User login
EMA panel backs peanut allergy desensitizing powder Palforzia
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
NMOSD challenges in children
, but have led to some uncertainty and confusion as well.
At the2020 CNS-ICNA Conjoint Meeting, held virtually this year, presenters discussed some of the challenges of differential diagnosis and treatment choice in pediatric NMOSD, which is easily confused with multiple sclerosis.
NMOSD used to be considered a monophasic disease restricted to the optic nerve and spinal cord, but is now known to affect other regions of the central nervous system and to relapse in some patients.
Diagnosis
The disease is often mediated by antibodies to the aquaporin-4 (AQP-4) water channel, but about 30% of adult patients lack the antibody, and AQP-4 seronegativity is more common in the pediatric population. Another common antibody found in 40%–50% of children with NMOSD targets myelin oligodendrocyte glycoprotein (MOG).
It is important to be aware that false negatives can occur in serology assays, and false positives are common, particularly in ELISA assays, Silvia N. Tenembaum, MD, said during her presentation. For those reasons, serology is not enough for a diagnosis. “Patients should also have compatible symptoms and MRI findings,” said Dr. Tenembaum, director of the pediatric neuroimmunology program at National Pediatric Hospital in Buenos Aires.
According to international consensus criteria, to be diagnosed with NMOSD, AQP-4 seropositive patients should also have at least one core clinical symptom: optic neuritis, acute myelitis, area postrema syndrome, other acute brainstem syndrome, symptomatic narcolepsy or acute diencephalic clinical syndrome, or symptomatic cerebral syndrome. AQP-4 seronegative patients or with unknown status should have at least two core symptoms, one of which must be optic neuritis, acute myelitis, or area postrema syndrome. Both conventional MRI and advanced new techniques are important for achieving differential diagnosis.
The most common symptom in children is optic neuritis, which occurs in 50%-70% of patients. Cerebral syndromes with or without encephalopathy and large tumefactive white matter lesions are also common, according to Dr. Tenembaum.
There are many conditions that mimic the spinal cord and optic nerve symptoms of NMOSD, which must be ruled out. One example is optic myelopathy and vision loss from late-onset biotinylase deficiency. It is critical to rule that out because it is treatable with supplements. Optic neuropathy, papillitis, and papilledema can also resemble NMOSD.
It is critical to achieve an early diagnosis of NMOSD in children, because some MS drugs can worsen NMOSD, according to Thaís Armangue, MD, PhD, head of neuroimmunology at SJD Barcelona Children’s Hospital, who also presented at the session. She pointed out that the MOG antibody, while common in children, is also associated with many demyelinating diseases. Some 50%-60% of children with acute disseminated encephalomyelitis (ADEM) have high titers of MOG antibodies. Although early studies suggested that persistent anti-MOG antibodies were associated with risk of developing MS, more recent studies show it predicts a non-MS disease course, particularly at titers greater than 1:1280, according to Dr. Tenembaum. Persistent anti-MOG antibodies are also associated with relapsing disease, but it is associated with other syndromes besides NMOSD. “The probability is that [MOG antibodies are] useful, but they cannot guide chronic immunotherapy, because even monophasic patients can last maybe 12 months before they become MOG negative, and we cannot wait so many months” to determine treatment course, said Dr. Tenembaum.
For monophasic ADEM or NMOSD, there is no need for chronic treatment. But children with MS and recurrent NMOSD require early chronic immunotherapy because specific therapies have been shown to improve prognosis.
Acute treatment
When it comes to acute treatment of NMOSD, the goal is to suppress the inflammatory attack but also to minimize long-term damage and optimize long-term neurological function. “The potential for irreversible injury with an attack is very high, and cumulative disabilities in NMOSD can result directly from attacks,” E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children at the University of Toronto, said during her talk.
IV steroids are generally the first choice, with a preference for methylprednisolone. Pediatric patients that are MOG antibody positive usually respond better and more quickly than do adults, with rapid daily improvements in mobility, vomiting, and eyesight. Dr. Yeh recommends weaning good responders off steroids because AQP-4 positive patients are likely to relapse without a steroid wean, and antibody testing may be unavailable or results may be delayed. The wean can range from 4 weeks to 4-6 months, depending on antibody status, likelihood of AQP-4 positivity, and clinical parameters.
Inadequate responses are usually pretty evident. If there is only light perception by day 4 or 5, or paralyzed patients are nonambulatory and achieve only twitchy movements by that time, second-line therapies should be considered, including therapeutic plasma exchange (TPE) with 5-7 exchanges or intravenous immunoglobulins (IVIg).
Dr. Yeh called for quick treatment. Whatever you do, “please do it sooner rather than later if you think there’s no response [to steroids],” Dr. Yeh said.
TPE is the first choice, according to Dr. Yeh. “There seems to be a fair amount of information that suggests that if you’re having difficulty getting a response to steroids, TPE can make a difference in these patients,” she said. But in some cases TPE may not be available, and IVIg can be attempted first. If it achieves no or only marginal improvement, TPE can be attempted later, but it must be kept in mind that TPE conducted too soon could wash out IVIg. Patients who get much better on IVIg can undergo a steroid wean, and then be evaluated for prophylactic therapy, said Dr. Yeh.
The evidence for IVIg is limited, reflecting the difficulty of studying treatments in rare populations. Still, when TPE is not available and the patient is quite impaired, IVIg makes sense to try. “Absence of evidence does not mean that the therapy doesn’t work, and I don’t think we should throw out the baby with the bath water,” said Dr. Yeh.
Although IVIg treatment is generally well tolerated, there have been a few serious adverse events, such as anaphylactic shock and aseptic meningitis, according to Andrea Savransky, MD, a pediatrician at National Pediatric Hospital in Buenos Aires, who also spoke at the session. “I think it is important to weigh the benefits against the risk,” Dr. Savransky said. She noted that TPE should not be taken lightly. One study showed more complications in pediatric patients than in adult patients, and it must be performed in specialized centers.
Emerging treaments
Tanuja Chitnis, MD, director of the Partners Pediatric MS Center at Massachusetts General Hospital, Boston, discussed some of the emerging treatments for pediatric NMOSD. Rituximab has been associated with success in some retrospective studies, but dosing should be personalized. Dr. Chitnis reported that B cells can return before 6 months, so she monitors B cells beginning 2 months after induction, redosing after 4 or 5 months rather than 6 if B cells return.
Nevertheless, relapses can still occur after rituximab therapy. “There is room for additional therapies to address this gap,” said Dr. Chitnis. Three new antibodies have received approval for treatment of NMOSD in adults. These include the complement inhibitor eculizumab, the IL-6 receptor antibody satralizumab, and the anti-CD19 antibody inebilizumab. Phase 3 clinical trials in children have been conducted for eculizumab and are in the planning stage for inebilizumab, and pediatric patients were included in pivotal trials for satralizumab.
Eculizumab treatment resulted in a 94.2% reduction in relapse risk in AQP4-positive adults. Satralizumab showed a 79% reduction in relapse risk among AQP-4 positive subjects with NMOSD or neuromyelitis optica and a 34% reduction in those who were AQP-4 negative. The pediatric subgroup had similar levels of response to adults, though the numbers were too small for a subgroup analysis.
In AQP-4 positive patients, inebilizumab treatment yielded a 77% reduction in relapse rate. In all patients, there was a 73% reduction.
For MOG antibody-positive patients with AQP-4 negative disease, novel therapies are at earlier stages of development. Typical MS therapies such as interferon beta and glatiramer acetate don’t seem to be effective. Some that have shown signs of efficacy include azathioprine, mycophenylate mofetil, rituximab, and IVIg infusion, but the state of the field is not encouraging. “This is an observation now being studied in larger cohorts, but in general I have not found that there’s a very strong response to any of these therapies, possibly with the exception of IVIg,” said Dr. Chitnis.
Dr. Tenembaum has no relevant financial disclosures. Dr. Armangue has received speaking honoraria from Novartis and travel expenses for scientific meetings from Merck, Biogen, and Roche. Dr. Yeh is on the scientific advisory board of Juno Therapeutics and has received research support from Biogen. Dr. Chitnis advises Biogen-Idec, Novartis, and Alexion, serves on clinical trial advisory boards for Novartis and Sanofi Aventis, and has received research support from Verily, EMD Serono, and Novartis. Dr. Savransky has received honoraria from Genzyme de Argentina SA.
, but have led to some uncertainty and confusion as well.
At the2020 CNS-ICNA Conjoint Meeting, held virtually this year, presenters discussed some of the challenges of differential diagnosis and treatment choice in pediatric NMOSD, which is easily confused with multiple sclerosis.
NMOSD used to be considered a monophasic disease restricted to the optic nerve and spinal cord, but is now known to affect other regions of the central nervous system and to relapse in some patients.
Diagnosis
The disease is often mediated by antibodies to the aquaporin-4 (AQP-4) water channel, but about 30% of adult patients lack the antibody, and AQP-4 seronegativity is more common in the pediatric population. Another common antibody found in 40%–50% of children with NMOSD targets myelin oligodendrocyte glycoprotein (MOG).
It is important to be aware that false negatives can occur in serology assays, and false positives are common, particularly in ELISA assays, Silvia N. Tenembaum, MD, said during her presentation. For those reasons, serology is not enough for a diagnosis. “Patients should also have compatible symptoms and MRI findings,” said Dr. Tenembaum, director of the pediatric neuroimmunology program at National Pediatric Hospital in Buenos Aires.
According to international consensus criteria, to be diagnosed with NMOSD, AQP-4 seropositive patients should also have at least one core clinical symptom: optic neuritis, acute myelitis, area postrema syndrome, other acute brainstem syndrome, symptomatic narcolepsy or acute diencephalic clinical syndrome, or symptomatic cerebral syndrome. AQP-4 seronegative patients or with unknown status should have at least two core symptoms, one of which must be optic neuritis, acute myelitis, or area postrema syndrome. Both conventional MRI and advanced new techniques are important for achieving differential diagnosis.
The most common symptom in children is optic neuritis, which occurs in 50%-70% of patients. Cerebral syndromes with or without encephalopathy and large tumefactive white matter lesions are also common, according to Dr. Tenembaum.
There are many conditions that mimic the spinal cord and optic nerve symptoms of NMOSD, which must be ruled out. One example is optic myelopathy and vision loss from late-onset biotinylase deficiency. It is critical to rule that out because it is treatable with supplements. Optic neuropathy, papillitis, and papilledema can also resemble NMOSD.
It is critical to achieve an early diagnosis of NMOSD in children, because some MS drugs can worsen NMOSD, according to Thaís Armangue, MD, PhD, head of neuroimmunology at SJD Barcelona Children’s Hospital, who also presented at the session. She pointed out that the MOG antibody, while common in children, is also associated with many demyelinating diseases. Some 50%-60% of children with acute disseminated encephalomyelitis (ADEM) have high titers of MOG antibodies. Although early studies suggested that persistent anti-MOG antibodies were associated with risk of developing MS, more recent studies show it predicts a non-MS disease course, particularly at titers greater than 1:1280, according to Dr. Tenembaum. Persistent anti-MOG antibodies are also associated with relapsing disease, but it is associated with other syndromes besides NMOSD. “The probability is that [MOG antibodies are] useful, but they cannot guide chronic immunotherapy, because even monophasic patients can last maybe 12 months before they become MOG negative, and we cannot wait so many months” to determine treatment course, said Dr. Tenembaum.
For monophasic ADEM or NMOSD, there is no need for chronic treatment. But children with MS and recurrent NMOSD require early chronic immunotherapy because specific therapies have been shown to improve prognosis.
Acute treatment
When it comes to acute treatment of NMOSD, the goal is to suppress the inflammatory attack but also to minimize long-term damage and optimize long-term neurological function. “The potential for irreversible injury with an attack is very high, and cumulative disabilities in NMOSD can result directly from attacks,” E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children at the University of Toronto, said during her talk.
IV steroids are generally the first choice, with a preference for methylprednisolone. Pediatric patients that are MOG antibody positive usually respond better and more quickly than do adults, with rapid daily improvements in mobility, vomiting, and eyesight. Dr. Yeh recommends weaning good responders off steroids because AQP-4 positive patients are likely to relapse without a steroid wean, and antibody testing may be unavailable or results may be delayed. The wean can range from 4 weeks to 4-6 months, depending on antibody status, likelihood of AQP-4 positivity, and clinical parameters.
Inadequate responses are usually pretty evident. If there is only light perception by day 4 or 5, or paralyzed patients are nonambulatory and achieve only twitchy movements by that time, second-line therapies should be considered, including therapeutic plasma exchange (TPE) with 5-7 exchanges or intravenous immunoglobulins (IVIg).
Dr. Yeh called for quick treatment. Whatever you do, “please do it sooner rather than later if you think there’s no response [to steroids],” Dr. Yeh said.
TPE is the first choice, according to Dr. Yeh. “There seems to be a fair amount of information that suggests that if you’re having difficulty getting a response to steroids, TPE can make a difference in these patients,” she said. But in some cases TPE may not be available, and IVIg can be attempted first. If it achieves no or only marginal improvement, TPE can be attempted later, but it must be kept in mind that TPE conducted too soon could wash out IVIg. Patients who get much better on IVIg can undergo a steroid wean, and then be evaluated for prophylactic therapy, said Dr. Yeh.
The evidence for IVIg is limited, reflecting the difficulty of studying treatments in rare populations. Still, when TPE is not available and the patient is quite impaired, IVIg makes sense to try. “Absence of evidence does not mean that the therapy doesn’t work, and I don’t think we should throw out the baby with the bath water,” said Dr. Yeh.
Although IVIg treatment is generally well tolerated, there have been a few serious adverse events, such as anaphylactic shock and aseptic meningitis, according to Andrea Savransky, MD, a pediatrician at National Pediatric Hospital in Buenos Aires, who also spoke at the session. “I think it is important to weigh the benefits against the risk,” Dr. Savransky said. She noted that TPE should not be taken lightly. One study showed more complications in pediatric patients than in adult patients, and it must be performed in specialized centers.
Emerging treaments
Tanuja Chitnis, MD, director of the Partners Pediatric MS Center at Massachusetts General Hospital, Boston, discussed some of the emerging treatments for pediatric NMOSD. Rituximab has been associated with success in some retrospective studies, but dosing should be personalized. Dr. Chitnis reported that B cells can return before 6 months, so she monitors B cells beginning 2 months after induction, redosing after 4 or 5 months rather than 6 if B cells return.
Nevertheless, relapses can still occur after rituximab therapy. “There is room for additional therapies to address this gap,” said Dr. Chitnis. Three new antibodies have received approval for treatment of NMOSD in adults. These include the complement inhibitor eculizumab, the IL-6 receptor antibody satralizumab, and the anti-CD19 antibody inebilizumab. Phase 3 clinical trials in children have been conducted for eculizumab and are in the planning stage for inebilizumab, and pediatric patients were included in pivotal trials for satralizumab.
