User login
For MD-IQ use only
This brain surgery was BYOS: Bring your own saxophone
Tumor vs. saxophone: The surgical grudge match
Brain surgery is a notoriously difficult task. There’s a reason we say, “Well, at least it’s not brain surgery” when we’re trying to convince someone that a task isn’t that tough. Make one wrong incision, cut the wrong neuron, and it’s goodbye higher cognitive function. And most people appreciate thinking. Crazy, right?
One would imagine that the act of brain surgery would become even more difficult when the patient brings his saxophone and plays it randomly throughout the operation. It’s a hospital, after all, not a jazz club. Patients don’t get to play musical instruments during other surgeries. Why should brain surgery patients get special treatment?
As it turns out, the musical performance was actually quite helpful. A man in Italy had a brain tumor in a particularly complex area, and he’s left-handed, which apparently makes the brain’s neural pathways much more complicated. Plus, he insisted that he retain his musical ability after the surgery. So he and his medical team had a crazy thought: Why not play the saxophone throughout the surgery? After all, according to head surgeon Christian Brogna, MD, playing an instrument means you understand music, which tests many higher cognitive functions such as coordination, mathematics, and memory.
And so, at various points throughout the 9-hour surgery, the patient played his saxophone for his doctors. Doing so allowed the surgeons to map the patient’s brain in a more complete and personalized fashion. With that extra knowledge, they were able to successfully remove the tumor while maintaining the patient’s musical ability, and the patient was discharged on Oct. 13, just 3 days after his operation.
While we’re happy the patient recovered, we do have to question his choice of music. During the surgery, he played the theme to the 1970 movie “Love Story” and the Italian national anthem. Perfectly fine pieces, no doubt, but the saxophone solo in “Jungleland” exists. And we could listen to that for 9 hours straight. In fact, we do that every Friday in the LOTME office.
Basketball has the Big Dance. Mosquitoes get the Big Sniff
In this week’s installment of our seemingly never-ending series, “Mosquitoes and the scientists who love them,” we visit The Rockefeller University in New York, where the olfactory capabilities of Aedes Aegypti – the primary vector species for Zika, dengue, yellow fever, and chikungunya – became the subject of a round robin–style tournament.

First things first, though. If you’re going to test mosquito noses, you have to give them something to smell. The researchers enrolled eight humans who were willing to wear nylon stockings on their forearms for 6 hours a day for multiple days. “Over the next few years, the researchers tested the nylons against each other in all possible pairings,” Leslie B. Vosshall, PhD, and associates said in a statement from the university. In other words, mosquito March Madness.
Nylons from different participants were hooked up in pairs to an olfactometer assay consisting of a plexiglass chamber divided into two tubes, each ending in a box that held a stocking. The mosquitoes were placed in the main chamber and observed as they flew down the tubes toward one stocking or the other.
Eventually, the “winner” of the “tournament” was Subject 33. And no, we don’t know why there was a Subject 33 since the study involved only eight participants. We do know that the nylons worn by Subject 33 were “four times more attractive to the mosquitoes than the next most-attractive study participant, and an astonishing 100 times more appealing than the least attractive, Subject 19,” according to the written statement.
Chemical analysis identified 50 molecular compounds that were elevated in the sebum of the high-attracting participants, and eventually the investigators discovered that mosquito magnets produced carboxylic acids at much higher levels than the less-attractive volunteers.
We could go on about the research team genetically engineering mosquitoes without odor receptors, but we have to save something for later. Tune in again next week for another exciting episode of “Mosquitoes and the scientists who love them.”
Are women better with words?
Men vs. Women is probably the oldest argument in the book, but there may now be movement. Researchers have been able not only to shift the advantage toward women, but also to use that knowledge to medical advantage.

When it comes to the matter of words and remembering them, women apparently have men beat. The margin is small, said lead author Marco Hirnstein, PhD, of the University of Bergen, Norway, but, after performing a meta-analysis of 168 published studies and PhD theses involving more than 350,000 participants, it’s pretty clear. The research supports women’s advantage over men in recall, verbal fluency (categorical and phonemic), and recognition.
So how is this information useful from a medical standpoint?
Dr. Hirnstein and colleagues suggested that this information can help in interpreting diagnostic assessment results. The example given was dementia diagnosis. Since women are underdiagnosed because their baseline exceeds average while men are overdiagnosed, taking gender and performance into account could clear up or catch cases that might otherwise slip through the cracks.
Now, let’s just put this part of the debate to rest and take this not only as a win for women but for science as well.
Tumor vs. saxophone: The surgical grudge match
Brain surgery is a notoriously difficult task. There’s a reason we say, “Well, at least it’s not brain surgery” when we’re trying to convince someone that a task isn’t that tough. Make one wrong incision, cut the wrong neuron, and it’s goodbye higher cognitive function. And most people appreciate thinking. Crazy, right?
One would imagine that the act of brain surgery would become even more difficult when the patient brings his saxophone and plays it randomly throughout the operation. It’s a hospital, after all, not a jazz club. Patients don’t get to play musical instruments during other surgeries. Why should brain surgery patients get special treatment?
As it turns out, the musical performance was actually quite helpful. A man in Italy had a brain tumor in a particularly complex area, and he’s left-handed, which apparently makes the brain’s neural pathways much more complicated. Plus, he insisted that he retain his musical ability after the surgery. So he and his medical team had a crazy thought: Why not play the saxophone throughout the surgery? After all, according to head surgeon Christian Brogna, MD, playing an instrument means you understand music, which tests many higher cognitive functions such as coordination, mathematics, and memory.
And so, at various points throughout the 9-hour surgery, the patient played his saxophone for his doctors. Doing so allowed the surgeons to map the patient’s brain in a more complete and personalized fashion. With that extra knowledge, they were able to successfully remove the tumor while maintaining the patient’s musical ability, and the patient was discharged on Oct. 13, just 3 days after his operation.
While we’re happy the patient recovered, we do have to question his choice of music. During the surgery, he played the theme to the 1970 movie “Love Story” and the Italian national anthem. Perfectly fine pieces, no doubt, but the saxophone solo in “Jungleland” exists. And we could listen to that for 9 hours straight. In fact, we do that every Friday in the LOTME office.
Basketball has the Big Dance. Mosquitoes get the Big Sniff
In this week’s installment of our seemingly never-ending series, “Mosquitoes and the scientists who love them,” we visit The Rockefeller University in New York, where the olfactory capabilities of Aedes Aegypti – the primary vector species for Zika, dengue, yellow fever, and chikungunya – became the subject of a round robin–style tournament.
First things first, though. If you’re going to test mosquito noses, you have to give them something to smell. The researchers enrolled eight humans who were willing to wear nylon stockings on their forearms for 6 hours a day for multiple days. “Over the next few years, the researchers tested the nylons against each other in all possible pairings,” Leslie B. Vosshall, PhD, and associates said in a statement from the university. In other words, mosquito March Madness.
Nylons from different participants were hooked up in pairs to an olfactometer assay consisting of a plexiglass chamber divided into two tubes, each ending in a box that held a stocking. The mosquitoes were placed in the main chamber and observed as they flew down the tubes toward one stocking or the other.
Eventually, the “winner” of the “tournament” was Subject 33. And no, we don’t know why there was a Subject 33 since the study involved only eight participants. We do know that the nylons worn by Subject 33 were “four times more attractive to the mosquitoes than the next most-attractive study participant, and an astonishing 100 times more appealing than the least attractive, Subject 19,” according to the written statement.
Chemical analysis identified 50 molecular compounds that were elevated in the sebum of the high-attracting participants, and eventually the investigators discovered that mosquito magnets produced carboxylic acids at much higher levels than the less-attractive volunteers.
We could go on about the research team genetically engineering mosquitoes without odor receptors, but we have to save something for later. Tune in again next week for another exciting episode of “Mosquitoes and the scientists who love them.”
Are women better with words?
Men vs. Women is probably the oldest argument in the book, but there may now be movement. Researchers have been able not only to shift the advantage toward women, but also to use that knowledge to medical advantage.
When it comes to the matter of words and remembering them, women apparently have men beat. The margin is small, said lead author Marco Hirnstein, PhD, of the University of Bergen, Norway, but, after performing a meta-analysis of 168 published studies and PhD theses involving more than 350,000 participants, it’s pretty clear. The research supports women’s advantage over men in recall, verbal fluency (categorical and phonemic), and recognition.
So how is this information useful from a medical standpoint?
Dr. Hirnstein and colleagues suggested that this information can help in interpreting diagnostic assessment results. The example given was dementia diagnosis. Since women are underdiagnosed because their baseline exceeds average while men are overdiagnosed, taking gender and performance into account could clear up or catch cases that might otherwise slip through the cracks.
Now, let’s just put this part of the debate to rest and take this not only as a win for women but for science as well.
Tumor vs. saxophone: The surgical grudge match
Brain surgery is a notoriously difficult task. There’s a reason we say, “Well, at least it’s not brain surgery” when we’re trying to convince someone that a task isn’t that tough. Make one wrong incision, cut the wrong neuron, and it’s goodbye higher cognitive function. And most people appreciate thinking. Crazy, right?
One would imagine that the act of brain surgery would become even more difficult when the patient brings his saxophone and plays it randomly throughout the operation. It’s a hospital, after all, not a jazz club. Patients don’t get to play musical instruments during other surgeries. Why should brain surgery patients get special treatment?
As it turns out, the musical performance was actually quite helpful. A man in Italy had a brain tumor in a particularly complex area, and he’s left-handed, which apparently makes the brain’s neural pathways much more complicated. Plus, he insisted that he retain his musical ability after the surgery. So he and his medical team had a crazy thought: Why not play the saxophone throughout the surgery? After all, according to head surgeon Christian Brogna, MD, playing an instrument means you understand music, which tests many higher cognitive functions such as coordination, mathematics, and memory.
And so, at various points throughout the 9-hour surgery, the patient played his saxophone for his doctors. Doing so allowed the surgeons to map the patient’s brain in a more complete and personalized fashion. With that extra knowledge, they were able to successfully remove the tumor while maintaining the patient’s musical ability, and the patient was discharged on Oct. 13, just 3 days after his operation.
While we’re happy the patient recovered, we do have to question his choice of music. During the surgery, he played the theme to the 1970 movie “Love Story” and the Italian national anthem. Perfectly fine pieces, no doubt, but the saxophone solo in “Jungleland” exists. And we could listen to that for 9 hours straight. In fact, we do that every Friday in the LOTME office.
Basketball has the Big Dance. Mosquitoes get the Big Sniff
In this week’s installment of our seemingly never-ending series, “Mosquitoes and the scientists who love them,” we visit The Rockefeller University in New York, where the olfactory capabilities of Aedes Aegypti – the primary vector species for Zika, dengue, yellow fever, and chikungunya – became the subject of a round robin–style tournament.
First things first, though. If you’re going to test mosquito noses, you have to give them something to smell. The researchers enrolled eight humans who were willing to wear nylon stockings on their forearms for 6 hours a day for multiple days. “Over the next few years, the researchers tested the nylons against each other in all possible pairings,” Leslie B. Vosshall, PhD, and associates said in a statement from the university. In other words, mosquito March Madness.
Nylons from different participants were hooked up in pairs to an olfactometer assay consisting of a plexiglass chamber divided into two tubes, each ending in a box that held a stocking. The mosquitoes were placed in the main chamber and observed as they flew down the tubes toward one stocking or the other.
Eventually, the “winner” of the “tournament” was Subject 33. And no, we don’t know why there was a Subject 33 since the study involved only eight participants. We do know that the nylons worn by Subject 33 were “four times more attractive to the mosquitoes than the next most-attractive study participant, and an astonishing 100 times more appealing than the least attractive, Subject 19,” according to the written statement.
Chemical analysis identified 50 molecular compounds that were elevated in the sebum of the high-attracting participants, and eventually the investigators discovered that mosquito magnets produced carboxylic acids at much higher levels than the less-attractive volunteers.
We could go on about the research team genetically engineering mosquitoes without odor receptors, but we have to save something for later. Tune in again next week for another exciting episode of “Mosquitoes and the scientists who love them.”
Are women better with words?
Men vs. Women is probably the oldest argument in the book, but there may now be movement. Researchers have been able not only to shift the advantage toward women, but also to use that knowledge to medical advantage.
When it comes to the matter of words and remembering them, women apparently have men beat. The margin is small, said lead author Marco Hirnstein, PhD, of the University of Bergen, Norway, but, after performing a meta-analysis of 168 published studies and PhD theses involving more than 350,000 participants, it’s pretty clear. The research supports women’s advantage over men in recall, verbal fluency (categorical and phonemic), and recognition.
So how is this information useful from a medical standpoint?
Dr. Hirnstein and colleagues suggested that this information can help in interpreting diagnostic assessment results. The example given was dementia diagnosis. Since women are underdiagnosed because their baseline exceeds average while men are overdiagnosed, taking gender and performance into account could clear up or catch cases that might otherwise slip through the cracks.
Now, let’s just put this part of the debate to rest and take this not only as a win for women but for science as well.
You and the skeptical patient: Who’s the doctor here?
“I spoke to him on many occasions about the dangers of COVID, but he just didn’t believe me,” said Dr. Hood, an internist in Lexington, Ky. “He just didn’t give me enough time to help him. He waited to let me know he was ill with COVID and took days to pick up the medicine. Unfortunately, he then passed away.”
The rise of the skeptical patient
It can be extremely frustrating for doctors when patients question or disbelieve their physician’s medical advice and explanations. And many physicians resent the amount of time they spend trying to explain or make their case, especially during a busy day. But patients’ skepticism about the validity of some treatments seems to be increasing.
“Patients are now more likely to have their own medical explanation for their complaint than they used to, and that can be bad for their health,” Dr. Hood said.
Dr. Hood sees medical cynicism as part of Americans’ growing distrust of experts, leveraged by easy access to the internet. “When people Google, they tend to look for support of their opinions, rather than arrive at a fully educated decision.”
Only about half of patients believe their physicians “provide fair and accurate treatment information all or most of the time,” according to a 2019 survey by the Pew Research Center.
Patients’ distrust has become more obvious during the COVID-19 pandemic, said John Schumann, MD, an internist with Oak Street Health, a practice with more than 500 physicians and other providers in 20 states, treating almost exclusively Medicare patients.
“The skeptics became more entrenched during the pandemic,” said Dr. Schumann, who is based in Tulsa, Okla. “They may think the COVID vaccines were approved too quickly, or believe the pandemic itself is a hoax.”
“There’s a lot of antiscience rhetoric now,” Dr. Schumann added. “I’d say about half of my patients are comfortable with science-based decisions and the other half are not.”
What are patients mistrustful about?
Patients’ suspicions of certain therapies began long before the pandemic. In dermatology, for example, some patients refuse to take topical steroids, said Steven R. Feldman, MD, a dermatologist in Winston-Salem, N.C.
“Their distrust is usually based on anecdotal stories they read about,” he noted. “Patients in other specialties are dead set against vaccinations.”
In addition to refusing treatments and inoculations, some patients ask for questionable regimens mentioned in the news. “Some patients have demanded hydroxychloroquine or Noromectin, drugs that are unproven in the treatment of COVID,” Dr. Schumann said. “We refuse to prescribe them.”
Dr. Hood said patients’ reluctance to follow medical advice can often be based on cost. “I have a patient who was more willing to save $20 than to save his life. But when the progression of his test results fit my predictions, he became more willing to take treatments. I had to wait for the opportune moment to convince him.”
Many naysayer patients keep their views to themselves, and physicians may be unaware that the patients are stonewalling. A 2006 study estimated that about 10%-16% of primary care patients actively resist medical authority.
Dr. Schumann cited patients who don’t want to hear an upsetting diagnosis. “Some patients might refuse to take a biopsy to see if they have cancer because they don’t want to know,” he said. “In many cases, they simply won’t get the biopsy and won’t tell the doctor that they didn’t.”
Sometimes skeptics’ arguments have merit
Some patients’ concerns can be valid, such as when they refuse to go on statins, said Zain Hakeem, DO, a physician in Austin, Tex.
“In some cases, I feel that statins are not necessary,” he said. “The science on statins for primary prevention is not strong, although they should be used for exceedingly high-risk patients.”
Certain patients, especially those with chronic conditions, do a great deal of research, using legitimate sources on the Web, and their research is well supported.
However, these patients can be overconfident in their conclusions. Several studies have shown that with just a little experience, people can replace beginners’ caution with a false sense of competence.
For example, “Patients may not weigh the risks correctly,” Dr. Hakeem said. “They can be more concerned about the risk of having their colon perforated during a colonoscopy, while the risk of cancer if they don’t have a colonoscopy is much higher.”
Some highly successful people may be more likely to trust their own medical instincts. When Steve Jobs, the founder of Apple, was diagnosed with pancreatic cancer in 2003, he put off surgery for 9 months while he tried to cure his disease with a vegan diet, acupuncture, herbs, bowel cleansings, and other remedies he read about. He died in 2011. Some experts believe that delay hastened his death.
Of course, not all physicians’ diagnoses or treatments are correct. One study indicated doctors’ diagnostic error rate could be as high as 15%. And just as patients can be overconfident in their conclusions, so can doctors. Another study found that physicians’ stated confidence in their diagnosis was only slightly affected by the inaccuracy of that diagnosis or the difficulty of the case.
Best ways to deal with cynical patients
Patients’ skepticism can frustrate doctors, reduce the efficiency of care delivery, and interfere with recovery. What can doctors do to deal with these problems?
1. Build the patient’s trust in you. “Getting patients to adhere to your advice involves making sure they feel they have a caring doctor whom they trust,” Dr. Feldman said.
“I want to show patients that I am entirely focused on them,” he added. “For example, I may rush to the door of the exam room from my last appointment, but I open the door very slowly and deliberately, because I want the patient to see that I won’t hurry with them.”
2. Spend time with the patient. Familiarity builds trust. Dr. Schumann said doctors at Oak Street Health see their patients an average of six to eight times a year, an unusually high number. “The more patients see their physicians, the more likely they are to trust them.”
3. Keep up to date. “I make sure I’m up to date with the literature, and I try to present a truthful message,” Dr. Hood said. “For instance, my research showed that inflammation played a strong role in developing complications from COVID, so I wrote a detailed treatment protocol aimed at the inflammation and the immune response, which has been very effective.”
4. Confront patients tactfully. Patients who do research on the Web don’t want to be scolded, Dr. Feldman said. In fact, he praises them, even if he doesn’t agree with their findings. “I might say: ‘What a relief to finally find patients who’ve taken the time to educate themselves before coming here.’ ”
Dr. Feldman is careful not to dispute patients’ conclusions. “Debating the issues is not an effective approach to get patients to trust you. The last thing you want to tell a patient is: ‘Listen to me! I’m an expert.’ People just dig in.”
However, it does help to give patients feedback. “I’m a big fan of patients arguing with me,” Dr. Hakeem said. “It means you can straighten out misunderstandings and improve decision-making.”
5. Explain your reasoning. “You need to communicate clearly and show them your thinking,” Dr. Hood said. “For instance, I’ll explain why a patient has a strong risk for heart attack.”
6. Acknowledge uncertainties. “The doctor may present the science as far more certain than it is,” Dr. Hakeem said. “If you don’t acknowledge the uncertainties, you could break the patient’s trust in you.”
7. Don’t use a lot of numbers. “Data is not a good tool to convince patients,” Dr. Feldman said. “The human brain isn’t designed to work that way.”
If you want to use numbers to show clinical risk, Dr. Hakeem advisd using natural frequencies, such as 10 out of 10,000, which is less confusing to the patient than the equivalent percentage of 0.1%.
It can be helpful to refer to familiar concepts. One way to understand a risk is to compare it with risks in daily life, such as the dangers of driving or falling in the shower, Dr. Hakeem added.
Dr. Feldman often refers to another person’s experience when presenting his medical advice. “I might say to the patient: ‘You remind me of another patient I had. They were sitting in the same chair you’re sitting in. They did really well on this drug, and I think it’s probably the best choice for you, too.’ ”
8. Adopt shared decision-making. This approach involves empowering the patient to become an equal partner in medical decisions. The patient is given information through portals and is encouraged to do research. Critics, however, say that most patients don’t want this degree of empowerment and would rather depend on the doctor’s advice.
Conclusion
It’s often impossible to get through to a skeptical patient, which can be disheartening for doctors. “Physicians want to do what is best for the patient, so when the patient doesn’t listen, they may take it personally,” Dr. Hood said. “But you always have to remember, the patient is the one with disease, and it’s up to the patient to open the door.”
Still, some skeptical patients ultimately change their minds. Dr. Schumann said patients who initially declined the COVID vaccine eventually decided to get it. “It often took them more than a year. but it’s never too late.”
A version of this article first appeared on Medscape.com.
“I spoke to him on many occasions about the dangers of COVID, but he just didn’t believe me,” said Dr. Hood, an internist in Lexington, Ky. “He just didn’t give me enough time to help him. He waited to let me know he was ill with COVID and took days to pick up the medicine. Unfortunately, he then passed away.”
The rise of the skeptical patient
It can be extremely frustrating for doctors when patients question or disbelieve their physician’s medical advice and explanations. And many physicians resent the amount of time they spend trying to explain or make their case, especially during a busy day. But patients’ skepticism about the validity of some treatments seems to be increasing.
“Patients are now more likely to have their own medical explanation for their complaint than they used to, and that can be bad for their health,” Dr. Hood said.
Dr. Hood sees medical cynicism as part of Americans’ growing distrust of experts, leveraged by easy access to the internet. “When people Google, they tend to look for support of their opinions, rather than arrive at a fully educated decision.”
Only about half of patients believe their physicians “provide fair and accurate treatment information all or most of the time,” according to a 2019 survey by the Pew Research Center.
Patients’ distrust has become more obvious during the COVID-19 pandemic, said John Schumann, MD, an internist with Oak Street Health, a practice with more than 500 physicians and other providers in 20 states, treating almost exclusively Medicare patients.
“The skeptics became more entrenched during the pandemic,” said Dr. Schumann, who is based in Tulsa, Okla. “They may think the COVID vaccines were approved too quickly, or believe the pandemic itself is a hoax.”
“There’s a lot of antiscience rhetoric now,” Dr. Schumann added. “I’d say about half of my patients are comfortable with science-based decisions and the other half are not.”
What are patients mistrustful about?
Patients’ suspicions of certain therapies began long before the pandemic. In dermatology, for example, some patients refuse to take topical steroids, said Steven R. Feldman, MD, a dermatologist in Winston-Salem, N.C.
“Their distrust is usually based on anecdotal stories they read about,” he noted. “Patients in other specialties are dead set against vaccinations.”
In addition to refusing treatments and inoculations, some patients ask for questionable regimens mentioned in the news. “Some patients have demanded hydroxychloroquine or Noromectin, drugs that are unproven in the treatment of COVID,” Dr. Schumann said. “We refuse to prescribe them.”
Dr. Hood said patients’ reluctance to follow medical advice can often be based on cost. “I have a patient who was more willing to save $20 than to save his life. But when the progression of his test results fit my predictions, he became more willing to take treatments. I had to wait for the opportune moment to convince him.”
Many naysayer patients keep their views to themselves, and physicians may be unaware that the patients are stonewalling. A 2006 study estimated that about 10%-16% of primary care patients actively resist medical authority.
Dr. Schumann cited patients who don’t want to hear an upsetting diagnosis. “Some patients might refuse to take a biopsy to see if they have cancer because they don’t want to know,” he said. “In many cases, they simply won’t get the biopsy and won’t tell the doctor that they didn’t.”
Sometimes skeptics’ arguments have merit
Some patients’ concerns can be valid, such as when they refuse to go on statins, said Zain Hakeem, DO, a physician in Austin, Tex.
“In some cases, I feel that statins are not necessary,” he said. “The science on statins for primary prevention is not strong, although they should be used for exceedingly high-risk patients.”
Certain patients, especially those with chronic conditions, do a great deal of research, using legitimate sources on the Web, and their research is well supported.
However, these patients can be overconfident in their conclusions. Several studies have shown that with just a little experience, people can replace beginners’ caution with a false sense of competence.
For example, “Patients may not weigh the risks correctly,” Dr. Hakeem said. “They can be more concerned about the risk of having their colon perforated during a colonoscopy, while the risk of cancer if they don’t have a colonoscopy is much higher.”
Some highly successful people may be more likely to trust their own medical instincts. When Steve Jobs, the founder of Apple, was diagnosed with pancreatic cancer in 2003, he put off surgery for 9 months while he tried to cure his disease with a vegan diet, acupuncture, herbs, bowel cleansings, and other remedies he read about. He died in 2011. Some experts believe that delay hastened his death.
Of course, not all physicians’ diagnoses or treatments are correct. One study indicated doctors’ diagnostic error rate could be as high as 15%. And just as patients can be overconfident in their conclusions, so can doctors. Another study found that physicians’ stated confidence in their diagnosis was only slightly affected by the inaccuracy of that diagnosis or the difficulty of the case.
Best ways to deal with cynical patients
Patients’ skepticism can frustrate doctors, reduce the efficiency of care delivery, and interfere with recovery. What can doctors do to deal with these problems?
1. Build the patient’s trust in you. “Getting patients to adhere to your advice involves making sure they feel they have a caring doctor whom they trust,” Dr. Feldman said.
“I want to show patients that I am entirely focused on them,” he added. “For example, I may rush to the door of the exam room from my last appointment, but I open the door very slowly and deliberately, because I want the patient to see that I won’t hurry with them.”
2. Spend time with the patient. Familiarity builds trust. Dr. Schumann said doctors at Oak Street Health see their patients an average of six to eight times a year, an unusually high number. “The more patients see their physicians, the more likely they are to trust them.”
3. Keep up to date. “I make sure I’m up to date with the literature, and I try to present a truthful message,” Dr. Hood said. “For instance, my research showed that inflammation played a strong role in developing complications from COVID, so I wrote a detailed treatment protocol aimed at the inflammation and the immune response, which has been very effective.”
4. Confront patients tactfully. Patients who do research on the Web don’t want to be scolded, Dr. Feldman said. In fact, he praises them, even if he doesn’t agree with their findings. “I might say: ‘What a relief to finally find patients who’ve taken the time to educate themselves before coming here.’ ”
Dr. Feldman is careful not to dispute patients’ conclusions. “Debating the issues is not an effective approach to get patients to trust you. The last thing you want to tell a patient is: ‘Listen to me! I’m an expert.’ People just dig in.”
However, it does help to give patients feedback. “I’m a big fan of patients arguing with me,” Dr. Hakeem said. “It means you can straighten out misunderstandings and improve decision-making.”
5. Explain your reasoning. “You need to communicate clearly and show them your thinking,” Dr. Hood said. “For instance, I’ll explain why a patient has a strong risk for heart attack.”
6. Acknowledge uncertainties. “The doctor may present the science as far more certain than it is,” Dr. Hakeem said. “If you don’t acknowledge the uncertainties, you could break the patient’s trust in you.”
7. Don’t use a lot of numbers. “Data is not a good tool to convince patients,” Dr. Feldman said. “The human brain isn’t designed to work that way.”
If you want to use numbers to show clinical risk, Dr. Hakeem advisd using natural frequencies, such as 10 out of 10,000, which is less confusing to the patient than the equivalent percentage of 0.1%.
It can be helpful to refer to familiar concepts. One way to understand a risk is to compare it with risks in daily life, such as the dangers of driving or falling in the shower, Dr. Hakeem added.
Dr. Feldman often refers to another person’s experience when presenting his medical advice. “I might say to the patient: ‘You remind me of another patient I had. They were sitting in the same chair you’re sitting in. They did really well on this drug, and I think it’s probably the best choice for you, too.’ ”
8. Adopt shared decision-making. This approach involves empowering the patient to become an equal partner in medical decisions. The patient is given information through portals and is encouraged to do research. Critics, however, say that most patients don’t want this degree of empowerment and would rather depend on the doctor’s advice.
Conclusion
It’s often impossible to get through to a skeptical patient, which can be disheartening for doctors. “Physicians want to do what is best for the patient, so when the patient doesn’t listen, they may take it personally,” Dr. Hood said. “But you always have to remember, the patient is the one with disease, and it’s up to the patient to open the door.”
Still, some skeptical patients ultimately change their minds. Dr. Schumann said patients who initially declined the COVID vaccine eventually decided to get it. “It often took them more than a year. but it’s never too late.”
A version of this article first appeared on Medscape.com.
“I spoke to him on many occasions about the dangers of COVID, but he just didn’t believe me,” said Dr. Hood, an internist in Lexington, Ky. “He just didn’t give me enough time to help him. He waited to let me know he was ill with COVID and took days to pick up the medicine. Unfortunately, he then passed away.”
The rise of the skeptical patient
It can be extremely frustrating for doctors when patients question or disbelieve their physician’s medical advice and explanations. And many physicians resent the amount of time they spend trying to explain or make their case, especially during a busy day. But patients’ skepticism about the validity of some treatments seems to be increasing.
“Patients are now more likely to have their own medical explanation for their complaint than they used to, and that can be bad for their health,” Dr. Hood said.
Dr. Hood sees medical cynicism as part of Americans’ growing distrust of experts, leveraged by easy access to the internet. “When people Google, they tend to look for support of their opinions, rather than arrive at a fully educated decision.”
Only about half of patients believe their physicians “provide fair and accurate treatment information all or most of the time,” according to a 2019 survey by the Pew Research Center.
Patients’ distrust has become more obvious during the COVID-19 pandemic, said John Schumann, MD, an internist with Oak Street Health, a practice with more than 500 physicians and other providers in 20 states, treating almost exclusively Medicare patients.
“The skeptics became more entrenched during the pandemic,” said Dr. Schumann, who is based in Tulsa, Okla. “They may think the COVID vaccines were approved too quickly, or believe the pandemic itself is a hoax.”
“There’s a lot of antiscience rhetoric now,” Dr. Schumann added. “I’d say about half of my patients are comfortable with science-based decisions and the other half are not.”
What are patients mistrustful about?
Patients’ suspicions of certain therapies began long before the pandemic. In dermatology, for example, some patients refuse to take topical steroids, said Steven R. Feldman, MD, a dermatologist in Winston-Salem, N.C.
“Their distrust is usually based on anecdotal stories they read about,” he noted. “Patients in other specialties are dead set against vaccinations.”
In addition to refusing treatments and inoculations, some patients ask for questionable regimens mentioned in the news. “Some patients have demanded hydroxychloroquine or Noromectin, drugs that are unproven in the treatment of COVID,” Dr. Schumann said. “We refuse to prescribe them.”
Dr. Hood said patients’ reluctance to follow medical advice can often be based on cost. “I have a patient who was more willing to save $20 than to save his life. But when the progression of his test results fit my predictions, he became more willing to take treatments. I had to wait for the opportune moment to convince him.”
Many naysayer patients keep their views to themselves, and physicians may be unaware that the patients are stonewalling. A 2006 study estimated that about 10%-16% of primary care patients actively resist medical authority.
Dr. Schumann cited patients who don’t want to hear an upsetting diagnosis. “Some patients might refuse to take a biopsy to see if they have cancer because they don’t want to know,” he said. “In many cases, they simply won’t get the biopsy and won’t tell the doctor that they didn’t.”
Sometimes skeptics’ arguments have merit
Some patients’ concerns can be valid, such as when they refuse to go on statins, said Zain Hakeem, DO, a physician in Austin, Tex.
“In some cases, I feel that statins are not necessary,” he said. “The science on statins for primary prevention is not strong, although they should be used for exceedingly high-risk patients.”
Certain patients, especially those with chronic conditions, do a great deal of research, using legitimate sources on the Web, and their research is well supported.
However, these patients can be overconfident in their conclusions. Several studies have shown that with just a little experience, people can replace beginners’ caution with a false sense of competence.
For example, “Patients may not weigh the risks correctly,” Dr. Hakeem said. “They can be more concerned about the risk of having their colon perforated during a colonoscopy, while the risk of cancer if they don’t have a colonoscopy is much higher.”
Some highly successful people may be more likely to trust their own medical instincts. When Steve Jobs, the founder of Apple, was diagnosed with pancreatic cancer in 2003, he put off surgery for 9 months while he tried to cure his disease with a vegan diet, acupuncture, herbs, bowel cleansings, and other remedies he read about. He died in 2011. Some experts believe that delay hastened his death.
Of course, not all physicians’ diagnoses or treatments are correct. One study indicated doctors’ diagnostic error rate could be as high as 15%. And just as patients can be overconfident in their conclusions, so can doctors. Another study found that physicians’ stated confidence in their diagnosis was only slightly affected by the inaccuracy of that diagnosis or the difficulty of the case.
Best ways to deal with cynical patients
Patients’ skepticism can frustrate doctors, reduce the efficiency of care delivery, and interfere with recovery. What can doctors do to deal with these problems?
1. Build the patient’s trust in you. “Getting patients to adhere to your advice involves making sure they feel they have a caring doctor whom they trust,” Dr. Feldman said.
“I want to show patients that I am entirely focused on them,” he added. “For example, I may rush to the door of the exam room from my last appointment, but I open the door very slowly and deliberately, because I want the patient to see that I won’t hurry with them.”
2. Spend time with the patient. Familiarity builds trust. Dr. Schumann said doctors at Oak Street Health see their patients an average of six to eight times a year, an unusually high number. “The more patients see their physicians, the more likely they are to trust them.”
3. Keep up to date. “I make sure I’m up to date with the literature, and I try to present a truthful message,” Dr. Hood said. “For instance, my research showed that inflammation played a strong role in developing complications from COVID, so I wrote a detailed treatment protocol aimed at the inflammation and the immune response, which has been very effective.”
4. Confront patients tactfully. Patients who do research on the Web don’t want to be scolded, Dr. Feldman said. In fact, he praises them, even if he doesn’t agree with their findings. “I might say: ‘What a relief to finally find patients who’ve taken the time to educate themselves before coming here.’ ”
Dr. Feldman is careful not to dispute patients’ conclusions. “Debating the issues is not an effective approach to get patients to trust you. The last thing you want to tell a patient is: ‘Listen to me! I’m an expert.’ People just dig in.”
However, it does help to give patients feedback. “I’m a big fan of patients arguing with me,” Dr. Hakeem said. “It means you can straighten out misunderstandings and improve decision-making.”
5. Explain your reasoning. “You need to communicate clearly and show them your thinking,” Dr. Hood said. “For instance, I’ll explain why a patient has a strong risk for heart attack.”
6. Acknowledge uncertainties. “The doctor may present the science as far more certain than it is,” Dr. Hakeem said. “If you don’t acknowledge the uncertainties, you could break the patient’s trust in you.”
7. Don’t use a lot of numbers. “Data is not a good tool to convince patients,” Dr. Feldman said. “The human brain isn’t designed to work that way.”
If you want to use numbers to show clinical risk, Dr. Hakeem advisd using natural frequencies, such as 10 out of 10,000, which is less confusing to the patient than the equivalent percentage of 0.1%.
It can be helpful to refer to familiar concepts. One way to understand a risk is to compare it with risks in daily life, such as the dangers of driving or falling in the shower, Dr. Hakeem added.
Dr. Feldman often refers to another person’s experience when presenting his medical advice. “I might say to the patient: ‘You remind me of another patient I had. They were sitting in the same chair you’re sitting in. They did really well on this drug, and I think it’s probably the best choice for you, too.’ ”
8. Adopt shared decision-making. This approach involves empowering the patient to become an equal partner in medical decisions. The patient is given information through portals and is encouraged to do research. Critics, however, say that most patients don’t want this degree of empowerment and would rather depend on the doctor’s advice.
Conclusion
It’s often impossible to get through to a skeptical patient, which can be disheartening for doctors. “Physicians want to do what is best for the patient, so when the patient doesn’t listen, they may take it personally,” Dr. Hood said. “But you always have to remember, the patient is the one with disease, and it’s up to the patient to open the door.”
Still, some skeptical patients ultimately change their minds. Dr. Schumann said patients who initially declined the COVID vaccine eventually decided to get it. “It often took them more than a year. but it’s never too late.”
A version of this article first appeared on Medscape.com.
A note from NORD
The National Organization for Rare Disorders (NORD)is tremendously grateful to the dedicated healthcare professionals who, despite long days and heavy workloads, continue to seek the latest information on medical advances that might be helpful to their patients. Please know that your commitment and support are tremendously important to the patients and families whom we serve.
As you may be aware, NORD is a nonprofit organization that was established in 1983 to provide advocacy, education, patient/family services and research on behalf of all Americans affected by rare diseases and the medical professionals providing their care.

