User login
New ILD, asthma, and COPD trials
This column presents a sampling of new and still-recruiting trials of interest to pulmonologists and their patients.
Trials are selected based primarily on these conditions: idiopathic pulmonary fibrosis/interstitial lung disease; chronic obstructive pulmonary disease (COPD); asthma; cystic fibrosis; infectious lung diseases; pulmonary artery hypertension; and lung cancer. Links to the studies and contact information are provided for each.
Idiopathic pulmonary fibrosis/interstitial lung disease
A Study to Evaluate Long-term Safety of Nintedanib in Children and Adolescents With Interstitial Lung Disease (InPedILD™-ON): NCT05285982
This nonrandomized, phase 3 study is open to children and adolescents between 6 and 17 years old who have interstitial lung disease with lung fibrosis. It is designed to test how well long-term treatment with nintedanib (a drug already used to treat lung fibrosis in adults) is tolerated in children and adolescents.
A total of 60 study participants will take nintedanib capsules twice a day for at least 2 years or until nintedanib or other treatment options become available outside of the study. There will be 9-11 site visits during the first 2 years and site visits every 3 months afterward.
Study physicians will collect information on any health problems of the participants. The primary outcome measure will be the incidence of treatment-emergent adverse events.
Location: 26 locations in the United States and internationally
Sponsor: Boehringer Ingelheim
Contact: clintriage.rdg@boehringer-ingelheim.com
Study start date: April 2022
Expected completion Date: May 2026
Asthma
A Phase 2, Single-Dose, Randomized, Active and Placebo Controlled, Four-Period, Cross-Over Study of the Safety and Efficacy of Intranasal Epinephrine After Administration of ARS-1 or Albuterol in Subjects With Persistent Asthma: NCT05363670
ARS-1 is a novel aqueous formulation of epinephrine nasal spray. The primary outcomes of this study will be the effect of ARS-1 versus albuterol and placebo from baseline to 1 hour on the difference in forced expiratory volume in 1 second based on area under the curve.
A total of 30 study participants (ages 12-65 years) will be recruited.
Location: Three U.S. locations in Florida, Maryland, and Ohio.
Sponsor: ARS Pharmaceuticals
Contact: rhasson@pacificlinkconsulting.com
Study start date: July 2022
Expected completion Date: November 2022
COPD
Treatment of Pneumocystitis in COPD (the TOPIC Study): NCT05418777
In this randomized, double-blind, placebo-controlled study, the primary outcome will be to determine if treating Pneumocystis jirovecii in acute exacerbations of COPD with confirmed P. jirovecii colonization has a beneficial clinical impact. As a secondary goal of the study, it will be determined if the addition of trimethoprim-sulfamethoxazole (TMP-SMX) to standard of care can decolonize these patients and if the decolonization is durable for at least 3 months.
A total of 30 participants aged 40-89 years will be randomized to receive either a suspension with the equivalent of one double-strength TMP-SMX or a suspension with placebo by mouth every 12 hours. If the participant is discharged prior to completing the 10-day course of the medication, they will be sent home with the remaining study medication and a medication diary which will be collected.
Location: William Beaumont Hospital, Royal Oak, Mich.
Sponsor: William Beaumont Hospitals
Contact: matthew.sims@beaumont.edu
Study start date: July 2022
Expected completion Date: August 2023
Inter-lobar Fissure Completion in Patients With Failed Bronchoscopic Lung Volume Reduction (SAVED-1): NCT05257681
This study is intended to be a pilot prospective controlled clinical trial to evaluate the potential role of a lung fissure completion with pleural adhesiolysis strategy (experimental intervention) in severe emphysema/COPD patients with failed bronchoscopic lung volume reduction via the use of endobronchial valves therapy.
In 20 select patients (ages 40-75 years), the lung fissure completion with adhesiolysis strategy will be performed by video-assisted thoracoscopic surgery guided stapling along the lung fissures to reduce collateral ventilation with adhesions removal. The primary outcomes will be to prove that interlobar fissures can be completed to at least 95% in severe emphysema patients with previously failed bronchoscopic lung volume reduction over a 2 year period and the occurrence of adverse events in that period. The surgery will be considered feasible if the target inter-lobar fissure can be completed in at least 90% of the patients enrolled. Secondary outcomes over 2 years will include quality of life improvement and the percentage of patients with significant changes in pulmonary function testing.
Location: Beth Deaconess Medical Center, Boston
Sponsor: Beth Israel Deaconess Medical Center
Contact: amajid@bidmc.harvard.edu
Study start date: May 2022
Expected completion Date: May 2024
This column presents a sampling of new and still-recruiting trials of interest to pulmonologists and their patients.
Trials are selected based primarily on these conditions: idiopathic pulmonary fibrosis/interstitial lung disease; chronic obstructive pulmonary disease (COPD); asthma; cystic fibrosis; infectious lung diseases; pulmonary artery hypertension; and lung cancer. Links to the studies and contact information are provided for each.
Idiopathic pulmonary fibrosis/interstitial lung disease
A Study to Evaluate Long-term Safety of Nintedanib in Children and Adolescents With Interstitial Lung Disease (InPedILD™-ON): NCT05285982
This nonrandomized, phase 3 study is open to children and adolescents between 6 and 17 years old who have interstitial lung disease with lung fibrosis. It is designed to test how well long-term treatment with nintedanib (a drug already used to treat lung fibrosis in adults) is tolerated in children and adolescents.
A total of 60 study participants will take nintedanib capsules twice a day for at least 2 years or until nintedanib or other treatment options become available outside of the study. There will be 9-11 site visits during the first 2 years and site visits every 3 months afterward.
Study physicians will collect information on any health problems of the participants. The primary outcome measure will be the incidence of treatment-emergent adverse events.
Location: 26 locations in the United States and internationally
Sponsor: Boehringer Ingelheim
Contact: clintriage.rdg@boehringer-ingelheim.com
Study start date: April 2022
Expected completion Date: May 2026
Asthma
A Phase 2, Single-Dose, Randomized, Active and Placebo Controlled, Four-Period, Cross-Over Study of the Safety and Efficacy of Intranasal Epinephrine After Administration of ARS-1 or Albuterol in Subjects With Persistent Asthma: NCT05363670
ARS-1 is a novel aqueous formulation of epinephrine nasal spray. The primary outcomes of this study will be the effect of ARS-1 versus albuterol and placebo from baseline to 1 hour on the difference in forced expiratory volume in 1 second based on area under the curve.
A total of 30 study participants (ages 12-65 years) will be recruited.
Location: Three U.S. locations in Florida, Maryland, and Ohio.
Sponsor: ARS Pharmaceuticals
Contact: rhasson@pacificlinkconsulting.com
Study start date: July 2022
Expected completion Date: November 2022
COPD
Treatment of Pneumocystitis in COPD (the TOPIC Study): NCT05418777
In this randomized, double-blind, placebo-controlled study, the primary outcome will be to determine if treating Pneumocystis jirovecii in acute exacerbations of COPD with confirmed P. jirovecii colonization has a beneficial clinical impact. As a secondary goal of the study, it will be determined if the addition of trimethoprim-sulfamethoxazole (TMP-SMX) to standard of care can decolonize these patients and if the decolonization is durable for at least 3 months.
A total of 30 participants aged 40-89 years will be randomized to receive either a suspension with the equivalent of one double-strength TMP-SMX or a suspension with placebo by mouth every 12 hours. If the participant is discharged prior to completing the 10-day course of the medication, they will be sent home with the remaining study medication and a medication diary which will be collected.
Location: William Beaumont Hospital, Royal Oak, Mich.
Sponsor: William Beaumont Hospitals
Contact: matthew.sims@beaumont.edu
Study start date: July 2022
Expected completion Date: August 2023
Inter-lobar Fissure Completion in Patients With Failed Bronchoscopic Lung Volume Reduction (SAVED-1): NCT05257681
This study is intended to be a pilot prospective controlled clinical trial to evaluate the potential role of a lung fissure completion with pleural adhesiolysis strategy (experimental intervention) in severe emphysema/COPD patients with failed bronchoscopic lung volume reduction via the use of endobronchial valves therapy.
In 20 select patients (ages 40-75 years), the lung fissure completion with adhesiolysis strategy will be performed by video-assisted thoracoscopic surgery guided stapling along the lung fissures to reduce collateral ventilation with adhesions removal. The primary outcomes will be to prove that interlobar fissures can be completed to at least 95% in severe emphysema patients with previously failed bronchoscopic lung volume reduction over a 2 year period and the occurrence of adverse events in that period. The surgery will be considered feasible if the target inter-lobar fissure can be completed in at least 90% of the patients enrolled. Secondary outcomes over 2 years will include quality of life improvement and the percentage of patients with significant changes in pulmonary function testing.
Location: Beth Deaconess Medical Center, Boston
Sponsor: Beth Israel Deaconess Medical Center
Contact: amajid@bidmc.harvard.edu
Study start date: May 2022
Expected completion Date: May 2024
This column presents a sampling of new and still-recruiting trials of interest to pulmonologists and their patients.
Trials are selected based primarily on these conditions: idiopathic pulmonary fibrosis/interstitial lung disease; chronic obstructive pulmonary disease (COPD); asthma; cystic fibrosis; infectious lung diseases; pulmonary artery hypertension; and lung cancer. Links to the studies and contact information are provided for each.
Idiopathic pulmonary fibrosis/interstitial lung disease
A Study to Evaluate Long-term Safety of Nintedanib in Children and Adolescents With Interstitial Lung Disease (InPedILD™-ON): NCT05285982
This nonrandomized, phase 3 study is open to children and adolescents between 6 and 17 years old who have interstitial lung disease with lung fibrosis. It is designed to test how well long-term treatment with nintedanib (a drug already used to treat lung fibrosis in adults) is tolerated in children and adolescents.
A total of 60 study participants will take nintedanib capsules twice a day for at least 2 years or until nintedanib or other treatment options become available outside of the study. There will be 9-11 site visits during the first 2 years and site visits every 3 months afterward.
Study physicians will collect information on any health problems of the participants. The primary outcome measure will be the incidence of treatment-emergent adverse events.
Location: 26 locations in the United States and internationally
Sponsor: Boehringer Ingelheim
Contact: clintriage.rdg@boehringer-ingelheim.com
Study start date: April 2022
Expected completion Date: May 2026
Asthma
A Phase 2, Single-Dose, Randomized, Active and Placebo Controlled, Four-Period, Cross-Over Study of the Safety and Efficacy of Intranasal Epinephrine After Administration of ARS-1 or Albuterol in Subjects With Persistent Asthma: NCT05363670
ARS-1 is a novel aqueous formulation of epinephrine nasal spray. The primary outcomes of this study will be the effect of ARS-1 versus albuterol and placebo from baseline to 1 hour on the difference in forced expiratory volume in 1 second based on area under the curve.
A total of 30 study participants (ages 12-65 years) will be recruited.
Location: Three U.S. locations in Florida, Maryland, and Ohio.
Sponsor: ARS Pharmaceuticals
Contact: rhasson@pacificlinkconsulting.com
Study start date: July 2022
Expected completion Date: November 2022
COPD
Treatment of Pneumocystitis in COPD (the TOPIC Study): NCT05418777
In this randomized, double-blind, placebo-controlled study, the primary outcome will be to determine if treating Pneumocystis jirovecii in acute exacerbations of COPD with confirmed P. jirovecii colonization has a beneficial clinical impact. As a secondary goal of the study, it will be determined if the addition of trimethoprim-sulfamethoxazole (TMP-SMX) to standard of care can decolonize these patients and if the decolonization is durable for at least 3 months.
A total of 30 participants aged 40-89 years will be randomized to receive either a suspension with the equivalent of one double-strength TMP-SMX or a suspension with placebo by mouth every 12 hours. If the participant is discharged prior to completing the 10-day course of the medication, they will be sent home with the remaining study medication and a medication diary which will be collected.
Location: William Beaumont Hospital, Royal Oak, Mich.
Sponsor: William Beaumont Hospitals
Contact: matthew.sims@beaumont.edu
Study start date: July 2022
Expected completion Date: August 2023
Inter-lobar Fissure Completion in Patients With Failed Bronchoscopic Lung Volume Reduction (SAVED-1): NCT05257681
This study is intended to be a pilot prospective controlled clinical trial to evaluate the potential role of a lung fissure completion with pleural adhesiolysis strategy (experimental intervention) in severe emphysema/COPD patients with failed bronchoscopic lung volume reduction via the use of endobronchial valves therapy.
In 20 select patients (ages 40-75 years), the lung fissure completion with adhesiolysis strategy will be performed by video-assisted thoracoscopic surgery guided stapling along the lung fissures to reduce collateral ventilation with adhesions removal. The primary outcomes will be to prove that interlobar fissures can be completed to at least 95% in severe emphysema patients with previously failed bronchoscopic lung volume reduction over a 2 year period and the occurrence of adverse events in that period. The surgery will be considered feasible if the target inter-lobar fissure can be completed in at least 90% of the patients enrolled. Secondary outcomes over 2 years will include quality of life improvement and the percentage of patients with significant changes in pulmonary function testing.
Location: Beth Deaconess Medical Center, Boston
Sponsor: Beth Israel Deaconess Medical Center
Contact: amajid@bidmc.harvard.edu
Study start date: May 2022
Expected completion Date: May 2024
Postdeployment Respiratory Health: The Roles of the Airborne Hazards and Open Burn Pit Registry and the Post-Deployment Cardiopulmonary Evaluation Network
Case Example
A 37-year-old female never smoker presents to your clinic with progressive dyspnea over the past 15 years. She reports dyspnea on exertion, wheezing, chronic nasal congestion, and difficulty sleeping that started a year after she returned from military deployment to Iraq. She has been unable to exercise, even at low intensity, for the past 5 years, despite being previously active. She has experienced some symptom improvement by taking an albuterol inhaler as needed, loratadine (10 mg), and fluticasone nasal spray (50 mcg). She occasionally uses famotidine for reflux (40 mg). She deployed to Southwest Asia for 12 months (2002-2003) and was primarily stationed in Qayyarah West, an Air Force base in the Mosul district in northern Iraq. She reports exposure during deployment to the fire in the Al-Mishraq sulfur mine, located approximately 25 km north of Qayyarah West, as well as dust storms and burn pits. She currently works as a medical assistant. Her examination is remarkable for normal bronchovesicular breath sounds without any wheezing or crackles on pulmonary evaluation. Her body mass index is 31. You obtain a chest radiograph and spirometry, which are both normal.
The veteran reports feeling frustrated as she has had multiple specialty evaluations in community clinics without receiving a diagnosis, despite worsening symptoms. She reports that she added her information to the Airborne Hazards and Open Burn Pit Registry (AHOBPR). She recently received a letter from the US Department of Veterans Affairs (VA) Post-Deployment Cardiopulmonary Evaluation Network (PDCEN) and is asking you whether she should participate in the PDCEN specialty evaluation. You are not familiar with the military experiences she has described or the programs she asks you about; however, you would like to know more to best care for your patient.
Background
The year 2021 marked the 20th anniversary of the September 11 attacks and the launch of the Global War on Terrorism. Almost 3 million US military personnel have been deployed in support of these operations along with about 300,000 US civilian contractors and thousands of troops from more than 40 nations.1-3
Respiratory hazards associated with deployment to Southwest Asia and Afghanistan are unique and varied. These exposures include blast injuries and a variety of particulate matter sources, such as burn pit combustion byproducts, aeroallergens, and dust storms.7,8,15,16 One air sampling study conducted at 15 deployment sites in Southwest Asia and Afghanistan found mean fine particulate matter (PM2.5) levels were as much as 10 times greater than sampling sites in both rural and urban cities in the United States; all sites sampled exceeded military exposure guidelines (65 µg/m3 for 1 year).17,18 Long-term exposure to PM2.5 has been associated with the development of chronic respiratory and cardiovascular disease; therefore, there has been considerable attention to the respiratory (and nonrespiratory) health of deployed military personnel.19
Concerns regarding the association between deployment and lung disease led to the creation of the national VA Airborne Hazards and Open Burn Pit Registry (AHOBPR) in 2014 and consists of (1) an online questionnaire to document deployment and medical history, exposure concerns, and symptoms; and (2) an optional in-person or virtual clinical health evaluation at the individual’s local VA medical center or military treatment facility (MTF). As of March 2022, more than 300,000 individuals have completed the online questionnaire of which about 30% declined the optional clinical health evaluation.
The clinical evaluation available to AHOBPR participants has not yet been described in the literature. Therefore, our objectives are to examine AHOBPR clinical evaluation data and review its application throughout the VA. In addition, we will also describe a parallel effort by the VA PDCEN, which is to provide comprehensive multiday clinical evaluations for unique AHOBPR participants with unexplained dyspnea and self-reported respiratory disease. A secondary aim of this publication is to disseminate information to health care professionals (HCPs) within and outside of the VA to aid in the referral and evaluation of previously deployed veterans who experience unexplained dyspnea.
AHOBPR Overview
The AHOBPR is an online questionnaire and optional in-person health evaluation that includes 7 major categories targeting deployment history, symptoms, medical history, health concerns, residential history, nonmilitary occupational history, nonmilitary environmental exposures, and health care utilization. The VA Defense Information Repository is used to obtain service dates for the service member/veteran, conflict involvement, and primary location during deployment. The questionnaire portion of the AHOBPR is administered online. It currently is open to all veterans who served in the Southwest Asia theater of operations (including Iraq, Kuwait, and Egypt) any time after August 2, 1990, or Afghanistan, Djibouti, Syria, or Uzbekistan after September 11, 2001. Veterans are eligible for completing the AHOBPR and optional health evaluation at no cost to the veteran regardless of VA benefits or whether they are currently enrolled in VA health care. Though the focus of the present manuscript is to profile a VA program, it is important to note that the US Department of Defense (DoD) is an active partner with the VA in the promotion of the AHOBPR to service members and similarly provides health evaluations for active-duty service members (including activating Reserve and Guard) through their local MTF.
We reviewed and analyzed AHOBPR operations and VA data from 2014 to 2020. Our analyses were limited to veterans seeking evaluation as well as their corresponding symptoms and HCP’s clinical impression from the electronic health record. As of September 20, 2021, 267,125 individuals completed the AHOBPR. The mean age was 43 years (range, 19-84), and the majority were male (86%) and served in the Army (58%). Open-air burn pits (91%), engine maintenance (38.8%), and convoy operations (71.7%) were the most common deployment-related exposures.
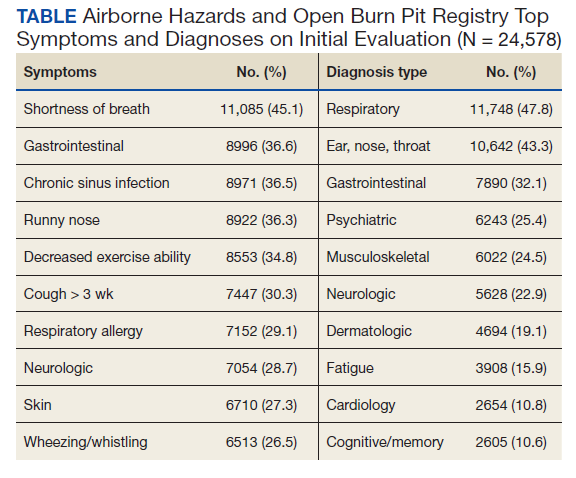
The optional in-person AHOBPR health evaluation may be requested by the veteran after completing the online questionnaire and is performed at the veteran’s local VA facility. The evaluation is most often completed by an environmental health clinician or primary care practitioner (PCP). A variety of resources are available to providers for training on this topic, including fact sheets, webinars, monthly calls, conferences, and accredited e-learning.20 As part of the clinical evaluation, the veteran’s chief concerns are assessed and evaluated. At the time of our analysis, 24,578 clinical examinations were performed across 126 VA medical facilities, with considerable geographic variation. Veterans receiving evaluations were predominantly male (89%) with a median age of 46.0 years (IQR, 15). Veterans’ major respiratory concerns included dyspnea (45.1%), decreased exercise ability (34.8%), and cough > 3 weeks (30.3%) (Table). After clinical evaluation by a VA or MTF HCP, 47.8% were found to have a respiratory diagnosis, including asthma (30.1%), COPD (12.8%), and bronchitis (11.9%).
Registry participants who opt to receive the clinical evaluation may benefit directly by undergoing a detailed clinical history and physical examination as well as having the opportunity to document their health concerns. For some, clinicians may need to refer veterans for additional specialty testing beyond this standard AHOBPR clinical evaluation. Although these evaluations can help address some of the veterans’ concerns, a substantial number may have unexplained respiratory symptoms that warrant further investigation.
Post-Deployment Cardiopulmonary Evaluation Network Clinical Evaluation
In May 2019, the VA established the Airborne Hazards and Burn Pits Center of Excellence (AHBPCE). One of the AHBPCE’s objectives is to deliver specialized care and consultation for veterans with concerns about their postdeployment health, including, but not limited to, unexplained dyspnea. To meet this objective, the AHBPCE developed the PDCEN, a national network consisting of specialty HCPs from 5 VA medical centers—located in San Francisco, California; Denver, Colorado; Baltimore, Maryland; Ann Arbor, Michigan; and East Orange, New Jersey. Collectively, the PDCEN has developed a standardized approach for the comprehensive clinical evaluation of unexplained dyspnea that is implemented uniformly across sites. Staff at the PDCEN screen the AHOBPR to identify veterans with features of respiratory disease and invite them to participate in an in-person evaluation at the nearest PDCEN site. Given the specialty expertise (detailed below) within the Network, the PDCEN focuses on complex cases that are resource intensive. To address complex cases of unexplained dyspnea, the PDCEN has developed a core clinical evaluation approach (Figure).
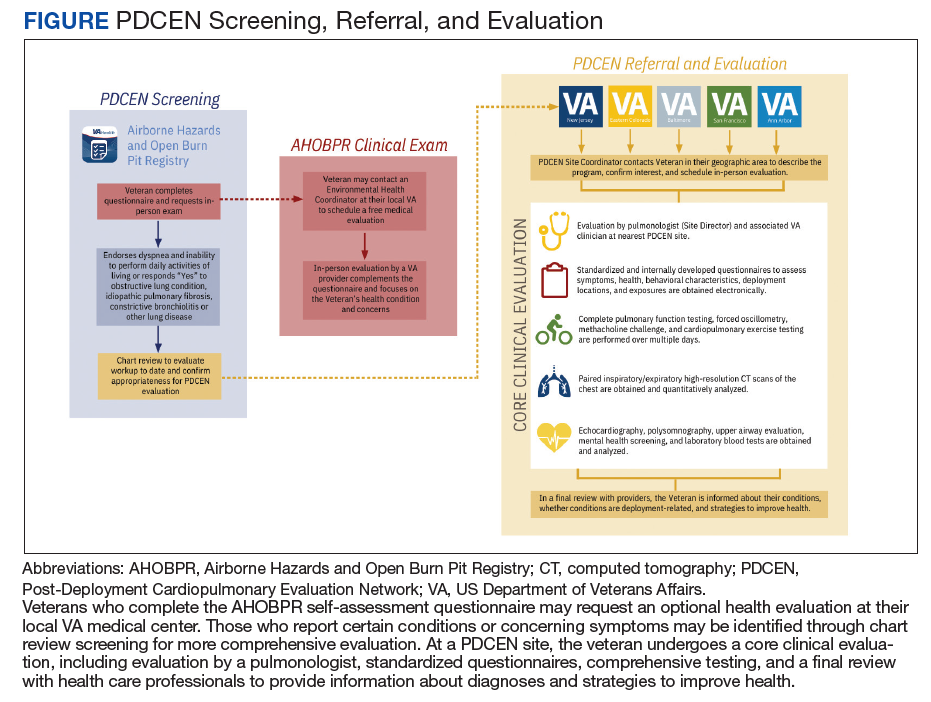
The first step in a veteran’s PDCEN evaluation entails a set of detailed questionnaires that request information about the veteran’s current respiratory, sleep, and mental health symptoms and any associated medical diagnoses. Questionnaires also identify potential exposures to military burn pits, sulfur mine and oil field fires, diesel exhaust fumes, dust storms, urban pollution, explosions/blasts, and chemical weapons. In addition, the questionnaires include deployment geographic location, which may inform future estimates of particulate matter exposure.21 Prior VA and non-VA evaluations and testing of their respiratory concerns are obtained for review. Exposure and health records from the DoD are also reviewed when available.
The next step in the PDCEN evaluation comprises comprehensive testing, including complete pulmonary function testing, methacholine challenge, cardiopulmonary exercise testing, forced oscillometry and exhaled nitric oxide testing, paired high-resolution inspiratory and expiratory chest computed tomography (CT) imaging, sinus CT imaging, direct flexible laryngoscopy, echocardiography, polysomnography, and laboratory blood testing. The testing process is managed by local site coordinators and varies by institution based on availability of each testing modality and subspecialist appointments.
Once testing is completed, the veteran is evaluated by a team of HCPs, including physicians from the disciplines of pulmonary medicine, environmental and occupational health, sleep medicine, otolaryngology and speech pathology, and mental health (when appropriate). After the clinical evaluation has been completed, this team of expert HCPs at each site convenes to provide a final summary review visit intended to be a comprehensive assessment of the veteran’s primary health concerns. The 3 primary objectives of this final review are to inform the veteran of (1) what respiratory and related conditions they have; (2) whether the conditions is/are deployment related; and (3) what treatments and/or follow-up care may enhance their current state of health in partnership with their local HCPs. The PDCEN does not provide ongoing management of any conditions identified during the veteran’s evaluation but communicates findings and recommendations to the veteran and their PCP for long-term care.
Discussion
The AHOBPR was established in response to mounting concerns that service members and veterans were experiencing adverse health effects that might be attributable to deployment-related exposures. Nearly half of all patients currently enrolled in the AHOBPR report dyspnea, and about one-third have decreased exercise tolerance and/or cough. Of those who completed the questionnaire and the subsequent in-person and generalized AHOBPR examination, our interim analysis showed that about half were assigned a respiratory diagnosis. Yet for many veterans, their breathing symptoms remained unexplained or did not respond to treatment.
While the AHOBPR and related examinations address the needs of many veterans, others may require more comprehensive examination. The PDCEN attends to the latter by providing more detailed and comprehensive clinical evaluations of veterans with deployment-related respiratory health concerns and seeks to learn from these evaluations by analyzing data obtained from veterans across sites. As such, the PDCEN hopes not only to improve the health of individual veterans, but also create standard practices for both VA and non-VA community evaluation of veterans exposed to respiratory hazards during deployment.
One of the major challenges in the field of postdeployment respiratory health is the lack of clear universal language or case definitions that encompass the veteran’s clinical concerns. In an influential case series published in 2011, 38 (77%) of 49 soldiers with history of airborne hazard exposure and unexplained exercise intolerance were reported to have histopathology consistent with constrictive bronchiolitis on surgical lung biopsy.14 Subsequent publications have described other histopathologic features in deployed military personnel, including granulomatous inflammation, interstitial lung disease, emphysema, and pleuritis.12-14 Reconciling these findings from surgical lung biopsy with the clinical presentation and noninvasive studies has proved difficult. Therefore, several groups of investigators have proposed terms, including postdeployment respiratory syndrome, deployment-related distal lung disease, and Iraq/Afghanistan War lung injury to describe the increased respiratory symptoms and variety of histopathologic and imaging findings in this population.9,12,22 At present, there remains a lack of consensus on terminology and case definitions as well as the role of military environmental exposures in exacerbating and/or causing these conditions. As HCPs, it is important to appreciate and acknowledge that the ambiguity and controversy pertaining to terminology, causation, and service connections are a common source of frustration experienced by veterans, which are increasingly reflected among reports in popular media and lay press.
A second and related challenge in the field of postdeployment respiratory health that contributes to veteran and HCP frustration is that many of the aforementioned abnormalities described on surgical lung biopsy are not readily identifiable on noninvasive tests, including traditional interpretation of pulmonary function tests or chest CT imaging.12-14,22 Thus, underlying conditions could be overlooked and veterans’ concerns and symptoms may be dismissed or misattributed to other comorbid conditions. While surgical lung biopsies may offer diagnostic clarity in identifying lung disease, there are significant procedural risks of surgical and anesthetic complications. Furthermore, a definitive diagnosis does not necessarily guarantee a clear treatment plan. For example, there are no current therapies approved by the US Food and Drug Administration for the treatment of constrictive bronchiolitis.
Research efforts are underway, including within the PDCEN, to evaluate a more sensitive and noninvasive assessment of the small airways that may even reduce or eliminate the need for surgical lung biopsy. In contrast to traditional pulmonary function testing, which is helpful for evaluation of the larger airways, forced oscillation technique can be used noninvasively, using pressure oscillations to evaluate for diseases of the smaller airways and has been used in the veteran population and in those exposed to dust from the World Trade Center disaster.23-25 Multiple breath washout technique provides a lung clearance index that is determined by the number of lung turnovers it takes to clear the lungs of an inert gas (eg, sulfur hexafluoride, nitrogen). Elevated lung clearance index values suggest ventilation heterogeneity and have been shown to be higher among deployed veterans with dyspnea.26,27 Finally, advanced CT analytic techniques may help identify functional small airways disease and are higher in deployed service members with constrictive bronchiolitis on surgical lung biopsy.28 These innovative noninvasive techniques are experimental but promising, especially as part of a broader evaluation of small airways disease.
AHOBPR clinical evaluations represent an initial step to better understand postdeployment health conditions available to all AHOBPR participants. The PDCEN clinical evaluation extends the AHOBPR evaluation by providing specialty care for certain veterans requiring more comprehensive evaluation while systematically collecting and analyzing clinical data to advance the field. The VA is committed to leveraging these data and all available expertise to provide a clear description of the spectrum of disease in this population and improve our ability to diagnose, follow, and treat respiratory health conditions occurring after deployment to Southwest Asia and Afghanistan.
