User login
Study outlines survival factors with nivolumab
Predictors of long-term survival of patients with advanced melanoma, renal cell carcinoma (RCC), non–small cell lung cancer (NSCLC), and other malignancies treated with nivolumab include the absence of liver or bone metastases, excellent baseline performance status, and the presence of grade 3 or greater treatment-related adverse events, investigators have found.
A secondary analysis of the phase 1 CA209-003 trial with expansion cohorts showed that, among 270 heavily pretreated patients with melanoma, RCC, and NSCLC who received single-agent nivolumab (Opdivo) during this trial, those with liver or bone metastases had a 69% higher risk for death within 5 years.
In contrast, patients with Eastern Cooperative Oncology Group (ECOG) performance status of 0 had a nearly threefold higher chance for survival, compared with patients with less favorable performance status scores, reported Suzanne L. Topalian, MD, from the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University in Baltimore and colleagues.
“The results of this study suggest that survival benefits reported in the more limited follow-up of recent nivolumab randomized clinical trials may persist for prolonged periods in some patients, extending to at least 5 years,” they wrote in JAMA Oncology.
In the CA209-003 trial, investigators enrolled patients 18 years or older with documented evidence of advanced melanoma, RCC, NSCLC, castration-resistant prostate cancer, or colorectal cancer. To be eligible, patients needed to have received 1-5 previous systemic therapies for advanced or recurrent cancer, measurable disease by Response Evaluation Criteria in Solid Tumors (RECIST) version 1.0, and an ECOG performance status of 0-2. The current survival analysis included data on 107 patients with melanoma, 34 with RCC, and 129 with NSCLC.
Estimated 5-year overall survival rates were 34.2% for patients with melanoma, 27.7% for patients with RCC, and 15.6% for patients with NSCLC. A multivariable analysis controlling for age, sex, performance status, metastatic disease, and number of prior therapies showed that the presence of either liver or bone metastases was associated with an odds ratio for 5-year survival of 0.31 (P = .02 and .04, respectively).
One factor favorably associated with survival included ECOG performance status 0 (OR, 2.74; P = .003). The investigators also found that treatment-related adverse events (AEs) were associated with longer overall survival, with a median of 19.8 months for patients with any grade of treatment-related event and 20.3 months for patients with grade 3 or greater events, compared with a median of 5.8 months for patients with no treatment-related events (P less than .001 for each comparison based on hazard ratios).
“Of note, patients in our study who developed treatment-related AEs, regardless of whether the AEs were deemed to have an immune-mediated causality, had significantly higher ORRs [overall response rates] and prolonged 5-year OS. These findings are reminiscent of some reports of anti–CTLA-4 therapy and align with other studies of anti–PD-1 therapies, “ Dr. Topalian and associates wrote.
The study and the secondary analysis were supported by Bristol-Myers Squibb. Dr. Topalian disclosed grants and travel reimbursements from Bristol-Myers Squibb and consulting fees with other entities. Multiple co-authors reported similar relationships. Four of the co-authors are Bristol-Myers Squibb employees.
SOURCE: Topalian SL et al. JAMA Oncology. 2019 Jul 25. doi: 10.1001/jamaoncol.2019.2187.
Although the existence of a subset of patients experiencing long-term survival certainly substantiates the role of PD-1/ PD-L1 checkpoint blockade in cancer immunotherapy, it is noteworthy to consider that these agents as monotherapy have not yielded sufficient activity and efficacy to replace standard-of-care therapy in the first line of therapy in advanced solid tumors, with the exception of NSCLC expressing high levels of PD-L1 and melanoma; emerging results also restrict monotherapy to stringently defined subsets of patients with gastric, esophageal, head and neck, and bladder cancers. Baseline predictive biomarkers have demonstrated distinct shortcomings, the first being their poor discriminatory ability and low negative predictive value. The clinician keen on securing the best possible outcome for his patients is thus left with the necessity for indiscriminate administration of PD-1/PD-L1 checkpoint inhibitors.
Unsurprisingly, the field of combination therapies using PD-1/PD-L1 checkpoint blockade as a backbone has been growing exponentially; a recent review shows more than 2,250 immunotherapy trials, 1,716 of which are investigating PD-1/ PD-L1 checkpoint inhibitors with more than 240 combination partners. Analysis of the pipeline also reveals a 67% increase in the number of active agents, amounting to more than 3,300, between September 2017 and September 2018. A noteworthy development is a 113% increase in cell therapies, and an increase of agents targeting neoantigens identified through bioinformatics analysis of an individual patient’s tumor, suggesting a shift toward increased personalization of immunotherapy. The observation that clinical development of immunotherapy agents has outstripped our understanding of the cancer-immune interactions advocates for renewed collective efforts in standardizing immune monitoring methods in clinical trials to identify immune evasion pathways that are dominant and to build novel trial designs able to efficiently enhance matching of patients with therapy.
Stefan Zimmermann, MD, and Solange Peters, MD, PhD, are from the Centre Hospitalier Universitaire Vaudois in Lausanne,Switzerland. Their remarks are excerpted and adapted from an editorial accompanying the study (JAMA Oncol. 2019 Jul 25. doi: 10.1001/jamaoncol.2019.2186). Dr. Zimmerman disclosed fees for advisory roles, travel grants, and clinical research support from Bristol-Myers Squibb and others. Dr. Peters disclosed fees for advisory board participation and/or lectures from Bristol-Myers Squibb and others.
Although the existence of a subset of patients experiencing long-term survival certainly substantiates the role of PD-1/ PD-L1 checkpoint blockade in cancer immunotherapy, it is noteworthy to consider that these agents as monotherapy have not yielded sufficient activity and efficacy to replace standard-of-care therapy in the first line of therapy in advanced solid tumors, with the exception of NSCLC expressing high levels of PD-L1 and melanoma; emerging results also restrict monotherapy to stringently defined subsets of patients with gastric, esophageal, head and neck, and bladder cancers. Baseline predictive biomarkers have demonstrated distinct shortcomings, the first being their poor discriminatory ability and low negative predictive value. The clinician keen on securing the best possible outcome for his patients is thus left with the necessity for indiscriminate administration of PD-1/PD-L1 checkpoint inhibitors.
Unsurprisingly, the field of combination therapies using PD-1/PD-L1 checkpoint blockade as a backbone has been growing exponentially; a recent review shows more than 2,250 immunotherapy trials, 1,716 of which are investigating PD-1/ PD-L1 checkpoint inhibitors with more than 240 combination partners. Analysis of the pipeline also reveals a 67% increase in the number of active agents, amounting to more than 3,300, between September 2017 and September 2018. A noteworthy development is a 113% increase in cell therapies, and an increase of agents targeting neoantigens identified through bioinformatics analysis of an individual patient’s tumor, suggesting a shift toward increased personalization of immunotherapy. The observation that clinical development of immunotherapy agents has outstripped our understanding of the cancer-immune interactions advocates for renewed collective efforts in standardizing immune monitoring methods in clinical trials to identify immune evasion pathways that are dominant and to build novel trial designs able to efficiently enhance matching of patients with therapy.
Stefan Zimmermann, MD, and Solange Peters, MD, PhD, are from the Centre Hospitalier Universitaire Vaudois in Lausanne,Switzerland. Their remarks are excerpted and adapted from an editorial accompanying the study (JAMA Oncol. 2019 Jul 25. doi: 10.1001/jamaoncol.2019.2186). Dr. Zimmerman disclosed fees for advisory roles, travel grants, and clinical research support from Bristol-Myers Squibb and others. Dr. Peters disclosed fees for advisory board participation and/or lectures from Bristol-Myers Squibb and others.
Although the existence of a subset of patients experiencing long-term survival certainly substantiates the role of PD-1/ PD-L1 checkpoint blockade in cancer immunotherapy, it is noteworthy to consider that these agents as monotherapy have not yielded sufficient activity and efficacy to replace standard-of-care therapy in the first line of therapy in advanced solid tumors, with the exception of NSCLC expressing high levels of PD-L1 and melanoma; emerging results also restrict monotherapy to stringently defined subsets of patients with gastric, esophageal, head and neck, and bladder cancers. Baseline predictive biomarkers have demonstrated distinct shortcomings, the first being their poor discriminatory ability and low negative predictive value. The clinician keen on securing the best possible outcome for his patients is thus left with the necessity for indiscriminate administration of PD-1/PD-L1 checkpoint inhibitors.
Unsurprisingly, the field of combination therapies using PD-1/PD-L1 checkpoint blockade as a backbone has been growing exponentially; a recent review shows more than 2,250 immunotherapy trials, 1,716 of which are investigating PD-1/ PD-L1 checkpoint inhibitors with more than 240 combination partners. Analysis of the pipeline also reveals a 67% increase in the number of active agents, amounting to more than 3,300, between September 2017 and September 2018. A noteworthy development is a 113% increase in cell therapies, and an increase of agents targeting neoantigens identified through bioinformatics analysis of an individual patient’s tumor, suggesting a shift toward increased personalization of immunotherapy. The observation that clinical development of immunotherapy agents has outstripped our understanding of the cancer-immune interactions advocates for renewed collective efforts in standardizing immune monitoring methods in clinical trials to identify immune evasion pathways that are dominant and to build novel trial designs able to efficiently enhance matching of patients with therapy.
Stefan Zimmermann, MD, and Solange Peters, MD, PhD, are from the Centre Hospitalier Universitaire Vaudois in Lausanne,Switzerland. Their remarks are excerpted and adapted from an editorial accompanying the study (JAMA Oncol. 2019 Jul 25. doi: 10.1001/jamaoncol.2019.2186). Dr. Zimmerman disclosed fees for advisory roles, travel grants, and clinical research support from Bristol-Myers Squibb and others. Dr. Peters disclosed fees for advisory board participation and/or lectures from Bristol-Myers Squibb and others.
Predictors of long-term survival of patients with advanced melanoma, renal cell carcinoma (RCC), non–small cell lung cancer (NSCLC), and other malignancies treated with nivolumab include the absence of liver or bone metastases, excellent baseline performance status, and the presence of grade 3 or greater treatment-related adverse events, investigators have found.
A secondary analysis of the phase 1 CA209-003 trial with expansion cohorts showed that, among 270 heavily pretreated patients with melanoma, RCC, and NSCLC who received single-agent nivolumab (Opdivo) during this trial, those with liver or bone metastases had a 69% higher risk for death within 5 years.
In contrast, patients with Eastern Cooperative Oncology Group (ECOG) performance status of 0 had a nearly threefold higher chance for survival, compared with patients with less favorable performance status scores, reported Suzanne L. Topalian, MD, from the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University in Baltimore and colleagues.
“The results of this study suggest that survival benefits reported in the more limited follow-up of recent nivolumab randomized clinical trials may persist for prolonged periods in some patients, extending to at least 5 years,” they wrote in JAMA Oncology.
In the CA209-003 trial, investigators enrolled patients 18 years or older with documented evidence of advanced melanoma, RCC, NSCLC, castration-resistant prostate cancer, or colorectal cancer. To be eligible, patients needed to have received 1-5 previous systemic therapies for advanced or recurrent cancer, measurable disease by Response Evaluation Criteria in Solid Tumors (RECIST) version 1.0, and an ECOG performance status of 0-2. The current survival analysis included data on 107 patients with melanoma, 34 with RCC, and 129 with NSCLC.
Estimated 5-year overall survival rates were 34.2% for patients with melanoma, 27.7% for patients with RCC, and 15.6% for patients with NSCLC. A multivariable analysis controlling for age, sex, performance status, metastatic disease, and number of prior therapies showed that the presence of either liver or bone metastases was associated with an odds ratio for 5-year survival of 0.31 (P = .02 and .04, respectively).
One factor favorably associated with survival included ECOG performance status 0 (OR, 2.74; P = .003). The investigators also found that treatment-related adverse events (AEs) were associated with longer overall survival, with a median of 19.8 months for patients with any grade of treatment-related event and 20.3 months for patients with grade 3 or greater events, compared with a median of 5.8 months for patients with no treatment-related events (P less than .001 for each comparison based on hazard ratios).
“Of note, patients in our study who developed treatment-related AEs, regardless of whether the AEs were deemed to have an immune-mediated causality, had significantly higher ORRs [overall response rates] and prolonged 5-year OS. These findings are reminiscent of some reports of anti–CTLA-4 therapy and align with other studies of anti–PD-1 therapies, “ Dr. Topalian and associates wrote.
The study and the secondary analysis were supported by Bristol-Myers Squibb. Dr. Topalian disclosed grants and travel reimbursements from Bristol-Myers Squibb and consulting fees with other entities. Multiple co-authors reported similar relationships. Four of the co-authors are Bristol-Myers Squibb employees.
SOURCE: Topalian SL et al. JAMA Oncology. 2019 Jul 25. doi: 10.1001/jamaoncol.2019.2187.
Predictors of long-term survival of patients with advanced melanoma, renal cell carcinoma (RCC), non–small cell lung cancer (NSCLC), and other malignancies treated with nivolumab include the absence of liver or bone metastases, excellent baseline performance status, and the presence of grade 3 or greater treatment-related adverse events, investigators have found.
A secondary analysis of the phase 1 CA209-003 trial with expansion cohorts showed that, among 270 heavily pretreated patients with melanoma, RCC, and NSCLC who received single-agent nivolumab (Opdivo) during this trial, those with liver or bone metastases had a 69% higher risk for death within 5 years.
In contrast, patients with Eastern Cooperative Oncology Group (ECOG) performance status of 0 had a nearly threefold higher chance for survival, compared with patients with less favorable performance status scores, reported Suzanne L. Topalian, MD, from the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University in Baltimore and colleagues.
“The results of this study suggest that survival benefits reported in the more limited follow-up of recent nivolumab randomized clinical trials may persist for prolonged periods in some patients, extending to at least 5 years,” they wrote in JAMA Oncology.
In the CA209-003 trial, investigators enrolled patients 18 years or older with documented evidence of advanced melanoma, RCC, NSCLC, castration-resistant prostate cancer, or colorectal cancer. To be eligible, patients needed to have received 1-5 previous systemic therapies for advanced or recurrent cancer, measurable disease by Response Evaluation Criteria in Solid Tumors (RECIST) version 1.0, and an ECOG performance status of 0-2. The current survival analysis included data on 107 patients with melanoma, 34 with RCC, and 129 with NSCLC.