As we approach NORD’s 40th anniversary, it is astonishing to realize how far we all have come since the early 1980s, when rare disease patients and their medical providers were essentially on their own to navigate the challenging waters of rare disease diagnosis and treatment.
Today, we are living in one of the most exciting periods in medical history, with innovative new diagnostics and treatments being developed or on the horizon. You’ll find information about these medical advances, as well as resources for yourself and your patients, on the NORD website including our Rare Disease Database, Video Library, CME programs and resources, and newsletter for medical professionals.
You’ll also find information about the annual NORD Rare Diseases and Orphan Products Breakthrough Summit, the largest annual conference for professionals and patients in the rare community, along with our annual conference specifically for patients and families, the “Living Rare, Living Stronger Family Forum.”
This issue of the Rare Neurological Diseases Special Report features articles from rare disease medical experts on specific diseases, including spinal muscular atrophy, Pompe disease, and Rett syndrome, as well as more general topics such as genetic therapies for neuromuscular diseases.
Also in this issue are articles on new and exciting initiatives such as the “NORD Rare Disease Centers of Excellence.” These 31 centers, geographically dispersed across the nation, represent an attempt to provide a strong, national network of support for both patients and medical professionals to promote earlier diagnosis and optimal care, regardless of location.
An interview in this issue with one of NORD’s longtime medical advisors and a leading rare disease expert provides advice for community physicians and other HCPs related to diagnosing rare diseases and approaches that may help shorten the diagnostic odyssey for patients. In addition, you can read about how patient advocacy organizations are collecting and managing a precious asset – patient data – to advance understanding of diseases, even extremely rare ones, and support research.
We are grateful for the work you do and for your commitment to your patients, including those with extremely rare or newly identified diseases. We invite you to visit the NORD website often, sign up for our newsletter for medical professionals and contact NORD at any time if we can be helpful to you.
Peter L. Saltonstall, president and CEO
National Organization for Rare Disorders (NORD)
The National Organization for Rare Disorders (NORD)is tremendously grateful to the dedicated healthcare professionals who, despite long days and heavy workloads, continue to seek the latest information on medical advances that might be helpful to their patients. Please know that your commitment and support are tremendously important to the patients and families whom we serve.
As you may be aware, NORD is a nonprofit organization that was established in 1983 to provide advocacy, education, patient/family services and research on behalf of all Americans affected by rare diseases and the medical professionals providing their care.
As we approach NORD’s 40th anniversary, it is astonishing to realize how far we all have come since the early 1980s, when rare disease patients and their medical providers were essentially on their own to navigate the challenging waters of rare disease diagnosis and treatment.
Today, we are living in one of the most exciting periods in medical history, with innovative new diagnostics and treatments being developed or on the horizon. You’ll find information about these medical advances, as well as resources for yourself and your patients, on the NORD website including our Rare Disease Database, Video Library, CME programs and resources, and newsletter for medical professionals.
You’ll also find information about the annual NORD Rare Diseases and Orphan Products Breakthrough Summit, the largest annual conference for professionals and patients in the rare community, along with our annual conference specifically for patients and families, the “Living Rare, Living Stronger Family Forum.”
This issue of the Rare Neurological Diseases Special Report features articles from rare disease medical experts on specific diseases, including spinal muscular atrophy, Pompe disease, and Rett syndrome, as well as more general topics such as genetic therapies for neuromuscular diseases.
Also in this issue are articles on new and exciting initiatives such as the “NORD Rare Disease Centers of Excellence.” These 31 centers, geographically dispersed across the nation, represent an attempt to provide a strong, national network of support for both patients and medical professionals to promote earlier diagnosis and optimal care, regardless of location.
An interview in this issue with one of NORD’s longtime medical advisors and a leading rare disease expert provides advice for community physicians and other HCPs related to diagnosing rare diseases and approaches that may help shorten the diagnostic odyssey for patients. In addition, you can read about how patient advocacy organizations are collecting and managing a precious asset – patient data – to advance understanding of diseases, even extremely rare ones, and support research.
We are grateful for the work you do and for your commitment to your patients, including those with extremely rare or newly identified diseases. We invite you to visit the NORD website often, sign up for our newsletter for medical professionals and contact NORD at any time if we can be helpful to you.
Peter L. Saltonstall, president and CEO
National Organization for Rare Disorders (NORD)
The National Organization for Rare Disorders (NORD)is tremendously grateful to the dedicated healthcare professionals who, despite long days and heavy workloads, continue to seek the latest information on medical advances that might be helpful to their patients. Please know that your commitment and support are tremendously important to the patients and families whom we serve.
As you may be aware, NORD is a nonprofit organization that was established in 1983 to provide advocacy, education, patient/family services and research on behalf of all Americans affected by rare diseases and the medical professionals providing their care.
As we approach NORD’s 40th anniversary, it is astonishing to realize how far we all have come since the early 1980s, when rare disease patients and their medical providers were essentially on their own to navigate the challenging waters of rare disease diagnosis and treatment.
Today, we are living in one of the most exciting periods in medical history, with innovative new diagnostics and treatments being developed or on the horizon. You’ll find information about these medical advances, as well as resources for yourself and your patients, on the NORD website including our Rare Disease Database, Video Library, CME programs and resources, and newsletter for medical professionals.
You’ll also find information about the annual NORD Rare Diseases and Orphan Products Breakthrough Summit, the largest annual conference for professionals and patients in the rare community, along with our annual conference specifically for patients and families, the “Living Rare, Living Stronger Family Forum.”
This issue of the Rare Neurological Diseases Special Report features articles from rare disease medical experts on specific diseases, including spinal muscular atrophy, Pompe disease, and Rett syndrome, as well as more general topics such as genetic therapies for neuromuscular diseases.
Also in this issue are articles on new and exciting initiatives such as the “NORD Rare Disease Centers of Excellence.” These 31 centers, geographically dispersed across the nation, represent an attempt to provide a strong, national network of support for both patients and medical professionals to promote earlier diagnosis and optimal care, regardless of location.
An interview in this issue with one of NORD’s longtime medical advisors and a leading rare disease expert provides advice for community physicians and other HCPs related to diagnosing rare diseases and approaches that may help shorten the diagnostic odyssey for patients. In addition, you can read about how patient advocacy organizations are collecting and managing a precious asset – patient data – to advance understanding of diseases, even extremely rare ones, and support research.
We are grateful for the work you do and for your commitment to your patients, including those with extremely rare or newly identified diseases. We invite you to visit the NORD website often, sign up for our newsletter for medical professionals and contact NORD at any time if we can be helpful to you.
Peter L. Saltonstall, president and CEO
National Organization for Rare Disorders (NORD)
Myasthenia gravis: Finding strength in treatment options
The term myasthenia gravis (MG), from the Latin “grave muscle weakness,” denotes the rare autoimmune disorder characterized by dysfunction at the neuromuscular junction.1 The clinical presentation of the disease is variable but most often includes ocular symptoms, such as ptosis and diplopia, bulbar weakness, and muscle fatigue upon exertion.2,3 Severe symptoms can lead to myasthenic crisis, in which generalized weakness can affect respiratory muscles, leading to possible intubation or death.2,3
Onset of disease ranges from childhood to late adulthood, and largely depends on the subgroup of disease and the age of the patient.4 Although complications from MG can arise, treatment methods have considerably reduced the risk of MG-associated mortality, with the current rate estimated to be 0.06 to 0.89 deaths for every 1 million person-years (that is, approximately 5% of cases).3,5
Pathophysiology
MG is caused by binding of autoimmune antibodies to postsynaptic receptors and by molecules that prevent signal transduction at the muscle endplate.2,4,6,7 The main culprit behind the pathology (in approximately 85% of cases) is an autoimmune antibody for the acetylcholine receptor (AChR); however, other offending antibodies – against muscle-specific serine kinases (MuSK), low-density lipoprotein receptor-related protein 4 (LRP4), and the proteoglycan agrin – are known, although at a lower frequency (in approximately 15% of cases).4,8 These antibodies prevent signal transmission by blocking, destroying, or disrupting the clustering of AChR at the muscle endplate, a necessary step in formation of the neuromuscular junction.4,8,9

The activity of these antibodies is key to understanding the importance of subgrouping the types of MG on the basis of antigen-specific autoimmune interactions. Specifically, the four categories of disease following a diagnosis of MG2,7 are:
- AChR antibody-positive.
- MuSK antibody-positive.
- LRP4 antibody-positive.
- Seronegative MG.
Classifying MG into subgroups gives insight into the functional expectations and potential treatment options for a given patient, although expectations can vary.2
Regrettably, the well-understood pathophysiology, diagnosis, and prognosis of MG have limited investigation and development of new therapies. Additionally, mainstay treatments, such as thymectomy and prednisone, work to alleviate symptoms for most patients, and have also contributed to periods of slowed research and development. However, treatment of refractory MG has, in recent years, become the subject of research on new therapeutic options, aimed at treating heterogeneous disease populations.10
In this review, we discuss the diagnosis of, and treatment options for, MG, and provide an update on promising options in the therapeutic pipeline.
Diagnosis
Distinguishing MG from other neuromuscular junction disorders is a pertinent step before treatment. Although the biomarkers discussed in this section are sensitive for making a diagnosis of MG, additional research is needed to classify seronegative patients who do not have circulating autoantibodies that are pathognomonic for MG.11

Upon clinical examination of observable myasthenic weakness, next steps would require assays for anti-AChR and anti-MuSK.1 If either of those tests are inconclusive, assays for anti-LRP4 are available (although the LRP4 antibody is also a marker in other neurological disorders).12
In the MG diagnostic algorithm, next steps include an electromyography repetitive stimulation test, which, if inconclusive, is followed by single-fiber electromyography.1 If any of these tests return positive, computed tomography or magnetic resonance imaging is necessary for thymus screening.
What follows this diagnostic schema is pharmacotherapeutic or surgical intervention to reduce, or even eliminate, symptoms of MG.1
Consensus on treatment standards
A quantitative assessment of best options for treating MG was conducted by leading experts,13 who reached consensus that primary outcomes in treating MG are reached when a patient presents without symptoms or limitations on daily activities; or has only slight weakness or fatigue in some muscles.13

