User login
Topical treatment with retinoid/benzoyl peroxide combination reduced acne scars
PARIS – Treatment with the fixed combination in a multicenter, randomized trial, Brigitte Dreno, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.

“To my knowledge, this is the first time that we have seen a topical therapy showing a reduction in atrophic acne scars,” said Dr. Dreno, professor and chair of the department of dermatology at Nantes (France) University Hospital.
She reported on 67 adolescents and adults with mainly moderate facial acne randomized to treat half their face with adapalene 0.3%/benzoyl peroxide 2.5% gel (Epiduo Forte) and the other half with the product’s vehicle daily for 6 months. Investigators were blinded as to which side was which. At baseline, patients averaged 40 acne lesions and 12 scars per half face.
The primary efficacy endpoint was the atrophic acne scar count per half face at week 24. At that point, the mean total was 9.5 scars on the active treatment side, compared with 13.3 on the control side. This translated to a statistically significant and clinically meaningful 15.5% decrease in scars with active treatment versus a 14.4% increase with vehicle. The between-side difference achieved statistical significance at week 1 and remained so at all follow-up visits through week 24.
By Scar Global Assessment at week 24, 32.9% of half faces treated with the combination product were rated clear or almost clear, compared with 16.4% with vehicle.
At 24 weeks, 24.1% of participants reported having moderately or very visible holes or indents on the active treatment side of their face, compared with 51.8% on the control side. The number of inflammatory acne lesions fell by 86.7% with the active treatment and 57.9% with vehicle over the course of 24 weeks. Again, the difference became statistically significant starting at week 1. By the Investigator’s Global Assessment at week 24, 64.2% of adapalene/benzoyl peroxide gel–treated faces were rated clear or almost clear, as were 19.4% with vehicle. In addition, 32% of patients reported a marked improvement in skin texture on their active treatment side at 24 weeks, as did 14% on the control side.
The salutary effect on acne scars documented with a topical therapy in this study represents a real advance in clinical care.
“Facial acne scars are a very important and difficult problem for our patients and also for dermatologists,” Dr. Dreno observed, adding that the evidence base for procedural interventions for acne scars, such as dermabrasion and laser resurfacing, is not top quality.
Not surprisingly with a topical retinoid, skin irritation was the most common treatment-emergent adverse event, reported by 14.9% of patients on their active treatment side and 6% with vehicle. This side effect was typically mild and resolved within the first 2-3 weeks.
The improvement in preexisting acne scars documented in this trial was probably caused by drug-induced remodeling of the dermal matrix, according to Dr. Dreno.
The study was funded by Galderma. Dr. Dreno reported receiving research grants from and/or serving as a consultant to Galderma, Bioderma, Pierre Fabre, and La Roche–Posay.
PARIS – Treatment with the fixed combination in a multicenter, randomized trial, Brigitte Dreno, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
“To my knowledge, this is the first time that we have seen a topical therapy showing a reduction in atrophic acne scars,” said Dr. Dreno, professor and chair of the department of dermatology at Nantes (France) University Hospital.
She reported on 67 adolescents and adults with mainly moderate facial acne randomized to treat half their face with adapalene 0.3%/benzoyl peroxide 2.5% gel (Epiduo Forte) and the other half with the product’s vehicle daily for 6 months. Investigators were blinded as to which side was which. At baseline, patients averaged 40 acne lesions and 12 scars per half face.
The primary efficacy endpoint was the atrophic acne scar count per half face at week 24. At that point, the mean total was 9.5 scars on the active treatment side, compared with 13.3 on the control side. This translated to a statistically significant and clinically meaningful 15.5% decrease in scars with active treatment versus a 14.4% increase with vehicle. The between-side difference achieved statistical significance at week 1 and remained so at all follow-up visits through week 24.
By Scar Global Assessment at week 24, 32.9% of half faces treated with the combination product were rated clear or almost clear, compared with 16.4% with vehicle.
At 24 weeks, 24.1% of participants reported having moderately or very visible holes or indents on the active treatment side of their face, compared with 51.8% on the control side. The number of inflammatory acne lesions fell by 86.7% with the active treatment and 57.9% with vehicle over the course of 24 weeks. Again, the difference became statistically significant starting at week 1. By the Investigator’s Global Assessment at week 24, 64.2% of adapalene/benzoyl peroxide gel–treated faces were rated clear or almost clear, as were 19.4% with vehicle. In addition, 32% of patients reported a marked improvement in skin texture on their active treatment side at 24 weeks, as did 14% on the control side.
The salutary effect on acne scars documented with a topical therapy in this study represents a real advance in clinical care.
“Facial acne scars are a very important and difficult problem for our patients and also for dermatologists,” Dr. Dreno observed, adding that the evidence base for procedural interventions for acne scars, such as dermabrasion and laser resurfacing, is not top quality.
Not surprisingly with a topical retinoid, skin irritation was the most common treatment-emergent adverse event, reported by 14.9% of patients on their active treatment side and 6% with vehicle. This side effect was typically mild and resolved within the first 2-3 weeks.
The improvement in preexisting acne scars documented in this trial was probably caused by drug-induced remodeling of the dermal matrix, according to Dr. Dreno.
The study was funded by Galderma. Dr. Dreno reported receiving research grants from and/or serving as a consultant to Galderma, Bioderma, Pierre Fabre, and La Roche–Posay.
PARIS – Treatment with the fixed combination in a multicenter, randomized trial, Brigitte Dreno, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
“To my knowledge, this is the first time that we have seen a topical therapy showing a reduction in atrophic acne scars,” said Dr. Dreno, professor and chair of the department of dermatology at Nantes (France) University Hospital.
She reported on 67 adolescents and adults with mainly moderate facial acne randomized to treat half their face with adapalene 0.3%/benzoyl peroxide 2.5% gel (Epiduo Forte) and the other half with the product’s vehicle daily for 6 months. Investigators were blinded as to which side was which. At baseline, patients averaged 40 acne lesions and 12 scars per half face.
The primary efficacy endpoint was the atrophic acne scar count per half face at week 24. At that point, the mean total was 9.5 scars on the active treatment side, compared with 13.3 on the control side. This translated to a statistically significant and clinically meaningful 15.5% decrease in scars with active treatment versus a 14.4% increase with vehicle. The between-side difference achieved statistical significance at week 1 and remained so at all follow-up visits through week 24.
By Scar Global Assessment at week 24, 32.9% of half faces treated with the combination product were rated clear or almost clear, compared with 16.4% with vehicle.
At 24 weeks, 24.1% of participants reported having moderately or very visible holes or indents on the active treatment side of their face, compared with 51.8% on the control side. The number of inflammatory acne lesions fell by 86.7% with the active treatment and 57.9% with vehicle over the course of 24 weeks. Again, the difference became statistically significant starting at week 1. By the Investigator’s Global Assessment at week 24, 64.2% of adapalene/benzoyl peroxide gel–treated faces were rated clear or almost clear, as were 19.4% with vehicle. In addition, 32% of patients reported a marked improvement in skin texture on their active treatment side at 24 weeks, as did 14% on the control side.
The salutary effect on acne scars documented with a topical therapy in this study represents a real advance in clinical care.
“Facial acne scars are a very important and difficult problem for our patients and also for dermatologists,” Dr. Dreno observed, adding that the evidence base for procedural interventions for acne scars, such as dermabrasion and laser resurfacing, is not top quality.
Not surprisingly with a topical retinoid, skin irritation was the most common treatment-emergent adverse event, reported by 14.9% of patients on their active treatment side and 6% with vehicle. This side effect was typically mild and resolved within the first 2-3 weeks.
The improvement in preexisting acne scars documented in this trial was probably caused by drug-induced remodeling of the dermal matrix, according to Dr. Dreno.
The study was funded by Galderma. Dr. Dreno reported receiving research grants from and/or serving as a consultant to Galderma, Bioderma, Pierre Fabre, and La Roche–Posay.
REPORTING FROM THE EADV CONGRESS
Key clinical point: A fixed combination adapalene 0.3%/benzoyl peroxide 2.5% gel reduced the number of preexisting facial atrophic acne scars and prevented new scar formation.
Major finding: Facial atrophic acne scar count dropped by 15.5% with 6 months of treatment with adapalene 0.3%/benzoyl peroxide 2.5% gel while increasing by 14.4% with vehicle.
Study details: This was a 6-month, prospective, multicenter, randomized, vehicle-controlled, split-face study involving 67 acne patients.
Disclosures: The study was funded by Galderma. The presenter reported receiving research grants from and/or serving as a consultant to Galderma, Bioderma, Pierre Fabre, and La Roche–Posay.
Serlopitant quells prurigo nodularis in phase 2 study
PARIS – The in a 127-patient, randomized, placebo-controlled trial, Sonja Stander, MD, said at the annual congress of the European Academy of Dermatology and Venereology.

She used her speaker’s platform not only to present key outcomes of the phase 2 study, but also to explain some of the underappreciated aspects of prurigo nodularis and how the results shed new light on the pathogenesis of the disease.
“There is a knowledge gap regarding this disease,” observed Dr. Stander, professor of dermatology at the University of Munster (Germany).
Prurigo nodularis is a chronic skin condition characterized by numerous intensely pruritic, symmetrically distributed, erosive nodular lesions. As Dr. Stander and her fellow members of the EADV Task Force Pruritus recently reported, prurigo nodularis should be considered as one of the clinical manifestations of chronic prurigo, hallmarks of which include neuronal sensitization to itch and development of an itch-scratch cycle (J Eur Acad Dermatol Venereol. 2018 Jul;32[7]:1059-65). At present, there is no approved treatment for prurigo nodularis in the United States or Europe.
Despite its name, prurigo nodularis is not just about the itch. Additional symptoms were frequently reported by participants in the serlopitant study. Indeed, while 97% of participants reported experiencing devilish pruritus, 52% reported a burning sensation on involved skin, 41% said the lesions were painful, and 36% indicated they were plagued by a stinging sensation. All of these disturbing sensations were significantly reduced with 8 weeks of serlopitant in the trial.

The clinical implications of these baseline findings are clear: “We have to ask not only about itch, but also about pain and burning and stinging, which are really an issue with these patients,” the dermatologist said.
Dr. Stander noted that prurigo nodularis has a large negative impact on quality of life as reflected in study participants’ mean baseline Dermatology Life Quality Index score of 61. And it’s a disease that sticks around: At enrollment, 38% of subjects had a 1- to 5-year history of prurigo nodularis, 20% had had the disease for 5-10 years, and fully 29% had had prurigo nodularis for longer than 10 years.
“This is not a chronic relapsing disease. These patients had prurigo nodularis all the time,” Dr. Stander said.
Consistent with the findings of other studies, half of patients with prurigo nodularis had an atopic predisposition as defined by an Erlangen Atopy Questionnaire score of 10 or higher.
Patients in the phase 2 study were randomized to either a 15-mg loading dose of oral serlopitant followed by 5 mg/day for 8 weeks or to placebo. All four of the most common manifestations of prurigo nodularis – itching, burning, pain, and stinging – were reduced to a significantly greater extent in the serlopitant group than with placebo. For example, the proportion of serlopitant-treated patients who rated their itching as none or mild went from zero at baseline to 54% at week 8, as compared with 26% among placebo-treated controls. After 8 weeks, 46% of serlopitant-treated patients rated their itching as moderate, severe, or very severe, as did 71% of controls.
Similarly, the proportion of patients in the serlopitant group who reported no or only a mild burning sensation climbed from 41% at baseline to 73% after 8 weeks. In the control group, the proportion improved from 36% to 47% over the course of 8 weeks. At week 8, 27% of patients on serlopitant characterized themselves as experiencing a moderate, severe, or very severe burning sensation; the rate was twice as high in controls.
Although the stinging sensation associated with prurigo nodularis was significantly reduced by serlopitant, the effect was less robust than with the other common sensory expressions of the disease. The proportion of patients with no or mild stinging increased by an absolute 23% after 8 weeks on serlopitant and by 6% with placebo. At week 8, 22% of patients treated with the neurokinin-1 receptor antagonist complained of a moderate to very severe stinging sensation, as did 40% of controls.
As a neurokinin-1 receptor antagonist, serlopitant inhibits substance P. The drug’s efficacy suggests that substance P plays a role in inducing the itch and other sensory symptoms of prurigo nodularis, according to Dr. Stander.
Based upon the favorable phase 2 results, multiple phase 3 clinical trials of serlopitant for prurigo nodularis are underway in the United States and elsewhere, including a year-long safety study.
Serlopitant is being developed by Menlo Therapeutics. Dr. Stander reported receiving research funding from and serving as a consultant to the company.
PARIS – The in a 127-patient, randomized, placebo-controlled trial, Sonja Stander, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
She used her speaker’s platform not only to present key outcomes of the phase 2 study, but also to explain some of the underappreciated aspects of prurigo nodularis and how the results shed new light on the pathogenesis of the disease.
“There is a knowledge gap regarding this disease,” observed Dr. Stander, professor of dermatology at the University of Munster (Germany).
Prurigo nodularis is a chronic skin condition characterized by numerous intensely pruritic, symmetrically distributed, erosive nodular lesions. As Dr. Stander and her fellow members of the EADV Task Force Pruritus recently reported, prurigo nodularis should be considered as one of the clinical manifestations of chronic prurigo, hallmarks of which include neuronal sensitization to itch and development of an itch-scratch cycle (J Eur Acad Dermatol Venereol. 2018 Jul;32[7]:1059-65). At present, there is no approved treatment for prurigo nodularis in the United States or Europe.
Despite its name, prurigo nodularis is not just about the itch. Additional symptoms were frequently reported by participants in the serlopitant study. Indeed, while 97% of participants reported experiencing devilish pruritus, 52% reported a burning sensation on involved skin, 41% said the lesions were painful, and 36% indicated they were plagued by a stinging sensation. All of these disturbing sensations were significantly reduced with 8 weeks of serlopitant in the trial.
The clinical implications of these baseline findings are clear: “We have to ask not only about itch, but also about pain and burning and stinging, which are really an issue with these patients,” the dermatologist said.
Dr. Stander noted that prurigo nodularis has a large negative impact on quality of life as reflected in study participants’ mean baseline Dermatology Life Quality Index score of 61. And it’s a disease that sticks around: At enrollment, 38% of subjects had a 1- to 5-year history of prurigo nodularis, 20% had had the disease for 5-10 years, and fully 29% had had prurigo nodularis for longer than 10 years.
“This is not a chronic relapsing disease. These patients had prurigo nodularis all the time,” Dr. Stander said.
Consistent with the findings of other studies, half of patients with prurigo nodularis had an atopic predisposition as defined by an Erlangen Atopy Questionnaire score of 10 or higher.
Patients in the phase 2 study were randomized to either a 15-mg loading dose of oral serlopitant followed by 5 mg/day for 8 weeks or to placebo. All four of the most common manifestations of prurigo nodularis – itching, burning, pain, and stinging – were reduced to a significantly greater extent in the serlopitant group than with placebo. For example, the proportion of serlopitant-treated patients who rated their itching as none or mild went from zero at baseline to 54% at week 8, as compared with 26% among placebo-treated controls. After 8 weeks, 46% of serlopitant-treated patients rated their itching as moderate, severe, or very severe, as did 71% of controls.