Estimated 5-year overall survival rates were 34.2% for patients with melanoma, 27.7% for patients with RCC, and 15.6% for patients with NSCLC. A multivariable analysis controlling for age, sex, performance status, metastatic disease, and number of prior therapies showed that the presence of either liver or bone metastases was associated with an odds ratio for 5-year survival of 0.31 (P = .02 and .04, respectively).
One factor favorably associated with survival included ECOG performance status 0 (OR, 2.74; P = .003). The investigators also found that treatment-related adverse events (AEs) were associated with longer overall survival, with a median of 19.8 months for patients with any grade of treatment-related event and 20.3 months for patients with grade 3 or greater events, compared with a median of 5.8 months for patients with no treatment-related events (P less than .001 for each comparison based on hazard ratios).
“Of note, patients in our study who developed treatment-related AEs, regardless of whether the AEs were deemed to have an immune-mediated causality, had significantly higher ORRs [overall response rates] and prolonged 5-year OS. These findings are reminiscent of some reports of anti–CTLA-4 therapy and align with other studies of anti–PD-1 therapies, “ Dr. Topalian and associates wrote.
The study and the secondary analysis were supported by Bristol-Myers Squibb. Dr. Topalian disclosed grants and travel reimbursements from Bristol-Myers Squibb and consulting fees with other entities. Multiple co-authors reported similar relationships. Four of the co-authors are Bristol-Myers Squibb employees.
SOURCE: Topalian SL et al. JAMA Oncology. 2019 Jul 25. doi: 10.1001/jamaoncol.2019.2187.
FROM JAMA ONCOLOGY
Cases of pediatric invasive melanoma have declined since 2002, study finds
AUSTIN – The compared with females. The risk of death is also significantly increased in black patients, other nonwhite patients, and in cases where surgery was not performed.
Those are key findings from a study that set out to investigate the incidence of pediatric melanoma over the last 2 decades and factors influencing survival. At the annual meeting of the Society for Pediatric Dermatology, one of the study authors, Spandana Maddukuri, said that pediatric melanoma is the most common skin cancer in the pediatric population, accounting for 1-3% of all pediatric malignancies and 1%-4% of all cases of melanoma (Pediatr Surg. 2013;48[11]:2207-13).
“Nonmodifiable risk factors are similar to those in adult melanoma and include fair skin, light hair and eye color, increased number of congenital nevi, and family history of melanoma,” said Ms. Maddukuri, a third-year student at New Jersey Medical School, Newark. “Environmental risk factors are similar to those in adult melanoma and include exposure to UV radiation. About 60% of children do not meet standard ABCDE [asymmetrical, border, color, diameter, evolving] diagnosis criteria, which often leads to delayed diagnosis.”
Some of the characteristics that are more commonly found in pediatric lesions include amelanosis, bleeding, uniform color, and variable diameter (J Am Acad Dermatol. 2013; 68[6]:913-25).
Ms. Maddukuri and colleagues queried the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database for cases of malignant melanoma that were diagnosed in individuals aged younger than 20 years between 2002 and 2015. After excluding all cases of adult melanoma and all cases of in situ melanoma, they included 1,620 patients in the final analysis and divided them into five age groups: less than 1 year, 1-4 years, 5-9 years, 10-14 years, and 15-19 years. They calculated the overall incidence rate per 100,000 population of pediatric melanoma based on data from the 2000 U.S. Census. Age-, sex-, and race-specific incidence rates were also calculated. Kaplan-Meier and Cox regression analyses to investigate disease-specific survival and risk factors.
With each successive age group, the investigators observed that incidence rate was significantly higher than that of the previous age group (P less than .005). “However, the most striking increase in incidence occurs between the age group of 10-14 and 15-19,” she said. “Sex also influenced incidence rates. Males had an incidence rate of 0.396 per 100,000 population while females had an incidence rate of 0.579 per 100,000 population.”
Race also influenced incidence rates. White patients had the highest incidence rate of 0.605 per 100,000 population, while blacks had the lowest incident rate at 0.042 per 100,000 population. American Indian and Alaska Native patients had incidence rates of 0.046 per 100,000 population, while Asians and Pacific Islanders had an incidence rate of 0.127 per 100,000 population.
The researchers found that increased survival was associated with white race, female sex, treatment with surgical intervention, and age older than 5 years. No differences in survival were observed regarding the primary anatomic location or extent of disease. The hazard ratio of death from invasive melanoma was significantly increased in males (HR, 2.34), black patients (HR, 3.96), other nonwhite patients (HR, 3.64), and in cases where surgery was not performed (HR, 6.04).
“It is surprising that, although incidence is significantly higher in white patients and females, compared to black patients and males, respectively, the risk of dying from melanoma is much higher in black patients and males,” Ms. Maddukuri said in an interview at the meeting. “Overall, the dermatologic community is on the right track in screening and diagnosing pediatric melanoma, as seen by the decreased incidence over the last 2 decades. However, increased awareness regarding pediatric melanoma is still encouraged. I believe we were able to identify certain populations that need more attention in terms of screening, diagnosis, and treatment, which are patients less than 5 years old, black and other nonwhite patients, and males.”
She acknowledged certain shortcomings of the study, including a limited clinical history of the patient population because of the nature of the database. She also said that further studies are required to investigate the contributing factors to decreasing incidence and to evaluate the relationship of the favorable prognostic factors to increased survival. The researchers are currently working on correlating incidence rates with UV exposure and geographical location.
They reported having no financial disclosures.
AUSTIN – The compared with females. The risk of death is also significantly increased in black patients, other nonwhite patients, and in cases where surgery was not performed.
Those are key findings from a study that set out to investigate the incidence of pediatric melanoma over the last 2 decades and factors influencing survival. At the annual meeting of the Society for Pediatric Dermatology, one of the study authors, Spandana Maddukuri, said that pediatric melanoma is the most common skin cancer in the pediatric population, accounting for 1-3% of all pediatric malignancies and 1%-4% of all cases of melanoma (Pediatr Surg. 2013;48[11]:2207-13).
“Nonmodifiable risk factors are similar to those in adult melanoma and include fair skin, light hair and eye color, increased number of congenital nevi, and family history of melanoma,” said Ms. Maddukuri, a third-year student at New Jersey Medical School, Newark. “Environmental risk factors are similar to those in adult melanoma and include exposure to UV radiation. About 60% of children do not meet standard ABCDE [asymmetrical, border, color, diameter, evolving] diagnosis criteria, which often leads to delayed diagnosis.”
Some of the characteristics that are more commonly found in pediatric lesions include amelanosis, bleeding, uniform color, and variable diameter (J Am Acad Dermatol. 2013; 68[6]:913-25).
Ms. Maddukuri and colleagues queried the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database for cases of malignant melanoma that were diagnosed in individuals aged younger than 20 years between 2002 and 2015. After excluding all cases of adult melanoma and all cases of in situ melanoma, they included 1,620 patients in the final analysis and divided them into five age groups: less than 1 year, 1-4 years, 5-9 years, 10-14 years, and 15-19 years. They calculated the overall incidence rate per 100,000 population of pediatric melanoma based on data from the 2000 U.S. Census. Age-, sex-, and race-specific incidence rates were also calculated. Kaplan-Meier and Cox regression analyses to investigate disease-specific survival and risk factors.
With each successive age group, the investigators observed that incidence rate was significantly higher than that of the previous age group (P less than .005). “However, the most striking increase in incidence occurs between the age group of 10-14 and 15-19,” she said. “Sex also influenced incidence rates. Males had an incidence rate of 0.396 per 100,000 population while females had an incidence rate of 0.579 per 100,000 population.”
Race also influenced incidence rates. White patients had the highest incidence rate of 0.605 per 100,000 population, while blacks had the lowest incident rate at 0.042 per 100,000 population. American Indian and Alaska Native patients had incidence rates of 0.046 per 100,000 population, while Asians and Pacific Islanders had an incidence rate of 0.127 per 100,000 population.
The researchers found that increased survival was associated with white race, female sex, treatment with surgical intervention, and age older than 5 years. No differences in survival were observed regarding the primary anatomic location or extent of disease. The hazard ratio of death from invasive melanoma was significantly increased in males (HR, 2.34), black patients (HR, 3.96), other nonwhite patients (HR, 3.64), and in cases where surgery was not performed (HR, 6.04).
“It is surprising that, although incidence is significantly higher in white patients and females, compared to black patients and males, respectively, the risk of dying from melanoma is much higher in black patients and males,” Ms. Maddukuri said in an interview at the meeting. “Overall, the dermatologic community is on the right track in screening and diagnosing pediatric melanoma, as seen by the decreased incidence over the last 2 decades. However, increased awareness regarding pediatric melanoma is still encouraged. I believe we were able to identify certain populations that need more attention in terms of screening, diagnosis, and treatment, which are patients less than 5 years old, black and other nonwhite patients, and males.”
She acknowledged certain shortcomings of the study, including a limited clinical history of the patient population because of the nature of the database. She also said that further studies are required to investigate the contributing factors to decreasing incidence and to evaluate the relationship of the favorable prognostic factors to increased survival. The researchers are currently working on correlating incidence rates with UV exposure and geographical location.
They reported having no financial disclosures.
AUSTIN – The compared with females. The risk of death is also significantly increased in black patients, other nonwhite patients, and in cases where surgery was not performed.
Those are key findings from a study that set out to investigate the incidence of pediatric melanoma over the last 2 decades and factors influencing survival. At the annual meeting of the Society for Pediatric Dermatology, one of the study authors, Spandana Maddukuri, said that pediatric melanoma is the most common skin cancer in the pediatric population, accounting for 1-3% of all pediatric malignancies and 1%-4% of all cases of melanoma (Pediatr Surg. 2013;48[11]:2207-13).
“Nonmodifiable risk factors are similar to those in adult melanoma and include fair skin, light hair and eye color, increased number of congenital nevi, and family history of melanoma,” said Ms. Maddukuri, a third-year student at New Jersey Medical School, Newark. “Environmental risk factors are similar to those in adult melanoma and include exposure to UV radiation. About 60% of children do not meet standard ABCDE [asymmetrical, border, color, diameter, evolving] diagnosis criteria, which often leads to delayed diagnosis.”
Some of the characteristics that are more commonly found in pediatric lesions include amelanosis, bleeding, uniform color, and variable diameter (J Am Acad Dermatol. 2013; 68[6]:913-25).
Ms. Maddukuri and colleagues queried the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database for cases of malignant melanoma that were diagnosed in individuals aged younger than 20 years between 2002 and 2015. After excluding all cases of adult melanoma and all cases of in situ melanoma, they included 1,620 patients in the final analysis and divided them into five age groups: less than 1 year, 1-4 years, 5-9 years, 10-14 years, and 15-19 years. They calculated the overall incidence rate per 100,000 population of pediatric melanoma based on data from the 2000 U.S. Census. Age-, sex-, and race-specific incidence rates were also calculated. Kaplan-Meier and Cox regression analyses to investigate disease-specific survival and risk factors.
With each successive age group, the investigators observed that incidence rate was significantly higher than that of the previous age group (P less than .005). “However, the most striking increase in incidence occurs between the age group of 10-14 and 15-19,” she said. “Sex also influenced incidence rates. Males had an incidence rate of 0.396 per 100,000 population while females had an incidence rate of 0.579 per 100,000 population.”
Race also influenced incidence rates. White patients had the highest incidence rate of 0.605 per 100,000 population, while blacks had the lowest incident rate at 0.042 per 100,000 population. American Indian and Alaska Native patients had incidence rates of 0.046 per 100,000 population, while Asians and Pacific Islanders had an incidence rate of 0.127 per 100,000 population.
The researchers found that increased survival was associated with white race, female sex, treatment with surgical intervention, and age older than 5 years. No differences in survival were observed regarding the primary anatomic location or extent of disease. The hazard ratio of death from invasive melanoma was significantly increased in males (HR, 2.34), black patients (HR, 3.96), other nonwhite patients (HR, 3.64), and in cases where surgery was not performed (HR, 6.04).
“It is surprising that, although incidence is significantly higher in white patients and females, compared to black patients and males, respectively, the risk of dying from melanoma is much higher in black patients and males,” Ms. Maddukuri said in an interview at the meeting. “Overall, the dermatologic community is on the right track in screening and diagnosing pediatric melanoma, as seen by the decreased incidence over the last 2 decades. However, increased awareness regarding pediatric melanoma is still encouraged. I believe we were able to identify certain populations that need more attention in terms of screening, diagnosis, and treatment, which are patients less than 5 years old, black and other nonwhite patients, and males.”
She acknowledged certain shortcomings of the study, including a limited clinical history of the patient population because of the nature of the database. She also said that further studies are required to investigate the contributing factors to decreasing incidence and to evaluate the relationship of the favorable prognostic factors to increased survival. The researchers are currently working on correlating incidence rates with UV exposure and geographical location.
They reported having no financial disclosures.
REPORTING FROM SPD 2019
IL-6, CRP are prognostic for checkpoint inhibition in melanoma
CHICAGO – according to post hoc analyses of data from three randomized CheckMate studies.
In 70 treatment-naive patients from the randomized phase 2 CheckMate 064 study who received sequential treatment with the programmed death-1 (PD-1) checkpoint inhibitor nivolumab (NIVO) followed by the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) checkpoint inhibitor ipilimumab (IPI), best overall response was modestly associated with lower baseline serum IL-6 (P = .087) and significantly associated with on-treatment IL-6 (P = .006). In 70 patients who received IPI then NIVO, best overall response was associated only with on-treatment IL-6 (P = .043), Jeffrey S. Weber, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology.
“This stimulated us to look at associations with survival ... and there apparently was a significant association with high IL-6 levels in the serum both pretreatment and on treatment in both arms, whether they got NIVO then IPI followed by NIVO maintenance, or IPI then NIVO, also followed by NIVO maintenance,” he said.
After adjusting for covariates, the hazard ratios for survival for baseline IL-6 below versus above the median were 7.81 and 1.07, in the groups, respectively. No deaths occurred in the NIVO-IPI group (thus, no HR), but the HR for survival based on on-treatment IL-6 below versus above the median in the IPI-NIVO group was 1.92.
“So initial conclusions: High baseline and on-treatment IL-6 levels in the serum were associated with poor survival,” said Dr. Weber, deputy director of the Perlmutter Cancer Center, New York University Langone Medical Center.
This finding prompted evaluation of additional samples from the randomized CheckMate 066 study, which compared dacarbazine chemotherapy (the standard of care at the time) and NIVO in 400 treatment-naive patients with BRAF wild-type disease.
