User login
Vaccine nonmedical exemptions creating metro ‘hotspots’
Recent increases in nonmedical exemptions (NMEs) to vaccination have created metropolitan “hotspots” with large numbers of unvaccinated children, according to a report published June 12 in PLoS Medicine.
although rates seem to have plateaued in some states since 2014. As a result of those increases, there were, during the 2016-2017 school year, 15 metro areas with kindergarten NME populations over 400, reported Jacqueline K. Olive, and her associates at Baylor College of Medicine. Their report was based on data from state health departments and the Centers for Disease Control and Prevention.
Leading the way was Maricopa County, Ariz., home of Phoenix and 2,947 unvaccinated kindergartners, which was more than triple the number in county/city No. 2, Salt Lake County/Salt Lake City (NME total: 956). Close behind in third was King County, Wash. (Seattle) at 940, followed by Multnomah County, Ore. (Portland) at 711 and Oakland County, Mich. (Troy) at 686, the investigators said.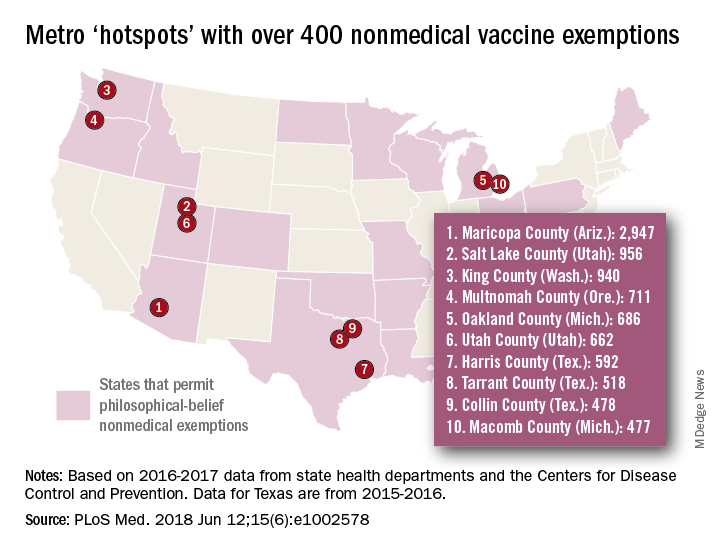
[There was only room for 10 in the map, so here are hotspots 11-15: Wayne County, Mich. (Detroit); Allegheny County, Pa. (Pittsburgh); Travis County, Tex. (Austin); Jackson County, Mo. (Kansas City); and Spokane County, Wash. (Spokane).]
In addition to the large-population hotspots, there are also a number of mainly rural counties with smaller populations but high NME rates. Eight of the 10 highest such rates can be found in Idaho, and at the top of that list is Camas County, which had an NME rate of 27% in 2016-2017, the researchers reported.
Analysis of the relationship between NMEs and MMR vaccination showed that “states with more NME students exhibited lower MMR vaccination rates. In contrast, states that have banned NMEs – Mississippi, California, and West Virginia – exhibit the highest MMR vaccine uptake and lowest incidence of vaccine preventable diseases,” the investigators wrote.
Ms. Olive and her associates said that there was no specific funding for the study and that no conflicts of interest existed.
SOURCE: Olive JK et al. PLoS Med. 2018 Jun 12;15(6): e1002578. doi: 10.1371/journal.pmed.1002578.
Recent increases in nonmedical exemptions (NMEs) to vaccination have created metropolitan “hotspots” with large numbers of unvaccinated children, according to a report published June 12 in PLoS Medicine.
although rates seem to have plateaued in some states since 2014. As a result of those increases, there were, during the 2016-2017 school year, 15 metro areas with kindergarten NME populations over 400, reported Jacqueline K. Olive, and her associates at Baylor College of Medicine. Their report was based on data from state health departments and the Centers for Disease Control and Prevention.
Leading the way was Maricopa County, Ariz., home of Phoenix and 2,947 unvaccinated kindergartners, which was more than triple the number in county/city No. 2, Salt Lake County/Salt Lake City (NME total: 956). Close behind in third was King County, Wash. (Seattle) at 940, followed by Multnomah County, Ore. (Portland) at 711 and Oakland County, Mich. (Troy) at 686, the investigators said.
[There was only room for 10 in the map, so here are hotspots 11-15: Wayne County, Mich. (Detroit); Allegheny County, Pa. (Pittsburgh); Travis County, Tex. (Austin); Jackson County, Mo. (Kansas City); and Spokane County, Wash. (Spokane).]
In addition to the large-population hotspots, there are also a number of mainly rural counties with smaller populations but high NME rates. Eight of the 10 highest such rates can be found in Idaho, and at the top of that list is Camas County, which had an NME rate of 27% in 2016-2017, the researchers reported.
Analysis of the relationship between NMEs and MMR vaccination showed that “states with more NME students exhibited lower MMR vaccination rates. In contrast, states that have banned NMEs – Mississippi, California, and West Virginia – exhibit the highest MMR vaccine uptake and lowest incidence of vaccine preventable diseases,” the investigators wrote.
Ms. Olive and her associates said that there was no specific funding for the study and that no conflicts of interest existed.
SOURCE: Olive JK et al. PLoS Med. 2018 Jun 12;15(6): e1002578. doi: 10.1371/journal.pmed.1002578.
Recent increases in nonmedical exemptions (NMEs) to vaccination have created metropolitan “hotspots” with large numbers of unvaccinated children, according to a report published June 12 in PLoS Medicine.
although rates seem to have plateaued in some states since 2014. As a result of those increases, there were, during the 2016-2017 school year, 15 metro areas with kindergarten NME populations over 400, reported Jacqueline K. Olive, and her associates at Baylor College of Medicine. Their report was based on data from state health departments and the Centers for Disease Control and Prevention.
Leading the way was Maricopa County, Ariz., home of Phoenix and 2,947 unvaccinated kindergartners, which was more than triple the number in county/city No. 2, Salt Lake County/Salt Lake City (NME total: 956). Close behind in third was King County, Wash. (Seattle) at 940, followed by Multnomah County, Ore. (Portland) at 711 and Oakland County, Mich. (Troy) at 686, the investigators said.
[There was only room for 10 in the map, so here are hotspots 11-15: Wayne County, Mich. (Detroit); Allegheny County, Pa. (Pittsburgh); Travis County, Tex. (Austin); Jackson County, Mo. (Kansas City); and Spokane County, Wash. (Spokane).]
In addition to the large-population hotspots, there are also a number of mainly rural counties with smaller populations but high NME rates. Eight of the 10 highest such rates can be found in Idaho, and at the top of that list is Camas County, which had an NME rate of 27% in 2016-2017, the researchers reported.
Analysis of the relationship between NMEs and MMR vaccination showed that “states with more NME students exhibited lower MMR vaccination rates. In contrast, states that have banned NMEs – Mississippi, California, and West Virginia – exhibit the highest MMR vaccine uptake and lowest incidence of vaccine preventable diseases,” the investigators wrote.
Ms. Olive and her associates said that there was no specific funding for the study and that no conflicts of interest existed.
SOURCE: Olive JK et al. PLoS Med. 2018 Jun 12;15(6): e1002578. doi: 10.1371/journal.pmed.1002578.
FROM PLOS MEDICINE
The demise of family dinners may play role in picky eating
My wife and I have dinner together almost every evening. There is a candle on the table regardless of the menu. And the meal begins with a toast, usually “To this chance to be together.” I can hear you muttering to yourself, “They must be one of those sappy, sweet hand-holding couples that appear to be joined at the hip.” Far from it, we lead very busy, active, but separate lives that only rarely intersect. But we make it a priority that one of those intersections occurs at a meal. For us, an evening dinner works best.
Listening to our friends, we have learned that an increasing number of them have drifted away from sharing a meal together. This phenomenon is surprising because most of them are retired, and time is not an issue. Of course, it is no secret that, for young overscheduled families, sitting down for a shared dining experience is becoming increasingly less frequent. Like some of you, I would like to claim that a return to family meal times would solve all of society’s ills. But some of the literature supporting this claim suggests shared family experiences in general, not particularly those associated with eating, may be just as important in supporting emotional health. But because everyone needs to eat, meals seem to me to be the easy target, low-hanging fruit if you will.
It is interesting that parents’ reports of their children’s eating patterns were validated by the behaviors videotaped by the researchers. But what is really interesting is that children who grew up in households where mealtimes followed a routine were more likely to be in the low–picky eating group. Routines included things like having a specific place times for eating, a habitual way of serving food, and other rituals such as saying grace.

Unfortunately, because this Michigan study began at age 4 years it doesn’t tell us if the worst picky eaters were that way from the beginning. I suspect that some were. But my hunch is that picky eaters who are managed in a home environment that includes mealtime rituals and puts dining together as a high priority are more likely to outgrow their pickiness.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater: A Guide for the Perplexed Parent.” Email him at pdnews@mdedge.com.
My wife and I have dinner together almost every evening. There is a candle on the table regardless of the menu. And the meal begins with a toast, usually “To this chance to be together.” I can hear you muttering to yourself, “They must be one of those sappy, sweet hand-holding couples that appear to be joined at the hip.” Far from it, we lead very busy, active, but separate lives that only rarely intersect. But we make it a priority that one of those intersections occurs at a meal. For us, an evening dinner works best.
Listening to our friends, we have learned that an increasing number of them have drifted away from sharing a meal together. This phenomenon is surprising because most of them are retired, and time is not an issue. Of course, it is no secret that, for young overscheduled families, sitting down for a shared dining experience is becoming increasingly less frequent. Like some of you, I would like to claim that a return to family meal times would solve all of society’s ills. But some of the literature supporting this claim suggests shared family experiences in general, not particularly those associated with eating, may be just as important in supporting emotional health. But because everyone needs to eat, meals seem to me to be the easy target, low-hanging fruit if you will.
It is interesting that parents’ reports of their children’s eating patterns were validated by the behaviors videotaped by the researchers. But what is really interesting is that children who grew up in households where mealtimes followed a routine were more likely to be in the low–picky eating group. Routines included things like having a specific place times for eating, a habitual way of serving food, and other rituals such as saying grace.
Unfortunately, because this Michigan study began at age 4 years it doesn’t tell us if the worst picky eaters were that way from the beginning. I suspect that some were. But my hunch is that picky eaters who are managed in a home environment that includes mealtime rituals and puts dining together as a high priority are more likely to outgrow their pickiness.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater: A Guide for the Perplexed Parent.” Email him at pdnews@mdedge.com.
My wife and I have dinner together almost every evening. There is a candle on the table regardless of the menu. And the meal begins with a toast, usually “To this chance to be together.” I can hear you muttering to yourself, “They must be one of those sappy, sweet hand-holding couples that appear to be joined at the hip.” Far from it, we lead very busy, active, but separate lives that only rarely intersect. But we make it a priority that one of those intersections occurs at a meal. For us, an evening dinner works best.
Listening to our friends, we have learned that an increasing number of them have drifted away from sharing a meal together. This phenomenon is surprising because most of them are retired, and time is not an issue. Of course, it is no secret that, for young overscheduled families, sitting down for a shared dining experience is becoming increasingly less frequent. Like some of you, I would like to claim that a return to family meal times would solve all of society’s ills. But some of the literature supporting this claim suggests shared family experiences in general, not particularly those associated with eating, may be just as important in supporting emotional health. But because everyone needs to eat, meals seem to me to be the easy target, low-hanging fruit if you will.
It is interesting that parents’ reports of their children’s eating patterns were validated by the behaviors videotaped by the researchers. But what is really interesting is that children who grew up in households where mealtimes followed a routine were more likely to be in the low–picky eating group. Routines included things like having a specific place times for eating, a habitual way of serving food, and other rituals such as saying grace.
Unfortunately, because this Michigan study began at age 4 years it doesn’t tell us if the worst picky eaters were that way from the beginning. I suspect that some were. But my hunch is that picky eaters who are managed in a home environment that includes mealtime rituals and puts dining together as a high priority are more likely to outgrow their pickiness.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater: A Guide for the Perplexed Parent.” Email him at pdnews@mdedge.com.
Youth with rhabdomyosarcoma see better survival with maintenance chemo
CHICAGO – , finds a phase 3 randomized controlled trial of the European Paediatric Soft Tissue Sarcoma Study Group (EpSSG).
Rhabdomyosarcoma is a rare but very aggressive tumor, lead study author Gianni Bisogno, MD, PhD, a professor at the University Hospital of Padova, Italy, and chair of the EpSSG, noted in a press briefing at the annual meeting of the American Society of Clinical Oncology, where the findings were reported. Among pediatric patients who achieve complete response to standard therapy, “we know that after 1 or 2 years, one-third of these children relapse, and most of them die,” he said.
The EpSSG trial, which took about 10 years to conduct, enrolled 371 patients aged 0-21 years with high-risk rhabdomyosarcoma who had had a complete response to standard intensive therapy. They were randomized evenly to stop treatment or to receive 6 months of maintenance treatment consisting of low-dose vinorelbine and cyclophosphamide.
