User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
Prolonged Antibiotics Risky for VLBW Infants
PHILADELPHIA – A week-long course of empiric antibiotic treatment in neonates may result in a higher subsequent rate of chronic lung disease, compared with infants treated for just 2 days, based on an association seen in a review of more than 900 very low birth weight newborns.
But this finding is not yet ready to definitively guide practice, as it came from a nonrandomized, retrospective study that may have failed to control for all possible confounding variables, Dr. Alexandra Novitsky said at the meeting
In her adjusted analysis, which controlled for several baseline variables, the 159 very low birth weight (VLBW) neonates who received a “long” course of empiric antibiotic treatment, usually for 7 days, had a statistically significant, twofold higher rate of also having chronic lung disease during follow-up, compared with the 747 neonates who received a “short” antibiotic course, usually for 2 days, said Dr. Novitsky, a neonatologist at Christiana Hospital in Newark, Del.
“It's too early to draw conclusions about changing therapy,” based on this finding, said Dr. David A. Paul, associate director of neonatology at Christiana Hospital, who collaborated on the analysis. “We did our best to control for possible confounders, and it still suggested that longer antibiotic treatment altered outcomes, but there may have been things [for which] we did not control,” he said in an interview. The next step is to design a prospective study and determine if changing the duration of empiric antibiotic therapy changes outcomes. “But the current findings raise concern that we should be cautious about the duration of treatment,” said Dr. Paul.
In the cases reviewed, each physician delivering care determined the duration of antibiotic treatment. Some may have opted for a longer course of treatment because they were concerned that “not all babies have culture-proven sepsis,” Dr. Paul said in an interview. The physicians “may have feared that the babies had infections that were missed in their blood cultures. They treated presumed sepsis,” he said.
Dr. Novitsky reviewed all the VLBW infants seen in the neonatal ICU at Christiana Hospital between July 2004 and June 2009. The regimen used on all neonates who received empiric antibiotic treatment consisted of ampicillin and gentamicin. The infants who received a longer antibiotic course had a significantly higher prevalence of several markers of a worse clinical profile, including lower birth weight, younger gestational age, a higher score for neonatal acute physiology (SNAP), and a lower 5-minute Apgar score. They also had higher rates of clinical chorioamnionitis, mechanical ventilation, and endotracheal tube colonization (endotracheal tubes underwent routine, weekly colonization assessments).
The infants who received a longer course of antibiotics also had a higher prevalence of antibiotic-resistant, gram-negative organisms colonizing their endotracheal tubes, a 6% rate compared with a 2% rate among the infants who received a short course of treatment – a significant difference. The two groups of infants had roughly identical prevalence rates of colonization with antibiotic-resistant gram-positive strains.
Dr. Novitsky defined the primary outcome evaluated in the analysis, chronic lung disease, as the need for supplemental oxygen by the infant at 36 weeks postmenstrual age. This outcome occurred in 185 of the 906 (20%) neonates in the study: 17% of the infants who received a short antibiotic course, and 36% of those who received a long course.
The multivariable analysis adjusted for differences in gestational age, SNAP score, Apgar score, maternal anti-biotic treatment, chorioamnionitis, preeclampsia, cesarean delivery, prolonged rupture of membranes, and need for mechanical ventilation. After adjustment, the two patient groups failed to show a significant difference in their rates of necrotizing enterocolitis or sepsis.
To further examine the relationship between duration of antibiotic treatment and chronic lung disease, Dr. Novitsky also presented the results of a subgroup analysis that focused on the 418 high-risk neonates in her study group, because of their delivery at 28 weeks' gestation or younger and their SNAP score of 8 or greater.
Within this subgroup, the adjusted rate for developing chronic lung disease ran 70% higher in the 108 infants who received a long course of antibiotics, compared with the 310 who received a short course, also a significant difference.
Dr. Novitsky and Dr. Paul said they had no relevant financial disclosures.
{kind=link}
But this finding is not yet ready to definitively guide practice.
Source DR. NOVITSKY
View on the News
Don't Overuse Antibiotics
The findings of this analysis suggest that physicians should not treat neonates with antibiotics when not necessary. If they do, they risk making the babies worse.
A neonatologist may be tempted to prescribe a more prolonged course of antibiotics out of fear that the infant may have an infection. To be cautious, she overtreats. These new data suggest that this practice can actually do harm. This is another reason not to overtreat.
It is reasonable to infer that the treating physician had seen something in some of these children to prompt the longer duration of treatment. The infant must have somehow seemed sicker. The physician may have been concerned that if antibiotic treatment stopped sooner, the neonate's condition would have worsened. The optimal duration of treatment is always something to think about.
It is plausible that just a few extra days of antibiotic treatment can make an important difference. A 2-day duration of treatment probably does not change the background flora in the esophagus as much as a 7-day course. Longer exposure to antibiotics can result in a higher rate of fungal infection, which can trigger increased inflammation.
RITA M. RYAN, M.D., is chief of neonatology at the Women & Children's Hospital of Buffalo (N.Y.). She made these comments in an interview. She said that she had no relevant financial disclosures.
PHILADELPHIA – A week-long course of empiric antibiotic treatment in neonates may result in a higher subsequent rate of chronic lung disease, compared with infants treated for just 2 days, based on an association seen in a review of more than 900 very low birth weight newborns.
But this finding is not yet ready to definitively guide practice, as it came from a nonrandomized, retrospective study that may have failed to control for all possible confounding variables, Dr. Alexandra Novitsky said at the meeting
In her adjusted analysis, which controlled for several baseline variables, the 159 very low birth weight (VLBW) neonates who received a “long” course of empiric antibiotic treatment, usually for 7 days, had a statistically significant, twofold higher rate of also having chronic lung disease during follow-up, compared with the 747 neonates who received a “short” antibiotic course, usually for 2 days, said Dr. Novitsky, a neonatologist at Christiana Hospital in Newark, Del.
“It's too early to draw conclusions about changing therapy,” based on this finding, said Dr. David A. Paul, associate director of neonatology at Christiana Hospital, who collaborated on the analysis. “We did our best to control for possible confounders, and it still suggested that longer antibiotic treatment altered outcomes, but there may have been things [for which] we did not control,” he said in an interview. The next step is to design a prospective study and determine if changing the duration of empiric antibiotic therapy changes outcomes. “But the current findings raise concern that we should be cautious about the duration of treatment,” said Dr. Paul.
In the cases reviewed, each physician delivering care determined the duration of antibiotic treatment. Some may have opted for a longer course of treatment because they were concerned that “not all babies have culture-proven sepsis,” Dr. Paul said in an interview. The physicians “may have feared that the babies had infections that were missed in their blood cultures. They treated presumed sepsis,” he said.
Dr. Novitsky reviewed all the VLBW infants seen in the neonatal ICU at Christiana Hospital between July 2004 and June 2009. The regimen used on all neonates who received empiric antibiotic treatment consisted of ampicillin and gentamicin. The infants who received a longer antibiotic course had a significantly higher prevalence of several markers of a worse clinical profile, including lower birth weight, younger gestational age, a higher score for neonatal acute physiology (SNAP), and a lower 5-minute Apgar score. They also had higher rates of clinical chorioamnionitis, mechanical ventilation, and endotracheal tube colonization (endotracheal tubes underwent routine, weekly colonization assessments).
The infants who received a longer course of antibiotics also had a higher prevalence of antibiotic-resistant, gram-negative organisms colonizing their endotracheal tubes, a 6% rate compared with a 2% rate among the infants who received a short course of treatment – a significant difference. The two groups of infants had roughly identical prevalence rates of colonization with antibiotic-resistant gram-positive strains.
Dr. Novitsky defined the primary outcome evaluated in the analysis, chronic lung disease, as the need for supplemental oxygen by the infant at 36 weeks postmenstrual age. This outcome occurred in 185 of the 906 (20%) neonates in the study: 17% of the infants who received a short antibiotic course, and 36% of those who received a long course.
The multivariable analysis adjusted for differences in gestational age, SNAP score, Apgar score, maternal anti-biotic treatment, chorioamnionitis, preeclampsia, cesarean delivery, prolonged rupture of membranes, and need for mechanical ventilation. After adjustment, the two patient groups failed to show a significant difference in their rates of necrotizing enterocolitis or sepsis.
