User login
Jury is out on universal screening for eating disorders
Eating disorders (binge eating disorder, bulimia nervosa, and anorexia nervosa) can cause “serious harms to physical and psychosocial health and take a tremendous toll on individuals and families,” task force member Lori Pbert, PhD, told this news organization.
“Screening for eating disorders has the potential to improve health by leading to early detection and effective treatment,” said Dr. Pbert, with the department of population and quantitative health sciences, University of Massachusetts, Worcester.
However, a “deep dive” into the available literature failed to turn up adequate evidence to recommend for or against routine screening for eating disorders for children and adolescents aged 10 years and older and for adults who have no signs or symptoms of an eating disorder or concerns about their eating and who have not previously been diagnosed with an eating disorder, Dr. Pbert said.
The task force, therefore, issued an “I” statement (insufficient evidence), meaning it cannot at this time recommend for or against screening for eating disorders.
An “I” statement is “fundamentally a call for more research,” Dr. Pbert noted.
Adolescents and adults who have signs and symptoms of an eating disorder – which include rapid weight loss; weight gain or pronounced deviation from growth trajectory; pubertal delay; bradycardia; oligomenorrhea; and amenorrhea – are not included in this recommendation.
The USPSTF recommendation statement and accompanying evidence report were published online March 15 in JAMA.
Clinical judgment key
In the absence of evidence, clinicians should use their judgment when determining whether or not to screen an individual patient for an eating disorder, Dr. Pbert advised.
One thing to consider is whether the patient is in a group at higher risk for eating disorders, such as athletes, females, young adults aged 18-29, and transgender individuals.
Another is whether the patient reports engaging in unhealthy weight control behaviors, such as fasting or skipping meals, Dr. Pbert said.
Importantly, any patient who has signs or symptoms of an eating disorder or is expressing concerns about their eating should be assessed and referred for appropriate care, Dr. Pbert said.
“The good news is that eating disorders can be treated,” she said.
Several organizations currently recommend screening in the context of monitoring changes in weight and other vital signs or signs and symptoms to determine whether a patient might have an eating disorder.
Dr. Pbert said it’s important to recognize that the USPSTF statement “doesn’t really conflict” with the recommendations of other organizations. “We all agree that patients who present with signs or symptoms of an eating disorder should be assessed further.”
Evidence gaps
The authors of an invited commentary in JAMA) say the task force has identified several “notable deficiencies” in the available data on screening for eating disorders.

“Directing attention to rigorous research to close this evidence gap will be important to find optimal approaches to identify patients with these complex disorders and improve their health outcomes,” write Evelyn Attia, MD, with Weill Cornell Medicine in New York, and Angela Guarda, MD, with Johns Hopkins University, Baltimore.
This “I” statement, they say, “highlights the need to prioritize research aimed at closing the evidence gap identified by USPSTF in a timely manner and underscores the need for new studies that address screening for eating disorders, treatment trials that enroll screen-detected populations from primary care settings, and screening in specific populations.
“Research on screening in primary care also should be paired with development and assessment of early brief intervention strategies for those individuals who screen positive, especially adolescents,” Dr. Attia and Dr. Guarda say.
Members of the USPSTF have disclosed no relevant financial relationships. Dr. Attia has received research support from the National Institute of Mental Health and the Hilda & Preston David Foundation; royalties from UpToDate; and has served as a clinical advisor to Equip Health. Dr. Guarda has received support from the Stephen and Jean Robinson Fund and research funding from the Klarman Family Foundation.
A version of this article first appeared on Medscape.com.
Eating disorders (binge eating disorder, bulimia nervosa, and anorexia nervosa) can cause “serious harms to physical and psychosocial health and take a tremendous toll on individuals and families,” task force member Lori Pbert, PhD, told this news organization.
“Screening for eating disorders has the potential to improve health by leading to early detection and effective treatment,” said Dr. Pbert, with the department of population and quantitative health sciences, University of Massachusetts, Worcester.
However, a “deep dive” into the available literature failed to turn up adequate evidence to recommend for or against routine screening for eating disorders for children and adolescents aged 10 years and older and for adults who have no signs or symptoms of an eating disorder or concerns about their eating and who have not previously been diagnosed with an eating disorder, Dr. Pbert said.
The task force, therefore, issued an “I” statement (insufficient evidence), meaning it cannot at this time recommend for or against screening for eating disorders.
An “I” statement is “fundamentally a call for more research,” Dr. Pbert noted.
Adolescents and adults who have signs and symptoms of an eating disorder – which include rapid weight loss; weight gain or pronounced deviation from growth trajectory; pubertal delay; bradycardia; oligomenorrhea; and amenorrhea – are not included in this recommendation.
The USPSTF recommendation statement and accompanying evidence report were published online March 15 in JAMA.
Clinical judgment key
In the absence of evidence, clinicians should use their judgment when determining whether or not to screen an individual patient for an eating disorder, Dr. Pbert advised.
One thing to consider is whether the patient is in a group at higher risk for eating disorders, such as athletes, females, young adults aged 18-29, and transgender individuals.
Another is whether the patient reports engaging in unhealthy weight control behaviors, such as fasting or skipping meals, Dr. Pbert said.
Importantly, any patient who has signs or symptoms of an eating disorder or is expressing concerns about their eating should be assessed and referred for appropriate care, Dr. Pbert said.
“The good news is that eating disorders can be treated,” she said.
Several organizations currently recommend screening in the context of monitoring changes in weight and other vital signs or signs and symptoms to determine whether a patient might have an eating disorder.
Dr. Pbert said it’s important to recognize that the USPSTF statement “doesn’t really conflict” with the recommendations of other organizations. “We all agree that patients who present with signs or symptoms of an eating disorder should be assessed further.”
Evidence gaps
The authors of an invited commentary in JAMA) say the task force has identified several “notable deficiencies” in the available data on screening for eating disorders.
“Directing attention to rigorous research to close this evidence gap will be important to find optimal approaches to identify patients with these complex disorders and improve their health outcomes,” write Evelyn Attia, MD, with Weill Cornell Medicine in New York, and Angela Guarda, MD, with Johns Hopkins University, Baltimore.
This “I” statement, they say, “highlights the need to prioritize research aimed at closing the evidence gap identified by USPSTF in a timely manner and underscores the need for new studies that address screening for eating disorders, treatment trials that enroll screen-detected populations from primary care settings, and screening in specific populations.
“Research on screening in primary care also should be paired with development and assessment of early brief intervention strategies for those individuals who screen positive, especially adolescents,” Dr. Attia and Dr. Guarda say.
Members of the USPSTF have disclosed no relevant financial relationships. Dr. Attia has received research support from the National Institute of Mental Health and the Hilda & Preston David Foundation; royalties from UpToDate; and has served as a clinical advisor to Equip Health. Dr. Guarda has received support from the Stephen and Jean Robinson Fund and research funding from the Klarman Family Foundation.
A version of this article first appeared on Medscape.com.
Eating disorders (binge eating disorder, bulimia nervosa, and anorexia nervosa) can cause “serious harms to physical and psychosocial health and take a tremendous toll on individuals and families,” task force member Lori Pbert, PhD, told this news organization.
“Screening for eating disorders has the potential to improve health by leading to early detection and effective treatment,” said Dr. Pbert, with the department of population and quantitative health sciences, University of Massachusetts, Worcester.
However, a “deep dive” into the available literature failed to turn up adequate evidence to recommend for or against routine screening for eating disorders for children and adolescents aged 10 years and older and for adults who have no signs or symptoms of an eating disorder or concerns about their eating and who have not previously been diagnosed with an eating disorder, Dr. Pbert said.
The task force, therefore, issued an “I” statement (insufficient evidence), meaning it cannot at this time recommend for or against screening for eating disorders.
An “I” statement is “fundamentally a call for more research,” Dr. Pbert noted.
Adolescents and adults who have signs and symptoms of an eating disorder – which include rapid weight loss; weight gain or pronounced deviation from growth trajectory; pubertal delay; bradycardia; oligomenorrhea; and amenorrhea – are not included in this recommendation.
The USPSTF recommendation statement and accompanying evidence report were published online March 15 in JAMA.
Clinical judgment key
In the absence of evidence, clinicians should use their judgment when determining whether or not to screen an individual patient for an eating disorder, Dr. Pbert advised.
One thing to consider is whether the patient is in a group at higher risk for eating disorders, such as athletes, females, young adults aged 18-29, and transgender individuals.
Another is whether the patient reports engaging in unhealthy weight control behaviors, such as fasting or skipping meals, Dr. Pbert said.
Importantly, any patient who has signs or symptoms of an eating disorder or is expressing concerns about their eating should be assessed and referred for appropriate care, Dr. Pbert said.
“The good news is that eating disorders can be treated,” she said.
Several organizations currently recommend screening in the context of monitoring changes in weight and other vital signs or signs and symptoms to determine whether a patient might have an eating disorder.
Dr. Pbert said it’s important to recognize that the USPSTF statement “doesn’t really conflict” with the recommendations of other organizations. “We all agree that patients who present with signs or symptoms of an eating disorder should be assessed further.”
Evidence gaps
The authors of an invited commentary in JAMA) say the task force has identified several “notable deficiencies” in the available data on screening for eating disorders.
“Directing attention to rigorous research to close this evidence gap will be important to find optimal approaches to identify patients with these complex disorders and improve their health outcomes,” write Evelyn Attia, MD, with Weill Cornell Medicine in New York, and Angela Guarda, MD, with Johns Hopkins University, Baltimore.
This “I” statement, they say, “highlights the need to prioritize research aimed at closing the evidence gap identified by USPSTF in a timely manner and underscores the need for new studies that address screening for eating disorders, treatment trials that enroll screen-detected populations from primary care settings, and screening in specific populations.
“Research on screening in primary care also should be paired with development and assessment of early brief intervention strategies for those individuals who screen positive, especially adolescents,” Dr. Attia and Dr. Guarda say.
Members of the USPSTF have disclosed no relevant financial relationships. Dr. Attia has received research support from the National Institute of Mental Health and the Hilda & Preston David Foundation; royalties from UpToDate; and has served as a clinical advisor to Equip Health. Dr. Guarda has received support from the Stephen and Jean Robinson Fund and research funding from the Klarman Family Foundation.
A version of this article first appeared on Medscape.com.
ACC looks to build inclusive, bully-free cardiology workplaces
The American College of Cardiology has issued a new health policy statement directed at eliminating the bias, discrimination, bullying, and harassment that hamstrings the delivery of quality cardiovascular care.
“We pay a lot of attention, of course, to our patients and patient care issues but our ability to care optimally for patients is limited if the workforce is handicapped in any way,” said Pamela S. Douglas, MD, of Duke University, Durham, N.C., who cochaired the writing committee.
