User login
Umbilical cord milking tied to severe IVH in very premature neonates
Delayed cord clamping and cutting is safer
LAS VEGAS – Umbilical cord milking can cause severe intraventricular hemorrhage (IVH) in very premature neonates and should not be performed on these cerebrovascularly fragile premature babies.

Just six of these procedures would be needed to cause a case of severe IVH in neonates born at 23-27 weeks’ gestation, Michael W. Varner, MD, said at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“Centers practicing umbilical cord milking should consider discontinuing this practice in infants 23-27 weeks’ gestation,” said Dr. Varner of the University of Utah, Salt Lake City.
The damage to the brains of very young preemies appears to be a direct result of the fluid overload caused by milking, he said. “From a mechanistic perspective, we can intuit that these findings are consistent with cord milking. This causes increasing venous return to the right atrium where it enters the foramen ovale and aorta. These very premature babies have more pulmonary vasoconstriction, which shunts more blood toward the brain. This results in fluctuations in flow in an immature brain with fragile germinal matrices and perhaps further compromised by chorioamnionitis inflammation, resulting in IVH.”
Premature Infants Receiving Milking or Delayed Cord Clamping (PREMOD2) was a noninferiority trial of umbilical cord milking compared to delayed cord clamping and cutting in preterm infants. Conducted at 11 sites in the United States and Europe, the study was halted prematurely when the data safety monitoring board determined that cord milking increased the risk of IVH in younger preemies and was no better than delayed cutting in the older preemies. The analysis presented at the meeting is the first public discussion of the data details.
The trial involved 474 premature neonates. They were randomized to placental transfusion via a 60-second delay in cord clamping and cutting or to umbilical cord milking, which involved grasping the cord and manually pushing the cord blood toward the infant four times before clamping. All participating sites received a video demonstrating the proper procedure. The cohort also was divided by gestational age: 23-27 weeks and 28-31 weeks.
The primary endpoint was a combination of severe IVH (grade 3 or higher) and neonatal death. Overall, the primary endpoint occurred in 29 of those randomized to cord milking (12%) and 20 randomized to delayed clamping (8%) – a significant difference.
This finding was largely driven by the treatment differences in the 23-27 week group, Dr. Varner said. Severe IVH occurred in 20 (22%) of those randomized to cord milking and five (6%) of those randomized to delayed clamping – a highly statistically significant difference with a P value of 0.0019.
In the 28-31 week group, there were no cases of severe IVH in the cord milking group, and three cases in the delayed clamping group; the difference was not statistically significant.
Overall, deaths were similar between the cord milking and cord clamping groups (17 and 15, respectively). Most of these deaths occurred in the younger group (14 in the cord milking group and 13 in the clamping group). There were five deaths in the older group: three in the cord milking group and two in the clamping group. None of these differences were statistically significant.
After seeing these data in a preplanned interim safety analysis, the Data Safety Monitoring Board stopped the study, saying that the intervention appeared dangerous for the younger babies, and no better than the delayed cutting and clamping for the older group, Dr. Varner said.
Since the trial was halted, investigators have been dissecting the data to identify any other intracranial hemorrhage risks particular to the infants. They found no significant differences in maternal characteristics at baseline, and – other than age and randomization– nothing significantly different between the infant groups. Severe persistent IVH occurred in almost 70% of the infants born at 23 weeks’ gestation but in only 7% in the delayed cord clamping group. The risks declined rapidly with increasing gestational age, although they were at all times greater than the risk of IVH in the cord clamping group.
“Looking at the data by gestational age, it’s clear that the majority of the severe IVH occurrences were in the 23 weekers, and also occurred in the first 7 days of life,” Dr. Varner said.
The cohort will be followed for at least another year, he added, as investigators track neurodevelopmental outcomes.
Investigators are particularly interested in differences in motor and language skills, as well as general cognitive development.
The study was sponsored by theEunice Kennedy Shriver National Institute of Child Health and Development. Neither Dr. Varner nor any of the coauthors had any financial declarations.
SOURCE: Katheria AC et al. The Pregnancy Meeting, late breaking abstract 1.
Delayed cord clamping and cutting is safer
Delayed cord clamping and cutting is safer
LAS VEGAS – Umbilical cord milking can cause severe intraventricular hemorrhage (IVH) in very premature neonates and should not be performed on these cerebrovascularly fragile premature babies.
Just six of these procedures would be needed to cause a case of severe IVH in neonates born at 23-27 weeks’ gestation, Michael W. Varner, MD, said at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“Centers practicing umbilical cord milking should consider discontinuing this practice in infants 23-27 weeks’ gestation,” said Dr. Varner of the University of Utah, Salt Lake City.
The damage to the brains of very young preemies appears to be a direct result of the fluid overload caused by milking, he said. “From a mechanistic perspective, we can intuit that these findings are consistent with cord milking. This causes increasing venous return to the right atrium where it enters the foramen ovale and aorta. These very premature babies have more pulmonary vasoconstriction, which shunts more blood toward the brain. This results in fluctuations in flow in an immature brain with fragile germinal matrices and perhaps further compromised by chorioamnionitis inflammation, resulting in IVH.”
Premature Infants Receiving Milking or Delayed Cord Clamping (PREMOD2) was a noninferiority trial of umbilical cord milking compared to delayed cord clamping and cutting in preterm infants. Conducted at 11 sites in the United States and Europe, the study was halted prematurely when the data safety monitoring board determined that cord milking increased the risk of IVH in younger preemies and was no better than delayed cutting in the older preemies. The analysis presented at the meeting is the first public discussion of the data details.
The trial involved 474 premature neonates. They were randomized to placental transfusion via a 60-second delay in cord clamping and cutting or to umbilical cord milking, which involved grasping the cord and manually pushing the cord blood toward the infant four times before clamping. All participating sites received a video demonstrating the proper procedure. The cohort also was divided by gestational age: 23-27 weeks and 28-31 weeks.
The primary endpoint was a combination of severe IVH (grade 3 or higher) and neonatal death. Overall, the primary endpoint occurred in 29 of those randomized to cord milking (12%) and 20 randomized to delayed clamping (8%) – a significant difference.
This finding was largely driven by the treatment differences in the 23-27 week group, Dr. Varner said. Severe IVH occurred in 20 (22%) of those randomized to cord milking and five (6%) of those randomized to delayed clamping – a highly statistically significant difference with a P value of 0.0019.
In the 28-31 week group, there were no cases of severe IVH in the cord milking group, and three cases in the delayed clamping group; the difference was not statistically significant.
Overall, deaths were similar between the cord milking and cord clamping groups (17 and 15, respectively). Most of these deaths occurred in the younger group (14 in the cord milking group and 13 in the clamping group). There were five deaths in the older group: three in the cord milking group and two in the clamping group. None of these differences were statistically significant.
After seeing these data in a preplanned interim safety analysis, the Data Safety Monitoring Board stopped the study, saying that the intervention appeared dangerous for the younger babies, and no better than the delayed cutting and clamping for the older group, Dr. Varner said.
Since the trial was halted, investigators have been dissecting the data to identify any other intracranial hemorrhage risks particular to the infants. They found no significant differences in maternal characteristics at baseline, and – other than age and randomization– nothing significantly different between the infant groups. Severe persistent IVH occurred in almost 70% of the infants born at 23 weeks’ gestation but in only 7% in the delayed cord clamping group. The risks declined rapidly with increasing gestational age, although they were at all times greater than the risk of IVH in the cord clamping group.
“Looking at the data by gestational age, it’s clear that the majority of the severe IVH occurrences were in the 23 weekers, and also occurred in the first 7 days of life,” Dr. Varner said.
The cohort will be followed for at least another year, he added, as investigators track neurodevelopmental outcomes.
Investigators are particularly interested in differences in motor and language skills, as well as general cognitive development.
The study was sponsored by theEunice Kennedy Shriver National Institute of Child Health and Development. Neither Dr. Varner nor any of the coauthors had any financial declarations.
SOURCE: Katheria AC et al. The Pregnancy Meeting, late breaking abstract 1.
LAS VEGAS – Umbilical cord milking can cause severe intraventricular hemorrhage (IVH) in very premature neonates and should not be performed on these cerebrovascularly fragile premature babies.
Just six of these procedures would be needed to cause a case of severe IVH in neonates born at 23-27 weeks’ gestation, Michael W. Varner, MD, said at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“Centers practicing umbilical cord milking should consider discontinuing this practice in infants 23-27 weeks’ gestation,” said Dr. Varner of the University of Utah, Salt Lake City.
The damage to the brains of very young preemies appears to be a direct result of the fluid overload caused by milking, he said. “From a mechanistic perspective, we can intuit that these findings are consistent with cord milking. This causes increasing venous return to the right atrium where it enters the foramen ovale and aorta. These very premature babies have more pulmonary vasoconstriction, which shunts more blood toward the brain. This results in fluctuations in flow in an immature brain with fragile germinal matrices and perhaps further compromised by chorioamnionitis inflammation, resulting in IVH.”
Premature Infants Receiving Milking or Delayed Cord Clamping (PREMOD2) was a noninferiority trial of umbilical cord milking compared to delayed cord clamping and cutting in preterm infants. Conducted at 11 sites in the United States and Europe, the study was halted prematurely when the data safety monitoring board determined that cord milking increased the risk of IVH in younger preemies and was no better than delayed cutting in the older preemies. The analysis presented at the meeting is the first public discussion of the data details.
The trial involved 474 premature neonates. They were randomized to placental transfusion via a 60-second delay in cord clamping and cutting or to umbilical cord milking, which involved grasping the cord and manually pushing the cord blood toward the infant four times before clamping. All participating sites received a video demonstrating the proper procedure. The cohort also was divided by gestational age: 23-27 weeks and 28-31 weeks.
The primary endpoint was a combination of severe IVH (grade 3 or higher) and neonatal death. Overall, the primary endpoint occurred in 29 of those randomized to cord milking (12%) and 20 randomized to delayed clamping (8%) – a significant difference.
This finding was largely driven by the treatment differences in the 23-27 week group, Dr. Varner said. Severe IVH occurred in 20 (22%) of those randomized to cord milking and five (6%) of those randomized to delayed clamping – a highly statistically significant difference with a P value of 0.0019.
In the 28-31 week group, there were no cases of severe IVH in the cord milking group, and three cases in the delayed clamping group; the difference was not statistically significant.