To further examine the relationship between duration of antibiotic treatment and chronic lung disease, Dr. Novitsky also presented the results of a subgroup analysis that focused on the 418 high-risk neonates in her study group, because of their delivery at 28 weeks' gestation or younger and their SNAP score of 8 or greater.
Within this subgroup, the adjusted rate for developing chronic lung disease ran 70% higher in the 108 infants who received a long course of antibiotics, compared with the 310 who received a short course, also a significant difference.
Dr. Novitsky and Dr. Paul said they had no relevant financial disclosures.
But this finding is not yet ready to definitively guide practice.
Source DR. NOVITSKY
View on the News
Don't Overuse Antibiotics
The findings of this analysis suggest that physicians should not treat neonates with antibiotics when not necessary. If they do, they risk making the babies worse.
A neonatologist may be tempted to prescribe a more prolonged course of antibiotics out of fear that the infant may have an infection. To be cautious, she overtreats. These new data suggest that this practice can actually do harm. This is another reason not to overtreat.
It is reasonable to infer that the treating physician had seen something in some of these children to prompt the longer duration of treatment. The infant must have somehow seemed sicker. The physician may have been concerned that if antibiotic treatment stopped sooner, the neonate's condition would have worsened. The optimal duration of treatment is always something to think about.
It is plausible that just a few extra days of antibiotic treatment can make an important difference. A 2-day duration of treatment probably does not change the background flora in the esophagus as much as a 7-day course. Longer exposure to antibiotics can result in a higher rate of fungal infection, which can trigger increased inflammation.
RITA M. RYAN, M.D., is chief of neonatology at the Women & Children's Hospital of Buffalo (N.Y.). She made these comments in an interview. She said that she had no relevant financial disclosures.
PHILADELPHIA – A week-long course of empiric antibiotic treatment in neonates may result in a higher subsequent rate of chronic lung disease, compared with infants treated for just 2 days, based on an association seen in a review of more than 900 very low birth weight newborns.
But this finding is not yet ready to definitively guide practice, as it came from a nonrandomized, retrospective study that may have failed to control for all possible confounding variables, Dr. Alexandra Novitsky said at the meeting
In her adjusted analysis, which controlled for several baseline variables, the 159 very low birth weight (VLBW) neonates who received a “long” course of empiric antibiotic treatment, usually for 7 days, had a statistically significant, twofold higher rate of also having chronic lung disease during follow-up, compared with the 747 neonates who received a “short” antibiotic course, usually for 2 days, said Dr. Novitsky, a neonatologist at Christiana Hospital in Newark, Del.
“It's too early to draw conclusions about changing therapy,” based on this finding, said Dr. David A. Paul, associate director of neonatology at Christiana Hospital, who collaborated on the analysis. “We did our best to control for possible confounders, and it still suggested that longer antibiotic treatment altered outcomes, but there may have been things [for which] we did not control,” he said in an interview. The next step is to design a prospective study and determine if changing the duration of empiric antibiotic therapy changes outcomes. “But the current findings raise concern that we should be cautious about the duration of treatment,” said Dr. Paul.
In the cases reviewed, each physician delivering care determined the duration of antibiotic treatment. Some may have opted for a longer course of treatment because they were concerned that “not all babies have culture-proven sepsis,” Dr. Paul said in an interview. The physicians “may have feared that the babies had infections that were missed in their blood cultures. They treated presumed sepsis,” he said.
Dr. Novitsky reviewed all the VLBW infants seen in the neonatal ICU at Christiana Hospital between July 2004 and June 2009. The regimen used on all neonates who received empiric antibiotic treatment consisted of ampicillin and gentamicin. The infants who received a longer antibiotic course had a significantly higher prevalence of several markers of a worse clinical profile, including lower birth weight, younger gestational age, a higher score for neonatal acute physiology (SNAP), and a lower 5-minute Apgar score. They also had higher rates of clinical chorioamnionitis, mechanical ventilation, and endotracheal tube colonization (endotracheal tubes underwent routine, weekly colonization assessments).
The infants who received a longer course of antibiotics also had a higher prevalence of antibiotic-resistant, gram-negative organisms colonizing their endotracheal tubes, a 6% rate compared with a 2% rate among the infants who received a short course of treatment – a significant difference. The two groups of infants had roughly identical prevalence rates of colonization with antibiotic-resistant gram-positive strains.
Dr. Novitsky defined the primary outcome evaluated in the analysis, chronic lung disease, as the need for supplemental oxygen by the infant at 36 weeks postmenstrual age. This outcome occurred in 185 of the 906 (20%) neonates in the study: 17% of the infants who received a short antibiotic course, and 36% of those who received a long course.
The multivariable analysis adjusted for differences in gestational age, SNAP score, Apgar score, maternal anti-biotic treatment, chorioamnionitis, preeclampsia, cesarean delivery, prolonged rupture of membranes, and need for mechanical ventilation. After adjustment, the two patient groups failed to show a significant difference in their rates of necrotizing enterocolitis or sepsis.
To further examine the relationship between duration of antibiotic treatment and chronic lung disease, Dr. Novitsky also presented the results of a subgroup analysis that focused on the 418 high-risk neonates in her study group, because of their delivery at 28 weeks' gestation or younger and their SNAP score of 8 or greater.
Within this subgroup, the adjusted rate for developing chronic lung disease ran 70% higher in the 108 infants who received a long course of antibiotics, compared with the 310 who received a short course, also a significant difference.
Dr. Novitsky and Dr. Paul said they had no relevant financial disclosures.
But this finding is not yet ready to definitively guide practice.
Source DR. NOVITSKY
View on the News
Don't Overuse Antibiotics
The findings of this analysis suggest that physicians should not treat neonates with antibiotics when not necessary. If they do, they risk making the babies worse.
A neonatologist may be tempted to prescribe a more prolonged course of antibiotics out of fear that the infant may have an infection. To be cautious, she overtreats. These new data suggest that this practice can actually do harm. This is another reason not to overtreat.
It is reasonable to infer that the treating physician had seen something in some of these children to prompt the longer duration of treatment. The infant must have somehow seemed sicker. The physician may have been concerned that if antibiotic treatment stopped sooner, the neonate's condition would have worsened. The optimal duration of treatment is always something to think about.
It is plausible that just a few extra days of antibiotic treatment can make an important difference. A 2-day duration of treatment probably does not change the background flora in the esophagus as much as a 7-day course. Longer exposure to antibiotics can result in a higher rate of fungal infection, which can trigger increased inflammation.
RITA M. RYAN, M.D., is chief of neonatology at the Women & Children's Hospital of Buffalo (N.Y.). She made these comments in an interview. She said that she had no relevant financial disclosures.
Early ICU Mobility Improves Patient Outcomes
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.

Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
FROM THE ANNUAL MEETING OF THE NATIONAL ASSOCIATION FOR MEDICAL DIRECTION OF RESPIRATORY CARE
Early ICU Mobility Improves Patient Outcomes
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
FROM THE ANNUAL MEETING OF THE NATIONAL ASSOCIATION FOR MEDICAL DIRECTION OF RESPIRATORY CARE
Early ICU Mobility Improves Patient Outcomes
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
LAS VEGAS – Early mobility aids faster and better recovery of patients in the intensive care unit, Dr. Russell R. Miller III said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
Fostering early mobility requires a "culture of mobility" in the respiratory intensive care unit, he said. "You need a strategy, a process of care and collaboration between all members" of the ICU team. "You need a distinct [ICU] culture to pull this off." Creating an ICU culture of mobility and reconditioning means improving teamwork among the ICU disciplines, linking effective teamwork with patient-focused outcomes, recognizing current practice patterns that interfere with achieving mobility, and ensuring that the process is reliable, said Dr. Miller, medical director of the respiratory ICU at Intermountain Healthcare in Salt Lake City.
Traditionally, ICU physicians paid little attention to patient mobility or to the role of neuromuscular function in patients with critical illness. But evidence reported over the past 10 years suggested that weakness and immobility in the ICU may diminish health-related quality of life over the long term. The mortality rate of patients during their first year following ICU discharge is likely twice their rate while in the ICU, and part of that is because of ICU inactivity, he said. Other causes of post-ICU mortality might include inflammatory muscle injury, sepsis, deconditioning, hyperglycemia, steroid treatment, and catabolism.
