User login
Third trimester Tdap vaccination raises antibodies in newborns
Immunization of pregnant women with the Tdap vaccine during weeks 27-30 of pregnancy yielded the higher concentration of protective pertussis toxin antibodies in neonates, compared with neonates not exposed to the vaccine, based on data from more than 600 pregnancies.

The Centers for Disease Control and Prevention recommends Tdap vaccination for pregnant women between 27 and 35 weeks’ gestation, but “data on pertussis antibody concentrations following maternal Tdap immunization are limited because of small cohort size or differing immunization schedules,” wrote C. Mary Healy, MD, of Baylor College of Medicine, Houston and her colleagues.
In an observational study published in JAMA, the researchers reviewed data from 626 pregnancies and births at a single tertiary care center in Texas. The average age of the mothers was 30 years; 41% were white, 27% Hispanic, 26% black, 5% Asian, and 1% another ethnicity. Of these, 312 received the Tdap vaccine at an average gestation of 31 weeks, while 314 women were not immunized.
Overall, the geometric mean concentration (GMC) of neonatal umbilical cord pertussis toxin antibodies among infants exposed to Tdap was 47.3 IU/mL, compared with 12.9 IU/mL for unexposed infants, yielding a GMC ratio of 3.6 (P less than .001).
In addition, pertussis toxin antibody concentrations of 15 IU/mL or higher, 30 IU/mL or higher, and 40 IU/mL or higher were significantly more common in Tdap-exposed vs. Tdap-unexposed neonates (86% vs. 37%, 72% vs. 17%, 59% vs. 12%, respectively).
The GMC of pertussis toxin antibodies was highest when the vaccine was given during weeks 27-30, after which the GMC declined, the researchers noted.
The study was limited by several factors including the observational design, which does not support causes and effect analysis, the use of data from a single center, and the lack of pre- and postimmunization serum samples for comparison, and the absence of data on women immunized during the second trimester, the researchers wrote.
However, the results support data from previous studies, and were strengthened by the large study population. The findings suggest that “following U.S. immunization recommendations and in accordance with current understanding of the kinetics of placental transfer, optimal time to administer Tdap vaccine to maximize pertussis toxin antibodies at birth may be early in the third trimester, with the window of 27 through 30 weeks of gestation yielding the highest cord blood levels,” the researchers said.
The study was supported in part by the Centers for Disease Control and Prevention. Dr. Healy disclosed relationships with Sanofi Pasteur, Novartis Vaccines, Pfizer, and Novavax.
SOURCE: Healy C et al. JAMA. 2018 Oct 9;320(14):1464-70.
Immunization of pregnant women with the Tdap vaccine during weeks 27-30 of pregnancy yielded the higher concentration of protective pertussis toxin antibodies in neonates, compared with neonates not exposed to the vaccine, based on data from more than 600 pregnancies.
The Centers for Disease Control and Prevention recommends Tdap vaccination for pregnant women between 27 and 35 weeks’ gestation, but “data on pertussis antibody concentrations following maternal Tdap immunization are limited because of small cohort size or differing immunization schedules,” wrote C. Mary Healy, MD, of Baylor College of Medicine, Houston and her colleagues.
In an observational study published in JAMA, the researchers reviewed data from 626 pregnancies and births at a single tertiary care center in Texas. The average age of the mothers was 30 years; 41% were white, 27% Hispanic, 26% black, 5% Asian, and 1% another ethnicity. Of these, 312 received the Tdap vaccine at an average gestation of 31 weeks, while 314 women were not immunized.
Overall, the geometric mean concentration (GMC) of neonatal umbilical cord pertussis toxin antibodies among infants exposed to Tdap was 47.3 IU/mL, compared with 12.9 IU/mL for unexposed infants, yielding a GMC ratio of 3.6 (P less than .001).
In addition, pertussis toxin antibody concentrations of 15 IU/mL or higher, 30 IU/mL or higher, and 40 IU/mL or higher were significantly more common in Tdap-exposed vs. Tdap-unexposed neonates (86% vs. 37%, 72% vs. 17%, 59% vs. 12%, respectively).
The GMC of pertussis toxin antibodies was highest when the vaccine was given during weeks 27-30, after which the GMC declined, the researchers noted.
The study was limited by several factors including the observational design, which does not support causes and effect analysis, the use of data from a single center, and the lack of pre- and postimmunization serum samples for comparison, and the absence of data on women immunized during the second trimester, the researchers wrote.
However, the results support data from previous studies, and were strengthened by the large study population. The findings suggest that “following U.S. immunization recommendations and in accordance with current understanding of the kinetics of placental transfer, optimal time to administer Tdap vaccine to maximize pertussis toxin antibodies at birth may be early in the third trimester, with the window of 27 through 30 weeks of gestation yielding the highest cord blood levels,” the researchers said.
The study was supported in part by the Centers for Disease Control and Prevention. Dr. Healy disclosed relationships with Sanofi Pasteur, Novartis Vaccines, Pfizer, and Novavax.
SOURCE: Healy C et al. JAMA. 2018 Oct 9;320(14):1464-70.
Immunization of pregnant women with the Tdap vaccine during weeks 27-30 of pregnancy yielded the higher concentration of protective pertussis toxin antibodies in neonates, compared with neonates not exposed to the vaccine, based on data from more than 600 pregnancies.
The Centers for Disease Control and Prevention recommends Tdap vaccination for pregnant women between 27 and 35 weeks’ gestation, but “data on pertussis antibody concentrations following maternal Tdap immunization are limited because of small cohort size or differing immunization schedules,” wrote C. Mary Healy, MD, of Baylor College of Medicine, Houston and her colleagues.
In an observational study published in JAMA, the researchers reviewed data from 626 pregnancies and births at a single tertiary care center in Texas. The average age of the mothers was 30 years; 41% were white, 27% Hispanic, 26% black, 5% Asian, and 1% another ethnicity. Of these, 312 received the Tdap vaccine at an average gestation of 31 weeks, while 314 women were not immunized.
Overall, the geometric mean concentration (GMC) of neonatal umbilical cord pertussis toxin antibodies among infants exposed to Tdap was 47.3 IU/mL, compared with 12.9 IU/mL for unexposed infants, yielding a GMC ratio of 3.6 (P less than .001).
In addition, pertussis toxin antibody concentrations of 15 IU/mL or higher, 30 IU/mL or higher, and 40 IU/mL or higher were significantly more common in Tdap-exposed vs. Tdap-unexposed neonates (86% vs. 37%, 72% vs. 17%, 59% vs. 12%, respectively).
The GMC of pertussis toxin antibodies was highest when the vaccine was given during weeks 27-30, after which the GMC declined, the researchers noted.
The study was limited by several factors including the observational design, which does not support causes and effect analysis, the use of data from a single center, and the lack of pre- and postimmunization serum samples for comparison, and the absence of data on women immunized during the second trimester, the researchers wrote.
However, the results support data from previous studies, and were strengthened by the large study population. The findings suggest that “following U.S. immunization recommendations and in accordance with current understanding of the kinetics of placental transfer, optimal time to administer Tdap vaccine to maximize pertussis toxin antibodies at birth may be early in the third trimester, with the window of 27 through 30 weeks of gestation yielding the highest cord blood levels,” the researchers said.
The study was supported in part by the Centers for Disease Control and Prevention. Dr. Healy disclosed relationships with Sanofi Pasteur, Novartis Vaccines, Pfizer, and Novavax.
SOURCE: Healy C et al. JAMA. 2018 Oct 9;320(14):1464-70.
FROM JAMA
Key clinical point:
Major finding: The geometric mean concentration of neonatal cord pertussis toxin antibodies was 47.3 IU/mL among newborns exposed to Tdap, compared with 12.9 IU/mL among unexposed (P less than .001).
Study details: The data come from an observational study of 626 pregnancies.
Disclosures: The study was supported in part by the Centers for Disease Control and Prevention. Dr. Healy disclosed relationships with Sanofi Pasteur, Novartis Vaccines, Pfizer, and Novavax.
Source: Healy C et al. JAMA. 2018 Oct 9;320(14):1464-70.
Pulmonary NP ensures care continuity, reduces readmissions
SAN ANTONIO – Unplanned whose discharge process involved a pulmonary nurse practitioner to coordinate continuity of care, a study of more than 70 patients has found.

Despite an increase over time in the rate of discharges, readmissions fell, Sarah Barry, CRNP, of Children’s Hospital of Philadelphia (CHOP), said at the annual meeting of the American College of Chest Physicians.
“The technology-dependent pediatric population who is going home with tracheostomy and ventilator dependence is at risk for hospital readmission, and having an advanced practice provider in a continuity role promotes adherence to our standards of practice and improves transition to home,” Ms. Barry said in an interview.
She noted previous research showing that 40% of 109 home mechanical ventilation patients discharged between 2003 and 2009 had unplanned readmissions, 28% of which occurred within the first month after discharge.
Nearly two thirds (64%) of those readmissions were related to a pulmonary and/or tracheostomy problem. That study also found that changes in condition management 1 week before discharge, such as medications, ventilator settings, or feeding regimens, was associated with unplanned readmission.
That research “makes us ask ourselves if our readmissions are avoidable and what can we do to get these kids home safe and to keep them home,” Ms. Barry told attendees, adding that CHOP was unhappy with their readmission rates.
“Kids were often not making it to their first pulmonary appointment, and it was a burden for these families,” she said. “We questioned whether or not having a nurse practitioner in a role to promote adherence to our standards would have a positive impact on our unplanned route.”
They evaluated the effect of such an NP on unplanned readmissions among tracheostomy/ventilator-supported children. The NP’s role was to track patients, mostly from the progressive care unit, who required a tracheostomy and ventilator and were expected to be discharged home or to a long-term care facility. The NP provided continuity for medical management and coordinated care at discharge.
“We also do not make changes for 2 weeks before discharge so that we can focus on all the other coordination that goes into getting these kids home,” Ms. Barry said.
She reviewed the patients’ electronic charts to record time to scheduled follow-up visit, days until hospital readmission, admitting diagnosis at readmission, and length of stay after readmission. With consideration for the time needed for transition into this new process, the population studied was assessed within three cohorts.
The first cohort comprised the 22 children discharged between April 2016 and March 2017, the full year before a pulmonary NP began coordinating the discharge process. These patients averaged 1.8 discharges per month with an initial follow-up of 2-12 weeks.
Just over a quarter (27%) of the first cohort were readmitted before their scheduled follow-up, ranging from 2 to 25 days after discharge. Five percent were readmitted within a week of discharge, and 27% were readmitted within a month; their average length of stay was 13 days after readmission. Most (83%) of these discharges were respiratory related while the other 17% were gastrointestinal related.
The second cohort involved the 11 patients discharged between April 2017 and August 2017, the first 5 months after a pulmonary NP began overseeing the discharge readiness process.
“We chose 5 months because it took about 5months for me to develop my own protocols and standards of practice,” Ms. Barry explained.
An average 2.2 discharges occurred monthly with 2-8 weeks of initial postdischarge follow-up. Though nearly half these children (45%) were readmitted before their scheduled follow-up, their length of stay was shorter, an average of 11 days.
Readmission within a week after discharge occurred among 27% of the children, and 45% of them were readmitted within a month of discharge. Sixty percent of these patients were readmitted for respiratory issues, compared with 40% with GI issues.
The third cohort included all 38 patients discharged from September 2017 to August 2018, the year after a pulmonary NP had become fully established in the continuity role, with an average 3.2 discharges occurred per month. Readmission rates were considerably lower: Eighteen percent of patients were readmitted before their scheduled follow-up appointment, which ranged from 1 to 13 weeks after discharge.
Five percent were readmitted within a week of discharge, and 24% were readmitted within a month, ranging from 1 to 26 days post discharge. But length of stay was shorter still at an average of 9 days.
The reasons for readmission varied more in this cohort: While 56% were respiratory related, 22% were related to fever, and 11% were related to neurodevelopment concerns or social reasons, such as necessary involvement of social services.
Ms. Barry’s colleague, Howard B. Panitch, MD, also on the staff of CHOP, noted during the discussion that the NP’s role is invaluable in “keeping the inpatient teams honest.
“She reminds her colleagues in critical care that you can’t make that ventilator change when on your way out the door or very close to discharge.”
Ms. Barry had no disclosures. No external funding was noted.
SOURCE: Barry S et al. CHEST 2018 Oct. doi: 10.1016/j.chest.2018.08.743.
SAN ANTONIO – Unplanned whose discharge process involved a pulmonary nurse practitioner to coordinate continuity of care, a study of more than 70 patients has found.
Despite an increase over time in the rate of discharges, readmissions fell, Sarah Barry, CRNP, of Children’s Hospital of Philadelphia (CHOP), said at the annual meeting of the American College of Chest Physicians.
“The technology-dependent pediatric population who is going home with tracheostomy and ventilator dependence is at risk for hospital readmission, and having an advanced practice provider in a continuity role promotes adherence to our standards of practice and improves transition to home,” Ms. Barry said in an interview.
She noted previous research showing that 40% of 109 home mechanical ventilation patients discharged between 2003 and 2009 had unplanned readmissions, 28% of which occurred within the first month after discharge.
Nearly two thirds (64%) of those readmissions were related to a pulmonary and/or tracheostomy problem. That study also found that changes in condition management 1 week before discharge, such as medications, ventilator settings, or feeding regimens, was associated with unplanned readmission.
That research “makes us ask ourselves if our readmissions are avoidable and what can we do to get these kids home safe and to keep them home,” Ms. Barry told attendees, adding that CHOP was unhappy with their readmission rates.
“Kids were often not making it to their first pulmonary appointment, and it was a burden for these families,” she said. “We questioned whether or not having a nurse practitioner in a role to promote adherence to our standards would have a positive impact on our unplanned route.”
They evaluated the effect of such an NP on unplanned readmissions among tracheostomy/ventilator-supported children. The NP’s role was to track patients, mostly from the progressive care unit, who required a tracheostomy and ventilator and were expected to be discharged home or to a long-term care facility. The NP provided continuity for medical management and coordinated care at discharge.
“We also do not make changes for 2 weeks before discharge so that we can focus on all the other coordination that goes into getting these kids home,” Ms. Barry said.
She reviewed the patients’ electronic charts to record time to scheduled follow-up visit, days until hospital readmission, admitting diagnosis at readmission, and length of stay after readmission. With consideration for the time needed for transition into this new process, the population studied was assessed within three cohorts.
The first cohort comprised the 22 children discharged between April 2016 and March 2017, the full year before a pulmonary NP began coordinating the discharge process. These patients averaged 1.8 discharges per month with an initial follow-up of 2-12 weeks.
Just over a quarter (27%) of the first cohort were readmitted before their scheduled follow-up, ranging from 2 to 25 days after discharge. Five percent were readmitted within a week of discharge, and 27% were readmitted within a month; their average length of stay was 13 days after readmission. Most (83%) of these discharges were respiratory related while the other 17% were gastrointestinal related.
The second cohort involved the 11 patients discharged between April 2017 and August 2017, the first 5 months after a pulmonary NP began overseeing the discharge readiness process.
“We chose 5 months because it took about 5months for me to develop my own protocols and standards of practice,” Ms. Barry explained.
An average 2.2 discharges occurred monthly with 2-8 weeks of initial postdischarge follow-up. Though nearly half these children (45%) were readmitted before their scheduled follow-up, their length of stay was shorter, an average of 11 days.
Readmission within a week after discharge occurred among 27% of the children, and 45% of them were readmitted within a month of discharge. Sixty percent of these patients were readmitted for respiratory issues, compared with 40% with GI issues.
The third cohort included all 38 patients discharged from September 2017 to August 2018, the year after a pulmonary NP had become fully established in the continuity role, with an average 3.2 discharges occurred per month. Readmission rates were considerably lower: Eighteen percent of patients were readmitted before their scheduled follow-up appointment, which ranged from 1 to 13 weeks after discharge.
Five percent were readmitted within a week of discharge, and 24% were readmitted within a month, ranging from 1 to 26 days post discharge. But length of stay was shorter still at an average of 9 days.
