User login
Palliative-Care Payment
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
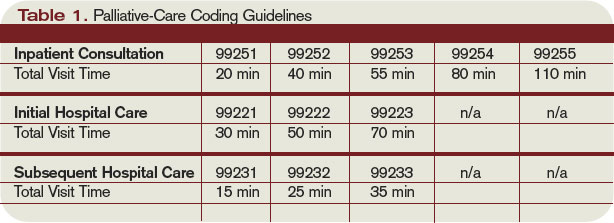
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
“Caregiver Culture” and End-of-Life Discussions
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
A Clinician's View: From Expert to Novice
Many of you are familiar with Patricia Benner’s book From Novice to Expert. It describes Benner’s application to nursing of the Dreyfus model of skill acquisition. The model posits that in the acquisition and development of a skill, a learner passes through five stages of proficiency: novice, advanced beginner, competent, proficient, and expert.
These stages reflect three different aspects of skilled performance. One is a transition from relying on abstract principles to the use of past concrete experiences as paradigms. The second is the change in your perception of a situation, which is seen less as a collection of equally relevant pieces and more as a complete whole in which only certain pieces are relevant. The third is a journey from being a detached observer to an involved participant. You no longer stand outside the situation—you’re now an integral part of it.
Nursing is a field with many different practice settings and specialties. Some nurses choose to stay in one setting and advance to the expert stage in that field. This takes many years and many experiences. Others choose to move into new areas, initiating a reverse expert-to-novice transition. I am one of those nurses.
I started my career as a geriatric nurse practitioner in a nursing home care unit at a VA medical center. I worked there for seven years. I went through Benner’s five stages and achieved expert status. I then decided it was time for a change and started a new journey on the inpatient hospice and palliative care unit at the same facility.
I chose to make this move for various reasons. Having been in foster homes as a child and having served in the army for four years, I was used to a life where change and growth were expected. I’m not afraid of change—to me, change is good. An opportunity for growth and new experiences and the challenges that come with them are rewarding to me.
But it wasn’t an easy move to make. As an expert in one area, you have confidence in what you’re doing. Some decisions are made quickly and instinctively—and they’re the right decisions. Becoming a novice again changes all of that. The confidence is no longer there; decisions take more thought, time, and effort.
This made me feel inefficient and uncomfortable at first in my new position. Instead of being able to act autonomously, I was once again dependent on others for guidance and direction. I had to open up to new ways of approaching things.
Having to “unlearn” things is a must when making a change like this. The examples I could cite are numerous, ranging from simple nursing concepts to important medical decisions. All levels of staff are involved in this expert-to-novice process. I learned important hospice and palliative care concepts from the housekeeper, the doctors, and every team member in between.
The director on my new unit would leave me notes, reminding me of certain key concepts to consider in palliative care and hospice cases. One very important note was “Cast a large net,” a reminder to ask open-ended questions when first approaching a patient and family, to get a feel for where they stood in their understanding of the diagnosis and prognosis. An example would be “Tell me what you know about your illness. And how do you feel about that?”
When presenting a statement or a question to dying patients, it’s important to let them guide the interaction rather than guiding it for them. These patients are no longer looking for treatment options in the hope of a cure or a longer life. They are now seeking peace, love, and acceptance. It’s not appropriate anymore to try to teach them about their illness and how to achieve a positive outcome. You must now have empathy for them and their death experience. You are seeking to help them accept death rather than fight it.
The unit provides not only hospice care but also palliative care. I didn’t fully realize or appreciate the differences between these two types of care until I started working on this unit. Palliative care focuses on reducing the severity of disease symptoms rather than providing a cure. The goals are to prevent and relieve suffering and to improve the patient’s quality of life. Nonhospice palliative care is offered along with curative and all other appropriate forms of medical management. It should not be confused with hospice care, which is palliative care delivered to those at the end of life.
When I worked in the nursing home setting, I often encountered palliative care and end-of-life situations. We did our best to meet these patients’ needs. We thought we were doing a good job, and I took exception to those who claimed otherwise. I now have a new level of understanding.
The mindset and milieu in a nursing home are quite different from those on my new unit. The nursing home environment is often very noisy and busy; the focus is usually on subacute conditions and rehabilitation. There are activities, therapies, lab and diagnostic tests, consults, rounds, and meetings.
On the hospice and palliative care unit, it is much quieter, and the pace is slower. We do quality-of-life meetings daily, spend time with families, and educate everyone involved on how to help the hospice patients achieve a more dignified and peaceful death.
One way to encourage this is by providing the patients and families with the pamphlet “Live and Die Healed.” It encourages the family to consider the following statements: Forgive me, I forgive you, I love you, Thank you, Goodbye, Let go, and Open up to what comes next. (The first five were written by Ira Byock, MD, former president of the American Academy of Hospice and Palliative Medicine. The last two were added by our hospice director, Deborah Grassman, ARNP.)
Death, I realize now, is a sacred event, and I am very happy that I decided to make this change in my nursing career. Not only is my mind more open, but my heart and soul are open as well. “If you don’t love yourself, then how can you love others?” is a question you’ve undoubtedly heard before. My new question is “If you don’t heal your own heart, then how can you help others heal their hearts?”
My heart was broken. Seven years ago, my sister died tragically, a victim of domestic violence. She was murdered—strangled in her bed by a jealous boyfriend—leaving behind four beautiful children. My hospice experience has helped me heal some of those wounds, and that is helping me heal others.
It has only been about 10 months since I started on this unit, but already I am no longer the rehab NP who would say “You’re a diabetic or cardiac patient—put that doughnut down” or “You’re an alcoholic. If you go out on pass and drink, we will do drug and alcohol testing when you return, and if the results are positive, we will discharge you.”
I now say instead, “I know you’re a diabetic and have heart disease, but you can have that doughnut” or “I know you’re an alcoholic, but would you like a beer or a glass of wine or anything else? You can have anything you want.”
It is very fulfilling to give people what they desire and need in their last days. I have never had so many people say “Thank you” and “God bless you.”
I still laugh and smile. I am still alive—and I actually feel more alive in this place. I treasure my life, my family, and my health much more now. I cry, too. There is no holding back. As a result of my expert-to-novice experience, I see and feel the human condition in a new light.
Ellen Thatcher is a Geriatric Nurse Practitioner on the Inpatient Hospice and Palliative Care Unit at Bay Pines VA Healthcare System in Bay Pines, Florida.
Many of you are familiar with Patricia Benner’s book From Novice to Expert. It describes Benner’s application to nursing of the Dreyfus model of skill acquisition. The model posits that in the acquisition and development of a skill, a learner passes through five stages of proficiency: novice, advanced beginner, competent, proficient, and expert.
These stages reflect three different aspects of skilled performance. One is a transition from relying on abstract principles to the use of past concrete experiences as paradigms. The second is the change in your perception of a situation, which is seen less as a collection of equally relevant pieces and more as a complete whole in which only certain pieces are relevant. The third is a journey from being a detached observer to an involved participant. You no longer stand outside the situation—you’re now an integral part of it.
Nursing is a field with many different practice settings and specialties. Some nurses choose to stay in one setting and advance to the expert stage in that field. This takes many years and many experiences. Others choose to move into new areas, initiating a reverse expert-to-novice transition. I am one of those nurses.
I started my career as a geriatric nurse practitioner in a nursing home care unit at a VA medical center. I worked there for seven years. I went through Benner’s five stages and achieved expert status. I then decided it was time for a change and started a new journey on the inpatient hospice and palliative care unit at the same facility.
I chose to make this move for various reasons. Having been in foster homes as a child and having served in the army for four years, I was used to a life where change and growth were expected. I’m not afraid of change—to me, change is good. An opportunity for growth and new experiences and the challenges that come with them are rewarding to me.
But it wasn’t an easy move to make. As an expert in one area, you have confidence in what you’re doing. Some decisions are made quickly and instinctively—and they’re the right decisions. Becoming a novice again changes all of that. The confidence is no longer there; decisions take more thought, time, and effort.
This made me feel inefficient and uncomfortable at first in my new position. Instead of being able to act autonomously, I was once again dependent on others for guidance and direction. I had to open up to new ways of approaching things.
Having to “unlearn” things is a must when making a change like this. The examples I could cite are numerous, ranging from simple nursing concepts to important medical decisions. All levels of staff are involved in this expert-to-novice process. I learned important hospice and palliative care concepts from the housekeeper, the doctors, and every team member in between.
The director on my new unit would leave me notes, reminding me of certain key concepts to consider in palliative care and hospice cases. One very important note was “Cast a large net,” a reminder to ask open-ended questions when first approaching a patient and family, to get a feel for where they stood in their understanding of the diagnosis and prognosis. An example would be “Tell me what you know about your illness. And how do you feel about that?”
When presenting a statement or a question to dying patients, it’s important to let them guide the interaction rather than guiding it for them. These patients are no longer looking for treatment options in the hope of a cure or a longer life. They are now seeking peace, love, and acceptance. It’s not appropriate anymore to try to teach them about their illness and how to achieve a positive outcome. You must now have empathy for them and their death experience. You are seeking to help them accept death rather than fight it.
The unit provides not only hospice care but also palliative care. I didn’t fully realize or appreciate the differences between these two types of care until I started working on this unit. Palliative care focuses on reducing the severity of disease symptoms rather than providing a cure. The goals are to prevent and relieve suffering and to improve the patient’s quality of life. Nonhospice palliative care is offered along with curative and all other appropriate forms of medical management. It should not be confused with hospice care, which is palliative care delivered to those at the end of life.
When I worked in the nursing home setting, I often encountered palliative care and end-of-life situations. We did our best to meet these patients’ needs. We thought we were doing a good job, and I took exception to those who claimed otherwise. I now have a new level of understanding.
The mindset and milieu in a nursing home are quite different from those on my new unit. The nursing home environment is often very noisy and busy; the focus is usually on subacute conditions and rehabilitation. There are activities, therapies, lab and diagnostic tests, consults, rounds, and meetings.
On the hospice and palliative care unit, it is much quieter, and the pace is slower. We do quality-of-life meetings daily, spend time with families, and educate everyone involved on how to help the hospice patients achieve a more dignified and peaceful death.
One way to encourage this is by providing the patients and families with the pamphlet “Live and Die Healed.” It encourages the family to consider the following statements: Forgive me, I forgive you, I love you, Thank you, Goodbye, Let go, and Open up to what comes next. (The first five were written by Ira Byock, MD, former president of the American Academy of Hospice and Palliative Medicine. The last two were added by our hospice director, Deborah Grassman, ARNP.)
Death, I realize now, is a sacred event, and I am very happy that I decided to make this change in my nursing career. Not only is my mind more open, but my heart and soul are open as well. “If you don’t love yourself, then how can you love others?” is a question you’ve undoubtedly heard before. My new question is “If you don’t heal your own heart, then how can you help others heal their hearts?”
My heart was broken. Seven years ago, my sister died tragically, a victim of domestic violence. She was murdered—strangled in her bed by a jealous boyfriend—leaving behind four beautiful children. My hospice experience has helped me heal some of those wounds, and that is helping me heal others.
It has only been about 10 months since I started on this unit, but already I am no longer the rehab NP who would say “You’re a diabetic or cardiac patient—put that doughnut down” or “You’re an alcoholic. If you go out on pass and drink, we will do drug and alcohol testing when you return, and if the results are positive, we will discharge you.”
I now say instead, “I know you’re a diabetic and have heart disease, but you can have that doughnut” or “I know you’re an alcoholic, but would you like a beer or a glass of wine or anything else? You can have anything you want.”
