User login
No benefits from bath emollients for childhood eczema
In a trial of 482 children with atopic dermatitis who were randomized to either use of prescribed emollient bath additives regularly for 12 months or no additives, in addition to usual care, there was no significant difference between the two groups in the patient-oriented eczema measure (POEM) – a score of symptoms in the previous week – for the first 16 weeks of treatment, reported Miriam Santer, MD, of the University of Southampton, England, and her coauthors. The mean POEM score was 7.5 in the bath additives group and 8.4 in the no bath additives group.
There also was no significant effect of emollient bath additives on the secondary outcomes, which included POEM over 52 weeks, dermatitis family impact, generic quality of life, number of eczema exacerbations, or topical corticosteroid or topical calcineurin inhibitor use.
The authors noted that there was the suggestion of benefit in children who bathed five or more times a week, and in children aged under 5 years, but in both cases, the numbers were small.
“Although there is evidence for the need for leave-on emollients and widespread clinical consensus around soap substitutes, there is less agreement about the potential additional benefits of bath additives and a dearth of evidence on their effectiveness,” wrote Dr. Santer and her associates. “Bath additives are, however, widely prescribed at a cost of more than 23 million pounds ($33 million US; 26 million euros) annually to the National Health Service in England.”
The bath emollients used in the study included Aveeno bath oil, and Oilatum bath additive and Balneum bath oil – products available largely in the United Kingdom – along with others. Adherence was reasonable, with 93% of participants in the emollient group using bath additives more than half or all the time, and 92% of those in the no bath additives group using them less than half the time or never.
The authors stressed that there was strong evidence that supported regular use of leave-on emollients, and clinical consensus around the use of emollients as soap substitutes. “These findings are timely for clinicians and prescribing advisers, as prescribing guidelines vary widely in their advice on the use of bath additives, and pressure on budgets has led to formularies becoming increasingly restrictive.”
The study was supported by the National Institute for Health Research. No conflicts of interest were declared.
SOURCE: Santer M et al. BMJ 2018 May 2. doi: 10.1136/bmj.k1332
The National Institute for Health and Care Excellence in the United Kingdom currently recommends regular use of “emollient wash products” for children with eczema, despite the fact that little good evidence of their benefit exists. It is therefore heartening that this study has largely addressed that evidence gap: There was no statistically significant difference between those children prescribed one of three bath additives in addition to standard care and those who received standard care alone.
However, there is still the question of whether younger children – particularly those who are bathed daily – might still benefit from bath emollients. Likewise, children who experience recurrent skin infections may derive some additional benefit from emollient bath additives with antiseptic properties.
Carsten Flohr, MD, is with the St. John’s Institute of Dermatology at Kings College London, and Amina Ahmed is a patient panel member at the Centre of Evidence-Based Dermatology in Nottingham, England. These comments are taken from an editorial accompanying the article by Santer et al. (BMJ. 2018 May 2. doi: 10.1136/bmj.k1791.) No conflicts of interest were declared.
The National Institute for Health and Care Excellence in the United Kingdom currently recommends regular use of “emollient wash products” for children with eczema, despite the fact that little good evidence of their benefit exists. It is therefore heartening that this study has largely addressed that evidence gap: There was no statistically significant difference between those children prescribed one of three bath additives in addition to standard care and those who received standard care alone.
However, there is still the question of whether younger children – particularly those who are bathed daily – might still benefit from bath emollients. Likewise, children who experience recurrent skin infections may derive some additional benefit from emollient bath additives with antiseptic properties.
Carsten Flohr, MD, is with the St. John’s Institute of Dermatology at Kings College London, and Amina Ahmed is a patient panel member at the Centre of Evidence-Based Dermatology in Nottingham, England. These comments are taken from an editorial accompanying the article by Santer et al. (BMJ. 2018 May 2. doi: 10.1136/bmj.k1791.) No conflicts of interest were declared.
The National Institute for Health and Care Excellence in the United Kingdom currently recommends regular use of “emollient wash products” for children with eczema, despite the fact that little good evidence of their benefit exists. It is therefore heartening that this study has largely addressed that evidence gap: There was no statistically significant difference between those children prescribed one of three bath additives in addition to standard care and those who received standard care alone.
However, there is still the question of whether younger children – particularly those who are bathed daily – might still benefit from bath emollients. Likewise, children who experience recurrent skin infections may derive some additional benefit from emollient bath additives with antiseptic properties.
Carsten Flohr, MD, is with the St. John’s Institute of Dermatology at Kings College London, and Amina Ahmed is a patient panel member at the Centre of Evidence-Based Dermatology in Nottingham, England. These comments are taken from an editorial accompanying the article by Santer et al. (BMJ. 2018 May 2. doi: 10.1136/bmj.k1791.) No conflicts of interest were declared.
In a trial of 482 children with atopic dermatitis who were randomized to either use of prescribed emollient bath additives regularly for 12 months or no additives, in addition to usual care, there was no significant difference between the two groups in the patient-oriented eczema measure (POEM) – a score of symptoms in the previous week – for the first 16 weeks of treatment, reported Miriam Santer, MD, of the University of Southampton, England, and her coauthors. The mean POEM score was 7.5 in the bath additives group and 8.4 in the no bath additives group.
There also was no significant effect of emollient bath additives on the secondary outcomes, which included POEM over 52 weeks, dermatitis family impact, generic quality of life, number of eczema exacerbations, or topical corticosteroid or topical calcineurin inhibitor use.
The authors noted that there was the suggestion of benefit in children who bathed five or more times a week, and in children aged under 5 years, but in both cases, the numbers were small.
“Although there is evidence for the need for leave-on emollients and widespread clinical consensus around soap substitutes, there is less agreement about the potential additional benefits of bath additives and a dearth of evidence on their effectiveness,” wrote Dr. Santer and her associates. “Bath additives are, however, widely prescribed at a cost of more than 23 million pounds ($33 million US; 26 million euros) annually to the National Health Service in England.”
The bath emollients used in the study included Aveeno bath oil, and Oilatum bath additive and Balneum bath oil – products available largely in the United Kingdom – along with others. Adherence was reasonable, with 93% of participants in the emollient group using bath additives more than half or all the time, and 92% of those in the no bath additives group using them less than half the time or never.
The authors stressed that there was strong evidence that supported regular use of leave-on emollients, and clinical consensus around the use of emollients as soap substitutes. “These findings are timely for clinicians and prescribing advisers, as prescribing guidelines vary widely in their advice on the use of bath additives, and pressure on budgets has led to formularies becoming increasingly restrictive.”
The study was supported by the National Institute for Health Research. No conflicts of interest were declared.
SOURCE: Santer M et al. BMJ 2018 May 2. doi: 10.1136/bmj.k1332
In a trial of 482 children with atopic dermatitis who were randomized to either use of prescribed emollient bath additives regularly for 12 months or no additives, in addition to usual care, there was no significant difference between the two groups in the patient-oriented eczema measure (POEM) – a score of symptoms in the previous week – for the first 16 weeks of treatment, reported Miriam Santer, MD, of the University of Southampton, England, and her coauthors. The mean POEM score was 7.5 in the bath additives group and 8.4 in the no bath additives group.
There also was no significant effect of emollient bath additives on the secondary outcomes, which included POEM over 52 weeks, dermatitis family impact, generic quality of life, number of eczema exacerbations, or topical corticosteroid or topical calcineurin inhibitor use.
The authors noted that there was the suggestion of benefit in children who bathed five or more times a week, and in children aged under 5 years, but in both cases, the numbers were small.
“Although there is evidence for the need for leave-on emollients and widespread clinical consensus around soap substitutes, there is less agreement about the potential additional benefits of bath additives and a dearth of evidence on their effectiveness,” wrote Dr. Santer and her associates. “Bath additives are, however, widely prescribed at a cost of more than 23 million pounds ($33 million US; 26 million euros) annually to the National Health Service in England.”
The bath emollients used in the study included Aveeno bath oil, and Oilatum bath additive and Balneum bath oil – products available largely in the United Kingdom – along with others. Adherence was reasonable, with 93% of participants in the emollient group using bath additives more than half or all the time, and 92% of those in the no bath additives group using them less than half the time or never.
The authors stressed that there was strong evidence that supported regular use of leave-on emollients, and clinical consensus around the use of emollients as soap substitutes. “These findings are timely for clinicians and prescribing advisers, as prescribing guidelines vary widely in their advice on the use of bath additives, and pressure on budgets has led to formularies becoming increasingly restrictive.”
The study was supported by the National Institute for Health Research. No conflicts of interest were declared.
SOURCE: Santer M et al. BMJ 2018 May 2. doi: 10.1136/bmj.k1332
FROM THE BMJ
Key clinical point: Emollient bath additives do not improve eczema scores in children.
Major finding: There was no significant difference in eczema scores between bath emollients or no bath emollients: the mean POEM score was 7.5 in the bath additives group and 8.4 in the no bath additives group.
Study details: An open-label randomized trial in 482 children with atopic dermatitis.
Disclosures: The study was supported by the National Institute for Health Research. No conflicts of interest were declared.
Source: Santer M et al. BMJ 2018 May 2. doi: 10.1136/bmj.k1332
‘You’re not going to tell my parents about this are you?’
You are on the front lines of the prevention, screening, and treatment decisions for adolescent substance use disorders. You often must choose whether to disclose information about substance use to parents and other concerned adults.
The risk of developing a substance use disorder increases dramatically the earlier an individual begins using a given substance.1 The neurobiology behind this risk is becoming increasingly clear. Young brains are undergoing crucial developmental processes, including synaptic pruning and myelination. The brain increasingly becomes more efficient in a staggered pattern, with limbic regions preceding frontal and executive regions, so we see adolescents with “more gas than brakes.” This has wisely been identified as developmentally appropriate, and even beneficial, rather than evidence that adolescents are somehow broken.2
Age-appropriate screening for substance use should occur as early as the preteen years and continue throughout adolescence. The most widely studied screening tools include the CRAFFT screening instrument and the Screening, Brief Intervention, and Referral to Treatment (SBIRT) approach.3,4 During formal and informal screening, you should lead with genuine concern for the well-being of the adolescent. Beginning a discussion with open-ended questions about substance use in the school and home is a way to build understanding of an adolescent’s environment prior to asking about personal use. While screening, consider well known risk factors including family history of substance use disorders, poor parental supervision, childhood maltreatment or abuse, low academic achievement, and untreated psychiatric disorders such as ADHD, depression, or anxiety, which may contribute to a higher likelihood or more rapid progression of a substance use disorder. Adolescents are more likely to disclose substance use when screening is done in private, rather than in the presence of a parent.5
Discussing the limits of confidentiality (generally when there is substantial risk of harm to self or others) with an adolescent shows respect and can be an expression of genuine care and concern. Once substance use or other risk-associated behaviors and choices are disclosed, you often may be asked not to share the information with parents. In some instances, privacy cannot be broken without consent. Be aware of your state laws governing parental and adolescent rights related to confidentiality.
You should strongly consider discussing substance use with the concerned adults when there are these red flags: daily use of any substance, any intravenous substance use, a score of 2 or higher on the CRAFFT, prescription medication misuse, or any change in medical status resulting from substance use, such as alcohol-related blackouts.
In most cases, adolescents should be informed of a decision to disclose substance use to their parents. Inviting adolescents to discuss how this will be done, including if the adolescent will be present, and whether you or the adolescent will disclose the use can be an opportunity to discuss their concerns. You should seek to understand if an adolescent has specific fears related to such a disclosure including careful consideration of any history of domestic violence or abuse.
Although adolescents increasingly identify with the opinions and values of their peers, it is a mistake to assume that they therefore do not value the opinions of their parents and the concerned adults in their lives. Parents play an integral role in preventing and treating adolescent substance use disorders. Except in rare instances of severe parent-child relationship problems or abuse, parents can and should be engaged as invaluable participants

Being aware of the legal and ethical obligations in treatment of adolescents presenting with any level of substance use, you can improve outcomes by thoughtfully inviting the participation of parents and other concerned adults into the prevention, screening, and treatment of adolescent substance use disorders.
Dr. Jackson is a child and adolescent psychiatrist at the University of Vermont, Burlington.
References
1. “Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings.” NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013).
2. “The Amazing Teen Brain,” Jay N. Geidd, Scientific American, May 2016.
3. Pediatrics 2011 Oct. doi: 10.1542/peds.2011-1754.
4. Alcohol Screening and Brief Intervention for Youth: A Practitioner’s Guide.
5. Pediatrics. 2016 Jul 1. doi: 10.1542/peds.2016-1211.
6. J Fam Commun. 2014 Jan 1:14(4):328-51.
7. J Clin Child Adolesc. Psychol. 2008;37(1):236-59.
8. J Child Adolesc Subst Abuse. 2015 May 4;24(3):155-65.
9. Arch Pediatr Adolesc Med. 2012;166(12):1132-9.
You are on the front lines of the prevention, screening, and treatment decisions for adolescent substance use disorders. You often must choose whether to disclose information about substance use to parents and other concerned adults.
The risk of developing a substance use disorder increases dramatically the earlier an individual begins using a given substance.1 The neurobiology behind this risk is becoming increasingly clear. Young brains are undergoing crucial developmental processes, including synaptic pruning and myelination. The brain increasingly becomes more efficient in a staggered pattern, with limbic regions preceding frontal and executive regions, so we see adolescents with “more gas than brakes.” This has wisely been identified as developmentally appropriate, and even beneficial, rather than evidence that adolescents are somehow broken.2
Age-appropriate screening for substance use should occur as early as the preteen years and continue throughout adolescence. The most widely studied screening tools include the CRAFFT screening instrument and the Screening, Brief Intervention, and Referral to Treatment (SBIRT) approach.3,4 During formal and informal screening, you should lead with genuine concern for the well-being of the adolescent. Beginning a discussion with open-ended questions about substance use in the school and home is a way to build understanding of an adolescent’s environment prior to asking about personal use. While screening, consider well known risk factors including family history of substance use disorders, poor parental supervision, childhood maltreatment or abuse, low academic achievement, and untreated psychiatric disorders such as ADHD, depression, or anxiety, which may contribute to a higher likelihood or more rapid progression of a substance use disorder. Adolescents are more likely to disclose substance use when screening is done in private, rather than in the presence of a parent.5
Discussing the limits of confidentiality (generally when there is substantial risk of harm to self or others) with an adolescent shows respect and can be an expression of genuine care and concern. Once substance use or other risk-associated behaviors and choices are disclosed, you often may be asked not to share the information with parents. In some instances, privacy cannot be broken without consent. Be aware of your state laws governing parental and adolescent rights related to confidentiality.
You should strongly consider discussing substance use with the concerned adults when there are these red flags: daily use of any substance, any intravenous substance use, a score of 2 or higher on the CRAFFT, prescription medication misuse, or any change in medical status resulting from substance use, such as alcohol-related blackouts.
