User login
Skip ultrasound in acute UTI in small children
MALMO, SWEDEN – Ultrasound of the kidneys and urinary tract in the acute phase of a first urinary tract infection in young children has an unacceptably high false-positive rate, Magdalena Okarska-Napierala, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.

“Sonography performed 2 weeks after treatment initiation seems to be more reliable,” said Dr. Okarska-Napierala, a pediatrician at the Medical University of Warsaw Children’s Hospital.
Broad agreement exists that imaging is warranted in all children with a first urinary tract infection (UTI), because this infection can be the first signal of a structural abnormality of the kidneys or urinary tract. Abdominal ultrasound is the first-choice imaging modality in this setting because it is noninvasive, widely available, and inexpensive. But there remains controversy – and guidelines differ – regarding when to perform the ultrasound in children with UTI who respond well to therapy. This was the impetus for Dr. Okarska-Napierala and her coinvestigators to launch a prospective, single-center study examining the issue.
“The theory beneath it is the possibility that diffuse inflammation affects the ultrasound picture of the kidneys and urinary tract and may give us false-positive results, so we shouldn’t base our decisions on those results,” she explained.
This theory has been provisionally confirmed by the preliminary results of the study, which is continuing to enroll patients.
To date, the study includes 48 children, mean age 10.4 months, hospitalized for their first UTI. Participation was restricted to patients with no known congenital abnormalities of the kidneys or urinary tract and who were not on antibiotics at enrollment. Of the 48 children, 44 had an Escherichia coli infection. The predominant treatment was a second-generation cephalosporin for a median of 10 days.
On day 1 of treatment all patients underwent an ultrasound exam evaluating kidney size, anterior-posterior renal pelvis diameter, and the urinary tract based upon a grading system for urinary tract dilation developed by multidisciplinary consensus (J Pediatr Urol. 2014 Dec;10[6]:982-98). The ultrasound exam was repeated 2 weeks later, and again 2 weeks after that.
The most striking findings were a significantly increased kidney size and more prevalent urinary tract dilation on the day 1 ultrasound exam than on repeat ultrasound 2 weeks later. The average length of the left and right kidneys was 67.0 and 64.5 mm, respectively, on day 1, dropping off to 64.3 and 62.0 mm at 2 weeks, with a smaller and statistically nonsignificant further drop-off to 61.9 and 60.0 mm on the week 4 ultrasound.
“We saw a strong correlation between initial kidney size and CRP [C-reactive protein] value: The higher the CRP you have initially, the bigger the kidneys. It’s an interesting finding, but not so very practical. The only practical conclusion is that if we perform ultrasound at this stage and the child has big kidneys, it doesn’t mean anything. We have to check it again later,” she said.
Also, the number of renal units with urinary tract dilation went from 29 on day 1 ultrasound to 20 at 2 weeks and 19 at 4 weeks. Of the 48 children, 28 had urinary tract dilation on day 1, compared with 18 at 2 weeks and 16 at 4 weeks.
“If we look at this practically, if we base our decision on the day 1 ultrasound we would qualify half of all children for voiding cystourethrography, which is harmful, but if we wait 2 weeks to do the ultrasound we would reduce this number by six children. So I think we can call this a clinically significant difference,” she continued.
Of the 48 children, 11 have undergone voiding cystourethrography, revealing 2 mild cases of vesicoureteral reflux, which is the most common congenital abnormality of the urinary tract.
“I would like to emphasize that there is no real benefit in performing an ultrasound exam in children in this acute phase of infection. And there is harm in that we have to repeat the exam later, the parents are worried, the doctor is worried,” Dr. Okarska-Napierala concluded.
She reported having no relevant financial conflicts, and the study was conducted free of commercial support.
MALMO, SWEDEN – Ultrasound of the kidneys and urinary tract in the acute phase of a first urinary tract infection in young children has an unacceptably high false-positive rate, Magdalena Okarska-Napierala, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Sonography performed 2 weeks after treatment initiation seems to be more reliable,” said Dr. Okarska-Napierala, a pediatrician at the Medical University of Warsaw Children’s Hospital.
Broad agreement exists that imaging is warranted in all children with a first urinary tract infection (UTI), because this infection can be the first signal of a structural abnormality of the kidneys or urinary tract. Abdominal ultrasound is the first-choice imaging modality in this setting because it is noninvasive, widely available, and inexpensive. But there remains controversy – and guidelines differ – regarding when to perform the ultrasound in children with UTI who respond well to therapy. This was the impetus for Dr. Okarska-Napierala and her coinvestigators to launch a prospective, single-center study examining the issue.
“The theory beneath it is the possibility that diffuse inflammation affects the ultrasound picture of the kidneys and urinary tract and may give us false-positive results, so we shouldn’t base our decisions on those results,” she explained.
This theory has been provisionally confirmed by the preliminary results of the study, which is continuing to enroll patients.
To date, the study includes 48 children, mean age 10.4 months, hospitalized for their first UTI. Participation was restricted to patients with no known congenital abnormalities of the kidneys or urinary tract and who were not on antibiotics at enrollment. Of the 48 children, 44 had an Escherichia coli infection. The predominant treatment was a second-generation cephalosporin for a median of 10 days.
On day 1 of treatment all patients underwent an ultrasound exam evaluating kidney size, anterior-posterior renal pelvis diameter, and the urinary tract based upon a grading system for urinary tract dilation developed by multidisciplinary consensus (J Pediatr Urol. 2014 Dec;10[6]:982-98). The ultrasound exam was repeated 2 weeks later, and again 2 weeks after that.
The most striking findings were a significantly increased kidney size and more prevalent urinary tract dilation on the day 1 ultrasound exam than on repeat ultrasound 2 weeks later. The average length of the left and right kidneys was 67.0 and 64.5 mm, respectively, on day 1, dropping off to 64.3 and 62.0 mm at 2 weeks, with a smaller and statistically nonsignificant further drop-off to 61.9 and 60.0 mm on the week 4 ultrasound.
“We saw a strong correlation between initial kidney size and CRP [C-reactive protein] value: The higher the CRP you have initially, the bigger the kidneys. It’s an interesting finding, but not so very practical. The only practical conclusion is that if we perform ultrasound at this stage and the child has big kidneys, it doesn’t mean anything. We have to check it again later,” she said.
Also, the number of renal units with urinary tract dilation went from 29 on day 1 ultrasound to 20 at 2 weeks and 19 at 4 weeks. Of the 48 children, 28 had urinary tract dilation on day 1, compared with 18 at 2 weeks and 16 at 4 weeks.
“If we look at this practically, if we base our decision on the day 1 ultrasound we would qualify half of all children for voiding cystourethrography, which is harmful, but if we wait 2 weeks to do the ultrasound we would reduce this number by six children. So I think we can call this a clinically significant difference,” she continued.
Of the 48 children, 11 have undergone voiding cystourethrography, revealing 2 mild cases of vesicoureteral reflux, which is the most common congenital abnormality of the urinary tract.
“I would like to emphasize that there is no real benefit in performing an ultrasound exam in children in this acute phase of infection. And there is harm in that we have to repeat the exam later, the parents are worried, the doctor is worried,” Dr. Okarska-Napierala concluded.
She reported having no relevant financial conflicts, and the study was conducted free of commercial support.
MALMO, SWEDEN – Ultrasound of the kidneys and urinary tract in the acute phase of a first urinary tract infection in young children has an unacceptably high false-positive rate, Magdalena Okarska-Napierala, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Sonography performed 2 weeks after treatment initiation seems to be more reliable,” said Dr. Okarska-Napierala, a pediatrician at the Medical University of Warsaw Children’s Hospital.
Broad agreement exists that imaging is warranted in all children with a first urinary tract infection (UTI), because this infection can be the first signal of a structural abnormality of the kidneys or urinary tract. Abdominal ultrasound is the first-choice imaging modality in this setting because it is noninvasive, widely available, and inexpensive. But there remains controversy – and guidelines differ – regarding when to perform the ultrasound in children with UTI who respond well to therapy. This was the impetus for Dr. Okarska-Napierala and her coinvestigators to launch a prospective, single-center study examining the issue.
“The theory beneath it is the possibility that diffuse inflammation affects the ultrasound picture of the kidneys and urinary tract and may give us false-positive results, so we shouldn’t base our decisions on those results,” she explained.
This theory has been provisionally confirmed by the preliminary results of the study, which is continuing to enroll patients.
To date, the study includes 48 children, mean age 10.4 months, hospitalized for their first UTI. Participation was restricted to patients with no known congenital abnormalities of the kidneys or urinary tract and who were not on antibiotics at enrollment. Of the 48 children, 44 had an Escherichia coli infection. The predominant treatment was a second-generation cephalosporin for a median of 10 days.
On day 1 of treatment all patients underwent an ultrasound exam evaluating kidney size, anterior-posterior renal pelvis diameter, and the urinary tract based upon a grading system for urinary tract dilation developed by multidisciplinary consensus (J Pediatr Urol. 2014 Dec;10[6]:982-98). The ultrasound exam was repeated 2 weeks later, and again 2 weeks after that.
The most striking findings were a significantly increased kidney size and more prevalent urinary tract dilation on the day 1 ultrasound exam than on repeat ultrasound 2 weeks later. The average length of the left and right kidneys was 67.0 and 64.5 mm, respectively, on day 1, dropping off to 64.3 and 62.0 mm at 2 weeks, with a smaller and statistically nonsignificant further drop-off to 61.9 and 60.0 mm on the week 4 ultrasound.
“We saw a strong correlation between initial kidney size and CRP [C-reactive protein] value: The higher the CRP you have initially, the bigger the kidneys. It’s an interesting finding, but not so very practical. The only practical conclusion is that if we perform ultrasound at this stage and the child has big kidneys, it doesn’t mean anything. We have to check it again later,” she said.
Also, the number of renal units with urinary tract dilation went from 29 on day 1 ultrasound to 20 at 2 weeks and 19 at 4 weeks. Of the 48 children, 28 had urinary tract dilation on day 1, compared with 18 at 2 weeks and 16 at 4 weeks.
“If we look at this practically, if we base our decision on the day 1 ultrasound we would qualify half of all children for voiding cystourethrography, which is harmful, but if we wait 2 weeks to do the ultrasound we would reduce this number by six children. So I think we can call this a clinically significant difference,” she continued.
Of the 48 children, 11 have undergone voiding cystourethrography, revealing 2 mild cases of vesicoureteral reflux, which is the most common congenital abnormality of the urinary tract.
“I would like to emphasize that there is no real benefit in performing an ultrasound exam in children in this acute phase of infection. And there is harm in that we have to repeat the exam later, the parents are worried, the doctor is worried,” Dr. Okarska-Napierala concluded.
She reported having no relevant financial conflicts, and the study was conducted free of commercial support.
REPORTING FROM ESPID 2018
Key clinical point:
Major finding: Average left kidney length dropped from 67.0 mm on treatment day 1 to 64.3 mm 2 weeks later.
Study details: This interim report from an ongoing, prospective, single-center study included 48 children up to age 3 years who were hospitalized for their first urinary tract infection.
Disclosures: The presenter reported no relevant financial conflicts.
Reducing risk of febrile convulsion after first dose of MMRV
MALMO, SWEDEN – Giving a combined MMR vaccine and a varicella vaccine separately on the same day in children with personal or family history of febrile convulsions while utilizing the more convenient MMRV vaccine in those without such a history showed promise as a means of reducing the overall risk of febrile convulsions attributable to vaccination, Corinne Willame said at the annual meeting of the European Society for Paediatric Infectious Diseases.

She presented a post hoc analysis of an enormous, German observational study that demonstrated an increased risk of hospitalization for febrile convulsions 5-12 days after receiving the first dose of the Priorix-Tetra MMRV vaccine, with no alternative plausible cause of the convulsions (Vaccine. 2014 Feb 3;32[6]:645-50).
The original study was conducted in more than 180,000 children under the age of 5 years, 90% of whom were 11- 23 months. The increased risk associated with MMRV, compared with MMR alone or MMR plus V separately on the same day, was similar in magnitude to what had previously been reported for the ProQuad MMRV vaccine, suggesting a class effect for the quadrivalent vaccines.
Because genetic predisposition is known to be associated with increased risk of febrile convulsions, Ms. Willame of GlaxoSmithKline in Wavre, Belgium, and her coinvestigators conducted an exploratory analysis investigating whether the presence of a personal or first-degree family history of febrile convulsions impacted the risk of developing febrile convulsions following a first dose of MMRV, compared with MMR alone or MMR and V administered separately on the same day. They found that indeed it did, according to Ms. Willame.
They analyzed the data in multiple ways. The first scenario compared the risk of febrile convulsions in 74,631 children 5-12 days after receiving the MMRV vaccine with a roughly equal number of children who received the MMR vaccine. Study subjects were matched for age, sex, month of vaccination, and insurance provider. The febrile convulsion incidence rate was 6.03 cases per 10,000 children in MMRV recipients and 2.55 per 10,000 in those who got MMR. Then they reanalyzed the data after subtracting all children with a baseline personal history of febrile convulsions from the pool of MMRV recipients: The febrile convulsion rate in the MMRV group dropped to 5.27 cases per 10,000.
Next, they did the same analysis in more than 64,000 matched children who got either MMRV or MMR plus V separately. For the whole cohort of MMRV recipients, the febrile convulsion rate was 6.53 cases per 10,000 vaccine recipients, dropping to 5.95 per 10,000 if children with a personal history of febrile convulsions were removed. The relative risk of febrile convulsions was 150% greater in the overall MMRV group than with MMR plus V, but only 58% greater when the children with a personal history of febrile seizures were excluded from the MMRV population.
Unfortunately, the parent study didn’t record whether a history of febrile convulsions was present in first-degree family members. The investigators therefore turned to the published literature on the subject and constructed conditional probability analyses based upon a 20%-40% likelihood of a positive family history in children with a personal history, and a 5% likelihood in those children without such a history. In this scenario, when children with a personal or hypothetical family history of febrile convulsions were subtracted from the MMRV group, the result was a febrile convulsion incidence rate of 3.27-4.41 cases per 10,000 MMRV recipients in the comparison with MMR and 3.63-4.95 per 10,000 in the comparison with MMR plus V.