The first strong suggestion that muscle wasting and weakness in ICU patients could have long-term effects during the year following discharge came in a 1-year follow-up study of 198 medical and surgical ICU patients treated in Toronto (N. Engl. J. Med. 2003;348:683-93). Subsequent reports began presenting evidence that early activity in ICU patients could be undertaken safely and could significantly reduce the duration of hospitalization (Crit. Care Med. 2006;34:A20).
Researchers reported results in 2009 from a prospective, randomized, multicenter U.S. study with 104 ICU patients showing that an early start to physical and occupational therapy led to a significant 50% decrease in the average number of days with delirium (Lancet 2009;373:1874-82). The 2009 report constituted the first evidence that early ICU mobility could have a meaningful impact on a clinical outcome, Dr. Miller said. Controlling delirium is crucial because each additional day a patient is delirious is linked with a 10% increased mortality risk, and length of stay for delirious patients averages 10 days longer. At least half of the patients who are delirious for more than 3 days develop long-term cognitive impairment, Dr. Miller said.
In his opinion, evidence now backs ICU mobilization for patients who are medically directed to bed rest (such as those with an unstable spine), coma patients, and patients with modest or severe hemodynamic instability. "All of these patients would have been considered excluded from mobilization in the ICU just 10 years ago," he said.
Other patients for whom mobilization should be considered, but in whom it is more challenging, include those with delirium, a history of stroke, a critical illness myoneuropathy, or a high fraction of inspired oxygen divided by positive end-expiratory pressure, as well as those on continuous dialysis, he said. But even among these patients, ICU staff should be "aggressive" in their approach to rehabilitation management, Dr. Miller said.
Staff also can help patients achieve early mobilization by avoiding overuse of sedation, minimizing narcotic use, and supporting breathing to prevent desaturation during activity. Staff members should not passively accept a patient’s refusal of activity, just as they would not automatically accept a patient’s refusal of an antibiotic or other any important intervention.
The intensity of activity should progress rapidly, although activity could be suspended for a day if a patient has an acute, unstable event. In patients who do not appear to have the strength for both reconditioning and weaning, reconditioning should take priority because it will make weaning easier.
Dr. Miller said that he had no disclosures relevant to this topic.
FROM THE ANNUAL MEETING OF THE NATIONAL ASSOCIATION FOR MEDICAL DIRECTION OF RESPIRATORY CARE
CT Trial Results Change Lung Cancer Screening Landscape
LAS VEGAS – The results from the National Lung Screening Trial constitute a "game changer" for lung cancer screening, Dr. James R. Jett said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
The study results, reported in a press release by the National Cancer Institute last November, "changed the landscape" for screening by showing that lung imaging by low-dose helical CT done annually for 3 years in people with a smoking history of least 30 pack-years cut their mortality rate from lung cancer during follow-up by 20%, compared with people who underwent three annual chest x-rays. "This is the biggest advance in lung cancer in my career, an absolutely stunning result," said Dr. Jett, a pulmonologist and lung cancer specialist at National Jewish Health in Denver.
The researchers who ran the National Lung Screening Trial will likely publish their full results this spring, after which annual screening of people who match the profile of those in the study should become the standard of care, Dr. Jett predicted.
The screening trial enrolled 53,454 current or former cigarette smokers aged 55-74 years, who had each accumulated at least 30 pack-years of smoking history but had quit within the previous 15 years. The more than 75,000 total screening events by CT and more than 73,000 total screens by chest x-ray yielded 24% positive CT images and 7% positive x-ray images. During roughly 144,000 person-years of follow-up in each arm, the mortality due to lung cancer reached 246 deaths per 100,000 person-years in the CT group and 308 deaths per 100,000 person-years in the x-ray group, a 20% absolute mortality reduction with CT screening that was statistically significant, and which led the trial’s Data and Safety Monitoring Board to stop the study and release the results.
The people screened by CT also had a 7% reduction in all-cause mortality, compared with those screened by x-ray, also a statistically significant difference.
As about 160,000 Americans die from lung cancer annually, a 20% cut in mortality from low-dose helical CT screening could potentially save about 32,000 lives a year in the United States alone. "That’s almost like eliminating all 40,000 breast cancer deaths each year," Dr. Jett said.
The results did not directly address the question of how long annual screening should continue. In the trial, screening stopped after three annual examinations because of limited financial resources, although despite that the study cost about $200 million, he said. But his review of the results identified no suggestion that in routine practice screening should stop after 3 years. "There was no drop in the number of cancers" during each sequential year of screening. "I don’t see anything that tells me you can stop [screening] after 3 years," he said.
"The biggest question is, can we afford" to do annual CT screening on the scale needed to include all people who fit the profile included in the trial.
A second issue is the safety of annual CT imaging, but Dr. Jett presented a brief analysis suggesting that it is safe. A low-dose CT scan involves a radiation exposure of about 0.65 mSv, less than 10% of the dose of a conventional chest CT, Dr. Jett said. With that level of exposure, annual low-dose CT imaging of currently smoking women aged 50 might cause an excess of 5 cancer deaths for every 10,000 people screened, compared with a background lung cancer mortality of 100 for every 10,000 people with no screening. Because screening could prevent 20% of these 100 deaths, it would avert more deaths that it might cause. For men, the risk: benefit ratio runs even higher because currently smoking men undergoing annual CT screening would have about 2 extra lung cancer deaths per 10,000 people due to the radiation exposure, compared with 110 per 10,000 without screening. Women face a higher risk from the radiation of screening than men because of the impact of chest radiation on breast cancer, Dr. Jett said.
Dr. Jett said that he has been an adviser to Genentech, Pfizer, and Bristol-Myers Squibb, and that he has a research grant pending from Oncimmune.
LAS VEGAS – The results from the National Lung Screening Trial constitute a "game changer" for lung cancer screening, Dr. James R. Jett said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
The study results, reported in a press release by the National Cancer Institute last November, "changed the landscape" for screening by showing that lung imaging by low-dose helical CT done annually for 3 years in people with a smoking history of least 30 pack-years cut their mortality rate from lung cancer during follow-up by 20%, compared with people who underwent three annual chest x-rays. "This is the biggest advance in lung cancer in my career, an absolutely stunning result," said Dr. Jett, a pulmonologist and lung cancer specialist at National Jewish Health in Denver.
The researchers who ran the National Lung Screening Trial will likely publish their full results this spring, after which annual screening of people who match the profile of those in the study should become the standard of care, Dr. Jett predicted.
The screening trial enrolled 53,454 current or former cigarette smokers aged 55-74 years, who had each accumulated at least 30 pack-years of smoking history but had quit within the previous 15 years. The more than 75,000 total screening events by CT and more than 73,000 total screens by chest x-ray yielded 24% positive CT images and 7% positive x-ray images. During roughly 144,000 person-years of follow-up in each arm, the mortality due to lung cancer reached 246 deaths per 100,000 person-years in the CT group and 308 deaths per 100,000 person-years in the x-ray group, a 20% absolute mortality reduction with CT screening that was statistically significant, and which led the trial’s Data and Safety Monitoring Board to stop the study and release the results.
The people screened by CT also had a 7% reduction in all-cause mortality, compared with those screened by x-ray, also a statistically significant difference.
As about 160,000 Americans die from lung cancer annually, a 20% cut in mortality from low-dose helical CT screening could potentially save about 32,000 lives a year in the United States alone. "That’s almost like eliminating all 40,000 breast cancer deaths each year," Dr. Jett said.
The results did not directly address the question of how long annual screening should continue. In the trial, screening stopped after three annual examinations because of limited financial resources, although despite that the study cost about $200 million, he said. But his review of the results identified no suggestion that in routine practice screening should stop after 3 years. "There was no drop in the number of cancers" during each sequential year of screening. "I don’t see anything that tells me you can stop [screening] after 3 years," he said.
"The biggest question is, can we afford" to do annual CT screening on the scale needed to include all people who fit the profile included in the trial.