In most cases, adolescents should be informed of a decision to disclose substance use to their parents. Inviting adolescents to discuss how this will be done, including if the adolescent will be present, and whether you or the adolescent will disclose the use can be an opportunity to discuss their concerns. You should seek to understand if an adolescent has specific fears related to such a disclosure including careful consideration of any history of domestic violence or abuse.
Although adolescents increasingly identify with the opinions and values of their peers, it is a mistake to assume that they therefore do not value the opinions of their parents and the concerned adults in their lives. Parents play an integral role in preventing and treating adolescent substance use disorders. Except in rare instances of severe parent-child relationship problems or abuse, parents can and should be engaged as invaluable participants
Being aware of the legal and ethical obligations in treatment of adolescents presenting with any level of substance use, you can improve outcomes by thoughtfully inviting the participation of parents and other concerned adults into the prevention, screening, and treatment of adolescent substance use disorders.
Dr. Jackson is a child and adolescent psychiatrist at the University of Vermont, Burlington.
References
1. “Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings.” NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013).
2. “The Amazing Teen Brain,” Jay N. Geidd, Scientific American, May 2016.
3. Pediatrics 2011 Oct. doi: 10.1542/peds.2011-1754.
4. Alcohol Screening and Brief Intervention for Youth: A Practitioner’s Guide.
5. Pediatrics. 2016 Jul 1. doi: 10.1542/peds.2016-1211.
6. J Fam Commun. 2014 Jan 1:14(4):328-51.
7. J Clin Child Adolesc. Psychol. 2008;37(1):236-59.
8. J Child Adolesc Subst Abuse. 2015 May 4;24(3):155-65.
9. Arch Pediatr Adolesc Med. 2012;166(12):1132-9.
You are on the front lines of the prevention, screening, and treatment decisions for adolescent substance use disorders. You often must choose whether to disclose information about substance use to parents and other concerned adults.
The risk of developing a substance use disorder increases dramatically the earlier an individual begins using a given substance.1 The neurobiology behind this risk is becoming increasingly clear. Young brains are undergoing crucial developmental processes, including synaptic pruning and myelination. The brain increasingly becomes more efficient in a staggered pattern, with limbic regions preceding frontal and executive regions, so we see adolescents with “more gas than brakes.” This has wisely been identified as developmentally appropriate, and even beneficial, rather than evidence that adolescents are somehow broken.2
Age-appropriate screening for substance use should occur as early as the preteen years and continue throughout adolescence. The most widely studied screening tools include the CRAFFT screening instrument and the Screening, Brief Intervention, and Referral to Treatment (SBIRT) approach.3,4 During formal and informal screening, you should lead with genuine concern for the well-being of the adolescent. Beginning a discussion with open-ended questions about substance use in the school and home is a way to build understanding of an adolescent’s environment prior to asking about personal use. While screening, consider well known risk factors including family history of substance use disorders, poor parental supervision, childhood maltreatment or abuse, low academic achievement, and untreated psychiatric disorders such as ADHD, depression, or anxiety, which may contribute to a higher likelihood or more rapid progression of a substance use disorder. Adolescents are more likely to disclose substance use when screening is done in private, rather than in the presence of a parent.5
Discussing the limits of confidentiality (generally when there is substantial risk of harm to self or others) with an adolescent shows respect and can be an expression of genuine care and concern. Once substance use or other risk-associated behaviors and choices are disclosed, you often may be asked not to share the information with parents. In some instances, privacy cannot be broken without consent. Be aware of your state laws governing parental and adolescent rights related to confidentiality.
You should strongly consider discussing substance use with the concerned adults when there are these red flags: daily use of any substance, any intravenous substance use, a score of 2 or higher on the CRAFFT, prescription medication misuse, or any change in medical status resulting from substance use, such as alcohol-related blackouts.
In most cases, adolescents should be informed of a decision to disclose substance use to their parents. Inviting adolescents to discuss how this will be done, including if the adolescent will be present, and whether you or the adolescent will disclose the use can be an opportunity to discuss their concerns. You should seek to understand if an adolescent has specific fears related to such a disclosure including careful consideration of any history of domestic violence or abuse.
Although adolescents increasingly identify with the opinions and values of their peers, it is a mistake to assume that they therefore do not value the opinions of their parents and the concerned adults in their lives. Parents play an integral role in preventing and treating adolescent substance use disorders. Except in rare instances of severe parent-child relationship problems or abuse, parents can and should be engaged as invaluable participants
Being aware of the legal and ethical obligations in treatment of adolescents presenting with any level of substance use, you can improve outcomes by thoughtfully inviting the participation of parents and other concerned adults into the prevention, screening, and treatment of adolescent substance use disorders.
Dr. Jackson is a child and adolescent psychiatrist at the University of Vermont, Burlington.
References
1. “Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings.” NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013).
2. “The Amazing Teen Brain,” Jay N. Geidd, Scientific American, May 2016.
3. Pediatrics 2011 Oct. doi: 10.1542/peds.2011-1754.
4. Alcohol Screening and Brief Intervention for Youth: A Practitioner’s Guide.
5. Pediatrics. 2016 Jul 1. doi: 10.1542/peds.2016-1211.
6. J Fam Commun. 2014 Jan 1:14(4):328-51.
7. J Clin Child Adolesc. Psychol. 2008;37(1):236-59.
8. J Child Adolesc Subst Abuse. 2015 May 4;24(3):155-65.
9. Arch Pediatr Adolesc Med. 2012;166(12):1132-9.
Low incidence of HS in children does not diminish importance of early diagnosis
a study has found.
“The relatively low disease burden must not overshadow the extreme quality of life impact this disease has on those afflicted with it,” noted Amit Garg, MD, and associates at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hyde Park, N.Y.
The clinical term “hidradenitis’ was used to locate pediatric patients within a multi-institutional database of 55 million patients participating in 27 integrated health care organizations whose records were active in the database between March 2014 and March 2017.
The standardized prevalence of HS among girls was 3.75 times greater than in boys (P less than .0001), and the condition was most common in those aged 15-17 years (72%) across each racial group. “HS disproportionately affects African American children and adolescents, who have a 3.5-fold greater standardized prevalence than do Caucasians,” the authors wrote. The report was published in the Journal of Investigative Dermatology. Specifically, the highest prevalence by race was found in females aged 15-17 years who were African American (525 per 100,000) and biracial (253 per 100,000).
The authors acknowledged the availability of limited existing HS pediatric data from case reports and small series, none of which provided descriptions of subgroups by gender, age, or race.
In their review of the existing literature, Dr. Garg and his associates noted several key observations that may further aid in clinical diagnosis of pediatric patients at greater risk of developing HS:
- HS appears most likely to be a post-adrenarche disease; children with the disease more frequently present with a hormonal imbalance compared with adults. In fact, HS in children may be a marker of precocious puberty, as noted in those presenting with adrenal hyperplasia and premature adrenarche.
- A separate population-based analysis revealed an association between HS and polycystic ovary syndrome.
- Pediatric patients diagnosed with HS are more likely to present with a family history of the condition, and those experiencing early onset appear likely to develop more widespread HS.
- A fivefold likelihood of HS in pediatric Down syndrome patients is also attributed to genetic mutations.
The higher incidence of HS among adults (0.1%) is likely due to largely postpubertal disease onset, the authors speculated. They acknowledged that delays in diagnosing adolescent HS could account for the difference in prevalence between pediatric and adult populations. According to one study cited by Dr. Garg and his colleagues, adults with HS may have symptoms as many as 7 years prior to receiving a diagnosis.
Findings in Dr. Garg’s study serve to reinforce those of previous studies on adult HS populations, which also cited higher prevalence among females, especially African American females.
The research was funded by an unrestricted educational grant from AbbVie. Dr. Garg has served as an adviser for and received honoraria from AbbVie; the remaining researchers had no relevant financial disclosures.
SOURCE: Garg A et al. J Investig Dermatol. 2018 Apr 2. doi: 10.1016/j.jid.2018.04.001.
a study has found.
“The relatively low disease burden must not overshadow the extreme quality of life impact this disease has on those afflicted with it,” noted Amit Garg, MD, and associates at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hyde Park, N.Y.
The clinical term “hidradenitis’ was used to locate pediatric patients within a multi-institutional database of 55 million patients participating in 27 integrated health care organizations whose records were active in the database between March 2014 and March 2017.
The standardized prevalence of HS among girls was 3.75 times greater than in boys (P less than .0001), and the condition was most common in those aged 15-17 years (72%) across each racial group. “HS disproportionately affects African American children and adolescents, who have a 3.5-fold greater standardized prevalence than do Caucasians,” the authors wrote. The report was published in the Journal of Investigative Dermatology. Specifically, the highest prevalence by race was found in females aged 15-17 years who were African American (525 per 100,000) and biracial (253 per 100,000).
The authors acknowledged the availability of limited existing HS pediatric data from case reports and small series, none of which provided descriptions of subgroups by gender, age, or race.
In their review of the existing literature, Dr. Garg and his associates noted several key observations that may further aid in clinical diagnosis of pediatric patients at greater risk of developing HS:
- HS appears most likely to be a post-adrenarche disease; children with the disease more frequently present with a hormonal imbalance compared with adults. In fact, HS in children may be a marker of precocious puberty, as noted in those presenting with adrenal hyperplasia and premature adrenarche.
- A separate population-based analysis revealed an association between HS and polycystic ovary syndrome.
- Pediatric patients diagnosed with HS are more likely to present with a family history of the condition, and those experiencing early onset appear likely to develop more widespread HS.
- A fivefold likelihood of HS in pediatric Down syndrome patients is also attributed to genetic mutations.
The higher incidence of HS among adults (0.1%) is likely due to largely postpubertal disease onset, the authors speculated. They acknowledged that delays in diagnosing adolescent HS could account for the difference in prevalence between pediatric and adult populations. According to one study cited by Dr. Garg and his colleagues, adults with HS may have symptoms as many as 7 years prior to receiving a diagnosis.
Findings in Dr. Garg’s study serve to reinforce those of previous studies on adult HS populations, which also cited higher prevalence among females, especially African American females.
The research was funded by an unrestricted educational grant from AbbVie. Dr. Garg has served as an adviser for and received honoraria from AbbVie; the remaining researchers had no relevant financial disclosures.
SOURCE: Garg A et al. J Investig Dermatol. 2018 Apr 2. doi: 10.1016/j.jid.2018.04.001.
a study has found.
“The relatively low disease burden must not overshadow the extreme quality of life impact this disease has on those afflicted with it,” noted Amit Garg, MD, and associates at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hyde Park, N.Y.
The clinical term “hidradenitis’ was used to locate pediatric patients within a multi-institutional database of 55 million patients participating in 27 integrated health care organizations whose records were active in the database between March 2014 and March 2017.
The standardized prevalence of HS among girls was 3.75 times greater than in boys (P less than .0001), and the condition was most common in those aged 15-17 years (72%) across each racial group. “HS disproportionately affects African American children and adolescents, who have a 3.5-fold greater standardized prevalence than do Caucasians,” the authors wrote. The report was published in the Journal of Investigative Dermatology. Specifically, the highest prevalence by race was found in females aged 15-17 years who were African American (525 per 100,000) and biracial (253 per 100,000).
The authors acknowledged the availability of limited existing HS pediatric data from case reports and small series, none of which provided descriptions of subgroups by gender, age, or race.
In their review of the existing literature, Dr. Garg and his associates noted several key observations that may further aid in clinical diagnosis of pediatric patients at greater risk of developing HS:
- HS appears most likely to be a post-adrenarche disease; children with the disease more frequently present with a hormonal imbalance compared with adults. In fact, HS in children may be a marker of precocious puberty, as noted in those presenting with adrenal hyperplasia and premature adrenarche.
- A separate population-based analysis revealed an association between HS and polycystic ovary syndrome.
- Pediatric patients diagnosed with HS are more likely to present with a family history of the condition, and those experiencing early onset appear likely to develop more widespread HS.
- A fivefold likelihood of HS in pediatric Down syndrome patients is also attributed to genetic mutations.
The higher incidence of HS among adults (0.1%) is likely due to largely postpubertal disease onset, the authors speculated. They acknowledged that delays in diagnosing adolescent HS could account for the difference in prevalence between pediatric and adult populations. According to one study cited by Dr. Garg and his colleagues, adults with HS may have symptoms as many as 7 years prior to receiving a diagnosis.
Findings in Dr. Garg’s study serve to reinforce those of previous studies on adult HS populations, which also cited higher prevalence among females, especially African American females.
The research was funded by an unrestricted educational grant from AbbVie. Dr. Garg has served as an adviser for and received honoraria from AbbVie; the remaining researchers had no relevant financial disclosures.
SOURCE: Garg A et al. J Investig Dermatol. 2018 Apr 2. doi: 10.1016/j.jid.2018.04.001.
FROM THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
Key clinical point: Onset of HS prior to age 10 years is extremely rate; more than two-thirds of cases occurred in teens aged 15-17 years.
Major finding: HS rates among girls are almost four times higher than those of boys; more than 70% of cases occurred in teens aged 15-17 years.
Study details: Cross-sectional population analysis of 1,240 pediatric patients sampled from a database of 55 million unique records.
Disclosures: The research was funded by an unrestricted educational grant from AbbVie. Dr. Garg has served as an adviser for and received honoraria from AbbVie; the remaining researchers had no relevant financial disclosures.
Source: Garg A et al. J Invest Dermatol. 2018 Apr 2. doi: 10.1016/j.jid.2018.04.001.
Consider caregiver oral health for children with bleeding disorders
SAN DIEGO – Caregiver oral health status is an identifiable risk factor that could be used to screen for poor oral health among children and young adults with bleeding disorders, results from a single-center suggest.
“We ask parents one simple question: ‘Have you had a cavity in the last year?’ If they say yes, we would be more concerned that their children would be more likely to have poor oral health,” Elizabeth Hastie said in an interview during a poster session at the biennial summit of the Thrombosis & Hemostasis Societies of North America.
Proper oral health may prevent joint disease and other conditions that predispose patients to bleeds, according to Ms. Hastie, a fourth-year medical student at Emory University, Atlanta. However, of the 147 hemophilia treatment centers in the United States, just 30% have a dentist on staff, while 90% of centers have expressed interest in increasing patient education in oral health.
In an effort to evaluate the dental habits, needs, and oral health issues of children and young adults up to age 18 with bleeding disorders, Ms. Hastie and her associates conducted a cross-sectional study of 226 patients who were evaluated by a staff dental hygienist at Children’s Healthcare of Atlanta Comprehensive Bleeding Disorders Clinic from May 2016 to October 2017.