Ms. Willame emphasized that her analysis must be considered hypothesis generating because it’s post hoc and relies upon published estimates of the prevalence of a positive family history of febrile convulsions. The febrile convulsion risk differences she found with the different vaccination strategies should be confirmed in studies that collect family history data of febrile seizures at an individual level.
Her study was funded by her employer, GlaxoSmithKline.
MALMO, SWEDEN – Giving a combined MMR vaccine and a varicella vaccine separately on the same day in children with personal or family history of febrile convulsions while utilizing the more convenient MMRV vaccine in those without such a history showed promise as a means of reducing the overall risk of febrile convulsions attributable to vaccination, Corinne Willame said at the annual meeting of the European Society for Paediatric Infectious Diseases.
She presented a post hoc analysis of an enormous, German observational study that demonstrated an increased risk of hospitalization for febrile convulsions 5-12 days after receiving the first dose of the Priorix-Tetra MMRV vaccine, with no alternative plausible cause of the convulsions (Vaccine. 2014 Feb 3;32[6]:645-50).
The original study was conducted in more than 180,000 children under the age of 5 years, 90% of whom were 11- 23 months. The increased risk associated with MMRV, compared with MMR alone or MMR plus V separately on the same day, was similar in magnitude to what had previously been reported for the ProQuad MMRV vaccine, suggesting a class effect for the quadrivalent vaccines.
Because genetic predisposition is known to be associated with increased risk of febrile convulsions, Ms. Willame of GlaxoSmithKline in Wavre, Belgium, and her coinvestigators conducted an exploratory analysis investigating whether the presence of a personal or first-degree family history of febrile convulsions impacted the risk of developing febrile convulsions following a first dose of MMRV, compared with MMR alone or MMR and V administered separately on the same day. They found that indeed it did, according to Ms. Willame.
They analyzed the data in multiple ways. The first scenario compared the risk of febrile convulsions in 74,631 children 5-12 days after receiving the MMRV vaccine with a roughly equal number of children who received the MMR vaccine. Study subjects were matched for age, sex, month of vaccination, and insurance provider. The febrile convulsion incidence rate was 6.03 cases per 10,000 children in MMRV recipients and 2.55 per 10,000 in those who got MMR. Then they reanalyzed the data after subtracting all children with a baseline personal history of febrile convulsions from the pool of MMRV recipients: The febrile convulsion rate in the MMRV group dropped to 5.27 cases per 10,000.
Next, they did the same analysis in more than 64,000 matched children who got either MMRV or MMR plus V separately. For the whole cohort of MMRV recipients, the febrile convulsion rate was 6.53 cases per 10,000 vaccine recipients, dropping to 5.95 per 10,000 if children with a personal history of febrile convulsions were removed. The relative risk of febrile convulsions was 150% greater in the overall MMRV group than with MMR plus V, but only 58% greater when the children with a personal history of febrile seizures were excluded from the MMRV population.
Unfortunately, the parent study didn’t record whether a history of febrile convulsions was present in first-degree family members. The investigators therefore turned to the published literature on the subject and constructed conditional probability analyses based upon a 20%-40% likelihood of a positive family history in children with a personal history, and a 5% likelihood in those children without such a history. In this scenario, when children with a personal or hypothetical family history of febrile convulsions were subtracted from the MMRV group, the result was a febrile convulsion incidence rate of 3.27-4.41 cases per 10,000 MMRV recipients in the comparison with MMR and 3.63-4.95 per 10,000 in the comparison with MMR plus V.
Ms. Willame emphasized that her analysis must be considered hypothesis generating because it’s post hoc and relies upon published estimates of the prevalence of a positive family history of febrile convulsions. The febrile convulsion risk differences she found with the different vaccination strategies should be confirmed in studies that collect family history data of febrile seizures at an individual level.
Her study was funded by her employer, GlaxoSmithKline.
MALMO, SWEDEN – Giving a combined MMR vaccine and a varicella vaccine separately on the same day in children with personal or family history of febrile convulsions while utilizing the more convenient MMRV vaccine in those without such a history showed promise as a means of reducing the overall risk of febrile convulsions attributable to vaccination, Corinne Willame said at the annual meeting of the European Society for Paediatric Infectious Diseases.
She presented a post hoc analysis of an enormous, German observational study that demonstrated an increased risk of hospitalization for febrile convulsions 5-12 days after receiving the first dose of the Priorix-Tetra MMRV vaccine, with no alternative plausible cause of the convulsions (Vaccine. 2014 Feb 3;32[6]:645-50).
The original study was conducted in more than 180,000 children under the age of 5 years, 90% of whom were 11- 23 months. The increased risk associated with MMRV, compared with MMR alone or MMR plus V separately on the same day, was similar in magnitude to what had previously been reported for the ProQuad MMRV vaccine, suggesting a class effect for the quadrivalent vaccines.
Because genetic predisposition is known to be associated with increased risk of febrile convulsions, Ms. Willame of GlaxoSmithKline in Wavre, Belgium, and her coinvestigators conducted an exploratory analysis investigating whether the presence of a personal or first-degree family history of febrile convulsions impacted the risk of developing febrile convulsions following a first dose of MMRV, compared with MMR alone or MMR and V administered separately on the same day. They found that indeed it did, according to Ms. Willame.
They analyzed the data in multiple ways. The first scenario compared the risk of febrile convulsions in 74,631 children 5-12 days after receiving the MMRV vaccine with a roughly equal number of children who received the MMR vaccine. Study subjects were matched for age, sex, month of vaccination, and insurance provider. The febrile convulsion incidence rate was 6.03 cases per 10,000 children in MMRV recipients and 2.55 per 10,000 in those who got MMR. Then they reanalyzed the data after subtracting all children with a baseline personal history of febrile convulsions from the pool of MMRV recipients: The febrile convulsion rate in the MMRV group dropped to 5.27 cases per 10,000.
Next, they did the same analysis in more than 64,000 matched children who got either MMRV or MMR plus V separately. For the whole cohort of MMRV recipients, the febrile convulsion rate was 6.53 cases per 10,000 vaccine recipients, dropping to 5.95 per 10,000 if children with a personal history of febrile convulsions were removed. The relative risk of febrile convulsions was 150% greater in the overall MMRV group than with MMR plus V, but only 58% greater when the children with a personal history of febrile seizures were excluded from the MMRV population.
Unfortunately, the parent study didn’t record whether a history of febrile convulsions was present in first-degree family members. The investigators therefore turned to the published literature on the subject and constructed conditional probability analyses based upon a 20%-40% likelihood of a positive family history in children with a personal history, and a 5% likelihood in those children without such a history. In this scenario, when children with a personal or hypothetical family history of febrile convulsions were subtracted from the MMRV group, the result was a febrile convulsion incidence rate of 3.27-4.41 cases per 10,000 MMRV recipients in the comparison with MMR and 3.63-4.95 per 10,000 in the comparison with MMR plus V.
Ms. Willame emphasized that her analysis must be considered hypothesis generating because it’s post hoc and relies upon published estimates of the prevalence of a positive family history of febrile convulsions. The febrile convulsion risk differences she found with the different vaccination strategies should be confirmed in studies that collect family history data of febrile seizures at an individual level.
Her study was funded by her employer, GlaxoSmithKline.
REPORTING FROM ESPID 2018
Key clinical point: The increased risk of febrile seizures associated with MMRV vaccine can probably be reduced by administering the MMR and varicella vaccines separately on the same day in children with a personal or family history of febrile seizures.
Major finding: The incidence rate of febrile seizures 5-12 days post MMRV vaccination was reduced from 6.53 to 3.63-4.95 cases per 10,000 vaccine recipients.
Study details: This was a post hoc analysis of an observational study of more than 180,000 German children.
Disclosures: The study was sponsored by GlaxoSmithKline and presented by a company employee.
Pediatric appendectomy fast track reduced LoS, narcotic use
Orlando – A significantly reduced length of stay and improved other measures of quality care, according to results from a recent single-center quality improvement project.
After implementation of the multidisciplinary clinical pathway, postoperative narcotic use decreased, while use of a standard antibiotic regimen increased, said Angela M. Kao, MD, a surgical resident with Carolinas Medical Center, Charlotte, N.C.
Of the patients treated according to the fast-track pathway, 90% were discharged within 8 hours of surgery or immediately after morning rounds with no increase in complications or readmissions, said Dr. Kao, who was named the Trainee Abstract Competition Winner based on this research presented at the American College of Surgeons Quality and Safety Conference.
While same-day discharge after laparoscopic appendectomy is safe for most children with nonperforated acute appendicitis, there is wide variability in its perioperative management, Dr. Kao said in an oral abstract presentation.
“At our institution, we noted that no standardized protocol existed for patients with noncomplicated appendicitis, leading to wide variations in postoperative length of stay,” she said.
In addition, preoperative antibiotics and postoperative pain regimens were largely based on provider preference, she added.
Accordingly, a multidisciplinary team used information from the American College of Surgeons National Surgical Quality Improvement Program Pediatric (NSQIP-P) to identify areas for improvement, including multimodal analgesia, standardization of antibiotics, early mobilization, and discharge initiated by nursing.
They also created a designated pre- and postoperative unit staffed by nurses trained in ERAS (Enhanced Recovery After Surgery), which greatly facilitated the goals of the project, Dr. Kao and her coauthors said.
The study results included 61 patients with noncomplicated acute appendicitis who underwent laparoscopic appendectomy after implementation of the fast-track pathway initiative. They were compared with a historical cohort of 58 patients treated in the year leading up to implementation of the pathway.
Dr. Kao and her colleagues found that 87% of fast-track patients received the standard recommended dosing of a third-generation cephalosporin and metronidazole, compared with just 13.8% among those in the period before the fast track’s implementation. In addition, duplicate antibiotic dosing was seen in 6.6% of cases, down from 49%.
Postoperative nausea was minimal, with 9% of fast-tracked patients requiring antiemetic, down from 18.9% in the previous period.
Postoperative IV narcotic use decreased from 86% to 54% because of the use of multimodal analgesia, Dr. Kao added.
Total hospital length of stay decreased 43% to a mean of 16 hours, and the postoperative length of stay decreased by 60% to a mean of 8 hours with no differences in complications or readmission, compared with the period before the fast track’s implementation, according to Dr. Kao.
Almost all of the fast-track patients (90.2%) were discharged within 8 hours or, in the case of procedures performed between midnight and 7 a.m., discharged immediately after morning rounds, according to data presented by the investigators.
“At our institution, a transition from patients discharged by the surgical team to nursing-initiated recovery and discharge was a key component,” Dr. Kao said at the meeting. “Earlier discharge was largely facilitated by nursing-initiated discharge, which allowed for more frequent evaluation of discharge readiness, compared to surgeon providers.”
Dr. Kao had no disclosures relevant to her presentation.
Orlando – A significantly reduced length of stay and improved other measures of quality care, according to results from a recent single-center quality improvement project.
After implementation of the multidisciplinary clinical pathway, postoperative narcotic use decreased, while use of a standard antibiotic regimen increased, said Angela M. Kao, MD, a surgical resident with Carolinas Medical Center, Charlotte, N.C.
Of the patients treated according to the fast-track pathway, 90% were discharged within 8 hours of surgery or immediately after morning rounds with no increase in complications or readmissions, said Dr. Kao, who was named the Trainee Abstract Competition Winner based on this research presented at the American College of Surgeons Quality and Safety Conference.
While same-day discharge after laparoscopic appendectomy is safe for most children with nonperforated acute appendicitis, there is wide variability in its perioperative management, Dr. Kao said in an oral abstract presentation.
“At our institution, we noted that no standardized protocol existed for patients with noncomplicated appendicitis, leading to wide variations in postoperative length of stay,” she said.
In addition, preoperative antibiotics and postoperative pain regimens were largely based on provider preference, she added.
Accordingly, a multidisciplinary team used information from the American College of Surgeons National Surgical Quality Improvement Program Pediatric (NSQIP-P) to identify areas for improvement, including multimodal analgesia, standardization of antibiotics, early mobilization, and discharge initiated by nursing.
They also created a designated pre- and postoperative unit staffed by nurses trained in ERAS (Enhanced Recovery After Surgery), which greatly facilitated the goals of the project, Dr. Kao and her coauthors said.
The study results included 61 patients with noncomplicated acute appendicitis who underwent laparoscopic appendectomy after implementation of the fast-track pathway initiative. They were compared with a historical cohort of 58 patients treated in the year leading up to implementation of the pathway.
Dr. Kao and her colleagues found that 87% of fast-track patients received the standard recommended dosing of a third-generation cephalosporin and metronidazole, compared with just 13.8% among those in the period before the fast track’s implementation. In addition, duplicate antibiotic dosing was seen in 6.6% of cases, down from 49%.
Postoperative nausea was minimal, with 9% of fast-tracked patients requiring antiemetic, down from 18.9% in the previous period.
Postoperative IV narcotic use decreased from 86% to 54% because of the use of multimodal analgesia, Dr. Kao added.
Total hospital length of stay decreased 43% to a mean of 16 hours, and the postoperative length of stay decreased by 60% to a mean of 8 hours with no differences in complications or readmission, compared with the period before the fast track’s implementation, according to Dr. Kao.
Almost all of the fast-track patients (90.2%) were discharged within 8 hours or, in the case of procedures performed between midnight and 7 a.m., discharged immediately after morning rounds, according to data presented by the investigators.
“At our institution, a transition from patients discharged by the surgical team to nursing-initiated recovery and discharge was a key component,” Dr. Kao said at the meeting. “Earlier discharge was largely facilitated by nursing-initiated discharge, which allowed for more frequent evaluation of discharge readiness, compared to surgeon providers.”
Dr. Kao had no disclosures relevant to her presentation.
Orlando – A significantly reduced length of stay and improved other measures of quality care, according to results from a recent single-center quality improvement project.
After implementation of the multidisciplinary clinical pathway, postoperative narcotic use decreased, while use of a standard antibiotic regimen increased, said Angela M. Kao, MD, a surgical resident with Carolinas Medical Center, Charlotte, N.C.
Of the patients treated according to the fast-track pathway, 90% were discharged within 8 hours of surgery or immediately after morning rounds with no increase in complications or readmissions, said Dr. Kao, who was named the Trainee Abstract Competition Winner based on this research presented at the American College of Surgeons Quality and Safety Conference.
While same-day discharge after laparoscopic appendectomy is safe for most children with nonperforated acute appendicitis, there is wide variability in its perioperative management, Dr. Kao said in an oral abstract presentation.
