User login
Optimizing Care for Veterans at Risk of Cancer From Camp Lejeune Water Exposure
Optimizing Care for Veterans at Risk of Cancer From Camp Lejeune Water Exposure
Clinical awareness of cancers associated with Camp Lejeune water contamination exposure remains limited despite legal and policy advances. Gaps persist in early symptom recognition and timely diagnostic evaluation before a definitive cancer diagnosis among exposed personnel. This may represent missed opportunities for earlier identification of volatile organic compounds (VOCs)-related cancers and for less invasive treatment options for veterans in this high-risk population.
Federal health care practitioners (HCPs), especially those in primary care and internal medicine, are uniquely positioned to bridge this gap. By improving the recognition of symptoms, pertinent physical examination findings, and implementing a diagnostic screening panel, HCPs can support accurate diagnoses and facilitate earlier treatment to improve health and quality of life for this population.
From 1953 to 1985, as many as 1 million military personnel, civilian workers, and their families stationed at US Marine Corps Base Camp Lejeune were unknowingly exposed to toxic and carcinogenic chemicals in drinking and bathing water.1 Three of the 8 main water sources on base were contaminated with VOCs, which are associated with multiple cancers.1-3
The US Department of Veterans Affairs (VA) recognizes 15 conditions associated with Camp Lejeune contaminated water exposure for VA benefits, including 10 cancers: adult leukemia; aplastic anemia and other myelodysplastic syndromes (MDS); bladder, esophageal, kidney, liver, breast (male and female), and lung cancers; multiple myeloma; and non-Hodgkin lymphoma (NHL).4
BACKGROUND
Established in 1942, Camp Lejeune is an important Marine Corps training installation. Between 1953 and 1985, multiple on-base water systems were contaminated with VOCs, including trichloroethylene (TCE), perchloroethylene (PCE), benzene, and vinyl chloride, due to improper waste disposal and industrial runoff from on- and off-base sources.5 Tarawa Terrace water treatment plant (WTP) was contaminated primarily with PCE from November 1957 to February 1987. Hadnot Point WTP was contaminated with TCE from August 1953 to December 1984, along with PCE, and benzene, toluene, ethylbenzene, and xylene (BTEX). Holcomb Boulevard WTP, established in 1972, was contaminated with TCE from June 1972 to February 1985.2 These contaminants entered the drinking and bathing water supply over decades, and exposure often occurred concurrently across = 1 VOC, compounding health risks.2,3 This prolonged 32-year VOC exposure window underlies current concerns regarding long-term cancer risk among affected service members, civilian employees, and family members. Epidemiologic research has found statistically significant associations between VOC exposure and multiple cancers, neurologic conditions, and reproductive issues.6 Specifically, TCE is associated with higher risks of hematologic cancers, multiple myeloma, NHL, and kidney cancer.3 PCE is linked with kidney cancer, benzene with multiple myeloma and NHL, and vinyl chloride with hepatobiliary cancers.3 A cohort mortality study compared Camp Lejeune personnel with a control group at Camp Pendleton from 1972 to 1985 and found a 3-fold higher incidence or mortality rate for kidney, esophageal, and female breast cancers, leukemia, and lymphoma among exposed Camp Lejeune personnel.6 Notably, personnel assigned to Camp Lejeune for as little as 6 months faced up to a 6-fold increase in cancer risk; the average military assignment between 1975 and 1985 was 18 months.3,6
Honoring America's Veterans and Caring for Camp Lejeune Families Act of 2012, the Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022, the Camp Lejeune Justice Act of 2022, and the pending Ensuring Justice for Camp Lejeune Victims Act of 2025 provide health care and legal resources for personnel and families affected by Camp Lejeune’s contaminated water.6-8 These laws acknowledge associations between exposure and specific health conditions and expanded health care, benefits, and legal recourse for affected veterans, survivors, and their families.8,9
CANCERS LINKED TO CAMP LEJEUNE
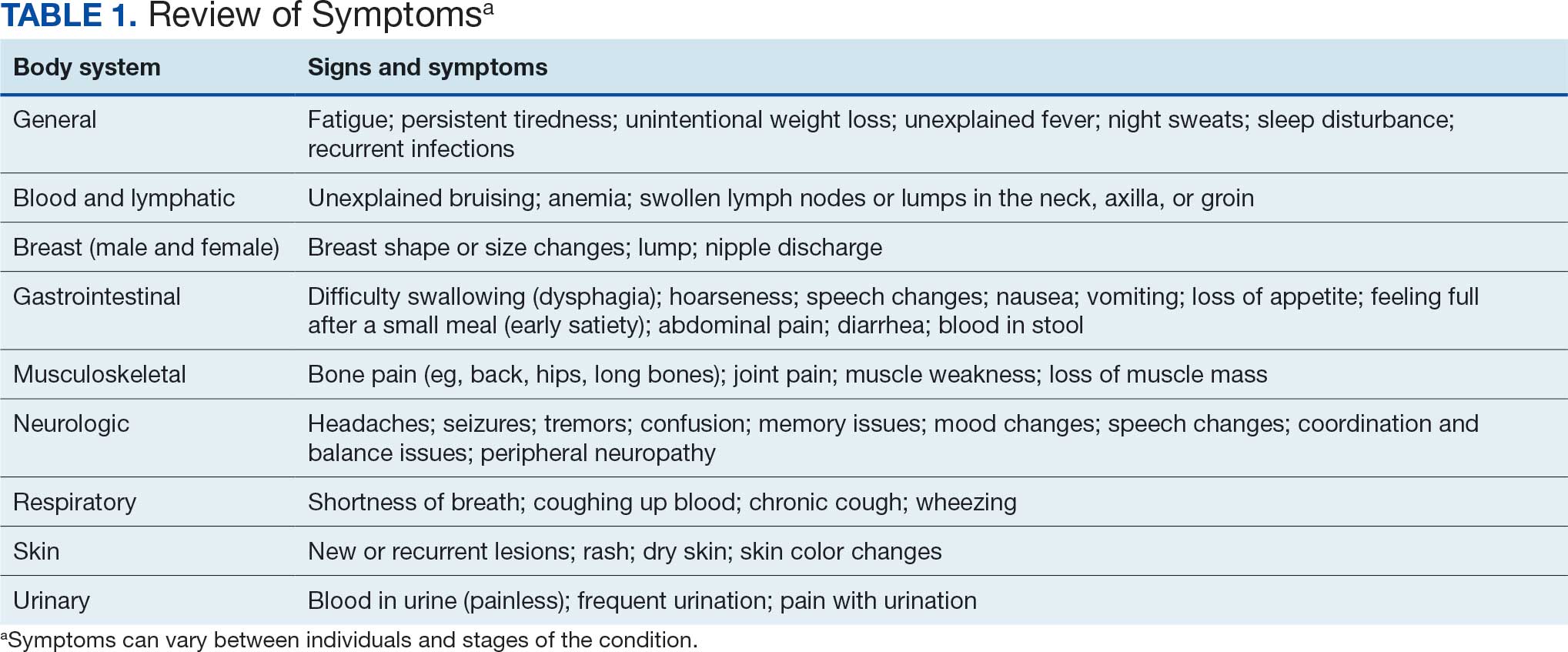
Camp Lejeune VOC-contaminated water exposure is associated with solid tumor and hematologic cancers. Symptoms, physical examination findings, and diagnostic considerations vary by cancer type (Table 1).
Bladder Cancer
The US incidence rate of bladder cancer for both males and females is 18 per 100,000 individuals per year, with a death rate of 4.1 per 100,000 individuals per year, and a 2.1% lifetime diagnosis risk.10 Personnel exposed to VOCs at Camp Lejeune had a 9% higher risk of developing bladder cancer and a 2% increased mortality compared with an unexposed control group at Camp Pendleton.1,7 Other bladder cancer subtypes at increased risk are papillary transitional cell carcinoma, nonpapillary transition cell carcinoma, and urothelial carcinoma.7 This is consistent with prior research that found PCE exposure is associated with an increased risk for bladder cancer.3,7,11 Smoking and tobacco use remain significant risk factors for bladder cancer.12
Symptomatology. The most common symptom associated with bladder cancer is painless hematuria (gross or microscopic). Other often delayed symptoms include urinary frequency, urgency, or nocturia.13,14
Diagnostics. Screening tests include urinalysis for hematuria, urine cytology, and cystoscopy with biopsy as the gold standard for diagnosis and staging.15,16
Kidney Cancer
The US incidence rate of kidney cancer and renal pelvis cancer for both males and females is 17.5 per 100,000 individuals per year, with a death rate of 3.4 per 100,000, and a 1.8% lifetime diagnosis risk.17 Camp Lejeune personnel exposed to VOCs had a 6% increased risk of developing kidney cancer and renal pelvis cancer and a 21% higher mortality risk compared with Camp Pendleton controls.1,7 Subtypes at risk include renal cell carcinoma and papillary carcinoma.7 This is consistent with prior research that found exposures to TCE and PCE are associated with a 3-fold increased risk of kidney cancer.3,7
Symptomatology. Hematuria, flank pain, and a palpable abdominal mass are common symptoms associated with kidney cancer. In advanced stages, other symptoms may include left-sided varicocele, anemia, weight loss, fatigue, fever, and night sweats.18
Diagnostics. Screening tests include urinalysis to assess the presence of blood, complete blood count (CBC) to assess anemia, calcium (elevated), and lactate dehydrogenase (LDH), which may be elevated. Imaging strategies include abdominal computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound.19
Esophageal Cancer
The US incidence rate of esophageal cancer for both males and females is 4.2 per 100,000 individuals per year, the death rate is 3.7 per 100,000 individuals per year, and a 0.5% lifetime diagnosis risk.20 VOC-exposed Camp Lejeune personnel had a 27% increased incidence and 25% increased mortality compared with the control group.1,7 Esophageal cancer subtypes at elevated risk include squamous cell carcinoma and adenocarcinoma. This is consistent with prior research that found Camp Lejeune water exposure is associated with a 3-fold increased risk for esophageal cancer.7 Additional risk factors include history of smoking and alcohol use.21
Symptomatology. Esophageal cancer is often asymptomatic with potential symptoms that include dysphagia, hoarseness, and weight loss in advanced disease.22
Diagnostics. Endoscopy with biopsy is the definitive method for diagnosis.23
Liver Cancer
The US incidence rate of liver cancer and intrahepatic bile duct cancer for both males and females is 9.4 per 100,000 individuals per year, with a death rate of 6.6 per 100,000 individuals per year, and a 1.1% lifetime diagnosis risk.24 VOC-exposed personnel had a 1% higher mortality than controls.1
Symptomatology. Liver cancer is often asymptomatic and appears in late stages.25 Common symptoms include right upper quadrant pain, early satiety, nausea, vomiting, loss of appetite, weight loss, ascites, jaundice, and abnormal bleeding or bruising.25,26
Diagnostics. Diagnostic tests may include an ultrasound, CT, or MRI. Additional laboratory testing may include liver function, a-fetoprotein blood, CBC, renal function, calcium, and hepatitis panel screening for hepatitis B and C.27,28
Lung Cancer
The US incidence rate of lung cancer for both males and females is 47.8 per 100,000 individuals per year, with a death rate of 31.5 per 100,000 individuals per year, and a 5.4% lifetime diagnosis risk.29 VOC-exposed personnel had a 16% increased risk and 19% higher mortality.1,7 Subtypes include large cell, small cell, non-small cell, squamous cell, and adenocarcinoma.7 Smoking is an additional risk factor.30
Symptomatology. Symptoms of lung cancer include cough, shortness of breath, chest pain worse with deep breathing, unexplained weight loss, fatigue, night sweats, and recurrent fevers. Advanced stages may metastasize or spread to the liver, bones, and brain.31
Diagnostics. Low-dose CT and chest X-ray are used for screening.32
Breast Cancer
The US incidence rate of female breast cancer is 130.8 per 100,000 individuals per year, with a death rate of 19.2 per 100,000 individuals per year, and a 13.0% lifetime risk of diagnosis.33 For female VOC-exposed personnel, there was an equal risk of developing breast cancer as the control group.1 However, exposed females at Camp Lejeune had a 23% higher mortality risk compared to the control group.7 Breast cancer subtypes among females include ductal carcinoma, lobular carcinoma, and ductal-lobular carcinoma.1
The US incidence rate of male breast cancer is 1.3 per 100,000 individuals per year, with a death rate of 0.3 per 100,000 individuals per year.34,35 The lifetime risk for males developing breast cancer is 137.7 per 100,000 and about 70 to 100 times less common in men than women.36
Male personnel exposed at Camp Lejeune had a 4% increased risk for developing breast cancer compared to Camp Pendleton.7 However, mortality was lower in the Camp Lejeune group.1 Although male breast cancer is rare, males at Camp Lejeune had a higher incidence, indicating a link between TCE, PCE, vinyl chloride exposures and male breast cancer.37 Male breast cancer is more often diagnosed in advanced stages than female breast cancer due to the lack of awareness or absence of routine screenings.38 The most common breast cancer type in males is invasive ductal carcinoma, accounting for 85% to 90% of cases; lobular carcinoma is the second most common type.39
Symptomatology. In both females and males, breast cancer symptoms include painless, firm mass or lump in the breast (left breast slightly more common than right), skin changes or dimpling, nipple retraction or turning inward, and nipple discharge. Breast cancer can spread to the lymph nodes and can be appreciated in axilla or clavicular regions.40
Diagnostics. The diagnostic evaluation for breast cancer is similar for females and males. It includes a clinical breast examination, diagnostic mammogram, and ultrasound.41 Mammograms can distinguish between gynecomastia and cancer, especially in males.42 A core or fine needle biopsy is needed to confirm diagnosis.41
Adult Leukemia
The US incidence rate of leukemia for both male and female was 14.4 per 100,000 individuals per year, with a death rate of 5.8 per 100,000 individuals per year, and a 1.5% lifetime diagnosis risk.43
VOC-exposed personnel had a 7% higher risk of developing leukemia and a 13% increased mortality risk compared with the control group.1,7 Subtypes of leukemia at risk included a 38% increased incidence of acute myeloid/monocytic leukemia (AML) and a 2% increased incidence of chronic lymphocytic leukemia (CLL).1 Benzene and TCE exposures are known risk factors for AML and other leukemias.7 Personnel at Camp Lejeune had 3 times the incidence or mortality for leukemia, specifically AML mortality at 20%.7 Smoking is an additional risk factor for certain leukemias, especially AML.30
Symptomatology. Symptoms associated with leukemia are often nonspecific and may include fatigue, pallor, easy bruising or bleeding (skin or gums), recurrent infections secondary to neutropenia, fever, night sweats, pain or feeling full after a small meal due to enlarged spleen or liver, and weight loss.44,45
Diagnostics. An initial screening includes a CBC with differential, a peripheral smear to detect the presence of blast cells, as well as Auer rods in myeloid blast cells in AML or smudge cells in CLL. Confirmatory tests may include bone marrow biopsy or flow cytometry. A referral to a hematologist is recommended for any suspected leukemia.46,47
Myelodysplastic Syndromes
Aplastic anemia and MDS are considered rare disorders.48 Aplastic anemia is a nonmalignant bone marrow failure disorder with pancytopenia and hypocellular bone marrow due to the loss of hematopoietic stem cells.48 MDS is a type of hematopoietic cancer where the bone marrow produces abnormal blood cells or does not make enough healthy cells.49 This can lead to an increased risk for infection, cytopenias, neutropenia, refractory anemia, and thrombocytopenia, and progression to AML in some patients.49
The reported US incidence of MDS from 1975 to 2013 was 6.7 per 100,000 for males and 3.7 per 100,000 for females.50 Benzene exposure is linked to MDS and a known cause of AML.1 VOC-exposed personnel had a 68% increased risk of developing MDS and a 2.3-fold increased mortality risk compared to controls.1,7
Symptomatology. Some patients are asymptomatic at diagnosis.51 Symptoms related to cytopenia include fatigue, pallor, purpura, petechiae, bleeding of skin, gum, or nose, recurrent infections, fever, bone pain, loss of appetite, and weight loss.50,51
Diagnostics. Initial workup includes a CBC with differential to assess for anemia, white blood cell and absolute neutrophil counts (low), and thrombocytopenia.52 A peripheral blood smear may show myeloid blast cells. A bone marrow aspiration and biopsy, flow cytometry, and cytogenetic or molecular testing may be performed. If MDS is suspected, a referral to a hematologist should be considered.52
Multiple Myeloma
The US incidence rate of multiple myeloma for both males and females is 7.3 per 100,000 individuals per year, with a mortality rate of 2.9 per 100,000 individuals per year, and a 0.8% lifetime diagnosis risk.53 VOC-exposed personnel had a 13% increased risk of developing multiple myeloma and an 8% increased mortality risk compared to unexposed personnel.1,7
Symptomatology. Multiple myeloma may be asymptomatic in early stages. The most common presenting symptom is bone pain, especially in the back, hips, and long bones, due to hypercalcemia from increased reabsorption, plasma cell tumor overgrowth in the bone marrow, and lytic lesions.54 Additional symptoms include fatigue and pallor related to anemia, leukopenia, thrombocytopenia, recurrent infections, extreme thirst, frequent urination, dehydration, confusion associated with hypercalcemia, peripheral neuropathy, loss of appetite, weight loss, and renal impairment or failure.54
Diagnostics. Testing considerations include a CBC with a peripheral blood smear to evaluate anemia and rouleaux formation of red blood cells (seen in > 50% of patients with multiple myeloma), comprehensive metabolic panel (CMP) to assess kidney function, calcium levels (elevated), serum and urine protein electrophoresis with immunofixation to detect monoclonal protein (detected in > 80% of patients with multiple myeloma) and Bence-Jones proteins, serum free light chain assay, and a bone marrow biopsy for diagnosis.55,56
MRI of the spine and pelvis is the most sensitive to detecting bone marrow involvement and focal lesions before lytic lesion progression occurs and for assessing spinal cord compression.57 PET/CT is more sensitive at detecting extramedullary disease, outside of the spine, and for patients that cannot undergo MRI.57 A whole-body low-dose CT, either alone or with PET, is more sensitive than an X-ray at detecting lytic lesions, fractures, or osteoporosis associated with multiple myeloma.57
Non-Hodgkin Lymphoma
The US incidence rate of NHL for both males and females are 18.7 per 100,000 individuals per year, the death rate is 4.9 per 100,000 individuals per year, and a 2% lifetime diagnosis risk.58 VOC-exposed personnel had a 1% higher risk of developing NHL and a decreased mortality risk compared to the control group.1,7 Specific NHL subtypes with increased risk in the exposed cohort are mantle cell (26%), follicular (7%), Burkitt (53%), and marginal zone B-cell (45%).7
Symptomatology. NHL often presents with painless lymphadenopathy or enlarged lymph nodes involving the cervical, axillary, inguinal regions.59,60 Other symptoms include frequent infections, unexplained bruising, weight loss, and “B symptoms,” such as fever and night sweats.59,60 Some patients develop a mediastinal mass in the thorax, which if large may lead to cough or shortness of breath.59
Diagnostics. The initial diagnostic workup includes CBC with differential and LDH, which may be elevated.60,61 Imaging may begin with a chest X-ray to assess for a mediastinal mass; however, CTs of the chest, abdomen, and pelvis provide more detail to better assess for NHL. Whole body PET/CT is considered the gold standard for assessing and staging systemic involvement. If enlarged lymph nodes are present, a biopsy can confirm the subtype of NHL.60,61
PHYSICAL EXAMINATION
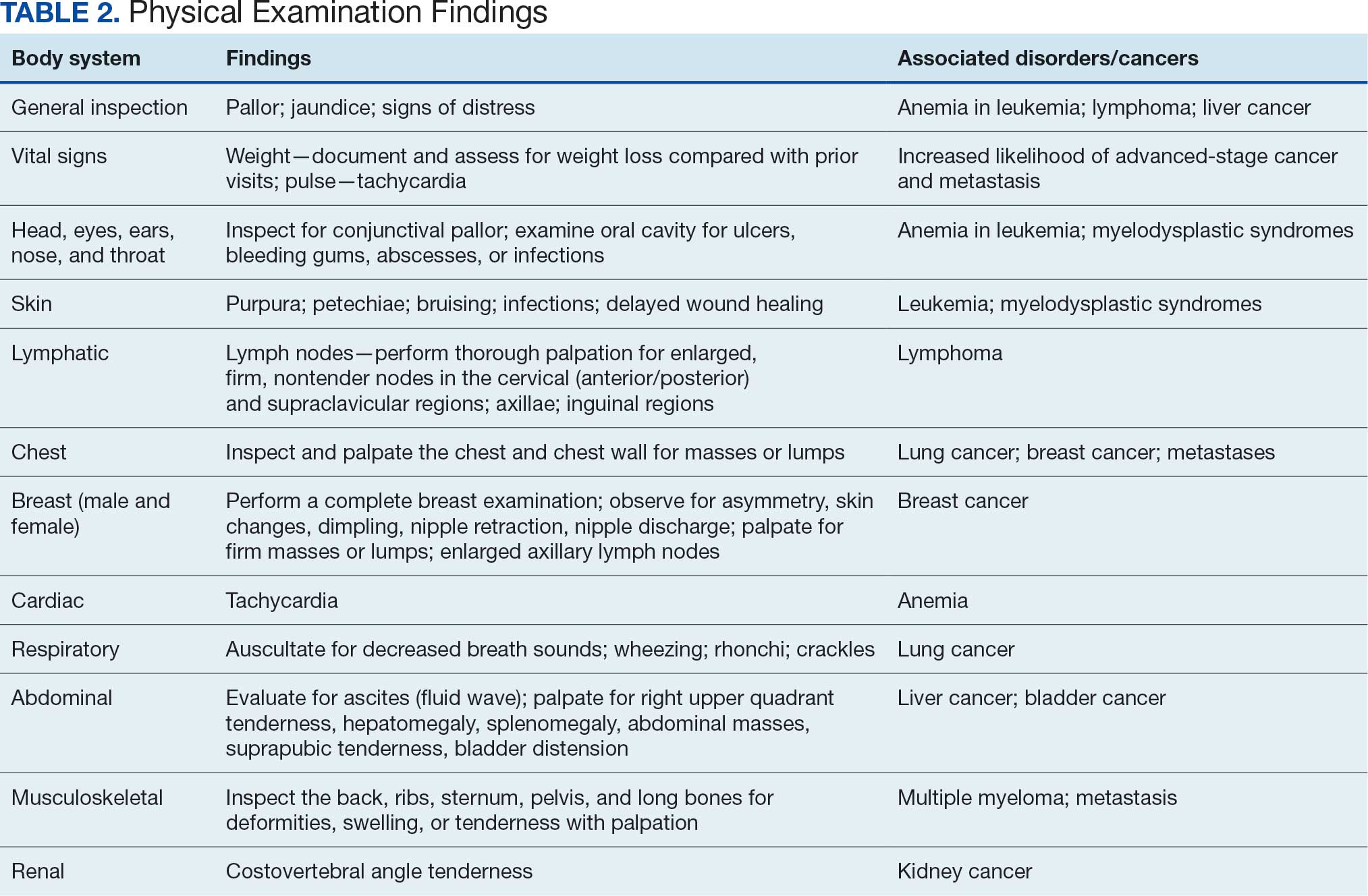
A focused physical examination may aid HCPs in early detection of the cancers associated with Camp Lejeune (Table 2). The physical examination can guide diagnostic testing and imaging for further assessment and workup for VOC-related cancers.
