User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
Early Days of Intracranial Stenting, Angioplasty Undergo Review
LOS ANGELES – Physicians using angioplasty and stenting to treat intracranial stenosis need to identify the best patients to receive these interventions, and make sure that the procedures are cost effective, Dr. Adnan I. Qureshi said at the International Stroke Conference.
During 2005-2007, a large sample of U.S. hospital data showed that out of an estimated 1.8 million patients with acute or chronic intracranial arterial disease, roughly 1,600 patients underwent intracranial angioplasty or received a stent in an intracranial artery, said Dr. Qureshi, professor and associate head of the neurology department at the University of Minnesota, Minneapolis. The sample, which included diagnostic- and procedure-code information on nearly 371,000 U.S. patients with a primary diagnosis of stroke or transient ischemic attack, also showed that the small number of patients who underwent intracranial angioplasty or received a stent had substantially higher hospital charges than did medically treated patients.

Stenting also produced generally good outcomes, with 76% of patients going home after their hospital discharge, 20% going on to a care facility, and 4% dying in hospital. Patients who underwent intracranial angioplasty had worse outcomes, with a 17% mortality rate and a 39% rate of discharge to a care facility, with 45% going home from the hospital (total is 101% due to rounding).
But the administrative database that supplied these data included no information on patients’ disease severity, making meaningful outcome comparisons impossible, Dr. Qureshi stressed.
"The data do not allow us to compare patients with similar disease severity. Worse outcomes may not be related to the procedure but to where these patients started from. The challenge is to apply these treatments to the patients who are most likely to benefit," he said in an interview. Until now, "technology has been the main focus. Other factors that play into outcomes, like patient selection and timely administration of the treatment, have taken a back seat.
"We need to closely monitor the outcomes of patients who undergo [intracranial stenting and angioplasty] because that is the only way we’ll find out whether patients truly benefit. Endovascular treatments are being used today without good evidence of who to use them on and when. The message we don’t want to come from our analysis is that intracranial angioplasty and stent placement don’t work. What muddies the picture is when you apply [these treatments] to patients who don’t benefit. We need to focus on treating the patients who will benefit. I think our data are a wake-up call for us to be sure we are properly [focused] on patient selection and on cost being offset by the benefit that patients receive."
Dr. Qureshi’s analysis used data collected in the Nationwide Inpatient Sample by the Healthcare Cost and Utilization Project of the Agency for Healthcare Research and Quality. During 2005-2007, of the 370,993 patients in the sample with a primary diagnostic code of stroke or transient ischemic attack, 158 patients underwent intracranial angioplasty and 169 received an intracranial stent. Those numbers extrapolate to nationwide levels of about 1,822,000 cases, with 791 patients undergoing angioplasty and 837 receiving an intracranial stent, Dr. Qureshi said at the meeting, sponsored by the American Heart Association.
Further analysis showed that intracranial interventions occurred primarily at large teaching hospitals. Hospitalization charges for patients undergoing primary intracranial angioplasty only averaged $88,000; and for patients undergoing angioplasty plus stenting, the charges averaged almost $61,000. In contrast, for the remaining patients in the database hospitalization charges averaged about $24,000. Among patients who underwent an intracranial intervention, the concurrent presence of heart failure, pneumonia, urinary tract infection, or an intracranial hemorrhage was linked with a significantly increased rate of death or disability.
"In today’s world, most patients who get this procedure had an ischemic event in the brain related to the stenosis, and most had already been tried on maximal medical therapy. The challenge is, at what point do you decide that you have exhausted the medical options and move to [an intervention]. The strategy of how these patients are managed has changed, but their outcomes have not shifted as much as we would like. We need to closely monitor outcomes," Dr. Qureshi said.
Dr. Qureshi said that he had no disclosures.
This study provides a snapshot of intracranial angioplasty and stenting for seriously stenotic arteries during 2005-2007 based on data from an administrative database. The results show that during that time, we began to see early signs that stenting and angioplasty were possible in intracranial arteries, just as they are for coronary or carotid arteries. The procedures generally were done in larger, more specialized institutions, such as comprehensive stroke centers.
Dr. Ralph L. Sacco |

The period covered was a time when operators learned how to do these procedures, and it was also a period of technical advances. The stents have changed with time. They have gotten better and smaller, and can now be manipulated to enter smaller arteries.
Current guidelines from the American Heart Association and American Stroke Association say that intracranial stenting and angioplasty should not be done unless all other treatments fail. Specifically, the guidelines published in January 2011 say that in patients with intracranial stenosis, "the usefulness of angioplasty and/or stent placement is unknown and is considered investigational" (Stroke 2011;42:227-76).
In addition, a large trial sponsored by the National Institutes of Health is now in progress comparing stenting and optimal medical therapy, the Stenting vs. Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial. Conventional medical therapy could include aspirin, clopidogrel, extended-release dipyridamole, aggressive statin therapy, and blood pressure control. Patients with symptomatic intracranial stenosis could also undergo regular monitoring with ultrasound, MR, CT, or angiography.