A second issue is the safety of annual CT imaging, but Dr. Jett presented a brief analysis suggesting that it is safe. A low-dose CT scan involves a radiation exposure of about 0.65 mSv, less than 10% of the dose of a conventional chest CT, Dr. Jett said. With that level of exposure, annual low-dose CT imaging of currently smoking women aged 50 might cause an excess of 5 cancer deaths for every 10,000 people screened, compared with a background lung cancer mortality of 100 for every 10,000 people with no screening. Because screening could prevent 20% of these 100 deaths, it would avert more deaths that it might cause. For men, the risk: benefit ratio runs even higher because currently smoking men undergoing annual CT screening would have about 2 extra lung cancer deaths per 10,000 people due to the radiation exposure, compared with 110 per 10,000 without screening. Women face a higher risk from the radiation of screening than men because of the impact of chest radiation on breast cancer, Dr. Jett said.
Dr. Jett said that he has been an adviser to Genentech, Pfizer, and Bristol-Myers Squibb, and that he has a research grant pending from Oncimmune.
LAS VEGAS – The results from the National Lung Screening Trial constitute a "game changer" for lung cancer screening, Dr. James R. Jett said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
The study results, reported in a press release by the National Cancer Institute last November, "changed the landscape" for screening by showing that lung imaging by low-dose helical CT done annually for 3 years in people with a smoking history of least 30 pack-years cut their mortality rate from lung cancer during follow-up by 20%, compared with people who underwent three annual chest x-rays. "This is the biggest advance in lung cancer in my career, an absolutely stunning result," said Dr. Jett, a pulmonologist and lung cancer specialist at National Jewish Health in Denver.
The researchers who ran the National Lung Screening Trial will likely publish their full results this spring, after which annual screening of people who match the profile of those in the study should become the standard of care, Dr. Jett predicted.
The screening trial enrolled 53,454 current or former cigarette smokers aged 55-74 years, who had each accumulated at least 30 pack-years of smoking history but had quit within the previous 15 years. The more than 75,000 total screening events by CT and more than 73,000 total screens by chest x-ray yielded 24% positive CT images and 7% positive x-ray images. During roughly 144,000 person-years of follow-up in each arm, the mortality due to lung cancer reached 246 deaths per 100,000 person-years in the CT group and 308 deaths per 100,000 person-years in the x-ray group, a 20% absolute mortality reduction with CT screening that was statistically significant, and which led the trial’s Data and Safety Monitoring Board to stop the study and release the results.
The people screened by CT also had a 7% reduction in all-cause mortality, compared with those screened by x-ray, also a statistically significant difference.
As about 160,000 Americans die from lung cancer annually, a 20% cut in mortality from low-dose helical CT screening could potentially save about 32,000 lives a year in the United States alone. "That’s almost like eliminating all 40,000 breast cancer deaths each year," Dr. Jett said.
The results did not directly address the question of how long annual screening should continue. In the trial, screening stopped after three annual examinations because of limited financial resources, although despite that the study cost about $200 million, he said. But his review of the results identified no suggestion that in routine practice screening should stop after 3 years. "There was no drop in the number of cancers" during each sequential year of screening. "I don’t see anything that tells me you can stop [screening] after 3 years," he said.
"The biggest question is, can we afford" to do annual CT screening on the scale needed to include all people who fit the profile included in the trial.
A second issue is the safety of annual CT imaging, but Dr. Jett presented a brief analysis suggesting that it is safe. A low-dose CT scan involves a radiation exposure of about 0.65 mSv, less than 10% of the dose of a conventional chest CT, Dr. Jett said. With that level of exposure, annual low-dose CT imaging of currently smoking women aged 50 might cause an excess of 5 cancer deaths for every 10,000 people screened, compared with a background lung cancer mortality of 100 for every 10,000 people with no screening. Because screening could prevent 20% of these 100 deaths, it would avert more deaths that it might cause. For men, the risk: benefit ratio runs even higher because currently smoking men undergoing annual CT screening would have about 2 extra lung cancer deaths per 10,000 people due to the radiation exposure, compared with 110 per 10,000 without screening. Women face a higher risk from the radiation of screening than men because of the impact of chest radiation on breast cancer, Dr. Jett said.
Dr. Jett said that he has been an adviser to Genentech, Pfizer, and Bristol-Myers Squibb, and that he has a research grant pending from Oncimmune.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE NATIONAL ASSOCIATION FOR MEDICAL DIRECTION OF RESPIRATORY CARE
CT Trial Results Change Lung Cancer Screening Landscape
LAS VEGAS – The results from the National Lung Screening Trial constitute a "game changer" for lung cancer screening, Dr. James R. Jett said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
The study results, reported in a press release by the National Cancer Institute last November, "changed the landscape" for screening by showing that lung imaging by low-dose helical CT done annually for 3 years in people with a smoking history of least 30 pack-years cut their mortality rate from lung cancer during follow-up by 20%, compared with people who underwent three annual chest x-rays. "This is the biggest advance in lung cancer in my career, an absolutely stunning result," said Dr. Jett, a pulmonologist and lung cancer specialist at National Jewish Health in Denver.
The researchers who ran the National Lung Screening Trial will likely publish their full results this spring, after which annual screening of people who match the profile of those in the study should become the standard of care, Dr. Jett predicted.
The screening trial enrolled 53,454 current or former cigarette smokers aged 55-74 years, who had each accumulated at least 30 pack-years of smoking history but had quit within the previous 15 years. The more than 75,000 total screening events by CT and more than 73,000 total screens by chest x-ray yielded 24% positive CT images and 7% positive x-ray images. During roughly 144,000 person-years of follow-up in each arm, the mortality due to lung cancer reached 246 deaths per 100,000 person-years in the CT group and 308 deaths per 100,000 person-years in the x-ray group, a 20% absolute mortality reduction with CT screening that was statistically significant, and which led the trial’s Data and Safety Monitoring Board to stop the study and release the results.
The people screened by CT also had a 7% reduction in all-cause mortality, compared with those screened by x-ray, also a statistically significant difference.
As about 160,000 Americans die from lung cancer annually, a 20% cut in mortality from low-dose helical CT screening could potentially save about 32,000 lives a year in the United States alone. "That’s almost like eliminating all 40,000 breast cancer deaths each year," Dr. Jett said.
The results did not directly address the question of how long annual screening should continue. In the trial, screening stopped after three annual examinations because of limited financial resources, although despite that the study cost about $200 million, he said. But his review of the results identified no suggestion that in routine practice screening should stop after 3 years. "There was no drop in the number of cancers" during each sequential year of screening. "I don’t see anything that tells me you can stop [screening] after 3 years," he said.
"The biggest question is, can we afford" to do annual CT screening on the scale needed to include all people who fit the profile included in the trial.
A second issue is the safety of annual CT imaging, but Dr. Jett presented a brief analysis suggesting that it is safe. A low-dose CT scan involves a radiation exposure of about 0.65 mSv, less than 10% of the dose of a conventional chest CT, Dr. Jett said. With that level of exposure, annual low-dose CT imaging of currently smoking women aged 50 might cause an excess of 5 cancer deaths for every 10,000 people screened, compared with a background lung cancer mortality of 100 for every 10,000 people with no screening. Because screening could prevent 20% of these 100 deaths, it would avert more deaths that it might cause. For men, the risk: benefit ratio runs even higher because currently smoking men undergoing annual CT screening would have about 2 extra lung cancer deaths per 10,000 people due to the radiation exposure, compared with 110 per 10,000 without screening. Women face a higher risk from the radiation of screening than men because of the impact of chest radiation on breast cancer, Dr. Jett said.
Dr. Jett said that he has been an adviser to Genentech, Pfizer, and Bristol-Myers Squibb, and that he has a research grant pending from Oncimmune.
LAS VEGAS – The results from the National Lung Screening Trial constitute a "game changer" for lung cancer screening, Dr. James R. Jett said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
The study results, reported in a press release by the National Cancer Institute last November, "changed the landscape" for screening by showing that lung imaging by low-dose helical CT done annually for 3 years in people with a smoking history of least 30 pack-years cut their mortality rate from lung cancer during follow-up by 20%, compared with people who underwent three annual chest x-rays. "This is the biggest advance in lung cancer in my career, an absolutely stunning result," said Dr. Jett, a pulmonologist and lung cancer specialist at National Jewish Health in Denver.
The researchers who ran the National Lung Screening Trial will likely publish their full results this spring, after which annual screening of people who match the profile of those in the study should become the standard of care, Dr. Jett predicted.