The document is the second in the ACC’s diversity inclusion initiative, following the 2019 report on equal compensation and opportunity in cardiology, but the foundation for the work actually started 5 years ago, she told this news organization.

“Unfortunately, COVID and other world events have created a climate in the United States where people don’t treat each other terribly well,” Dr. Douglas said. “It’s divisive and confrontational often, when it should be collaborative. So this document, at this time, was serendipitous but wonderful timing.”
The 2022 ACC Health Policy Statement on Building Respect, Civility, and Inclusion in the Cardiovascular Workforce was published online March 17 in the Journal of the American College of Cardiology.
The 63-page document provides 12 principles for building a better workplace, starting with the belief that civil behavior and respect are inherent in its core values of teamwork, collaboration, and professionalism.
The ACC calls on all organizations and individuals involved in providing cardiovascular care, education, or research to recognize the “ubiquity” of uncivil behavior and the continuum of bias, discrimination, bullying, and harassment (BDBH) that characterize it.
Some of the recommendations they offer to eliminate these behaviors include:
- Creating institutional policies and resources to ensure hiring decisions, evaluations, and departmental/program/center reviews are objective.
- Including assessments of personal behaviors related to respect and civility in performance reviews.
- Establishing confidential, fair, and transparent mechanisms for reporting and investigating individuals and/or departments suspected of BDBH.
- Adopting longitudinal metrics and accurate data collection to track progress and inform future policy and interventions.
- Encouraging independent evaluation of institutional culture and efforts to reduce BDBH.
- Celebrating those who promote and achieve excellence in reducing BDBH.
Patients behaving badly
What’s new, especially since the COVID-19 pandemic, is the number of patients who themselves engage in disrespectful and uncivil behavior, observed Dr. Douglas.
“As physicians, it was the patient’s always right. So you work to do backflips to accommodate the patient,” she said. “But when the patient says: I don’t want to be treated by anybody that comes from outside the United States, that’s not our society anymore. And that has to be addressed and dealt with.”
The policy statement features a suite of online tools and resources including 15 case examples and 30 sample policies from institutions that have been anonymized and some provide an action framework for addressing this type of patient behavior, Dr. Douglas said. An individual, for example, can ask the patient why they made the remark, explaining that the provider is qualified and someone they’d like to have care for their own family. If it was a trainee on the receiving end, it’s fair for them to go back to their supervisor, mentor, or training director.
“They should back you up and explain to the patient that it’s not who we are at this hospital and that they’re happy to provide care, but they are part of the hospital and need to obey the rules and environment in this hospital,” she said.
Writing committee cochair Michael J. Mack, MD, of Baylor Scott & White Health, Plano, Tex., told tthis news organization that “one of the concepts that I hadn’t heard before that resonated with me was the term ‘upstander’ – that you can’t just be a bystander and watch this happen and do nothing. If you’re witness to this in the workplace, if it’s gender bias or racial bias, you need to get involved and reach out to that individual and see what you can do to help and be a reporter of it.”
But it’s all too costly
Financial constraints are often cited as a reason not to focus on bias, discrimination, bullying, and harassment in the workplace or to shelve initiatives, but it’s a false argument, say Dr. Mack and Dr. Douglas.

“One of the case examples is a cardiology practice that is suffering a decline in finances, and the board makes the recommendation that the efforts at diversity and civil workplaces need to be the first to go,” Dr. Mack explained. “And the point that’s being made in this is you can’t afford not to do it because it ends up being more costly to the business in the long run.”
Part of that cost is associated with losing valuable employees that were contributing but left because there wasn’t a culture of respectfulness and positivity in their workplace. While that’s always been a risk, it’s become a particularly compelling issue because of the workforce shortages present 3 years on in the pandemic, he said.
“There’s a new reexamination to be sure that we have a positive work environment that people want to come to work at every day,” he said. “I run our Research Institute, and normally we have a 5% vacancy rate, and our unfilled-position rate is 25% right now.”
Health care is delivered as a team today, but if a member feels disrespected, or worse – harassed, bullied, or discriminated against – they’re not going to contribute at the top of their game, Dr. Douglas said.
“It’s very well documented that bad behavior exists and that it has negative consequences for patient care for institutions, who are at great risk legally and regulatory wise,” she said. “And the document makes that clear that that risk is increasing.”
Dr. Douglas pointed out that the Joint Commission now requires good behavior in institutions that it accredits and that the Accreditation Council for Graduate Medical Education requires education around professionalism and evidence that their trainees are treated as professionals.
Funding agencies like the National Institutes of Health have also jumped into this space, recently establishing a hotline to report harassment, discrimination, and bullying perpetrated by an NIH-funded investigator, and giving institutions 30 days to investigate.
“In the last 2 years they have defunded, taken away the grants of 75 investigators, compared to zero in the 5 years before that,” Dr. Douglas said. “So I think, even though the bad behavior may be escalating, the consequences are escalating too.”
The new “2022 ACC Health Policy Statement on Building Respect, Civility, and Inclusion in the Cardiovascular Workplace” will be discussed in a session at the ACC 2022 Scientific Sessions on April 2 at 4:15 p.m. ET.
A version of this article first appeared on Medscape.com.
The American College of Cardiology has issued a new health policy statement directed at eliminating the bias, discrimination, bullying, and harassment that hamstrings the delivery of quality cardiovascular care.
“We pay a lot of attention, of course, to our patients and patient care issues but our ability to care optimally for patients is limited if the workforce is handicapped in any way,” said Pamela S. Douglas, MD, of Duke University, Durham, N.C., who cochaired the writing committee.
The document is the second in the ACC’s diversity inclusion initiative, following the 2019 report on equal compensation and opportunity in cardiology, but the foundation for the work actually started 5 years ago, she told this news organization.
“Unfortunately, COVID and other world events have created a climate in the United States where people don’t treat each other terribly well,” Dr. Douglas said. “It’s divisive and confrontational often, when it should be collaborative. So this document, at this time, was serendipitous but wonderful timing.”
The 2022 ACC Health Policy Statement on Building Respect, Civility, and Inclusion in the Cardiovascular Workforce was published online March 17 in the Journal of the American College of Cardiology.
The 63-page document provides 12 principles for building a better workplace, starting with the belief that civil behavior and respect are inherent in its core values of teamwork, collaboration, and professionalism.
The ACC calls on all organizations and individuals involved in providing cardiovascular care, education, or research to recognize the “ubiquity” of uncivil behavior and the continuum of bias, discrimination, bullying, and harassment (BDBH) that characterize it.
Some of the recommendations they offer to eliminate these behaviors include:
- Creating institutional policies and resources to ensure hiring decisions, evaluations, and departmental/program/center reviews are objective.
- Including assessments of personal behaviors related to respect and civility in performance reviews.
- Establishing confidential, fair, and transparent mechanisms for reporting and investigating individuals and/or departments suspected of BDBH.
- Adopting longitudinal metrics and accurate data collection to track progress and inform future policy and interventions.
- Encouraging independent evaluation of institutional culture and efforts to reduce BDBH.
- Celebrating those who promote and achieve excellence in reducing BDBH.
Patients behaving badly
What’s new, especially since the COVID-19 pandemic, is the number of patients who themselves engage in disrespectful and uncivil behavior, observed Dr. Douglas.
“As physicians, it was the patient’s always right. So you work to do backflips to accommodate the patient,” she said. “But when the patient says: I don’t want to be treated by anybody that comes from outside the United States, that’s not our society anymore. And that has to be addressed and dealt with.”
The policy statement features a suite of online tools and resources including 15 case examples and 30 sample policies from institutions that have been anonymized and some provide an action framework for addressing this type of patient behavior, Dr. Douglas said. An individual, for example, can ask the patient why they made the remark, explaining that the provider is qualified and someone they’d like to have care for their own family. If it was a trainee on the receiving end, it’s fair for them to go back to their supervisor, mentor, or training director.
“They should back you up and explain to the patient that it’s not who we are at this hospital and that they’re happy to provide care, but they are part of the hospital and need to obey the rules and environment in this hospital,” she said.
Writing committee cochair Michael J. Mack, MD, of Baylor Scott & White Health, Plano, Tex., told tthis news organization that “one of the concepts that I hadn’t heard before that resonated with me was the term ‘upstander’ – that you can’t just be a bystander and watch this happen and do nothing. If you’re witness to this in the workplace, if it’s gender bias or racial bias, you need to get involved and reach out to that individual and see what you can do to help and be a reporter of it.”
But it’s all too costly
Financial constraints are often cited as a reason not to focus on bias, discrimination, bullying, and harassment in the workplace or to shelve initiatives, but it’s a false argument, say Dr. Mack and Dr. Douglas.
“One of the case examples is a cardiology practice that is suffering a decline in finances, and the board makes the recommendation that the efforts at diversity and civil workplaces need to be the first to go,” Dr. Mack explained. “And the point that’s being made in this is you can’t afford not to do it because it ends up being more costly to the business in the long run.”
Part of that cost is associated with losing valuable employees that were contributing but left because there wasn’t a culture of respectfulness and positivity in their workplace. While that’s always been a risk, it’s become a particularly compelling issue because of the workforce shortages present 3 years on in the pandemic, he said.
“There’s a new reexamination to be sure that we have a positive work environment that people want to come to work at every day,” he said. “I run our Research Institute, and normally we have a 5% vacancy rate, and our unfilled-position rate is 25% right now.”
Health care is delivered as a team today, but if a member feels disrespected, or worse – harassed, bullied, or discriminated against – they’re not going to contribute at the top of their game, Dr. Douglas said.
“It’s very well documented that bad behavior exists and that it has negative consequences for patient care for institutions, who are at great risk legally and regulatory wise,” she said. “And the document makes that clear that that risk is increasing.”
Dr. Douglas pointed out that the Joint Commission now requires good behavior in institutions that it accredits and that the Accreditation Council for Graduate Medical Education requires education around professionalism and evidence that their trainees are treated as professionals.
Funding agencies like the National Institutes of Health have also jumped into this space, recently establishing a hotline to report harassment, discrimination, and bullying perpetrated by an NIH-funded investigator, and giving institutions 30 days to investigate.
“In the last 2 years they have defunded, taken away the grants of 75 investigators, compared to zero in the 5 years before that,” Dr. Douglas said. “So I think, even though the bad behavior may be escalating, the consequences are escalating too.”
The new “2022 ACC Health Policy Statement on Building Respect, Civility, and Inclusion in the Cardiovascular Workplace” will be discussed in a session at the ACC 2022 Scientific Sessions on April 2 at 4:15 p.m. ET.
A version of this article first appeared on Medscape.com.
The American College of Cardiology has issued a new health policy statement directed at eliminating the bias, discrimination, bullying, and harassment that hamstrings the delivery of quality cardiovascular care.