My concern is whether some physicians are jumping to perform intracranial stenting or angioplasty too quickly. Even among the small number of patients who underwent these treatments in this study, we don’t know why their physicians concluded that they were failing medical treatment. Did these patients have a transient ischemic attack or a minor stroke just before their intervention? With the data used by Dr. Qureshi and his associates, we have no way to determine what indications led to the treatments used.
Some operators have become more technically proficient in treating intracranial arteries, but it will take more studies for us to learn which patients should appropriately get this treatment.
Ralph L. Sacco, M.D., is professor and chairman of neurology at the University of Miami. He said that he has been a consultant to Boehringer Ingelheim and Sanofi-Aventis.
This study provides a snapshot of intracranial angioplasty and stenting for seriously stenotic arteries during 2005-2007 based on data from an administrative database. The results show that during that time, we began to see early signs that stenting and angioplasty were possible in intracranial arteries, just as they are for coronary or carotid arteries. The procedures generally were done in larger, more specialized institutions, such as comprehensive stroke centers.
Dr. Ralph L. Sacco |
The period covered was a time when operators learned how to do these procedures, and it was also a period of technical advances. The stents have changed with time. They have gotten better and smaller, and can now be manipulated to enter smaller arteries.
Current guidelines from the American Heart Association and American Stroke Association say that intracranial stenting and angioplasty should not be done unless all other treatments fail. Specifically, the guidelines published in January 2011 say that in patients with intracranial stenosis, "the usefulness of angioplasty and/or stent placement is unknown and is considered investigational" (Stroke 2011;42:227-76).
In addition, a large trial sponsored by the National Institutes of Health is now in progress comparing stenting and optimal medical therapy, the Stenting vs. Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial. Conventional medical therapy could include aspirin, clopidogrel, extended-release dipyridamole, aggressive statin therapy, and blood pressure control. Patients with symptomatic intracranial stenosis could also undergo regular monitoring with ultrasound, MR, CT, or angiography.
My concern is whether some physicians are jumping to perform intracranial stenting or angioplasty too quickly. Even among the small number of patients who underwent these treatments in this study, we don’t know why their physicians concluded that they were failing medical treatment. Did these patients have a transient ischemic attack or a minor stroke just before their intervention? With the data used by Dr. Qureshi and his associates, we have no way to determine what indications led to the treatments used.
Some operators have become more technically proficient in treating intracranial arteries, but it will take more studies for us to learn which patients should appropriately get this treatment.
Ralph L. Sacco, M.D., is professor and chairman of neurology at the University of Miami. He said that he has been a consultant to Boehringer Ingelheim and Sanofi-Aventis.
This study provides a snapshot of intracranial angioplasty and stenting for seriously stenotic arteries during 2005-2007 based on data from an administrative database. The results show that during that time, we began to see early signs that stenting and angioplasty were possible in intracranial arteries, just as they are for coronary or carotid arteries. The procedures generally were done in larger, more specialized institutions, such as comprehensive stroke centers.
Dr. Ralph L. Sacco |
The period covered was a time when operators learned how to do these procedures, and it was also a period of technical advances. The stents have changed with time. They have gotten better and smaller, and can now be manipulated to enter smaller arteries.
Current guidelines from the American Heart Association and American Stroke Association say that intracranial stenting and angioplasty should not be done unless all other treatments fail. Specifically, the guidelines published in January 2011 say that in patients with intracranial stenosis, "the usefulness of angioplasty and/or stent placement is unknown and is considered investigational" (Stroke 2011;42:227-76).
In addition, a large trial sponsored by the National Institutes of Health is now in progress comparing stenting and optimal medical therapy, the Stenting vs. Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial. Conventional medical therapy could include aspirin, clopidogrel, extended-release dipyridamole, aggressive statin therapy, and blood pressure control. Patients with symptomatic intracranial stenosis could also undergo regular monitoring with ultrasound, MR, CT, or angiography.
My concern is whether some physicians are jumping to perform intracranial stenting or angioplasty too quickly. Even among the small number of patients who underwent these treatments in this study, we don’t know why their physicians concluded that they were failing medical treatment. Did these patients have a transient ischemic attack or a minor stroke just before their intervention? With the data used by Dr. Qureshi and his associates, we have no way to determine what indications led to the treatments used.
Some operators have become more technically proficient in treating intracranial arteries, but it will take more studies for us to learn which patients should appropriately get this treatment.
Ralph L. Sacco, M.D., is professor and chairman of neurology at the University of Miami. He said that he has been a consultant to Boehringer Ingelheim and Sanofi-Aventis.
LOS ANGELES – Physicians using angioplasty and stenting to treat intracranial stenosis need to identify the best patients to receive these interventions, and make sure that the procedures are cost effective, Dr. Adnan I. Qureshi said at the International Stroke Conference.
During 2005-2007, a large sample of U.S. hospital data showed that out of an estimated 1.8 million patients with acute or chronic intracranial arterial disease, roughly 1,600 patients underwent intracranial angioplasty or received a stent in an intracranial artery, said Dr. Qureshi, professor and associate head of the neurology department at the University of Minnesota, Minneapolis. The sample, which included diagnostic- and procedure-code information on nearly 371,000 U.S. patients with a primary diagnosis of stroke or transient ischemic attack, also showed that the small number of patients who underwent intracranial angioplasty or received a stent had substantially higher hospital charges than did medically treated patients.
