User login
Initial screening not enough to catch all cases of preterm congenital hypothyroidism
reported Niamh McGrath, MD, of the department of pediatric endocrinology at Children’s University Hospital, Dublin, and her associates in the Journal of Pediatrics.
In a population-based prospective review of 898,424 records between 2004 and 2016, Dr. McGrath and her associates identified all preterm infants less than 33 weeks diagnosed with congenital hypothyroidism and receiving treatment with levothyroxine. Of the infants screened, just 53 were selected to participate in the study, including 26 who were diagnosed at the first thyroid-stimulating hormone (TSH) screening and 27 who had delayed TSH elevation.
Gestational age ranged from 23 to 33 weeks, median birth weight measured 1.2 kg, median serum TSH concentration at the time of diagnosis was 78.3 mU/L, and median free thyroxine concentration was 8.9 pmol/L.
For half of the infants ultimately diagnosed, congenital hypothyroidism was not detected during the initial newborn screening. The authors also noted that 25% of patients with delayed TSH elevation had been exposed to iodine while undergoing surgery for necrotizing enterocolitis; after age 28 days, four of these infants were found to have elevated TSH. They cautioned that while this finding emphasizes the need for close monitoring and repeat screening of infants who have been exposed to iodine for up to 1 month following exposure, they could not be certain that the iodine exposure was responsible for the transient hypothyroidism in these patients.
Dr. McGrath and her associates emphasized the importance of repeat TSH screening for all preterm infants, noting that standard protocol screenings conducted just once at age 2 weeks or 4 weeks are not sufficient to effectively identify all cases of congenital hypothyroidism in which TSH elevation is delayed. Instead, they recommended measuring TSH on days 3-5 and at 1 week, 2 weeks, 4 weeks, and term-corrected gestational age.
“Our data are consistent with studies showing a high incidence of delayed TSH rise, particularly in very-low-birth-weight infants,” the authors wrote. They speculated that delays in detecting primary congenital hypothyroidism could be caused by the suppression of TSH secretion as a result of “hypothalamic-pituitary immaturity, medication administration, and effects of serious neonatal illness.” In fact, had standard, recommended 2-week-only screening protocols been followed with their patient population, fully 48% of infants with delayed TSH elevation would have been overlooked; half of these patients were later found to have decompensated hypothyroidism.
Neurodevelopmental disability caused by congenital hypothyroidism, which affects roughly 1 in every 2,000-4,000 births, is increasingly being prevented with newborn screenings that identify the condition early, but the incidence of congenital hypothyroidism has increased considerably in the past 20 years. The authors attribute this increase to the gradual change in screening cutoff levels and the rise in number of preterm infants who are surviving.
The need for a second screening, as well as appropriate timing and optimal TSH cutoff, are “subjects of active debate,” the authors wrote. The latest European screening guidelines recommend second screenings for preterm and low-birth-weight infants at either 2 weeks of age or 2 weeks following preliminary screening. Although they make no recommendations regarding additional screenings, American Academy of Pediatrics guidelines, published in 2006, cite a “disproportionate incidence” of delayed increase in TSH and congenital hypothyroidism in infants with very low birth weight. Dr. McGrath and her associates speculated that not all screening programs have adopted repeat screening of preterm infants, perhaps because of the low yield results, “the transient nature of most cases” detected, as well as conflicting long-term data on neurodevelopmental outcomes.
Dr. McGrath receives funding from the Children’s Fund for Health. The authors declared no conflicts of interest.
SOURCE: McGrath N et al. J Pediatr. 2018 Oct 24. doi: 10.1016/j.jpeds.2018.09.044.
reported Niamh McGrath, MD, of the department of pediatric endocrinology at Children’s University Hospital, Dublin, and her associates in the Journal of Pediatrics.
In a population-based prospective review of 898,424 records between 2004 and 2016, Dr. McGrath and her associates identified all preterm infants less than 33 weeks diagnosed with congenital hypothyroidism and receiving treatment with levothyroxine. Of the infants screened, just 53 were selected to participate in the study, including 26 who were diagnosed at the first thyroid-stimulating hormone (TSH) screening and 27 who had delayed TSH elevation.
Gestational age ranged from 23 to 33 weeks, median birth weight measured 1.2 kg, median serum TSH concentration at the time of diagnosis was 78.3 mU/L, and median free thyroxine concentration was 8.9 pmol/L.
For half of the infants ultimately diagnosed, congenital hypothyroidism was not detected during the initial newborn screening. The authors also noted that 25% of patients with delayed TSH elevation had been exposed to iodine while undergoing surgery for necrotizing enterocolitis; after age 28 days, four of these infants were found to have elevated TSH. They cautioned that while this finding emphasizes the need for close monitoring and repeat screening of infants who have been exposed to iodine for up to 1 month following exposure, they could not be certain that the iodine exposure was responsible for the transient hypothyroidism in these patients.
Dr. McGrath and her associates emphasized the importance of repeat TSH screening for all preterm infants, noting that standard protocol screenings conducted just once at age 2 weeks or 4 weeks are not sufficient to effectively identify all cases of congenital hypothyroidism in which TSH elevation is delayed. Instead, they recommended measuring TSH on days 3-5 and at 1 week, 2 weeks, 4 weeks, and term-corrected gestational age.
“Our data are consistent with studies showing a high incidence of delayed TSH rise, particularly in very-low-birth-weight infants,” the authors wrote. They speculated that delays in detecting primary congenital hypothyroidism could be caused by the suppression of TSH secretion as a result of “hypothalamic-pituitary immaturity, medication administration, and effects of serious neonatal illness.” In fact, had standard, recommended 2-week-only screening protocols been followed with their patient population, fully 48% of infants with delayed TSH elevation would have been overlooked; half of these patients were later found to have decompensated hypothyroidism.
Neurodevelopmental disability caused by congenital hypothyroidism, which affects roughly 1 in every 2,000-4,000 births, is increasingly being prevented with newborn screenings that identify the condition early, but the incidence of congenital hypothyroidism has increased considerably in the past 20 years. The authors attribute this increase to the gradual change in screening cutoff levels and the rise in number of preterm infants who are surviving.
The need for a second screening, as well as appropriate timing and optimal TSH cutoff, are “subjects of active debate,” the authors wrote. The latest European screening guidelines recommend second screenings for preterm and low-birth-weight infants at either 2 weeks of age or 2 weeks following preliminary screening. Although they make no recommendations regarding additional screenings, American Academy of Pediatrics guidelines, published in 2006, cite a “disproportionate incidence” of delayed increase in TSH and congenital hypothyroidism in infants with very low birth weight. Dr. McGrath and her associates speculated that not all screening programs have adopted repeat screening of preterm infants, perhaps because of the low yield results, “the transient nature of most cases” detected, as well as conflicting long-term data on neurodevelopmental outcomes.
Dr. McGrath receives funding from the Children’s Fund for Health. The authors declared no conflicts of interest.
SOURCE: McGrath N et al. J Pediatr. 2018 Oct 24. doi: 10.1016/j.jpeds.2018.09.044.
reported Niamh McGrath, MD, of the department of pediatric endocrinology at Children’s University Hospital, Dublin, and her associates in the Journal of Pediatrics.
In a population-based prospective review of 898,424 records between 2004 and 2016, Dr. McGrath and her associates identified all preterm infants less than 33 weeks diagnosed with congenital hypothyroidism and receiving treatment with levothyroxine. Of the infants screened, just 53 were selected to participate in the study, including 26 who were diagnosed at the first thyroid-stimulating hormone (TSH) screening and 27 who had delayed TSH elevation.
Gestational age ranged from 23 to 33 weeks, median birth weight measured 1.2 kg, median serum TSH concentration at the time of diagnosis was 78.3 mU/L, and median free thyroxine concentration was 8.9 pmol/L.
For half of the infants ultimately diagnosed, congenital hypothyroidism was not detected during the initial newborn screening. The authors also noted that 25% of patients with delayed TSH elevation had been exposed to iodine while undergoing surgery for necrotizing enterocolitis; after age 28 days, four of these infants were found to have elevated TSH. They cautioned that while this finding emphasizes the need for close monitoring and repeat screening of infants who have been exposed to iodine for up to 1 month following exposure, they could not be certain that the iodine exposure was responsible for the transient hypothyroidism in these patients.
Dr. McGrath and her associates emphasized the importance of repeat TSH screening for all preterm infants, noting that standard protocol screenings conducted just once at age 2 weeks or 4 weeks are not sufficient to effectively identify all cases of congenital hypothyroidism in which TSH elevation is delayed. Instead, they recommended measuring TSH on days 3-5 and at 1 week, 2 weeks, 4 weeks, and term-corrected gestational age.
“Our data are consistent with studies showing a high incidence of delayed TSH rise, particularly in very-low-birth-weight infants,” the authors wrote. They speculated that delays in detecting primary congenital hypothyroidism could be caused by the suppression of TSH secretion as a result of “hypothalamic-pituitary immaturity, medication administration, and effects of serious neonatal illness.” In fact, had standard, recommended 2-week-only screening protocols been followed with their patient population, fully 48% of infants with delayed TSH elevation would have been overlooked; half of these patients were later found to have decompensated hypothyroidism.
Neurodevelopmental disability caused by congenital hypothyroidism, which affects roughly 1 in every 2,000-4,000 births, is increasingly being prevented with newborn screenings that identify the condition early, but the incidence of congenital hypothyroidism has increased considerably in the past 20 years. The authors attribute this increase to the gradual change in screening cutoff levels and the rise in number of preterm infants who are surviving.
The need for a second screening, as well as appropriate timing and optimal TSH cutoff, are “subjects of active debate,” the authors wrote. The latest European screening guidelines recommend second screenings for preterm and low-birth-weight infants at either 2 weeks of age or 2 weeks following preliminary screening. Although they make no recommendations regarding additional screenings, American Academy of Pediatrics guidelines, published in 2006, cite a “disproportionate incidence” of delayed increase in TSH and congenital hypothyroidism in infants with very low birth weight. Dr. McGrath and her associates speculated that not all screening programs have adopted repeat screening of preterm infants, perhaps because of the low yield results, “the transient nature of most cases” detected, as well as conflicting long-term data on neurodevelopmental outcomes.
Dr. McGrath receives funding from the Children’s Fund for Health. The authors declared no conflicts of interest.
SOURCE: McGrath N et al. J Pediatr. 2018 Oct 24. doi: 10.1016/j.jpeds.2018.09.044.
FROM THE JOURNAL OF PEDIATRICS
Key clinical point: Periodic screenings are key to preventing permanent, decompensated hypothyroidism.
Major finding: High incidence of delayed TSH rise is common, especially in very-low-birth-weight infants.
Study details: A population-based prospective review of 898,424 records.
Disclosures: Dr. McGrath receives funding from the Children’s Fund for Health. The authors declared no conflicts of interest.
Source: McGrath N et al. J Pediatr. 2018 Oct 24. doi: 10.1016/j.jpeds.2018.09.044.
ACOG: First gynecologist visit between ages 13 and 15
The American College of Obstetricians and Gynecologists (ACOG) recommends that girls receive their first reproductive health visit between the ages of 13 and 15 years to discuss healthy relationships in addition to general reproductive health, according to a new committee opinion.