It is very fulfilling to give people what they desire and need in their last days. I have never had so many people say “Thank you” and “God bless you.”
I still laugh and smile. I am still alive—and I actually feel more alive in this place. I treasure my life, my family, and my health much more now. I cry, too. There is no holding back. As a result of my expert-to-novice experience, I see and feel the human condition in a new light.
Ellen Thatcher is a Geriatric Nurse Practitioner on the Inpatient Hospice and Palliative Care Unit at Bay Pines VA Healthcare System in Bay Pines, Florida.
Many of you are familiar with Patricia Benner’s book From Novice to Expert. It describes Benner’s application to nursing of the Dreyfus model of skill acquisition. The model posits that in the acquisition and development of a skill, a learner passes through five stages of proficiency: novice, advanced beginner, competent, proficient, and expert.
These stages reflect three different aspects of skilled performance. One is a transition from relying on abstract principles to the use of past concrete experiences as paradigms. The second is the change in your perception of a situation, which is seen less as a collection of equally relevant pieces and more as a complete whole in which only certain pieces are relevant. The third is a journey from being a detached observer to an involved participant. You no longer stand outside the situation—you’re now an integral part of it.
Nursing is a field with many different practice settings and specialties. Some nurses choose to stay in one setting and advance to the expert stage in that field. This takes many years and many experiences. Others choose to move into new areas, initiating a reverse expert-to-novice transition. I am one of those nurses.
I started my career as a geriatric nurse practitioner in a nursing home care unit at a VA medical center. I worked there for seven years. I went through Benner’s five stages and achieved expert status. I then decided it was time for a change and started a new journey on the inpatient hospice and palliative care unit at the same facility.
I chose to make this move for various reasons. Having been in foster homes as a child and having served in the army for four years, I was used to a life where change and growth were expected. I’m not afraid of change—to me, change is good. An opportunity for growth and new experiences and the challenges that come with them are rewarding to me.
But it wasn’t an easy move to make. As an expert in one area, you have confidence in what you’re doing. Some decisions are made quickly and instinctively—and they’re the right decisions. Becoming a novice again changes all of that. The confidence is no longer there; decisions take more thought, time, and effort.
This made me feel inefficient and uncomfortable at first in my new position. Instead of being able to act autonomously, I was once again dependent on others for guidance and direction. I had to open up to new ways of approaching things.
Having to “unlearn” things is a must when making a change like this. The examples I could cite are numerous, ranging from simple nursing concepts to important medical decisions. All levels of staff are involved in this expert-to-novice process. I learned important hospice and palliative care concepts from the housekeeper, the doctors, and every team member in between.
The director on my new unit would leave me notes, reminding me of certain key concepts to consider in palliative care and hospice cases. One very important note was “Cast a large net,” a reminder to ask open-ended questions when first approaching a patient and family, to get a feel for where they stood in their understanding of the diagnosis and prognosis. An example would be “Tell me what you know about your illness. And how do you feel about that?”
When presenting a statement or a question to dying patients, it’s important to let them guide the interaction rather than guiding it for them. These patients are no longer looking for treatment options in the hope of a cure or a longer life. They are now seeking peace, love, and acceptance. It’s not appropriate anymore to try to teach them about their illness and how to achieve a positive outcome. You must now have empathy for them and their death experience. You are seeking to help them accept death rather than fight it.
The unit provides not only hospice care but also palliative care. I didn’t fully realize or appreciate the differences between these two types of care until I started working on this unit. Palliative care focuses on reducing the severity of disease symptoms rather than providing a cure. The goals are to prevent and relieve suffering and to improve the patient’s quality of life. Nonhospice palliative care is offered along with curative and all other appropriate forms of medical management. It should not be confused with hospice care, which is palliative care delivered to those at the end of life.
When I worked in the nursing home setting, I often encountered palliative care and end-of-life situations. We did our best to meet these patients’ needs. We thought we were doing a good job, and I took exception to those who claimed otherwise. I now have a new level of understanding.
The mindset and milieu in a nursing home are quite different from those on my new unit. The nursing home environment is often very noisy and busy; the focus is usually on subacute conditions and rehabilitation. There are activities, therapies, lab and diagnostic tests, consults, rounds, and meetings.
On the hospice and palliative care unit, it is much quieter, and the pace is slower. We do quality-of-life meetings daily, spend time with families, and educate everyone involved on how to help the hospice patients achieve a more dignified and peaceful death.
One way to encourage this is by providing the patients and families with the pamphlet “Live and Die Healed.” It encourages the family to consider the following statements: Forgive me, I forgive you, I love you, Thank you, Goodbye, Let go, and Open up to what comes next. (The first five were written by Ira Byock, MD, former president of the American Academy of Hospice and Palliative Medicine. The last two were added by our hospice director, Deborah Grassman, ARNP.)
Death, I realize now, is a sacred event, and I am very happy that I decided to make this change in my nursing career. Not only is my mind more open, but my heart and soul are open as well. “If you don’t love yourself, then how can you love others?” is a question you’ve undoubtedly heard before. My new question is “If you don’t heal your own heart, then how can you help others heal their hearts?”
My heart was broken. Seven years ago, my sister died tragically, a victim of domestic violence. She was murdered—strangled in her bed by a jealous boyfriend—leaving behind four beautiful children. My hospice experience has helped me heal some of those wounds, and that is helping me heal others.
It has only been about 10 months since I started on this unit, but already I am no longer the rehab NP who would say “You’re a diabetic or cardiac patient—put that doughnut down” or “You’re an alcoholic. If you go out on pass and drink, we will do drug and alcohol testing when you return, and if the results are positive, we will discharge you.”
I now say instead, “I know you’re a diabetic and have heart disease, but you can have that doughnut” or “I know you’re an alcoholic, but would you like a beer or a glass of wine or anything else? You can have anything you want.”
It is very fulfilling to give people what they desire and need in their last days. I have never had so many people say “Thank you” and “God bless you.”
I still laugh and smile. I am still alive—and I actually feel more alive in this place. I treasure my life, my family, and my health much more now. I cry, too. There is no holding back. As a result of my expert-to-novice experience, I see and feel the human condition in a new light.
Ellen Thatcher is a Geriatric Nurse Practitioner on the Inpatient Hospice and Palliative Care Unit at Bay Pines VA Healthcare System in Bay Pines, Florida.
The DNR Dilemma

When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”

A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”
A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”
A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
When is the Best Time to Refer to Hospice?
End-of-Life Predictions

The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
Palliative Care Patience
As hospital-based palliative care programs continue to grow, palliative care specialists are eager to dispel misconceptions about their work.1 Quality palliative care management at the end of life is often mistakenly perceived as synonymous with adequate pain control, but controlling pain is just one of the facets of effectively moderating the intensity of patients’ and families’ suffering.
The cases narrated here illustrate some of the other common themes of good palliative care management at the end of life: aggressive symptom management, interdisciplinary teamwork, and attention to patients’ and families’ spiritual concerns. Active, respectful listening can help to identify and alleviate obstacles to a more humane end-of-life journey.
Time to Process the Big Picture
State-of-the-art medical therapy does not always address dying patients’ suffering, says Melissa Mahoney, MD, assistant professor of medicine at Emory University and co-director of the Palliative Care Consult Service at Emory Crawford Long Hospital in Atlanta. She experienced this firsthand with a request to consult with a 60-year-old woman who had been in and out of sub-acute rehabilitation facilities seeking pain relief for her spinal stenosis. During a recent rehab facility stay, she had become septic and was transferred to the hospital for dialysis and other treatments. When Dr. Mahoney met the patient, the woman had been saying that she wanted to die, and her family was supportive of her wishes.
During her first conversation with the patient, however, Dr. Mahoney was able to discern that when she said she wanted to die, the patient meant, “I’m in so much pain that I don’t want to live this way.” The first step for the palliative care team was to begin patient-controlled analgesia (PCA) with IV hydromorphone hydrochloride in an attempt to control her pain. The PCA worked—dramatically.
“The next day,” recalls Dr. Mahoney, “she was like a new person. She was able to cope with the idea of dialysis and was able to talk with her family and put things in perspective.”
The palliative care team followed the woman for months, as she continued a cycle of readmissions to both the sub-acute facility and the hospital. The difference from the previous scenario, however, was that the team could offer aggressive symptom management while encouraging the patient and her family to revisit quality of life issues. She eventually died in the hospital, but Dr. Mahoney believes that the palliative care team’s interventions and emphasis on communication helped the patient and her family to cope with the situation more effectively.
With pain under control, patients can begin to address such questions as What’s important to me now? How do I want to spend my days? Who would I want to speak for me if I can’t speak for myself? What are my end-of-life wishes?’
“None of those higher-level discussions can take place until someone can physically handle them,” emphasizes Dr. Mahoney. “The palliative care approach puts the focus back on the patient and on the family and away from the disease. It seeks to treat the person and hopefully ease suffering through the illness.”
Goals of Care Change with Time
Howard R. Epstein, MD, medical director, Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and a member of the SHM Palliative Care Task Force, notes that good palliative care incorporates ongoing discussions about patients’ and families’ goals of care. “Following diagnosis of a life-threatening illness, the initial goal might be ‘I want to be cured,’ ” he says. “But, if the disease progresses, then you need to have another discussion about goals of care. Hopefully, this is part of the process all along.”
Dr. Epstein participated in a particularly memorable case last fall, consulting with a patient who had metastatic renal cancer. Surgery had left him with an abdominal abscess, which surgeons were proposing to address with another procedure in order to prevent a potentially fatal infection. The palliative care team was called in to help Mr. A, who was only 50, decide on a care plan. During the care conference, says Dr. Epstein, Mr. A was alert and joking with his wife and indicated that he would rather go home with hospice care than undergo another surgery.
The team asked Mr. A about his goals. “He didn’t know how much time he had left,” recalls Dr. Epstein, “although he had a specific goal in mind: One of his four sons was getting married, and he wanted to be there for that. They were a very close-knit family.” Mr. A had been intensely engaged as a father all through his sons’ school years. They ranged in age from 19 to 30, and Mr. A was determined to remain close with them throughout his dying process.
The care team facilitated his return home with a PCA pump for pain and a link with a visiting hospice nurse and social worker. The case was followed by a reporter from the St. Paul Pioneer Press, and it was in those articles that Dr. Epstein learned more of Mr. A’s story. For instance, extended family members were pitching in to remodel the house; Mrs. A would have to sell it to cover her husband’s medical bills after he died. The engaged son later had to tell his father that his fiancée had canceled the wedding. Mr. A was able to allay his son’s guilt and fear about the canceled wedding and to be the kind of supportive father he had always been.
Because his goal of living until the wedding had changed, Mr. A was then able to focus on his other goal: having family with him as he died at home. And, indeed, Mr. A died a peaceful death a few weeks later surrounded by his whole family.
A Ship without a Captain
Pediatric hospitalists who handle palliative care recognize that, unlike adults’ end-of-life trajectories, which are usually a straight line, the trajectories of children with complex medical conditions tend to be more erratic between diagnosis and cure or death. As a result, their families spend a longer time relating to the medical system. The job of the palliative care team is to acknowledge the family’s experience and reframe that experience into a more egalitarian and satisfying one, including a comprehensive plan of care, says Margaret Hood, MD, senior pediatric hospitalist at MultiCare’s Mary Bridge Children’s Hospital in Tacoma, Wash. Thus, the interdisciplinary team at Mary Bridge meets with the family around a round table, where everyone’s input is given equal respect and weight.
