User login
Choosing Wisely Campaign Initiatives Grounded in Tenets of Hospital Medicine

The Choosing Wisely campaign is focused on better decision-making, improved quality, and decreased healthcare costs. Such focus on efficiency and cost-effectiveness also was part of the initial motivation for developing hospital medicine, says one of HM’s pioneering doctors.
Robert Wachter, MD, MHM, who heads the division of hospital medicine at the University of California at San Francisco, compares the current national obsession about healthcare waste with the medical quality and patient safety movements of the past decade.
“It’s the right time, the right message, and the right messenger,” says Dr. Wachter, who also chairs the American Board of Internal Medicine and sits on the board of the ABIM Foundation. “We’re a little scared about raised expectations. Delivering on them is going to be more difficult, even, than patient safety was, because ultimately it will require curtailing some income streams. You can’t reach the final outcome of cutting costs in healthcare without someone making less money.”
Dr. Wachter expects the medical community to hear “similar kinds of drumbeats about waste” from every corner of healthcare. “I think hospitalists should be active and enthusiastic partners in the Choosing Wisely campaign,” he says, “and leaders in American healthcare’s efforts to figure out how to purge waste from the system and decrease unnecessary expense.
The Choosing Wisely campaign is focused on better decision-making, improved quality, and decreased healthcare costs. Such focus on efficiency and cost-effectiveness also was part of the initial motivation for developing hospital medicine, says one of HM’s pioneering doctors.
Robert Wachter, MD, MHM, who heads the division of hospital medicine at the University of California at San Francisco, compares the current national obsession about healthcare waste with the medical quality and patient safety movements of the past decade.
“It’s the right time, the right message, and the right messenger,” says Dr. Wachter, who also chairs the American Board of Internal Medicine and sits on the board of the ABIM Foundation. “We’re a little scared about raised expectations. Delivering on them is going to be more difficult, even, than patient safety was, because ultimately it will require curtailing some income streams. You can’t reach the final outcome of cutting costs in healthcare without someone making less money.”
Dr. Wachter expects the medical community to hear “similar kinds of drumbeats about waste” from every corner of healthcare. “I think hospitalists should be active and enthusiastic partners in the Choosing Wisely campaign,” he says, “and leaders in American healthcare’s efforts to figure out how to purge waste from the system and decrease unnecessary expense.
The Choosing Wisely campaign is focused on better decision-making, improved quality, and decreased healthcare costs. Such focus on efficiency and cost-effectiveness also was part of the initial motivation for developing hospital medicine, says one of HM’s pioneering doctors.
Robert Wachter, MD, MHM, who heads the division of hospital medicine at the University of California at San Francisco, compares the current national obsession about healthcare waste with the medical quality and patient safety movements of the past decade.
“It’s the right time, the right message, and the right messenger,” says Dr. Wachter, who also chairs the American Board of Internal Medicine and sits on the board of the ABIM Foundation. “We’re a little scared about raised expectations. Delivering on them is going to be more difficult, even, than patient safety was, because ultimately it will require curtailing some income streams. You can’t reach the final outcome of cutting costs in healthcare without someone making less money.”
Dr. Wachter expects the medical community to hear “similar kinds of drumbeats about waste” from every corner of healthcare. “I think hospitalists should be active and enthusiastic partners in the Choosing Wisely campaign,” he says, “and leaders in American healthcare’s efforts to figure out how to purge waste from the system and decrease unnecessary expense.
Hospitalwide Reductions in Pediatric Patient Harm are Achievable

Clinical question: Can a broadly constructed improvement initiative significantly reduce serious safety events (SSEs)?
Study design: Single-institution quality-improvement initiative.
Setting: Cincinnati Children’s Hospital Medical Center.
Synopsis: A multidisciplinary team supported by leadership was formed to reduce SSEs across the hospital by 80% within four years. A consulting firm with expertise in the field was also engaged for this process. Multifaceted interventions were clustered according to perceived key drivers of change in the institution: error prevention systems, improved safety governance, cause analysis programs, lessons-learned programs, and specific tactical interventions.
SSEs per 10,000 adjusted patient-days decreased significantly, to a mean of 0.3 from 0.9 (P<0.0001) after implementation, while days between SSEs increased to a mean of 55.2 from 19.4 (P<0.0001).
This work represents one of the most robust single-center approaches to improving patient safety that has been published to date. The authors attribute much of their success to culture change, which required “relentless clarity of vision by the organization.” Although this substantially limits immediate generalizability of any of the specific interventions, the work stands on its own as a prime example of what may be accomplished through focused dedication to reducing patient harm.
Bottom line: Patient harm is preventable through a widespread and multifaceted institutional initiative.
Citation: Muething SE, Goudie A, Schoettker PJ, et al. Quality improvement initiative to reduce serious safety events and improve patient safety culture. Pediatrics. 2012;130:e423-431.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Can a broadly constructed improvement initiative significantly reduce serious safety events (SSEs)?
Study design: Single-institution quality-improvement initiative.
Setting: Cincinnati Children’s Hospital Medical Center.
Synopsis: A multidisciplinary team supported by leadership was formed to reduce SSEs across the hospital by 80% within four years. A consulting firm with expertise in the field was also engaged for this process. Multifaceted interventions were clustered according to perceived key drivers of change in the institution: error prevention systems, improved safety governance, cause analysis programs, lessons-learned programs, and specific tactical interventions.
SSEs per 10,000 adjusted patient-days decreased significantly, to a mean of 0.3 from 0.9 (P<0.0001) after implementation, while days between SSEs increased to a mean of 55.2 from 19.4 (P<0.0001).
This work represents one of the most robust single-center approaches to improving patient safety that has been published to date. The authors attribute much of their success to culture change, which required “relentless clarity of vision by the organization.” Although this substantially limits immediate generalizability of any of the specific interventions, the work stands on its own as a prime example of what may be accomplished through focused dedication to reducing patient harm.
Bottom line: Patient harm is preventable through a widespread and multifaceted institutional initiative.
Citation: Muething SE, Goudie A, Schoettker PJ, et al. Quality improvement initiative to reduce serious safety events and improve patient safety culture. Pediatrics. 2012;130:e423-431.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Can a broadly constructed improvement initiative significantly reduce serious safety events (SSEs)?
Study design: Single-institution quality-improvement initiative.
Setting: Cincinnati Children’s Hospital Medical Center.
Synopsis: A multidisciplinary team supported by leadership was formed to reduce SSEs across the hospital by 80% within four years. A consulting firm with expertise in the field was also engaged for this process. Multifaceted interventions were clustered according to perceived key drivers of change in the institution: error prevention systems, improved safety governance, cause analysis programs, lessons-learned programs, and specific tactical interventions.
SSEs per 10,000 adjusted patient-days decreased significantly, to a mean of 0.3 from 0.9 (P<0.0001) after implementation, while days between SSEs increased to a mean of 55.2 from 19.4 (P<0.0001).
This work represents one of the most robust single-center approaches to improving patient safety that has been published to date. The authors attribute much of their success to culture change, which required “relentless clarity of vision by the organization.” Although this substantially limits immediate generalizability of any of the specific interventions, the work stands on its own as a prime example of what may be accomplished through focused dedication to reducing patient harm.
Bottom line: Patient harm is preventable through a widespread and multifaceted institutional initiative.
Citation: Muething SE, Goudie A, Schoettker PJ, et al. Quality improvement initiative to reduce serious safety events and improve patient safety culture. Pediatrics. 2012;130:e423-431.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Post-Hospital Syndrome Contributes to Readmission Risk for Elderly
Post-hospital syndrome, as labeled in a recent, widely publicized opinion piece in the New England Journal of Medicine, is not a new concept, according to one hospitalist pioneer.1
Harlan Krumholz, MD, of the Yale School of Medicine in New Haven, Conn., writes in NEJM what others previously have described as “hospitalization-associated disability,” says Mark Williams, MD, MHM, chief of hospital medicine at Northwestern University School of Medicine and principal investigator of SHM’s Project BOOST (www.hospitalmedicine.org/boost).2
Dr. Krumholz found that the majority of 30-day readmissions for elderly patients with heart failure, pneumonia, or chronic obstructive pulmonary disease are for conditions other than the diagnosis named at discharge. He attributes this phenomenon to hospitalization-related sleep deprivation, malnourishment, pain and discomfort, cognition- and physical function-altering medications, deconditioning from bed rest or inactivity, and the experience of confronting stressful, mentally challenging situations in the hospital.1 Such stressors leave elderly patients with post-hospitalization disabilities comparable to a bad case of jet lag.
For Dr. Williams, the physical deterioration leading to rehospitalizations is better attributed to the underlying serious illness and comorbidities experienced by elderly patients—a kind of high-risk, post-illness syndrome. Prior research also has demonstrated the effects of bed rest for hospitalized elderly patients.
