User login
Quick Byte: Needle-free injections
A start-up operating out of MIT in Cambridge, Mass., called Portal Instruments has developed a needleless injection system.

The device, called PRIME, delivers medication into the bloodstream in a high-pressure stream that travels at Mach 0.7 – the speed of a jet. The makers signed a commercial deal in December 2017, and the device is expected to be available soon.
Reference
1. Kerrigan S. The 16 Most Remarkable Healthcare Innovations, Events, and Discoveries of 2018 For World Health Day. https://interestingengineering.com/the-16-most-remarkable-healthcare-innovations-events-and-discoveries-of-2018-for-world-health-day. April 7, 2018. Accessed June 4, 2018.
A start-up operating out of MIT in Cambridge, Mass., called Portal Instruments has developed a needleless injection system.
The device, called PRIME, delivers medication into the bloodstream in a high-pressure stream that travels at Mach 0.7 – the speed of a jet. The makers signed a commercial deal in December 2017, and the device is expected to be available soon.
Reference
1. Kerrigan S. The 16 Most Remarkable Healthcare Innovations, Events, and Discoveries of 2018 For World Health Day. https://interestingengineering.com/the-16-most-remarkable-healthcare-innovations-events-and-discoveries-of-2018-for-world-health-day. April 7, 2018. Accessed June 4, 2018.
A start-up operating out of MIT in Cambridge, Mass., called Portal Instruments has developed a needleless injection system.
The device, called PRIME, delivers medication into the bloodstream in a high-pressure stream that travels at Mach 0.7 – the speed of a jet. The makers signed a commercial deal in December 2017, and the device is expected to be available soon.
Reference
1. Kerrigan S. The 16 Most Remarkable Healthcare Innovations, Events, and Discoveries of 2018 For World Health Day. https://interestingengineering.com/the-16-most-remarkable-healthcare-innovations-events-and-discoveries-of-2018-for-world-health-day. April 7, 2018. Accessed June 4, 2018.
United States now over 100 measles cases for the year
according to the Centers for Disease Control and Prevention.
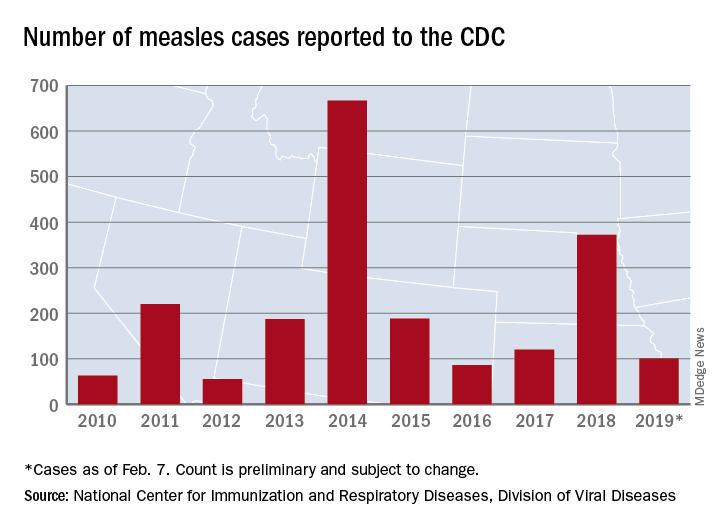
Just over half of the cases in 2019 have occurred in Clark County, Wash., which has reported 53 cases. That outbreak led Gov. Jay Inslee to declare a public health emergency for the entire state on Jan. 25.
The cases in Washington represent one of the five outbreaks – the CDC defines an outbreak as three or more cases – that have occurred so far this year, with three reported in New York State (Rockland County, Monroe County, and New York City) and one in Texas, which has been spread out over five counties, the CDC reported Feb. 11.
“These outbreaks are linked to travelers who brought measles back from other countries such as Israel and Ukraine, where large measles outbreaks are occurring,” the CDC noted. The other states with confirmed cases are California, Colorado, Connecticut, Georgia, Illinois, New Jersey, and Oregon.
In a video released Feb. 1, Surgeon General Jerome Adams stressed the importance of getting vaccinated and noted that an infected person can transmit the measles virus up to 4 days before he or she develops symptoms.
according to the Centers for Disease Control and Prevention.
Just over half of the cases in 2019 have occurred in Clark County, Wash., which has reported 53 cases. That outbreak led Gov. Jay Inslee to declare a public health emergency for the entire state on Jan. 25.
The cases in Washington represent one of the five outbreaks – the CDC defines an outbreak as three or more cases – that have occurred so far this year, with three reported in New York State (Rockland County, Monroe County, and New York City) and one in Texas, which has been spread out over five counties, the CDC reported Feb. 11.
“These outbreaks are linked to travelers who brought measles back from other countries such as Israel and Ukraine, where large measles outbreaks are occurring,” the CDC noted. The other states with confirmed cases are California, Colorado, Connecticut, Georgia, Illinois, New Jersey, and Oregon.
In a video released Feb. 1, Surgeon General Jerome Adams stressed the importance of getting vaccinated and noted that an infected person can transmit the measles virus up to 4 days before he or she develops symptoms.
according to the Centers for Disease Control and Prevention.
Just over half of the cases in 2019 have occurred in Clark County, Wash., which has reported 53 cases. That outbreak led Gov. Jay Inslee to declare a public health emergency for the entire state on Jan. 25.
The cases in Washington represent one of the five outbreaks – the CDC defines an outbreak as three or more cases – that have occurred so far this year, with three reported in New York State (Rockland County, Monroe County, and New York City) and one in Texas, which has been spread out over five counties, the CDC reported Feb. 11.
“These outbreaks are linked to travelers who brought measles back from other countries such as Israel and Ukraine, where large measles outbreaks are occurring,” the CDC noted. The other states with confirmed cases are California, Colorado, Connecticut, Georgia, Illinois, New Jersey, and Oregon.
In a video released Feb. 1, Surgeon General Jerome Adams stressed the importance of getting vaccinated and noted that an infected person can transmit the measles virus up to 4 days before he or she develops symptoms.
E-cig use reverses progress in reducing tobacco use in teens
A significant increase during 2017-2018 in e-cigarette use among U.S. youths has erased recent progress in reducing overall tobacco product use in this age group, a study from the Centers for Disease Control and Prevention has found.
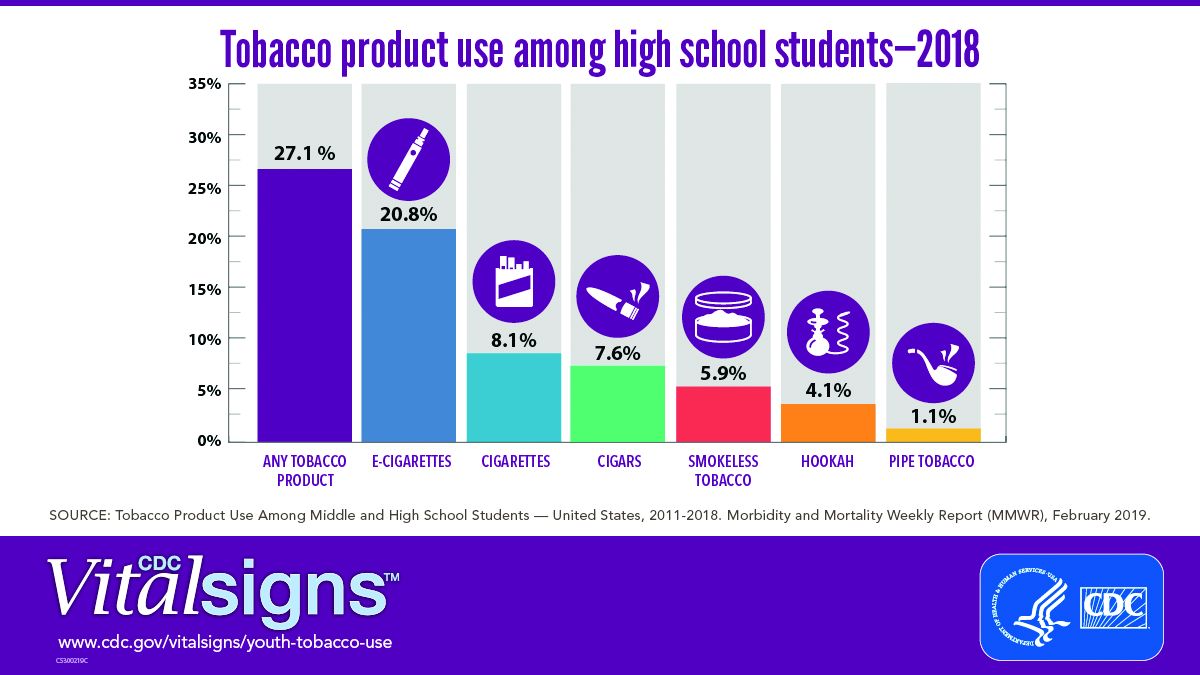
E-cigarettes are driving the trend. About 4 million high school students in the United States reported using any tobacco product in the last 30 days, and 3 million of them reported using e-cigarettes, according to a Vital Signs document published by the CDC on Feb. 11 in its Morbidity and Mortality Weekly Report.*
In addition, many high school students who use e-cigarettes use them often; 28% reported using the products at least 20 times in the past 28 days, up from 20% in 2017.
“Any use of any tobacco product is unsafe for teens,” Anne Schuchat, MD, principal deputy director of the CDC, said in a teleconference to present the findings. Nicotine is highly addictive and can harm brain development in youth, including capacity for learning, memory, and attention, she said.
The rise in e-cigarette use corresponds with the rise in marketing and availability of e-cigarette devices such as JUUL, which dispense nicotine via liquid refill pods available in flavors including strawberry and cotton candy, said Brian King, MPH, PhD, deputy director for research translation at the CDC’s Office on Smoking and Health.
“The advertising will lead a horse to water, the flavors will make them drink, and the nicotine will keep them coming back for more,” said Dr. King.
Approximately 27.1% of high school students and 7.2% of middle school students used a tobacco product in 2018, a significant increase from 2017 data, and with a major increase in e-cigarette use.
No change was noted in the use of other tobacco products, including cigarettes, from 2017 to 2018, according to the report. However, conventional cigarettes remained the most common companion product to e-cigarettes for youth who use two or more tobacco products (two in five high school students and one in three middle school students in 2018). From a demographic standpoint, e-cigarette use was highest among males, whites, and high school students.
Tobacco use in teens is trending in the direction of wiping out the progress made in recent years to reduce exposure to youths. The report noted, “The prevalence of e-cigarette use by U.S. high school students had peaked in 2015 before declining by 29% during 2015-2016 (from 16% to 11.3%); this decline was the first ever recorded for e-cigarette use among youths in the NYTS since monitoring began, and it was subsequently sustained during 2016-2017). However, current e-cigarette use increased by 77.8% among high school students and 48.5% among middle school students during 2017-2018, erasing the progress in reducing e-cigarette use, as well as any tobacco product use, that had occurred in prior years.”
The CDC and the Food and Drug Administration are taking action to curb the rise in e-cigarette use in youth in particular by seeking regulations to make the products less accessible, raising prices, and banning most flavorings, said Dr. Schuchat.
