User login
Cancer Data Trends 2025
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.

In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments

Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
The US Department of Veterans Affairs (VA) annually treats around 450,000 veterans with cancer and diagnoses an additional 56,000.1,2 Oral multikinase inhibitors (MKIs) are widely used as targeted therapies for many different malignancies. Despite the ease of oral administration, these agents are often accompanied by significant adverse effects (AEs) and drug-drug interactions.3,4 Common AEs include hypertension, cutaneous reactions, gastrointestinal disturbances, proteinuria, and fatigue. Some serious outcomes that may occur are myocardial infarction, thrombosis, nephrotic syndrome, hemorrhage, hepatotoxicity, and gastrointestinal events.5,6 Due to poor tolerability of these AEs, dose reductions, frequent therapy holds, and discontinuation of therapy may occur.
The US Food and Drug Administration recognizes dosing challenges with novel therapies and has created the Oncology Center of Excellence (OCE) Project Optimus initiative to reform dose optimization in oncology drug development. The initiative aims to shift the focus from establishing dose regimens based on the maximum tolerated doses of cytotoxic chemotherapeutics to an emphasis on maximum efficacy, safety, and tolerability, which better reflect real-world dosing.7,8
MKIs can be challenging to manage because of the frequent toxicity-related dose reductions, interruptions, and discontinuations. In a multicenter retrospective study, Schnadig et al investigated dosing characteristics of first-line sunitinib for advanced renal cell carcinoma (RCC) and found that, among 114 patients who experienced AEs while taking sunitinib, 39.5% had dose reductions, 5.3% delayed therapy, 18.4% required additional supportive medications, and 22.8% discontinued sunitinib.9 Overall survival and median progression-free survival of these patients were lower than reported by Motzer et al in a phase 3 clinical trial.10 Schnadig et al concluded that patients treated with sunitinib for RCC in the community setting required more frequent dose reductions and had less time on therapy compared with patients in clinical trials, which ultimately impacted clinical outcomes.9
At the VA North Texas Health Care System (VANTHCS), patients with cancer have difficulty tolerating MKIs and often require dose alterations and/or discontinuation because of drug intolerance rather than discontinuation due to progression. Frequent dose adjustments for toxicity management can place more strain on patients and health care resources because of additional appointments, clinician time, and emergency department visits. Escalating drug costs can also cause concern when prescription doses are unused or changed frequently.
To capture and quantify prescribing practices and dose adjustments, this study evaluated the tolerability of MKIs at VANTHCS. This analysis may also guide clinicians in the selection of starting doses as well as dose titration expectations to optimize MKI therapy.
METHODS
This single-center, retrospective chart review analyzed patients receiving oral oncology MKIs for various malignancies at VANTHCS between January 1, 2014, and October 31, 2024. Participants included adults aged ≥ 18 years with a prescription for axitinib, cabozantinib, lenvatinib, pazopanib, regorafenib, sorafenib, or sunitinib initiated by the hematology/oncology service at VANTHCS. Patients were included if they had follow-up documentation with the hematology/oncology service and/or other VANTHCS clinicians outlining their course of therapy after MKI initiation. Patients were excluded if they did not have sufficient follow-up documentation (eg, transferred care to a non-VA health care practitioner [HCP], moved to another VA health care system), were enrolled in clinical trials, or were prescribed an MKI from a Care in the Community (CITC) prescriber. Electronic health record review and data collection were performed using the VA Computerized Patient Record System and Research Electronic Data Capture. Data were collected from the time of initiation to cessation of therapy and included information regarding therapy changes, progressive disease, and date of death, when available. Data collected included age, sex, race, comorbidities, date of death, type of malignancy and subtypes, cancer stage, MKI used (ie, drug, dose, frequency, schedule, and indication), dates of medication changes (ie, start, adjustment, hold, discontinuation), concurrent antineoplastic treatments, and AEs documented at times of dose change or interruption.
The primary outcome was MKI tolerance determined using relative dose intensity (RDI) and mean and median time on therapy. Two methods are used to calculate RDI that vary in how they approach time on therapy as outlined in Hawn et al.11 This study used method 2, which accounts for holds in therapy by comparing the actual duration of treatment with the duration expected according to treatment protocol. Method 1 compares the prescribed dose with the administered dose and does not adjust for holds.11 Using method 2, the RDI in this study was calculated by dividing the total actual dose given by the total indicated dose for the malignancy being treated, which accounts for duration of treatment.

The total actual dose was the strength, frequency, and days on therapy for each time frame of treatment multiplied together. This method accounted for all dose adjustments and time periods of treatment holds, including patient self-adjustments, prescriber-directed adjustments, and nonadherence determined by HCP documentation and/or prescription data. Similarly, the indicated total dose was calculated by multiplying the indicated strength, frequency, and all days that treatment should have occurred (time from start to finish). Indicated doses were derived from the prescribing information for each malignancy with the exception of sunitinib, for which the off-label dose of 37.5 mg daily was considered a full dose.12,13 The total indicated dose for axitinib was calculated by considering the dose escalation schedule from the prescribing information.
Patients who required dose reductions due to renal/hepatic impairments or drug-drug interactions had their total indicated dose calculated using dose adjustments listed in the prescribing information. The mean RDI for each MKI agent was calculated by averaging the RDI for each prescription. The overall combined mean RDI included the means of all the MKIs reviewed to avoid skewing the results toward an MKI with more prescriptions. RDIs were also calculated for each cancer type for each agent. Additional descriptive secondary outcomes included rates of AEs and adjustments in doses.
RESULTS
Electronic data extraction identified 278 patients with 366 MKI prescriptions, of which 108 veterans with 158 MKI prescriptions were excluded. The top reason for exclusion was patients managed through CITC. Ultimately, 170 veterans with 208 MKI prescriptions managed by the VANTHCS hematology/oncology clinic were included (Table 1). Among patients receiving MKIs, the mean age was 72.7 years, 98% were male, and 99% had metastatic disease.
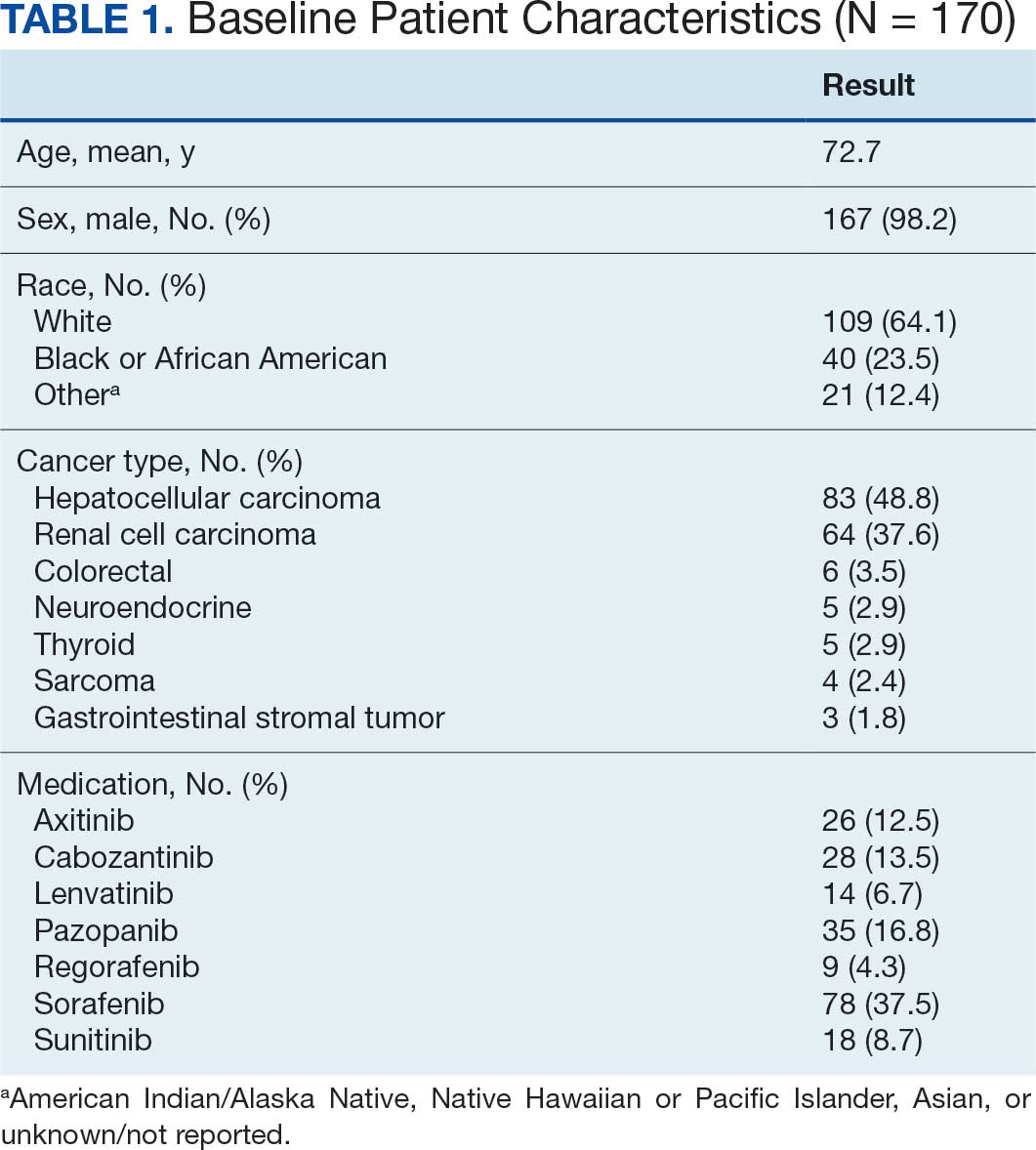
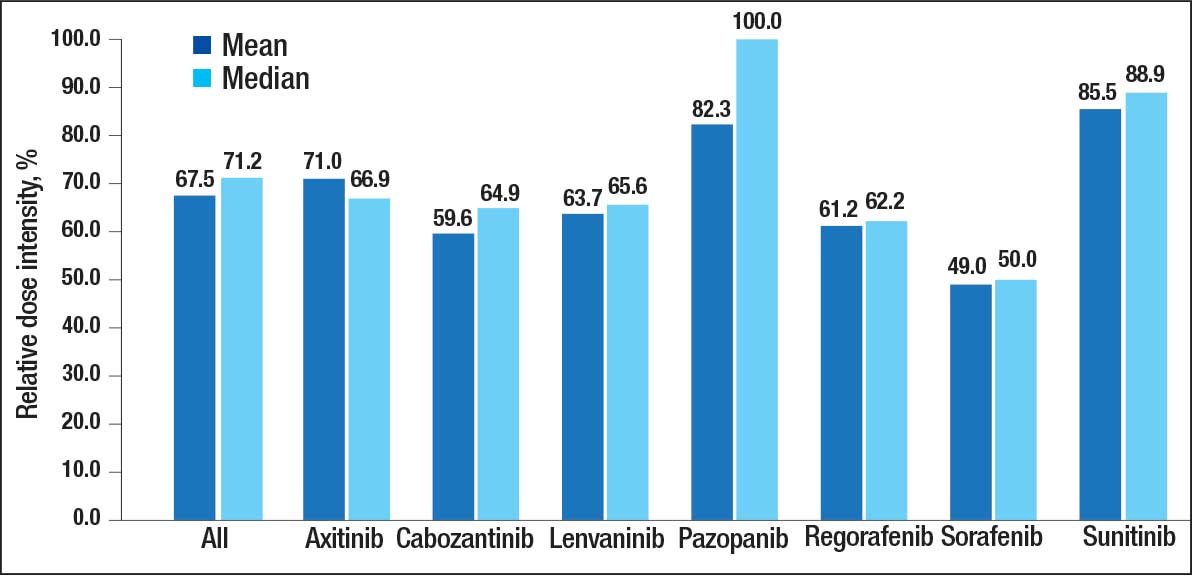
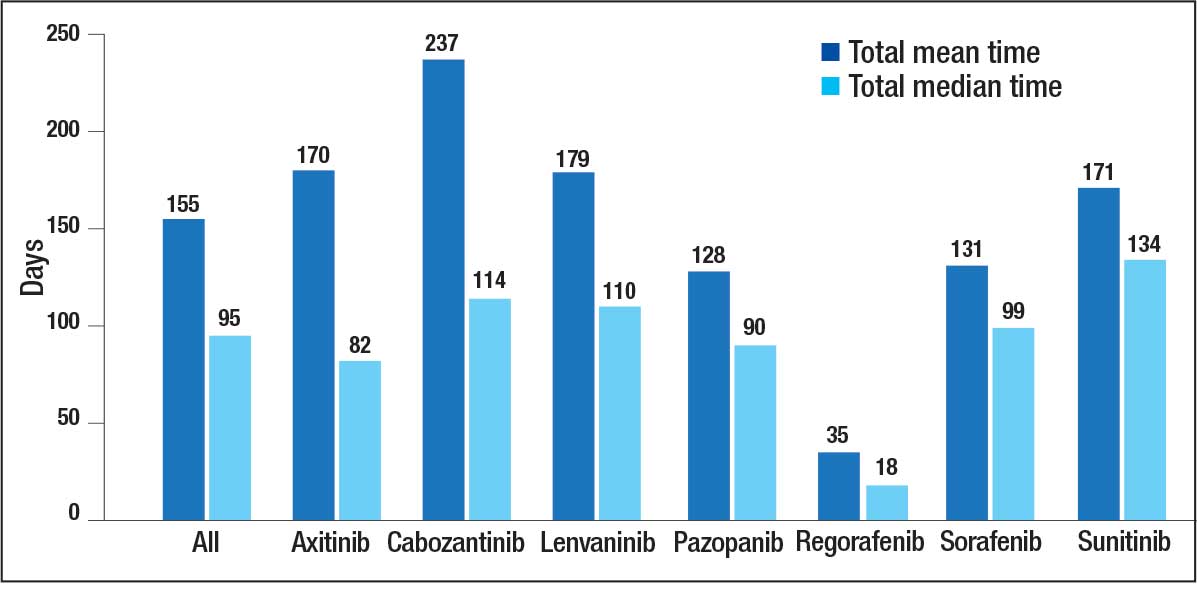
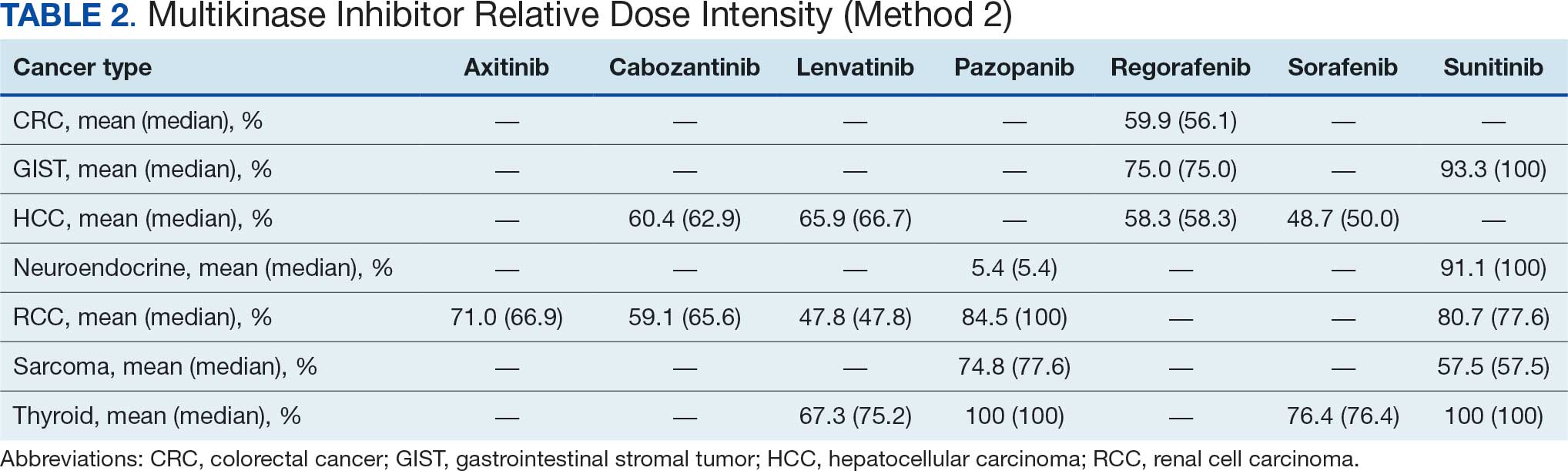
The overall combined mean MKI RDI was 67.5% using method 2 and ranged from 85.5% for sunitinib to 49.0% for sorafenib (Figure 1). Additional information regarding mean and median RDIs using method 2 is shown in Figure 1 and further subdivided by cancer type in Table 2. Median RDIs overall were similar to mean RDIs for most agents. Figure 2 indicates the mean and median time on therapy, reflecting time on therapy excluding days therapy was held. The overall combined mean and median days on therapy for all MKIs were 155 days and 95 days, respectively. Mean time on therapy depended on the agent used and ranged from 35 days (regorafenib) to 237 days (cabozantinib).
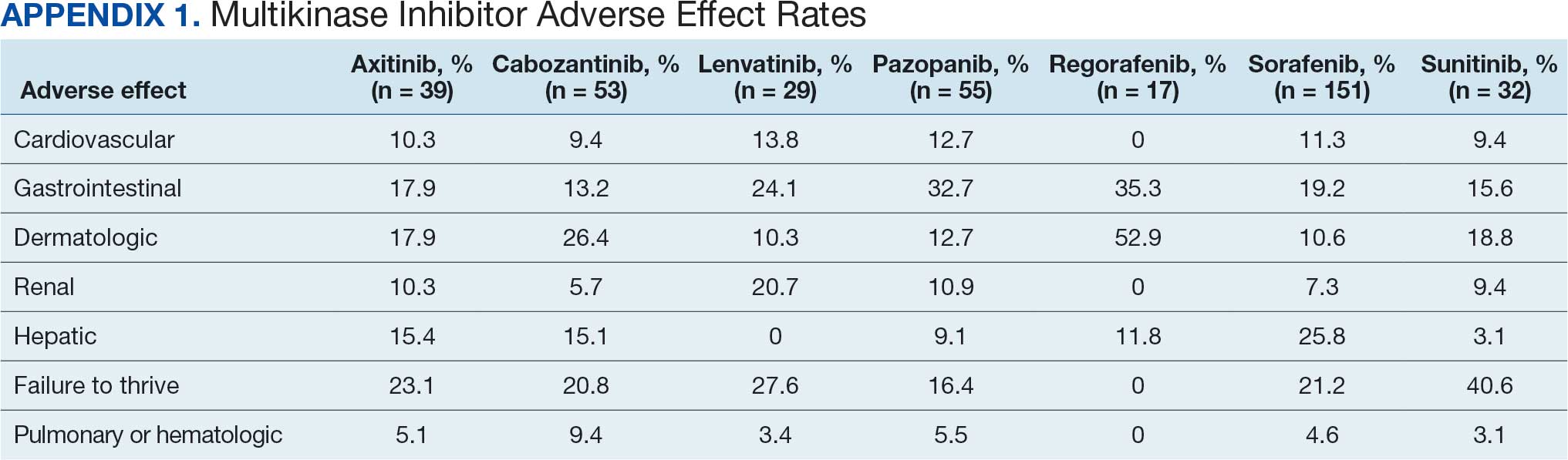
Of 208 MKI prescriptions, 127 (61.1%) were initiated at a reduced dose due to baseline concerns for tolerance such as performance status, frailty, and prior intolerance of other treatments. Eighty-one prescriptions (38.9%) were initiated at their indicated doses. Ninety prescriptions (43.3%) required dose reductions during treatment. Some MKI prescriptions had multiple dose increases and decreases, which is why RDI more accurately reflects dose adjustments. A total of 376 AEs that contributed to a dose adjustment, hold, or discontinuation occurred across all MKI prescriptions. The most common AEs were 82 failure-to-thrive events (21.8%) (fatigue, malaise, loss of appetite, reduced mobility, global decline), 79 gastrointestinal events (21.0%) (nausea, vomiting, diarrhea, abdominal pain), 62 dermatologic events (16.5%) (rash, hand-foot skin reactions, allergic response), 61 hepatic dysfunction events (16.2%) (liver enzyme elevations, hyperbilirubinemia), 40 cardiovascular events (10.6%) (hypertension, heart failure exacerbations, edema), and 33 renal dysfunction events (8.8%) (acute kidney injury, proteinuria) (Appendix 1).
