User login
For MD-IQ use only
Support for Policy Changes for Therapy Related to Homefront Missions
Recent natural disasters, civil disorder, and the COVID-19 pandemic response created an unprecedented demand for the US National Guard and Reserve components as well as active-duty personnel to serve on homefront missions critical to our nation. At times, those serving in these capacities are front and center to the most tragic events confronting our nation, and they frequently encounter tremendous suffering.
Recognizing the potential for these missions to create psychological sequela for those who serve on them, the authority for the Veterans Health Administration (VHA) vet centers to provide readjustment counseling services was broadened on December 30, 2021. Vet centers are community-based counseling centers that have traditionally served combat veterans, and broadening services reflects a major change in mission. Revised VHA Directive 1500(2) specifies that those who “served on active duty in response to a national emergency or major disaster declared by the President” or “served on active duty in the National Guard of a State under orders of the chief executive of that State in response to a disaster or civil disorder in such State” may now receive therapy at vet centers.1,2
As a result of this recent policy change, National Guard and active-duty Reserve service members now have parity with combat veterans to obtain therapy for symptoms arising as a result of their activation for service on homefront missions. As they seek care, we need to be ready so that these service members can obtain the best therapy services possible. Soldiers who served on homefront missions comprise a new cohort of service members now eligible for vet center therapy. Soldiers who served on homefront missions may present with issues that differ from those of combat veterans and veterans who have experienced military sexual trauma (MST), the populations treated by vet centers and other VHA mental health care clinics prior to this broadened authority. This article highlights some suggestions for service delivery to best meet the needs of this population.
Discussion
Available evidence-based therapies to treat posttraumatic stress disorder (PTSD) are effective regardless of whether the trauma occurred in combat, on the homefront, or in a civilian setting. The vet centers and VHA mental health services already have staff trained to deliver these therapy modalities and, in this sense, are ready to provide trauma-focused therapy treatment to soldiers with PTSD who served on homefront missions.
The broadened authority for the vet centers to provide readjustment services is necessary, as it corrects for a critical gap in services, but the importance of ensuring adequate staffing to meet the expected increased demand for services cannot be underscored. According to clinical practice guidelines for the treatment of PTSD, developed by the US Department of Veterans Affairs (VA) and the US Department of Defense (DoD), the therapies with the strongest evidence-based backing are prolonged exposure-based therapy (PE), cognitive processing therapy (CPT), and eye movement and desensitization reprocessing (EMDR).3 These therapy modalities, based on findings from clinical trials, are predicated on seeing a client for a sufficient number of sessions. Attendance at these sessions is recommended at least weekly to ensure adequate intensity of service delivery.4-7 According to the National Center for PTSD, PE typically involves 8 to 15 weekly or twice weekly sessions; CPT requires 8 to 14 or more weekly sessions, and EMDR is usually 4 to 12 weekly sessions.4-7
Ensuring adequate staffing is critical to offer these therapies at least weekly as the efficacies of these therapies are otherwise not proven if return session visits are stretched out over multiple weeks or months. The most recent clinical research has demonstrated that PTSD recovery can be expedited and there are lower patient dropout rates when sessions are massed or compressed so that multiple sessions are administered over 1 week.8-12 Providing these therapies in a massed format has shown to be as effective as when these therapies are provided weekly.
As the authority to treat soldiers serving on homefront missions is new, epidemiologic data do not yet exist to estimate the proportion of this population who will need treatment or present with PTSD, depression, anxiety, a substance use disorder, and/or comorbid conditions. Those with PTSD can benefit from PTSD evidence-based therapies already available for treatment. Others may benefit from treatments that are proven effective for their mental health diagnoses.
Therapists with experience primarily treating patients with PTSD related to combat or MST will need to be sensitive to the unique experiences of the National Guard and Reserve service members. For example, this component of soldiers served on COVID-19–related missions that provided food service support to nursing homes residents who were locked down from family members. As a result, they developed bonds with residents who later died. This may have been the first time that these soldiers witnessed death. If such a soldier is assessed and does not have PTSD but is nonetheless distressed, then the soldier may need alternate therapies, such as grief counseling. This need may be more pronounced for those soldiers who lost loved ones to COVID-19 while they served on these missions.
New Jersey Army National Guard soldiers provided food service support at the Woodland Behavioral and Nursing Center in Andover, New Jersey. These soldiers witnessed the unfortunate conditions in this facility, which included stacked bodies in a makeshift morgue during the height of the pandemic; however, they did not have the ability to make changes. The facility is under investigation for abuse and neglect of its residents.13
New Jersey National Guard soldiers supporting that facility and similar ones may have experienced moral injury, defined as “…perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations.”14 Importantly, when these soldiers present for therapy and express moral injury, their therapists need to be open to spiritual discourse. However, vet centers do not have chaplains on staff, so therapists must refer patients to chaplaincy services.
Among therapists with existing cultural competency for treating members of the military, some nuances exist for National Guard and Reserve service members. National Guard and Reserve component personnel already may feel that their problems are less important than those experienced by active-duty service members. Now that these soldiers have the eligibility to receive therapy, therapists may have to make extra efforts to both reassure this population that they are welcomed and to validate their need for services.
Special outreach efforts to those who served on historical National Guard and active-duty Reserve missions are a way to show good faith in serving these soldiers because they may have untreated PTSD or other undiagnosed mental health disorders related to earlier deployments, such as hurricane recovery missions. A study of disaster survivors found that the prevalence rate of severe and very severe psychological impact after a natural disaster was about 34%.15 Another epidemiologic study found that the prevalence rate of PTSD was 10% to 20% among disaster rescue workers.16 Specific data about the psychological problems of National Guard and Reserve components serving in disaster recovery are unavailable but is an area for future research.
Therapists who have treated active-duty service members and veterans who worked in mortuary services in a combat zone are used to hearing graphic details of horrifying scenes, but homefront experiences are different. Soldiers on homefront mortuary-based missions frequently reported being unable to forget the faces or the smell of dead bodies as they were stacked up and overwhelming the systems. Experienced vet center therapists should be prepared for the challenges in treating this new cohort of patients.
Conclusions
Now that National Guard and Reserve component soldiers who have responded to national and local emergencies are eligible for therapy, we need to be prepared to provide these services. In addition to addressing systemic staffing concerns, therapists need to be aware of the unique challenges faced by those who have served on homefront missions. These homefront missions have the potential to hit home for therapists.
1. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1550(2): readjustment counseling service. January 26, 2021. Accessed September 1, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9168
2. US Department of Veterans Affairs. Vet centers (readjustment counseling: vet center eligibility. Updated January 3, 2022. Accessed September 1, 2022. https://www.vetcenter.va.gov/eligibility.asp
3. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress reaction, version 3.0, 2017. Accessed September 1, 2022. https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal012418.pdf
4. US Department of Veterans Affairs, National Center for PTSD. Prolonged exposure (PE) therapy. Updated August 10, 2022. Accessed September 1, 2022. https://www.ptsd.va.gov/understand_tx/prolonged_exposure.asp
5. US Department of Veterans Affairs, National Center for PTSD. Cognitive processing therapy (CPT) for PTSD: how to help your loved one during treatment. Accessed September 1, 2022. https://www.ptsd.va.gov/publications/print/CPT_familyhandout.pdf
6. US Department of Veterans Affairs, National Center for PTSD. A provider’s guide to brief cognitive behavioral therapy. Accessed September 1, 2022. https://www.mirecc.va.gov/visn16/docs/Therapists_Guide_to_Brief_CBTManual.pdf
7. US Department of Veterans Affairs, National Center for PTSD. Eye movement desensitization and reprocessing (EMDR) for PTSD. Accessed September 1, 2022. https://www.ptsd.va.gov/understand_tx/emdr.asp
8. Wachen JS, Dondanville KA, Evans WR, Morris K, Cole A. Adjusting the timeframe of evidence-based therapies for PTSD-massed treatments. Curr Treat Options Psych. 2019;6(2):107-118. doi:10.1007/s40501-019-00169-9
9. Dell L, Sbisa AM, Forbes A, et al. Effect of massed v. standard prolonged exposure therapy on PTSD in military personnel and veterans: a non-inferiority randomised controlled trial [published online ahead of print, 2022 Apr 20]. Psychol Med. 2022;1-8. doi:10.1017/S0033291722000927
10. Held P, Kovacevic M, Petrey K, et al. Treating posttraumatic stress disorder at home in a single week using 1-week virtual massed cognitive processing therapy. J Trauma Stress. 2022;35(4):1215-1225. doi:10.1002/jts.22831
11. Yamokoski C, Flores H, Facemire V, Maieritsch K, Perez S, Fedynich A. Feasibility of an intensive outpatient treatment program for posttraumatic stress disorder within the veterans health care administration [published online ahead of print, 2022 Mar 7]. Psychol Serv. 2022;10.1037/ser0000628. doi:10.1037/ser0000628
12. Galovski TE, Werner KB, Weaver TL, et al. Massed cognitive processing therapy for posttraumatic stress disorder in women survivors of intimate partner violence. Psychol Trauma. 2022;14(5):769-779. doi:10.1037/tra0001100
13. Fallon S. NJ to send monitors into troubled nursing home that stacked bodies in makeshift morgue. Updated March 10, 2022. Accessed September 1, 2022. https://www.northjersey.com/story/news/health/2022/03/09/sussex-county-nj-nursing-home-monitors-covid-morgue/9447243002/
14. Litz BT, Stein N, Delaney E, et al. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin Psychol Rev. 2009;29(8):695-706. doi:10.1016/j.cpr.2009.07.003009
15. Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981-2001. Psychiatry. 2002;65(3):207-239. doi:10.1521/psyc.65.3.207.20173
16. Galea S, Nandi A, Vlahov D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol Rev. 2005;27:78-91. doi:10.1093/epirev/mxi003
Recent natural disasters, civil disorder, and the COVID-19 pandemic response created an unprecedented demand for the US National Guard and Reserve components as well as active-duty personnel to serve on homefront missions critical to our nation. At times, those serving in these capacities are front and center to the most tragic events confronting our nation, and they frequently encounter tremendous suffering.
Recognizing the potential for these missions to create psychological sequela for those who serve on them, the authority for the Veterans Health Administration (VHA) vet centers to provide readjustment counseling services was broadened on December 30, 2021. Vet centers are community-based counseling centers that have traditionally served combat veterans, and broadening services reflects a major change in mission. Revised VHA Directive 1500(2) specifies that those who “served on active duty in response to a national emergency or major disaster declared by the President” or “served on active duty in the National Guard of a State under orders of the chief executive of that State in response to a disaster or civil disorder in such State” may now receive therapy at vet centers.1,2
As a result of this recent policy change, National Guard and active-duty Reserve service members now have parity with combat veterans to obtain therapy for symptoms arising as a result of their activation for service on homefront missions. As they seek care, we need to be ready so that these service members can obtain the best therapy services possible. Soldiers who served on homefront missions comprise a new cohort of service members now eligible for vet center therapy. Soldiers who served on homefront missions may present with issues that differ from those of combat veterans and veterans who have experienced military sexual trauma (MST), the populations treated by vet centers and other VHA mental health care clinics prior to this broadened authority. This article highlights some suggestions for service delivery to best meet the needs of this population.
Discussion
Available evidence-based therapies to treat posttraumatic stress disorder (PTSD) are effective regardless of whether the trauma occurred in combat, on the homefront, or in a civilian setting. The vet centers and VHA mental health services already have staff trained to deliver these therapy modalities and, in this sense, are ready to provide trauma-focused therapy treatment to soldiers with PTSD who served on homefront missions.
The broadened authority for the vet centers to provide readjustment services is necessary, as it corrects for a critical gap in services, but the importance of ensuring adequate staffing to meet the expected increased demand for services cannot be underscored. According to clinical practice guidelines for the treatment of PTSD, developed by the US Department of Veterans Affairs (VA) and the US Department of Defense (DoD), the therapies with the strongest evidence-based backing are prolonged exposure-based therapy (PE), cognitive processing therapy (CPT), and eye movement and desensitization reprocessing (EMDR).3 These therapy modalities, based on findings from clinical trials, are predicated on seeing a client for a sufficient number of sessions. Attendance at these sessions is recommended at least weekly to ensure adequate intensity of service delivery.4-7 According to the National Center for PTSD, PE typically involves 8 to 15 weekly or twice weekly sessions; CPT requires 8 to 14 or more weekly sessions, and EMDR is usually 4 to 12 weekly sessions.4-7
Ensuring adequate staffing is critical to offer these therapies at least weekly as the efficacies of these therapies are otherwise not proven if return session visits are stretched out over multiple weeks or months. The most recent clinical research has demonstrated that PTSD recovery can be expedited and there are lower patient dropout rates when sessions are massed or compressed so that multiple sessions are administered over 1 week.8-12 Providing these therapies in a massed format has shown to be as effective as when these therapies are provided weekly.
As the authority to treat soldiers serving on homefront missions is new, epidemiologic data do not yet exist to estimate the proportion of this population who will need treatment or present with PTSD, depression, anxiety, a substance use disorder, and/or comorbid conditions. Those with PTSD can benefit from PTSD evidence-based therapies already available for treatment. Others may benefit from treatments that are proven effective for their mental health diagnoses.
Therapists with experience primarily treating patients with PTSD related to combat or MST will need to be sensitive to the unique experiences of the National Guard and Reserve service members. For example, this component of soldiers served on COVID-19–related missions that provided food service support to nursing homes residents who were locked down from family members. As a result, they developed bonds with residents who later died. This may have been the first time that these soldiers witnessed death. If such a soldier is assessed and does not have PTSD but is nonetheless distressed, then the soldier may need alternate therapies, such as grief counseling. This need may be more pronounced for those soldiers who lost loved ones to COVID-19 while they served on these missions.
New Jersey Army National Guard soldiers provided food service support at the Woodland Behavioral and Nursing Center in Andover, New Jersey. These soldiers witnessed the unfortunate conditions in this facility, which included stacked bodies in a makeshift morgue during the height of the pandemic; however, they did not have the ability to make changes. The facility is under investigation for abuse and neglect of its residents.13
New Jersey National Guard soldiers supporting that facility and similar ones may have experienced moral injury, defined as “…perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations.”14 Importantly, when these soldiers present for therapy and express moral injury, their therapists need to be open to spiritual discourse. However, vet centers do not have chaplains on staff, so therapists must refer patients to chaplaincy services.
Among therapists with existing cultural competency for treating members of the military, some nuances exist for National Guard and Reserve service members. National Guard and Reserve component personnel already may feel that their problems are less important than those experienced by active-duty service members. Now that these soldiers have the eligibility to receive therapy, therapists may have to make extra efforts to both reassure this population that they are welcomed and to validate their need for services.
Special outreach efforts to those who served on historical National Guard and active-duty Reserve missions are a way to show good faith in serving these soldiers because they may have untreated PTSD or other undiagnosed mental health disorders related to earlier deployments, such as hurricane recovery missions. A study of disaster survivors found that the prevalence rate of severe and very severe psychological impact after a natural disaster was about 34%.15 Another epidemiologic study found that the prevalence rate of PTSD was 10% to 20% among disaster rescue workers.16 Specific data about the psychological problems of National Guard and Reserve components serving in disaster recovery are unavailable but is an area for future research.
Therapists who have treated active-duty service members and veterans who worked in mortuary services in a combat zone are used to hearing graphic details of horrifying scenes, but homefront experiences are different. Soldiers on homefront mortuary-based missions frequently reported being unable to forget the faces or the smell of dead bodies as they were stacked up and overwhelming the systems. Experienced vet center therapists should be prepared for the challenges in treating this new cohort of patients.
Conclusions
Now that National Guard and Reserve component soldiers who have responded to national and local emergencies are eligible for therapy, we need to be prepared to provide these services. In addition to addressing systemic staffing concerns, therapists need to be aware of the unique challenges faced by those who have served on homefront missions. These homefront missions have the potential to hit home for therapists.
Recent natural disasters, civil disorder, and the COVID-19 pandemic response created an unprecedented demand for the US National Guard and Reserve components as well as active-duty personnel to serve on homefront missions critical to our nation. At times, those serving in these capacities are front and center to the most tragic events confronting our nation, and they frequently encounter tremendous suffering.
Recognizing the potential for these missions to create psychological sequela for those who serve on them, the authority for the Veterans Health Administration (VHA) vet centers to provide readjustment counseling services was broadened on December 30, 2021. Vet centers are community-based counseling centers that have traditionally served combat veterans, and broadening services reflects a major change in mission. Revised VHA Directive 1500(2) specifies that those who “served on active duty in response to a national emergency or major disaster declared by the President” or “served on active duty in the National Guard of a State under orders of the chief executive of that State in response to a disaster or civil disorder in such State” may now receive therapy at vet centers.1,2
As a result of this recent policy change, National Guard and active-duty Reserve service members now have parity with combat veterans to obtain therapy for symptoms arising as a result of their activation for service on homefront missions. As they seek care, we need to be ready so that these service members can obtain the best therapy services possible. Soldiers who served on homefront missions comprise a new cohort of service members now eligible for vet center therapy. Soldiers who served on homefront missions may present with issues that differ from those of combat veterans and veterans who have experienced military sexual trauma (MST), the populations treated by vet centers and other VHA mental health care clinics prior to this broadened authority. This article highlights some suggestions for service delivery to best meet the needs of this population.
Discussion
Available evidence-based therapies to treat posttraumatic stress disorder (PTSD) are effective regardless of whether the trauma occurred in combat, on the homefront, or in a civilian setting. The vet centers and VHA mental health services already have staff trained to deliver these therapy modalities and, in this sense, are ready to provide trauma-focused therapy treatment to soldiers with PTSD who served on homefront missions.
The broadened authority for the vet centers to provide readjustment services is necessary, as it corrects for a critical gap in services, but the importance of ensuring adequate staffing to meet the expected increased demand for services cannot be underscored. According to clinical practice guidelines for the treatment of PTSD, developed by the US Department of Veterans Affairs (VA) and the US Department of Defense (DoD), the therapies with the strongest evidence-based backing are prolonged exposure-based therapy (PE), cognitive processing therapy (CPT), and eye movement and desensitization reprocessing (EMDR).3 These therapy modalities, based on findings from clinical trials, are predicated on seeing a client for a sufficient number of sessions. Attendance at these sessions is recommended at least weekly to ensure adequate intensity of service delivery.4-7 According to the National Center for PTSD, PE typically involves 8 to 15 weekly or twice weekly sessions; CPT requires 8 to 14 or more weekly sessions, and EMDR is usually 4 to 12 weekly sessions.4-7
Ensuring adequate staffing is critical to offer these therapies at least weekly as the efficacies of these therapies are otherwise not proven if return session visits are stretched out over multiple weeks or months. The most recent clinical research has demonstrated that PTSD recovery can be expedited and there are lower patient dropout rates when sessions are massed or compressed so that multiple sessions are administered over 1 week.8-12 Providing these therapies in a massed format has shown to be as effective as when these therapies are provided weekly.
As the authority to treat soldiers serving on homefront missions is new, epidemiologic data do not yet exist to estimate the proportion of this population who will need treatment or present with PTSD, depression, anxiety, a substance use disorder, and/or comorbid conditions. Those with PTSD can benefit from PTSD evidence-based therapies already available for treatment. Others may benefit from treatments that are proven effective for their mental health diagnoses.
Therapists with experience primarily treating patients with PTSD related to combat or MST will need to be sensitive to the unique experiences of the National Guard and Reserve service members. For example, this component of soldiers served on COVID-19–related missions that provided food service support to nursing homes residents who were locked down from family members. As a result, they developed bonds with residents who later died. This may have been the first time that these soldiers witnessed death. If such a soldier is assessed and does not have PTSD but is nonetheless distressed, then the soldier may need alternate therapies, such as grief counseling. This need may be more pronounced for those soldiers who lost loved ones to COVID-19 while they served on these missions.
New Jersey Army National Guard soldiers provided food service support at the Woodland Behavioral and Nursing Center in Andover, New Jersey. These soldiers witnessed the unfortunate conditions in this facility, which included stacked bodies in a makeshift morgue during the height of the pandemic; however, they did not have the ability to make changes. The facility is under investigation for abuse and neglect of its residents.13
New Jersey National Guard soldiers supporting that facility and similar ones may have experienced moral injury, defined as “…perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations.”14 Importantly, when these soldiers present for therapy and express moral injury, their therapists need to be open to spiritual discourse. However, vet centers do not have chaplains on staff, so therapists must refer patients to chaplaincy services.
Among therapists with existing cultural competency for treating members of the military, some nuances exist for National Guard and Reserve service members. National Guard and Reserve component personnel already may feel that their problems are less important than those experienced by active-duty service members. Now that these soldiers have the eligibility to receive therapy, therapists may have to make extra efforts to both reassure this population that they are welcomed and to validate their need for services.
Special outreach efforts to those who served on historical National Guard and active-duty Reserve missions are a way to show good faith in serving these soldiers because they may have untreated PTSD or other undiagnosed mental health disorders related to earlier deployments, such as hurricane recovery missions. A study of disaster survivors found that the prevalence rate of severe and very severe psychological impact after a natural disaster was about 34%.15 Another epidemiologic study found that the prevalence rate of PTSD was 10% to 20% among disaster rescue workers.16 Specific data about the psychological problems of National Guard and Reserve components serving in disaster recovery are unavailable but is an area for future research.
Therapists who have treated active-duty service members and veterans who worked in mortuary services in a combat zone are used to hearing graphic details of horrifying scenes, but homefront experiences are different. Soldiers on homefront mortuary-based missions frequently reported being unable to forget the faces or the smell of dead bodies as they were stacked up and overwhelming the systems. Experienced vet center therapists should be prepared for the challenges in treating this new cohort of patients.
Conclusions
Now that National Guard and Reserve component soldiers who have responded to national and local emergencies are eligible for therapy, we need to be prepared to provide these services. In addition to addressing systemic staffing concerns, therapists need to be aware of the unique challenges faced by those who have served on homefront missions. These homefront missions have the potential to hit home for therapists.
1. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1550(2): readjustment counseling service. January 26, 2021. Accessed September 1, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9168
2. US Department of Veterans Affairs. Vet centers (readjustment counseling: vet center eligibility. Updated January 3, 2022. Accessed September 1, 2022. https://www.vetcenter.va.gov/eligibility.asp
3. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress reaction, version 3.0, 2017. Accessed September 1, 2022. https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal012418.pdf
4. US Department of Veterans Affairs, National Center for PTSD. Prolonged exposure (PE) therapy. Updated August 10, 2022. Accessed September 1, 2022. https://www.ptsd.va.gov/understand_tx/prolonged_exposure.asp
5. US Department of Veterans Affairs, National Center for PTSD. Cognitive processing therapy (CPT) for PTSD: how to help your loved one during treatment. Accessed September 1, 2022. https://www.ptsd.va.gov/publications/print/CPT_familyhandout.pdf
6. US Department of Veterans Affairs, National Center for PTSD. A provider’s guide to brief cognitive behavioral therapy. Accessed September 1, 2022. https://www.mirecc.va.gov/visn16/docs/Therapists_Guide_to_Brief_CBTManual.pdf
7. US Department of Veterans Affairs, National Center for PTSD. Eye movement desensitization and reprocessing (EMDR) for PTSD. Accessed September 1, 2022. https://www.ptsd.va.gov/understand_tx/emdr.asp
8. Wachen JS, Dondanville KA, Evans WR, Morris K, Cole A. Adjusting the timeframe of evidence-based therapies for PTSD-massed treatments. Curr Treat Options Psych. 2019;6(2):107-118. doi:10.1007/s40501-019-00169-9
9. Dell L, Sbisa AM, Forbes A, et al. Effect of massed v. standard prolonged exposure therapy on PTSD in military personnel and veterans: a non-inferiority randomised controlled trial [published online ahead of print, 2022 Apr 20]. Psychol Med. 2022;1-8. doi:10.1017/S0033291722000927
10. Held P, Kovacevic M, Petrey K, et al. Treating posttraumatic stress disorder at home in a single week using 1-week virtual massed cognitive processing therapy. J Trauma Stress. 2022;35(4):1215-1225. doi:10.1002/jts.22831
11. Yamokoski C, Flores H, Facemire V, Maieritsch K, Perez S, Fedynich A. Feasibility of an intensive outpatient treatment program for posttraumatic stress disorder within the veterans health care administration [published online ahead of print, 2022 Mar 7]. Psychol Serv. 2022;10.1037/ser0000628. doi:10.1037/ser0000628
12. Galovski TE, Werner KB, Weaver TL, et al. Massed cognitive processing therapy for posttraumatic stress disorder in women survivors of intimate partner violence. Psychol Trauma. 2022;14(5):769-779. doi:10.1037/tra0001100
13. Fallon S. NJ to send monitors into troubled nursing home that stacked bodies in makeshift morgue. Updated March 10, 2022. Accessed September 1, 2022. https://www.northjersey.com/story/news/health/2022/03/09/sussex-county-nj-nursing-home-monitors-covid-morgue/9447243002/
14. Litz BT, Stein N, Delaney E, et al. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin Psychol Rev. 2009;29(8):695-706. doi:10.1016/j.cpr.2009.07.003009
15. Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981-2001. Psychiatry. 2002;65(3):207-239. doi:10.1521/psyc.65.3.207.20173
16. Galea S, Nandi A, Vlahov D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol Rev. 2005;27:78-91. doi:10.1093/epirev/mxi003
1. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1550(2): readjustment counseling service. January 26, 2021. Accessed September 1, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9168
2. US Department of Veterans Affairs. Vet centers (readjustment counseling: vet center eligibility. Updated January 3, 2022. Accessed September 1, 2022. https://www.vetcenter.va.gov/eligibility.asp
3. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress reaction, version 3.0, 2017. Accessed September 1, 2022. https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal012418.pdf
4. US Department of Veterans Affairs, National Center for PTSD. Prolonged exposure (PE) therapy. Updated August 10, 2022. Accessed September 1, 2022. https://www.ptsd.va.gov/understand_tx/prolonged_exposure.asp
5. US Department of Veterans Affairs, National Center for PTSD. Cognitive processing therapy (CPT) for PTSD: how to help your loved one during treatment. Accessed September 1, 2022. https://www.ptsd.va.gov/publications/print/CPT_familyhandout.pdf
6. US Department of Veterans Affairs, National Center for PTSD. A provider’s guide to brief cognitive behavioral therapy. Accessed September 1, 2022. https://www.mirecc.va.gov/visn16/docs/Therapists_Guide_to_Brief_CBTManual.pdf
7. US Department of Veterans Affairs, National Center for PTSD. Eye movement desensitization and reprocessing (EMDR) for PTSD. Accessed September 1, 2022. https://www.ptsd.va.gov/understand_tx/emdr.asp
8. Wachen JS, Dondanville KA, Evans WR, Morris K, Cole A. Adjusting the timeframe of evidence-based therapies for PTSD-massed treatments. Curr Treat Options Psych. 2019;6(2):107-118. doi:10.1007/s40501-019-00169-9
9. Dell L, Sbisa AM, Forbes A, et al. Effect of massed v. standard prolonged exposure therapy on PTSD in military personnel and veterans: a non-inferiority randomised controlled trial [published online ahead of print, 2022 Apr 20]. Psychol Med. 2022;1-8. doi:10.1017/S0033291722000927
10. Held P, Kovacevic M, Petrey K, et al. Treating posttraumatic stress disorder at home in a single week using 1-week virtual massed cognitive processing therapy. J Trauma Stress. 2022;35(4):1215-1225. doi:10.1002/jts.22831
11. Yamokoski C, Flores H, Facemire V, Maieritsch K, Perez S, Fedynich A. Feasibility of an intensive outpatient treatment program for posttraumatic stress disorder within the veterans health care administration [published online ahead of print, 2022 Mar 7]. Psychol Serv. 2022;10.1037/ser0000628. doi:10.1037/ser0000628
12. Galovski TE, Werner KB, Weaver TL, et al. Massed cognitive processing therapy for posttraumatic stress disorder in women survivors of intimate partner violence. Psychol Trauma. 2022;14(5):769-779. doi:10.1037/tra0001100
13. Fallon S. NJ to send monitors into troubled nursing home that stacked bodies in makeshift morgue. Updated March 10, 2022. Accessed September 1, 2022. https://www.northjersey.com/story/news/health/2022/03/09/sussex-county-nj-nursing-home-monitors-covid-morgue/9447243002/
14. Litz BT, Stein N, Delaney E, et al. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin Psychol Rev. 2009;29(8):695-706. doi:10.1016/j.cpr.2009.07.003009
15. Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981-2001. Psychiatry. 2002;65(3):207-239. doi:10.1521/psyc.65.3.207.20173
16. Galea S, Nandi A, Vlahov D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol Rev. 2005;27:78-91. doi:10.1093/epirev/mxi003
A Veteran Presenting for Low Testosterone and Lower Urinary Tract Symptoms
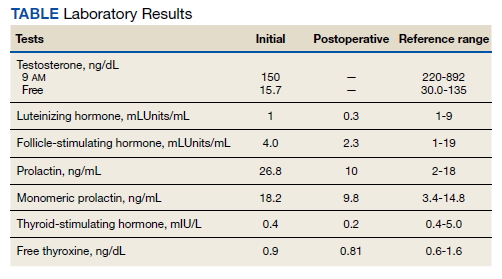
►Anish Bhatnagar, MD, Chief Medical Resident, Veterans Affairs Boston Healthcare System (VABHS) and Beth Israel Deaconess Medical Center (BIDMC): The patient noted erectile dysfunction starting 4 years ago, with accompanied decreased libido. However, until recently, he was able to achieve acceptable erectile capacity with medications. As part of his previous evaluations for erectile dysfunction, the patient had 2 total testosterone levels checked 6 months apart, both low at 150 ng/dL and 38.3 ng/dL (reference range, 220-892). The results of additional hormone studies are shown in the Table. Dr. Ananthakrishnan, can you help us interpret these laboratory results and tell us what tests you might order next?
►Sonia Ananthakrishnan, MD, Section of Endocrinology, Diabetes and Nutrition, Boston Medical Center (BMC) and Assistant Professor of Medicine, Boston University School of Medicine (BUSM): When patients present with signs of hypogonadism and an initial low morning testosterone levels, the next test should be a confirmatory repeat morning testosterone level as was done in this case. If this level is also low (for most assays < 300 ng/dL), further evaluation for primary vs secondary hypogonadism should be pursued with measurement of luteinizing hormone and follicle-stimulating hormone levels. Secondary hypogonadism should be suspected when these levels are low or inappropriately normal in the setting of a low testosterone level as in this patient. This patient does not appear to be on any medication or have reversible illnesses that we traditionally think of as possibly causing these hormone irregularities. Key examples include medications such as gonadotropin-releasing hormone analogs, glucocorticoids, and opioids, as well as conditions such as hyperprolactinemia, sleep apnea, diabetes mellitus, anorexia nervosa, or other chronic systemic illnesses, including cirrhosis or lung disease. In this setting, further evaluation of the patient’s anterior pituitary function should be undertaken. Initial screening tests showed mildly elevated prolactin and low normal thyroid-stimulating hormone levels, with a relatively normal free thyroxine. Given these abnormalities in the context of the patient’s total testosterone level < 150 ng/dL, magnetic resonance imaging (MRI) of the anterior pituitary is indicated, and what I would recommend next for evaluation of pituitary and/or hypothalamic tumor or infiltrative disease.1
►Dr. Bhatnagar: An MRI of the brain showed a large 2.7-cm sellar mass, with suprasellar extension and mass effect on the optic chiasm and pituitary infundibulum, partial extension into the right sphenoid sinus, and invasion into the right cavernous sinus. These findings were consistent with a pituitary macroadenoma. The patient was subsequently evaluated by a neurosurgeon who felt that because of the extension and compression of the mass, the patient would benefit from surgical resection.
Given his lower urinary tract symptoms, a prostate-specific antigen level was checked and returned elevated at 11.5 ng/mL. In the setting of these abnormalities, the patient underwent MRI of the abdomen, which noted a new 5.6-cm enhancing mass in the upper pole of his solitary right kidney, highly concerning for new RCC. After a multidisciplinary discussion, urology scheduled the patient for partial right nephrectomy first, with plans for pituitary resection only if the patient had adequate recovery following the urologic procedure.
Dr. Rifkin, this patient went straight from imaging to presumed diagnosis to planned surgical intervention without a confirmatory biopsy. In a patient who already has chronic kidney disease stage 4, why would we not want to pursue biopsy prior to this invasive procedure on his solitary kidney? In addition, given his baseline advanced renal disease, why pursue partial nephrectomy to delay initiation of hemodialysis instead of total nephrectomy and beginning hemodialysis?
►Ian Rifkin, MBBCh, PhD, MSc, Chief, Renal Section, VABHS, Section of Nephrology, BMC, and Associate Professor of Medicine, BUSM: In most cases, imaging alone is used to make a presumptive diagnosis of benign vs malignant renal masses. In one study, RCC was identified by MRI with 85% sensitivity and 76% specificity.2 However, as imaging and biopsy techniques have advanced, there are progressing discussions regarding the utility of biopsy. That being said, there are a number of situations in which patients currently undergo biopsy, particularly when there is diagnostic uncertainty.3 In this patient, with a history of RCC and imaging findings concerning for RCC, biopsy is unnecessary given the high clinical suspicion.
Regarding the choice of partial vs total nephrectomy, there are 2 important distinctions to be made. The first is that though it was previously felt that early initiation of dialysis improves survival, newer studies suggest that early initiation based off of glomerular filtration rate (GFR) offers no survival benefits compared to delayed initiation.4 Second, though there is less clinical data to support this, there is a signal toward the use of partial nephrectomy decreasing mortality compared to radical nephrectomy in management of RCC.5 In this patient, partial nephrectomy may not only increase rates of survival, but also delay initiation of dialysis.
►Dr. Bhatnagar: Prior to undergoing partial right nephrectomy, a morning cortisol level was found to be 5.8 μg/dL with an associated corticotropin (ACTH) level of 26 pg/mL. Dr. Ananthakrishnan, how would you interpret these laboratory results and what might you recommend prior to surgery?
►Dr. Ananthakrishnan: In a healthy patient, surgery often results in a several-fold increase in the secretion of cortisol to balance the unique stressors surgery places on the body.6 This patient is at increased risk for complete or partial adrenal insufficiency in the setting of both his pituitary macroadenoma as well as his previous left nephrectomy, which could have affected his left adrenal gland as well. Thus, this patient may not be able to mount the appropriate cortisol response needed to counter the stresses of surgery. His cortisol level is abnormally low for a morning value, with a relatively normal ACTH reference range of 6 to 50 pg/mL. He may have some degree of adrenal insufficiency, and thus will benefit from perioperative steroids.
►Dr. Bhatnagar: The patient was started on hydrocortisone and underwent a successful laparoscopic partial right nephrectomy. During the procedure, an estimated 2.5 L of blood was lost, with transfusion of 3 units of packed red blood cells. A surgical drain was left in the peritoneum. Postoperatively, he developed hypotension, requiring vasopressors and prolonged continuation of stress dosing of hydrocortisone. Over the next 4 days, the patient was weaned off vasopressors, and his creatinine level was noted to increase from a baseline of 1.8 mg/dL to 4.4 mg/dL.
Dr. Rifkin, how do you think about renal recovery in the patient postnephrectomy, and should we be concerned with the dramatic rise in his creatinine level?
►Dr. Rifkin: Removal of renal mass will result in an initial reduction of GFR proportional to the amount of functional renal tissue removed. However, in as early as 1 week, the residual nephrons begin to compensate through various mechanisms, such as modulation of efferent and afferent arterioles and renal tissue growth by hypertrophy and hyperplasia.7 In the acute setting, it may be difficult to distinguish an acute renal injury vs physiological GFR reduction postnephron loss, but often the initially elevated creatinine level may normalize/stabilize over time. Other markers of kidney function should concomitantly be monitored, including urine output, electrolyte/acid-base status, and urine sediment examination. In this patient, although his creatinine level may be elevated over the first few days, if his urine output remains robust and the urine sediment examination is normal, my concern for permanent kidney injury would be lessened.
►Dr. Bhatnagar: During the first 4 postoperative days the patient produced approximately 1 L of urine per day with a stable creatinine level. It is over this same time that the hydrocortisone was discontinued given improving hemodynamics. However, throughout postoperative day 5, the patient’s creatinine level acutely rose to a peak of 5.8 mg/dL. In addition, his urine output dramatically dropped to < 5 mL per hour, with blood clots noted in his Foley catheter. Dr. Rifkin, what is your differential for causing this acute change in both his creatinine level and urine output this far out from his procedure, and what might you do to help further evaluate?
►Dr. Rifkin: The most common cause of acute kidney injury in hospitalized patients is acute tubular necrosis (ATN).8 However, in this patient, who was recovering well postoperatively, was hemodynamically stable with a robust urine output, and in whom no apparent cause for ATN could be identified, other diagnoses were more likely. Considering the abrupt onset of oligo-anuria, the most likely diagnosis was urinary tract obstruction, particularly given the frank blood and blood clots that were present in the urine. Additional possibilities might be a late surgical complication or infection. Surgical complications could range from direct damage to the renal parenchyma to urinary leakage into the peritoneum from the site of anastomosis or tissue injury. Infections introduced either intraoperatively or developed postoperatively could also cause this sudden drop in urine output, though one would expect more systemic symptoms with this. Given that this patient has a surgical drain in place in the peritoneum, I would recommend testing the creatinine level in the peritoneal fluid drainage. If it is comparable to serum levels, this would argue against a urine leak, as we would expect the level to be significantly elevated in a leak. In addition, he should have imaging of the urinary tract followed by procedures to decompress the presumed obstructed urinary tract. These procedures might include either cystoscopy with ureteral stent placement or percutaneous nephrostomy, depending on the result of the imaging.
►Dr. Bhatnagar: The creatinine level obtained from the surgical drain was roughly equivalent to the serum creatinine, decreasing suspicion for a urine leak as the cause of his findings. Cystoscopy with ureteral stent placement was performed with subsequent increase in both urine output and concomitant decrease in serum creatinine.
Around this time, the patient also began to note blurry vision. Evaluation revealed difficulty with visual field confrontation in the right lower quadrant, right eye ptosis, right eye impaired adduction, absent abduction and impaired upgaze, but intact downgaze. Diplopia was present with gaze in all directions. His constellation of physical examination findings were concerning for a pathologic lesion partially involving cranial nerves II and III, with definitive involvement of cranial nerve VI, but sparing of cranial nerve IV. Repeat MRI of the brain showed hemorrhage into the sellar mass, with ongoing mass effect on the optic chiasm and extension into the sinuses (eAppendix). These findings were consistent with pituitary apoplexy. Dr. Ananthakrishnan, can you tell us more about pituitary apoplexy?
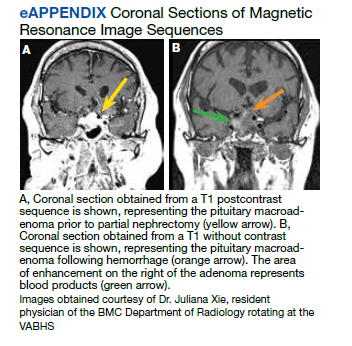
►Dr. Ananthakrishnan: Pituitary apoplexy is a clinical syndrome resulting from acute hemorrhage or infarction of the pituitary gland. It typically occurs in patients with preexisting pituitary adenomas and is characterized by the onset of headache, fever, vomiting, meningismus, decreased consciousness, and sometimes death. In addition, given the location of the pituitary gland within the sella, rapid changes in size can result in compression of cranial nerves III, IV, and VI, as well as the optic chiasm, resulting in ophthalmoplegia and visual disturbances as seen in this patient.9
There are a multitude of causes of pituitary apoplexy, including alterations in coagulopathy, pituitary stimulation (eg, dynamic pituitary hormone testing), and both acute increases and decreases in blood flow.10 This patient likely had an ischemic event due to changes in vascular perfusion, spurred by both his blood loss intraoperatively and ongoing hematuria. Management of pituitary apoplexy is dependent on the patient’s hemodynamics, mass effect symptoms, electrolyte balances, and hormone dysfunction. The decision for conservative management vs surgical intervention should be made in consultation with both neurosurgery and endocrinology. Once the patient is hemodynamically stable, the next step in evaluating this patient should be repeating his hormone studies.
►Dr. Bhatnagar: An assessment of pituitary function was consistent with values obtained preoperatively. After multidisciplinary discussions, surgery was deferred, and hydrocortisone was reinitiated to reduce inflammation caused by bleeding into the mass. As the ophthalmoplegia improved, this was transitioned to dexamethasone.
Twelve days after admission, he was discharged to a subacute rehabilitation center, with improvement in his ophthalmoplegia and stabilization of his creatinine level and urine output.
1. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536-2559. doi:10.1210/jc.2009-2354
2. Kay FU, Canvasser NE, Xi Y, et al. Diagnostic performance and interreader agreement of a standardized MR imaging approach in the prediction of small renal mass histology. Radiology. 2018;287(2):543-553. doi:10.1148/radiol.2018171557
3. Sahni VA, Silverman SG. Biopsy of renal masses: when and why. Cancer Imaging. 2009;9(1):44-55. doi:10.1102/1470-7330.2009.0005
4. Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609-619. doi:10.1056/NEJMoa1000552
5. Kunath F, Schmidt S, Krabbe L-M, et al. Partial nephrectomy versus radical nephrectomy for clinical localised renal masses. Cochrane Database Syst Rev. 2017;5(5):CD012045. doi:10.1002/14651858.CD012045.pub2
6. Kehlet H, Binder C. Adrenocortical function and clinical course during and after surgery in unsupplemented glucocorticoid-treated patients. Br J Anaesth. 1973;45(10):1043-1048. doi:10.1093/bja/45.10.1043
7. Chapman D, Moore R, Klarenbach S, Braam B. Residual renal function after partial or radical nephrectomy for renal cell carcinoma. Can Urol Assoc J. 2010;4(5):337-343. doi:10.5489/cuaj.909
8. Rahman M, Shad F, Smith MC. Acute kidney injury: a guide to diagnosis and management. Am Fam Physician. 2012;86(7):631-639.
9. Ranabir S, Baruah MP. Pituitary apoplexy. Indian J Endocrinol Metab. 2011;15(suppl 3):S188-S196. doi:10.4103/2230-8210.84862
10. Glezer A, Bronstein MD. Pituitary apoplexy: pathophysiology, diagnosis and management. Arch Endocrinol Metab. 2015;59(3):259-264. doi:10.1590/2359-3997000000047
►Anish Bhatnagar, MD, Chief Medical Resident, Veterans Affairs Boston Healthcare System (VABHS) and Beth Israel Deaconess Medical Center (BIDMC): The patient noted erectile dysfunction starting 4 years ago, with accompanied decreased libido. However, until recently, he was able to achieve acceptable erectile capacity with medications. As part of his previous evaluations for erectile dysfunction, the patient had 2 total testosterone levels checked 6 months apart, both low at 150 ng/dL and 38.3 ng/dL (reference range, 220-892). The results of additional hormone studies are shown in the Table. Dr. Ananthakrishnan, can you help us interpret these laboratory results and tell us what tests you might order next?
►Sonia Ananthakrishnan, MD, Section of Endocrinology, Diabetes and Nutrition, Boston Medical Center (BMC) and Assistant Professor of Medicine, Boston University School of Medicine (BUSM): When patients present with signs of hypogonadism and an initial low morning testosterone levels, the next test should be a confirmatory repeat morning testosterone level as was done in this case. If this level is also low (for most assays < 300 ng/dL), further evaluation for primary vs secondary hypogonadism should be pursued with measurement of luteinizing hormone and follicle-stimulating hormone levels. Secondary hypogonadism should be suspected when these levels are low or inappropriately normal in the setting of a low testosterone level as in this patient. This patient does not appear to be on any medication or have reversible illnesses that we traditionally think of as possibly causing these hormone irregularities. Key examples include medications such as gonadotropin-releasing hormone analogs, glucocorticoids, and opioids, as well as conditions such as hyperprolactinemia, sleep apnea, diabetes mellitus, anorexia nervosa, or other chronic systemic illnesses, including cirrhosis or lung disease. In this setting, further evaluation of the patient’s anterior pituitary function should be undertaken. Initial screening tests showed mildly elevated prolactin and low normal thyroid-stimulating hormone levels, with a relatively normal free thyroxine. Given these abnormalities in the context of the patient’s total testosterone level < 150 ng/dL, magnetic resonance imaging (MRI) of the anterior pituitary is indicated, and what I would recommend next for evaluation of pituitary and/or hypothalamic tumor or infiltrative disease.1
►Dr. Bhatnagar: An MRI of the brain showed a large 2.7-cm sellar mass, with suprasellar extension and mass effect on the optic chiasm and pituitary infundibulum, partial extension into the right sphenoid sinus, and invasion into the right cavernous sinus. These findings were consistent with a pituitary macroadenoma. The patient was subsequently evaluated by a neurosurgeon who felt that because of the extension and compression of the mass, the patient would benefit from surgical resection.
Given his lower urinary tract symptoms, a prostate-specific antigen level was checked and returned elevated at 11.5 ng/mL. In the setting of these abnormalities, the patient underwent MRI of the abdomen, which noted a new 5.6-cm enhancing mass in the upper pole of his solitary right kidney, highly concerning for new RCC. After a multidisciplinary discussion, urology scheduled the patient for partial right nephrectomy first, with plans for pituitary resection only if the patient had adequate recovery following the urologic procedure.
Dr. Rifkin, this patient went straight from imaging to presumed diagnosis to planned surgical intervention without a confirmatory biopsy. In a patient who already has chronic kidney disease stage 4, why would we not want to pursue biopsy prior to this invasive procedure on his solitary kidney? In addition, given his baseline advanced renal disease, why pursue partial nephrectomy to delay initiation of hemodialysis instead of total nephrectomy and beginning hemodialysis?
►Ian Rifkin, MBBCh, PhD, MSc, Chief, Renal Section, VABHS, Section of Nephrology, BMC, and Associate Professor of Medicine, BUSM: In most cases, imaging alone is used to make a presumptive diagnosis of benign vs malignant renal masses. In one study, RCC was identified by MRI with 85% sensitivity and 76% specificity.2 However, as imaging and biopsy techniques have advanced, there are progressing discussions regarding the utility of biopsy. That being said, there are a number of situations in which patients currently undergo biopsy, particularly when there is diagnostic uncertainty.3 In this patient, with a history of RCC and imaging findings concerning for RCC, biopsy is unnecessary given the high clinical suspicion.
Regarding the choice of partial vs total nephrectomy, there are 2 important distinctions to be made. The first is that though it was previously felt that early initiation of dialysis improves survival, newer studies suggest that early initiation based off of glomerular filtration rate (GFR) offers no survival benefits compared to delayed initiation.4 Second, though there is less clinical data to support this, there is a signal toward the use of partial nephrectomy decreasing mortality compared to radical nephrectomy in management of RCC.5 In this patient, partial nephrectomy may not only increase rates of survival, but also delay initiation of dialysis.
►Dr. Bhatnagar: Prior to undergoing partial right nephrectomy, a morning cortisol level was found to be 5.8 μg/dL with an associated corticotropin (ACTH) level of 26 pg/mL. Dr. Ananthakrishnan, how would you interpret these laboratory results and what might you recommend prior to surgery?
►Dr. Ananthakrishnan: In a healthy patient, surgery often results in a several-fold increase in the secretion of cortisol to balance the unique stressors surgery places on the body.6 This patient is at increased risk for complete or partial adrenal insufficiency in the setting of both his pituitary macroadenoma as well as his previous left nephrectomy, which could have affected his left adrenal gland as well. Thus, this patient may not be able to mount the appropriate cortisol response needed to counter the stresses of surgery. His cortisol level is abnormally low for a morning value, with a relatively normal ACTH reference range of 6 to 50 pg/mL. He may have some degree of adrenal insufficiency, and thus will benefit from perioperative steroids.
►Dr. Bhatnagar: The patient was started on hydrocortisone and underwent a successful laparoscopic partial right nephrectomy. During the procedure, an estimated 2.5 L of blood was lost, with transfusion of 3 units of packed red blood cells. A surgical drain was left in the peritoneum. Postoperatively, he developed hypotension, requiring vasopressors and prolonged continuation of stress dosing of hydrocortisone. Over the next 4 days, the patient was weaned off vasopressors, and his creatinine level was noted to increase from a baseline of 1.8 mg/dL to 4.4 mg/dL.
Dr. Rifkin, how do you think about renal recovery in the patient postnephrectomy, and should we be concerned with the dramatic rise in his creatinine level?
►Dr. Rifkin: Removal of renal mass will result in an initial reduction of GFR proportional to the amount of functional renal tissue removed. However, in as early as 1 week, the residual nephrons begin to compensate through various mechanisms, such as modulation of efferent and afferent arterioles and renal tissue growth by hypertrophy and hyperplasia.7 In the acute setting, it may be difficult to distinguish an acute renal injury vs physiological GFR reduction postnephron loss, but often the initially elevated creatinine level may normalize/stabilize over time. Other markers of kidney function should concomitantly be monitored, including urine output, electrolyte/acid-base status, and urine sediment examination. In this patient, although his creatinine level may be elevated over the first few days, if his urine output remains robust and the urine sediment examination is normal, my concern for permanent kidney injury would be lessened.
►Dr. Bhatnagar: During the first 4 postoperative days the patient produced approximately 1 L of urine per day with a stable creatinine level. It is over this same time that the hydrocortisone was discontinued given improving hemodynamics. However, throughout postoperative day 5, the patient’s creatinine level acutely rose to a peak of 5.8 mg/dL. In addition, his urine output dramatically dropped to < 5 mL per hour, with blood clots noted in his Foley catheter. Dr. Rifkin, what is your differential for causing this acute change in both his creatinine level and urine output this far out from his procedure, and what might you do to help further evaluate?
►Dr. Rifkin: The most common cause of acute kidney injury in hospitalized patients is acute tubular necrosis (ATN).8 However, in this patient, who was recovering well postoperatively, was hemodynamically stable with a robust urine output, and in whom no apparent cause for ATN could be identified, other diagnoses were more likely. Considering the abrupt onset of oligo-anuria, the most likely diagnosis was urinary tract obstruction, particularly given the frank blood and blood clots that were present in the urine. Additional possibilities might be a late surgical complication or infection. Surgical complications could range from direct damage to the renal parenchyma to urinary leakage into the peritoneum from the site of anastomosis or tissue injury. Infections introduced either intraoperatively or developed postoperatively could also cause this sudden drop in urine output, though one would expect more systemic symptoms with this. Given that this patient has a surgical drain in place in the peritoneum, I would recommend testing the creatinine level in the peritoneal fluid drainage. If it is comparable to serum levels, this would argue against a urine leak, as we would expect the level to be significantly elevated in a leak. In addition, he should have imaging of the urinary tract followed by procedures to decompress the presumed obstructed urinary tract. These procedures might include either cystoscopy with ureteral stent placement or percutaneous nephrostomy, depending on the result of the imaging.