Overall, deaths were similar between the cord milking and cord clamping groups (17 and 15, respectively). Most of these deaths occurred in the younger group (14 in the cord milking group and 13 in the clamping group). There were five deaths in the older group: three in the cord milking group and two in the clamping group. None of these differences were statistically significant.
After seeing these data in a preplanned interim safety analysis, the Data Safety Monitoring Board stopped the study, saying that the intervention appeared dangerous for the younger babies, and no better than the delayed cutting and clamping for the older group, Dr. Varner said.
Since the trial was halted, investigators have been dissecting the data to identify any other intracranial hemorrhage risks particular to the infants. They found no significant differences in maternal characteristics at baseline, and – other than age and randomization– nothing significantly different between the infant groups. Severe persistent IVH occurred in almost 70% of the infants born at 23 weeks’ gestation but in only 7% in the delayed cord clamping group. The risks declined rapidly with increasing gestational age, although they were at all times greater than the risk of IVH in the cord clamping group.
“Looking at the data by gestational age, it’s clear that the majority of the severe IVH occurrences were in the 23 weekers, and also occurred in the first 7 days of life,” Dr. Varner said.
The cohort will be followed for at least another year, he added, as investigators track neurodevelopmental outcomes.
Investigators are particularly interested in differences in motor and language skills, as well as general cognitive development.
The study was sponsored by theEunice Kennedy Shriver National Institute of Child Health and Development. Neither Dr. Varner nor any of the coauthors had any financial declarations.
SOURCE: Katheria AC et al. The Pregnancy Meeting, late breaking abstract 1.
REPORTING FROM THE PREGNANCY MEETING
FDA approves first interoperable insulin infusion pump
, for insulin delivery in children and adults with diabetes.

The pump delivers insulin under the skin at a variable or fixed rate. It can function on its own, or it can be digitally connected to automatically communicate with and receive drug-dosing commands from other diabetes management devices, such as automated insulin-dosing systems, the agency announced.
The approval was based on a review of performance data demonstrating that the device can deliver insulin accurately and reliably and at the rates and volumes programmed by the user. The agency also assessed the pump’s ability to connect reliably with other devices, as well as its cybersecurity and fail-safe modes.
Risks associated with the device were similar to those of other infusion pumps and include infection, bleeding, pain, or skin irritations. Blockages and air bubbles can occur in the tubing, which will affect drug delivery. Risks associated with incorrect drug delivery include hypo- and hyperglycemia as well as diabetic ketoacidosis.
“The marketing authorization of the [pump] has the potential to aid patients who seek more individualized diabetes therapy systems and opens the door for developers of future connected diabetes devices to get other safe and effective products to patients more efficiently,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
, for insulin delivery in children and adults with diabetes.
The pump delivers insulin under the skin at a variable or fixed rate. It can function on its own, or it can be digitally connected to automatically communicate with and receive drug-dosing commands from other diabetes management devices, such as automated insulin-dosing systems, the agency announced.
The approval was based on a review of performance data demonstrating that the device can deliver insulin accurately and reliably and at the rates and volumes programmed by the user. The agency also assessed the pump’s ability to connect reliably with other devices, as well as its cybersecurity and fail-safe modes.
Risks associated with the device were similar to those of other infusion pumps and include infection, bleeding, pain, or skin irritations. Blockages and air bubbles can occur in the tubing, which will affect drug delivery. Risks associated with incorrect drug delivery include hypo- and hyperglycemia as well as diabetic ketoacidosis.
“The marketing authorization of the [pump] has the potential to aid patients who seek more individualized diabetes therapy systems and opens the door for developers of future connected diabetes devices to get other safe and effective products to patients more efficiently,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
, for insulin delivery in children and adults with diabetes.
The pump delivers insulin under the skin at a variable or fixed rate. It can function on its own, or it can be digitally connected to automatically communicate with and receive drug-dosing commands from other diabetes management devices, such as automated insulin-dosing systems, the agency announced.
The approval was based on a review of performance data demonstrating that the device can deliver insulin accurately and reliably and at the rates and volumes programmed by the user. The agency also assessed the pump’s ability to connect reliably with other devices, as well as its cybersecurity and fail-safe modes.
Risks associated with the device were similar to those of other infusion pumps and include infection, bleeding, pain, or skin irritations. Blockages and air bubbles can occur in the tubing, which will affect drug delivery. Risks associated with incorrect drug delivery include hypo- and hyperglycemia as well as diabetic ketoacidosis.
“The marketing authorization of the [pump] has the potential to aid patients who seek more individualized diabetes therapy systems and opens the door for developers of future connected diabetes devices to get other safe and effective products to patients more efficiently,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
Flu season showing its staying power
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
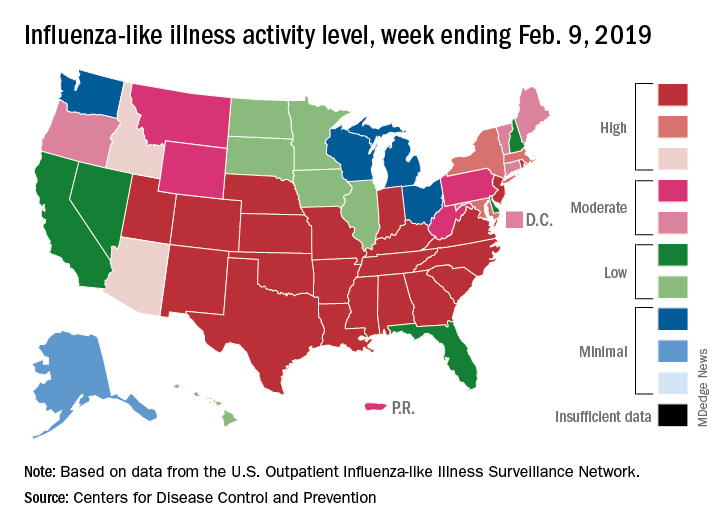
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
‘Telereferrals’ improved mental health referral follow-through
Children referred for mental health services in Los Angeles County using a telehealth referral were three times more likely to complete a community mental health clinic (CMHC) screening than children receiving conventional mental health referrals, a study found.

“Our findings highlight the importance of this initial access point for a successful referral to the CHMC,” Tumaini R. Coker, MD, MBA, of the University of Washington, Seattle, and Seattle Children’s Research Institute, and her colleagues wrote in Pediatrics. “We can hypothesize that the assistance from the telehealth care coordinator may have played an important role in access for families.”
Although this study was not powered to compare psychological health or quality-of-life differences, a larger study with a longer follow-up period may allow study of “variation in health outcomes … among a sample of all who were initially referred, particularly if the higher rates of access for children in the intervention translate into a greater proportion of children receiving services,” the authors wrote.
The research group partnered with two community mental health clinics (CMHCs) and six federally qualified health center clinics, the latter randomly assigned as control or intervention. The telehealth-enhanced referral process developed by the researchers involved patients at the intervention clinics viewing a video orientation to the CMHC and then participating in a live video conference for screening. Completion of the referral screening visit was the measure for CMHC access as a primary endpoint.
Among the 342 children, aged 5-12 years (average, 9 years), enrolled in the study, 87% were Latino, and 62% were boys.
Of children using the telehealth referral process, 80% completed an initial CMHC screening, compared to 64% of children receiving referrals via usual care procedures, resulting in three-times greater odds of a screening in the intervention group (adjusted odds ratio, 3.02).
It took approximately 6 more days for the telehealth-referred children to complete the screening.
“The increased time to the initial access point was anticipated for the intervention clinics because the telehealth care coordinator and CMHC staff held all the videoconference screening visits on a single preselected day each week,” which thereby limited availability of slots for screenings, Dr. Coker and her associates wrote.
Children who received telehealth-enabled referrals reported higher satisfaction levels with the referral system and with care, compared with those using usual care methods. Of the 342 children in the study, 213 were considered eligible to receive CMHC services. Reasons for ineligibility for services included presence of a developmental disability, lack of an mental health need, private health insurance coverage, a zip code outside of the CMHC’s catchment area, and not meeting income requirements.
Of those 213, 80% of the intervention group and 84% of controls subsequently had a mental health visit.
A study limitation is its personalization to the community partners involved, which may require different procedures in other settings, the authors noted. The study also did not look at the quality of mental health services received after initial screenings, precluding the ability to assess clinical outcomes. In addition, “the CMHCs did not involve the payers of mental health care for this population, limiting our capacity to identify barriers and system solutions that may improve the intervention’s sustainability,” the authors wrote.
The research was funded by grants from the Patient-Centered Outcomes Research Institute and the California Community Foundation. The authors reported having no relevant financial disclosures.
SOURCE: Coker TR et al. Pediatrics. 2019 Feb 15. doi: 10.1542/peds.2018-2738.
Despite the challenges of meeting patients’ and their families’ mental and behavioral needs, Coker et al. “had the courage to think outside the box to solve a practice and community need,” Susan J. Kressly, MD, is in private practice in Warrington, Pa., wrote in an accompanying editorial.
Some practices have been able to fully integrate a mental health service within their practice, usually on-site, but that model does not work for everyone. Space and privacy can be problematic, depending on the practice, and payment models can become complex, especially when mental health benefits are not managed by the same payer or through the same plan as other health insurance benefits, Dr. Kressly noted.
“The innovative model in this study combines a ‘soft hand-off’ referral model and takes advantage of telehealth technology for implementation,” she wrote. Families frequently do not follow through on recommendations and referrals, but practices can improve follow-through when they make personal introductions and appointments from their own practice. And using technology to do so can particularly resonate with the generations of children and parents now coming to pediatric practices.
“As pediatricians, we have a unique opportunity to provide care to families who are digital natives,” Dr. Kressly wrote. “As part of the family’s health care team, if we truly decide to put the patient and family at the center, pediatricians should examine their own hesitancy and trepidation regarding telehealth and technology-enabled communications and work to overcome them.”
Other ways to use telehealth beyond the referral system described by Coker et al. might include providing actual telepsychiatry visits at the child’s medical home or connecting families to local resources.
“Those practices that innovate to solve their problems by extending their medical home to include care teams outside their practice walls will likely see improved family satisfaction and, hopefully, improved outcomes,” Dr. Kressly suggested.
Dr. Kressly is in private practice in Warrington, Pa. She used no external funding and has no financial conflicts to report. These comments are condensed and summarized from her editorial accompanying the article by Coker et al (Pediatrics. 2019 Feb 15. doi: 10.1542/peds.2018-3765).
