User login
Respect is key when treating dermatologic conditions in transgender youth
LAKE TAHOE, CALIF. – The way Stanley Vance Jr., MD, sees it, the No. 1 priority in the care of transgender youth is respecting their gender identity.

“This can really help with rapport and also help them continue to engage with your care,” he said at the annual meeting of the Society for Pediatric Dermatology.
One of the first steps is to establish the patient’s chosen name and pronouns. “Ask, use, and be consistent,” said Dr. Vance, an adolescent medicine specialist at the University of California, San Francisco. “Taking it to another level, you can implement system-level tools to ensure that all of your staff consistently use the chosen name and pronouns. and working with the IT department to have a place in our electronic medical record to put the chosen name and preferred pronouns.”
In a study published in the Journal of Adolescent Health, researchers found that the use of chosen names and pronouns for transgender use was associated with reduced depressive symptoms, suicidal ideation, and suicidal behavior among transgender youth.
Dr. Vance, who also holds a staff position at the UCSF Child and Adolescent Clinic, went on to discuss dermatologic considerations for gender diverse youth. In transgender females, estrogens can reduce the quantity and density of body and facial hair, “but it doesn’t necessarily get rid of the hair, so we may refer to dermatology for hair removal or hair reduction. There can also be a decrease in sebum production, which can lead to dry skin for those who are at risk.”
Transgender females often seek laser hair removal or electrolysis to aid in “blendability,” or how they perceive as being female or feminine. “We know that this can help in psychosocial outcomes for these young people,” Dr. Vance said. “Another reason why hair reduction and removal may be important is preoperatively for vaginoplasty.”
In transgender males, testosterone increases male pattern hair growth and can increase male pattern hair loss. “Minoxidil does not interact with gender-affirming hormone treatment. If finasteride needs to be considered, it may interfere with the development of secondary sex characteristics.” Testosterone also increases sebum production and can increase acne, particularly in the first 6 months to 1 year after initiation, and with increased titration. “Some transmasculine youth may need oral isotretinoin, as stopping testosterone can be psychologically damaging,” Dr. Vance said.
“Unfortunately, the iPLEDGE program requirements can be perceived as gender nonaffirming, because patients must register by the sex assigned to them at birth, they must take pregnancy tests, and there can be provider assumptions about sexuality which does not equate with gender identity.”
He recommended having “open and honest” conversations with patients about the requirements and limitations of dispensing oral isotretinoin. “Assure the patient that you will be respectful and affirming of their gender identity while they’re in your office,” Dr. Vance advised. “If the patient has a mental health provider, you can strategize with them to reduce gender dysphoria around this process. Finally, advocating to change the system can not only be helpful for the patient in front of you, but for other patients who are in the same situation.”
He concluded his presentation by describing transgender youth as “some of the most resilient young people I’ve had the pleasure of working with.
“I think that we can all work to make sure they feel supported in who they are,” he said.
Dr. Vance reported having no relevant financial disclosures.
dbrunk@mdedge.com
LAKE TAHOE, CALIF. – The way Stanley Vance Jr., MD, sees it, the No. 1 priority in the care of transgender youth is respecting their gender identity.
“This can really help with rapport and also help them continue to engage with your care,” he said at the annual meeting of the Society for Pediatric Dermatology.
One of the first steps is to establish the patient’s chosen name and pronouns. “Ask, use, and be consistent,” said Dr. Vance, an adolescent medicine specialist at the University of California, San Francisco. “Taking it to another level, you can implement system-level tools to ensure that all of your staff consistently use the chosen name and pronouns. and working with the IT department to have a place in our electronic medical record to put the chosen name and preferred pronouns.”
In a study published in the Journal of Adolescent Health, researchers found that the use of chosen names and pronouns for transgender use was associated with reduced depressive symptoms, suicidal ideation, and suicidal behavior among transgender youth.
Dr. Vance, who also holds a staff position at the UCSF Child and Adolescent Clinic, went on to discuss dermatologic considerations for gender diverse youth. In transgender females, estrogens can reduce the quantity and density of body and facial hair, “but it doesn’t necessarily get rid of the hair, so we may refer to dermatology for hair removal or hair reduction. There can also be a decrease in sebum production, which can lead to dry skin for those who are at risk.”
Transgender females often seek laser hair removal or electrolysis to aid in “blendability,” or how they perceive as being female or feminine. “We know that this can help in psychosocial outcomes for these young people,” Dr. Vance said. “Another reason why hair reduction and removal may be important is preoperatively for vaginoplasty.”
In transgender males, testosterone increases male pattern hair growth and can increase male pattern hair loss. “Minoxidil does not interact with gender-affirming hormone treatment. If finasteride needs to be considered, it may interfere with the development of secondary sex characteristics.” Testosterone also increases sebum production and can increase acne, particularly in the first 6 months to 1 year after initiation, and with increased titration. “Some transmasculine youth may need oral isotretinoin, as stopping testosterone can be psychologically damaging,” Dr. Vance said.
“Unfortunately, the iPLEDGE program requirements can be perceived as gender nonaffirming, because patients must register by the sex assigned to them at birth, they must take pregnancy tests, and there can be provider assumptions about sexuality which does not equate with gender identity.”
He recommended having “open and honest” conversations with patients about the requirements and limitations of dispensing oral isotretinoin. “Assure the patient that you will be respectful and affirming of their gender identity while they’re in your office,” Dr. Vance advised. “If the patient has a mental health provider, you can strategize with them to reduce gender dysphoria around this process. Finally, advocating to change the system can not only be helpful for the patient in front of you, but for other patients who are in the same situation.”
He concluded his presentation by describing transgender youth as “some of the most resilient young people I’ve had the pleasure of working with.
“I think that we can all work to make sure they feel supported in who they are,” he said.
Dr. Vance reported having no relevant financial disclosures.
dbrunk@mdedge.com
LAKE TAHOE, CALIF. – The way Stanley Vance Jr., MD, sees it, the No. 1 priority in the care of transgender youth is respecting their gender identity.
“This can really help with rapport and also help them continue to engage with your care,” he said at the annual meeting of the Society for Pediatric Dermatology.
One of the first steps is to establish the patient’s chosen name and pronouns. “Ask, use, and be consistent,” said Dr. Vance, an adolescent medicine specialist at the University of California, San Francisco. “Taking it to another level, you can implement system-level tools to ensure that all of your staff consistently use the chosen name and pronouns. and working with the IT department to have a place in our electronic medical record to put the chosen name and preferred pronouns.”
In a study published in the Journal of Adolescent Health, researchers found that the use of chosen names and pronouns for transgender use was associated with reduced depressive symptoms, suicidal ideation, and suicidal behavior among transgender youth.
Dr. Vance, who also holds a staff position at the UCSF Child and Adolescent Clinic, went on to discuss dermatologic considerations for gender diverse youth. In transgender females, estrogens can reduce the quantity and density of body and facial hair, “but it doesn’t necessarily get rid of the hair, so we may refer to dermatology for hair removal or hair reduction. There can also be a decrease in sebum production, which can lead to dry skin for those who are at risk.”
Transgender females often seek laser hair removal or electrolysis to aid in “blendability,” or how they perceive as being female or feminine. “We know that this can help in psychosocial outcomes for these young people,” Dr. Vance said. “Another reason why hair reduction and removal may be important is preoperatively for vaginoplasty.”
In transgender males, testosterone increases male pattern hair growth and can increase male pattern hair loss. “Minoxidil does not interact with gender-affirming hormone treatment. If finasteride needs to be considered, it may interfere with the development of secondary sex characteristics.” Testosterone also increases sebum production and can increase acne, particularly in the first 6 months to 1 year after initiation, and with increased titration. “Some transmasculine youth may need oral isotretinoin, as stopping testosterone can be psychologically damaging,” Dr. Vance said.
“Unfortunately, the iPLEDGE program requirements can be perceived as gender nonaffirming, because patients must register by the sex assigned to them at birth, they must take pregnancy tests, and there can be provider assumptions about sexuality which does not equate with gender identity.”
He recommended having “open and honest” conversations with patients about the requirements and limitations of dispensing oral isotretinoin. “Assure the patient that you will be respectful and affirming of their gender identity while they’re in your office,” Dr. Vance advised. “If the patient has a mental health provider, you can strategize with them to reduce gender dysphoria around this process. Finally, advocating to change the system can not only be helpful for the patient in front of you, but for other patients who are in the same situation.”
He concluded his presentation by describing transgender youth as “some of the most resilient young people I’ve had the pleasure of working with.
“I think that we can all work to make sure they feel supported in who they are,” he said.
Dr. Vance reported having no relevant financial disclosures.
dbrunk@mdedge.com
EXPERT ANALYSIS FROM SPD 2018
Alcohol use during breastfeeding linked to cognitive harms in children
Risky or higher alcohol consumption while breastfeeding could be associated with poorer cognitive outcomes in children, according to a longitudinal cohort study.
In a paper published in Pediatrics, researchers analyzed data from 5,107 infants who were followed up every 2 years from Growing Up in Australia: The Longitudinal Study of Australian Children. They also examined other factors, such as information on mothers’ smoking and drinking habits during breastfeeding.
The analysis showed a significant association between increased maternal alcohol consumption and decreased nonverbal reasoning scores in children aged 6-7 years who had been breastfed at any time (95% confidence interval, –0.18 to –0.04; P = .01). The effect was independent of other factors that might have played a role, including prenatal alcohol consumption, maternal age, income, birth weight, head injury, and learning delay.
(95% CI, –0.20 to 0.17; P = .87), which the authors said supported the suggestion that the cognitive effects were the result of alcohol exposure through breast milk.
“This suggests that alcohol exposure through breast milk was responsible for cognitive reductions in breastfed infants rather than psychosocial or environmental factors surrounding maternal alcohol consumption,” wrote Louisa Gibson and Melanie Porter, PhD, of the department of psychology at Macquarie University in Sydney.
However, the association was no longer evident in children aged 8-11 years. The authors said that finding might be attributable to mediation by factors such as increased education.
In addition, Ms. Gibson and Dr. Porter did not find an association between smoking during breastfeeding and cognitive outcomes of the offspring.
The findings on breastfeeding and cognitive reductions in breastfed infants are consistent with animal studies showing that ethanol in breast milk can affect normal brain development.
“Increased cerebral cortex apoptosis and necrosis, for example, may disrupt higher order executive skills relied on in reasoning tasks,” the authors wrote. “Likewise, decreased myelination could reduce the processing speed needed to problem solve quickly.”
Children also might experience reduced cognition as a secondary effect of changes in feeding, nutritional intake, and sleep patterns that could themselves affect brain development, leading to behavioral changes that might “reduce exposure to enriching stimuli.”
However, the authors noted that the frequency and quantity of milk consumed, and the timing of alcohol consumption relative to breastfeeding, were not recorded as part of the study.
