
“This milestone in disease prevention and health promotion creates an opportunity to leverage information technology to make Healthy People come alive for all Americans in their communities and work places,” said HHS Chief Technology Officer Todd Park.
“The 'my HealthyPeople' applications challenge will help spur innovative approaches to helping communities track their progress using Health People objectives and targets as well as develop an agenda for health improvement.”
Healthy People 2010 is growing up. The Department of Health and Human Services has announced the birth of Healthy People 2020, a new generation of the nation's 10-year plan for health promotion and disease prevention.
“The launch of Healthy People 2020 comes at a critical time,” HHS Secretary Kathleen Sebelius said in a press statement. “Our challenge and opportunity is to avoid preventable disease from occurring in the first place.”
Because chronic diseases – like diabetes, heart disease, and cancer – account for 70% of deaths and consume 75% of national health spending, Healthy People 2020 stresses incorporating lifestyle changes that have repeatedly been proved to protect against those disorders. “Many of the risk factors that contribute to the development of these diseases are preventable,” said Dr. Howard Koh, assistant secretary for health. “Too many people are not reaching their full potential for health because of preventable conditions. Healthy People is the nation's road map and compass for better health, providing our society a vision for improving both the quantity and quality of life for all Americans.”
The team behind Healthy People 2020 began putting their plan together in 2007. The panel drew on input from public and private health officials, including experts in preventive medicine, representatives of more than 2,000 health organizations, and more than 8,000 public comments.
Healthy People 2020 isn't just intended for individuals, though, Dr. Jonathan Fielding said during a press briefing on the program's launch. Researchers, clinicians, educators and members of both public and private health care agencies need to band together to make the program a success, said Dr. Fielding, chairman of the Secretary's Advisory Committee on Health Promotion and Disease Prevention Objectives for 2020.
In response to the growing elderly segment of the American population, the new program includes a topic area for dementias, including Alzheimer's disease. Other new areas in the initiative are early and middle childhood and adolescent health; blood disorders and blood safety; genomics; global health; and health-related quality of life and well-being.
Like all children growing up in a technology-based society, Healthy People 2020 will incorporate the Internet and other technology media in both its message and its method. The newly designed Web site allows users to tailor information to their individual needs and look for evidence-based ways to put the program's recommendations to work in their lives.
Developers are also issuing a challenge to encourage the tech-savvy to create easy-to-use applications for those who are working with Healthy People 2020 objectives and community health data. Winning ideas will reap financial rewards – $4,000 in prize money is available.
“This milestone in disease prevention and health promotion creates an opportunity to leverage information technology to make Healthy People come alive for all Americans in their communities and work places,” said HHS Chief Technology Officer Todd Park.
“The 'my HealthyPeople' applications challenge will help spur innovative approaches to helping communities track their progress using Health People objectives and targets as well as develop an agenda for health improvement.”
Genetic Variants Confer Susceptibility to JIA
Major Finding: Two genetic variants with known associations to type 1 diabetes or celiac disease also predispose to juvenile idiopathic arthritis.
Data Source: DNA from 1,054 patients with juvenile idiopathic arthritis was compared with that of 3,129 healthy controls. Thirteen single nucleotide polymorphisms (SNPs) that already had confirmed associations with type 1 diabetes or celiac disease were investigated.
Disclosures: The study was sponsored by Arthritis Research U.K. and supported by the NIHR Manchester Biomedical Research Council. Genotype data used was funded by grants from the Medical Research Council and the Wellcome Trust. The authors said they had no relevant financial disclosures.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, U.K.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2169-72).
The researchers compared DNA from 1,054 patients with JIA with that of 3,129 healthy controls, focusing on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease. One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with JIA. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease. LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. It also has been linked to Ras signaling, a process important in cell growth, differentiation, and survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype. The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T-cell–independent induction of interferon gamma.
Although this gene has not been associated with ankylosing spondylitis, patients with enthesitis-related arthritis are prone to joint destruction in the spine and sacroiliac joints.
Major Finding: Two genetic variants with known associations to type 1 diabetes or celiac disease also predispose to juvenile idiopathic arthritis.
Data Source: DNA from 1,054 patients with juvenile idiopathic arthritis was compared with that of 3,129 healthy controls. Thirteen single nucleotide polymorphisms (SNPs) that already had confirmed associations with type 1 diabetes or celiac disease were investigated.
Disclosures: The study was sponsored by Arthritis Research U.K. and supported by the NIHR Manchester Biomedical Research Council. Genotype data used was funded by grants from the Medical Research Council and the Wellcome Trust. The authors said they had no relevant financial disclosures.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, U.K.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2169-72).
The researchers compared DNA from 1,054 patients with JIA with that of 3,129 healthy controls, focusing on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease. One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with JIA. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease. LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. It also has been linked to Ras signaling, a process important in cell growth, differentiation, and survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype. The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T-cell–independent induction of interferon gamma.
Although this gene has not been associated with ankylosing spondylitis, patients with enthesitis-related arthritis are prone to joint destruction in the spine and sacroiliac joints.
Major Finding: Two genetic variants with known associations to type 1 diabetes or celiac disease also predispose to juvenile idiopathic arthritis.
Data Source: DNA from 1,054 patients with juvenile idiopathic arthritis was compared with that of 3,129 healthy controls. Thirteen single nucleotide polymorphisms (SNPs) that already had confirmed associations with type 1 diabetes or celiac disease were investigated.
Disclosures: The study was sponsored by Arthritis Research U.K. and supported by the NIHR Manchester Biomedical Research Council. Genotype data used was funded by grants from the Medical Research Council and the Wellcome Trust. The authors said they had no relevant financial disclosures.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, U.K.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2169-72).
The researchers compared DNA from 1,054 patients with JIA with that of 3,129 healthy controls, focusing on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease. One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with JIA. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease. LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. It also has been linked to Ras signaling, a process important in cell growth, differentiation, and survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype. The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T-cell–independent induction of interferon gamma.
Although this gene has not been associated with ankylosing spondylitis, patients with enthesitis-related arthritis are prone to joint destruction in the spine and sacroiliac joints.
Genetic Variants May Confer Susceptibility to JIA
Major Finding: Two genetic variants with known associations to type 1 diabetes or celiac disease also predispose to juvenile idiopathic arthritis.
Data Source: DNA from 1,054 patients with juvenile idiopathic arthritis was compared with that of 3,129 healthy controls. Thirteen single nucleotide polymorphisms (SNPs) that already had confirmed associations with type 1 diabetes or celiac disease were investigated.
