User login
Emotional regulation training lowers risk of adolescents having sex
Emotional regulation (ER) skills training lowers the likelihood that young adolescents with mental health symptoms will have vaginal sex.
“The inclusion of ER training in a small-group behavioral intervention reduced sexual risk behaviors among seventh-graders with suspected mental health symptoms over a 2.5-year follow-up beyond that achieved with more traditional health education,” wrote Chistopher Houck, PhD, and his colleagues at Bradley Hasbro Children’s Research Center, Providence, R.I., in Pediatrics. “This was true across a range of behaviors, such as engaging in fewer condom-less sex acts, being less likely to have multiple partners, and being less likely to use substances before sex.”
Students in the study participated in one of two after school intervention programs, either ER or health promotion (HP). Both programs consisted of 12 twice-weekly, hour-long sessions composed of single-sex groups of 4-8 adolescents. Two follow-up sessions were provided for both groups at 6 and 12 months. Both interventions used identical techniques, such as interactive games, videos, group discussions, and workbook assignments. ER sessions focused more on recognizing feelings, strategies for reducing momentary emotional arousal, and sexual health topics. HP exclusively focused on health topics like sexual risk and substance abuse but did not include emotional education.
During the 30-month study, 63 in the ER group (31%) and 68 students in the HP group (39%) reported having vaginal sex for the first time. This equated to an adjusted hazard ratio that indicated a delay in vaginal sex in the ER group (0.61; 95% confidence interval,0.42-0.89). Overall, students in the ER group were much less likely to endorse risky sexual behaviors than did participants in the HP group: Students in the ER group were less likely to endorse any risky sexual behavior (adjusted odds ratio, 0.52; 95% CI, 0.32-0.84), to support having multiple partners within 6 months (aOR, 0.54; 95% CI, 0.30-0.99), and to support the use of drugs before sex (aOR, 0.42; 95% CI, 0.23-0.75). Students in the ER group also reported fewer condom-less sex acts, compared with students in the HP group (adjusted rate ratio, 0.36; 95% CI, 0.14-0.90).
According to Dr. Houck and his colleagues, this study had several limitations that are common to sexual risk studies. One limitation is the reliance on self-report data, which can be biased. Dr. Houck and his associates utilized computer-assisted self-interviews to minimize biases. Another, and potentially larger, limitation is that the study was powered to assess delay of vaginal sex. Part of the patient sample was not sexually experienced, which provided less power for comparisons to other sexual behaviors.
Dr. Houck and his colleagues also spoke to the potential that ER training has in reducing risky behaviors of adolescents, as well as the issues in implementing it.
“Because ER is a skill that could influence other adolescent risk behaviors, such as substance use, violence, and truancy, addressing ER during this sensitive period in adolescent development promises significant public health benefits,” they wrote. “The challenge is the scale-up and dissemination of ER interventions. Increasing the reach of programs in which health education is enhanced with emotion education may be an important step toward improving the lives of adolescents because they are prone to beginning risk behavior.”
Dr. Houck and his associates have no relevant financial disclosures. This study received funding from the National Institutes of Health and the Providence/Boston Center for AIDS Research.
SOURCE: Houck C et al. Pediatrics. 2018 May 10. doi: 10.1542/peds.2017-2525.
The work of Houck et al. provides an important contribution in understanding strategies to reduce sexually transmitted infections (STIs) and HIV in adolescents by utilizing emotional regulation skills.
By helping young people understand their emotions and how that relates to behavior in the context of a sexual encounter, the after school intervention program helped teens regulate positive and negative emotions. Specifically, it utilized three strategies: get out, let it out, and think it out. Games and role playing gave teens a chance to practice these strategies in scenarios of varying risk.
Teenagers who underwent emotional regulation training, rather than simply being taught about adolescent health topics, fared much better in reducing the transition to vaginal sex over a 30-month period.
Carol Ford, MD, and her colleague James Jaccard, PhD, pointed out the superiority of the emotional training, compared with just sexual health information.
“Together, these findings reveal the importance of gearing more attention toward emotions and the regulation of emotions when developing interventions aimed at influencing adolescent sexual behavior,” they wrote. “Behavioral decision theory implicates the role of adolescent cognitions about engaging in sex, norms and peer pressure, and adolescent image prototypes surrounding sex.”
More broadly, Dr. Ford and Dr. Jaccard, believe that this research is the beginning to designing better interventions.
“As we come to understand the types of cognitions and emotions that dominate working memory in high-risk sexual situations, we can effectively design interventions that help shape cognitive and affective appraisals and how youth process those appraisals when making choices.”
Carol Ford, MD, is the chief of the Craig-Dalsimer Division of Adolescent Medicine at the Children’s Hospital of Philadelphia; she holds the Orton P. Jackson Endowed Chair in Adolescent Medicine. James Jaccard, PhD, is a professor of social work at New York University Silver School of Social Work. This is a summary of their commentary that accompanied the article by Houck et al. (Pediatrics. 2018 May 10. doi: 10.1542/peds.2017-4143). They had no financial disclosures, and there was no external funding.
The work of Houck et al. provides an important contribution in understanding strategies to reduce sexually transmitted infections (STIs) and HIV in adolescents by utilizing emotional regulation skills.
By helping young people understand their emotions and how that relates to behavior in the context of a sexual encounter, the after school intervention program helped teens regulate positive and negative emotions. Specifically, it utilized three strategies: get out, let it out, and think it out. Games and role playing gave teens a chance to practice these strategies in scenarios of varying risk.
Teenagers who underwent emotional regulation training, rather than simply being taught about adolescent health topics, fared much better in reducing the transition to vaginal sex over a 30-month period.
Carol Ford, MD, and her colleague James Jaccard, PhD, pointed out the superiority of the emotional training, compared with just sexual health information.
“Together, these findings reveal the importance of gearing more attention toward emotions and the regulation of emotions when developing interventions aimed at influencing adolescent sexual behavior,” they wrote. “Behavioral decision theory implicates the role of adolescent cognitions about engaging in sex, norms and peer pressure, and adolescent image prototypes surrounding sex.”
More broadly, Dr. Ford and Dr. Jaccard, believe that this research is the beginning to designing better interventions.
“As we come to understand the types of cognitions and emotions that dominate working memory in high-risk sexual situations, we can effectively design interventions that help shape cognitive and affective appraisals and how youth process those appraisals when making choices.”
Carol Ford, MD, is the chief of the Craig-Dalsimer Division of Adolescent Medicine at the Children’s Hospital of Philadelphia; she holds the Orton P. Jackson Endowed Chair in Adolescent Medicine. James Jaccard, PhD, is a professor of social work at New York University Silver School of Social Work. This is a summary of their commentary that accompanied the article by Houck et al. (Pediatrics. 2018 May 10. doi: 10.1542/peds.2017-4143). They had no financial disclosures, and there was no external funding.
The work of Houck et al. provides an important contribution in understanding strategies to reduce sexually transmitted infections (STIs) and HIV in adolescents by utilizing emotional regulation skills.
By helping young people understand their emotions and how that relates to behavior in the context of a sexual encounter, the after school intervention program helped teens regulate positive and negative emotions. Specifically, it utilized three strategies: get out, let it out, and think it out. Games and role playing gave teens a chance to practice these strategies in scenarios of varying risk.
Teenagers who underwent emotional regulation training, rather than simply being taught about adolescent health topics, fared much better in reducing the transition to vaginal sex over a 30-month period.
Carol Ford, MD, and her colleague James Jaccard, PhD, pointed out the superiority of the emotional training, compared with just sexual health information.
“Together, these findings reveal the importance of gearing more attention toward emotions and the regulation of emotions when developing interventions aimed at influencing adolescent sexual behavior,” they wrote. “Behavioral decision theory implicates the role of adolescent cognitions about engaging in sex, norms and peer pressure, and adolescent image prototypes surrounding sex.”
More broadly, Dr. Ford and Dr. Jaccard, believe that this research is the beginning to designing better interventions.
“As we come to understand the types of cognitions and emotions that dominate working memory in high-risk sexual situations, we can effectively design interventions that help shape cognitive and affective appraisals and how youth process those appraisals when making choices.”
Carol Ford, MD, is the chief of the Craig-Dalsimer Division of Adolescent Medicine at the Children’s Hospital of Philadelphia; she holds the Orton P. Jackson Endowed Chair in Adolescent Medicine. James Jaccard, PhD, is a professor of social work at New York University Silver School of Social Work. This is a summary of their commentary that accompanied the article by Houck et al. (Pediatrics. 2018 May 10. doi: 10.1542/peds.2017-4143). They had no financial disclosures, and there was no external funding.
Emotional regulation (ER) skills training lowers the likelihood that young adolescents with mental health symptoms will have vaginal sex.
“The inclusion of ER training in a small-group behavioral intervention reduced sexual risk behaviors among seventh-graders with suspected mental health symptoms over a 2.5-year follow-up beyond that achieved with more traditional health education,” wrote Chistopher Houck, PhD, and his colleagues at Bradley Hasbro Children’s Research Center, Providence, R.I., in Pediatrics. “This was true across a range of behaviors, such as engaging in fewer condom-less sex acts, being less likely to have multiple partners, and being less likely to use substances before sex.”
Students in the study participated in one of two after school intervention programs, either ER or health promotion (HP). Both programs consisted of 12 twice-weekly, hour-long sessions composed of single-sex groups of 4-8 adolescents. Two follow-up sessions were provided for both groups at 6 and 12 months. Both interventions used identical techniques, such as interactive games, videos, group discussions, and workbook assignments. ER sessions focused more on recognizing feelings, strategies for reducing momentary emotional arousal, and sexual health topics. HP exclusively focused on health topics like sexual risk and substance abuse but did not include emotional education.
During the 30-month study, 63 in the ER group (31%) and 68 students in the HP group (39%) reported having vaginal sex for the first time. This equated to an adjusted hazard ratio that indicated a delay in vaginal sex in the ER group (0.61; 95% confidence interval,0.42-0.89). Overall, students in the ER group were much less likely to endorse risky sexual behaviors than did participants in the HP group: Students in the ER group were less likely to endorse any risky sexual behavior (adjusted odds ratio, 0.52; 95% CI, 0.32-0.84), to support having multiple partners within 6 months (aOR, 0.54; 95% CI, 0.30-0.99), and to support the use of drugs before sex (aOR, 0.42; 95% CI, 0.23-0.75). Students in the ER group also reported fewer condom-less sex acts, compared with students in the HP group (adjusted rate ratio, 0.36; 95% CI, 0.14-0.90).
According to Dr. Houck and his colleagues, this study had several limitations that are common to sexual risk studies. One limitation is the reliance on self-report data, which can be biased. Dr. Houck and his associates utilized computer-assisted self-interviews to minimize biases. Another, and potentially larger, limitation is that the study was powered to assess delay of vaginal sex. Part of the patient sample was not sexually experienced, which provided less power for comparisons to other sexual behaviors.
