User login
Risk Factor Engine Helps Personalize Risk Interventions
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.

Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.
Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.
Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION.
Risk Factor Engine Helps Personalize Risk Interventions
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.

Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.
Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.
Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION.
Risk Factor Engine Helps Personalize Risk Interventions
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.

Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.
Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
NEW YORK – Management of type 2 diabetes patients has shifted "from one-size-fits-all to recommendations that are more personalized," according to Dr. Patrick J. O’Connor, a family physician and senior clinical investigator at HealthPartners Research Foundation in Minneapolis.
From a risk-management perspective, that means assessing the role of each cardiovascular risk factor in a given patient and identifying which modifiable factor packs the biggest punch and is likely to yield the most benefit when changed, he said.
Cardiovascular events account for about two-thirds of all deaths in patients with type 2 diabetes, and most of a patient’s cardiovascular risk depends on age and sex, two risk factors that resist modification. The question then becomes which modifiable risk factor smoking, hypertension, hyperlipidemia, hemoglobin A1c level, and aspirin use – warrants initial attention.
The best way to find out is to run a risk-factor engine analysis on each patient. For the analysis, each of the patient’s actual values is run individually through a risk-assessment formula, each time substituting normal values for all the modifiable factors except one. This process helps to identify the modifiable factor that, if normalized, stands to most benefit the patient.
The best known risk-factor formulas are the Framingham Risk Score, and for patients with diabetes the score derived from data in the UK Prospective Diabetes Study (UKPDS). "No risk engines available today are perfect; the epidemiologic data [that the risk scoring formula derives from] may be out of date," he said. But among the risk formulas currently available, "the UKPDS is the most appropriate for patients with diabetes," and includes an entry for hemoglobin A1c.
Dr. O’Connor and his associates are in the process of producing a new risk-engine website designed for patients with diabetes.
Electronic medical records have made risk-engine assessments easy, because a physician can set up the electronic record to run the engine automatically using a patient’s stored risk-factor data.
For example, the UKPDS risk-scoring formula calculates that a 70-year-old man who doesn’t smoke and has had diabetes for 15 years with a hemoglobin A1c of 7.2%, a systolic blood pressure of 170 mm Hg, and moderate levels of total cholesterol and high density lipoprotein cholesterol has a 15% risk for a coronary heart disease event and a 21% risk for a stroke over the next 10 years. If his systolic pressure dropped to 140 mm Hg, his coronary event risk would fall to 13%, and his stroke risk would drop to 18% – modest declines.
An analysis like this might suggest that it is not worth the effort of undertaking the treatment required to cut the patient’s systolic pressure by 30 mm Hg to achieve such modest risk improvements.
On the other hand, if the same 70-year-old man also smoked at baseline, his 10-year coronary event risk would be 19% and his stroke risk 30%. It might be worth working with the patient to get him to stop smoking and to treat his systolic hypertension, as both actions would cut his 10-year stroke risk by an absolute value of 10%.
"Use the risk engine to get a sense of what the treatment should be. If the patient has little or no reversible risk, then stop. Not all interventions are of equal benefit to all patients at a given time," Dr. O’Connor noted.
Dr. O’Connor said he had no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION.
New Gestational Diabetes Criteria Predicted to Boost Incidence Rates
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
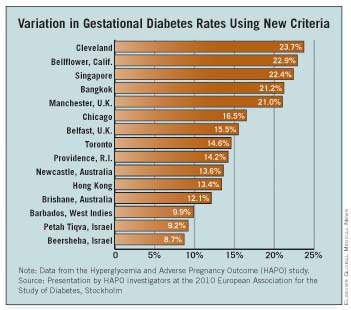
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).