Eculizumab treatment resulted in a 94.2% reduction in relapse risk in AQP4-positive adults. Satralizumab showed a 79% reduction in relapse risk among AQP-4 positive subjects with NMOSD or neuromyelitis optica and a 34% reduction in those who were AQP-4 negative. The pediatric subgroup had similar levels of response to adults, though the numbers were too small for a subgroup analysis.
In AQP-4 positive patients, inebilizumab treatment yielded a 77% reduction in relapse rate. In all patients, there was a 73% reduction.
For MOG antibody-positive patients with AQP-4 negative disease, novel therapies are at earlier stages of development. Typical MS therapies such as interferon beta and glatiramer acetate don’t seem to be effective. Some that have shown signs of efficacy include azathioprine, mycophenylate mofetil, rituximab, and IVIg infusion, but the state of the field is not encouraging. “This is an observation now being studied in larger cohorts, but in general I have not found that there’s a very strong response to any of these therapies, possibly with the exception of IVIg,” said Dr. Chitnis.
Dr. Tenembaum has no relevant financial disclosures. Dr. Armangue has received speaking honoraria from Novartis and travel expenses for scientific meetings from Merck, Biogen, and Roche. Dr. Yeh is on the scientific advisory board of Juno Therapeutics and has received research support from Biogen. Dr. Chitnis advises Biogen-Idec, Novartis, and Alexion, serves on clinical trial advisory boards for Novartis and Sanofi Aventis, and has received research support from Verily, EMD Serono, and Novartis. Dr. Savransky has received honoraria from Genzyme de Argentina SA.
, but have led to some uncertainty and confusion as well.
At the2020 CNS-ICNA Conjoint Meeting, held virtually this year, presenters discussed some of the challenges of differential diagnosis and treatment choice in pediatric NMOSD, which is easily confused with multiple sclerosis.
NMOSD used to be considered a monophasic disease restricted to the optic nerve and spinal cord, but is now known to affect other regions of the central nervous system and to relapse in some patients.
Diagnosis
The disease is often mediated by antibodies to the aquaporin-4 (AQP-4) water channel, but about 30% of adult patients lack the antibody, and AQP-4 seronegativity is more common in the pediatric population. Another common antibody found in 40%–50% of children with NMOSD targets myelin oligodendrocyte glycoprotein (MOG).
It is important to be aware that false negatives can occur in serology assays, and false positives are common, particularly in ELISA assays, Silvia N. Tenembaum, MD, said during her presentation. For those reasons, serology is not enough for a diagnosis. “Patients should also have compatible symptoms and MRI findings,” said Dr. Tenembaum, director of the pediatric neuroimmunology program at National Pediatric Hospital in Buenos Aires.
According to international consensus criteria, to be diagnosed with NMOSD, AQP-4 seropositive patients should also have at least one core clinical symptom: optic neuritis, acute myelitis, area postrema syndrome, other acute brainstem syndrome, symptomatic narcolepsy or acute diencephalic clinical syndrome, or symptomatic cerebral syndrome. AQP-4 seronegative patients or with unknown status should have at least two core symptoms, one of which must be optic neuritis, acute myelitis, or area postrema syndrome. Both conventional MRI and advanced new techniques are important for achieving differential diagnosis.
The most common symptom in children is optic neuritis, which occurs in 50%-70% of patients. Cerebral syndromes with or without encephalopathy and large tumefactive white matter lesions are also common, according to Dr. Tenembaum.
There are many conditions that mimic the spinal cord and optic nerve symptoms of NMOSD, which must be ruled out. One example is optic myelopathy and vision loss from late-onset biotinylase deficiency. It is critical to rule that out because it is treatable with supplements. Optic neuropathy, papillitis, and papilledema can also resemble NMOSD.
It is critical to achieve an early diagnosis of NMOSD in children, because some MS drugs can worsen NMOSD, according to Thaís Armangue, MD, PhD, head of neuroimmunology at SJD Barcelona Children’s Hospital, who also presented at the session. She pointed out that the MOG antibody, while common in children, is also associated with many demyelinating diseases. Some 50%-60% of children with acute disseminated encephalomyelitis (ADEM) have high titers of MOG antibodies. Although early studies suggested that persistent anti-MOG antibodies were associated with risk of developing MS, more recent studies show it predicts a non-MS disease course, particularly at titers greater than 1:1280, according to Dr. Tenembaum. Persistent anti-MOG antibodies are also associated with relapsing disease, but it is associated with other syndromes besides NMOSD. “The probability is that [MOG antibodies are] useful, but they cannot guide chronic immunotherapy, because even monophasic patients can last maybe 12 months before they become MOG negative, and we cannot wait so many months” to determine treatment course, said Dr. Tenembaum.
For monophasic ADEM or NMOSD, there is no need for chronic treatment. But children with MS and recurrent NMOSD require early chronic immunotherapy because specific therapies have been shown to improve prognosis.
Acute treatment
When it comes to acute treatment of NMOSD, the goal is to suppress the inflammatory attack but also to minimize long-term damage and optimize long-term neurological function. “The potential for irreversible injury with an attack is very high, and cumulative disabilities in NMOSD can result directly from attacks,” E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children at the University of Toronto, said during her talk.
IV steroids are generally the first choice, with a preference for methylprednisolone. Pediatric patients that are MOG antibody positive usually respond better and more quickly than do adults, with rapid daily improvements in mobility, vomiting, and eyesight. Dr. Yeh recommends weaning good responders off steroids because AQP-4 positive patients are likely to relapse without a steroid wean, and antibody testing may be unavailable or results may be delayed. The wean can range from 4 weeks to 4-6 months, depending on antibody status, likelihood of AQP-4 positivity, and clinical parameters.
Inadequate responses are usually pretty evident. If there is only light perception by day 4 or 5, or paralyzed patients are nonambulatory and achieve only twitchy movements by that time, second-line therapies should be considered, including therapeutic plasma exchange (TPE) with 5-7 exchanges or intravenous immunoglobulins (IVIg).
Dr. Yeh called for quick treatment. Whatever you do, “please do it sooner rather than later if you think there’s no response [to steroids],” Dr. Yeh said.
TPE is the first choice, according to Dr. Yeh. “There seems to be a fair amount of information that suggests that if you’re having difficulty getting a response to steroids, TPE can make a difference in these patients,” she said. But in some cases TPE may not be available, and IVIg can be attempted first. If it achieves no or only marginal improvement, TPE can be attempted later, but it must be kept in mind that TPE conducted too soon could wash out IVIg. Patients who get much better on IVIg can undergo a steroid wean, and then be evaluated for prophylactic therapy, said Dr. Yeh.
The evidence for IVIg is limited, reflecting the difficulty of studying treatments in rare populations. Still, when TPE is not available and the patient is quite impaired, IVIg makes sense to try. “Absence of evidence does not mean that the therapy doesn’t work, and I don’t think we should throw out the baby with the bath water,” said Dr. Yeh.
Although IVIg treatment is generally well tolerated, there have been a few serious adverse events, such as anaphylactic shock and aseptic meningitis, according to Andrea Savransky, MD, a pediatrician at National Pediatric Hospital in Buenos Aires, who also spoke at the session. “I think it is important to weigh the benefits against the risk,” Dr. Savransky said. She noted that TPE should not be taken lightly. One study showed more complications in pediatric patients than in adult patients, and it must be performed in specialized centers.
Emerging treaments
Tanuja Chitnis, MD, director of the Partners Pediatric MS Center at Massachusetts General Hospital, Boston, discussed some of the emerging treatments for pediatric NMOSD. Rituximab has been associated with success in some retrospective studies, but dosing should be personalized. Dr. Chitnis reported that B cells can return before 6 months, so she monitors B cells beginning 2 months after induction, redosing after 4 or 5 months rather than 6 if B cells return.
Nevertheless, relapses can still occur after rituximab therapy. “There is room for additional therapies to address this gap,” said Dr. Chitnis. Three new antibodies have received approval for treatment of NMOSD in adults. These include the complement inhibitor eculizumab, the IL-6 receptor antibody satralizumab, and the anti-CD19 antibody inebilizumab. Phase 3 clinical trials in children have been conducted for eculizumab and are in the planning stage for inebilizumab, and pediatric patients were included in pivotal trials for satralizumab.
Eculizumab treatment resulted in a 94.2% reduction in relapse risk in AQP4-positive adults. Satralizumab showed a 79% reduction in relapse risk among AQP-4 positive subjects with NMOSD or neuromyelitis optica and a 34% reduction in those who were AQP-4 negative. The pediatric subgroup had similar levels of response to adults, though the numbers were too small for a subgroup analysis.
In AQP-4 positive patients, inebilizumab treatment yielded a 77% reduction in relapse rate. In all patients, there was a 73% reduction.
For MOG antibody-positive patients with AQP-4 negative disease, novel therapies are at earlier stages of development. Typical MS therapies such as interferon beta and glatiramer acetate don’t seem to be effective. Some that have shown signs of efficacy include azathioprine, mycophenylate mofetil, rituximab, and IVIg infusion, but the state of the field is not encouraging. “This is an observation now being studied in larger cohorts, but in general I have not found that there’s a very strong response to any of these therapies, possibly with the exception of IVIg,” said Dr. Chitnis.
Dr. Tenembaum has no relevant financial disclosures. Dr. Armangue has received speaking honoraria from Novartis and travel expenses for scientific meetings from Merck, Biogen, and Roche. Dr. Yeh is on the scientific advisory board of Juno Therapeutics and has received research support from Biogen. Dr. Chitnis advises Biogen-Idec, Novartis, and Alexion, serves on clinical trial advisory boards for Novartis and Sanofi Aventis, and has received research support from Verily, EMD Serono, and Novartis. Dr. Savransky has received honoraria from Genzyme de Argentina SA.
FROM CNS-ICNA 2020
Worldwide measles vaccination is flagging
After almost 2 decades of progress, the global state of measles vaccination and measles mortality is deteriorating.
One of the most serious concerns of measles infection is its long-term neurological complications, including the fatal subacute sclerosing panencephalitis (SSPE) and measles inclusion-body encephalitis (MIBE), which is usually seen in immune deficient children. Although some efforts are being made to determine which patients might be most vulnerable to these outcomes, and to treat them, the best approach is still prevention and vaccination, according to Banu Anlar, MD, of Hacettepe University, Ankara, Turkey, who spoke during a session at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
Worldwide vaccination strategies have slipped in recent years, leading to upticks in measles cases and vaccination rates. As a result, in 2018 the World Health Organization postponed its goal of eliminating measles by 2020. Future eradication goals will likely need to be modified, according to Anaita Udwadia Hegde MD, a pediatric neurologist in Mumbai, India, who also presented at the session.
After measles deaths dropped 74% between 2000 and 2010, coinciding with widespread increases in vaccination, the WHO felt emboldened to deal the disease a knockout blow. In 2010, it held a Global Technical Consultation to determine the feasibility of an eradication campaign, which concluded it should be possible by 2020. Several characteristics of measles made that a reasonable goal: It is passed only among humans, with no known animal reservoir; natural infection grants lifelong immunity; there is only one serotype; the virus is genetically stable; the vaccine is safe and leads to 95%-97% seroconversion after two doses, which provides long-term protection against known genotypes; the disease is easily recognized and tested for; and it had been successfully eliminated already in some regions of the world.
As of 2017, analyses showed that the vaccination program saved the lives of about 1.5 million children. That was a cause for celebration, but the goal of eradication has remained elusive. Vaccination rates have trailed targets. In 2018, UNICEF and WHO estimated that 86% of children globally received the first measles vaccine, unchanged from 2010 and below the goal of 95%. Only 69% of children received the second dose, below the goal of 80%. Four countries in Europe lost their measles elimination status in 2018.
Other attempts to eradicate diseases have met with mixed results. The only full success was smallpox, eliminated in 1977. Similar efforts with polio, malaria, guinea worm, and now measles have all come up short. Those failures could complicate future efforts because global agencies and donors may be leery of past failures because of potential harm to their reputations, according to Dr. Hegde.
Such programs require sustained financial commitment and political support as well as local trust. Nevertheless, they must continue for ethical reasons, said Dr. Hegde, but also for economic ones: Every $1 spent on vaccination programs saves $58 in future costs in low- and middle-income countries. Missed childhood vaccination also results in future vulnerable teenagers and young adults, and these populations are much harder to reach and can drive large outbreaks.
Several factors are contributing to the global regression in vaccine coverage, according to Kristen Feemster, MD, MPH, a pediatric infectious disease physician and the global director of medical affairs at Merck. Globalization has enabled the spread of the disease. Most cases in the United States are imported by travelers to countries where the disease is endemic. “Measles can happen anywhere in the world, and when it does it can travel and spread. If you have an unvaccinated traveler who is exposed to measles abroad, they can return home and spread it to anyone else who is unvaccinated or not otherwise immune. When we see cases they’ve been sporadic, but if you return to a community where immunization rates are low, you have the potential for more sustained spread,” Dr. Feemster said during her presentation.
Why are so many travelers unvaccinated? A key reason is that vaccine hesitance is growing. Most affected individuals involved in outbreaks are unvaccinated, usually by choice rather than for medical reasons. Concerns continue over the measles vaccine and autism, growing out of the debunked studies of Andrew Wakefield. In one example, a Somali community in Minnesota experienced a higher than usual number of autism cases and parents sought reasons to explain it. They discovered the supposed connection between vaccination and autism, and Wakefield himself met with a group of them. The result was a drop in vaccination and, in 2011 and 2017, sizable measles outbreaks.
2020 has of course brought a fresh challenge to measles vaccine with the COVID-19 pandemic, which has reduced access to health care and shifted scientific and health care interest away from measles and other vaccine-preventable diseases. On the positive side, social distancing, mask wearing, and restricted movement are likely reducing exposure to measles, but reduced vaccination rates are likely to result in future outbreaks. “There’s been a significant decrease in rates for routine immunizations globally, so there’s a potential for yet another resurgence of measles and other vaccine-preventable diseases,” said Dr. Feemster.
Dr. Feemster is an employee of Merck. Dr. Anlar and Dr. Hegde did not disclose any relevant financial relationships.
After almost 2 decades of progress, the global state of measles vaccination and measles mortality is deteriorating.