Despite the challenges of meeting patients’ and their families’ mental and behavioral needs, Coker et al. “had the courage to think outside the box to solve a practice and community need,” Susan J. Kressly, MD, is in private practice in Warrington, Pa., wrote in an accompanying editorial.
Some practices have been able to fully integrate a mental health service within their practice, usually on-site, but that model does not work for everyone. Space and privacy can be problematic, depending on the practice, and payment models can become complex, especially when mental health benefits are not managed by the same payer or through the same plan as other health insurance benefits, Dr. Kressly noted.
“The innovative model in this study combines a ‘soft hand-off’ referral model and takes advantage of telehealth technology for implementation,” she wrote. Families frequently do not follow through on recommendations and referrals, but practices can improve follow-through when they make personal introductions and appointments from their own practice. And using technology to do so can particularly resonate with the generations of children and parents now coming to pediatric practices.
“As pediatricians, we have a unique opportunity to provide care to families who are digital natives,” Dr. Kressly wrote. “As part of the family’s health care team, if we truly decide to put the patient and family at the center, pediatricians should examine their own hesitancy and trepidation regarding telehealth and technology-enabled communications and work to overcome them.”
Other ways to use telehealth beyond the referral system described by Coker et al. might include providing actual telepsychiatry visits at the child’s medical home or connecting families to local resources.
“Those practices that innovate to solve their problems by extending their medical home to include care teams outside their practice walls will likely see improved family satisfaction and, hopefully, improved outcomes,” Dr. Kressly suggested.
Dr. Kressly is in private practice in Warrington, Pa. She used no external funding and has no financial conflicts to report. These comments are condensed and summarized from her editorial accompanying the article by Coker et al (Pediatrics. 2019 Feb 15. doi: 10.1542/peds.2018-3765).
Despite the challenges of meeting patients’ and their families’ mental and behavioral needs, Coker et al. “had the courage to think outside the box to solve a practice and community need,” Susan J. Kressly, MD, is in private practice in Warrington, Pa., wrote in an accompanying editorial.
Some practices have been able to fully integrate a mental health service within their practice, usually on-site, but that model does not work for everyone. Space and privacy can be problematic, depending on the practice, and payment models can become complex, especially when mental health benefits are not managed by the same payer or through the same plan as other health insurance benefits, Dr. Kressly noted.
“The innovative model in this study combines a ‘soft hand-off’ referral model and takes advantage of telehealth technology for implementation,” she wrote. Families frequently do not follow through on recommendations and referrals, but practices can improve follow-through when they make personal introductions and appointments from their own practice. And using technology to do so can particularly resonate with the generations of children and parents now coming to pediatric practices.
“As pediatricians, we have a unique opportunity to provide care to families who are digital natives,” Dr. Kressly wrote. “As part of the family’s health care team, if we truly decide to put the patient and family at the center, pediatricians should examine their own hesitancy and trepidation regarding telehealth and technology-enabled communications and work to overcome them.”
Other ways to use telehealth beyond the referral system described by Coker et al. might include providing actual telepsychiatry visits at the child’s medical home or connecting families to local resources.
“Those practices that innovate to solve their problems by extending their medical home to include care teams outside their practice walls will likely see improved family satisfaction and, hopefully, improved outcomes,” Dr. Kressly suggested.
Dr. Kressly is in private practice in Warrington, Pa. She used no external funding and has no financial conflicts to report. These comments are condensed and summarized from her editorial accompanying the article by Coker et al (Pediatrics. 2019 Feb 15. doi: 10.1542/peds.2018-3765).
Children referred for mental health services in Los Angeles County using a telehealth referral were three times more likely to complete a community mental health clinic (CMHC) screening than children receiving conventional mental health referrals, a study found.
“Our findings highlight the importance of this initial access point for a successful referral to the CHMC,” Tumaini R. Coker, MD, MBA, of the University of Washington, Seattle, and Seattle Children’s Research Institute, and her colleagues wrote in Pediatrics. “We can hypothesize that the assistance from the telehealth care coordinator may have played an important role in access for families.”
Although this study was not powered to compare psychological health or quality-of-life differences, a larger study with a longer follow-up period may allow study of “variation in health outcomes … among a sample of all who were initially referred, particularly if the higher rates of access for children in the intervention translate into a greater proportion of children receiving services,” the authors wrote.
The research group partnered with two community mental health clinics (CMHCs) and six federally qualified health center clinics, the latter randomly assigned as control or intervention. The telehealth-enhanced referral process developed by the researchers involved patients at the intervention clinics viewing a video orientation to the CMHC and then participating in a live video conference for screening. Completion of the referral screening visit was the measure for CMHC access as a primary endpoint.
Among the 342 children, aged 5-12 years (average, 9 years), enrolled in the study, 87% were Latino, and 62% were boys.
Of children using the telehealth referral process, 80% completed an initial CMHC screening, compared to 64% of children receiving referrals via usual care procedures, resulting in three-times greater odds of a screening in the intervention group (adjusted odds ratio, 3.02).
It took approximately 6 more days for the telehealth-referred children to complete the screening.
“The increased time to the initial access point was anticipated for the intervention clinics because the telehealth care coordinator and CMHC staff held all the videoconference screening visits on a single preselected day each week,” which thereby limited availability of slots for screenings, Dr. Coker and her associates wrote.
Children who received telehealth-enabled referrals reported higher satisfaction levels with the referral system and with care, compared with those using usual care methods. Of the 342 children in the study, 213 were considered eligible to receive CMHC services. Reasons for ineligibility for services included presence of a developmental disability, lack of an mental health need, private health insurance coverage, a zip code outside of the CMHC’s catchment area, and not meeting income requirements.
Of those 213, 80% of the intervention group and 84% of controls subsequently had a mental health visit.
A study limitation is its personalization to the community partners involved, which may require different procedures in other settings, the authors noted. The study also did not look at the quality of mental health services received after initial screenings, precluding the ability to assess clinical outcomes. In addition, “the CMHCs did not involve the payers of mental health care for this population, limiting our capacity to identify barriers and system solutions that may improve the intervention’s sustainability,” the authors wrote.
The research was funded by grants from the Patient-Centered Outcomes Research Institute and the California Community Foundation. The authors reported having no relevant financial disclosures.
SOURCE: Coker TR et al. Pediatrics. 2019 Feb 15. doi: 10.1542/peds.2018-2738.
Children referred for mental health services in Los Angeles County using a telehealth referral were three times more likely to complete a community mental health clinic (CMHC) screening than children receiving conventional mental health referrals, a study found.
“Our findings highlight the importance of this initial access point for a successful referral to the CHMC,” Tumaini R. Coker, MD, MBA, of the University of Washington, Seattle, and Seattle Children’s Research Institute, and her colleagues wrote in Pediatrics. “We can hypothesize that the assistance from the telehealth care coordinator may have played an important role in access for families.”
Although this study was not powered to compare psychological health or quality-of-life differences, a larger study with a longer follow-up period may allow study of “variation in health outcomes … among a sample of all who were initially referred, particularly if the higher rates of access for children in the intervention translate into a greater proportion of children receiving services,” the authors wrote.
The research group partnered with two community mental health clinics (CMHCs) and six federally qualified health center clinics, the latter randomly assigned as control or intervention. The telehealth-enhanced referral process developed by the researchers involved patients at the intervention clinics viewing a video orientation to the CMHC and then participating in a live video conference for screening. Completion of the referral screening visit was the measure for CMHC access as a primary endpoint.
Among the 342 children, aged 5-12 years (average, 9 years), enrolled in the study, 87% were Latino, and 62% were boys.
Of children using the telehealth referral process, 80% completed an initial CMHC screening, compared to 64% of children receiving referrals via usual care procedures, resulting in three-times greater odds of a screening in the intervention group (adjusted odds ratio, 3.02).
It took approximately 6 more days for the telehealth-referred children to complete the screening.
“The increased time to the initial access point was anticipated for the intervention clinics because the telehealth care coordinator and CMHC staff held all the videoconference screening visits on a single preselected day each week,” which thereby limited availability of slots for screenings, Dr. Coker and her associates wrote.
Children who received telehealth-enabled referrals reported higher satisfaction levels with the referral system and with care, compared with those using usual care methods. Of the 342 children in the study, 213 were considered eligible to receive CMHC services. Reasons for ineligibility for services included presence of a developmental disability, lack of an mental health need, private health insurance coverage, a zip code outside of the CMHC’s catchment area, and not meeting income requirements.
Of those 213, 80% of the intervention group and 84% of controls subsequently had a mental health visit.
A study limitation is its personalization to the community partners involved, which may require different procedures in other settings, the authors noted. The study also did not look at the quality of mental health services received after initial screenings, precluding the ability to assess clinical outcomes. In addition, “the CMHCs did not involve the payers of mental health care for this population, limiting our capacity to identify barriers and system solutions that may improve the intervention’s sustainability,” the authors wrote.
The research was funded by grants from the Patient-Centered Outcomes Research Institute and the California Community Foundation. The authors reported having no relevant financial disclosures.
SOURCE: Coker TR et al. Pediatrics. 2019 Feb 15. doi: 10.1542/peds.2018-2738.
FROM PEDIATRICS
Key clinical point: Use of telehealth referrals increased children’s access to mental health services in an urban county.
Major finding:
Study details: The findings are based on a multisite, randomized, controlled trial that included 342 children, aged 5-12 years, at two community mental health clinics and six federally qualified health center clinics in Los Angeles County.
Disclosures: The research was funded by the Patient-Centered Outcomes Research Institute and the California Community Foundation. The authors reported having no relevant financial disclosures.
Source: Coker TR et al. Pediatrics. 2019 Feb 15. doi: 10.1542/peds.2018-2738.

Inhibitor risk nears zero after 75 days in previously untreated hemophilia A
PRAGUE—For previously untreated patients (PUPs) with severe hemophilia A, the risk of developing factor VIII (FVIII) alloantibodies (inhibitors) becomes negligible after 75 exposure days, according to a recent study involving more than 1,000 infants.
This finding answers a long-standing and important question in the management of hemophilia A, reported lead author H. Marijke van den Berg, MD, PhD, of University Medical Centre in Utrecht, The Netherlands.
Inhibitor development is the biggest safety concern facing infants with severe hemophilia A because it affects 25%-35% of the patient population, but no previous studies have adequately described the associated risk profile, she noted.