Disclosures: The study was sponsored by Arthritis Research U.K. and supported by the NIHR Manchester Biomedical Research Council. Genotype data used were funded by grants from the Medical Research Council and the Wellcome Trust. The authors said they had no relevant financial disclosures.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, England, and colleagues.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2,169-72).
The researchers compared DNA from a total of 1,054 patients with juvenile idiopathic arthritis with that of 3,129 healthy controls. All the subjects were white.
The study focused on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease, according to the researchers.
One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with juvenile idiopathic arthritis. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease.
LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. In addition, LPP has been linked to Ras signaling, a process that is important to the functions of cell growth and differentiation, as well as survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype.
The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T cell–independent induction of interferon gamma.
Although this gene has not been associated with ankylosing spondylitis, patients with enthesitis-related arthritis are prone to joint destruction in the spine and sacroiliac joints.
“It is important to note that the numbers in this subgroup are small (61), so this finding should be interpreted with caution and will require validation in an independent cohort,” Dr. Hinks and her coauthors noted.
Major Finding: Two genetic variants with known associations to type 1 diabetes or celiac disease also predispose to juvenile idiopathic arthritis.
Data Source: DNA from 1,054 patients with juvenile idiopathic arthritis was compared with that of 3,129 healthy controls. Thirteen single nucleotide polymorphisms (SNPs) that already had confirmed associations with type 1 diabetes or celiac disease were investigated.
Disclosures: The study was sponsored by Arthritis Research U.K. and supported by the NIHR Manchester Biomedical Research Council. Genotype data used were funded by grants from the Medical Research Council and the Wellcome Trust. The authors said they had no relevant financial disclosures.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, England, and colleagues.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2,169-72).
The researchers compared DNA from a total of 1,054 patients with juvenile idiopathic arthritis with that of 3,129 healthy controls. All the subjects were white.
The study focused on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease, according to the researchers.
One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with juvenile idiopathic arthritis. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease.
LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. In addition, LPP has been linked to Ras signaling, a process that is important to the functions of cell growth and differentiation, as well as survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype.
The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T cell–independent induction of interferon gamma.
Although this gene has not been associated with ankylosing spondylitis, patients with enthesitis-related arthritis are prone to joint destruction in the spine and sacroiliac joints.
“It is important to note that the numbers in this subgroup are small (61), so this finding should be interpreted with caution and will require validation in an independent cohort,” Dr. Hinks and her coauthors noted.
Major Finding: Two genetic variants with known associations to type 1 diabetes or celiac disease also predispose to juvenile idiopathic arthritis.
Data Source: DNA from 1,054 patients with juvenile idiopathic arthritis was compared with that of 3,129 healthy controls. Thirteen single nucleotide polymorphisms (SNPs) that already had confirmed associations with type 1 diabetes or celiac disease were investigated.
Disclosures: The study was sponsored by Arthritis Research U.K. and supported by the NIHR Manchester Biomedical Research Council. Genotype data used were funded by grants from the Medical Research Council and the Wellcome Trust. The authors said they had no relevant financial disclosures.
Two genetic polymorphisms now appear to be associated with juvenile idiopathic arthritis as well as type 1 diabetes or celiac disease.
The finding lends credence to a growing idea that genetic variability in common loci can predispose a child to different autoimmune disorders, wrote Dr. Anne Hinks of the University of Manchester, England, and colleagues.
“The approach of targeting variants associated with other autoimmune diseases is already yielding insights into the genetic complexity underlying susceptibility to this serious childhood disease,” Dr. Hinks and her coauthors wrote (Ann. Rheum. Dis. 2010;69:2,169-72).
The researchers compared DNA from a total of 1,054 patients with juvenile idiopathic arthritis with that of 3,129 healthy controls. All the subjects were white.
The study focused on 13 single nucleotide polymorphisms (SNPs) that had already had confirmed associations with type 1 diabetes or celiac disease, according to the researchers.
One SNP on the preferred translocation partner in lipoma (LPP) gene (rs1464510) was significantly associated with juvenile idiopathic arthritis. Another SNP located in the ataxin 2 (ATXN2) gene was marginally associated with JIA, but the association was not significant.
The SNP lying in the LPP domain is particularly interesting, the authors noted, because that gene has a confirmed association with celiac disease.
LPP is integral in cell migration and adhesion and is a substrate of tyrosine phosphatase. In addition, LPP has been linked to Ras signaling, a process that is important to the functions of cell growth and differentiation, as well as survival.
A third SNP (rs17810546) located in the interleukin 12A gene (IL12A) was significantly associated with enthesitis-related arthritis. The IL12A gene has already been associated with celiac disease. The association with arthritis was a strong one, Dr. Hinks and her colleagues noted, but there were no other associations with any other JIA subtype.
The IL12A gene exerts a number of important influences, including encoding a cytokine necessary for the differentiation of T cells and T cell–independent induction of interferon gamma.
Although this gene has not been associated with ankylosing spondylitis, patients with enthesitis-related arthritis are prone to joint destruction in the spine and sacroiliac joints.
“It is important to note that the numbers in this subgroup are small (61), so this finding should be interpreted with caution and will require validation in an independent cohort,” Dr. Hinks and her coauthors noted.
Texas Center Ties Tort Reform to Lower Liability Costs
PALM BEACH, FLA. – Tort reform significantly decreased surgical malpractice lawsuits by nearly 80% in one Texas academic medical center.
The legislation, passed in 2003, also significantly reduced legal costs and malpractice insurance premiums for individual surgeons, Dr. Ronald Stewart said at the annual meeting of the Southern Surgical Association. In 2002, malpractice insurance premiums were $10,000 per surgeon. By 2010, the premium had dropped to $2,700, and it is projected to be $2,000 per surgeon in 2011.
"Obviously this is a complicated and potentially controversial issue," Dr. Stewart said in an interview. "However, our study was aimed at a simple question: Did the risk of surgical lawsuit decrease following tort reform? There’s no question in my mind that the legislation was directly responsible for these changes" in the surgery department of the University of Texas Health Sciences Center, said Dr. Stewart, the department’s interim chair. "Limiting economic incentives really does decrease malpractice case load and cost."
In 2003, Proposition 12 placed a $750,000 cap on noneconomic damages in medical malpractice lawsuits and limited an individual physician’s liability to $250,000. "UTHSCSA physicians’ liability is capped at $100,000, I believe, under the provision of public servant," Dr. Stewart said.
He and his colleagues compared prevalence, incidence, and risk and cost in general surgery and reviewed the frequency of lawsuits in the entire department (10 divisions) from 1992 to 2010. They used data from two hospital databases. One records all surgical procedures since 1979, and the other contains information on all malpractice claims filed since 1976.
