User login
Few states meet palliative care benchmark
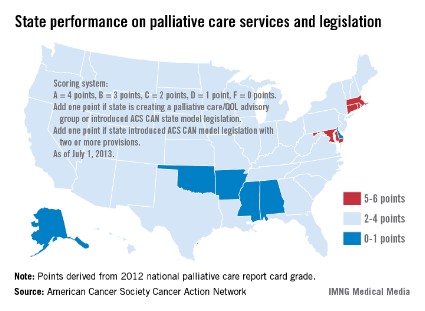
Only four states have effective strategies in place to improve access to and knowledge of palliative care services, the American Cancer Society Cancer Action Network reported.
The ACS CAN awarded top scores (5-6 points) to Connecticut, Maryland, Massachusetts, and Rhode Island using a scoring system that combines grades from the Center to Advance Palliative Care’s national palliative care report card with actions on model legislation.
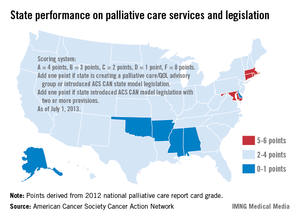
The four states passed laws "this session that focus on improving patient quality of life through palliative care," the ACS CAN noted, with Maryland finally crossing "the finish line with a palliative care bill after a 3-year effort."
The six states on the low end of the scoring range (0-1 points) were Alabama, Alaska, Arkansas, Delaware, Mississippi, and Oklahoma, the ACS CAN said in its report.
Palliative care is 1 of 10 legislative priority areas – including comprehensive smoke-free laws, tobacco taxes, restrictions on tanning bed use by minors, improved access to Medicaid, balanced pain policies, and time requirements for physical education in schools – measured by the ACS CAN. The network said that 38 states have reached benchmarks in three or fewer of the 10 areas, and that no states met the benchmarks in more than six areas.
"Many state legislatures are missing opportunities to enact laws and policies that could not only generate new revenue and long-term health savings, but also save lives," the ACS CAN said in a statement.
Only four states have effective strategies in place to improve access to and knowledge of palliative care services, the American Cancer Society Cancer Action Network reported.
The ACS CAN awarded top scores (5-6 points) to Connecticut, Maryland, Massachusetts, and Rhode Island using a scoring system that combines grades from the Center to Advance Palliative Care’s national palliative care report card with actions on model legislation.
The four states passed laws "this session that focus on improving patient quality of life through palliative care," the ACS CAN noted, with Maryland finally crossing "the finish line with a palliative care bill after a 3-year effort."
The six states on the low end of the scoring range (0-1 points) were Alabama, Alaska, Arkansas, Delaware, Mississippi, and Oklahoma, the ACS CAN said in its report.
Palliative care is 1 of 10 legislative priority areas – including comprehensive smoke-free laws, tobacco taxes, restrictions on tanning bed use by minors, improved access to Medicaid, balanced pain policies, and time requirements for physical education in schools – measured by the ACS CAN. The network said that 38 states have reached benchmarks in three or fewer of the 10 areas, and that no states met the benchmarks in more than six areas.
"Many state legislatures are missing opportunities to enact laws and policies that could not only generate new revenue and long-term health savings, but also save lives," the ACS CAN said in a statement.
Only four states have effective strategies in place to improve access to and knowledge of palliative care services, the American Cancer Society Cancer Action Network reported.
The ACS CAN awarded top scores (5-6 points) to Connecticut, Maryland, Massachusetts, and Rhode Island using a scoring system that combines grades from the Center to Advance Palliative Care’s national palliative care report card with actions on model legislation.
The four states passed laws "this session that focus on improving patient quality of life through palliative care," the ACS CAN noted, with Maryland finally crossing "the finish line with a palliative care bill after a 3-year effort."
The six states on the low end of the scoring range (0-1 points) were Alabama, Alaska, Arkansas, Delaware, Mississippi, and Oklahoma, the ACS CAN said in its report.
Palliative care is 1 of 10 legislative priority areas – including comprehensive smoke-free laws, tobacco taxes, restrictions on tanning bed use by minors, improved access to Medicaid, balanced pain policies, and time requirements for physical education in schools – measured by the ACS CAN. The network said that 38 states have reached benchmarks in three or fewer of the 10 areas, and that no states met the benchmarks in more than six areas.
"Many state legislatures are missing opportunities to enact laws and policies that could not only generate new revenue and long-term health savings, but also save lives," the ACS CAN said in a statement.
CHEST Foundation award project empowers patients and families through online palliative care resource
Designed to educate people about what palliative care is and what it offers, the website Palliative Care Services of Nebraska, www.palliativecarenebraska.com, states: "Palliative care is specialized medical care for people with serious life-limiting illnesses. Its focus lies in providing patients with relief from the symptoms, pain, and stress of illness, whatever the diagnosis. The goal is to improve quality of life for both the patient and the family."
That definition is one piece of a wealth of information available on the website, which was founded by Dr. Lisa Mansur, FCCP, recipient of The CHEST Foundation’s Roger C. Bone Advances in End-of-Life Care Award. In this instance, the term "end-of-life" care is slightly misleading because, as the website points out, "Palliative care is appropriate at any age and any stage in a serious illness and can be provided along with curative treatments." In this way it is different from its close cousin, hospice care, which is solely dedicated to comfort care when curative treatments are no longer appropriate or desired.
"The goal of the Palliative Care Services of Nebraska website is to empower people to learn and understand both the scientific and humanistic aspects of palliative care and to help them make informed decisions," she says. To that end, the site provides links to a wide array of articles, podcasts, and videos; a glossary of terms; and other resources for patients, families, caregivers, and medical professionals.
"Communication is a key tenet of palliative care," says Dr. Mansur. "Better communication equals better medicine." The emphasis on communication between patients, families, and doctors helps ensure that all needs – medical, emotional, spiritual, and practical – are fully met. In fact, Dr. Mansur calls what she and her colleagues practice "narrative medicine," with an emphasis on talking and listening rather than diagnosing and prescribing. That is not to say that patients do not receive treatment for their illness. If so desired, palliative care can work in concert with treatments meant to cure. But the focus is on the alleviation of symptoms, such as pain, fatigue, shortness of breath, loss of appetite, and anxiety or depression. Treatment might include medications along with things like massage and relaxation training. Palliative care focuses on the entire person, not just the illness. And it puts more choices in the patient’s hands.
A critical care specialist, Dr. Mansur recognized the need for palliative care in the critical care unit early in her career. She developed Palliative Care Services of Nebraska in 2010 in concert with Bryan Medical Center, where she is Director of Palliative Care, first as a hospital service with only one or two consultations a week. Since then the program has grown to accommodate up to 65 patients a week and includes an outpatient clinic, a staff of four advanced-practice nurses, and in-home visits for people who are too ill to come to the clinic. With her award from The CHEST Foundation, Dr. Mansur was able to greatly expand the website, which was launched in 2012.