“The impact of this is unknown, however, because not all women time their alcohol consumption to limit alcohol exposure, and unpredictable infant feeding patterns can interfere with timing attempts.”
Ms. Gibson and Dr. Porter reported no external funding and no conflicts of interest.
SOURCE: Gibson L et al. Pediatrics 2018 Jul 30. doi: 10.1542/peds.2017-4266.
This study represents an important step toward understanding the neurobiological and developmental risks associated with substance exposure during breastfeeding.
The finding of an association between maternal alcohol consumption during breastfeeding and later negative effects on child development are not surprising, given what already is known harmful effects of alcohol on the developing brain. There is no reason to think that these harmful effects might be limited to prenatal alcohol exposure.
“Previous recommendations that reveal limited alcohol consumption to be compatible with breastfeeding during critical periods of development ... may need to be reconsidered in light of this combined evidence,” wrote Lauren M. Jansson, MD.
Dr. Jansson is affiliated with the department of pediatrics at Johns Hopkins University, Baltimore. These comments are taken from an editorial (Pediatrics. 2018 Jul 30. doi: 10.1542/peds.2018-1377). She declared having no conflicts of interest.
This study represents an important step toward understanding the neurobiological and developmental risks associated with substance exposure during breastfeeding.
The finding of an association between maternal alcohol consumption during breastfeeding and later negative effects on child development are not surprising, given what already is known harmful effects of alcohol on the developing brain. There is no reason to think that these harmful effects might be limited to prenatal alcohol exposure.
“Previous recommendations that reveal limited alcohol consumption to be compatible with breastfeeding during critical periods of development ... may need to be reconsidered in light of this combined evidence,” wrote Lauren M. Jansson, MD.
Dr. Jansson is affiliated with the department of pediatrics at Johns Hopkins University, Baltimore. These comments are taken from an editorial (Pediatrics. 2018 Jul 30. doi: 10.1542/peds.2018-1377). She declared having no conflicts of interest.
This study represents an important step toward understanding the neurobiological and developmental risks associated with substance exposure during breastfeeding.
The finding of an association between maternal alcohol consumption during breastfeeding and later negative effects on child development are not surprising, given what already is known harmful effects of alcohol on the developing brain. There is no reason to think that these harmful effects might be limited to prenatal alcohol exposure.
“Previous recommendations that reveal limited alcohol consumption to be compatible with breastfeeding during critical periods of development ... may need to be reconsidered in light of this combined evidence,” wrote Lauren M. Jansson, MD.
Dr. Jansson is affiliated with the department of pediatrics at Johns Hopkins University, Baltimore. These comments are taken from an editorial (Pediatrics. 2018 Jul 30. doi: 10.1542/peds.2018-1377). She declared having no conflicts of interest.
Risky or higher alcohol consumption while breastfeeding could be associated with poorer cognitive outcomes in children, according to a longitudinal cohort study.
In a paper published in Pediatrics, researchers analyzed data from 5,107 infants who were followed up every 2 years from Growing Up in Australia: The Longitudinal Study of Australian Children. They also examined other factors, such as information on mothers’ smoking and drinking habits during breastfeeding.
The analysis showed a significant association between increased maternal alcohol consumption and decreased nonverbal reasoning scores in children aged 6-7 years who had been breastfed at any time (95% confidence interval, –0.18 to –0.04; P = .01). The effect was independent of other factors that might have played a role, including prenatal alcohol consumption, maternal age, income, birth weight, head injury, and learning delay.
(95% CI, –0.20 to 0.17; P = .87), which the authors said supported the suggestion that the cognitive effects were the result of alcohol exposure through breast milk.
“This suggests that alcohol exposure through breast milk was responsible for cognitive reductions in breastfed infants rather than psychosocial or environmental factors surrounding maternal alcohol consumption,” wrote Louisa Gibson and Melanie Porter, PhD, of the department of psychology at Macquarie University in Sydney.
However, the association was no longer evident in children aged 8-11 years. The authors said that finding might be attributable to mediation by factors such as increased education.
In addition, Ms. Gibson and Dr. Porter did not find an association between smoking during breastfeeding and cognitive outcomes of the offspring.
The findings on breastfeeding and cognitive reductions in breastfed infants are consistent with animal studies showing that ethanol in breast milk can affect normal brain development.
“Increased cerebral cortex apoptosis and necrosis, for example, may disrupt higher order executive skills relied on in reasoning tasks,” the authors wrote. “Likewise, decreased myelination could reduce the processing speed needed to problem solve quickly.”
Children also might experience reduced cognition as a secondary effect of changes in feeding, nutritional intake, and sleep patterns that could themselves affect brain development, leading to behavioral changes that might “reduce exposure to enriching stimuli.”
However, the authors noted that the frequency and quantity of milk consumed, and the timing of alcohol consumption relative to breastfeeding, were not recorded as part of the study.
“The impact of this is unknown, however, because not all women time their alcohol consumption to limit alcohol exposure, and unpredictable infant feeding patterns can interfere with timing attempts.”
Ms. Gibson and Dr. Porter reported no external funding and no conflicts of interest.
SOURCE: Gibson L et al. Pediatrics 2018 Jul 30. doi: 10.1542/peds.2017-4266.
Risky or higher alcohol consumption while breastfeeding could be associated with poorer cognitive outcomes in children, according to a longitudinal cohort study.
In a paper published in Pediatrics, researchers analyzed data from 5,107 infants who were followed up every 2 years from Growing Up in Australia: The Longitudinal Study of Australian Children. They also examined other factors, such as information on mothers’ smoking and drinking habits during breastfeeding.
The analysis showed a significant association between increased maternal alcohol consumption and decreased nonverbal reasoning scores in children aged 6-7 years who had been breastfed at any time (95% confidence interval, –0.18 to –0.04; P = .01). The effect was independent of other factors that might have played a role, including prenatal alcohol consumption, maternal age, income, birth weight, head injury, and learning delay.
(95% CI, –0.20 to 0.17; P = .87), which the authors said supported the suggestion that the cognitive effects were the result of alcohol exposure through breast milk.
“This suggests that alcohol exposure through breast milk was responsible for cognitive reductions in breastfed infants rather than psychosocial or environmental factors surrounding maternal alcohol consumption,” wrote Louisa Gibson and Melanie Porter, PhD, of the department of psychology at Macquarie University in Sydney.
However, the association was no longer evident in children aged 8-11 years. The authors said that finding might be attributable to mediation by factors such as increased education.
In addition, Ms. Gibson and Dr. Porter did not find an association between smoking during breastfeeding and cognitive outcomes of the offspring.
The findings on breastfeeding and cognitive reductions in breastfed infants are consistent with animal studies showing that ethanol in breast milk can affect normal brain development.
“Increased cerebral cortex apoptosis and necrosis, for example, may disrupt higher order executive skills relied on in reasoning tasks,” the authors wrote. “Likewise, decreased myelination could reduce the processing speed needed to problem solve quickly.”
Children also might experience reduced cognition as a secondary effect of changes in feeding, nutritional intake, and sleep patterns that could themselves affect brain development, leading to behavioral changes that might “reduce exposure to enriching stimuli.”
However, the authors noted that the frequency and quantity of milk consumed, and the timing of alcohol consumption relative to breastfeeding, were not recorded as part of the study.
“The impact of this is unknown, however, because not all women time their alcohol consumption to limit alcohol exposure, and unpredictable infant feeding patterns can interfere with timing attempts.”
Ms. Gibson and Dr. Porter reported no external funding and no conflicts of interest.
SOURCE: Gibson L et al. Pediatrics 2018 Jul 30. doi: 10.1542/peds.2017-4266.
FROM PEDIATRICS
Key clinical point: Alcohol consumption during breastfeeding might affect infants’ later cognitive outcomes.
Major finding: Children exposed to alcohol during breastfeeding showed lower decreased nonverbal reasoning scores (95% confidence interval, –0.18 to –0.04; P = .01).
Study details: A cohort study in 5,107 infants called Growing Up in Australia: The Longitudinal Study of Australian Children.
Disclosures: Ms. Gibson and Dr. Porter reported no external funding and no conflicts of interest.
Source: Gibson L et al. Pediatrics 2018 Jul 30. doi: 10.1542/peds.2017-4266.
Pediatric vitiligo primarily affects those aged 10-17
LAKE TAHOE, CALIF. – Among children and adolescents, vitiligo appears to predominately affect nonwhite boys and girls between the ages of 10 and 17 years, results from a large cross-sectional analysis demonstrated.

During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Jessica Haber, MD, said that, while it’s known vitiligo can have its onset in childhood, there have been no population-based analyses in the United States specific to children and adolescents with the condition.
“We wanted to examine disease burden in the U.S. specifically, because we have such a diverse population,” said Dr. Haber, a second-year resident in the department of dermatology at Northwell Health, New York.
For the study, she and her associates used IBM’s Explorys research analytics platform to conduct a cross-sectional analysis of more than 55 million unique patients across all census regions of the United States. There were 1,630 vitiligo cases identified from a total of 4,242,400 pediatric patients, for an overall standard prevalence of 0.04%, or 40.1 per 100,000 children and adolescents. The proportion of female and male patients with vitiligo was similar (49.1% and 50.9%, respectively), and nearly three-fourths (72.3%) were 10 years of age or older.
The researchers observed no significant difference in the prevalence of vitiligo between males and females (40.2 per 100,000 vs. 40 per 100,000, respectively). The standardized prevalence of vitiligo was greatest in pediatric patients who were of “other” races and ethnicities (including Asian, Hispanic, multiracial, and other; 69.1 per 100,000), followed by African Americans (51.5 per 100,000) and whites (37.9 per 100,000). There were too few vitiligo cases among biracial patients to determine standardized estimates, but the crude prevalence was greatest in this group (68.7 per 100,000).
Two factors could contribute to the increased prevalence of vitiligo observed in nonwhite children and adolescents, Dr. Haber said. One is selection bias.
“It has been reported that both children and adults with higher Fitzpatrick skin types tend to have increased morbidity of their vitiligo, so it may be a selection bias that these patients are seeking out treatment for their disease,” she said. (J Am Acad Dermatol. 2017;77[1]:1-13). That might explain some of our findings, as well.”
While the study findings “don’t necessarily change clinical practice, it is good for us to have a sense of the burden of disease in the pediatric patient population of vitiligo, and to be aware that this is a disease that predominately affects non-Caucasian children and adolescents,” Dr. Haber concluded.
She reported having no financial disclosures.
LAKE TAHOE, CALIF. – Among children and adolescents, vitiligo appears to predominately affect nonwhite boys and girls between the ages of 10 and 17 years, results from a large cross-sectional analysis demonstrated.
