User login
Heavy menstrual bleeding in teens often linked to bleeding disorders
Over one-third of adolescents presenting with heavy menstrual bleeding were diagnosed with a bleeding disorder after screening, according to results of a retrospective study.

The high incidence of bleeding disorders detected argues for routine screening of adolescents with heavy menstrual bleeding (HMB), Brooke O’Brien, MD, of the University of Queensland, Brisbane, Australia, and her colleagues wrote in the Journal of Pediatric & Adolescent Gynecology.
“These findings support comprehensive and systematic hemostatic evaluation in adolescents with HMB,” Dr. O’Brien and her colleagues wrote. “A higher level of awareness of bleeding disorders as a cause for HMB in adolescence, especially [von Willebrand disease] and platelet function disorders, is needed and close multidisciplinary collaboration between the pediatric and adolescent gynecologist and hematologist in a specialized tertiary center should be established in the management of these patients.”
In their study, Dr. O’Brien and her colleagues retrospectively evaluated 124 adolescents with HMB at a pediatric and adolescent gynecology tertiary care center between July 2007 and July 2017. Of these, 77 patients (62.1%) underwent screening for blood disorders.
The researchers found 27 adolescents overall were diagnosed with a blood disorder, which consisted of 35.0% of patients screened and 21.7% of all patients studied. Specifically, 14 of 27 patients (51.6%) screened were diagnosed with von Willebrand disease, 9 of 27 patients (33.3%) screened were found to have inherited platelet function disorders, 3 of 27 patients (11.1%) had inherited or acquired thrombocytopenia, and 1 of 27 patients (3.7%) had factor IX deficiency. The researchers also screened for iron deficiency and/or anemia and found 53 of 107 patients (49.5%) who were screened received a diagnosis, and 19 of 27 patients (70.3%) who were diagnosed with a bleeding disorder also had iron deficiency and/or anemia.
“In adolescents who are already known to have a bleeding disorder, consultation with a pediatric gynecologist and/or hematologist prior to menarche may be helpful to outline abnormal patterns of menstrual bleeding and to discuss options of treatment in the event of heavy menstrual bleeding,” Dr. O’Brien and her colleagues wrote.
Potential limitations in the study include the refractory nature of referrals at a tertiary care center potentially overestimating the prevalence of HMB in this population as well as the study’s retrospective design when investigating and measuring heavy menstrual bleeding, but researchers noted patients were reviewed and classified by a specialist pediatric hematologist.
The authors reported no relevant conflicts of interest.
SOURCE: O’Brien B et al. J Pediatr Adolesc Gynecol. 2018 Nov 22. doi: 10.1016/j.jpag.2018.11.005.
Over one-third of adolescents presenting with heavy menstrual bleeding were diagnosed with a bleeding disorder after screening, according to results of a retrospective study.
The high incidence of bleeding disorders detected argues for routine screening of adolescents with heavy menstrual bleeding (HMB), Brooke O’Brien, MD, of the University of Queensland, Brisbane, Australia, and her colleagues wrote in the Journal of Pediatric & Adolescent Gynecology.
“These findings support comprehensive and systematic hemostatic evaluation in adolescents with HMB,” Dr. O’Brien and her colleagues wrote. “A higher level of awareness of bleeding disorders as a cause for HMB in adolescence, especially [von Willebrand disease] and platelet function disorders, is needed and close multidisciplinary collaboration between the pediatric and adolescent gynecologist and hematologist in a specialized tertiary center should be established in the management of these patients.”
In their study, Dr. O’Brien and her colleagues retrospectively evaluated 124 adolescents with HMB at a pediatric and adolescent gynecology tertiary care center between July 2007 and July 2017. Of these, 77 patients (62.1%) underwent screening for blood disorders.
The researchers found 27 adolescents overall were diagnosed with a blood disorder, which consisted of 35.0% of patients screened and 21.7% of all patients studied. Specifically, 14 of 27 patients (51.6%) screened were diagnosed with von Willebrand disease, 9 of 27 patients (33.3%) screened were found to have inherited platelet function disorders, 3 of 27 patients (11.1%) had inherited or acquired thrombocytopenia, and 1 of 27 patients (3.7%) had factor IX deficiency. The researchers also screened for iron deficiency and/or anemia and found 53 of 107 patients (49.5%) who were screened received a diagnosis, and 19 of 27 patients (70.3%) who were diagnosed with a bleeding disorder also had iron deficiency and/or anemia.
“In adolescents who are already known to have a bleeding disorder, consultation with a pediatric gynecologist and/or hematologist prior to menarche may be helpful to outline abnormal patterns of menstrual bleeding and to discuss options of treatment in the event of heavy menstrual bleeding,” Dr. O’Brien and her colleagues wrote.
Potential limitations in the study include the refractory nature of referrals at a tertiary care center potentially overestimating the prevalence of HMB in this population as well as the study’s retrospective design when investigating and measuring heavy menstrual bleeding, but researchers noted patients were reviewed and classified by a specialist pediatric hematologist.
The authors reported no relevant conflicts of interest.
SOURCE: O’Brien B et al. J Pediatr Adolesc Gynecol. 2018 Nov 22. doi: 10.1016/j.jpag.2018.11.005.
Over one-third of adolescents presenting with heavy menstrual bleeding were diagnosed with a bleeding disorder after screening, according to results of a retrospective study.
The high incidence of bleeding disorders detected argues for routine screening of adolescents with heavy menstrual bleeding (HMB), Brooke O’Brien, MD, of the University of Queensland, Brisbane, Australia, and her colleagues wrote in the Journal of Pediatric & Adolescent Gynecology.
“These findings support comprehensive and systematic hemostatic evaluation in adolescents with HMB,” Dr. O’Brien and her colleagues wrote. “A higher level of awareness of bleeding disorders as a cause for HMB in adolescence, especially [von Willebrand disease] and platelet function disorders, is needed and close multidisciplinary collaboration between the pediatric and adolescent gynecologist and hematologist in a specialized tertiary center should be established in the management of these patients.”
In their study, Dr. O’Brien and her colleagues retrospectively evaluated 124 adolescents with HMB at a pediatric and adolescent gynecology tertiary care center between July 2007 and July 2017. Of these, 77 patients (62.1%) underwent screening for blood disorders.
The researchers found 27 adolescents overall were diagnosed with a blood disorder, which consisted of 35.0% of patients screened and 21.7% of all patients studied. Specifically, 14 of 27 patients (51.6%) screened were diagnosed with von Willebrand disease, 9 of 27 patients (33.3%) screened were found to have inherited platelet function disorders, 3 of 27 patients (11.1%) had inherited or acquired thrombocytopenia, and 1 of 27 patients (3.7%) had factor IX deficiency. The researchers also screened for iron deficiency and/or anemia and found 53 of 107 patients (49.5%) who were screened received a diagnosis, and 19 of 27 patients (70.3%) who were diagnosed with a bleeding disorder also had iron deficiency and/or anemia.
“In adolescents who are already known to have a bleeding disorder, consultation with a pediatric gynecologist and/or hematologist prior to menarche may be helpful to outline abnormal patterns of menstrual bleeding and to discuss options of treatment in the event of heavy menstrual bleeding,” Dr. O’Brien and her colleagues wrote.
Potential limitations in the study include the refractory nature of referrals at a tertiary care center potentially overestimating the prevalence of HMB in this population as well as the study’s retrospective design when investigating and measuring heavy menstrual bleeding, but researchers noted patients were reviewed and classified by a specialist pediatric hematologist.
The authors reported no relevant conflicts of interest.
SOURCE: O’Brien B et al. J Pediatr Adolesc Gynecol. 2018 Nov 22. doi: 10.1016/j.jpag.2018.11.005.
FROM THE JOURNAL OF PEDIATRIC & ADOLESCENT GYNECOLOGY
Key clinical point: More than one-third of adolescents with heavy menstrual bleeding were diagnosed with a bleeding disorder.
Major finding: After screening, 35% of women with heavy menstrual bleeding had a bleeding disorder; over half of those screened had von Willebrand disease.
Study details: A retrospective study of 124 adolescents at the Queensland Paediatric and Adolescent Gynaecology Service between July 2007 and July 2017.
Disclosures: The authors reported no relevant conflicts of interest.
Source: O’Brien B et al. J Pediatr Adolesc Gynecol. 2018 Nov 22 . doi: 10.1016/j.jpag.2018.11.005.
Teenagers with epilepsy may benefit from depression screening
NEW ORLEANS – Referral to a mental health provider is adequate for most patients with moderately severe symptoms of depression, but some patients may require active intervention during the clinical visit, said the researchers.
“We know that depression is more common in people with epilepsy, compared to the general population, but there is less information about depression in children and teens than adults, and little is known about the factors that increase the likelihood of depressive symptoms,” said Hillary Thomas, PhD, a pediatric psychologist at Children’s Medical Center in Dallas. “Depression screening should be routine at epilepsy treatment centers and can identify children and teens who would benefit from intervention.”
Following 2015 guidelines from the American Academy of Neurology, the Comprehensive Epilepsy Center at Children’s Health System in Dallas developed a behavioral health screening protocol for teens with epilepsy. The center aims to identify patients with depressive symptoms and ensure that they are referred to appropriate behavioral health practitioners. Clinicians also review the screening data and seizure variables for their potential implications for clinical care. Researchers at the center also seek to elucidate the relationship between depressive symptoms and seizure diagnosis and treatment.
As part of the protocol, Dr. Thomas and her colleagues administer the Patient Health Questionnaire-9 (adolescent version) to all patients aged 15-18 years during their visit to the epilepsy clinic. Patients with intellectual disability or other factors that prevent them from providing valid responses are excluded. If a patient’s PHQ-9 score indicates at least moderately severe depressive symptoms, or if he or she reports suicidal ideation, clinicians follow a specific response protocol that includes providing referrals, encouraging follow-up with the patient’s current mental health provider, and obtaining a suicide risk assessment from a psychologist or social worker. After the screener is completed, clinicians retrieve demographic and clinical data (e.g., seizure diagnosis, medication, number of clinic or emergency department visits) from the patient’s medical record and include them in a database for subsequent analysis.
Dr. Thomas and her colleagues presented data from 394 youth with epilepsy whom they had screened. Patients’ mean age was 16 years, and half of the population was female. The study population had rates of depression similar to those identified in previous studies, said Dr. Thomas. Approximately 87% of patients had minimal or mild depressive symptoms, and 8% had moderately severe depressive symptoms. Furthermore, 5% of the patients reported suicidal ideation or previous suicide attempt. Several of the patients with suicidal ideation had a current mental health provider, and the others required an in-clinic risk assessment. Overall, 13% of the population required behavioral health referral or intervention. When the researchers conducted chi-squared analysis, they found no significant association between seizure type and depression severity.
“Our results don’t mean that only 13% of the teens with epilepsy had depressive symptoms,” said Susan Arnold, MD, director of the Comprehensive Epilepsy Center and a coauthor of the study. “They indicate the significant percentage of teens whose level of depressive symptoms warranted behavioral health referrals or further evaluation or even intervention during a clinic visit. Health care providers need to be vigilant about continually screening children and teens for depression.” As part of each patient’s comprehensive care, epilepsy treatment centers should provide psychosocial teams that include social workers or psychologists, she added.
The investigators plan to continue analyzing the data for specific depression symptoms that are most common in teens. These symptoms could be the basis for developing additional resources for families, such as lists of warning signs and guides to symptom management, as well as group therapy and support groups.
SOURCE: Thomas HM et al. Abstract 1.388.
NEW ORLEANS – Referral to a mental health provider is adequate for most patients with moderately severe symptoms of depression, but some patients may require active intervention during the clinical visit, said the researchers.
“We know that depression is more common in people with epilepsy, compared to the general population, but there is less information about depression in children and teens than adults, and little is known about the factors that increase the likelihood of depressive symptoms,” said Hillary Thomas, PhD, a pediatric psychologist at Children’s Medical Center in Dallas. “Depression screening should be routine at epilepsy treatment centers and can identify children and teens who would benefit from intervention.”