Stenting also produced generally good outcomes, with 76% of patients going home after their hospital discharge, 20% going on to a care facility, and 4% dying in hospital. Patients who underwent intracranial angioplasty had worse outcomes, with a 17% mortality rate and a 39% rate of discharge to a care facility, with 45% going home from the hospital (total is 101% due to rounding).
But the administrative database that supplied these data included no information on patients’ disease severity, making meaningful outcome comparisons impossible, Dr. Qureshi stressed.
"The data do not allow us to compare patients with similar disease severity. Worse outcomes may not be related to the procedure but to where these patients started from. The challenge is to apply these treatments to the patients who are most likely to benefit," he said in an interview. Until now, "technology has been the main focus. Other factors that play into outcomes, like patient selection and timely administration of the treatment, have taken a back seat.
"We need to closely monitor the outcomes of patients who undergo [intracranial stenting and angioplasty] because that is the only way we’ll find out whether patients truly benefit. Endovascular treatments are being used today without good evidence of who to use them on and when. The message we don’t want to come from our analysis is that intracranial angioplasty and stent placement don’t work. What muddies the picture is when you apply [these treatments] to patients who don’t benefit. We need to focus on treating the patients who will benefit. I think our data are a wake-up call for us to be sure we are properly [focused] on patient selection and on cost being offset by the benefit that patients receive."
Dr. Qureshi’s analysis used data collected in the Nationwide Inpatient Sample by the Healthcare Cost and Utilization Project of the Agency for Healthcare Research and Quality. During 2005-2007, of the 370,993 patients in the sample with a primary diagnostic code of stroke or transient ischemic attack, 158 patients underwent intracranial angioplasty and 169 received an intracranial stent. Those numbers extrapolate to nationwide levels of about 1,822,000 cases, with 791 patients undergoing angioplasty and 837 receiving an intracranial stent, Dr. Qureshi said at the meeting, sponsored by the American Heart Association.
Further analysis showed that intracranial interventions occurred primarily at large teaching hospitals. Hospitalization charges for patients undergoing primary intracranial angioplasty only averaged $88,000; and for patients undergoing angioplasty plus stenting, the charges averaged almost $61,000. In contrast, for the remaining patients in the database hospitalization charges averaged about $24,000. Among patients who underwent an intracranial intervention, the concurrent presence of heart failure, pneumonia, urinary tract infection, or an intracranial hemorrhage was linked with a significantly increased rate of death or disability.
"In today’s world, most patients who get this procedure had an ischemic event in the brain related to the stenosis, and most had already been tried on maximal medical therapy. The challenge is, at what point do you decide that you have exhausted the medical options and move to [an intervention]. The strategy of how these patients are managed has changed, but their outcomes have not shifted as much as we would like. We need to closely monitor outcomes," Dr. Qureshi said.
Dr. Qureshi said that he had no disclosures.
LOS ANGELES – Physicians using angioplasty and stenting to treat intracranial stenosis need to identify the best patients to receive these interventions, and make sure that the procedures are cost effective, Dr. Adnan I. Qureshi said at the International Stroke Conference.
During 2005-2007, a large sample of U.S. hospital data showed that out of an estimated 1.8 million patients with acute or chronic intracranial arterial disease, roughly 1,600 patients underwent intracranial angioplasty or received a stent in an intracranial artery, said Dr. Qureshi, professor and associate head of the neurology department at the University of Minnesota, Minneapolis. The sample, which included diagnostic- and procedure-code information on nearly 371,000 U.S. patients with a primary diagnosis of stroke or transient ischemic attack, also showed that the small number of patients who underwent intracranial angioplasty or received a stent had substantially higher hospital charges than did medically treated patients.
Stenting also produced generally good outcomes, with 76% of patients going home after their hospital discharge, 20% going on to a care facility, and 4% dying in hospital. Patients who underwent intracranial angioplasty had worse outcomes, with a 17% mortality rate and a 39% rate of discharge to a care facility, with 45% going home from the hospital (total is 101% due to rounding).
But the administrative database that supplied these data included no information on patients’ disease severity, making meaningful outcome comparisons impossible, Dr. Qureshi stressed.
"The data do not allow us to compare patients with similar disease severity. Worse outcomes may not be related to the procedure but to where these patients started from. The challenge is to apply these treatments to the patients who are most likely to benefit," he said in an interview. Until now, "technology has been the main focus. Other factors that play into outcomes, like patient selection and timely administration of the treatment, have taken a back seat.
"We need to closely monitor the outcomes of patients who undergo [intracranial stenting and angioplasty] because that is the only way we’ll find out whether patients truly benefit. Endovascular treatments are being used today without good evidence of who to use them on and when. The message we don’t want to come from our analysis is that intracranial angioplasty and stent placement don’t work. What muddies the picture is when you apply [these treatments] to patients who don’t benefit. We need to focus on treating the patients who will benefit. I think our data are a wake-up call for us to be sure we are properly [focused] on patient selection and on cost being offset by the benefit that patients receive."
