User login
Palliative Consult
Hospital-based palliative care programs are gaining traction in the United States as studies show their efficacy in decreasing length of stay and improved quality of patient care.1,2 According to the American Hospital Association, 22% of all U.S. hospitals now have such programs.3 These programs—with their emphasis on coordinated, team-delivered care and communication—seem tailor-made for the expertise of hospitalists who are increasingly taking the lead to establish them at their institutions.
Through the SHM Web site (www.hospitalmedicine.org) and the Center to Advance Palliative Care (www.capc.org) ample resources exist for developing program infrastructure and acquiring on-site training (see www.capc.org/palliative-care-leadershipinitiative/overview).
There are unwritten protocols, however, that can make or break a palliative care service. Hospitalists involved with palliative care often find themselves relating to oncologists because many patients who have palliative care needs are undergoing inpatient curative treatments (such as brachytherapy) or are actively dying. Palliative care experts interviewed for this article agreed that in order to encourage referrals from their oncology colleagues, hospitalists must be attentive to oncologists’ concerns and to consultation etiquette.
“Palliative care has been something that oncologists traditionally think they do pretty well,” says David H. Lawson, MD, section chief, Medical Oncology at Emory Clinic. “I think there will be a lot of variability between oncologists about what they see as their province and what they see as open for someone else.”
—Diane E. Meier, MD
Assessing Oncologists’ Needs
During the organizational phase of a hospital-based palliative care service, it is advisable to meet with oncologists one-on-one, believes Charles F. von Gunten, MD, PhD, medical director of the Palliative Care Consultation Service at the University of California, San Diego, and director of the Center for Palliative Studies at San Diego Hospice and Palliative Care. “All consult services are fundamentally about providing advice to the managing physician when requested, about what is requested, and nothing else.”
He recommends that hospitalists involved in development of a hospital-based palliative care service find out how key oncologists at their hospital perceive the needs in the area of palliative care. “This may not match what the hospitalist thinks the oncologist needs, but that’s immaterial,” he cautions.
This advice squares with that of Steve Pantilat, MD, immediate past-president of SHM, and his team at the University of California, San Francisco. The palliative care service at UCSF is one of six Palliative Care Leadership Centers nationwide, so designated during an initiative launched two years ago by the Center to Advance Palliative Care. (The Robert Wood Johnson Foundation underwrites training activities at the six centers.) The issue in establishing palliative care services, says Dr. Pantilat, is “figuring out what would attract oncologists about such a program. What issues are most salient to them? Instead of saying, ‘I have a new service; would you please use it?’ You have to come in and say, ‘We’re thinking of starting this new service; how can we be of help to you?’ ”
Dr. Lawson agrees with Dr. von Gunten and Dr. Pantilat that hospitalists must develop communication with oncologists early during the start-up phase of a palliative care service. Hospitalists who offer palliative care services should also take time to familiarize themselves with patients’ treatment plans.
“I think there is going to be a learning curve for palliative care specialists,” says Dr. Lawson. “Part of that learning is to get some sense of how oncologists make decisions about whether to give chemo[therapy] or not. Oftentimes, there are pressures that might not be obvious.”
For instance, it may appear to a palliative care consultant that a certain patient should not undergo chemotherapy, but in fact the patient or the family may demand it.
Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, says the majority of consults she does are with oncology patients. She has found that attending Monday morning sign-out meetings with Emory oncologists has not only increased referrals to the palliative care service, but has added to her understanding of oncologists’ decision-making processes.
“When I go to weekly meetings, I hear the full spectrum of what they are doing. I see how oncologists work and how they decide about treatments,” she says. “It’s been a really good experience because I never would have seen this from the hospitalist viewpoint.”
Emory’s palliative care program was launched in November 2005 and has grown so quickly that they already need additional staff.
The Primary Client
The “key message” for a hospitalist when asked to do a palliative care consult is to remember that the client of a consultation service is the referring physician, points out geriatrician Diane E. Meier, MD, director of the Center to Advance Palliative Care and the director of the Hertzberg Palliative Care Institute at Mount Sinai School of Medicine in New York City. “As a geriatrician, if I call in an infectious disease consultant, I’m calling that physician to help me make decisions about my patient—not for that person to take over the care of my patient or to undermine my relationship to that patient. This is basic consultation etiquette, but physicians are often not taught in medical school or residency the difference between a primary care responsibility and a consultation responsibility.”
“The biggest mistake that people make in putting together palliative care services,” concurs Dr. von Gunten, “is thinking that the patient is the client. That isn’t true. It is the person requesting the consultation—meaning, the referring physician or the managing service. The patient is the secondary beneficiary.
“The language we use—‘my patient’—is fundamental to the practice of American medicine,” explains Dr. von Gunten. You have to respect that. If you go to someone’s home, you don’t redecorate it because you don’t like their taste. You do not comment on their choice of draperies or their choice of food. The same applies to medical consultations.” (See “Consult Etiquette for Palliative Care Services,” p. 33.)
Oncologists generally feel “very possessive” about their patients, adds Dr. von Gunten. Even though oncologists are technically also consultants (to the patient’s primary care physician), the pattern in American medicine is that oncologists treating patients acquire the status of a primary care physician. “So,” he says, “you treat them with that kind of respect, which means that you ask permission before you do things, and you don’t disparage what they are doing—either to their faces or to their patients or to other bystanders like nurses.”
Dr. Lawson agrees that oncologists often have a strong personal bond with their patients. “These personal feelings are often reciprocated by the patients and families,” he says. “Accepting another person [the hospitalist as palliative care consultant] into the equation can be difficult at times, even more so while the patient is still in the hospital and the oncologist is still around.”
The palliative care program at Emory is consult-driven. “The doctor has to agree to us getting involved, so I don’t get into territorial issues,” says Dr. Grossman. “When I do get involved with patients, the oncologists welcome me taking care of them and realize the benefit of what I’m doing. They see that my approach is collaborative.”
Dr. Grossman has been able to offer services to oncologists whose patients are receiving chemotherapy and experiencing significant symptoms, such as pain. When hospitalists on the hospital medicine service consult her about cancer patients, she calls the primary oncologist to familiarize herself with the patient’s background and to check if other treatments are available.
Strengths of Hospitalists
Palliative care should be distinguished from hospice or end-of-life care, although it can be concurrent. Palliative care needs—ranging from symptom management to alleviating psychological suffering—can exist at any point along the cancer care trajectory, notes Dr. von Gunten, who was a co-developer with Dr. Pantilat and others of the California Hospital Initiative in Palliative Services program to assist hospitals to develop palliative services.4
Hospitalists, says Dr. von Gunten, already possess some of the baseline skills needed to deliver palliative care: They’re based in the hospital and so have the opportunity to interact with patients and their families; they are experienced in hospital-based management of patients; they are experienced in teamwork with other providers also based in the hospital. The ability to be available to patients and physicians 24/7 is a real advantage in symptom management, says Dr. Lawson.
Because hospitalists by definition care for people who are not their primary care patients, the sophistication and sensitivity about working with one’s colleagues “is already inculcated,” observes Dr. Meier. In addition, “hospitalists understand that their responsibility to and relationship with the patient is only one piece of being a good doctor. Ensuring good care for a patient means very high level and high intensity communications with everyone involved in that patient’s care: all the other specialists, the primary care physician, and the floor team—the social workers, nurses, certified nursing assistants, dietary staff, and rehab and physiatry staff. Unless everyone is reading from the same page, the patient’s care will not be good. Very often, it’s the hospitalist or palliative care consultant who is at the center of the wheel, making sure that all the spokes are getting the same message,” she says.
Busy oncologists may call upon Dr. Grossman’s service to conduct family meetings about care plans. “Patients are very loyal to their oncologists, and they want their oncologists to be supportive of their decisions,” she notes. “I always explain to patients that my consultation was requested or supported by their oncologist. I am not there to cause more barriers; I’m there to have everybody on board and to understand where the patient is. We call everybody in—the social worker, the nurse, chaplaincy staff—because our approach is interdisciplinary and these are the essential members of our team.”
Dr. Grossman believes that hospitalists’ training in teamwork and communications are key to providing a good experience for oncology patients and their families. She is board certified in palliative care, which allows her to bring additional expertise to symptom support, including situations where she can help the dying process be as peaceful as possible—for both patient and family.
The issues important in palliative care—availability to patients, families, and referring physicians, ability to work in teams, and quality of care—dovetail with the primary goals of hospital medicine. Hospitalists’ palliative care services can thrive when they forge strong foundational relationships with their referring colleagues. TH
Gretchen Henkel regularly contributes to The Hospitalist.
References
- Selwyn PA, Rivard M, Kappell D, et al. Palliative care for AIDS at a large urban teaching hospital: program description and preliminary outcomes. J Palliat Med. 2003 Jun;6(3):461-474.
- Ryan A, Carter J, Lucas J, Berger J. You need not make the journey alone: overcoming impediments to providing palliative care in a public urban teaching hospital. Am J Hosp Palliat Care. 2002 May-June;19(3):171-180.
- The Case for Hospital-Based Palliative Care, published by the Center to Advance Palliative Care. Available online at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Last accessed March 22, 2006.
- Pantilat SZ, Rabow MW, Citko J, et al. Evaluating the California Hospital Initiative in Palliative Services. Arch Intern Med. 2006 Jan 23;166(2):227-230.
Hospital-based palliative care programs are gaining traction in the United States as studies show their efficacy in decreasing length of stay and improved quality of patient care.1,2 According to the American Hospital Association, 22% of all U.S. hospitals now have such programs.3 These programs—with their emphasis on coordinated, team-delivered care and communication—seem tailor-made for the expertise of hospitalists who are increasingly taking the lead to establish them at their institutions.
Through the SHM Web site (www.hospitalmedicine.org) and the Center to Advance Palliative Care (www.capc.org) ample resources exist for developing program infrastructure and acquiring on-site training (see www.capc.org/palliative-care-leadershipinitiative/overview).
There are unwritten protocols, however, that can make or break a palliative care service. Hospitalists involved with palliative care often find themselves relating to oncologists because many patients who have palliative care needs are undergoing inpatient curative treatments (such as brachytherapy) or are actively dying. Palliative care experts interviewed for this article agreed that in order to encourage referrals from their oncology colleagues, hospitalists must be attentive to oncologists’ concerns and to consultation etiquette.
“Palliative care has been something that oncologists traditionally think they do pretty well,” says David H. Lawson, MD, section chief, Medical Oncology at Emory Clinic. “I think there will be a lot of variability between oncologists about what they see as their province and what they see as open for someone else.”
—Diane E. Meier, MD
Assessing Oncologists’ Needs
During the organizational phase of a hospital-based palliative care service, it is advisable to meet with oncologists one-on-one, believes Charles F. von Gunten, MD, PhD, medical director of the Palliative Care Consultation Service at the University of California, San Diego, and director of the Center for Palliative Studies at San Diego Hospice and Palliative Care. “All consult services are fundamentally about providing advice to the managing physician when requested, about what is requested, and nothing else.”
He recommends that hospitalists involved in development of a hospital-based palliative care service find out how key oncologists at their hospital perceive the needs in the area of palliative care. “This may not match what the hospitalist thinks the oncologist needs, but that’s immaterial,” he cautions.
This advice squares with that of Steve Pantilat, MD, immediate past-president of SHM, and his team at the University of California, San Francisco. The palliative care service at UCSF is one of six Palliative Care Leadership Centers nationwide, so designated during an initiative launched two years ago by the Center to Advance Palliative Care. (The Robert Wood Johnson Foundation underwrites training activities at the six centers.) The issue in establishing palliative care services, says Dr. Pantilat, is “figuring out what would attract oncologists about such a program. What issues are most salient to them? Instead of saying, ‘I have a new service; would you please use it?’ You have to come in and say, ‘We’re thinking of starting this new service; how can we be of help to you?’ ”
Dr. Lawson agrees with Dr. von Gunten and Dr. Pantilat that hospitalists must develop communication with oncologists early during the start-up phase of a palliative care service. Hospitalists who offer palliative care services should also take time to familiarize themselves with patients’ treatment plans.
“I think there is going to be a learning curve for palliative care specialists,” says Dr. Lawson. “Part of that learning is to get some sense of how oncologists make decisions about whether to give chemo[therapy] or not. Oftentimes, there are pressures that might not be obvious.”
For instance, it may appear to a palliative care consultant that a certain patient should not undergo chemotherapy, but in fact the patient or the family may demand it.
Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, says the majority of consults she does are with oncology patients. She has found that attending Monday morning sign-out meetings with Emory oncologists has not only increased referrals to the palliative care service, but has added to her understanding of oncologists’ decision-making processes.
“When I go to weekly meetings, I hear the full spectrum of what they are doing. I see how oncologists work and how they decide about treatments,” she says. “It’s been a really good experience because I never would have seen this from the hospitalist viewpoint.”
Emory’s palliative care program was launched in November 2005 and has grown so quickly that they already need additional staff.
The Primary Client
The “key message” for a hospitalist when asked to do a palliative care consult is to remember that the client of a consultation service is the referring physician, points out geriatrician Diane E. Meier, MD, director of the Center to Advance Palliative Care and the director of the Hertzberg Palliative Care Institute at Mount Sinai School of Medicine in New York City. “As a geriatrician, if I call in an infectious disease consultant, I’m calling that physician to help me make decisions about my patient—not for that person to take over the care of my patient or to undermine my relationship to that patient. This is basic consultation etiquette, but physicians are often not taught in medical school or residency the difference between a primary care responsibility and a consultation responsibility.”
“The biggest mistake that people make in putting together palliative care services,” concurs Dr. von Gunten, “is thinking that the patient is the client. That isn’t true. It is the person requesting the consultation—meaning, the referring physician or the managing service. The patient is the secondary beneficiary.
“The language we use—‘my patient’—is fundamental to the practice of American medicine,” explains Dr. von Gunten. You have to respect that. If you go to someone’s home, you don’t redecorate it because you don’t like their taste. You do not comment on their choice of draperies or their choice of food. The same applies to medical consultations.” (See “Consult Etiquette for Palliative Care Services,” p. 33.)
Oncologists generally feel “very possessive” about their patients, adds Dr. von Gunten. Even though oncologists are technically also consultants (to the patient’s primary care physician), the pattern in American medicine is that oncologists treating patients acquire the status of a primary care physician. “So,” he says, “you treat them with that kind of respect, which means that you ask permission before you do things, and you don’t disparage what they are doing—either to their faces or to their patients or to other bystanders like nurses.”
Dr. Lawson agrees that oncologists often have a strong personal bond with their patients. “These personal feelings are often reciprocated by the patients and families,” he says. “Accepting another person [the hospitalist as palliative care consultant] into the equation can be difficult at times, even more so while the patient is still in the hospital and the oncologist is still around.”
The palliative care program at Emory is consult-driven. “The doctor has to agree to us getting involved, so I don’t get into territorial issues,” says Dr. Grossman. “When I do get involved with patients, the oncologists welcome me taking care of them and realize the benefit of what I’m doing. They see that my approach is collaborative.”
Dr. Grossman has been able to offer services to oncologists whose patients are receiving chemotherapy and experiencing significant symptoms, such as pain. When hospitalists on the hospital medicine service consult her about cancer patients, she calls the primary oncologist to familiarize herself with the patient’s background and to check if other treatments are available.
Strengths of Hospitalists
Palliative care should be distinguished from hospice or end-of-life care, although it can be concurrent. Palliative care needs—ranging from symptom management to alleviating psychological suffering—can exist at any point along the cancer care trajectory, notes Dr. von Gunten, who was a co-developer with Dr. Pantilat and others of the California Hospital Initiative in Palliative Services program to assist hospitals to develop palliative services.4
Hospitalists, says Dr. von Gunten, already possess some of the baseline skills needed to deliver palliative care: They’re based in the hospital and so have the opportunity to interact with patients and their families; they are experienced in hospital-based management of patients; they are experienced in teamwork with other providers also based in the hospital. The ability to be available to patients and physicians 24/7 is a real advantage in symptom management, says Dr. Lawson.
Because hospitalists by definition care for people who are not their primary care patients, the sophistication and sensitivity about working with one’s colleagues “is already inculcated,” observes Dr. Meier. In addition, “hospitalists understand that their responsibility to and relationship with the patient is only one piece of being a good doctor. Ensuring good care for a patient means very high level and high intensity communications with everyone involved in that patient’s care: all the other specialists, the primary care physician, and the floor team—the social workers, nurses, certified nursing assistants, dietary staff, and rehab and physiatry staff. Unless everyone is reading from the same page, the patient’s care will not be good. Very often, it’s the hospitalist or palliative care consultant who is at the center of the wheel, making sure that all the spokes are getting the same message,” she says.
Busy oncologists may call upon Dr. Grossman’s service to conduct family meetings about care plans. “Patients are very loyal to their oncologists, and they want their oncologists to be supportive of their decisions,” she notes. “I always explain to patients that my consultation was requested or supported by their oncologist. I am not there to cause more barriers; I’m there to have everybody on board and to understand where the patient is. We call everybody in—the social worker, the nurse, chaplaincy staff—because our approach is interdisciplinary and these are the essential members of our team.”
Dr. Grossman believes that hospitalists’ training in teamwork and communications are key to providing a good experience for oncology patients and their families. She is board certified in palliative care, which allows her to bring additional expertise to symptom support, including situations where she can help the dying process be as peaceful as possible—for both patient and family.
The issues important in palliative care—availability to patients, families, and referring physicians, ability to work in teams, and quality of care—dovetail with the primary goals of hospital medicine. Hospitalists’ palliative care services can thrive when they forge strong foundational relationships with their referring colleagues. TH
Gretchen Henkel regularly contributes to The Hospitalist.
References
- Selwyn PA, Rivard M, Kappell D, et al. Palliative care for AIDS at a large urban teaching hospital: program description and preliminary outcomes. J Palliat Med. 2003 Jun;6(3):461-474.
- Ryan A, Carter J, Lucas J, Berger J. You need not make the journey alone: overcoming impediments to providing palliative care in a public urban teaching hospital. Am J Hosp Palliat Care. 2002 May-June;19(3):171-180.
- The Case for Hospital-Based Palliative Care, published by the Center to Advance Palliative Care. Available online at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Last accessed March 22, 2006.
- Pantilat SZ, Rabow MW, Citko J, et al. Evaluating the California Hospital Initiative in Palliative Services. Arch Intern Med. 2006 Jan 23;166(2):227-230.