The Roger C. Bone award supports leadership in end-of-life care that stresses the importance of communication, compassion, and effective listening. The award honors the late Roger C. Bone, MD, Master FCCP, who wrote about ethical and humanistic issues surrounding end-of-life decisions and stressed the importance of communication between physicians and patients. For more information about The CHEST Foundation grants and awards program, contact Lee Ann Fulton at lfulton@chestnet.org.
Designed to educate people about what palliative care is and what it offers, the website Palliative Care Services of Nebraska, www.palliativecarenebraska.com, states: "Palliative care is specialized medical care for people with serious life-limiting illnesses. Its focus lies in providing patients with relief from the symptoms, pain, and stress of illness, whatever the diagnosis. The goal is to improve quality of life for both the patient and the family."
That definition is one piece of a wealth of information available on the website, which was founded by Dr. Lisa Mansur, FCCP, recipient of The CHEST Foundation’s Roger C. Bone Advances in End-of-Life Care Award. In this instance, the term "end-of-life" care is slightly misleading because, as the website points out, "Palliative care is appropriate at any age and any stage in a serious illness and can be provided along with curative treatments." In this way it is different from its close cousin, hospice care, which is solely dedicated to comfort care when curative treatments are no longer appropriate or desired.
"The goal of the Palliative Care Services of Nebraska website is to empower people to learn and understand both the scientific and humanistic aspects of palliative care and to help them make informed decisions," she says. To that end, the site provides links to a wide array of articles, podcasts, and videos; a glossary of terms; and other resources for patients, families, caregivers, and medical professionals.
"Communication is a key tenet of palliative care," says Dr. Mansur. "Better communication equals better medicine." The emphasis on communication between patients, families, and doctors helps ensure that all needs – medical, emotional, spiritual, and practical – are fully met. In fact, Dr. Mansur calls what she and her colleagues practice "narrative medicine," with an emphasis on talking and listening rather than diagnosing and prescribing. That is not to say that patients do not receive treatment for their illness. If so desired, palliative care can work in concert with treatments meant to cure. But the focus is on the alleviation of symptoms, such as pain, fatigue, shortness of breath, loss of appetite, and anxiety or depression. Treatment might include medications along with things like massage and relaxation training. Palliative care focuses on the entire person, not just the illness. And it puts more choices in the patient’s hands.
A critical care specialist, Dr. Mansur recognized the need for palliative care in the critical care unit early in her career. She developed Palliative Care Services of Nebraska in 2010 in concert with Bryan Medical Center, where she is Director of Palliative Care, first as a hospital service with only one or two consultations a week. Since then the program has grown to accommodate up to 65 patients a week and includes an outpatient clinic, a staff of four advanced-practice nurses, and in-home visits for people who are too ill to come to the clinic. With her award from The CHEST Foundation, Dr. Mansur was able to greatly expand the website, which was launched in 2012.
The Roger C. Bone award supports leadership in end-of-life care that stresses the importance of communication, compassion, and effective listening. The award honors the late Roger C. Bone, MD, Master FCCP, who wrote about ethical and humanistic issues surrounding end-of-life decisions and stressed the importance of communication between physicians and patients. For more information about The CHEST Foundation grants and awards program, contact Lee Ann Fulton at lfulton@chestnet.org.
Designed to educate people about what palliative care is and what it offers, the website Palliative Care Services of Nebraska, www.palliativecarenebraska.com, states: "Palliative care is specialized medical care for people with serious life-limiting illnesses. Its focus lies in providing patients with relief from the symptoms, pain, and stress of illness, whatever the diagnosis. The goal is to improve quality of life for both the patient and the family."
That definition is one piece of a wealth of information available on the website, which was founded by Dr. Lisa Mansur, FCCP, recipient of The CHEST Foundation’s Roger C. Bone Advances in End-of-Life Care Award. In this instance, the term "end-of-life" care is slightly misleading because, as the website points out, "Palliative care is appropriate at any age and any stage in a serious illness and can be provided along with curative treatments." In this way it is different from its close cousin, hospice care, which is solely dedicated to comfort care when curative treatments are no longer appropriate or desired.
"The goal of the Palliative Care Services of Nebraska website is to empower people to learn and understand both the scientific and humanistic aspects of palliative care and to help them make informed decisions," she says. To that end, the site provides links to a wide array of articles, podcasts, and videos; a glossary of terms; and other resources for patients, families, caregivers, and medical professionals.
"Communication is a key tenet of palliative care," says Dr. Mansur. "Better communication equals better medicine." The emphasis on communication between patients, families, and doctors helps ensure that all needs – medical, emotional, spiritual, and practical – are fully met. In fact, Dr. Mansur calls what she and her colleagues practice "narrative medicine," with an emphasis on talking and listening rather than diagnosing and prescribing. That is not to say that patients do not receive treatment for their illness. If so desired, palliative care can work in concert with treatments meant to cure. But the focus is on the alleviation of symptoms, such as pain, fatigue, shortness of breath, loss of appetite, and anxiety or depression. Treatment might include medications along with things like massage and relaxation training. Palliative care focuses on the entire person, not just the illness. And it puts more choices in the patient’s hands.
A critical care specialist, Dr. Mansur recognized the need for palliative care in the critical care unit early in her career. She developed Palliative Care Services of Nebraska in 2010 in concert with Bryan Medical Center, where she is Director of Palliative Care, first as a hospital service with only one or two consultations a week. Since then the program has grown to accommodate up to 65 patients a week and includes an outpatient clinic, a staff of four advanced-practice nurses, and in-home visits for people who are too ill to come to the clinic. With her award from The CHEST Foundation, Dr. Mansur was able to greatly expand the website, which was launched in 2012.
The Roger C. Bone award supports leadership in end-of-life care that stresses the importance of communication, compassion, and effective listening. The award honors the late Roger C. Bone, MD, Master FCCP, who wrote about ethical and humanistic issues surrounding end-of-life decisions and stressed the importance of communication between physicians and patients. For more information about The CHEST Foundation grants and awards program, contact Lee Ann Fulton at lfulton@chestnet.org.
Rising Medicare Spending for End-of-Life Care Brings Patients’ Wishes into Focus
A new report that shows ever-growing Medicare spending for chronically ill patients in the last two years of life can serve as a reminder for hospitalists to properly gauge patients’ wishes for end-of-life care, one of the authors says.
The brief from the Dartmouth Atlas Project [PDF] shows that from 2007 to 2010, average spending per patient in the last two years of life increased 15.2% to $69,947, and average spending in the last six months of life rose 13.4% to $36,392.
During the same three-year period, patients in their last six months of life were less likely to be hospitalized and logged more time in hospice care—21 days versus 18.3 days—reflecting the wishes of most patients to spend their last days in a homelike environment, the report notes. Accordingly, chronically ill Medicare patients were less likely to die in the hospital by the end of the study period.
David Goodman, MD, MS, co-principal investigator for Dartmouth Atlas of Health Care, says the growing use of hospice care and decreased hospitalization stays “aligns more closely with patients’ preferences.”