The reasons for readmission varied more in this cohort: While 56% were respiratory related, 22% were related to fever, and 11% were related to neurodevelopment concerns or social reasons, such as necessary involvement of social services.
Ms. Barry’s colleague, Howard B. Panitch, MD, also on the staff of CHOP, noted during the discussion that the NP’s role is invaluable in “keeping the inpatient teams honest.
“She reminds her colleagues in critical care that you can’t make that ventilator change when on your way out the door or very close to discharge.”
Ms. Barry had no disclosures. No external funding was noted.
SOURCE: Barry S et al. CHEST 2018 Oct. doi: 10.1016/j.chest.2018.08.743.
SAN ANTONIO – Unplanned whose discharge process involved a pulmonary nurse practitioner to coordinate continuity of care, a study of more than 70 patients has found.
Despite an increase over time in the rate of discharges, readmissions fell, Sarah Barry, CRNP, of Children’s Hospital of Philadelphia (CHOP), said at the annual meeting of the American College of Chest Physicians.
“The technology-dependent pediatric population who is going home with tracheostomy and ventilator dependence is at risk for hospital readmission, and having an advanced practice provider in a continuity role promotes adherence to our standards of practice and improves transition to home,” Ms. Barry said in an interview.
She noted previous research showing that 40% of 109 home mechanical ventilation patients discharged between 2003 and 2009 had unplanned readmissions, 28% of which occurred within the first month after discharge.
Nearly two thirds (64%) of those readmissions were related to a pulmonary and/or tracheostomy problem. That study also found that changes in condition management 1 week before discharge, such as medications, ventilator settings, or feeding regimens, was associated with unplanned readmission.
That research “makes us ask ourselves if our readmissions are avoidable and what can we do to get these kids home safe and to keep them home,” Ms. Barry told attendees, adding that CHOP was unhappy with their readmission rates.
“Kids were often not making it to their first pulmonary appointment, and it was a burden for these families,” she said. “We questioned whether or not having a nurse practitioner in a role to promote adherence to our standards would have a positive impact on our unplanned route.”
They evaluated the effect of such an NP on unplanned readmissions among tracheostomy/ventilator-supported children. The NP’s role was to track patients, mostly from the progressive care unit, who required a tracheostomy and ventilator and were expected to be discharged home or to a long-term care facility. The NP provided continuity for medical management and coordinated care at discharge.
“We also do not make changes for 2 weeks before discharge so that we can focus on all the other coordination that goes into getting these kids home,” Ms. Barry said.
She reviewed the patients’ electronic charts to record time to scheduled follow-up visit, days until hospital readmission, admitting diagnosis at readmission, and length of stay after readmission. With consideration for the time needed for transition into this new process, the population studied was assessed within three cohorts.
The first cohort comprised the 22 children discharged between April 2016 and March 2017, the full year before a pulmonary NP began coordinating the discharge process. These patients averaged 1.8 discharges per month with an initial follow-up of 2-12 weeks.
Just over a quarter (27%) of the first cohort were readmitted before their scheduled follow-up, ranging from 2 to 25 days after discharge. Five percent were readmitted within a week of discharge, and 27% were readmitted within a month; their average length of stay was 13 days after readmission. Most (83%) of these discharges were respiratory related while the other 17% were gastrointestinal related.
The second cohort involved the 11 patients discharged between April 2017 and August 2017, the first 5 months after a pulmonary NP began overseeing the discharge readiness process.
“We chose 5 months because it took about 5months for me to develop my own protocols and standards of practice,” Ms. Barry explained.
An average 2.2 discharges occurred monthly with 2-8 weeks of initial postdischarge follow-up. Though nearly half these children (45%) were readmitted before their scheduled follow-up, their length of stay was shorter, an average of 11 days.
Readmission within a week after discharge occurred among 27% of the children, and 45% of them were readmitted within a month of discharge. Sixty percent of these patients were readmitted for respiratory issues, compared with 40% with GI issues.
The third cohort included all 38 patients discharged from September 2017 to August 2018, the year after a pulmonary NP had become fully established in the continuity role, with an average 3.2 discharges occurred per month. Readmission rates were considerably lower: Eighteen percent of patients were readmitted before their scheduled follow-up appointment, which ranged from 1 to 13 weeks after discharge.
Five percent were readmitted within a week of discharge, and 24% were readmitted within a month, ranging from 1 to 26 days post discharge. But length of stay was shorter still at an average of 9 days.
The reasons for readmission varied more in this cohort: While 56% were respiratory related, 22% were related to fever, and 11% were related to neurodevelopment concerns or social reasons, such as necessary involvement of social services.
Ms. Barry’s colleague, Howard B. Panitch, MD, also on the staff of CHOP, noted during the discussion that the NP’s role is invaluable in “keeping the inpatient teams honest.
“She reminds her colleagues in critical care that you can’t make that ventilator change when on your way out the door or very close to discharge.”
Ms. Barry had no disclosures. No external funding was noted.
SOURCE: Barry S et al. CHEST 2018 Oct. doi: 10.1016/j.chest.2018.08.743.
REPORTING FROM CHEST 2018
Key clinical point: Use of pulmonary NP for continuity care decreases unplanned readmissions among pediatric tracheostomy/ventilator patients.
Major finding: Unplanned readmission rates declined from 27% to 18% before the patient’s first follow-up appointment.
Study details: A retrospective electronic chart review of 71 tracheostomy/ventilator-dependent children discharged between April 2016 and August 2018 at Children’s Hospital of Philadelphia.
Disclosures: Ms. Barry had no disclosures. No external funding was noted.
Source: Barry S et al. CHEST 2018 Oct. doi: 10.1016/j.chest.2018.08.743.
SSRIs linked to reduced height in risperidone-treated boys
according to results of an analysis reported in The Journal of Pediatrics.
The inverse association between SSRI use and height was particularly notable in boys undergoing puberty, according to the authors of the retrospective study. Follow-up into adulthood will be needed to see if the effects are reversible or have a negative impact on adult height.
“In the meantime, clinicians should continue to closely monitor children and adolescents starting antidepressant treatment to minimize side effects,” said Chadi A. Calarge, MD, of Baylor College of Medicine, Houston, and his coauthors.
These observations by Dr. Calarge and his colleagues were based on an analysis of 267 boys, of whom 190 had been treated with SSRIs. The boys had been in one of four previous studies, three of which included risperidone treatment for at least 6 or 12 months, and one small longitudinal observational study including children who had initiated risperidone in the month prior to enrollment. All four studies excluded subjects with chronic medical or neurologic conditions and those taking more than one antipsychotic medication.
Use of an SSRI was associated with reduced growth in height, particularly among boys in Tanner stages 3 and 4. “This effect is of a moderate magnitude of about 1 cm for every 1 year of treatment with SSRIs during adolescence,” Dr. Calarge and his coauthors said.
Among boys who took SSRIs continuously, the strongest inverse association with height z scores was in boys in Tanner stages 3 and 4 (r = –0.69; P less than .009). By contrast, this correlation was “negligible” in boys in Tanner stage 1 and stage 5, and there were only 5 boys of Tanner stage 2 in this analysis, the investigators said.
The mechanism by which SSRIs may have an effect on longitudinal growth has not been well investigated, according to Dr. Calarge and his coauthors. “Impaired growth hormone secretion or activity has been implicated, given that SSRIs alter serotonin signaling, which is known to control GH secretion.”
Funding for the study came from the National Institutes of Health, and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
SOURCE: Calarge CA et al. J Pediatr. 2018 Oct;201:245-51.
Although results of this secondary analysis require confirmation, they do underscore the need to consider how “complex combinations” of psychotropic agents may affect growth and development, according to Philip S. Zeitler, MD, PhD.
Such combinations are increasingly seen in the management of behavioral disorders in children and adolescents, Dr. Zeitler noted in a commentary on the findings by Calarge et al.
While side effects are well described for individual drugs used to treat youths with complex mental and behavioral disorders, the potential for side effects particular to combinations of these drugs are less well understood, he said.
The present study shows that in risperidone-treated youth, SSRI use was associated with decreased longitudinal growth. The estimated decrease of 1 cm per year of exposure to SSRIs suggests “a potentially significant decrease in adult height for peripubertal youth who are treated for many years,” according to the author.
“Unlike with stimulants, the decreased longitudinal growth was not associated with suppression of weight gain, suggesting an independent effect of SSRIs on growth during puberty,” he added.
Dr. Zeitler, of Aurora, Colo., is on the editorial board of The Journal of Pediatrics. His commentary on this study appeared in the October 2018 issue (J Pediatr. 2018;201:3). Dr. Zeitler also serves on the editorial board of the Journal of Clinical Endocrinology & Metabolism and Current Diabetes Reports, and is the editor-in-chief of Pediatric Diabetes. He reported serving on the data and safety monitoring board for Tolmar Pharmaceuticals, and serving as a consultant for Daiichi Sankyo, Merck, Boehringer-Ingelheim, and Janssen Pharmaceuticals.
Although results of this secondary analysis require confirmation, they do underscore the need to consider how “complex combinations” of psychotropic agents may affect growth and development, according to Philip S. Zeitler, MD, PhD.
Such combinations are increasingly seen in the management of behavioral disorders in children and adolescents, Dr. Zeitler noted in a commentary on the findings by Calarge et al.
While side effects are well described for individual drugs used to treat youths with complex mental and behavioral disorders, the potential for side effects particular to combinations of these drugs are less well understood, he said.
The present study shows that in risperidone-treated youth, SSRI use was associated with decreased longitudinal growth. The estimated decrease of 1 cm per year of exposure to SSRIs suggests “a potentially significant decrease in adult height for peripubertal youth who are treated for many years,” according to the author.
“Unlike with stimulants, the decreased longitudinal growth was not associated with suppression of weight gain, suggesting an independent effect of SSRIs on growth during puberty,” he added.
Dr. Zeitler, of Aurora, Colo., is on the editorial board of The Journal of Pediatrics. His commentary on this study appeared in the October 2018 issue (J Pediatr. 2018;201:3). Dr. Zeitler also serves on the editorial board of the Journal of Clinical Endocrinology & Metabolism and Current Diabetes Reports, and is the editor-in-chief of Pediatric Diabetes. He reported serving on the data and safety monitoring board for Tolmar Pharmaceuticals, and serving as a consultant for Daiichi Sankyo, Merck, Boehringer-Ingelheim, and Janssen Pharmaceuticals.
Although results of this secondary analysis require confirmation, they do underscore the need to consider how “complex combinations” of psychotropic agents may affect growth and development, according to Philip S. Zeitler, MD, PhD.
Such combinations are increasingly seen in the management of behavioral disorders in children and adolescents, Dr. Zeitler noted in a commentary on the findings by Calarge et al.
While side effects are well described for individual drugs used to treat youths with complex mental and behavioral disorders, the potential for side effects particular to combinations of these drugs are less well understood, he said.
The present study shows that in risperidone-treated youth, SSRI use was associated with decreased longitudinal growth. The estimated decrease of 1 cm per year of exposure to SSRIs suggests “a potentially significant decrease in adult height for peripubertal youth who are treated for many years,” according to the author.
“Unlike with stimulants, the decreased longitudinal growth was not associated with suppression of weight gain, suggesting an independent effect of SSRIs on growth during puberty,” he added.
Dr. Zeitler, of Aurora, Colo., is on the editorial board of The Journal of Pediatrics. His commentary on this study appeared in the October 2018 issue (J Pediatr. 2018;201:3). Dr. Zeitler also serves on the editorial board of the Journal of Clinical Endocrinology & Metabolism and Current Diabetes Reports, and is the editor-in-chief of Pediatric Diabetes. He reported serving on the data and safety monitoring board for Tolmar Pharmaceuticals, and serving as a consultant for Daiichi Sankyo, Merck, Boehringer-Ingelheim, and Janssen Pharmaceuticals.
according to results of an analysis reported in The Journal of Pediatrics.
The inverse association between SSRI use and height was particularly notable in boys undergoing puberty, according to the authors of the retrospective study. Follow-up into adulthood will be needed to see if the effects are reversible or have a negative impact on adult height.
“In the meantime, clinicians should continue to closely monitor children and adolescents starting antidepressant treatment to minimize side effects,” said Chadi A. Calarge, MD, of Baylor College of Medicine, Houston, and his coauthors.
These observations by Dr. Calarge and his colleagues were based on an analysis of 267 boys, of whom 190 had been treated with SSRIs. The boys had been in one of four previous studies, three of which included risperidone treatment for at least 6 or 12 months, and one small longitudinal observational study including children who had initiated risperidone in the month prior to enrollment. All four studies excluded subjects with chronic medical or neurologic conditions and those taking more than one antipsychotic medication.
Use of an SSRI was associated with reduced growth in height, particularly among boys in Tanner stages 3 and 4. “This effect is of a moderate magnitude of about 1 cm for every 1 year of treatment with SSRIs during adolescence,” Dr. Calarge and his coauthors said.
Among boys who took SSRIs continuously, the strongest inverse association with height z scores was in boys in Tanner stages 3 and 4 (r = –0.69; P less than .009). By contrast, this correlation was “negligible” in boys in Tanner stage 1 and stage 5, and there were only 5 boys of Tanner stage 2 in this analysis, the investigators said.
The mechanism by which SSRIs may have an effect on longitudinal growth has not been well investigated, according to Dr. Calarge and his coauthors. “Impaired growth hormone secretion or activity has been implicated, given that SSRIs alter serotonin signaling, which is known to control GH secretion.”
Funding for the study came from the National Institutes of Health, and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
SOURCE: Calarge CA et al. J Pediatr. 2018 Oct;201:245-51.
according to results of an analysis reported in The Journal of Pediatrics.
The inverse association between SSRI use and height was particularly notable in boys undergoing puberty, according to the authors of the retrospective study. Follow-up into adulthood will be needed to see if the effects are reversible or have a negative impact on adult height.
“In the meantime, clinicians should continue to closely monitor children and adolescents starting antidepressant treatment to minimize side effects,” said Chadi A. Calarge, MD, of Baylor College of Medicine, Houston, and his coauthors.
These observations by Dr. Calarge and his colleagues were based on an analysis of 267 boys, of whom 190 had been treated with SSRIs. The boys had been in one of four previous studies, three of which included risperidone treatment for at least 6 or 12 months, and one small longitudinal observational study including children who had initiated risperidone in the month prior to enrollment. All four studies excluded subjects with chronic medical or neurologic conditions and those taking more than one antipsychotic medication.
Use of an SSRI was associated with reduced growth in height, particularly among boys in Tanner stages 3 and 4. “This effect is of a moderate magnitude of about 1 cm for every 1 year of treatment with SSRIs during adolescence,” Dr. Calarge and his coauthors said.
Among boys who took SSRIs continuously, the strongest inverse association with height z scores was in boys in Tanner stages 3 and 4 (r = –0.69; P less than .009). By contrast, this correlation was “negligible” in boys in Tanner stage 1 and stage 5, and there were only 5 boys of Tanner stage 2 in this analysis, the investigators said.
The mechanism by which SSRIs may have an effect on longitudinal growth has not been well investigated, according to Dr. Calarge and his coauthors. “Impaired growth hormone secretion or activity has been implicated, given that SSRIs alter serotonin signaling, which is known to control GH secretion.”
Funding for the study came from the National Institutes of Health, and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
SOURCE: Calarge CA et al. J Pediatr. 2018 Oct;201:245-51.
FROM THE JOURNAL OF PEDIATRICS
Key clinical point: Among risperidone-treated boys, use of SSRIs was linked to reduced longitudinal growth, according to results of an analysis.
Major finding: The strongest inverse association between continuous SSRI use and height z scores was in boys in Tanner stages 3 and 4 (r = −0.69; P less than .009).
Study details: Retrospective analysis of 267 boys enrolled in four previous studies evaluating risperidone use.
Disclosures: Funding for the study came from the National Institutes of Health and other grants. One study coauthor reported funding support from Pfizer and Aeterna Zentaris.
Source: Calarge CA et al. J Pediatr. 2018;201:245-51.