The evaluation consisted of a 14-question survey derived from the American Academy of Pediatric Dentistry Caries–Risk Assessment Tool completed by the primary caregiver present during the visit and oral screening. The researchers extracted demographic and clinical characteristics from the patient’s chart and included age, race, county of residence, and bleeding disorder type and severity.
Nearly half of the patients (44%) reported they did not brush their teeth twice a day. Children younger than age 5 years were more likely to not brush their teeth twice a day, compared with children aged 5-14 years and young adults aged 15-18 years (57% vs. 44% and 31% respectively, P = .08).
More than one-quarter of patients (27%) reported not having a current dentist and 15% reported specific challenges with access to dental care including burdens related to distance, insurance coverage, and finding a provider willing to treat in the setting of their medical condition. Those who were Medicaid eligible or of low socioeconomic status were significantly more likely to report dental care access issues, compared with other patients (20% vs. 9%; P = .01).
Oral screening performed by the dental hygienist demonstrated significant oral pathology: 89% of patients had plaque accumulation, 57% had white spots or decalcifications, 37% had gingivitis, and 8% had suspicious lesions suggestive of dental caries.
The researchers also found that having a caregiver with active oral disease in the past 12 months increased the odds of suspicious lesions (odds ratio, 4.34), increased the odds of gingivitis (OR, 3.80), and decreased the odds of the patients’ brushing their teeth at least twice per day (OR, 0.17).
“Hopefully, if we can target those high-risk patients in clinic, we could reduce costs, the number of bleeds, the number of products and factor used, and potentially even morbidity in the future,” Ms. Hastie said.
She acknowledged certain limitations of the study, including its single-center design and the fact that a dental hygienist performed the majority of evaluations. She reported having no financial disclosures.
SAN DIEGO – Caregiver oral health status is an identifiable risk factor that could be used to screen for poor oral health among children and young adults with bleeding disorders, results from a single-center suggest.
“We ask parents one simple question: ‘Have you had a cavity in the last year?’ If they say yes, we would be more concerned that their children would be more likely to have poor oral health,” Elizabeth Hastie said in an interview during a poster session at the biennial summit of the Thrombosis & Hemostasis Societies of North America.
Proper oral health may prevent joint disease and other conditions that predispose patients to bleeds, according to Ms. Hastie, a fourth-year medical student at Emory University, Atlanta. However, of the 147 hemophilia treatment centers in the United States, just 30% have a dentist on staff, while 90% of centers have expressed interest in increasing patient education in oral health.
In an effort to evaluate the dental habits, needs, and oral health issues of children and young adults up to age 18 with bleeding disorders, Ms. Hastie and her associates conducted a cross-sectional study of 226 patients who were evaluated by a staff dental hygienist at Children’s Healthcare of Atlanta Comprehensive Bleeding Disorders Clinic from May 2016 to October 2017.
The evaluation consisted of a 14-question survey derived from the American Academy of Pediatric Dentistry Caries–Risk Assessment Tool completed by the primary caregiver present during the visit and oral screening. The researchers extracted demographic and clinical characteristics from the patient’s chart and included age, race, county of residence, and bleeding disorder type and severity.
Nearly half of the patients (44%) reported they did not brush their teeth twice a day. Children younger than age 5 years were more likely to not brush their teeth twice a day, compared with children aged 5-14 years and young adults aged 15-18 years (57% vs. 44% and 31% respectively, P = .08).
More than one-quarter of patients (27%) reported not having a current dentist and 15% reported specific challenges with access to dental care including burdens related to distance, insurance coverage, and finding a provider willing to treat in the setting of their medical condition. Those who were Medicaid eligible or of low socioeconomic status were significantly more likely to report dental care access issues, compared with other patients (20% vs. 9%; P = .01).
Oral screening performed by the dental hygienist demonstrated significant oral pathology: 89% of patients had plaque accumulation, 57% had white spots or decalcifications, 37% had gingivitis, and 8% had suspicious lesions suggestive of dental caries.
The researchers also found that having a caregiver with active oral disease in the past 12 months increased the odds of suspicious lesions (odds ratio, 4.34), increased the odds of gingivitis (OR, 3.80), and decreased the odds of the patients’ brushing their teeth at least twice per day (OR, 0.17).
“Hopefully, if we can target those high-risk patients in clinic, we could reduce costs, the number of bleeds, the number of products and factor used, and potentially even morbidity in the future,” Ms. Hastie said.
She acknowledged certain limitations of the study, including its single-center design and the fact that a dental hygienist performed the majority of evaluations. She reported having no financial disclosures.
SAN DIEGO – Caregiver oral health status is an identifiable risk factor that could be used to screen for poor oral health among children and young adults with bleeding disorders, results from a single-center suggest.
“We ask parents one simple question: ‘Have you had a cavity in the last year?’ If they say yes, we would be more concerned that their children would be more likely to have poor oral health,” Elizabeth Hastie said in an interview during a poster session at the biennial summit of the Thrombosis & Hemostasis Societies of North America.
Proper oral health may prevent joint disease and other conditions that predispose patients to bleeds, according to Ms. Hastie, a fourth-year medical student at Emory University, Atlanta. However, of the 147 hemophilia treatment centers in the United States, just 30% have a dentist on staff, while 90% of centers have expressed interest in increasing patient education in oral health.
In an effort to evaluate the dental habits, needs, and oral health issues of children and young adults up to age 18 with bleeding disorders, Ms. Hastie and her associates conducted a cross-sectional study of 226 patients who were evaluated by a staff dental hygienist at Children’s Healthcare of Atlanta Comprehensive Bleeding Disorders Clinic from May 2016 to October 2017.
The evaluation consisted of a 14-question survey derived from the American Academy of Pediatric Dentistry Caries–Risk Assessment Tool completed by the primary caregiver present during the visit and oral screening. The researchers extracted demographic and clinical characteristics from the patient’s chart and included age, race, county of residence, and bleeding disorder type and severity.
Nearly half of the patients (44%) reported they did not brush their teeth twice a day. Children younger than age 5 years were more likely to not brush their teeth twice a day, compared with children aged 5-14 years and young adults aged 15-18 years (57% vs. 44% and 31% respectively, P = .08).
More than one-quarter of patients (27%) reported not having a current dentist and 15% reported specific challenges with access to dental care including burdens related to distance, insurance coverage, and finding a provider willing to treat in the setting of their medical condition. Those who were Medicaid eligible or of low socioeconomic status were significantly more likely to report dental care access issues, compared with other patients (20% vs. 9%; P = .01).
Oral screening performed by the dental hygienist demonstrated significant oral pathology: 89% of patients had plaque accumulation, 57% had white spots or decalcifications, 37% had gingivitis, and 8% had suspicious lesions suggestive of dental caries.
The researchers also found that having a caregiver with active oral disease in the past 12 months increased the odds of suspicious lesions (odds ratio, 4.34), increased the odds of gingivitis (OR, 3.80), and decreased the odds of the patients’ brushing their teeth at least twice per day (OR, 0.17).
“Hopefully, if we can target those high-risk patients in clinic, we could reduce costs, the number of bleeds, the number of products and factor used, and potentially even morbidity in the future,” Ms. Hastie said.
She acknowledged certain limitations of the study, including its single-center design and the fact that a dental hygienist performed the majority of evaluations. She reported having no financial disclosures.
REPORTING FROM THSNA 2018
Key clinical point:
Major finding: Having a caregiver with active oral disease in the past 12 months increased the odds of the child having a suspicious lesion (OR 4.34) and gingivitis (OR 3.80).
Study details: A cross-sectional study of 226 pediatric patients who were evaluated by a dental hygienist.
Disclosures: Ms. Hastie reported having no financial disclosures.
Source: Hastie E et al. THSNA 2018, Poster 150.
Allergy, eczema common after pediatric solid organ transplantation
A total of 34% of children who underwent solid organ transplantation subsequently developed eczema, food allergy, rhinitis, eosinophilic gastrointestinal disease, or asthma, according to the results of a single-center retrospective cohort study.
Another 6.6% of patients developed autoimmunity, usually autoimmune cytopenia, inflammatory bowel disease, or vasculitis, wrote Nufar Marcus, MD, of the University of Toronto, and her associates.
Posttransplant allergy, autoimmunity, and immune-mediated disorders (PTAA) likely share a common pathogenesis “and may represent a unique state of post-transplant immune-dysregulation,” they wrote. The report was published in the Journal of Pediatrics.
The study included 273 children who underwent solid organ transplantation and were followed for a median 3.6 years (range, 1.7-6.3 years). None had immune-mediated conditions or allergies diagnosed at baseline. Posttransplantation allergies most commonly included eczema (51%), asthma (32%), food allergy (25%, including 5% with associated anaphylaxis), rhinitis (17%), and eosinophilic esophagitis, gastritis, or enteritis (13%).
Although only 31% of patients had information available on family history of allergy, those with a positive family history of allergy had a fivefold greater odds of posttransplantation PTAA, compared with other patients. Other risk factors for PTAA included female sex, young age at transplantation, eosinophilia, and a positive test for Epstein-Barr virus after transplantation, Dr. Marcus and associates said.
“The association of blood eosinophilia and PTAA reached statistical significance only when the transplant recipient was at least 6 months of age, demonstrating the nonspecific nature of abnormally high eosinophil counts during the first months of life,” they noted. The longer patients had eosinophilia after transplantation, the more likely they were to develop PTAA, “suggest[ing] a potential detrimental effect of prolonged activation of the eosinophilic-associated immune arms.”
Factors that appeared unlinked with PTAA included acute organ rejection, duration of posttransplantation steroidal treatment, organ type (living versus cadaveric), donor/recipient blood type and compatibility, infections besides Epstein-Barr virus, and posttransplant lymphoproliferative disease. “The specific type of post-transplantation immunosuppression regimen was neither associated nor protective of PTAA,” the investigators wrote. “However, a significant limitation was our inability to assess the effect of tacrolimus, as nearly all the cohort (97.8%) was treated with this medication.”
Ashley’s Angels fund provided support. The researchers reported having no conflicts of interest.
SOURCE: Marcus N et al. J Pediatr. 2018;196:154-60.
The study is one of several to highlight the occurrence of atopy and allergy following solid organ transplantation in children, Helen M. Evans, MBChB, wrote in an editorial accompanying the report by Marcus et al.
This report differed because it studied the differences in rates of atopy and allergy between transplanted solid organ groups. These occurred in 41% and 40% of liver and heart recipients, respectively, but in only 4% of kidney recipients. Atopy or allergy developed in 57% of multivisceral transplant patients, but the number of patients was very small (n = 7). The majority of the conditions developed within 1 year of transplantation.
The recent spike in these reports could signify better recognition of the problem or “the widespread switch of primary immunosuppression from cyclosporine to tacrolimus over the last few decades,” wrote Dr. Evans.
Most of these reports have been single-center retrospective studies, which are subject to inconsistent case definitions and recall bias, she noted. “The time is right for well-conducted multicenter prospective studies to better inform the true extent of these conditions after solid organ transplantation.”
In the meantime, transplantation centers should routinely track de novo eczema, allergy, and eosinophilic gastrointestinal disease in children being assessed for solid organ transplantation, and should take “rigorous” personal and family histories, said Dr. Evans. Ultimately, this work will help “minimize the risk of children developing these conditions” and “effectively treat them in the setting of immunosuppression after transplantation.”
Dr. Evans is a pediatric gastroenterologist at Starship Child Health in Aukland, New Zealand. She reported having no conflicts of interest. These comments summarize her editorial ( J Pediatr. 2018;196:10-11 ).
The study is one of several to highlight the occurrence of atopy and allergy following solid organ transplantation in children, Helen M. Evans, MBChB, wrote in an editorial accompanying the report by Marcus et al.
This report differed because it studied the differences in rates of atopy and allergy between transplanted solid organ groups. These occurred in 41% and 40% of liver and heart recipients, respectively, but in only 4% of kidney recipients. Atopy or allergy developed in 57% of multivisceral transplant patients, but the number of patients was very small (n = 7). The majority of the conditions developed within 1 year of transplantation.
The recent spike in these reports could signify better recognition of the problem or “the widespread switch of primary immunosuppression from cyclosporine to tacrolimus over the last few decades,” wrote Dr. Evans.
Most of these reports have been single-center retrospective studies, which are subject to inconsistent case definitions and recall bias, she noted. “The time is right for well-conducted multicenter prospective studies to better inform the true extent of these conditions after solid organ transplantation.”
In the meantime, transplantation centers should routinely track de novo eczema, allergy, and eosinophilic gastrointestinal disease in children being assessed for solid organ transplantation, and should take “rigorous” personal and family histories, said Dr. Evans. Ultimately, this work will help “minimize the risk of children developing these conditions” and “effectively treat them in the setting of immunosuppression after transplantation.”
Dr. Evans is a pediatric gastroenterologist at Starship Child Health in Aukland, New Zealand. She reported having no conflicts of interest. These comments summarize her editorial ( J Pediatr. 2018;196:10-11 ).
The study is one of several to highlight the occurrence of atopy and allergy following solid organ transplantation in children, Helen M. Evans, MBChB, wrote in an editorial accompanying the report by Marcus et al.
This report differed because it studied the differences in rates of atopy and allergy between transplanted solid organ groups. These occurred in 41% and 40% of liver and heart recipients, respectively, but in only 4% of kidney recipients. Atopy or allergy developed in 57% of multivisceral transplant patients, but the number of patients was very small (n = 7). The majority of the conditions developed within 1 year of transplantation.
The recent spike in these reports could signify better recognition of the problem or “the widespread switch of primary immunosuppression from cyclosporine to tacrolimus over the last few decades,” wrote Dr. Evans.
Most of these reports have been single-center retrospective studies, which are subject to inconsistent case definitions and recall bias, she noted. “The time is right for well-conducted multicenter prospective studies to better inform the true extent of these conditions after solid organ transplantation.”
In the meantime, transplantation centers should routinely track de novo eczema, allergy, and eosinophilic gastrointestinal disease in children being assessed for solid organ transplantation, and should take “rigorous” personal and family histories, said Dr. Evans. Ultimately, this work will help “minimize the risk of children developing these conditions” and “effectively treat them in the setting of immunosuppression after transplantation.”
Dr. Evans is a pediatric gastroenterologist at Starship Child Health in Aukland, New Zealand. She reported having no conflicts of interest. These comments summarize her editorial ( J Pediatr. 2018;196:10-11 ).
A total of 34% of children who underwent solid organ transplantation subsequently developed eczema, food allergy, rhinitis, eosinophilic gastrointestinal disease, or asthma, according to the results of a single-center retrospective cohort study.
Another 6.6% of patients developed autoimmunity, usually autoimmune cytopenia, inflammatory bowel disease, or vasculitis, wrote Nufar Marcus, MD, of the University of Toronto, and her associates.
