User login
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration

Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs
Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs
In leveraging existing, readily available evidence-based health care information (eg, systematic reviews, clinical practice guidelines), clinicians have historically made recommendations based on treatment responses of the average patient.1 Recently, this approach has been expanded into data-driven, evidence-based precision medical care for individuals across a wide range of disciplines and care settings. These precision medicine approaches use information related to an individual’s genes, environment, and lifestyle to tailor recommendations regarding prevention, diagnosis, and treatment.
Applying precision medicine approaches to the unique exposures and experiences of service members and veterans—particularly those who served in combat environments—through the incorporation of biopsychosocial factors into medical decision-making may be even more pertinent. This sentiment is reflected in Section 305 of the Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, which outlines the Precision Medicine Initiative of the US Department of Veterans Affairs (VA) to identify and validate brain and mental health biomarkers.2 Despite widespread consensus regarding the promise of precision medicine, large, rich datasets with elements pertaining to common military exposures such as traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are limited.
Existing datasets, most of which are relatively small or focus on specific cohorts (eg, older veterans, transitioning veterans), continue to create barriers to advancing precision medicine. For example, in classically designed clinical trials, analyses are generally conducted in a manner that may obfuscate efficacy among subcohorts of individuals, thereby underscoring the need to explore alternative strategies to unify existing datasets capable of revealing such heterogeneity.3 The evidence base for precision medical care is limited, drawing from published trials with relatively small sample sizes and even larger cohort studies have limited biomarker data. Additionally, these models are often exploratory during development, and to avoid statistical overfitting of an exploratory model, validation in similar datasets is needed—an added burden when data sources are small or underpowered to begin with.
A promising approach is to combine and harmonize the largest, most deeply characterized data sources from similar samples. Although combining such datasets may appear to require minimal time and effort, harmonizing similar variables in an evidence-based and replicable manner requires time and expertise, even when participant characteristics and outcomes are similar.4-7
Challenges related to harmonization are related to the wide range of strategies (eg, self-report questionnaires, clinical interviews, electronic health record review) used to measure common brain and mental health constructs, such as depression. Even when similar methods (eg, self-report measures) are implemented, challenges persist. For example, if a study used a depression measure that focused primarily on cognitive symptoms (eg, pessimism, self-dislike, suicidal ideation) and another study used a depression measure composed of items more heavily weighted towards somatic symptoms (eg, insomnia, loss of appetite, weight loss, decreased libido), combining their data could be challenging, particularly if researchers, clinicians, or administrators are interested in more than dichotomous outcomes (eg, depression vs no depression).8,9
To address this knowledge gap and harmonize multimodal data from varied sources, well-planned and reproducible curation is needed. Longitudinal cohort studies of service members and veterans with military combat and training exposure histories provide researchers and other stakeholders access to extant biopsychosocial data shown to affect risk for adverse health outcomes; however, efforts to facilitate individually tailored treatment or other precision medicine approaches would benefit from the synthesis of such datasets.10
Members of the VA Total Brain Diagnostics (TBD) team are engaged in harmonizing variables from the Long-Term Impact of Military-Relevant Brain Injury Consortium–Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC)11 and the Translational Research Center for TBI and Stress Disorders (TRACTS).12-21 While there is overlap across LIMBIC-CENC and TRACTS with respect to data domains, considerable data harmonization is needed to allow for future valid and meaningful analyses, particularly those involving multivariable predictors.
Data Sources
Both data sources for the TBD harmonization project, LIMBIC-CENC and TRACTS, include extensive, longitudinal data collected from relatively large cohorts of veterans and service members with combat exposure. Both studies collect detailed data related to potential brain injury history and include participants with and without a history of TBI. Similarly, both include extensive collection of fluid biomarkers and imaging data, as well as measures of biopsychosocial functioning.
Data collection sites for LIMBIC-CENC include 16 recruitment sites, 9 at VA medical centers (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego) and 7 at military treatment sites (Alexandria, San Diego, Tampa, Tacoma, Columbia, Coronado, Hinesville), in addition to 11 assessment sites (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego, Alexandria, Augusta). Data for TRACTS are collected at sites in Boston and Houston.
LIMBIC-CENC is a 12-year, 17-site cohort of service members and veteran participants with combat exposure who are well characterized at baseline and undergo annual reassessments. As of December 2025, > 3100 participants have been recruited, and nearly 90% remain in follow-up. Data collection includes > 6200 annual follow-up evaluations and > 1550 5-year re-evaluations, with 400 enrolled participants followed up annually.
TRACTS is a 16-year, 2-site cohort of veterans with combat exposure who complete comprehensive assessments at enrollment, undergo annual reassessments, and complete comprehensive reassessment every 5 years thereafter. As of December 2025, > 1075 participants have completed baseline (Time 1) assessments, > 600 have completed the 2-year re-evaluation (Time 2), > 175 have completed the 5-year re-evaluation (Time 3), and > 35 have completed 10-year evaluations (Time 4), with about 50 new participants added and 100 enrolled participants followed up annually. More data on participant characteristics are available for both LIMBIC-CENC and TRACTS in previous publications.11,22These 2 ongoing, prospective, longitudinal cohorts of service members and veterans offer access to a wide range of potential risk factors that can affect response to care and outcomes, including demographics (eg, age, sex), injury characteristics (eg, pre-exposure factors, exposure factors), biomarkers (eg, serum, saliva, brain imaging, evoked potentials), and functional measures (eg, computerized posturography, computerized eye tracking, sensory testing, clinical examination, neuropsychological assessments, symptom questionnaires).
Harmonization Strategy
Pooling and harmonizing data from large studies evaluating similar participant cohorts and conditions involves numerous steps to appropriately handle a variety of measurements and disparate variable names. The TBD team adapted a model data harmonization system developed by O’Neil et al through initial work harmonizing the Federal Interagency Traumatic Brain Injury Research Informatics System (FITBIR).4-7 This process was expanded and generalized by the research team to combine data from LIMBIC-CENC and TRACTS to create a single pooled dataset for analysis (Figure).
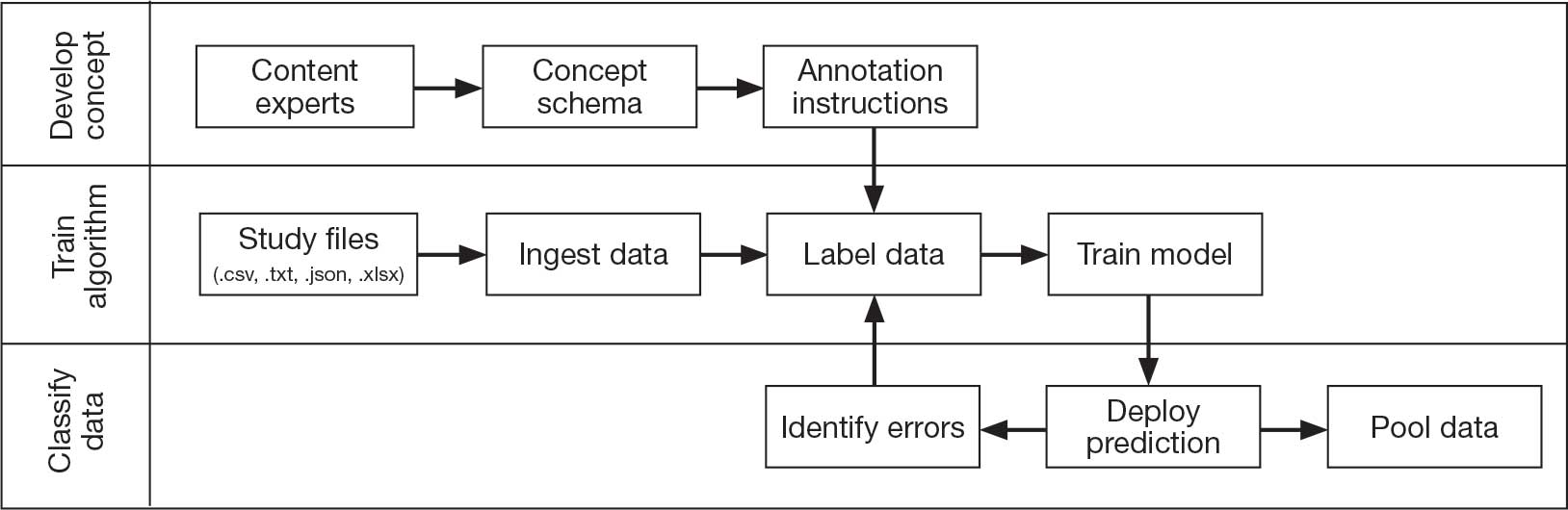
Injury Research database.
This approach was selected because it accommodates heterogeneous study designs (eg, cross-sectional, longitudinal, case-control), data collection methods (eg, clinical assessment, self-reported, objective blood, and imaging biomarkers), and various assessments of the same construct (ie, different measures of brain injury). While exact matches for data collection methods and measures may be easily harmonized, the timing of assessment, number of assessments, assessment tool version, and other factors must be considered. The goal was to harmonize data from LIMBIC-CENC and TRACTS to allow additional data sources to be harmonized and incorporated in the future.
Original data files from each study were reshaped to represent participant-level observations with 1 unique measurement per row. The measurement represents what information was collected and the value recorded represents the unique observation. These data are linked to metadata from the original study, which includes the study’s definition of each measurement, how it was collected, and any available information regarding when it was collected in reference to study enrollment or injury. Additional information on the file source, row, and column position of each data point was added to enable recreation of the original data as needed.
The resulting dataset was used to harmonize measurements from LIMBIC-CENC and TRACTS into a priori-defined schemas for brain- and mental health-relevant concepts, including TBI severity, PTSD, substance use, depression, suicidal ideation, and functioning (including cognitive, physical, and social functioning). This process was facilitated using natural language processing (NLP). Each study uniquely defines all measurements and provides written definitions with the data. Measurement definitions serve as records describing what was collected, how it was collected, and how the study may have uniquely defined information for its purposes. For example, definitions of exposure to brain injury and severity of brain injury may differ between studies, and the study-provided definition defines these differences.
Definitions were converted into numeric vectors through sentence embedding, a process that preserves the semantic meaning of the definition.23 Cosine similarity was used as the primary metric to compare the semantic textual similarity between pairs of measurement definitions. Cosine similarity ranges from 0 to 1, where 0 indicates no meaningful similarity and 1 indicates they have identical meanings.24 This approach leverages the relationship between the definitions of each measurement provided by a study and enables quick comparison of all pairwise combinations of measurement definitions between studies.
Subsets of similar measurements across studies were organized into a priori-defined schema. Clinical experts then reviewed each schema and further refined them into domains, (eg, mechanism of injury, clinical signs, acute symptoms) and subdomains (children), such as loss of consciousness, amnesia, and alteration of consciousness. This approach allows efficient handling of 2 specific cases that commonly occur when pooling and harmonizing datasets: (1) identifying the same measurement with differing names; and (2) identifying different measurements with definitions that each relate to the same domain.
The Table provides a general example of the schema for TBI severity. This was an iterative process in which clinical experts reviewed study-defined measurement definitions to develop general harmonized domains, and NLP techniques facilitated and accelerated identification and organization of measurements within these domains.
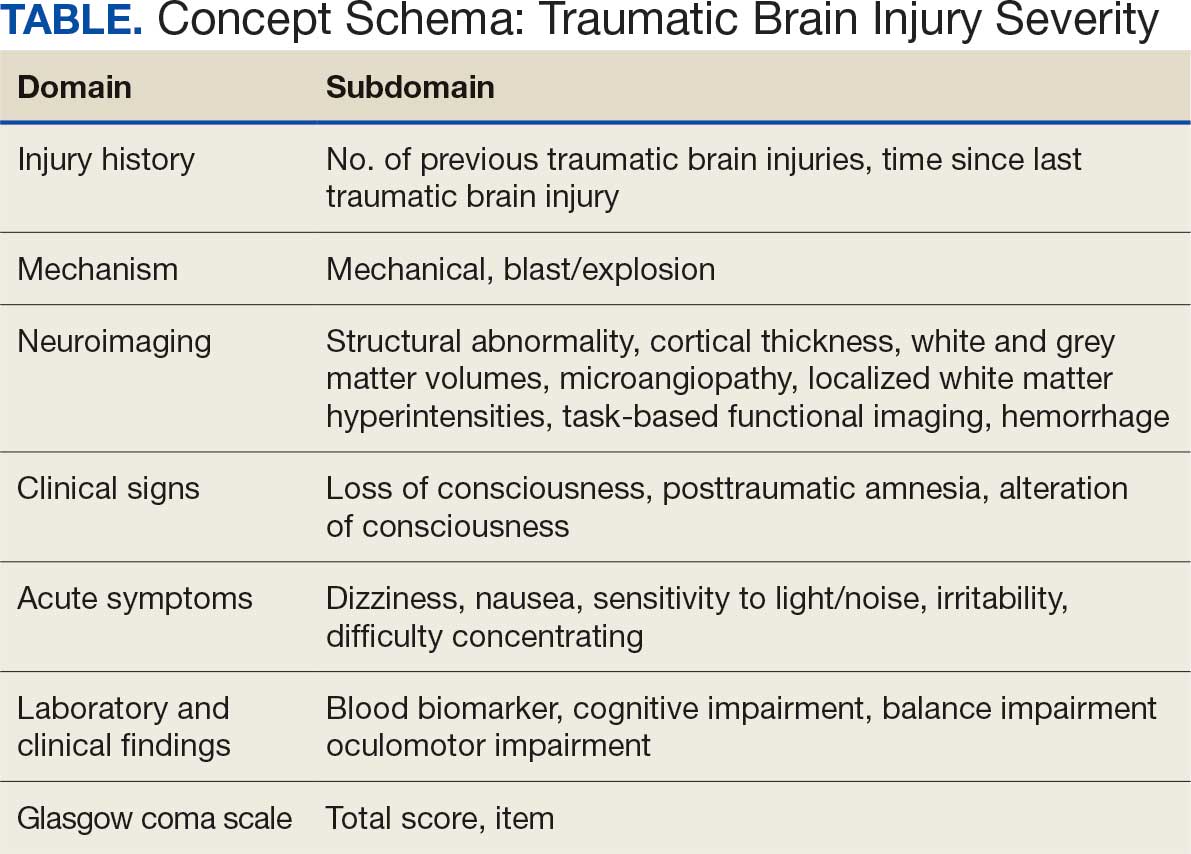
Expected Impact
Harmonization combining LIMBIC-CENC and TRACTS datasets is ongoing. Preliminary descriptive analyses of baseline cohort data indicate that harmonization across data sources is appropriate, given the lack of significant heterogeneity across sites and studies for most domains. Work by members of the TBD team is expected to lay the foundation for the use of existing and ongoing prospective, longitudinal datasets (eg, LIMBIC-CENC, TRACTS) and linked large datasets (eg, VA Informatics and Computing Infrastructure including electronic health records, VA Million Veteran Program, DaVINCI [US Department of Defense and VA Infrastructure for Clinical Intelligence]) to generate generalizable, clinically relevant information to advance precision brain and mental health care among service members and veterans.
By enhancing existing practice, this synthesized dataset has the potential to inform tailored and personalized medicine approaches designed to meet the needs of veterans and service members. These data will serve as the starting point for multivariable models examining the intersection of physiologic, behavioral, and environmental factors. The goal of this data harmonization effort is to better elucidate how clinicians and researchers can select optimal approaches for veterans and service members with TBI histories by accounting for a comprehensive set of physiologic, behavioral, and environmental factors in an individually tailored manner. These data may further extend existing clinical practice guideline approaches, inform shared decision-making, and enhance functional outcomes beyond those currently available.
Conclusions
Individuals who have served in the military have unique biopsychosocial exposures that are associated with brain and mental health disorders. To address these needs, the nationwide TBD team has initiated the creation of a unified, longitudinal dataset that includes harmonized measures from existing LIMBIC-CENC and TRACTS protocols. Initial data harmonization efforts are required to facilitate precision prognostics, diagnostics, and tailored interventions, with the goal of improving veterans’ brain and mental health and psychosocial functioning and enabling tailored and evidence-informed, individualized clinical care.
- The Promise of Precision Medicine. National Institutes of Health (NIH). Updated January 21, 2025. Accessed January 5, 2026. https://www.nih.gov/about-nih/nih-turning-discovery-into-health/promise-precision-medicine.
- Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, S 785, 116th Cong (2019-2020) Accessed January 5, 2026. https://www.congress.gov/bill/116th-congress/senate-bill/785
- Cheng C, Messerschmidt L, Bravo I, et al. A general primer for data harmonization. Sci Data. 2024;11:152. doi:10.1038/s41597-024-02956-3
- Neil M, Cameron D, Clauss K, et al. A proof-of-concept study demonstrating how FITBIR datasets can be harmonized to examine posttraumatic stress disorder-traumatic brain injury associations. J Behav Data Sci. 2024;4:45-62. doi:10.35566/jbds/oneil
- O’Neil ME, Cameron D, Krushnic D, et al. Using harmonized FITBIR datasets to examine associations between TBI history and cognitive functioning. Appl Neuropsychol Adult. doi:10.1080/23279095.2024.2401974
- O’Neil ME, Krushnic D, Clauss K, et al. Harmonizing federal interagency traumatic brain injury research data to examine depression and suicide-related outcomes. Rehabil Psychol. 2024;69:159-170. doi:10.1037/rep0000547
- O’Neil ME, Krushnic D, Walker WC, et al. Increased risk for clinically significant sleep disturbances in mild traumatic brain injury: an approach to leveraging the federal interagency traumatic brain injury research database. Brain Sci. 2024;14:921. doi:10.3390/brainsci14090921
- Uher R, Perlis RH, Placentino A, et al. Self-report and clinician-rated measures of depression severity: can one replace the other? Depress Anxiety. 2012;29:1043-1049. doi:10.1002/da.21993
- Hung CI, Weng LJ, Su YJ, et al. Depression and somatic symptoms scale: a new scale with both depression and somatic symptoms emphasized. Psychiatry Clin Neurosci. 2006;60:700-708. doi:10.1111/j.1440-1819.2006.01585.x
- Stewart IJ, Howard JT, Amuan ME, et al. Traumatic brain injury is associated with the subsequent risk of atrial fibrillation or atrial flutter. Heart Rhythm. 2025;22:661-667. doi:10.1016/j.hrthm.2024.09.019
- Cifu DX. Clinical research findings from the long-term impact of military-relevant brain injury consortium-chronic effects of neurotrauma consortium (LIMBIC-CENC) 2013-2021. Brain Inj. 2022;36:587-597.doi:10.1080/02699052.2022.2033843
- Fonda JR, Fredman L, Brogly SB, et al. Traumatic brain injury and attempted suicide among veterans of the wars in Iraq and Afghanistan. Am J Epidemiol. 2017;186:220-226. doi:10.1093/aje/kwx044
- Fortier CB, Amick MM, Kenna A, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime (BAT-L) clinical interview and the VA TBI screen. J Head Trauma Rehabil. 2015;30:E1-7. doi:10.1097/htr.0000000000000008
- Grande LJ, Robinson ME, Radigan LJ, et al. Verbal memory deficits in OEF/OIF/OND veterans exposed to blasts at close range. J Int Neuropsychol Soc. 2018;24:466-475. doi:10.1017/S1355617717001242
- Hayes JP, Logue MW, Sadeh N, et al. Mild traumatic brain injury is associated with reduced cortical thickness in those at risk for Alzheimer’s disease. Brain. 2017;140:813-825. doi:10.1093/brain/aww344
- Lippa SM, Fonda JR, Fortier CB, et al. Deployment-related psychiatric and behavioral conditions and their association with functional disability in OEF/OIF/OND veterans. J Trauma Stress. 2015;28:25-33. doi:10.1002/jts.21979
- McGlinchey RE, Milberg WP, Fonda JR, et al. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudinal prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Radigan LJ, McGlinchey RE, Milberg WP, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime and the VA Comprehensive TBI Evaluation. J Head Trauma Rehabil. 2018;33:E51-E55. doi:10.1097/htr.0000000000000361
- Sydnor VJ, Bouix S, Pasternak O, et al. Mild traumatic brain injury impacts associations between limbic system microstructure and post-traumatic stress disorder symptomatology. Neuroimage Clin. 2020;26:102190. doi:10.1016/j.nicl.2020.102190
- Van Etten EJ, Knight AR, Colaizzi TA, et al. Peritraumatic context and long-term outcomes of concussion. JAMA Netw Open. 2025;8:e2455622. doi:10.1001/jamanetworkopen.2024.55622
- Andrews RJ, Fonda JR, Levin LK, et al. Comprehensive analysis of the predictors of neurobehavioral symptom reporting in veterans. Neurology. 2018;91:e732-e745. doi:10.1212/wnl.0000000000006034
- McGlinchey RE, Milberg WP, Fonda JR, Fortier CB. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudional prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Reimers N, Gurevych I. Sentence-BERT: Sentence embeddings using Siamese BERT-Networks. 2019. Conference on Empirical Methods in Natural Language Processing.