“At our institution, we noted that no standardized protocol existed for patients with noncomplicated appendicitis, leading to wide variations in postoperative length of stay,” she said.
In addition, preoperative antibiotics and postoperative pain regimens were largely based on provider preference, she added.
Accordingly, a multidisciplinary team used information from the American College of Surgeons National Surgical Quality Improvement Program Pediatric (NSQIP-P) to identify areas for improvement, including multimodal analgesia, standardization of antibiotics, early mobilization, and discharge initiated by nursing.
They also created a designated pre- and postoperative unit staffed by nurses trained in ERAS (Enhanced Recovery After Surgery), which greatly facilitated the goals of the project, Dr. Kao and her coauthors said.
The study results included 61 patients with noncomplicated acute appendicitis who underwent laparoscopic appendectomy after implementation of the fast-track pathway initiative. They were compared with a historical cohort of 58 patients treated in the year leading up to implementation of the pathway.
Dr. Kao and her colleagues found that 87% of fast-track patients received the standard recommended dosing of a third-generation cephalosporin and metronidazole, compared with just 13.8% among those in the period before the fast track’s implementation. In addition, duplicate antibiotic dosing was seen in 6.6% of cases, down from 49%.
Postoperative nausea was minimal, with 9% of fast-tracked patients requiring antiemetic, down from 18.9% in the previous period.
Postoperative IV narcotic use decreased from 86% to 54% because of the use of multimodal analgesia, Dr. Kao added.
Total hospital length of stay decreased 43% to a mean of 16 hours, and the postoperative length of stay decreased by 60% to a mean of 8 hours with no differences in complications or readmission, compared with the period before the fast track’s implementation, according to Dr. Kao.
Almost all of the fast-track patients (90.2%) were discharged within 8 hours or, in the case of procedures performed between midnight and 7 a.m., discharged immediately after morning rounds, according to data presented by the investigators.
“At our institution, a transition from patients discharged by the surgical team to nursing-initiated recovery and discharge was a key component,” Dr. Kao said at the meeting. “Earlier discharge was largely facilitated by nursing-initiated discharge, which allowed for more frequent evaluation of discharge readiness, compared to surgeon providers.”
Dr. Kao had no disclosures relevant to her presentation.
REPORTING FROM ACSQSC 2018
Pseudotumor cerebri pediatric rates are rising
Pseudotumor cerebri, benign intracranial hypertension, and idiopathic intracranial hypertension are all terms to describe a syndrome of increased intracranial pressure, headaches, vision loss, or changes without an associated mass lesion.1 The condition was considered relatively rare, presenting most commonly in obese women in childbearing years. Surprisingly, 2

Obesity is the fastest growing morbidity among adolescents. The Centers for Disease Control and Prevention reported 32% of children 2-19 years were obese.1 This reality is impacting many areas of an adolescent’s health, but it also is changing the landscape of diseases that present in this age group. Although pediatric and adult pseudotumor cerebri always have had slightly varied features, many features were similar such as the papilledema, vision loss, headaches, and sixth nerve palsy. Obesity and female predominance tended to present more in the adult population, as many pediatric patients were not obese,2 and had fewer associated symptoms at the time of diagnosis, and the cause was thought to idiopathic.
Now, with the increase in obesity, more adolescents and more male patients are presenting with pseudotumor cerebri as a cause for their headache, and 57%-100% are obese, making it a compounding factor.3
Pediatric populations also are at risk of secondary pseudotumor cerebri, which is an increase in intracranial pressure from the use of medication, or other disease states such as anemia, kidney disease, or Down syndrome. Minocycline use is the most common medication cause and usually presents 1-2 months after normal use.4 Discontinuing the drug does lead to resolution. Retinoids, vitamin A products, growth hormone, and steroids also have been implicated. Given that acne is a common complaint amongst teens, knowledge of these side effects is important.4
In 2013, the criteria for diagnosis of pseudotumor cerebri was revised. Currently, the presence of papilledema, normal neurologic exam except for abnormal sixth cranial nerve, normal cerebral spinal fluid, elevated lumbar opening pressure, and normal imaging are needed for a definitive diagnosis. A probable diagnosis can be made if papilledema is not present but there abducens nerve palsy.2
In a routine physical exam, when I questioned a patient on any medication that was used daily, she replied she took ibuprofen daily for headaches and that she had been doing this for several months. Headaches were not in her chief complaints as she had learned to live with and ignore this symptom. Upon further evaluation, she was slightly overweight and has a questionable fundoscopic exam. After further evaluation by an ophthalmologist and a neurologist, pseudotumor cerebri was diagnosed.
Index of suspicion is key in correctly diagnosing patients, and understanding the changing landscape of medicine will lead to more thoughtful questioning during routine health exams and better outcomes for your patients.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. Am J Ophthalmol. 2015 Feb;159(2):344-52.e1.
2. Horm Res Paediatr. 2014;81(4):217-25.
3. Clin Imaging. 2018 May 24. doi: 10.1016/j.clinimag.2018.05.020.
4. Am J Ophthalmol. 1998 Jul;126(1):116-21.
5. Glob Pediatr Health. 2018. doi:10.1177/2333794X18785550.
Pseudotumor cerebri, benign intracranial hypertension, and idiopathic intracranial hypertension are all terms to describe a syndrome of increased intracranial pressure, headaches, vision loss, or changes without an associated mass lesion.1 The condition was considered relatively rare, presenting most commonly in obese women in childbearing years. Surprisingly, 2
Obesity is the fastest growing morbidity among adolescents. The Centers for Disease Control and Prevention reported 32% of children 2-19 years were obese.1 This reality is impacting many areas of an adolescent’s health, but it also is changing the landscape of diseases that present in this age group. Although pediatric and adult pseudotumor cerebri always have had slightly varied features, many features were similar such as the papilledema, vision loss, headaches, and sixth nerve palsy. Obesity and female predominance tended to present more in the adult population, as many pediatric patients were not obese,2 and had fewer associated symptoms at the time of diagnosis, and the cause was thought to idiopathic.
Now, with the increase in obesity, more adolescents and more male patients are presenting with pseudotumor cerebri as a cause for their headache, and 57%-100% are obese, making it a compounding factor.3
Pediatric populations also are at risk of secondary pseudotumor cerebri, which is an increase in intracranial pressure from the use of medication, or other disease states such as anemia, kidney disease, or Down syndrome. Minocycline use is the most common medication cause and usually presents 1-2 months after normal use.4 Discontinuing the drug does lead to resolution. Retinoids, vitamin A products, growth hormone, and steroids also have been implicated. Given that acne is a common complaint amongst teens, knowledge of these side effects is important.4
In 2013, the criteria for diagnosis of pseudotumor cerebri was revised. Currently, the presence of papilledema, normal neurologic exam except for abnormal sixth cranial nerve, normal cerebral spinal fluid, elevated lumbar opening pressure, and normal imaging are needed for a definitive diagnosis. A probable diagnosis can be made if papilledema is not present but there abducens nerve palsy.2
In a routine physical exam, when I questioned a patient on any medication that was used daily, she replied she took ibuprofen daily for headaches and that she had been doing this for several months. Headaches were not in her chief complaints as she had learned to live with and ignore this symptom. Upon further evaluation, she was slightly overweight and has a questionable fundoscopic exam. After further evaluation by an ophthalmologist and a neurologist, pseudotumor cerebri was diagnosed.
Index of suspicion is key in correctly diagnosing patients, and understanding the changing landscape of medicine will lead to more thoughtful questioning during routine health exams and better outcomes for your patients.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. Am J Ophthalmol. 2015 Feb;159(2):344-52.e1.
2. Horm Res Paediatr. 2014;81(4):217-25.
3. Clin Imaging. 2018 May 24. doi: 10.1016/j.clinimag.2018.05.020.
4. Am J Ophthalmol. 1998 Jul;126(1):116-21.
5. Glob Pediatr Health. 2018. doi:10.1177/2333794X18785550.
Pseudotumor cerebri, benign intracranial hypertension, and idiopathic intracranial hypertension are all terms to describe a syndrome of increased intracranial pressure, headaches, vision loss, or changes without an associated mass lesion.1 The condition was considered relatively rare, presenting most commonly in obese women in childbearing years. Surprisingly, 2
Obesity is the fastest growing morbidity among adolescents. The Centers for Disease Control and Prevention reported 32% of children 2-19 years were obese.1 This reality is impacting many areas of an adolescent’s health, but it also is changing the landscape of diseases that present in this age group. Although pediatric and adult pseudotumor cerebri always have had slightly varied features, many features were similar such as the papilledema, vision loss, headaches, and sixth nerve palsy. Obesity and female predominance tended to present more in the adult population, as many pediatric patients were not obese,2 and had fewer associated symptoms at the time of diagnosis, and the cause was thought to idiopathic.
Now, with the increase in obesity, more adolescents and more male patients are presenting with pseudotumor cerebri as a cause for their headache, and 57%-100% are obese, making it a compounding factor.3
Pediatric populations also are at risk of secondary pseudotumor cerebri, which is an increase in intracranial pressure from the use of medication, or other disease states such as anemia, kidney disease, or Down syndrome. Minocycline use is the most common medication cause and usually presents 1-2 months after normal use.4 Discontinuing the drug does lead to resolution. Retinoids, vitamin A products, growth hormone, and steroids also have been implicated. Given that acne is a common complaint amongst teens, knowledge of these side effects is important.4
In 2013, the criteria for diagnosis of pseudotumor cerebri was revised. Currently, the presence of papilledema, normal neurologic exam except for abnormal sixth cranial nerve, normal cerebral spinal fluid, elevated lumbar opening pressure, and normal imaging are needed for a definitive diagnosis. A probable diagnosis can be made if papilledema is not present but there abducens nerve palsy.2
In a routine physical exam, when I questioned a patient on any medication that was used daily, she replied she took ibuprofen daily for headaches and that she had been doing this for several months. Headaches were not in her chief complaints as she had learned to live with and ignore this symptom. Upon further evaluation, she was slightly overweight and has a questionable fundoscopic exam. After further evaluation by an ophthalmologist and a neurologist, pseudotumor cerebri was diagnosed.
Index of suspicion is key in correctly diagnosing patients, and understanding the changing landscape of medicine will lead to more thoughtful questioning during routine health exams and better outcomes for your patients.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. Am J Ophthalmol. 2015 Feb;159(2):344-52.e1.
2. Horm Res Paediatr. 2014;81(4):217-25.
3. Clin Imaging. 2018 May 24. doi: 10.1016/j.clinimag.2018.05.020.
4. Am J Ophthalmol. 1998 Jul;126(1):116-21.
5. Glob Pediatr Health. 2018. doi:10.1177/2333794X18785550.
New guidance offered for managing poorly controlled asthma in children
published in the Annals of Allergy, Asthma & Immunology.

“Although many children with asthma achieve symptom control with appropriate management, a substantial subset does not,” Bradley E. Chipps, MD, from the Capital Allergy & Respiratory Disease Center in Sacramento, Calif., and his colleagues wrote in the recommendations sponsored by the American College of Allergy, Asthma, and Immunology. “These children should undergo a step-up in care, but when and how to do that is not always straightforward. The Pediatric Asthma Yardstick is a practical resource for starting or adjusting controller therapy based on the options that are currently available for children, from infants to 18 years of age.”
In their recommendations, the authors grouped patients into age ranges of adolescent (12-18 years), school aged (6-11 years), and young children (5 years and under) as well as severity classifications.
Adolescents and school-aged children
For adolescents and school-aged children, step 1 was classified as intermittent asthma that can be controlled with low-dose inhaled corticosteroids (ICS) with short-acting beta2-agonist (SABA) for as-needed relief. Children considered for stepping up to the next therapy should show symptoms of mild persistent asthma that the authors recommended controlling with low-dose ICS, leukotriene receptor antagonist (LTRA), or low-dose theophylline with as-needed SABA.
In children 12-18 years with moderate persistent asthma (step 3), the authors recommended a combination of low-dose ICA and a long-acting beta2-agonist (LABA), while children 6-11 years should receive a medium dose of ICS; other considerations for school-aged children include a medium-high dose of ICS, a low-dose combination of ICS and LTRA, or low-dose ICS together with theophylline.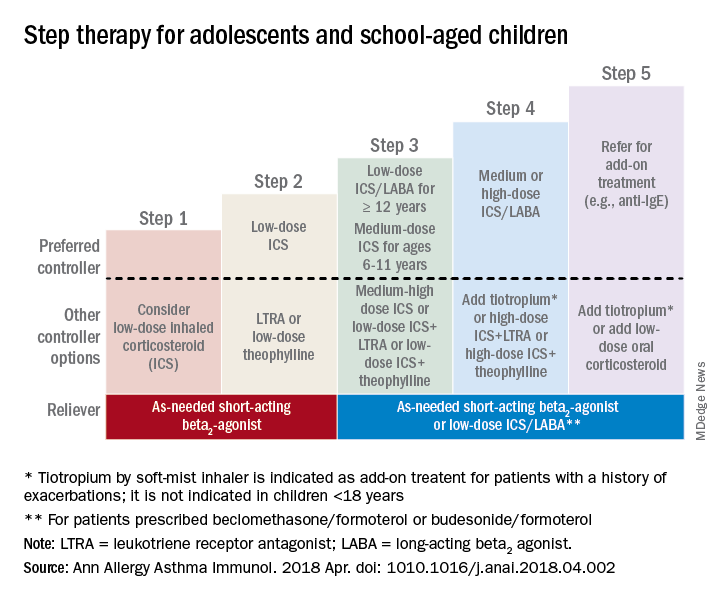
Adolescent or school-aged children with severe persistent asthma (step 4) should take a medium or high dose of ICS together with LABA, with the authors recommending adding tiotropium to a soft mist inhaler, combination high-dose ICS and LTRA, or a combination high-dose ICS and theophylline.
Dr. Chipps and his coauthors recommended children stepping up therapy beyond severe persistent asthma (step 5) should add on treatment such as low-dose oral corticosteroids, anti-immunoglobulin E therapy, and adding tiotropium to a soft-mist inhaler.
For adolescent and school-aged children going to steps 3-5, Dr. Chipps and his coauthors recommended prescribing as needed a short-acting beta2 agonist or low-dose ICS/LABA.
