User login
Speakers at HM13 Stress Overarching Reform, Day-to-Day Implementation

To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.

“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”

Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.

What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
Health-Care Journalists Tackle Barriers to Hospital Safety Records

The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Medical Centers Take Tips from Other Industries
Curriculums using Lean quality-improvement (QI) principles and techniques are becoming entrenched in medical teaching programs across the country.
A curriculum based on Lean QI is teaching medical residents at Boston Medical Center techniques based on successes in manufacturing and service industries, according to Charlene Weigel, MD, who now works as a hospitalist at Mount Auburn Hospital in Cambridge, Mass. Residents also are learning about implementation of Lean principles at the medical center, Dr. Weigel and co-authors report in a study published in the American Journal of Medical Quality.1
“In Week One, we gave an introduction to QI and explained what Lean means,” Dr. Weigel says. Three other interactive sessions explored such techniques as how to create process maps and root-cause analysis, and identifying steps that aren’t helpful. The 90 residents and eight Boston University School of Public Health students also created 17 group QI project plans. “The goal was for the QI classwork and ideas to become implemented in hospital QI projects, but logistically, we had to scale back expectations for that initial go-round,” Dr. Weigel says.
The medical center recently started a second cycle of the QI course, with students from the first cycle encouraged to continue their QI projects on their own. One group submitted its project as an Institute for Healthcare Improvement storyboard at a national meeting.
“The experience also exposed the residents to our interprofessional team structure, which reflects their future working relationships and professional roles in QI,” Dr. Weigel says.
Lean concepts also are the basis for the Perfecting Patient Care University (PPCU, www.prhi.org/perfecting-patient-care/what-is-ppc), a QI training program for health-care leaders and clinicians offered in a variety of formats by the Pittsburgh Regional Health Initiative, a regional health collaborative. An evaluation of outcomes at PPCU was published online in the American Journal of Medical Quality in April.2 The same journal also describes the curriculum, program evaluation, and lessons learned by SHM’s Quality and Safety Educators Academy (http://sites.hospitalmedicine.org/qsea), which provides training in QI and patient safety for teaching faculty.3 The academy, a 2.5-day course, is co-sponsored by the Alliance for Academic Internal Medicine.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Curriculums using Lean quality-improvement (QI) principles and techniques are becoming entrenched in medical teaching programs across the country.
A curriculum based on Lean QI is teaching medical residents at Boston Medical Center techniques based on successes in manufacturing and service industries, according to Charlene Weigel, MD, who now works as a hospitalist at Mount Auburn Hospital in Cambridge, Mass. Residents also are learning about implementation of Lean principles at the medical center, Dr. Weigel and co-authors report in a study published in the American Journal of Medical Quality.1
“In Week One, we gave an introduction to QI and explained what Lean means,” Dr. Weigel says. Three other interactive sessions explored such techniques as how to create process maps and root-cause analysis, and identifying steps that aren’t helpful. The 90 residents and eight Boston University School of Public Health students also created 17 group QI project plans. “The goal was for the QI classwork and ideas to become implemented in hospital QI projects, but logistically, we had to scale back expectations for that initial go-round,” Dr. Weigel says.
The medical center recently started a second cycle of the QI course, with students from the first cycle encouraged to continue their QI projects on their own. One group submitted its project as an Institute for Healthcare Improvement storyboard at a national meeting.
“The experience also exposed the residents to our interprofessional team structure, which reflects their future working relationships and professional roles in QI,” Dr. Weigel says.
Lean concepts also are the basis for the Perfecting Patient Care University (PPCU, www.prhi.org/perfecting-patient-care/what-is-ppc), a QI training program for health-care leaders and clinicians offered in a variety of formats by the Pittsburgh Regional Health Initiative, a regional health collaborative. An evaluation of outcomes at PPCU was published online in the American Journal of Medical Quality in April.2 The same journal also describes the curriculum, program evaluation, and lessons learned by SHM’s Quality and Safety Educators Academy (http://sites.hospitalmedicine.org/qsea), which provides training in QI and patient safety for teaching faculty.3 The academy, a 2.5-day course, is co-sponsored by the Alliance for Academic Internal Medicine.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Curriculums using Lean quality-improvement (QI) principles and techniques are becoming entrenched in medical teaching programs across the country.
A curriculum based on Lean QI is teaching medical residents at Boston Medical Center techniques based on successes in manufacturing and service industries, according to Charlene Weigel, MD, who now works as a hospitalist at Mount Auburn Hospital in Cambridge, Mass. Residents also are learning about implementation of Lean principles at the medical center, Dr. Weigel and co-authors report in a study published in the American Journal of Medical Quality.1
“In Week One, we gave an introduction to QI and explained what Lean means,” Dr. Weigel says. Three other interactive sessions explored such techniques as how to create process maps and root-cause analysis, and identifying steps that aren’t helpful. The 90 residents and eight Boston University School of Public Health students also created 17 group QI project plans. “The goal was for the QI classwork and ideas to become implemented in hospital QI projects, but logistically, we had to scale back expectations for that initial go-round,” Dr. Weigel says.
The medical center recently started a second cycle of the QI course, with students from the first cycle encouraged to continue their QI projects on their own. One group submitted its project as an Institute for Healthcare Improvement storyboard at a national meeting.
