Oritavancin and dalbavancin are long acting lipoglycopeptides indicated for the treatment of acute bacterial skin and skin structure infections (ABSSSI).1,2 Largely due to their long half-lives, prolonged tissue concentrations at sites of infection, tolerability, and minimal requirement for therapeutic drug monitoring, these agents are attractive options in outpatient settings.3,4 A 1- or 2-dose treatment of oritavancin and dalbavancin may be sufficient for conditions traditionally treated with outpatient parenteral antimicrobial therapy (OPAT) via peripherally inserted central catheter (PICC).
Limited research supports the use of dalbavancin and oritavancin for bone and joint infections, infective endocarditis, and bloodstream infections (BSIs). However, the US Food and Drug Administration has approved an indication for the treatment of ABSSSI.3-9 Dosing for these off-label indications varies but typically consists of an initial intravenous (IV) dose (1000 mg, 1200 mg, or 1500 mg), with a subsequent dose 1 to 2 weeks later or administered once weekly.6-10
Due in part to the recent availability of oritavancin and dalbavancin relative to the publication of practice guidelines, their appropriate place in therapy continues to evolve based on emerging literature.11,12 One potential barrier of use for these medications is their cost. Based on the number of doses administered, the 2022 estimated total acquisition cost of therapy for oritavancin and dalbavancin was $1014 to $4397 and $3046 to $7150, respectively (eAppendix). Despite the high acquisition costs, these agents do not require the placement of an indwelling central line, can be administered in outpatient settings, and require minimal therapeutic dose monitoring compared to vancomycin.13-15 This medication use evaluation (MUE) compared the total cost of treatment with oritavancin and dalbavancin vs therapies traditionally used for OPAT or prolonged IV inpatient therapy.
METHODS
This retrospective MUE was conducted at the Boise Veterans Affairs Medical Center (BVAMC), a level 2 facility with an extensive rural catchment area. BVAMC provides many OPAT services, including medications, supplies, and dressing changes after initial clinic or inpatient education. Contracted vendors may also assist with at-home nursing care using supplies provided by the BVAMC. Cases were identified using an internal database of OPAT patients and those who received oritavancin or dalbavancin between September 1, 2017, and November 1, 2022. Patients aged ≥ 18 years who received ≥ 1 dose of oritavancin or dalbavancin for ABSSSI, osteomyelitis/joint infections, endocarditis, and BSI were included. Comparator treatments consisting of ≥ 1 week of vancomycin or daptomycin for ABSSSI, osteomyelitis/joint infections, endocarditis, and BSI were identified through review of OPAT and Infectious Diseases service consults during the same timeframe. Patients were excluded if any antibiotic was prescribed by a non- VA clinician, if medications were not provided by OPAT, or if chart review did not identify an ABSSSI, osteomyelitis/ joint infection, or BSI diagnosis.
Electronic medical record review was conducted using a standardized data collection form (eAppendix). Data collected included demographics, infectious diagnosis, treatment administered, administration procedures and related visits and treatment locations, outcomes including clinical failure, adverse events (AEs), and hospital readmission.
Clinical failure was defined as readmission or death due to worsening infection or readmission secondary to a documented potential AE to the evaluated antibiotics within 90 days after initiation. Clinical failures excluded readmissions not associated with infection including comorbidities or elective procedures. AEs included new onset renal failure (serum creatinine ≥ 0.5 mg/dL), neutropenia (neutrophils ≤ 500), thrombocytopenia (platelets < 100,000), eosinophilia (> 15% eosinophils), or creatine phosphokinase > 10 times the upper limit of normal, and Clostridioides difficile (C. difficile) infection. Line complications included thrombophlebitis, local inflammation, or infection requiring line replacement (eAppendix).
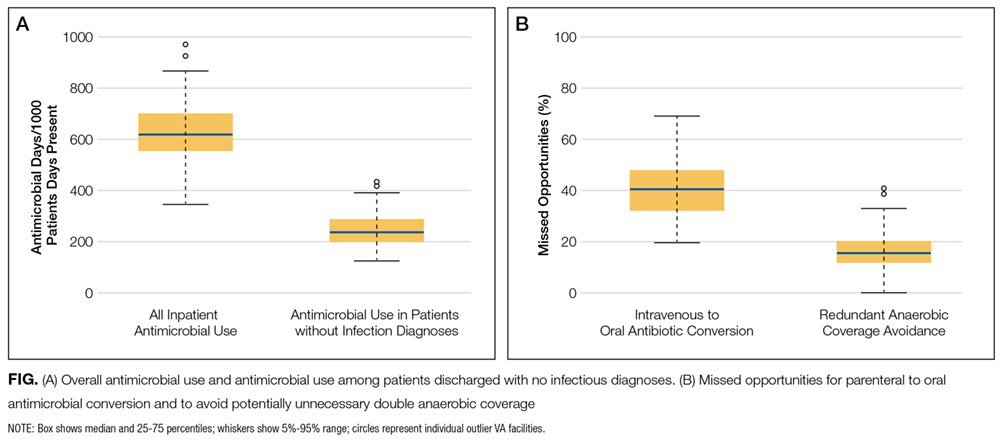
A cost-minimization approach was used to assess the total cost of treatment.16 Patients who received oritavancin or dalbavancin were matched with patients that received vancomycin and daptomycin for the same indication and about 1 month of initiation through the randomization function in Microsoft Excel. This accounted for changes in personnel, nonformulary drug approvals, cost, and changes in practice during the pandemic. Costs were calculated using a decision tree as a base model (Figure 1). In this model, each treatment dyad was assessed for the presence or absence of clinical failure, adverse event (medication and line complications), and treatment setting endpoints. Cost estimates were tabulated for each patient that received treatment using published VA data, literature, pharmacoeconomist guidance, or best faith effort based on workflow. 17-20 All cost estimates were based on 2022 figures or adjusted for inflation if obtained prior to 2022. Secondary endpoints of this analysis included estimated total cost of medication acquisition, administration supplies, laboratory monitoring, and human resources for OPAT visits or receiving home-health services.
This evaluation was classified by the BVAMC Medication Use Evaluation research determination subcommittee as a quality improvement project and was considered exempt from VA Human Subjects Research requirements based on the VA Policy Handbook guideline 1058.05.
RESULTS
The study identified 44 patients who received dalbavancin or oritavancin between September 1, 2017, and October 31, 2022. Thirty-nine patients were included in the analysis: 24 received oritavancin and 15 received dalbavancin and were matched by indication to 10 patients who received vancomycin and 8 patients who received daptomycin. Three patients could not be matched by indication of ABSSSI (Figure 2). Most patients were male, aged > 65 years, and were treated for osteomyelitis (Table 1). No patients were treated for infective endocarditis. A myriad of concomitant antibiotics were used to treat patients and culture results indicated that most infections treated with oritavancin and dalbavancin were polymicrobial.
The mean total cost of therapy per patient receiving oritavancin, dalbavancin, vancomycin, and daptomycin was $35,630, $59,612, $73,333, and $73,708, respectively (Figure 3). When stratified by indication, 27 patients (69%) in the oritavancin/dalbavancin group were treated for osteomyelitis/ joint infections (16 oritavancin, 11 dalbavancin), 9 patients (23%) were treated for BSI (6 oritavancin, 3 dalbavancin), and 3 patients (8%) were treated for ABSSSI (2 oritavancin, 1 dalbavancin). The mean cost per patient for osteomyelitis/joint infections with oritavancin, dalbavancin, vancomycin, and daptomycin was $34,678, $54,224, $87,488, and $85,044, respectively. The mean cost per patient for BSI for oritavancin, dalbavancin, vancomycin, and daptomycin was $35,048, $75,349, $40,305, and $68,068, respectively. The mean cost per patient for ABSSSI for oritavancin and dalbavancin was $44,771 and $71,672.51.
Estimated total drug cost represents the cost of drug acquisition, administration supplies, laboratory monitoring, and human resources for OPAT visits or receiving home health services. The mean cost per patient of drug-related therapy for oritavancin, dalbavancin, vancomycin, and daptomycin was $2203, $5924, $3637, and $7146, respectively (Table 2).
The mean cost per patient for osteomyelitis therapy for oritavancin, dalbavancin, vancomycin, and daptomycin was $2375, $6775, $4164, $8152, respectively. The mean cost of per patient for BSI treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $1737, $3475, $2409, and $1016, respectively. The mean cost per patient for oritavancin and dalbavancin for ABSSSI treatment, was $1553 and $3910, respectively.
Setting-related costs include expenses from inpatient admissions and postdischarge stays at community living centers (CLCs), skilled nursing facilities (SNFs), or rehabilitation facilities (RFs) for the duration of antimicrobial therapy. The mean setting-related therapy cost for osteomyelitis treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $27,852, $17,815, $83,324, and $72,856, respectively. The mean setting-related therapy cost per patient for BSI treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $33,310, $60,668, $37,734, and $67,074, respectively. The mean setting-related therapy cost per patient for ABSSSI treatment for oritavancin and dalbavancin was $43,218 and $67,762.00, respectively.
Six of 39 patients (15%) had clinical failure: 2 patients with oritavancin and 4 patients with dalbavancin. Four patients were readmitted for worsening infection and 2 for AEs. One patient (13%) in the daptomycin group had clinical failure due to readmission for worsening infection. There was no clinical failure with vancomycin. The costs associated with clinical failure per patient for oritavancin, dalbavancin, vancomycin, and daptomycin were $2925, $23,972, $0, and $3601, respectively (Table 3).
Thirty-eight patients (97%) who received oritavancin or dalbavancin had difficulty adhering to vancomycin or daptomycin OPAT. Oritavancin or dalbavancin was used in 10 patients (26%) who lacked support at home and 15 patients (38%) who had either a contraindication or previous failure with other antimicrobials, which were the most common explanations.
DISCUSSION
Long-acting lipoglycopeptides represent a potential alternative to home IV therapy that can avoid prolonged IV access with traditional OPAT. This offers significant advantages, allowing patients to be discharged from the hospital early, especially in rural areas with little OPAT infrastructure or those with logistic challenges. In this analysis, treatment with oritavancin for osteomyelitis, BSI, or ABSSSI, yielded an estimated cost savings of about $37,000 per patient, compared to treatment of matched indications with vancomycin and daptomycin. For every patient treated with dalbavancin for osteomyelitis, BSI, or ABSSSI, the cost savings was about $13,000 per patient, compared to treatment of matched indications for daptomycin and vancomycin. The estimated cost savings per patient for oritavancin was similar to previously published projections ($30,500 to $55,831).15
Cost savings were primarily driven by setting-related costs. The greatest contrast between the oritavancin and dalbavancin group compared to the vancomycin and daptomycin group was the length of stay in a postdischarge CLC, SNF, or RF setting. This analysis estimated that for every patient treated with oritavancin for osteomyelitis, the setting-related cost savings per patient was about $55,000 compared with vancomycin, and about $45,000 per patient compared with daptomycin. Furthermore, the estimated setting-related cost savings for osteomyelitis treatment with dalbavancin was about $65,000 compared with vancomycin and about $55,000 compared with daptomycin.
Clinical failure occurred with greater frequency in the oritavancin and dalbavancin groups (15%), compared with the vancomycin (0%) and daptomycin (13%) groups. Although the clinical failure rates in patients with osteomyelitis treated with oritavancin and dalbavancin compared with daptomycin were like those in previously published research (10%-30%), the rates of clinical failure for vancomycin in this analysis were lower than those in the oritavancin and dalbavancin group.8,21,22 The discrepancy in clinical failure rates between this analysis and previous research is likely due to selection bias. Based on the percentages of clinical failure found in the analysis, it is not surprising to note that the total clinical failure-related cost per patient was higher for oritavancin and dalbavancin compared to vancomycin, but similar between oritavancin and daptomycin.
This analysis also found that 15% of patients in the oritavancin and dalbavancin group experienced an AE compared to 10% of patients in the vancomycin group and none in the daptomycin group. In the oritavancin and dalbavancin group, the 2 most common AEs were infusion-related reactions and C. difficile colitis. Although infusion related reactions are easier to correspond to oritavancin and dalbavancin, it becomes difficult to definitively attribute the occurrence of C. difficile to these drugs as many patients were receiving concomitant antibiotics. Although not a primary or secondary objective, the rate of IV-line AEs were more prevalent in the vancomycin (10%), and daptomycin (13%) groups, compared to none in the oritavancin and dalbavancin group. This finding was expected; oritavancin and dalbavancin do not require a central IV line for administration.