“We pay a lot of attention, of course, to our patients and patient care issues but our ability to care optimally for patients is limited if the workforce is handicapped in any way,” said Pamela S. Douglas, MD, of Duke University, Durham, N.C., who cochaired the writing committee.
The document is the second in the ACC’s diversity inclusion initiative, following the 2019 report on equal compensation and opportunity in cardiology, but the foundation for the work actually started 5 years ago, she told this news organization.
“Unfortunately, COVID and other world events have created a climate in the United States where people don’t treat each other terribly well,” Dr. Douglas said. “It’s divisive and confrontational often, when it should be collaborative. So this document, at this time, was serendipitous but wonderful timing.”
The 2022 ACC Health Policy Statement on Building Respect, Civility, and Inclusion in the Cardiovascular Workforce was published online March 17 in the Journal of the American College of Cardiology.
The 63-page document provides 12 principles for building a better workplace, starting with the belief that civil behavior and respect are inherent in its core values of teamwork, collaboration, and professionalism.
The ACC calls on all organizations and individuals involved in providing cardiovascular care, education, or research to recognize the “ubiquity” of uncivil behavior and the continuum of bias, discrimination, bullying, and harassment (BDBH) that characterize it.
Some of the recommendations they offer to eliminate these behaviors include:
- Creating institutional policies and resources to ensure hiring decisions, evaluations, and departmental/program/center reviews are objective.
- Including assessments of personal behaviors related to respect and civility in performance reviews.
- Establishing confidential, fair, and transparent mechanisms for reporting and investigating individuals and/or departments suspected of BDBH.
- Adopting longitudinal metrics and accurate data collection to track progress and inform future policy and interventions.
- Encouraging independent evaluation of institutional culture and efforts to reduce BDBH.
- Celebrating those who promote and achieve excellence in reducing BDBH.
Patients behaving badly
What’s new, especially since the COVID-19 pandemic, is the number of patients who themselves engage in disrespectful and uncivil behavior, observed Dr. Douglas.
“As physicians, it was the patient’s always right. So you work to do backflips to accommodate the patient,” she said. “But when the patient says: I don’t want to be treated by anybody that comes from outside the United States, that’s not our society anymore. And that has to be addressed and dealt with.”
The policy statement features a suite of online tools and resources including 15 case examples and 30 sample policies from institutions that have been anonymized and some provide an action framework for addressing this type of patient behavior, Dr. Douglas said. An individual, for example, can ask the patient why they made the remark, explaining that the provider is qualified and someone they’d like to have care for their own family. If it was a trainee on the receiving end, it’s fair for them to go back to their supervisor, mentor, or training director.
“They should back you up and explain to the patient that it’s not who we are at this hospital and that they’re happy to provide care, but they are part of the hospital and need to obey the rules and environment in this hospital,” she said.
Writing committee cochair Michael J. Mack, MD, of Baylor Scott & White Health, Plano, Tex., told tthis news organization that “one of the concepts that I hadn’t heard before that resonated with me was the term ‘upstander’ – that you can’t just be a bystander and watch this happen and do nothing. If you’re witness to this in the workplace, if it’s gender bias or racial bias, you need to get involved and reach out to that individual and see what you can do to help and be a reporter of it.”
But it’s all too costly
Financial constraints are often cited as a reason not to focus on bias, discrimination, bullying, and harassment in the workplace or to shelve initiatives, but it’s a false argument, say Dr. Mack and Dr. Douglas.
“One of the case examples is a cardiology practice that is suffering a decline in finances, and the board makes the recommendation that the efforts at diversity and civil workplaces need to be the first to go,” Dr. Mack explained. “And the point that’s being made in this is you can’t afford not to do it because it ends up being more costly to the business in the long run.”
Part of that cost is associated with losing valuable employees that were contributing but left because there wasn’t a culture of respectfulness and positivity in their workplace. While that’s always been a risk, it’s become a particularly compelling issue because of the workforce shortages present 3 years on in the pandemic, he said.
“There’s a new reexamination to be sure that we have a positive work environment that people want to come to work at every day,” he said. “I run our Research Institute, and normally we have a 5% vacancy rate, and our unfilled-position rate is 25% right now.”
Health care is delivered as a team today, but if a member feels disrespected, or worse – harassed, bullied, or discriminated against – they’re not going to contribute at the top of their game, Dr. Douglas said.
“It’s very well documented that bad behavior exists and that it has negative consequences for patient care for institutions, who are at great risk legally and regulatory wise,” she said. “And the document makes that clear that that risk is increasing.”
Dr. Douglas pointed out that the Joint Commission now requires good behavior in institutions that it accredits and that the Accreditation Council for Graduate Medical Education requires education around professionalism and evidence that their trainees are treated as professionals.
Funding agencies like the National Institutes of Health have also jumped into this space, recently establishing a hotline to report harassment, discrimination, and bullying perpetrated by an NIH-funded investigator, and giving institutions 30 days to investigate.
“In the last 2 years they have defunded, taken away the grants of 75 investigators, compared to zero in the 5 years before that,” Dr. Douglas said. “So I think, even though the bad behavior may be escalating, the consequences are escalating too.”
The new “2022 ACC Health Policy Statement on Building Respect, Civility, and Inclusion in the Cardiovascular Workplace” will be discussed in a session at the ACC 2022 Scientific Sessions on April 2 at 4:15 p.m. ET.
A version of this article first appeared on Medscape.com.
FROM JACC
Children and COVID: CDC gives perspective on hospitalizations
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.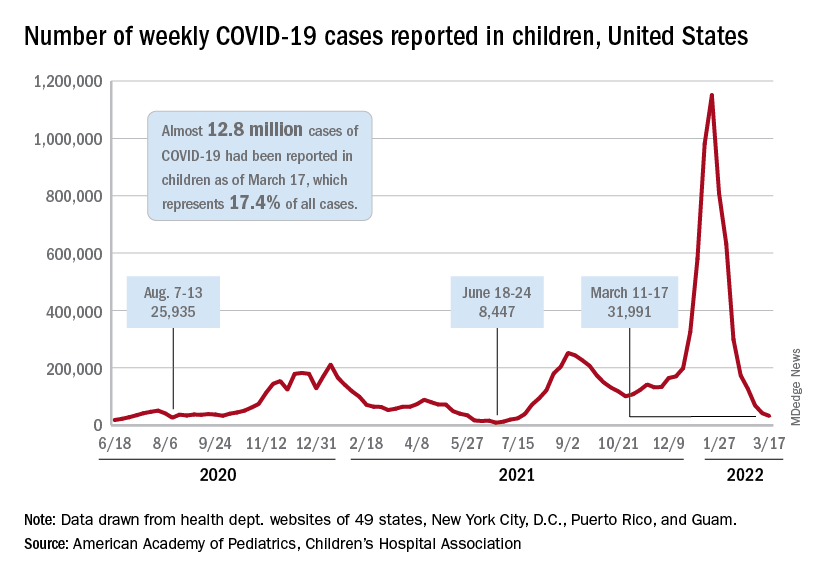
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
Racial disparities seen in pediatric postoperative mortality rates
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
FROM JAMA NETWORK OPEN
Knowns and unknowns about SSRI use during pregnancy in 2022
The last 15-20 years have brought enormous attention to the relevant clinical issues regarding prescribing antidepressants during pregnancy. Concern about the effects of fetal exposure to selective serotonin reuptake inhibitors (SSRIs) is appropriate given the consistent data that approximately 7% of women use antidepressants during pregnancy, and that risk for relapse of depression during pregnancy in women who have stopped antidepressants during pregnancy is very high.
We have learned so much from studies of relevant questions regarding SSRI exposure. Concerns about increased risk for organ malformation have been set aside. An extraordinary number of studies across a broad range of patients around the globe looked at the issue of risk for organ malformation following in utero SSRI exposure – even looking specifically at risk for cardiac malformations, which had been an earlier concern in the literature – with the evidence supporting absence of increased risk. Also clarified has been, first, the absence of risk of complications such as persistent pulmonary hypertension of the newborn (PPHN) and, second, a delineation of the prevalence and clinical implications of transient neonatal symptoms such as jitteriness and tachypnea in offspring of women who used antidepressants during pregnancy – so-called “poor neonatal adaptation syndrome.”

However, for so many clinicians and for patients, the missing piece in the risk-benefit equation has been the issue of long-term neurodevelopmental sequelae in children whose mothers used antidepressants during pregnancy. While the accumulated data have shown sparse evidence linking SSRI exposure with autism or attention-deficit/hyperactivity disorder (ADHD), the evidence has been mixed regarding neurobehavioral sequelae associated with fetal exposure using developmental outcomes such as language ability, cognition, academic performance, language, math, and other cognitive outcomes. As far back as the 1990s, colleagues in Canada failed to show a difference in neurobehavioral outcomes in 5- to 7-year-old children whose mothers used SSRIs or older tricyclic antidepressants during pregnancy compared to nonexposed women (N Engl J Med. 1997 Jan 23;336[4]:258-62). Even early on, it was noted that one of the strongest predictors of neurodevelopmental outcome was untreated maternal psychiatric illness.
Since those early studies and over the last decade, there have been numerous small studies with conflicting data regarding a whole host of neurodevelopmental outcomes with inconsistent methodologies, different assessments, and failure to control for the presence or absence of maternal psychiatric illness during pregnancy – one of the most critical predictors of neurodevelopmental outcome and one we are beginning to appreciate plays a very significant role.
Most recently, the authors of a very large population-based retrospective cohort study in Denmark linked population-based registries with obstetrical data and examined language and math performance among 575,369 public schoolchildren whose mothers used or didn’t use antidepressants during pregnancy (JAMA. 2021 Nov 2;326[17]:1725-35). These investigators found a decrease in mean test scores for language (53.4 vs. 56.6) and math (52.1 vs. 57.4) in children whose mothers received antidepressant prescriptions during pregnancy compared with children who did not have that exposure. However, when they adjusted for maternal psychiatric illness and other relevant confounders, the finding went to null for language (adjusted difference, –0.1; 95% confidence interval, –0.6 to 0.3), but did not for math (adjusted difference, −2.2; 95% CI, −2.7 to −1.6). The results ultimately showed a modest finding for exposure and a small decrement in mathematical performance. The takeaway is that antidepressant use may be a proxy for neurodevelopmental deficit but is unlikely to be the etiology or direct cause of that deficit.