Children 5 years and younger

In children 5 years and younger, intermittent asthma (step 1) should be considered if the child has infrequent or viral wheezing but few or no symptoms in the interim that can be controlled with as-needed SABA. These young children who show symptoms of mild persistent asthma (step 2) can be treated with daily low-dose ICS, with other controller options of LTRA or intermittent ICS.
Stepping up therapy from mild to moderate persistent asthma (step 3), young children should receive double the daily dose of low-dose ICS from the previous step or use the low-dose ICS together with LTRA; if children show symptoms of severe persistent asthma (step 4), they should continue their daily controller and be referred to a specialist; other considerations for controllers at this step included adding LTRA, adding intermittent ICS, or increasing ICS frequency.
Other factors to consider

Inconsistencies in response to medication can occur because of comorbid conditions such as obesity, rhinosinusitis, respiratory infection or gastroesophageal reflux; suboptimal inhaled drug delivery; or failure to comply with treatment because of not wanting to take medication (common in adolescents), belief that even controller medicine can be taken intermittently, family stress, cost including lack of insurance or medication not covered by insurance. “Before adjusting therapy, it is important to ensure that the child’s change in symptoms is due to asthma and not to any of these factors that need to be addressed,” Dr. Chipps and his colleagues wrote.
Collaboration among children, their parents, and clinicians is needed to achieve good asthma control because of the “variable presentation within individuals and within the population of children affected” with asthma, they wrote.
The article summarizing the guidelines was sponsored by the American College of Allergy, Asthma, and Immunology. Most of the authors report various financial relationships with companies including AstraZeneca, Aerocrine, Aviragen, Boehringer Ingelheim, Cephalon, Circassia, Commense, Genentech, GlaxoSmithKline, Greer, Meda, Merck, Mylan, Novartis, Patara, Regeneron, Sanofi, TEVA, Theravance, and Vectura Group. Dr. Farrar and Dr. Szefler had no financial interests to disclose.
SOURCE: Chipps BE et al. Ann Allergy Asthma Immunol. 2018 Apr. doi: 1010.1016/j.anai.2018.04.002.
published in the Annals of Allergy, Asthma & Immunology.
“Although many children with asthma achieve symptom control with appropriate management, a substantial subset does not,” Bradley E. Chipps, MD, from the Capital Allergy & Respiratory Disease Center in Sacramento, Calif., and his colleagues wrote in the recommendations sponsored by the American College of Allergy, Asthma, and Immunology. “These children should undergo a step-up in care, but when and how to do that is not always straightforward. The Pediatric Asthma Yardstick is a practical resource for starting or adjusting controller therapy based on the options that are currently available for children, from infants to 18 years of age.”
In their recommendations, the authors grouped patients into age ranges of adolescent (12-18 years), school aged (6-11 years), and young children (5 years and under) as well as severity classifications.
Adolescents and school-aged children
For adolescents and school-aged children, step 1 was classified as intermittent asthma that can be controlled with low-dose inhaled corticosteroids (ICS) with short-acting beta2-agonist (SABA) for as-needed relief. Children considered for stepping up to the next therapy should show symptoms of mild persistent asthma that the authors recommended controlling with low-dose ICS, leukotriene receptor antagonist (LTRA), or low-dose theophylline with as-needed SABA.
In children 12-18 years with moderate persistent asthma (step 3), the authors recommended a combination of low-dose ICA and a long-acting beta2-agonist (LABA), while children 6-11 years should receive a medium dose of ICS; other considerations for school-aged children include a medium-high dose of ICS, a low-dose combination of ICS and LTRA, or low-dose ICS together with theophylline.
Adolescent or school-aged children with severe persistent asthma (step 4) should take a medium or high dose of ICS together with LABA, with the authors recommending adding tiotropium to a soft mist inhaler, combination high-dose ICS and LTRA, or a combination high-dose ICS and theophylline.
Dr. Chipps and his coauthors recommended children stepping up therapy beyond severe persistent asthma (step 5) should add on treatment such as low-dose oral corticosteroids, anti-immunoglobulin E therapy, and adding tiotropium to a soft-mist inhaler.
For adolescent and school-aged children going to steps 3-5, Dr. Chipps and his coauthors recommended prescribing as needed a short-acting beta2 agonist or low-dose ICS/LABA.
Children 5 years and younger
In children 5 years and younger, intermittent asthma (step 1) should be considered if the child has infrequent or viral wheezing but few or no symptoms in the interim that can be controlled with as-needed SABA. These young children who show symptoms of mild persistent asthma (step 2) can be treated with daily low-dose ICS, with other controller options of LTRA or intermittent ICS.
Stepping up therapy from mild to moderate persistent asthma (step 3), young children should receive double the daily dose of low-dose ICS from the previous step or use the low-dose ICS together with LTRA; if children show symptoms of severe persistent asthma (step 4), they should continue their daily controller and be referred to a specialist; other considerations for controllers at this step included adding LTRA, adding intermittent ICS, or increasing ICS frequency.
Other factors to consider
Inconsistencies in response to medication can occur because of comorbid conditions such as obesity, rhinosinusitis, respiratory infection or gastroesophageal reflux; suboptimal inhaled drug delivery; or failure to comply with treatment because of not wanting to take medication (common in adolescents), belief that even controller medicine can be taken intermittently, family stress, cost including lack of insurance or medication not covered by insurance. “Before adjusting therapy, it is important to ensure that the child’s change in symptoms is due to asthma and not to any of these factors that need to be addressed,” Dr. Chipps and his colleagues wrote.
Collaboration among children, their parents, and clinicians is needed to achieve good asthma control because of the “variable presentation within individuals and within the population of children affected” with asthma, they wrote.
The article summarizing the guidelines was sponsored by the American College of Allergy, Asthma, and Immunology. Most of the authors report various financial relationships with companies including AstraZeneca, Aerocrine, Aviragen, Boehringer Ingelheim, Cephalon, Circassia, Commense, Genentech, GlaxoSmithKline, Greer, Meda, Merck, Mylan, Novartis, Patara, Regeneron, Sanofi, TEVA, Theravance, and Vectura Group. Dr. Farrar and Dr. Szefler had no financial interests to disclose.
SOURCE: Chipps BE et al. Ann Allergy Asthma Immunol. 2018 Apr. doi: 1010.1016/j.anai.2018.04.002.
published in the Annals of Allergy, Asthma & Immunology.
“Although many children with asthma achieve symptom control with appropriate management, a substantial subset does not,” Bradley E. Chipps, MD, from the Capital Allergy & Respiratory Disease Center in Sacramento, Calif., and his colleagues wrote in the recommendations sponsored by the American College of Allergy, Asthma, and Immunology. “These children should undergo a step-up in care, but when and how to do that is not always straightforward. The Pediatric Asthma Yardstick is a practical resource for starting or adjusting controller therapy based on the options that are currently available for children, from infants to 18 years of age.”
In their recommendations, the authors grouped patients into age ranges of adolescent (12-18 years), school aged (6-11 years), and young children (5 years and under) as well as severity classifications.
Adolescents and school-aged children
For adolescents and school-aged children, step 1 was classified as intermittent asthma that can be controlled with low-dose inhaled corticosteroids (ICS) with short-acting beta2-agonist (SABA) for as-needed relief. Children considered for stepping up to the next therapy should show symptoms of mild persistent asthma that the authors recommended controlling with low-dose ICS, leukotriene receptor antagonist (LTRA), or low-dose theophylline with as-needed SABA.
In children 12-18 years with moderate persistent asthma (step 3), the authors recommended a combination of low-dose ICA and a long-acting beta2-agonist (LABA), while children 6-11 years should receive a medium dose of ICS; other considerations for school-aged children include a medium-high dose of ICS, a low-dose combination of ICS and LTRA, or low-dose ICS together with theophylline.
Adolescent or school-aged children with severe persistent asthma (step 4) should take a medium or high dose of ICS together with LABA, with the authors recommending adding tiotropium to a soft mist inhaler, combination high-dose ICS and LTRA, or a combination high-dose ICS and theophylline.
Dr. Chipps and his coauthors recommended children stepping up therapy beyond severe persistent asthma (step 5) should add on treatment such as low-dose oral corticosteroids, anti-immunoglobulin E therapy, and adding tiotropium to a soft-mist inhaler.
For adolescent and school-aged children going to steps 3-5, Dr. Chipps and his coauthors recommended prescribing as needed a short-acting beta2 agonist or low-dose ICS/LABA.
Children 5 years and younger
In children 5 years and younger, intermittent asthma (step 1) should be considered if the child has infrequent or viral wheezing but few or no symptoms in the interim that can be controlled with as-needed SABA. These young children who show symptoms of mild persistent asthma (step 2) can be treated with daily low-dose ICS, with other controller options of LTRA or intermittent ICS.
Stepping up therapy from mild to moderate persistent asthma (step 3), young children should receive double the daily dose of low-dose ICS from the previous step or use the low-dose ICS together with LTRA; if children show symptoms of severe persistent asthma (step 4), they should continue their daily controller and be referred to a specialist; other considerations for controllers at this step included adding LTRA, adding intermittent ICS, or increasing ICS frequency.
Other factors to consider
Inconsistencies in response to medication can occur because of comorbid conditions such as obesity, rhinosinusitis, respiratory infection or gastroesophageal reflux; suboptimal inhaled drug delivery; or failure to comply with treatment because of not wanting to take medication (common in adolescents), belief that even controller medicine can be taken intermittently, family stress, cost including lack of insurance or medication not covered by insurance. “Before adjusting therapy, it is important to ensure that the child’s change in symptoms is due to asthma and not to any of these factors that need to be addressed,” Dr. Chipps and his colleagues wrote.
Collaboration among children, their parents, and clinicians is needed to achieve good asthma control because of the “variable presentation within individuals and within the population of children affected” with asthma, they wrote.
The article summarizing the guidelines was sponsored by the American College of Allergy, Asthma, and Immunology. Most of the authors report various financial relationships with companies including AstraZeneca, Aerocrine, Aviragen, Boehringer Ingelheim, Cephalon, Circassia, Commense, Genentech, GlaxoSmithKline, Greer, Meda, Merck, Mylan, Novartis, Patara, Regeneron, Sanofi, TEVA, Theravance, and Vectura Group. Dr. Farrar and Dr. Szefler had no financial interests to disclose.
SOURCE: Chipps BE et al. Ann Allergy Asthma Immunol. 2018 Apr. doi: 1010.1016/j.anai.2018.04.002.
FROM ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Early-onset atopic dermatitis linked to elevated risk for seasonal allergies and asthma
LAKE TAHOE, CALIF. – results from a large, retrospective cohort study demonstrated.
“The atopic march is characterized by a progression from atopic dermatitis, usually early in childhood, to subsequent development of allergic rhinitis and asthma, lead study author Joy Wan, MD, said at the annual meeting of the Society for Pediatric Dermatology. “It is thought that the skin acts as the site of primary sensitization through a defective epithelial barrier, which then allows for allergic sensitization to occur in the airways. It is estimated that 30%-60% of AD patients go on to develop asthma and/or allergic rhinitis. However, not all patients complete the so-called atopic march, and this variation in the risk of asthma and allergic rhinitis among AD patients is not very well understood. Better ways to risk stratify these patients are needed.”
One possible explanation for this variation in the risk of atopy in AD patients could be the timing of their dermatitis onset. “We know that atopic dermatitis begins in infancy, but it can start at any age,” said Dr. Wan, who is a fellow in the section of pediatric dermatology at the Children’s Hospital of Philadelphia. “There has been a distinction between early-onset versus late-onset AD. Some past studies have also suggested that there is an increased risk of asthma and allergic rhinitis in children who have early-onset AD before the age of 1 or 2. This suggests that perhaps the model of the atopic march varies between early- and late-onset AD. However, past studies have had several limitations. They’ve often had short durations of follow-up, they’ve only examined narrow ranges of age of onset for AD, and most of them have been designed to primarily evaluate other exposures and outcomes, rather than looking at the timing of AD onset itself.”
For the current study, Dr. Wan and her associates set out to examine the risk of seasonal allergies and asthma among children with AD with respect to the age of AD onset. They used data from the Pediatric Eczema Elective Registry (PEER), an ongoing, prospective U.S. cohort of more than 7,700 children with physician-confirmed AD (JAMA Dermatol. 2014 Jun;150:593-600). All registry participants had used pimecrolimus cream in the past, but children with lymphoproliferative disease were excluded from the registry, as were those with malignancy or those who required the use of systemic immunosuppression.
The researchers evaluated 3,966 subjects in PEER with at least 3 years of follow-up. The exposure of interest was age of AD onset, and they divided patients into three broad age categories: early onset (age 2 years or younger), mid onset (3-7 years), and late onset (8-17 years). Primary outcomes were prevalent seasonal allergies and asthma at the time of registry enrollment, and incident seasonal allergies and asthma during follow-up, assessed via patient surveys every 3 years.
The study population included high proportions of white and black children, and there was a slight predominance of females. The median age at PEER enrollment increased with advancing age of AD onset (5.2 years in the early-onset group vs. 8.2 years in the mid-onset group and 13.1 years in the late-onset group), while the duration of follow-up was fairly similar across the three groups (a median of about 8.3 months). Family history of AD was common across all three groups, while patients in the late-onset group tended to have better control of their AD, compared with their younger counterparts.
At baseline, the prevalence of seasonal allergies was highest among the early-onset group at 74.6%, compared with 69.9% among the mid-onset group and 70.1% among the late-onset group. After adjusting for sex, race, and age at registry enrollment, the relative risk for prevalent seasonal allergies was 9% lower in the mid-onset group (0.91) and 18% lower in the late-onset group (0.82), compared with those in the early-onset group. Next, Dr. Wan and her associates calculated the incidence of seasonal allergies among 1,054 patients who did not have allergies at baseline. The cumulative incidence was highest among the early-onset group (56.1%), followed by the mid-onset group (46.8%), and the late-onset group (30.6%). On adjusted analysis, the relative risk for seasonal allergies among patients who had no allergies at baseline was 18% lower in the mid-onset group (0.82) and 36% lower in the late-onset group (0.64), compared with those in the early-onset group.
In the analysis of asthma risk by age of AD onset, prevalence was highest among patients in the early-onset group at 51.5%, compared with 44.7% among the mid-onset age group and 43% among the late-onset age group. On adjusted analysis, the relative risk for asthma was 15% lower in the mid-onset group (0.85) and 29% lower in the late-onset group (0.71), compared with those in the early-onset group. Meanwhile, the cumulative incidence of asthma among patients without asthma at baseline was also highest in the early-onset group (39.2%), compared with 31.9% in the mid-onset group and 29.9% in the late-onset group.