Pharmacoeconomic literature continues to emerge with long-acting lipoglycopeptides. A 2024 Italian retrospective single-center analysis of 62 patients reported mean cost reductions > €3200 per patient (> $3400) given dalbavancin compared with the standard of care for ABSSSI or more deep-seeded infections such as osteomyelitis.23 A 2023 Spanish observational multicenter analysis of 124 patients with infective endocarditis demonstrated high efficacy, safety and cost-effectiveness with dalbavancin vs conventional treatments, with a mean savings of > €5548 per patient (> $6200).24 An analysis of the implementation of a dalbavancin order pathway for ABSSSI to avert inpatient admissions at 11 US emergency departments found a mean cost savings of $5133 per patient and $1211 per hospitalization day avoided, compared with inpatient usual care.25
Conversely, a multicenter, retrospective study of 209 patients in a community-based health care system failed to show a financial benefit for dalbavancin use when compared to standard of care for ABSSSI with higher readmission rates.26 Turco et al also reported increased cost results for 64 patients who received dalbavancin vs standard of care for ABSSSI.27 These discordant findings in ABSSSI studies may be impacted by the authors' patient selection choices and cost assumptions, especially with significantly cheaper oral alternatives. More data are needed to best identify the optimal therapeutic use for the long-acting lipoglycopeptides.
Limitations
The most significant limitation in this analysis was selection bias: 38 of 39 patients (97%) who received dalbavancin or oritavancin had a documented reason that described why OPAT therapy with traditional medications would not be optimal, including logistics, AEs, or clinical failures. Most patients treated with vancomycin and daptomycin were admitted into a SNF, RF, or CLC for the remainder of their treatment, allowing for closer monitoring and care compared to patients treated with oritavancin and dalbavancin, but at a greater cost. For patients sent to a community based SNF or RF, laboratory data were not available unless internally drawn or documented in the electronic medical record.
Additionally, not all cost data were available from VA sources; some were applied from literature, pharmacoeconomist, or best faith effort based on workflow. The cost data from third party contractors providing OPAT services to some BVAMC patients during the time frame of this analysis were not available. Due to its small sample size, outliers had the potential to affect averages reported and accuracy of the cost analysis. Emerging evidence suggests that daptomycin doses higher than the manufacturer-recommended regimen may be required for select indications, a factor that could affect cost, AEs, and efficacy outcomes.28 The acquisition cost of oritavancin and dalbavancin may vary by institution (ie, VA contract prices vs non- VA contract prices) and change over time. A current assessment of cost is needed to best visualize institutional benefit.
Finally, while the patient demographic of this MUE was highly representative of the demographic treated at the BVAMC (males aged >65 years), it may not be applicable to external patient populations. This analysis evaluated off-label indications for these medications. Consequently, this analysis would likely not be applicable to non-VA institution, as third-party payers (eg, insurance) are unlikely to cover medications for off-label indications.
CONCLUSIONS
This study found cost savings associated with the use of oritavancin and dalbavancin compared with vancomycin and daptomycin, particularly for the treatment of osteomyelitis. As safety and efficacy data continues to emerge, the use of long-acting lipoglycopeptides appears to be an increasingly attractive alternative option compared to traditional outpatient antimicrobial therapy, depending on the structure of the program. Larger, multicenter cost-effectiveness studies are needed to further establish the impact of these novel agents.
Cooper CC, Stein GE, Mitra S, Abubaker A, Havlichek DH. Long-acting lipoglycopeptides for the treatment of bone and joint infections. Surg Infect (Larchmt). 2021;22(8):771- 779. doi:10.1089/sur.2020.413
Simonetti O, Rizzetto G, Molinelli E, Cirioni O, Offidani A. Review: a safety profile of dalbavancin for on- and offlabel utilization. Ther Clin Risk Manag. 2021;17:223-232. doi:10.2147/TCRM.S271445
Bloem A, Bax HI, Yusuf E, Verkaik NJ. New-generation antibiotics for treatment of gram-positive infections: a review with focus on endocarditis and osteomyelitis. J Clin Med. 2021;10(8):1743. doi:10.3390/jcm10081743
Thomas G, Henao-Martínez AF, Franco-Paredes C, Chastain DB. Treatment of osteoarticular, cardiovascular, intravascular-catheter-related and other complicated infections with dalbavancin and oritavancin: a systematic review. Int J Antimicrob Agents. 2020;56(3):106069. doi:10.1016/j.ijantimicag.2020.106069
Rappo U, Puttagunta S, Shevchenko V, et al. Dalbavancin for the treatment of osteomyelitis in adult patients: a randomized clinical trial of efficacy and safety. Open Forum Infect Dis. 2018;6(1):ofy331. doi:10.1093/ofid/ofy331
Cain AR, Bremmer DN, Carr DR, et al. Effectiveness of dalbavancin compared with standard of care for the treatment of osteomyelitis: a real-world analysis. Open Forum Infect Dis. 2021;9(2):ofab589. doi:10.1093/ofid/ofab589
Van Hise NW, Chundi V, Didwania V, et al. Treatment of acute osteomyelitis with once-weekly oritavancin: a two-year, multicenter, retrospective study. Drugs Real World Outcomes. 2020;7(Suppl 1):41-45. doi:10.1007/s40801-020-00195-7
Cooper MM, Preslaski CR, Shihadeh KC, Hawkins KL, Jenkins TC. Multiple-dose dalbavancin regimens as the predominant treatment of deep-seated or endovascular infections: a scoping review. Open Forum Infect Dis. 2021;8(11):ofab486. doi:10.1093/ofid/ofab486
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2015;132(15):1435-1486. doi:10.1161/CIR.0000000000000296
Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin Infect Dis. 2015;61(6):e26-46. doi:10.1093/cid/civ482
Arrieta-Loitegui M, Caro-Teller JM, Ortiz-Pérez S, López- Medrano F, San Juan-Garrido R, Ferrari-Piquero JM. Effectiveness, safety, and cost analysis of dalbavancin in clinical practice. Eur J Hosp Pharm. 2022;29(1):55-58. doi:10.1136/ejhpharm-2020-002315
Pascale R, Maccaro A, Mikus E, et al. A retrospective multicentre study on dalbavancin effectiveness and cost-evaluation in sternotomic wound infection treatment: DALBA SWIT study. J Glob Antimicrob Resist. 2022;30:390-394. doi:10.1016/j.jgar.2022.07.018
Antosz K, Al-Hasan MN, Lu ZK, et at. Clinical utility and cost effectiveness of long-acting lipoglycopeptides used in deep seated infections among patients with social and economic barriers to care. Pharmacy (Basel). 2021;10(1):1. doi:10.3390/pharmacy10010001
Roberts MS. Economic aspects of evaluation. In: Friedman CP, Wyatt JC, eds. Evaluation Methods in Biomedical Informatics. 2nd ed. Springer; 2006:301-337.
Ektare V, Khachatryan A, Xue M, Dunne M, Johnson K, Stephens J. Assessing the economic value of avoiding hospital admissions by shifting the management of gram + acute bacterial skin and skin-structure infections to an outpatient care setting. J Med Econ. 2015;18(12):1092-1101. doi:10.3111/13696998.2015.1078339
Ruh CA, Parameswaran GI, Wojciechowski AL, Mergenhagen KA. Outcomes and pharmacoeconomic analysis of a home intravenous antibiotic infusion program in veterans. Clin Ther. 2015;37(11):2527-2535. doi:10.1016/j.clinthera.2015.09.009
Nakrani M, Yu D, Skikka M, et al. Comparison of vancomycin and daptomycin complications and interventions in outpatient parenteral antimicrobial therapy. Open Forum Infect Dis. 2020;7(Suppl 1):S361-S362. doi:10.1093/ofid/ofaa439.791
Scoble PJ, Reilly J, Tilloston GS. Real-world use of oritavancin for the treatment of osteomyelitis. Drugs Real World Outcomes. 2020;7(Suppl 1):46-54. doi:10.1007/s40801-020-00194-8
Segala D, Barbieri M, Di Nuzzo M, et al. Clinical, organizational, and pharmacoeconomic perspectives of dalbavancin vs standard of care in the infectious disease network. Glob Reg Health Technol Assess. 2024;11(Suppl 2):5-12. doi:10.33393/grhta.2024.3094
Gómez A, et al. EN-DALBACEN 2.0 Cohort: real-life study of dalbavancin as sequential/consolidation therapy in patients with infective endocarditis due to Gram-positive cocci. Int J Antimicrob Agents. 2023;62(3):106918. doi:10.1016/j.ijantimicag.2023.106918
LoVecchio F, McCarthy MW, Ye X, et al. Single intravenous dose dalbavancin pathway for the treatment of acute bacterial skin and skin structure infections: considerations for emergency department implementation and cost savings. J Emerg Med. 2024;67(2):e217-e229. doi:10.1016/j.jemermed.2024.03.003
Gonzalez J, Andrade DC, Niu J. Cost-consequence analysis of single-dose dalbavancin versus standard of care for the treatment of acute bacterial skin and skin structure infections in a multisite healthcare system. Clin Infect Dis. 2021;73(7):e1436-e1442. doi:10.1093/cid/ciaa1732
Turco NJ, Kane-Gill SL, Hernandez I, Oleksiuk LM, D’Amico F, Pickering AJ. A cost-minimization analysis of dalbavancin compared to conventional therapy for the outpatient treatment of acute bacterial skin and skin-structure infections. Expert Opin Pharmacother. 2018;19(4):319-325. doi:10.1080/14656566.2018.1442439
Jones TW, Jun AH, Michal JL, Olney WJ. High-dose daptomycin and clinical applications. Ann Pharmacother. 2021;55(11):1363-1378. doi:10.1177/1060028021991943
Danna Hanks, PharmD, MSHAa; Tomasz Z. Jodlowski, PharmD, BCPS, BCIDP, AAHIVPb; Karl Madaras-Kelly, PharmD, MPHb; Jennifer Diaz, PharmDb; Nicholas Vietri, MD, MSb
Author affiliations aSt. Luke’s Cancer Institute, Boise, Idaho bBoise Veterans Affairs Medical Center, Idaho
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Correspondence: Tomasz Jodlowski (tomasz.jodlowski@va.gov)
Fed Pract. 2025;42(6). Published online June 17. doi:10.12788/fp.0571
Danna Hanks, PharmD, MSHAa; Tomasz Z. Jodlowski, PharmD, BCPS, BCIDP, AAHIVPb; Karl Madaras-Kelly, PharmD, MPHb; Jennifer Diaz, PharmDb; Nicholas Vietri, MD, MSb
Author affiliations aSt. Luke’s Cancer Institute, Boise, Idaho bBoise Veterans Affairs Medical Center, Idaho
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Correspondence: Tomasz Jodlowski (tomasz.jodlowski@va.gov)
Fed Pract. 2025;42(6). Published online June 17. doi:10.12788/fp.0571
Author and Disclosure Information
Danna Hanks, PharmD, MSHAa; Tomasz Z. Jodlowski, PharmD, BCPS, BCIDP, AAHIVPb; Karl Madaras-Kelly, PharmD, MPHb; Jennifer Diaz, PharmDb; Nicholas Vietri, MD, MSb
Author affiliations aSt. Luke’s Cancer Institute, Boise, Idaho bBoise Veterans Affairs Medical Center, Idaho
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Correspondence: Tomasz Jodlowski (tomasz.jodlowski@va.gov)
Fed Pract. 2025;42(6). Published online June 17. doi:10.12788/fp.0571
Oritavancin and dalbavancin are long acting lipoglycopeptides indicated for the treatment of acute bacterial skin and skin structure infections (ABSSSI).1,2 Largely due to their long half-lives, prolonged tissue concentrations at sites of infection, tolerability, and minimal requirement for therapeutic drug monitoring, these agents are attractive options in outpatient settings.3,4 A 1- or 2-dose treatment of oritavancin and dalbavancin may be sufficient for conditions traditionally treated with outpatient parenteral antimicrobial therapy (OPAT) via peripherally inserted central catheter (PICC).