Dr. Hood recalls one case that was brought to her attention by a social worker. Amy (not her real name) had been born prematurely and had endured many medical problems in her first four years. Then, at age four, she started walking and talking; by age seven, she was reading at the fifth grade level. From ages seven to 10, Amy had minor problems, but she began deteriorating at age 10, when it was found that she had mitochondrial disease. The family had taken her to many specialists without any resolution to her problem and had been charging medical treatments to their credit cards. The social worker was concerned that the family would be devastated by bankruptcy.
The palliative care team organized a care conference attended by Amy’s primary care physician, palliative care team members, and other specialists. Although the care conference resulted in small adjustments to her care plan—a change in medication and the addition of one diagnostic test—the true change came when Amy’s mother turned to Dr. Hood and said, “You know, I thought you’d given up on us.”
That’s when it occurred to Dr. Hood that families like these, visiting specialist after specialist for their child’s complex medical conditions, are “on ‘a ship without a captain.’ Whether or not their children have life-limiting illnesses, they need a captain of the ship to help them navigate their journey,” she says.
Amy’s mother had been under the impression that the physicians were telling her there was nothing else to hope for. “You don’t give up hope,” asserts Dr. Hood. “You just change what you’re hoping for.”
Amy died three months after the palliative care conference, but took a Make-A-Wish Foundation trip to Disneyland and celebrated Christmas at home with her family. Her last wish, after Christmas, was to avoid re-entering the hospital, and this was honored as well.
There May Be More Time to Live
Attention to nuances embedded in patients’ stated wishes can sometimes result in a reversal of expectations about end of life. Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, was called by the hospitalist service last year to help facilitate transfer of a patient to hospice care.
In her 70s, the active woman had come to the hospital because a tumor mass was eroding through her breast tissue. The woman was avoiding treatment, including a biopsy, and appeared to be resolved to her fate. Based on her conversation with the emergency department (ED) attending, hospice was discussed and recommended; the patient was admitted primarily for IV antibiotics and care of her wound. In discussing goals of care with the patient, however, Dr. Grossman was able to elicit her reasons for refusing treatment. Ten years earlier, the patient had watched her daughter suffer with aggressive chemotherapy and radiation for her breast cancer. She told Dr. Grossman, “I’ve lived my life; I don’t want to go through all that.”
Knowing that breast cancer treatments have evolved in the past decade, Dr. Grossman asked the woman whether she would agree to a consultation with an oncologist to find out about less toxic treatment, including hormonal therapy. Subsequently, the patient decided to undergo a lumpectomy to increase her options. Dr. Grossman also prescribed a mild pain reliever for the woman, who had expressed fears about becoming addicted to pain medication (a common misperception in elderly patients). Upon discharge, the patient was feeling better physically, and she was optimistic about her future.
Despite the perceptions of the ED staff, the patient had not been hospice-appropriate. “No one had ever offered her the alternatives. In her mind, she saw chemotherapy as this terrible thing, and she just didn’t want to have that,” says Dr. Grossman. “So by listening to her we found out why she didn’t want chemotherapy, and we were able to encourage her to talk with the oncologist and the surgeon.”
I’m Afraid of What Comes after This Life
“Sometimes you find that patients and families are making decisions purely in a spiritual context,” notes Dr. Mahoney. “Until you know that, you can deliver clear and concise medical information and opinions and they won’t hear it. They may respect your opinion, but they will not take that into consideration when they’re making the decisions about themselves or a loved one because their spiritual belief system supersedes that factual information.”
Last year, Dr. Mahoney encountered a woman her late 50s with metastatic cancer. Her mother had died young of the same disease. The patient knew her disease was advanced and that she was facing the same thing her mother had faced. She, too, was leaving behind her daughters.
The patient, recalls Dr. Mahoney, had not filled out an advance directive and was having a difficult time talking with her family about her situation. It is Dr. Mahoney’s practice in such settings to ask people about their hopes and their fears, “because you can really gauge how someone sees their illness by asking those questions.”
The woman responded that she was very afraid of dying. “When I hear that answer, my next question is, ‘What do you fear? Do you fear that you might suffer?’ She said, ‘Oh no, no, I’m not afraid of that at all. Actually, I’ve sinned a lot in my life, and I’m afraid of what comes after this life.’ ”
Realizing that the woman was suffering spiritually, Dr. Mahoney called in her team’s chaplain to meet with the patient. During that meeting, the patient revealed to Chaplain Sandra Schaap that she had been the one to remove her mother from life support (her mother had not left an advance directive either). She was plagued by the fear of how she would be judged for that act. The chaplain was able to offer some comfort by sharing a benediction, which stated (among other things) that Christ would complete what we have left undone in this life.
“That conversation helped the patient see that she needed to complete her own advance directive so that her daughters wouldn’t go through the same thing that she had with her own mother,” says Dr. Mahoney.
Although Dr. Mahoney did not see the woman again, “I think we certainly set the framework for her and her family to be able to cope with what was coming. In the traditional medical model of disease treatment, I’m not sure that kind of detail would have come out. This woman would have left the hospital still carrying around that burden and [would have] had a very different life from that point,” she says.
Conclusion
“Every patient and family has a story of their illness and how it has impacted their lives,” Dr. Mahoney emphasizes. “Many times people are in the hospital for an acute problem, but they’ve suffered with an illness for years. There is a real opportunity to allow patients and families to tell their stories. People are often relieved when someone listens and can help put things in perspective. Palliative care specialists, by actively listening to patient and family concerns, can help relieve suffering on a physical, spiritual, and emotional level even when cure is not possible.” TH
In this issue Gretchen Henkel also writes about hospitalists who are overcommitted.
Reference
- Center to Advance Palliative Care. The case for hospital-based palliative care. Available at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Accessed on February 20, 2007.
As hospital-based palliative care programs continue to grow, palliative care specialists are eager to dispel misconceptions about their work.1 Quality palliative care management at the end of life is often mistakenly perceived as synonymous with adequate pain control, but controlling pain is just one of the facets of effectively moderating the intensity of patients’ and families’ suffering.
The cases narrated here illustrate some of the other common themes of good palliative care management at the end of life: aggressive symptom management, interdisciplinary teamwork, and attention to patients’ and families’ spiritual concerns. Active, respectful listening can help to identify and alleviate obstacles to a more humane end-of-life journey.
Time to Process the Big Picture
State-of-the-art medical therapy does not always address dying patients’ suffering, says Melissa Mahoney, MD, assistant professor of medicine at Emory University and co-director of the Palliative Care Consult Service at Emory Crawford Long Hospital in Atlanta. She experienced this firsthand with a request to consult with a 60-year-old woman who had been in and out of sub-acute rehabilitation facilities seeking pain relief for her spinal stenosis. During a recent rehab facility stay, she had become septic and was transferred to the hospital for dialysis and other treatments. When Dr. Mahoney met the patient, the woman had been saying that she wanted to die, and her family was supportive of her wishes.
During her first conversation with the patient, however, Dr. Mahoney was able to discern that when she said she wanted to die, the patient meant, “I’m in so much pain that I don’t want to live this way.” The first step for the palliative care team was to begin patient-controlled analgesia (PCA) with IV hydromorphone hydrochloride in an attempt to control her pain. The PCA worked—dramatically.
“The next day,” recalls Dr. Mahoney, “she was like a new person. She was able to cope with the idea of dialysis and was able to talk with her family and put things in perspective.”
The palliative care team followed the woman for months, as she continued a cycle of readmissions to both the sub-acute facility and the hospital. The difference from the previous scenario, however, was that the team could offer aggressive symptom management while encouraging the patient and her family to revisit quality of life issues. She eventually died in the hospital, but Dr. Mahoney believes that the palliative care team’s interventions and emphasis on communication helped the patient and her family to cope with the situation more effectively.
With pain under control, patients can begin to address such questions as What’s important to me now? How do I want to spend my days? Who would I want to speak for me if I can’t speak for myself? What are my end-of-life wishes?’
“None of those higher-level discussions can take place until someone can physically handle them,” emphasizes Dr. Mahoney. “The palliative care approach puts the focus back on the patient and on the family and away from the disease. It seeks to treat the person and hopefully ease suffering through the illness.”
Goals of Care Change with Time
Howard R. Epstein, MD, medical director, Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and a member of the SHM Palliative Care Task Force, notes that good palliative care incorporates ongoing discussions about patients’ and families’ goals of care. “Following diagnosis of a life-threatening illness, the initial goal might be ‘I want to be cured,’ ” he says. “But, if the disease progresses, then you need to have another discussion about goals of care. Hopefully, this is part of the process all along.”
Dr. Epstein participated in a particularly memorable case last fall, consulting with a patient who had metastatic renal cancer. Surgery had left him with an abdominal abscess, which surgeons were proposing to address with another procedure in order to prevent a potentially fatal infection. The palliative care team was called in to help Mr. A, who was only 50, decide on a care plan. During the care conference, says Dr. Epstein, Mr. A was alert and joking with his wife and indicated that he would rather go home with hospice care than undergo another surgery.
The team asked Mr. A about his goals. “He didn’t know how much time he had left,” recalls Dr. Epstein, “although he had a specific goal in mind: One of his four sons was getting married, and he wanted to be there for that. They were a very close-knit family.” Mr. A had been intensely engaged as a father all through his sons’ school years. They ranged in age from 19 to 30, and Mr. A was determined to remain close with them throughout his dying process.
The care team facilitated his return home with a PCA pump for pain and a link with a visiting hospice nurse and social worker. The case was followed by a reporter from the St. Paul Pioneer Press, and it was in those articles that Dr. Epstein learned more of Mr. A’s story. For instance, extended family members were pitching in to remodel the house; Mrs. A would have to sell it to cover her husband’s medical bills after he died. The engaged son later had to tell his father that his fiancée had canceled the wedding. Mr. A was able to allay his son’s guilt and fear about the canceled wedding and to be the kind of supportive father he had always been.
Because his goal of living until the wedding had changed, Mr. A was then able to focus on his other goal: having family with him as he died at home. And, indeed, Mr. A died a peaceful death a few weeks later surrounded by his whole family.
A Ship without a Captain
Pediatric hospitalists who handle palliative care recognize that, unlike adults’ end-of-life trajectories, which are usually a straight line, the trajectories of children with complex medical conditions tend to be more erratic between diagnosis and cure or death. As a result, their families spend a longer time relating to the medical system. The job of the palliative care team is to acknowledge the family’s experience and reframe that experience into a more egalitarian and satisfying one, including a comprehensive plan of care, says Margaret Hood, MD, senior pediatric hospitalist at MultiCare’s Mary Bridge Children’s Hospital in Tacoma, Wash. Thus, the interdisciplinary team at Mary Bridge meets with the family around a round table, where everyone’s input is given equal respect and weight.
Dr. Hood recalls one case that was brought to her attention by a social worker. Amy (not her real name) had been born prematurely and had endured many medical problems in her first four years. Then, at age four, she started walking and talking; by age seven, she was reading at the fifth grade level. From ages seven to 10, Amy had minor problems, but she began deteriorating at age 10, when it was found that she had mitochondrial disease. The family had taken her to many specialists without any resolution to her problem and had been charging medical treatments to their credit cards. The social worker was concerned that the family would be devastated by bankruptcy.
The palliative care team organized a care conference attended by Amy’s primary care physician, palliative care team members, and other specialists. Although the care conference resulted in small adjustments to her care plan—a change in medication and the addition of one diagnostic test—the true change came when Amy’s mother turned to Dr. Hood and said, “You know, I thought you’d given up on us.”
That’s when it occurred to Dr. Hood that families like these, visiting specialist after specialist for their child’s complex medical conditions, are “on ‘a ship without a captain.’ Whether or not their children have life-limiting illnesses, they need a captain of the ship to help them navigate their journey,” she says.