Proposed Diagnostic Screening Panel
Primary care and internal medicine HCPs have the opportunity to improve patient health outcomes by implementing a targeted diagnostic screening panel for identified veterans previously stationed at Camp Lejeune. Early identification of cancers associated with VOCs exposure can facilitate earlier treatment interventions and improve health and quality of life outcomes. The following diagnostic screening panel outlines a potential cost-effective strategy for evaluating and detecting the 10 cancers associated with VOC exposure in Camp Lejeune water.
Baseline Screening
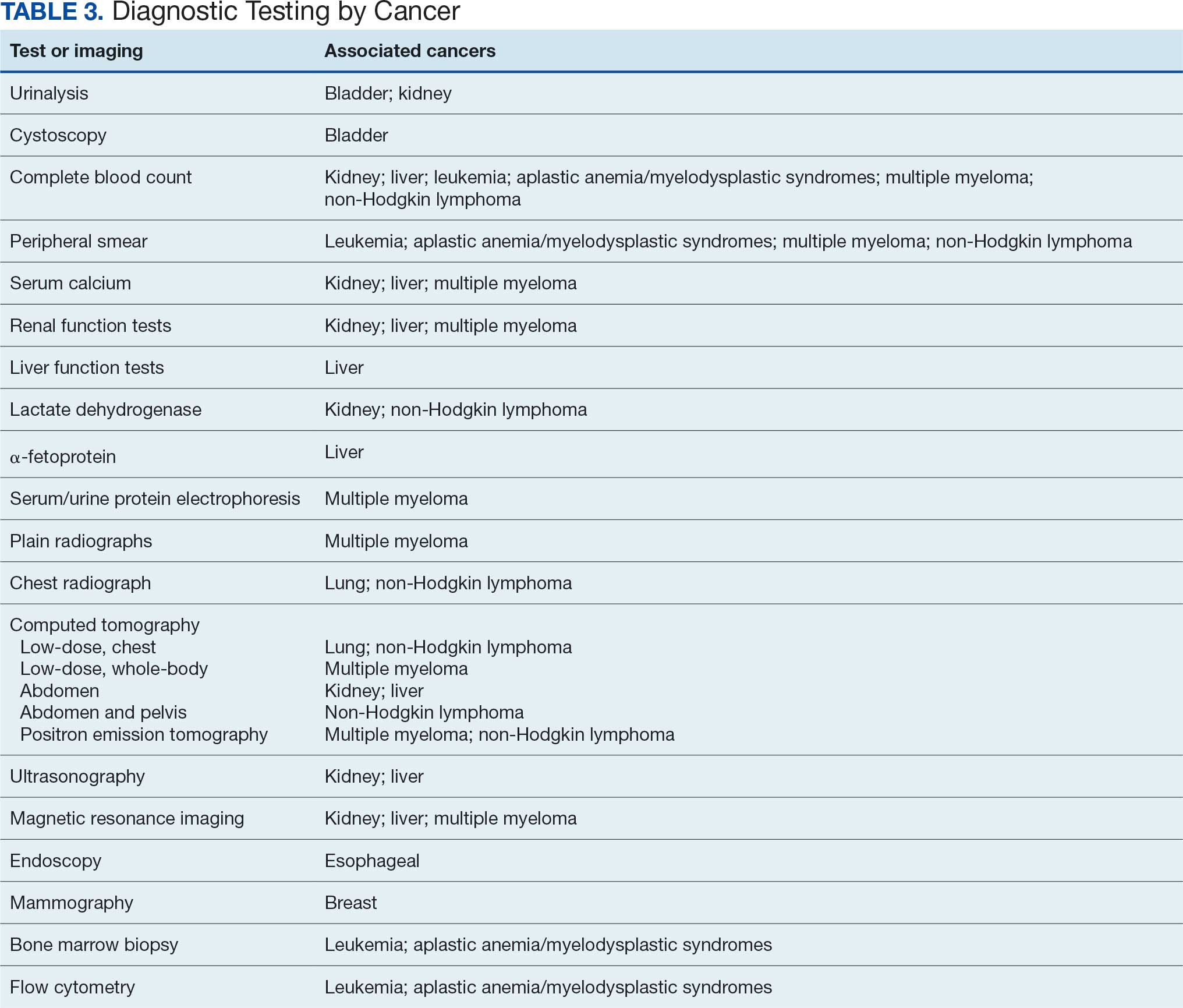
Implementing a diagnostic screening panel in this high-risk cohort can lead to earlier diagnosis, reduce mortality, and improve patient outcomes through early intervention, which in turn may result in less invasive treatment. This approach may also reduce health care costs by avoiding costs associated with delayed diagnosis and advanced-stage cancer care (Tables 3 and 4).
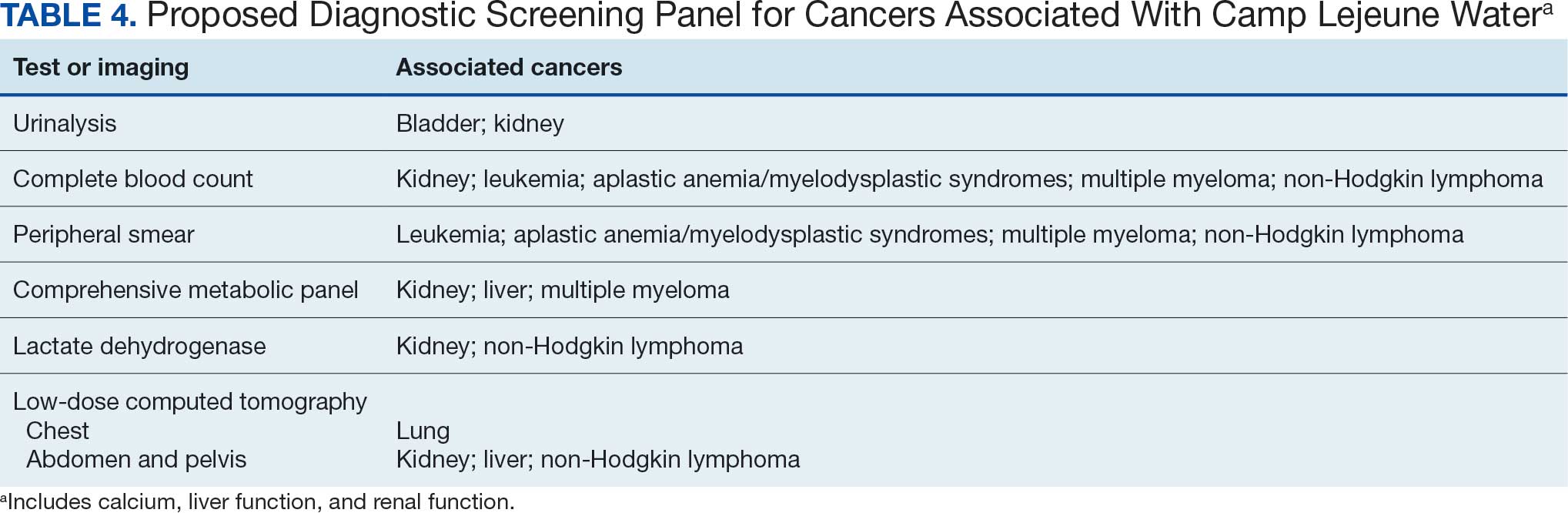
A baseline panel of tests for exposed veterans could include:
- A CBC with differential and peripheral smear to assess for anemia, leukemia, thrombocytopenia, and blast cells associated with leukemias, MDS, multiple myeloma, and NHL.19,46,47,52,55,56,60,61
- CMP evaluates calcium, total protein, renal and liver renal function. Elevated test results may indicate kidney or liver cancer or multiple myeloma.19,27,28,55,56
- LDH testing may reveal levels that are elevated from tissue damage or high cell turnover in kidney cancer, multiple myeloma, and NHL.19,55,56,60,61
- Urinalysis with microscopy may detect hematuria, proteinuria and cellular casts in bladder and kidney cancers.13,24,19
- Low-dose CTs of the chest, abdomen, and pelvis are recommended for early identification of any masses or lymphadenopathy in lung, kidney, liver cancers, and NHL.19,27,28,32,60,61
COST EFFICIENCY
Screening Panel Cost
According to the Medicare Clinical Laboratory Fee Schedule payment cap for 2018, the mean cost for the proposed blood workup was $35 (CBC, $10; CMP, $13; LDH, $8; urinalysis, $4).62 Medicare procedure price schedule for 2025 includes $351 for a CT of the abdomen and pelvis with and without contrast (Current Procedural Terminology [CPT] code 74177) and $187 for a CT of the chest with and without contrast (CPT code 71270).63,64 The total proposed diagnostic screening panel payment cost about $572.
Cancer Care Cost
The average cost for initial cancer care across all cancer sites from 2007 to 2013 was $43,516 per patient; Camp Lejeune-associated cancers ranged from $26,443 for bladder cancer to $89,947 for esophageal cancer care.64 Further, the last year of life cost across all cancer sites averaged $109,727, and Camp Lejeune-associated cancer types ranged from $76,101 for breast cancer to $169,588 for leukemia.65
CONCLUSIONS
From 1953 to 1985, up to 1 million military personnel, civilian workers, and their families stationed at Camp Lejeune were unknowingly exposed to toxic and carcinogenic VOCs, which are associated with = 10 cancers, including bladder, kidney, esophageal, liver, lung, breast, and hematologic malignancies.1-4 Some veterans may be asymptomatic, whereas others present with subtle or specific symptoms that can vary by individual and the type and stage of cancer. HCPs have an opportunity to improve patient outcomes through awareness in identifying symptoms associated with Camp Lejeune water exposure and performing a thorough baseline physical examination, especially noting lymphadenopathy, unexplained weight loss, or masses, which can guide further diagnostic evaluation. Timely screening can identify cancers earlier, reducing delays in care, mitigating the cost burden associated with advanced-stage cancer treatment, improving survival outcomes, and enhancing quality of life. Primary care and internal medicine HCPs specifically play a crucial role in early recognition, physical assessment, and appropriate screening tools. A proposed panel includes CBC with differential and peripheral smear, CMP, LDH, urinalysis, and low-dose CTs of the chest, abdomen and pelvis. Implementation should be guided by clinical judgment and patient-specific risk factors. The proposed diagnostic screening panel is a small price to pay for those who served in any capacity at Camp Lejeune.
- Bove FJ, Greek A, Gatiba R, et al. Cancer incidence among Marines and Navy personnel and civilian workers exposed to industrial solvents in drinking water at US Marine Corps Base Camp Lejeune: a cohort study. Environ Health Perspect. 2024;132:107008. doi:10.1289/EHP14966
- Maslia ML, Aral MM, Ruckart PZ, Bove FJ. Reconstructing historical VOC concentrations in drinking water for epidemiological studies at a US military base: summary of results. Water (Basel). 2016;8:449. doi:10.3390/w8100449
- Rosenfeld PE, Spaeth KR, McCarthy SJ, et al. Camp Lejeune Marine cancer risk assessment for exposure to contaminated drinking water from 1955 to 1987. Water Air Soil Pollut. 2024;235(2). doi:10.1007/s11270-023-06863-y
- US Department of Veterans Affairs, Veterans Health Administration. Camp Lejeune: past water contamination. Updated April 15, 2025. Accessed March 3, 2026. https://www.publichealth.va.gov/exposures/camp-lejeune/
- Jung K, Khan A, Mocharnuk R, et al. Clinical encounter with three cancer patients affected by groundwater contamination at Camp Lejeune: a case series and review of the literature. J Med Case Rep. 2022;16(1):272. doi:10.1186/s13256-022-03501-9
- Honoring America's Veterans and Caring for Camp Lejeune Familes Act of 2012, Pub L No. 112-154. Janey Ensminger Act. Congress.gov. Accessed April 15, 2026. https://ww.congress.gov/bill/112th-congress/house-bill/1627
- Bove FJ, Greek A, Gatiba R, et al. Evaluation of mortality among Marines, Navy personnel, and civilian workers exposed to contaminated drinking water at USMC Base Camp Lejeune: a cohort study. Environ Health. 2024;23(1):61. doi:10.1186/s12940-024-01099-7
- Honoring our PACT Act of 2022 (Pub L No. 117-168): expansion of health care eligibility and toxic exposure screenings. Congress.gov. Accessed March 3, 2026. https://www.congress.gov/bill/117th-congress/house-bill/3967
- Ensuring Justice for Camp Lejeune Victims Act of 2025. Congress.gov. Accessed March 24, 2026. https://www.congress.gov/bill/119th-congress/house-bill/4145
- SEER. Cancer stat facts: bladder cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/urinb.html
- Agency for Toxic Substances and Disease Registry. ATSDR assessment of the evidence for the drinking water contaminants at Camp Lejeune and specific cancers and other diseases. Published January 13, 2017. Accessed March 3, 2026. https://www.atsdr.cdc.gov/camp-lejeune/media/pdfs/2024/10/ATSDR_summary_of_the_evidence_for_causality_TCE_PCE_508.pdf
- National Cancer Institute. What is bladder cancer? Updated February 16, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder
- National Cancer Institute. Bladder cancer symptoms. Updated February 16, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder/symptoms
- American Cancer Society. Bladder cancer signs and symptoms. Updated March 12, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/bladder-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- National Cancer Institute. Bladder cancer screening. Updated April 27, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder/screening
- American Cancer Society. Tests for bladder cancer. Updated March 12, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/bladder-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: kidney and renal pelvis cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/kidrp.html
- American Cancer Society. Kidney cancer signs and symptoms. Updated May 1, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/kidney-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- American Cancer Society. Tests for kidney cancer. Updated May 1, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/kidney-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: esophageal cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/esoph.html
- Engel LS, Chow WH, Vaughan TL, et al. Population attributable risks of esophageal and gastric cancers.
J Natl Cancer Inst. 2003;95(18):1404-1413. doi:10.1093/jnci/djg047 - American Cancer Society. Signs and symptoms of esophageal cancer. Updated March 20, 2020. Accessed March 3, 2026. https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- American Cancer Society. Tests for esophageal cancer. Updated March 20, 2020. Accessed March 3, 2026. https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: liver and intrahepatic bile duct cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/livibd.html
- American Cancer Society. Signs and symptoms of liver cancer. Updated February 11, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/liver-cancer/detection-diagnosis-staging/signs-symptoms.html
- National Cancer Institute. What is liver cancer? Updated May 15, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/liver/what-is-liver-cancer
- American Cancer Society. Tests for liver cancer. Updated February 11, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/liver-cancer/detection-diagnosis-staging/how-diagnosed.html
- National Cancer Institute. Liver cancer screening. Updated May 15, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/liver/what-is-liver-cancer/screening
- SEER. Cancer stat facts: lung cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/lungb.html
- US Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. Accessed March 3, 2026. https://www.ncbi.nlm.nih.gov/books/NBK44695/pdf/Bookshelf_NBK44695.pdf
- American Cancer Society. Lung cancer signs and symptoms. Updated February 27, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/lung-cancer/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for lung cancer. Updated January 29, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/lung-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: female breast cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/breast.html
- SEER. SEER*Explorer breast incidence and mortality comparison. Updated July 2, 2025. Accessed March 3, 2026. https://seer.cancer.gov/statistics-network/explorer/application.html
- Susan G. Komen. Male breast cancer. Updated June 3, 2025. Accessed March 3, 2026. https://www.komen.org/breast-cancer/facts-statistics/male-breast-cancer/
- American Cancer Society. Key statistics for breast cancer in men. Updated January 16, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/about/key-statistics.html
- Ruckart PZ, Bove FJ, Shanley E 3rd, et al. Evaluation of contaminated drinking water and male breast cancer at Marine Corps Base Camp Lejeune, North Carolina: a case-control study. Environ Health. 2015;14:74. doi:10.1186/s12940-015-0061-4
- Culell P, Solernou L, Tarazona J, et al. Male breast cancer: a multicentric study. Breast J. 2007;13:213-215. doi:10.1111/j.1524-4741.2007.00412.x
- Giordano SH, Cohen DS, Buzdar AU, et al. Breast carcinoma in men: a population-based study. Cancer. 2004;101:51-57. doi:10.1002/cncr.20312
- American Cancer Society. Signs and symptoms of breast cancer in men. Updated April 27, 2018. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests to help diagnose breast cancer in men. Updated December 20, 2021. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/detection-diagnosis-staging/how-diagnosed.html
- Evans GF, Anthony T, Turnage RH, et al. The diagnostic accuracy of mammography in the evaluation of male breast disease. Am J Surg. 2001;181:96-100. doi:10.1016/S0002-9610(00)00571-7
- SEER. Cancer stat facts: leukemia. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/leuks.html
- American Cancer Society. Signs and symptoms of acute myeloid leukemia (AML). Updated March 20, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/acute-myeloid-leukemia/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Signs and symptoms of chronic lymphocytic leukemia (CLL). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/chronic-lymphocytic-leukemia/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for acute myeloid leukemia (AML). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/acute-myeloid-leukemia/detection-diagnosis-staging/how-diagnosed.html
- American Cancer Society. Tests for chronic lymphocytic leukemia (CLL). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/chronic-lymphocytic-leukemia/detection-diagnosis-staging/how-diagnosed.html
- Giudice V, Selleri C. Aplastic anemia: pathophysiology. Semin Hematol. 2022;59:13-20. doi:10.1053/j.seminhematol.2021.12.002
- National Cancer Institute. Myelodysplastic syndromes treatment (PDQ®)–patient version. Updated October 4, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/myeloproliferative/patient/myelodysplastic-treatment-pdq
- SEER. Cancer statistics review (CSR) 1975-2013: myelodysplastic syndromes. Accessed March 3, 2026. https://seer.cancer.gov/archive/csr/1975_2013/browse_csr.php?sectionSEL=30&pageSEL=sect_30_table.01
- American Cancer Society. Signs and symptoms of myelodysplastic syndrome (MDS). Updated November 21, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for myelodysplastic syndromes (MDS). Updated November 21, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: myeloma. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/mulmy.html
- American Cancer Society. Signs and symptoms of multiple myeloma. Updated February 28, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/multiple-myeloma/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for multiple myeloma. Updated February 28, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/multiple-myeloma/detection-diagnosis-staging/testing.html
- Laubach JP. Multiple myeloma: clinical features, laboratory manifestations, and diagnosis. UpToDate. Updated April 28, 2025. Accessed March 3, 2026. https://www.uptodate.com/contents/multiple-myeloma-clinical-features-laboratory-manifestations-and-diagnosis
- Hillengass J, Usmani S, Rajkumar SV, et al. International Myeloma Working Group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019;20:e302-e312. doi:10.1016/S1470-2045(19)30309-2
- SEER. Cancer stat facts: non-Hodgkin lymphoma. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/nhl.html
- American Cancer Society. Signs and symptoms of non-Hodgkin lymphoma. Updated February 15, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/detection-diagnosis-staging/signs-symptoms.html
- National Cancer Institute. Non-Hodgkin lymphoma treatment (PDQ®)–patient version. Updated August 22, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/lymphoma/patient/adult-nhl-treatment-pdq
- American Cancer Society. Tests for non-Hodgkin lymphoma. Updated February 15, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/detection-diagnosis-staging/how-diagnosed.html
- College of American Pathologists. Medicare clinical laboratory fee schedule. Published November 2017. Accessed March 3, 2026. https://documents.cap.org/documents/2018-final-medicare-clfs-rates.pdf
- Medicare.gov. Procedure price lookup for outpatient services. Accessed March 3, 2026. https://www.medicare.gov/procedure-price-lookup/cost/71270/
- Medicare.gov. Procedure price lookup for outpatient services. Accessed March 3, 2026. https://www.medicare.gov/procedure-price-lookup/cost/74177/
- National Cancer Institute. Cancer trends progress report: financial burden of cancer care. Updated April 2025. Accessed March 3, 2026. https://progressreport.cancer.gov/after/economic_burden
Clinical awareness of cancers associated with Camp Lejeune water contamination exposure remains limited despite legal and policy advances. Gaps persist in early symptom recognition and timely diagnostic evaluation before a definitive cancer diagnosis among exposed personnel. This may represent missed opportunities for earlier identification of volatile organic compounds (VOCs)-related cancers and for less invasive treatment options for veterans in this high-risk population.
Federal health care practitioners (HCPs), especially those in primary care and internal medicine, are uniquely positioned to bridge this gap. By improving the recognition of symptoms, pertinent physical examination findings, and implementing a diagnostic screening panel, HCPs can support accurate diagnoses and facilitate earlier treatment to improve health and quality of life for this population.