“We have targeted companies engaged in kid friendly marketing,” said Mitch Zeller, JD, director of the Center for Tobacco Products for the FDA.
In a statement published simultaneously with the Vital Signs study, FDA Commissioner Scott Gottlieb, MD, emphasized the link between e-cigarette use in teens and the potential for future tobacco use. “The kids using e-cigarettes are children who rejected conventional cigarettes, but don’t see the same stigma associated with the use of e-cigarettes. But now, having become exposed to nicotine through e-cigs, they will be more likely to smoke.” Dr. Gottlieb declared, “I will not allow a generation of children to become addicted to nicotine through e-cigarettes. We must stop the trends of youth e-cigarette use from continuing to build and will take whatever action is necessary to ensure these kids don’t become future smokers.” He reviewed steps taken in the past year by the FDA to counter tobacco use in teens but he warned of future actions that may need to be taken: “If these youth use trends continue, we’ll be forced to consider regulatory steps that could constrain or even foreclose the opportunities for currently addicted adult smokers to have the same level of access to these products that they now enjoy. I recognize that such a move could come with significant impacts to adult smokers.”
In the meantime, however, parents, teachers, community leaders, and health care providers are on the front lines and can make a difference in protecting youth and curbing nicotine use, Dr. King said.
One of the most important things clinicians can do is to ask young patients specifically about e-cigarette use, he emphasized. Learn and use the terminology the kids are using; ask, “Do you use JUUL?” If they are using these products, “make sure they know they are dangerous,” and can harm the developing brain, he said.
Although there are no currently approved medications to treat nicotine addiction in youth, research suggests that behavioral counseling, as well as reinforcement of the danger of nicotine from parents and other people of influence, can help, Dr. King said.
The Vital Signs report is based on data from the 2011-2018 National Youth Tobacco Survey, which assesses current use of cigarettes, cigars, smokeless tobacco, e-cigarettes, hookahs, pipe tobacco, and bidis among a nationally representative sample of middle and high school students in the United States. The findings were analyzed by the CDC, FDA, and the National Cancer Institute.
SOURCE: Gentzke AS et al. MMWR 2019 Feb 11. doi: 10.15585/mmwr.mm6806e1.
*Correction 2/13/2019 An earlier version of this article misstated the number of students using e-cigarettes as a proportion of all teen tobacco users.
A significant increase during 2017-2018 in e-cigarette use among U.S. youths has erased recent progress in reducing overall tobacco product use in this age group, a study from the Centers for Disease Control and Prevention has found.
E-cigarettes are driving the trend. About 4 million high school students in the United States reported using any tobacco product in the last 30 days, and 3 million of them reported using e-cigarettes, according to a Vital Signs document published by the CDC on Feb. 11 in its Morbidity and Mortality Weekly Report.*
In addition, many high school students who use e-cigarettes use them often; 28% reported using the products at least 20 times in the past 28 days, up from 20% in 2017.
“Any use of any tobacco product is unsafe for teens,” Anne Schuchat, MD, principal deputy director of the CDC, said in a teleconference to present the findings. Nicotine is highly addictive and can harm brain development in youth, including capacity for learning, memory, and attention, she said.
The rise in e-cigarette use corresponds with the rise in marketing and availability of e-cigarette devices such as JUUL, which dispense nicotine via liquid refill pods available in flavors including strawberry and cotton candy, said Brian King, MPH, PhD, deputy director for research translation at the CDC’s Office on Smoking and Health.
“The advertising will lead a horse to water, the flavors will make them drink, and the nicotine will keep them coming back for more,” said Dr. King.
Approximately 27.1% of high school students and 7.2% of middle school students used a tobacco product in 2018, a significant increase from 2017 data, and with a major increase in e-cigarette use.
No change was noted in the use of other tobacco products, including cigarettes, from 2017 to 2018, according to the report. However, conventional cigarettes remained the most common companion product to e-cigarettes for youth who use two or more tobacco products (two in five high school students and one in three middle school students in 2018). From a demographic standpoint, e-cigarette use was highest among males, whites, and high school students.
Tobacco use in teens is trending in the direction of wiping out the progress made in recent years to reduce exposure to youths. The report noted, “The prevalence of e-cigarette use by U.S. high school students had peaked in 2015 before declining by 29% during 2015-2016 (from 16% to 11.3%); this decline was the first ever recorded for e-cigarette use among youths in the NYTS since monitoring began, and it was subsequently sustained during 2016-2017). However, current e-cigarette use increased by 77.8% among high school students and 48.5% among middle school students during 2017-2018, erasing the progress in reducing e-cigarette use, as well as any tobacco product use, that had occurred in prior years.”
The CDC and the Food and Drug Administration are taking action to curb the rise in e-cigarette use in youth in particular by seeking regulations to make the products less accessible, raising prices, and banning most flavorings, said Dr. Schuchat.
“We have targeted companies engaged in kid friendly marketing,” said Mitch Zeller, JD, director of the Center for Tobacco Products for the FDA.
In a statement published simultaneously with the Vital Signs study, FDA Commissioner Scott Gottlieb, MD, emphasized the link between e-cigarette use in teens and the potential for future tobacco use. “The kids using e-cigarettes are children who rejected conventional cigarettes, but don’t see the same stigma associated with the use of e-cigarettes. But now, having become exposed to nicotine through e-cigs, they will be more likely to smoke.” Dr. Gottlieb declared, “I will not allow a generation of children to become addicted to nicotine through e-cigarettes. We must stop the trends of youth e-cigarette use from continuing to build and will take whatever action is necessary to ensure these kids don’t become future smokers.” He reviewed steps taken in the past year by the FDA to counter tobacco use in teens but he warned of future actions that may need to be taken: “If these youth use trends continue, we’ll be forced to consider regulatory steps that could constrain or even foreclose the opportunities for currently addicted adult smokers to have the same level of access to these products that they now enjoy. I recognize that such a move could come with significant impacts to adult smokers.”
In the meantime, however, parents, teachers, community leaders, and health care providers are on the front lines and can make a difference in protecting youth and curbing nicotine use, Dr. King said.
One of the most important things clinicians can do is to ask young patients specifically about e-cigarette use, he emphasized. Learn and use the terminology the kids are using; ask, “Do you use JUUL?” If they are using these products, “make sure they know they are dangerous,” and can harm the developing brain, he said.
Although there are no currently approved medications to treat nicotine addiction in youth, research suggests that behavioral counseling, as well as reinforcement of the danger of nicotine from parents and other people of influence, can help, Dr. King said.
The Vital Signs report is based on data from the 2011-2018 National Youth Tobacco Survey, which assesses current use of cigarettes, cigars, smokeless tobacco, e-cigarettes, hookahs, pipe tobacco, and bidis among a nationally representative sample of middle and high school students in the United States. The findings were analyzed by the CDC, FDA, and the National Cancer Institute.
SOURCE: Gentzke AS et al. MMWR 2019 Feb 11. doi: 10.15585/mmwr.mm6806e1.
*Correction 2/13/2019 An earlier version of this article misstated the number of students using e-cigarettes as a proportion of all teen tobacco users.
A significant increase during 2017-2018 in e-cigarette use among U.S. youths has erased recent progress in reducing overall tobacco product use in this age group, a study from the Centers for Disease Control and Prevention has found.
E-cigarettes are driving the trend. About 4 million high school students in the United States reported using any tobacco product in the last 30 days, and 3 million of them reported using e-cigarettes, according to a Vital Signs document published by the CDC on Feb. 11 in its Morbidity and Mortality Weekly Report.*
In addition, many high school students who use e-cigarettes use them often; 28% reported using the products at least 20 times in the past 28 days, up from 20% in 2017.
“Any use of any tobacco product is unsafe for teens,” Anne Schuchat, MD, principal deputy director of the CDC, said in a teleconference to present the findings. Nicotine is highly addictive and can harm brain development in youth, including capacity for learning, memory, and attention, she said.
The rise in e-cigarette use corresponds with the rise in marketing and availability of e-cigarette devices such as JUUL, which dispense nicotine via liquid refill pods available in flavors including strawberry and cotton candy, said Brian King, MPH, PhD, deputy director for research translation at the CDC’s Office on Smoking and Health.
“The advertising will lead a horse to water, the flavors will make them drink, and the nicotine will keep them coming back for more,” said Dr. King.
Approximately 27.1% of high school students and 7.2% of middle school students used a tobacco product in 2018, a significant increase from 2017 data, and with a major increase in e-cigarette use.
No change was noted in the use of other tobacco products, including cigarettes, from 2017 to 2018, according to the report. However, conventional cigarettes remained the most common companion product to e-cigarettes for youth who use two or more tobacco products (two in five high school students and one in three middle school students in 2018). From a demographic standpoint, e-cigarette use was highest among males, whites, and high school students.
Tobacco use in teens is trending in the direction of wiping out the progress made in recent years to reduce exposure to youths. The report noted, “The prevalence of e-cigarette use by U.S. high school students had peaked in 2015 before declining by 29% during 2015-2016 (from 16% to 11.3%); this decline was the first ever recorded for e-cigarette use among youths in the NYTS since monitoring began, and it was subsequently sustained during 2016-2017). However, current e-cigarette use increased by 77.8% among high school students and 48.5% among middle school students during 2017-2018, erasing the progress in reducing e-cigarette use, as well as any tobacco product use, that had occurred in prior years.”
The CDC and the Food and Drug Administration are taking action to curb the rise in e-cigarette use in youth in particular by seeking regulations to make the products less accessible, raising prices, and banning most flavorings, said Dr. Schuchat.
“We have targeted companies engaged in kid friendly marketing,” said Mitch Zeller, JD, director of the Center for Tobacco Products for the FDA.
In a statement published simultaneously with the Vital Signs study, FDA Commissioner Scott Gottlieb, MD, emphasized the link between e-cigarette use in teens and the potential for future tobacco use. “The kids using e-cigarettes are children who rejected conventional cigarettes, but don’t see the same stigma associated with the use of e-cigarettes. But now, having become exposed to nicotine through e-cigs, they will be more likely to smoke.” Dr. Gottlieb declared, “I will not allow a generation of children to become addicted to nicotine through e-cigarettes. We must stop the trends of youth e-cigarette use from continuing to build and will take whatever action is necessary to ensure these kids don’t become future smokers.” He reviewed steps taken in the past year by the FDA to counter tobacco use in teens but he warned of future actions that may need to be taken: “If these youth use trends continue, we’ll be forced to consider regulatory steps that could constrain or even foreclose the opportunities for currently addicted adult smokers to have the same level of access to these products that they now enjoy. I recognize that such a move could come with significant impacts to adult smokers.”
In the meantime, however, parents, teachers, community leaders, and health care providers are on the front lines and can make a difference in protecting youth and curbing nicotine use, Dr. King said.
One of the most important things clinicians can do is to ask young patients specifically about e-cigarette use, he emphasized. Learn and use the terminology the kids are using; ask, “Do you use JUUL?” If they are using these products, “make sure they know they are dangerous,” and can harm the developing brain, he said.
Although there are no currently approved medications to treat nicotine addiction in youth, research suggests that behavioral counseling, as well as reinforcement of the danger of nicotine from parents and other people of influence, can help, Dr. King said.