Results reported in the meeting’s plenary session showed that giving maintenance chemotherapy improved the 5-year overall survival rate by an absolute 12.8%, which translated to a near halving of the risk of death. And the maintenance regimen used was generally well tolerated.
“At the end of this long, not-easy study, we concluded that maintenance chemotherapy is an effective and well tolerated treatment for children with high-risk rhabdomyosarcoma,” Dr. Bisogno said.

There are three possibilities for its efficacy, he speculated. “It may be the duration, the type of drugs used, or the metronomic approach. Maybe altogether, these three different actions have a benefit to increase survival.
“Our group has decided this is the new standard treatment for patients. At least in Europe, we give standard intensive therapy and then we continue with 6 more months of low-dose chemotherapy,” Dr. Bisogno concluded. “We think that this approach – a new way of using old drugs – can be of interest also for other pediatric tumors.”
The trial is noteworthy in that it shows “how to successfully conduct large and important trials in rare diseases,” said ASCO Expert Warren Chow, MD.

The standard therapy for rhabdomyosarcomas is somewhat different in the United States, typically a regimen containing vincristine, actinomycin D, cyclophosphamide, and (more recently) irinotecan, he noted. “We have not been traditionally using maintenance chemo for any of the pediatric sarcomas, so this is a paradigm shift. These results will need to be tested with U.S.-based protocols before becoming standard of care in the United States. Also, we will need to determine if these results are applicable to patients older than 21 years of age who are considered high risk based solely on their age.
“Even with these caveats, this is the first significant treatment advance in this rare cancer in more than 30 years,” concluded Dr. Chow, a medical oncologist and clinical professor at City of Hope, Duarte, Calif. “No doubt, this trial was a home run.”
Study details
Patients enrolled in the EpSSG trial had had a complete response to the standard intensive therapy used in Europe: high-dose chemotherapy (ifosfamide, vincristine, and actinomycin D, with or without doxorubicin), radiation therapy, and surgery.
The maintenance chemotherapy consisted of a combination of low-dose intravenous vinorelbine given weekly and oral cyclophosphamide given daily. The 6-month duration was somewhat arbitrary, according to Dr. Bisogno. “We had to start somewhere. So when we started, we decided to use 6 months because there was some evidence in the past for regimens that long. In our next European trial, we are going to test different kinds and durations of maintenance because this is very important.”
The maintenance regimen was well tolerated compared with the regimen given during standard intensive therapy, with, for example, lower rates of grade 3 and 4 anemia (8.9% vs. 48.9%), neutropenia (80.6% vs. 91.6%), and thrombocytopenia (0.6% vs. 26.0%), which translated to less need for transfusions, and a lower rate of grade 3 or 4 infection (29.4% vs. 56.4%), Dr. Bisogno reported. There were no cases of grade 3 or 4 cardiac, hepatobiliary/pancreatic, or renal toxicity.
Relative to peers who stopped treatment after standard intensive therapy, patients who received maintenance treatment tended to have better disease-free survival (77.6% vs. 69.8%; hazard ratio, 0.68; P = .0613) and had significantly better overall survival (86.5% vs. 73.7%; hazard ratio, 0.52; P = .0111).
Dr. Bisogno disclosed that he has a consulting or advisory role with Clinigen Group, and receives travel, accommodations, and/or expenses from Jazz Pharmaceuticals. The study received funding from Fondazione Città della Speranza, Italy.
SOURCE: Bisogno et al. ASCO 2018 Abstract LBA2.
CHICAGO – , finds a phase 3 randomized controlled trial of the European Paediatric Soft Tissue Sarcoma Study Group (EpSSG).
Rhabdomyosarcoma is a rare but very aggressive tumor, lead study author Gianni Bisogno, MD, PhD, a professor at the University Hospital of Padova, Italy, and chair of the EpSSG, noted in a press briefing at the annual meeting of the American Society of Clinical Oncology, where the findings were reported. Among pediatric patients who achieve complete response to standard therapy, “we know that after 1 or 2 years, one-third of these children relapse, and most of them die,” he said.
The EpSSG trial, which took about 10 years to conduct, enrolled 371 patients aged 0-21 years with high-risk rhabdomyosarcoma who had had a complete response to standard intensive therapy. They were randomized evenly to stop treatment or to receive 6 months of maintenance treatment consisting of low-dose vinorelbine and cyclophosphamide.
Results reported in the meeting’s plenary session showed that giving maintenance chemotherapy improved the 5-year overall survival rate by an absolute 12.8%, which translated to a near halving of the risk of death. And the maintenance regimen used was generally well tolerated.
“At the end of this long, not-easy study, we concluded that maintenance chemotherapy is an effective and well tolerated treatment for children with high-risk rhabdomyosarcoma,” Dr. Bisogno said.
There are three possibilities for its efficacy, he speculated. “It may be the duration, the type of drugs used, or the metronomic approach. Maybe altogether, these three different actions have a benefit to increase survival.
“Our group has decided this is the new standard treatment for patients. At least in Europe, we give standard intensive therapy and then we continue with 6 more months of low-dose chemotherapy,” Dr. Bisogno concluded. “We think that this approach – a new way of using old drugs – can be of interest also for other pediatric tumors.”
The trial is noteworthy in that it shows “how to successfully conduct large and important trials in rare diseases,” said ASCO Expert Warren Chow, MD.
The standard therapy for rhabdomyosarcomas is somewhat different in the United States, typically a regimen containing vincristine, actinomycin D, cyclophosphamide, and (more recently) irinotecan, he noted. “We have not been traditionally using maintenance chemo for any of the pediatric sarcomas, so this is a paradigm shift. These results will need to be tested with U.S.-based protocols before becoming standard of care in the United States. Also, we will need to determine if these results are applicable to patients older than 21 years of age who are considered high risk based solely on their age.
“Even with these caveats, this is the first significant treatment advance in this rare cancer in more than 30 years,” concluded Dr. Chow, a medical oncologist and clinical professor at City of Hope, Duarte, Calif. “No doubt, this trial was a home run.”
Study details
Patients enrolled in the EpSSG trial had had a complete response to the standard intensive therapy used in Europe: high-dose chemotherapy (ifosfamide, vincristine, and actinomycin D, with or without doxorubicin), radiation therapy, and surgery.
The maintenance chemotherapy consisted of a combination of low-dose intravenous vinorelbine given weekly and oral cyclophosphamide given daily. The 6-month duration was somewhat arbitrary, according to Dr. Bisogno. “We had to start somewhere. So when we started, we decided to use 6 months because there was some evidence in the past for regimens that long. In our next European trial, we are going to test different kinds and durations of maintenance because this is very important.”
The maintenance regimen was well tolerated compared with the regimen given during standard intensive therapy, with, for example, lower rates of grade 3 and 4 anemia (8.9% vs. 48.9%), neutropenia (80.6% vs. 91.6%), and thrombocytopenia (0.6% vs. 26.0%), which translated to less need for transfusions, and a lower rate of grade 3 or 4 infection (29.4% vs. 56.4%), Dr. Bisogno reported. There were no cases of grade 3 or 4 cardiac, hepatobiliary/pancreatic, or renal toxicity.
Relative to peers who stopped treatment after standard intensive therapy, patients who received maintenance treatment tended to have better disease-free survival (77.6% vs. 69.8%; hazard ratio, 0.68; P = .0613) and had significantly better overall survival (86.5% vs. 73.7%; hazard ratio, 0.52; P = .0111).
Dr. Bisogno disclosed that he has a consulting or advisory role with Clinigen Group, and receives travel, accommodations, and/or expenses from Jazz Pharmaceuticals. The study received funding from Fondazione Città della Speranza, Italy.
SOURCE: Bisogno et al. ASCO 2018 Abstract LBA2.
CHICAGO – , finds a phase 3 randomized controlled trial of the European Paediatric Soft Tissue Sarcoma Study Group (EpSSG).
Rhabdomyosarcoma is a rare but very aggressive tumor, lead study author Gianni Bisogno, MD, PhD, a professor at the University Hospital of Padova, Italy, and chair of the EpSSG, noted in a press briefing at the annual meeting of the American Society of Clinical Oncology, where the findings were reported. Among pediatric patients who achieve complete response to standard therapy, “we know that after 1 or 2 years, one-third of these children relapse, and most of them die,” he said.
The EpSSG trial, which took about 10 years to conduct, enrolled 371 patients aged 0-21 years with high-risk rhabdomyosarcoma who had had a complete response to standard intensive therapy. They were randomized evenly to stop treatment or to receive 6 months of maintenance treatment consisting of low-dose vinorelbine and cyclophosphamide.
Results reported in the meeting’s plenary session showed that giving maintenance chemotherapy improved the 5-year overall survival rate by an absolute 12.8%, which translated to a near halving of the risk of death. And the maintenance regimen used was generally well tolerated.
“At the end of this long, not-easy study, we concluded that maintenance chemotherapy is an effective and well tolerated treatment for children with high-risk rhabdomyosarcoma,” Dr. Bisogno said.
There are three possibilities for its efficacy, he speculated. “It may be the duration, the type of drugs used, or the metronomic approach. Maybe altogether, these three different actions have a benefit to increase survival.
“Our group has decided this is the new standard treatment for patients. At least in Europe, we give standard intensive therapy and then we continue with 6 more months of low-dose chemotherapy,” Dr. Bisogno concluded. “We think that this approach – a new way of using old drugs – can be of interest also for other pediatric tumors.”
The trial is noteworthy in that it shows “how to successfully conduct large and important trials in rare diseases,” said ASCO Expert Warren Chow, MD.
The standard therapy for rhabdomyosarcomas is somewhat different in the United States, typically a regimen containing vincristine, actinomycin D, cyclophosphamide, and (more recently) irinotecan, he noted. “We have not been traditionally using maintenance chemo for any of the pediatric sarcomas, so this is a paradigm shift. These results will need to be tested with U.S.-based protocols before becoming standard of care in the United States. Also, we will need to determine if these results are applicable to patients older than 21 years of age who are considered high risk based solely on their age.
“Even with these caveats, this is the first significant treatment advance in this rare cancer in more than 30 years,” concluded Dr. Chow, a medical oncologist and clinical professor at City of Hope, Duarte, Calif. “No doubt, this trial was a home run.”
Study details
Patients enrolled in the EpSSG trial had had a complete response to the standard intensive therapy used in Europe: high-dose chemotherapy (ifosfamide, vincristine, and actinomycin D, with or without doxorubicin), radiation therapy, and surgery.
The maintenance chemotherapy consisted of a combination of low-dose intravenous vinorelbine given weekly and oral cyclophosphamide given daily. The 6-month duration was somewhat arbitrary, according to Dr. Bisogno. “We had to start somewhere. So when we started, we decided to use 6 months because there was some evidence in the past for regimens that long. In our next European trial, we are going to test different kinds and durations of maintenance because this is very important.”
The maintenance regimen was well tolerated compared with the regimen given during standard intensive therapy, with, for example, lower rates of grade 3 and 4 anemia (8.9% vs. 48.9%), neutropenia (80.6% vs. 91.6%), and thrombocytopenia (0.6% vs. 26.0%), which translated to less need for transfusions, and a lower rate of grade 3 or 4 infection (29.4% vs. 56.4%), Dr. Bisogno reported. There were no cases of grade 3 or 4 cardiac, hepatobiliary/pancreatic, or renal toxicity.
Relative to peers who stopped treatment after standard intensive therapy, patients who received maintenance treatment tended to have better disease-free survival (77.6% vs. 69.8%; hazard ratio, 0.68; P = .0613) and had significantly better overall survival (86.5% vs. 73.7%; hazard ratio, 0.52; P = .0111).
Dr. Bisogno disclosed that he has a consulting or advisory role with Clinigen Group, and receives travel, accommodations, and/or expenses from Jazz Pharmaceuticals. The study received funding from Fondazione Città della Speranza, Italy.
SOURCE: Bisogno et al. ASCO 2018 Abstract LBA2.
REPORTING FROM ASCO 2018
Key clinical point: Six months of maintenance chemotherapy improves survival in youth with high-risk rhabdomyosarcoma.
Major finding: Compared with counterparts not receiving any additional treatment, patients given maintenance low-dose vinorelbine and cyclophosphamide had better 5-year overall survival (86.5% vs. 73.7%; hazard ratio, 0.52).
Study details: A phase 3 randomized controlled trial among 371 patients aged 0-21 years with high-risk rhabdomyosarcoma who had had a complete response to standard intensive therapy.
Disclosures: Dr. Bisogno disclosed that he has a consulting or advisory role with Clinigen Group, and receives travel, accommodations, and/or expenses from Jazz Pharmaceuticals. The study received funding from Fondazione Città della Speranza, Italy.
Source: Bisogno et al. ASCO 2018, Abstract LBA2.
EULAR scientific program highlights spectrum of translational research
EULAR 2018’s scientific program in Amsterdam is packed with lectures, clinical and basic science symposia, workshops, and special interest sessions covering the full spectrum of rheumatic diseases, said Dr. Robert Landewé, chair of the Scientific Program Committee.