- Singhal A. Modern information retrieval: a brief overview. IEEE Data Eng Bull. 2001;24:34-43.
In leveraging existing, readily available evidence-based health care information (eg, systematic reviews, clinical practice guidelines), clinicians have historically made recommendations based on treatment responses of the average patient.1 Recently, this approach has been expanded into data-driven, evidence-based precision medical care for individuals across a wide range of disciplines and care settings. These precision medicine approaches use information related to an individual’s genes, environment, and lifestyle to tailor recommendations regarding prevention, diagnosis, and treatment.
Applying precision medicine approaches to the unique exposures and experiences of service members and veterans—particularly those who served in combat environments—through the incorporation of biopsychosocial factors into medical decision-making may be even more pertinent. This sentiment is reflected in Section 305 of the Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, which outlines the Precision Medicine Initiative of the US Department of Veterans Affairs (VA) to identify and validate brain and mental health biomarkers.2 Despite widespread consensus regarding the promise of precision medicine, large, rich datasets with elements pertaining to common military exposures such as traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are limited.
Existing datasets, most of which are relatively small or focus on specific cohorts (eg, older veterans, transitioning veterans), continue to create barriers to advancing precision medicine. For example, in classically designed clinical trials, analyses are generally conducted in a manner that may obfuscate efficacy among subcohorts of individuals, thereby underscoring the need to explore alternative strategies to unify existing datasets capable of revealing such heterogeneity.3 The evidence base for precision medical care is limited, drawing from published trials with relatively small sample sizes and even larger cohort studies have limited biomarker data. Additionally, these models are often exploratory during development, and to avoid statistical overfitting of an exploratory model, validation in similar datasets is needed—an added burden when data sources are small or underpowered to begin with.
A promising approach is to combine and harmonize the largest, most deeply characterized data sources from similar samples. Although combining such datasets may appear to require minimal time and effort, harmonizing similar variables in an evidence-based and replicable manner requires time and expertise, even when participant characteristics and outcomes are similar.4-7
Challenges related to harmonization are related to the wide range of strategies (eg, self-report questionnaires, clinical interviews, electronic health record review) used to measure common brain and mental health constructs, such as depression. Even when similar methods (eg, self-report measures) are implemented, challenges persist. For example, if a study used a depression measure that focused primarily on cognitive symptoms (eg, pessimism, self-dislike, suicidal ideation) and another study used a depression measure composed of items more heavily weighted towards somatic symptoms (eg, insomnia, loss of appetite, weight loss, decreased libido), combining their data could be challenging, particularly if researchers, clinicians, or administrators are interested in more than dichotomous outcomes (eg, depression vs no depression).8,9
To address this knowledge gap and harmonize multimodal data from varied sources, well-planned and reproducible curation is needed. Longitudinal cohort studies of service members and veterans with military combat and training exposure histories provide researchers and other stakeholders access to extant biopsychosocial data shown to affect risk for adverse health outcomes; however, efforts to facilitate individually tailored treatment or other precision medicine approaches would benefit from the synthesis of such datasets.10
Members of the VA Total Brain Diagnostics (TBD) team are engaged in harmonizing variables from the Long-Term Impact of Military-Relevant Brain Injury Consortium–Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC)11 and the Translational Research Center for TBI and Stress Disorders (TRACTS).12-21 While there is overlap across LIMBIC-CENC and TRACTS with respect to data domains, considerable data harmonization is needed to allow for future valid and meaningful analyses, particularly those involving multivariable predictors.
Data Sources
Both data sources for the TBD harmonization project, LIMBIC-CENC and TRACTS, include extensive, longitudinal data collected from relatively large cohorts of veterans and service members with combat exposure. Both studies collect detailed data related to potential brain injury history and include participants with and without a history of TBI. Similarly, both include extensive collection of fluid biomarkers and imaging data, as well as measures of biopsychosocial functioning.
Data collection sites for LIMBIC-CENC include 16 recruitment sites, 9 at VA medical centers (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego) and 7 at military treatment sites (Alexandria, San Diego, Tampa, Tacoma, Columbia, Coronado, Hinesville), in addition to 11 assessment sites (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego, Alexandria, Augusta). Data for TRACTS are collected at sites in Boston and Houston.
LIMBIC-CENC is a 12-year, 17-site cohort of service members and veteran participants with combat exposure who are well characterized at baseline and undergo annual reassessments. As of December 2025, > 3100 participants have been recruited, and nearly 90% remain in follow-up. Data collection includes > 6200 annual follow-up evaluations and > 1550 5-year re-evaluations, with 400 enrolled participants followed up annually.
TRACTS is a 16-year, 2-site cohort of veterans with combat exposure who complete comprehensive assessments at enrollment, undergo annual reassessments, and complete comprehensive reassessment every 5 years thereafter. As of December 2025, > 1075 participants have completed baseline (Time 1) assessments, > 600 have completed the 2-year re-evaluation (Time 2), > 175 have completed the 5-year re-evaluation (Time 3), and > 35 have completed 10-year evaluations (Time 4), with about 50 new participants added and 100 enrolled participants followed up annually. More data on participant characteristics are available for both LIMBIC-CENC and TRACTS in previous publications.11,22These 2 ongoing, prospective, longitudinal cohorts of service members and veterans offer access to a wide range of potential risk factors that can affect response to care and outcomes, including demographics (eg, age, sex), injury characteristics (eg, pre-exposure factors, exposure factors), biomarkers (eg, serum, saliva, brain imaging, evoked potentials), and functional measures (eg, computerized posturography, computerized eye tracking, sensory testing, clinical examination, neuropsychological assessments, symptom questionnaires).
Harmonization Strategy
Pooling and harmonizing data from large studies evaluating similar participant cohorts and conditions involves numerous steps to appropriately handle a variety of measurements and disparate variable names. The TBD team adapted a model data harmonization system developed by O’Neil et al through initial work harmonizing the Federal Interagency Traumatic Brain Injury Research Informatics System (FITBIR).4-7 This process was expanded and generalized by the research team to combine data from LIMBIC-CENC and TRACTS to create a single pooled dataset for analysis (Figure).
Injury Research database.
This approach was selected because it accommodates heterogeneous study designs (eg, cross-sectional, longitudinal, case-control), data collection methods (eg, clinical assessment, self-reported, objective blood, and imaging biomarkers), and various assessments of the same construct (ie, different measures of brain injury). While exact matches for data collection methods and measures may be easily harmonized, the timing of assessment, number of assessments, assessment tool version, and other factors must be considered. The goal was to harmonize data from LIMBIC-CENC and TRACTS to allow additional data sources to be harmonized and incorporated in the future.
Original data files from each study were reshaped to represent participant-level observations with 1 unique measurement per row. The measurement represents what information was collected and the value recorded represents the unique observation. These data are linked to metadata from the original study, which includes the study’s definition of each measurement, how it was collected, and any available information regarding when it was collected in reference to study enrollment or injury. Additional information on the file source, row, and column position of each data point was added to enable recreation of the original data as needed.
The resulting dataset was used to harmonize measurements from LIMBIC-CENC and TRACTS into a priori-defined schemas for brain- and mental health-relevant concepts, including TBI severity, PTSD, substance use, depression, suicidal ideation, and functioning (including cognitive, physical, and social functioning). This process was facilitated using natural language processing (NLP). Each study uniquely defines all measurements and provides written definitions with the data. Measurement definitions serve as records describing what was collected, how it was collected, and how the study may have uniquely defined information for its purposes. For example, definitions of exposure to brain injury and severity of brain injury may differ between studies, and the study-provided definition defines these differences.
Definitions were converted into numeric vectors through sentence embedding, a process that preserves the semantic meaning of the definition.23 Cosine similarity was used as the primary metric to compare the semantic textual similarity between pairs of measurement definitions. Cosine similarity ranges from 0 to 1, where 0 indicates no meaningful similarity and 1 indicates they have identical meanings.24 This approach leverages the relationship between the definitions of each measurement provided by a study and enables quick comparison of all pairwise combinations of measurement definitions between studies.
Subsets of similar measurements across studies were organized into a priori-defined schema. Clinical experts then reviewed each schema and further refined them into domains, (eg, mechanism of injury, clinical signs, acute symptoms) and subdomains (children), such as loss of consciousness, amnesia, and alteration of consciousness. This approach allows efficient handling of 2 specific cases that commonly occur when pooling and harmonizing datasets: (1) identifying the same measurement with differing names; and (2) identifying different measurements with definitions that each relate to the same domain.
The Table provides a general example of the schema for TBI severity. This was an iterative process in which clinical experts reviewed study-defined measurement definitions to develop general harmonized domains, and NLP techniques facilitated and accelerated identification and organization of measurements within these domains.
Expected Impact
Harmonization combining LIMBIC-CENC and TRACTS datasets is ongoing. Preliminary descriptive analyses of baseline cohort data indicate that harmonization across data sources is appropriate, given the lack of significant heterogeneity across sites and studies for most domains. Work by members of the TBD team is expected to lay the foundation for the use of existing and ongoing prospective, longitudinal datasets (eg, LIMBIC-CENC, TRACTS) and linked large datasets (eg, VA Informatics and Computing Infrastructure including electronic health records, VA Million Veteran Program, DaVINCI [US Department of Defense and VA Infrastructure for Clinical Intelligence]) to generate generalizable, clinically relevant information to advance precision brain and mental health care among service members and veterans.
By enhancing existing practice, this synthesized dataset has the potential to inform tailored and personalized medicine approaches designed to meet the needs of veterans and service members. These data will serve as the starting point for multivariable models examining the intersection of physiologic, behavioral, and environmental factors. The goal of this data harmonization effort is to better elucidate how clinicians and researchers can select optimal approaches for veterans and service members with TBI histories by accounting for a comprehensive set of physiologic, behavioral, and environmental factors in an individually tailored manner. These data may further extend existing clinical practice guideline approaches, inform shared decision-making, and enhance functional outcomes beyond those currently available.
Conclusions
Individuals who have served in the military have unique biopsychosocial exposures that are associated with brain and mental health disorders. To address these needs, the nationwide TBD team has initiated the creation of a unified, longitudinal dataset that includes harmonized measures from existing LIMBIC-CENC and TRACTS protocols. Initial data harmonization efforts are required to facilitate precision prognostics, diagnostics, and tailored interventions, with the goal of improving veterans’ brain and mental health and psychosocial functioning and enabling tailored and evidence-informed, individualized clinical care.
In leveraging existing, readily available evidence-based health care information (eg, systematic reviews, clinical practice guidelines), clinicians have historically made recommendations based on treatment responses of the average patient.1 Recently, this approach has been expanded into data-driven, evidence-based precision medical care for individuals across a wide range of disciplines and care settings. These precision medicine approaches use information related to an individual’s genes, environment, and lifestyle to tailor recommendations regarding prevention, diagnosis, and treatment.
Applying precision medicine approaches to the unique exposures and experiences of service members and veterans—particularly those who served in combat environments—through the incorporation of biopsychosocial factors into medical decision-making may be even more pertinent. This sentiment is reflected in Section 305 of the Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, which outlines the Precision Medicine Initiative of the US Department of Veterans Affairs (VA) to identify and validate brain and mental health biomarkers.2 Despite widespread consensus regarding the promise of precision medicine, large, rich datasets with elements pertaining to common military exposures such as traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are limited.
Existing datasets, most of which are relatively small or focus on specific cohorts (eg, older veterans, transitioning veterans), continue to create barriers to advancing precision medicine. For example, in classically designed clinical trials, analyses are generally conducted in a manner that may obfuscate efficacy among subcohorts of individuals, thereby underscoring the need to explore alternative strategies to unify existing datasets capable of revealing such heterogeneity.3 The evidence base for precision medical care is limited, drawing from published trials with relatively small sample sizes and even larger cohort studies have limited biomarker data. Additionally, these models are often exploratory during development, and to avoid statistical overfitting of an exploratory model, validation in similar datasets is needed—an added burden when data sources are small or underpowered to begin with.
A promising approach is to combine and harmonize the largest, most deeply characterized data sources from similar samples. Although combining such datasets may appear to require minimal time and effort, harmonizing similar variables in an evidence-based and replicable manner requires time and expertise, even when participant characteristics and outcomes are similar.4-7
Challenges related to harmonization are related to the wide range of strategies (eg, self-report questionnaires, clinical interviews, electronic health record review) used to measure common brain and mental health constructs, such as depression. Even when similar methods (eg, self-report measures) are implemented, challenges persist. For example, if a study used a depression measure that focused primarily on cognitive symptoms (eg, pessimism, self-dislike, suicidal ideation) and another study used a depression measure composed of items more heavily weighted towards somatic symptoms (eg, insomnia, loss of appetite, weight loss, decreased libido), combining their data could be challenging, particularly if researchers, clinicians, or administrators are interested in more than dichotomous outcomes (eg, depression vs no depression).8,9
To address this knowledge gap and harmonize multimodal data from varied sources, well-planned and reproducible curation is needed. Longitudinal cohort studies of service members and veterans with military combat and training exposure histories provide researchers and other stakeholders access to extant biopsychosocial data shown to affect risk for adverse health outcomes; however, efforts to facilitate individually tailored treatment or other precision medicine approaches would benefit from the synthesis of such datasets.10
Members of the VA Total Brain Diagnostics (TBD) team are engaged in harmonizing variables from the Long-Term Impact of Military-Relevant Brain Injury Consortium–Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC)11 and the Translational Research Center for TBI and Stress Disorders (TRACTS).12-21 While there is overlap across LIMBIC-CENC and TRACTS with respect to data domains, considerable data harmonization is needed to allow for future valid and meaningful analyses, particularly those involving multivariable predictors.
Data Sources
Both data sources for the TBD harmonization project, LIMBIC-CENC and TRACTS, include extensive, longitudinal data collected from relatively large cohorts of veterans and service members with combat exposure. Both studies collect detailed data related to potential brain injury history and include participants with and without a history of TBI. Similarly, both include extensive collection of fluid biomarkers and imaging data, as well as measures of biopsychosocial functioning.
Data collection sites for LIMBIC-CENC include 16 recruitment sites, 9 at VA medical centers (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego) and 7 at military treatment sites (Alexandria, San Diego, Tampa, Tacoma, Columbia, Coronado, Hinesville), in addition to 11 assessment sites (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego, Alexandria, Augusta). Data for TRACTS are collected at sites in Boston and Houston.
LIMBIC-CENC is a 12-year, 17-site cohort of service members and veteran participants with combat exposure who are well characterized at baseline and undergo annual reassessments. As of December 2025, > 3100 participants have been recruited, and nearly 90% remain in follow-up. Data collection includes > 6200 annual follow-up evaluations and > 1550 5-year re-evaluations, with 400 enrolled participants followed up annually.
TRACTS is a 16-year, 2-site cohort of veterans with combat exposure who complete comprehensive assessments at enrollment, undergo annual reassessments, and complete comprehensive reassessment every 5 years thereafter. As of December 2025, > 1075 participants have completed baseline (Time 1) assessments, > 600 have completed the 2-year re-evaluation (Time 2), > 175 have completed the 5-year re-evaluation (Time 3), and > 35 have completed 10-year evaluations (Time 4), with about 50 new participants added and 100 enrolled participants followed up annually. More data on participant characteristics are available for both LIMBIC-CENC and TRACTS in previous publications.11,22These 2 ongoing, prospective, longitudinal cohorts of service members and veterans offer access to a wide range of potential risk factors that can affect response to care and outcomes, including demographics (eg, age, sex), injury characteristics (eg, pre-exposure factors, exposure factors), biomarkers (eg, serum, saliva, brain imaging, evoked potentials), and functional measures (eg, computerized posturography, computerized eye tracking, sensory testing, clinical examination, neuropsychological assessments, symptom questionnaires).
Harmonization Strategy
Pooling and harmonizing data from large studies evaluating similar participant cohorts and conditions involves numerous steps to appropriately handle a variety of measurements and disparate variable names. The TBD team adapted a model data harmonization system developed by O’Neil et al through initial work harmonizing the Federal Interagency Traumatic Brain Injury Research Informatics System (FITBIR).4-7 This process was expanded and generalized by the research team to combine data from LIMBIC-CENC and TRACTS to create a single pooled dataset for analysis (Figure).
Injury Research database.
This approach was selected because it accommodates heterogeneous study designs (eg, cross-sectional, longitudinal, case-control), data collection methods (eg, clinical assessment, self-reported, objective blood, and imaging biomarkers), and various assessments of the same construct (ie, different measures of brain injury). While exact matches for data collection methods and measures may be easily harmonized, the timing of assessment, number of assessments, assessment tool version, and other factors must be considered. The goal was to harmonize data from LIMBIC-CENC and TRACTS to allow additional data sources to be harmonized and incorporated in the future.
Original data files from each study were reshaped to represent participant-level observations with 1 unique measurement per row. The measurement represents what information was collected and the value recorded represents the unique observation. These data are linked to metadata from the original study, which includes the study’s definition of each measurement, how it was collected, and any available information regarding when it was collected in reference to study enrollment or injury. Additional information on the file source, row, and column position of each data point was added to enable recreation of the original data as needed.
The resulting dataset was used to harmonize measurements from LIMBIC-CENC and TRACTS into a priori-defined schemas for brain- and mental health-relevant concepts, including TBI severity, PTSD, substance use, depression, suicidal ideation, and functioning (including cognitive, physical, and social functioning). This process was facilitated using natural language processing (NLP). Each study uniquely defines all measurements and provides written definitions with the data. Measurement definitions serve as records describing what was collected, how it was collected, and how the study may have uniquely defined information for its purposes. For example, definitions of exposure to brain injury and severity of brain injury may differ between studies, and the study-provided definition defines these differences.
Definitions were converted into numeric vectors through sentence embedding, a process that preserves the semantic meaning of the definition.23 Cosine similarity was used as the primary metric to compare the semantic textual similarity between pairs of measurement definitions. Cosine similarity ranges from 0 to 1, where 0 indicates no meaningful similarity and 1 indicates they have identical meanings.24 This approach leverages the relationship between the definitions of each measurement provided by a study and enables quick comparison of all pairwise combinations of measurement definitions between studies.
Subsets of similar measurements across studies were organized into a priori-defined schema. Clinical experts then reviewed each schema and further refined them into domains, (eg, mechanism of injury, clinical signs, acute symptoms) and subdomains (children), such as loss of consciousness, amnesia, and alteration of consciousness. This approach allows efficient handling of 2 specific cases that commonly occur when pooling and harmonizing datasets: (1) identifying the same measurement with differing names; and (2) identifying different measurements with definitions that each relate to the same domain.
The Table provides a general example of the schema for TBI severity. This was an iterative process in which clinical experts reviewed study-defined measurement definitions to develop general harmonized domains, and NLP techniques facilitated and accelerated identification and organization of measurements within these domains.
Expected Impact
Harmonization combining LIMBIC-CENC and TRACTS datasets is ongoing. Preliminary descriptive analyses of baseline cohort data indicate that harmonization across data sources is appropriate, given the lack of significant heterogeneity across sites and studies for most domains. Work by members of the TBD team is expected to lay the foundation for the use of existing and ongoing prospective, longitudinal datasets (eg, LIMBIC-CENC, TRACTS) and linked large datasets (eg, VA Informatics and Computing Infrastructure including electronic health records, VA Million Veteran Program, DaVINCI [US Department of Defense and VA Infrastructure for Clinical Intelligence]) to generate generalizable, clinically relevant information to advance precision brain and mental health care among service members and veterans.