Similarly, the proportion of patients in the serlopitant group who reported no or only a mild burning sensation climbed from 41% at baseline to 73% after 8 weeks. In the control group, the proportion improved from 36% to 47% over the course of 8 weeks. At week 8, 27% of patients on serlopitant characterized themselves as experiencing a moderate, severe, or very severe burning sensation; the rate was twice as high in controls.
Although the stinging sensation associated with prurigo nodularis was significantly reduced by serlopitant, the effect was less robust than with the other common sensory expressions of the disease. The proportion of patients with no or mild stinging increased by an absolute 23% after 8 weeks on serlopitant and by 6% with placebo. At week 8, 22% of patients treated with the neurokinin-1 receptor antagonist complained of a moderate to very severe stinging sensation, as did 40% of controls.
As a neurokinin-1 receptor antagonist, serlopitant inhibits substance P. The drug’s efficacy suggests that substance P plays a role in inducing the itch and other sensory symptoms of prurigo nodularis, according to Dr. Stander.
Based upon the favorable phase 2 results, multiple phase 3 clinical trials of serlopitant for prurigo nodularis are underway in the United States and elsewhere, including a year-long safety study.
Serlopitant is being developed by Menlo Therapeutics. Dr. Stander reported receiving research funding from and serving as a consultant to the company.
PARIS – The in a 127-patient, randomized, placebo-controlled trial, Sonja Stander, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
She used her speaker’s platform not only to present key outcomes of the phase 2 study, but also to explain some of the underappreciated aspects of prurigo nodularis and how the results shed new light on the pathogenesis of the disease.
“There is a knowledge gap regarding this disease,” observed Dr. Stander, professor of dermatology at the University of Munster (Germany).
Prurigo nodularis is a chronic skin condition characterized by numerous intensely pruritic, symmetrically distributed, erosive nodular lesions. As Dr. Stander and her fellow members of the EADV Task Force Pruritus recently reported, prurigo nodularis should be considered as one of the clinical manifestations of chronic prurigo, hallmarks of which include neuronal sensitization to itch and development of an itch-scratch cycle (J Eur Acad Dermatol Venereol. 2018 Jul;32[7]:1059-65). At present, there is no approved treatment for prurigo nodularis in the United States or Europe.
Despite its name, prurigo nodularis is not just about the itch. Additional symptoms were frequently reported by participants in the serlopitant study. Indeed, while 97% of participants reported experiencing devilish pruritus, 52% reported a burning sensation on involved skin, 41% said the lesions were painful, and 36% indicated they were plagued by a stinging sensation. All of these disturbing sensations were significantly reduced with 8 weeks of serlopitant in the trial.
The clinical implications of these baseline findings are clear: “We have to ask not only about itch, but also about pain and burning and stinging, which are really an issue with these patients,” the dermatologist said.
Dr. Stander noted that prurigo nodularis has a large negative impact on quality of life as reflected in study participants’ mean baseline Dermatology Life Quality Index score of 61. And it’s a disease that sticks around: At enrollment, 38% of subjects had a 1- to 5-year history of prurigo nodularis, 20% had had the disease for 5-10 years, and fully 29% had had prurigo nodularis for longer than 10 years.
“This is not a chronic relapsing disease. These patients had prurigo nodularis all the time,” Dr. Stander said.
Consistent with the findings of other studies, half of patients with prurigo nodularis had an atopic predisposition as defined by an Erlangen Atopy Questionnaire score of 10 or higher.
Patients in the phase 2 study were randomized to either a 15-mg loading dose of oral serlopitant followed by 5 mg/day for 8 weeks or to placebo. All four of the most common manifestations of prurigo nodularis – itching, burning, pain, and stinging – were reduced to a significantly greater extent in the serlopitant group than with placebo. For example, the proportion of serlopitant-treated patients who rated their itching as none or mild went from zero at baseline to 54% at week 8, as compared with 26% among placebo-treated controls. After 8 weeks, 46% of serlopitant-treated patients rated their itching as moderate, severe, or very severe, as did 71% of controls.
Similarly, the proportion of patients in the serlopitant group who reported no or only a mild burning sensation climbed from 41% at baseline to 73% after 8 weeks. In the control group, the proportion improved from 36% to 47% over the course of 8 weeks. At week 8, 27% of patients on serlopitant characterized themselves as experiencing a moderate, severe, or very severe burning sensation; the rate was twice as high in controls.
Although the stinging sensation associated with prurigo nodularis was significantly reduced by serlopitant, the effect was less robust than with the other common sensory expressions of the disease. The proportion of patients with no or mild stinging increased by an absolute 23% after 8 weeks on serlopitant and by 6% with placebo. At week 8, 22% of patients treated with the neurokinin-1 receptor antagonist complained of a moderate to very severe stinging sensation, as did 40% of controls.
As a neurokinin-1 receptor antagonist, serlopitant inhibits substance P. The drug’s efficacy suggests that substance P plays a role in inducing the itch and other sensory symptoms of prurigo nodularis, according to Dr. Stander.
Based upon the favorable phase 2 results, multiple phase 3 clinical trials of serlopitant for prurigo nodularis are underway in the United States and elsewhere, including a year-long safety study.
Serlopitant is being developed by Menlo Therapeutics. Dr. Stander reported receiving research funding from and serving as a consultant to the company.
REPORTING FROM THE EADV CONGRESS
Key clinical point: Serlopitant decreases the disruptive itch, burning, pain, and stinging of prurigo nodularis.
Major finding: The proportion of prurigo nodularis patients who rated their itching as none or mild went from zero at baseline to 54% after 8 weeks on oral serlopitant.
Study details: This 8-week, randomized, double-blind phase 2 study included 127 patients with prurigo nodularis who were randomized to oral serlopitant or placebo.
Disclosures: Serlopitant is being developed by Menlo Therapeutics. The presenter reported receiving research funding from and serving as a consultant to the company.
PEXIVAS trial results will likely change ANCA-associated vasculitis therapy
CHICAGO – Results of the landmark PEXIVAS study – far and away the largest randomized trial ever done in ANCA-associated vasculitis – will likely change treatment in a couple of major ways.

“I think this trial will have an impact on care. Based on these findings, physicians should strongly reconsider the utility of plasma exchange as a treatment for AAV [antineutrophil cytoplasmic antibody–associated vasculitis] patients and should now consider using lower cumulative doses of glucocorticoids for the treatment of severe AAV,” PEXIVAS coprincipal investigator Peter A. Merkel, MD, said at the annual meeting of the American College of Rheumatology.
That’s because the trial demonstrated that plasma exchange neither saved lives nor avoided end-stage renal disease, while utilization of oral glucocorticoids in doses substantially lower than the high-dose current standard significantly reduced the serious infection rate without causing less effective disease control, according to Dr. Merkel, chief of rheumatology and professor of medicine and epidemiology at the University of Pennsylvania in Philadelphia.
PEXIVAS comprised 704 patients with severe granulomatosis with polyangiitis or microscopic polyangiitis, making it more than twice as large as any other trial in AAV. This was a multicenter, international, open-label, randomized trial with a 2-by-2 factorial design. To qualify as having severe AAV, participants had to have an estimated glomerular filtration rate below 50 mL/min per 1.73 m2 and/or lung hemorrhage.
“This was in essence two trials embedded within one protocol in the factorial design,” he explained.
The impetus for this major clinical trial was a recognition that mortality due to AAV remains high, especially in the first year, with a clear unmet need for better, less toxic therapies. Indeed, it’s estimated that only 29% of deaths in the first year after diagnosis are due to the vasculitis disease itself, while over 50% of the mortality is caused by infection, much of it collateral damage from immunosuppressive therapies.
Dr. Merkel, who heads the National Institutes of Health–supported Vasculitis Clinical Research Consortium, said the time was right for a clinical trial aimed at improving patient management: “Clinical equipoise exists for the efficacy of both plasma exchange and reduced-dose glucocorticoids in ANCA-associated vasculitis.”
The patients underwent induction therapy with cyclophosphamide or rituximab (Rituxan) plus IV methylprednisolone. Then they were randomized to seven plasma exchange sessions in 14 days or no plasma exchange, and further randomized to conventional weight-based, high-dose oral glucocorticoids or a lower-dose regimen. Those on the reduced-dose regimen received 54% of the cumulative amount of glucocorticoids used in the standard-dose group through the first 3 months, and 61% over the course of 6 months. By week 4, those on the reduced-dose regimen were on an average of 25 mg/day, while those on standard therapy were on 50 mg/day. Adherence to assigned study arms exceeded 90%. Patients were followed prospectively for 1-7 years.
The primary endpoint, a composite of all-cause mortality or development of end-stage renal disease, occurred in 28% of patients on plasma exchange and 31% of those who did not undergo plasma exchange, a nonsignificant difference indicative of a lack of benefit for the intervention. No differential effect was seen in prespecified subgroups based on age, creatinine clearance, ANCA type, form of immunosuppression, or presence or absence of lung hemorrhage.
Further, the primary endpoint occurred in 28% of patients on reduced-dose glucocorticoids, compared with 26% on full-dose therapy; again, a nonsignificant difference, meaning lower-dose therapy didn’t result in less effective disease control. But it did result in a significant reduction in the prespecified endpoint of serious infections in the first year: 27% versus 33% with full-dose therapy, representing a 30% relative risk reduction.
Audience members wanted to know if there are any circumstances at all in which Dr. Merkel would now consider resorting to plasma exchange, such as maybe in AAV patients at the most extreme end of the severity spectrum.
“I’m not sure I should be the one dictating that; I think the world needs to see the data,” he replied.
That being said, he added, “I think these data are incredibly helpful to physicians and patients as they face this decision. I think plasma exchange is an expensive therapy and somewhat invasive. I think our results indicate that the benefit that we may have thought was there is not there.”
The study was sponsored by the National Institutes of Health, the Food and Drug Administration, the U.K. Medical Research Council and the National Institute for Health Research, the Canadian Institutes of Health Research, and the governments of France, Australia, and New Zealand. The presenter reported receiving research funding from the ACR, EULAR, FDA, NIH, Patient-Centered Outcomes Research Institute, and the Vasculitis Foundation. He also receives research funding from and/or serves as a consultant to more than a dozen pharmaceutical companies.
SOURCE: Merkel PA et al. Arthritis Rheumatol. 2018;70(Suppl 10):Abstract 2788.
CHICAGO – Results of the landmark PEXIVAS study – far and away the largest randomized trial ever done in ANCA-associated vasculitis – will likely change treatment in a couple of major ways.
“I think this trial will have an impact on care. Based on these findings, physicians should strongly reconsider the utility of plasma exchange as a treatment for AAV [antineutrophil cytoplasmic antibody–associated vasculitis] patients and should now consider using lower cumulative doses of glucocorticoids for the treatment of severe AAV,” PEXIVAS coprincipal investigator Peter A. Merkel, MD, said at the annual meeting of the American College of Rheumatology.
That’s because the trial demonstrated that plasma exchange neither saved lives nor avoided end-stage renal disease, while utilization of oral glucocorticoids in doses substantially lower than the high-dose current standard significantly reduced the serious infection rate without causing less effective disease control, according to Dr. Merkel, chief of rheumatology and professor of medicine and epidemiology at the University of Pennsylvania in Philadelphia.
PEXIVAS comprised 704 patients with severe granulomatosis with polyangiitis or microscopic polyangiitis, making it more than twice as large as any other trial in AAV. This was a multicenter, international, open-label, randomized trial with a 2-by-2 factorial design. To qualify as having severe AAV, participants had to have an estimated glomerular filtration rate below 50 mL/min per 1.73 m2 and/or lung hemorrhage.
“This was in essence two trials embedded within one protocol in the factorial design,” he explained.
The impetus for this major clinical trial was a recognition that mortality due to AAV remains high, especially in the first year, with a clear unmet need for better, less toxic therapies. Indeed, it’s estimated that only 29% of deaths in the first year after diagnosis are due to the vasculitis disease itself, while over 50% of the mortality is caused by infection, much of it collateral damage from immunosuppressive therapies.
Dr. Merkel, who heads the National Institutes of Health–supported Vasculitis Clinical Research Consortium, said the time was right for a clinical trial aimed at improving patient management: “Clinical equipoise exists for the efficacy of both plasma exchange and reduced-dose glucocorticoids in ANCA-associated vasculitis.”
The patients underwent induction therapy with cyclophosphamide or rituximab (Rituxan) plus IV methylprednisolone. Then they were randomized to seven plasma exchange sessions in 14 days or no plasma exchange, and further randomized to conventional weight-based, high-dose oral glucocorticoids or a lower-dose regimen. Those on the reduced-dose regimen received 54% of the cumulative amount of glucocorticoids used in the standard-dose group through the first 3 months, and 61% over the course of 6 months. By week 4, those on the reduced-dose regimen were on an average of 25 mg/day, while those on standard therapy were on 50 mg/day. Adherence to assigned study arms exceeded 90%. Patients were followed prospectively for 1-7 years.
The primary endpoint, a composite of all-cause mortality or development of end-stage renal disease, occurred in 28% of patients on plasma exchange and 31% of those who did not undergo plasma exchange, a nonsignificant difference indicative of a lack of benefit for the intervention. No differential effect was seen in prespecified subgroups based on age, creatinine clearance, ANCA type, form of immunosuppression, or presence or absence of lung hemorrhage.
Further, the primary endpoint occurred in 28% of patients on reduced-dose glucocorticoids, compared with 26% on full-dose therapy; again, a nonsignificant difference, meaning lower-dose therapy didn’t result in less effective disease control. But it did result in a significant reduction in the prespecified endpoint of serious infections in the first year: 27% versus 33% with full-dose therapy, representing a 30% relative risk reduction.
Audience members wanted to know if there are any circumstances at all in which Dr. Merkel would now consider resorting to plasma exchange, such as maybe in AAV patients at the most extreme end of the severity spectrum.
“I’m not sure I should be the one dictating that; I think the world needs to see the data,” he replied.
That being said, he added, “I think these data are incredibly helpful to physicians and patients as they face this decision. I think plasma exchange is an expensive therapy and somewhat invasive. I think our results indicate that the benefit that we may have thought was there is not there.”
The study was sponsored by the National Institutes of Health, the Food and Drug Administration, the U.K. Medical Research Council and the National Institute for Health Research, the Canadian Institutes of Health Research, and the governments of France, Australia, and New Zealand. The presenter reported receiving research funding from the ACR, EULAR, FDA, NIH, Patient-Centered Outcomes Research Institute, and the Vasculitis Foundation. He also receives research funding from and/or serves as a consultant to more than a dozen pharmaceutical companies.
SOURCE: Merkel PA et al. Arthritis Rheumatol. 2018;70(Suppl 10):Abstract 2788.
CHICAGO – Results of the landmark PEXIVAS study – far and away the largest randomized trial ever done in ANCA-associated vasculitis – will likely change treatment in a couple of major ways.
