User login
Protein discovery points the way to sepsis treatment

Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
AB blood type linked to cognitive impairment

Credit: Graham Colm
Individuals with type AB blood may be more likely than those with other blood types to develop memory loss in later years, according to a study published in Neurology.
Investigators found that people with AB blood were 82% more likely to develop cognitive impairment, which can lead to dementia.
Previous studies have shown that individuals with type O blood have a lower risk of heart disease and stroke, factors that can increase the risk of memory loss and dementia.
The new research was part of a larger study—the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study—of more than 30,000 subjects who were followed for an average of 3.4 years.
“Our study looks at blood type and risk of cognitive impairment, but several studies have shown that factors such as high blood pressure, high cholesterol, and diabetes increase the risk of cognitive impairment and dementia,” said Mary Cushman, MD, of the University of Vermont College of Medicine in Burlington.
“Blood type is also related to other vascular conditions like stroke, so the findings highlight the connections between vascular issues and brain health. More research is needed to confirm these results.”
Dr Cushman and her colleagues had set out to assess the relationship between ABO group, factor VIII (FVIII), and incident cognitive impairment in a large, prospective cohort of black and white adults in the US.
The team used cognitive domain tests to assess cognitive impairment. They identified 495 subjects who had no cognitive impairment at baseline but became impaired during follow-up. The investigators then compared these cases with 587 control subjects.
It turned out that subjects with AB blood made up 6% of the group that developed cognitive impairment, which is higher than the 4% of AB individuals found in the general population.
Multivariate analysis—adjusted for age, race, region, and sex—suggested that subjects with AB blood and those with higher FVIII had an increased risk of cognitive impairment. The odds ratios were 1.82 and 1.24, respectively.
Subjects with AB blood had a higher average level of FVIII than subjects with other blood types. The mean level of FVIII was 142 IU/dL among AB subjects and 104 IU/dL among subjects with type O blood.
However, the investigators also found that FVIII mediated only 18% of the association between AB blood type and cognitive impairment. ![]()
Credit: Graham Colm
Individuals with type AB blood may be more likely than those with other blood types to develop memory loss in later years, according to a study published in Neurology.
Investigators found that people with AB blood were 82% more likely to develop cognitive impairment, which can lead to dementia.
Previous studies have shown that individuals with type O blood have a lower risk of heart disease and stroke, factors that can increase the risk of memory loss and dementia.
The new research was part of a larger study—the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study—of more than 30,000 subjects who were followed for an average of 3.4 years.
“Our study looks at blood type and risk of cognitive impairment, but several studies have shown that factors such as high blood pressure, high cholesterol, and diabetes increase the risk of cognitive impairment and dementia,” said Mary Cushman, MD, of the University of Vermont College of Medicine in Burlington.
“Blood type is also related to other vascular conditions like stroke, so the findings highlight the connections between vascular issues and brain health. More research is needed to confirm these results.”
Dr Cushman and her colleagues had set out to assess the relationship between ABO group, factor VIII (FVIII), and incident cognitive impairment in a large, prospective cohort of black and white adults in the US.
The team used cognitive domain tests to assess cognitive impairment. They identified 495 subjects who had no cognitive impairment at baseline but became impaired during follow-up. The investigators then compared these cases with 587 control subjects.
It turned out that subjects with AB blood made up 6% of the group that developed cognitive impairment, which is higher than the 4% of AB individuals found in the general population.
Multivariate analysis—adjusted for age, race, region, and sex—suggested that subjects with AB blood and those with higher FVIII had an increased risk of cognitive impairment. The odds ratios were 1.82 and 1.24, respectively.
Subjects with AB blood had a higher average level of FVIII than subjects with other blood types. The mean level of FVIII was 142 IU/dL among AB subjects and 104 IU/dL among subjects with type O blood.
However, the investigators also found that FVIII mediated only 18% of the association between AB blood type and cognitive impairment. ![]()
Credit: Graham Colm
Individuals with type AB blood may be more likely than those with other blood types to develop memory loss in later years, according to a study published in Neurology.
Investigators found that people with AB blood were 82% more likely to develop cognitive impairment, which can lead to dementia.
Previous studies have shown that individuals with type O blood have a lower risk of heart disease and stroke, factors that can increase the risk of memory loss and dementia.
The new research was part of a larger study—the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study—of more than 30,000 subjects who were followed for an average of 3.4 years.
“Our study looks at blood type and risk of cognitive impairment, but several studies have shown that factors such as high blood pressure, high cholesterol, and diabetes increase the risk of cognitive impairment and dementia,” said Mary Cushman, MD, of the University of Vermont College of Medicine in Burlington.
“Blood type is also related to other vascular conditions like stroke, so the findings highlight the connections between vascular issues and brain health. More research is needed to confirm these results.”
Dr Cushman and her colleagues had set out to assess the relationship between ABO group, factor VIII (FVIII), and incident cognitive impairment in a large, prospective cohort of black and white adults in the US.
The team used cognitive domain tests to assess cognitive impairment. They identified 495 subjects who had no cognitive impairment at baseline but became impaired during follow-up. The investigators then compared these cases with 587 control subjects.
It turned out that subjects with AB blood made up 6% of the group that developed cognitive impairment, which is higher than the 4% of AB individuals found in the general population.
Multivariate analysis—adjusted for age, race, region, and sex—suggested that subjects with AB blood and those with higher FVIII had an increased risk of cognitive impairment. The odds ratios were 1.82 and 1.24, respectively.
Subjects with AB blood had a higher average level of FVIII than subjects with other blood types. The mean level of FVIII was 142 IU/dL among AB subjects and 104 IU/dL among subjects with type O blood.
However, the investigators also found that FVIII mediated only 18% of the association between AB blood type and cognitive impairment. ![]()
Spleen-like device could solve problems in treating sepsis
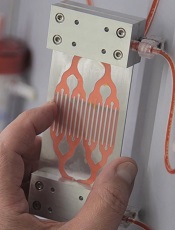
Credit: Wyss Institute
A device inspired by the human spleen could change the way we treat sepsis, researchers say.
This “biospleen” was able to cleanse human blood in lab tests and increase survival in animals with infected blood.
Experiments showed that, in a matter of hours, the biospleen can filter live and dead pathogens from the blood, as well as dangerous toxins released from the pathogens.