Regardless of the origins, is there anything hospitalists can do about this syndrome? “Absolutely,” Dr. Williams says. “Get elderly, hospitalized patients out of bed as quickly as possible, and be mindful of medications and their effects on elderly patients. But most hospitalists already think about these things when managing elderly patients.”
References
Post-hospital syndrome, as labeled in a recent, widely publicized opinion piece in the New England Journal of Medicine, is not a new concept, according to one hospitalist pioneer.1
Harlan Krumholz, MD, of the Yale School of Medicine in New Haven, Conn., writes in NEJM what others previously have described as “hospitalization-associated disability,” says Mark Williams, MD, MHM, chief of hospital medicine at Northwestern University School of Medicine and principal investigator of SHM’s Project BOOST (www.hospitalmedicine.org/boost).2
Dr. Krumholz found that the majority of 30-day readmissions for elderly patients with heart failure, pneumonia, or chronic obstructive pulmonary disease are for conditions other than the diagnosis named at discharge. He attributes this phenomenon to hospitalization-related sleep deprivation, malnourishment, pain and discomfort, cognition- and physical function-altering medications, deconditioning from bed rest or inactivity, and the experience of confronting stressful, mentally challenging situations in the hospital.1 Such stressors leave elderly patients with post-hospitalization disabilities comparable to a bad case of jet lag.
For Dr. Williams, the physical deterioration leading to rehospitalizations is better attributed to the underlying serious illness and comorbidities experienced by elderly patients—a kind of high-risk, post-illness syndrome. Prior research also has demonstrated the effects of bed rest for hospitalized elderly patients.
Regardless of the origins, is there anything hospitalists can do about this syndrome? “Absolutely,” Dr. Williams says. “Get elderly, hospitalized patients out of bed as quickly as possible, and be mindful of medications and their effects on elderly patients. But most hospitalists already think about these things when managing elderly patients.”
References
Post-hospital syndrome, as labeled in a recent, widely publicized opinion piece in the New England Journal of Medicine, is not a new concept, according to one hospitalist pioneer.1
Harlan Krumholz, MD, of the Yale School of Medicine in New Haven, Conn., writes in NEJM what others previously have described as “hospitalization-associated disability,” says Mark Williams, MD, MHM, chief of hospital medicine at Northwestern University School of Medicine and principal investigator of SHM’s Project BOOST (www.hospitalmedicine.org/boost).2
Dr. Krumholz found that the majority of 30-day readmissions for elderly patients with heart failure, pneumonia, or chronic obstructive pulmonary disease are for conditions other than the diagnosis named at discharge. He attributes this phenomenon to hospitalization-related sleep deprivation, malnourishment, pain and discomfort, cognition- and physical function-altering medications, deconditioning from bed rest or inactivity, and the experience of confronting stressful, mentally challenging situations in the hospital.1 Such stressors leave elderly patients with post-hospitalization disabilities comparable to a bad case of jet lag.
For Dr. Williams, the physical deterioration leading to rehospitalizations is better attributed to the underlying serious illness and comorbidities experienced by elderly patients—a kind of high-risk, post-illness syndrome. Prior research also has demonstrated the effects of bed rest for hospitalized elderly patients.
Regardless of the origins, is there anything hospitalists can do about this syndrome? “Absolutely,” Dr. Williams says. “Get elderly, hospitalized patients out of bed as quickly as possible, and be mindful of medications and their effects on elderly patients. But most hospitalists already think about these things when managing elderly patients.”
References
Hospital Medicine Experts Outline Criteria To Consider Before Growing Your Group
—Brian Hazen, MD, medical director, Inova Fairfax Hospital Group, Fairfax, Va.
Ilan Alhadeff, MD, SFHM, program medical director for Cogent HMG at Hackensack University Medical Center in Hackensack, N.J., pays a lot of attention to the work relative-value units (wRVUs) his hospitalists are producing and the number of encounters they’re tallying. But he’s not particularly worried about what he sees on a daily, weekly, or even monthly basis; he takes a monthslong view of his data when he wants to forecast whether he is going to need to think about adding staff.
“When you look at months, you can start seeing trends,” Dr. Alhadeff says. “Let’s say there’s 16 to 18 average encounters. If your average is 16, you’re saying, ‘OK, you’re on the lower end of your normal.’ And if your average is 18, you’re on the higher end of normal. But if you start seeing 18 every month, odds are you’re going to start getting to 19. So at that point, that’s raising the thought that we need to start thinking about bringing someone else on.”

It’s a dance HM group leaders around the country have to do when confronted with the age-old question: Should we expand our service? The answer is more art than science, experts say, as there is no standardized formula for knowing when your HM group should request more support from administration to add an FTE—or two or three. And, in a nod to the HM adage that if you’ve seen one HM group (HMG), then you’ve seen one HMG, the roadmap to expansion varies from place to place. But in a series of interviews with The Hospitalist, physicians, consultants, and management experts suggest there are broad themes that guide the process, including:
- Data. Dashboard metrics, such as average daily census (ADC), wRVUs, patient encounters, and length of stay (LOS), must be quantified. No discussion on expansion can be intelligibly made without a firm understanding of where a practice currently stands.
- Benchmarking. Collating figures isn’t enough. Measure your group against other local HMGs, regional groups, and national standards. SHM’s 2012 State of Hospital Medicine report is a good place to start.
- Scope or schedule. Pushing into new business lines (e.g. orthopedic comanagement) often requires new staff, as does adding shifts to provide 24-hour on-site coverage. Those arguments are different from the case to be made for expanding based on increased patient encounters.
- Physician buy-in. Group leaders cannot unilaterally determine it’s time to add staff, particularly in small-group settings in which hiring a new physician means taking revenue away from the existing group, if only in the short term. Talk with group members before embarking on expansion. Keep track of physician turnover. If hospitalists are leaving often, it could be a sign the group is understaffed.
- Administrative buy-in. If a group leader’s request for a new hire comes without months of conversation ahead of it, it’s likely too late. Prepare C-suite executives in advance about potential growth needs so the discussion does not feel like a surprise.
- Know your market. Don’t wait until a new active-adult community floods the hospital with patients to begin analyzing the impact new residents might have. The same goes for companies that are bringing thousands of new workers to an area.
- Prepare to do nothing. Too often, group leaders think the easiest solution is hiring a physician to lessen workload. Instead, exhaust improved efficiency options and infrastructure improvements that could accomplish the same goal.
“There is no one specific measure,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners Medical Group in St. Paul, Minn., and an SHM board member. “You have to look at it from several different aspects, and all or most need to line up and say that, yes, you could use more help.”
Practice Analysis
Dr. Kealey, board liaison to SHM’s Practice Analysis Committee, says that benchmarking might be among the most important first steps in determining the right time to grow a practice. Group leaders should keep in mind, though, that comparative analysis to outside measures is only step one of gauging a group’s performance.
“The external benchmarking is easy,” he says. “You can look at SHM survey data. There are a lot of places that will do local market surveys; that’s easy stuff to look at. It’s the internal stuff that’s a bit harder to make the case for, ‘OK, yes, I am a little below the national benchmarks, but here’s why.’”

In those instances, group leaders need to “look at the value equation” and engage hospital administrators in a discussion on why such metrics as wRVUs and ADC might not match local, regional, or national standards. Perhaps a hospital has a lower payor mix than the sample pool, or comparable regional institutions have a better mix of medical and surgical comanagement populations. Regardless of the details of the tailored explanation, the conversation must be one that’s ongoing between a group leader and the C-suite or it is likely to fail, Dr. Kealey says.
“It really gets to the partnership between the hospital and the hospitalist group and working together throughout the whole year, and not just looking at staffing needs, but looking at the hospital’s quality,” he adds. “It’s looking at [the hospital’s] ability to retain the surgeons and the specialists. It’s the leadership that you’re providing. It’s showing that you’re a real partner, so that when it does come time to make that value argument, that we need to grow...there is buy-in.
“If you’re not a true partner and you just come in as an adversary, I think your odds of success are not very high.”

Steve Sloan, MD, a partner at AIM Hospitalist Group of Westmont, Ill., says that group leaders would be wise to obtain input from all of their physicians before adding a new doctor, as each new hire impacts compensation for existing staff members. In Dr. Sloan’s 16-member group, 11 physicians are partners who discuss growth plans. The other doctors are on partnership tracks. And while that makes discussions more difficult than when nine physicians formed the group in 2007, up-front dialogue is crucial, Dr. Sloan says.
“We try to get all the partners together to make major decisions, such as hiring,” he says. “We don’t need everyone involved in every decision, but it’s not just one or two people making the decision.”
The conversation about growth also differs if new hires are needed to move the group into a new business line or if the group is adding staff to deal with its current patient load. Both require a business case for expansion to be made, but either way, codifying expectations with hospital clients is another way to streamline the growth process, says Dr. Alhadeff. His group contracts with his hospital to provide services and has the ability to autonomously add or delete staff as needed. Although personnel moves don’t require prior approval from the hospital, there is “an expected fiscal responsibility on our end and predetermined agreement do so.”