The screening trial enrolled 53,454 current or former cigarette smokers aged 55-74 years, who had each accumulated at least 30 pack-years of smoking history but had quit within the previous 15 years. The more than 75,000 total screening events by CT and more than 73,000 total screens by chest x-ray yielded 24% positive CT images and 7% positive x-ray images. During roughly 144,000 person-years of follow-up in each arm, the mortality due to lung cancer reached 246 deaths per 100,000 person-years in the CT group and 308 deaths per 100,000 person-years in the x-ray group, a 20% absolute mortality reduction with CT screening that was statistically significant, and which led the trial’s Data and Safety Monitoring Board to stop the study and release the results.
The people screened by CT also had a 7% reduction in all-cause mortality, compared with those screened by x-ray, also a statistically significant difference.
As about 160,000 Americans die from lung cancer annually, a 20% cut in mortality from low-dose helical CT screening could potentially save about 32,000 lives a year in the United States alone. "That’s almost like eliminating all 40,000 breast cancer deaths each year," Dr. Jett said.
The results did not directly address the question of how long annual screening should continue. In the trial, screening stopped after three annual examinations because of limited financial resources, although despite that the study cost about $200 million, he said. But his review of the results identified no suggestion that in routine practice screening should stop after 3 years. "There was no drop in the number of cancers" during each sequential year of screening. "I don’t see anything that tells me you can stop [screening] after 3 years," he said.
"The biggest question is, can we afford" to do annual CT screening on the scale needed to include all people who fit the profile included in the trial.
A second issue is the safety of annual CT imaging, but Dr. Jett presented a brief analysis suggesting that it is safe. A low-dose CT scan involves a radiation exposure of about 0.65 mSv, less than 10% of the dose of a conventional chest CT, Dr. Jett said. With that level of exposure, annual low-dose CT imaging of currently smoking women aged 50 might cause an excess of 5 cancer deaths for every 10,000 people screened, compared with a background lung cancer mortality of 100 for every 10,000 people with no screening. Because screening could prevent 20% of these 100 deaths, it would avert more deaths that it might cause. For men, the risk: benefit ratio runs even higher because currently smoking men undergoing annual CT screening would have about 2 extra lung cancer deaths per 10,000 people due to the radiation exposure, compared with 110 per 10,000 without screening. Women face a higher risk from the radiation of screening than men because of the impact of chest radiation on breast cancer, Dr. Jett said.
Dr. Jett said that he has been an adviser to Genentech, Pfizer, and Bristol-Myers Squibb, and that he has a research grant pending from Oncimmune.
LAS VEGAS – The results from the National Lung Screening Trial constitute a "game changer" for lung cancer screening, Dr. James R. Jett said at the annual meeting of the National Association for Medical Direction of Respiratory Care.
The study results, reported in a press release by the National Cancer Institute last November, "changed the landscape" for screening by showing that lung imaging by low-dose helical CT done annually for 3 years in people with a smoking history of least 30 pack-years cut their mortality rate from lung cancer during follow-up by 20%, compared with people who underwent three annual chest x-rays. "This is the biggest advance in lung cancer in my career, an absolutely stunning result," said Dr. Jett, a pulmonologist and lung cancer specialist at National Jewish Health in Denver.
The researchers who ran the National Lung Screening Trial will likely publish their full results this spring, after which annual screening of people who match the profile of those in the study should become the standard of care, Dr. Jett predicted.
The screening trial enrolled 53,454 current or former cigarette smokers aged 55-74 years, who had each accumulated at least 30 pack-years of smoking history but had quit within the previous 15 years. The more than 75,000 total screening events by CT and more than 73,000 total screens by chest x-ray yielded 24% positive CT images and 7% positive x-ray images. During roughly 144,000 person-years of follow-up in each arm, the mortality due to lung cancer reached 246 deaths per 100,000 person-years in the CT group and 308 deaths per 100,000 person-years in the x-ray group, a 20% absolute mortality reduction with CT screening that was statistically significant, and which led the trial’s Data and Safety Monitoring Board to stop the study and release the results.
The people screened by CT also had a 7% reduction in all-cause mortality, compared with those screened by x-ray, also a statistically significant difference.
As about 160,000 Americans die from lung cancer annually, a 20% cut in mortality from low-dose helical CT screening could potentially save about 32,000 lives a year in the United States alone. "That’s almost like eliminating all 40,000 breast cancer deaths each year," Dr. Jett said.
The results did not directly address the question of how long annual screening should continue. In the trial, screening stopped after three annual examinations because of limited financial resources, although despite that the study cost about $200 million, he said. But his review of the results identified no suggestion that in routine practice screening should stop after 3 years. "There was no drop in the number of cancers" during each sequential year of screening. "I don’t see anything that tells me you can stop [screening] after 3 years," he said.
"The biggest question is, can we afford" to do annual CT screening on the scale needed to include all people who fit the profile included in the trial.
A second issue is the safety of annual CT imaging, but Dr. Jett presented a brief analysis suggesting that it is safe. A low-dose CT scan involves a radiation exposure of about 0.65 mSv, less than 10% of the dose of a conventional chest CT, Dr. Jett said. With that level of exposure, annual low-dose CT imaging of currently smoking women aged 50 might cause an excess of 5 cancer deaths for every 10,000 people screened, compared with a background lung cancer mortality of 100 for every 10,000 people with no screening. Because screening could prevent 20% of these 100 deaths, it would avert more deaths that it might cause. For men, the risk: benefit ratio runs even higher because currently smoking men undergoing annual CT screening would have about 2 extra lung cancer deaths per 10,000 people due to the radiation exposure, compared with 110 per 10,000 without screening. Women face a higher risk from the radiation of screening than men because of the impact of chest radiation on breast cancer, Dr. Jett said.
Dr. Jett said that he has been an adviser to Genentech, Pfizer, and Bristol-Myers Squibb, and that he has a research grant pending from Oncimmune.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE NATIONAL ASSOCIATION FOR MEDICAL DIRECTION OF RESPIRATORY CARE
New Gestational Diabetes Criteria Predicted to Boost Incidence Rates
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).

But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
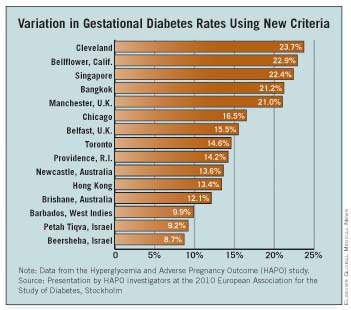
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION
New Gestational Diabetes Criteria Predicted to Boost Incidence Rates
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION
Home Health Care Cuts Hospitalizations in Patients With Chronic Diseases
NEW YORK – A patient-centered, medical-home approach to care for patients with multiple chronic diseases when they are discharged from the hospital and back in their own residences substantially cut their rate of hospital readmissions, suggesting that this new model of home-based medical care pays for itself by avoiding hospitalization costs.
"We think it’s very important for the U.S. health care system to move its focus from hospital to home, with care management that prevents unnecessary emergency department visits and hospital admissions," Dr. Eric C. Rackow said at the course.

"You can alter the outcomes at home [of patients with diabetes and other chronic diseases] if you keep patients healthier and more functional at home and out of the hospital," said Dr. Rackow, professor of medicine at New York University, and president and CEO of SeniorBridge, a company that provides medical services to patients when they are in their homes.
"We have health plan contracts where we have shown a 50% reduction in hospitalization and readmissions rates, producing a 50% drop in the cost per member per month," Dr. Rackow said in an interview. Although SeniorBridge is relatively unique in offering the services from a variety of health care professionals for in-home services to patients, the model is amenable to scale up, he said. "Doctors are the captains, but it’s the nurses, social workers, nutritionists, and pharmacists who actually are in the patients’ homes. Physicians can manage a large number of patients. It’s a cost-effective way to extend the physician’s reach."
To document the impact that home-based intervention can have, he presented data collected by SeniorBridge from 503 patients aged 65 years or older that the company managed during 2008-2010. Eighty-eight of these patients who had diabetes and multiple other chronic conditions had a hospital readmission rate of 21% during their first 30 days at home following discharge from their index hospitalization. The other 415 patients managed by SeniorBridge had multiple chronic conditions but no diabetes, and they had an 11% rehospitalization rate during their first 30 days at home. In contrast, a historic control of similar elderly Americans with multiple chronic conditions who did not receive comprehensive care at home following their hospital discharge had a 33% readmission rate, Dr. Rackow said.