Dr. Houck and his colleagues also spoke to the potential that ER training has in reducing risky behaviors of adolescents, as well as the issues in implementing it.
“Because ER is a skill that could influence other adolescent risk behaviors, such as substance use, violence, and truancy, addressing ER during this sensitive period in adolescent development promises significant public health benefits,” they wrote. “The challenge is the scale-up and dissemination of ER interventions. Increasing the reach of programs in which health education is enhanced with emotion education may be an important step toward improving the lives of adolescents because they are prone to beginning risk behavior.”
Dr. Houck and his associates have no relevant financial disclosures. This study received funding from the National Institutes of Health and the Providence/Boston Center for AIDS Research.
SOURCE: Houck C et al. Pediatrics. 2018 May 10. doi: 10.1542/peds.2017-2525.
Emotional regulation (ER) skills training lowers the likelihood that young adolescents with mental health symptoms will have vaginal sex.
“The inclusion of ER training in a small-group behavioral intervention reduced sexual risk behaviors among seventh-graders with suspected mental health symptoms over a 2.5-year follow-up beyond that achieved with more traditional health education,” wrote Chistopher Houck, PhD, and his colleagues at Bradley Hasbro Children’s Research Center, Providence, R.I., in Pediatrics. “This was true across a range of behaviors, such as engaging in fewer condom-less sex acts, being less likely to have multiple partners, and being less likely to use substances before sex.”
Students in the study participated in one of two after school intervention programs, either ER or health promotion (HP). Both programs consisted of 12 twice-weekly, hour-long sessions composed of single-sex groups of 4-8 adolescents. Two follow-up sessions were provided for both groups at 6 and 12 months. Both interventions used identical techniques, such as interactive games, videos, group discussions, and workbook assignments. ER sessions focused more on recognizing feelings, strategies for reducing momentary emotional arousal, and sexual health topics. HP exclusively focused on health topics like sexual risk and substance abuse but did not include emotional education.
During the 30-month study, 63 in the ER group (31%) and 68 students in the HP group (39%) reported having vaginal sex for the first time. This equated to an adjusted hazard ratio that indicated a delay in vaginal sex in the ER group (0.61; 95% confidence interval,0.42-0.89). Overall, students in the ER group were much less likely to endorse risky sexual behaviors than did participants in the HP group: Students in the ER group were less likely to endorse any risky sexual behavior (adjusted odds ratio, 0.52; 95% CI, 0.32-0.84), to support having multiple partners within 6 months (aOR, 0.54; 95% CI, 0.30-0.99), and to support the use of drugs before sex (aOR, 0.42; 95% CI, 0.23-0.75). Students in the ER group also reported fewer condom-less sex acts, compared with students in the HP group (adjusted rate ratio, 0.36; 95% CI, 0.14-0.90).
According to Dr. Houck and his colleagues, this study had several limitations that are common to sexual risk studies. One limitation is the reliance on self-report data, which can be biased. Dr. Houck and his associates utilized computer-assisted self-interviews to minimize biases. Another, and potentially larger, limitation is that the study was powered to assess delay of vaginal sex. Part of the patient sample was not sexually experienced, which provided less power for comparisons to other sexual behaviors.
Dr. Houck and his colleagues also spoke to the potential that ER training has in reducing risky behaviors of adolescents, as well as the issues in implementing it.
“Because ER is a skill that could influence other adolescent risk behaviors, such as substance use, violence, and truancy, addressing ER during this sensitive period in adolescent development promises significant public health benefits,” they wrote. “The challenge is the scale-up and dissemination of ER interventions. Increasing the reach of programs in which health education is enhanced with emotion education may be an important step toward improving the lives of adolescents because they are prone to beginning risk behavior.”
Dr. Houck and his associates have no relevant financial disclosures. This study received funding from the National Institutes of Health and the Providence/Boston Center for AIDS Research.
SOURCE: Houck C et al. Pediatrics. 2018 May 10. doi: 10.1542/peds.2017-2525.
FROM PEDIATRICS
Key clinical point: Emotional regulation (ER) training reduces the likelihood adolescents will have sex.
Major finding: There was a delay in vaginal sex in the ER group (adusted hazard ratio, 0.61; 95% confidence interval, 0.42-0.89), compared with the health promotion group.
Study details: The study included 420 seventh grade students aged 12-14 years from five urban Rhode Island middle schools between September 2009 and February 2012.
Disclosures: Dr. Houck and his associates have no relevant financial disclosures. This study received funding from the National Institutes of Health and the Providence/Boston Center for AIDS Research.
Source: Houck C et al. Pediatrics. 2018 May 10. doi: 10.1542/peds.2017-2525.
Responsive parenting intervention slows weight gain in infancy
TORONTO – Teaching parents of newborns to respond to eating and satiety cues in ways that promote self-regulation was associated with improvements in some weight outcomes at 3 years in a randomized clinical trial.
For the primary outcome of body mass index (BMI) z score at 3 years, a significant difference favoring the responsive parenting (RP) intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04). A longitudinal analysis examining the entire intervention period confirmed that the mean BMI group differences across seven study visits confirmed the effect of the RP intervention on BMI (P less than .001).
“We felt that the BMI z score and longitudinal growth analysis are probably the most sustained effects for an early-life intervention that have been recorded to date,” reported Ian M. Paul, MD, MSc, of Penn State University, Hershey. “While the differences between study groups were modest and not all achieved statistical significance, all favored the responsive-parenting intervention.”
Mean BMI percentile, a secondary outcome, was 47th for the RP group and 54th for controls, narrowly missing statistical significance (P = .07). Similarly, the percent of children deemed overweight at 3 years was 11.2% for the RP group and 19.8% for controls (P = .07), while 2.6% and 7.8%, respectively, were obese (P = .08).
No significant differences were seen in growth-related adverse events, such a weight-for-age less than the 5th percentile. The issue of “inducing” failure-to-thrive with a feeding intervention is a concern, said Dr. Paul, but there was no evidence for it in their study.
“One could question whether [the small differences seen between groups] are clinically significant, but if we look at how small differences have changed in the population over time and how those equate as far as longitudinal risk for cardiovascular outcomes and metabolic syndrome, etc., the small differences [we saw] might be important on a population level,” said Dr. Paul at the Pediatric Academic Societies meeting.
Study details
With upwards of one-quarter of U.S. children aged 2-5 years being overweight or obese, interventions to prevent rapid weight gain and reduce risk for overweight status in infancy are needed, noted Dr. Paul. Another reason to consider very early intervention, he added, is that infancy is a time of both “metabolic and behavioral plasticity.” However, most efforts to intervene early have, thus far, had limited success.
“Our responses to a baby crying are to feed that baby,” said Dr. Paul. This urge, along with others (such as “clear your plate”), evolved during times of food scarcity but persist now that we have inexpensive and palatable food, and promote rapid infant weight gain and increased obesity risk.
An alternative to those traditional parenting practices are responsive feeding and responsive parenting, he explained. “Responsive feeding and parenting requires prompt, developmentally appropriate responses to a child’s behaviors including hunger and satiety cues.”
In other studies, RP has been shown to foster cognitive, social, and emotional development. “The question we had was: Can responsive parenting reduce obesity risk?” he said.
The INSIGHT (Intervention Nurses Start Infants Growing on Healthy Trajectories) study is an ongoing, randomized clinical trial started in January 2012 comparing an RP intervention designed to prevent childhood obesity with a safety control, with the interventions matched on intensity and length.
Parent-child dyads were randomized 2 weeks after birth and were told that the purpose of the study was “to see if nurse visits to your home during your baby’s infancy can improve your ability to either respond to your child’s cues related to feeding and fussiness or improve your ability to provide a safe environment for your child and prevent injuries.”
A total of 279 primiparous mother-newborn dyads were studied. Most were white (89%) and non-Hispanic (94%), and the majority were married (75%). Mean prepregnancy BMI was 25.5 kg/m2.
“We chose first-time mothers because we thought they were more likely to listen to the parenting advice that we had to offer,” said Dr. Paul.
INSIGHT’s curriculum focused on RP in domains of infant feeding, sleep, interactive play, and emotion regulation. “We tried to promote self-regulation by setting limits but still being responsive in a variety of behavior domains,” Dr. Paul said. “So, for example…, for feeding we talked about exposure to healthy foods, shared feeding responsibility, for those that were bottle feeding we gave tips on size of bottle appropriate for the child and also not using bottle finishing practices. In the emotional and social regulation domain, we talked about alternatives to food to soothe, and emphasized embracing each child’s temperament and how to respond to different temperaments.”
Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
TORONTO – Teaching parents of newborns to respond to eating and satiety cues in ways that promote self-regulation was associated with improvements in some weight outcomes at 3 years in a randomized clinical trial.
For the primary outcome of body mass index (BMI) z score at 3 years, a significant difference favoring the responsive parenting (RP) intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04). A longitudinal analysis examining the entire intervention period confirmed that the mean BMI group differences across seven study visits confirmed the effect of the RP intervention on BMI (P less than .001).
“We felt that the BMI z score and longitudinal growth analysis are probably the most sustained effects for an early-life intervention that have been recorded to date,” reported Ian M. Paul, MD, MSc, of Penn State University, Hershey. “While the differences between study groups were modest and not all achieved statistical significance, all favored the responsive-parenting intervention.”
Mean BMI percentile, a secondary outcome, was 47th for the RP group and 54th for controls, narrowly missing statistical significance (P = .07). Similarly, the percent of children deemed overweight at 3 years was 11.2% for the RP group and 19.8% for controls (P = .07), while 2.6% and 7.8%, respectively, were obese (P = .08).
No significant differences were seen in growth-related adverse events, such a weight-for-age less than the 5th percentile. The issue of “inducing” failure-to-thrive with a feeding intervention is a concern, said Dr. Paul, but there was no evidence for it in their study.
“One could question whether [the small differences seen between groups] are clinically significant, but if we look at how small differences have changed in the population over time and how those equate as far as longitudinal risk for cardiovascular outcomes and metabolic syndrome, etc., the small differences [we saw] might be important on a population level,” said Dr. Paul at the Pediatric Academic Societies meeting.
Study details
With upwards of one-quarter of U.S. children aged 2-5 years being overweight or obese, interventions to prevent rapid weight gain and reduce risk for overweight status in infancy are needed, noted Dr. Paul. Another reason to consider very early intervention, he added, is that infancy is a time of both “metabolic and behavioral plasticity.” However, most efforts to intervene early have, thus far, had limited success.
“Our responses to a baby crying are to feed that baby,” said Dr. Paul. This urge, along with others (such as “clear your plate”), evolved during times of food scarcity but persist now that we have inexpensive and palatable food, and promote rapid infant weight gain and increased obesity risk.