“Most studies until now collected data until about 50 [exposure days] and not that far beyond,” Dr. van den Berg said at the annual congress of the European Association for Haemophilia and Allied Disorders. “So we were interested to see the serum plateau in our large cohort.”
Such a plateau would represent the time point at which risk of inhibitor development approaches zero.
Dr. van den Berg and her colleagues followed 1,038 PUPs with severe hemophilia A from first exposure to FVIII onward. Data were from drawn from the PedNet Registry. From the initial group, 943 patients (91%) were followed until 50 exposure days, and 899 (87%) were followed until 75 exposure days.
Inhibitor development was defined by a minimum of two positive inhibitor titers. In addition to determining the point in time of inhibitor development, the investigators performed a survival analysis for inhibitor incidence and reported median ages at first exposure and at exposure day 75.
The results showed that 298 out of 300 instances of inhibitor development occurred within 75 exposure days, and no inhibitors developed between exposure day 75 and 150. The final two instances occurred at exposure day 249 and 262, both with a low titer.
Median age at first exposure was 1.1 years, compared with 2.3 years at exposure day 75.
These findings suggest that risk of inhibitors is “near zero” after 75 days and that risk is approaching zero just 1 year after first exposure to FVIII, she said.
The results from this study could affect the design of future clinical trials for PUPs.
“Our recommendation will be to continue frequent [inhibitor] testing until 75 exposure days,” Dr. van den Berg said.
The time frame involved is very short, so close monitoring should be feasible for investigators, she noted.
Dr. van den Berg said that additional data, including Kaplan-Meier curves, would “hopefully” be published in a journal soon.
Dr. van den Berg reported having no relevant financial disclosures.
SOURCE: van den Berg HM et al. EAHAD 2019, Abstract OR05.
PRAGUE—For previously untreated patients (PUPs) with severe hemophilia A, the risk of developing factor VIII (FVIII) alloantibodies (inhibitors) becomes negligible after 75 exposure days, according to a recent study involving more than 1,000 infants.
This finding answers a long-standing and important question in the management of hemophilia A, reported lead author H. Marijke van den Berg, MD, PhD, of University Medical Centre in Utrecht, The Netherlands.
Inhibitor development is the biggest safety concern facing infants with severe hemophilia A because it affects 25%-35% of the patient population, but no previous studies have adequately described the associated risk profile, she noted.
“Most studies until now collected data until about 50 [exposure days] and not that far beyond,” Dr. van den Berg said at the annual congress of the European Association for Haemophilia and Allied Disorders. “So we were interested to see the serum plateau in our large cohort.”
Such a plateau would represent the time point at which risk of inhibitor development approaches zero.
Dr. van den Berg and her colleagues followed 1,038 PUPs with severe hemophilia A from first exposure to FVIII onward. Data were from drawn from the PedNet Registry. From the initial group, 943 patients (91%) were followed until 50 exposure days, and 899 (87%) were followed until 75 exposure days.
Inhibitor development was defined by a minimum of two positive inhibitor titers. In addition to determining the point in time of inhibitor development, the investigators performed a survival analysis for inhibitor incidence and reported median ages at first exposure and at exposure day 75.
The results showed that 298 out of 300 instances of inhibitor development occurred within 75 exposure days, and no inhibitors developed between exposure day 75 and 150. The final two instances occurred at exposure day 249 and 262, both with a low titer.
Median age at first exposure was 1.1 years, compared with 2.3 years at exposure day 75.
These findings suggest that risk of inhibitors is “near zero” after 75 days and that risk is approaching zero just 1 year after first exposure to FVIII, she said.
The results from this study could affect the design of future clinical trials for PUPs.
“Our recommendation will be to continue frequent [inhibitor] testing until 75 exposure days,” Dr. van den Berg said.
The time frame involved is very short, so close monitoring should be feasible for investigators, she noted.
Dr. van den Berg said that additional data, including Kaplan-Meier curves, would “hopefully” be published in a journal soon.
Dr. van den Berg reported having no relevant financial disclosures.
SOURCE: van den Berg HM et al. EAHAD 2019, Abstract OR05.
PRAGUE—For previously untreated patients (PUPs) with severe hemophilia A, the risk of developing factor VIII (FVIII) alloantibodies (inhibitors) becomes negligible after 75 exposure days, according to a recent study involving more than 1,000 infants.
This finding answers a long-standing and important question in the management of hemophilia A, reported lead author H. Marijke van den Berg, MD, PhD, of University Medical Centre in Utrecht, The Netherlands.
Inhibitor development is the biggest safety concern facing infants with severe hemophilia A because it affects 25%-35% of the patient population, but no previous studies have adequately described the associated risk profile, she noted.
“Most studies until now collected data until about 50 [exposure days] and not that far beyond,” Dr. van den Berg said at the annual congress of the European Association for Haemophilia and Allied Disorders. “So we were interested to see the serum plateau in our large cohort.”
Such a plateau would represent the time point at which risk of inhibitor development approaches zero.
Dr. van den Berg and her colleagues followed 1,038 PUPs with severe hemophilia A from first exposure to FVIII onward. Data were from drawn from the PedNet Registry. From the initial group, 943 patients (91%) were followed until 50 exposure days, and 899 (87%) were followed until 75 exposure days.
Inhibitor development was defined by a minimum of two positive inhibitor titers. In addition to determining the point in time of inhibitor development, the investigators performed a survival analysis for inhibitor incidence and reported median ages at first exposure and at exposure day 75.
The results showed that 298 out of 300 instances of inhibitor development occurred within 75 exposure days, and no inhibitors developed between exposure day 75 and 150. The final two instances occurred at exposure day 249 and 262, both with a low titer.
Median age at first exposure was 1.1 years, compared with 2.3 years at exposure day 75.
These findings suggest that risk of inhibitors is “near zero” after 75 days and that risk is approaching zero just 1 year after first exposure to FVIII, she said.
The results from this study could affect the design of future clinical trials for PUPs.
“Our recommendation will be to continue frequent [inhibitor] testing until 75 exposure days,” Dr. van den Berg said.
The time frame involved is very short, so close monitoring should be feasible for investigators, she noted.
Dr. van den Berg said that additional data, including Kaplan-Meier curves, would “hopefully” be published in a journal soon.
Dr. van den Berg reported having no relevant financial disclosures.
SOURCE: van den Berg HM et al. EAHAD 2019, Abstract OR05.
REPORTING FROM EAHAD 2019
Key clinical point: Major finding: Less than 1% of infants with severe hemophilia A developed inhibitors after 75 exposure days.
Study details: An observational study involving 1,038 previously untreated patients with severe hemophilia A, of which 899 (87%) were followed until 75 exposure days.
Disclosures: Dr. van den Berg reported having no relevant financial disclosures.
Source: van den Berg HM et al. EAHAD 2019, Abstract OR05.
Tranexamic acid shows improvements in heavy menstrual bleeding
new research suggests.
Writing in the Journal of Pediatric & Adolescent Gynecology, Sarah H. O’Brien, MD, from Nationwide Children’s Hospital and the Ohio State University, both in Columbus, and her coauthors presented the results of an open-label efficacy study of the competitive plasminogen inhibitor in 25 adolescent girls aged 10-19 years who attended pediatric hematology clinics for evaluation or management of heavy menstrual bleeding. The study participants were instructed to take 1,300 mg of tranexamic acid (two tablets) three times a day for up to 5 days during their monthly menstruation for three cycles.
The study found a significant improvement in mean menstrual impact questionnaire (MIQ) scores, which improved from a mean of 3 at baseline to 1.91 (P less than .001). Two-thirds of patients reported at least a one-point improvement from baseline, and all reported that this was clinically meaningful. At baseline, 84% of patients reported heavy to very heavy blood loss, but this decreased to 23% after treatment with tranexamic acid (P less than .001).
The study population included ten individuals (40%) with bleeding disorders. However, the researchers did not see a significant difference in response between those with bleeding disorders and those without.
While the treatment did not significantly affect school attendance (only 24% reported that their heavy bleeding limited school attendance), researchers did see a significant improvement in limitations on physical activities and on social and leisure activities. Patients who reported at baseline that their menstrual bleeding significantly affected their social and leisure activities had an average score improvement of 1.74, a greater than or equal to one point improvement. Participants also reported significant improvements in their Pictorial Blood Assessment Chart scores, which dropped from an average of 255 to 155 (P less than .001).
The treatment did not show any significant effects on hemoglobin or ferritin. The most common adverse events were sinonasal symptoms, such as nasal congestion, headache, and sinus pain, but no thrombotic or ocular adverse events were seen.
Dr. O’Brien and her coauthors wrote that one limitation of their study was using the MIQ score as their primary endpoint as opposed to a more objective measure, such as change in measured blood loss.
“However, a major factor that motivates patients with heavy menstrual bleeding to seek medical care is the negative impact of heavy menstrual bleeding on daily life,” they wrote.
The study drug was supplied by Ferring pharmaceuticals, and the study was supported by the Hemostasis and Thrombosis Research Society. One author disclosed receiving the Joan Fellowship in Pediatric Hemostasis and Thrombosis at Nationwide Children’s Hospital; no other authors said they had relevant financial disclosures.
SOURCE: O’Brien SH et al. J Pediatr Adol Gynec. 2019 Feb 4. doi: 10.1016/j.jpag.2019.01.009.
new research suggests.
Writing in the Journal of Pediatric & Adolescent Gynecology, Sarah H. O’Brien, MD, from Nationwide Children’s Hospital and the Ohio State University, both in Columbus, and her coauthors presented the results of an open-label efficacy study of the competitive plasminogen inhibitor in 25 adolescent girls aged 10-19 years who attended pediatric hematology clinics for evaluation or management of heavy menstrual bleeding. The study participants were instructed to take 1,300 mg of tranexamic acid (two tablets) three times a day for up to 5 days during their monthly menstruation for three cycles.
The study found a significant improvement in mean menstrual impact questionnaire (MIQ) scores, which improved from a mean of 3 at baseline to 1.91 (P less than .001). Two-thirds of patients reported at least a one-point improvement from baseline, and all reported that this was clinically meaningful. At baseline, 84% of patients reported heavy to very heavy blood loss, but this decreased to 23% after treatment with tranexamic acid (P less than .001).
The study population included ten individuals (40%) with bleeding disorders. However, the researchers did not see a significant difference in response between those with bleeding disorders and those without.