►Dr. Bhatnagar: The creatinine level obtained from the surgical drain was roughly equivalent to the serum creatinine, decreasing suspicion for a urine leak as the cause of his findings. Cystoscopy with ureteral stent placement was performed with subsequent increase in both urine output and concomitant decrease in serum creatinine.
Around this time, the patient also began to note blurry vision. Evaluation revealed difficulty with visual field confrontation in the right lower quadrant, right eye ptosis, right eye impaired adduction, absent abduction and impaired upgaze, but intact downgaze. Diplopia was present with gaze in all directions. His constellation of physical examination findings were concerning for a pathologic lesion partially involving cranial nerves II and III, with definitive involvement of cranial nerve VI, but sparing of cranial nerve IV. Repeat MRI of the brain showed hemorrhage into the sellar mass, with ongoing mass effect on the optic chiasm and extension into the sinuses (eAppendix). These findings were consistent with pituitary apoplexy. Dr. Ananthakrishnan, can you tell us more about pituitary apoplexy?
►Dr. Ananthakrishnan: Pituitary apoplexy is a clinical syndrome resulting from acute hemorrhage or infarction of the pituitary gland. It typically occurs in patients with preexisting pituitary adenomas and is characterized by the onset of headache, fever, vomiting, meningismus, decreased consciousness, and sometimes death. In addition, given the location of the pituitary gland within the sella, rapid changes in size can result in compression of cranial nerves III, IV, and VI, as well as the optic chiasm, resulting in ophthalmoplegia and visual disturbances as seen in this patient.9
There are a multitude of causes of pituitary apoplexy, including alterations in coagulopathy, pituitary stimulation (eg, dynamic pituitary hormone testing), and both acute increases and decreases in blood flow.10 This patient likely had an ischemic event due to changes in vascular perfusion, spurred by both his blood loss intraoperatively and ongoing hematuria. Management of pituitary apoplexy is dependent on the patient’s hemodynamics, mass effect symptoms, electrolyte balances, and hormone dysfunction. The decision for conservative management vs surgical intervention should be made in consultation with both neurosurgery and endocrinology. Once the patient is hemodynamically stable, the next step in evaluating this patient should be repeating his hormone studies.
►Dr. Bhatnagar: An assessment of pituitary function was consistent with values obtained preoperatively. After multidisciplinary discussions, surgery was deferred, and hydrocortisone was reinitiated to reduce inflammation caused by bleeding into the mass. As the ophthalmoplegia improved, this was transitioned to dexamethasone.
Twelve days after admission, he was discharged to a subacute rehabilitation center, with improvement in his ophthalmoplegia and stabilization of his creatinine level and urine output.
►Anish Bhatnagar, MD, Chief Medical Resident, Veterans Affairs Boston Healthcare System (VABHS) and Beth Israel Deaconess Medical Center (BIDMC): The patient noted erectile dysfunction starting 4 years ago, with accompanied decreased libido. However, until recently, he was able to achieve acceptable erectile capacity with medications. As part of his previous evaluations for erectile dysfunction, the patient had 2 total testosterone levels checked 6 months apart, both low at 150 ng/dL and 38.3 ng/dL (reference range, 220-892). The results of additional hormone studies are shown in the Table. Dr. Ananthakrishnan, can you help us interpret these laboratory results and tell us what tests you might order next?
►Sonia Ananthakrishnan, MD, Section of Endocrinology, Diabetes and Nutrition, Boston Medical Center (BMC) and Assistant Professor of Medicine, Boston University School of Medicine (BUSM): When patients present with signs of hypogonadism and an initial low morning testosterone levels, the next test should be a confirmatory repeat morning testosterone level as was done in this case. If this level is also low (for most assays < 300 ng/dL), further evaluation for primary vs secondary hypogonadism should be pursued with measurement of luteinizing hormone and follicle-stimulating hormone levels. Secondary hypogonadism should be suspected when these levels are low or inappropriately normal in the setting of a low testosterone level as in this patient. This patient does not appear to be on any medication or have reversible illnesses that we traditionally think of as possibly causing these hormone irregularities. Key examples include medications such as gonadotropin-releasing hormone analogs, glucocorticoids, and opioids, as well as conditions such as hyperprolactinemia, sleep apnea, diabetes mellitus, anorexia nervosa, or other chronic systemic illnesses, including cirrhosis or lung disease. In this setting, further evaluation of the patient’s anterior pituitary function should be undertaken. Initial screening tests showed mildly elevated prolactin and low normal thyroid-stimulating hormone levels, with a relatively normal free thyroxine. Given these abnormalities in the context of the patient’s total testosterone level < 150 ng/dL, magnetic resonance imaging (MRI) of the anterior pituitary is indicated, and what I would recommend next for evaluation of pituitary and/or hypothalamic tumor or infiltrative disease.1
►Dr. Bhatnagar: An MRI of the brain showed a large 2.7-cm sellar mass, with suprasellar extension and mass effect on the optic chiasm and pituitary infundibulum, partial extension into the right sphenoid sinus, and invasion into the right cavernous sinus. These findings were consistent with a pituitary macroadenoma. The patient was subsequently evaluated by a neurosurgeon who felt that because of the extension and compression of the mass, the patient would benefit from surgical resection.
Given his lower urinary tract symptoms, a prostate-specific antigen level was checked and returned elevated at 11.5 ng/mL. In the setting of these abnormalities, the patient underwent MRI of the abdomen, which noted a new 5.6-cm enhancing mass in the upper pole of his solitary right kidney, highly concerning for new RCC. After a multidisciplinary discussion, urology scheduled the patient for partial right nephrectomy first, with plans for pituitary resection only if the patient had adequate recovery following the urologic procedure.
Dr. Rifkin, this patient went straight from imaging to presumed diagnosis to planned surgical intervention without a confirmatory biopsy. In a patient who already has chronic kidney disease stage 4, why would we not want to pursue biopsy prior to this invasive procedure on his solitary kidney? In addition, given his baseline advanced renal disease, why pursue partial nephrectomy to delay initiation of hemodialysis instead of total nephrectomy and beginning hemodialysis?
►Ian Rifkin, MBBCh, PhD, MSc, Chief, Renal Section, VABHS, Section of Nephrology, BMC, and Associate Professor of Medicine, BUSM: In most cases, imaging alone is used to make a presumptive diagnosis of benign vs malignant renal masses. In one study, RCC was identified by MRI with 85% sensitivity and 76% specificity.2 However, as imaging and biopsy techniques have advanced, there are progressing discussions regarding the utility of biopsy. That being said, there are a number of situations in which patients currently undergo biopsy, particularly when there is diagnostic uncertainty.3 In this patient, with a history of RCC and imaging findings concerning for RCC, biopsy is unnecessary given the high clinical suspicion.
Regarding the choice of partial vs total nephrectomy, there are 2 important distinctions to be made. The first is that though it was previously felt that early initiation of dialysis improves survival, newer studies suggest that early initiation based off of glomerular filtration rate (GFR) offers no survival benefits compared to delayed initiation.4 Second, though there is less clinical data to support this, there is a signal toward the use of partial nephrectomy decreasing mortality compared to radical nephrectomy in management of RCC.5 In this patient, partial nephrectomy may not only increase rates of survival, but also delay initiation of dialysis.
►Dr. Bhatnagar: Prior to undergoing partial right nephrectomy, a morning cortisol level was found to be 5.8 μg/dL with an associated corticotropin (ACTH) level of 26 pg/mL. Dr. Ananthakrishnan, how would you interpret these laboratory results and what might you recommend prior to surgery?
►Dr. Ananthakrishnan: In a healthy patient, surgery often results in a several-fold increase in the secretion of cortisol to balance the unique stressors surgery places on the body.6 This patient is at increased risk for complete or partial adrenal insufficiency in the setting of both his pituitary macroadenoma as well as his previous left nephrectomy, which could have affected his left adrenal gland as well. Thus, this patient may not be able to mount the appropriate cortisol response needed to counter the stresses of surgery. His cortisol level is abnormally low for a morning value, with a relatively normal ACTH reference range of 6 to 50 pg/mL. He may have some degree of adrenal insufficiency, and thus will benefit from perioperative steroids.
►Dr. Bhatnagar: The patient was started on hydrocortisone and underwent a successful laparoscopic partial right nephrectomy. During the procedure, an estimated 2.5 L of blood was lost, with transfusion of 3 units of packed red blood cells. A surgical drain was left in the peritoneum. Postoperatively, he developed hypotension, requiring vasopressors and prolonged continuation of stress dosing of hydrocortisone. Over the next 4 days, the patient was weaned off vasopressors, and his creatinine level was noted to increase from a baseline of 1.8 mg/dL to 4.4 mg/dL.
Dr. Rifkin, how do you think about renal recovery in the patient postnephrectomy, and should we be concerned with the dramatic rise in his creatinine level?
►Dr. Rifkin: Removal of renal mass will result in an initial reduction of GFR proportional to the amount of functional renal tissue removed. However, in as early as 1 week, the residual nephrons begin to compensate through various mechanisms, such as modulation of efferent and afferent arterioles and renal tissue growth by hypertrophy and hyperplasia.7 In the acute setting, it may be difficult to distinguish an acute renal injury vs physiological GFR reduction postnephron loss, but often the initially elevated creatinine level may normalize/stabilize over time. Other markers of kidney function should concomitantly be monitored, including urine output, electrolyte/acid-base status, and urine sediment examination. In this patient, although his creatinine level may be elevated over the first few days, if his urine output remains robust and the urine sediment examination is normal, my concern for permanent kidney injury would be lessened.
►Dr. Bhatnagar: During the first 4 postoperative days the patient produced approximately 1 L of urine per day with a stable creatinine level. It is over this same time that the hydrocortisone was discontinued given improving hemodynamics. However, throughout postoperative day 5, the patient’s creatinine level acutely rose to a peak of 5.8 mg/dL. In addition, his urine output dramatically dropped to < 5 mL per hour, with blood clots noted in his Foley catheter. Dr. Rifkin, what is your differential for causing this acute change in both his creatinine level and urine output this far out from his procedure, and what might you do to help further evaluate?
►Dr. Rifkin: The most common cause of acute kidney injury in hospitalized patients is acute tubular necrosis (ATN).8 However, in this patient, who was recovering well postoperatively, was hemodynamically stable with a robust urine output, and in whom no apparent cause for ATN could be identified, other diagnoses were more likely. Considering the abrupt onset of oligo-anuria, the most likely diagnosis was urinary tract obstruction, particularly given the frank blood and blood clots that were present in the urine. Additional possibilities might be a late surgical complication or infection. Surgical complications could range from direct damage to the renal parenchyma to urinary leakage into the peritoneum from the site of anastomosis or tissue injury. Infections introduced either intraoperatively or developed postoperatively could also cause this sudden drop in urine output, though one would expect more systemic symptoms with this. Given that this patient has a surgical drain in place in the peritoneum, I would recommend testing the creatinine level in the peritoneal fluid drainage. If it is comparable to serum levels, this would argue against a urine leak, as we would expect the level to be significantly elevated in a leak. In addition, he should have imaging of the urinary tract followed by procedures to decompress the presumed obstructed urinary tract. These procedures might include either cystoscopy with ureteral stent placement or percutaneous nephrostomy, depending on the result of the imaging.
►Dr. Bhatnagar: The creatinine level obtained from the surgical drain was roughly equivalent to the serum creatinine, decreasing suspicion for a urine leak as the cause of his findings. Cystoscopy with ureteral stent placement was performed with subsequent increase in both urine output and concomitant decrease in serum creatinine.
Around this time, the patient also began to note blurry vision. Evaluation revealed difficulty with visual field confrontation in the right lower quadrant, right eye ptosis, right eye impaired adduction, absent abduction and impaired upgaze, but intact downgaze. Diplopia was present with gaze in all directions. His constellation of physical examination findings were concerning for a pathologic lesion partially involving cranial nerves II and III, with definitive involvement of cranial nerve VI, but sparing of cranial nerve IV. Repeat MRI of the brain showed hemorrhage into the sellar mass, with ongoing mass effect on the optic chiasm and extension into the sinuses (eAppendix). These findings were consistent with pituitary apoplexy. Dr. Ananthakrishnan, can you tell us more about pituitary apoplexy?
►Dr. Ananthakrishnan: Pituitary apoplexy is a clinical syndrome resulting from acute hemorrhage or infarction of the pituitary gland. It typically occurs in patients with preexisting pituitary adenomas and is characterized by the onset of headache, fever, vomiting, meningismus, decreased consciousness, and sometimes death. In addition, given the location of the pituitary gland within the sella, rapid changes in size can result in compression of cranial nerves III, IV, and VI, as well as the optic chiasm, resulting in ophthalmoplegia and visual disturbances as seen in this patient.9
There are a multitude of causes of pituitary apoplexy, including alterations in coagulopathy, pituitary stimulation (eg, dynamic pituitary hormone testing), and both acute increases and decreases in blood flow.10 This patient likely had an ischemic event due to changes in vascular perfusion, spurred by both his blood loss intraoperatively and ongoing hematuria. Management of pituitary apoplexy is dependent on the patient’s hemodynamics, mass effect symptoms, electrolyte balances, and hormone dysfunction. The decision for conservative management vs surgical intervention should be made in consultation with both neurosurgery and endocrinology. Once the patient is hemodynamically stable, the next step in evaluating this patient should be repeating his hormone studies.
►Dr. Bhatnagar: An assessment of pituitary function was consistent with values obtained preoperatively. After multidisciplinary discussions, surgery was deferred, and hydrocortisone was reinitiated to reduce inflammation caused by bleeding into the mass. As the ophthalmoplegia improved, this was transitioned to dexamethasone.
Twelve days after admission, he was discharged to a subacute rehabilitation center, with improvement in his ophthalmoplegia and stabilization of his creatinine level and urine output.
1. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536-2559. doi:10.1210/jc.2009-2354
2. Kay FU, Canvasser NE, Xi Y, et al. Diagnostic performance and interreader agreement of a standardized MR imaging approach in the prediction of small renal mass histology. Radiology. 2018;287(2):543-553. doi:10.1148/radiol.2018171557
3. Sahni VA, Silverman SG. Biopsy of renal masses: when and why. Cancer Imaging. 2009;9(1):44-55. doi:10.1102/1470-7330.2009.0005
4. Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609-619. doi:10.1056/NEJMoa1000552
5. Kunath F, Schmidt S, Krabbe L-M, et al. Partial nephrectomy versus radical nephrectomy for clinical localised renal masses. Cochrane Database Syst Rev. 2017;5(5):CD012045. doi:10.1002/14651858.CD012045.pub2
6. Kehlet H, Binder C. Adrenocortical function and clinical course during and after surgery in unsupplemented glucocorticoid-treated patients. Br J Anaesth. 1973;45(10):1043-1048. doi:10.1093/bja/45.10.1043
7. Chapman D, Moore R, Klarenbach S, Braam B. Residual renal function after partial or radical nephrectomy for renal cell carcinoma. Can Urol Assoc J. 2010;4(5):337-343. doi:10.5489/cuaj.909
8. Rahman M, Shad F, Smith MC. Acute kidney injury: a guide to diagnosis and management. Am Fam Physician. 2012;86(7):631-639.
9. Ranabir S, Baruah MP. Pituitary apoplexy. Indian J Endocrinol Metab. 2011;15(suppl 3):S188-S196. doi:10.4103/2230-8210.84862
10. Glezer A, Bronstein MD. Pituitary apoplexy: pathophysiology, diagnosis and management. Arch Endocrinol Metab. 2015;59(3):259-264. doi:10.1590/2359-3997000000047
1. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536-2559. doi:10.1210/jc.2009-2354
2. Kay FU, Canvasser NE, Xi Y, et al. Diagnostic performance and interreader agreement of a standardized MR imaging approach in the prediction of small renal mass histology. Radiology. 2018;287(2):543-553. doi:10.1148/radiol.2018171557
3. Sahni VA, Silverman SG. Biopsy of renal masses: when and why. Cancer Imaging. 2009;9(1):44-55. doi:10.1102/1470-7330.2009.0005
4. Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609-619. doi:10.1056/NEJMoa1000552
5. Kunath F, Schmidt S, Krabbe L-M, et al. Partial nephrectomy versus radical nephrectomy for clinical localised renal masses. Cochrane Database Syst Rev. 2017;5(5):CD012045. doi:10.1002/14651858.CD012045.pub2
6. Kehlet H, Binder C. Adrenocortical function and clinical course during and after surgery in unsupplemented glucocorticoid-treated patients. Br J Anaesth. 1973;45(10):1043-1048. doi:10.1093/bja/45.10.1043
7. Chapman D, Moore R, Klarenbach S, Braam B. Residual renal function after partial or radical nephrectomy for renal cell carcinoma. Can Urol Assoc J. 2010;4(5):337-343. doi:10.5489/cuaj.909
8. Rahman M, Shad F, Smith MC. Acute kidney injury: a guide to diagnosis and management. Am Fam Physician. 2012;86(7):631-639.
9. Ranabir S, Baruah MP. Pituitary apoplexy. Indian J Endocrinol Metab. 2011;15(suppl 3):S188-S196. doi:10.4103/2230-8210.84862
10. Glezer A, Bronstein MD. Pituitary apoplexy: pathophysiology, diagnosis and management. Arch Endocrinol Metab. 2015;59(3):259-264. doi:10.1590/2359-3997000000047
Psychedelics and the Military: What a Long, Strange Trip It’s Been
In 2019 the Defense Advanced Research Projects Agency invested $27 million in the Focused Pharma program to develop new, more efficacious, rapid-acting drugs, including hallucinogens.1 While Focused Pharma does not include human studies, the Veterans Health Administration’s (VHA) newly launched psychedelics program research does include clinical trials.2 When I read of these ambitious projects, I recalled 2 prescient memories from my youth.
The first memory was of a dinner table conversation between my father, then chief of pediatrics at a military hospital, and one of my older brothers, a burgeoning hippie. My father mentioned that the military was doing research on lysergic acid diethylamide (LSD), and my brother asked whether he could bring some home for my brother to try. My father looked up from the dinner table with incredulity and in an ironic monotone replied, “No you would not qualify for the research, you are not in the Army.”
The second was about 10 years later, when I visited the state psychiatric hospital where my father directed the adolescent ward. I saw a group of young adults watching test patterns on an old-fashioned television set. When I asked my father what was wrong with them, he shook his head and said, “Too much LSD.”
Albert Hoffman was a Sandoz chemist when in 1938 he serendipitously developed LSD while working on a fungus that grew on grain. LSD’s psychoactive properties were not discovered until 1943. About a decade later, as the Cold War chilled international relations, the Central Intelligence Agency (CIA) began conducting experiments on military personnel in the MKUltra program using LSD, electroshock, hypnosis, and other techniques to develop a mind control program before its rivals did.3
Beginning in the 1950s, the US government collaborated with pharmaceutical companies and research universities to develop LSD as part of a campaign of psychological warfare. Though planned to be used against enemies, the program instead exploited US service members to develop hallucinogens as a form of chemical warfare that could render enemy troops mentally incapacitated. That psychiatrists, who then (as now) led much of this research, raised a host of ethical concerns about dual roles, disclosure, and duty.4
Government investigations and academic studies have shown that even soldiers who volunteered for the research were not given adequate information about the nature of the experiments and the potential adverse effects, such as persisting flashbacks. The military’s research on LSD ended in 1963, not because of the unethical aspects of the research, but because the effects of LSD were so unpredictable that the drug could not be effectively weaponized. Like Tuskegee and other research abuses of the time, when the MKUltra program was exposed, there were congressional investigations.5 Later studies found that many of the active-duty research subjects experienced a plethora of lasting and serious psychiatric symptoms. VHA practitioners had to put back together many of these broken service members. This program was rife with violations of research ethics and human rights, and those abuses tainted the field of hallucinogenic research in US Department of Defense (DoD) and VHA circles for decades.5 These research abuses, in part, have led to hallucinogens being categorized as Schedule I controlled substances, effectively blocking federal funding for research until recently.
LSD, Psilocybin (4-phosphoryloxy-N,N-dimethyltryptamine), and 3,4-methylenedioxy-methamphetamine (MDMA), popularly known as psychedelics, are again receiving attention. However, the current investigations into psychedelics are vastly different—scientifically and ethically. The most important difference is that the context and leadership of these studies is not national security—it is health care.
The goal of this new wave of psychedelic research is not mind control or brain alteration, but liberation of the mind from cycles of rumination and trauma and empowerment to change patterns of self-destruction to affirmation of life. The impetus for this research is not international espionage but to find better treatments for chronic posttraumatic stress disorder, severe substance use disorders, and treatment-resistant depression that contribute to unquantifiable mental pain, psychosocial dysfunction, and an epidemic of suicide among military service members and veterans.6 Though we have some effective treatments for these often combat-inflicted maladies—primarily evidence-based psychotherapies—yet these treatments are not tolerable or safe, fast-acting, or long-lasting enough to succor each and every troubled soul. The success of ketamine, a dissociative drug, in relieving the most distressing service-connected psychiatric diagnoses has provided a proof of concept to reinvigorate the moribund hallucinogenic research idea.7
This dark chapter in US military research is a cautionary tale. The often quoted and more often ignored advice of the Spanish American philosopher George Santayana, “Those who cannot remember the past are condemned to repeat it,” should serve as the guiding principle of the new hallucinogenic research.8 Human subjects’ protections have exponentially improved since the days of the secret LSD project even for active-duty personnel. The Common Rule governs that all research participants are given adequate information that includes whatever is known about the risks and benefits of the research.10 Participants must provide full and free informed consent to enroll in these clinical trials, a consent that encompasses the right to withdraw from the research at any time without jeopardizing their careers, benefits, or ongoing health care.10
These rules, though, can be bent, broken, avoided, or worked around. Only the moral integrity of study personnel, administrators, oversight agencies, research compliance officers, and most important, principal investigators can assure that the rules are upheld and the rights they guarantee are respected.9 It would be a tragic shame if the promised hope for the relief of psychic pain went unrealized due to media hype, shared desperation of clinicians and patients, and conflicts of interests that today are more likely to come from profit-driven pharmaceutical companies than national security agencies. And for all of us in federal practice, remembering the sordid past forays with LSD can redeem the present research so future service members and veterans and the clinicians who care for them have better balms to heal the wounds of war.
1. US Department of Defense, Defense Advanced Research Projects Agency. Structure-guided drug design could yield fast-acting remedies for complex neuropsychiatric conditions. Accessed September 12, 2022. https://www.darpa.mil/news-events/2019-09-11#
2. Londono E. After six-decade hiatus, experimental psychedelic therapy returns to the VA. https://www.nytimes.com/2022/06/24/us/politics/psychedelic-therapy-veterans.html
3. Disbennett B. ‘This is the happy warrior, this is he:’ an analysis of CIA and military testing of LSD on non-consenting U.S. service-members and recovery through the VA disability system. Tennessee J Race, Gender, Social Justice. 2015;3(2):1-32. doi:10.2139/ssrn.2416478
4. Smith H. James Ketchum, who conducted mind-altering experiments on soldiers dies at 87. Accessed September 12, 2022. https://www.washingtonpost.com/local/obituaries/james-ketchum-who-conducted-mind-altering-experiments-on-soldiers-dies-at-87/2019/06/04/7b5ad322-86cc-11e9-a491-25df61c78dc4_story.html
5. Ross CA. LSD experiments by the United States Army. Hist Psychiatry. 2017;28(4):427-442. doi:10.1177/0957154X17717678
6. Albott CS, Lim KO, Forbes MK, et al. Efficacy, safety, and durability of repeated ketamine infusions of comorbid posttraumatic stress disorder and treatment resistant depression. Clin Psychiatry. 2018;79(3): 17m11634. doi:10.4088/JCP.17m11634
7. Shawler IC, Jordan CH, Jackson CA. Veteran and military mental health issues. Stat Pearls. Updated May 23, 2022. Accessed September 12, 2022. https://www.ncbi.nlm.nih.gov/books/NBK572092/#_NBK572092_pubdet_
8. Santayana G. The Life of Reason. 1905. Accessed September 12, 2022. https://www.gutenberg.org/files/15000/15000-h/15000-h.htm
9. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1200.05(2). Requirements for the protection of human subjects in research. Amended January 8, 2021. Accessed September 12, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=8171
10. US Department of Defense, Military Health System. Research protections. Accessed September 12, 2022. https://www.health.mil/About-MHS/OASDHA/Defense-Health-Agency/Research-and-Engineering/Research-Protections
In 2019 the Defense Advanced Research Projects Agency invested $27 million in the Focused Pharma program to develop new, more efficacious, rapid-acting drugs, including hallucinogens.1 While Focused Pharma does not include human studies, the Veterans Health Administration’s (VHA) newly launched psychedelics program research does include clinical trials.2 When I read of these ambitious projects, I recalled 2 prescient memories from my youth.