The group also keeps administrative stakeholders updated to make sure everyone is on the same page. Other groups might delineate in a contract what thresholds need to be met for expansion to be viable.
“It needs to be agreed upon,” Dr. Alhadeff says. “I like the flexibility of being able to determine within our company what we’re doing. But in answer to that, there are unintentional consequences. If we determine that we’re going to bring on someone else, and then we see after a few months that there is not enough volume to support this new physician, we could run into a problem. We will then have to make a financial decision, and the worst thing is to have to fire someone.”
Dr. Alhadeff also worries about the flipside: failing to hire when staff is overworked.
“We run that risk also,” he says. “We are walking a tightrope all the time, and we need to balance that tightrope.”

—Kenneth Hertz, FACMPE, principal, Medical Group Management Association Health Care Consulting Group, Denver
The Long View
Another tightrope is timing. Kenneth Hertz, FACMPE, principal of the Medical Group Management Association’s Health Care Consulting Group, says that it can take six months or longer to hire a physician, which means group leaders need to have a continual focus on whether growth is needed or will soon be needed. He suggests forecasting at least 12 to 18 months in advance to stay ahead of staffing needs.
Unfortunately, he says, analysis often gets put on hold in the shuffle of dealing with daily duties. “This is kind of generic to practice administrators, who are putting out fires almost every day. And when you’re putting out fires every day, you don’t have the luxury and the time to look out there and see what’s happening and know everything that’s going on,” he says. “They need to understand the importance of it and how all the pieces tie in together.”
Brian Hazen, MD, medical director of Inova Fairfax Hospital Group in Fairfax, Va., says an important approach is to realize growth isn’t always a good thing. HM group leaders often want to grow before they have stabilized their existing business lines, he says, and that can be the worst tack to take. He also notes that a group leader should ingratiate their program into the fabric of their hospital and not just rely on data to make the argument of the group’s value. That means putting hospitalists on committees, spearheading safety programs, and being seen as a partner in the institution.
“Job One is always patient safety and physician sanity,” he says. “If you are careful about growth and buy-in, and you do the committee work and support everybody so that you’re firmly entrenched in the hospital as a value, it’s much safer to grow. Growing for the sake of growing, you risk overexpansion, and that’s dangerous.”
Many hospitalist groups looking to grow will use locum tenens to bridge the staffing gap while they hire new employees (see “No Strings Attached,” December 2012, p. 36), but Dr. Hazen says without a longer view, that only serves as a Band-Aid.
Hertz, the consultant, often uses an analogy to show how important it is to be constantly planning ahead of the growth curve.
“It is a little bit like building roads,” he says. “Once you decide you need to add two lanes, by the time those are finished, you realize we really need to add two more lanes.”
Richard Quinn is a freelance writer in New Jersey.
—Brian Hazen, MD, medical director, Inova Fairfax Hospital Group, Fairfax, Va.
Ilan Alhadeff, MD, SFHM, program medical director for Cogent HMG at Hackensack University Medical Center in Hackensack, N.J., pays a lot of attention to the work relative-value units (wRVUs) his hospitalists are producing and the number of encounters they’re tallying. But he’s not particularly worried about what he sees on a daily, weekly, or even monthly basis; he takes a monthslong view of his data when he wants to forecast whether he is going to need to think about adding staff.
“When you look at months, you can start seeing trends,” Dr. Alhadeff says. “Let’s say there’s 16 to 18 average encounters. If your average is 16, you’re saying, ‘OK, you’re on the lower end of your normal.’ And if your average is 18, you’re on the higher end of normal. But if you start seeing 18 every month, odds are you’re going to start getting to 19. So at that point, that’s raising the thought that we need to start thinking about bringing someone else on.”
It’s a dance HM group leaders around the country have to do when confronted with the age-old question: Should we expand our service? The answer is more art than science, experts say, as there is no standardized formula for knowing when your HM group should request more support from administration to add an FTE—or two or three. And, in a nod to the HM adage that if you’ve seen one HM group (HMG), then you’ve seen one HMG, the roadmap to expansion varies from place to place. But in a series of interviews with The Hospitalist, physicians, consultants, and management experts suggest there are broad themes that guide the process, including:
- Data. Dashboard metrics, such as average daily census (ADC), wRVUs, patient encounters, and length of stay (LOS), must be quantified. No discussion on expansion can be intelligibly made without a firm understanding of where a practice currently stands.
- Benchmarking. Collating figures isn’t enough. Measure your group against other local HMGs, regional groups, and national standards. SHM’s 2012 State of Hospital Medicine report is a good place to start.
- Scope or schedule. Pushing into new business lines (e.g. orthopedic comanagement) often requires new staff, as does adding shifts to provide 24-hour on-site coverage. Those arguments are different from the case to be made for expanding based on increased patient encounters.
- Physician buy-in. Group leaders cannot unilaterally determine it’s time to add staff, particularly in small-group settings in which hiring a new physician means taking revenue away from the existing group, if only in the short term. Talk with group members before embarking on expansion. Keep track of physician turnover. If hospitalists are leaving often, it could be a sign the group is understaffed.
- Administrative buy-in. If a group leader’s request for a new hire comes without months of conversation ahead of it, it’s likely too late. Prepare C-suite executives in advance about potential growth needs so the discussion does not feel like a surprise.
- Know your market. Don’t wait until a new active-adult community floods the hospital with patients to begin analyzing the impact new residents might have. The same goes for companies that are bringing thousands of new workers to an area.
- Prepare to do nothing. Too often, group leaders think the easiest solution is hiring a physician to lessen workload. Instead, exhaust improved efficiency options and infrastructure improvements that could accomplish the same goal.
“There is no one specific measure,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners Medical Group in St. Paul, Minn., and an SHM board member. “You have to look at it from several different aspects, and all or most need to line up and say that, yes, you could use more help.”
Practice Analysis
Dr. Kealey, board liaison to SHM’s Practice Analysis Committee, says that benchmarking might be among the most important first steps in determining the right time to grow a practice. Group leaders should keep in mind, though, that comparative analysis to outside measures is only step one of gauging a group’s performance.
“The external benchmarking is easy,” he says. “You can look at SHM survey data. There are a lot of places that will do local market surveys; that’s easy stuff to look at. It’s the internal stuff that’s a bit harder to make the case for, ‘OK, yes, I am a little below the national benchmarks, but here’s why.’”
In those instances, group leaders need to “look at the value equation” and engage hospital administrators in a discussion on why such metrics as wRVUs and ADC might not match local, regional, or national standards. Perhaps a hospital has a lower payor mix than the sample pool, or comparable regional institutions have a better mix of medical and surgical comanagement populations. Regardless of the details of the tailored explanation, the conversation must be one that’s ongoing between a group leader and the C-suite or it is likely to fail, Dr. Kealey says.
“It really gets to the partnership between the hospital and the hospitalist group and working together throughout the whole year, and not just looking at staffing needs, but looking at the hospital’s quality,” he adds. “It’s looking at [the hospital’s] ability to retain the surgeons and the specialists. It’s the leadership that you’re providing. It’s showing that you’re a real partner, so that when it does come time to make that value argument, that we need to grow...there is buy-in.
“If you’re not a true partner and you just come in as an adversary, I think your odds of success are not very high.”
Steve Sloan, MD, a partner at AIM Hospitalist Group of Westmont, Ill., says that group leaders would be wise to obtain input from all of their physicians before adding a new doctor, as each new hire impacts compensation for existing staff members. In Dr. Sloan’s 16-member group, 11 physicians are partners who discuss growth plans. The other doctors are on partnership tracks. And while that makes discussions more difficult than when nine physicians formed the group in 2007, up-front dialogue is crucial, Dr. Sloan says.
“We try to get all the partners together to make major decisions, such as hiring,” he says. “We don’t need everyone involved in every decision, but it’s not just one or two people making the decision.”
The conversation about growth also differs if new hires are needed to move the group into a new business line or if the group is adding staff to deal with its current patient load. Both require a business case for expansion to be made, but either way, codifying expectations with hospital clients is another way to streamline the growth process, says Dr. Alhadeff. His group contracts with his hospital to provide services and has the ability to autonomously add or delete staff as needed. Although personnel moves don’t require prior approval from the hospital, there is “an expected fiscal responsibility on our end and predetermined agreement do so.”
The group also keeps administrative stakeholders updated to make sure everyone is on the same page. Other groups might delineate in a contract what thresholds need to be met for expansion to be viable.
“It needs to be agreed upon,” Dr. Alhadeff says. “I like the flexibility of being able to determine within our company what we’re doing. But in answer to that, there are unintentional consequences. If we determine that we’re going to bring on someone else, and then we see after a few months that there is not enough volume to support this new physician, we could run into a problem. We will then have to make a financial decision, and the worst thing is to have to fire someone.”
Dr. Alhadeff also worries about the flipside: failing to hire when staff is overworked.
“We run that risk also,” he says. “We are walking a tightrope all the time, and we need to balance that tightrope.”