“The experience also exposed the residents to our interprofessional team structure, which reflects their future working relationships and professional roles in QI,” Dr. Weigel says.
Lean concepts also are the basis for the Perfecting Patient Care University (PPCU, www.prhi.org/perfecting-patient-care/what-is-ppc), a QI training program for health-care leaders and clinicians offered in a variety of formats by the Pittsburgh Regional Health Initiative, a regional health collaborative. An evaluation of outcomes at PPCU was published online in the American Journal of Medical Quality in April.2 The same journal also describes the curriculum, program evaluation, and lessons learned by SHM’s Quality and Safety Educators Academy (http://sites.hospitalmedicine.org/qsea), which provides training in QI and patient safety for teaching faculty.3 The academy, a 2.5-day course, is co-sponsored by the Alliance for Academic Internal Medicine.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Hospitalists Can Get Ahead Through Quality and Patient Safety Initiatives
Are you a hospitalist who, on daily rounds, often thinks, “There’s got to be a better way to do this”? You might be just the type of person who can carve a niche for yourself in hospital quality and patient safety—and advance your career in the process.
Successful navigation of the quality-improvement (QI) and patient-safety domains, according to three veteran hospitalists, requires an initial passion and an incremental approach. Now is an especially good time, they agree, for young hospitalists to engage in these types of initiatives.
Why Do It?
In her capacity as president of the Mid-Atlantic Business Unit for Brentwood, Tenn.-based CogentHMG, Julia Wright, MD, SFHM, FACP, often encourages young recruits to consider participation in QI and patient-safety initiatives. She admits that the transition from residency to a busy HM practice, with its higher patient volumes and a faster pace, can be daunting at first. Still, she tries to cultivate interest in initiatives and establish a realistic timeframe for involvement.
There are many reasons to consider this as a career step. Dr. Wright says that quality and patient safety dovetail with hospitalists’ initial reasons for choosing medicine: to improve patients’ lives.
Janet Nagamine, RN, MD, SFHM, former patient safety officer and assistant chief of quality at Kaiser Permanente in Santa Clara, Calif., describes the fit this way: “I might be a good doctor, but as a hospitalist, I rely on many others within the system to deliver, so my patients can’t get good care until the entire system is running well,” she says. “There are all kinds of opportunities to fix our [hospital] system, and I really believe that hospitalists cannot separate themselves from that engagement.”
Elizabeth Gundersen, MD, FHM, of Fort Lauderdale, Fla., agrees that it’s a natural step to think about the ways to make a difference on a larger level. At her former institution, the University of Massachusetts (UMass) Medical School in Worcester, she parlayed her interest in QI to work her way up from ground-level hospitalist to associate chief of her division and quality officer for the hospital. “Physicians get a lot of satisfaction from helping individual patients,” she says. “One thing I really liked about getting involved with quality improvement was being able to make a difference for patients on a systems level.”
An Incremental Path
The path to her current position began with a very specific issue for Dr. Nagamine, an SHM board member who also serves as a Project BOOST co-investigator. “Although I have been doing patient safety since before they had a name for it, I didn’t start out saying that I wanted a career in quality and safety,” she says. “I was trying to take better care of my patients with diabetes, but controlling their glucose was extremely challenging because all the related variables—timing and amount of their insulin dosage, when and how much they had eaten—were charted in different places. This made it hard to adjust their insulin appropriately.”
It quickly became clear to Dr. Nagamine that the solution had to be systemic. She realized that something as basic as taking care of her patients with diabetes required multiple departments (i.e. dietary, nursing, and pharmacy) to furnish information in an integrated manner. So she joined the diabetes committee and went to work on the issue. She helped devise a flow chart that could be used by all relevant departments. A further evolution on the path emanated from one of her patients receiving the wrong medication. She joined the medication safety committee, became chair, “and the next thing you know, I’m in charge of patient safety, and an assistant chief of quality.”
Training Is Necessary
QI and patient-safety methodologies have become sophisticated disciplines in the past two decades, Dr. Wright says. Access to training in QI basics now is readily available to early-career hospitalists. For example, CogentHMG offers program support for QI so that anyone interested “doesn’t have to start from scratch anymore; we can help show them the way and support them in doing it.”
This month, HM13 (www.hospital medicine2013.org)—just outside Washington, D.C.—will offer multiple sessions on quality, as well as the “Initiating Quality Improvement Projects with Built-In Sustainment” workshop, led by Center for Comprehensive Access and Delivery Research and Evaluation (CADRE) core investigator Peter Kaboli, MD, MS, who will address sustainability.
Beyond methodological tools, success in quality and patient safety requires the ability to motivate people, often across multiple disciplines, Dr. Nagamine says. “If you want things to work better, you must invite the right people to the table. For example, we often forget to include key nonclinical stakeholders,” she adds.
When working with hospitals across the country to implement rapid-response tTeams, Dr. Nagamine often reminds them to invite the operators, or “key people,” in the process.
“If you put patient safety at the core of your initiative and create the context for that, most people will agree that it’s the right thing to do and will get on board, even if it’s an extra step for them,” she says. “Know your audience, listen to their perspective, and learn what matters to them. And to most people, it matters that they give good patient care.”