On adjusted analysis, the relative risk for asthma among this subset of patients was 4% lower in the mid-onset group (0.96) and 8% lower in the late-onset group (0.92), compared with those in the early-onset group, a difference that was not statistically significant. “One possible explanation for this is that asthma tends to develop soon after AD does, and the rates of developing asthma later on, as detected by our study, are nondifferential,” Dr. Wan said. “Another possibility is that the impact of early-onset versus late-onset AD is just different for asthma than it is for seasonal allergies.”
She acknowledged certain limitations of the study, including the risk of misclassification bias and limitations in recall with self-reported data, and the fact that the findings may not be generalizable to all patients with AD.
“Future studies with longer follow-up and studies of adult-onset AD will help extend our findings,” she concluded. “Nevertheless, our findings may inform how we risk stratify patients for AD treatment or atopic march prevention efforts in the future.”
PEER is funded by a grant from Valeant Pharmaceuticals, but Valeant had no role in this study. Dr. Wan reported having no financial disclosures. The study won an award at the meeting for best research presented by a dermatology resident or fellow.
LAKE TAHOE, CALIF. – results from a large, retrospective cohort study demonstrated.
“The atopic march is characterized by a progression from atopic dermatitis, usually early in childhood, to subsequent development of allergic rhinitis and asthma, lead study author Joy Wan, MD, said at the annual meeting of the Society for Pediatric Dermatology. “It is thought that the skin acts as the site of primary sensitization through a defective epithelial barrier, which then allows for allergic sensitization to occur in the airways. It is estimated that 30%-60% of AD patients go on to develop asthma and/or allergic rhinitis. However, not all patients complete the so-called atopic march, and this variation in the risk of asthma and allergic rhinitis among AD patients is not very well understood. Better ways to risk stratify these patients are needed.”
One possible explanation for this variation in the risk of atopy in AD patients could be the timing of their dermatitis onset. “We know that atopic dermatitis begins in infancy, but it can start at any age,” said Dr. Wan, who is a fellow in the section of pediatric dermatology at the Children’s Hospital of Philadelphia. “There has been a distinction between early-onset versus late-onset AD. Some past studies have also suggested that there is an increased risk of asthma and allergic rhinitis in children who have early-onset AD before the age of 1 or 2. This suggests that perhaps the model of the atopic march varies between early- and late-onset AD. However, past studies have had several limitations. They’ve often had short durations of follow-up, they’ve only examined narrow ranges of age of onset for AD, and most of them have been designed to primarily evaluate other exposures and outcomes, rather than looking at the timing of AD onset itself.”
For the current study, Dr. Wan and her associates set out to examine the risk of seasonal allergies and asthma among children with AD with respect to the age of AD onset. They used data from the Pediatric Eczema Elective Registry (PEER), an ongoing, prospective U.S. cohort of more than 7,700 children with physician-confirmed AD (JAMA Dermatol. 2014 Jun;150:593-600). All registry participants had used pimecrolimus cream in the past, but children with lymphoproliferative disease were excluded from the registry, as were those with malignancy or those who required the use of systemic immunosuppression.
The researchers evaluated 3,966 subjects in PEER with at least 3 years of follow-up. The exposure of interest was age of AD onset, and they divided patients into three broad age categories: early onset (age 2 years or younger), mid onset (3-7 years), and late onset (8-17 years). Primary outcomes were prevalent seasonal allergies and asthma at the time of registry enrollment, and incident seasonal allergies and asthma during follow-up, assessed via patient surveys every 3 years.
The study population included high proportions of white and black children, and there was a slight predominance of females. The median age at PEER enrollment increased with advancing age of AD onset (5.2 years in the early-onset group vs. 8.2 years in the mid-onset group and 13.1 years in the late-onset group), while the duration of follow-up was fairly similar across the three groups (a median of about 8.3 months). Family history of AD was common across all three groups, while patients in the late-onset group tended to have better control of their AD, compared with their younger counterparts.
At baseline, the prevalence of seasonal allergies was highest among the early-onset group at 74.6%, compared with 69.9% among the mid-onset group and 70.1% among the late-onset group. After adjusting for sex, race, and age at registry enrollment, the relative risk for prevalent seasonal allergies was 9% lower in the mid-onset group (0.91) and 18% lower in the late-onset group (0.82), compared with those in the early-onset group. Next, Dr. Wan and her associates calculated the incidence of seasonal allergies among 1,054 patients who did not have allergies at baseline. The cumulative incidence was highest among the early-onset group (56.1%), followed by the mid-onset group (46.8%), and the late-onset group (30.6%). On adjusted analysis, the relative risk for seasonal allergies among patients who had no allergies at baseline was 18% lower in the mid-onset group (0.82) and 36% lower in the late-onset group (0.64), compared with those in the early-onset group.
In the analysis of asthma risk by age of AD onset, prevalence was highest among patients in the early-onset group at 51.5%, compared with 44.7% among the mid-onset age group and 43% among the late-onset age group. On adjusted analysis, the relative risk for asthma was 15% lower in the mid-onset group (0.85) and 29% lower in the late-onset group (0.71), compared with those in the early-onset group. Meanwhile, the cumulative incidence of asthma among patients without asthma at baseline was also highest in the early-onset group (39.2%), compared with 31.9% in the mid-onset group and 29.9% in the late-onset group.
On adjusted analysis, the relative risk for asthma among this subset of patients was 4% lower in the mid-onset group (0.96) and 8% lower in the late-onset group (0.92), compared with those in the early-onset group, a difference that was not statistically significant. “One possible explanation for this is that asthma tends to develop soon after AD does, and the rates of developing asthma later on, as detected by our study, are nondifferential,” Dr. Wan said. “Another possibility is that the impact of early-onset versus late-onset AD is just different for asthma than it is for seasonal allergies.”
She acknowledged certain limitations of the study, including the risk of misclassification bias and limitations in recall with self-reported data, and the fact that the findings may not be generalizable to all patients with AD.
“Future studies with longer follow-up and studies of adult-onset AD will help extend our findings,” she concluded. “Nevertheless, our findings may inform how we risk stratify patients for AD treatment or atopic march prevention efforts in the future.”
PEER is funded by a grant from Valeant Pharmaceuticals, but Valeant had no role in this study. Dr. Wan reported having no financial disclosures. The study won an award at the meeting for best research presented by a dermatology resident or fellow.
LAKE TAHOE, CALIF. – results from a large, retrospective cohort study demonstrated.
“The atopic march is characterized by a progression from atopic dermatitis, usually early in childhood, to subsequent development of allergic rhinitis and asthma, lead study author Joy Wan, MD, said at the annual meeting of the Society for Pediatric Dermatology. “It is thought that the skin acts as the site of primary sensitization through a defective epithelial barrier, which then allows for allergic sensitization to occur in the airways. It is estimated that 30%-60% of AD patients go on to develop asthma and/or allergic rhinitis. However, not all patients complete the so-called atopic march, and this variation in the risk of asthma and allergic rhinitis among AD patients is not very well understood. Better ways to risk stratify these patients are needed.”
One possible explanation for this variation in the risk of atopy in AD patients could be the timing of their dermatitis onset. “We know that atopic dermatitis begins in infancy, but it can start at any age,” said Dr. Wan, who is a fellow in the section of pediatric dermatology at the Children’s Hospital of Philadelphia. “There has been a distinction between early-onset versus late-onset AD. Some past studies have also suggested that there is an increased risk of asthma and allergic rhinitis in children who have early-onset AD before the age of 1 or 2. This suggests that perhaps the model of the atopic march varies between early- and late-onset AD. However, past studies have had several limitations. They’ve often had short durations of follow-up, they’ve only examined narrow ranges of age of onset for AD, and most of them have been designed to primarily evaluate other exposures and outcomes, rather than looking at the timing of AD onset itself.”
For the current study, Dr. Wan and her associates set out to examine the risk of seasonal allergies and asthma among children with AD with respect to the age of AD onset. They used data from the Pediatric Eczema Elective Registry (PEER), an ongoing, prospective U.S. cohort of more than 7,700 children with physician-confirmed AD (JAMA Dermatol. 2014 Jun;150:593-600). All registry participants had used pimecrolimus cream in the past, but children with lymphoproliferative disease were excluded from the registry, as were those with malignancy or those who required the use of systemic immunosuppression.
The researchers evaluated 3,966 subjects in PEER with at least 3 years of follow-up. The exposure of interest was age of AD onset, and they divided patients into three broad age categories: early onset (age 2 years or younger), mid onset (3-7 years), and late onset (8-17 years). Primary outcomes were prevalent seasonal allergies and asthma at the time of registry enrollment, and incident seasonal allergies and asthma during follow-up, assessed via patient surveys every 3 years.
The study population included high proportions of white and black children, and there was a slight predominance of females. The median age at PEER enrollment increased with advancing age of AD onset (5.2 years in the early-onset group vs. 8.2 years in the mid-onset group and 13.1 years in the late-onset group), while the duration of follow-up was fairly similar across the three groups (a median of about 8.3 months). Family history of AD was common across all three groups, while patients in the late-onset group tended to have better control of their AD, compared with their younger counterparts.
At baseline, the prevalence of seasonal allergies was highest among the early-onset group at 74.6%, compared with 69.9% among the mid-onset group and 70.1% among the late-onset group. After adjusting for sex, race, and age at registry enrollment, the relative risk for prevalent seasonal allergies was 9% lower in the mid-onset group (0.91) and 18% lower in the late-onset group (0.82), compared with those in the early-onset group. Next, Dr. Wan and her associates calculated the incidence of seasonal allergies among 1,054 patients who did not have allergies at baseline. The cumulative incidence was highest among the early-onset group (56.1%), followed by the mid-onset group (46.8%), and the late-onset group (30.6%). On adjusted analysis, the relative risk for seasonal allergies among patients who had no allergies at baseline was 18% lower in the mid-onset group (0.82) and 36% lower in the late-onset group (0.64), compared with those in the early-onset group.
In the analysis of asthma risk by age of AD onset, prevalence was highest among patients in the early-onset group at 51.5%, compared with 44.7% among the mid-onset age group and 43% among the late-onset age group. On adjusted analysis, the relative risk for asthma was 15% lower in the mid-onset group (0.85) and 29% lower in the late-onset group (0.71), compared with those in the early-onset group. Meanwhile, the cumulative incidence of asthma among patients without asthma at baseline was also highest in the early-onset group (39.2%), compared with 31.9% in the mid-onset group and 29.9% in the late-onset group.
On adjusted analysis, the relative risk for asthma among this subset of patients was 4% lower in the mid-onset group (0.96) and 8% lower in the late-onset group (0.92), compared with those in the early-onset group, a difference that was not statistically significant. “One possible explanation for this is that asthma tends to develop soon after AD does, and the rates of developing asthma later on, as detected by our study, are nondifferential,” Dr. Wan said. “Another possibility is that the impact of early-onset versus late-onset AD is just different for asthma than it is for seasonal allergies.”
She acknowledged certain limitations of the study, including the risk of misclassification bias and limitations in recall with self-reported data, and the fact that the findings may not be generalizable to all patients with AD.
“Future studies with longer follow-up and studies of adult-onset AD will help extend our findings,” she concluded. “Nevertheless, our findings may inform how we risk stratify patients for AD treatment or atopic march prevention efforts in the future.”
PEER is funded by a grant from Valeant Pharmaceuticals, but Valeant had no role in this study. Dr. Wan reported having no financial disclosures. The study won an award at the meeting for best research presented by a dermatology resident or fellow.
AT SPD 2018
Treatments, disease affect spermatogonia in boys

Alkylating agents, hydroxyurea (HU), and certain non-malignant diseases can significantly deplete spermatogonial cell counts in young boys, according to research published in Human Reproduction.
Boys who received alkylating agents to treat cancer had significantly lower spermatogonial cell counts than control subjects or boys with malignant/nonmalignant diseases treated with non-alkylating agents.
Five of 6 SCD patients treated with HU had a totally depleted spermatogonial pool, and the remaining patient had a low spermatogonial cell count.
Five boys with non-malignant diseases who were not exposed to chemotherapy had significantly lower spermatogonial cell counts than controls.
“Our findings of a dramatic decrease in germ cell numbers in boys treated with alkylating agents and in sickle cell disease patients treated with hydroxyurea suggest that storing frozen testicular tissue from these boys should be performed before these treatments are initiated,” said study author Cecilia Petersen, MD, PhD, of Karolinska Institutet and University Hospital in Stockholm, Sweden.
“This needs to be communicated to physicians as well as patients and their parents or carers. However, until sperm that are able to fertilize eggs are produced from stored testicular tissue, we cannot confirm that germ cell quantity might determine the success of transplantation of the tissue in adulthood. Further research on this is needed to establish a realistic fertility preservation technique.”
Dr Petersen and her colleagues also noted that preserving testicular tissue may not be a viable option for boys who have low spermatogonial cell counts prior to treatment.
Patients and controls
For this study, the researchers analyzed testicular tissue from 32 boys facing treatments that carried a high risk of infertility—testicular irradiation, chemotherapy, or radiotherapy in advance of stem cell transplant.
Twenty boys had the tissue taken after initial chemotherapy, and 12 had it taken before starting any treatment.1
Eight patients had received chemotherapy with non-alkylating agents, 6 (all with malignancies) had received alkylating agents, and 6 (all with SCD) had received HU.
Diseases included acute lymphoblastic leukemia (n=6), SCD (n=6), acute myeloid leukemia (n=3), thalassemia major (n=3), neuroblastoma (n=2), juvenile myelomonocytic leukemia (n=2), myelodysplastic syndromes (n=2), primary immunodeficiency (n=2), Wilms tumor (n=1), adrenoleukodystrophy (n=1), hepatoblastoma (n=1), primitive neuroectodermal tumor (n=1), severe aplastic anemia (n=1), and Fanconi anemia (n=1).
The researchers compared samples from these 32 patients to 14 healthy testicular tissue samples stored in the biobank at the Karolinska University Hospital.
For both sample types, the team counted the number of spermatogonial cells found in a cross-section of seminiferous tubules.