The Vital Signs report is based on data from the 2011-2018 National Youth Tobacco Survey, which assesses current use of cigarettes, cigars, smokeless tobacco, e-cigarettes, hookahs, pipe tobacco, and bidis among a nationally representative sample of middle and high school students in the United States. The findings were analyzed by the CDC, FDA, and the National Cancer Institute.
SOURCE: Gentzke AS et al. MMWR 2019 Feb 11. doi: 10.15585/mmwr.mm6806e1.
*Correction 2/13/2019 An earlier version of this article misstated the number of students using e-cigarettes as a proportion of all teen tobacco users.
FROM CDC VITAL SIGNS REPORT
EC approves dasatinib plus chemo for kids with Ph+ ALL
The European Commission has approved dasatinib (Sprycel) for use in combination with chemotherapy for the treatment of pediatric patients with newly diagnosed, Philadelphia chromosome–positive (Ph+) acute lymphoblastic leukemia (ALL).
Dasatinib will be available in tablet form and as a powder for oral suspension, Bristol-Myers Squib said in a press release.
The approval was based on an event-free survival rate of 65.5% (95% confidence interval, 57.7-73.7) and an overall survival rate of 91.5% (95% CI, 84.2-95.5) in a phase 2 trial that evaluated the addition of dasatinib to a chemotherapy regimen modeled on a Berlin-Frankfurt-Münster high-risk backbone in pediatric patients with newly diagnosed Ph+ ALL.
Patients treated in the study (n = 106) were all aged younger than 18 years and received dasatinib at a daily dose of 60 mg/m2 on a continuous dosing regimen for up to 24 months, in combination with chemotherapy. About 77 % of patients (n = 82) received tablets exclusively; 23% of patients (n = 24) received the powder for oral suspension at least once.
Hematologic adverse events included grade 3 or 4 febrile neutropenia (75.5%), sepsis (23.6%), and bacteremia (24.5%). Nonhematologic, noninfectious grade 3 or 4 adverse events attributed to dasatinib and reported in more than 10% of patients included elevated ALT (21.7%) and AST (10.4%). Additional grade 3 or 4 adverse events attributed to dasatinib were pleural effusion (3.8%), edema (2.8%), hemorrhage (5.7%), and cardiac failure (0.8%). No events of pulmonary hypertension or pulmonary arterial hypertension were reported, the company said in the press release.
Dasatinib is already approved by the European Commission to treat children with Ph+ chronic myeloid leukemia in the chronic phase, which includes newly diagnosed patients and those with resistance or intolerance to imatinib.
The European Commission has approved dasatinib (Sprycel) for use in combination with chemotherapy for the treatment of pediatric patients with newly diagnosed, Philadelphia chromosome–positive (Ph+) acute lymphoblastic leukemia (ALL).
Dasatinib will be available in tablet form and as a powder for oral suspension, Bristol-Myers Squib said in a press release.
The approval was based on an event-free survival rate of 65.5% (95% confidence interval, 57.7-73.7) and an overall survival rate of 91.5% (95% CI, 84.2-95.5) in a phase 2 trial that evaluated the addition of dasatinib to a chemotherapy regimen modeled on a Berlin-Frankfurt-Münster high-risk backbone in pediatric patients with newly diagnosed Ph+ ALL.
Patients treated in the study (n = 106) were all aged younger than 18 years and received dasatinib at a daily dose of 60 mg/m2 on a continuous dosing regimen for up to 24 months, in combination with chemotherapy. About 77 % of patients (n = 82) received tablets exclusively; 23% of patients (n = 24) received the powder for oral suspension at least once.
Hematologic adverse events included grade 3 or 4 febrile neutropenia (75.5%), sepsis (23.6%), and bacteremia (24.5%). Nonhematologic, noninfectious grade 3 or 4 adverse events attributed to dasatinib and reported in more than 10% of patients included elevated ALT (21.7%) and AST (10.4%). Additional grade 3 or 4 adverse events attributed to dasatinib were pleural effusion (3.8%), edema (2.8%), hemorrhage (5.7%), and cardiac failure (0.8%). No events of pulmonary hypertension or pulmonary arterial hypertension were reported, the company said in the press release.
Dasatinib is already approved by the European Commission to treat children with Ph+ chronic myeloid leukemia in the chronic phase, which includes newly diagnosed patients and those with resistance or intolerance to imatinib.
The European Commission has approved dasatinib (Sprycel) for use in combination with chemotherapy for the treatment of pediatric patients with newly diagnosed, Philadelphia chromosome–positive (Ph+) acute lymphoblastic leukemia (ALL).
Dasatinib will be available in tablet form and as a powder for oral suspension, Bristol-Myers Squib said in a press release.
The approval was based on an event-free survival rate of 65.5% (95% confidence interval, 57.7-73.7) and an overall survival rate of 91.5% (95% CI, 84.2-95.5) in a phase 2 trial that evaluated the addition of dasatinib to a chemotherapy regimen modeled on a Berlin-Frankfurt-Münster high-risk backbone in pediatric patients with newly diagnosed Ph+ ALL.
Patients treated in the study (n = 106) were all aged younger than 18 years and received dasatinib at a daily dose of 60 mg/m2 on a continuous dosing regimen for up to 24 months, in combination with chemotherapy. About 77 % of patients (n = 82) received tablets exclusively; 23% of patients (n = 24) received the powder for oral suspension at least once.
Hematologic adverse events included grade 3 or 4 febrile neutropenia (75.5%), sepsis (23.6%), and bacteremia (24.5%). Nonhematologic, noninfectious grade 3 or 4 adverse events attributed to dasatinib and reported in more than 10% of patients included elevated ALT (21.7%) and AST (10.4%). Additional grade 3 or 4 adverse events attributed to dasatinib were pleural effusion (3.8%), edema (2.8%), hemorrhage (5.7%), and cardiac failure (0.8%). No events of pulmonary hypertension or pulmonary arterial hypertension were reported, the company said in the press release.
Dasatinib is already approved by the European Commission to treat children with Ph+ chronic myeloid leukemia in the chronic phase, which includes newly diagnosed patients and those with resistance or intolerance to imatinib.
Treatment missing for U.S. children with mental illness
according to data from a national survey of parents.

Among the estimated 7.7 million children with a treatable mental illness, 49.4% did not receive needed treatment from a psychiatrist, psychologist, psychiatric nurse, or clinical social worker in the previous 12 months, Daniel G. Whitney, PhD, and Mark D. Peterson, PhD, of the University of Michigan, Ann Arbor, wrote in JAMA Pediatrics.
State-level data from the National Survey of Children’s Health show considerable variation from the national average. North Carolina had the highest prevalence of nontreatment at 72.2% and Washington, D.C., had the lowest rate at 29.5%. The prevalence of at least one mental health disorder was highest in Maine (27.2%) and lowest in Hawaii (7.6%), the investigators reported.
Four states – Alabama, Mississippi, Oklahoma, and Utah – were in the top quartile for both mental health disorder prevalence and prevalence of children with a disorder who did not receive treatment, they noted.
“State-level practices and policies play a role in health care needs and use, which may help to explain the state variability observed in this study. Nevertheless, initiatives that assist systems of care coordination have demonstrated a reduction of mental health–related burdens across multiple domains,” Dr. Whitney and Dr. Peterson wrote.
SOURCE: Whitney DG et al. JAMA Pediatr. 2019 Feb 11. doi: 10.1001/jamapediatrics.2018.5399.
according to data from a national survey of parents.
Among the estimated 7.7 million children with a treatable mental illness, 49.4% did not receive needed treatment from a psychiatrist, psychologist, psychiatric nurse, or clinical social worker in the previous 12 months, Daniel G. Whitney, PhD, and Mark D. Peterson, PhD, of the University of Michigan, Ann Arbor, wrote in JAMA Pediatrics.
State-level data from the National Survey of Children’s Health show considerable variation from the national average. North Carolina had the highest prevalence of nontreatment at 72.2% and Washington, D.C., had the lowest rate at 29.5%. The prevalence of at least one mental health disorder was highest in Maine (27.2%) and lowest in Hawaii (7.6%), the investigators reported.
Four states – Alabama, Mississippi, Oklahoma, and Utah – were in the top quartile for both mental health disorder prevalence and prevalence of children with a disorder who did not receive treatment, they noted.
“State-level practices and policies play a role in health care needs and use, which may help to explain the state variability observed in this study. Nevertheless, initiatives that assist systems of care coordination have demonstrated a reduction of mental health–related burdens across multiple domains,” Dr. Whitney and Dr. Peterson wrote.
SOURCE: Whitney DG et al. JAMA Pediatr. 2019 Feb 11. doi: 10.1001/jamapediatrics.2018.5399.
according to data from a national survey of parents.
Among the estimated 7.7 million children with a treatable mental illness, 49.4% did not receive needed treatment from a psychiatrist, psychologist, psychiatric nurse, or clinical social worker in the previous 12 months, Daniel G. Whitney, PhD, and Mark D. Peterson, PhD, of the University of Michigan, Ann Arbor, wrote in JAMA Pediatrics.
State-level data from the National Survey of Children’s Health show considerable variation from the national average. North Carolina had the highest prevalence of nontreatment at 72.2% and Washington, D.C., had the lowest rate at 29.5%. The prevalence of at least one mental health disorder was highest in Maine (27.2%) and lowest in Hawaii (7.6%), the investigators reported.
Four states – Alabama, Mississippi, Oklahoma, and Utah – were in the top quartile for both mental health disorder prevalence and prevalence of children with a disorder who did not receive treatment, they noted.
“State-level practices and policies play a role in health care needs and use, which may help to explain the state variability observed in this study. Nevertheless, initiatives that assist systems of care coordination have demonstrated a reduction of mental health–related burdens across multiple domains,” Dr. Whitney and Dr. Peterson wrote.
SOURCE: Whitney DG et al. JAMA Pediatr. 2019 Feb 11. doi: 10.1001/jamapediatrics.2018.5399.
FROM JAMA PEDIATRICS
Use three phases of psychiatric disorders in children to guide treatment
BROOKLYN, N.Y. – , John T. Walkup, MD, said at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
After the onset of symptoms and over the course of time, those with untreated anxiety disorders are at risk for developing impairment in adaptation and coping, and also the development of maladaptive behaviors like substance abuse and suicidal behavior, said Dr. Walkup, chair of the department of psychiatry at Ann and Robert H. Lurie Children’s Hospital of Chicago.
The focus of his presentation was on the treatment of anxiety disorders in children, but Dr. Walkup said the impact of the three-tier progression is likely relevant to any psychiatric disorder that begins in childhood.
In essence, the scope of problems becomes more complicated over time, and without early treatment, children continue to be symptomatic. But they also develop a lifestyle based on avoidance coping and might engage in maladaptive behaviors, Dr. Walkup said. As a result, the complexity of treatment increases substantially beyond just symptom control.
Providing an example, Dr. Walkup described a child of 7 years of age with separation anxiety. If treated at the time symptoms begin, Dr. Walkup explained, cognitive-behavioral therapy and medication would be expected to be both straightforward and highly effective. If left untreated until age 14, the child might accumulate impairment in independent functioning (due to avoidance coping) at a particularly important time in development.