In utero efavirenz, dolutegravir exposure linked to childhood neurologic problems
SAN FRANCISCO – , according to a review of 3,747 children in the Surveillance Monitoring for ART Toxicities (SMARTT) study, an ongoing effort to monitor children exposed to antiretrovirals in the womb.
Overall, 237 children developed a neurologic complication at a mean age of 2; 16 of them were exposed to efavirenz. The study team estimated that 9.6% of children exposed to efavirenz had a neurological complication, versus 6.2% born to women on ART regimens without efavirenz. There was also a nonsignificant trend toward dolutegravir exposure and later neurological abnormalities, which occurred in four of 94 children exposed to the drug. Results were adjusted for maternal smoking and other risk factors.
No other safety signals were detected with the 19 other antiretrovirals analyzed in the study, lead investigator Claudia S. Crowell, MD, assistant professor of pediatrics at the University of Washington, Seattle, said at the annual scientific meeting on infectious diseases.
Efavirenz isn’t used much in the United States because there are more effective options with fewer side effects, but current guidelines recommend that women who are doing well on the drug stay on it while pregnant. Meanwhile, dolutegravir exposure at the time of conception was recently linked to an increased risk of neural tube defects in infants. The drug is commonly used in the United States, and guidelines have been strengthened to highlight the need for contraception use by women taking dolutegravir.
Dr. Crowell said she was surprised by her study’s findings, in part because efavirenz is not a teratogen. The work highlights how important it is to look beyond birth defects and follow children exposed to antiretrovirals for later problems. “We still haven’t determined what the safest regimen is for use in pregnancy,” she said.
Dr. Crowell explained the problem, and what her work means for practice in an interview at the meeting.
SOURCE: Crowell C et al. ID Week 2018 abstract LB5.
SAN FRANCISCO – , according to a review of 3,747 children in the Surveillance Monitoring for ART Toxicities (SMARTT) study, an ongoing effort to monitor children exposed to antiretrovirals in the womb.
Overall, 237 children developed a neurologic complication at a mean age of 2; 16 of them were exposed to efavirenz. The study team estimated that 9.6% of children exposed to efavirenz had a neurological complication, versus 6.2% born to women on ART regimens without efavirenz. There was also a nonsignificant trend toward dolutegravir exposure and later neurological abnormalities, which occurred in four of 94 children exposed to the drug. Results were adjusted for maternal smoking and other risk factors.
No other safety signals were detected with the 19 other antiretrovirals analyzed in the study, lead investigator Claudia S. Crowell, MD, assistant professor of pediatrics at the University of Washington, Seattle, said at the annual scientific meeting on infectious diseases.
Efavirenz isn’t used much in the United States because there are more effective options with fewer side effects, but current guidelines recommend that women who are doing well on the drug stay on it while pregnant. Meanwhile, dolutegravir exposure at the time of conception was recently linked to an increased risk of neural tube defects in infants. The drug is commonly used in the United States, and guidelines have been strengthened to highlight the need for contraception use by women taking dolutegravir.
Dr. Crowell said she was surprised by her study’s findings, in part because efavirenz is not a teratogen. The work highlights how important it is to look beyond birth defects and follow children exposed to antiretrovirals for later problems. “We still haven’t determined what the safest regimen is for use in pregnancy,” she said.
Dr. Crowell explained the problem, and what her work means for practice in an interview at the meeting.
SOURCE: Crowell C et al. ID Week 2018 abstract LB5.
SAN FRANCISCO – , according to a review of 3,747 children in the Surveillance Monitoring for ART Toxicities (SMARTT) study, an ongoing effort to monitor children exposed to antiretrovirals in the womb.
Overall, 237 children developed a neurologic complication at a mean age of 2; 16 of them were exposed to efavirenz. The study team estimated that 9.6% of children exposed to efavirenz had a neurological complication, versus 6.2% born to women on ART regimens without efavirenz. There was also a nonsignificant trend toward dolutegravir exposure and later neurological abnormalities, which occurred in four of 94 children exposed to the drug. Results were adjusted for maternal smoking and other risk factors.
No other safety signals were detected with the 19 other antiretrovirals analyzed in the study, lead investigator Claudia S. Crowell, MD, assistant professor of pediatrics at the University of Washington, Seattle, said at the annual scientific meeting on infectious diseases.
Efavirenz isn’t used much in the United States because there are more effective options with fewer side effects, but current guidelines recommend that women who are doing well on the drug stay on it while pregnant. Meanwhile, dolutegravir exposure at the time of conception was recently linked to an increased risk of neural tube defects in infants. The drug is commonly used in the United States, and guidelines have been strengthened to highlight the need for contraception use by women taking dolutegravir.
Dr. Crowell said she was surprised by her study’s findings, in part because efavirenz is not a teratogen. The work highlights how important it is to look beyond birth defects and follow children exposed to antiretrovirals for later problems. “We still haven’t determined what the safest regimen is for use in pregnancy,” she said.
Dr. Crowell explained the problem, and what her work means for practice in an interview at the meeting.
SOURCE: Crowell C et al. ID Week 2018 abstract LB5.
REPORTING FROM ID WEEK 2018

It’s time for universal CMV screening at birth
SAN FRANCISCO –
The reason is because most of the time the diagnosis of congenital cytomegalovirus is missed. Only about 10% of infants infected with the virus present with enlarged livers and other classic signs. Too often, the infection isn’t caught until later, when hearing loss and other neurologic sequelae reveal themselves, according to Fatima Kakkar, MD, a pediatric infectious disease specialist and researcher at the University of Montreal.
There are effective treatments – intravenous ganciclovir for 6 weeks or oral valganciclovir (Valcyte) for 6 months – that control the infection and reverse its effects.
People have tried to address the situation by screening children with hearing loss, in utero HIV exposure, or cytomegalovirus symptoms, but in a study Dr. Kakkar presented at IDWeek, an annual scientific meeting on infectious diseases, such targeted efforts still missed a lot of children.
Many think the answer is universal screening, and the Centers for Disease Control and Prevention are considering it. In a video interview at the meeting, Dr. Kakkar explained the issues, her study, and why universal screening is gaining support.
SOURCE: Kakkar F et al. IDWeek 2018, Abstract 115.
SAN FRANCISCO –
The reason is because most of the time the diagnosis of congenital cytomegalovirus is missed. Only about 10% of infants infected with the virus present with enlarged livers and other classic signs. Too often, the infection isn’t caught until later, when hearing loss and other neurologic sequelae reveal themselves, according to Fatima Kakkar, MD, a pediatric infectious disease specialist and researcher at the University of Montreal.
There are effective treatments – intravenous ganciclovir for 6 weeks or oral valganciclovir (Valcyte) for 6 months – that control the infection and reverse its effects.
People have tried to address the situation by screening children with hearing loss, in utero HIV exposure, or cytomegalovirus symptoms, but in a study Dr. Kakkar presented at IDWeek, an annual scientific meeting on infectious diseases, such targeted efforts still missed a lot of children.
Many think the answer is universal screening, and the Centers for Disease Control and Prevention are considering it. In a video interview at the meeting, Dr. Kakkar explained the issues, her study, and why universal screening is gaining support.
SOURCE: Kakkar F et al. IDWeek 2018, Abstract 115.
SAN FRANCISCO –
The reason is because most of the time the diagnosis of congenital cytomegalovirus is missed. Only about 10% of infants infected with the virus present with enlarged livers and other classic signs. Too often, the infection isn’t caught until later, when hearing loss and other neurologic sequelae reveal themselves, according to Fatima Kakkar, MD, a pediatric infectious disease specialist and researcher at the University of Montreal.
There are effective treatments – intravenous ganciclovir for 6 weeks or oral valganciclovir (Valcyte) for 6 months – that control the infection and reverse its effects.
People have tried to address the situation by screening children with hearing loss, in utero HIV exposure, or cytomegalovirus symptoms, but in a study Dr. Kakkar presented at IDWeek, an annual scientific meeting on infectious diseases, such targeted efforts still missed a lot of children.
Many think the answer is universal screening, and the Centers for Disease Control and Prevention are considering it. In a video interview at the meeting, Dr. Kakkar explained the issues, her study, and why universal screening is gaining support.
SOURCE: Kakkar F et al. IDWeek 2018, Abstract 115.
REPORTING FROM IDWEEK 2018

Opiate use tied to hepatitis C risk in youth
SAN FRANCISCO – A new study indicates young adults with opioid use disorder are seldom screened for hepatitis C virus infections; yet 11% of the subjects with opioid use disorder who were tested had been exposed to hepatitis C, and 6.8% had evidence of chronic hepatitis C infection.

Overall, 2.5% (6,812 subjects) of all subjects received hepatitis C testing and 122 (1.8%) tested positive. Based on health records, 23,345 had an ICD-9 code for any illicit drug use and 8.9% of those (2,090) were tested for HCV infection. Of the 933 subjects with an ICD-9 code for opioid use disorder, 35% were tested for HCV.
The results suggest that a group at significant risk of hepatitis C – those with opioid use disorder – is being overlooked in public health efforts to control the disease.
Clinicians may presume, “Oh, you just take opioids orally, you don’t inject drugs,” but oral opiate users can progress to intravenous drug use, Donna Futterman, MD, director of clinical pediatrics, Montefiore Medical Center, and professor of clinical pediatrics at Albert Einstein College of Medicine, both in New York, said during the press conference at the annual scientific meeting on infectious diseases.
Guidelines call for testing for hepatitis C only in individuals with known injected drug use, among other risk factors, but the research suggests that this significantly underestimates the population of teenagers and young adults who are at risk. Many who take opiates go on to use injectable drugs.
Another surprise finding in the study was that only 10.6% of those tested for hepatitis C had also been screened for human immunodeficiency virus (HIV).

The reasons for the low frequency of screening are likely complex, including lack of time, discomfort between the physician and patient, and concerns over privacy and stigma, according to Dr. Epstein, who emphasized the importance of communication to overcome such barriers.
“As a pediatrician, I try to be as open as possible with patients and let them know that anything they tell me is confidential. I start out discussing less private issues, things that are easier to talk about,” Dr. Epstein said.
But the results of the study also suggest that preconceived notions may be holding clinicians back from testing. “How can you test for hepatitis C and not think HIV?” Dr. Futterman said. “What is that differentiator in providers’ heads that makes them focus on one thing and not the other?”
SAN FRANCISCO – A new study indicates young adults with opioid use disorder are seldom screened for hepatitis C virus infections; yet 11% of the subjects with opioid use disorder who were tested had been exposed to hepatitis C, and 6.8% had evidence of chronic hepatitis C infection.
Overall, 2.5% (6,812 subjects) of all subjects received hepatitis C testing and 122 (1.8%) tested positive. Based on health records, 23,345 had an ICD-9 code for any illicit drug use and 8.9% of those (2,090) were tested for HCV infection. Of the 933 subjects with an ICD-9 code for opioid use disorder, 35% were tested for HCV.
The results suggest that a group at significant risk of hepatitis C – those with opioid use disorder – is being overlooked in public health efforts to control the disease.
Clinicians may presume, “Oh, you just take opioids orally, you don’t inject drugs,” but oral opiate users can progress to intravenous drug use, Donna Futterman, MD, director of clinical pediatrics, Montefiore Medical Center, and professor of clinical pediatrics at Albert Einstein College of Medicine, both in New York, said during the press conference at the annual scientific meeting on infectious diseases.
Guidelines call for testing for hepatitis C only in individuals with known injected drug use, among other risk factors, but the research suggests that this significantly underestimates the population of teenagers and young adults who are at risk. Many who take opiates go on to use injectable drugs.
Another surprise finding in the study was that only 10.6% of those tested for hepatitis C had also been screened for human immunodeficiency virus (HIV).
The reasons for the low frequency of screening are likely complex, including lack of time, discomfort between the physician and patient, and concerns over privacy and stigma, according to Dr. Epstein, who emphasized the importance of communication to overcome such barriers.
“As a pediatrician, I try to be as open as possible with patients and let them know that anything they tell me is confidential. I start out discussing less private issues, things that are easier to talk about,” Dr. Epstein said.
But the results of the study also suggest that preconceived notions may be holding clinicians back from testing. “How can you test for hepatitis C and not think HIV?” Dr. Futterman said. “What is that differentiator in providers’ heads that makes them focus on one thing and not the other?”
SAN FRANCISCO – A new study indicates young adults with opioid use disorder are seldom screened for hepatitis C virus infections; yet 11% of the subjects with opioid use disorder who were tested had been exposed to hepatitis C, and 6.8% had evidence of chronic hepatitis C infection.
Overall, 2.5% (6,812 subjects) of all subjects received hepatitis C testing and 122 (1.8%) tested positive. Based on health records, 23,345 had an ICD-9 code for any illicit drug use and 8.9% of those (2,090) were tested for HCV infection. Of the 933 subjects with an ICD-9 code for opioid use disorder, 35% were tested for HCV.
The results suggest that a group at significant risk of hepatitis C – those with opioid use disorder – is being overlooked in public health efforts to control the disease.
Clinicians may presume, “Oh, you just take opioids orally, you don’t inject drugs,” but oral opiate users can progress to intravenous drug use, Donna Futterman, MD, director of clinical pediatrics, Montefiore Medical Center, and professor of clinical pediatrics at Albert Einstein College of Medicine, both in New York, said during the press conference at the annual scientific meeting on infectious diseases.
Guidelines call for testing for hepatitis C only in individuals with known injected drug use, among other risk factors, but the research suggests that this significantly underestimates the population of teenagers and young adults who are at risk. Many who take opiates go on to use injectable drugs.
Another surprise finding in the study was that only 10.6% of those tested for hepatitis C had also been screened for human immunodeficiency virus (HIV).
The reasons for the low frequency of screening are likely complex, including lack of time, discomfort between the physician and patient, and concerns over privacy and stigma, according to Dr. Epstein, who emphasized the importance of communication to overcome such barriers.
“As a pediatrician, I try to be as open as possible with patients and let them know that anything they tell me is confidential. I start out discussing less private issues, things that are easier to talk about,” Dr. Epstein said.
But the results of the study also suggest that preconceived notions may be holding clinicians back from testing. “How can you test for hepatitis C and not think HIV?” Dr. Futterman said. “What is that differentiator in providers’ heads that makes them focus on one thing and not the other?”
REPORTING FROM ID WEEK 2018
Key clinical point: By focusing solely on injectable drug users, clinicians may miss many others who are at risk for hepatitis C infection.
Major finding: Among those with opiate use disorder, 11% tested positive for hepatitis C.
Study details: Survey of 269,124 teenagers and young adults visiting U.S. Federally Qualified Health Centers.
Disclosures: Dr. Epstein and Dr. Futterman have reported no conflicts of interest.
Stridor in the Pediatric Patient
The distinct features of the pediatric airway make respiratory failure an important concern independent of the underlying cause.
Cases
Case 1
It’s a busy shift on an unusually chilly and rainy July night. Emergency medical services (EMS) brings in a 9-month-old boy who woke up with a “squeaking” noise. His parents reported that he has had a fever, cough, rhinorrhea, and difficulty breathing for the past 2 days; however, they did not hear the noisy breathing until the night of presentation. When the patient is examined, it is noted that he has inspiratory stridor at rest, moderate subcostal retractions, and an occasional deep cough. Upper airway transmitted noises were present, but otherwise the patient had clear lungs.
The patient’s vital signs at presentation were: blood pressure (BP), 85/55 mm Hg; heart rate (HR), 163 beats/min; respiratory rate (RR), 55 breaths/min; and temperature (T), 101.8°F. Oxygen saturation was 90% on room air. The patient’s mother wants to know how the respiratory distress will be fixed and is inquiring if they will have to stay in the hospital overnight.
Case 2
As work begins on the child described above, EMS brings in a 3-year-old girl who appears to be in moderate-severe respiratory distress. Her parents report that she started to drool earlier in the day followed by coughing and occasional gagging. Her parents relay that they thought the symptoms were because of post-nasal drip due to her cold, but the respiratory distress seems to be getting worse, and she now has very noisy breathing and is reluctant to lay down. Upon examination, both inspiratory and expiratory stridor is heard, and it is noted that moderate subcostal retractions are present when the patient is supine.