The first memory was of a dinner table conversation between my father, then chief of pediatrics at a military hospital, and one of my older brothers, a burgeoning hippie. My father mentioned that the military was doing research on lysergic acid diethylamide (LSD), and my brother asked whether he could bring some home for my brother to try. My father looked up from the dinner table with incredulity and in an ironic monotone replied, “No you would not qualify for the research, you are not in the Army.”
The second was about 10 years later, when I visited the state psychiatric hospital where my father directed the adolescent ward. I saw a group of young adults watching test patterns on an old-fashioned television set. When I asked my father what was wrong with them, he shook his head and said, “Too much LSD.”
Albert Hoffman was a Sandoz chemist when in 1938 he serendipitously developed LSD while working on a fungus that grew on grain. LSD’s psychoactive properties were not discovered until 1943. About a decade later, as the Cold War chilled international relations, the Central Intelligence Agency (CIA) began conducting experiments on military personnel in the MKUltra program using LSD, electroshock, hypnosis, and other techniques to develop a mind control program before its rivals did.3
Beginning in the 1950s, the US government collaborated with pharmaceutical companies and research universities to develop LSD as part of a campaign of psychological warfare. Though planned to be used against enemies, the program instead exploited US service members to develop hallucinogens as a form of chemical warfare that could render enemy troops mentally incapacitated. That psychiatrists, who then (as now) led much of this research, raised a host of ethical concerns about dual roles, disclosure, and duty.4
Government investigations and academic studies have shown that even soldiers who volunteered for the research were not given adequate information about the nature of the experiments and the potential adverse effects, such as persisting flashbacks. The military’s research on LSD ended in 1963, not because of the unethical aspects of the research, but because the effects of LSD were so unpredictable that the drug could not be effectively weaponized. Like Tuskegee and other research abuses of the time, when the MKUltra program was exposed, there were congressional investigations.5 Later studies found that many of the active-duty research subjects experienced a plethora of lasting and serious psychiatric symptoms. VHA practitioners had to put back together many of these broken service members. This program was rife with violations of research ethics and human rights, and those abuses tainted the field of hallucinogenic research in US Department of Defense (DoD) and VHA circles for decades.5 These research abuses, in part, have led to hallucinogens being categorized as Schedule I controlled substances, effectively blocking federal funding for research until recently.
LSD, Psilocybin (4-phosphoryloxy-N,N-dimethyltryptamine), and 3,4-methylenedioxy-methamphetamine (MDMA), popularly known as psychedelics, are again receiving attention. However, the current investigations into psychedelics are vastly different—scientifically and ethically. The most important difference is that the context and leadership of these studies is not national security—it is health care.
The goal of this new wave of psychedelic research is not mind control or brain alteration, but liberation of the mind from cycles of rumination and trauma and empowerment to change patterns of self-destruction to affirmation of life. The impetus for this research is not international espionage but to find better treatments for chronic posttraumatic stress disorder, severe substance use disorders, and treatment-resistant depression that contribute to unquantifiable mental pain, psychosocial dysfunction, and an epidemic of suicide among military service members and veterans.6 Though we have some effective treatments for these often combat-inflicted maladies—primarily evidence-based psychotherapies—yet these treatments are not tolerable or safe, fast-acting, or long-lasting enough to succor each and every troubled soul. The success of ketamine, a dissociative drug, in relieving the most distressing service-connected psychiatric diagnoses has provided a proof of concept to reinvigorate the moribund hallucinogenic research idea.7
This dark chapter in US military research is a cautionary tale. The often quoted and more often ignored advice of the Spanish American philosopher George Santayana, “Those who cannot remember the past are condemned to repeat it,” should serve as the guiding principle of the new hallucinogenic research.8 Human subjects’ protections have exponentially improved since the days of the secret LSD project even for active-duty personnel. The Common Rule governs that all research participants are given adequate information that includes whatever is known about the risks and benefits of the research.10 Participants must provide full and free informed consent to enroll in these clinical trials, a consent that encompasses the right to withdraw from the research at any time without jeopardizing their careers, benefits, or ongoing health care.10
These rules, though, can be bent, broken, avoided, or worked around. Only the moral integrity of study personnel, administrators, oversight agencies, research compliance officers, and most important, principal investigators can assure that the rules are upheld and the rights they guarantee are respected.9 It would be a tragic shame if the promised hope for the relief of psychic pain went unrealized due to media hype, shared desperation of clinicians and patients, and conflicts of interests that today are more likely to come from profit-driven pharmaceutical companies than national security agencies. And for all of us in federal practice, remembering the sordid past forays with LSD can redeem the present research so future service members and veterans and the clinicians who care for them have better balms to heal the wounds of war.
In 2019 the Defense Advanced Research Projects Agency invested $27 million in the Focused Pharma program to develop new, more efficacious, rapid-acting drugs, including hallucinogens.1 While Focused Pharma does not include human studies, the Veterans Health Administration’s (VHA) newly launched psychedelics program research does include clinical trials.2 When I read of these ambitious projects, I recalled 2 prescient memories from my youth.
The first memory was of a dinner table conversation between my father, then chief of pediatrics at a military hospital, and one of my older brothers, a burgeoning hippie. My father mentioned that the military was doing research on lysergic acid diethylamide (LSD), and my brother asked whether he could bring some home for my brother to try. My father looked up from the dinner table with incredulity and in an ironic monotone replied, “No you would not qualify for the research, you are not in the Army.”
The second was about 10 years later, when I visited the state psychiatric hospital where my father directed the adolescent ward. I saw a group of young adults watching test patterns on an old-fashioned television set. When I asked my father what was wrong with them, he shook his head and said, “Too much LSD.”
Albert Hoffman was a Sandoz chemist when in 1938 he serendipitously developed LSD while working on a fungus that grew on grain. LSD’s psychoactive properties were not discovered until 1943. About a decade later, as the Cold War chilled international relations, the Central Intelligence Agency (CIA) began conducting experiments on military personnel in the MKUltra program using LSD, electroshock, hypnosis, and other techniques to develop a mind control program before its rivals did.3
Beginning in the 1950s, the US government collaborated with pharmaceutical companies and research universities to develop LSD as part of a campaign of psychological warfare. Though planned to be used against enemies, the program instead exploited US service members to develop hallucinogens as a form of chemical warfare that could render enemy troops mentally incapacitated. That psychiatrists, who then (as now) led much of this research, raised a host of ethical concerns about dual roles, disclosure, and duty.4
Government investigations and academic studies have shown that even soldiers who volunteered for the research were not given adequate information about the nature of the experiments and the potential adverse effects, such as persisting flashbacks. The military’s research on LSD ended in 1963, not because of the unethical aspects of the research, but because the effects of LSD were so unpredictable that the drug could not be effectively weaponized. Like Tuskegee and other research abuses of the time, when the MKUltra program was exposed, there were congressional investigations.5 Later studies found that many of the active-duty research subjects experienced a plethora of lasting and serious psychiatric symptoms. VHA practitioners had to put back together many of these broken service members. This program was rife with violations of research ethics and human rights, and those abuses tainted the field of hallucinogenic research in US Department of Defense (DoD) and VHA circles for decades.5 These research abuses, in part, have led to hallucinogens being categorized as Schedule I controlled substances, effectively blocking federal funding for research until recently.
LSD, Psilocybin (4-phosphoryloxy-N,N-dimethyltryptamine), and 3,4-methylenedioxy-methamphetamine (MDMA), popularly known as psychedelics, are again receiving attention. However, the current investigations into psychedelics are vastly different—scientifically and ethically. The most important difference is that the context and leadership of these studies is not national security—it is health care.
The goal of this new wave of psychedelic research is not mind control or brain alteration, but liberation of the mind from cycles of rumination and trauma and empowerment to change patterns of self-destruction to affirmation of life. The impetus for this research is not international espionage but to find better treatments for chronic posttraumatic stress disorder, severe substance use disorders, and treatment-resistant depression that contribute to unquantifiable mental pain, psychosocial dysfunction, and an epidemic of suicide among military service members and veterans.6 Though we have some effective treatments for these often combat-inflicted maladies—primarily evidence-based psychotherapies—yet these treatments are not tolerable or safe, fast-acting, or long-lasting enough to succor each and every troubled soul. The success of ketamine, a dissociative drug, in relieving the most distressing service-connected psychiatric diagnoses has provided a proof of concept to reinvigorate the moribund hallucinogenic research idea.7
This dark chapter in US military research is a cautionary tale. The often quoted and more often ignored advice of the Spanish American philosopher George Santayana, “Those who cannot remember the past are condemned to repeat it,” should serve as the guiding principle of the new hallucinogenic research.8 Human subjects’ protections have exponentially improved since the days of the secret LSD project even for active-duty personnel. The Common Rule governs that all research participants are given adequate information that includes whatever is known about the risks and benefits of the research.10 Participants must provide full and free informed consent to enroll in these clinical trials, a consent that encompasses the right to withdraw from the research at any time without jeopardizing their careers, benefits, or ongoing health care.10
These rules, though, can be bent, broken, avoided, or worked around. Only the moral integrity of study personnel, administrators, oversight agencies, research compliance officers, and most important, principal investigators can assure that the rules are upheld and the rights they guarantee are respected.9 It would be a tragic shame if the promised hope for the relief of psychic pain went unrealized due to media hype, shared desperation of clinicians and patients, and conflicts of interests that today are more likely to come from profit-driven pharmaceutical companies than national security agencies. And for all of us in federal practice, remembering the sordid past forays with LSD can redeem the present research so future service members and veterans and the clinicians who care for them have better balms to heal the wounds of war.
1. US Department of Defense, Defense Advanced Research Projects Agency. Structure-guided drug design could yield fast-acting remedies for complex neuropsychiatric conditions. Accessed September 12, 2022. https://www.darpa.mil/news-events/2019-09-11#
2. Londono E. After six-decade hiatus, experimental psychedelic therapy returns to the VA. https://www.nytimes.com/2022/06/24/us/politics/psychedelic-therapy-veterans.html
3. Disbennett B. ‘This is the happy warrior, this is he:’ an analysis of CIA and military testing of LSD on non-consenting U.S. service-members and recovery through the VA disability system. Tennessee J Race, Gender, Social Justice. 2015;3(2):1-32. doi:10.2139/ssrn.2416478
4. Smith H. James Ketchum, who conducted mind-altering experiments on soldiers dies at 87. Accessed September 12, 2022. https://www.washingtonpost.com/local/obituaries/james-ketchum-who-conducted-mind-altering-experiments-on-soldiers-dies-at-87/2019/06/04/7b5ad322-86cc-11e9-a491-25df61c78dc4_story.html
5. Ross CA. LSD experiments by the United States Army. Hist Psychiatry. 2017;28(4):427-442. doi:10.1177/0957154X17717678
6. Albott CS, Lim KO, Forbes MK, et al. Efficacy, safety, and durability of repeated ketamine infusions of comorbid posttraumatic stress disorder and treatment resistant depression. Clin Psychiatry. 2018;79(3): 17m11634. doi:10.4088/JCP.17m11634
7. Shawler IC, Jordan CH, Jackson CA. Veteran and military mental health issues. Stat Pearls. Updated May 23, 2022. Accessed September 12, 2022. https://www.ncbi.nlm.nih.gov/books/NBK572092/#_NBK572092_pubdet_
8. Santayana G. The Life of Reason. 1905. Accessed September 12, 2022. https://www.gutenberg.org/files/15000/15000-h/15000-h.htm
9. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1200.05(2). Requirements for the protection of human subjects in research. Amended January 8, 2021. Accessed September 12, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=8171
10. US Department of Defense, Military Health System. Research protections. Accessed September 12, 2022. https://www.health.mil/About-MHS/OASDHA/Defense-Health-Agency/Research-and-Engineering/Research-Protections
1. US Department of Defense, Defense Advanced Research Projects Agency. Structure-guided drug design could yield fast-acting remedies for complex neuropsychiatric conditions. Accessed September 12, 2022. https://www.darpa.mil/news-events/2019-09-11#
2. Londono E. After six-decade hiatus, experimental psychedelic therapy returns to the VA. https://www.nytimes.com/2022/06/24/us/politics/psychedelic-therapy-veterans.html
3. Disbennett B. ‘This is the happy warrior, this is he:’ an analysis of CIA and military testing of LSD on non-consenting U.S. service-members and recovery through the VA disability system. Tennessee J Race, Gender, Social Justice. 2015;3(2):1-32. doi:10.2139/ssrn.2416478
4. Smith H. James Ketchum, who conducted mind-altering experiments on soldiers dies at 87. Accessed September 12, 2022. https://www.washingtonpost.com/local/obituaries/james-ketchum-who-conducted-mind-altering-experiments-on-soldiers-dies-at-87/2019/06/04/7b5ad322-86cc-11e9-a491-25df61c78dc4_story.html
5. Ross CA. LSD experiments by the United States Army. Hist Psychiatry. 2017;28(4):427-442. doi:10.1177/0957154X17717678
6. Albott CS, Lim KO, Forbes MK, et al. Efficacy, safety, and durability of repeated ketamine infusions of comorbid posttraumatic stress disorder and treatment resistant depression. Clin Psychiatry. 2018;79(3): 17m11634. doi:10.4088/JCP.17m11634
7. Shawler IC, Jordan CH, Jackson CA. Veteran and military mental health issues. Stat Pearls. Updated May 23, 2022. Accessed September 12, 2022. https://www.ncbi.nlm.nih.gov/books/NBK572092/#_NBK572092_pubdet_
8. Santayana G. The Life of Reason. 1905. Accessed September 12, 2022. https://www.gutenberg.org/files/15000/15000-h/15000-h.htm
9. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1200.05(2). Requirements for the protection of human subjects in research. Amended January 8, 2021. Accessed September 12, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=8171
10. US Department of Defense, Military Health System. Research protections. Accessed September 12, 2022. https://www.health.mil/About-MHS/OASDHA/Defense-Health-Agency/Research-and-Engineering/Research-Protections
The truth about the ‘happy hormone’: Why we shouldn’t mess with dopamine
Google the word “dopamine” and you will learn that its nicknames are the “happy hormone” and the “pleasure molecule” and that it is among the most important chemicals in our brains. With The Guardian branding it “the Kim Kardashian of neurotransmitters,” dopamine has become a true pop-science darling – people across the globe have attempted to boost their mood with dopamine fasts and dopamine dressing.
A century ago, however, newly discovered dopamine was seen as an uninspiring chemical, nothing more than a precursor of noradrenaline. It took several stubborn and hardworking scientists to change that view.
Levodopa: An indifferent precursor
When Casimir Funk, PhD, a Polish biochemist and the discoverer of vitamins, first synthesized the dopamine precursor levodopa in 1911, he had no idea how important the molecule would prove to be in pharmacology and neurobiology. Nor did Markus Guggenheim, PhD, a Swiss biochemist, who isolated levodopa in 1913 from the seeds of a broad bean, Vicia faba. Dr. Guggenheim administered 1 g of levodopa to a rabbit, with no apparent negative consequences. He then prepared a larger dose (2.5 g) and tested it on himself. “Ten minutes after taking it, I felt very nauseous, I had to vomit twice,” he wrote in his paper. In the body, levodopa is converted into dopamine, which may act as an emetic – an effect Dr. Guggenheim didn’t understand. He simply abandoned his human study, erroneously concluding, on the basis of his animal research, that levodopa is “pharmacologically fairly indifferent.”
Around the same time, several scientists across Europe successfully synthesized dopamine, but those discoveries were shelved without much fanfare. For the next 3 decades, dopamine and levodopa were pushed into academic obscurity. Just before World War II, a group of German scientists showed that levodopa is metabolized to dopamine in the body, while another German researcher, Hermann Blaschko, MD, discovered that dopamine is an intermediary in the synthesis of noradrenaline. Even these findings, however, were not immediately accepted.
The dopamine story picked up pace in the post-war years with the observation that the hormone was present in various tissues and body fluids, although nowhere as abundantly as in the central nervous system. Intrigued, Dr. Blaschko, who (after escaping Nazi Germany, changing his name to Hugh, and starting work at Oxford [England] University) hypothesized that dopamine couldn’t be an unremarkable precursor of noradrenaline – it had to have some physiologic functions of its own. He asked his postdoctoral fellow, Oheh Hornykiewicz, MD, to test a few ideas. Dr. Hornykiewicz soon confirmed that dopamine lowered blood pressure in guinea pigs, proving that dopamine indeed had physiologic activity that was independent of other catecholamines.
Reserpine and rabbit ears
While Dr. Blaschko and Dr. Hornykiewicz were puzzling over dopamine’s physiologic role in the body, across the ocean at the National Heart Institute in Maryland, pharmacologist Bernard Brodie, PhD and colleagues were laying the groundwork for the discovery of dopamine’s starring role in the brain.
Spoiler alert: Dr. Brodie’s work showed that a new psychiatric drug known as reserpine was capable of fully depleting the brain’s stores of serotonin and – of greatest significance, as it turned out – mimicking the neuromuscular symptoms typical of Parkinson’s disease. The connection to dopamine would be made by new lab colleague Arvid Carlsson, MD, PhD, who would go on to win a Nobel Prize.
Derived from Rauwolfia serpentina (a plant that for centuries has been used in India for the treatment of mental illness, insomnia, and snake bites), reserpine was introduced in the West as a treatment for schizophrenia.
It worked marvels. In 1954, the press lauded the “dramatic” and seemingly “incredible”: results in treating “hopelessly insane patients.” Reserpine had a downside, however. Reports soon changed in tone regarding the drug’s severe side effects, including headaches, dizziness, vomiting, and, far more disturbingly, symptoms mimicking Parkinson’s disease, from muscular rigidity to tremors.
Dr. Brodie observed that, when reserpine was injected, animals became completely immobile. Serotonin nearly vanished from their brains, but bizarrely, drugs that spur serotonin production did not reverse the rabbits’ immobility.
Dr. Carlsson realized that other catecholamines must be involved in reserpine’s side effects, and he began to search for the culprits. He moved back to his native Sweden and ordered a spectrophotofluorimeter. In one of his experiments, Carlsson injected a pair of rabbits with reserpine, which caused the animals to become catatonic with flattened ears. After the researchers injected the animals with levodopa, within 15 minutes, the rabbits were hopping around, ears proudly vertical. “We were just as excited as the rabbits,” Dr. Carlsson later recalled in a 2016 interview. Dr. Carlsson realized that, because there was no noradrenaline in the rabbits’ brains, dopamine depletion must have been directly responsible for producing reserpine’s motor inhibitory effects.
Skeptics are silenced
In 1960, however, the medical community was not yet ready to accept that dopamine was anything but a boring intermediate between levodopa and noradrenaline. At a prestigious London symposium, Dr. Carlsson and his two colleagues presented their hypothesis that dopamine may be a neurotransmitter, thus implicating it in Parkinson’s disease. They were met with harsh criticism. Some of the experts said levodopa was nothing more than a poison. Dr. Carlsson later recalled facing “a profound and nearly unanimous skepticism regarding our points of view.”
That would soon change. Dr. Hornykiewicz, the biochemist who had earlier discovered dopamine’s BP-lowering effects, tested Dr. Carlsson’s ideas using the postmortem brains of Parkinson’s disease patients. It appeared Dr. Carlsson was right: Unlike in healthy brains, the striatum of patients with Parkinson’s disease contained almost no dopamine whatsoever. Beginning in 1961, in collaboration with neurologist Walther Birkmayer, MD, Hornykiewicz injected levodopa into 20 patients with Parkinson’s disease and observed a “miraculous” (albeit temporary) amelioration of rigidity, motionlessness, and speechlessness.
By the late 1960s, levodopa and dopamine were making headlines. A 1969 New York Times article described similar stunning improvements in patients with Parkinson’s disease who were treated with levodopa. A patient who had arrived at a hospital unable to speak, with hands clenched and rigid expression, was suddenly able to stride into his doctor’s office and even jog around. “I might say I’m a human being,” he told reporters. Although the treatment was expensive – equivalent to $210 in 2022 – physicians were deluged with requests for “dopa.” To this day, levodopa remains a gold standard in the treatment of Parkinson’s disease.
Still misunderstood
The history of dopamine, however, is not only about Parkinson’s disease but extends to the treatment of schizophrenia and addiction. When in the1940s a French military surgeon started giving a new antihistamine drug, promethazine, to prevent shock in soldiers undergoing surgery, he noticed a bizarre side effect: the soldiers would become euphoric yet oddly calm at the same time.
After the drug was modified by adding a chlorine atom and renamed chlorpromazine, it fast became a go-to treatment for psychosis. At the time, no one made the connection to dopamine. Contemporary doctors believed that it calmed people by lowering body temperature (common treatments for mental illness back in the day included swaddling patients in cold, wet sheets). Yet just like reserpine, chlorpromazine produced range of nasty side effects that closely mimicked Parkinson’s disease. This led a Dutch pharmacologist, Jacques van Rossum, to hypothesize that dopamine receptor blockade could explain chlorpromazine’s antipsychotic effects – an idea that remains widely accepted today.
In the 1970s, dopamine was linked with addiction through research on rodents, and this novel idea caught people’s imagination over the coming decades. A story on dopamine titled, “How We Get Addicted,” made the cover of Time in 1997.
Yet as the dopamine/addiction connection became widespread, it also became oversimplified. According to a 2015 article in Nature Reviews Neuroscience, a wave of low-quality research followed – nonreplicated, insufficient – which led the authors to conclude that we are “addicted to the dopamine theory of addiction.” Just about every pleasure under the sun was being attributed to dopamine, from eating delicious foods and playing computer games to sex, music, and hot showers. As recent science shows, however, dopamine is not simply about pleasure – it’s about reward prediction, response to stress, memory, learning, and even the functioning of the immune system. Since its first synthesis in the early 20th century, dopamine has often been misunderstood and oversimplified – and it seems the story is repeating itself now.
In one of his final interviews, Dr. Carlsson, who passed away in 2018 at the age of 95, warned about playing around with dopamine and, in particular, prescribing drugs that have an inhibitory action on this neurotransmitter. “Dopamine is involved in everything that happens in our brains – all its important functions,” he said.
We should be careful how we handle such a delicate and still little-known system.
A version of this article first appeared on Medscape.com.
Google the word “dopamine” and you will learn that its nicknames are the “happy hormone” and the “pleasure molecule” and that it is among the most important chemicals in our brains. With The Guardian branding it “the Kim Kardashian of neurotransmitters,” dopamine has become a true pop-science darling – people across the globe have attempted to boost their mood with dopamine fasts and dopamine dressing.
A century ago, however, newly discovered dopamine was seen as an uninspiring chemical, nothing more than a precursor of noradrenaline. It took several stubborn and hardworking scientists to change that view.
Levodopa: An indifferent precursor
When Casimir Funk, PhD, a Polish biochemist and the discoverer of vitamins, first synthesized the dopamine precursor levodopa in 1911, he had no idea how important the molecule would prove to be in pharmacology and neurobiology. Nor did Markus Guggenheim, PhD, a Swiss biochemist, who isolated levodopa in 1913 from the seeds of a broad bean, Vicia faba. Dr. Guggenheim administered 1 g of levodopa to a rabbit, with no apparent negative consequences. He then prepared a larger dose (2.5 g) and tested it on himself. “Ten minutes after taking it, I felt very nauseous, I had to vomit twice,” he wrote in his paper. In the body, levodopa is converted into dopamine, which may act as an emetic – an effect Dr. Guggenheim didn’t understand. He simply abandoned his human study, erroneously concluding, on the basis of his animal research, that levodopa is “pharmacologically fairly indifferent.”
Around the same time, several scientists across Europe successfully synthesized dopamine, but those discoveries were shelved without much fanfare. For the next 3 decades, dopamine and levodopa were pushed into academic obscurity. Just before World War II, a group of German scientists showed that levodopa is metabolized to dopamine in the body, while another German researcher, Hermann Blaschko, MD, discovered that dopamine is an intermediary in the synthesis of noradrenaline. Even these findings, however, were not immediately accepted.
The dopamine story picked up pace in the post-war years with the observation that the hormone was present in various tissues and body fluids, although nowhere as abundantly as in the central nervous system. Intrigued, Dr. Blaschko, who (after escaping Nazi Germany, changing his name to Hugh, and starting work at Oxford [England] University) hypothesized that dopamine couldn’t be an unremarkable precursor of noradrenaline – it had to have some physiologic functions of its own. He asked his postdoctoral fellow, Oheh Hornykiewicz, MD, to test a few ideas. Dr. Hornykiewicz soon confirmed that dopamine lowered blood pressure in guinea pigs, proving that dopamine indeed had physiologic activity that was independent of other catecholamines.
Reserpine and rabbit ears
While Dr. Blaschko and Dr. Hornykiewicz were puzzling over dopamine’s physiologic role in the body, across the ocean at the National Heart Institute in Maryland, pharmacologist Bernard Brodie, PhD and colleagues were laying the groundwork for the discovery of dopamine’s starring role in the brain.
Spoiler alert: Dr. Brodie’s work showed that a new psychiatric drug known as reserpine was capable of fully depleting the brain’s stores of serotonin and – of greatest significance, as it turned out – mimicking the neuromuscular symptoms typical of Parkinson’s disease. The connection to dopamine would be made by new lab colleague Arvid Carlsson, MD, PhD, who would go on to win a Nobel Prize.
Derived from Rauwolfia serpentina (a plant that for centuries has been used in India for the treatment of mental illness, insomnia, and snake bites), reserpine was introduced in the West as a treatment for schizophrenia.