While the treatment did not significantly affect school attendance (only 24% reported that their heavy bleeding limited school attendance), researchers did see a significant improvement in limitations on physical activities and on social and leisure activities. Patients who reported at baseline that their menstrual bleeding significantly affected their social and leisure activities had an average score improvement of 1.74, a greater than or equal to one point improvement. Participants also reported significant improvements in their Pictorial Blood Assessment Chart scores, which dropped from an average of 255 to 155 (P less than .001).
The treatment did not show any significant effects on hemoglobin or ferritin. The most common adverse events were sinonasal symptoms, such as nasal congestion, headache, and sinus pain, but no thrombotic or ocular adverse events were seen.
Dr. O’Brien and her coauthors wrote that one limitation of their study was using the MIQ score as their primary endpoint as opposed to a more objective measure, such as change in measured blood loss.
“However, a major factor that motivates patients with heavy menstrual bleeding to seek medical care is the negative impact of heavy menstrual bleeding on daily life,” they wrote.
The study drug was supplied by Ferring pharmaceuticals, and the study was supported by the Hemostasis and Thrombosis Research Society. One author disclosed receiving the Joan Fellowship in Pediatric Hemostasis and Thrombosis at Nationwide Children’s Hospital; no other authors said they had relevant financial disclosures.
SOURCE: O’Brien SH et al. J Pediatr Adol Gynec. 2019 Feb 4. doi: 10.1016/j.jpag.2019.01.009.
new research suggests.
Writing in the Journal of Pediatric & Adolescent Gynecology, Sarah H. O’Brien, MD, from Nationwide Children’s Hospital and the Ohio State University, both in Columbus, and her coauthors presented the results of an open-label efficacy study of the competitive plasminogen inhibitor in 25 adolescent girls aged 10-19 years who attended pediatric hematology clinics for evaluation or management of heavy menstrual bleeding. The study participants were instructed to take 1,300 mg of tranexamic acid (two tablets) three times a day for up to 5 days during their monthly menstruation for three cycles.
The study found a significant improvement in mean menstrual impact questionnaire (MIQ) scores, which improved from a mean of 3 at baseline to 1.91 (P less than .001). Two-thirds of patients reported at least a one-point improvement from baseline, and all reported that this was clinically meaningful. At baseline, 84% of patients reported heavy to very heavy blood loss, but this decreased to 23% after treatment with tranexamic acid (P less than .001).
The study population included ten individuals (40%) with bleeding disorders. However, the researchers did not see a significant difference in response between those with bleeding disorders and those without.
While the treatment did not significantly affect school attendance (only 24% reported that their heavy bleeding limited school attendance), researchers did see a significant improvement in limitations on physical activities and on social and leisure activities. Patients who reported at baseline that their menstrual bleeding significantly affected their social and leisure activities had an average score improvement of 1.74, a greater than or equal to one point improvement. Participants also reported significant improvements in their Pictorial Blood Assessment Chart scores, which dropped from an average of 255 to 155 (P less than .001).
The treatment did not show any significant effects on hemoglobin or ferritin. The most common adverse events were sinonasal symptoms, such as nasal congestion, headache, and sinus pain, but no thrombotic or ocular adverse events were seen.
Dr. O’Brien and her coauthors wrote that one limitation of their study was using the MIQ score as their primary endpoint as opposed to a more objective measure, such as change in measured blood loss.
“However, a major factor that motivates patients with heavy menstrual bleeding to seek medical care is the negative impact of heavy menstrual bleeding on daily life,” they wrote.
The study drug was supplied by Ferring pharmaceuticals, and the study was supported by the Hemostasis and Thrombosis Research Society. One author disclosed receiving the Joan Fellowship in Pediatric Hemostasis and Thrombosis at Nationwide Children’s Hospital; no other authors said they had relevant financial disclosures.
SOURCE: O’Brien SH et al. J Pediatr Adol Gynec. 2019 Feb 4. doi: 10.1016/j.jpag.2019.01.009.
FROM THE JOURNAL OF PEDIATRIC & ADOLESCENT GYNECOLOGY
Key clinical point: Tranexamic acid appears to improve quality of life for adolescents with heavy menstrual bleeding.
Major finding: Patients treated with tranexamic acid reported significant improvements in mean menstrual impact questionnaire scores.
Study details: Open-label efficacy study in 25 adolescent girls with heavy menstrual bleeding.
Disclosures: The study drug was supplied by Ferring pharmaceuticals, and the study was supported by the Hemostasis and Thrombosis Research Society. One author disclosed receiving the Joan Fellowship in Pediatric Hemostasis and Thrombosis at Nationwide Children’s Hospital; no other authors said they had relevant financial disclosures.
Source: O’Brien SH et al. J Pediatr Adol Gynec. 2019 Feb 4. doi: 10.1016/j.jpag.2019.01.009.
Conservatism spreads in prostate cancer
, the United States now has more than 100 measles cases for the year, e-cigarette use reverses progress in reducing teens’ tobacco use, and consider adopting the MESA 10-year coronary heart disease risk calculator.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
, the United States now has more than 100 measles cases for the year, e-cigarette use reverses progress in reducing teens’ tobacco use, and consider adopting the MESA 10-year coronary heart disease risk calculator.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
, the United States now has more than 100 measles cases for the year, e-cigarette use reverses progress in reducing teens’ tobacco use, and consider adopting the MESA 10-year coronary heart disease risk calculator.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Failure to launch can happen to college students
March often is the time of year when college freshmen truly begin to feel comfortable in their new settings. Many students report feeling excited to get back to campus after the long winter break, and once into their second semester, they feel more comfortable with the independence from family and high school supports. It also is a time for some college freshmen to return home after failing to manage this major transition.

Of the latter group, many will have had difficult months of depression, anxiety, or substance use, and most will be suffering from a deep sense of shame after failing to navigate this long-anticipated transition. Asking detailed questions about their academic challenges, social lives, self-care, and sleep while they were on campus will help you make thoughtful recommendations to your patients and their parents about how they might best get back on track.
Some students will report a great social experience, but academic struggles. They will report some normal ups and downs emotionally, but most of their distress will have been focused on their academic performance. Many 18-year-olds have not had to organize their time and effort around homework without the attention and support of parents and teachers. College often has much bigger classes, with less personal attention. There is a lot of assigned reading, but no regular incremental homework, only a major midterm and final exam, or a substantial paper. For a student who gets anxious about performance, or one with organizational challenges, this can lead to procrastination and poor performance.
Find out details about how they did academically. Did they fail one class or many classes? Did they receive some incompletes in their first semester and then struggle to catch up with them while keeping up with their second semester work? Did they have tutoring or support? Were they unrealistic about their course load? Or did they have their first serious relationship and not spend enough time on homework? Did they spend too much time partying with their new friends and not enough time sleeping and getting their homework done?
It is important to dig deeper if patients report regular or binge drug and alcohol use that interfered with their academic performance, as they may need more substantial substance use disorder treatment. Most students, though, will not have a substance use disorder. Instead, their academic failure could represent something as simple as the need for more academic support and time management support. Many schools have such programs to help students learn how to better manage their time and effort as they take fuller responsibility than they had for it in high school.
For other students, you will learn that their emotional distress preceded their academic troubles. The stress of the transition to college may be enough to trigger an episode of depression or to exacerbate a mood or anxiety disorder that was subclinical or in remission before school started. These students usually will report that sadness, intense anxiety, or loss of interest came early in their semester; perhaps they were even doing well academically when these problems started.
Ask about how their sleep was. Often they had difficulty falling asleep or woke up often at night, unlike most college students, whose sleep is compromised because they stay up late with new friends or because they are hard at work, but could easily sleep at any time.
Find out about their eating habits. Did they lose their appetite? Lose weight? Did they become preoccupied with weight or body image issues and begin restricting their intake? Eating disorders can begin in college when vulnerable students are stressed and have more control over their diet. While weight gain is more common in freshman year, it often is connected to poor stress management skills, and is more often a marker of a student who was struggling academically and then managing stress by overeating.
In the case where the distress came first, it is critical that your patients have a thorough psychiatric evaluation and treatment. It may be possible for them to return to school quickly, but it is most important that they are engaged in effective treatment and in at last partial remission before adding to their stress by attempting to return to school. Often, ambitious students and their parents need to hear this message very clearly from a pediatrician. A rushed return to school may be a set-up for a more protracted and difficult course of illness. For these students, it may be better to have a fresh start in a new semester. Help them (and their parents) to understand that they should use their time off to focus on treatment and good self-care so they might benefit from the many opportunities of college.
For a small minority of college students who do not succeed at college, their social withdrawal, academic deterioration, anxiety, and loss of interest in previous passions may occur alongside more serious psychiatric symptoms such as auditory hallucinations, paranoia, or grandiosity. Any time there is a suggestion of psychotic symptoms in a previously healthy person in the late teens or early 20s, a prompt comprehensive psychiatric evaluation is critical. These years are when most chronic psychotic disorders, such as schizophrenia, are likely to emerge. These patients require a thorough evaluation to distinguish these disorders from other illnesses, especially when they occur with substance use. And these patients require specialized care.
If your patient appears to have any psychotic symptoms, it is critical that you help the family find an excellent psychiatrist, or even a clinic that specializes in thought disorders so that he or she may get the best possible care early.

There is another class of students who withdraw from college who will need more comprehensive remediation, but not connected to any psychiatric diagnosis. Some young people may not be developmentally ready for college. These are your patients who often were excellent performers in high school, perhaps academically and athletically, but whose performance was more connected to pleasing important adults than to genuine motivating passions or sense of purpose. These young adults may have been drawn into the intense, results-oriented forces that are powerful in many of our high schools. If they did not have enough time or space to explore a host of interests, and to then manage the routine failures, setbacks, and disappointments that are essential to healthy adolescent development, they are going to run out of fuel in college. Such students often are quite dependent on their parents, and struggle with the independence college offers.

If your patients report that they could not muster the same intense work ethic they previously had, without any evidence of a psychiatric illness interfering with motivation, they may need time to finish the developmental work of cultivating a deep and rich sense of their own identity. Some students can do this at college, provided they, their parents and their school offer them adequate time before they have to declare a major. Other students will need to get a job and explore interests with a few courses at a community college, cultivating independence while learning about their own strengths and weaknesses and their genuine interests. This way, when they return to school, they will be motivated by a genuine sense of purpose and self-knowledge.