—Kenneth Hertz, FACMPE, principal, Medical Group Management Association Health Care Consulting Group, Denver
The Long View
Another tightrope is timing. Kenneth Hertz, FACMPE, principal of the Medical Group Management Association’s Health Care Consulting Group, says that it can take six months or longer to hire a physician, which means group leaders need to have a continual focus on whether growth is needed or will soon be needed. He suggests forecasting at least 12 to 18 months in advance to stay ahead of staffing needs.
Unfortunately, he says, analysis often gets put on hold in the shuffle of dealing with daily duties. “This is kind of generic to practice administrators, who are putting out fires almost every day. And when you’re putting out fires every day, you don’t have the luxury and the time to look out there and see what’s happening and know everything that’s going on,” he says. “They need to understand the importance of it and how all the pieces tie in together.”
Brian Hazen, MD, medical director of Inova Fairfax Hospital Group in Fairfax, Va., says an important approach is to realize growth isn’t always a good thing. HM group leaders often want to grow before they have stabilized their existing business lines, he says, and that can be the worst tack to take. He also notes that a group leader should ingratiate their program into the fabric of their hospital and not just rely on data to make the argument of the group’s value. That means putting hospitalists on committees, spearheading safety programs, and being seen as a partner in the institution.
“Job One is always patient safety and physician sanity,” he says. “If you are careful about growth and buy-in, and you do the committee work and support everybody so that you’re firmly entrenched in the hospital as a value, it’s much safer to grow. Growing for the sake of growing, you risk overexpansion, and that’s dangerous.”
Many hospitalist groups looking to grow will use locum tenens to bridge the staffing gap while they hire new employees (see “No Strings Attached,” December 2012, p. 36), but Dr. Hazen says without a longer view, that only serves as a Band-Aid.
Hertz, the consultant, often uses an analogy to show how important it is to be constantly planning ahead of the growth curve.
“It is a little bit like building roads,” he says. “Once you decide you need to add two lanes, by the time those are finished, you realize we really need to add two more lanes.”
Richard Quinn is a freelance writer in New Jersey.
—Brian Hazen, MD, medical director, Inova Fairfax Hospital Group, Fairfax, Va.
Ilan Alhadeff, MD, SFHM, program medical director for Cogent HMG at Hackensack University Medical Center in Hackensack, N.J., pays a lot of attention to the work relative-value units (wRVUs) his hospitalists are producing and the number of encounters they’re tallying. But he’s not particularly worried about what he sees on a daily, weekly, or even monthly basis; he takes a monthslong view of his data when he wants to forecast whether he is going to need to think about adding staff.
“When you look at months, you can start seeing trends,” Dr. Alhadeff says. “Let’s say there’s 16 to 18 average encounters. If your average is 16, you’re saying, ‘OK, you’re on the lower end of your normal.’ And if your average is 18, you’re on the higher end of normal. But if you start seeing 18 every month, odds are you’re going to start getting to 19. So at that point, that’s raising the thought that we need to start thinking about bringing someone else on.”
It’s a dance HM group leaders around the country have to do when confronted with the age-old question: Should we expand our service? The answer is more art than science, experts say, as there is no standardized formula for knowing when your HM group should request more support from administration to add an FTE—or two or three. And, in a nod to the HM adage that if you’ve seen one HM group (HMG), then you’ve seen one HMG, the roadmap to expansion varies from place to place. But in a series of interviews with The Hospitalist, physicians, consultants, and management experts suggest there are broad themes that guide the process, including:
- Data. Dashboard metrics, such as average daily census (ADC), wRVUs, patient encounters, and length of stay (LOS), must be quantified. No discussion on expansion can be intelligibly made without a firm understanding of where a practice currently stands.
- Benchmarking. Collating figures isn’t enough. Measure your group against other local HMGs, regional groups, and national standards. SHM’s 2012 State of Hospital Medicine report is a good place to start.
- Scope or schedule. Pushing into new business lines (e.g. orthopedic comanagement) often requires new staff, as does adding shifts to provide 24-hour on-site coverage. Those arguments are different from the case to be made for expanding based on increased patient encounters.
- Physician buy-in. Group leaders cannot unilaterally determine it’s time to add staff, particularly in small-group settings in which hiring a new physician means taking revenue away from the existing group, if only in the short term. Talk with group members before embarking on expansion. Keep track of physician turnover. If hospitalists are leaving often, it could be a sign the group is understaffed.
- Administrative buy-in. If a group leader’s request for a new hire comes without months of conversation ahead of it, it’s likely too late. Prepare C-suite executives in advance about potential growth needs so the discussion does not feel like a surprise.
- Know your market. Don’t wait until a new active-adult community floods the hospital with patients to begin analyzing the impact new residents might have. The same goes for companies that are bringing thousands of new workers to an area.
- Prepare to do nothing. Too often, group leaders think the easiest solution is hiring a physician to lessen workload. Instead, exhaust improved efficiency options and infrastructure improvements that could accomplish the same goal.
“There is no one specific measure,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners Medical Group in St. Paul, Minn., and an SHM board member. “You have to look at it from several different aspects, and all or most need to line up and say that, yes, you could use more help.”
Practice Analysis
Dr. Kealey, board liaison to SHM’s Practice Analysis Committee, says that benchmarking might be among the most important first steps in determining the right time to grow a practice. Group leaders should keep in mind, though, that comparative analysis to outside measures is only step one of gauging a group’s performance.
“The external benchmarking is easy,” he says. “You can look at SHM survey data. There are a lot of places that will do local market surveys; that’s easy stuff to look at. It’s the internal stuff that’s a bit harder to make the case for, ‘OK, yes, I am a little below the national benchmarks, but here’s why.’”
In those instances, group leaders need to “look at the value equation” and engage hospital administrators in a discussion on why such metrics as wRVUs and ADC might not match local, regional, or national standards. Perhaps a hospital has a lower payor mix than the sample pool, or comparable regional institutions have a better mix of medical and surgical comanagement populations. Regardless of the details of the tailored explanation, the conversation must be one that’s ongoing between a group leader and the C-suite or it is likely to fail, Dr. Kealey says.
“It really gets to the partnership between the hospital and the hospitalist group and working together throughout the whole year, and not just looking at staffing needs, but looking at the hospital’s quality,” he adds. “It’s looking at [the hospital’s] ability to retain the surgeons and the specialists. It’s the leadership that you’re providing. It’s showing that you’re a real partner, so that when it does come time to make that value argument, that we need to grow...there is buy-in.
“If you’re not a true partner and you just come in as an adversary, I think your odds of success are not very high.”
Steve Sloan, MD, a partner at AIM Hospitalist Group of Westmont, Ill., says that group leaders would be wise to obtain input from all of their physicians before adding a new doctor, as each new hire impacts compensation for existing staff members. In Dr. Sloan’s 16-member group, 11 physicians are partners who discuss growth plans. The other doctors are on partnership tracks. And while that makes discussions more difficult than when nine physicians formed the group in 2007, up-front dialogue is crucial, Dr. Sloan says.
“We try to get all the partners together to make major decisions, such as hiring,” he says. “We don’t need everyone involved in every decision, but it’s not just one or two people making the decision.”
The conversation about growth also differs if new hires are needed to move the group into a new business line or if the group is adding staff to deal with its current patient load. Both require a business case for expansion to be made, but either way, codifying expectations with hospital clients is another way to streamline the growth process, says Dr. Alhadeff. His group contracts with his hospital to provide services and has the ability to autonomously add or delete staff as needed. Although personnel moves don’t require prior approval from the hospital, there is “an expected fiscal responsibility on our end and predetermined agreement do so.”
The group also keeps administrative stakeholders updated to make sure everyone is on the same page. Other groups might delineate in a contract what thresholds need to be met for expansion to be viable.
“It needs to be agreed upon,” Dr. Alhadeff says. “I like the flexibility of being able to determine within our company what we’re doing. But in answer to that, there are unintentional consequences. If we determine that we’re going to bring on someone else, and then we see after a few months that there is not enough volume to support this new physician, we could run into a problem. We will then have to make a financial decision, and the worst thing is to have to fire someone.”
Dr. Alhadeff also worries about the flipside: failing to hire when staff is overworked.
“We run that risk also,” he says. “We are walking a tightrope all the time, and we need to balance that tightrope.”
—Kenneth Hertz, FACMPE, principal, Medical Group Management Association Health Care Consulting Group, Denver
The Long View
Another tightrope is timing. Kenneth Hertz, FACMPE, principal of the Medical Group Management Association’s Health Care Consulting Group, says that it can take six months or longer to hire a physician, which means group leaders need to have a continual focus on whether growth is needed or will soon be needed. He suggests forecasting at least 12 to 18 months in advance to stay ahead of staffing needs.
Unfortunately, he says, analysis often gets put on hold in the shuffle of dealing with daily duties. “This is kind of generic to practice administrators, who are putting out fires almost every day. And when you’re putting out fires every day, you don’t have the luxury and the time to look out there and see what’s happening and know everything that’s going on,” he says. “They need to understand the importance of it and how all the pieces tie in together.”