Amy’s mother had been under the impression that the physicians were telling her there was nothing else to hope for. “You don’t give up hope,” asserts Dr. Hood. “You just change what you’re hoping for.”
Amy died three months after the palliative care conference, but took a Make-A-Wish Foundation trip to Disneyland and celebrated Christmas at home with her family. Her last wish, after Christmas, was to avoid re-entering the hospital, and this was honored as well.
There May Be More Time to Live
Attention to nuances embedded in patients’ stated wishes can sometimes result in a reversal of expectations about end of life. Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, was called by the hospitalist service last year to help facilitate transfer of a patient to hospice care.
In her 70s, the active woman had come to the hospital because a tumor mass was eroding through her breast tissue. The woman was avoiding treatment, including a biopsy, and appeared to be resolved to her fate. Based on her conversation with the emergency department (ED) attending, hospice was discussed and recommended; the patient was admitted primarily for IV antibiotics and care of her wound. In discussing goals of care with the patient, however, Dr. Grossman was able to elicit her reasons for refusing treatment. Ten years earlier, the patient had watched her daughter suffer with aggressive chemotherapy and radiation for her breast cancer. She told Dr. Grossman, “I’ve lived my life; I don’t want to go through all that.”
Knowing that breast cancer treatments have evolved in the past decade, Dr. Grossman asked the woman whether she would agree to a consultation with an oncologist to find out about less toxic treatment, including hormonal therapy. Subsequently, the patient decided to undergo a lumpectomy to increase her options. Dr. Grossman also prescribed a mild pain reliever for the woman, who had expressed fears about becoming addicted to pain medication (a common misperception in elderly patients). Upon discharge, the patient was feeling better physically, and she was optimistic about her future.
Despite the perceptions of the ED staff, the patient had not been hospice-appropriate. “No one had ever offered her the alternatives. In her mind, she saw chemotherapy as this terrible thing, and she just didn’t want to have that,” says Dr. Grossman. “So by listening to her we found out why she didn’t want chemotherapy, and we were able to encourage her to talk with the oncologist and the surgeon.”
I’m Afraid of What Comes after This Life
“Sometimes you find that patients and families are making decisions purely in a spiritual context,” notes Dr. Mahoney. “Until you know that, you can deliver clear and concise medical information and opinions and they won’t hear it. They may respect your opinion, but they will not take that into consideration when they’re making the decisions about themselves or a loved one because their spiritual belief system supersedes that factual information.”
Last year, Dr. Mahoney encountered a woman her late 50s with metastatic cancer. Her mother had died young of the same disease. The patient knew her disease was advanced and that she was facing the same thing her mother had faced. She, too, was leaving behind her daughters.
The patient, recalls Dr. Mahoney, had not filled out an advance directive and was having a difficult time talking with her family about her situation. It is Dr. Mahoney’s practice in such settings to ask people about their hopes and their fears, “because you can really gauge how someone sees their illness by asking those questions.”
The woman responded that she was very afraid of dying. “When I hear that answer, my next question is, ‘What do you fear? Do you fear that you might suffer?’ She said, ‘Oh no, no, I’m not afraid of that at all. Actually, I’ve sinned a lot in my life, and I’m afraid of what comes after this life.’ ”
Realizing that the woman was suffering spiritually, Dr. Mahoney called in her team’s chaplain to meet with the patient. During that meeting, the patient revealed to Chaplain Sandra Schaap that she had been the one to remove her mother from life support (her mother had not left an advance directive either). She was plagued by the fear of how she would be judged for that act. The chaplain was able to offer some comfort by sharing a benediction, which stated (among other things) that Christ would complete what we have left undone in this life.
“That conversation helped the patient see that she needed to complete her own advance directive so that her daughters wouldn’t go through the same thing that she had with her own mother,” says Dr. Mahoney.
Although Dr. Mahoney did not see the woman again, “I think we certainly set the framework for her and her family to be able to cope with what was coming. In the traditional medical model of disease treatment, I’m not sure that kind of detail would have come out. This woman would have left the hospital still carrying around that burden and [would have] had a very different life from that point,” she says.
Conclusion
“Every patient and family has a story of their illness and how it has impacted their lives,” Dr. Mahoney emphasizes. “Many times people are in the hospital for an acute problem, but they’ve suffered with an illness for years. There is a real opportunity to allow patients and families to tell their stories. People are often relieved when someone listens and can help put things in perspective. Palliative care specialists, by actively listening to patient and family concerns, can help relieve suffering on a physical, spiritual, and emotional level even when cure is not possible.” TH
In this issue Gretchen Henkel also writes about hospitalists who are overcommitted.
Reference
- Center to Advance Palliative Care. The case for hospital-based palliative care. Available at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Accessed on February 20, 2007.
As hospital-based palliative care programs continue to grow, palliative care specialists are eager to dispel misconceptions about their work.1 Quality palliative care management at the end of life is often mistakenly perceived as synonymous with adequate pain control, but controlling pain is just one of the facets of effectively moderating the intensity of patients’ and families’ suffering.
The cases narrated here illustrate some of the other common themes of good palliative care management at the end of life: aggressive symptom management, interdisciplinary teamwork, and attention to patients’ and families’ spiritual concerns. Active, respectful listening can help to identify and alleviate obstacles to a more humane end-of-life journey.
Time to Process the Big Picture
State-of-the-art medical therapy does not always address dying patients’ suffering, says Melissa Mahoney, MD, assistant professor of medicine at Emory University and co-director of the Palliative Care Consult Service at Emory Crawford Long Hospital in Atlanta. She experienced this firsthand with a request to consult with a 60-year-old woman who had been in and out of sub-acute rehabilitation facilities seeking pain relief for her spinal stenosis. During a recent rehab facility stay, she had become septic and was transferred to the hospital for dialysis and other treatments. When Dr. Mahoney met the patient, the woman had been saying that she wanted to die, and her family was supportive of her wishes.
During her first conversation with the patient, however, Dr. Mahoney was able to discern that when she said she wanted to die, the patient meant, “I’m in so much pain that I don’t want to live this way.” The first step for the palliative care team was to begin patient-controlled analgesia (PCA) with IV hydromorphone hydrochloride in an attempt to control her pain. The PCA worked—dramatically.
“The next day,” recalls Dr. Mahoney, “she was like a new person. She was able to cope with the idea of dialysis and was able to talk with her family and put things in perspective.”
The palliative care team followed the woman for months, as she continued a cycle of readmissions to both the sub-acute facility and the hospital. The difference from the previous scenario, however, was that the team could offer aggressive symptom management while encouraging the patient and her family to revisit quality of life issues. She eventually died in the hospital, but Dr. Mahoney believes that the palliative care team’s interventions and emphasis on communication helped the patient and her family to cope with the situation more effectively.
With pain under control, patients can begin to address such questions as What’s important to me now? How do I want to spend my days? Who would I want to speak for me if I can’t speak for myself? What are my end-of-life wishes?’
“None of those higher-level discussions can take place until someone can physically handle them,” emphasizes Dr. Mahoney. “The palliative care approach puts the focus back on the patient and on the family and away from the disease. It seeks to treat the person and hopefully ease suffering through the illness.”
Goals of Care Change with Time
Howard R. Epstein, MD, medical director, Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and a member of the SHM Palliative Care Task Force, notes that good palliative care incorporates ongoing discussions about patients’ and families’ goals of care. “Following diagnosis of a life-threatening illness, the initial goal might be ‘I want to be cured,’ ” he says. “But, if the disease progresses, then you need to have another discussion about goals of care. Hopefully, this is part of the process all along.”
Dr. Epstein participated in a particularly memorable case last fall, consulting with a patient who had metastatic renal cancer. Surgery had left him with an abdominal abscess, which surgeons were proposing to address with another procedure in order to prevent a potentially fatal infection. The palliative care team was called in to help Mr. A, who was only 50, decide on a care plan. During the care conference, says Dr. Epstein, Mr. A was alert and joking with his wife and indicated that he would rather go home with hospice care than undergo another surgery.
The team asked Mr. A about his goals. “He didn’t know how much time he had left,” recalls Dr. Epstein, “although he had a specific goal in mind: One of his four sons was getting married, and he wanted to be there for that. They were a very close-knit family.” Mr. A had been intensely engaged as a father all through his sons’ school years. They ranged in age from 19 to 30, and Mr. A was determined to remain close with them throughout his dying process.
The care team facilitated his return home with a PCA pump for pain and a link with a visiting hospice nurse and social worker. The case was followed by a reporter from the St. Paul Pioneer Press, and it was in those articles that Dr. Epstein learned more of Mr. A’s story. For instance, extended family members were pitching in to remodel the house; Mrs. A would have to sell it to cover her husband’s medical bills after he died. The engaged son later had to tell his father that his fiancée had canceled the wedding. Mr. A was able to allay his son’s guilt and fear about the canceled wedding and to be the kind of supportive father he had always been.
Because his goal of living until the wedding had changed, Mr. A was then able to focus on his other goal: having family with him as he died at home. And, indeed, Mr. A died a peaceful death a few weeks later surrounded by his whole family.
A Ship without a Captain
Pediatric hospitalists who handle palliative care recognize that, unlike adults’ end-of-life trajectories, which are usually a straight line, the trajectories of children with complex medical conditions tend to be more erratic between diagnosis and cure or death. As a result, their families spend a longer time relating to the medical system. The job of the palliative care team is to acknowledge the family’s experience and reframe that experience into a more egalitarian and satisfying one, including a comprehensive plan of care, says Margaret Hood, MD, senior pediatric hospitalist at MultiCare’s Mary Bridge Children’s Hospital in Tacoma, Wash. Thus, the interdisciplinary team at Mary Bridge meets with the family around a round table, where everyone’s input is given equal respect and weight.
Dr. Hood recalls one case that was brought to her attention by a social worker. Amy (not her real name) had been born prematurely and had endured many medical problems in her first four years. Then, at age four, she started walking and talking; by age seven, she was reading at the fifth grade level. From ages seven to 10, Amy had minor problems, but she began deteriorating at age 10, when it was found that she had mitochondrial disease. The family had taken her to many specialists without any resolution to her problem and had been charging medical treatments to their credit cards. The social worker was concerned that the family would be devastated by bankruptcy.
The palliative care team organized a care conference attended by Amy’s primary care physician, palliative care team members, and other specialists. Although the care conference resulted in small adjustments to her care plan—a change in medication and the addition of one diagnostic test—the true change came when Amy’s mother turned to Dr. Hood and said, “You know, I thought you’d given up on us.”
That’s when it occurred to Dr. Hood that families like these, visiting specialist after specialist for their child’s complex medical conditions, are “on ‘a ship without a captain.’ Whether or not their children have life-limiting illnesses, they need a captain of the ship to help them navigate their journey,” she says.
Amy’s mother had been under the impression that the physicians were telling her there was nothing else to hope for. “You don’t give up hope,” asserts Dr. Hood. “You just change what you’re hoping for.”
Amy died three months after the palliative care conference, but took a Make-A-Wish Foundation trip to Disneyland and celebrated Christmas at home with her family. Her last wish, after Christmas, was to avoid re-entering the hospital, and this was honored as well.
There May Be More Time to Live
Attention to nuances embedded in patients’ stated wishes can sometimes result in a reversal of expectations about end of life. Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, was called by the hospitalist service last year to help facilitate transfer of a patient to hospice care.