Gretchen Henkel is a freelance writer in California.
Branch Out: QI and Patient-Safety Initiatives

Pick a passion. It’s best to choose an issue that’s important to you. “It has to be a
passion because much of the time it’s an uphill battle,” says Dr. Gundersen. She started with the issue of reducing readmissions, and with two colleagues pitched the idea of involving the UMass HM group in SHM’s Project BOOST. After that, she set out to become an expert on reducing readmissions, applying what she had learned to other successful initiatives.
Learn the lingo. Dr. Wright advises learning some of the most basic principles, such as Shewhart’s PDCA (Plan-Do-Check-Act) or Deming’s adaptation PDSA (Plan-Do-Study-Act) cycles; the quality tripod; and accessing resources made available from SHM. A member of SHM’s Hospital Quality and Patient Safety Committee, Dr. Wright says a subcommittee for leadership engagement has been created and furnishes tools and training for advancing quality initiatives. The Institute for Healthcare Improvement (www.ihi.org) also offers a wealth of measures, speaker series, and white papers on improvement in health care.
Start small. You can test your ability to work with interdisciplinary departments, often a prerequisite of many quality initiatives, by first joining a committee, Dr. Nagamine advises. “See how effective or persuasive you are in pitching an idea and seeing it through with other departments,” she says.
Brace for a marathon. “Most people,” Dr. Gundersen says, “do not hand you 100% of their cooperation and a budget you can work with.” It takes time to get buy-in, especially if you’re doing interdisciplinary initiatives. If possible, break your projects into achievable units. “Start with some quick wins. Small payoffs here and there can re-energize your team and eventually yield a larger payoff,” she says.
Limit sweat equity. It’s important to put in time at the start of a project to demonstrate your value, but if you’re constantly staying up late working on a project, consider pitching a compensated role to your boss. “Being a good citizen and volunteering for committees is one thing,” Dr. Nagamine cautions, “but taking on leadership roles in too many projects, without dedicated time, is not sustainable and can jeopardize the success of your projects.”
—Gretchen Henkel
Are you a hospitalist who, on daily rounds, often thinks, “There’s got to be a better way to do this”? You might be just the type of person who can carve a niche for yourself in hospital quality and patient safety—and advance your career in the process.
Successful navigation of the quality-improvement (QI) and patient-safety domains, according to three veteran hospitalists, requires an initial passion and an incremental approach. Now is an especially good time, they agree, for young hospitalists to engage in these types of initiatives.
Why Do It?
In her capacity as president of the Mid-Atlantic Business Unit for Brentwood, Tenn.-based CogentHMG, Julia Wright, MD, SFHM, FACP, often encourages young recruits to consider participation in QI and patient-safety initiatives. She admits that the transition from residency to a busy HM practice, with its higher patient volumes and a faster pace, can be daunting at first. Still, she tries to cultivate interest in initiatives and establish a realistic timeframe for involvement.
There are many reasons to consider this as a career step. Dr. Wright says that quality and patient safety dovetail with hospitalists’ initial reasons for choosing medicine: to improve patients’ lives.
Janet Nagamine, RN, MD, SFHM, former patient safety officer and assistant chief of quality at Kaiser Permanente in Santa Clara, Calif., describes the fit this way: “I might be a good doctor, but as a hospitalist, I rely on many others within the system to deliver, so my patients can’t get good care until the entire system is running well,” she says. “There are all kinds of opportunities to fix our [hospital] system, and I really believe that hospitalists cannot separate themselves from that engagement.”
Elizabeth Gundersen, MD, FHM, of Fort Lauderdale, Fla., agrees that it’s a natural step to think about the ways to make a difference on a larger level. At her former institution, the University of Massachusetts (UMass) Medical School in Worcester, she parlayed her interest in QI to work her way up from ground-level hospitalist to associate chief of her division and quality officer for the hospital. “Physicians get a lot of satisfaction from helping individual patients,” she says. “One thing I really liked about getting involved with quality improvement was being able to make a difference for patients on a systems level.”
An Incremental Path
The path to her current position began with a very specific issue for Dr. Nagamine, an SHM board member who also serves as a Project BOOST co-investigator. “Although I have been doing patient safety since before they had a name for it, I didn’t start out saying that I wanted a career in quality and safety,” she says. “I was trying to take better care of my patients with diabetes, but controlling their glucose was extremely challenging because all the related variables—timing and amount of their insulin dosage, when and how much they had eaten—were charted in different places. This made it hard to adjust their insulin appropriately.”
It quickly became clear to Dr. Nagamine that the solution had to be systemic. She realized that something as basic as taking care of her patients with diabetes required multiple departments (i.e. dietary, nursing, and pharmacy) to furnish information in an integrated manner. So she joined the diabetes committee and went to work on the issue. She helped devise a flow chart that could be used by all relevant departments. A further evolution on the path emanated from one of her patients receiving the wrong medication. She joined the medication safety committee, became chair, “and the next thing you know, I’m in charge of patient safety, and an assistant chief of quality.”