Brian Hazen, MD, medical director of Inova Fairfax Hospital Group in Fairfax, Va., says an important approach is to realize growth isn’t always a good thing. HM group leaders often want to grow before they have stabilized their existing business lines, he says, and that can be the worst tack to take. He also notes that a group leader should ingratiate their program into the fabric of their hospital and not just rely on data to make the argument of the group’s value. That means putting hospitalists on committees, spearheading safety programs, and being seen as a partner in the institution.
“Job One is always patient safety and physician sanity,” he says. “If you are careful about growth and buy-in, and you do the committee work and support everybody so that you’re firmly entrenched in the hospital as a value, it’s much safer to grow. Growing for the sake of growing, you risk overexpansion, and that’s dangerous.”
Many hospitalist groups looking to grow will use locum tenens to bridge the staffing gap while they hire new employees (see “No Strings Attached,” December 2012, p. 36), but Dr. Hazen says without a longer view, that only serves as a Band-Aid.
Hertz, the consultant, often uses an analogy to show how important it is to be constantly planning ahead of the growth curve.
“It is a little bit like building roads,” he says. “Once you decide you need to add two lanes, by the time those are finished, you realize we really need to add two more lanes.”
Richard Quinn is a freelance writer in New Jersey.
Win Whitcomb: Mortality Rates Become a Measuring Stick for Hospital Performance

—Blue Oyster Cult
The designers of the hospital value-based purchasing (HVBP) program sought to include outcomes measures in 2014, and when they did, mortality was their choice. Specifically, HVBP for fiscal-year 2014 (starting October 2013) will include 30-day mortality rates for myocardial infarction, heart failure, and pneumonia. The weighting for the mortality domain will be 25% (see Table 1).
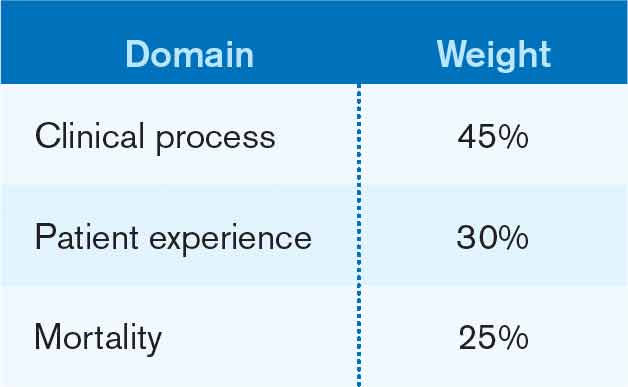
To review the requirements for the HVBP program in FY2014: All hospitals will have 1.25% of their Medicare inpatient payments withheld. They can earn back none, some, all, or an amount in excess of the 1.25%, depending on performance in the performance domains. To put it in perspective, 1.25% of Medicare inpatient payments for a 320-bed hospital are about $1 million. Such a hospital will have about $250,000 at risk in the mortality domain in FY2014.
Given the role hospitalists play in quality and safety initiatives, and the importance of medical record documentation in defining the risk of mortality and severity of illness, we can be crucial players in how our hospitals perform with regard to mortality.
Focus Areas for Mortality Reduction
Although many hospitalists might think that reducing mortality is like “boiling the ocean,” there are some areas where we can clearly focus our attention. There are four priority areas we should target in the coming years (also see Figure 1):
Reduce harm. This may take the form of reducing hospital-acquired infections, such as catheter-related UTIs, Clostridium difficile, and central-line-associated bloodstream infections, or reducing hospital-acquired VTE, falls, and delirium. Many hospital-acquired conditions have a collection, or bundle, of preventive practices. Hospitalists can work both in an institutional leadership capacity and in the course of daily clinical practice to implement bundles and best practices to reduce patient harm.
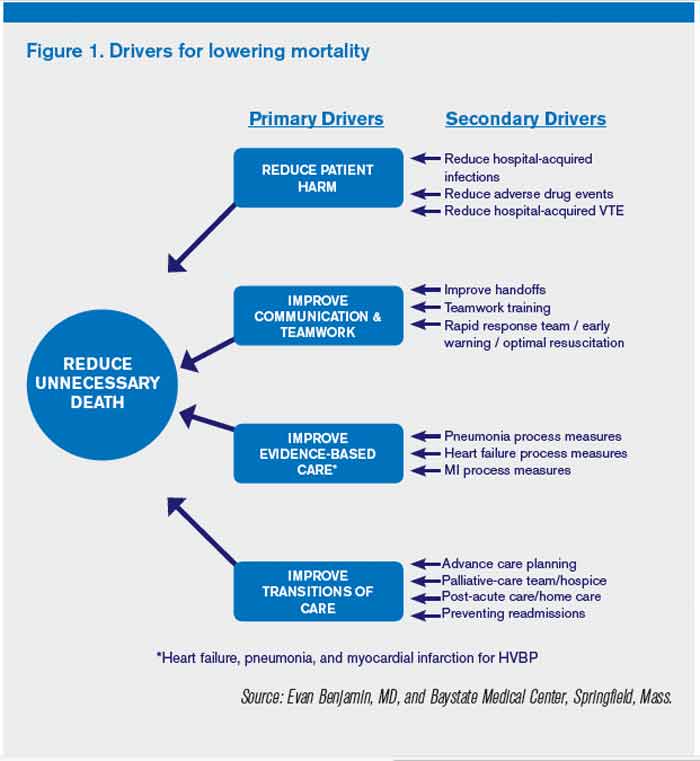
Improve teamwork. With hospitalists, “you started to have teams caring for inpatients in a coordinated way. So I regard this as [hospitalists] coming into their own, their vision of the future starting to really take hold,” said Brent James, coauthor of the recent Institute of Medicine report “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Partly, we’ve accomplished this through simply “showing up” and partly we’ve done it through becoming students of the art and science of teamwork. An example of teamwork training, developed by the Defense Department and the Agency for Healthcare Quality and Research (AHRQ), is TeamSTEPPS, which offers a systematic approach to cooperation, coordination, and communication among team members. Optimal patient resuscitation, in-hospital handoffs, rapid-response teams, and early-warning systems are essential pieces of teamwork that may reduce mortality.
Improve evidence-based care. This domain covers process measures aimed at optimizing care, including reducing mortality. For HVBP in particular, myocardial infarction, heart failure, and pneumonia are the focus.
Improve transitions of care. Best practices for care transitions and reducing readmissions, including advance-care planning, involvement of palliative care and hospice, and coordination with post-acute care, can be a key part of reducing 30-day mortality.
Documentation Integrity
Accurately capturing a patient’s condition in the medical record is crucial to assigning severity of illness and risk of mortality. Because mortality rates are severity-adjusted, accurate documentation is another important dimension to potentially improving a hospital’s performance with regard to the mortality domain. This is one more reason to work closely with your hospital’s documentation specialists.
Don’t Be Afraid...
Proponents of mortality as a quality measure point to it as the ultimate reflection of the care provided. While moving the needle might seem like a task too big to undertake, a disciplined approach to the elements of the driver diagram combined with a robust documentation program can provide your institution with a tangible focus on this definitive measure.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
—Blue Oyster Cult
The designers of the hospital value-based purchasing (HVBP) program sought to include outcomes measures in 2014, and when they did, mortality was their choice. Specifically, HVBP for fiscal-year 2014 (starting October 2013) will include 30-day mortality rates for myocardial infarction, heart failure, and pneumonia. The weighting for the mortality domain will be 25% (see Table 1).
To review the requirements for the HVBP program in FY2014: All hospitals will have 1.25% of their Medicare inpatient payments withheld. They can earn back none, some, all, or an amount in excess of the 1.25%, depending on performance in the performance domains. To put it in perspective, 1.25% of Medicare inpatient payments for a 320-bed hospital are about $1 million. Such a hospital will have about $250,000 at risk in the mortality domain in FY2014.
Given the role hospitalists play in quality and safety initiatives, and the importance of medical record documentation in defining the risk of mortality and severity of illness, we can be crucial players in how our hospitals perform with regard to mortality.
Focus Areas for Mortality Reduction
Although many hospitalists might think that reducing mortality is like “boiling the ocean,” there are some areas where we can clearly focus our attention. There are four priority areas we should target in the coming years (also see Figure 1):
Reduce harm. This may take the form of reducing hospital-acquired infections, such as catheter-related UTIs, Clostridium difficile, and central-line-associated bloodstream infections, or reducing hospital-acquired VTE, falls, and delirium. Many hospital-acquired conditions have a collection, or bundle, of preventive practices. Hospitalists can work both in an institutional leadership capacity and in the course of daily clinical practice to implement bundles and best practices to reduce patient harm.