One of the most serious concerns of measles infection is its long-term neurological complications, including the fatal subacute sclerosing panencephalitis (SSPE) and measles inclusion-body encephalitis (MIBE), which is usually seen in immune deficient children. Although some efforts are being made to determine which patients might be most vulnerable to these outcomes, and to treat them, the best approach is still prevention and vaccination, according to Banu Anlar, MD, of Hacettepe University, Ankara, Turkey, who spoke during a session at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
Worldwide vaccination strategies have slipped in recent years, leading to upticks in measles cases and vaccination rates. As a result, in 2018 the World Health Organization postponed its goal of eliminating measles by 2020. Future eradication goals will likely need to be modified, according to Anaita Udwadia Hegde MD, a pediatric neurologist in Mumbai, India, who also presented at the session.
After measles deaths dropped 74% between 2000 and 2010, coinciding with widespread increases in vaccination, the WHO felt emboldened to deal the disease a knockout blow. In 2010, it held a Global Technical Consultation to determine the feasibility of an eradication campaign, which concluded it should be possible by 2020. Several characteristics of measles made that a reasonable goal: It is passed only among humans, with no known animal reservoir; natural infection grants lifelong immunity; there is only one serotype; the virus is genetically stable; the vaccine is safe and leads to 95%-97% seroconversion after two doses, which provides long-term protection against known genotypes; the disease is easily recognized and tested for; and it had been successfully eliminated already in some regions of the world.
As of 2017, analyses showed that the vaccination program saved the lives of about 1.5 million children. That was a cause for celebration, but the goal of eradication has remained elusive. Vaccination rates have trailed targets. In 2018, UNICEF and WHO estimated that 86% of children globally received the first measles vaccine, unchanged from 2010 and below the goal of 95%. Only 69% of children received the second dose, below the goal of 80%. Four countries in Europe lost their measles elimination status in 2018.
Other attempts to eradicate diseases have met with mixed results. The only full success was smallpox, eliminated in 1977. Similar efforts with polio, malaria, guinea worm, and now measles have all come up short. Those failures could complicate future efforts because global agencies and donors may be leery of past failures because of potential harm to their reputations, according to Dr. Hegde.
Such programs require sustained financial commitment and political support as well as local trust. Nevertheless, they must continue for ethical reasons, said Dr. Hegde, but also for economic ones: Every $1 spent on vaccination programs saves $58 in future costs in low- and middle-income countries. Missed childhood vaccination also results in future vulnerable teenagers and young adults, and these populations are much harder to reach and can drive large outbreaks.
Several factors are contributing to the global regression in vaccine coverage, according to Kristen Feemster, MD, MPH, a pediatric infectious disease physician and the global director of medical affairs at Merck. Globalization has enabled the spread of the disease. Most cases in the United States are imported by travelers to countries where the disease is endemic. “Measles can happen anywhere in the world, and when it does it can travel and spread. If you have an unvaccinated traveler who is exposed to measles abroad, they can return home and spread it to anyone else who is unvaccinated or not otherwise immune. When we see cases they’ve been sporadic, but if you return to a community where immunization rates are low, you have the potential for more sustained spread,” Dr. Feemster said during her presentation.
Why are so many travelers unvaccinated? A key reason is that vaccine hesitance is growing. Most affected individuals involved in outbreaks are unvaccinated, usually by choice rather than for medical reasons. Concerns continue over the measles vaccine and autism, growing out of the debunked studies of Andrew Wakefield. In one example, a Somali community in Minnesota experienced a higher than usual number of autism cases and parents sought reasons to explain it. They discovered the supposed connection between vaccination and autism, and Wakefield himself met with a group of them. The result was a drop in vaccination and, in 2011 and 2017, sizable measles outbreaks.
2020 has of course brought a fresh challenge to measles vaccine with the COVID-19 pandemic, which has reduced access to health care and shifted scientific and health care interest away from measles and other vaccine-preventable diseases. On the positive side, social distancing, mask wearing, and restricted movement are likely reducing exposure to measles, but reduced vaccination rates are likely to result in future outbreaks. “There’s been a significant decrease in rates for routine immunizations globally, so there’s a potential for yet another resurgence of measles and other vaccine-preventable diseases,” said Dr. Feemster.
Dr. Feemster is an employee of Merck. Dr. Anlar and Dr. Hegde did not disclose any relevant financial relationships.
After almost 2 decades of progress, the global state of measles vaccination and measles mortality is deteriorating.
One of the most serious concerns of measles infection is its long-term neurological complications, including the fatal subacute sclerosing panencephalitis (SSPE) and measles inclusion-body encephalitis (MIBE), which is usually seen in immune deficient children. Although some efforts are being made to determine which patients might be most vulnerable to these outcomes, and to treat them, the best approach is still prevention and vaccination, according to Banu Anlar, MD, of Hacettepe University, Ankara, Turkey, who spoke during a session at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
Worldwide vaccination strategies have slipped in recent years, leading to upticks in measles cases and vaccination rates. As a result, in 2018 the World Health Organization postponed its goal of eliminating measles by 2020. Future eradication goals will likely need to be modified, according to Anaita Udwadia Hegde MD, a pediatric neurologist in Mumbai, India, who also presented at the session.
After measles deaths dropped 74% between 2000 and 2010, coinciding with widespread increases in vaccination, the WHO felt emboldened to deal the disease a knockout blow. In 2010, it held a Global Technical Consultation to determine the feasibility of an eradication campaign, which concluded it should be possible by 2020. Several characteristics of measles made that a reasonable goal: It is passed only among humans, with no known animal reservoir; natural infection grants lifelong immunity; there is only one serotype; the virus is genetically stable; the vaccine is safe and leads to 95%-97% seroconversion after two doses, which provides long-term protection against known genotypes; the disease is easily recognized and tested for; and it had been successfully eliminated already in some regions of the world.
As of 2017, analyses showed that the vaccination program saved the lives of about 1.5 million children. That was a cause for celebration, but the goal of eradication has remained elusive. Vaccination rates have trailed targets. In 2018, UNICEF and WHO estimated that 86% of children globally received the first measles vaccine, unchanged from 2010 and below the goal of 95%. Only 69% of children received the second dose, below the goal of 80%. Four countries in Europe lost their measles elimination status in 2018.
Other attempts to eradicate diseases have met with mixed results. The only full success was smallpox, eliminated in 1977. Similar efforts with polio, malaria, guinea worm, and now measles have all come up short. Those failures could complicate future efforts because global agencies and donors may be leery of past failures because of potential harm to their reputations, according to Dr. Hegde.
Such programs require sustained financial commitment and political support as well as local trust. Nevertheless, they must continue for ethical reasons, said Dr. Hegde, but also for economic ones: Every $1 spent on vaccination programs saves $58 in future costs in low- and middle-income countries. Missed childhood vaccination also results in future vulnerable teenagers and young adults, and these populations are much harder to reach and can drive large outbreaks.
Several factors are contributing to the global regression in vaccine coverage, according to Kristen Feemster, MD, MPH, a pediatric infectious disease physician and the global director of medical affairs at Merck. Globalization has enabled the spread of the disease. Most cases in the United States are imported by travelers to countries where the disease is endemic. “Measles can happen anywhere in the world, and when it does it can travel and spread. If you have an unvaccinated traveler who is exposed to measles abroad, they can return home and spread it to anyone else who is unvaccinated or not otherwise immune. When we see cases they’ve been sporadic, but if you return to a community where immunization rates are low, you have the potential for more sustained spread,” Dr. Feemster said during her presentation.
Why are so many travelers unvaccinated? A key reason is that vaccine hesitance is growing. Most affected individuals involved in outbreaks are unvaccinated, usually by choice rather than for medical reasons. Concerns continue over the measles vaccine and autism, growing out of the debunked studies of Andrew Wakefield. In one example, a Somali community in Minnesota experienced a higher than usual number of autism cases and parents sought reasons to explain it. They discovered the supposed connection between vaccination and autism, and Wakefield himself met with a group of them. The result was a drop in vaccination and, in 2011 and 2017, sizable measles outbreaks.
2020 has of course brought a fresh challenge to measles vaccine with the COVID-19 pandemic, which has reduced access to health care and shifted scientific and health care interest away from measles and other vaccine-preventable diseases. On the positive side, social distancing, mask wearing, and restricted movement are likely reducing exposure to measles, but reduced vaccination rates are likely to result in future outbreaks. “There’s been a significant decrease in rates for routine immunizations globally, so there’s a potential for yet another resurgence of measles and other vaccine-preventable diseases,” said Dr. Feemster.
Dr. Feemster is an employee of Merck. Dr. Anlar and Dr. Hegde did not disclose any relevant financial relationships.
FROM CNS-ICNA 2020
Latest week brings 44,000 more children with COVID-19
in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
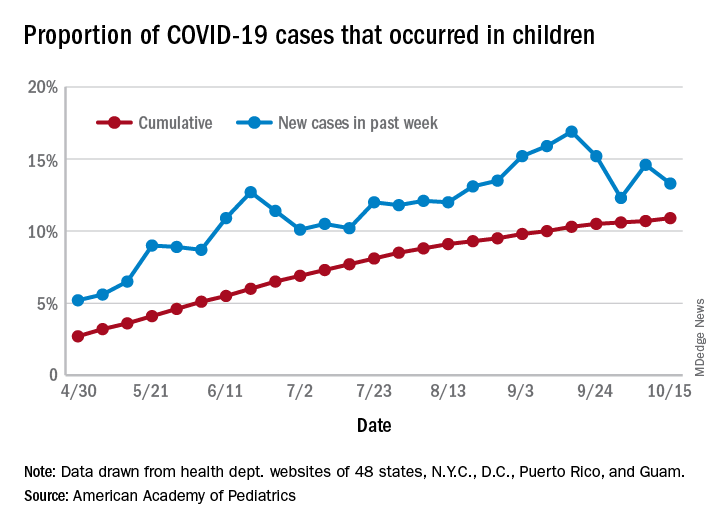
The total number of COVID-19 cases among children was 741,891 as of Oct. 15, which puts the cumulative proportion at 10.9% of the 6.8 million cases reported in all ages by 49 states (New York does not report ages), the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly COVID-19 report.
The 44,258 new cases in children represented 13.3% of all cases reported during the week ending Oct. 15, down from 14.6% the previous week (children make up almost 23% of the total U.S. population), the AAP/CHA data show.
Those data also indicate that there have been almost 986 cases of COVID-19 per 100,000 children in the United States. Corresponding rates among the states range from 181 per 100,000 in Vermont to 2,581 per 100,000 in North Dakota. Tennessee (2,277) and South Carolina (2,212) are the only other states above 2,000, according to the report.
California has reported the most child cases, 89,843 (1,010 per 100,000 children), so far, followed by Florida (44,199), Illinois (42,132), and Tennessee (40,137). Seven other states have had over 20,000 cases each, the AAP and CHA noted.
Measures of severe illness continue to be low, although the data are less comprehensive. Children represent only 1.7% of all COVID-19 hospitalizations (24 states and N.Y.C. reporting) and 0.07% of all deaths (42 states and N.Y.C. reporting). Thirteen states and D.C. have had no deaths yet, while Texas has reported three times as many (27) as any other state (Arizona is next with 9, although N.Y.C. has had 15), the AAP/CHA report said.
in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases among children was 741,891 as of Oct. 15, which puts the cumulative proportion at 10.9% of the 6.8 million cases reported in all ages by 49 states (New York does not report ages), the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly COVID-19 report.
The 44,258 new cases in children represented 13.3% of all cases reported during the week ending Oct. 15, down from 14.6% the previous week (children make up almost 23% of the total U.S. population), the AAP/CHA data show.
Those data also indicate that there have been almost 986 cases of COVID-19 per 100,000 children in the United States. Corresponding rates among the states range from 181 per 100,000 in Vermont to 2,581 per 100,000 in North Dakota. Tennessee (2,277) and South Carolina (2,212) are the only other states above 2,000, according to the report.
California has reported the most child cases, 89,843 (1,010 per 100,000 children), so far, followed by Florida (44,199), Illinois (42,132), and Tennessee (40,137). Seven other states have had over 20,000 cases each, the AAP and CHA noted.
Measures of severe illness continue to be low, although the data are less comprehensive. Children represent only 1.7% of all COVID-19 hospitalizations (24 states and N.Y.C. reporting) and 0.07% of all deaths (42 states and N.Y.C. reporting). Thirteen states and D.C. have had no deaths yet, while Texas has reported three times as many (27) as any other state (Arizona is next with 9, although N.Y.C. has had 15), the AAP/CHA report said.
in the United States, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases among children was 741,891 as of Oct. 15, which puts the cumulative proportion at 10.9% of the 6.8 million cases reported in all ages by 49 states (New York does not report ages), the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly COVID-19 report.
The 44,258 new cases in children represented 13.3% of all cases reported during the week ending Oct. 15, down from 14.6% the previous week (children make up almost 23% of the total U.S. population), the AAP/CHA data show.
Those data also indicate that there have been almost 986 cases of COVID-19 per 100,000 children in the United States. Corresponding rates among the states range from 181 per 100,000 in Vermont to 2,581 per 100,000 in North Dakota. Tennessee (2,277) and South Carolina (2,212) are the only other states above 2,000, according to the report.
California has reported the most child cases, 89,843 (1,010 per 100,000 children), so far, followed by Florida (44,199), Illinois (42,132), and Tennessee (40,137). Seven other states have had over 20,000 cases each, the AAP and CHA noted.
Measures of severe illness continue to be low, although the data are less comprehensive. Children represent only 1.7% of all COVID-19 hospitalizations (24 states and N.Y.C. reporting) and 0.07% of all deaths (42 states and N.Y.C. reporting). Thirteen states and D.C. have had no deaths yet, while Texas has reported three times as many (27) as any other state (Arizona is next with 9, although N.Y.C. has had 15), the AAP/CHA report said.
Women make progress in pediatric dermatology leadership
Women account for approximately 78% of the pediatric dermatology workforce, and continue to gain influence through increased numbers of leadership positions and published research, based on data from a review of professional society leaders, grant recipients, and annual meeting presenters from 2010 to 2019.
“Despite extensive research on gender equality in general dermatology, studies have yet to explore the evolving representation of women as leaders and researchers in pediatric dermatology, a field where the majority of board-certified physicians are women,” wrote Catherine Baker, MD, and colleagues. Dr. Baker was a medical student at Geisel School of Medicine at Dartmouth, Hanover, N.H., at the time of the study and is now a resident physician at Brigham and Women’s Hospital, Boston.
In a study published in Pediatric Dermatology, the researchers reviewed data on society leadership, research grants, and annual meeting speakers in order to evaluate the impact of women in pediatric dermatology.
Overall, the Society for Pediatric Dermatology has had 20 women presidents since its founding in 1975 (45%), and 7 of the last 10 since 2011 have been women (70%). The Pediatric Dermatology Research Alliance, founded in 2013, has two cochairs each year, and 75% have been women.