It worked marvels. In 1954, the press lauded the “dramatic” and seemingly “incredible”: results in treating “hopelessly insane patients.” Reserpine had a downside, however. Reports soon changed in tone regarding the drug’s severe side effects, including headaches, dizziness, vomiting, and, far more disturbingly, symptoms mimicking Parkinson’s disease, from muscular rigidity to tremors.
Dr. Brodie observed that, when reserpine was injected, animals became completely immobile. Serotonin nearly vanished from their brains, but bizarrely, drugs that spur serotonin production did not reverse the rabbits’ immobility.
Dr. Carlsson realized that other catecholamines must be involved in reserpine’s side effects, and he began to search for the culprits. He moved back to his native Sweden and ordered a spectrophotofluorimeter. In one of his experiments, Carlsson injected a pair of rabbits with reserpine, which caused the animals to become catatonic with flattened ears. After the researchers injected the animals with levodopa, within 15 minutes, the rabbits were hopping around, ears proudly vertical. “We were just as excited as the rabbits,” Dr. Carlsson later recalled in a 2016 interview. Dr. Carlsson realized that, because there was no noradrenaline in the rabbits’ brains, dopamine depletion must have been directly responsible for producing reserpine’s motor inhibitory effects.
Skeptics are silenced
In 1960, however, the medical community was not yet ready to accept that dopamine was anything but a boring intermediate between levodopa and noradrenaline. At a prestigious London symposium, Dr. Carlsson and his two colleagues presented their hypothesis that dopamine may be a neurotransmitter, thus implicating it in Parkinson’s disease. They were met with harsh criticism. Some of the experts said levodopa was nothing more than a poison. Dr. Carlsson later recalled facing “a profound and nearly unanimous skepticism regarding our points of view.”
That would soon change. Dr. Hornykiewicz, the biochemist who had earlier discovered dopamine’s BP-lowering effects, tested Dr. Carlsson’s ideas using the postmortem brains of Parkinson’s disease patients. It appeared Dr. Carlsson was right: Unlike in healthy brains, the striatum of patients with Parkinson’s disease contained almost no dopamine whatsoever. Beginning in 1961, in collaboration with neurologist Walther Birkmayer, MD, Hornykiewicz injected levodopa into 20 patients with Parkinson’s disease and observed a “miraculous” (albeit temporary) amelioration of rigidity, motionlessness, and speechlessness.
By the late 1960s, levodopa and dopamine were making headlines. A 1969 New York Times article described similar stunning improvements in patients with Parkinson’s disease who were treated with levodopa. A patient who had arrived at a hospital unable to speak, with hands clenched and rigid expression, was suddenly able to stride into his doctor’s office and even jog around. “I might say I’m a human being,” he told reporters. Although the treatment was expensive – equivalent to $210 in 2022 – physicians were deluged with requests for “dopa.” To this day, levodopa remains a gold standard in the treatment of Parkinson’s disease.
Still misunderstood
The history of dopamine, however, is not only about Parkinson’s disease but extends to the treatment of schizophrenia and addiction. When in the1940s a French military surgeon started giving a new antihistamine drug, promethazine, to prevent shock in soldiers undergoing surgery, he noticed a bizarre side effect: the soldiers would become euphoric yet oddly calm at the same time.
After the drug was modified by adding a chlorine atom and renamed chlorpromazine, it fast became a go-to treatment for psychosis. At the time, no one made the connection to dopamine. Contemporary doctors believed that it calmed people by lowering body temperature (common treatments for mental illness back in the day included swaddling patients in cold, wet sheets). Yet just like reserpine, chlorpromazine produced range of nasty side effects that closely mimicked Parkinson’s disease. This led a Dutch pharmacologist, Jacques van Rossum, to hypothesize that dopamine receptor blockade could explain chlorpromazine’s antipsychotic effects – an idea that remains widely accepted today.
In the 1970s, dopamine was linked with addiction through research on rodents, and this novel idea caught people’s imagination over the coming decades. A story on dopamine titled, “How We Get Addicted,” made the cover of Time in 1997.
Yet as the dopamine/addiction connection became widespread, it also became oversimplified. According to a 2015 article in Nature Reviews Neuroscience, a wave of low-quality research followed – nonreplicated, insufficient – which led the authors to conclude that we are “addicted to the dopamine theory of addiction.” Just about every pleasure under the sun was being attributed to dopamine, from eating delicious foods and playing computer games to sex, music, and hot showers. As recent science shows, however, dopamine is not simply about pleasure – it’s about reward prediction, response to stress, memory, learning, and even the functioning of the immune system. Since its first synthesis in the early 20th century, dopamine has often been misunderstood and oversimplified – and it seems the story is repeating itself now.
In one of his final interviews, Dr. Carlsson, who passed away in 2018 at the age of 95, warned about playing around with dopamine and, in particular, prescribing drugs that have an inhibitory action on this neurotransmitter. “Dopamine is involved in everything that happens in our brains – all its important functions,” he said.
We should be careful how we handle such a delicate and still little-known system.
A version of this article first appeared on Medscape.com.
Google the word “dopamine” and you will learn that its nicknames are the “happy hormone” and the “pleasure molecule” and that it is among the most important chemicals in our brains. With The Guardian branding it “the Kim Kardashian of neurotransmitters,” dopamine has become a true pop-science darling – people across the globe have attempted to boost their mood with dopamine fasts and dopamine dressing.
A century ago, however, newly discovered dopamine was seen as an uninspiring chemical, nothing more than a precursor of noradrenaline. It took several stubborn and hardworking scientists to change that view.
Levodopa: An indifferent precursor
When Casimir Funk, PhD, a Polish biochemist and the discoverer of vitamins, first synthesized the dopamine precursor levodopa in 1911, he had no idea how important the molecule would prove to be in pharmacology and neurobiology. Nor did Markus Guggenheim, PhD, a Swiss biochemist, who isolated levodopa in 1913 from the seeds of a broad bean, Vicia faba. Dr. Guggenheim administered 1 g of levodopa to a rabbit, with no apparent negative consequences. He then prepared a larger dose (2.5 g) and tested it on himself. “Ten minutes after taking it, I felt very nauseous, I had to vomit twice,” he wrote in his paper. In the body, levodopa is converted into dopamine, which may act as an emetic – an effect Dr. Guggenheim didn’t understand. He simply abandoned his human study, erroneously concluding, on the basis of his animal research, that levodopa is “pharmacologically fairly indifferent.”
Around the same time, several scientists across Europe successfully synthesized dopamine, but those discoveries were shelved without much fanfare. For the next 3 decades, dopamine and levodopa were pushed into academic obscurity. Just before World War II, a group of German scientists showed that levodopa is metabolized to dopamine in the body, while another German researcher, Hermann Blaschko, MD, discovered that dopamine is an intermediary in the synthesis of noradrenaline. Even these findings, however, were not immediately accepted.
The dopamine story picked up pace in the post-war years with the observation that the hormone was present in various tissues and body fluids, although nowhere as abundantly as in the central nervous system. Intrigued, Dr. Blaschko, who (after escaping Nazi Germany, changing his name to Hugh, and starting work at Oxford [England] University) hypothesized that dopamine couldn’t be an unremarkable precursor of noradrenaline – it had to have some physiologic functions of its own. He asked his postdoctoral fellow, Oheh Hornykiewicz, MD, to test a few ideas. Dr. Hornykiewicz soon confirmed that dopamine lowered blood pressure in guinea pigs, proving that dopamine indeed had physiologic activity that was independent of other catecholamines.
Reserpine and rabbit ears
While Dr. Blaschko and Dr. Hornykiewicz were puzzling over dopamine’s physiologic role in the body, across the ocean at the National Heart Institute in Maryland, pharmacologist Bernard Brodie, PhD and colleagues were laying the groundwork for the discovery of dopamine’s starring role in the brain.
Spoiler alert: Dr. Brodie’s work showed that a new psychiatric drug known as reserpine was capable of fully depleting the brain’s stores of serotonin and – of greatest significance, as it turned out – mimicking the neuromuscular symptoms typical of Parkinson’s disease. The connection to dopamine would be made by new lab colleague Arvid Carlsson, MD, PhD, who would go on to win a Nobel Prize.
Derived from Rauwolfia serpentina (a plant that for centuries has been used in India for the treatment of mental illness, insomnia, and snake bites), reserpine was introduced in the West as a treatment for schizophrenia.
It worked marvels. In 1954, the press lauded the “dramatic” and seemingly “incredible”: results in treating “hopelessly insane patients.” Reserpine had a downside, however. Reports soon changed in tone regarding the drug’s severe side effects, including headaches, dizziness, vomiting, and, far more disturbingly, symptoms mimicking Parkinson’s disease, from muscular rigidity to tremors.
Dr. Brodie observed that, when reserpine was injected, animals became completely immobile. Serotonin nearly vanished from their brains, but bizarrely, drugs that spur serotonin production did not reverse the rabbits’ immobility.
Dr. Carlsson realized that other catecholamines must be involved in reserpine’s side effects, and he began to search for the culprits. He moved back to his native Sweden and ordered a spectrophotofluorimeter. In one of his experiments, Carlsson injected a pair of rabbits with reserpine, which caused the animals to become catatonic with flattened ears. After the researchers injected the animals with levodopa, within 15 minutes, the rabbits were hopping around, ears proudly vertical. “We were just as excited as the rabbits,” Dr. Carlsson later recalled in a 2016 interview. Dr. Carlsson realized that, because there was no noradrenaline in the rabbits’ brains, dopamine depletion must have been directly responsible for producing reserpine’s motor inhibitory effects.
Skeptics are silenced
In 1960, however, the medical community was not yet ready to accept that dopamine was anything but a boring intermediate between levodopa and noradrenaline. At a prestigious London symposium, Dr. Carlsson and his two colleagues presented their hypothesis that dopamine may be a neurotransmitter, thus implicating it in Parkinson’s disease. They were met with harsh criticism. Some of the experts said levodopa was nothing more than a poison. Dr. Carlsson later recalled facing “a profound and nearly unanimous skepticism regarding our points of view.”
That would soon change. Dr. Hornykiewicz, the biochemist who had earlier discovered dopamine’s BP-lowering effects, tested Dr. Carlsson’s ideas using the postmortem brains of Parkinson’s disease patients. It appeared Dr. Carlsson was right: Unlike in healthy brains, the striatum of patients with Parkinson’s disease contained almost no dopamine whatsoever. Beginning in 1961, in collaboration with neurologist Walther Birkmayer, MD, Hornykiewicz injected levodopa into 20 patients with Parkinson’s disease and observed a “miraculous” (albeit temporary) amelioration of rigidity, motionlessness, and speechlessness.
By the late 1960s, levodopa and dopamine were making headlines. A 1969 New York Times article described similar stunning improvements in patients with Parkinson’s disease who were treated with levodopa. A patient who had arrived at a hospital unable to speak, with hands clenched and rigid expression, was suddenly able to stride into his doctor’s office and even jog around. “I might say I’m a human being,” he told reporters. Although the treatment was expensive – equivalent to $210 in 2022 – physicians were deluged with requests for “dopa.” To this day, levodopa remains a gold standard in the treatment of Parkinson’s disease.
Still misunderstood
The history of dopamine, however, is not only about Parkinson’s disease but extends to the treatment of schizophrenia and addiction. When in the1940s a French military surgeon started giving a new antihistamine drug, promethazine, to prevent shock in soldiers undergoing surgery, he noticed a bizarre side effect: the soldiers would become euphoric yet oddly calm at the same time.
After the drug was modified by adding a chlorine atom and renamed chlorpromazine, it fast became a go-to treatment for psychosis. At the time, no one made the connection to dopamine. Contemporary doctors believed that it calmed people by lowering body temperature (common treatments for mental illness back in the day included swaddling patients in cold, wet sheets). Yet just like reserpine, chlorpromazine produced range of nasty side effects that closely mimicked Parkinson’s disease. This led a Dutch pharmacologist, Jacques van Rossum, to hypothesize that dopamine receptor blockade could explain chlorpromazine’s antipsychotic effects – an idea that remains widely accepted today.
In the 1970s, dopamine was linked with addiction through research on rodents, and this novel idea caught people’s imagination over the coming decades. A story on dopamine titled, “How We Get Addicted,” made the cover of Time in 1997.
Yet as the dopamine/addiction connection became widespread, it also became oversimplified. According to a 2015 article in Nature Reviews Neuroscience, a wave of low-quality research followed – nonreplicated, insufficient – which led the authors to conclude that we are “addicted to the dopamine theory of addiction.” Just about every pleasure under the sun was being attributed to dopamine, from eating delicious foods and playing computer games to sex, music, and hot showers. As recent science shows, however, dopamine is not simply about pleasure – it’s about reward prediction, response to stress, memory, learning, and even the functioning of the immune system. Since its first synthesis in the early 20th century, dopamine has often been misunderstood and oversimplified – and it seems the story is repeating itself now.
In one of his final interviews, Dr. Carlsson, who passed away in 2018 at the age of 95, warned about playing around with dopamine and, in particular, prescribing drugs that have an inhibitory action on this neurotransmitter. “Dopamine is involved in everything that happens in our brains – all its important functions,” he said.
We should be careful how we handle such a delicate and still little-known system.
A version of this article first appeared on Medscape.com.
How do patients with chronic urticaria fare during pregnancy?
In addition, the rates of preterm births and medical problems of newborns in patients with CU are similar to those of the normal population and not linked to treatment used during pregnancy.
Those are the key findings from an analysis of new data from PREG-CU, an international, multicenter study of the Urticaria Centers of Reference and Excellence (UCARE) network. Results from the first PREG-CU analysis published in 2021 found that CU improved in about half of patients with CU during pregnancy. “However, two in five patients reported acute exacerbations of CU especially at the beginning and end of pregnancy,” investigators led by Emek Kocatürk, MD, of the department of dermatology and UCARE at Koç University School of Medicine, Istanbul, wrote in the new study, recently published in the Journal of the European Academy of Dermatology and Venereology.

“In addition, 1 in 10 pregnant CU patients required urticaria emergency care and 1 of 6 had angioedema during pregnancy,” they said. Risk factors for worsening CU during pregnancy, they added, were “mild disease and no angioedema before pregnancy, not taking treatment before pregnancy, chronic inducible urticaria, CU worsening during a previous pregnancy, stress as a driver of exacerbations, and treatment during pregnancy.”
Analysis involved 288 pregnant women
To optimize treatment of CU during pregnancy and to better understand how treatment affects pregnancy outcomes, the researchers analyzed 288 pregnancies in 288 women with CU from 13 countries and 21 centers worldwide. Their mean age at pregnancy was 32.1 years, and their mean duration of CU was 84.9 months. Prior to pregnancy, 35.7% of patients rated the severity of their CU symptoms as mild, 34.2% rated it as moderate, and 29.7% rated it as severe.
The researchers found that during pregnancy, 60% of patients used urticaria medication, including standard-dose second-generation H1-antihistamines (35.1%), first-generation H1-antihistamines (7.6%), high-dose second-generation H1-antihistamines (5.6%), and omalizumab (5.6%). The preterm birth rate was 10.2%, which was similar between patients who did and did not receive treatment during pregnancy (11.6% vs. 8.7%, respectively; P = .59).
On multivariate logistic regression, two predictors for preterm birth emerged: giving birth to twins (a 13.3-fold increased risk; P = .016) and emergency referrals for CU (a 4.3-fold increased risk; P =.016). The cesarean delivery rate was 51.3%, and more than 90% of newborns were healthy at birth. There was no link between any patient or disease characteristics or treatments and medical problems at birth.
In other findings, 78.8% of women with CU breastfed their babies. Of the 58 patients who did not breastfeed, 20.7% indicated severe urticaria/angioedema and/or taking medications as the main reason for not breastfeeding.
“Most CU patients use treatment during pregnancy and such treatments, especially second generation H1 antihistamines, seem to be safe during pregnancy regardless of the trimester,” the researchers concluded. “Outcomes of pregnancy in patients with CU were similar compared to the general population and not linked to treatment used during pregnancy. Notably, emergency referral for CU was an independent risk factor for preterm birth,” and the high cesarean delivery rate was “probably linked to comorbidities associated with the disease,” they added. “Overall, these findings suggest that patients should continue their treatments using an individualized dose to provide optimal symptom control.”
International guidelines
The authors noted that international guidelines for the management of urticaria published in 2022 suggest that modern second-generation H1-antihistamines should be used for pregnant patients, preferably loratadine with a possible extrapolation to desloratadine, cetirizine, or levocetirizine.
“Similarly, in this population, we found that cetirizine and loratadine were the most commonly used antihistamines, followed by levocetirizine and fexofenadine,” Dr. Kocatürk and colleagues wrote.
“Guidelines also suggest that the use of first-generation H1-antihistamines should be avoided given their sedative effects; but if these are to be given, it would be wise to know that use of first-generation H1-antihistamines immediately before parturition could cause respiratory depression and other adverse effects in the neonate,” they added, noting that chlorpheniramine and diphenhydramine are the first-generation H1-antihistamines with the greatest evidence of safety in pregnancy.
They acknowledged certain limitations of the analysis, including its retrospective design and the fact that there were no data on low birth weight, small for gestational age, or miscarriage rates. In addition, disease activity or severity during pregnancy and after birth were not monitored.
Asked to comment on these results, Raj Chovatiya, MD, PhD, who directs the center for eczema and itch in the department of dermatology at Northwestern University, Chicago, noted that despite a higher prevalence of CU among females compared with males, very little is known about how the condition is managed during pregnancy. “This retrospective study shows that most patients continue to utilize CU treatment during pregnancy (primarily second-generation antihistamines), with similar birth outcomes as the general population,” he said. “Interestingly, cesarean rates were higher among mothers with CU, and emergency CU referral was a risk factor for preterm birth. While additional prospective studies are needed, these results suggest that CU patients should be carefully managed, particularly during pregnancy, when treatment should be optimized.”
Dr. Kocatürk reported having received personal fees from Novartis, Ibrahim Etem-Menarini, and Sanofi, outside the submitted work. Many coauthors reported having numerous financial disclosures. Dr. Chovatiya disclosed that he is a consultant to, a speaker for, and/or a member of the advisory board for AbbVie, Arcutis, Arena, Incyte, Pfizer, Regeneron, and Sanofi Genzyme.
In addition, the rates of preterm births and medical problems of newborns in patients with CU are similar to those of the normal population and not linked to treatment used during pregnancy.
Those are the key findings from an analysis of new data from PREG-CU, an international, multicenter study of the Urticaria Centers of Reference and Excellence (UCARE) network. Results from the first PREG-CU analysis published in 2021 found that CU improved in about half of patients with CU during pregnancy. “However, two in five patients reported acute exacerbations of CU especially at the beginning and end of pregnancy,” investigators led by Emek Kocatürk, MD, of the department of dermatology and UCARE at Koç University School of Medicine, Istanbul, wrote in the new study, recently published in the Journal of the European Academy of Dermatology and Venereology.
“In addition, 1 in 10 pregnant CU patients required urticaria emergency care and 1 of 6 had angioedema during pregnancy,” they said. Risk factors for worsening CU during pregnancy, they added, were “mild disease and no angioedema before pregnancy, not taking treatment before pregnancy, chronic inducible urticaria, CU worsening during a previous pregnancy, stress as a driver of exacerbations, and treatment during pregnancy.”
Analysis involved 288 pregnant women
To optimize treatment of CU during pregnancy and to better understand how treatment affects pregnancy outcomes, the researchers analyzed 288 pregnancies in 288 women with CU from 13 countries and 21 centers worldwide. Their mean age at pregnancy was 32.1 years, and their mean duration of CU was 84.9 months. Prior to pregnancy, 35.7% of patients rated the severity of their CU symptoms as mild, 34.2% rated it as moderate, and 29.7% rated it as severe.
The researchers found that during pregnancy, 60% of patients used urticaria medication, including standard-dose second-generation H1-antihistamines (35.1%), first-generation H1-antihistamines (7.6%), high-dose second-generation H1-antihistamines (5.6%), and omalizumab (5.6%). The preterm birth rate was 10.2%, which was similar between patients who did and did not receive treatment during pregnancy (11.6% vs. 8.7%, respectively; P = .59).
On multivariate logistic regression, two predictors for preterm birth emerged: giving birth to twins (a 13.3-fold increased risk; P = .016) and emergency referrals for CU (a 4.3-fold increased risk; P =.016). The cesarean delivery rate was 51.3%, and more than 90% of newborns were healthy at birth. There was no link between any patient or disease characteristics or treatments and medical problems at birth.
In other findings, 78.8% of women with CU breastfed their babies. Of the 58 patients who did not breastfeed, 20.7% indicated severe urticaria/angioedema and/or taking medications as the main reason for not breastfeeding.
“Most CU patients use treatment during pregnancy and such treatments, especially second generation H1 antihistamines, seem to be safe during pregnancy regardless of the trimester,” the researchers concluded. “Outcomes of pregnancy in patients with CU were similar compared to the general population and not linked to treatment used during pregnancy. Notably, emergency referral for CU was an independent risk factor for preterm birth,” and the high cesarean delivery rate was “probably linked to comorbidities associated with the disease,” they added. “Overall, these findings suggest that patients should continue their treatments using an individualized dose to provide optimal symptom control.”
International guidelines
The authors noted that international guidelines for the management of urticaria published in 2022 suggest that modern second-generation H1-antihistamines should be used for pregnant patients, preferably loratadine with a possible extrapolation to desloratadine, cetirizine, or levocetirizine.
“Similarly, in this population, we found that cetirizine and loratadine were the most commonly used antihistamines, followed by levocetirizine and fexofenadine,” Dr. Kocatürk and colleagues wrote.
“Guidelines also suggest that the use of first-generation H1-antihistamines should be avoided given their sedative effects; but if these are to be given, it would be wise to know that use of first-generation H1-antihistamines immediately before parturition could cause respiratory depression and other adverse effects in the neonate,” they added, noting that chlorpheniramine and diphenhydramine are the first-generation H1-antihistamines with the greatest evidence of safety in pregnancy.
They acknowledged certain limitations of the analysis, including its retrospective design and the fact that there were no data on low birth weight, small for gestational age, or miscarriage rates. In addition, disease activity or severity during pregnancy and after birth were not monitored.
Asked to comment on these results, Raj Chovatiya, MD, PhD, who directs the center for eczema and itch in the department of dermatology at Northwestern University, Chicago, noted that despite a higher prevalence of CU among females compared with males, very little is known about how the condition is managed during pregnancy. “This retrospective study shows that most patients continue to utilize CU treatment during pregnancy (primarily second-generation antihistamines), with similar birth outcomes as the general population,” he said. “Interestingly, cesarean rates were higher among mothers with CU, and emergency CU referral was a risk factor for preterm birth. While additional prospective studies are needed, these results suggest that CU patients should be carefully managed, particularly during pregnancy, when treatment should be optimized.”
Dr. Kocatürk reported having received personal fees from Novartis, Ibrahim Etem-Menarini, and Sanofi, outside the submitted work. Many coauthors reported having numerous financial disclosures. Dr. Chovatiya disclosed that he is a consultant to, a speaker for, and/or a member of the advisory board for AbbVie, Arcutis, Arena, Incyte, Pfizer, Regeneron, and Sanofi Genzyme.
In addition, the rates of preterm births and medical problems of newborns in patients with CU are similar to those of the normal population and not linked to treatment used during pregnancy.
Those are the key findings from an analysis of new data from PREG-CU, an international, multicenter study of the Urticaria Centers of Reference and Excellence (UCARE) network. Results from the first PREG-CU analysis published in 2021 found that CU improved in about half of patients with CU during pregnancy. “However, two in five patients reported acute exacerbations of CU especially at the beginning and end of pregnancy,” investigators led by Emek Kocatürk, MD, of the department of dermatology and UCARE at Koç University School of Medicine, Istanbul, wrote in the new study, recently published in the Journal of the European Academy of Dermatology and Venereology.
“In addition, 1 in 10 pregnant CU patients required urticaria emergency care and 1 of 6 had angioedema during pregnancy,” they said. Risk factors for worsening CU during pregnancy, they added, were “mild disease and no angioedema before pregnancy, not taking treatment before pregnancy, chronic inducible urticaria, CU worsening during a previous pregnancy, stress as a driver of exacerbations, and treatment during pregnancy.”
Analysis involved 288 pregnant women
To optimize treatment of CU during pregnancy and to better understand how treatment affects pregnancy outcomes, the researchers analyzed 288 pregnancies in 288 women with CU from 13 countries and 21 centers worldwide. Their mean age at pregnancy was 32.1 years, and their mean duration of CU was 84.9 months. Prior to pregnancy, 35.7% of patients rated the severity of their CU symptoms as mild, 34.2% rated it as moderate, and 29.7% rated it as severe.
The researchers found that during pregnancy, 60% of patients used urticaria medication, including standard-dose second-generation H1-antihistamines (35.1%), first-generation H1-antihistamines (7.6%), high-dose second-generation H1-antihistamines (5.6%), and omalizumab (5.6%). The preterm birth rate was 10.2%, which was similar between patients who did and did not receive treatment during pregnancy (11.6% vs. 8.7%, respectively; P = .59).
On multivariate logistic regression, two predictors for preterm birth emerged: giving birth to twins (a 13.3-fold increased risk; P = .016) and emergency referrals for CU (a 4.3-fold increased risk; P =.016). The cesarean delivery rate was 51.3%, and more than 90% of newborns were healthy at birth. There was no link between any patient or disease characteristics or treatments and medical problems at birth.