Pyridostigmine, an acetylcholinesterase inhibitor, is recommended as part of the initial treatment plan for MG patients. Pyridostigmine prevents normal breakdown of acetylcholine, thus increasing acetylcholine levels and allowing signal transmission at the neuromuscular junction.14 Not all patients reach the aforementioned treatment goals when taking pyridostigmine, however; some require corticosteroids or immunosuppressive agents, or both, in addition.
Steroids, such as prednisone and prednisolone, occupy the second line in MG patients because of their ability to produce a rapid response, availability, and economy.1,15 Initial dosages of these medications are gradually adjusted to a maintenance dosage and schedule, as tolerated, to maintain control of symptoms.15
In MG patients who are in respiratory crisis, it is recommended that high-dosage prednisone be given in conjunction with plasmapheresis or intravenous immunoglobulin (IVIg).15 When the response to steroids is inadequate, adverse effects cannot be tolerated, or the patient experiences symptomatic relapse, nonsteroidal immunosuppressive agents are started.
Immunosuppressives are used to weaken the immune response or block production of self-antibodies. Several agents have been identified for use in MG, including azathioprine and mycophenolate mofetil; their use is limited, however, by a lack of supporting evidence from randomized clinical trials or the potential for serious adverse effects.13
Referral and specialized treatments. Patients who are refractory to all the aforementioned treatments should be referred to a physician who is expert in the management of MG. At this point, treatment guidelines recommend chronic IVIg infusion or plasmapheresis, which removes complement, cytokines, and antibodies from the blood.14 Additionally, monoclonal antibody therapies, such as eculizumab, have been shown to have efficacy in severe, refractory AChR antibody–positive generalized MG.16
Thymectomy has been a mainstay and, sometimes, first-line treatment of MG for nearly 80 years.15 The thymus has largely been implicated in the immunopathology of AChR-positive MG. Models suggest that increased expression of inflammatory factors causes an imbalance among immune cells, resulting in lymphofollicular hyperplasia or thymoma.17
Despite the growing body of evidence implicating the thymus in the progression of MG, some patients and physicians are reluctant to proceed with surgical intervention. This could be due to a disparity in surgical treatment options offered by surgeons, and facilities, with varying experience or ability to conduct newer techniques. Minimally invasive approaches, such as video-assisted thoracoscopic surgery and robotic thymectomy, have been found to be superior to traditional open surgical techniques.18,19 Minimally invasive techniques result in significantly fewer postoperative complications, less blood loss, and shorter length of hospital stay.19
In addition to the reduced risk offered by newer operative techniques, thymectomy has also been shown to have a beneficial effect by allowing the dosage of prednisone to be reduced in MG patients. In a randomized clinical trial conducted by Wolfe and coworkers,20 thymectomy produced improvement in two endpoints after 3 years in patients with nonthymomatous MG: the Quantitative MG Score and a lower average prednisone dosage. Although thymectomy is not a necessary precursor to remission in MG patients, it is still pertinent in reducing the adverse effects of long-term steroid use – providing objective evidence to support thymectomy as a treatment option.
Emerging therapies
Although conventional treatments for MG are well-established, 10% to 20% of MG patients remain refractory to therapeutic intervention.21 These patients are more susceptible to myasthenic crisis, which can result in hospitalization, intubation, and death.21 As mentioned, rescue therapies, including plasmapheresis and IVIg, are imperative to achieve remission of refractory MG, but such remission is unsustainable. Risks associated with these therapies, including contraindications and patient comorbidity, and their limited availability have prevented plasmapheresis and IVIg from being reliable interventions.12
These shortcomings, along with promising results from randomized clinical trials of newer modes of pharmacotherapeutic intervention, have increased interest in new therapies for MG. For example, complement pathway and neonatal Fc receptor (FcRn) inhibitors have recently shown promise in removing pathogenic autoimmune antibodies.18
Efgartigimod. FcRn is of interest in treating generalized MG because of its capacity to recycle and extend the half-life of IgG.22 Efgartigimod is a high-affinity FcRn inhibitor that simultaneously reduces IgG recycling and increases its degradation.22 This therapy is unique: it is highly selective for IgG, whereas other FcRn therapies are nonspecific, causing an undesirable decrease in other immunoglobulin and albumin levels.22 In December 2021, the Food and Drug Administration approved efgartigimod for the treatment of AChR-positive generalized MG.23
Zilucoplan is a subcutaneously administered complement inhibitor that has completed phase 3 clinical trials.18,24 The drug works by inhibiting cleavage of proteins C5a and C5b in the terminal complement complex, a necessary step in forming cytotoxic pores on targeted cells.18,24 Zilucoplan also prevents tissue damage and destruction of signal transmission at the postsynaptic membrane.25 Clinical trials have already established improvement in the Quantitative MG Score and the Myasthenia Gravis Activities of Daily Living Score in patients with generalized MG.18,24
Zilucoplan is similar to eculizumab, but targets a different binding site, allowing for treatment of heterogeneous MG populations who have a mutation in the eculizumab target antigen.26 Additionally, due to specific drug-body interactions, parameters for treatment using zilucoplan are broader than for therapies such as eculizumab. In a Zilucoplan press-release, the complement inhibitor showed statistically significant improvement in the treatment group of generalized, AChR-positive MG patients compared to the placebo group. Tolerability and safety was also a favorable finding in this study. However, a similar rate of treatment-emergent adverse events were recorded between the treatment group (76.7%) and placebo group (70.5%) which could indicate that the clinical application of this treatment is still forthcoming.27 If zilucoplan is approved by the FDA, it will be used earlier in disease progression and for a larger subset of patients.26
Nipocalimab is another immunoglobulin G1, FcRn antibody that reduces IgG levels in blood.27,28 A phase 2 clinical study in patients with AChR-positive or MuSK antibody–associated MG showed that 52% of patients who received nipocalimab had a significant reduction in the Myasthenia Gravis Activities of Daily Living Score 4 weeks after infusion.28 Phase 3 studies for adults with generalized MG are underway and are expected to conclude in April 2026.29
Looking forward
Despite emerging therapies aimed at treating IgG in both refractory and nonrefractory MG, there is still a need for research into biomarkers that further differentiate disease. Developing research into new biomarkers, such as circulating microRNAs, gives insight into the promise of personalized medicine, which can shape the landscape of MG and other disorders.30 As of August 2022, only two clinical trials are slated for investigation into new biomarkers for MG.
Although the treatment of MG might have once been considered stagnant, newer expert consensus and novel research are generating optimism for innovative therapies in coming years.
Mr. van der Eb is a second-year candidate in the master’s of science in applied life sciences program, Keck Graduate Institute, Claremont, Calif.; he has an associate’s degree in natural sciences from Pasadena City College, Calif., and a bachelor’s degree in biological sciences from the University of California, Irvine. Ms. Toruno is a graduate from the master’s of science in applied life sciences program, Keck Graduate Institute; she has a bachelor’s degree in psychology, with a minor in biological sciences, from the University of California, Irvine. Dr. Laird is director of clinical education and professor of practice for the master’s of science in physician assistant studies program, Keck Graduate Institute; he practices clinically in general and thoracic surgery.
References
1. Gilhus NE et al. Myasthenia gravis. Nat Rev Dis Primers. 2019 May 2;5(1):30. doi: 10.1038/s41572-019-0079-y.
2. Gilhus NE, Verschuuren JJ. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015 Oct;14(10):1023-36. doi: 10.1016/S1474-4422(15)00145-3.
3. Dresser L et al. Myasthenia gravis: Epidemiology, pathophysiology and clinical manifestations. J Clin Med. 2021 May;10(11):2235. doi: 10.3390/jcm10112235.
4. Iyer SR et al. The neuromuscular junction: Roles in aging and neuromuscular disease. Int J Mol Sci. 2021 Jul;22(15):8058. doi: 10.3390/ijms22158058.
5. Hehir MK, Silvestri NJ. Generalized myasthenia gravis: Classification, clinical presentation, natural history, and epidemiology. Neurol Clin. 2018 May;36(2):253-60. doi: 10.1016/j.ncl.2018.01.002.
6. Prüss H. Autoantibodies in neurological disease. Nat Rev Immunol. 2021 Dec;21(12):798-813. doi: 10.1038/s41577-021-00543-w.
7. Drachman DB et al. Myasthenic antibodies cross-link acetylcholine receptors to accelerate degradation. N Engl J Med. 1978 May 18;298(20):1116-22. doi: 10.1056/NEJM197805182982004.
8. Meriggioli MN. Myasthenia gravis with anti-acetylcholine receptor antibodies. Front Neurol Neurosci. 2009;26:94-108. doi: 10.1159/000212371.
9. Zhang HL, Peng HB. Mechanism of acetylcholine receptor cluster formation induced by DC electric field. PLoS One. 2011;6(10):e26805. doi: 10.1371/journal.pone.0026805.
10. Fichtner ML et al. Autoimmune pathology in myasthenia gravis disease subtypes is governed by divergent mechanisms of immunopathology. Front Immunol. 2020 May 27;11:776. doi: 10.3389/fimmu.2020.00776.
11. Tzartos JS et al. LRP4 antibodies in serum and CSF from amyotrophic lateral sclerosis patients. Ann Clin Transl Neurol. 2014 Feb;1(2):80-87. doi: 10.1002/acn3.26.
12. Narayanaswami P et al. International consensus guidance for management of myasthenia gravis: 2020 update. Neurology. 2021;96(3):114-22. doi: 10.1212/WNL.0000000000011124.
13. Cortés-Vicente E et al. Myasthenia gravis treatment updates. Curr Treat Options Neurol. 2020 Jul 15;22(8):24. doi: 10.1007/s11940-020-00632-6.
14. Tannemaat MR, Verschuuren JJGM. Emerging therapies for autoimmune myasthenia gravis: Towards treatment without corticosteroids. Neuromuscul Disord. 2020 Feb;30(2):111-9. doi: 10.1016/j.nmd.2019.12.003.
15. Silvestri NJ, Wolfe GI. Treatment-refractory myasthenia gravis. J Clin Neuromuscul Dis. 2014 Jun;15(4):167-78. doi: 10.1097/CND.0000000000000034.
16. Sanders DB et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology. 2016 Jul 26;87(4):419-25. doi: 10.1212/WNL.0000000000002790.
17. Evoli A, Meacci E. An update on thymectomy in myasthenia gravis. Expert Rev Neurother. 2019 Sep;19(9):823-33. doi: 10.1080/14737175.2019.1600404.
18. Habib AA et al. Update on immune-mediated therapies for myasthenia gravis. Muscle Nerve. 2020 Nov;62(5):579-92. doi: 10.1002/mus.26919.
19. O’Sullivan KE et al. A systematic review of robotic versus open and video assisted thoracoscopic surgery (VATS) approaches for thymectomy. Ann Cardiothorac Surg. 2019 Mar;8(2):174-93. doi: 10.21037/acs.2019.02.04.
20. Wolfe GI et al; MGTX Study Group. Randomized trial of thymectomy in myasthenia gravis. N Engl J Med. 2016;375(6):511-22. doi: 10.1056/NEJMoa1602489.
21. Schneider-Gold C et al. Understanding the burden of refractory myasthenia gravis. Ther Adv Neurol Disord. 2019 Mar 1;12:1756286419832242. doi: 10.1177/1756286419832242.
22. Howard JF Jr et al; . Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): A multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021 Jul;20(7):526-36. doi: 10.1016/S1474-4422(21)00159-9.
23. U.S. Food and Drug Administration. FDA approves new treatment for myasthenia gravis. News release. Dec 17, 2021. Accessed Feb 21, 2022. http://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-myasthenia-gravis.
24. Ra Pharmaceuticals. A phase 3, multicenter, randomized, double blind, placebo-controlled study to confirm the safety, tolerability, and efficacy of zilucoplan in subjects with generalized myasthenia gravis. ClinicalTrials.gov Identifier: NCT04115293. Updated Jan 28, 2022. Accessed Feb 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04115293.
25. Howard JF Jr et al. Zilucoplan: An investigational complement C5 inhibitor for the treatment of acetylcholine receptor autoantibody–positive generalized myasthenia gravis. Expert Opin Investig Drugs. 2021 May;30(5):483-93. doi: 10.1080/13543784.2021.1897567.
26. Albazli K et al. Complement inhibitor therapy for myasthenia gravis. Front Immunol. 2020 Jun 3;11:917. doi: 10.3389/fimmu.2020.00917.
27. UCB announces positive Phase 3 results for rozanolixizumab in generalized myasthenia gravis. UCB press release. December 10. 2021. Accessed August 15, 2022. https://www.ucb.com/stories-media/Press-Releases/article/UCB-announces-positive-Phase-3-results-for-rozanolixizumab-in-generalized-myasthenia-gravis.
28. Keller CW et al. Fc-receptor targeted therapies for the treatment of myasthenia gravis. Int J Mol Sci. 2021 May;22(11):5755. doi: 10.3390/ijms22115755.
29. Janssen Research & Development LLC. Phase 3, multicenter, randomized, double-blind, placebo-controlled study to evaluate the efficacy, safety, pharmacokinetics, and pharmacodynamics of nipocalimab administered to adults with generalized myasthenia gravis. ClinicalTrials.gov Identifier: NCT04951622. Updated Feb 17, 2022. Accessed Feb 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04951622.
30. Sabre L et al. Circulating miRNAs as potential biomarkers in myasthenia gravis: Tools for personalized medicine. Front Immunol. 2020 Mar 4;11:213. doi: 10.3389/fimmu.2020.00213.
The term myasthenia gravis (MG), from the Latin “grave muscle weakness,” denotes the rare autoimmune disorder characterized by dysfunction at the neuromuscular junction.1 The clinical presentation of the disease is variable but most often includes ocular symptoms, such as ptosis and diplopia, bulbar weakness, and muscle fatigue upon exertion.2,3 Severe symptoms can lead to myasthenic crisis, in which generalized weakness can affect respiratory muscles, leading to possible intubation or death.2,3
Onset of disease ranges from childhood to late adulthood, and largely depends on the subgroup of disease and the age of the patient.4 Although complications from MG can arise, treatment methods have considerably reduced the risk of MG-associated mortality, with the current rate estimated to be 0.06 to 0.89 deaths for every 1 million person-years (that is, approximately 5% of cases).3,5
Pathophysiology
MG is caused by binding of autoimmune antibodies to postsynaptic receptors and by molecules that prevent signal transduction at the muscle endplate.2,4,6,7 The main culprit behind the pathology (in approximately 85% of cases) is an autoimmune antibody for the acetylcholine receptor (AChR); however, other offending antibodies – against muscle-specific serine kinases (MuSK), low-density lipoprotein receptor-related protein 4 (LRP4), and the proteoglycan agrin – are known, although at a lower frequency (in approximately 15% of cases).4,8 These antibodies prevent signal transmission by blocking, destroying, or disrupting the clustering of AChR at the muscle endplate, a necessary step in formation of the neuromuscular junction.4,8,9
The activity of these antibodies is key to understanding the importance of subgrouping the types of MG on the basis of antigen-specific autoimmune interactions. Specifically, the four categories of disease following a diagnosis of MG2,7 are:
- AChR antibody-positive.
- MuSK antibody-positive.
- LRP4 antibody-positive.
- Seronegative MG.
Classifying MG into subgroups gives insight into the functional expectations and potential treatment options for a given patient, although expectations can vary.2
Regrettably, the well-understood pathophysiology, diagnosis, and prognosis of MG have limited investigation and development of new therapies. Additionally, mainstay treatments, such as thymectomy and prednisone, work to alleviate symptoms for most patients, and have also contributed to periods of slowed research and development. However, treatment of refractory MG has, in recent years, become the subject of research on new therapeutic options, aimed at treating heterogeneous disease populations.10
In this review, we discuss the diagnosis of, and treatment options for, MG, and provide an update on promising options in the therapeutic pipeline.
Diagnosis
Distinguishing MG from other neuromuscular junction disorders is a pertinent step before treatment. Although the biomarkers discussed in this section are sensitive for making a diagnosis of MG, additional research is needed to classify seronegative patients who do not have circulating autoantibodies that are pathognomonic for MG.11
Upon clinical examination of observable myasthenic weakness, next steps would require assays for anti-AChR and anti-MuSK.1 If either of those tests are inconclusive, assays for anti-LRP4 are available (although the LRP4 antibody is also a marker in other neurological disorders).12
In the MG diagnostic algorithm, next steps include an electromyography repetitive stimulation test, which, if inconclusive, is followed by single-fiber electromyography.1 If any of these tests return positive, computed tomography or magnetic resonance imaging is necessary for thymus screening.
What follows this diagnostic schema is pharmacotherapeutic or surgical intervention to reduce, or even eliminate, symptoms of MG.1
Consensus on treatment standards
A quantitative assessment of best options for treating MG was conducted by leading experts,13 who reached consensus that primary outcomes in treating MG are reached when a patient presents without symptoms or limitations on daily activities; or has only slight weakness or fatigue in some muscles.13
Pyridostigmine, an acetylcholinesterase inhibitor, is recommended as part of the initial treatment plan for MG patients. Pyridostigmine prevents normal breakdown of acetylcholine, thus increasing acetylcholine levels and allowing signal transmission at the neuromuscular junction.14 Not all patients reach the aforementioned treatment goals when taking pyridostigmine, however; some require corticosteroids or immunosuppressive agents, or both, in addition.
Steroids, such as prednisone and prednisolone, occupy the second line in MG patients because of their ability to produce a rapid response, availability, and economy.1,15 Initial dosages of these medications are gradually adjusted to a maintenance dosage and schedule, as tolerated, to maintain control of symptoms.15
In MG patients who are in respiratory crisis, it is recommended that high-dosage prednisone be given in conjunction with plasmapheresis or intravenous immunoglobulin (IVIg).15 When the response to steroids is inadequate, adverse effects cannot be tolerated, or the patient experiences symptomatic relapse, nonsteroidal immunosuppressive agents are started.
Immunosuppressives are used to weaken the immune response or block production of self-antibodies. Several agents have been identified for use in MG, including azathioprine and mycophenolate mofetil; their use is limited, however, by a lack of supporting evidence from randomized clinical trials or the potential for serious adverse effects.13
Referral and specialized treatments. Patients who are refractory to all the aforementioned treatments should be referred to a physician who is expert in the management of MG. At this point, treatment guidelines recommend chronic IVIg infusion or plasmapheresis, which removes complement, cytokines, and antibodies from the blood.14 Additionally, monoclonal antibody therapies, such as eculizumab, have been shown to have efficacy in severe, refractory AChR antibody–positive generalized MG.16
Thymectomy has been a mainstay and, sometimes, first-line treatment of MG for nearly 80 years.15 The thymus has largely been implicated in the immunopathology of AChR-positive MG. Models suggest that increased expression of inflammatory factors causes an imbalance among immune cells, resulting in lymphofollicular hyperplasia or thymoma.17
Despite the growing body of evidence implicating the thymus in the progression of MG, some patients and physicians are reluctant to proceed with surgical intervention. This could be due to a disparity in surgical treatment options offered by surgeons, and facilities, with varying experience or ability to conduct newer techniques. Minimally invasive approaches, such as video-assisted thoracoscopic surgery and robotic thymectomy, have been found to be superior to traditional open surgical techniques.18,19 Minimally invasive techniques result in significantly fewer postoperative complications, less blood loss, and shorter length of hospital stay.19
In addition to the reduced risk offered by newer operative techniques, thymectomy has also been shown to have a beneficial effect by allowing the dosage of prednisone to be reduced in MG patients. In a randomized clinical trial conducted by Wolfe and coworkers,20 thymectomy produced improvement in two endpoints after 3 years in patients with nonthymomatous MG: the Quantitative MG Score and a lower average prednisone dosage. Although thymectomy is not a necessary precursor to remission in MG patients, it is still pertinent in reducing the adverse effects of long-term steroid use – providing objective evidence to support thymectomy as a treatment option.
Emerging therapies
Although conventional treatments for MG are well-established, 10% to 20% of MG patients remain refractory to therapeutic intervention.21 These patients are more susceptible to myasthenic crisis, which can result in hospitalization, intubation, and death.21 As mentioned, rescue therapies, including plasmapheresis and IVIg, are imperative to achieve remission of refractory MG, but such remission is unsustainable. Risks associated with these therapies, including contraindications and patient comorbidity, and their limited availability have prevented plasmapheresis and IVIg from being reliable interventions.12
These shortcomings, along with promising results from randomized clinical trials of newer modes of pharmacotherapeutic intervention, have increased interest in new therapies for MG. For example, complement pathway and neonatal Fc receptor (FcRn) inhibitors have recently shown promise in removing pathogenic autoimmune antibodies.18
Efgartigimod. FcRn is of interest in treating generalized MG because of its capacity to recycle and extend the half-life of IgG.22 Efgartigimod is a high-affinity FcRn inhibitor that simultaneously reduces IgG recycling and increases its degradation.22 This therapy is unique: it is highly selective for IgG, whereas other FcRn therapies are nonspecific, causing an undesirable decrease in other immunoglobulin and albumin levels.22 In December 2021, the Food and Drug Administration approved efgartigimod for the treatment of AChR-positive generalized MG.23
Zilucoplan is a subcutaneously administered complement inhibitor that has completed phase 3 clinical trials.18,24 The drug works by inhibiting cleavage of proteins C5a and C5b in the terminal complement complex, a necessary step in forming cytotoxic pores on targeted cells.18,24 Zilucoplan also prevents tissue damage and destruction of signal transmission at the postsynaptic membrane.25 Clinical trials have already established improvement in the Quantitative MG Score and the Myasthenia Gravis Activities of Daily Living Score in patients with generalized MG.18,24
Zilucoplan is similar to eculizumab, but targets a different binding site, allowing for treatment of heterogeneous MG populations who have a mutation in the eculizumab target antigen.26 Additionally, due to specific drug-body interactions, parameters for treatment using zilucoplan are broader than for therapies such as eculizumab. In a Zilucoplan press-release, the complement inhibitor showed statistically significant improvement in the treatment group of generalized, AChR-positive MG patients compared to the placebo group. Tolerability and safety was also a favorable finding in this study. However, a similar rate of treatment-emergent adverse events were recorded between the treatment group (76.7%) and placebo group (70.5%) which could indicate that the clinical application of this treatment is still forthcoming.27 If zilucoplan is approved by the FDA, it will be used earlier in disease progression and for a larger subset of patients.26
Nipocalimab is another immunoglobulin G1, FcRn antibody that reduces IgG levels in blood.27,28 A phase 2 clinical study in patients with AChR-positive or MuSK antibody–associated MG showed that 52% of patients who received nipocalimab had a significant reduction in the Myasthenia Gravis Activities of Daily Living Score 4 weeks after infusion.28 Phase 3 studies for adults with generalized MG are underway and are expected to conclude in April 2026.29
Looking forward
Despite emerging therapies aimed at treating IgG in both refractory and nonrefractory MG, there is still a need for research into biomarkers that further differentiate disease. Developing research into new biomarkers, such as circulating microRNAs, gives insight into the promise of personalized medicine, which can shape the landscape of MG and other disorders.30 As of August 2022, only two clinical trials are slated for investigation into new biomarkers for MG.
Although the treatment of MG might have once been considered stagnant, newer expert consensus and novel research are generating optimism for innovative therapies in coming years.
Mr. van der Eb is a second-year candidate in the master’s of science in applied life sciences program, Keck Graduate Institute, Claremont, Calif.; he has an associate’s degree in natural sciences from Pasadena City College, Calif., and a bachelor’s degree in biological sciences from the University of California, Irvine. Ms. Toruno is a graduate from the master’s of science in applied life sciences program, Keck Graduate Institute; she has a bachelor’s degree in psychology, with a minor in biological sciences, from the University of California, Irvine. Dr. Laird is director of clinical education and professor of practice for the master’s of science in physician assistant studies program, Keck Graduate Institute; he practices clinically in general and thoracic surgery.
References
1. Gilhus NE et al. Myasthenia gravis. Nat Rev Dis Primers. 2019 May 2;5(1):30. doi: 10.1038/s41572-019-0079-y.
2. Gilhus NE, Verschuuren JJ. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015 Oct;14(10):1023-36. doi: 10.1016/S1474-4422(15)00145-3.
3. Dresser L et al. Myasthenia gravis: Epidemiology, pathophysiology and clinical manifestations. J Clin Med. 2021 May;10(11):2235. doi: 10.3390/jcm10112235.
4. Iyer SR et al. The neuromuscular junction: Roles in aging and neuromuscular disease. Int J Mol Sci. 2021 Jul;22(15):8058. doi: 10.3390/ijms22158058.
5. Hehir MK, Silvestri NJ. Generalized myasthenia gravis: Classification, clinical presentation, natural history, and epidemiology. Neurol Clin. 2018 May;36(2):253-60. doi: 10.1016/j.ncl.2018.01.002.
6. Prüss H. Autoantibodies in neurological disease. Nat Rev Immunol. 2021 Dec;21(12):798-813. doi: 10.1038/s41577-021-00543-w.
7. Drachman DB et al. Myasthenic antibodies cross-link acetylcholine receptors to accelerate degradation. N Engl J Med. 1978 May 18;298(20):1116-22. doi: 10.1056/NEJM197805182982004.
8. Meriggioli MN. Myasthenia gravis with anti-acetylcholine receptor antibodies. Front Neurol Neurosci. 2009;26:94-108. doi: 10.1159/000212371.
9. Zhang HL, Peng HB. Mechanism of acetylcholine receptor cluster formation induced by DC electric field. PLoS One. 2011;6(10):e26805. doi: 10.1371/journal.pone.0026805.
10. Fichtner ML et al. Autoimmune pathology in myasthenia gravis disease subtypes is governed by divergent mechanisms of immunopathology. Front Immunol. 2020 May 27;11:776. doi: 10.3389/fimmu.2020.00776.
11. Tzartos JS et al. LRP4 antibodies in serum and CSF from amyotrophic lateral sclerosis patients. Ann Clin Transl Neurol. 2014 Feb;1(2):80-87. doi: 10.1002/acn3.26.
12. Narayanaswami P et al. International consensus guidance for management of myasthenia gravis: 2020 update. Neurology. 2021;96(3):114-22. doi: 10.1212/WNL.0000000000011124.
13. Cortés-Vicente E et al. Myasthenia gravis treatment updates. Curr Treat Options Neurol. 2020 Jul 15;22(8):24. doi: 10.1007/s11940-020-00632-6.
14. Tannemaat MR, Verschuuren JJGM. Emerging therapies for autoimmune myasthenia gravis: Towards treatment without corticosteroids. Neuromuscul Disord. 2020 Feb;30(2):111-9. doi: 10.1016/j.nmd.2019.12.003.
15. Silvestri NJ, Wolfe GI. Treatment-refractory myasthenia gravis. J Clin Neuromuscul Dis. 2014 Jun;15(4):167-78. doi: 10.1097/CND.0000000000000034.
16. Sanders DB et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology. 2016 Jul 26;87(4):419-25. doi: 10.1212/WNL.0000000000002790.
17. Evoli A, Meacci E. An update on thymectomy in myasthenia gravis. Expert Rev Neurother. 2019 Sep;19(9):823-33. doi: 10.1080/14737175.2019.1600404.
18. Habib AA et al. Update on immune-mediated therapies for myasthenia gravis. Muscle Nerve. 2020 Nov;62(5):579-92. doi: 10.1002/mus.26919.
19. O’Sullivan KE et al. A systematic review of robotic versus open and video assisted thoracoscopic surgery (VATS) approaches for thymectomy. Ann Cardiothorac Surg. 2019 Mar;8(2):174-93. doi: 10.21037/acs.2019.02.04.
20. Wolfe GI et al; MGTX Study Group. Randomized trial of thymectomy in myasthenia gravis. N Engl J Med. 2016;375(6):511-22. doi: 10.1056/NEJMoa1602489.
21. Schneider-Gold C et al. Understanding the burden of refractory myasthenia gravis. Ther Adv Neurol Disord. 2019 Mar 1;12:1756286419832242. doi: 10.1177/1756286419832242.
22. Howard JF Jr et al; . Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): A multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021 Jul;20(7):526-36. doi: 10.1016/S1474-4422(21)00159-9.
23. U.S. Food and Drug Administration. FDA approves new treatment for myasthenia gravis. News release. Dec 17, 2021. Accessed Feb 21, 2022. http://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-myasthenia-gravis.
24. Ra Pharmaceuticals. A phase 3, multicenter, randomized, double blind, placebo-controlled study to confirm the safety, tolerability, and efficacy of zilucoplan in subjects with generalized myasthenia gravis. ClinicalTrials.gov Identifier: NCT04115293. Updated Jan 28, 2022. Accessed Feb 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04115293.
25. Howard JF Jr et al. Zilucoplan: An investigational complement C5 inhibitor for the treatment of acetylcholine receptor autoantibody–positive generalized myasthenia gravis. Expert Opin Investig Drugs. 2021 May;30(5):483-93. doi: 10.1080/13543784.2021.1897567.
26. Albazli K et al. Complement inhibitor therapy for myasthenia gravis. Front Immunol. 2020 Jun 3;11:917. doi: 10.3389/fimmu.2020.00917.
27. UCB announces positive Phase 3 results for rozanolixizumab in generalized myasthenia gravis. UCB press release. December 10. 2021. Accessed August 15, 2022. https://www.ucb.com/stories-media/Press-Releases/article/UCB-announces-positive-Phase-3-results-for-rozanolixizumab-in-generalized-myasthenia-gravis.
28. Keller CW et al. Fc-receptor targeted therapies for the treatment of myasthenia gravis. Int J Mol Sci. 2021 May;22(11):5755. doi: 10.3390/ijms22115755.
29. Janssen Research & Development LLC. Phase 3, multicenter, randomized, double-blind, placebo-controlled study to evaluate the efficacy, safety, pharmacokinetics, and pharmacodynamics of nipocalimab administered to adults with generalized myasthenia gravis. ClinicalTrials.gov Identifier: NCT04951622. Updated Feb 17, 2022. Accessed Feb 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04951622.
30. Sabre L et al. Circulating miRNAs as potential biomarkers in myasthenia gravis: Tools for personalized medicine. Front Immunol. 2020 Mar 4;11:213. doi: 10.3389/fimmu.2020.00213.
The term myasthenia gravis (MG), from the Latin “grave muscle weakness,” denotes the rare autoimmune disorder characterized by dysfunction at the neuromuscular junction.1 The clinical presentation of the disease is variable but most often includes ocular symptoms, such as ptosis and diplopia, bulbar weakness, and muscle fatigue upon exertion.2,3 Severe symptoms can lead to myasthenic crisis, in which generalized weakness can affect respiratory muscles, leading to possible intubation or death.2,3
Onset of disease ranges from childhood to late adulthood, and largely depends on the subgroup of disease and the age of the patient.4 Although complications from MG can arise, treatment methods have considerably reduced the risk of MG-associated mortality, with the current rate estimated to be 0.06 to 0.89 deaths for every 1 million person-years (that is, approximately 5% of cases).3,5
Pathophysiology
MG is caused by binding of autoimmune antibodies to postsynaptic receptors and by molecules that prevent signal transduction at the muscle endplate.2,4,6,7 The main culprit behind the pathology (in approximately 85% of cases) is an autoimmune antibody for the acetylcholine receptor (AChR); however, other offending antibodies – against muscle-specific serine kinases (MuSK), low-density lipoprotein receptor-related protein 4 (LRP4), and the proteoglycan agrin – are known, although at a lower frequency (in approximately 15% of cases).4,8 These antibodies prevent signal transmission by blocking, destroying, or disrupting the clustering of AChR at the muscle endplate, a necessary step in formation of the neuromuscular junction.4,8,9
The activity of these antibodies is key to understanding the importance of subgrouping the types of MG on the basis of antigen-specific autoimmune interactions. Specifically, the four categories of disease following a diagnosis of MG2,7 are:
- AChR antibody-positive.
- MuSK antibody-positive.
- LRP4 antibody-positive.
- Seronegative MG.
Classifying MG into subgroups gives insight into the functional expectations and potential treatment options for a given patient, although expectations can vary.2
Regrettably, the well-understood pathophysiology, diagnosis, and prognosis of MG have limited investigation and development of new therapies. Additionally, mainstay treatments, such as thymectomy and prednisone, work to alleviate symptoms for most patients, and have also contributed to periods of slowed research and development. However, treatment of refractory MG has, in recent years, become the subject of research on new therapeutic options, aimed at treating heterogeneous disease populations.10
In this review, we discuss the diagnosis of, and treatment options for, MG, and provide an update on promising options in the therapeutic pipeline.
Diagnosis
Distinguishing MG from other neuromuscular junction disorders is a pertinent step before treatment. Although the biomarkers discussed in this section are sensitive for making a diagnosis of MG, additional research is needed to classify seronegative patients who do not have circulating autoantibodies that are pathognomonic for MG.11
Upon clinical examination of observable myasthenic weakness, next steps would require assays for anti-AChR and anti-MuSK.1 If either of those tests are inconclusive, assays for anti-LRP4 are available (although the LRP4 antibody is also a marker in other neurological disorders).12
In the MG diagnostic algorithm, next steps include an electromyography repetitive stimulation test, which, if inconclusive, is followed by single-fiber electromyography.1 If any of these tests return positive, computed tomography or magnetic resonance imaging is necessary for thymus screening.
What follows this diagnostic schema is pharmacotherapeutic or surgical intervention to reduce, or even eliminate, symptoms of MG.1
Consensus on treatment standards
A quantitative assessment of best options for treating MG was conducted by leading experts,13 who reached consensus that primary outcomes in treating MG are reached when a patient presents without symptoms or limitations on daily activities; or has only slight weakness or fatigue in some muscles.13
Pyridostigmine, an acetylcholinesterase inhibitor, is recommended as part of the initial treatment plan for MG patients. Pyridostigmine prevents normal breakdown of acetylcholine, thus increasing acetylcholine levels and allowing signal transmission at the neuromuscular junction.14 Not all patients reach the aforementioned treatment goals when taking pyridostigmine, however; some require corticosteroids or immunosuppressive agents, or both, in addition.
Steroids, such as prednisone and prednisolone, occupy the second line in MG patients because of their ability to produce a rapid response, availability, and economy.1,15 Initial dosages of these medications are gradually adjusted to a maintenance dosage and schedule, as tolerated, to maintain control of symptoms.15
In MG patients who are in respiratory crisis, it is recommended that high-dosage prednisone be given in conjunction with plasmapheresis or intravenous immunoglobulin (IVIg).15 When the response to steroids is inadequate, adverse effects cannot be tolerated, or the patient experiences symptomatic relapse, nonsteroidal immunosuppressive agents are started.
Immunosuppressives are used to weaken the immune response or block production of self-antibodies. Several agents have been identified for use in MG, including azathioprine and mycophenolate mofetil; their use is limited, however, by a lack of supporting evidence from randomized clinical trials or the potential for serious adverse effects.13
Referral and specialized treatments. Patients who are refractory to all the aforementioned treatments should be referred to a physician who is expert in the management of MG. At this point, treatment guidelines recommend chronic IVIg infusion or plasmapheresis, which removes complement, cytokines, and antibodies from the blood.14 Additionally, monoclonal antibody therapies, such as eculizumab, have been shown to have efficacy in severe, refractory AChR antibody–positive generalized MG.16
Thymectomy has been a mainstay and, sometimes, first-line treatment of MG for nearly 80 years.15 The thymus has largely been implicated in the immunopathology of AChR-positive MG. Models suggest that increased expression of inflammatory factors causes an imbalance among immune cells, resulting in lymphofollicular hyperplasia or thymoma.17
Despite the growing body of evidence implicating the thymus in the progression of MG, some patients and physicians are reluctant to proceed with surgical intervention. This could be due to a disparity in surgical treatment options offered by surgeons, and facilities, with varying experience or ability to conduct newer techniques. Minimally invasive approaches, such as video-assisted thoracoscopic surgery and robotic thymectomy, have been found to be superior to traditional open surgical techniques.18,19 Minimally invasive techniques result in significantly fewer postoperative complications, less blood loss, and shorter length of hospital stay.19
In addition to the reduced risk offered by newer operative techniques, thymectomy has also been shown to have a beneficial effect by allowing the dosage of prednisone to be reduced in MG patients. In a randomized clinical trial conducted by Wolfe and coworkers,20 thymectomy produced improvement in two endpoints after 3 years in patients with nonthymomatous MG: the Quantitative MG Score and a lower average prednisone dosage. Although thymectomy is not a necessary precursor to remission in MG patients, it is still pertinent in reducing the adverse effects of long-term steroid use – providing objective evidence to support thymectomy as a treatment option.
Emerging therapies
Although conventional treatments for MG are well-established, 10% to 20% of MG patients remain refractory to therapeutic intervention.21 These patients are more susceptible to myasthenic crisis, which can result in hospitalization, intubation, and death.21 As mentioned, rescue therapies, including plasmapheresis and IVIg, are imperative to achieve remission of refractory MG, but such remission is unsustainable. Risks associated with these therapies, including contraindications and patient comorbidity, and their limited availability have prevented plasmapheresis and IVIg from being reliable interventions.12
These shortcomings, along with promising results from randomized clinical trials of newer modes of pharmacotherapeutic intervention, have increased interest in new therapies for MG. For example, complement pathway and neonatal Fc receptor (FcRn) inhibitors have recently shown promise in removing pathogenic autoimmune antibodies.18
Efgartigimod. FcRn is of interest in treating generalized MG because of its capacity to recycle and extend the half-life of IgG.22 Efgartigimod is a high-affinity FcRn inhibitor that simultaneously reduces IgG recycling and increases its degradation.22 This therapy is unique: it is highly selective for IgG, whereas other FcRn therapies are nonspecific, causing an undesirable decrease in other immunoglobulin and albumin levels.22 In December 2021, the Food and Drug Administration approved efgartigimod for the treatment of AChR-positive generalized MG.23
Zilucoplan is a subcutaneously administered complement inhibitor that has completed phase 3 clinical trials.18,24 The drug works by inhibiting cleavage of proteins C5a and C5b in the terminal complement complex, a necessary step in forming cytotoxic pores on targeted cells.18,24 Zilucoplan also prevents tissue damage and destruction of signal transmission at the postsynaptic membrane.25 Clinical trials have already established improvement in the Quantitative MG Score and the Myasthenia Gravis Activities of Daily Living Score in patients with generalized MG.18,24
Zilucoplan is similar to eculizumab, but targets a different binding site, allowing for treatment of heterogeneous MG populations who have a mutation in the eculizumab target antigen.26 Additionally, due to specific drug-body interactions, parameters for treatment using zilucoplan are broader than for therapies such as eculizumab. In a Zilucoplan press-release, the complement inhibitor showed statistically significant improvement in the treatment group of generalized, AChR-positive MG patients compared to the placebo group. Tolerability and safety was also a favorable finding in this study. However, a similar rate of treatment-emergent adverse events were recorded between the treatment group (76.7%) and placebo group (70.5%) which could indicate that the clinical application of this treatment is still forthcoming.27 If zilucoplan is approved by the FDA, it will be used earlier in disease progression and for a larger subset of patients.26
Nipocalimab is another immunoglobulin G1, FcRn antibody that reduces IgG levels in blood.27,28 A phase 2 clinical study in patients with AChR-positive or MuSK antibody–associated MG showed that 52% of patients who received nipocalimab had a significant reduction in the Myasthenia Gravis Activities of Daily Living Score 4 weeks after infusion.28 Phase 3 studies for adults with generalized MG are underway and are expected to conclude in April 2026.29
Looking forward
Despite emerging therapies aimed at treating IgG in both refractory and nonrefractory MG, there is still a need for research into biomarkers that further differentiate disease. Developing research into new biomarkers, such as circulating microRNAs, gives insight into the promise of personalized medicine, which can shape the landscape of MG and other disorders.30 As of August 2022, only two clinical trials are slated for investigation into new biomarkers for MG.
Although the treatment of MG might have once been considered stagnant, newer expert consensus and novel research are generating optimism for innovative therapies in coming years.
Mr. van der Eb is a second-year candidate in the master’s of science in applied life sciences program, Keck Graduate Institute, Claremont, Calif.; he has an associate’s degree in natural sciences from Pasadena City College, Calif., and a bachelor’s degree in biological sciences from the University of California, Irvine. Ms. Toruno is a graduate from the master’s of science in applied life sciences program, Keck Graduate Institute; she has a bachelor’s degree in psychology, with a minor in biological sciences, from the University of California, Irvine. Dr. Laird is director of clinical education and professor of practice for the master’s of science in physician assistant studies program, Keck Graduate Institute; he practices clinically in general and thoracic surgery.
References
1. Gilhus NE et al. Myasthenia gravis. Nat Rev Dis Primers. 2019 May 2;5(1):30. doi: 10.1038/s41572-019-0079-y.
2. Gilhus NE, Verschuuren JJ. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015 Oct;14(10):1023-36. doi: 10.1016/S1474-4422(15)00145-3.
3. Dresser L et al. Myasthenia gravis: Epidemiology, pathophysiology and clinical manifestations. J Clin Med. 2021 May;10(11):2235. doi: 10.3390/jcm10112235.
4. Iyer SR et al. The neuromuscular junction: Roles in aging and neuromuscular disease. Int J Mol Sci. 2021 Jul;22(15):8058. doi: 10.3390/ijms22158058.
5. Hehir MK, Silvestri NJ. Generalized myasthenia gravis: Classification, clinical presentation, natural history, and epidemiology. Neurol Clin. 2018 May;36(2):253-60. doi: 10.1016/j.ncl.2018.01.002.
6. Prüss H. Autoantibodies in neurological disease. Nat Rev Immunol. 2021 Dec;21(12):798-813. doi: 10.1038/s41577-021-00543-w.
7. Drachman DB et al. Myasthenic antibodies cross-link acetylcholine receptors to accelerate degradation. N Engl J Med. 1978 May 18;298(20):1116-22. doi: 10.1056/NEJM197805182982004.
8. Meriggioli MN. Myasthenia gravis with anti-acetylcholine receptor antibodies. Front Neurol Neurosci. 2009;26:94-108. doi: 10.1159/000212371.
9. Zhang HL, Peng HB. Mechanism of acetylcholine receptor cluster formation induced by DC electric field. PLoS One. 2011;6(10):e26805. doi: 10.1371/journal.pone.0026805.
10. Fichtner ML et al. Autoimmune pathology in myasthenia gravis disease subtypes is governed by divergent mechanisms of immunopathology. Front Immunol. 2020 May 27;11:776. doi: 10.3389/fimmu.2020.00776.
11. Tzartos JS et al. LRP4 antibodies in serum and CSF from amyotrophic lateral sclerosis patients. Ann Clin Transl Neurol. 2014 Feb;1(2):80-87. doi: 10.1002/acn3.26.
12. Narayanaswami P et al. International consensus guidance for management of myasthenia gravis: 2020 update. Neurology. 2021;96(3):114-22. doi: 10.1212/WNL.0000000000011124.
13. Cortés-Vicente E et al. Myasthenia gravis treatment updates. Curr Treat Options Neurol. 2020 Jul 15;22(8):24. doi: 10.1007/s11940-020-00632-6.
14. Tannemaat MR, Verschuuren JJGM. Emerging therapies for autoimmune myasthenia gravis: Towards treatment without corticosteroids. Neuromuscul Disord. 2020 Feb;30(2):111-9. doi: 10.1016/j.nmd.2019.12.003.
15. Silvestri NJ, Wolfe GI. Treatment-refractory myasthenia gravis. J Clin Neuromuscul Dis. 2014 Jun;15(4):167-78. doi: 10.1097/CND.0000000000000034.
16. Sanders DB et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology. 2016 Jul 26;87(4):419-25. doi: 10.1212/WNL.0000000000002790.
17. Evoli A, Meacci E. An update on thymectomy in myasthenia gravis. Expert Rev Neurother. 2019 Sep;19(9):823-33. doi: 10.1080/14737175.2019.1600404.
18. Habib AA et al. Update on immune-mediated therapies for myasthenia gravis. Muscle Nerve. 2020 Nov;62(5):579-92. doi: 10.1002/mus.26919.
19. O’Sullivan KE et al. A systematic review of robotic versus open and video assisted thoracoscopic surgery (VATS) approaches for thymectomy. Ann Cardiothorac Surg. 2019 Mar;8(2):174-93. doi: 10.21037/acs.2019.02.04.
20. Wolfe GI et al; MGTX Study Group. Randomized trial of thymectomy in myasthenia gravis. N Engl J Med. 2016;375(6):511-22. doi: 10.1056/NEJMoa1602489.
21. Schneider-Gold C et al. Understanding the burden of refractory myasthenia gravis. Ther Adv Neurol Disord. 2019 Mar 1;12:1756286419832242. doi: 10.1177/1756286419832242.
22. Howard JF Jr et al; . Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): A multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021 Jul;20(7):526-36. doi: 10.1016/S1474-4422(21)00159-9.
23. U.S. Food and Drug Administration. FDA approves new treatment for myasthenia gravis. News release. Dec 17, 2021. Accessed Feb 21, 2022. http://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-myasthenia-gravis.
24. Ra Pharmaceuticals. A phase 3, multicenter, randomized, double blind, placebo-controlled study to confirm the safety, tolerability, and efficacy of zilucoplan in subjects with generalized myasthenia gravis. ClinicalTrials.gov Identifier: NCT04115293. Updated Jan 28, 2022. Accessed Feb 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04115293.
25. Howard JF Jr et al. Zilucoplan: An investigational complement C5 inhibitor for the treatment of acetylcholine receptor autoantibody–positive generalized myasthenia gravis. Expert Opin Investig Drugs. 2021 May;30(5):483-93. doi: 10.1080/13543784.2021.1897567.
26. Albazli K et al. Complement inhibitor therapy for myasthenia gravis. Front Immunol. 2020 Jun 3;11:917. doi: 10.3389/fimmu.2020.00917.
27. UCB announces positive Phase 3 results for rozanolixizumab in generalized myasthenia gravis. UCB press release. December 10. 2021. Accessed August 15, 2022. https://www.ucb.com/stories-media/Press-Releases/article/UCB-announces-positive-Phase-3-results-for-rozanolixizumab-in-generalized-myasthenia-gravis.
28. Keller CW et al. Fc-receptor targeted therapies for the treatment of myasthenia gravis. Int J Mol Sci. 2021 May;22(11):5755. doi: 10.3390/ijms22115755.
29. Janssen Research & Development LLC. Phase 3, multicenter, randomized, double-blind, placebo-controlled study to evaluate the efficacy, safety, pharmacokinetics, and pharmacodynamics of nipocalimab administered to adults with generalized myasthenia gravis. ClinicalTrials.gov Identifier: NCT04951622. Updated Feb 17, 2022. Accessed Feb 21, 2022. https://clinicaltrials.gov/ct2/show/NCT04951622.
30. Sabre L et al. Circulating miRNAs as potential biomarkers in myasthenia gravis: Tools for personalized medicine. Front Immunol. 2020 Mar 4;11:213. doi: 10.3389/fimmu.2020.00213.

Vitamin D: Recent findings and implications for clinical practice
This transcript has been edited for clarity.
Hello. This is Dr JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. As a director of the Vitamin D and Omega-3 trial (VITAL), the largest randomized clinical trial in the world, I’m often asked, “How much vitamin D do we need, and should I take a vitamin D supplement?” I want to review the findings from recent randomized clinical trials and the implications for practice.
For a long time, vitamin D has been perceived as a magic bullet, a panacea, and a cure-all for many chronic health conditions such as cancer, cardiovascular disease, diabetes, bone fractures, cognitive decline, and depression. Many of the findings, though, have been from observational studies where a higher blood level of 25-hydroxy vitamin D has been linked to a lower risk for these health conditions.
We know in epidemiology that correlation doesn’t prove causation. Other factors could be involved; for example, people who have higher blood levels of vitamin D may have healthier diets, or they may be spending more time outdoors, being physically active and exposed to the sun. Some of these other factors could be lowering their risk.
When the randomized trials began to emerge, in many of these large-scale trials, the findings were generally neutral or null for cardiovascular disease, total cancer, diabetes, cognitive decline, depression, and many other health outcomes, including fracture. So, the question was asked, does this mean that vitamin D is not important to health?
To the contrary, these findings suggest that vitamin D is so essential to health that we need only small to moderate amounts of vitamin D. Vitamin D is very tightly regulated in the body – the metabolism and function of vitamin D. Even small to moderate amounts will meet the requirements for vitamin D and bone health and many other outcomes.
This is what the National Academy of Medicine, U.S. Preventive Services Task Force, and many other professional organizations have advised, that widespread screening for vitamin D deficiency and blanket universal supplementation with vitamin D would not be indicated.
The randomized trials of vitamin D, including the VITAL study, have generally not shown reductions in the major health outcomes. We found two exceptions in VITAL. We saw promising signals, including a 22% reduction in autoimmune conditions (rheumatoid arthritis and psoriasis) and a 17% reduction in advanced (metastatic or fatal) cancers. In meta-analyses of other large-scale randomized trials, the findings were a signal for a reduction in advanced cancers, even with very small doses of vitamin D (400-800 IUs daily). We tested 2,000 IUs daily in VITAL.
Overall, it’s recommended that small to moderate amounts of vitamin D are adequate, and among the healthy population, most people do not need screening or supplements.
The reduction in autoimmune diseases suggests that vitamin D may play a role in tamping down inflammation. The question has been raised about whether vitamin D is beneficial in reducing the severity of COVID illness, the need for hospitalization, and long COVID. We are looking at this question in a separate trial called VIVID (Vitamin D for COVID Trial) which tests a higher dose (> 3,000 IUs daily) of vitamin D. Those results will be available at the end of this year or early next year.
In other randomized trials of COVID and vitamin D, the results have been mixed and inconsistent, with no clear answer. During the COVID pandemic, I have generally advised that it’s reasonable to take 1,000-2,000 IUs of vitamin D daily as a form of insurance. This dose is known to be very safe. Over 5.3 years in the VITAL trial we saw that a dose of 2,000 IUs was very safe.
But it’s not essential to take a supplement. And overall, aside from some high-risk groups, most people do not need a supplement. The high-risk groups include patients in nursing homes who may have restricted diets and limited time out of doors. For people with malabsorption conditions such as Crohn’s disease, celiac disease, post–gastric bypass surgery, and those with osteoporosis who are on medications for osteoporosis, it’s still quite reasonable to prescribe calcium and vitamin D.
Recommendations for vitamin D in the generally healthy population really should focus on a healthy diet. The United States has a fortified food supply. Vitamin D is added to many foods, dairy products, and cereals, as well as beverages. Natural sources of vitamin D include fatty fish and wild mushrooms.
We should be looking at food labels (which now include vitamin D content) and try to get adequate vitamin D from our diet, and also do our best to spend time outdoors, being physically active, because it is of great benefit to our health. The general principle is that a dietary supplement will never be a substitute for a healthy diet or healthy lifestyle. And those other behaviors really should be the focus at this time.
Dr. Manson is professor of medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and chief of the division of preventive medicine at Brigham and Women’s Hospital, both in Boston. She has received infrastructure support from Mars Symbioscience for the COSMOS trial.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. As a director of the Vitamin D and Omega-3 trial (VITAL), the largest randomized clinical trial in the world, I’m often asked, “How much vitamin D do we need, and should I take a vitamin D supplement?” I want to review the findings from recent randomized clinical trials and the implications for practice.
For a long time, vitamin D has been perceived as a magic bullet, a panacea, and a cure-all for many chronic health conditions such as cancer, cardiovascular disease, diabetes, bone fractures, cognitive decline, and depression. Many of the findings, though, have been from observational studies where a higher blood level of 25-hydroxy vitamin D has been linked to a lower risk for these health conditions.
We know in epidemiology that correlation doesn’t prove causation. Other factors could be involved; for example, people who have higher blood levels of vitamin D may have healthier diets, or they may be spending more time outdoors, being physically active and exposed to the sun. Some of these other factors could be lowering their risk.
When the randomized trials began to emerge, in many of these large-scale trials, the findings were generally neutral or null for cardiovascular disease, total cancer, diabetes, cognitive decline, depression, and many other health outcomes, including fracture. So, the question was asked, does this mean that vitamin D is not important to health?
To the contrary, these findings suggest that vitamin D is so essential to health that we need only small to moderate amounts of vitamin D. Vitamin D is very tightly regulated in the body – the metabolism and function of vitamin D. Even small to moderate amounts will meet the requirements for vitamin D and bone health and many other outcomes.
This is what the National Academy of Medicine, U.S. Preventive Services Task Force, and many other professional organizations have advised, that widespread screening for vitamin D deficiency and blanket universal supplementation with vitamin D would not be indicated.
The randomized trials of vitamin D, including the VITAL study, have generally not shown reductions in the major health outcomes. We found two exceptions in VITAL. We saw promising signals, including a 22% reduction in autoimmune conditions (rheumatoid arthritis and psoriasis) and a 17% reduction in advanced (metastatic or fatal) cancers. In meta-analyses of other large-scale randomized trials, the findings were a signal for a reduction in advanced cancers, even with very small doses of vitamin D (400-800 IUs daily). We tested 2,000 IUs daily in VITAL.
Overall, it’s recommended that small to moderate amounts of vitamin D are adequate, and among the healthy population, most people do not need screening or supplements.
The reduction in autoimmune diseases suggests that vitamin D may play a role in tamping down inflammation. The question has been raised about whether vitamin D is beneficial in reducing the severity of COVID illness, the need for hospitalization, and long COVID. We are looking at this question in a separate trial called VIVID (Vitamin D for COVID Trial) which tests a higher dose (> 3,000 IUs daily) of vitamin D. Those results will be available at the end of this year or early next year.
In other randomized trials of COVID and vitamin D, the results have been mixed and inconsistent, with no clear answer. During the COVID pandemic, I have generally advised that it’s reasonable to take 1,000-2,000 IUs of vitamin D daily as a form of insurance. This dose is known to be very safe. Over 5.3 years in the VITAL trial we saw that a dose of 2,000 IUs was very safe.
But it’s not essential to take a supplement. And overall, aside from some high-risk groups, most people do not need a supplement. The high-risk groups include patients in nursing homes who may have restricted diets and limited time out of doors. For people with malabsorption conditions such as Crohn’s disease, celiac disease, post–gastric bypass surgery, and those with osteoporosis who are on medications for osteoporosis, it’s still quite reasonable to prescribe calcium and vitamin D.
Recommendations for vitamin D in the generally healthy population really should focus on a healthy diet. The United States has a fortified food supply. Vitamin D is added to many foods, dairy products, and cereals, as well as beverages. Natural sources of vitamin D include fatty fish and wild mushrooms.
We should be looking at food labels (which now include vitamin D content) and try to get adequate vitamin D from our diet, and also do our best to spend time outdoors, being physically active, because it is of great benefit to our health. The general principle is that a dietary supplement will never be a substitute for a healthy diet or healthy lifestyle. And those other behaviors really should be the focus at this time.
Dr. Manson is professor of medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and chief of the division of preventive medicine at Brigham and Women’s Hospital, both in Boston. She has received infrastructure support from Mars Symbioscience for the COSMOS trial.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. As a director of the Vitamin D and Omega-3 trial (VITAL), the largest randomized clinical trial in the world, I’m often asked, “How much vitamin D do we need, and should I take a vitamin D supplement?” I want to review the findings from recent randomized clinical trials and the implications for practice.
For a long time, vitamin D has been perceived as a magic bullet, a panacea, and a cure-all for many chronic health conditions such as cancer, cardiovascular disease, diabetes, bone fractures, cognitive decline, and depression. Many of the findings, though, have been from observational studies where a higher blood level of 25-hydroxy vitamin D has been linked to a lower risk for these health conditions.
We know in epidemiology that correlation doesn’t prove causation. Other factors could be involved; for example, people who have higher blood levels of vitamin D may have healthier diets, or they may be spending more time outdoors, being physically active and exposed to the sun. Some of these other factors could be lowering their risk.
When the randomized trials began to emerge, in many of these large-scale trials, the findings were generally neutral or null for cardiovascular disease, total cancer, diabetes, cognitive decline, depression, and many other health outcomes, including fracture. So, the question was asked, does this mean that vitamin D is not important to health?
To the contrary, these findings suggest that vitamin D is so essential to health that we need only small to moderate amounts of vitamin D. Vitamin D is very tightly regulated in the body – the metabolism and function of vitamin D. Even small to moderate amounts will meet the requirements for vitamin D and bone health and many other outcomes.
This is what the National Academy of Medicine, U.S. Preventive Services Task Force, and many other professional organizations have advised, that widespread screening for vitamin D deficiency and blanket universal supplementation with vitamin D would not be indicated.
The randomized trials of vitamin D, including the VITAL study, have generally not shown reductions in the major health outcomes. We found two exceptions in VITAL. We saw promising signals, including a 22% reduction in autoimmune conditions (rheumatoid arthritis and psoriasis) and a 17% reduction in advanced (metastatic or fatal) cancers. In meta-analyses of other large-scale randomized trials, the findings were a signal for a reduction in advanced cancers, even with very small doses of vitamin D (400-800 IUs daily). We tested 2,000 IUs daily in VITAL.
Overall, it’s recommended that small to moderate amounts of vitamin D are adequate, and among the healthy population, most people do not need screening or supplements.
The reduction in autoimmune diseases suggests that vitamin D may play a role in tamping down inflammation. The question has been raised about whether vitamin D is beneficial in reducing the severity of COVID illness, the need for hospitalization, and long COVID. We are looking at this question in a separate trial called VIVID (Vitamin D for COVID Trial) which tests a higher dose (> 3,000 IUs daily) of vitamin D. Those results will be available at the end of this year or early next year.
In other randomized trials of COVID and vitamin D, the results have been mixed and inconsistent, with no clear answer. During the COVID pandemic, I have generally advised that it’s reasonable to take 1,000-2,000 IUs of vitamin D daily as a form of insurance. This dose is known to be very safe. Over 5.3 years in the VITAL trial we saw that a dose of 2,000 IUs was very safe.
But it’s not essential to take a supplement. And overall, aside from some high-risk groups, most people do not need a supplement. The high-risk groups include patients in nursing homes who may have restricted diets and limited time out of doors. For people with malabsorption conditions such as Crohn’s disease, celiac disease, post–gastric bypass surgery, and those with osteoporosis who are on medications for osteoporosis, it’s still quite reasonable to prescribe calcium and vitamin D.
Recommendations for vitamin D in the generally healthy population really should focus on a healthy diet. The United States has a fortified food supply. Vitamin D is added to many foods, dairy products, and cereals, as well as beverages. Natural sources of vitamin D include fatty fish and wild mushrooms.
We should be looking at food labels (which now include vitamin D content) and try to get adequate vitamin D from our diet, and also do our best to spend time outdoors, being physically active, because it is of great benefit to our health. The general principle is that a dietary supplement will never be a substitute for a healthy diet or healthy lifestyle. And those other behaviors really should be the focus at this time.
Dr. Manson is professor of medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and chief of the division of preventive medicine at Brigham and Women’s Hospital, both in Boston. She has received infrastructure support from Mars Symbioscience for the COSMOS trial.
A version of this article first appeared on Medscape.com.
Dermatologists fear effects of Dobbs decision for patients on isotretinoin, methotrexate
More than 3 months after the Dobbs decision by the U.S. Supreme Court overturned Roe v. Wade and revoked the constitutional right to an abortion, Some have beefed up their already stringent instructions and lengthy conversations about avoiding pregnancy while on the medication.
The major fear is that a patient who is taking contraceptive precautions, in accordance with the isotretinoin risk-management program, iPLEDGE, but still becomes pregnant while on isotretinoin may find out about the pregnancy too late to undergo an abortion in her own state and may not be able to travel to another state – or the patient may live in a state where abortions are entirely prohibited and is unable to travel to another state.
Isotretinoin is marketed as Absorica, Absorica LD, Claravis, Amnesteem, Myorisan, and Zenatane; its former brand name was Accutane.
As of Oct. 7, a total of 14 states have banned most abortions, while 4 others have bans at 6, 15, 18, or 20 weeks. Attempts to restrict abortion on several other states are underway.