“We could compare the number of spermatogonia with those found in the healthy boys as a way to estimate the effect of medical treatment or the disease itself on the future fertility of a patient,” explained study author Jan-Bernd Stukenborg, PhD, of Karolinska Institutet and University Hospital.
Impact of treatment
There was no significant difference in the mean quantity of spermatogonia per transverse tubular cross-section (S/T) between patients exposed to non-alkylating agents (1.7 ± 1.0, n=8) and biobank controls (4.1 ± 4.6, n=14).
However, samples from patients who received alkylating agents had a significantly lower mean S/T value (0.2 ± 0.3, n=6) than samples from patients treated with non-alkylating agents (P=0.003) and biobank controls (P<0.001).
“We found that the numbers of germ cells present in the cross-sections of the seminiferous tubules were significantly depleted and close to 0 in patients treated with alkylating agents,” Dr Stukenborg said.
Samples from the SCD patients also had a significantly lower mean S/T value (0.3 ± 0.6, n=6) than biobank controls (P=0.003).
Dr Stukenborg noted that the germ cell pool was totally depleted in 5 of the boys with SCD, and the pool was “very low” in the sixth SCD patient.
“This was not seen in patients who had not started treatment or were treated with non-alkylating agents or in the biobank tissues,” Dr Stukenborg said.2
He and his colleagues noted that it is possible for germ cells to recover to normal levels after treatment that is highly toxic to the testes, but high doses of alkylating agents and radiotherapy to the testicles are strongly associated with permanent or long-term infertility.
“The first group of boys who received bone marrow transplants are now reaching their thirties,” said study author Kirsi Jahnukainen, MD, PhD, of Helsinki University Central Hospital in Finland.
“Recent data suggest they may have a high chance of their sperm production recovering, even if they received high-dose alkylating therapies, so long as they had no testicular irradiation.”
Impact of disease
The researchers also found evidence to suggest that, for some boys, their disease may have affected spermatogonial cell counts before any treatment began.
Five patients with non-malignant disease who had not been exposed to chemotherapy (3 with thalassemia major, 1 with Fanconi anemia, and 1 with primary immunodeficiency) had a significantly lower mean S/T value (0.4 ± 0.5) than controls (P=0.006).
“Among patients who had not been treated previously with chemotherapy, there were several boys with a low number of germ cells for their age,” Dr Jahnukainen said.
“This suggests that some non-malignant diseases that require bone marrow transplants may affect the fertility of young boys even before exposure to therapy that is toxic for the testes.”
The researchers noted that a limitation of this study was that biobank samples had no detailed information regarding previous medical treatments and testicular volumes.
1. Testicular tissue is taken from patients under general anesthesia. The surgeon removes approximately 20% of the tissue from the testicular capsule in one of the testicles. For this study, a third of the tissue was taken to the Karolinska Institutet for analysis.
2. A recent meta-analysis showed that normal testicular tissue samples of newborns contain approximately 2.5 germ cells per tubular cross-section. This number decreases to approximately 1.2 within the first 3 years of age, followed by an increase up to 2.6 germ cells per tubular cross-section at 6 to 7 years, reaching a plateau until the age of 11. At the onset of puberty, an increase of up to 7 spermatogonia per tubular cross-section could be observed.
Alkylating agents, hydroxyurea (HU), and certain non-malignant diseases can significantly deplete spermatogonial cell counts in young boys, according to research published in Human Reproduction.
Boys who received alkylating agents to treat cancer had significantly lower spermatogonial cell counts than control subjects or boys with malignant/nonmalignant diseases treated with non-alkylating agents.
Five of 6 SCD patients treated with HU had a totally depleted spermatogonial pool, and the remaining patient had a low spermatogonial cell count.
Five boys with non-malignant diseases who were not exposed to chemotherapy had significantly lower spermatogonial cell counts than controls.
“Our findings of a dramatic decrease in germ cell numbers in boys treated with alkylating agents and in sickle cell disease patients treated with hydroxyurea suggest that storing frozen testicular tissue from these boys should be performed before these treatments are initiated,” said study author Cecilia Petersen, MD, PhD, of Karolinska Institutet and University Hospital in Stockholm, Sweden.
“This needs to be communicated to physicians as well as patients and their parents or carers. However, until sperm that are able to fertilize eggs are produced from stored testicular tissue, we cannot confirm that germ cell quantity might determine the success of transplantation of the tissue in adulthood. Further research on this is needed to establish a realistic fertility preservation technique.”
Dr Petersen and her colleagues also noted that preserving testicular tissue may not be a viable option for boys who have low spermatogonial cell counts prior to treatment.
Patients and controls
For this study, the researchers analyzed testicular tissue from 32 boys facing treatments that carried a high risk of infertility—testicular irradiation, chemotherapy, or radiotherapy in advance of stem cell transplant.
Twenty boys had the tissue taken after initial chemotherapy, and 12 had it taken before starting any treatment.1
Eight patients had received chemotherapy with non-alkylating agents, 6 (all with malignancies) had received alkylating agents, and 6 (all with SCD) had received HU.
Diseases included acute lymphoblastic leukemia (n=6), SCD (n=6), acute myeloid leukemia (n=3), thalassemia major (n=3), neuroblastoma (n=2), juvenile myelomonocytic leukemia (n=2), myelodysplastic syndromes (n=2), primary immunodeficiency (n=2), Wilms tumor (n=1), adrenoleukodystrophy (n=1), hepatoblastoma (n=1), primitive neuroectodermal tumor (n=1), severe aplastic anemia (n=1), and Fanconi anemia (n=1).
The researchers compared samples from these 32 patients to 14 healthy testicular tissue samples stored in the biobank at the Karolinska University Hospital.
For both sample types, the team counted the number of spermatogonial cells found in a cross-section of seminiferous tubules.
“We could compare the number of spermatogonia with those found in the healthy boys as a way to estimate the effect of medical treatment or the disease itself on the future fertility of a patient,” explained study author Jan-Bernd Stukenborg, PhD, of Karolinska Institutet and University Hospital.
Impact of treatment
There was no significant difference in the mean quantity of spermatogonia per transverse tubular cross-section (S/T) between patients exposed to non-alkylating agents (1.7 ± 1.0, n=8) and biobank controls (4.1 ± 4.6, n=14).
However, samples from patients who received alkylating agents had a significantly lower mean S/T value (0.2 ± 0.3, n=6) than samples from patients treated with non-alkylating agents (P=0.003) and biobank controls (P<0.001).
“We found that the numbers of germ cells present in the cross-sections of the seminiferous tubules were significantly depleted and close to 0 in patients treated with alkylating agents,” Dr Stukenborg said.
Samples from the SCD patients also had a significantly lower mean S/T value (0.3 ± 0.6, n=6) than biobank controls (P=0.003).
Dr Stukenborg noted that the germ cell pool was totally depleted in 5 of the boys with SCD, and the pool was “very low” in the sixth SCD patient.
“This was not seen in patients who had not started treatment or were treated with non-alkylating agents or in the biobank tissues,” Dr Stukenborg said.2
He and his colleagues noted that it is possible for germ cells to recover to normal levels after treatment that is highly toxic to the testes, but high doses of alkylating agents and radiotherapy to the testicles are strongly associated with permanent or long-term infertility.
“The first group of boys who received bone marrow transplants are now reaching their thirties,” said study author Kirsi Jahnukainen, MD, PhD, of Helsinki University Central Hospital in Finland.
“Recent data suggest they may have a high chance of their sperm production recovering, even if they received high-dose alkylating therapies, so long as they had no testicular irradiation.”
Impact of disease
The researchers also found evidence to suggest that, for some boys, their disease may have affected spermatogonial cell counts before any treatment began.
Five patients with non-malignant disease who had not been exposed to chemotherapy (3 with thalassemia major, 1 with Fanconi anemia, and 1 with primary immunodeficiency) had a significantly lower mean S/T value (0.4 ± 0.5) than controls (P=0.006).
“Among patients who had not been treated previously with chemotherapy, there were several boys with a low number of germ cells for their age,” Dr Jahnukainen said.
“This suggests that some non-malignant diseases that require bone marrow transplants may affect the fertility of young boys even before exposure to therapy that is toxic for the testes.”
The researchers noted that a limitation of this study was that biobank samples had no detailed information regarding previous medical treatments and testicular volumes.
1. Testicular tissue is taken from patients under general anesthesia. The surgeon removes approximately 20% of the tissue from the testicular capsule in one of the testicles. For this study, a third of the tissue was taken to the Karolinska Institutet for analysis.
2. A recent meta-analysis showed that normal testicular tissue samples of newborns contain approximately 2.5 germ cells per tubular cross-section. This number decreases to approximately 1.2 within the first 3 years of age, followed by an increase up to 2.6 germ cells per tubular cross-section at 6 to 7 years, reaching a plateau until the age of 11. At the onset of puberty, an increase of up to 7 spermatogonia per tubular cross-section could be observed.
Alkylating agents, hydroxyurea (HU), and certain non-malignant diseases can significantly deplete spermatogonial cell counts in young boys, according to research published in Human Reproduction.
Boys who received alkylating agents to treat cancer had significantly lower spermatogonial cell counts than control subjects or boys with malignant/nonmalignant diseases treated with non-alkylating agents.
Five of 6 SCD patients treated with HU had a totally depleted spermatogonial pool, and the remaining patient had a low spermatogonial cell count.
Five boys with non-malignant diseases who were not exposed to chemotherapy had significantly lower spermatogonial cell counts than controls.
“Our findings of a dramatic decrease in germ cell numbers in boys treated with alkylating agents and in sickle cell disease patients treated with hydroxyurea suggest that storing frozen testicular tissue from these boys should be performed before these treatments are initiated,” said study author Cecilia Petersen, MD, PhD, of Karolinska Institutet and University Hospital in Stockholm, Sweden.
“This needs to be communicated to physicians as well as patients and their parents or carers. However, until sperm that are able to fertilize eggs are produced from stored testicular tissue, we cannot confirm that germ cell quantity might determine the success of transplantation of the tissue in adulthood. Further research on this is needed to establish a realistic fertility preservation technique.”
Dr Petersen and her colleagues also noted that preserving testicular tissue may not be a viable option for boys who have low spermatogonial cell counts prior to treatment.
Patients and controls
For this study, the researchers analyzed testicular tissue from 32 boys facing treatments that carried a high risk of infertility—testicular irradiation, chemotherapy, or radiotherapy in advance of stem cell transplant.
Twenty boys had the tissue taken after initial chemotherapy, and 12 had it taken before starting any treatment.1
Eight patients had received chemotherapy with non-alkylating agents, 6 (all with malignancies) had received alkylating agents, and 6 (all with SCD) had received HU.
Diseases included acute lymphoblastic leukemia (n=6), SCD (n=6), acute myeloid leukemia (n=3), thalassemia major (n=3), neuroblastoma (n=2), juvenile myelomonocytic leukemia (n=2), myelodysplastic syndromes (n=2), primary immunodeficiency (n=2), Wilms tumor (n=1), adrenoleukodystrophy (n=1), hepatoblastoma (n=1), primitive neuroectodermal tumor (n=1), severe aplastic anemia (n=1), and Fanconi anemia (n=1).
The researchers compared samples from these 32 patients to 14 healthy testicular tissue samples stored in the biobank at the Karolinska University Hospital.
For both sample types, the team counted the number of spermatogonial cells found in a cross-section of seminiferous tubules.
“We could compare the number of spermatogonia with those found in the healthy boys as a way to estimate the effect of medical treatment or the disease itself on the future fertility of a patient,” explained study author Jan-Bernd Stukenborg, PhD, of Karolinska Institutet and University Hospital.
Impact of treatment
There was no significant difference in the mean quantity of spermatogonia per transverse tubular cross-section (S/T) between patients exposed to non-alkylating agents (1.7 ± 1.0, n=8) and biobank controls (4.1 ± 4.6, n=14).
However, samples from patients who received alkylating agents had a significantly lower mean S/T value (0.2 ± 0.3, n=6) than samples from patients treated with non-alkylating agents (P=0.003) and biobank controls (P<0.001).
“We found that the numbers of germ cells present in the cross-sections of the seminiferous tubules were significantly depleted and close to 0 in patients treated with alkylating agents,” Dr Stukenborg said.
Samples from the SCD patients also had a significantly lower mean S/T value (0.3 ± 0.6, n=6) than biobank controls (P=0.003).
Dr Stukenborg noted that the germ cell pool was totally depleted in 5 of the boys with SCD, and the pool was “very low” in the sixth SCD patient.
“This was not seen in patients who had not started treatment or were treated with non-alkylating agents or in the biobank tissues,” Dr Stukenborg said.2
He and his colleagues noted that it is possible for germ cells to recover to normal levels after treatment that is highly toxic to the testes, but high doses of alkylating agents and radiotherapy to the testicles are strongly associated with permanent or long-term infertility.
“The first group of boys who received bone marrow transplants are now reaching their thirties,” said study author Kirsi Jahnukainen, MD, PhD, of Helsinki University Central Hospital in Finland.
“Recent data suggest they may have a high chance of their sperm production recovering, even if they received high-dose alkylating therapies, so long as they had no testicular irradiation.”
Impact of disease
The researchers also found evidence to suggest that, for some boys, their disease may have affected spermatogonial cell counts before any treatment began.
Five patients with non-malignant disease who had not been exposed to chemotherapy (3 with thalassemia major, 1 with Fanconi anemia, and 1 with primary immunodeficiency) had a significantly lower mean S/T value (0.4 ± 0.5) than controls (P=0.006).
“Among patients who had not been treated previously with chemotherapy, there were several boys with a low number of germ cells for their age,” Dr Jahnukainen said.
“This suggests that some non-malignant diseases that require bone marrow transplants may affect the fertility of young boys even before exposure to therapy that is toxic for the testes.”
The researchers noted that a limitation of this study was that biobank samples had no detailed information regarding previous medical treatments and testicular volumes.
1. Testicular tissue is taken from patients under general anesthesia. The surgeon removes approximately 20% of the tissue from the testicular capsule in one of the testicles. For this study, a third of the tissue was taken to the Karolinska Institutet for analysis.
2. A recent meta-analysis showed that normal testicular tissue samples of newborns contain approximately 2.5 germ cells per tubular cross-section. This number decreases to approximately 1.2 within the first 3 years of age, followed by an increase up to 2.6 germ cells per tubular cross-section at 6 to 7 years, reaching a plateau until the age of 11. At the onset of puberty, an increase of up to 7 spermatogonia per tubular cross-section could be observed.