Hospital-based palliative care programs are gaining traction in the United States as studies show their efficacy in decreasing length of stay and improved quality of patient care.1,2 According to the American Hospital Association, 22% of all U.S. hospitals now have such programs.3 These programs—with their emphasis on coordinated, team-delivered care and communication—seem tailor-made for the expertise of hospitalists who are increasingly taking the lead to establish them at their institutions.
Through the SHM Web site (www.hospitalmedicine.org) and the Center to Advance Palliative Care (www.capc.org) ample resources exist for developing program infrastructure and acquiring on-site training (see www.capc.org/palliative-care-leadershipinitiative/overview).
There are unwritten protocols, however, that can make or break a palliative care service. Hospitalists involved with palliative care often find themselves relating to oncologists because many patients who have palliative care needs are undergoing inpatient curative treatments (such as brachytherapy) or are actively dying. Palliative care experts interviewed for this article agreed that in order to encourage referrals from their oncology colleagues, hospitalists must be attentive to oncologists’ concerns and to consultation etiquette.
“Palliative care has been something that oncologists traditionally think they do pretty well,” says David H. Lawson, MD, section chief, Medical Oncology at Emory Clinic. “I think there will be a lot of variability between oncologists about what they see as their province and what they see as open for someone else.”
—Diane E. Meier, MD
Assessing Oncologists’ Needs
During the organizational phase of a hospital-based palliative care service, it is advisable to meet with oncologists one-on-one, believes Charles F. von Gunten, MD, PhD, medical director of the Palliative Care Consultation Service at the University of California, San Diego, and director of the Center for Palliative Studies at San Diego Hospice and Palliative Care. “All consult services are fundamentally about providing advice to the managing physician when requested, about what is requested, and nothing else.”
He recommends that hospitalists involved in development of a hospital-based palliative care service find out how key oncologists at their hospital perceive the needs in the area of palliative care. “This may not match what the hospitalist thinks the oncologist needs, but that’s immaterial,” he cautions.
This advice squares with that of Steve Pantilat, MD, immediate past-president of SHM, and his team at the University of California, San Francisco. The palliative care service at UCSF is one of six Palliative Care Leadership Centers nationwide, so designated during an initiative launched two years ago by the Center to Advance Palliative Care. (The Robert Wood Johnson Foundation underwrites training activities at the six centers.) The issue in establishing palliative care services, says Dr. Pantilat, is “figuring out what would attract oncologists about such a program. What issues are most salient to them? Instead of saying, ‘I have a new service; would you please use it?’ You have to come in and say, ‘We’re thinking of starting this new service; how can we be of help to you?’ ”
Dr. Lawson agrees with Dr. von Gunten and Dr. Pantilat that hospitalists must develop communication with oncologists early during the start-up phase of a palliative care service. Hospitalists who offer palliative care services should also take time to familiarize themselves with patients’ treatment plans.
“I think there is going to be a learning curve for palliative care specialists,” says Dr. Lawson. “Part of that learning is to get some sense of how oncologists make decisions about whether to give chemo[therapy] or not. Oftentimes, there are pressures that might not be obvious.”
For instance, it may appear to a palliative care consultant that a certain patient should not undergo chemotherapy, but in fact the patient or the family may demand it.
Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, says the majority of consults she does are with oncology patients. She has found that attending Monday morning sign-out meetings with Emory oncologists has not only increased referrals to the palliative care service, but has added to her understanding of oncologists’ decision-making processes.
“When I go to weekly meetings, I hear the full spectrum of what they are doing. I see how oncologists work and how they decide about treatments,” she says. “It’s been a really good experience because I never would have seen this from the hospitalist viewpoint.”
Emory’s palliative care program was launched in November 2005 and has grown so quickly that they already need additional staff.
The Primary Client
The “key message” for a hospitalist when asked to do a palliative care consult is to remember that the client of a consultation service is the referring physician, points out geriatrician Diane E. Meier, MD, director of the Center to Advance Palliative Care and the director of the Hertzberg Palliative Care Institute at Mount Sinai School of Medicine in New York City. “As a geriatrician, if I call in an infectious disease consultant, I’m calling that physician to help me make decisions about my patient—not for that person to take over the care of my patient or to undermine my relationship to that patient. This is basic consultation etiquette, but physicians are often not taught in medical school or residency the difference between a primary care responsibility and a consultation responsibility.”
“The biggest mistake that people make in putting together palliative care services,” concurs Dr. von Gunten, “is thinking that the patient is the client. That isn’t true. It is the person requesting the consultation—meaning, the referring physician or the managing service. The patient is the secondary beneficiary.
“The language we use—‘my patient’—is fundamental to the practice of American medicine,” explains Dr. von Gunten. You have to respect that. If you go to someone’s home, you don’t redecorate it because you don’t like their taste. You do not comment on their choice of draperies or their choice of food. The same applies to medical consultations.” (See “Consult Etiquette for Palliative Care Services,” p. 33.)
Oncologists generally feel “very possessive” about their patients, adds Dr. von Gunten. Even though oncologists are technically also consultants (to the patient’s primary care physician), the pattern in American medicine is that oncologists treating patients acquire the status of a primary care physician. “So,” he says, “you treat them with that kind of respect, which means that you ask permission before you do things, and you don’t disparage what they are doing—either to their faces or to their patients or to other bystanders like nurses.”
Dr. Lawson agrees that oncologists often have a strong personal bond with their patients. “These personal feelings are often reciprocated by the patients and families,” he says. “Accepting another person [the hospitalist as palliative care consultant] into the equation can be difficult at times, even more so while the patient is still in the hospital and the oncologist is still around.”
The palliative care program at Emory is consult-driven. “The doctor has to agree to us getting involved, so I don’t get into territorial issues,” says Dr. Grossman. “When I do get involved with patients, the oncologists welcome me taking care of them and realize the benefit of what I’m doing. They see that my approach is collaborative.”
Dr. Grossman has been able to offer services to oncologists whose patients are receiving chemotherapy and experiencing significant symptoms, such as pain. When hospitalists on the hospital medicine service consult her about cancer patients, she calls the primary oncologist to familiarize herself with the patient’s background and to check if other treatments are available.
Strengths of Hospitalists
Palliative care should be distinguished from hospice or end-of-life care, although it can be concurrent. Palliative care needs—ranging from symptom management to alleviating psychological suffering—can exist at any point along the cancer care trajectory, notes Dr. von Gunten, who was a co-developer with Dr. Pantilat and others of the California Hospital Initiative in Palliative Services program to assist hospitals to develop palliative services.4
Hospitalists, says Dr. von Gunten, already possess some of the baseline skills needed to deliver palliative care: They’re based in the hospital and so have the opportunity to interact with patients and their families; they are experienced in hospital-based management of patients; they are experienced in teamwork with other providers also based in the hospital. The ability to be available to patients and physicians 24/7 is a real advantage in symptom management, says Dr. Lawson.
Because hospitalists by definition care for people who are not their primary care patients, the sophistication and sensitivity about working with one’s colleagues “is already inculcated,” observes Dr. Meier. In addition, “hospitalists understand that their responsibility to and relationship with the patient is only one piece of being a good doctor. Ensuring good care for a patient means very high level and high intensity communications with everyone involved in that patient’s care: all the other specialists, the primary care physician, and the floor team—the social workers, nurses, certified nursing assistants, dietary staff, and rehab and physiatry staff. Unless everyone is reading from the same page, the patient’s care will not be good. Very often, it’s the hospitalist or palliative care consultant who is at the center of the wheel, making sure that all the spokes are getting the same message,” she says.
Busy oncologists may call upon Dr. Grossman’s service to conduct family meetings about care plans. “Patients are very loyal to their oncologists, and they want their oncologists to be supportive of their decisions,” she notes. “I always explain to patients that my consultation was requested or supported by their oncologist. I am not there to cause more barriers; I’m there to have everybody on board and to understand where the patient is. We call everybody in—the social worker, the nurse, chaplaincy staff—because our approach is interdisciplinary and these are the essential members of our team.”
Dr. Grossman believes that hospitalists’ training in teamwork and communications are key to providing a good experience for oncology patients and their families. She is board certified in palliative care, which allows her to bring additional expertise to symptom support, including situations where she can help the dying process be as peaceful as possible—for both patient and family.
The issues important in palliative care—availability to patients, families, and referring physicians, ability to work in teams, and quality of care—dovetail with the primary goals of hospital medicine. Hospitalists’ palliative care services can thrive when they forge strong foundational relationships with their referring colleagues. TH
Gretchen Henkel regularly contributes to The Hospitalist.
References
- Selwyn PA, Rivard M, Kappell D, et al. Palliative care for AIDS at a large urban teaching hospital: program description and preliminary outcomes. J Palliat Med. 2003 Jun;6(3):461-474.
- Ryan A, Carter J, Lucas J, Berger J. You need not make the journey alone: overcoming impediments to providing palliative care in a public urban teaching hospital. Am J Hosp Palliat Care. 2002 May-June;19(3):171-180.
- The Case for Hospital-Based Palliative Care, published by the Center to Advance Palliative Care. Available online at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Last accessed March 22, 2006.
- Pantilat SZ, Rabow MW, Citko J, et al. Evaluating the California Hospital Initiative in Palliative Services. Arch Intern Med. 2006 Jan 23;166(2):227-230.
SHM Establishes Palliative Care Task Force
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at cwhelan@medicine.bsd.uchicago.edu.
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.

Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at HalasyaL@trinity-health.org.
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at cwhelan@medicine.bsd.uchicago.edu.
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.
Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at HalasyaL@trinity-health.org.
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at cwhelan@medicine.bsd.uchicago.edu.
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.
Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at HalasyaL@trinity-health.org.
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
Palliative Care Services Offer New Horizons for Hospitalists
Howard Epstein, a hospitalist at Regions Hospital in St. Paul, MN, spent nearly 2 years planning an inpatient palliative care consultation service for Regions before its launch in January of this year. A multidisciplinary advisory committee met monthly to help with the planning, and Dr. Epstein, the embryonic program’s medical director, went before the hospital’s administration to make the clinical and financial case for supporting it.
“What we’re trying to do is to take the basic interdisciplinary approach pioneered in hospice and move it upstream,” to help relieve suffering in seriously ill patients before they need or qualify for hospice care, he explains. “I just knew I wanted to incorporate it into a hospitalist model,” and into the Hospitalist Services Division’s weekly block schedule.
After the service was launched, it became clear that the schedule did not allow for the significant time commitment required to do palliative care, so a new approach is planned for July. Dr. Epstein and 6 other hospitalists participating in the palliative care service will divide up weekly blocks of time. Half of their duties while on service will be devoted to palliative care and the other half to covering 1 hospital unit as a hospitalist, rather than the usual 2 units for hospitalists at Regions.
The palliative care service at Regions, which includes a half-time chaplain and social worker and a full-time nurse practitioner, responds to consultation requests by doctors and nurses from all of the hospital’s adult services. The service also admits patients from HealthPartners’ affiliated hospice program when they are hospitalized at Regions for short-term symptom management or respite care.
Key to long-term success lies in documenting improved clinical outcomes, patient, family, and provider satisfaction, financial savings, and enhanced patient throughput. “I’m optimistic we’ll be able to demonstrate significant value, but if we can’t, we’ll be hard-pressed to get continued support,” he says. This challenge, he adds, is similar to what the hospitalist service at Regions faced when it was launched in 1998.
Palliative care is not a new concept in medicine, but it has enjoyed dramatic growth in recent years. The American Hospital Association estimates that 17% of community hospitals and 26% of academic teaching hospitals in the United States now have either a palliative care consultation service or a dedicated unit, although the former is more common because it can be established with a smaller fiscal outlay.
Palliative care aims to relieve suffering, broadly defined, for patients living with chronic, advanced illnesses. State-of-the-art pain management is a major emphasis for the interdisciplinary palliative care team, but so are addressing the patient and family’s emotional, psychological and spiritual concerns related to the illness and offering guidance for making informed treatment decisions that reflect their values and goals for care. Palliative care services generally target all patients with advanced illness from the point of diagnosis, simultaneous with any other medical treatment regimens.
Two Medical Fields Growing Together
“I believe hospitalist practices and palliative care services are of necessity growing closer together,” says Susan Block, codirector of the Harvard Medical School Center for Palliative Care in Boston, MA. The Harvard Center provides intensive palliative care training for clinicians who also have an interest in teaching.
“If you run a palliative care consult service or a palliative care unit, you are operating much like a hospitalist, with a focus on hospital systems and workload issues, communication, and getting people out of the hospital,” Dr. Block says. At the same time, most hospitalists deal with end-of-life issues and the challenges of relieving symptoms such as pain, delirium, or anxiety every day, whether they view their role in those terms or not.
Stephanie Grossman, a hospitalist at Emory Healthcare in Atlanta, GA, says she discovered personal satisfaction as a young physician in having meaningful conversations about care goals with seriously ill patients and leading family conferences, despite the time pressures of the job. The head of the hospital medicine service at Emory, Mark Williams, MD, told Dr. Grossman there was a name for what she enjoyed doing: palliative care. He encouraged her, along with colleague Melissa Mahoney, to obtain additional training in developing such a program, starting with a 2003 conference in San Diego sponsored by the Center to Advance Palliative Care.
“I came back from San Diego feeling swept away by how it really was possible to develop a financially feasible program,” says Dr. Grossman. Back at Emory, she and Dr. Mahoney joined a palliative care task force formed by Dr. Williams, with representatives from geriatrics, nursing, social work, chaplaincy, finance, and administration. This group provided input for a business plan for the palliative care service that will start in September at Emory Crawford Long and Emory University hospitals.
The 2 hospitalists, who have become certified in palliative medicine, will divide a full-time position as codirectors of the inpatient palliative care service in alternating monthly blocks, along with additional teaching responsibilities. Their 4-year plan is to add additional staffing as the program grows and to work with a geriatrician to develop a palliative care fellowship program. The palliative care team, including a nurse, social worker, and chaplain, will conduct daily palliative care rounds and biweekly interdisciplinary case conferences at the 2 hospitals.
“We have a nurse practitioner involved to help us coordinate between the 2 sites. We’ll go to various departments and do some grand rounds to introduce and market the program,” Dr. Grossman notes. In addition to practicing a style of medicine that offers deeper personal interactions with patients, she is excited to be part of creating a new program. However, she emphasizes the importance of having an executive champion within the hospital who understands financing, institutional politics, and how to recruit other champions. “We’ve been lucky to enjoy the support of Dr. Williams and [Emory Chief Operating Officer] Pete Basler. Dr. Mahoney and I have been working with hospitalists for several years, but our work has all been clinical,” she says.
Another challenge for hospitalists interested in pursuing palliative care include the need to make sure their new responsibilities are not just an add-on to a full-time job. The hospital needs to commit resources for planning and implementing a palliative care program, including a percentage of the hospitalist’s time, Dr. Block says. “Zero FTEs is not viable in the long run,” she adds.
Physician billing for palliative care consults can help offset the costs of running a service, but it is unlikely to break even on billing alone, says Eva Chittenden, a hospitalist and palliative care physician at the University of California-San Francisco, which has operated a palliative care service since 1999. Dr. Chittenden is also part of the Palliative Care Leadership Center at UCSF, which offers 2-day intensive training programs 4 times a year for hospital teams that want to start or strengthen inpatient palliative care services.
In most cases, palliative care requires financial support from the hospital, although it’s not difficult to justify that support by showing cost avoidance, reduced lengths of stay, and improved clinical outcomes, with the help of tools developed by the Center to Advance Palliative Care, Dr. Chittenden says. Program development also challenges the hospitalist’s leadership and marketing skills.
A Process of Growing Involvement
“What often happens with hospitalists is that they start out exploring palliative care, and it becomes very compelling,” Dr. Block adds. “The more competent you get at it, the more compelling it becomes. They find deeper meaning in their work. And then they’re hooked.”
A hospitalist can seek additional training and then incorporate palliative care tools, concepts, and perspectives into his or her daily work. An interest in palliative care may lead to involvement with the hospital ethics committee, a seat on a palliative care advisory committee, or a role in standards or protocol development, as well as pursuit of specialty certification in hospice and palliative medicine.
Although hospitalists may be obvious candidates to participate in more formal palliative care program development, “incorporating palliative care into a routine hospitalist practice is not a trivial thing,” Dr. Block adds. For starters, it requires additional training. “Most hospitalists don’t have the competencies to practice expert palliative care if they don’t seek them out,” she says. But the opportunities are increasing, with growing palliative care fellowship opportunities nationwide.
Two hospitalists at Chandler Regional Medical Center in Chandler, AZ, are among the 4 physicians who serve on that facility’s 12-member interdisciplinary palliative care team, attending weekly team meetings to review active cases and brainstorm program development. Both have attended national palliative care conferences, reports the palliative care service’s nurse practitioner, Donna Nolde. The service consulted on 89 patients in March, and about 70% of those referrals came from hospitalists.
“As hospitalists, we often deal with issues of death and dying,” especially when working in the ICU or with referring oncologists, notes Chandler’s Mahmood Shahlapour. “We can sometimes step back and see the big picture when other doctors have trouble letting go.” Dr. Shahlapour believes palliative care is a logical extension of good internal medicine and will eventually become a bigger part of the training of internists.
An atypical path to palliative care is that of Glenda Hickman, MD, who was a hospitalist for the Denver, CO–based HealthONE system until one of the system’s hospitals asked her to take on the role of freelance palliative care consultant. Hickman, who also works part-time for Hospice of Metro Denver as a team medical director and picks up lecturing and teaching assignments, accepts consultations from 3 HealthONE hospitals and bills third-party payers for her consultations. Her husband is office manager and biller for her home-based business, and she carries a cell phone and pager to promptly answer referrals.
“I had a reputation for the touchy-feely aspects of medicine at the hospitals where I worked,” Dr. Hickman relates. “Dying patients would often get referred to me.” Based on her interests, Dr. Hickman sought training in palliative care, but she found it difficult to juggle with her full-time job as a hospitalist. “The heart of palliative care in a hospital is talking with patients and families. These conversations take a long time,” she says. When the hospital asked for her help in meeting its JCAHO requirements in pain management and palliative care, Dr. Hickman was willing to explore a model for how she could hang out a shingle as a solo practitioner.