During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Jessica Haber, MD, said that, while it’s known vitiligo can have its onset in childhood, there have been no population-based analyses in the United States specific to children and adolescents with the condition.
“We wanted to examine disease burden in the U.S. specifically, because we have such a diverse population,” said Dr. Haber, a second-year resident in the department of dermatology at Northwell Health, New York.
For the study, she and her associates used IBM’s Explorys research analytics platform to conduct a cross-sectional analysis of more than 55 million unique patients across all census regions of the United States. There were 1,630 vitiligo cases identified from a total of 4,242,400 pediatric patients, for an overall standard prevalence of 0.04%, or 40.1 per 100,000 children and adolescents. The proportion of female and male patients with vitiligo was similar (49.1% and 50.9%, respectively), and nearly three-fourths (72.3%) were 10 years of age or older.
The researchers observed no significant difference in the prevalence of vitiligo between males and females (40.2 per 100,000 vs. 40 per 100,000, respectively). The standardized prevalence of vitiligo was greatest in pediatric patients who were of “other” races and ethnicities (including Asian, Hispanic, multiracial, and other; 69.1 per 100,000), followed by African Americans (51.5 per 100,000) and whites (37.9 per 100,000). There were too few vitiligo cases among biracial patients to determine standardized estimates, but the crude prevalence was greatest in this group (68.7 per 100,000).
Two factors could contribute to the increased prevalence of vitiligo observed in nonwhite children and adolescents, Dr. Haber said. One is selection bias.
“It has been reported that both children and adults with higher Fitzpatrick skin types tend to have increased morbidity of their vitiligo, so it may be a selection bias that these patients are seeking out treatment for their disease,” she said. (J Am Acad Dermatol. 2017;77[1]:1-13). That might explain some of our findings, as well.”
While the study findings “don’t necessarily change clinical practice, it is good for us to have a sense of the burden of disease in the pediatric patient population of vitiligo, and to be aware that this is a disease that predominately affects non-Caucasian children and adolescents,” Dr. Haber concluded.
She reported having no financial disclosures.
LAKE TAHOE, CALIF. – Among children and adolescents, vitiligo appears to predominately affect nonwhite boys and girls between the ages of 10 and 17 years, results from a large cross-sectional analysis demonstrated.
During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Jessica Haber, MD, said that, while it’s known vitiligo can have its onset in childhood, there have been no population-based analyses in the United States specific to children and adolescents with the condition.
“We wanted to examine disease burden in the U.S. specifically, because we have such a diverse population,” said Dr. Haber, a second-year resident in the department of dermatology at Northwell Health, New York.
For the study, she and her associates used IBM’s Explorys research analytics platform to conduct a cross-sectional analysis of more than 55 million unique patients across all census regions of the United States. There were 1,630 vitiligo cases identified from a total of 4,242,400 pediatric patients, for an overall standard prevalence of 0.04%, or 40.1 per 100,000 children and adolescents. The proportion of female and male patients with vitiligo was similar (49.1% and 50.9%, respectively), and nearly three-fourths (72.3%) were 10 years of age or older.
The researchers observed no significant difference in the prevalence of vitiligo between males and females (40.2 per 100,000 vs. 40 per 100,000, respectively). The standardized prevalence of vitiligo was greatest in pediatric patients who were of “other” races and ethnicities (including Asian, Hispanic, multiracial, and other; 69.1 per 100,000), followed by African Americans (51.5 per 100,000) and whites (37.9 per 100,000). There were too few vitiligo cases among biracial patients to determine standardized estimates, but the crude prevalence was greatest in this group (68.7 per 100,000).
Two factors could contribute to the increased prevalence of vitiligo observed in nonwhite children and adolescents, Dr. Haber said. One is selection bias.
“It has been reported that both children and adults with higher Fitzpatrick skin types tend to have increased morbidity of their vitiligo, so it may be a selection bias that these patients are seeking out treatment for their disease,” she said. (J Am Acad Dermatol. 2017;77[1]:1-13). That might explain some of our findings, as well.”
While the study findings “don’t necessarily change clinical practice, it is good for us to have a sense of the burden of disease in the pediatric patient population of vitiligo, and to be aware that this is a disease that predominately affects non-Caucasian children and adolescents,” Dr. Haber concluded.
She reported having no financial disclosures.
REPORTING FROM SPD 2018
Key clinical point: Vitiligo appears to predominately affect nonwhite boys and girls 10 years of age and older in the pediatric population.
Major finding: Of pediatric patients with vitiligo, 72.3% were 10 years of age or older.
Study details: A cross-sectional analysis of 1,630 vitiligo cases identified from a total of 4,242,400 pediatric patients.
Disclosures: Dr. Haber reported having no relevant financial disclosures.
Fatigue linked to increased risk of ACL injury
SAN DIEGO – Fatigue increases anterior cruciate ligament injury risk in adolescent athletes, results from a field-based drop-jump study demonstrate.

“The number of ACL reconstructions that occur annually are on the rise, particularly in high school and adolescent aged athletes,” lead study author Mohsin S. Fidai, MD, said at the annual meeting of the American Orthopaedic Society for Sports Medicine. “About 70% of these are accounted for by noncontact injuries, the majority of which occur during jump landing. A number of risk factors that have previously been implicated in ACL injury include genetics and anatomy, but a modifiable risk factor is landing biomechanics.”
In 2005, researchers led by Timothy E. Hewett, PhD, determined biomechanical measures of neuromuscular control that might pose certain athletes to be at risk for ACL injury, particularly knee abduction and dynamic knee valgus during a drop-jump test (Am J Sports Med. 2005;33[4]:492-501). “Historically, these studies have required the use of sophisticated computer technology, which can be cumbersome from a time and cost perspective,” said Dr. Fidai, a third-year orthopedic surgery resident at Henry Ford Health System, Detroit.
In a more recent analysis, researchers validated a field-based drop vertical jump screening test for ACL injury (Phys Sportmed. 2016;44[1]:46-52). The sensitivity was 95%, the specificity was 46%, and it had a strong inter-rater reliability (k = 0.92; P less than .05).
The purpose of the current study was to evaluate the effect of fatigue on ACL injury risk using a field-based drop-jump test. “We hypothesized that fatigue would lead to greater dynamic knee valgus during a drop-jump test,” Dr. Fidai said. “We also wanted to identify individual characteristics which may place athletes at increased risk for ACL injury.”
The researchers recruited 85 athletes who competed in track and field, basketball, volleyball, and soccer. More than half (55%) were female, and the mean age was 15.4 years. They excluded athletes with any previous or current lower extremity injuries or neuromuscular deficits. Each athlete performed a maximum vertical jump, followed by a drop-jump test.
“We then fatigued all of our athletes with a standardized high-intensity fatigue protocol, and had each athlete perform another maximum vertical jump and drop-jump test,” Dr. Fidai said. “All drop-jumps were video recorded and sent to a number of orthopedic surgery residents, athletic trainers, and physical therapists for review.”
Of the 85 athletes, nearly half (45%) showed an increased risk for ACL injury after high-intensity aerobic activity. In addition, 68% of study participants were identified as having a medium or high risk for injury following the aerobic activity, compared with 44% at baseline. Dr. Fidai noted. “In the group of athletes with higher levels of fatigue, there is a significantly increased risk, compared with their counterparts with lower levels of fatigue.”
Specifically, 14 of the 22 athletes who demonstrated over 20% fatigue showed an increased ACL injury risk. Subgroup analysis revealed that female athletes and those older than age 15 were more likely to demonstrate an increased injury risk.
“The findings of this study advocate for changes to current neuromuscular training programs to incorporate fatigue resistance, as well as to raise awareness amongst physical therapists, athletic trainers, coaches, and athletes about the effect of fatigue on ACL injury risk,” Dr. Fidai concluded. “We can target vulnerable athletes, particularly female athletes, in an effort to negate some of those effects.”
The study’s principal investigator was Eric C. Makhni, MD. Dr. Makhni, an orthopedic surgeon in West Bloomfield, Mich., disclosed that he is a paid consultant for Smith & Nephew and that he receives publishing royalties from Springer. Dr. Fidai reported having no financial disclosures.
SAN DIEGO – Fatigue increases anterior cruciate ligament injury risk in adolescent athletes, results from a field-based drop-jump study demonstrate.
“The number of ACL reconstructions that occur annually are on the rise, particularly in high school and adolescent aged athletes,” lead study author Mohsin S. Fidai, MD, said at the annual meeting of the American Orthopaedic Society for Sports Medicine. “About 70% of these are accounted for by noncontact injuries, the majority of which occur during jump landing. A number of risk factors that have previously been implicated in ACL injury include genetics and anatomy, but a modifiable risk factor is landing biomechanics.”
In 2005, researchers led by Timothy E. Hewett, PhD, determined biomechanical measures of neuromuscular control that might pose certain athletes to be at risk for ACL injury, particularly knee abduction and dynamic knee valgus during a drop-jump test (Am J Sports Med. 2005;33[4]:492-501). “Historically, these studies have required the use of sophisticated computer technology, which can be cumbersome from a time and cost perspective,” said Dr. Fidai, a third-year orthopedic surgery resident at Henry Ford Health System, Detroit.
In a more recent analysis, researchers validated a field-based drop vertical jump screening test for ACL injury (Phys Sportmed. 2016;44[1]:46-52). The sensitivity was 95%, the specificity was 46%, and it had a strong inter-rater reliability (k = 0.92; P less than .05).
The purpose of the current study was to evaluate the effect of fatigue on ACL injury risk using a field-based drop-jump test. “We hypothesized that fatigue would lead to greater dynamic knee valgus during a drop-jump test,” Dr. Fidai said. “We also wanted to identify individual characteristics which may place athletes at increased risk for ACL injury.”
The researchers recruited 85 athletes who competed in track and field, basketball, volleyball, and soccer. More than half (55%) were female, and the mean age was 15.4 years. They excluded athletes with any previous or current lower extremity injuries or neuromuscular deficits. Each athlete performed a maximum vertical jump, followed by a drop-jump test.
“We then fatigued all of our athletes with a standardized high-intensity fatigue protocol, and had each athlete perform another maximum vertical jump and drop-jump test,” Dr. Fidai said. “All drop-jumps were video recorded and sent to a number of orthopedic surgery residents, athletic trainers, and physical therapists for review.”
Of the 85 athletes, nearly half (45%) showed an increased risk for ACL injury after high-intensity aerobic activity. In addition, 68% of study participants were identified as having a medium or high risk for injury following the aerobic activity, compared with 44% at baseline. Dr. Fidai noted. “In the group of athletes with higher levels of fatigue, there is a significantly increased risk, compared with their counterparts with lower levels of fatigue.”
Specifically, 14 of the 22 athletes who demonstrated over 20% fatigue showed an increased ACL injury risk. Subgroup analysis revealed that female athletes and those older than age 15 were more likely to demonstrate an increased injury risk.