Limited research supports the use of dalbavancin and oritavancin for bone and joint infections, infective endocarditis, and bloodstream infections (BSIs). However, the US Food and Drug Administration has approved an indication for the treatment of ABSSSI.3-9 Dosing for these off-label indications varies but typically consists of an initial intravenous (IV) dose (1000 mg, 1200 mg, or 1500 mg), with a subsequent dose 1 to 2 weeks later or administered once weekly.6-10
Due in part to the recent availability of oritavancin and dalbavancin relative to the publication of practice guidelines, their appropriate place in therapy continues to evolve based on emerging literature.11,12 One potential barrier of use for these medications is their cost. Based on the number of doses administered, the 2022 estimated total acquisition cost of therapy for oritavancin and dalbavancin was $1014 to $4397 and $3046 to $7150, respectively (eAppendix). Despite the high acquisition costs, these agents do not require the placement of an indwelling central line, can be administered in outpatient settings, and require minimal therapeutic dose monitoring compared to vancomycin.13-15 This medication use evaluation (MUE) compared the total cost of treatment with oritavancin and dalbavancin vs therapies traditionally used for OPAT or prolonged IV inpatient therapy.
METHODS
This retrospective MUE was conducted at the Boise Veterans Affairs Medical Center (BVAMC), a level 2 facility with an extensive rural catchment area. BVAMC provides many OPAT services, including medications, supplies, and dressing changes after initial clinic or inpatient education. Contracted vendors may also assist with at-home nursing care using supplies provided by the BVAMC. Cases were identified using an internal database of OPAT patients and those who received oritavancin or dalbavancin between September 1, 2017, and November 1, 2022. Patients aged ≥ 18 years who received ≥ 1 dose of oritavancin or dalbavancin for ABSSSI, osteomyelitis/joint infections, endocarditis, and BSI were included. Comparator treatments consisting of ≥ 1 week of vancomycin or daptomycin for ABSSSI, osteomyelitis/joint infections, endocarditis, and BSI were identified through review of OPAT and Infectious Diseases service consults during the same timeframe. Patients were excluded if any antibiotic was prescribed by a non- VA clinician, if medications were not provided by OPAT, or if chart review did not identify an ABSSSI, osteomyelitis/ joint infection, or BSI diagnosis.
Electronic medical record review was conducted using a standardized data collection form (eAppendix). Data collected included demographics, infectious diagnosis, treatment administered, administration procedures and related visits and treatment locations, outcomes including clinical failure, adverse events (AEs), and hospital readmission.
Clinical failure was defined as readmission or death due to worsening infection or readmission secondary to a documented potential AE to the evaluated antibiotics within 90 days after initiation. Clinical failures excluded readmissions not associated with infection including comorbidities or elective procedures. AEs included new onset renal failure (serum creatinine ≥ 0.5 mg/dL), neutropenia (neutrophils ≤ 500), thrombocytopenia (platelets < 100,000), eosinophilia (> 15% eosinophils), or creatine phosphokinase > 10 times the upper limit of normal, and Clostridioides difficile (C. difficile) infection. Line complications included thrombophlebitis, local inflammation, or infection requiring line replacement (eAppendix).
A cost-minimization approach was used to assess the total cost of treatment.16 Patients who received oritavancin or dalbavancin were matched with patients that received vancomycin and daptomycin for the same indication and about 1 month of initiation through the randomization function in Microsoft Excel. This accounted for changes in personnel, nonformulary drug approvals, cost, and changes in practice during the pandemic. Costs were calculated using a decision tree as a base model (Figure 1). In this model, each treatment dyad was assessed for the presence or absence of clinical failure, adverse event (medication and line complications), and treatment setting endpoints. Cost estimates were tabulated for each patient that received treatment using published VA data, literature, pharmacoeconomist guidance, or best faith effort based on workflow. 17-20 All cost estimates were based on 2022 figures or adjusted for inflation if obtained prior to 2022. Secondary endpoints of this analysis included estimated total cost of medication acquisition, administration supplies, laboratory monitoring, and human resources for OPAT visits or receiving home-health services.
This evaluation was classified by the BVAMC Medication Use Evaluation research determination subcommittee as a quality improvement project and was considered exempt from VA Human Subjects Research requirements based on the VA Policy Handbook guideline 1058.05.
RESULTS
The study identified 44 patients who received dalbavancin or oritavancin between September 1, 2017, and October 31, 2022. Thirty-nine patients were included in the analysis: 24 received oritavancin and 15 received dalbavancin and were matched by indication to 10 patients who received vancomycin and 8 patients who received daptomycin. Three patients could not be matched by indication of ABSSSI (Figure 2). Most patients were male, aged > 65 years, and were treated for osteomyelitis (Table 1). No patients were treated for infective endocarditis. A myriad of concomitant antibiotics were used to treat patients and culture results indicated that most infections treated with oritavancin and dalbavancin were polymicrobial.
The mean total cost of therapy per patient receiving oritavancin, dalbavancin, vancomycin, and daptomycin was $35,630, $59,612, $73,333, and $73,708, respectively (Figure 3). When stratified by indication, 27 patients (69%) in the oritavancin/dalbavancin group were treated for osteomyelitis/ joint infections (16 oritavancin, 11 dalbavancin), 9 patients (23%) were treated for BSI (6 oritavancin, 3 dalbavancin), and 3 patients (8%) were treated for ABSSSI (2 oritavancin, 1 dalbavancin). The mean cost per patient for osteomyelitis/joint infections with oritavancin, dalbavancin, vancomycin, and daptomycin was $34,678, $54,224, $87,488, and $85,044, respectively. The mean cost per patient for BSI for oritavancin, dalbavancin, vancomycin, and daptomycin was $35,048, $75,349, $40,305, and $68,068, respectively. The mean cost per patient for ABSSSI for oritavancin and dalbavancin was $44,771 and $71,672.51.
Estimated total drug cost represents the cost of drug acquisition, administration supplies, laboratory monitoring, and human resources for OPAT visits or receiving home health services. The mean cost per patient of drug-related therapy for oritavancin, dalbavancin, vancomycin, and daptomycin was $2203, $5924, $3637, and $7146, respectively (Table 2).
The mean cost per patient for osteomyelitis therapy for oritavancin, dalbavancin, vancomycin, and daptomycin was $2375, $6775, $4164, $8152, respectively. The mean cost of per patient for BSI treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $1737, $3475, $2409, and $1016, respectively. The mean cost per patient for oritavancin and dalbavancin for ABSSSI treatment, was $1553 and $3910, respectively.
Setting-related costs include expenses from inpatient admissions and postdischarge stays at community living centers (CLCs), skilled nursing facilities (SNFs), or rehabilitation facilities (RFs) for the duration of antimicrobial therapy. The mean setting-related therapy cost for osteomyelitis treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $27,852, $17,815, $83,324, and $72,856, respectively. The mean setting-related therapy cost per patient for BSI treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $33,310, $60,668, $37,734, and $67,074, respectively. The mean setting-related therapy cost per patient for ABSSSI treatment for oritavancin and dalbavancin was $43,218 and $67,762.00, respectively.
Six of 39 patients (15%) had clinical failure: 2 patients with oritavancin and 4 patients with dalbavancin. Four patients were readmitted for worsening infection and 2 for AEs. One patient (13%) in the daptomycin group had clinical failure due to readmission for worsening infection. There was no clinical failure with vancomycin. The costs associated with clinical failure per patient for oritavancin, dalbavancin, vancomycin, and daptomycin were $2925, $23,972, $0, and $3601, respectively (Table 3).
Thirty-eight patients (97%) who received oritavancin or dalbavancin had difficulty adhering to vancomycin or daptomycin OPAT. Oritavancin or dalbavancin was used in 10 patients (26%) who lacked support at home and 15 patients (38%) who had either a contraindication or previous failure with other antimicrobials, which were the most common explanations.
DISCUSSION
Long-acting lipoglycopeptides represent a potential alternative to home IV therapy that can avoid prolonged IV access with traditional OPAT. This offers significant advantages, allowing patients to be discharged from the hospital early, especially in rural areas with little OPAT infrastructure or those with logistic challenges. In this analysis, treatment with oritavancin for osteomyelitis, BSI, or ABSSSI, yielded an estimated cost savings of about $37,000 per patient, compared to treatment of matched indications with vancomycin and daptomycin. For every patient treated with dalbavancin for osteomyelitis, BSI, or ABSSSI, the cost savings was about $13,000 per patient, compared to treatment of matched indications for daptomycin and vancomycin. The estimated cost savings per patient for oritavancin was similar to previously published projections ($30,500 to $55,831).15
Cost savings were primarily driven by setting-related costs. The greatest contrast between the oritavancin and dalbavancin group compared to the vancomycin and daptomycin group was the length of stay in a postdischarge CLC, SNF, or RF setting. This analysis estimated that for every patient treated with oritavancin for osteomyelitis, the setting-related cost savings per patient was about $55,000 compared with vancomycin, and about $45,000 per patient compared with daptomycin. Furthermore, the estimated setting-related cost savings for osteomyelitis treatment with dalbavancin was about $65,000 compared with vancomycin and about $55,000 compared with daptomycin.
Clinical failure occurred with greater frequency in the oritavancin and dalbavancin groups (15%), compared with the vancomycin (0%) and daptomycin (13%) groups. Although the clinical failure rates in patients with osteomyelitis treated with oritavancin and dalbavancin compared with daptomycin were like those in previously published research (10%-30%), the rates of clinical failure for vancomycin in this analysis were lower than those in the oritavancin and dalbavancin group.8,21,22 The discrepancy in clinical failure rates between this analysis and previous research is likely due to selection bias. Based on the percentages of clinical failure found in the analysis, it is not surprising to note that the total clinical failure-related cost per patient was higher for oritavancin and dalbavancin compared to vancomycin, but similar between oritavancin and daptomycin.
This analysis also found that 15% of patients in the oritavancin and dalbavancin group experienced an AE compared to 10% of patients in the vancomycin group and none in the daptomycin group. In the oritavancin and dalbavancin group, the 2 most common AEs were infusion-related reactions and C. difficile colitis. Although infusion related reactions are easier to correspond to oritavancin and dalbavancin, it becomes difficult to definitively attribute the occurrence of C. difficile to these drugs as many patients were receiving concomitant antibiotics. Although not a primary or secondary objective, the rate of IV-line AEs were more prevalent in the vancomycin (10%), and daptomycin (13%) groups, compared to none in the oritavancin and dalbavancin group. This finding was expected; oritavancin and dalbavancin do not require a central IV line for administration.
Pharmacoeconomic literature continues to emerge with long-acting lipoglycopeptides. A 2024 Italian retrospective single-center analysis of 62 patients reported mean cost reductions > €3200 per patient (> $3400) given dalbavancin compared with the standard of care for ABSSSI or more deep-seeded infections such as osteomyelitis.23 A 2023 Spanish observational multicenter analysis of 124 patients with infective endocarditis demonstrated high efficacy, safety and cost-effectiveness with dalbavancin vs conventional treatments, with a mean savings of > €5548 per patient (> $6200).24 An analysis of the implementation of a dalbavancin order pathway for ABSSSI to avert inpatient admissions at 11 US emergency departments found a mean cost savings of $5133 per patient and $1211 per hospitalization day avoided, compared with inpatient usual care.25
Conversely, a multicenter, retrospective study of 209 patients in a community-based health care system failed to show a financial benefit for dalbavancin use when compared to standard of care for ABSSSI with higher readmission rates.26 Turco et al also reported increased cost results for 64 patients who received dalbavancin vs standard of care for ABSSSI.27 These discordant findings in ABSSSI studies may be impacted by the authors' patient selection choices and cost assumptions, especially with significantly cheaper oral alternatives. More data are needed to best identify the optimal therapeutic use for the long-acting lipoglycopeptides.
Limitations
The most significant limitation in this analysis was selection bias: 38 of 39 patients (97%) who received dalbavancin or oritavancin had a documented reason that described why OPAT therapy with traditional medications would not be optimal, including logistics, AEs, or clinical failures. Most patients treated with vancomycin and daptomycin were admitted into a SNF, RF, or CLC for the remainder of their treatment, allowing for closer monitoring and care compared to patients treated with oritavancin and dalbavancin, but at a greater cost. For patients sent to a community based SNF or RF, laboratory data were not available unless internally drawn or documented in the electronic medical record.
Additionally, not all cost data were available from VA sources; some were applied from literature, pharmacoeconomist, or best faith effort based on workflow. The cost data from third party contractors providing OPAT services to some BVAMC patients during the time frame of this analysis were not available. Due to its small sample size, outliers had the potential to affect averages reported and accuracy of the cost analysis. Emerging evidence suggests that daptomycin doses higher than the manufacturer-recommended regimen may be required for select indications, a factor that could affect cost, AEs, and efficacy outcomes.28 The acquisition cost of oritavancin and dalbavancin may vary by institution (ie, VA contract prices vs non- VA contract prices) and change over time. A current assessment of cost is needed to best visualize institutional benefit.