“I think this trial will have an impact on care. Based on these findings, physicians should strongly reconsider the utility of plasma exchange as a treatment for AAV [antineutrophil cytoplasmic antibody–associated vasculitis] patients and should now consider using lower cumulative doses of glucocorticoids for the treatment of severe AAV,” PEXIVAS coprincipal investigator Peter A. Merkel, MD, said at the annual meeting of the American College of Rheumatology.
That’s because the trial demonstrated that plasma exchange neither saved lives nor avoided end-stage renal disease, while utilization of oral glucocorticoids in doses substantially lower than the high-dose current standard significantly reduced the serious infection rate without causing less effective disease control, according to Dr. Merkel, chief of rheumatology and professor of medicine and epidemiology at the University of Pennsylvania in Philadelphia.
PEXIVAS comprised 704 patients with severe granulomatosis with polyangiitis or microscopic polyangiitis, making it more than twice as large as any other trial in AAV. This was a multicenter, international, open-label, randomized trial with a 2-by-2 factorial design. To qualify as having severe AAV, participants had to have an estimated glomerular filtration rate below 50 mL/min per 1.73 m2 and/or lung hemorrhage.
“This was in essence two trials embedded within one protocol in the factorial design,” he explained.
The impetus for this major clinical trial was a recognition that mortality due to AAV remains high, especially in the first year, with a clear unmet need for better, less toxic therapies. Indeed, it’s estimated that only 29% of deaths in the first year after diagnosis are due to the vasculitis disease itself, while over 50% of the mortality is caused by infection, much of it collateral damage from immunosuppressive therapies.
Dr. Merkel, who heads the National Institutes of Health–supported Vasculitis Clinical Research Consortium, said the time was right for a clinical trial aimed at improving patient management: “Clinical equipoise exists for the efficacy of both plasma exchange and reduced-dose glucocorticoids in ANCA-associated vasculitis.”
The patients underwent induction therapy with cyclophosphamide or rituximab (Rituxan) plus IV methylprednisolone. Then they were randomized to seven plasma exchange sessions in 14 days or no plasma exchange, and further randomized to conventional weight-based, high-dose oral glucocorticoids or a lower-dose regimen. Those on the reduced-dose regimen received 54% of the cumulative amount of glucocorticoids used in the standard-dose group through the first 3 months, and 61% over the course of 6 months. By week 4, those on the reduced-dose regimen were on an average of 25 mg/day, while those on standard therapy were on 50 mg/day. Adherence to assigned study arms exceeded 90%. Patients were followed prospectively for 1-7 years.
The primary endpoint, a composite of all-cause mortality or development of end-stage renal disease, occurred in 28% of patients on plasma exchange and 31% of those who did not undergo plasma exchange, a nonsignificant difference indicative of a lack of benefit for the intervention. No differential effect was seen in prespecified subgroups based on age, creatinine clearance, ANCA type, form of immunosuppression, or presence or absence of lung hemorrhage.
Further, the primary endpoint occurred in 28% of patients on reduced-dose glucocorticoids, compared with 26% on full-dose therapy; again, a nonsignificant difference, meaning lower-dose therapy didn’t result in less effective disease control. But it did result in a significant reduction in the prespecified endpoint of serious infections in the first year: 27% versus 33% with full-dose therapy, representing a 30% relative risk reduction.
Audience members wanted to know if there are any circumstances at all in which Dr. Merkel would now consider resorting to plasma exchange, such as maybe in AAV patients at the most extreme end of the severity spectrum.
“I’m not sure I should be the one dictating that; I think the world needs to see the data,” he replied.
That being said, he added, “I think these data are incredibly helpful to physicians and patients as they face this decision. I think plasma exchange is an expensive therapy and somewhat invasive. I think our results indicate that the benefit that we may have thought was there is not there.”
The study was sponsored by the National Institutes of Health, the Food and Drug Administration, the U.K. Medical Research Council and the National Institute for Health Research, the Canadian Institutes of Health Research, and the governments of France, Australia, and New Zealand. The presenter reported receiving research funding from the ACR, EULAR, FDA, NIH, Patient-Centered Outcomes Research Institute, and the Vasculitis Foundation. He also receives research funding from and/or serves as a consultant to more than a dozen pharmaceutical companies.
SOURCE: Merkel PA et al. Arthritis Rheumatol. 2018;70(Suppl 10):Abstract 2788.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point: Plasma exchange was without benefit and reduced-dose oral glucocorticoids safely decreased serious infections in ANCA-associated vasculitis.
Major finding: The rate of serious infections in the first year was 27% in patients on reduced-dose oral glucocorticoids and 33% with standard high-dose therapy, for a significant 30% relative risk reduction.
Study details: PEXIVAS was a multicenter, international, open-label, randomized trial with a 2-by-2 factorial design comprising 704 patients with severe ANCA-associated vasculitis.
Disclosures: The study was sponsored by the National Institutes of Health, the Food and Drug Administration, the U.K. Medical Research Council and the National Institute of Health Research, the Canadian Institutes of Health Research, and the governments of France, Australia, and New Zealand. The presenter reported receiving research funding from the ACR, EULAR, FDA, NIH, Patient-Centered Outcomes Research Institute, and the Vasculitis Foundation. He also receives research funding from and/or serves as a consultant to more than a dozen pharmaceutical companies.
Source: Merkel PA et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 2788.
Genetic risk factor found for RA-associated interstitial lung disease
CHICAGO – Rheumatoid arthritis–associated interstitial lung disease and idiopathic pulmonary fibrosis without RA share a common genetic underpinning whose hallmark is a gain-of-function MUC5B gene promoter variant that cranks up mucin production in the lungs, Pierre-Antoine Juge, MD, reported at the annual meeting of the American College of Rheumatology.

He presented a seven-country genetic case-control study of 620 patients with RA-associated interstitial lung disease (RA-ILD), 614 with RA but no ILD, and 5,448 unaffected controls. The key finding was that the MUC5B promoter variant rs35705950, already known to be the strongest genetic risk factor for idiopathic pulmonary fibrosis (IPF), also contributes substantially to the risk of RA-ILD.
Indeed, the presence of the MUC5B promoter variant in patients with RA proved to be associated with substantially higher risk of RA-ILD than the previously recognized risk factors for RA-ILD, including cigarette smoking and the human leukocyte antigen locus for RA, according to Dr. Juge, a rheumatologist at Bichat Hospital–Claude Bernard and Paris Diderot University.
MUC5B encodes for mucin production in the lungs. The increased risk of RA-ILD conferred by the presence of the MUC5B promoter variant was confined to the 41% of RA-ILD patients with a pattern of usual interstitial pneumonia (UIP) or possible UIP on high-resolution CT. The presence of the MUC5B promoter variant in RA patients was independently associated with an adjusted 6.1-fold increased risk of ILD with a UIP pattern on imaging – marked by honeycombing, reticular abnormalities, and subpleural involvement – compared with RA patients who didn’t possess the gain-of-function MUC5B variant. The risk of other types of RA-ILD wasn’t affected by the presence or absence of the MUC5B variant.
The MUC5B promoter variant was not a risk factor for development of RA.
These findings have potentially important implications for clinical practice, given that clinically significant ILD is present in about 10% of all RA patients and occult ILD is detectable using high-resolution CT in up to half of individuals with RA, Dr. Juge observed. Detection of the MUC5B promoter variant could be used to screen patients with RA for preclinical ILD. Also, there is now a sound rationale to study drugs known to be effective for IPF as potential treatments for RA-ILD, he said.
Dr. Juge reported having no financial conflicts regarding the study, which was sponsored by the National Institutes of Health, the U.S. Department of Defense, the French Rheumatology Society, the Japanese Society for the Promotion of Science, Fondation Arthritis, and the Nina Ireland Program for Lung Health.
In conjunction with his presentation in Chicago, the study was published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1801562).
SOURCE: Juge P-A et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1819.
CHICAGO – Rheumatoid arthritis–associated interstitial lung disease and idiopathic pulmonary fibrosis without RA share a common genetic underpinning whose hallmark is a gain-of-function MUC5B gene promoter variant that cranks up mucin production in the lungs, Pierre-Antoine Juge, MD, reported at the annual meeting of the American College of Rheumatology.
He presented a seven-country genetic case-control study of 620 patients with RA-associated interstitial lung disease (RA-ILD), 614 with RA but no ILD, and 5,448 unaffected controls. The key finding was that the MUC5B promoter variant rs35705950, already known to be the strongest genetic risk factor for idiopathic pulmonary fibrosis (IPF), also contributes substantially to the risk of RA-ILD.
Indeed, the presence of the MUC5B promoter variant in patients with RA proved to be associated with substantially higher risk of RA-ILD than the previously recognized risk factors for RA-ILD, including cigarette smoking and the human leukocyte antigen locus for RA, according to Dr. Juge, a rheumatologist at Bichat Hospital–Claude Bernard and Paris Diderot University.
MUC5B encodes for mucin production in the lungs. The increased risk of RA-ILD conferred by the presence of the MUC5B promoter variant was confined to the 41% of RA-ILD patients with a pattern of usual interstitial pneumonia (UIP) or possible UIP on high-resolution CT. The presence of the MUC5B promoter variant in RA patients was independently associated with an adjusted 6.1-fold increased risk of ILD with a UIP pattern on imaging – marked by honeycombing, reticular abnormalities, and subpleural involvement – compared with RA patients who didn’t possess the gain-of-function MUC5B variant. The risk of other types of RA-ILD wasn’t affected by the presence or absence of the MUC5B variant.
The MUC5B promoter variant was not a risk factor for development of RA.
These findings have potentially important implications for clinical practice, given that clinically significant ILD is present in about 10% of all RA patients and occult ILD is detectable using high-resolution CT in up to half of individuals with RA, Dr. Juge observed. Detection of the MUC5B promoter variant could be used to screen patients with RA for preclinical ILD. Also, there is now a sound rationale to study drugs known to be effective for IPF as potential treatments for RA-ILD, he said.
Dr. Juge reported having no financial conflicts regarding the study, which was sponsored by the National Institutes of Health, the U.S. Department of Defense, the French Rheumatology Society, the Japanese Society for the Promotion of Science, Fondation Arthritis, and the Nina Ireland Program for Lung Health.
In conjunction with his presentation in Chicago, the study was published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1801562).
SOURCE: Juge P-A et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1819.
CHICAGO – Rheumatoid arthritis–associated interstitial lung disease and idiopathic pulmonary fibrosis without RA share a common genetic underpinning whose hallmark is a gain-of-function MUC5B gene promoter variant that cranks up mucin production in the lungs, Pierre-Antoine Juge, MD, reported at the annual meeting of the American College of Rheumatology.
He presented a seven-country genetic case-control study of 620 patients with RA-associated interstitial lung disease (RA-ILD), 614 with RA but no ILD, and 5,448 unaffected controls. The key finding was that the MUC5B promoter variant rs35705950, already known to be the strongest genetic risk factor for idiopathic pulmonary fibrosis (IPF), also contributes substantially to the risk of RA-ILD.
Indeed, the presence of the MUC5B promoter variant in patients with RA proved to be associated with substantially higher risk of RA-ILD than the previously recognized risk factors for RA-ILD, including cigarette smoking and the human leukocyte antigen locus for RA, according to Dr. Juge, a rheumatologist at Bichat Hospital–Claude Bernard and Paris Diderot University.
MUC5B encodes for mucin production in the lungs. The increased risk of RA-ILD conferred by the presence of the MUC5B promoter variant was confined to the 41% of RA-ILD patients with a pattern of usual interstitial pneumonia (UIP) or possible UIP on high-resolution CT. The presence of the MUC5B promoter variant in RA patients was independently associated with an adjusted 6.1-fold increased risk of ILD with a UIP pattern on imaging – marked by honeycombing, reticular abnormalities, and subpleural involvement – compared with RA patients who didn’t possess the gain-of-function MUC5B variant. The risk of other types of RA-ILD wasn’t affected by the presence or absence of the MUC5B variant.
The MUC5B promoter variant was not a risk factor for development of RA.
These findings have potentially important implications for clinical practice, given that clinically significant ILD is present in about 10% of all RA patients and occult ILD is detectable using high-resolution CT in up to half of individuals with RA, Dr. Juge observed. Detection of the MUC5B promoter variant could be used to screen patients with RA for preclinical ILD. Also, there is now a sound rationale to study drugs known to be effective for IPF as potential treatments for RA-ILD, he said.
Dr. Juge reported having no financial conflicts regarding the study, which was sponsored by the National Institutes of Health, the U.S. Department of Defense, the French Rheumatology Society, the Japanese Society for the Promotion of Science, Fondation Arthritis, and the Nina Ireland Program for Lung Health.
In conjunction with his presentation in Chicago, the study was published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1801562).
SOURCE: Juge P-A et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1819.
REPORTING FROM THE ACR ANNUAL MEETING
Cannabis crimps teen cognitive development
BARCELONA – What would you predict has a greater detrimental effect on adolescent cognitive development: alcohol or cannabis use?

The evidence-based answer may come as a surprise. It certainly did for Patricia Conrod, PhD, who led the large population-based study that addressed the question.
“Generally, we found no effect of alcohol on cognitive development, which was a huge surprise to us. It might be related to the fact that the quantity of alcohol consumption in this young sample just wasn’t high enough to produce significant effects on cognitive development. But, to our surprise, we found rather significant effects of cannabis use on cognitive development,” she said at the annual congress of the European College of Neuropsychopharmacology.
Indeed, cannabis use proved to have detrimental effects on all four cognitive domains assessed in the study: working memory, perceptual reasoning, delayed recall, and inhibitory control, reported Dr. Conrod, professor of psychiatry at the University of Montreal.
Her recently study, published in the American Journal of Psychiatry, included 3,826 seventh-grade students at 31 Montreal-area schools. They constituted 5% of all students entering that grade in the greater Montreal area. Participants were prospectively assessed annually for 4 years regarding their use or nonuse of alcohol or cannabis and also underwent neurocognitive testing on the four domains of interest. The assessments were done on school computers with preservation of student confidentiality. Investigators used a Big Data approach to model the relationship between the extent of substance use and neurocognitive function variables over time.
Abstinent students were the best performers on the neurocognitive testing. Cannabis use, but not alcohol, in a given year was associated with concurrent adverse effects on all four cognitive domains. In addition, cannabis use showed evidence of having a neurotoxic lag effect on inhibitory control and working memory. This took the form of a lasting effect: A student who reported using cannabis 1 year but not the next showed impairment of inhibitory control and working memory during both years. And a student who used cannabis both years was even more impaired in those domains.
Dr. Conrod found the evidence of a neurotoxic effect of cannabis use on inhibitory control to be of particular concern because in earlier studies she established that impaired inhibitory control is a strong independent risk factor for subsequent substance use disorders.
”So what we’re seeing is indeed that early onset substance use is interfering with cognitive development, which now sets us up to be able to answer the question of whether evidence-based prevention protects cognitive development by delaying early onset of substance use. And over the longer term, does that protect young people against addiction?”