Another data analysis showed that 230 elderly SeniorBridge–treated patients with diabetes and multiple chronic diseases averaged 0.37 hospitalizations/year, and 1,486 elderly SeniorBridge-treated patients with multiple chronic diseases but no diabetes averaged 0.28 hospitalizations/year. By comparison, Medicare data showed a rate of 1.3 hospitalizations/year among similar patients receiving conventional care following a hospital discharge.
Multiple chronic illnesses are a hallmark of elderly patients with diabetes, affecting three-quarters of Americans 65 years or older with diabetes, Dr. Rackow said. The combination of diabetes, chronic obstructive pulmonary disease, and heart failure forms a common comorbidity constellation among elderly patients with diabetes, he noted.
Patients with several simultaneous chronic illnesses face special physical and cognitive challenges that pose problems for their self-directed care, he said. "The functional limitations [triggered by multiple chronic diseases] and the inability to self-manage tips patients and causes frequent hospitalizations." That’s why home medical services that aid a patient’s self management can have such a significant impact on rehospitalization rates.
Payment for SeniorBridge’s services has come from Medicaid, private insurers, and from long-term insurance policies. Medicare does not currently pay for these services, Dr. Rackow said.
Dr. Rackow is an employee, stockholder, and board member of SeniorBridge.
Here is a related video on "How Patients View Chronic Disease."
A good transition of care at the time of hospital discharge is critical in preventing some unnecessary readmissions. These would include inaccurate or incomplete discharge instructions, medication lists, follow-up information, and patient education on their disease and diet....
SeniorBridge appears to be a home-based care program for vulnerable elderly patients. I do not find it surprising that such a model may help prevent hospitalizations, and many chronic diseases (such as diabetes or heart failure) have high readmission rates that are unrelated to poor transitions per se – they are related to vulnerable patient populations that lack the capacity, health literacy, or economics to keep themselves out of the hospital with routine physician follow up. SeniorBridge is another alternative that may hold great promise. Whether it is truly cost effective remains to be seen based on the information in the article. We certainly cannot tell if the SeniorBridge patients are truly case matched to historical control or a different population altogether, so their self-reported information is probably rosier than real.
Nonetheless, if such programs (which function similarly to home hospice programs) provide enhanced services that are covered by insurance – hospitalists will gladly identify and refer vulnerable patients to these programs.
Franklin A. Michota, M.D., is the director of academic affairs in the Department of Hospital Medicine at the Cleveland Clinic. He reported no relevant conflicts of interest.
A good transition of care at the time of hospital discharge is critical in preventing some unnecessary readmissions. These would include inaccurate or incomplete discharge instructions, medication lists, follow-up information, and patient education on their disease and diet....
SeniorBridge appears to be a home-based care program for vulnerable elderly patients. I do not find it surprising that such a model may help prevent hospitalizations, and many chronic diseases (such as diabetes or heart failure) have high readmission rates that are unrelated to poor transitions per se – they are related to vulnerable patient populations that lack the capacity, health literacy, or economics to keep themselves out of the hospital with routine physician follow up. SeniorBridge is another alternative that may hold great promise. Whether it is truly cost effective remains to be seen based on the information in the article. We certainly cannot tell if the SeniorBridge patients are truly case matched to historical control or a different population altogether, so their self-reported information is probably rosier than real.
Nonetheless, if such programs (which function similarly to home hospice programs) provide enhanced services that are covered by insurance – hospitalists will gladly identify and refer vulnerable patients to these programs.
Franklin A. Michota, M.D., is the director of academic affairs in the Department of Hospital Medicine at the Cleveland Clinic. He reported no relevant conflicts of interest.
A good transition of care at the time of hospital discharge is critical in preventing some unnecessary readmissions. These would include inaccurate or incomplete discharge instructions, medication lists, follow-up information, and patient education on their disease and diet....
SeniorBridge appears to be a home-based care program for vulnerable elderly patients. I do not find it surprising that such a model may help prevent hospitalizations, and many chronic diseases (such as diabetes or heart failure) have high readmission rates that are unrelated to poor transitions per se – they are related to vulnerable patient populations that lack the capacity, health literacy, or economics to keep themselves out of the hospital with routine physician follow up. SeniorBridge is another alternative that may hold great promise. Whether it is truly cost effective remains to be seen based on the information in the article. We certainly cannot tell if the SeniorBridge patients are truly case matched to historical control or a different population altogether, so their self-reported information is probably rosier than real.
Nonetheless, if such programs (which function similarly to home hospice programs) provide enhanced services that are covered by insurance – hospitalists will gladly identify and refer vulnerable patients to these programs.
Franklin A. Michota, M.D., is the director of academic affairs in the Department of Hospital Medicine at the Cleveland Clinic. He reported no relevant conflicts of interest.
NEW YORK – A patient-centered, medical-home approach to care for patients with multiple chronic diseases when they are discharged from the hospital and back in their own residences substantially cut their rate of hospital readmissions, suggesting that this new model of home-based medical care pays for itself by avoiding hospitalization costs.
"We think it’s very important for the U.S. health care system to move its focus from hospital to home, with care management that prevents unnecessary emergency department visits and hospital admissions," Dr. Eric C. Rackow said at the course.
"You can alter the outcomes at home [of patients with diabetes and other chronic diseases] if you keep patients healthier and more functional at home and out of the hospital," said Dr. Rackow, professor of medicine at New York University, and president and CEO of SeniorBridge, a company that provides medical services to patients when they are in their homes.
"We have health plan contracts where we have shown a 50% reduction in hospitalization and readmissions rates, producing a 50% drop in the cost per member per month," Dr. Rackow said in an interview. Although SeniorBridge is relatively unique in offering the services from a variety of health care professionals for in-home services to patients, the model is amenable to scale up, he said. "Doctors are the captains, but it’s the nurses, social workers, nutritionists, and pharmacists who actually are in the patients’ homes. Physicians can manage a large number of patients. It’s a cost-effective way to extend the physician’s reach."
To document the impact that home-based intervention can have, he presented data collected by SeniorBridge from 503 patients aged 65 years or older that the company managed during 2008-2010. Eighty-eight of these patients who had diabetes and multiple other chronic conditions had a hospital readmission rate of 21% during their first 30 days at home following discharge from their index hospitalization. The other 415 patients managed by SeniorBridge had multiple chronic conditions but no diabetes, and they had an 11% rehospitalization rate during their first 30 days at home. In contrast, a historic control of similar elderly Americans with multiple chronic conditions who did not receive comprehensive care at home following their hospital discharge had a 33% readmission rate, Dr. Rackow said.
Another data analysis showed that 230 elderly SeniorBridge–treated patients with diabetes and multiple chronic diseases averaged 0.37 hospitalizations/year, and 1,486 elderly SeniorBridge-treated patients with multiple chronic diseases but no diabetes averaged 0.28 hospitalizations/year. By comparison, Medicare data showed a rate of 1.3 hospitalizations/year among similar patients receiving conventional care following a hospital discharge.
Multiple chronic illnesses are a hallmark of elderly patients with diabetes, affecting three-quarters of Americans 65 years or older with diabetes, Dr. Rackow said. The combination of diabetes, chronic obstructive pulmonary disease, and heart failure forms a common comorbidity constellation among elderly patients with diabetes, he noted.
Patients with several simultaneous chronic illnesses face special physical and cognitive challenges that pose problems for their self-directed care, he said. "The functional limitations [triggered by multiple chronic diseases] and the inability to self-manage tips patients and causes frequent hospitalizations." That’s why home medical services that aid a patient’s self management can have such a significant impact on rehospitalization rates.
Payment for SeniorBridge’s services has come from Medicaid, private insurers, and from long-term insurance policies. Medicare does not currently pay for these services, Dr. Rackow said.
Dr. Rackow is an employee, stockholder, and board member of SeniorBridge.
Here is a related video on "How Patients View Chronic Disease."