“To date, we don’t know of any specific effects of the Dobbs decision on isotretinoin prescribing, but with abortion access banned in many states, we anticipate that this could be a very real issue for individuals who accidentally become pregnant while taking isotretinoin,” said Ilona Frieden, MD, professor of dermatology and pediatrics at the University of California, San Francisco, and chair of the American Academy of Dermatology Association’s iPLEDGE Workgroup.
The iPLEDGE REMS (Risk Evaluation and Mitigation Strategy) is the Food and Drug Administration–required safety program that is in place to manage the risk of isotretinoin teratogenicity and minimize fetal exposure. The work group meets with the FDA and isotretinoin manufacturers to keep the program safe and operating smoothly. The iPLEDGE workgroup has not yet issued any specific statements on the implications of the Dobbs decision on prescribing isotretinoin.

But work on the issue is ongoing by the American Academy of Dermatology. In a statement issued in September, Mark D. Kaufmann, MD, president of the AAD, said that the academy “is continuing to work with its Patient Guidance for State Regulations Regarding Reproductive Health Task Force to help dermatologists best navigate state laws about how care should be implemented for patients who are or might become pregnant, and have been exposed to teratogenic medications.”
The task force, working with the academy, is “in the process of developing resources to help members better assist patients and have a productive and caring dialogue with them,” according to the statement. No specific timeline was given for when those resources might be available.
Methotrexate prescriptions
Also of concern are prescriptions for methotrexate, which is prescribed for psoriasis, atopic dermatitis, and other skin diseases. Soon after the Dobbs decision was announced on June 24, pharmacies began to require pharmacists in states that banned abortions to verify that a prescription for methotrexate was not intended for an abortion, since methotrexate is used in combination with misoprostol for termination of an early pregnancy.
The action was taken, spokespersons for several major pharmacies said, to comply with state laws. According to Kara Page, a CVS spokesperson: “Pharmacists are caught in the middle on this issue.” Laws in some states, she told this news organization, “restrict the dispensing of medications for the purpose of inducing an abortion. These laws, some of which include criminal penalties, have forced us to require pharmacists in these states to validate that the intended indication is not to terminate a pregnancy before they can fill a prescription for methotrexate.”
“New laws in various states require additional steps for dispensing certain prescriptions and apply to all pharmacies, including Walgreens,” Fraser Engerman, a spokesperson for Walgreens, told this news organization. “In these states, our pharmacists work closely with prescribers as needed, to fill lawful, clinically appropriate prescriptions. We provide ongoing training and information to help our pharmacists understand the latest requirements in their area, and with these supports, the expectation is they are empowered to fill these prescriptions.”
The iPLEDGE program has numerous requirements before a patient can begin isotretinoin treatment. Patients capable of becoming pregnant must agree to use two effective forms of birth control during the entire treatment period, which typically lasts 4 or 5 months, as well as 1 month before and 1 month after treatment, or commit to total abstinence during that time.
Perspective: A Georgia dermatologist
Howa Yeung, MD, MSc, assistant professor of dermatology at Emory University, Atlanta, who sees patients regularly, practices in Georgia, where abortion is now banned at about 6 weeks of pregnancy. Dr. Yeung worries that some dermatologists in Georgia and elsewhere may not even want to take the risk of prescribing isotretinoin, although the results in treating resistant acne are well documented.

That isn’t his only concern. “Some may not want to prescribe it to a patient who reports they are abstinent and instead require them to go on two forms [of contraception].” Or some women who are not sexually active with anyone who can get them pregnant may also be asked to go on contraception, he said. Abstinence is an alternative option in iPLEDGE.
In the past, he said, well before the Dobbs decision, some doctors have argued that iPLEDGE should not include abstinence as an option. That 2020 report was challenged by others who pointed out that removing the abstinence option would pose ethical issues and may disproportionately affect minorities and others.
Before the Dobbs decision, Dr. Yeung noted, dermatologists prescribing isotretinoin focused on pregnancy prevention but knew that if pregnancy accidentally occurred, abortion was available as an option. “The reality after the decision is, it may or may not be available to all our patients.”
Of the 14 states banning most abortions, 10 are clustered within the South and Southeast. A woman living in Arkansas, which bans most abortions, for example, is surrounded by 6 other states that do the same.
Perspective: An Arizona dermatologist
Christina Kranc, MD, is a general dermatologist in Phoenix and Scottsdale. Arizona now bans most abortions. However, this has not changed her practice much when prescribing isotretinoin, she told this news organization, because when selecting appropriate candidates for the medication, she is strict on the contraceptive requirement, and only very rarely agrees to a patient relying on abstinence.
And if a patient capable of becoming pregnant was only having sex with another patient capable of becoming pregnant? Dr. Kranc said she would still require contraception unless it was impossible for pregnancy to occur.
Among the many scenarios a dermatologist might have to consider are a lesbian cisgender woman who is having, or has only had, sexual activity with another cisgender women.
Perspective: A Connecticut dermatologist
The concern is not only about isotretinoin but all teratogenic drugs, according to Jane M. Grant-Kels, MD, vice chair of dermatology and professor of dermatology, pathology, and pediatrics at the University of Connecticut, Farmington. She often prescribes methotrexate, which is also teratogenic.