From 1953 to 1985, as many as 1 million military personnel, civilian workers, and their families stationed at US Marine Corps Base Camp Lejeune were unknowingly exposed to toxic and carcinogenic chemicals in drinking and bathing water.1 Three of the 8 main water sources on base were contaminated with VOCs, which are associated with multiple cancers.1-3
The US Department of Veterans Affairs (VA) recognizes 15 conditions associated with Camp Lejeune contaminated water exposure for VA benefits, including 10 cancers: adult leukemia; aplastic anemia and other myelodysplastic syndromes (MDS); bladder, esophageal, kidney, liver, breast (male and female), and lung cancers; multiple myeloma; and non-Hodgkin lymphoma (NHL).4
BACKGROUND
Established in 1942, Camp Lejeune is an important Marine Corps training installation. Between 1953 and 1985, multiple on-base water systems were contaminated with VOCs, including trichloroethylene (TCE), perchloroethylene (PCE), benzene, and vinyl chloride, due to improper waste disposal and industrial runoff from on- and off-base sources.5 Tarawa Terrace water treatment plant (WTP) was contaminated primarily with PCE from November 1957 to February 1987. Hadnot Point WTP was contaminated with TCE from August 1953 to December 1984, along with PCE, and benzene, toluene, ethylbenzene, and xylene (BTEX). Holcomb Boulevard WTP, established in 1972, was contaminated with TCE from June 1972 to February 1985.2 These contaminants entered the drinking and bathing water supply over decades, and exposure often occurred concurrently across = 1 VOC, compounding health risks.2,3 This prolonged 32-year VOC exposure window underlies current concerns regarding long-term cancer risk among affected service members, civilian employees, and family members. Epidemiologic research has found statistically significant associations between VOC exposure and multiple cancers, neurologic conditions, and reproductive issues.6 Specifically, TCE is associated with higher risks of hematologic cancers, multiple myeloma, NHL, and kidney cancer.3 PCE is linked with kidney cancer, benzene with multiple myeloma and NHL, and vinyl chloride with hepatobiliary cancers.3 A cohort mortality study compared Camp Lejeune personnel with a control group at Camp Pendleton from 1972 to 1985 and found a 3-fold higher incidence or mortality rate for kidney, esophageal, and female breast cancers, leukemia, and lymphoma among exposed Camp Lejeune personnel.6 Notably, personnel assigned to Camp Lejeune for as little as 6 months faced up to a 6-fold increase in cancer risk; the average military assignment between 1975 and 1985 was 18 months.3,6
Honoring America's Veterans and Caring for Camp Lejeune Families Act of 2012, the Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022, the Camp Lejeune Justice Act of 2022, and the pending Ensuring Justice for Camp Lejeune Victims Act of 2025 provide health care and legal resources for personnel and families affected by Camp Lejeune’s contaminated water.6-8 These laws acknowledge associations between exposure and specific health conditions and expanded health care, benefits, and legal recourse for affected veterans, survivors, and their families.8,9
CANCERS LINKED TO CAMP LEJEUNE
Camp Lejeune VOC-contaminated water exposure is associated with solid tumor and hematologic cancers. Symptoms, physical examination findings, and diagnostic considerations vary by cancer type (Table 1).
Bladder Cancer
The US incidence rate of bladder cancer for both males and females is 18 per 100,000 individuals per year, with a death rate of 4.1 per 100,000 individuals per year, and a 2.1% lifetime diagnosis risk.10 Personnel exposed to VOCs at Camp Lejeune had a 9% higher risk of developing bladder cancer and a 2% increased mortality compared with an unexposed control group at Camp Pendleton.1,7 Other bladder cancer subtypes at increased risk are papillary transitional cell carcinoma, nonpapillary transition cell carcinoma, and urothelial carcinoma.7 This is consistent with prior research that found PCE exposure is associated with an increased risk for bladder cancer.3,7,11 Smoking and tobacco use remain significant risk factors for bladder cancer.12
Symptomatology. The most common symptom associated with bladder cancer is painless hematuria (gross or microscopic). Other often delayed symptoms include urinary frequency, urgency, or nocturia.13,14
Diagnostics. Screening tests include urinalysis for hematuria, urine cytology, and cystoscopy with biopsy as the gold standard for diagnosis and staging.15,16
Kidney Cancer
The US incidence rate of kidney cancer and renal pelvis cancer for both males and females is 17.5 per 100,000 individuals per year, with a death rate of 3.4 per 100,000, and a 1.8% lifetime diagnosis risk.17 Camp Lejeune personnel exposed to VOCs had a 6% increased risk of developing kidney cancer and renal pelvis cancer and a 21% higher mortality risk compared with Camp Pendleton controls.1,7 Subtypes at risk include renal cell carcinoma and papillary carcinoma.7 This is consistent with prior research that found exposures to TCE and PCE are associated with a 3-fold increased risk of kidney cancer.3,7
Symptomatology. Hematuria, flank pain, and a palpable abdominal mass are common symptoms associated with kidney cancer. In advanced stages, other symptoms may include left-sided varicocele, anemia, weight loss, fatigue, fever, and night sweats.18
Diagnostics. Screening tests include urinalysis to assess the presence of blood, complete blood count (CBC) to assess anemia, calcium (elevated), and lactate dehydrogenase (LDH), which may be elevated. Imaging strategies include abdominal computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound.19
Esophageal Cancer
The US incidence rate of esophageal cancer for both males and females is 4.2 per 100,000 individuals per year, the death rate is 3.7 per 100,000 individuals per year, and a 0.5% lifetime diagnosis risk.20 VOC-exposed Camp Lejeune personnel had a 27% increased incidence and 25% increased mortality compared with the control group.1,7 Esophageal cancer subtypes at elevated risk include squamous cell carcinoma and adenocarcinoma. This is consistent with prior research that found Camp Lejeune water exposure is associated with a 3-fold increased risk for esophageal cancer.7 Additional risk factors include history of smoking and alcohol use.21
Symptomatology. Esophageal cancer is often asymptomatic with potential symptoms that include dysphagia, hoarseness, and weight loss in advanced disease.22
Diagnostics. Endoscopy with biopsy is the definitive method for diagnosis.23
Liver Cancer
The US incidence rate of liver cancer and intrahepatic bile duct cancer for both males and females is 9.4 per 100,000 individuals per year, with a death rate of 6.6 per 100,000 individuals per year, and a 1.1% lifetime diagnosis risk.24 VOC-exposed personnel had a 1% higher mortality than controls.1
Symptomatology. Liver cancer is often asymptomatic and appears in late stages.25 Common symptoms include right upper quadrant pain, early satiety, nausea, vomiting, loss of appetite, weight loss, ascites, jaundice, and abnormal bleeding or bruising.25,26
Diagnostics. Diagnostic tests may include an ultrasound, CT, or MRI. Additional laboratory testing may include liver function, a-fetoprotein blood, CBC, renal function, calcium, and hepatitis panel screening for hepatitis B and C.27,28
Lung Cancer
The US incidence rate of lung cancer for both males and females is 47.8 per 100,000 individuals per year, with a death rate of 31.5 per 100,000 individuals per year, and a 5.4% lifetime diagnosis risk.29 VOC-exposed personnel had a 16% increased risk and 19% higher mortality.1,7 Subtypes include large cell, small cell, non-small cell, squamous cell, and adenocarcinoma.7 Smoking is an additional risk factor.30
Symptomatology. Symptoms of lung cancer include cough, shortness of breath, chest pain worse with deep breathing, unexplained weight loss, fatigue, night sweats, and recurrent fevers. Advanced stages may metastasize or spread to the liver, bones, and brain.31
Diagnostics. Low-dose CT and chest X-ray are used for screening.32
Breast Cancer
The US incidence rate of female breast cancer is 130.8 per 100,000 individuals per year, with a death rate of 19.2 per 100,000 individuals per year, and a 13.0% lifetime risk of diagnosis.33 For female VOC-exposed personnel, there was an equal risk of developing breast cancer as the control group.1 However, exposed females at Camp Lejeune had a 23% higher mortality risk compared to the control group.7 Breast cancer subtypes among females include ductal carcinoma, lobular carcinoma, and ductal-lobular carcinoma.1
The US incidence rate of male breast cancer is 1.3 per 100,000 individuals per year, with a death rate of 0.3 per 100,000 individuals per year.34,35 The lifetime risk for males developing breast cancer is 137.7 per 100,000 and about 70 to 100 times less common in men than women.36
Male personnel exposed at Camp Lejeune had a 4% increased risk for developing breast cancer compared to Camp Pendleton.7 However, mortality was lower in the Camp Lejeune group.1 Although male breast cancer is rare, males at Camp Lejeune had a higher incidence, indicating a link between TCE, PCE, vinyl chloride exposures and male breast cancer.37 Male breast cancer is more often diagnosed in advanced stages than female breast cancer due to the lack of awareness or absence of routine screenings.38 The most common breast cancer type in males is invasive ductal carcinoma, accounting for 85% to 90% of cases; lobular carcinoma is the second most common type.39
Symptomatology. In both females and males, breast cancer symptoms include painless, firm mass or lump in the breast (left breast slightly more common than right), skin changes or dimpling, nipple retraction or turning inward, and nipple discharge. Breast cancer can spread to the lymph nodes and can be appreciated in axilla or clavicular regions.40
Diagnostics. The diagnostic evaluation for breast cancer is similar for females and males. It includes a clinical breast examination, diagnostic mammogram, and ultrasound.41 Mammograms can distinguish between gynecomastia and cancer, especially in males.42 A core or fine needle biopsy is needed to confirm diagnosis.41
Adult Leukemia
The US incidence rate of leukemia for both male and female was 14.4 per 100,000 individuals per year, with a death rate of 5.8 per 100,000 individuals per year, and a 1.5% lifetime diagnosis risk.43
VOC-exposed personnel had a 7% higher risk of developing leukemia and a 13% increased mortality risk compared with the control group.1,7 Subtypes of leukemia at risk included a 38% increased incidence of acute myeloid/monocytic leukemia (AML) and a 2% increased incidence of chronic lymphocytic leukemia (CLL).1 Benzene and TCE exposures are known risk factors for AML and other leukemias.7 Personnel at Camp Lejeune had 3 times the incidence or mortality for leukemia, specifically AML mortality at 20%.7 Smoking is an additional risk factor for certain leukemias, especially AML.30
Symptomatology. Symptoms associated with leukemia are often nonspecific and may include fatigue, pallor, easy bruising or bleeding (skin or gums), recurrent infections secondary to neutropenia, fever, night sweats, pain or feeling full after a small meal due to enlarged spleen or liver, and weight loss.44,45
Diagnostics. An initial screening includes a CBC with differential, a peripheral smear to detect the presence of blast cells, as well as Auer rods in myeloid blast cells in AML or smudge cells in CLL. Confirmatory tests may include bone marrow biopsy or flow cytometry. A referral to a hematologist is recommended for any suspected leukemia.46,47
Myelodysplastic Syndromes
Aplastic anemia and MDS are considered rare disorders.48 Aplastic anemia is a nonmalignant bone marrow failure disorder with pancytopenia and hypocellular bone marrow due to the loss of hematopoietic stem cells.48 MDS is a type of hematopoietic cancer where the bone marrow produces abnormal blood cells or does not make enough healthy cells.49 This can lead to an increased risk for infection, cytopenias, neutropenia, refractory anemia, and thrombocytopenia, and progression to AML in some patients.49
The reported US incidence of MDS from 1975 to 2013 was 6.7 per 100,000 for males and 3.7 per 100,000 for females.50 Benzene exposure is linked to MDS and a known cause of AML.1 VOC-exposed personnel had a 68% increased risk of developing MDS and a 2.3-fold increased mortality risk compared to controls.1,7
Symptomatology. Some patients are asymptomatic at diagnosis.51 Symptoms related to cytopenia include fatigue, pallor, purpura, petechiae, bleeding of skin, gum, or nose, recurrent infections, fever, bone pain, loss of appetite, and weight loss.50,51
Diagnostics. Initial workup includes a CBC with differential to assess for anemia, white blood cell and absolute neutrophil counts (low), and thrombocytopenia.52 A peripheral blood smear may show myeloid blast cells. A bone marrow aspiration and biopsy, flow cytometry, and cytogenetic or molecular testing may be performed. If MDS is suspected, a referral to a hematologist should be considered.52
Multiple Myeloma
The US incidence rate of multiple myeloma for both males and females is 7.3 per 100,000 individuals per year, with a mortality rate of 2.9 per 100,000 individuals per year, and a 0.8% lifetime diagnosis risk.53 VOC-exposed personnel had a 13% increased risk of developing multiple myeloma and an 8% increased mortality risk compared to unexposed personnel.1,7
Symptomatology. Multiple myeloma may be asymptomatic in early stages. The most common presenting symptom is bone pain, especially in the back, hips, and long bones, due to hypercalcemia from increased reabsorption, plasma cell tumor overgrowth in the bone marrow, and lytic lesions.54 Additional symptoms include fatigue and pallor related to anemia, leukopenia, thrombocytopenia, recurrent infections, extreme thirst, frequent urination, dehydration, confusion associated with hypercalcemia, peripheral neuropathy, loss of appetite, weight loss, and renal impairment or failure.54
Diagnostics. Testing considerations include a CBC with a peripheral blood smear to evaluate anemia and rouleaux formation of red blood cells (seen in > 50% of patients with multiple myeloma), comprehensive metabolic panel (CMP) to assess kidney function, calcium levels (elevated), serum and urine protein electrophoresis with immunofixation to detect monoclonal protein (detected in > 80% of patients with multiple myeloma) and Bence-Jones proteins, serum free light chain assay, and a bone marrow biopsy for diagnosis.55,56
MRI of the spine and pelvis is the most sensitive to detecting bone marrow involvement and focal lesions before lytic lesion progression occurs and for assessing spinal cord compression.57 PET/CT is more sensitive at detecting extramedullary disease, outside of the spine, and for patients that cannot undergo MRI.57 A whole-body low-dose CT, either alone or with PET, is more sensitive than an X-ray at detecting lytic lesions, fractures, or osteoporosis associated with multiple myeloma.57
Non-Hodgkin Lymphoma
The US incidence rate of NHL for both males and females are 18.7 per 100,000 individuals per year, the death rate is 4.9 per 100,000 individuals per year, and a 2% lifetime diagnosis risk.58 VOC-exposed personnel had a 1% higher risk of developing NHL and a decreased mortality risk compared to the control group.1,7 Specific NHL subtypes with increased risk in the exposed cohort are mantle cell (26%), follicular (7%), Burkitt (53%), and marginal zone B-cell (45%).7
Symptomatology. NHL often presents with painless lymphadenopathy or enlarged lymph nodes involving the cervical, axillary, inguinal regions.59,60 Other symptoms include frequent infections, unexplained bruising, weight loss, and “B symptoms,” such as fever and night sweats.59,60 Some patients develop a mediastinal mass in the thorax, which if large may lead to cough or shortness of breath.59
Diagnostics. The initial diagnostic workup includes CBC with differential and LDH, which may be elevated.60,61 Imaging may begin with a chest X-ray to assess for a mediastinal mass; however, CTs of the chest, abdomen, and pelvis provide more detail to better assess for NHL. Whole body PET/CT is considered the gold standard for assessing and staging systemic involvement. If enlarged lymph nodes are present, a biopsy can confirm the subtype of NHL.60,61
PHYSICAL EXAMINATION
A focused physical examination may aid HCPs in early detection of the cancers associated with Camp Lejeune (Table 2). The physical examination can guide diagnostic testing and imaging for further assessment and workup for VOC-related cancers.
Proposed Diagnostic Screening Panel
Primary care and internal medicine HCPs have the opportunity to improve patient health outcomes by implementing a targeted diagnostic screening panel for identified veterans previously stationed at Camp Lejeune. Early identification of cancers associated with VOCs exposure can facilitate earlier treatment interventions and improve health and quality of life outcomes. The following diagnostic screening panel outlines a potential cost-effective strategy for evaluating and detecting the 10 cancers associated with VOC exposure in Camp Lejeune water.
Baseline Screening
Implementing a diagnostic screening panel in this high-risk cohort can lead to earlier diagnosis, reduce mortality, and improve patient outcomes through early intervention, which in turn may result in less invasive treatment. This approach may also reduce health care costs by avoiding costs associated with delayed diagnosis and advanced-stage cancer care (Tables 3 and 4).
A baseline panel of tests for exposed veterans could include:
- A CBC with differential and peripheral smear to assess for anemia, leukemia, thrombocytopenia, and blast cells associated with leukemias, MDS, multiple myeloma, and NHL.19,46,47,52,55,56,60,61
- CMP evaluates calcium, total protein, renal and liver renal function. Elevated test results may indicate kidney or liver cancer or multiple myeloma.19,27,28,55,56
- LDH testing may reveal levels that are elevated from tissue damage or high cell turnover in kidney cancer, multiple myeloma, and NHL.19,55,56,60,61
- Urinalysis with microscopy may detect hematuria, proteinuria and cellular casts in bladder and kidney cancers.13,24,19
- Low-dose CTs of the chest, abdomen, and pelvis are recommended for early identification of any masses or lymphadenopathy in lung, kidney, liver cancers, and NHL.19,27,28,32,60,61
COST EFFICIENCY
Screening Panel Cost
According to the Medicare Clinical Laboratory Fee Schedule payment cap for 2018, the mean cost for the proposed blood workup was $35 (CBC, $10; CMP, $13; LDH, $8; urinalysis, $4).62 Medicare procedure price schedule for 2025 includes $351 for a CT of the abdomen and pelvis with and without contrast (Current Procedural Terminology [CPT] code 74177) and $187 for a CT of the chest with and without contrast (CPT code 71270).63,64 The total proposed diagnostic screening panel payment cost about $572.
Cancer Care Cost
The average cost for initial cancer care across all cancer sites from 2007 to 2013 was $43,516 per patient; Camp Lejeune-associated cancers ranged from $26,443 for bladder cancer to $89,947 for esophageal cancer care.64 Further, the last year of life cost across all cancer sites averaged $109,727, and Camp Lejeune-associated cancer types ranged from $76,101 for breast cancer to $169,588 for leukemia.65
CONCLUSIONS
From 1953 to 1985, up to 1 million military personnel, civilian workers, and their families stationed at Camp Lejeune were unknowingly exposed to toxic and carcinogenic VOCs, which are associated with = 10 cancers, including bladder, kidney, esophageal, liver, lung, breast, and hematologic malignancies.1-4 Some veterans may be asymptomatic, whereas others present with subtle or specific symptoms that can vary by individual and the type and stage of cancer. HCPs have an opportunity to improve patient outcomes through awareness in identifying symptoms associated with Camp Lejeune water exposure and performing a thorough baseline physical examination, especially noting lymphadenopathy, unexplained weight loss, or masses, which can guide further diagnostic evaluation. Timely screening can identify cancers earlier, reducing delays in care, mitigating the cost burden associated with advanced-stage cancer treatment, improving survival outcomes, and enhancing quality of life. Primary care and internal medicine HCPs specifically play a crucial role in early recognition, physical assessment, and appropriate screening tools. A proposed panel includes CBC with differential and peripheral smear, CMP, LDH, urinalysis, and low-dose CTs of the chest, abdomen and pelvis. Implementation should be guided by clinical judgment and patient-specific risk factors. The proposed diagnostic screening panel is a small price to pay for those who served in any capacity at Camp Lejeune.
Clinical awareness of cancers associated with Camp Lejeune water contamination exposure remains limited despite legal and policy advances. Gaps persist in early symptom recognition and timely diagnostic evaluation before a definitive cancer diagnosis among exposed personnel. This may represent missed opportunities for earlier identification of volatile organic compounds (VOCs)-related cancers and for less invasive treatment options for veterans in this high-risk population.
Federal health care practitioners (HCPs), especially those in primary care and internal medicine, are uniquely positioned to bridge this gap. By improving the recognition of symptoms, pertinent physical examination findings, and implementing a diagnostic screening panel, HCPs can support accurate diagnoses and facilitate earlier treatment to improve health and quality of life for this population.
From 1953 to 1985, as many as 1 million military personnel, civilian workers, and their families stationed at US Marine Corps Base Camp Lejeune were unknowingly exposed to toxic and carcinogenic chemicals in drinking and bathing water.1 Three of the 8 main water sources on base were contaminated with VOCs, which are associated with multiple cancers.1-3
The US Department of Veterans Affairs (VA) recognizes 15 conditions associated with Camp Lejeune contaminated water exposure for VA benefits, including 10 cancers: adult leukemia; aplastic anemia and other myelodysplastic syndromes (MDS); bladder, esophageal, kidney, liver, breast (male and female), and lung cancers; multiple myeloma; and non-Hodgkin lymphoma (NHL).4
BACKGROUND
Established in 1942, Camp Lejeune is an important Marine Corps training installation. Between 1953 and 1985, multiple on-base water systems were contaminated with VOCs, including trichloroethylene (TCE), perchloroethylene (PCE), benzene, and vinyl chloride, due to improper waste disposal and industrial runoff from on- and off-base sources.5 Tarawa Terrace water treatment plant (WTP) was contaminated primarily with PCE from November 1957 to February 1987. Hadnot Point WTP was contaminated with TCE from August 1953 to December 1984, along with PCE, and benzene, toluene, ethylbenzene, and xylene (BTEX). Holcomb Boulevard WTP, established in 1972, was contaminated with TCE from June 1972 to February 1985.2 These contaminants entered the drinking and bathing water supply over decades, and exposure often occurred concurrently across = 1 VOC, compounding health risks.2,3 This prolonged 32-year VOC exposure window underlies current concerns regarding long-term cancer risk among affected service members, civilian employees, and family members. Epidemiologic research has found statistically significant associations between VOC exposure and multiple cancers, neurologic conditions, and reproductive issues.6 Specifically, TCE is associated with higher risks of hematologic cancers, multiple myeloma, NHL, and kidney cancer.3 PCE is linked with kidney cancer, benzene with multiple myeloma and NHL, and vinyl chloride with hepatobiliary cancers.3 A cohort mortality study compared Camp Lejeune personnel with a control group at Camp Pendleton from 1972 to 1985 and found a 3-fold higher incidence or mortality rate for kidney, esophageal, and female breast cancers, leukemia, and lymphoma among exposed Camp Lejeune personnel.6 Notably, personnel assigned to Camp Lejeune for as little as 6 months faced up to a 6-fold increase in cancer risk; the average military assignment between 1975 and 1985 was 18 months.3,6
Honoring America's Veterans and Caring for Camp Lejeune Families Act of 2012, the Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022, the Camp Lejeune Justice Act of 2022, and the pending Ensuring Justice for Camp Lejeune Victims Act of 2025 provide health care and legal resources for personnel and families affected by Camp Lejeune’s contaminated water.6-8 These laws acknowledge associations between exposure and specific health conditions and expanded health care, benefits, and legal recourse for affected veterans, survivors, and their families.8,9
CANCERS LINKED TO CAMP LEJEUNE
Camp Lejeune VOC-contaminated water exposure is associated with solid tumor and hematologic cancers. Symptoms, physical examination findings, and diagnostic considerations vary by cancer type (Table 1).