“The findings of this study advocate for changes to current neuromuscular training programs to incorporate fatigue resistance, as well as to raise awareness amongst physical therapists, athletic trainers, coaches, and athletes about the effect of fatigue on ACL injury risk,” Dr. Fidai concluded. “We can target vulnerable athletes, particularly female athletes, in an effort to negate some of those effects.”
The study’s principal investigator was Eric C. Makhni, MD. Dr. Makhni, an orthopedic surgeon in West Bloomfield, Mich., disclosed that he is a paid consultant for Smith & Nephew and that he receives publishing royalties from Springer. Dr. Fidai reported having no financial disclosures.
SAN DIEGO – Fatigue increases anterior cruciate ligament injury risk in adolescent athletes, results from a field-based drop-jump study demonstrate.
“The number of ACL reconstructions that occur annually are on the rise, particularly in high school and adolescent aged athletes,” lead study author Mohsin S. Fidai, MD, said at the annual meeting of the American Orthopaedic Society for Sports Medicine. “About 70% of these are accounted for by noncontact injuries, the majority of which occur during jump landing. A number of risk factors that have previously been implicated in ACL injury include genetics and anatomy, but a modifiable risk factor is landing biomechanics.”
In 2005, researchers led by Timothy E. Hewett, PhD, determined biomechanical measures of neuromuscular control that might pose certain athletes to be at risk for ACL injury, particularly knee abduction and dynamic knee valgus during a drop-jump test (Am J Sports Med. 2005;33[4]:492-501). “Historically, these studies have required the use of sophisticated computer technology, which can be cumbersome from a time and cost perspective,” said Dr. Fidai, a third-year orthopedic surgery resident at Henry Ford Health System, Detroit.
In a more recent analysis, researchers validated a field-based drop vertical jump screening test for ACL injury (Phys Sportmed. 2016;44[1]:46-52). The sensitivity was 95%, the specificity was 46%, and it had a strong inter-rater reliability (k = 0.92; P less than .05).
The purpose of the current study was to evaluate the effect of fatigue on ACL injury risk using a field-based drop-jump test. “We hypothesized that fatigue would lead to greater dynamic knee valgus during a drop-jump test,” Dr. Fidai said. “We also wanted to identify individual characteristics which may place athletes at increased risk for ACL injury.”
The researchers recruited 85 athletes who competed in track and field, basketball, volleyball, and soccer. More than half (55%) were female, and the mean age was 15.4 years. They excluded athletes with any previous or current lower extremity injuries or neuromuscular deficits. Each athlete performed a maximum vertical jump, followed by a drop-jump test.
“We then fatigued all of our athletes with a standardized high-intensity fatigue protocol, and had each athlete perform another maximum vertical jump and drop-jump test,” Dr. Fidai said. “All drop-jumps were video recorded and sent to a number of orthopedic surgery residents, athletic trainers, and physical therapists for review.”
Of the 85 athletes, nearly half (45%) showed an increased risk for ACL injury after high-intensity aerobic activity. In addition, 68% of study participants were identified as having a medium or high risk for injury following the aerobic activity, compared with 44% at baseline. Dr. Fidai noted. “In the group of athletes with higher levels of fatigue, there is a significantly increased risk, compared with their counterparts with lower levels of fatigue.”
Specifically, 14 of the 22 athletes who demonstrated over 20% fatigue showed an increased ACL injury risk. Subgroup analysis revealed that female athletes and those older than age 15 were more likely to demonstrate an increased injury risk.
“The findings of this study advocate for changes to current neuromuscular training programs to incorporate fatigue resistance, as well as to raise awareness amongst physical therapists, athletic trainers, coaches, and athletes about the effect of fatigue on ACL injury risk,” Dr. Fidai concluded. “We can target vulnerable athletes, particularly female athletes, in an effort to negate some of those effects.”
The study’s principal investigator was Eric C. Makhni, MD. Dr. Makhni, an orthopedic surgeon in West Bloomfield, Mich., disclosed that he is a paid consultant for Smith & Nephew and that he receives publishing royalties from Springer. Dr. Fidai reported having no financial disclosures.
REPORTING FROM AOSSM 2018
Key clinical point: Athletes who experience fatigue as tested by a standardized assessment demonstrated increased risk of ACL injury.
Major finding: Nearly half of athletes (45%) showed an increased injury risk after high-intensity aerobic activity.
Study details: A field-based study of 85 athletes that used vertical and drop-jump assessments of each athlete, which were captured on video and reviewed by professional health observers.
Disclosures: Dr. Makhni disclosed that he is a paid consultant for Smith & Nephew and that he receives publishing royalties from Springer. Dr. Fidai reported having no financial disclosures.
HbA1c cutpoint predicts pediatric T1DM within a year
ORLANDO – Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year, according to investigators from The Environmental Determinants of Diabetes in the Young (TEDDY) study.

The risk is even greater if other factors – age at A1c test, month of A1c test, continent of residence, and the z-score for one antibody in particular, IA2A, a tyrosine phosphatase antigen protein – are taken into account, with an area under the curve (AUC) of about 0.97. The study team is developing an online risk calculator for clinicians so they can simply plug in the numbers.
But the 5.6% cutpoint works well even by itself, with an AUC of about 0.86. Among the children with genetic risk factors and islet cell autoantibodies who hit that mark in the study, the median time to diagnosis of type 1 diabetes mellitus (T1DM) was 7.1 months.
The point of the work is to catch disease onset early to prevent children from going into diabetic ketoacidosis.
The ultimate goal of TEDDY is to identify infectious agents, dietary factors, and other environmental agents that either trigger or protect against T1DM in genetically susceptible children, to develop strategies to prevent, delay, or even reverse T1DM. For more than a decade, the consortium has been following more than 8,000 children who screened positive at birth for genetic anomalies in the human leukocyte antigen region on their 6th chromosome, a major risk factor for T1DM. The team is following them to find out what puts them over the edge; A1c seems to be key.
Catching the disease early is a goal. Until now, the TEDDY team has used the development of pancreatic islet cell autoantibodies to trigger oral glucose tolerance tests (OGTTs) every 6 months.
The problem is that islet antibodies “are great at saying that you are going to get diabetes but not when. We have kids who have been multiple antibody positive now for 6, 7, 8 years” but who still haven’t developed T1DM. In the meantime, their parents have been dragging them in for OGTTs every 6 months for years, said lead investigator and TEDDY study coordinator Michael Killian, of the Pacific Northwest Research Institute, Seattle.
With the A1c cutpoint, it should be safe to hold off on direct glycemic surveillance until A1c levels reach 5.6%, and even safer when the full risk prediction model with 1A2A z-scores and other factors are available. Once children hit the parameters, it’s near certain they will develop T1DM within a year, so the findings should reduce the number of OGTT tests to just two or three. In the end, “we’ll get better compliance” with testing and still “catch these kids early,” Mr. Killian said at the annual scientific sessions of the American Diabetes Association.
Rare is the newborn who is screened for diabetes risk at birth, and even rarer is the child who is followed for autoantibodies. If the findings hold out, however, such early action could be the future.
“We envision a time” when newborns are screened for T1DM risk and followed for autoantibodies. Glycemic surveillance will kick in if they hit A1c levels of 5.6%, said William Hagopian, MD, PhD, clinical associate professor at the University of Washington, Seattle, and a TEDDY principal investigator.
Among the 8,000-plus children followed, 456 had persistent islet autoantibodies and at least three A1c tests in the prior 12 months; 104 progressed to T1DM and 352 did not. The mean age to islet autoantibody seroconversion was 43 months, and mean age to T1DM diagnosis was 73 months. The team ran a receiver operating curve analysis to identify the optimum A1c cutpoint, 5.6%.
The month of testing mattered, because “glycemia is higher in the winter, lower in the summer, and insulin sensitivity is lower in the winter, and higher in the summer,” Dr. Hagopian said. It probably has something to do with what the stresses of early human evolution bred into the genes.
The IA2A autoantibody z-score is the only number that will be cumbersome to plug into the upcoming online risk calculator. It’s the number of standard deviations off your reference lab’s mean. “You have to talk to the lab that does your IA2As to know what the standard deviation is,” Dr. Hagopian said.
The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
SOURCE: Killian M et al. ADA 2018, Abstract 162-LB
ORLANDO – Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year, according to investigators from The Environmental Determinants of Diabetes in the Young (TEDDY) study.
The risk is even greater if other factors – age at A1c test, month of A1c test, continent of residence, and the z-score for one antibody in particular, IA2A, a tyrosine phosphatase antigen protein – are taken into account, with an area under the curve (AUC) of about 0.97. The study team is developing an online risk calculator for clinicians so they can simply plug in the numbers.
But the 5.6% cutpoint works well even by itself, with an AUC of about 0.86. Among the children with genetic risk factors and islet cell autoantibodies who hit that mark in the study, the median time to diagnosis of type 1 diabetes mellitus (T1DM) was 7.1 months.
The point of the work is to catch disease onset early to prevent children from going into diabetic ketoacidosis.
The ultimate goal of TEDDY is to identify infectious agents, dietary factors, and other environmental agents that either trigger or protect against T1DM in genetically susceptible children, to develop strategies to prevent, delay, or even reverse T1DM. For more than a decade, the consortium has been following more than 8,000 children who screened positive at birth for genetic anomalies in the human leukocyte antigen region on their 6th chromosome, a major risk factor for T1DM. The team is following them to find out what puts them over the edge; A1c seems to be key.
Catching the disease early is a goal. Until now, the TEDDY team has used the development of pancreatic islet cell autoantibodies to trigger oral glucose tolerance tests (OGTTs) every 6 months.
The problem is that islet antibodies “are great at saying that you are going to get diabetes but not when. We have kids who have been multiple antibody positive now for 6, 7, 8 years” but who still haven’t developed T1DM. In the meantime, their parents have been dragging them in for OGTTs every 6 months for years, said lead investigator and TEDDY study coordinator Michael Killian, of the Pacific Northwest Research Institute, Seattle.
With the A1c cutpoint, it should be safe to hold off on direct glycemic surveillance until A1c levels reach 5.6%, and even safer when the full risk prediction model with 1A2A z-scores and other factors are available. Once children hit the parameters, it’s near certain they will develop T1DM within a year, so the findings should reduce the number of OGTT tests to just two or three. In the end, “we’ll get better compliance” with testing and still “catch these kids early,” Mr. Killian said at the annual scientific sessions of the American Diabetes Association.
Rare is the newborn who is screened for diabetes risk at birth, and even rarer is the child who is followed for autoantibodies. If the findings hold out, however, such early action could be the future.
“We envision a time” when newborns are screened for T1DM risk and followed for autoantibodies. Glycemic surveillance will kick in if they hit A1c levels of 5.6%, said William Hagopian, MD, PhD, clinical associate professor at the University of Washington, Seattle, and a TEDDY principal investigator.