Following 2015 guidelines from the American Academy of Neurology, the Comprehensive Epilepsy Center at Children’s Health System in Dallas developed a behavioral health screening protocol for teens with epilepsy. The center aims to identify patients with depressive symptoms and ensure that they are referred to appropriate behavioral health practitioners. Clinicians also review the screening data and seizure variables for their potential implications for clinical care. Researchers at the center also seek to elucidate the relationship between depressive symptoms and seizure diagnosis and treatment.
As part of the protocol, Dr. Thomas and her colleagues administer the Patient Health Questionnaire-9 (adolescent version) to all patients aged 15-18 years during their visit to the epilepsy clinic. Patients with intellectual disability or other factors that prevent them from providing valid responses are excluded. If a patient’s PHQ-9 score indicates at least moderately severe depressive symptoms, or if he or she reports suicidal ideation, clinicians follow a specific response protocol that includes providing referrals, encouraging follow-up with the patient’s current mental health provider, and obtaining a suicide risk assessment from a psychologist or social worker. After the screener is completed, clinicians retrieve demographic and clinical data (e.g., seizure diagnosis, medication, number of clinic or emergency department visits) from the patient’s medical record and include them in a database for subsequent analysis.
Dr. Thomas and her colleagues presented data from 394 youth with epilepsy whom they had screened. Patients’ mean age was 16 years, and half of the population was female. The study population had rates of depression similar to those identified in previous studies, said Dr. Thomas. Approximately 87% of patients had minimal or mild depressive symptoms, and 8% had moderately severe depressive symptoms. Furthermore, 5% of the patients reported suicidal ideation or previous suicide attempt. Several of the patients with suicidal ideation had a current mental health provider, and the others required an in-clinic risk assessment. Overall, 13% of the population required behavioral health referral or intervention. When the researchers conducted chi-squared analysis, they found no significant association between seizure type and depression severity.
“Our results don’t mean that only 13% of the teens with epilepsy had depressive symptoms,” said Susan Arnold, MD, director of the Comprehensive Epilepsy Center and a coauthor of the study. “They indicate the significant percentage of teens whose level of depressive symptoms warranted behavioral health referrals or further evaluation or even intervention during a clinic visit. Health care providers need to be vigilant about continually screening children and teens for depression.” As part of each patient’s comprehensive care, epilepsy treatment centers should provide psychosocial teams that include social workers or psychologists, she added.
The investigators plan to continue analyzing the data for specific depression symptoms that are most common in teens. These symptoms could be the basis for developing additional resources for families, such as lists of warning signs and guides to symptom management, as well as group therapy and support groups.
SOURCE: Thomas HM et al. Abstract 1.388.
NEW ORLEANS – Referral to a mental health provider is adequate for most patients with moderately severe symptoms of depression, but some patients may require active intervention during the clinical visit, said the researchers.
“We know that depression is more common in people with epilepsy, compared to the general population, but there is less information about depression in children and teens than adults, and little is known about the factors that increase the likelihood of depressive symptoms,” said Hillary Thomas, PhD, a pediatric psychologist at Children’s Medical Center in Dallas. “Depression screening should be routine at epilepsy treatment centers and can identify children and teens who would benefit from intervention.”
Following 2015 guidelines from the American Academy of Neurology, the Comprehensive Epilepsy Center at Children’s Health System in Dallas developed a behavioral health screening protocol for teens with epilepsy. The center aims to identify patients with depressive symptoms and ensure that they are referred to appropriate behavioral health practitioners. Clinicians also review the screening data and seizure variables for their potential implications for clinical care. Researchers at the center also seek to elucidate the relationship between depressive symptoms and seizure diagnosis and treatment.
As part of the protocol, Dr. Thomas and her colleagues administer the Patient Health Questionnaire-9 (adolescent version) to all patients aged 15-18 years during their visit to the epilepsy clinic. Patients with intellectual disability or other factors that prevent them from providing valid responses are excluded. If a patient’s PHQ-9 score indicates at least moderately severe depressive symptoms, or if he or she reports suicidal ideation, clinicians follow a specific response protocol that includes providing referrals, encouraging follow-up with the patient’s current mental health provider, and obtaining a suicide risk assessment from a psychologist or social worker. After the screener is completed, clinicians retrieve demographic and clinical data (e.g., seizure diagnosis, medication, number of clinic or emergency department visits) from the patient’s medical record and include them in a database for subsequent analysis.
Dr. Thomas and her colleagues presented data from 394 youth with epilepsy whom they had screened. Patients’ mean age was 16 years, and half of the population was female. The study population had rates of depression similar to those identified in previous studies, said Dr. Thomas. Approximately 87% of patients had minimal or mild depressive symptoms, and 8% had moderately severe depressive symptoms. Furthermore, 5% of the patients reported suicidal ideation or previous suicide attempt. Several of the patients with suicidal ideation had a current mental health provider, and the others required an in-clinic risk assessment. Overall, 13% of the population required behavioral health referral or intervention. When the researchers conducted chi-squared analysis, they found no significant association between seizure type and depression severity.
“Our results don’t mean that only 13% of the teens with epilepsy had depressive symptoms,” said Susan Arnold, MD, director of the Comprehensive Epilepsy Center and a coauthor of the study. “They indicate the significant percentage of teens whose level of depressive symptoms warranted behavioral health referrals or further evaluation or even intervention during a clinic visit. Health care providers need to be vigilant about continually screening children and teens for depression.” As part of each patient’s comprehensive care, epilepsy treatment centers should provide psychosocial teams that include social workers or psychologists, she added.
The investigators plan to continue analyzing the data for specific depression symptoms that are most common in teens. These symptoms could be the basis for developing additional resources for families, such as lists of warning signs and guides to symptom management, as well as group therapy and support groups.
SOURCE: Thomas HM et al. Abstract 1.388.
REPORTING FROM AES 2018
Key clinical point: Screening children with epilepsy regularly for depression may be advisable.
Major finding: About 13% of patients screened required referral or intervention.
Study details: Prospective study of 394 patients with epilepsy.
Disclosures: The investigators have no disclosures and received no funding for this study.
Source: Thomas HM et al. Abstract 1.388.
FDA approves congenital CMV diagnostic test
, a new test to be used as an aid in the diagnosis of congenital cytomegalovirus (CMV) in newborns less than 21 days of age.

The Alethia CMV Assay Test System detects CMV DNA from a saliva swab. Results from the test should be used only in conjunction with the results of other diagnostic tests and clinical information, according to an FDA statement.
“This test for detecting the virus, when used in conjunction with the results of other diagnostic tests, may help health care providers more quickly identify the virus in newborns,” said Timothy Stenzel, PhD, director of the Office of In Vitro Diagnostics and Radiological Health in the FDA’s Center for Devices and Radiological Health.
In a prospective clinical study, 1,472 saliva samples out of 1,475 samples collected from newborns were correctly identified by the device as negative for the presence of CMV DNA. Three samples were incorrectly identified as positive when they were negative. Five collected saliva specimens were correctly identified as positive for the presence of CMV DNA.
In a testing of 34 samples of archived specimens from babies known to be infected with CMV, all of the archived specimens were correctly identified by the device as positive for the presence of CMV DNA.
The FDA reviewed the Alethia CMV Assay Test System through a regulatory pathway established for novel, low- to moderate-risk devices. Along with this authorization, the FDA is establishing criteria, called special controls, which determine the requirements for demonstrating accuracy, reliability, and effectiveness of tests intended to be used as an aid in the diagnosis of congenital CMV infection.
With this new regulatory classification, subsequent devices of the same type with the same intended use may go through the FDA’s 510(k) process, whereby devices can obtain marketing authorization by demonstrating substantial equivalence to a previously approved device.
The FDA granted marketing authorization of the Alethia CMV Assay Test System to Meridian Bioscience.
, a new test to be used as an aid in the diagnosis of congenital cytomegalovirus (CMV) in newborns less than 21 days of age.
The Alethia CMV Assay Test System detects CMV DNA from a saliva swab. Results from the test should be used only in conjunction with the results of other diagnostic tests and clinical information, according to an FDA statement.
“This test for detecting the virus, when used in conjunction with the results of other diagnostic tests, may help health care providers more quickly identify the virus in newborns,” said Timothy Stenzel, PhD, director of the Office of In Vitro Diagnostics and Radiological Health in the FDA’s Center for Devices and Radiological Health.
In a prospective clinical study, 1,472 saliva samples out of 1,475 samples collected from newborns were correctly identified by the device as negative for the presence of CMV DNA. Three samples were incorrectly identified as positive when they were negative. Five collected saliva specimens were correctly identified as positive for the presence of CMV DNA.
In a testing of 34 samples of archived specimens from babies known to be infected with CMV, all of the archived specimens were correctly identified by the device as positive for the presence of CMV DNA.
The FDA reviewed the Alethia CMV Assay Test System through a regulatory pathway established for novel, low- to moderate-risk devices. Along with this authorization, the FDA is establishing criteria, called special controls, which determine the requirements for demonstrating accuracy, reliability, and effectiveness of tests intended to be used as an aid in the diagnosis of congenital CMV infection.
With this new regulatory classification, subsequent devices of the same type with the same intended use may go through the FDA’s 510(k) process, whereby devices can obtain marketing authorization by demonstrating substantial equivalence to a previously approved device.
The FDA granted marketing authorization of the Alethia CMV Assay Test System to Meridian Bioscience.
, a new test to be used as an aid in the diagnosis of congenital cytomegalovirus (CMV) in newborns less than 21 days of age.
The Alethia CMV Assay Test System detects CMV DNA from a saliva swab. Results from the test should be used only in conjunction with the results of other diagnostic tests and clinical information, according to an FDA statement.
“This test for detecting the virus, when used in conjunction with the results of other diagnostic tests, may help health care providers more quickly identify the virus in newborns,” said Timothy Stenzel, PhD, director of the Office of In Vitro Diagnostics and Radiological Health in the FDA’s Center for Devices and Radiological Health.
In a prospective clinical study, 1,472 saliva samples out of 1,475 samples collected from newborns were correctly identified by the device as negative for the presence of CMV DNA. Three samples were incorrectly identified as positive when they were negative. Five collected saliva specimens were correctly identified as positive for the presence of CMV DNA.
In a testing of 34 samples of archived specimens from babies known to be infected with CMV, all of the archived specimens were correctly identified by the device as positive for the presence of CMV DNA.
The FDA reviewed the Alethia CMV Assay Test System through a regulatory pathway established for novel, low- to moderate-risk devices. Along with this authorization, the FDA is establishing criteria, called special controls, which determine the requirements for demonstrating accuracy, reliability, and effectiveness of tests intended to be used as an aid in the diagnosis of congenital CMV infection.
With this new regulatory classification, subsequent devices of the same type with the same intended use may go through the FDA’s 510(k) process, whereby devices can obtain marketing authorization by demonstrating substantial equivalence to a previously approved device.
The FDA granted marketing authorization of the Alethia CMV Assay Test System to Meridian Bioscience.
Acute flaccid myelitis has unique MRI features
Acute flaccid myelitis appears to present most commonly as asymmetric weakness after respiratory viral infection and has distinctive MRI features that could help with early diagnosis.
In a paper published in JAMA Pediatrics, researchers presented the results of a retrospective case series of 45 children who were diagnosed between 2012 and 2016 with acute flaccid myelitis, or “pseudo polio,” using the Centers for Disease Control’s case definition.
Matthew J. Elrick, MD, PhD, of Johns Hopkins University, Baltimore, and his coauthors came up with a set of reproducible and distinctive features of acute flaccid myelitis. These were the presence of a prodromal fever or viral syndrome; weakness in a lower motor neuron pattern involving one or more limbs, neck, face, and/or bulbar muscles; supportive evidence either from MRI, nerve conduction studies, or cerebrospinal fluid; and the absence of objective sensory deficits, supratentorial white matter, cortical lesions greater than 1 cm in size, encephalopathy, elevated cerebrospinal fluid without pleocytosis, or any other alternative diagnosis.