Dr. Qureshi’s analysis used data collected in the Nationwide Inpatient Sample by the Healthcare Cost and Utilization Project of the Agency for Healthcare Research and Quality. During 2005-2007, of the 370,993 patients in the sample with a primary diagnostic code of stroke or transient ischemic attack, 158 patients underwent intracranial angioplasty and 169 received an intracranial stent. Those numbers extrapolate to nationwide levels of about 1,822,000 cases, with 791 patients undergoing angioplasty and 837 receiving an intracranial stent, Dr. Qureshi said at the meeting, sponsored by the American Heart Association.
Further analysis showed that intracranial interventions occurred primarily at large teaching hospitals. Hospitalization charges for patients undergoing primary intracranial angioplasty only averaged $88,000; and for patients undergoing angioplasty plus stenting, the charges averaged almost $61,000. In contrast, for the remaining patients in the database hospitalization charges averaged about $24,000. Among patients who underwent an intracranial intervention, the concurrent presence of heart failure, pneumonia, urinary tract infection, or an intracranial hemorrhage was linked with a significantly increased rate of death or disability.
"In today’s world, most patients who get this procedure had an ischemic event in the brain related to the stenosis, and most had already been tried on maximal medical therapy. The challenge is, at what point do you decide that you have exhausted the medical options and move to [an intervention]. The strategy of how these patients are managed has changed, but their outcomes have not shifted as much as we would like. We need to closely monitor outcomes," Dr. Qureshi said.
Dr. Qureshi said that he had no disclosures.
FROM THE INTERNATIONAL STROKE CONFERENCE
Major Finding: During 2005-2007, roughly 1,600 stroke or transient ischemic attack patients underwent intracranial angioplasty or stenting out of 1.8 million total U.S patients.
Data Source: The Nationwide Inpatient Sample, a 20% stratified sample of U.S. community hospitals that included 370,993 stroke or transient ischemic attack patients, including 327 who underwent intracranial angioplasty or stenting.
Disclosures: Dr. Qureshi said he had no disclosures.
Belimumab's FDA Approval Marks New Lupus-Treatment Era
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).

"I’ve been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug’s approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index (pdf), said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.

"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview." The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they’re on. If they flare a little, I’d first look to raise the dose of the drug they’re on before I go to a brand new biologic" such as belimumab. But we have a lot of patients where that [raising the dose] won’t work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won’t be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can’t adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug’s pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I’ve had to fight to get my patients access, even the ones who were very sick. The payer’s argument was that the drug was not approved for lupus. Now it’s the expensive drug that’s approved, but the inexpensive ones aren’t. Insurers will have trouble because if they say ‘Have you tried azathioprine or methotrexate?’ I can say ‘But those drugs are not approved for lupus.’ "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA’s announcement of belimumab’s approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company’s apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that’s clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies (pdf) that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).
"I’ve been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug’s approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index (pdf), said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview." The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they’re on. If they flare a little, I’d first look to raise the dose of the drug they’re on before I go to a brand new biologic" such as belimumab. But we have a lot of patients where that [raising the dose] won’t work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won’t be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can’t adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug’s pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I’ve had to fight to get my patients access, even the ones who were very sick. The payer’s argument was that the drug was not approved for lupus. Now it’s the expensive drug that’s approved, but the inexpensive ones aren’t. Insurers will have trouble because if they say ‘Have you tried azathioprine or methotrexate?’ I can say ‘But those drugs are not approved for lupus.’ "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA’s announcement of belimumab’s approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company’s apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that’s clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies (pdf) that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).
"I’ve been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug’s approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index (pdf), said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview." The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they’re on. If they flare a little, I’d first look to raise the dose of the drug they’re on before I go to a brand new biologic" such as belimumab. But we have a lot of patients where that [raising the dose] won’t work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won’t be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can’t adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug’s pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I’ve had to fight to get my patients access, even the ones who were very sick. The payer’s argument was that the drug was not approved for lupus. Now it’s the expensive drug that’s approved, but the inexpensive ones aren’t. Insurers will have trouble because if they say ‘Have you tried azathioprine or methotrexate?’ I can say ‘But those drugs are not approved for lupus.’ "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA’s announcement of belimumab’s approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company’s apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that’s clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies (pdf) that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
FROM THE FOOD AND DRUG ADMINISTRATION
Belimumab's FDA Approval Marks New Lupus-Treatment Era
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).

"I've been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug's approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index, said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview. The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they're on. If they flare a little, I'd first look to raise the dose of the drug they're on before I go to a brand new biologic such as belimumab. But we have a lot of patients where that [raising the dose] won't work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won't be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can't adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug's pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I've had to fight to get my patients access, even the ones who were very sick. The payer's argument was that the drug was not approved for lupus. Now it's the expensive drug that's approved, but the inexpensive ones aren't. Insurers will have trouble because if they say 'Have you tried azathioprine or methotrexate?' I can say 'But those drugs are not approved for lupus.' "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA's announcement of belimumab's approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.

"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company's apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that's clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).