Finally, while the patient demographic of this MUE was highly representative of the demographic treated at the BVAMC (males aged >65 years), it may not be applicable to external patient populations. This analysis evaluated off-label indications for these medications. Consequently, this analysis would likely not be applicable to non-VA institution, as third-party payers (eg, insurance) are unlikely to cover medications for off-label indications.
CONCLUSIONS
This study found cost savings associated with the use of oritavancin and dalbavancin compared with vancomycin and daptomycin, particularly for the treatment of osteomyelitis. As safety and efficacy data continues to emerge, the use of long-acting lipoglycopeptides appears to be an increasingly attractive alternative option compared to traditional outpatient antimicrobial therapy, depending on the structure of the program. Larger, multicenter cost-effectiveness studies are needed to further establish the impact of these novel agents.
Oritavancin and dalbavancin are long acting lipoglycopeptides indicated for the treatment of acute bacterial skin and skin structure infections (ABSSSI).1,2 Largely due to their long half-lives, prolonged tissue concentrations at sites of infection, tolerability, and minimal requirement for therapeutic drug monitoring, these agents are attractive options in outpatient settings.3,4 A 1- or 2-dose treatment of oritavancin and dalbavancin may be sufficient for conditions traditionally treated with outpatient parenteral antimicrobial therapy (OPAT) via peripherally inserted central catheter (PICC).
Limited research supports the use of dalbavancin and oritavancin for bone and joint infections, infective endocarditis, and bloodstream infections (BSIs). However, the US Food and Drug Administration has approved an indication for the treatment of ABSSSI.3-9 Dosing for these off-label indications varies but typically consists of an initial intravenous (IV) dose (1000 mg, 1200 mg, or 1500 mg), with a subsequent dose 1 to 2 weeks later or administered once weekly.6-10
Due in part to the recent availability of oritavancin and dalbavancin relative to the publication of practice guidelines, their appropriate place in therapy continues to evolve based on emerging literature.11,12 One potential barrier of use for these medications is their cost. Based on the number of doses administered, the 2022 estimated total acquisition cost of therapy for oritavancin and dalbavancin was $1014 to $4397 and $3046 to $7150, respectively (eAppendix). Despite the high acquisition costs, these agents do not require the placement of an indwelling central line, can be administered in outpatient settings, and require minimal therapeutic dose monitoring compared to vancomycin.13-15 This medication use evaluation (MUE) compared the total cost of treatment with oritavancin and dalbavancin vs therapies traditionally used for OPAT or prolonged IV inpatient therapy.
METHODS
This retrospective MUE was conducted at the Boise Veterans Affairs Medical Center (BVAMC), a level 2 facility with an extensive rural catchment area. BVAMC provides many OPAT services, including medications, supplies, and dressing changes after initial clinic or inpatient education. Contracted vendors may also assist with at-home nursing care using supplies provided by the BVAMC. Cases were identified using an internal database of OPAT patients and those who received oritavancin or dalbavancin between September 1, 2017, and November 1, 2022. Patients aged ≥ 18 years who received ≥ 1 dose of oritavancin or dalbavancin for ABSSSI, osteomyelitis/joint infections, endocarditis, and BSI were included. Comparator treatments consisting of ≥ 1 week of vancomycin or daptomycin for ABSSSI, osteomyelitis/joint infections, endocarditis, and BSI were identified through review of OPAT and Infectious Diseases service consults during the same timeframe. Patients were excluded if any antibiotic was prescribed by a non- VA clinician, if medications were not provided by OPAT, or if chart review did not identify an ABSSSI, osteomyelitis/ joint infection, or BSI diagnosis.
Electronic medical record review was conducted using a standardized data collection form (eAppendix). Data collected included demographics, infectious diagnosis, treatment administered, administration procedures and related visits and treatment locations, outcomes including clinical failure, adverse events (AEs), and hospital readmission.
Clinical failure was defined as readmission or death due to worsening infection or readmission secondary to a documented potential AE to the evaluated antibiotics within 90 days after initiation. Clinical failures excluded readmissions not associated with infection including comorbidities or elective procedures. AEs included new onset renal failure (serum creatinine ≥ 0.5 mg/dL), neutropenia (neutrophils ≤ 500), thrombocytopenia (platelets < 100,000), eosinophilia (> 15% eosinophils), or creatine phosphokinase > 10 times the upper limit of normal, and Clostridioides difficile (C. difficile) infection. Line complications included thrombophlebitis, local inflammation, or infection requiring line replacement (eAppendix).
A cost-minimization approach was used to assess the total cost of treatment.16 Patients who received oritavancin or dalbavancin were matched with patients that received vancomycin and daptomycin for the same indication and about 1 month of initiation through the randomization function in Microsoft Excel. This accounted for changes in personnel, nonformulary drug approvals, cost, and changes in practice during the pandemic. Costs were calculated using a decision tree as a base model (Figure 1). In this model, each treatment dyad was assessed for the presence or absence of clinical failure, adverse event (medication and line complications), and treatment setting endpoints. Cost estimates were tabulated for each patient that received treatment using published VA data, literature, pharmacoeconomist guidance, or best faith effort based on workflow. 17-20 All cost estimates were based on 2022 figures or adjusted for inflation if obtained prior to 2022. Secondary endpoints of this analysis included estimated total cost of medication acquisition, administration supplies, laboratory monitoring, and human resources for OPAT visits or receiving home-health services.
This evaluation was classified by the BVAMC Medication Use Evaluation research determination subcommittee as a quality improvement project and was considered exempt from VA Human Subjects Research requirements based on the VA Policy Handbook guideline 1058.05.
RESULTS
The study identified 44 patients who received dalbavancin or oritavancin between September 1, 2017, and October 31, 2022. Thirty-nine patients were included in the analysis: 24 received oritavancin and 15 received dalbavancin and were matched by indication to 10 patients who received vancomycin and 8 patients who received daptomycin. Three patients could not be matched by indication of ABSSSI (Figure 2). Most patients were male, aged > 65 years, and were treated for osteomyelitis (Table 1). No patients were treated for infective endocarditis. A myriad of concomitant antibiotics were used to treat patients and culture results indicated that most infections treated with oritavancin and dalbavancin were polymicrobial.
The mean total cost of therapy per patient receiving oritavancin, dalbavancin, vancomycin, and daptomycin was $35,630, $59,612, $73,333, and $73,708, respectively (Figure 3). When stratified by indication, 27 patients (69%) in the oritavancin/dalbavancin group were treated for osteomyelitis/ joint infections (16 oritavancin, 11 dalbavancin), 9 patients (23%) were treated for BSI (6 oritavancin, 3 dalbavancin), and 3 patients (8%) were treated for ABSSSI (2 oritavancin, 1 dalbavancin). The mean cost per patient for osteomyelitis/joint infections with oritavancin, dalbavancin, vancomycin, and daptomycin was $34,678, $54,224, $87,488, and $85,044, respectively. The mean cost per patient for BSI for oritavancin, dalbavancin, vancomycin, and daptomycin was $35,048, $75,349, $40,305, and $68,068, respectively. The mean cost per patient for ABSSSI for oritavancin and dalbavancin was $44,771 and $71,672.51.
Estimated total drug cost represents the cost of drug acquisition, administration supplies, laboratory monitoring, and human resources for OPAT visits or receiving home health services. The mean cost per patient of drug-related therapy for oritavancin, dalbavancin, vancomycin, and daptomycin was $2203, $5924, $3637, and $7146, respectively (Table 2).
The mean cost per patient for osteomyelitis therapy for oritavancin, dalbavancin, vancomycin, and daptomycin was $2375, $6775, $4164, $8152, respectively. The mean cost of per patient for BSI treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $1737, $3475, $2409, and $1016, respectively. The mean cost per patient for oritavancin and dalbavancin for ABSSSI treatment, was $1553 and $3910, respectively.
Setting-related costs include expenses from inpatient admissions and postdischarge stays at community living centers (CLCs), skilled nursing facilities (SNFs), or rehabilitation facilities (RFs) for the duration of antimicrobial therapy. The mean setting-related therapy cost for osteomyelitis treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $27,852, $17,815, $83,324, and $72,856, respectively. The mean setting-related therapy cost per patient for BSI treatment with oritavancin, dalbavancin, vancomycin, and daptomycin was $33,310, $60,668, $37,734, and $67,074, respectively. The mean setting-related therapy cost per patient for ABSSSI treatment for oritavancin and dalbavancin was $43,218 and $67,762.00, respectively.
Six of 39 patients (15%) had clinical failure: 2 patients with oritavancin and 4 patients with dalbavancin. Four patients were readmitted for worsening infection and 2 for AEs. One patient (13%) in the daptomycin group had clinical failure due to readmission for worsening infection. There was no clinical failure with vancomycin. The costs associated with clinical failure per patient for oritavancin, dalbavancin, vancomycin, and daptomycin were $2925, $23,972, $0, and $3601, respectively (Table 3).
Thirty-eight patients (97%) who received oritavancin or dalbavancin had difficulty adhering to vancomycin or daptomycin OPAT. Oritavancin or dalbavancin was used in 10 patients (26%) who lacked support at home and 15 patients (38%) who had either a contraindication or previous failure with other antimicrobials, which were the most common explanations.
DISCUSSION
Long-acting lipoglycopeptides represent a potential alternative to home IV therapy that can avoid prolonged IV access with traditional OPAT. This offers significant advantages, allowing patients to be discharged from the hospital early, especially in rural areas with little OPAT infrastructure or those with logistic challenges. In this analysis, treatment with oritavancin for osteomyelitis, BSI, or ABSSSI, yielded an estimated cost savings of about $37,000 per patient, compared to treatment of matched indications with vancomycin and daptomycin. For every patient treated with dalbavancin for osteomyelitis, BSI, or ABSSSI, the cost savings was about $13,000 per patient, compared to treatment of matched indications for daptomycin and vancomycin. The estimated cost savings per patient for oritavancin was similar to previously published projections ($30,500 to $55,831).15
Cost savings were primarily driven by setting-related costs. The greatest contrast between the oritavancin and dalbavancin group compared to the vancomycin and daptomycin group was the length of stay in a postdischarge CLC, SNF, or RF setting. This analysis estimated that for every patient treated with oritavancin for osteomyelitis, the setting-related cost savings per patient was about $55,000 compared with vancomycin, and about $45,000 per patient compared with daptomycin. Furthermore, the estimated setting-related cost savings for osteomyelitis treatment with dalbavancin was about $65,000 compared with vancomycin and about $55,000 compared with daptomycin.
Clinical failure occurred with greater frequency in the oritavancin and dalbavancin groups (15%), compared with the vancomycin (0%) and daptomycin (13%) groups. Although the clinical failure rates in patients with osteomyelitis treated with oritavancin and dalbavancin compared with daptomycin were like those in previously published research (10%-30%), the rates of clinical failure for vancomycin in this analysis were lower than those in the oritavancin and dalbavancin group.8,21,22 The discrepancy in clinical failure rates between this analysis and previous research is likely due to selection bias. Based on the percentages of clinical failure found in the analysis, it is not surprising to note that the total clinical failure-related cost per patient was higher for oritavancin and dalbavancin compared to vancomycin, but similar between oritavancin and daptomycin.
This analysis also found that 15% of patients in the oritavancin and dalbavancin group experienced an AE compared to 10% of patients in the vancomycin group and none in the daptomycin group. In the oritavancin and dalbavancin group, the 2 most common AEs were infusion-related reactions and C. difficile colitis. Although infusion related reactions are easier to correspond to oritavancin and dalbavancin, it becomes difficult to definitively attribute the occurrence of C. difficile to these drugs as many patients were receiving concomitant antibiotics. Although not a primary or secondary objective, the rate of IV-line AEs were more prevalent in the vancomycin (10%), and daptomycin (13%) groups, compared to none in the oritavancin and dalbavancin group. This finding was expected; oritavancin and dalbavancin do not require a central IV line for administration.