“The focus really needs to be on better diagnosis of patients’ preferences to reduce what has been well-documented as overutilization from the patient’s perspective,” Dr. Goodman says.
While costs and trends vary widely among regions and health-care systems, Dr. Goodman attributes the differences to local supplies of hospital beds and practice styles. For example, in regions with more beds, patients are more likely to spend time in the hospital near the end of life, he says. “There is definitely a national trend away from hospital care near the end of life,” he adds. “But that rate of change varies a lot from place to place. It’s helpful for hospitalists to understand where they fit on the spectrum.”
Visit our website for more information on end of life care.
A new report that shows ever-growing Medicare spending for chronically ill patients in the last two years of life can serve as a reminder for hospitalists to properly gauge patients’ wishes for end-of-life care, one of the authors says.
The brief from the Dartmouth Atlas Project [PDF] shows that from 2007 to 2010, average spending per patient in the last two years of life increased 15.2% to $69,947, and average spending in the last six months of life rose 13.4% to $36,392.
During the same three-year period, patients in their last six months of life were less likely to be hospitalized and logged more time in hospice care—21 days versus 18.3 days—reflecting the wishes of most patients to spend their last days in a homelike environment, the report notes. Accordingly, chronically ill Medicare patients were less likely to die in the hospital by the end of the study period.
David Goodman, MD, MS, co-principal investigator for Dartmouth Atlas of Health Care, says the growing use of hospice care and decreased hospitalization stays “aligns more closely with patients’ preferences.”
“The focus really needs to be on better diagnosis of patients’ preferences to reduce what has been well-documented as overutilization from the patient’s perspective,” Dr. Goodman says.
While costs and trends vary widely among regions and health-care systems, Dr. Goodman attributes the differences to local supplies of hospital beds and practice styles. For example, in regions with more beds, patients are more likely to spend time in the hospital near the end of life, he says. “There is definitely a national trend away from hospital care near the end of life,” he adds. “But that rate of change varies a lot from place to place. It’s helpful for hospitalists to understand where they fit on the spectrum.”
Visit our website for more information on end of life care.
A new report that shows ever-growing Medicare spending for chronically ill patients in the last two years of life can serve as a reminder for hospitalists to properly gauge patients’ wishes for end-of-life care, one of the authors says.
The brief from the Dartmouth Atlas Project [PDF] shows that from 2007 to 2010, average spending per patient in the last two years of life increased 15.2% to $69,947, and average spending in the last six months of life rose 13.4% to $36,392.
During the same three-year period, patients in their last six months of life were less likely to be hospitalized and logged more time in hospice care—21 days versus 18.3 days—reflecting the wishes of most patients to spend their last days in a homelike environment, the report notes. Accordingly, chronically ill Medicare patients were less likely to die in the hospital by the end of the study period.
David Goodman, MD, MS, co-principal investigator for Dartmouth Atlas of Health Care, says the growing use of hospice care and decreased hospitalization stays “aligns more closely with patients’ preferences.”
“The focus really needs to be on better diagnosis of patients’ preferences to reduce what has been well-documented as overutilization from the patient’s perspective,” Dr. Goodman says.
While costs and trends vary widely among regions and health-care systems, Dr. Goodman attributes the differences to local supplies of hospital beds and practice styles. For example, in regions with more beds, patients are more likely to spend time in the hospital near the end of life, he says. “There is definitely a national trend away from hospital care near the end of life,” he adds. “But that rate of change varies a lot from place to place. It’s helpful for hospitalists to understand where they fit on the spectrum.”
Visit our website for more information on end of life care.
Tigger and end-of-life talk
My wife texted, "Tigger is having problems. Call me."
Tigger is our beloved (and bouncy) 9½-year-old boxer. My wife had just finished putting our 16-month-old son down for his nap when she heard a commotion in the foyer. She looked downstairs and saw Tigger struggling to get up. She ran down the steps and sat down beside him. It was clear that his hind legs were not working. Wide-eyed, he looked terrified to her. As she stroked his back, he eventually settled down and rested for several minutes. After about 10 minutes, he was able to get up and slowly walk around the house.
I came home from work, followed shortly thereafter by one of our friends and two of his young boys. While my wife and I had drinks and pizza with our friend, and the boys and our daughter played in the yard. Tigger, normally in the center of the action, lay off to the side of the patio. When I brought out a bowl of food for him, he did not budge. This was a first – he has never passed up a meal. Instead, he usually looks to supplement his food with anything he can steal from unsuspecting members of our family.
That evening, my wife and I had a long conversation about Tigger. We were going to take him to the vet and have him evaluated, but we were very realistic about what we might find. On average, boxers live just shy of 10 years. We’ve noticed that he had been slowing down, and the events of that evening – keeping to himself and passing up dinner – made us concerned that the end was close. We agreed that our primary goal is to keep him comfortable. He is a valued member of our family, and we do not want him to suffer.
Thankfully, Tigger rebounded from that initial episode, although he had a similar episode in the weeks that followed. We know the end is coming for him and we are working to maximize our time with him. We are retelling stories from his younger days and enjoying some of his behavioral quirks (read: stealing food) more than we had in the past. Again, our focus remains on his comfort. When he appears to be struggling too much – when his pain and discomfort exceeds – we will make that difficult decision that most every pet owner has to eventually make.
These discussions made me think of the patients I have cared for over the years who were never encouraged to think in such terms about their own lives. Many were being treated for underlying malignancies, yet had no conversations with their physicians about goals of care or end-of-life decisions.
I have written in the past about the need for these discussions and how we, as physicians, often die differently from our patients. Allow this to be a reminder to everyone to discuss goals of care with your patients. The conversations are an important investment in your relationship with that patient and are vital to providing the best possible care for them.
Dr. Pistoria is chief of hospital medicine at Coordinated Health in Bethlehem, Pa., and an adviser to Hospitalist News. He believes that the best care is always personal.
My wife texted, "Tigger is having problems. Call me."
Tigger is our beloved (and bouncy) 9½-year-old boxer. My wife had just finished putting our 16-month-old son down for his nap when she heard a commotion in the foyer. She looked downstairs and saw Tigger struggling to get up. She ran down the steps and sat down beside him. It was clear that his hind legs were not working. Wide-eyed, he looked terrified to her. As she stroked his back, he eventually settled down and rested for several minutes. After about 10 minutes, he was able to get up and slowly walk around the house.
I came home from work, followed shortly thereafter by one of our friends and two of his young boys. While my wife and I had drinks and pizza with our friend, and the boys and our daughter played in the yard. Tigger, normally in the center of the action, lay off to the side of the patio. When I brought out a bowl of food for him, he did not budge. This was a first – he has never passed up a meal. Instead, he usually looks to supplement his food with anything he can steal from unsuspecting members of our family.
That evening, my wife and I had a long conversation about Tigger. We were going to take him to the vet and have him evaluated, but we were very realistic about what we might find. On average, boxers live just shy of 10 years. We’ve noticed that he had been slowing down, and the events of that evening – keeping to himself and passing up dinner – made us concerned that the end was close. We agreed that our primary goal is to keep him comfortable. He is a valued member of our family, and we do not want him to suffer.