The researchers detailed these experiments in Nature Medicine.
“Sepsis is a major medical threat, which is increasing because of antibiotic resistance,” said study author Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering in Boston, Massachusetts.
“We’re excited by the biospleen because it potentially provides a way to treat patients quickly without having to wait days to identify the source of infection, and it works equally well with antibiotic-resistant organisms. We hope to move this toward human testing [by] advancing to large animal studies as quickly as possible.”
The biospleen is a microfluidic device that works outside the body like a dialysis machine and removes living and dead microbes of all varieties, as well as toxins.
It consists of 2 adjacent, hollow channels that are connected to each other by a series of slits. One channel contains flowing blood, and the other has a saline solution that collects and removes the pathogens that travel through the slits.
Key to the success of the device are nanometer-sized magnetic beads coated with a genetically engineered version of the protein mannose binding lectin (MBL).
In its innate state, MBL has a branch-like “head” and a stick-like “tail.” The head binds to specific sugars on the surfaces of all sorts of bacteria, fungi, viruses, protozoa, and toxins, and the tail cues the immune system to destroy them.
However, other immune system proteins sometimes bind to the MBL tail and activate clotting and organ damage. So Dr Ingber and his colleagues used genetic engineering tools to lop off the tail and graft on a similar one from an antibody protein that does not cause these problems.
The team then attached the hybrid proteins to magnetic beads measuring 128 nanometers in diameter. These novel beads could be added to infected blood to bind to the pathogens and toxins without having to first identify the type of infectious agent.
The biospleen has a magnet that pulls the pathogen-coated magnetic beads through the channels to cleanse the blood flowing through the device, which can then be returned to the patient.
The researchers first tested the biospleen using human blood spiked with pathogens. They were able to filter blood faster than ever before, and the magnets efficiently pulled the beads—coated with pathogens—out of the blood.
More than 90% of key sepsis pathogens were bound and removed when the blood flowed through a single device at a rate of about 0.5 L to 1 L per hour. Many devices can be linked together to obtain levels required for human blood cleansing at dialysis-like rates.
Next, the researchers tested the device using rats infected with E coli, S aureus, and toxins—mimicking many of the bloodstream infections human sepsis patients experience. After 5 hours of filtering, about 90% of the bacteria and toxins were removed from the rats’ bloodstreams.
“We didn’t have to kill the pathogens,” said Michael Super, PhD, also of the Wyss Institute. “We just captured and removed them.”
What’s more, 90% of the treated animals survived, compared to 14% of the controls. And the modified MBL prevented the activation of complement factors and coagulation. ![]()
Credit: Wyss Institute
A device inspired by the human spleen could change the way we treat sepsis, researchers say.
This “biospleen” was able to cleanse human blood in lab tests and increase survival in animals with infected blood.
Experiments showed that, in a matter of hours, the biospleen can filter live and dead pathogens from the blood, as well as dangerous toxins released from the pathogens.
The researchers detailed these experiments in Nature Medicine.
“Sepsis is a major medical threat, which is increasing because of antibiotic resistance,” said study author Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering in Boston, Massachusetts.
“We’re excited by the biospleen because it potentially provides a way to treat patients quickly without having to wait days to identify the source of infection, and it works equally well with antibiotic-resistant organisms. We hope to move this toward human testing [by] advancing to large animal studies as quickly as possible.”
The biospleen is a microfluidic device that works outside the body like a dialysis machine and removes living and dead microbes of all varieties, as well as toxins.
It consists of 2 adjacent, hollow channels that are connected to each other by a series of slits. One channel contains flowing blood, and the other has a saline solution that collects and removes the pathogens that travel through the slits.
Key to the success of the device are nanometer-sized magnetic beads coated with a genetically engineered version of the protein mannose binding lectin (MBL).
In its innate state, MBL has a branch-like “head” and a stick-like “tail.” The head binds to specific sugars on the surfaces of all sorts of bacteria, fungi, viruses, protozoa, and toxins, and the tail cues the immune system to destroy them.
However, other immune system proteins sometimes bind to the MBL tail and activate clotting and organ damage. So Dr Ingber and his colleagues used genetic engineering tools to lop off the tail and graft on a similar one from an antibody protein that does not cause these problems.
The team then attached the hybrid proteins to magnetic beads measuring 128 nanometers in diameter. These novel beads could be added to infected blood to bind to the pathogens and toxins without having to first identify the type of infectious agent.
The biospleen has a magnet that pulls the pathogen-coated magnetic beads through the channels to cleanse the blood flowing through the device, which can then be returned to the patient.
The researchers first tested the biospleen using human blood spiked with pathogens. They were able to filter blood faster than ever before, and the magnets efficiently pulled the beads—coated with pathogens—out of the blood.
More than 90% of key sepsis pathogens were bound and removed when the blood flowed through a single device at a rate of about 0.5 L to 1 L per hour. Many devices can be linked together to obtain levels required for human blood cleansing at dialysis-like rates.
Next, the researchers tested the device using rats infected with E coli, S aureus, and toxins—mimicking many of the bloodstream infections human sepsis patients experience. After 5 hours of filtering, about 90% of the bacteria and toxins were removed from the rats’ bloodstreams.
“We didn’t have to kill the pathogens,” said Michael Super, PhD, also of the Wyss Institute. “We just captured and removed them.”
What’s more, 90% of the treated animals survived, compared to 14% of the controls. And the modified MBL prevented the activation of complement factors and coagulation. ![]()
Credit: Wyss Institute
A device inspired by the human spleen could change the way we treat sepsis, researchers say.
This “biospleen” was able to cleanse human blood in lab tests and increase survival in animals with infected blood.
Experiments showed that, in a matter of hours, the biospleen can filter live and dead pathogens from the blood, as well as dangerous toxins released from the pathogens.
The researchers detailed these experiments in Nature Medicine.
“Sepsis is a major medical threat, which is increasing because of antibiotic resistance,” said study author Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering in Boston, Massachusetts.
“We’re excited by the biospleen because it potentially provides a way to treat patients quickly without having to wait days to identify the source of infection, and it works equally well with antibiotic-resistant organisms. We hope to move this toward human testing [by] advancing to large animal studies as quickly as possible.”