Training Is Necessary
QI and patient-safety methodologies have become sophisticated disciplines in the past two decades, Dr. Wright says. Access to training in QI basics now is readily available to early-career hospitalists. For example, CogentHMG offers program support for QI so that anyone interested “doesn’t have to start from scratch anymore; we can help show them the way and support them in doing it.”
This month, HM13 (www.hospital medicine2013.org)—just outside Washington, D.C.—will offer multiple sessions on quality, as well as the “Initiating Quality Improvement Projects with Built-In Sustainment” workshop, led by Center for Comprehensive Access and Delivery Research and Evaluation (CADRE) core investigator Peter Kaboli, MD, MS, who will address sustainability.
Beyond methodological tools, success in quality and patient safety requires the ability to motivate people, often across multiple disciplines, Dr. Nagamine says. “If you want things to work better, you must invite the right people to the table. For example, we often forget to include key nonclinical stakeholders,” she adds.
When working with hospitals across the country to implement rapid-response tTeams, Dr. Nagamine often reminds them to invite the operators, or “key people,” in the process.
“If you put patient safety at the core of your initiative and create the context for that, most people will agree that it’s the right thing to do and will get on board, even if it’s an extra step for them,” she says. “Know your audience, listen to their perspective, and learn what matters to them. And to most people, it matters that they give good patient care.”
Gretchen Henkel is a freelance writer in California.
Branch Out: QI and Patient-Safety Initiatives
Pick a passion. It’s best to choose an issue that’s important to you. “It has to be a
passion because much of the time it’s an uphill battle,” says Dr. Gundersen. She started with the issue of reducing readmissions, and with two colleagues pitched the idea of involving the UMass HM group in SHM’s Project BOOST. After that, she set out to become an expert on reducing readmissions, applying what she had learned to other successful initiatives.
Learn the lingo. Dr. Wright advises learning some of the most basic principles, such as Shewhart’s PDCA (Plan-Do-Check-Act) or Deming’s adaptation PDSA (Plan-Do-Study-Act) cycles; the quality tripod; and accessing resources made available from SHM. A member of SHM’s Hospital Quality and Patient Safety Committee, Dr. Wright says a subcommittee for leadership engagement has been created and furnishes tools and training for advancing quality initiatives. The Institute for Healthcare Improvement (www.ihi.org) also offers a wealth of measures, speaker series, and white papers on improvement in health care.
Start small. You can test your ability to work with interdisciplinary departments, often a prerequisite of many quality initiatives, by first joining a committee, Dr. Nagamine advises. “See how effective or persuasive you are in pitching an idea and seeing it through with other departments,” she says.
Brace for a marathon. “Most people,” Dr. Gundersen says, “do not hand you 100% of their cooperation and a budget you can work with.” It takes time to get buy-in, especially if you’re doing interdisciplinary initiatives. If possible, break your projects into achievable units. “Start with some quick wins. Small payoffs here and there can re-energize your team and eventually yield a larger payoff,” she says.
Limit sweat equity. It’s important to put in time at the start of a project to demonstrate your value, but if you’re constantly staying up late working on a project, consider pitching a compensated role to your boss. “Being a good citizen and volunteering for committees is one thing,” Dr. Nagamine cautions, “but taking on leadership roles in too many projects, without dedicated time, is not sustainable and can jeopardize the success of your projects.”
—Gretchen Henkel
Are you a hospitalist who, on daily rounds, often thinks, “There’s got to be a better way to do this”? You might be just the type of person who can carve a niche for yourself in hospital quality and patient safety—and advance your career in the process.
Successful navigation of the quality-improvement (QI) and patient-safety domains, according to three veteran hospitalists, requires an initial passion and an incremental approach. Now is an especially good time, they agree, for young hospitalists to engage in these types of initiatives.
Why Do It?
In her capacity as president of the Mid-Atlantic Business Unit for Brentwood, Tenn.-based CogentHMG, Julia Wright, MD, SFHM, FACP, often encourages young recruits to consider participation in QI and patient-safety initiatives. She admits that the transition from residency to a busy HM practice, with its higher patient volumes and a faster pace, can be daunting at first. Still, she tries to cultivate interest in initiatives and establish a realistic timeframe for involvement.
There are many reasons to consider this as a career step. Dr. Wright says that quality and patient safety dovetail with hospitalists’ initial reasons for choosing medicine: to improve patients’ lives.
Janet Nagamine, RN, MD, SFHM, former patient safety officer and assistant chief of quality at Kaiser Permanente in Santa Clara, Calif., describes the fit this way: “I might be a good doctor, but as a hospitalist, I rely on many others within the system to deliver, so my patients can’t get good care until the entire system is running well,” she says. “There are all kinds of opportunities to fix our [hospital] system, and I really believe that hospitalists cannot separate themselves from that engagement.”
Elizabeth Gundersen, MD, FHM, of Fort Lauderdale, Fla., agrees that it’s a natural step to think about the ways to make a difference on a larger level. At her former institution, the University of Massachusetts (UMass) Medical School in Worcester, she parlayed her interest in QI to work her way up from ground-level hospitalist to associate chief of her division and quality officer for the hospital. “Physicians get a lot of satisfaction from helping individual patients,” she says. “One thing I really liked about getting involved with quality improvement was being able to make a difference for patients on a systems level.”