Thankfully, Tigger rebounded from that initial episode, although he had a similar episode in the weeks that followed. We know the end is coming for him and we are working to maximize our time with him. We are retelling stories from his younger days and enjoying some of his behavioral quirks (read: stealing food) more than we had in the past. Again, our focus remains on his comfort. When he appears to be struggling too much – when his pain and discomfort exceeds – we will make that difficult decision that most every pet owner has to eventually make.
These discussions made me think of the patients I have cared for over the years who were never encouraged to think in such terms about their own lives. Many were being treated for underlying malignancies, yet had no conversations with their physicians about goals of care or end-of-life decisions.
I have written in the past about the need for these discussions and how we, as physicians, often die differently from our patients. Allow this to be a reminder to everyone to discuss goals of care with your patients. The conversations are an important investment in your relationship with that patient and are vital to providing the best possible care for them.
Dr. Pistoria is chief of hospital medicine at Coordinated Health in Bethlehem, Pa., and an adviser to Hospitalist News. He believes that the best care is always personal.
My wife texted, "Tigger is having problems. Call me."
Tigger is our beloved (and bouncy) 9½-year-old boxer. My wife had just finished putting our 16-month-old son down for his nap when she heard a commotion in the foyer. She looked downstairs and saw Tigger struggling to get up. She ran down the steps and sat down beside him. It was clear that his hind legs were not working. Wide-eyed, he looked terrified to her. As she stroked his back, he eventually settled down and rested for several minutes. After about 10 minutes, he was able to get up and slowly walk around the house.
I came home from work, followed shortly thereafter by one of our friends and two of his young boys. While my wife and I had drinks and pizza with our friend, and the boys and our daughter played in the yard. Tigger, normally in the center of the action, lay off to the side of the patio. When I brought out a bowl of food for him, he did not budge. This was a first – he has never passed up a meal. Instead, he usually looks to supplement his food with anything he can steal from unsuspecting members of our family.
That evening, my wife and I had a long conversation about Tigger. We were going to take him to the vet and have him evaluated, but we were very realistic about what we might find. On average, boxers live just shy of 10 years. We’ve noticed that he had been slowing down, and the events of that evening – keeping to himself and passing up dinner – made us concerned that the end was close. We agreed that our primary goal is to keep him comfortable. He is a valued member of our family, and we do not want him to suffer.
Thankfully, Tigger rebounded from that initial episode, although he had a similar episode in the weeks that followed. We know the end is coming for him and we are working to maximize our time with him. We are retelling stories from his younger days and enjoying some of his behavioral quirks (read: stealing food) more than we had in the past. Again, our focus remains on his comfort. When he appears to be struggling too much – when his pain and discomfort exceeds – we will make that difficult decision that most every pet owner has to eventually make.
These discussions made me think of the patients I have cared for over the years who were never encouraged to think in such terms about their own lives. Many were being treated for underlying malignancies, yet had no conversations with their physicians about goals of care or end-of-life decisions.
I have written in the past about the need for these discussions and how we, as physicians, often die differently from our patients. Allow this to be a reminder to everyone to discuss goals of care with your patients. The conversations are an important investment in your relationship with that patient and are vital to providing the best possible care for them.
Dr. Pistoria is chief of hospital medicine at Coordinated Health in Bethlehem, Pa., and an adviser to Hospitalist News. He believes that the best care is always personal.

More hospitals providing palliative care
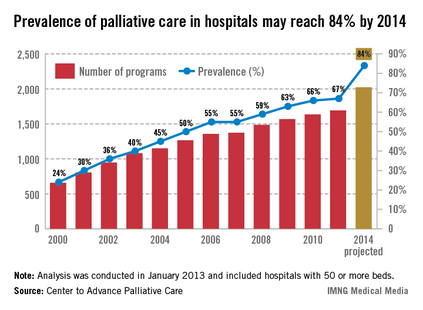
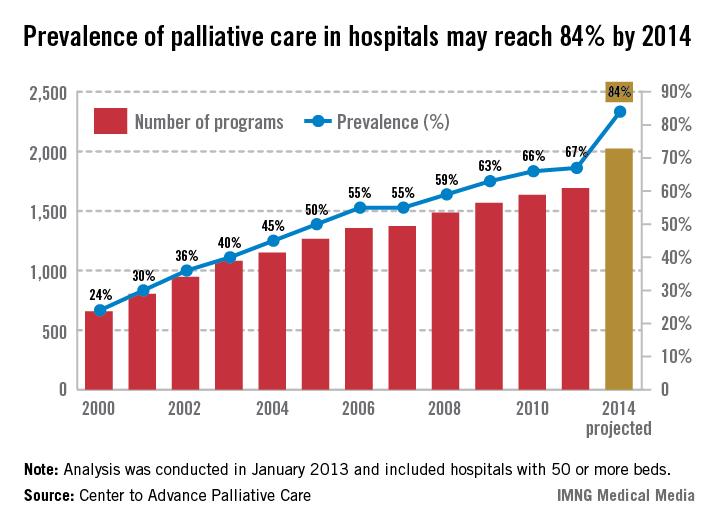
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
Palliative care training and associations with burnout in oncology fellows
ABSTRACT
Background Burnout among physicians can lead to decreased career satisfaction, physical and emotional exhaustion, and increased medical errors. In oncologists, high exposure to fatal illness is associated with burnout.
Methods The Maslach Burnout Inventory, measuring Emotional Exhaustion (EE), Depersonalization (DP), and Personal Accomplishment (PA), was administered to second-year US oncology fellows. Bivariate and multivariate analyses explored associations between burnout and fellow demographics, attitudes, and educational experiences.
Results A total of 254 fellows out of 402 eligible US fellows responded (63.2%) and 24.2% reported high EE, 30.0% reported high DP, and 26.8% reported low PA. Over half of the fellows reported burnout in at least one domain. Lower EE scores were associated with the fellows’ perceptions of having received better teaching, explicit teaching about certain end-of-life topics, and receipt of direct observation of goals-of-care discussions. Fellows who reported better overall teaching quality and more frequent observation of their skills had less depersonalization. Fellows who felt a responsibility to help patients at the end of life to prepare for death had higher PA.
Limitations This survey relies on the fellows’ self-reported perceptions without an objective measure for validation. Factors associated with burnout may not be causal. The number of analyses performed raises the concern for Type I errors; therefore, a stringent P value (.01) was used.
Conclusions Burnout is prevalent during oncology training. Higher-quality teaching is associated with less burnout among fellows. Fellowship programs should recognize the prevalence of burnout among oncology fellows as well as components of training that may protect against burnout.
*For a PDF of the full article, click on the link to the left of this introduction.
Life, Communication
ABSTRACT
Background Burnout among physicians can lead to decreased career satisfaction, physical and emotional exhaustion, and increased medical errors. In oncologists, high exposure to fatal illness is associated with burnout.