Case Conclusion
The veteran was referred to a PDCEN site and underwent a comprehensive multidisciplinary evaluation. Pulmonary function testing showed lung volumes and vital capacity within the predicted normal range, mild air trapping, and a low diffusion capacity for carbon monoxide. Methacholine challenge testing was normal; however, forced oscillometry suggested small airways obstruction. A high-resolution CT showed air trapping without parenchymal changes. Cardiopulmonary exercise testing demonstrated a peak exercise capacity within the predicted normal range but low breathing reserve. Otolaryngology evaluation including laryngoscopy suggested chronic nonallergic rhinitis.
At the end of the veteran’s evaluation, a summary review reported nonallergic rhinitis and distal airway obstruction consistent with small airways disease. Both were reported as most likely related to deployment given her significant environmental exposures and the temporal relationship with her deployment and symptom onset as well as lack of other identifiable causes. A more precise histopathologic diagnosis could be firmly established with a surgical lung biopsy, but after shared decision making with a PDCEN HCP, the patient declined to undergo this invasive procedure. After you review the summary review and recommendations from the PDCEN group, you start the veteran on intranasal steroids and a combined inhaled corticosteroid/long-acting β agonist inhaler as well as refer the veteran to pulmonary rehabilitation. After several weeks, she reports an improvement in sleep and nasal symptoms but continues to experience residual exercise intolerance.
This case serves as an example of the significant limitations that a previously active and healthy patient can develop after deployment to Southwest Asia and Afghanistan. Encouraging this veteran to complete the AHOBPR allowed her to be considered for a PDCEN evaluation that provided the opportunity to undergo a comprehensive noninvasive evaluation of her chronic dyspnea. In doing so, she obtained 2 important diagnoses and data from her evaluation will help establish best practices for standardized evaluations of respiratory concerns following deployment. Through the AHOBPR and PDCEN, the VA seeks to better understand postdeployment health conditions, their relationship to military and environmental exposures, and how best to diagnose and treat these conditions.
Acknowledgments
This work was supported by the US Department of Veterans Affairs (VA) Airborne Hazards and Burn Pits Center of Excellence (Public Law 115-929). The authors acknowledge support and contributions from Dr. Eric Shuping and leadership at VA’s Health Outcomes Military Exposures office as well as the New Jersey War Related Illness and Injury Study Center. In addition, we thank Erin McRoberts and Rajeev Swarup for their contributions to the Post-Deployment Cardiopulmonary Evaluation Network. Post-Deployment Cardiopulmonary Evaluation Network members:
Mehrdad Arjomandi, Caroline Davis, Michelle DeLuca, Nancy Eager, Courtney A. Eberhardt, Michael J. Falvo, Timothy Foley, Fiona A.S. Graff, Deborah Heaney, Stella E. Hines, Rachel E. Howard, Nisha Jani, Sheena Kamineni, Silpa Krefft, Mary L. Langlois, Helen Lozier, Simran K. Matharu, Anisa Moore, Lydia Patrick-DeLuca, Edward Pickering, Alexander Rabin, Michelle Robertson, Samantha L. Rogers, Aaron H. Schneider, Anand Shah, Anays Sotolongo, Jennifer H. Therkorn, Rebecca I. Toczylowski, Matthew Watson, Alison D. Wilczynski, Ian W. Wilson, Romi A. Yount.
1. Wenger J, O’Connell C, Cottrell L. Examination of recent deployment experience across the services and components. Exam. RAND Corporation; 2018. Accessed June 27, 2022. doi:10.7249/rr1928
2. Torreon BS. U.S. periods of war and dates of recent conflicts, RS21405. Congressional Research Service; 2017. June 5, 2020. Accessed June 27, 2022. https://crsreports.congress.gov/product/details?prodcode=RS21405
3. Dunigan M, Farmer CM, Burns RM, Hawks A, Setodji CM. Out of the shadows: the health and well-being of private contractors working in conflict environments. RAND Corporation; 2013. Accessed June 27, 2022. https://www.rand.org/pubs/research_reports/RR420.html
4. Szema AM, Peters MC, Weissinger KM, Gagliano CA, Chen JJ. New-onset asthma among soldiers serving in Iraq and Afghanistan. Allergy Asthma Proc. 2010;31(5):67-71. doi:10.2500/aap.2010.31.3383
5. Pugh MJ, Jaramillo CA, Leung KW, et al. Increasing prevalence of chronic lung disease in veterans of the wars in Iraq and Afghanistan. Mil Med. 2016;181(5):476-481. doi:10.7205/MILMED-D-15-00035
6. Falvo MJ, Osinubi OY, Sotolongo AM, Helmer DA. Airborne hazards exposure and respiratory health of Iraq and Afghanistan veterans. Epidemiol Rev. 2015;37:116-130. doi:10.1093/epirev/mxu009
7. McAndrew LM, Teichman RF, Osinubi OY, Jasien JV, Quigley KS. Environmental exposure and health of Operation Enduring Freedom/Operation Iraqi Freedom veterans. J Occup Environ Med. 2012;54(6):665-669. doi:10.1097/JOM.0b013e318255ba1b
8. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. doi:10.1093/aje/kwp287
9. Szema AM, Salihi W, Savary K, Chen JJ. Respiratory symptoms necessitating spirometry among soldiers with Iraq/Afghanistan war lung injury. J Occup Environ Med. 2011;53(9):961-965. doi:10.1097/JOM.0b013e31822c9f05
10. Committee on the Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan; Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. Accessed June 27, 2022. doi:10.17226/1320911. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. Accessed June 27, 2022. doi:10.17226/25837
12. Krefft SD, Wolff J, Zell-Baran L, et al. Respiratory diseases in post-9/11 military personnel following Southwest Asia deployment. J Occup Environ Med. 2020;62(5):337-343. doi:10.1097/JOM.0000000000001817
13. Gordetsky J, Kim C, Miller RF, Mehrad M. Non-necrotizing granulomatous pneumonitis and chronic pleuritis in soldiers deployed to Southwest Asia. Histopathology. 2020;77(3):453-459. doi:10.1111/his.14135
14. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. doi:10.1056/NEJMoa1101388
15. Helmer DA, Rossignol M, Blatt M, Agarwal R, Teichman R, Lange G. Health and exposure concerns of veterans deployed to Iraq and Afghanistan. J Occup Environ Med. 2007;49(5):475-480. doi:10.1097/JOM.0b013e318042d682
16. Kim YH, Warren SH, Kooter I, et al. Chemistry, lung toxicity and mutagenicity of burn pit smoke-related particulate matter. Part Fibre Toxicol. 2021;18(1):45. Published 2021 Dec 16. doi:10.1186/s12989-021-00435-w
17. Engelbrecht JP, McDonald EV, Gillies JA, Jayanty RK, Casuccio G, Gertler AW. Characterizing mineral dusts and other aerosols from the Middle East—Part 1: ambient sampling. Inhal Toxicol. 2009;21(4):297-326. doi:10.1080/08958370802464273
18. US Army Public Health Command. Technical guide 230: environmental health risk assessment and chemical exposure guidelines for deployed military personnel, 2013 revision. Accessed June 27, 2022. https://phc.amedd.army.mil/PHC%20Resource%20Library/TG230-DeploymentEHRA-and-MEGs-2013-Revision.pdf
19. Anderson JO, Thundiyil JG, Stolbach A. Clearing the air: a review of the effects of particulate matter air pollution on human health. J Med Toxicol. 2012;8(2):166-175. doi:10.1007/s13181-011-0203-1
20. Shuping E, Schneiderman A. Resources on environmental exposures for military veterans. Am Fam Physician. 2020;101(12):709-710.
21. Masri S, Garshick E, Coull BA, Koutrakis P. A novel calibration approach using satellite and visibility observations to estimate fine particulate matter exposures in Southwest Asia and Afghanistan. J Air Waste Manag Assoc. 2017;67(1):86-95. doi:10.1080/10962247.2016.1230079
22. Gutor SS, Richmond BW, Du RH, et al. Postdeployment respiratory syndrome in soldiers with chronic exertional dyspnea. Am J Surg Pathol. 2021;45(12):1587-1596. doi:10.1097/PAS.0000000000001757
23. Goldman MD, Saadeh C, Ross D. Clinical applications of forced oscillation to assess peripheral airway function. Respir Physiol Neurobiol. 2005;148(1-2):179-194. doi:10.1016/j.resp.2005.05.026
24. Butzko RP, Sotolongo AM, Helmer DA, et al. Forced oscillation technique in veterans with preserved spirometry and chronic respiratory symptoms. Respir Physiol Neurobiol. 2019;260:8-16. doi:10.1016/j.resp.2018.11.012
25. Oppenheimer BW, Goldring RM, Herberg ME, et al. Distal airway function in symptomatic subjects with normal spirometry following World Trade Center dust exposure. Chest. 2007;132(4):1275-1282. doi:10.1378/chest.07-0913
26. Zell-Baran LM, Krefft SD, Moore CM, Wolff J, Meehan R, Rose CS. Multiple breath washout: a noninvasive tool for identifying lung disease in symptomatic military deployers. Respir Med. 2021;176:106281. doi:10.1016/j.rmed.2020.106281
27. Krefft SD, Strand M, Smith J, Stroup C, Meehan R, Rose C. Utility of lung clearance index testing as a noninvasive marker of deployment-related lung disease. J Occup Environ Med. 2017;59(8):707-711. doi:10.1097/JOM.000000000000105828. Davis CW, Lopez CL, Bell AJ, et al. The severity of functional small airways disease in military personnel with constrictive bronchiolitis as measured by quantitative CT [published online ahead of print, 2022 May 24]. Am J Respir Crit Care Med. 2022;10.1164/rccm.202201-0153LE. doi:10.1164/rccm.202201-0153LE
Case Example
A 37-year-old female never smoker presents to your clinic with progressive dyspnea over the past 15 years. She reports dyspnea on exertion, wheezing, chronic nasal congestion, and difficulty sleeping that started a year after she returned from military deployment to Iraq. She has been unable to exercise, even at low intensity, for the past 5 years, despite being previously active. She has experienced some symptom improvement by taking an albuterol inhaler as needed, loratadine (10 mg), and fluticasone nasal spray (50 mcg). She occasionally uses famotidine for reflux (40 mg). She deployed to Southwest Asia for 12 months (2002-2003) and was primarily stationed in Qayyarah West, an Air Force base in the Mosul district in northern Iraq. She reports exposure during deployment to the fire in the Al-Mishraq sulfur mine, located approximately 25 km north of Qayyarah West, as well as dust storms and burn pits. She currently works as a medical assistant. Her examination is remarkable for normal bronchovesicular breath sounds without any wheezing or crackles on pulmonary evaluation. Her body mass index is 31. You obtain a chest radiograph and spirometry, which are both normal.
The veteran reports feeling frustrated as she has had multiple specialty evaluations in community clinics without receiving a diagnosis, despite worsening symptoms. She reports that she added her information to the Airborne Hazards and Open Burn Pit Registry (AHOBPR). She recently received a letter from the US Department of Veterans Affairs (VA) Post-Deployment Cardiopulmonary Evaluation Network (PDCEN) and is asking you whether she should participate in the PDCEN specialty evaluation. You are not familiar with the military experiences she has described or the programs she asks you about; however, you would like to know more to best care for your patient.
Background
The year 2021 marked the 20th anniversary of the September 11 attacks and the launch of the Global War on Terrorism. Almost 3 million US military personnel have been deployed in support of these operations along with about 300,000 US civilian contractors and thousands of troops from more than 40 nations.1-3
Respiratory hazards associated with deployment to Southwest Asia and Afghanistan are unique and varied. These exposures include blast injuries and a variety of particulate matter sources, such as burn pit combustion byproducts, aeroallergens, and dust storms.7,8,15,16 One air sampling study conducted at 15 deployment sites in Southwest Asia and Afghanistan found mean fine particulate matter (PM2.5) levels were as much as 10 times greater than sampling sites in both rural and urban cities in the United States; all sites sampled exceeded military exposure guidelines (65 µg/m3 for 1 year).17,18 Long-term exposure to PM2.5 has been associated with the development of chronic respiratory and cardiovascular disease; therefore, there has been considerable attention to the respiratory (and nonrespiratory) health of deployed military personnel.19
Concerns regarding the association between deployment and lung disease led to the creation of the national VA Airborne Hazards and Open Burn Pit Registry (AHOBPR) in 2014 and consists of (1) an online questionnaire to document deployment and medical history, exposure concerns, and symptoms; and (2) an optional in-person or virtual clinical health evaluation at the individual’s local VA medical center or military treatment facility (MTF). As of March 2022, more than 300,000 individuals have completed the online questionnaire of which about 30% declined the optional clinical health evaluation.
The clinical evaluation available to AHOBPR participants has not yet been described in the literature. Therefore, our objectives are to examine AHOBPR clinical evaluation data and review its application throughout the VA. In addition, we will also describe a parallel effort by the VA PDCEN, which is to provide comprehensive multiday clinical evaluations for unique AHOBPR participants with unexplained dyspnea and self-reported respiratory disease. A secondary aim of this publication is to disseminate information to health care professionals (HCPs) within and outside of the VA to aid in the referral and evaluation of previously deployed veterans who experience unexplained dyspnea.
AHOBPR Overview
The AHOBPR is an online questionnaire and optional in-person health evaluation that includes 7 major categories targeting deployment history, symptoms, medical history, health concerns, residential history, nonmilitary occupational history, nonmilitary environmental exposures, and health care utilization. The VA Defense Information Repository is used to obtain service dates for the service member/veteran, conflict involvement, and primary location during deployment. The questionnaire portion of the AHOBPR is administered online. It currently is open to all veterans who served in the Southwest Asia theater of operations (including Iraq, Kuwait, and Egypt) any time after August 2, 1990, or Afghanistan, Djibouti, Syria, or Uzbekistan after September 11, 2001. Veterans are eligible for completing the AHOBPR and optional health evaluation at no cost to the veteran regardless of VA benefits or whether they are currently enrolled in VA health care. Though the focus of the present manuscript is to profile a VA program, it is important to note that the US Department of Defense (DoD) is an active partner with the VA in the promotion of the AHOBPR to service members and similarly provides health evaluations for active-duty service members (including activating Reserve and Guard) through their local MTF.
We reviewed and analyzed AHOBPR operations and VA data from 2014 to 2020. Our analyses were limited to veterans seeking evaluation as well as their corresponding symptoms and HCP’s clinical impression from the electronic health record. As of September 20, 2021, 267,125 individuals completed the AHOBPR. The mean age was 43 years (range, 19-84), and the majority were male (86%) and served in the Army (58%). Open-air burn pits (91%), engine maintenance (38.8%), and convoy operations (71.7%) were the most common deployment-related exposures.
The optional in-person AHOBPR health evaluation may be requested by the veteran after completing the online questionnaire and is performed at the veteran’s local VA facility. The evaluation is most often completed by an environmental health clinician or primary care practitioner (PCP). A variety of resources are available to providers for training on this topic, including fact sheets, webinars, monthly calls, conferences, and accredited e-learning.20 As part of the clinical evaluation, the veteran’s chief concerns are assessed and evaluated. At the time of our analysis, 24,578 clinical examinations were performed across 126 VA medical facilities, with considerable geographic variation. Veterans receiving evaluations were predominantly male (89%) with a median age of 46.0 years (IQR, 15). Veterans’ major respiratory concerns included dyspnea (45.1%), decreased exercise ability (34.8%), and cough > 3 weeks (30.3%) (Table). After clinical evaluation by a VA or MTF HCP, 47.8% were found to have a respiratory diagnosis, including asthma (30.1%), COPD (12.8%), and bronchitis (11.9%).
Registry participants who opt to receive the clinical evaluation may benefit directly by undergoing a detailed clinical history and physical examination as well as having the opportunity to document their health concerns. For some, clinicians may need to refer veterans for additional specialty testing beyond this standard AHOBPR clinical evaluation. Although these evaluations can help address some of the veterans’ concerns, a substantial number may have unexplained respiratory symptoms that warrant further investigation.
Post-Deployment Cardiopulmonary Evaluation Network Clinical Evaluation
In May 2019, the VA established the Airborne Hazards and Burn Pits Center of Excellence (AHBPCE). One of the AHBPCE’s objectives is to deliver specialized care and consultation for veterans with concerns about their postdeployment health, including, but not limited to, unexplained dyspnea. To meet this objective, the AHBPCE developed the PDCEN, a national network consisting of specialty HCPs from 5 VA medical centers—located in San Francisco, California; Denver, Colorado; Baltimore, Maryland; Ann Arbor, Michigan; and East Orange, New Jersey. Collectively, the PDCEN has developed a standardized approach for the comprehensive clinical evaluation of unexplained dyspnea that is implemented uniformly across sites. Staff at the PDCEN screen the AHOBPR to identify veterans with features of respiratory disease and invite them to participate in an in-person evaluation at the nearest PDCEN site. Given the specialty expertise (detailed below) within the Network, the PDCEN focuses on complex cases that are resource intensive. To address complex cases of unexplained dyspnea, the PDCEN has developed a core clinical evaluation approach (Figure).
The first step in a veteran’s PDCEN evaluation entails a set of detailed questionnaires that request information about the veteran’s current respiratory, sleep, and mental health symptoms and any associated medical diagnoses. Questionnaires also identify potential exposures to military burn pits, sulfur mine and oil field fires, diesel exhaust fumes, dust storms, urban pollution, explosions/blasts, and chemical weapons. In addition, the questionnaires include deployment geographic location, which may inform future estimates of particulate matter exposure.21 Prior VA and non-VA evaluations and testing of their respiratory concerns are obtained for review. Exposure and health records from the DoD are also reviewed when available.
The next step in the PDCEN evaluation comprises comprehensive testing, including complete pulmonary function testing, methacholine challenge, cardiopulmonary exercise testing, forced oscillometry and exhaled nitric oxide testing, paired high-resolution inspiratory and expiratory chest computed tomography (CT) imaging, sinus CT imaging, direct flexible laryngoscopy, echocardiography, polysomnography, and laboratory blood testing. The testing process is managed by local site coordinators and varies by institution based on availability of each testing modality and subspecialist appointments.
Once testing is completed, the veteran is evaluated by a team of HCPs, including physicians from the disciplines of pulmonary medicine, environmental and occupational health, sleep medicine, otolaryngology and speech pathology, and mental health (when appropriate). After the clinical evaluation has been completed, this team of expert HCPs at each site convenes to provide a final summary review visit intended to be a comprehensive assessment of the veteran’s primary health concerns. The 3 primary objectives of this final review are to inform the veteran of (1) what respiratory and related conditions they have; (2) whether the conditions is/are deployment related; and (3) what treatments and/or follow-up care may enhance their current state of health in partnership with their local HCPs. The PDCEN does not provide ongoing management of any conditions identified during the veteran’s evaluation but communicates findings and recommendations to the veteran and their PCP for long-term care.
Discussion
The AHOBPR was established in response to mounting concerns that service members and veterans were experiencing adverse health effects that might be attributable to deployment-related exposures. Nearly half of all patients currently enrolled in the AHOBPR report dyspnea, and about one-third have decreased exercise tolerance and/or cough. Of those who completed the questionnaire and the subsequent in-person and generalized AHOBPR examination, our interim analysis showed that about half were assigned a respiratory diagnosis. Yet for many veterans, their breathing symptoms remained unexplained or did not respond to treatment.
While the AHOBPR and related examinations address the needs of many veterans, others may require more comprehensive examination. The PDCEN attends to the latter by providing more detailed and comprehensive clinical evaluations of veterans with deployment-related respiratory health concerns and seeks to learn from these evaluations by analyzing data obtained from veterans across sites. As such, the PDCEN hopes not only to improve the health of individual veterans, but also create standard practices for both VA and non-VA community evaluation of veterans exposed to respiratory hazards during deployment.
One of the major challenges in the field of postdeployment respiratory health is the lack of clear universal language or case definitions that encompass the veteran’s clinical concerns. In an influential case series published in 2011, 38 (77%) of 49 soldiers with history of airborne hazard exposure and unexplained exercise intolerance were reported to have histopathology consistent with constrictive bronchiolitis on surgical lung biopsy.14 Subsequent publications have described other histopathologic features in deployed military personnel, including granulomatous inflammation, interstitial lung disease, emphysema, and pleuritis.12-14 Reconciling these findings from surgical lung biopsy with the clinical presentation and noninvasive studies has proved difficult. Therefore, several groups of investigators have proposed terms, including postdeployment respiratory syndrome, deployment-related distal lung disease, and Iraq/Afghanistan War lung injury to describe the increased respiratory symptoms and variety of histopathologic and imaging findings in this population.9,12,22 At present, there remains a lack of consensus on terminology and case definitions as well as the role of military environmental exposures in exacerbating and/or causing these conditions. As HCPs, it is important to appreciate and acknowledge that the ambiguity and controversy pertaining to terminology, causation, and service connections are a common source of frustration experienced by veterans, which are increasingly reflected among reports in popular media and lay press.
A second and related challenge in the field of postdeployment respiratory health that contributes to veteran and HCP frustration is that many of the aforementioned abnormalities described on surgical lung biopsy are not readily identifiable on noninvasive tests, including traditional interpretation of pulmonary function tests or chest CT imaging.12-14,22 Thus, underlying conditions could be overlooked and veterans’ concerns and symptoms may be dismissed or misattributed to other comorbid conditions. While surgical lung biopsies may offer diagnostic clarity in identifying lung disease, there are significant procedural risks of surgical and anesthetic complications. Furthermore, a definitive diagnosis does not necessarily guarantee a clear treatment plan. For example, there are no current therapies approved by the US Food and Drug Administration for the treatment of constrictive bronchiolitis.
Research efforts are underway, including within the PDCEN, to evaluate a more sensitive and noninvasive assessment of the small airways that may even reduce or eliminate the need for surgical lung biopsy. In contrast to traditional pulmonary function testing, which is helpful for evaluation of the larger airways, forced oscillation technique can be used noninvasively, using pressure oscillations to evaluate for diseases of the smaller airways and has been used in the veteran population and in those exposed to dust from the World Trade Center disaster.23-25 Multiple breath washout technique provides a lung clearance index that is determined by the number of lung turnovers it takes to clear the lungs of an inert gas (eg, sulfur hexafluoride, nitrogen). Elevated lung clearance index values suggest ventilation heterogeneity and have been shown to be higher among deployed veterans with dyspnea.26,27 Finally, advanced CT analytic techniques may help identify functional small airways disease and are higher in deployed service members with constrictive bronchiolitis on surgical lung biopsy.28 These innovative noninvasive techniques are experimental but promising, especially as part of a broader evaluation of small airways disease.
AHOBPR clinical evaluations represent an initial step to better understand postdeployment health conditions available to all AHOBPR participants. The PDCEN clinical evaluation extends the AHOBPR evaluation by providing specialty care for certain veterans requiring more comprehensive evaluation while systematically collecting and analyzing clinical data to advance the field. The VA is committed to leveraging these data and all available expertise to provide a clear description of the spectrum of disease in this population and improve our ability to diagnose, follow, and treat respiratory health conditions occurring after deployment to Southwest Asia and Afghanistan.
Case Conclusion
The veteran was referred to a PDCEN site and underwent a comprehensive multidisciplinary evaluation. Pulmonary function testing showed lung volumes and vital capacity within the predicted normal range, mild air trapping, and a low diffusion capacity for carbon monoxide. Methacholine challenge testing was normal; however, forced oscillometry suggested small airways obstruction. A high-resolution CT showed air trapping without parenchymal changes. Cardiopulmonary exercise testing demonstrated a peak exercise capacity within the predicted normal range but low breathing reserve. Otolaryngology evaluation including laryngoscopy suggested chronic nonallergic rhinitis.
At the end of the veteran’s evaluation, a summary review reported nonallergic rhinitis and distal airway obstruction consistent with small airways disease. Both were reported as most likely related to deployment given her significant environmental exposures and the temporal relationship with her deployment and symptom onset as well as lack of other identifiable causes. A more precise histopathologic diagnosis could be firmly established with a surgical lung biopsy, but after shared decision making with a PDCEN HCP, the patient declined to undergo this invasive procedure. After you review the summary review and recommendations from the PDCEN group, you start the veteran on intranasal steroids and a combined inhaled corticosteroid/long-acting β agonist inhaler as well as refer the veteran to pulmonary rehabilitation. After several weeks, she reports an improvement in sleep and nasal symptoms but continues to experience residual exercise intolerance.
This case serves as an example of the significant limitations that a previously active and healthy patient can develop after deployment to Southwest Asia and Afghanistan. Encouraging this veteran to complete the AHOBPR allowed her to be considered for a PDCEN evaluation that provided the opportunity to undergo a comprehensive noninvasive evaluation of her chronic dyspnea. In doing so, she obtained 2 important diagnoses and data from her evaluation will help establish best practices for standardized evaluations of respiratory concerns following deployment. Through the AHOBPR and PDCEN, the VA seeks to better understand postdeployment health conditions, their relationship to military and environmental exposures, and how best to diagnose and treat these conditions.
Acknowledgments
This work was supported by the US Department of Veterans Affairs (VA) Airborne Hazards and Burn Pits Center of Excellence (Public Law 115-929). The authors acknowledge support and contributions from Dr. Eric Shuping and leadership at VA’s Health Outcomes Military Exposures office as well as the New Jersey War Related Illness and Injury Study Center. In addition, we thank Erin McRoberts and Rajeev Swarup for their contributions to the Post-Deployment Cardiopulmonary Evaluation Network. Post-Deployment Cardiopulmonary Evaluation Network members:
Mehrdad Arjomandi, Caroline Davis, Michelle DeLuca, Nancy Eager, Courtney A. Eberhardt, Michael J. Falvo, Timothy Foley, Fiona A.S. Graff, Deborah Heaney, Stella E. Hines, Rachel E. Howard, Nisha Jani, Sheena Kamineni, Silpa Krefft, Mary L. Langlois, Helen Lozier, Simran K. Matharu, Anisa Moore, Lydia Patrick-DeLuca, Edward Pickering, Alexander Rabin, Michelle Robertson, Samantha L. Rogers, Aaron H. Schneider, Anand Shah, Anays Sotolongo, Jennifer H. Therkorn, Rebecca I. Toczylowski, Matthew Watson, Alison D. Wilczynski, Ian W. Wilson, Romi A. Yount.
Case Example
A 37-year-old female never smoker presents to your clinic with progressive dyspnea over the past 15 years. She reports dyspnea on exertion, wheezing, chronic nasal congestion, and difficulty sleeping that started a year after she returned from military deployment to Iraq. She has been unable to exercise, even at low intensity, for the past 5 years, despite being previously active. She has experienced some symptom improvement by taking an albuterol inhaler as needed, loratadine (10 mg), and fluticasone nasal spray (50 mcg). She occasionally uses famotidine for reflux (40 mg). She deployed to Southwest Asia for 12 months (2002-2003) and was primarily stationed in Qayyarah West, an Air Force base in the Mosul district in northern Iraq. She reports exposure during deployment to the fire in the Al-Mishraq sulfur mine, located approximately 25 km north of Qayyarah West, as well as dust storms and burn pits. She currently works as a medical assistant. Her examination is remarkable for normal bronchovesicular breath sounds without any wheezing or crackles on pulmonary evaluation. Her body mass index is 31. You obtain a chest radiograph and spirometry, which are both normal.
The veteran reports feeling frustrated as she has had multiple specialty evaluations in community clinics without receiving a diagnosis, despite worsening symptoms. She reports that she added her information to the Airborne Hazards and Open Burn Pit Registry (AHOBPR). She recently received a letter from the US Department of Veterans Affairs (VA) Post-Deployment Cardiopulmonary Evaluation Network (PDCEN) and is asking you whether she should participate in the PDCEN specialty evaluation. You are not familiar with the military experiences she has described or the programs she asks you about; however, you would like to know more to best care for your patient.
Background
The year 2021 marked the 20th anniversary of the September 11 attacks and the launch of the Global War on Terrorism. Almost 3 million US military personnel have been deployed in support of these operations along with about 300,000 US civilian contractors and thousands of troops from more than 40 nations.1-3
Respiratory hazards associated with deployment to Southwest Asia and Afghanistan are unique and varied. These exposures include blast injuries and a variety of particulate matter sources, such as burn pit combustion byproducts, aeroallergens, and dust storms.7,8,15,16 One air sampling study conducted at 15 deployment sites in Southwest Asia and Afghanistan found mean fine particulate matter (PM2.5) levels were as much as 10 times greater than sampling sites in both rural and urban cities in the United States; all sites sampled exceeded military exposure guidelines (65 µg/m3 for 1 year).17,18 Long-term exposure to PM2.5 has been associated with the development of chronic respiratory and cardiovascular disease; therefore, there has been considerable attention to the respiratory (and nonrespiratory) health of deployed military personnel.19
Concerns regarding the association between deployment and lung disease led to the creation of the national VA Airborne Hazards and Open Burn Pit Registry (AHOBPR) in 2014 and consists of (1) an online questionnaire to document deployment and medical history, exposure concerns, and symptoms; and (2) an optional in-person or virtual clinical health evaluation at the individual’s local VA medical center or military treatment facility (MTF). As of March 2022, more than 300,000 individuals have completed the online questionnaire of which about 30% declined the optional clinical health evaluation.
The clinical evaluation available to AHOBPR participants has not yet been described in the literature. Therefore, our objectives are to examine AHOBPR clinical evaluation data and review its application throughout the VA. In addition, we will also describe a parallel effort by the VA PDCEN, which is to provide comprehensive multiday clinical evaluations for unique AHOBPR participants with unexplained dyspnea and self-reported respiratory disease. A secondary aim of this publication is to disseminate information to health care professionals (HCPs) within and outside of the VA to aid in the referral and evaluation of previously deployed veterans who experience unexplained dyspnea.