Again, baseline IL-6 levels (nondetectable vs. detectable) were associated with better overall survival (OS) in both groups (adjusted HRs, 1.79 and 1.54).
“So this is not a predictive marker, this is a baseline prognostic marker,” he said.
In the international, three-arm, randomized phase 3 CheckMate 067 study, which compared IPI, NIVO, and IPI+NIVO in 945 treatment-naive patients with either BRAF wild-type or BRAF mutated disease, baseline IL-6 levels (nondetectable vs. detectable) again were associated with better OS in all 3 arms (adjusted HRs, 3.13 for NIVO, 2.67 for NIVO+IPI, and 4.06 for IPI alone).
A multivariate analysis of data from the CheckMate 066 and 067 studies, with controlling for lactic acid deydrogenase, performance status, and disease stage, provided additional “impressive evidence” of IL-6 as a potent prognostic factor, Dr. Weber said.
“We then looked at CRP. I’ve always been interested in CRP because in a recent publication CRP was found to be associated with outcomes in patients who got PD-1, and the higher the CRP, the worse they did,” he said.
In CheckMate 064 there was modest association between lower baseline CRP and best overall response in both the NIVO-IPI and IPI-NIVO groups (P = .069 and 0.009, respectively), and on treatment, the association was really only seen in the IPI-NIVO group (P = .210 for NIVO-IPI and 0.015 for IPI-NIVO), in which the higher CRP levels were associated with progression or stability.
For survival, however, both baseline and on-treatment CRP levels were associated with OS; baseline serum CRP above the median was associated with shorter OS (HRs, 7.25 for NIVO-IPI and 1.53 for IPI-NIVO), and a similar trend was seen for on-treatment CRP (HRs, 1.60 and 2.0, respectively).
In CheckMate 066, the association between CRP and OS was also apparent, but not as impressive for NIVO alone (HR, 0.996) as it was for dacarbazine (HR, 1.90), and similar to CheckMate 064, higher baseline CRP levels were associated with shorter survival and were prognostic, he said.
In CheckMate 067, similar trends were seen across the treatment arms, and they were similar to those seen for IL-6, with higher baseline CRP levels (at or above median versus below) associated with shorter OS (HRs, 1.46 for NIVO, 1.26 for NIVO+IPI, and 1.48 for IPI alone).
To better understand how CRP might inhibit the effects of PD-1 and how it could have an immune effect – as also indicated by some prior data – Dr. Weber and colleagues conducted additional in vitro studies to examine the impact of exogenous CRP on T-cell function; they found that CRP affected the earliest steps in T-cell signaling and activation, thereby dampening antitumor immune responses.
Acute phase reactants such as CRP and chronic inflammatory proteins including IL-6 (which induces production of CRP from the liver) have been associated with poor prognosis in a variety of cancers, as well as with poor outcomes after anti–PD-1 or programmed death-ligand 1 (PD-L1) therapy in melanoma and other cancers, Dr. Weber said.
“In murine models of melanoma and pancreatic cancer, combined treatment with anti-IL-6 blockade and anti–PD-1/PD-L1 antibodies enhances antitumor immune responses and efficacy,” he explained, noting that the current analyses were undertaken based on those findings and on “a significant body of data” from other groups and from his own lab.
The current findings suggest that IL-6 and CRP may be prognostic for immune checkpoint inhibitor therapies in patients with melanoma, he said, adding that “blockade of IL-6 and CRP synthesis and/or activity in combination with immune checkpoint therapies may enhance responses and survival rates in patients with different cancers, including melanomas.”
To that end, an investigator-sponsored trial looking at IPI-NIVO with the IL-6–blocking antibody tocilizumab has been approved and will start accruing patients in the next few months, he said.
During a discussion of the findings at the meeting, Charles G. Drake, MD, PhD, associate director for clinical research at the Herbert Irving Comprehensive Cancer Center at Columbia University, New York, said that “Dr. Weber and his colleagues should be commended for really trying to show what CRP does to T-cell activation, and in the studies he showed us, it’s clearly negative.”
“But IL-6 is a pleiotropic cytokine. It will be very interesting to see what happens in the prospective clinical trial that he mentioned, in terms of all the other effects on CD-4 cells, neutrophils, and macrophages,” said Dr. Drake, who also is codirector of Columbia’s Cancer Immunotherapy Program. “Nevertheless, I think the data were clear that IL-6 and CRP are negative prognostic biomarkers in melanoma.”
Of note, the development of a biomarker identified in a trial typically takes many steps, but in the case of IL-6 – and perhaps even more so for CRP – the pathway is relatively short, Dr. Drake said.
“That’s because CRP is a validated and [Food and Drug Administration]–approved test; you can order it to assess cardiovascular risk in almost any hospital in the United States, and so the analyte – this part of the qualification – is done,” he explained. “I think if this was validated prospectively we could have CRP as a negative prognostic – not predictive – biomarker in melanoma, actually.”
Dr. Weber and Dr. Drake each reported relationships with numerous companies, including stock and other ownership interests and patents, consulting or advisory roles and/or receipt of honoraria, research funding to their respective institutions, and payment for travel, accommodations, and expenses
SOURCE: Weber J et al. ASCO 2019, Abstract 100.
CHICAGO – according to post hoc analyses of data from three randomized CheckMate studies.
In 70 treatment-naive patients from the randomized phase 2 CheckMate 064 study who received sequential treatment with the programmed death-1 (PD-1) checkpoint inhibitor nivolumab (NIVO) followed by the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) checkpoint inhibitor ipilimumab (IPI), best overall response was modestly associated with lower baseline serum IL-6 (P = .087) and significantly associated with on-treatment IL-6 (P = .006). In 70 patients who received IPI then NIVO, best overall response was associated only with on-treatment IL-6 (P = .043), Jeffrey S. Weber, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology.
“This stimulated us to look at associations with survival ... and there apparently was a significant association with high IL-6 levels in the serum both pretreatment and on treatment in both arms, whether they got NIVO then IPI followed by NIVO maintenance, or IPI then NIVO, also followed by NIVO maintenance,” he said.
After adjusting for covariates, the hazard ratios for survival for baseline IL-6 below versus above the median were 7.81 and 1.07, in the groups, respectively. No deaths occurred in the NIVO-IPI group (thus, no HR), but the HR for survival based on on-treatment IL-6 below versus above the median in the IPI-NIVO group was 1.92.
“So initial conclusions: High baseline and on-treatment IL-6 levels in the serum were associated with poor survival,” said Dr. Weber, deputy director of the Perlmutter Cancer Center, New York University Langone Medical Center.
This finding prompted evaluation of additional samples from the randomized CheckMate 066 study, which compared dacarbazine chemotherapy (the standard of care at the time) and NIVO in 400 treatment-naive patients with BRAF wild-type disease.
Again, baseline IL-6 levels (nondetectable vs. detectable) were associated with better overall survival (OS) in both groups (adjusted HRs, 1.79 and 1.54).
“So this is not a predictive marker, this is a baseline prognostic marker,” he said.
In the international, three-arm, randomized phase 3 CheckMate 067 study, which compared IPI, NIVO, and IPI+NIVO in 945 treatment-naive patients with either BRAF wild-type or BRAF mutated disease, baseline IL-6 levels (nondetectable vs. detectable) again were associated with better OS in all 3 arms (adjusted HRs, 3.13 for NIVO, 2.67 for NIVO+IPI, and 4.06 for IPI alone).
A multivariate analysis of data from the CheckMate 066 and 067 studies, with controlling for lactic acid deydrogenase, performance status, and disease stage, provided additional “impressive evidence” of IL-6 as a potent prognostic factor, Dr. Weber said.
“We then looked at CRP. I’ve always been interested in CRP because in a recent publication CRP was found to be associated with outcomes in patients who got PD-1, and the higher the CRP, the worse they did,” he said.
In CheckMate 064 there was modest association between lower baseline CRP and best overall response in both the NIVO-IPI and IPI-NIVO groups (P = .069 and 0.009, respectively), and on treatment, the association was really only seen in the IPI-NIVO group (P = .210 for NIVO-IPI and 0.015 for IPI-NIVO), in which the higher CRP levels were associated with progression or stability.
For survival, however, both baseline and on-treatment CRP levels were associated with OS; baseline serum CRP above the median was associated with shorter OS (HRs, 7.25 for NIVO-IPI and 1.53 for IPI-NIVO), and a similar trend was seen for on-treatment CRP (HRs, 1.60 and 2.0, respectively).
In CheckMate 066, the association between CRP and OS was also apparent, but not as impressive for NIVO alone (HR, 0.996) as it was for dacarbazine (HR, 1.90), and similar to CheckMate 064, higher baseline CRP levels were associated with shorter survival and were prognostic, he said.
In CheckMate 067, similar trends were seen across the treatment arms, and they were similar to those seen for IL-6, with higher baseline CRP levels (at or above median versus below) associated with shorter OS (HRs, 1.46 for NIVO, 1.26 for NIVO+IPI, and 1.48 for IPI alone).
To better understand how CRP might inhibit the effects of PD-1 and how it could have an immune effect – as also indicated by some prior data – Dr. Weber and colleagues conducted additional in vitro studies to examine the impact of exogenous CRP on T-cell function; they found that CRP affected the earliest steps in T-cell signaling and activation, thereby dampening antitumor immune responses.
Acute phase reactants such as CRP and chronic inflammatory proteins including IL-6 (which induces production of CRP from the liver) have been associated with poor prognosis in a variety of cancers, as well as with poor outcomes after anti–PD-1 or programmed death-ligand 1 (PD-L1) therapy in melanoma and other cancers, Dr. Weber said.
“In murine models of melanoma and pancreatic cancer, combined treatment with anti-IL-6 blockade and anti–PD-1/PD-L1 antibodies enhances antitumor immune responses and efficacy,” he explained, noting that the current analyses were undertaken based on those findings and on “a significant body of data” from other groups and from his own lab.
The current findings suggest that IL-6 and CRP may be prognostic for immune checkpoint inhibitor therapies in patients with melanoma, he said, adding that “blockade of IL-6 and CRP synthesis and/or activity in combination with immune checkpoint therapies may enhance responses and survival rates in patients with different cancers, including melanomas.”
To that end, an investigator-sponsored trial looking at IPI-NIVO with the IL-6–blocking antibody tocilizumab has been approved and will start accruing patients in the next few months, he said.
During a discussion of the findings at the meeting, Charles G. Drake, MD, PhD, associate director for clinical research at the Herbert Irving Comprehensive Cancer Center at Columbia University, New York, said that “Dr. Weber and his colleagues should be commended for really trying to show what CRP does to T-cell activation, and in the studies he showed us, it’s clearly negative.”
“But IL-6 is a pleiotropic cytokine. It will be very interesting to see what happens in the prospective clinical trial that he mentioned, in terms of all the other effects on CD-4 cells, neutrophils, and macrophages,” said Dr. Drake, who also is codirector of Columbia’s Cancer Immunotherapy Program. “Nevertheless, I think the data were clear that IL-6 and CRP are negative prognostic biomarkers in melanoma.”
Of note, the development of a biomarker identified in a trial typically takes many steps, but in the case of IL-6 – and perhaps even more so for CRP – the pathway is relatively short, Dr. Drake said.
“That’s because CRP is a validated and [Food and Drug Administration]–approved test; you can order it to assess cardiovascular risk in almost any hospital in the United States, and so the analyte – this part of the qualification – is done,” he explained. “I think if this was validated prospectively we could have CRP as a negative prognostic – not predictive – biomarker in melanoma, actually.”
Dr. Weber and Dr. Drake each reported relationships with numerous companies, including stock and other ownership interests and patents, consulting or advisory roles and/or receipt of honoraria, research funding to their respective institutions, and payment for travel, accommodations, and expenses
SOURCE: Weber J et al. ASCO 2019, Abstract 100.
CHICAGO – according to post hoc analyses of data from three randomized CheckMate studies.
In 70 treatment-naive patients from the randomized phase 2 CheckMate 064 study who received sequential treatment with the programmed death-1 (PD-1) checkpoint inhibitor nivolumab (NIVO) followed by the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) checkpoint inhibitor ipilimumab (IPI), best overall response was modestly associated with lower baseline serum IL-6 (P = .087) and significantly associated with on-treatment IL-6 (P = .006). In 70 patients who received IPI then NIVO, best overall response was associated only with on-treatment IL-6 (P = .043), Jeffrey S. Weber, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology.
“This stimulated us to look at associations with survival ... and there apparently was a significant association with high IL-6 levels in the serum both pretreatment and on treatment in both arms, whether they got NIVO then IPI followed by NIVO maintenance, or IPI then NIVO, also followed by NIVO maintenance,” he said.
After adjusting for covariates, the hazard ratios for survival for baseline IL-6 below versus above the median were 7.81 and 1.07, in the groups, respectively. No deaths occurred in the NIVO-IPI group (thus, no HR), but the HR for survival based on on-treatment IL-6 below versus above the median in the IPI-NIVO group was 1.92.
“So initial conclusions: High baseline and on-treatment IL-6 levels in the serum were associated with poor survival,” said Dr. Weber, deputy director of the Perlmutter Cancer Center, New York University Langone Medical Center.
This finding prompted evaluation of additional samples from the randomized CheckMate 066 study, which compared dacarbazine chemotherapy (the standard of care at the time) and NIVO in 400 treatment-naive patients with BRAF wild-type disease.
Again, baseline IL-6 levels (nondetectable vs. detectable) were associated with better overall survival (OS) in both groups (adjusted HRs, 1.79 and 1.54).
“So this is not a predictive marker, this is a baseline prognostic marker,” he said.
In the international, three-arm, randomized phase 3 CheckMate 067 study, which compared IPI, NIVO, and IPI+NIVO in 945 treatment-naive patients with either BRAF wild-type or BRAF mutated disease, baseline IL-6 levels (nondetectable vs. detectable) again were associated with better OS in all 3 arms (adjusted HRs, 3.13 for NIVO, 2.67 for NIVO+IPI, and 4.06 for IPI alone).
A multivariate analysis of data from the CheckMate 066 and 067 studies, with controlling for lactic acid deydrogenase, performance status, and disease stage, provided additional “impressive evidence” of IL-6 as a potent prognostic factor, Dr. Weber said.
“We then looked at CRP. I’ve always been interested in CRP because in a recent publication CRP was found to be associated with outcomes in patients who got PD-1, and the higher the CRP, the worse they did,” he said.