“In those kids, you can reduce their anxiety burden with acute treatments like [cognitive-behavioral therapy] or meds, but now you also have 7 or 8 years of accumulated impairment due to avoidance coping and parental accommodation,” Dr. Walkup said. “If those kids are going to catch up developmentally, they also need life skill support in addition to symptomatic treatment for their anxiety.”
In the case of any pediatric psychiatric disorder, early treatment has the potential to thwart progression to a more complex and treatment-resistant form, but anxiety is a particularly prominent example. In most children, anxiety is relatively easy to control if caught early but a greater challenge when fears are not contained and the child accumulates ongoing impairment.
The obstacle is that many children are not diagnosed at the time of onset, said Dr. Walkup. The solution, he suggested, is better training of pediatricians and other primary care physicians not only to identify those children but to initiate treatment in uncomplicated cases.
“The person who has that longitudinal relationship with the child is their primary care provider, and this is really the person who is going to do the best job in getting to these kids early and initiating treatment,” Dr. Walkup said.
“We have a program in Chicago where we have trained primary care physicians not only to treat anxiety and depression, but we have specifically focused them on the easiest cases in their caseload, the classic phenotypes,” Dr. Walkup reported. Using a collaborative care model, this approach has been effective in building the confidence of primary care clinicians and in reaching children when symptoms are easier to control.
Importantly, anti-anxiety medication delivered in primary care could be sufficient to help children to manage anxiety effectively when parents cooperate in helping their children manage their fears.
“People suggest that we always start with CBT, but there [are no data] to support that. I think it is a conclusion drawn from the fact that CBT works and medication has side effects,” Dr. Walkup said. He appreciates the evidence that CBT is effective, but he cautioned that this therapy is not available everywhere, and pharmacologic therapies may be as or potentially more effective for some anxiety symptoms like anxiety-related physical symptoms.
Conversely, some have expressed the opinion that drugs might be a better option in late adolescence, when the efficacy of CBT appears to diminish, but Dr. Walkup objected to that characterization as well.
“My sense is that if you treat a 7-year-old for symptoms that have lasted a year it’s very different from treating a 17-year-old who has had symptoms for a decade,” Dr. Walkup said. Referring back to the contention that psychiatric disease in children becomes more complicated with a longer duration, this might explain why “you don’t see as much immediate success” with CBT and medication in the older age groups even if this is an effective treatment tool.
Some psychiatric disorders in children, including anxiety, might resolve with age, but early recognition and treatment should be a goal because of the potential to reduce symptoms and avoidance coping, and improve long-term outcomes, Dr. Walkup reported. Ironically, it might not be just anxiety symptoms, but poor adaptation and coping that might be the most important driver of ongoing impairment.
Dr. Walkup has served as an unpaid adviser to the Anxiety Disorders of Association of America. In addition, he has received royalties from Wolters Kluwer for CME activity on childhood anxiety.
This story was updated 2/11/2019.
BROOKLYN, N.Y. – , John T. Walkup, MD, said at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
After the onset of symptoms and over the course of time, those with untreated anxiety disorders are at risk for developing impairment in adaptation and coping, and also the development of maladaptive behaviors like substance abuse and suicidal behavior, said Dr. Walkup, chair of the department of psychiatry at Ann and Robert H. Lurie Children’s Hospital of Chicago.
The focus of his presentation was on the treatment of anxiety disorders in children, but Dr. Walkup said the impact of the three-tier progression is likely relevant to any psychiatric disorder that begins in childhood.
In essence, the scope of problems becomes more complicated over time, and without early treatment, children continue to be symptomatic. But they also develop a lifestyle based on avoidance coping and might engage in maladaptive behaviors, Dr. Walkup said. As a result, the complexity of treatment increases substantially beyond just symptom control.
Providing an example, Dr. Walkup described a child of 7 years of age with separation anxiety. If treated at the time symptoms begin, Dr. Walkup explained, cognitive-behavioral therapy and medication would be expected to be both straightforward and highly effective. If left untreated until age 14, the child might accumulate impairment in independent functioning (due to avoidance coping) at a particularly important time in development.
“In those kids, you can reduce their anxiety burden with acute treatments like [cognitive-behavioral therapy] or meds, but now you also have 7 or 8 years of accumulated impairment due to avoidance coping and parental accommodation,” Dr. Walkup said. “If those kids are going to catch up developmentally, they also need life skill support in addition to symptomatic treatment for their anxiety.”
In the case of any pediatric psychiatric disorder, early treatment has the potential to thwart progression to a more complex and treatment-resistant form, but anxiety is a particularly prominent example. In most children, anxiety is relatively easy to control if caught early but a greater challenge when fears are not contained and the child accumulates ongoing impairment.
The obstacle is that many children are not diagnosed at the time of onset, said Dr. Walkup. The solution, he suggested, is better training of pediatricians and other primary care physicians not only to identify those children but to initiate treatment in uncomplicated cases.
“The person who has that longitudinal relationship with the child is their primary care provider, and this is really the person who is going to do the best job in getting to these kids early and initiating treatment,” Dr. Walkup said.
“We have a program in Chicago where we have trained primary care physicians not only to treat anxiety and depression, but we have specifically focused them on the easiest cases in their caseload, the classic phenotypes,” Dr. Walkup reported. Using a collaborative care model, this approach has been effective in building the confidence of primary care clinicians and in reaching children when symptoms are easier to control.
Importantly, anti-anxiety medication delivered in primary care could be sufficient to help children to manage anxiety effectively when parents cooperate in helping their children manage their fears.
“People suggest that we always start with CBT, but there [are no data] to support that. I think it is a conclusion drawn from the fact that CBT works and medication has side effects,” Dr. Walkup said. He appreciates the evidence that CBT is effective, but he cautioned that this therapy is not available everywhere, and pharmacologic therapies may be as or potentially more effective for some anxiety symptoms like anxiety-related physical symptoms.
Conversely, some have expressed the opinion that drugs might be a better option in late adolescence, when the efficacy of CBT appears to diminish, but Dr. Walkup objected to that characterization as well.
“My sense is that if you treat a 7-year-old for symptoms that have lasted a year it’s very different from treating a 17-year-old who has had symptoms for a decade,” Dr. Walkup said. Referring back to the contention that psychiatric disease in children becomes more complicated with a longer duration, this might explain why “you don’t see as much immediate success” with CBT and medication in the older age groups even if this is an effective treatment tool.
Some psychiatric disorders in children, including anxiety, might resolve with age, but early recognition and treatment should be a goal because of the potential to reduce symptoms and avoidance coping, and improve long-term outcomes, Dr. Walkup reported. Ironically, it might not be just anxiety symptoms, but poor adaptation and coping that might be the most important driver of ongoing impairment.
Dr. Walkup has served as an unpaid adviser to the Anxiety Disorders of Association of America. In addition, he has received royalties from Wolters Kluwer for CME activity on childhood anxiety.
This story was updated 2/11/2019.
BROOKLYN, N.Y. – , John T. Walkup, MD, said at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
After the onset of symptoms and over the course of time, those with untreated anxiety disorders are at risk for developing impairment in adaptation and coping, and also the development of maladaptive behaviors like substance abuse and suicidal behavior, said Dr. Walkup, chair of the department of psychiatry at Ann and Robert H. Lurie Children’s Hospital of Chicago.
The focus of his presentation was on the treatment of anxiety disorders in children, but Dr. Walkup said the impact of the three-tier progression is likely relevant to any psychiatric disorder that begins in childhood.
In essence, the scope of problems becomes more complicated over time, and without early treatment, children continue to be symptomatic. But they also develop a lifestyle based on avoidance coping and might engage in maladaptive behaviors, Dr. Walkup said. As a result, the complexity of treatment increases substantially beyond just symptom control.
Providing an example, Dr. Walkup described a child of 7 years of age with separation anxiety. If treated at the time symptoms begin, Dr. Walkup explained, cognitive-behavioral therapy and medication would be expected to be both straightforward and highly effective. If left untreated until age 14, the child might accumulate impairment in independent functioning (due to avoidance coping) at a particularly important time in development.
“In those kids, you can reduce their anxiety burden with acute treatments like [cognitive-behavioral therapy] or meds, but now you also have 7 or 8 years of accumulated impairment due to avoidance coping and parental accommodation,” Dr. Walkup said. “If those kids are going to catch up developmentally, they also need life skill support in addition to symptomatic treatment for their anxiety.”
In the case of any pediatric psychiatric disorder, early treatment has the potential to thwart progression to a more complex and treatment-resistant form, but anxiety is a particularly prominent example. In most children, anxiety is relatively easy to control if caught early but a greater challenge when fears are not contained and the child accumulates ongoing impairment.
The obstacle is that many children are not diagnosed at the time of onset, said Dr. Walkup. The solution, he suggested, is better training of pediatricians and other primary care physicians not only to identify those children but to initiate treatment in uncomplicated cases.
“The person who has that longitudinal relationship with the child is their primary care provider, and this is really the person who is going to do the best job in getting to these kids early and initiating treatment,” Dr. Walkup said.
“We have a program in Chicago where we have trained primary care physicians not only to treat anxiety and depression, but we have specifically focused them on the easiest cases in their caseload, the classic phenotypes,” Dr. Walkup reported. Using a collaborative care model, this approach has been effective in building the confidence of primary care clinicians and in reaching children when symptoms are easier to control.
Importantly, anti-anxiety medication delivered in primary care could be sufficient to help children to manage anxiety effectively when parents cooperate in helping their children manage their fears.
“People suggest that we always start with CBT, but there [are no data] to support that. I think it is a conclusion drawn from the fact that CBT works and medication has side effects,” Dr. Walkup said. He appreciates the evidence that CBT is effective, but he cautioned that this therapy is not available everywhere, and pharmacologic therapies may be as or potentially more effective for some anxiety symptoms like anxiety-related physical symptoms.
Conversely, some have expressed the opinion that drugs might be a better option in late adolescence, when the efficacy of CBT appears to diminish, but Dr. Walkup objected to that characterization as well.
“My sense is that if you treat a 7-year-old for symptoms that have lasted a year it’s very different from treating a 17-year-old who has had symptoms for a decade,” Dr. Walkup said. Referring back to the contention that psychiatric disease in children becomes more complicated with a longer duration, this might explain why “you don’t see as much immediate success” with CBT and medication in the older age groups even if this is an effective treatment tool.
Some psychiatric disorders in children, including anxiety, might resolve with age, but early recognition and treatment should be a goal because of the potential to reduce symptoms and avoidance coping, and improve long-term outcomes, Dr. Walkup reported. Ironically, it might not be just anxiety symptoms, but poor adaptation and coping that might be the most important driver of ongoing impairment.
Dr. Walkup has served as an unpaid adviser to the Anxiety Disorders of Association of America. In addition, he has received royalties from Wolters Kluwer for CME activity on childhood anxiety.
This story was updated 2/11/2019.
REPORTING FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
High prevalence of sleep problems in children with autism spectrum disorder
Children with a diagnosis of autism spectrum disorder or another developmental delay or disorder that includes autistic characteristics are twice as likely to have sleeping problems, a multisite case-control study has found.

The findings match up with previous similar studies, but this study is among the largest to measure sleeping problems in children with autism spectrum disorder (ASD) with two control groups.