AHOBPR Overview
The AHOBPR is an online questionnaire and optional in-person health evaluation that includes 7 major categories targeting deployment history, symptoms, medical history, health concerns, residential history, nonmilitary occupational history, nonmilitary environmental exposures, and health care utilization. The VA Defense Information Repository is used to obtain service dates for the service member/veteran, conflict involvement, and primary location during deployment. The questionnaire portion of the AHOBPR is administered online. It currently is open to all veterans who served in the Southwest Asia theater of operations (including Iraq, Kuwait, and Egypt) any time after August 2, 1990, or Afghanistan, Djibouti, Syria, or Uzbekistan after September 11, 2001. Veterans are eligible for completing the AHOBPR and optional health evaluation at no cost to the veteran regardless of VA benefits or whether they are currently enrolled in VA health care. Though the focus of the present manuscript is to profile a VA program, it is important to note that the US Department of Defense (DoD) is an active partner with the VA in the promotion of the AHOBPR to service members and similarly provides health evaluations for active-duty service members (including activating Reserve and Guard) through their local MTF.
We reviewed and analyzed AHOBPR operations and VA data from 2014 to 2020. Our analyses were limited to veterans seeking evaluation as well as their corresponding symptoms and HCP’s clinical impression from the electronic health record. As of September 20, 2021, 267,125 individuals completed the AHOBPR. The mean age was 43 years (range, 19-84), and the majority were male (86%) and served in the Army (58%). Open-air burn pits (91%), engine maintenance (38.8%), and convoy operations (71.7%) were the most common deployment-related exposures.
The optional in-person AHOBPR health evaluation may be requested by the veteran after completing the online questionnaire and is performed at the veteran’s local VA facility. The evaluation is most often completed by an environmental health clinician or primary care practitioner (PCP). A variety of resources are available to providers for training on this topic, including fact sheets, webinars, monthly calls, conferences, and accredited e-learning.20 As part of the clinical evaluation, the veteran’s chief concerns are assessed and evaluated. At the time of our analysis, 24,578 clinical examinations were performed across 126 VA medical facilities, with considerable geographic variation. Veterans receiving evaluations were predominantly male (89%) with a median age of 46.0 years (IQR, 15). Veterans’ major respiratory concerns included dyspnea (45.1%), decreased exercise ability (34.8%), and cough > 3 weeks (30.3%) (Table). After clinical evaluation by a VA or MTF HCP, 47.8% were found to have a respiratory diagnosis, including asthma (30.1%), COPD (12.8%), and bronchitis (11.9%).
Registry participants who opt to receive the clinical evaluation may benefit directly by undergoing a detailed clinical history and physical examination as well as having the opportunity to document their health concerns. For some, clinicians may need to refer veterans for additional specialty testing beyond this standard AHOBPR clinical evaluation. Although these evaluations can help address some of the veterans’ concerns, a substantial number may have unexplained respiratory symptoms that warrant further investigation.
Post-Deployment Cardiopulmonary Evaluation Network Clinical Evaluation
In May 2019, the VA established the Airborne Hazards and Burn Pits Center of Excellence (AHBPCE). One of the AHBPCE’s objectives is to deliver specialized care and consultation for veterans with concerns about their postdeployment health, including, but not limited to, unexplained dyspnea. To meet this objective, the AHBPCE developed the PDCEN, a national network consisting of specialty HCPs from 5 VA medical centers—located in San Francisco, California; Denver, Colorado; Baltimore, Maryland; Ann Arbor, Michigan; and East Orange, New Jersey. Collectively, the PDCEN has developed a standardized approach for the comprehensive clinical evaluation of unexplained dyspnea that is implemented uniformly across sites. Staff at the PDCEN screen the AHOBPR to identify veterans with features of respiratory disease and invite them to participate in an in-person evaluation at the nearest PDCEN site. Given the specialty expertise (detailed below) within the Network, the PDCEN focuses on complex cases that are resource intensive. To address complex cases of unexplained dyspnea, the PDCEN has developed a core clinical evaluation approach (Figure).
The first step in a veteran’s PDCEN evaluation entails a set of detailed questionnaires that request information about the veteran’s current respiratory, sleep, and mental health symptoms and any associated medical diagnoses. Questionnaires also identify potential exposures to military burn pits, sulfur mine and oil field fires, diesel exhaust fumes, dust storms, urban pollution, explosions/blasts, and chemical weapons. In addition, the questionnaires include deployment geographic location, which may inform future estimates of particulate matter exposure.21 Prior VA and non-VA evaluations and testing of their respiratory concerns are obtained for review. Exposure and health records from the DoD are also reviewed when available.
The next step in the PDCEN evaluation comprises comprehensive testing, including complete pulmonary function testing, methacholine challenge, cardiopulmonary exercise testing, forced oscillometry and exhaled nitric oxide testing, paired high-resolution inspiratory and expiratory chest computed tomography (CT) imaging, sinus CT imaging, direct flexible laryngoscopy, echocardiography, polysomnography, and laboratory blood testing. The testing process is managed by local site coordinators and varies by institution based on availability of each testing modality and subspecialist appointments.
Once testing is completed, the veteran is evaluated by a team of HCPs, including physicians from the disciplines of pulmonary medicine, environmental and occupational health, sleep medicine, otolaryngology and speech pathology, and mental health (when appropriate). After the clinical evaluation has been completed, this team of expert HCPs at each site convenes to provide a final summary review visit intended to be a comprehensive assessment of the veteran’s primary health concerns. The 3 primary objectives of this final review are to inform the veteran of (1) what respiratory and related conditions they have; (2) whether the conditions is/are deployment related; and (3) what treatments and/or follow-up care may enhance their current state of health in partnership with their local HCPs. The PDCEN does not provide ongoing management of any conditions identified during the veteran’s evaluation but communicates findings and recommendations to the veteran and their PCP for long-term care.
Discussion
The AHOBPR was established in response to mounting concerns that service members and veterans were experiencing adverse health effects that might be attributable to deployment-related exposures. Nearly half of all patients currently enrolled in the AHOBPR report dyspnea, and about one-third have decreased exercise tolerance and/or cough. Of those who completed the questionnaire and the subsequent in-person and generalized AHOBPR examination, our interim analysis showed that about half were assigned a respiratory diagnosis. Yet for many veterans, their breathing symptoms remained unexplained or did not respond to treatment.
While the AHOBPR and related examinations address the needs of many veterans, others may require more comprehensive examination. The PDCEN attends to the latter by providing more detailed and comprehensive clinical evaluations of veterans with deployment-related respiratory health concerns and seeks to learn from these evaluations by analyzing data obtained from veterans across sites. As such, the PDCEN hopes not only to improve the health of individual veterans, but also create standard practices for both VA and non-VA community evaluation of veterans exposed to respiratory hazards during deployment.
One of the major challenges in the field of postdeployment respiratory health is the lack of clear universal language or case definitions that encompass the veteran’s clinical concerns. In an influential case series published in 2011, 38 (77%) of 49 soldiers with history of airborne hazard exposure and unexplained exercise intolerance were reported to have histopathology consistent with constrictive bronchiolitis on surgical lung biopsy.14 Subsequent publications have described other histopathologic features in deployed military personnel, including granulomatous inflammation, interstitial lung disease, emphysema, and pleuritis.12-14 Reconciling these findings from surgical lung biopsy with the clinical presentation and noninvasive studies has proved difficult. Therefore, several groups of investigators have proposed terms, including postdeployment respiratory syndrome, deployment-related distal lung disease, and Iraq/Afghanistan War lung injury to describe the increased respiratory symptoms and variety of histopathologic and imaging findings in this population.9,12,22 At present, there remains a lack of consensus on terminology and case definitions as well as the role of military environmental exposures in exacerbating and/or causing these conditions. As HCPs, it is important to appreciate and acknowledge that the ambiguity and controversy pertaining to terminology, causation, and service connections are a common source of frustration experienced by veterans, which are increasingly reflected among reports in popular media and lay press.
A second and related challenge in the field of postdeployment respiratory health that contributes to veteran and HCP frustration is that many of the aforementioned abnormalities described on surgical lung biopsy are not readily identifiable on noninvasive tests, including traditional interpretation of pulmonary function tests or chest CT imaging.12-14,22 Thus, underlying conditions could be overlooked and veterans’ concerns and symptoms may be dismissed or misattributed to other comorbid conditions. While surgical lung biopsies may offer diagnostic clarity in identifying lung disease, there are significant procedural risks of surgical and anesthetic complications. Furthermore, a definitive diagnosis does not necessarily guarantee a clear treatment plan. For example, there are no current therapies approved by the US Food and Drug Administration for the treatment of constrictive bronchiolitis.
Research efforts are underway, including within the PDCEN, to evaluate a more sensitive and noninvasive assessment of the small airways that may even reduce or eliminate the need for surgical lung biopsy. In contrast to traditional pulmonary function testing, which is helpful for evaluation of the larger airways, forced oscillation technique can be used noninvasively, using pressure oscillations to evaluate for diseases of the smaller airways and has been used in the veteran population and in those exposed to dust from the World Trade Center disaster.23-25 Multiple breath washout technique provides a lung clearance index that is determined by the number of lung turnovers it takes to clear the lungs of an inert gas (eg, sulfur hexafluoride, nitrogen). Elevated lung clearance index values suggest ventilation heterogeneity and have been shown to be higher among deployed veterans with dyspnea.26,27 Finally, advanced CT analytic techniques may help identify functional small airways disease and are higher in deployed service members with constrictive bronchiolitis on surgical lung biopsy.28 These innovative noninvasive techniques are experimental but promising, especially as part of a broader evaluation of small airways disease.
AHOBPR clinical evaluations represent an initial step to better understand postdeployment health conditions available to all AHOBPR participants. The PDCEN clinical evaluation extends the AHOBPR evaluation by providing specialty care for certain veterans requiring more comprehensive evaluation while systematically collecting and analyzing clinical data to advance the field. The VA is committed to leveraging these data and all available expertise to provide a clear description of the spectrum of disease in this population and improve our ability to diagnose, follow, and treat respiratory health conditions occurring after deployment to Southwest Asia and Afghanistan.
Case Conclusion
The veteran was referred to a PDCEN site and underwent a comprehensive multidisciplinary evaluation. Pulmonary function testing showed lung volumes and vital capacity within the predicted normal range, mild air trapping, and a low diffusion capacity for carbon monoxide. Methacholine challenge testing was normal; however, forced oscillometry suggested small airways obstruction. A high-resolution CT showed air trapping without parenchymal changes. Cardiopulmonary exercise testing demonstrated a peak exercise capacity within the predicted normal range but low breathing reserve. Otolaryngology evaluation including laryngoscopy suggested chronic nonallergic rhinitis.
At the end of the veteran’s evaluation, a summary review reported nonallergic rhinitis and distal airway obstruction consistent with small airways disease. Both were reported as most likely related to deployment given her significant environmental exposures and the temporal relationship with her deployment and symptom onset as well as lack of other identifiable causes. A more precise histopathologic diagnosis could be firmly established with a surgical lung biopsy, but after shared decision making with a PDCEN HCP, the patient declined to undergo this invasive procedure. After you review the summary review and recommendations from the PDCEN group, you start the veteran on intranasal steroids and a combined inhaled corticosteroid/long-acting β agonist inhaler as well as refer the veteran to pulmonary rehabilitation. After several weeks, she reports an improvement in sleep and nasal symptoms but continues to experience residual exercise intolerance.
This case serves as an example of the significant limitations that a previously active and healthy patient can develop after deployment to Southwest Asia and Afghanistan. Encouraging this veteran to complete the AHOBPR allowed her to be considered for a PDCEN evaluation that provided the opportunity to undergo a comprehensive noninvasive evaluation of her chronic dyspnea. In doing so, she obtained 2 important diagnoses and data from her evaluation will help establish best practices for standardized evaluations of respiratory concerns following deployment. Through the AHOBPR and PDCEN, the VA seeks to better understand postdeployment health conditions, their relationship to military and environmental exposures, and how best to diagnose and treat these conditions.
Acknowledgments
This work was supported by the US Department of Veterans Affairs (VA) Airborne Hazards and Burn Pits Center of Excellence (Public Law 115-929). The authors acknowledge support and contributions from Dr. Eric Shuping and leadership at VA’s Health Outcomes Military Exposures office as well as the New Jersey War Related Illness and Injury Study Center. In addition, we thank Erin McRoberts and Rajeev Swarup for their contributions to the Post-Deployment Cardiopulmonary Evaluation Network. Post-Deployment Cardiopulmonary Evaluation Network members:
Mehrdad Arjomandi, Caroline Davis, Michelle DeLuca, Nancy Eager, Courtney A. Eberhardt, Michael J. Falvo, Timothy Foley, Fiona A.S. Graff, Deborah Heaney, Stella E. Hines, Rachel E. Howard, Nisha Jani, Sheena Kamineni, Silpa Krefft, Mary L. Langlois, Helen Lozier, Simran K. Matharu, Anisa Moore, Lydia Patrick-DeLuca, Edward Pickering, Alexander Rabin, Michelle Robertson, Samantha L. Rogers, Aaron H. Schneider, Anand Shah, Anays Sotolongo, Jennifer H. Therkorn, Rebecca I. Toczylowski, Matthew Watson, Alison D. Wilczynski, Ian W. Wilson, Romi A. Yount.
1. Wenger J, O’Connell C, Cottrell L. Examination of recent deployment experience across the services and components. Exam. RAND Corporation; 2018. Accessed June 27, 2022. doi:10.7249/rr1928
2. Torreon BS. U.S. periods of war and dates of recent conflicts, RS21405. Congressional Research Service; 2017. June 5, 2020. Accessed June 27, 2022. https://crsreports.congress.gov/product/details?prodcode=RS21405
3. Dunigan M, Farmer CM, Burns RM, Hawks A, Setodji CM. Out of the shadows: the health and well-being of private contractors working in conflict environments. RAND Corporation; 2013. Accessed June 27, 2022. https://www.rand.org/pubs/research_reports/RR420.html
4. Szema AM, Peters MC, Weissinger KM, Gagliano CA, Chen JJ. New-onset asthma among soldiers serving in Iraq and Afghanistan. Allergy Asthma Proc. 2010;31(5):67-71. doi:10.2500/aap.2010.31.3383
5. Pugh MJ, Jaramillo CA, Leung KW, et al. Increasing prevalence of chronic lung disease in veterans of the wars in Iraq and Afghanistan. Mil Med. 2016;181(5):476-481. doi:10.7205/MILMED-D-15-00035
6. Falvo MJ, Osinubi OY, Sotolongo AM, Helmer DA. Airborne hazards exposure and respiratory health of Iraq and Afghanistan veterans. Epidemiol Rev. 2015;37:116-130. doi:10.1093/epirev/mxu009
7. McAndrew LM, Teichman RF, Osinubi OY, Jasien JV, Quigley KS. Environmental exposure and health of Operation Enduring Freedom/Operation Iraqi Freedom veterans. J Occup Environ Med. 2012;54(6):665-669. doi:10.1097/JOM.0b013e318255ba1b
8. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. doi:10.1093/aje/kwp287
9. Szema AM, Salihi W, Savary K, Chen JJ. Respiratory symptoms necessitating spirometry among soldiers with Iraq/Afghanistan war lung injury. J Occup Environ Med. 2011;53(9):961-965. doi:10.1097/JOM.0b013e31822c9f05
10. Committee on the Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan; Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. Accessed June 27, 2022. doi:10.17226/1320911. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. Accessed June 27, 2022. doi:10.17226/25837
12. Krefft SD, Wolff J, Zell-Baran L, et al. Respiratory diseases in post-9/11 military personnel following Southwest Asia deployment. J Occup Environ Med. 2020;62(5):337-343. doi:10.1097/JOM.0000000000001817
13. Gordetsky J, Kim C, Miller RF, Mehrad M. Non-necrotizing granulomatous pneumonitis and chronic pleuritis in soldiers deployed to Southwest Asia. Histopathology. 2020;77(3):453-459. doi:10.1111/his.14135
14. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. doi:10.1056/NEJMoa1101388
15. Helmer DA, Rossignol M, Blatt M, Agarwal R, Teichman R, Lange G. Health and exposure concerns of veterans deployed to Iraq and Afghanistan. J Occup Environ Med. 2007;49(5):475-480. doi:10.1097/JOM.0b013e318042d682
16. Kim YH, Warren SH, Kooter I, et al. Chemistry, lung toxicity and mutagenicity of burn pit smoke-related particulate matter. Part Fibre Toxicol. 2021;18(1):45. Published 2021 Dec 16. doi:10.1186/s12989-021-00435-w
17. Engelbrecht JP, McDonald EV, Gillies JA, Jayanty RK, Casuccio G, Gertler AW. Characterizing mineral dusts and other aerosols from the Middle East—Part 1: ambient sampling. Inhal Toxicol. 2009;21(4):297-326. doi:10.1080/08958370802464273
18. US Army Public Health Command. Technical guide 230: environmental health risk assessment and chemical exposure guidelines for deployed military personnel, 2013 revision. Accessed June 27, 2022. https://phc.amedd.army.mil/PHC%20Resource%20Library/TG230-DeploymentEHRA-and-MEGs-2013-Revision.pdf
19. Anderson JO, Thundiyil JG, Stolbach A. Clearing the air: a review of the effects of particulate matter air pollution on human health. J Med Toxicol. 2012;8(2):166-175. doi:10.1007/s13181-011-0203-1
20. Shuping E, Schneiderman A. Resources on environmental exposures for military veterans. Am Fam Physician. 2020;101(12):709-710.
21. Masri S, Garshick E, Coull BA, Koutrakis P. A novel calibration approach using satellite and visibility observations to estimate fine particulate matter exposures in Southwest Asia and Afghanistan. J Air Waste Manag Assoc. 2017;67(1):86-95. doi:10.1080/10962247.2016.1230079
22. Gutor SS, Richmond BW, Du RH, et al. Postdeployment respiratory syndrome in soldiers with chronic exertional dyspnea. Am J Surg Pathol. 2021;45(12):1587-1596. doi:10.1097/PAS.0000000000001757
23. Goldman MD, Saadeh C, Ross D. Clinical applications of forced oscillation to assess peripheral airway function. Respir Physiol Neurobiol. 2005;148(1-2):179-194. doi:10.1016/j.resp.2005.05.026
24. Butzko RP, Sotolongo AM, Helmer DA, et al. Forced oscillation technique in veterans with preserved spirometry and chronic respiratory symptoms. Respir Physiol Neurobiol. 2019;260:8-16. doi:10.1016/j.resp.2018.11.012
25. Oppenheimer BW, Goldring RM, Herberg ME, et al. Distal airway function in symptomatic subjects with normal spirometry following World Trade Center dust exposure. Chest. 2007;132(4):1275-1282. doi:10.1378/chest.07-0913
26. Zell-Baran LM, Krefft SD, Moore CM, Wolff J, Meehan R, Rose CS. Multiple breath washout: a noninvasive tool for identifying lung disease in symptomatic military deployers. Respir Med. 2021;176:106281. doi:10.1016/j.rmed.2020.106281
27. Krefft SD, Strand M, Smith J, Stroup C, Meehan R, Rose C. Utility of lung clearance index testing as a noninvasive marker of deployment-related lung disease. J Occup Environ Med. 2017;59(8):707-711. doi:10.1097/JOM.000000000000105828. Davis CW, Lopez CL, Bell AJ, et al. The severity of functional small airways disease in military personnel with constrictive bronchiolitis as measured by quantitative CT [published online ahead of print, 2022 May 24]. Am J Respir Crit Care Med. 2022;10.1164/rccm.202201-0153LE. doi:10.1164/rccm.202201-0153LE
1. Wenger J, O’Connell C, Cottrell L. Examination of recent deployment experience across the services and components. Exam. RAND Corporation; 2018. Accessed June 27, 2022. doi:10.7249/rr1928
2. Torreon BS. U.S. periods of war and dates of recent conflicts, RS21405. Congressional Research Service; 2017. June 5, 2020. Accessed June 27, 2022. https://crsreports.congress.gov/product/details?prodcode=RS21405
3. Dunigan M, Farmer CM, Burns RM, Hawks A, Setodji CM. Out of the shadows: the health and well-being of private contractors working in conflict environments. RAND Corporation; 2013. Accessed June 27, 2022. https://www.rand.org/pubs/research_reports/RR420.html
4. Szema AM, Peters MC, Weissinger KM, Gagliano CA, Chen JJ. New-onset asthma among soldiers serving in Iraq and Afghanistan. Allergy Asthma Proc. 2010;31(5):67-71. doi:10.2500/aap.2010.31.3383
5. Pugh MJ, Jaramillo CA, Leung KW, et al. Increasing prevalence of chronic lung disease in veterans of the wars in Iraq and Afghanistan. Mil Med. 2016;181(5):476-481. doi:10.7205/MILMED-D-15-00035
6. Falvo MJ, Osinubi OY, Sotolongo AM, Helmer DA. Airborne hazards exposure and respiratory health of Iraq and Afghanistan veterans. Epidemiol Rev. 2015;37:116-130. doi:10.1093/epirev/mxu009
7. McAndrew LM, Teichman RF, Osinubi OY, Jasien JV, Quigley KS. Environmental exposure and health of Operation Enduring Freedom/Operation Iraqi Freedom veterans. J Occup Environ Med. 2012;54(6):665-669. doi:10.1097/JOM.0b013e318255ba1b
8. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. doi:10.1093/aje/kwp287
9. Szema AM, Salihi W, Savary K, Chen JJ. Respiratory symptoms necessitating spirometry among soldiers with Iraq/Afghanistan war lung injury. J Occup Environ Med. 2011;53(9):961-965. doi:10.1097/JOM.0b013e31822c9f05
10. Committee on the Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan; Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. Accessed June 27, 2022. doi:10.17226/1320911. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. Accessed June 27, 2022. doi:10.17226/25837
12. Krefft SD, Wolff J, Zell-Baran L, et al. Respiratory diseases in post-9/11 military personnel following Southwest Asia deployment. J Occup Environ Med. 2020;62(5):337-343. doi:10.1097/JOM.0000000000001817
13. Gordetsky J, Kim C, Miller RF, Mehrad M. Non-necrotizing granulomatous pneumonitis and chronic pleuritis in soldiers deployed to Southwest Asia. Histopathology. 2020;77(3):453-459. doi:10.1111/his.14135
14. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. doi:10.1056/NEJMoa1101388
15. Helmer DA, Rossignol M, Blatt M, Agarwal R, Teichman R, Lange G. Health and exposure concerns of veterans deployed to Iraq and Afghanistan. J Occup Environ Med. 2007;49(5):475-480. doi:10.1097/JOM.0b013e318042d682
16. Kim YH, Warren SH, Kooter I, et al. Chemistry, lung toxicity and mutagenicity of burn pit smoke-related particulate matter. Part Fibre Toxicol. 2021;18(1):45. Published 2021 Dec 16. doi:10.1186/s12989-021-00435-w
17. Engelbrecht JP, McDonald EV, Gillies JA, Jayanty RK, Casuccio G, Gertler AW. Characterizing mineral dusts and other aerosols from the Middle East—Part 1: ambient sampling. Inhal Toxicol. 2009;21(4):297-326. doi:10.1080/08958370802464273
18. US Army Public Health Command. Technical guide 230: environmental health risk assessment and chemical exposure guidelines for deployed military personnel, 2013 revision. Accessed June 27, 2022. https://phc.amedd.army.mil/PHC%20Resource%20Library/TG230-DeploymentEHRA-and-MEGs-2013-Revision.pdf
19. Anderson JO, Thundiyil JG, Stolbach A. Clearing the air: a review of the effects of particulate matter air pollution on human health. J Med Toxicol. 2012;8(2):166-175. doi:10.1007/s13181-011-0203-1
20. Shuping E, Schneiderman A. Resources on environmental exposures for military veterans. Am Fam Physician. 2020;101(12):709-710.
21. Masri S, Garshick E, Coull BA, Koutrakis P. A novel calibration approach using satellite and visibility observations to estimate fine particulate matter exposures in Southwest Asia and Afghanistan. J Air Waste Manag Assoc. 2017;67(1):86-95. doi:10.1080/10962247.2016.1230079
22. Gutor SS, Richmond BW, Du RH, et al. Postdeployment respiratory syndrome in soldiers with chronic exertional dyspnea. Am J Surg Pathol. 2021;45(12):1587-1596. doi:10.1097/PAS.0000000000001757
23. Goldman MD, Saadeh C, Ross D. Clinical applications of forced oscillation to assess peripheral airway function. Respir Physiol Neurobiol. 2005;148(1-2):179-194. doi:10.1016/j.resp.2005.05.026
24. Butzko RP, Sotolongo AM, Helmer DA, et al. Forced oscillation technique in veterans with preserved spirometry and chronic respiratory symptoms. Respir Physiol Neurobiol. 2019;260:8-16. doi:10.1016/j.resp.2018.11.012
25. Oppenheimer BW, Goldring RM, Herberg ME, et al. Distal airway function in symptomatic subjects with normal spirometry following World Trade Center dust exposure. Chest. 2007;132(4):1275-1282. doi:10.1378/chest.07-0913
26. Zell-Baran LM, Krefft SD, Moore CM, Wolff J, Meehan R, Rose CS. Multiple breath washout: a noninvasive tool for identifying lung disease in symptomatic military deployers. Respir Med. 2021;176:106281. doi:10.1016/j.rmed.2020.106281
27. Krefft SD, Strand M, Smith J, Stroup C, Meehan R, Rose C. Utility of lung clearance index testing as a noninvasive marker of deployment-related lung disease. J Occup Environ Med. 2017;59(8):707-711. doi:10.1097/JOM.000000000000105828. Davis CW, Lopez CL, Bell AJ, et al. The severity of functional small airways disease in military personnel with constrictive bronchiolitis as measured by quantitative CT [published online ahead of print, 2022 May 24]. Am J Respir Crit Care Med. 2022;10.1164/rccm.202201-0153LE. doi:10.1164/rccm.202201-0153LE
Addressing racial bias in pulse oximetry
Pulse oximetry is a vital monitoring tool in the ICU and in pulmonary medicine. Regrettably, re-emerging data show that pulse oximeters do not accurately measure blood oxygen levels in Black patients, presumably due to their skin tone. (i.e., low arterial oxygen saturation despite a seemingly normal pulse oximetry reading). While inaccuracy of pulse oximeter measurements in patients with darker skin has been recognized for decades, recent studies have highlighted this as an ongoing problem with potentially severe consequences for Black patients and other patients of color.
One recent study found that Black patients had almost three times the likelihood of occult hypoxemia compared with White patients (Sjoding, MW, et al. N Engl J Med. 2020;383[25]:2477-8).
Subsequent studies have confirmed this to be a widespread problem across various clinical settings in hundreds of hospitals (Wong AI, et al. JAMA Netw Open. 2021;4[11]:e2131674; Valbuena VS, et al. Chest. 2022;161[4]:971-8). A recent retrospective cohort study of patients with COVID-19 found that occult hypoxemia in Black and Hispanic patients was associated with delayed eligibility for potentially lifesaving COVID-19 therapies (Fawzy AF, et al. JAMA Intern Med. 2022; published online May 31, 2022).
Now that numerous studies have demonstrated the inaccuracy of pulse oximetry with the potential to cause harm to historically marginalized racial and ethnic groups, must we abandon the use of pulse oximetry? We would argue that pulse oximeters remain valuable tools, but for now, we must adapt our practice until better devices are widely adopted.
First, it is crucial that health professionals are aware that pulse oximeters may underestimate the true extent of hypoxemia for all patients, but particularly for patients with darker skin. Acknowledging this device flaw is essential to avoid harm to our patients.
Second, clinicians must have heightened skepticism for seemingly normal pulse oximetry values when caring for symptomatic patients at risk of occult hypoxemia.
Until better pulse oximeters are widely available, clinicians must consider workarounds aimed at ensuring timely identification of hypoxemia in Black patients and other patients of color.
These patients may need invasive monitoring of arterial oxygenation, including arterial blood gas checks or an arterial catheter. However, invasive monitoring comes at the cost of discomfort to patients and potential complications, such as vessel or nerve damage.

Invasive monitoring of patients at risk for occult hypoxemia is not an equitable or acceptable long-term solution for this problem. As advocates for patients, clinicians and professional organizations should lobby regulatory bodies to ensure pulse oximeters are accurate for all patients.
We must also call on government leaders to move this process forward. For example, in response to efforts by the United Kingdom’s Intensive Care Society, the Health Secretary of the UK, Sajid Javid, has called for a review of pulse oximeters as part of a larger review assessing structural issues in health care that lead to worse outcomes in racial and ethnic minorities (BBC News. https://www.bbc.com/news/uk-59363544. Published online Nov. 21, 2021).
Device companies are largely for-profit corporations with obligations to their shareholders. It seems that existing incentives are insufficient to motivate investment in less biased technology and real-world evaluations of their devices.
We previously called for buyers of pulse oximeters to change the incentives of device companies – that is, for “hospitals to commit to only purchasing pulse oximeters that have been shown to work equally well in patients of colour.” (Hidalgo DC, et al. Lancet Respir Med. 2021;9[4]:E37). And, indeed, we worry that hospitals are putting themselves at medicolegal risk by not raising their purchasing standards. Since it is now widely known that pulse oximeters are inaccurate in certain patients, could there be liability for hospitals that continue to use devices we know to be disproportionately inaccurate by race?

Device companies must commit to fixing racial bias in pulse oximeters. Change is feasible, and pulse oximeters can be redesigned to be accurate and reliable among all patients using existing technology that is decades-old.
In the 1960s and 1970s, Hewlett Packard worked with NASA to noninvasively measure oxygen saturation in astronauts (Moran-Thomas, M. Wired. Published online June 4, 2021. https://www.wired.com/story/pulse-oximeters-equity). The device was designed to work for all skin tones and could be calibrated based on an individual’s skin tone. However, Hewlett Packard moved away from medical devices in the 1980s, shelving their design while other companies took over the oximeter market.
Lastly, as new devices are designed, they must be proven to work for all patients. Testing should be conducted in real-world clinical settings using metrics aligned with clinical care, since we know testing in artificial environments may not generalize to critically ill patients. Testing standards historically used by the FDA, such as only requiring device testing in a small number of non-White individuals, may miss clinically relevant hypoxemia. Non-inferiority studies are particularly susceptible to poor design or under-powering, and rigorous standards are needed from unbiased sources.