DISCUSSION
The mean RDI of MKI prescriptions used in the veteran population at VANTHCS was about two-thirds of the indicated dose. These results indicate that most veterans required dose reductions and/or holds due to concerns over initial tolerance/performance status, worsening clinical condition, and/or intolerable AEs attributed to treatment. A retrospective study conducted by Denduluri et al suggested that an RDI of < 85% is a clinically meaningful reduction for traditional chemotherapy based on previous literature.14 However, it is less clear what RDI should be expected specifically for MKIs in real-world populations. The MKI phase 3 approval trials in RCC for axitinib, lenvatinib, and sunitinib found median RDIs of 89.4%, 69.6% to 70.4%, and 83.9%, respectively. Each trial cited dose reductions most commonly as the result of treatment-related AEs.15,16
Studies on the impact of RDIs on survival outcomes found that higher RDIs may improve overall and progression-free survival. Retrospective studies inspecting lenvatinib in hepatocellular carcinoma (HCC) indicated that an RDI > 70% in the initial 4 weeks resulted in favorable survival outcomes.17 Similarly, a retrospective study investigating sunitinib in RCC found that an RDI > 60% conferred favorable survival outcomes.18 Alghamdi et al noted that patients taking sorafenib for HCC who had RDI > 50% had a favorable trend in survival characteristics. Interestingly, the study found an RDI of 50% to 75% appeared to have better survival than an RDI > 75%.19 The authors of these studies hypothesized that additional dose reductions allowed for longer total time on therapy due to improved tolerability.17-19
This analysis found that the RDIs for most MKI agents at VANTHCS were < 85% and lower than the RDIs found in other review articles and phase 3 trials, with the exceptions of pazopanib in thyroid cancer and sunitinib in gastrointestinal stromal tumor (GIST), thyroid cancer, and neuroendocrine cancer. The reasons for the lower RDIs in this study are likely multifactorial, reflecting patient population characteristics, off-label dosing practices, and HCP experiences with these agents. Many veterans have chronic comorbidities that could contribute to reduced performance status and ability to tolerate these therapies. Despite attempts to preemptively reduce doses for patients and account for potential impaired tolerance, there were patients who required further dose reductions in our study.
Failure to thrive was the most common AE leading to dose adjustment or discontinuation, which illustrates the extensive effects these agents have on patient functioning in a real-world population. Notably though, the RDI for sunitinib was higher in this population because about half of patients were dosed using the off-label recommendation, whereas the prescribing information recommends a more intensive 6-week dosing cycle for certain cancer types.12,13,20 Sorafenib was also often dose-adjusted based on a pharmacokinetic study of sorafenib in renal/hepatic dysfunction, and the RDI likely reflects the off-label prescribing pattern.21
Patients with thyroid cancer were found to have higher RDIs compared with those receiving the same agents for other cancer types. Improved tolerability of MKIs in thyroid cancer may be due to a generally more tolerable disease course. Thyroid cancer is the most common cancer in individuals aged < 40 years, a population that is often more robust with fewer comorbidities. Moreover, the 5-year relative survival rate for thyroid cancer remains > 98%.22 This rate is in contrast to those for other cancer types such as HCC, with a 5-year relative survival rate of only 15%.23
It is challenging to compare the mean and median times on therapy found in this study with those in current literature, as this review included multiple different cancer types for each agent. However, the numbers are generally lower than durations of therapy found across the different disease states and further emphasize the difficulty in tolerating MKIs in the VANTHCS population. Regorafenib had a short duration of time on therapy, which highlights the importance of trials like ReDOS and initiatives such as OCE Project Optimus in helping improve tolerance.7,8,24
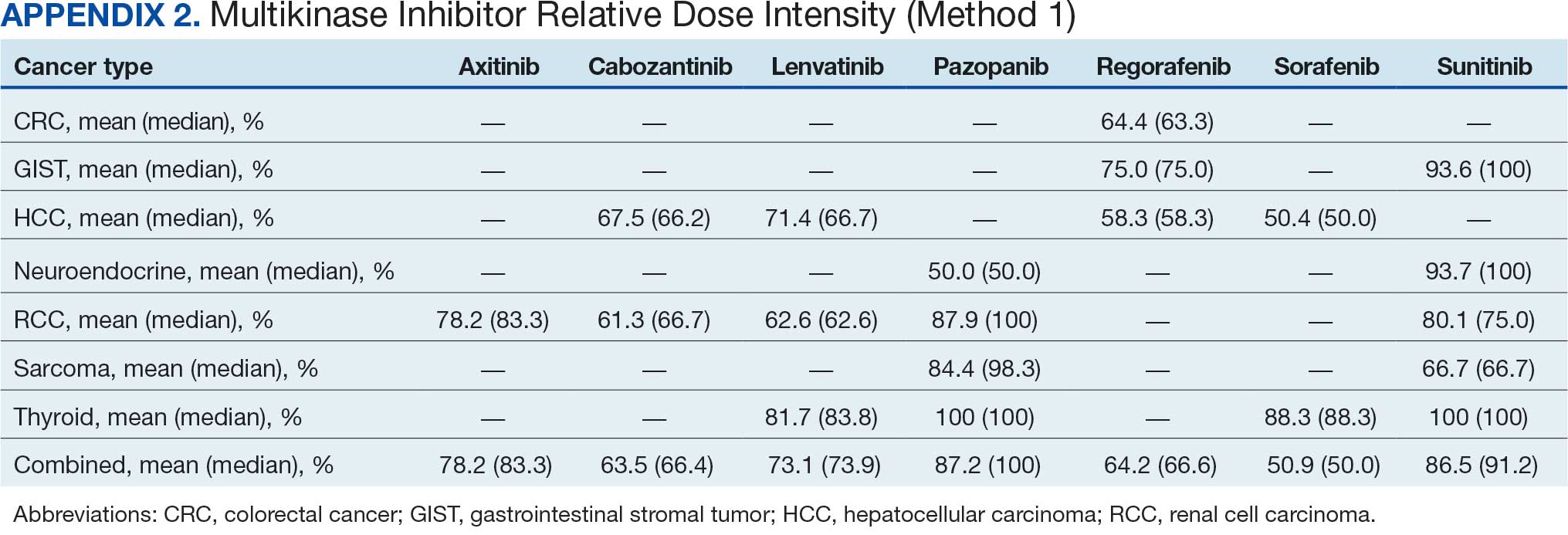
Comparing our results with other studies proved challenging because the RDI calculation methods were not specified. Calculating RDIs in this study using method 1, which does not account for holds, resulted in higher RDIs (Appendix 2). Using method 1, all MKIs had RDIs < 85%, except for pazopanib in thyroid cancer (100%) and RCC (87.9%), and sunitinib in GIST (93.6%), thyroid cancer (100%), and neuroendocrine cancer (93.7%). Notably, using method 1 increased the RDI for pazopanib in neuroendocrine cancer from 5.4% to 50.0%. The low RDI was attributed to a single veteran with a long hold duration, which demonstrates the discrepancy that can occur between the 2 methods.
Limitations
The retrospective design, lack of survival outcomes, and difficulty comparing results with other literature were limitations of this study. Because survival outcomes were not evaluated, future research should seek to investigate how RDIs and dose adjustments made among MKIs can affect survival outcomes in real-world populations. This veteran population with cancer often had multiple chronic comorbidities, which may have contributed to difficulty tolerating MKIs and could have impacted results. Disease-related factors may have influenced the poor tolerance of the MKIs and were not specifically accounted for. Adjustment for comorbidities was not possible because of discrepancies and/or incomplete diagnosis codes and Eastern Cooperative Oncology Group performance status scores documented in patient charts. Therefore, we decided not to report these findings due to potential inaccuracies.
CONCLUSIONS
Results of this study demonstrate that oncology MKI agents used at VANTHCS were difficult for patients to tolerate, leading to suboptimal dosing compared with indicated doses established in clinical trials and prescribing information. Clinicians may use these data to help guide clinical decision-making whenever initiating and managing MKI agents in this population. These findings reinforce that MKI agents are often difficult to tolerate in real-world practice, and indicated doses are often not achieved. Further studies should aim to investigate the effect that various RDIs have on overall survival. Further investigation into different dosing schemes for MKIs to improve tolerability and longer-term use may also prove beneficial.
This analysis may help guide clinicians to carefully approach dosing MKI agents in the veteran population. Given the RDI and AEs, more clinicians may consider starting at lower than indicated doses with the goal to titrate up as tolerated. Additionally, the results highlight the importance of considering palliative care consults and ensuring appropriate supportive care agents are preemptively engaged and adjusted as needed. Approaching dosing and titrations cautiously may help reduce the burden of management on the health care system.
- Frequently asked questions. VA National Oncology Program. 2025. Accessed December 15, 2025. https://www.cancer.va.gov/CANCER/faqs.html
- Torez L. Reigniting the cancer moonshot to beat cancer. VA News. April 20, 2023. Accessed April 6, 2026. https://news.va.gov/118378/reigniting-the-cancer-moonshot-to-beat-cancer
- Shah NN, Casella E, Capozzi D, et al. Improving the safety of oral chemotherapy at an academic medical center. J Oncol Pract. 2016;12:e71-e76. doi:10.1200/JOP.2015.007260
- Hussaarts KGAM, Veerman GDM, Jansman FGA, et al. Clinically relevant drug interactions with multikinase inhibitors: a review. Ther Adv Med Oncol. 2019;11:1758835918818347. doi:10.1177/1758835918818347
- Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8:262. doi:10.1038/s41392-023-01469-6
- Thomson RJ, Moshirfar M, Ronquillo Y. Tyrosine kinase inhibitors. In: StatPearls [Internet]. StatPearls Publishing; updated July 18, 2023. Accessed December 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK563322/
- Project Optimus. US Food and Drug Administration. Updated December 6, 2024. Accessed December 15, 2025. https://www.fda.gov/about-fda/oncology-center-excellence/project-optimus
- Optimizing the dosage of human prescription drugs and biological products for the treatment of oncologic diseases: Guidance for Industry. Docket number FDA-2022-D-2827. US Food and Drug Administration. August 2024. Accessed December 15, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/optimizing-dosage-human-prescription-drugs-and-biological-products-treatment-oncologic-diseases
- Schnadig ID, Hutson TE, Chung H, et al. Dosing patterns, toxicity, and outcomes in patients treated with first-line sunitinib for advanced renal cell carcinoma in community-based practices. Clin Genitourin Cancer. 2014;12:413-421. doi:10.1016/j.clgc.2014.06.015
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115-124. doi:10.1056/nejmoa065044
- Hawn C, Bansal D. Relative dose intensity in oncology trials: a discussion of two approaches. PharmaSUG. 2024. Accessed April 6, 2026. https://pharmasug.org/proceedings/2024/ST/PharmaSUG-2024-ST-297.pdf
- George S, Merriam P, Maki RG, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27:3154-3160. doi:10.1200/jco.2008.20.9890
- George S, Blay JY, Casali PG, et al. Clinical evaluation of continuous daily dosing of sunitinib malate in patients with advanced gastrointestinal stromal tumour after imatinib failure. Eur J Cancer. 2009;45:1959-1968. doi:10.1016/j.ejca.2009.02.011
- Denduluri N, Patt DA, Wang Y, et al. Dose delays, dose reductions, and relative dose intensity in patients with cancer who received adjuvant or neoadjuvant chemotherapy in community oncology practices. J Natl Compr Canc Netw. 2015;13:1383-1393. doi:10.6004/jnccn.2015.0166
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380:1103-1115. doi:10.1056/nejmoa1816047
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384:1289-1300. doi:10.1056/nejmoa2035716
- Kirino S, Tsuchiya K, Kurosaki M, et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PloS One. 2020;15:e0231828. doi:10.1371/journal.pone.0231828
- Ishihara H, Takagi T, Kondo T, et al. Decreased relative dose intensity during the early phase of treatment impacts the therapeutic efficacy of sunitinib in metastatic renal cell carcinoma. Jpn J Clin Oncol. 2018;48:667-672. doi:10.1093/jjco/hyy078
- Alghamdi MA, Amaro CP, Lee-Ying R, et al. Effect of sorafenib starting dose and dose intensity on survival in patients with hepatocellular carcinoma: results from a Canadian Multicenter Database. Cancer Med. 2020;9:4918-4928. doi:10.1002/cam4.3228
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295:2516-2524. doi:10.1001/jama.295.21.2516
- Miller AA, Murry DJ, Owzar K, et al. Phase I and pharmacokinetic study of sorafenib in patients with hepatic or renal dysfunction: CALGB 60301. J Clin Oncol. 2009;27:1800-1805. doi:10.1200/jco.2008.20.0931
- Boucai L, Zafereo M, Cabanillas ME. Thyroid cancer: a review. JAMA. 2024;331:425-435. doi:10.1001/jama.2023.26348
- Amin N, Anwar J, Sulaiman A, et al. Hepatocellular carcinoma: a comprehensive review. Diseases. 2025;13:207. doi:10.3390/diseases13070207
- Bekaii-Saab TS, Ou FS, Ahn DH, et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): a randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019;20:1070-1082. doi:10.1016/s1470-2045(19)30272-4
The US Department of Veterans Affairs (VA) annually treats around 450,000 veterans with cancer and diagnoses an additional 56,000.1,2 Oral multikinase inhibitors (MKIs) are widely used as targeted therapies for many different malignancies. Despite the ease of oral administration, these agents are often accompanied by significant adverse effects (AEs) and drug-drug interactions.3,4 Common AEs include hypertension, cutaneous reactions, gastrointestinal disturbances, proteinuria, and fatigue. Some serious outcomes that may occur are myocardial infarction, thrombosis, nephrotic syndrome, hemorrhage, hepatotoxicity, and gastrointestinal events.5,6 Due to poor tolerability of these AEs, dose reductions, frequent therapy holds, and discontinuation of therapy may occur.
The US Food and Drug Administration recognizes dosing challenges with novel therapies and has created the Oncology Center of Excellence (OCE) Project Optimus initiative to reform dose optimization in oncology drug development. The initiative aims to shift the focus from establishing dose regimens based on the maximum tolerated doses of cytotoxic chemotherapeutics to an emphasis on maximum efficacy, safety, and tolerability, which better reflect real-world dosing.7,8
MKIs can be challenging to manage because of the frequent toxicity-related dose reductions, interruptions, and discontinuations. In a multicenter retrospective study, Schnadig et al investigated dosing characteristics of first-line sunitinib for advanced renal cell carcinoma (RCC) and found that, among 114 patients who experienced AEs while taking sunitinib, 39.5% had dose reductions, 5.3% delayed therapy, 18.4% required additional supportive medications, and 22.8% discontinued sunitinib.9 Overall survival and median progression-free survival of these patients were lower than reported by Motzer et al in a phase 3 clinical trial.10 Schnadig et al concluded that patients treated with sunitinib for RCC in the community setting required more frequent dose reductions and had less time on therapy compared with patients in clinical trials, which ultimately impacted clinical outcomes.9
At the VA North Texas Health Care System (VANTHCS), patients with cancer have difficulty tolerating MKIs and often require dose alterations and/or discontinuation because of drug intolerance rather than discontinuation due to progression. Frequent dose adjustments for toxicity management can place more strain on patients and health care resources because of additional appointments, clinician time, and emergency department visits. Escalating drug costs can also cause concern when prescription doses are unused or changed frequently.
To capture and quantify prescribing practices and dose adjustments, this study evaluated the tolerability of MKIs at VANTHCS. This analysis may also guide clinicians in the selection of starting doses as well as dose titration expectations to optimize MKI therapy.
METHODS
This single-center, retrospective chart review analyzed patients receiving oral oncology MKIs for various malignancies at VANTHCS between January 1, 2014, and October 31, 2024. Participants included adults aged ≥ 18 years with a prescription for axitinib, cabozantinib, lenvatinib, pazopanib, regorafenib, sorafenib, or sunitinib initiated by the hematology/oncology service at VANTHCS. Patients were included if they had follow-up documentation with the hematology/oncology service and/or other VANTHCS clinicians outlining their course of therapy after MKI initiation. Patients were excluded if they did not have sufficient follow-up documentation (eg, transferred care to a non-VA health care practitioner [HCP], moved to another VA health care system), were enrolled in clinical trials, or were prescribed an MKI from a Care in the Community (CITC) prescriber. Electronic health record review and data collection were performed using the VA Computerized Patient Record System and Research Electronic Data Capture. Data were collected from the time of initiation to cessation of therapy and included information regarding therapy changes, progressive disease, and date of death, when available. Data collected included age, sex, race, comorbidities, date of death, type of malignancy and subtypes, cancer stage, MKI used (ie, drug, dose, frequency, schedule, and indication), dates of medication changes (ie, start, adjustment, hold, discontinuation), concurrent antineoplastic treatments, and AEs documented at times of dose change or interruption.
The primary outcome was MKI tolerance determined using relative dose intensity (RDI) and mean and median time on therapy. Two methods are used to calculate RDI that vary in how they approach time on therapy as outlined in Hawn et al.11 This study used method 2, which accounts for holds in therapy by comparing the actual duration of treatment with the duration expected according to treatment protocol. Method 1 compares the prescribed dose with the administered dose and does not adjust for holds.11 Using method 2, the RDI in this study was calculated by dividing the total actual dose given by the total indicated dose for the malignancy being treated, which accounts for duration of treatment.
The total actual dose was the strength, frequency, and days on therapy for each time frame of treatment multiplied together. This method accounted for all dose adjustments and time periods of treatment holds, including patient self-adjustments, prescriber-directed adjustments, and nonadherence determined by HCP documentation and/or prescription data. Similarly, the indicated total dose was calculated by multiplying the indicated strength, frequency, and all days that treatment should have occurred (time from start to finish). Indicated doses were derived from the prescribing information for each malignancy with the exception of sunitinib, for which the off-label dose of 37.5 mg daily was considered a full dose.12,13 The total indicated dose for axitinib was calculated by considering the dose escalation schedule from the prescribing information.
Patients who required dose reductions due to renal/hepatic impairments or drug-drug interactions had their total indicated dose calculated using dose adjustments listed in the prescribing information. The mean RDI for each MKI agent was calculated by averaging the RDI for each prescription. The overall combined mean RDI included the means of all the MKIs reviewed to avoid skewing the results toward an MKI with more prescriptions. RDIs were also calculated for each cancer type for each agent. Additional descriptive secondary outcomes included rates of AEs and adjustments in doses.
RESULTS
Electronic data extraction identified 278 patients with 366 MKI prescriptions, of which 108 veterans with 158 MKI prescriptions were excluded. The top reason for exclusion was patients managed through CITC. Ultimately, 170 veterans with 208 MKI prescriptions managed by the VANTHCS hematology/oncology clinic were included (Table 1). Among patients receiving MKIs, the mean age was 72.7 years, 98% were male, and 99% had metastatic disease.
The overall combined mean MKI RDI was 67.5% using method 2 and ranged from 85.5% for sunitinib to 49.0% for sorafenib (Figure 1). Additional information regarding mean and median RDIs using method 2 is shown in Figure 1 and further subdivided by cancer type in Table 2. Median RDIs overall were similar to mean RDIs for most agents. Figure 2 indicates the mean and median time on therapy, reflecting time on therapy excluding days therapy was held. The overall combined mean and median days on therapy for all MKIs were 155 days and 95 days, respectively. Mean time on therapy depended on the agent used and ranged from 35 days (regorafenib) to 237 days (cabozantinib).
Of 208 MKI prescriptions, 127 (61.1%) were initiated at a reduced dose due to baseline concerns for tolerance such as performance status, frailty, and prior intolerance of other treatments. Eighty-one prescriptions (38.9%) were initiated at their indicated doses. Ninety prescriptions (43.3%) required dose reductions during treatment. Some MKI prescriptions had multiple dose increases and decreases, which is why RDI more accurately reflects dose adjustments. A total of 376 AEs that contributed to a dose adjustment, hold, or discontinuation occurred across all MKI prescriptions. The most common AEs were 82 failure-to-thrive events (21.8%) (fatigue, malaise, loss of appetite, reduced mobility, global decline), 79 gastrointestinal events (21.0%) (nausea, vomiting, diarrhea, abdominal pain), 62 dermatologic events (16.5%) (rash, hand-foot skin reactions, allergic response), 61 hepatic dysfunction events (16.2%) (liver enzyme elevations, hyperbilirubinemia), 40 cardiovascular events (10.6%) (hypertension, heart failure exacerbations, edema), and 33 renal dysfunction events (8.8%) (acute kidney injury, proteinuria) (Appendix 1).