“ including physiologic differences, sleep disorders, developmental comorbidities, medical comorbidities causing sleep disruption, communication impairments, and behavioral disturbances,” Ann M. Reynolds, MD, of the University of Colorado and Children’s Hospital Colorado, both in Aurora, and her associates reported in Pediatrics.

“Children with ASD are more likely to have anxiety, which may predispose them to sleep problems,” the authors added.
The study evaluated sleep habits and problems in 1,987 children aged 2-5 years. The study population included 522 children with ASD, 228 children with other developmental delays and disorders that have ASD characteristics, 534 children with other developmental delays and disorders, and 703 children from the general population.
Parents completed the Children Sleep Habits Questionnaire (CSHQ), a 33-item assessment tool typically used with a total score cutoff of 41 and above for identification of children with sleep disorders. The researchers also used a second, more conservative cutoff of 48 – the cutoff for the highest quartile in the general population group – to avoid overidentification with the lower cutoff.
Scores were adjusted for maternal education and race/ethnicity, family income, child age and sex, and child cognitive scores on the Mullen Scales of Early Learning (MSEL). The researchers also adjusted for genetic and/or neurologic diagnoses, including Down syndrome, fragile X, Rett syndrome, tuberous sclerosis, cerebral palsy, and neurofibromatosis.
Autistic children tended to have lower MSEL scores than the other children. Both the autistic children and those with other developmental disorders and delays were more likely than those in the general population to have neurologic or genetic conditions.
Based on a cutoff score of 48, autistic children had more than double the odds of sleep problems, compared with children in the general population (adjusted odds ratio, 2.37; P = .001) and children with other developmental delays (aOR, 2.12; P = .001).
With a cutoff of 41, ASD children’s odds of sleep problems were 1.45 times greater than the general population (P = .023) and 1.75 times greater than those with developmental delays (P = .001).
But children with developmental delays who displayed autistic characteristics did not have not significantly different prevalence of sleep problems than children with ASD had.
“The phenotypic overlay between children with ASD and children with developmental delay with ASD [characteristics] may explain the similarities in sleep disturbance among these two groups,” the authors wrote. Both groups have “higher rates of obsessive-compulsive symptoms, self-injurious behavior, ADHD symptoms, and developmental and communication impairments” than children with developmental delays without autistic characteristics.
The research was funded by the Centers for Disease Control and Prevention, the National Institutes of Health, and the National Center for Advancing Translational Sciences Colorado Clinical and Translational Science Award. Dr Reynolds consults for Ovid Therapeutics regarding evaluation of sleep severity and improvement in clinical trials. No other authors had disclosures.
SOURCE: Reynolds AM et al. Pediatrics. 2019 Feb. 11. doi: 10.1542/peds.2018-0492.
We can help reduce night waking and improve sleep onset within 5-15 weeks after parents have been trained. “Successful behavioral programs include bedtime fading, teaching healthy sleep practices, and increasing a child’s physical activity during the day,” Catherine Lord, PhD, wrote. Although research supports melatonin as an effective intervention for helping children fall asleep and sleep longer, the high percentage of children in the study already taking melatonin reveals its limitations. “Thus, it is recommended that families try behavioral programs before trials with melatonin,” she wrote.
But families and providers can only work together to address sleep issues if providers ask about sleep concerns, help families implement interventions, and follow up with progress. “In most cases, this help does not have to come from sleep experts, but does require dedicated time and effort using the now-growing base of evidence about effective interventions,” she concluded.
These comments are condensed from an editorial (Pediatrics. 2019 Feb 11. doi: 10.1542/peds.2018-2629) by Dr. Lord , a professor of psychiatry and biobehavioral sciences at the University of California Los Angeles. Dr. Lord reports royalties from diagnostic instruments used in this study that were donated to a not-for-profit agency. She is supported by grants from the National Institutes of Health and Simons Foundation Autism Research Initiative.
We can help reduce night waking and improve sleep onset within 5-15 weeks after parents have been trained. “Successful behavioral programs include bedtime fading, teaching healthy sleep practices, and increasing a child’s physical activity during the day,” Catherine Lord, PhD, wrote. Although research supports melatonin as an effective intervention for helping children fall asleep and sleep longer, the high percentage of children in the study already taking melatonin reveals its limitations. “Thus, it is recommended that families try behavioral programs before trials with melatonin,” she wrote.
But families and providers can only work together to address sleep issues if providers ask about sleep concerns, help families implement interventions, and follow up with progress. “In most cases, this help does not have to come from sleep experts, but does require dedicated time and effort using the now-growing base of evidence about effective interventions,” she concluded.
These comments are condensed from an editorial (Pediatrics. 2019 Feb 11. doi: 10.1542/peds.2018-2629) by Dr. Lord , a professor of psychiatry and biobehavioral sciences at the University of California Los Angeles. Dr. Lord reports royalties from diagnostic instruments used in this study that were donated to a not-for-profit agency. She is supported by grants from the National Institutes of Health and Simons Foundation Autism Research Initiative.
We can help reduce night waking and improve sleep onset within 5-15 weeks after parents have been trained. “Successful behavioral programs include bedtime fading, teaching healthy sleep practices, and increasing a child’s physical activity during the day,” Catherine Lord, PhD, wrote. Although research supports melatonin as an effective intervention for helping children fall asleep and sleep longer, the high percentage of children in the study already taking melatonin reveals its limitations. “Thus, it is recommended that families try behavioral programs before trials with melatonin,” she wrote.
But families and providers can only work together to address sleep issues if providers ask about sleep concerns, help families implement interventions, and follow up with progress. “In most cases, this help does not have to come from sleep experts, but does require dedicated time and effort using the now-growing base of evidence about effective interventions,” she concluded.
These comments are condensed from an editorial (Pediatrics. 2019 Feb 11. doi: 10.1542/peds.2018-2629) by Dr. Lord , a professor of psychiatry and biobehavioral sciences at the University of California Los Angeles. Dr. Lord reports royalties from diagnostic instruments used in this study that were donated to a not-for-profit agency. She is supported by grants from the National Institutes of Health and Simons Foundation Autism Research Initiative.
Children with a diagnosis of autism spectrum disorder or another developmental delay or disorder that includes autistic characteristics are twice as likely to have sleeping problems, a multisite case-control study has found.
The findings match up with previous similar studies, but this study is among the largest to measure sleeping problems in children with autism spectrum disorder (ASD) with two control groups.
“ including physiologic differences, sleep disorders, developmental comorbidities, medical comorbidities causing sleep disruption, communication impairments, and behavioral disturbances,” Ann M. Reynolds, MD, of the University of Colorado and Children’s Hospital Colorado, both in Aurora, and her associates reported in Pediatrics.
“Children with ASD are more likely to have anxiety, which may predispose them to sleep problems,” the authors added.
The study evaluated sleep habits and problems in 1,987 children aged 2-5 years. The study population included 522 children with ASD, 228 children with other developmental delays and disorders that have ASD characteristics, 534 children with other developmental delays and disorders, and 703 children from the general population.
Parents completed the Children Sleep Habits Questionnaire (CSHQ), a 33-item assessment tool typically used with a total score cutoff of 41 and above for identification of children with sleep disorders. The researchers also used a second, more conservative cutoff of 48 – the cutoff for the highest quartile in the general population group – to avoid overidentification with the lower cutoff.
Scores were adjusted for maternal education and race/ethnicity, family income, child age and sex, and child cognitive scores on the Mullen Scales of Early Learning (MSEL). The researchers also adjusted for genetic and/or neurologic diagnoses, including Down syndrome, fragile X, Rett syndrome, tuberous sclerosis, cerebral palsy, and neurofibromatosis.
Autistic children tended to have lower MSEL scores than the other children. Both the autistic children and those with other developmental disorders and delays were more likely than those in the general population to have neurologic or genetic conditions.
Based on a cutoff score of 48, autistic children had more than double the odds of sleep problems, compared with children in the general population (adjusted odds ratio, 2.37; P = .001) and children with other developmental delays (aOR, 2.12; P = .001).
With a cutoff of 41, ASD children’s odds of sleep problems were 1.45 times greater than the general population (P = .023) and 1.75 times greater than those with developmental delays (P = .001).
But children with developmental delays who displayed autistic characteristics did not have not significantly different prevalence of sleep problems than children with ASD had.
“The phenotypic overlay between children with ASD and children with developmental delay with ASD [characteristics] may explain the similarities in sleep disturbance among these two groups,” the authors wrote. Both groups have “higher rates of obsessive-compulsive symptoms, self-injurious behavior, ADHD symptoms, and developmental and communication impairments” than children with developmental delays without autistic characteristics.
The research was funded by the Centers for Disease Control and Prevention, the National Institutes of Health, and the National Center for Advancing Translational Sciences Colorado Clinical and Translational Science Award. Dr Reynolds consults for Ovid Therapeutics regarding evaluation of sleep severity and improvement in clinical trials. No other authors had disclosures.
SOURCE: Reynolds AM et al. Pediatrics. 2019 Feb. 11. doi: 10.1542/peds.2018-0492.
Children with a diagnosis of autism spectrum disorder or another developmental delay or disorder that includes autistic characteristics are twice as likely to have sleeping problems, a multisite case-control study has found.
The findings match up with previous similar studies, but this study is among the largest to measure sleeping problems in children with autism spectrum disorder (ASD) with two control groups.
“ including physiologic differences, sleep disorders, developmental comorbidities, medical comorbidities causing sleep disruption, communication impairments, and behavioral disturbances,” Ann M. Reynolds, MD, of the University of Colorado and Children’s Hospital Colorado, both in Aurora, and her associates reported in Pediatrics.
“Children with ASD are more likely to have anxiety, which may predispose them to sleep problems,” the authors added.
The study evaluated sleep habits and problems in 1,987 children aged 2-5 years. The study population included 522 children with ASD, 228 children with other developmental delays and disorders that have ASD characteristics, 534 children with other developmental delays and disorders, and 703 children from the general population.
Parents completed the Children Sleep Habits Questionnaire (CSHQ), a 33-item assessment tool typically used with a total score cutoff of 41 and above for identification of children with sleep disorders. The researchers also used a second, more conservative cutoff of 48 – the cutoff for the highest quartile in the general population group – to avoid overidentification with the lower cutoff.
Scores were adjusted for maternal education and race/ethnicity, family income, child age and sex, and child cognitive scores on the Mullen Scales of Early Learning (MSEL). The researchers also adjusted for genetic and/or neurologic diagnoses, including Down syndrome, fragile X, Rett syndrome, tuberous sclerosis, cerebral palsy, and neurofibromatosis.
Autistic children tended to have lower MSEL scores than the other children. Both the autistic children and those with other developmental disorders and delays were more likely than those in the general population to have neurologic or genetic conditions.
Based on a cutoff score of 48, autistic children had more than double the odds of sleep problems, compared with children in the general population (adjusted odds ratio, 2.37; P = .001) and children with other developmental delays (aOR, 2.12; P = .001).
With a cutoff of 41, ASD children’s odds of sleep problems were 1.45 times greater than the general population (P = .023) and 1.75 times greater than those with developmental delays (P = .001).
But children with developmental delays who displayed autistic characteristics did not have not significantly different prevalence of sleep problems than children with ASD had.