Dr. Conrod and her coworkers are now in the process of obtaining answers to those questions in the large ongoing Canadian Institutes of Health Research-funded Co-Venture Trial. This randomized trial involving thousands of adolescent students used the investigators’ Preventure Program, a school-based, personality-targeted intervention for prevention of substance use and abuse.
The Preventure Program involves two 90-minute group sessions of manual-based cognitive-behavioral therapy. Students are invited to participate if they score at least one standard deviation above the school mean on one of four personality traits that have been shown to increase the risk of substance misuse and psychiatric disorders. The four personality traits are sensation seeking, impulsivity, anxiety sensitivity, and hopelessness. Typically, about 45% of students met that threshold, and 85% of those invited to participate in the program volunteered to do so. Students of similar personality type are grouped together for the targeted therapy sessions.
This brief coping skills intervention has been shown in multiple randomized trials around the world to reduce the likelihood of substance use in at-risk adolescents. For example, in an early trial involving 732 high school students in London, participation in the Preventure Program was associated with a 30% reduction in the likelihood of taking up the use of cannabis within the next 2 years, an 80% reduction in the likelihood of taking up cocaine, and a 50% reduction in the use of other drugs (Arch Gen Psychiatry. 2010 Jan;67[1]:85-93).
bjancin@mdedge.com
SOURCE: Conrod P. Am J Psychiatry. 2018 Oct 3. doi: 10.1176/appi.ajp.2018.18020202.
BARCELONA – What would you predict has a greater detrimental effect on adolescent cognitive development: alcohol or cannabis use?
The evidence-based answer may come as a surprise. It certainly did for Patricia Conrod, PhD, who led the large population-based study that addressed the question.
“Generally, we found no effect of alcohol on cognitive development, which was a huge surprise to us. It might be related to the fact that the quantity of alcohol consumption in this young sample just wasn’t high enough to produce significant effects on cognitive development. But, to our surprise, we found rather significant effects of cannabis use on cognitive development,” she said at the annual congress of the European College of Neuropsychopharmacology.
Indeed, cannabis use proved to have detrimental effects on all four cognitive domains assessed in the study: working memory, perceptual reasoning, delayed recall, and inhibitory control, reported Dr. Conrod, professor of psychiatry at the University of Montreal.
Her recently study, published in the American Journal of Psychiatry, included 3,826 seventh-grade students at 31 Montreal-area schools. They constituted 5% of all students entering that grade in the greater Montreal area. Participants were prospectively assessed annually for 4 years regarding their use or nonuse of alcohol or cannabis and also underwent neurocognitive testing on the four domains of interest. The assessments were done on school computers with preservation of student confidentiality. Investigators used a Big Data approach to model the relationship between the extent of substance use and neurocognitive function variables over time.
Abstinent students were the best performers on the neurocognitive testing. Cannabis use, but not alcohol, in a given year was associated with concurrent adverse effects on all four cognitive domains. In addition, cannabis use showed evidence of having a neurotoxic lag effect on inhibitory control and working memory. This took the form of a lasting effect: A student who reported using cannabis 1 year but not the next showed impairment of inhibitory control and working memory during both years. And a student who used cannabis both years was even more impaired in those domains.
Dr. Conrod found the evidence of a neurotoxic effect of cannabis use on inhibitory control to be of particular concern because in earlier studies she established that impaired inhibitory control is a strong independent risk factor for subsequent substance use disorders.
”So what we’re seeing is indeed that early onset substance use is interfering with cognitive development, which now sets us up to be able to answer the question of whether evidence-based prevention protects cognitive development by delaying early onset of substance use. And over the longer term, does that protect young people against addiction?”
Dr. Conrod and her coworkers are now in the process of obtaining answers to those questions in the large ongoing Canadian Institutes of Health Research-funded Co-Venture Trial. This randomized trial involving thousands of adolescent students used the investigators’ Preventure Program, a school-based, personality-targeted intervention for prevention of substance use and abuse.
The Preventure Program involves two 90-minute group sessions of manual-based cognitive-behavioral therapy. Students are invited to participate if they score at least one standard deviation above the school mean on one of four personality traits that have been shown to increase the risk of substance misuse and psychiatric disorders. The four personality traits are sensation seeking, impulsivity, anxiety sensitivity, and hopelessness. Typically, about 45% of students met that threshold, and 85% of those invited to participate in the program volunteered to do so. Students of similar personality type are grouped together for the targeted therapy sessions.
This brief coping skills intervention has been shown in multiple randomized trials around the world to reduce the likelihood of substance use in at-risk adolescents. For example, in an early trial involving 732 high school students in London, participation in the Preventure Program was associated with a 30% reduction in the likelihood of taking up the use of cannabis within the next 2 years, an 80% reduction in the likelihood of taking up cocaine, and a 50% reduction in the use of other drugs (Arch Gen Psychiatry. 2010 Jan;67[1]:85-93).
bjancin@mdedge.com
SOURCE: Conrod P. Am J Psychiatry. 2018 Oct 3. doi: 10.1176/appi.ajp.2018.18020202.
BARCELONA – What would you predict has a greater detrimental effect on adolescent cognitive development: alcohol or cannabis use?
The evidence-based answer may come as a surprise. It certainly did for Patricia Conrod, PhD, who led the large population-based study that addressed the question.
“Generally, we found no effect of alcohol on cognitive development, which was a huge surprise to us. It might be related to the fact that the quantity of alcohol consumption in this young sample just wasn’t high enough to produce significant effects on cognitive development. But, to our surprise, we found rather significant effects of cannabis use on cognitive development,” she said at the annual congress of the European College of Neuropsychopharmacology.
Indeed, cannabis use proved to have detrimental effects on all four cognitive domains assessed in the study: working memory, perceptual reasoning, delayed recall, and inhibitory control, reported Dr. Conrod, professor of psychiatry at the University of Montreal.
Her recently study, published in the American Journal of Psychiatry, included 3,826 seventh-grade students at 31 Montreal-area schools. They constituted 5% of all students entering that grade in the greater Montreal area. Participants were prospectively assessed annually for 4 years regarding their use or nonuse of alcohol or cannabis and also underwent neurocognitive testing on the four domains of interest. The assessments were done on school computers with preservation of student confidentiality. Investigators used a Big Data approach to model the relationship between the extent of substance use and neurocognitive function variables over time.
Abstinent students were the best performers on the neurocognitive testing. Cannabis use, but not alcohol, in a given year was associated with concurrent adverse effects on all four cognitive domains. In addition, cannabis use showed evidence of having a neurotoxic lag effect on inhibitory control and working memory. This took the form of a lasting effect: A student who reported using cannabis 1 year but not the next showed impairment of inhibitory control and working memory during both years. And a student who used cannabis both years was even more impaired in those domains.
Dr. Conrod found the evidence of a neurotoxic effect of cannabis use on inhibitory control to be of particular concern because in earlier studies she established that impaired inhibitory control is a strong independent risk factor for subsequent substance use disorders.
”So what we’re seeing is indeed that early onset substance use is interfering with cognitive development, which now sets us up to be able to answer the question of whether evidence-based prevention protects cognitive development by delaying early onset of substance use. And over the longer term, does that protect young people against addiction?”
Dr. Conrod and her coworkers are now in the process of obtaining answers to those questions in the large ongoing Canadian Institutes of Health Research-funded Co-Venture Trial. This randomized trial involving thousands of adolescent students used the investigators’ Preventure Program, a school-based, personality-targeted intervention for prevention of substance use and abuse.
The Preventure Program involves two 90-minute group sessions of manual-based cognitive-behavioral therapy. Students are invited to participate if they score at least one standard deviation above the school mean on one of four personality traits that have been shown to increase the risk of substance misuse and psychiatric disorders. The four personality traits are sensation seeking, impulsivity, anxiety sensitivity, and hopelessness. Typically, about 45% of students met that threshold, and 85% of those invited to participate in the program volunteered to do so. Students of similar personality type are grouped together for the targeted therapy sessions.
This brief coping skills intervention has been shown in multiple randomized trials around the world to reduce the likelihood of substance use in at-risk adolescents. For example, in an early trial involving 732 high school students in London, participation in the Preventure Program was associated with a 30% reduction in the likelihood of taking up the use of cannabis within the next 2 years, an 80% reduction in the likelihood of taking up cocaine, and a 50% reduction in the use of other drugs (Arch Gen Psychiatry. 2010 Jan;67[1]:85-93).
bjancin@mdedge.com
SOURCE: Conrod P. Am J Psychiatry. 2018 Oct 3. doi: 10.1176/appi.ajp.2018.18020202.
REPORTING FROM THE ECNP CONGRESS
Key clinical point:
Major finding: The observed neurotoxic effect on impulse control may spell future trouble.
Study details: This population-based study included 3,826 Montreal-area seventh graders who were prospectively assessed annually for 4 years regarding their cannabis and alcohol use and also underwent neurocognitive testing.
Disclosures: The study was funded by the Canadian Institutes of Health Research.
Source: Conrod P. Am J Psychiatry. 2018 Oct 3. doi: 10.1176/appi.ajp.2018.18020202.
Novel blood test brings RA prevention closer to reality
CHICAGO – A positive B cell clonality test in a peripheral blood sample predicts imminent onset of rheumatoid arthritis with a high degree of accuracy in at-risk individuals, Niek de Vries, MD, PhD, reported at the annual meeting of the American College of Rheumatology.

This finding, now confirmed twice over in separate validation studies, opens the door to trials of pharmacologic treatment aimed at preventing rheumatoid arthritis (RA).
“In my view, a positive test might be an indication for preventive treatment and retesting at 1 year to evaluate the treatment effect,” said Dr. de Vries, professor of rheumatology at the University of Amsterdam.
Many patients with RA experience a pre-RA phase marked by joint pain, the presence of RA-specific autoantibodies, IgM rheumatoid factor, and/or anticitrullinated protein antibodies, but no synovial inflammation. The challenge in attempting to develop RA preventive strategies targeting this population is that only about 28% of them go on to develop RA within 3 years. Exposing the entire preclinical-phase population to powerful antirheumatic drugs to try to prevent RA in the minority who are actually headed for overt disease is not an attractive strategy.
That’s why Dr. de Vries and his coinvestigators developed a method of B cell receptor (BCR) analysis using PCR and next-generation sequencing techniques. They determined that when a clone comprised more than 0.5% of the total B cell receptor population, it can be considered an expanded or dominant clone. They then demonstrated that when a patient in the pre-RA phase has five or more dominant clones in a peripheral blood sample, that can be considered a positive BCR test. In two published studies, they showed that a positive BCR test in the pre-RA stage accurately predicts onset of overt RA within the next several years (Ann Rheum Dis. 2017 Nov;76[11]:1924-30 and Ann Rheum Dis. 2018;77:151). They have also shown that at the time of RA onset, the BCR clones disappear from peripheral blood and reappear in the synovium.
At the ACR annual meeting, Dr. de Vries presented the results of a new BCR test validation study, this one involving 129 pre–RA-phase Dutch patients. The purpose of this study was to learn whether the BCR test is more predictive than clinical predictors such as the Risk Rule Model, and also to determine whether a higher number of dominant clones predicts RA onset even more accurately than the five-or-more clone threshold the investigators had been using. The answer to both questions proved to be yes.
Thirty-five percent of the 129 pre-RA subjects had a positive BCR test as defined by the presence of five or more expanded clones. A total of 75% of them went on to develop RA within the next 3 years. None of the BCR test-negative patients did. That result translated to a test sensitivity of 100%, a specificity of 87%, a positive predictive value of 71%, and a negative predictive value of 100%. A positive BCR blood test was associated with a 120-fold increased risk of an RA diagnosis within 3 years.
The investigators also compared outcomes in the 17% of study participants with a high degree of BCR test positivity, defined as the presence of nine or more expanded clones, versus the 18% of subjects whose positive BCR test had five to eight clones. Overall, 91% with a highly positive BCR test featuring nine or more clones developed RA within 3 years, compared with 55% of those with five to eight clones.
These findings permit categorization of pre-RA patients into three groups. Those with a negative BCR test can be reassured that their 3-year risk of developing RA is similar to the background risk in the general population. Those with a mid-range positive BCR test – that is, five to eight dominant clones – should probably be retested periodically, although the optimum interval is still under study. And patients with a highly positive BCR test might be candidates for preventive therapy.
Before RA-preventive therapy during the high-risk pre-RA phase can be introduced into routine clinical practice, however, several issues need to be resolved, Dr. de Vries continued. Although a single dose of rituximab (Rituxan) showed efficacy in a proof-of-concept study, that was off-label therapy. There is as yet no approved agent for prevention of RA in high-risk patients. Also, the risk/benefit ratio of preventive therapy will need to be determined. And rheumatologists will have to figure out how to identify these high-risk pre-RA individuals early, when preventive therapy is likely to most effective.
Several audience members observed that the Dutch investigators’ BCR test using PCR and next-generation sequencing is technically complex. They asked if the BCR results might correlate with any far more readily available serologic tests. The answer is no, according to Dr. de Vries.
“I think it’s very important to realize that what we test is the migration of B cells or plasmablast-like cells through the blood at the moment that we’re testing. This is completely different from a serological assessment of antibody production by plasma cells which are present in the bone marrow, which changes very little despite effective treatment. In contrast, if we test B cell migration while a patient gets corticosteroids we see an immediate disappearance of all these cells. So it’s a different parameter,” the rheumatologist explained.
The Dutch Arthritis Association funded the study. Dr. de Vries noted that he is a coinventor of the BCR test, the intellectual property rights for which belong to the University of Amsterdam. He receives research funding from Pfizer, Roche, Janssen, and GlaxoSmithKline.
SOURCE: de Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10). Abstract 835.
CHICAGO – A positive B cell clonality test in a peripheral blood sample predicts imminent onset of rheumatoid arthritis with a high degree of accuracy in at-risk individuals, Niek de Vries, MD, PhD, reported at the annual meeting of the American College of Rheumatology.
This finding, now confirmed twice over in separate validation studies, opens the door to trials of pharmacologic treatment aimed at preventing rheumatoid arthritis (RA).
“In my view, a positive test might be an indication for preventive treatment and retesting at 1 year to evaluate the treatment effect,” said Dr. de Vries, professor of rheumatology at the University of Amsterdam.
Many patients with RA experience a pre-RA phase marked by joint pain, the presence of RA-specific autoantibodies, IgM rheumatoid factor, and/or anticitrullinated protein antibodies, but no synovial inflammation. The challenge in attempting to develop RA preventive strategies targeting this population is that only about 28% of them go on to develop RA within 3 years. Exposing the entire preclinical-phase population to powerful antirheumatic drugs to try to prevent RA in the minority who are actually headed for overt disease is not an attractive strategy.