The researchers commented that, while the CDC case definition has helped with epidemiologic surveillance of acute flaccid myelitis, it may also pick up children with acute weakness caused by other conditions such as transverse myelitis, Guillain-Barré syndrome, ischemic myelopathy, and other myelopathies.
To identify clinical features that might help differentiate patients with acute flaccid myelitis, the researchers attempted to see how many alternative diagnoses were captured in the CDC case definition.
The patients in their study all presented with acute flaccid paralysis in at least one limb and with either an MRI showing a spinal cord lesion spanning one or more spinal segments but largely restricted to gray matter or pleocytosis of the cerebrospinal fluid. The researchers divided the cases into those who also met a well-defined alternative diagnosis – who they categorized as “acute flaccid myelitis with possible alternative diagnosis” (AFM-ad) – and those who were categorized as “restrictively defined AFM” (rAFM). Overall, 34 patients were classified as rAFM and 11 as AFM-ad.
Those in the rAFD group nearly all had asymmetric onset of symptoms, while those in the AFM-ad group were more likely to experience bilateral onset in their lower extremities, “reflecting the pattern of symptoms often seen in other causes of myelopathy such as transverse myelitis and ischemic injury,” the authors noted.
While both groups often presented with decreased muscle tone and reflexes, this was more likely to evolve to increased tone or hyperreflexia in the AFM-ad group. Patients with AFM-ad were also more likely to experience impaired bowel or bladder function.
On MRI, lesions were mostly or completely restricted to the spinal cord gray matter in patients with rAFM or to involve the dorsal pons. These patients did not have any supratentorial brain lesions.
Patients in the rAFM category also had lower cerebrospinal fluid protein values than those in the AFM-ad category, but this was the only cerebrospinal fluid difference between the two groups.
All patients categorized as having rAFM had an infectious prodrome – such as viral syndrome, fever, congestion, and cough – compared with 63.6% of the patients categorized as AFM-ad. The pathogen was identified in only 13 of the rAFM patients, and included 5 patients with enterovirus D68, 2 with unspecified enterovirus, 2 with rhinovirus, 2 with adenovirus, and 2 with mycoplasma. Of the three patients in the AFM-ad group whose pathogen was identified, one had an untyped rhinovirus/enterovirus and mycoplasma, one had a rhinovirus B, and one had enterovirus D68.
“These results highlight that the CDC case definition, while appropriately sensitive for epidemiologic ascertainment of possible AFM cases, also encompasses other neurologic diseases that can cause acute weakness,” the authors wrote. However, they acknowledged that acute flaccid myelitis was still poorly understood and their own definition of the disease may change as more children are diagnosed.
“We propose that the definition of rAFM presented here be used as a starting point for developing inclusion and exclusion criteria for future research studies of AFM,” they wrote.
The study was supported by Johns Hopkins University, the Bart McLean Fund for Neuroimmunology Research, and Project Restore. Two authors reported funding from private industry outside the submitted work and five reported support from or involvement with research and funding bodies.
SOURCE: Elrick MJ et al. JAMA Pediatr. 2018 Nov 30. doi: 10.1001/jamapediatrics.2018.4890.
Acute flaccid myelitis (AFM) initially presents subtly, complicating its diagnosis. Children present with a rapid onset of weakness that is associated with a febrile illness, which can be respiratory, gastrointestinal, or with symptoms of hand-foot-and-mouth disease. Given the lack of effective treatments, early diagnosis and monitoring are essential for mitigating the risk of respiratory decline and long-term complications.
While patient history and physical examination can provide clues to the presence of AFM, confirming the diagnosis requires lumbar puncture and MRI of the spinal cord. On MRI, diagnostic confirmation will come from findings of longitudinal, butterfly-shaped, anterior horn–predominant T2 and fluid-attenuated inversion recovery hyperintensities of the central gray matter.
Patients with suspected AFM should be hospitalized because they can rapidly deteriorate to the point of respiratory compromise, particularly those with upper extremity and bulbar weakness.
Sarah E. Hopkins, MD, is from the division of neurology at the Children’s Hospital of Philadelphia; Matthew J. Elrick, MD, PhD, is from the department of neurology at Johns Hopkins University, Baltimore; and Kevin Messacar, MD, is from the department of pediatrics at the Children’s Hospital Colorado. These comments are taken from an accompanying viewpoint (JAMA Pediatr. 2018 Nov 30. doi: 10.1001/jamapediatrics.2018.4896). Dr. Messacar reported support from the National Institutes of Health/National Institute of Allergy and Infectious and Dr. Hopkins reported support from the Centers for Disease Control and Prevention.
Acute flaccid myelitis (AFM) initially presents subtly, complicating its diagnosis. Children present with a rapid onset of weakness that is associated with a febrile illness, which can be respiratory, gastrointestinal, or with symptoms of hand-foot-and-mouth disease. Given the lack of effective treatments, early diagnosis and monitoring are essential for mitigating the risk of respiratory decline and long-term complications.
While patient history and physical examination can provide clues to the presence of AFM, confirming the diagnosis requires lumbar puncture and MRI of the spinal cord. On MRI, diagnostic confirmation will come from findings of longitudinal, butterfly-shaped, anterior horn–predominant T2 and fluid-attenuated inversion recovery hyperintensities of the central gray matter.
Patients with suspected AFM should be hospitalized because they can rapidly deteriorate to the point of respiratory compromise, particularly those with upper extremity and bulbar weakness.
Sarah E. Hopkins, MD, is from the division of neurology at the Children’s Hospital of Philadelphia; Matthew J. Elrick, MD, PhD, is from the department of neurology at Johns Hopkins University, Baltimore; and Kevin Messacar, MD, is from the department of pediatrics at the Children’s Hospital Colorado. These comments are taken from an accompanying viewpoint (JAMA Pediatr. 2018 Nov 30. doi: 10.1001/jamapediatrics.2018.4896). Dr. Messacar reported support from the National Institutes of Health/National Institute of Allergy and Infectious and Dr. Hopkins reported support from the Centers for Disease Control and Prevention.
Acute flaccid myelitis (AFM) initially presents subtly, complicating its diagnosis. Children present with a rapid onset of weakness that is associated with a febrile illness, which can be respiratory, gastrointestinal, or with symptoms of hand-foot-and-mouth disease. Given the lack of effective treatments, early diagnosis and monitoring are essential for mitigating the risk of respiratory decline and long-term complications.
While patient history and physical examination can provide clues to the presence of AFM, confirming the diagnosis requires lumbar puncture and MRI of the spinal cord. On MRI, diagnostic confirmation will come from findings of longitudinal, butterfly-shaped, anterior horn–predominant T2 and fluid-attenuated inversion recovery hyperintensities of the central gray matter.
Patients with suspected AFM should be hospitalized because they can rapidly deteriorate to the point of respiratory compromise, particularly those with upper extremity and bulbar weakness.
Sarah E. Hopkins, MD, is from the division of neurology at the Children’s Hospital of Philadelphia; Matthew J. Elrick, MD, PhD, is from the department of neurology at Johns Hopkins University, Baltimore; and Kevin Messacar, MD, is from the department of pediatrics at the Children’s Hospital Colorado. These comments are taken from an accompanying viewpoint (JAMA Pediatr. 2018 Nov 30. doi: 10.1001/jamapediatrics.2018.4896). Dr. Messacar reported support from the National Institutes of Health/National Institute of Allergy and Infectious and Dr. Hopkins reported support from the Centers for Disease Control and Prevention.
Acute flaccid myelitis appears to present most commonly as asymmetric weakness after respiratory viral infection and has distinctive MRI features that could help with early diagnosis.
In a paper published in JAMA Pediatrics, researchers presented the results of a retrospective case series of 45 children who were diagnosed between 2012 and 2016 with acute flaccid myelitis, or “pseudo polio,” using the Centers for Disease Control’s case definition.
Matthew J. Elrick, MD, PhD, of Johns Hopkins University, Baltimore, and his coauthors came up with a set of reproducible and distinctive features of acute flaccid myelitis. These were the presence of a prodromal fever or viral syndrome; weakness in a lower motor neuron pattern involving one or more limbs, neck, face, and/or bulbar muscles; supportive evidence either from MRI, nerve conduction studies, or cerebrospinal fluid; and the absence of objective sensory deficits, supratentorial white matter, cortical lesions greater than 1 cm in size, encephalopathy, elevated cerebrospinal fluid without pleocytosis, or any other alternative diagnosis.
The researchers commented that, while the CDC case definition has helped with epidemiologic surveillance of acute flaccid myelitis, it may also pick up children with acute weakness caused by other conditions such as transverse myelitis, Guillain-Barré syndrome, ischemic myelopathy, and other myelopathies.
To identify clinical features that might help differentiate patients with acute flaccid myelitis, the researchers attempted to see how many alternative diagnoses were captured in the CDC case definition.
The patients in their study all presented with acute flaccid paralysis in at least one limb and with either an MRI showing a spinal cord lesion spanning one or more spinal segments but largely restricted to gray matter or pleocytosis of the cerebrospinal fluid. The researchers divided the cases into those who also met a well-defined alternative diagnosis – who they categorized as “acute flaccid myelitis with possible alternative diagnosis” (AFM-ad) – and those who were categorized as “restrictively defined AFM” (rAFM). Overall, 34 patients were classified as rAFM and 11 as AFM-ad.
Those in the rAFD group nearly all had asymmetric onset of symptoms, while those in the AFM-ad group were more likely to experience bilateral onset in their lower extremities, “reflecting the pattern of symptoms often seen in other causes of myelopathy such as transverse myelitis and ischemic injury,” the authors noted.
While both groups often presented with decreased muscle tone and reflexes, this was more likely to evolve to increased tone or hyperreflexia in the AFM-ad group. Patients with AFM-ad were also more likely to experience impaired bowel or bladder function.
On MRI, lesions were mostly or completely restricted to the spinal cord gray matter in patients with rAFM or to involve the dorsal pons. These patients did not have any supratentorial brain lesions.
Patients in the rAFM category also had lower cerebrospinal fluid protein values than those in the AFM-ad category, but this was the only cerebrospinal fluid difference between the two groups.
All patients categorized as having rAFM had an infectious prodrome – such as viral syndrome, fever, congestion, and cough – compared with 63.6% of the patients categorized as AFM-ad. The pathogen was identified in only 13 of the rAFM patients, and included 5 patients with enterovirus D68, 2 with unspecified enterovirus, 2 with rhinovirus, 2 with adenovirus, and 2 with mycoplasma. Of the three patients in the AFM-ad group whose pathogen was identified, one had an untyped rhinovirus/enterovirus and mycoplasma, one had a rhinovirus B, and one had enterovirus D68.
“These results highlight that the CDC case definition, while appropriately sensitive for epidemiologic ascertainment of possible AFM cases, also encompasses other neurologic diseases that can cause acute weakness,” the authors wrote. However, they acknowledged that acute flaccid myelitis was still poorly understood and their own definition of the disease may change as more children are diagnosed.
“We propose that the definition of rAFM presented here be used as a starting point for developing inclusion and exclusion criteria for future research studies of AFM,” they wrote.
The study was supported by Johns Hopkins University, the Bart McLean Fund for Neuroimmunology Research, and Project Restore. Two authors reported funding from private industry outside the submitted work and five reported support from or involvement with research and funding bodies.
SOURCE: Elrick MJ et al. JAMA Pediatr. 2018 Nov 30. doi: 10.1001/jamapediatrics.2018.4890.
Acute flaccid myelitis appears to present most commonly as asymmetric weakness after respiratory viral infection and has distinctive MRI features that could help with early diagnosis.
In a paper published in JAMA Pediatrics, researchers presented the results of a retrospective case series of 45 children who were diagnosed between 2012 and 2016 with acute flaccid myelitis, or “pseudo polio,” using the Centers for Disease Control’s case definition.