Posttransplant allergy, autoimmunity, and immune-mediated disorders (PTAA) likely share a common pathogenesis “and may represent a unique state of post-transplant immune-dysregulation,” they wrote. The report was published in the Journal of Pediatrics.
The study included 273 children who underwent solid organ transplantation and were followed for a median 3.6 years (range, 1.7-6.3 years). None had immune-mediated conditions or allergies diagnosed at baseline. Posttransplantation allergies most commonly included eczema (51%), asthma (32%), food allergy (25%, including 5% with associated anaphylaxis), rhinitis (17%), and eosinophilic esophagitis, gastritis, or enteritis (13%).
Although only 31% of patients had information available on family history of allergy, those with a positive family history of allergy had a fivefold greater odds of posttransplantation PTAA, compared with other patients. Other risk factors for PTAA included female sex, young age at transplantation, eosinophilia, and a positive test for Epstein-Barr virus after transplantation, Dr. Marcus and associates said.
“The association of blood eosinophilia and PTAA reached statistical significance only when the transplant recipient was at least 6 months of age, demonstrating the nonspecific nature of abnormally high eosinophil counts during the first months of life,” they noted. The longer patients had eosinophilia after transplantation, the more likely they were to develop PTAA, “suggest[ing] a potential detrimental effect of prolonged activation of the eosinophilic-associated immune arms.”
Factors that appeared unlinked with PTAA included acute organ rejection, duration of posttransplantation steroidal treatment, organ type (living versus cadaveric), donor/recipient blood type and compatibility, infections besides Epstein-Barr virus, and posttransplant lymphoproliferative disease. “The specific type of post-transplantation immunosuppression regimen was neither associated nor protective of PTAA,” the investigators wrote. “However, a significant limitation was our inability to assess the effect of tacrolimus, as nearly all the cohort (97.8%) was treated with this medication.”
Ashley’s Angels fund provided support. The researchers reported having no conflicts of interest.
SOURCE: Marcus N et al. J Pediatr. 2018;196:154-60.
A total of 34% of children who underwent solid organ transplantation subsequently developed eczema, food allergy, rhinitis, eosinophilic gastrointestinal disease, or asthma, according to the results of a single-center retrospective cohort study.
Another 6.6% of patients developed autoimmunity, usually autoimmune cytopenia, inflammatory bowel disease, or vasculitis, wrote Nufar Marcus, MD, of the University of Toronto, and her associates.
Posttransplant allergy, autoimmunity, and immune-mediated disorders (PTAA) likely share a common pathogenesis “and may represent a unique state of post-transplant immune-dysregulation,” they wrote. The report was published in the Journal of Pediatrics.
The study included 273 children who underwent solid organ transplantation and were followed for a median 3.6 years (range, 1.7-6.3 years). None had immune-mediated conditions or allergies diagnosed at baseline. Posttransplantation allergies most commonly included eczema (51%), asthma (32%), food allergy (25%, including 5% with associated anaphylaxis), rhinitis (17%), and eosinophilic esophagitis, gastritis, or enteritis (13%).
Although only 31% of patients had information available on family history of allergy, those with a positive family history of allergy had a fivefold greater odds of posttransplantation PTAA, compared with other patients. Other risk factors for PTAA included female sex, young age at transplantation, eosinophilia, and a positive test for Epstein-Barr virus after transplantation, Dr. Marcus and associates said.
“The association of blood eosinophilia and PTAA reached statistical significance only when the transplant recipient was at least 6 months of age, demonstrating the nonspecific nature of abnormally high eosinophil counts during the first months of life,” they noted. The longer patients had eosinophilia after transplantation, the more likely they were to develop PTAA, “suggest[ing] a potential detrimental effect of prolonged activation of the eosinophilic-associated immune arms.”
Factors that appeared unlinked with PTAA included acute organ rejection, duration of posttransplantation steroidal treatment, organ type (living versus cadaveric), donor/recipient blood type and compatibility, infections besides Epstein-Barr virus, and posttransplant lymphoproliferative disease. “The specific type of post-transplantation immunosuppression regimen was neither associated nor protective of PTAA,” the investigators wrote. “However, a significant limitation was our inability to assess the effect of tacrolimus, as nearly all the cohort (97.8%) was treated with this medication.”
Ashley’s Angels fund provided support. The researchers reported having no conflicts of interest.
SOURCE: Marcus N et al. J Pediatr. 2018;196:154-60.
FROM JOURNAL OF PEDIATRICS
Key clinical point: Children undergoing solid organ transplantation often developed allergy or autoimmunity.
Major finding: Study details: Single-center retrospective cross-sectional study of 273 patients aged 18 and under who underwent solid organ transplantation followed for a median 3.6 years.
Disclosures: Ashley’s Angels fund provided support. The researchers reported having no conflicts of interest.
Source: Marcus N et al. J Pediatr. 2018;196:154-60.
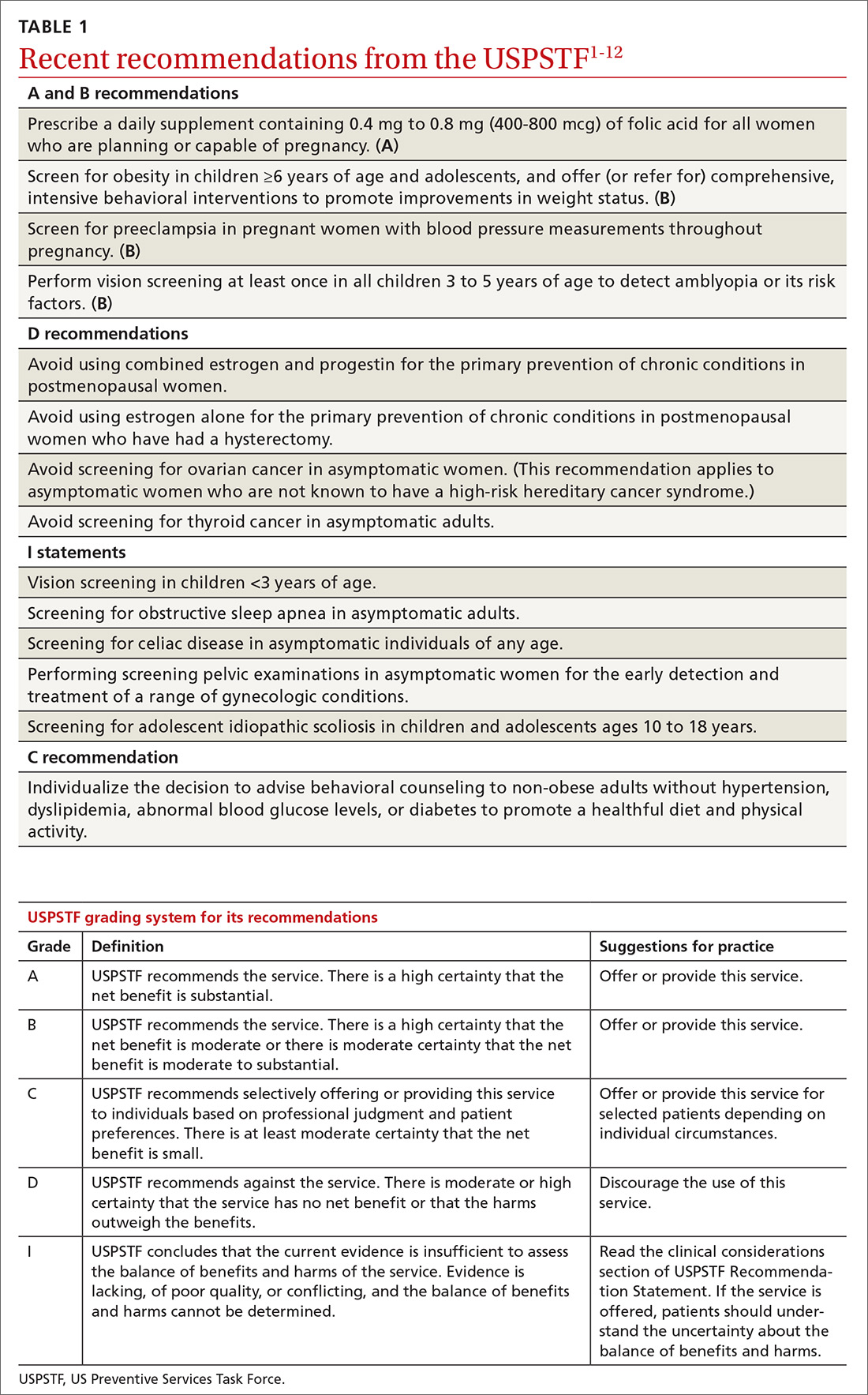
USPSTF update: New and revised recommendations
Over the past year the US Preventive Services Task Force made 14 recommendations on 12 conditions (TABLE 11-12). One of these pronouncements was the unusual reversal of a previous “D” recommendation against screening for scoliosis in adolescents, changing it to an “I” statement (insufficient evidence).
Affirmative recommendations
Four interventions were given an “A” or “B” recommendation this past year. Both grades signify a recommendation to perform the service, with “A” reflecting a higher level of certainty or a higher level of net benefit than “B.”
Recommend folic acid to prevent neural tube defects (A)
The evidence is very strong that folic acid intake prevents neural tube defects. In 2009 the Task Force recommended folic acid supplementation for women of childbearing age. In 2017 this recommendation was updated and slightly reworded to advise that all women who are planning a pregnancy or capable of becoming pregnant take a daily supplement containing 0.4 mg to 0.8 mg (400-800 mcg) of folic acid.
In the United States many grain products have been fortified with folic acid since 1996. This step has reduced the prevalence of neural tube defects from 10.7 cases per 10,000 live births to 7 cases per 10,000 live births in 2011.1 However, in spite of food fortification, most women in the United States do not consume the recommended daily amount of 0.4 mg (400 mcg) of folic acid. This supplementation is most important from one month before conception through the first 3 months of pregnancy.
Screen for obesity in children and adolescents (B)
Nearly 17% of children and adolescents ages 2 to 19 years in the United States are obese, and almost 32% are overweight or obese.2 Obesity is defined as a body mass index (BMI) ≥95th percentile, based on year-2000 growth charts published by the Centers for Disease Control and Prevention. Overweight is defined as a BMI between the 85th and 94th percentiles.
Obesity in children and adolescents is associated with many physical problems, including obstructive sleep apnea, orthopedic problems, high blood pressure, hyperlipidemia, and diabetes, as well as psychological harms from being teased and bullied. Obesity that continues into adulthood is associated with diabetes, cardiovascular disease, and orthopedic problems.
The Task Force found that intensive behavioral interventions for obesity in children ≥6 years of age and in adolescents can lead to moderate improvements in weight status for up to 12 months. Intensive behavioral interventions need to include at least 26 contact hours over 2 to 12 months. The recommendation statement includes a more detailed description of the types of programs that have evidence to support them.2
The Task Force did not recommend the use of either metformin or orlistat because of inadequate evidence on the harmful effects of metformin and because of sound evidence that orlistat causes moderate harms, such as abdominal pain, cramping, incontinence, and flatus.
Screen for preeclampsia (B), but dipstick testing is unreliable
Preeclampsia occurs in a little more than 3% of pregnancies in the United States.13 For the mother, this condition can lead to stroke, eclampsia, organ failure, and death; for the fetus, intrauterine growth retardation, preterm birth, low birth weight, and still birth. Preeclampsia is a leading cause of maternal mortality worldwide. Adverse health outcomes can be prevented by early detection of preeclampsia and by managing it appropriately.3
In 1996 the Task Force recommended screening for preeclampsia during pregnancy, and it reaffirmed that recommendation last year. The Task Force recommends taking blood pressure measurements at every prenatal visit, but does not recommend testing for urine protein with a dipstick because of the technique’s low accuracy.
Since 2014 the Task Force has also recommended using low-dose aspirin after Week 12 of pregnancy to prevent preeclampsia in women who are at high risk.14
Conduct vision screening in all children ages 3 to 5 years (B)
One of the more nuanced recommendations involves vision screening in children. The Task Force recently reaffirmed its 2011 recommendation to perform vision screening at least once in all children ages 3 to 5 years to detect amblyopia or its risk factors. But it found insufficient evidence to test children <3 years of age.
Amblyopia is a “functional reduction in visual acuity characterized by abnormal processing of visual images; [it is] established by the brain during a critical period of vision development.”4 Risk factors associated with the development of amblyopia include strabismus (ocular misalignment); vision loss caused by cataracts; refractive errors such as near and far sightedness, astigmatism (“blurred vision at any distance due to abnormal curvature of the cornea or lens”); and anisometropia (“asymmetric refractive error between the … eyes that causes image suppression in the eye with the larger error”). 4
Physical exam- and machine-based screening tests are available in the primary care setting (TABLE 2).4
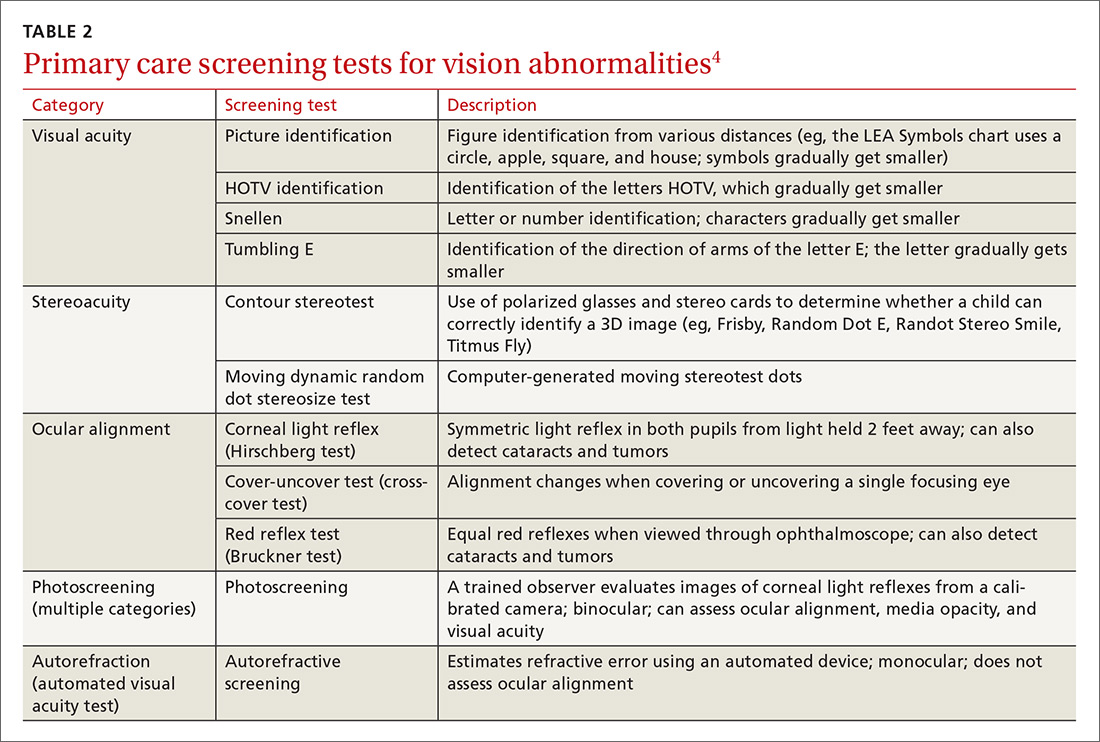
At first glance it appears that the Task Force recommends screening only for amblyopia, but the addition of “risk factors” implies a more comprehensive vision evaluation that would include visual acuity. This interpretation more closely aligns the Task Force recommendation with that of a joint report by the American Academy of Pediatrics, American Association for Pediatric Ophthalmology and Strabismus, American Academy of Certified Orthoptists, and American Academy of Ophthalmology, which recommends testing for a variety of vision problems in children.15 Nevertheless, the Task Force maintains that the evidence of benefit in testing more extensively before age 3 is insufficient, while the other organizations recommend starting testing at age 6 months.