In her 70s, the active woman had come to the hospital because a tumor mass was eroding through her breast tissue. The woman was avoiding treatment, including a biopsy, and appeared to be resolved to her fate. Based on her conversation with the emergency department (ED) attending, hospice was discussed and recommended; the patient was admitted primarily for IV antibiotics and care of her wound. In discussing goals of care with the patient, however, Dr. Grossman was able to elicit her reasons for refusing treatment. Ten years earlier, the patient had watched her daughter suffer with aggressive chemotherapy and radiation for her breast cancer. She told Dr. Grossman, “I’ve lived my life; I don’t want to go through all that.”
Knowing that breast cancer treatments have evolved in the past decade, Dr. Grossman asked the woman whether she would agree to a consultation with an oncologist to find out about less toxic treatment, including hormonal therapy. Subsequently, the patient decided to undergo a lumpectomy to increase her options. Dr. Grossman also prescribed a mild pain reliever for the woman, who had expressed fears about becoming addicted to pain medication (a common misperception in elderly patients). Upon discharge, the patient was feeling better physically, and she was optimistic about her future.
Despite the perceptions of the ED staff, the patient had not been hospice-appropriate. “No one had ever offered her the alternatives. In her mind, she saw chemotherapy as this terrible thing, and she just didn’t want to have that,” says Dr. Grossman. “So by listening to her we found out why she didn’t want chemotherapy, and we were able to encourage her to talk with the oncologist and the surgeon.”
I’m Afraid of What Comes after This Life
“Sometimes you find that patients and families are making decisions purely in a spiritual context,” notes Dr. Mahoney. “Until you know that, you can deliver clear and concise medical information and opinions and they won’t hear it. They may respect your opinion, but they will not take that into consideration when they’re making the decisions about themselves or a loved one because their spiritual belief system supersedes that factual information.”
Last year, Dr. Mahoney encountered a woman her late 50s with metastatic cancer. Her mother had died young of the same disease. The patient knew her disease was advanced and that she was facing the same thing her mother had faced. She, too, was leaving behind her daughters.
The patient, recalls Dr. Mahoney, had not filled out an advance directive and was having a difficult time talking with her family about her situation. It is Dr. Mahoney’s practice in such settings to ask people about their hopes and their fears, “because you can really gauge how someone sees their illness by asking those questions.”
The woman responded that she was very afraid of dying. “When I hear that answer, my next question is, ‘What do you fear? Do you fear that you might suffer?’ She said, ‘Oh no, no, I’m not afraid of that at all. Actually, I’ve sinned a lot in my life, and I’m afraid of what comes after this life.’ ”
Realizing that the woman was suffering spiritually, Dr. Mahoney called in her team’s chaplain to meet with the patient. During that meeting, the patient revealed to Chaplain Sandra Schaap that she had been the one to remove her mother from life support (her mother had not left an advance directive either). She was plagued by the fear of how she would be judged for that act. The chaplain was able to offer some comfort by sharing a benediction, which stated (among other things) that Christ would complete what we have left undone in this life.
“That conversation helped the patient see that she needed to complete her own advance directive so that her daughters wouldn’t go through the same thing that she had with her own mother,” says Dr. Mahoney.
Although Dr. Mahoney did not see the woman again, “I think we certainly set the framework for her and her family to be able to cope with what was coming. In the traditional medical model of disease treatment, I’m not sure that kind of detail would have come out. This woman would have left the hospital still carrying around that burden and [would have] had a very different life from that point,” she says.
Conclusion
“Every patient and family has a story of their illness and how it has impacted their lives,” Dr. Mahoney emphasizes. “Many times people are in the hospital for an acute problem, but they’ve suffered with an illness for years. There is a real opportunity to allow patients and families to tell their stories. People are often relieved when someone listens and can help put things in perspective. Palliative care specialists, by actively listening to patient and family concerns, can help relieve suffering on a physical, spiritual, and emotional level even when cure is not possible.” TH
In this issue Gretchen Henkel also writes about hospitalists who are overcommitted.
Reference
- Center to Advance Palliative Care. The case for hospital-based palliative care. Available at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Accessed on February 20, 2007.
World Hospice and Palliative Care Day

October 7, 2006, is World Hospice and Palliative Care Day. This day is dedicated to raising the visibility of palliative care within the global community and to providing opportunities to support hospice and palliative care in the form of a unified day of action.
According to official organizers, the event’s theme is “Access to care for all—highlighting the fact that everyone has a right to high-quality end-of-life care, but that more needs to be done to enable everyone to access it.” In creating World Hospice and Palliative Care Day 2006, the event’s organizers aim to raise awareness and understanding of the needs of those living with a terminal diagnosis, as well as the needs of their families. Other goals include calling attention to the need for increasing hospice and palliative care availability throughout the world and raising funds to be used in supporting these services.
Like the first World Hospice and Palliative Care Day, held in 2005, this event will be carried out in conjunction with Voices for Hospices, a global music effort that supports concerts held around the world to raise awareness of this important topic. The Voices for Hospices group is one of many supporters of this cause.
—World Hospice and Palliative Care Day 2006 Web site, Key Messages, page 1.
More than 1,000 events took place on World Hospice and Palliative Care Day 2005, and 74 countries supported the activities. Included in the 2005 event were a cycle rally in Nepal; art exhibitions in Australia, Hong Kong, and Austria; and palliative care conferences in Lithuania and Belarus. In addition, thousands of people from around the world signed a global petition calling for better quality care for people afflicted by terminal illness.
Hospitalists are asked frequently to lead and participate in initiatives meant to improve the identification and treatment of patients and families in need of palliative care. It is common knowledge that traditional medical training tends to focus on the efforts that must be made to cure and prevent illness. There are times when the first priority must be to look for a cure at all costs; however, it must be acknowledged that there are also times when the treatment of a patient’s symptoms should be looked upon as just as important. Conventional medical training frequently does not provide the tools needed to offer the best care for patients and their families when the latter goal becomes the higher priority.
This is why support of initiatives like World Hospice and Palliative Care Day can offer such value to the global community. Events like this one promote awareness of an important topic. For information and ideas on how to get involved in this or in future events, please consult www.worldday.org. Access the Web site’s “Get Involved” page for ideas on how to offer support. Suggested activities include campaigning, creating links and partnerships, and producing materials that will raise awareness.
On the “PR & Press” page of the Web site, in the “Key Messages 2006” section, the following question was posed: “What kinds of issues in general terms does World Hospice and Palliative Care Day hope to raise awareness of year on year?” One of the well-stated answers: “First and foremost we hope the Day helps to increase understanding of hospice and palliative care and how it supports those facing the end of life … . It’s not about ‘helping someone die’ but instead about helping someone to live as comfortably as possible with their illness. It’s about seeing them as [a] living person, not a dying patient. It’s supporting those closest to them and adding life to days, whether or not days can be added to lives.”
Smart Tools for QI Initiatives
SHM’s Quality Improvement Resource Rooms support hospitalists as QI leaders
The role and recognition of the hospitalist has evolved tremendously in the past 10 years, and hospitalists continue to be called upon to lead at their institutions, particularly in quality improvement initiatives. Based on their unique role within the hospital system (a job that requires interaction with many levels of hospital staff) hospitalists are clearly positioned to lead such efforts. As part of SHM’s dedication to promote the highest quality of care for the hospitalized patient, SHM’s Resource Rooms provide members and non-members alike access to information that will aid their knowledge in quality improvement around specific disease states. Currently, SHM provides four Resource Rooms: Venous Thromboembolism (VTE), Stroke, Antimicrobial Resistance (ABX), and Heart Failure. Two additional rooms, Geriatrics and Glycemic Control, will launch this fall.
Quality improvement for the patient will be successful if a systems-based multidisciplinary collaboration within the hospital is improved. Hospitalists are leading this challenging yet exciting opportunity to change the face of healthcare. It has been noted that medical school and residency training have failed to prepare the hospitalist for this leadership role. To this end, SHM provides users of the Resource Rooms with information describing how a specific disease state affects the population and explains why a hospitalist should act in initiating change, as well as what key knowledge, skills, and attitudes the hospitalist should possess. The user is offered information regarding didactic and bedside teaching, patient education, and opportunities for continuing medical education. These resources are useful for the novice as well as for the advanced hospitalist leader. Readers can also apply the concepts of these general mechanisms to any disease state they are seeking to improve at their institutions.
The QI workbook within each of the Resource Rooms is the most important feature and serves as a field guide to implementing a quality improvement program. The workbook includes the following aids:
- Essential first steps: garnering institutional support, assembling a team, developing team rules, and understanding the framework for improvement;
- Conducting an in-depth analysis of current processes and failures;
- Collecting data and devising metrics to assess the impact of your QI initiative;
- Moving from problems to solutions; and
- Continuing to improve: monitoring and learning from the process, as well as holding the gains and spreading your improvement
Other important resources that are common to all of the rooms and will aid in leading the QI efforts of the hospitalist are the educational features. Complex problems need multidisciplinary solutions. The “Improve” and “Educate” areas of the Resource Rooms include information that allow the hospitalist to teach and be taught. In the “Improve” section, a user can find QI Theory slide sets on the foundations of quality improvement initiatives and core measures on specific disease states.
Didactic sessions and teaching tools, as well as professional development, including core competencies and CME opportunities, are all present in the “Educate” feature of each room. For example, in the Heart Failure Resource Room, a didactic session slide set concerning the management of heart failure for hospitalized patients is provided. The slide set includes a heart failure overview that describes the epidemiology, etiologies, and objectives surrounding the management of acute congestive heart failure.
Evidence, improvement, and education tools designed to enhance inpatient outcomes can help the hospitalist develop and lead initiatives that can create a more cost-efficient approach to the treatment of hospitalized patients, while at the same time improving patient outcomes. SHM’s Quality Improvement Resource Rooms provide a compendium of resources to support the hospitalist who is embarking on this enormous task.
September Leadership Academy
New Level II a great success
The recently completed 4th SHM Leadership Academy was a true success in every sense of the word. The event was nearly a sellout, with 160 hospital medicine leaders arriving in Nashville, Tenn., in September to learn—from nationally respected leaders—tangible skills that they could take back to institute in their own practices.
The Leadership Academy Level I was designed to provide leaders in hospital medicine with the skills and resources required to lead and manage programs successfully both now and in the future. Small group sessions gave attendees a chance to interact with faculty and to share personal experiences from their own institutions. Nationally recognized speaker Jack Silversin, DMD, DrPH, presented his infamous broken squares activity, which kept the group energized and working together creatively to learn about effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and then apply them to everyday leadership and management challenges.


Another highlight was the self-evaluation session presented by David Javitch, PhD. His exercise gave everyone an opportunity to learn about their own personality traits and to practice working with extreme opposites, both in the workplace and in everyday life. Attendees continue to rave about the content of this meeting and are looking forward to enhancing their leadership skills by attending Level II courses, scheduled for fall 2007.
“No matter how many times I plan this course, I am amazed at the enthusiasm of the attendees and the new questions that they pose,” says Russell Holman, MD, SHM Leadership Academy course director.
Level II resulted from more than 300 Level I course evaluations that requested additional and ongoing leadership development activities. The Level II course focused on discussions about culture change, negotiation skills, and finance. Keynote speaker Leonard Marcus, PhD, defined the term “meta-leadership” in hospital medicine as a type of leadership that links individuals through their leader’s vision, creating enthusiastic followers.
The Level II course is a must have for those who want to expand upon leadership skills learned in Level I or for those who already have an MBA and want to improve upon leadership in clinical care. The skills discussed in this session are essential to effectively developing and implementing quality improvement programs, patient-safety initiatives, and other programs whose goal is to make system changes that improve patient care.
“The level of attendees participating in Level II was challenging,” says Dr. Holman. “It had us all—faculty and attendees alike—collaborating to answer questions from real-life experiences.”