Methods The Maslach Burnout Inventory, measuring Emotional Exhaustion (EE), Depersonalization (DP), and Personal Accomplishment (PA), was administered to second-year US oncology fellows. Bivariate and multivariate analyses explored associations between burnout and fellow demographics, attitudes, and educational experiences.
Results A total of 254 fellows out of 402 eligible US fellows responded (63.2%) and 24.2% reported high EE, 30.0% reported high DP, and 26.8% reported low PA. Over half of the fellows reported burnout in at least one domain. Lower EE scores were associated with the fellows’ perceptions of having received better teaching, explicit teaching about certain end-of-life topics, and receipt of direct observation of goals-of-care discussions. Fellows who reported better overall teaching quality and more frequent observation of their skills had less depersonalization. Fellows who felt a responsibility to help patients at the end of life to prepare for death had higher PA.
Limitations This survey relies on the fellows’ self-reported perceptions without an objective measure for validation. Factors associated with burnout may not be causal. The number of analyses performed raises the concern for Type I errors; therefore, a stringent P value (.01) was used.
Conclusions Burnout is prevalent during oncology training. Higher-quality teaching is associated with less burnout among fellows. Fellowship programs should recognize the prevalence of burnout among oncology fellows as well as components of training that may protect against burnout.
*For a PDF of the full article, click on the link to the left of this introduction.
ABSTRACT
Background Burnout among physicians can lead to decreased career satisfaction, physical and emotional exhaustion, and increased medical errors. In oncologists, high exposure to fatal illness is associated with burnout.
Methods The Maslach Burnout Inventory, measuring Emotional Exhaustion (EE), Depersonalization (DP), and Personal Accomplishment (PA), was administered to second-year US oncology fellows. Bivariate and multivariate analyses explored associations between burnout and fellow demographics, attitudes, and educational experiences.
Results A total of 254 fellows out of 402 eligible US fellows responded (63.2%) and 24.2% reported high EE, 30.0% reported high DP, and 26.8% reported low PA. Over half of the fellows reported burnout in at least one domain. Lower EE scores were associated with the fellows’ perceptions of having received better teaching, explicit teaching about certain end-of-life topics, and receipt of direct observation of goals-of-care discussions. Fellows who reported better overall teaching quality and more frequent observation of their skills had less depersonalization. Fellows who felt a responsibility to help patients at the end of life to prepare for death had higher PA.
Limitations This survey relies on the fellows’ self-reported perceptions without an objective measure for validation. Factors associated with burnout may not be causal. The number of analyses performed raises the concern for Type I errors; therefore, a stringent P value (.01) was used.
Conclusions Burnout is prevalent during oncology training. Higher-quality teaching is associated with less burnout among fellows. Fellowship programs should recognize the prevalence of burnout among oncology fellows as well as components of training that may protect against burnout.
*For a PDF of the full article, click on the link to the left of this introduction.
Life, Communication
Life, Communication
Checking up on advance care planning - and charting, too
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Earlier today our team was consulted to see an 85-year-old gentleman. A request was made that we conduct a family meeting to elicit the goals of care.
The patient had several underlying illnesses including diastolic heart failure, chronic renal insufficiency, and COPD. He was admitted after experiencing a complication from an outpatient procedure aimed at alleviating his chronic low back pain. After paging through his chart, it was clear that he suffered multiple setbacks throughout his admission, and that over the last 12 hours he was rapidly decompensating from hospital-acquired pneumonia and subsequent sepsis.
Though I was quite certain that his family had been approached about treatment goals, there was no documentation of this in the chart or reflection of these goals in the care plan. This was hospital day No. 32.
Two decades are behind us after being confronted with the impressive discord between what patients with advanced illnesses desire for themselves, what we think they want, and the actual care we deliver to them(JAMA 1995;274(20):1591-98). Where are we today when it comes to having dialogue with patients and families about advance care planning (ACP) or code status and our documentation of these critical decisions?
Recently, a study from 12 hospitals spanning Canada set out to see how often seriously ill elderly patients in the hospital were engaged in ACP (JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]). The mean age of the patients was 80 years, and they all had advanced illnesses that were not expected to be curable. Over 75% of the almost 300 patients enrolled reflected on end-of-life preferences prior to hospitalization, and only 12% were interested in life-prolonging care versus care that focused on quality of life. While in the prehospital period patients are completing advance directives (AD) and identifying a surrogate (48% and 73% respectively), the disconnect comes when looking at whether the documentation in the medical record is in agreement with patient preferences. It is not. The medical record accurately reflects the patient choice only 30% of the time. This led the invited commentary to declare that this disregard be classified as a medical error(JAMA Intern. Med. 2013 April 1 [doi: 10.1001/jamainternmed.2013.203]).
Are we the barriers to seeing ACP take place and properly chart the results?
Clearly that is part of the problem (the patient side of this equation will be explored in a future piece). In 2010, a group of hospitalists were audio-recorded during their initial encounter with a newly admitted patient (J. Gen. Intern. Med. 2011 26(4):359-66). During a total of 80 encounters, ACP was brought up less than 20% of the time. When it was addressed, the median length of a code status discussion was 1 minute. Prognosis was mentioned in only one encounter. No physician made a quantitative estimate of prognosis, nor did anyone make recommendations on whether or not CPR was medically appropriate.
Here is a sample from the recording with a hospitalist discussing code status with a patient diagnosed with cholangiocarcinoma:
Physician: "... If for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?"
Patient: "Yes."
Physician: "Yes. Okay. Okay. I think that’s all my questions."
How does the lack of ACP and documentation impact the hospitalist in 2013? Two big-ticket items come to mind: HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and 30-day readmissions. Both of these will be explored in the next column, along with what we can do to make both immediate and long-term positive impacts on ACP.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Health Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.

Timely palliative consult affects end-of-life care in gynecologic cancer patients
LOS ANGELES – A palliative care consultation within the last month of life improves a variety of end-of-life outcomes in patients dying from gynecologic cancers, based on a retrospective analysis.
Among the 100 patients studied, about one-fourth had a timely palliative care consultation, defined in one study as 14 days before death and in another study as 30 days before death, lead investigator Dr. Nicole S. Nevadunsky of Montefiore Medical Center, New York, reported at the annual meeting of the Society of Gynecologic Oncology.

Compared with their counterparts who had late or no consultations, patients who had timely consultations had lower scores for aggressive end-of-life events such as emergency department visits, chemotherapy, and death in an acute care setting.
In addition, in their last 14 days of life, this group had median direct inpatient hospital costs that were $5,106 less, and they were half as likely to be admitted.
"Our data suggest that early palliative medicine consultation results in decreased aggressive measures at the end of life [and] was associated with decreased direct inpatient costs for women who died from gynecologic malignancies," Dr. Nevadunsky noted. "Further research is needed to evaluate the quality of life in relation to [the aggressiveness of care] for patients and their families."