DISCUSSION
The mean RDI of MKI prescriptions used in the veteran population at VANTHCS was about two-thirds of the indicated dose. These results indicate that most veterans required dose reductions and/or holds due to concerns over initial tolerance/performance status, worsening clinical condition, and/or intolerable AEs attributed to treatment. A retrospective study conducted by Denduluri et al suggested that an RDI of < 85% is a clinically meaningful reduction for traditional chemotherapy based on previous literature.14 However, it is less clear what RDI should be expected specifically for MKIs in real-world populations. The MKI phase 3 approval trials in RCC for axitinib, lenvatinib, and sunitinib found median RDIs of 89.4%, 69.6% to 70.4%, and 83.9%, respectively. Each trial cited dose reductions most commonly as the result of treatment-related AEs.15,16
Studies on the impact of RDIs on survival outcomes found that higher RDIs may improve overall and progression-free survival. Retrospective studies inspecting lenvatinib in hepatocellular carcinoma (HCC) indicated that an RDI > 70% in the initial 4 weeks resulted in favorable survival outcomes.17 Similarly, a retrospective study investigating sunitinib in RCC found that an RDI > 60% conferred favorable survival outcomes.18 Alghamdi et al noted that patients taking sorafenib for HCC who had RDI > 50% had a favorable trend in survival characteristics. Interestingly, the study found an RDI of 50% to 75% appeared to have better survival than an RDI > 75%.19 The authors of these studies hypothesized that additional dose reductions allowed for longer total time on therapy due to improved tolerability.17-19
This analysis found that the RDIs for most MKI agents at VANTHCS were < 85% and lower than the RDIs found in other review articles and phase 3 trials, with the exceptions of pazopanib in thyroid cancer and sunitinib in gastrointestinal stromal tumor (GIST), thyroid cancer, and neuroendocrine cancer. The reasons for the lower RDIs in this study are likely multifactorial, reflecting patient population characteristics, off-label dosing practices, and HCP experiences with these agents. Many veterans have chronic comorbidities that could contribute to reduced performance status and ability to tolerate these therapies. Despite attempts to preemptively reduce doses for patients and account for potential impaired tolerance, there were patients who required further dose reductions in our study.
Failure to thrive was the most common AE leading to dose adjustment or discontinuation, which illustrates the extensive effects these agents have on patient functioning in a real-world population. Notably though, the RDI for sunitinib was higher in this population because about half of patients were dosed using the off-label recommendation, whereas the prescribing information recommends a more intensive 6-week dosing cycle for certain cancer types.12,13,20 Sorafenib was also often dose-adjusted based on a pharmacokinetic study of sorafenib in renal/hepatic dysfunction, and the RDI likely reflects the off-label prescribing pattern.21
Patients with thyroid cancer were found to have higher RDIs compared with those receiving the same agents for other cancer types. Improved tolerability of MKIs in thyroid cancer may be due to a generally more tolerable disease course. Thyroid cancer is the most common cancer in individuals aged < 40 years, a population that is often more robust with fewer comorbidities. Moreover, the 5-year relative survival rate for thyroid cancer remains > 98%.22 This rate is in contrast to those for other cancer types such as HCC, with a 5-year relative survival rate of only 15%.23
It is challenging to compare the mean and median times on therapy found in this study with those in current literature, as this review included multiple different cancer types for each agent. However, the numbers are generally lower than durations of therapy found across the different disease states and further emphasize the difficulty in tolerating MKIs in the VANTHCS population. Regorafenib had a short duration of time on therapy, which highlights the importance of trials like ReDOS and initiatives such as OCE Project Optimus in helping improve tolerance.7,8,24
Comparing our results with other studies proved challenging because the RDI calculation methods were not specified. Calculating RDIs in this study using method 1, which does not account for holds, resulted in higher RDIs (Appendix 2). Using method 1, all MKIs had RDIs < 85%, except for pazopanib in thyroid cancer (100%) and RCC (87.9%), and sunitinib in GIST (93.6%), thyroid cancer (100%), and neuroendocrine cancer (93.7%). Notably, using method 1 increased the RDI for pazopanib in neuroendocrine cancer from 5.4% to 50.0%. The low RDI was attributed to a single veteran with a long hold duration, which demonstrates the discrepancy that can occur between the 2 methods.
Limitations
The retrospective design, lack of survival outcomes, and difficulty comparing results with other literature were limitations of this study. Because survival outcomes were not evaluated, future research should seek to investigate how RDIs and dose adjustments made among MKIs can affect survival outcomes in real-world populations. This veteran population with cancer often had multiple chronic comorbidities, which may have contributed to difficulty tolerating MKIs and could have impacted results. Disease-related factors may have influenced the poor tolerance of the MKIs and were not specifically accounted for. Adjustment for comorbidities was not possible because of discrepancies and/or incomplete diagnosis codes and Eastern Cooperative Oncology Group performance status scores documented in patient charts. Therefore, we decided not to report these findings due to potential inaccuracies.
CONCLUSIONS
Results of this study demonstrate that oncology MKI agents used at VANTHCS were difficult for patients to tolerate, leading to suboptimal dosing compared with indicated doses established in clinical trials and prescribing information. Clinicians may use these data to help guide clinical decision-making whenever initiating and managing MKI agents in this population. These findings reinforce that MKI agents are often difficult to tolerate in real-world practice, and indicated doses are often not achieved. Further studies should aim to investigate the effect that various RDIs have on overall survival. Further investigation into different dosing schemes for MKIs to improve tolerability and longer-term use may also prove beneficial.
This analysis may help guide clinicians to carefully approach dosing MKI agents in the veteran population. Given the RDI and AEs, more clinicians may consider starting at lower than indicated doses with the goal to titrate up as tolerated. Additionally, the results highlight the importance of considering palliative care consults and ensuring appropriate supportive care agents are preemptively engaged and adjusted as needed. Approaching dosing and titrations cautiously may help reduce the burden of management on the health care system.
The US Department of Veterans Affairs (VA) annually treats around 450,000 veterans with cancer and diagnoses an additional 56,000.1,2 Oral multikinase inhibitors (MKIs) are widely used as targeted therapies for many different malignancies. Despite the ease of oral administration, these agents are often accompanied by significant adverse effects (AEs) and drug-drug interactions.3,4 Common AEs include hypertension, cutaneous reactions, gastrointestinal disturbances, proteinuria, and fatigue. Some serious outcomes that may occur are myocardial infarction, thrombosis, nephrotic syndrome, hemorrhage, hepatotoxicity, and gastrointestinal events.5,6 Due to poor tolerability of these AEs, dose reductions, frequent therapy holds, and discontinuation of therapy may occur.
The US Food and Drug Administration recognizes dosing challenges with novel therapies and has created the Oncology Center of Excellence (OCE) Project Optimus initiative to reform dose optimization in oncology drug development. The initiative aims to shift the focus from establishing dose regimens based on the maximum tolerated doses of cytotoxic chemotherapeutics to an emphasis on maximum efficacy, safety, and tolerability, which better reflect real-world dosing.7,8
MKIs can be challenging to manage because of the frequent toxicity-related dose reductions, interruptions, and discontinuations. In a multicenter retrospective study, Schnadig et al investigated dosing characteristics of first-line sunitinib for advanced renal cell carcinoma (RCC) and found that, among 114 patients who experienced AEs while taking sunitinib, 39.5% had dose reductions, 5.3% delayed therapy, 18.4% required additional supportive medications, and 22.8% discontinued sunitinib.9 Overall survival and median progression-free survival of these patients were lower than reported by Motzer et al in a phase 3 clinical trial.10 Schnadig et al concluded that patients treated with sunitinib for RCC in the community setting required more frequent dose reductions and had less time on therapy compared with patients in clinical trials, which ultimately impacted clinical outcomes.9
At the VA North Texas Health Care System (VANTHCS), patients with cancer have difficulty tolerating MKIs and often require dose alterations and/or discontinuation because of drug intolerance rather than discontinuation due to progression. Frequent dose adjustments for toxicity management can place more strain on patients and health care resources because of additional appointments, clinician time, and emergency department visits. Escalating drug costs can also cause concern when prescription doses are unused or changed frequently.
To capture and quantify prescribing practices and dose adjustments, this study evaluated the tolerability of MKIs at VANTHCS. This analysis may also guide clinicians in the selection of starting doses as well as dose titration expectations to optimize MKI therapy.
METHODS
This single-center, retrospective chart review analyzed patients receiving oral oncology MKIs for various malignancies at VANTHCS between January 1, 2014, and October 31, 2024. Participants included adults aged ≥ 18 years with a prescription for axitinib, cabozantinib, lenvatinib, pazopanib, regorafenib, sorafenib, or sunitinib initiated by the hematology/oncology service at VANTHCS. Patients were included if they had follow-up documentation with the hematology/oncology service and/or other VANTHCS clinicians outlining their course of therapy after MKI initiation. Patients were excluded if they did not have sufficient follow-up documentation (eg, transferred care to a non-VA health care practitioner [HCP], moved to another VA health care system), were enrolled in clinical trials, or were prescribed an MKI from a Care in the Community (CITC) prescriber. Electronic health record review and data collection were performed using the VA Computerized Patient Record System and Research Electronic Data Capture. Data were collected from the time of initiation to cessation of therapy and included information regarding therapy changes, progressive disease, and date of death, when available. Data collected included age, sex, race, comorbidities, date of death, type of malignancy and subtypes, cancer stage, MKI used (ie, drug, dose, frequency, schedule, and indication), dates of medication changes (ie, start, adjustment, hold, discontinuation), concurrent antineoplastic treatments, and AEs documented at times of dose change or interruption.
The primary outcome was MKI tolerance determined using relative dose intensity (RDI) and mean and median time on therapy. Two methods are used to calculate RDI that vary in how they approach time on therapy as outlined in Hawn et al.11 This study used method 2, which accounts for holds in therapy by comparing the actual duration of treatment with the duration expected according to treatment protocol. Method 1 compares the prescribed dose with the administered dose and does not adjust for holds.11 Using method 2, the RDI in this study was calculated by dividing the total actual dose given by the total indicated dose for the malignancy being treated, which accounts for duration of treatment.
The total actual dose was the strength, frequency, and days on therapy for each time frame of treatment multiplied together. This method accounted for all dose adjustments and time periods of treatment holds, including patient self-adjustments, prescriber-directed adjustments, and nonadherence determined by HCP documentation and/or prescription data. Similarly, the indicated total dose was calculated by multiplying the indicated strength, frequency, and all days that treatment should have occurred (time from start to finish). Indicated doses were derived from the prescribing information for each malignancy with the exception of sunitinib, for which the off-label dose of 37.5 mg daily was considered a full dose.12,13 The total indicated dose for axitinib was calculated by considering the dose escalation schedule from the prescribing information.
Patients who required dose reductions due to renal/hepatic impairments or drug-drug interactions had their total indicated dose calculated using dose adjustments listed in the prescribing information. The mean RDI for each MKI agent was calculated by averaging the RDI for each prescription. The overall combined mean RDI included the means of all the MKIs reviewed to avoid skewing the results toward an MKI with more prescriptions. RDIs were also calculated for each cancer type for each agent. Additional descriptive secondary outcomes included rates of AEs and adjustments in doses.
RESULTS
Electronic data extraction identified 278 patients with 366 MKI prescriptions, of which 108 veterans with 158 MKI prescriptions were excluded. The top reason for exclusion was patients managed through CITC. Ultimately, 170 veterans with 208 MKI prescriptions managed by the VANTHCS hematology/oncology clinic were included (Table 1). Among patients receiving MKIs, the mean age was 72.7 years, 98% were male, and 99% had metastatic disease.
The overall combined mean MKI RDI was 67.5% using method 2 and ranged from 85.5% for sunitinib to 49.0% for sorafenib (Figure 1). Additional information regarding mean and median RDIs using method 2 is shown in Figure 1 and further subdivided by cancer type in Table 2. Median RDIs overall were similar to mean RDIs for most agents. Figure 2 indicates the mean and median time on therapy, reflecting time on therapy excluding days therapy was held. The overall combined mean and median days on therapy for all MKIs were 155 days and 95 days, respectively. Mean time on therapy depended on the agent used and ranged from 35 days (regorafenib) to 237 days (cabozantinib).
Of 208 MKI prescriptions, 127 (61.1%) were initiated at a reduced dose due to baseline concerns for tolerance such as performance status, frailty, and prior intolerance of other treatments. Eighty-one prescriptions (38.9%) were initiated at their indicated doses. Ninety prescriptions (43.3%) required dose reductions during treatment. Some MKI prescriptions had multiple dose increases and decreases, which is why RDI more accurately reflects dose adjustments. A total of 376 AEs that contributed to a dose adjustment, hold, or discontinuation occurred across all MKI prescriptions. The most common AEs were 82 failure-to-thrive events (21.8%) (fatigue, malaise, loss of appetite, reduced mobility, global decline), 79 gastrointestinal events (21.0%) (nausea, vomiting, diarrhea, abdominal pain), 62 dermatologic events (16.5%) (rash, hand-foot skin reactions, allergic response), 61 hepatic dysfunction events (16.2%) (liver enzyme elevations, hyperbilirubinemia), 40 cardiovascular events (10.6%) (hypertension, heart failure exacerbations, edema), and 33 renal dysfunction events (8.8%) (acute kidney injury, proteinuria) (Appendix 1).
DISCUSSION
The mean RDI of MKI prescriptions used in the veteran population at VANTHCS was about two-thirds of the indicated dose. These results indicate that most veterans required dose reductions and/or holds due to concerns over initial tolerance/performance status, worsening clinical condition, and/or intolerable AEs attributed to treatment. A retrospective study conducted by Denduluri et al suggested that an RDI of < 85% is a clinically meaningful reduction for traditional chemotherapy based on previous literature.14 However, it is less clear what RDI should be expected specifically for MKIs in real-world populations. The MKI phase 3 approval trials in RCC for axitinib, lenvatinib, and sunitinib found median RDIs of 89.4%, 69.6% to 70.4%, and 83.9%, respectively. Each trial cited dose reductions most commonly as the result of treatment-related AEs.15,16
Studies on the impact of RDIs on survival outcomes found that higher RDIs may improve overall and progression-free survival. Retrospective studies inspecting lenvatinib in hepatocellular carcinoma (HCC) indicated that an RDI > 70% in the initial 4 weeks resulted in favorable survival outcomes.17 Similarly, a retrospective study investigating sunitinib in RCC found that an RDI > 60% conferred favorable survival outcomes.18 Alghamdi et al noted that patients taking sorafenib for HCC who had RDI > 50% had a favorable trend in survival characteristics. Interestingly, the study found an RDI of 50% to 75% appeared to have better survival than an RDI > 75%.19 The authors of these studies hypothesized that additional dose reductions allowed for longer total time on therapy due to improved tolerability.17-19
This analysis found that the RDIs for most MKI agents at VANTHCS were < 85% and lower than the RDIs found in other review articles and phase 3 trials, with the exceptions of pazopanib in thyroid cancer and sunitinib in gastrointestinal stromal tumor (GIST), thyroid cancer, and neuroendocrine cancer. The reasons for the lower RDIs in this study are likely multifactorial, reflecting patient population characteristics, off-label dosing practices, and HCP experiences with these agents. Many veterans have chronic comorbidities that could contribute to reduced performance status and ability to tolerate these therapies. Despite attempts to preemptively reduce doses for patients and account for potential impaired tolerance, there were patients who required further dose reductions in our study.
Failure to thrive was the most common AE leading to dose adjustment or discontinuation, which illustrates the extensive effects these agents have on patient functioning in a real-world population. Notably though, the RDI for sunitinib was higher in this population because about half of patients were dosed using the off-label recommendation, whereas the prescribing information recommends a more intensive 6-week dosing cycle for certain cancer types.12,13,20 Sorafenib was also often dose-adjusted based on a pharmacokinetic study of sorafenib in renal/hepatic dysfunction, and the RDI likely reflects the off-label prescribing pattern.21
Patients with thyroid cancer were found to have higher RDIs compared with those receiving the same agents for other cancer types. Improved tolerability of MKIs in thyroid cancer may be due to a generally more tolerable disease course. Thyroid cancer is the most common cancer in individuals aged < 40 years, a population that is often more robust with fewer comorbidities. Moreover, the 5-year relative survival rate for thyroid cancer remains > 98%.22 This rate is in contrast to those for other cancer types such as HCC, with a 5-year relative survival rate of only 15%.23
It is challenging to compare the mean and median times on therapy found in this study with those in current literature, as this review included multiple different cancer types for each agent. However, the numbers are generally lower than durations of therapy found across the different disease states and further emphasize the difficulty in tolerating MKIs in the VANTHCS population. Regorafenib had a short duration of time on therapy, which highlights the importance of trials like ReDOS and initiatives such as OCE Project Optimus in helping improve tolerance.7,8,24
Comparing our results with other studies proved challenging because the RDI calculation methods were not specified. Calculating RDIs in this study using method 1, which does not account for holds, resulted in higher RDIs (Appendix 2). Using method 1, all MKIs had RDIs < 85%, except for pazopanib in thyroid cancer (100%) and RCC (87.9%), and sunitinib in GIST (93.6%), thyroid cancer (100%), and neuroendocrine cancer (93.7%). Notably, using method 1 increased the RDI for pazopanib in neuroendocrine cancer from 5.4% to 50.0%. The low RDI was attributed to a single veteran with a long hold duration, which demonstrates the discrepancy that can occur between the 2 methods.
Limitations
The retrospective design, lack of survival outcomes, and difficulty comparing results with other literature were limitations of this study. Because survival outcomes were not evaluated, future research should seek to investigate how RDIs and dose adjustments made among MKIs can affect survival outcomes in real-world populations. This veteran population with cancer often had multiple chronic comorbidities, which may have contributed to difficulty tolerating MKIs and could have impacted results. Disease-related factors may have influenced the poor tolerance of the MKIs and were not specifically accounted for. Adjustment for comorbidities was not possible because of discrepancies and/or incomplete diagnosis codes and Eastern Cooperative Oncology Group performance status scores documented in patient charts. Therefore, we decided not to report these findings due to potential inaccuracies.
CONCLUSIONS
Results of this study demonstrate that oncology MKI agents used at VANTHCS were difficult for patients to tolerate, leading to suboptimal dosing compared with indicated doses established in clinical trials and prescribing information. Clinicians may use these data to help guide clinical decision-making whenever initiating and managing MKI agents in this population. These findings reinforce that MKI agents are often difficult to tolerate in real-world practice, and indicated doses are often not achieved. Further studies should aim to investigate the effect that various RDIs have on overall survival. Further investigation into different dosing schemes for MKIs to improve tolerability and longer-term use may also prove beneficial.
This analysis may help guide clinicians to carefully approach dosing MKI agents in the veteran population. Given the RDI and AEs, more clinicians may consider starting at lower than indicated doses with the goal to titrate up as tolerated. Additionally, the results highlight the importance of considering palliative care consults and ensuring appropriate supportive care agents are preemptively engaged and adjusted as needed. Approaching dosing and titrations cautiously may help reduce the burden of management on the health care system.