“More than 5,000 scientific abstracts were submitted, which is an absolute, all-time record,” Dr. Landewé said. Four experts scored each abstract, and only the top 7% were invited for oral presentation during abstract sessions or symposia, he explained in an interview.

Wednesday, June 13
A high point of the 2018 scientific program is Wednesday’s opening plenary session, which will feature abstracts that were handpicked by Dr. Landewé and Dr. Thomas Dörner, professor of rheumatology at Charite Universitätsmedizin, Berlin. “This session includes highly scored abstracts, including late-breakers, on current advances in therapeutics and disease classification,” said Dr. Dörner, who chaired this year’s Abstract Selection Committee.
The plenary abstract session will cover new findings on gout and cardiovascular disease from CANTOS (Canakinumab Anti-inflammatory Thrombosis Outcome Study), long-term mortality in patients with early RA from the COBRA (Combinatietherapie Bij Reumatoide Artritis) study, the use of zoledronic acid to treat knee osteoarthritis with bone lesions, and the relationship between bisphosphonate drug holidays and hip fracture risk. Researchers also will discuss baricitinib in systemic lupus erythematosus (SLE), the value of MRI when treating remitted RA to target, the validation of SLE classification criteria, and draft classification criteria for ANCA-associated vasculitides.
A notable clinical science session on Wednesday will cover cancer and inflammation, Dr. Landewé said. “This is a topic of increasing interest because cancer and inflammation share mutual pathways.”
Novel cancer therapies such as immune checkpoint inhibitors have improved outcomes across a range of tumor types, but also can induce rheumatic disease, he added. Accordingly, presenters will discuss inflammation as “friend” versus “foe” in cancer treatment, the role of tumor necrosis factor in cancer, and risk of malignancy among patients with RA.
Also on Wednesday, a session will tackle the relationship between psychological distress and pain in immune-mediated disease. “Pain is the major symptom of rheumatic diseases, and the role of the psyche remains poorly understood,” Dr. Landewé said. “But we know one thing for sure: There is an association, and speakers from outside the field of rheumatology will help explain.”
Attendees at this bench-to-bedside session will learn how distress appears to exacerbate arthritis pain and how managing psychological stress can help optimize outcomes in arthritis pain. Experts also will describe research on integrated brain pathways in pain and distress, as well as risk factors for cognitive impairment in RA.
Thursday, June 14

Topics in this session will include the use of estrogens and other hormonal therapies in patients with rheumatic disease, registry studies of rheumatologic conditions during pregnancy, and how clinicians can best discuss sexual concerns with their rheumatology patients.
Another clinical science session scheduled for Thursday afternoon will delve into structural damage progression in patients with axial spondyloarthritis, Dr. Landewé said. “Can we inhibit this structural progression? Can we show it? Does it make sense? And which drug company will win the battle to have the precedent?”
He hopes that Dr. Désirée van der Heijde of the Netherlands and Dr. Xenofon Baraliakos of Germany will help answer these questions when they discuss the latest evidence on identifying and treating clinically relevant structural progression. Also in this session, researchers will describe the combined effects of tumor necrosis factor inhibitors and NSAIDs on radiographic progression in ankylosing spondylitis, and MRI evidence supporting treating early axial spondyloarthritis to target with the goal of achieving sustained remission of inflammation.
Also on Thursday afternoon, a case-based session will take a deep dive into giant cell arteritis (GCA), Dr. Landewé noted. Attendees will learn about diagnosing and managing vision loss and stroke and the latest on corticosteroid therapy in GCA. The session also will cover biologics. “Giant cell arteritis has entered the field of biologicals!” said Dr. Landewé. “This has major implications for this disease and the clinical choices to be made.”
The past 5 decades have seen marked progress in the diagnosis and treatment of SLE, with corresponding improvements in survival and quality of life. “Still, lupus is awfully difficult,” Dr. Landewé said. “Therefore, we have planned a classical bench-to-bedside symposium to provide an all-inclusive look at current thinking and future developments.”
Talks during this Thursday afternoon session will cover the latest findings on the pathogenesis of SLE, the clinical significance of autoantibodies, distinguishing early SLE from mimics, and the role of blood-brain barrier permeability and neuropsychiatric manifestations of SLE and progressive systemic sclerosis.
Friday, June 15
For the first time, the scientific program also will include a clinical science session held jointly with the European Society of Musculoskeletal Radiology (ESSR). Dr. Joachim Sieper of Germany and ESSR President Dr. Monique Reijnierse of the Netherlands will cochair the Friday afternoon session on the role of MRI in rheumatology. Attendees from both organizations will learn when to use MRI in early and established RA and spondyloarthritis, and how to interpret the results, with abundant time built in for questions and answers. Dr. Landewé called the joint session “a test case” for exciting web-based interactions between EULAR and ESSR.
Another clinical science session on Friday afternoon will dive into the diagnosis of spondyloarthritis, which Dr. Landewé called “a matter of recognizing patterns, not ticking boxes on a list of criteria. This symposium leads you through the art of pattern recognition.”
Later on Friday afternoon, a session will explore advances in biologic therapy of small-vessel vasculitis, he added. “Biologic disease-modifying antirheumatic drugs [bDMARDs] are becoming more and more important in this area of expanding interest.” Experts will address complement inhibition in ANCA-associated vasculitis (AAV), the use of induction and maintenance rituximab in AAV, the evolving role of mepolizumab in eosinophilic granulomatosis with polyangiitis, survival in AAV, and the use of rituximab for treating children with granulomatosis with polyangiitis and microscopic polyangiitis.
Saturday, June 16
On Saturday, a bench-to-bedside session will cover gout and kidney function. “This is an area with important new insights,” Dr. Dörner said. Presenters will discuss the genetics of hyperuricemia, renal urate transporters, and the pros and cons of using xanthine oxidase inhibitors to treat chronic kidney disease. Researchers will also cover studies of impaired neutrophil chemotaxis in patients with chronic kidney disease and hyperuricemia, and the relationship between renal medullar hyperechogenicity and gout severity.
Also on Saturday, a clinical science session titled, “Rheumatoid arthritis: Is it all in your head?” will explore emerging data on the relationship between inflammation and depression. Patients with RA often face both clinical depression and social isolation, and these complex psychosocial conditions can worsen one another. “In addition to proper drug choice, treating RA effectively depends on how concomitant problems, such as nonspecific pain, depression, and social isolation, are coped with in a broad context,” Dr. Landewé said. “When it comes to optimal management, rheumatologists need to communicate and prescribe, not just prescribe.”
Christian Apfelbacher, PhD, of Germany will discuss prevention and treatment strategies and Dr. Jonathan Cavanagh of the United Kingdom will cover neuroimaging in RA. Researchers also will discuss new findings on pain, depression, and anxiety in patients recently diagnosed with RA.
Also on Saturday, a special session will cover EULAR’s initiatives to improve clinical approaches (ESSCA), Dr. Dörner noted. This effort has produced new or updated recommendations on topics such as vaccination, Sjögren’s syndrome, glucocorticoid therapy, and management of hand osteoarthritis, he said. “These recommendations follow a number of others and are expected to impact clinical science as well as clinical practice.”
EULAR 2018’s scientific program in Amsterdam is packed with lectures, clinical and basic science symposia, workshops, and special interest sessions covering the full spectrum of rheumatic diseases, said Dr. Robert Landewé, chair of the Scientific Program Committee.
“More than 5,000 scientific abstracts were submitted, which is an absolute, all-time record,” Dr. Landewé said. Four experts scored each abstract, and only the top 7% were invited for oral presentation during abstract sessions or symposia, he explained in an interview.
Wednesday, June 13
A high point of the 2018 scientific program is Wednesday’s opening plenary session, which will feature abstracts that were handpicked by Dr. Landewé and Dr. Thomas Dörner, professor of rheumatology at Charite Universitätsmedizin, Berlin. “This session includes highly scored abstracts, including late-breakers, on current advances in therapeutics and disease classification,” said Dr. Dörner, who chaired this year’s Abstract Selection Committee.
The plenary abstract session will cover new findings on gout and cardiovascular disease from CANTOS (Canakinumab Anti-inflammatory Thrombosis Outcome Study), long-term mortality in patients with early RA from the COBRA (Combinatietherapie Bij Reumatoide Artritis) study, the use of zoledronic acid to treat knee osteoarthritis with bone lesions, and the relationship between bisphosphonate drug holidays and hip fracture risk. Researchers also will discuss baricitinib in systemic lupus erythematosus (SLE), the value of MRI when treating remitted RA to target, the validation of SLE classification criteria, and draft classification criteria for ANCA-associated vasculitides.
A notable clinical science session on Wednesday will cover cancer and inflammation, Dr. Landewé said. “This is a topic of increasing interest because cancer and inflammation share mutual pathways.”
Novel cancer therapies such as immune checkpoint inhibitors have improved outcomes across a range of tumor types, but also can induce rheumatic disease, he added. Accordingly, presenters will discuss inflammation as “friend” versus “foe” in cancer treatment, the role of tumor necrosis factor in cancer, and risk of malignancy among patients with RA.
Also on Wednesday, a session will tackle the relationship between psychological distress and pain in immune-mediated disease. “Pain is the major symptom of rheumatic diseases, and the role of the psyche remains poorly understood,” Dr. Landewé said. “But we know one thing for sure: There is an association, and speakers from outside the field of rheumatology will help explain.”
Attendees at this bench-to-bedside session will learn how distress appears to exacerbate arthritis pain and how managing psychological stress can help optimize outcomes in arthritis pain. Experts also will describe research on integrated brain pathways in pain and distress, as well as risk factors for cognitive impairment in RA.
Thursday, June 14
Topics in this session will include the use of estrogens and other hormonal therapies in patients with rheumatic disease, registry studies of rheumatologic conditions during pregnancy, and how clinicians can best discuss sexual concerns with their rheumatology patients.
Another clinical science session scheduled for Thursday afternoon will delve into structural damage progression in patients with axial spondyloarthritis, Dr. Landewé said. “Can we inhibit this structural progression? Can we show it? Does it make sense? And which drug company will win the battle to have the precedent?”
He hopes that Dr. Désirée van der Heijde of the Netherlands and Dr. Xenofon Baraliakos of Germany will help answer these questions when they discuss the latest evidence on identifying and treating clinically relevant structural progression. Also in this session, researchers will describe the combined effects of tumor necrosis factor inhibitors and NSAIDs on radiographic progression in ankylosing spondylitis, and MRI evidence supporting treating early axial spondyloarthritis to target with the goal of achieving sustained remission of inflammation.
Also on Thursday afternoon, a case-based session will take a deep dive into giant cell arteritis (GCA), Dr. Landewé noted. Attendees will learn about diagnosing and managing vision loss and stroke and the latest on corticosteroid therapy in GCA. The session also will cover biologics. “Giant cell arteritis has entered the field of biologicals!” said Dr. Landewé. “This has major implications for this disease and the clinical choices to be made.”
The past 5 decades have seen marked progress in the diagnosis and treatment of SLE, with corresponding improvements in survival and quality of life. “Still, lupus is awfully difficult,” Dr. Landewé said. “Therefore, we have planned a classical bench-to-bedside symposium to provide an all-inclusive look at current thinking and future developments.”
Talks during this Thursday afternoon session will cover the latest findings on the pathogenesis of SLE, the clinical significance of autoantibodies, distinguishing early SLE from mimics, and the role of blood-brain barrier permeability and neuropsychiatric manifestations of SLE and progressive systemic sclerosis.
Friday, June 15
For the first time, the scientific program also will include a clinical science session held jointly with the European Society of Musculoskeletal Radiology (ESSR). Dr. Joachim Sieper of Germany and ESSR President Dr. Monique Reijnierse of the Netherlands will cochair the Friday afternoon session on the role of MRI in rheumatology. Attendees from both organizations will learn when to use MRI in early and established RA and spondyloarthritis, and how to interpret the results, with abundant time built in for questions and answers. Dr. Landewé called the joint session “a test case” for exciting web-based interactions between EULAR and ESSR.
Another clinical science session on Friday afternoon will dive into the diagnosis of spondyloarthritis, which Dr. Landewé called “a matter of recognizing patterns, not ticking boxes on a list of criteria. This symposium leads you through the art of pattern recognition.”
Later on Friday afternoon, a session will explore advances in biologic therapy of small-vessel vasculitis, he added. “Biologic disease-modifying antirheumatic drugs [bDMARDs] are becoming more and more important in this area of expanding interest.” Experts will address complement inhibition in ANCA-associated vasculitis (AAV), the use of induction and maintenance rituximab in AAV, the evolving role of mepolizumab in eosinophilic granulomatosis with polyangiitis, survival in AAV, and the use of rituximab for treating children with granulomatosis with polyangiitis and microscopic polyangiitis.
Saturday, June 16
On Saturday, a bench-to-bedside session will cover gout and kidney function. “This is an area with important new insights,” Dr. Dörner said. Presenters will discuss the genetics of hyperuricemia, renal urate transporters, and the pros and cons of using xanthine oxidase inhibitors to treat chronic kidney disease. Researchers will also cover studies of impaired neutrophil chemotaxis in patients with chronic kidney disease and hyperuricemia, and the relationship between renal medullar hyperechogenicity and gout severity.