“The phenotypic overlay between children with ASD and children with developmental delay with ASD [characteristics] may explain the similarities in sleep disturbance among these two groups,” the authors wrote. Both groups have “higher rates of obsessive-compulsive symptoms, self-injurious behavior, ADHD symptoms, and developmental and communication impairments” than children with developmental delays without autistic characteristics.
The research was funded by the Centers for Disease Control and Prevention, the National Institutes of Health, and the National Center for Advancing Translational Sciences Colorado Clinical and Translational Science Award. Dr Reynolds consults for Ovid Therapeutics regarding evaluation of sleep severity and improvement in clinical trials. No other authors had disclosures.
SOURCE: Reynolds AM et al. Pediatrics. 2019 Feb. 11. doi: 10.1542/peds.2018-0492.
FROM PEDIATRICS
Key clinical point: Sleeping problems are over twice as common in autistic children than in children in the general population.
Major finding: Children with ASD had 2.37 greater odds of sleep problems than did typically developing children.
Study details: Data from the Children Sleep Habits Questionnaire for 1,987 children, either typically developing, diagnosed with autism spectrum disorder, or diagnosed with other developmental disabilities.
Disclosures: The research was funded by the Centers for Disease Control and Prevention, the National Institutes of Health, and the National Center for Advancing Translational Sciences Colorado Clinical and Translational Science Award. Dr. Reynolds consults for Ovid Therapeutics regarding evaluation of sleep severity and improvement in clinical trials. No other authors had disclosures.
Source: Reynolds AM et al. Pediatrics. 2019 Feb 11. doi: 10.1542/peds.2018-0492.
LGBTQ youth struggle in foster or unstable housing situations
Lesbian, gay, bisexual, transgender, and questioning (LGBTQ) youth living in foster care or unstable housing are at greater risk for mental health problems, victimization, and getting into fights at school, compared with LGBTQ youth in stable housing and heterosexual youth in foster care, reported Laura Baums, PhD, of the University of Texas at Austin and her coauthors.
This was the finding of analyses of nested data of more than 493,000 students aged 10-18 years from the cross-sectional California Healthy Kids Survey for 2013-2015; 13% identified as LGBTQ. The analyses published in Pediatrics showed LGBTQ youth also were overrepresented in those living situations as compared with the general population.
Less than 1% of the overall sample was in foster care, but 30% of those youth identified as LGBTQ. About 4% of the overall sample lived in unstable housing, and 25% of those youth identified as LGBTQ. So the proportion of LGBTQ youth in foster care or unstable housing was two to three times greater than would be expected than the estimates of LGBTQ youth in nationally representative adolescent samples (that is 11%), Dr. Baums and her associates said.
LGBTQ youth in unstable housing reported lower grades, higher substance/alcohol abuse, higher rates of absenteeism, more fights in school, and more victimization, compared with heterosexual youth in unstable housing and LGBTQ youth in stable housing. Both LGBTQ youth in unstable housing and those in foster care reported higher rates of depression and suicidality in the past year, but the rates for depression were not different from LGBTQ youth in stable housing. Furthermore, African American LGBTQ youth in unstable housing showed poorer outcomes than non-Hispanic white LGBTQ youth in unstable housing, they said.
“” concluded Dr. Baums and her associates. “The findings of this study point to the need for care that is affirming and respectful of youth’s sexual orientation and gender identity.”
The authors reported no relevant financial disclosures. The study was funded by a Eunice Kennedy Shriver National Institute of Child Health and Human Development grant and supported by the Communities for Just Schools Fund and the Priscilla Pond Flawn Endowment at the university.
SOURCE: Baum L et al. Pediatrics. 2019 Feb 11. doi: 10.1542/peds.2017-4211.
Lesbian, gay, bisexual, transgender, and questioning (LGBTQ) youth living in foster care or unstable housing are at greater risk for mental health problems, victimization, and getting into fights at school, compared with LGBTQ youth in stable housing and heterosexual youth in foster care, reported Laura Baums, PhD, of the University of Texas at Austin and her coauthors.
This was the finding of analyses of nested data of more than 493,000 students aged 10-18 years from the cross-sectional California Healthy Kids Survey for 2013-2015; 13% identified as LGBTQ. The analyses published in Pediatrics showed LGBTQ youth also were overrepresented in those living situations as compared with the general population.
Less than 1% of the overall sample was in foster care, but 30% of those youth identified as LGBTQ. About 4% of the overall sample lived in unstable housing, and 25% of those youth identified as LGBTQ. So the proportion of LGBTQ youth in foster care or unstable housing was two to three times greater than would be expected than the estimates of LGBTQ youth in nationally representative adolescent samples (that is 11%), Dr. Baums and her associates said.
LGBTQ youth in unstable housing reported lower grades, higher substance/alcohol abuse, higher rates of absenteeism, more fights in school, and more victimization, compared with heterosexual youth in unstable housing and LGBTQ youth in stable housing. Both LGBTQ youth in unstable housing and those in foster care reported higher rates of depression and suicidality in the past year, but the rates for depression were not different from LGBTQ youth in stable housing. Furthermore, African American LGBTQ youth in unstable housing showed poorer outcomes than non-Hispanic white LGBTQ youth in unstable housing, they said.
“” concluded Dr. Baums and her associates. “The findings of this study point to the need for care that is affirming and respectful of youth’s sexual orientation and gender identity.”
The authors reported no relevant financial disclosures. The study was funded by a Eunice Kennedy Shriver National Institute of Child Health and Human Development grant and supported by the Communities for Just Schools Fund and the Priscilla Pond Flawn Endowment at the university.
SOURCE: Baum L et al. Pediatrics. 2019 Feb 11. doi: 10.1542/peds.2017-4211.
Lesbian, gay, bisexual, transgender, and questioning (LGBTQ) youth living in foster care or unstable housing are at greater risk for mental health problems, victimization, and getting into fights at school, compared with LGBTQ youth in stable housing and heterosexual youth in foster care, reported Laura Baums, PhD, of the University of Texas at Austin and her coauthors.
This was the finding of analyses of nested data of more than 493,000 students aged 10-18 years from the cross-sectional California Healthy Kids Survey for 2013-2015; 13% identified as LGBTQ. The analyses published in Pediatrics showed LGBTQ youth also were overrepresented in those living situations as compared with the general population.
Less than 1% of the overall sample was in foster care, but 30% of those youth identified as LGBTQ. About 4% of the overall sample lived in unstable housing, and 25% of those youth identified as LGBTQ. So the proportion of LGBTQ youth in foster care or unstable housing was two to three times greater than would be expected than the estimates of LGBTQ youth in nationally representative adolescent samples (that is 11%), Dr. Baums and her associates said.
LGBTQ youth in unstable housing reported lower grades, higher substance/alcohol abuse, higher rates of absenteeism, more fights in school, and more victimization, compared with heterosexual youth in unstable housing and LGBTQ youth in stable housing. Both LGBTQ youth in unstable housing and those in foster care reported higher rates of depression and suicidality in the past year, but the rates for depression were not different from LGBTQ youth in stable housing. Furthermore, African American LGBTQ youth in unstable housing showed poorer outcomes than non-Hispanic white LGBTQ youth in unstable housing, they said.
“” concluded Dr. Baums and her associates. “The findings of this study point to the need for care that is affirming and respectful of youth’s sexual orientation and gender identity.”
The authors reported no relevant financial disclosures. The study was funded by a Eunice Kennedy Shriver National Institute of Child Health and Human Development grant and supported by the Communities for Just Schools Fund and the Priscilla Pond Flawn Endowment at the university.
SOURCE: Baum L et al. Pediatrics. 2019 Feb 11. doi: 10.1542/peds.2017-4211.
FROM PEDIATRICS
PD-1 blockade plus CD19 CAR T boosts CAR T-cell persistence
SAN DIEGO – Checkpoint inhibition can be used safely and effectively with CD19-directed chimeric antigen receptor (CAR) T-cell therapy in children with relapsed B-cell acute lymphoblastic leukemia (ALL), and it may bolster CAR T-cell effects and persistence, suggest the findings in a series of 14 patients at the Children’s Hospital of Philadelphia.

Combined programmed death-1 (PD-1) blockade and CAR T-cell therapy appeared to have particular benefit in patients with early B-cell recovery and in those with bulky extramedullary disease, Shannon Maude, MD, PhD, reported during a press conference at the annual meeting of the American Society of Hematology.
The patients, aged 4-17 years with heavily pretreated relapsed B-ALL (13 patients) or B lymphoblastic lymphoma (1 patient), were treated with CD19-directed CAR T-cell therapy, including CTL019 in 4 patients and CTL119 in 10 patients, followed by pembrolizumab (in 13 patients) or nivolumab (in 1 patient).
Six patients received the combination therapy because of early B-cell recovery after initial CAR T-cell infusion, four patients had relapsed or refractory (R/R) bulky extramedullary disease, and four patients had failed to respond or relapsed after initial CAR T-cell therapy.
Three of the six with poor persistence of response reestablished B-cell aplasia (a reflection of CAR T-cell function) after reinfusion of the CAR T-cell product followed by infusion with PD-1 blockade, and they have “sustained CR [complete response] with B-cell aplasia, showing continued persistence of their CAR T cells,” said Dr. Maude, an attending physician in the Cancer Center at Children’s Hospital of Philadelphia.
Of the four patients with R/R bulky extramedullary disease, two patients had a partial response and two patients had CR, she said, explaining that it was hypothesized that the “PD-1 checkpoint pathway may be activated through the microenvironment in that extramedullary situation.”
However, all four patients who had partial or no response to initial CAR T-cell therapy progressed after PD-1 administration, she said, noting that “in one patient, this progression was marked by reduced CD19 expression, which was probably the mode of escape from CD19 CAR T cells.”
Prior studies have shown that patients who respond to CAR T-cell therapy have persistence of CD19 CAR T cells, whereas those with loss of CD19 CAR T cells within 6 months of infusion have a higher rate of relapse, Dr. Maude explained.
“Our hypothesis was that T cells, upon activation, may become exhausted through activation of immune checkpoint pathways, that one such pathway – PD-1 – may be involved in early loss of CD19 CAR T cells and therefore that the combination [of CD19 CAR T-cell therapy] with PD-1 checkpoint blockade may improve the function of the CAR T cells and their persistence,” she said.
The combined approach was well tolerated in this study, she said, noting that mild cytokine release syndrome symptoms and fever typical of CAR T-cell proliferative responses were observed in three patients within 2 days of starting pembrolizumab.
Other adverse effects associated with PD-1 inhibition, including acute pancreatitis, hypothyroidism, arthralgias, and urticaria, occurred in one patient each. There were four cases of grade 3-4 cytopenias that were deemed tolerable or reversible upon discontinuation.
“We show that PD-1 checkpoint inhibitors can be safely combined with CD19 CAR T-cell therapy and that this mechanism may be useful to improve CAR T-cell persistence,” Dr. Maude said.
These findings, which showed particular benefit in patients with poor persistence marked by early B-cell recovery and in those with R/R bulky extramedullary disease, should help inform future use of checkpoint inhibitors after CAR T-cell therapy, she added.
Dr. Maude reported financial ties to Novartis.
SOURCE: Li AM et al. ASH 2018, Abstract 556.