Improve teamwork. With hospitalists, “you started to have teams caring for inpatients in a coordinated way. So I regard this as [hospitalists] coming into their own, their vision of the future starting to really take hold,” said Brent James, coauthor of the recent Institute of Medicine report “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Partly, we’ve accomplished this through simply “showing up” and partly we’ve done it through becoming students of the art and science of teamwork. An example of teamwork training, developed by the Defense Department and the Agency for Healthcare Quality and Research (AHRQ), is TeamSTEPPS, which offers a systematic approach to cooperation, coordination, and communication among team members. Optimal patient resuscitation, in-hospital handoffs, rapid-response teams, and early-warning systems are essential pieces of teamwork that may reduce mortality.
Improve evidence-based care. This domain covers process measures aimed at optimizing care, including reducing mortality. For HVBP in particular, myocardial infarction, heart failure, and pneumonia are the focus.
Improve transitions of care. Best practices for care transitions and reducing readmissions, including advance-care planning, involvement of palliative care and hospice, and coordination with post-acute care, can be a key part of reducing 30-day mortality.
Documentation Integrity
Accurately capturing a patient’s condition in the medical record is crucial to assigning severity of illness and risk of mortality. Because mortality rates are severity-adjusted, accurate documentation is another important dimension to potentially improving a hospital’s performance with regard to the mortality domain. This is one more reason to work closely with your hospital’s documentation specialists.
Don’t Be Afraid...
Proponents of mortality as a quality measure point to it as the ultimate reflection of the care provided. While moving the needle might seem like a task too big to undertake, a disciplined approach to the elements of the driver diagram combined with a robust documentation program can provide your institution with a tangible focus on this definitive measure.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
—Blue Oyster Cult
The designers of the hospital value-based purchasing (HVBP) program sought to include outcomes measures in 2014, and when they did, mortality was their choice. Specifically, HVBP for fiscal-year 2014 (starting October 2013) will include 30-day mortality rates for myocardial infarction, heart failure, and pneumonia. The weighting for the mortality domain will be 25% (see Table 1).
To review the requirements for the HVBP program in FY2014: All hospitals will have 1.25% of their Medicare inpatient payments withheld. They can earn back none, some, all, or an amount in excess of the 1.25%, depending on performance in the performance domains. To put it in perspective, 1.25% of Medicare inpatient payments for a 320-bed hospital are about $1 million. Such a hospital will have about $250,000 at risk in the mortality domain in FY2014.
Given the role hospitalists play in quality and safety initiatives, and the importance of medical record documentation in defining the risk of mortality and severity of illness, we can be crucial players in how our hospitals perform with regard to mortality.
Focus Areas for Mortality Reduction
Although many hospitalists might think that reducing mortality is like “boiling the ocean,” there are some areas where we can clearly focus our attention. There are four priority areas we should target in the coming years (also see Figure 1):
Reduce harm. This may take the form of reducing hospital-acquired infections, such as catheter-related UTIs, Clostridium difficile, and central-line-associated bloodstream infections, or reducing hospital-acquired VTE, falls, and delirium. Many hospital-acquired conditions have a collection, or bundle, of preventive practices. Hospitalists can work both in an institutional leadership capacity and in the course of daily clinical practice to implement bundles and best practices to reduce patient harm.
Improve teamwork. With hospitalists, “you started to have teams caring for inpatients in a coordinated way. So I regard this as [hospitalists] coming into their own, their vision of the future starting to really take hold,” said Brent James, coauthor of the recent Institute of Medicine report “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Partly, we’ve accomplished this through simply “showing up” and partly we’ve done it through becoming students of the art and science of teamwork. An example of teamwork training, developed by the Defense Department and the Agency for Healthcare Quality and Research (AHRQ), is TeamSTEPPS, which offers a systematic approach to cooperation, coordination, and communication among team members. Optimal patient resuscitation, in-hospital handoffs, rapid-response teams, and early-warning systems are essential pieces of teamwork that may reduce mortality.
Improve evidence-based care. This domain covers process measures aimed at optimizing care, including reducing mortality. For HVBP in particular, myocardial infarction, heart failure, and pneumonia are the focus.
Improve transitions of care. Best practices for care transitions and reducing readmissions, including advance-care planning, involvement of palliative care and hospice, and coordination with post-acute care, can be a key part of reducing 30-day mortality.
Documentation Integrity
Accurately capturing a patient’s condition in the medical record is crucial to assigning severity of illness and risk of mortality. Because mortality rates are severity-adjusted, accurate documentation is another important dimension to potentially improving a hospital’s performance with regard to the mortality domain. This is one more reason to work closely with your hospital’s documentation specialists.
Don’t Be Afraid...
Proponents of mortality as a quality measure point to it as the ultimate reflection of the care provided. While moving the needle might seem like a task too big to undertake, a disciplined approach to the elements of the driver diagram combined with a robust documentation program can provide your institution with a tangible focus on this definitive measure.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Cardiologists Help Lower Readmission Rates for Hospitalized Heart Failure Patients
Data reported at the American Heart Association’s scientific sessions in Los Angeles in November suggest that when a cardiologist, rather than a hospitalist, is the attending physician for a hospitalized heart failure patient, readmission is less likely. Casey M. Lawler, MD, FACC, a cardiologist at the Minneapolis Heart Institute, says her center began establishing protocols to improve heart failure readmissions rates five years ago, after determining that many patients did not understand their diagnosis or treatment. “Thus, we became much more involved in post-discharge care,” including the phoning of discharged patients and follow-up with primary-care providers.
When the heart failure patients’ attending physicians were cardiologists, their readmission rate was 16%, versus 27.1% with hospitalists, even though their severity of illness was higher. Length of stay was similar for both groups and total mean costs were higher for the patients managed by cardiologists. “Although these results reveal that specialists have a positive impact on readmission rates, an overhaul to an entire healthcare system’s treatment of [heart failure] patients—from admission to post-discharge follow-up—is required to truly impact preventable readmissions,” Dr. Lawler asserted.
In the Minneapolis study, 65% of the 2,300 heart failure patients were managed by hospitalists, and 35% by cardiologists. A recent national survey of advanced heart failure programs found that cardiologists managed the care of acute HF patients more than 60 percent of the time.2
References
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- The Advisory Board Company. Mastering the cardiovascular care continuum: strategies for bridging divides among providers and across time. The Advisory Board Company website. Available at: http://www.advisory.com/Research/Cardiovascular-Roundtable/Studies/2012/Mastering-the-Cardiovascular-Care-Continuum. Accessed Jan. 8, 2013.
- Misky G, Carlson T, Klem P, et al. Development and implementation of a clinical care pathway for acute VTE reduces hospital utilization and cost at an urban tertiary care center [abstract]. J Hosp Med. 2012;7 Suppl 2:S66-S67.
- Versel N. Health IT holds key to better care integration. Information Week website. Available at: http://www.informationweek.com/healthcare/interoperability/health-it-holds-key-to-better-care-integ/240012443. Accessed Jan. 8, 2013.
- Office of Inspector General. Early Assessment Finds That CMS Faces Obstacles in Overseeing the Medicare EHR Incentive Program. Office of Inspector General website. Available at: https://oig.hhs.gov/oei/reports/oei-05-11-00250.asp. Accessed Jan. 8, 2013.
Data reported at the American Heart Association’s scientific sessions in Los Angeles in November suggest that when a cardiologist, rather than a hospitalist, is the attending physician for a hospitalized heart failure patient, readmission is less likely. Casey M. Lawler, MD, FACC, a cardiologist at the Minneapolis Heart Institute, says her center began establishing protocols to improve heart failure readmissions rates five years ago, after determining that many patients did not understand their diagnosis or treatment. “Thus, we became much more involved in post-discharge care,” including the phoning of discharged patients and follow-up with primary-care providers.
When the heart failure patients’ attending physicians were cardiologists, their readmission rate was 16%, versus 27.1% with hospitalists, even though their severity of illness was higher. Length of stay was similar for both groups and total mean costs were higher for the patients managed by cardiologists. “Although these results reveal that specialists have a positive impact on readmission rates, an overhaul to an entire healthcare system’s treatment of [heart failure] patients—from admission to post-discharge follow-up—is required to truly impact preventable readmissions,” Dr. Lawler asserted.
In the Minneapolis study, 65% of the 2,300 heart failure patients were managed by hospitalists, and 35% by cardiologists. A recent national survey of advanced heart failure programs found that cardiologists managed the care of acute HF patients more than 60 percent of the time.2
References
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- The Advisory Board Company. Mastering the cardiovascular care continuum: strategies for bridging divides among providers and across time. The Advisory Board Company website. Available at: http://www.advisory.com/Research/Cardiovascular-Roundtable/Studies/2012/Mastering-the-Cardiovascular-Care-Continuum. Accessed Jan. 8, 2013.
- Misky G, Carlson T, Klem P, et al. Development and implementation of a clinical care pathway for acute VTE reduces hospital utilization and cost at an urban tertiary care center [abstract]. J Hosp Med. 2012;7 Suppl 2:S66-S67.