By enhancing existing practice, this synthesized dataset has the potential to inform tailored and personalized medicine approaches designed to meet the needs of veterans and service members. These data will serve as the starting point for multivariable models examining the intersection of physiologic, behavioral, and environmental factors. The goal of this data harmonization effort is to better elucidate how clinicians and researchers can select optimal approaches for veterans and service members with TBI histories by accounting for a comprehensive set of physiologic, behavioral, and environmental factors in an individually tailored manner. These data may further extend existing clinical practice guideline approaches, inform shared decision-making, and enhance functional outcomes beyond those currently available.
Conclusions
Individuals who have served in the military have unique biopsychosocial exposures that are associated with brain and mental health disorders. To address these needs, the nationwide TBD team has initiated the creation of a unified, longitudinal dataset that includes harmonized measures from existing LIMBIC-CENC and TRACTS protocols. Initial data harmonization efforts are required to facilitate precision prognostics, diagnostics, and tailored interventions, with the goal of improving veterans’ brain and mental health and psychosocial functioning and enabling tailored and evidence-informed, individualized clinical care.
- The Promise of Precision Medicine. National Institutes of Health (NIH). Updated January 21, 2025. Accessed January 5, 2026. https://www.nih.gov/about-nih/nih-turning-discovery-into-health/promise-precision-medicine.
- Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, S 785, 116th Cong (2019-2020) Accessed January 5, 2026. https://www.congress.gov/bill/116th-congress/senate-bill/785
- Cheng C, Messerschmidt L, Bravo I, et al. A general primer for data harmonization. Sci Data. 2024;11:152. doi:10.1038/s41597-024-02956-3
- Neil M, Cameron D, Clauss K, et al. A proof-of-concept study demonstrating how FITBIR datasets can be harmonized to examine posttraumatic stress disorder-traumatic brain injury associations. J Behav Data Sci. 2024;4:45-62. doi:10.35566/jbds/oneil
- O’Neil ME, Cameron D, Krushnic D, et al. Using harmonized FITBIR datasets to examine associations between TBI history and cognitive functioning. Appl Neuropsychol Adult. doi:10.1080/23279095.2024.2401974
- O’Neil ME, Krushnic D, Clauss K, et al. Harmonizing federal interagency traumatic brain injury research data to examine depression and suicide-related outcomes. Rehabil Psychol. 2024;69:159-170. doi:10.1037/rep0000547
- O’Neil ME, Krushnic D, Walker WC, et al. Increased risk for clinically significant sleep disturbances in mild traumatic brain injury: an approach to leveraging the federal interagency traumatic brain injury research database. Brain Sci. 2024;14:921. doi:10.3390/brainsci14090921
- Uher R, Perlis RH, Placentino A, et al. Self-report and clinician-rated measures of depression severity: can one replace the other? Depress Anxiety. 2012;29:1043-1049. doi:10.1002/da.21993
- Hung CI, Weng LJ, Su YJ, et al. Depression and somatic symptoms scale: a new scale with both depression and somatic symptoms emphasized. Psychiatry Clin Neurosci. 2006;60:700-708. doi:10.1111/j.1440-1819.2006.01585.x
- Stewart IJ, Howard JT, Amuan ME, et al. Traumatic brain injury is associated with the subsequent risk of atrial fibrillation or atrial flutter. Heart Rhythm. 2025;22:661-667. doi:10.1016/j.hrthm.2024.09.019
- Cifu DX. Clinical research findings from the long-term impact of military-relevant brain injury consortium-chronic effects of neurotrauma consortium (LIMBIC-CENC) 2013-2021. Brain Inj. 2022;36:587-597.doi:10.1080/02699052.2022.2033843
- Fonda JR, Fredman L, Brogly SB, et al. Traumatic brain injury and attempted suicide among veterans of the wars in Iraq and Afghanistan. Am J Epidemiol. 2017;186:220-226. doi:10.1093/aje/kwx044
- Fortier CB, Amick MM, Kenna A, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime (BAT-L) clinical interview and the VA TBI screen. J Head Trauma Rehabil. 2015;30:E1-7. doi:10.1097/htr.0000000000000008
- Grande LJ, Robinson ME, Radigan LJ, et al. Verbal memory deficits in OEF/OIF/OND veterans exposed to blasts at close range. J Int Neuropsychol Soc. 2018;24:466-475. doi:10.1017/S1355617717001242
- Hayes JP, Logue MW, Sadeh N, et al. Mild traumatic brain injury is associated with reduced cortical thickness in those at risk for Alzheimer’s disease. Brain. 2017;140:813-825. doi:10.1093/brain/aww344
- Lippa SM, Fonda JR, Fortier CB, et al. Deployment-related psychiatric and behavioral conditions and their association with functional disability in OEF/OIF/OND veterans. J Trauma Stress. 2015;28:25-33. doi:10.1002/jts.21979
- McGlinchey RE, Milberg WP, Fonda JR, et al. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudinal prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Radigan LJ, McGlinchey RE, Milberg WP, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime and the VA Comprehensive TBI Evaluation. J Head Trauma Rehabil. 2018;33:E51-E55. doi:10.1097/htr.0000000000000361
- Sydnor VJ, Bouix S, Pasternak O, et al. Mild traumatic brain injury impacts associations between limbic system microstructure and post-traumatic stress disorder symptomatology. Neuroimage Clin. 2020;26:102190. doi:10.1016/j.nicl.2020.102190
- Van Etten EJ, Knight AR, Colaizzi TA, et al. Peritraumatic context and long-term outcomes of concussion. JAMA Netw Open. 2025;8:e2455622. doi:10.1001/jamanetworkopen.2024.55622
- Andrews RJ, Fonda JR, Levin LK, et al. Comprehensive analysis of the predictors of neurobehavioral symptom reporting in veterans. Neurology. 2018;91:e732-e745. doi:10.1212/wnl.0000000000006034
- McGlinchey RE, Milberg WP, Fonda JR, Fortier CB. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudional prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Reimers N, Gurevych I. Sentence-BERT: Sentence embeddings using Siamese BERT-Networks. 2019. Conference on Empirical Methods in Natural Language Processing.
- Singhal A. Modern information retrieval: a brief overview. IEEE Data Eng Bull. 2001;24:34-43.
- The Promise of Precision Medicine. National Institutes of Health (NIH). Updated January 21, 2025. Accessed January 5, 2026. https://www.nih.gov/about-nih/nih-turning-discovery-into-health/promise-precision-medicine.
- Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, S 785, 116th Cong (2019-2020) Accessed January 5, 2026. https://www.congress.gov/bill/116th-congress/senate-bill/785
- Cheng C, Messerschmidt L, Bravo I, et al. A general primer for data harmonization. Sci Data. 2024;11:152. doi:10.1038/s41597-024-02956-3
- Neil M, Cameron D, Clauss K, et al. A proof-of-concept study demonstrating how FITBIR datasets can be harmonized to examine posttraumatic stress disorder-traumatic brain injury associations. J Behav Data Sci. 2024;4:45-62. doi:10.35566/jbds/oneil
- O’Neil ME, Cameron D, Krushnic D, et al. Using harmonized FITBIR datasets to examine associations between TBI history and cognitive functioning. Appl Neuropsychol Adult. doi:10.1080/23279095.2024.2401974
- O’Neil ME, Krushnic D, Clauss K, et al. Harmonizing federal interagency traumatic brain injury research data to examine depression and suicide-related outcomes. Rehabil Psychol. 2024;69:159-170. doi:10.1037/rep0000547
- O’Neil ME, Krushnic D, Walker WC, et al. Increased risk for clinically significant sleep disturbances in mild traumatic brain injury: an approach to leveraging the federal interagency traumatic brain injury research database. Brain Sci. 2024;14:921. doi:10.3390/brainsci14090921
- Uher R, Perlis RH, Placentino A, et al. Self-report and clinician-rated measures of depression severity: can one replace the other? Depress Anxiety. 2012;29:1043-1049. doi:10.1002/da.21993
- Hung CI, Weng LJ, Su YJ, et al. Depression and somatic symptoms scale: a new scale with both depression and somatic symptoms emphasized. Psychiatry Clin Neurosci. 2006;60:700-708. doi:10.1111/j.1440-1819.2006.01585.x
- Stewart IJ, Howard JT, Amuan ME, et al. Traumatic brain injury is associated with the subsequent risk of atrial fibrillation or atrial flutter. Heart Rhythm. 2025;22:661-667. doi:10.1016/j.hrthm.2024.09.019
- Cifu DX. Clinical research findings from the long-term impact of military-relevant brain injury consortium-chronic effects of neurotrauma consortium (LIMBIC-CENC) 2013-2021. Brain Inj. 2022;36:587-597.doi:10.1080/02699052.2022.2033843
- Fonda JR, Fredman L, Brogly SB, et al. Traumatic brain injury and attempted suicide among veterans of the wars in Iraq and Afghanistan. Am J Epidemiol. 2017;186:220-226. doi:10.1093/aje/kwx044
- Fortier CB, Amick MM, Kenna A, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime (BAT-L) clinical interview and the VA TBI screen. J Head Trauma Rehabil. 2015;30:E1-7. doi:10.1097/htr.0000000000000008
- Grande LJ, Robinson ME, Radigan LJ, et al. Verbal memory deficits in OEF/OIF/OND veterans exposed to blasts at close range. J Int Neuropsychol Soc. 2018;24:466-475. doi:10.1017/S1355617717001242
- Hayes JP, Logue MW, Sadeh N, et al. Mild traumatic brain injury is associated with reduced cortical thickness in those at risk for Alzheimer’s disease. Brain. 2017;140:813-825. doi:10.1093/brain/aww344
- Lippa SM, Fonda JR, Fortier CB, et al. Deployment-related psychiatric and behavioral conditions and their association with functional disability in OEF/OIF/OND veterans. J Trauma Stress. 2015;28:25-33. doi:10.1002/jts.21979
- McGlinchey RE, Milberg WP, Fonda JR, et al. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudinal prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Radigan LJ, McGlinchey RE, Milberg WP, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime and the VA Comprehensive TBI Evaluation. J Head Trauma Rehabil. 2018;33:E51-E55. doi:10.1097/htr.0000000000000361
- Sydnor VJ, Bouix S, Pasternak O, et al. Mild traumatic brain injury impacts associations between limbic system microstructure and post-traumatic stress disorder symptomatology. Neuroimage Clin. 2020;26:102190. doi:10.1016/j.nicl.2020.102190
- Van Etten EJ, Knight AR, Colaizzi TA, et al. Peritraumatic context and long-term outcomes of concussion. JAMA Netw Open. 2025;8:e2455622. doi:10.1001/jamanetworkopen.2024.55622
- Andrews RJ, Fonda JR, Levin LK, et al. Comprehensive analysis of the predictors of neurobehavioral symptom reporting in veterans. Neurology. 2018;91:e732-e745. doi:10.1212/wnl.0000000000006034
- McGlinchey RE, Milberg WP, Fonda JR, Fortier CB. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudional prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Reimers N, Gurevych I. Sentence-BERT: Sentence embeddings using Siamese BERT-Networks. 2019. Conference on Empirical Methods in Natural Language Processing.
- Singhal A. Modern information retrieval: a brief overview. IEEE Data Eng Bull. 2001;24:34-43.
Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs
Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs

Trauma, Military Fitness, and Eating Disorders
Military culture may hold 2 salient risk factors for eating disorders: exposure to trauma and body condition standards. A recent study from the US Department of Veteran Affairs (VA) Salisbury Health Care System (VASHCS) found that veterans with posttraumatic stress disorder (PTSD) are more likely to report eating disturbances—particularly issues related to body dissatisfaction and dissatisfaction with eating habits. A 2019 study found that one-third of veterans who were overweight or obese screened positive for engaging in “making weight” behaviors during military service, or unhealthy weight control strategies. Frequently reported weight management behavior was excessive exercise, fasting/skipping meals, sitting in a sauna/wearing a latex suit, laxatives, diuretics, and vomiting.
Service members who are “normal” weight by civilian standards may be labeled “overweight” by the military. In a March 12 memo, Secretary of Defense Pete Hegseth ordered a US Department of Defense review of existing standards for physical fitness, body composition, and grooming. “Our troops will be fit — not fat. Our troops will look sharp — not sloppy. We seek only quality — not quotas. BOTTOM LINE: our @DeptofDefense will make standards HIGH & GREAT again — across the entire force,” he posted on X.
The desire to control weight to fit military standards, however, isn’t the only risk factor. Researchers at VASHCS surveyed 527 post-9/11 veterans (80.7% male) who typically deployed 1 or 2 times. All participants completed the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; the Neuro-Quality of Life in Neurological Disorders Positive Affect and Well-Being Scale (PAWB); and the Eating Disturbances Scale.
Nearly half (46%) of the sample met diagnostic criteria for a lifetime PTSD diagnosis. The study also reported significantly greater eating disturbances in veterans with a lifetime PTSD diagnosis than those without. Women reported significantly greater eating disturbances than men.
Most participants (80%) reported some level of dissatisfaction with their eating disturbances and 74% of participants reported feeling as if they were too fat.
Eating disturbances include refusing food, overexercising, overeating, and misusing laxatives or diuretic pills. Previous research that suggest that 10% to 15% of female veterans and 4% to 8% of male veterans report clinically significant disordered eating behaviors, especially binge eating. One study found that 78% of 45,477 overweight or obese veterans receiving care in VA facilities reported clinically significant binge eating. In a 2021 study, 254 veterans presenting for routine clinical care completed self‐report questionnaires assessing eating disorders, PTSD, depression, and shame, and 31% met probable criteria for bulimia nervosa, binge‐eating disorder, or purging disorder.
According to a 2023 study, eating disturbances that do not meet diagnostic criteria for a formal disorder can be problematic and may function as coping strategies for some facets of military life. The VASHCS researchers found that interventions focused on PAWB, such as acceptance and commitment therapy or compassion-focused therapy, may have potential as a protective factor. Including components that foster hope, optimism, and personal strength may positively mitigate the relationship between PTSD and eating disturbances. PAWB was significantly correlated with eating disturbances; individuals with a lifetime PTSD diagnosis reported significantly lower PAWB than those without.
Interventions grounded in positive psychology have shown promise. A group-based program found “noticeable” (although nonsignificant) improvements in optimistic thinking and treatment engagement. The study also cites that clinicians are beginning to incorporate positive psychology strategies (eg, gratitude journaling, goal setting, and “best possible self” visualization) as adjuncts to traditional treatments. Positive psychology, they write, holds “significant promise as a complementary approach to enhance recovery outcomes in both PTSD and eating disorders.”
Military culture may hold 2 salient risk factors for eating disorders: exposure to trauma and body condition standards. A recent study from the US Department of Veteran Affairs (VA) Salisbury Health Care System (VASHCS) found that veterans with posttraumatic stress disorder (PTSD) are more likely to report eating disturbances—particularly issues related to body dissatisfaction and dissatisfaction with eating habits. A 2019 study found that one-third of veterans who were overweight or obese screened positive for engaging in “making weight” behaviors during military service, or unhealthy weight control strategies. Frequently reported weight management behavior was excessive exercise, fasting/skipping meals, sitting in a sauna/wearing a latex suit, laxatives, diuretics, and vomiting.
Service members who are “normal” weight by civilian standards may be labeled “overweight” by the military. In a March 12 memo, Secretary of Defense Pete Hegseth ordered a US Department of Defense review of existing standards for physical fitness, body composition, and grooming. “Our troops will be fit — not fat. Our troops will look sharp — not sloppy. We seek only quality — not quotas. BOTTOM LINE: our @DeptofDefense will make standards HIGH & GREAT again — across the entire force,” he posted on X.
The desire to control weight to fit military standards, however, isn’t the only risk factor. Researchers at VASHCS surveyed 527 post-9/11 veterans (80.7% male) who typically deployed 1 or 2 times. All participants completed the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; the Neuro-Quality of Life in Neurological Disorders Positive Affect and Well-Being Scale (PAWB); and the Eating Disturbances Scale.
Nearly half (46%) of the sample met diagnostic criteria for a lifetime PTSD diagnosis. The study also reported significantly greater eating disturbances in veterans with a lifetime PTSD diagnosis than those without. Women reported significantly greater eating disturbances than men.
Most participants (80%) reported some level of dissatisfaction with their eating disturbances and 74% of participants reported feeling as if they were too fat.
Eating disturbances include refusing food, overexercising, overeating, and misusing laxatives or diuretic pills. Previous research that suggest that 10% to 15% of female veterans and 4% to 8% of male veterans report clinically significant disordered eating behaviors, especially binge eating. One study found that 78% of 45,477 overweight or obese veterans receiving care in VA facilities reported clinically significant binge eating. In a 2021 study, 254 veterans presenting for routine clinical care completed self‐report questionnaires assessing eating disorders, PTSD, depression, and shame, and 31% met probable criteria for bulimia nervosa, binge‐eating disorder, or purging disorder.
According to a 2023 study, eating disturbances that do not meet diagnostic criteria for a formal disorder can be problematic and may function as coping strategies for some facets of military life. The VASHCS researchers found that interventions focused on PAWB, such as acceptance and commitment therapy or compassion-focused therapy, may have potential as a protective factor. Including components that foster hope, optimism, and personal strength may positively mitigate the relationship between PTSD and eating disturbances. PAWB was significantly correlated with eating disturbances; individuals with a lifetime PTSD diagnosis reported significantly lower PAWB than those without.
Interventions grounded in positive psychology have shown promise. A group-based program found “noticeable” (although nonsignificant) improvements in optimistic thinking and treatment engagement. The study also cites that clinicians are beginning to incorporate positive psychology strategies (eg, gratitude journaling, goal setting, and “best possible self” visualization) as adjuncts to traditional treatments. Positive psychology, they write, holds “significant promise as a complementary approach to enhance recovery outcomes in both PTSD and eating disorders.”
Military culture may hold 2 salient risk factors for eating disorders: exposure to trauma and body condition standards. A recent study from the US Department of Veteran Affairs (VA) Salisbury Health Care System (VASHCS) found that veterans with posttraumatic stress disorder (PTSD) are more likely to report eating disturbances—particularly issues related to body dissatisfaction and dissatisfaction with eating habits. A 2019 study found that one-third of veterans who were overweight or obese screened positive for engaging in “making weight” behaviors during military service, or unhealthy weight control strategies. Frequently reported weight management behavior was excessive exercise, fasting/skipping meals, sitting in a sauna/wearing a latex suit, laxatives, diuretics, and vomiting.
Service members who are “normal” weight by civilian standards may be labeled “overweight” by the military. In a March 12 memo, Secretary of Defense Pete Hegseth ordered a US Department of Defense review of existing standards for physical fitness, body composition, and grooming. “Our troops will be fit — not fat. Our troops will look sharp — not sloppy. We seek only quality — not quotas. BOTTOM LINE: our @DeptofDefense will make standards HIGH & GREAT again — across the entire force,” he posted on X.
The desire to control weight to fit military standards, however, isn’t the only risk factor. Researchers at VASHCS surveyed 527 post-9/11 veterans (80.7% male) who typically deployed 1 or 2 times. All participants completed the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; the Neuro-Quality of Life in Neurological Disorders Positive Affect and Well-Being Scale (PAWB); and the Eating Disturbances Scale.
Nearly half (46%) of the sample met diagnostic criteria for a lifetime PTSD diagnosis. The study also reported significantly greater eating disturbances in veterans with a lifetime PTSD diagnosis than those without. Women reported significantly greater eating disturbances than men.
Most participants (80%) reported some level of dissatisfaction with their eating disturbances and 74% of participants reported feeling as if they were too fat.
Eating disturbances include refusing food, overexercising, overeating, and misusing laxatives or diuretic pills. Previous research that suggest that 10% to 15% of female veterans and 4% to 8% of male veterans report clinically significant disordered eating behaviors, especially binge eating. One study found that 78% of 45,477 overweight or obese veterans receiving care in VA facilities reported clinically significant binge eating. In a 2021 study, 254 veterans presenting for routine clinical care completed self‐report questionnaires assessing eating disorders, PTSD, depression, and shame, and 31% met probable criteria for bulimia nervosa, binge‐eating disorder, or purging disorder.