An alternative to those traditional parenting practices are responsive feeding and responsive parenting, he explained. “Responsive feeding and parenting requires prompt, developmentally appropriate responses to a child’s behaviors including hunger and satiety cues.”
In other studies, RP has been shown to foster cognitive, social, and emotional development. “The question we had was: Can responsive parenting reduce obesity risk?” he said.
The INSIGHT (Intervention Nurses Start Infants Growing on Healthy Trajectories) study is an ongoing, randomized clinical trial started in January 2012 comparing an RP intervention designed to prevent childhood obesity with a safety control, with the interventions matched on intensity and length.
Parent-child dyads were randomized 2 weeks after birth and were told that the purpose of the study was “to see if nurse visits to your home during your baby’s infancy can improve your ability to either respond to your child’s cues related to feeding and fussiness or improve your ability to provide a safe environment for your child and prevent injuries.”
A total of 279 primiparous mother-newborn dyads were studied. Most were white (89%) and non-Hispanic (94%), and the majority were married (75%). Mean prepregnancy BMI was 25.5 kg/m2.
“We chose first-time mothers because we thought they were more likely to listen to the parenting advice that we had to offer,” said Dr. Paul.
INSIGHT’s curriculum focused on RP in domains of infant feeding, sleep, interactive play, and emotion regulation. “We tried to promote self-regulation by setting limits but still being responsive in a variety of behavior domains,” Dr. Paul said. “So, for example…, for feeding we talked about exposure to healthy foods, shared feeding responsibility, for those that were bottle feeding we gave tips on size of bottle appropriate for the child and also not using bottle finishing practices. In the emotional and social regulation domain, we talked about alternatives to food to soothe, and emphasized embracing each child’s temperament and how to respond to different temperaments.”
Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
TORONTO – Teaching parents of newborns to respond to eating and satiety cues in ways that promote self-regulation was associated with improvements in some weight outcomes at 3 years in a randomized clinical trial.
For the primary outcome of body mass index (BMI) z score at 3 years, a significant difference favoring the responsive parenting (RP) intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04). A longitudinal analysis examining the entire intervention period confirmed that the mean BMI group differences across seven study visits confirmed the effect of the RP intervention on BMI (P less than .001).
“We felt that the BMI z score and longitudinal growth analysis are probably the most sustained effects for an early-life intervention that have been recorded to date,” reported Ian M. Paul, MD, MSc, of Penn State University, Hershey. “While the differences between study groups were modest and not all achieved statistical significance, all favored the responsive-parenting intervention.”
Mean BMI percentile, a secondary outcome, was 47th for the RP group and 54th for controls, narrowly missing statistical significance (P = .07). Similarly, the percent of children deemed overweight at 3 years was 11.2% for the RP group and 19.8% for controls (P = .07), while 2.6% and 7.8%, respectively, were obese (P = .08).
No significant differences were seen in growth-related adverse events, such a weight-for-age less than the 5th percentile. The issue of “inducing” failure-to-thrive with a feeding intervention is a concern, said Dr. Paul, but there was no evidence for it in their study.
“One could question whether [the small differences seen between groups] are clinically significant, but if we look at how small differences have changed in the population over time and how those equate as far as longitudinal risk for cardiovascular outcomes and metabolic syndrome, etc., the small differences [we saw] might be important on a population level,” said Dr. Paul at the Pediatric Academic Societies meeting.
Study details
With upwards of one-quarter of U.S. children aged 2-5 years being overweight or obese, interventions to prevent rapid weight gain and reduce risk for overweight status in infancy are needed, noted Dr. Paul. Another reason to consider very early intervention, he added, is that infancy is a time of both “metabolic and behavioral plasticity.” However, most efforts to intervene early have, thus far, had limited success.
“Our responses to a baby crying are to feed that baby,” said Dr. Paul. This urge, along with others (such as “clear your plate”), evolved during times of food scarcity but persist now that we have inexpensive and palatable food, and promote rapid infant weight gain and increased obesity risk.
An alternative to those traditional parenting practices are responsive feeding and responsive parenting, he explained. “Responsive feeding and parenting requires prompt, developmentally appropriate responses to a child’s behaviors including hunger and satiety cues.”
In other studies, RP has been shown to foster cognitive, social, and emotional development. “The question we had was: Can responsive parenting reduce obesity risk?” he said.
The INSIGHT (Intervention Nurses Start Infants Growing on Healthy Trajectories) study is an ongoing, randomized clinical trial started in January 2012 comparing an RP intervention designed to prevent childhood obesity with a safety control, with the interventions matched on intensity and length.
Parent-child dyads were randomized 2 weeks after birth and were told that the purpose of the study was “to see if nurse visits to your home during your baby’s infancy can improve your ability to either respond to your child’s cues related to feeding and fussiness or improve your ability to provide a safe environment for your child and prevent injuries.”
A total of 279 primiparous mother-newborn dyads were studied. Most were white (89%) and non-Hispanic (94%), and the majority were married (75%). Mean prepregnancy BMI was 25.5 kg/m2.
“We chose first-time mothers because we thought they were more likely to listen to the parenting advice that we had to offer,” said Dr. Paul.
INSIGHT’s curriculum focused on RP in domains of infant feeding, sleep, interactive play, and emotion regulation. “We tried to promote self-regulation by setting limits but still being responsive in a variety of behavior domains,” Dr. Paul said. “So, for example…, for feeding we talked about exposure to healthy foods, shared feeding responsibility, for those that were bottle feeding we gave tips on size of bottle appropriate for the child and also not using bottle finishing practices. In the emotional and social regulation domain, we talked about alternatives to food to soothe, and emphasized embracing each child’s temperament and how to respond to different temperaments.”
Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
REPORTING FROM PAS 2018
Key clinical point:
Major finding: For the primary outcome of body mass index z score at 3 years, a significant difference favoring the responsive parenting intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04).
Study details: A randomized clinical trial including 279 mother-newborn dyads.
Disclosures: Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
Cochrane report: HPV vaccine proves its worth in adolescent, young adult women
Two currently available human papillomavirus vaccines protect adolescents and young adult women without previous HPV disease from developing precancerous cervical lesions, according to data from more than 70,000 women followed for 8 years.
In a review published online by the Cochrane Library, Marc Arbyn, MD, of the Belgian Cancer Centre, Brussels, and his colleagues examined the effectiveness of two vaccines that target the HPV types 16 and 18, which account for most cases of cervical cancer. The researchers focused on the bivalent vaccine for HPV16 and HPV18 and the quadrivalent vaccine for HPV16, HPV18, and two additional HPV types associated with genital warts (HPV6 and HPV11). The review did not include data on the latest vaccine targeting nine HPV types because it has not been studied in a randomized, placebo-controlled trial.
The review comprised 26 studies and 73,428 women aged 15-45 years. The vaccine was most effective for young women aged 15-26 years.
The risk of serious adverse events was approximately 7% in control groups and vaccine groups across all ages (669 per 10,000 vs. 656 per 10,000, respectively). The mortality rate was 11 per 10,000 in control groups, compared with 14 per 10,000 in vaccine groups. The overall mortality was low, and no deaths reported in the studies were vaccine related, the researchers said, although mortality was greater in the vaccine groups among women older than 25 years.
The overall risk for precancerous lesions was not significantly different for women vaccinated between age 24 and 45 years versus unvaccinated women. However, the researchers found that the vaccines reduced the risk of precancerous lesions for HPV type 16 and 18 from 45 per 10, 000 to 14 per 10,000 in women aged 24 years and older who were previously negative for HPV 16 and 18.
The researchers found no significant impact on miscarriage rates, but they noted the need for additional research to examine the possible impact of vaccination on stillbirth and birth defects in children born to women who were vaccinated during pregnancy.
Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
SOURCE: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
Two currently available human papillomavirus vaccines protect adolescents and young adult women without previous HPV disease from developing precancerous cervical lesions, according to data from more than 70,000 women followed for 8 years.
In a review published online by the Cochrane Library, Marc Arbyn, MD, of the Belgian Cancer Centre, Brussels, and his colleagues examined the effectiveness of two vaccines that target the HPV types 16 and 18, which account for most cases of cervical cancer. The researchers focused on the bivalent vaccine for HPV16 and HPV18 and the quadrivalent vaccine for HPV16, HPV18, and two additional HPV types associated with genital warts (HPV6 and HPV11). The review did not include data on the latest vaccine targeting nine HPV types because it has not been studied in a randomized, placebo-controlled trial.
The review comprised 26 studies and 73,428 women aged 15-45 years. The vaccine was most effective for young women aged 15-26 years.
The risk of serious adverse events was approximately 7% in control groups and vaccine groups across all ages (669 per 10,000 vs. 656 per 10,000, respectively). The mortality rate was 11 per 10,000 in control groups, compared with 14 per 10,000 in vaccine groups. The overall mortality was low, and no deaths reported in the studies were vaccine related, the researchers said, although mortality was greater in the vaccine groups among women older than 25 years.
The overall risk for precancerous lesions was not significantly different for women vaccinated between age 24 and 45 years versus unvaccinated women. However, the researchers found that the vaccines reduced the risk of precancerous lesions for HPV type 16 and 18 from 45 per 10, 000 to 14 per 10,000 in women aged 24 years and older who were previously negative for HPV 16 and 18.
The researchers found no significant impact on miscarriage rates, but they noted the need for additional research to examine the possible impact of vaccination on stillbirth and birth defects in children born to women who were vaccinated during pregnancy.
Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
SOURCE: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
Two currently available human papillomavirus vaccines protect adolescents and young adult women without previous HPV disease from developing precancerous cervical lesions, according to data from more than 70,000 women followed for 8 years.
In a review published online by the Cochrane Library, Marc Arbyn, MD, of the Belgian Cancer Centre, Brussels, and his colleagues examined the effectiveness of two vaccines that target the HPV types 16 and 18, which account for most cases of cervical cancer. The researchers focused on the bivalent vaccine for HPV16 and HPV18 and the quadrivalent vaccine for HPV16, HPV18, and two additional HPV types associated with genital warts (HPV6 and HPV11). The review did not include data on the latest vaccine targeting nine HPV types because it has not been studied in a randomized, placebo-controlled trial.
The review comprised 26 studies and 73,428 women aged 15-45 years. The vaccine was most effective for young women aged 15-26 years.
The risk of serious adverse events was approximately 7% in control groups and vaccine groups across all ages (669 per 10,000 vs. 656 per 10,000, respectively). The mortality rate was 11 per 10,000 in control groups, compared with 14 per 10,000 in vaccine groups. The overall mortality was low, and no deaths reported in the studies were vaccine related, the researchers said, although mortality was greater in the vaccine groups among women older than 25 years.
The overall risk for precancerous lesions was not significantly different for women vaccinated between age 24 and 45 years versus unvaccinated women. However, the researchers found that the vaccines reduced the risk of precancerous lesions for HPV type 16 and 18 from 45 per 10, 000 to 14 per 10,000 in women aged 24 years and older who were previously negative for HPV 16 and 18.