Also on Saturday, a clinical science session titled, “Rheumatoid arthritis: Is it all in your head?” will explore emerging data on the relationship between inflammation and depression. Patients with RA often face both clinical depression and social isolation, and these complex psychosocial conditions can worsen one another. “In addition to proper drug choice, treating RA effectively depends on how concomitant problems, such as nonspecific pain, depression, and social isolation, are coped with in a broad context,” Dr. Landewé said. “When it comes to optimal management, rheumatologists need to communicate and prescribe, not just prescribe.”
Christian Apfelbacher, PhD, of Germany will discuss prevention and treatment strategies and Dr. Jonathan Cavanagh of the United Kingdom will cover neuroimaging in RA. Researchers also will discuss new findings on pain, depression, and anxiety in patients recently diagnosed with RA.
Also on Saturday, a special session will cover EULAR’s initiatives to improve clinical approaches (ESSCA), Dr. Dörner noted. This effort has produced new or updated recommendations on topics such as vaccination, Sjögren’s syndrome, glucocorticoid therapy, and management of hand osteoarthritis, he said. “These recommendations follow a number of others and are expected to impact clinical science as well as clinical practice.”
EULAR 2018’s scientific program in Amsterdam is packed with lectures, clinical and basic science symposia, workshops, and special interest sessions covering the full spectrum of rheumatic diseases, said Dr. Robert Landewé, chair of the Scientific Program Committee.
“More than 5,000 scientific abstracts were submitted, which is an absolute, all-time record,” Dr. Landewé said. Four experts scored each abstract, and only the top 7% were invited for oral presentation during abstract sessions or symposia, he explained in an interview.
Wednesday, June 13
A high point of the 2018 scientific program is Wednesday’s opening plenary session, which will feature abstracts that were handpicked by Dr. Landewé and Dr. Thomas Dörner, professor of rheumatology at Charite Universitätsmedizin, Berlin. “This session includes highly scored abstracts, including late-breakers, on current advances in therapeutics and disease classification,” said Dr. Dörner, who chaired this year’s Abstract Selection Committee.
The plenary abstract session will cover new findings on gout and cardiovascular disease from CANTOS (Canakinumab Anti-inflammatory Thrombosis Outcome Study), long-term mortality in patients with early RA from the COBRA (Combinatietherapie Bij Reumatoide Artritis) study, the use of zoledronic acid to treat knee osteoarthritis with bone lesions, and the relationship between bisphosphonate drug holidays and hip fracture risk. Researchers also will discuss baricitinib in systemic lupus erythematosus (SLE), the value of MRI when treating remitted RA to target, the validation of SLE classification criteria, and draft classification criteria for ANCA-associated vasculitides.
A notable clinical science session on Wednesday will cover cancer and inflammation, Dr. Landewé said. “This is a topic of increasing interest because cancer and inflammation share mutual pathways.”
Novel cancer therapies such as immune checkpoint inhibitors have improved outcomes across a range of tumor types, but also can induce rheumatic disease, he added. Accordingly, presenters will discuss inflammation as “friend” versus “foe” in cancer treatment, the role of tumor necrosis factor in cancer, and risk of malignancy among patients with RA.
Also on Wednesday, a session will tackle the relationship between psychological distress and pain in immune-mediated disease. “Pain is the major symptom of rheumatic diseases, and the role of the psyche remains poorly understood,” Dr. Landewé said. “But we know one thing for sure: There is an association, and speakers from outside the field of rheumatology will help explain.”
Attendees at this bench-to-bedside session will learn how distress appears to exacerbate arthritis pain and how managing psychological stress can help optimize outcomes in arthritis pain. Experts also will describe research on integrated brain pathways in pain and distress, as well as risk factors for cognitive impairment in RA.
Thursday, June 14
Topics in this session will include the use of estrogens and other hormonal therapies in patients with rheumatic disease, registry studies of rheumatologic conditions during pregnancy, and how clinicians can best discuss sexual concerns with their rheumatology patients.
Another clinical science session scheduled for Thursday afternoon will delve into structural damage progression in patients with axial spondyloarthritis, Dr. Landewé said. “Can we inhibit this structural progression? Can we show it? Does it make sense? And which drug company will win the battle to have the precedent?”
He hopes that Dr. Désirée van der Heijde of the Netherlands and Dr. Xenofon Baraliakos of Germany will help answer these questions when they discuss the latest evidence on identifying and treating clinically relevant structural progression. Also in this session, researchers will describe the combined effects of tumor necrosis factor inhibitors and NSAIDs on radiographic progression in ankylosing spondylitis, and MRI evidence supporting treating early axial spondyloarthritis to target with the goal of achieving sustained remission of inflammation.
Also on Thursday afternoon, a case-based session will take a deep dive into giant cell arteritis (GCA), Dr. Landewé noted. Attendees will learn about diagnosing and managing vision loss and stroke and the latest on corticosteroid therapy in GCA. The session also will cover biologics. “Giant cell arteritis has entered the field of biologicals!” said Dr. Landewé. “This has major implications for this disease and the clinical choices to be made.”
The past 5 decades have seen marked progress in the diagnosis and treatment of SLE, with corresponding improvements in survival and quality of life. “Still, lupus is awfully difficult,” Dr. Landewé said. “Therefore, we have planned a classical bench-to-bedside symposium to provide an all-inclusive look at current thinking and future developments.”
Talks during this Thursday afternoon session will cover the latest findings on the pathogenesis of SLE, the clinical significance of autoantibodies, distinguishing early SLE from mimics, and the role of blood-brain barrier permeability and neuropsychiatric manifestations of SLE and progressive systemic sclerosis.
Friday, June 15
For the first time, the scientific program also will include a clinical science session held jointly with the European Society of Musculoskeletal Radiology (ESSR). Dr. Joachim Sieper of Germany and ESSR President Dr. Monique Reijnierse of the Netherlands will cochair the Friday afternoon session on the role of MRI in rheumatology. Attendees from both organizations will learn when to use MRI in early and established RA and spondyloarthritis, and how to interpret the results, with abundant time built in for questions and answers. Dr. Landewé called the joint session “a test case” for exciting web-based interactions between EULAR and ESSR.
Another clinical science session on Friday afternoon will dive into the diagnosis of spondyloarthritis, which Dr. Landewé called “a matter of recognizing patterns, not ticking boxes on a list of criteria. This symposium leads you through the art of pattern recognition.”
Later on Friday afternoon, a session will explore advances in biologic therapy of small-vessel vasculitis, he added. “Biologic disease-modifying antirheumatic drugs [bDMARDs] are becoming more and more important in this area of expanding interest.” Experts will address complement inhibition in ANCA-associated vasculitis (AAV), the use of induction and maintenance rituximab in AAV, the evolving role of mepolizumab in eosinophilic granulomatosis with polyangiitis, survival in AAV, and the use of rituximab for treating children with granulomatosis with polyangiitis and microscopic polyangiitis.
Saturday, June 16
On Saturday, a bench-to-bedside session will cover gout and kidney function. “This is an area with important new insights,” Dr. Dörner said. Presenters will discuss the genetics of hyperuricemia, renal urate transporters, and the pros and cons of using xanthine oxidase inhibitors to treat chronic kidney disease. Researchers will also cover studies of impaired neutrophil chemotaxis in patients with chronic kidney disease and hyperuricemia, and the relationship between renal medullar hyperechogenicity and gout severity.
Also on Saturday, a clinical science session titled, “Rheumatoid arthritis: Is it all in your head?” will explore emerging data on the relationship between inflammation and depression. Patients with RA often face both clinical depression and social isolation, and these complex psychosocial conditions can worsen one another. “In addition to proper drug choice, treating RA effectively depends on how concomitant problems, such as nonspecific pain, depression, and social isolation, are coped with in a broad context,” Dr. Landewé said. “When it comes to optimal management, rheumatologists need to communicate and prescribe, not just prescribe.”
Christian Apfelbacher, PhD, of Germany will discuss prevention and treatment strategies and Dr. Jonathan Cavanagh of the United Kingdom will cover neuroimaging in RA. Researchers also will discuss new findings on pain, depression, and anxiety in patients recently diagnosed with RA.
Also on Saturday, a special session will cover EULAR’s initiatives to improve clinical approaches (ESSCA), Dr. Dörner noted. This effort has produced new or updated recommendations on topics such as vaccination, Sjögren’s syndrome, glucocorticoid therapy, and management of hand osteoarthritis, he said. “These recommendations follow a number of others and are expected to impact clinical science as well as clinical practice.”
EULAR pediatric sessions to highlight big data, personalized medicine
Personalized medicine, big data, and monogenic inflammatory diseases are just a few of the high points of pediatric rheumatology sessions at this year’s EULAR Congress.
EULAR Standing Committee Chairperson for Paediatric Rheumatology Berent J. Prakken, MD, PhD, said that a bench-to-bedside session on Wednesday afternoon would highlight how EULAR projects are driving advances in pediatric rheumatology.
Attendees will learn from Vicki Seyfert-Margolis, PhD, an internationally recognized expert in personalized medicine, about how digital tools can facilitate cross-border partnerships in pediatric rheumatology, Dr. Prakken said in an interview.
“This talk will be groundbreaking because it’s not just about another useful app,” said Dr. Prakken, professor of pediatric rheumatology and vice dean of education at University Medical Center Utrecht (the Netherlands). “Dr. Seyfert-Margolis will show how the digital revolution will change the way we communicate with patients, monitor disease, and develop novel models for clinical trials.”
The session will also cover work by the Understanding Childhood Arthritis Network (UCAN), created to facilitate international translational research in pediatric rheumatology. Speakers will describe how UCAN is helping to spur personalized medicine and working with the Pediatric Rheumatology International Trials Organization (PRINTO) to align bench and bedside perspectives.
Another program highlight is a Thursday afternoon session on connections between monogenic autoinflammatory and pediatric rheumatic diseases. “Groundbreaking studies of these rare genetic inflammatory diseases have provided important new insights that, in turn, have led to new therapeutic options,” said Dr. Prakken.

During the session, Joost Swart, MD, of Utrecht, the Netherlands, will discuss promising research on the intravenous use of mesenchymal stromal cells derived from bone marrow for the treatment of refractory juvenile idiopathic arthritis (JIA).
Dr. Swart, who helped pioneer the approach, will discuss the first phase I/II trial of its use in children. “This is a truly innovative way to handle refractory inflammation,” Dr. Prakken said.
The session on monogenic autoinflammatory diseases also will cover their clinical presentation in children and adults, their pathogenesis as compared with adult-onset rheumatic diseases, and emerging treatment options, according to Dr. Prakken.
On Friday afternoon, a pediatric session will feature big data science in pediatric rheumatology, a lightning-paced field that is generating new research and treatment paradigms.
Of special note, Salvatore Albani, MD, PhD, will discuss how the human immunome is revolutionizing personalized treatment of paediatric inflammatory diseases, Dr. Prakken said. “This is the first application of big data to develop a completely new, personalized map of the human immune system,” he added. “This technology has the potential to revolutionize human clinical immunology, and it may be the key to true precision medicine in inflammatory diseases.”
Other talks in the session will cover signaling pathways in childhood systemic lupus erythematosus (SLE), galectin-9 as a biomarker in juvenile dermatomyositis, and evidence from the phase 3 PRINTO trial on how best to taper corticosteroids in patients with new-onset juvenile dermatomyositis.
Another crucial topic in pediatric rheumatology is systemic hyperinflammation, a potentially life-threatening situation requiring rapid detection and treatment.
A Saturday morning session will dive deeply into this topic. First, Sebastiaan Vastert, MD, PhD, will share a birds-eye view of systemic inflammation in JIA, setting the stage for a discussion by Angelo Ravelli, MD, of challenges in diagnosing macrophage activation syndrome, which disproportionately affects JIA patients.
Also during the session, Fabrizio de Benedetti, MD, PhD, will review new findings on the pathogenesis of hyperinflammation and how they can guide therapeutic development. Rounding off the session, Rebecca Davies will present research on first-onset uveitis in patients receiving etanercept or methotrexate to treat JIA. “Attendees will learn new insights about diagnosing and treating systemic inflammation in children,” Dr. Prakken said.
Once the dust has settled on the EULAR Congress in Amsterdam, delegates can look forward to the 2019 EULAR Congress in Madrid, which will be held jointly with the Paediatric Rheumatology European Society, further integrating the fields of pediatric and adult rheumatology.
Personalized medicine, big data, and monogenic inflammatory diseases are just a few of the high points of pediatric rheumatology sessions at this year’s EULAR Congress.
EULAR Standing Committee Chairperson for Paediatric Rheumatology Berent J. Prakken, MD, PhD, said that a bench-to-bedside session on Wednesday afternoon would highlight how EULAR projects are driving advances in pediatric rheumatology.
Attendees will learn from Vicki Seyfert-Margolis, PhD, an internationally recognized expert in personalized medicine, about how digital tools can facilitate cross-border partnerships in pediatric rheumatology, Dr. Prakken said in an interview.