The patient’s vital signs at presentation were: BP, 89/58 mm Hg; HR, 144 beats/min; RR, 52 breaths/min; and T, 99.5°F. Oxygen saturation was 88% on room air. The nursing staff asked what to do next and why the 2 stridor cases are being managed so differently.
Stridor
Stridor is a high-pitched, harsh sound heard during respiration, predominantly during inspiration, as a result of turbulent air passage.1-3 Stridor is not a diagnosis in itself, but rather a sign of underlying acute or chronic etiology, which needs to be classified based on elicited history and examination.1,4 While the etiology of obstruction may be infectious, congenital, mechanical, or traumatic, the distinct features of the pediatric airway make respiratory failure an important concern independent of the underlying cause.
Anatomy
There are several anatomical differences unique to the pediatric airway that make children, especially infants under 1 year of age, more susceptible to airway obstruction.5,6The pediatric larynx is more anterior and superior and less fibrous than adults, thereby more compliant.6,7 The pediatric epiglottis is longer, omega-shaped, and softer, and the tongue is larger in comparison to the size of the oral cavity, resulting in obstructed airflow.6,7 Children also have a larger and more prominent occiput, causing mechanical obstruction by flexion of the neck when supine.6 While the cricoid cartilage was previously believed to be the narrowest portion of the airway, more recent measurement techniques have challenged this and shown that the glottic and subglottic areas may be narrower in children.7,8
Worsening obstruction resulting in a decreased airway radius leads to increased turbulence to air flow, which is explained by Poiseuille’s law.1,2,7 The resistance to airflow becomes inversely related to the fourth power of the radius, so even a small change in an already narrow pediatric airway can make a huge difference.5 In practice, this means 1 mm of mucosal edema will decrease the cross-sectional area of the airway by 75% and increase the resistance of airflow by a magnitude of 16 to 32 times depending on the level of turbulence.7The airway can be divided into extrathoracic and intrathoracic regions, separated by the vocal cords.13 Inspiratory stridor is typically due to extrathoracic obstruction and expiratory stridor is due to intrathoracic obstruction below the level of the cords. Biphasic stridor, however, may indicate a fixed obstruction at the level of the cords.2,3,5,9
Acute Differentials
The pediatric patient is at high risk for respiratory decompensation when the upper airway is acutely compromised. The history, physical examination, and phases of stridor can help determine the underlying diagnosis and definitive treatment plan.
Acute Croup
Acute croup (laryngotracheitis) is a clinical diagnosis based on acute onset of barky cough and inspiratory stridor.1 It is usually secondary to an infection, most commonly viral (parainfluenza virus), resulting in edema and increased secretions of the subglottic mucosa.7 The onset is typically preceded by upper respiratory illness (URI) symptoms, and is often worse at night or after waking from a nap.1 The peak incidence is between ages 6 months to 3 years. While croup is a clinical diagnosis, an anteroposterior X-ray will often show a steeple sign.7,10
Spasmodic Croup
Spasmodic croup is an atypical presentation usually seen in children 8 years or older without a preceding URI. Patients will wake up overnight with a harsh brass-like cough, stridor, and hoarse voice. The etiology is unclear, but often these patients have a history of atopy and respond in part to treatment with antihistamines.
Foreign Body Aspiration
All that is acutely stridulous is not croup. Stridor from foreign body aspiration is sudden in onset and children do not always present with a history suggestive of foreign body aspiration. Diagnosis requires a high index of suspicion because the event is often unwitnessed and typical patients are pre-verbal. The physical examination may reveal diminished air entry along with stridor. Diagnosis is made by obtaining an X-ray (lateral neck [Figure 1], lateral decubitus, or inspiratory/expiratory chest X-ray) or by bronchoscopy which is both diagnostic and therapeutic.7,10 Remember to always think of foreign body aspiration in children with acute stridor who have neither fever nor antecedent URI symptoms.

Bacterial Tracheitis
Bacterial tracheitis should be suspected in toxic appearing children who present with respiratory distress and stridor but who have a poor response to nebulized epinephrine. It is typically seen in toddlers and school-aged children, and like a viral tracheitis, presentation can be preceded by either URI or fever.10 Stridor is caused by subglottic edema and mucopurulent secretions in the airway.7,10 Infection is most commonly by S. aureus but initial antibiotic choice should be broad spectrum, and include a third-generation cephalosporin or beta-lactamase resistant penicillin.
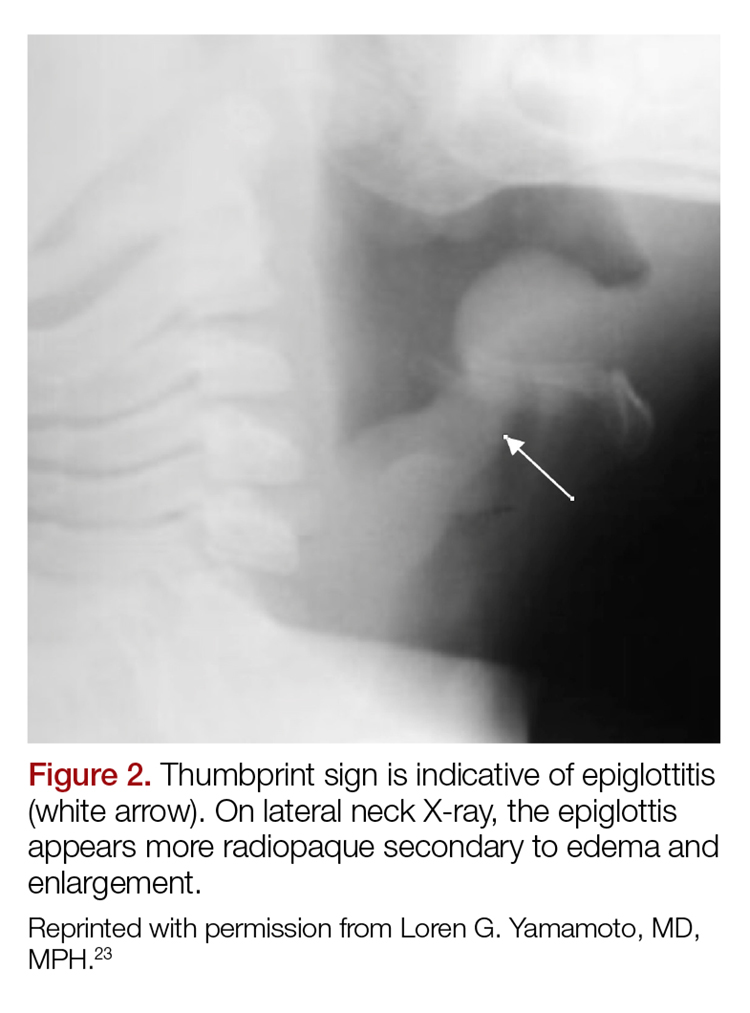
Epiglottitis
Epiglottitis is edema of the epiglottis, most commonly secondary to bacterial infection. The epidemiology of epiglottitis has changed dramatically since widespread immunization for H. influenza with a significantly decreased incidence and change in the average age of presentation to 14.6 years (previously 5.6 years).7 The clinical course begins with sore throat, dysphonia, refusal to eat and progressive difficulty handling secretions with eventual drooling, stridor, tripoding, and toxic appearance. Epiglottitis can be differentiated from croup and bacterial tracheitis because presentation typically lacks a cough.7,10,11 Diagnosis is made either by direct visualization of the epiglottis or a lateral neck X-ray showing a ‘thumb print’ sign (Figure 2).12 Emergency department treatment is similar to the management of the child with a partial foreign body occlusion and focuses on maintaining the airway and minimizing anything that agitates the patient. Intravenous (IV) antibiotic coverage is similar to bacterial tracheitis (third-generation cephalosporin or a beta-lactamase resistant penicillin).
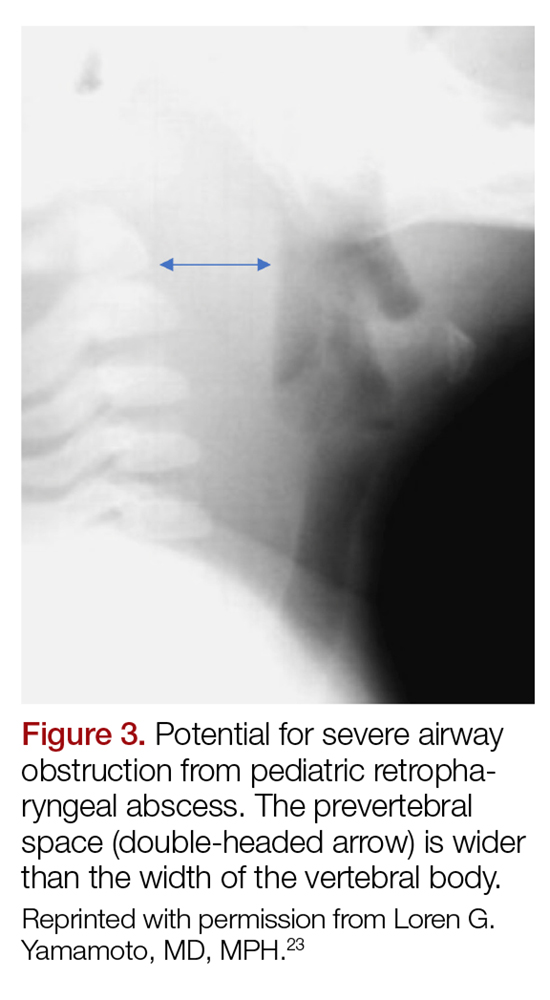
Retropharyngeal Abscess
The most common chief complaint of retropharyngeal abscess (RPA) is neck pain (38%) with fever. As such, it can clinically be mistaken for meningitis on initial presentation. Retropharyngeal abscess will present rarely with either stridor or associated respiratory distress, and it can also mimic croup on initial presentation. Physical examination findings which differentiate this entity include limited or painful neck extension (45%), torticollis (36.5%), and to a lesser extent limitation of neck flexion (12.5%).13 The median age at diagnosis is 36 months with 75% of patients less than 5 years. Typical presentation is insidious with fever and URI symptoms preceding onset. Diagnosis can be made with a lateral neck X-ray showing widening of the prevertebral space (Figure 3), but the gold standard diagnostic study is a computed tomography with contrast.14 Management is IV antibiotics covering aerobic and anaerobic bacteria (eg, ampicillin-sulbactam) ± surgical intervention.
Caustic Ingestion
Caustic ingestion is most commonly accidental and seen in children aged 12 months to 2 years. However, with recent fads, such as the “Tide Pod challenge” teenagers are also at risk. Airway compromise and stridor are secondary to mucosal injury and edema. Oral injury is not always a useful marker for significant distal injury. A complete evaluation of the upper airway and digestive tract within 48 hours after known/suspected caustic ingestion is recommended to assess full extent of damage.15
Chronic Differentials
Laryngomalacia
Laryngomalacia is a congenital weakness of laryngeal tissues, and it is the most common cause of both chronic stridor and neonatal stridor. It is characterized by progressive worsening of symptoms with crying/feeding and supine positioning. Diagnosis is made by bronchoscopy and management is conservative unless there are life threatening apneic or cyanotic events.7
Rings/Slings
There are many anatomic structures with the potential to cause extrinsic airway compression which present with stridor. This type of stridor is often biphasic. Examples include innominate artery compression, double aortic arch, aberrant subclavian artery, and pulmonary artery sling.7
Stridor presenting in children with a history of prematurity or prolonged intubation should raise concern for subglottic and tracheal stenosis.16
Evaluation
Regardless of the etiology of stridor, efforts should be made to keep the patient calm (ie, allow the parent to keep holding a young child, limit any examination not absolutely necessary). Much of the examination can be completed from a distance without disturbing the child.17 Observation of the inspiratory:expiratory (I:E) ratio can localize the level of airway obstruction. For example, an I:E ratio weighted toward a longer inspiration indicates an extrathoracic airway obstruction. Whereas an I:E with a prolonged expiratory phase is consistent with intrathoracic obstruction (eg, terminal bronchial obstruction).17
Another way to localize the level of obstruction is to look for changes in the voice; patients who present with a change in their voice have a subglottic partial obstruction such as croup. However, patients with a muffled voice or drooling have a supraglottic obstruction such as epiglottitis or RPA.17
Management
Management of stridor focuses on reducing airway obstruction, which is usually secondary to edema in the acute setting.
Viral Laryngotracheitis
Oral steroids are the mainstay of treatment. Research has shown dexamethasone is preferred over prednisolone.18-20 Steroids are not only useful in moderate to severe laryngotracheitis but also have a therapeutic role in children with mild laryngotracheitis.18 In hospital settings the parenteral formulation of dexamethasone can be safely given orally with good effect. There is no therapeutic advantage in acute laryngotracheitis to giving dexamethasone via either the IV or intramuscular route vs oral.21 In the outpatient setting, decadron tablets can be crushed and mixed in with a young child’s favorite soft food (eg, mashed potatoes or apple sauce). The authors recommend this strategy in lieu of prescribing dexamethasone suspension as its dilute concentration (1 mg/10 ml) results in a need for a child to receive a relatively large volume of a distasteful liquid. There is a wide therapeutic range of dexamethasone with studies documenting efficacy for laryngotracheitis in doses ranging from 0.15 mg/kg to 0.6 mg/kg. To date there are no large studies which demonstrate routine therapeutic utility of subsequent doses of dexamethasone. Nebulized budesonide (2.5 mg) can be given if oral steroids are not tolerated, however it is significantly more expensive.
Racemic epinephrine is the agent of choice for rapid onset of action in children who demonstrate stridor at rest. It causes vasoconstriction in the laryngeal mucosa, promotes bronchial smooth muscle relaxation, and thinning of bronchial secretions. It offers short-term relief of symptoms until steroids start to work. There is no rebound effect or worsening of symptoms once the epinephrine wears off, but children who receive this drug should be observed in the ED for a period of time (2-3 hours is standard of care in many hospitals) for return of symptoms.10,22 Patients who are persistently symptomatic 4 hours after administration of steroids or who require repeat doses of racemic epinephrine should be admitted for observation.10There are no contraindications to adjuvant treatments, such as antipyretics and non-sedating analgesics. Clinicians should maintain a high index of suspicion for anatomic airway anomalies that may need further evaluation/direct visualization in pediatric patients who present with repeated episodes of croup.10
Case Conclusions
Case 1
The 9-month-old boy with stridor was noted to have increased stridor while fussy, but even at rest some inspiratory stridor was present. A barky cough was noted in the examination room. The patient was placed on a monitor and a nebulized racemic epinephrine treatment was started. A single dose of oral dexamethasone was given shortly after presentation to the ED. Since the patient had inspiratory stridor at rest with associated tachypnea and hypoxia on initial presentation, a neck X-ray was obtained (Figure 4). Subglottic narrowing was identified on the imaging, but both the epiglottis and the prevertebral space were normal in appearance and no foreign bodies were visualized. The inspiratory stridor at rest, tachypnea, and mild hypoxia all improved after treatment, the patient was observed for 2 hours in the ED without recurrence of respiratory distress and was able to be discharged home with a diagnosis of acute croup.

Case 2
The 3-year-old girl was noted to be in significant positional respiratory distress, so the physician asked her parents to keep her calm in her position of comfort. She was calmly and quickly placed on a monitor with age-appropriate distraction techniques in place and advanced airway equipment at the bedside. A portable chest X-ray was obtained and revealed a coin was partially obstructing the trachea. Care was taken in the ED to avoid all interventions such as IV access that might upset the child so as not to inadvertently convert this partial airway obstruction to a complete obstruction. The otolaryngology team was called urgently, and the patient was transported to the operating room for foreign body removal in a controlled environment.