The recommendation, published online Oct. 24, emphasizes that such early visits provide opportunities for ob.gyns. to educate teenage girls and their guardians about age-appropriate health issues, such as sexual relationships, dating violence, and sexual coercion. Between the ages of 13 years and 15 years is an ideal window because middle school is a time that some adolescents develop their first romantic and sexual relationships (Obstet Gynecol. 2018; 132[5]:1317-18 doi: 10.1097/AOG.0000000000002946).
“Creating a nonjudgmental environment and educating staff on the unique concerns of adolescents are helpful ways to provide effective and appropriate care to this group of patients,” the authors wrote.
Ob.gyns. can use the early meeting to discuss key aspects of a healthy relationship with patients, including communication, self-respect, and mutual respect, while helping adolescents identify the characteristics of an unhealthy relationships such as dishonesty, intimidation, disrespect, and abuse, according to the opinion. As part of the discussion, ob.gyns. also may counsel patients to define their current relationship and their expectations for future relationships. Both relationships with and without sexual intimacy should be discussed, the opinion advises.
The recommendation reminds health care professionals to be mindful of federal and state confidentiality laws and that they be aware of mandatory reporting laws when intimate partner violence, teen dating violence, or statutory rape is suspected. In addition, the opinion notes that pregnant and parenting adolescents; lesbian, gay, bisexual, transgender, queer, or questioning (LGBTQ) individuals; and adolescents with physical and mental disabilities are at particular risk of disparities in the health care system.
“The promotion of healthy relationships in these groups requires the obstetrician-gynecologist to be aware of the unique barriers and hurdles to sexual and nonsexual expression, as well as to health care,” the opinion states. “Interventions to promote healthy relationships and a strong sexual health framework are more effective when started early and can affect indicators of long-term individual health and public health.”
The American College of Obstetricians and Gynecologists recommends that the first reproductive health visit occur between the ages of 13 and 15, and I agree with them. Often patients attending this appointment don’t have physical complaints, and we can focus on prevention and education. The visit can be about building the provider-patient relationship and may serve to ease fears and develop trust before visits for problem management.
There are a number of important health education topics to cover from puberty and menses to confidentiality and minor-access laws. Because many young people will begin to initiate romantic relationships during middle school, the topic of healthy relationships is critical. Unhealthy relationships, in their many forms, can have far reaching impacts on a young person’s health and wellness. For years, we’ve been talking with young people about preventing STIs or preventing unwanted pregnancy, but we’ve spent less energy working towards something.
I’m excited to see these recommendations and look forward to helping my younger patients think through relationships as important aspects of life and health, what they want from them, and how they can work towards them.
Melissa Kottke , MD is an obstetrician-gynecologist specializing in family planning and adolescent reproductive health at Emory University in Atlanta.
The American College of Obstetricians and Gynecologists recommends that the first reproductive health visit occur between the ages of 13 and 15, and I agree with them. Often patients attending this appointment don’t have physical complaints, and we can focus on prevention and education. The visit can be about building the provider-patient relationship and may serve to ease fears and develop trust before visits for problem management.
There are a number of important health education topics to cover from puberty and menses to confidentiality and minor-access laws. Because many young people will begin to initiate romantic relationships during middle school, the topic of healthy relationships is critical. Unhealthy relationships, in their many forms, can have far reaching impacts on a young person’s health and wellness. For years, we’ve been talking with young people about preventing STIs or preventing unwanted pregnancy, but we’ve spent less energy working towards something.
I’m excited to see these recommendations and look forward to helping my younger patients think through relationships as important aspects of life and health, what they want from them, and how they can work towards them.
Melissa Kottke , MD is an obstetrician-gynecologist specializing in family planning and adolescent reproductive health at Emory University in Atlanta.
The American College of Obstetricians and Gynecologists recommends that the first reproductive health visit occur between the ages of 13 and 15, and I agree with them. Often patients attending this appointment don’t have physical complaints, and we can focus on prevention and education. The visit can be about building the provider-patient relationship and may serve to ease fears and develop trust before visits for problem management.
There are a number of important health education topics to cover from puberty and menses to confidentiality and minor-access laws. Because many young people will begin to initiate romantic relationships during middle school, the topic of healthy relationships is critical. Unhealthy relationships, in their many forms, can have far reaching impacts on a young person’s health and wellness. For years, we’ve been talking with young people about preventing STIs or preventing unwanted pregnancy, but we’ve spent less energy working towards something.
I’m excited to see these recommendations and look forward to helping my younger patients think through relationships as important aspects of life and health, what they want from them, and how they can work towards them.
Melissa Kottke , MD is an obstetrician-gynecologist specializing in family planning and adolescent reproductive health at Emory University in Atlanta.
The American College of Obstetricians and Gynecologists (ACOG) recommends that girls receive their first reproductive health visit between the ages of 13 and 15 years to discuss healthy relationships in addition to general reproductive health, according to a new committee opinion.
The recommendation, published online Oct. 24, emphasizes that such early visits provide opportunities for ob.gyns. to educate teenage girls and their guardians about age-appropriate health issues, such as sexual relationships, dating violence, and sexual coercion. Between the ages of 13 years and 15 years is an ideal window because middle school is a time that some adolescents develop their first romantic and sexual relationships (Obstet Gynecol. 2018; 132[5]:1317-18 doi: 10.1097/AOG.0000000000002946).
“Creating a nonjudgmental environment and educating staff on the unique concerns of adolescents are helpful ways to provide effective and appropriate care to this group of patients,” the authors wrote.
Ob.gyns. can use the early meeting to discuss key aspects of a healthy relationship with patients, including communication, self-respect, and mutual respect, while helping adolescents identify the characteristics of an unhealthy relationships such as dishonesty, intimidation, disrespect, and abuse, according to the opinion. As part of the discussion, ob.gyns. also may counsel patients to define their current relationship and their expectations for future relationships. Both relationships with and without sexual intimacy should be discussed, the opinion advises.
The recommendation reminds health care professionals to be mindful of federal and state confidentiality laws and that they be aware of mandatory reporting laws when intimate partner violence, teen dating violence, or statutory rape is suspected. In addition, the opinion notes that pregnant and parenting adolescents; lesbian, gay, bisexual, transgender, queer, or questioning (LGBTQ) individuals; and adolescents with physical and mental disabilities are at particular risk of disparities in the health care system.
“The promotion of healthy relationships in these groups requires the obstetrician-gynecologist to be aware of the unique barriers and hurdles to sexual and nonsexual expression, as well as to health care,” the opinion states. “Interventions to promote healthy relationships and a strong sexual health framework are more effective when started early and can affect indicators of long-term individual health and public health.”
The American College of Obstetricians and Gynecologists (ACOG) recommends that girls receive their first reproductive health visit between the ages of 13 and 15 years to discuss healthy relationships in addition to general reproductive health, according to a new committee opinion.
The recommendation, published online Oct. 24, emphasizes that such early visits provide opportunities for ob.gyns. to educate teenage girls and their guardians about age-appropriate health issues, such as sexual relationships, dating violence, and sexual coercion. Between the ages of 13 years and 15 years is an ideal window because middle school is a time that some adolescents develop their first romantic and sexual relationships (Obstet Gynecol. 2018; 132[5]:1317-18 doi: 10.1097/AOG.0000000000002946).
“Creating a nonjudgmental environment and educating staff on the unique concerns of adolescents are helpful ways to provide effective and appropriate care to this group of patients,” the authors wrote.
Ob.gyns. can use the early meeting to discuss key aspects of a healthy relationship with patients, including communication, self-respect, and mutual respect, while helping adolescents identify the characteristics of an unhealthy relationships such as dishonesty, intimidation, disrespect, and abuse, according to the opinion. As part of the discussion, ob.gyns. also may counsel patients to define their current relationship and their expectations for future relationships. Both relationships with and without sexual intimacy should be discussed, the opinion advises.
The recommendation reminds health care professionals to be mindful of federal and state confidentiality laws and that they be aware of mandatory reporting laws when intimate partner violence, teen dating violence, or statutory rape is suspected. In addition, the opinion notes that pregnant and parenting adolescents; lesbian, gay, bisexual, transgender, queer, or questioning (LGBTQ) individuals; and adolescents with physical and mental disabilities are at particular risk of disparities in the health care system.
“The promotion of healthy relationships in these groups requires the obstetrician-gynecologist to be aware of the unique barriers and hurdles to sexual and nonsexual expression, as well as to health care,” the opinion states. “Interventions to promote healthy relationships and a strong sexual health framework are more effective when started early and can affect indicators of long-term individual health and public health.”
FROM OBSTETRICS & GYNECOLOGY
Full-dose quadrivalent flu vaccine shows increased efficacy in children
according to data from a randomized trial of nearly 2,000 children aged 6-35 months.

Data from previous studies have suggested that a full dose of vaccine may be more immunogenic in young children compared with a half dose, and Sanofi Pasteur has submitted a supplemental Biologics License Application to the Food and Drug Administration to allow use of the full 0.5-mL dose in children as young as 6 months, Monica Mercer, MD, of Sanofi Pasteur, said at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices in Atlanta.
Dr. Mercer presented findings from a phase IV randomized, observer-blinded study, in which the researchers assigned healthy children aged 6-35 months to receive Fluzone quadrivalent vaccine at a dose of 0.25 mL or 0.5 mL.
A total of 1,941 children (949 for the 0.25-mL dose and 992 for the 0.5-mL dose) were included in the safety analysis.
The most important safety outcome was to compare the rate of any fever, Dr. Mercer said at the meeting.
Overall, at 7 days after vaccination, the rate of fever was 11% for the half dose and 12% for the full dose, she said. The resulting difference of 0.84% met the criteria for noninferiority (less than 5%), she added.
In terms of safety, tenderness was the most frequently reported injection site reaction, noted in 47% of the half-dose group and 50% of the full-dose group. The rates of unsolicited adverse events were similar in both groups, the most common included diarrhea and cough, Dr. Mercer said.
No subjects in the full-dose group and three in the half-dose group discontinued the study because of adverse events. The only reported serious adverse event was one case of chronic urticaria in the half-dose group; no deaths were reported in either group.
As for efficacy, the full dose demonstrated noninferiority, compared with the half dose, against each of four strains: influenza A H1N1, influenza A H3N2, influenza B Victoria, and influenza B Yamagata. The geometric mean titers of the full and half doses for each of the four strains were, respectively, 310 and 214, 332 and 221, 348 and 261, and 349 and 243.
The potential action date for the supplemental Biologics License Application is January 2019, noted Dr. Mercer, who is employed by Sanofi Pasteur.
according to data from a randomized trial of nearly 2,000 children aged 6-35 months.
Data from previous studies have suggested that a full dose of vaccine may be more immunogenic in young children compared with a half dose, and Sanofi Pasteur has submitted a supplemental Biologics License Application to the Food and Drug Administration to allow use of the full 0.5-mL dose in children as young as 6 months, Monica Mercer, MD, of Sanofi Pasteur, said at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices in Atlanta.
Dr. Mercer presented findings from a phase IV randomized, observer-blinded study, in which the researchers assigned healthy children aged 6-35 months to receive Fluzone quadrivalent vaccine at a dose of 0.25 mL or 0.5 mL.