The percentage of women as lead authors of published research in pediatric dermatology increased significantly from 1983 to 2019; 71% of first authors and 65% of senior authors of papers in the journal Pediatric Dermatology in 2019 were women.
In addition, 26 of the 31 physicians (84%) who received SPD/PeDRA pilot project awards between 2008 and 2018 were women, as were 88% of SPD/PeDRA team/collaborative grant winners from 2016 to 2018.
However, named lectures at annual meetings remain an area in which women are underrepresented, the researchers wrote. Although women have been well represented at PeDRA meetings, accounting for 65% of plenary speakers, but they accounted for less than half (44%) of Hurwitz and Founders’ lectures at SPD annual meetings from 2010 to 2019.
The study findings were limited by a lack of data on nonbinary genders and the possibility of error in assessing gender based on name and online profiles, the researchers noted. However, the results suggest that women have increased their influence in pediatric dermatology through leadership and research, although a gender gap persists in roles as senior authors and named lecturers at meetings, they wrote.
Overall, “we expect increasing gender equity in these positions as women continue to play important roles as leaders and researchers in pediatric dermatology,” the researchers concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Baker C et al. Pediatr Dermatol. 2020 Jul 9. doi: 10.1111/pde.14266.
Women account for approximately 78% of the pediatric dermatology workforce, and continue to gain influence through increased numbers of leadership positions and published research, based on data from a review of professional society leaders, grant recipients, and annual meeting presenters from 2010 to 2019.
“Despite extensive research on gender equality in general dermatology, studies have yet to explore the evolving representation of women as leaders and researchers in pediatric dermatology, a field where the majority of board-certified physicians are women,” wrote Catherine Baker, MD, and colleagues. Dr. Baker was a medical student at Geisel School of Medicine at Dartmouth, Hanover, N.H., at the time of the study and is now a resident physician at Brigham and Women’s Hospital, Boston.
In a study published in Pediatric Dermatology, the researchers reviewed data on society leadership, research grants, and annual meeting speakers in order to evaluate the impact of women in pediatric dermatology.
Overall, the Society for Pediatric Dermatology has had 20 women presidents since its founding in 1975 (45%), and 7 of the last 10 since 2011 have been women (70%). The Pediatric Dermatology Research Alliance, founded in 2013, has two cochairs each year, and 75% have been women.
The percentage of women as lead authors of published research in pediatric dermatology increased significantly from 1983 to 2019; 71% of first authors and 65% of senior authors of papers in the journal Pediatric Dermatology in 2019 were women.
In addition, 26 of the 31 physicians (84%) who received SPD/PeDRA pilot project awards between 2008 and 2018 were women, as were 88% of SPD/PeDRA team/collaborative grant winners from 2016 to 2018.
However, named lectures at annual meetings remain an area in which women are underrepresented, the researchers wrote. Although women have been well represented at PeDRA meetings, accounting for 65% of plenary speakers, but they accounted for less than half (44%) of Hurwitz and Founders’ lectures at SPD annual meetings from 2010 to 2019.
The study findings were limited by a lack of data on nonbinary genders and the possibility of error in assessing gender based on name and online profiles, the researchers noted. However, the results suggest that women have increased their influence in pediatric dermatology through leadership and research, although a gender gap persists in roles as senior authors and named lecturers at meetings, they wrote.
Overall, “we expect increasing gender equity in these positions as women continue to play important roles as leaders and researchers in pediatric dermatology,” the researchers concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Baker C et al. Pediatr Dermatol. 2020 Jul 9. doi: 10.1111/pde.14266.
Women account for approximately 78% of the pediatric dermatology workforce, and continue to gain influence through increased numbers of leadership positions and published research, based on data from a review of professional society leaders, grant recipients, and annual meeting presenters from 2010 to 2019.
“Despite extensive research on gender equality in general dermatology, studies have yet to explore the evolving representation of women as leaders and researchers in pediatric dermatology, a field where the majority of board-certified physicians are women,” wrote Catherine Baker, MD, and colleagues. Dr. Baker was a medical student at Geisel School of Medicine at Dartmouth, Hanover, N.H., at the time of the study and is now a resident physician at Brigham and Women’s Hospital, Boston.
In a study published in Pediatric Dermatology, the researchers reviewed data on society leadership, research grants, and annual meeting speakers in order to evaluate the impact of women in pediatric dermatology.
Overall, the Society for Pediatric Dermatology has had 20 women presidents since its founding in 1975 (45%), and 7 of the last 10 since 2011 have been women (70%). The Pediatric Dermatology Research Alliance, founded in 2013, has two cochairs each year, and 75% have been women.
The percentage of women as lead authors of published research in pediatric dermatology increased significantly from 1983 to 2019; 71% of first authors and 65% of senior authors of papers in the journal Pediatric Dermatology in 2019 were women.
In addition, 26 of the 31 physicians (84%) who received SPD/PeDRA pilot project awards between 2008 and 2018 were women, as were 88% of SPD/PeDRA team/collaborative grant winners from 2016 to 2018.
However, named lectures at annual meetings remain an area in which women are underrepresented, the researchers wrote. Although women have been well represented at PeDRA meetings, accounting for 65% of plenary speakers, but they accounted for less than half (44%) of Hurwitz and Founders’ lectures at SPD annual meetings from 2010 to 2019.
The study findings were limited by a lack of data on nonbinary genders and the possibility of error in assessing gender based on name and online profiles, the researchers noted. However, the results suggest that women have increased their influence in pediatric dermatology through leadership and research, although a gender gap persists in roles as senior authors and named lecturers at meetings, they wrote.
Overall, “we expect increasing gender equity in these positions as women continue to play important roles as leaders and researchers in pediatric dermatology,” the researchers concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Baker C et al. Pediatr Dermatol. 2020 Jul 9. doi: 10.1111/pde.14266.
FROM PEDIATRIC DERMATOLOGY
Include irritability in ADHD suicidality risk assessments
Irritability appears to be a potent independent predictor of increased risk for suicidality in children and adolescents with ADHD, Tomer Levy, MD, said at the virtual congress of the European College of Neuropsychopharmacology.
While there is ample evidence that ADHD is associated with increased suicidality, Dr. Levy’s recent study involving 1,516 youths aged 6-17 years attending an outpatient ADHD clinic demonstrated that this increased risk is mediated by depression and irritability in roughly equal measures. Moreover, upon controlling for those two factors in a multivariate analysis, ADHD symptoms, per se, had no direct effect on risk of suicidality as defined by suidical ideation, attempts, or self-harm.
The clinical take-home message is that assessing irritability, as well as depression, may bolster an estimate of suicidality and help in managing suicidal risk in ADHD, according to Dr. Levy, a child and adolescent psychiatrist at the Hospital for Sick Children, Toronto, and head of behavioral regulation services at the Geha Mental Health Center in Petah Tikva, Israel.
The study included separate parent- and teacher-structured reports of the youths’ ADHD symptoms, suicidality, depression, irritability, and anxiety.
In multivariate analyses, parent-reported depression accounted for 39.1% of the association between ADHD symptoms and suicidality, while irritability symptoms mediated 36.8% of the total effect. In the teachers’ reports, depression and irritability symptoms accounted for 45.3% and 38.4% of the association. Anxiety symptoms mediated 19% of the relationship between ADHD and suicidality by parental report but had no significant impact on the association according to teacher report in the recently published study.
Dr. Levy noted that, in the DSM-5, irritability cuts across diagnostic categories. It is not only a core dimension of ADHD, but of the other externalizing disorders – conduct disorder and oppositional defiant disorder – as well, and also of neurodevelopmental, internalizing, and stress-related disorders.
Interventional studies aimed at dampening irritability as a potential strategy to reduce suicidality haven’t yet been done, but they deserve research priority status, in Dr. Levy’s view. Numerous functional dimensions that influence irritability are potential targets, including aggression, negative affect, low tolerance of frustration, skewed threat perception, and impaired self-regulation, according to the psychiatrist.
Most suicidal youths are attempting to cope with mental disorders. The most prevalent of these are major depressive disorder and dysthymia, followed by externalizing disorders. And among the externalizing disorders, conduct disorder stands out in terms of the magnitude of associated suicidality risk. In a large Taiwanese national study including 3,711 adolescents with conduct disorder and 14,844 age- and sex-matched controls, conduct disorder was associated with an adjusted 5.17-fold increased risk of subsequent suicide attempts over the next 10 years in a multivariate regression analysis adjusted for other psychiatric comorbidities and demographics.
In addition to depression, irritability symptoms, and conduct problems, other risk factors that should be part of a suicidality assessment in children and adolescents with ADHD include substance use, anxiety, poor family support, and bullying and/or being bullied. But, perhaps surprisingly, not impulsivity, Dr. Levy said.
“There is a widely held perception that impulsivity imparts a risk for suicidality, and especially in the transition from ideation to attempt. However, more recent evidence fails to show a convincing association,” according to Dr. Levy.
He reported having no financial conflicts regarding his presentation.
SOURCE: Levy T. ECNP 2020, Session EDU.02.
Irritability appears to be a potent independent predictor of increased risk for suicidality in children and adolescents with ADHD, Tomer Levy, MD, said at the virtual congress of the European College of Neuropsychopharmacology.
While there is ample evidence that ADHD is associated with increased suicidality, Dr. Levy’s recent study involving 1,516 youths aged 6-17 years attending an outpatient ADHD clinic demonstrated that this increased risk is mediated by depression and irritability in roughly equal measures. Moreover, upon controlling for those two factors in a multivariate analysis, ADHD symptoms, per se, had no direct effect on risk of suicidality as defined by suidical ideation, attempts, or self-harm.
The clinical take-home message is that assessing irritability, as well as depression, may bolster an estimate of suicidality and help in managing suicidal risk in ADHD, according to Dr. Levy, a child and adolescent psychiatrist at the Hospital for Sick Children, Toronto, and head of behavioral regulation services at the Geha Mental Health Center in Petah Tikva, Israel.
The study included separate parent- and teacher-structured reports of the youths’ ADHD symptoms, suicidality, depression, irritability, and anxiety.
In multivariate analyses, parent-reported depression accounted for 39.1% of the association between ADHD symptoms and suicidality, while irritability symptoms mediated 36.8% of the total effect. In the teachers’ reports, depression and irritability symptoms accounted for 45.3% and 38.4% of the association. Anxiety symptoms mediated 19% of the relationship between ADHD and suicidality by parental report but had no significant impact on the association according to teacher report in the recently published study.
Dr. Levy noted that, in the DSM-5, irritability cuts across diagnostic categories. It is not only a core dimension of ADHD, but of the other externalizing disorders – conduct disorder and oppositional defiant disorder – as well, and also of neurodevelopmental, internalizing, and stress-related disorders.
Interventional studies aimed at dampening irritability as a potential strategy to reduce suicidality haven’t yet been done, but they deserve research priority status, in Dr. Levy’s view. Numerous functional dimensions that influence irritability are potential targets, including aggression, negative affect, low tolerance of frustration, skewed threat perception, and impaired self-regulation, according to the psychiatrist.
Most suicidal youths are attempting to cope with mental disorders. The most prevalent of these are major depressive disorder and dysthymia, followed by externalizing disorders. And among the externalizing disorders, conduct disorder stands out in terms of the magnitude of associated suicidality risk. In a large Taiwanese national study including 3,711 adolescents with conduct disorder and 14,844 age- and sex-matched controls, conduct disorder was associated with an adjusted 5.17-fold increased risk of subsequent suicide attempts over the next 10 years in a multivariate regression analysis adjusted for other psychiatric comorbidities and demographics.
In addition to depression, irritability symptoms, and conduct problems, other risk factors that should be part of a suicidality assessment in children and adolescents with ADHD include substance use, anxiety, poor family support, and bullying and/or being bullied. But, perhaps surprisingly, not impulsivity, Dr. Levy said.
“There is a widely held perception that impulsivity imparts a risk for suicidality, and especially in the transition from ideation to attempt. However, more recent evidence fails to show a convincing association,” according to Dr. Levy.
He reported having no financial conflicts regarding his presentation.
SOURCE: Levy T. ECNP 2020, Session EDU.02.
Irritability appears to be a potent independent predictor of increased risk for suicidality in children and adolescents with ADHD, Tomer Levy, MD, said at the virtual congress of the European College of Neuropsychopharmacology.
While there is ample evidence that ADHD is associated with increased suicidality, Dr. Levy’s recent study involving 1,516 youths aged 6-17 years attending an outpatient ADHD clinic demonstrated that this increased risk is mediated by depression and irritability in roughly equal measures. Moreover, upon controlling for those two factors in a multivariate analysis, ADHD symptoms, per se, had no direct effect on risk of suicidality as defined by suidical ideation, attempts, or self-harm.
The clinical take-home message is that assessing irritability, as well as depression, may bolster an estimate of suicidality and help in managing suicidal risk in ADHD, according to Dr. Levy, a child and adolescent psychiatrist at the Hospital for Sick Children, Toronto, and head of behavioral regulation services at the Geha Mental Health Center in Petah Tikva, Israel.
The study included separate parent- and teacher-structured reports of the youths’ ADHD symptoms, suicidality, depression, irritability, and anxiety.
In multivariate analyses, parent-reported depression accounted for 39.1% of the association between ADHD symptoms and suicidality, while irritability symptoms mediated 36.8% of the total effect. In the teachers’ reports, depression and irritability symptoms accounted for 45.3% and 38.4% of the association. Anxiety symptoms mediated 19% of the relationship between ADHD and suicidality by parental report but had no significant impact on the association according to teacher report in the recently published study.
Dr. Levy noted that, in the DSM-5, irritability cuts across diagnostic categories. It is not only a core dimension of ADHD, but of the other externalizing disorders – conduct disorder and oppositional defiant disorder – as well, and also of neurodevelopmental, internalizing, and stress-related disorders.
Interventional studies aimed at dampening irritability as a potential strategy to reduce suicidality haven’t yet been done, but they deserve research priority status, in Dr. Levy’s view. Numerous functional dimensions that influence irritability are potential targets, including aggression, negative affect, low tolerance of frustration, skewed threat perception, and impaired self-regulation, according to the psychiatrist.
Most suicidal youths are attempting to cope with mental disorders. The most prevalent of these are major depressive disorder and dysthymia, followed by externalizing disorders. And among the externalizing disorders, conduct disorder stands out in terms of the magnitude of associated suicidality risk. In a large Taiwanese national study including 3,711 adolescents with conduct disorder and 14,844 age- and sex-matched controls, conduct disorder was associated with an adjusted 5.17-fold increased risk of subsequent suicide attempts over the next 10 years in a multivariate regression analysis adjusted for other psychiatric comorbidities and demographics.