In CheckMate 064 there was modest association between lower baseline CRP and best overall response in both the NIVO-IPI and IPI-NIVO groups (P = .069 and 0.009, respectively), and on treatment, the association was really only seen in the IPI-NIVO group (P = .210 for NIVO-IPI and 0.015 for IPI-NIVO), in which the higher CRP levels were associated with progression or stability.
For survival, however, both baseline and on-treatment CRP levels were associated with OS; baseline serum CRP above the median was associated with shorter OS (HRs, 7.25 for NIVO-IPI and 1.53 for IPI-NIVO), and a similar trend was seen for on-treatment CRP (HRs, 1.60 and 2.0, respectively).
In CheckMate 066, the association between CRP and OS was also apparent, but not as impressive for NIVO alone (HR, 0.996) as it was for dacarbazine (HR, 1.90), and similar to CheckMate 064, higher baseline CRP levels were associated with shorter survival and were prognostic, he said.
In CheckMate 067, similar trends were seen across the treatment arms, and they were similar to those seen for IL-6, with higher baseline CRP levels (at or above median versus below) associated with shorter OS (HRs, 1.46 for NIVO, 1.26 for NIVO+IPI, and 1.48 for IPI alone).
To better understand how CRP might inhibit the effects of PD-1 and how it could have an immune effect – as also indicated by some prior data – Dr. Weber and colleagues conducted additional in vitro studies to examine the impact of exogenous CRP on T-cell function; they found that CRP affected the earliest steps in T-cell signaling and activation, thereby dampening antitumor immune responses.
Acute phase reactants such as CRP and chronic inflammatory proteins including IL-6 (which induces production of CRP from the liver) have been associated with poor prognosis in a variety of cancers, as well as with poor outcomes after anti–PD-1 or programmed death-ligand 1 (PD-L1) therapy in melanoma and other cancers, Dr. Weber said.
“In murine models of melanoma and pancreatic cancer, combined treatment with anti-IL-6 blockade and anti–PD-1/PD-L1 antibodies enhances antitumor immune responses and efficacy,” he explained, noting that the current analyses were undertaken based on those findings and on “a significant body of data” from other groups and from his own lab.
The current findings suggest that IL-6 and CRP may be prognostic for immune checkpoint inhibitor therapies in patients with melanoma, he said, adding that “blockade of IL-6 and CRP synthesis and/or activity in combination with immune checkpoint therapies may enhance responses and survival rates in patients with different cancers, including melanomas.”
To that end, an investigator-sponsored trial looking at IPI-NIVO with the IL-6–blocking antibody tocilizumab has been approved and will start accruing patients in the next few months, he said.
During a discussion of the findings at the meeting, Charles G. Drake, MD, PhD, associate director for clinical research at the Herbert Irving Comprehensive Cancer Center at Columbia University, New York, said that “Dr. Weber and his colleagues should be commended for really trying to show what CRP does to T-cell activation, and in the studies he showed us, it’s clearly negative.”
“But IL-6 is a pleiotropic cytokine. It will be very interesting to see what happens in the prospective clinical trial that he mentioned, in terms of all the other effects on CD-4 cells, neutrophils, and macrophages,” said Dr. Drake, who also is codirector of Columbia’s Cancer Immunotherapy Program. “Nevertheless, I think the data were clear that IL-6 and CRP are negative prognostic biomarkers in melanoma.”
Of note, the development of a biomarker identified in a trial typically takes many steps, but in the case of IL-6 – and perhaps even more so for CRP – the pathway is relatively short, Dr. Drake said.
“That’s because CRP is a validated and [Food and Drug Administration]–approved test; you can order it to assess cardiovascular risk in almost any hospital in the United States, and so the analyte – this part of the qualification – is done,” he explained. “I think if this was validated prospectively we could have CRP as a negative prognostic – not predictive – biomarker in melanoma, actually.”
Dr. Weber and Dr. Drake each reported relationships with numerous companies, including stock and other ownership interests and patents, consulting or advisory roles and/or receipt of honoraria, research funding to their respective institutions, and payment for travel, accommodations, and expenses
SOURCE: Weber J et al. ASCO 2019, Abstract 100.
REPORTING FROM ASCO 2019
Another study supports safety of 2-cm margins for thick melanomas
based on data from a randomized, multicenter trial of 936 patients.
“Over time, and in light of the findings of several randomized studies, less extensive surgery for primary melanoma with tumor thickness greater than 2 mm has become more established,” and most recent guidelines recommend a 2-cm margin for these tumors, wrote Deborah Utjés, MD, of the Karolinska Institute in Stockholm and colleagues.
To reinforce the safety and effectiveness of the 2-cm margin, the researchers conducted an open-label, randomized trial of clinically staged melanoma patients aged 75 years and younger with localized cutaneous melanomas thicker than 2 mm, from January 1992 to May 2004. Patients were treated in Denmark, Estonia, Norway, and Sweden. The findings were published in the Lancet.
Patients were randomized to treatment with a 2-cm (471) or 4-cm excision margin (465). The melanomas were located on the trunk, upper extremities, or lower extremities.
The primary outcome of overall survival was similar between the groups. Over a median 20-year follow-up period, the death rate was approximately 50% in each group (49% in the 2-cm group and 51% in the 4-cm group). Disease-specific survival rates were similar as well. Of the 621 reported deaths, 397 were attributed to melanoma: 192 (48%) in the 2-cm group and 205 (52%) in the 4-cm group.
The study findings were limited by several factors, including a lower-than-expected number of patients, lack of nodal staging during the study period, and a focus only on the surgical margin without recording data on pathological excision margins.
However, the extended follow-up supports the safe use of the 2-cm margin for the treatment of melanomas thicker than 2 mm, the investigators wrote. In addition, results from an ongoing trial comparing 1-cm and 2-cm margins for melanomas at least 1 mm thick may yield more evidence to support still narrower surgical margins for some cutaneous melanomas.
The study notes that guidelines from organizations that include the American National Comprehensive Cancer Network and the American Academy of Dermatology recommend the 2-cm margin for tumors that are thicker than 2 mm.
The study was supported by the Swedish Cancer Society, Stockholm Cancer Society, Swedish Society for Medical Research, and the Stockholm County Council, and by funds from Radiumhemmet Research and Wallström. The authors reported no disclosures.
SOURCE: Utjés D et al. Lancet. 2019 Jul 4. doi: 10.1016/S0140-6736(19)31132-8.
based on data from a randomized, multicenter trial of 936 patients.
“Over time, and in light of the findings of several randomized studies, less extensive surgery for primary melanoma with tumor thickness greater than 2 mm has become more established,” and most recent guidelines recommend a 2-cm margin for these tumors, wrote Deborah Utjés, MD, of the Karolinska Institute in Stockholm and colleagues.
To reinforce the safety and effectiveness of the 2-cm margin, the researchers conducted an open-label, randomized trial of clinically staged melanoma patients aged 75 years and younger with localized cutaneous melanomas thicker than 2 mm, from January 1992 to May 2004. Patients were treated in Denmark, Estonia, Norway, and Sweden. The findings were published in the Lancet.
Patients were randomized to treatment with a 2-cm (471) or 4-cm excision margin (465). The melanomas were located on the trunk, upper extremities, or lower extremities.
The primary outcome of overall survival was similar between the groups. Over a median 20-year follow-up period, the death rate was approximately 50% in each group (49% in the 2-cm group and 51% in the 4-cm group). Disease-specific survival rates were similar as well. Of the 621 reported deaths, 397 were attributed to melanoma: 192 (48%) in the 2-cm group and 205 (52%) in the 4-cm group.
The study findings were limited by several factors, including a lower-than-expected number of patients, lack of nodal staging during the study period, and a focus only on the surgical margin without recording data on pathological excision margins.
However, the extended follow-up supports the safe use of the 2-cm margin for the treatment of melanomas thicker than 2 mm, the investigators wrote. In addition, results from an ongoing trial comparing 1-cm and 2-cm margins for melanomas at least 1 mm thick may yield more evidence to support still narrower surgical margins for some cutaneous melanomas.
The study notes that guidelines from organizations that include the American National Comprehensive Cancer Network and the American Academy of Dermatology recommend the 2-cm margin for tumors that are thicker than 2 mm.
The study was supported by the Swedish Cancer Society, Stockholm Cancer Society, Swedish Society for Medical Research, and the Stockholm County Council, and by funds from Radiumhemmet Research and Wallström. The authors reported no disclosures.
SOURCE: Utjés D et al. Lancet. 2019 Jul 4. doi: 10.1016/S0140-6736(19)31132-8.
based on data from a randomized, multicenter trial of 936 patients.
“Over time, and in light of the findings of several randomized studies, less extensive surgery for primary melanoma with tumor thickness greater than 2 mm has become more established,” and most recent guidelines recommend a 2-cm margin for these tumors, wrote Deborah Utjés, MD, of the Karolinska Institute in Stockholm and colleagues.
To reinforce the safety and effectiveness of the 2-cm margin, the researchers conducted an open-label, randomized trial of clinically staged melanoma patients aged 75 years and younger with localized cutaneous melanomas thicker than 2 mm, from January 1992 to May 2004. Patients were treated in Denmark, Estonia, Norway, and Sweden. The findings were published in the Lancet.
Patients were randomized to treatment with a 2-cm (471) or 4-cm excision margin (465). The melanomas were located on the trunk, upper extremities, or lower extremities.
The primary outcome of overall survival was similar between the groups. Over a median 20-year follow-up period, the death rate was approximately 50% in each group (49% in the 2-cm group and 51% in the 4-cm group). Disease-specific survival rates were similar as well. Of the 621 reported deaths, 397 were attributed to melanoma: 192 (48%) in the 2-cm group and 205 (52%) in the 4-cm group.
The study findings were limited by several factors, including a lower-than-expected number of patients, lack of nodal staging during the study period, and a focus only on the surgical margin without recording data on pathological excision margins.
However, the extended follow-up supports the safe use of the 2-cm margin for the treatment of melanomas thicker than 2 mm, the investigators wrote. In addition, results from an ongoing trial comparing 1-cm and 2-cm margins for melanomas at least 1 mm thick may yield more evidence to support still narrower surgical margins for some cutaneous melanomas.
The study notes that guidelines from organizations that include the American National Comprehensive Cancer Network and the American Academy of Dermatology recommend the 2-cm margin for tumors that are thicker than 2 mm.
The study was supported by the Swedish Cancer Society, Stockholm Cancer Society, Swedish Society for Medical Research, and the Stockholm County Council, and by funds from Radiumhemmet Research and Wallström. The authors reported no disclosures.
SOURCE: Utjés D et al. Lancet. 2019 Jul 4. doi: 10.1016/S0140-6736(19)31132-8.
FROM THE LANCET
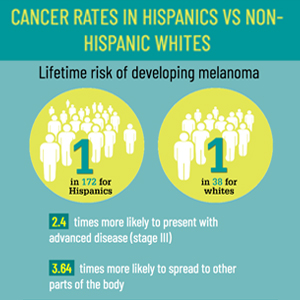
Infographic: Skin Cancer Stats in Hispanic Patients
Novel immune checkpoint holds ‘great promise’ as melanoma treatment target
MILAN – Ponciano D. Cruz Jr., MD, said at the World Congress of Dermatology.

Dr. Cruz, who along with colleagues discovered the immune checkpoint, have generated an anti–DC-HIL monoclonal antibody, which he said dramatically reduces melanoma growth and metastasis in animal models.
That antibody has also been shown to block the T-cell suppressor function of myeloid-derived suppressor cells (MDSCs), according to Dr. Cruz, who is with the department of dermatology at the University of Texas Southwestern Medical Center, Dallas.
“To date, we haven’t subjected our antibodies to clinical trials, but that will happen soon,” he said in an oral presentation at the meeting.
Also referred to as GPNMB, DC-HIL exists as a cell-bound receptor, and as a soluble factor secreted into circulation, according to Dr. Cruz.
In healthy subjects, DC-HIL is expressed in low levels by certain immune cells but is highly expressed by MDSCs in patients with melanoma, as well as other cancers including breast, colorectal, kidney, lung, and prostate cancers, he said. Those MDSCs expand exponentially as malignancies progress, he noted.
Soluble DC-HIL can be detected in the blood of many patients, and at increasing levels with metastasis, he added. DC-HIL–positive MDSC, and soluble DC-HIL, are blood markers that “may prognosticate the course and response to treatment of these cancers,” he said.
The researchers have demonstrated that DC-HIL inhibits T-cell activation by binding to its ligand, syndecan-4, on effector T cells, Dr. Cruz told attendees. “Thus, DC-HIL/syndecan-4 is a coinhibitory pathway akin to immune checkpoints CTLA4 [cytotoxic T-lymphocyte antigen 4] and PD-1 [programmed death-1],” he said.
In DC-HIL knockout mice, melanoma growth is suppressed in comparison to melanoma growth in wild-type mice, Dr. Cruz and colleagues have found in previous experiments. They subsequently found that their anti–DC-HIL monoclonal antibody reduced melanoma growth and metastasis in mice.
The antibody reversed the T-cell suppressor effect of MDSC in patients with metastatic melanoma and other cancers, he said.
Dr. Cruz has reported a disclosure (patents, royalties, other intellectual property) related to the use of anti–DC-HIL antibodies for cancer diagnosis, prognosis, and therapy.
MILAN – Ponciano D. Cruz Jr., MD, said at the World Congress of Dermatology.
Dr. Cruz, who along with colleagues discovered the immune checkpoint, have generated an anti–DC-HIL monoclonal antibody, which he said dramatically reduces melanoma growth and metastasis in animal models.
That antibody has also been shown to block the T-cell suppressor function of myeloid-derived suppressor cells (MDSCs), according to Dr. Cruz, who is with the department of dermatology at the University of Texas Southwestern Medical Center, Dallas.
“To date, we haven’t subjected our antibodies to clinical trials, but that will happen soon,” he said in an oral presentation at the meeting.
Also referred to as GPNMB, DC-HIL exists as a cell-bound receptor, and as a soluble factor secreted into circulation, according to Dr. Cruz.
In healthy subjects, DC-HIL is expressed in low levels by certain immune cells but is highly expressed by MDSCs in patients with melanoma, as well as other cancers including breast, colorectal, kidney, lung, and prostate cancers, he said. Those MDSCs expand exponentially as malignancies progress, he noted.