A total of 1,941 children (949 for the 0.25-mL dose and 992 for the 0.5-mL dose) were included in the safety analysis.
The most important safety outcome was to compare the rate of any fever, Dr. Mercer said at the meeting.
Overall, at 7 days after vaccination, the rate of fever was 11% for the half dose and 12% for the full dose, she said. The resulting difference of 0.84% met the criteria for noninferiority (less than 5%), she added.
In terms of safety, tenderness was the most frequently reported injection site reaction, noted in 47% of the half-dose group and 50% of the full-dose group. The rates of unsolicited adverse events were similar in both groups, the most common included diarrhea and cough, Dr. Mercer said.
No subjects in the full-dose group and three in the half-dose group discontinued the study because of adverse events. The only reported serious adverse event was one case of chronic urticaria in the half-dose group; no deaths were reported in either group.
As for efficacy, the full dose demonstrated noninferiority, compared with the half dose, against each of four strains: influenza A H1N1, influenza A H3N2, influenza B Victoria, and influenza B Yamagata. The geometric mean titers of the full and half doses for each of the four strains were, respectively, 310 and 214, 332 and 221, 348 and 261, and 349 and 243.
The potential action date for the supplemental Biologics License Application is January 2019, noted Dr. Mercer, who is employed by Sanofi Pasteur.
according to data from a randomized trial of nearly 2,000 children aged 6-35 months.
Data from previous studies have suggested that a full dose of vaccine may be more immunogenic in young children compared with a half dose, and Sanofi Pasteur has submitted a supplemental Biologics License Application to the Food and Drug Administration to allow use of the full 0.5-mL dose in children as young as 6 months, Monica Mercer, MD, of Sanofi Pasteur, said at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices in Atlanta.
Dr. Mercer presented findings from a phase IV randomized, observer-blinded study, in which the researchers assigned healthy children aged 6-35 months to receive Fluzone quadrivalent vaccine at a dose of 0.25 mL or 0.5 mL.
A total of 1,941 children (949 for the 0.25-mL dose and 992 for the 0.5-mL dose) were included in the safety analysis.
The most important safety outcome was to compare the rate of any fever, Dr. Mercer said at the meeting.
Overall, at 7 days after vaccination, the rate of fever was 11% for the half dose and 12% for the full dose, she said. The resulting difference of 0.84% met the criteria for noninferiority (less than 5%), she added.
In terms of safety, tenderness was the most frequently reported injection site reaction, noted in 47% of the half-dose group and 50% of the full-dose group. The rates of unsolicited adverse events were similar in both groups, the most common included diarrhea and cough, Dr. Mercer said.
No subjects in the full-dose group and three in the half-dose group discontinued the study because of adverse events. The only reported serious adverse event was one case of chronic urticaria in the half-dose group; no deaths were reported in either group.
As for efficacy, the full dose demonstrated noninferiority, compared with the half dose, against each of four strains: influenza A H1N1, influenza A H3N2, influenza B Victoria, and influenza B Yamagata. The geometric mean titers of the full and half doses for each of the four strains were, respectively, 310 and 214, 332 and 221, 348 and 261, and 349 and 243.
The potential action date for the supplemental Biologics License Application is January 2019, noted Dr. Mercer, who is employed by Sanofi Pasteur.
REPORTING FROM AN ACIP MEETING
Few clinical outcomes convincingly linked to sickle cell trait
Although sickle cell trait (SCT) has been linked to numerous adverse clinical outcomes in multiple studies, only a handful of those associations have strong supporting evidence, results of a systematic review suggest.
Venous and renal complications had the strongest evidence supporting an association with SCT, while exertion-related sudden death – perhaps the highest-profile potential complication of SCT – had moderate-strength evidence supporting a link, according to the review.
By contrast, most other associations between SCT and clinical outcomes had either low-strength evidence or insufficient data to support a link, according to Rakhi P. Naik, MD, of Johns Hopkins University, Baltimore, and coauthors of the review.
“Future rigorous studies are needed to address potential complications of SCT and to determine modifiers of risk,” they wrote. The report in the Annals of Internal Medicine.
The systematic review by Dr. Naik and colleagues focused on 41 studies, most of which were population-based cohort or case-control studies. They rated the evidence quality of each study and grouped 24 clinical outcomes of interest into six categories: exertion-related injury, renal, vascular, pediatric, surgery- and trauma-related outcomes, and mortality.
Exercise-related injury has received considerable attention, particularly in relation to the military and athletics.
The strength of evidence for a link between SCT and exertion-related death was low in their analysis, which included two studies evaluating the outcome. However, Dr. Naik and coauthors did note that SCT may be associated with a small absolute risk of exertion-related death in extreme conditions such a highly strenuous athletic training or the military.
“We do concur with the American Society of Hematology statement recommending against routine SCT screening in athletics and supporting the consistent use of universal precautions to mitigate exertion-related risk in all persons, regardless of SCT status,” they wrote.
Similarly, the absolute risk of exertional rhabdomyolysis in SCT is small and probably occurs only in high-intensity settings, with risk modified by other genetic and environmental factors, Dr. Naik and coauthors said, based on their analysis of two studies looking at this outcome.
Venous complications had a stronger body of evidence, including several studies showing high levels of procoagulants, which makes elevated venous thromboembolism risk plausible in individuals with SCT.
High-strength evidence linked pulmonary embolism, with or without deep-vein thrombosis, to SCT. In contrast, there was no increased risk of isolated deep-vein thrombosis in these individuals.
“The cause of this paradoxical observation is unknown but may be an increased risk for clot embolization in SCT,” Dr. Naik and colleagues wrote in a discussion of the results.
Renal outcomes were often attributed to SCT, and in this review, the authors said there was evidence to support SCT as a risk factor for both proteinuria and chronic kidney disease.
Out of six studies looking at proteinuria, the one high-quality study found a 1.86-fold increased risk for baseline albuminuria in African Americans with SCT versus those without, according to the review.
Out of four studies looking at chronic kidney disease, the two high-quality studies found 1.57- to 1.89-fold increased risk of those outcomes in African Americans with SCT.
Support for the study came in part from the National Human Genome Research Institute and the National Heart, Lung, and Blood Institute. The authors reported disclosures related to Novartis, Addmedica, and Global Blood Therapeutics, among others.
SOURCE: Naik RP et al. Ann Intern Med. 2018 Oct 30. doi:10.7326/M18-1161.
Although sickle cell trait (SCT) has been linked to numerous adverse clinical outcomes in multiple studies, only a handful of those associations have strong supporting evidence, results of a systematic review suggest.
Venous and renal complications had the strongest evidence supporting an association with SCT, while exertion-related sudden death – perhaps the highest-profile potential complication of SCT – had moderate-strength evidence supporting a link, according to the review.
By contrast, most other associations between SCT and clinical outcomes had either low-strength evidence or insufficient data to support a link, according to Rakhi P. Naik, MD, of Johns Hopkins University, Baltimore, and coauthors of the review.
“Future rigorous studies are needed to address potential complications of SCT and to determine modifiers of risk,” they wrote. The report in the Annals of Internal Medicine.
The systematic review by Dr. Naik and colleagues focused on 41 studies, most of which were population-based cohort or case-control studies. They rated the evidence quality of each study and grouped 24 clinical outcomes of interest into six categories: exertion-related injury, renal, vascular, pediatric, surgery- and trauma-related outcomes, and mortality.
Exercise-related injury has received considerable attention, particularly in relation to the military and athletics.
The strength of evidence for a link between SCT and exertion-related death was low in their analysis, which included two studies evaluating the outcome. However, Dr. Naik and coauthors did note that SCT may be associated with a small absolute risk of exertion-related death in extreme conditions such a highly strenuous athletic training or the military.
“We do concur with the American Society of Hematology statement recommending against routine SCT screening in athletics and supporting the consistent use of universal precautions to mitigate exertion-related risk in all persons, regardless of SCT status,” they wrote.
Similarly, the absolute risk of exertional rhabdomyolysis in SCT is small and probably occurs only in high-intensity settings, with risk modified by other genetic and environmental factors, Dr. Naik and coauthors said, based on their analysis of two studies looking at this outcome.
Venous complications had a stronger body of evidence, including several studies showing high levels of procoagulants, which makes elevated venous thromboembolism risk plausible in individuals with SCT.
High-strength evidence linked pulmonary embolism, with or without deep-vein thrombosis, to SCT. In contrast, there was no increased risk of isolated deep-vein thrombosis in these individuals.
“The cause of this paradoxical observation is unknown but may be an increased risk for clot embolization in SCT,” Dr. Naik and colleagues wrote in a discussion of the results.
Renal outcomes were often attributed to SCT, and in this review, the authors said there was evidence to support SCT as a risk factor for both proteinuria and chronic kidney disease.
Out of six studies looking at proteinuria, the one high-quality study found a 1.86-fold increased risk for baseline albuminuria in African Americans with SCT versus those without, according to the review.
Out of four studies looking at chronic kidney disease, the two high-quality studies found 1.57- to 1.89-fold increased risk of those outcomes in African Americans with SCT.
Support for the study came in part from the National Human Genome Research Institute and the National Heart, Lung, and Blood Institute. The authors reported disclosures related to Novartis, Addmedica, and Global Blood Therapeutics, among others.
SOURCE: Naik RP et al. Ann Intern Med. 2018 Oct 30. doi:10.7326/M18-1161.
Although sickle cell trait (SCT) has been linked to numerous adverse clinical outcomes in multiple studies, only a handful of those associations have strong supporting evidence, results of a systematic review suggest.
Venous and renal complications had the strongest evidence supporting an association with SCT, while exertion-related sudden death – perhaps the highest-profile potential complication of SCT – had moderate-strength evidence supporting a link, according to the review.
By contrast, most other associations between SCT and clinical outcomes had either low-strength evidence or insufficient data to support a link, according to Rakhi P. Naik, MD, of Johns Hopkins University, Baltimore, and coauthors of the review.
“Future rigorous studies are needed to address potential complications of SCT and to determine modifiers of risk,” they wrote. The report in the Annals of Internal Medicine.
The systematic review by Dr. Naik and colleagues focused on 41 studies, most of which were population-based cohort or case-control studies. They rated the evidence quality of each study and grouped 24 clinical outcomes of interest into six categories: exertion-related injury, renal, vascular, pediatric, surgery- and trauma-related outcomes, and mortality.
Exercise-related injury has received considerable attention, particularly in relation to the military and athletics.
The strength of evidence for a link between SCT and exertion-related death was low in their analysis, which included two studies evaluating the outcome. However, Dr. Naik and coauthors did note that SCT may be associated with a small absolute risk of exertion-related death in extreme conditions such a highly strenuous athletic training or the military.
“We do concur with the American Society of Hematology statement recommending against routine SCT screening in athletics and supporting the consistent use of universal precautions to mitigate exertion-related risk in all persons, regardless of SCT status,” they wrote.
Similarly, the absolute risk of exertional rhabdomyolysis in SCT is small and probably occurs only in high-intensity settings, with risk modified by other genetic and environmental factors, Dr. Naik and coauthors said, based on their analysis of two studies looking at this outcome.