That’s why Dr. de Vries and his coinvestigators developed a method of B cell receptor (BCR) analysis using PCR and next-generation sequencing techniques. They determined that when a clone comprised more than 0.5% of the total B cell receptor population, it can be considered an expanded or dominant clone. They then demonstrated that when a patient in the pre-RA phase has five or more dominant clones in a peripheral blood sample, that can be considered a positive BCR test. In two published studies, they showed that a positive BCR test in the pre-RA stage accurately predicts onset of overt RA within the next several years (Ann Rheum Dis. 2017 Nov;76[11]:1924-30 and Ann Rheum Dis. 2018;77:151). They have also shown that at the time of RA onset, the BCR clones disappear from peripheral blood and reappear in the synovium.
At the ACR annual meeting, Dr. de Vries presented the results of a new BCR test validation study, this one involving 129 pre–RA-phase Dutch patients. The purpose of this study was to learn whether the BCR test is more predictive than clinical predictors such as the Risk Rule Model, and also to determine whether a higher number of dominant clones predicts RA onset even more accurately than the five-or-more clone threshold the investigators had been using. The answer to both questions proved to be yes.
Thirty-five percent of the 129 pre-RA subjects had a positive BCR test as defined by the presence of five or more expanded clones. A total of 75% of them went on to develop RA within the next 3 years. None of the BCR test-negative patients did. That result translated to a test sensitivity of 100%, a specificity of 87%, a positive predictive value of 71%, and a negative predictive value of 100%. A positive BCR blood test was associated with a 120-fold increased risk of an RA diagnosis within 3 years.
The investigators also compared outcomes in the 17% of study participants with a high degree of BCR test positivity, defined as the presence of nine or more expanded clones, versus the 18% of subjects whose positive BCR test had five to eight clones. Overall, 91% with a highly positive BCR test featuring nine or more clones developed RA within 3 years, compared with 55% of those with five to eight clones.
These findings permit categorization of pre-RA patients into three groups. Those with a negative BCR test can be reassured that their 3-year risk of developing RA is similar to the background risk in the general population. Those with a mid-range positive BCR test – that is, five to eight dominant clones – should probably be retested periodically, although the optimum interval is still under study. And patients with a highly positive BCR test might be candidates for preventive therapy.
Before RA-preventive therapy during the high-risk pre-RA phase can be introduced into routine clinical practice, however, several issues need to be resolved, Dr. de Vries continued. Although a single dose of rituximab (Rituxan) showed efficacy in a proof-of-concept study, that was off-label therapy. There is as yet no approved agent for prevention of RA in high-risk patients. Also, the risk/benefit ratio of preventive therapy will need to be determined. And rheumatologists will have to figure out how to identify these high-risk pre-RA individuals early, when preventive therapy is likely to most effective.
Several audience members observed that the Dutch investigators’ BCR test using PCR and next-generation sequencing is technically complex. They asked if the BCR results might correlate with any far more readily available serologic tests. The answer is no, according to Dr. de Vries.
“I think it’s very important to realize that what we test is the migration of B cells or plasmablast-like cells through the blood at the moment that we’re testing. This is completely different from a serological assessment of antibody production by plasma cells which are present in the bone marrow, which changes very little despite effective treatment. In contrast, if we test B cell migration while a patient gets corticosteroids we see an immediate disappearance of all these cells. So it’s a different parameter,” the rheumatologist explained.
The Dutch Arthritis Association funded the study. Dr. de Vries noted that he is a coinventor of the BCR test, the intellectual property rights for which belong to the University of Amsterdam. He receives research funding from Pfizer, Roche, Janssen, and GlaxoSmithKline.
SOURCE: de Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10). Abstract 835.
CHICAGO – A positive B cell clonality test in a peripheral blood sample predicts imminent onset of rheumatoid arthritis with a high degree of accuracy in at-risk individuals, Niek de Vries, MD, PhD, reported at the annual meeting of the American College of Rheumatology.
This finding, now confirmed twice over in separate validation studies, opens the door to trials of pharmacologic treatment aimed at preventing rheumatoid arthritis (RA).
“In my view, a positive test might be an indication for preventive treatment and retesting at 1 year to evaluate the treatment effect,” said Dr. de Vries, professor of rheumatology at the University of Amsterdam.
Many patients with RA experience a pre-RA phase marked by joint pain, the presence of RA-specific autoantibodies, IgM rheumatoid factor, and/or anticitrullinated protein antibodies, but no synovial inflammation. The challenge in attempting to develop RA preventive strategies targeting this population is that only about 28% of them go on to develop RA within 3 years. Exposing the entire preclinical-phase population to powerful antirheumatic drugs to try to prevent RA in the minority who are actually headed for overt disease is not an attractive strategy.
That’s why Dr. de Vries and his coinvestigators developed a method of B cell receptor (BCR) analysis using PCR and next-generation sequencing techniques. They determined that when a clone comprised more than 0.5% of the total B cell receptor population, it can be considered an expanded or dominant clone. They then demonstrated that when a patient in the pre-RA phase has five or more dominant clones in a peripheral blood sample, that can be considered a positive BCR test. In two published studies, they showed that a positive BCR test in the pre-RA stage accurately predicts onset of overt RA within the next several years (Ann Rheum Dis. 2017 Nov;76[11]:1924-30 and Ann Rheum Dis. 2018;77:151). They have also shown that at the time of RA onset, the BCR clones disappear from peripheral blood and reappear in the synovium.
At the ACR annual meeting, Dr. de Vries presented the results of a new BCR test validation study, this one involving 129 pre–RA-phase Dutch patients. The purpose of this study was to learn whether the BCR test is more predictive than clinical predictors such as the Risk Rule Model, and also to determine whether a higher number of dominant clones predicts RA onset even more accurately than the five-or-more clone threshold the investigators had been using. The answer to both questions proved to be yes.
Thirty-five percent of the 129 pre-RA subjects had a positive BCR test as defined by the presence of five or more expanded clones. A total of 75% of them went on to develop RA within the next 3 years. None of the BCR test-negative patients did. That result translated to a test sensitivity of 100%, a specificity of 87%, a positive predictive value of 71%, and a negative predictive value of 100%. A positive BCR blood test was associated with a 120-fold increased risk of an RA diagnosis within 3 years.
The investigators also compared outcomes in the 17% of study participants with a high degree of BCR test positivity, defined as the presence of nine or more expanded clones, versus the 18% of subjects whose positive BCR test had five to eight clones. Overall, 91% with a highly positive BCR test featuring nine or more clones developed RA within 3 years, compared with 55% of those with five to eight clones.
These findings permit categorization of pre-RA patients into three groups. Those with a negative BCR test can be reassured that their 3-year risk of developing RA is similar to the background risk in the general population. Those with a mid-range positive BCR test – that is, five to eight dominant clones – should probably be retested periodically, although the optimum interval is still under study. And patients with a highly positive BCR test might be candidates for preventive therapy.
Before RA-preventive therapy during the high-risk pre-RA phase can be introduced into routine clinical practice, however, several issues need to be resolved, Dr. de Vries continued. Although a single dose of rituximab (Rituxan) showed efficacy in a proof-of-concept study, that was off-label therapy. There is as yet no approved agent for prevention of RA in high-risk patients. Also, the risk/benefit ratio of preventive therapy will need to be determined. And rheumatologists will have to figure out how to identify these high-risk pre-RA individuals early, when preventive therapy is likely to most effective.
Several audience members observed that the Dutch investigators’ BCR test using PCR and next-generation sequencing is technically complex. They asked if the BCR results might correlate with any far more readily available serologic tests. The answer is no, according to Dr. de Vries.
“I think it’s very important to realize that what we test is the migration of B cells or plasmablast-like cells through the blood at the moment that we’re testing. This is completely different from a serological assessment of antibody production by plasma cells which are present in the bone marrow, which changes very little despite effective treatment. In contrast, if we test B cell migration while a patient gets corticosteroids we see an immediate disappearance of all these cells. So it’s a different parameter,” the rheumatologist explained.
The Dutch Arthritis Association funded the study. Dr. de Vries noted that he is a coinventor of the BCR test, the intellectual property rights for which belong to the University of Amsterdam. He receives research funding from Pfizer, Roche, Janssen, and GlaxoSmithKline.
SOURCE: de Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10). Abstract 835.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point: A peripheral blood sample showing a high level of expanded B cell receptor clones accurately predicts looming onset of rheumatoid arthritis.
Major finding: Ninety-one percent of patients with a highly positive B cell receptor clonality blood test developed rheumatoid arthritis within the next 3 years.
Study details: This study included 129 patients deemed at high risk for developing rheumatoid arthritis who were followed for 3 years.
Disclosures: The Dutch Arthritis Association funded the study. The presenter noted that he is a coinventor of the B cell receptor blood test, the intellectual property rights for which belong to the University of Amsterdam.
Source: De Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 835.
Bipolar patients’ relatives face increased cardiovascular risk
BARCELONA – Young patients recently diagnosed with bipolar disorder are at double the 30-year risk of cardiovascular disease, compared with the general population, and their unaffected first-degree relatives are nearly as high risk, Klara Coello, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
The clinical implication of this finding is that unaffected first-degree relatives of patients with bipolar disorder – an affective disorder typically diagnosed at age 15-24 – should be targeted for intensified primary cardiovascular prevention, with a focus on smoking and dyslipidemia, both of which were more prevalent in these patients and their unaffected relatives than in the general population in her study, noted Dr. Coello, a doctoral candidate with the Copenhagen Affective Disorders Research Center at the University of Copenhagen.
She and her coinvestigators presented a cross-sectional study in which they calculated the 30-year Framingham Risk Scores for 221 patients recently diagnosed bipolar disorder – 95% of whom had been diagnosed within the past 2 years – along with 50 unaffected first-degree relatives and 119 age- and sex-matched controls. The investigators used the Framingham Risk Score because the widely used American Heart Association/American College of Cardiology Atherosclerotic Cardiovascular Disease Risk Estimator applies only to individuals aged 40 and up.
The key findings: The 30-year risk of cardiovascular disease for patients with bipolar was 98.5% greater than that of controls, and the calculated risk of the unaffected first-degree relatives was increased by 85.4%, compared with that of controls.
The Framingham Risk Score is determined on the basis of old-school cardiovascular risk factors, including age, gender, lipids, systolic blood pressure, diabetes, and smoking. 45% of the bipolar patients were smokers, as were 20% of their first-degree relatives and 13% of controls.
The Danish finding of increased cardiovascular risk in young adults with bipolar disorder recapitulates an American Heart Association Scientific Statement, which was published in Circulation (2015 Sep 8;132[10]:965-86). The statement was intended to alert clinicians that these affective disorders constitute “moderate-risk” conditions for arterial dysfunction prior to age 30 and for premature cardiovascular disease (CVD). The statement declared that this risk is likely mediated not only by the classic cardiovascular risk factors but also by disease-related inflammation, oxidative stress, sleep disruption, and the adverse metabolic effects of many psychotropic medications.
“The magnitude of increased risk for CVD in adulthood is substantial,” according to the AHA expert panel’s scientific statement.
Dr. Coello’s study only took into account levels of the traditional cardiovascular risk factors. Where the study broke new ground that hadn’t been explored in the AHA scientific statement, however, was in identifying unaffected first-degree relatives as an additional at-risk group.
She reported having no financial conflicts regarding her study, which constitutes her PhD thesis.
BARCELONA – Young patients recently diagnosed with bipolar disorder are at double the 30-year risk of cardiovascular disease, compared with the general population, and their unaffected first-degree relatives are nearly as high risk, Klara Coello, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
The clinical implication of this finding is that unaffected first-degree relatives of patients with bipolar disorder – an affective disorder typically diagnosed at age 15-24 – should be targeted for intensified primary cardiovascular prevention, with a focus on smoking and dyslipidemia, both of which were more prevalent in these patients and their unaffected relatives than in the general population in her study, noted Dr. Coello, a doctoral candidate with the Copenhagen Affective Disorders Research Center at the University of Copenhagen.
She and her coinvestigators presented a cross-sectional study in which they calculated the 30-year Framingham Risk Scores for 221 patients recently diagnosed bipolar disorder – 95% of whom had been diagnosed within the past 2 years – along with 50 unaffected first-degree relatives and 119 age- and sex-matched controls. The investigators used the Framingham Risk Score because the widely used American Heart Association/American College of Cardiology Atherosclerotic Cardiovascular Disease Risk Estimator applies only to individuals aged 40 and up.
The key findings: The 30-year risk of cardiovascular disease for patients with bipolar was 98.5% greater than that of controls, and the calculated risk of the unaffected first-degree relatives was increased by 85.4%, compared with that of controls.
The Framingham Risk Score is determined on the basis of old-school cardiovascular risk factors, including age, gender, lipids, systolic blood pressure, diabetes, and smoking. 45% of the bipolar patients were smokers, as were 20% of their first-degree relatives and 13% of controls.
The Danish finding of increased cardiovascular risk in young adults with bipolar disorder recapitulates an American Heart Association Scientific Statement, which was published in Circulation (2015 Sep 8;132[10]:965-86). The statement was intended to alert clinicians that these affective disorders constitute “moderate-risk” conditions for arterial dysfunction prior to age 30 and for premature cardiovascular disease (CVD). The statement declared that this risk is likely mediated not only by the classic cardiovascular risk factors but also by disease-related inflammation, oxidative stress, sleep disruption, and the adverse metabolic effects of many psychotropic medications.
“The magnitude of increased risk for CVD in adulthood is substantial,” according to the AHA expert panel’s scientific statement.
Dr. Coello’s study only took into account levels of the traditional cardiovascular risk factors. Where the study broke new ground that hadn’t been explored in the AHA scientific statement, however, was in identifying unaffected first-degree relatives as an additional at-risk group.
She reported having no financial conflicts regarding her study, which constitutes her PhD thesis.
BARCELONA – Young patients recently diagnosed with bipolar disorder are at double the 30-year risk of cardiovascular disease, compared with the general population, and their unaffected first-degree relatives are nearly as high risk, Klara Coello, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
The clinical implication of this finding is that unaffected first-degree relatives of patients with bipolar disorder – an affective disorder typically diagnosed at age 15-24 – should be targeted for intensified primary cardiovascular prevention, with a focus on smoking and dyslipidemia, both of which were more prevalent in these patients and their unaffected relatives than in the general population in her study, noted Dr. Coello, a doctoral candidate with the Copenhagen Affective Disorders Research Center at the University of Copenhagen.
She and her coinvestigators presented a cross-sectional study in which they calculated the 30-year Framingham Risk Scores for 221 patients recently diagnosed bipolar disorder – 95% of whom had been diagnosed within the past 2 years – along with 50 unaffected first-degree relatives and 119 age- and sex-matched controls. The investigators used the Framingham Risk Score because the widely used American Heart Association/American College of Cardiology Atherosclerotic Cardiovascular Disease Risk Estimator applies only to individuals aged 40 and up.
The key findings: The 30-year risk of cardiovascular disease for patients with bipolar was 98.5% greater than that of controls, and the calculated risk of the unaffected first-degree relatives was increased by 85.4%, compared with that of controls.
The Framingham Risk Score is determined on the basis of old-school cardiovascular risk factors, including age, gender, lipids, systolic blood pressure, diabetes, and smoking. 45% of the bipolar patients were smokers, as were 20% of their first-degree relatives and 13% of controls.