The biospleen is a microfluidic device that works outside the body like a dialysis machine and removes living and dead microbes of all varieties, as well as toxins.
It consists of 2 adjacent, hollow channels that are connected to each other by a series of slits. One channel contains flowing blood, and the other has a saline solution that collects and removes the pathogens that travel through the slits.
Key to the success of the device are nanometer-sized magnetic beads coated with a genetically engineered version of the protein mannose binding lectin (MBL).
In its innate state, MBL has a branch-like “head” and a stick-like “tail.” The head binds to specific sugars on the surfaces of all sorts of bacteria, fungi, viruses, protozoa, and toxins, and the tail cues the immune system to destroy them.
However, other immune system proteins sometimes bind to the MBL tail and activate clotting and organ damage. So Dr Ingber and his colleagues used genetic engineering tools to lop off the tail and graft on a similar one from an antibody protein that does not cause these problems.
The team then attached the hybrid proteins to magnetic beads measuring 128 nanometers in diameter. These novel beads could be added to infected blood to bind to the pathogens and toxins without having to first identify the type of infectious agent.
The biospleen has a magnet that pulls the pathogen-coated magnetic beads through the channels to cleanse the blood flowing through the device, which can then be returned to the patient.
The researchers first tested the biospleen using human blood spiked with pathogens. They were able to filter blood faster than ever before, and the magnets efficiently pulled the beads—coated with pathogens—out of the blood.
More than 90% of key sepsis pathogens were bound and removed when the blood flowed through a single device at a rate of about 0.5 L to 1 L per hour. Many devices can be linked together to obtain levels required for human blood cleansing at dialysis-like rates.
Next, the researchers tested the device using rats infected with E coli, S aureus, and toxins—mimicking many of the bloodstream infections human sepsis patients experience. After 5 hours of filtering, about 90% of the bacteria and toxins were removed from the rats’ bloodstreams.
“We didn’t have to kill the pathogens,” said Michael Super, PhD, also of the Wyss Institute. “We just captured and removed them.”
What’s more, 90% of the treated animals survived, compared to 14% of the controls. And the modified MBL prevented the activation of complement factors and coagulation. ![]()
FDA approves new treatment for PI

Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information. ![]()
Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information. ![]()
Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information. ![]()
Malaria parasites react to mosquito presence

(blue) in mosquito gut
Credit: Antoine Nicot
and Jacques Denoyelle
Experiments in canaries have shown that Plasmodium parasites react when non-infected mosquitoes bite their hosts, and the parasite responses increase transmission to the mosquito.
Like many other parasites, Plasmodium goes through a phase of chronic infection during which most of the parasites are in a dormant stage, and parasite numbers in the blood are very low.
Every now and then, however, the parasites “relapse,” and numbers increase, but the cause of this is not well understood.
So researchers set out to determine whether bites from non-infected mosquitoes can trigger relapses in Plasmodium during chronic infections, and whether relapses are associated with higher rates of transmission to the vector, ie, infection of the mosquitoes.
Sylvain Gandon, PhD, of the Université de Montpellier in France, and his colleagues described this research in PLOS Pathogens.
Specifically, the researchers studied the interaction between Plasmodium relictum, the parasite responsible for most cases of bird malaria in European songbirds, and its natural vector, a mosquito called Culex pipiens.
The team infected domestic canaries with P relictum and tested whether bites from uninfected Culex mosquitoes could trigger malaria relapses during chronic infection.
Indeed, parasite numbers in the blood routinely increased after the canaries were bitten. Moreover, the higher parasite loads following mosquito bites translated into higher infection rates in the mosquitoes.
The researchers therefore concluded that P relictum has the ability to boost its own transmission during the chronic phase of the vertebrate infection after being exposed to mosquito bites.
Although it is unclear if this also occurs in humans, the team suggested that better understanding of this phenomenon could eventually improve malaria control.
They also pointed out that many other pathogens alternate between acute and dormant phases. So better understanding of the ecological determinants and evolutionary forces governing parasite relapses could have wide-ranging applications. ![]()
(blue) in mosquito gut
Credit: Antoine Nicot
and Jacques Denoyelle
Experiments in canaries have shown that Plasmodium parasites react when non-infected mosquitoes bite their hosts, and the parasite responses increase transmission to the mosquito.
Like many other parasites, Plasmodium goes through a phase of chronic infection during which most of the parasites are in a dormant stage, and parasite numbers in the blood are very low.
Every now and then, however, the parasites “relapse,” and numbers increase, but the cause of this is not well understood.
So researchers set out to determine whether bites from non-infected mosquitoes can trigger relapses in Plasmodium during chronic infections, and whether relapses are associated with higher rates of transmission to the vector, ie, infection of the mosquitoes.
Sylvain Gandon, PhD, of the Université de Montpellier in France, and his colleagues described this research in PLOS Pathogens.
Specifically, the researchers studied the interaction between Plasmodium relictum, the parasite responsible for most cases of bird malaria in European songbirds, and its natural vector, a mosquito called Culex pipiens.
The team infected domestic canaries with P relictum and tested whether bites from uninfected Culex mosquitoes could trigger malaria relapses during chronic infection.
Indeed, parasite numbers in the blood routinely increased after the canaries were bitten. Moreover, the higher parasite loads following mosquito bites translated into higher infection rates in the mosquitoes.
The researchers therefore concluded that P relictum has the ability to boost its own transmission during the chronic phase of the vertebrate infection after being exposed to mosquito bites.
Although it is unclear if this also occurs in humans, the team suggested that better understanding of this phenomenon could eventually improve malaria control.
They also pointed out that many other pathogens alternate between acute and dormant phases. So better understanding of the ecological determinants and evolutionary forces governing parasite relapses could have wide-ranging applications. ![]()
(blue) in mosquito gut
Credit: Antoine Nicot
and Jacques Denoyelle
Experiments in canaries have shown that Plasmodium parasites react when non-infected mosquitoes bite their hosts, and the parasite responses increase transmission to the mosquito.
Like many other parasites, Plasmodium goes through a phase of chronic infection during which most of the parasites are in a dormant stage, and parasite numbers in the blood are very low.
Every now and then, however, the parasites “relapse,” and numbers increase, but the cause of this is not well understood.