The phrase “all work and no play” doesn’t describe any SHM meeting, and it certainly can’t be used in reference to the Leadership Academy. Attendees had an opportunity to network with fellow participants and exhibiting companies during the Monday night reception sponsored by Cogent Healthcare. Participants also had ample time to get out and experience some southern hospitality, while enjoying the spa, playing golf, touring on steamboats, dining, and shopping at the Gaylord Opryland Resort and Convention Center.
Leadership Academy Levels I and II were jam-packed with relevant materials and tools applicable to business and the real world. This is an outstanding opportunity for individuals just beginning their leadership journey and for those wanting to take their leadership skills to the next level.
Don’t miss out on the next opportunity to become a leader in hospital medicine. The next meeting will take place during the week of February 26–March 1, 2007, at the Gaylord Palms Resort and Convention Center in Orlando, Fla. Log on to www.hospitalmedicine.org or call (800) 843-3360 for more information.
October 7, 2006, is World Hospice and Palliative Care Day. This day is dedicated to raising the visibility of palliative care within the global community and to providing opportunities to support hospice and palliative care in the form of a unified day of action.
According to official organizers, the event’s theme is “Access to care for all—highlighting the fact that everyone has a right to high-quality end-of-life care, but that more needs to be done to enable everyone to access it.” In creating World Hospice and Palliative Care Day 2006, the event’s organizers aim to raise awareness and understanding of the needs of those living with a terminal diagnosis, as well as the needs of their families. Other goals include calling attention to the need for increasing hospice and palliative care availability throughout the world and raising funds to be used in supporting these services.
Like the first World Hospice and Palliative Care Day, held in 2005, this event will be carried out in conjunction with Voices for Hospices, a global music effort that supports concerts held around the world to raise awareness of this important topic. The Voices for Hospices group is one of many supporters of this cause.
—World Hospice and Palliative Care Day 2006 Web site, Key Messages, page 1.
More than 1,000 events took place on World Hospice and Palliative Care Day 2005, and 74 countries supported the activities. Included in the 2005 event were a cycle rally in Nepal; art exhibitions in Australia, Hong Kong, and Austria; and palliative care conferences in Lithuania and Belarus. In addition, thousands of people from around the world signed a global petition calling for better quality care for people afflicted by terminal illness.
Hospitalists are asked frequently to lead and participate in initiatives meant to improve the identification and treatment of patients and families in need of palliative care. It is common knowledge that traditional medical training tends to focus on the efforts that must be made to cure and prevent illness. There are times when the first priority must be to look for a cure at all costs; however, it must be acknowledged that there are also times when the treatment of a patient’s symptoms should be looked upon as just as important. Conventional medical training frequently does not provide the tools needed to offer the best care for patients and their families when the latter goal becomes the higher priority.
This is why support of initiatives like World Hospice and Palliative Care Day can offer such value to the global community. Events like this one promote awareness of an important topic. For information and ideas on how to get involved in this or in future events, please consult www.worldday.org. Access the Web site’s “Get Involved” page for ideas on how to offer support. Suggested activities include campaigning, creating links and partnerships, and producing materials that will raise awareness.
On the “PR & Press” page of the Web site, in the “Key Messages 2006” section, the following question was posed: “What kinds of issues in general terms does World Hospice and Palliative Care Day hope to raise awareness of year on year?” One of the well-stated answers: “First and foremost we hope the Day helps to increase understanding of hospice and palliative care and how it supports those facing the end of life … . It’s not about ‘helping someone die’ but instead about helping someone to live as comfortably as possible with their illness. It’s about seeing them as [a] living person, not a dying patient. It’s supporting those closest to them and adding life to days, whether or not days can be added to lives.”
Smart Tools for QI Initiatives
SHM’s Quality Improvement Resource Rooms support hospitalists as QI leaders
The role and recognition of the hospitalist has evolved tremendously in the past 10 years, and hospitalists continue to be called upon to lead at their institutions, particularly in quality improvement initiatives. Based on their unique role within the hospital system (a job that requires interaction with many levels of hospital staff) hospitalists are clearly positioned to lead such efforts. As part of SHM’s dedication to promote the highest quality of care for the hospitalized patient, SHM’s Resource Rooms provide members and non-members alike access to information that will aid their knowledge in quality improvement around specific disease states. Currently, SHM provides four Resource Rooms: Venous Thromboembolism (VTE), Stroke, Antimicrobial Resistance (ABX), and Heart Failure. Two additional rooms, Geriatrics and Glycemic Control, will launch this fall.
Quality improvement for the patient will be successful if a systems-based multidisciplinary collaboration within the hospital is improved. Hospitalists are leading this challenging yet exciting opportunity to change the face of healthcare. It has been noted that medical school and residency training have failed to prepare the hospitalist for this leadership role. To this end, SHM provides users of the Resource Rooms with information describing how a specific disease state affects the population and explains why a hospitalist should act in initiating change, as well as what key knowledge, skills, and attitudes the hospitalist should possess. The user is offered information regarding didactic and bedside teaching, patient education, and opportunities for continuing medical education. These resources are useful for the novice as well as for the advanced hospitalist leader. Readers can also apply the concepts of these general mechanisms to any disease state they are seeking to improve at their institutions.
The QI workbook within each of the Resource Rooms is the most important feature and serves as a field guide to implementing a quality improvement program. The workbook includes the following aids:
- Essential first steps: garnering institutional support, assembling a team, developing team rules, and understanding the framework for improvement;
- Conducting an in-depth analysis of current processes and failures;
- Collecting data and devising metrics to assess the impact of your QI initiative;
- Moving from problems to solutions; and
- Continuing to improve: monitoring and learning from the process, as well as holding the gains and spreading your improvement
Other important resources that are common to all of the rooms and will aid in leading the QI efforts of the hospitalist are the educational features. Complex problems need multidisciplinary solutions. The “Improve” and “Educate” areas of the Resource Rooms include information that allow the hospitalist to teach and be taught. In the “Improve” section, a user can find QI Theory slide sets on the foundations of quality improvement initiatives and core measures on specific disease states.
Didactic sessions and teaching tools, as well as professional development, including core competencies and CME opportunities, are all present in the “Educate” feature of each room. For example, in the Heart Failure Resource Room, a didactic session slide set concerning the management of heart failure for hospitalized patients is provided. The slide set includes a heart failure overview that describes the epidemiology, etiologies, and objectives surrounding the management of acute congestive heart failure.
Evidence, improvement, and education tools designed to enhance inpatient outcomes can help the hospitalist develop and lead initiatives that can create a more cost-efficient approach to the treatment of hospitalized patients, while at the same time improving patient outcomes. SHM’s Quality Improvement Resource Rooms provide a compendium of resources to support the hospitalist who is embarking on this enormous task.
September Leadership Academy
New Level II a great success
The recently completed 4th SHM Leadership Academy was a true success in every sense of the word. The event was nearly a sellout, with 160 hospital medicine leaders arriving in Nashville, Tenn., in September to learn—from nationally respected leaders—tangible skills that they could take back to institute in their own practices.
The Leadership Academy Level I was designed to provide leaders in hospital medicine with the skills and resources required to lead and manage programs successfully both now and in the future. Small group sessions gave attendees a chance to interact with faculty and to share personal experiences from their own institutions. Nationally recognized speaker Jack Silversin, DMD, DrPH, presented his infamous broken squares activity, which kept the group energized and working together creatively to learn about effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and then apply them to everyday leadership and management challenges.
Another highlight was the self-evaluation session presented by David Javitch, PhD. His exercise gave everyone an opportunity to learn about their own personality traits and to practice working with extreme opposites, both in the workplace and in everyday life. Attendees continue to rave about the content of this meeting and are looking forward to enhancing their leadership skills by attending Level II courses, scheduled for fall 2007.
“No matter how many times I plan this course, I am amazed at the enthusiasm of the attendees and the new questions that they pose,” says Russell Holman, MD, SHM Leadership Academy course director.
Level II resulted from more than 300 Level I course evaluations that requested additional and ongoing leadership development activities. The Level II course focused on discussions about culture change, negotiation skills, and finance. Keynote speaker Leonard Marcus, PhD, defined the term “meta-leadership” in hospital medicine as a type of leadership that links individuals through their leader’s vision, creating enthusiastic followers.
The Level II course is a must have for those who want to expand upon leadership skills learned in Level I or for those who already have an MBA and want to improve upon leadership in clinical care. The skills discussed in this session are essential to effectively developing and implementing quality improvement programs, patient-safety initiatives, and other programs whose goal is to make system changes that improve patient care.
“The level of attendees participating in Level II was challenging,” says Dr. Holman. “It had us all—faculty and attendees alike—collaborating to answer questions from real-life experiences.”
The phrase “all work and no play” doesn’t describe any SHM meeting, and it certainly can’t be used in reference to the Leadership Academy. Attendees had an opportunity to network with fellow participants and exhibiting companies during the Monday night reception sponsored by Cogent Healthcare. Participants also had ample time to get out and experience some southern hospitality, while enjoying the spa, playing golf, touring on steamboats, dining, and shopping at the Gaylord Opryland Resort and Convention Center.
Leadership Academy Levels I and II were jam-packed with relevant materials and tools applicable to business and the real world. This is an outstanding opportunity for individuals just beginning their leadership journey and for those wanting to take their leadership skills to the next level.
Don’t miss out on the next opportunity to become a leader in hospital medicine. The next meeting will take place during the week of February 26–March 1, 2007, at the Gaylord Palms Resort and Convention Center in Orlando, Fla. Log on to www.hospitalmedicine.org or call (800) 843-3360 for more information.
October 7, 2006, is World Hospice and Palliative Care Day. This day is dedicated to raising the visibility of palliative care within the global community and to providing opportunities to support hospice and palliative care in the form of a unified day of action.
According to official organizers, the event’s theme is “Access to care for all—highlighting the fact that everyone has a right to high-quality end-of-life care, but that more needs to be done to enable everyone to access it.” In creating World Hospice and Palliative Care Day 2006, the event’s organizers aim to raise awareness and understanding of the needs of those living with a terminal diagnosis, as well as the needs of their families. Other goals include calling attention to the need for increasing hospice and palliative care availability throughout the world and raising funds to be used in supporting these services.
Like the first World Hospice and Palliative Care Day, held in 2005, this event will be carried out in conjunction with Voices for Hospices, a global music effort that supports concerts held around the world to raise awareness of this important topic. The Voices for Hospices group is one of many supporters of this cause.
—World Hospice and Palliative Care Day 2006 Web site, Key Messages, page 1.
More than 1,000 events took place on World Hospice and Palliative Care Day 2005, and 74 countries supported the activities. Included in the 2005 event were a cycle rally in Nepal; art exhibitions in Australia, Hong Kong, and Austria; and palliative care conferences in Lithuania and Belarus. In addition, thousands of people from around the world signed a global petition calling for better quality care for people afflicted by terminal illness.
Hospitalists are asked frequently to lead and participate in initiatives meant to improve the identification and treatment of patients and families in need of palliative care. It is common knowledge that traditional medical training tends to focus on the efforts that must be made to cure and prevent illness. There are times when the first priority must be to look for a cure at all costs; however, it must be acknowledged that there are also times when the treatment of a patient’s symptoms should be looked upon as just as important. Conventional medical training frequently does not provide the tools needed to offer the best care for patients and their families when the latter goal becomes the higher priority.