Matthew J. Elrick, MD, PhD, of Johns Hopkins University, Baltimore, and his coauthors came up with a set of reproducible and distinctive features of acute flaccid myelitis. These were the presence of a prodromal fever or viral syndrome; weakness in a lower motor neuron pattern involving one or more limbs, neck, face, and/or bulbar muscles; supportive evidence either from MRI, nerve conduction studies, or cerebrospinal fluid; and the absence of objective sensory deficits, supratentorial white matter, cortical lesions greater than 1 cm in size, encephalopathy, elevated cerebrospinal fluid without pleocytosis, or any other alternative diagnosis.
The researchers commented that, while the CDC case definition has helped with epidemiologic surveillance of acute flaccid myelitis, it may also pick up children with acute weakness caused by other conditions such as transverse myelitis, Guillain-Barré syndrome, ischemic myelopathy, and other myelopathies.
To identify clinical features that might help differentiate patients with acute flaccid myelitis, the researchers attempted to see how many alternative diagnoses were captured in the CDC case definition.
The patients in their study all presented with acute flaccid paralysis in at least one limb and with either an MRI showing a spinal cord lesion spanning one or more spinal segments but largely restricted to gray matter or pleocytosis of the cerebrospinal fluid. The researchers divided the cases into those who also met a well-defined alternative diagnosis – who they categorized as “acute flaccid myelitis with possible alternative diagnosis” (AFM-ad) – and those who were categorized as “restrictively defined AFM” (rAFM). Overall, 34 patients were classified as rAFM and 11 as AFM-ad.
Those in the rAFD group nearly all had asymmetric onset of symptoms, while those in the AFM-ad group were more likely to experience bilateral onset in their lower extremities, “reflecting the pattern of symptoms often seen in other causes of myelopathy such as transverse myelitis and ischemic injury,” the authors noted.
While both groups often presented with decreased muscle tone and reflexes, this was more likely to evolve to increased tone or hyperreflexia in the AFM-ad group. Patients with AFM-ad were also more likely to experience impaired bowel or bladder function.
On MRI, lesions were mostly or completely restricted to the spinal cord gray matter in patients with rAFM or to involve the dorsal pons. These patients did not have any supratentorial brain lesions.
Patients in the rAFM category also had lower cerebrospinal fluid protein values than those in the AFM-ad category, but this was the only cerebrospinal fluid difference between the two groups.
All patients categorized as having rAFM had an infectious prodrome – such as viral syndrome, fever, congestion, and cough – compared with 63.6% of the patients categorized as AFM-ad. The pathogen was identified in only 13 of the rAFM patients, and included 5 patients with enterovirus D68, 2 with unspecified enterovirus, 2 with rhinovirus, 2 with adenovirus, and 2 with mycoplasma. Of the three patients in the AFM-ad group whose pathogen was identified, one had an untyped rhinovirus/enterovirus and mycoplasma, one had a rhinovirus B, and one had enterovirus D68.
“These results highlight that the CDC case definition, while appropriately sensitive for epidemiologic ascertainment of possible AFM cases, also encompasses other neurologic diseases that can cause acute weakness,” the authors wrote. However, they acknowledged that acute flaccid myelitis was still poorly understood and their own definition of the disease may change as more children are diagnosed.
“We propose that the definition of rAFM presented here be used as a starting point for developing inclusion and exclusion criteria for future research studies of AFM,” they wrote.
The study was supported by Johns Hopkins University, the Bart McLean Fund for Neuroimmunology Research, and Project Restore. Two authors reported funding from private industry outside the submitted work and five reported support from or involvement with research and funding bodies.
SOURCE: Elrick MJ et al. JAMA Pediatr. 2018 Nov 30. doi: 10.1001/jamapediatrics.2018.4890.
FROM JAMA PEDIATRICS
Key clinical point: Acute flaccid myelitis has distinct features that can distinguish it from other similar conditions.
Major finding: Asymmetric onset of symptoms and MRI signature can help distinguish acute flaccid myelitis from alternative diagnoses.
Study details: A retrospective case series in 45 children diagnosed with acute flaccid myelitis.
Disclosures: The study was supported by Johns Hopkins University, the Bart McLean Fund for Neuroimmunology Research, and Project Restore. Two authors reported funding from private industry outside the submitted work and five reported support from or involvement with research and funding bodies.
Source: Elrick MJ et al. JAMA Pediatr. 2018 Nov 30. doi: 10.1001/jamapediatrics.2018.4890.
Under Trump, number of uninsured kids rose for first time this decade
After years of steady decline, the number of U.S. children without health insurance rose by 276,000 in 2017, according to a Georgetown University report released Nov. 22.
While not a big jump statistically – the share of uninsured kids rose to 5% in 2017 from 4.7% a year earlier – it is still striking. The uninsured rate typically remains stable or drops during times of economic growth. In September, the U.S. unemployment rate hit its lowest level since 1969.
“The nation is going backwards on insuring kids and it is likely to get worse,” said Joan Alker, coauthor of the study and executive director of Georgetown’s Center for Children and Families in Washington.
Ms. Alker and other child health advocates place the blame for this change on the Trump administration and the Republican-controlled Congress, saying their policies and actions cast a pall on enrollment.
The number of children without coverage rose to 3.9 million in 2017 from about 3.6 million a year earlier, according to Census data analyzed by Georgetown. The overall uninsured rate for people of all ages – which plummeted from 2013 to 2016 following the health law’s implementation – remained unchanged at 8.8% last year.
The share of children with employer-sponsored coverage rose modestly in 2017, but not by enough to make up for the drop in children enrolling in Medicaid or getting coverage from Obamacare insurance exchanges, Ms. Alker said.
While no states made any significant gains in lowering children’s uninsured rate, nine states experienced significant increases. The biggest occurred in South Dakota (up from 4.7% to 6.2%), Utah (up from 6% to 7.3%), and Texas (from 9.8% to 10.7%).
More than one in five uninsured children nationwide live in Texas – about 835,000 kids – by far the highest number of any state.
Florida had 325,000 uninsured children last year, as its uninsured rate for that age group rose 0.7 percentage points to 7.3%. California had 301,000 children without insurance, though its number remained virtually unchanged, relative to the previous year.
Other states with significant increases were Georgia, Massachusetts, Ohio, Tennessee, and South Carolina.
The uninsured rates for children increased at nearly triple the rates in states that did not expand Medicaid under the Affordable Care Act, according to the report. Studies have shown that children whose parents are insured are more likely to have coverage.
The uninsured rate among Hispanic children was 7.8%, compared with 4.9% among whites and 4.6% among blacks overall. (Hispanics can be of any race.)
Georgetown has been tracking these figures since 2008 when 7.6 million children – or about 10% of kids – lacked health coverage.
Because nearly all low-income children are eligible for Medicaid or the federal Children’s Health Insurance Program, known as CHIP, the challenge is making sure parents are aware of the programs, getting them enrolled, and keeping them signed up as long as they are eligible, Ms. Alker said.
Congress let the CHIP program funding lapse for several months in 2017, putting states in a position of having to warn consumers that they would soon have to freeze enrollment. Congress restored federal funding in early in 2018.
In addition, low-income families were bombarded by news reports last year of Congress threatening to repeal the health law that expanded coverage to millions. In the past 2 years, the Trump administration has slashed funding to Obamacare navigators to help people sign up for coverage.
Ms. Alker also pointed to the Trump administration’s September proposal, known as the “public charge” rule, which could make it harder for legal immigrants to get green cards if they have received certain kinds of public assistance – including Medicaid, food stamps, and housing subsidies. Green cards allow them to live and work permanently in the United States.
OLE Health, a large health provider based in Napa Valley, Calif., that serves many immigrants, said it has seen patients disenroll from Medicaid in the past year. CEO Alicia Hardy said many have dropped coverage over fears the help could jeopardize their immigration status. “They are afraid of being deported.”
All those events could have deterred families from getting their kids covered. “The welcome mat has been pulled back and as a result we see more uninsured children,” Ms. Alker said.
She said the easiest way to change the trend would be for more states to expand Medicaid under the health law. A total of 14 states have yet to do so. Though the expansion largely affects adults, as parents enroll, their children are likely to follow.
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
After years of steady decline, the number of U.S. children without health insurance rose by 276,000 in 2017, according to a Georgetown University report released Nov. 22.
While not a big jump statistically – the share of uninsured kids rose to 5% in 2017 from 4.7% a year earlier – it is still striking. The uninsured rate typically remains stable or drops during times of economic growth. In September, the U.S. unemployment rate hit its lowest level since 1969.
“The nation is going backwards on insuring kids and it is likely to get worse,” said Joan Alker, coauthor of the study and executive director of Georgetown’s Center for Children and Families in Washington.
Ms. Alker and other child health advocates place the blame for this change on the Trump administration and the Republican-controlled Congress, saying their policies and actions cast a pall on enrollment.
The number of children without coverage rose to 3.9 million in 2017 from about 3.6 million a year earlier, according to Census data analyzed by Georgetown. The overall uninsured rate for people of all ages – which plummeted from 2013 to 2016 following the health law’s implementation – remained unchanged at 8.8% last year.
The share of children with employer-sponsored coverage rose modestly in 2017, but not by enough to make up for the drop in children enrolling in Medicaid or getting coverage from Obamacare insurance exchanges, Ms. Alker said.
While no states made any significant gains in lowering children’s uninsured rate, nine states experienced significant increases. The biggest occurred in South Dakota (up from 4.7% to 6.2%), Utah (up from 6% to 7.3%), and Texas (from 9.8% to 10.7%).
More than one in five uninsured children nationwide live in Texas – about 835,000 kids – by far the highest number of any state.
Florida had 325,000 uninsured children last year, as its uninsured rate for that age group rose 0.7 percentage points to 7.3%. California had 301,000 children without insurance, though its number remained virtually unchanged, relative to the previous year.
Other states with significant increases were Georgia, Massachusetts, Ohio, Tennessee, and South Carolina.
The uninsured rates for children increased at nearly triple the rates in states that did not expand Medicaid under the Affordable Care Act, according to the report. Studies have shown that children whose parents are insured are more likely to have coverage.
The uninsured rate among Hispanic children was 7.8%, compared with 4.9% among whites and 4.6% among blacks overall. (Hispanics can be of any race.)
Georgetown has been tracking these figures since 2008 when 7.6 million children – or about 10% of kids – lacked health coverage.
Because nearly all low-income children are eligible for Medicaid or the federal Children’s Health Insurance Program, known as CHIP, the challenge is making sure parents are aware of the programs, getting them enrolled, and keeping them signed up as long as they are eligible, Ms. Alker said.
Congress let the CHIP program funding lapse for several months in 2017, putting states in a position of having to warn consumers that they would soon have to freeze enrollment. Congress restored federal funding in early in 2018.
In addition, low-income families were bombarded by news reports last year of Congress threatening to repeal the health law that expanded coverage to millions. In the past 2 years, the Trump administration has slashed funding to Obamacare navigators to help people sign up for coverage.
Ms. Alker also pointed to the Trump administration’s September proposal, known as the “public charge” rule, which could make it harder for legal immigrants to get green cards if they have received certain kinds of public assistance – including Medicaid, food stamps, and housing subsidies. Green cards allow them to live and work permanently in the United States.
OLE Health, a large health provider based in Napa Valley, Calif., that serves many immigrants, said it has seen patients disenroll from Medicaid in the past year. CEO Alicia Hardy said many have dropped coverage over fears the help could jeopardize their immigration status. “They are afraid of being deported.”
All those events could have deterred families from getting their kids covered. “The welcome mat has been pulled back and as a result we see more uninsured children,” Ms. Alker said.
She said the easiest way to change the trend would be for more states to expand Medicaid under the health law. A total of 14 states have yet to do so. Though the expansion largely affects adults, as parents enroll, their children are likely to follow.
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
After years of steady decline, the number of U.S. children without health insurance rose by 276,000 in 2017, according to a Georgetown University report released Nov. 22.