So researchers set out to determine whether bites from non-infected mosquitoes can trigger relapses in Plasmodium during chronic infections, and whether relapses are associated with higher rates of transmission to the vector, ie, infection of the mosquitoes.
Sylvain Gandon, PhD, of the Université de Montpellier in France, and his colleagues described this research in PLOS Pathogens.
Specifically, the researchers studied the interaction between Plasmodium relictum, the parasite responsible for most cases of bird malaria in European songbirds, and its natural vector, a mosquito called Culex pipiens.
The team infected domestic canaries with P relictum and tested whether bites from uninfected Culex mosquitoes could trigger malaria relapses during chronic infection.
Indeed, parasite numbers in the blood routinely increased after the canaries were bitten. Moreover, the higher parasite loads following mosquito bites translated into higher infection rates in the mosquitoes.
The researchers therefore concluded that P relictum has the ability to boost its own transmission during the chronic phase of the vertebrate infection after being exposed to mosquito bites.
Although it is unclear if this also occurs in humans, the team suggested that better understanding of this phenomenon could eventually improve malaria control.
They also pointed out that many other pathogens alternate between acute and dormant phases. So better understanding of the ecological determinants and evolutionary forces governing parasite relapses could have wide-ranging applications. ![]()
Mutations linked to population disparities in cancers

Credit: NIGMS
Researchers have identified mutations in microRNAs (miRNAs) that are closely associated with certain global populations and have been implicated in cancers.
The group discovered 31 miRNAs containing variants that occur with different frequencies in African and non-African populations.
Seven of these miRNAs have been linked to the onset, progression, and spread of cancers with known health disparities between patients of European and African descent.
And a variant in one of these miRNAs is associated with a significantly increased risk of non-Hodgkin lymphoma (NHL).
These findings appear in BMC Medical Genomics.
To better understand miRNA diversity across the world, the researchers searched for miRNA variants in the genome sequences of 69 individuals from 14 populations in Europe, Asia, the Americas, and Africa. The samples included genetic material from diverse African populations, including 3 hunter-gatherer populations.
“We wanted to try to see if there was variability in miRNA that hadn’t been identified before,” said study author Renata A. Rawlings-Goss, PhD, of the University of Pennsylvania’s Perelman School of Medicine in Philadelphia.
Overall, the researchers found that miRNA sequences were similar across the populations they sampled. But they did identify 33 novel variants and found that variants in 31 miRNAs were population-differentiated.
The team searched available databases to see which genes these miRNAs were known to inhibit. Their query turned up a large proportion of genes involved in glucose and insulin metabolism, indicating a possible connection between diabetes risk and possessing one of these variants. The search also pointed to effects on genes implicated in cancers.
Specifically, 7 of the population-differentiated miRNAs are currently implicated as cancer biomarkers: hsa-mir-202, hsa-mir-423, hsa-mir-196a-2, hsa-mir-520h, hsa-mir-647, hsa-mir-943, and hsa-mir-1908.
Of particular interest was hsa-mir-202, which contained one of the most highly population-differentiated variants in the dataset and is under investigation as a marker for NHL and early stage breast cancer.
Recent research suggested that a T allele at SNP rs12355840 in hsa-mir-202 helps protect against death from breast cancer by increasing mature hsa-mir-202 expression levels, which leads to downregulation of its gene targets.
On the other hand, diminished expression of mature hsa-mir-202 in subjects harboring at least 1 non-T allele resulted in a significantly elevated risk of NHL (odds ratio=1.83, P=0.008).
Dr Rawlings-Goss and her colleagues found that African/African-American populations had a lower frequency of the T allele compared to European/Asian populations—26% vs 65%, on average. And this suggests decreased baseline expression levels of mature hsa-mir-202 in African populations.
“It’s becoming more and more apparent that miRNAs can have a broad-reaching and global effect on our health and adaptation to disease,” Dr Rawlings-Goss said. “Learning more about differences across populations could be helpful to doing early diagnostics and treating disease across diverse populations.” ![]()
Credit: NIGMS
Researchers have identified mutations in microRNAs (miRNAs) that are closely associated with certain global populations and have been implicated in cancers.
The group discovered 31 miRNAs containing variants that occur with different frequencies in African and non-African populations.
Seven of these miRNAs have been linked to the onset, progression, and spread of cancers with known health disparities between patients of European and African descent.
And a variant in one of these miRNAs is associated with a significantly increased risk of non-Hodgkin lymphoma (NHL).
These findings appear in BMC Medical Genomics.
To better understand miRNA diversity across the world, the researchers searched for miRNA variants in the genome sequences of 69 individuals from 14 populations in Europe, Asia, the Americas, and Africa. The samples included genetic material from diverse African populations, including 3 hunter-gatherer populations.
“We wanted to try to see if there was variability in miRNA that hadn’t been identified before,” said study author Renata A. Rawlings-Goss, PhD, of the University of Pennsylvania’s Perelman School of Medicine in Philadelphia.
Overall, the researchers found that miRNA sequences were similar across the populations they sampled. But they did identify 33 novel variants and found that variants in 31 miRNAs were population-differentiated.
The team searched available databases to see which genes these miRNAs were known to inhibit. Their query turned up a large proportion of genes involved in glucose and insulin metabolism, indicating a possible connection between diabetes risk and possessing one of these variants. The search also pointed to effects on genes implicated in cancers.
Specifically, 7 of the population-differentiated miRNAs are currently implicated as cancer biomarkers: hsa-mir-202, hsa-mir-423, hsa-mir-196a-2, hsa-mir-520h, hsa-mir-647, hsa-mir-943, and hsa-mir-1908.
Of particular interest was hsa-mir-202, which contained one of the most highly population-differentiated variants in the dataset and is under investigation as a marker for NHL and early stage breast cancer.
Recent research suggested that a T allele at SNP rs12355840 in hsa-mir-202 helps protect against death from breast cancer by increasing mature hsa-mir-202 expression levels, which leads to downregulation of its gene targets.
On the other hand, diminished expression of mature hsa-mir-202 in subjects harboring at least 1 non-T allele resulted in a significantly elevated risk of NHL (odds ratio=1.83, P=0.008).
Dr Rawlings-Goss and her colleagues found that African/African-American populations had a lower frequency of the T allele compared to European/Asian populations—26% vs 65%, on average. And this suggests decreased baseline expression levels of mature hsa-mir-202 in African populations.