An Incremental Path
The path to her current position began with a very specific issue for Dr. Nagamine, an SHM board member who also serves as a Project BOOST co-investigator. “Although I have been doing patient safety since before they had a name for it, I didn’t start out saying that I wanted a career in quality and safety,” she says. “I was trying to take better care of my patients with diabetes, but controlling their glucose was extremely challenging because all the related variables—timing and amount of their insulin dosage, when and how much they had eaten—were charted in different places. This made it hard to adjust their insulin appropriately.”
It quickly became clear to Dr. Nagamine that the solution had to be systemic. She realized that something as basic as taking care of her patients with diabetes required multiple departments (i.e. dietary, nursing, and pharmacy) to furnish information in an integrated manner. So she joined the diabetes committee and went to work on the issue. She helped devise a flow chart that could be used by all relevant departments. A further evolution on the path emanated from one of her patients receiving the wrong medication. She joined the medication safety committee, became chair, “and the next thing you know, I’m in charge of patient safety, and an assistant chief of quality.”
Training Is Necessary
QI and patient-safety methodologies have become sophisticated disciplines in the past two decades, Dr. Wright says. Access to training in QI basics now is readily available to early-career hospitalists. For example, CogentHMG offers program support for QI so that anyone interested “doesn’t have to start from scratch anymore; we can help show them the way and support them in doing it.”
This month, HM13 (www.hospital medicine2013.org)—just outside Washington, D.C.—will offer multiple sessions on quality, as well as the “Initiating Quality Improvement Projects with Built-In Sustainment” workshop, led by Center for Comprehensive Access and Delivery Research and Evaluation (CADRE) core investigator Peter Kaboli, MD, MS, who will address sustainability.
Beyond methodological tools, success in quality and patient safety requires the ability to motivate people, often across multiple disciplines, Dr. Nagamine says. “If you want things to work better, you must invite the right people to the table. For example, we often forget to include key nonclinical stakeholders,” she adds.
When working with hospitals across the country to implement rapid-response tTeams, Dr. Nagamine often reminds them to invite the operators, or “key people,” in the process.
“If you put patient safety at the core of your initiative and create the context for that, most people will agree that it’s the right thing to do and will get on board, even if it’s an extra step for them,” she says. “Know your audience, listen to their perspective, and learn what matters to them. And to most people, it matters that they give good patient care.”
Gretchen Henkel is a freelance writer in California.
Branch Out: QI and Patient-Safety Initiatives
Pick a passion. It’s best to choose an issue that’s important to you. “It has to be a
passion because much of the time it’s an uphill battle,” says Dr. Gundersen. She started with the issue of reducing readmissions, and with two colleagues pitched the idea of involving the UMass HM group in SHM’s Project BOOST. After that, she set out to become an expert on reducing readmissions, applying what she had learned to other successful initiatives.
Learn the lingo. Dr. Wright advises learning some of the most basic principles, such as Shewhart’s PDCA (Plan-Do-Check-Act) or Deming’s adaptation PDSA (Plan-Do-Study-Act) cycles; the quality tripod; and accessing resources made available from SHM. A member of SHM’s Hospital Quality and Patient Safety Committee, Dr. Wright says a subcommittee for leadership engagement has been created and furnishes tools and training for advancing quality initiatives. The Institute for Healthcare Improvement (www.ihi.org) also offers a wealth of measures, speaker series, and white papers on improvement in health care.
Start small. You can test your ability to work with interdisciplinary departments, often a prerequisite of many quality initiatives, by first joining a committee, Dr. Nagamine advises. “See how effective or persuasive you are in pitching an idea and seeing it through with other departments,” she says.
Brace for a marathon. “Most people,” Dr. Gundersen says, “do not hand you 100% of their cooperation and a budget you can work with.” It takes time to get buy-in, especially if you’re doing interdisciplinary initiatives. If possible, break your projects into achievable units. “Start with some quick wins. Small payoffs here and there can re-energize your team and eventually yield a larger payoff,” she says.
Limit sweat equity. It’s important to put in time at the start of a project to demonstrate your value, but if you’re constantly staying up late working on a project, consider pitching a compensated role to your boss. “Being a good citizen and volunteering for committees is one thing,” Dr. Nagamine cautions, “but taking on leadership roles in too many projects, without dedicated time, is not sustainable and can jeopardize the success of your projects.”
—Gretchen Henkel
Drive Change in an ACO

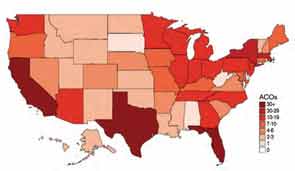
From informal polls I’ve recently conducted of hospitalists, many are not even aware they are part of an accountable-care organization (ACO). And if they are aware, they might not be engaging in meaningful dialogue with ACO leaders about their role in these organizations. But, in the long term, ACOs will need to bring hospitalists to the table in order to be successful.
Are You Part of an ACO?
David Muhlestein, who blogs for Health Affairs, tracks the growth of ACOs around the country. He states that, as of Jan. 31, there were 428 ACOs in the U.S. (see Figure 1).1 In terms of numbers, Florida, Texas, and California lead the nation with 42, 33, and 46 ACOs, respectively. So it is likely that you are part of an ACO. If you are unsure, ask your chief medical officer or president of the medical staff.