NEW YORK – A patient-centered, medical-home approach to care for patients with multiple chronic diseases when they are discharged from the hospital and back in their own residences substantially cut their rate of hospital readmissions, suggesting that this new model of home-based medical care pays for itself by avoiding hospitalization costs.
"We think it’s very important for the U.S. health care system to move its focus from hospital to home, with care management that prevents unnecessary emergency department visits and hospital admissions," Dr. Eric C. Rackow said at the course.
"You can alter the outcomes at home [of patients with diabetes and other chronic diseases] if you keep patients healthier and more functional at home and out of the hospital," said Dr. Rackow, professor of medicine at New York University, and president and CEO of SeniorBridge, a company that provides medical services to patients when they are in their homes.
"We have health plan contracts where we have shown a 50% reduction in hospitalization and readmissions rates, producing a 50% drop in the cost per member per month," Dr. Rackow said in an interview. Although SeniorBridge is relatively unique in offering the services from a variety of health care professionals for in-home services to patients, the model is amenable to scale up, he said. "Doctors are the captains, but it’s the nurses, social workers, nutritionists, and pharmacists who actually are in the patients’ homes. Physicians can manage a large number of patients. It’s a cost-effective way to extend the physician’s reach."
To document the impact that home-based intervention can have, he presented data collected by SeniorBridge from 503 patients aged 65 years or older that the company managed during 2008-2010. Eighty-eight of these patients who had diabetes and multiple other chronic conditions had a hospital readmission rate of 21% during their first 30 days at home following discharge from their index hospitalization. The other 415 patients managed by SeniorBridge had multiple chronic conditions but no diabetes, and they had an 11% rehospitalization rate during their first 30 days at home. In contrast, a historic control of similar elderly Americans with multiple chronic conditions who did not receive comprehensive care at home following their hospital discharge had a 33% readmission rate, Dr. Rackow said.
Another data analysis showed that 230 elderly SeniorBridge–treated patients with diabetes and multiple chronic diseases averaged 0.37 hospitalizations/year, and 1,486 elderly SeniorBridge-treated patients with multiple chronic diseases but no diabetes averaged 0.28 hospitalizations/year. By comparison, Medicare data showed a rate of 1.3 hospitalizations/year among similar patients receiving conventional care following a hospital discharge.
Multiple chronic illnesses are a hallmark of elderly patients with diabetes, affecting three-quarters of Americans 65 years or older with diabetes, Dr. Rackow said. The combination of diabetes, chronic obstructive pulmonary disease, and heart failure forms a common comorbidity constellation among elderly patients with diabetes, he noted.
Patients with several simultaneous chronic illnesses face special physical and cognitive challenges that pose problems for their self-directed care, he said. "The functional limitations [triggered by multiple chronic diseases] and the inability to self-manage tips patients and causes frequent hospitalizations." That’s why home medical services that aid a patient’s self management can have such a significant impact on rehospitalization rates.
Payment for SeniorBridge’s services has come from Medicaid, private insurers, and from long-term insurance policies. Medicare does not currently pay for these services, Dr. Rackow said.
Dr. Rackow is an employee, stockholder, and board member of SeniorBridge.
Here is a related video on "How Patients View Chronic Disease."
FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION
Major Finding: Patients aged 65 years or older with diabetes and multiple other chronic conditions had a 21% rehospitalization rate during the first 30 days following discharge from their index hospitalization when receiving home-management care, compared with a 33% rate in similar, historic control patients who did not receive such care.
Data Source: Eighty-eight patients aged 65 years or older with diabetes and multiple other chronic conditions treated by Senior Bridge during 2008-2010.
Disclosures: Dr. Rackow is an employee, stockholder, and board member of Senior Bridge.
Home Health Care Cuts Hospitalizations in Patients With Chronic Diseases
NEW YORK – A patient-centered, medical-home approach to care for patients with multiple chronic diseases when they are discharged from the hospital and back in their own residences substantially cut their rate of hospital readmissions, suggesting that this new model of home-based medical care pays for itself by avoiding hospitalization costs.
"We think it’s very important for the U.S. health care system to move its focus from hospital to home, with care management that prevents unnecessary emergency department visits and hospital admissions," Dr. Eric C. Rackow said at the course.
"You can alter the outcomes at home [of patients with diabetes and other chronic diseases] if you keep patients healthier and more functional at home and out of the hospital," said Dr. Rackow, professor of medicine at New York University, and president and CEO of SeniorBridge, a company that provides medical services to patients when they are in their homes.
"We have health plan contracts where we have shown a 50% reduction in hospitalization and readmissions rates, producing a 50% drop in the cost per member per month," Dr. Rackow said in an interview. Although SeniorBridge is relatively unique in offering the services from a variety of health care professionals for in-home services to patients, the model is amenable to scale up, he said. "Doctors are the captains, but it’s the nurses, social workers, nutritionists, and pharmacists who actually are in the patients’ homes. Physicians can manage a large number of patients. It’s a cost-effective way to extend the physician’s reach."
To document the impact that home-based intervention can have, he presented data collected by SeniorBridge from 503 patients aged 65 years or older that the company managed during 2008-2010. Eighty-eight of these patients who had diabetes and multiple other chronic conditions had a hospital readmission rate of 21% during their first 30 days at home following discharge from their index hospitalization. The other 415 patients managed by SeniorBridge had multiple chronic conditions but no diabetes, and they had an 11% rehospitalization rate during their first 30 days at home. In contrast, a historic control of similar elderly Americans with multiple chronic conditions who did not receive comprehensive care at home following their hospital discharge had a 33% readmission rate, Dr. Rackow said.
Another data analysis showed that 230 elderly SeniorBridge–treated patients with diabetes and multiple chronic diseases averaged 0.37 hospitalizations/year, and 1,486 elderly SeniorBridge-treated patients with multiple chronic diseases but no diabetes averaged 0.28 hospitalizations/year. By comparison, Medicare data showed a rate of 1.3 hospitalizations/year among similar patients receiving conventional care following a hospital discharge.
Multiple chronic illnesses are a hallmark of elderly patients with diabetes, affecting three-quarters of Americans 65 years or older with diabetes, Dr. Rackow said. The combination of diabetes, chronic obstructive pulmonary disease, and heart failure forms a common comorbidity constellation among elderly patients with diabetes, he noted.
Patients with several simultaneous chronic illnesses face special physical and cognitive challenges that pose problems for their self-directed care, he said. "The functional limitations [triggered by multiple chronic diseases] and the inability to self-manage tips patients and causes frequent hospitalizations." That’s why home medical services that aid a patient’s self management can have such a significant impact on rehospitalization rates.
Payment for SeniorBridge’s services has come from Medicaid, private insurers, and from long-term insurance policies. Medicare does not currently pay for these services, Dr. Rackow said.
Dr. Rackow is an employee, stockholder, and board member of SeniorBridge.
Here is a related video on "How Patients View Chronic Disease."
A good transition of care at the time of hospital discharge is critical in preventing some unnecessary readmissions. These would include inaccurate or incomplete discharge instructions, medication lists, follow-up information, and patient education on their disease and diet....
SeniorBridge appears to be a home-based care program for vulnerable elderly patients. I do not find it surprising that such a model may help prevent hospitalizations, and many chronic diseases (such as diabetes or heart failure) have high readmission rates that are unrelated to poor transitions per se – they are related to vulnerable patient populations that lack the capacity, health literacy, or economics to keep themselves out of the hospital with routine physician follow up. SeniorBridge is another alternative that may hold great promise. Whether it is truly cost effective remains to be seen based on the information in the article. We certainly cannot tell if the SeniorBridge patients are truly case matched to historical control or a different population altogether, so their self-reported information is probably rosier than real.
Nonetheless, if such programs (which function similarly to home hospice programs) provide enhanced services that are covered by insurance – hospitalists will gladly identify and refer vulnerable patients to these programs.
Franklin A. Michota, M.D., is the director of academic affairs in the Department of Hospital Medicine at the Cleveland Clinic. He reported no relevant conflicts of interest.
A good transition of care at the time of hospital discharge is critical in preventing some unnecessary readmissions. These would include inaccurate or incomplete discharge instructions, medication lists, follow-up information, and patient education on their disease and diet....