- Frequently asked questions. VA National Oncology Program. 2025. Accessed December 15, 2025. https://www.cancer.va.gov/CANCER/faqs.html
- Torez L. Reigniting the cancer moonshot to beat cancer. VA News. April 20, 2023. Accessed April 6, 2026. https://news.va.gov/118378/reigniting-the-cancer-moonshot-to-beat-cancer
- Shah NN, Casella E, Capozzi D, et al. Improving the safety of oral chemotherapy at an academic medical center. J Oncol Pract. 2016;12:e71-e76. doi:10.1200/JOP.2015.007260
- Hussaarts KGAM, Veerman GDM, Jansman FGA, et al. Clinically relevant drug interactions with multikinase inhibitors: a review. Ther Adv Med Oncol. 2019;11:1758835918818347. doi:10.1177/1758835918818347
- Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8:262. doi:10.1038/s41392-023-01469-6
- Thomson RJ, Moshirfar M, Ronquillo Y. Tyrosine kinase inhibitors. In: StatPearls [Internet]. StatPearls Publishing; updated July 18, 2023. Accessed December 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK563322/
- Project Optimus. US Food and Drug Administration. Updated December 6, 2024. Accessed December 15, 2025. https://www.fda.gov/about-fda/oncology-center-excellence/project-optimus
- Optimizing the dosage of human prescription drugs and biological products for the treatment of oncologic diseases: Guidance for Industry. Docket number FDA-2022-D-2827. US Food and Drug Administration. August 2024. Accessed December 15, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/optimizing-dosage-human-prescription-drugs-and-biological-products-treatment-oncologic-diseases
- Schnadig ID, Hutson TE, Chung H, et al. Dosing patterns, toxicity, and outcomes in patients treated with first-line sunitinib for advanced renal cell carcinoma in community-based practices. Clin Genitourin Cancer. 2014;12:413-421. doi:10.1016/j.clgc.2014.06.015
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115-124. doi:10.1056/nejmoa065044
- Hawn C, Bansal D. Relative dose intensity in oncology trials: a discussion of two approaches. PharmaSUG. 2024. Accessed April 6, 2026. https://pharmasug.org/proceedings/2024/ST/PharmaSUG-2024-ST-297.pdf
- George S, Merriam P, Maki RG, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27:3154-3160. doi:10.1200/jco.2008.20.9890
- George S, Blay JY, Casali PG, et al. Clinical evaluation of continuous daily dosing of sunitinib malate in patients with advanced gastrointestinal stromal tumour after imatinib failure. Eur J Cancer. 2009;45:1959-1968. doi:10.1016/j.ejca.2009.02.011
- Denduluri N, Patt DA, Wang Y, et al. Dose delays, dose reductions, and relative dose intensity in patients with cancer who received adjuvant or neoadjuvant chemotherapy in community oncology practices. J Natl Compr Canc Netw. 2015;13:1383-1393. doi:10.6004/jnccn.2015.0166
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380:1103-1115. doi:10.1056/nejmoa1816047
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384:1289-1300. doi:10.1056/nejmoa2035716
- Kirino S, Tsuchiya K, Kurosaki M, et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PloS One. 2020;15:e0231828. doi:10.1371/journal.pone.0231828
- Ishihara H, Takagi T, Kondo T, et al. Decreased relative dose intensity during the early phase of treatment impacts the therapeutic efficacy of sunitinib in metastatic renal cell carcinoma. Jpn J Clin Oncol. 2018;48:667-672. doi:10.1093/jjco/hyy078
- Alghamdi MA, Amaro CP, Lee-Ying R, et al. Effect of sorafenib starting dose and dose intensity on survival in patients with hepatocellular carcinoma: results from a Canadian Multicenter Database. Cancer Med. 2020;9:4918-4928. doi:10.1002/cam4.3228
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295:2516-2524. doi:10.1001/jama.295.21.2516
- Miller AA, Murry DJ, Owzar K, et al. Phase I and pharmacokinetic study of sorafenib in patients with hepatic or renal dysfunction: CALGB 60301. J Clin Oncol. 2009;27:1800-1805. doi:10.1200/jco.2008.20.0931
- Boucai L, Zafereo M, Cabanillas ME. Thyroid cancer: a review. JAMA. 2024;331:425-435. doi:10.1001/jama.2023.26348
- Amin N, Anwar J, Sulaiman A, et al. Hepatocellular carcinoma: a comprehensive review. Diseases. 2025;13:207. doi:10.3390/diseases13070207
- Bekaii-Saab TS, Ou FS, Ahn DH, et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): a randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019;20:1070-1082. doi:10.1016/s1470-2045(19)30272-4
- Frequently asked questions. VA National Oncology Program. 2025. Accessed December 15, 2025. https://www.cancer.va.gov/CANCER/faqs.html
- Torez L. Reigniting the cancer moonshot to beat cancer. VA News. April 20, 2023. Accessed April 6, 2026. https://news.va.gov/118378/reigniting-the-cancer-moonshot-to-beat-cancer
- Shah NN, Casella E, Capozzi D, et al. Improving the safety of oral chemotherapy at an academic medical center. J Oncol Pract. 2016;12:e71-e76. doi:10.1200/JOP.2015.007260
- Hussaarts KGAM, Veerman GDM, Jansman FGA, et al. Clinically relevant drug interactions with multikinase inhibitors: a review. Ther Adv Med Oncol. 2019;11:1758835918818347. doi:10.1177/1758835918818347
- Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8:262. doi:10.1038/s41392-023-01469-6
- Thomson RJ, Moshirfar M, Ronquillo Y. Tyrosine kinase inhibitors. In: StatPearls [Internet]. StatPearls Publishing; updated July 18, 2023. Accessed December 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK563322/
- Project Optimus. US Food and Drug Administration. Updated December 6, 2024. Accessed December 15, 2025. https://www.fda.gov/about-fda/oncology-center-excellence/project-optimus
- Optimizing the dosage of human prescription drugs and biological products for the treatment of oncologic diseases: Guidance for Industry. Docket number FDA-2022-D-2827. US Food and Drug Administration. August 2024. Accessed December 15, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/optimizing-dosage-human-prescription-drugs-and-biological-products-treatment-oncologic-diseases
- Schnadig ID, Hutson TE, Chung H, et al. Dosing patterns, toxicity, and outcomes in patients treated with first-line sunitinib for advanced renal cell carcinoma in community-based practices. Clin Genitourin Cancer. 2014;12:413-421. doi:10.1016/j.clgc.2014.06.015
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115-124. doi:10.1056/nejmoa065044
- Hawn C, Bansal D. Relative dose intensity in oncology trials: a discussion of two approaches. PharmaSUG. 2024. Accessed April 6, 2026. https://pharmasug.org/proceedings/2024/ST/PharmaSUG-2024-ST-297.pdf
- George S, Merriam P, Maki RG, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27:3154-3160. doi:10.1200/jco.2008.20.9890
- George S, Blay JY, Casali PG, et al. Clinical evaluation of continuous daily dosing of sunitinib malate in patients with advanced gastrointestinal stromal tumour after imatinib failure. Eur J Cancer. 2009;45:1959-1968. doi:10.1016/j.ejca.2009.02.011
- Denduluri N, Patt DA, Wang Y, et al. Dose delays, dose reductions, and relative dose intensity in patients with cancer who received adjuvant or neoadjuvant chemotherapy in community oncology practices. J Natl Compr Canc Netw. 2015;13:1383-1393. doi:10.6004/jnccn.2015.0166
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380:1103-1115. doi:10.1056/nejmoa1816047
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384:1289-1300. doi:10.1056/nejmoa2035716
- Kirino S, Tsuchiya K, Kurosaki M, et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PloS One. 2020;15:e0231828. doi:10.1371/journal.pone.0231828
- Ishihara H, Takagi T, Kondo T, et al. Decreased relative dose intensity during the early phase of treatment impacts the therapeutic efficacy of sunitinib in metastatic renal cell carcinoma. Jpn J Clin Oncol. 2018;48:667-672. doi:10.1093/jjco/hyy078
- Alghamdi MA, Amaro CP, Lee-Ying R, et al. Effect of sorafenib starting dose and dose intensity on survival in patients with hepatocellular carcinoma: results from a Canadian Multicenter Database. Cancer Med. 2020;9:4918-4928. doi:10.1002/cam4.3228
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295:2516-2524. doi:10.1001/jama.295.21.2516
- Miller AA, Murry DJ, Owzar K, et al. Phase I and pharmacokinetic study of sorafenib in patients with hepatic or renal dysfunction: CALGB 60301. J Clin Oncol. 2009;27:1800-1805. doi:10.1200/jco.2008.20.0931
- Boucai L, Zafereo M, Cabanillas ME. Thyroid cancer: a review. JAMA. 2024;331:425-435. doi:10.1001/jama.2023.26348
- Amin N, Anwar J, Sulaiman A, et al. Hepatocellular carcinoma: a comprehensive review. Diseases. 2025;13:207. doi:10.3390/diseases13070207
- Bekaii-Saab TS, Ou FS, Ahn DH, et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): a randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019;20:1070-1082. doi:10.1016/s1470-2045(19)30272-4
Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
Can Fecal Transplants Enhance Immunotherapy? New Evidence and Cautions
Can Fecal Transplants Enhance Immunotherapy? New Evidence and Cautions
A trio of new studies, published simultaneously in February in Nature Medicine, add to growing evidence that manipulating the gut microbiome may enhance responses to immunotherapy in selected patients with cancer.
In these small, early-phase studies involving patients with metastatic renal cell carcinoma (RCC), non-small cell lung cancer (NSCLC), and melanoma receiving immune checkpoint inhibitor (ICI) therapy, fecal microbiota transplantation (FMT) was associated with objective response rates that compared favorably with historical or prespecified benchmarks.
The idea that microbiome modulation via FMT “can augment immunotherapy efficacy is probably a good one and these studies certainly support that hypothesis,” said Diwakar Davar, MD, assistant professor of medicine and an oncologist/hematologist at the University of Pittsburgh, Pennsylvania, who wasn’t part of the new work.While “an intriguing approach and certainly worthy of further evaluation,” Davar cautioned that the latest studies are not robust enough to answer the question conclusively.
Although ICIs have improved outcomes for patients with melanoma, NSCLC, and RCC, many patients still do not respond or eventually develop resistance. A growing body of evidence suggests that the gut microbiome can influence the effectiveness of ICI therapy. However, much of this evidence comes from preclinical studies showing that modulating the microbiome via FMT can alter responses to immunotherapy, along with small proof-of-concept human studies — predominantly in melanoma — suggesting this approach may help overcome primary or acquired resistance to anti-PD-1 therapy.
The new studies aimed to build on this foundation by exploring whether FMT could improve ICI responses and clinical outcomes in patients with NSCLC, melanoma, and RCC.
In the phase 2, open-label FMT-LUMINate trial, researchers tested a healthy-donor FMT delivered as oral capsules before patients began immunotherapy. FMT capsules were produced using 80-100 g of feces per dose from screened healthy donors, and patients consumed 30-40 capsules while under supervision. The study included 20 patients with NSCLC and high PD-L1 tumor expression receiving FMT before standard first-line pembrolizumab monotherapy and 20 patients with cutaneous melanoma receiving FMT before ipilimumab plus nivolumab.
In the NSCLC cohort, 16 patients (80%) achieved an objective response. The 80% objective response rate exceeded the prespecified efficacy threshold of 64% and was higher than previously described historical data, which ranged from 39% to 46%, the study team noted.
In the melanoma cohort, FMT before nivolumab and ipilimumab yielded an objective response rate of 75%, also exceeding the historical expected response rates of 50% to 58% among patients receiving this ICI combination.
In patients with NSCLC, no grade 3 or higher adverse events were reported. However, grade 3 or higher adverse events were reported in 13 (65%) patients in the melanoma group, suggesting a potentially accelerated onset of immune-related adverse events. Researchers also observed a higher-than-expected frequency of myocarditis in melanoma patients (15%). These toxicities clustered among patients who had FMT donors enriched in Prevotella spp, highlighting the importance of donor selection for future trials, the researchers explained.
The team plans to assess the potential of FMT to overcome primary resistance to ICI as part of the phase 2 CanBiome2 randomized trial, which aims to enroll 128 patients.
The RCC Data
The other two studies focused on FMT in patients with metastatic RCC. In the phase 1 PERFORM study, 20 treatment-naive patients with metastatic RCC added encapsulated healthy-donor FMT to standard ICI-based regimens — most commonly ipilimumab plus nivolumab, with some patients receiving pembrolizumab plus axitinib or pembrolizumab plus lenvatinib.
The primary endpoint was safety defined by the incidence and severity of immune-related adverse events. The safety endpoint was met; 50% of patients (10 of 20) experienced grade 3 immune-related adverse events, and there were no serious FMT-related toxicities and no grade 4 or 5 events.
Among 18 evaluable patients, nine (50%) achieved an objective response, including two who had complete responses (11%). Notably, most treatment responders did not develop any grade 3 or higher immune-related adverse events, the researchers reported.
Finally, in the phase 2a TACITO trial, 45 patients with treatment-naive metastatic RCC were randomly allocated to receive donor FMT or placebo FMT. Patients received three administrations over 6 months — first via colonoscopy then as capsulized doses, alongside pembrolizumab plus axitinib.
The primary endpoint of 12-month progression-free survival narrowly missed statistical significance — 70% vs 41% (P = .053) — but suggested a benefit in the donor FMT group.
“We need more than 1 year to appreciate statistical significance in terms of progression-free survival,” study investigator Gianluca Ianiro, MD, PhD, with Catholic University of the Sacred Heart, Rome, told Medscape Medical News.
As for secondary endpoints, median progression-free survival was significantly longer with donor FMT (24.0 vs 9.0 months; hazard ratio, 0.50; P = .035) and the objective response rate was higher with donor FMT (52% vs 32%).
Why Might FMT Boost ICI Response?
Conceptually, FMT is intended to reshape the gut ecosystem in ways that favor antitumor immunity, and possibly reduce immune dysregulation.
Across these new studies, the mechanistic story is moving beyond the idea that more diversity is good and toward a model that suggests a benefit to removing or suppressing taxa associated with resistance or inflammatory toxicity.
For example, in the TACITO trial, microbiome analysis confirmed that acquisition or loss of specific bacterial strains was associated with 12-month progression-free survival.
Additionally, results of the FMT-LUMINate trial hinted that the therapeutic benefit of FMT may be driven by eliminating harmful bacteria present at baseline, most notably Enterocloster, Clostridium and Streptococcus spp.
“This bacterial depletion was associated with a favorable immunometabolic milieu,” the FMT-LUMINate researchers wrote. Additionally, the results suggest that “failure to eliminate baseline deleterious taxa may sustain an immunosuppressive metabolic and systemic immune milieu that compromises ICI responses.”
Is FMT Ready for Prime Time?
Ianiro told Medscape Medical News he “definitely” thinks microbiome modulation could eventually become part of standard immunotherapy regimens.
Although the “signal” of benefit is clearly there, Davar cautioned that it’s too early to justify routine, off-trial use of FMT specifically to improve ICI response.
“These remain small, proof-of-concept studies. They are not adequately powered trials of fecal transplants and multiple different covariates haven’t been considered,” Davar said.
The study researchers noted that issues around donor selection and availability, dosing schedules, product standardization, and safety risk stratification need to be resolved.
For example, TACITO’s real-world experience shows logistics can matter. Delays occurred due to capsule unavailability and other scheduling barriers, which led to late dosing and missed or shifted treatments in some patients.
That’s a reminder that scaling FMT for oncology would require robust manufacturing, distribution, and time-sensitive coordination with ICI start dates.
More broadly, “whether FMT is the most suitable method of essentially changing the gut microbiome remains unclear,” explained Davar, who suggested that engineered microbiome therapeutics or tailored therapies may be a preferable, more scalable and tailored long-term solution.
Overall, does this new research provide impetus to develop stool banks? “Probably not,” Davar said.
But is it a call for interested parties to think about clinical trials and experimental products that could influence the gut microbiome? “Those are all probably good ideas,” he said.
The PERFORM, TACITO and FMT-LUMINate trials had no commercial funding. Saman Maleki Vareki, PhD, of the PERFORM trial, is a cofounder of LND Therapeutics Inc and has submitted a US patent application related to FMT donor screening. Ianiro has received personal fees for acting as a speaker for Biocodex and Illumina and for acting as a consultant/advisor for Ferring Therapeutics. Arielle Elkrief, MD, of the FMT-LUMINate trial, has received honoraria from AstraZeneca, Merck, Bristol Myers Squibb, and EMD Serono; consulting fees from EverImmune, NECBio, and Sanofi-Pasteur; and is an inventor on a patent regarding the microbiome and immunotherapy response. Davar had no relevant disclosures.
A version of this article first appeared on Medscape.com.
A trio of new studies, published simultaneously in February in Nature Medicine, add to growing evidence that manipulating the gut microbiome may enhance responses to immunotherapy in selected patients with cancer.
In these small, early-phase studies involving patients with metastatic renal cell carcinoma (RCC), non-small cell lung cancer (NSCLC), and melanoma receiving immune checkpoint inhibitor (ICI) therapy, fecal microbiota transplantation (FMT) was associated with objective response rates that compared favorably with historical or prespecified benchmarks.
The idea that microbiome modulation via FMT “can augment immunotherapy efficacy is probably a good one and these studies certainly support that hypothesis,” said Diwakar Davar, MD, assistant professor of medicine and an oncologist/hematologist at the University of Pittsburgh, Pennsylvania, who wasn’t part of the new work.While “an intriguing approach and certainly worthy of further evaluation,” Davar cautioned that the latest studies are not robust enough to answer the question conclusively.
Although ICIs have improved outcomes for patients with melanoma, NSCLC, and RCC, many patients still do not respond or eventually develop resistance. A growing body of evidence suggests that the gut microbiome can influence the effectiveness of ICI therapy. However, much of this evidence comes from preclinical studies showing that modulating the microbiome via FMT can alter responses to immunotherapy, along with small proof-of-concept human studies — predominantly in melanoma — suggesting this approach may help overcome primary or acquired resistance to anti-PD-1 therapy.
The new studies aimed to build on this foundation by exploring whether FMT could improve ICI responses and clinical outcomes in patients with NSCLC, melanoma, and RCC.
In the phase 2, open-label FMT-LUMINate trial, researchers tested a healthy-donor FMT delivered as oral capsules before patients began immunotherapy. FMT capsules were produced using 80-100 g of feces per dose from screened healthy donors, and patients consumed 30-40 capsules while under supervision. The study included 20 patients with NSCLC and high PD-L1 tumor expression receiving FMT before standard first-line pembrolizumab monotherapy and 20 patients with cutaneous melanoma receiving FMT before ipilimumab plus nivolumab.
In the NSCLC cohort, 16 patients (80%) achieved an objective response. The 80% objective response rate exceeded the prespecified efficacy threshold of 64% and was higher than previously described historical data, which ranged from 39% to 46%, the study team noted.
In the melanoma cohort, FMT before nivolumab and ipilimumab yielded an objective response rate of 75%, also exceeding the historical expected response rates of 50% to 58% among patients receiving this ICI combination.
In patients with NSCLC, no grade 3 or higher adverse events were reported. However, grade 3 or higher adverse events were reported in 13 (65%) patients in the melanoma group, suggesting a potentially accelerated onset of immune-related adverse events. Researchers also observed a higher-than-expected frequency of myocarditis in melanoma patients (15%). These toxicities clustered among patients who had FMT donors enriched in Prevotella spp, highlighting the importance of donor selection for future trials, the researchers explained.
The team plans to assess the potential of FMT to overcome primary resistance to ICI as part of the phase 2 CanBiome2 randomized trial, which aims to enroll 128 patients.
The RCC Data
The other two studies focused on FMT in patients with metastatic RCC. In the phase 1 PERFORM study, 20 treatment-naive patients with metastatic RCC added encapsulated healthy-donor FMT to standard ICI-based regimens — most commonly ipilimumab plus nivolumab, with some patients receiving pembrolizumab plus axitinib or pembrolizumab plus lenvatinib.
The primary endpoint was safety defined by the incidence and severity of immune-related adverse events. The safety endpoint was met; 50% of patients (10 of 20) experienced grade 3 immune-related adverse events, and there were no serious FMT-related toxicities and no grade 4 or 5 events.
Among 18 evaluable patients, nine (50%) achieved an objective response, including two who had complete responses (11%). Notably, most treatment responders did not develop any grade 3 or higher immune-related adverse events, the researchers reported.
Finally, in the phase 2a TACITO trial, 45 patients with treatment-naive metastatic RCC were randomly allocated to receive donor FMT or placebo FMT. Patients received three administrations over 6 months — first via colonoscopy then as capsulized doses, alongside pembrolizumab plus axitinib.
The primary endpoint of 12-month progression-free survival narrowly missed statistical significance — 70% vs 41% (P = .053) — but suggested a benefit in the donor FMT group.
“We need more than 1 year to appreciate statistical significance in terms of progression-free survival,” study investigator Gianluca Ianiro, MD, PhD, with Catholic University of the Sacred Heart, Rome, told Medscape Medical News.
As for secondary endpoints, median progression-free survival was significantly longer with donor FMT (24.0 vs 9.0 months; hazard ratio, 0.50; P = .035) and the objective response rate was higher with donor FMT (52% vs 32%).
Why Might FMT Boost ICI Response?
Conceptually, FMT is intended to reshape the gut ecosystem in ways that favor antitumor immunity, and possibly reduce immune dysregulation.
Across these new studies, the mechanistic story is moving beyond the idea that more diversity is good and toward a model that suggests a benefit to removing or suppressing taxa associated with resistance or inflammatory toxicity.
For example, in the TACITO trial, microbiome analysis confirmed that acquisition or loss of specific bacterial strains was associated with 12-month progression-free survival.