Bladder Cancer
The US incidence rate of bladder cancer for both males and females is 18 per 100,000 individuals per year, with a death rate of 4.1 per 100,000 individuals per year, and a 2.1% lifetime diagnosis risk.10 Personnel exposed to VOCs at Camp Lejeune had a 9% higher risk of developing bladder cancer and a 2% increased mortality compared with an unexposed control group at Camp Pendleton.1,7 Other bladder cancer subtypes at increased risk are papillary transitional cell carcinoma, nonpapillary transition cell carcinoma, and urothelial carcinoma.7 This is consistent with prior research that found PCE exposure is associated with an increased risk for bladder cancer.3,7,11 Smoking and tobacco use remain significant risk factors for bladder cancer.12
Symptomatology. The most common symptom associated with bladder cancer is painless hematuria (gross or microscopic). Other often delayed symptoms include urinary frequency, urgency, or nocturia.13,14
Diagnostics. Screening tests include urinalysis for hematuria, urine cytology, and cystoscopy with biopsy as the gold standard for diagnosis and staging.15,16
Kidney Cancer
The US incidence rate of kidney cancer and renal pelvis cancer for both males and females is 17.5 per 100,000 individuals per year, with a death rate of 3.4 per 100,000, and a 1.8% lifetime diagnosis risk.17 Camp Lejeune personnel exposed to VOCs had a 6% increased risk of developing kidney cancer and renal pelvis cancer and a 21% higher mortality risk compared with Camp Pendleton controls.1,7 Subtypes at risk include renal cell carcinoma and papillary carcinoma.7 This is consistent with prior research that found exposures to TCE and PCE are associated with a 3-fold increased risk of kidney cancer.3,7
Symptomatology. Hematuria, flank pain, and a palpable abdominal mass are common symptoms associated with kidney cancer. In advanced stages, other symptoms may include left-sided varicocele, anemia, weight loss, fatigue, fever, and night sweats.18
Diagnostics. Screening tests include urinalysis to assess the presence of blood, complete blood count (CBC) to assess anemia, calcium (elevated), and lactate dehydrogenase (LDH), which may be elevated. Imaging strategies include abdominal computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound.19
Esophageal Cancer
The US incidence rate of esophageal cancer for both males and females is 4.2 per 100,000 individuals per year, the death rate is 3.7 per 100,000 individuals per year, and a 0.5% lifetime diagnosis risk.20 VOC-exposed Camp Lejeune personnel had a 27% increased incidence and 25% increased mortality compared with the control group.1,7 Esophageal cancer subtypes at elevated risk include squamous cell carcinoma and adenocarcinoma. This is consistent with prior research that found Camp Lejeune water exposure is associated with a 3-fold increased risk for esophageal cancer.7 Additional risk factors include history of smoking and alcohol use.21
Symptomatology. Esophageal cancer is often asymptomatic with potential symptoms that include dysphagia, hoarseness, and weight loss in advanced disease.22
Diagnostics. Endoscopy with biopsy is the definitive method for diagnosis.23
Liver Cancer
The US incidence rate of liver cancer and intrahepatic bile duct cancer for both males and females is 9.4 per 100,000 individuals per year, with a death rate of 6.6 per 100,000 individuals per year, and a 1.1% lifetime diagnosis risk.24 VOC-exposed personnel had a 1% higher mortality than controls.1
Symptomatology. Liver cancer is often asymptomatic and appears in late stages.25 Common symptoms include right upper quadrant pain, early satiety, nausea, vomiting, loss of appetite, weight loss, ascites, jaundice, and abnormal bleeding or bruising.25,26
Diagnostics. Diagnostic tests may include an ultrasound, CT, or MRI. Additional laboratory testing may include liver function, a-fetoprotein blood, CBC, renal function, calcium, and hepatitis panel screening for hepatitis B and C.27,28
Lung Cancer
The US incidence rate of lung cancer for both males and females is 47.8 per 100,000 individuals per year, with a death rate of 31.5 per 100,000 individuals per year, and a 5.4% lifetime diagnosis risk.29 VOC-exposed personnel had a 16% increased risk and 19% higher mortality.1,7 Subtypes include large cell, small cell, non-small cell, squamous cell, and adenocarcinoma.7 Smoking is an additional risk factor.30
Symptomatology. Symptoms of lung cancer include cough, shortness of breath, chest pain worse with deep breathing, unexplained weight loss, fatigue, night sweats, and recurrent fevers. Advanced stages may metastasize or spread to the liver, bones, and brain.31
Diagnostics. Low-dose CT and chest X-ray are used for screening.32
Breast Cancer
The US incidence rate of female breast cancer is 130.8 per 100,000 individuals per year, with a death rate of 19.2 per 100,000 individuals per year, and a 13.0% lifetime risk of diagnosis.33 For female VOC-exposed personnel, there was an equal risk of developing breast cancer as the control group.1 However, exposed females at Camp Lejeune had a 23% higher mortality risk compared to the control group.7 Breast cancer subtypes among females include ductal carcinoma, lobular carcinoma, and ductal-lobular carcinoma.1
The US incidence rate of male breast cancer is 1.3 per 100,000 individuals per year, with a death rate of 0.3 per 100,000 individuals per year.34,35 The lifetime risk for males developing breast cancer is 137.7 per 100,000 and about 70 to 100 times less common in men than women.36
Male personnel exposed at Camp Lejeune had a 4% increased risk for developing breast cancer compared to Camp Pendleton.7 However, mortality was lower in the Camp Lejeune group.1 Although male breast cancer is rare, males at Camp Lejeune had a higher incidence, indicating a link between TCE, PCE, vinyl chloride exposures and male breast cancer.37 Male breast cancer is more often diagnosed in advanced stages than female breast cancer due to the lack of awareness or absence of routine screenings.38 The most common breast cancer type in males is invasive ductal carcinoma, accounting for 85% to 90% of cases; lobular carcinoma is the second most common type.39
Symptomatology. In both females and males, breast cancer symptoms include painless, firm mass or lump in the breast (left breast slightly more common than right), skin changes or dimpling, nipple retraction or turning inward, and nipple discharge. Breast cancer can spread to the lymph nodes and can be appreciated in axilla or clavicular regions.40
Diagnostics. The diagnostic evaluation for breast cancer is similar for females and males. It includes a clinical breast examination, diagnostic mammogram, and ultrasound.41 Mammograms can distinguish between gynecomastia and cancer, especially in males.42 A core or fine needle biopsy is needed to confirm diagnosis.41
Adult Leukemia
The US incidence rate of leukemia for both male and female was 14.4 per 100,000 individuals per year, with a death rate of 5.8 per 100,000 individuals per year, and a 1.5% lifetime diagnosis risk.43
VOC-exposed personnel had a 7% higher risk of developing leukemia and a 13% increased mortality risk compared with the control group.1,7 Subtypes of leukemia at risk included a 38% increased incidence of acute myeloid/monocytic leukemia (AML) and a 2% increased incidence of chronic lymphocytic leukemia (CLL).1 Benzene and TCE exposures are known risk factors for AML and other leukemias.7 Personnel at Camp Lejeune had 3 times the incidence or mortality for leukemia, specifically AML mortality at 20%.7 Smoking is an additional risk factor for certain leukemias, especially AML.30
Symptomatology. Symptoms associated with leukemia are often nonspecific and may include fatigue, pallor, easy bruising or bleeding (skin or gums), recurrent infections secondary to neutropenia, fever, night sweats, pain or feeling full after a small meal due to enlarged spleen or liver, and weight loss.44,45
Diagnostics. An initial screening includes a CBC with differential, a peripheral smear to detect the presence of blast cells, as well as Auer rods in myeloid blast cells in AML or smudge cells in CLL. Confirmatory tests may include bone marrow biopsy or flow cytometry. A referral to a hematologist is recommended for any suspected leukemia.46,47
Myelodysplastic Syndromes
Aplastic anemia and MDS are considered rare disorders.48 Aplastic anemia is a nonmalignant bone marrow failure disorder with pancytopenia and hypocellular bone marrow due to the loss of hematopoietic stem cells.48 MDS is a type of hematopoietic cancer where the bone marrow produces abnormal blood cells or does not make enough healthy cells.49 This can lead to an increased risk for infection, cytopenias, neutropenia, refractory anemia, and thrombocytopenia, and progression to AML in some patients.49
The reported US incidence of MDS from 1975 to 2013 was 6.7 per 100,000 for males and 3.7 per 100,000 for females.50 Benzene exposure is linked to MDS and a known cause of AML.1 VOC-exposed personnel had a 68% increased risk of developing MDS and a 2.3-fold increased mortality risk compared to controls.1,7
Symptomatology. Some patients are asymptomatic at diagnosis.51 Symptoms related to cytopenia include fatigue, pallor, purpura, petechiae, bleeding of skin, gum, or nose, recurrent infections, fever, bone pain, loss of appetite, and weight loss.50,51
Diagnostics. Initial workup includes a CBC with differential to assess for anemia, white blood cell and absolute neutrophil counts (low), and thrombocytopenia.52 A peripheral blood smear may show myeloid blast cells. A bone marrow aspiration and biopsy, flow cytometry, and cytogenetic or molecular testing may be performed. If MDS is suspected, a referral to a hematologist should be considered.52
Multiple Myeloma
The US incidence rate of multiple myeloma for both males and females is 7.3 per 100,000 individuals per year, with a mortality rate of 2.9 per 100,000 individuals per year, and a 0.8% lifetime diagnosis risk.53 VOC-exposed personnel had a 13% increased risk of developing multiple myeloma and an 8% increased mortality risk compared to unexposed personnel.1,7
Symptomatology. Multiple myeloma may be asymptomatic in early stages. The most common presenting symptom is bone pain, especially in the back, hips, and long bones, due to hypercalcemia from increased reabsorption, plasma cell tumor overgrowth in the bone marrow, and lytic lesions.54 Additional symptoms include fatigue and pallor related to anemia, leukopenia, thrombocytopenia, recurrent infections, extreme thirst, frequent urination, dehydration, confusion associated with hypercalcemia, peripheral neuropathy, loss of appetite, weight loss, and renal impairment or failure.54
Diagnostics. Testing considerations include a CBC with a peripheral blood smear to evaluate anemia and rouleaux formation of red blood cells (seen in > 50% of patients with multiple myeloma), comprehensive metabolic panel (CMP) to assess kidney function, calcium levels (elevated), serum and urine protein electrophoresis with immunofixation to detect monoclonal protein (detected in > 80% of patients with multiple myeloma) and Bence-Jones proteins, serum free light chain assay, and a bone marrow biopsy for diagnosis.55,56
MRI of the spine and pelvis is the most sensitive to detecting bone marrow involvement and focal lesions before lytic lesion progression occurs and for assessing spinal cord compression.57 PET/CT is more sensitive at detecting extramedullary disease, outside of the spine, and for patients that cannot undergo MRI.57 A whole-body low-dose CT, either alone or with PET, is more sensitive than an X-ray at detecting lytic lesions, fractures, or osteoporosis associated with multiple myeloma.57
Non-Hodgkin Lymphoma
The US incidence rate of NHL for both males and females are 18.7 per 100,000 individuals per year, the death rate is 4.9 per 100,000 individuals per year, and a 2% lifetime diagnosis risk.58 VOC-exposed personnel had a 1% higher risk of developing NHL and a decreased mortality risk compared to the control group.1,7 Specific NHL subtypes with increased risk in the exposed cohort are mantle cell (26%), follicular (7%), Burkitt (53%), and marginal zone B-cell (45%).7
Symptomatology. NHL often presents with painless lymphadenopathy or enlarged lymph nodes involving the cervical, axillary, inguinal regions.59,60 Other symptoms include frequent infections, unexplained bruising, weight loss, and “B symptoms,” such as fever and night sweats.59,60 Some patients develop a mediastinal mass in the thorax, which if large may lead to cough or shortness of breath.59
Diagnostics. The initial diagnostic workup includes CBC with differential and LDH, which may be elevated.60,61 Imaging may begin with a chest X-ray to assess for a mediastinal mass; however, CTs of the chest, abdomen, and pelvis provide more detail to better assess for NHL. Whole body PET/CT is considered the gold standard for assessing and staging systemic involvement. If enlarged lymph nodes are present, a biopsy can confirm the subtype of NHL.60,61
PHYSICAL EXAMINATION
A focused physical examination may aid HCPs in early detection of the cancers associated with Camp Lejeune (Table 2). The physical examination can guide diagnostic testing and imaging for further assessment and workup for VOC-related cancers.
Proposed Diagnostic Screening Panel
Primary care and internal medicine HCPs have the opportunity to improve patient health outcomes by implementing a targeted diagnostic screening panel for identified veterans previously stationed at Camp Lejeune. Early identification of cancers associated with VOCs exposure can facilitate earlier treatment interventions and improve health and quality of life outcomes. The following diagnostic screening panel outlines a potential cost-effective strategy for evaluating and detecting the 10 cancers associated with VOC exposure in Camp Lejeune water.
Baseline Screening
Implementing a diagnostic screening panel in this high-risk cohort can lead to earlier diagnosis, reduce mortality, and improve patient outcomes through early intervention, which in turn may result in less invasive treatment. This approach may also reduce health care costs by avoiding costs associated with delayed diagnosis and advanced-stage cancer care (Tables 3 and 4).
A baseline panel of tests for exposed veterans could include:
- A CBC with differential and peripheral smear to assess for anemia, leukemia, thrombocytopenia, and blast cells associated with leukemias, MDS, multiple myeloma, and NHL.19,46,47,52,55,56,60,61
- CMP evaluates calcium, total protein, renal and liver renal function. Elevated test results may indicate kidney or liver cancer or multiple myeloma.19,27,28,55,56
- LDH testing may reveal levels that are elevated from tissue damage or high cell turnover in kidney cancer, multiple myeloma, and NHL.19,55,56,60,61
- Urinalysis with microscopy may detect hematuria, proteinuria and cellular casts in bladder and kidney cancers.13,24,19
- Low-dose CTs of the chest, abdomen, and pelvis are recommended for early identification of any masses or lymphadenopathy in lung, kidney, liver cancers, and NHL.19,27,28,32,60,61
COST EFFICIENCY
Screening Panel Cost
According to the Medicare Clinical Laboratory Fee Schedule payment cap for 2018, the mean cost for the proposed blood workup was $35 (CBC, $10; CMP, $13; LDH, $8; urinalysis, $4).62 Medicare procedure price schedule for 2025 includes $351 for a CT of the abdomen and pelvis with and without contrast (Current Procedural Terminology [CPT] code 74177) and $187 for a CT of the chest with and without contrast (CPT code 71270).63,64 The total proposed diagnostic screening panel payment cost about $572.
Cancer Care Cost
The average cost for initial cancer care across all cancer sites from 2007 to 2013 was $43,516 per patient; Camp Lejeune-associated cancers ranged from $26,443 for bladder cancer to $89,947 for esophageal cancer care.64 Further, the last year of life cost across all cancer sites averaged $109,727, and Camp Lejeune-associated cancer types ranged from $76,101 for breast cancer to $169,588 for leukemia.65
CONCLUSIONS
From 1953 to 1985, up to 1 million military personnel, civilian workers, and their families stationed at Camp Lejeune were unknowingly exposed to toxic and carcinogenic VOCs, which are associated with = 10 cancers, including bladder, kidney, esophageal, liver, lung, breast, and hematologic malignancies.1-4 Some veterans may be asymptomatic, whereas others present with subtle or specific symptoms that can vary by individual and the type and stage of cancer. HCPs have an opportunity to improve patient outcomes through awareness in identifying symptoms associated with Camp Lejeune water exposure and performing a thorough baseline physical examination, especially noting lymphadenopathy, unexplained weight loss, or masses, which can guide further diagnostic evaluation. Timely screening can identify cancers earlier, reducing delays in care, mitigating the cost burden associated with advanced-stage cancer treatment, improving survival outcomes, and enhancing quality of life. Primary care and internal medicine HCPs specifically play a crucial role in early recognition, physical assessment, and appropriate screening tools. A proposed panel includes CBC with differential and peripheral smear, CMP, LDH, urinalysis, and low-dose CTs of the chest, abdomen and pelvis. Implementation should be guided by clinical judgment and patient-specific risk factors. The proposed diagnostic screening panel is a small price to pay for those who served in any capacity at Camp Lejeune.
- Bove FJ, Greek A, Gatiba R, et al. Cancer incidence among Marines and Navy personnel and civilian workers exposed to industrial solvents in drinking water at US Marine Corps Base Camp Lejeune: a cohort study. Environ Health Perspect. 2024;132:107008. doi:10.1289/EHP14966
- Maslia ML, Aral MM, Ruckart PZ, Bove FJ. Reconstructing historical VOC concentrations in drinking water for epidemiological studies at a US military base: summary of results. Water (Basel). 2016;8:449. doi:10.3390/w8100449
- Rosenfeld PE, Spaeth KR, McCarthy SJ, et al. Camp Lejeune Marine cancer risk assessment for exposure to contaminated drinking water from 1955 to 1987. Water Air Soil Pollut. 2024;235(2). doi:10.1007/s11270-023-06863-y
- US Department of Veterans Affairs, Veterans Health Administration. Camp Lejeune: past water contamination. Updated April 15, 2025. Accessed March 3, 2026. https://www.publichealth.va.gov/exposures/camp-lejeune/
- Jung K, Khan A, Mocharnuk R, et al. Clinical encounter with three cancer patients affected by groundwater contamination at Camp Lejeune: a case series and review of the literature. J Med Case Rep. 2022;16(1):272. doi:10.1186/s13256-022-03501-9
- Honoring America's Veterans and Caring for Camp Lejeune Familes Act of 2012, Pub L No. 112-154. Janey Ensminger Act. Congress.gov. Accessed April 15, 2026. https://ww.congress.gov/bill/112th-congress/house-bill/1627
- Bove FJ, Greek A, Gatiba R, et al. Evaluation of mortality among Marines, Navy personnel, and civilian workers exposed to contaminated drinking water at USMC Base Camp Lejeune: a cohort study. Environ Health. 2024;23(1):61. doi:10.1186/s12940-024-01099-7
- Honoring our PACT Act of 2022 (Pub L No. 117-168): expansion of health care eligibility and toxic exposure screenings. Congress.gov. Accessed March 3, 2026. https://www.congress.gov/bill/117th-congress/house-bill/3967
- Ensuring Justice for Camp Lejeune Victims Act of 2025. Congress.gov. Accessed March 24, 2026. https://www.congress.gov/bill/119th-congress/house-bill/4145
- SEER. Cancer stat facts: bladder cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/urinb.html
- Agency for Toxic Substances and Disease Registry. ATSDR assessment of the evidence for the drinking water contaminants at Camp Lejeune and specific cancers and other diseases. Published January 13, 2017. Accessed March 3, 2026. https://www.atsdr.cdc.gov/camp-lejeune/media/pdfs/2024/10/ATSDR_summary_of_the_evidence_for_causality_TCE_PCE_508.pdf
- National Cancer Institute. What is bladder cancer? Updated February 16, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder
- National Cancer Institute. Bladder cancer symptoms. Updated February 16, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder/symptoms
- American Cancer Society. Bladder cancer signs and symptoms. Updated March 12, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/bladder-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- National Cancer Institute. Bladder cancer screening. Updated April 27, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder/screening
- American Cancer Society. Tests for bladder cancer. Updated March 12, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/bladder-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: kidney and renal pelvis cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/kidrp.html
- American Cancer Society. Kidney cancer signs and symptoms. Updated May 1, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/kidney-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- American Cancer Society. Tests for kidney cancer. Updated May 1, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/kidney-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: esophageal cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/esoph.html
- Engel LS, Chow WH, Vaughan TL, et al. Population attributable risks of esophageal and gastric cancers.