While not a big jump statistically – the share of uninsured kids rose to 5% in 2017 from 4.7% a year earlier – it is still striking. The uninsured rate typically remains stable or drops during times of economic growth. In September, the U.S. unemployment rate hit its lowest level since 1969.
“The nation is going backwards on insuring kids and it is likely to get worse,” said Joan Alker, coauthor of the study and executive director of Georgetown’s Center for Children and Families in Washington.
Ms. Alker and other child health advocates place the blame for this change on the Trump administration and the Republican-controlled Congress, saying their policies and actions cast a pall on enrollment.
The number of children without coverage rose to 3.9 million in 2017 from about 3.6 million a year earlier, according to Census data analyzed by Georgetown. The overall uninsured rate for people of all ages – which plummeted from 2013 to 2016 following the health law’s implementation – remained unchanged at 8.8% last year.
The share of children with employer-sponsored coverage rose modestly in 2017, but not by enough to make up for the drop in children enrolling in Medicaid or getting coverage from Obamacare insurance exchanges, Ms. Alker said.
While no states made any significant gains in lowering children’s uninsured rate, nine states experienced significant increases. The biggest occurred in South Dakota (up from 4.7% to 6.2%), Utah (up from 6% to 7.3%), and Texas (from 9.8% to 10.7%).
More than one in five uninsured children nationwide live in Texas – about 835,000 kids – by far the highest number of any state.
Florida had 325,000 uninsured children last year, as its uninsured rate for that age group rose 0.7 percentage points to 7.3%. California had 301,000 children without insurance, though its number remained virtually unchanged, relative to the previous year.
Other states with significant increases were Georgia, Massachusetts, Ohio, Tennessee, and South Carolina.
The uninsured rates for children increased at nearly triple the rates in states that did not expand Medicaid under the Affordable Care Act, according to the report. Studies have shown that children whose parents are insured are more likely to have coverage.
The uninsured rate among Hispanic children was 7.8%, compared with 4.9% among whites and 4.6% among blacks overall. (Hispanics can be of any race.)
Georgetown has been tracking these figures since 2008 when 7.6 million children – or about 10% of kids – lacked health coverage.
Because nearly all low-income children are eligible for Medicaid or the federal Children’s Health Insurance Program, known as CHIP, the challenge is making sure parents are aware of the programs, getting them enrolled, and keeping them signed up as long as they are eligible, Ms. Alker said.
Congress let the CHIP program funding lapse for several months in 2017, putting states in a position of having to warn consumers that they would soon have to freeze enrollment. Congress restored federal funding in early in 2018.
In addition, low-income families were bombarded by news reports last year of Congress threatening to repeal the health law that expanded coverage to millions. In the past 2 years, the Trump administration has slashed funding to Obamacare navigators to help people sign up for coverage.
Ms. Alker also pointed to the Trump administration’s September proposal, known as the “public charge” rule, which could make it harder for legal immigrants to get green cards if they have received certain kinds of public assistance – including Medicaid, food stamps, and housing subsidies. Green cards allow them to live and work permanently in the United States.
OLE Health, a large health provider based in Napa Valley, Calif., that serves many immigrants, said it has seen patients disenroll from Medicaid in the past year. CEO Alicia Hardy said many have dropped coverage over fears the help could jeopardize their immigration status. “They are afraid of being deported.”
All those events could have deterred families from getting their kids covered. “The welcome mat has been pulled back and as a result we see more uninsured children,” Ms. Alker said.
She said the easiest way to change the trend would be for more states to expand Medicaid under the health law. A total of 14 states have yet to do so. Though the expansion largely affects adults, as parents enroll, their children are likely to follow.
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Anthralin shows promise as second-line agent for pediatric alopecia areata
Given its limited systemic toxicity, , according to Sean Z. Wu, MD, of the department of dermatology, University of Cincinnati, and his associates.
In a retrospective study of 37 pediatric patients with AA, published in Pediatric Dermatology, Dr. Wu and his colleagues found that almost two-thirds experienced at least 50% regrowth of hair with topical anthralin treatment, but they described severe dermatitis and relapses as “potential drawbacks” of treatment.
The 37 patients were in the Cleveland Clinic AA areata database and began treatment with anthralin between 2004 and 2015, at aged 2-17 years (mean age 9). Over half (22) were females and most (31) were white. About 65% had patchy AA; the remainder had either alopecia totalis or alopecia universalis. Prior treatments included topical corticosteroids, minoxidil, and intralesional corticosteroids; four patients had not been treated previously. Patients were followed up from 51 days to more than 10 years, with a mean duration of 2.5 years. Treatment regimens, titrated up to achieve a mild to moderate dermatitis, included application of 0.5% cream for 5 minutes twice a week up to 1.0% cream for 30 minutes a day.
With topical anthralin, 12 (32%) of patients had complete scalp regrowth, 25 (68%) experienced at least 50% regrowth, and 5 (14%) had no response; in five patients, no follow-up information was available. Among those with at least 50% regrowth, the initial response was first noted at a mean of 3.4 months, and the mean time to maximal response was 15 months. This timeline suggests that treatment with anthralin should be continued beyond 1 year to ensure maximum beneficial results with hair regrowth, the authors wrote.
Factors associated with a positive response to treatment included less than 50% of scalp involvement. The two patients who used anthralin as monotherapy did not achieve a 50% scalp response, but the four treatment-naive patients were among those with at least 50% scalp regrowth, versus three of the five patients (60%) who had been treated previously with systemic steroids.
Two potential clinical limitations were noted during the study. Four patients had to stop treatment because of dermatitis, which suggests that patients and parents should be counseled about the potential for severe skin irritation with this treatment, the authors said. And among those who achieved at least 50% scalp regrowth, 16 of the 25 (64%) relapsed. The authors speculated that the effects of the drug could be temporary “or that the disease process may be able to overcome the anthralin effect over time.”
Dr. Wu and his coauthors cited the retrospective design and the small population size as major limitations of the study. Because some patients continued other treatments, it is “difficult to attribute scalp regrowth entirely to anthralin,” and variations in formulation and in treatment regimens are also factors to be considered, they cautioned. That AA has been found to spontaneously resolve, depending upon the severity of the disease, presents additional challenges for clinicians attempting to determine the extent to which anthralin offers therapeutic benefit, they pointed out.
In spite of the drug’s limitations, the authors concluded that the treatment was a safe and useful option as an “adjunct for those who fail first-line therapy with topical or intralesional corticosteroids.” They added that more work is needed to tailor treatment formulation, frequency, and duration to the specific needs of pediatric patients.
The authors had no relevant financial disclosures to report.
SOURCE: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
Given its limited systemic toxicity, , according to Sean Z. Wu, MD, of the department of dermatology, University of Cincinnati, and his associates.
In a retrospective study of 37 pediatric patients with AA, published in Pediatric Dermatology, Dr. Wu and his colleagues found that almost two-thirds experienced at least 50% regrowth of hair with topical anthralin treatment, but they described severe dermatitis and relapses as “potential drawbacks” of treatment.
The 37 patients were in the Cleveland Clinic AA areata database and began treatment with anthralin between 2004 and 2015, at aged 2-17 years (mean age 9). Over half (22) were females and most (31) were white. About 65% had patchy AA; the remainder had either alopecia totalis or alopecia universalis. Prior treatments included topical corticosteroids, minoxidil, and intralesional corticosteroids; four patients had not been treated previously. Patients were followed up from 51 days to more than 10 years, with a mean duration of 2.5 years. Treatment regimens, titrated up to achieve a mild to moderate dermatitis, included application of 0.5% cream for 5 minutes twice a week up to 1.0% cream for 30 minutes a day.
With topical anthralin, 12 (32%) of patients had complete scalp regrowth, 25 (68%) experienced at least 50% regrowth, and 5 (14%) had no response; in five patients, no follow-up information was available. Among those with at least 50% regrowth, the initial response was first noted at a mean of 3.4 months, and the mean time to maximal response was 15 months. This timeline suggests that treatment with anthralin should be continued beyond 1 year to ensure maximum beneficial results with hair regrowth, the authors wrote.
Factors associated with a positive response to treatment included less than 50% of scalp involvement. The two patients who used anthralin as monotherapy did not achieve a 50% scalp response, but the four treatment-naive patients were among those with at least 50% scalp regrowth, versus three of the five patients (60%) who had been treated previously with systemic steroids.
Two potential clinical limitations were noted during the study. Four patients had to stop treatment because of dermatitis, which suggests that patients and parents should be counseled about the potential for severe skin irritation with this treatment, the authors said. And among those who achieved at least 50% scalp regrowth, 16 of the 25 (64%) relapsed. The authors speculated that the effects of the drug could be temporary “or that the disease process may be able to overcome the anthralin effect over time.”
Dr. Wu and his coauthors cited the retrospective design and the small population size as major limitations of the study. Because some patients continued other treatments, it is “difficult to attribute scalp regrowth entirely to anthralin,” and variations in formulation and in treatment regimens are also factors to be considered, they cautioned. That AA has been found to spontaneously resolve, depending upon the severity of the disease, presents additional challenges for clinicians attempting to determine the extent to which anthralin offers therapeutic benefit, they pointed out.
In spite of the drug’s limitations, the authors concluded that the treatment was a safe and useful option as an “adjunct for those who fail first-line therapy with topical or intralesional corticosteroids.” They added that more work is needed to tailor treatment formulation, frequency, and duration to the specific needs of pediatric patients.
The authors had no relevant financial disclosures to report.
SOURCE: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
Given its limited systemic toxicity, , according to Sean Z. Wu, MD, of the department of dermatology, University of Cincinnati, and his associates.
In a retrospective study of 37 pediatric patients with AA, published in Pediatric Dermatology, Dr. Wu and his colleagues found that almost two-thirds experienced at least 50% regrowth of hair with topical anthralin treatment, but they described severe dermatitis and relapses as “potential drawbacks” of treatment.
The 37 patients were in the Cleveland Clinic AA areata database and began treatment with anthralin between 2004 and 2015, at aged 2-17 years (mean age 9). Over half (22) were females and most (31) were white. About 65% had patchy AA; the remainder had either alopecia totalis or alopecia universalis. Prior treatments included topical corticosteroids, minoxidil, and intralesional corticosteroids; four patients had not been treated previously. Patients were followed up from 51 days to more than 10 years, with a mean duration of 2.5 years. Treatment regimens, titrated up to achieve a mild to moderate dermatitis, included application of 0.5% cream for 5 minutes twice a week up to 1.0% cream for 30 minutes a day.
With topical anthralin, 12 (32%) of patients had complete scalp regrowth, 25 (68%) experienced at least 50% regrowth, and 5 (14%) had no response; in five patients, no follow-up information was available. Among those with at least 50% regrowth, the initial response was first noted at a mean of 3.4 months, and the mean time to maximal response was 15 months. This timeline suggests that treatment with anthralin should be continued beyond 1 year to ensure maximum beneficial results with hair regrowth, the authors wrote.
Factors associated with a positive response to treatment included less than 50% of scalp involvement. The two patients who used anthralin as monotherapy did not achieve a 50% scalp response, but the four treatment-naive patients were among those with at least 50% scalp regrowth, versus three of the five patients (60%) who had been treated previously with systemic steroids.
Two potential clinical limitations were noted during the study. Four patients had to stop treatment because of dermatitis, which suggests that patients and parents should be counseled about the potential for severe skin irritation with this treatment, the authors said. And among those who achieved at least 50% scalp regrowth, 16 of the 25 (64%) relapsed. The authors speculated that the effects of the drug could be temporary “or that the disease process may be able to overcome the anthralin effect over time.”
Dr. Wu and his coauthors cited the retrospective design and the small population size as major limitations of the study. Because some patients continued other treatments, it is “difficult to attribute scalp regrowth entirely to anthralin,” and variations in formulation and in treatment regimens are also factors to be considered, they cautioned. That AA has been found to spontaneously resolve, depending upon the severity of the disease, presents additional challenges for clinicians attempting to determine the extent to which anthralin offers therapeutic benefit, they pointed out.