While it is unclear how many gynecologic oncologists are also board certified in palliative care, "I think more clinicians actually do palliative medicine as part of their everyday practice," Dr. Nevadunsky said. Also, palliative care is truly a multidisciplinary undertaking involving, for example, nurses, pastoral care personnel, social workers, and others.
"As far as the best metric for palliative medicine, I think it is quality of life. But how to define that is extremely complicated and still evolving," she added.
"I think it’s an experience where the patient is getting what they want most out of things, and sometimes that’s saying to the patient, ‘If we can’t cure you, what is the most important thing to you?’ " she replied. "Each patient is different, and that’s what makes (defining quality of life) so complicated."
The American Society of Clinical Oncology recommends consideration of palliative care early in the course of metastatic or symptomatic disease.
"This is a very vague recommendation: who, what, when, where, how? How will patients respond to this? Who’s going to pay for this? What’s the patient going to get out of this?" Dr. Nevadunsky commented.
She and her colleagues studied 100 consecutive patients who died from gynecologic cancer between 2006 and 2009 and received care at Montefiore in the year before death.
In the first study, they defined a timely palliative care consultation as one occurring more than 30 days before death.
"The ideal timing for palliative medicine consultation is unknown; however, 30 days was chosen as the minimal exposure time because the standard metrics utilized to compare aggressive measures at the end of life included a minimum of 30 days," Dr. Nevadunsky explained.
"Overall, I was surprised to find that 49 of the 100 women actually had a palliative medicine consultation at some time or another during their care," she said.
However, the median number of days between consultation and death was 16, and only 18% of patients had a timely consultation.
Late diagnosis did not explain this finding, as less than 10% of patients received their diagnosis in the month before they died.
"The scope of this study was not inclusive to determine why this [late palliative care consultation] was happening," Dr. Nevadunsky said. Data showed that although the two groups were demographically similar, the patients who received a timely consultation were more likely to be married.
The group with timely consultations were less likely to receive aggressive end-of-life care, based on measures of eight indicators of aggressive care (0 vs. 2, P = .025).
The difference between those patients who had timely consultation and those with untimely or no consultation was greatest for the indicators of a hospital stay lasting more than 14 days in the last month of life (22% vs. 40%) and death in the acute care setting (28% vs. 45%).
In the second study, the investigators found that 29% of patients had a timely palliative care consultation, defined in this case as one occurring 14 days or more before death.
Patients with a timely consultation had lower median direct hospital inpatient costs per day in the last 30 days of life ($613 vs. $702, P = .02). They also had lower median direct hospital inpatient costs in the last 14 days overall ($0 vs. $5,106, P = .007) and on a per-day basis ($0 vs. $676, P = .007).
"The patients who had the timely consultations actually weren’t admitted to the hospital as often," Dr. Nevadunsky noted. In fact, they were half as likely to be admitted in the last 14 days (35% vs. 71%, P = .001).
"Shortcomings [of the study] include small numbers and the retrospective collection of data. Also, our study did not account for outpatient costs, including those assumed by families, or for those costs incurred by loss of time out of work by families to care for the patient," acknowledged Dr. Nevadunsky, who disclosed no relevant conflicts of interest.
LOS ANGELES – A palliative care consultation within the last month of life improves a variety of end-of-life outcomes in patients dying from gynecologic cancers, based on a retrospective analysis.
Among the 100 patients studied, about one-fourth had a timely palliative care consultation, defined in one study as 14 days before death and in another study as 30 days before death, lead investigator Dr. Nicole S. Nevadunsky of Montefiore Medical Center, New York, reported at the annual meeting of the Society of Gynecologic Oncology.
Compared with their counterparts who had late or no consultations, patients who had timely consultations had lower scores for aggressive end-of-life events such as emergency department visits, chemotherapy, and death in an acute care setting.
In addition, in their last 14 days of life, this group had median direct inpatient hospital costs that were $5,106 less, and they were half as likely to be admitted.
"Our data suggest that early palliative medicine consultation results in decreased aggressive measures at the end of life [and] was associated with decreased direct inpatient costs for women who died from gynecologic malignancies," Dr. Nevadunsky noted. "Further research is needed to evaluate the quality of life in relation to [the aggressiveness of care] for patients and their families."
While it is unclear how many gynecologic oncologists are also board certified in palliative care, "I think more clinicians actually do palliative medicine as part of their everyday practice," Dr. Nevadunsky said. Also, palliative care is truly a multidisciplinary undertaking involving, for example, nurses, pastoral care personnel, social workers, and others.
"As far as the best metric for palliative medicine, I think it is quality of life. But how to define that is extremely complicated and still evolving," she added.
"I think it’s an experience where the patient is getting what they want most out of things, and sometimes that’s saying to the patient, ‘If we can’t cure you, what is the most important thing to you?’ " she replied. "Each patient is different, and that’s what makes (defining quality of life) so complicated."
The American Society of Clinical Oncology recommends consideration of palliative care early in the course of metastatic or symptomatic disease.
"This is a very vague recommendation: who, what, when, where, how? How will patients respond to this? Who’s going to pay for this? What’s the patient going to get out of this?" Dr. Nevadunsky commented.
She and her colleagues studied 100 consecutive patients who died from gynecologic cancer between 2006 and 2009 and received care at Montefiore in the year before death.
In the first study, they defined a timely palliative care consultation as one occurring more than 30 days before death.
"The ideal timing for palliative medicine consultation is unknown; however, 30 days was chosen as the minimal exposure time because the standard metrics utilized to compare aggressive measures at the end of life included a minimum of 30 days," Dr. Nevadunsky explained.
"Overall, I was surprised to find that 49 of the 100 women actually had a palliative medicine consultation at some time or another during their care," she said.
However, the median number of days between consultation and death was 16, and only 18% of patients had a timely consultation.
Late diagnosis did not explain this finding, as less than 10% of patients received their diagnosis in the month before they died.
"The scope of this study was not inclusive to determine why this [late palliative care consultation] was happening," Dr. Nevadunsky said. Data showed that although the two groups were demographically similar, the patients who received a timely consultation were more likely to be married.
The group with timely consultations were less likely to receive aggressive end-of-life care, based on measures of eight indicators of aggressive care (0 vs. 2, P = .025).
The difference between those patients who had timely consultation and those with untimely or no consultation was greatest for the indicators of a hospital stay lasting more than 14 days in the last month of life (22% vs. 40%) and death in the acute care setting (28% vs. 45%).
In the second study, the investigators found that 29% of patients had a timely palliative care consultation, defined in this case as one occurring 14 days or more before death.
Patients with a timely consultation had lower median direct hospital inpatient costs per day in the last 30 days of life ($613 vs. $702, P = .02). They also had lower median direct hospital inpatient costs in the last 14 days overall ($0 vs. $5,106, P = .007) and on a per-day basis ($0 vs. $676, P = .007).
"The patients who had the timely consultations actually weren’t admitted to the hospital as often," Dr. Nevadunsky noted. In fact, they were half as likely to be admitted in the last 14 days (35% vs. 71%, P = .001).