The researchers found no significant impact on miscarriage rates, but they noted the need for additional research to examine the possible impact of vaccination on stillbirth and birth defects in children born to women who were vaccinated during pregnancy.
Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
SOURCE: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
FROM THE COCHRANE LIBRARY
Key clinical point:
Major finding: The vaccines reduced the risk of precancer caused by HPV16 and HPV18 from 341 per 10,000 to 157 per 10,000 (RR, 0.46).
Study details: The review was based on data from 26 studies including 73,428 women worldwide over 8 years.
Disclosures: The Cochrane Library sponsored the study. Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
Source: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
Retinal vessel diameter in children may offer window into future CVD risk
Body mass index, blood pressure, and physical activity all affect retinal vessel diameters, authors of the meta-analysis found.
The findings raise the possibility that, one day, clinicians could help “substantially counteract” the increasing burden of adult cardiovascular disease by diagnosing retinal microvascular impairments early in life, according to investigator Sabrina Köchli, MSc, and her colleagues with the department of sport, exercise, and health at the University of Basel (Switzerland).
“Regular retinal vessel screening may have the potential to be implemented in future medical examination programs to optimize therapy guidance in children and adolescents,” Ms. Köchli and her colleagues wrote in the journal Pediatrics.
The meta-analysis by Ms. Köchli and her coauthors included 11 studies looking at the association between BMI, blood pressure, or physical activity in children.
They found that higher BMI was associated with narrower retinal arteriolar diameters and wider venular diameters in 8 studies including a total of 5,003 participants. The pooled estimate effect size was –0.37 for the association between BMI and retinal arteriolar diameters and 0.35 for the association between BMI and retinal venular diameters, data showed.
Higher blood pressure likewise was associated with narrower retinal arteriolar diameters in 6 studies including 7,687 participants, with a pooled estimate of –0.63 for systolic blood pressure and –0.60 for diastolic blood pressure.
Several studies individually showed that physical activity was associated with retinal vessel diameters. For example, one German study of school children showing that physical inactivity was associated with a lower arteriolar-to-venular diameter. And an Australian study found that more time spent outdoors engaged in physical activity was tied to wider arteriolor diameters and that sedentary behavior was linked to narrower arteriolor diameters. However, because of differences among the studies in how physical activity or inactivity was measured, meta-analysis was not possible, the investigators said.
Retinal vessels, part of the cerebrovascular bed, have been described as a “window to the heart,” Ms. Köchli and her coauthors said in their report. Previous investigations have recently shown that retinal vessel diameters may predict cardiovascular outcomes in adults over the long term.
That suggests retinal vessel diameters are a “reproducible biomarker” that adds value in determining atherosclerotic cardiovascular disease risk, the authors commented.
“However, future researchers will have to ensure that retinal vessel imaging during childhood development has a prognostic value for the adult clinical outcome of pediatric populations,” they added.
No external funding was received for the study. Ms. Köchli and her coauthors had no financial disclosures or potential conflicts of interest to disclose.
SOURCE: Köchli S et al. Pediatrics. 2018;141(6):e20174090
Currently, retinal vessel diameters are not a strong contender for clinical risk prediction, Alan E. Simon, MD, and Matthew W. Gillman, MD, wrote in an editorial commenting on the study by Köchli et al.
However, the concept has “intuitive appeal because the eye provides the opportunity to view systemic arteries and veins directly,” wrote Dr. Simon and Dr. Gillman.
The association between childhood retinal vessel diameters and cardiovascular endpoints in adults has not been evaluated, understandably, because of the very long follow-up that would be required. And even though studies have suggested that there might be some small added benefit for women in adding adult retinal vessel diameters to other cardiovascular risk prediction scores, the same does not appear to be true for men.
Even if childhood retinal vessel diameters had strong predictive value, it’s still not clear whether the retinal vessel evaluation would be useful for pediatricians grouping patients into risk categories for strokes or heart attacks at some point in the future.
Likewise, using retinal vessel diameters as an outcome measure in clinical trials is not justified at present, although that could change in the future.
“As technological advances make this novel assessment more available to clinicians, we hope that such availability is accompanied by additional evidence for or against its usefulness among clinicians and researchers,” the authors said in the editorial.
Currently, retinal vessel diameters are not a strong contender for clinical risk prediction, Alan E. Simon, MD, and Matthew W. Gillman, MD, wrote in an editorial commenting on the study by Köchli et al.
However, the concept has “intuitive appeal because the eye provides the opportunity to view systemic arteries and veins directly,” wrote Dr. Simon and Dr. Gillman.
The association between childhood retinal vessel diameters and cardiovascular endpoints in adults has not been evaluated, understandably, because of the very long follow-up that would be required. And even though studies have suggested that there might be some small added benefit for women in adding adult retinal vessel diameters to other cardiovascular risk prediction scores, the same does not appear to be true for men.
Even if childhood retinal vessel diameters had strong predictive value, it’s still not clear whether the retinal vessel evaluation would be useful for pediatricians grouping patients into risk categories for strokes or heart attacks at some point in the future.
Likewise, using retinal vessel diameters as an outcome measure in clinical trials is not justified at present, although that could change in the future.
“As technological advances make this novel assessment more available to clinicians, we hope that such availability is accompanied by additional evidence for or against its usefulness among clinicians and researchers,” the authors said in the editorial.
Currently, retinal vessel diameters are not a strong contender for clinical risk prediction, Alan E. Simon, MD, and Matthew W. Gillman, MD, wrote in an editorial commenting on the study by Köchli et al.
However, the concept has “intuitive appeal because the eye provides the opportunity to view systemic arteries and veins directly,” wrote Dr. Simon and Dr. Gillman.
The association between childhood retinal vessel diameters and cardiovascular endpoints in adults has not been evaluated, understandably, because of the very long follow-up that would be required. And even though studies have suggested that there might be some small added benefit for women in adding adult retinal vessel diameters to other cardiovascular risk prediction scores, the same does not appear to be true for men.
Even if childhood retinal vessel diameters had strong predictive value, it’s still not clear whether the retinal vessel evaluation would be useful for pediatricians grouping patients into risk categories for strokes or heart attacks at some point in the future.
Likewise, using retinal vessel diameters as an outcome measure in clinical trials is not justified at present, although that could change in the future.
“As technological advances make this novel assessment more available to clinicians, we hope that such availability is accompanied by additional evidence for or against its usefulness among clinicians and researchers,” the authors said in the editorial.
Body mass index, blood pressure, and physical activity all affect retinal vessel diameters, authors of the meta-analysis found.
The findings raise the possibility that, one day, clinicians could help “substantially counteract” the increasing burden of adult cardiovascular disease by diagnosing retinal microvascular impairments early in life, according to investigator Sabrina Köchli, MSc, and her colleagues with the department of sport, exercise, and health at the University of Basel (Switzerland).
“Regular retinal vessel screening may have the potential to be implemented in future medical examination programs to optimize therapy guidance in children and adolescents,” Ms. Köchli and her colleagues wrote in the journal Pediatrics.
The meta-analysis by Ms. Köchli and her coauthors included 11 studies looking at the association between BMI, blood pressure, or physical activity in children.
They found that higher BMI was associated with narrower retinal arteriolar diameters and wider venular diameters in 8 studies including a total of 5,003 participants. The pooled estimate effect size was –0.37 for the association between BMI and retinal arteriolar diameters and 0.35 for the association between BMI and retinal venular diameters, data showed.
Higher blood pressure likewise was associated with narrower retinal arteriolar diameters in 6 studies including 7,687 participants, with a pooled estimate of –0.63 for systolic blood pressure and –0.60 for diastolic blood pressure.
Several studies individually showed that physical activity was associated with retinal vessel diameters. For example, one German study of school children showing that physical inactivity was associated with a lower arteriolar-to-venular diameter. And an Australian study found that more time spent outdoors engaged in physical activity was tied to wider arteriolor diameters and that sedentary behavior was linked to narrower arteriolor diameters. However, because of differences among the studies in how physical activity or inactivity was measured, meta-analysis was not possible, the investigators said.
Retinal vessels, part of the cerebrovascular bed, have been described as a “window to the heart,” Ms. Köchli and her coauthors said in their report. Previous investigations have recently shown that retinal vessel diameters may predict cardiovascular outcomes in adults over the long term.
That suggests retinal vessel diameters are a “reproducible biomarker” that adds value in determining atherosclerotic cardiovascular disease risk, the authors commented.
“However, future researchers will have to ensure that retinal vessel imaging during childhood development has a prognostic value for the adult clinical outcome of pediatric populations,” they added.
No external funding was received for the study. Ms. Köchli and her coauthors had no financial disclosures or potential conflicts of interest to disclose.
SOURCE: Köchli S et al. Pediatrics. 2018;141(6):e20174090
Body mass index, blood pressure, and physical activity all affect retinal vessel diameters, authors of the meta-analysis found.
The findings raise the possibility that, one day, clinicians could help “substantially counteract” the increasing burden of adult cardiovascular disease by diagnosing retinal microvascular impairments early in life, according to investigator Sabrina Köchli, MSc, and her colleagues with the department of sport, exercise, and health at the University of Basel (Switzerland).
“Regular retinal vessel screening may have the potential to be implemented in future medical examination programs to optimize therapy guidance in children and adolescents,” Ms. Köchli and her colleagues wrote in the journal Pediatrics.
The meta-analysis by Ms. Köchli and her coauthors included 11 studies looking at the association between BMI, blood pressure, or physical activity in children.
They found that higher BMI was associated with narrower retinal arteriolar diameters and wider venular diameters in 8 studies including a total of 5,003 participants. The pooled estimate effect size was –0.37 for the association between BMI and retinal arteriolar diameters and 0.35 for the association between BMI and retinal venular diameters, data showed.
Higher blood pressure likewise was associated with narrower retinal arteriolar diameters in 6 studies including 7,687 participants, with a pooled estimate of –0.63 for systolic blood pressure and –0.60 for diastolic blood pressure.
Several studies individually showed that physical activity was associated with retinal vessel diameters. For example, one German study of school children showing that physical inactivity was associated with a lower arteriolar-to-venular diameter. And an Australian study found that more time spent outdoors engaged in physical activity was tied to wider arteriolor diameters and that sedentary behavior was linked to narrower arteriolor diameters. However, because of differences among the studies in how physical activity or inactivity was measured, meta-analysis was not possible, the investigators said.
Retinal vessels, part of the cerebrovascular bed, have been described as a “window to the heart,” Ms. Köchli and her coauthors said in their report. Previous investigations have recently shown that retinal vessel diameters may predict cardiovascular outcomes in adults over the long term.
That suggests retinal vessel diameters are a “reproducible biomarker” that adds value in determining atherosclerotic cardiovascular disease risk, the authors commented.