The Danish finding of increased cardiovascular risk in young adults with bipolar disorder recapitulates an American Heart Association Scientific Statement, which was published in Circulation (2015 Sep 8;132[10]:965-86). The statement was intended to alert clinicians that these affective disorders constitute “moderate-risk” conditions for arterial dysfunction prior to age 30 and for premature cardiovascular disease (CVD). The statement declared that this risk is likely mediated not only by the classic cardiovascular risk factors but also by disease-related inflammation, oxidative stress, sleep disruption, and the adverse metabolic effects of many psychotropic medications.
“The magnitude of increased risk for CVD in adulthood is substantial,” according to the AHA expert panel’s scientific statement.
Dr. Coello’s study only took into account levels of the traditional cardiovascular risk factors. Where the study broke new ground that hadn’t been explored in the AHA scientific statement, however, was in identifying unaffected first-degree relatives as an additional at-risk group.
She reported having no financial conflicts regarding her study, which constitutes her PhD thesis.
REPORTING FROM THE ECNP CONGRESS
Key clinical point: The first-degree relatives of patients with bipolar disorder should be targeted for intensified primary cardiovascular prevention.
Major finding: Thirty-year cardiovascular risk was increased by 98.5% in recently diagnosed bipolar patients and by 85.4% in their unaffected first-degree relatives, compared with the general population.
Study details: This cross-sectional study involved calculation of 30-year Framingham Risk Scores for 221 patients recently diagnosed with bipolar disorder, 50 unaffected first-degree relatives, and 119 age- and sex-matched controls.
Disclosures: The study presenter reported having no financial conflicts of interest.
Big drinkers face newly appreciated massive health burden
BARCELONA – Individuals who regularly consume alcohol in quantities defined by the World Health Organization as “very high risk” face a daunting and yet widely underappreciated health burden, Rainer Spanagel, MD, observed at the annual congress of the European College of Neuropsychopharmacology.

He cited a recent study led by Jürgen Rehm, PhD, of the Centre for Addiction and Mental Health in Toronto in which the investigators estimated the prevalence of what the WHO has defined as a “very-high-risk drinking level” among people aged 15-65 years in 13 E.U. countries. The researchers then went on to determine the associated annual risk of disease and injury, as well as the effects on life expectancy.
“The numbers are so shocking that you have to take it seriously,” said Dr. Spanagel, chair of the department of psychopharmacology at the Central Institute of Mental Health in Mannheim, Germany.
Nearly 2 decades ago, the WHO defined very-high-risk level of alcohol consumption as more than 100 g/day of ethanol for men and more than 60 g/day for women. That translates to a threshold of 7.1 and 4.3 standard drinks – a 12-ounce beer, 5-ounce glass of wine, or 1.5-ounce serving of liquor – on a daily basis.
“This WHO categorization of drinking risk levels has been pretty much ignored in clinical trials and epidemiologic studies until 3 or 4 years ago,” according to Dr. Spanagel.
The study by Dr. Rehm and his colleagues suggests this has been a serious mistake. By using data from the WHO’s Global Information System on Alcohol and Health, as well as from clinical trials, the investigators determined that the prevalence of this level of alcohol consumption was less than 1% overall across 13 European countries. However, rates varied markedly: in excess of 4% in Ireland and more than 3.5% in the United Kingdom, compared with less than 0.5% in Germany, Sweden, Denmark, Finland, Hungary, and the Netherlands. The Czech Republic came in at about 3%, while Italy, Spain, France, and Austria had rates of more than 0.5% but less than 1%.
The investigators estimated that the risk of disease or injury associated with this very-high-risk drinking level was 13.5% per year. Based on data from nine E.U. countries, Dr. Rehm and his colleagues found that a very-high-risk level of alcohol consumption caused nearly 54% of all cases of hepatic cirrhosis in those countries, 41% of esophageal and oral cancers, and 44% of pancreatitis.
Life expectancy in the European Union stands at 80.6 years. compared with the general population. By comparison, all cancers considered together resulted in 10 years of life lost.
Dr. Spanagel is editor in chief of the journal Addiction Biology, in which this study appeared (Addict Biol. 2018 Jul;23[4]:961-8).
bjancin@mdedge.com
BARCELONA – Individuals who regularly consume alcohol in quantities defined by the World Health Organization as “very high risk” face a daunting and yet widely underappreciated health burden, Rainer Spanagel, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
He cited a recent study led by Jürgen Rehm, PhD, of the Centre for Addiction and Mental Health in Toronto in which the investigators estimated the prevalence of what the WHO has defined as a “very-high-risk drinking level” among people aged 15-65 years in 13 E.U. countries. The researchers then went on to determine the associated annual risk of disease and injury, as well as the effects on life expectancy.
“The numbers are so shocking that you have to take it seriously,” said Dr. Spanagel, chair of the department of psychopharmacology at the Central Institute of Mental Health in Mannheim, Germany.
Nearly 2 decades ago, the WHO defined very-high-risk level of alcohol consumption as more than 100 g/day of ethanol for men and more than 60 g/day for women. That translates to a threshold of 7.1 and 4.3 standard drinks – a 12-ounce beer, 5-ounce glass of wine, or 1.5-ounce serving of liquor – on a daily basis.
“This WHO categorization of drinking risk levels has been pretty much ignored in clinical trials and epidemiologic studies until 3 or 4 years ago,” according to Dr. Spanagel.
The study by Dr. Rehm and his colleagues suggests this has been a serious mistake. By using data from the WHO’s Global Information System on Alcohol and Health, as well as from clinical trials, the investigators determined that the prevalence of this level of alcohol consumption was less than 1% overall across 13 European countries. However, rates varied markedly: in excess of 4% in Ireland and more than 3.5% in the United Kingdom, compared with less than 0.5% in Germany, Sweden, Denmark, Finland, Hungary, and the Netherlands. The Czech Republic came in at about 3%, while Italy, Spain, France, and Austria had rates of more than 0.5% but less than 1%.
The investigators estimated that the risk of disease or injury associated with this very-high-risk drinking level was 13.5% per year. Based on data from nine E.U. countries, Dr. Rehm and his colleagues found that a very-high-risk level of alcohol consumption caused nearly 54% of all cases of hepatic cirrhosis in those countries, 41% of esophageal and oral cancers, and 44% of pancreatitis.
Life expectancy in the European Union stands at 80.6 years. compared with the general population. By comparison, all cancers considered together resulted in 10 years of life lost.
Dr. Spanagel is editor in chief of the journal Addiction Biology, in which this study appeared (Addict Biol. 2018 Jul;23[4]:961-8).
bjancin@mdedge.com
BARCELONA – Individuals who regularly consume alcohol in quantities defined by the World Health Organization as “very high risk” face a daunting and yet widely underappreciated health burden, Rainer Spanagel, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
He cited a recent study led by Jürgen Rehm, PhD, of the Centre for Addiction and Mental Health in Toronto in which the investigators estimated the prevalence of what the WHO has defined as a “very-high-risk drinking level” among people aged 15-65 years in 13 E.U. countries. The researchers then went on to determine the associated annual risk of disease and injury, as well as the effects on life expectancy.
“The numbers are so shocking that you have to take it seriously,” said Dr. Spanagel, chair of the department of psychopharmacology at the Central Institute of Mental Health in Mannheim, Germany.
Nearly 2 decades ago, the WHO defined very-high-risk level of alcohol consumption as more than 100 g/day of ethanol for men and more than 60 g/day for women. That translates to a threshold of 7.1 and 4.3 standard drinks – a 12-ounce beer, 5-ounce glass of wine, or 1.5-ounce serving of liquor – on a daily basis.
“This WHO categorization of drinking risk levels has been pretty much ignored in clinical trials and epidemiologic studies until 3 or 4 years ago,” according to Dr. Spanagel.
The study by Dr. Rehm and his colleagues suggests this has been a serious mistake. By using data from the WHO’s Global Information System on Alcohol and Health, as well as from clinical trials, the investigators determined that the prevalence of this level of alcohol consumption was less than 1% overall across 13 European countries. However, rates varied markedly: in excess of 4% in Ireland and more than 3.5% in the United Kingdom, compared with less than 0.5% in Germany, Sweden, Denmark, Finland, Hungary, and the Netherlands. The Czech Republic came in at about 3%, while Italy, Spain, France, and Austria had rates of more than 0.5% but less than 1%.
The investigators estimated that the risk of disease or injury associated with this very-high-risk drinking level was 13.5% per year. Based on data from nine E.U. countries, Dr. Rehm and his colleagues found that a very-high-risk level of alcohol consumption caused nearly 54% of all cases of hepatic cirrhosis in those countries, 41% of esophageal and oral cancers, and 44% of pancreatitis.
Life expectancy in the European Union stands at 80.6 years. compared with the general population. By comparison, all cancers considered together resulted in 10 years of life lost.
Dr. Spanagel is editor in chief of the journal Addiction Biology, in which this study appeared (Addict Biol. 2018 Jul;23[4]:961-8).
bjancin@mdedge.com
REPORTING FROM THE ECNP CONGRESS
This year’s top papers on mood disorders
BARCELONA – Among the handful of top publications on mood disorders during the first three-quarters of 2018 was a landmark comparison of the efficacy and acceptability of 21 antidepressants for acute treatment of major depressive disorder, Íria Grande, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.

Dr. Grande, a psychiatrist at the bipolar disorders clinic of the University of Barcelona, shared her personal top picks.
‘Antidepressants work’
This epic systematic review and network meta-analysis (Lancet. 2018 Apr 7;391[10128]:1357-66) encompassed 522 randomized double-blind trials with 116,477 participants with major depressive disorder assigned to 21 antidepressants or placebo, in some instances with an additional active comparator antidepressant arm. The report is a major extension of previous work by the same multinational group of investigators (Lancet. 2009 Feb 28;373[9665]:746-58), who initially scrutinized 12 older antidepressants in a total population only one-quarter the size of the updated analysis.
Based upon this vast randomized trial evidence, some of which came from unpublished studies tracked down by the investigators, the 21 antidepressants were rank-ordered in terms of effectiveness and acceptability. But in Dr. Grande’s view, the most important study finding wasn’t which antidepressant donned the crown of most effective or patient acceptable, it was the fact that all 21 drugs proved significantly more effective than placebo, with odds ratios ranging from 2.13 at the top end to 1.37 for reboxetine.
“The results showed antidepressants work. All of the antipsychiatry system is trying to show us that antidepressants do not work in major depression. Well, in this study, it has been proven that all antidepressants are more effective than placebo in major depressive disorder. I think social media should be made aware of that. (Lead investigator) Dr. Andrea Cipriani talked on the BBC about this article, and it had a high impact,” according to Dr. Grande.
All but three of the 21 antidepressants were deemed to be as acceptable as placebo, based upon study dropout rates. The exceptions were agomelatine and fluoxetine, which were 12%-14% more acceptable than placebo. “That’s strange, I think, but that’s what the clinical trial results showed,” she noted. The findings on clomipramine, which was 30% less acceptable than placebo, make sense, Dr. Grande said, “due to its muscarinic effects.”
She took issue with some of the specific study findings. For example, the two top-rated antidepressants in terms of efficacy were amitriptyline and mirtazapine, with odds ratios of 2.13 and 1.89, respectively.
“As a clinician, I don’t consider mirtazapine to be one of the best antidepressants, especially in major depression,” she said. “But these are the results, and as always, we have to adapt the evidence-based medicine and consider it from our clinical point of view.”
The investigators conducted a subanalysis restricted to placebo-controlled head-to-head studies with a comparator antidepressant which Dr. Grande found more interesting and informative than the overall analysis. In the head-to-head analysis, vortioxetine emerged as the top-rated antidepressant, both in efficacy, with an odds ratio of 2.0, as well as in acceptability.
Lithium vs. quetiapine
Finnish investigators used prospective national databases to examine the rates of psychiatric and all-cause hospitalization during a mean 7.2 years of follow-up in all 18,018 Finns hospitalized for bipolar disorder. The purpose was to assess the impact of various mood stabilizers on overall health outcomes in a real-world setting.
The big winner was lithium. In an analysis adjusted for concomitant psychotropic medications, duration of bipolar illness, and intervals of drug exposure and nonexposure, lithium was associated with the lowest risks of psychiatric rehospitalization and all-cause hospitalization, with relative risk reductions of 33% and 29%, respectively. In contrast, quetiapine, the most widely used antipsychotic agent, paled by comparison, achieving only an 8% reduction in the risk of psychiatric rehospitalization and a 7% decrease in all-cause hospitalization (JAMA Psychiatry. 2018 Apr 1;75[4]:347-55).
In addition, long-acting injectable antipsychotics were significantly more effective for prevention of hospitalization than oral antipsychotics.
“That is kind of shocking, because in some countries, long-acting injectables are not authorized and cannot be used. But I think after this article some regulatory changes are going to take place as a result,” Dr. Grande predicted.
“Another issue I thought was interesting, although it was not the main aim of the study, involved benzodiazepines. They increased the risk of hospitalizations, both for psychiatric illness and all other causes. So apart from giving lithium and long-acting injectable antipsychotics to our bipolar patients, we should also be really careful about the use of benzodiazepines,” she commented.
Intranasal esketamine for suicidality?
Esketamine nasal spray, a fast-acting N-methyl-D-aspartate antagonist whose application for marketing approval in combination with a standard oral antidepressant in treatment-resistant depression is now under Food and Drug Administration review, also is being developed for another indication: reduction of suicidality in patients at imminent suicide risk. In a proof-of-concept study, intranasal esketamine resulted in a significant reduction in suicidal thoughts 4 hours after administration, compared with usual care – but not at 24 hours (Am J Psychiatry. 2018 Jul 1;175[7]:620-30).
New and effective medications for this indication are sorely needed. The only drug approved for the indication of suicide prevention is clozapine.
‘Latest thinking’ on bipolar disorders
Dr. Grande coauthored a comprehensive review article on bipolar disorders that she recommended as worthwhile reading (Nat Rev Dis Primers. 2018 Mar 8;4:18008. doi: 10.1038/nrdp.2018.8).
“It covers all the latest thinking. It focuses on the early stages of the disorder, how epigenetic factors are essential, and many other topics, including the bipolarity index being developed at the University of Barcelona to classify drugs in terms of their capacity to prevent episodes of mania or depression in terms of number needed to treat and number needed to harm. It emphasizes the importance of intervening early and focusing on cognitive dysfunction,” Dr Grande said.
Psychedelics making a comeback
German and Swiss investigators used a facial expression discrimination task to demonstrate that psilocybin, a 5-hydroxytryptamine2A–receptor agonist, decreases connectivity between the amygdala and regions of the brain important in emotion processing, including the striatum and frontal pole. The investigators theorized that this might be the mechanism for the psychedelic’s apparent antidepressant effects (Eur Neuropsychopharmacol. 2018 Jun;28[6]:691-700).
Dr. Grande included this study in her top publications list because it reflects the rapidly growing rebirth of interest in psychedelics research among European psychiatrists.