Her advice for colleagues: “Whether you believe in abortion or not is irrelevant; it’s something you discuss with your patients.” She, too, fears that doctors in states banning abortions will stop prescribing these medications, “and that is very sad.”
For those practicing in states limiting or banning abortions, Dr. Grant-Kels said, “They need to have an even longer discussion with their patients about how serious this is.” Those doctors need to talk about not only two or three types of birth control, but also discuss with the patient about the potential need for travel, should pregnancy occur and abortion be the chosen option.
Although the newer biologics are an option for psoriasis, they are expensive. And, she said, many insurers require a step-therapy approach, and “want you to start with cheaper medications,” such as methotrexate. As a result, “in some states you won’t have access to the targeted therapies unless a patient fails something like methotrexate.”
Dr. Grant-Kels worries in particular about low-income women who may not have the means to travel to get an abortion.
Need for EC education
In a recent survey of 57 pediatric dermatologists who prescribe isotretinoin, only a third said they felt confident in their understanding of emergency contraception.
The authors of the study noted that the most common reasons for pregnancies during isotretinoin therapy reported to the FDA from 2011 to 2017 “included ineffective or inconsistent use” of contraceptives and “unsuccessful abstinence,” and recommended that physicians who prescribe isotretinoin update and increase their understanding of emergency contraception.
Dr. Yeung, Dr. Kranc, Dr. Grant-Kels, and Dr. Frieden reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
More than 3 months after the Dobbs decision by the U.S. Supreme Court overturned Roe v. Wade and revoked the constitutional right to an abortion, Some have beefed up their already stringent instructions and lengthy conversations about avoiding pregnancy while on the medication.
The major fear is that a patient who is taking contraceptive precautions, in accordance with the isotretinoin risk-management program, iPLEDGE, but still becomes pregnant while on isotretinoin may find out about the pregnancy too late to undergo an abortion in her own state and may not be able to travel to another state – or the patient may live in a state where abortions are entirely prohibited and is unable to travel to another state.
Isotretinoin is marketed as Absorica, Absorica LD, Claravis, Amnesteem, Myorisan, and Zenatane; its former brand name was Accutane.
As of Oct. 7, a total of 14 states have banned most abortions, while 4 others have bans at 6, 15, 18, or 20 weeks. Attempts to restrict abortion on several other states are underway.
“To date, we don’t know of any specific effects of the Dobbs decision on isotretinoin prescribing, but with abortion access banned in many states, we anticipate that this could be a very real issue for individuals who accidentally become pregnant while taking isotretinoin,” said Ilona Frieden, MD, professor of dermatology and pediatrics at the University of California, San Francisco, and chair of the American Academy of Dermatology Association’s iPLEDGE Workgroup.
The iPLEDGE REMS (Risk Evaluation and Mitigation Strategy) is the Food and Drug Administration–required safety program that is in place to manage the risk of isotretinoin teratogenicity and minimize fetal exposure. The work group meets with the FDA and isotretinoin manufacturers to keep the program safe and operating smoothly. The iPLEDGE workgroup has not yet issued any specific statements on the implications of the Dobbs decision on prescribing isotretinoin.
But work on the issue is ongoing by the American Academy of Dermatology. In a statement issued in September, Mark D. Kaufmann, MD, president of the AAD, said that the academy “is continuing to work with its Patient Guidance for State Regulations Regarding Reproductive Health Task Force to help dermatologists best navigate state laws about how care should be implemented for patients who are or might become pregnant, and have been exposed to teratogenic medications.”
The task force, working with the academy, is “in the process of developing resources to help members better assist patients and have a productive and caring dialogue with them,” according to the statement. No specific timeline was given for when those resources might be available.
Methotrexate prescriptions
Also of concern are prescriptions for methotrexate, which is prescribed for psoriasis, atopic dermatitis, and other skin diseases. Soon after the Dobbs decision was announced on June 24, pharmacies began to require pharmacists in states that banned abortions to verify that a prescription for methotrexate was not intended for an abortion, since methotrexate is used in combination with misoprostol for termination of an early pregnancy.
The action was taken, spokespersons for several major pharmacies said, to comply with state laws. According to Kara Page, a CVS spokesperson: “Pharmacists are caught in the middle on this issue.” Laws in some states, she told this news organization, “restrict the dispensing of medications for the purpose of inducing an abortion. These laws, some of which include criminal penalties, have forced us to require pharmacists in these states to validate that the intended indication is not to terminate a pregnancy before they can fill a prescription for methotrexate.”
“New laws in various states require additional steps for dispensing certain prescriptions and apply to all pharmacies, including Walgreens,” Fraser Engerman, a spokesperson for Walgreens, told this news organization. “In these states, our pharmacists work closely with prescribers as needed, to fill lawful, clinically appropriate prescriptions. We provide ongoing training and information to help our pharmacists understand the latest requirements in their area, and with these supports, the expectation is they are empowered to fill these prescriptions.”
The iPLEDGE program has numerous requirements before a patient can begin isotretinoin treatment. Patients capable of becoming pregnant must agree to use two effective forms of birth control during the entire treatment period, which typically lasts 4 or 5 months, as well as 1 month before and 1 month after treatment, or commit to total abstinence during that time.
Perspective: A Georgia dermatologist
Howa Yeung, MD, MSc, assistant professor of dermatology at Emory University, Atlanta, who sees patients regularly, practices in Georgia, where abortion is now banned at about 6 weeks of pregnancy. Dr. Yeung worries that some dermatologists in Georgia and elsewhere may not even want to take the risk of prescribing isotretinoin, although the results in treating resistant acne are well documented.
That isn’t his only concern. “Some may not want to prescribe it to a patient who reports they are abstinent and instead require them to go on two forms [of contraception].” Or some women who are not sexually active with anyone who can get them pregnant may also be asked to go on contraception, he said. Abstinence is an alternative option in iPLEDGE.
In the past, he said, well before the Dobbs decision, some doctors have argued that iPLEDGE should not include abstinence as an option. That 2020 report was challenged by others who pointed out that removing the abstinence option would pose ethical issues and may disproportionately affect minorities and others.
Before the Dobbs decision, Dr. Yeung noted, dermatologists prescribing isotretinoin focused on pregnancy prevention but knew that if pregnancy accidentally occurred, abortion was available as an option. “The reality after the decision is, it may or may not be available to all our patients.”
Of the 14 states banning most abortions, 10 are clustered within the South and Southeast. A woman living in Arkansas, which bans most abortions, for example, is surrounded by 6 other states that do the same.
Perspective: An Arizona dermatologist
Christina Kranc, MD, is a general dermatologist in Phoenix and Scottsdale. Arizona now bans most abortions. However, this has not changed her practice much when prescribing isotretinoin, she told this news organization, because when selecting appropriate candidates for the medication, she is strict on the contraceptive requirement, and only very rarely agrees to a patient relying on abstinence.
And if a patient capable of becoming pregnant was only having sex with another patient capable of becoming pregnant? Dr. Kranc said she would still require contraception unless it was impossible for pregnancy to occur.
Among the many scenarios a dermatologist might have to consider are a lesbian cisgender woman who is having, or has only had, sexual activity with another cisgender women.
Perspective: A Connecticut dermatologist
The concern is not only about isotretinoin but all teratogenic drugs, according to Jane M. Grant-Kels, MD, vice chair of dermatology and professor of dermatology, pathology, and pediatrics at the University of Connecticut, Farmington. She often prescribes methotrexate, which is also teratogenic.
Her advice for colleagues: “Whether you believe in abortion or not is irrelevant; it’s something you discuss with your patients.” She, too, fears that doctors in states banning abortions will stop prescribing these medications, “and that is very sad.”
For those practicing in states limiting or banning abortions, Dr. Grant-Kels said, “They need to have an even longer discussion with their patients about how serious this is.” Those doctors need to talk about not only two or three types of birth control, but also discuss with the patient about the potential need for travel, should pregnancy occur and abortion be the chosen option.
Although the newer biologics are an option for psoriasis, they are expensive. And, she said, many insurers require a step-therapy approach, and “want you to start with cheaper medications,” such as methotrexate. As a result, “in some states you won’t have access to the targeted therapies unless a patient fails something like methotrexate.”
Dr. Grant-Kels worries in particular about low-income women who may not have the means to travel to get an abortion.
Need for EC education
In a recent survey of 57 pediatric dermatologists who prescribe isotretinoin, only a third said they felt confident in their understanding of emergency contraception.
The authors of the study noted that the most common reasons for pregnancies during isotretinoin therapy reported to the FDA from 2011 to 2017 “included ineffective or inconsistent use” of contraceptives and “unsuccessful abstinence,” and recommended that physicians who prescribe isotretinoin update and increase their understanding of emergency contraception.
Dr. Yeung, Dr. Kranc, Dr. Grant-Kels, and Dr. Frieden reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
More than 3 months after the Dobbs decision by the U.S. Supreme Court overturned Roe v. Wade and revoked the constitutional right to an abortion, Some have beefed up their already stringent instructions and lengthy conversations about avoiding pregnancy while on the medication.
The major fear is that a patient who is taking contraceptive precautions, in accordance with the isotretinoin risk-management program, iPLEDGE, but still becomes pregnant while on isotretinoin may find out about the pregnancy too late to undergo an abortion in her own state and may not be able to travel to another state – or the patient may live in a state where abortions are entirely prohibited and is unable to travel to another state.
Isotretinoin is marketed as Absorica, Absorica LD, Claravis, Amnesteem, Myorisan, and Zenatane; its former brand name was Accutane.
As of Oct. 7, a total of 14 states have banned most abortions, while 4 others have bans at 6, 15, 18, or 20 weeks. Attempts to restrict abortion on several other states are underway.
“To date, we don’t know of any specific effects of the Dobbs decision on isotretinoin prescribing, but with abortion access banned in many states, we anticipate that this could be a very real issue for individuals who accidentally become pregnant while taking isotretinoin,” said Ilona Frieden, MD, professor of dermatology and pediatrics at the University of California, San Francisco, and chair of the American Academy of Dermatology Association’s iPLEDGE Workgroup.
The iPLEDGE REMS (Risk Evaluation and Mitigation Strategy) is the Food and Drug Administration–required safety program that is in place to manage the risk of isotretinoin teratogenicity and minimize fetal exposure. The work group meets with the FDA and isotretinoin manufacturers to keep the program safe and operating smoothly. The iPLEDGE workgroup has not yet issued any specific statements on the implications of the Dobbs decision on prescribing isotretinoin.
But work on the issue is ongoing by the American Academy of Dermatology. In a statement issued in September, Mark D. Kaufmann, MD, president of the AAD, said that the academy “is continuing to work with its Patient Guidance for State Regulations Regarding Reproductive Health Task Force to help dermatologists best navigate state laws about how care should be implemented for patients who are or might become pregnant, and have been exposed to teratogenic medications.”
The task force, working with the academy, is “in the process of developing resources to help members better assist patients and have a productive and caring dialogue with them,” according to the statement. No specific timeline was given for when those resources might be available.
Methotrexate prescriptions
Also of concern are prescriptions for methotrexate, which is prescribed for psoriasis, atopic dermatitis, and other skin diseases. Soon after the Dobbs decision was announced on June 24, pharmacies began to require pharmacists in states that banned abortions to verify that a prescription for methotrexate was not intended for an abortion, since methotrexate is used in combination with misoprostol for termination of an early pregnancy.
The action was taken, spokespersons for several major pharmacies said, to comply with state laws. According to Kara Page, a CVS spokesperson: “Pharmacists are caught in the middle on this issue.” Laws in some states, she told this news organization, “restrict the dispensing of medications for the purpose of inducing an abortion. These laws, some of which include criminal penalties, have forced us to require pharmacists in these states to validate that the intended indication is not to terminate a pregnancy before they can fill a prescription for methotrexate.”
“New laws in various states require additional steps for dispensing certain prescriptions and apply to all pharmacies, including Walgreens,” Fraser Engerman, a spokesperson for Walgreens, told this news organization. “In these states, our pharmacists work closely with prescribers as needed, to fill lawful, clinically appropriate prescriptions. We provide ongoing training and information to help our pharmacists understand the latest requirements in their area, and with these supports, the expectation is they are empowered to fill these prescriptions.”
The iPLEDGE program has numerous requirements before a patient can begin isotretinoin treatment. Patients capable of becoming pregnant must agree to use two effective forms of birth control during the entire treatment period, which typically lasts 4 or 5 months, as well as 1 month before and 1 month after treatment, or commit to total abstinence during that time.
Perspective: A Georgia dermatologist
Howa Yeung, MD, MSc, assistant professor of dermatology at Emory University, Atlanta, who sees patients regularly, practices in Georgia, where abortion is now banned at about 6 weeks of pregnancy. Dr. Yeung worries that some dermatologists in Georgia and elsewhere may not even want to take the risk of prescribing isotretinoin, although the results in treating resistant acne are well documented.
That isn’t his only concern. “Some may not want to prescribe it to a patient who reports they are abstinent and instead require them to go on two forms [of contraception].” Or some women who are not sexually active with anyone who can get them pregnant may also be asked to go on contraception, he said. Abstinence is an alternative option in iPLEDGE.
In the past, he said, well before the Dobbs decision, some doctors have argued that iPLEDGE should not include abstinence as an option. That 2020 report was challenged by others who pointed out that removing the abstinence option would pose ethical issues and may disproportionately affect minorities and others.
Before the Dobbs decision, Dr. Yeung noted, dermatologists prescribing isotretinoin focused on pregnancy prevention but knew that if pregnancy accidentally occurred, abortion was available as an option. “The reality after the decision is, it may or may not be available to all our patients.”
Of the 14 states banning most abortions, 10 are clustered within the South and Southeast. A woman living in Arkansas, which bans most abortions, for example, is surrounded by 6 other states that do the same.
Perspective: An Arizona dermatologist
Christina Kranc, MD, is a general dermatologist in Phoenix and Scottsdale. Arizona now bans most abortions. However, this has not changed her practice much when prescribing isotretinoin, she told this news organization, because when selecting appropriate candidates for the medication, she is strict on the contraceptive requirement, and only very rarely agrees to a patient relying on abstinence.
And if a patient capable of becoming pregnant was only having sex with another patient capable of becoming pregnant? Dr. Kranc said she would still require contraception unless it was impossible for pregnancy to occur.
Among the many scenarios a dermatologist might have to consider are a lesbian cisgender woman who is having, or has only had, sexual activity with another cisgender women.
Perspective: A Connecticut dermatologist
The concern is not only about isotretinoin but all teratogenic drugs, according to Jane M. Grant-Kels, MD, vice chair of dermatology and professor of dermatology, pathology, and pediatrics at the University of Connecticut, Farmington. She often prescribes methotrexate, which is also teratogenic.
Her advice for colleagues: “Whether you believe in abortion or not is irrelevant; it’s something you discuss with your patients.” She, too, fears that doctors in states banning abortions will stop prescribing these medications, “and that is very sad.”
For those practicing in states limiting or banning abortions, Dr. Grant-Kels said, “They need to have an even longer discussion with their patients about how serious this is.” Those doctors need to talk about not only two or three types of birth control, but also discuss with the patient about the potential need for travel, should pregnancy occur and abortion be the chosen option.
Although the newer biologics are an option for psoriasis, they are expensive. And, she said, many insurers require a step-therapy approach, and “want you to start with cheaper medications,” such as methotrexate. As a result, “in some states you won’t have access to the targeted therapies unless a patient fails something like methotrexate.”
Dr. Grant-Kels worries in particular about low-income women who may not have the means to travel to get an abortion.
Need for EC education
In a recent survey of 57 pediatric dermatologists who prescribe isotretinoin, only a third said they felt confident in their understanding of emergency contraception.
The authors of the study noted that the most common reasons for pregnancies during isotretinoin therapy reported to the FDA from 2011 to 2017 “included ineffective or inconsistent use” of contraceptives and “unsuccessful abstinence,” and recommended that physicians who prescribe isotretinoin update and increase their understanding of emergency contraception.
Dr. Yeung, Dr. Kranc, Dr. Grant-Kels, and Dr. Frieden reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dermatologists embrace low-dose oral minoxidil as hair loss adjunctive therapy
It’s not a new drug – it’s been available in topical form for hair loss since 1988 and was approved as an antihypertensive in 1979 – but .
The number of scholarly publications examining its use for hair loss has grown dramatically in the last 2 years: There were 2 in 2019, and that jumped to 17 in 2020 and 20 in 2021, with another 16 published so far this year, according to a PubMed search. An August article in The New York Times touting it as a potential cheap magic bullet is likely to drum up even more interest, said dermatologists.
The low-dose formulation is especially exciting for women, as there have been few great oral options for them, clinicians said.
Female hair loss “is devastating,” said Lily Talakoub, MD, adding that topical minoxidil (Rogaine), topical serums, and supplements “really do not provide the considerable growth that women really want to see.” Oral minoxidil is not approved by the U.S. Food and Drug Administration for hair loss, but “it has been shown in studies to cause the hairs to grow,” and has become a “lifeline” for women, said Dr. Talakoub, a dermatologist who is in private practice in McLean, Va.
“For many years we haven’t had anything new to tell patients medically,” said Lynne J. Goldberg, MD, professor of dermatology and pathology at Boston University School of Medicine. “Now, all of the sudden there’s a cheap, widely available efficacious medicine. That’s huge for female-pattern hair loss,” said Dr. Goldberg, who is also the director of the Boston Medical Center’s Hair Clinic.
“I’ve been using oral minoxidil for about 4 years with great success,” said dermatologist Eva Simmons-O’Brien, MD, who is in private practice in Towson, Md. She has used it primarily in women, mainly because she sees more women than men for hair loss.
Dr. Simmons-O’Brien said the excitement about low-dose oral minoxidil follows an increasing recognition in the medical and scientific community that hair loss is more than just a cosmetic issue.
Mechanism not fully understood
When minoxidil was first brought to market as an antihypertensive, clinicians noted hair growth in “balding patients,” which led to the development of the topical form. Even though it has been used for hair growth for decades, its mechanism of action is not fully understood. It is known that minoxidil is a vasodilator; it may also increase DNA synthesis and enhance cell proliferation, according to a review published in 2019.
“The positive effect of minoxidil on hair growth is mainly due to its metabolite, minoxidil sulfate, and the enzyme responsible for this conversion is sulfotransferase, which is located in hair follicles and varies in production among individuals,” write the authors, all affiliated with Mahidol University in Bangkok, Thailand.
Writing in the American Academy of Dermatology’s Dermatology World Insights and Inquiries, Warren R. Heymann, MD, observed that “even after decades of use,” how minoxidil improves alopecia is still not completely understood. He noted that a 2020 review found that minoxidil’s vasodilatory effects “are propagated by upregulation of vascular endothelial growth factor (VEGF), increasing cutaneous blood flow with resultant increase in oxygen and growth factor delivery to the hair follicle.” The medication prolongs the anagen phase and shortens the telogen phase, added Dr. Heymann, head of dermatology at Rowan University, Camden, N.J.
As an antihypertensive, minoxidil is given at 5-40 mg daily. Those doses have produced serious side effects such as sodium and fluid retention, ischemic heart disease, pericardial effusion, and pulmonary hypertension, according to the Thai researchers.
Those side effects have appeared to be rare with low-dose oral minoxidil. However, in JAAD Case Reports, South African researchers reported a case in which low-dose oral minoxidil may have led to cardiac side effects. A healthy 40-year-old woman, who after 3 weeks of treatment with 5% topical minoxidil, tacrolimus ointment 0.1%, clobetasol propionate ointment, 100 mg of doxycycline twice daily, and 0.25 mg of oral minoxidil daily, was hospitalized with full-body edema. An ultrasound showed fluid collections in the pericardium, pleural space, and abdomen. She also had a pleural effusion. The patient was given 40 mg of intravenous furosemide daily for 4 days, and the edema resolved.
“Having excluded other causes of pericardial effusion and anasarca in the previously healthy, young woman, we concluded that LDOM [low-dose oral minoxidil] was responsible for her clinical presentation,” write the authors.
A review of 17 studies published on-line in 2020 in the Journal of the American Academy of Dermatology found low-dose minoxidil to be safe and effective. Androgenetic alopecia was the most commonly studied, with doses of 0.25-1.25 mg proving to be effective and safe. It was also safe and effective for female-pattern hair loss, traction alopecia, chronic telogen effluvium, lichen planopilaris, alopecia areata, and permanent chemotherapy-induced alopecia.
The most common adverse effect was hypertrichosis. Other adverse events included postural hypotension and dizziness, lower-limb edema, and mild blood pressure changes.
In another multicenter, 1,404-patient safety study published in 2021 in JAAD, the authors found that hypertrichosis was the most frequent adverse event, reported by 15% of patients. Systemic adverse events included lightheadedness (1.7% of patients), fluid retention (1.3%), tachycardia (0.9%), headache (0.4%), periorbital edema (0.3%), and insomnia (0.2%). Only 29 patients (1.2%) withdrew because of these side effects.
“It definitely helps, and it’s relatively safe,” said Adam Friedman, MD, professor and chair of dermatology at George Washington University in Washington. “But I wouldn’t want to call it a game-changer,” he said, adding that it works best when used in combination with other therapies. He often uses it with a 5-alpha reductase inhibitor – finasteride (Propecia) or dutasteride (Avodart) – “rather than as a monotherapy,” said Dr. Friedman.
From Australia to around the globe
The first publication on low-dose oral minoxidil for hair loss was in December 2017. The pilot study in female-pattern hair loss was published in the International Journal of Dermatology by Rodney Sinclair, MBBS, MD, a Melbourne, Australia–based dermatologist.
Amy McMichael, MD, professor of dermatology at Wake Forest University, Winston-Salem, N.C., said she first heard Dr. Sinclair present his findings at an alopecia research meeting in Japan shortly before his initial publication.
“After that, I think all of us said, ‘Huh, this is interesting, and let’s try it, because we’re always looking for something more to help our patients,’” Dr. McMichael said, adding that she’s been prescribing low-dose minoxidil to her patients for 5 years.
She and colleagues at Wake Forest, along with Jerry Cooley, MD, a dermatologist in private practice in Charlotte, published a retrospective case series in March, looking at 105 adult patients – 80 women (ages 24-80) and 25 men (ages 19-63) – who were treated for androgenetic alopecia and/or telogen effluvium with oral minoxidil (dose range of 0.625–2.5 mg) once daily for a year, matched to 105 case controls.
Efficacy was based on the clinician’s assessment of clinical response and clinical photographic evaluation using a 3-point scale (worsening, stabilization, and improvement). Half of those treated demonstrated clinical improvement and 43% demonstrated stabilization. There was a significant difference (P < .001) in clinical response between those who received minoxidil and the controls.
Ideal patients?
Given its ease of use and low cost – $4-$12 for a 30-day supply of 2.5 mg tablets, according to GoodRX – low-dose minoxidil is a good fit for many patients, said dermatologists.
The best candidate is “a woman who’s perimenopausal or menopausal who’s got what we would say is moderate to severe loss of hair that’s kind of just starting,” said Dr. Simmons-O’Brien. The medication is not likely to grow hair where there is scarring already, however, she said.
“I tend to use it in people who either don’t want to do the topical minoxidil or have used it and have a lot of potential side effects from it,” like itching and irritation, said Dr. McMichael. She said oral minoxidil can also be helpful as an adjunct in patients with alopecia areata and that it can be used after anti-inflammatory treatments in central centrifugal cicatricial alopecia.
Dr. Goldberg said low-dose minoxidil would not be her first choice for female-pattern hair loss but that it’s “a great alternative” for people who can’t tolerate the topical form. Most of the women she has prescribed it to “have been pretty happy,” she added.
“I would be a little cautious in patients on a number of other medications,” Dr. Goldberg said, noting minoxidil’s potential systemic side effects.
Clinicians said they generally consult with a patient’s internist when they are starting them on oral minoxidil. “I always want to touch base with the primary care physician first,” said Dr. Friedman.
“If they’re on oral antihypertensive medications already, then I would ask them to talk to either their primary care physician or their cardiologist to make sure it’s okay to give this low dose,” said Dr. McMichael.
At the low doses, minoxidil rarely has any blood pressure–lowering effects, dermatologists said.
Women are usually started on 1.25 mg, while men can start at a higher, 2.5-mg dose, said clinicians.
Dr. Goldberg and Dr. Simmons-O’Brien said that recent additional warnings for finasteride about sexual side effects and the potential for suicide have changed the way they approach its use in young men, and that it has highlighted the potential for oral minoxidil as an alternative.
Oral minoxidil is rarely used as a monotherapy. “It takes a village” to address hair loss, said Dr. Simmons-O’Brien, noting that she likes to evaluate nutrition, vitamin D levels, and whether a patient is anemic or has thyroid disease when determining a course of action.
Dermatologists said they use oral minoxidil in combination with spironolactone, topical minoxidil, finasteride, or dutasteride. If patients are already on antihypertensives or at risk for excessive blood pressure–lowering effects of a combination that includes spironolactone, the dermatologists said again they will consult with a patient’s primary care physician first.
For women, the main limiting factor with oral minoxidil may be unwanted hair growth, usually on the face. Most of the clinicians interviewed for this story said they did not use spironolactone to counteract that hypertrichosis.
Dr. McMichael said she cautions African American women or women of African descent – who tend to have more body hair at baseline – that they should be aware of the potential for excess hair growth associated with low-dose minoxidil. She and other dermatologists interviewed for this story said they urge patients who are bothered by the excess hair to shave or wax or use other nonpharmacologic approaches.
The excess hair growth is less bothersome for men, they said.
Not a magic wand
Despite the increased profile and interest, oral minoxidil is not a cure-all, clinicians said.
“It’s important for patients to realize that hair loss can be complicated and there is no one magic wand,” said Dr. Simmons-O’Brien. Clinicians typically “are using several things to help encourage these follicular units to not miniaturize and disappear and create scars,” she said.
Dr. Friedman said he finds that patients have a hard time hearing that to continue to maintain growth, they have to take a medication for the rest of their life. “If you stop, you will have to start again,” he said.
Oral minoxidil, when used in combination with other therapies, will improve hair growth, said Dr. Goldberg. But it will not take someone back a decade, she said. “I try to temper expectations – promise a little and achieve more,” Dr. Goldberg said.
The study was independently supported. Dr. Smith and Dr. Jones report no relevant financial relationships. Dr. Simmons-O’Brien reports that she has received speaking fees from Isdin. Dr. McMichael disclosed relationships with Eli Lilly, Pfizer, Nutrafol, Revian, and UCB Pharma. Dr. Friedman, Dr. Goldberg, and Dr. Talakoub reported no disclosures.
A version of this article first appeared on Medscape.com.
It’s not a new drug – it’s been available in topical form for hair loss since 1988 and was approved as an antihypertensive in 1979 – but .
The number of scholarly publications examining its use for hair loss has grown dramatically in the last 2 years: There were 2 in 2019, and that jumped to 17 in 2020 and 20 in 2021, with another 16 published so far this year, according to a PubMed search. An August article in The New York Times touting it as a potential cheap magic bullet is likely to drum up even more interest, said dermatologists.
The low-dose formulation is especially exciting for women, as there have been few great oral options for them, clinicians said.
Female hair loss “is devastating,” said Lily Talakoub, MD, adding that topical minoxidil (Rogaine), topical serums, and supplements “really do not provide the considerable growth that women really want to see.” Oral minoxidil is not approved by the U.S. Food and Drug Administration for hair loss, but “it has been shown in studies to cause the hairs to grow,” and has become a “lifeline” for women, said Dr. Talakoub, a dermatologist who is in private practice in McLean, Va.
“For many years we haven’t had anything new to tell patients medically,” said Lynne J. Goldberg, MD, professor of dermatology and pathology at Boston University School of Medicine. “Now, all of the sudden there’s a cheap, widely available efficacious medicine. That’s huge for female-pattern hair loss,” said Dr. Goldberg, who is also the director of the Boston Medical Center’s Hair Clinic.
“I’ve been using oral minoxidil for about 4 years with great success,” said dermatologist Eva Simmons-O’Brien, MD, who is in private practice in Towson, Md. She has used it primarily in women, mainly because she sees more women than men for hair loss.
Dr. Simmons-O’Brien said the excitement about low-dose oral minoxidil follows an increasing recognition in the medical and scientific community that hair loss is more than just a cosmetic issue.
Mechanism not fully understood
When minoxidil was first brought to market as an antihypertensive, clinicians noted hair growth in “balding patients,” which led to the development of the topical form. Even though it has been used for hair growth for decades, its mechanism of action is not fully understood. It is known that minoxidil is a vasodilator; it may also increase DNA synthesis and enhance cell proliferation, according to a review published in 2019.
“The positive effect of minoxidil on hair growth is mainly due to its metabolite, minoxidil sulfate, and the enzyme responsible for this conversion is sulfotransferase, which is located in hair follicles and varies in production among individuals,” write the authors, all affiliated with Mahidol University in Bangkok, Thailand.
Writing in the American Academy of Dermatology’s Dermatology World Insights and Inquiries, Warren R. Heymann, MD, observed that “even after decades of use,” how minoxidil improves alopecia is still not completely understood. He noted that a 2020 review found that minoxidil’s vasodilatory effects “are propagated by upregulation of vascular endothelial growth factor (VEGF), increasing cutaneous blood flow with resultant increase in oxygen and growth factor delivery to the hair follicle.” The medication prolongs the anagen phase and shortens the telogen phase, added Dr. Heymann, head of dermatology at Rowan University, Camden, N.J.
As an antihypertensive, minoxidil is given at 5-40 mg daily. Those doses have produced serious side effects such as sodium and fluid retention, ischemic heart disease, pericardial effusion, and pulmonary hypertension, according to the Thai researchers.
Those side effects have appeared to be rare with low-dose oral minoxidil. However, in JAAD Case Reports, South African researchers reported a case in which low-dose oral minoxidil may have led to cardiac side effects. A healthy 40-year-old woman, who after 3 weeks of treatment with 5% topical minoxidil, tacrolimus ointment 0.1%, clobetasol propionate ointment, 100 mg of doxycycline twice daily, and 0.25 mg of oral minoxidil daily, was hospitalized with full-body edema. An ultrasound showed fluid collections in the pericardium, pleural space, and abdomen. She also had a pleural effusion. The patient was given 40 mg of intravenous furosemide daily for 4 days, and the edema resolved.
“Having excluded other causes of pericardial effusion and anasarca in the previously healthy, young woman, we concluded that LDOM [low-dose oral minoxidil] was responsible for her clinical presentation,” write the authors.
A review of 17 studies published on-line in 2020 in the Journal of the American Academy of Dermatology found low-dose minoxidil to be safe and effective. Androgenetic alopecia was the most commonly studied, with doses of 0.25-1.25 mg proving to be effective and safe. It was also safe and effective for female-pattern hair loss, traction alopecia, chronic telogen effluvium, lichen planopilaris, alopecia areata, and permanent chemotherapy-induced alopecia.
The most common adverse effect was hypertrichosis. Other adverse events included postural hypotension and dizziness, lower-limb edema, and mild blood pressure changes.
In another multicenter, 1,404-patient safety study published in 2021 in JAAD, the authors found that hypertrichosis was the most frequent adverse event, reported by 15% of patients. Systemic adverse events included lightheadedness (1.7% of patients), fluid retention (1.3%), tachycardia (0.9%), headache (0.4%), periorbital edema (0.3%), and insomnia (0.2%). Only 29 patients (1.2%) withdrew because of these side effects.
“It definitely helps, and it’s relatively safe,” said Adam Friedman, MD, professor and chair of dermatology at George Washington University in Washington. “But I wouldn’t want to call it a game-changer,” he said, adding that it works best when used in combination with other therapies. He often uses it with a 5-alpha reductase inhibitor – finasteride (Propecia) or dutasteride (Avodart) – “rather than as a monotherapy,” said Dr. Friedman.
From Australia to around the globe
The first publication on low-dose oral minoxidil for hair loss was in December 2017. The pilot study in female-pattern hair loss was published in the International Journal of Dermatology by Rodney Sinclair, MBBS, MD, a Melbourne, Australia–based dermatologist.
Amy McMichael, MD, professor of dermatology at Wake Forest University, Winston-Salem, N.C., said she first heard Dr. Sinclair present his findings at an alopecia research meeting in Japan shortly before his initial publication.
“After that, I think all of us said, ‘Huh, this is interesting, and let’s try it, because we’re always looking for something more to help our patients,’” Dr. McMichael said, adding that she’s been prescribing low-dose minoxidil to her patients for 5 years.
She and colleagues at Wake Forest, along with Jerry Cooley, MD, a dermatologist in private practice in Charlotte, published a retrospective case series in March, looking at 105 adult patients – 80 women (ages 24-80) and 25 men (ages 19-63) – who were treated for androgenetic alopecia and/or telogen effluvium with oral minoxidil (dose range of 0.625–2.5 mg) once daily for a year, matched to 105 case controls.
Efficacy was based on the clinician’s assessment of clinical response and clinical photographic evaluation using a 3-point scale (worsening, stabilization, and improvement). Half of those treated demonstrated clinical improvement and 43% demonstrated stabilization. There was a significant difference (P < .001) in clinical response between those who received minoxidil and the controls.
Ideal patients?
Given its ease of use and low cost – $4-$12 for a 30-day supply of 2.5 mg tablets, according to GoodRX – low-dose minoxidil is a good fit for many patients, said dermatologists.
The best candidate is “a woman who’s perimenopausal or menopausal who’s got what we would say is moderate to severe loss of hair that’s kind of just starting,” said Dr. Simmons-O’Brien. The medication is not likely to grow hair where there is scarring already, however, she said.
“I tend to use it in people who either don’t want to do the topical minoxidil or have used it and have a lot of potential side effects from it,” like itching and irritation, said Dr. McMichael. She said oral minoxidil can also be helpful as an adjunct in patients with alopecia areata and that it can be used after anti-inflammatory treatments in central centrifugal cicatricial alopecia.
Dr. Goldberg said low-dose minoxidil would not be her first choice for female-pattern hair loss but that it’s “a great alternative” for people who can’t tolerate the topical form. Most of the women she has prescribed it to “have been pretty happy,” she added.
“I would be a little cautious in patients on a number of other medications,” Dr. Goldberg said, noting minoxidil’s potential systemic side effects.
Clinicians said they generally consult with a patient’s internist when they are starting them on oral minoxidil. “I always want to touch base with the primary care physician first,” said Dr. Friedman.
“If they’re on oral antihypertensive medications already, then I would ask them to talk to either their primary care physician or their cardiologist to make sure it’s okay to give this low dose,” said Dr. McMichael.
At the low doses, minoxidil rarely has any blood pressure–lowering effects, dermatologists said.
Women are usually started on 1.25 mg, while men can start at a higher, 2.5-mg dose, said clinicians.
Dr. Goldberg and Dr. Simmons-O’Brien said that recent additional warnings for finasteride about sexual side effects and the potential for suicide have changed the way they approach its use in young men, and that it has highlighted the potential for oral minoxidil as an alternative.
Oral minoxidil is rarely used as a monotherapy. “It takes a village” to address hair loss, said Dr. Simmons-O’Brien, noting that she likes to evaluate nutrition, vitamin D levels, and whether a patient is anemic or has thyroid disease when determining a course of action.
Dermatologists said they use oral minoxidil in combination with spironolactone, topical minoxidil, finasteride, or dutasteride. If patients are already on antihypertensives or at risk for excessive blood pressure–lowering effects of a combination that includes spironolactone, the dermatologists said again they will consult with a patient’s primary care physician first.
For women, the main limiting factor with oral minoxidil may be unwanted hair growth, usually on the face. Most of the clinicians interviewed for this story said they did not use spironolactone to counteract that hypertrichosis.
Dr. McMichael said she cautions African American women or women of African descent – who tend to have more body hair at baseline – that they should be aware of the potential for excess hair growth associated with low-dose minoxidil. She and other dermatologists interviewed for this story said they urge patients who are bothered by the excess hair to shave or wax or use other nonpharmacologic approaches.
The excess hair growth is less bothersome for men, they said.
Not a magic wand
Despite the increased profile and interest, oral minoxidil is not a cure-all, clinicians said.
“It’s important for patients to realize that hair loss can be complicated and there is no one magic wand,” said Dr. Simmons-O’Brien. Clinicians typically “are using several things to help encourage these follicular units to not miniaturize and disappear and create scars,” she said.
Dr. Friedman said he finds that patients have a hard time hearing that to continue to maintain growth, they have to take a medication for the rest of their life. “If you stop, you will have to start again,” he said.
Oral minoxidil, when used in combination with other therapies, will improve hair growth, said Dr. Goldberg. But it will not take someone back a decade, she said. “I try to temper expectations – promise a little and achieve more,” Dr. Goldberg said.
The study was independently supported. Dr. Smith and Dr. Jones report no relevant financial relationships. Dr. Simmons-O’Brien reports that she has received speaking fees from Isdin. Dr. McMichael disclosed relationships with Eli Lilly, Pfizer, Nutrafol, Revian, and UCB Pharma. Dr. Friedman, Dr. Goldberg, and Dr. Talakoub reported no disclosures.
A version of this article first appeared on Medscape.com.
It’s not a new drug – it’s been available in topical form for hair loss since 1988 and was approved as an antihypertensive in 1979 – but .
The number of scholarly publications examining its use for hair loss has grown dramatically in the last 2 years: There were 2 in 2019, and that jumped to 17 in 2020 and 20 in 2021, with another 16 published so far this year, according to a PubMed search. An August article in The New York Times touting it as a potential cheap magic bullet is likely to drum up even more interest, said dermatologists.
The low-dose formulation is especially exciting for women, as there have been few great oral options for them, clinicians said.
Female hair loss “is devastating,” said Lily Talakoub, MD, adding that topical minoxidil (Rogaine), topical serums, and supplements “really do not provide the considerable growth that women really want to see.” Oral minoxidil is not approved by the U.S. Food and Drug Administration for hair loss, but “it has been shown in studies to cause the hairs to grow,” and has become a “lifeline” for women, said Dr. Talakoub, a dermatologist who is in private practice in McLean, Va.
“For many years we haven’t had anything new to tell patients medically,” said Lynne J. Goldberg, MD, professor of dermatology and pathology at Boston University School of Medicine. “Now, all of the sudden there’s a cheap, widely available efficacious medicine. That’s huge for female-pattern hair loss,” said Dr. Goldberg, who is also the director of the Boston Medical Center’s Hair Clinic.
“I’ve been using oral minoxidil for about 4 years with great success,” said dermatologist Eva Simmons-O’Brien, MD, who is in private practice in Towson, Md. She has used it primarily in women, mainly because she sees more women than men for hair loss.
Dr. Simmons-O’Brien said the excitement about low-dose oral minoxidil follows an increasing recognition in the medical and scientific community that hair loss is more than just a cosmetic issue.
Mechanism not fully understood
When minoxidil was first brought to market as an antihypertensive, clinicians noted hair growth in “balding patients,” which led to the development of the topical form. Even though it has been used for hair growth for decades, its mechanism of action is not fully understood. It is known that minoxidil is a vasodilator; it may also increase DNA synthesis and enhance cell proliferation, according to a review published in 2019.
“The positive effect of minoxidil on hair growth is mainly due to its metabolite, minoxidil sulfate, and the enzyme responsible for this conversion is sulfotransferase, which is located in hair follicles and varies in production among individuals,” write the authors, all affiliated with Mahidol University in Bangkok, Thailand.
Writing in the American Academy of Dermatology’s Dermatology World Insights and Inquiries, Warren R. Heymann, MD, observed that “even after decades of use,” how minoxidil improves alopecia is still not completely understood. He noted that a 2020 review found that minoxidil’s vasodilatory effects “are propagated by upregulation of vascular endothelial growth factor (VEGF), increasing cutaneous blood flow with resultant increase in oxygen and growth factor delivery to the hair follicle.” The medication prolongs the anagen phase and shortens the telogen phase, added Dr. Heymann, head of dermatology at Rowan University, Camden, N.J.
As an antihypertensive, minoxidil is given at 5-40 mg daily. Those doses have produced serious side effects such as sodium and fluid retention, ischemic heart disease, pericardial effusion, and pulmonary hypertension, according to the Thai researchers.
Those side effects have appeared to be rare with low-dose oral minoxidil. However, in JAAD Case Reports, South African researchers reported a case in which low-dose oral minoxidil may have led to cardiac side effects. A healthy 40-year-old woman, who after 3 weeks of treatment with 5% topical minoxidil, tacrolimus ointment 0.1%, clobetasol propionate ointment, 100 mg of doxycycline twice daily, and 0.25 mg of oral minoxidil daily, was hospitalized with full-body edema. An ultrasound showed fluid collections in the pericardium, pleural space, and abdomen. She also had a pleural effusion. The patient was given 40 mg of intravenous furosemide daily for 4 days, and the edema resolved.
“Having excluded other causes of pericardial effusion and anasarca in the previously healthy, young woman, we concluded that LDOM [low-dose oral minoxidil] was responsible for her clinical presentation,” write the authors.
A review of 17 studies published on-line in 2020 in the Journal of the American Academy of Dermatology found low-dose minoxidil to be safe and effective. Androgenetic alopecia was the most commonly studied, with doses of 0.25-1.25 mg proving to be effective and safe. It was also safe and effective for female-pattern hair loss, traction alopecia, chronic telogen effluvium, lichen planopilaris, alopecia areata, and permanent chemotherapy-induced alopecia.
The most common adverse effect was hypertrichosis. Other adverse events included postural hypotension and dizziness, lower-limb edema, and mild blood pressure changes.
In another multicenter, 1,404-patient safety study published in 2021 in JAAD, the authors found that hypertrichosis was the most frequent adverse event, reported by 15% of patients. Systemic adverse events included lightheadedness (1.7% of patients), fluid retention (1.3%), tachycardia (0.9%), headache (0.4%), periorbital edema (0.3%), and insomnia (0.2%). Only 29 patients (1.2%) withdrew because of these side effects.
“It definitely helps, and it’s relatively safe,” said Adam Friedman, MD, professor and chair of dermatology at George Washington University in Washington. “But I wouldn’t want to call it a game-changer,” he said, adding that it works best when used in combination with other therapies. He often uses it with a 5-alpha reductase inhibitor – finasteride (Propecia) or dutasteride (Avodart) – “rather than as a monotherapy,” said Dr. Friedman.
From Australia to around the globe
The first publication on low-dose oral minoxidil for hair loss was in December 2017. The pilot study in female-pattern hair loss was published in the International Journal of Dermatology by Rodney Sinclair, MBBS, MD, a Melbourne, Australia–based dermatologist.
Amy McMichael, MD, professor of dermatology at Wake Forest University, Winston-Salem, N.C., said she first heard Dr. Sinclair present his findings at an alopecia research meeting in Japan shortly before his initial publication.
“After that, I think all of us said, ‘Huh, this is interesting, and let’s try it, because we’re always looking for something more to help our patients,’” Dr. McMichael said, adding that she’s been prescribing low-dose minoxidil to her patients for 5 years.
She and colleagues at Wake Forest, along with Jerry Cooley, MD, a dermatologist in private practice in Charlotte, published a retrospective case series in March, looking at 105 adult patients – 80 women (ages 24-80) and 25 men (ages 19-63) – who were treated for androgenetic alopecia and/or telogen effluvium with oral minoxidil (dose range of 0.625–2.5 mg) once daily for a year, matched to 105 case controls.
Efficacy was based on the clinician’s assessment of clinical response and clinical photographic evaluation using a 3-point scale (worsening, stabilization, and improvement). Half of those treated demonstrated clinical improvement and 43% demonstrated stabilization. There was a significant difference (P < .001) in clinical response between those who received minoxidil and the controls.
Ideal patients?
Given its ease of use and low cost – $4-$12 for a 30-day supply of 2.5 mg tablets, according to GoodRX – low-dose minoxidil is a good fit for many patients, said dermatologists.
The best candidate is “a woman who’s perimenopausal or menopausal who’s got what we would say is moderate to severe loss of hair that’s kind of just starting,” said Dr. Simmons-O’Brien. The medication is not likely to grow hair where there is scarring already, however, she said.
“I tend to use it in people who either don’t want to do the topical minoxidil or have used it and have a lot of potential side effects from it,” like itching and irritation, said Dr. McMichael. She said oral minoxidil can also be helpful as an adjunct in patients with alopecia areata and that it can be used after anti-inflammatory treatments in central centrifugal cicatricial alopecia.
Dr. Goldberg said low-dose minoxidil would not be her first choice for female-pattern hair loss but that it’s “a great alternative” for people who can’t tolerate the topical form. Most of the women she has prescribed it to “have been pretty happy,” she added.
“I would be a little cautious in patients on a number of other medications,” Dr. Goldberg said, noting minoxidil’s potential systemic side effects.
Clinicians said they generally consult with a patient’s internist when they are starting them on oral minoxidil. “I always want to touch base with the primary care physician first,” said Dr. Friedman.
“If they’re on oral antihypertensive medications already, then I would ask them to talk to either their primary care physician or their cardiologist to make sure it’s okay to give this low dose,” said Dr. McMichael.
At the low doses, minoxidil rarely has any blood pressure–lowering effects, dermatologists said.
Women are usually started on 1.25 mg, while men can start at a higher, 2.5-mg dose, said clinicians.
Dr. Goldberg and Dr. Simmons-O’Brien said that recent additional warnings for finasteride about sexual side effects and the potential for suicide have changed the way they approach its use in young men, and that it has highlighted the potential for oral minoxidil as an alternative.
Oral minoxidil is rarely used as a monotherapy. “It takes a village” to address hair loss, said Dr. Simmons-O’Brien, noting that she likes to evaluate nutrition, vitamin D levels, and whether a patient is anemic or has thyroid disease when determining a course of action.
Dermatologists said they use oral minoxidil in combination with spironolactone, topical minoxidil, finasteride, or dutasteride. If patients are already on antihypertensives or at risk for excessive blood pressure–lowering effects of a combination that includes spironolactone, the dermatologists said again they will consult with a patient’s primary care physician first.
For women, the main limiting factor with oral minoxidil may be unwanted hair growth, usually on the face. Most of the clinicians interviewed for this story said they did not use spironolactone to counteract that hypertrichosis.
Dr. McMichael said she cautions African American women or women of African descent – who tend to have more body hair at baseline – that they should be aware of the potential for excess hair growth associated with low-dose minoxidil. She and other dermatologists interviewed for this story said they urge patients who are bothered by the excess hair to shave or wax or use other nonpharmacologic approaches.
The excess hair growth is less bothersome for men, they said.
Not a magic wand
Despite the increased profile and interest, oral minoxidil is not a cure-all, clinicians said.
“It’s important for patients to realize that hair loss can be complicated and there is no one magic wand,” said Dr. Simmons-O’Brien. Clinicians typically “are using several things to help encourage these follicular units to not miniaturize and disappear and create scars,” she said.
Dr. Friedman said he finds that patients have a hard time hearing that to continue to maintain growth, they have to take a medication for the rest of their life. “If you stop, you will have to start again,” he said.
Oral minoxidil, when used in combination with other therapies, will improve hair growth, said Dr. Goldberg. But it will not take someone back a decade, she said. “I try to temper expectations – promise a little and achieve more,” Dr. Goldberg said.
The study was independently supported. Dr. Smith and Dr. Jones report no relevant financial relationships. Dr. Simmons-O’Brien reports that she has received speaking fees from Isdin. Dr. McMichael disclosed relationships with Eli Lilly, Pfizer, Nutrafol, Revian, and UCB Pharma. Dr. Friedman, Dr. Goldberg, and Dr. Talakoub reported no disclosures.
A version of this article first appeared on Medscape.com.
The marked contrast in pandemic outcomes between Japan and the United States
This article was originally published Oct. 8 on Medscape Editor-In-Chief Eric Topol’s “Ground Truths” column on Substack.
Over time it has the least cumulative deaths per capita of any major country in the world. That’s without a zero-Covid policy or any national lockdowns, which is why I have not included China as a comparator.
Before we get into that data, let’s take a look at the age pyramids for Japan and the United States. The No. 1 risk factor for death from COVID-19 is advanced age, and you can see that in Japan about 25% of the population is age 65 and older, whereas in the United States that proportion is substantially reduced at 15%. Sure there are differences in comorbidities such as obesity and diabetes, but there is also the trade-off of a much higher population density in Japan.
Besides masks, which were distributed early on by the government to the population in Japan, there was the “Avoid the 3Cs” cluster-busting strategy, widely disseminated in the spring of 2020, leveraging Pareto’s 80-20 principle, long before there were any vaccines available. For a good portion of the pandemic, the Ministry of Foreign Affairs of Japan maintained a strict policy for border control, which while hard to quantify, may certainly have contributed to its success.
Besides these factors, once vaccines became available, Japan got the population with the primary series to 83% rapidly, even after getting a late start by many months compared with the United States, which has peaked at 68%. That’s a big gap.
But that gap got much worse when it came to boosters. Ninety-five percent of Japanese eligible compared with 40.8% of Americans have had a booster shot. Of note, that 95% in Japan pertains to the whole population. In the United States the percentage of people age 65 and older who have had two boosters is currently only 42%. I’ve previously reviewed the important lifesaving impact of two boosters among people age 65 and older from five independent studies during Omicron waves throughout the world.
Now let’s turn to cumulative fatalities in the two countries. There’s a huge, nearly ninefold difference, per capita. Using today’s Covid-19 Dashboard, there are cumulatively 45,533 deaths in Japan and 1,062,560 American deaths. That translates to 1 in 2,758 people in Japan compared with 1 in 315 Americans dying of COVID.
And if we look at excess mortality instead of confirmed COVID deaths, that enormous gap doesn’t change.
Obviously it would be good to have data for other COVID outcomes, such as hospitalizations, ICUs, and Long COVID, but they are not accessible.
Comparing Japan, the country that has fared the best, with the United States, one of the worst pandemic outcome results, leaves us with a sense that Prof Ian MacKay’s “Swiss cheese model” is the best explanation. It’s not just one thing. Masks, consistent evidence-based communication (3Cs) with attention to ventilation and air quality, and the outstanding uptake of vaccines and boosters all contributed to Japan’s success.
There is another factor to add to that model – Paxlovid. Its benefit of reducing hospitalizations and deaths for people over age 65 is unquestionable.
That’s why I had previously modified the Swiss cheese model to add Paxlovid.
But in the United States, where 15% of the population is 65 and older, they account for over 75% of the daily death toll, still in the range of 400 per day. Here, with a very high proportion of people age 65 and older left vulnerable without boosters, or primary vaccines, Paxlovid is only being given to less than 25% of the eligible (age 50+), and less people age 80 and older are getting Paxlovid than those age 45. The reasons that doctors are not prescribing it – worried about interactions for a 5-day course and rebound – are not substantiated.
Bottom line: In the United States we are not protecting our population anywhere near as well as Japan, as grossly evident by the fatalities among people at the highest risk. There needs to be far better uptake of boosters and use of Paxlovid in the age 65+ group, but the need for amped up protection is not at all restricted to this age subgroup. Across all age groups age 18 and over there is an 81% reduction of hospitalizations with two boosters with the most updated CDC data available, through the Omicron BA.5 wave.
No less the previous data through May 2022 showing protection from death across all ages with two boosters
And please don’t forget that around the world, over 20 million lives were saved, just in 2021, the first year of vaccines.
We can learn so much from a model country like Japan. Yes, we need nasal and variant-proof vaccines to effectively deal with the new variants that are already getting legs in places like XBB in Singapore and ones not on the radar yet. But right now we’ve got to do far better for people getting boosters and, when a person age 65 or older gets COVID, Paxlovid. Take a look at the Chris Hayes video segment when he pleaded for Americans to get a booster shot. Every day that vaccine waning of the U.S. population exceeds the small percentage of people who get a booster, our vulnerability increases. If we don’t get that on track, it’s likely going to be a rough winter ahead.
Dr. Topol is director of the Scripps Translational Science Institute in La Jolla, Calif. He has received research grants from the National Institutes of Health and reported conflicts of interest involving Dexcom, Illumina, Molecular Stethoscope, Quest Diagnostics, and Blue Cross Blue Shield Association. A version of this article appeared on Medscape.com.
This article was originally published Oct. 8 on Medscape Editor-In-Chief Eric Topol’s “Ground Truths” column on Substack.
Over time it has the least cumulative deaths per capita of any major country in the world. That’s without a zero-Covid policy or any national lockdowns, which is why I have not included China as a comparator.
Before we get into that data, let’s take a look at the age pyramids for Japan and the United States. The No. 1 risk factor for death from COVID-19 is advanced age, and you can see that in Japan about 25% of the population is age 65 and older, whereas in the United States that proportion is substantially reduced at 15%. Sure there are differences in comorbidities such as obesity and diabetes, but there is also the trade-off of a much higher population density in Japan.
Besides masks, which were distributed early on by the government to the population in Japan, there was the “Avoid the 3Cs” cluster-busting strategy, widely disseminated in the spring of 2020, leveraging Pareto’s 80-20 principle, long before there were any vaccines available. For a good portion of the pandemic, the Ministry of Foreign Affairs of Japan maintained a strict policy for border control, which while hard to quantify, may certainly have contributed to its success.
Besides these factors, once vaccines became available, Japan got the population with the primary series to 83% rapidly, even after getting a late start by many months compared with the United States, which has peaked at 68%. That’s a big gap.
But that gap got much worse when it came to boosters. Ninety-five percent of Japanese eligible compared with 40.8% of Americans have had a booster shot. Of note, that 95% in Japan pertains to the whole population. In the United States the percentage of people age 65 and older who have had two boosters is currently only 42%. I’ve previously reviewed the important lifesaving impact of two boosters among people age 65 and older from five independent studies during Omicron waves throughout the world.
Now let’s turn to cumulative fatalities in the two countries. There’s a huge, nearly ninefold difference, per capita. Using today’s Covid-19 Dashboard, there are cumulatively 45,533 deaths in Japan and 1,062,560 American deaths. That translates to 1 in 2,758 people in Japan compared with 1 in 315 Americans dying of COVID.
And if we look at excess mortality instead of confirmed COVID deaths, that enormous gap doesn’t change.
Obviously it would be good to have data for other COVID outcomes, such as hospitalizations, ICUs, and Long COVID, but they are not accessible.
Comparing Japan, the country that has fared the best, with the United States, one of the worst pandemic outcome results, leaves us with a sense that Prof Ian MacKay’s “Swiss cheese model” is the best explanation. It’s not just one thing. Masks, consistent evidence-based communication (3Cs) with attention to ventilation and air quality, and the outstanding uptake of vaccines and boosters all contributed to Japan’s success.
There is another factor to add to that model – Paxlovid. Its benefit of reducing hospitalizations and deaths for people over age 65 is unquestionable.
That’s why I had previously modified the Swiss cheese model to add Paxlovid.
But in the United States, where 15% of the population is 65 and older, they account for over 75% of the daily death toll, still in the range of 400 per day. Here, with a very high proportion of people age 65 and older left vulnerable without boosters, or primary vaccines, Paxlovid is only being given to less than 25% of the eligible (age 50+), and less people age 80 and older are getting Paxlovid than those age 45. The reasons that doctors are not prescribing it – worried about interactions for a 5-day course and rebound – are not substantiated.
Bottom line: In the United States we are not protecting our population anywhere near as well as Japan, as grossly evident by the fatalities among people at the highest risk. There needs to be far better uptake of boosters and use of Paxlovid in the age 65+ group, but the need for amped up protection is not at all restricted to this age subgroup. Across all age groups age 18 and over there is an 81% reduction of hospitalizations with two boosters with the most updated CDC data available, through the Omicron BA.5 wave.
No less the previous data through May 2022 showing protection from death across all ages with two boosters
And please don’t forget that around the world, over 20 million lives were saved, just in 2021, the first year of vaccines.
We can learn so much from a model country like Japan. Yes, we need nasal and variant-proof vaccines to effectively deal with the new variants that are already getting legs in places like XBB in Singapore and ones not on the radar yet. But right now we’ve got to do far better for people getting boosters and, when a person age 65 or older gets COVID, Paxlovid. Take a look at the Chris Hayes video segment when he pleaded for Americans to get a booster shot. Every day that vaccine waning of the U.S. population exceeds the small percentage of people who get a booster, our vulnerability increases. If we don’t get that on track, it’s likely going to be a rough winter ahead.
Dr. Topol is director of the Scripps Translational Science Institute in La Jolla, Calif. He has received research grants from the National Institutes of Health and reported conflicts of interest involving Dexcom, Illumina, Molecular Stethoscope, Quest Diagnostics, and Blue Cross Blue Shield Association. A version of this article appeared on Medscape.com.
This article was originally published Oct. 8 on Medscape Editor-In-Chief Eric Topol’s “Ground Truths” column on Substack.
Over time it has the least cumulative deaths per capita of any major country in the world. That’s without a zero-Covid policy or any national lockdowns, which is why I have not included China as a comparator.
Before we get into that data, let’s take a look at the age pyramids for Japan and the United States. The No. 1 risk factor for death from COVID-19 is advanced age, and you can see that in Japan about 25% of the population is age 65 and older, whereas in the United States that proportion is substantially reduced at 15%. Sure there are differences in comorbidities such as obesity and diabetes, but there is also the trade-off of a much higher population density in Japan.
Besides masks, which were distributed early on by the government to the population in Japan, there was the “Avoid the 3Cs” cluster-busting strategy, widely disseminated in the spring of 2020, leveraging Pareto’s 80-20 principle, long before there were any vaccines available. For a good portion of the pandemic, the Ministry of Foreign Affairs of Japan maintained a strict policy for border control, which while hard to quantify, may certainly have contributed to its success.
Besides these factors, once vaccines became available, Japan got the population with the primary series to 83% rapidly, even after getting a late start by many months compared with the United States, which has peaked at 68%. That’s a big gap.
But that gap got much worse when it came to boosters. Ninety-five percent of Japanese eligible compared with 40.8% of Americans have had a booster shot. Of note, that 95% in Japan pertains to the whole population. In the United States the percentage of people age 65 and older who have had two boosters is currently only 42%. I’ve previously reviewed the important lifesaving impact of two boosters among people age 65 and older from five independent studies during Omicron waves throughout the world.
Now let’s turn to cumulative fatalities in the two countries. There’s a huge, nearly ninefold difference, per capita. Using today’s Covid-19 Dashboard, there are cumulatively 45,533 deaths in Japan and 1,062,560 American deaths. That translates to 1 in 2,758 people in Japan compared with 1 in 315 Americans dying of COVID.
And if we look at excess mortality instead of confirmed COVID deaths, that enormous gap doesn’t change.
Obviously it would be good to have data for other COVID outcomes, such as hospitalizations, ICUs, and Long COVID, but they are not accessible.
Comparing Japan, the country that has fared the best, with the United States, one of the worst pandemic outcome results, leaves us with a sense that Prof Ian MacKay’s “Swiss cheese model” is the best explanation. It’s not just one thing. Masks, consistent evidence-based communication (3Cs) with attention to ventilation and air quality, and the outstanding uptake of vaccines and boosters all contributed to Japan’s success.
There is another factor to add to that model – Paxlovid. Its benefit of reducing hospitalizations and deaths for people over age 65 is unquestionable.
That’s why I had previously modified the Swiss cheese model to add Paxlovid.
But in the United States, where 15% of the population is 65 and older, they account for over 75% of the daily death toll, still in the range of 400 per day. Here, with a very high proportion of people age 65 and older left vulnerable without boosters, or primary vaccines, Paxlovid is only being given to less than 25% of the eligible (age 50+), and less people age 80 and older are getting Paxlovid than those age 45. The reasons that doctors are not prescribing it – worried about interactions for a 5-day course and rebound – are not substantiated.
Bottom line: In the United States we are not protecting our population anywhere near as well as Japan, as grossly evident by the fatalities among people at the highest risk. There needs to be far better uptake of boosters and use of Paxlovid in the age 65+ group, but the need for amped up protection is not at all restricted to this age subgroup. Across all age groups age 18 and over there is an 81% reduction of hospitalizations with two boosters with the most updated CDC data available, through the Omicron BA.5 wave.
No less the previous data through May 2022 showing protection from death across all ages with two boosters
And please don’t forget that around the world, over 20 million lives were saved, just in 2021, the first year of vaccines.
We can learn so much from a model country like Japan. Yes, we need nasal and variant-proof vaccines to effectively deal with the new variants that are already getting legs in places like XBB in Singapore and ones not on the radar yet. But right now we’ve got to do far better for people getting boosters and, when a person age 65 or older gets COVID, Paxlovid. Take a look at the Chris Hayes video segment when he pleaded for Americans to get a booster shot. Every day that vaccine waning of the U.S. population exceeds the small percentage of people who get a booster, our vulnerability increases. If we don’t get that on track, it’s likely going to be a rough winter ahead.
Dr. Topol is director of the Scripps Translational Science Institute in La Jolla, Calif. He has received research grants from the National Institutes of Health and reported conflicts of interest involving Dexcom, Illumina, Molecular Stethoscope, Quest Diagnostics, and Blue Cross Blue Shield Association. A version of this article appeared on Medscape.com.
Keep menstrual cramps away the dietary prevention way
Foods for thought: Menstrual cramp prevention
For those who menstruate, it’s typical for that time of the month to bring cravings for things that may give a serotonin boost that eases the rise in stress hormones. Chocolate and other foods high in sugar fall into that category, but they could actually be adding to the problem.