Negative “D” recommendations
Equally as important as affirmative recommendations for effective interventions are the “D” recommendations advising against interventions that are ineffective or cause more harm than benefits. This past year, the Task Force recommended against 4 interventions. Two pertain to the use of estrogen or combined estrogen and progestin for the primary prevention of chronic conditions in postmenopausal women.5 This topic has been discussed in a recent JFP audiocast. Also receiving “D” recommendations were screening for ovarian cancer in asymptomatic women,6 discussed in another JFP audiocast, and screening for thyroid cancer in asymptomatic adults.7
The “D” recommendation for thyroid cancer screening was based on the low incidence of thyroid cancer, the evidence showing no change in mortality after the introduction of population-based screening, and the likelihood of overdiagnosis and overtreatment that would result from screening. The screening tests considered by the Task Force included neck palpation and ultrasound.7
Insufficient evidence
In addition to the previously mentioned “I” statement on vision screening for children <3 years of age,4 4 other interventions lacked sufficient evidence that the Task Force could use in determining relative levels of harms and benefits. These interventions were screening for obstructive sleep apnea in asymptomatic adults,8 screening for celiac disease in asymptomatic patients of all ages,9 screening with a pelvic examination in asymptomatic women,10 and screening for adolescent idiopathic scoliosis in children and adolescents ages 10 to 18 years.11
The lack of evidence regarding the value of a routine pelvic exam for asymptomatic women is surprising given how often this procedure is performed. The Task Force defined a pelvic exam as an “assessment of the external genitalia, internal speculum examination, bimanual palpation, and rectovaginal examination.”10 The Task Force found very little evidence on the accuracy and effectiveness of this exam for a range of gynecologic conditions other than cervical cancer, gonorrhea, and chlamydia, for which screening is recommended.10
The “I” statement on screening for adolescent idiopathic scoliosis in children and adolescents is an unusual revision of a “D” recommendation from 2004. At that time, the Task Force found that treatment of adolescent idiopathic scoliosis leads to health benefits in only a small proportion of individuals and that there are harms of treatment such as unnecessary bracing and referral to specialty care. For the most recent evidence report, the Task Force used a new methodology to assess treatment harms and concluded that the evidence is now inadequate. That finding, along with new evidence that “suggests that brace treatment can interrupt or slow scoliosis progression” led the Task Force to move away from a “D” recommendation.11
The enigmatic “C” recommendation
Perhaps the most difficult recommendation category to understand and implement is the “C” recommendation. With a “C” intervention, there is moderate certainty that the net benefit of universal implementation would be very small; but there are some individuals who might benefit from it, and physicians should offer it selectively.
The Task Force made one “C” recommendation over the past year: for adults who are not obese and who do not have other cardiovascular disease (CVD) risks, the net gain in referring them to behavioral counseling to promote a healthful diet and physical activity is small. However, the harms from such referrals are also small. Counseling interventions can result in healthier habits and in small improvements in intermediate outcomes, such as blood pressure, cholesterol levels, and weight. The effect on overall CVD mortality, though, has been minimal.12 The Task Force concluded that “[those] who are interested and ready to make behavioral changes may be most likely to benefit from behavioral counseling.”
1. USPSTF. Folic acid for the prevention of neural tube defects: preventive medication. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/folic-acid-for-the-prevention-of-neural-tube-defects-preventive-medication. Accessed March 22, 2018.
2. USPSTF. Obesity in children and adolescents: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/obesity-in-children-and-adolescents-screening1. Accessed March 22, 2018.
3. USPSTF. Preeclampsia: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/preeclampsia-screening1. Accessed March 22, 2018.
4. USPSTF. Vision in children ages 6 months to 5 years: Screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/vision-in-children-ages-6-months-to-5-years-screening. Accessed March 22, 2018.
5. USPSTF. Hormone therapy in postmenopausal women: primary prevention of chronic conditions. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/menopausal-hormone-therapy-preventive-medication1. Accessed March 24, 2018.
6. USPSTF. Ovarian cancer: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/ovarian-cancer-screening1. Accessed March 24, 2018.
7. USPSTF. Thyroid cancer: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/thyroid-cancer-screening1. Accessed March 22, 2018.
8. USPSTF. Obstructive sleep apnea in adults: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/obstructive-sleep-apnea-in-adults-screening. Accessed March 22, 2018.
9. USPSTF. Celiac disease: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/celiac-disease-screening. Accessed March 24, 2018.
10. USPSTF. Gynecological conditions: periodic screening with the pelvic examination. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/gynecological-conditions-screening-with-the-pelvic-examination. Accessed March 22, 2018.
11. USPSTF. Adolescent idiopathic scoliosis: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/adolescent-idiopathic-scoliosis-screening1. Accessed March 22, 2018.
12. USPSTF. Healthful diet and physical activity for cardiovascular disease prevention in adults without known risk factors: behavioral counseling. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/healthful-diet-and-physical-activity-for-cardiovascular-disease-prevention-in-adults-without-known-risk-factors-behavioral-counseling. Accessed March 22, 2018.
13. Ananth CV, Keyes KM, Wapner RJ. Pre-eclampsia rates in the United States, 1980-2010: age-period-cohort analysis. BMJ. 2013;347:f6564.
14. USPSTF. Low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: preventive medication. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/low-dose-aspirin-use-for-the-prevention-of-morbidity-and-mortality-from-preeclampsia-preventive-medication. Accessed March 22, 2018.
15. Donahue SP, Baker CN; Committee on Practice and Ambulatory Medicine, American Academy of Pediatrics; Section on Ophthalmology, American Academy of Pediatrics; American Association of Certified Orthoptists; American Association for Pediatric Ophthalmology and Strabismus; American Academy of Ophthalmology. Procedures for the evaluation of the visual system by pediatricians. Pediatrics. 2016;137.2015-3597.
Over the past year the US Preventive Services Task Force made 14 recommendations on 12 conditions (TABLE 11-12). One of these pronouncements was the unusual reversal of a previous “D” recommendation against screening for scoliosis in adolescents, changing it to an “I” statement (insufficient evidence).
Affirmative recommendations
Four interventions were given an “A” or “B” recommendation this past year. Both grades signify a recommendation to perform the service, with “A” reflecting a higher level of certainty or a higher level of net benefit than “B.”
Recommend folic acid to prevent neural tube defects (A)
The evidence is very strong that folic acid intake prevents neural tube defects. In 2009 the Task Force recommended folic acid supplementation for women of childbearing age. In 2017 this recommendation was updated and slightly reworded to advise that all women who are planning a pregnancy or capable of becoming pregnant take a daily supplement containing 0.4 mg to 0.8 mg (400-800 mcg) of folic acid.
In the United States many grain products have been fortified with folic acid since 1996. This step has reduced the prevalence of neural tube defects from 10.7 cases per 10,000 live births to 7 cases per 10,000 live births in 2011.1 However, in spite of food fortification, most women in the United States do not consume the recommended daily amount of 0.4 mg (400 mcg) of folic acid. This supplementation is most important from one month before conception through the first 3 months of pregnancy.
Screen for obesity in children and adolescents (B)
Nearly 17% of children and adolescents ages 2 to 19 years in the United States are obese, and almost 32% are overweight or obese.2 Obesity is defined as a body mass index (BMI) ≥95th percentile, based on year-2000 growth charts published by the Centers for Disease Control and Prevention. Overweight is defined as a BMI between the 85th and 94th percentiles.
Obesity in children and adolescents is associated with many physical problems, including obstructive sleep apnea, orthopedic problems, high blood pressure, hyperlipidemia, and diabetes, as well as psychological harms from being teased and bullied. Obesity that continues into adulthood is associated with diabetes, cardiovascular disease, and orthopedic problems.
The Task Force found that intensive behavioral interventions for obesity in children ≥6 years of age and in adolescents can lead to moderate improvements in weight status for up to 12 months. Intensive behavioral interventions need to include at least 26 contact hours over 2 to 12 months. The recommendation statement includes a more detailed description of the types of programs that have evidence to support them.2
The Task Force did not recommend the use of either metformin or orlistat because of inadequate evidence on the harmful effects of metformin and because of sound evidence that orlistat causes moderate harms, such as abdominal pain, cramping, incontinence, and flatus.
Screen for preeclampsia (B), but dipstick testing is unreliable
Preeclampsia occurs in a little more than 3% of pregnancies in the United States.13 For the mother, this condition can lead to stroke, eclampsia, organ failure, and death; for the fetus, intrauterine growth retardation, preterm birth, low birth weight, and still birth. Preeclampsia is a leading cause of maternal mortality worldwide. Adverse health outcomes can be prevented by early detection of preeclampsia and by managing it appropriately.3
In 1996 the Task Force recommended screening for preeclampsia during pregnancy, and it reaffirmed that recommendation last year. The Task Force recommends taking blood pressure measurements at every prenatal visit, but does not recommend testing for urine protein with a dipstick because of the technique’s low accuracy.
Since 2014 the Task Force has also recommended using low-dose aspirin after Week 12 of pregnancy to prevent preeclampsia in women who are at high risk.14
Conduct vision screening in all children ages 3 to 5 years (B)
One of the more nuanced recommendations involves vision screening in children. The Task Force recently reaffirmed its 2011 recommendation to perform vision screening at least once in all children ages 3 to 5 years to detect amblyopia or its risk factors. But it found insufficient evidence to test children <3 years of age.
Amblyopia is a “functional reduction in visual acuity characterized by abnormal processing of visual images; [it is] established by the brain during a critical period of vision development.”4 Risk factors associated with the development of amblyopia include strabismus (ocular misalignment); vision loss caused by cataracts; refractive errors such as near and far sightedness, astigmatism (“blurred vision at any distance due to abnormal curvature of the cornea or lens”); and anisometropia (“asymmetric refractive error between the … eyes that causes image suppression in the eye with the larger error”). 4
Physical exam- and machine-based screening tests are available in the primary care setting (TABLE 2).4
At first glance it appears that the Task Force recommends screening only for amblyopia, but the addition of “risk factors” implies a more comprehensive vision evaluation that would include visual acuity. This interpretation more closely aligns the Task Force recommendation with that of a joint report by the American Academy of Pediatrics, American Association for Pediatric Ophthalmology and Strabismus, American Academy of Certified Orthoptists, and American Academy of Ophthalmology, which recommends testing for a variety of vision problems in children.15 Nevertheless, the Task Force maintains that the evidence of benefit in testing more extensively before age 3 is insufficient, while the other organizations recommend starting testing at age 6 months.
Negative “D” recommendations
Equally as important as affirmative recommendations for effective interventions are the “D” recommendations advising against interventions that are ineffective or cause more harm than benefits. This past year, the Task Force recommended against 4 interventions. Two pertain to the use of estrogen or combined estrogen and progestin for the primary prevention of chronic conditions in postmenopausal women.5 This topic has been discussed in a recent JFP audiocast. Also receiving “D” recommendations were screening for ovarian cancer in asymptomatic women,6 discussed in another JFP audiocast, and screening for thyroid cancer in asymptomatic adults.7
The “D” recommendation for thyroid cancer screening was based on the low incidence of thyroid cancer, the evidence showing no change in mortality after the introduction of population-based screening, and the likelihood of overdiagnosis and overtreatment that would result from screening. The screening tests considered by the Task Force included neck palpation and ultrasound.7
Insufficient evidence
In addition to the previously mentioned “I” statement on vision screening for children <3 years of age,4 4 other interventions lacked sufficient evidence that the Task Force could use in determining relative levels of harms and benefits. These interventions were screening for obstructive sleep apnea in asymptomatic adults,8 screening for celiac disease in asymptomatic patients of all ages,9 screening with a pelvic examination in asymptomatic women,10 and screening for adolescent idiopathic scoliosis in children and adolescents ages 10 to 18 years.11
The lack of evidence regarding the value of a routine pelvic exam for asymptomatic women is surprising given how often this procedure is performed. The Task Force defined a pelvic exam as an “assessment of the external genitalia, internal speculum examination, bimanual palpation, and rectovaginal examination.”10 The Task Force found very little evidence on the accuracy and effectiveness of this exam for a range of gynecologic conditions other than cervical cancer, gonorrhea, and chlamydia, for which screening is recommended.10
The “I” statement on screening for adolescent idiopathic scoliosis in children and adolescents is an unusual revision of a “D” recommendation from 2004. At that time, the Task Force found that treatment of adolescent idiopathic scoliosis leads to health benefits in only a small proportion of individuals and that there are harms of treatment such as unnecessary bracing and referral to specialty care. For the most recent evidence report, the Task Force used a new methodology to assess treatment harms and concluded that the evidence is now inadequate. That finding, along with new evidence that “suggests that brace treatment can interrupt or slow scoliosis progression” led the Task Force to move away from a “D” recommendation.11
The enigmatic “C” recommendation
Perhaps the most difficult recommendation category to understand and implement is the “C” recommendation. With a “C” intervention, there is moderate certainty that the net benefit of universal implementation would be very small; but there are some individuals who might benefit from it, and physicians should offer it selectively.
The Task Force made one “C” recommendation over the past year: for adults who are not obese and who do not have other cardiovascular disease (CVD) risks, the net gain in referring them to behavioral counseling to promote a healthful diet and physical activity is small. However, the harms from such referrals are also small. Counseling interventions can result in healthier habits and in small improvements in intermediate outcomes, such as blood pressure, cholesterol levels, and weight. The effect on overall CVD mortality, though, has been minimal.12 The Task Force concluded that “[those] who are interested and ready to make behavioral changes may be most likely to benefit from behavioral counseling.”