Venous complications had a stronger body of evidence, including several studies showing high levels of procoagulants, which makes elevated venous thromboembolism risk plausible in individuals with SCT.
High-strength evidence linked pulmonary embolism, with or without deep-vein thrombosis, to SCT. In contrast, there was no increased risk of isolated deep-vein thrombosis in these individuals.
“The cause of this paradoxical observation is unknown but may be an increased risk for clot embolization in SCT,” Dr. Naik and colleagues wrote in a discussion of the results.
Renal outcomes were often attributed to SCT, and in this review, the authors said there was evidence to support SCT as a risk factor for both proteinuria and chronic kidney disease.
Out of six studies looking at proteinuria, the one high-quality study found a 1.86-fold increased risk for baseline albuminuria in African Americans with SCT versus those without, according to the review.
Out of four studies looking at chronic kidney disease, the two high-quality studies found 1.57- to 1.89-fold increased risk of those outcomes in African Americans with SCT.
Support for the study came in part from the National Human Genome Research Institute and the National Heart, Lung, and Blood Institute. The authors reported disclosures related to Novartis, Addmedica, and Global Blood Therapeutics, among others.
SOURCE: Naik RP et al. Ann Intern Med. 2018 Oct 30. doi:10.7326/M18-1161.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point:
Major finding: Risks of 1.57-fold and higher were seen in high-quality studies linking SCT to venous and renal complications, while studies of moderate quality suggested small absolute risks of exertion-related mortality or rhabdomyolysis.
Study details: A systematic review including 41 mostly population-based cohort or case-control studies looking at 24 clinical outcomes of interest.
Disclosures: Support for the study came in part from the National Human Genome Research Institute and the National Heart, Lung, and Blood Institute. The authors reported disclosures related to Novartis, Addmedica, and Global Blood Therapeutics, among others.
Source: Naik RP et al. Ann Intern Med. 2018 Oct 30. doi:10.7326/M18-1161.
Kids and guns: Injury costs rose as incidence fell
Hospital costs for children with firearm-related injuries rose from 2006 to 2014, while the incidence of emergency department visits declined over the same period, according to the first national study of such visits in children.
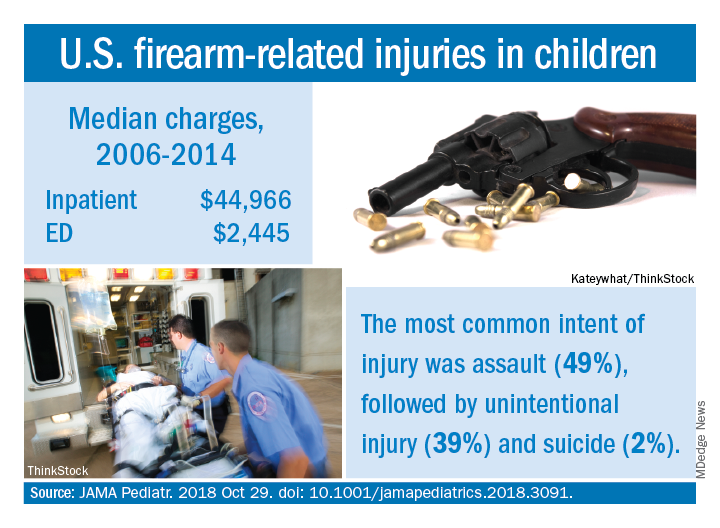
Median charges were $2,445 for an ED visit and $44,966 for inpatient management of individuals under 18 years of age for the entire study period, with both increasing over time and all data adjusted to 2018 dollars. The median charge for an ED visit rose from over $2,100 in 2006 to under $2,900 in 2014, while the inpatient median increased from approximately $43,000 to about $59,000. Total charges for firearm-related injuries in children were $2.5 billion during 2006-2014, with a mean of $270 million a year, Faiz Gani, MBBS, and Joseph K. Canner, MHS, said in JAMA Pediatrics.
The overall incidence of ED visits was 11.3/100,000 children under 18 years of age for the study period, with a steady decline seen from 2006, when incidence was about 15 visits/100,000, to 10/100,000 in 2014. The rate had dropped to about 7.5 visits/100,000 in 2013 before increasing in 2014, Dr. Gani and Mr. Canner of Johns Hopkins University, Baltimore, said based on data for 75,086 visits from the Nationwide Emergency Medicine Sample.
A trend observed throughout the course of the study was the higher incidence of ED visits among males, which was consistently more than five times higher than that of females. The highest incidence by age group was 85.9/100,000 for males aged 15-17 years. The most common intent of injury was assault at 49%, with unintentional injury next at 39% and suicide at 2%, the investigators reported.
This “first and largest nationally representative study” demonstrates the “substantial clinical and financial burden associated with firearm-related injuries among pediatric patients. Moving forward, additional resources and funds should be allocated to the study of firearm-related injuries. Only through further understanding of the social, political, and health-related risk factors for these injuries can we develop and implement effective policies to address this public health concern, wrote Dr. Gani and Mr. Canner, who reported no conflicts of interest.
SOURCE: JAMA Pediatr. 2018 Oct 29. doi: 10.1001/jamapediatrics.2018.3091.
Hospital costs for children with firearm-related injuries rose from 2006 to 2014, while the incidence of emergency department visits declined over the same period, according to the first national study of such visits in children.
Median charges were $2,445 for an ED visit and $44,966 for inpatient management of individuals under 18 years of age for the entire study period, with both increasing over time and all data adjusted to 2018 dollars. The median charge for an ED visit rose from over $2,100 in 2006 to under $2,900 in 2014, while the inpatient median increased from approximately $43,000 to about $59,000. Total charges for firearm-related injuries in children were $2.5 billion during 2006-2014, with a mean of $270 million a year, Faiz Gani, MBBS, and Joseph K. Canner, MHS, said in JAMA Pediatrics.
The overall incidence of ED visits was 11.3/100,000 children under 18 years of age for the study period, with a steady decline seen from 2006, when incidence was about 15 visits/100,000, to 10/100,000 in 2014. The rate had dropped to about 7.5 visits/100,000 in 2013 before increasing in 2014, Dr. Gani and Mr. Canner of Johns Hopkins University, Baltimore, said based on data for 75,086 visits from the Nationwide Emergency Medicine Sample.
A trend observed throughout the course of the study was the higher incidence of ED visits among males, which was consistently more than five times higher than that of females. The highest incidence by age group was 85.9/100,000 for males aged 15-17 years. The most common intent of injury was assault at 49%, with unintentional injury next at 39% and suicide at 2%, the investigators reported.
This “first and largest nationally representative study” demonstrates the “substantial clinical and financial burden associated with firearm-related injuries among pediatric patients. Moving forward, additional resources and funds should be allocated to the study of firearm-related injuries. Only through further understanding of the social, political, and health-related risk factors for these injuries can we develop and implement effective policies to address this public health concern, wrote Dr. Gani and Mr. Canner, who reported no conflicts of interest.
SOURCE: JAMA Pediatr. 2018 Oct 29. doi: 10.1001/jamapediatrics.2018.3091.
Hospital costs for children with firearm-related injuries rose from 2006 to 2014, while the incidence of emergency department visits declined over the same period, according to the first national study of such visits in children.
Median charges were $2,445 for an ED visit and $44,966 for inpatient management of individuals under 18 years of age for the entire study period, with both increasing over time and all data adjusted to 2018 dollars. The median charge for an ED visit rose from over $2,100 in 2006 to under $2,900 in 2014, while the inpatient median increased from approximately $43,000 to about $59,000. Total charges for firearm-related injuries in children were $2.5 billion during 2006-2014, with a mean of $270 million a year, Faiz Gani, MBBS, and Joseph K. Canner, MHS, said in JAMA Pediatrics.
The overall incidence of ED visits was 11.3/100,000 children under 18 years of age for the study period, with a steady decline seen from 2006, when incidence was about 15 visits/100,000, to 10/100,000 in 2014. The rate had dropped to about 7.5 visits/100,000 in 2013 before increasing in 2014, Dr. Gani and Mr. Canner of Johns Hopkins University, Baltimore, said based on data for 75,086 visits from the Nationwide Emergency Medicine Sample.
A trend observed throughout the course of the study was the higher incidence of ED visits among males, which was consistently more than five times higher than that of females. The highest incidence by age group was 85.9/100,000 for males aged 15-17 years. The most common intent of injury was assault at 49%, with unintentional injury next at 39% and suicide at 2%, the investigators reported.
This “first and largest nationally representative study” demonstrates the “substantial clinical and financial burden associated with firearm-related injuries among pediatric patients. Moving forward, additional resources and funds should be allocated to the study of firearm-related injuries. Only through further understanding of the social, political, and health-related risk factors for these injuries can we develop and implement effective policies to address this public health concern, wrote Dr. Gani and Mr. Canner, who reported no conflicts of interest.
SOURCE: JAMA Pediatr. 2018 Oct 29. doi: 10.1001/jamapediatrics.2018.3091.
FROM JAMA PEDIATRICS
Team tracks changes in height, weight in pediatric ALL
New research suggests several factors may be associated with the risk of short stature and excess weight gain in children with acute lymphoblastic leukemia (ALL).
Researchers found that patients who were younger at ALL diagnosis had an increased risk of becoming overweight or obese both during and after therapy.
Patients had an increased risk of short stature after therapy if they were older at diagnosis or had standard or high-risk disease, higher white blood cell counts at diagnosis, and central nervous system disease.
The researchers reported these findings in Cancer.
The team looked at 372 children with ALL, reviewing changes in their body mass index (BMI), weight, and height from diagnosis to 5 years after treatment ended.
The patients were treated with the Total XV protocol between 2000 and 2007 (NCT00137111). They received 6 weeks of induction therapy, 8 weeks of consolidation, and continuation for 120 weeks in females and 146 weeks in males.
BMI changes
Roughly a quarter of patients were overweight or obese at diagnosis, but that increased to roughly half of patients by the time they had been off therapy for 5 years.
“Over the whole population that was studied, we found statistically significant weight gain even during remission-induction therapy,” said study author Hiroto Inaba, MD, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
Patients’ median BMI z scores increased significantly during induction (P<0.001) and reinduction (P=0.001) with glucocorticoid therapy as well as in the first year after therapy ended (P=0.006).
At various points during treatment, there were significant differences in BMI z scores according to sex, race, and disease risk group. However, these differences were not present after therapy.
On the other hand, there were significant differences in BMI z scores according to age both during and after therapy.
Between week 21 of treatment and 3 years after therapy ended, patients who were ages 2 to 9 at diagnosis had median BMI z scores that were significantly higher than scores of patients who were age 10 or older at diagnosis (P≤0.033 for all time points).
The researchers also found that patients who were of a healthy weight or underweight at the time of diagnosis had a significantly higher risk of becoming overweight or obese during or after therapy if they were ages 2 to 9 at diagnosis, compared to the older patients (P=0.001).
Height changes
The researchers found that height z scores declined during treatment and improved after it ended, although z scores “never improved to the levels noted at the time of diagnosis.”
Median height z scores at the end of induction and in continuation weeks 1 to 21 were significantly higher in patients age 10 or older at diagnosis than in patients ages to 2 to 9 at diagnosis (P≤0.038 for all time points).