According to a 2023 study, eating disturbances that do not meet diagnostic criteria for a formal disorder can be problematic and may function as coping strategies for some facets of military life. The VASHCS researchers found that interventions focused on PAWB, such as acceptance and commitment therapy or compassion-focused therapy, may have potential as a protective factor. Including components that foster hope, optimism, and personal strength may positively mitigate the relationship between PTSD and eating disturbances. PAWB was significantly correlated with eating disturbances; individuals with a lifetime PTSD diagnosis reported significantly lower PAWB than those without.
Interventions grounded in positive psychology have shown promise. A group-based program found “noticeable” (although nonsignificant) improvements in optimistic thinking and treatment engagement. The study also cites that clinicians are beginning to incorporate positive psychology strategies (eg, gratitude journaling, goal setting, and “best possible self” visualization) as adjuncts to traditional treatments. Positive psychology, they write, holds “significant promise as a complementary approach to enhance recovery outcomes in both PTSD and eating disorders.”

'Distress is the Norm': How Oncologists Can Open the Door to Patient Mental Health
'Distress is the Norm': How Oncologists Can Open the Door to Patient Mental Health
For patients with cancer, the determining factor in whether they pursue mental health services is often whether their oncologist explicitly says it is a good idea, a psychologist said during the July Association of VA Hematology and Oncology (AVAHO) seminar in Long Beach, California, on treating veterans with renal cell carcinoma (RCC).
Kysa Christie, PhD, of the West Los Angeles Veterans Affairs Medical Center, presented findings from a 2018 study in which researchers asked Swiss patients with cancer whether their oncologist discussed their emotional health with them.
In terms of boosting intake, it did not matter if oncologists acknowledged distress or pointed out that psychosocial services existed. Instead, a direct recommendation made a difference, increasing the likelihood of using the services over a 4-month period after initial assessment (odds ratio, 6.27).
“What it took was, ‘I really recommend this. This is something that I would want you to try,’” Christie said.
Oncologists are crucial links between patients and mental health services, Christie said: “If people don’t ask about [distress], you’re not going to see it, but it’s there. Distress is the norm, right? It is not a weakness. It is something that we expect to see.”
Christie noted that an estimated 20% of cancer patients have major depressive disorder, and 35% to 40% have a diagnosable psychiatric condition. RCC shows disproportionately high rates of mental strain. According to Christie, research suggests that about three-fourths of the population report elevated levels of distress as evidenced by patients who scored ≥ 5 on the NCCN Distress Thermometer. Patients with cancer have an estimated 20% higher risk of suicide, especially during the first 12 months after diagnosis and at end of life, she added.
“Early during a diagnosis phase, where you’re having a lot of tests being done, you know something is happening. But you don’t know what,” Christie said. “It could be very serious. That’s just a lot of stress to hold and not know how to plan for.”
After diagnosis, routine could set in and lower distress, she said. Then terminal illness may spike it back up again. Does mental health treatment work in patients with cancer?
“There’s a really strong body of evidence-based treatments for depression, anxiety, adjustment disorders, and coping with different cancers,” Christie said. But it is a step too far to expect patients to ask for help while they are juggling appointments, tests, infusions, and more. “It’s a big ask, right? It’s setting people up for failure.”
To help, Christie said she is embedded with a medical oncology team and routinely talks with the staff about which patients may need help. “One thing I like to do is try to have brief visits with veterans and introduce myself when they come to clinic. I treat it like an opt-out rather than an opt-in program: I’ll just pop into the exam room. They don’t have to ask to see me.”
Christie focuses on open-ended questions and talks about resources ranging from support groups and brief appointments to extensive individual therapy.
Another approach is a strategy known as the “warm handoff,” when an oncologist directly introduces a patient to a mental health professional. “It’s a transfer of care in front of the veteran: It’s much more time-efficient than putting in a referral.”
Christie explained how this can work. A clinician will ask her to meet with a patient during an appointment, perhaps in a couple minutes.
“Then I pop into the room, and the oncologist says, ‘Thanks for joining us. This is Mr. Jones. He has been experiencing feelings of anxiety and sadness, and we’d appreciate your help in exploring some options that might help.’ I turn to the patient and ask, ‘What more would you add?’ Then I either take Mr. Jones back to my office or stay in clinic, and we’re off to the races.”
Christie reported no disclosures.
For patients with cancer, the determining factor in whether they pursue mental health services is often whether their oncologist explicitly says it is a good idea, a psychologist said during the July Association of VA Hematology and Oncology (AVAHO) seminar in Long Beach, California, on treating veterans with renal cell carcinoma (RCC).
Kysa Christie, PhD, of the West Los Angeles Veterans Affairs Medical Center, presented findings from a 2018 study in which researchers asked Swiss patients with cancer whether their oncologist discussed their emotional health with them.
In terms of boosting intake, it did not matter if oncologists acknowledged distress or pointed out that psychosocial services existed. Instead, a direct recommendation made a difference, increasing the likelihood of using the services over a 4-month period after initial assessment (odds ratio, 6.27).
“What it took was, ‘I really recommend this. This is something that I would want you to try,’” Christie said.
Oncologists are crucial links between patients and mental health services, Christie said: “If people don’t ask about [distress], you’re not going to see it, but it’s there. Distress is the norm, right? It is not a weakness. It is something that we expect to see.”
Christie noted that an estimated 20% of cancer patients have major depressive disorder, and 35% to 40% have a diagnosable psychiatric condition. RCC shows disproportionately high rates of mental strain. According to Christie, research suggests that about three-fourths of the population report elevated levels of distress as evidenced by patients who scored ≥ 5 on the NCCN Distress Thermometer. Patients with cancer have an estimated 20% higher risk of suicide, especially during the first 12 months after diagnosis and at end of life, she added.
“Early during a diagnosis phase, where you’re having a lot of tests being done, you know something is happening. But you don’t know what,” Christie said. “It could be very serious. That’s just a lot of stress to hold and not know how to plan for.”
After diagnosis, routine could set in and lower distress, she said. Then terminal illness may spike it back up again. Does mental health treatment work in patients with cancer?
“There’s a really strong body of evidence-based treatments for depression, anxiety, adjustment disorders, and coping with different cancers,” Christie said. But it is a step too far to expect patients to ask for help while they are juggling appointments, tests, infusions, and more. “It’s a big ask, right? It’s setting people up for failure.”
To help, Christie said she is embedded with a medical oncology team and routinely talks with the staff about which patients may need help. “One thing I like to do is try to have brief visits with veterans and introduce myself when they come to clinic. I treat it like an opt-out rather than an opt-in program: I’ll just pop into the exam room. They don’t have to ask to see me.”
Christie focuses on open-ended questions and talks about resources ranging from support groups and brief appointments to extensive individual therapy.
Another approach is a strategy known as the “warm handoff,” when an oncologist directly introduces a patient to a mental health professional. “It’s a transfer of care in front of the veteran: It’s much more time-efficient than putting in a referral.”
Christie explained how this can work. A clinician will ask her to meet with a patient during an appointment, perhaps in a couple minutes.
“Then I pop into the room, and the oncologist says, ‘Thanks for joining us. This is Mr. Jones. He has been experiencing feelings of anxiety and sadness, and we’d appreciate your help in exploring some options that might help.’ I turn to the patient and ask, ‘What more would you add?’ Then I either take Mr. Jones back to my office or stay in clinic, and we’re off to the races.”
Christie reported no disclosures.
For patients with cancer, the determining factor in whether they pursue mental health services is often whether their oncologist explicitly says it is a good idea, a psychologist said during the July Association of VA Hematology and Oncology (AVAHO) seminar in Long Beach, California, on treating veterans with renal cell carcinoma (RCC).
Kysa Christie, PhD, of the West Los Angeles Veterans Affairs Medical Center, presented findings from a 2018 study in which researchers asked Swiss patients with cancer whether their oncologist discussed their emotional health with them.
In terms of boosting intake, it did not matter if oncologists acknowledged distress or pointed out that psychosocial services existed. Instead, a direct recommendation made a difference, increasing the likelihood of using the services over a 4-month period after initial assessment (odds ratio, 6.27).
“What it took was, ‘I really recommend this. This is something that I would want you to try,’” Christie said.
Oncologists are crucial links between patients and mental health services, Christie said: “If people don’t ask about [distress], you’re not going to see it, but it’s there. Distress is the norm, right? It is not a weakness. It is something that we expect to see.”
Christie noted that an estimated 20% of cancer patients have major depressive disorder, and 35% to 40% have a diagnosable psychiatric condition. RCC shows disproportionately high rates of mental strain. According to Christie, research suggests that about three-fourths of the population report elevated levels of distress as evidenced by patients who scored ≥ 5 on the NCCN Distress Thermometer. Patients with cancer have an estimated 20% higher risk of suicide, especially during the first 12 months after diagnosis and at end of life, she added.
“Early during a diagnosis phase, where you’re having a lot of tests being done, you know something is happening. But you don’t know what,” Christie said. “It could be very serious. That’s just a lot of stress to hold and not know how to plan for.”
After diagnosis, routine could set in and lower distress, she said. Then terminal illness may spike it back up again. Does mental health treatment work in patients with cancer?
“There’s a really strong body of evidence-based treatments for depression, anxiety, adjustment disorders, and coping with different cancers,” Christie said. But it is a step too far to expect patients to ask for help while they are juggling appointments, tests, infusions, and more. “It’s a big ask, right? It’s setting people up for failure.”
To help, Christie said she is embedded with a medical oncology team and routinely talks with the staff about which patients may need help. “One thing I like to do is try to have brief visits with veterans and introduce myself when they come to clinic. I treat it like an opt-out rather than an opt-in program: I’ll just pop into the exam room. They don’t have to ask to see me.”
Christie focuses on open-ended questions and talks about resources ranging from support groups and brief appointments to extensive individual therapy.
Another approach is a strategy known as the “warm handoff,” when an oncologist directly introduces a patient to a mental health professional. “It’s a transfer of care in front of the veteran: It’s much more time-efficient than putting in a referral.”
Christie explained how this can work. A clinician will ask her to meet with a patient during an appointment, perhaps in a couple minutes.
“Then I pop into the room, and the oncologist says, ‘Thanks for joining us. This is Mr. Jones. He has been experiencing feelings of anxiety and sadness, and we’d appreciate your help in exploring some options that might help.’ I turn to the patient and ask, ‘What more would you add?’ Then I either take Mr. Jones back to my office or stay in clinic, and we’re off to the races.”
Christie reported no disclosures.
'Distress is the Norm': How Oncologists Can Open the Door to Patient Mental Health
'Distress is the Norm': How Oncologists Can Open the Door to Patient Mental Health

What They Want and What They Need: The End-of-Life Conflict
What They Want and What They Need: The End-of-Life Conflict
When contemplating the state of ethical dialogue in our modern world, the philosopher Alasdair MacIntyre had this to say: “I can only answer the question, ‘What am I to do?’ If I can answer the prior question ‘Of what story or stories do I find myself a part?’”1 That is, our ethics must proceed from our understanding of ourselves, others, and the world. David Hume might scoff, but we do need an “is” to appreciate and grasp our “ought.” This is just as true for medical ethics as it is for the rest of life. Questions about what we should do in medicine should draw us to deeper questions about identity and purpose.
In this issue, Ruskin et al present a tragic case of a man who spent his later years walking the line between life and a self-chosen death.2 After enduring the chronic decline of Parkinson disease, he faced a final diagnosis of glioblastoma. The patient enrolled in hospice while considering how he might move elsewhere to avail himself of assisted suicide. Before he had a chance to do that, he was admitted to an inpatient hospice unit where he weakened further. In the throes of what may have been delirium or a last effort to enact his wish of a hastened death, he attempted suicide on the hospice unit. He survived only to die days later from the cancer.
The authors reflect on the complexities of this case, including the distress of a clinician who may want to satisfy a veteran’s wish but cannot due to legal constraints, and the challenges of identifying pathologic suicidal ideation from an earnest and rational desire for a hastened death. How should they handle these conversations? They conclude by suggesting ways clinicians may assess and respond to requests for a hastened death, recognizing that assisted suicide remains illegal within the Veterans Health Administration (VHA).
Clinicians can return to the foundation of our profession to better consider these questions. The case report authors acknowledge this but avoid learning from what the conflict might teach us: “The inability to help veterans achieve their care preferences [to receive a hastened death] conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.” Before feeling like they have failed the veteran, a clinician must ask if it is really within their scope of practice to end someone’s life. While it is true that “the mission of VHA’s [Palliative and Hospice Care] program is to honor veterans’ preferences for care,” this mission exists within a greater context of appreciating that not all preferences can or should be honored.3 An obvious example is when a veteran requests an intervention that is not clinically indicated (eg, antibiotics for a viral infection). Clinicians are not bound to honor this preference; not because there is a law directing the clinicians’ decision making (there is not) but because there is a standard of care that accounts for but can supersede the veteran’s preference.
Is assisted suicide ever clinically indicated? While the answer shifts depending on the jurisdiction, the case report authors acknowledge why the preference for assisted suicide cannot be honored in a VHA facility: it is against the law.4 However, as they explain, this is insufficient to assuage the moral distress that might arise for some clinicians who want to fulfill a veteran’s request. They recommend several different strategies for clinicians to consider when receiving a request for assisted suicide. Distress in the form of cognitive dissonance may also arise from the tension that exists between stopping some forms of suicide while assisting in others.
While it is important to assess whether the request for a hastened death is driven by an untreated symptom or mental illness, this will only get a clinician so far when the request is made in earnest with no remediable drivers. While I cannot argue the point here, I accept that there are forms of suicide which are rational. However, that alone is insufficient to justify the act or assist someone with it; we must assess the good that the rational choice seeks to realize.5 If suicide can be rational, clinicians should ask whether it is within the goals of medicine to assist in suicide. The authors seem to take it for granted that the distressed clinician in the case hopes to hasten this veteran’s death or at least refer him to someone who could. Perhaps his suicide attempt on the hospice unit was, in part, a consequence of being incapable of offering such assistance. These presuppositions should be considered explicitly to better align one’s practice both with the mission of VHA and with the goals of medicine.
One way to do this is to consider whether we can cast assisted suicide as a medical therapy. Sulmasy proposes the provisional “canons of therapy” which might guide clinicians in assessing medical therapies.6 This article distinguishes 3 types of clinically and ethically distinct practices. I have split his first canon (proportionality) into 2 for the sake of clarity.
Priority: Do the benefits outweigh the burdens of the intervention?
The challenge of assessing priority when considering assisted suicide is that we cannot explain any benefits or burdens that might accrue after death; it is beyond our knowledge and informed consent is impossible. While there is always some uncertainty in discerning the benefits and burdens of an intervention, death presents an insurmountable procedural problem for informed consent to assisted suicide.
Fit: Are the means appropriate for the outcome of interest?
The outcomes of interest when considering assisted suicide are many—many—they range from symptom relief or avoidance to reclaiming dignity. In the case described by Ruskin et al, the interdisciplinary team offered the veteran a number of interventions to assuage his symptoms. Dignity therapy may have been employed as a meaningful, useful way of bringing closure to a life.7,8 Ultimately, however, some distress, particularly existential distress, may be intractable and clinicians must commit, as they did in this case, to doing what they can to remedy other symptoms and not abandon the veteran. Suicide is a tempting option because it may eliminate some of these concerns, but one must first grapple with the ethical question of whether suicide is ever an appropriate way to pursue any of these outcomes. Addressing that question is beyond the scope of this commentary, but both clinicians and patients should consider whether and why suicide should be considered appropriate and whether it is appropriate for the medical profession to assist with it.
Parsimony: Is this the least invasive, least burdensome intervention available?
In US jurisdictions where it is legal, assisted suicide is considered an intervention of last resort. Assisted suicide seems to be neither invasive (it involves taking medications) nor burdensome: the medications usually work quickly and without adverse effects, although there are risks (eg, vomiting). Broadening our view beyond the individual reveals something different.
In a cultural sense, assisted suicide is invasive. It changes how clinicians and patients consider health and medical care. We no longer have the profession of medicine with another intervention in the toolbox; we have a totally different profession which now intends death instead of health for its patients. It changes medicine and society at large profoundly. This makes it culturally invasive.
Furthermore, although the veteran in the case recurrently grappled with the choice of suicide, most people do not. They live by default. Offering assisted suicide, even in broad, general terms, may still leave them deciding to live, but the offer has also taken from them the possibility of living by default. They must justify their choice if only to themselves, considering the reasons they continue to pursue life-prolonging treatment and incur financial, emotional, and physical costs for their family. This is a dangerous cultural burden ironically imposed by the offer of more choices.9 Clinicians, by offering assisted suicide even if a patient declines it, also affirm the reasonableness of ending one’s life given the circumstances. That affirmation may be burdensome (eg, “They see my life as not worth living”) rather than validating.10
Restoration: Will this intervention help to restore the patient overall (even if not immediately)?
It would seem restoration is impossible for someone who is dying. Dying is terrible and so one possibility would be to hasten the process with assisted suicide. If health is in view, though, clinicians could recognize that restoration is always possible as long as someone is alive.
For someone dying, restoration may look like symptom relief (restoring bodily distress) which in turn may restore one’s capacity to sleep or to converse with loved ones. Assisted suicide does not fit in this paradigm. Is it intended to help patients sustain and restore their health, whatever amount they have (this is what the hospice and psychiatric services attempted to do in the case). Or is it intended to help patients pursue whatever goals seem good to the patient even those goals which conflict with health? Happily, most patients want their health sustained or restored so there is usually no conflict. As medical technology advances, though, conflicts arise: Should a clinician prescribe stimulants to enhance a healthy student’s wakefulness during final exams? Should a clinician engineer embryos to provide parents with a particular kind of child? Should a clinician end a patient’s life? Assisted suicide is obviously not aimed at restoration. It is a concession to the intractability of one’s disease and disability and one’s impending death. Without clarity and agreement on the goal of medicine, the default provision of care centers instead on satisfying patient preferences whatever they are.
Holism: Does the intervention prioritize the whole patient (vs prioritizing a part for the sake of the whole)?
Clinicians offering assisted suicide suggest that providing a death on a patient’s own terms restores autonomy and brings coherence to a life narrative that, at its end, is fraught with tragedy. This is what it looks like to honor “the whole patient.” A clinician must scrutinize that judgment to determine whether the patient meets statutory criteria for assisted suicide. The impulse underlying the moral distress described by Ruskin et al and many other clinicians is that a patient’s judgment, once determined to be sound, should trump a clinician’s judgment about what is best for the patient’s health and whether there are limits on what the clinician can do to satisfy a patient’s preferences. Ironically, assisted suicide prioritizes a patient’s judgment about how their life should end above other considerations, namely, that medicine has traditionally sought the patient’s good by sustaining and restoring their health, not by intending and causing their death. Notably, there was no lack of holism in the care provided the veteran in the case both before and after his suicide attempt.
Discretion: What are the limits of the intervention itself? What is the scope of medicine in general? What is the limit of one’s own individual knowledge and skill?
Assisted suicide has a substantial limit: it does not offer relief from suffering because there will be no one left alive to experience relief. Assisted suicide cannot achieve anything for the patient because they are dead by the time they fully receive what has been given. This profound limit makes assisted suicide unlike anything else offered in medicine and should give clinicians pause before adopting it, prompting them to grapple with whether causing a patient’s death is within the scope of medicine. If so, how did this come to be after thousands of years to the contrary across cultures and traditions, and what justifies this change? Finally, clinicians must contend with the limits of informed consent.
This brief reflection on how clinicians should consider medical therapies brings us back to MacIntyre’s exhortation: We cannot decide what to do until we have discerned the story to which we belong. One way of telling the story of medicine is to tell it with the techniques front and center: we prescribe, we operate, we irradiate, make the numbers go in the right direction, cure infections, and shrink masses. We can also tell that story by rejoicing that technology is giving us increasing control over our bodies and we can put that power to whatever use we desire. Often that will align with health, but it may not and that is for many patients increasingly acceptable. There is another, better story to tell: the profession of medicine exists to help people sustain and restore health, whatever bit of it they have and even as they lay dying. All those things just listed may help clinicians in that pursuit or they may not, given the specific context.