Business is growing, although the workload fluctuates widely. However, while Dr. Hickman works alongside social workers and chaplains at the hospitals, the biggest drawback has been the lack of a formal, interdisciplinary team. “This is high-maintenance, high-emotion work. It can be a big drain, and I don’t have a designated team with which to share the burden. My goal is to run a full palliative care team for the hospital,” she says, and there are signs that HealthONE eventually may move in that direction.
“It’s not that hospitalists can’t do palliative care. I did. I was so drawn to it and to trying to do it right, which meant I was trying to do 2 jobs at once,” she adds. Hospitalists can also participate by recognizing when their patients need the extra attention of a palliative care specialist. “Identifying who those patients are is a huge skill by itself.”
Resources for Getting Started in Palliative Care
The Center to Advance Palliative Care (CAPC) at Mount Sinai School of Medicine in New York City offers a comprehensive national resource for palliative care development in hospitals, including how to make the financial case. Its next national seminar is October 17 to 19 in San Diego, CA. CAPC also supports 6 regional Palliative Care Leadership Centers, including one with a hospitalist emphasis at the University of California-San Francisco, scheduled to run through June 2006. For more information on CAPC’s resources and leadership centers, call 202-201-2670 or visit www.capc.org.
Larry Beresford can be contacted at larryberesford@hotmail.com.
Other Helpful Resources
- For information on the Education in Palliative and End-of-Life Care (EPEC) curriculum, visit www.epec.net.
- The American Board of Hospice and Palliative Medicine will offer its next specialty certifying examination in November of 2005. For eligibility or other questions, call 301-439-8001 or visit www.abhpm.org.
- The American Association of Hospice and Palliative Medicine offers education and training resources, including an annual assembly scheduled for February 8 to 11, 2006, in Nashville, TN; visit www.aahpm.org.
- Harvard’s Center for Palliative Care offers a 2-week intensive training course, with an emphasis on teaching, in April and November every year. For information, call 617-724-9509, send email to pallcare@partners.org, or visit www.hms.harvard.edu/cdi/pallcare/.
- The Veterans Administration also offers palliative care resources, fellowship opportunities and other information; visit www.hospice.va.gov.
Howard Epstein, a hospitalist at Regions Hospital in St. Paul, MN, spent nearly 2 years planning an inpatient palliative care consultation service for Regions before its launch in January of this year. A multidisciplinary advisory committee met monthly to help with the planning, and Dr. Epstein, the embryonic program’s medical director, went before the hospital’s administration to make the clinical and financial case for supporting it.
“What we’re trying to do is to take the basic interdisciplinary approach pioneered in hospice and move it upstream,” to help relieve suffering in seriously ill patients before they need or qualify for hospice care, he explains. “I just knew I wanted to incorporate it into a hospitalist model,” and into the Hospitalist Services Division’s weekly block schedule.
After the service was launched, it became clear that the schedule did not allow for the significant time commitment required to do palliative care, so a new approach is planned for July. Dr. Epstein and 6 other hospitalists participating in the palliative care service will divide up weekly blocks of time. Half of their duties while on service will be devoted to palliative care and the other half to covering 1 hospital unit as a hospitalist, rather than the usual 2 units for hospitalists at Regions.
The palliative care service at Regions, which includes a half-time chaplain and social worker and a full-time nurse practitioner, responds to consultation requests by doctors and nurses from all of the hospital’s adult services. The service also admits patients from HealthPartners’ affiliated hospice program when they are hospitalized at Regions for short-term symptom management or respite care.
Key to long-term success lies in documenting improved clinical outcomes, patient, family, and provider satisfaction, financial savings, and enhanced patient throughput. “I’m optimistic we’ll be able to demonstrate significant value, but if we can’t, we’ll be hard-pressed to get continued support,” he says. This challenge, he adds, is similar to what the hospitalist service at Regions faced when it was launched in 1998.
Palliative care is not a new concept in medicine, but it has enjoyed dramatic growth in recent years. The American Hospital Association estimates that 17% of community hospitals and 26% of academic teaching hospitals in the United States now have either a palliative care consultation service or a dedicated unit, although the former is more common because it can be established with a smaller fiscal outlay.
Palliative care aims to relieve suffering, broadly defined, for patients living with chronic, advanced illnesses. State-of-the-art pain management is a major emphasis for the interdisciplinary palliative care team, but so are addressing the patient and family’s emotional, psychological and spiritual concerns related to the illness and offering guidance for making informed treatment decisions that reflect their values and goals for care. Palliative care services generally target all patients with advanced illness from the point of diagnosis, simultaneous with any other medical treatment regimens.
Two Medical Fields Growing Together
“I believe hospitalist practices and palliative care services are of necessity growing closer together,” says Susan Block, codirector of the Harvard Medical School Center for Palliative Care in Boston, MA. The Harvard Center provides intensive palliative care training for clinicians who also have an interest in teaching.
“If you run a palliative care consult service or a palliative care unit, you are operating much like a hospitalist, with a focus on hospital systems and workload issues, communication, and getting people out of the hospital,” Dr. Block says. At the same time, most hospitalists deal with end-of-life issues and the challenges of relieving symptoms such as pain, delirium, or anxiety every day, whether they view their role in those terms or not.
Stephanie Grossman, a hospitalist at Emory Healthcare in Atlanta, GA, says she discovered personal satisfaction as a young physician in having meaningful conversations about care goals with seriously ill patients and leading family conferences, despite the time pressures of the job. The head of the hospital medicine service at Emory, Mark Williams, MD, told Dr. Grossman there was a name for what she enjoyed doing: palliative care. He encouraged her, along with colleague Melissa Mahoney, to obtain additional training in developing such a program, starting with a 2003 conference in San Diego sponsored by the Center to Advance Palliative Care.
“I came back from San Diego feeling swept away by how it really was possible to develop a financially feasible program,” says Dr. Grossman. Back at Emory, she and Dr. Mahoney joined a palliative care task force formed by Dr. Williams, with representatives from geriatrics, nursing, social work, chaplaincy, finance, and administration. This group provided input for a business plan for the palliative care service that will start in September at Emory Crawford Long and Emory University hospitals.
The 2 hospitalists, who have become certified in palliative medicine, will divide a full-time position as codirectors of the inpatient palliative care service in alternating monthly blocks, along with additional teaching responsibilities. Their 4-year plan is to add additional staffing as the program grows and to work with a geriatrician to develop a palliative care fellowship program. The palliative care team, including a nurse, social worker, and chaplain, will conduct daily palliative care rounds and biweekly interdisciplinary case conferences at the 2 hospitals.
“We have a nurse practitioner involved to help us coordinate between the 2 sites. We’ll go to various departments and do some grand rounds to introduce and market the program,” Dr. Grossman notes. In addition to practicing a style of medicine that offers deeper personal interactions with patients, she is excited to be part of creating a new program. However, she emphasizes the importance of having an executive champion within the hospital who understands financing, institutional politics, and how to recruit other champions. “We’ve been lucky to enjoy the support of Dr. Williams and [Emory Chief Operating Officer] Pete Basler. Dr. Mahoney and I have been working with hospitalists for several years, but our work has all been clinical,” she says.
Another challenge for hospitalists interested in pursuing palliative care include the need to make sure their new responsibilities are not just an add-on to a full-time job. The hospital needs to commit resources for planning and implementing a palliative care program, including a percentage of the hospitalist’s time, Dr. Block says. “Zero FTEs is not viable in the long run,” she adds.
Physician billing for palliative care consults can help offset the costs of running a service, but it is unlikely to break even on billing alone, says Eva Chittenden, a hospitalist and palliative care physician at the University of California-San Francisco, which has operated a palliative care service since 1999. Dr. Chittenden is also part of the Palliative Care Leadership Center at UCSF, which offers 2-day intensive training programs 4 times a year for hospital teams that want to start or strengthen inpatient palliative care services.
In most cases, palliative care requires financial support from the hospital, although it’s not difficult to justify that support by showing cost avoidance, reduced lengths of stay, and improved clinical outcomes, with the help of tools developed by the Center to Advance Palliative Care, Dr. Chittenden says. Program development also challenges the hospitalist’s leadership and marketing skills.
A Process of Growing Involvement
“What often happens with hospitalists is that they start out exploring palliative care, and it becomes very compelling,” Dr. Block adds. “The more competent you get at it, the more compelling it becomes. They find deeper meaning in their work. And then they’re hooked.”
A hospitalist can seek additional training and then incorporate palliative care tools, concepts, and perspectives into his or her daily work. An interest in palliative care may lead to involvement with the hospital ethics committee, a seat on a palliative care advisory committee, or a role in standards or protocol development, as well as pursuit of specialty certification in hospice and palliative medicine.
Although hospitalists may be obvious candidates to participate in more formal palliative care program development, “incorporating palliative care into a routine hospitalist practice is not a trivial thing,” Dr. Block adds. For starters, it requires additional training. “Most hospitalists don’t have the competencies to practice expert palliative care if they don’t seek them out,” she says. But the opportunities are increasing, with growing palliative care fellowship opportunities nationwide.
Two hospitalists at Chandler Regional Medical Center in Chandler, AZ, are among the 4 physicians who serve on that facility’s 12-member interdisciplinary palliative care team, attending weekly team meetings to review active cases and brainstorm program development. Both have attended national palliative care conferences, reports the palliative care service’s nurse practitioner, Donna Nolde. The service consulted on 89 patients in March, and about 70% of those referrals came from hospitalists.
“As hospitalists, we often deal with issues of death and dying,” especially when working in the ICU or with referring oncologists, notes Chandler’s Mahmood Shahlapour. “We can sometimes step back and see the big picture when other doctors have trouble letting go.” Dr. Shahlapour believes palliative care is a logical extension of good internal medicine and will eventually become a bigger part of the training of internists.
An atypical path to palliative care is that of Glenda Hickman, MD, who was a hospitalist for the Denver, CO–based HealthONE system until one of the system’s hospitals asked her to take on the role of freelance palliative care consultant. Hickman, who also works part-time for Hospice of Metro Denver as a team medical director and picks up lecturing and teaching assignments, accepts consultations from 3 HealthONE hospitals and bills third-party payers for her consultations. Her husband is office manager and biller for her home-based business, and she carries a cell phone and pager to promptly answer referrals.
“I had a reputation for the touchy-feely aspects of medicine at the hospitals where I worked,” Dr. Hickman relates. “Dying patients would often get referred to me.” Based on her interests, Dr. Hickman sought training in palliative care, but she found it difficult to juggle with her full-time job as a hospitalist. “The heart of palliative care in a hospital is talking with patients and families. These conversations take a long time,” she says. When the hospital asked for her help in meeting its JCAHO requirements in pain management and palliative care, Dr. Hickman was willing to explore a model for how she could hang out a shingle as a solo practitioner.
Business is growing, although the workload fluctuates widely. However, while Dr. Hickman works alongside social workers and chaplains at the hospitals, the biggest drawback has been the lack of a formal, interdisciplinary team. “This is high-maintenance, high-emotion work. It can be a big drain, and I don’t have a designated team with which to share the burden. My goal is to run a full palliative care team for the hospital,” she says, and there are signs that HealthONE eventually may move in that direction.
“It’s not that hospitalists can’t do palliative care. I did. I was so drawn to it and to trying to do it right, which meant I was trying to do 2 jobs at once,” she adds. Hospitalists can also participate by recognizing when their patients need the extra attention of a palliative care specialist. “Identifying who those patients are is a huge skill by itself.”
Resources for Getting Started in Palliative Care
The Center to Advance Palliative Care (CAPC) at Mount Sinai School of Medicine in New York City offers a comprehensive national resource for palliative care development in hospitals, including how to make the financial case. Its next national seminar is October 17 to 19 in San Diego, CA. CAPC also supports 6 regional Palliative Care Leadership Centers, including one with a hospitalist emphasis at the University of California-San Francisco, scheduled to run through June 2006. For more information on CAPC’s resources and leadership centers, call 202-201-2670 or visit www.capc.org.
Larry Beresford can be contacted at larryberesford@hotmail.com.
Other Helpful Resources
- For information on the Education in Palliative and End-of-Life Care (EPEC) curriculum, visit www.epec.net.
- The American Board of Hospice and Palliative Medicine will offer its next specialty certifying examination in November of 2005. For eligibility or other questions, call 301-439-8001 or visit www.abhpm.org.
- The American Association of Hospice and Palliative Medicine offers education and training resources, including an annual assembly scheduled for February 8 to 11, 2006, in Nashville, TN; visit www.aahpm.org.
- Harvard’s Center for Palliative Care offers a 2-week intensive training course, with an emphasis on teaching, in April and November every year. For information, call 617-724-9509, send email to pallcare@partners.org, or visit www.hms.harvard.edu/cdi/pallcare/.
- The Veterans Administration also offers palliative care resources, fellowship opportunities and other information; visit www.hospice.va.gov.
Howard Epstein, a hospitalist at Regions Hospital in St. Paul, MN, spent nearly 2 years planning an inpatient palliative care consultation service for Regions before its launch in January of this year. A multidisciplinary advisory committee met monthly to help with the planning, and Dr. Epstein, the embryonic program’s medical director, went before the hospital’s administration to make the clinical and financial case for supporting it.
“What we’re trying to do is to take the basic interdisciplinary approach pioneered in hospice and move it upstream,” to help relieve suffering in seriously ill patients before they need or qualify for hospice care, he explains. “I just knew I wanted to incorporate it into a hospitalist model,” and into the Hospitalist Services Division’s weekly block schedule.
After the service was launched, it became clear that the schedule did not allow for the significant time commitment required to do palliative care, so a new approach is planned for July. Dr. Epstein and 6 other hospitalists participating in the palliative care service will divide up weekly blocks of time. Half of their duties while on service will be devoted to palliative care and the other half to covering 1 hospital unit as a hospitalist, rather than the usual 2 units for hospitalists at Regions.
The palliative care service at Regions, which includes a half-time chaplain and social worker and a full-time nurse practitioner, responds to consultation requests by doctors and nurses from all of the hospital’s adult services. The service also admits patients from HealthPartners’ affiliated hospice program when they are hospitalized at Regions for short-term symptom management or respite care.
Key to long-term success lies in documenting improved clinical outcomes, patient, family, and provider satisfaction, financial savings, and enhanced patient throughput. “I’m optimistic we’ll be able to demonstrate significant value, but if we can’t, we’ll be hard-pressed to get continued support,” he says. This challenge, he adds, is similar to what the hospitalist service at Regions faced when it was launched in 1998.
Palliative care is not a new concept in medicine, but it has enjoyed dramatic growth in recent years. The American Hospital Association estimates that 17% of community hospitals and 26% of academic teaching hospitals in the United States now have either a palliative care consultation service or a dedicated unit, although the former is more common because it can be established with a smaller fiscal outlay.
Palliative care aims to relieve suffering, broadly defined, for patients living with chronic, advanced illnesses. State-of-the-art pain management is a major emphasis for the interdisciplinary palliative care team, but so are addressing the patient and family’s emotional, psychological and spiritual concerns related to the illness and offering guidance for making informed treatment decisions that reflect their values and goals for care. Palliative care services generally target all patients with advanced illness from the point of diagnosis, simultaneous with any other medical treatment regimens.
Two Medical Fields Growing Together
“I believe hospitalist practices and palliative care services are of necessity growing closer together,” says Susan Block, codirector of the Harvard Medical School Center for Palliative Care in Boston, MA. The Harvard Center provides intensive palliative care training for clinicians who also have an interest in teaching.
“If you run a palliative care consult service or a palliative care unit, you are operating much like a hospitalist, with a focus on hospital systems and workload issues, communication, and getting people out of the hospital,” Dr. Block says. At the same time, most hospitalists deal with end-of-life issues and the challenges of relieving symptoms such as pain, delirium, or anxiety every day, whether they view their role in those terms or not.
Stephanie Grossman, a hospitalist at Emory Healthcare in Atlanta, GA, says she discovered personal satisfaction as a young physician in having meaningful conversations about care goals with seriously ill patients and leading family conferences, despite the time pressures of the job. The head of the hospital medicine service at Emory, Mark Williams, MD, told Dr. Grossman there was a name for what she enjoyed doing: palliative care. He encouraged her, along with colleague Melissa Mahoney, to obtain additional training in developing such a program, starting with a 2003 conference in San Diego sponsored by the Center to Advance Palliative Care.
“I came back from San Diego feeling swept away by how it really was possible to develop a financially feasible program,” says Dr. Grossman. Back at Emory, she and Dr. Mahoney joined a palliative care task force formed by Dr. Williams, with representatives from geriatrics, nursing, social work, chaplaincy, finance, and administration. This group provided input for a business plan for the palliative care service that will start in September at Emory Crawford Long and Emory University hospitals.
The 2 hospitalists, who have become certified in palliative medicine, will divide a full-time position as codirectors of the inpatient palliative care service in alternating monthly blocks, along with additional teaching responsibilities. Their 4-year plan is to add additional staffing as the program grows and to work with a geriatrician to develop a palliative care fellowship program. The palliative care team, including a nurse, social worker, and chaplain, will conduct daily palliative care rounds and biweekly interdisciplinary case conferences at the 2 hospitals.
“We have a nurse practitioner involved to help us coordinate between the 2 sites. We’ll go to various departments and do some grand rounds to introduce and market the program,” Dr. Grossman notes. In addition to practicing a style of medicine that offers deeper personal interactions with patients, she is excited to be part of creating a new program. However, she emphasizes the importance of having an executive champion within the hospital who understands financing, institutional politics, and how to recruit other champions. “We’ve been lucky to enjoy the support of Dr. Williams and [Emory Chief Operating Officer] Pete Basler. Dr. Mahoney and I have been working with hospitalists for several years, but our work has all been clinical,” she says.
Another challenge for hospitalists interested in pursuing palliative care include the need to make sure their new responsibilities are not just an add-on to a full-time job. The hospital needs to commit resources for planning and implementing a palliative care program, including a percentage of the hospitalist’s time, Dr. Block says. “Zero FTEs is not viable in the long run,” she adds.
Physician billing for palliative care consults can help offset the costs of running a service, but it is unlikely to break even on billing alone, says Eva Chittenden, a hospitalist and palliative care physician at the University of California-San Francisco, which has operated a palliative care service since 1999. Dr. Chittenden is also part of the Palliative Care Leadership Center at UCSF, which offers 2-day intensive training programs 4 times a year for hospital teams that want to start or strengthen inpatient palliative care services.