Pharmacoeconomic literature continues to emerge with long-acting lipoglycopeptides. A 2024 Italian retrospective single-center analysis of 62 patients reported mean cost reductions > €3200 per patient (> $3400) given dalbavancin compared with the standard of care for ABSSSI or more deep-seeded infections such as osteomyelitis.23 A 2023 Spanish observational multicenter analysis of 124 patients with infective endocarditis demonstrated high efficacy, safety and cost-effectiveness with dalbavancin vs conventional treatments, with a mean savings of > €5548 per patient (> $6200).24 An analysis of the implementation of a dalbavancin order pathway for ABSSSI to avert inpatient admissions at 11 US emergency departments found a mean cost savings of $5133 per patient and $1211 per hospitalization day avoided, compared with inpatient usual care.25
Conversely, a multicenter, retrospective study of 209 patients in a community-based health care system failed to show a financial benefit for dalbavancin use when compared to standard of care for ABSSSI with higher readmission rates.26 Turco et al also reported increased cost results for 64 patients who received dalbavancin vs standard of care for ABSSSI.27 These discordant findings in ABSSSI studies may be impacted by the authors' patient selection choices and cost assumptions, especially with significantly cheaper oral alternatives. More data are needed to best identify the optimal therapeutic use for the long-acting lipoglycopeptides.
Limitations
The most significant limitation in this analysis was selection bias: 38 of 39 patients (97%) who received dalbavancin or oritavancin had a documented reason that described why OPAT therapy with traditional medications would not be optimal, including logistics, AEs, or clinical failures. Most patients treated with vancomycin and daptomycin were admitted into a SNF, RF, or CLC for the remainder of their treatment, allowing for closer monitoring and care compared to patients treated with oritavancin and dalbavancin, but at a greater cost. For patients sent to a community based SNF or RF, laboratory data were not available unless internally drawn or documented in the electronic medical record.
Additionally, not all cost data were available from VA sources; some were applied from literature, pharmacoeconomist, or best faith effort based on workflow. The cost data from third party contractors providing OPAT services to some BVAMC patients during the time frame of this analysis were not available. Due to its small sample size, outliers had the potential to affect averages reported and accuracy of the cost analysis. Emerging evidence suggests that daptomycin doses higher than the manufacturer-recommended regimen may be required for select indications, a factor that could affect cost, AEs, and efficacy outcomes.28 The acquisition cost of oritavancin and dalbavancin may vary by institution (ie, VA contract prices vs non- VA contract prices) and change over time. A current assessment of cost is needed to best visualize institutional benefit.
Finally, while the patient demographic of this MUE was highly representative of the demographic treated at the BVAMC (males aged >65 years), it may not be applicable to external patient populations. This analysis evaluated off-label indications for these medications. Consequently, this analysis would likely not be applicable to non-VA institution, as third-party payers (eg, insurance) are unlikely to cover medications for off-label indications.
CONCLUSIONS
This study found cost savings associated with the use of oritavancin and dalbavancin compared with vancomycin and daptomycin, particularly for the treatment of osteomyelitis. As safety and efficacy data continues to emerge, the use of long-acting lipoglycopeptides appears to be an increasingly attractive alternative option compared to traditional outpatient antimicrobial therapy, depending on the structure of the program. Larger, multicenter cost-effectiveness studies are needed to further establish the impact of these novel agents.
Cooper CC, Stein GE, Mitra S, Abubaker A, Havlichek DH. Long-acting lipoglycopeptides for the treatment of bone and joint infections. Surg Infect (Larchmt). 2021;22(8):771- 779. doi:10.1089/sur.2020.413
Simonetti O, Rizzetto G, Molinelli E, Cirioni O, Offidani A. Review: a safety profile of dalbavancin for on- and offlabel utilization. Ther Clin Risk Manag. 2021;17:223-232. doi:10.2147/TCRM.S271445
Bloem A, Bax HI, Yusuf E, Verkaik NJ. New-generation antibiotics for treatment of gram-positive infections: a review with focus on endocarditis and osteomyelitis. J Clin Med. 2021;10(8):1743. doi:10.3390/jcm10081743
Thomas G, Henao-Martínez AF, Franco-Paredes C, Chastain DB. Treatment of osteoarticular, cardiovascular, intravascular-catheter-related and other complicated infections with dalbavancin and oritavancin: a systematic review. Int J Antimicrob Agents. 2020;56(3):106069. doi:10.1016/j.ijantimicag.2020.106069
Rappo U, Puttagunta S, Shevchenko V, et al. Dalbavancin for the treatment of osteomyelitis in adult patients: a randomized clinical trial of efficacy and safety. Open Forum Infect Dis. 2018;6(1):ofy331. doi:10.1093/ofid/ofy331
Cain AR, Bremmer DN, Carr DR, et al. Effectiveness of dalbavancin compared with standard of care for the treatment of osteomyelitis: a real-world analysis. Open Forum Infect Dis. 2021;9(2):ofab589. doi:10.1093/ofid/ofab589
Van Hise NW, Chundi V, Didwania V, et al. Treatment of acute osteomyelitis with once-weekly oritavancin: a two-year, multicenter, retrospective study. Drugs Real World Outcomes. 2020;7(Suppl 1):41-45. doi:10.1007/s40801-020-00195-7
Cooper MM, Preslaski CR, Shihadeh KC, Hawkins KL, Jenkins TC. Multiple-dose dalbavancin regimens as the predominant treatment of deep-seated or endovascular infections: a scoping review. Open Forum Infect Dis. 2021;8(11):ofab486. doi:10.1093/ofid/ofab486
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2015;132(15):1435-1486. doi:10.1161/CIR.0000000000000296
Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin Infect Dis. 2015;61(6):e26-46. doi:10.1093/cid/civ482
Arrieta-Loitegui M, Caro-Teller JM, Ortiz-Pérez S, López- Medrano F, San Juan-Garrido R, Ferrari-Piquero JM. Effectiveness, safety, and cost analysis of dalbavancin in clinical practice. Eur J Hosp Pharm. 2022;29(1):55-58. doi:10.1136/ejhpharm-2020-002315
Pascale R, Maccaro A, Mikus E, et al. A retrospective multicentre study on dalbavancin effectiveness and cost-evaluation in sternotomic wound infection treatment: DALBA SWIT study. J Glob Antimicrob Resist. 2022;30:390-394. doi:10.1016/j.jgar.2022.07.018
Antosz K, Al-Hasan MN, Lu ZK, et at. Clinical utility and cost effectiveness of long-acting lipoglycopeptides used in deep seated infections among patients with social and economic barriers to care. Pharmacy (Basel). 2021;10(1):1. doi:10.3390/pharmacy10010001
Roberts MS. Economic aspects of evaluation. In: Friedman CP, Wyatt JC, eds. Evaluation Methods in Biomedical Informatics. 2nd ed. Springer; 2006:301-337.
Ektare V, Khachatryan A, Xue M, Dunne M, Johnson K, Stephens J. Assessing the economic value of avoiding hospital admissions by shifting the management of gram + acute bacterial skin and skin-structure infections to an outpatient care setting. J Med Econ. 2015;18(12):1092-1101. doi:10.3111/13696998.2015.1078339
Ruh CA, Parameswaran GI, Wojciechowski AL, Mergenhagen KA. Outcomes and pharmacoeconomic analysis of a home intravenous antibiotic infusion program in veterans. Clin Ther. 2015;37(11):2527-2535. doi:10.1016/j.clinthera.2015.09.009
Nakrani M, Yu D, Skikka M, et al. Comparison of vancomycin and daptomycin complications and interventions in outpatient parenteral antimicrobial therapy. Open Forum Infect Dis. 2020;7(Suppl 1):S361-S362. doi:10.1093/ofid/ofaa439.791
Scoble PJ, Reilly J, Tilloston GS. Real-world use of oritavancin for the treatment of osteomyelitis. Drugs Real World Outcomes. 2020;7(Suppl 1):46-54. doi:10.1007/s40801-020-00194-8
Segala D, Barbieri M, Di Nuzzo M, et al. Clinical, organizational, and pharmacoeconomic perspectives of dalbavancin vs standard of care in the infectious disease network. Glob Reg Health Technol Assess. 2024;11(Suppl 2):5-12. doi:10.33393/grhta.2024.3094
Gómez A, et al. EN-DALBACEN 2.0 Cohort: real-life study of dalbavancin as sequential/consolidation therapy in patients with infective endocarditis due to Gram-positive cocci. Int J Antimicrob Agents. 2023;62(3):106918. doi:10.1016/j.ijantimicag.2023.106918
LoVecchio F, McCarthy MW, Ye X, et al. Single intravenous dose dalbavancin pathway for the treatment of acute bacterial skin and skin structure infections: considerations for emergency department implementation and cost savings. J Emerg Med. 2024;67(2):e217-e229. doi:10.1016/j.jemermed.2024.03.003
Gonzalez J, Andrade DC, Niu J. Cost-consequence analysis of single-dose dalbavancin versus standard of care for the treatment of acute bacterial skin and skin structure infections in a multisite healthcare system. Clin Infect Dis. 2021;73(7):e1436-e1442. doi:10.1093/cid/ciaa1732
Turco NJ, Kane-Gill SL, Hernandez I, Oleksiuk LM, D’Amico F, Pickering AJ. A cost-minimization analysis of dalbavancin compared to conventional therapy for the outpatient treatment of acute bacterial skin and skin-structure infections. Expert Opin Pharmacother. 2018;19(4):319-325. doi:10.1080/14656566.2018.1442439
Jones TW, Jun AH, Michal JL, Olney WJ. High-dose daptomycin and clinical applications. Ann Pharmacother. 2021;55(11):1363-1378. doi:10.1177/1060028021991943
Cooper CC, Stein GE, Mitra S, Abubaker A, Havlichek DH. Long-acting lipoglycopeptides for the treatment of bone and joint infections. Surg Infect (Larchmt). 2021;22(8):771- 779. doi:10.1089/sur.2020.413
Simonetti O, Rizzetto G, Molinelli E, Cirioni O, Offidani A. Review: a safety profile of dalbavancin for on- and offlabel utilization. Ther Clin Risk Manag. 2021;17:223-232. doi:10.2147/TCRM.S271445
Bloem A, Bax HI, Yusuf E, Verkaik NJ. New-generation antibiotics for treatment of gram-positive infections: a review with focus on endocarditis and osteomyelitis. J Clin Med. 2021;10(8):1743. doi:10.3390/jcm10081743
Thomas G, Henao-Martínez AF, Franco-Paredes C, Chastain DB. Treatment of osteoarticular, cardiovascular, intravascular-catheter-related and other complicated infections with dalbavancin and oritavancin: a systematic review. Int J Antimicrob Agents. 2020;56(3):106069. doi:10.1016/j.ijantimicag.2020.106069
Rappo U, Puttagunta S, Shevchenko V, et al. Dalbavancin for the treatment of osteomyelitis in adult patients: a randomized clinical trial of efficacy and safety. Open Forum Infect Dis. 2018;6(1):ofy331. doi:10.1093/ofid/ofy331
Cain AR, Bremmer DN, Carr DR, et al. Effectiveness of dalbavancin compared with standard of care for the treatment of osteomyelitis: a real-world analysis. Open Forum Infect Dis. 2021;9(2):ofab589. doi:10.1093/ofid/ofab589
Van Hise NW, Chundi V, Didwania V, et al. Treatment of acute osteomyelitis with once-weekly oritavancin: a two-year, multicenter, retrospective study. Drugs Real World Outcomes. 2020;7(Suppl 1):41-45. doi:10.1007/s40801-020-00195-7
Cooper MM, Preslaski CR, Shihadeh KC, Hawkins KL, Jenkins TC. Multiple-dose dalbavancin regimens as the predominant treatment of deep-seated or endovascular infections: a scoping review. Open Forum Infect Dis. 2021;8(11):ofab486. doi:10.1093/ofid/ofab486
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2015;132(15):1435-1486. doi:10.1161/CIR.0000000000000296
Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin Infect Dis. 2015;61(6):e26-46. doi:10.1093/cid/civ482
Arrieta-Loitegui M, Caro-Teller JM, Ortiz-Pérez S, López- Medrano F, San Juan-Garrido R, Ferrari-Piquero JM. Effectiveness, safety, and cost analysis of dalbavancin in clinical practice. Eur J Hosp Pharm. 2022;29(1):55-58. doi:10.1136/ejhpharm-2020-002315
Pascale R, Maccaro A, Mikus E, et al. A retrospective multicentre study on dalbavancin effectiveness and cost-evaluation in sternotomic wound infection treatment: DALBA SWIT study. J Glob Antimicrob Resist. 2022;30:390-394. doi:10.1016/j.jgar.2022.07.018
Antosz K, Al-Hasan MN, Lu ZK, et at. Clinical utility and cost effectiveness of long-acting lipoglycopeptides used in deep seated infections among patients with social and economic barriers to care. Pharmacy (Basel). 2021;10(1):1. doi:10.3390/pharmacy10010001
Roberts MS. Economic aspects of evaluation. In: Friedman CP, Wyatt JC, eds. Evaluation Methods in Biomedical Informatics. 2nd ed. Springer; 2006:301-337.