Ruskin et al tell a story of clinicians living in the tension of wanting to satisfy the desires their patients bring to them but must settle for the best that medicine can provide. Medical intervention as preference satisfaction is a story we have been living and practicing for 50 years since Beauchamp and Childress described the 4-principle framework for biomedical ethics: respect for autonomy, justice, nonmaleficence, beneficence.
Medicine-as-preference-satisfaction conflicts with the VHA mission to “honor America’s veterans by providing exceptional health care that improves their health and well-being.” VHA does not owe veterans whatever they request. VHA owes them exceptional health care. When a patient comes to a clinician, a clinician owes them a bounded set of things in service to their health. The dissonance a clinician might experience in trying to discern whether a patient’s death can serve that patient’s own health should signal a need to step back and reflect on how they understand the foundations of medical practice.
I do not disagree with the authors in their general approach to how clinicians might discuss this with patients who request a hastened death. I also seek to assuage symptoms, validate emotions, and remain steadfast through someone’s dying. I also affirm my commitment as a physician to care for a person’s health which, while someone is dying, usually entails managing symptoms. It never entails ending someone’s life. The clinicians in the case did an excellent job caring for this veteran and could not have done better by helping him end his life.
- MacIntyre A. After Virtue: A Study in Moral Theory. 3rd ed. 2007.
- Ruskin A, Bauer M, Alrojolah L. Managing requests for medical aid in dying within the US Department of Veterans Affairs Health Care System. Fed Pract. 2026;43:238-242. doi:10.12788/fp.0739
- VHA Directive 1139: Palliative care consult teams and Veterans Integrated Service Network Leads. September 9, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9930
- Assisted Suicide Funding Restriction Act of 1997. 42 USC § 14401.
- Safranek JP. Autonomy and assisted suicide the execution of freedom. Hastings Cent Rep. 1998;28:32-36. doi:10.2307/3528611
- Sulmasy DP. The last low whispers of our dead: when is it ethically justifiable to render a patient unconscious until death? Theor Med Bioeth. 2018;39:233-263. doi:10.1007/s11017-018-9459-7
- Chochinov HM. Dying, Dignity, and new horizons in palliative end-of-life care. CA Cancer J Clin. 2006;56:84-103. doi:10.3322/canjclin.56.2.84
- Chochinov HM. Intensive caring: reminding families they matter. J Palliat Med. 2024;27:152-155.
- Velleman JD. Against the right to die. J Med Philos. 1992;17:665-681.
- Peace WJ. Comfort Care as Denial of Personhood. Hastings Cent Rep. 2012;42:14-17. doi:10.1002/hast.38
When contemplating the state of ethical dialogue in our modern world, the philosopher Alasdair MacIntyre had this to say: “I can only answer the question, ‘What am I to do?’ If I can answer the prior question ‘Of what story or stories do I find myself a part?’”1 That is, our ethics must proceed from our understanding of ourselves, others, and the world. David Hume might scoff, but we do need an “is” to appreciate and grasp our “ought.” This is just as true for medical ethics as it is for the rest of life. Questions about what we should do in medicine should draw us to deeper questions about identity and purpose.
In this issue, Ruskin et al present a tragic case of a man who spent his later years walking the line between life and a self-chosen death.2 After enduring the chronic decline of Parkinson disease, he faced a final diagnosis of glioblastoma. The patient enrolled in hospice while considering how he might move elsewhere to avail himself of assisted suicide. Before he had a chance to do that, he was admitted to an inpatient hospice unit where he weakened further. In the throes of what may have been delirium or a last effort to enact his wish of a hastened death, he attempted suicide on the hospice unit. He survived only to die days later from the cancer.
The authors reflect on the complexities of this case, including the distress of a clinician who may want to satisfy a veteran’s wish but cannot due to legal constraints, and the challenges of identifying pathologic suicidal ideation from an earnest and rational desire for a hastened death. How should they handle these conversations? They conclude by suggesting ways clinicians may assess and respond to requests for a hastened death, recognizing that assisted suicide remains illegal within the Veterans Health Administration (VHA).
Clinicians can return to the foundation of our profession to better consider these questions. The case report authors acknowledge this but avoid learning from what the conflict might teach us: “The inability to help veterans achieve their care preferences [to receive a hastened death] conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.” Before feeling like they have failed the veteran, a clinician must ask if it is really within their scope of practice to end someone’s life. While it is true that “the mission of VHA’s [Palliative and Hospice Care] program is to honor veterans’ preferences for care,” this mission exists within a greater context of appreciating that not all preferences can or should be honored.3 An obvious example is when a veteran requests an intervention that is not clinically indicated (eg, antibiotics for a viral infection). Clinicians are not bound to honor this preference; not because there is a law directing the clinicians’ decision making (there is not) but because there is a standard of care that accounts for but can supersede the veteran’s preference.
Is assisted suicide ever clinically indicated? While the answer shifts depending on the jurisdiction, the case report authors acknowledge why the preference for assisted suicide cannot be honored in a VHA facility: it is against the law.4 However, as they explain, this is insufficient to assuage the moral distress that might arise for some clinicians who want to fulfill a veteran’s request. They recommend several different strategies for clinicians to consider when receiving a request for assisted suicide. Distress in the form of cognitive dissonance may also arise from the tension that exists between stopping some forms of suicide while assisting in others.
While it is important to assess whether the request for a hastened death is driven by an untreated symptom or mental illness, this will only get a clinician so far when the request is made in earnest with no remediable drivers. While I cannot argue the point here, I accept that there are forms of suicide which are rational. However, that alone is insufficient to justify the act or assist someone with it; we must assess the good that the rational choice seeks to realize.5 If suicide can be rational, clinicians should ask whether it is within the goals of medicine to assist in suicide. The authors seem to take it for granted that the distressed clinician in the case hopes to hasten this veteran’s death or at least refer him to someone who could. Perhaps his suicide attempt on the hospice unit was, in part, a consequence of being incapable of offering such assistance. These presuppositions should be considered explicitly to better align one’s practice both with the mission of VHA and with the goals of medicine.
One way to do this is to consider whether we can cast assisted suicide as a medical therapy. Sulmasy proposes the provisional “canons of therapy” which might guide clinicians in assessing medical therapies.6 This article distinguishes 3 types of clinically and ethically distinct practices. I have split his first canon (proportionality) into 2 for the sake of clarity.
Priority: Do the benefits outweigh the burdens of the intervention?
The challenge of assessing priority when considering assisted suicide is that we cannot explain any benefits or burdens that might accrue after death; it is beyond our knowledge and informed consent is impossible. While there is always some uncertainty in discerning the benefits and burdens of an intervention, death presents an insurmountable procedural problem for informed consent to assisted suicide.
Fit: Are the means appropriate for the outcome of interest?
The outcomes of interest when considering assisted suicide are many—many—they range from symptom relief or avoidance to reclaiming dignity. In the case described by Ruskin et al, the interdisciplinary team offered the veteran a number of interventions to assuage his symptoms. Dignity therapy may have been employed as a meaningful, useful way of bringing closure to a life.7,8 Ultimately, however, some distress, particularly existential distress, may be intractable and clinicians must commit, as they did in this case, to doing what they can to remedy other symptoms and not abandon the veteran. Suicide is a tempting option because it may eliminate some of these concerns, but one must first grapple with the ethical question of whether suicide is ever an appropriate way to pursue any of these outcomes. Addressing that question is beyond the scope of this commentary, but both clinicians and patients should consider whether and why suicide should be considered appropriate and whether it is appropriate for the medical profession to assist with it.
Parsimony: Is this the least invasive, least burdensome intervention available?
In US jurisdictions where it is legal, assisted suicide is considered an intervention of last resort. Assisted suicide seems to be neither invasive (it involves taking medications) nor burdensome: the medications usually work quickly and without adverse effects, although there are risks (eg, vomiting). Broadening our view beyond the individual reveals something different.
In a cultural sense, assisted suicide is invasive. It changes how clinicians and patients consider health and medical care. We no longer have the profession of medicine with another intervention in the toolbox; we have a totally different profession which now intends death instead of health for its patients. It changes medicine and society at large profoundly. This makes it culturally invasive.
Furthermore, although the veteran in the case recurrently grappled with the choice of suicide, most people do not. They live by default. Offering assisted suicide, even in broad, general terms, may still leave them deciding to live, but the offer has also taken from them the possibility of living by default. They must justify their choice if only to themselves, considering the reasons they continue to pursue life-prolonging treatment and incur financial, emotional, and physical costs for their family. This is a dangerous cultural burden ironically imposed by the offer of more choices.9 Clinicians, by offering assisted suicide even if a patient declines it, also affirm the reasonableness of ending one’s life given the circumstances. That affirmation may be burdensome (eg, “They see my life as not worth living”) rather than validating.10
Restoration: Will this intervention help to restore the patient overall (even if not immediately)?
It would seem restoration is impossible for someone who is dying. Dying is terrible and so one possibility would be to hasten the process with assisted suicide. If health is in view, though, clinicians could recognize that restoration is always possible as long as someone is alive.
For someone dying, restoration may look like symptom relief (restoring bodily distress) which in turn may restore one’s capacity to sleep or to converse with loved ones. Assisted suicide does not fit in this paradigm. Is it intended to help patients sustain and restore their health, whatever amount they have (this is what the hospice and psychiatric services attempted to do in the case). Or is it intended to help patients pursue whatever goals seem good to the patient even those goals which conflict with health? Happily, most patients want their health sustained or restored so there is usually no conflict. As medical technology advances, though, conflicts arise: Should a clinician prescribe stimulants to enhance a healthy student’s wakefulness during final exams? Should a clinician engineer embryos to provide parents with a particular kind of child? Should a clinician end a patient’s life? Assisted suicide is obviously not aimed at restoration. It is a concession to the intractability of one’s disease and disability and one’s impending death. Without clarity and agreement on the goal of medicine, the default provision of care centers instead on satisfying patient preferences whatever they are.
Holism: Does the intervention prioritize the whole patient (vs prioritizing a part for the sake of the whole)?
Clinicians offering assisted suicide suggest that providing a death on a patient’s own terms restores autonomy and brings coherence to a life narrative that, at its end, is fraught with tragedy. This is what it looks like to honor “the whole patient.” A clinician must scrutinize that judgment to determine whether the patient meets statutory criteria for assisted suicide. The impulse underlying the moral distress described by Ruskin et al and many other clinicians is that a patient’s judgment, once determined to be sound, should trump a clinician’s judgment about what is best for the patient’s health and whether there are limits on what the clinician can do to satisfy a patient’s preferences. Ironically, assisted suicide prioritizes a patient’s judgment about how their life should end above other considerations, namely, that medicine has traditionally sought the patient’s good by sustaining and restoring their health, not by intending and causing their death. Notably, there was no lack of holism in the care provided the veteran in the case both before and after his suicide attempt.
Discretion: What are the limits of the intervention itself? What is the scope of medicine in general? What is the limit of one’s own individual knowledge and skill?
Assisted suicide has a substantial limit: it does not offer relief from suffering because there will be no one left alive to experience relief. Assisted suicide cannot achieve anything for the patient because they are dead by the time they fully receive what has been given. This profound limit makes assisted suicide unlike anything else offered in medicine and should give clinicians pause before adopting it, prompting them to grapple with whether causing a patient’s death is within the scope of medicine. If so, how did this come to be after thousands of years to the contrary across cultures and traditions, and what justifies this change? Finally, clinicians must contend with the limits of informed consent.
This brief reflection on how clinicians should consider medical therapies brings us back to MacIntyre’s exhortation: We cannot decide what to do until we have discerned the story to which we belong. One way of telling the story of medicine is to tell it with the techniques front and center: we prescribe, we operate, we irradiate, make the numbers go in the right direction, cure infections, and shrink masses. We can also tell that story by rejoicing that technology is giving us increasing control over our bodies and we can put that power to whatever use we desire. Often that will align with health, but it may not and that is for many patients increasingly acceptable. There is another, better story to tell: the profession of medicine exists to help people sustain and restore health, whatever bit of it they have and even as they lay dying. All those things just listed may help clinicians in that pursuit or they may not, given the specific context.
Ruskin et al tell a story of clinicians living in the tension of wanting to satisfy the desires their patients bring to them but must settle for the best that medicine can provide. Medical intervention as preference satisfaction is a story we have been living and practicing for 50 years since Beauchamp and Childress described the 4-principle framework for biomedical ethics: respect for autonomy, justice, nonmaleficence, beneficence.
Medicine-as-preference-satisfaction conflicts with the VHA mission to “honor America’s veterans by providing exceptional health care that improves their health and well-being.” VHA does not owe veterans whatever they request. VHA owes them exceptional health care. When a patient comes to a clinician, a clinician owes them a bounded set of things in service to their health. The dissonance a clinician might experience in trying to discern whether a patient’s death can serve that patient’s own health should signal a need to step back and reflect on how they understand the foundations of medical practice.
I do not disagree with the authors in their general approach to how clinicians might discuss this with patients who request a hastened death. I also seek to assuage symptoms, validate emotions, and remain steadfast through someone’s dying. I also affirm my commitment as a physician to care for a person’s health which, while someone is dying, usually entails managing symptoms. It never entails ending someone’s life. The clinicians in the case did an excellent job caring for this veteran and could not have done better by helping him end his life.
When contemplating the state of ethical dialogue in our modern world, the philosopher Alasdair MacIntyre had this to say: “I can only answer the question, ‘What am I to do?’ If I can answer the prior question ‘Of what story or stories do I find myself a part?’”1 That is, our ethics must proceed from our understanding of ourselves, others, and the world. David Hume might scoff, but we do need an “is” to appreciate and grasp our “ought.” This is just as true for medical ethics as it is for the rest of life. Questions about what we should do in medicine should draw us to deeper questions about identity and purpose.
In this issue, Ruskin et al present a tragic case of a man who spent his later years walking the line between life and a self-chosen death.2 After enduring the chronic decline of Parkinson disease, he faced a final diagnosis of glioblastoma. The patient enrolled in hospice while considering how he might move elsewhere to avail himself of assisted suicide. Before he had a chance to do that, he was admitted to an inpatient hospice unit where he weakened further. In the throes of what may have been delirium or a last effort to enact his wish of a hastened death, he attempted suicide on the hospice unit. He survived only to die days later from the cancer.
The authors reflect on the complexities of this case, including the distress of a clinician who may want to satisfy a veteran’s wish but cannot due to legal constraints, and the challenges of identifying pathologic suicidal ideation from an earnest and rational desire for a hastened death. How should they handle these conversations? They conclude by suggesting ways clinicians may assess and respond to requests for a hastened death, recognizing that assisted suicide remains illegal within the Veterans Health Administration (VHA).
Clinicians can return to the foundation of our profession to better consider these questions. The case report authors acknowledge this but avoid learning from what the conflict might teach us: “The inability to help veterans achieve their care preferences [to receive a hastened death] conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.” Before feeling like they have failed the veteran, a clinician must ask if it is really within their scope of practice to end someone’s life. While it is true that “the mission of VHA’s [Palliative and Hospice Care] program is to honor veterans’ preferences for care,” this mission exists within a greater context of appreciating that not all preferences can or should be honored.3 An obvious example is when a veteran requests an intervention that is not clinically indicated (eg, antibiotics for a viral infection). Clinicians are not bound to honor this preference; not because there is a law directing the clinicians’ decision making (there is not) but because there is a standard of care that accounts for but can supersede the veteran’s preference.
Is assisted suicide ever clinically indicated? While the answer shifts depending on the jurisdiction, the case report authors acknowledge why the preference for assisted suicide cannot be honored in a VHA facility: it is against the law.4 However, as they explain, this is insufficient to assuage the moral distress that might arise for some clinicians who want to fulfill a veteran’s request. They recommend several different strategies for clinicians to consider when receiving a request for assisted suicide. Distress in the form of cognitive dissonance may also arise from the tension that exists between stopping some forms of suicide while assisting in others.
While it is important to assess whether the request for a hastened death is driven by an untreated symptom or mental illness, this will only get a clinician so far when the request is made in earnest with no remediable drivers. While I cannot argue the point here, I accept that there are forms of suicide which are rational. However, that alone is insufficient to justify the act or assist someone with it; we must assess the good that the rational choice seeks to realize.5 If suicide can be rational, clinicians should ask whether it is within the goals of medicine to assist in suicide. The authors seem to take it for granted that the distressed clinician in the case hopes to hasten this veteran’s death or at least refer him to someone who could. Perhaps his suicide attempt on the hospice unit was, in part, a consequence of being incapable of offering such assistance. These presuppositions should be considered explicitly to better align one’s practice both with the mission of VHA and with the goals of medicine.
One way to do this is to consider whether we can cast assisted suicide as a medical therapy. Sulmasy proposes the provisional “canons of therapy” which might guide clinicians in assessing medical therapies.6 This article distinguishes 3 types of clinically and ethically distinct practices. I have split his first canon (proportionality) into 2 for the sake of clarity.
Priority: Do the benefits outweigh the burdens of the intervention?
The challenge of assessing priority when considering assisted suicide is that we cannot explain any benefits or burdens that might accrue after death; it is beyond our knowledge and informed consent is impossible. While there is always some uncertainty in discerning the benefits and burdens of an intervention, death presents an insurmountable procedural problem for informed consent to assisted suicide.
Fit: Are the means appropriate for the outcome of interest?
The outcomes of interest when considering assisted suicide are many—many—they range from symptom relief or avoidance to reclaiming dignity. In the case described by Ruskin et al, the interdisciplinary team offered the veteran a number of interventions to assuage his symptoms. Dignity therapy may have been employed as a meaningful, useful way of bringing closure to a life.7,8 Ultimately, however, some distress, particularly existential distress, may be intractable and clinicians must commit, as they did in this case, to doing what they can to remedy other symptoms and not abandon the veteran. Suicide is a tempting option because it may eliminate some of these concerns, but one must first grapple with the ethical question of whether suicide is ever an appropriate way to pursue any of these outcomes. Addressing that question is beyond the scope of this commentary, but both clinicians and patients should consider whether and why suicide should be considered appropriate and whether it is appropriate for the medical profession to assist with it.
Parsimony: Is this the least invasive, least burdensome intervention available?
In US jurisdictions where it is legal, assisted suicide is considered an intervention of last resort. Assisted suicide seems to be neither invasive (it involves taking medications) nor burdensome: the medications usually work quickly and without adverse effects, although there are risks (eg, vomiting). Broadening our view beyond the individual reveals something different.
In a cultural sense, assisted suicide is invasive. It changes how clinicians and patients consider health and medical care. We no longer have the profession of medicine with another intervention in the toolbox; we have a totally different profession which now intends death instead of health for its patients. It changes medicine and society at large profoundly. This makes it culturally invasive.
Furthermore, although the veteran in the case recurrently grappled with the choice of suicide, most people do not. They live by default. Offering assisted suicide, even in broad, general terms, may still leave them deciding to live, but the offer has also taken from them the possibility of living by default. They must justify their choice if only to themselves, considering the reasons they continue to pursue life-prolonging treatment and incur financial, emotional, and physical costs for their family. This is a dangerous cultural burden ironically imposed by the offer of more choices.9 Clinicians, by offering assisted suicide even if a patient declines it, also affirm the reasonableness of ending one’s life given the circumstances. That affirmation may be burdensome (eg, “They see my life as not worth living”) rather than validating.10
Restoration: Will this intervention help to restore the patient overall (even if not immediately)?
It would seem restoration is impossible for someone who is dying. Dying is terrible and so one possibility would be to hasten the process with assisted suicide. If health is in view, though, clinicians could recognize that restoration is always possible as long as someone is alive.