With that said, patients and their doctors can be reassured with respect to how much we have learned about SSRIs during pregnancy across the last decade. Yet there are appropriate concerns about long-term neurodevelopmental sequelae in this patient population. I think that what we can say in 2022 is that there is a growing appreciation for the effect of maternal psychiatric illness on long-term outcomes in children and the effect of maternal psychiatric illness on risk for postpartum depression, which we know influences long-term neurodevelopmental outcomes in children. Perhaps more than in years past, there is now also an appreciation of the effect of a dysregulated stress axis on the intrauterine fetal neuronal programming, which is perhaps the newest frontier, and which may hold the answers with respect to how to weigh the effect of maternal psychiatric illness on decisions about psychotropic use during pregnancy. But for today, there is an appreciation that exposure to maternal psychopathology is not a benign exposure.
Although some of the data remain incomplete, in 2022, patients will continue to make individual decisions based on the available data, factoring in the effect of maternal adversity in a more deliberate way and with a refined lens through with which to see their options with respect to using or not using SSRIs during pregnancy.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at obnews@mdedge.com.
The last 15-20 years have brought enormous attention to the relevant clinical issues regarding prescribing antidepressants during pregnancy. Concern about the effects of fetal exposure to selective serotonin reuptake inhibitors (SSRIs) is appropriate given the consistent data that approximately 7% of women use antidepressants during pregnancy, and that risk for relapse of depression during pregnancy in women who have stopped antidepressants during pregnancy is very high.
We have learned so much from studies of relevant questions regarding SSRI exposure. Concerns about increased risk for organ malformation have been set aside. An extraordinary number of studies across a broad range of patients around the globe looked at the issue of risk for organ malformation following in utero SSRI exposure – even looking specifically at risk for cardiac malformations, which had been an earlier concern in the literature – with the evidence supporting absence of increased risk. Also clarified has been, first, the absence of risk of complications such as persistent pulmonary hypertension of the newborn (PPHN) and, second, a delineation of the prevalence and clinical implications of transient neonatal symptoms such as jitteriness and tachypnea in offspring of women who used antidepressants during pregnancy – so-called “poor neonatal adaptation syndrome.”
However, for so many clinicians and for patients, the missing piece in the risk-benefit equation has been the issue of long-term neurodevelopmental sequelae in children whose mothers used antidepressants during pregnancy. While the accumulated data have shown sparse evidence linking SSRI exposure with autism or attention-deficit/hyperactivity disorder (ADHD), the evidence has been mixed regarding neurobehavioral sequelae associated with fetal exposure using developmental outcomes such as language ability, cognition, academic performance, language, math, and other cognitive outcomes. As far back as the 1990s, colleagues in Canada failed to show a difference in neurobehavioral outcomes in 5- to 7-year-old children whose mothers used SSRIs or older tricyclic antidepressants during pregnancy compared to nonexposed women (N Engl J Med. 1997 Jan 23;336[4]:258-62). Even early on, it was noted that one of the strongest predictors of neurodevelopmental outcome was untreated maternal psychiatric illness.
Since those early studies and over the last decade, there have been numerous small studies with conflicting data regarding a whole host of neurodevelopmental outcomes with inconsistent methodologies, different assessments, and failure to control for the presence or absence of maternal psychiatric illness during pregnancy – one of the most critical predictors of neurodevelopmental outcome and one we are beginning to appreciate plays a very significant role.
Most recently, the authors of a very large population-based retrospective cohort study in Denmark linked population-based registries with obstetrical data and examined language and math performance among 575,369 public schoolchildren whose mothers used or didn’t use antidepressants during pregnancy (JAMA. 2021 Nov 2;326[17]:1725-35). These investigators found a decrease in mean test scores for language (53.4 vs. 56.6) and math (52.1 vs. 57.4) in children whose mothers received antidepressant prescriptions during pregnancy compared with children who did not have that exposure. However, when they adjusted for maternal psychiatric illness and other relevant confounders, the finding went to null for language (adjusted difference, –0.1; 95% confidence interval, –0.6 to 0.3), but did not for math (adjusted difference, −2.2; 95% CI, −2.7 to −1.6). The results ultimately showed a modest finding for exposure and a small decrement in mathematical performance. The takeaway is that antidepressant use may be a proxy for neurodevelopmental deficit but is unlikely to be the etiology or direct cause of that deficit.
With that said, patients and their doctors can be reassured with respect to how much we have learned about SSRIs during pregnancy across the last decade. Yet there are appropriate concerns about long-term neurodevelopmental sequelae in this patient population. I think that what we can say in 2022 is that there is a growing appreciation for the effect of maternal psychiatric illness on long-term outcomes in children and the effect of maternal psychiatric illness on risk for postpartum depression, which we know influences long-term neurodevelopmental outcomes in children. Perhaps more than in years past, there is now also an appreciation of the effect of a dysregulated stress axis on the intrauterine fetal neuronal programming, which is perhaps the newest frontier, and which may hold the answers with respect to how to weigh the effect of maternal psychiatric illness on decisions about psychotropic use during pregnancy. But for today, there is an appreciation that exposure to maternal psychopathology is not a benign exposure.
Although some of the data remain incomplete, in 2022, patients will continue to make individual decisions based on the available data, factoring in the effect of maternal adversity in a more deliberate way and with a refined lens through with which to see their options with respect to using or not using SSRIs during pregnancy.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at obnews@mdedge.com.
The last 15-20 years have brought enormous attention to the relevant clinical issues regarding prescribing antidepressants during pregnancy. Concern about the effects of fetal exposure to selective serotonin reuptake inhibitors (SSRIs) is appropriate given the consistent data that approximately 7% of women use antidepressants during pregnancy, and that risk for relapse of depression during pregnancy in women who have stopped antidepressants during pregnancy is very high.
We have learned so much from studies of relevant questions regarding SSRI exposure. Concerns about increased risk for organ malformation have been set aside. An extraordinary number of studies across a broad range of patients around the globe looked at the issue of risk for organ malformation following in utero SSRI exposure – even looking specifically at risk for cardiac malformations, which had been an earlier concern in the literature – with the evidence supporting absence of increased risk. Also clarified has been, first, the absence of risk of complications such as persistent pulmonary hypertension of the newborn (PPHN) and, second, a delineation of the prevalence and clinical implications of transient neonatal symptoms such as jitteriness and tachypnea in offspring of women who used antidepressants during pregnancy – so-called “poor neonatal adaptation syndrome.”
However, for so many clinicians and for patients, the missing piece in the risk-benefit equation has been the issue of long-term neurodevelopmental sequelae in children whose mothers used antidepressants during pregnancy. While the accumulated data have shown sparse evidence linking SSRI exposure with autism or attention-deficit/hyperactivity disorder (ADHD), the evidence has been mixed regarding neurobehavioral sequelae associated with fetal exposure using developmental outcomes such as language ability, cognition, academic performance, language, math, and other cognitive outcomes. As far back as the 1990s, colleagues in Canada failed to show a difference in neurobehavioral outcomes in 5- to 7-year-old children whose mothers used SSRIs or older tricyclic antidepressants during pregnancy compared to nonexposed women (N Engl J Med. 1997 Jan 23;336[4]:258-62). Even early on, it was noted that one of the strongest predictors of neurodevelopmental outcome was untreated maternal psychiatric illness.
Since those early studies and over the last decade, there have been numerous small studies with conflicting data regarding a whole host of neurodevelopmental outcomes with inconsistent methodologies, different assessments, and failure to control for the presence or absence of maternal psychiatric illness during pregnancy – one of the most critical predictors of neurodevelopmental outcome and one we are beginning to appreciate plays a very significant role.
Most recently, the authors of a very large population-based retrospective cohort study in Denmark linked population-based registries with obstetrical data and examined language and math performance among 575,369 public schoolchildren whose mothers used or didn’t use antidepressants during pregnancy (JAMA. 2021 Nov 2;326[17]:1725-35). These investigators found a decrease in mean test scores for language (53.4 vs. 56.6) and math (52.1 vs. 57.4) in children whose mothers received antidepressant prescriptions during pregnancy compared with children who did not have that exposure. However, when they adjusted for maternal psychiatric illness and other relevant confounders, the finding went to null for language (adjusted difference, –0.1; 95% confidence interval, –0.6 to 0.3), but did not for math (adjusted difference, −2.2; 95% CI, −2.7 to −1.6). The results ultimately showed a modest finding for exposure and a small decrement in mathematical performance. The takeaway is that antidepressant use may be a proxy for neurodevelopmental deficit but is unlikely to be the etiology or direct cause of that deficit.
With that said, patients and their doctors can be reassured with respect to how much we have learned about SSRIs during pregnancy across the last decade. Yet there are appropriate concerns about long-term neurodevelopmental sequelae in this patient population. I think that what we can say in 2022 is that there is a growing appreciation for the effect of maternal psychiatric illness on long-term outcomes in children and the effect of maternal psychiatric illness on risk for postpartum depression, which we know influences long-term neurodevelopmental outcomes in children. Perhaps more than in years past, there is now also an appreciation of the effect of a dysregulated stress axis on the intrauterine fetal neuronal programming, which is perhaps the newest frontier, and which may hold the answers with respect to how to weigh the effect of maternal psychiatric illness on decisions about psychotropic use during pregnancy. But for today, there is an appreciation that exposure to maternal psychopathology is not a benign exposure.
Although some of the data remain incomplete, in 2022, patients will continue to make individual decisions based on the available data, factoring in the effect of maternal adversity in a more deliberate way and with a refined lens through with which to see their options with respect to using or not using SSRIs during pregnancy.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at obnews@mdedge.com.
Access without a portal
I don’t have a patient portal. Probably never will.
This isn’t an attempt at “information blocking,” or intentional noncompliance, or a rebellious streak against the CURES act.
It’s practical: I can’t afford it.

I’m a small one-doc practice. My overhead is high, my profit margin is razor thin. In the sudden spike of COVID-19– and war-related inflation, my gas and office supply costs have gone up, but I’m in a field where I can’t raise my own prices to compensate. The restaurants and grocery stores near me can, but I can’t because of the way insurance works.
With that background, I don’t have the money to set up a patient portal for people to be able to get their notes, test results, anything.
This isn’t to say that I withhold things from patients. If they want a copy of my note, or their MRI report, or whatever, they’re welcome to it. I’m happy to fax it to them, or put it in the mail, or have them come by and pick it up.
I have no desire to keep information from patients. I actually try to stay on top of it, calling them with test results within 24 hours of receiving them and arranging follow-ups quickly when needed.
That’s one of the pluses of my dinky practice – I generally know my patients and can make decisions quickly on the next step once results come in. They don’t get tossed in a box to be reviewed in a few days. I take pride in staying on top of things – isn’t that how we all want to be treated when we’re on the other side of the desk?
Politicians like to say how much America depends on small businesses and how important we are to the economy. They love to do photo ops at a newly opened ice cream place or small barbecue joint. But if you’re a doctor in a small practice, you often get treated the same way the Mega-Med Group (“287 doctors! 19 specialties! 37 offices! No waiting!”) is treated. They can afford to have a digital portal, so why can’t you?