"Shortcomings [of the study] include small numbers and the retrospective collection of data. Also, our study did not account for outpatient costs, including those assumed by families, or for those costs incurred by loss of time out of work by families to care for the patient," acknowledged Dr. Nevadunsky, who disclosed no relevant conflicts of interest.
LOS ANGELES – A palliative care consultation within the last month of life improves a variety of end-of-life outcomes in patients dying from gynecologic cancers, based on a retrospective analysis.
Among the 100 patients studied, about one-fourth had a timely palliative care consultation, defined in one study as 14 days before death and in another study as 30 days before death, lead investigator Dr. Nicole S. Nevadunsky of Montefiore Medical Center, New York, reported at the annual meeting of the Society of Gynecologic Oncology.
Compared with their counterparts who had late or no consultations, patients who had timely consultations had lower scores for aggressive end-of-life events such as emergency department visits, chemotherapy, and death in an acute care setting.
In addition, in their last 14 days of life, this group had median direct inpatient hospital costs that were $5,106 less, and they were half as likely to be admitted.
"Our data suggest that early palliative medicine consultation results in decreased aggressive measures at the end of life [and] was associated with decreased direct inpatient costs for women who died from gynecologic malignancies," Dr. Nevadunsky noted. "Further research is needed to evaluate the quality of life in relation to [the aggressiveness of care] for patients and their families."
While it is unclear how many gynecologic oncologists are also board certified in palliative care, "I think more clinicians actually do palliative medicine as part of their everyday practice," Dr. Nevadunsky said. Also, palliative care is truly a multidisciplinary undertaking involving, for example, nurses, pastoral care personnel, social workers, and others.
"As far as the best metric for palliative medicine, I think it is quality of life. But how to define that is extremely complicated and still evolving," she added.
"I think it’s an experience where the patient is getting what they want most out of things, and sometimes that’s saying to the patient, ‘If we can’t cure you, what is the most important thing to you?’ " she replied. "Each patient is different, and that’s what makes (defining quality of life) so complicated."
The American Society of Clinical Oncology recommends consideration of palliative care early in the course of metastatic or symptomatic disease.
"This is a very vague recommendation: who, what, when, where, how? How will patients respond to this? Who’s going to pay for this? What’s the patient going to get out of this?" Dr. Nevadunsky commented.
She and her colleagues studied 100 consecutive patients who died from gynecologic cancer between 2006 and 2009 and received care at Montefiore in the year before death.
In the first study, they defined a timely palliative care consultation as one occurring more than 30 days before death.
"The ideal timing for palliative medicine consultation is unknown; however, 30 days was chosen as the minimal exposure time because the standard metrics utilized to compare aggressive measures at the end of life included a minimum of 30 days," Dr. Nevadunsky explained.
"Overall, I was surprised to find that 49 of the 100 women actually had a palliative medicine consultation at some time or another during their care," she said.
However, the median number of days between consultation and death was 16, and only 18% of patients had a timely consultation.
Late diagnosis did not explain this finding, as less than 10% of patients received their diagnosis in the month before they died.
"The scope of this study was not inclusive to determine why this [late palliative care consultation] was happening," Dr. Nevadunsky said. Data showed that although the two groups were demographically similar, the patients who received a timely consultation were more likely to be married.
The group with timely consultations were less likely to receive aggressive end-of-life care, based on measures of eight indicators of aggressive care (0 vs. 2, P = .025).
The difference between those patients who had timely consultation and those with untimely or no consultation was greatest for the indicators of a hospital stay lasting more than 14 days in the last month of life (22% vs. 40%) and death in the acute care setting (28% vs. 45%).
In the second study, the investigators found that 29% of patients had a timely palliative care consultation, defined in this case as one occurring 14 days or more before death.
Patients with a timely consultation had lower median direct hospital inpatient costs per day in the last 30 days of life ($613 vs. $702, P = .02). They also had lower median direct hospital inpatient costs in the last 14 days overall ($0 vs. $5,106, P = .007) and on a per-day basis ($0 vs. $676, P = .007).
"The patients who had the timely consultations actually weren’t admitted to the hospital as often," Dr. Nevadunsky noted. In fact, they were half as likely to be admitted in the last 14 days (35% vs. 71%, P = .001).
"Shortcomings [of the study] include small numbers and the retrospective collection of data. Also, our study did not account for outpatient costs, including those assumed by families, or for those costs incurred by loss of time out of work by families to care for the patient," acknowledged Dr. Nevadunsky, who disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING ON WOMEN'S CANCER
Major finding: Patients receiving timely palliative care had lower scores for aggressive care at the end of life (0 vs. 2) and, in their last 14 days, had lower median direct inpatient hospital costs ($0 vs. $5,106) and were half as likely to be admitted (35% vs. 71%).
Data source: A pair of retrospective cohort studies among 100 patients who died from gynecologic cancers.
Disclosures: Dr. Nevadunsky disclosed no relevant conflicts of interest.

Lower costs documented in hospitals with palliative care programs
NEW ORLEANS – Hospitals with palliative care programs had lower treatment intensity on average at the end of life than did those without palliative care, in a national sample of 3,593 hospitals.
ICU length of stay in the last 6 months of life was 0.4 days shorter (P less than .001) and hospice length of stay 1.6 days longer (P = .013) at hospitals with palliative care versus those without.
The study strengthens claims that palliative care cuts costs, and is the first to examine the impact of palliative care in such a large national sample of hospitals, Jay R. Horton said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Prior studies focused on the effects of palliative care. Mr. Horton’s study considers outcomes for the entire older adult population in the hospital.

The researchers considered data from 3,593 hospitals with a palliative care status noted on the 2008 American Hospital Association survey. In all, 1,657 hospitals had palliative care programs and 1,936 hospitals did not. The researchers then linked the hospital data with the data from the Dartmouth Atlas on 896,097 fee-for-service Medicare patients, aged 67-99 years, with one or more chronic illnesses, who died in 2007. Patients were assigned to a hospital where they received the majority of their care in the last 2 years of life.
Covariates predictive of outcomes such as age, sex, race and comorbidities were already corrected for in the Dartmouth Atlas. Propensity scoring was used for variables predictive of outcomes or the presence of palliative care in the AHA survey such as Joint Commission Accreditation and total bed count. Finally, propensity scores were used to reweight the sample to reduce selection bias.
The effect of palliative care would very likely be stronger if the data had identified those patients who actually received palliative care, said Mr. Horton , director of the palliative care consult service at The Lilian and Benjamin Hertzberg Palliative Care Institute, Icahn School of Medicine at Mount Sinai Hospital, New York. Ongoing research uses data from the National Palliative Care Registry to better identify palliative care programs and socioeconomic factors to further reduce potential selection bias.
Treatment intensity for patients with serious illness varies widely across the country. One study showed that more than 40% of the variation is due to the supply of specialists and hospital capacity (BMJ 2002;325:961-4). Put another way, the greater the supply of physicians, the greater the utilization, even after adjustment for factors that should drive utilization, such as patient preference and disease severity.