"I've been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug's approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index, said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview. The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they're on. If they flare a little, I'd first look to raise the dose of the drug they're on before I go to a brand new biologic such as belimumab. But we have a lot of patients where that [raising the dose] won't work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won't be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can't adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug's pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I've had to fight to get my patients access, even the ones who were very sick. The payer's argument was that the drug was not approved for lupus. Now it's the expensive drug that's approved, but the inexpensive ones aren't. Insurers will have trouble because if they say 'Have you tried azathioprine or methotrexate?' I can say 'But those drugs are not approved for lupus.' "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA's announcement of belimumab's approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company's apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that's clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).
"I've been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug's approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index, said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview. The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they're on. If they flare a little, I'd first look to raise the dose of the drug they're on before I go to a brand new biologic such as belimumab. But we have a lot of patients where that [raising the dose] won't work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won't be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can't adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug's pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I've had to fight to get my patients access, even the ones who were very sick. The payer's argument was that the drug was not approved for lupus. Now it's the expensive drug that's approved, but the inexpensive ones aren't. Insurers will have trouble because if they say 'Have you tried azathioprine or methotrexate?' I can say 'But those drugs are not approved for lupus.' "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA's announcement of belimumab's approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company's apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that's clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
FROM THE FOOD AND DRUG ADMINISTRATION
Belimumab's FDA Approval Marks New Lupus-Treatment Era
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).
"I’ve been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug’s approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index (pdf), said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview." The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they’re on. If they flare a little, I’d first look to raise the dose of the drug they’re on before I go to a brand new biologic" such as belimumab. But we have a lot of patients where that [raising the dose] won’t work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won’t be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can’t adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug’s pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I’ve had to fight to get my patients access, even the ones who were very sick. The payer’s argument was that the drug was not approved for lupus. Now it’s the expensive drug that’s approved, but the inexpensive ones aren’t. Insurers will have trouble because if they say ‘Have you tried azathioprine or methotrexate?’ I can say ‘But those drugs are not approved for lupus.’ "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA’s announcement of belimumab’s approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company’s apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that’s clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies (pdf) that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).
"I’ve been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug’s approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index (pdf), said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview." The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they’re on. If they flare a little, I’d first look to raise the dose of the drug they’re on before I go to a brand new biologic" such as belimumab. But we have a lot of patients where that [raising the dose] won’t work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won’t be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can’t adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug’s pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I’ve had to fight to get my patients access, even the ones who were very sick. The payer’s argument was that the drug was not approved for lupus. Now it’s the expensive drug that’s approved, but the inexpensive ones aren’t. Insurers will have trouble because if they say ‘Have you tried azathioprine or methotrexate?’ I can say ‘But those drugs are not approved for lupus.’ "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA’s announcement of belimumab’s approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company’s apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that’s clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies (pdf) that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
The announcement late on March 9 from the Food and Drug Administration that it had approved belimumab as a treatment for systemic lupus erythematosus, the first new treatment approved for this disease in more than 50 years, produced reaction among lupus specialists that ran the gamut from unrestrained elation to somewhat more restrained enthusiasm.
Regardless of the degree of caution experts might have about the efficacy of belimumab and the consequences of its widespread use, there was no denying that its approval marked a milestone for the management of patients with systemic lupus erythematosus (SLE).
"I’ve been calling my friends and going yippee. This is a historic day for lupus patients," said Dr. Joan T. Merrill, professor of medicine and chair of the clinical pharmacology research program at the Oklahoma Medical Research Foundation in Oklahoma City, who participated in the belimumab trials and exemplified a more enthusiastic take on the drug’s approval.
A more cautious but still welcoming view came from Dr. David Wofsy, who was not involved in the belimumab studies. "I expect the drug will be widely used in lupus, given the great, unmet need for new therapies. But patients and physicians need to remain cognizant of the fact that roughly half of the subjects in the trials did not achieve the desired clinical outcome" a novel measure designed specifically for the two pivotal belimumab trials, the SLE Responder Index (pdf), said Dr. Wofsy, a professor of rheumatology at the University of California, San Francisco.
"Moreover, at this point, there is relatively little information about the effect of belimumab in patients with the most serious manifestations of lupus," such as active nephritis and central nervous system manifestations, Dr. Wofsy said in an interview." The majority of patients in the belimumab trials had cutaneous manifestations, musculoskeletal manifestations, or both, so we are beginning to understand the potential benefit of the drug in these patients. It will take time and undoubtedly more trials before we know how the drug will perform in patients with other manifestations.
"There is understandably great excitement about this landmark achievement, but patients and physicians will be well served if they remain realistic in their expectations and cautious in their use of a new agent," Dr. Wofsy said.
Dr. Merrill applied less caution in her assessment of the role belimumab will fill once physicians start prescribing it.
"I believe it will be tried in many [SLE] patients over the next year," she said in an interview. "I will certainly try it in many of my patients. The majority of lupus patients will flare sooner or later on the medicine they’re on. If they flare a little, I’d first look to raise the dose of the drug they’re on before I go to a brand new biologic" such as belimumab. But we have a lot of patients where that [raising the dose] won’t work, and they deserve a chance to try" the new drug. "The data from the trials show us that belimumab won’t be the perfect drug for every patient, but there may be a substantial number of patients who may be helped. A patient doing well on a less expensive drug is not a candidate for changing treatment to belimumab, but there are many patients who are candidates."