“It’s becoming more and more apparent that miRNAs can have a broad-reaching and global effect on our health and adaptation to disease,” Dr Rawlings-Goss said. “Learning more about differences across populations could be helpful to doing early diagnostics and treating disease across diverse populations.” ![]()
Credit: NIGMS
Researchers have identified mutations in microRNAs (miRNAs) that are closely associated with certain global populations and have been implicated in cancers.
The group discovered 31 miRNAs containing variants that occur with different frequencies in African and non-African populations.
Seven of these miRNAs have been linked to the onset, progression, and spread of cancers with known health disparities between patients of European and African descent.
And a variant in one of these miRNAs is associated with a significantly increased risk of non-Hodgkin lymphoma (NHL).
These findings appear in BMC Medical Genomics.
To better understand miRNA diversity across the world, the researchers searched for miRNA variants in the genome sequences of 69 individuals from 14 populations in Europe, Asia, the Americas, and Africa. The samples included genetic material from diverse African populations, including 3 hunter-gatherer populations.
“We wanted to try to see if there was variability in miRNA that hadn’t been identified before,” said study author Renata A. Rawlings-Goss, PhD, of the University of Pennsylvania’s Perelman School of Medicine in Philadelphia.
Overall, the researchers found that miRNA sequences were similar across the populations they sampled. But they did identify 33 novel variants and found that variants in 31 miRNAs were population-differentiated.
The team searched available databases to see which genes these miRNAs were known to inhibit. Their query turned up a large proportion of genes involved in glucose and insulin metabolism, indicating a possible connection between diabetes risk and possessing one of these variants. The search also pointed to effects on genes implicated in cancers.
Specifically, 7 of the population-differentiated miRNAs are currently implicated as cancer biomarkers: hsa-mir-202, hsa-mir-423, hsa-mir-196a-2, hsa-mir-520h, hsa-mir-647, hsa-mir-943, and hsa-mir-1908.
Of particular interest was hsa-mir-202, which contained one of the most highly population-differentiated variants in the dataset and is under investigation as a marker for NHL and early stage breast cancer.
Recent research suggested that a T allele at SNP rs12355840 in hsa-mir-202 helps protect against death from breast cancer by increasing mature hsa-mir-202 expression levels, which leads to downregulation of its gene targets.
On the other hand, diminished expression of mature hsa-mir-202 in subjects harboring at least 1 non-T allele resulted in a significantly elevated risk of NHL (odds ratio=1.83, P=0.008).
Dr Rawlings-Goss and her colleagues found that African/African-American populations had a lower frequency of the T allele compared to European/Asian populations—26% vs 65%, on average. And this suggests decreased baseline expression levels of mature hsa-mir-202 in African populations.
“It’s becoming more and more apparent that miRNAs can have a broad-reaching and global effect on our health and adaptation to disease,” Dr Rawlings-Goss said. “Learning more about differences across populations could be helpful to doing early diagnostics and treating disease across diverse populations.” ![]()
Database details international research regulations
The National Institutes of Health has launched an online public database called ClinRegs, which includes country-specific information on
clinical research regulations.
ClinRegs currently provides information for 12 countries, but additional countries will likely be added in the future.
The goal of ClinRegs is to make it easier for investigators to find and understand country-specific requirements on topics such as clinical trial application submission and ethics committee approvals.
The database allows users to review regulatory requirements in 7 topic areas, including informed consent practices and trial sponsorship.
The site was created—and will be updated—by the National Institute of Allergy and Infectious Diseases. ![]()
The National Institutes of Health has launched an online public database called ClinRegs, which includes country-specific information on
clinical research regulations.
ClinRegs currently provides information for 12 countries, but additional countries will likely be added in the future.
The goal of ClinRegs is to make it easier for investigators to find and understand country-specific requirements on topics such as clinical trial application submission and ethics committee approvals.
The database allows users to review regulatory requirements in 7 topic areas, including informed consent practices and trial sponsorship.
The site was created—and will be updated—by the National Institute of Allergy and Infectious Diseases. ![]()
The National Institutes of Health has launched an online public database called ClinRegs, which includes country-specific information on
clinical research regulations.
ClinRegs currently provides information for 12 countries, but additional countries will likely be added in the future.
The goal of ClinRegs is to make it easier for investigators to find and understand country-specific requirements on topics such as clinical trial application submission and ethics committee approvals.
The database allows users to review regulatory requirements in 7 topic areas, including informed consent practices and trial sponsorship.
The site was created—and will be updated—by the National Institute of Allergy and Infectious Diseases. ![]()
Fats may hold key to new malaria treatment
Credit: Stuart Hay
Scientists believe they have discovered a weak spot in the malaria life cycle that could be exploited to prevent the disease from spreading.
The team found that female malaria parasites take on fat differently than male parasites.
And the protein gABCG2, which controls the transport of fat molecules, plays a key role in malaria parasite survival.
Phuong Tran, PhD, of Australia National University in Canberra, and his colleagues recounted these findings in Nature Communications.
The researchers noted that ATP-binding cassette transporters are known to play key roles in drug resistance. And the genome of the Plasmodium falciparum parasite encodes multiple members of this family, including gABCG2, which is transcribed predominantly in the gametocyte stage.
So the team used gene deletion and tagging to investigate the expression, localization, and function of gABCG2. They found that gABCG2 was only present in female gametocytes—in a single, lipid-like structure.
“Female parasites build a deposit of fat in a localized spot, which is controlled by gABCG2,” said study author Alexander Maier, PhD, of Australia National University.
“However, malaria genetically modified to have no gABCG2 did not accumulate fat in the same way, and crucially, struggled to survive in the mosquito.”
Cell lines in which gABCG2 was knocked out produced more gametocytes of both sexes, but they showed a reduction in cholesteryl esters, diacylglycerols, and triacylglycerols.
The researchers therefore concluded that gABCG2 regulates gametocyte numbers and the accumulation of neutral lipids, which are likely important for parasite development in the insect stages of the parasite life cycle.
Dr Tran said this discovery could lead to new malaria drugs based on current drugs that influence fat digestion.