For someone dying, restoration may look like symptom relief (restoring bodily distress) which in turn may restore one’s capacity to sleep or to converse with loved ones. Assisted suicide does not fit in this paradigm. Is it intended to help patients sustain and restore their health, whatever amount they have (this is what the hospice and psychiatric services attempted to do in the case). Or is it intended to help patients pursue whatever goals seem good to the patient even those goals which conflict with health? Happily, most patients want their health sustained or restored so there is usually no conflict. As medical technology advances, though, conflicts arise: Should a clinician prescribe stimulants to enhance a healthy student’s wakefulness during final exams? Should a clinician engineer embryos to provide parents with a particular kind of child? Should a clinician end a patient’s life? Assisted suicide is obviously not aimed at restoration. It is a concession to the intractability of one’s disease and disability and one’s impending death. Without clarity and agreement on the goal of medicine, the default provision of care centers instead on satisfying patient preferences whatever they are.
Holism: Does the intervention prioritize the whole patient (vs prioritizing a part for the sake of the whole)?
Clinicians offering assisted suicide suggest that providing a death on a patient’s own terms restores autonomy and brings coherence to a life narrative that, at its end, is fraught with tragedy. This is what it looks like to honor “the whole patient.” A clinician must scrutinize that judgment to determine whether the patient meets statutory criteria for assisted suicide. The impulse underlying the moral distress described by Ruskin et al and many other clinicians is that a patient’s judgment, once determined to be sound, should trump a clinician’s judgment about what is best for the patient’s health and whether there are limits on what the clinician can do to satisfy a patient’s preferences. Ironically, assisted suicide prioritizes a patient’s judgment about how their life should end above other considerations, namely, that medicine has traditionally sought the patient’s good by sustaining and restoring their health, not by intending and causing their death. Notably, there was no lack of holism in the care provided the veteran in the case both before and after his suicide attempt.
Discretion: What are the limits of the intervention itself? What is the scope of medicine in general? What is the limit of one’s own individual knowledge and skill?
Assisted suicide has a substantial limit: it does not offer relief from suffering because there will be no one left alive to experience relief. Assisted suicide cannot achieve anything for the patient because they are dead by the time they fully receive what has been given. This profound limit makes assisted suicide unlike anything else offered in medicine and should give clinicians pause before adopting it, prompting them to grapple with whether causing a patient’s death is within the scope of medicine. If so, how did this come to be after thousands of years to the contrary across cultures and traditions, and what justifies this change? Finally, clinicians must contend with the limits of informed consent.
This brief reflection on how clinicians should consider medical therapies brings us back to MacIntyre’s exhortation: We cannot decide what to do until we have discerned the story to which we belong. One way of telling the story of medicine is to tell it with the techniques front and center: we prescribe, we operate, we irradiate, make the numbers go in the right direction, cure infections, and shrink masses. We can also tell that story by rejoicing that technology is giving us increasing control over our bodies and we can put that power to whatever use we desire. Often that will align with health, but it may not and that is for many patients increasingly acceptable. There is another, better story to tell: the profession of medicine exists to help people sustain and restore health, whatever bit of it they have and even as they lay dying. All those things just listed may help clinicians in that pursuit or they may not, given the specific context.
Ruskin et al tell a story of clinicians living in the tension of wanting to satisfy the desires their patients bring to them but must settle for the best that medicine can provide. Medical intervention as preference satisfaction is a story we have been living and practicing for 50 years since Beauchamp and Childress described the 4-principle framework for biomedical ethics: respect for autonomy, justice, nonmaleficence, beneficence.
Medicine-as-preference-satisfaction conflicts with the VHA mission to “honor America’s veterans by providing exceptional health care that improves their health and well-being.” VHA does not owe veterans whatever they request. VHA owes them exceptional health care. When a patient comes to a clinician, a clinician owes them a bounded set of things in service to their health. The dissonance a clinician might experience in trying to discern whether a patient’s death can serve that patient’s own health should signal a need to step back and reflect on how they understand the foundations of medical practice.
I do not disagree with the authors in their general approach to how clinicians might discuss this with patients who request a hastened death. I also seek to assuage symptoms, validate emotions, and remain steadfast through someone’s dying. I also affirm my commitment as a physician to care for a person’s health which, while someone is dying, usually entails managing symptoms. It never entails ending someone’s life. The clinicians in the case did an excellent job caring for this veteran and could not have done better by helping him end his life.
- MacIntyre A. After Virtue: A Study in Moral Theory. 3rd ed. 2007.
- Ruskin A, Bauer M, Alrojolah L. Managing requests for medical aid in dying within the US Department of Veterans Affairs Health Care System. Fed Pract. 2026;43:238-242. doi:10.12788/fp.0739
- VHA Directive 1139: Palliative care consult teams and Veterans Integrated Service Network Leads. September 9, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9930
- Assisted Suicide Funding Restriction Act of 1997. 42 USC § 14401.
- Safranek JP. Autonomy and assisted suicide the execution of freedom. Hastings Cent Rep. 1998;28:32-36. doi:10.2307/3528611
- Sulmasy DP. The last low whispers of our dead: when is it ethically justifiable to render a patient unconscious until death? Theor Med Bioeth. 2018;39:233-263. doi:10.1007/s11017-018-9459-7
- Chochinov HM. Dying, Dignity, and new horizons in palliative end-of-life care. CA Cancer J Clin. 2006;56:84-103. doi:10.3322/canjclin.56.2.84
- Chochinov HM. Intensive caring: reminding families they matter. J Palliat Med. 2024;27:152-155.
- Velleman JD. Against the right to die. J Med Philos. 1992;17:665-681.
- Peace WJ. Comfort Care as Denial of Personhood. Hastings Cent Rep. 2012;42:14-17. doi:10.1002/hast.38
- MacIntyre A. After Virtue: A Study in Moral Theory. 3rd ed. 2007.
- Ruskin A, Bauer M, Alrojolah L. Managing requests for medical aid in dying within the US Department of Veterans Affairs Health Care System. Fed Pract. 2026;43:238-242. doi:10.12788/fp.0739
- VHA Directive 1139: Palliative care consult teams and Veterans Integrated Service Network Leads. September 9, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9930
- Assisted Suicide Funding Restriction Act of 1997. 42 USC § 14401.
- Safranek JP. Autonomy and assisted suicide the execution of freedom. Hastings Cent Rep. 1998;28:32-36. doi:10.2307/3528611
- Sulmasy DP. The last low whispers of our dead: when is it ethically justifiable to render a patient unconscious until death? Theor Med Bioeth. 2018;39:233-263. doi:10.1007/s11017-018-9459-7
- Chochinov HM. Dying, Dignity, and new horizons in palliative end-of-life care. CA Cancer J Clin. 2006;56:84-103. doi:10.3322/canjclin.56.2.84
- Chochinov HM. Intensive caring: reminding families they matter. J Palliat Med. 2024;27:152-155.
- Velleman JD. Against the right to die. J Med Philos. 1992;17:665-681.
- Peace WJ. Comfort Care as Denial of Personhood. Hastings Cent Rep. 2012;42:14-17. doi:10.1002/hast.38
What They Want and What They Need: The End-of-Life Conflict
What They Want and What They Need: The End-of-Life Conflict
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
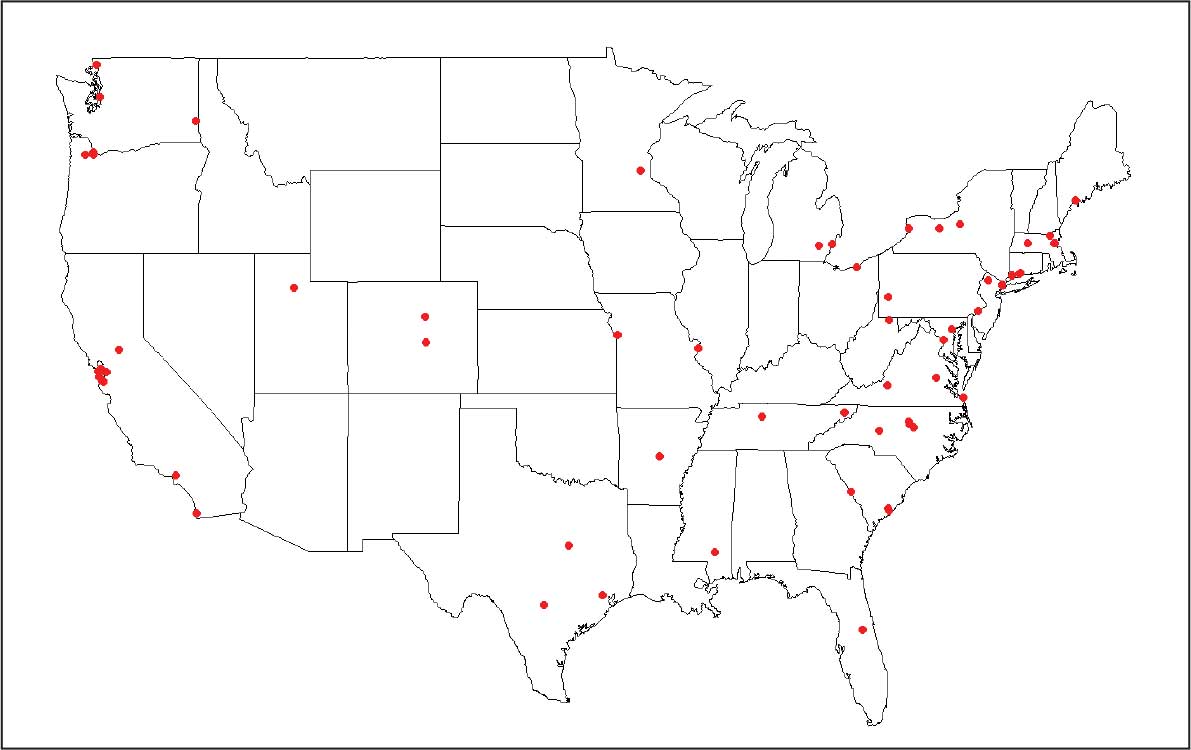
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health

Military Sexual Trauma is 'Persistently Prevalent'
Military sexual trauma (MST) remained “persistently prevalent” between 2013 and 2026, experiencing a slight overall increase from 7.6% to 8.2% in the time period, according to a research letter written by researchers from Yale University and the Veterans Affairs (VA) Connecticut Healthcare System and published in JAMA Psychiatry. Prevalence among female veterans jumped from 32.4% to 43.3%, with many citing MST as a factor in their decision to leave military service earlier than planned.
The researchers analyzed data from 3 independent nationally representative cohorts of veterans surveyed as part of the National Health and Resilience in Veterans Study. In 2025 and 2026, 189 veterans reported sexual harassment and 80 veterans reported sexual assault. Among female veterans, 128 (42.7%) reported harassment and 55 (21.2%) reported assault; 61 male veterans (3.6%) reported harassment and 25 (1.4%) reported assault.
Many veterans experienced multiple MSTs. In 2025 and 2026, 61 women and 23 men reported 2 or 3 occurrences of MST, and 57 (42 women, 15 men) reported ≥ 4 occurrences. Most indicated ≥ 1 MST occurrence was perpetrated by a higher-ranking military member. Women were more likely to report ≥ 2 MST occurrences and MST perpetrated by a higher-ranking military member, according to the letter.
MST can have potentially disproportionate consequences for women in terms of military workforce composition, leadership representation, and long-term force readiness, the researchers say. Findings based on 2024 national veteran population data suggest that roughly 1 in 6 women and 1 in 100 men will leave military service after MST.
History of MST has been independently associated with elevated risk for suicidal thoughts and behaviors, including future suicidal intent. In this study, compared with veterans without MST, those with MST had nearly triple the rates of past-year suicidal ideation and > 4 times the rates of lifetime suicide attempt. They were also significantly more likely to indicate future suicidal intent (6.9% vs 1.2%). Predicted probabilities of suicidal ideation (34.2% vs 28.3%) and suicide attempt (18.5% vs 13.4%) were significantly higher among females than males.
Female service members who experienced MST are also nearly 3 times more likely to have moderate to severe posttraumatic stress disorder (PTSD) symptoms, compared with female service members who did not experience MST. Women veterans who report MST and have PTSD are also more likely to have comorbid mental health diagnoses, including major depression, anxiety, eating disorders, and substance use disorders.
The researchers claim the research is the first nationally representative characterization of MST contextual features and updated estimates of treatment utilization. They found that fewer than half of survivors received MST-related treatment.
In 2021, President Biden directed the US Department of Defense to establish the Independent Review Commission on Sexual Assault in the Military (IRC). An overview of the IRC commission findings underscored the need for screening. The increased risk of suicidal thoughts and behaviors, it says, makes “integration of crosscutting prevention initiatives within MST care and suicide prevention at VA” critical.
The Veterans Health Administration universal MST screening program is part of a web of MST-related services. Analysis of medical record data demonstrates that the program yields clinically meaningful information, and increases the likelihood of mental health treatment. Despite the barriers to care for all MST survivors noted in qualitative studies, the commission report says, quantitative research agrees that veterans with a positive MST screen are more likely to engage in health care in VA.
Military sexual trauma (MST) remained “persistently prevalent” between 2013 and 2026, experiencing a slight overall increase from 7.6% to 8.2% in the time period, according to a research letter written by researchers from Yale University and the Veterans Affairs (VA) Connecticut Healthcare System and published in JAMA Psychiatry. Prevalence among female veterans jumped from 32.4% to 43.3%, with many citing MST as a factor in their decision to leave military service earlier than planned.
The researchers analyzed data from 3 independent nationally representative cohorts of veterans surveyed as part of the National Health and Resilience in Veterans Study. In 2025 and 2026, 189 veterans reported sexual harassment and 80 veterans reported sexual assault. Among female veterans, 128 (42.7%) reported harassment and 55 (21.2%) reported assault; 61 male veterans (3.6%) reported harassment and 25 (1.4%) reported assault.
Many veterans experienced multiple MSTs. In 2025 and 2026, 61 women and 23 men reported 2 or 3 occurrences of MST, and 57 (42 women, 15 men) reported ≥ 4 occurrences. Most indicated ≥ 1 MST occurrence was perpetrated by a higher-ranking military member. Women were more likely to report ≥ 2 MST occurrences and MST perpetrated by a higher-ranking military member, according to the letter.
MST can have potentially disproportionate consequences for women in terms of military workforce composition, leadership representation, and long-term force readiness, the researchers say. Findings based on 2024 national veteran population data suggest that roughly 1 in 6 women and 1 in 100 men will leave military service after MST.
History of MST has been independently associated with elevated risk for suicidal thoughts and behaviors, including future suicidal intent. In this study, compared with veterans without MST, those with MST had nearly triple the rates of past-year suicidal ideation and > 4 times the rates of lifetime suicide attempt. They were also significantly more likely to indicate future suicidal intent (6.9% vs 1.2%). Predicted probabilities of suicidal ideation (34.2% vs 28.3%) and suicide attempt (18.5% vs 13.4%) were significantly higher among females than males.
Female service members who experienced MST are also nearly 3 times more likely to have moderate to severe posttraumatic stress disorder (PTSD) symptoms, compared with female service members who did not experience MST. Women veterans who report MST and have PTSD are also more likely to have comorbid mental health diagnoses, including major depression, anxiety, eating disorders, and substance use disorders.
The researchers claim the research is the first nationally representative characterization of MST contextual features and updated estimates of treatment utilization. They found that fewer than half of survivors received MST-related treatment.
In 2021, President Biden directed the US Department of Defense to establish the Independent Review Commission on Sexual Assault in the Military (IRC). An overview of the IRC commission findings underscored the need for screening. The increased risk of suicidal thoughts and behaviors, it says, makes “integration of crosscutting prevention initiatives within MST care and suicide prevention at VA” critical.
The Veterans Health Administration universal MST screening program is part of a web of MST-related services. Analysis of medical record data demonstrates that the program yields clinically meaningful information, and increases the likelihood of mental health treatment. Despite the barriers to care for all MST survivors noted in qualitative studies, the commission report says, quantitative research agrees that veterans with a positive MST screen are more likely to engage in health care in VA.
Military sexual trauma (MST) remained “persistently prevalent” between 2013 and 2026, experiencing a slight overall increase from 7.6% to 8.2% in the time period, according to a research letter written by researchers from Yale University and the Veterans Affairs (VA) Connecticut Healthcare System and published in JAMA Psychiatry. Prevalence among female veterans jumped from 32.4% to 43.3%, with many citing MST as a factor in their decision to leave military service earlier than planned.
The researchers analyzed data from 3 independent nationally representative cohorts of veterans surveyed as part of the National Health and Resilience in Veterans Study. In 2025 and 2026, 189 veterans reported sexual harassment and 80 veterans reported sexual assault. Among female veterans, 128 (42.7%) reported harassment and 55 (21.2%) reported assault; 61 male veterans (3.6%) reported harassment and 25 (1.4%) reported assault.
Many veterans experienced multiple MSTs. In 2025 and 2026, 61 women and 23 men reported 2 or 3 occurrences of MST, and 57 (42 women, 15 men) reported ≥ 4 occurrences. Most indicated ≥ 1 MST occurrence was perpetrated by a higher-ranking military member. Women were more likely to report ≥ 2 MST occurrences and MST perpetrated by a higher-ranking military member, according to the letter.
MST can have potentially disproportionate consequences for women in terms of military workforce composition, leadership representation, and long-term force readiness, the researchers say. Findings based on 2024 national veteran population data suggest that roughly 1 in 6 women and 1 in 100 men will leave military service after MST.
History of MST has been independently associated with elevated risk for suicidal thoughts and behaviors, including future suicidal intent. In this study, compared with veterans without MST, those with MST had nearly triple the rates of past-year suicidal ideation and > 4 times the rates of lifetime suicide attempt. They were also significantly more likely to indicate future suicidal intent (6.9% vs 1.2%). Predicted probabilities of suicidal ideation (34.2% vs 28.3%) and suicide attempt (18.5% vs 13.4%) were significantly higher among females than males.
Female service members who experienced MST are also nearly 3 times more likely to have moderate to severe posttraumatic stress disorder (PTSD) symptoms, compared with female service members who did not experience MST. Women veterans who report MST and have PTSD are also more likely to have comorbid mental health diagnoses, including major depression, anxiety, eating disorders, and substance use disorders.
The researchers claim the research is the first nationally representative characterization of MST contextual features and updated estimates of treatment utilization. They found that fewer than half of survivors received MST-related treatment.
In 2021, President Biden directed the US Department of Defense to establish the Independent Review Commission on Sexual Assault in the Military (IRC). An overview of the IRC commission findings underscored the need for screening. The increased risk of suicidal thoughts and behaviors, it says, makes “integration of crosscutting prevention initiatives within MST care and suicide prevention at VA” critical.
The Veterans Health Administration universal MST screening program is part of a web of MST-related services. Analysis of medical record data demonstrates that the program yields clinically meaningful information, and increases the likelihood of mental health treatment. Despite the barriers to care for all MST survivors noted in qualitative studies, the commission report says, quantitative research agrees that veterans with a positive MST screen are more likely to engage in health care in VA.