What remains less clear today is the possible role of belimumab as initial therapy. "There are no treatment algorithms in SLE; there is no clinical trial evidence to know which drug to start first," Dr. Merrill said. A patient with SLE and predominant arthritis symptoms might initially get started on methotrexate, but if that is only partially effective, it would be reasonable to use belimumab as the next step, she said. An SLE patient who presents with a significant rash as the predominant symptom might start on methotrexate or another oral immunosuppressant, and again, belimumab could later be added if needed. Or the patient may be intolerant of such drugs as azathioprine or mycophenolate, prompting a faster progression to belimumab. Hydroxychloroquine monotherapy usually can’t adequately control substantial SLE symptoms.
Although the two companies that will jointly market belimumab (Benlysta), Human Genome Sciences and GlaxoSmithKline, have not yet announced the drug’s pricing, expectations are that it will be high. "There is no such thing as a cheap biologic," especially while it remains on patent, Dr. Merrill noted. But the world of drug options for treating SLE is somewhat unique, because virtually none of the standard-of-care options has labeling for SLE.
"For many years, insurers refused to cover expensive biologics" for SLE patients, Dr. Merrill said. "I’ve had to fight to get my patients access, even the ones who were very sick. The payer’s argument was that the drug was not approved for lupus. Now it’s the expensive drug that’s approved, but the inexpensive ones aren’t. Insurers will have trouble because if they say ‘Have you tried azathioprine or methotrexate?’ I can say ‘But those drugs are not approved for lupus.’ "
The United States "is struggling to figure out how to solve the cost of medical care. In the meantime, my strong conviction is that lupus patients, like any other patient, should have access to the best care available. If that proves to be belimumab, then so be it," Dr. Wofsy said.
A notable feature of the FDA’s announcement of belimumab’s approval was the agency noting that African American SLE patients and those of African heritage "did not appear to respond to treatment with belimumab" in the two pivotal studies. The FDA noted that the companies developing belimumab agreed to run a new study to specifically address this issue in greater detail.
"The trials done were not powered to address the efficacy of belimumab in African Americans, but the lack of an encouraging signal in this population can only be described as very disappointing, given that this population is disproportionately affected by SLE. The company’s apparent commitment to answer this question definitely in a new trial is very important and to their credit," Dr. Wofsy said.
But citing the difficulty of presuming a genetic profile in individual patients who might have a particular racial identity, Dr. Merrill drew a different conclusion. "In my opinion, the data do not support any limitation excluding African Americans" from treatment with belimumab. "Everyone has a different genetic mix. Data that focus on race are very unscientific. I think that all patients deserve a chance to be tried on a treatment that’s clearly showed widespread safety, compared with other drugs that are used for standard of care but have lots of side effects."
The labeling issued by the companies (pdf) that will market belimumab lists a recommended dosage for each belimumab infusion as 10 mg/kg, every 2 weeks for the first three doses followed by new doses every 4 weeks, the dosage that gave the best results in the pivotal trials. But physicians will need to take a flexible attitude on dosage as they start treating patients, Dr. Merrill said. Although she will start some patients on 10 mg/kg, she might start with a lower dosage in patients she is nervous about and then slowly raise the dosage, and, if a patient remains symptomatic but well tolerates 10 mg/kg, she would also consider increasing the dosage higher, she said.
Dr. Merrill said that she has been a consultant to and has received research support from Human Genome Sciences and GlaxoSmithKline, as well as from many other companies. Dr. Wofsy has been a consultant to Bristol Myers Squibb and has received research support from several drug companies.
Dr. Wofsy has consulted for Human Genome Sciences and GlaxoSmithKline, as well as other companies involved in lupus drug development.
FROM THE FOOD AND DRUG ADMINISTRATION
Retrievable Stents Produce Fast Recanalization in Acute Stroke
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.

"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |

I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
FROM THE ANNUAL INTERNATIONAL STROKE CONFERENCE
Major Finding: Treatment of acute ischemic stroke patients with retrievable stents led to a 91% recanalization rate using an average of 1.4 passes per patient in a procedure that lasted an average of 45 minutes.
Data Source: A series of 89 patients with acute ischemic stroke who underwent treatment with a retrievable stent at one of three hospitals in Barcelona during March 2008–December 2010.
Disclosures: Dr. Aleu said that she and her associates had no disclosures.
Retrievable Stents Produce Fast Recanalization in Acute Stroke
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
FROM THE ANNUAL INTERNATIONAL STROKE CONFERENCE
Major Finding: Treatment of acute ischemic stroke patients with retrievable stents led to a 91% recanalization rate using an average of 1.4 passes per patient in a procedure that lasted an average of 45 minutes.
Data Source: A series of 89 patients with acute ischemic stroke who underwent treatment with a retrievable stent at one of three hospitals in Barcelona during March 2008–December 2010.
Disclosures: Dr. Aleu said that she and her associates had no disclosures.
Retrievable Stents Produce Fast Recanalization in Acute Stroke
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
Stent retrievers are the next generation of revascularization tools for acute stroke patients. They will improve the efficacy of clot removal. The average of 1.4 passes per patient and a deployment time of less than a minute that Dr. Aleu reported is incredible, compared with the four to five passes usually needed with the Merci retriever or the prolonged time required to remove a clot with the Penumbra device. Retrievable stents are very deliverable and deployable and allow you to more easily get through the loops of the cerebral arteries.