“If we can target the molecule gABCG2 and kill the females, then we can stop the fertilization, which will stop the development and transmission of the disease,” he said. “It may even lead to a vaccine for malaria.” ![]()
Credit: Stuart Hay
Scientists believe they have discovered a weak spot in the malaria life cycle that could be exploited to prevent the disease from spreading.
The team found that female malaria parasites take on fat differently than male parasites.
And the protein gABCG2, which controls the transport of fat molecules, plays a key role in malaria parasite survival.
Phuong Tran, PhD, of Australia National University in Canberra, and his colleagues recounted these findings in Nature Communications.
The researchers noted that ATP-binding cassette transporters are known to play key roles in drug resistance. And the genome of the Plasmodium falciparum parasite encodes multiple members of this family, including gABCG2, which is transcribed predominantly in the gametocyte stage.
So the team used gene deletion and tagging to investigate the expression, localization, and function of gABCG2. They found that gABCG2 was only present in female gametocytes—in a single, lipid-like structure.
“Female parasites build a deposit of fat in a localized spot, which is controlled by gABCG2,” said study author Alexander Maier, PhD, of Australia National University.
“However, malaria genetically modified to have no gABCG2 did not accumulate fat in the same way, and crucially, struggled to survive in the mosquito.”
Cell lines in which gABCG2 was knocked out produced more gametocytes of both sexes, but they showed a reduction in cholesteryl esters, diacylglycerols, and triacylglycerols.
The researchers therefore concluded that gABCG2 regulates gametocyte numbers and the accumulation of neutral lipids, which are likely important for parasite development in the insect stages of the parasite life cycle.
Dr Tran said this discovery could lead to new malaria drugs based on current drugs that influence fat digestion.
“If we can target the molecule gABCG2 and kill the females, then we can stop the fertilization, which will stop the development and transmission of the disease,” he said. “It may even lead to a vaccine for malaria.” ![]()
Credit: Stuart Hay
Scientists believe they have discovered a weak spot in the malaria life cycle that could be exploited to prevent the disease from spreading.
The team found that female malaria parasites take on fat differently than male parasites.
And the protein gABCG2, which controls the transport of fat molecules, plays a key role in malaria parasite survival.
Phuong Tran, PhD, of Australia National University in Canberra, and his colleagues recounted these findings in Nature Communications.
The researchers noted that ATP-binding cassette transporters are known to play key roles in drug resistance. And the genome of the Plasmodium falciparum parasite encodes multiple members of this family, including gABCG2, which is transcribed predominantly in the gametocyte stage.
So the team used gene deletion and tagging to investigate the expression, localization, and function of gABCG2. They found that gABCG2 was only present in female gametocytes—in a single, lipid-like structure.
“Female parasites build a deposit of fat in a localized spot, which is controlled by gABCG2,” said study author Alexander Maier, PhD, of Australia National University.
“However, malaria genetically modified to have no gABCG2 did not accumulate fat in the same way, and crucially, struggled to survive in the mosquito.”
Cell lines in which gABCG2 was knocked out produced more gametocytes of both sexes, but they showed a reduction in cholesteryl esters, diacylglycerols, and triacylglycerols.
The researchers therefore concluded that gABCG2 regulates gametocyte numbers and the accumulation of neutral lipids, which are likely important for parasite development in the insect stages of the parasite life cycle.
Dr Tran said this discovery could lead to new malaria drugs based on current drugs that influence fat digestion.
“If we can target the molecule gABCG2 and kill the females, then we can stop the fertilization, which will stop the development and transmission of the disease,” he said. “It may even lead to a vaccine for malaria.”
Re-analyses of RCTs may reveal different conclusions

Credit: Darren Baker
A new study suggests that as many as a third of randomized clinical trials (RCTs) could be re-analyzed in ways that modify their conclusions.
The study also indicates that such re-analyses are extremely rare, due to many researchers’ unwillingness to share data.
“There is a real need for researchers to provide access to their raw data for others to analyze,” said John Ioannidis, MD, DSc, of the Stanford Prevention Research Center in California.
“Without this access, and possibly incentives to perform this work, there is increasing lack of trust in whether the results of published, randomized trials are credible and can be taken at face value.”
Dr Ioannidis and his colleagues used the MEDLINE database to evaluate re-analyses of RCTs and detailed their findings in JAMA. A related editorial is also available in the journal.
The team searched for articles written in English describing the re-analysis of raw data used in previously published RCTs. Meta-analyses were excluded from the study, as were studies testing a different hypothesis than the original trial.
The researchers screened nearly 3000 articles of potential interest and read the full text of 226. Of these, 37 were ultimately included in the study. Thirty-two of them had an overlap of at least 1 author from the original paper.
New conclusions
Thirteen of the re-analyses (35% of the total) came to conclusions that differed from those of the original trial with regard to who could benefit from the tested medication or intervention.
Three concluded that the patient population to treat should be different from the one recommended by the original study. One concluded that fewer patients should be treated. And the remaining 9 indicated that more patients should be treated.
The differences between the original RCTs and the re-analyses often occurred because the researchers conducting the re-analyses used different statistical or analytical methods, ways of defining outcomes, or ways of handling missing data.
For example, an RCT on the treatment of bleeding esophageal varices concluded that sclerotherapy reduced mortality but didn’t prevent rebleeding.
The re-analysis, which used a different statistical model of risk, suggested the treatment did prevent rebleeding but didn’t reduce mortality. The new conclusion suggested the intervention would be most appropriate for patients with rebleeding, rather than those at the highest risk of death from the condition.
Another study investigated the best way to deliver an erythropoiesis-stimulating medication to anemia patients by comparing a fixed dose administered once every 3 weeks with weight-based weekly dosing. In the re-analysis, the conclusion changed when investigators used an updated hemoglobin threshold level to determine when therapy should be initiated.
“The high proportion of re-analyses reaching different conclusions than the original papers may be partly an artifact,” Dr Ioannidis said. “By that I mean that, in the current environment, re-analyses that reach exactly the same results as the original would have great difficulty getting published.”
“However, making the raw data of trials available for re-analyses is essential not only for re-evaluating whether the original claims were correct, but also for using these data to perform additional analyses of interest and combined analyses.”
In this way, existing raw data could be used to explore new clinical questions and might occasionally eliminate the need to conduct new trials.