In most cases, palliative care requires financial support from the hospital, although it’s not difficult to justify that support by showing cost avoidance, reduced lengths of stay, and improved clinical outcomes, with the help of tools developed by the Center to Advance Palliative Care, Dr. Chittenden says. Program development also challenges the hospitalist’s leadership and marketing skills.
A Process of Growing Involvement
“What often happens with hospitalists is that they start out exploring palliative care, and it becomes very compelling,” Dr. Block adds. “The more competent you get at it, the more compelling it becomes. They find deeper meaning in their work. And then they’re hooked.”
A hospitalist can seek additional training and then incorporate palliative care tools, concepts, and perspectives into his or her daily work. An interest in palliative care may lead to involvement with the hospital ethics committee, a seat on a palliative care advisory committee, or a role in standards or protocol development, as well as pursuit of specialty certification in hospice and palliative medicine.
Although hospitalists may be obvious candidates to participate in more formal palliative care program development, “incorporating palliative care into a routine hospitalist practice is not a trivial thing,” Dr. Block adds. For starters, it requires additional training. “Most hospitalists don’t have the competencies to practice expert palliative care if they don’t seek them out,” she says. But the opportunities are increasing, with growing palliative care fellowship opportunities nationwide.
Two hospitalists at Chandler Regional Medical Center in Chandler, AZ, are among the 4 physicians who serve on that facility’s 12-member interdisciplinary palliative care team, attending weekly team meetings to review active cases and brainstorm program development. Both have attended national palliative care conferences, reports the palliative care service’s nurse practitioner, Donna Nolde. The service consulted on 89 patients in March, and about 70% of those referrals came from hospitalists.
“As hospitalists, we often deal with issues of death and dying,” especially when working in the ICU or with referring oncologists, notes Chandler’s Mahmood Shahlapour. “We can sometimes step back and see the big picture when other doctors have trouble letting go.” Dr. Shahlapour believes palliative care is a logical extension of good internal medicine and will eventually become a bigger part of the training of internists.
An atypical path to palliative care is that of Glenda Hickman, MD, who was a hospitalist for the Denver, CO–based HealthONE system until one of the system’s hospitals asked her to take on the role of freelance palliative care consultant. Hickman, who also works part-time for Hospice of Metro Denver as a team medical director and picks up lecturing and teaching assignments, accepts consultations from 3 HealthONE hospitals and bills third-party payers for her consultations. Her husband is office manager and biller for her home-based business, and she carries a cell phone and pager to promptly answer referrals.
“I had a reputation for the touchy-feely aspects of medicine at the hospitals where I worked,” Dr. Hickman relates. “Dying patients would often get referred to me.” Based on her interests, Dr. Hickman sought training in palliative care, but she found it difficult to juggle with her full-time job as a hospitalist. “The heart of palliative care in a hospital is talking with patients and families. These conversations take a long time,” she says. When the hospital asked for her help in meeting its JCAHO requirements in pain management and palliative care, Dr. Hickman was willing to explore a model for how she could hang out a shingle as a solo practitioner.
Business is growing, although the workload fluctuates widely. However, while Dr. Hickman works alongside social workers and chaplains at the hospitals, the biggest drawback has been the lack of a formal, interdisciplinary team. “This is high-maintenance, high-emotion work. It can be a big drain, and I don’t have a designated team with which to share the burden. My goal is to run a full palliative care team for the hospital,” she says, and there are signs that HealthONE eventually may move in that direction.
“It’s not that hospitalists can’t do palliative care. I did. I was so drawn to it and to trying to do it right, which meant I was trying to do 2 jobs at once,” she adds. Hospitalists can also participate by recognizing when their patients need the extra attention of a palliative care specialist. “Identifying who those patients are is a huge skill by itself.”
Resources for Getting Started in Palliative Care
The Center to Advance Palliative Care (CAPC) at Mount Sinai School of Medicine in New York City offers a comprehensive national resource for palliative care development in hospitals, including how to make the financial case. Its next national seminar is October 17 to 19 in San Diego, CA. CAPC also supports 6 regional Palliative Care Leadership Centers, including one with a hospitalist emphasis at the University of California-San Francisco, scheduled to run through June 2006. For more information on CAPC’s resources and leadership centers, call 202-201-2670 or visit www.capc.org.
Larry Beresford can be contacted at larryberesford@hotmail.com.
Other Helpful Resources
- For information on the Education in Palliative and End-of-Life Care (EPEC) curriculum, visit www.epec.net.
- The American Board of Hospice and Palliative Medicine will offer its next specialty certifying examination in November of 2005. For eligibility or other questions, call 301-439-8001 or visit www.abhpm.org.
- The American Association of Hospice and Palliative Medicine offers education and training resources, including an annual assembly scheduled for February 8 to 11, 2006, in Nashville, TN; visit www.aahpm.org.
- Harvard’s Center for Palliative Care offers a 2-week intensive training course, with an emphasis on teaching, in April and November every year. For information, call 617-724-9509, send email to pallcare@partners.org, or visit www.hms.harvard.edu/cdi/pallcare/.
- The Veterans Administration also offers palliative care resources, fellowship opportunities and other information; visit www.hospice.va.gov.
Withholding nutrition at the end of life: Clinical and ethical issues
Elder abuse and neglect: What physicians can and should do
Improving the care of patients dying of heart failure
Defining Effective Clinician Roles in End-of-Life Care
OBJECTIVE: Our goal was to determine primary care clinician perceptions of what is important to the provision of quality end-of-life care.
STUDY DESIGN: We used ethnography, a qualitative research method involving the use of open-ended semistructured interviews.
POPULATION: We included 38 family practice residency faculty from 9 community residency programs of the Affiliated Family Practice Residency Network, Department of Family Medicine, University of Washington School of Medicine.
OUTCOMES MEASURED: The roles described by interviewees when discussing their best practices while delivering end-of-life care were compiled.
RESULTS: Primary care clinicians organize their delivery of quality end-of-life care predominantly through their relationships with patients and families. They play 3 roles when providing end-of-life care. As consultants, clinicians provide expert medical advice and treatment. As collaborators, they seek to understand the patient and family experience. Seasoned clinicians act as guides, using their personal intuitive knowledge of patient and family to facilitate everyone’s growth when providing end-of-life care.
CONCLUSIONS: Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve end-of-life care for patients, families, and clinicians.
- Exemplary end-of-life care is organized around relationships, meaning, and roles.
- Knowledge and skills are essential but are not how exemplary end-of-life care is organized.
- Clinicians providing end-of-life care play 3 roles: consultant, collaborator, and guide.
- Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve care.
Modern medicine has dramatically improved the length and quality of life for countless persons but has also created problems in integrating these advances with end-of-life care. Although 70% of Americans want to die in their own home supported by family, 74% of Americans currently die in institutions.1,2 Clearly, there is a disparity between patient preferences and the end-of-life services provided in America.
Most recommendations for the provision of quality end-of-life care are based on unresearched expert opinion that identifies problems and offers solutions.3-5 Studies have explored communication strategies,6 satisfaction levels with care,7 perceptions of management issues,8 and attitudes toward both death and dying patients.9 Yet little research addresses how practicing community clinicians develop the appropriate relationships and integrate the requisite knowledge, skills, and attitudes to provide quality end-of-life care.
The relationship between clinician, patient, and family and the personal meaning of events for each participant greatly influence end-of-life care.10 Although most commentary on physician roles and relationships in end-of-life care also reflects unresearched expert opinion,11-13 Steinmetz and Gabel14,15 theorized a model that was later validated against the experience of practicing family physicians. The role of the clinician in the successful provision of quality care has not been systematically researched and remains a major challenge to improving end-of-life care. We describe an exploratory qualitative study to determine the perceptions of practicing clinicians regarding quality end-of-life care.
Methods
With approval from the Human Subjects Committee of the University of Washington School of Medicine, faculty were recruited from 9 community programs in the Affiliated Family Practice Residency Network of the Department of Family Medicine. Twenty semistructured long interviews were conducted from a convenience sample at 3 residency sites.16 An additional 8 semistructured interviews and 2 focus groups (10 participants) further explored the data. Thus, a total of 38 clinicians participated in the study. Demographic characteristics of the study cohort have been published previously.10
We conducted the initial 20 interviews using open-ended questions designed to uncover faculty perceptions of quality end-of-life care. The questions explored may be found in the Table. Nonspecific prompts such as “tell me more” were used to enrich data and avoid interviewer bias. The interview was rehearsed with a medical school faculty expert in ethnographic research, field tested, and adjusted before final use. The interviews were audio-recorded and transcribed into qualitative research software.17
Throughout the interview process, the investigators met weekly to compare findings, discuss emerging categories, and jointly code the transcripts for model development using the process of grounded theory described by Glaser and Strauss.18 Common themes, communication and educational issues, and roles and relationships were identified. Data were constantly compared and winnowed to facilitate manageability; data collection and analysis occurred simultaneously.19,20 Common themes are published elsewhere.10 We report and discuss the analysis of the data pertaining to clinician roles and relationships.
We employed the following 3 strategies to assess the methodologic validity of the study and face validity of the themes and models emerging from the data analysis.
TABLE
INTERVIEW QUESTIONS
Remember a case in which you provided care for a patient and family facing a chronic, progressive, terminal illness:
|
Methodologic validation
The themes, models, and 2 interview transcripts were reviewed by 2 expert consultants with experience in qualitative research on end-of-life care and chronic debilitating disease. They assessed the validity of the research process and model development.21,22 These experts confirmed the methodologic approach, affirmed that the transcripts supported the coded model, and noted that the results were consistent with their own past research experience.
Face validity faculty interviews
Long interviews were conducted with a convenience sample of 8 faculty at 2 other residency sites. Researchers described the previous interview process and presented a written summary of the roles and relationship model coded from the data. Dialogue was encouraged with nonspecific prompts to enrich the data and avoid interviewer bias. Interviews were recorded, transcribed, and coded by the researchers to assess face validity and further develop the roles and relationship model using a grounded theory approach.
Face validity focus groups
Two focus groups were conducted with a total of 10 faculty at 2 additional sites. The entire model (themes, communication, roles, and relationships) was presented, and dialogue was encouraged. The researchers recorded, transcribed, and reviewed the focus groups to further assess face validity and refine the model.
Content validity
In a manner identical to that of the focus groups, the researchers presented the entire model at 2 of the 3 sites where faculty provided the initial 20 interviews. These sessions were audiotaped, transcribed, and reviewed by the researchers. The model presented was considered a valid, clinically plausible summary of the content of the initial interviews.
Results
Content analysis of the roles and relationships described by the study cohort revealed 3 distinct clinician roles in the provision of end-of-life care that we termed “consultant,” “collaborator,” and “guide.” All roles were viewed as important; none was more valuable than another; and the roles appeared to build on each other, often merging. Roles were implemented fluidly, with clinicians moving from one role to another as circumstances dictated. Although clinicians tended to describe successful cases, they freely discussed the challenges of end-of-life care, noting that less-than-ideal results were frequent. Thus, the models were described as “best practice” rather than routine care.
Consultant
The consultant provides expert medical information to the patient and family based on the biomedical model and the disease process. The power of the consultant role emanates from the clinician’s medical authority and special knowledge. The consultant presents information to help the patient and family understand the diagnosis, prognosis, and treatment. Once this knowledge is understood, the patient and family determine its meaning to them and decide on treatment. If the patient or family cannot decide or understand the medical implications of their particular situation, the consultant decides based on the medical facts.
A pediatrician illustrated the application of the consultant role in 2 situations involving newborns with severe heart anomalies. Here the physician describes the difficulty of using only medical facts to assist the family in deciding whether to discontinue the ventilator: “I remember saying: ‘The only thing that’s keeping the baby alive at this point is the ventilator. How do you feel about making the decision to turn that off?’ I remember it was a very cruel thing to have them make the decision.”
The physician continued: “Next time I said: ‘We have to sit down and talk about how your baby is doing because he died, and I’m going to turn off the machines now.’ I don’t think we should put them in the position of having to make this decision. We should make this decision and tell them what we’re going to do.” In this situation the clinician employed biomedical expertise to determine the appropriate medical care and outcome for the patient and family. In both cases the decision centered on continuing or discontinuing a medical intervention (respirator) and avoided discussion of the parents’ affective experience. Hallmarks of the consultant role include a biomedical focus, disease-centered decision-making processes, and the clinician’s assumption of authority based on biomedical expertise.
Collaborator
The collaborator exchanges information with the patient and family to promote a common understanding of the diagnosis and illness experience, working with them to choose a treatment path. The collaborator incorporates all components of the consultant role and additionally requires the clinician to understand the patient/family experience. The collaborator considers patient and family issues that need to be addressed to understand the medical facts, appreciates their past experiences with serious illness, determines what information would be difficult for them to accept but would benefit them if they were challenged to confront it, and recognizes that the patient and family hold ultimate responsibility for making treatment decisions.
The following quotes exemplify collaborative clinical care. In the first example, the physician steps outside his comfort zone to provide medical care based on the expressed wishes of a 30-year-old man dying of an advanced brain tumor: “The issue for me was letting go of control. He was going 4 hours away to a fishing cabin and going on a boat. I was really nervous…what if he all of a sudden crashed there? It took me a while to get used to the idea that he needs to be able to do what he enjoys doing, and everybody knows that there’s a risk.”
In a second example, the physician describes collaborating with the family of an 85-year-old woman suffering a massive stroke: “Having heard from the family that they understand that Grandma has had a big stroke and isn’t going to survive…then what wishes do Grandma and the family have? Have they ever discussed this sort of situation?”
In both these examples an understanding of the patient/family experience directs the clinician toward appropriate end-of-life care and is a major source of the collaborator’s power.
Guide
As a guide, the clinician actively and personally seeks solutions for the patient based not only on the medical facts (consultant) and the patient’s values and preferences (collaborator) but also on the guide’s greater understanding of the medical context. In essence, the guide not only knows why and where the patient and family prefer to go but also how to get there.
The following quote demonstrates a clinical application of the guide role. The physician first collaborates to understand the resistance of a terminally ill patient to hospice care:
“They had been very resistant to hospice for reasons that I wasn’t quite clear on. It wasn’t until I was in the home and listened to them talk that I realized they viewed hospice as ‘people are giving up on him.’ I think nobody really was talking to the patient about whether he was willing to give up or if he was ready to die.
“Once patient and family concerns were understood, the guide role was employed: I told the wife and family, ‘We’ve maxed out our medical therapies. There’s not much more we can do for him physically, but perhaps there’s something we can do for him spiritually and emotionally.’ When it was presented to them that way, they were much more understanding. We talked about hospice philosophy and looking at death as a part of life, saying: ‘That we’re not going to resuscitate does not mean do not treat.’ That’s where I came in more as the guide and said: ‘This is what I think is reasonable. What are your expectations? What do you want, Billy? And what do you want, as far as [his] wife and kids?”
The guide role requires that the clinician interpret the patient’s experience, integrate this interpretation with the clinician’s understanding of the clinical situation, and make a recommendation based on the guide’s personal and professional understanding of the situation. The power of the guide role emanates from the clinician’s understanding of how to use the medical system to see that the goals of patient and family are realized.
Discussion
The results of our study are consistent with reports over the past 3 decades by researchers, educators, and social critics who have explored how health professionals provide end-of-life care.23-29 Despite their varying perspectives, all reflect a common theme: the need to provide care based on the unique illness experience and values of the patient and family. The majority of clinicians in our study spoke of the importance of their relationships with patients and families. More than 50% of all interview commentary addressed clinician issues of relationship and personal meaning when providing end-of-life care.
The descriptions of consultant,30 collaborator,31,32 and guide33 confirm previous theoretical discussions regarding the nature of roles and relationships between patients and physicians. The guide is the most complex of the roles described by our study cohort and lends itself to ambivalence on the part of clinicians, in light of its potential to be misunderstood as paternalism. Yet, given the vulnerability and dependence of many patients who are terminally ill, the guide provides these patients with structure, safety, support, and care—based on the patients’ values and goals—reminiscent of the role of a nurturing parent.34
The personal nature of the decisions the guide facilitates reflects the reality of medicine as a moral enterprise.34,35 Having generally witnessed many more deaths than the patient, the guide has knowledge regarding the processes of dying and medical systems that is instrumental in assuring that the desires of the patient and family are realized. A knowledge of patient and family, an appreciation of the futility of the medical situation, and an insight into the process and systems of dying afford the clinician an opportunity to shape the death experience; as Nuland36 described: “Each of us needs a guide who knows us as well as he knows the pathways by which we can approach death.”
Facility with these roles may be a function of personal talent, introspection, and experience. The physicians studied reported that competence with these roles grew over time through delivering endof-life care and learning from patients, families, and other caregivers. Less experienced clinicians tended to describe the consultant and collaborator roles only. Clinicians describing the guide role had been in practice at least a decade and thus were at least 17 years into their training and practice in medicine. Apparently, expertise in all 3 roles requires not only excellent technical diagnostic and treatment skills but also the complex integrated skills of relational knowledge and caring gained through experience.
Our data indicate that relationship, meaning, and roles are primary moderators of the organization of exemplary end-of-life care. Yet, it appears to take nearly 2 decades for physicians to gain the confidence in their knowledge, skills, and attitudes necessary to comfortably guide patients and families through the nuances of end-of-life care. How to successfully educate clinicians to use such a model earlier is beyond our scope but appears crucial to improving training efforts. Current attempts to teach end-of-life care do not develop and explore the complex integrative domains of relational knowledge37-40 described in our study. Studies of educational interventions that stress the importance of the relational aspects of end-of-life care appear warranted.
To facilitate skill acquisition, the authors propose the steps diagrammed in the Figure to assist clinicians in providing quality end-of-life care. We believe the time spent determining patient-centered goals and the roles and relationships required by the clinician should at least equal the time spent determining which tests and treatments to provide. At the end of life, when tests and treatments result in fewer benefits and greater risks and burdens, determining patient and family needs and goals becomes increasingly important as management changes from cure to care.