This is why support of initiatives like World Hospice and Palliative Care Day can offer such value to the global community. Events like this one promote awareness of an important topic. For information and ideas on how to get involved in this or in future events, please consult www.worldday.org. Access the Web site’s “Get Involved” page for ideas on how to offer support. Suggested activities include campaigning, creating links and partnerships, and producing materials that will raise awareness.
On the “PR & Press” page of the Web site, in the “Key Messages 2006” section, the following question was posed: “What kinds of issues in general terms does World Hospice and Palliative Care Day hope to raise awareness of year on year?” One of the well-stated answers: “First and foremost we hope the Day helps to increase understanding of hospice and palliative care and how it supports those facing the end of life … . It’s not about ‘helping someone die’ but instead about helping someone to live as comfortably as possible with their illness. It’s about seeing them as [a] living person, not a dying patient. It’s supporting those closest to them and adding life to days, whether or not days can be added to lives.”
Smart Tools for QI Initiatives
SHM’s Quality Improvement Resource Rooms support hospitalists as QI leaders
The role and recognition of the hospitalist has evolved tremendously in the past 10 years, and hospitalists continue to be called upon to lead at their institutions, particularly in quality improvement initiatives. Based on their unique role within the hospital system (a job that requires interaction with many levels of hospital staff) hospitalists are clearly positioned to lead such efforts. As part of SHM’s dedication to promote the highest quality of care for the hospitalized patient, SHM’s Resource Rooms provide members and non-members alike access to information that will aid their knowledge in quality improvement around specific disease states. Currently, SHM provides four Resource Rooms: Venous Thromboembolism (VTE), Stroke, Antimicrobial Resistance (ABX), and Heart Failure. Two additional rooms, Geriatrics and Glycemic Control, will launch this fall.
Quality improvement for the patient will be successful if a systems-based multidisciplinary collaboration within the hospital is improved. Hospitalists are leading this challenging yet exciting opportunity to change the face of healthcare. It has been noted that medical school and residency training have failed to prepare the hospitalist for this leadership role. To this end, SHM provides users of the Resource Rooms with information describing how a specific disease state affects the population and explains why a hospitalist should act in initiating change, as well as what key knowledge, skills, and attitudes the hospitalist should possess. The user is offered information regarding didactic and bedside teaching, patient education, and opportunities for continuing medical education. These resources are useful for the novice as well as for the advanced hospitalist leader. Readers can also apply the concepts of these general mechanisms to any disease state they are seeking to improve at their institutions.
The QI workbook within each of the Resource Rooms is the most important feature and serves as a field guide to implementing a quality improvement program. The workbook includes the following aids:
- Essential first steps: garnering institutional support, assembling a team, developing team rules, and understanding the framework for improvement;
- Conducting an in-depth analysis of current processes and failures;
- Collecting data and devising metrics to assess the impact of your QI initiative;
- Moving from problems to solutions; and
- Continuing to improve: monitoring and learning from the process, as well as holding the gains and spreading your improvement
Other important resources that are common to all of the rooms and will aid in leading the QI efforts of the hospitalist are the educational features. Complex problems need multidisciplinary solutions. The “Improve” and “Educate” areas of the Resource Rooms include information that allow the hospitalist to teach and be taught. In the “Improve” section, a user can find QI Theory slide sets on the foundations of quality improvement initiatives and core measures on specific disease states.
Didactic sessions and teaching tools, as well as professional development, including core competencies and CME opportunities, are all present in the “Educate” feature of each room. For example, in the Heart Failure Resource Room, a didactic session slide set concerning the management of heart failure for hospitalized patients is provided. The slide set includes a heart failure overview that describes the epidemiology, etiologies, and objectives surrounding the management of acute congestive heart failure.
Evidence, improvement, and education tools designed to enhance inpatient outcomes can help the hospitalist develop and lead initiatives that can create a more cost-efficient approach to the treatment of hospitalized patients, while at the same time improving patient outcomes. SHM’s Quality Improvement Resource Rooms provide a compendium of resources to support the hospitalist who is embarking on this enormous task.
September Leadership Academy
New Level II a great success
The recently completed 4th SHM Leadership Academy was a true success in every sense of the word. The event was nearly a sellout, with 160 hospital medicine leaders arriving in Nashville, Tenn., in September to learn—from nationally respected leaders—tangible skills that they could take back to institute in their own practices.
The Leadership Academy Level I was designed to provide leaders in hospital medicine with the skills and resources required to lead and manage programs successfully both now and in the future. Small group sessions gave attendees a chance to interact with faculty and to share personal experiences from their own institutions. Nationally recognized speaker Jack Silversin, DMD, DrPH, presented his infamous broken squares activity, which kept the group energized and working together creatively to learn about effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and then apply them to everyday leadership and management challenges.
Another highlight was the self-evaluation session presented by David Javitch, PhD. His exercise gave everyone an opportunity to learn about their own personality traits and to practice working with extreme opposites, both in the workplace and in everyday life. Attendees continue to rave about the content of this meeting and are looking forward to enhancing their leadership skills by attending Level II courses, scheduled for fall 2007.
“No matter how many times I plan this course, I am amazed at the enthusiasm of the attendees and the new questions that they pose,” says Russell Holman, MD, SHM Leadership Academy course director.
Level II resulted from more than 300 Level I course evaluations that requested additional and ongoing leadership development activities. The Level II course focused on discussions about culture change, negotiation skills, and finance. Keynote speaker Leonard Marcus, PhD, defined the term “meta-leadership” in hospital medicine as a type of leadership that links individuals through their leader’s vision, creating enthusiastic followers.
The Level II course is a must have for those who want to expand upon leadership skills learned in Level I or for those who already have an MBA and want to improve upon leadership in clinical care. The skills discussed in this session are essential to effectively developing and implementing quality improvement programs, patient-safety initiatives, and other programs whose goal is to make system changes that improve patient care.
“The level of attendees participating in Level II was challenging,” says Dr. Holman. “It had us all—faculty and attendees alike—collaborating to answer questions from real-life experiences.”
The phrase “all work and no play” doesn’t describe any SHM meeting, and it certainly can’t be used in reference to the Leadership Academy. Attendees had an opportunity to network with fellow participants and exhibiting companies during the Monday night reception sponsored by Cogent Healthcare. Participants also had ample time to get out and experience some southern hospitality, while enjoying the spa, playing golf, touring on steamboats, dining, and shopping at the Gaylord Opryland Resort and Convention Center.
Leadership Academy Levels I and II were jam-packed with relevant materials and tools applicable to business and the real world. This is an outstanding opportunity for individuals just beginning their leadership journey and for those wanting to take their leadership skills to the next level.
Don’t miss out on the next opportunity to become a leader in hospital medicine. The next meeting will take place during the week of February 26–March 1, 2007, at the Gaylord Palms Resort and Convention Center in Orlando, Fla. Log on to www.hospitalmedicine.org or call (800) 843-3360 for more information.
'I'm not that sick!' Overcoming the barriers to hospice discussions
How do we decide when a patient with nonmalignant disease is eligible for hospice care?
Each hospice has its own policy, but Medicare requires 6 months or less life expectancy for certification of eligibility and reimbursement. Other important criteria include patient and family understanding and wishes.
Evidence-based guidelines for determining prognosis in some noncancer diseases have been developed. However, despite their widespread use, limited data exist to support their accuracy (strength of recommendation: B). Moreover, a high degree of prognostic accuracy may be unattainable given the unpredictable course of common noncancer chronic diseases. Hospice eligibility for patients with nonmalignant disease is based on clinical judgment.
Refer to hospice when goals are focused on quality of life rather than intervention
Nancy Havas, MD
Medical Collage of Wisconsin, Milwaukee
Hospice referral with a nonmalignant diagnosis is challenging but essential to quality patient care. Between episodes of disease exacerbations, we need to take an active role in discussing goals of care, remembering that some patients and families need “permission” to palliative goals rather than continuing with aggressive interventions. My gauge of when to refer to hospice is when the goals of care become focused on quality of life and staying out of the hospital rather than intervention in the disease course. Most patients underuse the benefits that a hospice referral can provide, and while some patients outlive the 6-month criteria for hospice care, this benefit can be renewed if the patient still meets the criteria.
Evidence summary
Hospices have varying admission criteria. However, according to US law, patients must be certified to be “terminally ill” with a prognosis of less than 6 months to live in order to qualify for the Medicare hospice benefit.1 US law and Medicare regulations specify that an attending physician and the accepting hospice medical director must agree to the prognosis for certification of eligibility.
Brickner et al’s survey2 demonstrated that physicians find accurate prognostication difficult. Furthermore, many of the common noncancer diseases have erratic and unpredictable courses, making prognosis even harder. Indeed, patients with noncancer diagnoses are typically admitted to hospices later in their terminal course, 3 resulting in increased inpatient hospital stays4 and ultimately lower patient and family satisfaction. 5 The difficulties inherent in prognostication were underscored by a study that found patients with non-cancer diagnoses to be much more likely to be discharged from hospice alive.6
The National Hospice Organization (NHO) has created guidelines7 for determining prognosis in selected noncancer diseases including heart disease, pulmonary disease, dementia, HIV, liver disease, renal disease, stroke, coma, and amyotrophic lateral sclerosis (ALS). To validate these guidelines, one group identified 2607 patients who meet the NHO guidelines.8 Only 655 (25%) were dead within 6 months. The estimated median survival of these identified patients was 804 days. When every potential prognostic criterion was met (far more than NHO standards) only 19 of the 2607 patients qualified for hospice, and yet 10 of them were still alive at 6 months. Unlike many cancers, in which there is a steady terminal decline, diseases such as chronic obstructive pulmonary disease, congestive heart failure, and liver failure are characterized by a baseline of moderate functioning with intermittent—often life-threatening—exacerbations.
A recent Clinical Inquiry9 addressed the issue of hospice care for patients with late-stage Alzheimer’s disease. That evidence-based answer concluded that criteria superior to the NHO guidelines or clinical judgment had been established for prognosis of Alzheimer’s disease. However, using those improved criteria yielded only marginally more accurate prognostication. At best, 71% of the patients predicted to live less than 6 months did so, but only if the patients had progressed through the disease in an orderly fashion. For the larger subset of patients, those who did not progress through Alzheimer’s in a predictable way, only 30% of the patients actually died within 6 months.
Recommendations from others
The NHO7 provides parameters to help determine a 6-month life expectancy. The “General Guidelines for Determining Prognosis” are summarized in the TABLE. Further details of the “general guidelines” as well as guidelines for prognosis in specific diseases (heart disease, pulmonary disease, dementia, HIV, liver disease, renal disease, stroke, coma, and ALS) are outlined by the NHO.7
TABLE
Hospice criteria
Patients should meet all of the following criteria:
|
1. Social Security Act. 55 FR 50834 (1990), as amended at 57 FR 36017 (1992) (codified at 42 CFR 418.22).
2. Brickner L, Scannell K, Marquet S, Ackerson L. Barriers to hospice care and referrals: survey of physicians’ knowledge, attitudes, and perceptions in a health maintenance organization. J Palliat Med 2004;7:411-418.
3. Farnon C, Hofmann M. Factors contributing to late hospice admission and proposals for change. Am J Hosp Palliat Care 1997;14:212-218.
4. Miller SC, Kinzbrunner B, Pettit P, Williams JR. How does the timing of hospice referral influence hospice care in the last days of life? J Am Geriatr Soc 2003;51:798-806.
5. Rickerson E, Harrold J, Kapo J, Carroll JT, Casarett D. Timing of hospice referral and families’ perceptions of services: are earlier hospice referrals better? J Am Geriatr Soc 2005;53:819-523.