“However, future researchers will have to ensure that retinal vessel imaging during childhood development has a prognostic value for the adult clinical outcome of pediatric populations,” they added.
No external funding was received for the study. Ms. Köchli and her coauthors had no financial disclosures or potential conflicts of interest to disclose.
SOURCE: Köchli S et al. Pediatrics. 2018;141(6):e20174090
Key clinical point: In children, retinal vessel diameters may be sensitive biomarkers for cardiovascular risk stratification.
Major finding: BMI was associated with retinal arteriolar and venular diameters; blood pressure also was associated with retinal arteriolar diameters.
Study details: A meta-analysis of 11 studies.
Disclosures: No external funding was received for the study. Authors reported that they had no financial disclosures or potential conflicts of interest.
Source: Köchli S et al. Pediatrics. 2018;141(6):e20174090.
Unusual skin reactions to aluminum patch test seen in some children
Instead of the usual eczematous reaction confined to the test area, they exhibited erythema and papules distant from the test area.
In one girl, the reaction consisted of erythematous itchy papules across much of her back on day 2, and by day 4, there were even papules on her chest. In the other girl, erythema, infiltration, and occasional papules covered the whole patch area, and erythematous papules also were seen at some distance from the test area, Nadia Raison-Peyron, MD, of Saint-Eloi Hospital, Montpellier, France, and her colleagues, reported in Pediatric Dermatology.
Biopsies were not performed because of the girls’ young age.
SOURCE: Raison-Peyron N et al. Pediatr Dermatol. 2018. doi: 10.1111/pde.13481.
Instead of the usual eczematous reaction confined to the test area, they exhibited erythema and papules distant from the test area.
In one girl, the reaction consisted of erythematous itchy papules across much of her back on day 2, and by day 4, there were even papules on her chest. In the other girl, erythema, infiltration, and occasional papules covered the whole patch area, and erythematous papules also were seen at some distance from the test area, Nadia Raison-Peyron, MD, of Saint-Eloi Hospital, Montpellier, France, and her colleagues, reported in Pediatric Dermatology.
Biopsies were not performed because of the girls’ young age.
SOURCE: Raison-Peyron N et al. Pediatr Dermatol. 2018. doi: 10.1111/pde.13481.
Instead of the usual eczematous reaction confined to the test area, they exhibited erythema and papules distant from the test area.
In one girl, the reaction consisted of erythematous itchy papules across much of her back on day 2, and by day 4, there were even papules on her chest. In the other girl, erythema, infiltration, and occasional papules covered the whole patch area, and erythematous papules also were seen at some distance from the test area, Nadia Raison-Peyron, MD, of Saint-Eloi Hospital, Montpellier, France, and her colleagues, reported in Pediatric Dermatology.
Biopsies were not performed because of the girls’ young age.
SOURCE: Raison-Peyron N et al. Pediatr Dermatol. 2018. doi: 10.1111/pde.13481.
FROM PEDIATRIC DERMATOLOGY
About sex, adults aren’t talking or kids aren’t listening
TORONTO – Almost half of adolescents (45%) reported that their primary care providers (PCPs) do not routinely ask them about sex, and only 13% report they’ve been offered screening for sexually transmitted infections (STIs), according to a survey study presented at the Pediatric Academic Societies meeting.
And it appears the teenagers aren’t even listening to much of what their parents are saying on the subject: The survey also found that 90% of parents reported that they talk to their adolescents about sex, but only 39% of adolescents reported the same.
Regarding the discrepancy between the parents’ and adolescents’ responses, “Our best guess is that parents may have mentioned sex with their adolescents at some point, but the conversation was not meaningful enough to register on the adolescents’ radars! That type of discussion is probably best had more than once and in more than one way,”she said in an interview.
The adolescents, aged 13-17 years, and parents of adolescents attending the 2017 Minnesota State Fair were invited to complete an 18-question anonymous survey. The teens were queried whether they had seen a PCP in the last year and asked about their discussions about sexual activity and STIs with their physicians and parents. Parents were asked about their knowledge of discussions the teens had with their PCPs and their own discussions with their children. A total of 582 adolescents and 516 parents completed the survey.

One-quarter of parents who completed the survey felt that PCPs should not discuss sex with their teens.
“I think that primary care physicians have a lot to cover when doing preventive health visits with adolescents, and talking about sex is not necessarily an easy or comfortable thing to do and so may be something that falls to a lower priority. And it certainly doesn’t help if parents are not supportive of the concept of confidential adolescent care,” Dr. Schneider related.
“We were very surprised to see that 25% of parents did not feel that PCPs should be discussing sex with their child. I think that we need to next work on getting the parents on board and building an expectation that adolescents, when visiting their PCP, will have confidential discussions about sexual health,” she said.
TORONTO – Almost half of adolescents (45%) reported that their primary care providers (PCPs) do not routinely ask them about sex, and only 13% report they’ve been offered screening for sexually transmitted infections (STIs), according to a survey study presented at the Pediatric Academic Societies meeting.
And it appears the teenagers aren’t even listening to much of what their parents are saying on the subject: The survey also found that 90% of parents reported that they talk to their adolescents about sex, but only 39% of adolescents reported the same.
Regarding the discrepancy between the parents’ and adolescents’ responses, “Our best guess is that parents may have mentioned sex with their adolescents at some point, but the conversation was not meaningful enough to register on the adolescents’ radars! That type of discussion is probably best had more than once and in more than one way,”she said in an interview.
The adolescents, aged 13-17 years, and parents of adolescents attending the 2017 Minnesota State Fair were invited to complete an 18-question anonymous survey. The teens were queried whether they had seen a PCP in the last year and asked about their discussions about sexual activity and STIs with their physicians and parents. Parents were asked about their knowledge of discussions the teens had with their PCPs and their own discussions with their children. A total of 582 adolescents and 516 parents completed the survey.
One-quarter of parents who completed the survey felt that PCPs should not discuss sex with their teens.
“I think that primary care physicians have a lot to cover when doing preventive health visits with adolescents, and talking about sex is not necessarily an easy or comfortable thing to do and so may be something that falls to a lower priority. And it certainly doesn’t help if parents are not supportive of the concept of confidential adolescent care,” Dr. Schneider related.
“We were very surprised to see that 25% of parents did not feel that PCPs should be discussing sex with their child. I think that we need to next work on getting the parents on board and building an expectation that adolescents, when visiting their PCP, will have confidential discussions about sexual health,” she said.
TORONTO – Almost half of adolescents (45%) reported that their primary care providers (PCPs) do not routinely ask them about sex, and only 13% report they’ve been offered screening for sexually transmitted infections (STIs), according to a survey study presented at the Pediatric Academic Societies meeting.
And it appears the teenagers aren’t even listening to much of what their parents are saying on the subject: The survey also found that 90% of parents reported that they talk to their adolescents about sex, but only 39% of adolescents reported the same.
Regarding the discrepancy between the parents’ and adolescents’ responses, “Our best guess is that parents may have mentioned sex with their adolescents at some point, but the conversation was not meaningful enough to register on the adolescents’ radars! That type of discussion is probably best had more than once and in more than one way,”she said in an interview.
The adolescents, aged 13-17 years, and parents of adolescents attending the 2017 Minnesota State Fair were invited to complete an 18-question anonymous survey. The teens were queried whether they had seen a PCP in the last year and asked about their discussions about sexual activity and STIs with their physicians and parents. Parents were asked about their knowledge of discussions the teens had with their PCPs and their own discussions with their children. A total of 582 adolescents and 516 parents completed the survey.
One-quarter of parents who completed the survey felt that PCPs should not discuss sex with their teens.
“I think that primary care physicians have a lot to cover when doing preventive health visits with adolescents, and talking about sex is not necessarily an easy or comfortable thing to do and so may be something that falls to a lower priority. And it certainly doesn’t help if parents are not supportive of the concept of confidential adolescent care,” Dr. Schneider related.
“We were very surprised to see that 25% of parents did not feel that PCPs should be discussing sex with their child. I think that we need to next work on getting the parents on board and building an expectation that adolescents, when visiting their PCP, will have confidential discussions about sexual health,” she said.
Key clinical point:
Major finding: Of the adolescents who responded to the survey, 45% said their PCPs don’t routinely discuss sex with them, and only 13% reported being offered screening for STIs.
Study details: Survey study including 582 adolescents aged 13-17 years and 516 parents of adolescents.
Disclosures: Dr. Schneider reported no financial conflicts of interest.
Off-label prescribing of SGAs in children varies by diagnosis
TORONTO – On-label prescribing of second-generation antipsychotics in hospitalized pediatric patients with bipolar disorder and schizophrenia was greater than off-label prescribing, but not for patients with autism spectrum disorder, results from a single-center study showed.
“There is an increasing trend for using second-generation antipsychotics (SGAs) in children,” lead study author Debra V. McQuade, MD, PhD, said in an interview in advance of the Pediatric Academic Societies meeting. “This trend has already been widely acknowledged as concerning, due to the relatively high adverse event burden associated with them. Also, and perhaps more concerning, the great majority of these prescriptions are prescribed as ‘off-label’ (without Food and Drug Administration approval or indication). This is true in all settings, whether outpatient or inpatient. And, this off-label use is really high – usually reported as 60%-95% of all SGA prescriptions to children. We wanted to understand more about this practice of off-label prescribing of SGAs to children – to understand what drives it, to see if there were any organizing principles that might help to better explain it.”
Dr. McQuade and her associates found that for the three diagnostic groups overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001). Prescriptions for patients with bipolar disorder and schizophrenia followed this pattern, with on-label and off-label prescribing rates of 73% vs. 27%, for bipolar disorder, and 85% vs. 14% for schizophrenia. However, this prescription pattern was reversed for patients with autism spectrum disorder (35% vs. 64%; P less than .001), a finding that the researchers did not expect.

She said that while off-label prescribing of SGAs to pediatric patients remains widespread and is a concerning trend, the study findings suggested that prescribers “do select and prescribe SGAs in ways that are directly or indirectly influenced by FDA guidelines, mitigating risk to their pediatric patients.” Dr. McQuade acknowledged certain weaknesses of the study, including the fact that it was limited to one hospital setting and by the small number of prescribers who contributed to the overall pool of data.
She reported having no relevant financial disclosures.
TORONTO – On-label prescribing of second-generation antipsychotics in hospitalized pediatric patients with bipolar disorder and schizophrenia was greater than off-label prescribing, but not for patients with autism spectrum disorder, results from a single-center study showed.