Over the past year the US Preventive Services Task Force made 14 recommendations on 12 conditions (TABLE 11-12). One of these pronouncements was the unusual reversal of a previous “D” recommendation against screening for scoliosis in adolescents, changing it to an “I” statement (insufficient evidence).
Affirmative recommendations
Four interventions were given an “A” or “B” recommendation this past year. Both grades signify a recommendation to perform the service, with “A” reflecting a higher level of certainty or a higher level of net benefit than “B.”
Recommend folic acid to prevent neural tube defects (A)
The evidence is very strong that folic acid intake prevents neural tube defects. In 2009 the Task Force recommended folic acid supplementation for women of childbearing age. In 2017 this recommendation was updated and slightly reworded to advise that all women who are planning a pregnancy or capable of becoming pregnant take a daily supplement containing 0.4 mg to 0.8 mg (400-800 mcg) of folic acid.
In the United States many grain products have been fortified with folic acid since 1996. This step has reduced the prevalence of neural tube defects from 10.7 cases per 10,000 live births to 7 cases per 10,000 live births in 2011.1 However, in spite of food fortification, most women in the United States do not consume the recommended daily amount of 0.4 mg (400 mcg) of folic acid. This supplementation is most important from one month before conception through the first 3 months of pregnancy.
Screen for obesity in children and adolescents (B)
Nearly 17% of children and adolescents ages 2 to 19 years in the United States are obese, and almost 32% are overweight or obese.2 Obesity is defined as a body mass index (BMI) ≥95th percentile, based on year-2000 growth charts published by the Centers for Disease Control and Prevention. Overweight is defined as a BMI between the 85th and 94th percentiles.
Obesity in children and adolescents is associated with many physical problems, including obstructive sleep apnea, orthopedic problems, high blood pressure, hyperlipidemia, and diabetes, as well as psychological harms from being teased and bullied. Obesity that continues into adulthood is associated with diabetes, cardiovascular disease, and orthopedic problems.
The Task Force found that intensive behavioral interventions for obesity in children ≥6 years of age and in adolescents can lead to moderate improvements in weight status for up to 12 months. Intensive behavioral interventions need to include at least 26 contact hours over 2 to 12 months. The recommendation statement includes a more detailed description of the types of programs that have evidence to support them.2
The Task Force did not recommend the use of either metformin or orlistat because of inadequate evidence on the harmful effects of metformin and because of sound evidence that orlistat causes moderate harms, such as abdominal pain, cramping, incontinence, and flatus.
Screen for preeclampsia (B), but dipstick testing is unreliable
Preeclampsia occurs in a little more than 3% of pregnancies in the United States.13 For the mother, this condition can lead to stroke, eclampsia, organ failure, and death; for the fetus, intrauterine growth retardation, preterm birth, low birth weight, and still birth. Preeclampsia is a leading cause of maternal mortality worldwide. Adverse health outcomes can be prevented by early detection of preeclampsia and by managing it appropriately.3
In 1996 the Task Force recommended screening for preeclampsia during pregnancy, and it reaffirmed that recommendation last year. The Task Force recommends taking blood pressure measurements at every prenatal visit, but does not recommend testing for urine protein with a dipstick because of the technique’s low accuracy.
Since 2014 the Task Force has also recommended using low-dose aspirin after Week 12 of pregnancy to prevent preeclampsia in women who are at high risk.14
Conduct vision screening in all children ages 3 to 5 years (B)
One of the more nuanced recommendations involves vision screening in children. The Task Force recently reaffirmed its 2011 recommendation to perform vision screening at least once in all children ages 3 to 5 years to detect amblyopia or its risk factors. But it found insufficient evidence to test children <3 years of age.
Amblyopia is a “functional reduction in visual acuity characterized by abnormal processing of visual images; [it is] established by the brain during a critical period of vision development.”4 Risk factors associated with the development of amblyopia include strabismus (ocular misalignment); vision loss caused by cataracts; refractive errors such as near and far sightedness, astigmatism (“blurred vision at any distance due to abnormal curvature of the cornea or lens”); and anisometropia (“asymmetric refractive error between the … eyes that causes image suppression in the eye with the larger error”). 4
Physical exam- and machine-based screening tests are available in the primary care setting (TABLE 2).4
At first glance it appears that the Task Force recommends screening only for amblyopia, but the addition of “risk factors” implies a more comprehensive vision evaluation that would include visual acuity. This interpretation more closely aligns the Task Force recommendation with that of a joint report by the American Academy of Pediatrics, American Association for Pediatric Ophthalmology and Strabismus, American Academy of Certified Orthoptists, and American Academy of Ophthalmology, which recommends testing for a variety of vision problems in children.15 Nevertheless, the Task Force maintains that the evidence of benefit in testing more extensively before age 3 is insufficient, while the other organizations recommend starting testing at age 6 months.
Negative “D” recommendations
Equally as important as affirmative recommendations for effective interventions are the “D” recommendations advising against interventions that are ineffective or cause more harm than benefits. This past year, the Task Force recommended against 4 interventions. Two pertain to the use of estrogen or combined estrogen and progestin for the primary prevention of chronic conditions in postmenopausal women.5 This topic has been discussed in a recent JFP audiocast. Also receiving “D” recommendations were screening for ovarian cancer in asymptomatic women,6 discussed in another JFP audiocast, and screening for thyroid cancer in asymptomatic adults.7
The “D” recommendation for thyroid cancer screening was based on the low incidence of thyroid cancer, the evidence showing no change in mortality after the introduction of population-based screening, and the likelihood of overdiagnosis and overtreatment that would result from screening. The screening tests considered by the Task Force included neck palpation and ultrasound.7
Insufficient evidence
In addition to the previously mentioned “I” statement on vision screening for children <3 years of age,4 4 other interventions lacked sufficient evidence that the Task Force could use in determining relative levels of harms and benefits. These interventions were screening for obstructive sleep apnea in asymptomatic adults,8 screening for celiac disease in asymptomatic patients of all ages,9 screening with a pelvic examination in asymptomatic women,10 and screening for adolescent idiopathic scoliosis in children and adolescents ages 10 to 18 years.11
The lack of evidence regarding the value of a routine pelvic exam for asymptomatic women is surprising given how often this procedure is performed. The Task Force defined a pelvic exam as an “assessment of the external genitalia, internal speculum examination, bimanual palpation, and rectovaginal examination.”10 The Task Force found very little evidence on the accuracy and effectiveness of this exam for a range of gynecologic conditions other than cervical cancer, gonorrhea, and chlamydia, for which screening is recommended.10
The “I” statement on screening for adolescent idiopathic scoliosis in children and adolescents is an unusual revision of a “D” recommendation from 2004. At that time, the Task Force found that treatment of adolescent idiopathic scoliosis leads to health benefits in only a small proportion of individuals and that there are harms of treatment such as unnecessary bracing and referral to specialty care. For the most recent evidence report, the Task Force used a new methodology to assess treatment harms and concluded that the evidence is now inadequate. That finding, along with new evidence that “suggests that brace treatment can interrupt or slow scoliosis progression” led the Task Force to move away from a “D” recommendation.11
The enigmatic “C” recommendation
Perhaps the most difficult recommendation category to understand and implement is the “C” recommendation. With a “C” intervention, there is moderate certainty that the net benefit of universal implementation would be very small; but there are some individuals who might benefit from it, and physicians should offer it selectively.
The Task Force made one “C” recommendation over the past year: for adults who are not obese and who do not have other cardiovascular disease (CVD) risks, the net gain in referring them to behavioral counseling to promote a healthful diet and physical activity is small. However, the harms from such referrals are also small. Counseling interventions can result in healthier habits and in small improvements in intermediate outcomes, such as blood pressure, cholesterol levels, and weight. The effect on overall CVD mortality, though, has been minimal.12 The Task Force concluded that “[those] who are interested and ready to make behavioral changes may be most likely to benefit from behavioral counseling.”
1. USPSTF. Folic acid for the prevention of neural tube defects: preventive medication. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/folic-acid-for-the-prevention-of-neural-tube-defects-preventive-medication. Accessed March 22, 2018.
2. USPSTF. Obesity in children and adolescents: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/obesity-in-children-and-adolescents-screening1. Accessed March 22, 2018.
3. USPSTF. Preeclampsia: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/preeclampsia-screening1. Accessed March 22, 2018.
4. USPSTF. Vision in children ages 6 months to 5 years: Screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/vision-in-children-ages-6-months-to-5-years-screening. Accessed March 22, 2018.
5. USPSTF. Hormone therapy in postmenopausal women: primary prevention of chronic conditions. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/menopausal-hormone-therapy-preventive-medication1. Accessed March 24, 2018.
6. USPSTF. Ovarian cancer: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/ovarian-cancer-screening1. Accessed March 24, 2018.
7. USPSTF. Thyroid cancer: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/thyroid-cancer-screening1. Accessed March 22, 2018.
8. USPSTF. Obstructive sleep apnea in adults: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/obstructive-sleep-apnea-in-adults-screening. Accessed March 22, 2018.
9. USPSTF. Celiac disease: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/celiac-disease-screening. Accessed March 24, 2018.
10. USPSTF. Gynecological conditions: periodic screening with the pelvic examination. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/gynecological-conditions-screening-with-the-pelvic-examination. Accessed March 22, 2018.
11. USPSTF. Adolescent idiopathic scoliosis: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/adolescent-idiopathic-scoliosis-screening1. Accessed March 22, 2018.
12. USPSTF. Healthful diet and physical activity for cardiovascular disease prevention in adults without known risk factors: behavioral counseling. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/healthful-diet-and-physical-activity-for-cardiovascular-disease-prevention-in-adults-without-known-risk-factors-behavioral-counseling. Accessed March 22, 2018.
13. Ananth CV, Keyes KM, Wapner RJ. Pre-eclampsia rates in the United States, 1980-2010: age-period-cohort analysis. BMJ. 2013;347:f6564.
14. USPSTF. Low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: preventive medication. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/low-dose-aspirin-use-for-the-prevention-of-morbidity-and-mortality-from-preeclampsia-preventive-medication. Accessed March 22, 2018.
15. Donahue SP, Baker CN; Committee on Practice and Ambulatory Medicine, American Academy of Pediatrics; Section on Ophthalmology, American Academy of Pediatrics; American Association of Certified Orthoptists; American Association for Pediatric Ophthalmology and Strabismus; American Academy of Ophthalmology. Procedures for the evaluation of the visual system by pediatricians. Pediatrics. 2016;137.2015-3597.
1. USPSTF. Folic acid for the prevention of neural tube defects: preventive medication. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/folic-acid-for-the-prevention-of-neural-tube-defects-preventive-medication. Accessed March 22, 2018.
2. USPSTF. Obesity in children and adolescents: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/obesity-in-children-and-adolescents-screening1. Accessed March 22, 2018.
3. USPSTF. Preeclampsia: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/preeclampsia-screening1. Accessed March 22, 2018.
4. USPSTF. Vision in children ages 6 months to 5 years: Screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/vision-in-children-ages-6-months-to-5-years-screening. Accessed March 22, 2018.
5. USPSTF. Hormone therapy in postmenopausal women: primary prevention of chronic conditions. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/menopausal-hormone-therapy-preventive-medication1. Accessed March 24, 2018.
6. USPSTF. Ovarian cancer: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/ovarian-cancer-screening1. Accessed March 24, 2018.
7. USPSTF. Thyroid cancer: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/thyroid-cancer-screening1. Accessed March 22, 2018.
8. USPSTF. Obstructive sleep apnea in adults: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/obstructive-sleep-apnea-in-adults-screening. Accessed March 22, 2018.
9. USPSTF. Celiac disease: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/celiac-disease-screening. Accessed March 24, 2018.
10. USPSTF. Gynecological conditions: periodic screening with the pelvic examination. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/gynecological-conditions-screening-with-the-pelvic-examination. Accessed March 22, 2018.
11. USPSTF. Adolescent idiopathic scoliosis: screening. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/adolescent-idiopathic-scoliosis-screening1. Accessed March 22, 2018.
12. USPSTF. Healthful diet and physical activity for cardiovascular disease prevention in adults without known risk factors: behavioral counseling. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/healthful-diet-and-physical-activity-for-cardiovascular-disease-prevention-in-adults-without-known-risk-factors-behavioral-counseling. Accessed March 22, 2018.
13. Ananth CV, Keyes KM, Wapner RJ. Pre-eclampsia rates in the United States, 1980-2010: age-period-cohort analysis. BMJ. 2013;347:f6564.
14. USPSTF. Low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: preventive medication. Available at: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/low-dose-aspirin-use-for-the-prevention-of-morbidity-and-mortality-from-preeclampsia-preventive-medication. Accessed March 22, 2018.
15. Donahue SP, Baker CN; Committee on Practice and Ambulatory Medicine, American Academy of Pediatrics; Section on Ophthalmology, American Academy of Pediatrics; American Association of Certified Orthoptists; American Association for Pediatric Ophthalmology and Strabismus; American Academy of Ophthalmology. Procedures for the evaluation of the visual system by pediatricians. Pediatrics. 2016;137.2015-3597.
From The Journal of Family Practice | 2018;67(5):294-296,298-299.

One-fifth of Medicaid kids receive mental health diagnoses
Twenty percent of children insured by Medicaid received a psychiatric diagnosis before 8 years of age, according to data from more than 35,000 Medicaid-insured children in a mid-Atlantic state.
Previous cross-sectional studies have addressed trends in psychiatric treatment of children. “However, little is known about the longitudinal patterns of pediatric use of psychiatric services,” wrote Dinci Pennap, MPH, of the University of Maryland, Baltimore, and her colleagues.
By the age of 8 years, 20% of the children had received a psychiatric diagnosis; 58% of these diagnoses were behavioral. The most common psychiatric diagnoses were ADHD (44%) and learning disorder (32%).
In addition, 10% (2,196) of children had received psychotropic medications. Of those receiving psychotropic medications, 81% received a single medication, 16% received two medications, and 4% received three medications for 60 days or more, the researchers said. Girls were significantly more likely than boys to be diagnosed with adjustment disorder (22% vs. 15%, respectively) or anxiety disorder (7% vs. 4%, respectively). Boys were significantly more likely than girls to be diagnosed with ADHD (30% vs. 22%).
the researchers said.
The study findings were limited by several factors, including the use of clinician-reported diagnoses rather than research-identified diagnoses and the possible lack of generalizability to Medicaid populations in other regions or to privately insured children, the researchers noted. However, the results captured long-term psychotropic use and “highlight the need for safety and outcomes research, particularly for health outcomes such as metabolic imbalance, weight gain, and sleep disturbances after initiation of psychotropic medication for very young children.”