Liability cost was defined as any monetary award to a plaintiff, legal cost as the cost incurred defending the suits, and total litigation as the sum of those costs.
From July 1992 to June 2010, 98,513 surgical procedures were performed and 28 lawsuits were filed. Most (25) were filed from 1992 to 2003 (the prereform period). About half (13) were decided in favor of the plaintiff, and the remainder in favor of the surgeon. The liability cost of the suits was $5.56 million and the legal cost $1.6 million – for a total litigation bill of $7.16 million. The annualized cost was almost $600,000.
Of the three suits filed since 2004, one is still pending, and there were no plaintiff payouts in the other two, according to Dr. Stewart. Total legal costs of $3,345 translate into about $500 per year.
Besides frequency and cost, prevalence also significantly decreased, he said. Before tort reform, malpractice suit prevalence was 40/100,000 surgeons. After tort reform, it was 8/100,000, for a relative reduction of almost 80% (risk reduction, 0.21).
These changes led directly to the significant reductions in malpractice insurance premiums, which dropped by $8,000 per surgeon, Dr. Stewart said.
His cost analysis didn’t control for any confounding factors, such as improved disclosure, decreased errors, or quality improvement practices. "These factors may have been responsible for some decreased malpractice lawsuits, but it is very likely that tort reform was the primary driver for the observed decrease," he said.
The study did more than simply point out cost savings, said Dr. Benjamin Li, a discussant with Louisiana State University Health Sciences Center. "It does not even measure more indirect costs, such as the practice of defensive medicine, the cost of recruiting surgeons into a high-risk medical malpractice environment, and the loss of opportunity to correct systems errors due to the inhibition of open discussion of medical errors for fear of malpractice suits," he said.
Tort reform can improve the physician/patient relationship, Dr. Stewart said in an interview. "I believe a major problem of the tort system was that it fostered an adversarial relationship between surgeon and patient, which, when present, is directly counter to good patient care."
However, he noted, not everyone believes the law was – and remains – a good one. The Texas Trial Lawyers Association declined to comment on the issue, referring questions instead to Texas Watch, which defines itself as "a nonpartisan, advocacy organization working to improve consumer and insurance protections for Texas families ... providing a counter to wealthy special interest lobby efforts."
The decrease in lawsuits, plaintiff payouts, and malpractice premiums is no surprise to Alex Winslow, executive director of Texas Watch. "The question is what that really means," he said in an interview. "While insurance companies and physicians are shielded and make more money, patients continue to suffer the burden of crushing medical errors. This does not mean there are less medical errors; it just means that patients have no means to hold doctors accountable."
There are no data showing that the quality of health care services or medical errors has decreased since tort reform passed, Mr. Winslow said. "Nationwide, this is still a real problem, and in Texas there is no evidence that the quality of care has gotten better."
While the statewide statistics may not be in evidence, Dr. Stewart described his institution’s experience with quality improvement since tort reform. "At least within our system, these malpractice cost savings have translated directly into spending on patient quality and safety initiatives – hopefully, directly benefiting our patients and improving the quality of care."
Proponents of the law say the more favorable legal climate has expanded health care services and drawn more physicians to the state – a claim Mr. Winslow contested. "Underserved areas continue to struggle to attract physicians to serve their population, and Texas ranks close to the bottom in terms of physicians per capita." Doctors are coming, he said, but only to metropolitan areas that already have a good supply. "We continue to lag well behind the rest of the country in per capita physician supply. Physician supply is failing to keep up with population growth."
However, the Texas Alliance for Patient Access – a statewide coalition of doctors, hospitals, clinics, nursing homes, and physician liability insurers – asserts that physician supply and medical services have increased since 2003. "Overall, Texas has enjoyed a 62% greater growth rate in newly licensed physicians in the past 3 years, compared to 3 years preceding reform," according to TAPA documents supplied by spokesman Jon Opelt. Other statistics he provided support the claim that underserved areas are benefiting from the law.
• Twenty-four rural counties added at least one general surgeon, and 11 added their first general surgeon.
• Twelve rural counties added at least one orthopedic surgeon, and nine counties added their first orthopedic surgeon.
• Six Texas counties added their first neurosurgeon; two of those counties are rural.
• Fifteen rural counties added a cardiologist or cardiovascular surgeon, including 11 that added their first cardiologist.
• The ranks of rural obstetricians have grown by 27%. Twenty-two rural counties added an obstetrician and 10 counties added their first OB.
Twenty-three rural counties have added at least one emergency medicine physician, and 18 added their first emergency room doctor.
Texas voters seem to favor the law, according to a survey of 501 randomly selected registered voters conducted in September by the group Texans Against Lawsuit Abuse. Most survey respondents (62%) thought recent legal reforms have been a good thing because they have helped bring thousands of new physician specialists to Texas, allowed hospitals to provide expanded medical care, and reduced questionable lawsuits so people with legitimate malpractice claims could have their cases heard, a press release stated.
Dr. Stewart said his study can’t address these complex political issues, but he believes that "tort reform in Texas sets the stage for improved access to surgical care, reduces cost, and allows more effective quality and performance improvement initiatives."
Dr. Stewart had no relevant financial disclosures.
PALM BEACH, FLA. – Tort reform significantly decreased surgical malpractice lawsuits by nearly 80% in one Texas academic medical center.
The legislation, passed in 2003, also significantly reduced legal costs and malpractice insurance premiums for individual surgeons, Dr. Ronald Stewart said at the annual meeting of the Southern Surgical Association. In 2002, malpractice insurance premiums were $10,000 per surgeon. By 2010, the premium had dropped to $2,700, and it is projected to be $2,000 per surgeon in 2011.
"Obviously this is a complicated and potentially controversial issue," Dr. Stewart said in an interview. "However, our study was aimed at a simple question: Did the risk of surgical lawsuit decrease following tort reform? There’s no question in my mind that the legislation was directly responsible for these changes" in the surgery department of the University of Texas Health Sciences Center, said Dr. Stewart, the department’s interim chair. "Limiting economic incentives really does decrease malpractice case load and cost."
In 2003, Proposition 12 placed a $750,000 cap on noneconomic damages in medical malpractice lawsuits and limited an individual physician’s liability to $250,000. "UTHSCSA physicians’ liability is capped at $100,000, I believe, under the provision of public servant," Dr. Stewart said.
He and his colleagues compared prevalence, incidence, and risk and cost in general surgery and reviewed the frequency of lawsuits in the entire department (10 divisions) from 1992 to 2010. They used data from two hospital databases. One records all surgical procedures since 1979, and the other contains information on all malpractice claims filed since 1976.