In spite of the drug’s limitations, the authors concluded that the treatment was a safe and useful option as an “adjunct for those who fail first-line therapy with topical or intralesional corticosteroids.” They added that more work is needed to tailor treatment formulation, frequency, and duration to the specific needs of pediatric patients.
The authors had no relevant financial disclosures to report.
SOURCE: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
FROM PEDIATRIC DERMATOLOGY
Key clinical point: Additional research is needed to pinpoint protocols for optimal formulation, dosage, and duration of anthralin in pediatric patients.
Major finding: At least 50% regrowth of scalp hair was achieved in 68% of patients treated with topical anthralin.
Study details: A retrospective chart review of 37 patients with alopecia areata who started treatment at a mean age of 9 years.
Disclosures: The authors reported no relevant financial disclosures.
Source: Wu SZ et al. Pediatr Dermatol. 2018;35:817-20.
Infant mortality generally unchanged in 2016
Infant mortality in the United Sates dropped very slightly from 2015 to 2016 and has not changed significantly since 2011, according to the National Center for Health Statistics.
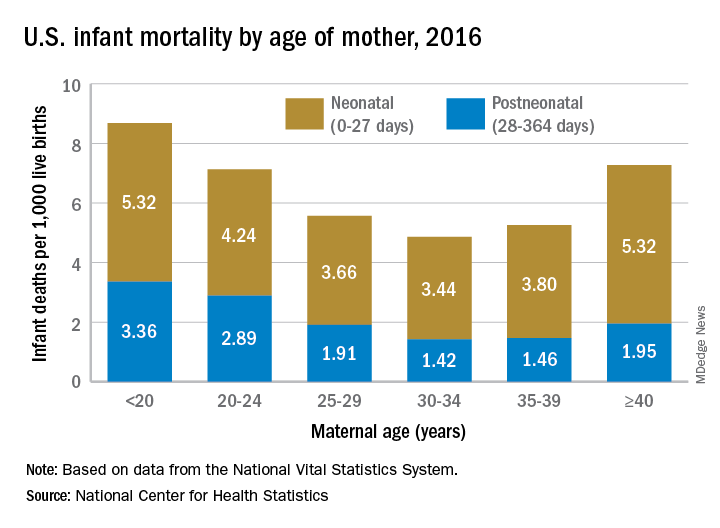
Overall infant mortality was 5.87 per 1,000 live births in 2016, which was not significantly less than the 2015 rate of 5.90 per 1,000 or the rate of 6.07 per 1,000 recorded in 2011, the NCHS said in a recent Data Brief. The rate for 2016 works out to 3.88 per 1,000 for the neonatal period (0-27 days) and 1.99 per 1,000 during the postneonatal period (28-364 days).
The rate was lowest for mothers aged 30-34 years (4.86 per 1,000) and highest for those under 20 years (8.69). All overall rates by maternal age were significantly different from each other, except for those of mothers aged 20-24 years (7.13) and those aged 40 years and over (7.27). Neonatal mortality was highest for the under-20 group and the 40-and-over group at 5.32 per 1,000, with the difference between them coming during the postneonatal period: 3.36 for those under 20 and 1.95 for the 40-and-overs, the NCHS investigators reported based on data from the National Vital Statistics System.
The leading cause of death during the neonatal period in 2016 was low birth weight at 98 per 1,000 live births, with congenital malformations second at 86 per 1,000. The leading cause of death in the postneonatal period was congenital malformations at 36 per 1,000, followed by sudden infant death syndrome (35 per 1,000), unintentional injuries (27 per 1,000), diseases of the circulatory system (9 per 1,000), and homicide (6 per 1,000), they added.
Infant mortality in the United Sates dropped very slightly from 2015 to 2016 and has not changed significantly since 2011, according to the National Center for Health Statistics.
Overall infant mortality was 5.87 per 1,000 live births in 2016, which was not significantly less than the 2015 rate of 5.90 per 1,000 or the rate of 6.07 per 1,000 recorded in 2011, the NCHS said in a recent Data Brief. The rate for 2016 works out to 3.88 per 1,000 for the neonatal period (0-27 days) and 1.99 per 1,000 during the postneonatal period (28-364 days).
The rate was lowest for mothers aged 30-34 years (4.86 per 1,000) and highest for those under 20 years (8.69). All overall rates by maternal age were significantly different from each other, except for those of mothers aged 20-24 years (7.13) and those aged 40 years and over (7.27). Neonatal mortality was highest for the under-20 group and the 40-and-over group at 5.32 per 1,000, with the difference between them coming during the postneonatal period: 3.36 for those under 20 and 1.95 for the 40-and-overs, the NCHS investigators reported based on data from the National Vital Statistics System.
The leading cause of death during the neonatal period in 2016 was low birth weight at 98 per 1,000 live births, with congenital malformations second at 86 per 1,000. The leading cause of death in the postneonatal period was congenital malformations at 36 per 1,000, followed by sudden infant death syndrome (35 per 1,000), unintentional injuries (27 per 1,000), diseases of the circulatory system (9 per 1,000), and homicide (6 per 1,000), they added.
Infant mortality in the United Sates dropped very slightly from 2015 to 2016 and has not changed significantly since 2011, according to the National Center for Health Statistics.
Overall infant mortality was 5.87 per 1,000 live births in 2016, which was not significantly less than the 2015 rate of 5.90 per 1,000 or the rate of 6.07 per 1,000 recorded in 2011, the NCHS said in a recent Data Brief. The rate for 2016 works out to 3.88 per 1,000 for the neonatal period (0-27 days) and 1.99 per 1,000 during the postneonatal period (28-364 days).
The rate was lowest for mothers aged 30-34 years (4.86 per 1,000) and highest for those under 20 years (8.69). All overall rates by maternal age were significantly different from each other, except for those of mothers aged 20-24 years (7.13) and those aged 40 years and over (7.27). Neonatal mortality was highest for the under-20 group and the 40-and-over group at 5.32 per 1,000, with the difference between them coming during the postneonatal period: 3.36 for those under 20 and 1.95 for the 40-and-overs, the NCHS investigators reported based on data from the National Vital Statistics System.
The leading cause of death during the neonatal period in 2016 was low birth weight at 98 per 1,000 live births, with congenital malformations second at 86 per 1,000. The leading cause of death in the postneonatal period was congenital malformations at 36 per 1,000, followed by sudden infant death syndrome (35 per 1,000), unintentional injuries (27 per 1,000), diseases of the circulatory system (9 per 1,000), and homicide (6 per 1,000), they added.
Child gun deaths lowest in states with strictest firearm laws
ORLANDO – and laws restricting children’s access to firearms are linked to reduced pediatric firearm suicide rates, according to research.

“State-level legislation could play an important role in reducing pediatric firearm-related deaths,” concluded Jordan S. Taylor, MD, of Stanford (Calif.) University and his colleagues.
Dr. Taylor earned top honors among the American Academy of Pediatrics (AAP) Council on Injury, Violence and Poison Prevention research abstracts when he presented his findings at the annual meeting of the American Academy of Pediatrics.
Firearm injuries account for the second leading cause of death among U.S. children: 3,155 youth ages 19 years and younger died from gunshot injuries in 2016, and more than 17,000 were injured. Yet state laws governing the purchase, ownership, carriage, and storage of guns vary widely across the country. Dr. Taylor and his colleagues conducted two studies to assess the effects of firearm legislation on firearm-related injuries and deaths in U.S. children.
In their first study, they analyzed pediatric inpatient admissions for firearm injuries in 2012 relative to the stringency of state firearm legislation. They relied on five data sources for the analysis: the Kids’ Inpatient Database (KID), the Healthcare Cost and Utilization Project, the Agency for Healthcare Research and Quality, the U.S. Census Bureau, and the 2013 Brady scorecard.
The Brady scorecard provides scores for each state based on the presence and strictness of firearm-related laws, including legislation on background checks, ability of dangerous individuals to purchase guns, trafficking laws, and laws governing the sales, carrying, and purchasing of firearms.
The 10 states with the strictest laws (highest Brady scores) are California, Connecticut, Delaware, Hawaii, Illinois, Maryland, Massachusetts, New Jersey, New York, and Rhode Island. The 10 states with the lowest scores (least-strict legislation) are Alaska, Arizona, Arkansas, Florida, Kentucky, Louisiana, Montana, Nevada, Virginia, and Wyoming.
Among the 6,941 youth (aged 0-20 years) hospitalized in 2012 for firearm injuries, 7% died. More than a third of these (36%) occurred in the South, 25% in the Midwest, 22% in the West, and 17% in the Northeast.
Children most likely to be injured were boys, older children, black and Latino children, and children living in low-income zip codes.
The Midwest and South, which have lower average Brady scores (more lax legislation on guns), had 8.30 injuries per 100,000 children, compared with 7.54 injuries per 100,000 children in the Northeast and West, which have higher average Brady scores (more stringent gun laws). This was a difference of 0.76 injuries per 100,000 children (95% confidence interval, 0.38-1.13; P less than 0.001).
Then the researchers conducted a second analysis that looked specifically at firearm mortality within the context of both child access prevention (CAP) laws and states’ Brady scores. CAP laws include safe storage laws and gun lock laws, for example.
This analysis used the Web-Based Injury Statistics Query and Reporting System to capture pediatric firearm deaths from 2014-2015 and compared these to the 2014 Brady scores and CAP laws.
An estimated 2,715 child gun deaths occurred during the study period, of which 62% were homicides and 31% were suicides. The researchers identified “a significant negative correlation between states’ firearm legislation stringency and pediatric firearm mortality (Spearman correlation coefficient = –0.66) and between presence of CAP laws and firearm suicide rates (Spearman correlation coefficient = –0.56).”
Dr. Taylor said in an interview, “states that have both types of child access prevention laws [had] suicide rates four times lower than states that did not have either of those.”
Positive correlations also showed up between unemployment rate and firearm homicide rate (Spearman correlation coefficient = 0.55) and teen tobacco use and firearm suicide rate (Spearman correlation coefficient = 0.50).
The association between Brady scores and pediatric mortality from firearms remained significant after adjustment for poverty, unemployment, and substance abuse (P less than .01). Similarly, the association between the pediatric firearm suicide rate and CAP laws remained significant after controlling for socioeconomic factors and other firearm legislation (P less than .01).
In a video interview, Dr. Taylor discussed his research findings and their importance in clinical practice.
“It’s absolutely important for pediatricians to talk to families about firearms in their home and also in the homes of their friends that they visit,” Dr. Taylor said. “We try to approach it as a public health issue similar to seat belts and car seats.”
No external funding was used, and Dr. Taylor reported no conflicts of interest.
ORLANDO – and laws restricting children’s access to firearms are linked to reduced pediatric firearm suicide rates, according to research.
“State-level legislation could play an important role in reducing pediatric firearm-related deaths,” concluded Jordan S. Taylor, MD, of Stanford (Calif.) University and his colleagues.
Dr. Taylor earned top honors among the American Academy of Pediatrics (AAP) Council on Injury, Violence and Poison Prevention research abstracts when he presented his findings at the annual meeting of the American Academy of Pediatrics.
Firearm injuries account for the second leading cause of death among U.S. children: 3,155 youth ages 19 years and younger died from gunshot injuries in 2016, and more than 17,000 were injured. Yet state laws governing the purchase, ownership, carriage, and storage of guns vary widely across the country. Dr. Taylor and his colleagues conducted two studies to assess the effects of firearm legislation on firearm-related injuries and deaths in U.S. children.
In their first study, they analyzed pediatric inpatient admissions for firearm injuries in 2012 relative to the stringency of state firearm legislation. They relied on five data sources for the analysis: the Kids’ Inpatient Database (KID), the Healthcare Cost and Utilization Project, the Agency for Healthcare Research and Quality, the U.S. Census Bureau, and the 2013 Brady scorecard.