Or not doing my best to care for them.
Like Avis, I may not be No. 1, but I sure try harder.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I don’t have a patient portal. Probably never will.
This isn’t an attempt at “information blocking,” or intentional noncompliance, or a rebellious streak against the CURES act.
It’s practical: I can’t afford it.
I’m a small one-doc practice. My overhead is high, my profit margin is razor thin. In the sudden spike of COVID-19– and war-related inflation, my gas and office supply costs have gone up, but I’m in a field where I can’t raise my own prices to compensate. The restaurants and grocery stores near me can, but I can’t because of the way insurance works.
With that background, I don’t have the money to set up a patient portal for people to be able to get their notes, test results, anything.
This isn’t to say that I withhold things from patients. If they want a copy of my note, or their MRI report, or whatever, they’re welcome to it. I’m happy to fax it to them, or put it in the mail, or have them come by and pick it up.
I have no desire to keep information from patients. I actually try to stay on top of it, calling them with test results within 24 hours of receiving them and arranging follow-ups quickly when needed.
That’s one of the pluses of my dinky practice – I generally know my patients and can make decisions quickly on the next step once results come in. They don’t get tossed in a box to be reviewed in a few days. I take pride in staying on top of things – isn’t that how we all want to be treated when we’re on the other side of the desk?
Politicians like to say how much America depends on small businesses and how important we are to the economy. They love to do photo ops at a newly opened ice cream place or small barbecue joint. But if you’re a doctor in a small practice, you often get treated the same way the Mega-Med Group (“287 doctors! 19 specialties! 37 offices! No waiting!”) is treated. They can afford to have a digital portal, so why can’t you?
Or not doing my best to care for them.
Like Avis, I may not be No. 1, but I sure try harder.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I don’t have a patient portal. Probably never will.
This isn’t an attempt at “information blocking,” or intentional noncompliance, or a rebellious streak against the CURES act.
It’s practical: I can’t afford it.
I’m a small one-doc practice. My overhead is high, my profit margin is razor thin. In the sudden spike of COVID-19– and war-related inflation, my gas and office supply costs have gone up, but I’m in a field where I can’t raise my own prices to compensate. The restaurants and grocery stores near me can, but I can’t because of the way insurance works.
With that background, I don’t have the money to set up a patient portal for people to be able to get their notes, test results, anything.
This isn’t to say that I withhold things from patients. If they want a copy of my note, or their MRI report, or whatever, they’re welcome to it. I’m happy to fax it to them, or put it in the mail, or have them come by and pick it up.
I have no desire to keep information from patients. I actually try to stay on top of it, calling them with test results within 24 hours of receiving them and arranging follow-ups quickly when needed.
That’s one of the pluses of my dinky practice – I generally know my patients and can make decisions quickly on the next step once results come in. They don’t get tossed in a box to be reviewed in a few days. I take pride in staying on top of things – isn’t that how we all want to be treated when we’re on the other side of the desk?
Politicians like to say how much America depends on small businesses and how important we are to the economy. They love to do photo ops at a newly opened ice cream place or small barbecue joint. But if you’re a doctor in a small practice, you often get treated the same way the Mega-Med Group (“287 doctors! 19 specialties! 37 offices! No waiting!”) is treated. They can afford to have a digital portal, so why can’t you?
Or not doing my best to care for them.
Like Avis, I may not be No. 1, but I sure try harder.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
New guidance on cannabis use for treatment-resistant epilepsy
A recent review article draws from existing clinical trials and clinical experience in New South Wales, Australia, to fill this gap with interim guidance for both pediatric and adult patients. The article was published in the British Journal of Clinical Pharmacology.
The only current U.S. guidelines are from the American Academy of Neurology’s position statement on the use of medical cannabis for neurologic disorders and the American Epilepsy Society’s position statement on cannabis as a treatment for epileptic seizures. The AAN statement “highlights the current evidence, which currently only supports [Food and Drug Administration]–approved CBD [cannabidiol] (Epidiolex) for specific epilepsy syndromes,” said Daniel Freedman, DO, an assistant professor of neurology at the University of Texas at Austin and coauthor of the AAN’s position statement.
“Rescheduling marijuana will enable researchers to study CBD, THC [tetrahydrocannabinol], and other cannabinoids in high-quality studies so that we can better understand what works and for which conditions,” said Dr. Freedman, who was not involved in the Australian guidance document. He noted that little consensus exists because little evidence exists outside the handful of trials for Epidiolex.
“There are some patients with epilepsy that can benefit from high-quality, pharmaceutical-grade CBD products,” Dr. Freedman said. “These patients need to be carefully identified by a neurologist or epileptologist and prescribed a legal, safe, quality-controlled, and FDA-regulated product.”
Appropriate patient populations
Drug-resistant epilepsy, defined as failure of two appropriate antiseizure medications, affects an estimated one third of people with epilepsy, the new guideline notes. Though many over-the-counter products are available at dispensaries in the 33 U.S. states that allow use of cannabis for medical purposes, Epidiolex (cannabidiol) is the only FDA-approved drug for epilepsy that contains a substance derived from cannabis and the only one for which evidence from randomized, controlled trials exists.
Dr. Freedman notes that hemp-derived CBD oils are classified differently in the United States than marijuana-derived CBD oil, including Epidiolex, and are loosely regulated supplements or food additives commonly seen, for example at gas station.
“The point I drive home to patients is that you wouldn’t get your antibiotics from a gas station, so please don’t get your seizure medication from there,” Dr. Freedman said. “Studies have been done on ‘over-the-counter’ CBD oils and shown that they have variable quality, sometimes no detectable CBD, and sometimes other chemicals added like THC.”
Studies of Epidiolex showed that cannabidiol more effectively reduced seizure frequency than placebo for pediatric patients with Dravet syndrome (42% reduction) and for pediatric and adult patients with Lennox-Gastaut syndrome (39% reduction) or tuberous sclerosis complex (49% reduction). Efficacy was similar across dosing from 10-50 mg/kg per day, but higher doses involved higher rates of serious adverse events.
No reliable evidence in humans exists for THC or other cannabinoids in treating epilepsy.
The Australian guidance recommends limiting cannabis treatment to patients with severe drug-resistant epilepsy; a diagnosis of Dravet syndrome, Lennox-Gastaut syndrome, or tuberous sclerosis complex; and previous treatment with four approved antiseizure medications and/or the ketogenic diet, epilepsy surgery, or neurostimulator. The authors provide specific criteria for each of these conditions and then address exceptional cases that may be considered outside that criteria, such as patients under 2 years old, severe epilepsy with extended or repeated hospitalization or ICU admission, or a dangerous seizure type. The review also includes a detailed list of exclusion criteria for CBD medicine use.
The authors advised a thorough consent process before prescribing any cannabinoids, including therapeutic goals and stopping criteria; the lack of evidence available on dosing, efficacy, and side effects; and the potential for dependence or withdrawal. Consent discussions should also note whether the products are unregistered and not covered by external payers (anything other than Epidiolex currently), any activity restrictions, and any implications for occupational drug screening.
Considerations for unapproved cannabinoids
The authors note several factors to consider if prescribing or recommending a nonapproved, nonregulated cannabis medicine, including the ”differences between registered plant-derived cannabis medicines, synthetic cannabis medicines, and unregistered hemp-derived products.” Epidiolex is plant derived while other cannabis-derived medications (Marinol, Syndos, and Cesamet) that have been approved for nonepilepsy conditions, such as nausea associated with chemotherapy, are synthetic.
The guidance document notes several reasons to use a regulated medication instead of an unregulated product:
- Manufacturing processes can differ for unregulated products, including inconsistency in batches and unknown shelf life.
- Quality control processes, including risk of impurities, are much better with regulated products, which also have a system in place for safety recalls.
- More scientific evidence is available for regulated products.
- Safety surveillance reporting is more robust and standardized for regulated products whereas adverse event reporting is less reliable for unregulated products.
- Nonregulated products are rarely covered by insurance or other reimbursement.
Legal considerations will also vary by jurisdiction. ”Right now in the U.S. we have a confused legality where state level programs are still technically illegal at the federal level and I imagine there are some quality differences amongst dispensaries and states,” Dr. Freedman said. “Whenever there is disagreement between state and federal laws, this creates tension for our patients.” He noted, for example, that a patient using a CBD product that contains THC may, even if legal in their state, be confiscated by the Transportation Security Administration at an airport since it is not FDA approved and is not legal, according to the Drug Enforcement Agency.
The authors noted that inadequate data on long-term CBD use and data on neurodevelopmental effects of THC in children, teens, and young adults means THC products should be contraindicated for these age groups. (Epidiolex has less than 2% THC.) Drug interactions should also be considered, particularly for clobazam, CYP3A4 inhibitors or inducers (including St. John’s wort), digoxin, or a mechanistic target of rapamycin inhibitor.
Dr. Freedman said that most neurologists are comfortable prescribing Epidiolex since it has FDA approval while prescribing unapproved products varies more in the field. “Now that many states have compassionate use programs for medical marijuana, some neurologists do this as well,” Dr. Freedman said. Patients often ask about unregulated CBD or CBD+THC products because they’re seen as “natural and therefore better than manufactured pharmaceuticals.”
“I think this is the naturalistic fallacy at work and try to educate my patients on that since our only high-level data to show marijuana products work for epilepsy comes from a pharmaceutical company,” Dr. Freedman said. “My reasons for hesitating on compassionate use are that there is often THC, with variable amounts of concentration, and we know that THC can harm the developing pediatric brain.”
Dosing and adverse effects
Pediatric and adult dosing differences need to be considered, and “patient response (efficacy and toxicity) to these medications varies widely,” the authors noted. They advised getting serum transaminases (ALT and AST) and total bilirubin levels before beginning treatment. All patients should begin Epidiolex at a low dose, such as 2-5 mg/kg per day of CBD in two divided doses, the authors advise, and titrate slowly while monitoring for side effects (no more than 5 mg/kg per day per week). The current dosing range for CBD is 5-20 mg/kg per day in two divided doses, with higher rates involving more risk of adverse events.
“Note that some cannabinoids auto-inhibit their own metabolism and some have active metabolites with longer half-lives,” the authors wrote. “Therefore, dose or frequency may need to be reduced over time, unless tolerance occurs.” These doses, specific to Epidiolex, “cannot necessarily be applied to other oral CBD formulations or other types of epilepsy.” This guidance also does not apply to inhaled or transdermal routes of administration.
The most common adverse events were sleepiness – which occurred in up to 60% of trial participants – as well as diarrhea, decreases in appetite and weight, and drug interactions. Risk of hepatotoxicity means there’s a need to monitor liver function and adjust dosing for patients with moderate or severe hepatic impairment. “Other short-term side effects reported only with THC-containing cannabinoid compounds include increased risk of cardiac and cerebrovascular events, anxiety and psychosis risk, dependency, and withdrawal,” the authors wrote.