About 90% of adolescent girls have menstrual pain, and it’s the leading cause of school absences for the demographic. Muscle relaxers and PMS pills are usually the recommended solution to alleviating menstrual cramps, but what if the patient doesn’t want to take any medicine?
Serah Sannoh of Rutgers University wanted to find another way to relieve her menstrual pains. The literature review she presented at the annual meeting of the North American Menopause Society found multiple studies that examined dietary patterns that resulted in menstrual pain.
In Ms. Sannoh’s analysis, she looked at how certain foods have an effect on cramps. Do they contribute to the pain or reduce it? Diets high in processed foods, oils, sugars, salt, and omega-6 fatty acids promote inflammation in the muscles around the uterus. Thus, cramps.
The answer, sometimes, is not to add a medicine but to change our daily practices, she suggested. Foods high in omega-3 fatty acids helped reduce pain, and those who practiced a vegan diet had the lowest muscle inflammation rates. So more salmon and fewer Swedish Fish.
Stage 1 of the robot apocalypse is already upon us
The mere mention of a robot apocalypse is enough to conjure images of terrifying robot soldiers with Austrian accents harvesting and killing humanity while the survivors live blissfully in a simulation and do low-gravity kung fu with high-profile Hollywood actors. They’ll even take over the navy.

Reality is often less exciting than the movies, but rest assured, the robots will not be denied their dominion of Earth. Our future robot overlords are simply taking a more subtle, less dramatic route toward their ultimate subjugation of mankind: They’re making us all sad and burned out.
The research pulls from work conducted in multiple countries to paint a picture of a humanity filled with anxiety about jobs as robotic automation grows more common. In India, a survey of automobile manufacturing works showed that working alongside industrial robots was linked with greater reports of burnout and workplace incivility. In Singapore, a group of college students randomly assigned to read one of three articles – one about the use of robots in business, a generic article about robots, or an article unrelated to robots – were then surveyed about their job security concerns. Three guesses as to which group was most worried.
In addition, the researchers analyzed 185 U.S. metropolitan areas for robot prevalence alongside use of job-recruiting websites and found that the more robots a city used, the more common job searches were. Unemployment rates weren’t affected, suggesting people had job insecurity because of robots. Sure, there could be other, nonrobotic reasons for this, but that’s no fun. We’re here because we fear our future android rulers.
It’s not all doom and gloom, fortunately. In an online experiment, the study authors found that self-affirmation exercises, such as writing down characteristics or values important to us, can overcome the existential fears and lessen concern about robots in the workplace. One of the authors noted that, while some fear is justified, “media reports on new technologies like robots and algorithms tend to be apocalyptic in nature, so people may develop an irrational fear about them.”
Oops. Our bad.
Apocalypse, stage 2: Leaping oral superorganisms
The terms of our secret agreement with the shadowy-but-powerful dental-industrial complex stipulate that LOTME can only cover tooth-related news once a year. This is that once a year.
Since we’ve already dealt with a robot apocalypse, how about a sci-fi horror story? A story with a “cross-kingdom partnership” in which assemblages of bacteria and fungi perform feats greater than either could achieve on its own. A story in which new microscopy technologies allow “scientists to visualize the behavior of living microbes in real time,” according to a statement from the University of Pennsylvania, Philadelphia.
While looking at saliva samples from toddlers with severe tooth decay, lead author Zhi Ren and associates “noticed the bacteria and fungi forming these assemblages and developing motions we never thought they would possess: a ‘walking-like’ and ‘leaping-like’ mobility. … It’s almost like a new organism – a superorganism – with new functions,” said senior author Hyun Koo, DDS, PhD, of Penn Dental Medicine.
Did he say “mobility”? He did, didn’t he?
To study these alleged superorganisms, they set up a laboratory system “using the bacteria, fungi, and a tooth-like material, all incubated in human saliva,” the university explained.
“Incubated in human saliva.” There’s a phrase you don’t see every day.
It only took a few hours for the investigators to observe the bacterial/fungal assemblages making leaps of more than 100 microns across the tooth-like material. “That is more than 200 times their own body length,” Dr. Ren said, “making them even better than most vertebrates, relative to body size. For example, tree frogs and grasshoppers can leap forward about 50 times and 20 times their own body length, respectively.”
So, will it be the robots or the evil superorganisms? Let us give you a word of advice: Always bet on bacteria.
Foods for thought: Menstrual cramp prevention
For those who menstruate, it’s typical for that time of the month to bring cravings for things that may give a serotonin boost that eases the rise in stress hormones. Chocolate and other foods high in sugar fall into that category, but they could actually be adding to the problem.
About 90% of adolescent girls have menstrual pain, and it’s the leading cause of school absences for the demographic. Muscle relaxers and PMS pills are usually the recommended solution to alleviating menstrual cramps, but what if the patient doesn’t want to take any medicine?
Serah Sannoh of Rutgers University wanted to find another way to relieve her menstrual pains. The literature review she presented at the annual meeting of the North American Menopause Society found multiple studies that examined dietary patterns that resulted in menstrual pain.
In Ms. Sannoh’s analysis, she looked at how certain foods have an effect on cramps. Do they contribute to the pain or reduce it? Diets high in processed foods, oils, sugars, salt, and omega-6 fatty acids promote inflammation in the muscles around the uterus. Thus, cramps.
The answer, sometimes, is not to add a medicine but to change our daily practices, she suggested. Foods high in omega-3 fatty acids helped reduce pain, and those who practiced a vegan diet had the lowest muscle inflammation rates. So more salmon and fewer Swedish Fish.
Stage 1 of the robot apocalypse is already upon us
The mere mention of a robot apocalypse is enough to conjure images of terrifying robot soldiers with Austrian accents harvesting and killing humanity while the survivors live blissfully in a simulation and do low-gravity kung fu with high-profile Hollywood actors. They’ll even take over the navy.
Reality is often less exciting than the movies, but rest assured, the robots will not be denied their dominion of Earth. Our future robot overlords are simply taking a more subtle, less dramatic route toward their ultimate subjugation of mankind: They’re making us all sad and burned out.
The research pulls from work conducted in multiple countries to paint a picture of a humanity filled with anxiety about jobs as robotic automation grows more common. In India, a survey of automobile manufacturing works showed that working alongside industrial robots was linked with greater reports of burnout and workplace incivility. In Singapore, a group of college students randomly assigned to read one of three articles – one about the use of robots in business, a generic article about robots, or an article unrelated to robots – were then surveyed about their job security concerns. Three guesses as to which group was most worried.
In addition, the researchers analyzed 185 U.S. metropolitan areas for robot prevalence alongside use of job-recruiting websites and found that the more robots a city used, the more common job searches were. Unemployment rates weren’t affected, suggesting people had job insecurity because of robots. Sure, there could be other, nonrobotic reasons for this, but that’s no fun. We’re here because we fear our future android rulers.
It’s not all doom and gloom, fortunately. In an online experiment, the study authors found that self-affirmation exercises, such as writing down characteristics or values important to us, can overcome the existential fears and lessen concern about robots in the workplace. One of the authors noted that, while some fear is justified, “media reports on new technologies like robots and algorithms tend to be apocalyptic in nature, so people may develop an irrational fear about them.”
Oops. Our bad.
Apocalypse, stage 2: Leaping oral superorganisms
The terms of our secret agreement with the shadowy-but-powerful dental-industrial complex stipulate that LOTME can only cover tooth-related news once a year. This is that once a year.
Since we’ve already dealt with a robot apocalypse, how about a sci-fi horror story? A story with a “cross-kingdom partnership” in which assemblages of bacteria and fungi perform feats greater than either could achieve on its own. A story in which new microscopy technologies allow “scientists to visualize the behavior of living microbes in real time,” according to a statement from the University of Pennsylvania, Philadelphia.
While looking at saliva samples from toddlers with severe tooth decay, lead author Zhi Ren and associates “noticed the bacteria and fungi forming these assemblages and developing motions we never thought they would possess: a ‘walking-like’ and ‘leaping-like’ mobility. … It’s almost like a new organism – a superorganism – with new functions,” said senior author Hyun Koo, DDS, PhD, of Penn Dental Medicine.
Did he say “mobility”? He did, didn’t he?
To study these alleged superorganisms, they set up a laboratory system “using the bacteria, fungi, and a tooth-like material, all incubated in human saliva,” the university explained.
“Incubated in human saliva.” There’s a phrase you don’t see every day.
It only took a few hours for the investigators to observe the bacterial/fungal assemblages making leaps of more than 100 microns across the tooth-like material. “That is more than 200 times their own body length,” Dr. Ren said, “making them even better than most vertebrates, relative to body size. For example, tree frogs and grasshoppers can leap forward about 50 times and 20 times their own body length, respectively.”
So, will it be the robots or the evil superorganisms? Let us give you a word of advice: Always bet on bacteria.
Foods for thought: Menstrual cramp prevention
For those who menstruate, it’s typical for that time of the month to bring cravings for things that may give a serotonin boost that eases the rise in stress hormones. Chocolate and other foods high in sugar fall into that category, but they could actually be adding to the problem.
About 90% of adolescent girls have menstrual pain, and it’s the leading cause of school absences for the demographic. Muscle relaxers and PMS pills are usually the recommended solution to alleviating menstrual cramps, but what if the patient doesn’t want to take any medicine?
Serah Sannoh of Rutgers University wanted to find another way to relieve her menstrual pains. The literature review she presented at the annual meeting of the North American Menopause Society found multiple studies that examined dietary patterns that resulted in menstrual pain.
In Ms. Sannoh’s analysis, she looked at how certain foods have an effect on cramps. Do they contribute to the pain or reduce it? Diets high in processed foods, oils, sugars, salt, and omega-6 fatty acids promote inflammation in the muscles around the uterus. Thus, cramps.
The answer, sometimes, is not to add a medicine but to change our daily practices, she suggested. Foods high in omega-3 fatty acids helped reduce pain, and those who practiced a vegan diet had the lowest muscle inflammation rates. So more salmon and fewer Swedish Fish.
Stage 1 of the robot apocalypse is already upon us
The mere mention of a robot apocalypse is enough to conjure images of terrifying robot soldiers with Austrian accents harvesting and killing humanity while the survivors live blissfully in a simulation and do low-gravity kung fu with high-profile Hollywood actors. They’ll even take over the navy.
Reality is often less exciting than the movies, but rest assured, the robots will not be denied their dominion of Earth. Our future robot overlords are simply taking a more subtle, less dramatic route toward their ultimate subjugation of mankind: They’re making us all sad and burned out.
The research pulls from work conducted in multiple countries to paint a picture of a humanity filled with anxiety about jobs as robotic automation grows more common. In India, a survey of automobile manufacturing works showed that working alongside industrial robots was linked with greater reports of burnout and workplace incivility. In Singapore, a group of college students randomly assigned to read one of three articles – one about the use of robots in business, a generic article about robots, or an article unrelated to robots – were then surveyed about their job security concerns. Three guesses as to which group was most worried.
In addition, the researchers analyzed 185 U.S. metropolitan areas for robot prevalence alongside use of job-recruiting websites and found that the more robots a city used, the more common job searches were. Unemployment rates weren’t affected, suggesting people had job insecurity because of robots. Sure, there could be other, nonrobotic reasons for this, but that’s no fun. We’re here because we fear our future android rulers.
It’s not all doom and gloom, fortunately. In an online experiment, the study authors found that self-affirmation exercises, such as writing down characteristics or values important to us, can overcome the existential fears and lessen concern about robots in the workplace. One of the authors noted that, while some fear is justified, “media reports on new technologies like robots and algorithms tend to be apocalyptic in nature, so people may develop an irrational fear about them.”
Oops. Our bad.
Apocalypse, stage 2: Leaping oral superorganisms
The terms of our secret agreement with the shadowy-but-powerful dental-industrial complex stipulate that LOTME can only cover tooth-related news once a year. This is that once a year.
Since we’ve already dealt with a robot apocalypse, how about a sci-fi horror story? A story with a “cross-kingdom partnership” in which assemblages of bacteria and fungi perform feats greater than either could achieve on its own. A story in which new microscopy technologies allow “scientists to visualize the behavior of living microbes in real time,” according to a statement from the University of Pennsylvania, Philadelphia.
While looking at saliva samples from toddlers with severe tooth decay, lead author Zhi Ren and associates “noticed the bacteria and fungi forming these assemblages and developing motions we never thought they would possess: a ‘walking-like’ and ‘leaping-like’ mobility. … It’s almost like a new organism – a superorganism – with new functions,” said senior author Hyun Koo, DDS, PhD, of Penn Dental Medicine.
Did he say “mobility”? He did, didn’t he?
To study these alleged superorganisms, they set up a laboratory system “using the bacteria, fungi, and a tooth-like material, all incubated in human saliva,” the university explained.
“Incubated in human saliva.” There’s a phrase you don’t see every day.
It only took a few hours for the investigators to observe the bacterial/fungal assemblages making leaps of more than 100 microns across the tooth-like material. “That is more than 200 times their own body length,” Dr. Ren said, “making them even better than most vertebrates, relative to body size. For example, tree frogs and grasshoppers can leap forward about 50 times and 20 times their own body length, respectively.”
So, will it be the robots or the evil superorganisms? Let us give you a word of advice: Always bet on bacteria.

Randomized, Double-Blind Placebo-Controlled Trial to Assess the Effect of Probiotics on Irritable Bowel Syndrome in Veterans With Gulf War Illness
About 700,000 US military personnel were deployed in Operation Desert Storm (August 1990 to March 1991).1 Almost 30 years since the war, a large number of these veterans continue to experience a complex of symptoms of unknown etiology called Gulf War illness (GWI), which significantly affects health and quality of life (QOL). The lack of clear etiology of the illness has impaired research to find specific treatments and has further exacerbated the stress among veterans. GWI typically includes a mixture of chronic headache, cognitive difficulties, widespread pain, unexplained fatigue, memory and concentration problems, as well as chronic respiratory and gastrointestinal (GI) symptoms.2 Abdominal pain and alteration of bowel habits are also symptoms typical of irritable bowel syndrome (IBS). It has been estimated that IBS occurs in up to 30% of Gulf War veterans.3
The etiology of IBS is unknown. Possible mechanisms include visceral hypersensitivity, altered gut motor function, aberrant brain-gut interaction, and psychological factors, perhaps with a genetic predisposition.4 Gastroenteritis has been reported as a triggering mechanism in up to one-third of patients with IBS.5 Gastroenteritis can alter the gut microbiota and has been reported to be a significant risk factor for the development of IBS.6 In one study of Operation Desert Shield soldiers, > 50% of military personnel developed acute gastroenteritis while on duty.7 A high prevalence of extra-intestinal symptoms also has been reported, including fatigue, headache, joint pains, and anxiety, in Gulf War veterans with IBS. These extra-intestinal symptoms of IBS are consistent with the reported GWI symptoms. Change in gut microbiota also has been associated with many of the extra-intestinal symptoms of IBS, especially fatigue.8,9 Gut microbiota are known to change with travel, stress, and a change in diet, all potential factors that are relevant to Gulf War veterans. This would suggest that an imbalance in the gut microbiota, ie, dysbiosis, may play a role in the pathogenesis of both IBS and GWI. Dysbiosis could be a risk factor for or alternatively a consequence of GWI.
A systematic review highlighted the heterogeneity of the gut microbiota in patients with IBS.10 Overall, Enterobacteriaceae, Lactobacillaceae, and Bacteroides were increased, whereas Clostridiales, Faecalibacterium, and Bifidobacterium were decreased in patients with IBS compared with controls. Gut microbiota also has been associated with cognitive changes, anxiety, and depression—symptoms associated with IBS and are part of the GWI.
If altered gut microbiota contributes to the etiopathogenesis of IBS, its restoration of with probiotics should help. Probiotics are live organisms that when ingested may improve health by promoting the growth of naturally occurring flora and establishing a healthy gut flora. Probiotics have several mechanisms of actions. Probiotics work in the lumen of the gut by producing antibacterial molecules and enhancing the mucosal barrier.11 Probiotics also may produce metabolic compounds that alter the intestinal microbiota and improve intestinal barrier function.12 Probiotics also have been shown to activate receptors in the enteric nervous system with the potential to promote pain relief in the setting of visceral hyperalgesia.13,14 The anti-inflammatory properties of probiotics potentially could modulate the basic pathophysiology of IBS and improve motility, visceral hypersensitivity, and brain-gut interaction.15 Furthermore, significant gut dysbiosis has been shown with GWI; suggesting that probiotics may have a role in its management.16,17
Probiotics have not been studied in Gulf War veterans with IBS. We performed a prospective, double-blind placebo-controlled study to determine the efficacy of a commercially available probiotic containing 8 strains of bacteria (De Simone Formulation; formally known as VSL#3 and Visbiome) on symptoms of IBS and GWI. This probiotic was selected as the overall literature suggested benefit of combination probiotics in IBS, and VSL#3 has been shown to be efficacious in ulcerative colitis and microscopic colitis.18-20
Methods
Veterans who served in Operation Desert Storm (August 1990 to March 1991) and enrolled at the George E. Wahlen Veterans Affairs (VA) Medical Center (GEWVAMC), Salt Lake City, Utah, were eligible for the study. The inclusion criteria were: veterans aged ≥ 35 years; ≥ 2 nonintestinal GWI symptoms (eg, fatigue, joint pains, insomnia, general stiffness, and headache); IBS diagnosis based on the Rome III criteria; IBS symptoms > 6 months; normal gross appearance of the colonic mucosa; negative markers for celiac disease and inflammatory bowel disease (IBD); normal thyroid function; and serum calcium levels.21 Those who had a clinically significant cardiac, pulmonary, hepatic or renal dysfunction; history of/or presence of systemic malignancy; current evidence of celiac disease or IBD; unstable/significant psychiatric disease; recent change in GI medications; current pregnancy; or use of antibiotics or probiotics within the past 1 month were excluded. Subjects were enrolled from a list of veterans with GWI from the GEWVAMC Gulf War registry; referrals to gastroenterology clinics for IBS from internal medicine clinics; and posted advertisements.
Protocol
After written informed consent was obtained, each veteran was verified to have IBS and ≥ 2 GWI symptoms. All veterans had the following tests and panels: complete blood count, erythrocyte sedimentation rate, serum comprehensive metabolic panel, thyroid-stimulating hormone, tissue transglutaminase, stool test for ova and parasite, giardia antigen, and clostridia toxins to exclude organic cause of GI symptoms. Colonoscopy was performed in all veterans to exclude IBD, and to rule out microscopic or lymphocytic colitis.
Randomization was computer generated and maintained by the study pharmacist so that study personnel and patients were blinded to the trial groups. All investigators were blinded and allocation was concealed. The medication was supplied in a numbered container by the pharmacist after patient enrollment. After a 2-week run-in period, veterans were randomized (1:1) to receive either 1 sachet of probiotic (De Simone Formulation; formally known as VSL#3 and Visbiome) or placebo once daily for 8 weeks.
Each probiotic packet contains 900 billion probiotic bacteria per sachet.11 This formulation contained 8 viable strains of bacteria: 4 strains of Lactobacillus (L acidophilus, L plantarum, L paracasei, L delbrueckii subsp. bulgaricus); 3 strains of Bifidobacteria (Bifidobacterium breve, B lactis, B infantis); and 1 strain of Streptococcus thermophilus. This formulation had been commercialized and studied as VSL#3 and is currently available in the United States under the Visbiome trade name. While branding changed during the study, the formulation did not. The investigational medicine (VSL#3, Visbiome, and placebo) were shipped from the manufacturer Dupont/Danisco in Madison, Wisconsin. The subjects received placebo or probiotic (VSL#3/Visbiome) and both were identical in appearance. The medication was supplied in a numbered container by the pharmacist after patient enrollment.
Measures
Veterans completed the bowel disease questionnaire to record baseline bowel habits.22 All veterans recorded daily bowel symptoms to confirm the presence of IBS during the 2-week pretreatment period, at baseline, and at the end of the 8-week treatment. The symptoms assessed included severity of abdominal pain (0, none to 100, severe); severity of bloating (0, none to 100, severe); stool frequency; Bristol stool scale (1, very hard to 7, watery); severity of diarrhea (0, none to 100, severe); severity of constipation (0, none to 100, severe); satisfaction with bowel habits (0, none to 100, severe); and IBS affecting or interfering with life (0, none to 100, severe). The bowel symptom score is the sum of the 5 symptom scores.23,24
IBS-specific QOL (IBS-QOL) was recorded at baseline and at the end of treatment.25 The IBS-QOL consists of a 34-item validated disease-specific questionnaire that measures 8 domains relevant to subjects with IBS: dysphoria, interference with activity, body image, health worry, food avoidance, social reaction, sexual life, and relationships. We used the Somatic Symptom Checklist to detect the following extra-intestinal symptoms that are common among veterans with GWI: headache, backache, wheeziness, insomnia, bad breath, fatigue, general stiffness, dizziness, weakness, sensitivity to hot and cold, palpitation, and tightness in chest. Subjects rated symptoms on a scale of 1 to 5: how often (1, none; 2, monthly; 3, once weekly; 4, several times weekly; 5, daily), and how bothersome (1, not at all to 5, extremely).26
Subjects completed the Posttraumatic Stress Disorder (PTSD) Checklist–Military, which is specific to military experience with 17 items on a 1 to 5 scale (1, not at all to 5, extremely). Scores were summed to produce a total symptom severity score (range, 17-85).27 Subjects also completed the Brief Symptom Inventory 18 (BSI-18) during the baseline evaluation.28 BSI-18 measures subjects’ reported overall psychological distress. It assesses 3 symptoms dimensions (somatization, depression, and anxiety) and a global severity index. The raw scores were transferred to normative T scores based on samples of nonpatient normal men and women.

Symptom data were compared after 8 weeks of treatment. The primary study endpoint was change in bowel symptom score. The secondary endpoints were mean change in symptoms, QOL, extra-intestinal symptoms, and PTSD score. The study was approved by the Salt Lake City Veterans Affairs Medical Center and the University of Utah Institutional Review Board and registered in ClinicalTrials.gov (NCT03078530).
Statistical Methods
Comparisons of the probiotic vs placebo groups for demographic variable were analyzed using a 2-sample t test for continuous variables, and with a χ2 test or Fisher exact test for categorical variables. The primary and secondary outcome variables were recorded daily for 2 weeks as pretreatment baseline and for 2 weeks at the end of treatment. These symptoms were recorded as ordered categorical variables, which were then averaged across the week to produce a continuous measurement for statistical analysis. For the primary outcome of GI symptoms, posttreatment comparisons were made between the study groups using a 2-sample t test of the baseline vs posttreatment values. All P values were calculated for 2-sided comparisons. The planned sample size in our study protocol was to recruit 40 individuals per group in order to achieve 80% power to detect a 30% improvement between baseline and end of treatment in the primary bowel symptom score. This study recruited 53 subjects. With this sample size, the study had 80% power to detect a 0.8 SD in any of the outcomes.
Results
We screened 101 veterans with IBS and GWI; 39 veterans did not fulfill the inclusion/exclusion criteria, 22 declined to participate or did not complete the screening questionnaires and tests, and 9 were lost to follow-up. Sixty-two participants were randomized in a double-blind placebo-controlled study design; 9 dropped out before the end of the study. Data were analyzed from 53 veterans who completed the study, 29 in the placebo group and 24 in the probiotic group (Figure 1). The cohort was primarily male with a mean (SD) age of 55 (8) years (range, 42-73) (Table 1).
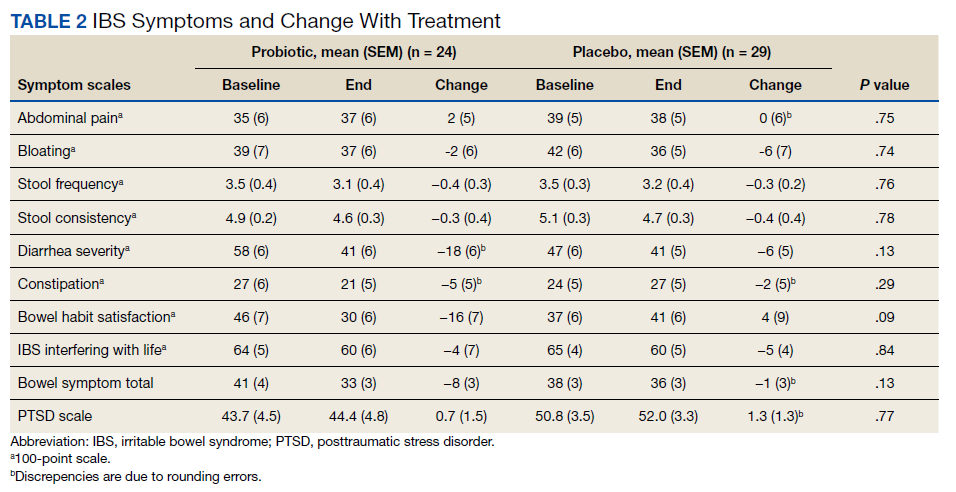
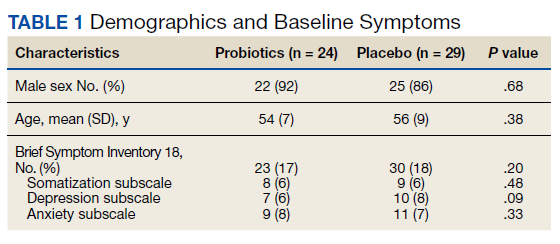
Overall, the treatment was well tolerated. All subjects were contacted every 2 weeks during the study to check for adverse effects, but no serious events were reported. There were no differences at baseline in any of the BSI-18 subscale scores in veterans between the groups. There was a greater mean (SEM) improvement of diarrhea severity in the probiotic group compared with the placebo group: 18 (6), a 31% improvement, vs 6 (5), a 13% improvement, respectively; however, the difference was not statistically significance (P = .13) (Table 2). There also was a greater mean (SEM) improvement in satisfaction of bowel habits in the probiotic group compared with the placebo group: 16 (7), a 35% improvement vs 4 (9), an 8% worsening; this also was not statistically significant (P = .09). There was no difference in the change of IBS-QOL before and after treatment in either group (Figure 2). There was no improvement in any of the symptoms of GWI (all P ≥ .06) (Appendix).
Discussion
GWI is a complex multisystem illness of unknown etiology. There was high prevalence of diarrhea during deployment, and veterans were exposed to several physical, environmental, and mental stresses of the war.3 A change in gut microbiota can occur during deployment due to diet changes, environmental and physical stress, and GI infections.29 These changes would suggest that manipulation of gut microbiota might offer a new modality of treatment of IBS and GWI. We evaluated the effect of a high-potency multistrain probiotic in veterans with IBS and GWI. We did not detect any statistically significant differences between the probiotic and placebo groups on bowel symptom score and individual symptoms of IBS and on QOL. Also, there was no improvement for the other symptoms of GWI. To our knowledge, this is the first study evaluating the effect of probiotics in veterans with IBS and GWI. Our results are consistent with the literature on probiotics and IBS.