Among the 8,000-plus children followed, 456 had persistent islet autoantibodies and at least three A1c tests in the prior 12 months; 104 progressed to T1DM and 352 did not. The mean age to islet autoantibody seroconversion was 43 months, and mean age to T1DM diagnosis was 73 months. The team ran a receiver operating curve analysis to identify the optimum A1c cutpoint, 5.6%.
The month of testing mattered, because “glycemia is higher in the winter, lower in the summer, and insulin sensitivity is lower in the winter, and higher in the summer,” Dr. Hagopian said. It probably has something to do with what the stresses of early human evolution bred into the genes.
The IA2A autoantibody z-score is the only number that will be cumbersome to plug into the upcoming online risk calculator. It’s the number of standard deviations off your reference lab’s mean. “You have to talk to the lab that does your IA2As to know what the standard deviation is,” Dr. Hagopian said.
The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
SOURCE: Killian M et al. ADA 2018, Abstract 162-LB
ORLANDO – Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year, according to investigators from The Environmental Determinants of Diabetes in the Young (TEDDY) study.
The risk is even greater if other factors – age at A1c test, month of A1c test, continent of residence, and the z-score for one antibody in particular, IA2A, a tyrosine phosphatase antigen protein – are taken into account, with an area under the curve (AUC) of about 0.97. The study team is developing an online risk calculator for clinicians so they can simply plug in the numbers.
But the 5.6% cutpoint works well even by itself, with an AUC of about 0.86. Among the children with genetic risk factors and islet cell autoantibodies who hit that mark in the study, the median time to diagnosis of type 1 diabetes mellitus (T1DM) was 7.1 months.
The point of the work is to catch disease onset early to prevent children from going into diabetic ketoacidosis.
The ultimate goal of TEDDY is to identify infectious agents, dietary factors, and other environmental agents that either trigger or protect against T1DM in genetically susceptible children, to develop strategies to prevent, delay, or even reverse T1DM. For more than a decade, the consortium has been following more than 8,000 children who screened positive at birth for genetic anomalies in the human leukocyte antigen region on their 6th chromosome, a major risk factor for T1DM. The team is following them to find out what puts them over the edge; A1c seems to be key.
Catching the disease early is a goal. Until now, the TEDDY team has used the development of pancreatic islet cell autoantibodies to trigger oral glucose tolerance tests (OGTTs) every 6 months.
The problem is that islet antibodies “are great at saying that you are going to get diabetes but not when. We have kids who have been multiple antibody positive now for 6, 7, 8 years” but who still haven’t developed T1DM. In the meantime, their parents have been dragging them in for OGTTs every 6 months for years, said lead investigator and TEDDY study coordinator Michael Killian, of the Pacific Northwest Research Institute, Seattle.
With the A1c cutpoint, it should be safe to hold off on direct glycemic surveillance until A1c levels reach 5.6%, and even safer when the full risk prediction model with 1A2A z-scores and other factors are available. Once children hit the parameters, it’s near certain they will develop T1DM within a year, so the findings should reduce the number of OGTT tests to just two or three. In the end, “we’ll get better compliance” with testing and still “catch these kids early,” Mr. Killian said at the annual scientific sessions of the American Diabetes Association.
Rare is the newborn who is screened for diabetes risk at birth, and even rarer is the child who is followed for autoantibodies. If the findings hold out, however, such early action could be the future.
“We envision a time” when newborns are screened for T1DM risk and followed for autoantibodies. Glycemic surveillance will kick in if they hit A1c levels of 5.6%, said William Hagopian, MD, PhD, clinical associate professor at the University of Washington, Seattle, and a TEDDY principal investigator.
Among the 8,000-plus children followed, 456 had persistent islet autoantibodies and at least three A1c tests in the prior 12 months; 104 progressed to T1DM and 352 did not. The mean age to islet autoantibody seroconversion was 43 months, and mean age to T1DM diagnosis was 73 months. The team ran a receiver operating curve analysis to identify the optimum A1c cutpoint, 5.6%.
The month of testing mattered, because “glycemia is higher in the winter, lower in the summer, and insulin sensitivity is lower in the winter, and higher in the summer,” Dr. Hagopian said. It probably has something to do with what the stresses of early human evolution bred into the genes.
The IA2A autoantibody z-score is the only number that will be cumbersome to plug into the upcoming online risk calculator. It’s the number of standard deviations off your reference lab’s mean. “You have to talk to the lab that does your IA2As to know what the standard deviation is,” Dr. Hagopian said.
The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
SOURCE: Killian M et al. ADA 2018, Abstract 162-LB
FROM ADA 2018
Key clinical point: Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year.
Major finding: Among the children with genetic risk factors and islet cell autoantibodies who hit that mark, the median time to diagnosis was 7.1 months.
Study details: The findings are from more than 400 children in The Environmental Determinants of Diabetes in the Young (TEDDY) cohort.
Disclosures: The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
Source: Killian M et al. ADA 2018, Abstract 162-LB.
Timely culture reports lower LOS for neonatal fever
ATLANTA – An adjustment in the culture reporting schedule at Texas Children’s Hospital, Houston, helped reduce the average length of stay for neonatal fever from 48 to 43 hours, without increasing readmissions for serious bacterial infections, according to a review presented at the Pediatric Hospital Medicine meeting.

Investigators there were working to meet the goals of the Reducing Excessive Variability in Infant Sepsis Evaluation project (REVISE), a national collaboration aimed at improving care. One of the goals is to reduce the length of stay (LOS) for neonatal fever to fewer than 30 hours for low-risk infants and fewer than 42 hours among high-risk infants.
The traditional standard is to keep children in the hospital for 48 hours to rule out sepsis, but that thinking has begun to change amid evidence that blood cultures generally do not need that long to turn positive, among other findings, said investigator Huay-Ying Lo, MD, a pediatrician at Texas Children’s.
“At our institution,” which admits more than 200 NF cases annually, “we have order sets for neonatal fever, and we’re actually doing pretty well” meeting most of the REVISE goals, “so we decided to focus on reducing length of stay,” she said at the meeting.
Evidence of the safety and cost savings of earlier discharge was presented to providers, and weekly emails reminded them of the early discharge goal and updated them on the current average LOS for NF.
Dr. Lo and her team also brainstormed with providers to identify problems. “One of the barriers they consistently mentioned was the timing of cultures being reported out from the microbiology lab. A lot of time, people were just waiting for the report to say no growth for 36 hours or whatever it was going to be,” she said.
That led to talks with the microbiology department. Blood cultures were already automated, so there wasn’t much that needed to be done. Urine cultures were read manually three to four times a day after the initial incubation period. However, after an initial Gram stain, CSF cultures were read manually only one or two times a day – whenever somebody had time. The hours were random, and sometimes results were not reported until the evening, which meant the child had to spend another night in the hospital.
The lab director agreed that it was a problem, and standardized procedures to read cultures twice a day, at 7 a.m. and 2 p.m. “The times we agreed upon; 7 a.m. works really well for morning discharge, and at 2 p.m., the day team is still there and can get kids out that day,” Dr. Lo explained.
. Among infants 7-60 days old admitted with NF – excluding ill-appearing children and those with comorbidities that increased the risk of infections – the mean LOS fell from 48 hours among 144 infants treated before the intervention, to 43 hours among 157 treated afterward (P = .001), and “we didn’t have any more readmission for serious bacterial infections,” Dr. Lo said.
“We want to reduce it further. If we get to 42 hours, we’ll be pretty happy.” Updating discharge criteria, and letting providers know how their LOS’s compare with their peers’ might help. “I’m sure some people are more conservative and some a little more liberal,” she said.
There was no industry funding for the work, and the investigators had no disclosures. The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
ATLANTA – An adjustment in the culture reporting schedule at Texas Children’s Hospital, Houston, helped reduce the average length of stay for neonatal fever from 48 to 43 hours, without increasing readmissions for serious bacterial infections, according to a review presented at the Pediatric Hospital Medicine meeting.
Investigators there were working to meet the goals of the Reducing Excessive Variability in Infant Sepsis Evaluation project (REVISE), a national collaboration aimed at improving care. One of the goals is to reduce the length of stay (LOS) for neonatal fever to fewer than 30 hours for low-risk infants and fewer than 42 hours among high-risk infants.
The traditional standard is to keep children in the hospital for 48 hours to rule out sepsis, but that thinking has begun to change amid evidence that blood cultures generally do not need that long to turn positive, among other findings, said investigator Huay-Ying Lo, MD, a pediatrician at Texas Children’s.
“At our institution,” which admits more than 200 NF cases annually, “we have order sets for neonatal fever, and we’re actually doing pretty well” meeting most of the REVISE goals, “so we decided to focus on reducing length of stay,” she said at the meeting.
Evidence of the safety and cost savings of earlier discharge was presented to providers, and weekly emails reminded them of the early discharge goal and updated them on the current average LOS for NF.
Dr. Lo and her team also brainstormed with providers to identify problems. “One of the barriers they consistently mentioned was the timing of cultures being reported out from the microbiology lab. A lot of time, people were just waiting for the report to say no growth for 36 hours or whatever it was going to be,” she said.
That led to talks with the microbiology department. Blood cultures were already automated, so there wasn’t much that needed to be done. Urine cultures were read manually three to four times a day after the initial incubation period. However, after an initial Gram stain, CSF cultures were read manually only one or two times a day – whenever somebody had time. The hours were random, and sometimes results were not reported until the evening, which meant the child had to spend another night in the hospital.
The lab director agreed that it was a problem, and standardized procedures to read cultures twice a day, at 7 a.m. and 2 p.m. “The times we agreed upon; 7 a.m. works really well for morning discharge, and at 2 p.m., the day team is still there and can get kids out that day,” Dr. Lo explained.
. Among infants 7-60 days old admitted with NF – excluding ill-appearing children and those with comorbidities that increased the risk of infections – the mean LOS fell from 48 hours among 144 infants treated before the intervention, to 43 hours among 157 treated afterward (P = .001), and “we didn’t have any more readmission for serious bacterial infections,” Dr. Lo said.
“We want to reduce it further. If we get to 42 hours, we’ll be pretty happy.” Updating discharge criteria, and letting providers know how their LOS’s compare with their peers’ might help. “I’m sure some people are more conservative and some a little more liberal,” she said.
There was no industry funding for the work, and the investigators had no disclosures. The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
ATLANTA – An adjustment in the culture reporting schedule at Texas Children’s Hospital, Houston, helped reduce the average length of stay for neonatal fever from 48 to 43 hours, without increasing readmissions for serious bacterial infections, according to a review presented at the Pediatric Hospital Medicine meeting.