Though no withdrawal syndrome has been linked to stopping CBD, the authors suggested decreasing the dose by 10% every 2 days if stopping is not urgent.
“The key points to this issue are that CBD and all marijuana products need to be safe and regulated,” Dr. Freedman said. “Any claims about them need to be backed by high-quality evidence looking at that specific product for that specific condition.”
Dr. Freedman noted the need for children to receive treatment from clinicians with expertise in their specific condition since many other evidence-based treatments exist even for patients with epilepsy syndromes that are difficult to treat, such as other medications, surgery, and specialized diets.
“We need to fix the inconsistent regulation between over-the-counter CBD products, state dispensaries, and federal laws,” Dr. Freedman added. “Any medicine being used to treat children should be held to the same FDA standard of safety and efficacy.”
Dr. Freedman and the authors had no conflicts of interest. No external funding was noted.
A recent review article draws from existing clinical trials and clinical experience in New South Wales, Australia, to fill this gap with interim guidance for both pediatric and adult patients. The article was published in the British Journal of Clinical Pharmacology.
The only current U.S. guidelines are from the American Academy of Neurology’s position statement on the use of medical cannabis for neurologic disorders and the American Epilepsy Society’s position statement on cannabis as a treatment for epileptic seizures. The AAN statement “highlights the current evidence, which currently only supports [Food and Drug Administration]–approved CBD [cannabidiol] (Epidiolex) for specific epilepsy syndromes,” said Daniel Freedman, DO, an assistant professor of neurology at the University of Texas at Austin and coauthor of the AAN’s position statement.
“Rescheduling marijuana will enable researchers to study CBD, THC [tetrahydrocannabinol], and other cannabinoids in high-quality studies so that we can better understand what works and for which conditions,” said Dr. Freedman, who was not involved in the Australian guidance document. He noted that little consensus exists because little evidence exists outside the handful of trials for Epidiolex.
“There are some patients with epilepsy that can benefit from high-quality, pharmaceutical-grade CBD products,” Dr. Freedman said. “These patients need to be carefully identified by a neurologist or epileptologist and prescribed a legal, safe, quality-controlled, and FDA-regulated product.”
Appropriate patient populations
Drug-resistant epilepsy, defined as failure of two appropriate antiseizure medications, affects an estimated one third of people with epilepsy, the new guideline notes. Though many over-the-counter products are available at dispensaries in the 33 U.S. states that allow use of cannabis for medical purposes, Epidiolex (cannabidiol) is the only FDA-approved drug for epilepsy that contains a substance derived from cannabis and the only one for which evidence from randomized, controlled trials exists.
Dr. Freedman notes that hemp-derived CBD oils are classified differently in the United States than marijuana-derived CBD oil, including Epidiolex, and are loosely regulated supplements or food additives commonly seen, for example at gas station.
“The point I drive home to patients is that you wouldn’t get your antibiotics from a gas station, so please don’t get your seizure medication from there,” Dr. Freedman said. “Studies have been done on ‘over-the-counter’ CBD oils and shown that they have variable quality, sometimes no detectable CBD, and sometimes other chemicals added like THC.”
Studies of Epidiolex showed that cannabidiol more effectively reduced seizure frequency than placebo for pediatric patients with Dravet syndrome (42% reduction) and for pediatric and adult patients with Lennox-Gastaut syndrome (39% reduction) or tuberous sclerosis complex (49% reduction). Efficacy was similar across dosing from 10-50 mg/kg per day, but higher doses involved higher rates of serious adverse events.
No reliable evidence in humans exists for THC or other cannabinoids in treating epilepsy.
The Australian guidance recommends limiting cannabis treatment to patients with severe drug-resistant epilepsy; a diagnosis of Dravet syndrome, Lennox-Gastaut syndrome, or tuberous sclerosis complex; and previous treatment with four approved antiseizure medications and/or the ketogenic diet, epilepsy surgery, or neurostimulator. The authors provide specific criteria for each of these conditions and then address exceptional cases that may be considered outside that criteria, such as patients under 2 years old, severe epilepsy with extended or repeated hospitalization or ICU admission, or a dangerous seizure type. The review also includes a detailed list of exclusion criteria for CBD medicine use.
The authors advised a thorough consent process before prescribing any cannabinoids, including therapeutic goals and stopping criteria; the lack of evidence available on dosing, efficacy, and side effects; and the potential for dependence or withdrawal. Consent discussions should also note whether the products are unregistered and not covered by external payers (anything other than Epidiolex currently), any activity restrictions, and any implications for occupational drug screening.
Considerations for unapproved cannabinoids
The authors note several factors to consider if prescribing or recommending a nonapproved, nonregulated cannabis medicine, including the ”differences between registered plant-derived cannabis medicines, synthetic cannabis medicines, and unregistered hemp-derived products.” Epidiolex is plant derived while other cannabis-derived medications (Marinol, Syndos, and Cesamet) that have been approved for nonepilepsy conditions, such as nausea associated with chemotherapy, are synthetic.
The guidance document notes several reasons to use a regulated medication instead of an unregulated product:
- Manufacturing processes can differ for unregulated products, including inconsistency in batches and unknown shelf life.
- Quality control processes, including risk of impurities, are much better with regulated products, which also have a system in place for safety recalls.
- More scientific evidence is available for regulated products.
- Safety surveillance reporting is more robust and standardized for regulated products whereas adverse event reporting is less reliable for unregulated products.
- Nonregulated products are rarely covered by insurance or other reimbursement.
Legal considerations will also vary by jurisdiction. ”Right now in the U.S. we have a confused legality where state level programs are still technically illegal at the federal level and I imagine there are some quality differences amongst dispensaries and states,” Dr. Freedman said. “Whenever there is disagreement between state and federal laws, this creates tension for our patients.” He noted, for example, that a patient using a CBD product that contains THC may, even if legal in their state, be confiscated by the Transportation Security Administration at an airport since it is not FDA approved and is not legal, according to the Drug Enforcement Agency.
The authors noted that inadequate data on long-term CBD use and data on neurodevelopmental effects of THC in children, teens, and young adults means THC products should be contraindicated for these age groups. (Epidiolex has less than 2% THC.) Drug interactions should also be considered, particularly for clobazam, CYP3A4 inhibitors or inducers (including St. John’s wort), digoxin, or a mechanistic target of rapamycin inhibitor.
Dr. Freedman said that most neurologists are comfortable prescribing Epidiolex since it has FDA approval while prescribing unapproved products varies more in the field. “Now that many states have compassionate use programs for medical marijuana, some neurologists do this as well,” Dr. Freedman said. Patients often ask about unregulated CBD or CBD+THC products because they’re seen as “natural and therefore better than manufactured pharmaceuticals.”
“I think this is the naturalistic fallacy at work and try to educate my patients on that since our only high-level data to show marijuana products work for epilepsy comes from a pharmaceutical company,” Dr. Freedman said. “My reasons for hesitating on compassionate use are that there is often THC, with variable amounts of concentration, and we know that THC can harm the developing pediatric brain.”
Dosing and adverse effects
Pediatric and adult dosing differences need to be considered, and “patient response (efficacy and toxicity) to these medications varies widely,” the authors noted. They advised getting serum transaminases (ALT and AST) and total bilirubin levels before beginning treatment. All patients should begin Epidiolex at a low dose, such as 2-5 mg/kg per day of CBD in two divided doses, the authors advise, and titrate slowly while monitoring for side effects (no more than 5 mg/kg per day per week). The current dosing range for CBD is 5-20 mg/kg per day in two divided doses, with higher rates involving more risk of adverse events.
“Note that some cannabinoids auto-inhibit their own metabolism and some have active metabolites with longer half-lives,” the authors wrote. “Therefore, dose or frequency may need to be reduced over time, unless tolerance occurs.” These doses, specific to Epidiolex, “cannot necessarily be applied to other oral CBD formulations or other types of epilepsy.” This guidance also does not apply to inhaled or transdermal routes of administration.
The most common adverse events were sleepiness – which occurred in up to 60% of trial participants – as well as diarrhea, decreases in appetite and weight, and drug interactions. Risk of hepatotoxicity means there’s a need to monitor liver function and adjust dosing for patients with moderate or severe hepatic impairment. “Other short-term side effects reported only with THC-containing cannabinoid compounds include increased risk of cardiac and cerebrovascular events, anxiety and psychosis risk, dependency, and withdrawal,” the authors wrote.
Though no withdrawal syndrome has been linked to stopping CBD, the authors suggested decreasing the dose by 10% every 2 days if stopping is not urgent.
“The key points to this issue are that CBD and all marijuana products need to be safe and regulated,” Dr. Freedman said. “Any claims about them need to be backed by high-quality evidence looking at that specific product for that specific condition.”
Dr. Freedman noted the need for children to receive treatment from clinicians with expertise in their specific condition since many other evidence-based treatments exist even for patients with epilepsy syndromes that are difficult to treat, such as other medications, surgery, and specialized diets.
“We need to fix the inconsistent regulation between over-the-counter CBD products, state dispensaries, and federal laws,” Dr. Freedman added. “Any medicine being used to treat children should be held to the same FDA standard of safety and efficacy.”
Dr. Freedman and the authors had no conflicts of interest. No external funding was noted.
A recent review article draws from existing clinical trials and clinical experience in New South Wales, Australia, to fill this gap with interim guidance for both pediatric and adult patients. The article was published in the British Journal of Clinical Pharmacology.
The only current U.S. guidelines are from the American Academy of Neurology’s position statement on the use of medical cannabis for neurologic disorders and the American Epilepsy Society’s position statement on cannabis as a treatment for epileptic seizures. The AAN statement “highlights the current evidence, which currently only supports [Food and Drug Administration]–approved CBD [cannabidiol] (Epidiolex) for specific epilepsy syndromes,” said Daniel Freedman, DO, an assistant professor of neurology at the University of Texas at Austin and coauthor of the AAN’s position statement.
“Rescheduling marijuana will enable researchers to study CBD, THC [tetrahydrocannabinol], and other cannabinoids in high-quality studies so that we can better understand what works and for which conditions,” said Dr. Freedman, who was not involved in the Australian guidance document. He noted that little consensus exists because little evidence exists outside the handful of trials for Epidiolex.
“There are some patients with epilepsy that can benefit from high-quality, pharmaceutical-grade CBD products,” Dr. Freedman said. “These patients need to be carefully identified by a neurologist or epileptologist and prescribed a legal, safe, quality-controlled, and FDA-regulated product.”