In other findings, 78.8% of women with CU breastfed their babies. Of the 58 patients who did not breastfeed, 20.7% indicated severe urticaria/angioedema and/or taking medications as the main reason for not breastfeeding.
“Most CU patients use treatment during pregnancy and such treatments, especially second generation H1 antihistamines, seem to be safe during pregnancy regardless of the trimester,” the researchers concluded. “Outcomes of pregnancy in patients with CU were similar compared to the general population and not linked to treatment used during pregnancy. Notably, emergency referral for CU was an independent risk factor for preterm birth,” and the high cesarean delivery rate was “probably linked to comorbidities associated with the disease,” they added. “Overall, these findings suggest that patients should continue their treatments using an individualized dose to provide optimal symptom control.”
International guidelines
The authors noted that international guidelines for the management of urticaria published in 2022 suggest that modern second-generation H1-antihistamines should be used for pregnant patients, preferably loratadine with a possible extrapolation to desloratadine, cetirizine, or levocetirizine.
“Similarly, in this population, we found that cetirizine and loratadine were the most commonly used antihistamines, followed by levocetirizine and fexofenadine,” Dr. Kocatürk and colleagues wrote.
“Guidelines also suggest that the use of first-generation H1-antihistamines should be avoided given their sedative effects; but if these are to be given, it would be wise to know that use of first-generation H1-antihistamines immediately before parturition could cause respiratory depression and other adverse effects in the neonate,” they added, noting that chlorpheniramine and diphenhydramine are the first-generation H1-antihistamines with the greatest evidence of safety in pregnancy.
They acknowledged certain limitations of the analysis, including its retrospective design and the fact that there were no data on low birth weight, small for gestational age, or miscarriage rates. In addition, disease activity or severity during pregnancy and after birth were not monitored.
Asked to comment on these results, Raj Chovatiya, MD, PhD, who directs the center for eczema and itch in the department of dermatology at Northwestern University, Chicago, noted that despite a higher prevalence of CU among females compared with males, very little is known about how the condition is managed during pregnancy. “This retrospective study shows that most patients continue to utilize CU treatment during pregnancy (primarily second-generation antihistamines), with similar birth outcomes as the general population,” he said. “Interestingly, cesarean rates were higher among mothers with CU, and emergency CU referral was a risk factor for preterm birth. While additional prospective studies are needed, these results suggest that CU patients should be carefully managed, particularly during pregnancy, when treatment should be optimized.”
Dr. Kocatürk reported having received personal fees from Novartis, Ibrahim Etem-Menarini, and Sanofi, outside the submitted work. Many coauthors reported having numerous financial disclosures. Dr. Chovatiya disclosed that he is a consultant to, a speaker for, and/or a member of the advisory board for AbbVie, Arcutis, Arena, Incyte, Pfizer, Regeneron, and Sanofi Genzyme.
FROM JEADV

Roselyn Tso confirmed to head Indian Health Service
It took 609 days, but the US Senate has finally (unanimously) confirmed President Biden’s choice to head the Indian Health Service (IHS: Roselyn Tso.)
President Biden nominated Tso in March 2022, and she was formally sworn in on September 27, 2022. The long-awaited confirmation filled a space that hadn’t had a permanent director since Michael Weahkee, a Pueblo of Zuni citizen, stepped down in 2021. In the interim, Elizabeth Fowler, of the Comanche Nation, served as acting director.
Tso’s resume includes almost 40 years of professional experience working at all levels of the IHS. Before taking over as IHS director, she led the IHS Navajo area, the largest IHS regional area, managing more than 4000 employees and a budget of nearly $1 billion.
She also brings “decades of lived experience as a member of the Navajo Nation,” she said in a 40-minute Senate hearing with the US Senate Committee on Indian Affairs in May.
The first Navajo Nation citizen to head the IHS (and only the second woman to do so), Tso introduced herself in Navajo: Deeschii’nii (Start of the Red Streak People) and born for Hashk’aa hadzohi (Yucca Fruit Strung Out). “This is a historic achievement for all of our Navajo people and tribal nations across the country,” Navajo Nation President Jonathan Nez said. “To have one of our own Navajo members in the highest position with IHS is remarkable.”
Tso spoke of having to “navigate the services provided by the Agency for myself, family, and friends.” Her personal and professional backgrounds, she said, help her understand how patients experience the system and how that can be improved. “The health care provided at IHS is critical for those we serve. I understand this not just because I work there,” she said. “My family relies on IHS. My friends rely on IHS. I rely on the IHS.”
The long lacuna in confirming a permanent IHS director left the Native peoples particularly vulnerable—when the COVID-19 pandemic essentially worsened the existing problems they faced, such as diabetes mellitus and cancer. Life expectancy for Native people fell by more than 6 years between 2019 and 2021, to 65 years, compared with the US average of 76 years.
Without a full-time IHS leader, the National Council of Urban Indian Health said in a statement, tribal nations and other Native health care providers struggled to raise and address the issues they were facing amid the pandemic. “Since the resignation of Rear Admiral Weahkee, there have been countless requests from Indian Country calling on Congress and the Administration to nominate a new IHS director to address the growing health disparities experienced by AI/ANs.”
Tso laid out her priorities in her May testimony: creating a more unified health care system using the latest technology to develop centralized systems; improving accountability, transparency, and patient safety; addressing workforce needs and challenges, improving recruitment and retention.
Meeting her goals, she noted, would take “strong partnerships and communication with our Tribal partners…. Each tribe has unique needs, and those needs cannot be met if you do not understand them.”
Last year, President Joseph R. Biden asked Congress to significantly increase IHS funding, but his proposal was cut to $400 million. “For years, IHS has been funded at a rate that is far below its level of need, and the results of this historical neglect can be seen in the disparities in health outcomes for AI/AN people,” William Smith, Valdez Native Tribe, Chairman of the National Indian Health Board (NIHB), wrote to the Senate Committee on Indian Affairs, on the topic of the next IHS director. “Perhaps one of the greatest challenges facing the [Indian, tribal and urban] system is the chronic and severe underfunding and budgetary instability for health care and public health services infrastructure and delivery. Since its creation in 1955, IHS has been chronically underfunded, with annual appropriations never exceeding 50% of demonstrated need. This underfunding has contributed to substandard investment in health delivery systems, some of the worst health disparities among any US population and a severe lack of public health infrastructure and services for our people. At the start of the COVID-19 pandemic these vulnerabilities were starkly exposed and while Congress moved decisively to invest into Tribal health and public health, the new Director must work to maintain these one-time investments.”
Stacy Bohlen, NIHB chief executive, told The Oklahoman that tribal leaders will look to Tso to press Congress for more money and to secure mandatory full funding for IHS—in contrast with the current annual appropriations, where Congress includes IHS in much larger budget bills. “When those bills stall, so does the money tribal clinics need to pay employees and suppliers,” making it hard to recruit and retain employees. “In the Indian Health System,” Bohlen says, “we simply can’t afford that kind of vulnerability.”
Securing advance appropriations and, ultimately, full mandatory funding for IHS, Smith wrote in his letter to the Senate committee, “fulfills the commitment made to our people generations ago and breaks down the systemic healthcare funding inequities the federal government tolerates for Tribes.”
Tso emphasized her intent to “improve the physical, mental, social, and spiritual health and well-being of all American Indians and Alaskan Natives served by the Agency.” Tso “understands the healthcare needs that many first people of this country deal with,” President Nez said. “Her work ethic, value system and approach to problem solving demonstrates the resilience of Indigenous peoples and the commitment to combat the systemic inequities that impact tribal nations.”
It took 609 days, but the US Senate has finally (unanimously) confirmed President Biden’s choice to head the Indian Health Service (IHS: Roselyn Tso.)
President Biden nominated Tso in March 2022, and she was formally sworn in on September 27, 2022. The long-awaited confirmation filled a space that hadn’t had a permanent director since Michael Weahkee, a Pueblo of Zuni citizen, stepped down in 2021. In the interim, Elizabeth Fowler, of the Comanche Nation, served as acting director.
Tso’s resume includes almost 40 years of professional experience working at all levels of the IHS. Before taking over as IHS director, she led the IHS Navajo area, the largest IHS regional area, managing more than 4000 employees and a budget of nearly $1 billion.
She also brings “decades of lived experience as a member of the Navajo Nation,” she said in a 40-minute Senate hearing with the US Senate Committee on Indian Affairs in May.
The first Navajo Nation citizen to head the IHS (and only the second woman to do so), Tso introduced herself in Navajo: Deeschii’nii (Start of the Red Streak People) and born for Hashk’aa hadzohi (Yucca Fruit Strung Out). “This is a historic achievement for all of our Navajo people and tribal nations across the country,” Navajo Nation President Jonathan Nez said. “To have one of our own Navajo members in the highest position with IHS is remarkable.”
Tso spoke of having to “navigate the services provided by the Agency for myself, family, and friends.” Her personal and professional backgrounds, she said, help her understand how patients experience the system and how that can be improved. “The health care provided at IHS is critical for those we serve. I understand this not just because I work there,” she said. “My family relies on IHS. My friends rely on IHS. I rely on the IHS.”
The long lacuna in confirming a permanent IHS director left the Native peoples particularly vulnerable—when the COVID-19 pandemic essentially worsened the existing problems they faced, such as diabetes mellitus and cancer. Life expectancy for Native people fell by more than 6 years between 2019 and 2021, to 65 years, compared with the US average of 76 years.
Without a full-time IHS leader, the National Council of Urban Indian Health said in a statement, tribal nations and other Native health care providers struggled to raise and address the issues they were facing amid the pandemic. “Since the resignation of Rear Admiral Weahkee, there have been countless requests from Indian Country calling on Congress and the Administration to nominate a new IHS director to address the growing health disparities experienced by AI/ANs.”
Tso laid out her priorities in her May testimony: creating a more unified health care system using the latest technology to develop centralized systems; improving accountability, transparency, and patient safety; addressing workforce needs and challenges, improving recruitment and retention.
Meeting her goals, she noted, would take “strong partnerships and communication with our Tribal partners…. Each tribe has unique needs, and those needs cannot be met if you do not understand them.”
Last year, President Joseph R. Biden asked Congress to significantly increase IHS funding, but his proposal was cut to $400 million. “For years, IHS has been funded at a rate that is far below its level of need, and the results of this historical neglect can be seen in the disparities in health outcomes for AI/AN people,” William Smith, Valdez Native Tribe, Chairman of the National Indian Health Board (NIHB), wrote to the Senate Committee on Indian Affairs, on the topic of the next IHS director. “Perhaps one of the greatest challenges facing the [Indian, tribal and urban] system is the chronic and severe underfunding and budgetary instability for health care and public health services infrastructure and delivery. Since its creation in 1955, IHS has been chronically underfunded, with annual appropriations never exceeding 50% of demonstrated need. This underfunding has contributed to substandard investment in health delivery systems, some of the worst health disparities among any US population and a severe lack of public health infrastructure and services for our people. At the start of the COVID-19 pandemic these vulnerabilities were starkly exposed and while Congress moved decisively to invest into Tribal health and public health, the new Director must work to maintain these one-time investments.”
Stacy Bohlen, NIHB chief executive, told The Oklahoman that tribal leaders will look to Tso to press Congress for more money and to secure mandatory full funding for IHS—in contrast with the current annual appropriations, where Congress includes IHS in much larger budget bills. “When those bills stall, so does the money tribal clinics need to pay employees and suppliers,” making it hard to recruit and retain employees. “In the Indian Health System,” Bohlen says, “we simply can’t afford that kind of vulnerability.”
Securing advance appropriations and, ultimately, full mandatory funding for IHS, Smith wrote in his letter to the Senate committee, “fulfills the commitment made to our people generations ago and breaks down the systemic healthcare funding inequities the federal government tolerates for Tribes.”
Tso emphasized her intent to “improve the physical, mental, social, and spiritual health and well-being of all American Indians and Alaskan Natives served by the Agency.” Tso “understands the healthcare needs that many first people of this country deal with,” President Nez said. “Her work ethic, value system and approach to problem solving demonstrates the resilience of Indigenous peoples and the commitment to combat the systemic inequities that impact tribal nations.”
It took 609 days, but the US Senate has finally (unanimously) confirmed President Biden’s choice to head the Indian Health Service (IHS: Roselyn Tso.)
President Biden nominated Tso in March 2022, and she was formally sworn in on September 27, 2022. The long-awaited confirmation filled a space that hadn’t had a permanent director since Michael Weahkee, a Pueblo of Zuni citizen, stepped down in 2021. In the interim, Elizabeth Fowler, of the Comanche Nation, served as acting director.
Tso’s resume includes almost 40 years of professional experience working at all levels of the IHS. Before taking over as IHS director, she led the IHS Navajo area, the largest IHS regional area, managing more than 4000 employees and a budget of nearly $1 billion.
She also brings “decades of lived experience as a member of the Navajo Nation,” she said in a 40-minute Senate hearing with the US Senate Committee on Indian Affairs in May.
The first Navajo Nation citizen to head the IHS (and only the second woman to do so), Tso introduced herself in Navajo: Deeschii’nii (Start of the Red Streak People) and born for Hashk’aa hadzohi (Yucca Fruit Strung Out). “This is a historic achievement for all of our Navajo people and tribal nations across the country,” Navajo Nation President Jonathan Nez said. “To have one of our own Navajo members in the highest position with IHS is remarkable.”
Tso spoke of having to “navigate the services provided by the Agency for myself, family, and friends.” Her personal and professional backgrounds, she said, help her understand how patients experience the system and how that can be improved. “The health care provided at IHS is critical for those we serve. I understand this not just because I work there,” she said. “My family relies on IHS. My friends rely on IHS. I rely on the IHS.”
The long lacuna in confirming a permanent IHS director left the Native peoples particularly vulnerable—when the COVID-19 pandemic essentially worsened the existing problems they faced, such as diabetes mellitus and cancer. Life expectancy for Native people fell by more than 6 years between 2019 and 2021, to 65 years, compared with the US average of 76 years.
Without a full-time IHS leader, the National Council of Urban Indian Health said in a statement, tribal nations and other Native health care providers struggled to raise and address the issues they were facing amid the pandemic. “Since the resignation of Rear Admiral Weahkee, there have been countless requests from Indian Country calling on Congress and the Administration to nominate a new IHS director to address the growing health disparities experienced by AI/ANs.”
Tso laid out her priorities in her May testimony: creating a more unified health care system using the latest technology to develop centralized systems; improving accountability, transparency, and patient safety; addressing workforce needs and challenges, improving recruitment and retention.
Meeting her goals, she noted, would take “strong partnerships and communication with our Tribal partners…. Each tribe has unique needs, and those needs cannot be met if you do not understand them.”
Last year, President Joseph R. Biden asked Congress to significantly increase IHS funding, but his proposal was cut to $400 million. “For years, IHS has been funded at a rate that is far below its level of need, and the results of this historical neglect can be seen in the disparities in health outcomes for AI/AN people,” William Smith, Valdez Native Tribe, Chairman of the National Indian Health Board (NIHB), wrote to the Senate Committee on Indian Affairs, on the topic of the next IHS director. “Perhaps one of the greatest challenges facing the [Indian, tribal and urban] system is the chronic and severe underfunding and budgetary instability for health care and public health services infrastructure and delivery. Since its creation in 1955, IHS has been chronically underfunded, with annual appropriations never exceeding 50% of demonstrated need. This underfunding has contributed to substandard investment in health delivery systems, some of the worst health disparities among any US population and a severe lack of public health infrastructure and services for our people. At the start of the COVID-19 pandemic these vulnerabilities were starkly exposed and while Congress moved decisively to invest into Tribal health and public health, the new Director must work to maintain these one-time investments.”
Stacy Bohlen, NIHB chief executive, told The Oklahoman that tribal leaders will look to Tso to press Congress for more money and to secure mandatory full funding for IHS—in contrast with the current annual appropriations, where Congress includes IHS in much larger budget bills. “When those bills stall, so does the money tribal clinics need to pay employees and suppliers,” making it hard to recruit and retain employees. “In the Indian Health System,” Bohlen says, “we simply can’t afford that kind of vulnerability.”
Securing advance appropriations and, ultimately, full mandatory funding for IHS, Smith wrote in his letter to the Senate committee, “fulfills the commitment made to our people generations ago and breaks down the systemic healthcare funding inequities the federal government tolerates for Tribes.”
Tso emphasized her intent to “improve the physical, mental, social, and spiritual health and well-being of all American Indians and Alaskan Natives served by the Agency.” Tso “understands the healthcare needs that many first people of this country deal with,” President Nez said. “Her work ethic, value system and approach to problem solving demonstrates the resilience of Indigenous peoples and the commitment to combat the systemic inequities that impact tribal nations.”
Antioxidant-rich diet may reduce Helicobacter pylori risk
People who eat a balanced diet with sufficient antioxidants from fruits and vegetables may face reduced risks for Heliobacter pylori infections, according to a new report.
In particular, patients with an H. pylori infection were more likely to score lower on the Dietary Antioxidant Index (DAI), which was created to consider a diet’s entire antioxidant profile.
“Available evidence indicates that diet has an important role in developing H. pylori infection. Therefore, protective dietary factors are important from a public health point of view,” Farzad Shidfar, a professor of nutrition at the Iran University of Medical Sciences, Tehran, and member of the university’s colorectal research center, and colleagues write.
“While some nutritional research has widely focused on single nutrients or foods in diet-disease relations, the overall diet could be more informative because humans typically consume a combination of nutrients and foods,” they write. “Dietary indices such as DAI are one of the approaches for this purpose.”
The study was published online in BMC Gastroenterology.
Measuring antioxidant intake
Previous research has indicated an inverse association between the DAI and inflammatory diseases, the study authors write, including gastric cancer, colorectal cancer, nonalcoholic fatty liver disease, and obesity. Studies have also indicated that H. pylori infection is related to deficiencies in vitamins A, C, and E, which have antioxidant properties.
In a case-control study, the research team compared the dietary intake of 148 patients with H. pylori to 302 healthy controls without infection. The patients in the H. pylori–positive group were recruited between June 2021 and November 2021 from the gastroenterology clinic at Rasoul-e-Akram Hospital in Tehran, where they were newly diagnosed with active infection and not yet under treatment.
The researchers calculated the DAI based on dietary intake information from a validated, 168-item food frequency questionnaire used in Iran. The participants were asked about their dietary intake based on the average day, week, month, and year. They also discussed serving sizes of food items, and to increase the accuracy of estimates, interviewers showed household measurements or serving sizes to confirm the measurements with participants.
The average age of the study participants was 39 years, and about 60% were women. Compared with the healthy controls, those with H. pylori were significantly older, had higher body mass index, and smoked more.
Overall, patients with H. pylori had a significantly lower intake of vitamin A, vitamin E, manganese, and selenium. Other differences in dietary intake – for vitamin C and zinc – were not significant.
The average total DAI was significantly higher in the healthy controls, at 7.67, as compared with 3.57 in the patients with H. pylori. The risk for infection decreased as continuous DAI increased.
After adjusting for several variables, the researchers found that participants with less than the median DAI values had an increased risk of developing an H. pylori infection.
“A balanced diet, especially high consumption of fruits and vegetables, might protect people against the consequences of H. pylori infection,” the study authors write. “On the contrary, a diet full of carbohydrates and sweets is related to a higher H. pylori infection prevalence.”
Why a good diet may help combat infection
The findings are consistent with other studies that have noted a higher intake of fruits and vegetables among healthy people compared with those who have H. pylori infections, the study authors write. Animal studies have also indicated that taking vitamins A, C, and E and selenium can lead to a reduction in H. pylori growth.
“Several biologically plausible reasons may explain why dietary antioxidants might be, either directly or indirectly, a protective factor against H. pylori infection,” the researchers write. “It is well-known that antioxidants, with their free radical scavenging activities, can inhibit the growth of H. pylori.”
H. pylori is urease-positive and can synthesize a large amount of urease for ammonia production to neutralize gastric acid, which allows it to colonize in the stomach epithelium, the study authors write. Vitamin C inhibits urease activity and improves the stimulation of granulocytes, macrophages, lymphocytes, and immunoglobulin production. Other nutrients, such as zinc, may inhibit the urease enzyme and prevent H. pylori adhesion to gastric tissues, they write.
“Dietary elements have previously been shown to dramatically alter pathogenic responses to H. pylori infections,” Richard Peek Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn., told this news organization.
Dr. Peek, who wasn’t involved with this study, and colleagues found that iron deficiency is linked with altered bile metabolism, which can promote H. pylori–induced gastric carcinogenesis.
“The current study is important, as it suggests that shifting to a diet rich in antioxidants may be beneficial in terms of H. pylori infection,” he said.
At the same time, Dr. Peek expressed caution about generalizing the results across populations.
“Most of the persons enrolled in this study were likely infected with H. pylori as children,” he noted. “Therefore, the inverse role of antioxidant-rich diets and H. pylori infection must be interpreted with caution.”
Future studies should confirm the findings in other groups and determine whether antioxidant-rich diets limit the diseases caused by H. pylori infection, Dr. Peek added.
The study was not funded by any research center, and the authors declared no conflicts of interest. Dr. Peek reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
People who eat a balanced diet with sufficient antioxidants from fruits and vegetables may face reduced risks for Heliobacter pylori infections, according to a new report.
In particular, patients with an H. pylori infection were more likely to score lower on the Dietary Antioxidant Index (DAI), which was created to consider a diet’s entire antioxidant profile.
“Available evidence indicates that diet has an important role in developing H. pylori infection. Therefore, protective dietary factors are important from a public health point of view,” Farzad Shidfar, a professor of nutrition at the Iran University of Medical Sciences, Tehran, and member of the university’s colorectal research center, and colleagues write.
“While some nutritional research has widely focused on single nutrients or foods in diet-disease relations, the overall diet could be more informative because humans typically consume a combination of nutrients and foods,” they write. “Dietary indices such as DAI are one of the approaches for this purpose.”
The study was published online in BMC Gastroenterology.
Measuring antioxidant intake
Previous research has indicated an inverse association between the DAI and inflammatory diseases, the study authors write, including gastric cancer, colorectal cancer, nonalcoholic fatty liver disease, and obesity. Studies have also indicated that H. pylori infection is related to deficiencies in vitamins A, C, and E, which have antioxidant properties.
In a case-control study, the research team compared the dietary intake of 148 patients with H. pylori to 302 healthy controls without infection. The patients in the H. pylori–positive group were recruited between June 2021 and November 2021 from the gastroenterology clinic at Rasoul-e-Akram Hospital in Tehran, where they were newly diagnosed with active infection and not yet under treatment.
The researchers calculated the DAI based on dietary intake information from a validated, 168-item food frequency questionnaire used in Iran. The participants were asked about their dietary intake based on the average day, week, month, and year. They also discussed serving sizes of food items, and to increase the accuracy of estimates, interviewers showed household measurements or serving sizes to confirm the measurements with participants.
The average age of the study participants was 39 years, and about 60% were women. Compared with the healthy controls, those with H. pylori were significantly older, had higher body mass index, and smoked more.
Overall, patients with H. pylori had a significantly lower intake of vitamin A, vitamin E, manganese, and selenium. Other differences in dietary intake – for vitamin C and zinc – were not significant.
The average total DAI was significantly higher in the healthy controls, at 7.67, as compared with 3.57 in the patients with H. pylori. The risk for infection decreased as continuous DAI increased.
After adjusting for several variables, the researchers found that participants with less than the median DAI values had an increased risk of developing an H. pylori infection.
“A balanced diet, especially high consumption of fruits and vegetables, might protect people against the consequences of H. pylori infection,” the study authors write. “On the contrary, a diet full of carbohydrates and sweets is related to a higher H. pylori infection prevalence.”
Why a good diet may help combat infection
The findings are consistent with other studies that have noted a higher intake of fruits and vegetables among healthy people compared with those who have H. pylori infections, the study authors write. Animal studies have also indicated that taking vitamins A, C, and E and selenium can lead to a reduction in H. pylori growth.
“Several biologically plausible reasons may explain why dietary antioxidants might be, either directly or indirectly, a protective factor against H. pylori infection,” the researchers write. “It is well-known that antioxidants, with their free radical scavenging activities, can inhibit the growth of H. pylori.”
H. pylori is urease-positive and can synthesize a large amount of urease for ammonia production to neutralize gastric acid, which allows it to colonize in the stomach epithelium, the study authors write. Vitamin C inhibits urease activity and improves the stimulation of granulocytes, macrophages, lymphocytes, and immunoglobulin production. Other nutrients, such as zinc, may inhibit the urease enzyme and prevent H. pylori adhesion to gastric tissues, they write.
“Dietary elements have previously been shown to dramatically alter pathogenic responses to H. pylori infections,” Richard Peek Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn., told this news organization.
Dr. Peek, who wasn’t involved with this study, and colleagues found that iron deficiency is linked with altered bile metabolism, which can promote H. pylori–induced gastric carcinogenesis.
“The current study is important, as it suggests that shifting to a diet rich in antioxidants may be beneficial in terms of H. pylori infection,” he said.
At the same time, Dr. Peek expressed caution about generalizing the results across populations.
“Most of the persons enrolled in this study were likely infected with H. pylori as children,” he noted. “Therefore, the inverse role of antioxidant-rich diets and H. pylori infection must be interpreted with caution.”
Future studies should confirm the findings in other groups and determine whether antioxidant-rich diets limit the diseases caused by H. pylori infection, Dr. Peek added.