FIGURE
FLOW DIAGRAM FOR CLINICIAN ROLES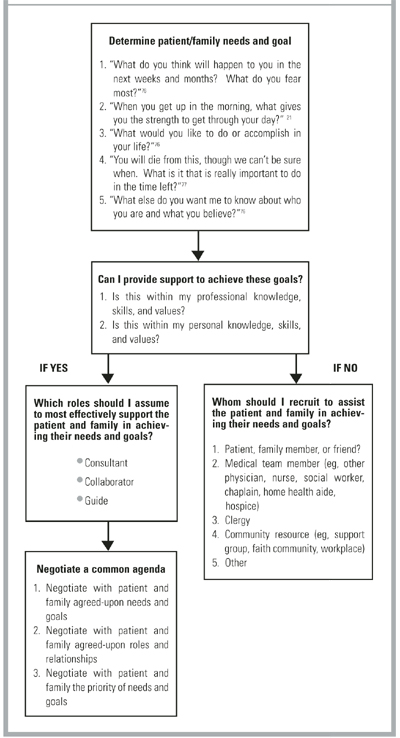
Limitations
This study is limited by a study sample of primary care, family practice faculty who geographically represent all practice in the Pacific Northwest and are predominantly Euro-American in ethnicity. The majority are family physicians, with the remainder pediatricians, internists, and a small number of nurse practitioners and physician assistants. Although no significant differences in terms of roles, relationships, and personal meanings between professional groups were noted, whether these findings are transferable to other primary care clinicians in community practice is unknown. Whether non–primary care specialists and clinicians of differing ethnicity or geographic region would respond differently is unknown. Generalizing these findings to non–primary care clinicians and clinicians of color requires further research.
Conclusions
Given the enormity of social and cultural values that make death a taboo topic, it is unclear how any single reform can easily overcome the multiple barriers to improved end-of-life care. Whether it is possible to teach attitudes and values, such as empathy and self-reflection, is uncertain, though promising curricula and research exist.41-42 If primary care physicians and other professionals improve their knowledge, skills, and attitudes in the delivery of such care, the ultimate effect on improving the experience of patients and families will require further study.
Acknowledgments
We wish to thank the Emily Davie and Joseph S. Kornfeld Foundation and The Nathan Cummings Foundation, New York, which provided generous grants that made our study and article possible. Additionally, we thank Phyllis Silverman, PhD, Harvard University, for her early counsel and advice; Tom Taylor, MD, PhD, University of Washington School of Medicine, for his thoughtful input into the study design, his sage guidance, and his review of the manuscript; Jeanne Quint Benoliel, DNS, Professor Emeritus, University of Washington School of Nursing, for her inspiration and review of the study design and results; and Greg Guldin, PhD, Pacific Lutheran University, for his thoughtful review of the manuscript.
1. The George Gallup International Institute. Spiritual beliefs and the dying process: a report on a national survey. Princeton, NJ: George Gallup International Institute;1997.
2. Field MJ, Cassel CK, eds. Approaching death: improving care at the end of life: Committee on Care at the End of Life, Division of Health Care Services, Institute of Medicine. Washington, DC: National Academy Press; 1997.
3. Schonwetter RS, Hawke W, Knight CF, eds. Hospice and palliative medicine core curriculum and review syllabus: American Academy of Hospice and Palliative Medicine. Dubuque, Iowa: Kendall/Hunt; 1999.
4. Emanuel LL, von Gunten CF, Ferris FD. The education for physicians on end-of-life care (EPEC) curriculum. Chicago, Ill: American Medical Association; 1999.
5. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744-49.
6. Todd C, Still A. General practitioners’ strategies and tactics of communication with the terminally ill. Fam Pract 1993;10:268-76.
7. Blyth AC. Audit of terminal care in a general practice. BMJ 1990;300:983-86.
8. Goodlin SJ, Jette AM, Lynn J, Wasson JH. Community physicians describe management issues for patients expected to live less than twelve months. J Palliat Care 1998;14:30-35.
9. Durand RP, Dickinson GE, Sumner DE, Lancaster CG. Family physicians’ attitudes toward death and the terminally-ill patient. Fam Pract Res J 1990;9:123-29.
10. Farber SJ, Egnew TR, Herman-Bertsch JL. Issues in end-of-life care: family practice faculty perceptions. J Fam Pract 1999;49:525-30.
11. Brewin TB. Not TLC but FPI. J R Soc Med 1990;83:172-75.
12. Mitchell G. The role of the general practitioner in palliative care. Aust Fam Physician 1994;23:1233-39.
13. Ogle KS, Plum JD. The role of the primary care physician in the care of the terminally ill. Clin Geriatr Med 1996;12:267-77.
14. Steinmetz D, Gabel LL. The family physician’s role in caring for the dying patient and family: a comprehensive theoretical model. Fam Pract 1992;9:433-36.
15. Steinmetz D, Walsh M, Gabel LL, Williams PT. Family physicians’ involvement with dying patients and their families. Arch Fam Med 1993;2:753-61.
16. Crabtree BF, Miller WL. A qualitative approach to primary care research: the long interview. Fam Med 1991;23:145-51.
17. Seidel J, Friese S, Leonard DC. The Ethnograph version 4.0 . Amherst, Mass: Qualis Research Associates; 1995.
18. Glaser B, Strauss A. The discovery of grounded theory. New York, NY: Aldine; 1967.
19. Strauss A, Corbin C. Basics of qualitative research. Newbury Park, Calif: Sage; 1990.
20. Wolcott HF. Writing up qualitative research. Newbury Park, Calif: Sage; 1990.
21. Benoliel JQ. Advancing nursing science: qualitative approaches. West J Nurs Res 1984;6:1-8.
22. Taylor TR, Gordon MJ, Ashworth CD. A systems perspective on clinical management. Behav Sci 1984;29:233-47.
23. Glaser BG, Strauss AL. Awareness of dying. Chicago, Ill: Aldine; 1965.
24. Kubler-Ross E. On death and dying. New York, NY: MacMillan; 1969.
25. Weisman A. On dying and denying: a psychiatric study on terminality. New York, NY: Behavioral Publications; 1972.
26. Saunders C, Baines M. Living with dying. New York, NY: Oxford University Press; 1983.
27. Corbin JM, Strauss AL. Unending work and care: managing chronic illness at home. San Francisco, Calif: Jossey-Bass; 1988.
28. Broyard A. Intoxicated by my illness. New York, NY: Potter; 1992.
29. Callahan D. Troubled dream of life. New York, NY: Simon & Schuster; 1993.
30. Balint J, Shelton W. Regaining the initiative: forging a new model of the patient-physician relationship. JAMA 1996;275:887-91.
31. Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med 1983;98:228-34.
32. Stewart M, Brown JB, Weston WW, McWhinney IR, Freeman TR. Patient centered medicine: transforming the clinical method. Thousand Oaks, Calif: Sage; 1995.
33. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA 1992;267:2221-26.
34. Cassell EJ. The nature of suffering and the goals of medicine. New York, NY: Oxford University Press; 1991.
35. Veatch RM. Contemporary bioethics and the demise of modern medicine. In Ormiston G, Sassower R, eds. Prescriptions: the dissemination of medical authority. New York, NY: Greenwood Press; 1990;23-39.
36. Nuland S. How we die. New York, NY: Knopf; 1994.
37. Rogers CR. Client-centered therapy: its current practice, implications, and theory. Boston, Mass: Houghton Mifflin; 1951.
38. Buber M. I and thou. New York, NY: MacMillan; 1974.
39. Mayeroff M. On caring. New York, NY: HarperPerennial; 1990.
40. Kleinman A, Kleinman J. Suffering and its professional transformation: toward an ethnography of interpersonal experience. Cult Med Psychiatry 1991;15:275-301.
41. Novack DH, Suchman AL, Clark W, Epstein RM, Najberg E, Kaplan C. Calibrating the physician: personal awareness and effective patient care. JAMA 1997;278:502-09.
42. Epstein RM. Mindful practice. JAMA 1999;282:833-39.
OBJECTIVE: Our goal was to determine primary care clinician perceptions of what is important to the provision of quality end-of-life care.
STUDY DESIGN: We used ethnography, a qualitative research method involving the use of open-ended semistructured interviews.
POPULATION: We included 38 family practice residency faculty from 9 community residency programs of the Affiliated Family Practice Residency Network, Department of Family Medicine, University of Washington School of Medicine.
OUTCOMES MEASURED: The roles described by interviewees when discussing their best practices while delivering end-of-life care were compiled.
RESULTS: Primary care clinicians organize their delivery of quality end-of-life care predominantly through their relationships with patients and families. They play 3 roles when providing end-of-life care. As consultants, clinicians provide expert medical advice and treatment. As collaborators, they seek to understand the patient and family experience. Seasoned clinicians act as guides, using their personal intuitive knowledge of patient and family to facilitate everyone’s growth when providing end-of-life care.
CONCLUSIONS: Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve end-of-life care for patients, families, and clinicians.
- Exemplary end-of-life care is organized around relationships, meaning, and roles.
- Knowledge and skills are essential but are not how exemplary end-of-life care is organized.
- Clinicians providing end-of-life care play 3 roles: consultant, collaborator, and guide.
- Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve care.
Modern medicine has dramatically improved the length and quality of life for countless persons but has also created problems in integrating these advances with end-of-life care. Although 70% of Americans want to die in their own home supported by family, 74% of Americans currently die in institutions.1,2 Clearly, there is a disparity between patient preferences and the end-of-life services provided in America.
Most recommendations for the provision of quality end-of-life care are based on unresearched expert opinion that identifies problems and offers solutions.3-5 Studies have explored communication strategies,6 satisfaction levels with care,7 perceptions of management issues,8 and attitudes toward both death and dying patients.9 Yet little research addresses how practicing community clinicians develop the appropriate relationships and integrate the requisite knowledge, skills, and attitudes to provide quality end-of-life care.
The relationship between clinician, patient, and family and the personal meaning of events for each participant greatly influence end-of-life care.10 Although most commentary on physician roles and relationships in end-of-life care also reflects unresearched expert opinion,11-13 Steinmetz and Gabel14,15 theorized a model that was later validated against the experience of practicing family physicians. The role of the clinician in the successful provision of quality care has not been systematically researched and remains a major challenge to improving end-of-life care. We describe an exploratory qualitative study to determine the perceptions of practicing clinicians regarding quality end-of-life care.
Methods
With approval from the Human Subjects Committee of the University of Washington School of Medicine, faculty were recruited from 9 community programs in the Affiliated Family Practice Residency Network of the Department of Family Medicine. Twenty semistructured long interviews were conducted from a convenience sample at 3 residency sites.16 An additional 8 semistructured interviews and 2 focus groups (10 participants) further explored the data. Thus, a total of 38 clinicians participated in the study. Demographic characteristics of the study cohort have been published previously.10
We conducted the initial 20 interviews using open-ended questions designed to uncover faculty perceptions of quality end-of-life care. The questions explored may be found in the Table. Nonspecific prompts such as “tell me more” were used to enrich data and avoid interviewer bias. The interview was rehearsed with a medical school faculty expert in ethnographic research, field tested, and adjusted before final use. The interviews were audio-recorded and transcribed into qualitative research software.17
Throughout the interview process, the investigators met weekly to compare findings, discuss emerging categories, and jointly code the transcripts for model development using the process of grounded theory described by Glaser and Strauss.18 Common themes, communication and educational issues, and roles and relationships were identified. Data were constantly compared and winnowed to facilitate manageability; data collection and analysis occurred simultaneously.19,20 Common themes are published elsewhere.10 We report and discuss the analysis of the data pertaining to clinician roles and relationships.
We employed the following 3 strategies to assess the methodologic validity of the study and face validity of the themes and models emerging from the data analysis.
TABLE
INTERVIEW QUESTIONS
Remember a case in which you provided care for a patient and family facing a chronic, progressive, terminal illness:
|
Methodologic validation
The themes, models, and 2 interview transcripts were reviewed by 2 expert consultants with experience in qualitative research on end-of-life care and chronic debilitating disease. They assessed the validity of the research process and model development.21,22 These experts confirmed the methodologic approach, affirmed that the transcripts supported the coded model, and noted that the results were consistent with their own past research experience.
Face validity faculty interviews
Long interviews were conducted with a convenience sample of 8 faculty at 2 other residency sites. Researchers described the previous interview process and presented a written summary of the roles and relationship model coded from the data. Dialogue was encouraged with nonspecific prompts to enrich the data and avoid interviewer bias. Interviews were recorded, transcribed, and coded by the researchers to assess face validity and further develop the roles and relationship model using a grounded theory approach.
Face validity focus groups
Two focus groups were conducted with a total of 10 faculty at 2 additional sites. The entire model (themes, communication, roles, and relationships) was presented, and dialogue was encouraged. The researchers recorded, transcribed, and reviewed the focus groups to further assess face validity and refine the model.
Content validity
In a manner identical to that of the focus groups, the researchers presented the entire model at 2 of the 3 sites where faculty provided the initial 20 interviews. These sessions were audiotaped, transcribed, and reviewed by the researchers. The model presented was considered a valid, clinically plausible summary of the content of the initial interviews.
Results
Content analysis of the roles and relationships described by the study cohort revealed 3 distinct clinician roles in the provision of end-of-life care that we termed “consultant,” “collaborator,” and “guide.” All roles were viewed as important; none was more valuable than another; and the roles appeared to build on each other, often merging. Roles were implemented fluidly, with clinicians moving from one role to another as circumstances dictated. Although clinicians tended to describe successful cases, they freely discussed the challenges of end-of-life care, noting that less-than-ideal results were frequent. Thus, the models were described as “best practice” rather than routine care.
Consultant
The consultant provides expert medical information to the patient and family based on the biomedical model and the disease process. The power of the consultant role emanates from the clinician’s medical authority and special knowledge. The consultant presents information to help the patient and family understand the diagnosis, prognosis, and treatment. Once this knowledge is understood, the patient and family determine its meaning to them and decide on treatment. If the patient or family cannot decide or understand the medical implications of their particular situation, the consultant decides based on the medical facts.
A pediatrician illustrated the application of the consultant role in 2 situations involving newborns with severe heart anomalies. Here the physician describes the difficulty of using only medical facts to assist the family in deciding whether to discontinue the ventilator: “I remember saying: ‘The only thing that’s keeping the baby alive at this point is the ventilator. How do you feel about making the decision to turn that off?’ I remember it was a very cruel thing to have them make the decision.”
The physician continued: “Next time I said: ‘We have to sit down and talk about how your baby is doing because he died, and I’m going to turn off the machines now.’ I don’t think we should put them in the position of having to make this decision. We should make this decision and tell them what we’re going to do.” In this situation the clinician employed biomedical expertise to determine the appropriate medical care and outcome for the patient and family. In both cases the decision centered on continuing or discontinuing a medical intervention (respirator) and avoided discussion of the parents’ affective experience. Hallmarks of the consultant role include a biomedical focus, disease-centered decision-making processes, and the clinician’s assumption of authority based on biomedical expertise.
Collaborator
The collaborator exchanges information with the patient and family to promote a common understanding of the diagnosis and illness experience, working with them to choose a treatment path. The collaborator incorporates all components of the consultant role and additionally requires the clinician to understand the patient/family experience. The collaborator considers patient and family issues that need to be addressed to understand the medical facts, appreciates their past experiences with serious illness, determines what information would be difficult for them to accept but would benefit them if they were challenged to confront it, and recognizes that the patient and family hold ultimate responsibility for making treatment decisions.
The following quotes exemplify collaborative clinical care. In the first example, the physician steps outside his comfort zone to provide medical care based on the expressed wishes of a 30-year-old man dying of an advanced brain tumor: “The issue for me was letting go of control. He was going 4 hours away to a fishing cabin and going on a boat. I was really nervous…what if he all of a sudden crashed there? It took me a while to get used to the idea that he needs to be able to do what he enjoys doing, and everybody knows that there’s a risk.”
In a second example, the physician describes collaborating with the family of an 85-year-old woman suffering a massive stroke: “Having heard from the family that they understand that Grandma has had a big stroke and isn’t going to survive…then what wishes do Grandma and the family have? Have they ever discussed this sort of situation?”
In both these examples an understanding of the patient/family experience directs the clinician toward appropriate end-of-life care and is a major source of the collaborator’s power.
Guide
As a guide, the clinician actively and personally seeks solutions for the patient based not only on the medical facts (consultant) and the patient’s values and preferences (collaborator) but also on the guide’s greater understanding of the medical context. In essence, the guide not only knows why and where the patient and family prefer to go but also how to get there.
The following quote demonstrates a clinical application of the guide role. The physician first collaborates to understand the resistance of a terminally ill patient to hospice care:
“They had been very resistant to hospice for reasons that I wasn’t quite clear on. It wasn’t until I was in the home and listened to them talk that I realized they viewed hospice as ‘people are giving up on him.’ I think nobody really was talking to the patient about whether he was willing to give up or if he was ready to die.
“Once patient and family concerns were understood, the guide role was employed: I told the wife and family, ‘We’ve maxed out our medical therapies. There’s not much more we can do for him physically, but perhaps there’s something we can do for him spiritually and emotionally.’ When it was presented to them that way, they were much more understanding. We talked about hospice philosophy and looking at death as a part of life, saying: ‘That we’re not going to resuscitate does not mean do not treat.’ That’s where I came in more as the guide and said: ‘This is what I think is reasonable. What are your expectations? What do you want, Billy? And what do you want, as far as [his] wife and kids?”
The guide role requires that the clinician interpret the patient’s experience, integrate this interpretation with the clinician’s understanding of the clinical situation, and make a recommendation based on the guide’s personal and professional understanding of the situation. The power of the guide role emanates from the clinician’s understanding of how to use the medical system to see that the goals of patient and family are realized.
Discussion
The results of our study are consistent with reports over the past 3 decades by researchers, educators, and social critics who have explored how health professionals provide end-of-life care.23-29 Despite their varying perspectives, all reflect a common theme: the need to provide care based on the unique illness experience and values of the patient and family. The majority of clinicians in our study spoke of the importance of their relationships with patients and families. More than 50% of all interview commentary addressed clinician issues of relationship and personal meaning when providing end-of-life care.
The descriptions of consultant,30 collaborator,31,32 and guide33 confirm previous theoretical discussions regarding the nature of roles and relationships between patients and physicians. The guide is the most complex of the roles described by our study cohort and lends itself to ambivalence on the part of clinicians, in light of its potential to be misunderstood as paternalism. Yet, given the vulnerability and dependence of many patients who are terminally ill, the guide provides these patients with structure, safety, support, and care—based on the patients’ values and goals—reminiscent of the role of a nurturing parent.34
The personal nature of the decisions the guide facilitates reflects the reality of medicine as a moral enterprise.34,35 Having generally witnessed many more deaths than the patient, the guide has knowledge regarding the processes of dying and medical systems that is instrumental in assuring that the desires of the patient and family are realized. A knowledge of patient and family, an appreciation of the futility of the medical situation, and an insight into the process and systems of dying afford the clinician an opportunity to shape the death experience; as Nuland36 described: “Each of us needs a guide who knows us as well as he knows the pathways by which we can approach death.”