Dr. Adnan H. Siddiqui |
I have used the Solitaire stent myself on about a dozen patients at the State University of New York at Buffalo, as part of the multicenter Solitaire FR With the Intention of Thrombectomy (SWIFT) study, which is randomizing 200 acute stroke patients to clot removal with either the Solitaire stent or the Merci retriever. So far, we do not have any outcome results that we can report, but I have found this retrievable stent to be much more torqueable and navigable than other intracerebral devices. If we can produce results that are similar to what Dr. Aleu reported in the Barcelona series then I would be happy.
With 47% of patients having a modified Rankin score of 2 or less at 3-month follow-up they have approach the 50% level that I believe is the next goal for endovascular treatment of acute stroke. So far, the best outcomes achieved using other devices has been 40%-45% of patients achieving this level of recovery. Having 50% of patients recover this way is the next benchmark we must aim for in multicenter, randomized, controlled trials.
Adnan H. Siddiqui, M.D., is a neurosurgeon and director of the stroke program at the State University of New York at Buffalo. He said he has served as a consultant to ev3, the company that markets the Solitaire retrievable stent.
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
LOS ANGELES – Using retrievable stents to remove occluding clots from the cerebral arteries of acute, ischemic-stroke patients produced a high rate of recanalization and good safety in 3-month follow-up of 74 patients, the largest series of stroke patients treated this way yet reported.
Removing clots from acute stroke patients using retrievable stents also required less time and fewer passes, with an average procedure duration of 45 minutes, Dr. Aitziber Aleu said at the International Stroke Conference.
"The advantage of stentrievers [retrievable stents] is that they are very easy to use and are faster to recanalize with fewer passes," said Dr. Aleu, an interventional neurologist at Germans Trias i Pujol University Hospital, Barcelona. "You get the vessel open faster, compared with some of the older devices, and you get higher recanalization rates." Retrievable stents "are now our first-line approach for acute stroke patients," she said in an interview.
The series of 89 patients she reported underwent treatment with a retrievable stent at Hospital Germans Trias i Pujol or one of two other hospitals in the Barcelona area during March 2008 to December 2010. The operators used either of two different brands of retrievable stents, the Solitaire or the Trevo, on roughly equal numbers of patients.
The average age of the 89 patients in the reported series was 66 years, and their average NIH Stroke Scale score at baseline was 18, ranging from 15-22. Prior to stent placement, 48% of the patients had received treatment with tissue plasminogen activator. The most common location of the occluding clot was in the M1 segment of the middle cerebral artery, in 44% of patients. The occluding clot occurred in the vertebrobasilar artery in 15%, the terminal region of the interior cerebral artery in 14%, and 14% of patients had tandem occlusions in both the proximal region of the internal cerebral artery and in the middle cerebral artery.
The average recanalization procedure took 45 minutes, with a range of 27-60 minutes, and each procedure required an average of 1.4 stent passes to remove the occluding blood clot. Stent deployment usually lasted less than a minute before retrieval, and the operators had no episodes of failed deployment. Stent treatment resulted in successful recanalization in 81 patients (91%), with 70% achieving a Thrombolysis in Cerebral Infarction flow rate of III, and 21% achieving TICI II flow.
The investigators identified neurologic improvement 1 day after treatment in 28 patients (32%), and by 1 week after treatment 6 patients (7%) had died.
When she made her report, Dr. Aleu had 3-month follow-up results for 74 patients. At that time, 35 patients (47%) had a modified Rankin score of 2 or less, and 15 patients (20%) had died. During 3-month follow-up, 9% of the 74 patients had a symptomatic intracerebral hemorrhage.
Dr. Aleu said that she and her associates on the study had no disclosures.
FROM THE ANNUAL INTERNATIONAL STROKE CONFERENCE
Major Finding: Treatment of acute ischemic stroke patients with retrievable stents led to a 91% recanalization rate using an average of 1.4 passes per patient in a procedure that lasted an average of 45 minutes.
Data Source: A series of 89 patients with acute ischemic stroke who underwent treatment with a retrievable stent at one of three hospitals in Barcelona during March 2008–December 2010.
Disclosures: Dr. Aleu said that she and her associates had no disclosures.
Set of Symptoms Identified to Flag Stroke Risk
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."

Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
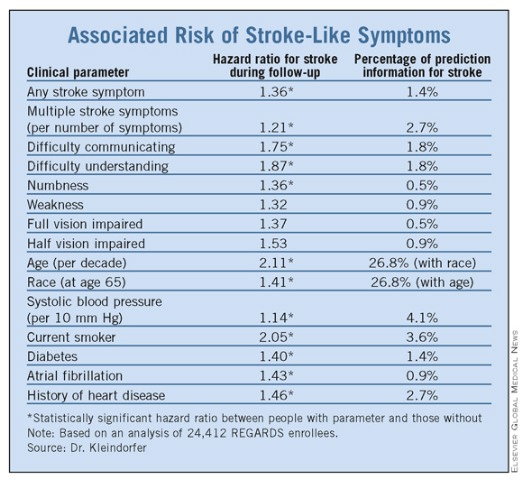
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
FROM THE INTERNATIONAL STROKE CONFERENCE
Major Finding: People without a known history of stroke or transient ischemic attack had a 36% relatively increased risk for a future stroke if they had a strokelike symptom.