Liability cost was defined as any monetary award to a plaintiff, legal cost as the cost incurred defending the suits, and total litigation as the sum of those costs.
From July 1992 to June 2010, 98,513 surgical procedures were performed and 28 lawsuits were filed. Most (25) were filed from 1992 to 2003 (the prereform period). About half (13) were decided in favor of the plaintiff, and the remainder in favor of the surgeon. The liability cost of the suits was $5.56 million and the legal cost $1.6 million – for a total litigation bill of $7.16 million. The annualized cost was almost $600,000.
Of the three suits filed since 2004, one is still pending, and there were no plaintiff payouts in the other two, according to Dr. Stewart. Total legal costs of $3,345 translate into about $500 per year.
Besides frequency and cost, prevalence also significantly decreased, he said. Before tort reform, malpractice suit prevalence was 40/100,000 surgeons. After tort reform, it was 8/100,000, for a relative reduction of almost 80% (risk reduction, 0.21).
These changes led directly to the significant reductions in malpractice insurance premiums, which dropped by $8,000 per surgeon, Dr. Stewart said.
His cost analysis didn’t control for any confounding factors, such as improved disclosure, decreased errors, or quality improvement practices. "These factors may have been responsible for some decreased malpractice lawsuits, but it is very likely that tort reform was the primary driver for the observed decrease," he said.
The study did more than simply point out cost savings, said Dr. Benjamin Li, a discussant with Louisiana State University Health Sciences Center. "It does not even measure more indirect costs, such as the practice of defensive medicine, the cost of recruiting surgeons into a high-risk medical malpractice environment, and the loss of opportunity to correct systems errors due to the inhibition of open discussion of medical errors for fear of malpractice suits," he said.
Tort reform can improve the physician/patient relationship, Dr. Stewart said in an interview. "I believe a major problem of the tort system was that it fostered an adversarial relationship between surgeon and patient, which, when present, is directly counter to good patient care."
However, he noted, not everyone believes the law was – and remains – a good one. The Texas Trial Lawyers Association declined to comment on the issue, referring questions instead to Texas Watch, which defines itself as "a nonpartisan, advocacy organization working to improve consumer and insurance protections for Texas families ... providing a counter to wealthy special interest lobby efforts."
The decrease in lawsuits, plaintiff payouts, and malpractice premiums is no surprise to Alex Winslow, executive director of Texas Watch. "The question is what that really means," he said in an interview. "While insurance companies and physicians are shielded and make more money, patients continue to suffer the burden of crushing medical errors. This does not mean there are less medical errors; it just means that patients have no means to hold doctors accountable."
There are no data showing that the quality of health care services or medical errors has decreased since tort reform passed, Mr. Winslow said. "Nationwide, this is still a real problem, and in Texas there is no evidence that the quality of care has gotten better."
While the statewide statistics may not be in evidence, Dr. Stewart described his institution’s experience with quality improvement since tort reform. "At least within our system, these malpractice cost savings have translated directly into spending on patient quality and safety initiatives – hopefully, directly benefiting our patients and improving the quality of care."
Proponents of the law say the more favorable legal climate has expanded health care services and drawn more physicians to the state – a claim Mr. Winslow contested. "Underserved areas continue to struggle to attract physicians to serve their population, and Texas ranks close to the bottom in terms of physicians per capita." Doctors are coming, he said, but only to metropolitan areas that already have a good supply. "We continue to lag well behind the rest of the country in per capita physician supply. Physician supply is failing to keep up with population growth."
However, the Texas Alliance for Patient Access – a statewide coalition of doctors, hospitals, clinics, nursing homes, and physician liability insurers – asserts that physician supply and medical services have increased since 2003. "Overall, Texas has enjoyed a 62% greater growth rate in newly licensed physicians in the past 3 years, compared to 3 years preceding reform," according to TAPA documents supplied by spokesman Jon Opelt. Other statistics he provided support the claim that underserved areas are benefiting from the law.
• Twenty-four rural counties added at least one general surgeon, and 11 added their first general surgeon.
• Twelve rural counties added at least one orthopedic surgeon, and nine counties added their first orthopedic surgeon.
• Six Texas counties added their first neurosurgeon; two of those counties are rural.
• Fifteen rural counties added a cardiologist or cardiovascular surgeon, including 11 that added their first cardiologist.
• The ranks of rural obstetricians have grown by 27%. Twenty-two rural counties added an obstetrician and 10 counties added their first OB.
Twenty-three rural counties have added at least one emergency medicine physician, and 18 added their first emergency room doctor.
Texas voters seem to favor the law, according to a survey of 501 randomly selected registered voters conducted in September by the group Texans Against Lawsuit Abuse. Most survey respondents (62%) thought recent legal reforms have been a good thing because they have helped bring thousands of new physician specialists to Texas, allowed hospitals to provide expanded medical care, and reduced questionable lawsuits so people with legitimate malpractice claims could have their cases heard, a press release stated.
Dr. Stewart said his study can’t address these complex political issues, but he believes that "tort reform in Texas sets the stage for improved access to surgical care, reduces cost, and allows more effective quality and performance improvement initiatives."
Dr. Stewart had no relevant financial disclosures.
PALM BEACH, FLA. – Tort reform significantly decreased surgical malpractice lawsuits by nearly 80% in one Texas academic medical center.
The legislation, passed in 2003, also significantly reduced legal costs and malpractice insurance premiums for individual surgeons, Dr. Ronald Stewart said at the annual meeting of the Southern Surgical Association. In 2002, malpractice insurance premiums were $10,000 per surgeon. By 2010, the premium had dropped to $2,700, and it is projected to be $2,000 per surgeon in 2011.
"Obviously this is a complicated and potentially controversial issue," Dr. Stewart said in an interview. "However, our study was aimed at a simple question: Did the risk of surgical lawsuit decrease following tort reform? There’s no question in my mind that the legislation was directly responsible for these changes" in the surgery department of the University of Texas Health Sciences Center, said Dr. Stewart, the department’s interim chair. "Limiting economic incentives really does decrease malpractice case load and cost."
In 2003, Proposition 12 placed a $750,000 cap on noneconomic damages in medical malpractice lawsuits and limited an individual physician’s liability to $250,000. "UTHSCSA physicians’ liability is capped at $100,000, I believe, under the provision of public servant," Dr. Stewart said.
He and his colleagues compared prevalence, incidence, and risk and cost in general surgery and reviewed the frequency of lawsuits in the entire department (10 divisions) from 1992 to 2010. They used data from two hospital databases. One records all surgical procedures since 1979, and the other contains information on all malpractice claims filed since 1976.