"This supply-sensitive care, as it is sometimes called, is at the discretion of clinicians and to a certain extent at the discretion of patients, but more troubling is that much of this care may be unnecessary," said Mr. Horton.
Mr. Horton reported having no financial disclosures.
NEW ORLEANS – Hospitals with palliative care programs had lower treatment intensity on average at the end of life than did those without palliative care, in a national sample of 3,593 hospitals.
ICU length of stay in the last 6 months of life was 0.4 days shorter (P less than .001) and hospice length of stay 1.6 days longer (P = .013) at hospitals with palliative care versus those without.
The study strengthens claims that palliative care cuts costs, and is the first to examine the impact of palliative care in such a large national sample of hospitals, Jay R. Horton said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Prior studies focused on the effects of palliative care. Mr. Horton’s study considers outcomes for the entire older adult population in the hospital.
The researchers considered data from 3,593 hospitals with a palliative care status noted on the 2008 American Hospital Association survey. In all, 1,657 hospitals had palliative care programs and 1,936 hospitals did not. The researchers then linked the hospital data with the data from the Dartmouth Atlas on 896,097 fee-for-service Medicare patients, aged 67-99 years, with one or more chronic illnesses, who died in 2007. Patients were assigned to a hospital where they received the majority of their care in the last 2 years of life.
Covariates predictive of outcomes such as age, sex, race and comorbidities were already corrected for in the Dartmouth Atlas. Propensity scoring was used for variables predictive of outcomes or the presence of palliative care in the AHA survey such as Joint Commission Accreditation and total bed count. Finally, propensity scores were used to reweight the sample to reduce selection bias.
The effect of palliative care would very likely be stronger if the data had identified those patients who actually received palliative care, said Mr. Horton , director of the palliative care consult service at The Lilian and Benjamin Hertzberg Palliative Care Institute, Icahn School of Medicine at Mount Sinai Hospital, New York. Ongoing research uses data from the National Palliative Care Registry to better identify palliative care programs and socioeconomic factors to further reduce potential selection bias.
Treatment intensity for patients with serious illness varies widely across the country. One study showed that more than 40% of the variation is due to the supply of specialists and hospital capacity (BMJ 2002;325:961-4). Put another way, the greater the supply of physicians, the greater the utilization, even after adjustment for factors that should drive utilization, such as patient preference and disease severity.
"This supply-sensitive care, as it is sometimes called, is at the discretion of clinicians and to a certain extent at the discretion of patients, but more troubling is that much of this care may be unnecessary," said Mr. Horton.
Mr. Horton reported having no financial disclosures.
NEW ORLEANS – Hospitals with palliative care programs had lower treatment intensity on average at the end of life than did those without palliative care, in a national sample of 3,593 hospitals.
ICU length of stay in the last 6 months of life was 0.4 days shorter (P less than .001) and hospice length of stay 1.6 days longer (P = .013) at hospitals with palliative care versus those without.
The study strengthens claims that palliative care cuts costs, and is the first to examine the impact of palliative care in such a large national sample of hospitals, Jay R. Horton said at the annual meeting of the American Academy of Hospice and Palliative Medicine.
Prior studies focused on the effects of palliative care. Mr. Horton’s study considers outcomes for the entire older adult population in the hospital.
The researchers considered data from 3,593 hospitals with a palliative care status noted on the 2008 American Hospital Association survey. In all, 1,657 hospitals had palliative care programs and 1,936 hospitals did not. The researchers then linked the hospital data with the data from the Dartmouth Atlas on 896,097 fee-for-service Medicare patients, aged 67-99 years, with one or more chronic illnesses, who died in 2007. Patients were assigned to a hospital where they received the majority of their care in the last 2 years of life.
Covariates predictive of outcomes such as age, sex, race and comorbidities were already corrected for in the Dartmouth Atlas. Propensity scoring was used for variables predictive of outcomes or the presence of palliative care in the AHA survey such as Joint Commission Accreditation and total bed count. Finally, propensity scores were used to reweight the sample to reduce selection bias.
The effect of palliative care would very likely be stronger if the data had identified those patients who actually received palliative care, said Mr. Horton , director of the palliative care consult service at The Lilian and Benjamin Hertzberg Palliative Care Institute, Icahn School of Medicine at Mount Sinai Hospital, New York. Ongoing research uses data from the National Palliative Care Registry to better identify palliative care programs and socioeconomic factors to further reduce potential selection bias.
Treatment intensity for patients with serious illness varies widely across the country. One study showed that more than 40% of the variation is due to the supply of specialists and hospital capacity (BMJ 2002;325:961-4). Put another way, the greater the supply of physicians, the greater the utilization, even after adjustment for factors that should drive utilization, such as patient preference and disease severity.
"This supply-sensitive care, as it is sometimes called, is at the discretion of clinicians and to a certain extent at the discretion of patients, but more troubling is that much of this care may be unnecessary," said Mr. Horton.
Mr. Horton reported having no financial disclosures.
AT THE AAHPM ANNUAL ASSEMBLY
Major finding: ICU length of stay in the last 6 months of life was 0.4 days shorter and hospice length of stay was 1.6 days longer at hospitals with palliative care (P less than .001, P = .013).
Data source: A retrospective analysis of 3,593 hospitals with palliative care data.
Disclosures: Mr. Horton reported having no financial disclosures.

SPIKES protocol offers guidance for 'active listening' when talking to cancer patients
Mr. William Goeren provides personal insight and practical tips for communicating with cancer patients using the SPIKES method. Mr. Goeren is a recent cancer survivor and director of clinical services at CancerCare, a national nonprofit organization that provides counseling, educational programs, and practical and financial assistance to people affected by cancer.
The Oncology Practice Summit was the 8th annual meeting of Community Oncology, the journal of clinical issues in community practice. The conference was hosted this year by Community Oncology as well as The Journal of Supportive Oncology and The Oncology Report.
Mr. William Goeren provides personal insight and practical tips for communicating with cancer patients using the SPIKES method. Mr. Goeren is a recent cancer survivor and director of clinical services at CancerCare, a national nonprofit organization that provides counseling, educational programs, and practical and financial assistance to people affected by cancer.
The Oncology Practice Summit was the 8th annual meeting of Community Oncology, the journal of clinical issues in community practice. The conference was hosted this year by Community Oncology as well as The Journal of Supportive Oncology and The Oncology Report.
Mr. William Goeren provides personal insight and practical tips for communicating with cancer patients using the SPIKES method. Mr. Goeren is a recent cancer survivor and director of clinical services at CancerCare, a national nonprofit organization that provides counseling, educational programs, and practical and financial assistance to people affected by cancer.
The Oncology Practice Summit was the 8th annual meeting of Community Oncology, the journal of clinical issues in community practice. The conference was hosted this year by Community Oncology as well as The Journal of Supportive Oncology and The Oncology Report.