Indeed, elsewhere at the ECNP congress David J. Nutt, DM, declared, “We now have the beginnings of some swinging of the pendulum back in a modern direction. Over the last 10 years there have been a small number of open studies, all done with psilocybin, which is somewhat easier to use than LSD. There are studies in OCD [obsessive-compulsive disorder], tobacco dependence, alcoholism, resistant depression, end-of-life mood changes with cancer and other terminal diseases, and at least two ongoing randomized trials in resistant depression.”
Dr. Nutt, professor of neuropsychopharmacology at Imperial College London, was senior author of the first proof-of-concept study of psilocybin accompanied by psychologic support as a novel therapy for moderate to severe treatment-resistant major depression (Lancet Psychiatry. 2016 Jul;3[7]:619-27).
Methylphenidate ineffective for treatment of acute mania
The MEMAP study was a randomized, double-blind, placebo-controlled multicenter clinical trial testing what has been called the vigilance regulation model of mania. This model hypothesized that unstable regulation of wakefulness figures prominently in the pathogenesis of both mania and attention-deficit/hyperactivity disorder. If true, investigators reasoned, then 2.5 days of methylphenidate at 20-40 mg/day should have a rapid antimanic effect similar to the drug’s benefits in ADHD. Dr. Grande had been a skeptic, and indeed, the trial was halted early for futility (Eur Neuropsychopharmacol. 2018 Jan;28[1]:185-94).
She reported serving as a paid speaker for Lunbeck, Ferrer, GlaxoSmithKline, and Janssen. Her own research is funded by the Spanish Ministry of Economy and Competitiveness.
BARCELONA – Among the handful of top publications on mood disorders during the first three-quarters of 2018 was a landmark comparison of the efficacy and acceptability of 21 antidepressants for acute treatment of major depressive disorder, Íria Grande, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Dr. Grande, a psychiatrist at the bipolar disorders clinic of the University of Barcelona, shared her personal top picks.
‘Antidepressants work’
This epic systematic review and network meta-analysis (Lancet. 2018 Apr 7;391[10128]:1357-66) encompassed 522 randomized double-blind trials with 116,477 participants with major depressive disorder assigned to 21 antidepressants or placebo, in some instances with an additional active comparator antidepressant arm. The report is a major extension of previous work by the same multinational group of investigators (Lancet. 2009 Feb 28;373[9665]:746-58), who initially scrutinized 12 older antidepressants in a total population only one-quarter the size of the updated analysis.
Based upon this vast randomized trial evidence, some of which came from unpublished studies tracked down by the investigators, the 21 antidepressants were rank-ordered in terms of effectiveness and acceptability. But in Dr. Grande’s view, the most important study finding wasn’t which antidepressant donned the crown of most effective or patient acceptable, it was the fact that all 21 drugs proved significantly more effective than placebo, with odds ratios ranging from 2.13 at the top end to 1.37 for reboxetine.
“The results showed antidepressants work. All of the antipsychiatry system is trying to show us that antidepressants do not work in major depression. Well, in this study, it has been proven that all antidepressants are more effective than placebo in major depressive disorder. I think social media should be made aware of that. (Lead investigator) Dr. Andrea Cipriani talked on the BBC about this article, and it had a high impact,” according to Dr. Grande.
All but three of the 21 antidepressants were deemed to be as acceptable as placebo, based upon study dropout rates. The exceptions were agomelatine and fluoxetine, which were 12%-14% more acceptable than placebo. “That’s strange, I think, but that’s what the clinical trial results showed,” she noted. The findings on clomipramine, which was 30% less acceptable than placebo, make sense, Dr. Grande said, “due to its muscarinic effects.”
She took issue with some of the specific study findings. For example, the two top-rated antidepressants in terms of efficacy were amitriptyline and mirtazapine, with odds ratios of 2.13 and 1.89, respectively.
“As a clinician, I don’t consider mirtazapine to be one of the best antidepressants, especially in major depression,” she said. “But these are the results, and as always, we have to adapt the evidence-based medicine and consider it from our clinical point of view.”
The investigators conducted a subanalysis restricted to placebo-controlled head-to-head studies with a comparator antidepressant which Dr. Grande found more interesting and informative than the overall analysis. In the head-to-head analysis, vortioxetine emerged as the top-rated antidepressant, both in efficacy, with an odds ratio of 2.0, as well as in acceptability.
Lithium vs. quetiapine
Finnish investigators used prospective national databases to examine the rates of psychiatric and all-cause hospitalization during a mean 7.2 years of follow-up in all 18,018 Finns hospitalized for bipolar disorder. The purpose was to assess the impact of various mood stabilizers on overall health outcomes in a real-world setting.
The big winner was lithium. In an analysis adjusted for concomitant psychotropic medications, duration of bipolar illness, and intervals of drug exposure and nonexposure, lithium was associated with the lowest risks of psychiatric rehospitalization and all-cause hospitalization, with relative risk reductions of 33% and 29%, respectively. In contrast, quetiapine, the most widely used antipsychotic agent, paled by comparison, achieving only an 8% reduction in the risk of psychiatric rehospitalization and a 7% decrease in all-cause hospitalization (JAMA Psychiatry. 2018 Apr 1;75[4]:347-55).
In addition, long-acting injectable antipsychotics were significantly more effective for prevention of hospitalization than oral antipsychotics.
“That is kind of shocking, because in some countries, long-acting injectables are not authorized and cannot be used. But I think after this article some regulatory changes are going to take place as a result,” Dr. Grande predicted.
“Another issue I thought was interesting, although it was not the main aim of the study, involved benzodiazepines. They increased the risk of hospitalizations, both for psychiatric illness and all other causes. So apart from giving lithium and long-acting injectable antipsychotics to our bipolar patients, we should also be really careful about the use of benzodiazepines,” she commented.
Intranasal esketamine for suicidality?
Esketamine nasal spray, a fast-acting N-methyl-D-aspartate antagonist whose application for marketing approval in combination with a standard oral antidepressant in treatment-resistant depression is now under Food and Drug Administration review, also is being developed for another indication: reduction of suicidality in patients at imminent suicide risk. In a proof-of-concept study, intranasal esketamine resulted in a significant reduction in suicidal thoughts 4 hours after administration, compared with usual care – but not at 24 hours (Am J Psychiatry. 2018 Jul 1;175[7]:620-30).
New and effective medications for this indication are sorely needed. The only drug approved for the indication of suicide prevention is clozapine.
‘Latest thinking’ on bipolar disorders
Dr. Grande coauthored a comprehensive review article on bipolar disorders that she recommended as worthwhile reading (Nat Rev Dis Primers. 2018 Mar 8;4:18008. doi: 10.1038/nrdp.2018.8).
“It covers all the latest thinking. It focuses on the early stages of the disorder, how epigenetic factors are essential, and many other topics, including the bipolarity index being developed at the University of Barcelona to classify drugs in terms of their capacity to prevent episodes of mania or depression in terms of number needed to treat and number needed to harm. It emphasizes the importance of intervening early and focusing on cognitive dysfunction,” Dr Grande said.
Psychedelics making a comeback
German and Swiss investigators used a facial expression discrimination task to demonstrate that psilocybin, a 5-hydroxytryptamine2A–receptor agonist, decreases connectivity between the amygdala and regions of the brain important in emotion processing, including the striatum and frontal pole. The investigators theorized that this might be the mechanism for the psychedelic’s apparent antidepressant effects (Eur Neuropsychopharmacol. 2018 Jun;28[6]:691-700).
Dr. Grande included this study in her top publications list because it reflects the rapidly growing rebirth of interest in psychedelics research among European psychiatrists.
Indeed, elsewhere at the ECNP congress David J. Nutt, DM, declared, “We now have the beginnings of some swinging of the pendulum back in a modern direction. Over the last 10 years there have been a small number of open studies, all done with psilocybin, which is somewhat easier to use than LSD. There are studies in OCD [obsessive-compulsive disorder], tobacco dependence, alcoholism, resistant depression, end-of-life mood changes with cancer and other terminal diseases, and at least two ongoing randomized trials in resistant depression.”
Dr. Nutt, professor of neuropsychopharmacology at Imperial College London, was senior author of the first proof-of-concept study of psilocybin accompanied by psychologic support as a novel therapy for moderate to severe treatment-resistant major depression (Lancet Psychiatry. 2016 Jul;3[7]:619-27).
Methylphenidate ineffective for treatment of acute mania
The MEMAP study was a randomized, double-blind, placebo-controlled multicenter clinical trial testing what has been called the vigilance regulation model of mania. This model hypothesized that unstable regulation of wakefulness figures prominently in the pathogenesis of both mania and attention-deficit/hyperactivity disorder. If true, investigators reasoned, then 2.5 days of methylphenidate at 20-40 mg/day should have a rapid antimanic effect similar to the drug’s benefits in ADHD. Dr. Grande had been a skeptic, and indeed, the trial was halted early for futility (Eur Neuropsychopharmacol. 2018 Jan;28[1]:185-94).
She reported serving as a paid speaker for Lunbeck, Ferrer, GlaxoSmithKline, and Janssen. Her own research is funded by the Spanish Ministry of Economy and Competitiveness.
BARCELONA – Among the handful of top publications on mood disorders during the first three-quarters of 2018 was a landmark comparison of the efficacy and acceptability of 21 antidepressants for acute treatment of major depressive disorder, Íria Grande, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Dr. Grande, a psychiatrist at the bipolar disorders clinic of the University of Barcelona, shared her personal top picks.
‘Antidepressants work’
This epic systematic review and network meta-analysis (Lancet. 2018 Apr 7;391[10128]:1357-66) encompassed 522 randomized double-blind trials with 116,477 participants with major depressive disorder assigned to 21 antidepressants or placebo, in some instances with an additional active comparator antidepressant arm. The report is a major extension of previous work by the same multinational group of investigators (Lancet. 2009 Feb 28;373[9665]:746-58), who initially scrutinized 12 older antidepressants in a total population only one-quarter the size of the updated analysis.
Based upon this vast randomized trial evidence, some of which came from unpublished studies tracked down by the investigators, the 21 antidepressants were rank-ordered in terms of effectiveness and acceptability. But in Dr. Grande’s view, the most important study finding wasn’t which antidepressant donned the crown of most effective or patient acceptable, it was the fact that all 21 drugs proved significantly more effective than placebo, with odds ratios ranging from 2.13 at the top end to 1.37 for reboxetine.
“The results showed antidepressants work. All of the antipsychiatry system is trying to show us that antidepressants do not work in major depression. Well, in this study, it has been proven that all antidepressants are more effective than placebo in major depressive disorder. I think social media should be made aware of that. (Lead investigator) Dr. Andrea Cipriani talked on the BBC about this article, and it had a high impact,” according to Dr. Grande.
All but three of the 21 antidepressants were deemed to be as acceptable as placebo, based upon study dropout rates. The exceptions were agomelatine and fluoxetine, which were 12%-14% more acceptable than placebo. “That’s strange, I think, but that’s what the clinical trial results showed,” she noted. The findings on clomipramine, which was 30% less acceptable than placebo, make sense, Dr. Grande said, “due to its muscarinic effects.”
She took issue with some of the specific study findings. For example, the two top-rated antidepressants in terms of efficacy were amitriptyline and mirtazapine, with odds ratios of 2.13 and 1.89, respectively.
“As a clinician, I don’t consider mirtazapine to be one of the best antidepressants, especially in major depression,” she said. “But these are the results, and as always, we have to adapt the evidence-based medicine and consider it from our clinical point of view.”
The investigators conducted a subanalysis restricted to placebo-controlled head-to-head studies with a comparator antidepressant which Dr. Grande found more interesting and informative than the overall analysis. In the head-to-head analysis, vortioxetine emerged as the top-rated antidepressant, both in efficacy, with an odds ratio of 2.0, as well as in acceptability.
Lithium vs. quetiapine
Finnish investigators used prospective national databases to examine the rates of psychiatric and all-cause hospitalization during a mean 7.2 years of follow-up in all 18,018 Finns hospitalized for bipolar disorder. The purpose was to assess the impact of various mood stabilizers on overall health outcomes in a real-world setting.
The big winner was lithium. In an analysis adjusted for concomitant psychotropic medications, duration of bipolar illness, and intervals of drug exposure and nonexposure, lithium was associated with the lowest risks of psychiatric rehospitalization and all-cause hospitalization, with relative risk reductions of 33% and 29%, respectively. In contrast, quetiapine, the most widely used antipsychotic agent, paled by comparison, achieving only an 8% reduction in the risk of psychiatric rehospitalization and a 7% decrease in all-cause hospitalization (JAMA Psychiatry. 2018 Apr 1;75[4]:347-55).
In addition, long-acting injectable antipsychotics were significantly more effective for prevention of hospitalization than oral antipsychotics.
“That is kind of shocking, because in some countries, long-acting injectables are not authorized and cannot be used. But I think after this article some regulatory changes are going to take place as a result,” Dr. Grande predicted.
“Another issue I thought was interesting, although it was not the main aim of the study, involved benzodiazepines. They increased the risk of hospitalizations, both for psychiatric illness and all other causes. So apart from giving lithium and long-acting injectable antipsychotics to our bipolar patients, we should also be really careful about the use of benzodiazepines,” she commented.
Intranasal esketamine for suicidality?
Esketamine nasal spray, a fast-acting N-methyl-D-aspartate antagonist whose application for marketing approval in combination with a standard oral antidepressant in treatment-resistant depression is now under Food and Drug Administration review, also is being developed for another indication: reduction of suicidality in patients at imminent suicide risk. In a proof-of-concept study, intranasal esketamine resulted in a significant reduction in suicidal thoughts 4 hours after administration, compared with usual care – but not at 24 hours (Am J Psychiatry. 2018 Jul 1;175[7]:620-30).
New and effective medications for this indication are sorely needed. The only drug approved for the indication of suicide prevention is clozapine.
‘Latest thinking’ on bipolar disorders
Dr. Grande coauthored a comprehensive review article on bipolar disorders that she recommended as worthwhile reading (Nat Rev Dis Primers. 2018 Mar 8;4:18008. doi: 10.1038/nrdp.2018.8).
“It covers all the latest thinking. It focuses on the early stages of the disorder, how epigenetic factors are essential, and many other topics, including the bipolarity index being developed at the University of Barcelona to classify drugs in terms of their capacity to prevent episodes of mania or depression in terms of number needed to treat and number needed to harm. It emphasizes the importance of intervening early and focusing on cognitive dysfunction,” Dr Grande said.
Psychedelics making a comeback
German and Swiss investigators used a facial expression discrimination task to demonstrate that psilocybin, a 5-hydroxytryptamine2A–receptor agonist, decreases connectivity between the amygdala and regions of the brain important in emotion processing, including the striatum and frontal pole. The investigators theorized that this might be the mechanism for the psychedelic’s apparent antidepressant effects (Eur Neuropsychopharmacol. 2018 Jun;28[6]:691-700).