The probiotic formulation used in our study has been evaluated in patients with IBS previously. Kim and colleagues found that after 8 weeks of treatment of patients with diarrhea-predominant IBS with VSL#3, there was improvement in bloating, but no effect was found on abdominal pain, gas, or urgency.30 A subsequent study by the same investigators on patients with all types of IBS found that VSL#3 showed no effect on abdominal pain, stool frequency and consistency, or on bloating, but there was improvement in flatulence.31 Another study that evaluated the effect of VSL#3 on symptoms of diarrhea-predominant IBS and QOL found improvement in IBS symptoms from baseline in both the probiotic and the placebo groups, but the difference between the 2 groups was not statistically significant.32 Similarly, Wong and colleagues performed a double-blind, placebo-controlled mechanistic study to evaluate the effect of VSL#3. They found improvement in bowel symptom score, abdominal pain intensity, and satisfaction with bowel habits with both the VSL#3 and placebo group but similar to our study, the differences were not statistically significant.
Several reviews have evaluated the efficacy of probiotics for IBS. A 2010 review found evidence that probiotics trended toward improved IBS symptoms compared with placebo.33 The 2014 follow-up by the same authors demonstrated that overall, probiotics improved global symptoms of IBS and multistrain probiotics were more effective.20 A third meta-analysis from the same group found evidence that multistrain probiotics seemed to have a beneficial effect but could not definitively conclude that probiotics are efficacious in improving IBS symptoms.34 Other authors also have seen inconsistent effects of probiotics compared with placebo on global symptoms, abdominal pain, and bloating after performing systematic reviews of the literature.35-38 Although several reviews support that multistrain probiotics are more effective, they fail to conclude which combinations are more efficacious.
The effect of probiotics on QOL has not been investigated by many studies.37 In our study, we did not find significant improvement in QOL in the probiotic group, which is in line with 2 previous studies that showed no effect on IBS QOL of VSL#3 vs placebo.32,39 Most of the research reports that multistrain probiotics are more effective than using a single strain.34,35,40Bifidobacterium and Lactobacillus are the most commonly used bacteria in the multistrain probiotics that have shown their positive effect on IBS.35,41 The probiotic used in our study contained other species along with these 2 microorganisms.
The dose and duration of treatment of probiotics also has been debated. In one meta-analysis, the investigators found that studies of ≥ 8 weeks were more likely to show a positive effect; 4 of the 7 studies with statistically significant improvement in IBS symptoms were longer than 8 weeks.35 However, another meta-analysis based on 35 randomized controlled trials found that there was not a statistically significant difference between groups treated for > 4 weeks vs < 4 weeks.42 In addition, another meta-analysis of VSL#3 on IBS in children and adults also found no difference in results based on the duration of treatment of probiotics.43 Similar to our study, 3 other studies of VSL#3 treated patients for 8 weeks and found no statistically significant effect.30-32 In the past, VSL#3 has been used at dosages of 450 or 900 billion bacteria per day.
An individual’s response to probiotics may depend on the subtype of IBS. However, most of the studies, like ours, included groups of all subtypes. It may be that probiotics are more effective in patients with moderate-to-severe symptoms. Most of our patients had milder symptoms, and we cannot discount how subjects with more severe disease may have responded to the drug. Interestingly, one study demonstrated that Lactobacillus was more effective in patients with moderately severe abdominal pain compared with mild symptoms.44
In our study, the probiotic did not improve PTSD symptoms or other extra-intestinal symptoms common in IBS and GWI. Similar to our study, Wong and colleagues did not find significant improvement of psychological and sleep scores after treatment with VSL#3.6 Similarly, there is evidence that alteration in gut microbiota is associated with health and diseases, but what specific alterations occur and whether they can be improved with probiotics remains unknown.45
Limitations
The inconsistent response to probiotics in various studies may be due to IBS heterogeneity. Furthermore, there are demographic differences between Gulf War veterans and patients enrolled in other studies: Gulf War veterans are predominantly male, many were deployed abroad and had a history of gastroenteritis during deployment, and were exposed to stressful situations.46 These factors may be involved in triggering or maintaining IBS in Gulf War veterans. A further limitation of our randomized trial is the relatively small sample size.
Conclusions
This study did not demonstrate statistically significant improvement in symptoms of IBS or improvement in QOL after treatment with a multistrain probiotic. We also did not find any improvement in symptoms of GWI or PTSD. There was no difference in psychological scores between the placebo and treatment groups, and it is unlikely that psychological factors confounded the response to treatment in this study.
The effectiveness of a probiotic may depend on the baseline gut microbiome of the individual and depend on the strain, amount, and frequency of bacteria used. A lack of response of the probiotics does not exclude gut viruses and fungi having a role in exacerbating GWI symptoms. It is also possible that the bacteria present or the dose of the probiotic used was not sufficient to improve symptoms. So far, the definitive benefit of probiotics has been demonstrated for only a few preparations, and none are approved by the US Food and Drug Administration for any disease. More research is needed to determine whether probiotics have any role in the treatment of IBS and GWI.
Acknowledgments
AKT received grant support from the US Department of Veterans Affairs and the US Department of Defense (W81XWH-10-1-0593, W81XWH-15-1-0636). We thank Keith G. Tolman, MD, for assistance in editing the initial proposal and for periodic consultation. We thank the manufacturer of the probiotic for supplying the active drug and the placebo. The manufacture of the probiotic had no role in the design and conduct of the study, analysis and interpretation of the data, and in the preparation of the manuscript.
1. O’Shea EF, Cotter PD, Stanton C, Ross RP, Hill C. Production of bioactive substances by intestinal bacteria as a basis for explaining probiotic mechanisms: bacteriocins and conjugated linoleic acid. Int J Food Microbiol. 2012;152(3):189-205. doi:10.1016/j.ijfoodmicro.2011.05.025.
2. Kamiya T, Wang L, Forsythe P, et al. Inhibitory effects of Lactobacillus reuteri on visceral pain induced by colorectal distension in Sprague-Dawley rats. Gut. 2006;55(2):191-196. doi:10.1136/gut.2005.070987.
3. Verdu EF, Bercik P, Verma-Gandhu M, et al. Specific probiotic therapy attenuates antibiotic induced visceral hypersensitivity in mice. Gut. 2006;55(2):182-190. doi:10.1136/gut.2005.066100
4. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044-1060. doi:10.1111/apt.15001.
5. Niu HL, Xiao JY. The efficacy and safety of probiotics in patients with irritable bowel syndrome: Evidence based on 35 randomized controlled trials. Int J Surg. 2020;75:116-127. doi:10.1016/j.ijsu.2020.01.142.
6. Wong RK, Yang C, Song GH, Wong J, Ho KY. Melatonin regulation as a possible mechanism for probiotic (VSL#3) in irritable bowel syndrome: a randomized double-blinded placebo study. Dig Dis Sci. 2015;60(1):186-194. doi:10.1007/s10620-014-3299-8.
7. Hyams KC, Bourgeois AL, Merrell BR, et al. Diarrheal disease during Operation Desert Shield. N Engl J Med. 1991;325(20):1423-1428. doi:10.1056/NEJM199111143252006 8. Clancy RL, Gleeson M, Cox A, et al. Reversal in fatigued athletes of a defect in interferon gamma secretion after administration of Lactobacillus acidophilus. Br J Sports Med. 2006;40(4):351-354. doi:10.1136/bjsm.2005.024364
9. Sullivan A, Nord CE, Evengard B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutr J. 2009;8:4. doi:10.1186/1475-2891-8-4
10. Pittayanon R, Lau JT, Yuan Y, et al. Gut microbiota in patients with irritable bowel syndrome—a systematic review. Gastroenterology. 2019;157(1):97-108. doi:10.1053/j.gastro.2019.03.049
11. Rao RK, Samak G. Protection and restitution of gut barrier by probiotics: nutritional and clinical implications. Curr Nutr Food Sci. 2013;9(2):99-107. doi:10.2174/1573401311309020004
12. O´Shea EF, Cotter PD, Stanton C, Ross RP, Hill C. Production of bioactive substances by intestinal bacteria as a basis for explaining probiotic mechanisms: bacteriocins and conjugated linoleic acid. Int J Food Microbiol. 2012;152(3):189-205. doi:10.1016/j.ijfoodmicro.2011.05.025
13. Kamiya T, Wang L, Forsythe P, et al. Inhibitory effects of Lactobacillus reuteri on visceral pain induced by colorectal distension in Sprague-Dawley rats. Gut. 2006;55(2):191-196. doi:10.1136/gut.2005.070987
14. Verdu EF, Bercik P, Verma-Gandhu M, et al. Specific probiotic therapy attenuates antibiotic induced visceral hypersensitivity in mice. Gut. 2006;55(2):182-190. doi:10.1136/gut.2005.06610015. O´Mahony L, McCarthy J, Kelly P, et al. Lactobacillus and bifidobacterium in irritable bowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterology. 2005;128(3):541-551. doi:10.1053/j.gastro.2004.11.050
16. Alhasson F, Das S, Seth R, et al. Altered gut microbiome in a mouse model of Gulf War Illness causes neuroinflammation and intestinal injury via leaky gut and TLR4 activation. PLoS One. 2017;12(3):e0172914. doi:10.1371/journal.pone.0172914.17. Janulewicz PA, Seth RK, Carlson JM, et al. The gut-microbiome in Gulf War veterans: a preliminary report. Int J Environ Res Public Health. 2019;16(19). doi:10.3390/ijerph16193751
18. Dang X, Xu M, Liu D, Zhou D, Yang W. Assessing the efficacy and safety of fecal microbiota transplantation and probiotic VSL#3 for active ulcerative colitis: a systematic review and meta-analysis. PLoS One. 2020;15(3):e0228846. doi:10.1371/journal.pone.0228846
19. Ford AC, Quigley EM, Lacy BE, et al. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: systematic review and meta-analysis. Am J Gastroenterol. 2014;109(10):1547-1561; quiz 1546, 1562. doi:10.1038/ajg.2014.202
20. Rohatgi S, Ahuja V, Makharia GK, et al. VSL#3 induces and maintains short-term clinical response in patients with active microscopic colitis: a two-phase randomised clinical trial. BMJ Open Gastroenterol. 2015;2(1):e000018. doi:10.1136/bmjgast-2014-000018
21. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480-1491. doi:10.1053/j.gastro.2005.11.061
22. Talley NJ, Phillips SF, Melton J, 3rd, Wiltgen C, Zinsmeister AR. A patient questionnaire to identify bowel disease. Ann Intern Med. 1989;111(8):671-674. doi:10.7326/0003-4819-111-8-671
23. Bensoussan A, Talley NJ, Hing M, Menzies R, Guo A, Ngu M. Treatment of irritable bowel syndrome with Chinese herbal medicine: a randomized controlled trial. JAMA. 1998;280(18):1585-1589. doi:10.1001/jama.280.18.1585
24. Francis CY, Morris J, Whorwell PJ. The irritable bowel severity scoring system: a simple method of monitoring irritable bowel syndrome and its progress. Aliment Pharmacol Ther. 1997;11(2):395-402. doi:10.1046/j.1365-2036.1997.142318000.x
25. Patrick DL, Drossman DA, Frederick IO, DiCesare J, Puder KL. Quality of life in persons with irritable bowel syndrome: development and validation of a new measure. Dig Dis Sci. 1998;43(2):400-411. doi:10.1023/a:1018831127942
26. Attanasio V, Andrasik F, Blanchard EB, Arena JG. Psychometric properties of the SUNYA revision of the Psychosomatic Symptom Checklist. J Behav Med. 1984;7(2):247-257. doi:10.1007/BF00845390
27. Weathers F, Litz B, Herman D, Huska J, Keane T. The PTSD Checklist (PCL): reliability, validity, and diagnostic utility. Accessed August 25, 2022. https://www.researchgate.net/publication/291448760_The_PTSD_Checklist_PCL_Reliability_validity_and_diagnostic_utility
28. Derogatis L. Brief Symptom Inventory-18 (BSI-18): Administration, Scoring, and Procedure Manual. Ed 3 ed. National Computer Systems; 2000.
29. Stamps BW, Lyon WJ, Irvin AP, Kelley-Loughnane N, Goodson MS. A pilot study of the effect of deployment on the gut microbiome and traveler´s diarrhea susceptibility. Front Cell Infect Microbiol. 2020;10:589297. doi:10.3389/fcimb.2020.589297
30. Kim HJ, Camilleri M, McKinzie S, et al. A randomized controlled trial of a probiotic, VSL#3, on gut transit and symptoms in diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2003;17(7):895-904. doi:10.1046/j.1365-2036.2003.01543.x
31. Kim HJ, Vazquez Roque MI, Camilleri M, et al. A randomized controlled trial of a probiotic combination VSL# 3 and placebo in irritable bowel syndrome with bloating. Neurogastroenterol Motil. 2005;17(5):687-696. doi:10.1111/j.1365-2982.2005.00695.x32. Michail S, Kenche H. Gut microbiota is not modified by randomized, double-blind, placebo-controlled trial of vsl#3 in diarrhea-predominant irritable bowel syndrome. Probiotics Antimicrob Proteins. 2011;3(1):1-7. doi:10.1007/s12602-010-9059-y
33. Moayyedi P, Ford AC, Talley NJ, et al. The efficacy of probiotics in the treatment of irritable bowel syndrome: a systematic review. Gut. 2010;59(3):325-332. doi:10.1136/gut.2008.167270

34. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044-1060. doi:10.1111/apt.15001
35. Dale HF, Rasmussen SH, Asiller OO, Lied GA. Probiotics in irritable bowel syndrome: an up-to-date systematic review. Nutrients. 2019;11(9). doi:10.3390/nu11092048
36. Didari T, Mozaffari S, Nikfar S, Abdollahi M. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J Gastroenterol. 2015;21(10):3072-84. doi:10.3748/wjg.v21.i10.3072
37. Hungin APS, Mitchell CR, Whorwell P, et al. Systematic review: probiotics in the management of lower gastrointestinal symptoms—an updated evidence-based international consensus. Aliment Pharmacol Ther. 2018;47(8):1054-1070. doi:10.1111/apt.14539
38. Niu HL, Xiao JY. The efficacy and safety of probiotics in patients with irritable bowel syndrome: evidence based on 35 randomized controlled trials. Int J Surg. 2020;75:116-127. doi:10.1016/j.ijsu.2020.01.142
39. Wong RK, Yang C, Song GH, Wong J, Ho KY. Melatonin regulation as a possible mechanism for probiotic (VSL#3) in irritable bowel syndrome: a randomized double-blinded placebo study. Dig Dis Sci. 2015;60(1):186-194. doi:10.1007/s10620-014-3299-8
40. Ford AC, Moayyedi P, Lacy BE, et al. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Am J Gastroenterol. 2014;109(suppl 1):S2-26; quiz S27. doi: 10.1038/ajg.2014.187
41. Simren M, Barbara G, Flint HJ, et al. Intestinal microbiota in functional bowel disorders: a Rome foundation report. Gut. 2013;62(1):159-76. doi:10.1136/gutjnl-2012-302167
42. Ki Cha B, Mun Jung S, Hwan Choi C, et al. The effect of a multispecies probiotic mixture on the symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. J Clin Gastroenterol. 2012;46(3):220-7. doi:10.1097/MCG.0b013e31823712b1
43. Connell M, Shin A, James-Stevenson T, Xu H, Imperiale TF, Herron J. Systematic review and meta-analysis: Efficacy of patented probiotic, VSL#3, in irritable bowel syndrome. Neurogastroenterol Motil. 2018;30(12):e13427. doi:10.1111/nmo.13427
44. Lyra A, Hillila M, Huttunen T, et al. Irritable bowel syndrome symptom severity improves equally with probiotic and placebo. World J Gastroenterol. 2016;22(48):10631-10642. doi:10.3748/wjg.v22.i48.10631
45. Sanders ME, Guarner F, Guerrant R, et al. An update on the use and investigation of probiotics in health and disease. Gut. 2013;62(5):787-796. doi:10.1136/gutjnl-2012-302504
46. Tuteja AK. Deployment-associated functional gastrointestinal disorders: do we know the etiology? Dig Dis Sci. 2011;56(11):3109-3111. doi:10.1007/s10620-011-1856-y
About 700,000 US military personnel were deployed in Operation Desert Storm (August 1990 to March 1991).1 Almost 30 years since the war, a large number of these veterans continue to experience a complex of symptoms of unknown etiology called Gulf War illness (GWI), which significantly affects health and quality of life (QOL). The lack of clear etiology of the illness has impaired research to find specific treatments and has further exacerbated the stress among veterans. GWI typically includes a mixture of chronic headache, cognitive difficulties, widespread pain, unexplained fatigue, memory and concentration problems, as well as chronic respiratory and gastrointestinal (GI) symptoms.2 Abdominal pain and alteration of bowel habits are also symptoms typical of irritable bowel syndrome (IBS). It has been estimated that IBS occurs in up to 30% of Gulf War veterans.3
The etiology of IBS is unknown. Possible mechanisms include visceral hypersensitivity, altered gut motor function, aberrant brain-gut interaction, and psychological factors, perhaps with a genetic predisposition.4 Gastroenteritis has been reported as a triggering mechanism in up to one-third of patients with IBS.5 Gastroenteritis can alter the gut microbiota and has been reported to be a significant risk factor for the development of IBS.6 In one study of Operation Desert Shield soldiers, > 50% of military personnel developed acute gastroenteritis while on duty.7 A high prevalence of extra-intestinal symptoms also has been reported, including fatigue, headache, joint pains, and anxiety, in Gulf War veterans with IBS. These extra-intestinal symptoms of IBS are consistent with the reported GWI symptoms. Change in gut microbiota also has been associated with many of the extra-intestinal symptoms of IBS, especially fatigue.8,9 Gut microbiota are known to change with travel, stress, and a change in diet, all potential factors that are relevant to Gulf War veterans. This would suggest that an imbalance in the gut microbiota, ie, dysbiosis, may play a role in the pathogenesis of both IBS and GWI. Dysbiosis could be a risk factor for or alternatively a consequence of GWI.
A systematic review highlighted the heterogeneity of the gut microbiota in patients with IBS.10 Overall, Enterobacteriaceae, Lactobacillaceae, and Bacteroides were increased, whereas Clostridiales, Faecalibacterium, and Bifidobacterium were decreased in patients with IBS compared with controls. Gut microbiota also has been associated with cognitive changes, anxiety, and depression—symptoms associated with IBS and are part of the GWI.
If altered gut microbiota contributes to the etiopathogenesis of IBS, its restoration of with probiotics should help. Probiotics are live organisms that when ingested may improve health by promoting the growth of naturally occurring flora and establishing a healthy gut flora. Probiotics have several mechanisms of actions. Probiotics work in the lumen of the gut by producing antibacterial molecules and enhancing the mucosal barrier.11 Probiotics also may produce metabolic compounds that alter the intestinal microbiota and improve intestinal barrier function.12 Probiotics also have been shown to activate receptors in the enteric nervous system with the potential to promote pain relief in the setting of visceral hyperalgesia.13,14 The anti-inflammatory properties of probiotics potentially could modulate the basic pathophysiology of IBS and improve motility, visceral hypersensitivity, and brain-gut interaction.15 Furthermore, significant gut dysbiosis has been shown with GWI; suggesting that probiotics may have a role in its management.16,17
Probiotics have not been studied in Gulf War veterans with IBS. We performed a prospective, double-blind placebo-controlled study to determine the efficacy of a commercially available probiotic containing 8 strains of bacteria (De Simone Formulation; formally known as VSL#3 and Visbiome) on symptoms of IBS and GWI. This probiotic was selected as the overall literature suggested benefit of combination probiotics in IBS, and VSL#3 has been shown to be efficacious in ulcerative colitis and microscopic colitis.18-20
Methods
Veterans who served in Operation Desert Storm (August 1990 to March 1991) and enrolled at the George E. Wahlen Veterans Affairs (VA) Medical Center (GEWVAMC), Salt Lake City, Utah, were eligible for the study. The inclusion criteria were: veterans aged ≥ 35 years; ≥ 2 nonintestinal GWI symptoms (eg, fatigue, joint pains, insomnia, general stiffness, and headache); IBS diagnosis based on the Rome III criteria; IBS symptoms > 6 months; normal gross appearance of the colonic mucosa; negative markers for celiac disease and inflammatory bowel disease (IBD); normal thyroid function; and serum calcium levels.21 Those who had a clinically significant cardiac, pulmonary, hepatic or renal dysfunction; history of/or presence of systemic malignancy; current evidence of celiac disease or IBD; unstable/significant psychiatric disease; recent change in GI medications; current pregnancy; or use of antibiotics or probiotics within the past 1 month were excluded. Subjects were enrolled from a list of veterans with GWI from the GEWVAMC Gulf War registry; referrals to gastroenterology clinics for IBS from internal medicine clinics; and posted advertisements.
Protocol
After written informed consent was obtained, each veteran was verified to have IBS and ≥ 2 GWI symptoms. All veterans had the following tests and panels: complete blood count, erythrocyte sedimentation rate, serum comprehensive metabolic panel, thyroid-stimulating hormone, tissue transglutaminase, stool test for ova and parasite, giardia antigen, and clostridia toxins to exclude organic cause of GI symptoms. Colonoscopy was performed in all veterans to exclude IBD, and to rule out microscopic or lymphocytic colitis.
Randomization was computer generated and maintained by the study pharmacist so that study personnel and patients were blinded to the trial groups. All investigators were blinded and allocation was concealed. The medication was supplied in a numbered container by the pharmacist after patient enrollment. After a 2-week run-in period, veterans were randomized (1:1) to receive either 1 sachet of probiotic (De Simone Formulation; formally known as VSL#3 and Visbiome) or placebo once daily for 8 weeks.
Each probiotic packet contains 900 billion probiotic bacteria per sachet.11 This formulation contained 8 viable strains of bacteria: 4 strains of Lactobacillus (L acidophilus, L plantarum, L paracasei, L delbrueckii subsp. bulgaricus); 3 strains of Bifidobacteria (Bifidobacterium breve, B lactis, B infantis); and 1 strain of Streptococcus thermophilus. This formulation had been commercialized and studied as VSL#3 and is currently available in the United States under the Visbiome trade name. While branding changed during the study, the formulation did not. The investigational medicine (VSL#3, Visbiome, and placebo) were shipped from the manufacturer Dupont/Danisco in Madison, Wisconsin. The subjects received placebo or probiotic (VSL#3/Visbiome) and both were identical in appearance. The medication was supplied in a numbered container by the pharmacist after patient enrollment.
Measures
Veterans completed the bowel disease questionnaire to record baseline bowel habits.22 All veterans recorded daily bowel symptoms to confirm the presence of IBS during the 2-week pretreatment period, at baseline, and at the end of the 8-week treatment. The symptoms assessed included severity of abdominal pain (0, none to 100, severe); severity of bloating (0, none to 100, severe); stool frequency; Bristol stool scale (1, very hard to 7, watery); severity of diarrhea (0, none to 100, severe); severity of constipation (0, none to 100, severe); satisfaction with bowel habits (0, none to 100, severe); and IBS affecting or interfering with life (0, none to 100, severe). The bowel symptom score is the sum of the 5 symptom scores.23,24
IBS-specific QOL (IBS-QOL) was recorded at baseline and at the end of treatment.25 The IBS-QOL consists of a 34-item validated disease-specific questionnaire that measures 8 domains relevant to subjects with IBS: dysphoria, interference with activity, body image, health worry, food avoidance, social reaction, sexual life, and relationships. We used the Somatic Symptom Checklist to detect the following extra-intestinal symptoms that are common among veterans with GWI: headache, backache, wheeziness, insomnia, bad breath, fatigue, general stiffness, dizziness, weakness, sensitivity to hot and cold, palpitation, and tightness in chest. Subjects rated symptoms on a scale of 1 to 5: how often (1, none; 2, monthly; 3, once weekly; 4, several times weekly; 5, daily), and how bothersome (1, not at all to 5, extremely).26
Subjects completed the Posttraumatic Stress Disorder (PTSD) Checklist–Military, which is specific to military experience with 17 items on a 1 to 5 scale (1, not at all to 5, extremely). Scores were summed to produce a total symptom severity score (range, 17-85).27 Subjects also completed the Brief Symptom Inventory 18 (BSI-18) during the baseline evaluation.28 BSI-18 measures subjects’ reported overall psychological distress. It assesses 3 symptoms dimensions (somatization, depression, and anxiety) and a global severity index. The raw scores were transferred to normative T scores based on samples of nonpatient normal men and women.
Symptom data were compared after 8 weeks of treatment. The primary study endpoint was change in bowel symptom score. The secondary endpoints were mean change in symptoms, QOL, extra-intestinal symptoms, and PTSD score. The study was approved by the Salt Lake City Veterans Affairs Medical Center and the University of Utah Institutional Review Board and registered in ClinicalTrials.gov (NCT03078530).
Statistical Methods
Comparisons of the probiotic vs placebo groups for demographic variable were analyzed using a 2-sample t test for continuous variables, and with a χ2 test or Fisher exact test for categorical variables. The primary and secondary outcome variables were recorded daily for 2 weeks as pretreatment baseline and for 2 weeks at the end of treatment. These symptoms were recorded as ordered categorical variables, which were then averaged across the week to produce a continuous measurement for statistical analysis. For the primary outcome of GI symptoms, posttreatment comparisons were made between the study groups using a 2-sample t test of the baseline vs posttreatment values. All P values were calculated for 2-sided comparisons. The planned sample size in our study protocol was to recruit 40 individuals per group in order to achieve 80% power to detect a 30% improvement between baseline and end of treatment in the primary bowel symptom score. This study recruited 53 subjects. With this sample size, the study had 80% power to detect a 0.8 SD in any of the outcomes.
Results
We screened 101 veterans with IBS and GWI; 39 veterans did not fulfill the inclusion/exclusion criteria, 22 declined to participate or did not complete the screening questionnaires and tests, and 9 were lost to follow-up. Sixty-two participants were randomized in a double-blind placebo-controlled study design; 9 dropped out before the end of the study. Data were analyzed from 53 veterans who completed the study, 29 in the placebo group and 24 in the probiotic group (Figure 1). The cohort was primarily male with a mean (SD) age of 55 (8) years (range, 42-73) (Table 1).
Overall, the treatment was well tolerated. All subjects were contacted every 2 weeks during the study to check for adverse effects, but no serious events were reported. There were no differences at baseline in any of the BSI-18 subscale scores in veterans between the groups. There was a greater mean (SEM) improvement of diarrhea severity in the probiotic group compared with the placebo group: 18 (6), a 31% improvement, vs 6 (5), a 13% improvement, respectively; however, the difference was not statistically significance (P = .13) (Table 2). There also was a greater mean (SEM) improvement in satisfaction of bowel habits in the probiotic group compared with the placebo group: 16 (7), a 35% improvement vs 4 (9), an 8% worsening; this also was not statistically significant (P = .09). There was no difference in the change of IBS-QOL before and after treatment in either group (Figure 2). There was no improvement in any of the symptoms of GWI (all P ≥ .06) (Appendix).
Discussion
GWI is a complex multisystem illness of unknown etiology. There was high prevalence of diarrhea during deployment, and veterans were exposed to several physical, environmental, and mental stresses of the war.3 A change in gut microbiota can occur during deployment due to diet changes, environmental and physical stress, and GI infections.29 These changes would suggest that manipulation of gut microbiota might offer a new modality of treatment of IBS and GWI. We evaluated the effect of a high-potency multistrain probiotic in veterans with IBS and GWI. We did not detect any statistically significant differences between the probiotic and placebo groups on bowel symptom score and individual symptoms of IBS and on QOL. Also, there was no improvement for the other symptoms of GWI. To our knowledge, this is the first study evaluating the effect of probiotics in veterans with IBS and GWI. Our results are consistent with the literature on probiotics and IBS.
The probiotic formulation used in our study has been evaluated in patients with IBS previously. Kim and colleagues found that after 8 weeks of treatment of patients with diarrhea-predominant IBS with VSL#3, there was improvement in bloating, but no effect was found on abdominal pain, gas, or urgency.30 A subsequent study by the same investigators on patients with all types of IBS found that VSL#3 showed no effect on abdominal pain, stool frequency and consistency, or on bloating, but there was improvement in flatulence.31 Another study that evaluated the effect of VSL#3 on symptoms of diarrhea-predominant IBS and QOL found improvement in IBS symptoms from baseline in both the probiotic and the placebo groups, but the difference between the 2 groups was not statistically significant.32 Similarly, Wong and colleagues performed a double-blind, placebo-controlled mechanistic study to evaluate the effect of VSL#3. They found improvement in bowel symptom score, abdominal pain intensity, and satisfaction with bowel habits with both the VSL#3 and placebo group but similar to our study, the differences were not statistically significant.
Several reviews have evaluated the efficacy of probiotics for IBS. A 2010 review found evidence that probiotics trended toward improved IBS symptoms compared with placebo.33 The 2014 follow-up by the same authors demonstrated that overall, probiotics improved global symptoms of IBS and multistrain probiotics were more effective.20 A third meta-analysis from the same group found evidence that multistrain probiotics seemed to have a beneficial effect but could not definitively conclude that probiotics are efficacious in improving IBS symptoms.34 Other authors also have seen inconsistent effects of probiotics compared with placebo on global symptoms, abdominal pain, and bloating after performing systematic reviews of the literature.35-38 Although several reviews support that multistrain probiotics are more effective, they fail to conclude which combinations are more efficacious.
The effect of probiotics on QOL has not been investigated by many studies.37 In our study, we did not find significant improvement in QOL in the probiotic group, which is in line with 2 previous studies that showed no effect on IBS QOL of VSL#3 vs placebo.32,39 Most of the research reports that multistrain probiotics are more effective than using a single strain.34,35,40Bifidobacterium and Lactobacillus are the most commonly used bacteria in the multistrain probiotics that have shown their positive effect on IBS.35,41 The probiotic used in our study contained other species along with these 2 microorganisms.
The dose and duration of treatment of probiotics also has been debated. In one meta-analysis, the investigators found that studies of ≥ 8 weeks were more likely to show a positive effect; 4 of the 7 studies with statistically significant improvement in IBS symptoms were longer than 8 weeks.35 However, another meta-analysis based on 35 randomized controlled trials found that there was not a statistically significant difference between groups treated for > 4 weeks vs < 4 weeks.42 In addition, another meta-analysis of VSL#3 on IBS in children and adults also found no difference in results based on the duration of treatment of probiotics.43 Similar to our study, 3 other studies of VSL#3 treated patients for 8 weeks and found no statistically significant effect.30-32 In the past, VSL#3 has been used at dosages of 450 or 900 billion bacteria per day.
An individual’s response to probiotics may depend on the subtype of IBS. However, most of the studies, like ours, included groups of all subtypes. It may be that probiotics are more effective in patients with moderate-to-severe symptoms. Most of our patients had milder symptoms, and we cannot discount how subjects with more severe disease may have responded to the drug. Interestingly, one study demonstrated that Lactobacillus was more effective in patients with moderately severe abdominal pain compared with mild symptoms.44
In our study, the probiotic did not improve PTSD symptoms or other extra-intestinal symptoms common in IBS and GWI. Similar to our study, Wong and colleagues did not find significant improvement of psychological and sleep scores after treatment with VSL#3.6 Similarly, there is evidence that alteration in gut microbiota is associated with health and diseases, but what specific alterations occur and whether they can be improved with probiotics remains unknown.45
Limitations
The inconsistent response to probiotics in various studies may be due to IBS heterogeneity. Furthermore, there are demographic differences between Gulf War veterans and patients enrolled in other studies: Gulf War veterans are predominantly male, many were deployed abroad and had a history of gastroenteritis during deployment, and were exposed to stressful situations.46 These factors may be involved in triggering or maintaining IBS in Gulf War veterans. A further limitation of our randomized trial is the relatively small sample size.
Conclusions
This study did not demonstrate statistically significant improvement in symptoms of IBS or improvement in QOL after treatment with a multistrain probiotic. We also did not find any improvement in symptoms of GWI or PTSD. There was no difference in psychological scores between the placebo and treatment groups, and it is unlikely that psychological factors confounded the response to treatment in this study.
The effectiveness of a probiotic may depend on the baseline gut microbiome of the individual and depend on the strain, amount, and frequency of bacteria used. A lack of response of the probiotics does not exclude gut viruses and fungi having a role in exacerbating GWI symptoms. It is also possible that the bacteria present or the dose of the probiotic used was not sufficient to improve symptoms. So far, the definitive benefit of probiotics has been demonstrated for only a few preparations, and none are approved by the US Food and Drug Administration for any disease. More research is needed to determine whether probiotics have any role in the treatment of IBS and GWI.
Acknowledgments
AKT received grant support from the US Department of Veterans Affairs and the US Department of Defense (W81XWH-10-1-0593, W81XWH-15-1-0636). We thank Keith G. Tolman, MD, for assistance in editing the initial proposal and for periodic consultation. We thank the manufacturer of the probiotic for supplying the active drug and the placebo. The manufacture of the probiotic had no role in the design and conduct of the study, analysis and interpretation of the data, and in the preparation of the manuscript.
About 700,000 US military personnel were deployed in Operation Desert Storm (August 1990 to March 1991).1 Almost 30 years since the war, a large number of these veterans continue to experience a complex of symptoms of unknown etiology called Gulf War illness (GWI), which significantly affects health and quality of life (QOL). The lack of clear etiology of the illness has impaired research to find specific treatments and has further exacerbated the stress among veterans. GWI typically includes a mixture of chronic headache, cognitive difficulties, widespread pain, unexplained fatigue, memory and concentration problems, as well as chronic respiratory and gastrointestinal (GI) symptoms.2 Abdominal pain and alteration of bowel habits are also symptoms typical of irritable bowel syndrome (IBS). It has been estimated that IBS occurs in up to 30% of Gulf War veterans.3
The etiology of IBS is unknown. Possible mechanisms include visceral hypersensitivity, altered gut motor function, aberrant brain-gut interaction, and psychological factors, perhaps with a genetic predisposition.4 Gastroenteritis has been reported as a triggering mechanism in up to one-third of patients with IBS.5 Gastroenteritis can alter the gut microbiota and has been reported to be a significant risk factor for the development of IBS.6 In one study of Operation Desert Shield soldiers, > 50% of military personnel developed acute gastroenteritis while on duty.7 A high prevalence of extra-intestinal symptoms also has been reported, including fatigue, headache, joint pains, and anxiety, in Gulf War veterans with IBS. These extra-intestinal symptoms of IBS are consistent with the reported GWI symptoms. Change in gut microbiota also has been associated with many of the extra-intestinal symptoms of IBS, especially fatigue.8,9 Gut microbiota are known to change with travel, stress, and a change in diet, all potential factors that are relevant to Gulf War veterans. This would suggest that an imbalance in the gut microbiota, ie, dysbiosis, may play a role in the pathogenesis of both IBS and GWI. Dysbiosis could be a risk factor for or alternatively a consequence of GWI.
A systematic review highlighted the heterogeneity of the gut microbiota in patients with IBS.10 Overall, Enterobacteriaceae, Lactobacillaceae, and Bacteroides were increased, whereas Clostridiales, Faecalibacterium, and Bifidobacterium were decreased in patients with IBS compared with controls. Gut microbiota also has been associated with cognitive changes, anxiety, and depression—symptoms associated with IBS and are part of the GWI.
If altered gut microbiota contributes to the etiopathogenesis of IBS, its restoration of with probiotics should help. Probiotics are live organisms that when ingested may improve health by promoting the growth of naturally occurring flora and establishing a healthy gut flora. Probiotics have several mechanisms of actions. Probiotics work in the lumen of the gut by producing antibacterial molecules and enhancing the mucosal barrier.11 Probiotics also may produce metabolic compounds that alter the intestinal microbiota and improve intestinal barrier function.12 Probiotics also have been shown to activate receptors in the enteric nervous system with the potential to promote pain relief in the setting of visceral hyperalgesia.13,14 The anti-inflammatory properties of probiotics potentially could modulate the basic pathophysiology of IBS and improve motility, visceral hypersensitivity, and brain-gut interaction.15 Furthermore, significant gut dysbiosis has been shown with GWI; suggesting that probiotics may have a role in its management.16,17
Probiotics have not been studied in Gulf War veterans with IBS. We performed a prospective, double-blind placebo-controlled study to determine the efficacy of a commercially available probiotic containing 8 strains of bacteria (De Simone Formulation; formally known as VSL#3 and Visbiome) on symptoms of IBS and GWI. This probiotic was selected as the overall literature suggested benefit of combination probiotics in IBS, and VSL#3 has been shown to be efficacious in ulcerative colitis and microscopic colitis.18-20
Methods
Veterans who served in Operation Desert Storm (August 1990 to March 1991) and enrolled at the George E. Wahlen Veterans Affairs (VA) Medical Center (GEWVAMC), Salt Lake City, Utah, were eligible for the study. The inclusion criteria were: veterans aged ≥ 35 years; ≥ 2 nonintestinal GWI symptoms (eg, fatigue, joint pains, insomnia, general stiffness, and headache); IBS diagnosis based on the Rome III criteria; IBS symptoms > 6 months; normal gross appearance of the colonic mucosa; negative markers for celiac disease and inflammatory bowel disease (IBD); normal thyroid function; and serum calcium levels.21 Those who had a clinically significant cardiac, pulmonary, hepatic or renal dysfunction; history of/or presence of systemic malignancy; current evidence of celiac disease or IBD; unstable/significant psychiatric disease; recent change in GI medications; current pregnancy; or use of antibiotics or probiotics within the past 1 month were excluded. Subjects were enrolled from a list of veterans with GWI from the GEWVAMC Gulf War registry; referrals to gastroenterology clinics for IBS from internal medicine clinics; and posted advertisements.
Protocol
After written informed consent was obtained, each veteran was verified to have IBS and ≥ 2 GWI symptoms. All veterans had the following tests and panels: complete blood count, erythrocyte sedimentation rate, serum comprehensive metabolic panel, thyroid-stimulating hormone, tissue transglutaminase, stool test for ova and parasite, giardia antigen, and clostridia toxins to exclude organic cause of GI symptoms. Colonoscopy was performed in all veterans to exclude IBD, and to rule out microscopic or lymphocytic colitis.
Randomization was computer generated and maintained by the study pharmacist so that study personnel and patients were blinded to the trial groups. All investigators were blinded and allocation was concealed. The medication was supplied in a numbered container by the pharmacist after patient enrollment. After a 2-week run-in period, veterans were randomized (1:1) to receive either 1 sachet of probiotic (De Simone Formulation; formally known as VSL#3 and Visbiome) or placebo once daily for 8 weeks.
Each probiotic packet contains 900 billion probiotic bacteria per sachet.11 This formulation contained 8 viable strains of bacteria: 4 strains of Lactobacillus (L acidophilus, L plantarum, L paracasei, L delbrueckii subsp. bulgaricus); 3 strains of Bifidobacteria (Bifidobacterium breve, B lactis, B infantis); and 1 strain of Streptococcus thermophilus. This formulation had been commercialized and studied as VSL#3 and is currently available in the United States under the Visbiome trade name. While branding changed during the study, the formulation did not. The investigational medicine (VSL#3, Visbiome, and placebo) were shipped from the manufacturer Dupont/Danisco in Madison, Wisconsin. The subjects received placebo or probiotic (VSL#3/Visbiome) and both were identical in appearance. The medication was supplied in a numbered container by the pharmacist after patient enrollment.
Measures
Veterans completed the bowel disease questionnaire to record baseline bowel habits.22 All veterans recorded daily bowel symptoms to confirm the presence of IBS during the 2-week pretreatment period, at baseline, and at the end of the 8-week treatment. The symptoms assessed included severity of abdominal pain (0, none to 100, severe); severity of bloating (0, none to 100, severe); stool frequency; Bristol stool scale (1, very hard to 7, watery); severity of diarrhea (0, none to 100, severe); severity of constipation (0, none to 100, severe); satisfaction with bowel habits (0, none to 100, severe); and IBS affecting or interfering with life (0, none to 100, severe). The bowel symptom score is the sum of the 5 symptom scores.23,24
IBS-specific QOL (IBS-QOL) was recorded at baseline and at the end of treatment.25 The IBS-QOL consists of a 34-item validated disease-specific questionnaire that measures 8 domains relevant to subjects with IBS: dysphoria, interference with activity, body image, health worry, food avoidance, social reaction, sexual life, and relationships. We used the Somatic Symptom Checklist to detect the following extra-intestinal symptoms that are common among veterans with GWI: headache, backache, wheeziness, insomnia, bad breath, fatigue, general stiffness, dizziness, weakness, sensitivity to hot and cold, palpitation, and tightness in chest. Subjects rated symptoms on a scale of 1 to 5: how often (1, none; 2, monthly; 3, once weekly; 4, several times weekly; 5, daily), and how bothersome (1, not at all to 5, extremely).26
Subjects completed the Posttraumatic Stress Disorder (PTSD) Checklist–Military, which is specific to military experience with 17 items on a 1 to 5 scale (1, not at all to 5, extremely). Scores were summed to produce a total symptom severity score (range, 17-85).27 Subjects also completed the Brief Symptom Inventory 18 (BSI-18) during the baseline evaluation.28 BSI-18 measures subjects’ reported overall psychological distress. It assesses 3 symptoms dimensions (somatization, depression, and anxiety) and a global severity index. The raw scores were transferred to normative T scores based on samples of nonpatient normal men and women.
Symptom data were compared after 8 weeks of treatment. The primary study endpoint was change in bowel symptom score. The secondary endpoints were mean change in symptoms, QOL, extra-intestinal symptoms, and PTSD score. The study was approved by the Salt Lake City Veterans Affairs Medical Center and the University of Utah Institutional Review Board and registered in ClinicalTrials.gov (NCT03078530).
Statistical Methods
Comparisons of the probiotic vs placebo groups for demographic variable were analyzed using a 2-sample t test for continuous variables, and with a χ2 test or Fisher exact test for categorical variables. The primary and secondary outcome variables were recorded daily for 2 weeks as pretreatment baseline and for 2 weeks at the end of treatment. These symptoms were recorded as ordered categorical variables, which were then averaged across the week to produce a continuous measurement for statistical analysis. For the primary outcome of GI symptoms, posttreatment comparisons were made between the study groups using a 2-sample t test of the baseline vs posttreatment values. All P values were calculated for 2-sided comparisons. The planned sample size in our study protocol was to recruit 40 individuals per group in order to achieve 80% power to detect a 30% improvement between baseline and end of treatment in the primary bowel symptom score. This study recruited 53 subjects. With this sample size, the study had 80% power to detect a 0.8 SD in any of the outcomes.
Results
We screened 101 veterans with IBS and GWI; 39 veterans did not fulfill the inclusion/exclusion criteria, 22 declined to participate or did not complete the screening questionnaires and tests, and 9 were lost to follow-up. Sixty-two participants were randomized in a double-blind placebo-controlled study design; 9 dropped out before the end of the study. Data were analyzed from 53 veterans who completed the study, 29 in the placebo group and 24 in the probiotic group (Figure 1). The cohort was primarily male with a mean (SD) age of 55 (8) years (range, 42-73) (Table 1).
Overall, the treatment was well tolerated. All subjects were contacted every 2 weeks during the study to check for adverse effects, but no serious events were reported. There were no differences at baseline in any of the BSI-18 subscale scores in veterans between the groups. There was a greater mean (SEM) improvement of diarrhea severity in the probiotic group compared with the placebo group: 18 (6), a 31% improvement, vs 6 (5), a 13% improvement, respectively; however, the difference was not statistically significance (P = .13) (Table 2). There also was a greater mean (SEM) improvement in satisfaction of bowel habits in the probiotic group compared with the placebo group: 16 (7), a 35% improvement vs 4 (9), an 8% worsening; this also was not statistically significant (P = .09). There was no difference in the change of IBS-QOL before and after treatment in either group (Figure 2). There was no improvement in any of the symptoms of GWI (all P ≥ .06) (Appendix).
Discussion
GWI is a complex multisystem illness of unknown etiology. There was high prevalence of diarrhea during deployment, and veterans were exposed to several physical, environmental, and mental stresses of the war.3 A change in gut microbiota can occur during deployment due to diet changes, environmental and physical stress, and GI infections.29 These changes would suggest that manipulation of gut microbiota might offer a new modality of treatment of IBS and GWI. We evaluated the effect of a high-potency multistrain probiotic in veterans with IBS and GWI. We did not detect any statistically significant differences between the probiotic and placebo groups on bowel symptom score and individual symptoms of IBS and on QOL. Also, there was no improvement for the other symptoms of GWI. To our knowledge, this is the first study evaluating the effect of probiotics in veterans with IBS and GWI. Our results are consistent with the literature on probiotics and IBS.
The probiotic formulation used in our study has been evaluated in patients with IBS previously. Kim and colleagues found that after 8 weeks of treatment of patients with diarrhea-predominant IBS with VSL#3, there was improvement in bloating, but no effect was found on abdominal pain, gas, or urgency.30 A subsequent study by the same investigators on patients with all types of IBS found that VSL#3 showed no effect on abdominal pain, stool frequency and consistency, or on bloating, but there was improvement in flatulence.31 Another study that evaluated the effect of VSL#3 on symptoms of diarrhea-predominant IBS and QOL found improvement in IBS symptoms from baseline in both the probiotic and the placebo groups, but the difference between the 2 groups was not statistically significant.32 Similarly, Wong and colleagues performed a double-blind, placebo-controlled mechanistic study to evaluate the effect of VSL#3. They found improvement in bowel symptom score, abdominal pain intensity, and satisfaction with bowel habits with both the VSL#3 and placebo group but similar to our study, the differences were not statistically significant.
Several reviews have evaluated the efficacy of probiotics for IBS. A 2010 review found evidence that probiotics trended toward improved IBS symptoms compared with placebo.33 The 2014 follow-up by the same authors demonstrated that overall, probiotics improved global symptoms of IBS and multistrain probiotics were more effective.20 A third meta-analysis from the same group found evidence that multistrain probiotics seemed to have a beneficial effect but could not definitively conclude that probiotics are efficacious in improving IBS symptoms.34 Other authors also have seen inconsistent effects of probiotics compared with placebo on global symptoms, abdominal pain, and bloating after performing systematic reviews of the literature.35-38 Although several reviews support that multistrain probiotics are more effective, they fail to conclude which combinations are more efficacious.
The effect of probiotics on QOL has not been investigated by many studies.37 In our study, we did not find significant improvement in QOL in the probiotic group, which is in line with 2 previous studies that showed no effect on IBS QOL of VSL#3 vs placebo.32,39 Most of the research reports that multistrain probiotics are more effective than using a single strain.34,35,40Bifidobacterium and Lactobacillus are the most commonly used bacteria in the multistrain probiotics that have shown their positive effect on IBS.35,41 The probiotic used in our study contained other species along with these 2 microorganisms.
The dose and duration of treatment of probiotics also has been debated. In one meta-analysis, the investigators found that studies of ≥ 8 weeks were more likely to show a positive effect; 4 of the 7 studies with statistically significant improvement in IBS symptoms were longer than 8 weeks.35 However, another meta-analysis based on 35 randomized controlled trials found that there was not a statistically significant difference between groups treated for > 4 weeks vs < 4 weeks.42 In addition, another meta-analysis of VSL#3 on IBS in children and adults also found no difference in results based on the duration of treatment of probiotics.43 Similar to our study, 3 other studies of VSL#3 treated patients for 8 weeks and found no statistically significant effect.30-32 In the past, VSL#3 has been used at dosages of 450 or 900 billion bacteria per day.
An individual’s response to probiotics may depend on the subtype of IBS. However, most of the studies, like ours, included groups of all subtypes. It may be that probiotics are more effective in patients with moderate-to-severe symptoms. Most of our patients had milder symptoms, and we cannot discount how subjects with more severe disease may have responded to the drug. Interestingly, one study demonstrated that Lactobacillus was more effective in patients with moderately severe abdominal pain compared with mild symptoms.44
In our study, the probiotic did not improve PTSD symptoms or other extra-intestinal symptoms common in IBS and GWI. Similar to our study, Wong and colleagues did not find significant improvement of psychological and sleep scores after treatment with VSL#3.6 Similarly, there is evidence that alteration in gut microbiota is associated with health and diseases, but what specific alterations occur and whether they can be improved with probiotics remains unknown.45
Limitations
The inconsistent response to probiotics in various studies may be due to IBS heterogeneity. Furthermore, there are demographic differences between Gulf War veterans and patients enrolled in other studies: Gulf War veterans are predominantly male, many were deployed abroad and had a history of gastroenteritis during deployment, and were exposed to stressful situations.46 These factors may be involved in triggering or maintaining IBS in Gulf War veterans. A further limitation of our randomized trial is the relatively small sample size.
Conclusions
This study did not demonstrate statistically significant improvement in symptoms of IBS or improvement in QOL after treatment with a multistrain probiotic. We also did not find any improvement in symptoms of GWI or PTSD. There was no difference in psychological scores between the placebo and treatment groups, and it is unlikely that psychological factors confounded the response to treatment in this study.
The effectiveness of a probiotic may depend on the baseline gut microbiome of the individual and depend on the strain, amount, and frequency of bacteria used. A lack of response of the probiotics does not exclude gut viruses and fungi having a role in exacerbating GWI symptoms. It is also possible that the bacteria present or the dose of the probiotic used was not sufficient to improve symptoms. So far, the definitive benefit of probiotics has been demonstrated for only a few preparations, and none are approved by the US Food and Drug Administration for any disease. More research is needed to determine whether probiotics have any role in the treatment of IBS and GWI.
Acknowledgments
AKT received grant support from the US Department of Veterans Affairs and the US Department of Defense (W81XWH-10-1-0593, W81XWH-15-1-0636). We thank Keith G. Tolman, MD, for assistance in editing the initial proposal and for periodic consultation. We thank the manufacturer of the probiotic for supplying the active drug and the placebo. The manufacture of the probiotic had no role in the design and conduct of the study, analysis and interpretation of the data, and in the preparation of the manuscript.
1. O’Shea EF, Cotter PD, Stanton C, Ross RP, Hill C. Production of bioactive substances by intestinal bacteria as a basis for explaining probiotic mechanisms: bacteriocins and conjugated linoleic acid. Int J Food Microbiol. 2012;152(3):189-205. doi:10.1016/j.ijfoodmicro.2011.05.025.
2. Kamiya T, Wang L, Forsythe P, et al. Inhibitory effects of Lactobacillus reuteri on visceral pain induced by colorectal distension in Sprague-Dawley rats. Gut. 2006;55(2):191-196. doi:10.1136/gut.2005.070987.
3. Verdu EF, Bercik P, Verma-Gandhu M, et al. Specific probiotic therapy attenuates antibiotic induced visceral hypersensitivity in mice. Gut. 2006;55(2):182-190. doi:10.1136/gut.2005.066100
4. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044-1060. doi:10.1111/apt.15001.
5. Niu HL, Xiao JY. The efficacy and safety of probiotics in patients with irritable bowel syndrome: Evidence based on 35 randomized controlled trials. Int J Surg. 2020;75:116-127. doi:10.1016/j.ijsu.2020.01.142.
6. Wong RK, Yang C, Song GH, Wong J, Ho KY. Melatonin regulation as a possible mechanism for probiotic (VSL#3) in irritable bowel syndrome: a randomized double-blinded placebo study. Dig Dis Sci. 2015;60(1):186-194. doi:10.1007/s10620-014-3299-8.
7. Hyams KC, Bourgeois AL, Merrell BR, et al. Diarrheal disease during Operation Desert Shield. N Engl J Med. 1991;325(20):1423-1428. doi:10.1056/NEJM199111143252006 8. Clancy RL, Gleeson M, Cox A, et al. Reversal in fatigued athletes of a defect in interferon gamma secretion after administration of Lactobacillus acidophilus. Br J Sports Med. 2006;40(4):351-354. doi:10.1136/bjsm.2005.024364
9. Sullivan A, Nord CE, Evengard B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutr J. 2009;8:4. doi:10.1186/1475-2891-8-4
10. Pittayanon R, Lau JT, Yuan Y, et al. Gut microbiota in patients with irritable bowel syndrome—a systematic review. Gastroenterology. 2019;157(1):97-108. doi:10.1053/j.gastro.2019.03.049
11. Rao RK, Samak G. Protection and restitution of gut barrier by probiotics: nutritional and clinical implications. Curr Nutr Food Sci. 2013;9(2):99-107. doi:10.2174/1573401311309020004
12. O´Shea EF, Cotter PD, Stanton C, Ross RP, Hill C. Production of bioactive substances by intestinal bacteria as a basis for explaining probiotic mechanisms: bacteriocins and conjugated linoleic acid. Int J Food Microbiol. 2012;152(3):189-205. doi:10.1016/j.ijfoodmicro.2011.05.025
13. Kamiya T, Wang L, Forsythe P, et al. Inhibitory effects of Lactobacillus reuteri on visceral pain induced by colorectal distension in Sprague-Dawley rats. Gut. 2006;55(2):191-196. doi:10.1136/gut.2005.070987
14. Verdu EF, Bercik P, Verma-Gandhu M, et al. Specific probiotic therapy attenuates antibiotic induced visceral hypersensitivity in mice. Gut. 2006;55(2):182-190. doi:10.1136/gut.2005.06610015. O´Mahony L, McCarthy J, Kelly P, et al. Lactobacillus and bifidobacterium in irritable bowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterology. 2005;128(3):541-551. doi:10.1053/j.gastro.2004.11.050
16. Alhasson F, Das S, Seth R, et al. Altered gut microbiome in a mouse model of Gulf War Illness causes neuroinflammation and intestinal injury via leaky gut and TLR4 activation. PLoS One. 2017;12(3):e0172914. doi:10.1371/journal.pone.0172914.17. Janulewicz PA, Seth RK, Carlson JM, et al. The gut-microbiome in Gulf War veterans: a preliminary report. Int J Environ Res Public Health. 2019;16(19). doi:10.3390/ijerph16193751
18. Dang X, Xu M, Liu D, Zhou D, Yang W. Assessing the efficacy and safety of fecal microbiota transplantation and probiotic VSL#3 for active ulcerative colitis: a systematic review and meta-analysis. PLoS One. 2020;15(3):e0228846. doi:10.1371/journal.pone.0228846
19. Ford AC, Quigley EM, Lacy BE, et al. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: systematic review and meta-analysis. Am J Gastroenterol. 2014;109(10):1547-1561; quiz 1546, 1562. doi:10.1038/ajg.2014.202
20. Rohatgi S, Ahuja V, Makharia GK, et al. VSL#3 induces and maintains short-term clinical response in patients with active microscopic colitis: a two-phase randomised clinical trial. BMJ Open Gastroenterol. 2015;2(1):e000018. doi:10.1136/bmjgast-2014-000018
21. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480-1491. doi:10.1053/j.gastro.2005.11.061
22. Talley NJ, Phillips SF, Melton J, 3rd, Wiltgen C, Zinsmeister AR. A patient questionnaire to identify bowel disease. Ann Intern Med. 1989;111(8):671-674. doi:10.7326/0003-4819-111-8-671
23. Bensoussan A, Talley NJ, Hing M, Menzies R, Guo A, Ngu M. Treatment of irritable bowel syndrome with Chinese herbal medicine: a randomized controlled trial. JAMA. 1998;280(18):1585-1589. doi:10.1001/jama.280.18.1585
24. Francis CY, Morris J, Whorwell PJ. The irritable bowel severity scoring system: a simple method of monitoring irritable bowel syndrome and its progress. Aliment Pharmacol Ther. 1997;11(2):395-402. doi:10.1046/j.1365-2036.1997.142318000.x
25. Patrick DL, Drossman DA, Frederick IO, DiCesare J, Puder KL. Quality of life in persons with irritable bowel syndrome: development and validation of a new measure. Dig Dis Sci. 1998;43(2):400-411. doi:10.1023/a:1018831127942
26. Attanasio V, Andrasik F, Blanchard EB, Arena JG. Psychometric properties of the SUNYA revision of the Psychosomatic Symptom Checklist. J Behav Med. 1984;7(2):247-257. doi:10.1007/BF00845390
27. Weathers F, Litz B, Herman D, Huska J, Keane T. The PTSD Checklist (PCL): reliability, validity, and diagnostic utility. Accessed August 25, 2022. https://www.researchgate.net/publication/291448760_The_PTSD_Checklist_PCL_Reliability_validity_and_diagnostic_utility
28. Derogatis L. Brief Symptom Inventory-18 (BSI-18): Administration, Scoring, and Procedure Manual. Ed 3 ed. National Computer Systems; 2000.
29. Stamps BW, Lyon WJ, Irvin AP, Kelley-Loughnane N, Goodson MS. A pilot study of the effect of deployment on the gut microbiome and traveler´s diarrhea susceptibility. Front Cell Infect Microbiol. 2020;10:589297. doi:10.3389/fcimb.2020.589297
30. Kim HJ, Camilleri M, McKinzie S, et al. A randomized controlled trial of a probiotic, VSL#3, on gut transit and symptoms in diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2003;17(7):895-904. doi:10.1046/j.1365-2036.2003.01543.x
31. Kim HJ, Vazquez Roque MI, Camilleri M, et al. A randomized controlled trial of a probiotic combination VSL# 3 and placebo in irritable bowel syndrome with bloating. Neurogastroenterol Motil. 2005;17(5):687-696. doi:10.1111/j.1365-2982.2005.00695.x32. Michail S, Kenche H. Gut microbiota is not modified by randomized, double-blind, placebo-controlled trial of vsl#3 in diarrhea-predominant irritable bowel syndrome. Probiotics Antimicrob Proteins. 2011;3(1):1-7. doi:10.1007/s12602-010-9059-y
33. Moayyedi P, Ford AC, Talley NJ, et al. The efficacy of probiotics in the treatment of irritable bowel syndrome: a systematic review. Gut. 2010;59(3):325-332. doi:10.1136/gut.2008.167270
34. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044-1060. doi:10.1111/apt.15001
35. Dale HF, Rasmussen SH, Asiller OO, Lied GA. Probiotics in irritable bowel syndrome: an up-to-date systematic review. Nutrients. 2019;11(9). doi:10.3390/nu11092048
36. Didari T, Mozaffari S, Nikfar S, Abdollahi M. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J Gastroenterol. 2015;21(10):3072-84. doi:10.3748/wjg.v21.i10.3072
37. Hungin APS, Mitchell CR, Whorwell P, et al. Systematic review: probiotics in the management of lower gastrointestinal symptoms—an updated evidence-based international consensus. Aliment Pharmacol Ther. 2018;47(8):1054-1070. doi:10.1111/apt.14539
38. Niu HL, Xiao JY. The efficacy and safety of probiotics in patients with irritable bowel syndrome: evidence based on 35 randomized controlled trials. Int J Surg. 2020;75:116-127. doi:10.1016/j.ijsu.2020.01.142
39. Wong RK, Yang C, Song GH, Wong J, Ho KY. Melatonin regulation as a possible mechanism for probiotic (VSL#3) in irritable bowel syndrome: a randomized double-blinded placebo study. Dig Dis Sci. 2015;60(1):186-194. doi:10.1007/s10620-014-3299-8
40. Ford AC, Moayyedi P, Lacy BE, et al. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Am J Gastroenterol. 2014;109(suppl 1):S2-26; quiz S27. doi: 10.1038/ajg.2014.187
41. Simren M, Barbara G, Flint HJ, et al. Intestinal microbiota in functional bowel disorders: a Rome foundation report. Gut. 2013;62(1):159-76. doi:10.1136/gutjnl-2012-302167
42. Ki Cha B, Mun Jung S, Hwan Choi C, et al. The effect of a multispecies probiotic mixture on the symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. J Clin Gastroenterol. 2012;46(3):220-7. doi:10.1097/MCG.0b013e31823712b1
43. Connell M, Shin A, James-Stevenson T, Xu H, Imperiale TF, Herron J. Systematic review and meta-analysis: Efficacy of patented probiotic, VSL#3, in irritable bowel syndrome. Neurogastroenterol Motil. 2018;30(12):e13427. doi:10.1111/nmo.13427
44. Lyra A, Hillila M, Huttunen T, et al. Irritable bowel syndrome symptom severity improves equally with probiotic and placebo. World J Gastroenterol. 2016;22(48):10631-10642. doi:10.3748/wjg.v22.i48.10631
45. Sanders ME, Guarner F, Guerrant R, et al. An update on the use and investigation of probiotics in health and disease. Gut. 2013;62(5):787-796. doi:10.1136/gutjnl-2012-302504
46. Tuteja AK. Deployment-associated functional gastrointestinal disorders: do we know the etiology? Dig Dis Sci. 2011;56(11):3109-3111. doi:10.1007/s10620-011-1856-y
1. O’Shea EF, Cotter PD, Stanton C, Ross RP, Hill C. Production of bioactive substances by intestinal bacteria as a basis for explaining probiotic mechanisms: bacteriocins and conjugated linoleic acid. Int J Food Microbiol. 2012;152(3):189-205. doi:10.1016/j.ijfoodmicro.2011.05.025.
2. Kamiya T, Wang L, Forsythe P, et al. Inhibitory effects of Lactobacillus reuteri on visceral pain induced by colorectal distension in Sprague-Dawley rats. Gut. 2006;55(2):191-196. doi:10.1136/gut.2005.070987.
3. Verdu EF, Bercik P, Verma-Gandhu M, et al. Specific probiotic therapy attenuates antibiotic induced visceral hypersensitivity in mice. Gut. 2006;55(2):182-190. doi:10.1136/gut.2005.066100
4. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044-1060. doi:10.1111/apt.15001.
5. Niu HL, Xiao JY. The efficacy and safety of probiotics in patients with irritable bowel syndrome: Evidence based on 35 randomized controlled trials. Int J Surg. 2020;75:116-127. doi:10.1016/j.ijsu.2020.01.142.
6. Wong RK, Yang C, Song GH, Wong J, Ho KY. Melatonin regulation as a possible mechanism for probiotic (VSL#3) in irritable bowel syndrome: a randomized double-blinded placebo study. Dig Dis Sci. 2015;60(1):186-194. doi:10.1007/s10620-014-3299-8.
7. Hyams KC, Bourgeois AL, Merrell BR, et al. Diarrheal disease during Operation Desert Shield. N Engl J Med. 1991;325(20):1423-1428. doi:10.1056/NEJM199111143252006 8. Clancy RL, Gleeson M, Cox A, et al. Reversal in fatigued athletes of a defect in interferon gamma secretion after administration of Lactobacillus acidophilus. Br J Sports Med. 2006;40(4):351-354. doi:10.1136/bjsm.2005.024364
9. Sullivan A, Nord CE, Evengard B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutr J. 2009;8:4. doi:10.1186/1475-2891-8-4
10. Pittayanon R, Lau JT, Yuan Y, et al. Gut microbiota in patients with irritable bowel syndrome—a systematic review. Gastroenterology. 2019;157(1):97-108. doi:10.1053/j.gastro.2019.03.049
11. Rao RK, Samak G. Protection and restitution of gut barrier by probiotics: nutritional and clinical implications. Curr Nutr Food Sci. 2013;9(2):99-107. doi:10.2174/1573401311309020004
12. O´Shea EF, Cotter PD, Stanton C, Ross RP, Hill C. Production of bioactive substances by intestinal bacteria as a basis for explaining probiotic mechanisms: bacteriocins and conjugated linoleic acid. Int J Food Microbiol. 2012;152(3):189-205. doi:10.1016/j.ijfoodmicro.2011.05.025
13. Kamiya T, Wang L, Forsythe P, et al. Inhibitory effects of Lactobacillus reuteri on visceral pain induced by colorectal distension in Sprague-Dawley rats. Gut. 2006;55(2):191-196. doi:10.1136/gut.2005.070987
14. Verdu EF, Bercik P, Verma-Gandhu M, et al. Specific probiotic therapy attenuates antibiotic induced visceral hypersensitivity in mice. Gut. 2006;55(2):182-190. doi:10.1136/gut.2005.06610015. O´Mahony L, McCarthy J, Kelly P, et al. Lactobacillus and bifidobacterium in irritable bowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterology. 2005;128(3):541-551. doi:10.1053/j.gastro.2004.11.050
16. Alhasson F, Das S, Seth R, et al. Altered gut microbiome in a mouse model of Gulf War Illness causes neuroinflammation and intestinal injury via leaky gut and TLR4 activation. PLoS One. 2017;12(3):e0172914. doi:10.1371/journal.pone.0172914.17. Janulewicz PA, Seth RK, Carlson JM, et al. The gut-microbiome in Gulf War veterans: a preliminary report. Int J Environ Res Public Health. 2019;16(19). doi:10.3390/ijerph16193751
18. Dang X, Xu M, Liu D, Zhou D, Yang W. Assessing the efficacy and safety of fecal microbiota transplantation and probiotic VSL#3 for active ulcerative colitis: a systematic review and meta-analysis. PLoS One. 2020;15(3):e0228846. doi:10.1371/journal.pone.0228846
19. Ford AC, Quigley EM, Lacy BE, et al. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: systematic review and meta-analysis. Am J Gastroenterol. 2014;109(10):1547-1561; quiz 1546, 1562. doi:10.1038/ajg.2014.202
20. Rohatgi S, Ahuja V, Makharia GK, et al. VSL#3 induces and maintains short-term clinical response in patients with active microscopic colitis: a two-phase randomised clinical trial. BMJ Open Gastroenterol. 2015;2(1):e000018. doi:10.1136/bmjgast-2014-000018
21. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480-1491. doi:10.1053/j.gastro.2005.11.061
22. Talley NJ, Phillips SF, Melton J, 3rd, Wiltgen C, Zinsmeister AR. A patient questionnaire to identify bowel disease. Ann Intern Med. 1989;111(8):671-674. doi:10.7326/0003-4819-111-8-671
23. Bensoussan A, Talley NJ, Hing M, Menzies R, Guo A, Ngu M. Treatment of irritable bowel syndrome with Chinese herbal medicine: a randomized controlled trial. JAMA. 1998;280(18):1585-1589. doi:10.1001/jama.280.18.1585
24. Francis CY, Morris J, Whorwell PJ. The irritable bowel severity scoring system: a simple method of monitoring irritable bowel syndrome and its progress. Aliment Pharmacol Ther. 1997;11(2):395-402. doi:10.1046/j.1365-2036.1997.142318000.x
25. Patrick DL, Drossman DA, Frederick IO, DiCesare J, Puder KL. Quality of life in persons with irritable bowel syndrome: development and validation of a new measure. Dig Dis Sci. 1998;43(2):400-411. doi:10.1023/a:1018831127942
26. Attanasio V, Andrasik F, Blanchard EB, Arena JG. Psychometric properties of the SUNYA revision of the Psychosomatic Symptom Checklist. J Behav Med. 1984;7(2):247-257. doi:10.1007/BF00845390
27. Weathers F, Litz B, Herman D, Huska J, Keane T. The PTSD Checklist (PCL): reliability, validity, and diagnostic utility. Accessed August 25, 2022. https://www.researchgate.net/publication/291448760_The_PTSD_Checklist_PCL_Reliability_validity_and_diagnostic_utility
28. Derogatis L. Brief Symptom Inventory-18 (BSI-18): Administration, Scoring, and Procedure Manual. Ed 3 ed. National Computer Systems; 2000.
29. Stamps BW, Lyon WJ, Irvin AP, Kelley-Loughnane N, Goodson MS. A pilot study of the effect of deployment on the gut microbiome and traveler´s diarrhea susceptibility. Front Cell Infect Microbiol. 2020;10:589297. doi:10.3389/fcimb.2020.589297
30. Kim HJ, Camilleri M, McKinzie S, et al. A randomized controlled trial of a probiotic, VSL#3, on gut transit and symptoms in diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2003;17(7):895-904. doi:10.1046/j.1365-2036.2003.01543.x
31. Kim HJ, Vazquez Roque MI, Camilleri M, et al. A randomized controlled trial of a probiotic combination VSL# 3 and placebo in irritable bowel syndrome with bloating. Neurogastroenterol Motil. 2005;17(5):687-696. doi:10.1111/j.1365-2982.2005.00695.x32. Michail S, Kenche H. Gut microbiota is not modified by randomized, double-blind, placebo-controlled trial of vsl#3 in diarrhea-predominant irritable bowel syndrome. Probiotics Antimicrob Proteins. 2011;3(1):1-7. doi:10.1007/s12602-010-9059-y
33. Moayyedi P, Ford AC, Talley NJ, et al. The efficacy of probiotics in the treatment of irritable bowel syndrome: a systematic review. Gut. 2010;59(3):325-332. doi:10.1136/gut.2008.167270
34. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044-1060. doi:10.1111/apt.15001
35. Dale HF, Rasmussen SH, Asiller OO, Lied GA. Probiotics in irritable bowel syndrome: an up-to-date systematic review. Nutrients. 2019;11(9). doi:10.3390/nu11092048
36. Didari T, Mozaffari S, Nikfar S, Abdollahi M. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J Gastroenterol. 2015;21(10):3072-84. doi:10.3748/wjg.v21.i10.3072
37. Hungin APS, Mitchell CR, Whorwell P, et al. Systematic review: probiotics in the management of lower gastrointestinal symptoms—an updated evidence-based international consensus. Aliment Pharmacol Ther. 2018;47(8):1054-1070. doi:10.1111/apt.14539
38. Niu HL, Xiao JY. The efficacy and safety of probiotics in patients with irritable bowel syndrome: evidence based on 35 randomized controlled trials. Int J Surg. 2020;75:116-127. doi:10.1016/j.ijsu.2020.01.142
39. Wong RK, Yang C, Song GH, Wong J, Ho KY. Melatonin regulation as a possible mechanism for probiotic (VSL#3) in irritable bowel syndrome: a randomized double-blinded placebo study. Dig Dis Sci. 2015;60(1):186-194. doi:10.1007/s10620-014-3299-8
40. Ford AC, Moayyedi P, Lacy BE, et al. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Am J Gastroenterol. 2014;109(suppl 1):S2-26; quiz S27. doi: 10.1038/ajg.2014.187
41. Simren M, Barbara G, Flint HJ, et al. Intestinal microbiota in functional bowel disorders: a Rome foundation report. Gut. 2013;62(1):159-76. doi:10.1136/gutjnl-2012-302167
42. Ki Cha B, Mun Jung S, Hwan Choi C, et al. The effect of a multispecies probiotic mixture on the symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. J Clin Gastroenterol. 2012;46(3):220-7. doi:10.1097/MCG.0b013e31823712b1
43. Connell M, Shin A, James-Stevenson T, Xu H, Imperiale TF, Herron J. Systematic review and meta-analysis: Efficacy of patented probiotic, VSL#3, in irritable bowel syndrome. Neurogastroenterol Motil. 2018;30(12):e13427. doi:10.1111/nmo.13427
44. Lyra A, Hillila M, Huttunen T, et al. Irritable bowel syndrome symptom severity improves equally with probiotic and placebo. World J Gastroenterol. 2016;22(48):10631-10642. doi:10.3748/wjg.v22.i48.10631
45. Sanders ME, Guarner F, Guerrant R, et al. An update on the use and investigation of probiotics in health and disease. Gut. 2013;62(5):787-796. doi:10.1136/gutjnl-2012-302504
46. Tuteja AK. Deployment-associated functional gastrointestinal disorders: do we know the etiology? Dig Dis Sci. 2011;56(11):3109-3111. doi:10.1007/s10620-011-1856-y