While potential solutions are currently being evaluated, the fact remains that the inaccuracy of pulse oximeters has been known for decades without any meaningful action taken to correct the problem.
As Valeria Valbuena, author of a study demonstrating inaccuracy of pulse oximetry in patients about to undergo ECMO, points out, “Using White patients as the standard in biomedical design has led to both differential care and innovation inertia for optimizing the way devices and algorithms work for patients of racial and ethnic minoritized groups” (Valbuena VS. JAMA Intern Med. 2022. doi: 10.1001/jamainternmed.2022.1903).
We know that hypoxemia is dangerous for our patients and that this is only one example of the long-standing systemic racism leading to harm in historically marginalized racial and ethnic groups. It is unacceptable that the devices we rely on to care for our patients are disproportionately inaccurate in non-White patients.
We hope that with increased awareness of this problem, meaningful action will be taken by device companies to ensure pulse oximeters work accurately for all patients.
From the Division of Pulmonary and Critical Care, Department of Medicine and the Center for Bioethics and Social Sciences in Medicine, University of Michigan Medical School (Drs. Harlan and Valley), and the Institute for Healthcare Policy and Innovation (Dr. Valley), University of Michigan, Ann Arbor, MI; and the Division of Pulmonary Sciences and Critical Care Medicine, University of Colorado School of Medicine, Aurora, CO (Dr. Colon Hidalgo).
Pulse oximetry is a vital monitoring tool in the ICU and in pulmonary medicine. Regrettably, re-emerging data show that pulse oximeters do not accurately measure blood oxygen levels in Black patients, presumably due to their skin tone. (i.e., low arterial oxygen saturation despite a seemingly normal pulse oximetry reading). While inaccuracy of pulse oximeter measurements in patients with darker skin has been recognized for decades, recent studies have highlighted this as an ongoing problem with potentially severe consequences for Black patients and other patients of color.
One recent study found that Black patients had almost three times the likelihood of occult hypoxemia compared with White patients (Sjoding, MW, et al. N Engl J Med. 2020;383[25]:2477-8).
Subsequent studies have confirmed this to be a widespread problem across various clinical settings in hundreds of hospitals (Wong AI, et al. JAMA Netw Open. 2021;4[11]:e2131674; Valbuena VS, et al. Chest. 2022;161[4]:971-8). A recent retrospective cohort study of patients with COVID-19 found that occult hypoxemia in Black and Hispanic patients was associated with delayed eligibility for potentially lifesaving COVID-19 therapies (Fawzy AF, et al. JAMA Intern Med. 2022; published online May 31, 2022).
Now that numerous studies have demonstrated the inaccuracy of pulse oximetry with the potential to cause harm to historically marginalized racial and ethnic groups, must we abandon the use of pulse oximetry? We would argue that pulse oximeters remain valuable tools, but for now, we must adapt our practice until better devices are widely adopted.
First, it is crucial that health professionals are aware that pulse oximeters may underestimate the true extent of hypoxemia for all patients, but particularly for patients with darker skin. Acknowledging this device flaw is essential to avoid harm to our patients.
Second, clinicians must have heightened skepticism for seemingly normal pulse oximetry values when caring for symptomatic patients at risk of occult hypoxemia.
Until better pulse oximeters are widely available, clinicians must consider workarounds aimed at ensuring timely identification of hypoxemia in Black patients and other patients of color.
These patients may need invasive monitoring of arterial oxygenation, including arterial blood gas checks or an arterial catheter. However, invasive monitoring comes at the cost of discomfort to patients and potential complications, such as vessel or nerve damage.
Invasive monitoring of patients at risk for occult hypoxemia is not an equitable or acceptable long-term solution for this problem. As advocates for patients, clinicians and professional organizations should lobby regulatory bodies to ensure pulse oximeters are accurate for all patients.
We must also call on government leaders to move this process forward. For example, in response to efforts by the United Kingdom’s Intensive Care Society, the Health Secretary of the UK, Sajid Javid, has called for a review of pulse oximeters as part of a larger review assessing structural issues in health care that lead to worse outcomes in racial and ethnic minorities (BBC News. https://www.bbc.com/news/uk-59363544. Published online Nov. 21, 2021).
Device companies are largely for-profit corporations with obligations to their shareholders. It seems that existing incentives are insufficient to motivate investment in less biased technology and real-world evaluations of their devices.
We previously called for buyers of pulse oximeters to change the incentives of device companies – that is, for “hospitals to commit to only purchasing pulse oximeters that have been shown to work equally well in patients of colour.” (Hidalgo DC, et al. Lancet Respir Med. 2021;9[4]:E37). And, indeed, we worry that hospitals are putting themselves at medicolegal risk by not raising their purchasing standards. Since it is now widely known that pulse oximeters are inaccurate in certain patients, could there be liability for hospitals that continue to use devices we know to be disproportionately inaccurate by race?
Device companies must commit to fixing racial bias in pulse oximeters. Change is feasible, and pulse oximeters can be redesigned to be accurate and reliable among all patients using existing technology that is decades-old.
In the 1960s and 1970s, Hewlett Packard worked with NASA to noninvasively measure oxygen saturation in astronauts (Moran-Thomas, M. Wired. Published online June 4, 2021. https://www.wired.com/story/pulse-oximeters-equity). The device was designed to work for all skin tones and could be calibrated based on an individual’s skin tone. However, Hewlett Packard moved away from medical devices in the 1980s, shelving their design while other companies took over the oximeter market.
Lastly, as new devices are designed, they must be proven to work for all patients. Testing should be conducted in real-world clinical settings using metrics aligned with clinical care, since we know testing in artificial environments may not generalize to critically ill patients. Testing standards historically used by the FDA, such as only requiring device testing in a small number of non-White individuals, may miss clinically relevant hypoxemia. Non-inferiority studies are particularly susceptible to poor design or under-powering, and rigorous standards are needed from unbiased sources.
While potential solutions are currently being evaluated, the fact remains that the inaccuracy of pulse oximeters has been known for decades without any meaningful action taken to correct the problem.
As Valeria Valbuena, author of a study demonstrating inaccuracy of pulse oximetry in patients about to undergo ECMO, points out, “Using White patients as the standard in biomedical design has led to both differential care and innovation inertia for optimizing the way devices and algorithms work for patients of racial and ethnic minoritized groups” (Valbuena VS. JAMA Intern Med. 2022. doi: 10.1001/jamainternmed.2022.1903).
We know that hypoxemia is dangerous for our patients and that this is only one example of the long-standing systemic racism leading to harm in historically marginalized racial and ethnic groups. It is unacceptable that the devices we rely on to care for our patients are disproportionately inaccurate in non-White patients.
We hope that with increased awareness of this problem, meaningful action will be taken by device companies to ensure pulse oximeters work accurately for all patients.
From the Division of Pulmonary and Critical Care, Department of Medicine and the Center for Bioethics and Social Sciences in Medicine, University of Michigan Medical School (Drs. Harlan and Valley), and the Institute for Healthcare Policy and Innovation (Dr. Valley), University of Michigan, Ann Arbor, MI; and the Division of Pulmonary Sciences and Critical Care Medicine, University of Colorado School of Medicine, Aurora, CO (Dr. Colon Hidalgo).
Pulse oximetry is a vital monitoring tool in the ICU and in pulmonary medicine. Regrettably, re-emerging data show that pulse oximeters do not accurately measure blood oxygen levels in Black patients, presumably due to their skin tone. (i.e., low arterial oxygen saturation despite a seemingly normal pulse oximetry reading). While inaccuracy of pulse oximeter measurements in patients with darker skin has been recognized for decades, recent studies have highlighted this as an ongoing problem with potentially severe consequences for Black patients and other patients of color.
One recent study found that Black patients had almost three times the likelihood of occult hypoxemia compared with White patients (Sjoding, MW, et al. N Engl J Med. 2020;383[25]:2477-8).
Subsequent studies have confirmed this to be a widespread problem across various clinical settings in hundreds of hospitals (Wong AI, et al. JAMA Netw Open. 2021;4[11]:e2131674; Valbuena VS, et al. Chest. 2022;161[4]:971-8). A recent retrospective cohort study of patients with COVID-19 found that occult hypoxemia in Black and Hispanic patients was associated with delayed eligibility for potentially lifesaving COVID-19 therapies (Fawzy AF, et al. JAMA Intern Med. 2022; published online May 31, 2022).
Now that numerous studies have demonstrated the inaccuracy of pulse oximetry with the potential to cause harm to historically marginalized racial and ethnic groups, must we abandon the use of pulse oximetry? We would argue that pulse oximeters remain valuable tools, but for now, we must adapt our practice until better devices are widely adopted.
First, it is crucial that health professionals are aware that pulse oximeters may underestimate the true extent of hypoxemia for all patients, but particularly for patients with darker skin. Acknowledging this device flaw is essential to avoid harm to our patients.
Second, clinicians must have heightened skepticism for seemingly normal pulse oximetry values when caring for symptomatic patients at risk of occult hypoxemia.
Until better pulse oximeters are widely available, clinicians must consider workarounds aimed at ensuring timely identification of hypoxemia in Black patients and other patients of color.
These patients may need invasive monitoring of arterial oxygenation, including arterial blood gas checks or an arterial catheter. However, invasive monitoring comes at the cost of discomfort to patients and potential complications, such as vessel or nerve damage.
Invasive monitoring of patients at risk for occult hypoxemia is not an equitable or acceptable long-term solution for this problem. As advocates for patients, clinicians and professional organizations should lobby regulatory bodies to ensure pulse oximeters are accurate for all patients.
We must also call on government leaders to move this process forward. For example, in response to efforts by the United Kingdom’s Intensive Care Society, the Health Secretary of the UK, Sajid Javid, has called for a review of pulse oximeters as part of a larger review assessing structural issues in health care that lead to worse outcomes in racial and ethnic minorities (BBC News. https://www.bbc.com/news/uk-59363544. Published online Nov. 21, 2021).
Device companies are largely for-profit corporations with obligations to their shareholders. It seems that existing incentives are insufficient to motivate investment in less biased technology and real-world evaluations of their devices.
We previously called for buyers of pulse oximeters to change the incentives of device companies – that is, for “hospitals to commit to only purchasing pulse oximeters that have been shown to work equally well in patients of colour.” (Hidalgo DC, et al. Lancet Respir Med. 2021;9[4]:E37). And, indeed, we worry that hospitals are putting themselves at medicolegal risk by not raising their purchasing standards. Since it is now widely known that pulse oximeters are inaccurate in certain patients, could there be liability for hospitals that continue to use devices we know to be disproportionately inaccurate by race?
Device companies must commit to fixing racial bias in pulse oximeters. Change is feasible, and pulse oximeters can be redesigned to be accurate and reliable among all patients using existing technology that is decades-old.
In the 1960s and 1970s, Hewlett Packard worked with NASA to noninvasively measure oxygen saturation in astronauts (Moran-Thomas, M. Wired. Published online June 4, 2021. https://www.wired.com/story/pulse-oximeters-equity). The device was designed to work for all skin tones and could be calibrated based on an individual’s skin tone. However, Hewlett Packard moved away from medical devices in the 1980s, shelving their design while other companies took over the oximeter market.
Lastly, as new devices are designed, they must be proven to work for all patients. Testing should be conducted in real-world clinical settings using metrics aligned with clinical care, since we know testing in artificial environments may not generalize to critically ill patients. Testing standards historically used by the FDA, such as only requiring device testing in a small number of non-White individuals, may miss clinically relevant hypoxemia. Non-inferiority studies are particularly susceptible to poor design or under-powering, and rigorous standards are needed from unbiased sources.
While potential solutions are currently being evaluated, the fact remains that the inaccuracy of pulse oximeters has been known for decades without any meaningful action taken to correct the problem.
As Valeria Valbuena, author of a study demonstrating inaccuracy of pulse oximetry in patients about to undergo ECMO, points out, “Using White patients as the standard in biomedical design has led to both differential care and innovation inertia for optimizing the way devices and algorithms work for patients of racial and ethnic minoritized groups” (Valbuena VS. JAMA Intern Med. 2022. doi: 10.1001/jamainternmed.2022.1903).
We know that hypoxemia is dangerous for our patients and that this is only one example of the long-standing systemic racism leading to harm in historically marginalized racial and ethnic groups. It is unacceptable that the devices we rely on to care for our patients are disproportionately inaccurate in non-White patients.
We hope that with increased awareness of this problem, meaningful action will be taken by device companies to ensure pulse oximeters work accurately for all patients.
From the Division of Pulmonary and Critical Care, Department of Medicine and the Center for Bioethics and Social Sciences in Medicine, University of Michigan Medical School (Drs. Harlan and Valley), and the Institute for Healthcare Policy and Innovation (Dr. Valley), University of Michigan, Ann Arbor, MI; and the Division of Pulmonary Sciences and Critical Care Medicine, University of Colorado School of Medicine, Aurora, CO (Dr. Colon Hidalgo).
Registry launched to reach more patients with PF
The Pulmonary Fibrosis Foundation (PFF) has launched a new initiative in which they hope to capture a far more diverse representation of patients with pulmonary fibrosis (PF) than the current registry allows them to do, a press release from the PFF indicated.
“The existing registry we have – the PFF Patient Registry – is limited to our care centers, which are primarily academic clinical institutions and we have only a few thousand patients within that registry,” Junelle Speller, MBA, vice president of the PFF Registry, told this news organization.
“We wanted to go beyond these care centers and capture patients in community centers, and in rural settings to provide a more complete understanding of patients with this disease and, of course, have a larger sample size,” she added.
“ across all parts of the United States and, most importantly, accelerate the research on PF toward improving earlier diagnosis, treatment, and outcomes for these patients,” Ms. Speller said.
Passive versus active
The PFF Community Registry differs in its structure and purpose from the PFF Patient Registry, as Ms. Speller explained. First, the PFF Patient Registry, established in 2016, is “passive” in its nature in that whatever information is entered into a patient’s electronic medical record or clinical chart on a routine office visit is abstracted and captured in the registry. By contrast, the PFF Community Registry is asking for self-reported data from patients, “so it’s more of an ‘active’ registry and will give us a chance to have a bidirectional connection with participants, provide email updates and newsletters, and give patients an opportunity to participate in future studies within the registry as well as in clinical trials,” she noted.
The two registries still overlap in that both capture demographic data on patients’ medical and family histories as well as any medications patients may be taking, but the Community Registry will also capture information with respect to education, employment, patient-reported outcomes, and quality of life metrics. “It will also let us know how patients feel about continued education on the disease itself and patient participation in support groups,” Ms. Speller observed.
The Community Registry will also collect information from lung transplant recipients who have had PF or any other form of interstitial lung disease (ILD) as well as information from caregivers and family members affected by the patient’s disease. As Ms. Speller noted, both PF and other forms of ILD (of which there are more than 200 types) are all characterized by inflammation or scarring in the lung. “Patients are often misdiagnosed, and it can take months, even years, to identify the disease,” Ms. Speller said.
From there, it can be a very long and difficult road ahead, with no cure in sight, although several antifibrotic drugs do help slow disease progression. Typically, onset is around the age of 60 and symptoms include chronic dry cough, fatigue, shortness of breath, weakness, discomfort in the chest, and sometimes unexplained weight loss. Some patients do have a history of smoking, but not all, Ms. Speller noted. So far, registry data suggest PF largely occurs in White patients.
“We’re very excited about the Community Registry, particularly about reaching into communities that we haven’t been able to reach with our existing registry,” Ms. Speller noted. “The rural population in particular is often underserved, so we are really looking forward to capturing data from these patients as well as those from community centers within smaller and larger cities,” she observed.
“A powerful aspect of the Community Registry is that we can use the information gained from it to understand the experience of individuals living with PF, and how it impacts their lives and those of their families and caregivers,” Kevin Flaherty, MD, steering committee chair, PFF Registry, said in a statement.
“Researchers can also look at the data to better understand fibrotic lung diseases and learn about effective approaches to improve patient care,” he added.
Patients who wish to join the PFF Community Registry can sign up at pffregistry.org. To learn more about PF and its risk factors, readers are invited to visit www.AboutPF.org. More than 250,000 patients in the United States are living with either PF or other types of ILD.
Ms. Speller and Dr. Flaherty disclosed no financial conflicts of interest. The PFF Registry is supported by its founding partner, Genentech, Visionary Partner, United Therapeutics, and its sustaining partner, Boehringer Ingelheim, as well as many donors.
A version of this article first appeared on Medscape.com.
This article was updated 8/8/22.
The Pulmonary Fibrosis Foundation (PFF) has launched a new initiative in which they hope to capture a far more diverse representation of patients with pulmonary fibrosis (PF) than the current registry allows them to do, a press release from the PFF indicated.
“The existing registry we have – the PFF Patient Registry – is limited to our care centers, which are primarily academic clinical institutions and we have only a few thousand patients within that registry,” Junelle Speller, MBA, vice president of the PFF Registry, told this news organization.
“We wanted to go beyond these care centers and capture patients in community centers, and in rural settings to provide a more complete understanding of patients with this disease and, of course, have a larger sample size,” she added.
“ across all parts of the United States and, most importantly, accelerate the research on PF toward improving earlier diagnosis, treatment, and outcomes for these patients,” Ms. Speller said.
Passive versus active
The PFF Community Registry differs in its structure and purpose from the PFF Patient Registry, as Ms. Speller explained. First, the PFF Patient Registry, established in 2016, is “passive” in its nature in that whatever information is entered into a patient’s electronic medical record or clinical chart on a routine office visit is abstracted and captured in the registry. By contrast, the PFF Community Registry is asking for self-reported data from patients, “so it’s more of an ‘active’ registry and will give us a chance to have a bidirectional connection with participants, provide email updates and newsletters, and give patients an opportunity to participate in future studies within the registry as well as in clinical trials,” she noted.
The two registries still overlap in that both capture demographic data on patients’ medical and family histories as well as any medications patients may be taking, but the Community Registry will also capture information with respect to education, employment, patient-reported outcomes, and quality of life metrics. “It will also let us know how patients feel about continued education on the disease itself and patient participation in support groups,” Ms. Speller observed.
The Community Registry will also collect information from lung transplant recipients who have had PF or any other form of interstitial lung disease (ILD) as well as information from caregivers and family members affected by the patient’s disease. As Ms. Speller noted, both PF and other forms of ILD (of which there are more than 200 types) are all characterized by inflammation or scarring in the lung. “Patients are often misdiagnosed, and it can take months, even years, to identify the disease,” Ms. Speller said.
From there, it can be a very long and difficult road ahead, with no cure in sight, although several antifibrotic drugs do help slow disease progression. Typically, onset is around the age of 60 and symptoms include chronic dry cough, fatigue, shortness of breath, weakness, discomfort in the chest, and sometimes unexplained weight loss. Some patients do have a history of smoking, but not all, Ms. Speller noted. So far, registry data suggest PF largely occurs in White patients.
“We’re very excited about the Community Registry, particularly about reaching into communities that we haven’t been able to reach with our existing registry,” Ms. Speller noted. “The rural population in particular is often underserved, so we are really looking forward to capturing data from these patients as well as those from community centers within smaller and larger cities,” she observed.
“A powerful aspect of the Community Registry is that we can use the information gained from it to understand the experience of individuals living with PF, and how it impacts their lives and those of their families and caregivers,” Kevin Flaherty, MD, steering committee chair, PFF Registry, said in a statement.
“Researchers can also look at the data to better understand fibrotic lung diseases and learn about effective approaches to improve patient care,” he added.
Patients who wish to join the PFF Community Registry can sign up at pffregistry.org. To learn more about PF and its risk factors, readers are invited to visit www.AboutPF.org. More than 250,000 patients in the United States are living with either PF or other types of ILD.
Ms. Speller and Dr. Flaherty disclosed no financial conflicts of interest. The PFF Registry is supported by its founding partner, Genentech, Visionary Partner, United Therapeutics, and its sustaining partner, Boehringer Ingelheim, as well as many donors.
A version of this article first appeared on Medscape.com.
This article was updated 8/8/22.
The Pulmonary Fibrosis Foundation (PFF) has launched a new initiative in which they hope to capture a far more diverse representation of patients with pulmonary fibrosis (PF) than the current registry allows them to do, a press release from the PFF indicated.
“The existing registry we have – the PFF Patient Registry – is limited to our care centers, which are primarily academic clinical institutions and we have only a few thousand patients within that registry,” Junelle Speller, MBA, vice president of the PFF Registry, told this news organization.
“We wanted to go beyond these care centers and capture patients in community centers, and in rural settings to provide a more complete understanding of patients with this disease and, of course, have a larger sample size,” she added.
“ across all parts of the United States and, most importantly, accelerate the research on PF toward improving earlier diagnosis, treatment, and outcomes for these patients,” Ms. Speller said.
Passive versus active
The PFF Community Registry differs in its structure and purpose from the PFF Patient Registry, as Ms. Speller explained. First, the PFF Patient Registry, established in 2016, is “passive” in its nature in that whatever information is entered into a patient’s electronic medical record or clinical chart on a routine office visit is abstracted and captured in the registry. By contrast, the PFF Community Registry is asking for self-reported data from patients, “so it’s more of an ‘active’ registry and will give us a chance to have a bidirectional connection with participants, provide email updates and newsletters, and give patients an opportunity to participate in future studies within the registry as well as in clinical trials,” she noted.
The two registries still overlap in that both capture demographic data on patients’ medical and family histories as well as any medications patients may be taking, but the Community Registry will also capture information with respect to education, employment, patient-reported outcomes, and quality of life metrics. “It will also let us know how patients feel about continued education on the disease itself and patient participation in support groups,” Ms. Speller observed.
The Community Registry will also collect information from lung transplant recipients who have had PF or any other form of interstitial lung disease (ILD) as well as information from caregivers and family members affected by the patient’s disease. As Ms. Speller noted, both PF and other forms of ILD (of which there are more than 200 types) are all characterized by inflammation or scarring in the lung. “Patients are often misdiagnosed, and it can take months, even years, to identify the disease,” Ms. Speller said.
From there, it can be a very long and difficult road ahead, with no cure in sight, although several antifibrotic drugs do help slow disease progression. Typically, onset is around the age of 60 and symptoms include chronic dry cough, fatigue, shortness of breath, weakness, discomfort in the chest, and sometimes unexplained weight loss. Some patients do have a history of smoking, but not all, Ms. Speller noted. So far, registry data suggest PF largely occurs in White patients.
“We’re very excited about the Community Registry, particularly about reaching into communities that we haven’t been able to reach with our existing registry,” Ms. Speller noted. “The rural population in particular is often underserved, so we are really looking forward to capturing data from these patients as well as those from community centers within smaller and larger cities,” she observed.
“A powerful aspect of the Community Registry is that we can use the information gained from it to understand the experience of individuals living with PF, and how it impacts their lives and those of their families and caregivers,” Kevin Flaherty, MD, steering committee chair, PFF Registry, said in a statement.
“Researchers can also look at the data to better understand fibrotic lung diseases and learn about effective approaches to improve patient care,” he added.
Patients who wish to join the PFF Community Registry can sign up at pffregistry.org. To learn more about PF and its risk factors, readers are invited to visit www.AboutPF.org. More than 250,000 patients in the United States are living with either PF or other types of ILD.
Ms. Speller and Dr. Flaherty disclosed no financial conflicts of interest. The PFF Registry is supported by its founding partner, Genentech, Visionary Partner, United Therapeutics, and its sustaining partner, Boehringer Ingelheim, as well as many donors.
A version of this article first appeared on Medscape.com.
This article was updated 8/8/22.
Robotic bronchoscopy 2022
Over the last several years, hundreds of millions of dollars have been spent on robotic bronchoscopy systems in the United States. The release of robotic scopes was made to great fanfare, translating into the market being infiltrated with these systems. With base costs in the hundreds of thousands of dollars, robotic bronchoscope systems are easily the most expensive singular capital investment in the bronchoscopy suite. I frequently get asked questions from those who have not yet made that purchase: “Should I buy a robot?” “How could I justify a new robot purchase to my hospital?” “Is the hype real?” These are complex questions to answer. Before one can answer, I think it’s best to look back on the last 2 decades of bronchoscopy for peripheral lung nodules to get a better understanding of the value proposition robotic bronchoscopes may offer.
Guided bronchoscopy for lung nodules has significantly evolved over the past 2 decades, shifting diagnostic procedures from interventional radiologist to the pulmonologist. Some of these advances were based in redesigns of the bronchoscope (ultrathin bronchoscopy) or application of technology to the bronchoscope (radial EBUS, virtual bronchoscopy); but, these were not broadly applicable to the pulmonology community at large. It was not until the development of electromagnetic navigational bronchoscopy (ENB) that widespread adoption of bronchoscopy for lung nodules occurred. By and large, ENB fueled a rapid expansion of nodule bronchoscopy, mainly due to its ease of use and novel approach. Initial studies of ENB had impressive results; however, studies were criticized for having small numbers, inadequate follow-up, spurious definitions of yield, and that they were being done at highly specialized centers. The NAVIGATE trial was launched to address these criticisms among “real world” conditions. Sponsored by Medtronic, it studied ENB (superDimension platform, v6.0 or higher) across 29 academic and medical centers in the United States, enrolling over 1,000 patients (Folch EE, et al. J Thorac Oncol. 2019;14[3]:445-58. Epub 2018 Nov 23), and reported a diagnostic yield of 73%.

This led to a drive to improve upon yield, resulting in development of new technologies specifically designed to address some of the factors thought associated with diminished yield, and, out of this, robotic bronchoscopy was born. These factors included CT scan-body registration divergence, deflection of the extended working channel (EWC) by rigid biopsy tools, and inability to accurately “aim” the EWC-biopsy tool at the nodule; these were especially problematic in nodules not associated with airways. Robotic scopes were specifically designed to reach into the peripheral lung airways similar to an EWC, but with better structural integrity and steerability. This tip integrity would resist tool-related displacement, and steerability would allow for improved targeting of nodules during the biopsy.
There are two robots approved by the FDA at the time of this writing (Auris Monarch, Intuitive Ion), with a third awaiting FDA clearance (Noah Galaxy). In general, though the engineering of the robotic scopes to improve structural tip integrity are similar, the approach to navigation and targeting vary significantly. The Monarch platform uses electromagnetic guidance, similar to other traditional ENB platforms. The Ion platform does not use ENB; instead, it uses fiberoptic shape sensing technology, which analyzes the shape and orientation of the scope to provide location information. There are potential advantages to shape sensing, the most notable being the absence of electromagnetics; this allows for use of fluoroscopy during the procedure, which otherwise would have interfered with ENB-based navigation. There are other subtle differences between the two robots. The Monarch uses a scope-in-scope design, with a robotic scope contained within a robotic sheath; the Ion uses a single robotic scope. The Ion scope diameter is 3.5 mm, whereas the Monarch diameter is 4.4 mm; this may be a potential advantage when having to navigate through smaller airways.
So, which robot is better suited to reach peripheral nodules more consistently and accurately? I get asked this question a lot, since I have both platforms at my institution. But, answering with my own opinion based on my institution’s anecdotal experience would be irresponsible. I’m more of a “what does the data show?” person. Luckily, we do have clinical trials in both robot technologies. It should be noted here that there will likely never be a head-to-head randomized trial, so evaluating published studies with each platform is going to be the best method we have for comparison going forward, albeit an imperfect one. It should also be noted that many of the early robotic bronchoscopy trials have to be looked at with caution, as yield definitions tended not to be conservative and/or the follow-up of non-malignant was not robust. With that in mind, let’s review representative high-quality studies for each platform.
The best study to date using the Ion platform came out of Memorial Sloan Kettering Cancer Center (Kalchiem-Dekel O, et al. Chest. 2022;161[2];572-82). This single-site study reported on 159 nodule biopsies, with the primary outcome being diagnostic yield. The patients had 1 year of follow-up, and the definition of yield was conservative. The average lesion size was 18 mm, and nodule locations and characteristics were representative of real-world conditions. Overall diagnostic yield was 81.7%; however, it dropped to under 70% for nodules under 20 mm in size.
The largest study to date using the Monarch platform was also a single center study, this from the University of Chicago (Agrawal, et al. Ann Thorac Surg. 2022 Jan 17;S0003-4975(22)00042-X. Online ahead of print). This study included 124 nodules with at least 12 months of follow-up; diagnostic yield definition was conservative. Median nodule size was 20.5 mm, with distribution and characteristics representative of real-world conditions. Overall accuracy was 77%, and, similar to the Ion study, dropped to under 70% when nodule size was smaller than 20 mm.
Overall, both robot studies seemed to show a modest improvement in diagnostic yield when compared with ENB, and their outcomes were overall similar. It is important to remember that these were studies of each center’s first experiences with early versions of each technology; over time, the technology will continue to improve, as will operator skill and experience, and with that, perhaps improvements in yield will be seen, as well.
Interestingly, both studies evaluated target localization using radial EBUS (rEBUS), which also allowed for airway-nodule relationships to be reported. In Kalchiem-Dekel’s study, 85% of cases used rEBUS to determine localization, and, of these, 91.2% of cases showed accurate localization. In Agrawal’s study, rEBUS was used in all cases with a reported localization of 94%. In both, yield did not seem to be affected by airway-nodule relationships, perhaps explained by more robust tip control of the robotic scope. However, localization did not equate to yield in all cases, which brings up a very important question: Can the yield of robotic bronchoscopy be further improved with better real-time on-board imaging, such as CBCT scanning or C-arm based tomography? Currently, there is a study using 3D technology (Cios 3D Mobile Spin) in conjunction with the Ion platform to evaluate this.
So, let’s circle back to where we started. I think if you look at the totality of the data, it is clear that the robotic platforms currently offer a modest improvement in diagnostic yield over traditional ENB, with individual performances that are somewhat equivalent despite differences in design and operation. But does this improvement in yield justify the cost? Individual hospitals will have to make that decision. The capital cost and per-use price of the scope is significant, which has to be balanced against each center’s current performance with non-robotic bronchoscopy.