The study was not funded by any research center, and the authors declared no conflicts of interest. Dr. Peek reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
People who eat a balanced diet with sufficient antioxidants from fruits and vegetables may face reduced risks for Heliobacter pylori infections, according to a new report.
In particular, patients with an H. pylori infection were more likely to score lower on the Dietary Antioxidant Index (DAI), which was created to consider a diet’s entire antioxidant profile.
“Available evidence indicates that diet has an important role in developing H. pylori infection. Therefore, protective dietary factors are important from a public health point of view,” Farzad Shidfar, a professor of nutrition at the Iran University of Medical Sciences, Tehran, and member of the university’s colorectal research center, and colleagues write.
“While some nutritional research has widely focused on single nutrients or foods in diet-disease relations, the overall diet could be more informative because humans typically consume a combination of nutrients and foods,” they write. “Dietary indices such as DAI are one of the approaches for this purpose.”
The study was published online in BMC Gastroenterology.
Measuring antioxidant intake
Previous research has indicated an inverse association between the DAI and inflammatory diseases, the study authors write, including gastric cancer, colorectal cancer, nonalcoholic fatty liver disease, and obesity. Studies have also indicated that H. pylori infection is related to deficiencies in vitamins A, C, and E, which have antioxidant properties.
In a case-control study, the research team compared the dietary intake of 148 patients with H. pylori to 302 healthy controls without infection. The patients in the H. pylori–positive group were recruited between June 2021 and November 2021 from the gastroenterology clinic at Rasoul-e-Akram Hospital in Tehran, where they were newly diagnosed with active infection and not yet under treatment.
The researchers calculated the DAI based on dietary intake information from a validated, 168-item food frequency questionnaire used in Iran. The participants were asked about their dietary intake based on the average day, week, month, and year. They also discussed serving sizes of food items, and to increase the accuracy of estimates, interviewers showed household measurements or serving sizes to confirm the measurements with participants.
The average age of the study participants was 39 years, and about 60% were women. Compared with the healthy controls, those with H. pylori were significantly older, had higher body mass index, and smoked more.
Overall, patients with H. pylori had a significantly lower intake of vitamin A, vitamin E, manganese, and selenium. Other differences in dietary intake – for vitamin C and zinc – were not significant.
The average total DAI was significantly higher in the healthy controls, at 7.67, as compared with 3.57 in the patients with H. pylori. The risk for infection decreased as continuous DAI increased.
After adjusting for several variables, the researchers found that participants with less than the median DAI values had an increased risk of developing an H. pylori infection.
“A balanced diet, especially high consumption of fruits and vegetables, might protect people against the consequences of H. pylori infection,” the study authors write. “On the contrary, a diet full of carbohydrates and sweets is related to a higher H. pylori infection prevalence.”
Why a good diet may help combat infection
The findings are consistent with other studies that have noted a higher intake of fruits and vegetables among healthy people compared with those who have H. pylori infections, the study authors write. Animal studies have also indicated that taking vitamins A, C, and E and selenium can lead to a reduction in H. pylori growth.
“Several biologically plausible reasons may explain why dietary antioxidants might be, either directly or indirectly, a protective factor against H. pylori infection,” the researchers write. “It is well-known that antioxidants, with their free radical scavenging activities, can inhibit the growth of H. pylori.”
H. pylori is urease-positive and can synthesize a large amount of urease for ammonia production to neutralize gastric acid, which allows it to colonize in the stomach epithelium, the study authors write. Vitamin C inhibits urease activity and improves the stimulation of granulocytes, macrophages, lymphocytes, and immunoglobulin production. Other nutrients, such as zinc, may inhibit the urease enzyme and prevent H. pylori adhesion to gastric tissues, they write.
“Dietary elements have previously been shown to dramatically alter pathogenic responses to H. pylori infections,” Richard Peek Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn., told this news organization.
Dr. Peek, who wasn’t involved with this study, and colleagues found that iron deficiency is linked with altered bile metabolism, which can promote H. pylori–induced gastric carcinogenesis.
“The current study is important, as it suggests that shifting to a diet rich in antioxidants may be beneficial in terms of H. pylori infection,” he said.
At the same time, Dr. Peek expressed caution about generalizing the results across populations.
“Most of the persons enrolled in this study were likely infected with H. pylori as children,” he noted. “Therefore, the inverse role of antioxidant-rich diets and H. pylori infection must be interpreted with caution.”
Future studies should confirm the findings in other groups and determine whether antioxidant-rich diets limit the diseases caused by H. pylori infection, Dr. Peek added.
The study was not funded by any research center, and the authors declared no conflicts of interest. Dr. Peek reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM BMC GASTROENTEROLOGY
COMMENT & CONTROVERSY
Misoprostol: Clinical pharmacology in obstetrics and gynecology
ROBERT L. BARBIERI, MD (JULY 2022)
Outcomes from my practice’s pilot study
In his recent editorial, Dr. Barbieri addressed the important topic of office-based cervical ripening prior to inpatient induction of labor. In order to decrease the length of labor and increase the success of vaginal delivery, the cervical factor is of prime importance. Patients with an unfavorable cervix (Bishop score of ≥6) are more likely to experience longer labor, risk of infection, fetal distress, etc, and may end up with an unwanted cesarean delivery. To prevent the above, numerous approaches (mechanical methods, double-balloon catheter, laminaria, misoprostol among others) have been discussed.
The inclusion criteria for office-based cervical ripening are low-risk patients, singleton pregnancies between 39 and 40 weeks of gestation, and cephalic presentation. The details of inclusion and exclusion criteria have to be determined by each practice individually. Our practice went a step further. We performed a small pilot study to assess the safety and efficacy of office cervical ripening in low-risk primigravid patients with low Bishop scores who were not scheduled for induction in anticipation of labor. Ten primigravid patients with poor Bishop scores (6 or less) were administered 50 µg misoprostol at 39+ weeks of pregnancy in the office setting. Bishop scores were taken twice per week until delivery. In 7 out of 10 patients, the Bishop score became favorable within a week of treatment, and in 3 patients the Bishop score remained the same. Three out of 10 patients experienced self-limited episodes of uterine contractility, and 2 of the patients went into labor within 3 days of using misoprostol. All patients were delivered within 2 weeks of treatment without an induction: 8 delivered vaginally, and 2 by cesarean delivery.2
Cesarean delivery was done for fetal distress (1 case) and prolonged second stage of labor (1 case). All neonates were born in satisfactory condition with Apgar scores between 7 and 10. Our preliminary results demonstrated marked improvement in cervical ripening judged by the Bishop score in 70% of patients.2
A prospective randomized study should be performed with the following agenda:
- Does late pregnancy medical cervical ripening in low-risk patients affect labor course and cesarean delivery rate?
- What is the optimal dose and route of administration of misoprostol?3,4
References
- Barbieri R. Office-based ambulatory cervical ripening prior to in patient induction of labor. OBG Manag. 2021;33:9-13.
- Petrikovsky B. Should cervical ripening become routine in primigravid low risk patients [In press]. Neonat Int Care. 2022:1, 4-6.
- Sharami SH, Milani F, Faraji R. Comparison of 25 µg sublingual and 50 µg intravaginal misoprostol for cervical ripening and labor: a randomized controlled equivalence trial. Arch Med. 2014:10:653-656.
- Barbieri R. Misoprostol: clinical pharmacology in obstetrics and gynecology. OBG Manag. 2022:34:7, 8-12.
B. Petrikovsky, MD, PhD
New Hyde Park, New York
Dr. Barbieri responds
I appreciate that Dr. Petrikovsky took time from a busy practice to provide our readers with his very innovative idea. I agree with him that a clinical trial is warranted to test the effects of late pregnancy medical cervical ripening in low-risk patients on labor course and birth outcome. Maybe one of our readers will take on the challenge to complete such a trial! ●
Misoprostol: Clinical pharmacology in obstetrics and gynecology
ROBERT L. BARBIERI, MD (JULY 2022)
Outcomes from my practice’s pilot study
In his recent editorial, Dr. Barbieri addressed the important topic of office-based cervical ripening prior to inpatient induction of labor. In order to decrease the length of labor and increase the success of vaginal delivery, the cervical factor is of prime importance. Patients with an unfavorable cervix (Bishop score of ≥6) are more likely to experience longer labor, risk of infection, fetal distress, etc, and may end up with an unwanted cesarean delivery. To prevent the above, numerous approaches (mechanical methods, double-balloon catheter, laminaria, misoprostol among others) have been discussed.
The inclusion criteria for office-based cervical ripening are low-risk patients, singleton pregnancies between 39 and 40 weeks of gestation, and cephalic presentation. The details of inclusion and exclusion criteria have to be determined by each practice individually. Our practice went a step further. We performed a small pilot study to assess the safety and efficacy of office cervical ripening in low-risk primigravid patients with low Bishop scores who were not scheduled for induction in anticipation of labor. Ten primigravid patients with poor Bishop scores (6 or less) were administered 50 µg misoprostol at 39+ weeks of pregnancy in the office setting. Bishop scores were taken twice per week until delivery. In 7 out of 10 patients, the Bishop score became favorable within a week of treatment, and in 3 patients the Bishop score remained the same. Three out of 10 patients experienced self-limited episodes of uterine contractility, and 2 of the patients went into labor within 3 days of using misoprostol. All patients were delivered within 2 weeks of treatment without an induction: 8 delivered vaginally, and 2 by cesarean delivery.2
Cesarean delivery was done for fetal distress (1 case) and prolonged second stage of labor (1 case). All neonates were born in satisfactory condition with Apgar scores between 7 and 10. Our preliminary results demonstrated marked improvement in cervical ripening judged by the Bishop score in 70% of patients.2
A prospective randomized study should be performed with the following agenda:
- Does late pregnancy medical cervical ripening in low-risk patients affect labor course and cesarean delivery rate?
- What is the optimal dose and route of administration of misoprostol?3,4
References
- Barbieri R. Office-based ambulatory cervical ripening prior to in patient induction of labor. OBG Manag. 2021;33:9-13.
- Petrikovsky B. Should cervical ripening become routine in primigravid low risk patients [In press]. Neonat Int Care. 2022:1, 4-6.
- Sharami SH, Milani F, Faraji R. Comparison of 25 µg sublingual and 50 µg intravaginal misoprostol for cervical ripening and labor: a randomized controlled equivalence trial. Arch Med. 2014:10:653-656.
- Barbieri R. Misoprostol: clinical pharmacology in obstetrics and gynecology. OBG Manag. 2022:34:7, 8-12.
B. Petrikovsky, MD, PhD
New Hyde Park, New York
Dr. Barbieri responds
I appreciate that Dr. Petrikovsky took time from a busy practice to provide our readers with his very innovative idea. I agree with him that a clinical trial is warranted to test the effects of late pregnancy medical cervical ripening in low-risk patients on labor course and birth outcome. Maybe one of our readers will take on the challenge to complete such a trial! ●
Misoprostol: Clinical pharmacology in obstetrics and gynecology
ROBERT L. BARBIERI, MD (JULY 2022)
Outcomes from my practice’s pilot study
In his recent editorial, Dr. Barbieri addressed the important topic of office-based cervical ripening prior to inpatient induction of labor. In order to decrease the length of labor and increase the success of vaginal delivery, the cervical factor is of prime importance. Patients with an unfavorable cervix (Bishop score of ≥6) are more likely to experience longer labor, risk of infection, fetal distress, etc, and may end up with an unwanted cesarean delivery. To prevent the above, numerous approaches (mechanical methods, double-balloon catheter, laminaria, misoprostol among others) have been discussed.
The inclusion criteria for office-based cervical ripening are low-risk patients, singleton pregnancies between 39 and 40 weeks of gestation, and cephalic presentation. The details of inclusion and exclusion criteria have to be determined by each practice individually. Our practice went a step further. We performed a small pilot study to assess the safety and efficacy of office cervical ripening in low-risk primigravid patients with low Bishop scores who were not scheduled for induction in anticipation of labor. Ten primigravid patients with poor Bishop scores (6 or less) were administered 50 µg misoprostol at 39+ weeks of pregnancy in the office setting. Bishop scores were taken twice per week until delivery. In 7 out of 10 patients, the Bishop score became favorable within a week of treatment, and in 3 patients the Bishop score remained the same. Three out of 10 patients experienced self-limited episodes of uterine contractility, and 2 of the patients went into labor within 3 days of using misoprostol. All patients were delivered within 2 weeks of treatment without an induction: 8 delivered vaginally, and 2 by cesarean delivery.2
Cesarean delivery was done for fetal distress (1 case) and prolonged second stage of labor (1 case). All neonates were born in satisfactory condition with Apgar scores between 7 and 10. Our preliminary results demonstrated marked improvement in cervical ripening judged by the Bishop score in 70% of patients.2
A prospective randomized study should be performed with the following agenda:
- Does late pregnancy medical cervical ripening in low-risk patients affect labor course and cesarean delivery rate?
- What is the optimal dose and route of administration of misoprostol?3,4
References
- Barbieri R. Office-based ambulatory cervical ripening prior to in patient induction of labor. OBG Manag. 2021;33:9-13.
- Petrikovsky B. Should cervical ripening become routine in primigravid low risk patients [In press]. Neonat Int Care. 2022:1, 4-6.
- Sharami SH, Milani F, Faraji R. Comparison of 25 µg sublingual and 50 µg intravaginal misoprostol for cervical ripening and labor: a randomized controlled equivalence trial. Arch Med. 2014:10:653-656.
- Barbieri R. Misoprostol: clinical pharmacology in obstetrics and gynecology. OBG Manag. 2022:34:7, 8-12.
B. Petrikovsky, MD, PhD
New Hyde Park, New York
Dr. Barbieri responds
I appreciate that Dr. Petrikovsky took time from a busy practice to provide our readers with his very innovative idea. I agree with him that a clinical trial is warranted to test the effects of late pregnancy medical cervical ripening in low-risk patients on labor course and birth outcome. Maybe one of our readers will take on the challenge to complete such a trial! ●
Clinical psychoeconomics: Accounting for money matters in psychiatric assessment and treatment
Despite money’s central role in our psychic lives, many trainees – and some seasoned practitioners – skirt around financial issues. Some clinicians confess that inquiring about patients’ finances feels “too personal.” They fear that asking about money could suggest that the clinician is primarily concerned with getting paid. Some clinicians feel that looking into patients’ finances might be unprofessional, outside one’s scope of practice. But it is not.

Trainees often receive little guidance concerning money matters in patients’ lives and treatments, considerations we have labeled clinical psychoeconomics. Considerable evidence suggests that financial concerns often provoke emotional distress and dysfunctional behaviors, and directly influence patient’s health care decisions. Financial issues also influence how clinicians view and react to patients.
We have recently reviewed (and illustrated through case vignettes) how money matters might impact psychiatric assessment, case formulation, treatment planning, and ongoing psychiatric treatments including psychotherapies.1 Consider how money affects people’s lives: Money helps people meet multiple practical, psychological, and social needs by enabling them to obtain food, clothing, shelter, other material goods, services, discretionary time, and opportunities. And money strongly influences relationships. Regardless of poverty or wealth, thoughts and behaviors connected to acquiring, possessing, and disposing of money, and feelings accompanying these processes such as greed, neediness, envy, pride, shame, guilt, and self-satisfaction often underly intrapsychic and interpersonal conflicts.

Individuals constantly engage in numerous simultaneous conscious, preconscious, and unconscious neuro-economic trade-offs that determine goals, efforts, and timing. Many are financially influenced. Money influences how virtually all patients seek, receive, and sustain their mental health care including psychotherapy.
Money problems can be associated with insecurity, impotence, feeling unloved, and lack of freedom or subjugation. Individuals may resent how they’re forced to acquire money, and feel shamed or morally injured by their jobs, financial dependence on other family members, public assistance, or their questionable ways of obtaining money.
Impoverished individuals may face choosing between food, housing, medications, and medical care. Domestically abused individuals may reluctantly remain with their abusers, risking physical harm or death rather than face destitution. Some families tolerate severely disabled individuals at home because they rely on their disability checks and caregiver payments. Suicides may turn on how individuals forecast financial repercussions affecting their families. Desires to avoid debt may lead to treatment avoidance.
Individuals with enough money to get by face daily financially related choices involving competing needs, desires, values, and loyalties. They may experience conflicts concerning spending on necessities vs. indulgences or spending on oneself vs. significant others.
Whereas some wealthy individuals may assume unwarranted airs of superiority and entitlement, others may feel guilty about wealth, or fearful that others like them only for their money. Individuals on the receiving end of wealth may feel emotionally and behaviorally manipulated by their benefactors.
Assessment
Assessments should consider how financial matters have shaped patients’ early psychological development as well their current lives. How do patients’ emotions, thoughts, and behaviors reflect money matters? What money-related pathologies are evident? What aspects of the patient’s “financial world” seem modifiable?
Financial questions should be posed colloquially. Screeners include: “Where do you live?”, “Who’s in the home?”, “How do you (all) manage financially?”, “What do you all do for a living?”, “How do you make ends meet?”, and “What financial problems are you facing?” Clinicians can quickly learn about patients’ financial self-sufficiencies, individuals for whom they bear financial responsibility, and others they rely on for support, for example, relatives. If patients avoid answering such questions forthrightly, particularly when financial arrangements are “complicated,” clinicians will want to revisit these issues later after establishing a firmer alliance but continue to wonder about the meaning of the patient’s reluctance.
When explicit, patients, families, and couples are fully aware of the conflicts but have difficulty resolving financial disputes. When conflicts are implicit, money problems may be unacknowledged, avoided, denied, or minimized. Conflicts concerning money are often transmitted trans-generationally.
Psychopathological conditions unequivocally linked to money include compulsive shopping, gambling disorders, miserly hoarding, impulse buying, and spending sprees during hypomanic and manic states. Mounting debts may create progressively insurmountable sources of distress. Money can be weaponized to sadistically create enticement, envy, or deprivation. Some monetarily antisocial individuals compromise interpersonal relationships as well as treatments. Individuals with alcohol/substance use disorders may spend so much on substances that little is left for necessities. Financially needy individuals may engage in morally questionable behaviors they might otherwise shun.
Case formulation and treatment planning
Incorporating money matters into case formulations entails demonstrating how financial concerns influenced maladaptive development and distort current attitudes, perceptions, and behaviors.
Concurrently, clinicians should acknowledge patients’ reality-based fiscal decisions, appreciating cultural and family value differences concerning how money should be acquired and spent. Since money often determines frequency and duration of treatment visits, clinicians are ethically obligated to discuss with patients what they might expect from different medications and psychotherapies, and their comparative costs.
Money matters’ impact on psychotherapies
Money matters often affect transference and countertransference reactions. Some reactions stem from how patients and clinicians compare their own financial situations with those of the other.
To help identify and ameliorate money-related countertransference responses, clinicians can reflect on questions such as: “How comfortable are you with people who are much poorer or richer than you are?” “How comfortable are you with impoverished individuals or with multimillionaires or their children?” And “why?” For trainees, all these reactions should be discussed in supervision.
Conclusions
To summarize, four clinical psychoeconomic issues should be routinely assessed and factored into psychiatric case formulations and treatment plans: how financial issues 1) have impacted patients’ psychological development; 2) impact patients’ current lives; 3) are likely to impact access, type, intensity, and duration of treatment visits; and 4) might provoke money-related transference and countertransference concerns.
In advising patients about treatment options, clinicians should discuss each treatment’s relative effectiveness and estimated costs of care. Patients’ decisions will likely be heavily influenced by financial considerations.
Dr. Yager is based in the department of psychiatry, University of Colorado at Denver, Aurora. Dr. Kay is based in the department of psychiatry, Wright State University, Dayton, Ohio. No external funds were received for this project, and the authors have no conflicts to disclose.
Reference
1. Yager J and Kay J. Money matters in psychiatric assessment, case formulation, treatment planning, and ongoing psychotherapy: Clinical psychoeconomics. J Nerv Ment Dis. 2022 Jun 10. doi: 10.1097/NMD.0000000000001552.
Despite money’s central role in our psychic lives, many trainees – and some seasoned practitioners – skirt around financial issues. Some clinicians confess that inquiring about patients’ finances feels “too personal.” They fear that asking about money could suggest that the clinician is primarily concerned with getting paid. Some clinicians feel that looking into patients’ finances might be unprofessional, outside one’s scope of practice. But it is not.
Trainees often receive little guidance concerning money matters in patients’ lives and treatments, considerations we have labeled clinical psychoeconomics. Considerable evidence suggests that financial concerns often provoke emotional distress and dysfunctional behaviors, and directly influence patient’s health care decisions. Financial issues also influence how clinicians view and react to patients.
We have recently reviewed (and illustrated through case vignettes) how money matters might impact psychiatric assessment, case formulation, treatment planning, and ongoing psychiatric treatments including psychotherapies.1 Consider how money affects people’s lives: Money helps people meet multiple practical, psychological, and social needs by enabling them to obtain food, clothing, shelter, other material goods, services, discretionary time, and opportunities. And money strongly influences relationships. Regardless of poverty or wealth, thoughts and behaviors connected to acquiring, possessing, and disposing of money, and feelings accompanying these processes such as greed, neediness, envy, pride, shame, guilt, and self-satisfaction often underly intrapsychic and interpersonal conflicts.
Individuals constantly engage in numerous simultaneous conscious, preconscious, and unconscious neuro-economic trade-offs that determine goals, efforts, and timing. Many are financially influenced. Money influences how virtually all patients seek, receive, and sustain their mental health care including psychotherapy.
Money problems can be associated with insecurity, impotence, feeling unloved, and lack of freedom or subjugation. Individuals may resent how they’re forced to acquire money, and feel shamed or morally injured by their jobs, financial dependence on other family members, public assistance, or their questionable ways of obtaining money.
Impoverished individuals may face choosing between food, housing, medications, and medical care. Domestically abused individuals may reluctantly remain with their abusers, risking physical harm or death rather than face destitution. Some families tolerate severely disabled individuals at home because they rely on their disability checks and caregiver payments. Suicides may turn on how individuals forecast financial repercussions affecting their families. Desires to avoid debt may lead to treatment avoidance.
Individuals with enough money to get by face daily financially related choices involving competing needs, desires, values, and loyalties. They may experience conflicts concerning spending on necessities vs. indulgences or spending on oneself vs. significant others.
Whereas some wealthy individuals may assume unwarranted airs of superiority and entitlement, others may feel guilty about wealth, or fearful that others like them only for their money. Individuals on the receiving end of wealth may feel emotionally and behaviorally manipulated by their benefactors.
Assessment
Assessments should consider how financial matters have shaped patients’ early psychological development as well their current lives. How do patients’ emotions, thoughts, and behaviors reflect money matters? What money-related pathologies are evident? What aspects of the patient’s “financial world” seem modifiable?
Financial questions should be posed colloquially. Screeners include: “Where do you live?”, “Who’s in the home?”, “How do you (all) manage financially?”, “What do you all do for a living?”, “How do you make ends meet?”, and “What financial problems are you facing?” Clinicians can quickly learn about patients’ financial self-sufficiencies, individuals for whom they bear financial responsibility, and others they rely on for support, for example, relatives. If patients avoid answering such questions forthrightly, particularly when financial arrangements are “complicated,” clinicians will want to revisit these issues later after establishing a firmer alliance but continue to wonder about the meaning of the patient’s reluctance.
When explicit, patients, families, and couples are fully aware of the conflicts but have difficulty resolving financial disputes. When conflicts are implicit, money problems may be unacknowledged, avoided, denied, or minimized. Conflicts concerning money are often transmitted trans-generationally.
Psychopathological conditions unequivocally linked to money include compulsive shopping, gambling disorders, miserly hoarding, impulse buying, and spending sprees during hypomanic and manic states. Mounting debts may create progressively insurmountable sources of distress. Money can be weaponized to sadistically create enticement, envy, or deprivation. Some monetarily antisocial individuals compromise interpersonal relationships as well as treatments. Individuals with alcohol/substance use disorders may spend so much on substances that little is left for necessities. Financially needy individuals may engage in morally questionable behaviors they might otherwise shun.
Case formulation and treatment planning
Incorporating money matters into case formulations entails demonstrating how financial concerns influenced maladaptive development and distort current attitudes, perceptions, and behaviors.
Concurrently, clinicians should acknowledge patients’ reality-based fiscal decisions, appreciating cultural and family value differences concerning how money should be acquired and spent. Since money often determines frequency and duration of treatment visits, clinicians are ethically obligated to discuss with patients what they might expect from different medications and psychotherapies, and their comparative costs.
Money matters’ impact on psychotherapies
Money matters often affect transference and countertransference reactions. Some reactions stem from how patients and clinicians compare their own financial situations with those of the other.
To help identify and ameliorate money-related countertransference responses, clinicians can reflect on questions such as: “How comfortable are you with people who are much poorer or richer than you are?” “How comfortable are you with impoverished individuals or with multimillionaires or their children?” And “why?” For trainees, all these reactions should be discussed in supervision.
Conclusions
To summarize, four clinical psychoeconomic issues should be routinely assessed and factored into psychiatric case formulations and treatment plans: how financial issues 1) have impacted patients’ psychological development; 2) impact patients’ current lives; 3) are likely to impact access, type, intensity, and duration of treatment visits; and 4) might provoke money-related transference and countertransference concerns.
In advising patients about treatment options, clinicians should discuss each treatment’s relative effectiveness and estimated costs of care. Patients’ decisions will likely be heavily influenced by financial considerations.