Questions abound about availability, legality of new cannabis-derived epilepsy drug
The first-ever federal approval of a marijuana-derived drug, Epidiolex (cannabidiol), comes with a cloud of complications.

Epidiolex is an oral solution of purified cannabidiol (CBD), a component of the marijuana plant that does not make people high.
According to the results of a phase 3 trial in patients with Lennox-Gastaut syndrome published earlier this year, median monthly drop seizures fell by 43.9% in a Epidiolex group compared with 21.8% in a placebo group (Lancet. 2018;391[10125]:1085-96). A 2017 study found that patients with Dravet syndrome who took the drug had fewer median convulsive seizures per month, dropping from 12.4 to 5.9, while there was barely a difference for the placebo group (N Engl J Med. 2017;376:2011-20). In both trials, patients received Epidiolex as an add-on treatment.
“There definitely are side effects such as sleepiness, abnormal liver function values, and other things that people will have to watch out for, such as interactions with other drugs,” Jacqueline A. French, MD, professor of neurology at New York University and chief scientific officer of the Epilepsy Foundation, said in an interview. “But it will definitely be a great benefit to some and a benefit to many.”
It’s not clear how the drug works, she said.
Greenwich Biosciences, the U.S. subsidiary of British drug maker GW Pharmaceuticals, plans to market Epidiolex this fall, spokesman Steve Schultz said in an interview. First, however, the U.S. Drug Enforcement Agency must reschedule the drug so it doesn’t fall under federal antimarijuana laws. It has 90 days after the FDA approval to do so, and its rescheduling is expected.
Then the focus will turn to the states, which have a crazy quilt of laws about marijuana and its medical use. “We’ve worked with the state legislators to enact laws or to modify laws to allow for our medicine to be made available,” Mr. Schultz said. “There may be one or two that we’re still working on.”
At issue: States and the District of Columbia have a wide variety of laws that appear to affect the sale of Epidiolex.
According to the website procon.org, 30 states and the District of Columbia allow medical marijuana, although the laws vary regarding what is allowed and do not address cannabis-derived pharmaceuticals.
Another 17 states have laws that address CBD specifically, often with language that allows its use to treat epilepsy in all or specific cases, according to procon.org.

In Oklahoma, an anticannabis law excludes “from the definition of marijuana ‘any federal Food and Drug Administration–approved cannabidiol drug or substance.’ ”
North Carolina attorney Rod Kight, who represents businesses in the cannabis industry, predicts that “once the federal government [via the DEA] changes the law, the states will fall in line. The only thing that would prevent them would be a lack of understanding of what’s going on.”
Meanwhile, many sellers of CBD-based products continue to promote their use as treatments for epilepsy and many other conditions.
Legal exceptions made by states for FDA-approved CBD-based drugs could affect access to unapproved CBD-based products. It’s also possible that Epidiolex could hurt sellers of cannabis products in other ways. “They’ll now have to compete with a drug made to a specific strength and purity, and that’s probably going to have some impact on their business,” William J. McNichol, adjunct professor at Rutgers Law School, Camden, N.J., said in an interview. “If you have a choice, are you going to choose aspirin I made myself in my artisan aspirin factory that the FDA never saw? Or aspirin made by Bayer?”

What’s next? For one, the FDA’s approval of Epidiolex seems likely to open the door for more cannabis-based medications. “The FDA is quite open to evaluating cannabinoid-based medicines as long as they go through their process,” said Mr. Schultz, the Greenwich Biosciences spokesman.
As for the legal front, Mr. Kight said potential changes in federal law could expand the legality of cannabis-based products by allowing them when they’re derived from “industrial hemp.” This could mean that patients with epilepsy will have more legal ways to buy CBD products.
Regardless of the legal situation, Mr. Kight said, “a physician can explain to patients across the board about how CBD might benefit them. The physician can say there are extract products that are out there and available over the counter.”
As for the maker of Epidiolex, GW Pharmaceuticals is recruiting for a phase 3 trial of a cannabinoid treatment for tuberous sclerosis complex, Mr. Schultz said. The results are due in the first half of 2019.
The company is also conducting cannabinoid research in the areas of autism and Rett syndrome, Mr. Schultz said, adding: “We also have done work in schizophrenia and in oncology and glioblastoma.”
Mr. Kight disclosed that he represents companies in the cannabis industry. Dr. French is president of the Epilepsy Study Consortium and disclosed working with multiple drug makers in the epilepsy field, including GW Pharmaceuticals. Dr. French receives fixed compensation by the consortium and is not paid by any pharmaceutical company. Mr. McNichol reported no relevant disclosures.
The first-ever federal approval of a marijuana-derived drug, Epidiolex (cannabidiol), comes with a cloud of complications.
Epidiolex is an oral solution of purified cannabidiol (CBD), a component of the marijuana plant that does not make people high.
According to the results of a phase 3 trial in patients with Lennox-Gastaut syndrome published earlier this year, median monthly drop seizures fell by 43.9% in a Epidiolex group compared with 21.8% in a placebo group (Lancet. 2018;391[10125]:1085-96). A 2017 study found that patients with Dravet syndrome who took the drug had fewer median convulsive seizures per month, dropping from 12.4 to 5.9, while there was barely a difference for the placebo group (N Engl J Med. 2017;376:2011-20). In both trials, patients received Epidiolex as an add-on treatment.
“There definitely are side effects such as sleepiness, abnormal liver function values, and other things that people will have to watch out for, such as interactions with other drugs,” Jacqueline A. French, MD, professor of neurology at New York University and chief scientific officer of the Epilepsy Foundation, said in an interview. “But it will definitely be a great benefit to some and a benefit to many.”
It’s not clear how the drug works, she said.
Greenwich Biosciences, the U.S. subsidiary of British drug maker GW Pharmaceuticals, plans to market Epidiolex this fall, spokesman Steve Schultz said in an interview. First, however, the U.S. Drug Enforcement Agency must reschedule the drug so it doesn’t fall under federal antimarijuana laws. It has 90 days after the FDA approval to do so, and its rescheduling is expected.
Then the focus will turn to the states, which have a crazy quilt of laws about marijuana and its medical use. “We’ve worked with the state legislators to enact laws or to modify laws to allow for our medicine to be made available,” Mr. Schultz said. “There may be one or two that we’re still working on.”
At issue: States and the District of Columbia have a wide variety of laws that appear to affect the sale of Epidiolex.
According to the website procon.org, 30 states and the District of Columbia allow medical marijuana, although the laws vary regarding what is allowed and do not address cannabis-derived pharmaceuticals.
Another 17 states have laws that address CBD specifically, often with language that allows its use to treat epilepsy in all or specific cases, according to procon.org.
In Oklahoma, an anticannabis law excludes “from the definition of marijuana ‘any federal Food and Drug Administration–approved cannabidiol drug or substance.’ ”
North Carolina attorney Rod Kight, who represents businesses in the cannabis industry, predicts that “once the federal government [via the DEA] changes the law, the states will fall in line. The only thing that would prevent them would be a lack of understanding of what’s going on.”
Meanwhile, many sellers of CBD-based products continue to promote their use as treatments for epilepsy and many other conditions.
Legal exceptions made by states for FDA-approved CBD-based drugs could affect access to unapproved CBD-based products. It’s also possible that Epidiolex could hurt sellers of cannabis products in other ways. “They’ll now have to compete with a drug made to a specific strength and purity, and that’s probably going to have some impact on their business,” William J. McNichol, adjunct professor at Rutgers Law School, Camden, N.J., said in an interview. “If you have a choice, are you going to choose aspirin I made myself in my artisan aspirin factory that the FDA never saw? Or aspirin made by Bayer?”
What’s next? For one, the FDA’s approval of Epidiolex seems likely to open the door for more cannabis-based medications. “The FDA is quite open to evaluating cannabinoid-based medicines as long as they go through their process,” said Mr. Schultz, the Greenwich Biosciences spokesman.
As for the legal front, Mr. Kight said potential changes in federal law could expand the legality of cannabis-based products by allowing them when they’re derived from “industrial hemp.” This could mean that patients with epilepsy will have more legal ways to buy CBD products.
Regardless of the legal situation, Mr. Kight said, “a physician can explain to patients across the board about how CBD might benefit them. The physician can say there are extract products that are out there and available over the counter.”
As for the maker of Epidiolex, GW Pharmaceuticals is recruiting for a phase 3 trial of a cannabinoid treatment for tuberous sclerosis complex, Mr. Schultz said. The results are due in the first half of 2019.
The company is also conducting cannabinoid research in the areas of autism and Rett syndrome, Mr. Schultz said, adding: “We also have done work in schizophrenia and in oncology and glioblastoma.”
Mr. Kight disclosed that he represents companies in the cannabis industry. Dr. French is president of the Epilepsy Study Consortium and disclosed working with multiple drug makers in the epilepsy field, including GW Pharmaceuticals. Dr. French receives fixed compensation by the consortium and is not paid by any pharmaceutical company. Mr. McNichol reported no relevant disclosures.
The first-ever federal approval of a marijuana-derived drug, Epidiolex (cannabidiol), comes with a cloud of complications.
Epidiolex is an oral solution of purified cannabidiol (CBD), a component of the marijuana plant that does not make people high.
According to the results of a phase 3 trial in patients with Lennox-Gastaut syndrome published earlier this year, median monthly drop seizures fell by 43.9% in a Epidiolex group compared with 21.8% in a placebo group (Lancet. 2018;391[10125]:1085-96). A 2017 study found that patients with Dravet syndrome who took the drug had fewer median convulsive seizures per month, dropping from 12.4 to 5.9, while there was barely a difference for the placebo group (N Engl J Med. 2017;376:2011-20). In both trials, patients received Epidiolex as an add-on treatment.
“There definitely are side effects such as sleepiness, abnormal liver function values, and other things that people will have to watch out for, such as interactions with other drugs,” Jacqueline A. French, MD, professor of neurology at New York University and chief scientific officer of the Epilepsy Foundation, said in an interview. “But it will definitely be a great benefit to some and a benefit to many.”
It’s not clear how the drug works, she said.
Greenwich Biosciences, the U.S. subsidiary of British drug maker GW Pharmaceuticals, plans to market Epidiolex this fall, spokesman Steve Schultz said in an interview. First, however, the U.S. Drug Enforcement Agency must reschedule the drug so it doesn’t fall under federal antimarijuana laws. It has 90 days after the FDA approval to do so, and its rescheduling is expected.
Then the focus will turn to the states, which have a crazy quilt of laws about marijuana and its medical use. “We’ve worked with the state legislators to enact laws or to modify laws to allow for our medicine to be made available,” Mr. Schultz said. “There may be one or two that we’re still working on.”
At issue: States and the District of Columbia have a wide variety of laws that appear to affect the sale of Epidiolex.
According to the website procon.org, 30 states and the District of Columbia allow medical marijuana, although the laws vary regarding what is allowed and do not address cannabis-derived pharmaceuticals.
Another 17 states have laws that address CBD specifically, often with language that allows its use to treat epilepsy in all or specific cases, according to procon.org.
In Oklahoma, an anticannabis law excludes “from the definition of marijuana ‘any federal Food and Drug Administration–approved cannabidiol drug or substance.’ ”
North Carolina attorney Rod Kight, who represents businesses in the cannabis industry, predicts that “once the federal government [via the DEA] changes the law, the states will fall in line. The only thing that would prevent them would be a lack of understanding of what’s going on.”
Meanwhile, many sellers of CBD-based products continue to promote their use as treatments for epilepsy and many other conditions.
Legal exceptions made by states for FDA-approved CBD-based drugs could affect access to unapproved CBD-based products. It’s also possible that Epidiolex could hurt sellers of cannabis products in other ways. “They’ll now have to compete with a drug made to a specific strength and purity, and that’s probably going to have some impact on their business,” William J. McNichol, adjunct professor at Rutgers Law School, Camden, N.J., said in an interview. “If you have a choice, are you going to choose aspirin I made myself in my artisan aspirin factory that the FDA never saw? Or aspirin made by Bayer?”
What’s next? For one, the FDA’s approval of Epidiolex seems likely to open the door for more cannabis-based medications. “The FDA is quite open to evaluating cannabinoid-based medicines as long as they go through their process,” said Mr. Schultz, the Greenwich Biosciences spokesman.
As for the legal front, Mr. Kight said potential changes in federal law could expand the legality of cannabis-based products by allowing them when they’re derived from “industrial hemp.” This could mean that patients with epilepsy will have more legal ways to buy CBD products.
Regardless of the legal situation, Mr. Kight said, “a physician can explain to patients across the board about how CBD might benefit them. The physician can say there are extract products that are out there and available over the counter.”
As for the maker of Epidiolex, GW Pharmaceuticals is recruiting for a phase 3 trial of a cannabinoid treatment for tuberous sclerosis complex, Mr. Schultz said. The results are due in the first half of 2019.
The company is also conducting cannabinoid research in the areas of autism and Rett syndrome, Mr. Schultz said, adding: “We also have done work in schizophrenia and in oncology and glioblastoma.”
Mr. Kight disclosed that he represents companies in the cannabis industry. Dr. French is president of the Epilepsy Study Consortium and disclosed working with multiple drug makers in the epilepsy field, including GW Pharmaceuticals. Dr. French receives fixed compensation by the consortium and is not paid by any pharmaceutical company. Mr. McNichol reported no relevant disclosures.
How to bring behavioral care into your office
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).

Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.

There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.

Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).
Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.
There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
There is consensus within both the medical and public health communities that an integrated model of health care, in which behavioral health is integrated into primary care settings, is the optimal way to improve the health of a population (not just treat disease) while managing costs and improving the patient’s experience of care. Such a model is especially compelling for pediatric care.
There are 74 million children under 18 years in the United States and the prevalence of psychiatric disorders in youth is 20%, or 15 million; after vaccinations and following development, managing psychiatric symptoms is the most common issue in pediatric primary care.
While some psychiatric illnesses can be well managed by primary care clinicians alone, some illnesses require specialized therapy or more complex pharmacologic treatment. Untreated or inadequately treated childhood mental illness can lead to a longer and worse course of illness, academic difficulties, emergence of associated illnesses (such as substance use disorders), and legal problems. For those children with chronic medical conditions, emotional disorders cause distress, and affect adherence and family functioning. We will discuss some practical strategies to begin to bring behavioral health care into the pediatric primary care setting.