Additionally, results of the FMT-LUMINate trial hinted that the therapeutic benefit of FMT may be driven by eliminating harmful bacteria present at baseline, most notably Enterocloster, Clostridium and Streptococcus spp.
“This bacterial depletion was associated with a favorable immunometabolic milieu,” the FMT-LUMINate researchers wrote. Additionally, the results suggest that “failure to eliminate baseline deleterious taxa may sustain an immunosuppressive metabolic and systemic immune milieu that compromises ICI responses.”
Is FMT Ready for Prime Time?
Ianiro told Medscape Medical News he “definitely” thinks microbiome modulation could eventually become part of standard immunotherapy regimens.
Although the “signal” of benefit is clearly there, Davar cautioned that it’s too early to justify routine, off-trial use of FMT specifically to improve ICI response.
“These remain small, proof-of-concept studies. They are not adequately powered trials of fecal transplants and multiple different covariates haven’t been considered,” Davar said.
The study researchers noted that issues around donor selection and availability, dosing schedules, product standardization, and safety risk stratification need to be resolved.
For example, TACITO’s real-world experience shows logistics can matter. Delays occurred due to capsule unavailability and other scheduling barriers, which led to late dosing and missed or shifted treatments in some patients.
That’s a reminder that scaling FMT for oncology would require robust manufacturing, distribution, and time-sensitive coordination with ICI start dates.
More broadly, “whether FMT is the most suitable method of essentially changing the gut microbiome remains unclear,” explained Davar, who suggested that engineered microbiome therapeutics or tailored therapies may be a preferable, more scalable and tailored long-term solution.
Overall, does this new research provide impetus to develop stool banks? “Probably not,” Davar said.
But is it a call for interested parties to think about clinical trials and experimental products that could influence the gut microbiome? “Those are all probably good ideas,” he said.
The PERFORM, TACITO and FMT-LUMINate trials had no commercial funding. Saman Maleki Vareki, PhD, of the PERFORM trial, is a cofounder of LND Therapeutics Inc and has submitted a US patent application related to FMT donor screening. Ianiro has received personal fees for acting as a speaker for Biocodex and Illumina and for acting as a consultant/advisor for Ferring Therapeutics. Arielle Elkrief, MD, of the FMT-LUMINate trial, has received honoraria from AstraZeneca, Merck, Bristol Myers Squibb, and EMD Serono; consulting fees from EverImmune, NECBio, and Sanofi-Pasteur; and is an inventor on a patent regarding the microbiome and immunotherapy response. Davar had no relevant disclosures.
A version of this article first appeared on Medscape.com.
A trio of new studies, published simultaneously in February in Nature Medicine, add to growing evidence that manipulating the gut microbiome may enhance responses to immunotherapy in selected patients with cancer.
In these small, early-phase studies involving patients with metastatic renal cell carcinoma (RCC), non-small cell lung cancer (NSCLC), and melanoma receiving immune checkpoint inhibitor (ICI) therapy, fecal microbiota transplantation (FMT) was associated with objective response rates that compared favorably with historical or prespecified benchmarks.
The idea that microbiome modulation via FMT “can augment immunotherapy efficacy is probably a good one and these studies certainly support that hypothesis,” said Diwakar Davar, MD, assistant professor of medicine and an oncologist/hematologist at the University of Pittsburgh, Pennsylvania, who wasn’t part of the new work.While “an intriguing approach and certainly worthy of further evaluation,” Davar cautioned that the latest studies are not robust enough to answer the question conclusively.
Although ICIs have improved outcomes for patients with melanoma, NSCLC, and RCC, many patients still do not respond or eventually develop resistance. A growing body of evidence suggests that the gut microbiome can influence the effectiveness of ICI therapy. However, much of this evidence comes from preclinical studies showing that modulating the microbiome via FMT can alter responses to immunotherapy, along with small proof-of-concept human studies — predominantly in melanoma — suggesting this approach may help overcome primary or acquired resistance to anti-PD-1 therapy.
The new studies aimed to build on this foundation by exploring whether FMT could improve ICI responses and clinical outcomes in patients with NSCLC, melanoma, and RCC.
In the phase 2, open-label FMT-LUMINate trial, researchers tested a healthy-donor FMT delivered as oral capsules before patients began immunotherapy. FMT capsules were produced using 80-100 g of feces per dose from screened healthy donors, and patients consumed 30-40 capsules while under supervision. The study included 20 patients with NSCLC and high PD-L1 tumor expression receiving FMT before standard first-line pembrolizumab monotherapy and 20 patients with cutaneous melanoma receiving FMT before ipilimumab plus nivolumab.
In the NSCLC cohort, 16 patients (80%) achieved an objective response. The 80% objective response rate exceeded the prespecified efficacy threshold of 64% and was higher than previously described historical data, which ranged from 39% to 46%, the study team noted.
In the melanoma cohort, FMT before nivolumab and ipilimumab yielded an objective response rate of 75%, also exceeding the historical expected response rates of 50% to 58% among patients receiving this ICI combination.
In patients with NSCLC, no grade 3 or higher adverse events were reported. However, grade 3 or higher adverse events were reported in 13 (65%) patients in the melanoma group, suggesting a potentially accelerated onset of immune-related adverse events. Researchers also observed a higher-than-expected frequency of myocarditis in melanoma patients (15%). These toxicities clustered among patients who had FMT donors enriched in Prevotella spp, highlighting the importance of donor selection for future trials, the researchers explained.
The team plans to assess the potential of FMT to overcome primary resistance to ICI as part of the phase 2 CanBiome2 randomized trial, which aims to enroll 128 patients.
The RCC Data
The other two studies focused on FMT in patients with metastatic RCC. In the phase 1 PERFORM study, 20 treatment-naive patients with metastatic RCC added encapsulated healthy-donor FMT to standard ICI-based regimens — most commonly ipilimumab plus nivolumab, with some patients receiving pembrolizumab plus axitinib or pembrolizumab plus lenvatinib.
The primary endpoint was safety defined by the incidence and severity of immune-related adverse events. The safety endpoint was met; 50% of patients (10 of 20) experienced grade 3 immune-related adverse events, and there were no serious FMT-related toxicities and no grade 4 or 5 events.
Among 18 evaluable patients, nine (50%) achieved an objective response, including two who had complete responses (11%). Notably, most treatment responders did not develop any grade 3 or higher immune-related adverse events, the researchers reported.
Finally, in the phase 2a TACITO trial, 45 patients with treatment-naive metastatic RCC were randomly allocated to receive donor FMT or placebo FMT. Patients received three administrations over 6 months — first via colonoscopy then as capsulized doses, alongside pembrolizumab plus axitinib.
The primary endpoint of 12-month progression-free survival narrowly missed statistical significance — 70% vs 41% (P = .053) — but suggested a benefit in the donor FMT group.
“We need more than 1 year to appreciate statistical significance in terms of progression-free survival,” study investigator Gianluca Ianiro, MD, PhD, with Catholic University of the Sacred Heart, Rome, told Medscape Medical News.
As for secondary endpoints, median progression-free survival was significantly longer with donor FMT (24.0 vs 9.0 months; hazard ratio, 0.50; P = .035) and the objective response rate was higher with donor FMT (52% vs 32%).
Why Might FMT Boost ICI Response?
Conceptually, FMT is intended to reshape the gut ecosystem in ways that favor antitumor immunity, and possibly reduce immune dysregulation.
Across these new studies, the mechanistic story is moving beyond the idea that more diversity is good and toward a model that suggests a benefit to removing or suppressing taxa associated with resistance or inflammatory toxicity.
For example, in the TACITO trial, microbiome analysis confirmed that acquisition or loss of specific bacterial strains was associated with 12-month progression-free survival.
Additionally, results of the FMT-LUMINate trial hinted that the therapeutic benefit of FMT may be driven by eliminating harmful bacteria present at baseline, most notably Enterocloster, Clostridium and Streptococcus spp.
“This bacterial depletion was associated with a favorable immunometabolic milieu,” the FMT-LUMINate researchers wrote. Additionally, the results suggest that “failure to eliminate baseline deleterious taxa may sustain an immunosuppressive metabolic and systemic immune milieu that compromises ICI responses.”
Is FMT Ready for Prime Time?
Ianiro told Medscape Medical News he “definitely” thinks microbiome modulation could eventually become part of standard immunotherapy regimens.
Although the “signal” of benefit is clearly there, Davar cautioned that it’s too early to justify routine, off-trial use of FMT specifically to improve ICI response.
“These remain small, proof-of-concept studies. They are not adequately powered trials of fecal transplants and multiple different covariates haven’t been considered,” Davar said.
The study researchers noted that issues around donor selection and availability, dosing schedules, product standardization, and safety risk stratification need to be resolved.
For example, TACITO’s real-world experience shows logistics can matter. Delays occurred due to capsule unavailability and other scheduling barriers, which led to late dosing and missed or shifted treatments in some patients.
That’s a reminder that scaling FMT for oncology would require robust manufacturing, distribution, and time-sensitive coordination with ICI start dates.
More broadly, “whether FMT is the most suitable method of essentially changing the gut microbiome remains unclear,” explained Davar, who suggested that engineered microbiome therapeutics or tailored therapies may be a preferable, more scalable and tailored long-term solution.
Overall, does this new research provide impetus to develop stool banks? “Probably not,” Davar said.
But is it a call for interested parties to think about clinical trials and experimental products that could influence the gut microbiome? “Those are all probably good ideas,” he said.
The PERFORM, TACITO and FMT-LUMINate trials had no commercial funding. Saman Maleki Vareki, PhD, of the PERFORM trial, is a cofounder of LND Therapeutics Inc and has submitted a US patent application related to FMT donor screening. Ianiro has received personal fees for acting as a speaker for Biocodex and Illumina and for acting as a consultant/advisor for Ferring Therapeutics. Arielle Elkrief, MD, of the FMT-LUMINate trial, has received honoraria from AstraZeneca, Merck, Bristol Myers Squibb, and EMD Serono; consulting fees from EverImmune, NECBio, and Sanofi-Pasteur; and is an inventor on a patent regarding the microbiome and immunotherapy response. Davar had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Can Fecal Transplants Enhance Immunotherapy? New Evidence and Cautions
Can Fecal Transplants Enhance Immunotherapy? New Evidence and Cautions
Fecal Microbiota Transplant Safety Goal Met in Kidney Cancer
Fecal Microbiota Transplant Safety Goal Met in Kidney Cancer
TOPLINE:
Healthy donor fecal microbiota transplantation (FMT) combined with immune checkpoint inhibitors (ICI) in metastatic renal cell carcinoma demonstrated safety with a 50% objective response rate and no grade 4-5 toxicities. Successful engraftment of diverse, anti-inflammatory microbiota correlated with improved clinical response and reduced immune-related adverse events.
METHODOLOGY:
- Many patients with metastatic renal cell carcinoma who take ICI experience immune-related adverse events that may require treatment interruption. Recent studies have provided proof of concept for microbiome modulation as a therapeutic adjunct in metastatic renal cell carcinoma, with FMT showing efficacy in resolving TKI-induced toxicities. However, the safety and clinical activity of healthy donor FMT in metastatic renal cell carcinoma remained unexplored, and its mechanism of action was unclear prior to this study.
- The new phase 1 trial enrolled 20 treatment-naive patients with metastatic renal cell carcinoma classified as intermediate-risk or poor-risk disease, who received encapsulated healthy donor FMT (LND101) combined with ipilimumab plus nivolumab (n = 16), pembrolizumab plus axitinib (n = 3), or pembrolizumab plus lenvatinib (n = 1).
- Participants underwent polyethylene glycol bowel preparation before receiving one full dose (36-40 capsules containing 80-100 g of stool) and two half-doses (20-25 capsules each containing 50-60 g of stool) of FMT from rigorously screened healthy donors.
- The primary endpoint was safety assessed through incidence and severity of immune-related adverse events, while secondary endpoints included objective response rate by response evaluation criteria in solid tumors version 1.1, gut microbiome changes, immune correlates, and quality of life.
- Analysis included longitudinal monitoring of stool and blood samples at five timepoints: baseline, week 1 post-FMT, week 4, week 7, and week 10, with a median follow-up of 21.9 months.
TAKEAWAY:
- The safety endpoint was met, with half (10 of 20) of patients experiencing grade 3 immune-related adverse events and no serious FMT-related toxicities or grade 4-5 immune-related adverse events. One patient (5%) reported experiencing an FMT-related grade 1 gastrointestinal event.
- Among evaluable patients (n = 18), the objective response rate was 50% (9 of 18), including two complete responses (11%; 2 of 18), while 67% (12 of 18) achieved clinical benefit defined as complete response, partial response, or stable disease for at least 6 months.
- Higher alpha diversity and greater functional engraftment of short-chain fatty acid-producing and anti-inflammatory taxa correlated with protection from severe immune-related adverse events (P = .041) and improved therapeutic response (P = .006).
- Expansion of Segatella copri above 10 counts per million at 10 weeks post-FMT predicted severe toxicity in patients receiving ipilimumab plus nivolumab, regardless of donor or recipient microbiota origin.
IN PRACTICE:
These findings demonstrate the safety and potential for functional microbiome engraftment to optimize response and minimize toxicity in ICI-treated [metastatic renal cell carcinoma]. Together, our results underscore the importance of functional donor screening and targeted modulation of the microbiome in optimizing the safety and efficacy of next-generation immune-based therapies,” wrote the authors of the study.
SOURCE:
The study was led by Ricardo Fernandes, Behnam Jabbarizadeh, and Adnan Rajeh, London Health Sciences Centre, London, Ontario, Canada. It was published online on January 28 in Nature Medicine.
LIMITATIONS:
According to the authors, the study’s primary limitation was its small sample size, which was not powered to define the ideal donor microbiome composition for enhancing immunotherapy efficacy without additional toxicities. The single-center design and highly selected patient population may limit external generalizability, requiring validation in larger, multicenter trials to refine donor selection criteria and clarify microbiome-immunity mechanisms.
DISCLOSURES:
The clinical trial was primarily funded through philanthropic donations to co-authors Saman Maleki Vareki and Fernandes through the London Health Sciences Foundation clinical trials program. Vareki and Michael Silverman, another co-author, reported having US Patent application no. 63/913,940 related to FMT donor screening. Vareki reported receiving grants from the Lotte and John Hecht Memorial Foundation, the Weston Family Foundation, and the Canadian Institutes of Health Research. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Healthy donor fecal microbiota transplantation (FMT) combined with immune checkpoint inhibitors (ICI) in metastatic renal cell carcinoma demonstrated safety with a 50% objective response rate and no grade 4-5 toxicities. Successful engraftment of diverse, anti-inflammatory microbiota correlated with improved clinical response and reduced immune-related adverse events.
METHODOLOGY:
- Many patients with metastatic renal cell carcinoma who take ICI experience immune-related adverse events that may require treatment interruption. Recent studies have provided proof of concept for microbiome modulation as a therapeutic adjunct in metastatic renal cell carcinoma, with FMT showing efficacy in resolving TKI-induced toxicities. However, the safety and clinical activity of healthy donor FMT in metastatic renal cell carcinoma remained unexplored, and its mechanism of action was unclear prior to this study.
- The new phase 1 trial enrolled 20 treatment-naive patients with metastatic renal cell carcinoma classified as intermediate-risk or poor-risk disease, who received encapsulated healthy donor FMT (LND101) combined with ipilimumab plus nivolumab (n = 16), pembrolizumab plus axitinib (n = 3), or pembrolizumab plus lenvatinib (n = 1).
- Participants underwent polyethylene glycol bowel preparation before receiving one full dose (36-40 capsules containing 80-100 g of stool) and two half-doses (20-25 capsules each containing 50-60 g of stool) of FMT from rigorously screened healthy donors.
- The primary endpoint was safety assessed through incidence and severity of immune-related adverse events, while secondary endpoints included objective response rate by response evaluation criteria in solid tumors version 1.1, gut microbiome changes, immune correlates, and quality of life.
- Analysis included longitudinal monitoring of stool and blood samples at five timepoints: baseline, week 1 post-FMT, week 4, week 7, and week 10, with a median follow-up of 21.9 months.
TAKEAWAY:
- The safety endpoint was met, with half (10 of 20) of patients experiencing grade 3 immune-related adverse events and no serious FMT-related toxicities or grade 4-5 immune-related adverse events. One patient (5%) reported experiencing an FMT-related grade 1 gastrointestinal event.
- Among evaluable patients (n = 18), the objective response rate was 50% (9 of 18), including two complete responses (11%; 2 of 18), while 67% (12 of 18) achieved clinical benefit defined as complete response, partial response, or stable disease for at least 6 months.
- Higher alpha diversity and greater functional engraftment of short-chain fatty acid-producing and anti-inflammatory taxa correlated with protection from severe immune-related adverse events (P = .041) and improved therapeutic response (P = .006).
- Expansion of Segatella copri above 10 counts per million at 10 weeks post-FMT predicted severe toxicity in patients receiving ipilimumab plus nivolumab, regardless of donor or recipient microbiota origin.
IN PRACTICE:
These findings demonstrate the safety and potential for functional microbiome engraftment to optimize response and minimize toxicity in ICI-treated [metastatic renal cell carcinoma]. Together, our results underscore the importance of functional donor screening and targeted modulation of the microbiome in optimizing the safety and efficacy of next-generation immune-based therapies,” wrote the authors of the study.
SOURCE:
The study was led by Ricardo Fernandes, Behnam Jabbarizadeh, and Adnan Rajeh, London Health Sciences Centre, London, Ontario, Canada. It was published online on January 28 in Nature Medicine.
LIMITATIONS:
According to the authors, the study’s primary limitation was its small sample size, which was not powered to define the ideal donor microbiome composition for enhancing immunotherapy efficacy without additional toxicities. The single-center design and highly selected patient population may limit external generalizability, requiring validation in larger, multicenter trials to refine donor selection criteria and clarify microbiome-immunity mechanisms.
DISCLOSURES:
The clinical trial was primarily funded through philanthropic donations to co-authors Saman Maleki Vareki and Fernandes through the London Health Sciences Foundation clinical trials program. Vareki and Michael Silverman, another co-author, reported having US Patent application no. 63/913,940 related to FMT donor screening. Vareki reported receiving grants from the Lotte and John Hecht Memorial Foundation, the Weston Family Foundation, and the Canadian Institutes of Health Research. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Healthy donor fecal microbiota transplantation (FMT) combined with immune checkpoint inhibitors (ICI) in metastatic renal cell carcinoma demonstrated safety with a 50% objective response rate and no grade 4-5 toxicities. Successful engraftment of diverse, anti-inflammatory microbiota correlated with improved clinical response and reduced immune-related adverse events.
METHODOLOGY:
- Many patients with metastatic renal cell carcinoma who take ICI experience immune-related adverse events that may require treatment interruption. Recent studies have provided proof of concept for microbiome modulation as a therapeutic adjunct in metastatic renal cell carcinoma, with FMT showing efficacy in resolving TKI-induced toxicities. However, the safety and clinical activity of healthy donor FMT in metastatic renal cell carcinoma remained unexplored, and its mechanism of action was unclear prior to this study.
- The new phase 1 trial enrolled 20 treatment-naive patients with metastatic renal cell carcinoma classified as intermediate-risk or poor-risk disease, who received encapsulated healthy donor FMT (LND101) combined with ipilimumab plus nivolumab (n = 16), pembrolizumab plus axitinib (n = 3), or pembrolizumab plus lenvatinib (n = 1).
- Participants underwent polyethylene glycol bowel preparation before receiving one full dose (36-40 capsules containing 80-100 g of stool) and two half-doses (20-25 capsules each containing 50-60 g of stool) of FMT from rigorously screened healthy donors.
- The primary endpoint was safety assessed through incidence and severity of immune-related adverse events, while secondary endpoints included objective response rate by response evaluation criteria in solid tumors version 1.1, gut microbiome changes, immune correlates, and quality of life.
- Analysis included longitudinal monitoring of stool and blood samples at five timepoints: baseline, week 1 post-FMT, week 4, week 7, and week 10, with a median follow-up of 21.9 months.
TAKEAWAY:
- The safety endpoint was met, with half (10 of 20) of patients experiencing grade 3 immune-related adverse events and no serious FMT-related toxicities or grade 4-5 immune-related adverse events. One patient (5%) reported experiencing an FMT-related grade 1 gastrointestinal event.
- Among evaluable patients (n = 18), the objective response rate was 50% (9 of 18), including two complete responses (11%; 2 of 18), while 67% (12 of 18) achieved clinical benefit defined as complete response, partial response, or stable disease for at least 6 months.