However, the median height z scores at 5 years off therapy were significantly higher for the younger patients than for the older patients (P=0.011).
The median height z scores were higher for patients with low-risk disease than for standard- or high-risk patients in weeks 17, 21, 48, and 146 of treatment and at 1 to 3 years after therapy ended (P≤0.024 for all time points).
At 3 years to 5 years after treatment ended, the median height z scores were significantly higher among patients with white blood cell counts below 50 × 109/L at diagnosis (P≤0.018 for all time points).
Patients without central nervous system disease had significantly higher median height z scores at 3 years after treatment ended (P=0.029).
Males had significantly higher median height z scores than females in weeks 96 and 120 of therapy (P≤0.009 for both time points).
And white patients had higher median height z scores than black patients at 2 to 4 years after treatment ended (P≤0.027 for all time points).
Implications
To address the issue of excess weight gain in ALL patients, the researchers suggested early interventions, such as education about proper diet and exercise.
“When you look at the literature of childhood obesity prevention for the general population, there are interventions that could also help ALL patients,” said study author Emily Browne, of St. Jude.
“But we need to adapt those recommendations to take the cancer therapy into account.”
For the issue of height, the researchers recommended evaluating certain patients for growth hormone deficiency.
The team also noted that further study is needed to determine whether emerging therapeutic approaches can reduce toxicities without compromising antileukemic effects.
“We are hoping new therapeutic options can decrease intensity of chemotherapy and keep normal tissues intact,” Dr. Inaba said. “But until then, we’re collaborating with multiple clinical departments to help ensure a good, quality cure and a good quality of life in survivorship.”
This research was supported by grants from the National Institutes of Health and ALSAC, the fundraising and awareness organization of St. Jude.
New research suggests several factors may be associated with the risk of short stature and excess weight gain in children with acute lymphoblastic leukemia (ALL).
Researchers found that patients who were younger at ALL diagnosis had an increased risk of becoming overweight or obese both during and after therapy.
Patients had an increased risk of short stature after therapy if they were older at diagnosis or had standard or high-risk disease, higher white blood cell counts at diagnosis, and central nervous system disease.
The researchers reported these findings in Cancer.
The team looked at 372 children with ALL, reviewing changes in their body mass index (BMI), weight, and height from diagnosis to 5 years after treatment ended.
The patients were treated with the Total XV protocol between 2000 and 2007 (NCT00137111). They received 6 weeks of induction therapy, 8 weeks of consolidation, and continuation for 120 weeks in females and 146 weeks in males.
BMI changes
Roughly a quarter of patients were overweight or obese at diagnosis, but that increased to roughly half of patients by the time they had been off therapy for 5 years.
“Over the whole population that was studied, we found statistically significant weight gain even during remission-induction therapy,” said study author Hiroto Inaba, MD, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
Patients’ median BMI z scores increased significantly during induction (P<0.001) and reinduction (P=0.001) with glucocorticoid therapy as well as in the first year after therapy ended (P=0.006).
At various points during treatment, there were significant differences in BMI z scores according to sex, race, and disease risk group. However, these differences were not present after therapy.
On the other hand, there were significant differences in BMI z scores according to age both during and after therapy.
Between week 21 of treatment and 3 years after therapy ended, patients who were ages 2 to 9 at diagnosis had median BMI z scores that were significantly higher than scores of patients who were age 10 or older at diagnosis (P≤0.033 for all time points).
The researchers also found that patients who were of a healthy weight or underweight at the time of diagnosis had a significantly higher risk of becoming overweight or obese during or after therapy if they were ages 2 to 9 at diagnosis, compared to the older patients (P=0.001).
Height changes
The researchers found that height z scores declined during treatment and improved after it ended, although z scores “never improved to the levels noted at the time of diagnosis.”
Median height z scores at the end of induction and in continuation weeks 1 to 21 were significantly higher in patients age 10 or older at diagnosis than in patients ages to 2 to 9 at diagnosis (P≤0.038 for all time points).
However, the median height z scores at 5 years off therapy were significantly higher for the younger patients than for the older patients (P=0.011).
The median height z scores were higher for patients with low-risk disease than for standard- or high-risk patients in weeks 17, 21, 48, and 146 of treatment and at 1 to 3 years after therapy ended (P≤0.024 for all time points).
At 3 years to 5 years after treatment ended, the median height z scores were significantly higher among patients with white blood cell counts below 50 × 109/L at diagnosis (P≤0.018 for all time points).
Patients without central nervous system disease had significantly higher median height z scores at 3 years after treatment ended (P=0.029).
Males had significantly higher median height z scores than females in weeks 96 and 120 of therapy (P≤0.009 for both time points).
And white patients had higher median height z scores than black patients at 2 to 4 years after treatment ended (P≤0.027 for all time points).
Implications
To address the issue of excess weight gain in ALL patients, the researchers suggested early interventions, such as education about proper diet and exercise.
“When you look at the literature of childhood obesity prevention for the general population, there are interventions that could also help ALL patients,” said study author Emily Browne, of St. Jude.
“But we need to adapt those recommendations to take the cancer therapy into account.”
For the issue of height, the researchers recommended evaluating certain patients for growth hormone deficiency.
The team also noted that further study is needed to determine whether emerging therapeutic approaches can reduce toxicities without compromising antileukemic effects.
“We are hoping new therapeutic options can decrease intensity of chemotherapy and keep normal tissues intact,” Dr. Inaba said. “But until then, we’re collaborating with multiple clinical departments to help ensure a good, quality cure and a good quality of life in survivorship.”
This research was supported by grants from the National Institutes of Health and ALSAC, the fundraising and awareness organization of St. Jude.
New research suggests several factors may be associated with the risk of short stature and excess weight gain in children with acute lymphoblastic leukemia (ALL).
Researchers found that patients who were younger at ALL diagnosis had an increased risk of becoming overweight or obese both during and after therapy.
Patients had an increased risk of short stature after therapy if they were older at diagnosis or had standard or high-risk disease, higher white blood cell counts at diagnosis, and central nervous system disease.
The researchers reported these findings in Cancer.
The team looked at 372 children with ALL, reviewing changes in their body mass index (BMI), weight, and height from diagnosis to 5 years after treatment ended.
The patients were treated with the Total XV protocol between 2000 and 2007 (NCT00137111). They received 6 weeks of induction therapy, 8 weeks of consolidation, and continuation for 120 weeks in females and 146 weeks in males.
BMI changes
Roughly a quarter of patients were overweight or obese at diagnosis, but that increased to roughly half of patients by the time they had been off therapy for 5 years.
“Over the whole population that was studied, we found statistically significant weight gain even during remission-induction therapy,” said study author Hiroto Inaba, MD, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
Patients’ median BMI z scores increased significantly during induction (P<0.001) and reinduction (P=0.001) with glucocorticoid therapy as well as in the first year after therapy ended (P=0.006).
At various points during treatment, there were significant differences in BMI z scores according to sex, race, and disease risk group. However, these differences were not present after therapy.
On the other hand, there were significant differences in BMI z scores according to age both during and after therapy.
Between week 21 of treatment and 3 years after therapy ended, patients who were ages 2 to 9 at diagnosis had median BMI z scores that were significantly higher than scores of patients who were age 10 or older at diagnosis (P≤0.033 for all time points).
The researchers also found that patients who were of a healthy weight or underweight at the time of diagnosis had a significantly higher risk of becoming overweight or obese during or after therapy if they were ages 2 to 9 at diagnosis, compared to the older patients (P=0.001).
Height changes
The researchers found that height z scores declined during treatment and improved after it ended, although z scores “never improved to the levels noted at the time of diagnosis.”
Median height z scores at the end of induction and in continuation weeks 1 to 21 were significantly higher in patients age 10 or older at diagnosis than in patients ages to 2 to 9 at diagnosis (P≤0.038 for all time points).
However, the median height z scores at 5 years off therapy were significantly higher for the younger patients than for the older patients (P=0.011).
The median height z scores were higher for patients with low-risk disease than for standard- or high-risk patients in weeks 17, 21, 48, and 146 of treatment and at 1 to 3 years after therapy ended (P≤0.024 for all time points).
At 3 years to 5 years after treatment ended, the median height z scores were significantly higher among patients with white blood cell counts below 50 × 109/L at diagnosis (P≤0.018 for all time points).
Patients without central nervous system disease had significantly higher median height z scores at 3 years after treatment ended (P=0.029).
Males had significantly higher median height z scores than females in weeks 96 and 120 of therapy (P≤0.009 for both time points).
And white patients had higher median height z scores than black patients at 2 to 4 years after treatment ended (P≤0.027 for all time points).
Implications
To address the issue of excess weight gain in ALL patients, the researchers suggested early interventions, such as education about proper diet and exercise.
“When you look at the literature of childhood obesity prevention for the general population, there are interventions that could also help ALL patients,” said study author Emily Browne, of St. Jude.
“But we need to adapt those recommendations to take the cancer therapy into account.”
For the issue of height, the researchers recommended evaluating certain patients for growth hormone deficiency.
The team also noted that further study is needed to determine whether emerging therapeutic approaches can reduce toxicities without compromising antileukemic effects.
“We are hoping new therapeutic options can decrease intensity of chemotherapy and keep normal tissues intact,” Dr. Inaba said. “But until then, we’re collaborating with multiple clinical departments to help ensure a good, quality cure and a good quality of life in survivorship.”
This research was supported by grants from the National Institutes of Health and ALSAC, the fundraising and awareness organization of St. Jude.
Talk to adolescents about sexual assault
SEATTLE – Recent events have highlighted the issue of sexual assault in adolescents. But the onus still is on psychiatrists and other clinicians to ask patients whether they’ve ever been a victim of sexual assault or other kinds of trauma, according to an expert.
“It turns out that these experiences are common for kids, and they’re very correlated with the development of all kinds of psychiatric disorders. And if we ask, they will tell us. If we don’t ask they probably won’t,” said Lucy Berliner, director of the Harborview Center for Sexual Assault and Traumatic Stress, who discussed the epidemiology of sexual trauma in adolescents at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
A common misconception is that victims of sexual assault have endured multiple, chronic traumas. A more common scenario, however, is a single incident, much like the one described by Christine Blasey Ford, PhD, in her testimony before Congress, and clinicians should be more on the lookout for such cases. “I think those young people get a little bit lost,” Ms. Berliner said at the meeting.
Unlike the incident described by Dr. Ford, coercion often was not physical. Fifty-two percent of the time, the adolescents experienced abuse by authority figures, such as an assault by a teacher or coach, or even someone who used social advantage such as being older or more popular. In 17% of the cases, the victim was drugged or unconscious. Physical restraint was reported in 20% of cases. Weapons were involved only 7% of the time.
Twenty-eight percent of the adolescents were victims of a teenager, compared with 54% who attributed the assault to an adult. Overall, 72% of the subjects presented at an emergency department rather than a counseling clinic, which suggests that screening in medical environments also is a key factor in identifying and responding to people who have been assaulted.
All study subjects were offered counseling, but the uptake was low: The median was 2 sessions.