- Versel N. Health IT holds key to better care integration. Information Week website. Available at: http://www.informationweek.com/healthcare/interoperability/health-it-holds-key-to-better-care-integ/240012443. Accessed Jan. 8, 2013.
- Office of Inspector General. Early Assessment Finds That CMS Faces Obstacles in Overseeing the Medicare EHR Incentive Program. Office of Inspector General website. Available at: https://oig.hhs.gov/oei/reports/oei-05-11-00250.asp. Accessed Jan. 8, 2013.
Data reported at the American Heart Association’s scientific sessions in Los Angeles in November suggest that when a cardiologist, rather than a hospitalist, is the attending physician for a hospitalized heart failure patient, readmission is less likely. Casey M. Lawler, MD, FACC, a cardiologist at the Minneapolis Heart Institute, says her center began establishing protocols to improve heart failure readmissions rates five years ago, after determining that many patients did not understand their diagnosis or treatment. “Thus, we became much more involved in post-discharge care,” including the phoning of discharged patients and follow-up with primary-care providers.
When the heart failure patients’ attending physicians were cardiologists, their readmission rate was 16%, versus 27.1% with hospitalists, even though their severity of illness was higher. Length of stay was similar for both groups and total mean costs were higher for the patients managed by cardiologists. “Although these results reveal that specialists have a positive impact on readmission rates, an overhaul to an entire healthcare system’s treatment of [heart failure] patients—from admission to post-discharge follow-up—is required to truly impact preventable readmissions,” Dr. Lawler asserted.
In the Minneapolis study, 65% of the 2,300 heart failure patients were managed by hospitalists, and 35% by cardiologists. A recent national survey of advanced heart failure programs found that cardiologists managed the care of acute HF patients more than 60 percent of the time.2
References
- Enguidanos S, Vesper E, Lorenz K. 30-day readmissions among seriously ill older adults. J Palliat Med. 2012;15(12):1356-1361.
- The Advisory Board Company. Mastering the cardiovascular care continuum: strategies for bridging divides among providers and across time. The Advisory Board Company website. Available at: http://www.advisory.com/Research/Cardiovascular-Roundtable/Studies/2012/Mastering-the-Cardiovascular-Care-Continuum. Accessed Jan. 8, 2013.
- Misky G, Carlson T, Klem P, et al. Development and implementation of a clinical care pathway for acute VTE reduces hospital utilization and cost at an urban tertiary care center [abstract]. J Hosp Med. 2012;7 Suppl 2:S66-S67.
- Versel N. Health IT holds key to better care integration. Information Week website. Available at: http://www.informationweek.com/healthcare/interoperability/health-it-holds-key-to-better-care-integ/240012443. Accessed Jan. 8, 2013.
- Office of Inspector General. Early Assessment Finds That CMS Faces Obstacles in Overseeing the Medicare EHR Incentive Program. Office of Inspector General website. Available at: https://oig.hhs.gov/oei/reports/oei-05-11-00250.asp. Accessed Jan. 8, 2013.
ONLINE EXCLUSIVE: American Pain Society Board Member Discusses Opioid Risks, Rewards, and Why Continuing Education is a Must
Click here to listen to Scott Strassels, PhD, PharmD, BCPS, an assistant professor in the College of Pharmacy at the University of Texas at Austin and a board member of the American Pain Society, discuss the risks and rewards of opioid therapies, and why continuing education is important for all clinicians.
Click here to listen to Scott Strassels, PhD, PharmD, BCPS, an assistant professor in the College of Pharmacy at the University of Texas at Austin and a board member of the American Pain Society, discuss the risks and rewards of opioid therapies, and why continuing education is important for all clinicians.
Click here to listen to Scott Strassels, PhD, PharmD, BCPS, an assistant professor in the College of Pharmacy at the University of Texas at Austin and a board member of the American Pain Society, discuss the risks and rewards of opioid therapies, and why continuing education is important for all clinicians.
Quality Improvement Project Helps Hospital Patients Get Needed Prescriptions
A quality-improvement (QI) project to give high-risk patients ready access to prescribed medications at the time of hospital discharge achieved an 86% success rate, according to an abstract poster presented at HM12 in San Diego last April.1
Lead author Elizabeth Le, MD, then a resident at the University of California at San Francisco Medical Center (UCSF) and now a practicing hospitalist at the Veterans Administration Medical Center in Palo Alto, Calif., says the multidisciplinary “brown bag medications” project involved training house staff to recognize patients at risk. Staff meetings and rounds were used to identify appropriate candidates—those with limited mobility or cognitive issues, lacking insurance coverage or financial resources, a history of medication noncompliance, or leaving the hospital against medical advice—as well as those prescribed medications with a greater urgency for administration on schedule, such as anticoagulants or antibiotics.
About one-quarter of patients on the unit where this approach was first tested were found to need the service, which involved faxing prescriptions to an outpatient pharmacy across the street from the hospital for either pick-up by the family or delivery to the patient’s hospital room. For those with financial impediments, hospital social workers and case managers explored other options, including the social work department’s discretionary use fund, to pay for the drugs.
Dr. Le believes the project could be replicated in other facilities that lack access to in-house pharmacy services at discharge. She recommends involving social workers and case managers in the planning.
At UCSF, recent EHR implementation has automated the ordering of medications, but the challenge of recognizing who could benefit from extra help in obtaining their discharge medications remains a critical issue for hospitals trying to bring readmissions under control.
For more information about the brown bag medications program, contact Dr. Le at Elizabeth.Le@va.gov.
References
A quality-improvement (QI) project to give high-risk patients ready access to prescribed medications at the time of hospital discharge achieved an 86% success rate, according to an abstract poster presented at HM12 in San Diego last April.1
Lead author Elizabeth Le, MD, then a resident at the University of California at San Francisco Medical Center (UCSF) and now a practicing hospitalist at the Veterans Administration Medical Center in Palo Alto, Calif., says the multidisciplinary “brown bag medications” project involved training house staff to recognize patients at risk. Staff meetings and rounds were used to identify appropriate candidates—those with limited mobility or cognitive issues, lacking insurance coverage or financial resources, a history of medication noncompliance, or leaving the hospital against medical advice—as well as those prescribed medications with a greater urgency for administration on schedule, such as anticoagulants or antibiotics.
About one-quarter of patients on the unit where this approach was first tested were found to need the service, which involved faxing prescriptions to an outpatient pharmacy across the street from the hospital for either pick-up by the family or delivery to the patient’s hospital room. For those with financial impediments, hospital social workers and case managers explored other options, including the social work department’s discretionary use fund, to pay for the drugs.
Dr. Le believes the project could be replicated in other facilities that lack access to in-house pharmacy services at discharge. She recommends involving social workers and case managers in the planning.
At UCSF, recent EHR implementation has automated the ordering of medications, but the challenge of recognizing who could benefit from extra help in obtaining their discharge medications remains a critical issue for hospitals trying to bring readmissions under control.
For more information about the brown bag medications program, contact Dr. Le at Elizabeth.Le@va.gov.
References
A quality-improvement (QI) project to give high-risk patients ready access to prescribed medications at the time of hospital discharge achieved an 86% success rate, according to an abstract poster presented at HM12 in San Diego last April.1
Lead author Elizabeth Le, MD, then a resident at the University of California at San Francisco Medical Center (UCSF) and now a practicing hospitalist at the Veterans Administration Medical Center in Palo Alto, Calif., says the multidisciplinary “brown bag medications” project involved training house staff to recognize patients at risk. Staff meetings and rounds were used to identify appropriate candidates—those with limited mobility or cognitive issues, lacking insurance coverage or financial resources, a history of medication noncompliance, or leaving the hospital against medical advice—as well as those prescribed medications with a greater urgency for administration on schedule, such as anticoagulants or antibiotics.
About one-quarter of patients on the unit where this approach was first tested were found to need the service, which involved faxing prescriptions to an outpatient pharmacy across the street from the hospital for either pick-up by the family or delivery to the patient’s hospital room. For those with financial impediments, hospital social workers and case managers explored other options, including the social work department’s discretionary use fund, to pay for the drugs.
Dr. Le believes the project could be replicated in other facilities that lack access to in-house pharmacy services at discharge. She recommends involving social workers and case managers in the planning.
At UCSF, recent EHR implementation has automated the ordering of medications, but the challenge of recognizing who could benefit from extra help in obtaining their discharge medications remains a critical issue for hospitals trying to bring readmissions under control.
For more information about the brown bag medications program, contact Dr. Le at Elizabeth.Le@va.gov.
References
Smartphones Distract Hospital Staff on Rounds
Smartphone use by hospitalists and other hospital staff is becoming ubiquitous, with a recent survey showing 72% of physicians using these devices at work.1 At the same time, concerns are being raised about clinical distractions and threats to patient privacy, even while such benefits as rapid access to colleagues, medical references, and patient records are touted.