- Higher alpha diversity and greater functional engraftment of short-chain fatty acid-producing and anti-inflammatory taxa correlated with protection from severe immune-related adverse events (P = .041) and improved therapeutic response (P = .006).
- Expansion of Segatella copri above 10 counts per million at 10 weeks post-FMT predicted severe toxicity in patients receiving ipilimumab plus nivolumab, regardless of donor or recipient microbiota origin.
IN PRACTICE:
These findings demonstrate the safety and potential for functional microbiome engraftment to optimize response and minimize toxicity in ICI-treated [metastatic renal cell carcinoma]. Together, our results underscore the importance of functional donor screening and targeted modulation of the microbiome in optimizing the safety and efficacy of next-generation immune-based therapies,” wrote the authors of the study.
SOURCE:
The study was led by Ricardo Fernandes, Behnam Jabbarizadeh, and Adnan Rajeh, London Health Sciences Centre, London, Ontario, Canada. It was published online on January 28 in Nature Medicine.
LIMITATIONS:
According to the authors, the study’s primary limitation was its small sample size, which was not powered to define the ideal donor microbiome composition for enhancing immunotherapy efficacy without additional toxicities. The single-center design and highly selected patient population may limit external generalizability, requiring validation in larger, multicenter trials to refine donor selection criteria and clarify microbiome-immunity mechanisms.
DISCLOSURES:
The clinical trial was primarily funded through philanthropic donations to co-authors Saman Maleki Vareki and Fernandes through the London Health Sciences Foundation clinical trials program. Vareki and Michael Silverman, another co-author, reported having US Patent application no. 63/913,940 related to FMT donor screening. Vareki reported receiving grants from the Lotte and John Hecht Memorial Foundation, the Weston Family Foundation, and the Canadian Institutes of Health Research. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Fecal Microbiota Transplant Safety Goal Met in Kidney Cancer
Fecal Microbiota Transplant Safety Goal Met in Kidney Cancer
Rising Kidney Cancer Cases and Emerging Treatments for Veterans
Rising Kidney Cancer Cases and Emerging Treatments for Veterans
Click here to view more from Cancer Data Trends 2025.
1. American Cancer Society website. Key Statistics About Kidney Cancer. Revised May 2024. Accessed December 18, 2024. https://www.cancer.org/cancer/types/kidney-cancer/about/key-statistics.html
2. American Cancer Society website. Cancer Facts & Figures 2024. 2024—First Year the US Expects More than 2M New Cases of Cancer. Published January 17, 2024. Accessed December 18, 2024. https://www.cancer.org/research/acs-research-news/facts-and-figures-2024.html
3.United States Department of Veterans Affairs factsheet. Pact Act & Gulf War, Post-911 Era Veterans. Published July 2023. Accessed December 18, 2024. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.va.gov/files/2023-08/PACT%20Act%20and%20Gulf%20War%2C%20Post-911%20Veterans%20NEW%20July%202023.pdf
4. Li M, Li L, Zheng J, Li Z, Li S, Wang K, Chen X. Liquid biopsy at the frontier in renal cell carcinoma: recent analysis of techniques and clinical application. Mol Cancer. 2023 Feb 21;22(1):37. doi:10.1186/s12943-023-01745-7
5. Bellman NL. Incidental Finding of Renal Cell Carcinoma: Detected by a Thrombus in the Inferior Vena Cava. Journal of Diagnostic Medical Sonography. 2015;31(2):118-121. doi:10.1177/8756479314546691
6. Brown JT. Adjuvant Therapy for Non-Clear Cell Renal Cell Carcinoma—The Ascent Continues. JAMA Network Open. 2024 Aug 1;7(8):e2425251. doi:10.1001/jamanetworkopen.2024.25251
7. Siva S, Louie AV, Kotecha R, et al. Stereotactic body radiotherapy for primary renal cell carcinoma: a systematic review and practice guideline from the International Society of Stereotactic Radiosurgery (ISRS). Lancet Oncol. 2024 Jan;25(1):e18-e28. doi: 10.1016/S1470-2045(23)00513-2.
8. Choueiri TK, Tomczak P, Park SH, et al; for the KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi:10.1056/NEJMoa2312695
9. Bytnar JA, McGlynn KA, Kern SQ, Shriver CD, Zhu K. Incidence rates of bladder and kidney cancers among US military servicemen: comparison with the rates in the general US population. Eur J Cancer Prev. 2024 Nov 1;33(6):505-511. doi:10.1097/CEJ.0000000000000886
Click here to view more from Cancer Data Trends 2025.
Click here to view more from Cancer Data Trends 2025.
1. American Cancer Society website. Key Statistics About Kidney Cancer. Revised May 2024. Accessed December 18, 2024. https://www.cancer.org/cancer/types/kidney-cancer/about/key-statistics.html
2. American Cancer Society website. Cancer Facts & Figures 2024. 2024—First Year the US Expects More than 2M New Cases of Cancer. Published January 17, 2024. Accessed December 18, 2024. https://www.cancer.org/research/acs-research-news/facts-and-figures-2024.html
3.United States Department of Veterans Affairs factsheet. Pact Act & Gulf War, Post-911 Era Veterans. Published July 2023. Accessed December 18, 2024. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.va.gov/files/2023-08/PACT%20Act%20and%20Gulf%20War%2C%20Post-911%20Veterans%20NEW%20July%202023.pdf
4. Li M, Li L, Zheng J, Li Z, Li S, Wang K, Chen X. Liquid biopsy at the frontier in renal cell carcinoma: recent analysis of techniques and clinical application. Mol Cancer. 2023 Feb 21;22(1):37. doi:10.1186/s12943-023-01745-7
5. Bellman NL. Incidental Finding of Renal Cell Carcinoma: Detected by a Thrombus in the Inferior Vena Cava. Journal of Diagnostic Medical Sonography. 2015;31(2):118-121. doi:10.1177/8756479314546691
6. Brown JT. Adjuvant Therapy for Non-Clear Cell Renal Cell Carcinoma—The Ascent Continues. JAMA Network Open. 2024 Aug 1;7(8):e2425251. doi:10.1001/jamanetworkopen.2024.25251
7. Siva S, Louie AV, Kotecha R, et al. Stereotactic body radiotherapy for primary renal cell carcinoma: a systematic review and practice guideline from the International Society of Stereotactic Radiosurgery (ISRS). Lancet Oncol. 2024 Jan;25(1):e18-e28. doi: 10.1016/S1470-2045(23)00513-2.
8. Choueiri TK, Tomczak P, Park SH, et al; for the KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi:10.1056/NEJMoa2312695
9. Bytnar JA, McGlynn KA, Kern SQ, Shriver CD, Zhu K. Incidence rates of bladder and kidney cancers among US military servicemen: comparison with the rates in the general US population. Eur J Cancer Prev. 2024 Nov 1;33(6):505-511. doi:10.1097/CEJ.0000000000000886
1. American Cancer Society website. Key Statistics About Kidney Cancer. Revised May 2024. Accessed December 18, 2024. https://www.cancer.org/cancer/types/kidney-cancer/about/key-statistics.html
2. American Cancer Society website. Cancer Facts & Figures 2024. 2024—First Year the US Expects More than 2M New Cases of Cancer. Published January 17, 2024. Accessed December 18, 2024. https://www.cancer.org/research/acs-research-news/facts-and-figures-2024.html
3.United States Department of Veterans Affairs factsheet. Pact Act & Gulf War, Post-911 Era Veterans. Published July 2023. Accessed December 18, 2024. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.va.gov/files/2023-08/PACT%20Act%20and%20Gulf%20War%2C%20Post-911%20Veterans%20NEW%20July%202023.pdf
4. Li M, Li L, Zheng J, Li Z, Li S, Wang K, Chen X. Liquid biopsy at the frontier in renal cell carcinoma: recent analysis of techniques and clinical application. Mol Cancer. 2023 Feb 21;22(1):37. doi:10.1186/s12943-023-01745-7
5. Bellman NL. Incidental Finding of Renal Cell Carcinoma: Detected by a Thrombus in the Inferior Vena Cava. Journal of Diagnostic Medical Sonography. 2015;31(2):118-121. doi:10.1177/8756479314546691
6. Brown JT. Adjuvant Therapy for Non-Clear Cell Renal Cell Carcinoma—The Ascent Continues. JAMA Network Open. 2024 Aug 1;7(8):e2425251. doi:10.1001/jamanetworkopen.2024.25251
7. Siva S, Louie AV, Kotecha R, et al. Stereotactic body radiotherapy for primary renal cell carcinoma: a systematic review and practice guideline from the International Society of Stereotactic Radiosurgery (ISRS). Lancet Oncol. 2024 Jan;25(1):e18-e28. doi: 10.1016/S1470-2045(23)00513-2.
8. Choueiri TK, Tomczak P, Park SH, et al; for the KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi:10.1056/NEJMoa2312695
9. Bytnar JA, McGlynn KA, Kern SQ, Shriver CD, Zhu K. Incidence rates of bladder and kidney cancers among US military servicemen: comparison with the rates in the general US population. Eur J Cancer Prev. 2024 Nov 1;33(6):505-511. doi:10.1097/CEJ.0000000000000886
Rising Kidney Cancer Cases and Emerging Treatments for Veterans
Rising Kidney Cancer Cases and Emerging Treatments for Veterans




SBRT: A New Front-Runner in Treating Localized Renal Cell Carcinoma?
For patients with primary localized renal cell carcinoma (RCC), especially those who aren’t good candidates for surgery, noninvasive or minimally invasive ablative treatments have emerged as important options. These ablative treatments include radiofrequency ablation (RFA), microwave ablation, cryoablation, and the relative new-comer stereotactic body radiotherapy (SBRT).
But how do these approaches stack up against each other?
A recent meta-analysis published in Lancet Oncology found that SBRT appears to be equally safe and potentially more effective than other ablative treatment options for localized RCC.
“Our findings suggest that SBRT might offer a particularly advantageous option for treating larger renal cell carcinoma tumors, yielding the highest local control rates among ablative options with comparatively low rates of severe complications,” Srinivas Raman, MD, Department of Radiation Oncology, Princess Margaret Cancer Centre, Toronto, Ontario, Canada, and colleagues wrote.
Outside experts who spoke with Medscape Medical News said SBRT should likely play a larger role in the management of early-stage RCC.
“Given its noninvasive nature, favorable toxicity profile, and comparable renal outcomes, SBRT warrants broader adoption,” said Shankar Siva, PhD, MBBS, a radiation oncologist at the Peter MacCallum Cancer Centre and professor at the University of Melbourne, both in Melbourne, Australia.
This new analysis is “helpful as it provides reassurance and further strong quality data to present in multidisciplinary renal rounds and tumor boards to consider the use of SBRT as an alternative to other ablative technique,” said Joelle Helou, MD, MSc, radiation oncologist, Verspeeten Family Cancer Centre, and assistant professor, Department of Oncology, Western University, both in London, Ontario, Canada.
Filling a Knowledge Gap
RCC is the most common malignancy of the kidney, accounting for > 90% of all renal malignancies. Worldwide, the incidence of RCC has continued to rise, with a 2% annual rate of increase over the past two decades.
The conventional treatment of choice is radical or partial nephrectomy; however, not all patients are ideally suited for surgery, especially those who are older or have compromised kidney function or comorbid conditions.
Ablative therapies have been integrated into clinical guidelines as evidence-based interventions to treat primary RCC. These therapies include RFA and microwave ablation — two minimally invasive thermal ablation techniques that use heat to destroy the tumor tissue — and cryoablation, which uses extreme cold to destroy the tumor tissue.
Studies have generally found similar outcomes with RFA and microwave ablation, with the choice of treatment often guided by what’s available and operator expertise. The US and European guidelines recommend these treatments, particularly for smaller tumors (< 4 cm), citing their effectiveness and minimal invasiveness.
SBRT is a relatively new noninvasive option that delivers highly focused radiation doses to the tumor across multiple sessions and may be particularly suited to larger tumors (≥ 4 cm).
National Comprehensive Cancer Network guidelines state that SBRT may be considered for nonoptimal surgical candidates with stage I, II, or III kidney cancer.
However, comparative data on these four techniques has been limited until now.
What Did the Meta-Analysis Find?
Raman and colleagues performed a systematic review and meta-analysis pooled data from 133 studies involving 8910 patients (mean age, 68 years) with localized RCC treated with one of the four ablative therapies.
Overall, across the four ablative approaches, local control rates were very similar at 1 year, ranging from 95% for cryoablation to 99% for SBRT, and at 2 years, ranging from 94% for cryoablation to 97% for SBRT. At 5 years, however, there was a slightly greater separation in outcomes favoring SBRT (95%) and RFA (92%) compared with cryoablation (90%) and microwave ablation (86%).
Although all four techniques demonstrated similar local control for small tumors measuring < 4 cm, the approaches began to diverge for larger tumors measuring ≥ 4 cm at 1, 2, and 5 years. At 5 years, for instance, SBRT had the highest local control rate (93%), outperforming RFA (79%), microwave ablation (82%), and cryoablation (85%).
Looking at survival outcomes, cancer-specific survival was 100% at 1 year across all treatments. At 5 years, small differences in cancer-specific survival were observed. For smaller tumors, cancer-specific survival ranged from 100% for both SBRT and RFA to 97% for microwave ablation and 98% for cryoablation. For larger tumors, the cancer-specific survival rate was 100% for microwave ablation, 95% for SBRT, and 94% for cryoablation.
These small differences in cancer-specific survival likely reflect differences in patient and tumor characteristics across the treatment groups, the study authors said.
Notably, patients treated with SBRT were older than those treated with microwave ablation and RFA, while also having the largest tumors, which have consistently been shown to be associated with worse local control, greater propensity for regional and distant metastases, worse survival outcomes, and increased treatment-related toxicity, the authors explained.
There were no significant differences in the rate of grade 1-2 adverse events between the ablative methods, although grade 3-4 adverse events occurred in a significantly higher proportion of patients treated with cryoablation (3%) than in those who received RFA and SBRT (2%) or microwave ablation (1%). Baseline or change in renal function, as measured by estimated glomerular filtration rate, did not differ between the ablative techniques.
Overall, the findings reinforce that, although typically offered to older patients with worse baseline renal function and much larger tumors, “SBRT maintained high effectiveness at 1, 2, and 5 years compared to thermal ablation,” Siva told Medscape Medical News.
SBRT in Clinical Practice?
Despite the mounting evidence in favor of SBRT for primary localized RCC unsuitable for surgery, “there is still some reluctance from urologists, mainly, to refer patients for consideration of SBRT,” Helou told Medscape Medical News.
This hesitance is reflected in the meta-analysis, he noted, with SBRT being the least performed ablative therapy (612 patients). Cryoablation was the most common technique used in 3726 patients, followed by RFA (2503 patients) and microwave ablation (2069 patients).
The “compelling efficacy and safety data suggest SBRT should play a larger role in managing early-stage RCC in nonsurgical candidates, particularly for larger tumors where it offers excellent long-term local control,” said Siva, who led the phase 2 FASTTRACK II study evaluating SBRT in patients with inoperable or high-risk primary RCC.
Despite patients having larger than average tumors (4.6 cm) compared with those in many other trials, Siva and colleagues reported a 100% local control rate following SBRT and no patient deaths from cancer during the study period.
The FASTTRACK II study marked “an inflection point for SBRT, and [the approach] is now slowly getting traction,” Chad Tang, MD, radiation oncologist, MD Anderson Cancer Center, Houston, told Medscape Medical News.
Overall, Raman and colleagues said decisions about ablative therapy should be “precisely tailored to the individual patient’s clinical condition and treatment objectives.” Treatment selection should, for instance, depend on tumor size, location, patient comorbidities, availability of a technique, institutional and physician expertise, and patient preference.
Looking ahead, randomized controlled trials across larger patient populations are needed to further elucidate the long-term cancer and survival outcomes associated with these ablative treatments. Research comparing ablative methods with surgery and surveillance as well as exploring other relevant clinical outcomes, such as cost-effectiveness and quality of life, should be performed as well.
“Prospective randomized trials remain essential to further refine the position of SBRT in clinical practice in patients who are surgical candidates,” Siva told Medscape Medical News.
This research had no commercial funding. Raman reported receiving personal fees from AstraZeneca, Sanofi, Knight Pharmaceuticals, Verity Pharma, and Tersera, and grants from Knight Therapeutics, AstraZeneca, and Varian. Siva reported financial relationships with AstraZeneca and Telix Pharmaceuticals. Helou and Tang had no relevant disclosures.
For patients with primary localized renal cell carcinoma (RCC), especially those who aren’t good candidates for surgery, noninvasive or minimally invasive ablative treatments have emerged as important options. These ablative treatments include radiofrequency ablation (RFA), microwave ablation, cryoablation, and the relative new-comer stereotactic body radiotherapy (SBRT).
But how do these approaches stack up against each other?
A recent meta-analysis published in Lancet Oncology found that SBRT appears to be equally safe and potentially more effective than other ablative treatment options for localized RCC.
“Our findings suggest that SBRT might offer a particularly advantageous option for treating larger renal cell carcinoma tumors, yielding the highest local control rates among ablative options with comparatively low rates of severe complications,” Srinivas Raman, MD, Department of Radiation Oncology, Princess Margaret Cancer Centre, Toronto, Ontario, Canada, and colleagues wrote.
Outside experts who spoke with Medscape Medical News said SBRT should likely play a larger role in the management of early-stage RCC.
“Given its noninvasive nature, favorable toxicity profile, and comparable renal outcomes, SBRT warrants broader adoption,” said Shankar Siva, PhD, MBBS, a radiation oncologist at the Peter MacCallum Cancer Centre and professor at the University of Melbourne, both in Melbourne, Australia.
This new analysis is “helpful as it provides reassurance and further strong quality data to present in multidisciplinary renal rounds and tumor boards to consider the use of SBRT as an alternative to other ablative technique,” said Joelle Helou, MD, MSc, radiation oncologist, Verspeeten Family Cancer Centre, and assistant professor, Department of Oncology, Western University, both in London, Ontario, Canada.
Filling a Knowledge Gap
RCC is the most common malignancy of the kidney, accounting for > 90% of all renal malignancies. Worldwide, the incidence of RCC has continued to rise, with a 2% annual rate of increase over the past two decades.
The conventional treatment of choice is radical or partial nephrectomy; however, not all patients are ideally suited for surgery, especially those who are older or have compromised kidney function or comorbid conditions.
Ablative therapies have been integrated into clinical guidelines as evidence-based interventions to treat primary RCC. These therapies include RFA and microwave ablation — two minimally invasive thermal ablation techniques that use heat to destroy the tumor tissue — and cryoablation, which uses extreme cold to destroy the tumor tissue.
Studies have generally found similar outcomes with RFA and microwave ablation, with the choice of treatment often guided by what’s available and operator expertise. The US and European guidelines recommend these treatments, particularly for smaller tumors (< 4 cm), citing their effectiveness and minimal invasiveness.
SBRT is a relatively new noninvasive option that delivers highly focused radiation doses to the tumor across multiple sessions and may be particularly suited to larger tumors (≥ 4 cm).
National Comprehensive Cancer Network guidelines state that SBRT may be considered for nonoptimal surgical candidates with stage I, II, or III kidney cancer.
However, comparative data on these four techniques has been limited until now.
What Did the Meta-Analysis Find?
Raman and colleagues performed a systematic review and meta-analysis pooled data from 133 studies involving 8910 patients (mean age, 68 years) with localized RCC treated with one of the four ablative therapies.
Overall, across the four ablative approaches, local control rates were very similar at 1 year, ranging from 95% for cryoablation to 99% for SBRT, and at 2 years, ranging from 94% for cryoablation to 97% for SBRT. At 5 years, however, there was a slightly greater separation in outcomes favoring SBRT (95%) and RFA (92%) compared with cryoablation (90%) and microwave ablation (86%).
Although all four techniques demonstrated similar local control for small tumors measuring < 4 cm, the approaches began to diverge for larger tumors measuring ≥ 4 cm at 1, 2, and 5 years. At 5 years, for instance, SBRT had the highest local control rate (93%), outperforming RFA (79%), microwave ablation (82%), and cryoablation (85%).
Looking at survival outcomes, cancer-specific survival was 100% at 1 year across all treatments. At 5 years, small differences in cancer-specific survival were observed. For smaller tumors, cancer-specific survival ranged from 100% for both SBRT and RFA to 97% for microwave ablation and 98% for cryoablation. For larger tumors, the cancer-specific survival rate was 100% for microwave ablation, 95% for SBRT, and 94% for cryoablation.