In addition to depression, irritability symptoms, and conduct problems, other risk factors that should be part of a suicidality assessment in children and adolescents with ADHD include substance use, anxiety, poor family support, and bullying and/or being bullied. But, perhaps surprisingly, not impulsivity, Dr. Levy said.
“There is a widely held perception that impulsivity imparts a risk for suicidality, and especially in the transition from ideation to attempt. However, more recent evidence fails to show a convincing association,” according to Dr. Levy.
He reported having no financial conflicts regarding his presentation.
SOURCE: Levy T. ECNP 2020, Session EDU.02.
FROM ECNP 2020
Key clinical point: Assessment of irritability symptoms and depression may be helpful in managing suicidality risk in ADHD.
Major finding: Parent- and teacher-reported depression and irritability symptoms mediated up to 84% of the association between pediatric ADHD and suicidality.
Study details: This cross-sectional study examined the role of irritability, depression, and anxiety in suicidality among 1,516 children and adolescents at an outpatient ADHD clinic.
Disclosures: The presenter reported having no financial conflicts regarding his study.
Source: Levy T. ECNP 2020, Session EDU.02.
Irritable Baby With Weight Loss and a Periorificial and Truncal Rash
The Diagnosis: Acrodermatitis Enteropathica
Acrodermatitis enteropathica (AE) was the presumptive diagnosis. Oral supplementation with zinc sulfate 3 mg/kg/d was started immediately after a zinc level was ordered. A low zinc level of 15 µg/dL (reference range, 56-134 µg/dL) eventually was obtained. The lesions began to fade in 2 days along with return of normal feeding and disposition, and the patient was discharged with continued zinc supplementation.
Acrodermatitis enteropathica is an autosomal-recessive condition resulting in severe zinc deficiency caused by a defect of dietary zinc absorption in the duodenum and jejunum.1 It occurs in 1 in 500,000 individuals with no gender or racial predilection. It can be acquired or inherited.2 Recognition of clinical symptoms is essential due to potential death if untreated. Zinc is an important trace element required for the proper functioning of all cells and plays a large role in the metabolism of protein, carbohydrates, and vitamin A. Zinc deficiency impairs immune function, leading to bacterial infections. It also is a cofactor of numerous metal enzymes such as alkaline phosphatase, RNA polymerase, and numerous digestive enzymes.3
Our laboratory analysis revealed low alkaline phosphatase and zinc levels, which led to the diagnosis of AE; unfortunately, these levels can be ambiguous.4 There are many causes of acquired zinc deficiency, including premature birth, low birth weight, zinc deficiency in maternal milk, exclusive parenteral nutrition, malabsorption syndromes such as Crohn disease and celiac disease, alcoholism, low calcium and phytate (cereal grain) diet, and kwashiorkor.5 The hereditary deficiency of zinc classically is known as AE and is caused by an autosomal-recessive mutation of the SLC39A4 gene on chromosome arm 8q24.3, which determines a congenital partial or total deficiency of the zinc transporter protein ZIP4.6
The clinical manifestations of acquired zinc deficiency and AE are similar and consist of 3 essential symptoms: periorificial dermatitis, alopecia, and diarrhea. Unfortunately, this clinical triad is complete in only 20% of patients with AE.3 For example, our patient was too young for an alopecia determination. The disease typically presents with eczematous papules and sometimes vesiculobullous or pustular lesions located around perioral and acral areas (Figure 1) as well as the anogenital region (Figures 2 and 3). The severity of the skin lesions is variable.7 Our patient also presented with eczematous truncal papules on the chest (Figure 4). Acrodermatitis enteropathica usually presents during childhood after weaning. Along with the aforementioned skin findings, other symptoms in infancy can include diarrhea, mood changes, and anorexia. In school-aged children and toddlers, zinc deficiency is characterized by growth retardation, alopecia, weight loss, and recurrent infections.




In the differential diagnosis, the clinical presentation of biotin deficiency involves abnormalities of the hair, skin, nails, and central nervous system (eg, seizures, ataxia, deafness).8 Cystic fibrosis presentation depends on the multiorgan involvement, but neonates often present with failure to thrive.9 Essential fatty acid deficiency presents clinically as dermatitis, alopecia, and thrombocytopenia, but a complete blood cell count with platelets was within reference range in our patient.10 Langerhans cell histiocytosis presents with perineal and postauricular lesions, but the skin biopsy did not confirm this diagnosis in our patient.11 Histopathologic examination of the buttock biopsy in our patient revealed nonspecific epidermal hyperplasia with acanthosis as well as clustered necrotic keratinocytes with vacuolization and parakeratosis.
Most clinicians who suspect AE treat with a therapeutic supplementation of zinc sulfate 3 mg/kg/d while awaiting laboratory results. Acrodermatitis enteropathica is a rare condition, and early recognition of skin findings is important because misdiagnosis can lead to infections, malnutrition, and possibly death.
- Sehgal VN, Jain S. Acrodermatitis enteropathica. Clin Dermatol. 2000;18:745-748.
- Van Wouwe JP. Clinical and laboratory assessment of zinc deficiency in Dutch children: a review. Biol Trace Elem Res. 1995;49:211-225.
- Maverakis E, Fung MA, Lynch PJ, et al. Acrodermatitis enteropathica and an overview of zinc metabolism. J Am Acad Dermatol. 2007;56:116-124.
- Van Wouwe JP. Clinical and laboratory diagnosis of acrodermatitis enteropathica. Eur J Pediatr. 1989;149:2-8.
- Perafán-Riveros C, França LF, Alves AC, et al. Acrodermatitisenteropathica: case report and review of the literature. Pediatr Dermatol. 2002;19:426-431.
- Kury S, Dréno B, Bézieau S, et al. Identification of SLC39A4, a gene involved in acrodermatitis enteropathica. Nat Genet. 2002;31:239-240.
- Nistor N, Ciontu L, Frasinariu OE, et al. Acrodermatitis enteropathica: a case report. Medicine. 2016;95:E3553.
- Gratias T. Biotin deficiency. Medscape website. https://emedicine.medscape.com/article/984803-overview. Updated October 22, 2018. Accessed October 15, 2020.
- Sharma G. Cystic fibrosis. Medscape website. https://emedicine.medscape.com/article/1001602-overview. Updated September 28, 2018. Accessed October 15, 2020.
- Morley JE. Essential fatty acid deficiency. Merck Manual website. https://www.merckmanuals.com/professional/nutritional-disorders/undernutrition/essential-fatty-acid-deficiency. Updated January 2020. Accessed October 15, 2020.
- Shea CR. Langerhans cell histiocytosis. Medscape website. https://emedicine.medscape.com/article/1100579-overview. Updated June 12, 2020. Accessed October 15, 2020.
The Diagnosis: Acrodermatitis Enteropathica
Acrodermatitis enteropathica (AE) was the presumptive diagnosis. Oral supplementation with zinc sulfate 3 mg/kg/d was started immediately after a zinc level was ordered. A low zinc level of 15 µg/dL (reference range, 56-134 µg/dL) eventually was obtained. The lesions began to fade in 2 days along with return of normal feeding and disposition, and the patient was discharged with continued zinc supplementation.
Acrodermatitis enteropathica is an autosomal-recessive condition resulting in severe zinc deficiency caused by a defect of dietary zinc absorption in the duodenum and jejunum.1 It occurs in 1 in 500,000 individuals with no gender or racial predilection. It can be acquired or inherited.2 Recognition of clinical symptoms is essential due to potential death if untreated. Zinc is an important trace element required for the proper functioning of all cells and plays a large role in the metabolism of protein, carbohydrates, and vitamin A. Zinc deficiency impairs immune function, leading to bacterial infections. It also is a cofactor of numerous metal enzymes such as alkaline phosphatase, RNA polymerase, and numerous digestive enzymes.3
Our laboratory analysis revealed low alkaline phosphatase and zinc levels, which led to the diagnosis of AE; unfortunately, these levels can be ambiguous.4 There are many causes of acquired zinc deficiency, including premature birth, low birth weight, zinc deficiency in maternal milk, exclusive parenteral nutrition, malabsorption syndromes such as Crohn disease and celiac disease, alcoholism, low calcium and phytate (cereal grain) diet, and kwashiorkor.5 The hereditary deficiency of zinc classically is known as AE and is caused by an autosomal-recessive mutation of the SLC39A4 gene on chromosome arm 8q24.3, which determines a congenital partial or total deficiency of the zinc transporter protein ZIP4.6
The clinical manifestations of acquired zinc deficiency and AE are similar and consist of 3 essential symptoms: periorificial dermatitis, alopecia, and diarrhea. Unfortunately, this clinical triad is complete in only 20% of patients with AE.3 For example, our patient was too young for an alopecia determination. The disease typically presents with eczematous papules and sometimes vesiculobullous or pustular lesions located around perioral and acral areas (Figure 1) as well as the anogenital region (Figures 2 and 3). The severity of the skin lesions is variable.7 Our patient also presented with eczematous truncal papules on the chest (Figure 4). Acrodermatitis enteropathica usually presents during childhood after weaning. Along with the aforementioned skin findings, other symptoms in infancy can include diarrhea, mood changes, and anorexia. In school-aged children and toddlers, zinc deficiency is characterized by growth retardation, alopecia, weight loss, and recurrent infections.
In the differential diagnosis, the clinical presentation of biotin deficiency involves abnormalities of the hair, skin, nails, and central nervous system (eg, seizures, ataxia, deafness).8 Cystic fibrosis presentation depends on the multiorgan involvement, but neonates often present with failure to thrive.9 Essential fatty acid deficiency presents clinically as dermatitis, alopecia, and thrombocytopenia, but a complete blood cell count with platelets was within reference range in our patient.10 Langerhans cell histiocytosis presents with perineal and postauricular lesions, but the skin biopsy did not confirm this diagnosis in our patient.11 Histopathologic examination of the buttock biopsy in our patient revealed nonspecific epidermal hyperplasia with acanthosis as well as clustered necrotic keratinocytes with vacuolization and parakeratosis.
Most clinicians who suspect AE treat with a therapeutic supplementation of zinc sulfate 3 mg/kg/d while awaiting laboratory results. Acrodermatitis enteropathica is a rare condition, and early recognition of skin findings is important because misdiagnosis can lead to infections, malnutrition, and possibly death.
The Diagnosis: Acrodermatitis Enteropathica
Acrodermatitis enteropathica (AE) was the presumptive diagnosis. Oral supplementation with zinc sulfate 3 mg/kg/d was started immediately after a zinc level was ordered. A low zinc level of 15 µg/dL (reference range, 56-134 µg/dL) eventually was obtained. The lesions began to fade in 2 days along with return of normal feeding and disposition, and the patient was discharged with continued zinc supplementation.
Acrodermatitis enteropathica is an autosomal-recessive condition resulting in severe zinc deficiency caused by a defect of dietary zinc absorption in the duodenum and jejunum.1 It occurs in 1 in 500,000 individuals with no gender or racial predilection. It can be acquired or inherited.2 Recognition of clinical symptoms is essential due to potential death if untreated. Zinc is an important trace element required for the proper functioning of all cells and plays a large role in the metabolism of protein, carbohydrates, and vitamin A. Zinc deficiency impairs immune function, leading to bacterial infections. It also is a cofactor of numerous metal enzymes such as alkaline phosphatase, RNA polymerase, and numerous digestive enzymes.3
Our laboratory analysis revealed low alkaline phosphatase and zinc levels, which led to the diagnosis of AE; unfortunately, these levels can be ambiguous.4 There are many causes of acquired zinc deficiency, including premature birth, low birth weight, zinc deficiency in maternal milk, exclusive parenteral nutrition, malabsorption syndromes such as Crohn disease and celiac disease, alcoholism, low calcium and phytate (cereal grain) diet, and kwashiorkor.5 The hereditary deficiency of zinc classically is known as AE and is caused by an autosomal-recessive mutation of the SLC39A4 gene on chromosome arm 8q24.3, which determines a congenital partial or total deficiency of the zinc transporter protein ZIP4.6
The clinical manifestations of acquired zinc deficiency and AE are similar and consist of 3 essential symptoms: periorificial dermatitis, alopecia, and diarrhea. Unfortunately, this clinical triad is complete in only 20% of patients with AE.3 For example, our patient was too young for an alopecia determination. The disease typically presents with eczematous papules and sometimes vesiculobullous or pustular lesions located around perioral and acral areas (Figure 1) as well as the anogenital region (Figures 2 and 3). The severity of the skin lesions is variable.7 Our patient also presented with eczematous truncal papules on the chest (Figure 4). Acrodermatitis enteropathica usually presents during childhood after weaning. Along with the aforementioned skin findings, other symptoms in infancy can include diarrhea, mood changes, and anorexia. In school-aged children and toddlers, zinc deficiency is characterized by growth retardation, alopecia, weight loss, and recurrent infections.
In the differential diagnosis, the clinical presentation of biotin deficiency involves abnormalities of the hair, skin, nails, and central nervous system (eg, seizures, ataxia, deafness).8 Cystic fibrosis presentation depends on the multiorgan involvement, but neonates often present with failure to thrive.9 Essential fatty acid deficiency presents clinically as dermatitis, alopecia, and thrombocytopenia, but a complete blood cell count with platelets was within reference range in our patient.10 Langerhans cell histiocytosis presents with perineal and postauricular lesions, but the skin biopsy did not confirm this diagnosis in our patient.11 Histopathologic examination of the buttock biopsy in our patient revealed nonspecific epidermal hyperplasia with acanthosis as well as clustered necrotic keratinocytes with vacuolization and parakeratosis.
Most clinicians who suspect AE treat with a therapeutic supplementation of zinc sulfate 3 mg/kg/d while awaiting laboratory results. Acrodermatitis enteropathica is a rare condition, and early recognition of skin findings is important because misdiagnosis can lead to infections, malnutrition, and possibly death.
- Sehgal VN, Jain S. Acrodermatitis enteropathica. Clin Dermatol. 2000;18:745-748.
- Van Wouwe JP. Clinical and laboratory assessment of zinc deficiency in Dutch children: a review. Biol Trace Elem Res. 1995;49:211-225.
- Maverakis E, Fung MA, Lynch PJ, et al. Acrodermatitis enteropathica and an overview of zinc metabolism. J Am Acad Dermatol. 2007;56:116-124.
- Van Wouwe JP. Clinical and laboratory diagnosis of acrodermatitis enteropathica. Eur J Pediatr. 1989;149:2-8.
- Perafán-Riveros C, França LF, Alves AC, et al. Acrodermatitisenteropathica: case report and review of the literature. Pediatr Dermatol. 2002;19:426-431.
- Kury S, Dréno B, Bézieau S, et al. Identification of SLC39A4, a gene involved in acrodermatitis enteropathica. Nat Genet. 2002;31:239-240.
- Nistor N, Ciontu L, Frasinariu OE, et al. Acrodermatitis enteropathica: a case report. Medicine. 2016;95:E3553.
- Gratias T. Biotin deficiency. Medscape website. https://emedicine.medscape.com/article/984803-overview. Updated October 22, 2018. Accessed October 15, 2020.
- Sharma G. Cystic fibrosis. Medscape website. https://emedicine.medscape.com/article/1001602-overview. Updated September 28, 2018. Accessed October 15, 2020.
- Morley JE. Essential fatty acid deficiency. Merck Manual website. https://www.merckmanuals.com/professional/nutritional-disorders/undernutrition/essential-fatty-acid-deficiency. Updated January 2020. Accessed October 15, 2020.
- Shea CR. Langerhans cell histiocytosis. Medscape website. https://emedicine.medscape.com/article/1100579-overview. Updated June 12, 2020. Accessed October 15, 2020.
- Sehgal VN, Jain S. Acrodermatitis enteropathica. Clin Dermatol. 2000;18:745-748.
- Van Wouwe JP. Clinical and laboratory assessment of zinc deficiency in Dutch children: a review. Biol Trace Elem Res. 1995;49:211-225.
- Maverakis E, Fung MA, Lynch PJ, et al. Acrodermatitis enteropathica and an overview of zinc metabolism. J Am Acad Dermatol. 2007;56:116-124.
- Van Wouwe JP. Clinical and laboratory diagnosis of acrodermatitis enteropathica. Eur J Pediatr. 1989;149:2-8.
- Perafán-Riveros C, França LF, Alves AC, et al. Acrodermatitisenteropathica: case report and review of the literature. Pediatr Dermatol. 2002;19:426-431.
- Kury S, Dréno B, Bézieau S, et al. Identification of SLC39A4, a gene involved in acrodermatitis enteropathica. Nat Genet. 2002;31:239-240.
- Nistor N, Ciontu L, Frasinariu OE, et al. Acrodermatitis enteropathica: a case report. Medicine. 2016;95:E3553.
- Gratias T. Biotin deficiency. Medscape website. https://emedicine.medscape.com/article/984803-overview. Updated October 22, 2018. Accessed October 15, 2020.
- Sharma G. Cystic fibrosis. Medscape website. https://emedicine.medscape.com/article/1001602-overview. Updated September 28, 2018. Accessed October 15, 2020.
- Morley JE. Essential fatty acid deficiency. Merck Manual website. https://www.merckmanuals.com/professional/nutritional-disorders/undernutrition/essential-fatty-acid-deficiency. Updated January 2020. Accessed October 15, 2020.
- Shea CR. Langerhans cell histiocytosis. Medscape website. https://emedicine.medscape.com/article/1100579-overview. Updated June 12, 2020. Accessed October 15, 2020.

A 4-month-old infant boy presented to the pediatric hospital unit with a rash, fever, and failure to thrive. Prior to admission, the patient was treated for impetigo by a community dermatologist. After not responding to treatment, he was admitted and given intravenous acyclovir for 1 day by the pediatric hospitalist, and the dermatology service was consulted. The parents reported the patient had diarrhea for 1 month and a worsening rash over the last 2 weeks. The mother was breastfeeding. Physical examination revealed a fever (temperature, 38.9°C [102°F]) and an irritable infant whose growth curve had fallen from the 50th to 15th percentile since the 2-month well-baby examination. He had a fine, red, papular truncal rash with confluent plaques in a periorificial distribution that spared the inguinal skin folds, with some vesicles in a herpetiform presentation on the thighs as well as inflammation on the feet and hands. A complete blood cell count was within reference range, but the alkaline phosphatase level was low at 53 U/L (reference range, 72–307 U/L). A herpes simplex virus test was negative. A human immunodeficiency virus test and skin biopsy were performed.

New Americans: Considerations for culturally collaborative care
Adam is a 14-year-old who presents for “behavioral concerns” as recommended by his teacher. He is in the eighth grade and is struggling academically and socially. He has intermittent outbursts and poor engagement with other children, and often refuses to do schoolwork. He is seen in the outpatient primary care clinic, usually with his mother and two older siblings, one of whom typically translates for his Arabic-speaking mother. Adam is bilingual, although he prefers Arabic. It is difficult to understand the presenting concern as Adam states that he is doing well and is unsure why the teacher would have made such a report. Mother notes that she does not see these behaviors at home either.
What must we consider? Are there potential barriers, alternate ways to engage, and what role may culture have?
There are many things to consider in the above case, including language barriers, nuanced interactions, and cultural expectations and norms. To understand the scope, statistics reveal that the United States leads the world in its immigrant population with about 44.8 million foreign-born persons in 2018, which accounts for approximately 13.7% of the U.S. population.1 In 2019, 30,000 refugees were resettled in the United States.2 In 2017, immigrant children made up 27% (19.6 million) of U.S. children, of which second-generation children (born in the United States to immigrant parents) were the vast majority at 16.7 million.3 Given this information, 
Culture is defined as a set of shared beliefs, norms, values, and behaviors exhibited by a group. Culture plays a role and impacts children in various ways throughout their development. Health care providers would benefit from aspiring to exude cultural humility – learning with and from patients and their families with openness, kindness, and a desire for collaboration. The provider also must consider a family’s history of migration as the response to migration may vary based on age, personal experiences, age at which migration occurred, language abilities, and amount of cultural engagement in the new country (i.e. acculturation).4,5
Cultural framework model
One example of a potential framework to use to engage within a cultural context includes the LEARN (Listen, Explain, Acknowledge, Recommend, Negotiate) model,6,7 which initially was developed to be used within a family medicine clinic. It includes the following:
Listen with sympathy and understanding to the patient’s perception of the problem. Try to understand their perspective of symptoms through considering their thoughts regarding etiology and treatment options.
Explain your perception of the problem. Have a dialogue about what you perceive is the likely cause based on a medical perspective.
Acknowledge and discuss the differences and similarities. Engage in open conversation while being cognizant that there may be similarities and differences in the perception you may have versus your patient’s perception. Try to find areas that can be engaged in and an alliance built upon, as well as respectfully and humbly addressing any concerns about potentially harmful patient understandings.
Recommend treatment. Present a treatment recommendation that considers both yours and the patient’s perspectives.
Negotiate agreement. Discuss, collaborate, and finalize a treatment plan that considers a biopsychosocial and spiritual/religious model of care that is patient-centered and personalized such that the main goal is optimal health and wellness for the patient/family.
The following are tips to consider in the life-long process of becoming more culturally aware:
- Be willing to learn with your patients and be thoughtful about your own feelings/thoughts/behaviors that may be positively or negatively impacting those interactions.
- Be aware of your own identity and what that may contribute to the clinical space.
- Recognize that you are not meant to know everything, but being open to the journey and learning process will go a long way.
- Try to shift the focus from paternalistic medicine to collaborative and patient-centered approaches.
The case at hand
In returning to our case and applying the LEARN model and cultural humility, we may be able to uncover more of the story. Adam is seen at a subsequent appointment, and you determine it best to obtain an in-person interpreter for this appointment. As you listen to the story, you learn that his father was killed early in Adam’s life, his mother has suffered from depression, and they moved here 3 years ago from a refugee camp, where most of their family continues to reside. He notes that at times he feels that he is back in that space and that he also feels frustrated. He is accustomed to doing well academically, but English has been difficult to learn.

You explain your understanding and acknowledge concerns for his past experiences playing a role, the importance of having community supports, and that learning a new language is challenging. You recommend that the school offer culturally appropriate interventions, trauma-informed assessments, and English-language opportunities. Adam and his mother note willingness to engage in this plan but would like to speak to their local religious leader as well.
Collaborating in a manner similar to this will likely build a therapeutic alliance between the patient, their family, and caretakers, thus leading to improved outcomes.
For further reading, consider AACAP Finding Mental Healthcare for Children of Immigrants and the American Academy of Pediatrics Providing Culturally Effective Care Toolkit.
Dr. Abdul-Karim, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. “Key findings about U.S. immigrants.” Pew Research Center, Washington, D.C. (2020)
2. “Key facts about refugees to the U.S.” Pew Research Center, Washington, D.C. (2019)
3. “Immigrant Children.” Child Trends, Bethesda, MD (2018).
4. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed. (Philadelphia: Lippincott Williams & Wilkins, 2015, pp. 139-45).
5. Lewis’sChild and Adolescent Psychiatry: A Comprehensive Textbook, 5th ed. (Philadelphia: Lippincott Williams & Wilkins, 2017, pp. 111-22).
6. Berlin EA, Fowkes WA Jr.A teaching framework for cross-cultural health care. Application in family practice. West J Med 1983;139(6):934-8.
7. Paediatr Child Health. 2018 Feb;23(1):66-9.
Adam is a 14-year-old who presents for “behavioral concerns” as recommended by his teacher. He is in the eighth grade and is struggling academically and socially. He has intermittent outbursts and poor engagement with other children, and often refuses to do schoolwork. He is seen in the outpatient primary care clinic, usually with his mother and two older siblings, one of whom typically translates for his Arabic-speaking mother. Adam is bilingual, although he prefers Arabic. It is difficult to understand the presenting concern as Adam states that he is doing well and is unsure why the teacher would have made such a report. Mother notes that she does not see these behaviors at home either.
What must we consider? Are there potential barriers, alternate ways to engage, and what role may culture have?
There are many things to consider in the above case, including language barriers, nuanced interactions, and cultural expectations and norms. To understand the scope, statistics reveal that the United States leads the world in its immigrant population with about 44.8 million foreign-born persons in 2018, which accounts for approximately 13.7% of the U.S. population.1 In 2019, 30,000 refugees were resettled in the United States.2 In 2017, immigrant children made up 27% (19.6 million) of U.S. children, of which second-generation children (born in the United States to immigrant parents) were the vast majority at 16.7 million.3 Given this information,
Culture is defined as a set of shared beliefs, norms, values, and behaviors exhibited by a group. Culture plays a role and impacts children in various ways throughout their development. Health care providers would benefit from aspiring to exude cultural humility – learning with and from patients and their families with openness, kindness, and a desire for collaboration. The provider also must consider a family’s history of migration as the response to migration may vary based on age, personal experiences, age at which migration occurred, language abilities, and amount of cultural engagement in the new country (i.e. acculturation).4,5
Cultural framework model
One example of a potential framework to use to engage within a cultural context includes the LEARN (Listen, Explain, Acknowledge, Recommend, Negotiate) model,6,7 which initially was developed to be used within a family medicine clinic. It includes the following:
Listen with sympathy and understanding to the patient’s perception of the problem. Try to understand their perspective of symptoms through considering their thoughts regarding etiology and treatment options.
Explain your perception of the problem. Have a dialogue about what you perceive is the likely cause based on a medical perspective.
Acknowledge and discuss the differences and similarities. Engage in open conversation while being cognizant that there may be similarities and differences in the perception you may have versus your patient’s perception. Try to find areas that can be engaged in and an alliance built upon, as well as respectfully and humbly addressing any concerns about potentially harmful patient understandings.
Recommend treatment. Present a treatment recommendation that considers both yours and the patient’s perspectives.
Negotiate agreement. Discuss, collaborate, and finalize a treatment plan that considers a biopsychosocial and spiritual/religious model of care that is patient-centered and personalized such that the main goal is optimal health and wellness for the patient/family.
The following are tips to consider in the life-long process of becoming more culturally aware:
- Be willing to learn with your patients and be thoughtful about your own feelings/thoughts/behaviors that may be positively or negatively impacting those interactions.
- Be aware of your own identity and what that may contribute to the clinical space.
- Recognize that you are not meant to know everything, but being open to the journey and learning process will go a long way.
- Try to shift the focus from paternalistic medicine to collaborative and patient-centered approaches.
The case at hand
In returning to our case and applying the LEARN model and cultural humility, we may be able to uncover more of the story. Adam is seen at a subsequent appointment, and you determine it best to obtain an in-person interpreter for this appointment. As you listen to the story, you learn that his father was killed early in Adam’s life, his mother has suffered from depression, and they moved here 3 years ago from a refugee camp, where most of their family continues to reside. He notes that at times he feels that he is back in that space and that he also feels frustrated. He is accustomed to doing well academically, but English has been difficult to learn.
You explain your understanding and acknowledge concerns for his past experiences playing a role, the importance of having community supports, and that learning a new language is challenging. You recommend that the school offer culturally appropriate interventions, trauma-informed assessments, and English-language opportunities. Adam and his mother note willingness to engage in this plan but would like to speak to their local religious leader as well.
Collaborating in a manner similar to this will likely build a therapeutic alliance between the patient, their family, and caretakers, thus leading to improved outcomes.
For further reading, consider AACAP Finding Mental Healthcare for Children of Immigrants and the American Academy of Pediatrics Providing Culturally Effective Care Toolkit.
Dr. Abdul-Karim, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. “Key findings about U.S. immigrants.” Pew Research Center, Washington, D.C. (2020)
2. “Key facts about refugees to the U.S.” Pew Research Center, Washington, D.C. (2019)
3. “Immigrant Children.” Child Trends, Bethesda, MD (2018).
4. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed. (Philadelphia: Lippincott Williams & Wilkins, 2015, pp. 139-45).
5. Lewis’sChild and Adolescent Psychiatry: A Comprehensive Textbook, 5th ed. (Philadelphia: Lippincott Williams & Wilkins, 2017, pp. 111-22).
6. Berlin EA, Fowkes WA Jr.A teaching framework for cross-cultural health care. Application in family practice. West J Med 1983;139(6):934-8.
7. Paediatr Child Health. 2018 Feb;23(1):66-9.
Adam is a 14-year-old who presents for “behavioral concerns” as recommended by his teacher. He is in the eighth grade and is struggling academically and socially. He has intermittent outbursts and poor engagement with other children, and often refuses to do schoolwork. He is seen in the outpatient primary care clinic, usually with his mother and two older siblings, one of whom typically translates for his Arabic-speaking mother. Adam is bilingual, although he prefers Arabic. It is difficult to understand the presenting concern as Adam states that he is doing well and is unsure why the teacher would have made such a report. Mother notes that she does not see these behaviors at home either.
What must we consider? Are there potential barriers, alternate ways to engage, and what role may culture have?
There are many things to consider in the above case, including language barriers, nuanced interactions, and cultural expectations and norms. To understand the scope, statistics reveal that the United States leads the world in its immigrant population with about 44.8 million foreign-born persons in 2018, which accounts for approximately 13.7% of the U.S. population.1 In 2019, 30,000 refugees were resettled in the United States.2 In 2017, immigrant children made up 27% (19.6 million) of U.S. children, of which second-generation children (born in the United States to immigrant parents) were the vast majority at 16.7 million.3 Given this information,
Culture is defined as a set of shared beliefs, norms, values, and behaviors exhibited by a group. Culture plays a role and impacts children in various ways throughout their development. Health care providers would benefit from aspiring to exude cultural humility – learning with and from patients and their families with openness, kindness, and a desire for collaboration. The provider also must consider a family’s history of migration as the response to migration may vary based on age, personal experiences, age at which migration occurred, language abilities, and amount of cultural engagement in the new country (i.e. acculturation).4,5
Cultural framework model
One example of a potential framework to use to engage within a cultural context includes the LEARN (Listen, Explain, Acknowledge, Recommend, Negotiate) model,6,7 which initially was developed to be used within a family medicine clinic. It includes the following:
Listen with sympathy and understanding to the patient’s perception of the problem. Try to understand their perspective of symptoms through considering their thoughts regarding etiology and treatment options.
Explain your perception of the problem. Have a dialogue about what you perceive is the likely cause based on a medical perspective.
Acknowledge and discuss the differences and similarities. Engage in open conversation while being cognizant that there may be similarities and differences in the perception you may have versus your patient’s perception. Try to find areas that can be engaged in and an alliance built upon, as well as respectfully and humbly addressing any concerns about potentially harmful patient understandings.
Recommend treatment. Present a treatment recommendation that considers both yours and the patient’s perspectives.
Negotiate agreement. Discuss, collaborate, and finalize a treatment plan that considers a biopsychosocial and spiritual/religious model of care that is patient-centered and personalized such that the main goal is optimal health and wellness for the patient/family.
The following are tips to consider in the life-long process of becoming more culturally aware:
- Be willing to learn with your patients and be thoughtful about your own feelings/thoughts/behaviors that may be positively or negatively impacting those interactions.
- Be aware of your own identity and what that may contribute to the clinical space.
- Recognize that you are not meant to know everything, but being open to the journey and learning process will go a long way.
- Try to shift the focus from paternalistic medicine to collaborative and patient-centered approaches.
The case at hand
In returning to our case and applying the LEARN model and cultural humility, we may be able to uncover more of the story. Adam is seen at a subsequent appointment, and you determine it best to obtain an in-person interpreter for this appointment. As you listen to the story, you learn that his father was killed early in Adam’s life, his mother has suffered from depression, and they moved here 3 years ago from a refugee camp, where most of their family continues to reside. He notes that at times he feels that he is back in that space and that he also feels frustrated. He is accustomed to doing well academically, but English has been difficult to learn.
You explain your understanding and acknowledge concerns for his past experiences playing a role, the importance of having community supports, and that learning a new language is challenging. You recommend that the school offer culturally appropriate interventions, trauma-informed assessments, and English-language opportunities. Adam and his mother note willingness to engage in this plan but would like to speak to their local religious leader as well.
Collaborating in a manner similar to this will likely build a therapeutic alliance between the patient, their family, and caretakers, thus leading to improved outcomes.
For further reading, consider AACAP Finding Mental Healthcare for Children of Immigrants and the American Academy of Pediatrics Providing Culturally Effective Care Toolkit.
Dr. Abdul-Karim, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. “Key findings about U.S. immigrants.” Pew Research Center, Washington, D.C. (2020)
2. “Key facts about refugees to the U.S.” Pew Research Center, Washington, D.C. (2019)
3. “Immigrant Children.” Child Trends, Bethesda, MD (2018).
4. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed. (Philadelphia: Lippincott Williams & Wilkins, 2015, pp. 139-45).
5. Lewis’sChild and Adolescent Psychiatry: A Comprehensive Textbook, 5th ed. (Philadelphia: Lippincott Williams & Wilkins, 2017, pp. 111-22).
6. Berlin EA, Fowkes WA Jr.A teaching framework for cross-cultural health care. Application in family practice. West J Med 1983;139(6):934-8.
7. Paediatr Child Health. 2018 Feb;23(1):66-9.
A teen presents with a severe, tender rash on the extremities
“There’s rue for you, and here’s some for me; we may call it herb of grace o’ Sundays. O, you must wear your rue with a difference.”
— Ophelia in Hamlet by William Shakespeare
The patient was admitted to the hospital for IV fluids, pain control, and observation. The following day she admitted using the leaves of a plant on the trail as a bug repellent, as one time was taught by her grandfather. She rubbed some of the leaves on the brother as well. The grandfather shared some pictures of the bushes, and the plant was identified as Ruta graveolens.

The blisters were deroofed, cleaned with saline, and wrapped with triamcinolone ointment and petrolatum. The patient was also started on a prednisone taper and received analgesics for the severe pain.
Ruta graveolens also known as common rue or herb of grace, is an ornamental plant from the Rutaceae family. This plant is also used as a medicinal herb, condiment, and as an insect repellent. If ingested in large doses, it can cause severe abdominal pain and vomiting. It also can be hepatotoxic.
The herb contains furocumarines, such as 8-methoxypsoralen and 5-methoxypsoralen and furoquinoline alkaloids. These chemicals when exposed to UVA radiation cause cell injury and inflammation of the skin. This is considered a phototoxic reaction of the skin, compared with allergic reactions, such as poison ivy dermatitis, which need a prior sensitization to the allergen for the T cells to be activated and cause injury in the skin. Other common plants and fruits that can cause phytophotodermatitis include citrus fruits, figs, carrots, celery, parsnips, parsley, and other wildflowers like hogweed.

Depending on the degree of injury, the patients can be treated with topical corticosteroids, petrolatum wraps, and pain control. In severe cases like our patient, systemic prednisone may help stop the progression of the lesions and help with the inflammation. Skin hyperpigmentation after the initial injury may take months to clear, and some patient can develop scars.
The differential diagnosis should include severe bullous contact dermatitis like exposure to urushiol in poison ivy; second- and third-degree burns; severe medications reactions such Stevens-Johnson syndrome or toxic epidermal necrolysis, and inmunobullous diseases such as bullous lupus erythematosus, pemphigus vulgaris, or bullous pemphigoid. If there is no history of exposure or there are any other systemic symptoms, consider performing a skin biopsy of one of the lesions.
In this patient’s case, the history of exposure and skin findings helped the dermatologist on call make the right diagnosis.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
J Burn Care Res. 2018 Oct 23;39(6):1064-6.
Dermatitis. 2007 Mar;18(1):52-5.
BMJ Case Rep. 2015 Dec 23;2015:bcr2015213388.
“There’s rue for you, and here’s some for me; we may call it herb of grace o’ Sundays. O, you must wear your rue with a difference.”
— Ophelia in Hamlet by William Shakespeare
The patient was admitted to the hospital for IV fluids, pain control, and observation. The following day she admitted using the leaves of a plant on the trail as a bug repellent, as one time was taught by her grandfather. She rubbed some of the leaves on the brother as well. The grandfather shared some pictures of the bushes, and the plant was identified as Ruta graveolens.
The blisters were deroofed, cleaned with saline, and wrapped with triamcinolone ointment and petrolatum. The patient was also started on a prednisone taper and received analgesics for the severe pain.
Ruta graveolens also known as common rue or herb of grace, is an ornamental plant from the Rutaceae family. This plant is also used as a medicinal herb, condiment, and as an insect repellent. If ingested in large doses, it can cause severe abdominal pain and vomiting. It also can be hepatotoxic.
The herb contains furocumarines, such as 8-methoxypsoralen and 5-methoxypsoralen and furoquinoline alkaloids. These chemicals when exposed to UVA radiation cause cell injury and inflammation of the skin. This is considered a phototoxic reaction of the skin, compared with allergic reactions, such as poison ivy dermatitis, which need a prior sensitization to the allergen for the T cells to be activated and cause injury in the skin. Other common plants and fruits that can cause phytophotodermatitis include citrus fruits, figs, carrots, celery, parsnips, parsley, and other wildflowers like hogweed.
Depending on the degree of injury, the patients can be treated with topical corticosteroids, petrolatum wraps, and pain control. In severe cases like our patient, systemic prednisone may help stop the progression of the lesions and help with the inflammation. Skin hyperpigmentation after the initial injury may take months to clear, and some patient can develop scars.
The differential diagnosis should include severe bullous contact dermatitis like exposure to urushiol in poison ivy; second- and third-degree burns; severe medications reactions such Stevens-Johnson syndrome or toxic epidermal necrolysis, and inmunobullous diseases such as bullous lupus erythematosus, pemphigus vulgaris, or bullous pemphigoid. If there is no history of exposure or there are any other systemic symptoms, consider performing a skin biopsy of one of the lesions.
In this patient’s case, the history of exposure and skin findings helped the dermatologist on call make the right diagnosis.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
J Burn Care Res. 2018 Oct 23;39(6):1064-6.
Dermatitis. 2007 Mar;18(1):52-5.
BMJ Case Rep. 2015 Dec 23;2015:bcr2015213388.
“There’s rue for you, and here’s some for me; we may call it herb of grace o’ Sundays. O, you must wear your rue with a difference.”
— Ophelia in Hamlet by William Shakespeare
The patient was admitted to the hospital for IV fluids, pain control, and observation. The following day she admitted using the leaves of a plant on the trail as a bug repellent, as one time was taught by her grandfather. She rubbed some of the leaves on the brother as well. The grandfather shared some pictures of the bushes, and the plant was identified as Ruta graveolens.
The blisters were deroofed, cleaned with saline, and wrapped with triamcinolone ointment and petrolatum. The patient was also started on a prednisone taper and received analgesics for the severe pain.
Ruta graveolens also known as common rue or herb of grace, is an ornamental plant from the Rutaceae family. This plant is also used as a medicinal herb, condiment, and as an insect repellent. If ingested in large doses, it can cause severe abdominal pain and vomiting. It also can be hepatotoxic.
The herb contains furocumarines, such as 8-methoxypsoralen and 5-methoxypsoralen and furoquinoline alkaloids. These chemicals when exposed to UVA radiation cause cell injury and inflammation of the skin. This is considered a phototoxic reaction of the skin, compared with allergic reactions, such as poison ivy dermatitis, which need a prior sensitization to the allergen for the T cells to be activated and cause injury in the skin. Other common plants and fruits that can cause phytophotodermatitis include citrus fruits, figs, carrots, celery, parsnips, parsley, and other wildflowers like hogweed.
Depending on the degree of injury, the patients can be treated with topical corticosteroids, petrolatum wraps, and pain control. In severe cases like our patient, systemic prednisone may help stop the progression of the lesions and help with the inflammation. Skin hyperpigmentation after the initial injury may take months to clear, and some patient can develop scars.
The differential diagnosis should include severe bullous contact dermatitis like exposure to urushiol in poison ivy; second- and third-degree burns; severe medications reactions such Stevens-Johnson syndrome or toxic epidermal necrolysis, and inmunobullous diseases such as bullous lupus erythematosus, pemphigus vulgaris, or bullous pemphigoid. If there is no history of exposure or there are any other systemic symptoms, consider performing a skin biopsy of one of the lesions.
In this patient’s case, the history of exposure and skin findings helped the dermatologist on call make the right diagnosis.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
J Burn Care Res. 2018 Oct 23;39(6):1064-6.
Dermatitis. 2007 Mar;18(1):52-5.
BMJ Case Rep. 2015 Dec 23;2015:bcr2015213388.

She started taking lithium for depression and anxiety 3 weeks prior to her developing the rash. She denies taking any other medications, supplements, or recreational drugs.
She denied any prior history of photosensitivity, no history of mouth ulcers, joint pain, muscle weakness, hair loss, or any other symptoms.
Besides her brother, there are no other affected family members, and no history of immune bullous disorders or other skin conditions.
On physical exam, the girl appears in a lot of pain and is uncomfortable. The skin is red and hot, and there are tense bullae on the neck, arms, and legs. There are no ocular or mucosal lesions.
Manners matter
Have you been surprised and impressed by a child who says after a visit, “Thank you, Doctor [Howard]”? While it may seem antiquated to teach such manners to children these days, there are several important benefits to this education.

Manners serve important functions in benefiting a person’s group with cohesiveness and the individuals themselves with acceptance in the group. Use of manners instantly suggests a more trustworthy person.
There are three main categories of manners: hygiene, courtesy, and cultural norm manners.
Hygiene manners, from using the toilet to refraining from picking one’s nose, have obvious health benefits of not spreading disease. Hygiene manners take time to teach, but parents are motivated and helped by natural reactions of disgust that even infants recognize.
Courtesy manners, on the other hand, are habits of self-control and good-faith behaviors that signal that one is putting the interests of others ahead of one’s own for the moment. Taking another’s comfort into account, basic to kindness and respect, does not require agreeing with or submitting to the other. Courtesy manners require a developing self-awareness (I can choose to act this way) and awareness of social status (I am not more important than everyone else) that begins in toddlerhood. Modeling manners around the child is the most important way to teach courtesy. Parents usually start actively teaching the child to say “please” and “thank you,” and show pride in this apparent “demonstration of appreciation” even when it is simply reinforced behavior at first. The delight of grandparents reinforces both the parents and children, and reflects manners as building tribe cohesiveness.
Good manners become a habit
Manners such as warm greetings, a firm handshake (before COVID-19), and prompt thanks are most believable when occurring promptly when appropriate – when they come from habit. This immediate reaction, a result of so-called “fast thinking,” develops when behaviors learned from “slow thinking” are instilled early and often until they are automatic. The other benefit of this overlearning is that the behavior then looks unambivalent; a lag of too many milliseconds makes the recipient doubt genuineness.
Parents often ask us how to handle their child‘s rude or disrespectful behavior. Praise for manners is a simple start. Toddlers and preschoolers are taught manners best by adult modeling, but also by reinforcement and praise for the basics: to say “Hello,” ask “Please,” and say “Thank you,” “Excuse me,” “You’re welcome,” or “Would you help me, please?” The behaviors also include avoiding raising one’s voice, suppressing interrupting, and apologizing when appropriate. Even shy children can learn eye contact by making a game of figuring out the other’s eye color. Shaming, yelling, and punishing for poor manners usually backfires because it shows disrespect of the child who will likely give this back.
Older children can be taught to offer other people the opportunity to go through a door first, to be first to select a seat, speak first and without interruption, or order first. There are daily opportunities for these manners of showing respect. Opening doors for others, or standing when a guest enters the room are more formal but still appreciated. Parents who use and expect courtesy manners with everyone – irrespective of gender, race, ethnicity, or role as a server versus professional – show that they value others and build antiracism.

School age is a time to learn to wait before speaking to consider whether what they say could be experienced as hurtful to the other person. This requires taking someone else’s point of view, an ability that emerges around age 6 years and can be promoted when parents review with their child “How would you feel if it were you?” Role playing common scenarios of how to behave and speak when seeing a person who looks or acts different is also effective. Avoiding interrupting may be more difficult for very talkative or impulsive children, especially those with ADHD. Practicing waiting for permission to speak by being handed a “talking stick” at the dinner table can be good practice for everyone.
Manners are a group asset
Beyond personal benefits, manners are the basis of a civil society. Cultural norm manners are particular to groups, helping members feel affiliated, as well as identifying those with different manners as “other.”
Teens are particularly likely to use a different code of behavior to fit in with a subgroup. This may be acceptable if restricted to within their group (such as swear words) or within certain agreed-upon limits with family members. But teens need to understand the value of learning, practicing, and using manners for their own, as well as their group’s and nation’s, well-being.
As a developmental-behavioral pediatrician, I have cared for many children with intellectual disabilities and autism spectrum disorder (ASD). Deficits in social interaction skills are a basic criterion for the diagnosis of ASD. Overtraining is especially needed for children with ASD whose mirror movements, social attention, and imitation are weak. For children with these conditions, making manners a strong habit takes more effort but is even more vital than for neurotypical children. Temple Grandin, a famous adult with ASD, has described how her mother taught her manners as a survival skill. She reports incorporating manners very consciously and methodically because they did not come naturally. Children with even rote social skills are liked better by peers and teachers, their atypical behaviors is better tolerated, and they get more positive feedback that encourages integration inside and outside the classroom. Manners may make the difference between being allowed in or expelled from classrooms, libraries, clubs, teams, or religious institutions. When it is time to get a job, social skills are the key factor for employment for these individuals and a significant help for neurotypical individuals as well. Failure to signal socially appropriate behavior can make a person appear threatening and has had the rare but tragic result of rough or fatal handling by police.
Has the teaching of manners waned? Perhaps, because, for some families, the child is being socialized mostly by nonfamily caregivers who have low use of manners. Some parents have made teaching manners a low priority or even resisted using manners themselves as inauthentic. This may reflect prioritizing a “laid-back” lifestyle and speaking crudely as a sign of independence, perhaps in reaction to lack of autonomy at work. Mastering the careful interactions developed over time to avoid invoking an aggressive response depend on direct feedback from reactions of the recipient. With so much of our communication done electronically, asynchronously, even anonymously, the usual feedback has been reduced. Practicing curses, insults, and put-downs online easily extends to in-person interactions without the perpetrator even noticing and are generally reinforced and repeated without parental supervision. Disrespectful behavior from community leaders also reduces the threshold for society.
When people are ignorant of or choose not to use manners they may be perceived as “other” and hostile. This may lead to distrust, dislike, and lowered ability to find the common ground needed for making decisions that benefit the greater society. Oliver Wendell Holmes said “Under bad manners ... lies very commonly an overestimate of our special individuality, as distinguished from our generic humanity (“The Professor at the Breakfast Table,” 1858). Working for major goals that benefit all of humanity is essential to survival in our highly interconnected world. Considering all of humanity is a difficult concept for children, and even for many adults, but it starts with using civil behavior at home, in school, and in one’s community.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Have you been surprised and impressed by a child who says after a visit, “Thank you, Doctor [Howard]”? While it may seem antiquated to teach such manners to children these days, there are several important benefits to this education.
Manners serve important functions in benefiting a person’s group with cohesiveness and the individuals themselves with acceptance in the group. Use of manners instantly suggests a more trustworthy person.
There are three main categories of manners: hygiene, courtesy, and cultural norm manners.
Hygiene manners, from using the toilet to refraining from picking one’s nose, have obvious health benefits of not spreading disease. Hygiene manners take time to teach, but parents are motivated and helped by natural reactions of disgust that even infants recognize.
Courtesy manners, on the other hand, are habits of self-control and good-faith behaviors that signal that one is putting the interests of others ahead of one’s own for the moment. Taking another’s comfort into account, basic to kindness and respect, does not require agreeing with or submitting to the other. Courtesy manners require a developing self-awareness (I can choose to act this way) and awareness of social status (I am not more important than everyone else) that begins in toddlerhood. Modeling manners around the child is the most important way to teach courtesy. Parents usually start actively teaching the child to say “please” and “thank you,” and show pride in this apparent “demonstration of appreciation” even when it is simply reinforced behavior at first. The delight of grandparents reinforces both the parents and children, and reflects manners as building tribe cohesiveness.
Good manners become a habit
Manners such as warm greetings, a firm handshake (before COVID-19), and prompt thanks are most believable when occurring promptly when appropriate – when they come from habit. This immediate reaction, a result of so-called “fast thinking,” develops when behaviors learned from “slow thinking” are instilled early and often until they are automatic. The other benefit of this overlearning is that the behavior then looks unambivalent; a lag of too many milliseconds makes the recipient doubt genuineness.
Parents often ask us how to handle their child‘s rude or disrespectful behavior. Praise for manners is a simple start. Toddlers and preschoolers are taught manners best by adult modeling, but also by reinforcement and praise for the basics: to say “Hello,” ask “Please,” and say “Thank you,” “Excuse me,” “You’re welcome,” or “Would you help me, please?” The behaviors also include avoiding raising one’s voice, suppressing interrupting, and apologizing when appropriate. Even shy children can learn eye contact by making a game of figuring out the other’s eye color. Shaming, yelling, and punishing for poor manners usually backfires because it shows disrespect of the child who will likely give this back.
Older children can be taught to offer other people the opportunity to go through a door first, to be first to select a seat, speak first and without interruption, or order first. There are daily opportunities for these manners of showing respect. Opening doors for others, or standing when a guest enters the room are more formal but still appreciated. Parents who use and expect courtesy manners with everyone – irrespective of gender, race, ethnicity, or role as a server versus professional – show that they value others and build antiracism.
School age is a time to learn to wait before speaking to consider whether what they say could be experienced as hurtful to the other person. This requires taking someone else’s point of view, an ability that emerges around age 6 years and can be promoted when parents review with their child “How would you feel if it were you?” Role playing common scenarios of how to behave and speak when seeing a person who looks or acts different is also effective. Avoiding interrupting may be more difficult for very talkative or impulsive children, especially those with ADHD. Practicing waiting for permission to speak by being handed a “talking stick” at the dinner table can be good practice for everyone.
Manners are a group asset
Beyond personal benefits, manners are the basis of a civil society. Cultural norm manners are particular to groups, helping members feel affiliated, as well as identifying those with different manners as “other.”
Teens are particularly likely to use a different code of behavior to fit in with a subgroup. This may be acceptable if restricted to within their group (such as swear words) or within certain agreed-upon limits with family members. But teens need to understand the value of learning, practicing, and using manners for their own, as well as their group’s and nation’s, well-being.
As a developmental-behavioral pediatrician, I have cared for many children with intellectual disabilities and autism spectrum disorder (ASD). Deficits in social interaction skills are a basic criterion for the diagnosis of ASD. Overtraining is especially needed for children with ASD whose mirror movements, social attention, and imitation are weak. For children with these conditions, making manners a strong habit takes more effort but is even more vital than for neurotypical children. Temple Grandin, a famous adult with ASD, has described how her mother taught her manners as a survival skill. She reports incorporating manners very consciously and methodically because they did not come naturally. Children with even rote social skills are liked better by peers and teachers, their atypical behaviors is better tolerated, and they get more positive feedback that encourages integration inside and outside the classroom. Manners may make the difference between being allowed in or expelled from classrooms, libraries, clubs, teams, or religious institutions. When it is time to get a job, social skills are the key factor for employment for these individuals and a significant help for neurotypical individuals as well. Failure to signal socially appropriate behavior can make a person appear threatening and has had the rare but tragic result of rough or fatal handling by police.
Has the teaching of manners waned? Perhaps, because, for some families, the child is being socialized mostly by nonfamily caregivers who have low use of manners. Some parents have made teaching manners a low priority or even resisted using manners themselves as inauthentic. This may reflect prioritizing a “laid-back” lifestyle and speaking crudely as a sign of independence, perhaps in reaction to lack of autonomy at work. Mastering the careful interactions developed over time to avoid invoking an aggressive response depend on direct feedback from reactions of the recipient. With so much of our communication done electronically, asynchronously, even anonymously, the usual feedback has been reduced. Practicing curses, insults, and put-downs online easily extends to in-person interactions without the perpetrator even noticing and are generally reinforced and repeated without parental supervision. Disrespectful behavior from community leaders also reduces the threshold for society.
When people are ignorant of or choose not to use manners they may be perceived as “other” and hostile. This may lead to distrust, dislike, and lowered ability to find the common ground needed for making decisions that benefit the greater society. Oliver Wendell Holmes said “Under bad manners ... lies very commonly an overestimate of our special individuality, as distinguished from our generic humanity (“The Professor at the Breakfast Table,” 1858). Working for major goals that benefit all of humanity is essential to survival in our highly interconnected world. Considering all of humanity is a difficult concept for children, and even for many adults, but it starts with using civil behavior at home, in school, and in one’s community.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Have you been surprised and impressed by a child who says after a visit, “Thank you, Doctor [Howard]”? While it may seem antiquated to teach such manners to children these days, there are several important benefits to this education.
Manners serve important functions in benefiting a person’s group with cohesiveness and the individuals themselves with acceptance in the group. Use of manners instantly suggests a more trustworthy person.
There are three main categories of manners: hygiene, courtesy, and cultural norm manners.
Hygiene manners, from using the toilet to refraining from picking one’s nose, have obvious health benefits of not spreading disease. Hygiene manners take time to teach, but parents are motivated and helped by natural reactions of disgust that even infants recognize.
Courtesy manners, on the other hand, are habits of self-control and good-faith behaviors that signal that one is putting the interests of others ahead of one’s own for the moment. Taking another’s comfort into account, basic to kindness and respect, does not require agreeing with or submitting to the other. Courtesy manners require a developing self-awareness (I can choose to act this way) and awareness of social status (I am not more important than everyone else) that begins in toddlerhood. Modeling manners around the child is the most important way to teach courtesy. Parents usually start actively teaching the child to say “please” and “thank you,” and show pride in this apparent “demonstration of appreciation” even when it is simply reinforced behavior at first. The delight of grandparents reinforces both the parents and children, and reflects manners as building tribe cohesiveness.
Good manners become a habit
Manners such as warm greetings, a firm handshake (before COVID-19), and prompt thanks are most believable when occurring promptly when appropriate – when they come from habit. This immediate reaction, a result of so-called “fast thinking,” develops when behaviors learned from “slow thinking” are instilled early and often until they are automatic. The other benefit of this overlearning is that the behavior then looks unambivalent; a lag of too many milliseconds makes the recipient doubt genuineness.
Parents often ask us how to handle their child‘s rude or disrespectful behavior. Praise for manners is a simple start. Toddlers and preschoolers are taught manners best by adult modeling, but also by reinforcement and praise for the basics: to say “Hello,” ask “Please,” and say “Thank you,” “Excuse me,” “You’re welcome,” or “Would you help me, please?” The behaviors also include avoiding raising one’s voice, suppressing interrupting, and apologizing when appropriate. Even shy children can learn eye contact by making a game of figuring out the other’s eye color. Shaming, yelling, and punishing for poor manners usually backfires because it shows disrespect of the child who will likely give this back.
Older children can be taught to offer other people the opportunity to go through a door first, to be first to select a seat, speak first and without interruption, or order first. There are daily opportunities for these manners of showing respect. Opening doors for others, or standing when a guest enters the room are more formal but still appreciated. Parents who use and expect courtesy manners with everyone – irrespective of gender, race, ethnicity, or role as a server versus professional – show that they value others and build antiracism.
School age is a time to learn to wait before speaking to consider whether what they say could be experienced as hurtful to the other person. This requires taking someone else’s point of view, an ability that emerges around age 6 years and can be promoted when parents review with their child “How would you feel if it were you?” Role playing common scenarios of how to behave and speak when seeing a person who looks or acts different is also effective. Avoiding interrupting may be more difficult for very talkative or impulsive children, especially those with ADHD. Practicing waiting for permission to speak by being handed a “talking stick” at the dinner table can be good practice for everyone.
Manners are a group asset
Beyond personal benefits, manners are the basis of a civil society. Cultural norm manners are particular to groups, helping members feel affiliated, as well as identifying those with different manners as “other.”
Teens are particularly likely to use a different code of behavior to fit in with a subgroup. This may be acceptable if restricted to within their group (such as swear words) or within certain agreed-upon limits with family members. But teens need to understand the value of learning, practicing, and using manners for their own, as well as their group’s and nation’s, well-being.
As a developmental-behavioral pediatrician, I have cared for many children with intellectual disabilities and autism spectrum disorder (ASD). Deficits in social interaction skills are a basic criterion for the diagnosis of ASD. Overtraining is especially needed for children with ASD whose mirror movements, social attention, and imitation are weak. For children with these conditions, making manners a strong habit takes more effort but is even more vital than for neurotypical children. Temple Grandin, a famous adult with ASD, has described how her mother taught her manners as a survival skill. She reports incorporating manners very consciously and methodically because they did not come naturally. Children with even rote social skills are liked better by peers and teachers, their atypical behaviors is better tolerated, and they get more positive feedback that encourages integration inside and outside the classroom. Manners may make the difference between being allowed in or expelled from classrooms, libraries, clubs, teams, or religious institutions. When it is time to get a job, social skills are the key factor for employment for these individuals and a significant help for neurotypical individuals as well. Failure to signal socially appropriate behavior can make a person appear threatening and has had the rare but tragic result of rough or fatal handling by police.
Has the teaching of manners waned? Perhaps, because, for some families, the child is being socialized mostly by nonfamily caregivers who have low use of manners. Some parents have made teaching manners a low priority or even resisted using manners themselves as inauthentic. This may reflect prioritizing a “laid-back” lifestyle and speaking crudely as a sign of independence, perhaps in reaction to lack of autonomy at work. Mastering the careful interactions developed over time to avoid invoking an aggressive response depend on direct feedback from reactions of the recipient. With so much of our communication done electronically, asynchronously, even anonymously, the usual feedback has been reduced. Practicing curses, insults, and put-downs online easily extends to in-person interactions without the perpetrator even noticing and are generally reinforced and repeated without parental supervision. Disrespectful behavior from community leaders also reduces the threshold for society.
When people are ignorant of or choose not to use manners they may be perceived as “other” and hostile. This may lead to distrust, dislike, and lowered ability to find the common ground needed for making decisions that benefit the greater society. Oliver Wendell Holmes said “Under bad manners ... lies very commonly an overestimate of our special individuality, as distinguished from our generic humanity (“The Professor at the Breakfast Table,” 1858). Working for major goals that benefit all of humanity is essential to survival in our highly interconnected world. Considering all of humanity is a difficult concept for children, and even for many adults, but it starts with using civil behavior at home, in school, and in one’s community.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.