Ektare V, Khachatryan A, Xue M, Dunne M, Johnson K, Stephens J. Assessing the economic value of avoiding hospital admissions by shifting the management of gram + acute bacterial skin and skin-structure infections to an outpatient care setting. J Med Econ. 2015;18(12):1092-1101. doi:10.3111/13696998.2015.1078339
Ruh CA, Parameswaran GI, Wojciechowski AL, Mergenhagen KA. Outcomes and pharmacoeconomic analysis of a home intravenous antibiotic infusion program in veterans. Clin Ther. 2015;37(11):2527-2535. doi:10.1016/j.clinthera.2015.09.009
Nakrani M, Yu D, Skikka M, et al. Comparison of vancomycin and daptomycin complications and interventions in outpatient parenteral antimicrobial therapy. Open Forum Infect Dis. 2020;7(Suppl 1):S361-S362. doi:10.1093/ofid/ofaa439.791
Scoble PJ, Reilly J, Tilloston GS. Real-world use of oritavancin for the treatment of osteomyelitis. Drugs Real World Outcomes. 2020;7(Suppl 1):46-54. doi:10.1007/s40801-020-00194-8
Segala D, Barbieri M, Di Nuzzo M, et al. Clinical, organizational, and pharmacoeconomic perspectives of dalbavancin vs standard of care in the infectious disease network. Glob Reg Health Technol Assess. 2024;11(Suppl 2):5-12. doi:10.33393/grhta.2024.3094
Gómez A, et al. EN-DALBACEN 2.0 Cohort: real-life study of dalbavancin as sequential/consolidation therapy in patients with infective endocarditis due to Gram-positive cocci. Int J Antimicrob Agents. 2023;62(3):106918. doi:10.1016/j.ijantimicag.2023.106918
LoVecchio F, McCarthy MW, Ye X, et al. Single intravenous dose dalbavancin pathway for the treatment of acute bacterial skin and skin structure infections: considerations for emergency department implementation and cost savings. J Emerg Med. 2024;67(2):e217-e229. doi:10.1016/j.jemermed.2024.03.003
Gonzalez J, Andrade DC, Niu J. Cost-consequence analysis of single-dose dalbavancin versus standard of care for the treatment of acute bacterial skin and skin structure infections in a multisite healthcare system. Clin Infect Dis. 2021;73(7):e1436-e1442. doi:10.1093/cid/ciaa1732
Turco NJ, Kane-Gill SL, Hernandez I, Oleksiuk LM, D’Amico F, Pickering AJ. A cost-minimization analysis of dalbavancin compared to conventional therapy for the outpatient treatment of acute bacterial skin and skin-structure infections. Expert Opin Pharmacother. 2018;19(4):319-325. doi:10.1080/14656566.2018.1442439
Jones TW, Jun AH, Michal JL, Olney WJ. High-dose daptomycin and clinical applications. Ann Pharmacother. 2021;55(11):1363-1378. doi:10.1177/1060028021991943
Inpatient antimicrobial utilization measures are associated with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
BACKGROUND: Antimicrobial stewardship programs (ASPs) have been advocated to improve antimicrobial utilization, but program implementation is variable.
OBJECTIVE: To determine associations of ASPs with facility characteristics and inpatient antimicrobial utilization measures in the Veterans Affairs (VA) system in 2012.
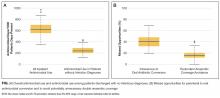
DESIGN: In 2012, the VA administered a survey on antimicrobial stewardship practices to designated ASP contacts at VA acute-care hospitals. From the survey, we identified 34 variables across three domains (evidence, organizational context, and facilitation) that were assessed, using multivariable LASSO (least absolute shrinkage and selection operator) regression, against four antimicrobial utilization measures: aggregate acute care antimicrobial use, antimicrobial use in patients with noninfectious primary discharge diagnoses, missed opportunities to convert from parenteral to oral antimicrobial therapy, and double anaerobic coverage.
SETTING: All 130 VA facilities with acute care services.
RESULTS: Variables associated with at least three favorable changes in antimicrobial utilization included presence of postgraduate physician/pharmacy training programs, number of antimicrobial-specific order sets, frequency of systematic de-escalation review, presence of pharmacists and/or infectious diseases (ID) attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist. Variables associated with two unfavorable measures included bed size, the level of engagement with VA Antimicrobial Stewardship Task Force online resources, and utilization of antimicrobial stop orders.
CONCLUSIONS: Formalization of ASP processes and presence of pharmacy and ID expertise are associated with favorable utilization. Systematic de-escalation review and order set establishment may be high-yield interventions.
Also in JHM
High prevalence of inappropriate benzodiazepine and sedative hypnotic prescriptions among hospitalized older adults
AUTHORS: Elisabeth Anna Pek, MD, Andrew Remfry, MD, Ciara Pendrith, MSc, Chris Fan-Lun, BScPhm, R. Sacha Bhatia, MD, and Christine Soong, MD, MSc, SFHM
Incidence, predictors, and outcomes of hospital-acquired anemia
AUTHORS: Anil N. Makam, MD, MAS, Oanh K. Nguyen, MD, MAS, Christopher Clark, MPA, and Ethan A. Halm, MD, MPH
Association between radiologic incidental findings and resource utilization in patients admitted with chest pain in an urban medical center
AUTHORS: Venkat P. Gundareddy, MD, MPH, SFHM, Nisa M. Maruthur, MD, MHS, Abednego Chibungu, MD, Preetam Bollampally, MD, Regina Landis, MS, abd Shaker M. Eid, MD, MBA
Clinical utility of routine CBC testing in patients with community-acquired pneumonia
AUTHORS: Neelaysh Vukkadala, BS, and Andrew Auerbach, MD, MPH, SFHM
Overuse of troponin? A comprehensive evaluation of testing in a large hospital system
Inpatient antimicrobial utilization measures are associated with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
Inpatient antimicrobial utilization measures are associated with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
BACKGROUND: Antimicrobial stewardship programs (ASPs) have been advocated to improve antimicrobial utilization, but program implementation is variable.
OBJECTIVE: To determine associations of ASPs with facility characteristics and inpatient antimicrobial utilization measures in the Veterans Affairs (VA) system in 2012.
DESIGN: In 2012, the VA administered a survey on antimicrobial stewardship practices to designated ASP contacts at VA acute-care hospitals. From the survey, we identified 34 variables across three domains (evidence, organizational context, and facilitation) that were assessed, using multivariable LASSO (least absolute shrinkage and selection operator) regression, against four antimicrobial utilization measures: aggregate acute care antimicrobial use, antimicrobial use in patients with noninfectious primary discharge diagnoses, missed opportunities to convert from parenteral to oral antimicrobial therapy, and double anaerobic coverage.
SETTING: All 130 VA facilities with acute care services.
RESULTS: Variables associated with at least three favorable changes in antimicrobial utilization included presence of postgraduate physician/pharmacy training programs, number of antimicrobial-specific order sets, frequency of systematic de-escalation review, presence of pharmacists and/or infectious diseases (ID) attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist. Variables associated with two unfavorable measures included bed size, the level of engagement with VA Antimicrobial Stewardship Task Force online resources, and utilization of antimicrobial stop orders.
CONCLUSIONS: Formalization of ASP processes and presence of pharmacy and ID expertise are associated with favorable utilization. Systematic de-escalation review and order set establishment may be high-yield interventions.
Also in JHM
High prevalence of inappropriate benzodiazepine and sedative hypnotic prescriptions among hospitalized older adults
AUTHORS: Elisabeth Anna Pek, MD, Andrew Remfry, MD, Ciara Pendrith, MSc, Chris Fan-Lun, BScPhm, R. Sacha Bhatia, MD, and Christine Soong, MD, MSc, SFHM
Incidence, predictors, and outcomes of hospital-acquired anemia
AUTHORS: Anil N. Makam, MD, MAS, Oanh K. Nguyen, MD, MAS, Christopher Clark, MPA, and Ethan A. Halm, MD, MPH
Association between radiologic incidental findings and resource utilization in patients admitted with chest pain in an urban medical center
AUTHORS: Venkat P. Gundareddy, MD, MPH, SFHM, Nisa M. Maruthur, MD, MHS, Abednego Chibungu, MD, Preetam Bollampally, MD, Regina Landis, MS, abd Shaker M. Eid, MD, MBA
Clinical utility of routine CBC testing in patients with community-acquired pneumonia
AUTHORS: Neelaysh Vukkadala, BS, and Andrew Auerbach, MD, MPH, SFHM
Overuse of troponin? A comprehensive evaluation of testing in a large hospital system
BACKGROUND: Antimicrobial stewardship programs (ASPs) have been advocated to improve antimicrobial utilization, but program implementation is variable.
OBJECTIVE: To determine associations of ASPs with facility characteristics and inpatient antimicrobial utilization measures in the Veterans Affairs (VA) system in 2012.
DESIGN: In 2012, the VA administered a survey on antimicrobial stewardship practices to designated ASP contacts at VA acute-care hospitals. From the survey, we identified 34 variables across three domains (evidence, organizational context, and facilitation) that were assessed, using multivariable LASSO (least absolute shrinkage and selection operator) regression, against four antimicrobial utilization measures: aggregate acute care antimicrobial use, antimicrobial use in patients with noninfectious primary discharge diagnoses, missed opportunities to convert from parenteral to oral antimicrobial therapy, and double anaerobic coverage.
SETTING: All 130 VA facilities with acute care services.
RESULTS: Variables associated with at least three favorable changes in antimicrobial utilization included presence of postgraduate physician/pharmacy training programs, number of antimicrobial-specific order sets, frequency of systematic de-escalation review, presence of pharmacists and/or infectious diseases (ID) attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist. Variables associated with two unfavorable measures included bed size, the level of engagement with VA Antimicrobial Stewardship Task Force online resources, and utilization of antimicrobial stop orders.
CONCLUSIONS: Formalization of ASP processes and presence of pharmacy and ID expertise are associated with favorable utilization. Systematic de-escalation review and order set establishment may be high-yield interventions.
Also in JHM
High prevalence of inappropriate benzodiazepine and sedative hypnotic prescriptions among hospitalized older adults
AUTHORS: Elisabeth Anna Pek, MD, Andrew Remfry, MD, Ciara Pendrith, MSc, Chris Fan-Lun, BScPhm, R. Sacha Bhatia, MD, and Christine Soong, MD, MSc, SFHM
Incidence, predictors, and outcomes of hospital-acquired anemia
AUTHORS: Anil N. Makam, MD, MAS, Oanh K. Nguyen, MD, MAS, Christopher Clark, MPA, and Ethan A. Halm, MD, MPH
Association between radiologic incidental findings and resource utilization in patients admitted with chest pain in an urban medical center
AUTHORS: Venkat P. Gundareddy, MD, MPH, SFHM, Nisa M. Maruthur, MD, MHS, Abednego Chibungu, MD, Preetam Bollampally, MD, Regina Landis, MS, abd Shaker M. Eid, MD, MBA
Clinical utility of routine CBC testing in patients with community-acquired pneumonia
AUTHORS: Neelaysh Vukkadala, BS, and Andrew Auerbach, MD, MPH, SFHM
Overuse of troponin? A comprehensive evaluation of testing in a large hospital system
Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
The deleterious impact of inappropriate and/or excessive antimicrobial usage is well recognized. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that at least 2 million people become infected with antimicrobial-resistant bacteria with 23,000 subsequent deaths and at least $1 billion in excess medical costs per year.1
In response, many healthcare organizations have developed antimicrobial stewardship programs (ASPs). Guidelines co-sponsored by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America, as well as recent statements from the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,all recommend core ASP elements.2-5 The guidelines provide general recommendations on ASP structure, strategies, and activities. The recommended ASP structure is a team of physicians and pharmacists that collaborates with facility governing committees and other stakeholders to optimize antimicrobial use. While personnel with expertise in infectious diseases (ID) often lead ASPs, hospitalists are also recognized as key contributors, especially in quality improvement.6,7 Recommended strategies include prospective audit of antimicrobial use with intervention and feedback and formulary restriction with preauthorization. Recommended activities include education, creation of guidelines, clinical pathways, and order forms, and programs to promote de-escalation and conversion from parenteral (IV) to oral (PO) antimicrobial therapy. However, limited evidence exists regarding the effectiveness of these ASP core elements.8,9 While Cochrane reviews found clear evidence that particular stewardship strategies (eg, audit and feedback, formulary restriction, guidelines implemented with or without feedback, protocols, computerized decision support) can be effective in reducing antimicrobial usage and improving clinical outcomes over the long term, little evidence exists favoring 1 strategy over another.8 Furthermore, most individual studies of ASPs are single-center, making their conclusions less generalizable.