“This talk will be groundbreaking because it’s not just about another useful app,” said Dr. Prakken, professor of pediatric rheumatology and vice dean of education at University Medical Center Utrecht (the Netherlands). “Dr. Seyfert-Margolis will show how the digital revolution will change the way we communicate with patients, monitor disease, and develop novel models for clinical trials.”
The session will also cover work by the Understanding Childhood Arthritis Network (UCAN), created to facilitate international translational research in pediatric rheumatology. Speakers will describe how UCAN is helping to spur personalized medicine and working with the Pediatric Rheumatology International Trials Organization (PRINTO) to align bench and bedside perspectives.
Another program highlight is a Thursday afternoon session on connections between monogenic autoinflammatory and pediatric rheumatic diseases. “Groundbreaking studies of these rare genetic inflammatory diseases have provided important new insights that, in turn, have led to new therapeutic options,” said Dr. Prakken.
During the session, Joost Swart, MD, of Utrecht, the Netherlands, will discuss promising research on the intravenous use of mesenchymal stromal cells derived from bone marrow for the treatment of refractory juvenile idiopathic arthritis (JIA).
Dr. Swart, who helped pioneer the approach, will discuss the first phase I/II trial of its use in children. “This is a truly innovative way to handle refractory inflammation,” Dr. Prakken said.
The session on monogenic autoinflammatory diseases also will cover their clinical presentation in children and adults, their pathogenesis as compared with adult-onset rheumatic diseases, and emerging treatment options, according to Dr. Prakken.
On Friday afternoon, a pediatric session will feature big data science in pediatric rheumatology, a lightning-paced field that is generating new research and treatment paradigms.
Of special note, Salvatore Albani, MD, PhD, will discuss how the human immunome is revolutionizing personalized treatment of paediatric inflammatory diseases, Dr. Prakken said. “This is the first application of big data to develop a completely new, personalized map of the human immune system,” he added. “This technology has the potential to revolutionize human clinical immunology, and it may be the key to true precision medicine in inflammatory diseases.”
Other talks in the session will cover signaling pathways in childhood systemic lupus erythematosus (SLE), galectin-9 as a biomarker in juvenile dermatomyositis, and evidence from the phase 3 PRINTO trial on how best to taper corticosteroids in patients with new-onset juvenile dermatomyositis.
Another crucial topic in pediatric rheumatology is systemic hyperinflammation, a potentially life-threatening situation requiring rapid detection and treatment.
A Saturday morning session will dive deeply into this topic. First, Sebastiaan Vastert, MD, PhD, will share a birds-eye view of systemic inflammation in JIA, setting the stage for a discussion by Angelo Ravelli, MD, of challenges in diagnosing macrophage activation syndrome, which disproportionately affects JIA patients.
Also during the session, Fabrizio de Benedetti, MD, PhD, will review new findings on the pathogenesis of hyperinflammation and how they can guide therapeutic development. Rounding off the session, Rebecca Davies will present research on first-onset uveitis in patients receiving etanercept or methotrexate to treat JIA. “Attendees will learn new insights about diagnosing and treating systemic inflammation in children,” Dr. Prakken said.
Once the dust has settled on the EULAR Congress in Amsterdam, delegates can look forward to the 2019 EULAR Congress in Madrid, which will be held jointly with the Paediatric Rheumatology European Society, further integrating the fields of pediatric and adult rheumatology.
Personalized medicine, big data, and monogenic inflammatory diseases are just a few of the high points of pediatric rheumatology sessions at this year’s EULAR Congress.
EULAR Standing Committee Chairperson for Paediatric Rheumatology Berent J. Prakken, MD, PhD, said that a bench-to-bedside session on Wednesday afternoon would highlight how EULAR projects are driving advances in pediatric rheumatology.
Attendees will learn from Vicki Seyfert-Margolis, PhD, an internationally recognized expert in personalized medicine, about how digital tools can facilitate cross-border partnerships in pediatric rheumatology, Dr. Prakken said in an interview.
“This talk will be groundbreaking because it’s not just about another useful app,” said Dr. Prakken, professor of pediatric rheumatology and vice dean of education at University Medical Center Utrecht (the Netherlands). “Dr. Seyfert-Margolis will show how the digital revolution will change the way we communicate with patients, monitor disease, and develop novel models for clinical trials.”
The session will also cover work by the Understanding Childhood Arthritis Network (UCAN), created to facilitate international translational research in pediatric rheumatology. Speakers will describe how UCAN is helping to spur personalized medicine and working with the Pediatric Rheumatology International Trials Organization (PRINTO) to align bench and bedside perspectives.
Another program highlight is a Thursday afternoon session on connections between monogenic autoinflammatory and pediatric rheumatic diseases. “Groundbreaking studies of these rare genetic inflammatory diseases have provided important new insights that, in turn, have led to new therapeutic options,” said Dr. Prakken.
During the session, Joost Swart, MD, of Utrecht, the Netherlands, will discuss promising research on the intravenous use of mesenchymal stromal cells derived from bone marrow for the treatment of refractory juvenile idiopathic arthritis (JIA).
Dr. Swart, who helped pioneer the approach, will discuss the first phase I/II trial of its use in children. “This is a truly innovative way to handle refractory inflammation,” Dr. Prakken said.
The session on monogenic autoinflammatory diseases also will cover their clinical presentation in children and adults, their pathogenesis as compared with adult-onset rheumatic diseases, and emerging treatment options, according to Dr. Prakken.
On Friday afternoon, a pediatric session will feature big data science in pediatric rheumatology, a lightning-paced field that is generating new research and treatment paradigms.
Of special note, Salvatore Albani, MD, PhD, will discuss how the human immunome is revolutionizing personalized treatment of paediatric inflammatory diseases, Dr. Prakken said. “This is the first application of big data to develop a completely new, personalized map of the human immune system,” he added. “This technology has the potential to revolutionize human clinical immunology, and it may be the key to true precision medicine in inflammatory diseases.”
Other talks in the session will cover signaling pathways in childhood systemic lupus erythematosus (SLE), galectin-9 as a biomarker in juvenile dermatomyositis, and evidence from the phase 3 PRINTO trial on how best to taper corticosteroids in patients with new-onset juvenile dermatomyositis.
Another crucial topic in pediatric rheumatology is systemic hyperinflammation, a potentially life-threatening situation requiring rapid detection and treatment.
A Saturday morning session will dive deeply into this topic. First, Sebastiaan Vastert, MD, PhD, will share a birds-eye view of systemic inflammation in JIA, setting the stage for a discussion by Angelo Ravelli, MD, of challenges in diagnosing macrophage activation syndrome, which disproportionately affects JIA patients.
Also during the session, Fabrizio de Benedetti, MD, PhD, will review new findings on the pathogenesis of hyperinflammation and how they can guide therapeutic development. Rounding off the session, Rebecca Davies will present research on first-onset uveitis in patients receiving etanercept or methotrexate to treat JIA. “Attendees will learn new insights about diagnosing and treating systemic inflammation in children,” Dr. Prakken said.
Once the dust has settled on the EULAR Congress in Amsterdam, delegates can look forward to the 2019 EULAR Congress in Madrid, which will be held jointly with the Paediatric Rheumatology European Society, further integrating the fields of pediatric and adult rheumatology.
Dasatinib outcomes similar to imatinib in pediatric Ph+ ALL

Dasatinib used during induction and consolidation in the Children’s Oncology Group (COG) AALL0622 trial provided early response rates for children with Ph-positive (Ph+) acute lymphoblastic leukemia (ALL), according to investigators.
But the early response rates did not improve event-free survival (EFS) compared to the use of consolidation imatinib in the AALL0031 study.
Incidence of cranial relapse was more than doubled in AALL0622 compared to AALL0031.
The investigators believe the incidence of cranial relapse may explain the results of AALL0622.
“We cannot yet conclude that the current dasatinib plus chemotherapy combination is better than imatinib plus chemotherapy,” the authors stated.
AALL0622 was designed to be an improvement on AALL0031, which demonstrated that adding the tyrosine kinase inhibitor (TKI) imatinib to intensive chemotherapy in the consolidation phase significantly improved survival for children with Ph+ ALL.
In AALL0622 dasatinib was given early in induction (day 15) and then in consolidation with the hope that patients could achieve early remission.
Another departure from AALL0031 was that cranial irradiation was not provided for control of central nervous system (CNS) metastasis. Because dasatinib accumulates in the CNS, which is a ‘sanctuary site’ for leukemia, it was presumed that patients could benefit from a TKI yet be spared from cranial irradiation.
As expected, adding dasatinib mid-induction provided a complete remission rate of 98% at the end of induction (day 29), which was better than the 89% seen in AALL0031.
In addition, more patients in AALL0622 showed minimal residual disease (MRD) <0.01% at the end of induction: 59% vs 25% in AALL0031 (P <0.001). At the end of consolidation, corresponding rates were 89% vs 71% for AALL0031.
For the primary outcome, 3-year EFS was 84.6% for patients in AALL0622 in standard-risk patients. Five-year OS and EFS rates were 86% and 60%, respectively.
In patients with overt brain metastasis (CNS3 status), 5-year CNS relapse was 15% for patients in the AALL0622 study vs 6.6% for patients in the AALL031 study.
However, 5-year OS rates were similar in the two groups of patients: 86% for AALL0622 vs 81% for AALL0031.
HSCT
AALL0622 allowed the use of hematopoietic stem cell transplantation (HSCT) in high-risk patients as well as in standard-risk patients with a sibling donor.
Five-year OS and EFS for standard-risk patients (19% underwent HSCT at first remission) and high-risk patients (91% underwent HSCT in first remission) were similar.
Children who did not undergo HSCT had a similar 5-year OS of 88%, which suggested that children with Ph+ ALL should not undergo transplantation at first remission.
Samples from a subset of patients was analyzed for IKZF1 mutations and correlated with outcomes.
Five-year OS was 80% in those harboring the mutation versus 100% who had the wild-type gene (P=0.04); 4-year EFS was also significantly lower—10% vs 82% (P=0.04).
Screening for IKZF1 may be used to identify high-risk patients suitable for HSCT and/or alternate treatment, the authors note.
The investigators reported their findings in The Journal of Clinical Oncology.
Dasatinib used during induction and consolidation in the Children’s Oncology Group (COG) AALL0622 trial provided early response rates for children with Ph-positive (Ph+) acute lymphoblastic leukemia (ALL), according to investigators.
But the early response rates did not improve event-free survival (EFS) compared to the use of consolidation imatinib in the AALL0031 study.
Incidence of cranial relapse was more than doubled in AALL0622 compared to AALL0031.
The investigators believe the incidence of cranial relapse may explain the results of AALL0622.
“We cannot yet conclude that the current dasatinib plus chemotherapy combination is better than imatinib plus chemotherapy,” the authors stated.
AALL0622 was designed to be an improvement on AALL0031, which demonstrated that adding the tyrosine kinase inhibitor (TKI) imatinib to intensive chemotherapy in the consolidation phase significantly improved survival for children with Ph+ ALL.
In AALL0622 dasatinib was given early in induction (day 15) and then in consolidation with the hope that patients could achieve early remission.
Another departure from AALL0031 was that cranial irradiation was not provided for control of central nervous system (CNS) metastasis. Because dasatinib accumulates in the CNS, which is a ‘sanctuary site’ for leukemia, it was presumed that patients could benefit from a TKI yet be spared from cranial irradiation.
As expected, adding dasatinib mid-induction provided a complete remission rate of 98% at the end of induction (day 29), which was better than the 89% seen in AALL0031.
In addition, more patients in AALL0622 showed minimal residual disease (MRD) <0.01% at the end of induction: 59% vs 25% in AALL0031 (P <0.001). At the end of consolidation, corresponding rates were 89% vs 71% for AALL0031.
For the primary outcome, 3-year EFS was 84.6% for patients in AALL0622 in standard-risk patients. Five-year OS and EFS rates were 86% and 60%, respectively.
In patients with overt brain metastasis (CNS3 status), 5-year CNS relapse was 15% for patients in the AALL0622 study vs 6.6% for patients in the AALL031 study.
However, 5-year OS rates were similar in the two groups of patients: 86% for AALL0622 vs 81% for AALL0031.
HSCT
AALL0622 allowed the use of hematopoietic stem cell transplantation (HSCT) in high-risk patients as well as in standard-risk patients with a sibling donor.
Five-year OS and EFS for standard-risk patients (19% underwent HSCT at first remission) and high-risk patients (91% underwent HSCT in first remission) were similar.
Children who did not undergo HSCT had a similar 5-year OS of 88%, which suggested that children with Ph+ ALL should not undergo transplantation at first remission.
Samples from a subset of patients was analyzed for IKZF1 mutations and correlated with outcomes.
Five-year OS was 80% in those harboring the mutation versus 100% who had the wild-type gene (P=0.04); 4-year EFS was also significantly lower—10% vs 82% (P=0.04).
Screening for IKZF1 may be used to identify high-risk patients suitable for HSCT and/or alternate treatment, the authors note.