Dr. Pennap had no financial conflicts to disclose. One of the study coauthors disclosed research grants from the National Institutes of Health.
SOURCE: Pennap D et al. JAMA Pediatr. 2018. doi: 10.1001/jamapediatrics.2018.0240.
Twenty percent of children insured by Medicaid received a psychiatric diagnosis before 8 years of age, according to data from more than 35,000 Medicaid-insured children in a mid-Atlantic state.
Previous cross-sectional studies have addressed trends in psychiatric treatment of children. “However, little is known about the longitudinal patterns of pediatric use of psychiatric services,” wrote Dinci Pennap, MPH, of the University of Maryland, Baltimore, and her colleagues.
By the age of 8 years, 20% of the children had received a psychiatric diagnosis; 58% of these diagnoses were behavioral. The most common psychiatric diagnoses were ADHD (44%) and learning disorder (32%).
In addition, 10% (2,196) of children had received psychotropic medications. Of those receiving psychotropic medications, 81% received a single medication, 16% received two medications, and 4% received three medications for 60 days or more, the researchers said. Girls were significantly more likely than boys to be diagnosed with adjustment disorder (22% vs. 15%, respectively) or anxiety disorder (7% vs. 4%, respectively). Boys were significantly more likely than girls to be diagnosed with ADHD (30% vs. 22%).
the researchers said.
The study findings were limited by several factors, including the use of clinician-reported diagnoses rather than research-identified diagnoses and the possible lack of generalizability to Medicaid populations in other regions or to privately insured children, the researchers noted. However, the results captured long-term psychotropic use and “highlight the need for safety and outcomes research, particularly for health outcomes such as metabolic imbalance, weight gain, and sleep disturbances after initiation of psychotropic medication for very young children.”
Dr. Pennap had no financial conflicts to disclose. One of the study coauthors disclosed research grants from the National Institutes of Health.
SOURCE: Pennap D et al. JAMA Pediatr. 2018. doi: 10.1001/jamapediatrics.2018.0240.
Twenty percent of children insured by Medicaid received a psychiatric diagnosis before 8 years of age, according to data from more than 35,000 Medicaid-insured children in a mid-Atlantic state.
Previous cross-sectional studies have addressed trends in psychiatric treatment of children. “However, little is known about the longitudinal patterns of pediatric use of psychiatric services,” wrote Dinci Pennap, MPH, of the University of Maryland, Baltimore, and her colleagues.
By the age of 8 years, 20% of the children had received a psychiatric diagnosis; 58% of these diagnoses were behavioral. The most common psychiatric diagnoses were ADHD (44%) and learning disorder (32%).
In addition, 10% (2,196) of children had received psychotropic medications. Of those receiving psychotropic medications, 81% received a single medication, 16% received two medications, and 4% received three medications for 60 days or more, the researchers said. Girls were significantly more likely than boys to be diagnosed with adjustment disorder (22% vs. 15%, respectively) or anxiety disorder (7% vs. 4%, respectively). Boys were significantly more likely than girls to be diagnosed with ADHD (30% vs. 22%).
the researchers said.
The study findings were limited by several factors, including the use of clinician-reported diagnoses rather than research-identified diagnoses and the possible lack of generalizability to Medicaid populations in other regions or to privately insured children, the researchers noted. However, the results captured long-term psychotropic use and “highlight the need for safety and outcomes research, particularly for health outcomes such as metabolic imbalance, weight gain, and sleep disturbances after initiation of psychotropic medication for very young children.”
Dr. Pennap had no financial conflicts to disclose. One of the study coauthors disclosed research grants from the National Institutes of Health.
SOURCE: Pennap D et al. JAMA Pediatr. 2018. doi: 10.1001/jamapediatrics.2018.0240.
FROM JAMA PEDIATRICS
Key clinical point: More safety and outcome data are needed for young children receiving psychiatric medications.
Major finding: Twenty percent of Medicaid-insured children in a mid-Atlantic state were diagnosed with a psychiatric disorder before 8 years of age.
Study details: The data come from a longitudinal study of 35,244 children insured with Medicaid born in 2007 in a mid-Atlantic state.
Disclosures: Dr. Pennap had no financial conflicts to disclose. One of the study coauthors disclosed research grants from the National Institutes of Health.
Source: Pennap D et al. JAMA Pediatr. 2018. doi: 10.1001/jamapediatrics.2018.0240.
CHMP backs approval of dasatinib for kids

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended changes to the marketing authorization for dasatinib (Sprycel).
The CHMP is recommending approval for dasatinib as a treatment for pediatric patients with newly diagnosed, Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML) in chronic phase (CP) or Ph+ CML-CP that is resistant or intolerant to prior therapy, including imatinib.
The CHMP has also recommended approval of a new formulation of dasatinib—a powder for oral suspension (PFOS)—for use in pediatric patients.
Dasatinib is already approved in the European Union to treat adults with:
- Newly diagnosed Ph+ CML-CP
- Chronic, accelerated, or blast phase CML with resistance or intolerance to prior therapy, including imatinib
- Ph+ acute lymphoblastic leukemia and lymphoid blast CML with resistance or intolerance to prior therapy.
The CHMP’s opinion on dasatinib for pediatric patients will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, the commission will grant a centralized marketing authorization that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
The CHMP’s opinion on dasatinib for pediatric patients is supported by 2 studies. Results from the phase 1 study (NCT00306202) were published in the Journal of Clinical Oncology in 2013. Phase 2 (NCT00777036) results were published in the same journal this year.
Phase 1
The phase 1 trial included 17 patients with CML-CP, all of whom had received prior imatinib.
Eleven patients received dasatinib at a starting dose of 60 mg/m2 once daily, and 6 received the drug at a starting dose of 80 mg/m2 once daily. Dose escalation was allowed based on tolerance and response. The median duration of treatment was 24.1 months (range, 2.3 to 50.6 months).
The 60 mg/m2 starting dose appeared more tolerable than 80 mg/m2 dose.
Drug-related adverse events (AEs) occurring in at least 20% of patients included neutropenia (82.4%), anemia (70.6%), thrombocytopenia (64.7%), nausea (29.4%), headache (35.3%), diarrhea (23.5%), and pain in extremity (23.5%). Grade 3-4 AEs included neutropenia (23.5%), thrombocytopenia (11.8%), and headache (5.9%). There were no drug-related deaths.
Ninety-four percent of patients achieved a complete hematologic response (CHR), 88% had a major cytogenetic response (MCyR), 82% had a complete cytogenetic response (CCyR), 47% had a major molecular response (MMR), and 24% had a complete molecular response (CMR).
Patients who received the lower starting dose of dasatinib had lower rates of cumulative CCyR (72.7% vs 100%) and CHR (90.9% vs 100%) but higher rates of cumulative MMR (54.5% vs 33.3%) and CMR (27.3% vs 16.7).
The median progression-free survival (PFS) and overall survival (OS) had not been reached at last follow-up. At 24 months, the estimated PFS was 61%, and the estimated OS was 88%.
Phase 2
The phase 2 trial included 29 patients with imatinib-resistant/intolerant CML-CP and 84 with newly diagnosed CML-CP.
The previously treated patients received dasatinib tablets. Newly diagnosed patients were treated with dasatinib tablets (n=51) or PFOS (n=33). Patients who started on PFOS could switch to tablets after receiving PFOS for at least 1 year. Sixty-seven percent of patients on PFOS switched to tablets due to patient preference.
The average daily dose of dasatinib was 58.18 mg/m2 in the previously treated patients and 59.84 mg/m2 in the newly diagnosed patients (for both tablets and PFOS). The median duration of treatment was 49.91 months (range, 1.9 to 90.2) and 42.30 months (range, 0.1 to 75.2), respectively.
Rates of confirmed CHR (at any time) were 93% in the previously treated patients and 96% in the newly diagnosed patients.
At 12 months, previously treated patients had an MMR rate of 41% and a CMR rate of 7%. In newly diagnosed patients, MMR was 52%, and CMR was 8%.
At 24 months, previously treated patients had an MMR rate of 55% and a CMR rate of 17%. In the newly diagnosed patients, MMR was 70%, and CMR was 21%.
The rate of MCyR at any time was 89.7% in all previously treated patients and 90% when the researchers excluded patients with MCyR or unknown cytogenetic status at baseline.
The rate of CCyR at any time was 94% in all newly diagnosed patients and 93.9% when the researchers excluded patients with CCyR or unknown cytogenetic status at baseline.
The median PFS and OS had not been reached at last follow-up. The estimated 48-month PFS was 78% in the previously treated patients and 93% in the newly diagnosed patients. The estimated 48-month OS was 96% and 100%, respectively.
Dasatinib-related AEs occurring in at least 10% of the previously treated patients included nausea/vomiting (31%), myalgia/arthralgia (17%), fatigue (14%), rash (14%), diarrhea (14%), hemorrhage (10%), bone growth and development events (10%), and shortness of breath (10%).
Dasatinib-related AEs occurring in at least 10% of the newly diagnosed patients included nausea/vomiting (20%), myalgia/arthralgia (10%), fatigue (11%), rash (19%), diarrhea (18%), and hemorrhage (10%).
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended changes to the marketing authorization for dasatinib (Sprycel).
The CHMP is recommending approval for dasatinib as a treatment for pediatric patients with newly diagnosed, Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML) in chronic phase (CP) or Ph+ CML-CP that is resistant or intolerant to prior therapy, including imatinib.
The CHMP has also recommended approval of a new formulation of dasatinib—a powder for oral suspension (PFOS)—for use in pediatric patients.
Dasatinib is already approved in the European Union to treat adults with:
- Newly diagnosed Ph+ CML-CP
- Chronic, accelerated, or blast phase CML with resistance or intolerance to prior therapy, including imatinib
- Ph+ acute lymphoblastic leukemia and lymphoid blast CML with resistance or intolerance to prior therapy.
The CHMP’s opinion on dasatinib for pediatric patients will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, the commission will grant a centralized marketing authorization that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
The CHMP’s opinion on dasatinib for pediatric patients is supported by 2 studies. Results from the phase 1 study (NCT00306202) were published in the Journal of Clinical Oncology in 2013. Phase 2 (NCT00777036) results were published in the same journal this year.
Phase 1
The phase 1 trial included 17 patients with CML-CP, all of whom had received prior imatinib.
Eleven patients received dasatinib at a starting dose of 60 mg/m2 once daily, and 6 received the drug at a starting dose of 80 mg/m2 once daily. Dose escalation was allowed based on tolerance and response. The median duration of treatment was 24.1 months (range, 2.3 to 50.6 months).
The 60 mg/m2 starting dose appeared more tolerable than 80 mg/m2 dose.
Drug-related adverse events (AEs) occurring in at least 20% of patients included neutropenia (82.4%), anemia (70.6%), thrombocytopenia (64.7%), nausea (29.4%), headache (35.3%), diarrhea (23.5%), and pain in extremity (23.5%). Grade 3-4 AEs included neutropenia (23.5%), thrombocytopenia (11.8%), and headache (5.9%). There were no drug-related deaths.
Ninety-four percent of patients achieved a complete hematologic response (CHR), 88% had a major cytogenetic response (MCyR), 82% had a complete cytogenetic response (CCyR), 47% had a major molecular response (MMR), and 24% had a complete molecular response (CMR).
Patients who received the lower starting dose of dasatinib had lower rates of cumulative CCyR (72.7% vs 100%) and CHR (90.9% vs 100%) but higher rates of cumulative MMR (54.5% vs 33.3%) and CMR (27.3% vs 16.7).
The median progression-free survival (PFS) and overall survival (OS) had not been reached at last follow-up. At 24 months, the estimated PFS was 61%, and the estimated OS was 88%.
Phase 2
The phase 2 trial included 29 patients with imatinib-resistant/intolerant CML-CP and 84 with newly diagnosed CML-CP.
The previously treated patients received dasatinib tablets. Newly diagnosed patients were treated with dasatinib tablets (n=51) or PFOS (n=33). Patients who started on PFOS could switch to tablets after receiving PFOS for at least 1 year. Sixty-seven percent of patients on PFOS switched to tablets due to patient preference.
The average daily dose of dasatinib was 58.18 mg/m2 in the previously treated patients and 59.84 mg/m2 in the newly diagnosed patients (for both tablets and PFOS). The median duration of treatment was 49.91 months (range, 1.9 to 90.2) and 42.30 months (range, 0.1 to 75.2), respectively.
Rates of confirmed CHR (at any time) were 93% in the previously treated patients and 96% in the newly diagnosed patients.
At 12 months, previously treated patients had an MMR rate of 41% and a CMR rate of 7%. In newly diagnosed patients, MMR was 52%, and CMR was 8%.
At 24 months, previously treated patients had an MMR rate of 55% and a CMR rate of 17%. In the newly diagnosed patients, MMR was 70%, and CMR was 21%.
The rate of MCyR at any time was 89.7% in all previously treated patients and 90% when the researchers excluded patients with MCyR or unknown cytogenetic status at baseline.
The rate of CCyR at any time was 94% in all newly diagnosed patients and 93.9% when the researchers excluded patients with CCyR or unknown cytogenetic status at baseline.
The median PFS and OS had not been reached at last follow-up. The estimated 48-month PFS was 78% in the previously treated patients and 93% in the newly diagnosed patients. The estimated 48-month OS was 96% and 100%, respectively.
Dasatinib-related AEs occurring in at least 10% of the previously treated patients included nausea/vomiting (31%), myalgia/arthralgia (17%), fatigue (14%), rash (14%), diarrhea (14%), hemorrhage (10%), bone growth and development events (10%), and shortness of breath (10%).
Dasatinib-related AEs occurring in at least 10% of the newly diagnosed patients included nausea/vomiting (20%), myalgia/arthralgia (10%), fatigue (11%), rash (19%), diarrhea (18%), and hemorrhage (10%).
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended changes to the marketing authorization for dasatinib (Sprycel).
The CHMP is recommending approval for dasatinib as a treatment for pediatric patients with newly diagnosed, Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML) in chronic phase (CP) or Ph+ CML-CP that is resistant or intolerant to prior therapy, including imatinib.
The CHMP has also recommended approval of a new formulation of dasatinib—a powder for oral suspension (PFOS)—for use in pediatric patients.
Dasatinib is already approved in the European Union to treat adults with:
- Newly diagnosed Ph+ CML-CP
- Chronic, accelerated, or blast phase CML with resistance or intolerance to prior therapy, including imatinib
- Ph+ acute lymphoblastic leukemia and lymphoid blast CML with resistance or intolerance to prior therapy.
The CHMP’s opinion on dasatinib for pediatric patients will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, the commission will grant a centralized marketing authorization that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
The CHMP’s opinion on dasatinib for pediatric patients is supported by 2 studies. Results from the phase 1 study (NCT00306202) were published in the Journal of Clinical Oncology in 2013. Phase 2 (NCT00777036) results were published in the same journal this year.