“My guess is that in the beginning, a lot of people say, ‘I just want to put it behind me, or I want to try to figure it out myself,’ and it only comes around later, in mental health settings, where these kids are in there for some type of psychiatric disorder. And unless we ask, we’re not going to find out (about a previous assault), and we won’t be able to give them the help that would help them with this psychiatric disorder,” said Ms. Berliner, also a clinical associate professor at the University of Washington School of Social Work in Seattle.
Clinicians might not ask about these experiences, she said, because of fears of triggering raw emotions. But such fears are unfounded, she stated. “We need to get over ourselves,” Ms. Berliner said. “If we don’t create the opportunity, why would they tell us? And if they don’t want to tell us, they won’t. But you can’t traumatize a kid by talking about something that’s already actually happened to them.”
That point can even extend to the legal system. Also during the session, Emily Petersen, senior deputy prosecuting attorney in the Special Assault Unit in King County, Washington, emphasized that, in her experience, young people who are victims of sexual and other forms of assault are resilient – and they will not be traumatized by speaking with a prosecutor or to police about their experiences.
But the legal system cannot provide healing, she and Ms. Berliner noted. That must come from the victim’s support system. “These experiences don’t have to define victims of sexual assault as long as the adults in their lives are responding appropriately to them,” Ms. Petersen said.
Ms. Berliner and Ms. Petersen disclosed no conflicts of interest.
SEATTLE – Recent events have highlighted the issue of sexual assault in adolescents. But the onus still is on psychiatrists and other clinicians to ask patients whether they’ve ever been a victim of sexual assault or other kinds of trauma, according to an expert.
“It turns out that these experiences are common for kids, and they’re very correlated with the development of all kinds of psychiatric disorders. And if we ask, they will tell us. If we don’t ask they probably won’t,” said Lucy Berliner, director of the Harborview Center for Sexual Assault and Traumatic Stress, who discussed the epidemiology of sexual trauma in adolescents at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
A common misconception is that victims of sexual assault have endured multiple, chronic traumas. A more common scenario, however, is a single incident, much like the one described by Christine Blasey Ford, PhD, in her testimony before Congress, and clinicians should be more on the lookout for such cases. “I think those young people get a little bit lost,” Ms. Berliner said at the meeting.
Unlike the incident described by Dr. Ford, coercion often was not physical. Fifty-two percent of the time, the adolescents experienced abuse by authority figures, such as an assault by a teacher or coach, or even someone who used social advantage such as being older or more popular. In 17% of the cases, the victim was drugged or unconscious. Physical restraint was reported in 20% of cases. Weapons were involved only 7% of the time.
Twenty-eight percent of the adolescents were victims of a teenager, compared with 54% who attributed the assault to an adult. Overall, 72% of the subjects presented at an emergency department rather than a counseling clinic, which suggests that screening in medical environments also is a key factor in identifying and responding to people who have been assaulted.
All study subjects were offered counseling, but the uptake was low: The median was 2 sessions.
“My guess is that in the beginning, a lot of people say, ‘I just want to put it behind me, or I want to try to figure it out myself,’ and it only comes around later, in mental health settings, where these kids are in there for some type of psychiatric disorder. And unless we ask, we’re not going to find out (about a previous assault), and we won’t be able to give them the help that would help them with this psychiatric disorder,” said Ms. Berliner, also a clinical associate professor at the University of Washington School of Social Work in Seattle.
Clinicians might not ask about these experiences, she said, because of fears of triggering raw emotions. But such fears are unfounded, she stated. “We need to get over ourselves,” Ms. Berliner said. “If we don’t create the opportunity, why would they tell us? And if they don’t want to tell us, they won’t. But you can’t traumatize a kid by talking about something that’s already actually happened to them.”
That point can even extend to the legal system. Also during the session, Emily Petersen, senior deputy prosecuting attorney in the Special Assault Unit in King County, Washington, emphasized that, in her experience, young people who are victims of sexual and other forms of assault are resilient – and they will not be traumatized by speaking with a prosecutor or to police about their experiences.
But the legal system cannot provide healing, she and Ms. Berliner noted. That must come from the victim’s support system. “These experiences don’t have to define victims of sexual assault as long as the adults in their lives are responding appropriately to them,” Ms. Petersen said.
Ms. Berliner and Ms. Petersen disclosed no conflicts of interest.
SEATTLE – Recent events have highlighted the issue of sexual assault in adolescents. But the onus still is on psychiatrists and other clinicians to ask patients whether they’ve ever been a victim of sexual assault or other kinds of trauma, according to an expert.
“It turns out that these experiences are common for kids, and they’re very correlated with the development of all kinds of psychiatric disorders. And if we ask, they will tell us. If we don’t ask they probably won’t,” said Lucy Berliner, director of the Harborview Center for Sexual Assault and Traumatic Stress, who discussed the epidemiology of sexual trauma in adolescents at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
A common misconception is that victims of sexual assault have endured multiple, chronic traumas. A more common scenario, however, is a single incident, much like the one described by Christine Blasey Ford, PhD, in her testimony before Congress, and clinicians should be more on the lookout for such cases. “I think those young people get a little bit lost,” Ms. Berliner said at the meeting.
Unlike the incident described by Dr. Ford, coercion often was not physical. Fifty-two percent of the time, the adolescents experienced abuse by authority figures, such as an assault by a teacher or coach, or even someone who used social advantage such as being older or more popular. In 17% of the cases, the victim was drugged or unconscious. Physical restraint was reported in 20% of cases. Weapons were involved only 7% of the time.
Twenty-eight percent of the adolescents were victims of a teenager, compared with 54% who attributed the assault to an adult. Overall, 72% of the subjects presented at an emergency department rather than a counseling clinic, which suggests that screening in medical environments also is a key factor in identifying and responding to people who have been assaulted.
All study subjects were offered counseling, but the uptake was low: The median was 2 sessions.
“My guess is that in the beginning, a lot of people say, ‘I just want to put it behind me, or I want to try to figure it out myself,’ and it only comes around later, in mental health settings, where these kids are in there for some type of psychiatric disorder. And unless we ask, we’re not going to find out (about a previous assault), and we won’t be able to give them the help that would help them with this psychiatric disorder,” said Ms. Berliner, also a clinical associate professor at the University of Washington School of Social Work in Seattle.
Clinicians might not ask about these experiences, she said, because of fears of triggering raw emotions. But such fears are unfounded, she stated. “We need to get over ourselves,” Ms. Berliner said. “If we don’t create the opportunity, why would they tell us? And if they don’t want to tell us, they won’t. But you can’t traumatize a kid by talking about something that’s already actually happened to them.”
That point can even extend to the legal system. Also during the session, Emily Petersen, senior deputy prosecuting attorney in the Special Assault Unit in King County, Washington, emphasized that, in her experience, young people who are victims of sexual and other forms of assault are resilient – and they will not be traumatized by speaking with a prosecutor or to police about their experiences.
But the legal system cannot provide healing, she and Ms. Berliner noted. That must come from the victim’s support system. “These experiences don’t have to define victims of sexual assault as long as the adults in their lives are responding appropriately to them,” Ms. Petersen said.
Ms. Berliner and Ms. Petersen disclosed no conflicts of interest.
REPORTING FROM AACAP 2018
FDA approves Xyrem to treat children with narcolepsy
The Food and Drug Administration has cleared Xyrem (sodium oxybate) oral solution to treat cataplexy and excessive daytime sleepiness in patients ages 7-17 with narcolepsy.

The central nervous system depressant previously had been approved to treat cataplexy in adults with narcolepsy.
The current approval was granted by the FDA under a Priority Review designation. Xyrem also received the FDA’s Orphan Drug designation, which is intended to encourage the development of drugs for rare diseases.
The agency noted in a press release, however, that the drug would continue to be available only through risk evaluation mitigation strategy (REMS) programs because of “the risk of serious outcomes resulting from inappropriate prescribing, misuse, abuse and diversion.” Xyrem either alone or in combination with other CNS depressants may be associated with reactions including seizure, respiratory depression, decreases in the level of consciousness, coma, and death, the FDA said.
The most common adverse reactions in pediatric patients were enuresis, nausea, headache, vomiting, weight decrease, decreased appetite, and dizziness.
For more information on prescribing Xyrem for pediatric patients, see the revised labeling information on the FDA website.
The Food and Drug Administration has cleared Xyrem (sodium oxybate) oral solution to treat cataplexy and excessive daytime sleepiness in patients ages 7-17 with narcolepsy.
The central nervous system depressant previously had been approved to treat cataplexy in adults with narcolepsy.
The current approval was granted by the FDA under a Priority Review designation. Xyrem also received the FDA’s Orphan Drug designation, which is intended to encourage the development of drugs for rare diseases.
The agency noted in a press release, however, that the drug would continue to be available only through risk evaluation mitigation strategy (REMS) programs because of “the risk of serious outcomes resulting from inappropriate prescribing, misuse, abuse and diversion.” Xyrem either alone or in combination with other CNS depressants may be associated with reactions including seizure, respiratory depression, decreases in the level of consciousness, coma, and death, the FDA said.
The most common adverse reactions in pediatric patients were enuresis, nausea, headache, vomiting, weight decrease, decreased appetite, and dizziness.
For more information on prescribing Xyrem for pediatric patients, see the revised labeling information on the FDA website.
The Food and Drug Administration has cleared Xyrem (sodium oxybate) oral solution to treat cataplexy and excessive daytime sleepiness in patients ages 7-17 with narcolepsy.
The central nervous system depressant previously had been approved to treat cataplexy in adults with narcolepsy.
The current approval was granted by the FDA under a Priority Review designation. Xyrem also received the FDA’s Orphan Drug designation, which is intended to encourage the development of drugs for rare diseases.
The agency noted in a press release, however, that the drug would continue to be available only through risk evaluation mitigation strategy (REMS) programs because of “the risk of serious outcomes resulting from inappropriate prescribing, misuse, abuse and diversion.” Xyrem either alone or in combination with other CNS depressants may be associated with reactions including seizure, respiratory depression, decreases in the level of consciousness, coma, and death, the FDA said.
The most common adverse reactions in pediatric patients were enuresis, nausea, headache, vomiting, weight decrease, decreased appetite, and dizziness.
For more information on prescribing Xyrem for pediatric patients, see the revised labeling information on the FDA website.
Collaborative approach for suicidal youth helps providers, too
SEATTLE – When it comes to treating children and adolescents who have experienced trauma and present suicidality, it is not just the patients who need support. Clinicians also experience grave anxiety when dealing with a traumatized child exhibiting suicidal behavior. The Collaborative Assessment and Management of Suicide (CAMS) framework can help clinicians or health care workers manage the care of these challenging patients.

CAMS is well established in adults with suicidal behavior, but it is unproven in youth and adolescents. The key is to its success in younger patients will be whether the program is developmentally appropriate, according to Molly C. Adrian, PhD, assistant professor of psychiatry and behavioral medicine at the University of Washington, Seattle. Dr. Adrian discussed CAMS and its potential applications at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
The CAMS approach emphasizes cooperation between the therapist and patient. “Adolescents are seeking autonomy and independence, and so it’s a good fit philosophically that you would partner alongside the teen as opposed to starting in a more adversarial sort of way – not that we as therapists ever do that. But it can be more tense when suicide is on the table and you feel unprepared,” Dr. Adrian said.
Seattle Children’s Hospital is persuaded enough to make CAMS part of its standard of care, Dr. Adrian said.