“Failure to launch” is a critical symptom at a key transitional moment. Pediatric providers can be essential to their patients and families by clarifying the nature of the difficulty and coordinating a reasonable plan to get these young adults back on track to healthy adulthood.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
March often is the time of year when college freshmen truly begin to feel comfortable in their new settings. Many students report feeling excited to get back to campus after the long winter break, and once into their second semester, they feel more comfortable with the independence from family and high school supports. It also is a time for some college freshmen to return home after failing to manage this major transition.
Of the latter group, many will have had difficult months of depression, anxiety, or substance use, and most will be suffering from a deep sense of shame after failing to navigate this long-anticipated transition. Asking detailed questions about their academic challenges, social lives, self-care, and sleep while they were on campus will help you make thoughtful recommendations to your patients and their parents about how they might best get back on track.
Some students will report a great social experience, but academic struggles. They will report some normal ups and downs emotionally, but most of their distress will have been focused on their academic performance. Many 18-year-olds have not had to organize their time and effort around homework without the attention and support of parents and teachers. College often has much bigger classes, with less personal attention. There is a lot of assigned reading, but no regular incremental homework, only a major midterm and final exam, or a substantial paper. For a student who gets anxious about performance, or one with organizational challenges, this can lead to procrastination and poor performance.
Find out details about how they did academically. Did they fail one class or many classes? Did they receive some incompletes in their first semester and then struggle to catch up with them while keeping up with their second semester work? Did they have tutoring or support? Were they unrealistic about their course load? Or did they have their first serious relationship and not spend enough time on homework? Did they spend too much time partying with their new friends and not enough time sleeping and getting their homework done?
It is important to dig deeper if patients report regular or binge drug and alcohol use that interfered with their academic performance, as they may need more substantial substance use disorder treatment. Most students, though, will not have a substance use disorder. Instead, their academic failure could represent something as simple as the need for more academic support and time management support. Many schools have such programs to help students learn how to better manage their time and effort as they take fuller responsibility than they had for it in high school.
For other students, you will learn that their emotional distress preceded their academic troubles. The stress of the transition to college may be enough to trigger an episode of depression or to exacerbate a mood or anxiety disorder that was subclinical or in remission before school started. These students usually will report that sadness, intense anxiety, or loss of interest came early in their semester; perhaps they were even doing well academically when these problems started.
Ask about how their sleep was. Often they had difficulty falling asleep or woke up often at night, unlike most college students, whose sleep is compromised because they stay up late with new friends or because they are hard at work, but could easily sleep at any time.
Find out about their eating habits. Did they lose their appetite? Lose weight? Did they become preoccupied with weight or body image issues and begin restricting their intake? Eating disorders can begin in college when vulnerable students are stressed and have more control over their diet. While weight gain is more common in freshman year, it often is connected to poor stress management skills, and is more often a marker of a student who was struggling academically and then managing stress by overeating.
In the case where the distress came first, it is critical that your patients have a thorough psychiatric evaluation and treatment. It may be possible for them to return to school quickly, but it is most important that they are engaged in effective treatment and in at last partial remission before adding to their stress by attempting to return to school. Often, ambitious students and their parents need to hear this message very clearly from a pediatrician. A rushed return to school may be a set-up for a more protracted and difficult course of illness. For these students, it may be better to have a fresh start in a new semester. Help them (and their parents) to understand that they should use their time off to focus on treatment and good self-care so they might benefit from the many opportunities of college.
For a small minority of college students who do not succeed at college, their social withdrawal, academic deterioration, anxiety, and loss of interest in previous passions may occur alongside more serious psychiatric symptoms such as auditory hallucinations, paranoia, or grandiosity. Any time there is a suggestion of psychotic symptoms in a previously healthy person in the late teens or early 20s, a prompt comprehensive psychiatric evaluation is critical. These years are when most chronic psychotic disorders, such as schizophrenia, are likely to emerge. These patients require a thorough evaluation to distinguish these disorders from other illnesses, especially when they occur with substance use. And these patients require specialized care.
If your patient appears to have any psychotic symptoms, it is critical that you help the family find an excellent psychiatrist, or even a clinic that specializes in thought disorders so that he or she may get the best possible care early.
There is another class of students who withdraw from college who will need more comprehensive remediation, but not connected to any psychiatric diagnosis. Some young people may not be developmentally ready for college. These are your patients who often were excellent performers in high school, perhaps academically and athletically, but whose performance was more connected to pleasing important adults than to genuine motivating passions or sense of purpose. These young adults may have been drawn into the intense, results-oriented forces that are powerful in many of our high schools. If they did not have enough time or space to explore a host of interests, and to then manage the routine failures, setbacks, and disappointments that are essential to healthy adolescent development, they are going to run out of fuel in college. Such students often are quite dependent on their parents, and struggle with the independence college offers.
If your patients report that they could not muster the same intense work ethic they previously had, without any evidence of a psychiatric illness interfering with motivation, they may need time to finish the developmental work of cultivating a deep and rich sense of their own identity. Some students can do this at college, provided they, their parents and their school offer them adequate time before they have to declare a major. Other students will need to get a job and explore interests with a few courses at a community college, cultivating independence while learning about their own strengths and weaknesses and their genuine interests. This way, when they return to school, they will be motivated by a genuine sense of purpose and self-knowledge.
“Failure to launch” is a critical symptom at a key transitional moment. Pediatric providers can be essential to their patients and families by clarifying the nature of the difficulty and coordinating a reasonable plan to get these young adults back on track to healthy adulthood.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
March often is the time of year when college freshmen truly begin to feel comfortable in their new settings. Many students report feeling excited to get back to campus after the long winter break, and once into their second semester, they feel more comfortable with the independence from family and high school supports. It also is a time for some college freshmen to return home after failing to manage this major transition.
Of the latter group, many will have had difficult months of depression, anxiety, or substance use, and most will be suffering from a deep sense of shame after failing to navigate this long-anticipated transition. Asking detailed questions about their academic challenges, social lives, self-care, and sleep while they were on campus will help you make thoughtful recommendations to your patients and their parents about how they might best get back on track.
Some students will report a great social experience, but academic struggles. They will report some normal ups and downs emotionally, but most of their distress will have been focused on their academic performance. Many 18-year-olds have not had to organize their time and effort around homework without the attention and support of parents and teachers. College often has much bigger classes, with less personal attention. There is a lot of assigned reading, but no regular incremental homework, only a major midterm and final exam, or a substantial paper. For a student who gets anxious about performance, or one with organizational challenges, this can lead to procrastination and poor performance.
Find out details about how they did academically. Did they fail one class or many classes? Did they receive some incompletes in their first semester and then struggle to catch up with them while keeping up with their second semester work? Did they have tutoring or support? Were they unrealistic about their course load? Or did they have their first serious relationship and not spend enough time on homework? Did they spend too much time partying with their new friends and not enough time sleeping and getting their homework done?
It is important to dig deeper if patients report regular or binge drug and alcohol use that interfered with their academic performance, as they may need more substantial substance use disorder treatment. Most students, though, will not have a substance use disorder. Instead, their academic failure could represent something as simple as the need for more academic support and time management support. Many schools have such programs to help students learn how to better manage their time and effort as they take fuller responsibility than they had for it in high school.
For other students, you will learn that their emotional distress preceded their academic troubles. The stress of the transition to college may be enough to trigger an episode of depression or to exacerbate a mood or anxiety disorder that was subclinical or in remission before school started. These students usually will report that sadness, intense anxiety, or loss of interest came early in their semester; perhaps they were even doing well academically when these problems started.
Ask about how their sleep was. Often they had difficulty falling asleep or woke up often at night, unlike most college students, whose sleep is compromised because they stay up late with new friends or because they are hard at work, but could easily sleep at any time.
Find out about their eating habits. Did they lose their appetite? Lose weight? Did they become preoccupied with weight or body image issues and begin restricting their intake? Eating disorders can begin in college when vulnerable students are stressed and have more control over their diet. While weight gain is more common in freshman year, it often is connected to poor stress management skills, and is more often a marker of a student who was struggling academically and then managing stress by overeating.
In the case where the distress came first, it is critical that your patients have a thorough psychiatric evaluation and treatment. It may be possible for them to return to school quickly, but it is most important that they are engaged in effective treatment and in at last partial remission before adding to their stress by attempting to return to school. Often, ambitious students and their parents need to hear this message very clearly from a pediatrician. A rushed return to school may be a set-up for a more protracted and difficult course of illness. For these students, it may be better to have a fresh start in a new semester. Help them (and their parents) to understand that they should use their time off to focus on treatment and good self-care so they might benefit from the many opportunities of college.
For a small minority of college students who do not succeed at college, their social withdrawal, academic deterioration, anxiety, and loss of interest in previous passions may occur alongside more serious psychiatric symptoms such as auditory hallucinations, paranoia, or grandiosity. Any time there is a suggestion of psychotic symptoms in a previously healthy person in the late teens or early 20s, a prompt comprehensive psychiatric evaluation is critical. These years are when most chronic psychotic disorders, such as schizophrenia, are likely to emerge. These patients require a thorough evaluation to distinguish these disorders from other illnesses, especially when they occur with substance use. And these patients require specialized care.
If your patient appears to have any psychotic symptoms, it is critical that you help the family find an excellent psychiatrist, or even a clinic that specializes in thought disorders so that he or she may get the best possible care early.
There is another class of students who withdraw from college who will need more comprehensive remediation, but not connected to any psychiatric diagnosis. Some young people may not be developmentally ready for college. These are your patients who often were excellent performers in high school, perhaps academically and athletically, but whose performance was more connected to pleasing important adults than to genuine motivating passions or sense of purpose. These young adults may have been drawn into the intense, results-oriented forces that are powerful in many of our high schools. If they did not have enough time or space to explore a host of interests, and to then manage the routine failures, setbacks, and disappointments that are essential to healthy adolescent development, they are going to run out of fuel in college. Such students often are quite dependent on their parents, and struggle with the independence college offers.
If your patients report that they could not muster the same intense work ethic they previously had, without any evidence of a psychiatric illness interfering with motivation, they may need time to finish the developmental work of cultivating a deep and rich sense of their own identity. Some students can do this at college, provided they, their parents and their school offer them adequate time before they have to declare a major. Other students will need to get a job and explore interests with a few courses at a community college, cultivating independence while learning about their own strengths and weaknesses and their genuine interests. This way, when they return to school, they will be motivated by a genuine sense of purpose and self-knowledge.