But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION
New Gestational Diabetes Criteria Predicted to Boost Incidence Rates
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
NEW YORK – The incidence of gestational diabetes will rise substantially now that the American Diabetes Association has formally adopted new diagnostic criteria, especially in selected regions where pregnant woman may be older or have a higher prevalence of obesity.
Among the 15 geographically diverse communities that participated in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, the results of which led to the new ADA guidelines, the incidence of gestational diabetes ran as high as 24%, in Cleveland, while also reaching a low of 9%, in two communities in Israel. The overall gestational diabetes incidence rate in HAPO averaged 16%, Dr. Boyd E. Metzger said at the meeting sponsored by the American Diabetes Association, strikingly above the 7% rate documented as recently as 2005 in a large group of women from southern California (Diabetes Care 2008;31:899-904).
But Dr. Metzger also expressed optimism that most of the added new cases of gestational diabetes that the new criteria identify will respond to lifestyle management, and that the net result of broader diagnosis and treatment will be a substantially reduced rate of adverse sequelae.
"The mild gestational diabetes that makes up the expanded population should be patients we can successfully manage with less expensive," lifestyle treatment, said Dr. Metzger, a professor of nutrition and metabolism at Northwestern University in Chicago. The increased numbers may also include "a modest increase in those who need drug treatment." In general, "a more aggressive approach to diagnosis and treatment should lead to a reduction in complications of gestational diabetes. It would be disappointing if we can’t achieve in the real world what the research study showed," he said in an interview at a.
The new gestational diabetes diagnostic criteria received formal adoption from the American Diabetes Association in the group’s annual position statement on Standards of Medical Care in Diabetes, published in January (Diabetes Care 2011;34:S11-S61). The Standards’ section on the detection and diagnosis of gestational diabetes cited the 2008 HAPO study (N. Engl. J. Med. 2008;358:1991-2002) as the basis for the new diagnostic criteria. An initial proposal of the new criteria came from the International Association of Diabetes and Pregnancy Study Groups Consensus Panel last year, which recommended criteria to identify a woman with gestational diabetes if at week 24-28 her fasting plasma glucose was at least 92 mg/dL, or her plasma glucose 1 hour after an oral glucose challenge was at least 180 mg/dL, or her plasma glucose 2 hours after the glucose challenge was at least 153 mg/dL.
The new criteria "are not very different from the old ADA criteria. The biggest single difference is that any one of these criteria diagnoses an abnormal glucose level rather than requiring woman to meet at least two of the criteria," said Dr. Metzger, lead author for both HAPO and for the IADPSG. This easing to allow diagnosis based on just one criterion "accounts for a lot of the increase in numbers," he said. In the HAPO findings from more than 23,000 women, the fasting plasma glucose criterion diagnosed 8.3% of the women as having gestational diabetes, the 1-hour post-challenge plasma glucose level identified an additional 5.7% of women with gestational diabetes, and the 2-hour post-challenge glucose level identified another 2.1% with gestational diabetes, together totaling just over 16% with the diagnosis.
Data documenting the broad range of geographic variation in gestational diabetes incidence appeared in a report presented by a group of HAPO investigators, including Dr. Metzger, last September at the annual meeting of the European Association for the Study of Diabetes in Stockholm. Five of the 15 HAP sites had rates of 21%-24%, led by Cleveland with the highest rate and followed by Bellflower, Ca.; Singapore; Bangkok; and Manchester, U.K. Two different communities contributing data in Israel both had 9% rates, with the remaining eight sites having gestational diabetes rates of 10%-17%.
Having new diagnostic criteria also raises the question of whether treatment goals will need changing. "We would like to get women [diagnosed with gestational diabetes] to a fasting plasma glucose of 90 mg/dL or below. When the diagnostic threshold is 92 mg/dL, if we don’t get them to below then we are not changing their risk," Dr. Metzger said. But "we are not proponents of oral agents" for treating gestational diabetes.
"I don’t have a lot of experience using the new criteria," he admitted. "We just introduced them [at Northwestern University Medical Center] in January," after their official endorsement from the ADA, Dr. Metzger said. "We don’t yet have the data to make new treatment recommendations. The right treatment targets will need to be defined by results from additional studies."
Dr. Metzger said that he had no disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN DIABETES ASSOCIATION