How ACOs Work
All ACOs seek to manage a group, or population, of patients as efficiently as possible while maintaining or improving quality of care. For Medicare ACOs, the goal is to bring together hospitals and physicians in order to share savings derived from efficiencies in care. But before any savings can be shared, the Medicare ACO must demonstrate that it achieved high-quality care across four domains, totaling 33 individual quality measures. (see Table 1)
Main Flavors of ACOs
There are two types of ACOs: private ACOs and Medicare ACOs. Prior to Medicare ACOs, which were launched in January 2012, there were 150 private-sector ACOs, and this number continues to grow. Private ACOs represent a heterogeneous group in terms of reimbursement model. Some operate under shared savings programs; others use full or partial capitation, bundled payments, and/or other types of arrangements. But nearly all ACOs operate under the premise that the incentives used to make care more efficient and less costly can only be applied if measurable quality is maintained or improved. ACOs do not pay doctors or hospitals more unless high quality is demonstrated.
ACO Quality Measures and Hospitalists
Most of the 33 quality measures required by Medicare ACOs are based in ambulatory practice. These include measures related to blood pressure, immunizations, cancer, and fall-risk screening, and measures for diabetics, such as lipids and hemoglobin A1C. However, there are a few measures for which hospitalists should share in accountability, including:
- All-cause hospital readmission rate—risk-standardized;
- Ambulatory sensitive condition hospital admission rates (CHF, COPD); and
- Medication reconciliation after discharge from an inpatient facility.
Four Key Actions for Hospitalists
Hospitalists make a significant contribution to the quality and the financial performance of ACOs. In addition to the quality metrics cited above, hospitalists impact the inpatient portion of the overall population’s cost of care. Furthermore, hospitalists are vital partners in the care coordination required for an ACO to be successful.
Here are four actions I suggest taking in order for your hospitalist group to be effective as participants in an ACO:
- Have a representative from your group participate in ACO committees that address hospital utilization and related matters, such as care coordination impacting pre- and post-hospital care.
- Learn how to work with ACO case managers on care transitions, including post-discharge follow-up and information transfer.
- Understand an ACO’s approach to engagement of and coordination with post-acute-care facilities. The ability of a post-acute facility, such a skilled nursing facility, to accept patients who have complex care needs, to manage changes in condition in the facility when appropriate, and to send complete information upon transfer to the hospital are important strategies for an ACO’s success.
- Understand how an ACO reports quality and cost performance and how savings will be shared among participants.
Mindset Change
If hospitalists are part of the chain of ACO physicians and providers held accountable for the health of a population of patients, we must work more closely with the medical home/neighborhood, post-acute-care facilities, and home-care providers. The change in mindset will occur only if we have a set of tools to get the job done, such as case managers and information technology, and the appropriate incentives to support better care coordination. I encourage my fellow hospitalists to make things happen, instead of taking a passive role in this monumental transformation.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
From informal polls I’ve recently conducted of hospitalists, many are not even aware they are part of an accountable-care organization (ACO). And if they are aware, they might not be engaging in meaningful dialogue with ACO leaders about their role in these organizations. But, in the long term, ACOs will need to bring hospitalists to the table in order to be successful.
Are You Part of an ACO?
David Muhlestein, who blogs for Health Affairs, tracks the growth of ACOs around the country. He states that, as of Jan. 31, there were 428 ACOs in the U.S. (see Figure 1).1 In terms of numbers, Florida, Texas, and California lead the nation with 42, 33, and 46 ACOs, respectively. So it is likely that you are part of an ACO. If you are unsure, ask your chief medical officer or president of the medical staff.
How ACOs Work
All ACOs seek to manage a group, or population, of patients as efficiently as possible while maintaining or improving quality of care. For Medicare ACOs, the goal is to bring together hospitals and physicians in order to share savings derived from efficiencies in care. But before any savings can be shared, the Medicare ACO must demonstrate that it achieved high-quality care across four domains, totaling 33 individual quality measures. (see Table 1)
Main Flavors of ACOs
There are two types of ACOs: private ACOs and Medicare ACOs. Prior to Medicare ACOs, which were launched in January 2012, there were 150 private-sector ACOs, and this number continues to grow. Private ACOs represent a heterogeneous group in terms of reimbursement model. Some operate under shared savings programs; others use full or partial capitation, bundled payments, and/or other types of arrangements. But nearly all ACOs operate under the premise that the incentives used to make care more efficient and less costly can only be applied if measurable quality is maintained or improved. ACOs do not pay doctors or hospitals more unless high quality is demonstrated.
ACO Quality Measures and Hospitalists
Most of the 33 quality measures required by Medicare ACOs are based in ambulatory practice. These include measures related to blood pressure, immunizations, cancer, and fall-risk screening, and measures for diabetics, such as lipids and hemoglobin A1C. However, there are a few measures for which hospitalists should share in accountability, including:
- All-cause hospital readmission rate—risk-standardized;
- Ambulatory sensitive condition hospital admission rates (CHF, COPD); and
- Medication reconciliation after discharge from an inpatient facility.