SeniorBridge appears to be a home-based care program for vulnerable elderly patients. I do not find it surprising that such a model may help prevent hospitalizations, and many chronic diseases (such as diabetes or heart failure) have high readmission rates that are unrelated to poor transitions per se – they are related to vulnerable patient populations that lack the capacity, health literacy, or economics to keep themselves out of the hospital with routine physician follow up. SeniorBridge is another alternative that may hold great promise. Whether it is truly cost effective remains to be seen based on the information in the article. We certainly cannot tell if the SeniorBridge patients are truly case matched to historical control or a different population altogether, so their self-reported information is probably rosier than real.
Nonetheless, if such programs (which function similarly to home hospice programs) provide enhanced services that are covered by insurance – hospitalists will gladly identify and refer vulnerable patients to these programs.
Franklin A. Michota, M.D., is the director of academic affairs in the Department of Hospital Medicine at the Cleveland Clinic. He reported no relevant conflicts of interest.
A good transition of care at the time of hospital discharge is critical in preventing some unnecessary readmissions. These would include inaccurate or incomplete discharge instructions, medication lists, follow-up information, and patient education on their disease and diet....
SeniorBridge appears to be a home-based care program for vulnerable elderly patients. I do not find it surprising that such a model may help prevent hospitalizations, and many chronic diseases (such as diabetes or heart failure) have high readmission rates that are unrelated to poor transitions per se – they are related to vulnerable patient populations that lack the capacity, health literacy, or economics to keep themselves out of the hospital with routine physician follow up. SeniorBridge is another alternative that may hold great promise. Whether it is truly cost effective remains to be seen based on the information in the article. We certainly cannot tell if the SeniorBridge patients are truly case matched to historical control or a different population altogether, so their self-reported information is probably rosier than real.
Nonetheless, if such programs (which function similarly to home hospice programs) provide enhanced services that are covered by insurance – hospitalists will gladly identify and refer vulnerable patients to these programs.
Franklin A. Michota, M.D., is the director of academic affairs in the Department of Hospital Medicine at the Cleveland Clinic. He reported no relevant conflicts of interest.
NEW YORK – A patient-centered, medical-home approach to care for patients with multiple chronic diseases when they are discharged from the hospital and back in their own residences substantially cut their rate of hospital readmissions, suggesting that this new model of home-based medical care pays for itself by avoiding hospitalization costs.
"We think it’s very important for the U.S. health care system to move its focus from hospital to home, with care management that prevents unnecessary emergency department visits and hospital admissions," Dr. Eric C. Rackow said at the course.
"You can alter the outcomes at home [of patients with diabetes and other chronic diseases] if you keep patients healthier and more functional at home and out of the hospital," said Dr. Rackow, professor of medicine at New York University, and president and CEO of SeniorBridge, a company that provides medical services to patients when they are in their homes.
"We have health plan contracts where we have shown a 50% reduction in hospitalization and readmissions rates, producing a 50% drop in the cost per member per month," Dr. Rackow said in an interview. Although SeniorBridge is relatively unique in offering the services from a variety of health care professionals for in-home services to patients, the model is amenable to scale up, he said. "Doctors are the captains, but it’s the nurses, social workers, nutritionists, and pharmacists who actually are in the patients’ homes. Physicians can manage a large number of patients. It’s a cost-effective way to extend the physician’s reach."
To document the impact that home-based intervention can have, he presented data collected by SeniorBridge from 503 patients aged 65 years or older that the company managed during 2008-2010. Eighty-eight of these patients who had diabetes and multiple other chronic conditions had a hospital readmission rate of 21% during their first 30 days at home following discharge from their index hospitalization. The other 415 patients managed by SeniorBridge had multiple chronic conditions but no diabetes, and they had an 11% rehospitalization rate during their first 30 days at home. In contrast, a historic control of similar elderly Americans with multiple chronic conditions who did not receive comprehensive care at home following their hospital discharge had a 33% readmission rate, Dr. Rackow said.
Another data analysis showed that 230 elderly SeniorBridge–treated patients with diabetes and multiple chronic diseases averaged 0.37 hospitalizations/year, and 1,486 elderly SeniorBridge-treated patients with multiple chronic diseases but no diabetes averaged 0.28 hospitalizations/year. By comparison, Medicare data showed a rate of 1.3 hospitalizations/year among similar patients receiving conventional care following a hospital discharge.
Multiple chronic illnesses are a hallmark of elderly patients with diabetes, affecting three-quarters of Americans 65 years or older with diabetes, Dr. Rackow said. The combination of diabetes, chronic obstructive pulmonary disease, and heart failure forms a common comorbidity constellation among elderly patients with diabetes, he noted.
Patients with several simultaneous chronic illnesses face special physical and cognitive challenges that pose problems for their self-directed care, he said. "The functional limitations [triggered by multiple chronic diseases] and the inability to self-manage tips patients and causes frequent hospitalizations." That’s why home medical services that aid a patient’s self management can have such a significant impact on rehospitalization rates.
Payment for SeniorBridge’s services has come from Medicaid, private insurers, and from long-term insurance policies. Medicare does not currently pay for these services, Dr. Rackow said.
Dr. Rackow is an employee, stockholder, and board member of SeniorBridge.
Here is a related video on "How Patients View Chronic Disease."
NEW YORK – A patient-centered, medical-home approach to care for patients with multiple chronic diseases when they are discharged from the hospital and back in their own residences substantially cut their rate of hospital readmissions, suggesting that this new model of home-based medical care pays for itself by avoiding hospitalization costs.
"We think it’s very important for the U.S. health care system to move its focus from hospital to home, with care management that prevents unnecessary emergency department visits and hospital admissions," Dr. Eric C. Rackow said at the course.
"You can alter the outcomes at home [of patients with diabetes and other chronic diseases] if you keep patients healthier and more functional at home and out of the hospital," said Dr. Rackow, professor of medicine at New York University, and president and CEO of SeniorBridge, a company that provides medical services to patients when they are in their homes.
"We have health plan contracts where we have shown a 50% reduction in hospitalization and readmissions rates, producing a 50% drop in the cost per member per month," Dr. Rackow said in an interview. Although SeniorBridge is relatively unique in offering the services from a variety of health care professionals for in-home services to patients, the model is amenable to scale up, he said. "Doctors are the captains, but it’s the nurses, social workers, nutritionists, and pharmacists who actually are in the patients’ homes. Physicians can manage a large number of patients. It’s a cost-effective way to extend the physician’s reach."
To document the impact that home-based intervention can have, he presented data collected by SeniorBridge from 503 patients aged 65 years or older that the company managed during 2008-2010. Eighty-eight of these patients who had diabetes and multiple other chronic conditions had a hospital readmission rate of 21% during their first 30 days at home following discharge from their index hospitalization. The other 415 patients managed by SeniorBridge had multiple chronic conditions but no diabetes, and they had an 11% rehospitalization rate during their first 30 days at home. In contrast, a historic control of similar elderly Americans with multiple chronic conditions who did not receive comprehensive care at home following their hospital discharge had a 33% readmission rate, Dr. Rackow said.
Another data analysis showed that 230 elderly SeniorBridge–treated patients with diabetes and multiple chronic diseases averaged 0.37 hospitalizations/year, and 1,486 elderly SeniorBridge-treated patients with multiple chronic diseases but no diabetes averaged 0.28 hospitalizations/year. By comparison, Medicare data showed a rate of 1.3 hospitalizations/year among similar patients receiving conventional care following a hospital discharge.
Multiple chronic illnesses are a hallmark of elderly patients with diabetes, affecting three-quarters of Americans 65 years or older with diabetes, Dr. Rackow said. The combination of diabetes, chronic obstructive pulmonary disease, and heart failure forms a common comorbidity constellation among elderly patients with diabetes, he noted.
Patients with several simultaneous chronic illnesses face special physical and cognitive challenges that pose problems for their self-directed care, he said. "The functional limitations [triggered by multiple chronic diseases] and the inability to self-manage tips patients and causes frequent hospitalizations." That’s why home medical services that aid a patient’s self management can have such a significant impact on rehospitalization rates.
Payment for SeniorBridge’s services has come from Medicaid, private insurers, and from long-term insurance policies. Medicare does not currently pay for these services, Dr. Rackow said.
Dr. Rackow is an employee, stockholder, and board member of SeniorBridge.
Here is a related video on "How Patients View Chronic Disease."
FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION