User login
Ultrasound method predicts liver complications in pediatric transplant
HOUSTON – An ultrasound method for assessing liver stiffness might be useful for predicting which pediatric patients will develop a life-threatening complication of hematopoietic stem cell transplantation.

Shear wave elastography values predicted severe hepatic sinusoidal obstruction syndrome/veno-occlusive disease (SOS/VOD) at least 4 days before standard diagnostic criteria in most patients treated in a small, prospective, two-center study, Sherwin S. Chan, MD, PhD, said at the Transplantation & Cellular Therapy Meetings.
Early identification of SOS/VOD using elastography could be beneficial in light of data showing that timing is critical in the administration of defibrotide, a treatment recommended for severe and very severe patients, according to Dr. Chan, vice chair of radiology for the University of Missouri at Kansas City.
“If you’re able to initiate it early, you can really increase day 100 survival,” Dr. Chan said in an oral presentation.
The data presented included 54 pediatric patients undergoing transplantation at one of two institutions.
At one site, the patients underwent shear wave elastography evaluation 10 days before the conditioning regimen began, and again at 5 and 14 days after the transplant. At the other site, patients with suspected SOS/VOD were enrolled and underwent elastography every other day for up to 10 exams.
Those are very different imaging protocols, Dr. Chan acknowledged in his presentation, noting that the studies started independently and data were pooled as investigators at the two institutions became aware of one another’s work.
A total of 16 patients, or 30%, developed SOS/VOD, Dr. Chan reported. Of those 16 cases, 12 (75%) were severe or very severe by the recent European Society for Blood and Marrow Transplantation (EBMT) criteria.
Increased shear wave elastography velocity was the best predictor of severe SOS/VOD, according to Dr. Chan, with a cutoff value of 1.65 m/s being 92% sensitive and 67% specific for severe SOS/VOD.
That threshold was passed at least 4 days before severe grading or death in 9 out of the 12 severe cases, he added.
Accordingly, a prospective, multicenter trial has been initiated at a number of U.S. centers to investigate whether the findings of this study are generalizable to other patient populations, Dr. Chan said at the meeting held by the American Society of Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research. At this meeting, the American Society for Blood and Marrow Transplantation announced a new name for the society: American Society for Transplantation and Cellular Therapy.
That prospective, multicenter trial is supported by Jazz Pharmaceuticals, according to Dr. Chan, who reported consulting with Jazz Pharmaceuticals in his disclosure statement.
SOURCE: Chan SS et al. TCT 2019, Abstract 55.
HOUSTON – An ultrasound method for assessing liver stiffness might be useful for predicting which pediatric patients will develop a life-threatening complication of hematopoietic stem cell transplantation.
Shear wave elastography values predicted severe hepatic sinusoidal obstruction syndrome/veno-occlusive disease (SOS/VOD) at least 4 days before standard diagnostic criteria in most patients treated in a small, prospective, two-center study, Sherwin S. Chan, MD, PhD, said at the Transplantation & Cellular Therapy Meetings.
Early identification of SOS/VOD using elastography could be beneficial in light of data showing that timing is critical in the administration of defibrotide, a treatment recommended for severe and very severe patients, according to Dr. Chan, vice chair of radiology for the University of Missouri at Kansas City.
“If you’re able to initiate it early, you can really increase day 100 survival,” Dr. Chan said in an oral presentation.
The data presented included 54 pediatric patients undergoing transplantation at one of two institutions.
At one site, the patients underwent shear wave elastography evaluation 10 days before the conditioning regimen began, and again at 5 and 14 days after the transplant. At the other site, patients with suspected SOS/VOD were enrolled and underwent elastography every other day for up to 10 exams.
Those are very different imaging protocols, Dr. Chan acknowledged in his presentation, noting that the studies started independently and data were pooled as investigators at the two institutions became aware of one another’s work.
A total of 16 patients, or 30%, developed SOS/VOD, Dr. Chan reported. Of those 16 cases, 12 (75%) were severe or very severe by the recent European Society for Blood and Marrow Transplantation (EBMT) criteria.
Increased shear wave elastography velocity was the best predictor of severe SOS/VOD, according to Dr. Chan, with a cutoff value of 1.65 m/s being 92% sensitive and 67% specific for severe SOS/VOD.
That threshold was passed at least 4 days before severe grading or death in 9 out of the 12 severe cases, he added.
Accordingly, a prospective, multicenter trial has been initiated at a number of U.S. centers to investigate whether the findings of this study are generalizable to other patient populations, Dr. Chan said at the meeting held by the American Society of Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research. At this meeting, the American Society for Blood and Marrow Transplantation announced a new name for the society: American Society for Transplantation and Cellular Therapy.
That prospective, multicenter trial is supported by Jazz Pharmaceuticals, according to Dr. Chan, who reported consulting with Jazz Pharmaceuticals in his disclosure statement.
SOURCE: Chan SS et al. TCT 2019, Abstract 55.
HOUSTON – An ultrasound method for assessing liver stiffness might be useful for predicting which pediatric patients will develop a life-threatening complication of hematopoietic stem cell transplantation.
Shear wave elastography values predicted severe hepatic sinusoidal obstruction syndrome/veno-occlusive disease (SOS/VOD) at least 4 days before standard diagnostic criteria in most patients treated in a small, prospective, two-center study, Sherwin S. Chan, MD, PhD, said at the Transplantation & Cellular Therapy Meetings.
Early identification of SOS/VOD using elastography could be beneficial in light of data showing that timing is critical in the administration of defibrotide, a treatment recommended for severe and very severe patients, according to Dr. Chan, vice chair of radiology for the University of Missouri at Kansas City.
“If you’re able to initiate it early, you can really increase day 100 survival,” Dr. Chan said in an oral presentation.
The data presented included 54 pediatric patients undergoing transplantation at one of two institutions.
At one site, the patients underwent shear wave elastography evaluation 10 days before the conditioning regimen began, and again at 5 and 14 days after the transplant. At the other site, patients with suspected SOS/VOD were enrolled and underwent elastography every other day for up to 10 exams.
Those are very different imaging protocols, Dr. Chan acknowledged in his presentation, noting that the studies started independently and data were pooled as investigators at the two institutions became aware of one another’s work.
A total of 16 patients, or 30%, developed SOS/VOD, Dr. Chan reported. Of those 16 cases, 12 (75%) were severe or very severe by the recent European Society for Blood and Marrow Transplantation (EBMT) criteria.
Increased shear wave elastography velocity was the best predictor of severe SOS/VOD, according to Dr. Chan, with a cutoff value of 1.65 m/s being 92% sensitive and 67% specific for severe SOS/VOD.
That threshold was passed at least 4 days before severe grading or death in 9 out of the 12 severe cases, he added.
Accordingly, a prospective, multicenter trial has been initiated at a number of U.S. centers to investigate whether the findings of this study are generalizable to other patient populations, Dr. Chan said at the meeting held by the American Society of Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research. At this meeting, the American Society for Blood and Marrow Transplantation announced a new name for the society: American Society for Transplantation and Cellular Therapy.
That prospective, multicenter trial is supported by Jazz Pharmaceuticals, according to Dr. Chan, who reported consulting with Jazz Pharmaceuticals in his disclosure statement.
SOURCE: Chan SS et al. TCT 2019, Abstract 55.
REPORTING FROM TCT 2019
Palliative care has improved for critically ill children, but challenges remain
SAN DIEGO – and is more common among older children, female children, and those with government insurance or at a high risk of mortality. The findings come from a retrospective analysis of data from 52 hospitals, which included ICU admissions (except neonatal ICU) during 2007-2018.

The good news is that palliative care consultations have increased, with consultations in less than 1% of cases at the start of the study and rising quickly to more than 7% in 2018.
“In the adult world, palliative care has expanded in recent decades, and I think now that it’s coming to the pediatric world, it’ll just continue to go up,” said Siobhan O’Keefe, MD, in an interview. Dr. O’Keefe is with Children’s Hospital Colorado, Aurora. She presented the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
More work needs to be done, she said. “We are not uniformly using palliative care for critically ill children in the U.S., and it varies across institutions. That’s probably not the ideal situation,” said Dr. O’Keefe. The study did not track palliative care versus the presence of board-certified palliative care physicians or palliative care fellowships, but she suspects they would correlate.
Dr. O’Keefe called for physicians to think beyond the patient, to family members and caregivers. “We need to focus on family outcomes, how they are taking care of children with moderate disability, and incorporate that into our outcomes,” she said. Previous research has shown family members to be at risk of anxiety, depression, unemployment, and financial distress.
The researchers analyzed data from 740,890 patients with 1,024,666 hospitalizations (82% had one hospitalization). They divided subjects into three cohorts, one of which was a category of patients with criteria for palliative care based on previous research (PC-ICU). The PC-ICU cohort included patients with an expected length of stay more than 2 weeks, patients receiving extracorporeal membrane oxygenation (ECMO), severe brain injuries, acute respiratory failure with serious comorbidity, hematologic or oncologic disease, metabolic disease, renal failure that required continuous renal replacement therapy, hepatic failure, or serious chromosomal abnormality. A second cohort included chronic complex conditions not found in the PC-ICU cohort (additional criteria), and a third cohort had no criteria for palliative care.
Thirty percent of hospitalizations met the PC-ICU cohort criteria, 40% met the additional cohort criteria, and 30% fell in the no criteria cohort. The PC-ICU group had the highest mortality, at 8.03%, compared with 1.08% in the additional criteria group and 0.34% in the no criteria group (P less than .00001).
Palliative care consultations occurred more frequently in 5-12 year olds (odds ratio 1.06; 95% confidence interval, 1.01-1.13) and in those aged 13 years or older (OR, 1.38; 95% CI, 1.3-1.46), in females (OR, 1.13; 95% CI, 1.06-1.15), and in patients with government insurance (OR, 1.23; 95% CI, 1.17-1.29). Compared with those in the no criteria cohort, PC-ICU patients were more likely to receive a palliative care consult (OR, 75.5; 95% CI, 60.4-94.3), as were those in the additional criteria group (OR, 19.1; 95% CI, 15.3-23.9).
Cross-institutional palliative care frequency varied widely among patients in the PC-ICU group, ranging from 0% to 44%. The frequency ranged from 0% to 12% across institutions for patients in the additional criteria group.
SOURCE: O’Keefe S et al. Critical Care Congress 2019, Abstract 418.
SAN DIEGO – and is more common among older children, female children, and those with government insurance or at a high risk of mortality. The findings come from a retrospective analysis of data from 52 hospitals, which included ICU admissions (except neonatal ICU) during 2007-2018.
The good news is that palliative care consultations have increased, with consultations in less than 1% of cases at the start of the study and rising quickly to more than 7% in 2018.
“In the adult world, palliative care has expanded in recent decades, and I think now that it’s coming to the pediatric world, it’ll just continue to go up,” said Siobhan O’Keefe, MD, in an interview. Dr. O’Keefe is with Children’s Hospital Colorado, Aurora. She presented the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
More work needs to be done, she said. “We are not uniformly using palliative care for critically ill children in the U.S., and it varies across institutions. That’s probably not the ideal situation,” said Dr. O’Keefe. The study did not track palliative care versus the presence of board-certified palliative care physicians or palliative care fellowships, but she suspects they would correlate.
Dr. O’Keefe called for physicians to think beyond the patient, to family members and caregivers. “We need to focus on family outcomes, how they are taking care of children with moderate disability, and incorporate that into our outcomes,” she said. Previous research has shown family members to be at risk of anxiety, depression, unemployment, and financial distress.
The researchers analyzed data from 740,890 patients with 1,024,666 hospitalizations (82% had one hospitalization). They divided subjects into three cohorts, one of which was a category of patients with criteria for palliative care based on previous research (PC-ICU). The PC-ICU cohort included patients with an expected length of stay more than 2 weeks, patients receiving extracorporeal membrane oxygenation (ECMO), severe brain injuries, acute respiratory failure with serious comorbidity, hematologic or oncologic disease, metabolic disease, renal failure that required continuous renal replacement therapy, hepatic failure, or serious chromosomal abnormality. A second cohort included chronic complex conditions not found in the PC-ICU cohort (additional criteria), and a third cohort had no criteria for palliative care.
Thirty percent of hospitalizations met the PC-ICU cohort criteria, 40% met the additional cohort criteria, and 30% fell in the no criteria cohort. The PC-ICU group had the highest mortality, at 8.03%, compared with 1.08% in the additional criteria group and 0.34% in the no criteria group (P less than .00001).
Palliative care consultations occurred more frequently in 5-12 year olds (odds ratio 1.06; 95% confidence interval, 1.01-1.13) and in those aged 13 years or older (OR, 1.38; 95% CI, 1.3-1.46), in females (OR, 1.13; 95% CI, 1.06-1.15), and in patients with government insurance (OR, 1.23; 95% CI, 1.17-1.29). Compared with those in the no criteria cohort, PC-ICU patients were more likely to receive a palliative care consult (OR, 75.5; 95% CI, 60.4-94.3), as were those in the additional criteria group (OR, 19.1; 95% CI, 15.3-23.9).
Cross-institutional palliative care frequency varied widely among patients in the PC-ICU group, ranging from 0% to 44%. The frequency ranged from 0% to 12% across institutions for patients in the additional criteria group.
SOURCE: O’Keefe S et al. Critical Care Congress 2019, Abstract 418.
SAN DIEGO – and is more common among older children, female children, and those with government insurance or at a high risk of mortality. The findings come from a retrospective analysis of data from 52 hospitals, which included ICU admissions (except neonatal ICU) during 2007-2018.
The good news is that palliative care consultations have increased, with consultations in less than 1% of cases at the start of the study and rising quickly to more than 7% in 2018.
“In the adult world, palliative care has expanded in recent decades, and I think now that it’s coming to the pediatric world, it’ll just continue to go up,” said Siobhan O’Keefe, MD, in an interview. Dr. O’Keefe is with Children’s Hospital Colorado, Aurora. She presented the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
More work needs to be done, she said. “We are not uniformly using palliative care for critically ill children in the U.S., and it varies across institutions. That’s probably not the ideal situation,” said Dr. O’Keefe. The study did not track palliative care versus the presence of board-certified palliative care physicians or palliative care fellowships, but she suspects they would correlate.
Dr. O’Keefe called for physicians to think beyond the patient, to family members and caregivers. “We need to focus on family outcomes, how they are taking care of children with moderate disability, and incorporate that into our outcomes,” she said. Previous research has shown family members to be at risk of anxiety, depression, unemployment, and financial distress.
The researchers analyzed data from 740,890 patients with 1,024,666 hospitalizations (82% had one hospitalization). They divided subjects into three cohorts, one of which was a category of patients with criteria for palliative care based on previous research (PC-ICU). The PC-ICU cohort included patients with an expected length of stay more than 2 weeks, patients receiving extracorporeal membrane oxygenation (ECMO), severe brain injuries, acute respiratory failure with serious comorbidity, hematologic or oncologic disease, metabolic disease, renal failure that required continuous renal replacement therapy, hepatic failure, or serious chromosomal abnormality. A second cohort included chronic complex conditions not found in the PC-ICU cohort (additional criteria), and a third cohort had no criteria for palliative care.
Thirty percent of hospitalizations met the PC-ICU cohort criteria, 40% met the additional cohort criteria, and 30% fell in the no criteria cohort. The PC-ICU group had the highest mortality, at 8.03%, compared with 1.08% in the additional criteria group and 0.34% in the no criteria group (P less than .00001).
Palliative care consultations occurred more frequently in 5-12 year olds (odds ratio 1.06; 95% confidence interval, 1.01-1.13) and in those aged 13 years or older (OR, 1.38; 95% CI, 1.3-1.46), in females (OR, 1.13; 95% CI, 1.06-1.15), and in patients with government insurance (OR, 1.23; 95% CI, 1.17-1.29). Compared with those in the no criteria cohort, PC-ICU patients were more likely to receive a palliative care consult (OR, 75.5; 95% CI, 60.4-94.3), as were those in the additional criteria group (OR, 19.1; 95% CI, 15.3-23.9).
Cross-institutional palliative care frequency varied widely among patients in the PC-ICU group, ranging from 0% to 44%. The frequency ranged from 0% to 12% across institutions for patients in the additional criteria group.
SOURCE: O’Keefe S et al. Critical Care Congress 2019, Abstract 418.
REPORTING FROM CCC48
Influenza activity continues to increase
The 2018-2019 flu season is showing no signs of decline as activity measures continued to increase into mid-February, according to the Centers for Disease Control and Prevention.
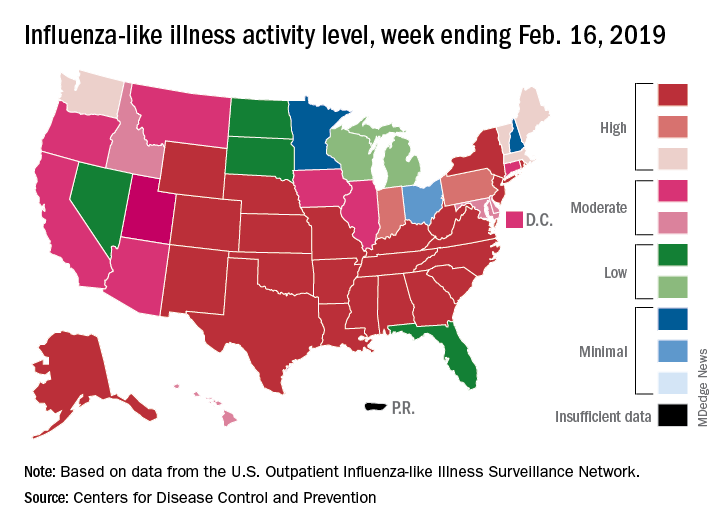
Eight of the last 10 flu seasons had already reached their peak before mid-February, but another rise brought the proportion of outpatient visits for influenza-like illness (ILI) to 5.1% for the week ending Feb. 16, compared with 4.8% the week before, the CDC’s influenza division reported Feb. 22. ILI is defined as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.
The week also brought more ILI to more states, as the number reporting an activity level of 10 on the CDC’s 1-10 scale rose from 21 to 24 and the number in the high range of 8-10 increased from 26 to 30. Another seven states – including California, which was at level 5 the previous week – and the District of Columbia were at level 7 for the current reporting week, the CDC said.
Two flu-related pediatric deaths occurred during the week ending Feb. 16 and another five were reported from previous weeks, which brings the total to 41 for the 2018-2019 season. Data for influenza deaths at all ages, which are reported a week later, show that 205 occurred in the week ending Feb. 9, with reporting 75% complete. There were 236 total deaths for the week ending Feb. 2 (94% reporting) and 218 deaths during the week ending Jan. 26 (99% reporting), the CDC said.
The 2018-2019 flu season is showing no signs of decline as activity measures continued to increase into mid-February, according to the Centers for Disease Control and Prevention.
Eight of the last 10 flu seasons had already reached their peak before mid-February, but another rise brought the proportion of outpatient visits for influenza-like illness (ILI) to 5.1% for the week ending Feb. 16, compared with 4.8% the week before, the CDC’s influenza division reported Feb. 22. ILI is defined as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.
The week also brought more ILI to more states, as the number reporting an activity level of 10 on the CDC’s 1-10 scale rose from 21 to 24 and the number in the high range of 8-10 increased from 26 to 30. Another seven states – including California, which was at level 5 the previous week – and the District of Columbia were at level 7 for the current reporting week, the CDC said.
Two flu-related pediatric deaths occurred during the week ending Feb. 16 and another five were reported from previous weeks, which brings the total to 41 for the 2018-2019 season. Data for influenza deaths at all ages, which are reported a week later, show that 205 occurred in the week ending Feb. 9, with reporting 75% complete. There were 236 total deaths for the week ending Feb. 2 (94% reporting) and 218 deaths during the week ending Jan. 26 (99% reporting), the CDC said.
The 2018-2019 flu season is showing no signs of decline as activity measures continued to increase into mid-February, according to the Centers for Disease Control and Prevention.
Eight of the last 10 flu seasons had already reached their peak before mid-February, but another rise brought the proportion of outpatient visits for influenza-like illness (ILI) to 5.1% for the week ending Feb. 16, compared with 4.8% the week before, the CDC’s influenza division reported Feb. 22. ILI is defined as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.
The week also brought more ILI to more states, as the number reporting an activity level of 10 on the CDC’s 1-10 scale rose from 21 to 24 and the number in the high range of 8-10 increased from 26 to 30. Another seven states – including California, which was at level 5 the previous week – and the District of Columbia were at level 7 for the current reporting week, the CDC said.
Two flu-related pediatric deaths occurred during the week ending Feb. 16 and another five were reported from previous weeks, which brings the total to 41 for the 2018-2019 season. Data for influenza deaths at all ages, which are reported a week later, show that 205 occurred in the week ending Feb. 9, with reporting 75% complete. There were 236 total deaths for the week ending Feb. 2 (94% reporting) and 218 deaths during the week ending Jan. 26 (99% reporting), the CDC said.
Pseudoscience redux
My most recent column discussed the problem of pseudoscience that pervades some corners of the Internet. Personally, I respond to pseudoscience primarily by trying to provide accurate and less-biased information. I recognize that not everyone approaches decision making by seeking more information. When dealing a diverse public, a medical professional needs to have other approaches in the armamentarium.1 When dealing with other physicians, I am less flexible. Either the profession of medicine believes in science or it doesn’t.
![]()
Since that column was published, there have been major developments. There are measles outbreaks in the states of Washington and New York, and more than 100 deaths from a measles epidemic in the Philippines. The World Health Organization has made vaccine hesitancy one of its ten threats to global health in 2019.
Facebook has indicated that it might demote the priority and frequency with which it recommends articles that promulgate anti-vax information and conspiracy theories.2 Facebook isn’t doing this because it has had an epiphany; it has come under pressure for its role in the spread of misinformation. Current legislation was written before the rise of social media, when Internet Service Providers were primarily conduits to transfer bits and bytes between computers. Those ISPs were not liable for the content of the transmitted Web pages. Facebook, by producing what it called a newsfeed and by making personalized suggestions for other websites to browse, doesn’t fit the passive model of an ISP.
For alleged violations of user’s privacy, Facebook might be subject to billion dollar fines, according to a Washington Post article.3 Still, for a company whose revenue is $4 billion per month and whose stock market value is $400 billion, paying a billion dollar fine for years of alleged misbehaviors that have enabled it to become a giant empire is, “in the scheme of things ... a speeding ticket” in the parlance of the penultimate scene of the movie The Social Network. The real financial risk is people deciding they can’t trust the platform and going elsewhere.
Authorities in the United Kingdom in February 2019 released a highly critical, 108-page report about fake news, which said, “Facebook should not be allowed to behave like ‘digital gangsters’ in the online world.”4 The U.K. report urges new regulations to deal with privacy breaches and with fake news. It endeavors to create a duty for social media companies to combat the spread of misinformation.
Then the Wall Street Journal reported that Pinterest has stopped returning results for searches related to vaccination.5 Pinterest realized that most of the shared images on its platform cautioned against vaccination, which contradicts the recommendations of medical experts. Unable to otherwise combat the flow of misinformation, the company apparently has decided to eliminate returning results, pro or con, for any search terms related to vaccines.

While lamenting the public’s inability to distinguish misinformation on the Internet, I’ve also been observing the factors that lead physicians astray. I expect physicians, as trained scientists and as professionals, to be able to assimilate new information and change their practices accordingly. Those who do research on the translation of technology find that, this doesn’t happen with any regularity.
The February 2019 issue of Hospital Pediatrics has four items on the topic of treating bronchiolitis, including two research articles, a brief report, and a commentary. That is obviously a relevant topic this time of year. The impression after reading those four items is that hospitalists don’t really know how to best treat the most common illness they encounter. And even when they “know” how to do it, many factors distort the science. Those factors are highlighted in the article on barriers to minimizing viral testing.6
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. “Discussing immunization with vaccine-hesitant parents requires caring, individualized approach,” by Jeff Craven, Pediatric News, Nov. 7, 2018; “How do you get anti-vaxxers to vaccinate their kids? Talk to them – for hours,” by Nadine Gartner, Washington Post, Feb. 19, 2019.
2. “Facebook will consider removing or demoting anti-vaccination recommendations amid backlash,” by Taylor Telford, Washington Post, Feb. 15, 2019.
3. “U.S. regulators have met to discuss imposing a record-setting fine against Facebook for privacy violations,” by Tony Romm and Elizabeth Dwoskin, Washington Post, Jan. 18, 2019; “Report: Facebook, FTC discussing ‘multibillion dollar’ fine,” by Associated Press.
4. “Disinformation and ‘fake news’: Final Report,” House of Commons, Feb. 18, 2019, p. 42, item 139.
5. “Pinterest blocks vaccination searches in move to control the conversation,” by Robert McMillan and Daniela Hernandez, The Wall Street Journal, Feb. 20, 2019.
6. “Barriers to minimizing respiratory viral testing in bronchiolitis: Physician perceptions on testing practices,” by MZ Huang et al. Hospital Pediatrics 2019 Feb. doi: 10.1542/hpeds.2018-0108.
My most recent column discussed the problem of pseudoscience that pervades some corners of the Internet. Personally, I respond to pseudoscience primarily by trying to provide accurate and less-biased information. I recognize that not everyone approaches decision making by seeking more information. When dealing a diverse public, a medical professional needs to have other approaches in the armamentarium.1 When dealing with other physicians, I am less flexible. Either the profession of medicine believes in science or it doesn’t.
![]()
Since that column was published, there have been major developments. There are measles outbreaks in the states of Washington and New York, and more than 100 deaths from a measles epidemic in the Philippines. The World Health Organization has made vaccine hesitancy one of its ten threats to global health in 2019.
Facebook has indicated that it might demote the priority and frequency with which it recommends articles that promulgate anti-vax information and conspiracy theories.2 Facebook isn’t doing this because it has had an epiphany; it has come under pressure for its role in the spread of misinformation. Current legislation was written before the rise of social media, when Internet Service Providers were primarily conduits to transfer bits and bytes between computers. Those ISPs were not liable for the content of the transmitted Web pages. Facebook, by producing what it called a newsfeed and by making personalized suggestions for other websites to browse, doesn’t fit the passive model of an ISP.
For alleged violations of user’s privacy, Facebook might be subject to billion dollar fines, according to a Washington Post article.3 Still, for a company whose revenue is $4 billion per month and whose stock market value is $400 billion, paying a billion dollar fine for years of alleged misbehaviors that have enabled it to become a giant empire is, “in the scheme of things ... a speeding ticket” in the parlance of the penultimate scene of the movie The Social Network. The real financial risk is people deciding they can’t trust the platform and going elsewhere.
Authorities in the United Kingdom in February 2019 released a highly critical, 108-page report about fake news, which said, “Facebook should not be allowed to behave like ‘digital gangsters’ in the online world.”4 The U.K. report urges new regulations to deal with privacy breaches and with fake news. It endeavors to create a duty for social media companies to combat the spread of misinformation.
Then the Wall Street Journal reported that Pinterest has stopped returning results for searches related to vaccination.5 Pinterest realized that most of the shared images on its platform cautioned against vaccination, which contradicts the recommendations of medical experts. Unable to otherwise combat the flow of misinformation, the company apparently has decided to eliminate returning results, pro or con, for any search terms related to vaccines.
While lamenting the public’s inability to distinguish misinformation on the Internet, I’ve also been observing the factors that lead physicians astray. I expect physicians, as trained scientists and as professionals, to be able to assimilate new information and change their practices accordingly. Those who do research on the translation of technology find that, this doesn’t happen with any regularity.
The February 2019 issue of Hospital Pediatrics has four items on the topic of treating bronchiolitis, including two research articles, a brief report, and a commentary. That is obviously a relevant topic this time of year. The impression after reading those four items is that hospitalists don’t really know how to best treat the most common illness they encounter. And even when they “know” how to do it, many factors distort the science. Those factors are highlighted in the article on barriers to minimizing viral testing.6
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. “Discussing immunization with vaccine-hesitant parents requires caring, individualized approach,” by Jeff Craven, Pediatric News, Nov. 7, 2018; “How do you get anti-vaxxers to vaccinate their kids? Talk to them – for hours,” by Nadine Gartner, Washington Post, Feb. 19, 2019.
2. “Facebook will consider removing or demoting anti-vaccination recommendations amid backlash,” by Taylor Telford, Washington Post, Feb. 15, 2019.
3. “U.S. regulators have met to discuss imposing a record-setting fine against Facebook for privacy violations,” by Tony Romm and Elizabeth Dwoskin, Washington Post, Jan. 18, 2019; “Report: Facebook, FTC discussing ‘multibillion dollar’ fine,” by Associated Press.
4. “Disinformation and ‘fake news’: Final Report,” House of Commons, Feb. 18, 2019, p. 42, item 139.
5. “Pinterest blocks vaccination searches in move to control the conversation,” by Robert McMillan and Daniela Hernandez, The Wall Street Journal, Feb. 20, 2019.
6. “Barriers to minimizing respiratory viral testing in bronchiolitis: Physician perceptions on testing practices,” by MZ Huang et al. Hospital Pediatrics 2019 Feb. doi: 10.1542/hpeds.2018-0108.
My most recent column discussed the problem of pseudoscience that pervades some corners of the Internet. Personally, I respond to pseudoscience primarily by trying to provide accurate and less-biased information. I recognize that not everyone approaches decision making by seeking more information. When dealing a diverse public, a medical professional needs to have other approaches in the armamentarium.1 When dealing with other physicians, I am less flexible. Either the profession of medicine believes in science or it doesn’t.
![]()
Since that column was published, there have been major developments. There are measles outbreaks in the states of Washington and New York, and more than 100 deaths from a measles epidemic in the Philippines. The World Health Organization has made vaccine hesitancy one of its ten threats to global health in 2019.
Facebook has indicated that it might demote the priority and frequency with which it recommends articles that promulgate anti-vax information and conspiracy theories.2 Facebook isn’t doing this because it has had an epiphany; it has come under pressure for its role in the spread of misinformation. Current legislation was written before the rise of social media, when Internet Service Providers were primarily conduits to transfer bits and bytes between computers. Those ISPs were not liable for the content of the transmitted Web pages. Facebook, by producing what it called a newsfeed and by making personalized suggestions for other websites to browse, doesn’t fit the passive model of an ISP.
For alleged violations of user’s privacy, Facebook might be subject to billion dollar fines, according to a Washington Post article.3 Still, for a company whose revenue is $4 billion per month and whose stock market value is $400 billion, paying a billion dollar fine for years of alleged misbehaviors that have enabled it to become a giant empire is, “in the scheme of things ... a speeding ticket” in the parlance of the penultimate scene of the movie The Social Network. The real financial risk is people deciding they can’t trust the platform and going elsewhere.
Authorities in the United Kingdom in February 2019 released a highly critical, 108-page report about fake news, which said, “Facebook should not be allowed to behave like ‘digital gangsters’ in the online world.”4 The U.K. report urges new regulations to deal with privacy breaches and with fake news. It endeavors to create a duty for social media companies to combat the spread of misinformation.
Then the Wall Street Journal reported that Pinterest has stopped returning results for searches related to vaccination.5 Pinterest realized that most of the shared images on its platform cautioned against vaccination, which contradicts the recommendations of medical experts. Unable to otherwise combat the flow of misinformation, the company apparently has decided to eliminate returning results, pro or con, for any search terms related to vaccines.
While lamenting the public’s inability to distinguish misinformation on the Internet, I’ve also been observing the factors that lead physicians astray. I expect physicians, as trained scientists and as professionals, to be able to assimilate new information and change their practices accordingly. Those who do research on the translation of technology find that, this doesn’t happen with any regularity.
The February 2019 issue of Hospital Pediatrics has four items on the topic of treating bronchiolitis, including two research articles, a brief report, and a commentary. That is obviously a relevant topic this time of year. The impression after reading those four items is that hospitalists don’t really know how to best treat the most common illness they encounter. And even when they “know” how to do it, many factors distort the science. Those factors are highlighted in the article on barriers to minimizing viral testing.6
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. “Discussing immunization with vaccine-hesitant parents requires caring, individualized approach,” by Jeff Craven, Pediatric News, Nov. 7, 2018; “How do you get anti-vaxxers to vaccinate their kids? Talk to them – for hours,” by Nadine Gartner, Washington Post, Feb. 19, 2019.
2. “Facebook will consider removing or demoting anti-vaccination recommendations amid backlash,” by Taylor Telford, Washington Post, Feb. 15, 2019.
3. “U.S. regulators have met to discuss imposing a record-setting fine against Facebook for privacy violations,” by Tony Romm and Elizabeth Dwoskin, Washington Post, Jan. 18, 2019; “Report: Facebook, FTC discussing ‘multibillion dollar’ fine,” by Associated Press.
4. “Disinformation and ‘fake news’: Final Report,” House of Commons, Feb. 18, 2019, p. 42, item 139.
5. “Pinterest blocks vaccination searches in move to control the conversation,” by Robert McMillan and Daniela Hernandez, The Wall Street Journal, Feb. 20, 2019.
6. “Barriers to minimizing respiratory viral testing in bronchiolitis: Physician perceptions on testing practices,” by MZ Huang et al. Hospital Pediatrics 2019 Feb. doi: 10.1542/hpeds.2018-0108.
Experts: Consider enteral therapy in CD, with caveats
LAS VEGAS – Temporarily switching to an enteral diet – without solid food – has the potential to reverse Crohn’s disease (CD), especially in children, a panel of experts told gastroenterologists here.
They acknowledged the controversial treatment requires strict adherence and can be impossible for some patients to tolerate. But it can be successful too, said gastroenterologist Lindsey G. Albenberg, DO, of Children’s Hospital of Philadelphia, where enteral nutrition therapy (ENT) is commonly used in patients with CD.
“Parents are obviously thrilled that there’s no exposure to immunosuppressive medications,” she said in a discussion about ENT at the Crohn’s & Colitis Congress - a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Typically, we provide 80%-90% of calorie needs through a polymeric formula by mouth. If we see clinical response at 4-6 weeks or even earlier, then we will pursue a course of about 8-12 weeks.”
Research into the best role for ENT therapy in CD is limited. A 2018 Cochrane Library review found there’s “very low quality evidence” suggesting that ENT is better than steroids to induce remission in children. It also found there’s “very low quality evidence” that steroids are better than ENT in adults with CD (Cochrane Database Syst Rev. 2018 Apr 1. doi: 10.1002/14651858.CD000542.pub3).
According to clinician-scientist James D. Lewis, MD, MSCE, of the University of Pennsylvania, Philadelphia, ENT “has gotten a bad name in some ways because of a meta-analysis showing it was inferior to corticosteroids to induce remission.” In fact, he said, studies “didn’t look at mucosal healing and pooled together adults and children.”
In children, he said, the treatment seems to clearly be effective. The picture is less promising in adults. “Presumably that’s because those of you who are parents probably have more control over your young children than your own behavior,” he said, referring to management of food intake.
In adults, “there’s no reason to think it wouldn’t work,” he said. “But trying to convince adults to give up food is really challenging.”
Children who try ENT are often required to use a nasogastric feeding tube, an approach that adults tend to avoid. In kids, “it’s a question of knowing your patient,” said gastroenterologist David Suskind, MD, of Seattle Children’s Hospital. “If the patient says, ‘There’s no way you’ll put a nasal gastric tube in, and no way I will drink it [the ENT supplement],’ this may not be the best therapy. If they’re interested, we push forward. We get much better efficacy because the patients will do what we’re asking.”
Several panelists recommended that patients use polymeric formulations instead of elemental formulations because they’re more palatable. It can be a struggle, however, to stick with the treatment.
Kelly Issokson, MS, RD, CNSC, a dietitian with Cedars-Sinai Medical Center in Los Angeles, tried an ENT therapy for 30 days in order to understand what patients experience and said it was “very challenging.”
“When you sit down to a meal, you anticipate it, you start to salivate. With shakes, it was a lot more clinical,” she said. “The other thing I struggled with was texture and having it be so sweet. I’d freeze [the shakes] into ice cube trays and popsicles. That helped break the monotony. It changes the flavor and cuts the sweetness.”
Ms. Issokson urges her patients to stick with ENT for the entire period of therapy. “Studies show when patients introduce real foods the efficacy of inducing remission goes down. We recommend 100% calories and proteins coming from the formula,” she said. That means “no coffee, no broth, no tea, no nothing but the formula. Most of our patients are able to do that exclusively.”
Toward the end of therapy, around week 8 or 11, some patients tell her they crave food like soup. “I say OK, have a tiny bit,” she said, “but remember, this is only temporary. We’re almost at the end. Try to be 100% exclusive.”
Dr. Albenberg and Dr. Suskind report no disclosures. Ms. Issokson reports consulting fees (speaking and teaching) from AGA, Crohn’s & Colitis Foundation, Academy of Nutrition and Dietetics, and United Ostomy Association. Dr. Lewis reports many relationships – including consulting fees, ownership interest, and grant/research support – with Eli Lilly, Bristol‐Myers Squibb, Gilead, and others.
Correction, 2/22/19: An earlier version of this article misidentified the person in the first photo above.
LAS VEGAS – Temporarily switching to an enteral diet – without solid food – has the potential to reverse Crohn’s disease (CD), especially in children, a panel of experts told gastroenterologists here.
They acknowledged the controversial treatment requires strict adherence and can be impossible for some patients to tolerate. But it can be successful too, said gastroenterologist Lindsey G. Albenberg, DO, of Children’s Hospital of Philadelphia, where enteral nutrition therapy (ENT) is commonly used in patients with CD.
“Parents are obviously thrilled that there’s no exposure to immunosuppressive medications,” she said in a discussion about ENT at the Crohn’s & Colitis Congress - a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Typically, we provide 80%-90% of calorie needs through a polymeric formula by mouth. If we see clinical response at 4-6 weeks or even earlier, then we will pursue a course of about 8-12 weeks.”
Research into the best role for ENT therapy in CD is limited. A 2018 Cochrane Library review found there’s “very low quality evidence” suggesting that ENT is better than steroids to induce remission in children. It also found there’s “very low quality evidence” that steroids are better than ENT in adults with CD (Cochrane Database Syst Rev. 2018 Apr 1. doi: 10.1002/14651858.CD000542.pub3).
According to clinician-scientist James D. Lewis, MD, MSCE, of the University of Pennsylvania, Philadelphia, ENT “has gotten a bad name in some ways because of a meta-analysis showing it was inferior to corticosteroids to induce remission.” In fact, he said, studies “didn’t look at mucosal healing and pooled together adults and children.”
In children, he said, the treatment seems to clearly be effective. The picture is less promising in adults. “Presumably that’s because those of you who are parents probably have more control over your young children than your own behavior,” he said, referring to management of food intake.
In adults, “there’s no reason to think it wouldn’t work,” he said. “But trying to convince adults to give up food is really challenging.”
Children who try ENT are often required to use a nasogastric feeding tube, an approach that adults tend to avoid. In kids, “it’s a question of knowing your patient,” said gastroenterologist David Suskind, MD, of Seattle Children’s Hospital. “If the patient says, ‘There’s no way you’ll put a nasal gastric tube in, and no way I will drink it [the ENT supplement],’ this may not be the best therapy. If they’re interested, we push forward. We get much better efficacy because the patients will do what we’re asking.”
Several panelists recommended that patients use polymeric formulations instead of elemental formulations because they’re more palatable. It can be a struggle, however, to stick with the treatment.
Kelly Issokson, MS, RD, CNSC, a dietitian with Cedars-Sinai Medical Center in Los Angeles, tried an ENT therapy for 30 days in order to understand what patients experience and said it was “very challenging.”
“When you sit down to a meal, you anticipate it, you start to salivate. With shakes, it was a lot more clinical,” she said. “The other thing I struggled with was texture and having it be so sweet. I’d freeze [the shakes] into ice cube trays and popsicles. That helped break the monotony. It changes the flavor and cuts the sweetness.”
Ms. Issokson urges her patients to stick with ENT for the entire period of therapy. “Studies show when patients introduce real foods the efficacy of inducing remission goes down. We recommend 100% calories and proteins coming from the formula,” she said. That means “no coffee, no broth, no tea, no nothing but the formula. Most of our patients are able to do that exclusively.”
Toward the end of therapy, around week 8 or 11, some patients tell her they crave food like soup. “I say OK, have a tiny bit,” she said, “but remember, this is only temporary. We’re almost at the end. Try to be 100% exclusive.”
Dr. Albenberg and Dr. Suskind report no disclosures. Ms. Issokson reports consulting fees (speaking and teaching) from AGA, Crohn’s & Colitis Foundation, Academy of Nutrition and Dietetics, and United Ostomy Association. Dr. Lewis reports many relationships – including consulting fees, ownership interest, and grant/research support – with Eli Lilly, Bristol‐Myers Squibb, Gilead, and others.
Correction, 2/22/19: An earlier version of this article misidentified the person in the first photo above.
LAS VEGAS – Temporarily switching to an enteral diet – without solid food – has the potential to reverse Crohn’s disease (CD), especially in children, a panel of experts told gastroenterologists here.
They acknowledged the controversial treatment requires strict adherence and can be impossible for some patients to tolerate. But it can be successful too, said gastroenterologist Lindsey G. Albenberg, DO, of Children’s Hospital of Philadelphia, where enteral nutrition therapy (ENT) is commonly used in patients with CD.
“Parents are obviously thrilled that there’s no exposure to immunosuppressive medications,” she said in a discussion about ENT at the Crohn’s & Colitis Congress - a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Typically, we provide 80%-90% of calorie needs through a polymeric formula by mouth. If we see clinical response at 4-6 weeks or even earlier, then we will pursue a course of about 8-12 weeks.”
Research into the best role for ENT therapy in CD is limited. A 2018 Cochrane Library review found there’s “very low quality evidence” suggesting that ENT is better than steroids to induce remission in children. It also found there’s “very low quality evidence” that steroids are better than ENT in adults with CD (Cochrane Database Syst Rev. 2018 Apr 1. doi: 10.1002/14651858.CD000542.pub3).
According to clinician-scientist James D. Lewis, MD, MSCE, of the University of Pennsylvania, Philadelphia, ENT “has gotten a bad name in some ways because of a meta-analysis showing it was inferior to corticosteroids to induce remission.” In fact, he said, studies “didn’t look at mucosal healing and pooled together adults and children.”
In children, he said, the treatment seems to clearly be effective. The picture is less promising in adults. “Presumably that’s because those of you who are parents probably have more control over your young children than your own behavior,” he said, referring to management of food intake.
In adults, “there’s no reason to think it wouldn’t work,” he said. “But trying to convince adults to give up food is really challenging.”
Children who try ENT are often required to use a nasogastric feeding tube, an approach that adults tend to avoid. In kids, “it’s a question of knowing your patient,” said gastroenterologist David Suskind, MD, of Seattle Children’s Hospital. “If the patient says, ‘There’s no way you’ll put a nasal gastric tube in, and no way I will drink it [the ENT supplement],’ this may not be the best therapy. If they’re interested, we push forward. We get much better efficacy because the patients will do what we’re asking.”
Several panelists recommended that patients use polymeric formulations instead of elemental formulations because they’re more palatable. It can be a struggle, however, to stick with the treatment.
Kelly Issokson, MS, RD, CNSC, a dietitian with Cedars-Sinai Medical Center in Los Angeles, tried an ENT therapy for 30 days in order to understand what patients experience and said it was “very challenging.”
“When you sit down to a meal, you anticipate it, you start to salivate. With shakes, it was a lot more clinical,” she said. “The other thing I struggled with was texture and having it be so sweet. I’d freeze [the shakes] into ice cube trays and popsicles. That helped break the monotony. It changes the flavor and cuts the sweetness.”
Ms. Issokson urges her patients to stick with ENT for the entire period of therapy. “Studies show when patients introduce real foods the efficacy of inducing remission goes down. We recommend 100% calories and proteins coming from the formula,” she said. That means “no coffee, no broth, no tea, no nothing but the formula. Most of our patients are able to do that exclusively.”
Toward the end of therapy, around week 8 or 11, some patients tell her they crave food like soup. “I say OK, have a tiny bit,” she said, “but remember, this is only temporary. We’re almost at the end. Try to be 100% exclusive.”
Dr. Albenberg and Dr. Suskind report no disclosures. Ms. Issokson reports consulting fees (speaking and teaching) from AGA, Crohn’s & Colitis Foundation, Academy of Nutrition and Dietetics, and United Ostomy Association. Dr. Lewis reports many relationships – including consulting fees, ownership interest, and grant/research support – with Eli Lilly, Bristol‐Myers Squibb, Gilead, and others.
Correction, 2/22/19: An earlier version of this article misidentified the person in the first photo above.
EXPERT ANALYSIS FROM THE CROHN’S & COLITIS CONGRESS
Trametinib effectively treats case of giant congenital melanocytic nevus
according to a case report presented in Pediatrics.
Her nevus covered most of her back and much of her torso and had thickened significantly over the years since initial presentation to the point of disfigurement, even invading the fascia and musculature of the trunk and pelvis, reported Adnan Mir, MD, PhD, of the University of Texas Southwestern Medical Center, Dallas, and his coauthors. Furthermore, she presented with intractable pruritus and pain that interfered with sleep and responded minimally to treatments. Although initial immunohistochemical staining and gene sequencing did not reveal any mutations, such as BRAF V600E, further testing uncovered an AKAP9-BRAF fusion.
There are few if any effective ways of treating GCMNs. With that knowledge, as well as general theories of the mechanism GCMNs in mind, the patient’s health care team decided to try a 0.5-mg daily dose of trametinib when she was 7 years old. Her pruritus and pain resolved completely, and after 6 months of treatment with trametinib, repeat MRI “revealed decreased thickening of the dermis and near resolutions of muscular invasion.” According to the patient’s family, her quality of life improved dramatically.
SOURCE: Mir A et al. Pediatrics. 2019;143(3):e20182469.
according to a case report presented in Pediatrics.
Her nevus covered most of her back and much of her torso and had thickened significantly over the years since initial presentation to the point of disfigurement, even invading the fascia and musculature of the trunk and pelvis, reported Adnan Mir, MD, PhD, of the University of Texas Southwestern Medical Center, Dallas, and his coauthors. Furthermore, she presented with intractable pruritus and pain that interfered with sleep and responded minimally to treatments. Although initial immunohistochemical staining and gene sequencing did not reveal any mutations, such as BRAF V600E, further testing uncovered an AKAP9-BRAF fusion.
There are few if any effective ways of treating GCMNs. With that knowledge, as well as general theories of the mechanism GCMNs in mind, the patient’s health care team decided to try a 0.5-mg daily dose of trametinib when she was 7 years old. Her pruritus and pain resolved completely, and after 6 months of treatment with trametinib, repeat MRI “revealed decreased thickening of the dermis and near resolutions of muscular invasion.” According to the patient’s family, her quality of life improved dramatically.
SOURCE: Mir A et al. Pediatrics. 2019;143(3):e20182469.
according to a case report presented in Pediatrics.
Her nevus covered most of her back and much of her torso and had thickened significantly over the years since initial presentation to the point of disfigurement, even invading the fascia and musculature of the trunk and pelvis, reported Adnan Mir, MD, PhD, of the University of Texas Southwestern Medical Center, Dallas, and his coauthors. Furthermore, she presented with intractable pruritus and pain that interfered with sleep and responded minimally to treatments. Although initial immunohistochemical staining and gene sequencing did not reveal any mutations, such as BRAF V600E, further testing uncovered an AKAP9-BRAF fusion.
There are few if any effective ways of treating GCMNs. With that knowledge, as well as general theories of the mechanism GCMNs in mind, the patient’s health care team decided to try a 0.5-mg daily dose of trametinib when she was 7 years old. Her pruritus and pain resolved completely, and after 6 months of treatment with trametinib, repeat MRI “revealed decreased thickening of the dermis and near resolutions of muscular invasion.” According to the patient’s family, her quality of life improved dramatically.
SOURCE: Mir A et al. Pediatrics. 2019;143(3):e20182469.
FROM PEDIATRICS
Child suicides rock Kentucky county; lack of access to care burdens rural Arizona
The people of Fayette County, Ky., reportedly have experienced five suicides by children in the last year. The latest suicide occurred several weeks ago and involved a 12-year-old girl. This followed the suicides of children aged 10, 11, 13, and 14 years.

The deaths are not related, and there seems to be no connection to race or gender. All involved hanging, and one child might have been bullied.
The cases reflect a disturbing trend in Kentucky and across the country. In 2015, 25% of suicides of children under 17 years in Kentucky involved those aged 10-14, a 14% increase from 4 years earlier. The percentage of 6th-grade students who have thought about or planned their suicide also has climbed in recent years.
Fayette County Coroner Gary W. Ginn said the deaths in Kentucky provide another example of how events in life that might be less traumatic to adults can cause mental anguish for children, anguish which can lead some to take their own lives.
“We should be very worried to have this many cases, but we should not be hopeless,“ said Susan H. Pollack, MD, a pediatrician at the University of Kentucky Children’s Hospital, Lexington, in an interview with the Lexington Herald-Leader. She added that resources and programs are available but that stronger support systems focusing on youth are needed.
“Our families have limited options when their child needs a higher level of care. ... Local agencies often have a wait list,” Fayette County Public Schools spokeswoman Lisa Deffendall said in the article. “We have made referrals and seen it take weeks for children to get the help they need. Where do families turn when their child is in crisis? Who provides care when school is not in session?”
Rural Arizona facing crisis
Living in rural areas can prove isolating, and gaining access to health care, including mental health care, can be challenging. A segment presented on KOLD News 13 in Tucson provided yet another examples of the mental health crisis in rural America.
Cochise County is an area of about 6,200 square miles in the southeast corner of Arizona. The area, which is about eight times bigger than New York City, is home to about 125,000 people. For those with mental health issues, it’s a bleak place to live, with only two psychiatrists available and no mental health facility.
“It’s as if we got a fire going that we can’t put out,” said James P. Reed, DO, in an interview. He is one of the two psychiatrists practicing in the county. In the last 2 months alone, 64 new people have sought his help, and he has had to turn many away.
Dr. Reed has been practicing in the country for 35 years, which gives him a longer-term perspective. “It’s so much worse now. I don’t know what it is, if it’s a consequence of our society and the direction it’s going. I just can’t put my finger on it.”
The main reason behind the paucity of mental health professionals comes down to economics. Burdened with student loan debts after graduation from medical school, the low salaries of rural positions cripple the recruitment of psychiatrists and other medical professionals.
In Cochise County, as elsewhere, the main refuge for people with mental illness is jail. “We have people in there [who] really shouldn’t be in there,” said Cochise County Sheriff Mark J. Dannels. “These people need special help that I can’t provide to them. It’s almost a misjustice to have them in our jail. Unfortunately, there’s no other place to put them.”
Perils of involuntary mental health holds
South Dakota is one of five states where jailing people with mental illness is part of a deliberate strategy, and the state’s new governor wants to change the practice.
“They’re not criminals,” Gov. Kristi Noem said in an article published in the Sioux Falls Argus Leader. “They’re having a crisis at a point in time when they need to be observed, but unfortunately, in a lot of communities, that’s the only option that folks have.”
The article cited the case of Nick Johnson, a 14-year-old whose mental health struggles include the loss of control that can include aggressiveness. Although not charged with any offense, the response had been stints in the Minnehaha County Juvenile Detention Center. “It feels like I’m in prison,” Nick said. “Why would a kid have to go through that?”
National advocacy groups have criticized the practice of imprisoning people with mental illness, and local jail officials have complained that their facilities have not been designed to deliver mental health treatment. “If you look at it from a strictly medical perspective, being in a jail setting is almost guaranteed to make somebody’s mental health crisis worse, not better,” said Lisa Dailey, legislative and policy counsel for the Treatment Advocacy Center, a national nonprofit that surveys and ranks states for their mental health policies. “It’s the worst possible thing you could do.” The report said the other states that take this approach toward people with mental illness are Texas, Wyoming, New Mexico, and North Dakota.
Cutbacks may hit recovery centers
Idaho’s nine crisis centers are in peril in the first year of the administration of Gov. Brad Little. The centers, located in nine of the state’s cities, collectively had requested about $890,000 from the Idaho Millennium Fund that would enable them to stabilize precarious financing and improve outreach efforts in surrounding rural communities.
However, as the Idaho Statesman reported, the funding request did not make it to the governor’s budget recommendation for 2020. Instead, the governor intends to use the Millennium Fund funds to expand Medicaid coverage. The consequence of the lack of state financial support could be the shuttering of all nine centers. If that happens, it would be much harder for those in the throes of or recovering from addiction or mental health issues to find the support they need.
“[The centers’] continued survival has been something of a miracle already,” said Norma Jaeger, executive director of Recovery Idaho. The organization had submitted the funding request on behalf of the nine centers. “Hopefully, a better funding solution is on the horizon,” said Ms. Jaeger.
Some in government disagree with that view, contending that the ongoing use of the Millennium Fund was never in the plans and that the centers were expected to seek other nongovernmental sources of funding. This tact is contrary to the traditional state funding of mental health and substance abuse programs. The legality of the move is being considered by the state Supreme Court.
Mental health and religious faith
A recent article in the Philadelphia Inquirer related the downsides and upsides of religious belief in the struggle against depression. The article discussed Yashi Brown, who at age 20, dealt with a bout of depression that led to manic episodes and contemplation of suicide. To her dismay, Ms. Brown found that her Jehovah’s Witness faith community was of little help.
Twenty years later, Ms. Brown, who now works as a mental health advocate in Los Angeles, better understands why relying on the faith’s teachings did not work. “I was in the throes of a manic episode,” she said. “I didn’t even have the tools to say a prayer.”
Ms. Brown’s experience highlights the burden faced by some religious traditions in helping church members with mental health issues. Instead of receiving tangible care from mental health professionals, those who are suffering can be told to rely on faith alone. The fallout is especially profound for African Americans like Ms. Brown, research shows. African Americans are 20% more likely to experience serious psychological distress than their white counterparts but are less likely to seek help – even if they can financially afford it.
The racial/ethnic disparities in health care that affect African Americans partly explains this reticence to seek treatment. Another factor is the multigenerational acceptance among some African Americans of mental trauma as a normal part of life, according to Meagan McLeod, a pastor and spiritual care director for Friends Hospital, a psychiatric hospital in northeast Philadelphia. “The idea is, if prayer worked for our ancestors when we were in slavery, then prayer has to be able to work now,” said Ms. McLeod.
Meanwhile, the article said, mental health professionals and clergy think that faith and mental health treatment “can – and should – work together. Research suggests higher levels of religiosity or spirituality are associated with lower rates of depression, anxiety, substance use disorder, and suicidal thoughts. Prayer can have the same calming effects as meditation,” such as both lowering blood pressure and respiratory rates. Incorporating religious approaches into the mental health treatment of African American patients might be particularly helpful, the article said.
The people of Fayette County, Ky., reportedly have experienced five suicides by children in the last year. The latest suicide occurred several weeks ago and involved a 12-year-old girl. This followed the suicides of children aged 10, 11, 13, and 14 years.
The deaths are not related, and there seems to be no connection to race or gender. All involved hanging, and one child might have been bullied.
The cases reflect a disturbing trend in Kentucky and across the country. In 2015, 25% of suicides of children under 17 years in Kentucky involved those aged 10-14, a 14% increase from 4 years earlier. The percentage of 6th-grade students who have thought about or planned their suicide also has climbed in recent years.
Fayette County Coroner Gary W. Ginn said the deaths in Kentucky provide another example of how events in life that might be less traumatic to adults can cause mental anguish for children, anguish which can lead some to take their own lives.
“We should be very worried to have this many cases, but we should not be hopeless,“ said Susan H. Pollack, MD, a pediatrician at the University of Kentucky Children’s Hospital, Lexington, in an interview with the Lexington Herald-Leader. She added that resources and programs are available but that stronger support systems focusing on youth are needed.
“Our families have limited options when their child needs a higher level of care. ... Local agencies often have a wait list,” Fayette County Public Schools spokeswoman Lisa Deffendall said in the article. “We have made referrals and seen it take weeks for children to get the help they need. Where do families turn when their child is in crisis? Who provides care when school is not in session?”
Rural Arizona facing crisis
Living in rural areas can prove isolating, and gaining access to health care, including mental health care, can be challenging. A segment presented on KOLD News 13 in Tucson provided yet another examples of the mental health crisis in rural America.
Cochise County is an area of about 6,200 square miles in the southeast corner of Arizona. The area, which is about eight times bigger than New York City, is home to about 125,000 people. For those with mental health issues, it’s a bleak place to live, with only two psychiatrists available and no mental health facility.
“It’s as if we got a fire going that we can’t put out,” said James P. Reed, DO, in an interview. He is one of the two psychiatrists practicing in the county. In the last 2 months alone, 64 new people have sought his help, and he has had to turn many away.
Dr. Reed has been practicing in the country for 35 years, which gives him a longer-term perspective. “It’s so much worse now. I don’t know what it is, if it’s a consequence of our society and the direction it’s going. I just can’t put my finger on it.”
The main reason behind the paucity of mental health professionals comes down to economics. Burdened with student loan debts after graduation from medical school, the low salaries of rural positions cripple the recruitment of psychiatrists and other medical professionals.
In Cochise County, as elsewhere, the main refuge for people with mental illness is jail. “We have people in there [who] really shouldn’t be in there,” said Cochise County Sheriff Mark J. Dannels. “These people need special help that I can’t provide to them. It’s almost a misjustice to have them in our jail. Unfortunately, there’s no other place to put them.”
Perils of involuntary mental health holds
South Dakota is one of five states where jailing people with mental illness is part of a deliberate strategy, and the state’s new governor wants to change the practice.
“They’re not criminals,” Gov. Kristi Noem said in an article published in the Sioux Falls Argus Leader. “They’re having a crisis at a point in time when they need to be observed, but unfortunately, in a lot of communities, that’s the only option that folks have.”
The article cited the case of Nick Johnson, a 14-year-old whose mental health struggles include the loss of control that can include aggressiveness. Although not charged with any offense, the response had been stints in the Minnehaha County Juvenile Detention Center. “It feels like I’m in prison,” Nick said. “Why would a kid have to go through that?”
National advocacy groups have criticized the practice of imprisoning people with mental illness, and local jail officials have complained that their facilities have not been designed to deliver mental health treatment. “If you look at it from a strictly medical perspective, being in a jail setting is almost guaranteed to make somebody’s mental health crisis worse, not better,” said Lisa Dailey, legislative and policy counsel for the Treatment Advocacy Center, a national nonprofit that surveys and ranks states for their mental health policies. “It’s the worst possible thing you could do.” The report said the other states that take this approach toward people with mental illness are Texas, Wyoming, New Mexico, and North Dakota.
Cutbacks may hit recovery centers
Idaho’s nine crisis centers are in peril in the first year of the administration of Gov. Brad Little. The centers, located in nine of the state’s cities, collectively had requested about $890,000 from the Idaho Millennium Fund that would enable them to stabilize precarious financing and improve outreach efforts in surrounding rural communities.
However, as the Idaho Statesman reported, the funding request did not make it to the governor’s budget recommendation for 2020. Instead, the governor intends to use the Millennium Fund funds to expand Medicaid coverage. The consequence of the lack of state financial support could be the shuttering of all nine centers. If that happens, it would be much harder for those in the throes of or recovering from addiction or mental health issues to find the support they need.
“[The centers’] continued survival has been something of a miracle already,” said Norma Jaeger, executive director of Recovery Idaho. The organization had submitted the funding request on behalf of the nine centers. “Hopefully, a better funding solution is on the horizon,” said Ms. Jaeger.
Some in government disagree with that view, contending that the ongoing use of the Millennium Fund was never in the plans and that the centers were expected to seek other nongovernmental sources of funding. This tact is contrary to the traditional state funding of mental health and substance abuse programs. The legality of the move is being considered by the state Supreme Court.
Mental health and religious faith
A recent article in the Philadelphia Inquirer related the downsides and upsides of religious belief in the struggle against depression. The article discussed Yashi Brown, who at age 20, dealt with a bout of depression that led to manic episodes and contemplation of suicide. To her dismay, Ms. Brown found that her Jehovah’s Witness faith community was of little help.
Twenty years later, Ms. Brown, who now works as a mental health advocate in Los Angeles, better understands why relying on the faith’s teachings did not work. “I was in the throes of a manic episode,” she said. “I didn’t even have the tools to say a prayer.”
Ms. Brown’s experience highlights the burden faced by some religious traditions in helping church members with mental health issues. Instead of receiving tangible care from mental health professionals, those who are suffering can be told to rely on faith alone. The fallout is especially profound for African Americans like Ms. Brown, research shows. African Americans are 20% more likely to experience serious psychological distress than their white counterparts but are less likely to seek help – even if they can financially afford it.
The racial/ethnic disparities in health care that affect African Americans partly explains this reticence to seek treatment. Another factor is the multigenerational acceptance among some African Americans of mental trauma as a normal part of life, according to Meagan McLeod, a pastor and spiritual care director for Friends Hospital, a psychiatric hospital in northeast Philadelphia. “The idea is, if prayer worked for our ancestors when we were in slavery, then prayer has to be able to work now,” said Ms. McLeod.
Meanwhile, the article said, mental health professionals and clergy think that faith and mental health treatment “can – and should – work together. Research suggests higher levels of religiosity or spirituality are associated with lower rates of depression, anxiety, substance use disorder, and suicidal thoughts. Prayer can have the same calming effects as meditation,” such as both lowering blood pressure and respiratory rates. Incorporating religious approaches into the mental health treatment of African American patients might be particularly helpful, the article said.
The people of Fayette County, Ky., reportedly have experienced five suicides by children in the last year. The latest suicide occurred several weeks ago and involved a 12-year-old girl. This followed the suicides of children aged 10, 11, 13, and 14 years.
The deaths are not related, and there seems to be no connection to race or gender. All involved hanging, and one child might have been bullied.
The cases reflect a disturbing trend in Kentucky and across the country. In 2015, 25% of suicides of children under 17 years in Kentucky involved those aged 10-14, a 14% increase from 4 years earlier. The percentage of 6th-grade students who have thought about or planned their suicide also has climbed in recent years.
Fayette County Coroner Gary W. Ginn said the deaths in Kentucky provide another example of how events in life that might be less traumatic to adults can cause mental anguish for children, anguish which can lead some to take their own lives.
“We should be very worried to have this many cases, but we should not be hopeless,“ said Susan H. Pollack, MD, a pediatrician at the University of Kentucky Children’s Hospital, Lexington, in an interview with the Lexington Herald-Leader. She added that resources and programs are available but that stronger support systems focusing on youth are needed.
“Our families have limited options when their child needs a higher level of care. ... Local agencies often have a wait list,” Fayette County Public Schools spokeswoman Lisa Deffendall said in the article. “We have made referrals and seen it take weeks for children to get the help they need. Where do families turn when their child is in crisis? Who provides care when school is not in session?”
Rural Arizona facing crisis
Living in rural areas can prove isolating, and gaining access to health care, including mental health care, can be challenging. A segment presented on KOLD News 13 in Tucson provided yet another examples of the mental health crisis in rural America.
Cochise County is an area of about 6,200 square miles in the southeast corner of Arizona. The area, which is about eight times bigger than New York City, is home to about 125,000 people. For those with mental health issues, it’s a bleak place to live, with only two psychiatrists available and no mental health facility.
“It’s as if we got a fire going that we can’t put out,” said James P. Reed, DO, in an interview. He is one of the two psychiatrists practicing in the county. In the last 2 months alone, 64 new people have sought his help, and he has had to turn many away.
Dr. Reed has been practicing in the country for 35 years, which gives him a longer-term perspective. “It’s so much worse now. I don’t know what it is, if it’s a consequence of our society and the direction it’s going. I just can’t put my finger on it.”
The main reason behind the paucity of mental health professionals comes down to economics. Burdened with student loan debts after graduation from medical school, the low salaries of rural positions cripple the recruitment of psychiatrists and other medical professionals.
In Cochise County, as elsewhere, the main refuge for people with mental illness is jail. “We have people in there [who] really shouldn’t be in there,” said Cochise County Sheriff Mark J. Dannels. “These people need special help that I can’t provide to them. It’s almost a misjustice to have them in our jail. Unfortunately, there’s no other place to put them.”
Perils of involuntary mental health holds
South Dakota is one of five states where jailing people with mental illness is part of a deliberate strategy, and the state’s new governor wants to change the practice.
“They’re not criminals,” Gov. Kristi Noem said in an article published in the Sioux Falls Argus Leader. “They’re having a crisis at a point in time when they need to be observed, but unfortunately, in a lot of communities, that’s the only option that folks have.”
The article cited the case of Nick Johnson, a 14-year-old whose mental health struggles include the loss of control that can include aggressiveness. Although not charged with any offense, the response had been stints in the Minnehaha County Juvenile Detention Center. “It feels like I’m in prison,” Nick said. “Why would a kid have to go through that?”
National advocacy groups have criticized the practice of imprisoning people with mental illness, and local jail officials have complained that their facilities have not been designed to deliver mental health treatment. “If you look at it from a strictly medical perspective, being in a jail setting is almost guaranteed to make somebody’s mental health crisis worse, not better,” said Lisa Dailey, legislative and policy counsel for the Treatment Advocacy Center, a national nonprofit that surveys and ranks states for their mental health policies. “It’s the worst possible thing you could do.” The report said the other states that take this approach toward people with mental illness are Texas, Wyoming, New Mexico, and North Dakota.
Cutbacks may hit recovery centers
Idaho’s nine crisis centers are in peril in the first year of the administration of Gov. Brad Little. The centers, located in nine of the state’s cities, collectively had requested about $890,000 from the Idaho Millennium Fund that would enable them to stabilize precarious financing and improve outreach efforts in surrounding rural communities.
However, as the Idaho Statesman reported, the funding request did not make it to the governor’s budget recommendation for 2020. Instead, the governor intends to use the Millennium Fund funds to expand Medicaid coverage. The consequence of the lack of state financial support could be the shuttering of all nine centers. If that happens, it would be much harder for those in the throes of or recovering from addiction or mental health issues to find the support they need.
“[The centers’] continued survival has been something of a miracle already,” said Norma Jaeger, executive director of Recovery Idaho. The organization had submitted the funding request on behalf of the nine centers. “Hopefully, a better funding solution is on the horizon,” said Ms. Jaeger.
Some in government disagree with that view, contending that the ongoing use of the Millennium Fund was never in the plans and that the centers were expected to seek other nongovernmental sources of funding. This tact is contrary to the traditional state funding of mental health and substance abuse programs. The legality of the move is being considered by the state Supreme Court.
Mental health and religious faith
A recent article in the Philadelphia Inquirer related the downsides and upsides of religious belief in the struggle against depression. The article discussed Yashi Brown, who at age 20, dealt with a bout of depression that led to manic episodes and contemplation of suicide. To her dismay, Ms. Brown found that her Jehovah’s Witness faith community was of little help.
Twenty years later, Ms. Brown, who now works as a mental health advocate in Los Angeles, better understands why relying on the faith’s teachings did not work. “I was in the throes of a manic episode,” she said. “I didn’t even have the tools to say a prayer.”
Ms. Brown’s experience highlights the burden faced by some religious traditions in helping church members with mental health issues. Instead of receiving tangible care from mental health professionals, those who are suffering can be told to rely on faith alone. The fallout is especially profound for African Americans like Ms. Brown, research shows. African Americans are 20% more likely to experience serious psychological distress than their white counterparts but are less likely to seek help – even if they can financially afford it.
The racial/ethnic disparities in health care that affect African Americans partly explains this reticence to seek treatment. Another factor is the multigenerational acceptance among some African Americans of mental trauma as a normal part of life, according to Meagan McLeod, a pastor and spiritual care director for Friends Hospital, a psychiatric hospital in northeast Philadelphia. “The idea is, if prayer worked for our ancestors when we were in slavery, then prayer has to be able to work now,” said Ms. McLeod.
Meanwhile, the article said, mental health professionals and clergy think that faith and mental health treatment “can – and should – work together. Research suggests higher levels of religiosity or spirituality are associated with lower rates of depression, anxiety, substance use disorder, and suicidal thoughts. Prayer can have the same calming effects as meditation,” such as both lowering blood pressure and respiratory rates. Incorporating religious approaches into the mental health treatment of African American patients might be particularly helpful, the article said.
Sildenafil associated with persistent pulmonary hypertension in neonates with early IUGR
LAS VEGAS – Increased rates of persistent neonatal pulmonary hypertension in neonates put the brakes on STRIDER, an international placebo-controlled study looking at sildenafil as a treatment for early-onset intrauterine growth restriction (IUGR).

The study’s independent data safety monitoring board halted STRIDER (Sildenafil Therapy in Dismal Prognosis Early-Onset Fetal Growth Restriction) last July, after an interim safety analysis identified possible fetal harm and no signal of benefit over placebo, Dr. Anouk Pels reported at the annual meeting of the Society for Maternal-Fetal Medicine. The late-breaking presentation at the meeting revealed the first outcome data details.
The board had “serious concerns that sildenafil may cause harm to newborn children. … Given the results , it is extremely unlikely that any benefit could be shown on the primary endpoint if the trial is continued to its completion,” said Dr. Pels of the University of Amsterdam. “Our recommendation is not to use sildenafil for this indication in pregnant women.”
Although the link remains as-yet unproven, pulmonary hypertension among sildenafil-exposed neonates is biologically plausible, she said. It could have been a symptomatic rebound response to the discontinuation of constant intrauterine sildenafil exposure – or it could have been a hint of something more profound. Like the genital vasculature, pulmonary vasculature is a target of the drug. Intrauterine exposure to sildenafil could theoretically alter its development.
“It’s possible that sildenafil may be causing structural changes in the pulmonary vasculature of fetuses. This needs to be explored further, and we will do so by performing additional analyses on autopsy data and placental histology.”
STRIDER involved 261 pregnant women diagnosed with severe early-onset fetal growth restriction. They were randomized to sildenafil 25 mg or placebo three times daily until delivery or 32 weeks’ gestation. A safety analysis was conducted after every 50 patients were enrolled. The preplanned interim analysis was conducted after half of the cohort had been enrolled and received at least one dose of the study medication.
The primary outcome was a composite measure of neonatal mortality or major neonatal morbidity at hospital discharge.
Gestational age at baseline was about 24.6 weeks, and the estimated fetal weight by ultrasound, 465 g. About 45% of pregnancies had evidence of a notching in the uterine artery. In about 42%, the pulsatility index of the umbilical artery was above the 95th percentile; the pulsatility index of the middle cerebral artery was below the 5% percentile in about 70% of cases.
About a quarter of the women had a diagnosis of pregnancy-induced hypertension, and another quarter, preeclampsia. Women used the study medication for a mean of 22 days.
There were no significant between-group differences in maternal outcomes. Median gestational age at delivery was 28 weeks in both groups. About 10% in each group experienced new-onset pregnancy-induced hypertension; About a quarter of each group developed new-onset preeclampsia or HELLP (hemolysis, elevated liver enzymes, low platelet count). There were no between-group differences in the number of maternal antihypertensives prescribed.
The primary combined outcome of neonatal mortality or major neonatal morbidity occurred in 66 of the sildenafil-exposed neonates and 58 of the placebo-exposed infants (61% vs. 54%) – not a significant difference. Fetal death occurred in 23 and 29 pregnancies, respectively (21% and 27%); neonatal death occurred in 21 and 11, respectively (19% and 10%). Overall, fetal/neonatal mortality was similar between the sildenafil and placebo groups (41% and 37%, respectively).
Of the 64 sildenafil-exposed neonates who survived to hospital discharge, 22 exhibited clinically relevant morbidity. Of the 67 in the placebo-treated group who survived to hospital discharge, 18 had clinically relevant morbidity. Overall, 42 in the sildenafil group and 49 of the placebo group survived to hospital discharge without relevant morbidity.
There were a number of secondary outcomes, none exhibiting any significant between-group differences. These included the median weights of those who experienced intrauterine death (425 g and 350 g), median live birth weight (725 g and 783 g), intraventricular hemorrhage of grade II or IV (3% and 2%), periventricular hemorrhage grade II or higher (0%, both groups), necrotizing enterocolitis grade II or higher (7% and 8%), and at least one culture-proven or clinical infection (41% and 33%).
The significantly higher rates of pulmonary hypertension in the sildenafil-exposed neonates was the showstopper. Almost half of the 21 who died had proven pulmonary hypertension (10), as did 6 of the 64 who survived – an excess of 16 cases. Of proven cases, 11 were persistent pulmonary hypertension. There were also two cases of sepsis-associated pulmonary hypertension and four cases of bronchopulmonary dysplasia associated with the disorder. In the placebo-exposed group, pulmonary hypertension occurred in 3 of the 11 deaths and 1 of the 67 who survived. Of proven cases, two were persistent pulmonary hypertension. There was no sepsis-associated pulmonary hypertension, but there were three cases of bronchopulmonary dysplasia associated with the disorder. Some children had both persistent pulmonary hypertension and bronchopulmonary dysplasia.
“While there was no difference in the primary outcomes or in overall mortality, there were more cases of pulmonary hypertension in the sildenafil group,” Dr. Pels said. “We can speculate on the cause, whether it was related to sildenafil and why, or whether it was simply chance. This is the reason we need to conduct more in-depth analyses of these data.”
Funding came from federal health agencies and universities in the countries where STRIDER was conducted, including New Zealand, Australia, the United Kingdom, Ireland, and the Netherlands. Dr. Pels had no relevant financial disclosures.
SOURCE: Pels A et al. The Pregnancy Meeting, Late-Breaker 2.
LAS VEGAS – Increased rates of persistent neonatal pulmonary hypertension in neonates put the brakes on STRIDER, an international placebo-controlled study looking at sildenafil as a treatment for early-onset intrauterine growth restriction (IUGR).
The study’s independent data safety monitoring board halted STRIDER (Sildenafil Therapy in Dismal Prognosis Early-Onset Fetal Growth Restriction) last July, after an interim safety analysis identified possible fetal harm and no signal of benefit over placebo, Dr. Anouk Pels reported at the annual meeting of the Society for Maternal-Fetal Medicine. The late-breaking presentation at the meeting revealed the first outcome data details.
The board had “serious concerns that sildenafil may cause harm to newborn children. … Given the results , it is extremely unlikely that any benefit could be shown on the primary endpoint if the trial is continued to its completion,” said Dr. Pels of the University of Amsterdam. “Our recommendation is not to use sildenafil for this indication in pregnant women.”
Although the link remains as-yet unproven, pulmonary hypertension among sildenafil-exposed neonates is biologically plausible, she said. It could have been a symptomatic rebound response to the discontinuation of constant intrauterine sildenafil exposure – or it could have been a hint of something more profound. Like the genital vasculature, pulmonary vasculature is a target of the drug. Intrauterine exposure to sildenafil could theoretically alter its development.
“It’s possible that sildenafil may be causing structural changes in the pulmonary vasculature of fetuses. This needs to be explored further, and we will do so by performing additional analyses on autopsy data and placental histology.”
STRIDER involved 261 pregnant women diagnosed with severe early-onset fetal growth restriction. They were randomized to sildenafil 25 mg or placebo three times daily until delivery or 32 weeks’ gestation. A safety analysis was conducted after every 50 patients were enrolled. The preplanned interim analysis was conducted after half of the cohort had been enrolled and received at least one dose of the study medication.
The primary outcome was a composite measure of neonatal mortality or major neonatal morbidity at hospital discharge.
Gestational age at baseline was about 24.6 weeks, and the estimated fetal weight by ultrasound, 465 g. About 45% of pregnancies had evidence of a notching in the uterine artery. In about 42%, the pulsatility index of the umbilical artery was above the 95th percentile; the pulsatility index of the middle cerebral artery was below the 5% percentile in about 70% of cases.
About a quarter of the women had a diagnosis of pregnancy-induced hypertension, and another quarter, preeclampsia. Women used the study medication for a mean of 22 days.
There were no significant between-group differences in maternal outcomes. Median gestational age at delivery was 28 weeks in both groups. About 10% in each group experienced new-onset pregnancy-induced hypertension; About a quarter of each group developed new-onset preeclampsia or HELLP (hemolysis, elevated liver enzymes, low platelet count). There were no between-group differences in the number of maternal antihypertensives prescribed.
The primary combined outcome of neonatal mortality or major neonatal morbidity occurred in 66 of the sildenafil-exposed neonates and 58 of the placebo-exposed infants (61% vs. 54%) – not a significant difference. Fetal death occurred in 23 and 29 pregnancies, respectively (21% and 27%); neonatal death occurred in 21 and 11, respectively (19% and 10%). Overall, fetal/neonatal mortality was similar between the sildenafil and placebo groups (41% and 37%, respectively).
Of the 64 sildenafil-exposed neonates who survived to hospital discharge, 22 exhibited clinically relevant morbidity. Of the 67 in the placebo-treated group who survived to hospital discharge, 18 had clinically relevant morbidity. Overall, 42 in the sildenafil group and 49 of the placebo group survived to hospital discharge without relevant morbidity.
There were a number of secondary outcomes, none exhibiting any significant between-group differences. These included the median weights of those who experienced intrauterine death (425 g and 350 g), median live birth weight (725 g and 783 g), intraventricular hemorrhage of grade II or IV (3% and 2%), periventricular hemorrhage grade II or higher (0%, both groups), necrotizing enterocolitis grade II or higher (7% and 8%), and at least one culture-proven or clinical infection (41% and 33%).
The significantly higher rates of pulmonary hypertension in the sildenafil-exposed neonates was the showstopper. Almost half of the 21 who died had proven pulmonary hypertension (10), as did 6 of the 64 who survived – an excess of 16 cases. Of proven cases, 11 were persistent pulmonary hypertension. There were also two cases of sepsis-associated pulmonary hypertension and four cases of bronchopulmonary dysplasia associated with the disorder. In the placebo-exposed group, pulmonary hypertension occurred in 3 of the 11 deaths and 1 of the 67 who survived. Of proven cases, two were persistent pulmonary hypertension. There was no sepsis-associated pulmonary hypertension, but there were three cases of bronchopulmonary dysplasia associated with the disorder. Some children had both persistent pulmonary hypertension and bronchopulmonary dysplasia.
“While there was no difference in the primary outcomes or in overall mortality, there were more cases of pulmonary hypertension in the sildenafil group,” Dr. Pels said. “We can speculate on the cause, whether it was related to sildenafil and why, or whether it was simply chance. This is the reason we need to conduct more in-depth analyses of these data.”
Funding came from federal health agencies and universities in the countries where STRIDER was conducted, including New Zealand, Australia, the United Kingdom, Ireland, and the Netherlands. Dr. Pels had no relevant financial disclosures.
SOURCE: Pels A et al. The Pregnancy Meeting, Late-Breaker 2.
LAS VEGAS – Increased rates of persistent neonatal pulmonary hypertension in neonates put the brakes on STRIDER, an international placebo-controlled study looking at sildenafil as a treatment for early-onset intrauterine growth restriction (IUGR).
The study’s independent data safety monitoring board halted STRIDER (Sildenafil Therapy in Dismal Prognosis Early-Onset Fetal Growth Restriction) last July, after an interim safety analysis identified possible fetal harm and no signal of benefit over placebo, Dr. Anouk Pels reported at the annual meeting of the Society for Maternal-Fetal Medicine. The late-breaking presentation at the meeting revealed the first outcome data details.
The board had “serious concerns that sildenafil may cause harm to newborn children. … Given the results , it is extremely unlikely that any benefit could be shown on the primary endpoint if the trial is continued to its completion,” said Dr. Pels of the University of Amsterdam. “Our recommendation is not to use sildenafil for this indication in pregnant women.”