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
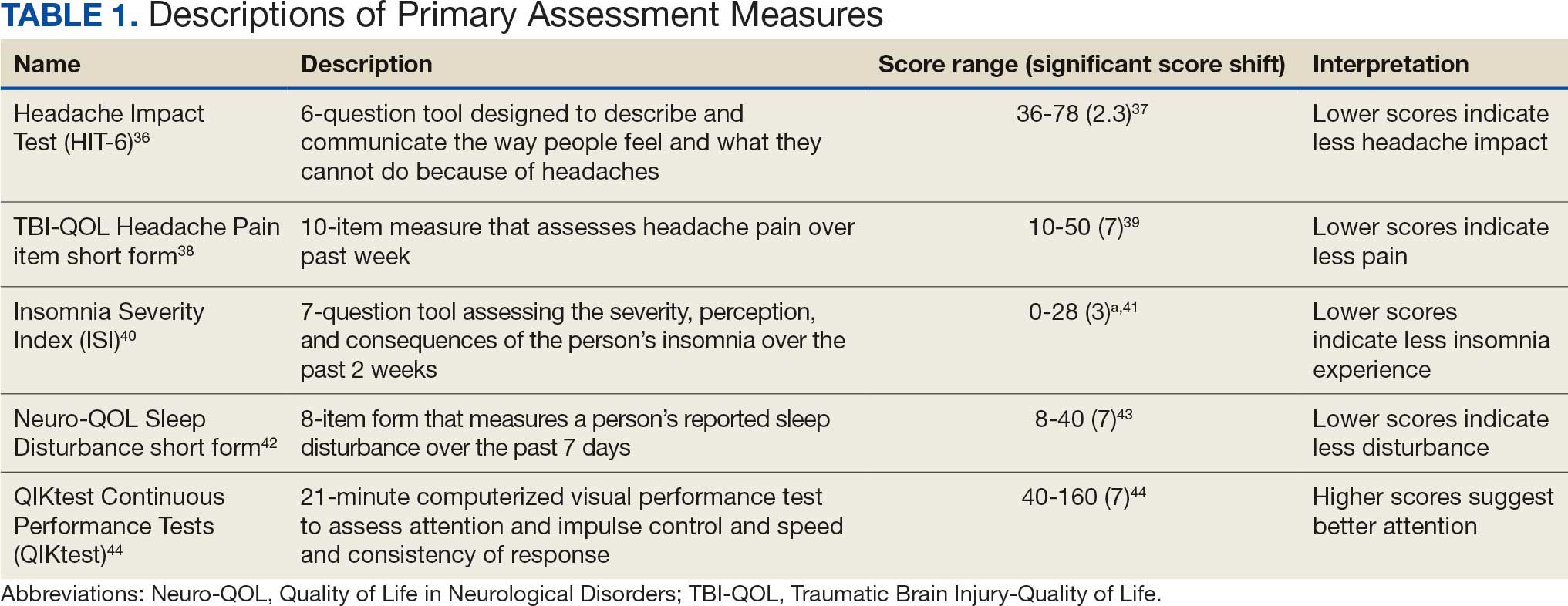
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
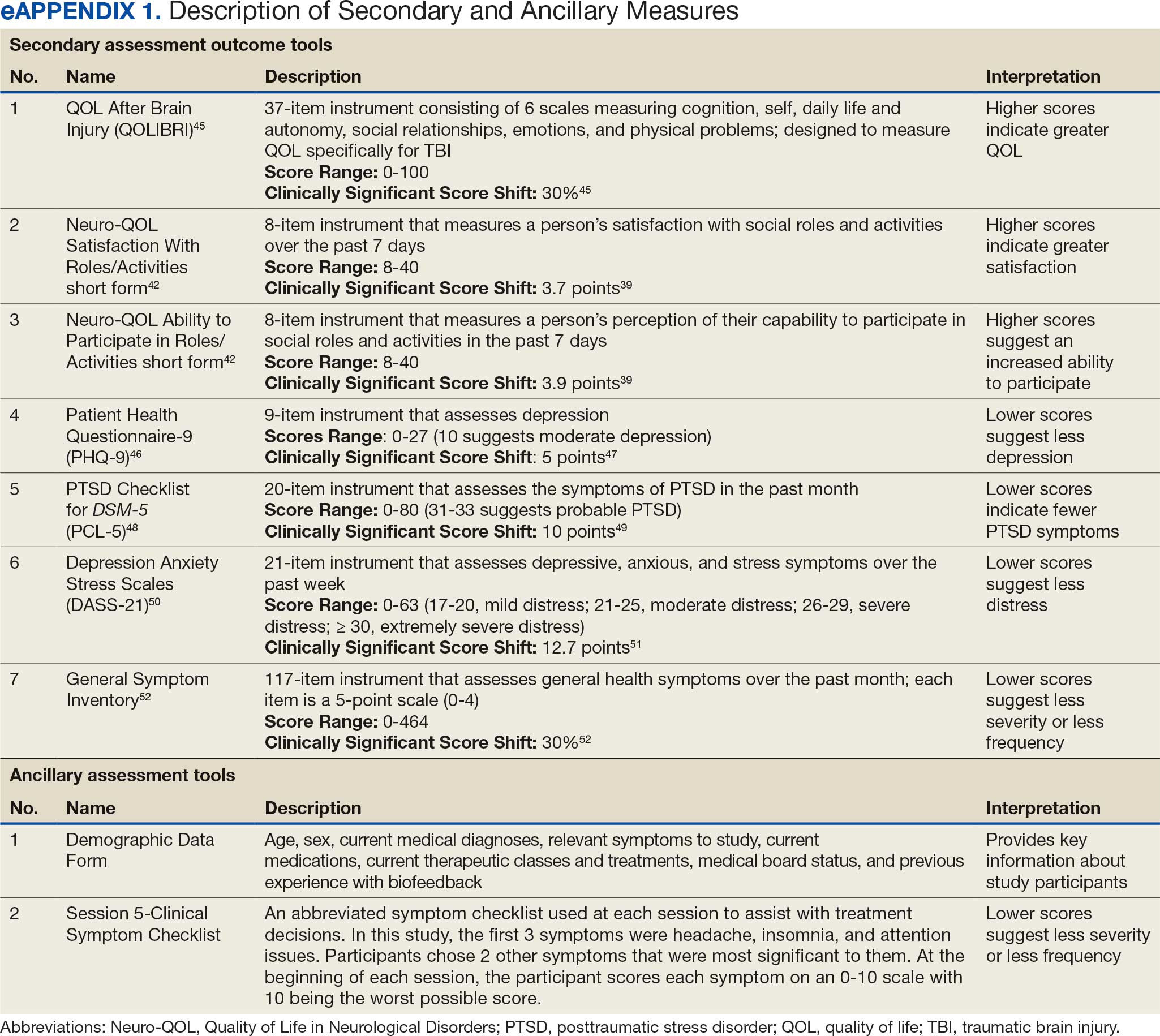
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
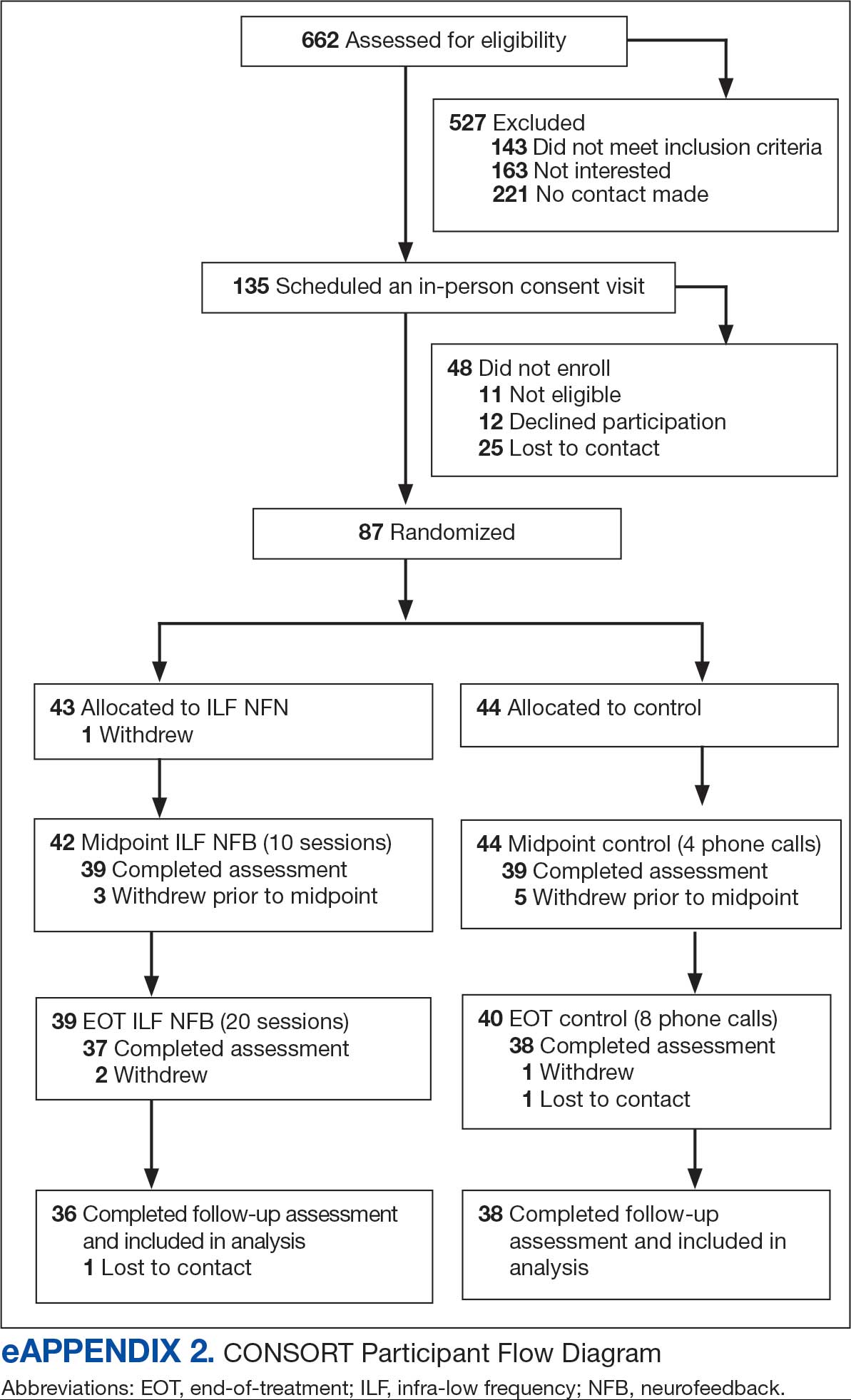
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
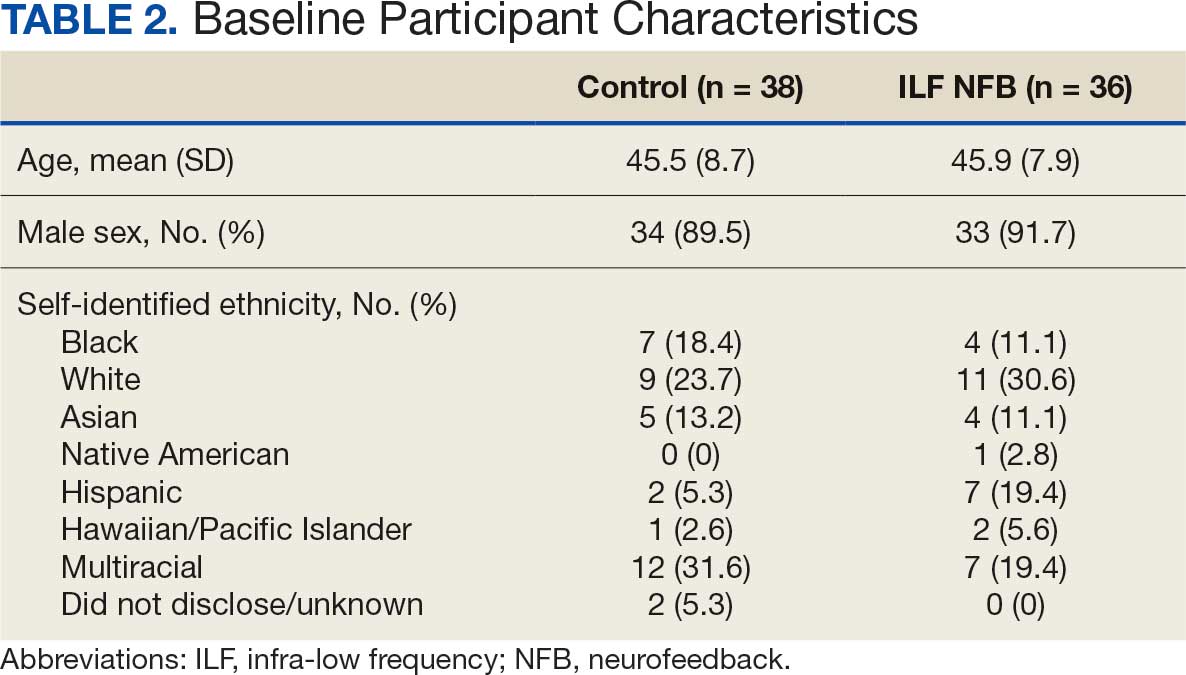
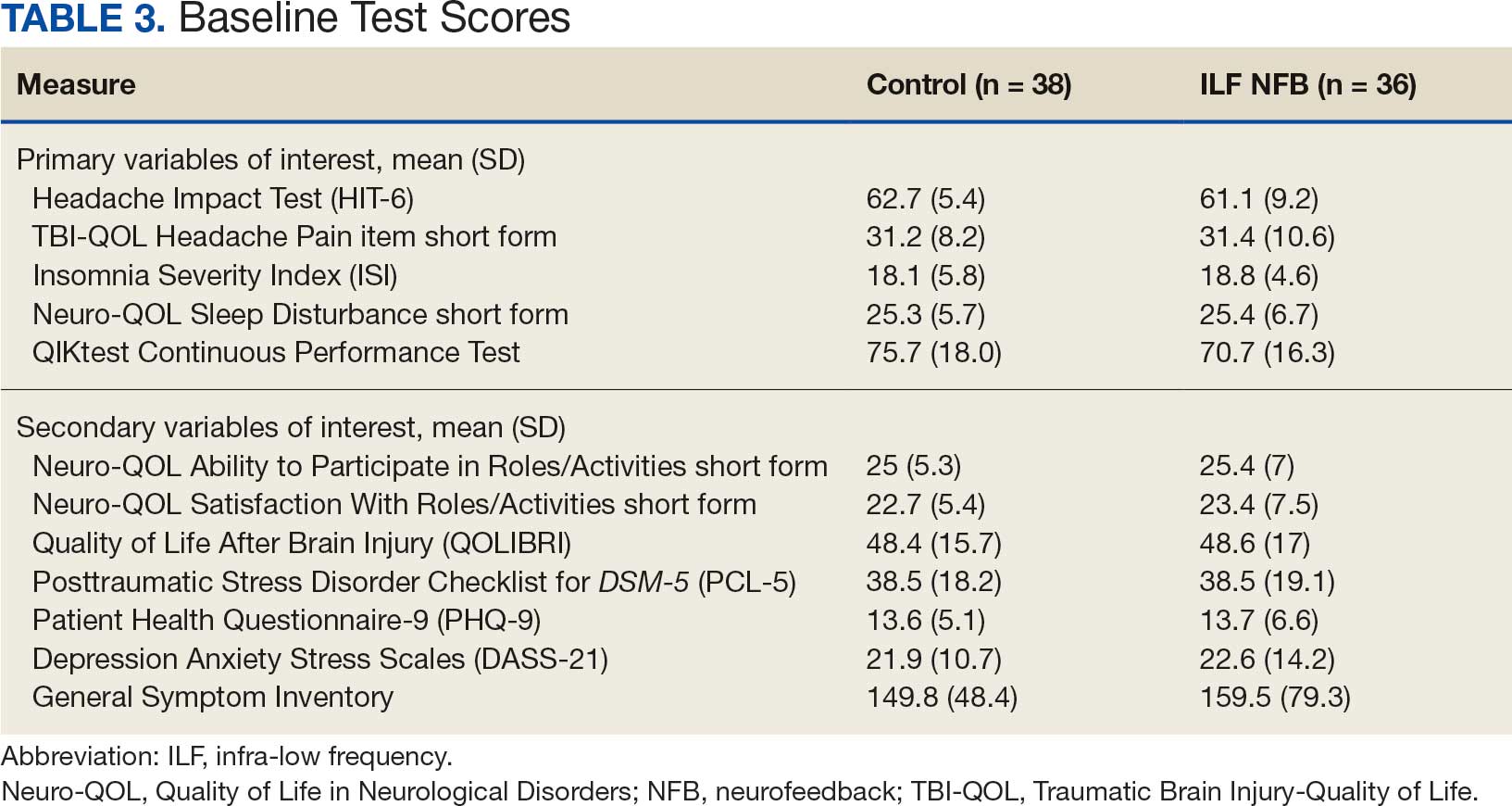
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
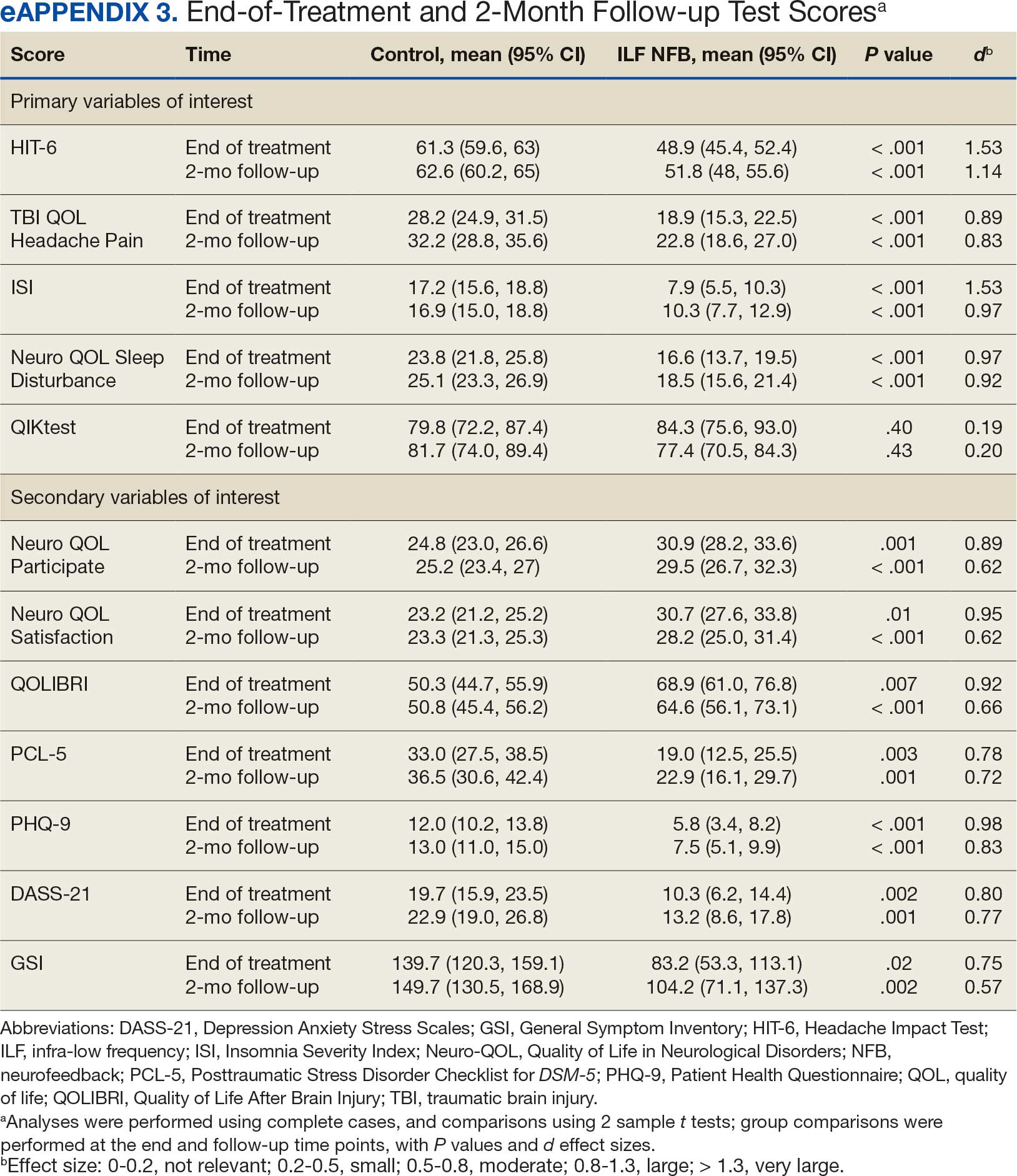
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
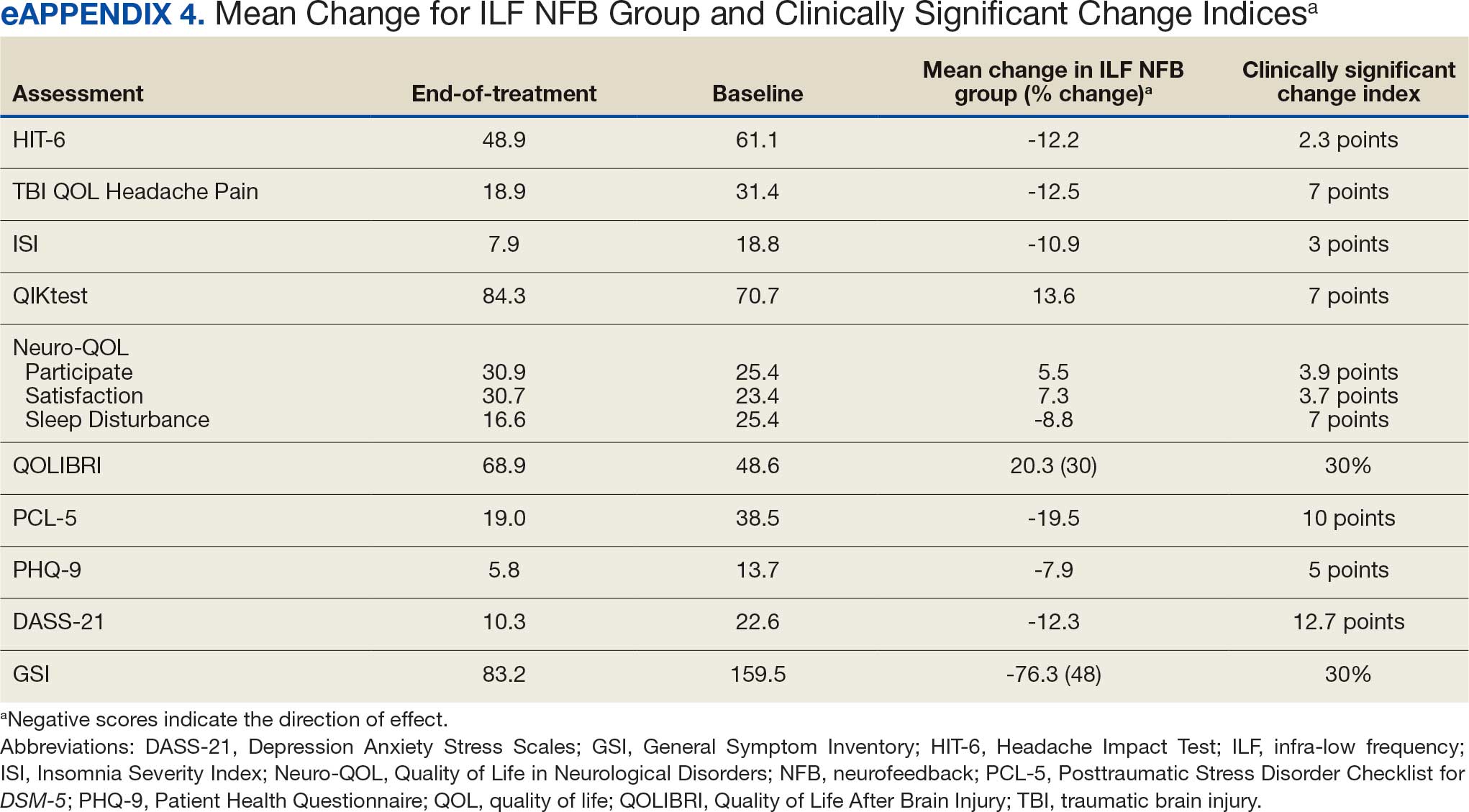
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms

State Firearm Laws Linked to Veteran Suicide Rates
TOPLINE: Among veterans and demographically matched nonveterans from 2002 to 2019, higher state household firearm ownership was associated with higher rates of deaths by suicide, while greater state firearm law restrictiveness was associated with lower rates of deaths by suicide. In 2017 to 2019 models, these associations were seen for both veterans and matched nonveterans and driven primarily by firearm deaths by suicide rates.