Start by implementing behavioral health screening into annual and sick visits. Broad instruments, such as the Pediatric Symptom Checklist (PSC, 35 items) or the Child Behavior Check List (CBCL, 113 items) can be filled out by caregivers in the waiting room or online before a visit, and can suggest specific disorders or simply the need for a full psychiatric assessment. Electronic medical records may have publicly available questionnaires such as PSC built into their software, facilitating use of a tablet or home computer, and may ease scoring and downloading of results. Depending on the structure of your practice, you could have one clinician in charge of managing screening. You may become comfortable diagnosing certain disorders, such as ADHD, a major depressive episode, or an anxiety disorder, and you may begin medication treatment when appropriate. You can use instruments developed for specific disease entities (such as ADHD, obsessive compulsive disorder [OCD], anxiety, or depression) to monitor your patient’s treatment response, and they may be done virtually to minimize unnecessary visits.
Treatment algorithms for most psychiatric illnesses are available through the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry, and can guide you through the early stages of treatment. Psychotherapy is the first-line treatment for mild to moderate anxiety and mood disorders, and it is critical to the treatment of more severe disorders. Difficulty in finding a therapist who is skilled in a specific treatment, is a good fit, and accepts insurance can be a significant barrier to care. Establishing a coordinated relationship with a team of therapists can facilitate referrals. Some states have programs in which primary care physicians can have telephone consultations with mental health clinicians or to access referral services for therapy, such as the Massachusetts Child Psychiatry Access Project.
If you have a busy enough practice, consider bringing a social worker or psychologist to work with you. Such a clinician could perform diagnostic assessments, ongoing therapy, parent guidance, family work, or care coordination. Consider how to make it cost-effective for this clinician and your group, whether by inviting that person to sublet one of your offices, or having that person directly employed by you and benefiting from your office staff and patient flow. Many states now reimburse for screening and these funds could contribute to the expense of a social worker. This approach would bring you from coordination to true colocation, which greatly improves the likelihood of compliance with therapy, enhances coordination of a patient’s care, creates opportunities for ongoing education between disciplines, and diminishes stigma of acknowledging a mental illness. Anxiety disorders are the most common illnesses of youth, with mood disorders emerging in adolescence, and substance use disorders in later adolescence. Consider this in seeking a clinician with a specific interest or skill set (such as cognitive behavioral therapy for anxiety or mood problems, dialectical behavior therapy for chronic suicidality, or motivational interviewing for substance abuse).
Beyond diagnosing and treating psychiatric illness in your patients, a primary care pediatric setting with integrated behavioral health would improve the health of our young patients by investing in prevention and parental support. Universal prevention efforts are a hallmark of good pediatric care, from vaccines to educating parents and children about injury prevention (bike helmets, smoke detectors, and car seats) and risky behaviors (smoking). Educate your patients and their parents about best practices to promote good mental health, from good sleep hygiene to regular exercise and healthy stress management techniques. You could use posters and pamphlets, videos and smartphone apps, or screening instruments and discussion.
If you invest in a colocated mental health clinician, you can expand your prevention efforts beyond the universal. Screen for a family history of anxiety, mood, and substance use disorders, and screen for adverse childhood experiences scores. Chronic stress and a family history of specific psychiatric illnesses significantly increase the risk of specific illnesses in your patients. There are evidence-based interventions that can be used to prevent the emergence of many disorders in young people at specific risk. For example, parents who have struggled with anxiety can learn specific strategies for managing their children’s anxiety, significantly lowering the risk of anxiety disorders in their children. These skills can be taught individually or in groups, depending on the prevalence in your practice. Those insurers who reimburse for therapy have a reimbursement schedule for work with parents as well.
There may be funds available to support your investment in integrated care. Under the Affordable Care Act, Medicaid enhanced funding for Health Homes for enrolled children. There have been federal grants for primary care offices to engage in different levels of integration and measure outcomes (Project LAUNCH – Linking Actions for Unmet Needs in Children’s Health). There may be funding at the state level or from private foundations dedicated to public health research and initiatives. Even if you do not invest in procuring outside funding, you should consider how to measure patient outcomes once you are making any efforts at integrating behavioral health care into your practice. Outcome measures include questionnaire scores, treatment adherence, number of school absences, number of office or ED visits, or global measurements, such as the Child Global Assessment Scale (CGAS). Such data can inform you about how to adjust your approach, and could contribute to the larger effort to understand what strategies are most effective and feasible. Addressing the behavioral health needs of your patients could meaningfully contribute to the efforts to make the vision of integrated care – that which truly promotes health in our young people – a reality.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics at Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
Mandated 1-hour sepsis care protocol lowers mortality in children
A bundle of blood cultures, broad-spectrum antibiotics, and intravenous fluid replacement reduces risk of in-hospital mortality among children with sepsis if all three forms of management are initiated within an hour, according to a cohort study published in JAMA.

Although published guidelines already recommend prompt initiation of these three elements of care, a mandate created in New York in 2013 called for these interventions to be initiated in children within 1 hour of sepsis recognition. The newly published cohort study shows a mortality benefit when this is done.
In the study, which evaluated the impact of the bundle as well as each of the components in 1,179 pediatric patients with sepsis treated at 54 hospitals, the risk-adjusted odds ratio of in-hospital mortality was 0.59 (P = .02) among patients receiving the mandated protocol, compared with those who did not.
When provided within 1 hour, none of the individual components of the bundles were associated with a significant reduction of risk-adjusted, in-hospital mortality by themselves. However, there were trends for benefit with blood cultures (OR, 0.73; P = .1) and broad-spectrum antibiotics (OR, 0.78; P = .18). There was no trend for administration of intravenous fluids (OR, 0.88; P = .56), for which the mandate specified 20 mL/kg.
Although 46.5% of patients received intravenous fluids, 62.8% received broad-spectrum antibiotics, and blood cultures were obtained in 67.7% of the children within 1 hour, only 24.9% were managed with the entire sepsis bundle. Across hospitals, the proportion of children completing the bundle ranged from 7.3% to 46.1%.
Bundle completion was more common in hospitals already treating a relatively high volume of pediatric patients and in those with pediatric specialty services, but the study authors noted that this was not a linear relationship. Rather, they called this association “hypothesis generating” and speculated that other factors might also be important.
The children in this cohort ranged in age from under 1 month to 17 years. Slightly more than half were aged 6 years or older and nearly one-third were older than 12 years. Nearly 45% had no comorbidities. Slightly more than one-third had a malignancy or were immunosuppressed.
None of the study authors reported any relevant financial relationships with industry.
SOURCE: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.
The data published by Evans et al support a protocol approach to sepsis management in children as well as prompt delivery of the components outlined in the New York state mandate, according to an accompanying editorial written by Robert J. Vinci, MD, of Boston Medical Center, and Elliot Melendez, MD, of Johns Hopkins All Children’s Hospital, St. Petersburg, Fla. However, it cannot be determined from this study whether it is prompt delivery of these three mandated components or a more rigorous approach to pediatric sepsis management that deserves the most credit for the mortality benefit.
“Organizations that undertake quality improvement initiatives may have systems of care that promote the bundle completion, which then leads to improved outcomes,” they wrote. As a result, bundle completion may be a marker of expertise in managing critically ill children. They agreed that the data support the tested protocol, but they questioned whether this is sufficient.
“Organizations should be cautious about merely adopting a bundle of care without ensuring they have a universal culture of safety and quality that is adopted and supported from front-line clinical caregivers to organizational leaders and administrators,” they stated.
Dr. Vinci and Dr. Melendez had no disclosures to report.
SOURCE: JAMA. 2018;320(4):345-346. doi:10.1001/jama.2018.9183.
The data published by Evans et al support a protocol approach to sepsis management in children as well as prompt delivery of the components outlined in the New York state mandate, according to an accompanying editorial written by Robert J. Vinci, MD, of Boston Medical Center, and Elliot Melendez, MD, of Johns Hopkins All Children’s Hospital, St. Petersburg, Fla. However, it cannot be determined from this study whether it is prompt delivery of these three mandated components or a more rigorous approach to pediatric sepsis management that deserves the most credit for the mortality benefit.
“Organizations that undertake quality improvement initiatives may have systems of care that promote the bundle completion, which then leads to improved outcomes,” they wrote. As a result, bundle completion may be a marker of expertise in managing critically ill children. They agreed that the data support the tested protocol, but they questioned whether this is sufficient.
“Organizations should be cautious about merely adopting a bundle of care without ensuring they have a universal culture of safety and quality that is adopted and supported from front-line clinical caregivers to organizational leaders and administrators,” they stated.
Dr. Vinci and Dr. Melendez had no disclosures to report.
SOURCE: JAMA. 2018;320(4):345-346. doi:10.1001/jama.2018.9183.
The data published by Evans et al support a protocol approach to sepsis management in children as well as prompt delivery of the components outlined in the New York state mandate, according to an accompanying editorial written by Robert J. Vinci, MD, of Boston Medical Center, and Elliot Melendez, MD, of Johns Hopkins All Children’s Hospital, St. Petersburg, Fla. However, it cannot be determined from this study whether it is prompt delivery of these three mandated components or a more rigorous approach to pediatric sepsis management that deserves the most credit for the mortality benefit.
“Organizations that undertake quality improvement initiatives may have systems of care that promote the bundle completion, which then leads to improved outcomes,” they wrote. As a result, bundle completion may be a marker of expertise in managing critically ill children. They agreed that the data support the tested protocol, but they questioned whether this is sufficient.
“Organizations should be cautious about merely adopting a bundle of care without ensuring they have a universal culture of safety and quality that is adopted and supported from front-line clinical caregivers to organizational leaders and administrators,” they stated.
Dr. Vinci and Dr. Melendez had no disclosures to report.
SOURCE: JAMA. 2018;320(4):345-346. doi:10.1001/jama.2018.9183.
A bundle of blood cultures, broad-spectrum antibiotics, and intravenous fluid replacement reduces risk of in-hospital mortality among children with sepsis if all three forms of management are initiated within an hour, according to a cohort study published in JAMA.
Although published guidelines already recommend prompt initiation of these three elements of care, a mandate created in New York in 2013 called for these interventions to be initiated in children within 1 hour of sepsis recognition. The newly published cohort study shows a mortality benefit when this is done.
In the study, which evaluated the impact of the bundle as well as each of the components in 1,179 pediatric patients with sepsis treated at 54 hospitals, the risk-adjusted odds ratio of in-hospital mortality was 0.59 (P = .02) among patients receiving the mandated protocol, compared with those who did not.
When provided within 1 hour, none of the individual components of the bundles were associated with a significant reduction of risk-adjusted, in-hospital mortality by themselves. However, there were trends for benefit with blood cultures (OR, 0.73; P = .1) and broad-spectrum antibiotics (OR, 0.78; P = .18). There was no trend for administration of intravenous fluids (OR, 0.88; P = .56), for which the mandate specified 20 mL/kg.
Although 46.5% of patients received intravenous fluids, 62.8% received broad-spectrum antibiotics, and blood cultures were obtained in 67.7% of the children within 1 hour, only 24.9% were managed with the entire sepsis bundle. Across hospitals, the proportion of children completing the bundle ranged from 7.3% to 46.1%.
Bundle completion was more common in hospitals already treating a relatively high volume of pediatric patients and in those with pediatric specialty services, but the study authors noted that this was not a linear relationship. Rather, they called this association “hypothesis generating” and speculated that other factors might also be important.
The children in this cohort ranged in age from under 1 month to 17 years. Slightly more than half were aged 6 years or older and nearly one-third were older than 12 years. Nearly 45% had no comorbidities. Slightly more than one-third had a malignancy or were immunosuppressed.
None of the study authors reported any relevant financial relationships with industry.
SOURCE: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.
A bundle of blood cultures, broad-spectrum antibiotics, and intravenous fluid replacement reduces risk of in-hospital mortality among children with sepsis if all three forms of management are initiated within an hour, according to a cohort study published in JAMA.
Although published guidelines already recommend prompt initiation of these three elements of care, a mandate created in New York in 2013 called for these interventions to be initiated in children within 1 hour of sepsis recognition. The newly published cohort study shows a mortality benefit when this is done.
In the study, which evaluated the impact of the bundle as well as each of the components in 1,179 pediatric patients with sepsis treated at 54 hospitals, the risk-adjusted odds ratio of in-hospital mortality was 0.59 (P = .02) among patients receiving the mandated protocol, compared with those who did not.
When provided within 1 hour, none of the individual components of the bundles were associated with a significant reduction of risk-adjusted, in-hospital mortality by themselves. However, there were trends for benefit with blood cultures (OR, 0.73; P = .1) and broad-spectrum antibiotics (OR, 0.78; P = .18). There was no trend for administration of intravenous fluids (OR, 0.88; P = .56), for which the mandate specified 20 mL/kg.
Although 46.5% of patients received intravenous fluids, 62.8% received broad-spectrum antibiotics, and blood cultures were obtained in 67.7% of the children within 1 hour, only 24.9% were managed with the entire sepsis bundle. Across hospitals, the proportion of children completing the bundle ranged from 7.3% to 46.1%.
Bundle completion was more common in hospitals already treating a relatively high volume of pediatric patients and in those with pediatric specialty services, but the study authors noted that this was not a linear relationship. Rather, they called this association “hypothesis generating” and speculated that other factors might also be important.
The children in this cohort ranged in age from under 1 month to 17 years. Slightly more than half were aged 6 years or older and nearly one-third were older than 12 years. Nearly 45% had no comorbidities. Slightly more than one-third had a malignancy or were immunosuppressed.
None of the study authors reported any relevant financial relationships with industry.
SOURCE: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.
FROM JAMA
Key clinical point: Delivery of all three parts of the bundled pediatric sepsis management protocol was required for a mortality benefit.
Major finding: With timely delivery of the complete bundle, the odds ratio for in-hospital mortality was reduced 41% (OR, 0.59; P = .02).
Study details: A cohort study including 1,179 pediatric patients with sepsis at 54 New York hospitals.
Disclosures: None of the study authors reported any relevant financial relationships with industry.
Source: Evans IVR et al. JAMA. 2018 Jul 24. doi:10.1001/jama.2018.9071.