1. Bjornson CL, Johnson DW. Croup. Lancet. 2008;371(9609):329-339. doi:10.1016/S0140-6736(08)60170-1.
2. Escobar ML, Needleman J. Stridor. Pediatr Rev. 2015;36(3):135-137. doi:10.1542/pir.36-3-135.
3. Pfleger A, Eber E. Assessment and causes of stridor. Paediatr Respir Rev. 2016;18:64-72. doi:10.1016/j.prrv.2015.10.003.
4. Boudewyns A, Claes J, Van de Heyning P. Clinical practice: an approach to stridor in infants and children. Eur J Pediatr. 2010;169(2):135-141. doi:10.1007/s00431-009-1044-7.
5. Kelley PB, Simon JE. Racemic epinephrine use in croup and disposition. Am J Emerg Med. 1992;10(3):181-183.
6. Mandal A, Kabra SK, Lodha R. Upper airway obstruction in children. Indian J Pediatr. 2015;82(8):737-744.
7. Marchese A, Langhan ML. Management of airway obstruction and stridor in pediatric patients. Pediatr Emerg Med Pract. 2017;14(11):1-24.
8. Wani TM, Bissonnette B, Rafiq Malik M, et al. Age-based analysis of pediatric upper airway dimensions using computed tomography imaging. Pediatr Pulmonol. 2016;51(3):267-271. doi:10.1002/ppul.23232.
9. Donaldson D, Poleski D, Knipple E, et al. Intramuscular versus oral dexamethasone for the treatment of moderate-to-severe croup: a randomized, double-blind trial. Acad Emerg Med. 2003;10(1):16-21.
10. Boudewyns A, Claes J, Van de Heyning P. Clinical practice: an approach to stridor in infants and children. Eur J Pediatr. 2010;169(2):135-141. doi:10.1007/s00431-009-1044-7.
11. Tibballs J, Watson T. Symptoms and signs differentiating croup and epiglottitis. J Paediatr Child Health. 2011;47(3):77-82. doi:10.1111/j.1440-1754.2010.01892.x.
12. Sobol SE, Zapata S. Epiglottitis and croup. Otolaryngol Clin North Am. 2008;41(3):551-566. doi:10.1016/j.otc.2008.01.012.
13. Craig FW, Schunk JE. Retropharyngeal abscess in children: clinical presentation, utility of imaging, and current management. Pediatrics. 2003;111(6 Pt 1):1394-1398.
14. Roberson DW. Pediatric retropharyngeal abscesses. Clin Pediatr Emerg Med. 2004;5(1):37-40.
15. Riffat F, Cheng A. Pediatric caustic ingestion: 50 consecutive cases and a review of the literature. Dis Esophagus. 2009;22(1):89-94. doi:10.1111/j.1442-2050.2008.00867.x.
16. Daniel SJ. The upper airway: congenital malformations. Paediatr Respir Revi. 2006;7 Suppl 1:S260-S263.
17. Arutyunyan H, Spangler M. Pediatric upper airway obstruction. Peds RAP Web site. https://www.hippoed.com/peds/rap/episode/pedsrapfebruary/pediatricupper. Published February 2018. Accessed August 31, 2018.
18. Bjornson CL, Klassen TP, Williamson J, et al; Pediatric Emergency Research Canada Network. A randomized trial of a single dose of oral dexamethasone for mild croup. N Engl J Med. 2004;351(13):1306-1313.
19. Fifoot AA, Ting JY. Comparison between single-dose oral prednisolone and oral dexamethasone in the treatment of croup: a randomized, double-blinded clinical trial. Emerg Med Australas. 2007;19(1):51-58.
20. Sparrow A, Geelhoed G. Prednisolone versus dexamethasone in croup: a randomised equivalence trial. Arch Dis Child. 2005;91(7):580-583.
21. Donaldson D, Poleski D, Knipple E, et al. Intramuscular versus oral dexamethasone for the treatment of moderate-to-severe croup: a randomized, double-blind trial. Acad Emerg Med. 2003;10(1):16-21.
22. Kelley PB, Simon JE. Racemic epinephrine use in croup and disposition. Am J Emerg Med. 1992;10(3):181-183.
23. Yamamoto LG. Test your skill in reading pediatric lateral necks. University of Hawaii Web site. https://www.hawaii.edu/medicine/pediatrics/pemxray/v2c20.html. Accessed September 13, 2018.
The distinct features of the pediatric airway make respiratory failure an important concern independent of the underlying cause.
The distinct features of the pediatric airway make respiratory failure an important concern independent of the underlying cause.
Cases
Case 1
It’s a busy shift on an unusually chilly and rainy July night. Emergency medical services (EMS) brings in a 9-month-old boy who woke up with a “squeaking” noise. His parents reported that he has had a fever, cough, rhinorrhea, and difficulty breathing for the past 2 days; however, they did not hear the noisy breathing until the night of presentation. When the patient is examined, it is noted that he has inspiratory stridor at rest, moderate subcostal retractions, and an occasional deep cough. Upper airway transmitted noises were present, but otherwise the patient had clear lungs.
The patient’s vital signs at presentation were: blood pressure (BP), 85/55 mm Hg; heart rate (HR), 163 beats/min; respiratory rate (RR), 55 breaths/min; and temperature (T), 101.8°F. Oxygen saturation was 90% on room air. The patient’s mother wants to know how the respiratory distress will be fixed and is inquiring if they will have to stay in the hospital overnight.
Case 2
As work begins on the child described above, EMS brings in a 3-year-old girl who appears to be in moderate-severe respiratory distress. Her parents report that she started to drool earlier in the day followed by coughing and occasional gagging. Her parents relay that they thought the symptoms were because of post-nasal drip due to her cold, but the respiratory distress seems to be getting worse, and she now has very noisy breathing and is reluctant to lay down. Upon examination, both inspiratory and expiratory stridor is heard, and it is noted that moderate subcostal retractions are present when the patient is supine.
The patient’s vital signs at presentation were: BP, 89/58 mm Hg; HR, 144 beats/min; RR, 52 breaths/min; and T, 99.5°F. Oxygen saturation was 88% on room air. The nursing staff asked what to do next and why the 2 stridor cases are being managed so differently.
Stridor
Stridor is a high-pitched, harsh sound heard during respiration, predominantly during inspiration, as a result of turbulent air passage.1-3 Stridor is not a diagnosis in itself, but rather a sign of underlying acute or chronic etiology, which needs to be classified based on elicited history and examination.1,4 While the etiology of obstruction may be infectious, congenital, mechanical, or traumatic, the distinct features of the pediatric airway make respiratory failure an important concern independent of the underlying cause.
Anatomy
There are several anatomical differences unique to the pediatric airway that make children, especially infants under 1 year of age, more susceptible to airway obstruction.5,6The pediatric larynx is more anterior and superior and less fibrous than adults, thereby more compliant.6,7 The pediatric epiglottis is longer, omega-shaped, and softer, and the tongue is larger in comparison to the size of the oral cavity, resulting in obstructed airflow.6,7 Children also have a larger and more prominent occiput, causing mechanical obstruction by flexion of the neck when supine.6 While the cricoid cartilage was previously believed to be the narrowest portion of the airway, more recent measurement techniques have challenged this and shown that the glottic and subglottic areas may be narrower in children.7,8
Worsening obstruction resulting in a decreased airway radius leads to increased turbulence to air flow, which is explained by Poiseuille’s law.1,2,7 The resistance to airflow becomes inversely related to the fourth power of the radius, so even a small change in an already narrow pediatric airway can make a huge difference.5 In practice, this means 1 mm of mucosal edema will decrease the cross-sectional area of the airway by 75% and increase the resistance of airflow by a magnitude of 16 to 32 times depending on the level of turbulence.7The airway can be divided into extrathoracic and intrathoracic regions, separated by the vocal cords.13 Inspiratory stridor is typically due to extrathoracic obstruction and expiratory stridor is due to intrathoracic obstruction below the level of the cords. Biphasic stridor, however, may indicate a fixed obstruction at the level of the cords.2,3,5,9
Acute Differentials
The pediatric patient is at high risk for respiratory decompensation when the upper airway is acutely compromised. The history, physical examination, and phases of stridor can help determine the underlying diagnosis and definitive treatment plan.
Acute Croup
Acute croup (laryngotracheitis) is a clinical diagnosis based on acute onset of barky cough and inspiratory stridor.1 It is usually secondary to an infection, most commonly viral (parainfluenza virus), resulting in edema and increased secretions of the subglottic mucosa.7 The onset is typically preceded by upper respiratory illness (URI) symptoms, and is often worse at night or after waking from a nap.1 The peak incidence is between ages 6 months to 3 years. While croup is a clinical diagnosis, an anteroposterior X-ray will often show a steeple sign.7,10
Spasmodic Croup
Spasmodic croup is an atypical presentation usually seen in children 8 years or older without a preceding URI. Patients will wake up overnight with a harsh brass-like cough, stridor, and hoarse voice. The etiology is unclear, but often these patients have a history of atopy and respond in part to treatment with antihistamines.
Foreign Body Aspiration
All that is acutely stridulous is not croup. Stridor from foreign body aspiration is sudden in onset and children do not always present with a history suggestive of foreign body aspiration. Diagnosis requires a high index of suspicion because the event is often unwitnessed and typical patients are pre-verbal. The physical examination may reveal diminished air entry along with stridor. Diagnosis is made by obtaining an X-ray (lateral neck [Figure 1], lateral decubitus, or inspiratory/expiratory chest X-ray) or by bronchoscopy which is both diagnostic and therapeutic.7,10 Remember to always think of foreign body aspiration in children with acute stridor who have neither fever nor antecedent URI symptoms.
Bacterial Tracheitis
Bacterial tracheitis should be suspected in toxic appearing children who present with respiratory distress and stridor but who have a poor response to nebulized epinephrine. It is typically seen in toddlers and school-aged children, and like a viral tracheitis, presentation can be preceded by either URI or fever.10 Stridor is caused by subglottic edema and mucopurulent secretions in the airway.7,10 Infection is most commonly by S. aureus but initial antibiotic choice should be broad spectrum, and include a third-generation cephalosporin or beta-lactamase resistant penicillin.
Epiglottitis
Epiglottitis is edema of the epiglottis, most commonly secondary to bacterial infection. The epidemiology of epiglottitis has changed dramatically since widespread immunization for H. influenza with a significantly decreased incidence and change in the average age of presentation to 14.6 years (previously 5.6 years).7 The clinical course begins with sore throat, dysphonia, refusal to eat and progressive difficulty handling secretions with eventual drooling, stridor, tripoding, and toxic appearance. Epiglottitis can be differentiated from croup and bacterial tracheitis because presentation typically lacks a cough.7,10,11 Diagnosis is made either by direct visualization of the epiglottis or a lateral neck X-ray showing a ‘thumb print’ sign (Figure 2).12 Emergency department treatment is similar to the management of the child with a partial foreign body occlusion and focuses on maintaining the airway and minimizing anything that agitates the patient. Intravenous (IV) antibiotic coverage is similar to bacterial tracheitis (third-generation cephalosporin or a beta-lactamase resistant penicillin).
Retropharyngeal Abscess
The most common chief complaint of retropharyngeal abscess (RPA) is neck pain (38%) with fever. As such, it can clinically be mistaken for meningitis on initial presentation. Retropharyngeal abscess will present rarely with either stridor or associated respiratory distress, and it can also mimic croup on initial presentation. Physical examination findings which differentiate this entity include limited or painful neck extension (45%), torticollis (36.5%), and to a lesser extent limitation of neck flexion (12.5%).13 The median age at diagnosis is 36 months with 75% of patients less than 5 years. Typical presentation is insidious with fever and URI symptoms preceding onset. Diagnosis can be made with a lateral neck X-ray showing widening of the prevertebral space (Figure 3), but the gold standard diagnostic study is a computed tomography with contrast.14 Management is IV antibiotics covering aerobic and anaerobic bacteria (eg, ampicillin-sulbactam) ± surgical intervention.
Caustic Ingestion
Caustic ingestion is most commonly accidental and seen in children aged 12 months to 2 years. However, with recent fads, such as the “Tide Pod challenge” teenagers are also at risk. Airway compromise and stridor are secondary to mucosal injury and edema. Oral injury is not always a useful marker for significant distal injury. A complete evaluation of the upper airway and digestive tract within 48 hours after known/suspected caustic ingestion is recommended to assess full extent of damage.15
Chronic Differentials
Laryngomalacia
Laryngomalacia is a congenital weakness of laryngeal tissues, and it is the most common cause of both chronic stridor and neonatal stridor. It is characterized by progressive worsening of symptoms with crying/feeding and supine positioning. Diagnosis is made by bronchoscopy and management is conservative unless there are life threatening apneic or cyanotic events.7
Rings/Slings
There are many anatomic structures with the potential to cause extrinsic airway compression which present with stridor. This type of stridor is often biphasic. Examples include innominate artery compression, double aortic arch, aberrant subclavian artery, and pulmonary artery sling.7
Stridor presenting in children with a history of prematurity or prolonged intubation should raise concern for subglottic and tracheal stenosis.16
Evaluation
Regardless of the etiology of stridor, efforts should be made to keep the patient calm (ie, allow the parent to keep holding a young child, limit any examination not absolutely necessary). Much of the examination can be completed from a distance without disturbing the child.17 Observation of the inspiratory:expiratory (I:E) ratio can localize the level of airway obstruction. For example, an I:E ratio weighted toward a longer inspiration indicates an extrathoracic airway obstruction. Whereas an I:E with a prolonged expiratory phase is consistent with intrathoracic obstruction (eg, terminal bronchial obstruction).17
Another way to localize the level of obstruction is to look for changes in the voice; patients who present with a change in their voice have a subglottic partial obstruction such as croup. However, patients with a muffled voice or drooling have a supraglottic obstruction such as epiglottitis or RPA.17
Management
Management of stridor focuses on reducing airway obstruction, which is usually secondary to edema in the acute setting.
Viral Laryngotracheitis
Oral steroids are the mainstay of treatment. Research has shown dexamethasone is preferred over prednisolone.18-20 Steroids are not only useful in moderate to severe laryngotracheitis but also have a therapeutic role in children with mild laryngotracheitis.18 In hospital settings the parenteral formulation of dexamethasone can be safely given orally with good effect. There is no therapeutic advantage in acute laryngotracheitis to giving dexamethasone via either the IV or intramuscular route vs oral.21 In the outpatient setting, decadron tablets can be crushed and mixed in with a young child’s favorite soft food (eg, mashed potatoes or apple sauce). The authors recommend this strategy in lieu of prescribing dexamethasone suspension as its dilute concentration (1 mg/10 ml) results in a need for a child to receive a relatively large volume of a distasteful liquid. There is a wide therapeutic range of dexamethasone with studies documenting efficacy for laryngotracheitis in doses ranging from 0.15 mg/kg to 0.6 mg/kg. To date there are no large studies which demonstrate routine therapeutic utility of subsequent doses of dexamethasone. Nebulized budesonide (2.5 mg) can be given if oral steroids are not tolerated, however it is significantly more expensive.
Racemic epinephrine is the agent of choice for rapid onset of action in children who demonstrate stridor at rest. It causes vasoconstriction in the laryngeal mucosa, promotes bronchial smooth muscle relaxation, and thinning of bronchial secretions. It offers short-term relief of symptoms until steroids start to work. There is no rebound effect or worsening of symptoms once the epinephrine wears off, but children who receive this drug should be observed in the ED for a period of time (2-3 hours is standard of care in many hospitals) for return of symptoms.10,22 Patients who are persistently symptomatic 4 hours after administration of steroids or who require repeat doses of racemic epinephrine should be admitted for observation.10There are no contraindications to adjuvant treatments, such as antipyretics and non-sedating analgesics. Clinicians should maintain a high index of suspicion for anatomic airway anomalies that may need further evaluation/direct visualization in pediatric patients who present with repeated episodes of croup.10
Case Conclusions
Case 1
The 9-month-old boy with stridor was noted to have increased stridor while fussy, but even at rest some inspiratory stridor was present. A barky cough was noted in the examination room. The patient was placed on a monitor and a nebulized racemic epinephrine treatment was started. A single dose of oral dexamethasone was given shortly after presentation to the ED. Since the patient had inspiratory stridor at rest with associated tachypnea and hypoxia on initial presentation, a neck X-ray was obtained (Figure 4). Subglottic narrowing was identified on the imaging, but both the epiglottis and the prevertebral space were normal in appearance and no foreign bodies were visualized. The inspiratory stridor at rest, tachypnea, and mild hypoxia all improved after treatment, the patient was observed for 2 hours in the ED without recurrence of respiratory distress and was able to be discharged home with a diagnosis of acute croup.