Dr. Yager is based in the department of psychiatry, University of Colorado at Denver, Aurora. Dr. Kay is based in the department of psychiatry, Wright State University, Dayton, Ohio. No external funds were received for this project, and the authors have no conflicts to disclose.
Reference
1. Yager J and Kay J. Money matters in psychiatric assessment, case formulation, treatment planning, and ongoing psychotherapy: Clinical psychoeconomics. J Nerv Ment Dis. 2022 Jun 10. doi: 10.1097/NMD.0000000000001552.
Despite money’s central role in our psychic lives, many trainees – and some seasoned practitioners – skirt around financial issues. Some clinicians confess that inquiring about patients’ finances feels “too personal.” They fear that asking about money could suggest that the clinician is primarily concerned with getting paid. Some clinicians feel that looking into patients’ finances might be unprofessional, outside one’s scope of practice. But it is not.
Trainees often receive little guidance concerning money matters in patients’ lives and treatments, considerations we have labeled clinical psychoeconomics. Considerable evidence suggests that financial concerns often provoke emotional distress and dysfunctional behaviors, and directly influence patient’s health care decisions. Financial issues also influence how clinicians view and react to patients.
We have recently reviewed (and illustrated through case vignettes) how money matters might impact psychiatric assessment, case formulation, treatment planning, and ongoing psychiatric treatments including psychotherapies.1 Consider how money affects people’s lives: Money helps people meet multiple practical, psychological, and social needs by enabling them to obtain food, clothing, shelter, other material goods, services, discretionary time, and opportunities. And money strongly influences relationships. Regardless of poverty or wealth, thoughts and behaviors connected to acquiring, possessing, and disposing of money, and feelings accompanying these processes such as greed, neediness, envy, pride, shame, guilt, and self-satisfaction often underly intrapsychic and interpersonal conflicts.
Individuals constantly engage in numerous simultaneous conscious, preconscious, and unconscious neuro-economic trade-offs that determine goals, efforts, and timing. Many are financially influenced. Money influences how virtually all patients seek, receive, and sustain their mental health care including psychotherapy.
Money problems can be associated with insecurity, impotence, feeling unloved, and lack of freedom or subjugation. Individuals may resent how they’re forced to acquire money, and feel shamed or morally injured by their jobs, financial dependence on other family members, public assistance, or their questionable ways of obtaining money.
Impoverished individuals may face choosing between food, housing, medications, and medical care. Domestically abused individuals may reluctantly remain with their abusers, risking physical harm or death rather than face destitution. Some families tolerate severely disabled individuals at home because they rely on their disability checks and caregiver payments. Suicides may turn on how individuals forecast financial repercussions affecting their families. Desires to avoid debt may lead to treatment avoidance.
Individuals with enough money to get by face daily financially related choices involving competing needs, desires, values, and loyalties. They may experience conflicts concerning spending on necessities vs. indulgences or spending on oneself vs. significant others.
Whereas some wealthy individuals may assume unwarranted airs of superiority and entitlement, others may feel guilty about wealth, or fearful that others like them only for their money. Individuals on the receiving end of wealth may feel emotionally and behaviorally manipulated by their benefactors.
Assessment
Assessments should consider how financial matters have shaped patients’ early psychological development as well their current lives. How do patients’ emotions, thoughts, and behaviors reflect money matters? What money-related pathologies are evident? What aspects of the patient’s “financial world” seem modifiable?
Financial questions should be posed colloquially. Screeners include: “Where do you live?”, “Who’s in the home?”, “How do you (all) manage financially?”, “What do you all do for a living?”, “How do you make ends meet?”, and “What financial problems are you facing?” Clinicians can quickly learn about patients’ financial self-sufficiencies, individuals for whom they bear financial responsibility, and others they rely on for support, for example, relatives. If patients avoid answering such questions forthrightly, particularly when financial arrangements are “complicated,” clinicians will want to revisit these issues later after establishing a firmer alliance but continue to wonder about the meaning of the patient’s reluctance.
When explicit, patients, families, and couples are fully aware of the conflicts but have difficulty resolving financial disputes. When conflicts are implicit, money problems may be unacknowledged, avoided, denied, or minimized. Conflicts concerning money are often transmitted trans-generationally.
Psychopathological conditions unequivocally linked to money include compulsive shopping, gambling disorders, miserly hoarding, impulse buying, and spending sprees during hypomanic and manic states. Mounting debts may create progressively insurmountable sources of distress. Money can be weaponized to sadistically create enticement, envy, or deprivation. Some monetarily antisocial individuals compromise interpersonal relationships as well as treatments. Individuals with alcohol/substance use disorders may spend so much on substances that little is left for necessities. Financially needy individuals may engage in morally questionable behaviors they might otherwise shun.
Case formulation and treatment planning
Incorporating money matters into case formulations entails demonstrating how financial concerns influenced maladaptive development and distort current attitudes, perceptions, and behaviors.
Concurrently, clinicians should acknowledge patients’ reality-based fiscal decisions, appreciating cultural and family value differences concerning how money should be acquired and spent. Since money often determines frequency and duration of treatment visits, clinicians are ethically obligated to discuss with patients what they might expect from different medications and psychotherapies, and their comparative costs.
Money matters’ impact on psychotherapies
Money matters often affect transference and countertransference reactions. Some reactions stem from how patients and clinicians compare their own financial situations with those of the other.
To help identify and ameliorate money-related countertransference responses, clinicians can reflect on questions such as: “How comfortable are you with people who are much poorer or richer than you are?” “How comfortable are you with impoverished individuals or with multimillionaires or their children?” And “why?” For trainees, all these reactions should be discussed in supervision.
Conclusions
To summarize, four clinical psychoeconomic issues should be routinely assessed and factored into psychiatric case formulations and treatment plans: how financial issues 1) have impacted patients’ psychological development; 2) impact patients’ current lives; 3) are likely to impact access, type, intensity, and duration of treatment visits; and 4) might provoke money-related transference and countertransference concerns.
In advising patients about treatment options, clinicians should discuss each treatment’s relative effectiveness and estimated costs of care. Patients’ decisions will likely be heavily influenced by financial considerations.
Dr. Yager is based in the department of psychiatry, University of Colorado at Denver, Aurora. Dr. Kay is based in the department of psychiatry, Wright State University, Dayton, Ohio. No external funds were received for this project, and the authors have no conflicts to disclose.
Reference
1. Yager J and Kay J. Money matters in psychiatric assessment, case formulation, treatment planning, and ongoing psychotherapy: Clinical psychoeconomics. J Nerv Ment Dis. 2022 Jun 10. doi: 10.1097/NMD.0000000000001552.
Long-term antidepressant use tied to an increase in CVD, mortality risk
The investigators drew on 10-year data from the UK Biobank on over 220,000 adults and compared the risk of developing adverse health outcomes among those taking antidepressants with the risk among those who were not taking antidepressants.
After adjusting for preexisting risk factors, they found that 10-year antidepressant use was associated with a twofold higher risk of CHD, an almost-twofold higher risk of CVD as well as CVD mortality, a higher risk of cerebrovascular disease, and more than double the risk of all-cause mortality.
On the other hand, at 10 years, antidepressant use was associated with a 23% lower risk of developing hypertension and a 32% lower risk of diabetes.
The main culprits were mirtazapine, venlafaxine, duloxetine, and trazodone, although SSRIs were also tied to increased risk.
“Our message for clinicians is that prescribing of antidepressants in the long term may not be harm free [and] we hope that this study will help doctors and patients have more informed conversations when they weigh up the potential risks and benefits of treatments for depression,” study investigator Narinder Bansal, MD, honorary research fellow, Centre for Academic Health and Centre for Academic Primary Care, University of Bristol (England), said in a news release.
“Regardless of whether the drugs are the underlying cause of these problems, our findings emphasize the importance of proactive cardiovascular monitoring and prevention in patients who have depression and are on antidepressants, given that both have been associated with higher risks,” she added.
The study was published online in the British Journal of Psychiatry Open.
Monitoring of CVD risk ‘critical’
Antidepressants are among the most widely prescribed drugs; 70 million prescriptions were dispensed in 2018 alone, representing a doubling of prescriptions for these agents in a decade, the investigators noted. “This striking rise in prescribing is attributed to long-term treatment rather than an increased incidence of depression.”
Most trials that have assessed antidepressant efficacy have been “poorly suited to examining adverse outcomes.” One reason for this is that many of the trials are short-term studies. Since depression is “strongly associated” with CVD risk factors, “careful assessment of the long-term cardiometabolic effects of antidepressant treatment is critical.”
Moreover, information about “a wide range of prospectively measured confounders ... is needed to provide robust estimates of the risks associated with long-term antidepressant use,” the authors noted.
The researchers examined the association between antidepressant use and four cardiometabolic morbidity outcomes – diabetes, hypertension, cerebrovascular disease, and CHD. In addition, they assessed two mortality outcomes – CVD mortality and all-cause mortality. Participants were divided into cohorts on the basis of outcome of interest.
The dataset contains detailed information on socioeconomic status, demographics, anthropometric, behavioral, and biochemical risk factors, disability, and health status and is linked to datasets of primary care records and deaths.
The study included 222,121 participants whose data had been linked to primary care records during 2018 (median age of participants, 56-57 years). About half were women, and 96% were of White ethnicity.
Participants were excluded if they had been prescribed antidepressants 12 months or less before baseline, if they had previously been diagnosed for the outcome of interest, if they had been previously prescribed psychotropic drugs, if they used cardiometabolic drugs at baseline, or if they had undergone treatment with antidepressant polytherapy.
Potential confounders included age, gender, body mass index, waist/hip ratio, smoking and alcohol intake status, physical activity, parental history of outcome, biochemical and hematologic biomarkers, socioeconomic status, and long-term illness, disability, or infirmity.
Mechanism unclear
By the end of the 5- and 10-year follow-up periods, an average of 8% and 6% of participants in each cohort, respectively, had been prescribed an antidepressant. SSRIs constituted the most commonly prescribed class (80%-82%), and citalopram was the most commonly prescribed SSRI (46%-47%). Mirtazapine was the most frequently prescribed non-SSRI antidepressant (44%-46%).
At 5 years, any antidepressant use was associated with an increased risk for diabetes, CHD, and all-cause mortality, but the findings were attenuated after further adjustment for confounders. In fact, SSRIs were associated with a reduced risk of diabetes at 5 years (hazard ratio, 0.64; 95% confidence interval, 0.49-0.83).
At 10 years, SSRIs were associated with an increased risk of cerebrovascular disease, CVD mortality, and all-cause mortality; non-SSRIs were associated with an increased risk of CHD, CVD, and all-cause mortality.
On the other hand, SSRIs were associated with a decrease in risk of diabetes and hypertension at 10 years (HR, 0.68; 95% CI, 0.53-0.87; and HR, 0.77; 95% CI, 0.66-0.89, respectively).
“While we have taken into account a wide range of pre-existing risk factors for cardiovascular disease, including those that are linked to depression such as excess weight, smoking, and low physical activity, it is difficult to fully control for the effects of depression in this kind of study, partly because there is considerable variability in the recording of depression severity in primary care,” said Dr. Bansal.
“This is important because many people taking antidepressants such as mirtazapine, venlafaxine, duloxetine and trazodone may have a more severe depression. This makes it difficult to fully separate the effects of the depression from the effects of medication,” she said.
Further research “is needed to assess whether the associations we have seen are genuinely due to the drugs; and, if so, why this might be,” she added.
Strengths, limitations
Commenting on the study, Roger McIntyre, MD, professor of psychiatry and pharmacology and head of the mood disorders psychopharmacology unit at the University of Toronto,, discussed the strengths and weaknesses of the study.

The UK Biobank is a “well-described, well-phenotyped dataset of good quality,” said Dr. McIntyre, chairperson and executive director of the Brain and Cognitive Discover Foundation, Toronto, who was not involved with the study. Another strength is the “impressive number of variables the database contains, which enabled the authors to go much deeper into the topics.”
A “significant limitation” is the confounding that is inherent to the disorder itself – “people with depression have a much higher intrinsic risk of CVD, [cerebrovascular disease], and cardiovascular mortality,” Dr. McIntyre noted.
The researchers did not adjust for trauma or childhood maltreatment, “which are the biggest risk factors for both depression and CVD; and drug and alcohol misuse were also not accounted for.”
Additionally, “to determine whether something is an association or potentially causative, it must satisfy the Bradford-Hill criteria,” said Dr. McIntyre. “Since we’re moving more toward using these big databases and because we depend on them to give us long-term perspectives, we would want to see coherent, compelling Bradford-Hill criteria regarding causation. If you don’t have any, that’s fine too, but then it’s important to make clear that there is no clear causative line, just an association.”
The research was funded by the National Institute of Health Research School for Primary Care Research and was supported by the NI Biomedical Research Centre at University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol. Dr. McIntyre has received research grant support from CI/GACD/National Natural Science Foundation of China and the Milken Institute and speaker/consultation fees from numerous companies. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
The investigators drew on 10-year data from the UK Biobank on over 220,000 adults and compared the risk of developing adverse health outcomes among those taking antidepressants with the risk among those who were not taking antidepressants.
After adjusting for preexisting risk factors, they found that 10-year antidepressant use was associated with a twofold higher risk of CHD, an almost-twofold higher risk of CVD as well as CVD mortality, a higher risk of cerebrovascular disease, and more than double the risk of all-cause mortality.
On the other hand, at 10 years, antidepressant use was associated with a 23% lower risk of developing hypertension and a 32% lower risk of diabetes.
The main culprits were mirtazapine, venlafaxine, duloxetine, and trazodone, although SSRIs were also tied to increased risk.
“Our message for clinicians is that prescribing of antidepressants in the long term may not be harm free [and] we hope that this study will help doctors and patients have more informed conversations when they weigh up the potential risks and benefits of treatments for depression,” study investigator Narinder Bansal, MD, honorary research fellow, Centre for Academic Health and Centre for Academic Primary Care, University of Bristol (England), said in a news release.
“Regardless of whether the drugs are the underlying cause of these problems, our findings emphasize the importance of proactive cardiovascular monitoring and prevention in patients who have depression and are on antidepressants, given that both have been associated with higher risks,” she added.
The study was published online in the British Journal of Psychiatry Open.
Monitoring of CVD risk ‘critical’
Antidepressants are among the most widely prescribed drugs; 70 million prescriptions were dispensed in 2018 alone, representing a doubling of prescriptions for these agents in a decade, the investigators noted. “This striking rise in prescribing is attributed to long-term treatment rather than an increased incidence of depression.”
Most trials that have assessed antidepressant efficacy have been “poorly suited to examining adverse outcomes.” One reason for this is that many of the trials are short-term studies. Since depression is “strongly associated” with CVD risk factors, “careful assessment of the long-term cardiometabolic effects of antidepressant treatment is critical.”
Moreover, information about “a wide range of prospectively measured confounders ... is needed to provide robust estimates of the risks associated with long-term antidepressant use,” the authors noted.
The researchers examined the association between antidepressant use and four cardiometabolic morbidity outcomes – diabetes, hypertension, cerebrovascular disease, and CHD. In addition, they assessed two mortality outcomes – CVD mortality and all-cause mortality. Participants were divided into cohorts on the basis of outcome of interest.
The dataset contains detailed information on socioeconomic status, demographics, anthropometric, behavioral, and biochemical risk factors, disability, and health status and is linked to datasets of primary care records and deaths.
The study included 222,121 participants whose data had been linked to primary care records during 2018 (median age of participants, 56-57 years). About half were women, and 96% were of White ethnicity.
Participants were excluded if they had been prescribed antidepressants 12 months or less before baseline, if they had previously been diagnosed for the outcome of interest, if they had been previously prescribed psychotropic drugs, if they used cardiometabolic drugs at baseline, or if they had undergone treatment with antidepressant polytherapy.
Potential confounders included age, gender, body mass index, waist/hip ratio, smoking and alcohol intake status, physical activity, parental history of outcome, biochemical and hematologic biomarkers, socioeconomic status, and long-term illness, disability, or infirmity.
Mechanism unclear
By the end of the 5- and 10-year follow-up periods, an average of 8% and 6% of participants in each cohort, respectively, had been prescribed an antidepressant. SSRIs constituted the most commonly prescribed class (80%-82%), and citalopram was the most commonly prescribed SSRI (46%-47%). Mirtazapine was the most frequently prescribed non-SSRI antidepressant (44%-46%).
At 5 years, any antidepressant use was associated with an increased risk for diabetes, CHD, and all-cause mortality, but the findings were attenuated after further adjustment for confounders. In fact, SSRIs were associated with a reduced risk of diabetes at 5 years (hazard ratio, 0.64; 95% confidence interval, 0.49-0.83).
At 10 years, SSRIs were associated with an increased risk of cerebrovascular disease, CVD mortality, and all-cause mortality; non-SSRIs were associated with an increased risk of CHD, CVD, and all-cause mortality.
On the other hand, SSRIs were associated with a decrease in risk of diabetes and hypertension at 10 years (HR, 0.68; 95% CI, 0.53-0.87; and HR, 0.77; 95% CI, 0.66-0.89, respectively).
“While we have taken into account a wide range of pre-existing risk factors for cardiovascular disease, including those that are linked to depression such as excess weight, smoking, and low physical activity, it is difficult to fully control for the effects of depression in this kind of study, partly because there is considerable variability in the recording of depression severity in primary care,” said Dr. Bansal.
“This is important because many people taking antidepressants such as mirtazapine, venlafaxine, duloxetine and trazodone may have a more severe depression. This makes it difficult to fully separate the effects of the depression from the effects of medication,” she said.
Further research “is needed to assess whether the associations we have seen are genuinely due to the drugs; and, if so, why this might be,” she added.
Strengths, limitations
Commenting on the study, Roger McIntyre, MD, professor of psychiatry and pharmacology and head of the mood disorders psychopharmacology unit at the University of Toronto,, discussed the strengths and weaknesses of the study.
The UK Biobank is a “well-described, well-phenotyped dataset of good quality,” said Dr. McIntyre, chairperson and executive director of the Brain and Cognitive Discover Foundation, Toronto, who was not involved with the study. Another strength is the “impressive number of variables the database contains, which enabled the authors to go much deeper into the topics.”
A “significant limitation” is the confounding that is inherent to the disorder itself – “people with depression have a much higher intrinsic risk of CVD, [cerebrovascular disease], and cardiovascular mortality,” Dr. McIntyre noted.
The researchers did not adjust for trauma or childhood maltreatment, “which are the biggest risk factors for both depression and CVD; and drug and alcohol misuse were also not accounted for.”
Additionally, “to determine whether something is an association or potentially causative, it must satisfy the Bradford-Hill criteria,” said Dr. McIntyre. “Since we’re moving more toward using these big databases and because we depend on them to give us long-term perspectives, we would want to see coherent, compelling Bradford-Hill criteria regarding causation. If you don’t have any, that’s fine too, but then it’s important to make clear that there is no clear causative line, just an association.”
The research was funded by the National Institute of Health Research School for Primary Care Research and was supported by the NI Biomedical Research Centre at University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol. Dr. McIntyre has received research grant support from CI/GACD/National Natural Science Foundation of China and the Milken Institute and speaker/consultation fees from numerous companies. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
The investigators drew on 10-year data from the UK Biobank on over 220,000 adults and compared the risk of developing adverse health outcomes among those taking antidepressants with the risk among those who were not taking antidepressants.
After adjusting for preexisting risk factors, they found that 10-year antidepressant use was associated with a twofold higher risk of CHD, an almost-twofold higher risk of CVD as well as CVD mortality, a higher risk of cerebrovascular disease, and more than double the risk of all-cause mortality.
On the other hand, at 10 years, antidepressant use was associated with a 23% lower risk of developing hypertension and a 32% lower risk of diabetes.
The main culprits were mirtazapine, venlafaxine, duloxetine, and trazodone, although SSRIs were also tied to increased risk.
“Our message for clinicians is that prescribing of antidepressants in the long term may not be harm free [and] we hope that this study will help doctors and patients have more informed conversations when they weigh up the potential risks and benefits of treatments for depression,” study investigator Narinder Bansal, MD, honorary research fellow, Centre for Academic Health and Centre for Academic Primary Care, University of Bristol (England), said in a news release.
“Regardless of whether the drugs are the underlying cause of these problems, our findings emphasize the importance of proactive cardiovascular monitoring and prevention in patients who have depression and are on antidepressants, given that both have been associated with higher risks,” she added.
The study was published online in the British Journal of Psychiatry Open.
Monitoring of CVD risk ‘critical’
Antidepressants are among the most widely prescribed drugs; 70 million prescriptions were dispensed in 2018 alone, representing a doubling of prescriptions for these agents in a decade, the investigators noted. “This striking rise in prescribing is attributed to long-term treatment rather than an increased incidence of depression.”
Most trials that have assessed antidepressant efficacy have been “poorly suited to examining adverse outcomes.” One reason for this is that many of the trials are short-term studies. Since depression is “strongly associated” with CVD risk factors, “careful assessment of the long-term cardiometabolic effects of antidepressant treatment is critical.”
Moreover, information about “a wide range of prospectively measured confounders ... is needed to provide robust estimates of the risks associated with long-term antidepressant use,” the authors noted.
The researchers examined the association between antidepressant use and four cardiometabolic morbidity outcomes – diabetes, hypertension, cerebrovascular disease, and CHD. In addition, they assessed two mortality outcomes – CVD mortality and all-cause mortality. Participants were divided into cohorts on the basis of outcome of interest.
The dataset contains detailed information on socioeconomic status, demographics, anthropometric, behavioral, and biochemical risk factors, disability, and health status and is linked to datasets of primary care records and deaths.
The study included 222,121 participants whose data had been linked to primary care records during 2018 (median age of participants, 56-57 years). About half were women, and 96% were of White ethnicity.
Participants were excluded if they had been prescribed antidepressants 12 months or less before baseline, if they had previously been diagnosed for the outcome of interest, if they had been previously prescribed psychotropic drugs, if they used cardiometabolic drugs at baseline, or if they had undergone treatment with antidepressant polytherapy.
Potential confounders included age, gender, body mass index, waist/hip ratio, smoking and alcohol intake status, physical activity, parental history of outcome, biochemical and hematologic biomarkers, socioeconomic status, and long-term illness, disability, or infirmity.
Mechanism unclear
By the end of the 5- and 10-year follow-up periods, an average of 8% and 6% of participants in each cohort, respectively, had been prescribed an antidepressant. SSRIs constituted the most commonly prescribed class (80%-82%), and citalopram was the most commonly prescribed SSRI (46%-47%). Mirtazapine was the most frequently prescribed non-SSRI antidepressant (44%-46%).
At 5 years, any antidepressant use was associated with an increased risk for diabetes, CHD, and all-cause mortality, but the findings were attenuated after further adjustment for confounders. In fact, SSRIs were associated with a reduced risk of diabetes at 5 years (hazard ratio, 0.64; 95% confidence interval, 0.49-0.83).
At 10 years, SSRIs were associated with an increased risk of cerebrovascular disease, CVD mortality, and all-cause mortality; non-SSRIs were associated with an increased risk of CHD, CVD, and all-cause mortality.
On the other hand, SSRIs were associated with a decrease in risk of diabetes and hypertension at 10 years (HR, 0.68; 95% CI, 0.53-0.87; and HR, 0.77; 95% CI, 0.66-0.89, respectively).
“While we have taken into account a wide range of pre-existing risk factors for cardiovascular disease, including those that are linked to depression such as excess weight, smoking, and low physical activity, it is difficult to fully control for the effects of depression in this kind of study, partly because there is considerable variability in the recording of depression severity in primary care,” said Dr. Bansal.
“This is important because many people taking antidepressants such as mirtazapine, venlafaxine, duloxetine and trazodone may have a more severe depression. This makes it difficult to fully separate the effects of the depression from the effects of medication,” she said.
Further research “is needed to assess whether the associations we have seen are genuinely due to the drugs; and, if so, why this might be,” she added.
Strengths, limitations
Commenting on the study, Roger McIntyre, MD, professor of psychiatry and pharmacology and head of the mood disorders psychopharmacology unit at the University of Toronto,, discussed the strengths and weaknesses of the study.
The UK Biobank is a “well-described, well-phenotyped dataset of good quality,” said Dr. McIntyre, chairperson and executive director of the Brain and Cognitive Discover Foundation, Toronto, who was not involved with the study. Another strength is the “impressive number of variables the database contains, which enabled the authors to go much deeper into the topics.”
A “significant limitation” is the confounding that is inherent to the disorder itself – “people with depression have a much higher intrinsic risk of CVD, [cerebrovascular disease], and cardiovascular mortality,” Dr. McIntyre noted.
The researchers did not adjust for trauma or childhood maltreatment, “which are the biggest risk factors for both depression and CVD; and drug and alcohol misuse were also not accounted for.”
Additionally, “to determine whether something is an association or potentially causative, it must satisfy the Bradford-Hill criteria,” said Dr. McIntyre. “Since we’re moving more toward using these big databases and because we depend on them to give us long-term perspectives, we would want to see coherent, compelling Bradford-Hill criteria regarding causation. If you don’t have any, that’s fine too, but then it’s important to make clear that there is no clear causative line, just an association.”
The research was funded by the National Institute of Health Research School for Primary Care Research and was supported by the NI Biomedical Research Centre at University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol. Dr. McIntyre has received research grant support from CI/GACD/National Natural Science Foundation of China and the Milken Institute and speaker/consultation fees from numerous companies. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
FROM THE BRITISH JOURNAL OF PSYCHIATRY OPEN