Four Key Actions for Hospitalists
Hospitalists make a significant contribution to the quality and the financial performance of ACOs. In addition to the quality metrics cited above, hospitalists impact the inpatient portion of the overall population’s cost of care. Furthermore, hospitalists are vital partners in the care coordination required for an ACO to be successful.
Here are four actions I suggest taking in order for your hospitalist group to be effective as participants in an ACO:
- Have a representative from your group participate in ACO committees that address hospital utilization and related matters, such as care coordination impacting pre- and post-hospital care.
- Learn how to work with ACO case managers on care transitions, including post-discharge follow-up and information transfer.
- Understand an ACO’s approach to engagement of and coordination with post-acute-care facilities. The ability of a post-acute facility, such a skilled nursing facility, to accept patients who have complex care needs, to manage changes in condition in the facility when appropriate, and to send complete information upon transfer to the hospital are important strategies for an ACO’s success.
- Understand how an ACO reports quality and cost performance and how savings will be shared among participants.
Mindset Change
If hospitalists are part of the chain of ACO physicians and providers held accountable for the health of a population of patients, we must work more closely with the medical home/neighborhood, post-acute-care facilities, and home-care providers. The change in mindset will occur only if we have a set of tools to get the job done, such as case managers and information technology, and the appropriate incentives to support better care coordination. I encourage my fellow hospitalists to make things happen, instead of taking a passive role in this monumental transformation.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
From informal polls I’ve recently conducted of hospitalists, many are not even aware they are part of an accountable-care organization (ACO). And if they are aware, they might not be engaging in meaningful dialogue with ACO leaders about their role in these organizations. But, in the long term, ACOs will need to bring hospitalists to the table in order to be successful.
Are You Part of an ACO?
David Muhlestein, who blogs for Health Affairs, tracks the growth of ACOs around the country. He states that, as of Jan. 31, there were 428 ACOs in the U.S. (see Figure 1).1 In terms of numbers, Florida, Texas, and California lead the nation with 42, 33, and 46 ACOs, respectively. So it is likely that you are part of an ACO. If you are unsure, ask your chief medical officer or president of the medical staff.
How ACOs Work
All ACOs seek to manage a group, or population, of patients as efficiently as possible while maintaining or improving quality of care. For Medicare ACOs, the goal is to bring together hospitals and physicians in order to share savings derived from efficiencies in care. But before any savings can be shared, the Medicare ACO must demonstrate that it achieved high-quality care across four domains, totaling 33 individual quality measures. (see Table 1)
Main Flavors of ACOs
There are two types of ACOs: private ACOs and Medicare ACOs. Prior to Medicare ACOs, which were launched in January 2012, there were 150 private-sector ACOs, and this number continues to grow. Private ACOs represent a heterogeneous group in terms of reimbursement model. Some operate under shared savings programs; others use full or partial capitation, bundled payments, and/or other types of arrangements. But nearly all ACOs operate under the premise that the incentives used to make care more efficient and less costly can only be applied if measurable quality is maintained or improved. ACOs do not pay doctors or hospitals more unless high quality is demonstrated.
ACO Quality Measures and Hospitalists
Most of the 33 quality measures required by Medicare ACOs are based in ambulatory practice. These include measures related to blood pressure, immunizations, cancer, and fall-risk screening, and measures for diabetics, such as lipids and hemoglobin A1C. However, there are a few measures for which hospitalists should share in accountability, including:
- All-cause hospital readmission rate—risk-standardized;
- Ambulatory sensitive condition hospital admission rates (CHF, COPD); and
- Medication reconciliation after discharge from an inpatient facility.
Four Key Actions for Hospitalists
Hospitalists make a significant contribution to the quality and the financial performance of ACOs. In addition to the quality metrics cited above, hospitalists impact the inpatient portion of the overall population’s cost of care. Furthermore, hospitalists are vital partners in the care coordination required for an ACO to be successful.
Here are four actions I suggest taking in order for your hospitalist group to be effective as participants in an ACO:
- Have a representative from your group participate in ACO committees that address hospital utilization and related matters, such as care coordination impacting pre- and post-hospital care.
- Learn how to work with ACO case managers on care transitions, including post-discharge follow-up and information transfer.
- Understand an ACO’s approach to engagement of and coordination with post-acute-care facilities. The ability of a post-acute facility, such a skilled nursing facility, to accept patients who have complex care needs, to manage changes in condition in the facility when appropriate, and to send complete information upon transfer to the hospital are important strategies for an ACO’s success.
- Understand how an ACO reports quality and cost performance and how savings will be shared among participants.