Case 2
The 3-year-old girl was noted to be in significant positional respiratory distress, so the physician asked her parents to keep her calm in her position of comfort. She was calmly and quickly placed on a monitor with age-appropriate distraction techniques in place and advanced airway equipment at the bedside. A portable chest X-ray was obtained and revealed a coin was partially obstructing the trachea. Care was taken in the ED to avoid all interventions such as IV access that might upset the child so as not to inadvertently convert this partial airway obstruction to a complete obstruction. The otolaryngology team was called urgently, and the patient was transported to the operating room for foreign body removal in a controlled environment.
Cases
Case 1
It’s a busy shift on an unusually chilly and rainy July night. Emergency medical services (EMS) brings in a 9-month-old boy who woke up with a “squeaking” noise. His parents reported that he has had a fever, cough, rhinorrhea, and difficulty breathing for the past 2 days; however, they did not hear the noisy breathing until the night of presentation. When the patient is examined, it is noted that he has inspiratory stridor at rest, moderate subcostal retractions, and an occasional deep cough. Upper airway transmitted noises were present, but otherwise the patient had clear lungs.
The patient’s vital signs at presentation were: blood pressure (BP), 85/55 mm Hg; heart rate (HR), 163 beats/min; respiratory rate (RR), 55 breaths/min; and temperature (T), 101.8°F. Oxygen saturation was 90% on room air. The patient’s mother wants to know how the respiratory distress will be fixed and is inquiring if they will have to stay in the hospital overnight.
Case 2
As work begins on the child described above, EMS brings in a 3-year-old girl who appears to be in moderate-severe respiratory distress. Her parents report that she started to drool earlier in the day followed by coughing and occasional gagging. Her parents relay that they thought the symptoms were because of post-nasal drip due to her cold, but the respiratory distress seems to be getting worse, and she now has very noisy breathing and is reluctant to lay down. Upon examination, both inspiratory and expiratory stridor is heard, and it is noted that moderate subcostal retractions are present when the patient is supine.
The patient’s vital signs at presentation were: BP, 89/58 mm Hg; HR, 144 beats/min; RR, 52 breaths/min; and T, 99.5°F. Oxygen saturation was 88% on room air. The nursing staff asked what to do next and why the 2 stridor cases are being managed so differently.
Stridor
Stridor is a high-pitched, harsh sound heard during respiration, predominantly during inspiration, as a result of turbulent air passage.1-3 Stridor is not a diagnosis in itself, but rather a sign of underlying acute or chronic etiology, which needs to be classified based on elicited history and examination.1,4 While the etiology of obstruction may be infectious, congenital, mechanical, or traumatic, the distinct features of the pediatric airway make respiratory failure an important concern independent of the underlying cause.
Anatomy
There are several anatomical differences unique to the pediatric airway that make children, especially infants under 1 year of age, more susceptible to airway obstruction.5,6The pediatric larynx is more anterior and superior and less fibrous than adults, thereby more compliant.6,7 The pediatric epiglottis is longer, omega-shaped, and softer, and the tongue is larger in comparison to the size of the oral cavity, resulting in obstructed airflow.6,7 Children also have a larger and more prominent occiput, causing mechanical obstruction by flexion of the neck when supine.6 While the cricoid cartilage was previously believed to be the narrowest portion of the airway, more recent measurement techniques have challenged this and shown that the glottic and subglottic areas may be narrower in children.7,8
Worsening obstruction resulting in a decreased airway radius leads to increased turbulence to air flow, which is explained by Poiseuille’s law.1,2,7 The resistance to airflow becomes inversely related to the fourth power of the radius, so even a small change in an already narrow pediatric airway can make a huge difference.5 In practice, this means 1 mm of mucosal edema will decrease the cross-sectional area of the airway by 75% and increase the resistance of airflow by a magnitude of 16 to 32 times depending on the level of turbulence.7The airway can be divided into extrathoracic and intrathoracic regions, separated by the vocal cords.13 Inspiratory stridor is typically due to extrathoracic obstruction and expiratory stridor is due to intrathoracic obstruction below the level of the cords. Biphasic stridor, however, may indicate a fixed obstruction at the level of the cords.2,3,5,9
Acute Differentials
The pediatric patient is at high risk for respiratory decompensation when the upper airway is acutely compromised. The history, physical examination, and phases of stridor can help determine the underlying diagnosis and definitive treatment plan.
Acute Croup
Acute croup (laryngotracheitis) is a clinical diagnosis based on acute onset of barky cough and inspiratory stridor.1 It is usually secondary to an infection, most commonly viral (parainfluenza virus), resulting in edema and increased secretions of the subglottic mucosa.7 The onset is typically preceded by upper respiratory illness (URI) symptoms, and is often worse at night or after waking from a nap.1 The peak incidence is between ages 6 months to 3 years. While croup is a clinical diagnosis, an anteroposterior X-ray will often show a steeple sign.7,10
Spasmodic Croup
Spasmodic croup is an atypical presentation usually seen in children 8 years or older without a preceding URI. Patients will wake up overnight with a harsh brass-like cough, stridor, and hoarse voice. The etiology is unclear, but often these patients have a history of atopy and respond in part to treatment with antihistamines.
Foreign Body Aspiration
All that is acutely stridulous is not croup. Stridor from foreign body aspiration is sudden in onset and children do not always present with a history suggestive of foreign body aspiration. Diagnosis requires a high index of suspicion because the event is often unwitnessed and typical patients are pre-verbal. The physical examination may reveal diminished air entry along with stridor. Diagnosis is made by obtaining an X-ray (lateral neck [Figure 1], lateral decubitus, or inspiratory/expiratory chest X-ray) or by bronchoscopy which is both diagnostic and therapeutic.7,10 Remember to always think of foreign body aspiration in children with acute stridor who have neither fever nor antecedent URI symptoms.
Bacterial Tracheitis
Bacterial tracheitis should be suspected in toxic appearing children who present with respiratory distress and stridor but who have a poor response to nebulized epinephrine. It is typically seen in toddlers and school-aged children, and like a viral tracheitis, presentation can be preceded by either URI or fever.10 Stridor is caused by subglottic edema and mucopurulent secretions in the airway.7,10 Infection is most commonly by S. aureus but initial antibiotic choice should be broad spectrum, and include a third-generation cephalosporin or beta-lactamase resistant penicillin.
Epiglottitis
Epiglottitis is edema of the epiglottis, most commonly secondary to bacterial infection. The epidemiology of epiglottitis has changed dramatically since widespread immunization for H. influenza with a significantly decreased incidence and change in the average age of presentation to 14.6 years (previously 5.6 years).7 The clinical course begins with sore throat, dysphonia, refusal to eat and progressive difficulty handling secretions with eventual drooling, stridor, tripoding, and toxic appearance. Epiglottitis can be differentiated from croup and bacterial tracheitis because presentation typically lacks a cough.7,10,11 Diagnosis is made either by direct visualization of the epiglottis or a lateral neck X-ray showing a ‘thumb print’ sign (Figure 2).12 Emergency department treatment is similar to the management of the child with a partial foreign body occlusion and focuses on maintaining the airway and minimizing anything that agitates the patient. Intravenous (IV) antibiotic coverage is similar to bacterial tracheitis (third-generation cephalosporin or a beta-lactamase resistant penicillin).
Retropharyngeal Abscess
The most common chief complaint of retropharyngeal abscess (RPA) is neck pain (38%) with fever. As such, it can clinically be mistaken for meningitis on initial presentation. Retropharyngeal abscess will present rarely with either stridor or associated respiratory distress, and it can also mimic croup on initial presentation. Physical examination findings which differentiate this entity include limited or painful neck extension (45%), torticollis (36.5%), and to a lesser extent limitation of neck flexion (12.5%).13 The median age at diagnosis is 36 months with 75% of patients less than 5 years. Typical presentation is insidious with fever and URI symptoms preceding onset. Diagnosis can be made with a lateral neck X-ray showing widening of the prevertebral space (Figure 3), but the gold standard diagnostic study is a computed tomography with contrast.14 Management is IV antibiotics covering aerobic and anaerobic bacteria (eg, ampicillin-sulbactam) ± surgical intervention.
Caustic Ingestion
Caustic ingestion is most commonly accidental and seen in children aged 12 months to 2 years. However, with recent fads, such as the “Tide Pod challenge” teenagers are also at risk. Airway compromise and stridor are secondary to mucosal injury and edema. Oral injury is not always a useful marker for significant distal injury. A complete evaluation of the upper airway and digestive tract within 48 hours after known/suspected caustic ingestion is recommended to assess full extent of damage.15
Chronic Differentials
Laryngomalacia
Laryngomalacia is a congenital weakness of laryngeal tissues, and it is the most common cause of both chronic stridor and neonatal stridor. It is characterized by progressive worsening of symptoms with crying/feeding and supine positioning. Diagnosis is made by bronchoscopy and management is conservative unless there are life threatening apneic or cyanotic events.7
Rings/Slings
There are many anatomic structures with the potential to cause extrinsic airway compression which present with stridor. This type of stridor is often biphasic. Examples include innominate artery compression, double aortic arch, aberrant subclavian artery, and pulmonary artery sling.7
Stridor presenting in children with a history of prematurity or prolonged intubation should raise concern for subglottic and tracheal stenosis.16
Evaluation
Regardless of the etiology of stridor, efforts should be made to keep the patient calm (ie, allow the parent to keep holding a young child, limit any examination not absolutely necessary). Much of the examination can be completed from a distance without disturbing the child.17 Observation of the inspiratory:expiratory (I:E) ratio can localize the level of airway obstruction. For example, an I:E ratio weighted toward a longer inspiration indicates an extrathoracic airway obstruction. Whereas an I:E with a prolonged expiratory phase is consistent with intrathoracic obstruction (eg, terminal bronchial obstruction).17
Another way to localize the level of obstruction is to look for changes in the voice; patients who present with a change in their voice have a subglottic partial obstruction such as croup. However, patients with a muffled voice or drooling have a supraglottic obstruction such as epiglottitis or RPA.17
Management
Management of stridor focuses on reducing airway obstruction, which is usually secondary to edema in the acute setting.
Viral Laryngotracheitis
Oral steroids are the mainstay of treatment. Research has shown dexamethasone is preferred over prednisolone.18-20 Steroids are not only useful in moderate to severe laryngotracheitis but also have a therapeutic role in children with mild laryngotracheitis.18 In hospital settings the parenteral formulation of dexamethasone can be safely given orally with good effect. There is no therapeutic advantage in acute laryngotracheitis to giving dexamethasone via either the IV or intramuscular route vs oral.21 In the outpatient setting, decadron tablets can be crushed and mixed in with a young child’s favorite soft food (eg, mashed potatoes or apple sauce). The authors recommend this strategy in lieu of prescribing dexamethasone suspension as its dilute concentration (1 mg/10 ml) results in a need for a child to receive a relatively large volume of a distasteful liquid. There is a wide therapeutic range of dexamethasone with studies documenting efficacy for laryngotracheitis in doses ranging from 0.15 mg/kg to 0.6 mg/kg. To date there are no large studies which demonstrate routine therapeutic utility of subsequent doses of dexamethasone. Nebulized budesonide (2.5 mg) can be given if oral steroids are not tolerated, however it is significantly more expensive.
Racemic epinephrine is the agent of choice for rapid onset of action in children who demonstrate stridor at rest. It causes vasoconstriction in the laryngeal mucosa, promotes bronchial smooth muscle relaxation, and thinning of bronchial secretions. It offers short-term relief of symptoms until steroids start to work. There is no rebound effect or worsening of symptoms once the epinephrine wears off, but children who receive this drug should be observed in the ED for a period of time (2-3 hours is standard of care in many hospitals) for return of symptoms.10,22 Patients who are persistently symptomatic 4 hours after administration of steroids or who require repeat doses of racemic epinephrine should be admitted for observation.10There are no contraindications to adjuvant treatments, such as antipyretics and non-sedating analgesics. Clinicians should maintain a high index of suspicion for anatomic airway anomalies that may need further evaluation/direct visualization in pediatric patients who present with repeated episodes of croup.10
Case Conclusions
Case 1
The 9-month-old boy with stridor was noted to have increased stridor while fussy, but even at rest some inspiratory stridor was present. A barky cough was noted in the examination room. The patient was placed on a monitor and a nebulized racemic epinephrine treatment was started. A single dose of oral dexamethasone was given shortly after presentation to the ED. Since the patient had inspiratory stridor at rest with associated tachypnea and hypoxia on initial presentation, a neck X-ray was obtained (Figure 4). Subglottic narrowing was identified on the imaging, but both the epiglottis and the prevertebral space were normal in appearance and no foreign bodies were visualized. The inspiratory stridor at rest, tachypnea, and mild hypoxia all improved after treatment, the patient was observed for 2 hours in the ED without recurrence of respiratory distress and was able to be discharged home with a diagnosis of acute croup.
Case 2
The 3-year-old girl was noted to be in significant positional respiratory distress, so the physician asked her parents to keep her calm in her position of comfort. She was calmly and quickly placed on a monitor with age-appropriate distraction techniques in place and advanced airway equipment at the bedside. A portable chest X-ray was obtained and revealed a coin was partially obstructing the trachea. Care was taken in the ED to avoid all interventions such as IV access that might upset the child so as not to inadvertently convert this partial airway obstruction to a complete obstruction. The otolaryngology team was called urgently, and the patient was transported to the operating room for foreign body removal in a controlled environment.
1. Bjornson CL, Johnson DW. Croup. Lancet. 2008;371(9609):329-339. doi:10.1016/S0140-6736(08)60170-1.
2. Escobar ML, Needleman J. Stridor. Pediatr Rev. 2015;36(3):135-137. doi:10.1542/pir.36-3-135.
3. Pfleger A, Eber E. Assessment and causes of stridor. Paediatr Respir Rev. 2016;18:64-72. doi:10.1016/j.prrv.2015.10.003.
4. Boudewyns A, Claes J, Van de Heyning P. Clinical practice: an approach to stridor in infants and children. Eur J Pediatr. 2010;169(2):135-141. doi:10.1007/s00431-009-1044-7.
5. Kelley PB, Simon JE. Racemic epinephrine use in croup and disposition. Am J Emerg Med. 1992;10(3):181-183.
6. Mandal A, Kabra SK, Lodha R. Upper airway obstruction in children. Indian J Pediatr. 2015;82(8):737-744.
7. Marchese A, Langhan ML. Management of airway obstruction and stridor in pediatric patients. Pediatr Emerg Med Pract. 2017;14(11):1-24.
8. Wani TM, Bissonnette B, Rafiq Malik M, et al. Age-based analysis of pediatric upper airway dimensions using computed tomography imaging. Pediatr Pulmonol. 2016;51(3):267-271. doi:10.1002/ppul.23232.
9. Donaldson D, Poleski D, Knipple E, et al. Intramuscular versus oral dexamethasone for the treatment of moderate-to-severe croup: a randomized, double-blind trial. Acad Emerg Med. 2003;10(1):16-21.
10. Boudewyns A, Claes J, Van de Heyning P. Clinical practice: an approach to stridor in infants and children. Eur J Pediatr. 2010;169(2):135-141. doi:10.1007/s00431-009-1044-7.
11. Tibballs J, Watson T. Symptoms and signs differentiating croup and epiglottitis. J Paediatr Child Health. 2011;47(3):77-82. doi:10.1111/j.1440-1754.2010.01892.x.
12. Sobol SE, Zapata S. Epiglottitis and croup. Otolaryngol Clin North Am. 2008;41(3):551-566. doi:10.1016/j.otc.2008.01.012.