To date, there have been over 25,000 robotic procedures performed in the United States, so enthusiasm across diverse centers is being maintained. Whether this enthusiasm is driven by yield or novelty, or both, I’m not sure. With other nonrobotic platforms having reached, or soon to reach, the market, this is a good time to be in the business of bronchoscopy.
Dr. Cicenia is in the Section of Bronchoscopy at Cleveland Clinic’s Respiratory Institute, Cleveland, Ohio.
Over the last several years, hundreds of millions of dollars have been spent on robotic bronchoscopy systems in the United States. The release of robotic scopes was made to great fanfare, translating into the market being infiltrated with these systems. With base costs in the hundreds of thousands of dollars, robotic bronchoscope systems are easily the most expensive singular capital investment in the bronchoscopy suite. I frequently get asked questions from those who have not yet made that purchase: “Should I buy a robot?” “How could I justify a new robot purchase to my hospital?” “Is the hype real?” These are complex questions to answer. Before one can answer, I think it’s best to look back on the last 2 decades of bronchoscopy for peripheral lung nodules to get a better understanding of the value proposition robotic bronchoscopes may offer.
Guided bronchoscopy for lung nodules has significantly evolved over the past 2 decades, shifting diagnostic procedures from interventional radiologist to the pulmonologist. Some of these advances were based in redesigns of the bronchoscope (ultrathin bronchoscopy) or application of technology to the bronchoscope (radial EBUS, virtual bronchoscopy); but, these were not broadly applicable to the pulmonology community at large. It was not until the development of electromagnetic navigational bronchoscopy (ENB) that widespread adoption of bronchoscopy for lung nodules occurred. By and large, ENB fueled a rapid expansion of nodule bronchoscopy, mainly due to its ease of use and novel approach. Initial studies of ENB had impressive results; however, studies were criticized for having small numbers, inadequate follow-up, spurious definitions of yield, and that they were being done at highly specialized centers. The NAVIGATE trial was launched to address these criticisms among “real world” conditions. Sponsored by Medtronic, it studied ENB (superDimension platform, v6.0 or higher) across 29 academic and medical centers in the United States, enrolling over 1,000 patients (Folch EE, et al. J Thorac Oncol. 2019;14[3]:445-58. Epub 2018 Nov 23), and reported a diagnostic yield of 73%.
This led to a drive to improve upon yield, resulting in development of new technologies specifically designed to address some of the factors thought associated with diminished yield, and, out of this, robotic bronchoscopy was born. These factors included CT scan-body registration divergence, deflection of the extended working channel (EWC) by rigid biopsy tools, and inability to accurately “aim” the EWC-biopsy tool at the nodule; these were especially problematic in nodules not associated with airways. Robotic scopes were specifically designed to reach into the peripheral lung airways similar to an EWC, but with better structural integrity and steerability. This tip integrity would resist tool-related displacement, and steerability would allow for improved targeting of nodules during the biopsy.
There are two robots approved by the FDA at the time of this writing (Auris Monarch, Intuitive Ion), with a third awaiting FDA clearance (Noah Galaxy). In general, though the engineering of the robotic scopes to improve structural tip integrity are similar, the approach to navigation and targeting vary significantly. The Monarch platform uses electromagnetic guidance, similar to other traditional ENB platforms. The Ion platform does not use ENB; instead, it uses fiberoptic shape sensing technology, which analyzes the shape and orientation of the scope to provide location information. There are potential advantages to shape sensing, the most notable being the absence of electromagnetics; this allows for use of fluoroscopy during the procedure, which otherwise would have interfered with ENB-based navigation. There are other subtle differences between the two robots. The Monarch uses a scope-in-scope design, with a robotic scope contained within a robotic sheath; the Ion uses a single robotic scope. The Ion scope diameter is 3.5 mm, whereas the Monarch diameter is 4.4 mm; this may be a potential advantage when having to navigate through smaller airways.
So, which robot is better suited to reach peripheral nodules more consistently and accurately? I get asked this question a lot, since I have both platforms at my institution. But, answering with my own opinion based on my institution’s anecdotal experience would be irresponsible. I’m more of a “what does the data show?” person. Luckily, we do have clinical trials in both robot technologies. It should be noted here that there will likely never be a head-to-head randomized trial, so evaluating published studies with each platform is going to be the best method we have for comparison going forward, albeit an imperfect one. It should also be noted that many of the early robotic bronchoscopy trials have to be looked at with caution, as yield definitions tended not to be conservative and/or the follow-up of non-malignant was not robust. With that in mind, let’s review representative high-quality studies for each platform.
The best study to date using the Ion platform came out of Memorial Sloan Kettering Cancer Center (Kalchiem-Dekel O, et al. Chest. 2022;161[2];572-82). This single-site study reported on 159 nodule biopsies, with the primary outcome being diagnostic yield. The patients had 1 year of follow-up, and the definition of yield was conservative. The average lesion size was 18 mm, and nodule locations and characteristics were representative of real-world conditions. Overall diagnostic yield was 81.7%; however, it dropped to under 70% for nodules under 20 mm in size.
The largest study to date using the Monarch platform was also a single center study, this from the University of Chicago (Agrawal, et al. Ann Thorac Surg. 2022 Jan 17;S0003-4975(22)00042-X. Online ahead of print). This study included 124 nodules with at least 12 months of follow-up; diagnostic yield definition was conservative. Median nodule size was 20.5 mm, with distribution and characteristics representative of real-world conditions. Overall accuracy was 77%, and, similar to the Ion study, dropped to under 70% when nodule size was smaller than 20 mm.
Overall, both robot studies seemed to show a modest improvement in diagnostic yield when compared with ENB, and their outcomes were overall similar. It is important to remember that these were studies of each center’s first experiences with early versions of each technology; over time, the technology will continue to improve, as will operator skill and experience, and with that, perhaps improvements in yield will be seen, as well.
Interestingly, both studies evaluated target localization using radial EBUS (rEBUS), which also allowed for airway-nodule relationships to be reported. In Kalchiem-Dekel’s study, 85% of cases used rEBUS to determine localization, and, of these, 91.2% of cases showed accurate localization. In Agrawal’s study, rEBUS was used in all cases with a reported localization of 94%. In both, yield did not seem to be affected by airway-nodule relationships, perhaps explained by more robust tip control of the robotic scope. However, localization did not equate to yield in all cases, which brings up a very important question: Can the yield of robotic bronchoscopy be further improved with better real-time on-board imaging, such as CBCT scanning or C-arm based tomography? Currently, there is a study using 3D technology (Cios 3D Mobile Spin) in conjunction with the Ion platform to evaluate this.
So, let’s circle back to where we started. I think if you look at the totality of the data, it is clear that the robotic platforms currently offer a modest improvement in diagnostic yield over traditional ENB, with individual performances that are somewhat equivalent despite differences in design and operation. But does this improvement in yield justify the cost? Individual hospitals will have to make that decision. The capital cost and per-use price of the scope is significant, which has to be balanced against each center’s current performance with non-robotic bronchoscopy.
To date, there have been over 25,000 robotic procedures performed in the United States, so enthusiasm across diverse centers is being maintained. Whether this enthusiasm is driven by yield or novelty, or both, I’m not sure. With other nonrobotic platforms having reached, or soon to reach, the market, this is a good time to be in the business of bronchoscopy.
Dr. Cicenia is in the Section of Bronchoscopy at Cleveland Clinic’s Respiratory Institute, Cleveland, Ohio.
Over the last several years, hundreds of millions of dollars have been spent on robotic bronchoscopy systems in the United States. The release of robotic scopes was made to great fanfare, translating into the market being infiltrated with these systems. With base costs in the hundreds of thousands of dollars, robotic bronchoscope systems are easily the most expensive singular capital investment in the bronchoscopy suite. I frequently get asked questions from those who have not yet made that purchase: “Should I buy a robot?” “How could I justify a new robot purchase to my hospital?” “Is the hype real?” These are complex questions to answer. Before one can answer, I think it’s best to look back on the last 2 decades of bronchoscopy for peripheral lung nodules to get a better understanding of the value proposition robotic bronchoscopes may offer.
Guided bronchoscopy for lung nodules has significantly evolved over the past 2 decades, shifting diagnostic procedures from interventional radiologist to the pulmonologist. Some of these advances were based in redesigns of the bronchoscope (ultrathin bronchoscopy) or application of technology to the bronchoscope (radial EBUS, virtual bronchoscopy); but, these were not broadly applicable to the pulmonology community at large. It was not until the development of electromagnetic navigational bronchoscopy (ENB) that widespread adoption of bronchoscopy for lung nodules occurred. By and large, ENB fueled a rapid expansion of nodule bronchoscopy, mainly due to its ease of use and novel approach. Initial studies of ENB had impressive results; however, studies were criticized for having small numbers, inadequate follow-up, spurious definitions of yield, and that they were being done at highly specialized centers. The NAVIGATE trial was launched to address these criticisms among “real world” conditions. Sponsored by Medtronic, it studied ENB (superDimension platform, v6.0 or higher) across 29 academic and medical centers in the United States, enrolling over 1,000 patients (Folch EE, et al. J Thorac Oncol. 2019;14[3]:445-58. Epub 2018 Nov 23), and reported a diagnostic yield of 73%.
This led to a drive to improve upon yield, resulting in development of new technologies specifically designed to address some of the factors thought associated with diminished yield, and, out of this, robotic bronchoscopy was born. These factors included CT scan-body registration divergence, deflection of the extended working channel (EWC) by rigid biopsy tools, and inability to accurately “aim” the EWC-biopsy tool at the nodule; these were especially problematic in nodules not associated with airways. Robotic scopes were specifically designed to reach into the peripheral lung airways similar to an EWC, but with better structural integrity and steerability. This tip integrity would resist tool-related displacement, and steerability would allow for improved targeting of nodules during the biopsy.
There are two robots approved by the FDA at the time of this writing (Auris Monarch, Intuitive Ion), with a third awaiting FDA clearance (Noah Galaxy). In general, though the engineering of the robotic scopes to improve structural tip integrity are similar, the approach to navigation and targeting vary significantly. The Monarch platform uses electromagnetic guidance, similar to other traditional ENB platforms. The Ion platform does not use ENB; instead, it uses fiberoptic shape sensing technology, which analyzes the shape and orientation of the scope to provide location information. There are potential advantages to shape sensing, the most notable being the absence of electromagnetics; this allows for use of fluoroscopy during the procedure, which otherwise would have interfered with ENB-based navigation. There are other subtle differences between the two robots. The Monarch uses a scope-in-scope design, with a robotic scope contained within a robotic sheath; the Ion uses a single robotic scope. The Ion scope diameter is 3.5 mm, whereas the Monarch diameter is 4.4 mm; this may be a potential advantage when having to navigate through smaller airways.
So, which robot is better suited to reach peripheral nodules more consistently and accurately? I get asked this question a lot, since I have both platforms at my institution. But, answering with my own opinion based on my institution’s anecdotal experience would be irresponsible. I’m more of a “what does the data show?” person. Luckily, we do have clinical trials in both robot technologies. It should be noted here that there will likely never be a head-to-head randomized trial, so evaluating published studies with each platform is going to be the best method we have for comparison going forward, albeit an imperfect one. It should also be noted that many of the early robotic bronchoscopy trials have to be looked at with caution, as yield definitions tended not to be conservative and/or the follow-up of non-malignant was not robust. With that in mind, let’s review representative high-quality studies for each platform.
The best study to date using the Ion platform came out of Memorial Sloan Kettering Cancer Center (Kalchiem-Dekel O, et al. Chest. 2022;161[2];572-82). This single-site study reported on 159 nodule biopsies, with the primary outcome being diagnostic yield. The patients had 1 year of follow-up, and the definition of yield was conservative. The average lesion size was 18 mm, and nodule locations and characteristics were representative of real-world conditions. Overall diagnostic yield was 81.7%; however, it dropped to under 70% for nodules under 20 mm in size.
The largest study to date using the Monarch platform was also a single center study, this from the University of Chicago (Agrawal, et al. Ann Thorac Surg. 2022 Jan 17;S0003-4975(22)00042-X. Online ahead of print). This study included 124 nodules with at least 12 months of follow-up; diagnostic yield definition was conservative. Median nodule size was 20.5 mm, with distribution and characteristics representative of real-world conditions. Overall accuracy was 77%, and, similar to the Ion study, dropped to under 70% when nodule size was smaller than 20 mm.
Overall, both robot studies seemed to show a modest improvement in diagnostic yield when compared with ENB, and their outcomes were overall similar. It is important to remember that these were studies of each center’s first experiences with early versions of each technology; over time, the technology will continue to improve, as will operator skill and experience, and with that, perhaps improvements in yield will be seen, as well.
Interestingly, both studies evaluated target localization using radial EBUS (rEBUS), which also allowed for airway-nodule relationships to be reported. In Kalchiem-Dekel’s study, 85% of cases used rEBUS to determine localization, and, of these, 91.2% of cases showed accurate localization. In Agrawal’s study, rEBUS was used in all cases with a reported localization of 94%. In both, yield did not seem to be affected by airway-nodule relationships, perhaps explained by more robust tip control of the robotic scope. However, localization did not equate to yield in all cases, which brings up a very important question: Can the yield of robotic bronchoscopy be further improved with better real-time on-board imaging, such as CBCT scanning or C-arm based tomography? Currently, there is a study using 3D technology (Cios 3D Mobile Spin) in conjunction with the Ion platform to evaluate this.
So, let’s circle back to where we started. I think if you look at the totality of the data, it is clear that the robotic platforms currently offer a modest improvement in diagnostic yield over traditional ENB, with individual performances that are somewhat equivalent despite differences in design and operation. But does this improvement in yield justify the cost? Individual hospitals will have to make that decision. The capital cost and per-use price of the scope is significant, which has to be balanced against each center’s current performance with non-robotic bronchoscopy.
To date, there have been over 25,000 robotic procedures performed in the United States, so enthusiasm across diverse centers is being maintained. Whether this enthusiasm is driven by yield or novelty, or both, I’m not sure. With other nonrobotic platforms having reached, or soon to reach, the market, this is a good time to be in the business of bronchoscopy.
Dr. Cicenia is in the Section of Bronchoscopy at Cleveland Clinic’s Respiratory Institute, Cleveland, Ohio.
New Omicron COVID boosters coming soon: What to know now
– a month ahead of schedule, the Biden administration announced this week.
Moderna has signed a $1.74 billion federal contract to supply 66 million initial doses of the “bivalent” booster, which includes the original “ancestral” virus strain and elements of the Omicron BA.4 and BA.5 variants. Pfizer also announced a $3.2 billion U.S. agreement for another 105 million shots. Both vaccine suppliers have signed options to provide millions more boosters in the months ahead.
About 83.5% of Americans have received at least one COVID-19 shot, with 71.5% fully vaccinated with the initial series, 48% receiving one booster shot, and 31% two boosters, according to the CDC. With about 130,000 new COVID cases per day, and about 440 deaths, officials say the updated boosters may help rein in those figures by targeting the highly transmissible and widely circulating Omicron strains.
Federal health officials are still hammering out details of guidelines and recommendations of who should get the boosters, which are expected to come from the CDC and FDA. For now, authorities have decided not to expand eligibility for second boosters of the existing vaccines – now recommended only for adults over 50 and those 12 and older with immune deficiencies. Children 5 through 11 are advised to receive a single booster, 5 months after their initial vaccine series.
For a preview of what to expect from the CDC and FDA, this news organization spoke with Keri Althoff, PhD, an epidemiologist at Johns Hopkins University, Baltimore.
Q: Based on what we know now, who should be getting one of these new bivalent boosters?A: Of course, there is a process here regarding the specific recommendations, but it appears there will likely be a recommendation for all individuals to get this bivalent booster, similar to the first booster. And there will likely be a recommended time frame as to time since the last booster.
Right now, we have a recommendation for adults over the age of 50 or adults who are at higher risk for severe COVID-related illness [to get] a second booster. For them, there will probably be a timeline that says you should get the booster if you’re X amount of months or more from your second booster; or X amount of months or more from your first booster, if you’ve only had one.
Q: What about pregnant women or those being treated for chronic health conditions?A: I would imagine that once this bivalent booster becomes available, it will be recommended for all adults.
Q: And for children?A: That’s a good question. It’s something I have been digging into, [and] I think parents are really interested in this. Most kids, 5 and above, are supposed to be boosted with one shot right now, if they’re X amount of days from their primary vaccine series. Of course those 6 months to 4.99 years are not yet eligible [for boosters].
As a parent, I would love to see my children become eligible for the bivalent booster. It would be great if these boosters are conveying some additional protection that the kids could get access to before we send them off to school this fall. But there are questions as to whether or not that is going to happen.
Q: If you never received a booster, but only the preliminary vaccine series, do you need to get those earlier boosters before having the new bivalent booster shot?A: I don’t think they will likely make that a requirement – to restrict the bivalent booster only to those who are already boosted or up to date on their vaccines at the time the bivalent booster becomes available. But that will be up to the [CDC] vaccine recommendation committee to decide.
Q: Are there any new risks associated with these boosters, since they were developed so rapidly?A: No. We continue to monitor this technology, and with all the mRNA vaccines that have been delivered, you have seen all that monitoring play out with the detection, for example, of different forms of inflammation of the heart tissue and who that may impact. So, those monitoring systems work, and they work really, really well, so we can detect those things. And we know these vaccines are definitely safe.
Q: Some health experts are concerned “vaccine fatigue” will have an impact on the booster campaign. What’s your take?A: We have seen this fatigue in the proportion of individuals who are boosted with a first booster and even boosted with a second. But having those earlier boosters along with this new bivalent booster is important, because essentially, what we’re doing is really priming the immune system.
We’re trying to expedite the process of getting people’s immune system up to speed so that when the virus comes our way – as we know it will, because [of] these Omicron strains that are highly infectious and really whipping through our communities – we’re able to get the highest level of population immunity, you don’t end up in the hospital.
Q: What other challenges do you see in persuading Americans to get another round of boosters?A: One of the things that I’ve been hearing a lot, which I get very nervous about, is people saying: “Oh, I got fully vaccinated, I did or did not get the booster, and I had COVID anyway and it was really nothing, it didn’t feel like much to me, and so I’m not going to be boosted anymore.” We are not in a place quite yet where those guidelines are being rolled back in any way, shape, or form. We still have highly vulnerable people to severe disease and death in our communities, and we’re seeing hundreds of deaths every day.
There are consequences, even if it isn’t in severity of disease, meaning hospitalization and death. And let’s not let the actual quality of the vaccine being so successful that it can keep you out of the hospital. Don’t mistake that for “I don’t need another one.”
Q: Unlike the flu shot, which is reformulated each year to match circulating strains, the new COVID boosters offer protection against older strains as well as the newer ones. Why?A: It’s all about creating a broader immune response in individuals so that as more strains emerge, which they likely will, we can create a broader population immune response [to all strains]. Our individual bodies are seeing differences in these strains through vaccination that helps everyone stay healthy.
Q: There haven’t been clinical trials of these new mRNA boosters. How strong is the evidence that they will be effective against the emerging Omicron variants?A: There have been some studies – some great studies – looking at things like neutralizing antibodies, which we use as a surrogate for clinical trials. But that is not the same as studying the outcome of interest, which would be hospitalizations. So, part of the challenge is to be able to say: “Okay, this is what we know about the safety and effectiveness of the prior vaccines ... and how can we relate that to outcomes with these new boosters at an earlier stage [before] clinical data is available?”
Q: How long will the new boosters’ protections last – do we know yet?A: That timing is still a question, but of course what plays a big role in that is what COVID strains are circulating. If we prep these boosters that are Omicron specific, and then we have something totally new emerge ... we have to be more nimble because the variants are outpacing what we’re able to do.
This turns out to be a bit of a game of probability – the more infection we have, the more replication of the virus; the more replication, the more opportunity for mutations and subsequent variants.
Q: What about a combined flu-COVID vaccine; is that on the horizon?A: My children, who like most children do not like vaccines, always tell me: “Mom, why can’t they just put the influenza vaccine and the COVID vaccine into the same shot?” And I’m like: “Oh, from your lips to some scientist’s ears.”
At a time like this, where mRNA technology has totally disrupted what we can do with vaccines, in such a good way, I think we should push for the limits, because that would be incredible.
Q: If you’ve received a non-mRNA COVID vaccine, like those produced by Johnson & Johnson and Novavax, should you also get an mRNA booster?A: Right now, the CDC guidelines do state that if your primary vaccine series was not with an mRNA vaccine then being boosted with an mRNA is a fine thing to do, and it’s actually encouraged. So that’s not going to change with the bivalent booster.
Q: Is it okay to get a flu shot and a COVID booster at the same time, as the Centers for Disease Control and Prevention has recommended with past vaccines?A: I don’t anticipate there being recommendations against that. But I would also say watch for the recommendations that come out this fall on the bivalent boosters.
I do hope in the recommendations the CDC makes about the COVID boosters, they will say think about also getting your influenza vaccine, too. You could also get your COVID booster first, then by October get your influenza vaccine.
Q: Once you’re fully boosted, is it safe to stop wearing a mask, social distancing, avoiding crowded indoor spaces, and taking other precautions to avoid COVID-19?A: The virus is going to do what it does, which is infect whomever it can, and make them sick. So, if you see a lot of community transmission – you know who is ill with COVID in your kids’ schools, you know in your workplace and when people go out – that still signals there’s some increases in the circulation of virus. So, look at that to understand what your risk is.
If you know someone or have a colleague who is currently pregnant or immune suppressed, think about how you can protect them with mask-wearing, even if it’s just when you’re in one-on-one closed-door meetings with that individual.
So, your masking question is an important one, and it’s important for people to continue to hang onto those masks and wear them the week before you go see Grandma, for instance, to further reduce your risk so you don’t bring anything to here.
The high-level community risk nationwide is high right now. COVID is here.
A version of this article first appeared on WebMd.com.
– a month ahead of schedule, the Biden administration announced this week.
Moderna has signed a $1.74 billion federal contract to supply 66 million initial doses of the “bivalent” booster, which includes the original “ancestral” virus strain and elements of the Omicron BA.4 and BA.5 variants. Pfizer also announced a $3.2 billion U.S. agreement for another 105 million shots. Both vaccine suppliers have signed options to provide millions more boosters in the months ahead.
About 83.5% of Americans have received at least one COVID-19 shot, with 71.5% fully vaccinated with the initial series, 48% receiving one booster shot, and 31% two boosters, according to the CDC. With about 130,000 new COVID cases per day, and about 440 deaths, officials say the updated boosters may help rein in those figures by targeting the highly transmissible and widely circulating Omicron strains.
Federal health officials are still hammering out details of guidelines and recommendations of who should get the boosters, which are expected to come from the CDC and FDA. For now, authorities have decided not to expand eligibility for second boosters of the existing vaccines – now recommended only for adults over 50 and those 12 and older with immune deficiencies. Children 5 through 11 are advised to receive a single booster, 5 months after their initial vaccine series.
For a preview of what to expect from the CDC and FDA, this news organization spoke with Keri Althoff, PhD, an epidemiologist at Johns Hopkins University, Baltimore.
Q: Based on what we know now, who should be getting one of these new bivalent boosters?A: Of course, there is a process here regarding the specific recommendations, but it appears there will likely be a recommendation for all individuals to get this bivalent booster, similar to the first booster. And there will likely be a recommended time frame as to time since the last booster.
Right now, we have a recommendation for adults over the age of 50 or adults who are at higher risk for severe COVID-related illness [to get] a second booster. For them, there will probably be a timeline that says you should get the booster if you’re X amount of months or more from your second booster; or X amount of months or more from your first booster, if you’ve only had one.
Q: What about pregnant women or those being treated for chronic health conditions?A: I would imagine that once this bivalent booster becomes available, it will be recommended for all adults.
Q: And for children?A: That’s a good question. It’s something I have been digging into, [and] I think parents are really interested in this. Most kids, 5 and above, are supposed to be boosted with one shot right now, if they’re X amount of days from their primary vaccine series. Of course those 6 months to 4.99 years are not yet eligible [for boosters].
As a parent, I would love to see my children become eligible for the bivalent booster. It would be great if these boosters are conveying some additional protection that the kids could get access to before we send them off to school this fall. But there are questions as to whether or not that is going to happen.
Q: If you never received a booster, but only the preliminary vaccine series, do you need to get those earlier boosters before having the new bivalent booster shot?A: I don’t think they will likely make that a requirement – to restrict the bivalent booster only to those who are already boosted or up to date on their vaccines at the time the bivalent booster becomes available. But that will be up to the [CDC] vaccine recommendation committee to decide.
Q: Are there any new risks associated with these boosters, since they were developed so rapidly?A: No. We continue to monitor this technology, and with all the mRNA vaccines that have been delivered, you have seen all that monitoring play out with the detection, for example, of different forms of inflammation of the heart tissue and who that may impact. So, those monitoring systems work, and they work really, really well, so we can detect those things. And we know these vaccines are definitely safe.
Q: Some health experts are concerned “vaccine fatigue” will have an impact on the booster campaign. What’s your take?A: We have seen this fatigue in the proportion of individuals who are boosted with a first booster and even boosted with a second. But having those earlier boosters along with this new bivalent booster is important, because essentially, what we’re doing is really priming the immune system.
We’re trying to expedite the process of getting people’s immune system up to speed so that when the virus comes our way – as we know it will, because [of] these Omicron strains that are highly infectious and really whipping through our communities – we’re able to get the highest level of population immunity, you don’t end up in the hospital.
Q: What other challenges do you see in persuading Americans to get another round of boosters?A: One of the things that I’ve been hearing a lot, which I get very nervous about, is people saying: “Oh, I got fully vaccinated, I did or did not get the booster, and I had COVID anyway and it was really nothing, it didn’t feel like much to me, and so I’m not going to be boosted anymore.” We are not in a place quite yet where those guidelines are being rolled back in any way, shape, or form. We still have highly vulnerable people to severe disease and death in our communities, and we’re seeing hundreds of deaths every day.
There are consequences, even if it isn’t in severity of disease, meaning hospitalization and death. And let’s not let the actual quality of the vaccine being so successful that it can keep you out of the hospital. Don’t mistake that for “I don’t need another one.”
Q: Unlike the flu shot, which is reformulated each year to match circulating strains, the new COVID boosters offer protection against older strains as well as the newer ones. Why?A: It’s all about creating a broader immune response in individuals so that as more strains emerge, which they likely will, we can create a broader population immune response [to all strains]. Our individual bodies are seeing differences in these strains through vaccination that helps everyone stay healthy.
Q: There haven’t been clinical trials of these new mRNA boosters. How strong is the evidence that they will be effective against the emerging Omicron variants?A: There have been some studies – some great studies – looking at things like neutralizing antibodies, which we use as a surrogate for clinical trials. But that is not the same as studying the outcome of interest, which would be hospitalizations. So, part of the challenge is to be able to say: “Okay, this is what we know about the safety and effectiveness of the prior vaccines ... and how can we relate that to outcomes with these new boosters at an earlier stage [before] clinical data is available?”
Q: How long will the new boosters’ protections last – do we know yet?A: That timing is still a question, but of course what plays a big role in that is what COVID strains are circulating. If we prep these boosters that are Omicron specific, and then we have something totally new emerge ... we have to be more nimble because the variants are outpacing what we’re able to do.
This turns out to be a bit of a game of probability – the more infection we have, the more replication of the virus; the more replication, the more opportunity for mutations and subsequent variants.
Q: What about a combined flu-COVID vaccine; is that on the horizon?A: My children, who like most children do not like vaccines, always tell me: “Mom, why can’t they just put the influenza vaccine and the COVID vaccine into the same shot?” And I’m like: “Oh, from your lips to some scientist’s ears.”
At a time like this, where mRNA technology has totally disrupted what we can do with vaccines, in such a good way, I think we should push for the limits, because that would be incredible.
Q: If you’ve received a non-mRNA COVID vaccine, like those produced by Johnson & Johnson and Novavax, should you also get an mRNA booster?A: Right now, the CDC guidelines do state that if your primary vaccine series was not with an mRNA vaccine then being boosted with an mRNA is a fine thing to do, and it’s actually encouraged. So that’s not going to change with the bivalent booster.
Q: Is it okay to get a flu shot and a COVID booster at the same time, as the Centers for Disease Control and Prevention has recommended with past vaccines?A: I don’t anticipate there being recommendations against that. But I would also say watch for the recommendations that come out this fall on the bivalent boosters.
I do hope in the recommendations the CDC makes about the COVID boosters, they will say think about also getting your influenza vaccine, too. You could also get your COVID booster first, then by October get your influenza vaccine.
Q: Once you’re fully boosted, is it safe to stop wearing a mask, social distancing, avoiding crowded indoor spaces, and taking other precautions to avoid COVID-19?A: The virus is going to do what it does, which is infect whomever it can, and make them sick. So, if you see a lot of community transmission – you know who is ill with COVID in your kids’ schools, you know in your workplace and when people go out – that still signals there’s some increases in the circulation of virus. So, look at that to understand what your risk is.
If you know someone or have a colleague who is currently pregnant or immune suppressed, think about how you can protect them with mask-wearing, even if it’s just when you’re in one-on-one closed-door meetings with that individual.
So, your masking question is an important one, and it’s important for people to continue to hang onto those masks and wear them the week before you go see Grandma, for instance, to further reduce your risk so you don’t bring anything to here.
The high-level community risk nationwide is high right now. COVID is here.
A version of this article first appeared on WebMd.com.
– a month ahead of schedule, the Biden administration announced this week.
Moderna has signed a $1.74 billion federal contract to supply 66 million initial doses of the “bivalent” booster, which includes the original “ancestral” virus strain and elements of the Omicron BA.4 and BA.5 variants. Pfizer also announced a $3.2 billion U.S. agreement for another 105 million shots. Both vaccine suppliers have signed options to provide millions more boosters in the months ahead.
About 83.5% of Americans have received at least one COVID-19 shot, with 71.5% fully vaccinated with the initial series, 48% receiving one booster shot, and 31% two boosters, according to the CDC. With about 130,000 new COVID cases per day, and about 440 deaths, officials say the updated boosters may help rein in those figures by targeting the highly transmissible and widely circulating Omicron strains.