Mindset Change
If hospitalists are part of the chain of ACO physicians and providers held accountable for the health of a population of patients, we must work more closely with the medical home/neighborhood, post-acute-care facilities, and home-care providers. The change in mindset will occur only if we have a set of tools to get the job done, such as case managers and information technology, and the appropriate incentives to support better care coordination. I encourage my fellow hospitalists to make things happen, instead of taking a passive role in this monumental transformation.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Win Whitcomb: Front-Line Hospitalists Fight Against Health Care-Associated Infections (HAIs)

2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
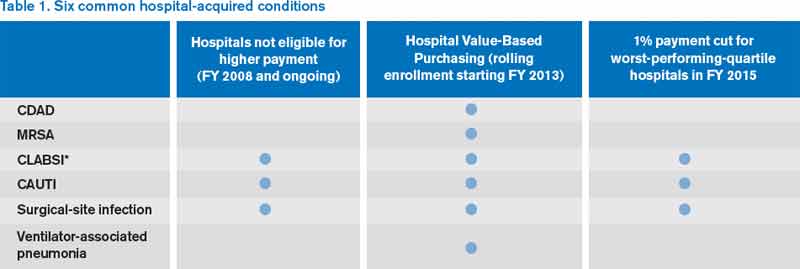
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
Bob Wachter Puts Forward Spin on Patient Safety, Quality of Care at HM13

Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
ONLINE EXCLUSIVE: The Medical Director of the National Alliance on Mental Illness Spotlights Hospitalist Communication, Attention to Discharge Details
Click here to listen to Dr. Duckworth
Click here to listen to Dr. Duckworth
Click here to listen to Dr. Duckworth
Robotic Vaporizers Reduce Hospital Bacterial Infections
Paired, robotlike devices that disperse a bleaching disinfectant into the air of hospital rooms, then detoxify the disinfecting chemical, were found to be highly effective at killing and preventing the spread of “superbug” bacteria, according to research from Johns Hopkins Hospital published in Clinical Infectious Diseases.5 Hydrogen peroxide vaporizers were first deployed in Singapore hospitals in 2002 during an outbreak of severe acute respiratory syndrome (SARS).
Almost half of a study group of 6,350 patients in and out of 180 hospital rooms over a two-and-a-half-year period received the enhanced cleaning technology, while the others received routine cleaning only. Manufactured by Bioquell Inc. of Horsham, Pa. (www.bioquell.com), each device is about the size of a washing machine. They were deployed in hospital rooms with sealed vents, dispersing a thin film of hydrogen peroxide across all exposed surfaces, equipment, floors, and walls. This approach reduced by 64% the number of patients who later became contaminated with any of the most common drug-resistant organisms, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, Clostridium difficile, and Acinetobacter baumannii.
Spreading the bleaching vapor this way “represents a major technological advance in preventing the spread of dangerous bacteria inside hospital rooms,” says senior investigator Trish Perl, MD, MSc, professor of medicine and an infectious disease specialist at Johns Hopkins. The hospital announced in December that it would begin decontaminating isolation rooms with these devices as standard practice starting in January.
Reference
Paired, robotlike devices that disperse a bleaching disinfectant into the air of hospital rooms, then detoxify the disinfecting chemical, were found to be highly effective at killing and preventing the spread of “superbug” bacteria, according to research from Johns Hopkins Hospital published in Clinical Infectious Diseases.5 Hydrogen peroxide vaporizers were first deployed in Singapore hospitals in 2002 during an outbreak of severe acute respiratory syndrome (SARS).
Almost half of a study group of 6,350 patients in and out of 180 hospital rooms over a two-and-a-half-year period received the enhanced cleaning technology, while the others received routine cleaning only. Manufactured by Bioquell Inc. of Horsham, Pa. (www.bioquell.com), each device is about the size of a washing machine. They were deployed in hospital rooms with sealed vents, dispersing a thin film of hydrogen peroxide across all exposed surfaces, equipment, floors, and walls. This approach reduced by 64% the number of patients who later became contaminated with any of the most common drug-resistant organisms, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, Clostridium difficile, and Acinetobacter baumannii.
Spreading the bleaching vapor this way “represents a major technological advance in preventing the spread of dangerous bacteria inside hospital rooms,” says senior investigator Trish Perl, MD, MSc, professor of medicine and an infectious disease specialist at Johns Hopkins. The hospital announced in December that it would begin decontaminating isolation rooms with these devices as standard practice starting in January.
Reference
Paired, robotlike devices that disperse a bleaching disinfectant into the air of hospital rooms, then detoxify the disinfecting chemical, were found to be highly effective at killing and preventing the spread of “superbug” bacteria, according to research from Johns Hopkins Hospital published in Clinical Infectious Diseases.5 Hydrogen peroxide vaporizers were first deployed in Singapore hospitals in 2002 during an outbreak of severe acute respiratory syndrome (SARS).
Almost half of a study group of 6,350 patients in and out of 180 hospital rooms over a two-and-a-half-year period received the enhanced cleaning technology, while the others received routine cleaning only. Manufactured by Bioquell Inc. of Horsham, Pa. (www.bioquell.com), each device is about the size of a washing machine. They were deployed in hospital rooms with sealed vents, dispersing a thin film of hydrogen peroxide across all exposed surfaces, equipment, floors, and walls. This approach reduced by 64% the number of patients who later became contaminated with any of the most common drug-resistant organisms, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, Clostridium difficile, and Acinetobacter baumannii.
Spreading the bleaching vapor this way “represents a major technological advance in preventing the spread of dangerous bacteria inside hospital rooms,” says senior investigator Trish Perl, MD, MSc, professor of medicine and an infectious disease specialist at Johns Hopkins. The hospital announced in December that it would begin decontaminating isolation rooms with these devices as standard practice starting in January.
Reference
Society of Hospital Medicine Launches Online Training Program for Hospitalists
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)