13. Craig FW, Schunk JE. Retropharyngeal abscess in children: clinical presentation, utility of imaging, and current management. Pediatrics. 2003;111(6 Pt 1):1394-1398.
14. Roberson DW. Pediatric retropharyngeal abscesses. Clin Pediatr Emerg Med. 2004;5(1):37-40.
15. Riffat F, Cheng A. Pediatric caustic ingestion: 50 consecutive cases and a review of the literature. Dis Esophagus. 2009;22(1):89-94. doi:10.1111/j.1442-2050.2008.00867.x.
16. Daniel SJ. The upper airway: congenital malformations. Paediatr Respir Revi. 2006;7 Suppl 1:S260-S263.
17. Arutyunyan H, Spangler M. Pediatric upper airway obstruction. Peds RAP Web site. https://www.hippoed.com/peds/rap/episode/pedsrapfebruary/pediatricupper. Published February 2018. Accessed August 31, 2018.
18. Bjornson CL, Klassen TP, Williamson J, et al; Pediatric Emergency Research Canada Network. A randomized trial of a single dose of oral dexamethasone for mild croup. N Engl J Med. 2004;351(13):1306-1313.
19. Fifoot AA, Ting JY. Comparison between single-dose oral prednisolone and oral dexamethasone in the treatment of croup: a randomized, double-blinded clinical trial. Emerg Med Australas. 2007;19(1):51-58.
20. Sparrow A, Geelhoed G. Prednisolone versus dexamethasone in croup: a randomised equivalence trial. Arch Dis Child. 2005;91(7):580-583.
21. Donaldson D, Poleski D, Knipple E, et al. Intramuscular versus oral dexamethasone for the treatment of moderate-to-severe croup: a randomized, double-blind trial. Acad Emerg Med. 2003;10(1):16-21.
22. Kelley PB, Simon JE. Racemic epinephrine use in croup and disposition. Am J Emerg Med. 1992;10(3):181-183.
23. Yamamoto LG. Test your skill in reading pediatric lateral necks. University of Hawaii Web site. https://www.hawaii.edu/medicine/pediatrics/pemxray/v2c20.html. Accessed September 13, 2018.
1. Bjornson CL, Johnson DW. Croup. Lancet. 2008;371(9609):329-339. doi:10.1016/S0140-6736(08)60170-1.
2. Escobar ML, Needleman J. Stridor. Pediatr Rev. 2015;36(3):135-137. doi:10.1542/pir.36-3-135.
3. Pfleger A, Eber E. Assessment and causes of stridor. Paediatr Respir Rev. 2016;18:64-72. doi:10.1016/j.prrv.2015.10.003.
4. Boudewyns A, Claes J, Van de Heyning P. Clinical practice: an approach to stridor in infants and children. Eur J Pediatr. 2010;169(2):135-141. doi:10.1007/s00431-009-1044-7.
5. Kelley PB, Simon JE. Racemic epinephrine use in croup and disposition. Am J Emerg Med. 1992;10(3):181-183.
6. Mandal A, Kabra SK, Lodha R. Upper airway obstruction in children. Indian J Pediatr. 2015;82(8):737-744.
7. Marchese A, Langhan ML. Management of airway obstruction and stridor in pediatric patients. Pediatr Emerg Med Pract. 2017;14(11):1-24.
8. Wani TM, Bissonnette B, Rafiq Malik M, et al. Age-based analysis of pediatric upper airway dimensions using computed tomography imaging. Pediatr Pulmonol. 2016;51(3):267-271. doi:10.1002/ppul.23232.
9. Donaldson D, Poleski D, Knipple E, et al. Intramuscular versus oral dexamethasone for the treatment of moderate-to-severe croup: a randomized, double-blind trial. Acad Emerg Med. 2003;10(1):16-21.
10. Boudewyns A, Claes J, Van de Heyning P. Clinical practice: an approach to stridor in infants and children. Eur J Pediatr. 2010;169(2):135-141. doi:10.1007/s00431-009-1044-7.
11. Tibballs J, Watson T. Symptoms and signs differentiating croup and epiglottitis. J Paediatr Child Health. 2011;47(3):77-82. doi:10.1111/j.1440-1754.2010.01892.x.
12. Sobol SE, Zapata S. Epiglottitis and croup. Otolaryngol Clin North Am. 2008;41(3):551-566. doi:10.1016/j.otc.2008.01.012.
13. Craig FW, Schunk JE. Retropharyngeal abscess in children: clinical presentation, utility of imaging, and current management. Pediatrics. 2003;111(6 Pt 1):1394-1398.
14. Roberson DW. Pediatric retropharyngeal abscesses. Clin Pediatr Emerg Med. 2004;5(1):37-40.
15. Riffat F, Cheng A. Pediatric caustic ingestion: 50 consecutive cases and a review of the literature. Dis Esophagus. 2009;22(1):89-94. doi:10.1111/j.1442-2050.2008.00867.x.
16. Daniel SJ. The upper airway: congenital malformations. Paediatr Respir Revi. 2006;7 Suppl 1:S260-S263.
17. Arutyunyan H, Spangler M. Pediatric upper airway obstruction. Peds RAP Web site. https://www.hippoed.com/peds/rap/episode/pedsrapfebruary/pediatricupper. Published February 2018. Accessed August 31, 2018.
18. Bjornson CL, Klassen TP, Williamson J, et al; Pediatric Emergency Research Canada Network. A randomized trial of a single dose of oral dexamethasone for mild croup. N Engl J Med. 2004;351(13):1306-1313.
19. Fifoot AA, Ting JY. Comparison between single-dose oral prednisolone and oral dexamethasone in the treatment of croup: a randomized, double-blinded clinical trial. Emerg Med Australas. 2007;19(1):51-58.
20. Sparrow A, Geelhoed G. Prednisolone versus dexamethasone in croup: a randomised equivalence trial. Arch Dis Child. 2005;91(7):580-583.
21. Donaldson D, Poleski D, Knipple E, et al. Intramuscular versus oral dexamethasone for the treatment of moderate-to-severe croup: a randomized, double-blind trial. Acad Emerg Med. 2003;10(1):16-21.
22. Kelley PB, Simon JE. Racemic epinephrine use in croup and disposition. Am J Emerg Med. 1992;10(3):181-183.
23. Yamamoto LG. Test your skill in reading pediatric lateral necks. University of Hawaii Web site. https://www.hawaii.edu/medicine/pediatrics/pemxray/v2c20.html. Accessed September 13, 2018.
Obesity in early childhood promotes obese adolescence
Most obese adolescents first became obese between the ages of 2 and 6 years, based on data from approximately 50,000 children in Germany.

Identifying periods of weight gain in childhood can help develop intervention and prevention strategies to reduce the risk of obesity in adolescence, wrote Mandy Geserick, MSc, of the University of Leipzig, Germany, and her colleagues in the New England Journal of Medicine.
To assess the timing of weight gain in early childhood, the researchers reviewed data from a German patient registry designed to monitor growth data. The study population included 51,505 children who had at least one visit to a pediatrician between birth and age 14 years and a second visit between age 15 and 19 years.
Overall, the probability of being overweight or obese in adolescence was 29% among children who gained more weight in the preschool years, between the ages of 2 and 6 years (defined as a change in body mass index [BMI] of 0.2 or more to less than 2.0), compared with 20% among children whose preschool weight remained stable (defined as a change in BMI of more than −0.2 to less than 0.2) – a relative risk of 1.43.
“A total of 83% of the children with obesity at the age of 4 were overweight or obese in adolescence, and only 17% returned to a normal weight,” they wrote. In addition, 44% of children who were born large for gestational age were overweight or obese in adolescence.
“A practical clinical implication of our study results would be surveillance for BMI acceleration, which should be recognized before 6 years of age, even in the absence of obesity,” the researchers wrote.
The study findings were limited by several factors including the variation in the number of visits, the lack of data on many children beyond the age of 14 years, and the lack of data on parental weight and perinatal risk factors associated with obesity, the researchers noted. However, the results were strengthened by the large, population-based design, and support the study hypothesis that obesity develops in early childhood and, once present, persists into adolescence.
“The specific dynamics and patterns of BMI in this early childhood period, rather than the absolute BMI, appear to be important factors in identifying children at risk for obesity later in life,” the researchers wrote. “It is therefore important for health care professionals, educational staff, and parents to become more sensitive to this critical time period.”
The study was supported by the German Research Council for the Clinical Research Center; the Federal Ministry of Education and Research; and the University of Leipzig, which was supported by the European Union, the European Regional Development Fund, and the Free State of Saxony within the framework of the excellence initiative. The CrescNet registry infrastructure was supported by grants from Hexal, Novo Nordisk, Merck Serono, Lilly Deutschland, Pfizer, and Ipsen Pharma. Dr. Geserick had no financial conflicts to report.
SOURCE: Geserick M et al. N Engl J Med. 2018 Oct 3. doi: 10.1056/NEJMoa1803527.
Most normal-weight children remained in the normal range throughout childhood, but the association between obesity by the age of 5 years and obese adolescence is a “new and important” finding, Michael S. Freemark, MD, wrote in an accompanying editorial (N Engl J Med. 2018 Oct 3. doi: 10.1056/NEJMe1811305).
Although body mass index (BMI) generally decreases by age 5-6 years before increasing through adolescence, data from previous studies have shown that “an early or exaggerated ‘adiposity rebound’ portends an increased risk of obesity in later childhood and adolescence,” he wrote.
In this study, BMI increase between age 2 and 6 years was the strongest predictor of obesity in adolescence. Although the study was not designed to show causality, the results support the idea of a window of opportunity for intervention for children at increased risk for obesity, Dr. Freemark wrote. “The finding that the risk of adolescent obesity manifests by 3 to 5 years of age suggests that nutritional counseling should be considered when exaggerated weight gain persists or emerges after 2 years of age; it would be of value to test the efficacy of early dietary intervention in an appropriate trial.
“Counseling could be applied preemptively for families in which the parents are overweight, particularly if there is a history of maternal diabetes or smoking,” he added.
Dr. Freemark is affiliated with the division of pediatric endocrinology and diabetes at Duke University, Durham, N.C. He disclosed grants from Rhythm Pharmaceuticals, the American Heart Association, and the Humanitarian Innovation Fund and European Commission, as well as personal fees from Springer Publishing outside the submitted work.
Most normal-weight children remained in the normal range throughout childhood, but the association between obesity by the age of 5 years and obese adolescence is a “new and important” finding, Michael S. Freemark, MD, wrote in an accompanying editorial (N Engl J Med. 2018 Oct 3. doi: 10.1056/NEJMe1811305).
Although body mass index (BMI) generally decreases by age 5-6 years before increasing through adolescence, data from previous studies have shown that “an early or exaggerated ‘adiposity rebound’ portends an increased risk of obesity in later childhood and adolescence,” he wrote.
In this study, BMI increase between age 2 and 6 years was the strongest predictor of obesity in adolescence. Although the study was not designed to show causality, the results support the idea of a window of opportunity for intervention for children at increased risk for obesity, Dr. Freemark wrote. “The finding that the risk of adolescent obesity manifests by 3 to 5 years of age suggests that nutritional counseling should be considered when exaggerated weight gain persists or emerges after 2 years of age; it would be of value to test the efficacy of early dietary intervention in an appropriate trial.
“Counseling could be applied preemptively for families in which the parents are overweight, particularly if there is a history of maternal diabetes or smoking,” he added.
Dr. Freemark is affiliated with the division of pediatric endocrinology and diabetes at Duke University, Durham, N.C. He disclosed grants from Rhythm Pharmaceuticals, the American Heart Association, and the Humanitarian Innovation Fund and European Commission, as well as personal fees from Springer Publishing outside the submitted work.
Most normal-weight children remained in the normal range throughout childhood, but the association between obesity by the age of 5 years and obese adolescence is a “new and important” finding, Michael S. Freemark, MD, wrote in an accompanying editorial (N Engl J Med. 2018 Oct 3. doi: 10.1056/NEJMe1811305).
Although body mass index (BMI) generally decreases by age 5-6 years before increasing through adolescence, data from previous studies have shown that “an early or exaggerated ‘adiposity rebound’ portends an increased risk of obesity in later childhood and adolescence,” he wrote.
In this study, BMI increase between age 2 and 6 years was the strongest predictor of obesity in adolescence. Although the study was not designed to show causality, the results support the idea of a window of opportunity for intervention for children at increased risk for obesity, Dr. Freemark wrote. “The finding that the risk of adolescent obesity manifests by 3 to 5 years of age suggests that nutritional counseling should be considered when exaggerated weight gain persists or emerges after 2 years of age; it would be of value to test the efficacy of early dietary intervention in an appropriate trial.
“Counseling could be applied preemptively for families in which the parents are overweight, particularly if there is a history of maternal diabetes or smoking,” he added.
Dr. Freemark is affiliated with the division of pediatric endocrinology and diabetes at Duke University, Durham, N.C. He disclosed grants from Rhythm Pharmaceuticals, the American Heart Association, and the Humanitarian Innovation Fund and European Commission, as well as personal fees from Springer Publishing outside the submitted work.
Most obese adolescents first became obese between the ages of 2 and 6 years, based on data from approximately 50,000 children in Germany.
Identifying periods of weight gain in childhood can help develop intervention and prevention strategies to reduce the risk of obesity in adolescence, wrote Mandy Geserick, MSc, of the University of Leipzig, Germany, and her colleagues in the New England Journal of Medicine.
To assess the timing of weight gain in early childhood, the researchers reviewed data from a German patient registry designed to monitor growth data. The study population included 51,505 children who had at least one visit to a pediatrician between birth and age 14 years and a second visit between age 15 and 19 years.
Overall, the probability of being overweight or obese in adolescence was 29% among children who gained more weight in the preschool years, between the ages of 2 and 6 years (defined as a change in body mass index [BMI] of 0.2 or more to less than 2.0), compared with 20% among children whose preschool weight remained stable (defined as a change in BMI of more than −0.2 to less than 0.2) – a relative risk of 1.43.
“A total of 83% of the children with obesity at the age of 4 were overweight or obese in adolescence, and only 17% returned to a normal weight,” they wrote. In addition, 44% of children who were born large for gestational age were overweight or obese in adolescence.
“A practical clinical implication of our study results would be surveillance for BMI acceleration, which should be recognized before 6 years of age, even in the absence of obesity,” the researchers wrote.
The study findings were limited by several factors including the variation in the number of visits, the lack of data on many children beyond the age of 14 years, and the lack of data on parental weight and perinatal risk factors associated with obesity, the researchers noted. However, the results were strengthened by the large, population-based design, and support the study hypothesis that obesity develops in early childhood and, once present, persists into adolescence.
“The specific dynamics and patterns of BMI in this early childhood period, rather than the absolute BMI, appear to be important factors in identifying children at risk for obesity later in life,” the researchers wrote. “It is therefore important for health care professionals, educational staff, and parents to become more sensitive to this critical time period.”
The study was supported by the German Research Council for the Clinical Research Center; the Federal Ministry of Education and Research; and the University of Leipzig, which was supported by the European Union, the European Regional Development Fund, and the Free State of Saxony within the framework of the excellence initiative. The CrescNet registry infrastructure was supported by grants from Hexal, Novo Nordisk, Merck Serono, Lilly Deutschland, Pfizer, and Ipsen Pharma. Dr. Geserick had no financial conflicts to report.
SOURCE: Geserick M et al. N Engl J Med. 2018 Oct 3. doi: 10.1056/NEJMoa1803527.
Most obese adolescents first became obese between the ages of 2 and 6 years, based on data from approximately 50,000 children in Germany.
Identifying periods of weight gain in childhood can help develop intervention and prevention strategies to reduce the risk of obesity in adolescence, wrote Mandy Geserick, MSc, of the University of Leipzig, Germany, and her colleagues in the New England Journal of Medicine.
To assess the timing of weight gain in early childhood, the researchers reviewed data from a German patient registry designed to monitor growth data. The study population included 51,505 children who had at least one visit to a pediatrician between birth and age 14 years and a second visit between age 15 and 19 years.