These small differences in cancer-specific survival likely reflect differences in patient and tumor characteristics across the treatment groups, the study authors said.
Notably, patients treated with SBRT were older than those treated with microwave ablation and RFA, while also having the largest tumors, which have consistently been shown to be associated with worse local control, greater propensity for regional and distant metastases, worse survival outcomes, and increased treatment-related toxicity, the authors explained.
There were no significant differences in the rate of grade 1-2 adverse events between the ablative methods, although grade 3-4 adverse events occurred in a significantly higher proportion of patients treated with cryoablation (3%) than in those who received RFA and SBRT (2%) or microwave ablation (1%). Baseline or change in renal function, as measured by estimated glomerular filtration rate, did not differ between the ablative techniques.
Overall, the findings reinforce that, although typically offered to older patients with worse baseline renal function and much larger tumors, “SBRT maintained high effectiveness at 1, 2, and 5 years compared to thermal ablation,” Siva told Medscape Medical News.
SBRT in Clinical Practice?
Despite the mounting evidence in favor of SBRT for primary localized RCC unsuitable for surgery, “there is still some reluctance from urologists, mainly, to refer patients for consideration of SBRT,” Helou told Medscape Medical News.
This hesitance is reflected in the meta-analysis, he noted, with SBRT being the least performed ablative therapy (612 patients). Cryoablation was the most common technique used in 3726 patients, followed by RFA (2503 patients) and microwave ablation (2069 patients).
The “compelling efficacy and safety data suggest SBRT should play a larger role in managing early-stage RCC in nonsurgical candidates, particularly for larger tumors where it offers excellent long-term local control,” said Siva, who led the phase 2 FASTTRACK II study evaluating SBRT in patients with inoperable or high-risk primary RCC.
Despite patients having larger than average tumors (4.6 cm) compared with those in many other trials, Siva and colleagues reported a 100% local control rate following SBRT and no patient deaths from cancer during the study period.
The FASTTRACK II study marked “an inflection point for SBRT, and [the approach] is now slowly getting traction,” Chad Tang, MD, radiation oncologist, MD Anderson Cancer Center, Houston, told Medscape Medical News.
Overall, Raman and colleagues said decisions about ablative therapy should be “precisely tailored to the individual patient’s clinical condition and treatment objectives.” Treatment selection should, for instance, depend on tumor size, location, patient comorbidities, availability of a technique, institutional and physician expertise, and patient preference.
Looking ahead, randomized controlled trials across larger patient populations are needed to further elucidate the long-term cancer and survival outcomes associated with these ablative treatments. Research comparing ablative methods with surgery and surveillance as well as exploring other relevant clinical outcomes, such as cost-effectiveness and quality of life, should be performed as well.
“Prospective randomized trials remain essential to further refine the position of SBRT in clinical practice in patients who are surgical candidates,” Siva told Medscape Medical News.
This research had no commercial funding. Raman reported receiving personal fees from AstraZeneca, Sanofi, Knight Pharmaceuticals, Verity Pharma, and Tersera, and grants from Knight Therapeutics, AstraZeneca, and Varian. Siva reported financial relationships with AstraZeneca and Telix Pharmaceuticals. Helou and Tang had no relevant disclosures.
For patients with primary localized renal cell carcinoma (RCC), especially those who aren’t good candidates for surgery, noninvasive or minimally invasive ablative treatments have emerged as important options. These ablative treatments include radiofrequency ablation (RFA), microwave ablation, cryoablation, and the relative new-comer stereotactic body radiotherapy (SBRT).
But how do these approaches stack up against each other?
A recent meta-analysis published in Lancet Oncology found that SBRT appears to be equally safe and potentially more effective than other ablative treatment options for localized RCC.
“Our findings suggest that SBRT might offer a particularly advantageous option for treating larger renal cell carcinoma tumors, yielding the highest local control rates among ablative options with comparatively low rates of severe complications,” Srinivas Raman, MD, Department of Radiation Oncology, Princess Margaret Cancer Centre, Toronto, Ontario, Canada, and colleagues wrote.
Outside experts who spoke with Medscape Medical News said SBRT should likely play a larger role in the management of early-stage RCC.
“Given its noninvasive nature, favorable toxicity profile, and comparable renal outcomes, SBRT warrants broader adoption,” said Shankar Siva, PhD, MBBS, a radiation oncologist at the Peter MacCallum Cancer Centre and professor at the University of Melbourne, both in Melbourne, Australia.
This new analysis is “helpful as it provides reassurance and further strong quality data to present in multidisciplinary renal rounds and tumor boards to consider the use of SBRT as an alternative to other ablative technique,” said Joelle Helou, MD, MSc, radiation oncologist, Verspeeten Family Cancer Centre, and assistant professor, Department of Oncology, Western University, both in London, Ontario, Canada.
Filling a Knowledge Gap
RCC is the most common malignancy of the kidney, accounting for > 90% of all renal malignancies. Worldwide, the incidence of RCC has continued to rise, with a 2% annual rate of increase over the past two decades.
The conventional treatment of choice is radical or partial nephrectomy; however, not all patients are ideally suited for surgery, especially those who are older or have compromised kidney function or comorbid conditions.
Ablative therapies have been integrated into clinical guidelines as evidence-based interventions to treat primary RCC. These therapies include RFA and microwave ablation — two minimally invasive thermal ablation techniques that use heat to destroy the tumor tissue — and cryoablation, which uses extreme cold to destroy the tumor tissue.
Studies have generally found similar outcomes with RFA and microwave ablation, with the choice of treatment often guided by what’s available and operator expertise. The US and European guidelines recommend these treatments, particularly for smaller tumors (< 4 cm), citing their effectiveness and minimal invasiveness.
SBRT is a relatively new noninvasive option that delivers highly focused radiation doses to the tumor across multiple sessions and may be particularly suited to larger tumors (≥ 4 cm).
National Comprehensive Cancer Network guidelines state that SBRT may be considered for nonoptimal surgical candidates with stage I, II, or III kidney cancer.
However, comparative data on these four techniques has been limited until now.
What Did the Meta-Analysis Find?
Raman and colleagues performed a systematic review and meta-analysis pooled data from 133 studies involving 8910 patients (mean age, 68 years) with localized RCC treated with one of the four ablative therapies.
Overall, across the four ablative approaches, local control rates were very similar at 1 year, ranging from 95% for cryoablation to 99% for SBRT, and at 2 years, ranging from 94% for cryoablation to 97% for SBRT. At 5 years, however, there was a slightly greater separation in outcomes favoring SBRT (95%) and RFA (92%) compared with cryoablation (90%) and microwave ablation (86%).
Although all four techniques demonstrated similar local control for small tumors measuring < 4 cm, the approaches began to diverge for larger tumors measuring ≥ 4 cm at 1, 2, and 5 years. At 5 years, for instance, SBRT had the highest local control rate (93%), outperforming RFA (79%), microwave ablation (82%), and cryoablation (85%).
Looking at survival outcomes, cancer-specific survival was 100% at 1 year across all treatments. At 5 years, small differences in cancer-specific survival were observed. For smaller tumors, cancer-specific survival ranged from 100% for both SBRT and RFA to 97% for microwave ablation and 98% for cryoablation. For larger tumors, the cancer-specific survival rate was 100% for microwave ablation, 95% for SBRT, and 94% for cryoablation.
These small differences in cancer-specific survival likely reflect differences in patient and tumor characteristics across the treatment groups, the study authors said.
Notably, patients treated with SBRT were older than those treated with microwave ablation and RFA, while also having the largest tumors, which have consistently been shown to be associated with worse local control, greater propensity for regional and distant metastases, worse survival outcomes, and increased treatment-related toxicity, the authors explained.
There were no significant differences in the rate of grade 1-2 adverse events between the ablative methods, although grade 3-4 adverse events occurred in a significantly higher proportion of patients treated with cryoablation (3%) than in those who received RFA and SBRT (2%) or microwave ablation (1%). Baseline or change in renal function, as measured by estimated glomerular filtration rate, did not differ between the ablative techniques.
Overall, the findings reinforce that, although typically offered to older patients with worse baseline renal function and much larger tumors, “SBRT maintained high effectiveness at 1, 2, and 5 years compared to thermal ablation,” Siva told Medscape Medical News.
SBRT in Clinical Practice?
Despite the mounting evidence in favor of SBRT for primary localized RCC unsuitable for surgery, “there is still some reluctance from urologists, mainly, to refer patients for consideration of SBRT,” Helou told Medscape Medical News.
This hesitance is reflected in the meta-analysis, he noted, with SBRT being the least performed ablative therapy (612 patients). Cryoablation was the most common technique used in 3726 patients, followed by RFA (2503 patients) and microwave ablation (2069 patients).
The “compelling efficacy and safety data suggest SBRT should play a larger role in managing early-stage RCC in nonsurgical candidates, particularly for larger tumors where it offers excellent long-term local control,” said Siva, who led the phase 2 FASTTRACK II study evaluating SBRT in patients with inoperable or high-risk primary RCC.
Despite patients having larger than average tumors (4.6 cm) compared with those in many other trials, Siva and colleagues reported a 100% local control rate following SBRT and no patient deaths from cancer during the study period.
The FASTTRACK II study marked “an inflection point for SBRT, and [the approach] is now slowly getting traction,” Chad Tang, MD, radiation oncologist, MD Anderson Cancer Center, Houston, told Medscape Medical News.
Overall, Raman and colleagues said decisions about ablative therapy should be “precisely tailored to the individual patient’s clinical condition and treatment objectives.” Treatment selection should, for instance, depend on tumor size, location, patient comorbidities, availability of a technique, institutional and physician expertise, and patient preference.
Looking ahead, randomized controlled trials across larger patient populations are needed to further elucidate the long-term cancer and survival outcomes associated with these ablative treatments. Research comparing ablative methods with surgery and surveillance as well as exploring other relevant clinical outcomes, such as cost-effectiveness and quality of life, should be performed as well.
“Prospective randomized trials remain essential to further refine the position of SBRT in clinical practice in patients who are surgical candidates,” Siva told Medscape Medical News.
This research had no commercial funding. Raman reported receiving personal fees from AstraZeneca, Sanofi, Knight Pharmaceuticals, Verity Pharma, and Tersera, and grants from Knight Therapeutics, AstraZeneca, and Varian. Siva reported financial relationships with AstraZeneca and Telix Pharmaceuticals. Helou and Tang had no relevant disclosures.
New Cancer Drugs: Do Patients Prefer Faster Access or Clinical Benefit?
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
When the Food and Drug Administration (FDA) grants cancer drugs accelerated approval, a key aim is to provide patients faster access to therapies that can benefit them.
The downside of a speedier approval timeline, however, is that it’s often not yet clear whether the new drugs will actually allow a patient to live longer or better. Information on overall survival and quality of life typically comes years later, after drugs undergo confirmatory trials, or sometimes not at all, if companies fail to conduct these trials.
During this waiting period, patients may be receiving a cancer drug that provides no real clinical benefit but comes with a host of toxicities.
In fact, the odds are about as good as a coin flip. For cancer drugs that have confirmatory trial data, more than half don’t ultimately provide an overall survival or quality of life benefit.
Inherent to the accelerated approval process is the assumption that patients are willing to accept this uncertainty in exchange for faster access.
But is that really the case?
The researchers asked about 870 adults with experience of cancer challenges — either their own cancer diagnosis or that of family or a close friend — whether they valued faster access or certainty that a drug really works.
In the study, participants imagined they had been diagnosed with cancer and could choose between two cancer drugs under investigation in clinical trials but with uncertain effectiveness, and a current standard treatment. Participants had to make a series of choices based on five scenarios.
The first two scenarios were based on the impact of the current standard treatment: A patient’s life expectancy on the standard treatment (6 months up to 3 years), and a patient’s physical health on the standard treatment (functional status restricted only during strenuous activities up to completely disabled).
The remaining three scenarios dealt with the two new drugs: The effect of the new drugs on a surrogate endpoint, progression-free survival (whether the drugs slowed tumor growth for an extra month or 5 additional months compared with the standard treatment), certainty that slowing tumor growth will improve survival (very low to high), and the wait time to access the drugs (immediately to as long as 2 years).
The researchers assessed the relative importance of survival benefit certainty vs wait time and how that balance shifted depending on the different scenarios.
Overall, the researchers found that, if there was no evidence linking the surrogate endpoint (progression-free survival) to overall survival, patients were willing to wait about 8 months for weak evidence of an overall survival benefit (ie, low certainty the drug will extend survival by 1-5 months), about 16 months for moderate certainty, and almost 22 months for high certainty.
Despite a willingness to wait for greater certainty, participants did value speed as well. Overall, respondents showed a strong preference against a 1-year delay in FDA approval time. People who were aged 55 years or more and were non-White individuals made less than $40,000 year as well as those with the lowest life expectancy on a current standard treatment were most sensitive to wait times while those with better functional status and longer life expectancies on a current treatment were less sensitive to longer wait times.
“Our results indicate that some patients (except those with the poorest prognoses) would find the additional time required to generate evidence on the survival benefit of new cancer drugs an acceptable tradeoff,” the study authors concluded.
Although people do place high value on timely access to new cancer drugs, especially if there are limited treatment options, many are willing to wait for greater certainty that a new drug provides an overall survival benefit, lead author Robin Forrest, MSc, with the Department of Health Policy, London School of Economics in England, said in an interview.
In the study, respondents also did not place significant value on whether the drug substantially slowed cancer growth. “In other words, substantial progression-free survival benefit of a drug did not compensate for lack of certainty about a drug’s benefit on survival in respondents’ drug choices,” the authors explained.
“In an effort to move quickly, we have accepted progression-free survival [as a surrogate endpoint],” Jyoti D. Patel, MD, oncologist with Northwestern Memorial Hospital, Chicago, Illinois, who wasn’t involved in the study. But a growing body of evidence indicates that progression-free survival is often a poor surrogate for overall survival. And what this study suggests is that “patients uniformly care about improvements in overall survival and the quality of that survival,” Patel said.
Bishal Gyawali, MD, PhD, was not surprised by the findings.
“I always thought this was the real-world scenario, but the problem is the voices of ordinary patients are not heard,” Gyawali, with Queen’s University, Kingston, Ontario, Canada, who also wasn’t involved in the study, said in an interview.
“What is heard is the loud noise of ‘we need access now, today, yesterday’ — ‘we don’t care if the drug doesn’t improve overall survival, we just need a drug, any drug’ — ‘we don’t care how much it costs, we need access today,’ ” Gyawali said. “Not saying this is wrong, but this is not the representation of all patients.”
However, the voices of patients who are more cautious and want evidence of benefit before accepting toxicities don’t make headlines, he added.
What this survey means from a policy perspective, said Gyawali, is that accelerated approvals that do not mandate survival endpoint in confirmatory trials are ignoring the need of many patients who prioritize certainty of benefit over speed of access.
The study was funded by the London School of Economics and Political Science Phelan United States Centre. Forrest had no relevant disclosures. Gyawali has received consulting fees from Vivio Health. Patel has various relationships with AbbVie, Anheart, AstraZeneca, Bristol-Myers Squibb, Guardant, Tempus, Sanofi, BluePrint, Takeda, and Gilead.
A version of this article first appeared on Medscape.com.
FROM THE LANCET ONCOLOGY
Inside the Patient-Oncologist Bond: Why It’s Often So Strong
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Cannabis in Cancer: What Oncologists and Patients Should Know
first, and oncologists may be hesitant to broach the topic with their patients.
Updated guidelines from the American Society of Clinical Oncology (ASCO) on the use of cannabis and cannabinoids in adults with cancer stress that it’s an important conversation to have.
According to the ASCO expert panel, access to and use of cannabis alongside cancer care have outpaced the science on evidence-based indications, and overall high-quality data on the effects of cannabis during cancer care are lacking. While several observational studies support cannabis use to help ease chemotherapy-related nausea and vomiting, the literature remains more divided on other potential benefits, such as alleviating cancer pain and sleep problems, and some evidence points to potential downsides of cannabis use.
Oncologists should “absolutely talk to patients” about cannabis, Brooke Worster, MD, medical director for the Master of Science in Medical Cannabis Science & Business program at Thomas Jefferson University, Philadelphia, told Medscape Medical News.
“Patients are interested, and they are going to find access to information. As a medical professional, it’s our job to help guide them through these spaces in a safe, nonjudgmental way.”
But, Worster noted, oncologists don’t have to be experts on cannabis to begin the conversation with patients.
So, “let yourself off the hook,” Worster urged.
Plus, avoiding the conversation won’t stop patients from using cannabis. In a recent study, Worster and her colleagues found that nearly one third of patients at 12 National Cancer Institute-designated cancer centers had used cannabis since their diagnosis — most often for sleep disturbance, pain, stress, and anxiety. Most (60%) felt somewhat or extremely comfortable talking to their healthcare provider about it, but only 21.5% said they had done so. Even fewer — about 10% — had talked to their treating oncologist.
Because patients may not discuss cannabis use, it’s especially important for oncologists to open up a line of communication, said Worster, also the enterprise director of supportive oncology at the Thomas Jefferson University.
Evidence on Cannabis During Cancer Care
A substantial proportion of people with cancer believe cannabis can help manage cancer-related symptoms.
In Worster’s recent survey study, regardless of whether patients had used cannabis, almost 90% of those surveyed reported a perceived benefit. Although 65% also reported perceived risks for cannabis use, including difficulty concentrating, lung damage, and impaired memory, the perceived benefits outweighed the risks.
Despite generally positive perceptions, the overall literature on the benefits of cannabis in patients with cancer paints a less clear picture.
The ASCO guidelines, which were based on 13 systematic reviews and five additional primary studies, reported that cannabis can improve refractory, chemotherapy-induced nausea or vomiting when added to guideline-concordant antiemetic regimens, but that there is no clear evidence of benefit or harm for other supportive care outcomes.
The “certainty of evidence for most outcomes was low or very low,” the ASCO authors wrote.
The ASCO experts explained that, outside the context of a clinical trial, the evidence is not sufficient to recommend cannabis or cannabinoids for managing cancer pain, sleep issues, appetite loss, or anxiety and depression. For these outcomes, some studies indicate a benefit, while others don’t.
Real-world data from a large registry study, for instance, have indicated that medical cannabis is “a safe and effective complementary treatment for pain relief in patients with cancer.” However, a 2020 meta-analysis found that, in studies with a low risk for bias, adding cannabinoids to opioids did not reduce cancer pain in adults with advanced cancer.
There can be downsides to cannabis use, too. In one recent study, some patients reported feeling worse physically and psychologically compared with those who didn’t use cannabis. Another study found that oral cannabis was associated with “bothersome” side effects, including sedation, dizziness, and transient anxiety.
The ASCO guidelines also made it clear that cannabis or cannabinoids should not be used as cancer-directed treatment, outside of a clinical trial.
Talking to Patients About Cannabis
Given the level of evidence and patient interest in cannabis, it is important for oncologists to raise the topic of cannabis use with their patients.
To help inform decision-making and approaches to care, the ASCO guidelines suggest that oncologists can guide care themselves or direct patients to appropriate “unbiased, evidence-based” resources. For those who use cannabis or cannabinoids outside of evidence-based indications or clinician recommendations, it’s important to explore patients’ goals, educate them, and try to minimize harm.
One strategy for broaching the topic, Worster suggested, is to simply ask patients if they have tried or considered trying cannabis to control symptoms like nausea and vomiting, loss of appetite, or cancer pain.
The conversation with patients should then include an overview of the potential benefits and potential risks for cannabis use as well as risk reduction strategies, Worster noted.
But “approach it in an open and nonjudgmental frame of mind,” she said. “Just have a conversation.”
Discussing the formulation and concentration of tetrahydrocannabinol (THC) and cannabidiol (CBD) in products matters as well.
Will the product be inhaled, ingested, or topical? Inhaled cannabis is not ideal but is sometimes what patients have access to, Worster explained. Inhaled formulations tend to have faster onset, which might be preferable for treating chemotherapy-related nausea and vomiting, whereas edible formulations may take a while to start working.
It’s also important to warn patients about taking too much, she said, explaining that inhaling THC at higher doses can increase the risk for cardiovascular effects, anxiety, paranoia, panic, and psychosis.
CBD, on the other hand, is anti-inflammatory, but early data suggest it may blunt immune responses in high doses and should be used cautiously by patients receiving immunotherapy.
