User login
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
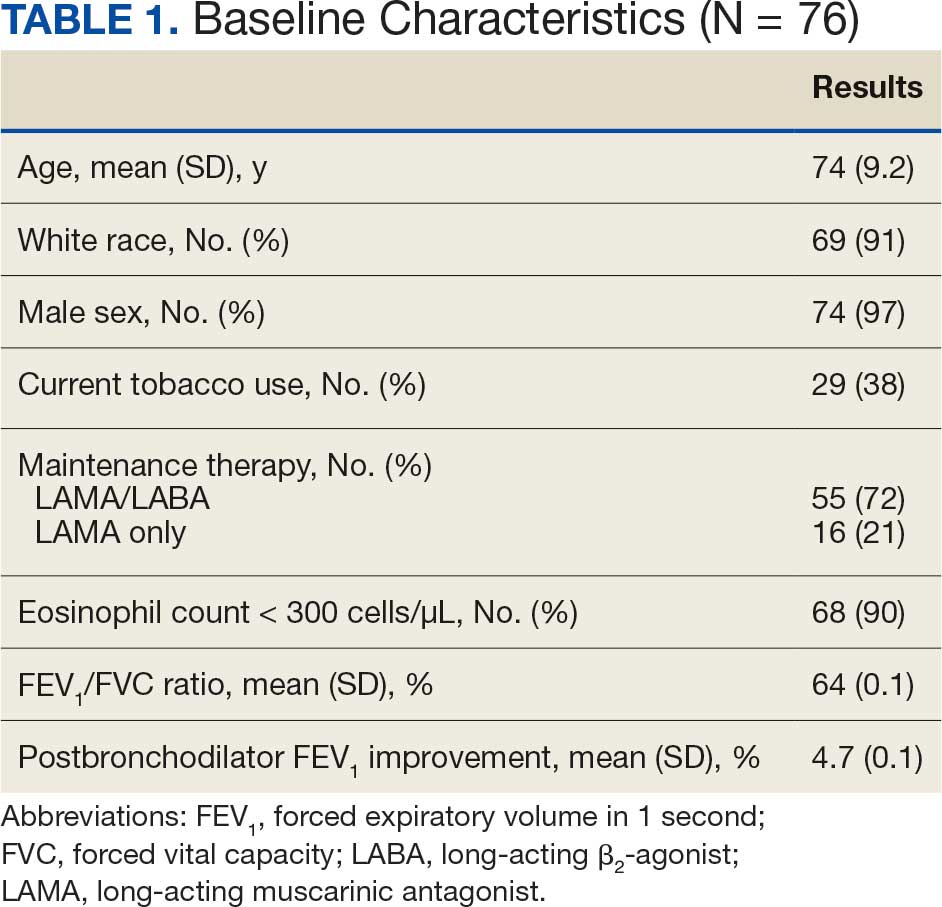
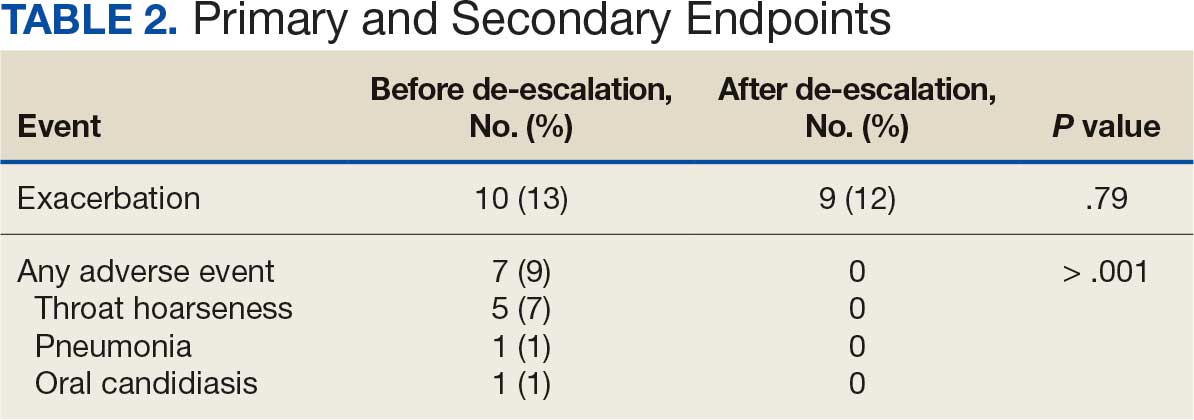
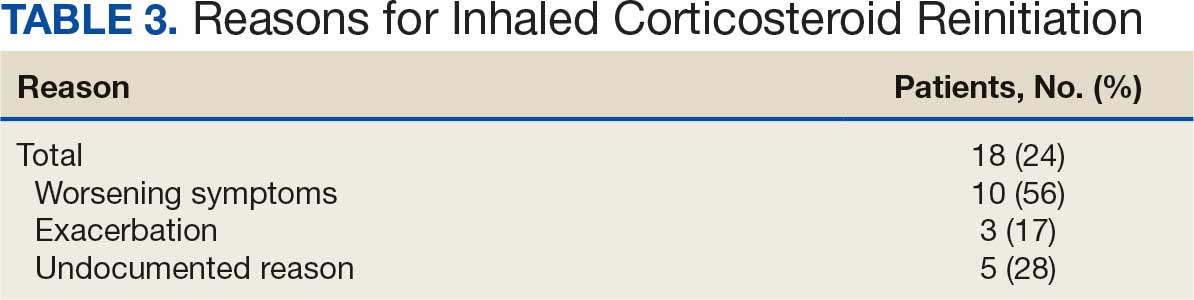
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events