“There is an increasing trend for using second-generation antipsychotics (SGAs) in children,” lead study author Debra V. McQuade, MD, PhD, said in an interview in advance of the Pediatric Academic Societies meeting. “This trend has already been widely acknowledged as concerning, due to the relatively high adverse event burden associated with them. Also, and perhaps more concerning, the great majority of these prescriptions are prescribed as ‘off-label’ (without Food and Drug Administration approval or indication). This is true in all settings, whether outpatient or inpatient. And, this off-label use is really high – usually reported as 60%-95% of all SGA prescriptions to children. We wanted to understand more about this practice of off-label prescribing of SGAs to children – to understand what drives it, to see if there were any organizing principles that might help to better explain it.”
Dr. McQuade and her associates found that for the three diagnostic groups overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001). Prescriptions for patients with bipolar disorder and schizophrenia followed this pattern, with on-label and off-label prescribing rates of 73% vs. 27%, for bipolar disorder, and 85% vs. 14% for schizophrenia. However, this prescription pattern was reversed for patients with autism spectrum disorder (35% vs. 64%; P less than .001), a finding that the researchers did not expect.
She said that while off-label prescribing of SGAs to pediatric patients remains widespread and is a concerning trend, the study findings suggested that prescribers “do select and prescribe SGAs in ways that are directly or indirectly influenced by FDA guidelines, mitigating risk to their pediatric patients.” Dr. McQuade acknowledged certain weaknesses of the study, including the fact that it was limited to one hospital setting and by the small number of prescribers who contributed to the overall pool of data.
She reported having no relevant financial disclosures.
TORONTO – On-label prescribing of second-generation antipsychotics in hospitalized pediatric patients with bipolar disorder and schizophrenia was greater than off-label prescribing, but not for patients with autism spectrum disorder, results from a single-center study showed.
“There is an increasing trend for using second-generation antipsychotics (SGAs) in children,” lead study author Debra V. McQuade, MD, PhD, said in an interview in advance of the Pediatric Academic Societies meeting. “This trend has already been widely acknowledged as concerning, due to the relatively high adverse event burden associated with them. Also, and perhaps more concerning, the great majority of these prescriptions are prescribed as ‘off-label’ (without Food and Drug Administration approval or indication). This is true in all settings, whether outpatient or inpatient. And, this off-label use is really high – usually reported as 60%-95% of all SGA prescriptions to children. We wanted to understand more about this practice of off-label prescribing of SGAs to children – to understand what drives it, to see if there were any organizing principles that might help to better explain it.”
Dr. McQuade and her associates found that for the three diagnostic groups overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001). Prescriptions for patients with bipolar disorder and schizophrenia followed this pattern, with on-label and off-label prescribing rates of 73% vs. 27%, for bipolar disorder, and 85% vs. 14% for schizophrenia. However, this prescription pattern was reversed for patients with autism spectrum disorder (35% vs. 64%; P less than .001), a finding that the researchers did not expect.
She said that while off-label prescribing of SGAs to pediatric patients remains widespread and is a concerning trend, the study findings suggested that prescribers “do select and prescribe SGAs in ways that are directly or indirectly influenced by FDA guidelines, mitigating risk to their pediatric patients.” Dr. McQuade acknowledged certain weaknesses of the study, including the fact that it was limited to one hospital setting and by the small number of prescribers who contributed to the overall pool of data.
She reported having no relevant financial disclosures.
Key clinical point:
Major finding: Overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001), but this prescription pattern did not hold true for patients with autism spectrum disorder.
Study details: A retrospective review of 86 hospitalized pediatric inpatients with a diagnosis of autism spectrum disorder, bipolar disorder, or schizophrenia.
Disclosures: Dr. McQuade reported having no financial disclosures.
Reduce referrals: Skip eye chart with automated vision checker for kids
TORONTO – Using an automated photorefractor-based vision screening in preschool-age children reduced referrals to ophthalmologists and optometrists by one-third, compared with standard chart-based screening, according to a nonrandomized trial conducted in Boston. The handheld device that was used requires minimal cooperation from the child and also checks ocular alignment.
“This device requires almost zero cooperation from the child. The nurse or assistant holds the device and the child has to look at it for about two seconds, as opposed to several minutes to do a chart-based test,” reported Louis Vernacchio, MD, at the 2018 Pediatric Academic Societies meeting.

They found a 33.7% decline in initial ophthalmology and optometry visits after practices switched from chart-based vision screening to the hand-held screening device.
“Optometry and ophthalmology is the No. 1 specialist to whom our patients of all ages are referred to in our pediatric network, and the No. 1 diagnosis was normal vision, so in most cases, there’s nothing wrong, and they’re clogging up the system.”
Instrument-based vision screening has been shown to have high sensitivity and specificity, compared with ophthalmic vision screening, and has much better testability in young children than traditional eye chart–based screening.
In previously reported data, Dr. Vernacchio’s group showed that, with instrument-based vision screening, completed screening rates among children aged 3-5 years improved. The most marked improvement was in the 3-year-olds, among whom completed screening rates increased from 39% with chart-based screening to 87% with instrument screening. (Modest JR et al. Pediatrics. 2017 Jul;140[1]. pii: e20163745.) Family satisfaction is also improved with the automated method.
The automated vision screening device used in the study was the Spot Vision Screener produced by Welch Allyn.
“Our nurses are in heaven with these devices, so besides the billing that you can do, you can save staff time and easily justify the cost of the device. My office now has 4 or 5 of these devices because it just saves so much time to have them readily available.”
Professional societies endorse automated vision screening
Amblyopia is seen in 2 or 3 children per 100 in the United States, reported Dr. Vernacchio. Chart-based vision screening is notoriously difficult to accomplish in young children and there is both a risk of missing amblyopia in those who do not cooperate and a risk of overreferral because of poor performance on the test.
Recently, the American Academy of Pediatrics, the U.S. Preventive Services Task Force, and others have endorsed the use of instrument-based vision screening in place of chart-based screening for children aged 3-5 years based on evidence of improved testability and acceptable sensitivity and specificity.
The Spot Vision Screener has a retail cost between $6000 and $7000, according to Dr. Vernacchio. “Many” insurance companies will pay a separate fee for vision screening using an instrument, but others bundle the screening into a well visit, he noted.
“So, you can actually calculate the time to recover the cost of the device based on your payer practices,” he said. Another option is a smart phone app that uses a subscription model, in which the test results are interpreted by the company within a few minutes with a per test charge of about .99 cents.
“The Holy Grail is whether this process will reduce the incidence of amblyopia,” said Dr. Vernacchio. That study is next on his to-do list, he said, but “it’s going to take longer to answer that question.”
The authors reported no conflicts of interest. There was no external funding.
TORONTO – Using an automated photorefractor-based vision screening in preschool-age children reduced referrals to ophthalmologists and optometrists by one-third, compared with standard chart-based screening, according to a nonrandomized trial conducted in Boston. The handheld device that was used requires minimal cooperation from the child and also checks ocular alignment.
“This device requires almost zero cooperation from the child. The nurse or assistant holds the device and the child has to look at it for about two seconds, as opposed to several minutes to do a chart-based test,” reported Louis Vernacchio, MD, at the 2018 Pediatric Academic Societies meeting.
They found a 33.7% decline in initial ophthalmology and optometry visits after practices switched from chart-based vision screening to the hand-held screening device.
“Optometry and ophthalmology is the No. 1 specialist to whom our patients of all ages are referred to in our pediatric network, and the No. 1 diagnosis was normal vision, so in most cases, there’s nothing wrong, and they’re clogging up the system.”
Instrument-based vision screening has been shown to have high sensitivity and specificity, compared with ophthalmic vision screening, and has much better testability in young children than traditional eye chart–based screening.
In previously reported data, Dr. Vernacchio’s group showed that, with instrument-based vision screening, completed screening rates among children aged 3-5 years improved. The most marked improvement was in the 3-year-olds, among whom completed screening rates increased from 39% with chart-based screening to 87% with instrument screening. (Modest JR et al. Pediatrics. 2017 Jul;140[1]. pii: e20163745.) Family satisfaction is also improved with the automated method.
The automated vision screening device used in the study was the Spot Vision Screener produced by Welch Allyn.
“Our nurses are in heaven with these devices, so besides the billing that you can do, you can save staff time and easily justify the cost of the device. My office now has 4 or 5 of these devices because it just saves so much time to have them readily available.”
Professional societies endorse automated vision screening
Amblyopia is seen in 2 or 3 children per 100 in the United States, reported Dr. Vernacchio. Chart-based vision screening is notoriously difficult to accomplish in young children and there is both a risk of missing amblyopia in those who do not cooperate and a risk of overreferral because of poor performance on the test.
Recently, the American Academy of Pediatrics, the U.S. Preventive Services Task Force, and others have endorsed the use of instrument-based vision screening in place of chart-based screening for children aged 3-5 years based on evidence of improved testability and acceptable sensitivity and specificity.
The Spot Vision Screener has a retail cost between $6000 and $7000, according to Dr. Vernacchio. “Many” insurance companies will pay a separate fee for vision screening using an instrument, but others bundle the screening into a well visit, he noted.
“So, you can actually calculate the time to recover the cost of the device based on your payer practices,” he said. Another option is a smart phone app that uses a subscription model, in which the test results are interpreted by the company within a few minutes with a per test charge of about .99 cents.
“The Holy Grail is whether this process will reduce the incidence of amblyopia,” said Dr. Vernacchio. That study is next on his to-do list, he said, but “it’s going to take longer to answer that question.”
The authors reported no conflicts of interest. There was no external funding.
TORONTO – Using an automated photorefractor-based vision screening in preschool-age children reduced referrals to ophthalmologists and optometrists by one-third, compared with standard chart-based screening, according to a nonrandomized trial conducted in Boston. The handheld device that was used requires minimal cooperation from the child and also checks ocular alignment.
“This device requires almost zero cooperation from the child. The nurse or assistant holds the device and the child has to look at it for about two seconds, as opposed to several minutes to do a chart-based test,” reported Louis Vernacchio, MD, at the 2018 Pediatric Academic Societies meeting.
They found a 33.7% decline in initial ophthalmology and optometry visits after practices switched from chart-based vision screening to the hand-held screening device.
“Optometry and ophthalmology is the No. 1 specialist to whom our patients of all ages are referred to in our pediatric network, and the No. 1 diagnosis was normal vision, so in most cases, there’s nothing wrong, and they’re clogging up the system.”
Instrument-based vision screening has been shown to have high sensitivity and specificity, compared with ophthalmic vision screening, and has much better testability in young children than traditional eye chart–based screening.
In previously reported data, Dr. Vernacchio’s group showed that, with instrument-based vision screening, completed screening rates among children aged 3-5 years improved. The most marked improvement was in the 3-year-olds, among whom completed screening rates increased from 39% with chart-based screening to 87% with instrument screening. (Modest JR et al. Pediatrics. 2017 Jul;140[1]. pii: e20163745.) Family satisfaction is also improved with the automated method.
The automated vision screening device used in the study was the Spot Vision Screener produced by Welch Allyn.