Worster noted that as laws change and the science advances, new cannabis products and formulations will emerge, as will artificial intelligence tools for helping to guide patients and clinicians in optimal use of cannabis for cancer care. State websites are a particularly helpful tool for providing state-specific medical education related to cannabis laws and use, as well, she said.
The bottom line, she said, is that talking to patients about the ins and outs of cannabis use “really matters.”
Worster disclosed that she is a medical consultant for EO Care.
A version of this article appeared on Medscape.com.
first, and oncologists may be hesitant to broach the topic with their patients.
Updated guidelines from the American Society of Clinical Oncology (ASCO) on the use of cannabis and cannabinoids in adults with cancer stress that it’s an important conversation to have.
According to the ASCO expert panel, access to and use of cannabis alongside cancer care have outpaced the science on evidence-based indications, and overall high-quality data on the effects of cannabis during cancer care are lacking. While several observational studies support cannabis use to help ease chemotherapy-related nausea and vomiting, the literature remains more divided on other potential benefits, such as alleviating cancer pain and sleep problems, and some evidence points to potential downsides of cannabis use.
Oncologists should “absolutely talk to patients” about cannabis, Brooke Worster, MD, medical director for the Master of Science in Medical Cannabis Science & Business program at Thomas Jefferson University, Philadelphia, told Medscape Medical News.
“Patients are interested, and they are going to find access to information. As a medical professional, it’s our job to help guide them through these spaces in a safe, nonjudgmental way.”
But, Worster noted, oncologists don’t have to be experts on cannabis to begin the conversation with patients.
So, “let yourself off the hook,” Worster urged.
Plus, avoiding the conversation won’t stop patients from using cannabis. In a recent study, Worster and her colleagues found that nearly one third of patients at 12 National Cancer Institute-designated cancer centers had used cannabis since their diagnosis — most often for sleep disturbance, pain, stress, and anxiety. Most (60%) felt somewhat or extremely comfortable talking to their healthcare provider about it, but only 21.5% said they had done so. Even fewer — about 10% — had talked to their treating oncologist.
Because patients may not discuss cannabis use, it’s especially important for oncologists to open up a line of communication, said Worster, also the enterprise director of supportive oncology at the Thomas Jefferson University.
Evidence on Cannabis During Cancer Care
A substantial proportion of people with cancer believe cannabis can help manage cancer-related symptoms.
In Worster’s recent survey study, regardless of whether patients had used cannabis, almost 90% of those surveyed reported a perceived benefit. Although 65% also reported perceived risks for cannabis use, including difficulty concentrating, lung damage, and impaired memory, the perceived benefits outweighed the risks.
Despite generally positive perceptions, the overall literature on the benefits of cannabis in patients with cancer paints a less clear picture.
The ASCO guidelines, which were based on 13 systematic reviews and five additional primary studies, reported that cannabis can improve refractory, chemotherapy-induced nausea or vomiting when added to guideline-concordant antiemetic regimens, but that there is no clear evidence of benefit or harm for other supportive care outcomes.
The “certainty of evidence for most outcomes was low or very low,” the ASCO authors wrote.
The ASCO experts explained that, outside the context of a clinical trial, the evidence is not sufficient to recommend cannabis or cannabinoids for managing cancer pain, sleep issues, appetite loss, or anxiety and depression. For these outcomes, some studies indicate a benefit, while others don’t.
Real-world data from a large registry study, for instance, have indicated that medical cannabis is “a safe and effective complementary treatment for pain relief in patients with cancer.” However, a 2020 meta-analysis found that, in studies with a low risk for bias, adding cannabinoids to opioids did not reduce cancer pain in adults with advanced cancer.
There can be downsides to cannabis use, too. In one recent study, some patients reported feeling worse physically and psychologically compared with those who didn’t use cannabis. Another study found that oral cannabis was associated with “bothersome” side effects, including sedation, dizziness, and transient anxiety.
The ASCO guidelines also made it clear that cannabis or cannabinoids should not be used as cancer-directed treatment, outside of a clinical trial.
Talking to Patients About Cannabis
Given the level of evidence and patient interest in cannabis, it is important for oncologists to raise the topic of cannabis use with their patients.
To help inform decision-making and approaches to care, the ASCO guidelines suggest that oncologists can guide care themselves or direct patients to appropriate “unbiased, evidence-based” resources. For those who use cannabis or cannabinoids outside of evidence-based indications or clinician recommendations, it’s important to explore patients’ goals, educate them, and try to minimize harm.
One strategy for broaching the topic, Worster suggested, is to simply ask patients if they have tried or considered trying cannabis to control symptoms like nausea and vomiting, loss of appetite, or cancer pain.
The conversation with patients should then include an overview of the potential benefits and potential risks for cannabis use as well as risk reduction strategies, Worster noted.
But “approach it in an open and nonjudgmental frame of mind,” she said. “Just have a conversation.”
Discussing the formulation and concentration of tetrahydrocannabinol (THC) and cannabidiol (CBD) in products matters as well.
Will the product be inhaled, ingested, or topical? Inhaled cannabis is not ideal but is sometimes what patients have access to, Worster explained. Inhaled formulations tend to have faster onset, which might be preferable for treating chemotherapy-related nausea and vomiting, whereas edible formulations may take a while to start working.
It’s also important to warn patients about taking too much, she said, explaining that inhaling THC at higher doses can increase the risk for cardiovascular effects, anxiety, paranoia, panic, and psychosis.
CBD, on the other hand, is anti-inflammatory, but early data suggest it may blunt immune responses in high doses and should be used cautiously by patients receiving immunotherapy.
Worster noted that as laws change and the science advances, new cannabis products and formulations will emerge, as will artificial intelligence tools for helping to guide patients and clinicians in optimal use of cannabis for cancer care. State websites are a particularly helpful tool for providing state-specific medical education related to cannabis laws and use, as well, she said.
The bottom line, she said, is that talking to patients about the ins and outs of cannabis use “really matters.”
Worster disclosed that she is a medical consultant for EO Care.
A version of this article appeared on Medscape.com.
first, and oncologists may be hesitant to broach the topic with their patients.
Updated guidelines from the American Society of Clinical Oncology (ASCO) on the use of cannabis and cannabinoids in adults with cancer stress that it’s an important conversation to have.
According to the ASCO expert panel, access to and use of cannabis alongside cancer care have outpaced the science on evidence-based indications, and overall high-quality data on the effects of cannabis during cancer care are lacking. While several observational studies support cannabis use to help ease chemotherapy-related nausea and vomiting, the literature remains more divided on other potential benefits, such as alleviating cancer pain and sleep problems, and some evidence points to potential downsides of cannabis use.
Oncologists should “absolutely talk to patients” about cannabis, Brooke Worster, MD, medical director for the Master of Science in Medical Cannabis Science & Business program at Thomas Jefferson University, Philadelphia, told Medscape Medical News.
“Patients are interested, and they are going to find access to information. As a medical professional, it’s our job to help guide them through these spaces in a safe, nonjudgmental way.”
But, Worster noted, oncologists don’t have to be experts on cannabis to begin the conversation with patients.
So, “let yourself off the hook,” Worster urged.
Plus, avoiding the conversation won’t stop patients from using cannabis. In a recent study, Worster and her colleagues found that nearly one third of patients at 12 National Cancer Institute-designated cancer centers had used cannabis since their diagnosis — most often for sleep disturbance, pain, stress, and anxiety. Most (60%) felt somewhat or extremely comfortable talking to their healthcare provider about it, but only 21.5% said they had done so. Even fewer — about 10% — had talked to their treating oncologist.
Because patients may not discuss cannabis use, it’s especially important for oncologists to open up a line of communication, said Worster, also the enterprise director of supportive oncology at the Thomas Jefferson University.
Evidence on Cannabis During Cancer Care
A substantial proportion of people with cancer believe cannabis can help manage cancer-related symptoms.
In Worster’s recent survey study, regardless of whether patients had used cannabis, almost 90% of those surveyed reported a perceived benefit. Although 65% also reported perceived risks for cannabis use, including difficulty concentrating, lung damage, and impaired memory, the perceived benefits outweighed the risks.
Despite generally positive perceptions, the overall literature on the benefits of cannabis in patients with cancer paints a less clear picture.
The ASCO guidelines, which were based on 13 systematic reviews and five additional primary studies, reported that cannabis can improve refractory, chemotherapy-induced nausea or vomiting when added to guideline-concordant antiemetic regimens, but that there is no clear evidence of benefit or harm for other supportive care outcomes.
The “certainty of evidence for most outcomes was low or very low,” the ASCO authors wrote.
The ASCO experts explained that, outside the context of a clinical trial, the evidence is not sufficient to recommend cannabis or cannabinoids for managing cancer pain, sleep issues, appetite loss, or anxiety and depression. For these outcomes, some studies indicate a benefit, while others don’t.
Real-world data from a large registry study, for instance, have indicated that medical cannabis is “a safe and effective complementary treatment for pain relief in patients with cancer.” However, a 2020 meta-analysis found that, in studies with a low risk for bias, adding cannabinoids to opioids did not reduce cancer pain in adults with advanced cancer.
There can be downsides to cannabis use, too. In one recent study, some patients reported feeling worse physically and psychologically compared with those who didn’t use cannabis. Another study found that oral cannabis was associated with “bothersome” side effects, including sedation, dizziness, and transient anxiety.
The ASCO guidelines also made it clear that cannabis or cannabinoids should not be used as cancer-directed treatment, outside of a clinical trial.
Talking to Patients About Cannabis
Given the level of evidence and patient interest in cannabis, it is important for oncologists to raise the topic of cannabis use with their patients.
To help inform decision-making and approaches to care, the ASCO guidelines suggest that oncologists can guide care themselves or direct patients to appropriate “unbiased, evidence-based” resources. For those who use cannabis or cannabinoids outside of evidence-based indications or clinician recommendations, it’s important to explore patients’ goals, educate them, and try to minimize harm.
One strategy for broaching the topic, Worster suggested, is to simply ask patients if they have tried or considered trying cannabis to control symptoms like nausea and vomiting, loss of appetite, or cancer pain.
The conversation with patients should then include an overview of the potential benefits and potential risks for cannabis use as well as risk reduction strategies, Worster noted.
But “approach it in an open and nonjudgmental frame of mind,” she said. “Just have a conversation.”
Discussing the formulation and concentration of tetrahydrocannabinol (THC) and cannabidiol (CBD) in products matters as well.
Will the product be inhaled, ingested, or topical? Inhaled cannabis is not ideal but is sometimes what patients have access to, Worster explained. Inhaled formulations tend to have faster onset, which might be preferable for treating chemotherapy-related nausea and vomiting, whereas edible formulations may take a while to start working.
It’s also important to warn patients about taking too much, she said, explaining that inhaling THC at higher doses can increase the risk for cardiovascular effects, anxiety, paranoia, panic, and psychosis.
CBD, on the other hand, is anti-inflammatory, but early data suggest it may blunt immune responses in high doses and should be used cautiously by patients receiving immunotherapy.
Worster noted that as laws change and the science advances, new cannabis products and formulations will emerge, as will artificial intelligence tools for helping to guide patients and clinicians in optimal use of cannabis for cancer care. State websites are a particularly helpful tool for providing state-specific medical education related to cannabis laws and use, as well, she said.
The bottom line, she said, is that talking to patients about the ins and outs of cannabis use “really matters.”
Worster disclosed that she is a medical consultant for EO Care.
A version of this article appeared on Medscape.com.
Risk Assessment Tool Can Help Predict Fractures in Cancer
TOPLINE:
METHODOLOGY:
- Cancer-specific guidelines recommend using FRAX to assess fracture risk, but its applicability in patients with cancer remains unclear.
- This retrospective cohort study included 9877 patients with cancer (mean age, 67.1 years) and 45,875 matched control individuals without cancer (mean age, 66.2 years). All participants had dual-energy x-ray absorptiometry (DXA) scans.
- Researchers collected data on bone mineral density and fractures. The 10-year probabilities of major osteoporotic fractures and hip fractures were calculated using FRAX, and the observed 10-year probabilities of these fractures were compared with FRAX-derived probabilities.
- Compared with individuals without cancer, patients with cancer had a shorter mean follow-up duration (8.5 vs 7.6 years), a slightly higher mean body mass index, and a higher percentage of parental hip fractures (7.0% vs 8.2%); additionally, patients with cancer were more likely to have secondary causes of osteoporosis (10% vs 38.4%) and less likely to receive osteoporosis medication (9.9% vs 4.2%).
TAKEAWAY:
- Compared with individuals without cancer, patients with cancer had a significantly higher incidence rate of major fractures (12.9 vs 14.5 per 1000 person-years) and hip fractures (3.5 vs 4.2 per 1000 person-years).
- FRAX with bone mineral density exhibited excellent calibration for predicting major osteoporotic fractures (slope, 1.03) and hip fractures (0.97) in patients with cancer, regardless of the site of cancer diagnosis. FRAX without bone mineral density, however, underestimated the risk for both major (0.87) and hip fractures (0.72).
- In patients with cancer, FRAX with bone mineral density findings were associated with incident major osteoporotic fractures (hazard ratio [HR] per SD, 1.84) and hip fractures (HR per SD, 3.61).
- When models were adjusted for FRAX with bone mineral density, patients with cancer had an increased risk for both major osteoporotic fractures (HR, 1.17) and hip fractures (HR, 1.30). No difference was found in the risk for fracture between patients with and individuals without cancer when the models were adjusted for FRAX without bone mineral density, even when considering osteoporosis medication use.
IN PRACTICE:
“This retrospective cohort study demonstrates that individuals with cancer are at higher risk of fracture than individuals without cancer and that FRAX, particularly with BMD [bone mineral density], may accurately predict fracture risk in this population. These results, along with the known mortality risk of osteoporotic fractures among cancer survivors, further emphasize the clinical importance of closing the current osteoporosis care gap among cancer survivors,” the authors wrote.
SOURCE:
This study, led by Carrie Ye, MD, MPH, University of Alberta, Edmonton, Alberta, Canada, was published online in JAMA Oncology.
LIMITATIONS:
This study cohort included a selected group of cancer survivors who were referred for DXA scans and may not represent the general cancer population. The cohort consisted predominantly of women, limiting the generalizability to men with cancer. Given the heterogeneity of the population, the findings may not be applicable to all cancer subgroups. Information on cancer stage or the presence of bone metastases at the time of fracture risk assessment was lacking, which could have affected the findings.
DISCLOSURES:
This study was funded by the CancerCare Manitoba Foundation. Three authors reported having ties with various sources, including two who received grants from various organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Cancer-specific guidelines recommend using FRAX to assess fracture risk, but its applicability in patients with cancer remains unclear.
- This retrospective cohort study included 9877 patients with cancer (mean age, 67.1 years) and 45,875 matched control individuals without cancer (mean age, 66.2 years). All participants had dual-energy x-ray absorptiometry (DXA) scans.
- Researchers collected data on bone mineral density and fractures. The 10-year probabilities of major osteoporotic fractures and hip fractures were calculated using FRAX, and the observed 10-year probabilities of these fractures were compared with FRAX-derived probabilities.
- Compared with individuals without cancer, patients with cancer had a shorter mean follow-up duration (8.5 vs 7.6 years), a slightly higher mean body mass index, and a higher percentage of parental hip fractures (7.0% vs 8.2%); additionally, patients with cancer were more likely to have secondary causes of osteoporosis (10% vs 38.4%) and less likely to receive osteoporosis medication (9.9% vs 4.2%).
TAKEAWAY:
- Compared with individuals without cancer, patients with cancer had a significantly higher incidence rate of major fractures (12.9 vs 14.5 per 1000 person-years) and hip fractures (3.5 vs 4.2 per 1000 person-years).
- FRAX with bone mineral density exhibited excellent calibration for predicting major osteoporotic fractures (slope, 1.03) and hip fractures (0.97) in patients with cancer, regardless of the site of cancer diagnosis. FRAX without bone mineral density, however, underestimated the risk for both major (0.87) and hip fractures (0.72).
- In patients with cancer, FRAX with bone mineral density findings were associated with incident major osteoporotic fractures (hazard ratio [HR] per SD, 1.84) and hip fractures (HR per SD, 3.61).
- When models were adjusted for FRAX with bone mineral density, patients with cancer had an increased risk for both major osteoporotic fractures (HR, 1.17) and hip fractures (HR, 1.30). No difference was found in the risk for fracture between patients with and individuals without cancer when the models were adjusted for FRAX without bone mineral density, even when considering osteoporosis medication use.
IN PRACTICE:
“This retrospective cohort study demonstrates that individuals with cancer are at higher risk of fracture than individuals without cancer and that FRAX, particularly with BMD [bone mineral density], may accurately predict fracture risk in this population. These results, along with the known mortality risk of osteoporotic fractures among cancer survivors, further emphasize the clinical importance of closing the current osteoporosis care gap among cancer survivors,” the authors wrote.
SOURCE:
This study, led by Carrie Ye, MD, MPH, University of Alberta, Edmonton, Alberta, Canada, was published online in JAMA Oncology.
LIMITATIONS:
This study cohort included a selected group of cancer survivors who were referred for DXA scans and may not represent the general cancer population. The cohort consisted predominantly of women, limiting the generalizability to men with cancer. Given the heterogeneity of the population, the findings may not be applicable to all cancer subgroups. Information on cancer stage or the presence of bone metastases at the time of fracture risk assessment was lacking, which could have affected the findings.
DISCLOSURES:
This study was funded by the CancerCare Manitoba Foundation. Three authors reported having ties with various sources, including two who received grants from various organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Cancer-specific guidelines recommend using FRAX to assess fracture risk, but its applicability in patients with cancer remains unclear.
- This retrospective cohort study included 9877 patients with cancer (mean age, 67.1 years) and 45,875 matched control individuals without cancer (mean age, 66.2 years). All participants had dual-energy x-ray absorptiometry (DXA) scans.
- Researchers collected data on bone mineral density and fractures. The 10-year probabilities of major osteoporotic fractures and hip fractures were calculated using FRAX, and the observed 10-year probabilities of these fractures were compared with FRAX-derived probabilities.
- Compared with individuals without cancer, patients with cancer had a shorter mean follow-up duration (8.5 vs 7.6 years), a slightly higher mean body mass index, and a higher percentage of parental hip fractures (7.0% vs 8.2%); additionally, patients with cancer were more likely to have secondary causes of osteoporosis (10% vs 38.4%) and less likely to receive osteoporosis medication (9.9% vs 4.2%).
TAKEAWAY:
- Compared with individuals without cancer, patients with cancer had a significantly higher incidence rate of major fractures (12.9 vs 14.5 per 1000 person-years) and hip fractures (3.5 vs 4.2 per 1000 person-years).
- FRAX with bone mineral density exhibited excellent calibration for predicting major osteoporotic fractures (slope, 1.03) and hip fractures (0.97) in patients with cancer, regardless of the site of cancer diagnosis. FRAX without bone mineral density, however, underestimated the risk for both major (0.87) and hip fractures (0.72).
- In patients with cancer, FRAX with bone mineral density findings were associated with incident major osteoporotic fractures (hazard ratio [HR] per SD, 1.84) and hip fractures (HR per SD, 3.61).
- When models were adjusted for FRAX with bone mineral density, patients with cancer had an increased risk for both major osteoporotic fractures (HR, 1.17) and hip fractures (HR, 1.30). No difference was found in the risk for fracture between patients with and individuals without cancer when the models were adjusted for FRAX without bone mineral density, even when considering osteoporosis medication use.
IN PRACTICE:
“This retrospective cohort study demonstrates that individuals with cancer are at higher risk of fracture than individuals without cancer and that FRAX, particularly with BMD [bone mineral density], may accurately predict fracture risk in this population. These results, along with the known mortality risk of osteoporotic fractures among cancer survivors, further emphasize the clinical importance of closing the current osteoporosis care gap among cancer survivors,” the authors wrote.
SOURCE:
This study, led by Carrie Ye, MD, MPH, University of Alberta, Edmonton, Alberta, Canada, was published online in JAMA Oncology.
LIMITATIONS:
This study cohort included a selected group of cancer survivors who were referred for DXA scans and may not represent the general cancer population. The cohort consisted predominantly of women, limiting the generalizability to men with cancer. Given the heterogeneity of the population, the findings may not be applicable to all cancer subgroups. Information on cancer stage or the presence of bone metastases at the time of fracture risk assessment was lacking, which could have affected the findings.
DISCLOSURES:
This study was funded by the CancerCare Manitoba Foundation. Three authors reported having ties with various sources, including two who received grants from various organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.