Federal health officials are still hammering out details of guidelines and recommendations of who should get the boosters, which are expected to come from the CDC and FDA. For now, authorities have decided not to expand eligibility for second boosters of the existing vaccines – now recommended only for adults over 50 and those 12 and older with immune deficiencies. Children 5 through 11 are advised to receive a single booster, 5 months after their initial vaccine series.
For a preview of what to expect from the CDC and FDA, this news organization spoke with Keri Althoff, PhD, an epidemiologist at Johns Hopkins University, Baltimore.
Q: Based on what we know now, who should be getting one of these new bivalent boosters?A: Of course, there is a process here regarding the specific recommendations, but it appears there will likely be a recommendation for all individuals to get this bivalent booster, similar to the first booster. And there will likely be a recommended time frame as to time since the last booster.
Right now, we have a recommendation for adults over the age of 50 or adults who are at higher risk for severe COVID-related illness [to get] a second booster. For them, there will probably be a timeline that says you should get the booster if you’re X amount of months or more from your second booster; or X amount of months or more from your first booster, if you’ve only had one.
Q: What about pregnant women or those being treated for chronic health conditions?A: I would imagine that once this bivalent booster becomes available, it will be recommended for all adults.
Q: And for children?A: That’s a good question. It’s something I have been digging into, [and] I think parents are really interested in this. Most kids, 5 and above, are supposed to be boosted with one shot right now, if they’re X amount of days from their primary vaccine series. Of course those 6 months to 4.99 years are not yet eligible [for boosters].
As a parent, I would love to see my children become eligible for the bivalent booster. It would be great if these boosters are conveying some additional protection that the kids could get access to before we send them off to school this fall. But there are questions as to whether or not that is going to happen.
Q: If you never received a booster, but only the preliminary vaccine series, do you need to get those earlier boosters before having the new bivalent booster shot?A: I don’t think they will likely make that a requirement – to restrict the bivalent booster only to those who are already boosted or up to date on their vaccines at the time the bivalent booster becomes available. But that will be up to the [CDC] vaccine recommendation committee to decide.
Q: Are there any new risks associated with these boosters, since they were developed so rapidly?A: No. We continue to monitor this technology, and with all the mRNA vaccines that have been delivered, you have seen all that monitoring play out with the detection, for example, of different forms of inflammation of the heart tissue and who that may impact. So, those monitoring systems work, and they work really, really well, so we can detect those things. And we know these vaccines are definitely safe.
Q: Some health experts are concerned “vaccine fatigue” will have an impact on the booster campaign. What’s your take?A: We have seen this fatigue in the proportion of individuals who are boosted with a first booster and even boosted with a second. But having those earlier boosters along with this new bivalent booster is important, because essentially, what we’re doing is really priming the immune system.
We’re trying to expedite the process of getting people’s immune system up to speed so that when the virus comes our way – as we know it will, because [of] these Omicron strains that are highly infectious and really whipping through our communities – we’re able to get the highest level of population immunity, you don’t end up in the hospital.
Q: What other challenges do you see in persuading Americans to get another round of boosters?A: One of the things that I’ve been hearing a lot, which I get very nervous about, is people saying: “Oh, I got fully vaccinated, I did or did not get the booster, and I had COVID anyway and it was really nothing, it didn’t feel like much to me, and so I’m not going to be boosted anymore.” We are not in a place quite yet where those guidelines are being rolled back in any way, shape, or form. We still have highly vulnerable people to severe disease and death in our communities, and we’re seeing hundreds of deaths every day.
There are consequences, even if it isn’t in severity of disease, meaning hospitalization and death. And let’s not let the actual quality of the vaccine being so successful that it can keep you out of the hospital. Don’t mistake that for “I don’t need another one.”
Q: Unlike the flu shot, which is reformulated each year to match circulating strains, the new COVID boosters offer protection against older strains as well as the newer ones. Why?A: It’s all about creating a broader immune response in individuals so that as more strains emerge, which they likely will, we can create a broader population immune response [to all strains]. Our individual bodies are seeing differences in these strains through vaccination that helps everyone stay healthy.
Q: There haven’t been clinical trials of these new mRNA boosters. How strong is the evidence that they will be effective against the emerging Omicron variants?A: There have been some studies – some great studies – looking at things like neutralizing antibodies, which we use as a surrogate for clinical trials. But that is not the same as studying the outcome of interest, which would be hospitalizations. So, part of the challenge is to be able to say: “Okay, this is what we know about the safety and effectiveness of the prior vaccines ... and how can we relate that to outcomes with these new boosters at an earlier stage [before] clinical data is available?”
Q: How long will the new boosters’ protections last – do we know yet?A: That timing is still a question, but of course what plays a big role in that is what COVID strains are circulating. If we prep these boosters that are Omicron specific, and then we have something totally new emerge ... we have to be more nimble because the variants are outpacing what we’re able to do.
This turns out to be a bit of a game of probability – the more infection we have, the more replication of the virus; the more replication, the more opportunity for mutations and subsequent variants.
Q: What about a combined flu-COVID vaccine; is that on the horizon?A: My children, who like most children do not like vaccines, always tell me: “Mom, why can’t they just put the influenza vaccine and the COVID vaccine into the same shot?” And I’m like: “Oh, from your lips to some scientist’s ears.”
At a time like this, where mRNA technology has totally disrupted what we can do with vaccines, in such a good way, I think we should push for the limits, because that would be incredible.
Q: If you’ve received a non-mRNA COVID vaccine, like those produced by Johnson & Johnson and Novavax, should you also get an mRNA booster?A: Right now, the CDC guidelines do state that if your primary vaccine series was not with an mRNA vaccine then being boosted with an mRNA is a fine thing to do, and it’s actually encouraged. So that’s not going to change with the bivalent booster.
Q: Is it okay to get a flu shot and a COVID booster at the same time, as the Centers for Disease Control and Prevention has recommended with past vaccines?A: I don’t anticipate there being recommendations against that. But I would also say watch for the recommendations that come out this fall on the bivalent boosters.
I do hope in the recommendations the CDC makes about the COVID boosters, they will say think about also getting your influenza vaccine, too. You could also get your COVID booster first, then by October get your influenza vaccine.
Q: Once you’re fully boosted, is it safe to stop wearing a mask, social distancing, avoiding crowded indoor spaces, and taking other precautions to avoid COVID-19?A: The virus is going to do what it does, which is infect whomever it can, and make them sick. So, if you see a lot of community transmission – you know who is ill with COVID in your kids’ schools, you know in your workplace and when people go out – that still signals there’s some increases in the circulation of virus. So, look at that to understand what your risk is.
If you know someone or have a colleague who is currently pregnant or immune suppressed, think about how you can protect them with mask-wearing, even if it’s just when you’re in one-on-one closed-door meetings with that individual.
So, your masking question is an important one, and it’s important for people to continue to hang onto those masks and wear them the week before you go see Grandma, for instance, to further reduce your risk so you don’t bring anything to here.
The high-level community risk nationwide is high right now. COVID is here.
A version of this article first appeared on WebMd.com.
COVID-19 and IPF: Fundamental similarities found
An AI-guided analysis of more than 1,000 human lung transcriptomic datasets found that COVID-19 resembles idiopathic pulmonary fibrosis (IPF) at a fundamental level, according to a study published in eBiomedicine, part of The Lancet Discovery Science.
In the aftermath of COVID-19, a significant number of patients develop a fibrotic lung disease, for which insights into pathogenesis, disease models, or treatment options are lacking, according to researchers Dr. Sinha and colleagues. This long-haul form of the disease culminates in a fibrotic type of interstitial lung disease (ILD). While the actual prevalence of post–COVID-19 ILD (PCLD) is still emerging, early analysis indicates that more than a third of COVID-19 survivors develop fibrotic abnormalities, according to the authors.
Previous research has shown that one of the important determinants for PCLD is the duration of disease. Among patients who developed fibrosis, approximately 4% of patients had a disease duration of less than 1 week; approximately 24% had a disease duration between 1 and 3 weeks; and around 61% had a disease duration longer than 3 weeks, the authors stated.
The lung transcriptomic datasets compared in their study were associated with various lung conditions. The researchers used two viral pandemic signatures (ViP and sViP) and one COVID lung-derived signature. They found that the resemblances included that COVID-19 recapitulates the gene expression patterns (ViP and IPF signatures), cytokine storm (IL15-centric), and the AT2 cytopathic changes, for example, injury, DNA damage, arrest in a transient, damage-induced progenitor state, and senescence-associated secretory phenotype (SASP).
In laboratory experiments, Dr. Sinha and colleagues were able to induce these same immunocytopathic features in preclinical COVID-19 models (human adult lung organoid and hamster) and to reverse them in the hamster model with effective anti–CoV-2 therapeutics.
PPI-network analyses pinpointed endoplasmic reticulum (ER) stress as one of the shared early triggers of both IPF and COVID-19, and immunohistochemistry studies validated the same in the lungs of deceased subjects with COVID-19 and the SARS-CoV-2–challenged hamster lungs. Additionally, lungs from transgenic mice, in which ER stress was induced specifically in the AT2 cells, faithfully recapitulated the host immune response and alveolar cytopathic changes that are induced by SARS-CoV-2.
stated corresponding author Pradipta Ghosh, MD, professor in the departments of medicine and cellular and molecular medicine, University of California, San Diego. “If proven in prospective studies, this biomarker could indicate who is at greatest risk for progressive fibrosis and may require lung transplantation,” she said in an interview.
Dr. Ghosh stated further, “When it comes to therapeutics in COVID lung or IPF, we also found that shared fundamental pathogenic mechanisms present excellent opportunities for developing therapeutics that can arrest the fibrogenic drivers in both diseases. One clue that emerged is a specific cytokine that is at the heart of the smoldering inflammation which is invariably associated with fibrosis. That is interleukin 15 [IL-15] and its receptor.” Dr. Ghosh observed that there are two Food and Drug Administration–approved drugs for IPF. “None are very effective in arresting this invariably fatal disease. Hence, finding better options to treat IPF is an urgent and an unmet need.”
Preclinical testing of hypotheses, Dr. Ghosh said, is next on the path to clinical trials. “We have the advantage of using human lung organoids (mini-lungs grown using stem cells) in a dish, adding additional cells to the system (like fibroblasts and immune cells), infecting them with the virus, or subjecting them to the IL-15 cytokine and monitoring lung fibrosis progression in a dish. Anti–IL-15 therapy can then be initiated to observe reversal of the fibrogenic cascade.” Hamsters have also been shown to provide appropriate models for mimicking lung fibrosis, Dr. Ghosh said.
“The report by Sinha and colleagues describes the fascinating similarities between drivers of post-COVID lung disease and idiopathic pulmonary fibrosis,” stated David Bowton, MD, professor emeritus, section on critical care, department of anesthesiology, Wake Forest University, Winston-Salem, N.C., in an interview. He added that, “Central to the mechanisms of induction of fibrosis in both disorders appears to be endoplasmic reticulum stress in alveolar type II cells (AT2). ER stress induces the unfolded protein response (UPR) that halts protein translation and promotes the degradation of misfolded proteins. Prolonged UPR can reprogram the cell or trigger apoptosis pathways. ER stress in the lung has been reported in a variety of cell lines including AT2 in IPF, bronchial and alveolar epithelial cells in asthma and [chronic obstructive pulmonary disease], and endothelial cells in pulmonary hypertension.”
Dr. Bowton commented further, including a caution, “Sinha and colleagues suggest that the identification of these gene signatures and mechanisms will be a fruitful avenue for developing effective therapeutics for IPF and other fibrotic lung diseases. I am hopeful that these data may offer clues that expedite this process. However, the redundancy of triggers for effector pathways in biologic systems argues that, even if successful, this will be [a] long and fraught process.”
The research study was supported by National Institutes of Health grants and funding from the Tobacco-Related Disease Research Program.
Dr. Sinha, Dr. Ghosh, and Dr. Bowton reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
An AI-guided analysis of more than 1,000 human lung transcriptomic datasets found that COVID-19 resembles idiopathic pulmonary fibrosis (IPF) at a fundamental level, according to a study published in eBiomedicine, part of The Lancet Discovery Science.
In the aftermath of COVID-19, a significant number of patients develop a fibrotic lung disease, for which insights into pathogenesis, disease models, or treatment options are lacking, according to researchers Dr. Sinha and colleagues. This long-haul form of the disease culminates in a fibrotic type of interstitial lung disease (ILD). While the actual prevalence of post–COVID-19 ILD (PCLD) is still emerging, early analysis indicates that more than a third of COVID-19 survivors develop fibrotic abnormalities, according to the authors.
Previous research has shown that one of the important determinants for PCLD is the duration of disease. Among patients who developed fibrosis, approximately 4% of patients had a disease duration of less than 1 week; approximately 24% had a disease duration between 1 and 3 weeks; and around 61% had a disease duration longer than 3 weeks, the authors stated.
The lung transcriptomic datasets compared in their study were associated with various lung conditions. The researchers used two viral pandemic signatures (ViP and sViP) and one COVID lung-derived signature. They found that the resemblances included that COVID-19 recapitulates the gene expression patterns (ViP and IPF signatures), cytokine storm (IL15-centric), and the AT2 cytopathic changes, for example, injury, DNA damage, arrest in a transient, damage-induced progenitor state, and senescence-associated secretory phenotype (SASP).
In laboratory experiments, Dr. Sinha and colleagues were able to induce these same immunocytopathic features in preclinical COVID-19 models (human adult lung organoid and hamster) and to reverse them in the hamster model with effective anti–CoV-2 therapeutics.
PPI-network analyses pinpointed endoplasmic reticulum (ER) stress as one of the shared early triggers of both IPF and COVID-19, and immunohistochemistry studies validated the same in the lungs of deceased subjects with COVID-19 and the SARS-CoV-2–challenged hamster lungs. Additionally, lungs from transgenic mice, in which ER stress was induced specifically in the AT2 cells, faithfully recapitulated the host immune response and alveolar cytopathic changes that are induced by SARS-CoV-2.
stated corresponding author Pradipta Ghosh, MD, professor in the departments of medicine and cellular and molecular medicine, University of California, San Diego. “If proven in prospective studies, this biomarker could indicate who is at greatest risk for progressive fibrosis and may require lung transplantation,” she said in an interview.
Dr. Ghosh stated further, “When it comes to therapeutics in COVID lung or IPF, we also found that shared fundamental pathogenic mechanisms present excellent opportunities for developing therapeutics that can arrest the fibrogenic drivers in both diseases. One clue that emerged is a specific cytokine that is at the heart of the smoldering inflammation which is invariably associated with fibrosis. That is interleukin 15 [IL-15] and its receptor.” Dr. Ghosh observed that there are two Food and Drug Administration–approved drugs for IPF. “None are very effective in arresting this invariably fatal disease. Hence, finding better options to treat IPF is an urgent and an unmet need.”
Preclinical testing of hypotheses, Dr. Ghosh said, is next on the path to clinical trials. “We have the advantage of using human lung organoids (mini-lungs grown using stem cells) in a dish, adding additional cells to the system (like fibroblasts and immune cells), infecting them with the virus, or subjecting them to the IL-15 cytokine and monitoring lung fibrosis progression in a dish. Anti–IL-15 therapy can then be initiated to observe reversal of the fibrogenic cascade.” Hamsters have also been shown to provide appropriate models for mimicking lung fibrosis, Dr. Ghosh said.
“The report by Sinha and colleagues describes the fascinating similarities between drivers of post-COVID lung disease and idiopathic pulmonary fibrosis,” stated David Bowton, MD, professor emeritus, section on critical care, department of anesthesiology, Wake Forest University, Winston-Salem, N.C., in an interview. He added that, “Central to the mechanisms of induction of fibrosis in both disorders appears to be endoplasmic reticulum stress in alveolar type II cells (AT2). ER stress induces the unfolded protein response (UPR) that halts protein translation and promotes the degradation of misfolded proteins. Prolonged UPR can reprogram the cell or trigger apoptosis pathways. ER stress in the lung has been reported in a variety of cell lines including AT2 in IPF, bronchial and alveolar epithelial cells in asthma and [chronic obstructive pulmonary disease], and endothelial cells in pulmonary hypertension.”
Dr. Bowton commented further, including a caution, “Sinha and colleagues suggest that the identification of these gene signatures and mechanisms will be a fruitful avenue for developing effective therapeutics for IPF and other fibrotic lung diseases. I am hopeful that these data may offer clues that expedite this process. However, the redundancy of triggers for effector pathways in biologic systems argues that, even if successful, this will be [a] long and fraught process.”
The research study was supported by National Institutes of Health grants and funding from the Tobacco-Related Disease Research Program.
Dr. Sinha, Dr. Ghosh, and Dr. Bowton reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
An AI-guided analysis of more than 1,000 human lung transcriptomic datasets found that COVID-19 resembles idiopathic pulmonary fibrosis (IPF) at a fundamental level, according to a study published in eBiomedicine, part of The Lancet Discovery Science.
In the aftermath of COVID-19, a significant number of patients develop a fibrotic lung disease, for which insights into pathogenesis, disease models, or treatment options are lacking, according to researchers Dr. Sinha and colleagues. This long-haul form of the disease culminates in a fibrotic type of interstitial lung disease (ILD). While the actual prevalence of post–COVID-19 ILD (PCLD) is still emerging, early analysis indicates that more than a third of COVID-19 survivors develop fibrotic abnormalities, according to the authors.
Previous research has shown that one of the important determinants for PCLD is the duration of disease. Among patients who developed fibrosis, approximately 4% of patients had a disease duration of less than 1 week; approximately 24% had a disease duration between 1 and 3 weeks; and around 61% had a disease duration longer than 3 weeks, the authors stated.
The lung transcriptomic datasets compared in their study were associated with various lung conditions. The researchers used two viral pandemic signatures (ViP and sViP) and one COVID lung-derived signature. They found that the resemblances included that COVID-19 recapitulates the gene expression patterns (ViP and IPF signatures), cytokine storm (IL15-centric), and the AT2 cytopathic changes, for example, injury, DNA damage, arrest in a transient, damage-induced progenitor state, and senescence-associated secretory phenotype (SASP).
In laboratory experiments, Dr. Sinha and colleagues were able to induce these same immunocytopathic features in preclinical COVID-19 models (human adult lung organoid and hamster) and to reverse them in the hamster model with effective anti–CoV-2 therapeutics.
PPI-network analyses pinpointed endoplasmic reticulum (ER) stress as one of the shared early triggers of both IPF and COVID-19, and immunohistochemistry studies validated the same in the lungs of deceased subjects with COVID-19 and the SARS-CoV-2–challenged hamster lungs. Additionally, lungs from transgenic mice, in which ER stress was induced specifically in the AT2 cells, faithfully recapitulated the host immune response and alveolar cytopathic changes that are induced by SARS-CoV-2.
stated corresponding author Pradipta Ghosh, MD, professor in the departments of medicine and cellular and molecular medicine, University of California, San Diego. “If proven in prospective studies, this biomarker could indicate who is at greatest risk for progressive fibrosis and may require lung transplantation,” she said in an interview.
Dr. Ghosh stated further, “When it comes to therapeutics in COVID lung or IPF, we also found that shared fundamental pathogenic mechanisms present excellent opportunities for developing therapeutics that can arrest the fibrogenic drivers in both diseases. One clue that emerged is a specific cytokine that is at the heart of the smoldering inflammation which is invariably associated with fibrosis. That is interleukin 15 [IL-15] and its receptor.” Dr. Ghosh observed that there are two Food and Drug Administration–approved drugs for IPF. “None are very effective in arresting this invariably fatal disease. Hence, finding better options to treat IPF is an urgent and an unmet need.”
Preclinical testing of hypotheses, Dr. Ghosh said, is next on the path to clinical trials. “We have the advantage of using human lung organoids (mini-lungs grown using stem cells) in a dish, adding additional cells to the system (like fibroblasts and immune cells), infecting them with the virus, or subjecting them to the IL-15 cytokine and monitoring lung fibrosis progression in a dish. Anti–IL-15 therapy can then be initiated to observe reversal of the fibrogenic cascade.” Hamsters have also been shown to provide appropriate models for mimicking lung fibrosis, Dr. Ghosh said.
“The report by Sinha and colleagues describes the fascinating similarities between drivers of post-COVID lung disease and idiopathic pulmonary fibrosis,” stated David Bowton, MD, professor emeritus, section on critical care, department of anesthesiology, Wake Forest University, Winston-Salem, N.C., in an interview. He added that, “Central to the mechanisms of induction of fibrosis in both disorders appears to be endoplasmic reticulum stress in alveolar type II cells (AT2). ER stress induces the unfolded protein response (UPR) that halts protein translation and promotes the degradation of misfolded proteins. Prolonged UPR can reprogram the cell or trigger apoptosis pathways. ER stress in the lung has been reported in a variety of cell lines including AT2 in IPF, bronchial and alveolar epithelial cells in asthma and [chronic obstructive pulmonary disease], and endothelial cells in pulmonary hypertension.”
Dr. Bowton commented further, including a caution, “Sinha and colleagues suggest that the identification of these gene signatures and mechanisms will be a fruitful avenue for developing effective therapeutics for IPF and other fibrotic lung diseases. I am hopeful that these data may offer clues that expedite this process. However, the redundancy of triggers for effector pathways in biologic systems argues that, even if successful, this will be [a] long and fraught process.”
The research study was supported by National Institutes of Health grants and funding from the Tobacco-Related Disease Research Program.
Dr. Sinha, Dr. Ghosh, and Dr. Bowton reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM eBIOMEDICINE
Death risk doubles for Black infants with bronchopulmonary dysplasia
Infants with bronchopulmonary dysplasia (BPD) who were born to Black mothers were significantly more likely to die or to have a longer hospital stay than infants of other ethnicities, based on data from more than 800 infants.
The overall incidence of BPD is rising, in part because of improved survival for extremely preterm infants, wrote Tamorah R. Lewis, MD, of the University of Missouri, Kansas City, and colleagues.
Previous studies suggest that racial disparities may affect outcomes for preterm infants with a range of neonatal morbidities during neonatal ICU (NICU) hospitalization, including respiratory distress syndrome, intraventricular hemorrhage, and necrotizing enterocolitis. However, the association of racial disparities with outcomes for preterm infants with BPD remains unclear, they said.
In a study published in JAMA Pediatrics, the researchers, on behalf of the Bronchopulmonary Dysplasia Collaborative, reviewed data from 834 preterm infants enrolled in the BPD Collaborative registry from Jan. 1, 2015, to July 19, 2021, at eight centers in the United States.
The study infants were born at less than 32 weeks’ gestation and were diagnosed with severe BPD according to the 2001 National Institutes of Health Consensus Criteria. The study population included 276 Black infants and 558 white infants. The median gestational age was 24 weeks, and 41% of the infants were female.
The primary outcomes were infant death and length of hospital stay.
Although death was infrequent (4% overall), Black maternal race was significantly associated with an increased risk of death from BPD (adjusted odds ratio, 2.1). Black maternal race also was significantly associated with a longer hospital stay for the infants, with an adjusted between-group difference of 10 days.
Infants of Black mothers also were more likely than those with White mothers to receive invasive respiratory support at the time of delivery. Black infants were more likely than White infants to have lower gestational age, lower birth weight and length, and smaller head circumference.
However, the proportions of cesarean deliveries, gender distribution, and infants small for gestational age were similar between Black and White infant groups. Medication exposure at 36 weeks postmenstrual age (PMA) also was similar for Black and White infants, and 50% of patients overall were treated with nasal continuous positive airway pressure at 36 weeks’ PMA. Awareness of the increased risk of death and longer hospital stay for Black infants is critical, “given the highly variable outcomes for patients with BPD and the uncertainty regarding demographic factors that contribute to late respiratory morbidity in severe BPD,” the researchers wrote.
The study findings were limited by several factors including variations among study centers in the identification and recording of maternal race, lack of data on paternal race, and the focus specifically on Black maternal race and not other ethnicities. Given the documented health disparities for Black individuals in the United States, “we restricted our cohort to only those patients born to Black or White mothers to estimate the association of Black maternal race and adverse in-hospital outcomes in infants with severe BPD,” the researchers wrote
Other limitations include the lack of data surrounding infant death and inability to adjust for all potential modifiers of BPD pathogenesis and progression, such as BPD comorbidities.
Prospective studies are needed to identify the sociodemographic mechanisms that may contribute to health outcome disparities for Black infants with severe BPD, the researchers emphasized.
In the meantime, the results highlight the need for more attention to variations in care for infants with BPD of different races, and approaches to family-centered care should consider “the precise needs of high-risk, structurally disadvantaged families while informing the design of prospective trials that improve outcomes for high-risk subgroups of children with severe BPD,” they concluded.
Data raise questions about the origin of disparities
The current study findings contribute to the knowledge and awareness of disparities in the high-risk NICU population, Nicolas A. Bamat, MD, and colleagues wrote in an accompanying editorial. “Further, their findings oppose the central tendency in the literature: that infants of Black mothers have less severe lung disease of prematurity during the birth hospitalization.”
The editorial authors noted that the study’s inclusion of racial characteristics as confounding variables to assess the effect of race on health “can imply questionable assumptions about where in a causal pathway racism begins to exert an effect,” whether after a diagnosis of BPD, during pregnancy in response to inequitable obstetric care, or “centuries ago, propagating forward through the shared experience of communities oppressed by the legacy of racism and its ongoing contemporary manifestations.”
The editorial authors added that, “in lung disease of prematurity, few variables are reliable antecedents to race as an exposure. Complex adjustment is necessary to reduce bias in targeted research questions.” However, the current study findings highlight the need to move toward more equitable neonatal care, and to prioritize interventions to reduce racial health disparities at the level of the NICU as well as at the hospital and government policy levels.
Consider range of contributing factors and confounders
The current study is important because “it is imperative to measure racial outcomes in health care in order to highlight and address disparities and biases,” Tim Joos, MD, said in an interview. However, “it can be difficult to determine how much race is a factor in itself versus a proxy for other important characteristics, such as socioeconomic status and level of education, that can confound the results.”
In the current study, the twofold-increased death rate in the premature infants of Black mothers is concerning and deserves further attention, Dr. Joos said. “The 10-day longer length of stay for infants of Black mothers seems quite shocking at first glance, but because of the long hospital stays for these extremely premature infants in general, it is about 7% longer than the infants born to White mothers.”
The take-home message is that this difference is still significant, and can reflect many factors including disease severity and complications, need for feeding assistance, teaching, and setting up home supports, said Dr. Joos.
As for additional research, “it would be useful for hospitals to break down why the differences exist, although I worry a provider or institution will feel they need to discharge Black families sooner to avoid being biased. Family preference and comfort level should be given high priority,” he emphasized.
The study received no outside funding, but lead author Dr. Lewis was supported by the National Institute on Child Health and Development and the Robert Wood Johnson Foundation. Several coauthors were supported by other grants from the National Institutes of Health. Dr. Barnat and one coauthor were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Joos had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Infants with bronchopulmonary dysplasia (BPD) who were born to Black mothers were significantly more likely to die or to have a longer hospital stay than infants of other ethnicities, based on data from more than 800 infants.
The overall incidence of BPD is rising, in part because of improved survival for extremely preterm infants, wrote Tamorah R. Lewis, MD, of the University of Missouri, Kansas City, and colleagues.
Previous studies suggest that racial disparities may affect outcomes for preterm infants with a range of neonatal morbidities during neonatal ICU (NICU) hospitalization, including respiratory distress syndrome, intraventricular hemorrhage, and necrotizing enterocolitis. However, the association of racial disparities with outcomes for preterm infants with BPD remains unclear, they said.
In a study published in JAMA Pediatrics, the researchers, on behalf of the Bronchopulmonary Dysplasia Collaborative, reviewed data from 834 preterm infants enrolled in the BPD Collaborative registry from Jan. 1, 2015, to July 19, 2021, at eight centers in the United States.
The study infants were born at less than 32 weeks’ gestation and were diagnosed with severe BPD according to the 2001 National Institutes of Health Consensus Criteria. The study population included 276 Black infants and 558 white infants. The median gestational age was 24 weeks, and 41% of the infants were female.
The primary outcomes were infant death and length of hospital stay.
Although death was infrequent (4% overall), Black maternal race was significantly associated with an increased risk of death from BPD (adjusted odds ratio, 2.1). Black maternal race also was significantly associated with a longer hospital stay for the infants, with an adjusted between-group difference of 10 days.
Infants of Black mothers also were more likely than those with White mothers to receive invasive respiratory support at the time of delivery. Black infants were more likely than White infants to have lower gestational age, lower birth weight and length, and smaller head circumference.
However, the proportions of cesarean deliveries, gender distribution, and infants small for gestational age were similar between Black and White infant groups. Medication exposure at 36 weeks postmenstrual age (PMA) also was similar for Black and White infants, and 50% of patients overall were treated with nasal continuous positive airway pressure at 36 weeks’ PMA. Awareness of the increased risk of death and longer hospital stay for Black infants is critical, “given the highly variable outcomes for patients with BPD and the uncertainty regarding demographic factors that contribute to late respiratory morbidity in severe BPD,” the researchers wrote.
The study findings were limited by several factors including variations among study centers in the identification and recording of maternal race, lack of data on paternal race, and the focus specifically on Black maternal race and not other ethnicities. Given the documented health disparities for Black individuals in the United States, “we restricted our cohort to only those patients born to Black or White mothers to estimate the association of Black maternal race and adverse in-hospital outcomes in infants with severe BPD,” the researchers wrote
Other limitations include the lack of data surrounding infant death and inability to adjust for all potential modifiers of BPD pathogenesis and progression, such as BPD comorbidities.
Prospective studies are needed to identify the sociodemographic mechanisms that may contribute to health outcome disparities for Black infants with severe BPD, the researchers emphasized.
In the meantime, the results highlight the need for more attention to variations in care for infants with BPD of different races, and approaches to family-centered care should consider “the precise needs of high-risk, structurally disadvantaged families while informing the design of prospective trials that improve outcomes for high-risk subgroups of children with severe BPD,” they concluded.