“Our nurses are in heaven with these devices, so besides the billing that you can do, you can save staff time and easily justify the cost of the device. My office now has 4 or 5 of these devices because it just saves so much time to have them readily available.”
Professional societies endorse automated vision screening
Amblyopia is seen in 2 or 3 children per 100 in the United States, reported Dr. Vernacchio. Chart-based vision screening is notoriously difficult to accomplish in young children and there is both a risk of missing amblyopia in those who do not cooperate and a risk of overreferral because of poor performance on the test.
Recently, the American Academy of Pediatrics, the U.S. Preventive Services Task Force, and others have endorsed the use of instrument-based vision screening in place of chart-based screening for children aged 3-5 years based on evidence of improved testability and acceptable sensitivity and specificity.
The Spot Vision Screener has a retail cost between $6000 and $7000, according to Dr. Vernacchio. “Many” insurance companies will pay a separate fee for vision screening using an instrument, but others bundle the screening into a well visit, he noted.
“So, you can actually calculate the time to recover the cost of the device based on your payer practices,” he said. Another option is a smart phone app that uses a subscription model, in which the test results are interpreted by the company within a few minutes with a per test charge of about .99 cents.
“The Holy Grail is whether this process will reduce the incidence of amblyopia,” said Dr. Vernacchio. That study is next on his to-do list, he said, but “it’s going to take longer to answer that question.”
The authors reported no conflicts of interest. There was no external funding.
Key clinical point: Switching from a chart-based to an instrument-based vision screening reduced unnecessary pediatric eye care referrals.
Major finding: Use of an automated vision screening system reduced referrals for pediatric eye care by 33.7%.
Study details: A nonrandomized analysis of referral patterns from January 2015 to June 2015 from 12 pediatric primary care practices, with findings compared with a prior time period before the vision screening device was used.
Disclosures: The authors reported no conflicts of interest. There was no external funding
Safety and support experiences of transgender and gender nonconforming youth explored
TORONTO – Youth with nonbinary identities – those that are beyond or outside of the categories of male/man and female/woman – feel significantly safer and more supported at school, compared with their transgender and gender nonconforming peers with binary identities, results from a survey of more than 300 youth showed.
“There has been little research specifically about the experiences of transgender and gender nonconforming youth that have nonbinary identities,” lead study author Brittany Allen, MD, said in an interview in advance of the Pediatric Academic Societies meeting.

Dr. Allen, a pediatrician at the University of Wisconsin–Madison, and her associates conducted an online survey of 311 transgender, nonbinary, and gender nonconforming youth in the state who ranged aged 12-22 years. Study participants were asked about their school safety and support experiences, and the researchers used Wilcoxon rank-sum tests to compare Likert scale responses among youth who reported nonbinary identities with those who reported binary identities. On the 1-5 scale, 1 meant “strongly agree” while 5 meant “strongly disagree.”
Dr. Allen, who is also comedical director of the Pediatric and Adolescent Transgender Health Clinic at American Family Children’s Hospital, Madison, reported that 311 young people completed more than 70% of the survey. Of those, 287 identified as having either binary (164; 57%) or nonbinary (123; 43%) gender identities. That percentage of those reporting nonbinary identities “is striking,” she said, and is “a much higher percentage than seen in adult studies of transgender and gender nonconforming people.”
Compared with respondents with binary identities, those with nonbinary identities were more often Caucasian/White (81% vs. 65% for those with binary identities; P = .003) and less likely to qualify for free lunch (28% vs. 55%; P = .001). Both binary and nonbinary groups reported similar school attendance and belonging. However, compared with the binary group, the nonbinary group reported significantly higher ratings of school safety (Likert score of 2.62 vs. 2.96, respectively; P = .0078) and peer support (Likert score of 2.54 vs. 2.87; P = .0139) and also were more likely to report being able to access adult support at school if needed (Likert score of 2.31 vs. 2.66; P = .0085).
“The primary message is that many transgender or gender nonconforming youth have identities outside of a gender binary and that transgender and gender nonconforming youth with different gender identities may have different strengths and challenges in different settings,” Dr. Allen said.
“Our work shows that nonbinary youth have relative safety and support at school compared to their transgender and gender nonconforming peers with binary identities – though it’s important to note that transgender and gender nonconforming youth overall are still at high risk of school harassment and violence. Interventions to promote school safety for youth of all gender identities should consider that transgender and gender nonconforming youth with different gender identities have different risks related to school safety and support.”
She acknowledged certain limitations of the study, including the fact that the researchers used a convenience sample to recruit participants, “which means that we may not have reached transgender and gender nonconforming youth that were less connected to support services or transgender and gender nonconforming peers,” Dr. Allen said. “This study also specifically assessed transgender and gender nonconforming youth; we did not have a comparison group of cisgender participants for comparison due to our study design.”
The study was funded by the National Institutes of Health, the Baldwin Wisconsin Ideas Endowment, the University of Wisconsin Advancing Health Equity and Diversity initiative, and the Wisconsin Partnership Program. Dr. Allen reported having no financial disclosures.
TORONTO – Youth with nonbinary identities – those that are beyond or outside of the categories of male/man and female/woman – feel significantly safer and more supported at school, compared with their transgender and gender nonconforming peers with binary identities, results from a survey of more than 300 youth showed.
“There has been little research specifically about the experiences of transgender and gender nonconforming youth that have nonbinary identities,” lead study author Brittany Allen, MD, said in an interview in advance of the Pediatric Academic Societies meeting.
Dr. Allen, a pediatrician at the University of Wisconsin–Madison, and her associates conducted an online survey of 311 transgender, nonbinary, and gender nonconforming youth in the state who ranged aged 12-22 years. Study participants were asked about their school safety and support experiences, and the researchers used Wilcoxon rank-sum tests to compare Likert scale responses among youth who reported nonbinary identities with those who reported binary identities. On the 1-5 scale, 1 meant “strongly agree” while 5 meant “strongly disagree.”
Dr. Allen, who is also comedical director of the Pediatric and Adolescent Transgender Health Clinic at American Family Children’s Hospital, Madison, reported that 311 young people completed more than 70% of the survey. Of those, 287 identified as having either binary (164; 57%) or nonbinary (123; 43%) gender identities. That percentage of those reporting nonbinary identities “is striking,” she said, and is “a much higher percentage than seen in adult studies of transgender and gender nonconforming people.”
Compared with respondents with binary identities, those with nonbinary identities were more often Caucasian/White (81% vs. 65% for those with binary identities; P = .003) and less likely to qualify for free lunch (28% vs. 55%; P = .001). Both binary and nonbinary groups reported similar school attendance and belonging. However, compared with the binary group, the nonbinary group reported significantly higher ratings of school safety (Likert score of 2.62 vs. 2.96, respectively; P = .0078) and peer support (Likert score of 2.54 vs. 2.87; P = .0139) and also were more likely to report being able to access adult support at school if needed (Likert score of 2.31 vs. 2.66; P = .0085).
“The primary message is that many transgender or gender nonconforming youth have identities outside of a gender binary and that transgender and gender nonconforming youth with different gender identities may have different strengths and challenges in different settings,” Dr. Allen said.
“Our work shows that nonbinary youth have relative safety and support at school compared to their transgender and gender nonconforming peers with binary identities – though it’s important to note that transgender and gender nonconforming youth overall are still at high risk of school harassment and violence. Interventions to promote school safety for youth of all gender identities should consider that transgender and gender nonconforming youth with different gender identities have different risks related to school safety and support.”
She acknowledged certain limitations of the study, including the fact that the researchers used a convenience sample to recruit participants, “which means that we may not have reached transgender and gender nonconforming youth that were less connected to support services or transgender and gender nonconforming peers,” Dr. Allen said. “This study also specifically assessed transgender and gender nonconforming youth; we did not have a comparison group of cisgender participants for comparison due to our study design.”
The study was funded by the National Institutes of Health, the Baldwin Wisconsin Ideas Endowment, the University of Wisconsin Advancing Health Equity and Diversity initiative, and the Wisconsin Partnership Program. Dr. Allen reported having no financial disclosures.
TORONTO – Youth with nonbinary identities – those that are beyond or outside of the categories of male/man and female/woman – feel significantly safer and more supported at school, compared with their transgender and gender nonconforming peers with binary identities, results from a survey of more than 300 youth showed.
“There has been little research specifically about the experiences of transgender and gender nonconforming youth that have nonbinary identities,” lead study author Brittany Allen, MD, said in an interview in advance of the Pediatric Academic Societies meeting.
Dr. Allen, a pediatrician at the University of Wisconsin–Madison, and her associates conducted an online survey of 311 transgender, nonbinary, and gender nonconforming youth in the state who ranged aged 12-22 years. Study participants were asked about their school safety and support experiences, and the researchers used Wilcoxon rank-sum tests to compare Likert scale responses among youth who reported nonbinary identities with those who reported binary identities. On the 1-5 scale, 1 meant “strongly agree” while 5 meant “strongly disagree.”
Dr. Allen, who is also comedical director of the Pediatric and Adolescent Transgender Health Clinic at American Family Children’s Hospital, Madison, reported that 311 young people completed more than 70% of the survey. Of those, 287 identified as having either binary (164; 57%) or nonbinary (123; 43%) gender identities. That percentage of those reporting nonbinary identities “is striking,” she said, and is “a much higher percentage than seen in adult studies of transgender and gender nonconforming people.”
Compared with respondents with binary identities, those with nonbinary identities were more often Caucasian/White (81% vs. 65% for those with binary identities; P = .003) and less likely to qualify for free lunch (28% vs. 55%; P = .001). Both binary and nonbinary groups reported similar school attendance and belonging. However, compared with the binary group, the nonbinary group reported significantly higher ratings of school safety (Likert score of 2.62 vs. 2.96, respectively; P = .0078) and peer support (Likert score of 2.54 vs. 2.87; P = .0139) and also were more likely to report being able to access adult support at school if needed (Likert score of 2.31 vs. 2.66; P = .0085).
“The primary message is that many transgender or gender nonconforming youth have identities outside of a gender binary and that transgender and gender nonconforming youth with different gender identities may have different strengths and challenges in different settings,” Dr. Allen said.
“Our work shows that nonbinary youth have relative safety and support at school compared to their transgender and gender nonconforming peers with binary identities – though it’s important to note that transgender and gender nonconforming youth overall are still at high risk of school harassment and violence. Interventions to promote school safety for youth of all gender identities should consider that transgender and gender nonconforming youth with different gender identities have different risks related to school safety and support.”
She acknowledged certain limitations of the study, including the fact that the researchers used a convenience sample to recruit participants, “which means that we may not have reached transgender and gender nonconforming youth that were less connected to support services or transgender and gender nonconforming peers,” Dr. Allen said. “This study also specifically assessed transgender and gender nonconforming youth; we did not have a comparison group of cisgender participants for comparison due to our study design.”