SAN DIEGO – Checkpoint inhibition can be used safely and effectively with CD19-directed chimeric antigen receptor (CAR) T-cell therapy in children with relapsed B-cell acute lymphoblastic leukemia (ALL), and it may bolster CAR T-cell effects and persistence, suggest the findings in a series of 14 patients at the Children’s Hospital of Philadelphia.
Combined programmed death-1 (PD-1) blockade and CAR T-cell therapy appeared to have particular benefit in patients with early B-cell recovery and in those with bulky extramedullary disease, Shannon Maude, MD, PhD, reported during a press conference at the annual meeting of the American Society of Hematology.
The patients, aged 4-17 years with heavily pretreated relapsed B-ALL (13 patients) or B lymphoblastic lymphoma (1 patient), were treated with CD19-directed CAR T-cell therapy, including CTL019 in 4 patients and CTL119 in 10 patients, followed by pembrolizumab (in 13 patients) or nivolumab (in 1 patient).
Six patients received the combination therapy because of early B-cell recovery after initial CAR T-cell infusion, four patients had relapsed or refractory (R/R) bulky extramedullary disease, and four patients had failed to respond or relapsed after initial CAR T-cell therapy.
Three of the six with poor persistence of response reestablished B-cell aplasia (a reflection of CAR T-cell function) after reinfusion of the CAR T-cell product followed by infusion with PD-1 blockade, and they have “sustained CR [complete response] with B-cell aplasia, showing continued persistence of their CAR T cells,” said Dr. Maude, an attending physician in the Cancer Center at Children’s Hospital of Philadelphia.
Of the four patients with R/R bulky extramedullary disease, two patients had a partial response and two patients had CR, she said, explaining that it was hypothesized that the “PD-1 checkpoint pathway may be activated through the microenvironment in that extramedullary situation.”
However, all four patients who had partial or no response to initial CAR T-cell therapy progressed after PD-1 administration, she said, noting that “in one patient, this progression was marked by reduced CD19 expression, which was probably the mode of escape from CD19 CAR T cells.”
Prior studies have shown that patients who respond to CAR T-cell therapy have persistence of CD19 CAR T cells, whereas those with loss of CD19 CAR T cells within 6 months of infusion have a higher rate of relapse, Dr. Maude explained.
“Our hypothesis was that T cells, upon activation, may become exhausted through activation of immune checkpoint pathways, that one such pathway – PD-1 – may be involved in early loss of CD19 CAR T cells and therefore that the combination [of CD19 CAR T-cell therapy] with PD-1 checkpoint blockade may improve the function of the CAR T cells and their persistence,” she said.
The combined approach was well tolerated in this study, she said, noting that mild cytokine release syndrome symptoms and fever typical of CAR T-cell proliferative responses were observed in three patients within 2 days of starting pembrolizumab.
Other adverse effects associated with PD-1 inhibition, including acute pancreatitis, hypothyroidism, arthralgias, and urticaria, occurred in one patient each. There were four cases of grade 3-4 cytopenias that were deemed tolerable or reversible upon discontinuation.
“We show that PD-1 checkpoint inhibitors can be safely combined with CD19 CAR T-cell therapy and that this mechanism may be useful to improve CAR T-cell persistence,” Dr. Maude said.
These findings, which showed particular benefit in patients with poor persistence marked by early B-cell recovery and in those with R/R bulky extramedullary disease, should help inform future use of checkpoint inhibitors after CAR T-cell therapy, she added.
Dr. Maude reported financial ties to Novartis.
SOURCE: Li AM et al. ASH 2018, Abstract 556.
SAN DIEGO – Checkpoint inhibition can be used safely and effectively with CD19-directed chimeric antigen receptor (CAR) T-cell therapy in children with relapsed B-cell acute lymphoblastic leukemia (ALL), and it may bolster CAR T-cell effects and persistence, suggest the findings in a series of 14 patients at the Children’s Hospital of Philadelphia.
Combined programmed death-1 (PD-1) blockade and CAR T-cell therapy appeared to have particular benefit in patients with early B-cell recovery and in those with bulky extramedullary disease, Shannon Maude, MD, PhD, reported during a press conference at the annual meeting of the American Society of Hematology.
The patients, aged 4-17 years with heavily pretreated relapsed B-ALL (13 patients) or B lymphoblastic lymphoma (1 patient), were treated with CD19-directed CAR T-cell therapy, including CTL019 in 4 patients and CTL119 in 10 patients, followed by pembrolizumab (in 13 patients) or nivolumab (in 1 patient).
Six patients received the combination therapy because of early B-cell recovery after initial CAR T-cell infusion, four patients had relapsed or refractory (R/R) bulky extramedullary disease, and four patients had failed to respond or relapsed after initial CAR T-cell therapy.
Three of the six with poor persistence of response reestablished B-cell aplasia (a reflection of CAR T-cell function) after reinfusion of the CAR T-cell product followed by infusion with PD-1 blockade, and they have “sustained CR [complete response] with B-cell aplasia, showing continued persistence of their CAR T cells,” said Dr. Maude, an attending physician in the Cancer Center at Children’s Hospital of Philadelphia.
Of the four patients with R/R bulky extramedullary disease, two patients had a partial response and two patients had CR, she said, explaining that it was hypothesized that the “PD-1 checkpoint pathway may be activated through the microenvironment in that extramedullary situation.”
However, all four patients who had partial or no response to initial CAR T-cell therapy progressed after PD-1 administration, she said, noting that “in one patient, this progression was marked by reduced CD19 expression, which was probably the mode of escape from CD19 CAR T cells.”
Prior studies have shown that patients who respond to CAR T-cell therapy have persistence of CD19 CAR T cells, whereas those with loss of CD19 CAR T cells within 6 months of infusion have a higher rate of relapse, Dr. Maude explained.
“Our hypothesis was that T cells, upon activation, may become exhausted through activation of immune checkpoint pathways, that one such pathway – PD-1 – may be involved in early loss of CD19 CAR T cells and therefore that the combination [of CD19 CAR T-cell therapy] with PD-1 checkpoint blockade may improve the function of the CAR T cells and their persistence,” she said.
The combined approach was well tolerated in this study, she said, noting that mild cytokine release syndrome symptoms and fever typical of CAR T-cell proliferative responses were observed in three patients within 2 days of starting pembrolizumab.
Other adverse effects associated with PD-1 inhibition, including acute pancreatitis, hypothyroidism, arthralgias, and urticaria, occurred in one patient each. There were four cases of grade 3-4 cytopenias that were deemed tolerable or reversible upon discontinuation.
“We show that PD-1 checkpoint inhibitors can be safely combined with CD19 CAR T-cell therapy and that this mechanism may be useful to improve CAR T-cell persistence,” Dr. Maude said.
These findings, which showed particular benefit in patients with poor persistence marked by early B-cell recovery and in those with R/R bulky extramedullary disease, should help inform future use of checkpoint inhibitors after CAR T-cell therapy, she added.
Dr. Maude reported financial ties to Novartis.
SOURCE: Li AM et al. ASH 2018, Abstract 556.
REPORTING FROM ASH 2018
Key clinical point: Major finding: Three of six patients with poor CAR T-cell persistence had a complete response after treatment with the combination therapy. Study details: A clinical study of 14 patients with relapsed B-ALL.
Disclosures: Dr. Maude reported financial relationships with Novartis.
Source: Li AM et al. ASH 2018, Abstract 556.
What is your diagnosis?
It most commonly affects young girls. The pathogenesis of LAHS is thought to involve a sporadic, autosomal dominant mutation that leads to a defect between the hair cuticle and the inner root sheath.1 This defect results in the hair being poorly anchored to the scalp, and therefore easily and painlessly plucked or lost during normal hair care.

The classic presentation of LAHS is that of hair thinning and hair that may be unruly and/or lackluster; the hair rarely, if ever, requires cutting.2 The key feature is the ability to easily and painlessly pluck hairs from the patient’s scalp. The affected area is limited to the scalp, and loss of eyebrows, eyelashes, and body hair should not be seen.
Diagnosis and consideration of the differential
The diagnosis of LAHS can in some cases be made on history and physical exam alone. Patients with LAHS typically will show hair thinning with or without dullness or unruliness. They lack evidence of scalp inflammation, such as erythema, scale, pruritus, and pain. Areas of hair thinning or aberration are typically not well demarcated, and there are typically not areas of complete hair loss. There is no scarring or atrophy of the scalp itself.

Diagnostic tests include the “hair pull test,” as well as trichogram testing. In the “hair pull test” a provider grasps a set of hair at the proximal shaft near the scalp. The traction applied should result in the painless and easy extraction of more than 10% of grasped hairs in a patient with LAHS. Removal of less than 10% of hair is a normal finding, as patients without LAHS typically have about 10% of their scalp hair in the telogen phase at any given time, which would result in removal during the hair pull test.3 In trichography, plucked hairs are examined under magnification, with or without the use of selective dyes. Cinnamaldehyde is a dye that stains citrulline, which is abundant in the inner root sheath, and can be a tool in identifying its presence and/or aberrations.4 A trichogram of the pulled hairs in a patient with LAHS may classically show ruffled appearance of the cuticle, misshapen anagen hair bulbs, and absence of the inner root sheath.5 Examination under magnification also allows providers to better identify telogen versus anagen hairs, which aids in the diagnosis. By carefully considering the patient history, physical exam, and results of additional hair tests, providers can make the diagnosis of LAHS and avoid unnecessary blood work and invasive procedures like scalp biopsies.
The differential diagnosis of hair loss frequently includes alopecia areata. However, in alopecia areata, patients typically have sharply demarcated areas of hair loss, which may involve the eyebrows, eyelids, and body hairs. In alopecia areata, providers may be able to identify the “exclamation point sign” in which the hair shaft thins proximally, leading to the appearance of more pigmented, thicker hairs floating above the scalp.
Telogen effluvium is a condition in which a medical illness or stress, such as systemic illness, surgery, severe emotional distress, childbirth, dietary changes, or another traumatic event, causes a disruption in the natural cycle of hair growth such that the percentage of hairs in the telogen phase increases from about 10% to up to 70%.6 Unlike in LAHS, in which shed hairs are in the anagen phase, the hair that is shed in telogen effluvium is in the telogen phase and will have a different appearance when magnified.
Anagen effluvium, loss of hairs in their growing phase, is typically associated with chemotherapy. The hairs become broken and fractured at the shaft leading to breakage at different points throughout the scalp. Affected areas can include the eyebrows, eyelashes, and body hair. In the absence of a history of administration of a chemotherapy agent (or other drug known to trigger hair loss), the diagnosis of anagen effluvium should not be made.
Patients with trichotillosis (also known as trichotillomania) present with areas of hair loss caused by intentional or subconscious hair pulling. It is considered a psychological condition that can be associated with obsessive compulsive disorder, although the presence of a secondary psychological diagnosis is not required. Providers may see irregular geometric shapes of hair loss, and on close inspection see broken hair shafts of different lengths. Patients most often pull hair from their scalps (over 70% of patients), but also can pull eyelashes, eyebrow hairs, and pubic hairs.7
Treatment
LAHS is self-limited and does not necessitate treatment. However, if patients or parents feel there is significant disease burden, perhaps with poor effects on quality of life or with psychosocial impairment, treatment with minoxidil 5% solution has been studied with some success reported in the literature.1,8,9
Ms. Natsis is a medical student at the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Ms. Natsis and Dr. Eichenfield had no relevant financial disclosures. Email them at pdnews@mdedge.com.