Liability cost was defined as any monetary award to a plaintiff, legal cost as the cost incurred defending the suits, and total litigation as the sum of those costs.
From July 1992 to June 2010, 98,513 surgical procedures were performed and 28 lawsuits were filed. Most (25) were filed from 1992 to 2003 (the prereform period). About half (13) were decided in favor of the plaintiff, and the remainder in favor of the surgeon. The liability cost of the suits was $5.56 million and the legal cost $1.6 million – for a total litigation bill of $7.16 million. The annualized cost was almost $600,000.
Of the three suits filed since 2004, one is still pending, and there were no plaintiff payouts in the other two, according to Dr. Stewart. Total legal costs of $3,345 translate into about $500 per year.
Besides frequency and cost, prevalence also significantly decreased, he said. Before tort reform, malpractice suit prevalence was 40/100,000 surgeons. After tort reform, it was 8/100,000, for a relative reduction of almost 80% (risk reduction, 0.21).
These changes led directly to the significant reductions in malpractice insurance premiums, which dropped by $8,000 per surgeon, Dr. Stewart said.
His cost analysis didn’t control for any confounding factors, such as improved disclosure, decreased errors, or quality improvement practices. "These factors may have been responsible for some decreased malpractice lawsuits, but it is very likely that tort reform was the primary driver for the observed decrease," he said.
The study did more than simply point out cost savings, said Dr. Benjamin Li, a discussant with Louisiana State University Health Sciences Center. "It does not even measure more indirect costs, such as the practice of defensive medicine, the cost of recruiting surgeons into a high-risk medical malpractice environment, and the loss of opportunity to correct systems errors due to the inhibition of open discussion of medical errors for fear of malpractice suits," he said.
Tort reform can improve the physician/patient relationship, Dr. Stewart said in an interview. "I believe a major problem of the tort system was that it fostered an adversarial relationship between surgeon and patient, which, when present, is directly counter to good patient care."
However, he noted, not everyone believes the law was – and remains – a good one. The Texas Trial Lawyers Association declined to comment on the issue, referring questions instead to Texas Watch, which defines itself as "a nonpartisan, advocacy organization working to improve consumer and insurance protections for Texas families ... providing a counter to wealthy special interest lobby efforts."
The decrease in lawsuits, plaintiff payouts, and malpractice premiums is no surprise to Alex Winslow, executive director of Texas Watch. "The question is what that really means," he said in an interview. "While insurance companies and physicians are shielded and make more money, patients continue to suffer the burden of crushing medical errors. This does not mean there are less medical errors; it just means that patients have no means to hold doctors accountable."
There are no data showing that the quality of health care services or medical errors has decreased since tort reform passed, Mr. Winslow said. "Nationwide, this is still a real problem, and in Texas there is no evidence that the quality of care has gotten better."
While the statewide statistics may not be in evidence, Dr. Stewart described his institution’s experience with quality improvement since tort reform. "At least within our system, these malpractice cost savings have translated directly into spending on patient quality and safety initiatives – hopefully, directly benefiting our patients and improving the quality of care."
Proponents of the law say the more favorable legal climate has expanded health care services and drawn more physicians to the state – a claim Mr. Winslow contested. "Underserved areas continue to struggle to attract physicians to serve their population, and Texas ranks close to the bottom in terms of physicians per capita." Doctors are coming, he said, but only to metropolitan areas that already have a good supply. "We continue to lag well behind the rest of the country in per capita physician supply. Physician supply is failing to keep up with population growth."
However, the Texas Alliance for Patient Access – a statewide coalition of doctors, hospitals, clinics, nursing homes, and physician liability insurers – asserts that physician supply and medical services have increased since 2003. "Overall, Texas has enjoyed a 62% greater growth rate in newly licensed physicians in the past 3 years, compared to 3 years preceding reform," according to TAPA documents supplied by spokesman Jon Opelt. Other statistics he provided support the claim that underserved areas are benefiting from the law.
• Twenty-four rural counties added at least one general surgeon, and 11 added their first general surgeon.
• Twelve rural counties added at least one orthopedic surgeon, and nine counties added their first orthopedic surgeon.
• Six Texas counties added their first neurosurgeon; two of those counties are rural.
• Fifteen rural counties added a cardiologist or cardiovascular surgeon, including 11 that added their first cardiologist.
• The ranks of rural obstetricians have grown by 27%. Twenty-two rural counties added an obstetrician and 10 counties added their first OB.
Twenty-three rural counties have added at least one emergency medicine physician, and 18 added their first emergency room doctor.
Texas voters seem to favor the law, according to a survey of 501 randomly selected registered voters conducted in September by the group Texans Against Lawsuit Abuse. Most survey respondents (62%) thought recent legal reforms have been a good thing because they have helped bring thousands of new physician specialists to Texas, allowed hospitals to provide expanded medical care, and reduced questionable lawsuits so people with legitimate malpractice claims could have their cases heard, a press release stated.
Dr. Stewart said his study can’t address these complex political issues, but he believes that "tort reform in Texas sets the stage for improved access to surgical care, reduces cost, and allows more effective quality and performance improvement initiatives."
Dr. Stewart had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Texas Center Ties Tort Reform to Lower Liability Costs
PALM BEACH, FLA. – Tort reform significantly decreased surgical malpractice lawsuits by nearly 80% in one Texas academic medical center.
The legislation, passed in 2003, also significantly reduced legal costs and malpractice insurance premiums for individual surgeons, Dr. Ronald Stewart said at the annual meeting of the Southern Surgical Association. In 2002, malpractice insurance premiums were $10,000 per surgeon. By 2010, the premium had dropped to $2,700, and it is projected to be $2,000 per surgeon in 2011.
"Obviously this is a complicated and potentially controversial issue," Dr. Stewart said in an interview. "However, our study was aimed at a simple question: Did the risk of surgical lawsuit decrease following tort reform? There’s no question in my mind that the legislation was directly responsible for these changes" in the surgery department of the University of Texas Health Sciences Center, said Dr. Stewart, the department’s interim chair. "Limiting economic incentives really does decrease malpractice case load and cost."
In 2003, Proposition 12 placed a $750,000 cap on noneconomic damages in medical malpractice lawsuits and limited an individual physician’s liability to $250,000. "UTHSCSA physicians’ liability is capped at $100,000, I believe, under the provision of public servant," Dr. Stewart said.