Overall, the probability of being overweight or obese in adolescence was 29% among children who gained more weight in the preschool years, between the ages of 2 and 6 years (defined as a change in body mass index [BMI] of 0.2 or more to less than 2.0), compared with 20% among children whose preschool weight remained stable (defined as a change in BMI of more than −0.2 to less than 0.2) – a relative risk of 1.43.
“A total of 83% of the children with obesity at the age of 4 were overweight or obese in adolescence, and only 17% returned to a normal weight,” they wrote. In addition, 44% of children who were born large for gestational age were overweight or obese in adolescence.
“A practical clinical implication of our study results would be surveillance for BMI acceleration, which should be recognized before 6 years of age, even in the absence of obesity,” the researchers wrote.
The study findings were limited by several factors including the variation in the number of visits, the lack of data on many children beyond the age of 14 years, and the lack of data on parental weight and perinatal risk factors associated with obesity, the researchers noted. However, the results were strengthened by the large, population-based design, and support the study hypothesis that obesity develops in early childhood and, once present, persists into adolescence.
“The specific dynamics and patterns of BMI in this early childhood period, rather than the absolute BMI, appear to be important factors in identifying children at risk for obesity later in life,” the researchers wrote. “It is therefore important for health care professionals, educational staff, and parents to become more sensitive to this critical time period.”
The study was supported by the German Research Council for the Clinical Research Center; the Federal Ministry of Education and Research; and the University of Leipzig, which was supported by the European Union, the European Regional Development Fund, and the Free State of Saxony within the framework of the excellence initiative. The CrescNet registry infrastructure was supported by grants from Hexal, Novo Nordisk, Merck Serono, Lilly Deutschland, Pfizer, and Ipsen Pharma. Dr. Geserick had no financial conflicts to report.
SOURCE: Geserick M et al. N Engl J Med. 2018 Oct 3. doi: 10.1056/NEJMoa1803527.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Of children who were obese at age 4 years, 83% were overweight or obese in adolescence.
Study details: The data come from a retrospective study of 51,505 children in Germany.
Disclosures: The study was supported by the German Research Council for the Clinical Research Center; the Federal Ministry of Education and Research; and the University of Leipzig, which was supported by the European Union, the European Regional Development Fund, and the Free State of Saxony within the framework of the excellence initiative. The CrescNet registry infrastructure was supported by grants from Hexal, Novo Nordisk, Merck Serono, Lilly Deutschland, Pfizer, and Ipsen Pharma. Dr. Geserick had no financial conflicts to report.
Source: Geserick M et al. N Engl J Med. 2018 Oct 3. doi: 10.1056/NEJMoa1803527.
Teens who vape are likely to add cigarette smoking
instead of substituting one for the other, according to research published in Nicotine & Tobacco Research.

“Our work provides more evidence that young people who use e-cigarettes progress to smoking cigarettes in the future,” Michael S. Dunbar, PhD, a behavioral scientist at the RAND Corp. stated in a press release. “This study also suggests that teens don’t substitute vaping products for cigarettes. Instead, they go on to use both products more frequently as they get older.”
Dr. Dunbar and his colleagues followed 2,039 adolescents aged 16-20 years who were originally enrolled in a Los Angeles–based substance use prevention program in sixth and seventh grade (2008) and completed annual Web-based surveys during 2015-2017 on their use of e-cigarettes (EC), cigarettes, alcohol, and marijuana. They also answered questions about their mental health with questions about anxiety and depression. The researchers used two models to measures associations between different factors.
The first model showed an association between EC and cigarette use. Then other factors, such as alcohol use, were introduced. Alcohol use was associated with increased cigarette use, and cigarette use was associated with increased use of alcohol. When introducing marijuana as a factor, associations remained between cigarette use and EC use, with higher EC use associated with greater marijuana use and vice versa. Greater cigarette use, however, was not predictive of later marijuana use. There was no association between EC use and mental health, but more cigarette use was associated with poorer mental health.
Under the second model, there was a moderate to strong association between EC use and cigarette use, and participants with greater EC use and greater cigarette use also reported higher alcohol use. There also was a significant between-person association with higher EC use, cigarette use, and marijuana use. There was a small negative association between mental health and cigarette use, but not with mental health and EC use,the researchers said.
“For young people, using these products may actually lead to more harm in the long run,” Dr. Dunbar said in the press release. “This highlights the importance of taking steps to prevent youth from vaping in the first place. One way to do this could be to limit e-cigarette and other tobacco advertising in kid-accessible spaces.”
This study was funded by grants from the National Institute of Alcohol Abuse and Alcoholism. The authors reported no relevant conflicts of interest.
SOURCE: Dunbar MS et al. Nicotine Tob Res. 2018 Oct 3. doi: 10.1093/ntr/nty179.
instead of substituting one for the other, according to research published in Nicotine & Tobacco Research.
“Our work provides more evidence that young people who use e-cigarettes progress to smoking cigarettes in the future,” Michael S. Dunbar, PhD, a behavioral scientist at the RAND Corp. stated in a press release. “This study also suggests that teens don’t substitute vaping products for cigarettes. Instead, they go on to use both products more frequently as they get older.”
Dr. Dunbar and his colleagues followed 2,039 adolescents aged 16-20 years who were originally enrolled in a Los Angeles–based substance use prevention program in sixth and seventh grade (2008) and completed annual Web-based surveys during 2015-2017 on their use of e-cigarettes (EC), cigarettes, alcohol, and marijuana. They also answered questions about their mental health with questions about anxiety and depression. The researchers used two models to measures associations between different factors.
The first model showed an association between EC and cigarette use. Then other factors, such as alcohol use, were introduced. Alcohol use was associated with increased cigarette use, and cigarette use was associated with increased use of alcohol. When introducing marijuana as a factor, associations remained between cigarette use and EC use, with higher EC use associated with greater marijuana use and vice versa. Greater cigarette use, however, was not predictive of later marijuana use. There was no association between EC use and mental health, but more cigarette use was associated with poorer mental health.
Under the second model, there was a moderate to strong association between EC use and cigarette use, and participants with greater EC use and greater cigarette use also reported higher alcohol use. There also was a significant between-person association with higher EC use, cigarette use, and marijuana use. There was a small negative association between mental health and cigarette use, but not with mental health and EC use,the researchers said.
“For young people, using these products may actually lead to more harm in the long run,” Dr. Dunbar said in the press release. “This highlights the importance of taking steps to prevent youth from vaping in the first place. One way to do this could be to limit e-cigarette and other tobacco advertising in kid-accessible spaces.”
This study was funded by grants from the National Institute of Alcohol Abuse and Alcoholism. The authors reported no relevant conflicts of interest.
SOURCE: Dunbar MS et al. Nicotine Tob Res. 2018 Oct 3. doi: 10.1093/ntr/nty179.
instead of substituting one for the other, according to research published in Nicotine & Tobacco Research.
“Our work provides more evidence that young people who use e-cigarettes progress to smoking cigarettes in the future,” Michael S. Dunbar, PhD, a behavioral scientist at the RAND Corp. stated in a press release. “This study also suggests that teens don’t substitute vaping products for cigarettes. Instead, they go on to use both products more frequently as they get older.”
Dr. Dunbar and his colleagues followed 2,039 adolescents aged 16-20 years who were originally enrolled in a Los Angeles–based substance use prevention program in sixth and seventh grade (2008) and completed annual Web-based surveys during 2015-2017 on their use of e-cigarettes (EC), cigarettes, alcohol, and marijuana. They also answered questions about their mental health with questions about anxiety and depression. The researchers used two models to measures associations between different factors.
The first model showed an association between EC and cigarette use. Then other factors, such as alcohol use, were introduced. Alcohol use was associated with increased cigarette use, and cigarette use was associated with increased use of alcohol. When introducing marijuana as a factor, associations remained between cigarette use and EC use, with higher EC use associated with greater marijuana use and vice versa. Greater cigarette use, however, was not predictive of later marijuana use. There was no association between EC use and mental health, but more cigarette use was associated with poorer mental health.
Under the second model, there was a moderate to strong association between EC use and cigarette use, and participants with greater EC use and greater cigarette use also reported higher alcohol use. There also was a significant between-person association with higher EC use, cigarette use, and marijuana use. There was a small negative association between mental health and cigarette use, but not with mental health and EC use,the researchers said.
“For young people, using these products may actually lead to more harm in the long run,” Dr. Dunbar said in the press release. “This highlights the importance of taking steps to prevent youth from vaping in the first place. One way to do this could be to limit e-cigarette and other tobacco advertising in kid-accessible spaces.”
This study was funded by grants from the National Institute of Alcohol Abuse and Alcoholism. The authors reported no relevant conflicts of interest.
SOURCE: Dunbar MS et al. Nicotine Tob Res. 2018 Oct 3. doi: 10.1093/ntr/nty179.
FROM NICOTINE & TOBACCO RESEARCH
Key clinical point: Adolescents who use e-cigarettes are more likely to progress to cigarette use, while continuing to vape.
Major finding: There was a significant bidirectional association between e-cigarette use and cigarette use, and some third factors such as alcohol use, marijuana use, and mental health.
Study details: A longitudinal study of adolescents aged 16-20 years enrolled in a substance use prevention program.
Disclosures: This study was funded by grants from the National Institute of Alcohol Abuse and Alcoholism. The authors reported no relevant conflicts of interest.
Source: Dunbar MS et al. Nicotine Tob Res. 2018 Oct 3. doi: 10.1093/ntr/nty179.
Ice pops improved parents’ ratings of ED quality
SAN DIEGO – Simply offering an ice pop to children who are receiving care in an ED boosts satisfaction scores and physician ratings by their children’s parents, according to data presented at the annual meeting of the American College of Emergency Physicians.

Patient experience and subsequently patient satisfaction scores “have become an increasingly important component of health care delivery. ... Does [the act of] administering Popsicles actually make us better clinicians?” asked Ryan Finn, MD, of the Mayo Clinic, Rochester, Minn., who presented these data.
Exploring low-cost ways to improve patient experience and, by extension, patient satisfaction led to this study of an ice pop intervention, Dr. Finn explained. The study design was simple. During a 3-month period, all children under the age of 14 years (mean age, 6 years) who visited the ED on an even numbered date were offered an ice pop. On odd numbered dates, no ice pop was given. There were no other differences in care.
Parent perceptions of care were assessed with the proprietary Press Ganey patient satisfaction survey. Although a completed survey was submitted for less than 5% of the more than 4,500 patients treated during the study period, differences between the groups still reached statistical significance.
When parents were asked to rate physicians on concern for their child’s comfort, 74% of the group given ice pops and 58% of the group given no ice pops gave favorable responses (P less than.05). The parents of children in the ice pop group also were significantly more likely to rate physicians favorably for their courtesy (77% vs. 62%; P less than .04) and for their willingness to take the time to listen (84% vs. 57%; P less than .03).
Overall rating of care (64% vs. 61%) and likelihood of recommending the ED to others (66% vs. 59%) did not approach statistical significance, according to Dr. Finn.
There are numerous potential advantages to improving the patient experience and boosting patient satisfaction in the ED, as is the case in other areas of the hospital. Even if medical care is of high quality, patient satisfaction does not necessarily follow. Although this single-center study had limitations, such as the low survey completion rate, the measurable effects of the ice pop intervention encourages this direction of research.
“Further studies should increase sample size, assess age group subsets, and assess return on investment for this and other low-cost interventions with the potential to alter patient perceptions,” Dr. Finn said. Because patient satisfaction can be reasonably expected to favorably affect quality of care assessments, he indicated that this is a reasonable target for quality improvement strategies.
SAN DIEGO – Simply offering an ice pop to children who are receiving care in an ED boosts satisfaction scores and physician ratings by their children’s parents, according to data presented at the annual meeting of the American College of Emergency Physicians.
Patient experience and subsequently patient satisfaction scores “have become an increasingly important component of health care delivery. ... Does [the act of] administering Popsicles actually make us better clinicians?” asked Ryan Finn, MD, of the Mayo Clinic, Rochester, Minn., who presented these data.
Exploring low-cost ways to improve patient experience and, by extension, patient satisfaction led to this study of an ice pop intervention, Dr. Finn explained. The study design was simple. During a 3-month period, all children under the age of 14 years (mean age, 6 years) who visited the ED on an even numbered date were offered an ice pop. On odd numbered dates, no ice pop was given. There were no other differences in care.
Parent perceptions of care were assessed with the proprietary Press Ganey patient satisfaction survey. Although a completed survey was submitted for less than 5% of the more than 4,500 patients treated during the study period, differences between the groups still reached statistical significance.
When parents were asked to rate physicians on concern for their child’s comfort, 74% of the group given ice pops and 58% of the group given no ice pops gave favorable responses (P less than.05). The parents of children in the ice pop group also were significantly more likely to rate physicians favorably for their courtesy (77% vs. 62%; P less than .04) and for their willingness to take the time to listen (84% vs. 57%; P less than .03).
Overall rating of care (64% vs. 61%) and likelihood of recommending the ED to others (66% vs. 59%) did not approach statistical significance, according to Dr. Finn.
There are numerous potential advantages to improving the patient experience and boosting patient satisfaction in the ED, as is the case in other areas of the hospital. Even if medical care is of high quality, patient satisfaction does not necessarily follow. Although this single-center study had limitations, such as the low survey completion rate, the measurable effects of the ice pop intervention encourages this direction of research.
“Further studies should increase sample size, assess age group subsets, and assess return on investment for this and other low-cost interventions with the potential to alter patient perceptions,” Dr. Finn said. Because patient satisfaction can be reasonably expected to favorably affect quality of care assessments, he indicated that this is a reasonable target for quality improvement strategies.
SAN DIEGO – Simply offering an ice pop to children who are receiving care in an ED boosts satisfaction scores and physician ratings by their children’s parents, according to data presented at the annual meeting of the American College of Emergency Physicians.
Patient experience and subsequently patient satisfaction scores “have become an increasingly important component of health care delivery. ... Does [the act of] administering Popsicles actually make us better clinicians?” asked Ryan Finn, MD, of the Mayo Clinic, Rochester, Minn., who presented these data.
Exploring low-cost ways to improve patient experience and, by extension, patient satisfaction led to this study of an ice pop intervention, Dr. Finn explained. The study design was simple. During a 3-month period, all children under the age of 14 years (mean age, 6 years) who visited the ED on an even numbered date were offered an ice pop. On odd numbered dates, no ice pop was given. There were no other differences in care.
Parent perceptions of care were assessed with the proprietary Press Ganey patient satisfaction survey. Although a completed survey was submitted for less than 5% of the more than 4,500 patients treated during the study period, differences between the groups still reached statistical significance.
When parents were asked to rate physicians on concern for their child’s comfort, 74% of the group given ice pops and 58% of the group given no ice pops gave favorable responses (P less than.05). The parents of children in the ice pop group also were significantly more likely to rate physicians favorably for their courtesy (77% vs. 62%; P less than .04) and for their willingness to take the time to listen (84% vs. 57%; P less than .03).
Overall rating of care (64% vs. 61%) and likelihood of recommending the ED to others (66% vs. 59%) did not approach statistical significance, according to Dr. Finn.
There are numerous potential advantages to improving the patient experience and boosting patient satisfaction in the ED, as is the case in other areas of the hospital. Even if medical care is of high quality, patient satisfaction does not necessarily follow. Although this single-center study had limitations, such as the low survey completion rate, the measurable effects of the ice pop intervention encourages this direction of research.
“Further studies should increase sample size, assess age group subsets, and assess return on investment for this and other low-cost interventions with the potential to alter patient perceptions,” Dr. Finn said. Because patient satisfaction can be reasonably expected to favorably affect quality of care assessments, he indicated that this is a reasonable target for quality improvement strategies.
FROM ACEP18
Key clinical point: Providing an ice pop to children in the ED boosted satisfaction scores.
Major finding: The parents of children given ice pops ranked physicians higher on measures of courtesy and concern.
Study details: Prospective, controlled study of survey results completed by 5% of more than 4,500 patients.
Disclosures: Dr. Finn reported no financial relationships relevant to this study.