J Natl Cancer Inst. 2003;95(18):1404-1413. doi:10.1093/jnci/djg047 - American Cancer Society. Signs and symptoms of esophageal cancer. Updated March 20, 2020. Accessed March 3, 2026. https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- American Cancer Society. Tests for esophageal cancer. Updated March 20, 2020. Accessed March 3, 2026. https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: liver and intrahepatic bile duct cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/livibd.html
- American Cancer Society. Signs and symptoms of liver cancer. Updated February 11, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/liver-cancer/detection-diagnosis-staging/signs-symptoms.html
- National Cancer Institute. What is liver cancer? Updated May 15, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/liver/what-is-liver-cancer
- American Cancer Society. Tests for liver cancer. Updated February 11, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/liver-cancer/detection-diagnosis-staging/how-diagnosed.html
- National Cancer Institute. Liver cancer screening. Updated May 15, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/liver/what-is-liver-cancer/screening
- SEER. Cancer stat facts: lung cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/lungb.html
- US Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. Accessed March 3, 2026. https://www.ncbi.nlm.nih.gov/books/NBK44695/pdf/Bookshelf_NBK44695.pdf
- American Cancer Society. Lung cancer signs and symptoms. Updated February 27, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/lung-cancer/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for lung cancer. Updated January 29, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/lung-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: female breast cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/breast.html
- SEER. SEER*Explorer breast incidence and mortality comparison. Updated July 2, 2025. Accessed March 3, 2026. https://seer.cancer.gov/statistics-network/explorer/application.html
- Susan G. Komen. Male breast cancer. Updated June 3, 2025. Accessed March 3, 2026. https://www.komen.org/breast-cancer/facts-statistics/male-breast-cancer/
- American Cancer Society. Key statistics for breast cancer in men. Updated January 16, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/about/key-statistics.html
- Ruckart PZ, Bove FJ, Shanley E 3rd, et al. Evaluation of contaminated drinking water and male breast cancer at Marine Corps Base Camp Lejeune, North Carolina: a case-control study. Environ Health. 2015;14:74. doi:10.1186/s12940-015-0061-4
- Culell P, Solernou L, Tarazona J, et al. Male breast cancer: a multicentric study. Breast J. 2007;13:213-215. doi:10.1111/j.1524-4741.2007.00412.x
- Giordano SH, Cohen DS, Buzdar AU, et al. Breast carcinoma in men: a population-based study. Cancer. 2004;101:51-57. doi:10.1002/cncr.20312
- American Cancer Society. Signs and symptoms of breast cancer in men. Updated April 27, 2018. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests to help diagnose breast cancer in men. Updated December 20, 2021. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/detection-diagnosis-staging/how-diagnosed.html
- Evans GF, Anthony T, Turnage RH, et al. The diagnostic accuracy of mammography in the evaluation of male breast disease. Am J Surg. 2001;181:96-100. doi:10.1016/S0002-9610(00)00571-7
- SEER. Cancer stat facts: leukemia. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/leuks.html
- American Cancer Society. Signs and symptoms of acute myeloid leukemia (AML). Updated March 20, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/acute-myeloid-leukemia/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Signs and symptoms of chronic lymphocytic leukemia (CLL). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/chronic-lymphocytic-leukemia/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for acute myeloid leukemia (AML). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/acute-myeloid-leukemia/detection-diagnosis-staging/how-diagnosed.html
- American Cancer Society. Tests for chronic lymphocytic leukemia (CLL). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/chronic-lymphocytic-leukemia/detection-diagnosis-staging/how-diagnosed.html
- Giudice V, Selleri C. Aplastic anemia: pathophysiology. Semin Hematol. 2022;59:13-20. doi:10.1053/j.seminhematol.2021.12.002
- National Cancer Institute. Myelodysplastic syndromes treatment (PDQ®)–patient version. Updated October 4, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/myeloproliferative/patient/myelodysplastic-treatment-pdq
- SEER. Cancer statistics review (CSR) 1975-2013: myelodysplastic syndromes. Accessed March 3, 2026. https://seer.cancer.gov/archive/csr/1975_2013/browse_csr.php?sectionSEL=30&pageSEL=sect_30_table.01
- American Cancer Society. Signs and symptoms of myelodysplastic syndrome (MDS). Updated November 21, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for myelodysplastic syndromes (MDS). Updated November 21, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: myeloma. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/mulmy.html
- American Cancer Society. Signs and symptoms of multiple myeloma. Updated February 28, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/multiple-myeloma/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for multiple myeloma. Updated February 28, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/multiple-myeloma/detection-diagnosis-staging/testing.html
- Laubach JP. Multiple myeloma: clinical features, laboratory manifestations, and diagnosis. UpToDate. Updated April 28, 2025. Accessed March 3, 2026. https://www.uptodate.com/contents/multiple-myeloma-clinical-features-laboratory-manifestations-and-diagnosis
- Hillengass J, Usmani S, Rajkumar SV, et al. International Myeloma Working Group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019;20:e302-e312. doi:10.1016/S1470-2045(19)30309-2
- SEER. Cancer stat facts: non-Hodgkin lymphoma. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/nhl.html
- American Cancer Society. Signs and symptoms of non-Hodgkin lymphoma. Updated February 15, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/detection-diagnosis-staging/signs-symptoms.html
- National Cancer Institute. Non-Hodgkin lymphoma treatment (PDQ®)–patient version. Updated August 22, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/lymphoma/patient/adult-nhl-treatment-pdq
- American Cancer Society. Tests for non-Hodgkin lymphoma. Updated February 15, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/detection-diagnosis-staging/how-diagnosed.html
- College of American Pathologists. Medicare clinical laboratory fee schedule. Published November 2017. Accessed March 3, 2026. https://documents.cap.org/documents/2018-final-medicare-clfs-rates.pdf
- Medicare.gov. Procedure price lookup for outpatient services. Accessed March 3, 2026. https://www.medicare.gov/procedure-price-lookup/cost/71270/
- Medicare.gov. Procedure price lookup for outpatient services. Accessed March 3, 2026. https://www.medicare.gov/procedure-price-lookup/cost/74177/
- National Cancer Institute. Cancer trends progress report: financial burden of cancer care. Updated April 2025. Accessed March 3, 2026. https://progressreport.cancer.gov/after/economic_burden
- Bove FJ, Greek A, Gatiba R, et al. Cancer incidence among Marines and Navy personnel and civilian workers exposed to industrial solvents in drinking water at US Marine Corps Base Camp Lejeune: a cohort study. Environ Health Perspect. 2024;132:107008. doi:10.1289/EHP14966
- Maslia ML, Aral MM, Ruckart PZ, Bove FJ. Reconstructing historical VOC concentrations in drinking water for epidemiological studies at a US military base: summary of results. Water (Basel). 2016;8:449. doi:10.3390/w8100449
- Rosenfeld PE, Spaeth KR, McCarthy SJ, et al. Camp Lejeune Marine cancer risk assessment for exposure to contaminated drinking water from 1955 to 1987. Water Air Soil Pollut. 2024;235(2). doi:10.1007/s11270-023-06863-y
- US Department of Veterans Affairs, Veterans Health Administration. Camp Lejeune: past water contamination. Updated April 15, 2025. Accessed March 3, 2026. https://www.publichealth.va.gov/exposures/camp-lejeune/
- Jung K, Khan A, Mocharnuk R, et al. Clinical encounter with three cancer patients affected by groundwater contamination at Camp Lejeune: a case series and review of the literature. J Med Case Rep. 2022;16(1):272. doi:10.1186/s13256-022-03501-9
- Honoring America's Veterans and Caring for Camp Lejeune Familes Act of 2012, Pub L No. 112-154. Janey Ensminger Act. Congress.gov. Accessed April 15, 2026. https://ww.congress.gov/bill/112th-congress/house-bill/1627
- Bove FJ, Greek A, Gatiba R, et al. Evaluation of mortality among Marines, Navy personnel, and civilian workers exposed to contaminated drinking water at USMC Base Camp Lejeune: a cohort study. Environ Health. 2024;23(1):61. doi:10.1186/s12940-024-01099-7
- Honoring our PACT Act of 2022 (Pub L No. 117-168): expansion of health care eligibility and toxic exposure screenings. Congress.gov. Accessed March 3, 2026. https://www.congress.gov/bill/117th-congress/house-bill/3967
- Ensuring Justice for Camp Lejeune Victims Act of 2025. Congress.gov. Accessed March 24, 2026. https://www.congress.gov/bill/119th-congress/house-bill/4145
- SEER. Cancer stat facts: bladder cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/urinb.html
- Agency for Toxic Substances and Disease Registry. ATSDR assessment of the evidence for the drinking water contaminants at Camp Lejeune and specific cancers and other diseases. Published January 13, 2017. Accessed March 3, 2026. https://www.atsdr.cdc.gov/camp-lejeune/media/pdfs/2024/10/ATSDR_summary_of_the_evidence_for_causality_TCE_PCE_508.pdf
- National Cancer Institute. What is bladder cancer? Updated February 16, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder
- National Cancer Institute. Bladder cancer symptoms. Updated February 16, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder/symptoms
- American Cancer Society. Bladder cancer signs and symptoms. Updated March 12, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/bladder-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- National Cancer Institute. Bladder cancer screening. Updated April 27, 2023. Accessed March 3, 2026. https://www.cancer.gov/types/bladder/screening
- American Cancer Society. Tests for bladder cancer. Updated March 12, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/bladder-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: kidney and renal pelvis cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/kidrp.html
- American Cancer Society. Kidney cancer signs and symptoms. Updated May 1, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/kidney-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- American Cancer Society. Tests for kidney cancer. Updated May 1, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/kidney-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: esophageal cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/esoph.html
- Engel LS, Chow WH, Vaughan TL, et al. Population attributable risks of esophageal and gastric cancers.
J Natl Cancer Inst. 2003;95(18):1404-1413. doi:10.1093/jnci/djg047 - American Cancer Society. Signs and symptoms of esophageal cancer. Updated March 20, 2020. Accessed March 3, 2026. https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/signs-and-symptoms.html
- American Cancer Society. Tests for esophageal cancer. Updated March 20, 2020. Accessed March 3, 2026. https://www.cancer.org/cancer/types/esophagus-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: liver and intrahepatic bile duct cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/livibd.html
- American Cancer Society. Signs and symptoms of liver cancer. Updated February 11, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/liver-cancer/detection-diagnosis-staging/signs-symptoms.html
- National Cancer Institute. What is liver cancer? Updated May 15, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/liver/what-is-liver-cancer
- American Cancer Society. Tests for liver cancer. Updated February 11, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/liver-cancer/detection-diagnosis-staging/how-diagnosed.html
- National Cancer Institute. Liver cancer screening. Updated May 15, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/liver/what-is-liver-cancer/screening
- SEER. Cancer stat facts: lung cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/lungb.html
- US Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. Accessed March 3, 2026. https://www.ncbi.nlm.nih.gov/books/NBK44695/pdf/Bookshelf_NBK44695.pdf
- American Cancer Society. Lung cancer signs and symptoms. Updated February 27, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/lung-cancer/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for lung cancer. Updated January 29, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/lung-cancer/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: female breast cancer. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/breast.html
- SEER. SEER*Explorer breast incidence and mortality comparison. Updated July 2, 2025. Accessed March 3, 2026. https://seer.cancer.gov/statistics-network/explorer/application.html
- Susan G. Komen. Male breast cancer. Updated June 3, 2025. Accessed March 3, 2026. https://www.komen.org/breast-cancer/facts-statistics/male-breast-cancer/
- American Cancer Society. Key statistics for breast cancer in men. Updated January 16, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/about/key-statistics.html
- Ruckart PZ, Bove FJ, Shanley E 3rd, et al. Evaluation of contaminated drinking water and male breast cancer at Marine Corps Base Camp Lejeune, North Carolina: a case-control study. Environ Health. 2015;14:74. doi:10.1186/s12940-015-0061-4
- Culell P, Solernou L, Tarazona J, et al. Male breast cancer: a multicentric study. Breast J. 2007;13:213-215. doi:10.1111/j.1524-4741.2007.00412.x
- Giordano SH, Cohen DS, Buzdar AU, et al. Breast carcinoma in men: a population-based study. Cancer. 2004;101:51-57. doi:10.1002/cncr.20312
- American Cancer Society. Signs and symptoms of breast cancer in men. Updated April 27, 2018. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests to help diagnose breast cancer in men. Updated December 20, 2021. Accessed March 3, 2026. https://www.cancer.org/cancer/types/breast-cancer-in-men/detection-diagnosis-staging/how-diagnosed.html
- Evans GF, Anthony T, Turnage RH, et al. The diagnostic accuracy of mammography in the evaluation of male breast disease. Am J Surg. 2001;181:96-100. doi:10.1016/S0002-9610(00)00571-7
- SEER. Cancer stat facts: leukemia. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/leuks.html
- American Cancer Society. Signs and symptoms of acute myeloid leukemia (AML). Updated March 20, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/acute-myeloid-leukemia/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Signs and symptoms of chronic lymphocytic leukemia (CLL). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/chronic-lymphocytic-leukemia/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for acute myeloid leukemia (AML). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/acute-myeloid-leukemia/detection-diagnosis-staging/how-diagnosed.html
- American Cancer Society. Tests for chronic lymphocytic leukemia (CLL). Updated March 4, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/chronic-lymphocytic-leukemia/detection-diagnosis-staging/how-diagnosed.html
- Giudice V, Selleri C. Aplastic anemia: pathophysiology. Semin Hematol. 2022;59:13-20. doi:10.1053/j.seminhematol.2021.12.002
- National Cancer Institute. Myelodysplastic syndromes treatment (PDQ®)–patient version. Updated October 4, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/myeloproliferative/patient/myelodysplastic-treatment-pdq
- SEER. Cancer statistics review (CSR) 1975-2013: myelodysplastic syndromes. Accessed March 3, 2026. https://seer.cancer.gov/archive/csr/1975_2013/browse_csr.php?sectionSEL=30&pageSEL=sect_30_table.01
- American Cancer Society. Signs and symptoms of myelodysplastic syndrome (MDS). Updated November 21, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for myelodysplastic syndromes (MDS). Updated November 21, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/detection-diagnosis-staging/how-diagnosed.html
- SEER. Cancer stat facts: myeloma. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/mulmy.html
- American Cancer Society. Signs and symptoms of multiple myeloma. Updated February 28, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/multiple-myeloma/detection-diagnosis-staging/signs-symptoms.html
- American Cancer Society. Tests for multiple myeloma. Updated February 28, 2025. Accessed March 3, 2026. https://www.cancer.org/cancer/types/multiple-myeloma/detection-diagnosis-staging/testing.html
- Laubach JP. Multiple myeloma: clinical features, laboratory manifestations, and diagnosis. UpToDate. Updated April 28, 2025. Accessed March 3, 2026. https://www.uptodate.com/contents/multiple-myeloma-clinical-features-laboratory-manifestations-and-diagnosis
- Hillengass J, Usmani S, Rajkumar SV, et al. International Myeloma Working Group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019;20:e302-e312. doi:10.1016/S1470-2045(19)30309-2
- SEER. Cancer stat facts: non-Hodgkin lymphoma. Accessed March 3, 2026. https://seer.cancer.gov/statfacts/html/nhl.html
- American Cancer Society. Signs and symptoms of non-Hodgkin lymphoma. Updated February 15, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/detection-diagnosis-staging/signs-symptoms.html
- National Cancer Institute. Non-Hodgkin lymphoma treatment (PDQ®)–patient version. Updated August 22, 2024. Accessed March 3, 2026. https://www.cancer.gov/types/lymphoma/patient/adult-nhl-treatment-pdq
- American Cancer Society. Tests for non-Hodgkin lymphoma. Updated February 15, 2024. Accessed March 3, 2026. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/detection-diagnosis-staging/how-diagnosed.html
- College of American Pathologists. Medicare clinical laboratory fee schedule. Published November 2017. Accessed March 3, 2026. https://documents.cap.org/documents/2018-final-medicare-clfs-rates.pdf
- Medicare.gov. Procedure price lookup for outpatient services. Accessed March 3, 2026. https://www.medicare.gov/procedure-price-lookup/cost/71270/
- Medicare.gov. Procedure price lookup for outpatient services. Accessed March 3, 2026. https://www.medicare.gov/procedure-price-lookup/cost/74177/
- National Cancer Institute. Cancer trends progress report: financial burden of cancer care. Updated April 2025. Accessed March 3, 2026. https://progressreport.cancer.gov/after/economic_burden
Optimizing Care for Veterans at Risk of Cancer From Camp Lejeune Water Exposure
Optimizing Care for Veterans at Risk of Cancer From Camp Lejeune Water Exposure

Geographic Clusters Show Uneven Cancer Screening in the US
Geographic Clusters Show Uneven Cancer Screening in the US
TOPLINE:
An analysis of 3142 US counties revealed that county-level screening for breast, cervical, and colorectal cancer increased overall between 1997 and 2019; however, despite the reduced geographic variation, persistently high-screening clusters remained in the Northeast, whereas persistently low-screening clusters remained in the Southwest.
METHODOLOGY:
- Cancer screening reduces mortality. Despite guideline recommendation, the uptake of breast, cervical, and colorectal cancer screening in the US falls short of national goals and varies across sociodemographic groups. To date, only a few studies have examined geographic and temporal patterns of screening.
- To address this gap, researchers conducted a cross-sectional study using an ecological panel design to analyze county-level screening prevalence across 3142 US mainland counties from 1997 to 2019, deriving prevalence estimates from Behavioral Risk Factor Surveillance System (BRFSS) and National Health Interview Survey (NHIS) data over 3- to 5-year periods.
- Spatial autocorrelation analyses, including Global Moran I and the bivariate local indicator of spatial autocorrelation, were performed to assess geographic clusters of cancer screening within each period. Four types of local geographic clusters of county-level cancer screening were identified: counties with persistently high screening rates, counties with persistently low screening rates, counties in which screening rates decreased from high to low, and counties in which screening rates increased from low to high.
- Screening prevalence was compared across multiple time windows for different modalities (mammography, a Papanicolaou test, colonoscopy, colorectal cancer test, endoscopy, and a fecal occult blood test [FOBT]). Overall, 3101 counties were analyzed for mammography and the Papanicolaou test, 3107 counties for colonoscopy, 3100 counties for colorectal cancer test, 3089 counties for endoscopy, and 3090 counties for the FOBT.
TAKEAWAY:
- Overall screening prevalence increased from 1997 to 2019, and global spatial autocorrelation declined over time. For instance, the distribution of mammography screening became 83% more uniform in more recent years (Moran I, 0.57 in 1997-1999 vs 0.10 in 2017-2019). Similarly, Papanicolaou test screening became more uniform in more recent years (Moran I, 0.44 vs. 0.07). These changes indicate reduced geographic heterogeneity.
- Colonoscopy and endoscopy use increased, surpassing a 50% prevalence in many counties for 2010; however, FOBT use declined. Spatial clustering also attenuated, with a 23.4% declined in Moran I for colonoscopy from 2011-2016 to 2017-2019, a 12.3% decline in the colorectal cancer test from 2004-2007 to 2008-2010, and a 14.0% decline for endoscopy from 2004-2007 to 2008-2010.
- Persistently high-/high-screening clusters were concentrated in the Northeast for mammography and colorectal cancer screening and in the East for Papanicolaou test screening, whereas persistently low-/low-screening clusters were concentrated in the Southwest for the same modalities.
- Clusters of low- and high-screening counties were more disadvantaged -- with lower socioeconomic status and a higher proportion of non-White residents -- than other cluster types, suggesting some improvement in screening uptake in more disadvantaged areas. Counties with persistently low screening exhibited greater socioeconomic disadvantages -- lower media household income, higher poverty, lower home values, and lower educational attainment -- than those with persistently high screening.
IN PRACTICE:
"This cross-sectional study found that despite secular increases that reduced geographic variation in screening, local clusters of high and low screening persisted in the Northeast and Southwest US, respectively. Future studies could incorporate health care access characteristics to explain why areas of low screening did not catch up to optimize cancer screening practice," the authors wrote.
SOURCE:
The study, led by Pranoti Pradhan, PhD, Harvard T.H. Chan School of Public Health, Boston, was published online in JAMA Network Open.
LIMITATIONS:
The county-level estimates were modeled using BRFSS, NHIS, and US Census data, which might be susceptible to sampling biases despite corrections for nonresponse and noncoverage. Researchers lacked data on specific health systems characteristics that may have directly driven changes in prevalence and were restricted to using screening time intervals available from the Small Area Estimates for Cancer-Relates Measures from the National Cancer Institute, rather than those according to US Preventive Services Task Force guidelines. Additionally, the spatial cluster method was sensitive to county size and arrangement, which may have influenced local cluster detection.
DISCLOSURES:
This research was supported by the T32 Cancer Prevention and Control Funding Fellowship and T32 Cancer Epidemiology Fellowship at the Harvard T.H. Chan School of Public Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An analysis of 3142 US counties revealed that county-level screening for breast, cervical, and colorectal cancer increased overall between 1997 and 2019; however, despite the reduced geographic variation, persistently high-screening clusters remained in the Northeast, whereas persistently low-screening clusters remained in the Southwest.
METHODOLOGY:
- Cancer screening reduces mortality. Despite guideline recommendation, the uptake of breast, cervical, and colorectal cancer screening in the US falls short of national goals and varies across sociodemographic groups. To date, only a few studies have examined geographic and temporal patterns of screening.
- To address this gap, researchers conducted a cross-sectional study using an ecological panel design to analyze county-level screening prevalence across 3142 US mainland counties from 1997 to 2019, deriving prevalence estimates from Behavioral Risk Factor Surveillance System (BRFSS) and National Health Interview Survey (NHIS) data over 3- to 5-year periods.
- Spatial autocorrelation analyses, including Global Moran I and the bivariate local indicator of spatial autocorrelation, were performed to assess geographic clusters of cancer screening within each period. Four types of local geographic clusters of county-level cancer screening were identified: counties with persistently high screening rates, counties with persistently low screening rates, counties in which screening rates decreased from high to low, and counties in which screening rates increased from low to high.
- Screening prevalence was compared across multiple time windows for different modalities (mammography, a Papanicolaou test, colonoscopy, colorectal cancer test, endoscopy, and a fecal occult blood test [FOBT]). Overall, 3101 counties were analyzed for mammography and the Papanicolaou test, 3107 counties for colonoscopy, 3100 counties for colorectal cancer test, 3089 counties for endoscopy, and 3090 counties for the FOBT.
TAKEAWAY:
- Overall screening prevalence increased from 1997 to 2019, and global spatial autocorrelation declined over time. For instance, the distribution of mammography screening became 83% more uniform in more recent years (Moran I, 0.57 in 1997-1999 vs 0.10 in 2017-2019). Similarly, Papanicolaou test screening became more uniform in more recent years (Moran I, 0.44 vs. 0.07). These changes indicate reduced geographic heterogeneity.
- Colonoscopy and endoscopy use increased, surpassing a 50% prevalence in many counties for 2010; however, FOBT use declined. Spatial clustering also attenuated, with a 23.4% declined in Moran I for colonoscopy from 2011-2016 to 2017-2019, a 12.3% decline in the colorectal cancer test from 2004-2007 to 2008-2010, and a 14.0% decline for endoscopy from 2004-2007 to 2008-2010.
- Persistently high-/high-screening clusters were concentrated in the Northeast for mammography and colorectal cancer screening and in the East for Papanicolaou test screening, whereas persistently low-/low-screening clusters were concentrated in the Southwest for the same modalities.
- Clusters of low- and high-screening counties were more disadvantaged -- with lower socioeconomic status and a higher proportion of non-White residents -- than other cluster types, suggesting some improvement in screening uptake in more disadvantaged areas. Counties with persistently low screening exhibited greater socioeconomic disadvantages -- lower media household income, higher poverty, lower home values, and lower educational attainment -- than those with persistently high screening.