Data raise questions about the origin of disparities
The current study findings contribute to the knowledge and awareness of disparities in the high-risk NICU population, Nicolas A. Bamat, MD, and colleagues wrote in an accompanying editorial. “Further, their findings oppose the central tendency in the literature: that infants of Black mothers have less severe lung disease of prematurity during the birth hospitalization.”
The editorial authors noted that the study’s inclusion of racial characteristics as confounding variables to assess the effect of race on health “can imply questionable assumptions about where in a causal pathway racism begins to exert an effect,” whether after a diagnosis of BPD, during pregnancy in response to inequitable obstetric care, or “centuries ago, propagating forward through the shared experience of communities oppressed by the legacy of racism and its ongoing contemporary manifestations.”
The editorial authors added that, “in lung disease of prematurity, few variables are reliable antecedents to race as an exposure. Complex adjustment is necessary to reduce bias in targeted research questions.” However, the current study findings highlight the need to move toward more equitable neonatal care, and to prioritize interventions to reduce racial health disparities at the level of the NICU as well as at the hospital and government policy levels.
Consider range of contributing factors and confounders
The current study is important because “it is imperative to measure racial outcomes in health care in order to highlight and address disparities and biases,” Tim Joos, MD, said in an interview. However, “it can be difficult to determine how much race is a factor in itself versus a proxy for other important characteristics, such as socioeconomic status and level of education, that can confound the results.”
In the current study, the twofold-increased death rate in the premature infants of Black mothers is concerning and deserves further attention, Dr. Joos said. “The 10-day longer length of stay for infants of Black mothers seems quite shocking at first glance, but because of the long hospital stays for these extremely premature infants in general, it is about 7% longer than the infants born to White mothers.”
The take-home message is that this difference is still significant, and can reflect many factors including disease severity and complications, need for feeding assistance, teaching, and setting up home supports, said Dr. Joos.
As for additional research, “it would be useful for hospitals to break down why the differences exist, although I worry a provider or institution will feel they need to discharge Black families sooner to avoid being biased. Family preference and comfort level should be given high priority,” he emphasized.
The study received no outside funding, but lead author Dr. Lewis was supported by the National Institute on Child Health and Development and the Robert Wood Johnson Foundation. Several coauthors were supported by other grants from the National Institutes of Health. Dr. Barnat and one coauthor were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Joos had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Infants with bronchopulmonary dysplasia (BPD) who were born to Black mothers were significantly more likely to die or to have a longer hospital stay than infants of other ethnicities, based on data from more than 800 infants.
The overall incidence of BPD is rising, in part because of improved survival for extremely preterm infants, wrote Tamorah R. Lewis, MD, of the University of Missouri, Kansas City, and colleagues.
Previous studies suggest that racial disparities may affect outcomes for preterm infants with a range of neonatal morbidities during neonatal ICU (NICU) hospitalization, including respiratory distress syndrome, intraventricular hemorrhage, and necrotizing enterocolitis. However, the association of racial disparities with outcomes for preterm infants with BPD remains unclear, they said.
In a study published in JAMA Pediatrics, the researchers, on behalf of the Bronchopulmonary Dysplasia Collaborative, reviewed data from 834 preterm infants enrolled in the BPD Collaborative registry from Jan. 1, 2015, to July 19, 2021, at eight centers in the United States.
The study infants were born at less than 32 weeks’ gestation and were diagnosed with severe BPD according to the 2001 National Institutes of Health Consensus Criteria. The study population included 276 Black infants and 558 white infants. The median gestational age was 24 weeks, and 41% of the infants were female.
The primary outcomes were infant death and length of hospital stay.
Although death was infrequent (4% overall), Black maternal race was significantly associated with an increased risk of death from BPD (adjusted odds ratio, 2.1). Black maternal race also was significantly associated with a longer hospital stay for the infants, with an adjusted between-group difference of 10 days.
Infants of Black mothers also were more likely than those with White mothers to receive invasive respiratory support at the time of delivery. Black infants were more likely than White infants to have lower gestational age, lower birth weight and length, and smaller head circumference.
However, the proportions of cesarean deliveries, gender distribution, and infants small for gestational age were similar between Black and White infant groups. Medication exposure at 36 weeks postmenstrual age (PMA) also was similar for Black and White infants, and 50% of patients overall were treated with nasal continuous positive airway pressure at 36 weeks’ PMA. Awareness of the increased risk of death and longer hospital stay for Black infants is critical, “given the highly variable outcomes for patients with BPD and the uncertainty regarding demographic factors that contribute to late respiratory morbidity in severe BPD,” the researchers wrote.
The study findings were limited by several factors including variations among study centers in the identification and recording of maternal race, lack of data on paternal race, and the focus specifically on Black maternal race and not other ethnicities. Given the documented health disparities for Black individuals in the United States, “we restricted our cohort to only those patients born to Black or White mothers to estimate the association of Black maternal race and adverse in-hospital outcomes in infants with severe BPD,” the researchers wrote
Other limitations include the lack of data surrounding infant death and inability to adjust for all potential modifiers of BPD pathogenesis and progression, such as BPD comorbidities.
Prospective studies are needed to identify the sociodemographic mechanisms that may contribute to health outcome disparities for Black infants with severe BPD, the researchers emphasized.
In the meantime, the results highlight the need for more attention to variations in care for infants with BPD of different races, and approaches to family-centered care should consider “the precise needs of high-risk, structurally disadvantaged families while informing the design of prospective trials that improve outcomes for high-risk subgroups of children with severe BPD,” they concluded.
Data raise questions about the origin of disparities
The current study findings contribute to the knowledge and awareness of disparities in the high-risk NICU population, Nicolas A. Bamat, MD, and colleagues wrote in an accompanying editorial. “Further, their findings oppose the central tendency in the literature: that infants of Black mothers have less severe lung disease of prematurity during the birth hospitalization.”
The editorial authors noted that the study’s inclusion of racial characteristics as confounding variables to assess the effect of race on health “can imply questionable assumptions about where in a causal pathway racism begins to exert an effect,” whether after a diagnosis of BPD, during pregnancy in response to inequitable obstetric care, or “centuries ago, propagating forward through the shared experience of communities oppressed by the legacy of racism and its ongoing contemporary manifestations.”
The editorial authors added that, “in lung disease of prematurity, few variables are reliable antecedents to race as an exposure. Complex adjustment is necessary to reduce bias in targeted research questions.” However, the current study findings highlight the need to move toward more equitable neonatal care, and to prioritize interventions to reduce racial health disparities at the level of the NICU as well as at the hospital and government policy levels.
Consider range of contributing factors and confounders
The current study is important because “it is imperative to measure racial outcomes in health care in order to highlight and address disparities and biases,” Tim Joos, MD, said in an interview. However, “it can be difficult to determine how much race is a factor in itself versus a proxy for other important characteristics, such as socioeconomic status and level of education, that can confound the results.”
In the current study, the twofold-increased death rate in the premature infants of Black mothers is concerning and deserves further attention, Dr. Joos said. “The 10-day longer length of stay for infants of Black mothers seems quite shocking at first glance, but because of the long hospital stays for these extremely premature infants in general, it is about 7% longer than the infants born to White mothers.”
The take-home message is that this difference is still significant, and can reflect many factors including disease severity and complications, need for feeding assistance, teaching, and setting up home supports, said Dr. Joos.
As for additional research, “it would be useful for hospitals to break down why the differences exist, although I worry a provider or institution will feel they need to discharge Black families sooner to avoid being biased. Family preference and comfort level should be given high priority,” he emphasized.
The study received no outside funding, but lead author Dr. Lewis was supported by the National Institute on Child Health and Development and the Robert Wood Johnson Foundation. Several coauthors were supported by other grants from the National Institutes of Health. Dr. Barnat and one coauthor were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Joos had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
FROM JAMA PEDIATRICS
Author Q&A: Intravenous Immunoglobulin for Treatment of COVID-19 in Select Patients
Dr. George Sakoulas is an infectious diseases clinician at Sharp Memorial Hospital in San Diego and professor of pediatrics at the University of California, San Diego School of Medicine. He was the lead investigator in a study published in the May/June 2022 issue of JCOM that found that, when allocated to the appropriate patient type, intravenous immunoglobulin can reduce hospital costs for COVID-19 care. 1 He joined JCOM’s Editor-in-Chief, Dr. Ebrahim Barkoudah, to discuss the study’s background and highlight its main findings.
The following has been edited for length and clarity.
Dr. Barkoudah Dr. Sakoulas is an investigator and a clinician, bridging both worlds to bring the best evidence to our patients. We’re discussing his new article regarding intravenous immunoglobulin in treating nonventilated COVID-19 patients with moderate-to-severe hypoxia. Dr. Sakoulas, could you please share with our readers the clinical question your study addressed and what your work around COVID-19 management means for clinical practice?
Dr. Sakoulas Thank you. I’m an infectious disease physician. I’ve been treating patients with viral acute respiratory distress syndrome for almost 20 years as an ID doctor. Most of these cases are due to influenza or other viruses. And from time to time, anecdotally and supported by some literature, we’ve been using IVIG, or intravenous immunoglobulin, in some of these cases. And again, I can report anecdotal success with that over the years.
So when COVID emerged in March of 2020, we deployed IVIG in a couple of patients early who were heading downhill. Remember, in March of 2020, we didn’t have the knowledge of steroids helping, patients being ventilated very promptly, and we saw some patients who made a turnaround after treatment with IVIG. We were able to get some support from an industry sponsor and perform and publish a pilot study, enrolling patients early in the pandemic. That study actually showed benefits, which then led the sponsor to fund a phase 3 multicenter clinical trial. Unfortunately, a couple of things happened. First, the trial was designed with the knowledge we had in April of 2020, and again, this is before steroids, before we incorporated proning patients in the ICU, or started ventilating people early. So there were some management changes and evolutions and improvements that happened. And second, the trial was enrolling a very broad repertoire of patients. There were no age limitations, and the trial, ultimately a phase 3 multicenter trial, failed to meet its endpoint.
There were some trends for benefit in younger patients, and as the trial was ongoing, we continued to evolve our knowledge, and we really honed it down to seeing a benefit of using IVIG in patients with COVID with specific criteria in mind. They had to be relatively younger patients, under 65, and not have any major comorbidities. In other words, they weren’t dialysis patients or end-stage disease patients, heart failure patients, cancer or malignancy patients. So, you know, we’re looking at the patients under 65 with obesity, diabetes, and hypertension, who are rapidly declining, going from room air to BiPAP or high-flow oxygen in a short amount of time. And we learned that when using IVIG early, we actually saw patients improve and turn around.
What this article in JCOM highlighted was, number one, incorporating that outcome or that patient type and then looking at the cost of hospitalization of patients who received IVIG versus those that did not. There were 2 groups that were studied. One was the group of patients in that original pilot trial that I discussed who were randomized to receive 1 or the other prospectively; it was an unblinded randomized study. And the second group was a matched case-control study where we had patients treated with IVIG matched by age and comorbidity status and level of hypoxia to patients that did not receive IVIG. We saw a financial benefit in shortening or reducing hospitalizations, really coming down to getting rid of that 20% tail of patients that wound up going to the ICU, getting intubated, and using a high amount of hospital resources that would ramp up the cost of hospitalization. We saw great mitigation of that with IVIG, and even with a small subset of patients, we were able to show a benefit.
Dr. Barkoudah Any thoughts on where we can implement the new findings from your article in our practice at the moment, knowing we now have practice guidelines and protocols to treat COVID-19? There was a tangible benefit in treating the patients the way you approached it in your important work. Could you share with us what would be implementable at the moment?
Dr. Sakoulas I think, fortunately, with the increasing host immunity in the population and decreased virulence of the virus, perhaps we won’t see as many patients of the type that were in these trials going forward, but I suspect we will perhaps in the unvaccinated patients that remain. I believe one-third of the United States is not vaccinated. So there is certainly a vulnerable group of people out there. Potentially, an unvaccinated patient who winds up getting very sick, the patient who is relatively young—what I’m looking at is the 30- to 65-year-old obese, hypertensive, or diabetic patient who comes in and, despite the steroids and the antivirals, rapidly deteriorates into requiring high-flow oxygen. I think implementing IVIG in that patient type would be helpful. I don’t think it’s going to be as helpful in patients who are very elderly, because I think the mechanism of the disease is different in an 80-year-old versus a 50-year-old patient. So again, hopefully, it will not amount to a lot of patients, but I still suspect hospitals are going to see, perhaps in the fall, when they’re expecting a greater number of cases, a trickling of patients that do meet the criteria that I described.
Dr. Barkoudah JCOM’s audience are the QI implementers and hospital leadership. And what caught my eye in your article is your perspective on the pharmacoeconomics of treating COVID-19, and I really appreciate your looking at the cost aspect. Would you talk about the economics of inpatient care, the total care that we provide now that we’re in the age of tocilizumab, and the current state of multiple layers of therapy?
Dr. Sakoulas The reason to look at the economics of it is because IVIG—which is actually not a drug, it’s a blood product—is very expensive. So, we received a considerable amount of administrative pushback implementing this treatment at the beginning outside of the clinical trial setting because it hadn’t been studied on a large scale and because the cost was so high, even though, as a clinician at the bedside, I was seeing a benefit in patients. This study came out of my trying to demonstrate to the folks that are keeping the economics of medicine in mind that, in fact, investing several thousand dollars of treatment in IVIG will save you cost of care, the cost of an ICU bed, the cost of a ventilator, and the cost even of ECMO, which is hugely expensive.
If you look at the numbers in the study, for two-thirds or three-quarters of the patients, your cost of care is actually greater than the controls because you’re giving them IVIG, and it’s increasing the cost of their care, even though three-quarters of the patients are going to do just as well without it. It’s that 20% to 25% of patients that really are going to benefit from it, where you’re reducing your cost of care so much, and you’re getting rid of that very, very expensive 20%, that there’s a cost savings across the board per patient. So, it’s hard to understand when you say you’re losing money on three-quarters of the patients, you’re only saving money on a quarter of the patients, but that cost of saving on that small subset is so substantial it’s really impacting all numbers.
Also, abandoning the outlier principle is sort of an underlying theme in how we think of things. We tend to ignore outliers, not consider them, but I think we really have to pay attention to the more extreme cases because those patients are the ones that drive not just the financial cost of care. Remember, if you’re down to 1 ventilator and you can cut down the use of scarce ICU resources, the cost is sort of even beyond the cost of money. It’s the cost of resources that may become scarce in some settings. So, I think it speaks to that as well.
A lot of the drugs that we use, for example, tocilizumab, were able to be studied in thousands of patients. If you look at the absolute numbers, the benefit of tocilizumab from a magnitude standpoint—low to mid twenties to high twenties—you know, reducing mortality from 29% to 24%. I mean, just take a step back and think about that. Even though it’s statistically significant, try telling a patient, “Well, I’m going to give you this treatment that’s going to reduce mortality from 29% to 24%.” You know, that doesn’t really change anything from a clinical significance standpoint. But they have a P value less than .05, which is our standard, and they were able to do a study with thousands of patients. We didn’t have that luxury with IVIG. No one studied thousands of patients, only retrospectively, and those retrospective studies don’t get the attention because they’re considered biased with all their limitations. But I think one of the difficulties we have here is the balance between statistical and clinical significance. For example, in our pilot study, our ventilation rate was 58% with the non-IVIG patients versus 14% for IVIG patients. So you might say, magnitude-wise, that’s a big number, but the statistical significance of it is borderline because of small numbers.
Anyway, that’s a challenge that we have as clinicians trying to incorporate what’s published—the balancing of statistics, absolute numbers, and practicalities of delivering care. And I think this study highlights some of the nuances that go into that incorporation and those clinical decisions.
Dr. Barkoudah Would you mind sharing with our audience how we can make the connection between the medical outcomes and pharmacoeconomics findings from your article and link it to the bedside and treatment of our patients?
Dr. Sakoulas One of the points this article brings out is the importance of bringing together not just level 1A data, but also small studies with data such as this, where the magnitude of the effect is pretty big but you lose the statistics because of the small numbers. And then also the patients’ aspects of things. I think, as a bedside clinician, you appreciate things, the nuances, much sooner than what percolates out from a level 1A study. Case in point, in the sponsored phase 3 study that we did, and in some other studies that were prospectively done as well, these studies of IVIG simply had an enrollment of patients that was very broad, and not every patient benefits from the same therapy. A great example of this is the sepsis trials with Xigris and those types of agents that failed. You know, there are clinicians to this day who believe that there is a subset of patients that benefit from agents like this. The IVIG story falls a little bit into that category. It comes down to trying to identify the subset of patients that might benefit. And I think we’ve outlined this subset pretty well in our study: the younger, obese diabetic or hypertensive patient who’s rapidly declining.
It really brings together the need to not necessarily toss out these smaller studies, but kind of summarize everything together, and clinicians who are bedside, who are more in tune with the nuances of individual decisions at the individual patient level, might better appreciate these kinds of data. But I think we all have to put it together. IVIG does not make treatment guidelines at national levels and so forth. It’s not even listed in many of them. But there are patients out there who, if you ask them specifically how they felt, including a friend of mine who received the medication, there’s no question from their end, how they felt about this treatment option. Now, some people will get it and will not benefit. We just have to be really tuned into the fact that the same drug does not have the same result for every patient. And just to consider this in the high-risk patients that we talked about in our study.
Dr. Barkoudah While we were prepping for this interview, you made an analogy regarding clinical evidence along the lines of, “Do we need randomized clinical trials to do a parachute-type of experiment,” and we chatted about clinical wisdom. Would you mind sharing with our readers your thoughts on that?
Dr. Sakoulas Sometimes, we try a treatment and it’s very obvious for that particular patient that it helped them. Then you study the treatment in a large trial setting and it doesn’t work. For us bedside clinicians, there are some interventions sometimes that do appear as beneficial as a parachute would be, but yet, there has never been a randomized clinical trial proving that parachutes work. Again, a part of the challenge we have is patients are so different, their immunology is different, the pathogen infecting them is different, the time they present is different. Some present early, some present late. There are just so many moving parts to treating an infection that only a subset of people are going to benefit. And sometimes as clinicians, we’re so nuanced, that we identify a specific subset of patients where we know we can help them. And it’s so obvious for us, like a parachute would be, but to people who are looking at the world from 30,000 feet, they don’t necessarily grasp that because, when you look at all comers, it doesn’t show a benefit.
So the problem is that now those treatments that might help a subset of patients are being denied, and the subset of patients that are going to benefit never get the treatment. Now we have to balance that with a lot of stuff that went on during the pandemic with, you know, ivermectin, hydroxychloroquine, and people pushing those things. Someone asked me once what I thought about hydroxychloroquine, and I said, “Well, somebody in the lab probably showed that it was beneficial, analogous to lighting tissue paper on fire on a plate and taking a cup of water and putting the fire out. Well, now, if you take that cup of water to the Caldor fire that’s burning in California on thousands of acres, you’re not going to be able to put the fire out with that cup of water.” So while it might work in the lab, it’s truly not going to work in a clinical setting. We have to balance individualizing care for patients with some information people are pushing out there that may not be necessarily translatable to the clinical setting.
I think there’s nothing better than being at the bedside, though, and being able to implement something and seeing what works. And really, experience goes a long way in being able to individually treat a patient optimally.
Dr. Barkoudah Thank you for everything you do at the bedside and your work on improving the treatment we have and how we can leverage knowledge to treat our patients. Thank you very much for your time and your scholarly contribution. We appreciate it and I hope the work will continue. We will keep working on treating COVID-19 patients with the best knowledge we have.
Q&A participants: George Sakoulas, MD, Sharp Rees-Stealy Medical Group, La Jolla, CA, and University of California San Diego School of Medicine, San Diego, CA; and Ebrahim Barkoudah, MD, MPH, Department of Medicine, Brigham and Women’s Hospital, Boston, MA.
Disclosures: None reported.
1. Poremba M, Dehner M, Perreiter A, et al. Intravenous immunoglobulin in treating nonventilated COVID-19 patients with moderate-to-severe hypoxia: a pharmacoeconomic analysis. J Clin Outcomes Manage. 2022;29(3):123-129. doi:10.12788/jcom.0094
Dr. George Sakoulas is an infectious diseases clinician at Sharp Memorial Hospital in San Diego and professor of pediatrics at the University of California, San Diego School of Medicine. He was the lead investigator in a study published in the May/June 2022 issue of JCOM that found that, when allocated to the appropriate patient type, intravenous immunoglobulin can reduce hospital costs for COVID-19 care. 1 He joined JCOM’s Editor-in-Chief, Dr. Ebrahim Barkoudah, to discuss the study’s background and highlight its main findings.
The following has been edited for length and clarity.
Dr. Barkoudah Dr. Sakoulas is an investigator and a clinician, bridging both worlds to bring the best evidence to our patients. We’re discussing his new article regarding intravenous immunoglobulin in treating nonventilated COVID-19 patients with moderate-to-severe hypoxia. Dr. Sakoulas, could you please share with our readers the clinical question your study addressed and what your work around COVID-19 management means for clinical practice?
Dr. Sakoulas Thank you. I’m an infectious disease physician. I’ve been treating patients with viral acute respiratory distress syndrome for almost 20 years as an ID doctor. Most of these cases are due to influenza or other viruses. And from time to time, anecdotally and supported by some literature, we’ve been using IVIG, or intravenous immunoglobulin, in some of these cases. And again, I can report anecdotal success with that over the years.
So when COVID emerged in March of 2020, we deployed IVIG in a couple of patients early who were heading downhill. Remember, in March of 2020, we didn’t have the knowledge of steroids helping, patients being ventilated very promptly, and we saw some patients who made a turnaround after treatment with IVIG. We were able to get some support from an industry sponsor and perform and publish a pilot study, enrolling patients early in the pandemic. That study actually showed benefits, which then led the sponsor to fund a phase 3 multicenter clinical trial. Unfortunately, a couple of things happened. First, the trial was designed with the knowledge we had in April of 2020, and again, this is before steroids, before we incorporated proning patients in the ICU, or started ventilating people early. So there were some management changes and evolutions and improvements that happened. And second, the trial was enrolling a very broad repertoire of patients. There were no age limitations, and the trial, ultimately a phase 3 multicenter trial, failed to meet its endpoint.
There were some trends for benefit in younger patients, and as the trial was ongoing, we continued to evolve our knowledge, and we really honed it down to seeing a benefit of using IVIG in patients with COVID with specific criteria in mind. They had to be relatively younger patients, under 65, and not have any major comorbidities. In other words, they weren’t dialysis patients or end-stage disease patients, heart failure patients, cancer or malignancy patients. So, you know, we’re looking at the patients under 65 with obesity, diabetes, and hypertension, who are rapidly declining, going from room air to BiPAP or high-flow oxygen in a short amount of time. And we learned that when using IVIG early, we actually saw patients improve and turn around.
What this article in JCOM highlighted was, number one, incorporating that outcome or that patient type and then looking at the cost of hospitalization of patients who received IVIG versus those that did not. There were 2 groups that were studied. One was the group of patients in that original pilot trial that I discussed who were randomized to receive 1 or the other prospectively; it was an unblinded randomized study. And the second group was a matched case-control study where we had patients treated with IVIG matched by age and comorbidity status and level of hypoxia to patients that did not receive IVIG. We saw a financial benefit in shortening or reducing hospitalizations, really coming down to getting rid of that 20% tail of patients that wound up going to the ICU, getting intubated, and using a high amount of hospital resources that would ramp up the cost of hospitalization. We saw great mitigation of that with IVIG, and even with a small subset of patients, we were able to show a benefit.
Dr. Barkoudah Any thoughts on where we can implement the new findings from your article in our practice at the moment, knowing we now have practice guidelines and protocols to treat COVID-19? There was a tangible benefit in treating the patients the way you approached it in your important work. Could you share with us what would be implementable at the moment?
Dr. Sakoulas I think, fortunately, with the increasing host immunity in the population and decreased virulence of the virus, perhaps we won’t see as many patients of the type that were in these trials going forward, but I suspect we will perhaps in the unvaccinated patients that remain. I believe one-third of the United States is not vaccinated. So there is certainly a vulnerable group of people out there. Potentially, an unvaccinated patient who winds up getting very sick, the patient who is relatively young—what I’m looking at is the 30- to 65-year-old obese, hypertensive, or diabetic patient who comes in and, despite the steroids and the antivirals, rapidly deteriorates into requiring high-flow oxygen. I think implementing IVIG in that patient type would be helpful. I don’t think it’s going to be as helpful in patients who are very elderly, because I think the mechanism of the disease is different in an 80-year-old versus a 50-year-old patient. So again, hopefully, it will not amount to a lot of patients, but I still suspect hospitals are going to see, perhaps in the fall, when they’re expecting a greater number of cases, a trickling of patients that do meet the criteria that I described.
Dr. Barkoudah JCOM’s audience are the QI implementers and hospital leadership. And what caught my eye in your article is your perspective on the pharmacoeconomics of treating COVID-19, and I really appreciate your looking at the cost aspect. Would you talk about the economics of inpatient care, the total care that we provide now that we’re in the age of tocilizumab, and the current state of multiple layers of therapy?
Dr. Sakoulas The reason to look at the economics of it is because IVIG—which is actually not a drug, it’s a blood product—is very expensive. So, we received a considerable amount of administrative pushback implementing this treatment at the beginning outside of the clinical trial setting because it hadn’t been studied on a large scale and because the cost was so high, even though, as a clinician at the bedside, I was seeing a benefit in patients. This study came out of my trying to demonstrate to the folks that are keeping the economics of medicine in mind that, in fact, investing several thousand dollars of treatment in IVIG will save you cost of care, the cost of an ICU bed, the cost of a ventilator, and the cost even of ECMO, which is hugely expensive.
If you look at the numbers in the study, for two-thirds or three-quarters of the patients, your cost of care is actually greater than the controls because you’re giving them IVIG, and it’s increasing the cost of their care, even though three-quarters of the patients are going to do just as well without it. It’s that 20% to 25% of patients that really are going to benefit from it, where you’re reducing your cost of care so much, and you’re getting rid of that very, very expensive 20%, that there’s a cost savings across the board per patient. So, it’s hard to understand when you say you’re losing money on three-quarters of the patients, you’re only saving money on a quarter of the patients, but that cost of saving on that small subset is so substantial it’s really impacting all numbers.
Also, abandoning the outlier principle is sort of an underlying theme in how we think of things. We tend to ignore outliers, not consider them, but I think we really have to pay attention to the more extreme cases because those patients are the ones that drive not just the financial cost of care. Remember, if you’re down to 1 ventilator and you can cut down the use of scarce ICU resources, the cost is sort of even beyond the cost of money. It’s the cost of resources that may become scarce in some settings. So, I think it speaks to that as well.
A lot of the drugs that we use, for example, tocilizumab, were able to be studied in thousands of patients. If you look at the absolute numbers, the benefit of tocilizumab from a magnitude standpoint—low to mid twenties to high twenties—you know, reducing mortality from 29% to 24%. I mean, just take a step back and think about that. Even though it’s statistically significant, try telling a patient, “Well, I’m going to give you this treatment that’s going to reduce mortality from 29% to 24%.” You know, that doesn’t really change anything from a clinical significance standpoint. But they have a P value less than .05, which is our standard, and they were able to do a study with thousands of patients. We didn’t have that luxury with IVIG. No one studied thousands of patients, only retrospectively, and those retrospective studies don’t get the attention because they’re considered biased with all their limitations. But I think one of the difficulties we have here is the balance between statistical and clinical significance. For example, in our pilot study, our ventilation rate was 58% with the non-IVIG patients versus 14% for IVIG patients. So you might say, magnitude-wise, that’s a big number, but the statistical significance of it is borderline because of small numbers.
Anyway, that’s a challenge that we have as clinicians trying to incorporate what’s published—the balancing of statistics, absolute numbers, and practicalities of delivering care. And I think this study highlights some of the nuances that go into that incorporation and those clinical decisions.
Dr. Barkoudah Would you mind sharing with our audience how we can make the connection between the medical outcomes and pharmacoeconomics findings from your article and link it to the bedside and treatment of our patients?
Dr. Sakoulas One of the points this article brings out is the importance of bringing together not just level 1A data, but also small studies with data such as this, where the magnitude of the effect is pretty big but you lose the statistics because of the small numbers. And then also the patients’ aspects of things. I think, as a bedside clinician, you appreciate things, the nuances, much sooner than what percolates out from a level 1A study. Case in point, in the sponsored phase 3 study that we did, and in some other studies that were prospectively done as well, these studies of IVIG simply had an enrollment of patients that was very broad, and not every patient benefits from the same therapy. A great example of this is the sepsis trials with Xigris and those types of agents that failed. You know, there are clinicians to this day who believe that there is a subset of patients that benefit from agents like this. The IVIG story falls a little bit into that category. It comes down to trying to identify the subset of patients that might benefit. And I think we’ve outlined this subset pretty well in our study: the younger, obese diabetic or hypertensive patient who’s rapidly declining.
It really brings together the need to not necessarily toss out these smaller studies, but kind of summarize everything together, and clinicians who are bedside, who are more in tune with the nuances of individual decisions at the individual patient level, might better appreciate these kinds of data. But I think we all have to put it together. IVIG does not make treatment guidelines at national levels and so forth. It’s not even listed in many of them. But there are patients out there who, if you ask them specifically how they felt, including a friend of mine who received the medication, there’s no question from their end, how they felt about this treatment option. Now, some people will get it and will not benefit. We just have to be really tuned into the fact that the same drug does not have the same result for every patient. And just to consider this in the high-risk patients that we talked about in our study.
Dr. Barkoudah While we were prepping for this interview, you made an analogy regarding clinical evidence along the lines of, “Do we need randomized clinical trials to do a parachute-type of experiment,” and we chatted about clinical wisdom. Would you mind sharing with our readers your thoughts on that?