Phase 1
The phase 1 trial included 17 patients with CML-CP, all of whom had received prior imatinib.
Eleven patients received dasatinib at a starting dose of 60 mg/m2 once daily, and 6 received the drug at a starting dose of 80 mg/m2 once daily. Dose escalation was allowed based on tolerance and response. The median duration of treatment was 24.1 months (range, 2.3 to 50.6 months).
The 60 mg/m2 starting dose appeared more tolerable than 80 mg/m2 dose.
Drug-related adverse events (AEs) occurring in at least 20% of patients included neutropenia (82.4%), anemia (70.6%), thrombocytopenia (64.7%), nausea (29.4%), headache (35.3%), diarrhea (23.5%), and pain in extremity (23.5%). Grade 3-4 AEs included neutropenia (23.5%), thrombocytopenia (11.8%), and headache (5.9%). There were no drug-related deaths.
Ninety-four percent of patients achieved a complete hematologic response (CHR), 88% had a major cytogenetic response (MCyR), 82% had a complete cytogenetic response (CCyR), 47% had a major molecular response (MMR), and 24% had a complete molecular response (CMR).
Patients who received the lower starting dose of dasatinib had lower rates of cumulative CCyR (72.7% vs 100%) and CHR (90.9% vs 100%) but higher rates of cumulative MMR (54.5% vs 33.3%) and CMR (27.3% vs 16.7).
The median progression-free survival (PFS) and overall survival (OS) had not been reached at last follow-up. At 24 months, the estimated PFS was 61%, and the estimated OS was 88%.
Phase 2
The phase 2 trial included 29 patients with imatinib-resistant/intolerant CML-CP and 84 with newly diagnosed CML-CP.
The previously treated patients received dasatinib tablets. Newly diagnosed patients were treated with dasatinib tablets (n=51) or PFOS (n=33). Patients who started on PFOS could switch to tablets after receiving PFOS for at least 1 year. Sixty-seven percent of patients on PFOS switched to tablets due to patient preference.
The average daily dose of dasatinib was 58.18 mg/m2 in the previously treated patients and 59.84 mg/m2 in the newly diagnosed patients (for both tablets and PFOS). The median duration of treatment was 49.91 months (range, 1.9 to 90.2) and 42.30 months (range, 0.1 to 75.2), respectively.
Rates of confirmed CHR (at any time) were 93% in the previously treated patients and 96% in the newly diagnosed patients.
At 12 months, previously treated patients had an MMR rate of 41% and a CMR rate of 7%. In newly diagnosed patients, MMR was 52%, and CMR was 8%.
At 24 months, previously treated patients had an MMR rate of 55% and a CMR rate of 17%. In the newly diagnosed patients, MMR was 70%, and CMR was 21%.
The rate of MCyR at any time was 89.7% in all previously treated patients and 90% when the researchers excluded patients with MCyR or unknown cytogenetic status at baseline.
The rate of CCyR at any time was 94% in all newly diagnosed patients and 93.9% when the researchers excluded patients with CCyR or unknown cytogenetic status at baseline.
The median PFS and OS had not been reached at last follow-up. The estimated 48-month PFS was 78% in the previously treated patients and 93% in the newly diagnosed patients. The estimated 48-month OS was 96% and 100%, respectively.
Dasatinib-related AEs occurring in at least 10% of the previously treated patients included nausea/vomiting (31%), myalgia/arthralgia (17%), fatigue (14%), rash (14%), diarrhea (14%), hemorrhage (10%), bone growth and development events (10%), and shortness of breath (10%).
Dasatinib-related AEs occurring in at least 10% of the newly diagnosed patients included nausea/vomiting (20%), myalgia/arthralgia (10%), fatigue (11%), rash (19%), diarrhea (18%), and hemorrhage (10%).
VIDEO: To boost newborn breastfeeding rates, hide the EHR formula order
AUSTIN, TEXAS – When the check box for ordering formula for newborns was removed as a standard newborn order option in the electronic health record (EHR), rates of exclusive breastfeeding climbed significantly in Los Angeles County hospitals, according to a recent study.
“The saying, ‘out of sight, out of mind’ cannot be overstated when it comes to physician order entry,” wrote Ramy Eskander, MD, and his colleagues in the poster accompanying the presentation at the annual clinical and scientific sessions of the American College of Obstetricians and Gynecologists.
In a video interview, Dr. Eskander said that he and his colleagues at the University of California, Los Angeles, were looking for an intervention that would use the EHR as a quality improvement tool.
What they decided to do was to see “how could we possibly ‘get in the way’ and have an intervention between the provider and the patient that didn’t necessarily involve much work on the provider’s end, that had a significant impact on the back end,” he said. What they ended up doing was remove the order to request formula for mothers from the physician order set in the EHR.
Study data were collected in three stages for the academic tertiary care hospital within the Los Angeles County Department of Health Services system.
First, Dr. Eskander and his colleagues collected baseline data from January to July of 2016. Then, data were collected from July to the end of 2016, while a campaign was underway to bring staff and patients up to speed on the benefits of exclusive breastfeeding. There were no statistically significant differences in the rates of exclusive breastfeeding on discharge between these two time periods, when rates hovered between 30% and 40%.
The final data collection period began in January 2017. At that time, the option to order formula for a newborn was removed as an option for the EHR newborn order set.
“When we did that, providers weren’t looking at the possibility of having that easy check box right there to fill in … and we know that when people have to go through more steps, they invariably don’t do it,” Dr. Eskander said.
He and his colleagues saw an almost immediate . Once the formula order was removed, breastfeeding rates rose from 40.57% to 53.90% (P less than .001). Rates have been sustained since the removal of the EHR option for formula.
There was no difference in how infants fared after the intervention, said Dr. Eskander. “The outcomes for those infants was identical. There were no increased NICU admissions, there were no increased poor outcomes.”
Length of stay remained the same as well. “The babies were being discharged in the same state of health, just more of them were getting breast milk only, and we know the benefits that tends to portend,” he added.
There was some initial grumbling when the formula order was pulled from the newborn order set, he conceded. “The providers were not very happy about having to look for the newborn order for formula.” However, it took just about a month for the new workflow to seem normal, he said.
Dr. Eskander envisions a future where the EHR is “smart” enough to prompt appropriate orders and interventions for serious conditions such as preeclampsia. The electronic record, he said, could recognize the maternal diagnosis “and immediately create a system and structure around that mother to be able to help protect her and her baby. ... then having those diagnoses be able to drive outcomes can be very significant.”
Dr. Eskander reported no relevant financial disclosures.
SOURCE: Eskander, R et al. ACOG 2018, Abstract 31I.
AUSTIN, TEXAS – When the check box for ordering formula for newborns was removed as a standard newborn order option in the electronic health record (EHR), rates of exclusive breastfeeding climbed significantly in Los Angeles County hospitals, according to a recent study.
“The saying, ‘out of sight, out of mind’ cannot be overstated when it comes to physician order entry,” wrote Ramy Eskander, MD, and his colleagues in the poster accompanying the presentation at the annual clinical and scientific sessions of the American College of Obstetricians and Gynecologists.
In a video interview, Dr. Eskander said that he and his colleagues at the University of California, Los Angeles, were looking for an intervention that would use the EHR as a quality improvement tool.
What they decided to do was to see “how could we possibly ‘get in the way’ and have an intervention between the provider and the patient that didn’t necessarily involve much work on the provider’s end, that had a significant impact on the back end,” he said. What they ended up doing was remove the order to request formula for mothers from the physician order set in the EHR.
Study data were collected in three stages for the academic tertiary care hospital within the Los Angeles County Department of Health Services system.
First, Dr. Eskander and his colleagues collected baseline data from January to July of 2016. Then, data were collected from July to the end of 2016, while a campaign was underway to bring staff and patients up to speed on the benefits of exclusive breastfeeding. There were no statistically significant differences in the rates of exclusive breastfeeding on discharge between these two time periods, when rates hovered between 30% and 40%.
The final data collection period began in January 2017. At that time, the option to order formula for a newborn was removed as an option for the EHR newborn order set.
“When we did that, providers weren’t looking at the possibility of having that easy check box right there to fill in … and we know that when people have to go through more steps, they invariably don’t do it,” Dr. Eskander said.
He and his colleagues saw an almost immediate . Once the formula order was removed, breastfeeding rates rose from 40.57% to 53.90% (P less than .001). Rates have been sustained since the removal of the EHR option for formula.
There was no difference in how infants fared after the intervention, said Dr. Eskander. “The outcomes for those infants was identical. There were no increased NICU admissions, there were no increased poor outcomes.”
Length of stay remained the same as well. “The babies were being discharged in the same state of health, just more of them were getting breast milk only, and we know the benefits that tends to portend,” he added.
There was some initial grumbling when the formula order was pulled from the newborn order set, he conceded. “The providers were not very happy about having to look for the newborn order for formula.” However, it took just about a month for the new workflow to seem normal, he said.
Dr. Eskander envisions a future where the EHR is “smart” enough to prompt appropriate orders and interventions for serious conditions such as preeclampsia. The electronic record, he said, could recognize the maternal diagnosis “and immediately create a system and structure around that mother to be able to help protect her and her baby. ... then having those diagnoses be able to drive outcomes can be very significant.”
Dr. Eskander reported no relevant financial disclosures.
SOURCE: Eskander, R et al. ACOG 2018, Abstract 31I.
AUSTIN, TEXAS – When the check box for ordering formula for newborns was removed as a standard newborn order option in the electronic health record (EHR), rates of exclusive breastfeeding climbed significantly in Los Angeles County hospitals, according to a recent study.
“The saying, ‘out of sight, out of mind’ cannot be overstated when it comes to physician order entry,” wrote Ramy Eskander, MD, and his colleagues in the poster accompanying the presentation at the annual clinical and scientific sessions of the American College of Obstetricians and Gynecologists.
In a video interview, Dr. Eskander said that he and his colleagues at the University of California, Los Angeles, were looking for an intervention that would use the EHR as a quality improvement tool.
What they decided to do was to see “how could we possibly ‘get in the way’ and have an intervention between the provider and the patient that didn’t necessarily involve much work on the provider’s end, that had a significant impact on the back end,” he said. What they ended up doing was remove the order to request formula for mothers from the physician order set in the EHR.
Study data were collected in three stages for the academic tertiary care hospital within the Los Angeles County Department of Health Services system.
First, Dr. Eskander and his colleagues collected baseline data from January to July of 2016. Then, data were collected from July to the end of 2016, while a campaign was underway to bring staff and patients up to speed on the benefits of exclusive breastfeeding. There were no statistically significant differences in the rates of exclusive breastfeeding on discharge between these two time periods, when rates hovered between 30% and 40%.
The final data collection period began in January 2017. At that time, the option to order formula for a newborn was removed as an option for the EHR newborn order set.
“When we did that, providers weren’t looking at the possibility of having that easy check box right there to fill in … and we know that when people have to go through more steps, they invariably don’t do it,” Dr. Eskander said.
He and his colleagues saw an almost immediate . Once the formula order was removed, breastfeeding rates rose from 40.57% to 53.90% (P less than .001). Rates have been sustained since the removal of the EHR option for formula.
There was no difference in how infants fared after the intervention, said Dr. Eskander. “The outcomes for those infants was identical. There were no increased NICU admissions, there were no increased poor outcomes.”
Length of stay remained the same as well. “The babies were being discharged in the same state of health, just more of them were getting breast milk only, and we know the benefits that tends to portend,” he added.
There was some initial grumbling when the formula order was pulled from the newborn order set, he conceded. “The providers were not very happy about having to look for the newborn order for formula.” However, it took just about a month for the new workflow to seem normal, he said.
Dr. Eskander envisions a future where the EHR is “smart” enough to prompt appropriate orders and interventions for serious conditions such as preeclampsia. The electronic record, he said, could recognize the maternal diagnosis “and immediately create a system and structure around that mother to be able to help protect her and her baby. ... then having those diagnoses be able to drive outcomes can be very significant.”
Dr. Eskander reported no relevant financial disclosures.
SOURCE: Eskander, R et al. ACOG 2018, Abstract 31I.
REPORTING FROM ACOG 2018

New law allows Maryland students to use sunscreen at school
In early April, Maryland Governor Larry Hogan signed HB 427 into law, making Maryland the second state in 2018 to ensure that state policy allows students to possess and use sunscreen at school.
“The passing of this bill helps encourage children to develop sun-safe behaviors early on, like sunscreen application,” American Society for Dermatologic Surgery Association president Lisa Donofrio, MD, said in a statement issued by the ASDSA. “Maryland’s efforts reinforce the importance of teaching children the risks of sun exposure during outdoor activities and how to best avoid skin cancer,” she added.
ASDSA worked with the Maryland Dermatologic Society in advocating for passage of the law. In the statement, ASDSA Board Member Lawrence Green, MD, of Rockville, Maryland, who testified in favor of SB 217, said, “allowing children to put on sunscreen before recess … would really help protect them from the dangers of the sun.”
More information about SUNucate is available here.
In early April, Maryland Governor Larry Hogan signed HB 427 into law, making Maryland the second state in 2018 to ensure that state policy allows students to possess and use sunscreen at school.
“The passing of this bill helps encourage children to develop sun-safe behaviors early on, like sunscreen application,” American Society for Dermatologic Surgery Association president Lisa Donofrio, MD, said in a statement issued by the ASDSA. “Maryland’s efforts reinforce the importance of teaching children the risks of sun exposure during outdoor activities and how to best avoid skin cancer,” she added.
ASDSA worked with the Maryland Dermatologic Society in advocating for passage of the law. In the statement, ASDSA Board Member Lawrence Green, MD, of Rockville, Maryland, who testified in favor of SB 217, said, “allowing children to put on sunscreen before recess … would really help protect them from the dangers of the sun.”
More information about SUNucate is available here.
In early April, Maryland Governor Larry Hogan signed HB 427 into law, making Maryland the second state in 2018 to ensure that state policy allows students to possess and use sunscreen at school.
“The passing of this bill helps encourage children to develop sun-safe behaviors early on, like sunscreen application,” American Society for Dermatologic Surgery Association president Lisa Donofrio, MD, said in a statement issued by the ASDSA. “Maryland’s efforts reinforce the importance of teaching children the risks of sun exposure during outdoor activities and how to best avoid skin cancer,” she added.
ASDSA worked with the Maryland Dermatologic Society in advocating for passage of the law. In the statement, ASDSA Board Member Lawrence Green, MD, of Rockville, Maryland, who testified in favor of SB 217, said, “allowing children to put on sunscreen before recess … would really help protect them from the dangers of the sun.”
More information about SUNucate is available here.