IN PRACTICE:
"This cross-sectional study found that despite secular increases that reduced geographic variation in screening, local clusters of high and low screening persisted in the Northeast and Southwest US, respectively. Future studies could incorporate health care access characteristics to explain why areas of low screening did not catch up to optimize cancer screening practice," the authors wrote.
SOURCE:
The study, led by Pranoti Pradhan, PhD, Harvard T.H. Chan School of Public Health, Boston, was published online in JAMA Network Open.
LIMITATIONS:
The county-level estimates were modeled using BRFSS, NHIS, and US Census data, which might be susceptible to sampling biases despite corrections for nonresponse and noncoverage. Researchers lacked data on specific health systems characteristics that may have directly driven changes in prevalence and were restricted to using screening time intervals available from the Small Area Estimates for Cancer-Relates Measures from the National Cancer Institute, rather than those according to US Preventive Services Task Force guidelines. Additionally, the spatial cluster method was sensitive to county size and arrangement, which may have influenced local cluster detection.
DISCLOSURES:
This research was supported by the T32 Cancer Prevention and Control Funding Fellowship and T32 Cancer Epidemiology Fellowship at the Harvard T.H. Chan School of Public Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An analysis of 3142 US counties revealed that county-level screening for breast, cervical, and colorectal cancer increased overall between 1997 and 2019; however, despite the reduced geographic variation, persistently high-screening clusters remained in the Northeast, whereas persistently low-screening clusters remained in the Southwest.
METHODOLOGY:
- Cancer screening reduces mortality. Despite guideline recommendation, the uptake of breast, cervical, and colorectal cancer screening in the US falls short of national goals and varies across sociodemographic groups. To date, only a few studies have examined geographic and temporal patterns of screening.
- To address this gap, researchers conducted a cross-sectional study using an ecological panel design to analyze county-level screening prevalence across 3142 US mainland counties from 1997 to 2019, deriving prevalence estimates from Behavioral Risk Factor Surveillance System (BRFSS) and National Health Interview Survey (NHIS) data over 3- to 5-year periods.
- Spatial autocorrelation analyses, including Global Moran I and the bivariate local indicator of spatial autocorrelation, were performed to assess geographic clusters of cancer screening within each period. Four types of local geographic clusters of county-level cancer screening were identified: counties with persistently high screening rates, counties with persistently low screening rates, counties in which screening rates decreased from high to low, and counties in which screening rates increased from low to high.
- Screening prevalence was compared across multiple time windows for different modalities (mammography, a Papanicolaou test, colonoscopy, colorectal cancer test, endoscopy, and a fecal occult blood test [FOBT]). Overall, 3101 counties were analyzed for mammography and the Papanicolaou test, 3107 counties for colonoscopy, 3100 counties for colorectal cancer test, 3089 counties for endoscopy, and 3090 counties for the FOBT.
TAKEAWAY:
- Overall screening prevalence increased from 1997 to 2019, and global spatial autocorrelation declined over time. For instance, the distribution of mammography screening became 83% more uniform in more recent years (Moran I, 0.57 in 1997-1999 vs 0.10 in 2017-2019). Similarly, Papanicolaou test screening became more uniform in more recent years (Moran I, 0.44 vs. 0.07). These changes indicate reduced geographic heterogeneity.
- Colonoscopy and endoscopy use increased, surpassing a 50% prevalence in many counties for 2010; however, FOBT use declined. Spatial clustering also attenuated, with a 23.4% declined in Moran I for colonoscopy from 2011-2016 to 2017-2019, a 12.3% decline in the colorectal cancer test from 2004-2007 to 2008-2010, and a 14.0% decline for endoscopy from 2004-2007 to 2008-2010.
- Persistently high-/high-screening clusters were concentrated in the Northeast for mammography and colorectal cancer screening and in the East for Papanicolaou test screening, whereas persistently low-/low-screening clusters were concentrated in the Southwest for the same modalities.
- Clusters of low- and high-screening counties were more disadvantaged -- with lower socioeconomic status and a higher proportion of non-White residents -- than other cluster types, suggesting some improvement in screening uptake in more disadvantaged areas. Counties with persistently low screening exhibited greater socioeconomic disadvantages -- lower media household income, higher poverty, lower home values, and lower educational attainment -- than those with persistently high screening.
IN PRACTICE:
"This cross-sectional study found that despite secular increases that reduced geographic variation in screening, local clusters of high and low screening persisted in the Northeast and Southwest US, respectively. Future studies could incorporate health care access characteristics to explain why areas of low screening did not catch up to optimize cancer screening practice," the authors wrote.
SOURCE:
The study, led by Pranoti Pradhan, PhD, Harvard T.H. Chan School of Public Health, Boston, was published online in JAMA Network Open.
LIMITATIONS:
The county-level estimates were modeled using BRFSS, NHIS, and US Census data, which might be susceptible to sampling biases despite corrections for nonresponse and noncoverage. Researchers lacked data on specific health systems characteristics that may have directly driven changes in prevalence and were restricted to using screening time intervals available from the Small Area Estimates for Cancer-Relates Measures from the National Cancer Institute, rather than those according to US Preventive Services Task Force guidelines. Additionally, the spatial cluster method was sensitive to county size and arrangement, which may have influenced local cluster detection.
DISCLOSURES:
This research was supported by the T32 Cancer Prevention and Control Funding Fellowship and T32 Cancer Epidemiology Fellowship at the Harvard T.H. Chan School of Public Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Geographic Clusters Show Uneven Cancer Screening in the US
Geographic Clusters Show Uneven Cancer Screening in the US

Artificial Intelligence Shows Promise in Detecting Missed Interval Breast Cancer on Screening Mammograms
TOPLINE:
An artificial intelligence (AI) system flagged high-risk areas on mammograms for potentially missed interval breast cancers (IBCs), which radiologists had also retrospectively identified as abnormal. Moreover, the AI detected a substantial number of IBCs that manual review had overlooked.
METHODOLOGY:
- Researchers conducted a retrospective analysis of 119 IBC screening mammograms of women (mean age, 57.3 years) with a high breast density (Breast Imaging Reporting and Data System [BI-RADS] c/d, 63.0%) using data retrieved from Cancer Registries of Eastern Switzerland and Grisons-Glarus databases.
- A recorded tumour was classified as IBC when an invasive or in situ BC was diagnosed within 24 months after a normal screening mammogram.
- Three radiologists retrospectively assessed the mammograms for visible signs of BC, which were then classified as either potentially missed IBCs or IBCs without retrospective abnormalities on the basis of consensus conference recommendations of radiologists.
- An AI system generated two scores (a scale of 0 to 100): a case score reflecting the likelihood that the mammogram currently harbours cancer and a risk score estimating the probability of a BC diagnosis within 2 years.
TAKEAWAY:
- Radiologists classified 68.9% of IBCs as those having no retrospective abnormalities and assigned significantly higher BI-RADS scores to the remaining 31.1% of potentially missed IBCs (P < .05).
- Potentially missed IBCs received significantly higher AI case scores (mean, 54.1 vs 23.1; P < .05) and were assigned to a higher risk category (48.7% vs 14.6%; P < .05) than IBCs without retrospective abnormalities.
- Of all IBC cases, 46.2% received an AI case score > 25, 25.2% scored > 50, and 13.4% scored > 75.
- Potentially missed IBCs scored widely between low and high risk and case scores, whereas IBCs without retrospective abnormalities scored low case and risk scores. Specifically, 73.0% of potentially missed IBCs vs 34.1% of IBCs without retrospective abnormalities had case scores > 25, 51.4% vs 13.4% had case scores > 50, and 29.7% vs 6.1% had case scores > 75.
IN PRACTICE:
“Our research highlights that an AI system can identify BC signs in relevant portions of IBC screening mammograms and thus potentially reduce the number of IBCs in an MSP [mammography screening program] that currently does not utilize an AI system,” the authors of the study concluded, adding that “it can identify some IBCs that are not visible to humans (IBCs without retrospective abnormalities).”
SOURCE:
This study was led by Jonas Subelack, Chair of Health Economics, Policy and Management, School of Medicine, University of St. Gallen, St. Gallen, Switzerland. It was published online in European Radiology.
LIMITATIONS:
The retrospective study design inherently limited causal conclusions. Without access to diagnostic mammograms or the detailed position of BC, researchers could not evaluate whether AI-marked lesions corresponded to later detected BCs.
DISCLOSURES:
This research was funded by the Cancer League of Eastern Switzerland. One author reported receiving consulting and speaker fees from iCAD.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An artificial intelligence (AI) system flagged high-risk areas on mammograms for potentially missed interval breast cancers (IBCs), which radiologists had also retrospectively identified as abnormal. Moreover, the AI detected a substantial number of IBCs that manual review had overlooked.
METHODOLOGY:
- Researchers conducted a retrospective analysis of 119 IBC screening mammograms of women (mean age, 57.3 years) with a high breast density (Breast Imaging Reporting and Data System [BI-RADS] c/d, 63.0%) using data retrieved from Cancer Registries of Eastern Switzerland and Grisons-Glarus databases.
- A recorded tumour was classified as IBC when an invasive or in situ BC was diagnosed within 24 months after a normal screening mammogram.
- Three radiologists retrospectively assessed the mammograms for visible signs of BC, which were then classified as either potentially missed IBCs or IBCs without retrospective abnormalities on the basis of consensus conference recommendations of radiologists.
- An AI system generated two scores (a scale of 0 to 100): a case score reflecting the likelihood that the mammogram currently harbours cancer and a risk score estimating the probability of a BC diagnosis within 2 years.
TAKEAWAY:
- Radiologists classified 68.9% of IBCs as those having no retrospective abnormalities and assigned significantly higher BI-RADS scores to the remaining 31.1% of potentially missed IBCs (P < .05).
- Potentially missed IBCs received significantly higher AI case scores (mean, 54.1 vs 23.1; P < .05) and were assigned to a higher risk category (48.7% vs 14.6%; P < .05) than IBCs without retrospective abnormalities.
- Of all IBC cases, 46.2% received an AI case score > 25, 25.2% scored > 50, and 13.4% scored > 75.
- Potentially missed IBCs scored widely between low and high risk and case scores, whereas IBCs without retrospective abnormalities scored low case and risk scores. Specifically, 73.0% of potentially missed IBCs vs 34.1% of IBCs without retrospective abnormalities had case scores > 25, 51.4% vs 13.4% had case scores > 50, and 29.7% vs 6.1% had case scores > 75.
IN PRACTICE:
“Our research highlights that an AI system can identify BC signs in relevant portions of IBC screening mammograms and thus potentially reduce the number of IBCs in an MSP [mammography screening program] that currently does not utilize an AI system,” the authors of the study concluded, adding that “it can identify some IBCs that are not visible to humans (IBCs without retrospective abnormalities).”
SOURCE:
This study was led by Jonas Subelack, Chair of Health Economics, Policy and Management, School of Medicine, University of St. Gallen, St. Gallen, Switzerland. It was published online in European Radiology.
LIMITATIONS:
The retrospective study design inherently limited causal conclusions. Without access to diagnostic mammograms or the detailed position of BC, researchers could not evaluate whether AI-marked lesions corresponded to later detected BCs.
DISCLOSURES:
This research was funded by the Cancer League of Eastern Switzerland. One author reported receiving consulting and speaker fees from iCAD.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An artificial intelligence (AI) system flagged high-risk areas on mammograms for potentially missed interval breast cancers (IBCs), which radiologists had also retrospectively identified as abnormal. Moreover, the AI detected a substantial number of IBCs that manual review had overlooked.
METHODOLOGY:
- Researchers conducted a retrospective analysis of 119 IBC screening mammograms of women (mean age, 57.3 years) with a high breast density (Breast Imaging Reporting and Data System [BI-RADS] c/d, 63.0%) using data retrieved from Cancer Registries of Eastern Switzerland and Grisons-Glarus databases.
- A recorded tumour was classified as IBC when an invasive or in situ BC was diagnosed within 24 months after a normal screening mammogram.
- Three radiologists retrospectively assessed the mammograms for visible signs of BC, which were then classified as either potentially missed IBCs or IBCs without retrospective abnormalities on the basis of consensus conference recommendations of radiologists.
- An AI system generated two scores (a scale of 0 to 100): a case score reflecting the likelihood that the mammogram currently harbours cancer and a risk score estimating the probability of a BC diagnosis within 2 years.
TAKEAWAY:
- Radiologists classified 68.9% of IBCs as those having no retrospective abnormalities and assigned significantly higher BI-RADS scores to the remaining 31.1% of potentially missed IBCs (P < .05).
- Potentially missed IBCs received significantly higher AI case scores (mean, 54.1 vs 23.1; P < .05) and were assigned to a higher risk category (48.7% vs 14.6%; P < .05) than IBCs without retrospective abnormalities.
- Of all IBC cases, 46.2% received an AI case score > 25, 25.2% scored > 50, and 13.4% scored > 75.
- Potentially missed IBCs scored widely between low and high risk and case scores, whereas IBCs without retrospective abnormalities scored low case and risk scores. Specifically, 73.0% of potentially missed IBCs vs 34.1% of IBCs without retrospective abnormalities had case scores > 25, 51.4% vs 13.4% had case scores > 50, and 29.7% vs 6.1% had case scores > 75.
IN PRACTICE:
“Our research highlights that an AI system can identify BC signs in relevant portions of IBC screening mammograms and thus potentially reduce the number of IBCs in an MSP [mammography screening program] that currently does not utilize an AI system,” the authors of the study concluded, adding that “it can identify some IBCs that are not visible to humans (IBCs without retrospective abnormalities).”
SOURCE:
This study was led by Jonas Subelack, Chair of Health Economics, Policy and Management, School of Medicine, University of St. Gallen, St. Gallen, Switzerland. It was published online in European Radiology.
LIMITATIONS:
The retrospective study design inherently limited causal conclusions. Without access to diagnostic mammograms or the detailed position of BC, researchers could not evaluate whether AI-marked lesions corresponded to later detected BCs.
DISCLOSURES:
This research was funded by the Cancer League of Eastern Switzerland. One author reported receiving consulting and speaker fees from iCAD.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.

Cancer Data Trends 2025
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.

In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments

Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Women who undergo surgery for breast cancer often hear that they should take it easy with exercise during recovery. But new research looking at intense strength training puts that advice into question.
The study, of nearly 200 women who’d undergone lumpectomy or mastectomy, found that a 3-month weight-training program helped patients make substantial gains in strength, mobility, balance, and body composition.
And while previous studies have examined resistance exercise during breast cancer surgery recovery, this program pumped up the intensity: Most women progressed to deadlifting 100 to 200 pounds, even though few had ever performed strength training before.
“Most of these patients can do a lot more than we think,” said principal investigator Colin Champ, MD, director of the Exercise Oncology and Resiliency Center at Allegheny Health Network in Pittsburgh.
The findings were presented at The American Society of Breast Surgeons (ASBrS) Annual Meeting, held in Seattle from April 29 to May 3.
Pumping Up the Intensity
For the analysis, Champ and his colleagues pooled the results of 3 small prospective studies of their strength conditioning program, including one that previously reported no worsening in patients’ lymphedema, and instead, showed signs of improvement.
The researchers evaluated program participants’ physical and functional gains and whether any of those parameters differed by the extent of their breast cancer surgery.
In total, there were 197 participants, including 85 who’d undergone mastectomies and 112 who’d had lumpectomies; 26 patients also had axillary lymph node dissection.
All of the women attended the same 3-month supervised strength-training program, starting at various points in their recovery process. Nearly half started at 3 months postdiagnosis.
According to Champ, the program addresses a full range of motion, with the exercise intensity building over a short period — similar to what professional athletes do in early training. The specific exercises include split squats, dumbbell presses, and dumbbell rows, done 3 days per week, for about 45-60 minutes.
Most participants, Champ said, start with deadlifting around 70 pounds (lifting weight from the floor to hip level). “If you can carry groceries, you can deadlift 60 or 70 pounds,” he noted.
Each month, the weight and sets increase, while the repetitions decrease.
“We just had a woman in her 70s who deadlifted about 200 pounds” as the program progressed, Champ said.
Benefits Regardless of Surgery Type
Women in the current analysis underwent baseline and post-program testing of body composition and functional parameters, including strength, mobility, and balance. Mastectomy patients (median age, 51 years) were younger than lumpectomy patients (median age, 59 years). They were also more likely to have had chemotherapy (45% vs 27%).
Overall, Champ’s team found that both surgery groups showed statistically significant improvements in muscle and body fat percentages over the course of the program, with muscle mass increasing by 1 percentage point on average and body fat declining by 1.5 percentage points.
Similarly, functional movement scores, grip strength, loads lifted, and balance skills also improved, with comparable benefits regardless of surgery type or whether lymph node dissection was performed.
By the end of the program’s third week, Champ said, most women could deadlift 100-pound weights. And by the 3-month mark, many were able to lift 200-pound loads.
Champ called the results empowering, and he hopes they help reframe the traditional mindset that intense strength training is too heavy a lift after breast cancer surgery.
A surgical oncologist who was not involved in the study agreed.
“This gives us something concrete to say to patients,” said Tina Hieken, MD, of the Mayo Clinic in Rochester, Minnesota. “We have more data to say it’s safe for you to exercise.’’
Hieken, who chaired the meeting’s scientific program committee, also noted that the findings pertain to women of all baseline fitness levels.
For her part, Hieken already encourages patients to walk for exercise and spend time outdoors — in part for the mental well-being benefits.
With patients facing so much uncertainty after a cancer diagnosis, she said, “this is something an individual can take control of.”
Champ and Hieken had no disclosures.
A version of this article first appeared on Medscape.com.
Women who undergo surgery for breast cancer often hear that they should take it easy with exercise during recovery. But new research looking at intense strength training puts that advice into question.
The study, of nearly 200 women who’d undergone lumpectomy or mastectomy, found that a 3-month weight-training program helped patients make substantial gains in strength, mobility, balance, and body composition.
And while previous studies have examined resistance exercise during breast cancer surgery recovery, this program pumped up the intensity: Most women progressed to deadlifting 100 to 200 pounds, even though few had ever performed strength training before.
“Most of these patients can do a lot more than we think,” said principal investigator Colin Champ, MD, director of the Exercise Oncology and Resiliency Center at Allegheny Health Network in Pittsburgh.
The findings were presented at The American Society of Breast Surgeons (ASBrS) Annual Meeting, held in Seattle from April 29 to May 3.
Pumping Up the Intensity
For the analysis, Champ and his colleagues pooled the results of 3 small prospective studies of their strength conditioning program, including one that previously reported no worsening in patients’ lymphedema, and instead, showed signs of improvement.
The researchers evaluated program participants’ physical and functional gains and whether any of those parameters differed by the extent of their breast cancer surgery.
In total, there were 197 participants, including 85 who’d undergone mastectomies and 112 who’d had lumpectomies; 26 patients also had axillary lymph node dissection.
All of the women attended the same 3-month supervised strength-training program, starting at various points in their recovery process. Nearly half started at 3 months postdiagnosis.
According to Champ, the program addresses a full range of motion, with the exercise intensity building over a short period — similar to what professional athletes do in early training. The specific exercises include split squats, dumbbell presses, and dumbbell rows, done 3 days per week, for about 45-60 minutes.
Most participants, Champ said, start with deadlifting around 70 pounds (lifting weight from the floor to hip level). “If you can carry groceries, you can deadlift 60 or 70 pounds,” he noted.
Each month, the weight and sets increase, while the repetitions decrease.
“We just had a woman in her 70s who deadlifted about 200 pounds” as the program progressed, Champ said.
Benefits Regardless of Surgery Type
Women in the current analysis underwent baseline and post-program testing of body composition and functional parameters, including strength, mobility, and balance. Mastectomy patients (median age, 51 years) were younger than lumpectomy patients (median age, 59 years). They were also more likely to have had chemotherapy (45% vs 27%).
Overall, Champ’s team found that both surgery groups showed statistically significant improvements in muscle and body fat percentages over the course of the program, with muscle mass increasing by 1 percentage point on average and body fat declining by 1.5 percentage points.
Similarly, functional movement scores, grip strength, loads lifted, and balance skills also improved, with comparable benefits regardless of surgery type or whether lymph node dissection was performed.
By the end of the program’s third week, Champ said, most women could deadlift 100-pound weights. And by the 3-month mark, many were able to lift 200-pound loads.
Champ called the results empowering, and he hopes they help reframe the traditional mindset that intense strength training is too heavy a lift after breast cancer surgery.
A surgical oncologist who was not involved in the study agreed.
“This gives us something concrete to say to patients,” said Tina Hieken, MD, of the Mayo Clinic in Rochester, Minnesota. “We have more data to say it’s safe for you to exercise.’’
Hieken, who chaired the meeting’s scientific program committee, also noted that the findings pertain to women of all baseline fitness levels.
For her part, Hieken already encourages patients to walk for exercise and spend time outdoors — in part for the mental well-being benefits.
With patients facing so much uncertainty after a cancer diagnosis, she said, “this is something an individual can take control of.”
Champ and Hieken had no disclosures.
A version of this article first appeared on Medscape.com.
Women who undergo surgery for breast cancer often hear that they should take it easy with exercise during recovery. But new research looking at intense strength training puts that advice into question.
The study, of nearly 200 women who’d undergone lumpectomy or mastectomy, found that a 3-month weight-training program helped patients make substantial gains in strength, mobility, balance, and body composition.
And while previous studies have examined resistance exercise during breast cancer surgery recovery, this program pumped up the intensity: Most women progressed to deadlifting 100 to 200 pounds, even though few had ever performed strength training before.
“Most of these patients can do a lot more than we think,” said principal investigator Colin Champ, MD, director of the Exercise Oncology and Resiliency Center at Allegheny Health Network in Pittsburgh.
The findings were presented at The American Society of Breast Surgeons (ASBrS) Annual Meeting, held in Seattle from April 29 to May 3.
Pumping Up the Intensity
For the analysis, Champ and his colleagues pooled the results of 3 small prospective studies of their strength conditioning program, including one that previously reported no worsening in patients’ lymphedema, and instead, showed signs of improvement.