In 2012, the VA National Antimicrobial Stewardship Task Force (ASTF), in conjunction with the VA Healthcare Analysis and Information Group (HAIG) administered a survey on the characteristics of ASPs at all 130 acute care VA facilities (Appendix A). We used these survey results to build an implementation model and then assess associations between facility-level variables and 4 antimicrobial utilization measures.
METHODS
Survey and Data
In 2011, the ASTF was chartered to develop, deploy, and monitor a strategic plan for optimizing antimicrobial therapy management. Monthly educational webinars and sample policies were offered to all facilities, including a sample business plan for stewardship and policies to encourage de-escalation from broad-spectrum antimicrobials, promote conversion from parenteral to oral antimicrobial therapy, avoid unnecessary double anaerobic coverage, and mitigate unnecessary antimicrobial usage in the context of Clostridium difficile infection.10
At the time that ASTF was chartered, the understanding of how ASP structures across VA facilities operated was limited. Hence, to capture baseline institutional characteristics and stewardship activities, ASTF and HAIG developed an inventory assessment of ASPs that was distributed online in November 2012. All 130 VA facilities providing inpatient acute care services responded.
We derived 57 facility characteristics relevant to antimicrobial utilization and conducted a series of factor analyses to simplify the complex dataset, and identify underlying latent constructs. We categorized resulting factors into domains of evidence, context, or facilitation as guided by the Promoting Action on Research Implementation in Health Services framework.11 Briefly, the evidence domain describes how the facility uses codified and noncodified sources of knowledge (eg, research evidence, clinical experience). Organizational context comprises a facility’s characteristics that ensure a more conducive environment to put evidence into practice (eg, supportive leadership, organizational structure, evaluative systems). Facilitation emphasizes a facility personnel’s “state of preparedness” and receptivity to implementation.
Using factor analysis to identify facility factors as correlates of the outcomes, we first examined polychoric correlations among facility characteristics to assess multicollinearity. We performed independent component analysis to create latent constructs of variables that were defined by factor loadings (that indicated the proportion of variance accounted for by the construct) and uniqueness factors (that determined how well the variables were interpreted by the construct). Factors retained included variables that had uniqueness values of less than 0.7 and factor loadings greater than 0.3. Those associated with uniqueness values greater than 0.7 were left as single items, as were characteristics deemed a priori to be particularly important to antimicrobial stewardship. Factor scales that had only 2 items were converted into indices, while factor scores were generated for those factors that contained 3 or more items.12-15
Data for facility-level antimicrobial utilization measures were obtained from the VA Corporate Data Warehouse from calendar year 2012. The analysis was conducted within the VA Informatics and Computing Infrastructure. All study procedures were approved by the VA Central Institutional Review Board.
Measures
Four utilization measures were defined as dependent measures: overall antimicrobial use; antimicrobial use in patients with non-infectious discharge diagnoses; missed opportunities to convert from parenteral to oral antimicrobial therapy; and missed opportunities to avoid double anaerobic coverage with metronidazole.
Overall antimicrobial use was defined as total acute care (ie, medical/surgical/intensive care) antibacterial use for each facility aggregated as per CDC National Healthcare Safety Network Antimicrobial Use Option guidelines (antimicrobial days per 1000 patient days present). A subanalysis of overall antimicrobial use was restricted to antimicrobial use among patients without an infection-related discharge diagnosis, as we surmised that this measure may capture a greater proportion of potentially unnecessary antimicrobial use. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)16 codes for infectious processes were identified by a combination of those classified previously in the literature,17 and those identified by finding the descendants of all infections named in the Systematized Nomenclature of Medicine--Clinical Terms.18 Next, all remaining codes for principal discharge diagnoses for which antimicrobials were administered were reviewed for potential indications for systemic antibacterial use. Discharges were considered noninfectious if no codes were identified when systemic antimicrobials were or could be indicated. For this measure, antimicrobial days were not counted if administered on or 1 day after the calendar day of surgery warranting antimicrobial prophylaxis.
Missed opportunities for conversion from parenteral to oral (IV to PO) formulations of highly bioavailable oral antimicrobials (ciprofloxacin, levofloxacin, moxifloxacin, azithromycin, clindamycin, linezolid, metronidazole, and fluconazole) were defined as the percentage of days of unnecessary IV therapy that were given when PO therapy could have been used among patients who were not in intensive care units at the time of antimicrobial administration who were receiving other oral medications, using previously described methodology.19Missed opportunities for avoiding redundant anaerobic coverage with metronidazole were defined as the percentage of days in which patients receiving metronidazole also receivedantibiotics with activity against anaerobic bacteria, specifically beta-lactam/beta-lactamase inhibitors, carbapenems, cefotetan/cefoxitin, clindamycin, moxifloxacin, or tigecycline), using previously described methodology.20 Patients for whom C. difficile testing was either ordered or positive within the prior 28 days (indicating potential clinical concern for C. difficile infection) were excluded from this endpoint.
Analysis
The variables derived above were entered into a multivariable model for each of the 4 antimicrobial utilization measures. The least absolute shrinkage and selection operator (LASSO) regression was used to determine significant associations between variables and individual utilization measures.21 LASSO was chosen because it offers advantages over traditional subset selection approaches in large multivariable analyses by assessing covariates simultaneously rather than sequentially, supporting prediction rather than estimation of effect.22P values were not reported as they are not useful in determining statistical significance in this methodology. A tuning parameter of 0.025 was determined for the model based on a cross-validation approach. Significant variables remaining in the model were reported with the percent change in each utilization measure per unit change in the variable of interest. For binary factors, percent change was reported according to whether the variable was present or not. For ordinal variables, percent change was reported according to incremental increase in ordinal score. For continuous variables or variables represented by factor or index scores, percent change was reported per each 25% increase in the range of the score.
RESULTS
Inpatient Facility Antimicrobial Stewardship Characteristics and Antimicrobial Utilization
Frequencies of key facility characteristics that contributed to variable development are included in Table 1. Full survey results across all facilities are included in Appendix B. Factor analysis reduced the total number of variables to 32; however, we also included hospital size and VA complexity score. Thus, 34 variables were evaluated for association with antimicrobial utilization measures: 4 in the evidence domain, 23 in the context domain, and 7 in the facilitation domain (Table 2).
Table 1
Table 1 (continued)
Median facility antimicrobial use was 619 antimicrobial days per 1000 days present (interquartile range [IQR], 554-700; overall range, 346-974). Median facility noninfectious antimicrobial use was 236 per 1000 days present (IQR, 200-286). Missed opportunities for conversion from IV to PO antimicrobial therapy were common, with a median facility value of 40.4% (391/969) of potentially eligible days of therapy (IQR, 32.2-47.8%). Missed opportunities to avoid double anaerobic coverage were less common (median 15.3% (186/1214) of potentially eligible days of therapy (IQR, 11.8%-20.2%; Figure).
Overall Antimicrobial Use
Four variables were associated with decreased overall antimicrobial use, although with small magnitude of change: presence of postgraduate physician/pharmacy training programs (0.03% decrease per quarter increase in factor score; on the order of 0.2 antimicrobial days per 1000 patient days present), presence of pharmacists and/or ID attendings on general medicine ward teams (0.02% decrease per quarter increase in index score), frequency of systematic de-escalation review (0.01% decrease per ordinal increase in score), and degree of involvement of ID physicians and/or fellows in antimicrobial approvals (0.007% decrease per quarter increase in index score). No variables were associated with increased overall antimicrobial use.
Table 2
Table 2 (continued)
Antimicrobial Use among Discharges without Infectious Diagnoses
Six variables were associated with decreased antimicrobial use in patients without infectious discharge diagnoses, while 4 variables were associated with increased use. Variables associated with the greatest magnitude of decreased use included facility educational programs for prudent antimicrobial use (1.8% on the order of 4 antimicrobial days per 1000 patient days present), frequency of systematic de-escalation review (1.5% per incremental increase in score), and whether a facility’s lead antimicrobial stewardship pharmacist had ID training (1.3%). Also significantly associated with decreased use was a factor summarizing the presence of 4 condition-specific stewardship processes (de-escalation policies, policies for addressing antimicrobial use in the context of C. difficile infection, blood culture review, and automatic ID consults for certain conditions) (0.6% per quarter increase in factor score range), the extent to which postgraduate physician/pharmacy training programs were present (0.6% per quarter increase in factor score range), and the number of electronic antimicrobial-specific order sets present (0.4% per order set). The variables associated with increased use of antimicrobials included the presence of antimicrobial stop orders (4.6%), the degree to which non-ID physicians were involved in antimicrobial approvals (0.7% per increase in ordinal score), the level engagement with ASTF online resources (0.6% per quarter increase in factor score range), and hospital size (0.6% per 50-bed increase).
Figure
Missed Opportunities for Parenteral to Oral Antimicrobial Conversion
Missed opportunities for IV to PO antimicrobial conversion had the largest number of significant associations with organizational variables: 14 variables were associated with fewer missed opportunities, while 5 were associated with greater missed opportunities. Variables associated with the largest reductions in missed opportunities for IV to PO conversion included having guidelines for antimicrobial duration (12.8%), participating in regional stewardship collaboratives (8.1%), number of antimicrobial-specific order sets (6.0% per order set), ID training of the ASP pharmacist (4.9%), and VA facility complexity designation (4.2% per quarter increase in score indicating greater complexity).23 Variables associated with more missed opportunities included stop orders (11.7%), overall perceived receptiveness to antimicrobial stewardship among clinical services (9.4%), the degree of engagement with ASTF online resources (6.9% per quarter increase in factor score range), educational programs for prudent antimicrobial use (4.1%), and hospital size (1.0% per 50-bed increase).
Missed Opportunities for Avoidance of Double Anaerobic Coverage
Four variables were associated with more avoidance of double anaerobic coverage: ID training of the lead ASP pharmacist (8.8%), presence of pharmacists and/or ID attendings on acute care ward teams (6.2% per quarter increase in index score), degree of ID pharmacist involvement in antimicrobial approvals, ranging from not at all (score=0) to both weekdays and nights/weekends (score=2; 4.3% per ordinal increase), and the number of antimicrobial-specific order sets (1.5% per order set). No variables were associated with less avoidance of double anaerobic coverage.
Variables Associated with Multiple Favorable or Unfavorable Antimicrobial Utilization Measures
To better assess the consistency of the relationship between organizational variables and measures of antimicrobial use, we tabulated variables that were associated with at least 3 potentially favorable (ie, reduced overall or noninfectious antimicrobial use or fewer missed opportunities) measures. Altogether, 5 variables satisfied this criterion: the presence of postgraduate physician/pharmacy training programs, the number of antimicrobial-specific order sets, frequency of systematic de-escalation review, the presence of pharmacists and/or ID attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist (Table 3). Three other variables were associated with at least 2 unfavorable measures: hospital size, the degree to which the facility engaged with ASTF online resources, and presence of antimicrobial stop orders.
Table 3
DISCUSSION
Variability in ASP implementation across VA allowed us to assess the relationship between ASP and facility elements and baseline patterns of antimicrobial utilization. Hospitalists and hospital policy-makers are becoming more and more engaged in inpatient antimicrobial stewardship. While our results suggest that having pharmacists and/or physicians with formal ID training participate in everyday inpatient activities can favorably improve antimicrobial utilization, considerable input into stewardship can be made by hospitalists and policy makers. In particular, based on this work, the highest yield from an organizational standpoint may be in working to develop order sets within the electronic medical record and systematic efforts to promote de-escalation of broad-spectrum therapy, as well as encouraging hospital administration to devote specific physician and pharmacy salary support to stewardship efforts.