Facility with these roles may be a function of personal talent, introspection, and experience. The physicians studied reported that competence with these roles grew over time through delivering endof-life care and learning from patients, families, and other caregivers. Less experienced clinicians tended to describe the consultant and collaborator roles only. Clinicians describing the guide role had been in practice at least a decade and thus were at least 17 years into their training and practice in medicine. Apparently, expertise in all 3 roles requires not only excellent technical diagnostic and treatment skills but also the complex integrated skills of relational knowledge and caring gained through experience.
Our data indicate that relationship, meaning, and roles are primary moderators of the organization of exemplary end-of-life care. Yet, it appears to take nearly 2 decades for physicians to gain the confidence in their knowledge, skills, and attitudes necessary to comfortably guide patients and families through the nuances of end-of-life care. How to successfully educate clinicians to use such a model earlier is beyond our scope but appears crucial to improving training efforts. Current attempts to teach end-of-life care do not develop and explore the complex integrative domains of relational knowledge37-40 described in our study. Studies of educational interventions that stress the importance of the relational aspects of end-of-life care appear warranted.
To facilitate skill acquisition, the authors propose the steps diagrammed in the Figure to assist clinicians in providing quality end-of-life care. We believe the time spent determining patient-centered goals and the roles and relationships required by the clinician should at least equal the time spent determining which tests and treatments to provide. At the end of life, when tests and treatments result in fewer benefits and greater risks and burdens, determining patient and family needs and goals becomes increasingly important as management changes from cure to care.
FIGURE
FLOW DIAGRAM FOR CLINICIAN ROLES
Limitations
This study is limited by a study sample of primary care, family practice faculty who geographically represent all practice in the Pacific Northwest and are predominantly Euro-American in ethnicity. The majority are family physicians, with the remainder pediatricians, internists, and a small number of nurse practitioners and physician assistants. Although no significant differences in terms of roles, relationships, and personal meanings between professional groups were noted, whether these findings are transferable to other primary care clinicians in community practice is unknown. Whether non–primary care specialists and clinicians of differing ethnicity or geographic region would respond differently is unknown. Generalizing these findings to non–primary care clinicians and clinicians of color requires further research.
Conclusions
Given the enormity of social and cultural values that make death a taboo topic, it is unclear how any single reform can easily overcome the multiple barriers to improved end-of-life care. Whether it is possible to teach attitudes and values, such as empathy and self-reflection, is uncertain, though promising curricula and research exist.41-42 If primary care physicians and other professionals improve their knowledge, skills, and attitudes in the delivery of such care, the ultimate effect on improving the experience of patients and families will require further study.
Acknowledgments
We wish to thank the Emily Davie and Joseph S. Kornfeld Foundation and The Nathan Cummings Foundation, New York, which provided generous grants that made our study and article possible. Additionally, we thank Phyllis Silverman, PhD, Harvard University, for her early counsel and advice; Tom Taylor, MD, PhD, University of Washington School of Medicine, for his thoughtful input into the study design, his sage guidance, and his review of the manuscript; Jeanne Quint Benoliel, DNS, Professor Emeritus, University of Washington School of Nursing, for her inspiration and review of the study design and results; and Greg Guldin, PhD, Pacific Lutheran University, for his thoughtful review of the manuscript.
OBJECTIVE: Our goal was to determine primary care clinician perceptions of what is important to the provision of quality end-of-life care.
STUDY DESIGN: We used ethnography, a qualitative research method involving the use of open-ended semistructured interviews.
POPULATION: We included 38 family practice residency faculty from 9 community residency programs of the Affiliated Family Practice Residency Network, Department of Family Medicine, University of Washington School of Medicine.
OUTCOMES MEASURED: The roles described by interviewees when discussing their best practices while delivering end-of-life care were compiled.
RESULTS: Primary care clinicians organize their delivery of quality end-of-life care predominantly through their relationships with patients and families. They play 3 roles when providing end-of-life care. As consultants, clinicians provide expert medical advice and treatment. As collaborators, they seek to understand the patient and family experience. Seasoned clinicians act as guides, using their personal intuitive knowledge of patient and family to facilitate everyone’s growth when providing end-of-life care.
CONCLUSIONS: Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve end-of-life care for patients, families, and clinicians.
- Exemplary end-of-life care is organized around relationships, meaning, and roles.
- Knowledge and skills are essential but are not how exemplary end-of-life care is organized.
- Clinicians providing end-of-life care play 3 roles: consultant, collaborator, and guide.
- Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve care.
Modern medicine has dramatically improved the length and quality of life for countless persons but has also created problems in integrating these advances with end-of-life care. Although 70% of Americans want to die in their own home supported by family, 74% of Americans currently die in institutions.1,2 Clearly, there is a disparity between patient preferences and the end-of-life services provided in America.
Most recommendations for the provision of quality end-of-life care are based on unresearched expert opinion that identifies problems and offers solutions.3-5 Studies have explored communication strategies,6 satisfaction levels with care,7 perceptions of management issues,8 and attitudes toward both death and dying patients.9 Yet little research addresses how practicing community clinicians develop the appropriate relationships and integrate the requisite knowledge, skills, and attitudes to provide quality end-of-life care.
The relationship between clinician, patient, and family and the personal meaning of events for each participant greatly influence end-of-life care.10 Although most commentary on physician roles and relationships in end-of-life care also reflects unresearched expert opinion,11-13 Steinmetz and Gabel14,15 theorized a model that was later validated against the experience of practicing family physicians. The role of the clinician in the successful provision of quality care has not been systematically researched and remains a major challenge to improving end-of-life care. We describe an exploratory qualitative study to determine the perceptions of practicing clinicians regarding quality end-of-life care.
Methods
With approval from the Human Subjects Committee of the University of Washington School of Medicine, faculty were recruited from 9 community programs in the Affiliated Family Practice Residency Network of the Department of Family Medicine. Twenty semistructured long interviews were conducted from a convenience sample at 3 residency sites.16 An additional 8 semistructured interviews and 2 focus groups (10 participants) further explored the data. Thus, a total of 38 clinicians participated in the study. Demographic characteristics of the study cohort have been published previously.10
We conducted the initial 20 interviews using open-ended questions designed to uncover faculty perceptions of quality end-of-life care. The questions explored may be found in the Table. Nonspecific prompts such as “tell me more” were used to enrich data and avoid interviewer bias. The interview was rehearsed with a medical school faculty expert in ethnographic research, field tested, and adjusted before final use. The interviews were audio-recorded and transcribed into qualitative research software.17
Throughout the interview process, the investigators met weekly to compare findings, discuss emerging categories, and jointly code the transcripts for model development using the process of grounded theory described by Glaser and Strauss.18 Common themes, communication and educational issues, and roles and relationships were identified. Data were constantly compared and winnowed to facilitate manageability; data collection and analysis occurred simultaneously.19,20 Common themes are published elsewhere.10 We report and discuss the analysis of the data pertaining to clinician roles and relationships.
We employed the following 3 strategies to assess the methodologic validity of the study and face validity of the themes and models emerging from the data analysis.
TABLE
INTERVIEW QUESTIONS
Remember a case in which you provided care for a patient and family facing a chronic, progressive, terminal illness:
|
Methodologic validation
The themes, models, and 2 interview transcripts were reviewed by 2 expert consultants with experience in qualitative research on end-of-life care and chronic debilitating disease. They assessed the validity of the research process and model development.21,22 These experts confirmed the methodologic approach, affirmed that the transcripts supported the coded model, and noted that the results were consistent with their own past research experience.
Face validity faculty interviews
Long interviews were conducted with a convenience sample of 8 faculty at 2 other residency sites. Researchers described the previous interview process and presented a written summary of the roles and relationship model coded from the data. Dialogue was encouraged with nonspecific prompts to enrich the data and avoid interviewer bias. Interviews were recorded, transcribed, and coded by the researchers to assess face validity and further develop the roles and relationship model using a grounded theory approach.
Face validity focus groups
Two focus groups were conducted with a total of 10 faculty at 2 additional sites. The entire model (themes, communication, roles, and relationships) was presented, and dialogue was encouraged. The researchers recorded, transcribed, and reviewed the focus groups to further assess face validity and refine the model.
Content validity
In a manner identical to that of the focus groups, the researchers presented the entire model at 2 of the 3 sites where faculty provided the initial 20 interviews. These sessions were audiotaped, transcribed, and reviewed by the researchers. The model presented was considered a valid, clinically plausible summary of the content of the initial interviews.
Results
Content analysis of the roles and relationships described by the study cohort revealed 3 distinct clinician roles in the provision of end-of-life care that we termed “consultant,” “collaborator,” and “guide.” All roles were viewed as important; none was more valuable than another; and the roles appeared to build on each other, often merging. Roles were implemented fluidly, with clinicians moving from one role to another as circumstances dictated. Although clinicians tended to describe successful cases, they freely discussed the challenges of end-of-life care, noting that less-than-ideal results were frequent. Thus, the models were described as “best practice” rather than routine care.
Consultant
The consultant provides expert medical information to the patient and family based on the biomedical model and the disease process. The power of the consultant role emanates from the clinician’s medical authority and special knowledge. The consultant presents information to help the patient and family understand the diagnosis, prognosis, and treatment. Once this knowledge is understood, the patient and family determine its meaning to them and decide on treatment. If the patient or family cannot decide or understand the medical implications of their particular situation, the consultant decides based on the medical facts.
A pediatrician illustrated the application of the consultant role in 2 situations involving newborns with severe heart anomalies. Here the physician describes the difficulty of using only medical facts to assist the family in deciding whether to discontinue the ventilator: “I remember saying: ‘The only thing that’s keeping the baby alive at this point is the ventilator. How do you feel about making the decision to turn that off?’ I remember it was a very cruel thing to have them make the decision.”
The physician continued: “Next time I said: ‘We have to sit down and talk about how your baby is doing because he died, and I’m going to turn off the machines now.’ I don’t think we should put them in the position of having to make this decision. We should make this decision and tell them what we’re going to do.” In this situation the clinician employed biomedical expertise to determine the appropriate medical care and outcome for the patient and family. In both cases the decision centered on continuing or discontinuing a medical intervention (respirator) and avoided discussion of the parents’ affective experience. Hallmarks of the consultant role include a biomedical focus, disease-centered decision-making processes, and the clinician’s assumption of authority based on biomedical expertise.
Collaborator
The collaborator exchanges information with the patient and family to promote a common understanding of the diagnosis and illness experience, working with them to choose a treatment path. The collaborator incorporates all components of the consultant role and additionally requires the clinician to understand the patient/family experience. The collaborator considers patient and family issues that need to be addressed to understand the medical facts, appreciates their past experiences with serious illness, determines what information would be difficult for them to accept but would benefit them if they were challenged to confront it, and recognizes that the patient and family hold ultimate responsibility for making treatment decisions.
The following quotes exemplify collaborative clinical care. In the first example, the physician steps outside his comfort zone to provide medical care based on the expressed wishes of a 30-year-old man dying of an advanced brain tumor: “The issue for me was letting go of control. He was going 4 hours away to a fishing cabin and going on a boat. I was really nervous…what if he all of a sudden crashed there? It took me a while to get used to the idea that he needs to be able to do what he enjoys doing, and everybody knows that there’s a risk.”
In a second example, the physician describes collaborating with the family of an 85-year-old woman suffering a massive stroke: “Having heard from the family that they understand that Grandma has had a big stroke and isn’t going to survive…then what wishes do Grandma and the family have? Have they ever discussed this sort of situation?”
In both these examples an understanding of the patient/family experience directs the clinician toward appropriate end-of-life care and is a major source of the collaborator’s power.
Guide
As a guide, the clinician actively and personally seeks solutions for the patient based not only on the medical facts (consultant) and the patient’s values and preferences (collaborator) but also on the guide’s greater understanding of the medical context. In essence, the guide not only knows why and where the patient and family prefer to go but also how to get there.
The following quote demonstrates a clinical application of the guide role. The physician first collaborates to understand the resistance of a terminally ill patient to hospice care:
“They had been very resistant to hospice for reasons that I wasn’t quite clear on. It wasn’t until I was in the home and listened to them talk that I realized they viewed hospice as ‘people are giving up on him.’ I think nobody really was talking to the patient about whether he was willing to give up or if he was ready to die.
“Once patient and family concerns were understood, the guide role was employed: I told the wife and family, ‘We’ve maxed out our medical therapies. There’s not much more we can do for him physically, but perhaps there’s something we can do for him spiritually and emotionally.’ When it was presented to them that way, they were much more understanding. We talked about hospice philosophy and looking at death as a part of life, saying: ‘That we’re not going to resuscitate does not mean do not treat.’ That’s where I came in more as the guide and said: ‘This is what I think is reasonable. What are your expectations? What do you want, Billy? And what do you want, as far as [his] wife and kids?”
The guide role requires that the clinician interpret the patient’s experience, integrate this interpretation with the clinician’s understanding of the clinical situation, and make a recommendation based on the guide’s personal and professional understanding of the situation. The power of the guide role emanates from the clinician’s understanding of how to use the medical system to see that the goals of patient and family are realized.
Discussion
The results of our study are consistent with reports over the past 3 decades by researchers, educators, and social critics who have explored how health professionals provide end-of-life care.23-29 Despite their varying perspectives, all reflect a common theme: the need to provide care based on the unique illness experience and values of the patient and family. The majority of clinicians in our study spoke of the importance of their relationships with patients and families. More than 50% of all interview commentary addressed clinician issues of relationship and personal meaning when providing end-of-life care.
The descriptions of consultant,30 collaborator,31,32 and guide33 confirm previous theoretical discussions regarding the nature of roles and relationships between patients and physicians. The guide is the most complex of the roles described by our study cohort and lends itself to ambivalence on the part of clinicians, in light of its potential to be misunderstood as paternalism. Yet, given the vulnerability and dependence of many patients who are terminally ill, the guide provides these patients with structure, safety, support, and care—based on the patients’ values and goals—reminiscent of the role of a nurturing parent.34
The personal nature of the decisions the guide facilitates reflects the reality of medicine as a moral enterprise.34,35 Having generally witnessed many more deaths than the patient, the guide has knowledge regarding the processes of dying and medical systems that is instrumental in assuring that the desires of the patient and family are realized. A knowledge of patient and family, an appreciation of the futility of the medical situation, and an insight into the process and systems of dying afford the clinician an opportunity to shape the death experience; as Nuland36 described: “Each of us needs a guide who knows us as well as he knows the pathways by which we can approach death.”
Facility with these roles may be a function of personal talent, introspection, and experience. The physicians studied reported that competence with these roles grew over time through delivering endof-life care and learning from patients, families, and other caregivers. Less experienced clinicians tended to describe the consultant and collaborator roles only. Clinicians describing the guide role had been in practice at least a decade and thus were at least 17 years into their training and practice in medicine. Apparently, expertise in all 3 roles requires not only excellent technical diagnostic and treatment skills but also the complex integrated skills of relational knowledge and caring gained through experience.
Our data indicate that relationship, meaning, and roles are primary moderators of the organization of exemplary end-of-life care. Yet, it appears to take nearly 2 decades for physicians to gain the confidence in their knowledge, skills, and attitudes necessary to comfortably guide patients and families through the nuances of end-of-life care. How to successfully educate clinicians to use such a model earlier is beyond our scope but appears crucial to improving training efforts. Current attempts to teach end-of-life care do not develop and explore the complex integrative domains of relational knowledge37-40 described in our study. Studies of educational interventions that stress the importance of the relational aspects of end-of-life care appear warranted.
To facilitate skill acquisition, the authors propose the steps diagrammed in the Figure to assist clinicians in providing quality end-of-life care. We believe the time spent determining patient-centered goals and the roles and relationships required by the clinician should at least equal the time spent determining which tests and treatments to provide. At the end of life, when tests and treatments result in fewer benefits and greater risks and burdens, determining patient and family needs and goals becomes increasingly important as management changes from cure to care.
FIGURE
FLOW DIAGRAM FOR CLINICIAN ROLES
Limitations
This study is limited by a study sample of primary care, family practice faculty who geographically represent all practice in the Pacific Northwest and are predominantly Euro-American in ethnicity. The majority are family physicians, with the remainder pediatricians, internists, and a small number of nurse practitioners and physician assistants. Although no significant differences in terms of roles, relationships, and personal meanings between professional groups were noted, whether these findings are transferable to other primary care clinicians in community practice is unknown. Whether non–primary care specialists and clinicians of differing ethnicity or geographic region would respond differently is unknown. Generalizing these findings to non–primary care clinicians and clinicians of color requires further research.
Conclusions
Given the enormity of social and cultural values that make death a taboo topic, it is unclear how any single reform can easily overcome the multiple barriers to improved end-of-life care. Whether it is possible to teach attitudes and values, such as empathy and self-reflection, is uncertain, though promising curricula and research exist.41-42 If primary care physicians and other professionals improve their knowledge, skills, and attitudes in the delivery of such care, the ultimate effect on improving the experience of patients and families will require further study.
Acknowledgments
We wish to thank the Emily Davie and Joseph S. Kornfeld Foundation and The Nathan Cummings Foundation, New York, which provided generous grants that made our study and article possible. Additionally, we thank Phyllis Silverman, PhD, Harvard University, for her early counsel and advice; Tom Taylor, MD, PhD, University of Washington School of Medicine, for his thoughtful input into the study design, his sage guidance, and his review of the manuscript; Jeanne Quint Benoliel, DNS, Professor Emeritus, University of Washington School of Nursing, for her inspiration and review of the study design and results; and Greg Guldin, PhD, Pacific Lutheran University, for his thoughtful review of the manuscript.
1. The George Gallup International Institute. Spiritual beliefs and the dying process: a report on a national survey. Princeton, NJ: George Gallup International Institute;1997.
2. Field MJ, Cassel CK, eds. Approaching death: improving care at the end of life: Committee on Care at the End of Life, Division of Health Care Services, Institute of Medicine. Washington, DC: National Academy Press; 1997.