Soluble DC-HIL can be detected in the blood of many patients, and at increasing levels with metastasis, he added. DC-HIL–positive MDSC, and soluble DC-HIL, are blood markers that “may prognosticate the course and response to treatment of these cancers,” he said.
The researchers have demonstrated that DC-HIL inhibits T-cell activation by binding to its ligand, syndecan-4, on effector T cells, Dr. Cruz told attendees. “Thus, DC-HIL/syndecan-4 is a coinhibitory pathway akin to immune checkpoints CTLA4 [cytotoxic T-lymphocyte antigen 4] and PD-1 [programmed death-1],” he said.
In DC-HIL knockout mice, melanoma growth is suppressed in comparison to melanoma growth in wild-type mice, Dr. Cruz and colleagues have found in previous experiments. They subsequently found that their anti–DC-HIL monoclonal antibody reduced melanoma growth and metastasis in mice.
The antibody reversed the T-cell suppressor effect of MDSC in patients with metastatic melanoma and other cancers, he said.
Dr. Cruz has reported a disclosure (patents, royalties, other intellectual property) related to the use of anti–DC-HIL antibodies for cancer diagnosis, prognosis, and therapy.
MILAN – Ponciano D. Cruz Jr., MD, said at the World Congress of Dermatology.
Dr. Cruz, who along with colleagues discovered the immune checkpoint, have generated an anti–DC-HIL monoclonal antibody, which he said dramatically reduces melanoma growth and metastasis in animal models.
That antibody has also been shown to block the T-cell suppressor function of myeloid-derived suppressor cells (MDSCs), according to Dr. Cruz, who is with the department of dermatology at the University of Texas Southwestern Medical Center, Dallas.
“To date, we haven’t subjected our antibodies to clinical trials, but that will happen soon,” he said in an oral presentation at the meeting.
Also referred to as GPNMB, DC-HIL exists as a cell-bound receptor, and as a soluble factor secreted into circulation, according to Dr. Cruz.
In healthy subjects, DC-HIL is expressed in low levels by certain immune cells but is highly expressed by MDSCs in patients with melanoma, as well as other cancers including breast, colorectal, kidney, lung, and prostate cancers, he said. Those MDSCs expand exponentially as malignancies progress, he noted.
Soluble DC-HIL can be detected in the blood of many patients, and at increasing levels with metastasis, he added. DC-HIL–positive MDSC, and soluble DC-HIL, are blood markers that “may prognosticate the course and response to treatment of these cancers,” he said.
The researchers have demonstrated that DC-HIL inhibits T-cell activation by binding to its ligand, syndecan-4, on effector T cells, Dr. Cruz told attendees. “Thus, DC-HIL/syndecan-4 is a coinhibitory pathway akin to immune checkpoints CTLA4 [cytotoxic T-lymphocyte antigen 4] and PD-1 [programmed death-1],” he said.
In DC-HIL knockout mice, melanoma growth is suppressed in comparison to melanoma growth in wild-type mice, Dr. Cruz and colleagues have found in previous experiments. They subsequently found that their anti–DC-HIL monoclonal antibody reduced melanoma growth and metastasis in mice.
The antibody reversed the T-cell suppressor effect of MDSC in patients with metastatic melanoma and other cancers, he said.
Dr. Cruz has reported a disclosure (patents, royalties, other intellectual property) related to the use of anti–DC-HIL antibodies for cancer diagnosis, prognosis, and therapy.
EXPERT ANALYSIS FROM WCD2019
Sequential dermoscopy imaging helps find melanomas early
WAIKOLOA, HAWAII – Sequential dermoscopy imaging (SDI) is a valuable strategy for diagnosing melanomas early and with better sensitivity and specificity, compared with biopsy decisions based solely on the ugly duckling sign, the ABCDs of melanoma, or other aspects of lesion morphology, Michael A. Marchetti, MD, said at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.

SDI entails obtaining repeated dermoscopy images over time in order to detect subtle changes. It is typically done short term, over the course of 3-4 months, or longer term, over a period of 6 months to years, with long-term SDI being reserved for monitoring of less suspicious lesions, often in patients with an atypical mole syndrome.
SDI improves diagnostic specificity by dramatically reducing excision of benign pigmented lesions: in one large Belgian study, by up to 75% (Br J Dermatol. 2012 Oct;167[4]:778-86).
Short-term SDI also improves diagnostic sensitivity. That’s because it enables early identification of clinically featureless melanomas that are detected solely based upon change over a 3-month follow-up period. The operative principle here is that 93%-96% of melanomas will show change on dermoscopy within 3 months, while 99% of unchanged melanocytic lesions are benign. Since 16% of benign nevi will change within 3 months, that means 10%-30% of changed lesions are melanomas.
“If there is any change – it doesn’t matter what the change is, but the two images look different – that should lead to a biopsy,” explained Dr. Marchetti, a dermatologist at Memorial Sloan Kettering Cancer Center, New York.
As a result of this improved sensitivity and specificity, SDI has been shown to reduce the cost per melanoma diagnosis by about 40% (PLoS One. 2014 Oct 14;9[10]:e109339. doi: 10.1371/journal.pone.0109339).
Dr. Marchetti considers SDI a second-level diagnostic test for individual equivocal lesions. His first-level diagnostic tool is total-body photography.
SDI needs to be done by scrupulous examination of digital photographic images side-by-side on a computer monitor. A basic rule of SDI is that it should never be used to monitor raised or palpable lesions.
“The only thing you can monitor is something that’s flat,” he stressed.
Nor should SDI be used to monitor lesions with a peripheral globular pattern. And very slow-growing melanomas could potentially be missed by short-term SDI, so suspected lentigo maligna should be monitored for a minimum of 12 months, according to Dr. Marchetti.
Not every patient with an equivocal melanocytic lesion is a good candidate for SDI. It’s a monitoring strategy that should be reserved for reliable patients who will come back in 3 months. “If a patient doesn’t come back I take that very seriously. We call or send a letter,” Dr. Marchetti said.
Moreover, even in a patient who is a good candidate for SDI, he always offers the option of biopsy today rather than short-term monitoring.
SDI employed in conjunction with total-body photography is an extremely effective means of monitoring patients at very high risk for melanoma, Dr. Marchetti said. The power of this combination was illustrated in a prospective Australian study of 311 patients with a history of invasive melanoma plus either a high-risk genetic mutation or a strong family history. During a median follow-up of 3.5 years, 75 melanomas were detected, 14 of them at the baseline visit. The median thickness of melanomas detected post baseline was in situ. Thirty-nine percent of melanomas were detected using SDI and 38% via total body photography. Roughly one in five biopsied melanocytic lesions proved to be melanoma. Of note, five of the melanomas were more than 1 mm in Breslow thickness: Three of them were histologically desmoplastic, and the other two had nodular components (JAMA Dermatol. 2014 Aug;150(8):819-27).
For dermatologists who need to brush up on their dermoscopy skills, Dr. Marchetti recommended dermoscopedia as a useful, free resource.
Legal implications of monitoring via photography
“People often get worked up about this, but I’m not aware of a lawsuit alleging missed melanoma using baseline photography as evidence. And patients, in my experience, are universally appreciative of the use of imaging, although admittedly my experience is biased because people generally come to me for imaging,” Dr. Marchetti said.
He makes a point of telling every patient who opts for short-term SDI that, although the lesion has no features of concern now, it’s important to return promptly for reexamination should any changes occur.
Dr. Marchetti reported having no financial conflicts regarding his presentation.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Sequential dermoscopy imaging (SDI) is a valuable strategy for diagnosing melanomas early and with better sensitivity and specificity, compared with biopsy decisions based solely on the ugly duckling sign, the ABCDs of melanoma, or other aspects of lesion morphology, Michael A. Marchetti, MD, said at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
SDI entails obtaining repeated dermoscopy images over time in order to detect subtle changes. It is typically done short term, over the course of 3-4 months, or longer term, over a period of 6 months to years, with long-term SDI being reserved for monitoring of less suspicious lesions, often in patients with an atypical mole syndrome.
SDI improves diagnostic specificity by dramatically reducing excision of benign pigmented lesions: in one large Belgian study, by up to 75% (Br J Dermatol. 2012 Oct;167[4]:778-86).
Short-term SDI also improves diagnostic sensitivity. That’s because it enables early identification of clinically featureless melanomas that are detected solely based upon change over a 3-month follow-up period. The operative principle here is that 93%-96% of melanomas will show change on dermoscopy within 3 months, while 99% of unchanged melanocytic lesions are benign. Since 16% of benign nevi will change within 3 months, that means 10%-30% of changed lesions are melanomas.
“If there is any change – it doesn’t matter what the change is, but the two images look different – that should lead to a biopsy,” explained Dr. Marchetti, a dermatologist at Memorial Sloan Kettering Cancer Center, New York.
As a result of this improved sensitivity and specificity, SDI has been shown to reduce the cost per melanoma diagnosis by about 40% (PLoS One. 2014 Oct 14;9[10]:e109339. doi: 10.1371/journal.pone.0109339).
Dr. Marchetti considers SDI a second-level diagnostic test for individual equivocal lesions. His first-level diagnostic tool is total-body photography.
SDI needs to be done by scrupulous examination of digital photographic images side-by-side on a computer monitor. A basic rule of SDI is that it should never be used to monitor raised or palpable lesions.
“The only thing you can monitor is something that’s flat,” he stressed.
Nor should SDI be used to monitor lesions with a peripheral globular pattern. And very slow-growing melanomas could potentially be missed by short-term SDI, so suspected lentigo maligna should be monitored for a minimum of 12 months, according to Dr. Marchetti.
Not every patient with an equivocal melanocytic lesion is a good candidate for SDI. It’s a monitoring strategy that should be reserved for reliable patients who will come back in 3 months. “If a patient doesn’t come back I take that very seriously. We call or send a letter,” Dr. Marchetti said.
Moreover, even in a patient who is a good candidate for SDI, he always offers the option of biopsy today rather than short-term monitoring.
SDI employed in conjunction with total-body photography is an extremely effective means of monitoring patients at very high risk for melanoma, Dr. Marchetti said. The power of this combination was illustrated in a prospective Australian study of 311 patients with a history of invasive melanoma plus either a high-risk genetic mutation or a strong family history. During a median follow-up of 3.5 years, 75 melanomas were detected, 14 of them at the baseline visit. The median thickness of melanomas detected post baseline was in situ. Thirty-nine percent of melanomas were detected using SDI and 38% via total body photography. Roughly one in five biopsied melanocytic lesions proved to be melanoma. Of note, five of the melanomas were more than 1 mm in Breslow thickness: Three of them were histologically desmoplastic, and the other two had nodular components (JAMA Dermatol. 2014 Aug;150(8):819-27).
For dermatologists who need to brush up on their dermoscopy skills, Dr. Marchetti recommended dermoscopedia as a useful, free resource.
Legal implications of monitoring via photography
“People often get worked up about this, but I’m not aware of a lawsuit alleging missed melanoma using baseline photography as evidence. And patients, in my experience, are universally appreciative of the use of imaging, although admittedly my experience is biased because people generally come to me for imaging,” Dr. Marchetti said.
He makes a point of telling every patient who opts for short-term SDI that, although the lesion has no features of concern now, it’s important to return promptly for reexamination should any changes occur.
Dr. Marchetti reported having no financial conflicts regarding his presentation.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Sequential dermoscopy imaging (SDI) is a valuable strategy for diagnosing melanomas early and with better sensitivity and specificity, compared with biopsy decisions based solely on the ugly duckling sign, the ABCDs of melanoma, or other aspects of lesion morphology, Michael A. Marchetti, MD, said at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
SDI entails obtaining repeated dermoscopy images over time in order to detect subtle changes. It is typically done short term, over the course of 3-4 months, or longer term, over a period of 6 months to years, with long-term SDI being reserved for monitoring of less suspicious lesions, often in patients with an atypical mole syndrome.
SDI improves diagnostic specificity by dramatically reducing excision of benign pigmented lesions: in one large Belgian study, by up to 75% (Br J Dermatol. 2012 Oct;167[4]:778-86).
Short-term SDI also improves diagnostic sensitivity. That’s because it enables early identification of clinically featureless melanomas that are detected solely based upon change over a 3-month follow-up period. The operative principle here is that 93%-96% of melanomas will show change on dermoscopy within 3 months, while 99% of unchanged melanocytic lesions are benign. Since 16% of benign nevi will change within 3 months, that means 10%-30% of changed lesions are melanomas.
“If there is any change – it doesn’t matter what the change is, but the two images look different – that should lead to a biopsy,” explained Dr. Marchetti, a dermatologist at Memorial Sloan Kettering Cancer Center, New York.
As a result of this improved sensitivity and specificity, SDI has been shown to reduce the cost per melanoma diagnosis by about 40% (PLoS One. 2014 Oct 14;9[10]:e109339. doi: 10.1371/journal.pone.0109339).
Dr. Marchetti considers SDI a second-level diagnostic test for individual equivocal lesions. His first-level diagnostic tool is total-body photography.
SDI needs to be done by scrupulous examination of digital photographic images side-by-side on a computer monitor. A basic rule of SDI is that it should never be used to monitor raised or palpable lesions.
“The only thing you can monitor is something that’s flat,” he stressed.
Nor should SDI be used to monitor lesions with a peripheral globular pattern. And very slow-growing melanomas could potentially be missed by short-term SDI, so suspected lentigo maligna should be monitored for a minimum of 12 months, according to Dr. Marchetti.
Not every patient with an equivocal melanocytic lesion is a good candidate for SDI. It’s a monitoring strategy that should be reserved for reliable patients who will come back in 3 months. “If a patient doesn’t come back I take that very seriously. We call or send a letter,” Dr. Marchetti said.
Moreover, even in a patient who is a good candidate for SDI, he always offers the option of biopsy today rather than short-term monitoring.
SDI employed in conjunction with total-body photography is an extremely effective means of monitoring patients at very high risk for melanoma, Dr. Marchetti said. The power of this combination was illustrated in a prospective Australian study of 311 patients with a history of invasive melanoma plus either a high-risk genetic mutation or a strong family history. During a median follow-up of 3.5 years, 75 melanomas were detected, 14 of them at the baseline visit. The median thickness of melanomas detected post baseline was in situ. Thirty-nine percent of melanomas were detected using SDI and 38% via total body photography. Roughly one in five biopsied melanocytic lesions proved to be melanoma. Of note, five of the melanomas were more than 1 mm in Breslow thickness: Three of them were histologically desmoplastic, and the other two had nodular components (JAMA Dermatol. 2014 Aug;150(8):819-27).