CAMS is a framework for patient management that has no prerequisites for the therapeutic approach. “It’s principle driven, not protocol driven. Clinicians can use whatever specific interventions they feel are appropriate for the drivers (of the suicidality). What we’re trying to change is the approach to the suicidal patient, so that it is not an anxiety-provoking, terrifying experience for the clinician – because we know that a suicidal patient is the most anxiety-provoking task for clinicians,” Dr. Adrian said. “We want clinicians to feel prepared and protected in providing the elements of care,” Dr. Adrian said in an interview.
The framework incorporates a suicide-status form (SSF), which assesses theory-driven and epidemiologically guided risk factors and helps to identify the drivers or the reasons why suicide is compelling to the patient. Those drivers then help inform crisis prevention efforts and the selection of interventions.
Three randomized, controlled trials have demonstrated the efficacy of CAMS over standard of care in adult patients, showing that the SSF is an effective assessment tool and that CAMS reduces suicidal ideation and leads to decreases in distress, depression, and hopelessness. There are no randomized, controlled trials showing its efficacy in children, but Seattle Children’s Hospital is conducting a pilot study in 12 youth and have found a 40% response rate at 8 weeks.
The SSF gauges the patient’s status and trajectory, while the CAMS therapeutic worksheet helps to distinguish direct and indirect drivers of suicidal behavior. In cases in which trauma symptoms or experiences are tied to suicidal behavior, they receive priority for treatment. The framework provides for discussion of options and treatment choice through collaboration between the clinician and the patient.
The patient and clinician fill out an SSF in the first session and use it to create a crisis convention plan, which includes gaining a commitment to treatment, removing or restricting access to lethal means, and incorporating parental monitoring.
Dr. Adrian is hopeful that the CAMS framework will help health care workers address suicidality in traumatized youth and adolescents. Currently, they may feel intimidated by a stricken child’s issues. “You don’t want to be responsible for a child dying, so you may overrespond with an intervention like an emergency department evaluation or an inpatient hospitalization that may be iatrogenic – there are data coming out from adults that hospitalization contributes to suicide risk above and beyond other risk factors,” Dr. Adrian said.
CAMS is simple and flexible, according to Dr. Adrian, and can be used by psychiatrists, social workers, substance use counselors, and others. At Seattle Children’s Hospital, clinicians have embraced it. “They feel it changes their practice. It gets to the heart of the matter quickly, and they feel more confident having that framework,” Dr. Adrian said.
Dr. Adrian has no conflicts of interest or disclosures.
SEATTLE – When it comes to treating children and adolescents who have experienced trauma and present suicidality, it is not just the patients who need support. Clinicians also experience grave anxiety when dealing with a traumatized child exhibiting suicidal behavior. The Collaborative Assessment and Management of Suicide (CAMS) framework can help clinicians or health care workers manage the care of these challenging patients.
CAMS is well established in adults with suicidal behavior, but it is unproven in youth and adolescents. The key is to its success in younger patients will be whether the program is developmentally appropriate, according to Molly C. Adrian, PhD, assistant professor of psychiatry and behavioral medicine at the University of Washington, Seattle. Dr. Adrian discussed CAMS and its potential applications at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
The CAMS approach emphasizes cooperation between the therapist and patient. “Adolescents are seeking autonomy and independence, and so it’s a good fit philosophically that you would partner alongside the teen as opposed to starting in a more adversarial sort of way – not that we as therapists ever do that. But it can be more tense when suicide is on the table and you feel unprepared,” Dr. Adrian said.
Seattle Children’s Hospital is persuaded enough to make CAMS part of its standard of care, Dr. Adrian said.
CAMS is a framework for patient management that has no prerequisites for the therapeutic approach. “It’s principle driven, not protocol driven. Clinicians can use whatever specific interventions they feel are appropriate for the drivers (of the suicidality). What we’re trying to change is the approach to the suicidal patient, so that it is not an anxiety-provoking, terrifying experience for the clinician – because we know that a suicidal patient is the most anxiety-provoking task for clinicians,” Dr. Adrian said. “We want clinicians to feel prepared and protected in providing the elements of care,” Dr. Adrian said in an interview.
The framework incorporates a suicide-status form (SSF), which assesses theory-driven and epidemiologically guided risk factors and helps to identify the drivers or the reasons why suicide is compelling to the patient. Those drivers then help inform crisis prevention efforts and the selection of interventions.
Three randomized, controlled trials have demonstrated the efficacy of CAMS over standard of care in adult patients, showing that the SSF is an effective assessment tool and that CAMS reduces suicidal ideation and leads to decreases in distress, depression, and hopelessness. There are no randomized, controlled trials showing its efficacy in children, but Seattle Children’s Hospital is conducting a pilot study in 12 youth and have found a 40% response rate at 8 weeks.
The SSF gauges the patient’s status and trajectory, while the CAMS therapeutic worksheet helps to distinguish direct and indirect drivers of suicidal behavior. In cases in which trauma symptoms or experiences are tied to suicidal behavior, they receive priority for treatment. The framework provides for discussion of options and treatment choice through collaboration between the clinician and the patient.
The patient and clinician fill out an SSF in the first session and use it to create a crisis convention plan, which includes gaining a commitment to treatment, removing or restricting access to lethal means, and incorporating parental monitoring.
Dr. Adrian is hopeful that the CAMS framework will help health care workers address suicidality in traumatized youth and adolescents. Currently, they may feel intimidated by a stricken child’s issues. “You don’t want to be responsible for a child dying, so you may overrespond with an intervention like an emergency department evaluation or an inpatient hospitalization that may be iatrogenic – there are data coming out from adults that hospitalization contributes to suicide risk above and beyond other risk factors,” Dr. Adrian said.
CAMS is simple and flexible, according to Dr. Adrian, and can be used by psychiatrists, social workers, substance use counselors, and others. At Seattle Children’s Hospital, clinicians have embraced it. “They feel it changes their practice. It gets to the heart of the matter quickly, and they feel more confident having that framework,” Dr. Adrian said.
Dr. Adrian has no conflicts of interest or disclosures.
SEATTLE – When it comes to treating children and adolescents who have experienced trauma and present suicidality, it is not just the patients who need support. Clinicians also experience grave anxiety when dealing with a traumatized child exhibiting suicidal behavior. The Collaborative Assessment and Management of Suicide (CAMS) framework can help clinicians or health care workers manage the care of these challenging patients.
CAMS is well established in adults with suicidal behavior, but it is unproven in youth and adolescents. The key is to its success in younger patients will be whether the program is developmentally appropriate, according to Molly C. Adrian, PhD, assistant professor of psychiatry and behavioral medicine at the University of Washington, Seattle. Dr. Adrian discussed CAMS and its potential applications at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
The CAMS approach emphasizes cooperation between the therapist and patient. “Adolescents are seeking autonomy and independence, and so it’s a good fit philosophically that you would partner alongside the teen as opposed to starting in a more adversarial sort of way – not that we as therapists ever do that. But it can be more tense when suicide is on the table and you feel unprepared,” Dr. Adrian said.
Seattle Children’s Hospital is persuaded enough to make CAMS part of its standard of care, Dr. Adrian said.
CAMS is a framework for patient management that has no prerequisites for the therapeutic approach. “It’s principle driven, not protocol driven. Clinicians can use whatever specific interventions they feel are appropriate for the drivers (of the suicidality). What we’re trying to change is the approach to the suicidal patient, so that it is not an anxiety-provoking, terrifying experience for the clinician – because we know that a suicidal patient is the most anxiety-provoking task for clinicians,” Dr. Adrian said. “We want clinicians to feel prepared and protected in providing the elements of care,” Dr. Adrian said in an interview.
The framework incorporates a suicide-status form (SSF), which assesses theory-driven and epidemiologically guided risk factors and helps to identify the drivers or the reasons why suicide is compelling to the patient. Those drivers then help inform crisis prevention efforts and the selection of interventions.
Three randomized, controlled trials have demonstrated the efficacy of CAMS over standard of care in adult patients, showing that the SSF is an effective assessment tool and that CAMS reduces suicidal ideation and leads to decreases in distress, depression, and hopelessness. There are no randomized, controlled trials showing its efficacy in children, but Seattle Children’s Hospital is conducting a pilot study in 12 youth and have found a 40% response rate at 8 weeks.
The SSF gauges the patient’s status and trajectory, while the CAMS therapeutic worksheet helps to distinguish direct and indirect drivers of suicidal behavior. In cases in which trauma symptoms or experiences are tied to suicidal behavior, they receive priority for treatment. The framework provides for discussion of options and treatment choice through collaboration between the clinician and the patient.
The patient and clinician fill out an SSF in the first session and use it to create a crisis convention plan, which includes gaining a commitment to treatment, removing or restricting access to lethal means, and incorporating parental monitoring.
Dr. Adrian is hopeful that the CAMS framework will help health care workers address suicidality in traumatized youth and adolescents. Currently, they may feel intimidated by a stricken child’s issues. “You don’t want to be responsible for a child dying, so you may overrespond with an intervention like an emergency department evaluation or an inpatient hospitalization that may be iatrogenic – there are data coming out from adults that hospitalization contributes to suicide risk above and beyond other risk factors,” Dr. Adrian said.
CAMS is simple and flexible, according to Dr. Adrian, and can be used by psychiatrists, social workers, substance use counselors, and others. At Seattle Children’s Hospital, clinicians have embraced it. “They feel it changes their practice. It gets to the heart of the matter quickly, and they feel more confident having that framework,” Dr. Adrian said.
Dr. Adrian has no conflicts of interest or disclosures.
FROM AACAP 2018
How to help crying infants
Babies evolved to cry to get their needs met and adults evolved to be aroused by the sound. Perfect match, right? But crying/fussing was rated the No. 1 hardest part of parenting for 0- to 3-year-olds in our data from more than 68,000 parents.

As clinicians, we become amazingly immune to the crying in our offices, but hopefully not to crying as a concern of parents. Our training directs us to look for pathology such as under- or overfeeding, infection, gastroesophageal reflux disease (GERD), volvulus, a hair tourniquet, or an injury as causes of crying. Having ruled these out, the bigger task is making sure that parents learn to read their infants’ crying and find ways to console them. Learning to handle crying can be tense, frustrating, and upsetting for parents, but success is ultimately satisfying and an important part of the reciprocal interaction that builds attachment for both parent and child.
“Developmental crying” is a great term for explaining crying in the first 3 months to families, as it is age related. The acronym PURPLE was created to teach about this normal crying.
- “P” is for peak of crying – babies may cry more each week, most in month 2, then less in months 3-5.
- “U” is for unexpected – crying can come and go without explanation.
- “R” is for resists soothing – babies may not stop crying no matter what is tried.
- “P” is for pain-like face – babies appear to be in pain, even if they are not.
- “L” is for long lasting – crying can last 5 hours a day or more.
- “E” is for evening – the baby might cry more in the late afternoon and evening.
The 1- to 2-week visit is a key time to teach parents about the expected upcoming crying and ways to manage it. I lean on the evidence-based steps for soothing, using the 5 S’s described by Harvey Karp, MD, based on the wisdom of T. Berry Brazelton, MD. These include:
- Swaddling in a wrap that constrains arms and legs.