In a study published in the Journal of Hospital Medicine, Rachel Katz-Sidlow, MD, of the department of pediatrics at Jacobi Medical Center in Bronx, N.Y., and colleagues surveyed residents’ and attendings’ perceptions of the use of smartphones during inpatient rounds, both their own and observed behaviors of colleagues.2 Fifty-seven percent of residents and 28% of faculty reported using smartphones during inpatient rounds, while significantly higher percentages observed other team members doing so.
The most common smartphone uses were for patient care, but doctors also use them to read and reply to personal texts and emails, as well as for non-patient-care-related Web searches. The authors observe that smartphones “introduce another source of interruption, multitasking, and distraction into the hospital environment,” with potential negative consequences.
Nineteen percent of residents believed they had missed important clinical information because of smartphone distraction during rounds. After seeing the survey results, Jacobi Medical Center instituted a smartphone policy in February 2012, essentially requiring personal mobile communication devices to be silenced at the start of rounds, except for patient care communication or urgent family matters, Dr. Katz-Sidlow wrote in an email to the The Hospitalist.
Confirmation of the spread of communication technology in the hospital toward smartphones and away from traditional pagers comes from data presented at the American Academy of Pediatrics conference in New Orleans in October by Stephanie Kuhlmann, MD, pediatric hospitalist at the University of Kansas at Wichita.3 Dr. Kuhlmann conducted an electronic survey of pediatric hospitalists, with 60% reporting that they receive work-related text messages. Twelve percent sent more than 10 text messages per shift, while 40% expressed concern about HIPAA violations. Most text messages are not encrypted, and many hospitals have yet to implement appropriately secure programs and policies, Dr. Kuhlmann says.
“Hospitals need to be aware of this trend and need to find a way to secure these text messages,” she adds.
Another recent survey by the Orem, Utah-based firm KLAS Research found that while 70% of clinicians report using smartphones or tablets to look up electronic patient records, they are less likely to input information into the EHR on these devices because of the difficulty of entering data on their small screens.4
References
- Dolan B. 72 percent of US physicians use smartphones. Mobi Health News website. Available at: http://mobihealthnews.com/7505/72-percent-of-us-physicians-use-smartphones/. Accessed Dec. 8, 2012.
- Katz-Sidlow RJ, Ludwig A, Millers S, Sidlow R. Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595-599.
- Miller NS. Text messages are a growing trend among pediatric hospitalists. Pediatric News Digital Network website. Available at: http://www.pediatricnews.com/news/top-news/single-article/text-messages-are-a-growing-trend-among-pediatric-hospitalists/3dabf7208c75c44d36f368a83221d320.html. Accessed Nov. 1, 2012.
- Westerlind E. Mobile healthcare applications: can enterprise vendors keep up? KLAS website. Available at: http://www.klasresearch.com/KLASreports. Accessed Dec. 8, 2012.
Smartphone use by hospitalists and other hospital staff is becoming ubiquitous, with a recent survey showing 72% of physicians using these devices at work.1 At the same time, concerns are being raised about clinical distractions and threats to patient privacy, even while such benefits as rapid access to colleagues, medical references, and patient records are touted.
In a study published in the Journal of Hospital Medicine, Rachel Katz-Sidlow, MD, of the department of pediatrics at Jacobi Medical Center in Bronx, N.Y., and colleagues surveyed residents’ and attendings’ perceptions of the use of smartphones during inpatient rounds, both their own and observed behaviors of colleagues.2 Fifty-seven percent of residents and 28% of faculty reported using smartphones during inpatient rounds, while significantly higher percentages observed other team members doing so.
The most common smartphone uses were for patient care, but doctors also use them to read and reply to personal texts and emails, as well as for non-patient-care-related Web searches. The authors observe that smartphones “introduce another source of interruption, multitasking, and distraction into the hospital environment,” with potential negative consequences.
Nineteen percent of residents believed they had missed important clinical information because of smartphone distraction during rounds. After seeing the survey results, Jacobi Medical Center instituted a smartphone policy in February 2012, essentially requiring personal mobile communication devices to be silenced at the start of rounds, except for patient care communication or urgent family matters, Dr. Katz-Sidlow wrote in an email to the The Hospitalist.
Confirmation of the spread of communication technology in the hospital toward smartphones and away from traditional pagers comes from data presented at the American Academy of Pediatrics conference in New Orleans in October by Stephanie Kuhlmann, MD, pediatric hospitalist at the University of Kansas at Wichita.3 Dr. Kuhlmann conducted an electronic survey of pediatric hospitalists, with 60% reporting that they receive work-related text messages. Twelve percent sent more than 10 text messages per shift, while 40% expressed concern about HIPAA violations. Most text messages are not encrypted, and many hospitals have yet to implement appropriately secure programs and policies, Dr. Kuhlmann says.
“Hospitals need to be aware of this trend and need to find a way to secure these text messages,” she adds.
Another recent survey by the Orem, Utah-based firm KLAS Research found that while 70% of clinicians report using smartphones or tablets to look up electronic patient records, they are less likely to input information into the EHR on these devices because of the difficulty of entering data on their small screens.4
References
- Dolan B. 72 percent of US physicians use smartphones. Mobi Health News website. Available at: http://mobihealthnews.com/7505/72-percent-of-us-physicians-use-smartphones/. Accessed Dec. 8, 2012.
- Katz-Sidlow RJ, Ludwig A, Millers S, Sidlow R. Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595-599.
- Miller NS. Text messages are a growing trend among pediatric hospitalists. Pediatric News Digital Network website. Available at: http://www.pediatricnews.com/news/top-news/single-article/text-messages-are-a-growing-trend-among-pediatric-hospitalists/3dabf7208c75c44d36f368a83221d320.html. Accessed Nov. 1, 2012.
- Westerlind E. Mobile healthcare applications: can enterprise vendors keep up? KLAS website. Available at: http://www.klasresearch.com/KLASreports. Accessed Dec. 8, 2012.
Smartphone use by hospitalists and other hospital staff is becoming ubiquitous, with a recent survey showing 72% of physicians using these devices at work.1 At the same time, concerns are being raised about clinical distractions and threats to patient privacy, even while such benefits as rapid access to colleagues, medical references, and patient records are touted.
In a study published in the Journal of Hospital Medicine, Rachel Katz-Sidlow, MD, of the department of pediatrics at Jacobi Medical Center in Bronx, N.Y., and colleagues surveyed residents’ and attendings’ perceptions of the use of smartphones during inpatient rounds, both their own and observed behaviors of colleagues.2 Fifty-seven percent of residents and 28% of faculty reported using smartphones during inpatient rounds, while significantly higher percentages observed other team members doing so.
The most common smartphone uses were for patient care, but doctors also use them to read and reply to personal texts and emails, as well as for non-patient-care-related Web searches. The authors observe that smartphones “introduce another source of interruption, multitasking, and distraction into the hospital environment,” with potential negative consequences.
Nineteen percent of residents believed they had missed important clinical information because of smartphone distraction during rounds. After seeing the survey results, Jacobi Medical Center instituted a smartphone policy in February 2012, essentially requiring personal mobile communication devices to be silenced at the start of rounds, except for patient care communication or urgent family matters, Dr. Katz-Sidlow wrote in an email to the The Hospitalist.
Confirmation of the spread of communication technology in the hospital toward smartphones and away from traditional pagers comes from data presented at the American Academy of Pediatrics conference in New Orleans in October by Stephanie Kuhlmann, MD, pediatric hospitalist at the University of Kansas at Wichita.3 Dr. Kuhlmann conducted an electronic survey of pediatric hospitalists, with 60% reporting that they receive work-related text messages. Twelve percent sent more than 10 text messages per shift, while 40% expressed concern about HIPAA violations. Most text messages are not encrypted, and many hospitals have yet to implement appropriately secure programs and policies, Dr. Kuhlmann says.
“Hospitals need to be aware of this trend and need to find a way to secure these text messages,” she adds.
Another recent survey by the Orem, Utah-based firm KLAS Research found that while 70% of clinicians report using smartphones or tablets to look up electronic patient records, they are less likely to input information into the EHR on these devices because of the difficulty of entering data on their small screens.4
References
- Dolan B. 72 percent of US physicians use smartphones. Mobi Health News website. Available at: http://mobihealthnews.com/7505/72-percent-of-us-physicians-use-smartphones/. Accessed Dec. 8, 2012.
- Katz-Sidlow RJ, Ludwig A, Millers S, Sidlow R. Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595-599.
- Miller NS. Text messages are a growing trend among pediatric hospitalists. Pediatric News Digital Network website. Available at: http://www.pediatricnews.com/news/top-news/single-article/text-messages-are-a-growing-trend-among-pediatric-hospitalists/3dabf7208c75c44d36f368a83221d320.html. Accessed Nov. 1, 2012.
- Westerlind E. Mobile healthcare applications: can enterprise vendors keep up? KLAS website. Available at: http://www.klasresearch.com/KLASreports. Accessed Dec. 8, 2012.
Society for Hospital Medicine Compiles List of Don'ts for Hospitalists
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.