Dr. Sakoulas Sometimes, we try a treatment and it’s very obvious for that particular patient that it helped them. Then you study the treatment in a large trial setting and it doesn’t work. For us bedside clinicians, there are some interventions sometimes that do appear as beneficial as a parachute would be, but yet, there has never been a randomized clinical trial proving that parachutes work. Again, a part of the challenge we have is patients are so different, their immunology is different, the pathogen infecting them is different, the time they present is different. Some present early, some present late. There are just so many moving parts to treating an infection that only a subset of people are going to benefit. And sometimes as clinicians, we’re so nuanced, that we identify a specific subset of patients where we know we can help them. And it’s so obvious for us, like a parachute would be, but to people who are looking at the world from 30,000 feet, they don’t necessarily grasp that because, when you look at all comers, it doesn’t show a benefit.
So the problem is that now those treatments that might help a subset of patients are being denied, and the subset of patients that are going to benefit never get the treatment. Now we have to balance that with a lot of stuff that went on during the pandemic with, you know, ivermectin, hydroxychloroquine, and people pushing those things. Someone asked me once what I thought about hydroxychloroquine, and I said, “Well, somebody in the lab probably showed that it was beneficial, analogous to lighting tissue paper on fire on a plate and taking a cup of water and putting the fire out. Well, now, if you take that cup of water to the Caldor fire that’s burning in California on thousands of acres, you’re not going to be able to put the fire out with that cup of water.” So while it might work in the lab, it’s truly not going to work in a clinical setting. We have to balance individualizing care for patients with some information people are pushing out there that may not be necessarily translatable to the clinical setting.
I think there’s nothing better than being at the bedside, though, and being able to implement something and seeing what works. And really, experience goes a long way in being able to individually treat a patient optimally.
Dr. Barkoudah Thank you for everything you do at the bedside and your work on improving the treatment we have and how we can leverage knowledge to treat our patients. Thank you very much for your time and your scholarly contribution. We appreciate it and I hope the work will continue. We will keep working on treating COVID-19 patients with the best knowledge we have.
Q&A participants: George Sakoulas, MD, Sharp Rees-Stealy Medical Group, La Jolla, CA, and University of California San Diego School of Medicine, San Diego, CA; and Ebrahim Barkoudah, MD, MPH, Department of Medicine, Brigham and Women’s Hospital, Boston, MA.
Disclosures: None reported.
Dr. George Sakoulas is an infectious diseases clinician at Sharp Memorial Hospital in San Diego and professor of pediatrics at the University of California, San Diego School of Medicine. He was the lead investigator in a study published in the May/June 2022 issue of JCOM that found that, when allocated to the appropriate patient type, intravenous immunoglobulin can reduce hospital costs for COVID-19 care. 1 He joined JCOM’s Editor-in-Chief, Dr. Ebrahim Barkoudah, to discuss the study’s background and highlight its main findings.
The following has been edited for length and clarity.
Dr. Barkoudah Dr. Sakoulas is an investigator and a clinician, bridging both worlds to bring the best evidence to our patients. We’re discussing his new article regarding intravenous immunoglobulin in treating nonventilated COVID-19 patients with moderate-to-severe hypoxia. Dr. Sakoulas, could you please share with our readers the clinical question your study addressed and what your work around COVID-19 management means for clinical practice?
Dr. Sakoulas Thank you. I’m an infectious disease physician. I’ve been treating patients with viral acute respiratory distress syndrome for almost 20 years as an ID doctor. Most of these cases are due to influenza or other viruses. And from time to time, anecdotally and supported by some literature, we’ve been using IVIG, or intravenous immunoglobulin, in some of these cases. And again, I can report anecdotal success with that over the years.
So when COVID emerged in March of 2020, we deployed IVIG in a couple of patients early who were heading downhill. Remember, in March of 2020, we didn’t have the knowledge of steroids helping, patients being ventilated very promptly, and we saw some patients who made a turnaround after treatment with IVIG. We were able to get some support from an industry sponsor and perform and publish a pilot study, enrolling patients early in the pandemic. That study actually showed benefits, which then led the sponsor to fund a phase 3 multicenter clinical trial. Unfortunately, a couple of things happened. First, the trial was designed with the knowledge we had in April of 2020, and again, this is before steroids, before we incorporated proning patients in the ICU, or started ventilating people early. So there were some management changes and evolutions and improvements that happened. And second, the trial was enrolling a very broad repertoire of patients. There were no age limitations, and the trial, ultimately a phase 3 multicenter trial, failed to meet its endpoint.
There were some trends for benefit in younger patients, and as the trial was ongoing, we continued to evolve our knowledge, and we really honed it down to seeing a benefit of using IVIG in patients with COVID with specific criteria in mind. They had to be relatively younger patients, under 65, and not have any major comorbidities. In other words, they weren’t dialysis patients or end-stage disease patients, heart failure patients, cancer or malignancy patients. So, you know, we’re looking at the patients under 65 with obesity, diabetes, and hypertension, who are rapidly declining, going from room air to BiPAP or high-flow oxygen in a short amount of time. And we learned that when using IVIG early, we actually saw patients improve and turn around.
What this article in JCOM highlighted was, number one, incorporating that outcome or that patient type and then looking at the cost of hospitalization of patients who received IVIG versus those that did not. There were 2 groups that were studied. One was the group of patients in that original pilot trial that I discussed who were randomized to receive 1 or the other prospectively; it was an unblinded randomized study. And the second group was a matched case-control study where we had patients treated with IVIG matched by age and comorbidity status and level of hypoxia to patients that did not receive IVIG. We saw a financial benefit in shortening or reducing hospitalizations, really coming down to getting rid of that 20% tail of patients that wound up going to the ICU, getting intubated, and using a high amount of hospital resources that would ramp up the cost of hospitalization. We saw great mitigation of that with IVIG, and even with a small subset of patients, we were able to show a benefit.
Dr. Barkoudah Any thoughts on where we can implement the new findings from your article in our practice at the moment, knowing we now have practice guidelines and protocols to treat COVID-19? There was a tangible benefit in treating the patients the way you approached it in your important work. Could you share with us what would be implementable at the moment?
Dr. Sakoulas I think, fortunately, with the increasing host immunity in the population and decreased virulence of the virus, perhaps we won’t see as many patients of the type that were in these trials going forward, but I suspect we will perhaps in the unvaccinated patients that remain. I believe one-third of the United States is not vaccinated. So there is certainly a vulnerable group of people out there. Potentially, an unvaccinated patient who winds up getting very sick, the patient who is relatively young—what I’m looking at is the 30- to 65-year-old obese, hypertensive, or diabetic patient who comes in and, despite the steroids and the antivirals, rapidly deteriorates into requiring high-flow oxygen. I think implementing IVIG in that patient type would be helpful. I don’t think it’s going to be as helpful in patients who are very elderly, because I think the mechanism of the disease is different in an 80-year-old versus a 50-year-old patient. So again, hopefully, it will not amount to a lot of patients, but I still suspect hospitals are going to see, perhaps in the fall, when they’re expecting a greater number of cases, a trickling of patients that do meet the criteria that I described.
Dr. Barkoudah JCOM’s audience are the QI implementers and hospital leadership. And what caught my eye in your article is your perspective on the pharmacoeconomics of treating COVID-19, and I really appreciate your looking at the cost aspect. Would you talk about the economics of inpatient care, the total care that we provide now that we’re in the age of tocilizumab, and the current state of multiple layers of therapy?
Dr. Sakoulas The reason to look at the economics of it is because IVIG—which is actually not a drug, it’s a blood product—is very expensive. So, we received a considerable amount of administrative pushback implementing this treatment at the beginning outside of the clinical trial setting because it hadn’t been studied on a large scale and because the cost was so high, even though, as a clinician at the bedside, I was seeing a benefit in patients. This study came out of my trying to demonstrate to the folks that are keeping the economics of medicine in mind that, in fact, investing several thousand dollars of treatment in IVIG will save you cost of care, the cost of an ICU bed, the cost of a ventilator, and the cost even of ECMO, which is hugely expensive.
If you look at the numbers in the study, for two-thirds or three-quarters of the patients, your cost of care is actually greater than the controls because you’re giving them IVIG, and it’s increasing the cost of their care, even though three-quarters of the patients are going to do just as well without it. It’s that 20% to 25% of patients that really are going to benefit from it, where you’re reducing your cost of care so much, and you’re getting rid of that very, very expensive 20%, that there’s a cost savings across the board per patient. So, it’s hard to understand when you say you’re losing money on three-quarters of the patients, you’re only saving money on a quarter of the patients, but that cost of saving on that small subset is so substantial it’s really impacting all numbers.
Also, abandoning the outlier principle is sort of an underlying theme in how we think of things. We tend to ignore outliers, not consider them, but I think we really have to pay attention to the more extreme cases because those patients are the ones that drive not just the financial cost of care. Remember, if you’re down to 1 ventilator and you can cut down the use of scarce ICU resources, the cost is sort of even beyond the cost of money. It’s the cost of resources that may become scarce in some settings. So, I think it speaks to that as well.
A lot of the drugs that we use, for example, tocilizumab, were able to be studied in thousands of patients. If you look at the absolute numbers, the benefit of tocilizumab from a magnitude standpoint—low to mid twenties to high twenties—you know, reducing mortality from 29% to 24%. I mean, just take a step back and think about that. Even though it’s statistically significant, try telling a patient, “Well, I’m going to give you this treatment that’s going to reduce mortality from 29% to 24%.” You know, that doesn’t really change anything from a clinical significance standpoint. But they have a P value less than .05, which is our standard, and they were able to do a study with thousands of patients. We didn’t have that luxury with IVIG. No one studied thousands of patients, only retrospectively, and those retrospective studies don’t get the attention because they’re considered biased with all their limitations. But I think one of the difficulties we have here is the balance between statistical and clinical significance. For example, in our pilot study, our ventilation rate was 58% with the non-IVIG patients versus 14% for IVIG patients. So you might say, magnitude-wise, that’s a big number, but the statistical significance of it is borderline because of small numbers.
Anyway, that’s a challenge that we have as clinicians trying to incorporate what’s published—the balancing of statistics, absolute numbers, and practicalities of delivering care. And I think this study highlights some of the nuances that go into that incorporation and those clinical decisions.
Dr. Barkoudah Would you mind sharing with our audience how we can make the connection between the medical outcomes and pharmacoeconomics findings from your article and link it to the bedside and treatment of our patients?
Dr. Sakoulas One of the points this article brings out is the importance of bringing together not just level 1A data, but also small studies with data such as this, where the magnitude of the effect is pretty big but you lose the statistics because of the small numbers. And then also the patients’ aspects of things. I think, as a bedside clinician, you appreciate things, the nuances, much sooner than what percolates out from a level 1A study. Case in point, in the sponsored phase 3 study that we did, and in some other studies that were prospectively done as well, these studies of IVIG simply had an enrollment of patients that was very broad, and not every patient benefits from the same therapy. A great example of this is the sepsis trials with Xigris and those types of agents that failed. You know, there are clinicians to this day who believe that there is a subset of patients that benefit from agents like this. The IVIG story falls a little bit into that category. It comes down to trying to identify the subset of patients that might benefit. And I think we’ve outlined this subset pretty well in our study: the younger, obese diabetic or hypertensive patient who’s rapidly declining.
It really brings together the need to not necessarily toss out these smaller studies, but kind of summarize everything together, and clinicians who are bedside, who are more in tune with the nuances of individual decisions at the individual patient level, might better appreciate these kinds of data. But I think we all have to put it together. IVIG does not make treatment guidelines at national levels and so forth. It’s not even listed in many of them. But there are patients out there who, if you ask them specifically how they felt, including a friend of mine who received the medication, there’s no question from their end, how they felt about this treatment option. Now, some people will get it and will not benefit. We just have to be really tuned into the fact that the same drug does not have the same result for every patient. And just to consider this in the high-risk patients that we talked about in our study.
Dr. Barkoudah While we were prepping for this interview, you made an analogy regarding clinical evidence along the lines of, “Do we need randomized clinical trials to do a parachute-type of experiment,” and we chatted about clinical wisdom. Would you mind sharing with our readers your thoughts on that?
Dr. Sakoulas Sometimes, we try a treatment and it’s very obvious for that particular patient that it helped them. Then you study the treatment in a large trial setting and it doesn’t work. For us bedside clinicians, there are some interventions sometimes that do appear as beneficial as a parachute would be, but yet, there has never been a randomized clinical trial proving that parachutes work. Again, a part of the challenge we have is patients are so different, their immunology is different, the pathogen infecting them is different, the time they present is different. Some present early, some present late. There are just so many moving parts to treating an infection that only a subset of people are going to benefit. And sometimes as clinicians, we’re so nuanced, that we identify a specific subset of patients where we know we can help them. And it’s so obvious for us, like a parachute would be, but to people who are looking at the world from 30,000 feet, they don’t necessarily grasp that because, when you look at all comers, it doesn’t show a benefit.
So the problem is that now those treatments that might help a subset of patients are being denied, and the subset of patients that are going to benefit never get the treatment. Now we have to balance that with a lot of stuff that went on during the pandemic with, you know, ivermectin, hydroxychloroquine, and people pushing those things. Someone asked me once what I thought about hydroxychloroquine, and I said, “Well, somebody in the lab probably showed that it was beneficial, analogous to lighting tissue paper on fire on a plate and taking a cup of water and putting the fire out. Well, now, if you take that cup of water to the Caldor fire that’s burning in California on thousands of acres, you’re not going to be able to put the fire out with that cup of water.” So while it might work in the lab, it’s truly not going to work in a clinical setting. We have to balance individualizing care for patients with some information people are pushing out there that may not be necessarily translatable to the clinical setting.
I think there’s nothing better than being at the bedside, though, and being able to implement something and seeing what works. And really, experience goes a long way in being able to individually treat a patient optimally.
Dr. Barkoudah Thank you for everything you do at the bedside and your work on improving the treatment we have and how we can leverage knowledge to treat our patients. Thank you very much for your time and your scholarly contribution. We appreciate it and I hope the work will continue. We will keep working on treating COVID-19 patients with the best knowledge we have.
Q&A participants: George Sakoulas, MD, Sharp Rees-Stealy Medical Group, La Jolla, CA, and University of California San Diego School of Medicine, San Diego, CA; and Ebrahim Barkoudah, MD, MPH, Department of Medicine, Brigham and Women’s Hospital, Boston, MA.
Disclosures: None reported.
1. Poremba M, Dehner M, Perreiter A, et al. Intravenous immunoglobulin in treating nonventilated COVID-19 patients with moderate-to-severe hypoxia: a pharmacoeconomic analysis. J Clin Outcomes Manage. 2022;29(3):123-129. doi:10.12788/jcom.0094
1. Poremba M, Dehner M, Perreiter A, et al. Intravenous immunoglobulin in treating nonventilated COVID-19 patients with moderate-to-severe hypoxia: a pharmacoeconomic analysis. J Clin Outcomes Manage. 2022;29(3):123-129. doi:10.12788/jcom.0094
Race-specific spirometry may miss emphysema diagnoses
An overreliance on spirometry to identify emphysema led to missed cases in Black individuals, particularly men, based on a secondary data analysis of 2,674 people.
“Over the last few years, there has been growing debate around the use of race adjustment in diagnostic algorithms and equations commonly used in medicine,” lead author Gabrielle Yi-Hui Liu, MD, said in an interview. “Whereas, previously it was common to accept racial or ethnic differences in clinical measures and outcomes as inherent differences among populations, there is now more recognition of how racism, socioeconomic status, and environmental exposures can cause these racial differences. Our initial interest in this study was to examine how the use of race-specific spirometry reference equations, and the use of spirometry in general, may be contributing to racial disparities.”
“Previous studies have suggested that the use of race-specific equations in spirometry can exacerbate racial inequities in healthcare outcomes by under-recognition of early disease in Black adults, and this study adds to that evidence,” said Suman Pal, MBBS, of the University of New Mexico, Albuquerque, in an interview.
“By examining the crucial ways in which systemic factors in medicine, such as race-specific equations, exacerbate racial inequities in healthcare, this study is a timely analysis in a moment of national reckoning of structural racism,” said Dr. Pal, who was not involved in the study.
In a study published in Annals of Internal Medicine, Dr. Liu and colleagues at Northwestern University, Chicago, conducted a secondary analysis of data from the CARDIA Lung study (Coronary Artery Risk Development In Young Adults).
The primary outcome of the study was the prevalence of emphysema among participants with various measures of normal spirometry results, stratified by sex and race. The normal results included an forced expiratory volume in 1 second (FEV1)–forced vital capacity (FVC) ratio greater than or equal to 0.7 or greater than or equal to the lower limit of normal. The participants also were stratified by FEV1 percent predicted, using race-specific reference equations, for FEV1 between 80% and 99% of predicted, or an FEV1 between 100% and 120% of predicted.
The study population included 485 Black men, 762 Black women, 659 White men, and 768 White women who received both a CT scan (in 2010-2011) and spirometry (obtained in 2015-2016) in the CARDIA study. The mean age of the participants at the spirometry exam was 55 years.
A total of 5.3% of the participants had emphysema after stratifying by FEV1-FVC ratio. The prevalence was significantly higher for Black men, compared with White men (12.3% vs. 4.0%; relative risk, 3.0), and for Black women, compared with White women (5.0% vs. 2.6%; RR, 1.9).
The association between Black race and emphysema risk persisted but decreased when the researchers used a race-neutral estimate.
When the participants were stratified by race-specific FEV1 percent predicted, 6.5% of individuals with a race-specific FEV1 between 80% and 99% had emphysema. After controlling for factors including age and smoking, emphysema was significantly more prevalent in Black men versus White men (15.5% vs. 4.0%) and in Black women, compared with White women (6.6% vs. 3.4%).
The racial difference persisted in men with a race-specific FEV1 between 100% and 120% of predicted. Of these, 4.0% had emphysema. The prevalence was significantly higher in Black men, compared with White men (13.9% vs. 2.2%), but similar between Black women and White women (2.6% vs. 2.0%).
The use of race-neutral equations reduced, but did not eliminate, these disparities, the researchers said.
The findings were limited by the lack of CT imaging data from the same visit as the final spirometry collection, the researchers noted. “Given that imaging was obtained 5 years before spirometry and emphysema is an irreversible finding, this may have led to an overall underestimation of the prevalence of emphysema.”
Spirometry alone misses cases
“We were surprised by the substantial rates of emphysema we saw among Black men in our cohort with normal spirometry,” Dr. Liu said in an interview. “We did not expect to find than more than one in eight Black men with an FEV1 between 100% and 120% predicted would have emphysema – a rate more than six times higher than White men with the same range of FEV1.”
“One takeaway is that we are likely missing a lot of people with impaired respiratory health or true lung disease by only using spirometry to diagnose COPD,” said Dr. Liu. In clinical practice, “physicians should consider ordering CT scans on patients with normal spirometry who have respiratory symptoms such as cough or shortness of breath. If emphysema is found, physicians should discuss mitigating any potential risk factors and consider the use of COPD medications such as inhalers.
“Our findings also support using race-neutral reference equations to interpret spirometry instead of race-specific equations. Racial disparities in rates of emphysema among those with ‘normal’ FEV1 [between 80% and 120% predicted], were attenuated or eliminated when race-neutral equations were used to calculate FEV1. This suggests that race-specific equations are normalizing worse lung health in Black adults,” Dr. Liu explained.
“We need to continue research into additional tools that can be used to assess respiratory health and diagnose COPD, while keeping in mind how these tools may affect racial disparities,” said Dr. Liu. “Our study suggests that our reliance on spirometry measures such as FEV1/FVC ratio and FEV1 is missing a number of people with respiratory symptoms and CT evidence of lung disease, and that this is disproportionately affecting Black adults in the United States.” Looking ahead, “it is important to find better tools to identify people with impaired respiratory health or early manifestations of disease so we can intercept chronic lung disease before it becomes clinically apparent and patients have sustained significant lung damage.”
The CARDIA study was supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Dr. Liu was supported by a grant from the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Pal had no financial conflicts to disclose.
*This article was updated 7/22/2022.
An overreliance on spirometry to identify emphysema led to missed cases in Black individuals, particularly men, based on a secondary data analysis of 2,674 people.
“Over the last few years, there has been growing debate around the use of race adjustment in diagnostic algorithms and equations commonly used in medicine,” lead author Gabrielle Yi-Hui Liu, MD, said in an interview. “Whereas, previously it was common to accept racial or ethnic differences in clinical measures and outcomes as inherent differences among populations, there is now more recognition of how racism, socioeconomic status, and environmental exposures can cause these racial differences. Our initial interest in this study was to examine how the use of race-specific spirometry reference equations, and the use of spirometry in general, may be contributing to racial disparities.”
“Previous studies have suggested that the use of race-specific equations in spirometry can exacerbate racial inequities in healthcare outcomes by under-recognition of early disease in Black adults, and this study adds to that evidence,” said Suman Pal, MBBS, of the University of New Mexico, Albuquerque, in an interview.
“By examining the crucial ways in which systemic factors in medicine, such as race-specific equations, exacerbate racial inequities in healthcare, this study is a timely analysis in a moment of national reckoning of structural racism,” said Dr. Pal, who was not involved in the study.
In a study published in Annals of Internal Medicine, Dr. Liu and colleagues at Northwestern University, Chicago, conducted a secondary analysis of data from the CARDIA Lung study (Coronary Artery Risk Development In Young Adults).
The primary outcome of the study was the prevalence of emphysema among participants with various measures of normal spirometry results, stratified by sex and race. The normal results included an forced expiratory volume in 1 second (FEV1)–forced vital capacity (FVC) ratio greater than or equal to 0.7 or greater than or equal to the lower limit of normal. The participants also were stratified by FEV1 percent predicted, using race-specific reference equations, for FEV1 between 80% and 99% of predicted, or an FEV1 between 100% and 120% of predicted.
The study population included 485 Black men, 762 Black women, 659 White men, and 768 White women who received both a CT scan (in 2010-2011) and spirometry (obtained in 2015-2016) in the CARDIA study. The mean age of the participants at the spirometry exam was 55 years.
A total of 5.3% of the participants had emphysema after stratifying by FEV1-FVC ratio. The prevalence was significantly higher for Black men, compared with White men (12.3% vs. 4.0%; relative risk, 3.0), and for Black women, compared with White women (5.0% vs. 2.6%; RR, 1.9).
The association between Black race and emphysema risk persisted but decreased when the researchers used a race-neutral estimate.
When the participants were stratified by race-specific FEV1 percent predicted, 6.5% of individuals with a race-specific FEV1 between 80% and 99% had emphysema. After controlling for factors including age and smoking, emphysema was significantly more prevalent in Black men versus White men (15.5% vs. 4.0%) and in Black women, compared with White women (6.6% vs. 3.4%).
The racial difference persisted in men with a race-specific FEV1 between 100% and 120% of predicted. Of these, 4.0% had emphysema. The prevalence was significantly higher in Black men, compared with White men (13.9% vs. 2.2%), but similar between Black women and White women (2.6% vs. 2.0%).
The use of race-neutral equations reduced, but did not eliminate, these disparities, the researchers said.
The findings were limited by the lack of CT imaging data from the same visit as the final spirometry collection, the researchers noted. “Given that imaging was obtained 5 years before spirometry and emphysema is an irreversible finding, this may have led to an overall underestimation of the prevalence of emphysema.”
Spirometry alone misses cases
“We were surprised by the substantial rates of emphysema we saw among Black men in our cohort with normal spirometry,” Dr. Liu said in an interview. “We did not expect to find than more than one in eight Black men with an FEV1 between 100% and 120% predicted would have emphysema – a rate more than six times higher than White men with the same range of FEV1.”
“One takeaway is that we are likely missing a lot of people with impaired respiratory health or true lung disease by only using spirometry to diagnose COPD,” said Dr. Liu. In clinical practice, “physicians should consider ordering CT scans on patients with normal spirometry who have respiratory symptoms such as cough or shortness of breath. If emphysema is found, physicians should discuss mitigating any potential risk factors and consider the use of COPD medications such as inhalers.
“Our findings also support using race-neutral reference equations to interpret spirometry instead of race-specific equations. Racial disparities in rates of emphysema among those with ‘normal’ FEV1 [between 80% and 120% predicted], were attenuated or eliminated when race-neutral equations were used to calculate FEV1. This suggests that race-specific equations are normalizing worse lung health in Black adults,” Dr. Liu explained.
“We need to continue research into additional tools that can be used to assess respiratory health and diagnose COPD, while keeping in mind how these tools may affect racial disparities,” said Dr. Liu. “Our study suggests that our reliance on spirometry measures such as FEV1/FVC ratio and FEV1 is missing a number of people with respiratory symptoms and CT evidence of lung disease, and that this is disproportionately affecting Black adults in the United States.” Looking ahead, “it is important to find better tools to identify people with impaired respiratory health or early manifestations of disease so we can intercept chronic lung disease before it becomes clinically apparent and patients have sustained significant lung damage.”
The CARDIA study was supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Dr. Liu was supported by a grant from the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Pal had no financial conflicts to disclose.
*This article was updated 7/22/2022.
An overreliance on spirometry to identify emphysema led to missed cases in Black individuals, particularly men, based on a secondary data analysis of 2,674 people.
“Over the last few years, there has been growing debate around the use of race adjustment in diagnostic algorithms and equations commonly used in medicine,” lead author Gabrielle Yi-Hui Liu, MD, said in an interview. “Whereas, previously it was common to accept racial or ethnic differences in clinical measures and outcomes as inherent differences among populations, there is now more recognition of how racism, socioeconomic status, and environmental exposures can cause these racial differences. Our initial interest in this study was to examine how the use of race-specific spirometry reference equations, and the use of spirometry in general, may be contributing to racial disparities.”
“Previous studies have suggested that the use of race-specific equations in spirometry can exacerbate racial inequities in healthcare outcomes by under-recognition of early disease in Black adults, and this study adds to that evidence,” said Suman Pal, MBBS, of the University of New Mexico, Albuquerque, in an interview.
“By examining the crucial ways in which systemic factors in medicine, such as race-specific equations, exacerbate racial inequities in healthcare, this study is a timely analysis in a moment of national reckoning of structural racism,” said Dr. Pal, who was not involved in the study.
In a study published in Annals of Internal Medicine, Dr. Liu and colleagues at Northwestern University, Chicago, conducted a secondary analysis of data from the CARDIA Lung study (Coronary Artery Risk Development In Young Adults).
The primary outcome of the study was the prevalence of emphysema among participants with various measures of normal spirometry results, stratified by sex and race. The normal results included an forced expiratory volume in 1 second (FEV1)–forced vital capacity (FVC) ratio greater than or equal to 0.7 or greater than or equal to the lower limit of normal. The participants also were stratified by FEV1 percent predicted, using race-specific reference equations, for FEV1 between 80% and 99% of predicted, or an FEV1 between 100% and 120% of predicted.
The study population included 485 Black men, 762 Black women, 659 White men, and 768 White women who received both a CT scan (in 2010-2011) and spirometry (obtained in 2015-2016) in the CARDIA study. The mean age of the participants at the spirometry exam was 55 years.
A total of 5.3% of the participants had emphysema after stratifying by FEV1-FVC ratio. The prevalence was significantly higher for Black men, compared with White men (12.3% vs. 4.0%; relative risk, 3.0), and for Black women, compared with White women (5.0% vs. 2.6%; RR, 1.9).
The association between Black race and emphysema risk persisted but decreased when the researchers used a race-neutral estimate.
When the participants were stratified by race-specific FEV1 percent predicted, 6.5% of individuals with a race-specific FEV1 between 80% and 99% had emphysema. After controlling for factors including age and smoking, emphysema was significantly more prevalent in Black men versus White men (15.5% vs. 4.0%) and in Black women, compared with White women (6.6% vs. 3.4%).
The racial difference persisted in men with a race-specific FEV1 between 100% and 120% of predicted. Of these, 4.0% had emphysema. The prevalence was significantly higher in Black men, compared with White men (13.9% vs. 2.2%), but similar between Black women and White women (2.6% vs. 2.0%).
The use of race-neutral equations reduced, but did not eliminate, these disparities, the researchers said.
The findings were limited by the lack of CT imaging data from the same visit as the final spirometry collection, the researchers noted. “Given that imaging was obtained 5 years before spirometry and emphysema is an irreversible finding, this may have led to an overall underestimation of the prevalence of emphysema.”
Spirometry alone misses cases
“We were surprised by the substantial rates of emphysema we saw among Black men in our cohort with normal spirometry,” Dr. Liu said in an interview. “We did not expect to find than more than one in eight Black men with an FEV1 between 100% and 120% predicted would have emphysema – a rate more than six times higher than White men with the same range of FEV1.”
“One takeaway is that we are likely missing a lot of people with impaired respiratory health or true lung disease by only using spirometry to diagnose COPD,” said Dr. Liu. In clinical practice, “physicians should consider ordering CT scans on patients with normal spirometry who have respiratory symptoms such as cough or shortness of breath. If emphysema is found, physicians should discuss mitigating any potential risk factors and consider the use of COPD medications such as inhalers.
“Our findings also support using race-neutral reference equations to interpret spirometry instead of race-specific equations. Racial disparities in rates of emphysema among those with ‘normal’ FEV1 [between 80% and 120% predicted], were attenuated or eliminated when race-neutral equations were used to calculate FEV1. This suggests that race-specific equations are normalizing worse lung health in Black adults,” Dr. Liu explained.
“We need to continue research into additional tools that can be used to assess respiratory health and diagnose COPD, while keeping in mind how these tools may affect racial disparities,” said Dr. Liu. “Our study suggests that our reliance on spirometry measures such as FEV1/FVC ratio and FEV1 is missing a number of people with respiratory symptoms and CT evidence of lung disease, and that this is disproportionately affecting Black adults in the United States.” Looking ahead, “it is important to find better tools to identify people with impaired respiratory health or early manifestations of disease so we can intercept chronic lung disease before it becomes clinically apparent and patients have sustained significant lung damage.”
The CARDIA study was supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Dr. Liu was supported by a grant from the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Pal had no financial conflicts to disclose.
*This article was updated 7/22/2022.
FROM ANNALS OF INTERNAL MEDICINE