Data Source: Review of prospectively collected data on 24,412 American people without a history of stroke or transient ischemic attack enrolled in the REGARDS study.
Disclosures: Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
Set of Symptoms Identified to Flag Stroke Risk
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
FROM THE INTERNATIONAL STROKE CONFERENCE
Major Finding: People without a known history of stroke or transient ischemic attack had a 36% relatively increased risk for a future stroke if they had a strokelike symptom.
Data Source: Review of prospectively collected data on 24,412 American people without a history of stroke or transient ischemic attack enrolled in the REGARDS study.
Disclosures: Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
Set of Symptoms Identified to Flag Stroke Risk
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
LOS ANGELES – Several strokelike symptoms worked as strong risk factors for future strokes in patients with no history of strokes or transient ischemic attacks in a prospective study of more than 24,000 Americans.
"A history of strokelike symptoms appears to be a powerful risk factor for future stroke," Dr. Dawn O. Kleindorfer said at the International Stroke Conference. "Having any strokelike symptom was as predictive for future stroke as diabetes or atrial fibrillation. Having four or more strokelike symptoms is higher risk than any other risk factor."
Although these findings need confirmation and additional study, she envisioned eventually using these findings to create a new risk-factor screen for the general adult population.
People without a known history of stroke who have strokelike symptoms "are a group that hasn’t been well described before. They are at increased risk for stroke, but [today] they don’t get any kind of diagnosis. If we could design a way to ask questions that would predict the stroke risk in these patients, find them, and get them to medical care, we may help people at high stroke risk," said Dr. Kleindorfer, director of the division of vascular neurology at the University of Cincinnati. "This is not something to use yet; it needs more development. But eventually this could be part of general health assessment," she said in an interview.
Prior findings by Dr. Kleindorfer and her associates showed that 18% of Americans from the general public who had no known history of stroke or transient ischemic attack had at least one strokelike symptom either currently or in the past.
If the stroke-symptom questions undergo further validation, "we would have a way to be aggressive [in screening], like screening blood pressure. But this is even more powerful. It could be used at anything from public health fairs to assessing high-risk populations," commented Dr. Pooja Khatri, a neurologist and stroke specialist at the University of Cincinnati who has not been involved in this research.
The six questions ask about the sudden onset of painless hemibody weakness, painless hemibody numbness, difficulty understanding, difficulty speaking, loss of vision in one or both eyes, and loss of hemifield vision. These six questions derived from the Questionnaire for Verifying Stroke-Free Status (Stroke 2000;31:1076-80), Dr. Kleindorfer said in an interview.
The new study involved participants from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, which enrolled more than 30,000 white and African American U.S. residents, aged 45 years or older, during 2003-2007. The new analysis included 24,412 REGARDS enrollees, and excluded those who reported a history of stroke or transient ischemic attack. The researchers followed the study group for a median of 4.4 years, during which time this group had 381 incident strokes.
In an analysis that adjusted for the standard elements of the Framingham Stroke Risk Score, the researchers identified three strokelike symptoms significantly linked with an increased risk for incident stroke: Difficulty speaking, difficulty understanding, and numbness (see chart). These three symptoms each contributed approximately 2%, 2%, and 1%, respectively, of total stroke risk, making them at least as important to risk as diabetes and atrial fibrillation, which each contributed approximately 1% of total risk.
Each of the other three strokelike symptoms – weakness, half vision, and total vision impairment – did not individually have a statistically significant link to stroke incidence. However, collectively having a single strokelike symptom of any type increased a person’s relative risk for stroke by 36%, and represented more than 1% of total stroke risk. Among people with more than one strokelike symptom, each additional symptom increased stroke risk by a relative, statistically significant 21%, and overall multiple symptoms constituted nearly 3% of all stroke risk. These numbers meant that if a person had four strokelike symptoms, their relative risk of an incident stroke during 4.4 years of follow-up more than doubled, Dr. Kleindorfer said.
She noted her surprise that weakness was not a significant risk factor for later stroke. "I would have expected weakness to be the best predictor [of risk], but perhaps the people who suddenly couldn’t walk sought care and were diagnosed with stroke and were therefore excluded from the study," she said.
Dr. Kleindorfer also cautioned that the strokelike symptoms she studied could have resulted from causes other than a previously unrecognized stroke, such as seizure, syncope, migraine, psychiatric disease, ocular disease, low back pain, and dementia.
Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.
FROM THE INTERNATIONAL STROKE CONFERENCE
Major Finding: People without a known history of stroke or transient ischemic attack had a 36% relatively increased risk for a future stroke if they had a strokelike symptom.
Data Source: Review of prospectively collected data on 24,412 American people without a history of stroke or transient ischemic attack enrolled in the REGARDS study.
Disclosures: Dr. Kleindorfer said that she has been a consultant to Genentech and Boehringer Ingelheim. Dr. Khatri said that she had no disclosures.