“Failure to launch” is a critical symptom at a key transitional moment. Pediatric providers can be essential to their patients and families by clarifying the nature of the difficulty and coordinating a reasonable plan to get these young adults back on track to healthy adulthood.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
Adenovirus: More than just another viral illness
The mother of three looked tired and little worried. She wasn’t one to bring her kids to the pediatrician’s office with every minor illness, but her youngest had 3 days of fever, runny nose, cough, and little of her normal energy.

The pediatrician entered the room and smiled sympathetically.
“We ran tests for flu and RSV [respiratory syncytial virus] and it’s neither of those so. ...”
“So it’s just a virus that we don’t routinely test for and it’s going to need to run its course,” the mother finished his sentence. She knew the drill.
Before the doctor could leave the room though, the mother had one more question. “You don’t think it could be adenovirus do you?”
Most years, influenza and RSV command center stage, and adenovirus is relegated to the wings. It is not so much lack of disease or morbidity, but rather lack of recognition. Yes, we all learned in medical school that it is a cause of epidemic keratoconjunctivitis, but many adenoviral infections are clinically indistinguishable from infections caused by other viruses. Common symptoms – fever, cough, sore throat, and malaise – overlap with those caused by influenza. Like rhinovirus, adenovirus can cause common cold symptoms. Like RSV, it can cause bronchiolitis. Just like parainfluenza, it can cause croup. It can cause a pertussislike syndrome with prolonged cough, and enteric adenoviruses, especially types 40 and 41, cause gastroenteritis that mimics norovirus or rotavirus infection.
Testing for adenovirus is not readily available or routine in most pediatricians’ offices, and while many hospitals and reference labs offer adenovirus polymerase chain reaction testing as part of a comprehensive respiratory virus panel, the test can be expensive and unlikely to change management in most ambulatory patients. This makes it difficult to count the number of adenoviruses annually.
This winter though, adenovirus was in the news ... repeatedly. In November 2018, CBS News reported that a University of Maryland freshman had died of an adenovirus-related illness. The family of Olivia Paregol told reporters that she was being treated for Crohn’s disease. Immune suppression is one recognized risk factor for more severe adenoviral disease; underlying heart and lung disease are others. Testing at the Centers for Disease Control and Prevention revealed that the student and several others on campus were infected with adenovirus type 7, a strain that has been associated with outbreaks of acute, severe respiratory illness in military recruits. As of Jan. 24, 2019, university officials reported 42 confirmed cases of adenovirus in University of Maryland students, 13 of which were confirmed as adenovirus 7.
Adenovirus type 7 also caused an outbreak at a pediatric long-term care facility in New Jersey late last year. Between Sept. 26 and Nov. 11, 2018, 36 residents and 1 staff member became ill. Eleven individuals died. In an unrelated outbreak at a second pediatric long-term care facility, 17 residents were affected between Oct. 20 and Dec. 10, 2018. Adenovirus 3 was identified and all children recovered.
Between October 2013 and July 2014, public health officials in Oregon identified an increase in adenoviral infections in people with respiratory illness. Sixty-nine percent were hospitalized (136/198), 31% needed intensive care, and 18% were mechanically ventilated. Multiple types of adenovirus were recovered but the most common was adenovirus 7 (Emerg Infect Dis. 2016. doi: 10.3201/eid2206.151898).

Depending on your perspective, measures to prevent the spread of adenovirus are elegantly simple, evidence-based, public health intervention or maddeningly little more than common sense. Wash your hands often with soap and water. Avoid touching your eyes, mouth, and nose with unwashed hands. Avoid close contact with people who are sick. The latter is easier if those who are sick stay home. Prior to the start of the most recent academic semester at the University of Maryland, university officials urged students who were sick not to return to campus but to stay at home to rest and recover. Those who fell ill on campus were urged to return home via nonpublic transportation if possible. Those who stayed on campus were advised to stay in their living spaces and clean high-touch surfaces with bleach. Like other nonenveloped viruses, adenovirus is not easily destroyed by many commonly used disinfectants. Under ideal conditions, it can survive on surfaces – remaining infectious – for up to 3 months.
Back at the pediatrician’s office, “We need an adenovirus vaccine,” the mother said as she picked up her child and headed for the door.
There is, in fact, a live oral vaccine that protects against adenovirus types 4 and 7. It is only approved for use in United States military personnel aged 17-50 years and it is given to all recruits as soon as they enter basic training. It works too. Before vaccine was available, up to 80% of recruits became infected during their initial training, half of those developing significant illness and a quarter being hospitalized. When the current vaccine was introduced in 2011, there was a 100-fold decrease in adenovirus-related disease burden (from 5.8 to 0.02 cases per 1,000 person-weeks, P less than .0001). That translates to 1 death, 1,100-2,700 hospitalizations and 13,000 febrile illnesses prevented each year (Clin Infect Dis. 2014 Oct 1. doi: 10.1093/cid/ciu507).
Some experts have suggested that adenovirus vaccine could be useful in civilian populations, too, but I question what the public reception would be. We have safe influenza vaccines that reduce the need for hospitalization and reduce mortality from influenza, but we still can’t convince some people to immunize themselves and their children. In the last 4 years, flu vaccination rates among children have remained just shy of 60% and adult rates are even lower. Collectively, we don’t seem to be ready to relinquish – or at least diminish – the annual suffering that goes with flu. I have to wonder if the same would be true for adenovirus.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
The mother of three looked tired and little worried. She wasn’t one to bring her kids to the pediatrician’s office with every minor illness, but her youngest had 3 days of fever, runny nose, cough, and little of her normal energy.
The pediatrician entered the room and smiled sympathetically.
“We ran tests for flu and RSV [respiratory syncytial virus] and it’s neither of those so. ...”
“So it’s just a virus that we don’t routinely test for and it’s going to need to run its course,” the mother finished his sentence. She knew the drill.
Before the doctor could leave the room though, the mother had one more question. “You don’t think it could be adenovirus do you?”
Most years, influenza and RSV command center stage, and adenovirus is relegated to the wings. It is not so much lack of disease or morbidity, but rather lack of recognition. Yes, we all learned in medical school that it is a cause of epidemic keratoconjunctivitis, but many adenoviral infections are clinically indistinguishable from infections caused by other viruses. Common symptoms – fever, cough, sore throat, and malaise – overlap with those caused by influenza. Like rhinovirus, adenovirus can cause common cold symptoms. Like RSV, it can cause bronchiolitis. Just like parainfluenza, it can cause croup. It can cause a pertussislike syndrome with prolonged cough, and enteric adenoviruses, especially types 40 and 41, cause gastroenteritis that mimics norovirus or rotavirus infection.
Testing for adenovirus is not readily available or routine in most pediatricians’ offices, and while many hospitals and reference labs offer adenovirus polymerase chain reaction testing as part of a comprehensive respiratory virus panel, the test can be expensive and unlikely to change management in most ambulatory patients. This makes it difficult to count the number of adenoviruses annually.
This winter though, adenovirus was in the news ... repeatedly. In November 2018, CBS News reported that a University of Maryland freshman had died of an adenovirus-related illness. The family of Olivia Paregol told reporters that she was being treated for Crohn’s disease. Immune suppression is one recognized risk factor for more severe adenoviral disease; underlying heart and lung disease are others. Testing at the Centers for Disease Control and Prevention revealed that the student and several others on campus were infected with adenovirus type 7, a strain that has been associated with outbreaks of acute, severe respiratory illness in military recruits. As of Jan. 24, 2019, university officials reported 42 confirmed cases of adenovirus in University of Maryland students, 13 of which were confirmed as adenovirus 7.
Adenovirus type 7 also caused an outbreak at a pediatric long-term care facility in New Jersey late last year. Between Sept. 26 and Nov. 11, 2018, 36 residents and 1 staff member became ill. Eleven individuals died. In an unrelated outbreak at a second pediatric long-term care facility, 17 residents were affected between Oct. 20 and Dec. 10, 2018. Adenovirus 3 was identified and all children recovered.
Between October 2013 and July 2014, public health officials in Oregon identified an increase in adenoviral infections in people with respiratory illness. Sixty-nine percent were hospitalized (136/198), 31% needed intensive care, and 18% were mechanically ventilated. Multiple types of adenovirus were recovered but the most common was adenovirus 7 (Emerg Infect Dis. 2016. doi: 10.3201/eid2206.151898).
Depending on your perspective, measures to prevent the spread of adenovirus are elegantly simple, evidence-based, public health intervention or maddeningly little more than common sense. Wash your hands often with soap and water. Avoid touching your eyes, mouth, and nose with unwashed hands. Avoid close contact with people who are sick. The latter is easier if those who are sick stay home. Prior to the start of the most recent academic semester at the University of Maryland, university officials urged students who were sick not to return to campus but to stay at home to rest and recover. Those who fell ill on campus were urged to return home via nonpublic transportation if possible. Those who stayed on campus were advised to stay in their living spaces and clean high-touch surfaces with bleach. Like other nonenveloped viruses, adenovirus is not easily destroyed by many commonly used disinfectants. Under ideal conditions, it can survive on surfaces – remaining infectious – for up to 3 months.
Back at the pediatrician’s office, “We need an adenovirus vaccine,” the mother said as she picked up her child and headed for the door.
There is, in fact, a live oral vaccine that protects against adenovirus types 4 and 7. It is only approved for use in United States military personnel aged 17-50 years and it is given to all recruits as soon as they enter basic training. It works too. Before vaccine was available, up to 80% of recruits became infected during their initial training, half of those developing significant illness and a quarter being hospitalized. When the current vaccine was introduced in 2011, there was a 100-fold decrease in adenovirus-related disease burden (from 5.8 to 0.02 cases per 1,000 person-weeks, P less than .0001). That translates to 1 death, 1,100-2,700 hospitalizations and 13,000 febrile illnesses prevented each year (Clin Infect Dis. 2014 Oct 1. doi: 10.1093/cid/ciu507).
Some experts have suggested that adenovirus vaccine could be useful in civilian populations, too, but I question what the public reception would be. We have safe influenza vaccines that reduce the need for hospitalization and reduce mortality from influenza, but we still can’t convince some people to immunize themselves and their children. In the last 4 years, flu vaccination rates among children have remained just shy of 60% and adult rates are even lower. Collectively, we don’t seem to be ready to relinquish – or at least diminish – the annual suffering that goes with flu. I have to wonder if the same would be true for adenovirus.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
The mother of three looked tired and little worried. She wasn’t one to bring her kids to the pediatrician’s office with every minor illness, but her youngest had 3 days of fever, runny nose, cough, and little of her normal energy.