The investigators reported their findings in The Journal of Clinical Oncology.
Dasatinib used during induction and consolidation in the Children’s Oncology Group (COG) AALL0622 trial provided early response rates for children with Ph-positive (Ph+) acute lymphoblastic leukemia (ALL), according to investigators.
But the early response rates did not improve event-free survival (EFS) compared to the use of consolidation imatinib in the AALL0031 study.
Incidence of cranial relapse was more than doubled in AALL0622 compared to AALL0031.
The investigators believe the incidence of cranial relapse may explain the results of AALL0622.
“We cannot yet conclude that the current dasatinib plus chemotherapy combination is better than imatinib plus chemotherapy,” the authors stated.
AALL0622 was designed to be an improvement on AALL0031, which demonstrated that adding the tyrosine kinase inhibitor (TKI) imatinib to intensive chemotherapy in the consolidation phase significantly improved survival for children with Ph+ ALL.
In AALL0622 dasatinib was given early in induction (day 15) and then in consolidation with the hope that patients could achieve early remission.
Another departure from AALL0031 was that cranial irradiation was not provided for control of central nervous system (CNS) metastasis. Because dasatinib accumulates in the CNS, which is a ‘sanctuary site’ for leukemia, it was presumed that patients could benefit from a TKI yet be spared from cranial irradiation.
As expected, adding dasatinib mid-induction provided a complete remission rate of 98% at the end of induction (day 29), which was better than the 89% seen in AALL0031.
In addition, more patients in AALL0622 showed minimal residual disease (MRD) <0.01% at the end of induction: 59% vs 25% in AALL0031 (P <0.001). At the end of consolidation, corresponding rates were 89% vs 71% for AALL0031.
For the primary outcome, 3-year EFS was 84.6% for patients in AALL0622 in standard-risk patients. Five-year OS and EFS rates were 86% and 60%, respectively.
In patients with overt brain metastasis (CNS3 status), 5-year CNS relapse was 15% for patients in the AALL0622 study vs 6.6% for patients in the AALL031 study.
However, 5-year OS rates were similar in the two groups of patients: 86% for AALL0622 vs 81% for AALL0031.
HSCT
AALL0622 allowed the use of hematopoietic stem cell transplantation (HSCT) in high-risk patients as well as in standard-risk patients with a sibling donor.
Five-year OS and EFS for standard-risk patients (19% underwent HSCT at first remission) and high-risk patients (91% underwent HSCT in first remission) were similar.
Children who did not undergo HSCT had a similar 5-year OS of 88%, which suggested that children with Ph+ ALL should not undergo transplantation at first remission.
Samples from a subset of patients was analyzed for IKZF1 mutations and correlated with outcomes.
Five-year OS was 80% in those harboring the mutation versus 100% who had the wild-type gene (P=0.04); 4-year EFS was also significantly lower—10% vs 82% (P=0.04).
Screening for IKZF1 may be used to identify high-risk patients suitable for HSCT and/or alternate treatment, the authors note.
The investigators reported their findings in The Journal of Clinical Oncology.
Allergies linked to autism spectrum disorder in children
The prevalence of food, respiratory, and skin allergy is greater in U.S. children with autism spectrum disorder (ASD) than in U.S. children without the disorder, according to findings published June 8 in JAMA Network Open.
An analysis of data from the National Health Interview Survey found that the weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Survey data were collected between 1997 and 2016, and included patients aged 3-17 years. Allergic conditions were defined by the respondent, usually a parent, answering in the affirmative that the child had any kind of food, digestive, respiratory, or skin allergy in the past 12 months. ASD was defined based on an affirmative response to a question asking whether the child received an ASD diagnosis from a health professional. The question was asked as part of a 10-condition checklist from 1997 to 2013, and as a standalone item from 2014 onward, with revised wording to distinguish autism, Asperger’s disorder, pervasive developmental disorder, and ASD, wrote Guifeng Xu, MD, of the department of epidemiology at the University of Iowa, Iowa City, and her coauthors.
Of the 199,520 children included in the study, 8,734 had food allergy, 24,555 had respiratory allergy, and 19,399 had skin allergy. An ASD diagnosis was reported in 1,868 children. The weighted prevalence was 4.31% for food allergy (95% confidence interval, 4.20%-4.43%), 12.15% for respiratory allergy (95% CI, 11.92%-12.38%), and 9.91% for skin allergy (95% CI, 9.72%-10.10%), the authors said.
Children with ASD were more likely than were children without ASD to have food allergy, respiratory allergy, and skin allergy (P less than .001). After adjustment for factors including age, sex, ethnicity, and family education level, the odds ratio of ASD was more than double among children with food allergy, compared with those without food allergy (odds ratio, 2.72; 95% CI, 2.26-3.28; P less than .001).
Respiratory allergy and skin allergy also were significantly associated with ASD, but to a lesser degree, with an OR of 1.53 (95% CI, 1.32-1.78; P less than .001) for respiratory allergy and 1.80 (95% CI, 1.55-2.09; P less than .001) for skin allergy, Dr. Xu and her colleagues reported.
,” though the underlying mechanisms still need to be identified, the authors wrote.
Particularly striking were the connections found between ASD and food allergy. “Although the underlying mechanisms for the observed association between food allergy and ASD remain to be elucidated, the gut-brain-behavior axis could be one of the potential mechanisms,” Dr. Xu and her coauthors wrote. “Previous studies found higher prevalence of gastrointestinal symptoms among children with ASD.”
Limitations to the study include possible recall bias and misreporting, as well as an absence of information about onset of allergy and ASD diagnosis.
“Large prospective cohort studies starting from birth or early life are needed to confirm our findings,” the authors concluded.
No conflicts of interest were reported.
SOURCE: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
The results of this study add to a “growing body of literature supporting an immune-mediated subtype of autism spectrum disorder (ASD),” Christopher J. McDougle, MD, wrote in an editorial published with the study.
Although prior studies have identified an association between ASD and respiratory and skin allergy, this study is “the first to document the association of food allergy with ASD with confidence, in part based on the large sample size they accessed,” he said (JAMA Network Open. 2018;1[2]:e180280. doi: 10.1001/jamanetworkopen.2018.0280).

Dr. McDougle is affiliated with the Lurie Center for Autism at Massachusetts General Hospital.
The results of this study add to a “growing body of literature supporting an immune-mediated subtype of autism spectrum disorder (ASD),” Christopher J. McDougle, MD, wrote in an editorial published with the study.
Although prior studies have identified an association between ASD and respiratory and skin allergy, this study is “the first to document the association of food allergy with ASD with confidence, in part based on the large sample size they accessed,” he said (JAMA Network Open. 2018;1[2]:e180280. doi: 10.1001/jamanetworkopen.2018.0280).
Dr. McDougle is affiliated with the Lurie Center for Autism at Massachusetts General Hospital.
The results of this study add to a “growing body of literature supporting an immune-mediated subtype of autism spectrum disorder (ASD),” Christopher J. McDougle, MD, wrote in an editorial published with the study.
Although prior studies have identified an association between ASD and respiratory and skin allergy, this study is “the first to document the association of food allergy with ASD with confidence, in part based on the large sample size they accessed,” he said (JAMA Network Open. 2018;1[2]:e180280. doi: 10.1001/jamanetworkopen.2018.0280).
Dr. McDougle is affiliated with the Lurie Center for Autism at Massachusetts General Hospital.
The prevalence of food, respiratory, and skin allergy is greater in U.S. children with autism spectrum disorder (ASD) than in U.S. children without the disorder, according to findings published June 8 in JAMA Network Open.
An analysis of data from the National Health Interview Survey found that the weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Survey data were collected between 1997 and 2016, and included patients aged 3-17 years. Allergic conditions were defined by the respondent, usually a parent, answering in the affirmative that the child had any kind of food, digestive, respiratory, or skin allergy in the past 12 months. ASD was defined based on an affirmative response to a question asking whether the child received an ASD diagnosis from a health professional. The question was asked as part of a 10-condition checklist from 1997 to 2013, and as a standalone item from 2014 onward, with revised wording to distinguish autism, Asperger’s disorder, pervasive developmental disorder, and ASD, wrote Guifeng Xu, MD, of the department of epidemiology at the University of Iowa, Iowa City, and her coauthors.
Of the 199,520 children included in the study, 8,734 had food allergy, 24,555 had respiratory allergy, and 19,399 had skin allergy. An ASD diagnosis was reported in 1,868 children. The weighted prevalence was 4.31% for food allergy (95% confidence interval, 4.20%-4.43%), 12.15% for respiratory allergy (95% CI, 11.92%-12.38%), and 9.91% for skin allergy (95% CI, 9.72%-10.10%), the authors said.
Children with ASD were more likely than were children without ASD to have food allergy, respiratory allergy, and skin allergy (P less than .001). After adjustment for factors including age, sex, ethnicity, and family education level, the odds ratio of ASD was more than double among children with food allergy, compared with those without food allergy (odds ratio, 2.72; 95% CI, 2.26-3.28; P less than .001).
Respiratory allergy and skin allergy also were significantly associated with ASD, but to a lesser degree, with an OR of 1.53 (95% CI, 1.32-1.78; P less than .001) for respiratory allergy and 1.80 (95% CI, 1.55-2.09; P less than .001) for skin allergy, Dr. Xu and her colleagues reported.
,” though the underlying mechanisms still need to be identified, the authors wrote.
Particularly striking were the connections found between ASD and food allergy. “Although the underlying mechanisms for the observed association between food allergy and ASD remain to be elucidated, the gut-brain-behavior axis could be one of the potential mechanisms,” Dr. Xu and her coauthors wrote. “Previous studies found higher prevalence of gastrointestinal symptoms among children with ASD.”
Limitations to the study include possible recall bias and misreporting, as well as an absence of information about onset of allergy and ASD diagnosis.
“Large prospective cohort studies starting from birth or early life are needed to confirm our findings,” the authors concluded.
No conflicts of interest were reported.
SOURCE: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
The prevalence of food, respiratory, and skin allergy is greater in U.S. children with autism spectrum disorder (ASD) than in U.S. children without the disorder, according to findings published June 8 in JAMA Network Open.
An analysis of data from the National Health Interview Survey found that the weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Survey data were collected between 1997 and 2016, and included patients aged 3-17 years. Allergic conditions were defined by the respondent, usually a parent, answering in the affirmative that the child had any kind of food, digestive, respiratory, or skin allergy in the past 12 months. ASD was defined based on an affirmative response to a question asking whether the child received an ASD diagnosis from a health professional. The question was asked as part of a 10-condition checklist from 1997 to 2013, and as a standalone item from 2014 onward, with revised wording to distinguish autism, Asperger’s disorder, pervasive developmental disorder, and ASD, wrote Guifeng Xu, MD, of the department of epidemiology at the University of Iowa, Iowa City, and her coauthors.
Of the 199,520 children included in the study, 8,734 had food allergy, 24,555 had respiratory allergy, and 19,399 had skin allergy. An ASD diagnosis was reported in 1,868 children. The weighted prevalence was 4.31% for food allergy (95% confidence interval, 4.20%-4.43%), 12.15% for respiratory allergy (95% CI, 11.92%-12.38%), and 9.91% for skin allergy (95% CI, 9.72%-10.10%), the authors said.
Children with ASD were more likely than were children without ASD to have food allergy, respiratory allergy, and skin allergy (P less than .001). After adjustment for factors including age, sex, ethnicity, and family education level, the odds ratio of ASD was more than double among children with food allergy, compared with those without food allergy (odds ratio, 2.72; 95% CI, 2.26-3.28; P less than .001).
Respiratory allergy and skin allergy also were significantly associated with ASD, but to a lesser degree, with an OR of 1.53 (95% CI, 1.32-1.78; P less than .001) for respiratory allergy and 1.80 (95% CI, 1.55-2.09; P less than .001) for skin allergy, Dr. Xu and her colleagues reported.
,” though the underlying mechanisms still need to be identified, the authors wrote.
Particularly striking were the connections found between ASD and food allergy. “Although the underlying mechanisms for the observed association between food allergy and ASD remain to be elucidated, the gut-brain-behavior axis could be one of the potential mechanisms,” Dr. Xu and her coauthors wrote. “Previous studies found higher prevalence of gastrointestinal symptoms among children with ASD.”
Limitations to the study include possible recall bias and misreporting, as well as an absence of information about onset of allergy and ASD diagnosis.
“Large prospective cohort studies starting from birth or early life are needed to confirm our findings,” the authors concluded.
No conflicts of interest were reported.
SOURCE: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
FROM JAMA NETWORK OPEN
Key clinical point: The prevalence of food, respiratory, and skin allergy was greater in children with autism spectrum disorder (ASD).
Major finding: The weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Study details: A population-based study of 199,520 children aged 3-17 years in the National Health Interview Survey.
Disclosures: No conflicts of interest were reported.
Source: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
App found to improve quality of life for families of premature infants
TORONTO – Significant improvement in quality of life was observed in neonatal ICU families using the PreeMe+You app, preliminary results from a two-center study showed.