The researchers evaluated program participants’ physical and functional gains and whether any of those parameters differed by the extent of their breast cancer surgery.
In total, there were 197 participants, including 85 who’d undergone mastectomies and 112 who’d had lumpectomies; 26 patients also had axillary lymph node dissection.
All of the women attended the same 3-month supervised strength-training program, starting at various points in their recovery process. Nearly half started at 3 months postdiagnosis.
According to Champ, the program addresses a full range of motion, with the exercise intensity building over a short period — similar to what professional athletes do in early training. The specific exercises include split squats, dumbbell presses, and dumbbell rows, done 3 days per week, for about 45-60 minutes.
Most participants, Champ said, start with deadlifting around 70 pounds (lifting weight from the floor to hip level). “If you can carry groceries, you can deadlift 60 or 70 pounds,” he noted.
Each month, the weight and sets increase, while the repetitions decrease.
“We just had a woman in her 70s who deadlifted about 200 pounds” as the program progressed, Champ said.
Benefits Regardless of Surgery Type
Women in the current analysis underwent baseline and post-program testing of body composition and functional parameters, including strength, mobility, and balance. Mastectomy patients (median age, 51 years) were younger than lumpectomy patients (median age, 59 years). They were also more likely to have had chemotherapy (45% vs 27%).
Overall, Champ’s team found that both surgery groups showed statistically significant improvements in muscle and body fat percentages over the course of the program, with muscle mass increasing by 1 percentage point on average and body fat declining by 1.5 percentage points.
Similarly, functional movement scores, grip strength, loads lifted, and balance skills also improved, with comparable benefits regardless of surgery type or whether lymph node dissection was performed.
By the end of the program’s third week, Champ said, most women could deadlift 100-pound weights. And by the 3-month mark, many were able to lift 200-pound loads.
Champ called the results empowering, and he hopes they help reframe the traditional mindset that intense strength training is too heavy a lift after breast cancer surgery.
A surgical oncologist who was not involved in the study agreed.
“This gives us something concrete to say to patients,” said Tina Hieken, MD, of the Mayo Clinic in Rochester, Minnesota. “We have more data to say it’s safe for you to exercise.’’
Hieken, who chaired the meeting’s scientific program committee, also noted that the findings pertain to women of all baseline fitness levels.
For her part, Hieken already encourages patients to walk for exercise and spend time outdoors — in part for the mental well-being benefits.
With patients facing so much uncertainty after a cancer diagnosis, she said, “this is something an individual can take control of.”
Champ and Hieken had no disclosures.
A version of this article first appeared on Medscape.com.
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Wildfire Smoke Linked to Potential Risks for Some Cancers
Wildfire smoke exposure may be associated with increased risks for multiple types of cancer, suggests an analysis of prospective cohort data from over 90,000 individuals.
To determine how this widespread pollution might be affecting cancer risk, senior author Shuguang Leng, MBBS, PhD, and colleagues analyzed data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. That prospective national study enrolled approximately 154,000 participants between 1993 and 2001 and tracked cancer incidence through 2018. Of these, 91,460 participants had wildfire smoke exposure data and were included in the analysis.
During the 2006-2018 exposure period, the investigators identified incident cases of 242 ovarian, 800 colorectal, 896 bladder, 1696 hematopoietic, 1739 breast, and 1758 lung cancers, as well as 1127 melanoma cases. The median 36-month moving average for wildfire smoke PM2.5 (fine particulate matter) across the cohort was 0.37 µg/m3.
Wildfire smoke exposure was significantly associated with increased risks for lung, colorectal, breast, bladder, and hematopoietic cancer, according to the results of the study presented by Leng at American Association for Cancer Research (AACR) Annual Meeting 2026.
Each 1 µg/m3 increase in the 36-month moving average of wildfire smoke PM2.5 was associated with a 63% higher risk for hematopoietic cancer (HR, 1.63; 95% CI, 1.02-2.60), a nearly twofold higher risk for lung cancer (hazard ratio [HR], 1.92; 95% CI, 1.18-3.15), more than twofold higher risks for breast cancer (HR, 2.09; 95% CI, 1.34-3.26) and colorectal cancer (HR, 2.31; 95% CI, 1.11-4.81), and a more than threefold higher risk for bladder cancer (HR, 3.49; 95% CI, 1.66-7.34). No significant associations were observed for ovarian cancer or melanoma.
The investigators quantified wildfire smoke exposure at each participant’s residence on a monthly basis using three measures: near-ground wildfire smoke PM2.5, wildfire smoke black carbon, and satellite-derived wildfire smoke plume-day counts, with measurements available from 2006 until first cancer diagnosis or last contact.
Given evidence that 3 years of air pollution exposure can influence the development of epidermal growth factor receptor-positive lung adenocarcinoma, the team modeled exposure as a time-varying variable using 36-month moving averages preceding each month. HRs were estimated using Cox proportional hazards models stratified by study center, with restricted cubic splines applied to evaluate dose-response relationships. Models were adjusted for age, sex, race and ethnicity, education, smoking history, BMI, and trial arm.
All five cancer types linked with wildfire smoke exposure showed linear dose-response relationships, Leng noted, “which means the higher the exposure, the higher the cancer risk.”
Results based on wildfire smoke plume-day counts were generally consistent with those for PM2.5, while associations for black carbon exposure were observed only for breast and bladder cancers.
With wildfires on the rise, these findings suggest that the resulting smoke may become a “major driver for cancer burden in the US in the coming decades,” said Leng, of the University of New Mexico Comprehensive Cancer Center, Albuquerque, New Mexico.
“Wildfire smoke has become a major source of air pollution in the United States,” he continued. Large fires in the US are three times more common than they were 50 years ago, and the “tons of toxicants and particles” released by these fires “can travel hundreds of miles to affect communities far away.”
The investigators also conducted histology-specific analyses, finding that adenocarcinoma showed the strongest association with wildfire smoke among lung cancer subtypes. Among colorectal cancers, proximal tumors appeared more sensitive to wildfire smoke exposure, while among bladder cancers, the association was strongest for muscle-invasive disease.
Wildfire Smoke Exposure Expected to Rise
Under even the most conservative climate projections, wildfire smoke exposure in the US is expected to rise over the next 20-30 years, Leng said.
Annual average wildfire smoke PM2.5 levels, currently estimated at around 0.5 µg/m3, could rise to 1 µg/m3. Based on the study’s dose-response data, this would correspond to substantially greater cancer risk.
There will be “a much larger area” of the US exposed “at a much higher dose,” Leng predicted.
Mitigating the Risks of Wildfire Smoke
This is a “strong hypothesis-generating study,” Jun Wu, PhD, professor of environmental and occupational health at the UC Irvine Program in Public Health, Irvine, California, told Medscape Medical News.
“This is one of the first large, prospective US cohort studies to examine wildfire smoke specifically in relation to cancer risk, especially cancer sites beyond the lung,” Wu said. “A major strength is that the PLCO platform has around 91,000 participants with longitudinal follow-up and detailed covariate data, including smoking history, which is often a weak point in previous air pollution-cancer studies.”
According to Wu, who was not involved in the analysis but recently published data linking wildfire smoke exposure to preterm birth, the reported risks for colorectal, breast, bladder, and hematopoietic cancers represent novel contributions to the literature. However, she cautioned against viewing the specific HRs as a precise estimates of risk due to wide confidence intervals.
The findings should encourage individuals, public health officials, and clinicians to mitigate the risks of wildfire smoke, Wu said.
Specifically, she suggested that public health assessments expand beyond acute outcomes like emergency department visits to include long-term endpoints such as cancer, while community clean-air shelters need to be made more widely available.
She advised clinicians to incorporate wildfire exposure into routine patient histories and to provide vulnerable patients — such as those with asthma, chronic obstructive pulmonary disease, heart failure, or pregnancy — with smoke-season action plans.
Risk mitigation begins with awareness, according to Wu, who advised individuals check their local air quality index on AirNow.gov or PurpleAir.
On smoky days, she suggested prioritizing indoor air quality by keeping windows closed and running air purifiers. If going outside on such days is necessary, she suggested an N95 or KN95 mask, as these offer “meaningful protection,” while cloth and surgical masks do not.
These preventive steps may have once been out of the ordinary, Wu said, but the risk for wildfire smoke exposure is becoming a part of everyday life.
“The common thread is a shift in framing,” Wu said. “Wildfire smoke has traditionally been treated as an acute event, but the emerging evidence points to a chronic environmental exposure. Both our clinical and public health systems have room to grow into that reality.”
The analysis was funded by the National Institutes of Health. The investigators and Wu reported having no conflicts of interest.
This article was previously published on Medscape.
Wildfire smoke exposure may be associated with increased risks for multiple types of cancer, suggests an analysis of prospective cohort data from over 90,000 individuals.
To determine how this widespread pollution might be affecting cancer risk, senior author Shuguang Leng, MBBS, PhD, and colleagues analyzed data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. That prospective national study enrolled approximately 154,000 participants between 1993 and 2001 and tracked cancer incidence through 2018. Of these, 91,460 participants had wildfire smoke exposure data and were included in the analysis.
During the 2006-2018 exposure period, the investigators identified incident cases of 242 ovarian, 800 colorectal, 896 bladder, 1696 hematopoietic, 1739 breast, and 1758 lung cancers, as well as 1127 melanoma cases. The median 36-month moving average for wildfire smoke PM2.5 (fine particulate matter) across the cohort was 0.37 µg/m3.
Wildfire smoke exposure was significantly associated with increased risks for lung, colorectal, breast, bladder, and hematopoietic cancer, according to the results of the study presented by Leng at American Association for Cancer Research (AACR) Annual Meeting 2026.
Each 1 µg/m3 increase in the 36-month moving average of wildfire smoke PM2.5 was associated with a 63% higher risk for hematopoietic cancer (HR, 1.63; 95% CI, 1.02-2.60), a nearly twofold higher risk for lung cancer (hazard ratio [HR], 1.92; 95% CI, 1.18-3.15), more than twofold higher risks for breast cancer (HR, 2.09; 95% CI, 1.34-3.26) and colorectal cancer (HR, 2.31; 95% CI, 1.11-4.81), and a more than threefold higher risk for bladder cancer (HR, 3.49; 95% CI, 1.66-7.34). No significant associations were observed for ovarian cancer or melanoma.
The investigators quantified wildfire smoke exposure at each participant’s residence on a monthly basis using three measures: near-ground wildfire smoke PM2.5, wildfire smoke black carbon, and satellite-derived wildfire smoke plume-day counts, with measurements available from 2006 until first cancer diagnosis or last contact.
Given evidence that 3 years of air pollution exposure can influence the development of epidermal growth factor receptor-positive lung adenocarcinoma, the team modeled exposure as a time-varying variable using 36-month moving averages preceding each month. HRs were estimated using Cox proportional hazards models stratified by study center, with restricted cubic splines applied to evaluate dose-response relationships. Models were adjusted for age, sex, race and ethnicity, education, smoking history, BMI, and trial arm.
All five cancer types linked with wildfire smoke exposure showed linear dose-response relationships, Leng noted, “which means the higher the exposure, the higher the cancer risk.”
Results based on wildfire smoke plume-day counts were generally consistent with those for PM2.5, while associations for black carbon exposure were observed only for breast and bladder cancers.
With wildfires on the rise, these findings suggest that the resulting smoke may become a “major driver for cancer burden in the US in the coming decades,” said Leng, of the University of New Mexico Comprehensive Cancer Center, Albuquerque, New Mexico.
“Wildfire smoke has become a major source of air pollution in the United States,” he continued. Large fires in the US are three times more common than they were 50 years ago, and the “tons of toxicants and particles” released by these fires “can travel hundreds of miles to affect communities far away.”
The investigators also conducted histology-specific analyses, finding that adenocarcinoma showed the strongest association with wildfire smoke among lung cancer subtypes. Among colorectal cancers, proximal tumors appeared more sensitive to wildfire smoke exposure, while among bladder cancers, the association was strongest for muscle-invasive disease.
Wildfire Smoke Exposure Expected to Rise
Under even the most conservative climate projections, wildfire smoke exposure in the US is expected to rise over the next 20-30 years, Leng said.
Annual average wildfire smoke PM2.5 levels, currently estimated at around 0.5 µg/m3, could rise to 1 µg/m3. Based on the study’s dose-response data, this would correspond to substantially greater cancer risk.
There will be “a much larger area” of the US exposed “at a much higher dose,” Leng predicted.
Mitigating the Risks of Wildfire Smoke
This is a “strong hypothesis-generating study,” Jun Wu, PhD, professor of environmental and occupational health at the UC Irvine Program in Public Health, Irvine, California, told Medscape Medical News.
“This is one of the first large, prospective US cohort studies to examine wildfire smoke specifically in relation to cancer risk, especially cancer sites beyond the lung,” Wu said. “A major strength is that the PLCO platform has around 91,000 participants with longitudinal follow-up and detailed covariate data, including smoking history, which is often a weak point in previous air pollution-cancer studies.”
According to Wu, who was not involved in the analysis but recently published data linking wildfire smoke exposure to preterm birth, the reported risks for colorectal, breast, bladder, and hematopoietic cancers represent novel contributions to the literature. However, she cautioned against viewing the specific HRs as a precise estimates of risk due to wide confidence intervals.
The findings should encourage individuals, public health officials, and clinicians to mitigate the risks of wildfire smoke, Wu said.
Specifically, she suggested that public health assessments expand beyond acute outcomes like emergency department visits to include long-term endpoints such as cancer, while community clean-air shelters need to be made more widely available.
She advised clinicians to incorporate wildfire exposure into routine patient histories and to provide vulnerable patients — such as those with asthma, chronic obstructive pulmonary disease, heart failure, or pregnancy — with smoke-season action plans.
Risk mitigation begins with awareness, according to Wu, who advised individuals check their local air quality index on AirNow.gov or PurpleAir.
On smoky days, she suggested prioritizing indoor air quality by keeping windows closed and running air purifiers. If going outside on such days is necessary, she suggested an N95 or KN95 mask, as these offer “meaningful protection,” while cloth and surgical masks do not.
These preventive steps may have once been out of the ordinary, Wu said, but the risk for wildfire smoke exposure is becoming a part of everyday life.
“The common thread is a shift in framing,” Wu said. “Wildfire smoke has traditionally been treated as an acute event, but the emerging evidence points to a chronic environmental exposure. Both our clinical and public health systems have room to grow into that reality.”
The analysis was funded by the National Institutes of Health. The investigators and Wu reported having no conflicts of interest.
This article was previously published on Medscape.
Wildfire smoke exposure may be associated with increased risks for multiple types of cancer, suggests an analysis of prospective cohort data from over 90,000 individuals.
To determine how this widespread pollution might be affecting cancer risk, senior author Shuguang Leng, MBBS, PhD, and colleagues analyzed data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. That prospective national study enrolled approximately 154,000 participants between 1993 and 2001 and tracked cancer incidence through 2018. Of these, 91,460 participants had wildfire smoke exposure data and were included in the analysis.
During the 2006-2018 exposure period, the investigators identified incident cases of 242 ovarian, 800 colorectal, 896 bladder, 1696 hematopoietic, 1739 breast, and 1758 lung cancers, as well as 1127 melanoma cases. The median 36-month moving average for wildfire smoke PM2.5 (fine particulate matter) across the cohort was 0.37 µg/m3.
Wildfire smoke exposure was significantly associated with increased risks for lung, colorectal, breast, bladder, and hematopoietic cancer, according to the results of the study presented by Leng at American Association for Cancer Research (AACR) Annual Meeting 2026.
Each 1 µg/m3 increase in the 36-month moving average of wildfire smoke PM2.5 was associated with a 63% higher risk for hematopoietic cancer (HR, 1.63; 95% CI, 1.02-2.60), a nearly twofold higher risk for lung cancer (hazard ratio [HR], 1.92; 95% CI, 1.18-3.15), more than twofold higher risks for breast cancer (HR, 2.09; 95% CI, 1.34-3.26) and colorectal cancer (HR, 2.31; 95% CI, 1.11-4.81), and a more than threefold higher risk for bladder cancer (HR, 3.49; 95% CI, 1.66-7.34). No significant associations were observed for ovarian cancer or melanoma.
The investigators quantified wildfire smoke exposure at each participant’s residence on a monthly basis using three measures: near-ground wildfire smoke PM2.5, wildfire smoke black carbon, and satellite-derived wildfire smoke plume-day counts, with measurements available from 2006 until first cancer diagnosis or last contact.
Given evidence that 3 years of air pollution exposure can influence the development of epidermal growth factor receptor-positive lung adenocarcinoma, the team modeled exposure as a time-varying variable using 36-month moving averages preceding each month. HRs were estimated using Cox proportional hazards models stratified by study center, with restricted cubic splines applied to evaluate dose-response relationships. Models were adjusted for age, sex, race and ethnicity, education, smoking history, BMI, and trial arm.
All five cancer types linked with wildfire smoke exposure showed linear dose-response relationships, Leng noted, “which means the higher the exposure, the higher the cancer risk.”
Results based on wildfire smoke plume-day counts were generally consistent with those for PM2.5, while associations for black carbon exposure were observed only for breast and bladder cancers.
With wildfires on the rise, these findings suggest that the resulting smoke may become a “major driver for cancer burden in the US in the coming decades,” said Leng, of the University of New Mexico Comprehensive Cancer Center, Albuquerque, New Mexico.
“Wildfire smoke has become a major source of air pollution in the United States,” he continued. Large fires in the US are three times more common than they were 50 years ago, and the “tons of toxicants and particles” released by these fires “can travel hundreds of miles to affect communities far away.”
The investigators also conducted histology-specific analyses, finding that adenocarcinoma showed the strongest association with wildfire smoke among lung cancer subtypes. Among colorectal cancers, proximal tumors appeared more sensitive to wildfire smoke exposure, while among bladder cancers, the association was strongest for muscle-invasive disease.
Wildfire Smoke Exposure Expected to Rise
Under even the most conservative climate projections, wildfire smoke exposure in the US is expected to rise over the next 20-30 years, Leng said.
Annual average wildfire smoke PM2.5 levels, currently estimated at around 0.5 µg/m3, could rise to 1 µg/m3. Based on the study’s dose-response data, this would correspond to substantially greater cancer risk.
There will be “a much larger area” of the US exposed “at a much higher dose,” Leng predicted.
Mitigating the Risks of Wildfire Smoke
This is a “strong hypothesis-generating study,” Jun Wu, PhD, professor of environmental and occupational health at the UC Irvine Program in Public Health, Irvine, California, told Medscape Medical News.
“This is one of the first large, prospective US cohort studies to examine wildfire smoke specifically in relation to cancer risk, especially cancer sites beyond the lung,” Wu said. “A major strength is that the PLCO platform has around 91,000 participants with longitudinal follow-up and detailed covariate data, including smoking history, which is often a weak point in previous air pollution-cancer studies.”
According to Wu, who was not involved in the analysis but recently published data linking wildfire smoke exposure to preterm birth, the reported risks for colorectal, breast, bladder, and hematopoietic cancers represent novel contributions to the literature. However, she cautioned against viewing the specific HRs as a precise estimates of risk due to wide confidence intervals.
The findings should encourage individuals, public health officials, and clinicians to mitigate the risks of wildfire smoke, Wu said.
Specifically, she suggested that public health assessments expand beyond acute outcomes like emergency department visits to include long-term endpoints such as cancer, while community clean-air shelters need to be made more widely available.
She advised clinicians to incorporate wildfire exposure into routine patient histories and to provide vulnerable patients — such as those with asthma, chronic obstructive pulmonary disease, heart failure, or pregnancy — with smoke-season action plans.
Risk mitigation begins with awareness, according to Wu, who advised individuals check their local air quality index on AirNow.gov or PurpleAir.
On smoky days, she suggested prioritizing indoor air quality by keeping windows closed and running air purifiers. If going outside on such days is necessary, she suggested an N95 or KN95 mask, as these offer “meaningful protection,” while cloth and surgical masks do not.
These preventive steps may have once been out of the ordinary, Wu said, but the risk for wildfire smoke exposure is becoming a part of everyday life.
“The common thread is a shift in framing,” Wu said. “Wildfire smoke has traditionally been treated as an acute event, but the emerging evidence points to a chronic environmental exposure. Both our clinical and public health systems have room to grow into that reality.”
The analysis was funded by the National Institutes of Health. The investigators and Wu reported having no conflicts of interest.
This article was previously published on Medscape.
Vet Prostate Cancer Survivors Face Hidden Breast Cancer Risk
Vet Prostate Cancer Survivors Face Hidden Breast Cancer Risk
TOPLINE:
Among 1.3 million male veterans treated for prostate cancer, 11,327 (0.86%) developed breast cancer an average of 5.4 years after initial diagnosis. Younger age at prostate cancer diagnosis, metastatic disease, androgen deprivation therapy (ADT), radiation treatment, and prolonged use of certain cardiovascular disease (CVD) medications were associated with increased risk for breast cancer.
METHODOLOGY:
- Researchers used a retrospective cohort design in Veterans Health Administration (VHA) care, pulling data from the Veterans Affairs (VA) Prostate Cancer Data Core at the VA Corporate Data Warehouse.
- Participants included 1,314,492 male veterans with prostate cancer treated at VHA facilities from January 1, 2000, to March 12, 2024.
- Exposure definitions included prostate cancer treatments (ADT, anti-androgen treatment, radiation-brachytherapy, and platinum chemotherapy) and CVD medications (furosemide, spironolactone, digoxin) captured via inpatient/outpatient/fee-based pharmacy and Current Procedural Terminology codes.
- Analysis measured time from prostate cancer diagnosis to breast cancer diagnosis, death, or March 12, 2024, applying Cox proportional hazards and Fine-Gray competing risk methods, with a sensitivity analysis adding body mass index (BMI) after excluding 71,718 missing values.
TAKEAWAY:
- Metastatic prostate cancer at diagnosis more than doubled the risk for breast cancer compared to nonmetastatic disease (hazard ratio [HR], 2.03; 95% CI, 1.90-2.17; P < .0001; subdistribution hazard ratio [SHR], 1.68; 95% CI, 1.57-1.81; P < .0001).