The pediatrician entered the room and smiled sympathetically.
“We ran tests for flu and RSV [respiratory syncytial virus] and it’s neither of those so. ...”
“So it’s just a virus that we don’t routinely test for and it’s going to need to run its course,” the mother finished his sentence. She knew the drill.
Before the doctor could leave the room though, the mother had one more question. “You don’t think it could be adenovirus do you?”
Most years, influenza and RSV command center stage, and adenovirus is relegated to the wings. It is not so much lack of disease or morbidity, but rather lack of recognition. Yes, we all learned in medical school that it is a cause of epidemic keratoconjunctivitis, but many adenoviral infections are clinically indistinguishable from infections caused by other viruses. Common symptoms – fever, cough, sore throat, and malaise – overlap with those caused by influenza. Like rhinovirus, adenovirus can cause common cold symptoms. Like RSV, it can cause bronchiolitis. Just like parainfluenza, it can cause croup. It can cause a pertussislike syndrome with prolonged cough, and enteric adenoviruses, especially types 40 and 41, cause gastroenteritis that mimics norovirus or rotavirus infection.
Testing for adenovirus is not readily available or routine in most pediatricians’ offices, and while many hospitals and reference labs offer adenovirus polymerase chain reaction testing as part of a comprehensive respiratory virus panel, the test can be expensive and unlikely to change management in most ambulatory patients. This makes it difficult to count the number of adenoviruses annually.
This winter though, adenovirus was in the news ... repeatedly. In November 2018, CBS News reported that a University of Maryland freshman had died of an adenovirus-related illness. The family of Olivia Paregol told reporters that she was being treated for Crohn’s disease. Immune suppression is one recognized risk factor for more severe adenoviral disease; underlying heart and lung disease are others. Testing at the Centers for Disease Control and Prevention revealed that the student and several others on campus were infected with adenovirus type 7, a strain that has been associated with outbreaks of acute, severe respiratory illness in military recruits. As of Jan. 24, 2019, university officials reported 42 confirmed cases of adenovirus in University of Maryland students, 13 of which were confirmed as adenovirus 7.
Adenovirus type 7 also caused an outbreak at a pediatric long-term care facility in New Jersey late last year. Between Sept. 26 and Nov. 11, 2018, 36 residents and 1 staff member became ill. Eleven individuals died. In an unrelated outbreak at a second pediatric long-term care facility, 17 residents were affected between Oct. 20 and Dec. 10, 2018. Adenovirus 3 was identified and all children recovered.
Between October 2013 and July 2014, public health officials in Oregon identified an increase in adenoviral infections in people with respiratory illness. Sixty-nine percent were hospitalized (136/198), 31% needed intensive care, and 18% were mechanically ventilated. Multiple types of adenovirus were recovered but the most common was adenovirus 7 (Emerg Infect Dis. 2016. doi: 10.3201/eid2206.151898).
Depending on your perspective, measures to prevent the spread of adenovirus are elegantly simple, evidence-based, public health intervention or maddeningly little more than common sense. Wash your hands often with soap and water. Avoid touching your eyes, mouth, and nose with unwashed hands. Avoid close contact with people who are sick. The latter is easier if those who are sick stay home. Prior to the start of the most recent academic semester at the University of Maryland, university officials urged students who were sick not to return to campus but to stay at home to rest and recover. Those who fell ill on campus were urged to return home via nonpublic transportation if possible. Those who stayed on campus were advised to stay in their living spaces and clean high-touch surfaces with bleach. Like other nonenveloped viruses, adenovirus is not easily destroyed by many commonly used disinfectants. Under ideal conditions, it can survive on surfaces – remaining infectious – for up to 3 months.
Back at the pediatrician’s office, “We need an adenovirus vaccine,” the mother said as she picked up her child and headed for the door.
There is, in fact, a live oral vaccine that protects against adenovirus types 4 and 7. It is only approved for use in United States military personnel aged 17-50 years and it is given to all recruits as soon as they enter basic training. It works too. Before vaccine was available, up to 80% of recruits became infected during their initial training, half of those developing significant illness and a quarter being hospitalized. When the current vaccine was introduced in 2011, there was a 100-fold decrease in adenovirus-related disease burden (from 5.8 to 0.02 cases per 1,000 person-weeks, P less than .0001). That translates to 1 death, 1,100-2,700 hospitalizations and 13,000 febrile illnesses prevented each year (Clin Infect Dis. 2014 Oct 1. doi: 10.1093/cid/ciu507).
Some experts have suggested that adenovirus vaccine could be useful in civilian populations, too, but I question what the public reception would be. We have safe influenza vaccines that reduce the need for hospitalization and reduce mortality from influenza, but we still can’t convince some people to immunize themselves and their children. In the last 4 years, flu vaccination rates among children have remained just shy of 60% and adult rates are even lower. Collectively, we don’t seem to be ready to relinquish – or at least diminish – the annual suffering that goes with flu. I have to wonder if the same would be true for adenovirus.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Interactive parenting, life skill intervention improves self-esteem in teen mothers
than did those who received standard care, according to Joanne E. Cox, MD, director of primary care at Boston Children’s Hospital and Harvard Medical School, and her associates.
A total of 140 mothers who were aged less than 19 years when they delivered and whose child was aged less than 12 months were included in the study published in Pediatrics. Of this group, 72 received the intervention, which included a series of five 1-hour, one-on-one, interactive modules adapted from the Nurturing and Ansell-Casey Life Skills curricula, delivered over the infant’s first 15 months, in addition to standard teen-tot clinic care. The remaining 68 mothers received teen-tot care alone.
While overall maternal self-esteem decreased in both the intervention and control groups when measured at 36 months, the intervention group experienced a significantly smaller decrease from baseline (P = .011). Similarly, the intervention group had higher scores regarding preparedness for motherhood (P = .011), acceptance of infant (P = .008), and expected relationship with infant (P = .029).
Of the 52 mothers in the intervention group and 48 mothers in the control group for whom pregnancy data was available at 36 months, 42% in the intervention group had a repeat pregnancy, compared with 67% in the control group (adjusted odds ratio, 0.20; 95% confidence interval, 0.06-0.75; P = .017).
The study findings “highlight the positive impact of pairing medical services with comprehensive social services and parenting education and can inform future policy and services for teen parents. These positive effects also have potential to improve long-term outcomes for teens and their children,” Dr. Cox and her associates concluded.
The study authors reported no conflicts of interest. The study was supported in part by a grant from the Office of Adolescent Pregnancy Programs, the Edgerley Family Endowment, a Leadership Education in Adolescent Health training grant, the Maternal and Child Health Bureau, and the Health Resources and Services Administration.
lfranki@mdedge.com
SOURCE: Cox JE et al. Pediatrics. 2019 Feb 12. doi: 10.1542/peds.2018-2303.
than did those who received standard care, according to Joanne E. Cox, MD, director of primary care at Boston Children’s Hospital and Harvard Medical School, and her associates.
A total of 140 mothers who were aged less than 19 years when they delivered and whose child was aged less than 12 months were included in the study published in Pediatrics. Of this group, 72 received the intervention, which included a series of five 1-hour, one-on-one, interactive modules adapted from the Nurturing and Ansell-Casey Life Skills curricula, delivered over the infant’s first 15 months, in addition to standard teen-tot clinic care. The remaining 68 mothers received teen-tot care alone.
While overall maternal self-esteem decreased in both the intervention and control groups when measured at 36 months, the intervention group experienced a significantly smaller decrease from baseline (P = .011). Similarly, the intervention group had higher scores regarding preparedness for motherhood (P = .011), acceptance of infant (P = .008), and expected relationship with infant (P = .029).
Of the 52 mothers in the intervention group and 48 mothers in the control group for whom pregnancy data was available at 36 months, 42% in the intervention group had a repeat pregnancy, compared with 67% in the control group (adjusted odds ratio, 0.20; 95% confidence interval, 0.06-0.75; P = .017).
The study findings “highlight the positive impact of pairing medical services with comprehensive social services and parenting education and can inform future policy and services for teen parents. These positive effects also have potential to improve long-term outcomes for teens and their children,” Dr. Cox and her associates concluded.
The study authors reported no conflicts of interest. The study was supported in part by a grant from the Office of Adolescent Pregnancy Programs, the Edgerley Family Endowment, a Leadership Education in Adolescent Health training grant, the Maternal and Child Health Bureau, and the Health Resources and Services Administration.
lfranki@mdedge.com
SOURCE: Cox JE et al. Pediatrics. 2019 Feb 12. doi: 10.1542/peds.2018-2303.
than did those who received standard care, according to Joanne E. Cox, MD, director of primary care at Boston Children’s Hospital and Harvard Medical School, and her associates.
A total of 140 mothers who were aged less than 19 years when they delivered and whose child was aged less than 12 months were included in the study published in Pediatrics. Of this group, 72 received the intervention, which included a series of five 1-hour, one-on-one, interactive modules adapted from the Nurturing and Ansell-Casey Life Skills curricula, delivered over the infant’s first 15 months, in addition to standard teen-tot clinic care. The remaining 68 mothers received teen-tot care alone.
While overall maternal self-esteem decreased in both the intervention and control groups when measured at 36 months, the intervention group experienced a significantly smaller decrease from baseline (P = .011). Similarly, the intervention group had higher scores regarding preparedness for motherhood (P = .011), acceptance of infant (P = .008), and expected relationship with infant (P = .029).
Of the 52 mothers in the intervention group and 48 mothers in the control group for whom pregnancy data was available at 36 months, 42% in the intervention group had a repeat pregnancy, compared with 67% in the control group (adjusted odds ratio, 0.20; 95% confidence interval, 0.06-0.75; P = .017).
The study findings “highlight the positive impact of pairing medical services with comprehensive social services and parenting education and can inform future policy and services for teen parents. These positive effects also have potential to improve long-term outcomes for teens and their children,” Dr. Cox and her associates concluded.
The study authors reported no conflicts of interest. The study was supported in part by a grant from the Office of Adolescent Pregnancy Programs, the Edgerley Family Endowment, a Leadership Education in Adolescent Health training grant, the Maternal and Child Health Bureau, and the Health Resources and Services Administration.
lfranki@mdedge.com
SOURCE: Cox JE et al. Pediatrics. 2019 Feb 12. doi: 10.1542/peds.2018-2303.
FROM PEDIATRICS