“NICU time is stressful,” one of the study authors, Abigail Whitney, said at the Pediatric Academic Societies annual meeting. “With the birth of a preterm infant, parents are often quickly transitioned into the role of becoming a parent much sooner and in much different circumstances than they might have anticipated. Parents have reported feelings of isolation, alienation, and insecurity in the parental role while in the NICU. Studies have shown that interventions that engage parents in their infant’s progress can decrease parental stress and anxiety, increase positive parent-infant interaction, and even reduce the infant’s length of stay. Also, with advancing technology there has been a push to find ways to use mobile technology to help parents balance engaging with their infant with the rest of their busy lives.”

In a study overseen by PreeMe+You’s chief medical expert, Bree Andrews, MD, MPH, Ms. Whitney and her associates administered the app to 48 families at either the University of Chicago Medicine Comer Children’s Hospital NICU or the Evanston Hospital NICU to assess readiness for using mobile technologies at the bedside. All families were recommended by a child life specialist who identified families who might be interested in using something like PreeMe+You. They excluded any families that were currently involved with child and family services, those with an infant younger than 7 days old, those whose child required escalation of care or upcoming surgeries, and those whose infant was over 37 weeks’ gestation.
First, the researchers briefed NICU staff about the study at charge nurse meetings, faculty meetings, and daily huddles for 2 weeks before first enrollment. “We did this knowing that parents might go to their nurses or doctors about how to answer specific questions within the app, or maybe want to learn more about a certain topic they learned from PreeMe+You,” Ms. Whitney said.
Data measurements included the PreeMe+You composite survey, which pulled questions from the Fragile Infant Parent Readiness Evaluation (FIPRE) and the NICU Parent Risk Evaluation and Engagement Model and Instrument (PREEMI). “We also included additional questions about technology use and capacity, as well as the PedsQL [Pediatric Quality of Life Inventory] Family Impact Module to assess parental quality of life throughout the study,” she said.

Over a period of 9 months, the researchers collected 153 quality of life measurements from 48 families. Of these, 48 occurred at enrollment, 23 occurred less than 1 week after enrollment, 30 occurred 1-2 weeks after enrollment, 28 occurred 3-4 weeks after enrollment, and 24 occurred 4 weeks or more after enrollment. By study closure, the researchers had follow-up data on 44 of the 48 families. The average gestational age at birth was 29.3 weeks, the average day of life at enrollment was 25.4, and the average birth weight was 1,280 grams.
On the app’s composite survey, 14.6% “agreed” and 79.2% “strongly agreed” that they were currently using a smart phone or tablet to look for information about preemies/NICU on the Internet, and about half “agreed” or “strongly agreed” (27.1% and 33.3%, respectively) that they spent more than 30 minutes per week looking up information about their NICU baby online. Nearly all families “agreed” or “strongly agreed” (14.6% and 85.4%) that they had a smart phone or tablet for Internet use in the NICU, and nearly all “agreed” or “strongly agreed” (33.3% and 62.5%) that having an app at the NICU bedside/home would be helpful. “This showed us that families were ready to use technology and interested in something like PreeMe+You at the bedside,” Ms. Whitney said.
At the time of study enrollment, 12 were in the purple stage, 8 were in the blue stage, 19 infants were in the orange stage, and 9 were in the yellow stage. Ms. Whitney reported that based on the PedsQL Family Impact Module, 35 of the 44 families showed increased quality of life functionality after participating in the study. This change was significant, with a P value of .001. Improvements were seen in the measure’s eight domains (physical, emotional, social, cognitive, communication, worry, daily activities, and family relationship functionality). “We saw increases across all of the domains based on how long the parents had been using the app,” Ms. Whitney said. “We found the biggest increase in quality of life in families of babies born less than 25 weeks’ gestational age, those born 25-26 weeks gestational age, those born 27-28 weeks gestational age, and those born 33-37 weeks gestational age. We are encouraged to see some of these quality of life changes in some of the earliest-born gestation babies because these are presumably the families that would have the longest time to go in the NICU and could benefit the most from using an app like PreeMe+You.”
She acknowledged certain limitations of the study, including the fact that it was conducted in two NICUs, “and we definitely need more comparisons to look at the natural trajectory of quality of life changes while families are in the NICU. Also, all of the families enrolled in our study had access to a research team that checked in with them weekly. In the real world, PreeMe+You would probably be self-guided.” Going forward, PreeMe+You plans to include additional features to give parents more self-guidance, making it easier for them to interact and partner with their baby’s medical team.
Funding for the study was provided by the Bucksbaum Institute for Clinical Excellence. Ms. Whitney was supported by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases.
TORONTO – Significant improvement in quality of life was observed in neonatal ICU families using the PreeMe+You app, preliminary results from a two-center study showed.
“NICU time is stressful,” one of the study authors, Abigail Whitney, said at the Pediatric Academic Societies annual meeting. “With the birth of a preterm infant, parents are often quickly transitioned into the role of becoming a parent much sooner and in much different circumstances than they might have anticipated. Parents have reported feelings of isolation, alienation, and insecurity in the parental role while in the NICU. Studies have shown that interventions that engage parents in their infant’s progress can decrease parental stress and anxiety, increase positive parent-infant interaction, and even reduce the infant’s length of stay. Also, with advancing technology there has been a push to find ways to use mobile technology to help parents balance engaging with their infant with the rest of their busy lives.”
In a study overseen by PreeMe+You’s chief medical expert, Bree Andrews, MD, MPH, Ms. Whitney and her associates administered the app to 48 families at either the University of Chicago Medicine Comer Children’s Hospital NICU or the Evanston Hospital NICU to assess readiness for using mobile technologies at the bedside. All families were recommended by a child life specialist who identified families who might be interested in using something like PreeMe+You. They excluded any families that were currently involved with child and family services, those with an infant younger than 7 days old, those whose child required escalation of care or upcoming surgeries, and those whose infant was over 37 weeks’ gestation.
First, the researchers briefed NICU staff about the study at charge nurse meetings, faculty meetings, and daily huddles for 2 weeks before first enrollment. “We did this knowing that parents might go to their nurses or doctors about how to answer specific questions within the app, or maybe want to learn more about a certain topic they learned from PreeMe+You,” Ms. Whitney said.
Data measurements included the PreeMe+You composite survey, which pulled questions from the Fragile Infant Parent Readiness Evaluation (FIPRE) and the NICU Parent Risk Evaluation and Engagement Model and Instrument (PREEMI). “We also included additional questions about technology use and capacity, as well as the PedsQL [Pediatric Quality of Life Inventory] Family Impact Module to assess parental quality of life throughout the study,” she said.
Over a period of 9 months, the researchers collected 153 quality of life measurements from 48 families. Of these, 48 occurred at enrollment, 23 occurred less than 1 week after enrollment, 30 occurred 1-2 weeks after enrollment, 28 occurred 3-4 weeks after enrollment, and 24 occurred 4 weeks or more after enrollment. By study closure, the researchers had follow-up data on 44 of the 48 families. The average gestational age at birth was 29.3 weeks, the average day of life at enrollment was 25.4, and the average birth weight was 1,280 grams.
On the app’s composite survey, 14.6% “agreed” and 79.2% “strongly agreed” that they were currently using a smart phone or tablet to look for information about preemies/NICU on the Internet, and about half “agreed” or “strongly agreed” (27.1% and 33.3%, respectively) that they spent more than 30 minutes per week looking up information about their NICU baby online. Nearly all families “agreed” or “strongly agreed” (14.6% and 85.4%) that they had a smart phone or tablet for Internet use in the NICU, and nearly all “agreed” or “strongly agreed” (33.3% and 62.5%) that having an app at the NICU bedside/home would be helpful. “This showed us that families were ready to use technology and interested in something like PreeMe+You at the bedside,” Ms. Whitney said.
At the time of study enrollment, 12 were in the purple stage, 8 were in the blue stage, 19 infants were in the orange stage, and 9 were in the yellow stage. Ms. Whitney reported that based on the PedsQL Family Impact Module, 35 of the 44 families showed increased quality of life functionality after participating in the study. This change was significant, with a P value of .001. Improvements were seen in the measure’s eight domains (physical, emotional, social, cognitive, communication, worry, daily activities, and family relationship functionality). “We saw increases across all of the domains based on how long the parents had been using the app,” Ms. Whitney said. “We found the biggest increase in quality of life in families of babies born less than 25 weeks’ gestational age, those born 25-26 weeks gestational age, those born 27-28 weeks gestational age, and those born 33-37 weeks gestational age. We are encouraged to see some of these quality of life changes in some of the earliest-born gestation babies because these are presumably the families that would have the longest time to go in the NICU and could benefit the most from using an app like PreeMe+You.”
She acknowledged certain limitations of the study, including the fact that it was conducted in two NICUs, “and we definitely need more comparisons to look at the natural trajectory of quality of life changes while families are in the NICU. Also, all of the families enrolled in our study had access to a research team that checked in with them weekly. In the real world, PreeMe+You would probably be self-guided.” Going forward, PreeMe+You plans to include additional features to give parents more self-guidance, making it easier for them to interact and partner with their baby’s medical team.
Funding for the study was provided by the Bucksbaum Institute for Clinical Excellence. Ms. Whitney was supported by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases.
TORONTO – Significant improvement in quality of life was observed in neonatal ICU families using the PreeMe+You app, preliminary results from a two-center study showed.
“NICU time is stressful,” one of the study authors, Abigail Whitney, said at the Pediatric Academic Societies annual meeting. “With the birth of a preterm infant, parents are often quickly transitioned into the role of becoming a parent much sooner and in much different circumstances than they might have anticipated. Parents have reported feelings of isolation, alienation, and insecurity in the parental role while in the NICU. Studies have shown that interventions that engage parents in their infant’s progress can decrease parental stress and anxiety, increase positive parent-infant interaction, and even reduce the infant’s length of stay. Also, with advancing technology there has been a push to find ways to use mobile technology to help parents balance engaging with their infant with the rest of their busy lives.”
In a study overseen by PreeMe+You’s chief medical expert, Bree Andrews, MD, MPH, Ms. Whitney and her associates administered the app to 48 families at either the University of Chicago Medicine Comer Children’s Hospital NICU or the Evanston Hospital NICU to assess readiness for using mobile technologies at the bedside. All families were recommended by a child life specialist who identified families who might be interested in using something like PreeMe+You. They excluded any families that were currently involved with child and family services, those with an infant younger than 7 days old, those whose child required escalation of care or upcoming surgeries, and those whose infant was over 37 weeks’ gestation.
First, the researchers briefed NICU staff about the study at charge nurse meetings, faculty meetings, and daily huddles for 2 weeks before first enrollment. “We did this knowing that parents might go to their nurses or doctors about how to answer specific questions within the app, or maybe want to learn more about a certain topic they learned from PreeMe+You,” Ms. Whitney said.
Data measurements included the PreeMe+You composite survey, which pulled questions from the Fragile Infant Parent Readiness Evaluation (FIPRE) and the NICU Parent Risk Evaluation and Engagement Model and Instrument (PREEMI). “We also included additional questions about technology use and capacity, as well as the PedsQL [Pediatric Quality of Life Inventory] Family Impact Module to assess parental quality of life throughout the study,” she said.
Over a period of 9 months, the researchers collected 153 quality of life measurements from 48 families. Of these, 48 occurred at enrollment, 23 occurred less than 1 week after enrollment, 30 occurred 1-2 weeks after enrollment, 28 occurred 3-4 weeks after enrollment, and 24 occurred 4 weeks or more after enrollment. By study closure, the researchers had follow-up data on 44 of the 48 families. The average gestational age at birth was 29.3 weeks, the average day of life at enrollment was 25.4, and the average birth weight was 1,280 grams.
On the app’s composite survey, 14.6% “agreed” and 79.2% “strongly agreed” that they were currently using a smart phone or tablet to look for information about preemies/NICU on the Internet, and about half “agreed” or “strongly agreed” (27.1% and 33.3%, respectively) that they spent more than 30 minutes per week looking up information about their NICU baby online. Nearly all families “agreed” or “strongly agreed” (14.6% and 85.4%) that they had a smart phone or tablet for Internet use in the NICU, and nearly all “agreed” or “strongly agreed” (33.3% and 62.5%) that having an app at the NICU bedside/home would be helpful. “This showed us that families were ready to use technology and interested in something like PreeMe+You at the bedside,” Ms. Whitney said.
At the time of study enrollment, 12 were in the purple stage, 8 were in the blue stage, 19 infants were in the orange stage, and 9 were in the yellow stage. Ms. Whitney reported that based on the PedsQL Family Impact Module, 35 of the 44 families showed increased quality of life functionality after participating in the study. This change was significant, with a P value of .001. Improvements were seen in the measure’s eight domains (physical, emotional, social, cognitive, communication, worry, daily activities, and family relationship functionality). “We saw increases across all of the domains based on how long the parents had been using the app,” Ms. Whitney said. “We found the biggest increase in quality of life in families of babies born less than 25 weeks’ gestational age, those born 25-26 weeks gestational age, those born 27-28 weeks gestational age, and those born 33-37 weeks gestational age. We are encouraged to see some of these quality of life changes in some of the earliest-born gestation babies because these are presumably the families that would have the longest time to go in the NICU and could benefit the most from using an app like PreeMe+You.”