Appropriate patient populations
Drug-resistant epilepsy, defined as failure of two appropriate antiseizure medications, affects an estimated one third of people with epilepsy, the new guideline notes. Though many over-the-counter products are available at dispensaries in the 33 U.S. states that allow use of cannabis for medical purposes, Epidiolex (cannabidiol) is the only FDA-approved drug for epilepsy that contains a substance derived from cannabis and the only one for which evidence from randomized, controlled trials exists.
Dr. Freedman notes that hemp-derived CBD oils are classified differently in the United States than marijuana-derived CBD oil, including Epidiolex, and are loosely regulated supplements or food additives commonly seen, for example at gas station.
“The point I drive home to patients is that you wouldn’t get your antibiotics from a gas station, so please don’t get your seizure medication from there,” Dr. Freedman said. “Studies have been done on ‘over-the-counter’ CBD oils and shown that they have variable quality, sometimes no detectable CBD, and sometimes other chemicals added like THC.”
Studies of Epidiolex showed that cannabidiol more effectively reduced seizure frequency than placebo for pediatric patients with Dravet syndrome (42% reduction) and for pediatric and adult patients with Lennox-Gastaut syndrome (39% reduction) or tuberous sclerosis complex (49% reduction). Efficacy was similar across dosing from 10-50 mg/kg per day, but higher doses involved higher rates of serious adverse events.
No reliable evidence in humans exists for THC or other cannabinoids in treating epilepsy.
The Australian guidance recommends limiting cannabis treatment to patients with severe drug-resistant epilepsy; a diagnosis of Dravet syndrome, Lennox-Gastaut syndrome, or tuberous sclerosis complex; and previous treatment with four approved antiseizure medications and/or the ketogenic diet, epilepsy surgery, or neurostimulator. The authors provide specific criteria for each of these conditions and then address exceptional cases that may be considered outside that criteria, such as patients under 2 years old, severe epilepsy with extended or repeated hospitalization or ICU admission, or a dangerous seizure type. The review also includes a detailed list of exclusion criteria for CBD medicine use.
The authors advised a thorough consent process before prescribing any cannabinoids, including therapeutic goals and stopping criteria; the lack of evidence available on dosing, efficacy, and side effects; and the potential for dependence or withdrawal. Consent discussions should also note whether the products are unregistered and not covered by external payers (anything other than Epidiolex currently), any activity restrictions, and any implications for occupational drug screening.
Considerations for unapproved cannabinoids
The authors note several factors to consider if prescribing or recommending a nonapproved, nonregulated cannabis medicine, including the ”differences between registered plant-derived cannabis medicines, synthetic cannabis medicines, and unregistered hemp-derived products.” Epidiolex is plant derived while other cannabis-derived medications (Marinol, Syndos, and Cesamet) that have been approved for nonepilepsy conditions, such as nausea associated with chemotherapy, are synthetic.
The guidance document notes several reasons to use a regulated medication instead of an unregulated product:
- Manufacturing processes can differ for unregulated products, including inconsistency in batches and unknown shelf life.
- Quality control processes, including risk of impurities, are much better with regulated products, which also have a system in place for safety recalls.
- More scientific evidence is available for regulated products.
- Safety surveillance reporting is more robust and standardized for regulated products whereas adverse event reporting is less reliable for unregulated products.
- Nonregulated products are rarely covered by insurance or other reimbursement.
Legal considerations will also vary by jurisdiction. ”Right now in the U.S. we have a confused legality where state level programs are still technically illegal at the federal level and I imagine there are some quality differences amongst dispensaries and states,” Dr. Freedman said. “Whenever there is disagreement between state and federal laws, this creates tension for our patients.” He noted, for example, that a patient using a CBD product that contains THC may, even if legal in their state, be confiscated by the Transportation Security Administration at an airport since it is not FDA approved and is not legal, according to the Drug Enforcement Agency.
The authors noted that inadequate data on long-term CBD use and data on neurodevelopmental effects of THC in children, teens, and young adults means THC products should be contraindicated for these age groups. (Epidiolex has less than 2% THC.) Drug interactions should also be considered, particularly for clobazam, CYP3A4 inhibitors or inducers (including St. John’s wort), digoxin, or a mechanistic target of rapamycin inhibitor.
Dr. Freedman said that most neurologists are comfortable prescribing Epidiolex since it has FDA approval while prescribing unapproved products varies more in the field. “Now that many states have compassionate use programs for medical marijuana, some neurologists do this as well,” Dr. Freedman said. Patients often ask about unregulated CBD or CBD+THC products because they’re seen as “natural and therefore better than manufactured pharmaceuticals.”
“I think this is the naturalistic fallacy at work and try to educate my patients on that since our only high-level data to show marijuana products work for epilepsy comes from a pharmaceutical company,” Dr. Freedman said. “My reasons for hesitating on compassionate use are that there is often THC, with variable amounts of concentration, and we know that THC can harm the developing pediatric brain.”
Dosing and adverse effects
Pediatric and adult dosing differences need to be considered, and “patient response (efficacy and toxicity) to these medications varies widely,” the authors noted. They advised getting serum transaminases (ALT and AST) and total bilirubin levels before beginning treatment. All patients should begin Epidiolex at a low dose, such as 2-5 mg/kg per day of CBD in two divided doses, the authors advise, and titrate slowly while monitoring for side effects (no more than 5 mg/kg per day per week). The current dosing range for CBD is 5-20 mg/kg per day in two divided doses, with higher rates involving more risk of adverse events.
“Note that some cannabinoids auto-inhibit their own metabolism and some have active metabolites with longer half-lives,” the authors wrote. “Therefore, dose or frequency may need to be reduced over time, unless tolerance occurs.” These doses, specific to Epidiolex, “cannot necessarily be applied to other oral CBD formulations or other types of epilepsy.” This guidance also does not apply to inhaled or transdermal routes of administration.
The most common adverse events were sleepiness – which occurred in up to 60% of trial participants – as well as diarrhea, decreases in appetite and weight, and drug interactions. Risk of hepatotoxicity means there’s a need to monitor liver function and adjust dosing for patients with moderate or severe hepatic impairment. “Other short-term side effects reported only with THC-containing cannabinoid compounds include increased risk of cardiac and cerebrovascular events, anxiety and psychosis risk, dependency, and withdrawal,” the authors wrote.
Though no withdrawal syndrome has been linked to stopping CBD, the authors suggested decreasing the dose by 10% every 2 days if stopping is not urgent.
“The key points to this issue are that CBD and all marijuana products need to be safe and regulated,” Dr. Freedman said. “Any claims about them need to be backed by high-quality evidence looking at that specific product for that specific condition.”
Dr. Freedman noted the need for children to receive treatment from clinicians with expertise in their specific condition since many other evidence-based treatments exist even for patients with epilepsy syndromes that are difficult to treat, such as other medications, surgery, and specialized diets.
“We need to fix the inconsistent regulation between over-the-counter CBD products, state dispensaries, and federal laws,” Dr. Freedman added. “Any medicine being used to treat children should be held to the same FDA standard of safety and efficacy.”
Dr. Freedman and the authors had no conflicts of interest. No external funding was noted.
FROM THE BRITISH JOURNAL OF CLINICAL PHARMACOLOGY
Intermittent fasting good for weight loss, at least short term
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE REVIEWS: ENDOCRINOLOGY
Mild COVID-19 infection linked to later type 2 diabetes
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA
Third-party vendor physicians more likely to prescribe antibiotics during acute care telehealth visits
Third-party vendor physicians appear to be more much more likely than their system-employed counterparts to prescribe antibiotics during acute care telehealth visits for acute respiratory infection (ARI), according to a study in the Journal of Telemedicine and Telecare.
As health systems expand their direct-to-consumer (DTC) virtual care, the quality of that care seems to vary, write the authors. Patients with ARI symptoms make up about one-third of virtual visits. Prescribing practice is a commonly cited measure of care quality for ARI, which is usually viral and rarely benefits from antibiotics.
“When providing care through telehealth, hospital-affiliated emergency physicians practiced better antibiotic stewardship than vendor-supplied, non–hospital-affiliated physicians,” lead study author Kathleen Li, MD, MS, a clinical lecturer in the department of emergency medicine at the University of Michigan, Ann Arbor, told this news organization.
“We had a sense that a difference existed, but the magnitude of the difference was larger than expected,” she said.
Dr. Li and her colleagues retrospectively analyzed on-demand telehealth visits available to health system employees and dependents of a large urban academic health system from March 2018, when the service began, through July 2019.
All 16 affiliated physicians providing ARI care were board-certified in emergency medicine, compared with 2 (8%) of the 25 unaffiliated (vendor-employed) physicians. Most unaffiliated physicians were known to be board-certified in family medicine, internal medicine, or pediatrics.
Unaffiliated physicians were not given access to the health system’s electronic medical record. Instead, all their patient histories, exams, assessments, plans, impressions, and discharge instructions were scanned into the electronic medical record system by other staff the next day.
Unaffiliated doctors were more than twice as likely to prescribe antibiotics
The researchers extracted data on all 257 virtual ARI visits from the electronic health record system, including prescriptions and medication therapeutic class. They performed multivariable logistic regression, adjusting for patient age and time of visit (weekday vs. weekend; day vs. overnight).
Antibiotic prescription rates were similar between weekday and weekend visits, and between day and night visits. Regardless of provider status, older patients were more likely to be prescribed antibiotics (P = .01).
Overall, affiliated physicians prescribed antibiotics during 18% of visits, whereas vendor physicians prescribed antibiotics during 37% of visits. After adjustments, the odds were 2.3 times higher that a patient in a telehealth visit with a vendor provider would be prescribed antibiotics (95% confidence interval, 1.1-4.5).
The predicted antibiotic prescribing rate for ARI was 19% (95% confidence interval, 13%-25%) for affiliated providers vs. 35% (95% CI, 22%-47%) for unaffiliated providers, an average marginal effect of 15% (95% CI, 2%-29%). The difference was even greater (average marginal effect 20%, 95% CI, 4%-35%) when children and patients over 65 were excluded.
Consistent, high-quality care and antibiotic stewardship are needed in all settings
Three experts who were not involved in the study commented on the study.
Joshua W. Elder, MD, MPH, MHS, medical director of Telehealth Express Care (direct-to-consumer telemedicine) at UC Davis Health in Sacramento, Calif., said, “An important unanswered question is how factors such as communication (policy and procedures, practice guidelines), connection (electronic health records), and reimbursement and incentives that health system and vendor-based providers received impacted this outcome.
“As the volume of virtual practices grows, most health systems will need to create a hybrid between health-system-employed and vendor-and/or-payer-supplied physicians,” he added. “Finding ways to create similar quality and outcomes will be essential in the evolving digital health infrastructure being developed.”
Charles Teixeira, DO, an infectious disease specialist at the Medical University of South Carolina in Charleston, said that this study highlighted the need to consistently provide high-quality, evidence-based care regardless of the encounter setting.