- Younger age at prostate cancer diagnosis was associated with increased risk for breast cancer (HR, 0.97; 95% CI, 0.97-0.98; P < .0001; SHR, 0.957; 95% CI, 0.955-0.959; P < .0001), indicating that for each additional year of age at diagnosis, the risk decreased.
- Continuation of CVD medications after prostate cancer diagnosis was associated with increased risk for breast cancer: furosemide (HR, 1.51; 95% CI, 1.39-1.63; P < .0001; SHR, 1.21; 95% CI, 1.12-1.31; P < .0001), spironolactone (HR, 1.36; 95% CI, 1.15-1.61; P = .0004; SHR, 1.23; 95% CI, 1.04-1.47; P = .0174), and digoxin (HR, 1.49; 95% CI, 1.29-1.72; P < .0001; SHR, 1.26; 95% CI, 1.10-1.46; P = .0015).
- Radiation therapy and ADT were associated with increased risk for breast cancer (radiation: HR, 1.06; 95% CI, 1.02-1.11; P = .0088; SHR, 1.10; 95% CI, 1.05-1.15; P < .0001; ADT: HR, 1.24; 95% CI, 1.17-1.32; P < .0001; SHR, 1.28; 95% CI, 1.20-1.37; P < .0001), while abiraterone was associated with decreased risk (HR, 0.36; 95% CI, 0.31-0.42; P < .0001; SHR, 0.39; 95% CI, 0.34-0.45; P < .0001).
IN PRACTICE:
"While there is a lack of data, male veterans with previous prostate cancer are at an elevated risk of breast cancer (0.87%), than their civilian counterparts (0.14%),” the authors wrote. “To address the current gap in knowledge and data, this study leveraged an existing large cohort of male veterans with prostate cancer and examined factors associated with increased risk of male breast cancer."
SOURCE:
The study was led by Erum Z. Whyne, VA North Texas Health Care System in Dallas, and Haekyung Jeon-Slaughter, University of Texas Southwestern Medical Center in Dallas. It was published online in The Prostate.
LIMITATIONS:
Though the study findings are based on large, representative data from male veterans with previously diagnosed prostate cancer, the results might not be generalizable to the overall male breast cancer population. As a retrospective cohort study, results may be biased and causality is difficult to establish. The study did not examine other known risk factors for male breast cancer incidence, such as family history, BRCA2 mutations, and military environmental exposure due to lack of data. BMI had missingness of 5.46% (n = 71,718) and was not included as a covariate in the final model, though sensitivity analysis showed it was not significantly associated with increased risk for male breast cancer.
DISCLOSURES:
The research was supported using resources and facilities of the VA Informatics and Computing Infrastructure (VINCI), VA HSR RES 13-457. The VA North Texas Health Care System Institutional Review Board approved the study and waived informed consent. No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE:
Among 1.3 million male veterans treated for prostate cancer, 11,327 (0.86%) developed breast cancer an average of 5.4 years after initial diagnosis. Younger age at prostate cancer diagnosis, metastatic disease, androgen deprivation therapy (ADT), radiation treatment, and prolonged use of certain cardiovascular disease (CVD) medications were associated with increased risk for breast cancer.
METHODOLOGY:
- Researchers used a retrospective cohort design in Veterans Health Administration (VHA) care, pulling data from the Veterans Affairs (VA) Prostate Cancer Data Core at the VA Corporate Data Warehouse.
- Participants included 1,314,492 male veterans with prostate cancer treated at VHA facilities from January 1, 2000, to March 12, 2024.
- Exposure definitions included prostate cancer treatments (ADT, anti-androgen treatment, radiation-brachytherapy, and platinum chemotherapy) and CVD medications (furosemide, spironolactone, digoxin) captured via inpatient/outpatient/fee-based pharmacy and Current Procedural Terminology codes.
- Analysis measured time from prostate cancer diagnosis to breast cancer diagnosis, death, or March 12, 2024, applying Cox proportional hazards and Fine-Gray competing risk methods, with a sensitivity analysis adding body mass index (BMI) after excluding 71,718 missing values.
TAKEAWAY:
- Metastatic prostate cancer at diagnosis more than doubled the risk for breast cancer compared to nonmetastatic disease (hazard ratio [HR], 2.03; 95% CI, 1.90-2.17; P < .0001; subdistribution hazard ratio [SHR], 1.68; 95% CI, 1.57-1.81; P < .0001).
- Younger age at prostate cancer diagnosis was associated with increased risk for breast cancer (HR, 0.97; 95% CI, 0.97-0.98; P < .0001; SHR, 0.957; 95% CI, 0.955-0.959; P < .0001), indicating that for each additional year of age at diagnosis, the risk decreased.
- Continuation of CVD medications after prostate cancer diagnosis was associated with increased risk for breast cancer: furosemide (HR, 1.51; 95% CI, 1.39-1.63; P < .0001; SHR, 1.21; 95% CI, 1.12-1.31; P < .0001), spironolactone (HR, 1.36; 95% CI, 1.15-1.61; P = .0004; SHR, 1.23; 95% CI, 1.04-1.47; P = .0174), and digoxin (HR, 1.49; 95% CI, 1.29-1.72; P < .0001; SHR, 1.26; 95% CI, 1.10-1.46; P = .0015).
- Radiation therapy and ADT were associated with increased risk for breast cancer (radiation: HR, 1.06; 95% CI, 1.02-1.11; P = .0088; SHR, 1.10; 95% CI, 1.05-1.15; P < .0001; ADT: HR, 1.24; 95% CI, 1.17-1.32; P < .0001; SHR, 1.28; 95% CI, 1.20-1.37; P < .0001), while abiraterone was associated with decreased risk (HR, 0.36; 95% CI, 0.31-0.42; P < .0001; SHR, 0.39; 95% CI, 0.34-0.45; P < .0001).
IN PRACTICE:
"While there is a lack of data, male veterans with previous prostate cancer are at an elevated risk of breast cancer (0.87%), than their civilian counterparts (0.14%),” the authors wrote. “To address the current gap in knowledge and data, this study leveraged an existing large cohort of male veterans with prostate cancer and examined factors associated with increased risk of male breast cancer."
SOURCE:
The study was led by Erum Z. Whyne, VA North Texas Health Care System in Dallas, and Haekyung Jeon-Slaughter, University of Texas Southwestern Medical Center in Dallas. It was published online in The Prostate.
LIMITATIONS:
Though the study findings are based on large, representative data from male veterans with previously diagnosed prostate cancer, the results might not be generalizable to the overall male breast cancer population. As a retrospective cohort study, results may be biased and causality is difficult to establish. The study did not examine other known risk factors for male breast cancer incidence, such as family history, BRCA2 mutations, and military environmental exposure due to lack of data. BMI had missingness of 5.46% (n = 71,718) and was not included as a covariate in the final model, though sensitivity analysis showed it was not significantly associated with increased risk for male breast cancer.
DISCLOSURES:
The research was supported using resources and facilities of the VA Informatics and Computing Infrastructure (VINCI), VA HSR RES 13-457. The VA North Texas Health Care System Institutional Review Board approved the study and waived informed consent. No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE:
Among 1.3 million male veterans treated for prostate cancer, 11,327 (0.86%) developed breast cancer an average of 5.4 years after initial diagnosis. Younger age at prostate cancer diagnosis, metastatic disease, androgen deprivation therapy (ADT), radiation treatment, and prolonged use of certain cardiovascular disease (CVD) medications were associated with increased risk for breast cancer.
METHODOLOGY:
- Researchers used a retrospective cohort design in Veterans Health Administration (VHA) care, pulling data from the Veterans Affairs (VA) Prostate Cancer Data Core at the VA Corporate Data Warehouse.
- Participants included 1,314,492 male veterans with prostate cancer treated at VHA facilities from January 1, 2000, to March 12, 2024.
- Exposure definitions included prostate cancer treatments (ADT, anti-androgen treatment, radiation-brachytherapy, and platinum chemotherapy) and CVD medications (furosemide, spironolactone, digoxin) captured via inpatient/outpatient/fee-based pharmacy and Current Procedural Terminology codes.
- Analysis measured time from prostate cancer diagnosis to breast cancer diagnosis, death, or March 12, 2024, applying Cox proportional hazards and Fine-Gray competing risk methods, with a sensitivity analysis adding body mass index (BMI) after excluding 71,718 missing values.
TAKEAWAY:
- Metastatic prostate cancer at diagnosis more than doubled the risk for breast cancer compared to nonmetastatic disease (hazard ratio [HR], 2.03; 95% CI, 1.90-2.17; P < .0001; subdistribution hazard ratio [SHR], 1.68; 95% CI, 1.57-1.81; P < .0001).
- Younger age at prostate cancer diagnosis was associated with increased risk for breast cancer (HR, 0.97; 95% CI, 0.97-0.98; P < .0001; SHR, 0.957; 95% CI, 0.955-0.959; P < .0001), indicating that for each additional year of age at diagnosis, the risk decreased.
- Continuation of CVD medications after prostate cancer diagnosis was associated with increased risk for breast cancer: furosemide (HR, 1.51; 95% CI, 1.39-1.63; P < .0001; SHR, 1.21; 95% CI, 1.12-1.31; P < .0001), spironolactone (HR, 1.36; 95% CI, 1.15-1.61; P = .0004; SHR, 1.23; 95% CI, 1.04-1.47; P = .0174), and digoxin (HR, 1.49; 95% CI, 1.29-1.72; P < .0001; SHR, 1.26; 95% CI, 1.10-1.46; P = .0015).
- Radiation therapy and ADT were associated with increased risk for breast cancer (radiation: HR, 1.06; 95% CI, 1.02-1.11; P = .0088; SHR, 1.10; 95% CI, 1.05-1.15; P < .0001; ADT: HR, 1.24; 95% CI, 1.17-1.32; P < .0001; SHR, 1.28; 95% CI, 1.20-1.37; P < .0001), while abiraterone was associated with decreased risk (HR, 0.36; 95% CI, 0.31-0.42; P < .0001; SHR, 0.39; 95% CI, 0.34-0.45; P < .0001).
IN PRACTICE:
"While there is a lack of data, male veterans with previous prostate cancer are at an elevated risk of breast cancer (0.87%), than their civilian counterparts (0.14%),” the authors wrote. “To address the current gap in knowledge and data, this study leveraged an existing large cohort of male veterans with prostate cancer and examined factors associated with increased risk of male breast cancer."
SOURCE:
The study was led by Erum Z. Whyne, VA North Texas Health Care System in Dallas, and Haekyung Jeon-Slaughter, University of Texas Southwestern Medical Center in Dallas. It was published online in The Prostate.
LIMITATIONS:
Though the study findings are based on large, representative data from male veterans with previously diagnosed prostate cancer, the results might not be generalizable to the overall male breast cancer population. As a retrospective cohort study, results may be biased and causality is difficult to establish. The study did not examine other known risk factors for male breast cancer incidence, such as family history, BRCA2 mutations, and military environmental exposure due to lack of data. BMI had missingness of 5.46% (n = 71,718) and was not included as a covariate in the final model, though sensitivity analysis showed it was not significantly associated with increased risk for male breast cancer.
DISCLOSURES:
The research was supported using resources and facilities of the VA Informatics and Computing Infrastructure (VINCI), VA HSR RES 13-457. The VA North Texas Health Care System Institutional Review Board approved the study and waived informed consent. No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Vet Prostate Cancer Survivors Face Hidden Breast Cancer Risk
Vet Prostate Cancer Survivors Face Hidden Breast Cancer Risk
Housing Support May Boost CRC Screening in Vets Experiencing Homelessness
TOPLINE: Among Veterans Health Administration (VHA) patients experiencing homelessness, gaining housing is linked to higher 24-month colorectal (CRC) and breast cancer screening completion. In cohorts of 117,619 veterans eligible for colorectal screening and 6517 veterans eligible for breast cancer screening veterans, screening occurs in 36.1% and 47.9% after housing gain vs 18.8% and 23.7% if homelessness persists.
METHODOLOGY
A retrospective cohort study examined all veterans experiencing homelessness who received care at the VHA from 2011 to 2021 and were eligible for but not up to date on CRC and breast cancer screening.
117,619 veterans experiencing homelessness were eligible for but not up to date on CRC screening (aged 50-75 years without prior cancer diagnosis, inflammatory bowel disease, or colectomy) and 6517 veterans experiencing homelessness were eligible for but not up to date on breast cancer screening (women aged 50-75 years without prior cancer diagnosis, lumpectomy, or mastectomy) were included at their index clinic visit.
Exposure was defined as gaining housing within 24 months following index clinic visit, identified through the Homeless Screening Clinical Reminder, US Department of Veterans Affairs (VA) Homeless Operations, Management, and Evaluation System assessments, or US Department of Housing and Urban Development—VA Supportive Housing program move-in dates.
Primary outcome were undergoing screening for CRC (colonoscopy, flexible sigmoidoscopy, computed tomography colonography, barium enema, or stool-based study) or breast cancer (mammogram) that was at a VHA facility or paid by VA within 24 months following index clinic visit.
TAKEAWAY
Among veterans who gained housing, 36.1% underwent CRC screening and 47.9% underwent breast cancer screening during the 24-month observation period, compared with 18.8% and 23.7% of veterans, respectively, among those who remained homeless.
Veterans who gained housing had 2.3 times the adjusted hazard ratio (aHR) of undergoing CRC screening compared with those who remained homeless (AHR, 2.3; 95% CI, 2.2-2.3; P < .001).
Veterans who gained housing had 2.4 times the adjusted hazard of undergoing breast cancer screening compared with those who remained homeless (AHR, 2.4; 95% CI, 2.2-2.7; P < .001).
Median (interquartile range [IQR]) time from index visit to cancer screening was 8 months (4-15) for CRC screening and 8 months (3-14) for breast cancer screening; median (IQR) time from gaining housing to screening was 4 months (1-9) and 3 months (1-8), respectively.
IN PRACTICE: Veterans experiencing homelessness who gain housing have higher rates of cancer screening. “This finding supports promotion of housing to improve health outcomes for homeless individuals," wrote the authors of the study.
SOURCE: The study was led by researchers at the University of California, San Francisco. It was published online in Annals of Family Medicine.
LIMITATIONS: Residual unmeasured confounding was likely due to the observational design of this study, because veterans able to navigate services to obtain housing may also be more likely to complete preventive care. Housing transitions may be misclassified because the Homeless Screening Clinical Reminder was not designed to track changes and may not be administered to veterans already identified as experiencing homelessness. The study did not capture data for screening completed outside VHA or that was not paid for by it. The study cohort only includes veterans with VHA contact, which may limit generalizability.
DISCLOSURES: Benioff Homelessness and Housing Initiative provided grant support for the work; Project Grant K24AG046372 was also awarded to Kushel for the study. Decker is a National Clinician Scholar with salary support from the US Department of Veterans Affairs and reported receiving personal fees from Moon Surgical. Kanzaria and Kushel are faculty members of the Benioff Homelessness and Housing Initiative; Kanzaria also reported advisory work for Amae Health. Kushel is listed as serving on boards including Housing California, National Homelessness Law Center, and Steinberg Institute; other authors reported no conflicts.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Among Veterans Health Administration (VHA) patients experiencing homelessness, gaining housing is linked to higher 24-month colorectal (CRC) and breast cancer screening completion. In cohorts of 117,619 veterans eligible for colorectal screening and 6517 veterans eligible for breast cancer screening veterans, screening occurs in 36.1% and 47.9% after housing gain vs 18.8% and 23.7% if homelessness persists.
METHODOLOGY
A retrospective cohort study examined all veterans experiencing homelessness who received care at the VHA from 2011 to 2021 and were eligible for but not up to date on CRC and breast cancer screening.
117,619 veterans experiencing homelessness were eligible for but not up to date on CRC screening (aged 50-75 years without prior cancer diagnosis, inflammatory bowel disease, or colectomy) and 6517 veterans experiencing homelessness were eligible for but not up to date on breast cancer screening (women aged 50-75 years without prior cancer diagnosis, lumpectomy, or mastectomy) were included at their index clinic visit.
Exposure was defined as gaining housing within 24 months following index clinic visit, identified through the Homeless Screening Clinical Reminder, US Department of Veterans Affairs (VA) Homeless Operations, Management, and Evaluation System assessments, or US Department of Housing and Urban Development—VA Supportive Housing program move-in dates.
Primary outcome were undergoing screening for CRC (colonoscopy, flexible sigmoidoscopy, computed tomography colonography, barium enema, or stool-based study) or breast cancer (mammogram) that was at a VHA facility or paid by VA within 24 months following index clinic visit.
TAKEAWAY
Among veterans who gained housing, 36.1% underwent CRC screening and 47.9% underwent breast cancer screening during the 24-month observation period, compared with 18.8% and 23.7% of veterans, respectively, among those who remained homeless.
Veterans who gained housing had 2.3 times the adjusted hazard ratio (aHR) of undergoing CRC screening compared with those who remained homeless (AHR, 2.3; 95% CI, 2.2-2.3; P < .001).
Veterans who gained housing had 2.4 times the adjusted hazard of undergoing breast cancer screening compared with those who remained homeless (AHR, 2.4; 95% CI, 2.2-2.7; P < .001).
Median (interquartile range [IQR]) time from index visit to cancer screening was 8 months (4-15) for CRC screening and 8 months (3-14) for breast cancer screening; median (IQR) time from gaining housing to screening was 4 months (1-9) and 3 months (1-8), respectively.
IN PRACTICE: Veterans experiencing homelessness who gain housing have higher rates of cancer screening. “This finding supports promotion of housing to improve health outcomes for homeless individuals," wrote the authors of the study.
SOURCE: The study was led by researchers at the University of California, San Francisco. It was published online in Annals of Family Medicine.
LIMITATIONS: Residual unmeasured confounding was likely due to the observational design of this study, because veterans able to navigate services to obtain housing may also be more likely to complete preventive care. Housing transitions may be misclassified because the Homeless Screening Clinical Reminder was not designed to track changes and may not be administered to veterans already identified as experiencing homelessness. The study did not capture data for screening completed outside VHA or that was not paid for by it. The study cohort only includes veterans with VHA contact, which may limit generalizability.
DISCLOSURES: Benioff Homelessness and Housing Initiative provided grant support for the work; Project Grant K24AG046372 was also awarded to Kushel for the study. Decker is a National Clinician Scholar with salary support from the US Department of Veterans Affairs and reported receiving personal fees from Moon Surgical. Kanzaria and Kushel are faculty members of the Benioff Homelessness and Housing Initiative; Kanzaria also reported advisory work for Amae Health. Kushel is listed as serving on boards including Housing California, National Homelessness Law Center, and Steinberg Institute; other authors reported no conflicts.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Among Veterans Health Administration (VHA) patients experiencing homelessness, gaining housing is linked to higher 24-month colorectal (CRC) and breast cancer screening completion. In cohorts of 117,619 veterans eligible for colorectal screening and 6517 veterans eligible for breast cancer screening veterans, screening occurs in 36.1% and 47.9% after housing gain vs 18.8% and 23.7% if homelessness persists.
METHODOLOGY
A retrospective cohort study examined all veterans experiencing homelessness who received care at the VHA from 2011 to 2021 and were eligible for but not up to date on CRC and breast cancer screening.
117,619 veterans experiencing homelessness were eligible for but not up to date on CRC screening (aged 50-75 years without prior cancer diagnosis, inflammatory bowel disease, or colectomy) and 6517 veterans experiencing homelessness were eligible for but not up to date on breast cancer screening (women aged 50-75 years without prior cancer diagnosis, lumpectomy, or mastectomy) were included at their index clinic visit.
Exposure was defined as gaining housing within 24 months following index clinic visit, identified through the Homeless Screening Clinical Reminder, US Department of Veterans Affairs (VA) Homeless Operations, Management, and Evaluation System assessments, or US Department of Housing and Urban Development—VA Supportive Housing program move-in dates.
Primary outcome were undergoing screening for CRC (colonoscopy, flexible sigmoidoscopy, computed tomography colonography, barium enema, or stool-based study) or breast cancer (mammogram) that was at a VHA facility or paid by VA within 24 months following index clinic visit.
TAKEAWAY
Among veterans who gained housing, 36.1% underwent CRC screening and 47.9% underwent breast cancer screening during the 24-month observation period, compared with 18.8% and 23.7% of veterans, respectively, among those who remained homeless.
Veterans who gained housing had 2.3 times the adjusted hazard ratio (aHR) of undergoing CRC screening compared with those who remained homeless (AHR, 2.3; 95% CI, 2.2-2.3; P < .001).
Veterans who gained housing had 2.4 times the adjusted hazard of undergoing breast cancer screening compared with those who remained homeless (AHR, 2.4; 95% CI, 2.2-2.7; P < .001).
Median (interquartile range [IQR]) time from index visit to cancer screening was 8 months (4-15) for CRC screening and 8 months (3-14) for breast cancer screening; median (IQR) time from gaining housing to screening was 4 months (1-9) and 3 months (1-8), respectively.
IN PRACTICE: Veterans experiencing homelessness who gain housing have higher rates of cancer screening. “This finding supports promotion of housing to improve health outcomes for homeless individuals," wrote the authors of the study.
SOURCE: The study was led by researchers at the University of California, San Francisco. It was published online in Annals of Family Medicine.
LIMITATIONS: Residual unmeasured confounding was likely due to the observational design of this study, because veterans able to navigate services to obtain housing may also be more likely to complete preventive care. Housing transitions may be misclassified because the Homeless Screening Clinical Reminder was not designed to track changes and may not be administered to veterans already identified as experiencing homelessness. The study did not capture data for screening completed outside VHA or that was not paid for by it. The study cohort only includes veterans with VHA contact, which may limit generalizability.
DISCLOSURES: Benioff Homelessness and Housing Initiative provided grant support for the work; Project Grant K24AG046372 was also awarded to Kushel for the study. Decker is a National Clinician Scholar with salary support from the US Department of Veterans Affairs and reported receiving personal fees from Moon Surgical. Kanzaria and Kushel are faculty members of the Benioff Homelessness and Housing Initiative; Kanzaria also reported advisory work for Amae Health. Kushel is listed as serving on boards including Housing California, National Homelessness Law Center, and Steinberg Institute; other authors reported no conflicts.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.