Although the link remains as-yet unproven, pulmonary hypertension among sildenafil-exposed neonates is biologically plausible, she said. It could have been a symptomatic rebound response to the discontinuation of constant intrauterine sildenafil exposure – or it could have been a hint of something more profound. Like the genital vasculature, pulmonary vasculature is a target of the drug. Intrauterine exposure to sildenafil could theoretically alter its development.
“It’s possible that sildenafil may be causing structural changes in the pulmonary vasculature of fetuses. This needs to be explored further, and we will do so by performing additional analyses on autopsy data and placental histology.”
STRIDER involved 261 pregnant women diagnosed with severe early-onset fetal growth restriction. They were randomized to sildenafil 25 mg or placebo three times daily until delivery or 32 weeks’ gestation. A safety analysis was conducted after every 50 patients were enrolled. The preplanned interim analysis was conducted after half of the cohort had been enrolled and received at least one dose of the study medication.
The primary outcome was a composite measure of neonatal mortality or major neonatal morbidity at hospital discharge.
Gestational age at baseline was about 24.6 weeks, and the estimated fetal weight by ultrasound, 465 g. About 45% of pregnancies had evidence of a notching in the uterine artery. In about 42%, the pulsatility index of the umbilical artery was above the 95th percentile; the pulsatility index of the middle cerebral artery was below the 5% percentile in about 70% of cases.
About a quarter of the women had a diagnosis of pregnancy-induced hypertension, and another quarter, preeclampsia. Women used the study medication for a mean of 22 days.
There were no significant between-group differences in maternal outcomes. Median gestational age at delivery was 28 weeks in both groups. About 10% in each group experienced new-onset pregnancy-induced hypertension; About a quarter of each group developed new-onset preeclampsia or HELLP (hemolysis, elevated liver enzymes, low platelet count). There were no between-group differences in the number of maternal antihypertensives prescribed.
The primary combined outcome of neonatal mortality or major neonatal morbidity occurred in 66 of the sildenafil-exposed neonates and 58 of the placebo-exposed infants (61% vs. 54%) – not a significant difference. Fetal death occurred in 23 and 29 pregnancies, respectively (21% and 27%); neonatal death occurred in 21 and 11, respectively (19% and 10%). Overall, fetal/neonatal mortality was similar between the sildenafil and placebo groups (41% and 37%, respectively).
Of the 64 sildenafil-exposed neonates who survived to hospital discharge, 22 exhibited clinically relevant morbidity. Of the 67 in the placebo-treated group who survived to hospital discharge, 18 had clinically relevant morbidity. Overall, 42 in the sildenafil group and 49 of the placebo group survived to hospital discharge without relevant morbidity.
There were a number of secondary outcomes, none exhibiting any significant between-group differences. These included the median weights of those who experienced intrauterine death (425 g and 350 g), median live birth weight (725 g and 783 g), intraventricular hemorrhage of grade II or IV (3% and 2%), periventricular hemorrhage grade II or higher (0%, both groups), necrotizing enterocolitis grade II or higher (7% and 8%), and at least one culture-proven or clinical infection (41% and 33%).
The significantly higher rates of pulmonary hypertension in the sildenafil-exposed neonates was the showstopper. Almost half of the 21 who died had proven pulmonary hypertension (10), as did 6 of the 64 who survived – an excess of 16 cases. Of proven cases, 11 were persistent pulmonary hypertension. There were also two cases of sepsis-associated pulmonary hypertension and four cases of bronchopulmonary dysplasia associated with the disorder. In the placebo-exposed group, pulmonary hypertension occurred in 3 of the 11 deaths and 1 of the 67 who survived. Of proven cases, two were persistent pulmonary hypertension. There was no sepsis-associated pulmonary hypertension, but there were three cases of bronchopulmonary dysplasia associated with the disorder. Some children had both persistent pulmonary hypertension and bronchopulmonary dysplasia.
“While there was no difference in the primary outcomes or in overall mortality, there were more cases of pulmonary hypertension in the sildenafil group,” Dr. Pels said. “We can speculate on the cause, whether it was related to sildenafil and why, or whether it was simply chance. This is the reason we need to conduct more in-depth analyses of these data.”
Funding came from federal health agencies and universities in the countries where STRIDER was conducted, including New Zealand, Australia, the United Kingdom, Ireland, and the Netherlands. Dr. Pels had no relevant financial disclosures.
SOURCE: Pels A et al. The Pregnancy Meeting, Late-Breaker 2.
REPORTING FROM THE PREGNANCY MEETING
Key clinical point:
Major finding: There were 16 cases of persistent pulmonary hypertension in the treated group and four in the placebo group.
Study details: The randomized study involved 261 pregnant women treated with sildenafil for early-onset intrauterine growth restriction.
Disclosures: Funding agencies and universities in the countries involved in the trial contributed to funding. Dr. Pels had no relevant financial disclosures.
Source: Pels A et al. The Pregnancy Meeting, Late-Breaker 2.
Measles: 26 new cases reported last week
according to the Centers for Disease Control and Prevention.
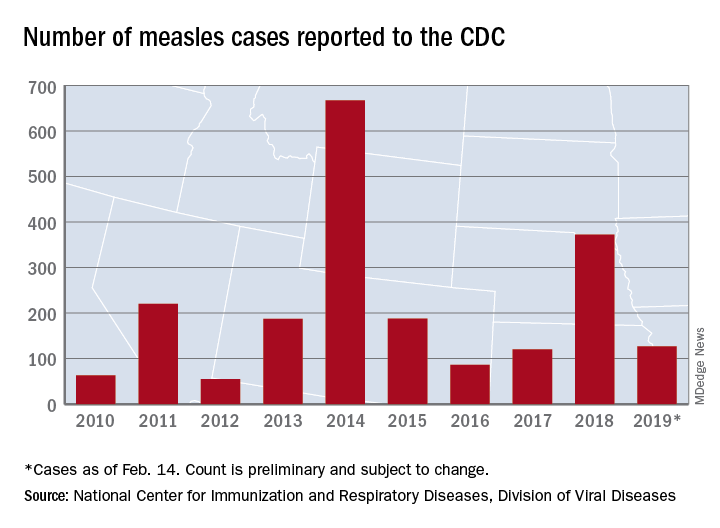
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
Enterovirus in at-risk children associated with later celiac disease
“We found a significant association between exposure to enterovirus and subsequent risk of celiac disease,” wrote lead author Christian R. Kahrs of the University of Oslo and his coauthors, adding that “adenovirus was not associated with celiac disease.” The study was published in the BMJ.
From 2001 to 2007, 46,939 newborns in Norway were screened for the HLA-DQ2/DQ8 genotype, which is associated with an increased risk of celiac disease. The genotype was identified in 912 children, and blood and stool sample collection began at 3 months. Children who were still contributing blood samples by 2014-2016 were invited to be screened for celiac disease.
Of the 220 children screened, 25 were diagnosed with celiac disease. Enterovirus was detected in 370 (17%) of the 2,135 stool samples and was more frequent in children who developed celiac disease antibodies than in matched controls (adjusted odds ratio, 1.49; 95% confidence interval, 1.07-2.06; P = .02). There was a significant association between later development of celiac disease and the commonly identified enterovirus A (aOR, 1.62; 95% CI, 1.04-2.53; P = .03) and enterovirus B (aOR, 2.27; 95% CI, 1.33-3.88; P = .003). No adenovirus types were associated with development of celiac disease.
The authors acknowledged their study’s limitations, including the possibility that children might be diagnosed with celiac disease later than the study’s roughly 10-year follow-up and the limited number of children with the disease despite a large number of analyzed samples. They noted that, “given the limited number of cases, we call for corroboration in similar studies and preferably interventional studies to reach conclusions about causality.”
The study was funded by the Research Council of Norway, the Project for the Conceptual Development of Research Organization, and the Norwegian Coeliac Society. Two authors reported grant support from trusts and foundations in Norway and Switzerland; no conflicts of interest were reported.
SOURCE: Kahrs CR et al. BMJ. 2019 Feb 13. doi: 10.1136/bmj.l231.
“We found a significant association between exposure to enterovirus and subsequent risk of celiac disease,” wrote lead author Christian R. Kahrs of the University of Oslo and his coauthors, adding that “adenovirus was not associated with celiac disease.” The study was published in the BMJ.
From 2001 to 2007, 46,939 newborns in Norway were screened for the HLA-DQ2/DQ8 genotype, which is associated with an increased risk of celiac disease. The genotype was identified in 912 children, and blood and stool sample collection began at 3 months. Children who were still contributing blood samples by 2014-2016 were invited to be screened for celiac disease.
Of the 220 children screened, 25 were diagnosed with celiac disease. Enterovirus was detected in 370 (17%) of the 2,135 stool samples and was more frequent in children who developed celiac disease antibodies than in matched controls (adjusted odds ratio, 1.49; 95% confidence interval, 1.07-2.06; P = .02). There was a significant association between later development of celiac disease and the commonly identified enterovirus A (aOR, 1.62; 95% CI, 1.04-2.53; P = .03) and enterovirus B (aOR, 2.27; 95% CI, 1.33-3.88; P = .003). No adenovirus types were associated with development of celiac disease.
The authors acknowledged their study’s limitations, including the possibility that children might be diagnosed with celiac disease later than the study’s roughly 10-year follow-up and the limited number of children with the disease despite a large number of analyzed samples. They noted that, “given the limited number of cases, we call for corroboration in similar studies and preferably interventional studies to reach conclusions about causality.”
The study was funded by the Research Council of Norway, the Project for the Conceptual Development of Research Organization, and the Norwegian Coeliac Society. Two authors reported grant support from trusts and foundations in Norway and Switzerland; no conflicts of interest were reported.
SOURCE: Kahrs CR et al. BMJ. 2019 Feb 13. doi: 10.1136/bmj.l231.
“We found a significant association between exposure to enterovirus and subsequent risk of celiac disease,” wrote lead author Christian R. Kahrs of the University of Oslo and his coauthors, adding that “adenovirus was not associated with celiac disease.” The study was published in the BMJ.
From 2001 to 2007, 46,939 newborns in Norway were screened for the HLA-DQ2/DQ8 genotype, which is associated with an increased risk of celiac disease. The genotype was identified in 912 children, and blood and stool sample collection began at 3 months. Children who were still contributing blood samples by 2014-2016 were invited to be screened for celiac disease.
Of the 220 children screened, 25 were diagnosed with celiac disease. Enterovirus was detected in 370 (17%) of the 2,135 stool samples and was more frequent in children who developed celiac disease antibodies than in matched controls (adjusted odds ratio, 1.49; 95% confidence interval, 1.07-2.06; P = .02). There was a significant association between later development of celiac disease and the commonly identified enterovirus A (aOR, 1.62; 95% CI, 1.04-2.53; P = .03) and enterovirus B (aOR, 2.27; 95% CI, 1.33-3.88; P = .003). No adenovirus types were associated with development of celiac disease.
The authors acknowledged their study’s limitations, including the possibility that children might be diagnosed with celiac disease later than the study’s roughly 10-year follow-up and the limited number of children with the disease despite a large number of analyzed samples. They noted that, “given the limited number of cases, we call for corroboration in similar studies and preferably interventional studies to reach conclusions about causality.”
The study was funded by the Research Council of Norway, the Project for the Conceptual Development of Research Organization, and the Norwegian Coeliac Society. Two authors reported grant support from trusts and foundations in Norway and Switzerland; no conflicts of interest were reported.
SOURCE: Kahrs CR et al. BMJ. 2019 Feb 13. doi: 10.1136/bmj.l231.
FROM THE BMJ