The study was funded by the National Institutes of Health, the Baldwin Wisconsin Ideas Endowment, the University of Wisconsin Advancing Health Equity and Diversity initiative, and the Wisconsin Partnership Program. Dr. Allen reported having no financial disclosures.
Key clinical point: Nonbinary youth felt significantly safer and more supported at school, compared with transgender peers with binary identities.
Major finding: Compared with the binary group, the nonbinary group reported significantly higher ratings of school safety (Likert score of 2.62 vs. 2.96, respectively) and peer support (Likert score of 2.54 vs. 2.87).
Study details: An online survey of 311 transgender, nonbinary, and gender nonconforming youth in Wisconsin who aged 12-22 years.
Disclosures: The study was funded by the National Institutes of Health, the Baldwin Wisconsin Ideas Endowment, the University of Wisconsin Advancing Health Equity and Diversity initiative, and the Wisconsin Partnership Program. Dr. Allen reported having no financial disclosures.
Relapse rate drives stem cell transplant failure in pediatric ALL patients
Relapse was the main impediment to successful hematopoietic stem cell transplant (HSCT) in high-risk pediatric acute lymphocytic leukemia (ALL), according to one of the largest single-center experiences reported to date.
The effects of relapse were especially evident for patients with haploidentical donors; these patients had a 3-year cumulative relapse incidence of 47% and event-free survival rate of 35%, both significantly higher than what was seen in other transplant recipients treated at the same center.
The findings, recently published in the journal Biology of Blood and Marrow Transplantation, suggest a substantial unmet need in the treatment of high-risk patients in first remission.
“Newer methods to improve graft-versus-leukemia effect are being tested and will need to be incorporated into the management of high-risk patients,” Asaf D. Yanir, MD, and coauthors at Baylor College of Medicine in Houston said in the report.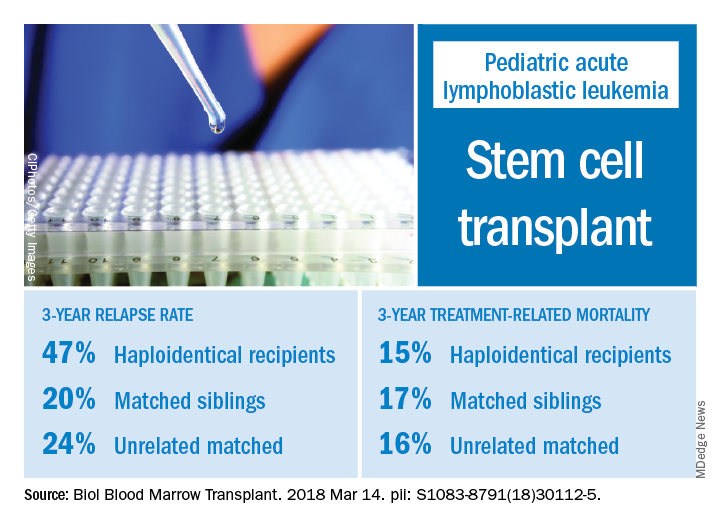
Dr. Yanir and colleagues reported recent outcomes for 124 patients who had undergone HSCT for ALL at their center during 2008-2016. That group included 20 haploidentical transplant recipients, 48 patients with matched sibling donors, and 56 with unrelated matched donors.
The 3-year cumulative incidence of relapse was 47% for haploidentical recipients, compared with 20% for matched sibling donors recipients and 24% for unrelated matched donors recipients (P = .02), according to their findings.
The main cause of HSCT failure was relapse, occurring in 47% of haploidentical transplant recipients, compared with 20% for those with matched sibling donors and 24% for those with unrelated matched donors (P = .02).
Those findings are in line with other studies showing inferior outcomes following haploidentical donor HSCT. However, in contrast to those studies, Dr. Yanir and colleagues did find a rate of treatment-related mortality comparable with other transplant approaches. The 3-year incidence of treatment-related mortality was 15% for the haploidentical group and, similarly, 17% in the matched sibling donor group and 16% in the unrelated matched donor group.
That lower rate of treatment-related mortality in the haploidentical group may be caused by improvements in procedures and supportive care. “Unfortunately, the benefits gained by reducing treatment-related mortality were offset by the high rate of relapse, which remains the main obstacle to successful haploidentical donor HSCT,” Dr. Yanir and coauthors wrote in their report.
New strategies are being studied to retain the graft-versus-leukemia effect or enhance it in patients who’ve undergone haploidentical HSCT, such as selectively depleting alloreactive T cells while sparing other immune effectors, investigators wrote.
“Given evolving practices, it is important to continually evaluate the projected event-free survival for pediatric ALL following HSCT, based on the donor type used,” they wrote.
Dr. Yanir and coauthors had no financial disclosures or conflicts of interest to report.
SOURCE: Yanir AD et al. Biol Blood Marrow Transplant. 2018 Mar 14. doi: 10.1016/j.bbmt.2018.03.001.
Relapse was the main impediment to successful hematopoietic stem cell transplant (HSCT) in high-risk pediatric acute lymphocytic leukemia (ALL), according to one of the largest single-center experiences reported to date.
The effects of relapse were especially evident for patients with haploidentical donors; these patients had a 3-year cumulative relapse incidence of 47% and event-free survival rate of 35%, both significantly higher than what was seen in other transplant recipients treated at the same center.
The findings, recently published in the journal Biology of Blood and Marrow Transplantation, suggest a substantial unmet need in the treatment of high-risk patients in first remission.
“Newer methods to improve graft-versus-leukemia effect are being tested and will need to be incorporated into the management of high-risk patients,” Asaf D. Yanir, MD, and coauthors at Baylor College of Medicine in Houston said in the report.
Dr. Yanir and colleagues reported recent outcomes for 124 patients who had undergone HSCT for ALL at their center during 2008-2016. That group included 20 haploidentical transplant recipients, 48 patients with matched sibling donors, and 56 with unrelated matched donors.
The 3-year cumulative incidence of relapse was 47% for haploidentical recipients, compared with 20% for matched sibling donors recipients and 24% for unrelated matched donors recipients (P = .02), according to their findings.
The main cause of HSCT failure was relapse, occurring in 47% of haploidentical transplant recipients, compared with 20% for those with matched sibling donors and 24% for those with unrelated matched donors (P = .02).
Those findings are in line with other studies showing inferior outcomes following haploidentical donor HSCT. However, in contrast to those studies, Dr. Yanir and colleagues did find a rate of treatment-related mortality comparable with other transplant approaches. The 3-year incidence of treatment-related mortality was 15% for the haploidentical group and, similarly, 17% in the matched sibling donor group and 16% in the unrelated matched donor group.
That lower rate of treatment-related mortality in the haploidentical group may be caused by improvements in procedures and supportive care. “Unfortunately, the benefits gained by reducing treatment-related mortality were offset by the high rate of relapse, which remains the main obstacle to successful haploidentical donor HSCT,” Dr. Yanir and coauthors wrote in their report.
New strategies are being studied to retain the graft-versus-leukemia effect or enhance it in patients who’ve undergone haploidentical HSCT, such as selectively depleting alloreactive T cells while sparing other immune effectors, investigators wrote.
“Given evolving practices, it is important to continually evaluate the projected event-free survival for pediatric ALL following HSCT, based on the donor type used,” they wrote.
Dr. Yanir and coauthors had no financial disclosures or conflicts of interest to report.
SOURCE: Yanir AD et al. Biol Blood Marrow Transplant. 2018 Mar 14. doi: 10.1016/j.bbmt.2018.03.001.
Relapse was the main impediment to successful hematopoietic stem cell transplant (HSCT) in high-risk pediatric acute lymphocytic leukemia (ALL), according to one of the largest single-center experiences reported to date.
The effects of relapse were especially evident for patients with haploidentical donors; these patients had a 3-year cumulative relapse incidence of 47% and event-free survival rate of 35%, both significantly higher than what was seen in other transplant recipients treated at the same center.
The findings, recently published in the journal Biology of Blood and Marrow Transplantation, suggest a substantial unmet need in the treatment of high-risk patients in first remission.
“Newer methods to improve graft-versus-leukemia effect are being tested and will need to be incorporated into the management of high-risk patients,” Asaf D. Yanir, MD, and coauthors at Baylor College of Medicine in Houston said in the report.
Dr. Yanir and colleagues reported recent outcomes for 124 patients who had undergone HSCT for ALL at their center during 2008-2016. That group included 20 haploidentical transplant recipients, 48 patients with matched sibling donors, and 56 with unrelated matched donors.
The 3-year cumulative incidence of relapse was 47% for haploidentical recipients, compared with 20% for matched sibling donors recipients and 24% for unrelated matched donors recipients (P = .02), according to their findings.
The main cause of HSCT failure was relapse, occurring in 47% of haploidentical transplant recipients, compared with 20% for those with matched sibling donors and 24% for those with unrelated matched donors (P = .02).
Those findings are in line with other studies showing inferior outcomes following haploidentical donor HSCT. However, in contrast to those studies, Dr. Yanir and colleagues did find a rate of treatment-related mortality comparable with other transplant approaches. The 3-year incidence of treatment-related mortality was 15% for the haploidentical group and, similarly, 17% in the matched sibling donor group and 16% in the unrelated matched donor group.
That lower rate of treatment-related mortality in the haploidentical group may be caused by improvements in procedures and supportive care. “Unfortunately, the benefits gained by reducing treatment-related mortality were offset by the high rate of relapse, which remains the main obstacle to successful haploidentical donor HSCT,” Dr. Yanir and coauthors wrote in their report.
New strategies are being studied to retain the graft-versus-leukemia effect or enhance it in patients who’ve undergone haploidentical HSCT, such as selectively depleting alloreactive T cells while sparing other immune effectors, investigators wrote.
“Given evolving practices, it is important to continually evaluate the projected event-free survival for pediatric ALL following HSCT, based on the donor type used,” they wrote.
Dr. Yanir and coauthors had no financial disclosures or conflicts of interest to report.
SOURCE: Yanir AD et al. Biol Blood Marrow Transplant. 2018 Mar 14. doi: 10.1016/j.bbmt.2018.03.001.
FROM BIOLOGY OF BLOOD AND MARROW TRANSPLANTATION
Key clinical point: In pediatric acute lymphocytic leukemia (ALL) patients, relapse is the main barrier to successful hematopoietic stem cell transplant (HSCT), especially for those who receive haploidentical donor grafts.
Major finding: The main cause of HSCT failure was relapse, occurring in 47% of haploidentical transplant recipients, compared with 20% for those with matched sibling donors and 24% for those with unrelated matched donors (P = .02).
Study details: A retrospective analysis of 124 transplants performed at a single center during 2008-2016.
Disclosures: Authors had no financial disclosures or conflicts of interest to report.
Source: Yanir AD et al. Biol Blood Marrow Transplant. doi: 10.1016/j.bbmt.2018.03.001.