For dermatologists who need to brush up on their dermoscopy skills, Dr. Marchetti recommended dermoscopedia as a useful, free resource.
Legal implications of monitoring via photography
“People often get worked up about this, but I’m not aware of a lawsuit alleging missed melanoma using baseline photography as evidence. And patients, in my experience, are universally appreciative of the use of imaging, although admittedly my experience is biased because people generally come to me for imaging,” Dr. Marchetti said.
He makes a point of telling every patient who opts for short-term SDI that, although the lesion has no features of concern now, it’s important to return promptly for reexamination should any changes occur.
Dr. Marchetti reported having no financial conflicts regarding his presentation.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
REPORTING FROM SDEF HAWAII DERMATOLOGY SEMINAR
Phototherapy: Is It Still Important?
Phototherapy has been used to treat skin diseases for millennia. From the Incas to the ancient Greeks and Egyptians, nearly every major civilization has attempted to harness the sun, with some even worshipping it for its healing powers.1 Today, phototherapy remains as important as ever. Despite the technological advances that have brought about biologic medications, small molecule inhibitors, and elegant vehicle delivery systems, phototherapy continues to be a valuable tool in the dermatologist’s armamentarium.
Patient Access to Phototherapy
An important step in successfully managing any disease is access to treatment. In today’s health care landscape, therapeutic decisions frequently are dictated by a patient’s financial situation as well as by the discretion of payers. Costly medications such as biologics often are not accessible to patients on government insurance who fall into the Medicare “donut hole” and may be denied by insurance companies for a myriad of reasons. Luckily, phototherapy typically is well covered and is even a first-line treatment option for some conditions, such as mycosis fungoides.
Nevertheless, phototherapy also has its own unique accessibility hurdles. The time-consuming nature of office-based phototherapy treatment is the main barrier, and many patients find it difficult to incorporate treatments into their daily lives. Additionally, office-based phototherapy units often are clustered in major cities, making access more difficult for rural patients. Because light-responsive conditions often are chronic and may require a lifetime of treatment, home phototherapy units are now being recognized as cost-effective treatment options and are increasingly covered by insurance. In fact, one study comparing psoriasis patients treated with home narrowband UVB (NB-UVB) vs outpatient NB-UVB found that in-home treatment was equally as effective as office-based treatment at a similar cost.2 Because studies comparing the effectiveness of office-based vs home-based phototherapy treatment are underway for various other diseases, hopefully more patients will be able to receive home units, thus increasing access to safe and effective treatment.
Wide Range of Treatment Indications
Another merit of phototherapy is its ability to be used in almost all patient populations. It is one of the few modalities whose indications span the entire length of the human lifetime—from pediatric atopic dermatitis to chronic pruritus in elderly patients. Phototherapy also is one of the few treatment options that is safe to use in patients with an active malignancy or in patients who have multiple other medical conditions. Comorbidities including congestive heart failure, chronic infections, and demyelinating disorders often prevent the use of oral and injectable medications for immune-mediated disorders such as psoriasis or atopic dermatitis. In patients with multiple comorbidities whose disease remains uncontrolled despite an adequate topical regimen, phototherapy is one of the few effective treatment options that remain. Additionally, there is a considerable number of patients who prefer external treatments for cutaneous diseases. For these patients, phototherapy offers the opportunity to control skin conditions without the use of an internal medication.
Favorable Safety Profile
Phototherapy is a largely benign intervention with an excellent safety profile. Its main potential adverse events include erythema, pruritus, xerosis, recurrence of herpes simplex virus infection, and premature skin aging. The effects of phototherapy on skin carcinogenesis have long been controversial; however, data suggest a clear distinction in risk between treatment with NB-UVB and psoralen plus UVA (PUVA). A systematic review of psoriasis patients treated with phototherapy found no evidence to suggest an increased risk of melanoma or nonmelanoma skin cancer with NB-UVB treatment.3 The same cannot be said for psoriasis patients treated with PUVA, who were noted to have a higher incidence of nonmelanoma skin cancer than the general population. This increased risk was more substantial in American cohorts than in European cohorts, likely due to multiple factors including variable skin types and treatment regimens. Increased rates of melanoma also were noted in American PUVA cohorts, with no similar increase seen in their European counterparts.3
Broad vs Targeted Therapies
Targeted therapies have dominated the health care landscape over the last few years, with the majority of new medications being highly focused and only efficacious in a few conditions. One of phototherapy’s greatest strengths is its lack of specificity. Because the field of dermatology is filled with rare, overlapping, and often poorly understood diseases, nonspecific treatment options are needed to fill the gaps. Many generalized skin conditions may lack treatment options indicated by the US Food and Drug Administration. Phototherapy is the ultimate untargeted intervention and may be broadly used for a wide range of cutaneous conditions. Although classically utilized for atopic dermatitis and psoriasis, NB-UVB also can effectively treat generalized pruritus, vitiligo, urticaria, and seborrheic dermatitis.4 Not to be outdone, PUVA has shown success in treating more than 50 different dermatologic conditions including lichen planus, alopecia areata, and mycosis fungoides.
Final Thoughts
Phototherapy is a safe, accessible, and widely applicable treatment for a range of cutaneous disorders. Although more precisely engineered internal therapies have begun to replace UV light in psoriasis and atopic dermatitis, phototherapy likely will always remain an ideal treatment for a wide cohort of patients. Between increased access to home units and the continued validation of its excellent safety record, the future of phototherapy is looking bright.
- Grzybowski A, Sak J, Pawlikowski J. A brief report on the history of phototherapy. Clin Dermatol. 2016;34:532-537.
- Koek MB, Sigurdsson V, van Weelden H, et al. Cost effectiveness of home ultraviolet B phototherapy for psoriasis: economic evaluation of a randomised controlled trial (PLUTO study). BMJ. 2010;340:c1490.
- Archier E, Devaux S, Castela E, et al. Carcinogenic risks of psoralen UV-A therapy and narrowband UV-B therapy in chronic plaque psoriasis: a systematic literature review. J Eur Acad Dermatol Venereol. 2012;26(suppl 3):22-31.
- Gambichler T, Breuckmann F, Boms S, et al. Narrowband UVB phototherapy in skin conditions beyond psoriasis. J Am Acad Dermatol. 2005;52:660-670.
- Ledo E, Ledo A. Phototherapy, photochemotherapy, and photodynamic therapy: unapproved uses or indications. Clin Dermatol. 2000;18:77-86.
Phototherapy has been used to treat skin diseases for millennia. From the Incas to the ancient Greeks and Egyptians, nearly every major civilization has attempted to harness the sun, with some even worshipping it for its healing powers.1 Today, phototherapy remains as important as ever. Despite the technological advances that have brought about biologic medications, small molecule inhibitors, and elegant vehicle delivery systems, phototherapy continues to be a valuable tool in the dermatologist’s armamentarium.
Patient Access to Phototherapy
An important step in successfully managing any disease is access to treatment. In today’s health care landscape, therapeutic decisions frequently are dictated by a patient’s financial situation as well as by the discretion of payers. Costly medications such as biologics often are not accessible to patients on government insurance who fall into the Medicare “donut hole” and may be denied by insurance companies for a myriad of reasons. Luckily, phototherapy typically is well covered and is even a first-line treatment option for some conditions, such as mycosis fungoides.
Nevertheless, phototherapy also has its own unique accessibility hurdles. The time-consuming nature of office-based phototherapy treatment is the main barrier, and many patients find it difficult to incorporate treatments into their daily lives. Additionally, office-based phototherapy units often are clustered in major cities, making access more difficult for rural patients. Because light-responsive conditions often are chronic and may require a lifetime of treatment, home phototherapy units are now being recognized as cost-effective treatment options and are increasingly covered by insurance. In fact, one study comparing psoriasis patients treated with home narrowband UVB (NB-UVB) vs outpatient NB-UVB found that in-home treatment was equally as effective as office-based treatment at a similar cost.2 Because studies comparing the effectiveness of office-based vs home-based phototherapy treatment are underway for various other diseases, hopefully more patients will be able to receive home units, thus increasing access to safe and effective treatment.
Wide Range of Treatment Indications
Another merit of phototherapy is its ability to be used in almost all patient populations. It is one of the few modalities whose indications span the entire length of the human lifetime—from pediatric atopic dermatitis to chronic pruritus in elderly patients. Phototherapy also is one of the few treatment options that is safe to use in patients with an active malignancy or in patients who have multiple other medical conditions. Comorbidities including congestive heart failure, chronic infections, and demyelinating disorders often prevent the use of oral and injectable medications for immune-mediated disorders such as psoriasis or atopic dermatitis. In patients with multiple comorbidities whose disease remains uncontrolled despite an adequate topical regimen, phototherapy is one of the few effective treatment options that remain. Additionally, there is a considerable number of patients who prefer external treatments for cutaneous diseases. For these patients, phototherapy offers the opportunity to control skin conditions without the use of an internal medication.
Favorable Safety Profile
Phototherapy is a largely benign intervention with an excellent safety profile. Its main potential adverse events include erythema, pruritus, xerosis, recurrence of herpes simplex virus infection, and premature skin aging. The effects of phototherapy on skin carcinogenesis have long been controversial; however, data suggest a clear distinction in risk between treatment with NB-UVB and psoralen plus UVA (PUVA). A systematic review of psoriasis patients treated with phototherapy found no evidence to suggest an increased risk of melanoma or nonmelanoma skin cancer with NB-UVB treatment.3 The same cannot be said for psoriasis patients treated with PUVA, who were noted to have a higher incidence of nonmelanoma skin cancer than the general population. This increased risk was more substantial in American cohorts than in European cohorts, likely due to multiple factors including variable skin types and treatment regimens. Increased rates of melanoma also were noted in American PUVA cohorts, with no similar increase seen in their European counterparts.3
Broad vs Targeted Therapies
Targeted therapies have dominated the health care landscape over the last few years, with the majority of new medications being highly focused and only efficacious in a few conditions. One of phototherapy’s greatest strengths is its lack of specificity. Because the field of dermatology is filled with rare, overlapping, and often poorly understood diseases, nonspecific treatment options are needed to fill the gaps. Many generalized skin conditions may lack treatment options indicated by the US Food and Drug Administration. Phototherapy is the ultimate untargeted intervention and may be broadly used for a wide range of cutaneous conditions. Although classically utilized for atopic dermatitis and psoriasis, NB-UVB also can effectively treat generalized pruritus, vitiligo, urticaria, and seborrheic dermatitis.4 Not to be outdone, PUVA has shown success in treating more than 50 different dermatologic conditions including lichen planus, alopecia areata, and mycosis fungoides.
Final Thoughts
Phototherapy is a safe, accessible, and widely applicable treatment for a range of cutaneous disorders. Although more precisely engineered internal therapies have begun to replace UV light in psoriasis and atopic dermatitis, phototherapy likely will always remain an ideal treatment for a wide cohort of patients. Between increased access to home units and the continued validation of its excellent safety record, the future of phototherapy is looking bright.
Phototherapy has been used to treat skin diseases for millennia. From the Incas to the ancient Greeks and Egyptians, nearly every major civilization has attempted to harness the sun, with some even worshipping it for its healing powers.1 Today, phototherapy remains as important as ever. Despite the technological advances that have brought about biologic medications, small molecule inhibitors, and elegant vehicle delivery systems, phototherapy continues to be a valuable tool in the dermatologist’s armamentarium.
Patient Access to Phototherapy
An important step in successfully managing any disease is access to treatment. In today’s health care landscape, therapeutic decisions frequently are dictated by a patient’s financial situation as well as by the discretion of payers. Costly medications such as biologics often are not accessible to patients on government insurance who fall into the Medicare “donut hole” and may be denied by insurance companies for a myriad of reasons. Luckily, phototherapy typically is well covered and is even a first-line treatment option for some conditions, such as mycosis fungoides.
Nevertheless, phototherapy also has its own unique accessibility hurdles. The time-consuming nature of office-based phototherapy treatment is the main barrier, and many patients find it difficult to incorporate treatments into their daily lives. Additionally, office-based phototherapy units often are clustered in major cities, making access more difficult for rural patients. Because light-responsive conditions often are chronic and may require a lifetime of treatment, home phototherapy units are now being recognized as cost-effective treatment options and are increasingly covered by insurance. In fact, one study comparing psoriasis patients treated with home narrowband UVB (NB-UVB) vs outpatient NB-UVB found that in-home treatment was equally as effective as office-based treatment at a similar cost.2 Because studies comparing the effectiveness of office-based vs home-based phototherapy treatment are underway for various other diseases, hopefully more patients will be able to receive home units, thus increasing access to safe and effective treatment.
Wide Range of Treatment Indications
Another merit of phototherapy is its ability to be used in almost all patient populations. It is one of the few modalities whose indications span the entire length of the human lifetime—from pediatric atopic dermatitis to chronic pruritus in elderly patients. Phototherapy also is one of the few treatment options that is safe to use in patients with an active malignancy or in patients who have multiple other medical conditions. Comorbidities including congestive heart failure, chronic infections, and demyelinating disorders often prevent the use of oral and injectable medications for immune-mediated disorders such as psoriasis or atopic dermatitis. In patients with multiple comorbidities whose disease remains uncontrolled despite an adequate topical regimen, phototherapy is one of the few effective treatment options that remain. Additionally, there is a considerable number of patients who prefer external treatments for cutaneous diseases. For these patients, phototherapy offers the opportunity to control skin conditions without the use of an internal medication.
Favorable Safety Profile
Phototherapy is a largely benign intervention with an excellent safety profile. Its main potential adverse events include erythema, pruritus, xerosis, recurrence of herpes simplex virus infection, and premature skin aging. The effects of phototherapy on skin carcinogenesis have long been controversial; however, data suggest a clear distinction in risk between treatment with NB-UVB and psoralen plus UVA (PUVA). A systematic review of psoriasis patients treated with phototherapy found no evidence to suggest an increased risk of melanoma or nonmelanoma skin cancer with NB-UVB treatment.3 The same cannot be said for psoriasis patients treated with PUVA, who were noted to have a higher incidence of nonmelanoma skin cancer than the general population. This increased risk was more substantial in American cohorts than in European cohorts, likely due to multiple factors including variable skin types and treatment regimens. Increased rates of melanoma also were noted in American PUVA cohorts, with no similar increase seen in their European counterparts.3
Broad vs Targeted Therapies
Targeted therapies have dominated the health care landscape over the last few years, with the majority of new medications being highly focused and only efficacious in a few conditions. One of phototherapy’s greatest strengths is its lack of specificity. Because the field of dermatology is filled with rare, overlapping, and often poorly understood diseases, nonspecific treatment options are needed to fill the gaps. Many generalized skin conditions may lack treatment options indicated by the US Food and Drug Administration. Phototherapy is the ultimate untargeted intervention and may be broadly used for a wide range of cutaneous conditions. Although classically utilized for atopic dermatitis and psoriasis, NB-UVB also can effectively treat generalized pruritus, vitiligo, urticaria, and seborrheic dermatitis.4 Not to be outdone, PUVA has shown success in treating more than 50 different dermatologic conditions including lichen planus, alopecia areata, and mycosis fungoides.