He and his colleagues compared prevalence, incidence, and risk and cost in general surgery and reviewed the frequency of lawsuits in the entire department (10 divisions) from 1992 to 2010. They used data from two hospital databases. One records all surgical procedures since 1979, and the other contains information on all malpractice claims filed since 1976.
Liability cost was defined as any monetary award to a plaintiff, legal cost as the cost incurred defending the suits, and total litigation as the sum of those costs.
From July 1992 to June 2010, 98,513 surgical procedures were performed and 28 lawsuits were filed. Most (25) were filed from 1992 to 2003 (the prereform period). About half (13) were decided in favor of the plaintiff, and the remainder in favor of the surgeon. The liability cost of the suits was $5.56 million and the legal cost $1.6 million – for a total litigation bill of $7.16 million. The annualized cost was almost $600,000.
Of the three suits filed since 2004, one is still pending, and there were no plaintiff payouts in the other two, according to Dr. Stewart. Total legal costs of $3,345 translate into about $500 per year.
Besides frequency and cost, prevalence also significantly decreased, he said. Before tort reform, malpractice suit prevalence was 40/100,000 surgeons. After tort reform, it was 8/100,000, for a relative reduction of almost 80% (risk reduction, 0.21).
These changes led directly to the significant reductions in malpractice insurance premiums, which dropped by $8,000 per surgeon, Dr. Stewart said.
His cost analysis didn’t control for any confounding factors, such as improved disclosure, decreased errors, or quality improvement practices. "These factors may have been responsible for some decreased malpractice lawsuits, but it is very likely that tort reform was the primary driver for the observed decrease," he said.
The study did more than simply point out cost savings, said Dr. Benjamin Li, a discussant with Louisiana State University Health Sciences Center. "It does not even measure more indirect costs, such as the practice of defensive medicine, the cost of recruiting surgeons into a high-risk medical malpractice environment, and the loss of opportunity to correct systems errors due to the inhibition of open discussion of medical errors for fear of malpractice suits," he said.
Tort reform can improve the physician/patient relationship, Dr. Stewart said in an interview. "I believe a major problem of the tort system was that it fostered an adversarial relationship between surgeon and patient, which, when present, is directly counter to good patient care."
However, he noted, not everyone believes the law was – and remains – a good one. The Texas Trial Lawyers Association declined to comment on the issue, referring questions instead to Texas Watch, which defines itself as "a nonpartisan, advocacy organization working to improve consumer and insurance protections for Texas families ... providing a counter to wealthy special interest lobby efforts."
The decrease in lawsuits, plaintiff payouts, and malpractice premiums is no surprise to Alex Winslow, executive director of Texas Watch. "The question is what that really means," he said in an interview. "While insurance companies and physicians are shielded and make more money, patients continue to suffer the burden of crushing medical errors. This does not mean there are less medical errors; it just means that patients have no means to hold doctors accountable."
There are no data showing that the quality of health care services or medical errors has decreased since tort reform passed, Mr. Winslow said. "Nationwide, this is still a real problem, and in Texas there is no evidence that the quality of care has gotten better."
While the statewide statistics may not be in evidence, Dr. Stewart described his institution’s experience with quality improvement since tort reform. "At least within our system, these malpractice cost savings have translated directly into spending on patient quality and safety initiatives – hopefully, directly benefiting our patients and improving the quality of care."
Proponents of the law say the more favorable legal climate has expanded health care services and drawn more physicians to the state – a claim Mr. Winslow contested. "Underserved areas continue to struggle to attract physicians to serve their population, and Texas ranks close to the bottom in terms of physicians per capita." Doctors are coming, he said, but only to metropolitan areas that already have a good supply. "We continue to lag well behind the rest of the country in per capita physician supply. Physician supply is failing to keep up with population growth."
However, the Texas Alliance for Patient Access – a statewide coalition of doctors, hospitals, clinics, nursing homes, and physician liability insurers – asserts that physician supply and medical services have increased since 2003. "Overall, Texas has enjoyed a 62% greater growth rate in newly licensed physicians in the past 3 years, compared to 3 years preceding reform," according to TAPA documents supplied by spokesman Jon Opelt. Other statistics he provided support the claim that underserved areas are benefiting from the law.
• Twenty-four rural counties added at least one general surgeon, and 11 added their first general surgeon.
• Twelve rural counties added at least one orthopedic surgeon, and nine counties added their first orthopedic surgeon.
• Six Texas counties added their first neurosurgeon; two of those counties are rural.
• Fifteen rural counties added a cardiologist or cardiovascular surgeon, including 11 that added their first cardiologist.
• The ranks of rural obstetricians have grown by 27%. Twenty-two rural counties added an obstetrician and 10 counties added their first OB.
Twenty-three rural counties have added at least one emergency medicine physician, and 18 added their first emergency room doctor.
Texas voters seem to favor the law, according to a survey of 501 randomly selected registered voters conducted in September by the group Texans Against Lawsuit Abuse. Most survey respondents (62%) thought recent legal reforms have been a good thing because they have helped bring thousands of new physician specialists to Texas, allowed hospitals to provide expanded medical care, and reduced questionable lawsuits so people with legitimate malpractice claims could have their cases heard, a press release stated.
Dr. Stewart said his study can’t address these complex political issues, but he believes that "tort reform in Texas sets the stage for improved access to surgical care, reduces cost, and allows more effective quality and performance improvement initiatives."
Dr. Stewart had no relevant financial disclosures.
PALM BEACH, FLA. – Tort reform significantly decreased surgical malpractice lawsuits by nearly 80% in one Texas academic medical center.
The legislation, passed in 2003, also significantly reduced legal costs and malpractice insurance premiums for individual surgeons, Dr. Ronald Stewart said at the annual meeting of the Southern Surgical Association. In 2002, malpractice insurance premiums were $10,000 per surgeon. By 2010, the premium had dropped to $2,700, and it is projected to be $2,000 per surgeon in 2011.
"Obviously this is a complicated and potentially controversial issue," Dr. Stewart said in an interview. "However, our study was aimed at a simple question: Did the risk of surgical lawsuit decrease following tort reform? There’s no question in my mind that the legislation was directly responsible for these changes" in the surgery department of the University of Texas Health Sciences Center, said Dr. Stewart, the department’s interim chair. "Limiting economic incentives really does decrease malpractice case load and cost."
In 2003, Proposition 12 placed a $750,000 cap on noneconomic damages in medical malpractice lawsuits and limited an individual physician’s liability to $250,000. "UTHSCSA physicians’ liability is capped at $100,000, I believe, under the provision of public servant," Dr. Stewart said.