Investigators there were working to meet the goals of the Reducing Excessive Variability in Infant Sepsis Evaluation project (REVISE), a national collaboration aimed at improving care. One of the goals is to reduce the length of stay (LOS) for neonatal fever to fewer than 30 hours for low-risk infants and fewer than 42 hours among high-risk infants.
The traditional standard is to keep children in the hospital for 48 hours to rule out sepsis, but that thinking has begun to change amid evidence that blood cultures generally do not need that long to turn positive, among other findings, said investigator Huay-Ying Lo, MD, a pediatrician at Texas Children’s.
“At our institution,” which admits more than 200 NF cases annually, “we have order sets for neonatal fever, and we’re actually doing pretty well” meeting most of the REVISE goals, “so we decided to focus on reducing length of stay,” she said at the meeting.
Evidence of the safety and cost savings of earlier discharge was presented to providers, and weekly emails reminded them of the early discharge goal and updated them on the current average LOS for NF.
Dr. Lo and her team also brainstormed with providers to identify problems. “One of the barriers they consistently mentioned was the timing of cultures being reported out from the microbiology lab. A lot of time, people were just waiting for the report to say no growth for 36 hours or whatever it was going to be,” she said.
That led to talks with the microbiology department. Blood cultures were already automated, so there wasn’t much that needed to be done. Urine cultures were read manually three to four times a day after the initial incubation period. However, after an initial Gram stain, CSF cultures were read manually only one or two times a day – whenever somebody had time. The hours were random, and sometimes results were not reported until the evening, which meant the child had to spend another night in the hospital.
The lab director agreed that it was a problem, and standardized procedures to read cultures twice a day, at 7 a.m. and 2 p.m. “The times we agreed upon; 7 a.m. works really well for morning discharge, and at 2 p.m., the day team is still there and can get kids out that day,” Dr. Lo explained.
. Among infants 7-60 days old admitted with NF – excluding ill-appearing children and those with comorbidities that increased the risk of infections – the mean LOS fell from 48 hours among 144 infants treated before the intervention, to 43 hours among 157 treated afterward (P = .001), and “we didn’t have any more readmission for serious bacterial infections,” Dr. Lo said.
“We want to reduce it further. If we get to 42 hours, we’ll be pretty happy.” Updating discharge criteria, and letting providers know how their LOS’s compare with their peers’ might help. “I’m sure some people are more conservative and some a little more liberal,” she said.
There was no industry funding for the work, and the investigators had no disclosures. The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
REPORTING FROM PHM 2018
Key clinical point: An adjustment in the culture reporting schedule at Texas Children’s Hospital, Houston, helped reduce the average length of stay for neonatal fever, without increasing readmissions for serious bacterial infections.
Major finding: The mean length of stay fell from 48 hours among 144 infants treated before the intervention, to 43 hours among 157 treated afterward (P = .001).
Study details: Pre/post analysis of quality improvement project.
Disclosures: There was no industry funding for the work, and the investigators had no disclosures.

Asthma medication ratio identifies high-risk pediatric patients
ATLANTA – An according to researchers from the Medical University of South Carolina (MUSC), Charleston.

The asthma medication ratio (AMR) – the number of prescriptions for controller medications divided by the number of prescriptions for both controller and rescue medications – has been around for a while, but it’s mostly been used as a quality metric. The new study shows that it’s also useful in the clinic to identify children who could benefit from extra attention.
A perfect ratio of 1 means that control is good without rescue inhalers. The ratio falls as the number of rescue inhalers goes up, signaling poorer control. Children with a ratio below 0.5 are considered high risk; they’d hit that mark if, for instance, they were prescribed one control medication such as fluticasone propionate (Flovent) and two albuterol rescue inhalers in a month.
If control is good, “you should only need a rescue inhaler very, very sporadically;” high-risk children probably need a higher dose of their controller, or help with compliance, explained lead investigator Annie L. Andrews, MD, associate professor of pediatrics at MUSC.
The university uses the EPIC records system, which incorporates prescription data from Surescripts, so the number of asthma medication fills is already available. The system just needs to be adjusted to calculate and report AMRs monthly, something Dr. Andrews and her team are working on. “The information is right there, but it’s an untapped resource,” she said. “We just need to crunch the numbers, and operationalize it. Why are we waiting until kids are in the hospital” to intervene?
Dr. Andrews presented a proof-of-concept study at the Pediatric Hospital Medicine meeting. Her team identified 214,452 asthma patients aged 2-17 years with at least one claim for an inhaled corticosteroid in the Truven MarketScan Medicaid database from 2013-14.
They calculated AMRs for each child every 3 months over a 15-month period. About 9% of children at any given time had AMRs below 0.5.
The first AMR was at or above 0.5 in 93,512 children; 18.1% had a subsequent asthma-related event, meaning an ED visit or hospitalization, during the course of the study. Among the 17,635 children with an initial AMR below 0.5, 25% had asthma-related events. The initial AMR couldn’t be calculated in 103,305 children, which likely meant they had less-active disease. Those children had the lowest proportion of asthma events, at 13.9%.
An AMR below 0.5 nearly doubled the risk of an asthma-related hospitalization or ED visit in the subsequent 3 months, with an odds ratios ranging from 1.7 to 1.9, compared with other children. The findings were statistically significant.
In short, serial AMRs helped predict exacerbations among Medicaid children. The team showed the same trend among commercially insured children in a recently published study. The only difference was that Medicaid children had a higher proportion of high-risk AMRs, and a higher number of asthma events (Am J Manag Care. 2018 Jun;24[6]:294-300). Together, the studies validate “the rolling 3-month AMR as an appropriate method for identifying children at high risk for imminent exacerbation,” the investigators concluded.
With automatic AMR reporting already in the works at MUSC, “we are now trying to figure out how to intervene. Do we just tell providers who their high-risk kids are and let them figure out how to contact families, or do we use this information to contact families directly? That’s kind of what I favor: ‘Hey, your kid just popped up as high risk, so let’s figure out what you need. Do you need a new prescription or a reminder to see your doctor?’ ” Dr. Andrews said.
Her team is developing a mobile app to communicate with families.
The mean age in the study was 7.9 years; 59% of the children were boys, and 41% were black.
The work was funded by the National Institutes of Health, among others. Dr. Andrews had no disclosures. The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
ATLANTA – An according to researchers from the Medical University of South Carolina (MUSC), Charleston.
The asthma medication ratio (AMR) – the number of prescriptions for controller medications divided by the number of prescriptions for both controller and rescue medications – has been around for a while, but it’s mostly been used as a quality metric. The new study shows that it’s also useful in the clinic to identify children who could benefit from extra attention.
A perfect ratio of 1 means that control is good without rescue inhalers. The ratio falls as the number of rescue inhalers goes up, signaling poorer control. Children with a ratio below 0.5 are considered high risk; they’d hit that mark if, for instance, they were prescribed one control medication such as fluticasone propionate (Flovent) and two albuterol rescue inhalers in a month.
If control is good, “you should only need a rescue inhaler very, very sporadically;” high-risk children probably need a higher dose of their controller, or help with compliance, explained lead investigator Annie L. Andrews, MD, associate professor of pediatrics at MUSC.
The university uses the EPIC records system, which incorporates prescription data from Surescripts, so the number of asthma medication fills is already available. The system just needs to be adjusted to calculate and report AMRs monthly, something Dr. Andrews and her team are working on. “The information is right there, but it’s an untapped resource,” she said. “We just need to crunch the numbers, and operationalize it. Why are we waiting until kids are in the hospital” to intervene?
Dr. Andrews presented a proof-of-concept study at the Pediatric Hospital Medicine meeting. Her team identified 214,452 asthma patients aged 2-17 years with at least one claim for an inhaled corticosteroid in the Truven MarketScan Medicaid database from 2013-14.
They calculated AMRs for each child every 3 months over a 15-month period. About 9% of children at any given time had AMRs below 0.5.
The first AMR was at or above 0.5 in 93,512 children; 18.1% had a subsequent asthma-related event, meaning an ED visit or hospitalization, during the course of the study. Among the 17,635 children with an initial AMR below 0.5, 25% had asthma-related events. The initial AMR couldn’t be calculated in 103,305 children, which likely meant they had less-active disease. Those children had the lowest proportion of asthma events, at 13.9%.
An AMR below 0.5 nearly doubled the risk of an asthma-related hospitalization or ED visit in the subsequent 3 months, with an odds ratios ranging from 1.7 to 1.9, compared with other children. The findings were statistically significant.
In short, serial AMRs helped predict exacerbations among Medicaid children. The team showed the same trend among commercially insured children in a recently published study. The only difference was that Medicaid children had a higher proportion of high-risk AMRs, and a higher number of asthma events (Am J Manag Care. 2018 Jun;24[6]:294-300). Together, the studies validate “the rolling 3-month AMR as an appropriate method for identifying children at high risk for imminent exacerbation,” the investigators concluded.
With automatic AMR reporting already in the works at MUSC, “we are now trying to figure out how to intervene. Do we just tell providers who their high-risk kids are and let them figure out how to contact families, or do we use this information to contact families directly? That’s kind of what I favor: ‘Hey, your kid just popped up as high risk, so let’s figure out what you need. Do you need a new prescription or a reminder to see your doctor?’ ” Dr. Andrews said.
Her team is developing a mobile app to communicate with families.
The mean age in the study was 7.9 years; 59% of the children were boys, and 41% were black.
The work was funded by the National Institutes of Health, among others. Dr. Andrews had no disclosures. The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
ATLANTA – An according to researchers from the Medical University of South Carolina (MUSC), Charleston.
The asthma medication ratio (AMR) – the number of prescriptions for controller medications divided by the number of prescriptions for both controller and rescue medications – has been around for a while, but it’s mostly been used as a quality metric. The new study shows that it’s also useful in the clinic to identify children who could benefit from extra attention.
A perfect ratio of 1 means that control is good without rescue inhalers. The ratio falls as the number of rescue inhalers goes up, signaling poorer control. Children with a ratio below 0.5 are considered high risk; they’d hit that mark if, for instance, they were prescribed one control medication such as fluticasone propionate (Flovent) and two albuterol rescue inhalers in a month.
If control is good, “you should only need a rescue inhaler very, very sporadically;” high-risk children probably need a higher dose of their controller, or help with compliance, explained lead investigator Annie L. Andrews, MD, associate professor of pediatrics at MUSC.
The university uses the EPIC records system, which incorporates prescription data from Surescripts, so the number of asthma medication fills is already available. The system just needs to be adjusted to calculate and report AMRs monthly, something Dr. Andrews and her team are working on. “The information is right there, but it’s an untapped resource,” she said. “We just need to crunch the numbers, and operationalize it. Why are we waiting until kids are in the hospital” to intervene?