METHODOLOGY:
US state-level data across 6 consecutive 3-year periods from 2002-2019, stratified suicide rates by veteran status (veteran vs matched nonveterans) and method (firearm vs nonfirearm).
Data sources included US Department of Veterans Affairs (VA) Office of Mental Health and Suicide Prevention counts matched to the National Death Index, plus Centers for Disease Control suicide counts and population estimates by sex and age.
Participants included veterans with state- and period-specific death suicide counts and population denominators from the VetPop model, and a matched nonveteran comparison created by comparing state deaths by suicide data to veterans’ age and gender distributions.
Exposure measures included annual state household firearm ownership rate estimates carried forward to 2017-2019, and a 7-item state firearm policy restrictiveness index derived from the RAND Corporation state firearm law database.
TAKEAWAY:
Average death by suicide rates from 2002-2019 were 28.2 per 100,000 for veterans and 27.5 per 100,000 for matched nonveterans, with most deaths involving a firearm.
Across states, the maximum average death by suicide rate was about 3 times the minimum over the study period, and veteran and matched nonveteran state patterns aligned closely.
Higher household firearm ownership was associated with higher firearm death by suicide rates for veterans and matched nonveterans from 2017-2019.
Greater firearm law restrictiveness, equivalent to 3 additional restrictive laws, was associated with fewer firearm deaths by suicide for veterans and matched nonveterans from 2017-2019.
IN PRACTICE: “The results suggest that changes to state firearm laws and policies should be investigated as a possibly cost-effective primary prevention strategy for reducing suicide rates among veterans and nonveterans,” the authors wrote.
SOURCE:The study was led by Andrew R. Morral, PhD, RAND Corporation in Arlington, Virginia, and Terry L. Schell, PhD, and Adam Scherling, RAND Corporation in Santa Monica, California and published online in Injury Prevention.
LIMITATIONS: The estimates are correlational and should not be interpreted as causal effect estimates, as most interstate variation in gun ownership and firearm laws predates the beginning of the available VA death by suicide data, limiting the analytical approach to identify causal effects. VA does not share microdata on veteran suicide, requiring construction of a matched comparison sample of nonveterans by estimating veteran decedent removal from general population suicide totals within cells of a 5-way table based on publicly released 3-way tables, introducing imprecision. Veteran suicide counts are known to undercount suicides among veterans who separated from the military prior to 1974, likely resulting in a slight underestimate of veteran suicide rates for the oldest cohort of veterans, particularly in earlier study periods. Restricting analysis to identify modeled effects solely through limited changes in state firearm ownership and policies during the study period yields imprecise effect estimates.
DISCLOSURES: This work received support from a grant provided by The RAND Epstein Family Veterans Policy Research Institute, established through a contribution from Daniel J. Epstein via the Epstein Family Foundation. Neither the Institute, the Foundation, nor Mr. Epstein participated in the design, conduct, analysis, or drafting of this report. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Among veterans and demographically matched nonveterans from 2002 to 2019, higher state household firearm ownership was associated with higher rates of deaths by suicide, while greater state firearm law restrictiveness was associated with lower rates of deaths by suicide. In 2017 to 2019 models, these associations were seen for both veterans and matched nonveterans and driven primarily by firearm deaths by suicide rates.
METHODOLOGY:
US state-level data across 6 consecutive 3-year periods from 2002-2019, stratified suicide rates by veteran status (veteran vs matched nonveterans) and method (firearm vs nonfirearm).
Data sources included US Department of Veterans Affairs (VA) Office of Mental Health and Suicide Prevention counts matched to the National Death Index, plus Centers for Disease Control suicide counts and population estimates by sex and age.
Participants included veterans with state- and period-specific death suicide counts and population denominators from the VetPop model, and a matched nonveteran comparison created by comparing state deaths by suicide data to veterans’ age and gender distributions.
Exposure measures included annual state household firearm ownership rate estimates carried forward to 2017-2019, and a 7-item state firearm policy restrictiveness index derived from the RAND Corporation state firearm law database.
TAKEAWAY:
Average death by suicide rates from 2002-2019 were 28.2 per 100,000 for veterans and 27.5 per 100,000 for matched nonveterans, with most deaths involving a firearm.
Across states, the maximum average death by suicide rate was about 3 times the minimum over the study period, and veteran and matched nonveteran state patterns aligned closely.
Higher household firearm ownership was associated with higher firearm death by suicide rates for veterans and matched nonveterans from 2017-2019.
Greater firearm law restrictiveness, equivalent to 3 additional restrictive laws, was associated with fewer firearm deaths by suicide for veterans and matched nonveterans from 2017-2019.
IN PRACTICE: “The results suggest that changes to state firearm laws and policies should be investigated as a possibly cost-effective primary prevention strategy for reducing suicide rates among veterans and nonveterans,” the authors wrote.
SOURCE:The study was led by Andrew R. Morral, PhD, RAND Corporation in Arlington, Virginia, and Terry L. Schell, PhD, and Adam Scherling, RAND Corporation in Santa Monica, California and published online in Injury Prevention.
LIMITATIONS: The estimates are correlational and should not be interpreted as causal effect estimates, as most interstate variation in gun ownership and firearm laws predates the beginning of the available VA death by suicide data, limiting the analytical approach to identify causal effects. VA does not share microdata on veteran suicide, requiring construction of a matched comparison sample of nonveterans by estimating veteran decedent removal from general population suicide totals within cells of a 5-way table based on publicly released 3-way tables, introducing imprecision. Veteran suicide counts are known to undercount suicides among veterans who separated from the military prior to 1974, likely resulting in a slight underestimate of veteran suicide rates for the oldest cohort of veterans, particularly in earlier study periods. Restricting analysis to identify modeled effects solely through limited changes in state firearm ownership and policies during the study period yields imprecise effect estimates.
DISCLOSURES: This work received support from a grant provided by The RAND Epstein Family Veterans Policy Research Institute, established through a contribution from Daniel J. Epstein via the Epstein Family Foundation. Neither the Institute, the Foundation, nor Mr. Epstein participated in the design, conduct, analysis, or drafting of this report. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Among veterans and demographically matched nonveterans from 2002 to 2019, higher state household firearm ownership was associated with higher rates of deaths by suicide, while greater state firearm law restrictiveness was associated with lower rates of deaths by suicide. In 2017 to 2019 models, these associations were seen for both veterans and matched nonveterans and driven primarily by firearm deaths by suicide rates.
METHODOLOGY:
US state-level data across 6 consecutive 3-year periods from 2002-2019, stratified suicide rates by veteran status (veteran vs matched nonveterans) and method (firearm vs nonfirearm).
Data sources included US Department of Veterans Affairs (VA) Office of Mental Health and Suicide Prevention counts matched to the National Death Index, plus Centers for Disease Control suicide counts and population estimates by sex and age.
Participants included veterans with state- and period-specific death suicide counts and population denominators from the VetPop model, and a matched nonveteran comparison created by comparing state deaths by suicide data to veterans’ age and gender distributions.
Exposure measures included annual state household firearm ownership rate estimates carried forward to 2017-2019, and a 7-item state firearm policy restrictiveness index derived from the RAND Corporation state firearm law database.
TAKEAWAY:
Average death by suicide rates from 2002-2019 were 28.2 per 100,000 for veterans and 27.5 per 100,000 for matched nonveterans, with most deaths involving a firearm.
Across states, the maximum average death by suicide rate was about 3 times the minimum over the study period, and veteran and matched nonveteran state patterns aligned closely.
Higher household firearm ownership was associated with higher firearm death by suicide rates for veterans and matched nonveterans from 2017-2019.
Greater firearm law restrictiveness, equivalent to 3 additional restrictive laws, was associated with fewer firearm deaths by suicide for veterans and matched nonveterans from 2017-2019.
IN PRACTICE: “The results suggest that changes to state firearm laws and policies should be investigated as a possibly cost-effective primary prevention strategy for reducing suicide rates among veterans and nonveterans,” the authors wrote.
SOURCE:The study was led by Andrew R. Morral, PhD, RAND Corporation in Arlington, Virginia, and Terry L. Schell, PhD, and Adam Scherling, RAND Corporation in Santa Monica, California and published online in Injury Prevention.
LIMITATIONS: The estimates are correlational and should not be interpreted as causal effect estimates, as most interstate variation in gun ownership and firearm laws predates the beginning of the available VA death by suicide data, limiting the analytical approach to identify causal effects. VA does not share microdata on veteran suicide, requiring construction of a matched comparison sample of nonveterans by estimating veteran decedent removal from general population suicide totals within cells of a 5-way table based on publicly released 3-way tables, introducing imprecision. Veteran suicide counts are known to undercount suicides among veterans who separated from the military prior to 1974, likely resulting in a slight underestimate of veteran suicide rates for the oldest cohort of veterans, particularly in earlier study periods. Restricting analysis to identify modeled effects solely through limited changes in state firearm ownership and policies during the study period yields imprecise effect estimates.
DISCLOSURES: This work received support from a grant provided by The RAND Epstein Family Veterans Policy Research Institute, established through a contribution from Daniel J. Epstein via the Epstein Family Foundation. Neither the Institute, the Foundation, nor Mr. Epstein participated in the design, conduct, analysis, or drafting of this report. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Impact of Blast Exposures
Blast exposure has been associated with a wide range of negative outcomes, including alterations in brain structure and function, poorer cognitive functioning, and increased severity of psychiatric and health symptoms. Long-term effects also include chronic secondary downstream effects, such as neuroinflammation, neurotoxicity, cellular senescence, and neurodegeneration.
Now, a recent US Department of Veterans Affairs (VA) study of 114 post-9/11 combat veterans suggests that lifetime blast exposure severity is independently associated with accelerated epigenetic aging, even after accounting for PTSD and TBI. The field of epigenetics refers to how environment influences genes by changing the chemicals attached to them.
This cross-sectional study analyzed participants enrolled in 2 coordinated VA research protocols: the Chronic Effects of Neurotrauma Consortium Study 34 and the Post-Deployment Mental Health Study. Researchers measured biological aging using DunedinPACE, an epigenetic biomarker derived from whole-blood DNA methylation data.
Greater blast exposure severity was significantly associated with faster DunedinPACE. Mild TBI history was also independently associated with faster aging, whereas PTSD diagnosis was not. No significant interaction effects were observed. Exploratory analyses suggested that higher-intensity and more frequent blast exposures contributed to more accelerated aging.
The researchers said their findings suggest that accelerated biological aging may represent a pathway linking blast exposure to increased vulnerability for age-related disease and could inform early identification of at-risk veterans.
Preclinical work has “undeniably demonstrated that primary blast forces can directly induce neurotrauma with associated, ongoing symptoms,” according to the authors of a 2024 study. “[H]owever, these findings have not translated into clinical work.” Most human studies of blast exposure use data obtained from assessments of TBI. That approach is limited, they said, because blast exposure does not always result in symptoms of concussion or TBI, and clinical symptoms of TBI are not necessary for blast-induced neurotrauma to occur.
Moreover, understanding how and why blast exposure often results in negative consequences is still lagging, and interventions and treatments have lagged comparatively, the researchers noted. In large part, they added, this is because there is no broadly endorsed definition of blast exposure. They illustrated their point with examples of terms used in earlier research: blast TBI, primary blast TBI, pressure severity, distance from the blast, and frequency of exposure. The lack of standardized language, they suggested, “prevents synthesis of existing literature into a cohesive understanding of the field.”
Those researchers called for concerted and collaborative efforts to advance the study of blast exposure, including developing a standardized definition of blast exposure and curating an empirical literature base allowing clear comparisons of results across studies. They also urged raising awareness about blast-related negative outcomes with education at all levels: continuing education opportunities, round tables at annual conference meetings, grand rounds in hospital or academic medical center settings, and journal clubs.
Blast exposure has been associated with a wide range of negative outcomes, including alterations in brain structure and function, poorer cognitive functioning, and increased severity of psychiatric and health symptoms. Long-term effects also include chronic secondary downstream effects, such as neuroinflammation, neurotoxicity, cellular senescence, and neurodegeneration.
Now, a recent US Department of Veterans Affairs (VA) study of 114 post-9/11 combat veterans suggests that lifetime blast exposure severity is independently associated with accelerated epigenetic aging, even after accounting for PTSD and TBI. The field of epigenetics refers to how environment influences genes by changing the chemicals attached to them.
This cross-sectional study analyzed participants enrolled in 2 coordinated VA research protocols: the Chronic Effects of Neurotrauma Consortium Study 34 and the Post-Deployment Mental Health Study. Researchers measured biological aging using DunedinPACE, an epigenetic biomarker derived from whole-blood DNA methylation data.
Greater blast exposure severity was significantly associated with faster DunedinPACE. Mild TBI history was also independently associated with faster aging, whereas PTSD diagnosis was not. No significant interaction effects were observed. Exploratory analyses suggested that higher-intensity and more frequent blast exposures contributed to more accelerated aging.
The researchers said their findings suggest that accelerated biological aging may represent a pathway linking blast exposure to increased vulnerability for age-related disease and could inform early identification of at-risk veterans.
Preclinical work has “undeniably demonstrated that primary blast forces can directly induce neurotrauma with associated, ongoing symptoms,” according to the authors of a 2024 study. “[H]owever, these findings have not translated into clinical work.” Most human studies of blast exposure use data obtained from assessments of TBI. That approach is limited, they said, because blast exposure does not always result in symptoms of concussion or TBI, and clinical symptoms of TBI are not necessary for blast-induced neurotrauma to occur.
Moreover, understanding how and why blast exposure often results in negative consequences is still lagging, and interventions and treatments have lagged comparatively, the researchers noted. In large part, they added, this is because there is no broadly endorsed definition of blast exposure. They illustrated their point with examples of terms used in earlier research: blast TBI, primary blast TBI, pressure severity, distance from the blast, and frequency of exposure. The lack of standardized language, they suggested, “prevents synthesis of existing literature into a cohesive understanding of the field.”
Those researchers called for concerted and collaborative efforts to advance the study of blast exposure, including developing a standardized definition of blast exposure and curating an empirical literature base allowing clear comparisons of results across studies. They also urged raising awareness about blast-related negative outcomes with education at all levels: continuing education opportunities, round tables at annual conference meetings, grand rounds in hospital or academic medical center settings, and journal clubs.
Blast exposure has been associated with a wide range of negative outcomes, including alterations in brain structure and function, poorer cognitive functioning, and increased severity of psychiatric and health symptoms. Long-term effects also include chronic secondary downstream effects, such as neuroinflammation, neurotoxicity, cellular senescence, and neurodegeneration.
Now, a recent US Department of Veterans Affairs (VA) study of 114 post-9/11 combat veterans suggests that lifetime blast exposure severity is independently associated with accelerated epigenetic aging, even after accounting for PTSD and TBI. The field of epigenetics refers to how environment influences genes by changing the chemicals attached to them.
This cross-sectional study analyzed participants enrolled in 2 coordinated VA research protocols: the Chronic Effects of Neurotrauma Consortium Study 34 and the Post-Deployment Mental Health Study. Researchers measured biological aging using DunedinPACE, an epigenetic biomarker derived from whole-blood DNA methylation data.
Greater blast exposure severity was significantly associated with faster DunedinPACE. Mild TBI history was also independently associated with faster aging, whereas PTSD diagnosis was not. No significant interaction effects were observed. Exploratory analyses suggested that higher-intensity and more frequent blast exposures contributed to more accelerated aging.
The researchers said their findings suggest that accelerated biological aging may represent a pathway linking blast exposure to increased vulnerability for age-related disease and could inform early identification of at-risk veterans.
Preclinical work has “undeniably demonstrated that primary blast forces can directly induce neurotrauma with associated, ongoing symptoms,” according to the authors of a 2024 study. “[H]owever, these findings have not translated into clinical work.” Most human studies of blast exposure use data obtained from assessments of TBI. That approach is limited, they said, because blast exposure does not always result in symptoms of concussion or TBI, and clinical symptoms of TBI are not necessary for blast-induced neurotrauma to occur.
Moreover, understanding how and why blast exposure often results in negative consequences is still lagging, and interventions and treatments have lagged comparatively, the researchers noted. In large part, they added, this is because there is no broadly endorsed definition of blast exposure. They illustrated their point with examples of terms used in earlier research: blast TBI, primary blast TBI, pressure severity, distance from the blast, and frequency of exposure. The lack of standardized language, they suggested, “prevents synthesis of existing literature into a cohesive understanding of the field.”
Those researchers called for concerted and collaborative efforts to advance the study of blast exposure, including developing a standardized definition of blast exposure and curating an empirical literature base allowing clear comparisons of results across studies. They also urged raising awareness about blast-related negative outcomes with education at all levels: continuing education opportunities, round tables at annual conference meetings, grand rounds in hospital or academic medical center settings, and journal clubs.