Credit: Darren Baker
A new study suggests that as many as a third of randomized clinical trials (RCTs) could be re-analyzed in ways that modify their conclusions.
The study also indicates that such re-analyses are extremely rare, due to many researchers’ unwillingness to share data.
“There is a real need for researchers to provide access to their raw data for others to analyze,” said John Ioannidis, MD, DSc, of the Stanford Prevention Research Center in California.
“Without this access, and possibly incentives to perform this work, there is increasing lack of trust in whether the results of published, randomized trials are credible and can be taken at face value.”
Dr Ioannidis and his colleagues used the MEDLINE database to evaluate re-analyses of RCTs and detailed their findings in JAMA. A related editorial is also available in the journal.
The team searched for articles written in English describing the re-analysis of raw data used in previously published RCTs. Meta-analyses were excluded from the study, as were studies testing a different hypothesis than the original trial.
The researchers screened nearly 3000 articles of potential interest and read the full text of 226. Of these, 37 were ultimately included in the study. Thirty-two of them had an overlap of at least 1 author from the original paper.
New conclusions
Thirteen of the re-analyses (35% of the total) came to conclusions that differed from those of the original trial with regard to who could benefit from the tested medication or intervention.
Three concluded that the patient population to treat should be different from the one recommended by the original study. One concluded that fewer patients should be treated. And the remaining 9 indicated that more patients should be treated.
The differences between the original RCTs and the re-analyses often occurred because the researchers conducting the re-analyses used different statistical or analytical methods, ways of defining outcomes, or ways of handling missing data.
For example, an RCT on the treatment of bleeding esophageal varices concluded that sclerotherapy reduced mortality but didn’t prevent rebleeding.
The re-analysis, which used a different statistical model of risk, suggested the treatment did prevent rebleeding but didn’t reduce mortality. The new conclusion suggested the intervention would be most appropriate for patients with rebleeding, rather than those at the highest risk of death from the condition.
Another study investigated the best way to deliver an erythropoiesis-stimulating medication to anemia patients by comparing a fixed dose administered once every 3 weeks with weight-based weekly dosing. In the re-analysis, the conclusion changed when investigators used an updated hemoglobin threshold level to determine when therapy should be initiated.
“The high proportion of re-analyses reaching different conclusions than the original papers may be partly an artifact,” Dr Ioannidis said. “By that I mean that, in the current environment, re-analyses that reach exactly the same results as the original would have great difficulty getting published.”
“However, making the raw data of trials available for re-analyses is essential not only for re-evaluating whether the original claims were correct, but also for using these data to perform additional analyses of interest and combined analyses.”
In this way, existing raw data could be used to explore new clinical questions and might occasionally eliminate the need to conduct new trials.
Credit: Darren Baker
A new study suggests that as many as a third of randomized clinical trials (RCTs) could be re-analyzed in ways that modify their conclusions.
The study also indicates that such re-analyses are extremely rare, due to many researchers’ unwillingness to share data.
“There is a real need for researchers to provide access to their raw data for others to analyze,” said John Ioannidis, MD, DSc, of the Stanford Prevention Research Center in California.
“Without this access, and possibly incentives to perform this work, there is increasing lack of trust in whether the results of published, randomized trials are credible and can be taken at face value.”
Dr Ioannidis and his colleagues used the MEDLINE database to evaluate re-analyses of RCTs and detailed their findings in JAMA. A related editorial is also available in the journal.
The team searched for articles written in English describing the re-analysis of raw data used in previously published RCTs. Meta-analyses were excluded from the study, as were studies testing a different hypothesis than the original trial.
The researchers screened nearly 3000 articles of potential interest and read the full text of 226. Of these, 37 were ultimately included in the study. Thirty-two of them had an overlap of at least 1 author from the original paper.
New conclusions
Thirteen of the re-analyses (35% of the total) came to conclusions that differed from those of the original trial with regard to who could benefit from the tested medication or intervention.
Three concluded that the patient population to treat should be different from the one recommended by the original study. One concluded that fewer patients should be treated. And the remaining 9 indicated that more patients should be treated.
The differences between the original RCTs and the re-analyses often occurred because the researchers conducting the re-analyses used different statistical or analytical methods, ways of defining outcomes, or ways of handling missing data.
For example, an RCT on the treatment of bleeding esophageal varices concluded that sclerotherapy reduced mortality but didn’t prevent rebleeding.
The re-analysis, which used a different statistical model of risk, suggested the treatment did prevent rebleeding but didn’t reduce mortality. The new conclusion suggested the intervention would be most appropriate for patients with rebleeding, rather than those at the highest risk of death from the condition.
Another study investigated the best way to deliver an erythropoiesis-stimulating medication to anemia patients by comparing a fixed dose administered once every 3 weeks with weight-based weekly dosing. In the re-analysis, the conclusion changed when investigators used an updated hemoglobin threshold level to determine when therapy should be initiated.
“The high proportion of re-analyses reaching different conclusions than the original papers may be partly an artifact,” Dr Ioannidis said. “By that I mean that, in the current environment, re-analyses that reach exactly the same results as the original would have great difficulty getting published.”
“However, making the raw data of trials available for re-analyses is essential not only for re-evaluating whether the original claims were correct, but also for using these data to perform additional analyses of interest and combined analyses.”
In this way, existing raw data could be used to explore new clinical questions and might occasionally eliminate the need to conduct new trials.
Overcoming an obstacle to RBC development

Researchers have discovered a natural barrier to hematopoiesis and a way to circumvent it, according to a paper published in Blood.
The group found that components of the exosome complex—exosc8 and exosc9—suppress red blood cell (RBC) maturation.
“From a fundamental perspective, this is very important because this mechanism counteracts the development of precursor cells into red blood cells, thereby establishing a balance between developed cells and the progenitor population,” said study author Emery Bresnick, PhD, of the UW School of Medicine and Public Health in Madison, Wisconsin.
“In the context of translation, if you want to maximize the output of end-stage red blood cells, which we’re not able to do at this time, our study provides a rational approach involving lowering the levels of these subunits.”
Specifically, the researchers found that GATA-1 and Foxo3 can repress the exosome components, thereby allowing for RBC maturation.
The barrier explained
Dr Bresnick and his colleagues noted that the primary obstacle in converting hematopoietic stem cells into RBCs involves late-stage maturation.