Dr. Andrews presented a proof-of-concept study at the Pediatric Hospital Medicine meeting. Her team identified 214,452 asthma patients aged 2-17 years with at least one claim for an inhaled corticosteroid in the Truven MarketScan Medicaid database from 2013-14.
They calculated AMRs for each child every 3 months over a 15-month period. About 9% of children at any given time had AMRs below 0.5.
The first AMR was at or above 0.5 in 93,512 children; 18.1% had a subsequent asthma-related event, meaning an ED visit or hospitalization, during the course of the study. Among the 17,635 children with an initial AMR below 0.5, 25% had asthma-related events. The initial AMR couldn’t be calculated in 103,305 children, which likely meant they had less-active disease. Those children had the lowest proportion of asthma events, at 13.9%.
An AMR below 0.5 nearly doubled the risk of an asthma-related hospitalization or ED visit in the subsequent 3 months, with an odds ratios ranging from 1.7 to 1.9, compared with other children. The findings were statistically significant.
In short, serial AMRs helped predict exacerbations among Medicaid children. The team showed the same trend among commercially insured children in a recently published study. The only difference was that Medicaid children had a higher proportion of high-risk AMRs, and a higher number of asthma events (Am J Manag Care. 2018 Jun;24[6]:294-300). Together, the studies validate “the rolling 3-month AMR as an appropriate method for identifying children at high risk for imminent exacerbation,” the investigators concluded.
With automatic AMR reporting already in the works at MUSC, “we are now trying to figure out how to intervene. Do we just tell providers who their high-risk kids are and let them figure out how to contact families, or do we use this information to contact families directly? That’s kind of what I favor: ‘Hey, your kid just popped up as high risk, so let’s figure out what you need. Do you need a new prescription or a reminder to see your doctor?’ ” Dr. Andrews said.
Her team is developing a mobile app to communicate with families.
The mean age in the study was 7.9 years; 59% of the children were boys, and 41% were black.
The work was funded by the National Institutes of Health, among others. Dr. Andrews had no disclosures. The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
REPORTING FROM PHM 2018
Key clinical point: The asthma medication ratio is useful in the clinic to identify children who could benefit from extra attention.
Major finding: About 9% of children at any given time had AMRs below 0.5, meaning they were at high risk for acute exacerbations.
Study details: Review of more than 200,000 pediatric asthma patients on Medicaid
Disclosures: The work was funded by the National Institutes of Health, among others. The study lead had no disclosures.
Short-course IV antibiotics okay for newborn bacteremic UTI
ATLANTA – A short course of IV antibiotics – 7 days or less – is fine for most infants with uncomplicated bacteremic urinary tract infections, according to a review of 116 children younger than 60 days.
How long to treat bacteremic UTIs in the very young has been debated in pediatrics for a while, with some centers opting for a few days and others for 2 weeks or more. Shorter courses reduce length of stay, costs, and complications, but there hasn’t been much research to see whether they work as well.

The new investigation has suggested they do. “Young infants with bacteremic UTI who received less than or equal to 7 days of IV antibiotic therapy did not have more recurrent UTIs,” compared “to infants who received longer courses. Short course IV therapy with early conversion to oral antibiotics may be considered in this population,” said lead investigator Sanyukta Desai, MD, at the Pediatric Hospital Medicine meeting.
The team compared outcomes of 58 infants treated for 7 days or less to outcomes of 58 infants treated for more than 7 days at 11 children’s hospitals scattered across the United States.
Urine was collected by catheter, and each child grew the same organism in their blood and urine cultures, confirming the diagnosis of bacteremic UTI. Children with bacterial meningitis, or suspected of having it, were excluded. The subjects had all been admitted through the ED.
There was quite a bit of variation among the 11 hospitals, with the proportion of children treated with short courses ranging from 10% to 81%.
As for the results, two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days. None of them developed meningitis, and none required ICU admission. Propensity-score matching revealed an odds ratio for recurrence that favored shorter treatment, but it wasn’t statistically significant.
The mean length of stay was 5 days in the short-course arm and 11 days in the long-course arm. There were no serious adverse events within 30 days of the index admission in either group.
Among the recurrences, the two children in the short-course arm were initially treated for 3 and 5 days. Both were older than 28 days at their initial presentation, and both had vesicoureteral reflux of at least grade 2, which was not diagnosed in one child until after the recurrence. The other child had been on prophylactic trimethoprim/sulfamethoxazole before the recurrence.
The four recurrent cases in the long arm initially received either 10 or 14 days of IV antibiotics. Two children had grade 4 vesicoureteral reflux and had been on prophylactic amoxicillin.
Infants treated with longer antibiotic courses were more likely to be under 28 days old, appear ill at presentation, have had bacteremia for more than 24 hours, and have and grow out pathogens other than Escherichia coli. The two groups were otherwise balanced for sex, prematurity, complex chronic conditions, and known genitourinary anomalies.
With such low event rates, the study wasn’t powered to detect small but potentially meaningful differences in outcomes, and further work is needed to define which children would benefit from longer treatment courses. Even so, “it was reassuring that patients did well in both arms,” said Dr. Desai, a clinical fellow in the division of hospital medicine at Cincinnati Children’s Hospital.
“At our institution with uncomplicated UTI, we wait to see what the culture grows.” If there’s an oral antibiotic that will work, “we send [infants] home in 3-4 days. We haven’t had any poor outcomes, even when they’re bacteremic,” she said.
The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
ATLANTA – A short course of IV antibiotics – 7 days or less – is fine for most infants with uncomplicated bacteremic urinary tract infections, according to a review of 116 children younger than 60 days.
How long to treat bacteremic UTIs in the very young has been debated in pediatrics for a while, with some centers opting for a few days and others for 2 weeks or more. Shorter courses reduce length of stay, costs, and complications, but there hasn’t been much research to see whether they work as well.
The new investigation has suggested they do. “Young infants with bacteremic UTI who received less than or equal to 7 days of IV antibiotic therapy did not have more recurrent UTIs,” compared “to infants who received longer courses. Short course IV therapy with early conversion to oral antibiotics may be considered in this population,” said lead investigator Sanyukta Desai, MD, at the Pediatric Hospital Medicine meeting.
The team compared outcomes of 58 infants treated for 7 days or less to outcomes of 58 infants treated for more than 7 days at 11 children’s hospitals scattered across the United States.
Urine was collected by catheter, and each child grew the same organism in their blood and urine cultures, confirming the diagnosis of bacteremic UTI. Children with bacterial meningitis, or suspected of having it, were excluded. The subjects had all been admitted through the ED.
There was quite a bit of variation among the 11 hospitals, with the proportion of children treated with short courses ranging from 10% to 81%.
As for the results, two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days. None of them developed meningitis, and none required ICU admission. Propensity-score matching revealed an odds ratio for recurrence that favored shorter treatment, but it wasn’t statistically significant.
The mean length of stay was 5 days in the short-course arm and 11 days in the long-course arm. There were no serious adverse events within 30 days of the index admission in either group.
Among the recurrences, the two children in the short-course arm were initially treated for 3 and 5 days. Both were older than 28 days at their initial presentation, and both had vesicoureteral reflux of at least grade 2, which was not diagnosed in one child until after the recurrence. The other child had been on prophylactic trimethoprim/sulfamethoxazole before the recurrence.
The four recurrent cases in the long arm initially received either 10 or 14 days of IV antibiotics. Two children had grade 4 vesicoureteral reflux and had been on prophylactic amoxicillin.
Infants treated with longer antibiotic courses were more likely to be under 28 days old, appear ill at presentation, have had bacteremia for more than 24 hours, and have and grow out pathogens other than Escherichia coli. The two groups were otherwise balanced for sex, prematurity, complex chronic conditions, and known genitourinary anomalies.
With such low event rates, the study wasn’t powered to detect small but potentially meaningful differences in outcomes, and further work is needed to define which children would benefit from longer treatment courses. Even so, “it was reassuring that patients did well in both arms,” said Dr. Desai, a clinical fellow in the division of hospital medicine at Cincinnati Children’s Hospital.
“At our institution with uncomplicated UTI, we wait to see what the culture grows.” If there’s an oral antibiotic that will work, “we send [infants] home in 3-4 days. We haven’t had any poor outcomes, even when they’re bacteremic,” she said.
The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
ATLANTA – A short course of IV antibiotics – 7 days or less – is fine for most infants with uncomplicated bacteremic urinary tract infections, according to a review of 116 children younger than 60 days.
How long to treat bacteremic UTIs in the very young has been debated in pediatrics for a while, with some centers opting for a few days and others for 2 weeks or more. Shorter courses reduce length of stay, costs, and complications, but there hasn’t been much research to see whether they work as well.
The new investigation has suggested they do. “Young infants with bacteremic UTI who received less than or equal to 7 days of IV antibiotic therapy did not have more recurrent UTIs,” compared “to infants who received longer courses. Short course IV therapy with early conversion to oral antibiotics may be considered in this population,” said lead investigator Sanyukta Desai, MD, at the Pediatric Hospital Medicine meeting.
The team compared outcomes of 58 infants treated for 7 days or less to outcomes of 58 infants treated for more than 7 days at 11 children’s hospitals scattered across the United States.
Urine was collected by catheter, and each child grew the same organism in their blood and urine cultures, confirming the diagnosis of bacteremic UTI. Children with bacterial meningitis, or suspected of having it, were excluded. The subjects had all been admitted through the ED.
There was quite a bit of variation among the 11 hospitals, with the proportion of children treated with short courses ranging from 10% to 81%.
As for the results, two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days. None of them developed meningitis, and none required ICU admission. Propensity-score matching revealed an odds ratio for recurrence that favored shorter treatment, but it wasn’t statistically significant.
The mean length of stay was 5 days in the short-course arm and 11 days in the long-course arm. There were no serious adverse events within 30 days of the index admission in either group.
Among the recurrences, the two children in the short-course arm were initially treated for 3 and 5 days. Both were older than 28 days at their initial presentation, and both had vesicoureteral reflux of at least grade 2, which was not diagnosed in one child until after the recurrence. The other child had been on prophylactic trimethoprim/sulfamethoxazole before the recurrence.
The four recurrent cases in the long arm initially received either 10 or 14 days of IV antibiotics. Two children had grade 4 vesicoureteral reflux and had been on prophylactic amoxicillin.
Infants treated with longer antibiotic courses were more likely to be under 28 days old, appear ill at presentation, have had bacteremia for more than 24 hours, and have and grow out pathogens other than Escherichia coli. The two groups were otherwise balanced for sex, prematurity, complex chronic conditions, and known genitourinary anomalies.
With such low event rates, the study wasn’t powered to detect small but potentially meaningful differences in outcomes, and further work is needed to define which children would benefit from longer treatment courses. Even so, “it was reassuring that patients did well in both arms,” said Dr. Desai, a clinical fellow in the division of hospital medicine at Cincinnati Children’s Hospital.