Final Thoughts
Phototherapy is a safe, accessible, and widely applicable treatment for a range of cutaneous disorders. Although more precisely engineered internal therapies have begun to replace UV light in psoriasis and atopic dermatitis, phototherapy likely will always remain an ideal treatment for a wide cohort of patients. Between increased access to home units and the continued validation of its excellent safety record, the future of phototherapy is looking bright.
- Grzybowski A, Sak J, Pawlikowski J. A brief report on the history of phototherapy. Clin Dermatol. 2016;34:532-537.
- Koek MB, Sigurdsson V, van Weelden H, et al. Cost effectiveness of home ultraviolet B phototherapy for psoriasis: economic evaluation of a randomised controlled trial (PLUTO study). BMJ. 2010;340:c1490.
- Archier E, Devaux S, Castela E, et al. Carcinogenic risks of psoralen UV-A therapy and narrowband UV-B therapy in chronic plaque psoriasis: a systematic literature review. J Eur Acad Dermatol Venereol. 2012;26(suppl 3):22-31.
- Gambichler T, Breuckmann F, Boms S, et al. Narrowband UVB phototherapy in skin conditions beyond psoriasis. J Am Acad Dermatol. 2005;52:660-670.
- Ledo E, Ledo A. Phototherapy, photochemotherapy, and photodynamic therapy: unapproved uses or indications. Clin Dermatol. 2000;18:77-86.
- Grzybowski A, Sak J, Pawlikowski J. A brief report on the history of phototherapy. Clin Dermatol. 2016;34:532-537.
- Koek MB, Sigurdsson V, van Weelden H, et al. Cost effectiveness of home ultraviolet B phototherapy for psoriasis: economic evaluation of a randomised controlled trial (PLUTO study). BMJ. 2010;340:c1490.
- Archier E, Devaux S, Castela E, et al. Carcinogenic risks of psoralen UV-A therapy and narrowband UV-B therapy in chronic plaque psoriasis: a systematic literature review. J Eur Acad Dermatol Venereol. 2012;26(suppl 3):22-31.
- Gambichler T, Breuckmann F, Boms S, et al. Narrowband UVB phototherapy in skin conditions beyond psoriasis. J Am Acad Dermatol. 2005;52:660-670.
- Ledo E, Ledo A. Phototherapy, photochemotherapy, and photodynamic therapy: unapproved uses or indications. Clin Dermatol. 2000;18:77-86.

Five rules for evaluating melanonychia
WAIKOLOA, HAWAII – Many dermatologists find melanonychia to be intimidating. The clinical features are ambiguous, and the prospect of doing a painful nail apparatus biopsy can be daunting for the inexperienced. As a result, the biopsy gets delayed and melanoma of the nail is often initially a missed diagnosis, not uncommonly for years, with devastating consequences.

Here are five at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Rule #1: Always look beyond the nail
When a light-skinned person presents with more than one nail with pigmentation, the likelihood that one of them is melanoma is much less than if there is only one nail with melanonychia, according to Dr. Jellinek, a dermatologist in private practice in East Greenwich, R.I.
Also, be sure to look at the skin and mucosa. Consider the medications the patients may be taking: For example, cyclophosphamide (Cytoxan) is notorious for causing nail changes as a side effect. A past medical history of lichen planus, carpal tunnel syndrome, Addison disease, or other conditions may explain the melanonychia.

Laugier-Hunziker syndrome is a condition worth getting to know. It’s an acquired disorder characterized longitudinal melanonychia and other pigmentary changes, which may include diffuse hyperpigmentation of the orolabial mucosa, ocular pigment, and/or pigmented palmoplantar lesions. It’s said to be rare, but Dr. Jellinek disagrees.
“Learn this one if you don’t know it. I see a case about every 2 weeks. It’s not heritable and not associated with any other medical condition,” he said.
Rule #2: Your dermatoscope is great for nails
What Dr. Jellinek considers to be among the all-time best papers on the value of dermoscopy for nail pigmentation was authored by French investigators. They analyzed 148 consecutive cases of longitudinal melanonychia and concluded that the dermoscopic combination of a brown background coupled with irregular longitudinal lines in terms of color, spacing, diameter, and/or lack of parallelism strongly suggests melanoma. A micro-Hutchinson’s sign, while a rare finding, occurred only in melanoma, where it represented periungual spread of a radial growth phase malignancy (Arch Dermatol. 2002 Oct;138[10]:1327-33).
“I think nail dermoscopy is most helpful for subungual hemorrhage. I average one referral per week for hemorrhage under the nail. On dermoscopy it’s as if someone took paint and threw it at the nail. Purple to brown blood spots, with no background color. This should be a doorway diagnosis of hemorrhage,” Dr. Jellinek said.
Rule #3: Know when you don’t know
“This is really the key for me,” the dermatologist commented. “There are automatic cases for biopsy, and more commonly routine cases for reassurance. But the gray zone, when you know you don’t know, is the key decision making moment.”
When something just doesn’t feel right, there’s absolutely nothing wrong with getting a second opinion, he stressed.
“It’s worthwhile getting to know people whose opinions you trust. There’s a saying I like to teach our fellows: ‘Never worry alone.’ So if you’re worried about someone, listen to that inner voice. There’s no shame in getting a second opinion. It’s great! Patients are never upset, either. They feel really well taken care of,” he said.
Rule #4: Don’t wimp out when a biopsy is warranted
Many dermatologists hem and haw about doing a biopsy for a concerning lesion on the nail, when they wouldn’t hesitate to biopsy a similarly suspicious lesion on the face.
But it’s essential to biopsy the right area, he added. For longitudinal melanonychia, that’s the matrix. The nail plate is the wrong place; a biopsy obtained there will result in an inappropriate benign diagnosis.

“The starter set is to do a punch biopsy. This is your gateway drug to the world of nail surgery. Lots of dermatologists are intimidated by nail surgery, but if you can do any minor surgery, you can do a punch of the matrix. All it takes is a little practice. And if all you can do is punch biopsies, you’re good for your career. If you can do that, you’re golden. There are people who’ve just done punch biopsies for their whole career and they don’t miss melanomas,” he said.
Step one is to undermine the proximal nail fold using a pediatric elevator, which costs only about $30. “If you’re going to do a lot of nail surgery, they’re really helpful,” he said.
There’s no need at all to evulse the nail. Just make oblique incisions in the proximal nail fold in order to reflect it and look at the matrix. A 3-mm punch is standard, directed right over the origin of the pigment. Resist the temptation to force or squeeze the specimen in order to extract it. Instead, use really fine-tipped scissors to nibble at the base of the specimen, then gently pull it out, making an effort to keep the nail plate attached to the digit and avoid getting it stuck up in the punch.
Rule #5: Have dermatopathologists extensively experienced with nail pathology on your Rolodex
The histopathologic findings present in early subungual melanoma in situ are often too subtle for general dermatopathologists to appreciate, in Dr. Jellinek’s experience. He cited other investigators’ study of 18 cases of subungual melanoma in situ, all marked by longitudinal melanonychia. Only half showed the classic giveaway on the original nail matrix biopsy, consisting of a significantly increased number of atypical melanocytes with marked nuclear atypia. Blatant pagetoid spread was infrequent. However, all 18 cases displayed a novel, more subtle, and previously undescribed finding: haphazard and uneven distribution of atypical solitary melanocytes with variably sized and shaped hyperchromatic nuclei (J Cutan Pathol. 2016 Jan;43[1]:41-52).
Dr. Jellinek reported having no financial conflicts regarding his presentation. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Many dermatologists find melanonychia to be intimidating. The clinical features are ambiguous, and the prospect of doing a painful nail apparatus biopsy can be daunting for the inexperienced. As a result, the biopsy gets delayed and melanoma of the nail is often initially a missed diagnosis, not uncommonly for years, with devastating consequences.
Here are five at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Rule #1: Always look beyond the nail
When a light-skinned person presents with more than one nail with pigmentation, the likelihood that one of them is melanoma is much less than if there is only one nail with melanonychia, according to Dr. Jellinek, a dermatologist in private practice in East Greenwich, R.I.
Also, be sure to look at the skin and mucosa. Consider the medications the patients may be taking: For example, cyclophosphamide (Cytoxan) is notorious for causing nail changes as a side effect. A past medical history of lichen planus, carpal tunnel syndrome, Addison disease, or other conditions may explain the melanonychia.
Laugier-Hunziker syndrome is a condition worth getting to know. It’s an acquired disorder characterized longitudinal melanonychia and other pigmentary changes, which may include diffuse hyperpigmentation of the orolabial mucosa, ocular pigment, and/or pigmented palmoplantar lesions. It’s said to be rare, but Dr. Jellinek disagrees.
“Learn this one if you don’t know it. I see a case about every 2 weeks. It’s not heritable and not associated with any other medical condition,” he said.
Rule #2: Your dermatoscope is great for nails
What Dr. Jellinek considers to be among the all-time best papers on the value of dermoscopy for nail pigmentation was authored by French investigators. They analyzed 148 consecutive cases of longitudinal melanonychia and concluded that the dermoscopic combination of a brown background coupled with irregular longitudinal lines in terms of color, spacing, diameter, and/or lack of parallelism strongly suggests melanoma. A micro-Hutchinson’s sign, while a rare finding, occurred only in melanoma, where it represented periungual spread of a radial growth phase malignancy (Arch Dermatol. 2002 Oct;138[10]:1327-33).
“I think nail dermoscopy is most helpful for subungual hemorrhage. I average one referral per week for hemorrhage under the nail. On dermoscopy it’s as if someone took paint and threw it at the nail. Purple to brown blood spots, with no background color. This should be a doorway diagnosis of hemorrhage,” Dr. Jellinek said.
Rule #3: Know when you don’t know
“This is really the key for me,” the dermatologist commented. “There are automatic cases for biopsy, and more commonly routine cases for reassurance. But the gray zone, when you know you don’t know, is the key decision making moment.”
When something just doesn’t feel right, there’s absolutely nothing wrong with getting a second opinion, he stressed.
“It’s worthwhile getting to know people whose opinions you trust. There’s a saying I like to teach our fellows: ‘Never worry alone.’ So if you’re worried about someone, listen to that inner voice. There’s no shame in getting a second opinion. It’s great! Patients are never upset, either. They feel really well taken care of,” he said.
Rule #4: Don’t wimp out when a biopsy is warranted
Many dermatologists hem and haw about doing a biopsy for a concerning lesion on the nail, when they wouldn’t hesitate to biopsy a similarly suspicious lesion on the face.
But it’s essential to biopsy the right area, he added. For longitudinal melanonychia, that’s the matrix. The nail plate is the wrong place; a biopsy obtained there will result in an inappropriate benign diagnosis.
“The starter set is to do a punch biopsy. This is your gateway drug to the world of nail surgery. Lots of dermatologists are intimidated by nail surgery, but if you can do any minor surgery, you can do a punch of the matrix. All it takes is a little practice. And if all you can do is punch biopsies, you’re good for your career. If you can do that, you’re golden. There are people who’ve just done punch biopsies for their whole career and they don’t miss melanomas,” he said.
Step one is to undermine the proximal nail fold using a pediatric elevator, which costs only about $30. “If you’re going to do a lot of nail surgery, they’re really helpful,” he said.
There’s no need at all to evulse the nail. Just make oblique incisions in the proximal nail fold in order to reflect it and look at the matrix. A 3-mm punch is standard, directed right over the origin of the pigment. Resist the temptation to force or squeeze the specimen in order to extract it. Instead, use really fine-tipped scissors to nibble at the base of the specimen, then gently pull it out, making an effort to keep the nail plate attached to the digit and avoid getting it stuck up in the punch.
Rule #5: Have dermatopathologists extensively experienced with nail pathology on your Rolodex
The histopathologic findings present in early subungual melanoma in situ are often too subtle for general dermatopathologists to appreciate, in Dr. Jellinek’s experience. He cited other investigators’ study of 18 cases of subungual melanoma in situ, all marked by longitudinal melanonychia. Only half showed the classic giveaway on the original nail matrix biopsy, consisting of a significantly increased number of atypical melanocytes with marked nuclear atypia. Blatant pagetoid spread was infrequent. However, all 18 cases displayed a novel, more subtle, and previously undescribed finding: haphazard and uneven distribution of atypical solitary melanocytes with variably sized and shaped hyperchromatic nuclei (J Cutan Pathol. 2016 Jan;43[1]:41-52).
Dr. Jellinek reported having no financial conflicts regarding his presentation. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Many dermatologists find melanonychia to be intimidating. The clinical features are ambiguous, and the prospect of doing a painful nail apparatus biopsy can be daunting for the inexperienced. As a result, the biopsy gets delayed and melanoma of the nail is often initially a missed diagnosis, not uncommonly for years, with devastating consequences.
Here are five at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Rule #1: Always look beyond the nail
When a light-skinned person presents with more than one nail with pigmentation, the likelihood that one of them is melanoma is much less than if there is only one nail with melanonychia, according to Dr. Jellinek, a dermatologist in private practice in East Greenwich, R.I.
Also, be sure to look at the skin and mucosa. Consider the medications the patients may be taking: For example, cyclophosphamide (Cytoxan) is notorious for causing nail changes as a side effect. A past medical history of lichen planus, carpal tunnel syndrome, Addison disease, or other conditions may explain the melanonychia.
Laugier-Hunziker syndrome is a condition worth getting to know. It’s an acquired disorder characterized longitudinal melanonychia and other pigmentary changes, which may include diffuse hyperpigmentation of the orolabial mucosa, ocular pigment, and/or pigmented palmoplantar lesions. It’s said to be rare, but Dr. Jellinek disagrees.