The Brady scorecard provides scores for each state based on the presence and strictness of firearm-related laws, including legislation on background checks, ability of dangerous individuals to purchase guns, trafficking laws, and laws governing the sales, carrying, and purchasing of firearms.
The 10 states with the strictest laws (highest Brady scores) are California, Connecticut, Delaware, Hawaii, Illinois, Maryland, Massachusetts, New Jersey, New York, and Rhode Island. The 10 states with the lowest scores (least-strict legislation) are Alaska, Arizona, Arkansas, Florida, Kentucky, Louisiana, Montana, Nevada, Virginia, and Wyoming.
Among the 6,941 youth (aged 0-20 years) hospitalized in 2012 for firearm injuries, 7% died. More than a third of these (36%) occurred in the South, 25% in the Midwest, 22% in the West, and 17% in the Northeast.
Children most likely to be injured were boys, older children, black and Latino children, and children living in low-income zip codes.
The Midwest and South, which have lower average Brady scores (more lax legislation on guns), had 8.30 injuries per 100,000 children, compared with 7.54 injuries per 100,000 children in the Northeast and West, which have higher average Brady scores (more stringent gun laws). This was a difference of 0.76 injuries per 100,000 children (95% confidence interval, 0.38-1.13; P less than 0.001).
Then the researchers conducted a second analysis that looked specifically at firearm mortality within the context of both child access prevention (CAP) laws and states’ Brady scores. CAP laws include safe storage laws and gun lock laws, for example.
This analysis used the Web-Based Injury Statistics Query and Reporting System to capture pediatric firearm deaths from 2014-2015 and compared these to the 2014 Brady scores and CAP laws.
An estimated 2,715 child gun deaths occurred during the study period, of which 62% were homicides and 31% were suicides. The researchers identified “a significant negative correlation between states’ firearm legislation stringency and pediatric firearm mortality (Spearman correlation coefficient = –0.66) and between presence of CAP laws and firearm suicide rates (Spearman correlation coefficient = –0.56).”
Dr. Taylor said in an interview, “states that have both types of child access prevention laws [had] suicide rates four times lower than states that did not have either of those.”
Positive correlations also showed up between unemployment rate and firearm homicide rate (Spearman correlation coefficient = 0.55) and teen tobacco use and firearm suicide rate (Spearman correlation coefficient = 0.50).
The association between Brady scores and pediatric mortality from firearms remained significant after adjustment for poverty, unemployment, and substance abuse (P less than .01). Similarly, the association between the pediatric firearm suicide rate and CAP laws remained significant after controlling for socioeconomic factors and other firearm legislation (P less than .01).
In a video interview, Dr. Taylor discussed his research findings and their importance in clinical practice.
“It’s absolutely important for pediatricians to talk to families about firearms in their home and also in the homes of their friends that they visit,” Dr. Taylor said. “We try to approach it as a public health issue similar to seat belts and car seats.”
No external funding was used, and Dr. Taylor reported no conflicts of interest.
ORLANDO – and laws restricting children’s access to firearms are linked to reduced pediatric firearm suicide rates, according to research.
“State-level legislation could play an important role in reducing pediatric firearm-related deaths,” concluded Jordan S. Taylor, MD, of Stanford (Calif.) University and his colleagues.
Dr. Taylor earned top honors among the American Academy of Pediatrics (AAP) Council on Injury, Violence and Poison Prevention research abstracts when he presented his findings at the annual meeting of the American Academy of Pediatrics.
Firearm injuries account for the second leading cause of death among U.S. children: 3,155 youth ages 19 years and younger died from gunshot injuries in 2016, and more than 17,000 were injured. Yet state laws governing the purchase, ownership, carriage, and storage of guns vary widely across the country. Dr. Taylor and his colleagues conducted two studies to assess the effects of firearm legislation on firearm-related injuries and deaths in U.S. children.
In their first study, they analyzed pediatric inpatient admissions for firearm injuries in 2012 relative to the stringency of state firearm legislation. They relied on five data sources for the analysis: the Kids’ Inpatient Database (KID), the Healthcare Cost and Utilization Project, the Agency for Healthcare Research and Quality, the U.S. Census Bureau, and the 2013 Brady scorecard.
The Brady scorecard provides scores for each state based on the presence and strictness of firearm-related laws, including legislation on background checks, ability of dangerous individuals to purchase guns, trafficking laws, and laws governing the sales, carrying, and purchasing of firearms.
The 10 states with the strictest laws (highest Brady scores) are California, Connecticut, Delaware, Hawaii, Illinois, Maryland, Massachusetts, New Jersey, New York, and Rhode Island. The 10 states with the lowest scores (least-strict legislation) are Alaska, Arizona, Arkansas, Florida, Kentucky, Louisiana, Montana, Nevada, Virginia, and Wyoming.
Among the 6,941 youth (aged 0-20 years) hospitalized in 2012 for firearm injuries, 7% died. More than a third of these (36%) occurred in the South, 25% in the Midwest, 22% in the West, and 17% in the Northeast.
Children most likely to be injured were boys, older children, black and Latino children, and children living in low-income zip codes.
The Midwest and South, which have lower average Brady scores (more lax legislation on guns), had 8.30 injuries per 100,000 children, compared with 7.54 injuries per 100,000 children in the Northeast and West, which have higher average Brady scores (more stringent gun laws). This was a difference of 0.76 injuries per 100,000 children (95% confidence interval, 0.38-1.13; P less than 0.001).
Then the researchers conducted a second analysis that looked specifically at firearm mortality within the context of both child access prevention (CAP) laws and states’ Brady scores. CAP laws include safe storage laws and gun lock laws, for example.
This analysis used the Web-Based Injury Statistics Query and Reporting System to capture pediatric firearm deaths from 2014-2015 and compared these to the 2014 Brady scores and CAP laws.
An estimated 2,715 child gun deaths occurred during the study period, of which 62% were homicides and 31% were suicides. The researchers identified “a significant negative correlation between states’ firearm legislation stringency and pediatric firearm mortality (Spearman correlation coefficient = –0.66) and between presence of CAP laws and firearm suicide rates (Spearman correlation coefficient = –0.56).”
Dr. Taylor said in an interview, “states that have both types of child access prevention laws [had] suicide rates four times lower than states that did not have either of those.”
Positive correlations also showed up between unemployment rate and firearm homicide rate (Spearman correlation coefficient = 0.55) and teen tobacco use and firearm suicide rate (Spearman correlation coefficient = 0.50).
The association between Brady scores and pediatric mortality from firearms remained significant after adjustment for poverty, unemployment, and substance abuse (P less than .01). Similarly, the association between the pediatric firearm suicide rate and CAP laws remained significant after controlling for socioeconomic factors and other firearm legislation (P less than .01).
In a video interview, Dr. Taylor discussed his research findings and their importance in clinical practice.
“It’s absolutely important for pediatricians to talk to families about firearms in their home and also in the homes of their friends that they visit,” Dr. Taylor said. “We try to approach it as a public health issue similar to seat belts and car seats.”
No external funding was used, and Dr. Taylor reported no conflicts of interest.
REPORTING FROM AAP 2018
Key clinical point: Stricter state firearm legislation was associated with reduced firearm-related pediatric mortality.
Major finding: 8.3 injuries per 100,000 children occurred in the Midwest and South, compared with 7.5 injuries per 100,000 children in the Northeast and West.
Study details: The findings are based on two separate analyses that analyzed state Brady scores along with 6,941 firearm-related hospitalizations in 2012 and 2,715 pediatric deaths from firearms in 2014-2015.
Disclosures: No external funding was used, and Dr. Taylor reported no conflicts of interest.
What is your diagnosis? - December 2018
A KOH (potassium hydroxide) test done at the visit was negative as well as a fungal culture of each toenail.

The patient was diagnosed with congenital malalignment of the great toenails (CMGTN) based on history and morphologic appearance.
Congenital malalignment of the great toenails is an underrecognized and underreported nail disorder characterized by lateral deviation of the nail plate, which is not parallel to the longitudinal axis of the distal phalanx.1 The cause is unknown. Some reports suggest a genetic cause being transmitted in an autosomal dominant fashion with variable expression.2 There have been reports of CMGTN in monozygotic and dizygotic twins making this theory likely.3 Other authors consider an external cause such as amniotic bands, neonatal asphyxia, vascular malformations, and uterine pressure. This condition also has been reported in patients with Rubinstein-Taybi syndrome.4
The nail changes can occur at birth but in some cases, such as our patient, the nails become dystrophic months to years after birth. Characteristic nail changes include shorter, discolored, hyperkeratotic nails with transverse groove or ridges. In some cases, the dystrophic nails may cause inflammation and tenderness and is the most common cause of ingrown toenails in children.
The differential diagnosis includes onychomycosis, traumatic nails, nail psoriasis, pachyonychia congenital (PC), and onychomadesis. Onychomycosis can present with white or yellow discoloration of the nail that in some cases can be associated with nail breakage, hyperkeratosis, onycholysis, and subungual debris. Either fungal culture or periodic acid shift stain of nail clippings can help confirm or exclude this diagnosis. Psoriatic nails present with nail pits, oils spots, and onycholysis. Traumatic nail changes may occur from using small shoes and trauma from running or playing soccer, and presents with subungual hemorrhage and nail dystrophy of the first or second toenail. PC is a genetic disorder caused by a mutation in certain keratin proteins of the skin (k6a, k6b, K16 and K17). These patients usually have other skin findings including palmoplantar keratoderma, white plaques on the mouth, and skin cysts (steatocystoma multiplex and vellus hair cysts). Nail changes characteristic of PC includes subungual hyperkeratosis that causes a wedge shape thickening of the nail bed (pincer nails).5 Onychomadesis can be seen after viral infections such as hand-foot-mouth disease or in patients taking chemotherapy drugs that affect nail growth.
CMGTN usually resolves with time, but some patients with severe deviation and paronychia may need surgical correction.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
1. Dermatol Online J. 2014 Jan 15;20(1):21251.
2. J Dtsch Dermatol Ges. 2012 May;10(5):326-30.
3. J Am Acad Dermatol. 2007 Oct;57(4):711-5.
4. Pediatr Dermatol. 2004 Jan-Feb;21(1):44-7.
5. Curr Opin Pediatr. 2014 Aug;26(4):440-5.
6. Skin Appendage Disord. 2018 Oct;4(4):230-5.
A KOH (potassium hydroxide) test done at the visit was negative as well as a fungal culture of each toenail.
The patient was diagnosed with congenital malalignment of the great toenails (CMGTN) based on history and morphologic appearance.
Congenital malalignment of the great toenails is an underrecognized and underreported nail disorder characterized by lateral deviation of the nail plate, which is not parallel to the longitudinal axis of the distal phalanx.1 The cause is unknown. Some reports suggest a genetic cause being transmitted in an autosomal dominant fashion with variable expression.2 There have been reports of CMGTN in monozygotic and dizygotic twins making this theory likely.3 Other authors consider an external cause such as amniotic bands, neonatal asphyxia, vascular malformations, and uterine pressure. This condition also has been reported in patients with Rubinstein-Taybi syndrome.4
The nail changes can occur at birth but in some cases, such as our patient, the nails become dystrophic months to years after birth. Characteristic nail changes include shorter, discolored, hyperkeratotic nails with transverse groove or ridges. In some cases, the dystrophic nails may cause inflammation and tenderness and is the most common cause of ingrown toenails in children.
The differential diagnosis includes onychomycosis, traumatic nails, nail psoriasis, pachyonychia congenital (PC), and onychomadesis. Onychomycosis can present with white or yellow discoloration of the nail that in some cases can be associated with nail breakage, hyperkeratosis, onycholysis, and subungual debris. Either fungal culture or periodic acid shift stain of nail clippings can help confirm or exclude this diagnosis. Psoriatic nails present with nail pits, oils spots, and onycholysis. Traumatic nail changes may occur from using small shoes and trauma from running or playing soccer, and presents with subungual hemorrhage and nail dystrophy of the first or second toenail. PC is a genetic disorder caused by a mutation in certain keratin proteins of the skin (k6a, k6b, K16 and K17). These patients usually have other skin findings including palmoplantar keratoderma, white plaques on the mouth, and skin cysts (steatocystoma multiplex and vellus hair cysts). Nail changes characteristic of PC includes subungual hyperkeratosis that causes a wedge shape thickening of the nail bed (pincer nails).5 Onychomadesis can be seen after viral infections such as hand-foot-mouth disease or in patients taking chemotherapy drugs that affect nail growth.