3. Schonwetter RS, Hawke W, Knight CF, eds. Hospice and palliative medicine core curriculum and review syllabus: American Academy of Hospice and Palliative Medicine. Dubuque, Iowa: Kendall/Hunt; 1999.
4. Emanuel LL, von Gunten CF, Ferris FD. The education for physicians on end-of-life care (EPEC) curriculum. Chicago, Ill: American Medical Association; 1999.
5. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744-49.
6. Todd C, Still A. General practitioners’ strategies and tactics of communication with the terminally ill. Fam Pract 1993;10:268-76.
7. Blyth AC. Audit of terminal care in a general practice. BMJ 1990;300:983-86.
8. Goodlin SJ, Jette AM, Lynn J, Wasson JH. Community physicians describe management issues for patients expected to live less than twelve months. J Palliat Care 1998;14:30-35.
9. Durand RP, Dickinson GE, Sumner DE, Lancaster CG. Family physicians’ attitudes toward death and the terminally-ill patient. Fam Pract Res J 1990;9:123-29.
10. Farber SJ, Egnew TR, Herman-Bertsch JL. Issues in end-of-life care: family practice faculty perceptions. J Fam Pract 1999;49:525-30.
11. Brewin TB. Not TLC but FPI. J R Soc Med 1990;83:172-75.
12. Mitchell G. The role of the general practitioner in palliative care. Aust Fam Physician 1994;23:1233-39.
13. Ogle KS, Plum JD. The role of the primary care physician in the care of the terminally ill. Clin Geriatr Med 1996;12:267-77.
14. Steinmetz D, Gabel LL. The family physician’s role in caring for the dying patient and family: a comprehensive theoretical model. Fam Pract 1992;9:433-36.
15. Steinmetz D, Walsh M, Gabel LL, Williams PT. Family physicians’ involvement with dying patients and their families. Arch Fam Med 1993;2:753-61.
16. Crabtree BF, Miller WL. A qualitative approach to primary care research: the long interview. Fam Med 1991;23:145-51.
17. Seidel J, Friese S, Leonard DC. The Ethnograph version 4.0 . Amherst, Mass: Qualis Research Associates; 1995.
18. Glaser B, Strauss A. The discovery of grounded theory. New York, NY: Aldine; 1967.
19. Strauss A, Corbin C. Basics of qualitative research. Newbury Park, Calif: Sage; 1990.
20. Wolcott HF. Writing up qualitative research. Newbury Park, Calif: Sage; 1990.
21. Benoliel JQ. Advancing nursing science: qualitative approaches. West J Nurs Res 1984;6:1-8.
22. Taylor TR, Gordon MJ, Ashworth CD. A systems perspective on clinical management. Behav Sci 1984;29:233-47.
23. Glaser BG, Strauss AL. Awareness of dying. Chicago, Ill: Aldine; 1965.
24. Kubler-Ross E. On death and dying. New York, NY: MacMillan; 1969.
25. Weisman A. On dying and denying: a psychiatric study on terminality. New York, NY: Behavioral Publications; 1972.
26. Saunders C, Baines M. Living with dying. New York, NY: Oxford University Press; 1983.
27. Corbin JM, Strauss AL. Unending work and care: managing chronic illness at home. San Francisco, Calif: Jossey-Bass; 1988.
28. Broyard A. Intoxicated by my illness. New York, NY: Potter; 1992.
29. Callahan D. Troubled dream of life. New York, NY: Simon & Schuster; 1993.
30. Balint J, Shelton W. Regaining the initiative: forging a new model of the patient-physician relationship. JAMA 1996;275:887-91.
31. Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med 1983;98:228-34.
32. Stewart M, Brown JB, Weston WW, McWhinney IR, Freeman TR. Patient centered medicine: transforming the clinical method. Thousand Oaks, Calif: Sage; 1995.
33. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA 1992;267:2221-26.
34. Cassell EJ. The nature of suffering and the goals of medicine. New York, NY: Oxford University Press; 1991.
35. Veatch RM. Contemporary bioethics and the demise of modern medicine. In Ormiston G, Sassower R, eds. Prescriptions: the dissemination of medical authority. New York, NY: Greenwood Press; 1990;23-39.
36. Nuland S. How we die. New York, NY: Knopf; 1994.
37. Rogers CR. Client-centered therapy: its current practice, implications, and theory. Boston, Mass: Houghton Mifflin; 1951.
38. Buber M. I and thou. New York, NY: MacMillan; 1974.
39. Mayeroff M. On caring. New York, NY: HarperPerennial; 1990.
40. Kleinman A, Kleinman J. Suffering and its professional transformation: toward an ethnography of interpersonal experience. Cult Med Psychiatry 1991;15:275-301.
41. Novack DH, Suchman AL, Clark W, Epstein RM, Najberg E, Kaplan C. Calibrating the physician: personal awareness and effective patient care. JAMA 1997;278:502-09.
42. Epstein RM. Mindful practice. JAMA 1999;282:833-39.
1. The George Gallup International Institute. Spiritual beliefs and the dying process: a report on a national survey. Princeton, NJ: George Gallup International Institute;1997.
2. Field MJ, Cassel CK, eds. Approaching death: improving care at the end of life: Committee on Care at the End of Life, Division of Health Care Services, Institute of Medicine. Washington, DC: National Academy Press; 1997.
3. Schonwetter RS, Hawke W, Knight CF, eds. Hospice and palliative medicine core curriculum and review syllabus: American Academy of Hospice and Palliative Medicine. Dubuque, Iowa: Kendall/Hunt; 1999.
4. Emanuel LL, von Gunten CF, Ferris FD. The education for physicians on end-of-life care (EPEC) curriculum. Chicago, Ill: American Medical Association; 1999.
5. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744-49.
6. Todd C, Still A. General practitioners’ strategies and tactics of communication with the terminally ill. Fam Pract 1993;10:268-76.
7. Blyth AC. Audit of terminal care in a general practice. BMJ 1990;300:983-86.
8. Goodlin SJ, Jette AM, Lynn J, Wasson JH. Community physicians describe management issues for patients expected to live less than twelve months. J Palliat Care 1998;14:30-35.
9. Durand RP, Dickinson GE, Sumner DE, Lancaster CG. Family physicians’ attitudes toward death and the terminally-ill patient. Fam Pract Res J 1990;9:123-29.
10. Farber SJ, Egnew TR, Herman-Bertsch JL. Issues in end-of-life care: family practice faculty perceptions. J Fam Pract 1999;49:525-30.
11. Brewin TB. Not TLC but FPI. J R Soc Med 1990;83:172-75.
12. Mitchell G. The role of the general practitioner in palliative care. Aust Fam Physician 1994;23:1233-39.
13. Ogle KS, Plum JD. The role of the primary care physician in the care of the terminally ill. Clin Geriatr Med 1996;12:267-77.
14. Steinmetz D, Gabel LL. The family physician’s role in caring for the dying patient and family: a comprehensive theoretical model. Fam Pract 1992;9:433-36.
15. Steinmetz D, Walsh M, Gabel LL, Williams PT. Family physicians’ involvement with dying patients and their families. Arch Fam Med 1993;2:753-61.
16. Crabtree BF, Miller WL. A qualitative approach to primary care research: the long interview. Fam Med 1991;23:145-51.
17. Seidel J, Friese S, Leonard DC. The Ethnograph version 4.0 . Amherst, Mass: Qualis Research Associates; 1995.
18. Glaser B, Strauss A. The discovery of grounded theory. New York, NY: Aldine; 1967.
19. Strauss A, Corbin C. Basics of qualitative research. Newbury Park, Calif: Sage; 1990.
20. Wolcott HF. Writing up qualitative research. Newbury Park, Calif: Sage; 1990.
21. Benoliel JQ. Advancing nursing science: qualitative approaches. West J Nurs Res 1984;6:1-8.
22. Taylor TR, Gordon MJ, Ashworth CD. A systems perspective on clinical management. Behav Sci 1984;29:233-47.
23. Glaser BG, Strauss AL. Awareness of dying. Chicago, Ill: Aldine; 1965.
24. Kubler-Ross E. On death and dying. New York, NY: MacMillan; 1969.
25. Weisman A. On dying and denying: a psychiatric study on terminality. New York, NY: Behavioral Publications; 1972.
26. Saunders C, Baines M. Living with dying. New York, NY: Oxford University Press; 1983.
27. Corbin JM, Strauss AL. Unending work and care: managing chronic illness at home. San Francisco, Calif: Jossey-Bass; 1988.
28. Broyard A. Intoxicated by my illness. New York, NY: Potter; 1992.
29. Callahan D. Troubled dream of life. New York, NY: Simon & Schuster; 1993.
30. Balint J, Shelton W. Regaining the initiative: forging a new model of the patient-physician relationship. JAMA 1996;275:887-91.
31. Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med 1983;98:228-34.
32. Stewart M, Brown JB, Weston WW, McWhinney IR, Freeman TR. Patient centered medicine: transforming the clinical method. Thousand Oaks, Calif: Sage; 1995.
33. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA 1992;267:2221-26.
34. Cassell EJ. The nature of suffering and the goals of medicine. New York, NY: Oxford University Press; 1991.
35. Veatch RM. Contemporary bioethics and the demise of modern medicine. In Ormiston G, Sassower R, eds. Prescriptions: the dissemination of medical authority. New York, NY: Greenwood Press; 1990;23-39.
36. Nuland S. How we die. New York, NY: Knopf; 1994.
37. Rogers CR. Client-centered therapy: its current practice, implications, and theory. Boston, Mass: Houghton Mifflin; 1951.
38. Buber M. I and thou. New York, NY: MacMillan; 1974.
39. Mayeroff M. On caring. New York, NY: HarperPerennial; 1990.
40. Kleinman A, Kleinman J. Suffering and its professional transformation: toward an ethnography of interpersonal experience. Cult Med Psychiatry 1991;15:275-301.
41. Novack DH, Suchman AL, Clark W, Epstein RM, Najberg E, Kaplan C. Calibrating the physician: personal awareness and effective patient care. JAMA 1997;278:502-09.
42. Epstein RM. Mindful practice. JAMA 1999;282:833-39.
Home care: What a physician needs to know
Palliative care for the elderly
I was confused by Dr Gross’s case discussion1 in The Art of Medicine until I realized that his moral dilemma was not whether he should use warfarin to prevent strokes in an elderly patient with atrial fibrillation and gastrointestinal (GI) bleeding. His real dilemma was the conflict between what our medical school training tells us to do and what our hearts tell us to do. Fortunately, palliative medicine is now teaching us that we can follow our hearts and let go of these dilemmas. I believe the case presented is a perfect example.
In the case discussion a woman, Mrs Lopez, had multiple strokes. GI bleeding was a complication of warfarin therapy and a possible malignancy. Dr Gross’s heart told him not to be too aggressive in his testing and treatments. Mrs Lopez and her family agreed “not to embark on an elaborate search.” What was missed, perhaps, was the opportunity to more fully discuss her directives for care. What was also missed at the time was the identification that Mrs Lopez was terminally ill. She was terminal because her life was clearly coming to an end. The ability to cure and fix was no longer realistic. Some of her directives were clear: Dr Gross mentioned that Mrs Lopez accepted life’s uncertainties. Her philosophy seemed to be summed up in the phrase: What will be, will be. So a reasonable choice was palliative care, with an aggressive focus on keeping her comfortable and controlling distressing symptoms. GI bleeding is emotionally distressing and can cause weakness, fatigue, dyspnea, and chest pain, if coronary artery disease is present. The moral principle of “do no harm” would uphold the decision not to give her anything (such as warfarin) that increased the risk of GI bleeding. Aspirin might have been included in this decision, especially given aspirin’s limited possible benefit. Transfusions were appropriate treatment for the anemia resulting from the bleeding. Repeated strokes confirmed the terminal nature of her condition. She might die with the next stroke or she might live to have another one. As Mrs Lopez said, “Si dios quiere.”
The goals to reduce suffering, to control her symptoms, and to maximize her comfort could have made Dr Gross’s dilemma disappear. With these goals in mind he might have reacted to the next stroke in a different way. The goals and the ethical principles of beneficence and doing no harm would have supported his decision not to admit her to the intensive care unit again. The time for cure and fix was past. Central lines and nasogastric tubes were inappropriate for the patient, who was terminal and now hoped for a peaceful, comfortable, dignified death. Dr Gross did come to this realization. But he could have avoided the emotionally charged decision to discontinue Mrs Lopez’s treatments by not starting them.
Death need not be the enemy physicians hide from at all costs. Death is part of life. Physicians can help their patients and families a great deal by recognizing when the dying process is starting. The dilemma described by Dr Gross reflects physicians’ reluctance to let go of curing and fixing as the only goals of care. The principles and philosophy of palliative medicine can help physicians get out of apparent moral clinical dilemmas, especially those based on different treatments aimed at fixing what cannot be fixed. Palliative medicine goals remove the dilemma by upholding the physician’s role in looking at the whole patient, the whole picture, and recognizing the need for appropriate end-of-life care. Planning a good peaceful death may create the perfect outcome.
George F. Davis, MD
Albany, New York
- Gross PR. A rock and a hard place. J Fam Pract 2000; 49:863-64.
The preceding letter was referred to Dr Gross who responded as follows:
I applaud Dr Davis for drawing attention to the value of palliative care. I’m afraid, however, that in his eagerness to prescribe palliative care to resolve the quandry I described, he missed the exact location of the “rock and hard place” I spoke of.
My dilemma was not so much a conflict between “what our medical school training tells us to do and what our hearts tell us to do”; rather, it was an uncertainty within my own heart and mind as to which course of action would lead to a better life for my patient.
In this situation—an elderly patient with atrial fibrillation and gastrointestinal bleeding—both heart and medical training speak with 1 voice: Do not anticoagulate. The dilemma is that this clear choice carries its own substantial risk—a stroke that can cripple if it does not kill. After she suffered 1 stroke, then 2, I worried that Mrs Lopez’s next event could lead not only to death but to months of hemiparesis before she perished—and wondered whether I was doing all I could to avert that disaster. Therefore, the thrust of my piece was that clinical uncertainty leads us to second-guess high-stakes decisions, and even wise choices can lead to unhappy outcomes.
I wholeheartedly agree with Dr Davis that palliative care should become our focus as patients near the end of their lives. Perhaps I could have been more exhaustive in my discussions with Mrs Lopez and her family. They did know that she had a terminal condition; we had discussed her wishes regarding resuscitation. Had I recognized at the moment of her last stroke that her situation would quickly deteriorate it would have been easy to spare her the nasogastric tube and central line. Given that she had just bounced back from a similar episode 2 weeks before, I found that call more difficult to make.
Our work as physicians offers us limitless opportunities to establish high standards for ourselves as we minister to our patients. Having set the bar, we may find that reaching it in every situation can be extraordinarily difficult. Just as we look for ways to comfort our patients, I hope that physicians can find ways to share, listen, and comfort one another when we try our best and still fall short.
Paul R. Gross, MD
St. Joseph’s Medical Center
Yonkers, New York
I was confused by Dr Gross’s case discussion1 in The Art of Medicine until I realized that his moral dilemma was not whether he should use warfarin to prevent strokes in an elderly patient with atrial fibrillation and gastrointestinal (GI) bleeding. His real dilemma was the conflict between what our medical school training tells us to do and what our hearts tell us to do. Fortunately, palliative medicine is now teaching us that we can follow our hearts and let go of these dilemmas. I believe the case presented is a perfect example.
In the case discussion a woman, Mrs Lopez, had multiple strokes. GI bleeding was a complication of warfarin therapy and a possible malignancy. Dr Gross’s heart told him not to be too aggressive in his testing and treatments. Mrs Lopez and her family agreed “not to embark on an elaborate search.” What was missed, perhaps, was the opportunity to more fully discuss her directives for care. What was also missed at the time was the identification that Mrs Lopez was terminally ill. She was terminal because her life was clearly coming to an end. The ability to cure and fix was no longer realistic. Some of her directives were clear: Dr Gross mentioned that Mrs Lopez accepted life’s uncertainties. Her philosophy seemed to be summed up in the phrase: What will be, will be. So a reasonable choice was palliative care, with an aggressive focus on keeping her comfortable and controlling distressing symptoms. GI bleeding is emotionally distressing and can cause weakness, fatigue, dyspnea, and chest pain, if coronary artery disease is present. The moral principle of “do no harm” would uphold the decision not to give her anything (such as warfarin) that increased the risk of GI bleeding. Aspirin might have been included in this decision, especially given aspirin’s limited possible benefit. Transfusions were appropriate treatment for the anemia resulting from the bleeding. Repeated strokes confirmed the terminal nature of her condition. She might die with the next stroke or she might live to have another one. As Mrs Lopez said, “Si dios quiere.”
The goals to reduce suffering, to control her symptoms, and to maximize her comfort could have made Dr Gross’s dilemma disappear. With these goals in mind he might have reacted to the next stroke in a different way. The goals and the ethical principles of beneficence and doing no harm would have supported his decision not to admit her to the intensive care unit again. The time for cure and fix was past. Central lines and nasogastric tubes were inappropriate for the patient, who was terminal and now hoped for a peaceful, comfortable, dignified death. Dr Gross did come to this realization. But he could have avoided the emotionally charged decision to discontinue Mrs Lopez’s treatments by not starting them.
Death need not be the enemy physicians hide from at all costs. Death is part of life. Physicians can help their patients and families a great deal by recognizing when the dying process is starting. The dilemma described by Dr Gross reflects physicians’ reluctance to let go of curing and fixing as the only goals of care. The principles and philosophy of palliative medicine can help physicians get out of apparent moral clinical dilemmas, especially those based on different treatments aimed at fixing what cannot be fixed. Palliative medicine goals remove the dilemma by upholding the physician’s role in looking at the whole patient, the whole picture, and recognizing the need for appropriate end-of-life care. Planning a good peaceful death may create the perfect outcome.
George F. Davis, MD
Albany, New York
- Gross PR. A rock and a hard place. J Fam Pract 2000; 49:863-64.
The preceding letter was referred to Dr Gross who responded as follows:
I applaud Dr Davis for drawing attention to the value of palliative care. I’m afraid, however, that in his eagerness to prescribe palliative care to resolve the quandry I described, he missed the exact location of the “rock and hard place” I spoke of.
My dilemma was not so much a conflict between “what our medical school training tells us to do and what our hearts tell us to do”; rather, it was an uncertainty within my own heart and mind as to which course of action would lead to a better life for my patient.