References
1. Arch Dermatol. 2002;138(4):501-6.
2. Int J Trichology. 2010;2(2):96-100.
3. Pediatric Dermatol. 2016:33(50):507-10.
4. Dermatol Clin. 1986;14:745-51.
5. Arch Dermatol. 2009;145(10):1123-8.
6. J Clin Diagn Res. 2015;9(9):WE01-3.
7. Am J Psychiatry. 2016;173(9):868-74.
8. Australas J Dermatol. 2018;59:e286-e287.
9. Pediatr Dermatol. 2014;31:389-90.
It most commonly affects young girls. The pathogenesis of LAHS is thought to involve a sporadic, autosomal dominant mutation that leads to a defect between the hair cuticle and the inner root sheath.1 This defect results in the hair being poorly anchored to the scalp, and therefore easily and painlessly plucked or lost during normal hair care.
The classic presentation of LAHS is that of hair thinning and hair that may be unruly and/or lackluster; the hair rarely, if ever, requires cutting.2 The key feature is the ability to easily and painlessly pluck hairs from the patient’s scalp. The affected area is limited to the scalp, and loss of eyebrows, eyelashes, and body hair should not be seen.
Diagnosis and consideration of the differential
The diagnosis of LAHS can in some cases be made on history and physical exam alone. Patients with LAHS typically will show hair thinning with or without dullness or unruliness. They lack evidence of scalp inflammation, such as erythema, scale, pruritus, and pain. Areas of hair thinning or aberration are typically not well demarcated, and there are typically not areas of complete hair loss. There is no scarring or atrophy of the scalp itself.
Diagnostic tests include the “hair pull test,” as well as trichogram testing. In the “hair pull test” a provider grasps a set of hair at the proximal shaft near the scalp. The traction applied should result in the painless and easy extraction of more than 10% of grasped hairs in a patient with LAHS. Removal of less than 10% of hair is a normal finding, as patients without LAHS typically have about 10% of their scalp hair in the telogen phase at any given time, which would result in removal during the hair pull test.3 In trichography, plucked hairs are examined under magnification, with or without the use of selective dyes. Cinnamaldehyde is a dye that stains citrulline, which is abundant in the inner root sheath, and can be a tool in identifying its presence and/or aberrations.4 A trichogram of the pulled hairs in a patient with LAHS may classically show ruffled appearance of the cuticle, misshapen anagen hair bulbs, and absence of the inner root sheath.5 Examination under magnification also allows providers to better identify telogen versus anagen hairs, which aids in the diagnosis. By carefully considering the patient history, physical exam, and results of additional hair tests, providers can make the diagnosis of LAHS and avoid unnecessary blood work and invasive procedures like scalp biopsies.
The differential diagnosis of hair loss frequently includes alopecia areata. However, in alopecia areata, patients typically have sharply demarcated areas of hair loss, which may involve the eyebrows, eyelids, and body hairs. In alopecia areata, providers may be able to identify the “exclamation point sign” in which the hair shaft thins proximally, leading to the appearance of more pigmented, thicker hairs floating above the scalp.
Telogen effluvium is a condition in which a medical illness or stress, such as systemic illness, surgery, severe emotional distress, childbirth, dietary changes, or another traumatic event, causes a disruption in the natural cycle of hair growth such that the percentage of hairs in the telogen phase increases from about 10% to up to 70%.6 Unlike in LAHS, in which shed hairs are in the anagen phase, the hair that is shed in telogen effluvium is in the telogen phase and will have a different appearance when magnified.
Anagen effluvium, loss of hairs in their growing phase, is typically associated with chemotherapy. The hairs become broken and fractured at the shaft leading to breakage at different points throughout the scalp. Affected areas can include the eyebrows, eyelashes, and body hair. In the absence of a history of administration of a chemotherapy agent (or other drug known to trigger hair loss), the diagnosis of anagen effluvium should not be made.
Patients with trichotillosis (also known as trichotillomania) present with areas of hair loss caused by intentional or subconscious hair pulling. It is considered a psychological condition that can be associated with obsessive compulsive disorder, although the presence of a secondary psychological diagnosis is not required. Providers may see irregular geometric shapes of hair loss, and on close inspection see broken hair shafts of different lengths. Patients most often pull hair from their scalps (over 70% of patients), but also can pull eyelashes, eyebrow hairs, and pubic hairs.7
Treatment
LAHS is self-limited and does not necessitate treatment. However, if patients or parents feel there is significant disease burden, perhaps with poor effects on quality of life or with psychosocial impairment, treatment with minoxidil 5% solution has been studied with some success reported in the literature.1,8,9
Ms. Natsis is a medical student at the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Ms. Natsis and Dr. Eichenfield had no relevant financial disclosures. Email them at pdnews@mdedge.com.
References
1. Arch Dermatol. 2002;138(4):501-6.
2. Int J Trichology. 2010;2(2):96-100.
3. Pediatric Dermatol. 2016:33(50):507-10.
4. Dermatol Clin. 1986;14:745-51.
5. Arch Dermatol. 2009;145(10):1123-8.
6. J Clin Diagn Res. 2015;9(9):WE01-3.
7. Am J Psychiatry. 2016;173(9):868-74.
8. Australas J Dermatol. 2018;59:e286-e287.
9. Pediatr Dermatol. 2014;31:389-90.
It most commonly affects young girls. The pathogenesis of LAHS is thought to involve a sporadic, autosomal dominant mutation that leads to a defect between the hair cuticle and the inner root sheath.1 This defect results in the hair being poorly anchored to the scalp, and therefore easily and painlessly plucked or lost during normal hair care.
The classic presentation of LAHS is that of hair thinning and hair that may be unruly and/or lackluster; the hair rarely, if ever, requires cutting.2 The key feature is the ability to easily and painlessly pluck hairs from the patient’s scalp. The affected area is limited to the scalp, and loss of eyebrows, eyelashes, and body hair should not be seen.
Diagnosis and consideration of the differential
The diagnosis of LAHS can in some cases be made on history and physical exam alone. Patients with LAHS typically will show hair thinning with or without dullness or unruliness. They lack evidence of scalp inflammation, such as erythema, scale, pruritus, and pain. Areas of hair thinning or aberration are typically not well demarcated, and there are typically not areas of complete hair loss. There is no scarring or atrophy of the scalp itself.
Diagnostic tests include the “hair pull test,” as well as trichogram testing. In the “hair pull test” a provider grasps a set of hair at the proximal shaft near the scalp. The traction applied should result in the painless and easy extraction of more than 10% of grasped hairs in a patient with LAHS. Removal of less than 10% of hair is a normal finding, as patients without LAHS typically have about 10% of their scalp hair in the telogen phase at any given time, which would result in removal during the hair pull test.3 In trichography, plucked hairs are examined under magnification, with or without the use of selective dyes. Cinnamaldehyde is a dye that stains citrulline, which is abundant in the inner root sheath, and can be a tool in identifying its presence and/or aberrations.4 A trichogram of the pulled hairs in a patient with LAHS may classically show ruffled appearance of the cuticle, misshapen anagen hair bulbs, and absence of the inner root sheath.5 Examination under magnification also allows providers to better identify telogen versus anagen hairs, which aids in the diagnosis. By carefully considering the patient history, physical exam, and results of additional hair tests, providers can make the diagnosis of LAHS and avoid unnecessary blood work and invasive procedures like scalp biopsies.
The differential diagnosis of hair loss frequently includes alopecia areata. However, in alopecia areata, patients typically have sharply demarcated areas of hair loss, which may involve the eyebrows, eyelids, and body hairs. In alopecia areata, providers may be able to identify the “exclamation point sign” in which the hair shaft thins proximally, leading to the appearance of more pigmented, thicker hairs floating above the scalp.
Telogen effluvium is a condition in which a medical illness or stress, such as systemic illness, surgery, severe emotional distress, childbirth, dietary changes, or another traumatic event, causes a disruption in the natural cycle of hair growth such that the percentage of hairs in the telogen phase increases from about 10% to up to 70%.6 Unlike in LAHS, in which shed hairs are in the anagen phase, the hair that is shed in telogen effluvium is in the telogen phase and will have a different appearance when magnified.
Anagen effluvium, loss of hairs in their growing phase, is typically associated with chemotherapy. The hairs become broken and fractured at the shaft leading to breakage at different points throughout the scalp. Affected areas can include the eyebrows, eyelashes, and body hair. In the absence of a history of administration of a chemotherapy agent (or other drug known to trigger hair loss), the diagnosis of anagen effluvium should not be made.
Patients with trichotillosis (also known as trichotillomania) present with areas of hair loss caused by intentional or subconscious hair pulling. It is considered a psychological condition that can be associated with obsessive compulsive disorder, although the presence of a secondary psychological diagnosis is not required. Providers may see irregular geometric shapes of hair loss, and on close inspection see broken hair shafts of different lengths. Patients most often pull hair from their scalps (over 70% of patients), but also can pull eyelashes, eyebrow hairs, and pubic hairs.7
Treatment
LAHS is self-limited and does not necessitate treatment. However, if patients or parents feel there is significant disease burden, perhaps with poor effects on quality of life or with psychosocial impairment, treatment with minoxidil 5% solution has been studied with some success reported in the literature.1,8,9
Ms. Natsis is a medical student at the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Ms. Natsis and Dr. Eichenfield had no relevant financial disclosures. Email them at pdnews@mdedge.com.
References
1. Arch Dermatol. 2002;138(4):501-6.
2. Int J Trichology. 2010;2(2):96-100.
3. Pediatric Dermatol. 2016:33(50):507-10.
4. Dermatol Clin. 1986;14:745-51.
5. Arch Dermatol. 2009;145(10):1123-8.
6. J Clin Diagn Res. 2015;9(9):WE01-3.
7. Am J Psychiatry. 2016;173(9):868-74.
8. Australas J Dermatol. 2018;59:e286-e287.
9. Pediatr Dermatol. 2014;31:389-90.
A 5-year-old female is brought to clinic for hair loss. The mother reports that when styling her daughter's hair, she has noticed areas of hair thinning, especially at the temples and at the occiput. The mother denies scale, pruritus, and erythema. The patient reports that her scalp does not hurt. She has never had a haircut because her hair hasn't grown long enough to cut. There is no history of specific bald spots. The patient has no personal history of psoriasis, seborrheic dermatitis, or autoimmune disease. No picking has been noted, and there is no history of compulsive behaviors or anxiety. The patient's mother has a history of Graves disease. The mother reports that the patient's older sister may have had hair thinning when she was younger as well, but no longer has thin hair.

The patient was previously seen by another provider who prescribed hydrocortisone 2.5% ointment, which the mother has been applying nightly without improvement.
The child is otherwise medically well and thriving, with no recent change in activity level and with growth parameters consistently around the 75th percentile for height and weight. On physical exam, the patient has blondish, fine hair with areas of poorly demarcated hair thinning at the left temple and at the occiput. The hair remaining at the occiput is normal in texture. There are no areas of complete hair loss. There is no scale, erythema, or abnormal pigmentation, and no cervical or occipital adenopathy. The patient has intact eyebrows and eyelashes.