- Side or stomach holding (but not for sleeping).
- Shushing sounds of voice, radio static, fan, air conditioner, or car ride.
- Swinging gently (point out to never shake a baby).
- Sucking on a pacifier, finger, or hand.
Because babies change state slowly and also respond to high caregiver emotion such as anxiety, it is important for parents to take some deep breaths and give each “S” several minutes to have an effect.
Some of our patients will go beyond typical crying to colic, defined as crying for at least 3 hours per day, at least 3 days per week, starting before 3 months post term. While typically easing by age 3 months, colic can in nightmare cases persist to age 1 year. Needless to say, prolonged crying can be an enormous stress for families. Researchers in the Fussy Baby Network consulting on infant crying have found value in a family prescription for REST: Reassurance, Empathy, Support, and Time away. Reassurance that the child is not ill should be provided after a careful history, including asking why parents think the baby is crying, and a physical exam, even if we think we can tell at a glance that the baby is okay. Remember that every parent’s first concern is whether the baby is okay, and crying indicates otherwise. Parents are counting on us for a thorough exam before we reassure them. Exhausted new parents deserve empathy – acknowledgment of how difficult, scary, and maddening it is to not be able to console their newborns.
While friends are saying “You must be so happy!” after a child is born, ambivalence (What have I done to my life?) is very common, but not easy to admit. We can point out that the typical age at which parents report “loving” their infants is actually more like 6 weeks, when they finally smile! To acknowledge ambivalence, I may say, “When you feel like throwing him out the window, it’s okay to lay him in the crib and put on headphones for a few minutes.” Music, meditation, yoga, or exercise are break activities that also can reduce parent stress.
Support for the parents is one of the most important protections for children at all ages, but can’t be assumed. Unfortunately, crying tends to increase beginning at 2 weeks post term, right when the partner returns to work or relatives leave. It is important to ask, “Who is helping you with the baby?” Just having a partner doesn’t mean that person is taking a turn! Fathers may be afraid of holding a baby, or may have no experience and try to defer. We need to encourage fathers in all aspects of care but especially to “find at least one way to console your baby.” Sometimes mothers “rescue” dads too quickly. While mothers may have both more experience with infants and the magic of breastfeeding for consoling, depriving fathers of working through the struggle of managing crying can result in their developing less confidence in caregiving. It also can cause them to miss out on supporting the mother at this delicate time, a chance to profoundly strengthen the partnership.
Taking into account the importance for parents of finding ways to console crying babies, getting some “time away” can be helpful, especially if crying goes on for months. Maybe those friends who asked, “What can I do to help?” could come over for an hour in the evening (peak crying time) to hold the baby. This also can be a chance for parent time together, a newly rare commodity.

Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Babies evolved to cry to get their needs met and adults evolved to be aroused by the sound. Perfect match, right? But crying/fussing was rated the No. 1 hardest part of parenting for 0- to 3-year-olds in our data from more than 68,000 parents.
As clinicians, we become amazingly immune to the crying in our offices, but hopefully not to crying as a concern of parents. Our training directs us to look for pathology such as under- or overfeeding, infection, gastroesophageal reflux disease (GERD), volvulus, a hair tourniquet, or an injury as causes of crying. Having ruled these out, the bigger task is making sure that parents learn to read their infants’ crying and find ways to console them. Learning to handle crying can be tense, frustrating, and upsetting for parents, but success is ultimately satisfying and an important part of the reciprocal interaction that builds attachment for both parent and child.
“Developmental crying” is a great term for explaining crying in the first 3 months to families, as it is age related. The acronym PURPLE was created to teach about this normal crying.
- “P” is for peak of crying – babies may cry more each week, most in month 2, then less in months 3-5.
- “U” is for unexpected – crying can come and go without explanation.
- “R” is for resists soothing – babies may not stop crying no matter what is tried.
- “P” is for pain-like face – babies appear to be in pain, even if they are not.
- “L” is for long lasting – crying can last 5 hours a day or more.
- “E” is for evening – the baby might cry more in the late afternoon and evening.
The 1- to 2-week visit is a key time to teach parents about the expected upcoming crying and ways to manage it. I lean on the evidence-based steps for soothing, using the 5 S’s described by Harvey Karp, MD, based on the wisdom of T. Berry Brazelton, MD. These include:
- Swaddling in a wrap that constrains arms and legs.
- Side or stomach holding (but not for sleeping).
- Shushing sounds of voice, radio static, fan, air conditioner, or car ride.
- Swinging gently (point out to never shake a baby).
- Sucking on a pacifier, finger, or hand.
Because babies change state slowly and also respond to high caregiver emotion such as anxiety, it is important for parents to take some deep breaths and give each “S” several minutes to have an effect.
Some of our patients will go beyond typical crying to colic, defined as crying for at least 3 hours per day, at least 3 days per week, starting before 3 months post term. While typically easing by age 3 months, colic can in nightmare cases persist to age 1 year. Needless to say, prolonged crying can be an enormous stress for families. Researchers in the Fussy Baby Network consulting on infant crying have found value in a family prescription for REST: Reassurance, Empathy, Support, and Time away. Reassurance that the child is not ill should be provided after a careful history, including asking why parents think the baby is crying, and a physical exam, even if we think we can tell at a glance that the baby is okay. Remember that every parent’s first concern is whether the baby is okay, and crying indicates otherwise. Parents are counting on us for a thorough exam before we reassure them. Exhausted new parents deserve empathy – acknowledgment of how difficult, scary, and maddening it is to not be able to console their newborns.
While friends are saying “You must be so happy!” after a child is born, ambivalence (What have I done to my life?) is very common, but not easy to admit. We can point out that the typical age at which parents report “loving” their infants is actually more like 6 weeks, when they finally smile! To acknowledge ambivalence, I may say, “When you feel like throwing him out the window, it’s okay to lay him in the crib and put on headphones for a few minutes.” Music, meditation, yoga, or exercise are break activities that also can reduce parent stress.
Support for the parents is one of the most important protections for children at all ages, but can’t be assumed. Unfortunately, crying tends to increase beginning at 2 weeks post term, right when the partner returns to work or relatives leave. It is important to ask, “Who is helping you with the baby?” Just having a partner doesn’t mean that person is taking a turn! Fathers may be afraid of holding a baby, or may have no experience and try to defer. We need to encourage fathers in all aspects of care but especially to “find at least one way to console your baby.” Sometimes mothers “rescue” dads too quickly. While mothers may have both more experience with infants and the magic of breastfeeding for consoling, depriving fathers of working through the struggle of managing crying can result in their developing less confidence in caregiving. It also can cause them to miss out on supporting the mother at this delicate time, a chance to profoundly strengthen the partnership.
Taking into account the importance for parents of finding ways to console crying babies, getting some “time away” can be helpful, especially if crying goes on for months. Maybe those friends who asked, “What can I do to help?” could come over for an hour in the evening (peak crying time) to hold the baby. This also can be a chance for parent time together, a newly rare commodity.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Babies evolved to cry to get their needs met and adults evolved to be aroused by the sound. Perfect match, right? But crying/fussing was rated the No. 1 hardest part of parenting for 0- to 3-year-olds in our data from more than 68,000 parents.
As clinicians, we become amazingly immune to the crying in our offices, but hopefully not to crying as a concern of parents. Our training directs us to look for pathology such as under- or overfeeding, infection, gastroesophageal reflux disease (GERD), volvulus, a hair tourniquet, or an injury as causes of crying. Having ruled these out, the bigger task is making sure that parents learn to read their infants’ crying and find ways to console them. Learning to handle crying can be tense, frustrating, and upsetting for parents, but success is ultimately satisfying and an important part of the reciprocal interaction that builds attachment for both parent and child.
“Developmental crying” is a great term for explaining crying in the first 3 months to families, as it is age related. The acronym PURPLE was created to teach about this normal crying.
- “P” is for peak of crying – babies may cry more each week, most in month 2, then less in months 3-5.
- “U” is for unexpected – crying can come and go without explanation.
- “R” is for resists soothing – babies may not stop crying no matter what is tried.
- “P” is for pain-like face – babies appear to be in pain, even if they are not.
- “L” is for long lasting – crying can last 5 hours a day or more.
- “E” is for evening – the baby might cry more in the late afternoon and evening.
The 1- to 2-week visit is a key time to teach parents about the expected upcoming crying and ways to manage it. I lean on the evidence-based steps for soothing, using the 5 S’s described by Harvey Karp, MD, based on the wisdom of T. Berry Brazelton, MD. These include:
- Swaddling in a wrap that constrains arms and legs.
- Side or stomach holding (but not for sleeping).
- Shushing sounds of voice, radio static, fan, air conditioner, or car ride.
- Swinging gently (point out to never shake a baby).
- Sucking on a pacifier, finger, or hand.
Because babies change state slowly and also respond to high caregiver emotion such as anxiety, it is important for parents to take some deep breaths and give each “S” several minutes to have an effect.
Some of our patients will go beyond typical crying to colic, defined as crying for at least 3 hours per day, at least 3 days per week, starting before 3 months post term. While typically easing by age 3 months, colic can in nightmare cases persist to age 1 year. Needless to say, prolonged crying can be an enormous stress for families. Researchers in the Fussy Baby Network consulting on infant crying have found value in a family prescription for REST: Reassurance, Empathy, Support, and Time away. Reassurance that the child is not ill should be provided after a careful history, including asking why parents think the baby is crying, and a physical exam, even if we think we can tell at a glance that the baby is okay. Remember that every parent’s first concern is whether the baby is okay, and crying indicates otherwise. Parents are counting on us for a thorough exam before we reassure them. Exhausted new parents deserve empathy – acknowledgment of how difficult, scary, and maddening it is to not be able to console their newborns.
While friends are saying “You must be so happy!” after a child is born, ambivalence (What have I done to my life?) is very common, but not easy to admit. We can point out that the typical age at which parents report “loving” their infants is actually more like 6 weeks, when they finally smile! To acknowledge ambivalence, I may say, “When you feel like throwing him out the window, it’s okay to lay him in the crib and put on headphones for a few minutes.” Music, meditation, yoga, or exercise are break activities that also can reduce parent stress.
Support for the parents is one of the most important protections for children at all ages, but can’t be assumed. Unfortunately, crying tends to increase beginning at 2 weeks post term, right when the partner returns to work or relatives leave. It is important to ask, “Who is helping you with the baby?” Just having a partner doesn’t mean that person is taking a turn! Fathers may be afraid of holding a baby, or may have no experience and try to defer. We need to encourage fathers in all aspects of care but especially to “find at least one way to console your baby.” Sometimes mothers “rescue” dads too quickly. While mothers may have both more experience with infants and the magic of breastfeeding for consoling, depriving fathers of working through the struggle of managing crying can result in their developing less confidence in caregiving. It also can cause them to miss out on supporting the mother at this delicate time, a chance to profoundly strengthen the partnership.
Taking into account the importance for parents of finding ways to console crying babies, getting some “time away” can be helpful, especially if crying goes on for months. Maybe those friends who asked, “What can I do to help?” could come over for an hour in the evening (peak crying time) to hold the baby. This also can be a chance for parent time together, a newly rare commodity.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.