In this situation—an elderly patient with atrial fibrillation and gastrointestinal bleeding—both heart and medical training speak with 1 voice: Do not anticoagulate. The dilemma is that this clear choice carries its own substantial risk—a stroke that can cripple if it does not kill. After she suffered 1 stroke, then 2, I worried that Mrs Lopez’s next event could lead not only to death but to months of hemiparesis before she perished—and wondered whether I was doing all I could to avert that disaster. Therefore, the thrust of my piece was that clinical uncertainty leads us to second-guess high-stakes decisions, and even wise choices can lead to unhappy outcomes.
I wholeheartedly agree with Dr Davis that palliative care should become our focus as patients near the end of their lives. Perhaps I could have been more exhaustive in my discussions with Mrs Lopez and her family. They did know that she had a terminal condition; we had discussed her wishes regarding resuscitation. Had I recognized at the moment of her last stroke that her situation would quickly deteriorate it would have been easy to spare her the nasogastric tube and central line. Given that she had just bounced back from a similar episode 2 weeks before, I found that call more difficult to make.
Our work as physicians offers us limitless opportunities to establish high standards for ourselves as we minister to our patients. Having set the bar, we may find that reaching it in every situation can be extraordinarily difficult. Just as we look for ways to comfort our patients, I hope that physicians can find ways to share, listen, and comfort one another when we try our best and still fall short.
Paul R. Gross, MD
St. Joseph’s Medical Center
Yonkers, New York
I was confused by Dr Gross’s case discussion1 in The Art of Medicine until I realized that his moral dilemma was not whether he should use warfarin to prevent strokes in an elderly patient with atrial fibrillation and gastrointestinal (GI) bleeding. His real dilemma was the conflict between what our medical school training tells us to do and what our hearts tell us to do. Fortunately, palliative medicine is now teaching us that we can follow our hearts and let go of these dilemmas. I believe the case presented is a perfect example.
In the case discussion a woman, Mrs Lopez, had multiple strokes. GI bleeding was a complication of warfarin therapy and a possible malignancy. Dr Gross’s heart told him not to be too aggressive in his testing and treatments. Mrs Lopez and her family agreed “not to embark on an elaborate search.” What was missed, perhaps, was the opportunity to more fully discuss her directives for care. What was also missed at the time was the identification that Mrs Lopez was terminally ill. She was terminal because her life was clearly coming to an end. The ability to cure and fix was no longer realistic. Some of her directives were clear: Dr Gross mentioned that Mrs Lopez accepted life’s uncertainties. Her philosophy seemed to be summed up in the phrase: What will be, will be. So a reasonable choice was palliative care, with an aggressive focus on keeping her comfortable and controlling distressing symptoms. GI bleeding is emotionally distressing and can cause weakness, fatigue, dyspnea, and chest pain, if coronary artery disease is present. The moral principle of “do no harm” would uphold the decision not to give her anything (such as warfarin) that increased the risk of GI bleeding. Aspirin might have been included in this decision, especially given aspirin’s limited possible benefit. Transfusions were appropriate treatment for the anemia resulting from the bleeding. Repeated strokes confirmed the terminal nature of her condition. She might die with the next stroke or she might live to have another one. As Mrs Lopez said, “Si dios quiere.”
The goals to reduce suffering, to control her symptoms, and to maximize her comfort could have made Dr Gross’s dilemma disappear. With these goals in mind he might have reacted to the next stroke in a different way. The goals and the ethical principles of beneficence and doing no harm would have supported his decision not to admit her to the intensive care unit again. The time for cure and fix was past. Central lines and nasogastric tubes were inappropriate for the patient, who was terminal and now hoped for a peaceful, comfortable, dignified death. Dr Gross did come to this realization. But he could have avoided the emotionally charged decision to discontinue Mrs Lopez’s treatments by not starting them.
Death need not be the enemy physicians hide from at all costs. Death is part of life. Physicians can help their patients and families a great deal by recognizing when the dying process is starting. The dilemma described by Dr Gross reflects physicians’ reluctance to let go of curing and fixing as the only goals of care. The principles and philosophy of palliative medicine can help physicians get out of apparent moral clinical dilemmas, especially those based on different treatments aimed at fixing what cannot be fixed. Palliative medicine goals remove the dilemma by upholding the physician’s role in looking at the whole patient, the whole picture, and recognizing the need for appropriate end-of-life care. Planning a good peaceful death may create the perfect outcome.
George F. Davis, MD
Albany, New York
- Gross PR. A rock and a hard place. J Fam Pract 2000; 49:863-64.
The preceding letter was referred to Dr Gross who responded as follows:
I applaud Dr Davis for drawing attention to the value of palliative care. I’m afraid, however, that in his eagerness to prescribe palliative care to resolve the quandry I described, he missed the exact location of the “rock and hard place” I spoke of.
My dilemma was not so much a conflict between “what our medical school training tells us to do and what our hearts tell us to do”; rather, it was an uncertainty within my own heart and mind as to which course of action would lead to a better life for my patient.
In this situation—an elderly patient with atrial fibrillation and gastrointestinal bleeding—both heart and medical training speak with 1 voice: Do not anticoagulate. The dilemma is that this clear choice carries its own substantial risk—a stroke that can cripple if it does not kill. After she suffered 1 stroke, then 2, I worried that Mrs Lopez’s next event could lead not only to death but to months of hemiparesis before she perished—and wondered whether I was doing all I could to avert that disaster. Therefore, the thrust of my piece was that clinical uncertainty leads us to second-guess high-stakes decisions, and even wise choices can lead to unhappy outcomes.
I wholeheartedly agree with Dr Davis that palliative care should become our focus as patients near the end of their lives. Perhaps I could have been more exhaustive in my discussions with Mrs Lopez and her family. They did know that she had a terminal condition; we had discussed her wishes regarding resuscitation. Had I recognized at the moment of her last stroke that her situation would quickly deteriorate it would have been easy to spare her the nasogastric tube and central line. Given that she had just bounced back from a similar episode 2 weeks before, I found that call more difficult to make.
Our work as physicians offers us limitless opportunities to establish high standards for ourselves as we minister to our patients. Having set the bar, we may find that reaching it in every situation can be extraordinarily difficult. Just as we look for ways to comfort our patients, I hope that physicians can find ways to share, listen, and comfort one another when we try our best and still fall short.
Paul R. Gross, MD
St. Joseph’s Medical Center
Yonkers, New York
Which pharmacologic therapies are effective in preventing acute mountain sickness?
BACKGROUND: Acute mountain sickness results in symptoms such as headache, loss of appetite, nausea, fatigue, insomnia, and increased mortality in the first few days of exertion at high altitudes. Acetazolamide and dexamethasone have been recommended as treatments to prevent acute mountain sickness, although their efficacy and tolerability have not been well established.
DATA SOURCE: Thirty-three clinical trials comparing any pharmacologic treatment with placebo for the prevention of acute mountain sickness were identified through a comprehensive search of MEDLINE, EMBASE, the Cochrane Library, a high altitude bibliography Web site, and the bibliographies of retrieved reports and review articles. Of these trials, 18 reported complete prevention of acute mountain sickness as an outcome and as related to ascents to 4050 to 5890 meters (13300 to 19300 feet). These were included in a qualitative analysis of efficacy for any pharmacologic treatment (all 18 trials) and statistical meta-analyses for dexamethasone (8 trials representing 161 subjects) and acetazolamide (9 trials representing 295 subjects).
STUDY DESIGN AND VALIDITY: Only one author determined whether studies met inclusion criteria. All 3 authors read the included articles for validity, applying the 3-item 5-point Oxford score. The mean quality score was 3 (range=2-5). A total of 17 of the 33 trials used an adequate method of blinding. Validity was not a criteria for inclusion in the review. Following the qualitative analysis of efficacy, relative benefit (relative risk [RR] of prevention of mountain sickness) and numbers needed to treat (NNTs) were calculated for 2 interventions, dexamethasone and acetazolamide. Although the studies were rated for validity using previously tested criteria, no information on study limitations is given with which to judge the direction of effect. Using more than one author to determine eligibility would have minimized investigator bias. Although included studies varied in their definitions of acute mountain sickness, the results were homogenous. The investigators limited the outcome to complete prevention of symptoms. This conservative approach would underestimate the efficacy of the treatments making any significant benefit more likely to be real. Unfortunately, no information is provided on the subjects in the trials, including information such as age, sex, training, smoking status, and other risk factors for acute mountain sickness. This information would have helped generalize the study results.
OUTCOMES MEASURED: The primary outcome measured was complete prevention of acute mountain sickness according to the definition used in each of the original studies. Although reported for some of the studies, the reduction in symptom severity was not considered a criterion for efficacy in this study. Secondary outcomes included prevention of headache, nausea, insomnia, and dizziness, and the development of adverse drug reactions.
RESULTS: In 8 trials of dexamethasone (n=161) and 9 of acetazolamide (n=295), all with exposure above 4000 meters, single daily doses of dexamethasone 8 mg, 12 mg, and 16 mg or acetazolamide 750 mg were all more efficacious than placebo (NNT=3 for both). Smaller doses (dexamethasone 0.5 and 2 mg in one trial, acetazolamide 500 mg in 3 trials) did not prevent mountain sickness over placebo. Five trials of acetazolamide reported symptom end points including insomnia, headache, nausea, and dizziness; all results favored acetazolamide (NNT=3-6). Both dexamethasone and acetazolamide demonstrated a trend toward greater efficacy (lower NNT) with faster ascent rates. There was no relative benefit (RR for prophylaxis=1) for trials with ascent rates below approximately 500 meters per day; but there was a five- to six-fold relative benefit for prophylaxis at the highest ascent rates. Regarding adverse effects, subjects in 2 of 5 studies were more likely to experience depression on weaning of dexamethasone (overall RR=4.5). Acetazolamide was associated with polyuria (RR=4.2) and paraesthesia (RR=4.0).
Both dexamethasone 8 to 16 mg and acetazolamide 750 mg per day are effective for preventing acute mountain sickness. Despite US Food and Drug Administration approval, 500 mg per day of acetazolamide is not effective in preventing all symptoms. Side effects are mild for both drugs, but the potential for depression with abrupt cessation of dexamethasone may warrant weaning doses after exposure. There is no apparent benefit to therapy if ascension rates are less than 500 meters per day. Unfortunately, this study does not guide the clinician in selecting high- or low-risk patients in terms of demographics or lifestyle factors, and it does not it clarify how soon to start either medication before the ascent.
BACKGROUND: Acute mountain sickness results in symptoms such as headache, loss of appetite, nausea, fatigue, insomnia, and increased mortality in the first few days of exertion at high altitudes. Acetazolamide and dexamethasone have been recommended as treatments to prevent acute mountain sickness, although their efficacy and tolerability have not been well established.
DATA SOURCE: Thirty-three clinical trials comparing any pharmacologic treatment with placebo for the prevention of acute mountain sickness were identified through a comprehensive search of MEDLINE, EMBASE, the Cochrane Library, a high altitude bibliography Web site, and the bibliographies of retrieved reports and review articles. Of these trials, 18 reported complete prevention of acute mountain sickness as an outcome and as related to ascents to 4050 to 5890 meters (13300 to 19300 feet). These were included in a qualitative analysis of efficacy for any pharmacologic treatment (all 18 trials) and statistical meta-analyses for dexamethasone (8 trials representing 161 subjects) and acetazolamide (9 trials representing 295 subjects).
STUDY DESIGN AND VALIDITY: Only one author determined whether studies met inclusion criteria. All 3 authors read the included articles for validity, applying the 3-item 5-point Oxford score. The mean quality score was 3 (range=2-5). A total of 17 of the 33 trials used an adequate method of blinding. Validity was not a criteria for inclusion in the review. Following the qualitative analysis of efficacy, relative benefit (relative risk [RR] of prevention of mountain sickness) and numbers needed to treat (NNTs) were calculated for 2 interventions, dexamethasone and acetazolamide. Although the studies were rated for validity using previously tested criteria, no information on study limitations is given with which to judge the direction of effect. Using more than one author to determine eligibility would have minimized investigator bias. Although included studies varied in their definitions of acute mountain sickness, the results were homogenous. The investigators limited the outcome to complete prevention of symptoms. This conservative approach would underestimate the efficacy of the treatments making any significant benefit more likely to be real. Unfortunately, no information is provided on the subjects in the trials, including information such as age, sex, training, smoking status, and other risk factors for acute mountain sickness. This information would have helped generalize the study results.
OUTCOMES MEASURED: The primary outcome measured was complete prevention of acute mountain sickness according to the definition used in each of the original studies. Although reported for some of the studies, the reduction in symptom severity was not considered a criterion for efficacy in this study. Secondary outcomes included prevention of headache, nausea, insomnia, and dizziness, and the development of adverse drug reactions.
RESULTS: In 8 trials of dexamethasone (n=161) and 9 of acetazolamide (n=295), all with exposure above 4000 meters, single daily doses of dexamethasone 8 mg, 12 mg, and 16 mg or acetazolamide 750 mg were all more efficacious than placebo (NNT=3 for both). Smaller doses (dexamethasone 0.5 and 2 mg in one trial, acetazolamide 500 mg in 3 trials) did not prevent mountain sickness over placebo. Five trials of acetazolamide reported symptom end points including insomnia, headache, nausea, and dizziness; all results favored acetazolamide (NNT=3-6). Both dexamethasone and acetazolamide demonstrated a trend toward greater efficacy (lower NNT) with faster ascent rates. There was no relative benefit (RR for prophylaxis=1) for trials with ascent rates below approximately 500 meters per day; but there was a five- to six-fold relative benefit for prophylaxis at the highest ascent rates. Regarding adverse effects, subjects in 2 of 5 studies were more likely to experience depression on weaning of dexamethasone (overall RR=4.5). Acetazolamide was associated with polyuria (RR=4.2) and paraesthesia (RR=4.0).
Both dexamethasone 8 to 16 mg and acetazolamide 750 mg per day are effective for preventing acute mountain sickness. Despite US Food and Drug Administration approval, 500 mg per day of acetazolamide is not effective in preventing all symptoms. Side effects are mild for both drugs, but the potential for depression with abrupt cessation of dexamethasone may warrant weaning doses after exposure. There is no apparent benefit to therapy if ascension rates are less than 500 meters per day. Unfortunately, this study does not guide the clinician in selecting high- or low-risk patients in terms of demographics or lifestyle factors, and it does not it clarify how soon to start either medication before the ascent.
BACKGROUND: Acute mountain sickness results in symptoms such as headache, loss of appetite, nausea, fatigue, insomnia, and increased mortality in the first few days of exertion at high altitudes. Acetazolamide and dexamethasone have been recommended as treatments to prevent acute mountain sickness, although their efficacy and tolerability have not been well established.
DATA SOURCE: Thirty-three clinical trials comparing any pharmacologic treatment with placebo for the prevention of acute mountain sickness were identified through a comprehensive search of MEDLINE, EMBASE, the Cochrane Library, a high altitude bibliography Web site, and the bibliographies of retrieved reports and review articles. Of these trials, 18 reported complete prevention of acute mountain sickness as an outcome and as related to ascents to 4050 to 5890 meters (13300 to 19300 feet). These were included in a qualitative analysis of efficacy for any pharmacologic treatment (all 18 trials) and statistical meta-analyses for dexamethasone (8 trials representing 161 subjects) and acetazolamide (9 trials representing 295 subjects).
STUDY DESIGN AND VALIDITY: Only one author determined whether studies met inclusion criteria. All 3 authors read the included articles for validity, applying the 3-item 5-point Oxford score. The mean quality score was 3 (range=2-5). A total of 17 of the 33 trials used an adequate method of blinding. Validity was not a criteria for inclusion in the review. Following the qualitative analysis of efficacy, relative benefit (relative risk [RR] of prevention of mountain sickness) and numbers needed to treat (NNTs) were calculated for 2 interventions, dexamethasone and acetazolamide. Although the studies were rated for validity using previously tested criteria, no information on study limitations is given with which to judge the direction of effect. Using more than one author to determine eligibility would have minimized investigator bias. Although included studies varied in their definitions of acute mountain sickness, the results were homogenous. The investigators limited the outcome to complete prevention of symptoms. This conservative approach would underestimate the efficacy of the treatments making any significant benefit more likely to be real. Unfortunately, no information is provided on the subjects in the trials, including information such as age, sex, training, smoking status, and other risk factors for acute mountain sickness. This information would have helped generalize the study results.
OUTCOMES MEASURED: The primary outcome measured was complete prevention of acute mountain sickness according to the definition used in each of the original studies. Although reported for some of the studies, the reduction in symptom severity was not considered a criterion for efficacy in this study. Secondary outcomes included prevention of headache, nausea, insomnia, and dizziness, and the development of adverse drug reactions.
RESULTS: In 8 trials of dexamethasone (n=161) and 9 of acetazolamide (n=295), all with exposure above 4000 meters, single daily doses of dexamethasone 8 mg, 12 mg, and 16 mg or acetazolamide 750 mg were all more efficacious than placebo (NNT=3 for both). Smaller doses (dexamethasone 0.5 and 2 mg in one trial, acetazolamide 500 mg in 3 trials) did not prevent mountain sickness over placebo. Five trials of acetazolamide reported symptom end points including insomnia, headache, nausea, and dizziness; all results favored acetazolamide (NNT=3-6). Both dexamethasone and acetazolamide demonstrated a trend toward greater efficacy (lower NNT) with faster ascent rates. There was no relative benefit (RR for prophylaxis=1) for trials with ascent rates below approximately 500 meters per day; but there was a five- to six-fold relative benefit for prophylaxis at the highest ascent rates. Regarding adverse effects, subjects in 2 of 5 studies were more likely to experience depression on weaning of dexamethasone (overall RR=4.5). Acetazolamide was associated with polyuria (RR=4.2) and paraesthesia (RR=4.0).
Both dexamethasone 8 to 16 mg and acetazolamide 750 mg per day are effective for preventing acute mountain sickness. Despite US Food and Drug Administration approval, 500 mg per day of acetazolamide is not effective in preventing all symptoms. Side effects are mild for both drugs, but the potential for depression with abrupt cessation of dexamethasone may warrant weaning doses after exposure. There is no apparent benefit to therapy if ascension rates are less than 500 meters per day. Unfortunately, this study does not guide the clinician in selecting high- or low-risk patients in terms of demographics or lifestyle factors, and it does not it clarify how soon to start either medication before the ascent.