6. Kutner JS, Meyer SA, Beaty BL, Kassner CT, Nowels DE, Beehler C. Outcomes and characteristics of patients discharged alive from hospice. J Am Geriatr Soc 2004;52:1337-1342.
7. National Hospice Organization Standards and Accreditation Committee Medical Guidelines Task Force. Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases. Hosp J 1996;11:47-63.
8. Fox E, Landrum-McNiff K, Zhong Z, Dawson NV, Wu AW, Lynn J. Evaluation of prognostic criteria for determining hospice eligibility in patients with advanced lung, heart, or liver disease. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatments. JAMA 1999;282:1638-1645
9. Modi S, Moore C, Shah K. Which late-stage Alzheimer’s patients should be referred for hospice care? J Fam Pract 2005;54:984-986.
Each hospice has its own policy, but Medicare requires 6 months or less life expectancy for certification of eligibility and reimbursement. Other important criteria include patient and family understanding and wishes.
Evidence-based guidelines for determining prognosis in some noncancer diseases have been developed. However, despite their widespread use, limited data exist to support their accuracy (strength of recommendation: B). Moreover, a high degree of prognostic accuracy may be unattainable given the unpredictable course of common noncancer chronic diseases. Hospice eligibility for patients with nonmalignant disease is based on clinical judgment.
Refer to hospice when goals are focused on quality of life rather than intervention
Nancy Havas, MD
Medical Collage of Wisconsin, Milwaukee
Hospice referral with a nonmalignant diagnosis is challenging but essential to quality patient care. Between episodes of disease exacerbations, we need to take an active role in discussing goals of care, remembering that some patients and families need “permission” to palliative goals rather than continuing with aggressive interventions. My gauge of when to refer to hospice is when the goals of care become focused on quality of life and staying out of the hospital rather than intervention in the disease course. Most patients underuse the benefits that a hospice referral can provide, and while some patients outlive the 6-month criteria for hospice care, this benefit can be renewed if the patient still meets the criteria.
Evidence summary
Hospices have varying admission criteria. However, according to US law, patients must be certified to be “terminally ill” with a prognosis of less than 6 months to live in order to qualify for the Medicare hospice benefit.1 US law and Medicare regulations specify that an attending physician and the accepting hospice medical director must agree to the prognosis for certification of eligibility.
Brickner et al’s survey2 demonstrated that physicians find accurate prognostication difficult. Furthermore, many of the common noncancer diseases have erratic and unpredictable courses, making prognosis even harder. Indeed, patients with noncancer diagnoses are typically admitted to hospices later in their terminal course, 3 resulting in increased inpatient hospital stays4 and ultimately lower patient and family satisfaction. 5 The difficulties inherent in prognostication were underscored by a study that found patients with non-cancer diagnoses to be much more likely to be discharged from hospice alive.6
The National Hospice Organization (NHO) has created guidelines7 for determining prognosis in selected noncancer diseases including heart disease, pulmonary disease, dementia, HIV, liver disease, renal disease, stroke, coma, and amyotrophic lateral sclerosis (ALS). To validate these guidelines, one group identified 2607 patients who meet the NHO guidelines.8 Only 655 (25%) were dead within 6 months. The estimated median survival of these identified patients was 804 days. When every potential prognostic criterion was met (far more than NHO standards) only 19 of the 2607 patients qualified for hospice, and yet 10 of them were still alive at 6 months. Unlike many cancers, in which there is a steady terminal decline, diseases such as chronic obstructive pulmonary disease, congestive heart failure, and liver failure are characterized by a baseline of moderate functioning with intermittent—often life-threatening—exacerbations.
A recent Clinical Inquiry9 addressed the issue of hospice care for patients with late-stage Alzheimer’s disease. That evidence-based answer concluded that criteria superior to the NHO guidelines or clinical judgment had been established for prognosis of Alzheimer’s disease. However, using those improved criteria yielded only marginally more accurate prognostication. At best, 71% of the patients predicted to live less than 6 months did so, but only if the patients had progressed through the disease in an orderly fashion. For the larger subset of patients, those who did not progress through Alzheimer’s in a predictable way, only 30% of the patients actually died within 6 months.
Recommendations from others
The NHO7 provides parameters to help determine a 6-month life expectancy. The “General Guidelines for Determining Prognosis” are summarized in the TABLE. Further details of the “general guidelines” as well as guidelines for prognosis in specific diseases (heart disease, pulmonary disease, dementia, HIV, liver disease, renal disease, stroke, coma, and ALS) are outlined by the NHO.7
TABLE
Hospice criteria
Patients should meet all of the following criteria:
|
Each hospice has its own policy, but Medicare requires 6 months or less life expectancy for certification of eligibility and reimbursement. Other important criteria include patient and family understanding and wishes.
Evidence-based guidelines for determining prognosis in some noncancer diseases have been developed. However, despite their widespread use, limited data exist to support their accuracy (strength of recommendation: B). Moreover, a high degree of prognostic accuracy may be unattainable given the unpredictable course of common noncancer chronic diseases. Hospice eligibility for patients with nonmalignant disease is based on clinical judgment.
Refer to hospice when goals are focused on quality of life rather than intervention
Nancy Havas, MD
Medical Collage of Wisconsin, Milwaukee
Hospice referral with a nonmalignant diagnosis is challenging but essential to quality patient care. Between episodes of disease exacerbations, we need to take an active role in discussing goals of care, remembering that some patients and families need “permission” to palliative goals rather than continuing with aggressive interventions. My gauge of when to refer to hospice is when the goals of care become focused on quality of life and staying out of the hospital rather than intervention in the disease course. Most patients underuse the benefits that a hospice referral can provide, and while some patients outlive the 6-month criteria for hospice care, this benefit can be renewed if the patient still meets the criteria.
Evidence summary
Hospices have varying admission criteria. However, according to US law, patients must be certified to be “terminally ill” with a prognosis of less than 6 months to live in order to qualify for the Medicare hospice benefit.1 US law and Medicare regulations specify that an attending physician and the accepting hospice medical director must agree to the prognosis for certification of eligibility.
Brickner et al’s survey2 demonstrated that physicians find accurate prognostication difficult. Furthermore, many of the common noncancer diseases have erratic and unpredictable courses, making prognosis even harder. Indeed, patients with noncancer diagnoses are typically admitted to hospices later in their terminal course, 3 resulting in increased inpatient hospital stays4 and ultimately lower patient and family satisfaction. 5 The difficulties inherent in prognostication were underscored by a study that found patients with non-cancer diagnoses to be much more likely to be discharged from hospice alive.6
The National Hospice Organization (NHO) has created guidelines7 for determining prognosis in selected noncancer diseases including heart disease, pulmonary disease, dementia, HIV, liver disease, renal disease, stroke, coma, and amyotrophic lateral sclerosis (ALS). To validate these guidelines, one group identified 2607 patients who meet the NHO guidelines.8 Only 655 (25%) were dead within 6 months. The estimated median survival of these identified patients was 804 days. When every potential prognostic criterion was met (far more than NHO standards) only 19 of the 2607 patients qualified for hospice, and yet 10 of them were still alive at 6 months. Unlike many cancers, in which there is a steady terminal decline, diseases such as chronic obstructive pulmonary disease, congestive heart failure, and liver failure are characterized by a baseline of moderate functioning with intermittent—often life-threatening—exacerbations.
A recent Clinical Inquiry9 addressed the issue of hospice care for patients with late-stage Alzheimer’s disease. That evidence-based answer concluded that criteria superior to the NHO guidelines or clinical judgment had been established for prognosis of Alzheimer’s disease. However, using those improved criteria yielded only marginally more accurate prognostication. At best, 71% of the patients predicted to live less than 6 months did so, but only if the patients had progressed through the disease in an orderly fashion. For the larger subset of patients, those who did not progress through Alzheimer’s in a predictable way, only 30% of the patients actually died within 6 months.
Recommendations from others
The NHO7 provides parameters to help determine a 6-month life expectancy. The “General Guidelines for Determining Prognosis” are summarized in the TABLE. Further details of the “general guidelines” as well as guidelines for prognosis in specific diseases (heart disease, pulmonary disease, dementia, HIV, liver disease, renal disease, stroke, coma, and ALS) are outlined by the NHO.7
TABLE
Hospice criteria
Patients should meet all of the following criteria:
|
1. Social Security Act. 55 FR 50834 (1990), as amended at 57 FR 36017 (1992) (codified at 42 CFR 418.22).
2. Brickner L, Scannell K, Marquet S, Ackerson L. Barriers to hospice care and referrals: survey of physicians’ knowledge, attitudes, and perceptions in a health maintenance organization. J Palliat Med 2004;7:411-418.
3. Farnon C, Hofmann M. Factors contributing to late hospice admission and proposals for change. Am J Hosp Palliat Care 1997;14:212-218.
4. Miller SC, Kinzbrunner B, Pettit P, Williams JR. How does the timing of hospice referral influence hospice care in the last days of life? J Am Geriatr Soc 2003;51:798-806.
5. Rickerson E, Harrold J, Kapo J, Carroll JT, Casarett D. Timing of hospice referral and families’ perceptions of services: are earlier hospice referrals better? J Am Geriatr Soc 2005;53:819-523.
6. Kutner JS, Meyer SA, Beaty BL, Kassner CT, Nowels DE, Beehler C. Outcomes and characteristics of patients discharged alive from hospice. J Am Geriatr Soc 2004;52:1337-1342.
7. National Hospice Organization Standards and Accreditation Committee Medical Guidelines Task Force. Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases. Hosp J 1996;11:47-63.
8. Fox E, Landrum-McNiff K, Zhong Z, Dawson NV, Wu AW, Lynn J. Evaluation of prognostic criteria for determining hospice eligibility in patients with advanced lung, heart, or liver disease. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatments. JAMA 1999;282:1638-1645
9. Modi S, Moore C, Shah K. Which late-stage Alzheimer’s patients should be referred for hospice care? J Fam Pract 2005;54:984-986.
1. Social Security Act. 55 FR 50834 (1990), as amended at 57 FR 36017 (1992) (codified at 42 CFR 418.22).
2. Brickner L, Scannell K, Marquet S, Ackerson L. Barriers to hospice care and referrals: survey of physicians’ knowledge, attitudes, and perceptions in a health maintenance organization. J Palliat Med 2004;7:411-418.
3. Farnon C, Hofmann M. Factors contributing to late hospice admission and proposals for change. Am J Hosp Palliat Care 1997;14:212-218.
4. Miller SC, Kinzbrunner B, Pettit P, Williams JR. How does the timing of hospice referral influence hospice care in the last days of life? J Am Geriatr Soc 2003;51:798-806.
5. Rickerson E, Harrold J, Kapo J, Carroll JT, Casarett D. Timing of hospice referral and families’ perceptions of services: are earlier hospice referrals better? J Am Geriatr Soc 2005;53:819-523.
6. Kutner JS, Meyer SA, Beaty BL, Kassner CT, Nowels DE, Beehler C. Outcomes and characteristics of patients discharged alive from hospice. J Am Geriatr Soc 2004;52:1337-1342.
7. National Hospice Organization Standards and Accreditation Committee Medical Guidelines Task Force. Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases. Hosp J 1996;11:47-63.
8. Fox E, Landrum-McNiff K, Zhong Z, Dawson NV, Wu AW, Lynn J. Evaluation of prognostic criteria for determining hospice eligibility in patients with advanced lung, heart, or liver disease. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatments. JAMA 1999;282:1638-1645
9. Modi S, Moore C, Shah K. Which late-stage Alzheimer’s patients should be referred for hospice care? J Fam Pract 2005;54:984-986.
Evidence-based answers from the Family Physicians Inquiries Network