She acknowledged certain limitations of the study, including the fact that it was conducted in two NICUs, “and we definitely need more comparisons to look at the natural trajectory of quality of life changes while families are in the NICU. Also, all of the families enrolled in our study had access to a research team that checked in with them weekly. In the real world, PreeMe+You would probably be self-guided.” Going forward, PreeMe+You plans to include additional features to give parents more self-guidance, making it easier for them to interact and partner with their baby’s medical team.
Funding for the study was provided by the Bucksbaum Institute for Clinical Excellence. Ms. Whitney was supported by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases.
REPORTING FROM PAS 2018
Key clinical point:
Major finding: In all, 35 of the 44 families showed increased quality of life functionality, based on the PedsQL Family Impact Module (P = .001).
Study details: A two-center study of 44 families with premature infants intended to assess readiness for using mobile technologies at the bedside.
Disclosures: Funding for the study was provided by the Bucksbaum Institute for Clinical Excellence. Ms. Whitney was supported by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases.
Youth tobacco use shows ‘promising declines’
according to the Centers for Disease Control and Prevention.
The prevalence of current tobacco use – defined as use on 1 or more days in the past 30 days – among high schoolers fell from 24.2% in 2011 to 19.6% in 2017, and middle school use decreased from 7.5% to 5.6% over that same time. That means the number of youth tobacco users went from almost 4.6 million in 2011 to slightly more than 3.6 million in 2017, Teresa W. Wang, PhD, and her associates said in the Morbidity and Mortality Weekly Report.
Almost half (47%) of the high school students who used tobacco in 2017 used two or more products, as did two out of five (42%) middle schoolers. That year, black high school students were less likely to use any tobacco product (14.2%) than were whites (22.7%) and Hispanics (16.7%). E-cigarettes were the most popular form of tobacco among white and Hispanic high schoolers, while cigars were the most commonly used form among blacks, they reported based on data from the National Youth Tobacco Surveys, which had sample sizes of 18,766 in 2011 and 17,872 in 2017.
“Despite promising declines in tobacco use, far too many young people continue to use tobacco products, including e-cigarettes,” CDC Director Robert R. Redfield, MD, said in a written statement accompanying the report. “Comprehensive, sustained strategies can help prevent and reduce tobacco use and protect our nation’s youth from this preventable health risk.”
In a separate statement, FDA Commissioner Scott Gottlieb, MD, said, “We are working hard to develop a pathway to put products like e-cigarettes through an appropriate series of regulatory gates to properly evaluate them as an alternative for adults who still want to get access to satisfying levels of nicotine, without all the risks associated with lighting tobacco on fire. And we will continue to encourage the development of potentially less harmful forms of nicotine delivery for currently addicted adult smokers. … But these public health opportunities are put at risk if all we do is hook another generation of kids on nicotine and tobacco products through alternatives like e-cigarettes.”
SOURCE: Wang TW et al. MMWR. 2018;67(22):629-33.
according to the Centers for Disease Control and Prevention.
The prevalence of current tobacco use – defined as use on 1 or more days in the past 30 days – among high schoolers fell from 24.2% in 2011 to 19.6% in 2017, and middle school use decreased from 7.5% to 5.6% over that same time. That means the number of youth tobacco users went from almost 4.6 million in 2011 to slightly more than 3.6 million in 2017, Teresa W. Wang, PhD, and her associates said in the Morbidity and Mortality Weekly Report.
Almost half (47%) of the high school students who used tobacco in 2017 used two or more products, as did two out of five (42%) middle schoolers. That year, black high school students were less likely to use any tobacco product (14.2%) than were whites (22.7%) and Hispanics (16.7%). E-cigarettes were the most popular form of tobacco among white and Hispanic high schoolers, while cigars were the most commonly used form among blacks, they reported based on data from the National Youth Tobacco Surveys, which had sample sizes of 18,766 in 2011 and 17,872 in 2017.
“Despite promising declines in tobacco use, far too many young people continue to use tobacco products, including e-cigarettes,” CDC Director Robert R. Redfield, MD, said in a written statement accompanying the report. “Comprehensive, sustained strategies can help prevent and reduce tobacco use and protect our nation’s youth from this preventable health risk.”
In a separate statement, FDA Commissioner Scott Gottlieb, MD, said, “We are working hard to develop a pathway to put products like e-cigarettes through an appropriate series of regulatory gates to properly evaluate them as an alternative for adults who still want to get access to satisfying levels of nicotine, without all the risks associated with lighting tobacco on fire. And we will continue to encourage the development of potentially less harmful forms of nicotine delivery for currently addicted adult smokers. … But these public health opportunities are put at risk if all we do is hook another generation of kids on nicotine and tobacco products through alternatives like e-cigarettes.”
SOURCE: Wang TW et al. MMWR. 2018;67(22):629-33.
according to the Centers for Disease Control and Prevention.
The prevalence of current tobacco use – defined as use on 1 or more days in the past 30 days – among high schoolers fell from 24.2% in 2011 to 19.6% in 2017, and middle school use decreased from 7.5% to 5.6% over that same time. That means the number of youth tobacco users went from almost 4.6 million in 2011 to slightly more than 3.6 million in 2017, Teresa W. Wang, PhD, and her associates said in the Morbidity and Mortality Weekly Report.
Almost half (47%) of the high school students who used tobacco in 2017 used two or more products, as did two out of five (42%) middle schoolers. That year, black high school students were less likely to use any tobacco product (14.2%) than were whites (22.7%) and Hispanics (16.7%). E-cigarettes were the most popular form of tobacco among white and Hispanic high schoolers, while cigars were the most commonly used form among blacks, they reported based on data from the National Youth Tobacco Surveys, which had sample sizes of 18,766 in 2011 and 17,872 in 2017.
“Despite promising declines in tobacco use, far too many young people continue to use tobacco products, including e-cigarettes,” CDC Director Robert R. Redfield, MD, said in a written statement accompanying the report. “Comprehensive, sustained strategies can help prevent and reduce tobacco use and protect our nation’s youth from this preventable health risk.”
In a separate statement, FDA Commissioner Scott Gottlieb, MD, said, “We are working hard to develop a pathway to put products like e-cigarettes through an appropriate series of regulatory gates to properly evaluate them as an alternative for adults who still want to get access to satisfying levels of nicotine, without all the risks associated with lighting tobacco on fire. And we will continue to encourage the development of potentially less harmful forms of nicotine delivery for currently addicted adult smokers. … But these public health opportunities are put at risk if all we do is hook another generation of kids on nicotine and tobacco products through alternatives like e-cigarettes.”
SOURCE: Wang TW et al. MMWR. 2018;67(22):629-33.
FROM MMWR
Marijuana’s perceived approval ratings on the rise
Parents’ disapproval of marijuana use has dropped since 1979 – at least that’s what their teenage children say, according to results of the 2017 Monitoring the Future survey.
The approximately 13,500 12th graders involved in the 2017 survey believe that their parents are much less likely to disapprove of marijuana use, compared with the students who responded to the survey during 1976-1979. At that time, 15% of the 12th graders said that their parents would not disapprove of using marijuana once or twice, but by 2017 the number had made a statistically significant rise to 23%, Richard A. Miech, PhD, and his associates said in their report on the 2017 survey.
Perceived approval of occasional marijuana use, which had garnered only an 8% share of respondents in 1976-1979, was up to a significantly higher 17% in 2017, and regular use went from 4% to 13%, said Dr. Miech and his associates, of the University of Michigan Institute for Social Research, Ann Arbor.
Parents’ increased acceptance of marijuana, as perceived by the 12th-grade students, was not matched for other substances. Disapproval for smoking one or more packs of cigarettes a day, for example, climbed from 89% in 1976-1979 to 92% in 2017, while disapproval of weekend binge drinking rose just a bit, going from 85% to 86%, they said.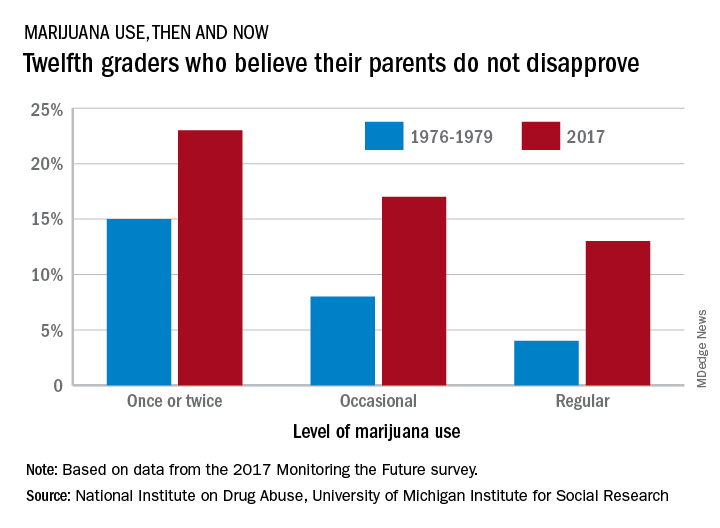
Measures of parental disapproval were reintroduced into the survey in 2017 after being removed in 1979 – the survey began in 1975 – “because students’ responses varied little over time and across drugs,” Dr. Miech and his associates noted. “Today’s parents of 12th graders have more experience with drug use than did parents in the late 1970s [and] population attitudes toward marijuana use across all ages are becoming more lenient,” they wrote.
The 2017 edition of the annual survey, which is funded by the National Institute on Drug Abuse, is based on reports from almost 44,000 students in 8th, 10th, and 12th grade in 360 public and private secondary schools across the country.
Parents’ disapproval of marijuana use has dropped since 1979 – at least that’s what their teenage children say, according to results of the 2017 Monitoring the Future survey.
The approximately 13,500 12th graders involved in the 2017 survey believe that their parents are much less likely to disapprove of marijuana use, compared with the students who responded to the survey during 1976-1979. At that time, 15% of the 12th graders said that their parents would not disapprove of using marijuana once or twice, but by 2017 the number had made a statistically significant rise to 23%, Richard A. Miech, PhD, and his associates said in their report on the 2017 survey.
Perceived approval of occasional marijuana use, which had garnered only an 8% share of respondents in 1976-1979, was up to a significantly higher 17% in 2017, and regular use went from 4% to 13%, said Dr. Miech and his associates, of the University of Michigan Institute for Social Research, Ann Arbor.
Parents’ increased acceptance of marijuana, as perceived by the 12th-grade students, was not matched for other substances. Disapproval for smoking one or more packs of cigarettes a day, for example, climbed from 89% in 1976-1979 to 92% in 2017, while disapproval of weekend binge drinking rose just a bit, going from 85% to 86%, they said.
Measures of parental disapproval were reintroduced into the survey in 2017 after being removed in 1979 – the survey began in 1975 – “because students’ responses varied little over time and across drugs,” Dr. Miech and his associates noted. “Today’s parents of 12th graders have more experience with drug use than did parents in the late 1970s [and] population attitudes toward marijuana use across all ages are becoming more lenient,” they wrote.
The 2017 edition of the annual survey, which is funded by the National Institute on Drug Abuse, is based on reports from almost 44,000 students in 8th, 10th, and 12th grade in 360 public and private secondary schools across the country.
Parents’ disapproval of marijuana use has dropped since 1979 – at least that’s what their teenage children say, according to results of the 2017 Monitoring the Future survey.
The approximately 13,500 12th graders involved in the 2017 survey believe that their parents are much less likely to disapprove of marijuana use, compared with the students who responded to the survey during 1976-1979. At that time, 15% of the 12th graders said that their parents would not disapprove of using marijuana once or twice, but by 2017 the number had made a statistically significant rise to 23%, Richard A. Miech, PhD, and his associates said in their report on the 2017 survey.
Perceived approval of occasional marijuana use, which had garnered only an 8% share of respondents in 1976-1979, was up to a significantly higher 17% in 2017, and regular use went from 4% to 13%, said Dr. Miech and his associates, of the University of Michigan Institute for Social Research, Ann Arbor.
Parents’ increased acceptance of marijuana, as perceived by the 12th-grade students, was not matched for other substances. Disapproval for smoking one or more packs of cigarettes a day, for example, climbed from 89% in 1976-1979 to 92% in 2017, while disapproval of weekend binge drinking rose just a bit, going from 85% to 86%, they said.
Measures of parental disapproval were reintroduced into the survey in 2017 after being removed in 1979 – the survey began in 1975 – “because students’ responses varied little over time and across drugs,” Dr. Miech and his associates noted. “Today’s parents of 12th graders have more experience with drug use than did parents in the late 1970s [and] population attitudes toward marijuana use across all ages are becoming more lenient,” they wrote.
The 2017 edition of the annual survey, which is funded by the National Institute on Drug Abuse, is based on reports from almost 44,000 students in 8th, 10th, and 12th grade in 360 public and private secondary schools across the country.