“It was important to compare the prescribing practices for commonly used medications, especially those as important as antibiotics,” he added. “Overprescribing antibiotics can have a progressive, long-term effect on a community and increase the risk for patients to develop multidrug-resistant bacteria.”
Jeffrey A. Linder, MD, MPH, the chief of general internal medicine and geriatrics in the department of medicine at Northwestern University in Chicago, commended the authors for investigating the quality of telehealth.
“The major limitation,” he found, “is that the investigators lumped all ARI visits – including those that are potentially antibiotic appropriate (e.g., otitis media, pharyngitis, sinusitis), those that are non–antibiotic appropriate (e.g., bronchitis, influenza, laryngitis, URI, viral syndrome), and those that are nonspecific symptoms (e.g., cough, congestion, fever, sore throat) – into the same category.”
No clinical information was collected or presented that would enable the reader to tell if these two groups of physicians were evaluating different patient populations or even if they just diagnosed patients differently,” he added.
“Our study did not delve into why we saw the difference,” Dr. Li explained. “Exploring potential reasons further will have important implications for how to optimally deliver care via telehealth.”
All authors and independent experts have disclosed no relevant financial relationships. The study received no financial support.
A version of this article first appeared on Medscape.com.
Third-party vendor physicians appear to be more much more likely than their system-employed counterparts to prescribe antibiotics during acute care telehealth visits for acute respiratory infection (ARI), according to a study in the Journal of Telemedicine and Telecare.
As health systems expand their direct-to-consumer (DTC) virtual care, the quality of that care seems to vary, write the authors. Patients with ARI symptoms make up about one-third of virtual visits. Prescribing practice is a commonly cited measure of care quality for ARI, which is usually viral and rarely benefits from antibiotics.
“When providing care through telehealth, hospital-affiliated emergency physicians practiced better antibiotic stewardship than vendor-supplied, non–hospital-affiliated physicians,” lead study author Kathleen Li, MD, MS, a clinical lecturer in the department of emergency medicine at the University of Michigan, Ann Arbor, told this news organization.
“We had a sense that a difference existed, but the magnitude of the difference was larger than expected,” she said.
Dr. Li and her colleagues retrospectively analyzed on-demand telehealth visits available to health system employees and dependents of a large urban academic health system from March 2018, when the service began, through July 2019.
All 16 affiliated physicians providing ARI care were board-certified in emergency medicine, compared with 2 (8%) of the 25 unaffiliated (vendor-employed) physicians. Most unaffiliated physicians were known to be board-certified in family medicine, internal medicine, or pediatrics.
Unaffiliated physicians were not given access to the health system’s electronic medical record. Instead, all their patient histories, exams, assessments, plans, impressions, and discharge instructions were scanned into the electronic medical record system by other staff the next day.
Unaffiliated doctors were more than twice as likely to prescribe antibiotics
The researchers extracted data on all 257 virtual ARI visits from the electronic health record system, including prescriptions and medication therapeutic class. They performed multivariable logistic regression, adjusting for patient age and time of visit (weekday vs. weekend; day vs. overnight).
Antibiotic prescription rates were similar between weekday and weekend visits, and between day and night visits. Regardless of provider status, older patients were more likely to be prescribed antibiotics (P = .01).
Overall, affiliated physicians prescribed antibiotics during 18% of visits, whereas vendor physicians prescribed antibiotics during 37% of visits. After adjustments, the odds were 2.3 times higher that a patient in a telehealth visit with a vendor provider would be prescribed antibiotics (95% confidence interval, 1.1-4.5).
The predicted antibiotic prescribing rate for ARI was 19% (95% confidence interval, 13%-25%) for affiliated providers vs. 35% (95% CI, 22%-47%) for unaffiliated providers, an average marginal effect of 15% (95% CI, 2%-29%). The difference was even greater (average marginal effect 20%, 95% CI, 4%-35%) when children and patients over 65 were excluded.
Consistent, high-quality care and antibiotic stewardship are needed in all settings
Three experts who were not involved in the study commented on the study.
Joshua W. Elder, MD, MPH, MHS, medical director of Telehealth Express Care (direct-to-consumer telemedicine) at UC Davis Health in Sacramento, Calif., said, “An important unanswered question is how factors such as communication (policy and procedures, practice guidelines), connection (electronic health records), and reimbursement and incentives that health system and vendor-based providers received impacted this outcome.
“As the volume of virtual practices grows, most health systems will need to create a hybrid between health-system-employed and vendor-and/or-payer-supplied physicians,” he added. “Finding ways to create similar quality and outcomes will be essential in the evolving digital health infrastructure being developed.”
Charles Teixeira, DO, an infectious disease specialist at the Medical University of South Carolina in Charleston, said that this study highlighted the need to consistently provide high-quality, evidence-based care regardless of the encounter setting.
“It was important to compare the prescribing practices for commonly used medications, especially those as important as antibiotics,” he added. “Overprescribing antibiotics can have a progressive, long-term effect on a community and increase the risk for patients to develop multidrug-resistant bacteria.”
Jeffrey A. Linder, MD, MPH, the chief of general internal medicine and geriatrics in the department of medicine at Northwestern University in Chicago, commended the authors for investigating the quality of telehealth.
“The major limitation,” he found, “is that the investigators lumped all ARI visits – including those that are potentially antibiotic appropriate (e.g., otitis media, pharyngitis, sinusitis), those that are non–antibiotic appropriate (e.g., bronchitis, influenza, laryngitis, URI, viral syndrome), and those that are nonspecific symptoms (e.g., cough, congestion, fever, sore throat) – into the same category.”
No clinical information was collected or presented that would enable the reader to tell if these two groups of physicians were evaluating different patient populations or even if they just diagnosed patients differently,” he added.
“Our study did not delve into why we saw the difference,” Dr. Li explained. “Exploring potential reasons further will have important implications for how to optimally deliver care via telehealth.”
All authors and independent experts have disclosed no relevant financial relationships. The study received no financial support.
A version of this article first appeared on Medscape.com.
Third-party vendor physicians appear to be more much more likely than their system-employed counterparts to prescribe antibiotics during acute care telehealth visits for acute respiratory infection (ARI), according to a study in the Journal of Telemedicine and Telecare.
As health systems expand their direct-to-consumer (DTC) virtual care, the quality of that care seems to vary, write the authors. Patients with ARI symptoms make up about one-third of virtual visits. Prescribing practice is a commonly cited measure of care quality for ARI, which is usually viral and rarely benefits from antibiotics.
“When providing care through telehealth, hospital-affiliated emergency physicians practiced better antibiotic stewardship than vendor-supplied, non–hospital-affiliated physicians,” lead study author Kathleen Li, MD, MS, a clinical lecturer in the department of emergency medicine at the University of Michigan, Ann Arbor, told this news organization.
“We had a sense that a difference existed, but the magnitude of the difference was larger than expected,” she said.
Dr. Li and her colleagues retrospectively analyzed on-demand telehealth visits available to health system employees and dependents of a large urban academic health system from March 2018, when the service began, through July 2019.
All 16 affiliated physicians providing ARI care were board-certified in emergency medicine, compared with 2 (8%) of the 25 unaffiliated (vendor-employed) physicians. Most unaffiliated physicians were known to be board-certified in family medicine, internal medicine, or pediatrics.
Unaffiliated physicians were not given access to the health system’s electronic medical record. Instead, all their patient histories, exams, assessments, plans, impressions, and discharge instructions were scanned into the electronic medical record system by other staff the next day.
Unaffiliated doctors were more than twice as likely to prescribe antibiotics
The researchers extracted data on all 257 virtual ARI visits from the electronic health record system, including prescriptions and medication therapeutic class. They performed multivariable logistic regression, adjusting for patient age and time of visit (weekday vs. weekend; day vs. overnight).
Antibiotic prescription rates were similar between weekday and weekend visits, and between day and night visits. Regardless of provider status, older patients were more likely to be prescribed antibiotics (P = .01).
Overall, affiliated physicians prescribed antibiotics during 18% of visits, whereas vendor physicians prescribed antibiotics during 37% of visits. After adjustments, the odds were 2.3 times higher that a patient in a telehealth visit with a vendor provider would be prescribed antibiotics (95% confidence interval, 1.1-4.5).
The predicted antibiotic prescribing rate for ARI was 19% (95% confidence interval, 13%-25%) for affiliated providers vs. 35% (95% CI, 22%-47%) for unaffiliated providers, an average marginal effect of 15% (95% CI, 2%-29%). The difference was even greater (average marginal effect 20%, 95% CI, 4%-35%) when children and patients over 65 were excluded.
Consistent, high-quality care and antibiotic stewardship are needed in all settings
Three experts who were not involved in the study commented on the study.
Joshua W. Elder, MD, MPH, MHS, medical director of Telehealth Express Care (direct-to-consumer telemedicine) at UC Davis Health in Sacramento, Calif., said, “An important unanswered question is how factors such as communication (policy and procedures, practice guidelines), connection (electronic health records), and reimbursement and incentives that health system and vendor-based providers received impacted this outcome.
“As the volume of virtual practices grows, most health systems will need to create a hybrid between health-system-employed and vendor-and/or-payer-supplied physicians,” he added. “Finding ways to create similar quality and outcomes will be essential in the evolving digital health infrastructure being developed.”
Charles Teixeira, DO, an infectious disease specialist at the Medical University of South Carolina in Charleston, said that this study highlighted the need to consistently provide high-quality, evidence-based care regardless of the encounter setting.
“It was important to compare the prescribing practices for commonly used medications, especially those as important as antibiotics,” he added. “Overprescribing antibiotics can have a progressive, long-term effect on a community and increase the risk for patients to develop multidrug-resistant bacteria.”
Jeffrey A. Linder, MD, MPH, the chief of general internal medicine and geriatrics in the department of medicine at Northwestern University in Chicago, commended the authors for investigating the quality of telehealth.
“The major limitation,” he found, “is that the investigators lumped all ARI visits – including those that are potentially antibiotic appropriate (e.g., otitis media, pharyngitis, sinusitis), those that are non–antibiotic appropriate (e.g., bronchitis, influenza, laryngitis, URI, viral syndrome), and those that are nonspecific symptoms (e.g., cough, congestion, fever, sore throat) – into the same category.”
No clinical information was collected or presented that would enable the reader to tell if these two groups of physicians were evaluating different patient populations or even if they just diagnosed patients differently,” he added.
“Our study did not delve into why we saw the difference,” Dr. Li explained. “Exploring potential reasons further will have important implications for how to optimally deliver care via telehealth.”
All authors and independent experts have disclosed no relevant financial relationships. The study received no financial support.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF TELEMEDICINE AND TELECARE