Dr. Grande included this study in her top publications list because it reflects the rapidly growing rebirth of interest in psychedelics research among European psychiatrists.
Indeed, elsewhere at the ECNP congress David J. Nutt, DM, declared, “We now have the beginnings of some swinging of the pendulum back in a modern direction. Over the last 10 years there have been a small number of open studies, all done with psilocybin, which is somewhat easier to use than LSD. There are studies in OCD [obsessive-compulsive disorder], tobacco dependence, alcoholism, resistant depression, end-of-life mood changes with cancer and other terminal diseases, and at least two ongoing randomized trials in resistant depression.”
Dr. Nutt, professor of neuropsychopharmacology at Imperial College London, was senior author of the first proof-of-concept study of psilocybin accompanied by psychologic support as a novel therapy for moderate to severe treatment-resistant major depression (Lancet Psychiatry. 2016 Jul;3[7]:619-27).
Methylphenidate ineffective for treatment of acute mania
The MEMAP study was a randomized, double-blind, placebo-controlled multicenter clinical trial testing what has been called the vigilance regulation model of mania. This model hypothesized that unstable regulation of wakefulness figures prominently in the pathogenesis of both mania and attention-deficit/hyperactivity disorder. If true, investigators reasoned, then 2.5 days of methylphenidate at 20-40 mg/day should have a rapid antimanic effect similar to the drug’s benefits in ADHD. Dr. Grande had been a skeptic, and indeed, the trial was halted early for futility (Eur Neuropsychopharmacol. 2018 Jan;28[1]:185-94).
She reported serving as a paid speaker for Lunbeck, Ferrer, GlaxoSmithKline, and Janssen. Her own research is funded by the Spanish Ministry of Economy and Competitiveness.
REPORTING FROM THE ECNP CONGRESS
Improve cognitive symptoms of depression to boost work productivity
BARCELONA – (Assessment in Work Productivity and the Relationship with Cognitive Symptoms).

“We found that as patients rated themselves as improved in terms of cognition – ‘I can think better,’ ‘I can focus,’ ‘I’m concentrating better’ – there was a strong correlation at 12 weeks and later extended to 1 year with improved work productivity by as much as 75%. It’s pretty dramatic,” lead investigator Pratap Chokka, MD, said in an interview at the annual congress of the European College of Neuropsychopharmacology.
AtWoRK was a multicenter, open-label, naturalistic intervention study in which 219 gainfully employed Canadian adults with major depressive disorder (MDD) who had presented to primary care physicians or psychiatrists were placed on vortioxetine (Trintellex) flexibly dosed at 10-20 mg/day and scheduled for routine follow-up visits every 4 weeks for 52 weeks.
This was a patient population with severe depression, severe cognitive dysfunction, severe anxiety, and substantial functional impairment as reflected in their baseline scores on a variety of validated measures (see graphic). The study was designed to emulate real-world clinical practice.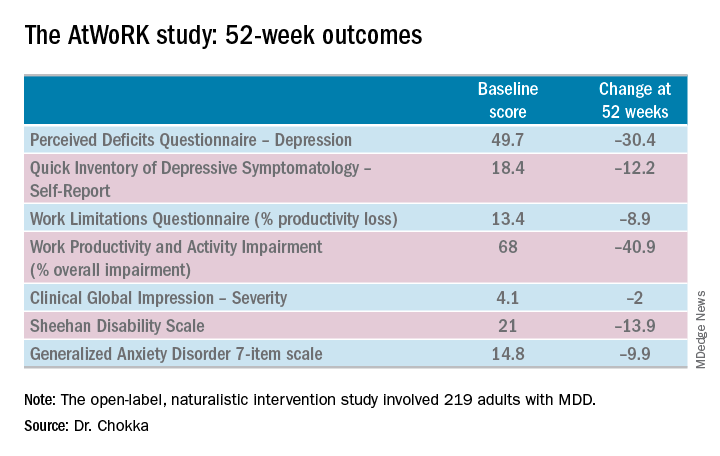
“We know that patients with depression are very impaired in terms of work productivity. Depressed patients really suffer from absenteeism and presenteeism [reduced productivity at work caused by depression]. And very few naturalistic studies have been done in working patients with depression,” according to Dr. Chokka. “The randomized trials are really important. They show us that a drug is working. But in terms of the real world that I work in, I need to have effectiveness: Does the drug work in patients with comorbid conditions, problems in their home lives, who are maybe drinking alcohol? Those are cases we’d rule out from participation in the RCTs.”
“The patients in our study walked into our clinics saying, ‘You know what, doctor, my mind isn’t working very good. I’m depressed, I can’t think, I can’t focus, I’m missing work, my boss is on my case, I’m making errors. I need help.’ These are the kinds of practicalities we wanted to address,” explained Dr. Chokka, a psychiatrist at Grey Nuns Community Hospital in Edmonton, Can.
The primary endpoint in AtWoRK was the correlation between changes in patients’ self-reported cognitive symptoms on the 20-item Perceived Deficits Questionnaire–Depression (PDQ-D-20) and changes in work productivity loss measured on the Work Limitations Questionnaire (WLQ) at week 12. Those 12-week results were recently published (CNS Spectr. 2018 May 24:1-10). At the ECNP congress, Dr. Chokka presented the expanded 52-week outcomes.
The correlation between change from baseline to week 12 in PDQ-D-20 and change in WLQ was strong (r = 0.606), and it remained strong at week 52 (r = 0.731; P less than .001).
At 52 weeks on vortioxetine, 77% of patients fulfilled criteria for MDD response, which required at least a 50% reduction in Quick Inventory of Depressive Symptomatology – Self-Report (QIDS-SR) score from baseline, and 56% for disease remission, which meant the QIDS-SR score was 5 or less. The response and remission rates were 71% and 45%, respectively, in the 107 subjects for whom the drug was the first treatment for their current MDD episode and 83% and 67% for the 112 switched to vortioxetine at study outset because the antidepressant they’d been on was ineffective.
Subjects also displayed significant improvement at 12 and 52 weeks in mood as assessed using QIDS-SR and global functioning as measured using the Sheehan Disability Scale (SDS). Of note, however, improvement in cognitive symptoms was independent of and not predictive of improvement in overall depressive symptoms on the QIDS-SR. Nor did improvement in depressive symptoms predict functional outcomes as assessed by the WLQ or SDS.
In Dr. Chokka’s view, these findings have clear implications for clinical practice: “In the past we thought that, if we can get the mood better, things will all get better. We now we know that treating depression is about more than just getting the mood better.”
Vortioxetine is an antidepressant with multiple agonist and antagonist effects on various 5-HT serotonin receptors.
The AtWoRK study was supported by Lundbeck Canada. Dr. Chokka reported receiving research grants from and serving on advisory boards and as a speaker for that company and others.
SOURCE: Chokka P. ECNP, P.022.
BARCELONA – (Assessment in Work Productivity and the Relationship with Cognitive Symptoms).
“We found that as patients rated themselves as improved in terms of cognition – ‘I can think better,’ ‘I can focus,’ ‘I’m concentrating better’ – there was a strong correlation at 12 weeks and later extended to 1 year with improved work productivity by as much as 75%. It’s pretty dramatic,” lead investigator Pratap Chokka, MD, said in an interview at the annual congress of the European College of Neuropsychopharmacology.
AtWoRK was a multicenter, open-label, naturalistic intervention study in which 219 gainfully employed Canadian adults with major depressive disorder (MDD) who had presented to primary care physicians or psychiatrists were placed on vortioxetine (Trintellex) flexibly dosed at 10-20 mg/day and scheduled for routine follow-up visits every 4 weeks for 52 weeks.
This was a patient population with severe depression, severe cognitive dysfunction, severe anxiety, and substantial functional impairment as reflected in their baseline scores on a variety of validated measures (see graphic). The study was designed to emulate real-world clinical practice.
“We know that patients with depression are very impaired in terms of work productivity. Depressed patients really suffer from absenteeism and presenteeism [reduced productivity at work caused by depression]. And very few naturalistic studies have been done in working patients with depression,” according to Dr. Chokka. “The randomized trials are really important. They show us that a drug is working. But in terms of the real world that I work in, I need to have effectiveness: Does the drug work in patients with comorbid conditions, problems in their home lives, who are maybe drinking alcohol? Those are cases we’d rule out from participation in the RCTs.”
“The patients in our study walked into our clinics saying, ‘You know what, doctor, my mind isn’t working very good. I’m depressed, I can’t think, I can’t focus, I’m missing work, my boss is on my case, I’m making errors. I need help.’ These are the kinds of practicalities we wanted to address,” explained Dr. Chokka, a psychiatrist at Grey Nuns Community Hospital in Edmonton, Can.
The primary endpoint in AtWoRK was the correlation between changes in patients’ self-reported cognitive symptoms on the 20-item Perceived Deficits Questionnaire–Depression (PDQ-D-20) and changes in work productivity loss measured on the Work Limitations Questionnaire (WLQ) at week 12. Those 12-week results were recently published (CNS Spectr. 2018 May 24:1-10). At the ECNP congress, Dr. Chokka presented the expanded 52-week outcomes.
The correlation between change from baseline to week 12 in PDQ-D-20 and change in WLQ was strong (r = 0.606), and it remained strong at week 52 (r = 0.731; P less than .001).
At 52 weeks on vortioxetine, 77% of patients fulfilled criteria for MDD response, which required at least a 50% reduction in Quick Inventory of Depressive Symptomatology – Self-Report (QIDS-SR) score from baseline, and 56% for disease remission, which meant the QIDS-SR score was 5 or less. The response and remission rates were 71% and 45%, respectively, in the 107 subjects for whom the drug was the first treatment for their current MDD episode and 83% and 67% for the 112 switched to vortioxetine at study outset because the antidepressant they’d been on was ineffective.
Subjects also displayed significant improvement at 12 and 52 weeks in mood as assessed using QIDS-SR and global functioning as measured using the Sheehan Disability Scale (SDS). Of note, however, improvement in cognitive symptoms was independent of and not predictive of improvement in overall depressive symptoms on the QIDS-SR. Nor did improvement in depressive symptoms predict functional outcomes as assessed by the WLQ or SDS.
In Dr. Chokka’s view, these findings have clear implications for clinical practice: “In the past we thought that, if we can get the mood better, things will all get better. We now we know that treating depression is about more than just getting the mood better.”
Vortioxetine is an antidepressant with multiple agonist and antagonist effects on various 5-HT serotonin receptors.
The AtWoRK study was supported by Lundbeck Canada. Dr. Chokka reported receiving research grants from and serving on advisory boards and as a speaker for that company and others.
SOURCE: Chokka P. ECNP, P.022.
BARCELONA – (Assessment in Work Productivity and the Relationship with Cognitive Symptoms).
“We found that as patients rated themselves as improved in terms of cognition – ‘I can think better,’ ‘I can focus,’ ‘I’m concentrating better’ – there was a strong correlation at 12 weeks and later extended to 1 year with improved work productivity by as much as 75%. It’s pretty dramatic,” lead investigator Pratap Chokka, MD, said in an interview at the annual congress of the European College of Neuropsychopharmacology.
AtWoRK was a multicenter, open-label, naturalistic intervention study in which 219 gainfully employed Canadian adults with major depressive disorder (MDD) who had presented to primary care physicians or psychiatrists were placed on vortioxetine (Trintellex) flexibly dosed at 10-20 mg/day and scheduled for routine follow-up visits every 4 weeks for 52 weeks.
This was a patient population with severe depression, severe cognitive dysfunction, severe anxiety, and substantial functional impairment as reflected in their baseline scores on a variety of validated measures (see graphic). The study was designed to emulate real-world clinical practice.
“We know that patients with depression are very impaired in terms of work productivity. Depressed patients really suffer from absenteeism and presenteeism [reduced productivity at work caused by depression]. And very few naturalistic studies have been done in working patients with depression,” according to Dr. Chokka. “The randomized trials are really important. They show us that a drug is working. But in terms of the real world that I work in, I need to have effectiveness: Does the drug work in patients with comorbid conditions, problems in their home lives, who are maybe drinking alcohol? Those are cases we’d rule out from participation in the RCTs.”
“The patients in our study walked into our clinics saying, ‘You know what, doctor, my mind isn’t working very good. I’m depressed, I can’t think, I can’t focus, I’m missing work, my boss is on my case, I’m making errors. I need help.’ These are the kinds of practicalities we wanted to address,” explained Dr. Chokka, a psychiatrist at Grey Nuns Community Hospital in Edmonton, Can.
The primary endpoint in AtWoRK was the correlation between changes in patients’ self-reported cognitive symptoms on the 20-item Perceived Deficits Questionnaire–Depression (PDQ-D-20) and changes in work productivity loss measured on the Work Limitations Questionnaire (WLQ) at week 12. Those 12-week results were recently published (CNS Spectr. 2018 May 24:1-10). At the ECNP congress, Dr. Chokka presented the expanded 52-week outcomes.
The correlation between change from baseline to week 12 in PDQ-D-20 and change in WLQ was strong (r = 0.606), and it remained strong at week 52 (r = 0.731; P less than .001).
At 52 weeks on vortioxetine, 77% of patients fulfilled criteria for MDD response, which required at least a 50% reduction in Quick Inventory of Depressive Symptomatology – Self-Report (QIDS-SR) score from baseline, and 56% for disease remission, which meant the QIDS-SR score was 5 or less. The response and remission rates were 71% and 45%, respectively, in the 107 subjects for whom the drug was the first treatment for their current MDD episode and 83% and 67% for the 112 switched to vortioxetine at study outset because the antidepressant they’d been on was ineffective.
Subjects also displayed significant improvement at 12 and 52 weeks in mood as assessed using QIDS-SR and global functioning as measured using the Sheehan Disability Scale (SDS). Of note, however, improvement in cognitive symptoms was independent of and not predictive of improvement in overall depressive symptoms on the QIDS-SR. Nor did improvement in depressive symptoms predict functional outcomes as assessed by the WLQ or SDS.
In Dr. Chokka’s view, these findings have clear implications for clinical practice: “In the past we thought that, if we can get the mood better, things will all get better. We now we know that treating depression is about more than just getting the mood better.”
Vortioxetine is an antidepressant with multiple agonist and antagonist effects on various 5-HT serotonin receptors.
The AtWoRK study was supported by Lundbeck Canada. Dr. Chokka reported receiving research grants from and serving on advisory boards and as a speaker for that company and others.
SOURCE: Chokka P. ECNP, P.022.
REPORTING FROM THE ECNP CONGRESS
Key clinical point: Treat cognitive symptoms of depression to improve impaired work productivity.
Major finding: Impaired work productivity in depressed patients improved greatly in response to reduction in cognitive symptoms, but not with enhanced mood.
Study details: A 52-week, multicenter, open-label study in which 219 employed adults with major depression were placed on vortioxetine and serially assessed for changes in cognitive dysfunction, mood, and work productivity.
Disclosures: The AtWoRK study was supported by Lundbeck Canada. The presenter reported receiving research grants from and serving on advisory boards and as a speaker for that company and others.
Source: Chokka P. ECNP, P.022.