“At our institution with uncomplicated UTI, we wait to see what the culture grows.” If there’s an oral antibiotic that will work, “we send [infants] home in 3-4 days. We haven’t had any poor outcomes, even when they’re bacteremic,” she said.
The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
REPORTING FROM PHM 2018
Key clinical point:
Major finding: Two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days.
Study details: Review of 116 infants.
Disclosures: The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
Study explores adolescents’ views on their skin tone, pressure to tan
LAKE TAHOE, CALIF. –

During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Shivani Patel, MD, said that prior research on skin color had focused mainly on adults and its impact on self-esteem and perceived attractiveness, yet little data are available on perceptions of skin color among adolescents.
“During puberty, adolescents receive pressure from friends, family, and social media to conform to a certain acceptable standard of skin tone,” said Dr. Patel, a chief resident in the department of dermatology at Johns Hopkins University, Baltimore. “They will often engage in risky behaviors such as tanning bed use, suntanning, and use of skin lightening creams.”
In an effort to characterize the attitudes of adolescents about their skin tone, she and her associates recruited 50 patients aged 12-19 years who were seen at the Johns Hopkins dermatology clinics. Slightly more than half (56%) were female. They were asked to complete surveys on their use of sunscreen, tanning beds, and skin-lightening creams, as well as to report any family or friends who have used these interventions.
Next, the researchers used Pantone’s Capsure device to record each subject’s skin tone according to a palate of 110 skin colors available from Pantone’s SkinTone Guide, which is intended to match and reproduce lifelike skin tones in a variety of industries. The adolescents were then given the palette and asked which skin tone they felt best represented their skin and which skin tone they wished they had. These differences were compared with their objective measurement by the study team.
Of all respondents, 20% indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001), a feeling they said started around the age of 12 years and stemmed from perceived pressure from friends and celebrity figures. Those who suntanned were more likely to wear sunscreen (P less than .01), a finding “that was reassuring and showed that they are aware of sunscreen and sun safety,” Dr. Patel said. However, about half of the respondents reported never wearing sunscreen and only two reported wearing sunscreen daily. No one reported using tanning beds, but 8% reported that a family member used them. One adolescent reported using skin lightening creams, and three reported that their mothers used them.
The researchers also found that black and Asian study participants were significantly more likely to desire a skin tone lighter than what they perceived their skin tone to be, while white participants were significantly more likely to desire a darker skin tone (P less than .011 for both associations).
The findings suggest that sun safety initiatives should target prepubertal patients before they engage in risky behaviors, Dr. Patel said. She acknowledged that the small sample size is a limitation of the study, but said that she and her associates hope to conduct a larger-scale analysis.
She reported having no financial disclosures.
LAKE TAHOE, CALIF. –
During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Shivani Patel, MD, said that prior research on skin color had focused mainly on adults and its impact on self-esteem and perceived attractiveness, yet little data are available on perceptions of skin color among adolescents.
“During puberty, adolescents receive pressure from friends, family, and social media to conform to a certain acceptable standard of skin tone,” said Dr. Patel, a chief resident in the department of dermatology at Johns Hopkins University, Baltimore. “They will often engage in risky behaviors such as tanning bed use, suntanning, and use of skin lightening creams.”
In an effort to characterize the attitudes of adolescents about their skin tone, she and her associates recruited 50 patients aged 12-19 years who were seen at the Johns Hopkins dermatology clinics. Slightly more than half (56%) were female. They were asked to complete surveys on their use of sunscreen, tanning beds, and skin-lightening creams, as well as to report any family or friends who have used these interventions.
Next, the researchers used Pantone’s Capsure device to record each subject’s skin tone according to a palate of 110 skin colors available from Pantone’s SkinTone Guide, which is intended to match and reproduce lifelike skin tones in a variety of industries. The adolescents were then given the palette and asked which skin tone they felt best represented their skin and which skin tone they wished they had. These differences were compared with their objective measurement by the study team.
Of all respondents, 20% indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001), a feeling they said started around the age of 12 years and stemmed from perceived pressure from friends and celebrity figures. Those who suntanned were more likely to wear sunscreen (P less than .01), a finding “that was reassuring and showed that they are aware of sunscreen and sun safety,” Dr. Patel said. However, about half of the respondents reported never wearing sunscreen and only two reported wearing sunscreen daily. No one reported using tanning beds, but 8% reported that a family member used them. One adolescent reported using skin lightening creams, and three reported that their mothers used them.
The researchers also found that black and Asian study participants were significantly more likely to desire a skin tone lighter than what they perceived their skin tone to be, while white participants were significantly more likely to desire a darker skin tone (P less than .011 for both associations).
The findings suggest that sun safety initiatives should target prepubertal patients before they engage in risky behaviors, Dr. Patel said. She acknowledged that the small sample size is a limitation of the study, but said that she and her associates hope to conduct a larger-scale analysis.
She reported having no financial disclosures.
LAKE TAHOE, CALIF. –
During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Shivani Patel, MD, said that prior research on skin color had focused mainly on adults and its impact on self-esteem and perceived attractiveness, yet little data are available on perceptions of skin color among adolescents.
“During puberty, adolescents receive pressure from friends, family, and social media to conform to a certain acceptable standard of skin tone,” said Dr. Patel, a chief resident in the department of dermatology at Johns Hopkins University, Baltimore. “They will often engage in risky behaviors such as tanning bed use, suntanning, and use of skin lightening creams.”
In an effort to characterize the attitudes of adolescents about their skin tone, she and her associates recruited 50 patients aged 12-19 years who were seen at the Johns Hopkins dermatology clinics. Slightly more than half (56%) were female. They were asked to complete surveys on their use of sunscreen, tanning beds, and skin-lightening creams, as well as to report any family or friends who have used these interventions.
Next, the researchers used Pantone’s Capsure device to record each subject’s skin tone according to a palate of 110 skin colors available from Pantone’s SkinTone Guide, which is intended to match and reproduce lifelike skin tones in a variety of industries. The adolescents were then given the palette and asked which skin tone they felt best represented their skin and which skin tone they wished they had. These differences were compared with their objective measurement by the study team.
Of all respondents, 20% indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001), a feeling they said started around the age of 12 years and stemmed from perceived pressure from friends and celebrity figures. Those who suntanned were more likely to wear sunscreen (P less than .01), a finding “that was reassuring and showed that they are aware of sunscreen and sun safety,” Dr. Patel said. However, about half of the respondents reported never wearing sunscreen and only two reported wearing sunscreen daily. No one reported using tanning beds, but 8% reported that a family member used them. One adolescent reported using skin lightening creams, and three reported that their mothers used them.
The researchers also found that black and Asian study participants were significantly more likely to desire a skin tone lighter than what they perceived their skin tone to be, while white participants were significantly more likely to desire a darker skin tone (P less than .011 for both associations).
The findings suggest that sun safety initiatives should target prepubertal patients before they engage in risky behaviors, Dr. Patel said. She acknowledged that the small sample size is a limitation of the study, but said that she and her associates hope to conduct a larger-scale analysis.
She reported having no financial disclosures.
REPORTING FROM SPD 2018
Key clinical point: Sun safety initiatives should target prepubertal patients before they engage in risky behaviors.
Major finding: One in five adolescents indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001).
Study details: A survey of 50 patients aged 12-19 years.
Disclosures: Dr. Patel reported having no financial disclosures.
Preterm birth rate ‘is on the rise again’
After several years of decline, the incidence of preterm births in the United States “is on the rise again,” according to the National Center for Health Statistics.
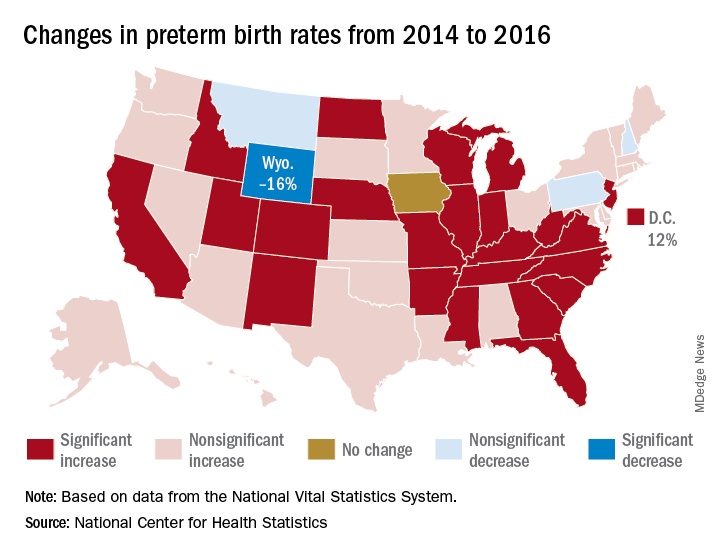
That 3% increase was spread pretty evenly: 23 states and the District of Columbia experienced statistically significant increases from 2014 to 2016, and 22 other states also had increases, although these were not statistically significant. One state, Iowa, had no change; three states – Montana, New Hampshire, and Pennsylvania – had nonsignificant declines, and Wyoming was the only state with a statistically significant drop (16%) in preterm birth incidence, they said based on data from the National Vital Statistics System.
The largest increase, 12%, was seen in the District of Columbia, followed by Idaho and North Dakota at 10% and Arkansas, New Mexico, and West Virginia at 9%, the researchers reported.
After several years of decline, the incidence of preterm births in the United States “is on the rise again,” according to the National Center for Health Statistics.
That 3% increase was spread pretty evenly: 23 states and the District of Columbia experienced statistically significant increases from 2014 to 2016, and 22 other states also had increases, although these were not statistically significant. One state, Iowa, had no change; three states – Montana, New Hampshire, and Pennsylvania – had nonsignificant declines, and Wyoming was the only state with a statistically significant drop (16%) in preterm birth incidence, they said based on data from the National Vital Statistics System.
The largest increase, 12%, was seen in the District of Columbia, followed by Idaho and North Dakota at 10% and Arkansas, New Mexico, and West Virginia at 9%, the researchers reported.
After several years of decline, the incidence of preterm births in the United States “is on the rise again,” according to the National Center for Health Statistics.
That 3% increase was spread pretty evenly: 23 states and the District of Columbia experienced statistically significant increases from 2014 to 2016, and 22 other states also had increases, although these were not statistically significant. One state, Iowa, had no change; three states – Montana, New Hampshire, and Pennsylvania – had nonsignificant declines, and Wyoming was the only state with a statistically significant drop (16%) in preterm birth incidence, they said based on data from the National Vital Statistics System.
The largest increase, 12%, was seen in the District of Columbia, followed by Idaho and North Dakota at 10% and Arkansas, New Mexico, and West Virginia at 9%, the researchers reported.