“The problem isn’t simply getting erythroid precursors produced by the bucket, but understanding how these cells systematically lose their nuclei and organelles to become a red blood cell, the final product,” Dr Bresnick said.
“This is the bottleneck, even in the stem cell world of embryonic and induced pluripotent stem cells. We know little about how the cell orchestrates the intricate processes that constitute late-stage maturation.”
At the end of RBC development, the erythroid precursor must eject its own genetic material via enucleation. Although it’s clear why enucleation is important (making the cell more flexible and allowing it to carry more oxygen), exactly how the cell does it has been unclear.
Besides ejecting the nucleus, the cell must be cleared of other organelles, such as the endoplasmic reticulum and mitochondria. This process (autophagy) is linked to a pair of transcription factors—GATA1 and Foxo3—that control gene expression important in RBC development.
Because they knew GATA1 and Foxo3 promote autophagy, Dr Bresnick and his colleagues wondered if the proteins these transcription factors repress play an important role in cell maturation.
This led them to identify exosc8 and exosc9, two units of the exosome that ultimately established the development barrier.
The researchers plan to continue studying the exosome because many RNAs in the cell are not degraded by the exosome. Determining exactly how the exosome decides what RNA to dispose of may provide an even better understanding of the newly discovered barrier.
“One goal we have is to establish the specific RNA targets the exosome is regulating that are responsible for the blockade,” Dr Bresnick said. “In doing so, we might even uncover targets that are easier to manipulate than the exosome itself.”
Researchers have discovered a natural barrier to hematopoiesis and a way to circumvent it, according to a paper published in Blood.
The group found that components of the exosome complex—exosc8 and exosc9—suppress red blood cell (RBC) maturation.
“From a fundamental perspective, this is very important because this mechanism counteracts the development of precursor cells into red blood cells, thereby establishing a balance between developed cells and the progenitor population,” said study author Emery Bresnick, PhD, of the UW School of Medicine and Public Health in Madison, Wisconsin.
“In the context of translation, if you want to maximize the output of end-stage red blood cells, which we’re not able to do at this time, our study provides a rational approach involving lowering the levels of these subunits.”
Specifically, the researchers found that GATA-1 and Foxo3 can repress the exosome components, thereby allowing for RBC maturation.
The barrier explained
Dr Bresnick and his colleagues noted that the primary obstacle in converting hematopoietic stem cells into RBCs involves late-stage maturation.
“The problem isn’t simply getting erythroid precursors produced by the bucket, but understanding how these cells systematically lose their nuclei and organelles to become a red blood cell, the final product,” Dr Bresnick said.
“This is the bottleneck, even in the stem cell world of embryonic and induced pluripotent stem cells. We know little about how the cell orchestrates the intricate processes that constitute late-stage maturation.”
At the end of RBC development, the erythroid precursor must eject its own genetic material via enucleation. Although it’s clear why enucleation is important (making the cell more flexible and allowing it to carry more oxygen), exactly how the cell does it has been unclear.
Besides ejecting the nucleus, the cell must be cleared of other organelles, such as the endoplasmic reticulum and mitochondria. This process (autophagy) is linked to a pair of transcription factors—GATA1 and Foxo3—that control gene expression important in RBC development.
Because they knew GATA1 and Foxo3 promote autophagy, Dr Bresnick and his colleagues wondered if the proteins these transcription factors repress play an important role in cell maturation.
This led them to identify exosc8 and exosc9, two units of the exosome that ultimately established the development barrier.
The researchers plan to continue studying the exosome because many RNAs in the cell are not degraded by the exosome. Determining exactly how the exosome decides what RNA to dispose of may provide an even better understanding of the newly discovered barrier.
“One goal we have is to establish the specific RNA targets the exosome is regulating that are responsible for the blockade,” Dr Bresnick said. “In doing so, we might even uncover targets that are easier to manipulate than the exosome itself.”
Researchers have discovered a natural barrier to hematopoiesis and a way to circumvent it, according to a paper published in Blood.
The group found that components of the exosome complex—exosc8 and exosc9—suppress red blood cell (RBC) maturation.
“From a fundamental perspective, this is very important because this mechanism counteracts the development of precursor cells into red blood cells, thereby establishing a balance between developed cells and the progenitor population,” said study author Emery Bresnick, PhD, of the UW School of Medicine and Public Health in Madison, Wisconsin.
“In the context of translation, if you want to maximize the output of end-stage red blood cells, which we’re not able to do at this time, our study provides a rational approach involving lowering the levels of these subunits.”
Specifically, the researchers found that GATA-1 and Foxo3 can repress the exosome components, thereby allowing for RBC maturation.
The barrier explained
Dr Bresnick and his colleagues noted that the primary obstacle in converting hematopoietic stem cells into RBCs involves late-stage maturation.
“The problem isn’t simply getting erythroid precursors produced by the bucket, but understanding how these cells systematically lose their nuclei and organelles to become a red blood cell, the final product,” Dr Bresnick said.
“This is the bottleneck, even in the stem cell world of embryonic and induced pluripotent stem cells. We know little about how the cell orchestrates the intricate processes that constitute late-stage maturation.”
At the end of RBC development, the erythroid precursor must eject its own genetic material via enucleation. Although it’s clear why enucleation is important (making the cell more flexible and allowing it to carry more oxygen), exactly how the cell does it has been unclear.
Besides ejecting the nucleus, the cell must be cleared of other organelles, such as the endoplasmic reticulum and mitochondria. This process (autophagy) is linked to a pair of transcription factors—GATA1 and Foxo3—that control gene expression important in RBC development.
Because they knew GATA1 and Foxo3 promote autophagy, Dr Bresnick and his colleagues wondered if the proteins these transcription factors repress play an important role in cell maturation.
This led them to identify exosc8 and exosc9, two units of the exosome that ultimately established the development barrier.
The researchers plan to continue studying the exosome because many RNAs in the cell are not degraded by the exosome. Determining exactly how the exosome decides what RNA to dispose of may provide an even better understanding of the newly discovered barrier.
“One goal we have is to establish the specific RNA targets the exosome is regulating that are responsible for the blockade,” Dr Bresnick said. “In doing so, we might even uncover targets that are easier to manipulate than the exosome itself.”