CMGTN usually resolves with time, but some patients with severe deviation and paronychia may need surgical correction.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
1. Dermatol Online J. 2014 Jan 15;20(1):21251.
2. J Dtsch Dermatol Ges. 2012 May;10(5):326-30.
3. J Am Acad Dermatol. 2007 Oct;57(4):711-5.
4. Pediatr Dermatol. 2004 Jan-Feb;21(1):44-7.
5. Curr Opin Pediatr. 2014 Aug;26(4):440-5.
6. Skin Appendage Disord. 2018 Oct;4(4):230-5.
A KOH (potassium hydroxide) test done at the visit was negative as well as a fungal culture of each toenail.
The patient was diagnosed with congenital malalignment of the great toenails (CMGTN) based on history and morphologic appearance.
Congenital malalignment of the great toenails is an underrecognized and underreported nail disorder characterized by lateral deviation of the nail plate, which is not parallel to the longitudinal axis of the distal phalanx.1 The cause is unknown. Some reports suggest a genetic cause being transmitted in an autosomal dominant fashion with variable expression.2 There have been reports of CMGTN in monozygotic and dizygotic twins making this theory likely.3 Other authors consider an external cause such as amniotic bands, neonatal asphyxia, vascular malformations, and uterine pressure. This condition also has been reported in patients with Rubinstein-Taybi syndrome.4
The nail changes can occur at birth but in some cases, such as our patient, the nails become dystrophic months to years after birth. Characteristic nail changes include shorter, discolored, hyperkeratotic nails with transverse groove or ridges. In some cases, the dystrophic nails may cause inflammation and tenderness and is the most common cause of ingrown toenails in children.
The differential diagnosis includes onychomycosis, traumatic nails, nail psoriasis, pachyonychia congenital (PC), and onychomadesis. Onychomycosis can present with white or yellow discoloration of the nail that in some cases can be associated with nail breakage, hyperkeratosis, onycholysis, and subungual debris. Either fungal culture or periodic acid shift stain of nail clippings can help confirm or exclude this diagnosis. Psoriatic nails present with nail pits, oils spots, and onycholysis. Traumatic nail changes may occur from using small shoes and trauma from running or playing soccer, and presents with subungual hemorrhage and nail dystrophy of the first or second toenail. PC is a genetic disorder caused by a mutation in certain keratin proteins of the skin (k6a, k6b, K16 and K17). These patients usually have other skin findings including palmoplantar keratoderma, white plaques on the mouth, and skin cysts (steatocystoma multiplex and vellus hair cysts). Nail changes characteristic of PC includes subungual hyperkeratosis that causes a wedge shape thickening of the nail bed (pincer nails).5 Onychomadesis can be seen after viral infections such as hand-foot-mouth disease or in patients taking chemotherapy drugs that affect nail growth.
CMGTN usually resolves with time, but some patients with severe deviation and paronychia may need surgical correction.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
1. Dermatol Online J. 2014 Jan 15;20(1):21251.
2. J Dtsch Dermatol Ges. 2012 May;10(5):326-30.
3. J Am Acad Dermatol. 2007 Oct;57(4):711-5.
4. Pediatr Dermatol. 2004 Jan-Feb;21(1):44-7.
5. Curr Opin Pediatr. 2014 Aug;26(4):440-5.
6. Skin Appendage Disord. 2018 Oct;4(4):230-5.
A 4-year-old boy is brought to our pediatric dermatology clinic by his mother with the concern of difficult to treat toenail fungus.

The mother reported that she started noticing the toenail changes at around 8 months of age, and it has been progressively getting worse.
He has been treated with several courses of topical antifungals and 3 months of oral terbinafine without success.
A fungal culture done 1 year prior showed slight growth of Cladosporium Sp., but the nails failed to improve after systemic therapy. He denied any associated pain or inflammation. He likes playing softball and plays soccer sometimes. The mother is very worried because the father also has a history of onychomycosis that he has not been able to clear for years.
On physical exam, he is a very pleasant young boy. His cutaneous exam is normal including hair and teeth except for thickening of the bilateral first toenails associated with transverse ridging and yellow discoloration.
Sofa and bed injuries very common among young children
ORLANDO – Injuries related to beds and sofas in children aged under 5 years occur more than twice as frequently than injuries related to stairs, according to new research.
“Findings from our analysis reveal that it is an important source of injury to young children and a leading cause of trauma to infants,” concluded David S. Liu, of Baylor College of Medicine, Houston, who presented the findings at the annual meeting of the American Academy of Pediatrics.
“The rate of bed- and sofa-related injuries is increasing, which underscores the need for increased prevention efforts, including parental education and improved safety design, to decrease soft furniture injuries among young children,” Mr. Liu and his colleagues wrote.
The researchers used the National Electronic Injury Surveillance System of the U.S. Consumer Product Safety Commission to conduct a retrospective analysis of injuries related to sofas and beds from 2007 to 2016.
They found that an estimated 2.3 million children aged under 5 years were treated for injuries related to soft furniture during those years, an average of 230,026 injuries a year, or 115 injuries per 10,000 children. To the surprise of the researchers, injuries related to beds and sofas were the most common types of accidental injury in that age group, occurring 2.5 times more often than stair-related injuries, which occurred at a rate of 47 per 10,000 population.
Boys were slightly more likely to be injured, making up 56% of all the cases. Soft tissue/internal organ injuries were most common, comprising 28% of all injuries, followed by lacerations in 24% of cases, abrasions in 15%, and fractures in 14%.
More than half the children (61%) sustained injuries to the head or face, and 3% were hospitalized for their injuries. Although infants (under 1 year old) only accounted for 28% of children injured, they were twice as likely to be hospitalized than older children.
The researchers also identified increases in injuries over the time period studied. Bed-related injuries increased 17% from 2007 to 2016, and sofa/couch-related injuries increased 17% during that period.
Although the vast majority of children were treated and released, approximately 4% of children were admitted or treated and transferred to another facility. Overall, an estimated 3,361 children died during the 9-year period, translating to a little over 370 children a year.
In a video interview, Mr. Liu discussed the implications of these findings.
“We know how dangerous car accidents and staircases are, and we often recommend car seats and stair gates for those,” Mr. Liu said. “Obviously we can’t put a gate or a barrier on every single sofa, couch, and bed in America, so as clinicians and parents, the best we can do is keep aware of how dangerous these items are. Just because of their soft nature doesn’t mean they’re inherently safer.”
The researchers reported no disclosures and the research received no external funding.
ORLANDO – Injuries related to beds and sofas in children aged under 5 years occur more than twice as frequently than injuries related to stairs, according to new research.
“Findings from our analysis reveal that it is an important source of injury to young children and a leading cause of trauma to infants,” concluded David S. Liu, of Baylor College of Medicine, Houston, who presented the findings at the annual meeting of the American Academy of Pediatrics.
“The rate of bed- and sofa-related injuries is increasing, which underscores the need for increased prevention efforts, including parental education and improved safety design, to decrease soft furniture injuries among young children,” Mr. Liu and his colleagues wrote.
The researchers used the National Electronic Injury Surveillance System of the U.S. Consumer Product Safety Commission to conduct a retrospective analysis of injuries related to sofas and beds from 2007 to 2016.
They found that an estimated 2.3 million children aged under 5 years were treated for injuries related to soft furniture during those years, an average of 230,026 injuries a year, or 115 injuries per 10,000 children. To the surprise of the researchers, injuries related to beds and sofas were the most common types of accidental injury in that age group, occurring 2.5 times more often than stair-related injuries, which occurred at a rate of 47 per 10,000 population.
Boys were slightly more likely to be injured, making up 56% of all the cases. Soft tissue/internal organ injuries were most common, comprising 28% of all injuries, followed by lacerations in 24% of cases, abrasions in 15%, and fractures in 14%.
More than half the children (61%) sustained injuries to the head or face, and 3% were hospitalized for their injuries. Although infants (under 1 year old) only accounted for 28% of children injured, they were twice as likely to be hospitalized than older children.
The researchers also identified increases in injuries over the time period studied. Bed-related injuries increased 17% from 2007 to 2016, and sofa/couch-related injuries increased 17% during that period.
Although the vast majority of children were treated and released, approximately 4% of children were admitted or treated and transferred to another facility. Overall, an estimated 3,361 children died during the 9-year period, translating to a little over 370 children a year.
In a video interview, Mr. Liu discussed the implications of these findings.
“We know how dangerous car accidents and staircases are, and we often recommend car seats and stair gates for those,” Mr. Liu said. “Obviously we can’t put a gate or a barrier on every single sofa, couch, and bed in America, so as clinicians and parents, the best we can do is keep aware of how dangerous these items are. Just because of their soft nature doesn’t mean they’re inherently safer.”
The researchers reported no disclosures and the research received no external funding.
ORLANDO – Injuries related to beds and sofas in children aged under 5 years occur more than twice as frequently than injuries related to stairs, according to new research.
“Findings from our analysis reveal that it is an important source of injury to young children and a leading cause of trauma to infants,” concluded David S. Liu, of Baylor College of Medicine, Houston, who presented the findings at the annual meeting of the American Academy of Pediatrics.
“The rate of bed- and sofa-related injuries is increasing, which underscores the need for increased prevention efforts, including parental education and improved safety design, to decrease soft furniture injuries among young children,” Mr. Liu and his colleagues wrote.
The researchers used the National Electronic Injury Surveillance System of the U.S. Consumer Product Safety Commission to conduct a retrospective analysis of injuries related to sofas and beds from 2007 to 2016.
They found that an estimated 2.3 million children aged under 5 years were treated for injuries related to soft furniture during those years, an average of 230,026 injuries a year, or 115 injuries per 10,000 children. To the surprise of the researchers, injuries related to beds and sofas were the most common types of accidental injury in that age group, occurring 2.5 times more often than stair-related injuries, which occurred at a rate of 47 per 10,000 population.
Boys were slightly more likely to be injured, making up 56% of all the cases. Soft tissue/internal organ injuries were most common, comprising 28% of all injuries, followed by lacerations in 24% of cases, abrasions in 15%, and fractures in 14%.
More than half the children (61%) sustained injuries to the head or face, and 3% were hospitalized for their injuries. Although infants (under 1 year old) only accounted for 28% of children injured, they were twice as likely to be hospitalized than older children.
The researchers also identified increases in injuries over the time period studied. Bed-related injuries increased 17% from 2007 to 2016, and sofa/couch-related injuries increased 17% during that period.
Although the vast majority of children were treated and released, approximately 4% of children were admitted or treated and transferred to another facility. Overall, an estimated 3,361 children died during the 9-year period, translating to a little over 370 children a year.
In a video interview, Mr. Liu discussed the implications of these findings.
“We know how dangerous car accidents and staircases are, and we often recommend car seats and stair gates for those,” Mr. Liu said. “Obviously we can’t put a gate or a barrier on every single sofa, couch, and bed in America, so as clinicians and parents, the best we can do is keep aware of how dangerous these items are. Just because of their soft nature doesn’t mean they’re inherently safer.”
The researchers reported no disclosures and the research received no external funding.
REPORTING FROM AAP 2018
Key clinical point: Injuries from beds and sofas/couches are common in children aged under 5 years, occurring 2.5 times more frequently than stairs-related injuries.
Major finding: An estimated 115 bed/sofa-related injuries per 10,000 children occur every year.
Study details: The findings are based on a retrospective analysis of injuries related to sofas and beds from 2007 to 2016.
Disclosures: The researchers reported no disclosures and the research received no external funding.