He and his colleagues compared prevalence, incidence, and risk and cost in general surgery and reviewed the frequency of lawsuits in the entire department (10 divisions) from 1992 to 2010. They used data from two hospital databases. One records all surgical procedures since 1979, and the other contains information on all malpractice claims filed since 1976.
Liability cost was defined as any monetary award to a plaintiff, legal cost as the cost incurred defending the suits, and total litigation as the sum of those costs.
From July 1992 to June 2010, 98,513 surgical procedures were performed and 28 lawsuits were filed. Most (25) were filed from 1992 to 2003 (the prereform period). About half (13) were decided in favor of the plaintiff, and the remainder in favor of the surgeon. The liability cost of the suits was $5.56 million and the legal cost $1.6 million – for a total litigation bill of $7.16 million. The annualized cost was almost $600,000.
Of the three suits filed since 2004, one is still pending, and there were no plaintiff payouts in the other two, according to Dr. Stewart. Total legal costs of $3,345 translate into about $500 per year.
Besides frequency and cost, prevalence also significantly decreased, he said. Before tort reform, malpractice suit prevalence was 40/100,000 surgeons. After tort reform, it was 8/100,000, for a relative reduction of almost 80% (risk reduction, 0.21).
These changes led directly to the significant reductions in malpractice insurance premiums, which dropped by $8,000 per surgeon, Dr. Stewart said.
His cost analysis didn’t control for any confounding factors, such as improved disclosure, decreased errors, or quality improvement practices. "These factors may have been responsible for some decreased malpractice lawsuits, but it is very likely that tort reform was the primary driver for the observed decrease," he said.
The study did more than simply point out cost savings, said Dr. Benjamin Li, a discussant with Louisiana State University Health Sciences Center. "It does not even measure more indirect costs, such as the practice of defensive medicine, the cost of recruiting surgeons into a high-risk medical malpractice environment, and the loss of opportunity to correct systems errors due to the inhibition of open discussion of medical errors for fear of malpractice suits," he said.
Tort reform can improve the physician/patient relationship, Dr. Stewart said in an interview. "I believe a major problem of the tort system was that it fostered an adversarial relationship between surgeon and patient, which, when present, is directly counter to good patient care."
However, he noted, not everyone believes the law was – and remains – a good one. The Texas Trial Lawyers Association declined to comment on the issue, referring questions instead to Texas Watch, which defines itself as "a nonpartisan, advocacy organization working to improve consumer and insurance protections for Texas families ... providing a counter to wealthy special interest lobby efforts."
The decrease in lawsuits, plaintiff payouts, and malpractice premiums is no surprise to Alex Winslow, executive director of Texas Watch. "The question is what that really means," he said in an interview. "While insurance companies and physicians are shielded and make more money, patients continue to suffer the burden of crushing medical errors. This does not mean there are less medical errors; it just means that patients have no means to hold doctors accountable."
There are no data showing that the quality of health care services or medical errors has decreased since tort reform passed, Mr. Winslow said. "Nationwide, this is still a real problem, and in Texas there is no evidence that the quality of care has gotten better."
While the statewide statistics may not be in evidence, Dr. Stewart described his institution’s experience with quality improvement since tort reform. "At least within our system, these malpractice cost savings have translated directly into spending on patient quality and safety initiatives – hopefully, directly benefiting our patients and improving the quality of care."
Proponents of the law say the more favorable legal climate has expanded health care services and drawn more physicians to the state – a claim Mr. Winslow contested. "Underserved areas continue to struggle to attract physicians to serve their population, and Texas ranks close to the bottom in terms of physicians per capita." Doctors are coming, he said, but only to metropolitan areas that already have a good supply. "We continue to lag well behind the rest of the country in per capita physician supply. Physician supply is failing to keep up with population growth."
However, the Texas Alliance for Patient Access – a statewide coalition of doctors, hospitals, clinics, nursing homes, and physician liability insurers – asserts that physician supply and medical services have increased since 2003. "Overall, Texas has enjoyed a 62% greater growth rate in newly licensed physicians in the past 3 years, compared to 3 years preceding reform," according to TAPA documents supplied by spokesman Jon Opelt. Other statistics he provided support the claim that underserved areas are benefiting from the law.
• Twenty-four rural counties added at least one general surgeon, and 11 added their first general surgeon.
• Twelve rural counties added at least one orthopedic surgeon, and nine counties added their first orthopedic surgeon.
• Six Texas counties added their first neurosurgeon; two of those counties are rural.
• Fifteen rural counties added a cardiologist or cardiovascular surgeon, including 11 that added their first cardiologist.
• The ranks of rural obstetricians have grown by 27%. Twenty-two rural counties added an obstetrician and 10 counties added their first OB.
Twenty-three rural counties have added at least one emergency medicine physician, and 18 added their first emergency room doctor.
Texas voters seem to favor the law, according to a survey of 501 randomly selected registered voters conducted in September by the group Texans Against Lawsuit Abuse. Most survey respondents (62%) thought recent legal reforms have been a good thing because they have helped bring thousands of new physician specialists to Texas, allowed hospitals to provide expanded medical care, and reduced questionable lawsuits so people with legitimate malpractice claims could have their cases heard, a press release stated.
Dr. Stewart said his study can’t address these complex political issues, but he believes that "tort reform in Texas sets the stage for improved access to surgical care, reduces cost, and allows more effective quality and performance improvement initiatives."
Dr. Stewart had no relevant financial disclosures.
PALM BEACH, FLA. – Tort reform significantly decreased surgical malpractice lawsuits by nearly 80% in one Texas academic medical center.
The legislation, passed in 2003, also significantly reduced legal costs and malpractice insurance premiums for individual surgeons, Dr. Ronald Stewart said at the annual meeting of the Southern Surgical Association. In 2002, malpractice insurance premiums were $10,000 per surgeon. By 2010, the premium had dropped to $2,700, and it is projected to be $2,000 per surgeon in 2011.
"Obviously this is a complicated and potentially controversial issue," Dr. Stewart said in an interview. "However, our study was aimed at a simple question: Did the risk of surgical lawsuit decrease following tort reform? There’s no question in my mind that the legislation was directly responsible for these changes" in the surgery department of the University of Texas Health Sciences Center, said Dr. Stewart, the department’s interim chair. "Limiting economic incentives really does decrease malpractice case load and cost."
In 2003, Proposition 12 placed a $750,000 cap on noneconomic damages in medical malpractice lawsuits and limited an individual physician’s liability to $250,000. "UTHSCSA physicians’ liability is capped at $100,000, I believe, under the provision of public servant," Dr. Stewart said.