“Learn this one if you don’t know it. I see a case about every 2 weeks. It’s not heritable and not associated with any other medical condition,” he said.
Rule #2: Your dermatoscope is great for nails
What Dr. Jellinek considers to be among the all-time best papers on the value of dermoscopy for nail pigmentation was authored by French investigators. They analyzed 148 consecutive cases of longitudinal melanonychia and concluded that the dermoscopic combination of a brown background coupled with irregular longitudinal lines in terms of color, spacing, diameter, and/or lack of parallelism strongly suggests melanoma. A micro-Hutchinson’s sign, while a rare finding, occurred only in melanoma, where it represented periungual spread of a radial growth phase malignancy (Arch Dermatol. 2002 Oct;138[10]:1327-33).
“I think nail dermoscopy is most helpful for subungual hemorrhage. I average one referral per week for hemorrhage under the nail. On dermoscopy it’s as if someone took paint and threw it at the nail. Purple to brown blood spots, with no background color. This should be a doorway diagnosis of hemorrhage,” Dr. Jellinek said.
Rule #3: Know when you don’t know
“This is really the key for me,” the dermatologist commented. “There are automatic cases for biopsy, and more commonly routine cases for reassurance. But the gray zone, when you know you don’t know, is the key decision making moment.”
When something just doesn’t feel right, there’s absolutely nothing wrong with getting a second opinion, he stressed.
“It’s worthwhile getting to know people whose opinions you trust. There’s a saying I like to teach our fellows: ‘Never worry alone.’ So if you’re worried about someone, listen to that inner voice. There’s no shame in getting a second opinion. It’s great! Patients are never upset, either. They feel really well taken care of,” he said.
Rule #4: Don’t wimp out when a biopsy is warranted
Many dermatologists hem and haw about doing a biopsy for a concerning lesion on the nail, when they wouldn’t hesitate to biopsy a similarly suspicious lesion on the face.
But it’s essential to biopsy the right area, he added. For longitudinal melanonychia, that’s the matrix. The nail plate is the wrong place; a biopsy obtained there will result in an inappropriate benign diagnosis.
“The starter set is to do a punch biopsy. This is your gateway drug to the world of nail surgery. Lots of dermatologists are intimidated by nail surgery, but if you can do any minor surgery, you can do a punch of the matrix. All it takes is a little practice. And if all you can do is punch biopsies, you’re good for your career. If you can do that, you’re golden. There are people who’ve just done punch biopsies for their whole career and they don’t miss melanomas,” he said.
Step one is to undermine the proximal nail fold using a pediatric elevator, which costs only about $30. “If you’re going to do a lot of nail surgery, they’re really helpful,” he said.
There’s no need at all to evulse the nail. Just make oblique incisions in the proximal nail fold in order to reflect it and look at the matrix. A 3-mm punch is standard, directed right over the origin of the pigment. Resist the temptation to force or squeeze the specimen in order to extract it. Instead, use really fine-tipped scissors to nibble at the base of the specimen, then gently pull it out, making an effort to keep the nail plate attached to the digit and avoid getting it stuck up in the punch.
Rule #5: Have dermatopathologists extensively experienced with nail pathology on your Rolodex
The histopathologic findings present in early subungual melanoma in situ are often too subtle for general dermatopathologists to appreciate, in Dr. Jellinek’s experience. He cited other investigators’ study of 18 cases of subungual melanoma in situ, all marked by longitudinal melanonychia. Only half showed the classic giveaway on the original nail matrix biopsy, consisting of a significantly increased number of atypical melanocytes with marked nuclear atypia. Blatant pagetoid spread was infrequent. However, all 18 cases displayed a novel, more subtle, and previously undescribed finding: haphazard and uneven distribution of atypical solitary melanocytes with variably sized and shaped hyperchromatic nuclei (J Cutan Pathol. 2016 Jan;43[1]:41-52).
Dr. Jellinek reported having no financial conflicts regarding his presentation. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Entrectinib exhibits activity in children with solid tumors
Entrectinib demonstrated “very promising” antitumor activity in children and adolescents with recurrent or refractory solid tumors, according to an investigator involved in a phase 1/1b trial.
Twelve of 29 patients enrolled in the trial have responded to entrectinib. All responders had fusions in genes targeted by the drug – NTRK1/2/3 (TRKA/B/C), ROS1, or ALK – or an ALK mutation.
Details of this study are scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Giles W. Robinson, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn., discussed the study during a press briefing in advance of the meeting.
“Entrectinib is an oral and potent inhibitor of the TRKA/B/C, ROS1, and ALK proteins, but it also penetrates into the brain to reach tumors in the brain and spine, which can be a hard area to get drugs to,” Dr. Robinson explained.
“Promising clinical activity was initially seen in the adult solid tumor patients with target rearrangements, and it was encouraging to see these patients also had responses when the tumors were located in their brains. And what got us really excited as pediatric oncologists was that a variety of pediatric cancers harbor these fusions and mutations within certain tumors.”
With this in mind, Dr. Robinson and colleagues conducted a phase 1/1b study (NCT02650401) of entrectinib in 29 patients with recurrent or refractory solid tumors, including central nervous system (CNS) tumors.
The patients’ median age was 7 years (range, 0-20 years), and roughly half of them were male (n = 15). Patients were diagnosed with neuroblastoma (n = 16), high-grade glioma (n = 5), inflammatory myofibroblastic tumors (n = 3), infantile fibrosarcoma (n = 2), CNS embryonal tumor (n = 1), melanoma (n = 1), and synovial sarcoma (n = 1).
In the dose-finding portion of the trial, patients received entrectinib at 250 mg/m2 (n = 3), 400 mg/m2 (n = 3), 550 mg/m2 (n = 7), or 750 mg/m2 (n = 3).
In the phase 1b portion, patients received entrectinib at 550 mg/m2 (n = 7) – the recommended dose – or 400 mg/m2 (n = 6) if they were unable to swallow intact capsules.
Dr. Robinson said entrectinib was “quite well tolerated” overall, but he did not present any data on adverse events. He did say dose-limiting toxicities included fatigue, elevated creatinine levels, dysgeusia resulting in loss of taste, weight gain, and, in one patient, pulmonary edema.
“Entrectinib produced striking, rapid, and durable responses in all children with refractory CNS and solid tumors that actually harbored these fusions in NTRK1/2/3, ROS1, or ALK,” Dr. Robinson said. “It also produced a significant response in one ALK-mutated neuroblastoma patient. [N]o responses were seen in tumors lacking aberrations in the target kinases.”
In all, 12 patients responded. The three complete responders had an ALK F1174L mutation, an ALK fusion, and an NTRK fusion, respectively. Five partial responders had NTRK fusions, three had ROS1 fusions, and one had an ALK fusion.
Three responders discontinued treatment. Ten patients were still receiving entrectinib at last follow-up, and 11 patients had died.
Progression-free survival was significantly longer among patients who had fusions than among those who did not (P less than .0001).
“To sum up, entrectinib really is very promising,” Dr. Robinson said. “It has very promising antitumor activity and progression-free survival but [only] in patients with target gene fusions.”
Dr. Robinson said this trial is ongoing, but it is now limited to patients with fusions targeted by entrectinib.
The trial is sponsored by Hoffman-La Roche Ltd. and supported by Alex’s Lemonade Stand Center of Excellence. Dr. Robinson has relationships with Lilly, Genentech/Roche, and Novartis.
SOURCE: Robinson GW et al. ASCO 2019. Abstract 10009.
Entrectinib demonstrated “very promising” antitumor activity in children and adolescents with recurrent or refractory solid tumors, according to an investigator involved in a phase 1/1b trial.
Twelve of 29 patients enrolled in the trial have responded to entrectinib. All responders had fusions in genes targeted by the drug – NTRK1/2/3 (TRKA/B/C), ROS1, or ALK – or an ALK mutation.
Details of this study are scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Giles W. Robinson, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn., discussed the study during a press briefing in advance of the meeting.
“Entrectinib is an oral and potent inhibitor of the TRKA/B/C, ROS1, and ALK proteins, but it also penetrates into the brain to reach tumors in the brain and spine, which can be a hard area to get drugs to,” Dr. Robinson explained.
“Promising clinical activity was initially seen in the adult solid tumor patients with target rearrangements, and it was encouraging to see these patients also had responses when the tumors were located in their brains. And what got us really excited as pediatric oncologists was that a variety of pediatric cancers harbor these fusions and mutations within certain tumors.”
With this in mind, Dr. Robinson and colleagues conducted a phase 1/1b study (NCT02650401) of entrectinib in 29 patients with recurrent or refractory solid tumors, including central nervous system (CNS) tumors.
The patients’ median age was 7 years (range, 0-20 years), and roughly half of them were male (n = 15). Patients were diagnosed with neuroblastoma (n = 16), high-grade glioma (n = 5), inflammatory myofibroblastic tumors (n = 3), infantile fibrosarcoma (n = 2), CNS embryonal tumor (n = 1), melanoma (n = 1), and synovial sarcoma (n = 1).
In the dose-finding portion of the trial, patients received entrectinib at 250 mg/m2 (n = 3), 400 mg/m2 (n = 3), 550 mg/m2 (n = 7), or 750 mg/m2 (n = 3).
In the phase 1b portion, patients received entrectinib at 550 mg/m2 (n = 7) – the recommended dose – or 400 mg/m2 (n = 6) if they were unable to swallow intact capsules.
Dr. Robinson said entrectinib was “quite well tolerated” overall, but he did not present any data on adverse events. He did say dose-limiting toxicities included fatigue, elevated creatinine levels, dysgeusia resulting in loss of taste, weight gain, and, in one patient, pulmonary edema.
“Entrectinib produced striking, rapid, and durable responses in all children with refractory CNS and solid tumors that actually harbored these fusions in NTRK1/2/3, ROS1, or ALK,” Dr. Robinson said. “It also produced a significant response in one ALK-mutated neuroblastoma patient. [N]o responses were seen in tumors lacking aberrations in the target kinases.”
In all, 12 patients responded. The three complete responders had an ALK F1174L mutation, an ALK fusion, and an NTRK fusion, respectively. Five partial responders had NTRK fusions, three had ROS1 fusions, and one had an ALK fusion.
Three responders discontinued treatment. Ten patients were still receiving entrectinib at last follow-up, and 11 patients had died.
Progression-free survival was significantly longer among patients who had fusions than among those who did not (P less than .0001).
“To sum up, entrectinib really is very promising,” Dr. Robinson said. “It has very promising antitumor activity and progression-free survival but [only] in patients with target gene fusions.”
Dr. Robinson said this trial is ongoing, but it is now limited to patients with fusions targeted by entrectinib.
The trial is sponsored by Hoffman-La Roche Ltd. and supported by Alex’s Lemonade Stand Center of Excellence. Dr. Robinson has relationships with Lilly, Genentech/Roche, and Novartis.
SOURCE: Robinson GW et al. ASCO 2019. Abstract 10009.
Entrectinib demonstrated “very promising” antitumor activity in children and adolescents with recurrent or refractory solid tumors, according to an investigator involved in a phase 1/1b trial.
Twelve of 29 patients enrolled in the trial have responded to entrectinib. All responders had fusions in genes targeted by the drug – NTRK1/2/3 (TRKA/B/C), ROS1, or ALK – or an ALK mutation.
Details of this study are scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Giles W. Robinson, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn., discussed the study during a press briefing in advance of the meeting.
“Entrectinib is an oral and potent inhibitor of the TRKA/B/C, ROS1, and ALK proteins, but it also penetrates into the brain to reach tumors in the brain and spine, which can be a hard area to get drugs to,” Dr. Robinson explained.
“Promising clinical activity was initially seen in the adult solid tumor patients with target rearrangements, and it was encouraging to see these patients also had responses when the tumors were located in their brains. And what got us really excited as pediatric oncologists was that a variety of pediatric cancers harbor these fusions and mutations within certain tumors.”
With this in mind, Dr. Robinson and colleagues conducted a phase 1/1b study (NCT02650401) of entrectinib in 29 patients with recurrent or refractory solid tumors, including central nervous system (CNS) tumors.
The patients’ median age was 7 years (range, 0-20 years), and roughly half of them were male (n = 15). Patients were diagnosed with neuroblastoma (n = 16), high-grade glioma (n = 5), inflammatory myofibroblastic tumors (n = 3), infantile fibrosarcoma (n = 2), CNS embryonal tumor (n = 1), melanoma (n = 1), and synovial sarcoma (n = 1).
In the dose-finding portion of the trial, patients received entrectinib at 250 mg/m2 (n = 3), 400 mg/m2 (n = 3), 550 mg/m2 (n = 7), or 750 mg/m2 (n = 3).
In the phase 1b portion, patients received entrectinib at 550 mg/m2 (n = 7) – the recommended dose – or 400 mg/m2 (n = 6) if they were unable to swallow intact capsules.
Dr. Robinson said entrectinib was “quite well tolerated” overall, but he did not present any data on adverse events. He did say dose-limiting toxicities included fatigue, elevated creatinine levels, dysgeusia resulting in loss of taste, weight gain, and, in one patient, pulmonary edema.
“Entrectinib produced striking, rapid, and durable responses in all children with refractory CNS and solid tumors that actually harbored these fusions in NTRK1/2/3, ROS1, or ALK,” Dr. Robinson said. “It also produced a significant response in one ALK-mutated neuroblastoma patient. [N]o responses were seen in tumors lacking aberrations in the target kinases.”
In all, 12 patients responded. The three complete responders had an ALK F1174L mutation, an ALK fusion, and an NTRK fusion, respectively. Five partial responders had NTRK fusions, three had ROS1 fusions, and one had an ALK fusion.
Three responders discontinued treatment. Ten patients were still receiving entrectinib at last follow-up, and 11 patients had died.
Progression-free survival was significantly longer among patients who had fusions than among those who did not (P less than .0001).
“To sum up, entrectinib really is very promising,” Dr. Robinson said. “It has very promising antitumor activity and progression-free survival but [only] in patients with target gene fusions.”
Dr. Robinson said this trial is ongoing, but it is now limited to patients with fusions targeted by entrectinib.
The trial is sponsored by Hoffman-La Roche Ltd. and supported by Alex’s Lemonade Stand Center of Excellence. Dr. Robinson has relationships with Lilly, Genentech/Roche, and Novartis.
SOURCE: Robinson GW et al. ASCO 2019. Abstract 10009.
REPORTING FROM ASCO 2019