He and his colleagues compared prevalence, incidence, and risk and cost in general surgery and reviewed the frequency of lawsuits in the entire department (10 divisions) from 1992 to 2010. They used data from two hospital databases. One records all surgical procedures since 1979, and the other contains information on all malpractice claims filed since 1976.
Liability cost was defined as any monetary award to a plaintiff, legal cost as the cost incurred defending the suits, and total litigation as the sum of those costs.
From July 1992 to June 2010, 98,513 surgical procedures were performed and 28 lawsuits were filed. Most (25) were filed from 1992 to 2003 (the prereform period). About half (13) were decided in favor of the plaintiff, and the remainder in favor of the surgeon. The liability cost of the suits was $5.56 million and the legal cost $1.6 million – for a total litigation bill of $7.16 million. The annualized cost was almost $600,000.
Of the three suits filed since 2004, one is still pending, and there were no plaintiff payouts in the other two, according to Dr. Stewart. Total legal costs of $3,345 translate into about $500 per year.
Besides frequency and cost, prevalence also significantly decreased, he said. Before tort reform, malpractice suit prevalence was 40/100,000 surgeons. After tort reform, it was 8/100,000, for a relative reduction of almost 80% (risk reduction, 0.21).
These changes led directly to the significant reductions in malpractice insurance premiums, which dropped by $8,000 per surgeon, Dr. Stewart said.
His cost analysis didn’t control for any confounding factors, such as improved disclosure, decreased errors, or quality improvement practices. "These factors may have been responsible for some decreased malpractice lawsuits, but it is very likely that tort reform was the primary driver for the observed decrease," he said.
The study did more than simply point out cost savings, said Dr. Benjamin Li, a discussant with Louisiana State University Health Sciences Center. "It does not even measure more indirect costs, such as the practice of defensive medicine, the cost of recruiting surgeons into a high-risk medical malpractice environment, and the loss of opportunity to correct systems errors due to the inhibition of open discussion of medical errors for fear of malpractice suits," he said.
Tort reform can improve the physician/patient relationship, Dr. Stewart said in an interview. "I believe a major problem of the tort system was that it fostered an adversarial relationship between surgeon and patient, which, when present, is directly counter to good patient care."
However, he noted, not everyone believes the law was – and remains – a good one. The Texas Trial Lawyers Association declined to comment on the issue, referring questions instead to Texas Watch, which defines itself as "a nonpartisan, advocacy organization working to improve consumer and insurance protections for Texas families ... providing a counter to wealthy special interest lobby efforts."
The decrease in lawsuits, plaintiff payouts, and malpractice premiums is no surprise to Alex Winslow, executive director of Texas Watch. "The question is what that really means," he said in an interview. "While insurance companies and physicians are shielded and make more money, patients continue to suffer the burden of crushing medical errors. This does not mean there are less medical errors; it just means that patients have no means to hold doctors accountable."
There are no data showing that the quality of health care services or medical errors has decreased since tort reform passed, Mr. Winslow said. "Nationwide, this is still a real problem, and in Texas there is no evidence that the quality of care has gotten better."
While the statewide statistics may not be in evidence, Dr. Stewart described his institution’s experience with quality improvement since tort reform. "At least within our system, these malpractice cost savings have translated directly into spending on patient quality and safety initiatives – hopefully, directly benefiting our patients and improving the quality of care."
Proponents of the law say the more favorable legal climate has expanded health care services and drawn more physicians to the state – a claim Mr. Winslow contested. "Underserved areas continue to struggle to attract physicians to serve their population, and Texas ranks close to the bottom in terms of physicians per capita." Doctors are coming, he said, but only to metropolitan areas that already have a good supply. "We continue to lag well behind the rest of the country in per capita physician supply. Physician supply is failing to keep up with population growth."
However, the Texas Alliance for Patient Access – a statewide coalition of doctors, hospitals, clinics, nursing homes, and physician liability insurers – asserts that physician supply and medical services have increased since 2003. "Overall, Texas has enjoyed a 62% greater growth rate in newly licensed physicians in the past 3 years, compared to 3 years preceding reform," according to TAPA documents supplied by spokesman Jon Opelt. Other statistics he provided support the claim that underserved areas are benefiting from the law.
• Twenty-four rural counties added at least one general surgeon, and 11 added their first general surgeon.
• Twelve rural counties added at least one orthopedic surgeon, and nine counties added their first orthopedic surgeon.
• Six Texas counties added their first neurosurgeon; two of those counties are rural.
• Fifteen rural counties added a cardiologist or cardiovascular surgeon, including 11 that added their first cardiologist.
• The ranks of rural obstetricians have grown by 27%. Twenty-two rural counties added an obstetrician and 10 counties added their first OB.
Twenty-three rural counties have added at least one emergency medicine physician, and 18 added their first emergency room doctor.
Texas voters seem to favor the law, according to a survey of 501 randomly selected registered voters conducted in September by the group Texans Against Lawsuit Abuse. Most survey respondents (62%) thought recent legal reforms have been a good thing because they have helped bring thousands of new physician specialists to Texas, allowed hospitals to provide expanded medical care, and reduced questionable lawsuits so people with legitimate malpractice claims could have their cases heard, a press release stated.
Dr. Stewart said his study can’t address these complex political issues, but he believes that "tort reform in Texas sets the stage for improved access to surgical care, reduces cost, and allows more effective quality and performance improvement initiatives."
Dr. Stewart had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Tort reform decreased legal costs and the prevalence of malpractice suits in a Texas academic medical center.
Data Source: The prevalence of suits decreased by 80% after the 2003 tort reform legislation; associated legal costs decreased from $7 million to less than $4,000.
Disclosures: Dr. Stewart had no relevant financial disclosures.
Poor Long-Term Outcomes Suggest Need to Revisit Diabetic Foot Care
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.

"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
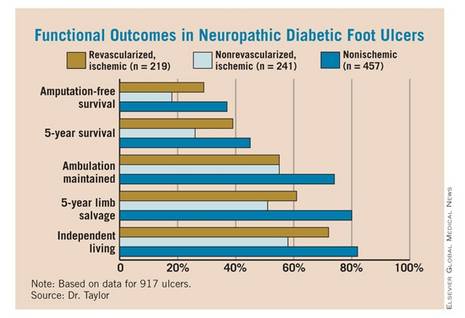
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.
"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.
"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Poor Long-Term Outcomes Suggest Need to Revisit Diabetic Foot Care
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.
"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.
"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.
"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Only 35% of revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation because of the ulcer.
Data Source: A review of 917 diabetic foot ulcers in 706 patients.
Disclosures: Dr. Spence Taylor had no financial disclosures.