While we noted that finding the ASTF online resources helpful was associated with potentially unfavorable antimicrobial utilization, we speculate that this may represent reverse causality due to facilities recognizing that their antimicrobial usage is suboptimal and thus seeking out sample ASTF policies to implement. The association between the presence of automatic stop orders and potentially unfavorable antimicrobial utilization is less clear since the timeframe was not specified in the survey; it may be that setting stop orders too far in advance may promote an environment in which critical thinking about antimicrobial de-escalation is not encouraged or timely. The larger magnitude of association between ASP characteristics and antimicrobial usage among patients without infectious discharge diagnoses versus overall antimicrobial usage also suggests that clinical situations where infection was of low enough suspicion to not even have the providers eventually list an infectious diagnosis on their discharge summaries may be particularly malleable to ASP interventions, though further exploration is needed in determining how useful this utilization measure may be as a marker for inappropriate antimicrobial use.
Our results complement those of Pakyz et al.24 who surveyed 44 academic medical facilities in March 2013 to develop an ASP intensity score and correlate this score and its specific components to overall and targeted antimicrobial use. This study found that the overall ASP intensity score was not significantly associated with total or targeted antimicrobial use. However, ASP strategies were more associated with decreased total and targeted antimicrobial use than were specific ASP resources. In particular, the presence of a preauthorization strategy was associated with decreased targeted antimicrobial use. Our particular findings that order set establishment and de-escalation efforts are associated with multiple antibiotic outcomes also line up with the findings of Schuts et al,who performed a meta-analysis of the effects of meeting antimicrobial stewardship objectives and found that achieving guideline concordance (such as through establishment of order sets) and successfully de-escalating antimicrobial therapy was associated with reduced mortality.25,26 This meta-analysis, however, was limited by low rigor of its studies and potential for reverse causality. While our study has the advantages of capturing an entire national network of 130 acute care facilities with a 100% response rate, it, too, is limited by a number of issues, most notably by the fact that the survey was not specifically designed for the analysis of antimicrobial utilization measures, patient-level risk stratification was not available, the VA population does not reflect the U.S. population at-large, recall bias, and that antimicrobial prescribing and stewardship practices have evolved in VA since 2012. Furthermore, all of the antimicrobial utilization measures studied are imperfect at capturing inappropriate antibiotic use; in particular, our reliance on principal ICD-9 codes for noninfectious outcomes requires prospective validation. Many survey questions were subjective and subject to misinterpretation; other unmeasured confounders may also be present. Causality cannot be inferred from association. Nevertheless, our findings support many core indicators for hospital ASP recommended by the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,3,4 most notably, having personnel with ID training involved in stewardship and establishing a formal procedure for ASP review for the appropriateness of an antimicrobial at or after 48 hours from the initial order.
In summary, the VA has made efforts to advance the practice of antimicrobial stewardship system-wide, including a 2014 directive that all VA facilities have an ASP,27 since the 2012 HAIG assessment reported considerable variability in antimicrobial utilization and antimicrobial stewardship activities. Our study identifies areas of stewardship that may correlate with, positively or negatively, antimicrobial utilization measures that will require further investigation. A repeat and more detailed antimicrobial stewardship survey was recently completed and will help VA gauge ongoing effects of ASTF activities. We hope to re-evaluate our model with newer data when available.
Acknowledgments
The authors wish to thank Michael Fletcher, Jaime Lopez, and Catherine Loc-Carrillo for their administrative and organizational support of the project and Allison Kelly, MD, for her pivotal role in survey development and distribution. This work was supported by the VA Health Services Research and Development Service Collaborative Research to Enhance and Advance Transformation and Excellence (CREATE) Initiative; Cognitive Support Informatics for Antimicrobial Stewardshipproject (CRE 12-313).
Disclosure
The authors report no financial conflicts of interest.
1. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/drugresistance/threat-report-2013/. Published 2013. Accessed January 7, 2016. 2. Dellit TH, Owens RC, McGowan JE Jr, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159-177. PubMed 3. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html. Published 2015. Accessed January 7, 2016. 4. Pollack LA, Plachouras D, Gruhler H, Sinkowitz-Cochran R. Transatlantic taskforce on antimicrobial resistance (TATFAR) summary of the modified Delphi process for common structure and process indicators for hospital antimicrobial stewardship programs. http://www.cdc.gov/drugresistance/pdf/summary_of_tatfar_recommendation_1.pdf. Published 2015. Accessed January 7, 2016. 5. Barlam TF, Cosgrove SE, Abbo LM, MacDougal C, Schuetz AN, Septimus EJ, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. PubMed 6. Rohde JM, Jacobsen D, Rosenberg DJ. Role of the hospitalist in antimicrobial stewardship: a review of work completed and description of a multisite collaborative. Clin Ther. 2013;35(6):751-757. PubMed 7. Mack MR, Rohde JM, Jacobsen D, Barron JR, Ko C, Goonewardene M, et al. Engaging hospitalists in antimicrobial stewardship: lessons from a multihosopital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed 8. Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013;4:CD003543. PubMed 9. Filice G, Drekonja D, Wilt TJ, Greer N, Butler M, Wagner B. Antimicrobial stewardship programs in inpatient settings: a systematic review. Washington, DC: Department of Veterans Affairs Health Services Research and Development. http://www.hsrd.research.va.gov/publications/esp/antimicrobial.pdf. Published 2013. Accessed January 7, 2016. 10. Graber CJ, Madaras-Kelly K, Jones MM, Neuhauser MM, Goetz MB. Unnecessary antimicrobial use in the context of Clostridium difficile infection: a call to arms for the Veterans Affairs Antimicrobial Stewardship Task Force. Infect Control Hosp Epidemiol. 2013(6);34:651-653. PubMed 11. Rycroft-Malone J. The PARIHS framework--a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297-304. PubMed 12. Chou AF, Graber CJ, Jones MM, Zhang Y, Goetz MB, Madaras-Kelly K, et al. Specifying an implementation framework for VA antimicrobial stewardship programs. Oral presentation at the VA HSR&D/QUERI National Conference, July 8-9, 2015. Washington, DC: U.S. Department of Veterans Affairs. http://www.hsrd.research.va.gov/meetings/2015/abstract-display.cfm?RecordID=862. Accessed July 5, 2016. 13. Bartholomew DJ. Factor analysis for categorical data. J R Stat Soc. 1980;42:293-321. 14. Flanagan M, Ramanujam R, Sutherland J, Vaughn T, Diekema D, Doebbeling BN. Development and validation of measures to assess prevention and control of AMR in hospitals. Med Care. 2007;45(6): 537-544. PubMed 15. Kline P. An easy guide to factor analysis. New York: Routledge, 1994. 16. Centers for Disease Control and Prevention, National Center for Health Statistics. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Atlanta GA: Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/icd/icd9cm.htm. Published 2013. Accessed January 7, 2016. 17. Huttner B, Jones M, Huttner A, Rubin M, Samore MH. Antibiotic prescription practices for pneumonia, skin and soft tissue infections and urinary tract infections throughout the US Veterans Affairs system. J Antimicrob Chemother. 2013;68(10):2393-2399. PubMed 18. National Institutes of Health. SNOMED Clinical Terms (SNOMED CT). Bethesda, MD: U.S. National Library of Medicine. https://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html. NIH website. Published 2009. Accessed January 7. 2016. 19. Jones M, Huttner B, Madaras-Kelly K, Nechodom K, Nielson C, Bidwell Goetz M, et al. Parenteral to oral conversion of fluoroquinolones: low-hanging fruit for antimicrobial stewardship programs? Infect Control Hosp Epidemiol 2012;33(4): 362-367. PubMed 20. Huttner B, Jones M, Rubin MA, Madaras-Kelly K, Nielson C, Goetz MB, et al. Double trouble: how big a problem is redundant anaerobic antibiotic coverage in Veterans Affairs medical centres? J Antimicrob Chemother. 2012;67(6):1537-1539. PubMed 21. Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc B. 1996;58:267-288. 22. Taylor J, Tibshirani RJ. Statistical learning and selective inference. Proc Natl Acad Sci U S A. 2015;112(25):7629-7634. PubMed 23. VHA Office of Productivity, Efficiency, and Staffing. Facility Complexity Levels. Department of Veterans Affairs website. http://opes.vssc.med.va.gov/FacilityComplexityLevels/Pages/default.aspx. Published 2008. Accessed January 7, 2016. 24. Pakyz AL, Moczygemba LR, Wang H, Stevens MP, Edmond MB. An evaluation of the association between an antimicrobial stewardship score and antimicrobial usage. J Antimicrob Chemother. 2015;70(5):1588-1591. PubMed 25. Schuts EC, Hulscher ME, Mouton JW, Verduin CM, Stuart JW, Overdiek HW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):847-856. PubMed 26. Graber CJ, Goetz MB. Next steps for antimicrobial stewardship. Lancet Infect Dis. 2016;16(7):764-765. PubMed 27. Petzel RA. VHA Directive 1031: Antimicrobial stewardship programs (ASP). Washington, DC: Department of Veterans Affairs.http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2964. Published January 22, 2014. Accessed July 5, 2016.
The deleterious impact of inappropriate and/or excessive antimicrobial usage is well recognized. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that at least 2 million people become infected with antimicrobial-resistant bacteria with 23,000 subsequent deaths and at least $1 billion in excess medical costs per year.1
In response, many healthcare organizations have developed antimicrobial stewardship programs (ASPs). Guidelines co-sponsored by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America, as well as recent statements from the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,all recommend core ASP elements.2-5 The guidelines provide general recommendations on ASP structure, strategies, and activities. The recommended ASP structure is a team of physicians and pharmacists that collaborates with facility governing committees and other stakeholders to optimize antimicrobial use. While personnel with expertise in infectious diseases (ID) often lead ASPs, hospitalists are also recognized as key contributors, especially in quality improvement.6,7 Recommended strategies include prospective audit of antimicrobial use with intervention and feedback and formulary restriction with preauthorization. Recommended activities include education, creation of guidelines, clinical pathways, and order forms, and programs to promote de-escalation and conversion from parenteral (IV) to oral (PO) antimicrobial therapy. However, limited evidence exists regarding the effectiveness of these ASP core elements.8,9 While Cochrane reviews found clear evidence that particular stewardship strategies (eg, audit and feedback, formulary restriction, guidelines implemented with or without feedback, protocols, computerized decision support) can be effective in reducing antimicrobial usage and improving clinical outcomes over the long term, little evidence exists favoring 1 strategy over another.8 Furthermore, most individual studies of ASPs are single-center, making their conclusions less generalizable.
In 2012, the VA National Antimicrobial Stewardship Task Force (ASTF), in conjunction with the VA Healthcare Analysis and Information Group (HAIG) administered a survey on the characteristics of ASPs at all 130 acute care VA facilities (Appendix A). We used these survey results to build an implementation model and then assess associations between facility-level variables and 4 antimicrobial utilization measures.
METHODS
Survey and Data
In 2011, the ASTF was chartered to develop, deploy, and monitor a strategic plan for optimizing antimicrobial therapy management. Monthly educational webinars and sample policies were offered to all facilities, including a sample business plan for stewardship and policies to encourage de-escalation from broad-spectrum antimicrobials, promote conversion from parenteral to oral antimicrobial therapy, avoid unnecessary double anaerobic coverage, and mitigate unnecessary antimicrobial usage in the context of Clostridium difficile infection.10
At the time that ASTF was chartered, the understanding of how ASP structures across VA facilities operated was limited. Hence, to capture baseline institutional characteristics and stewardship activities, ASTF and HAIG developed an inventory assessment of ASPs that was distributed online in November 2012. All 130 VA facilities providing inpatient acute care services responded.
We derived 57 facility characteristics relevant to antimicrobial utilization and conducted a series of factor analyses to simplify the complex dataset, and identify underlying latent constructs. We categorized resulting factors into domains of evidence, context, or facilitation as guided by the Promoting Action on Research Implementation in Health Services framework.11 Briefly, the evidence domain describes how the facility uses codified and noncodified sources of knowledge (eg, research evidence, clinical experience). Organizational context comprises a facility’s characteristics that ensure a more conducive environment to put evidence into practice (eg, supportive leadership, organizational structure, evaluative systems). Facilitation emphasizes a facility personnel’s “state of preparedness” and receptivity to implementation.
Using factor analysis to identify facility factors as correlates of the outcomes, we first examined polychoric correlations among facility characteristics to assess multicollinearity. We performed independent component analysis to create latent constructs of variables that were defined by factor loadings (that indicated the proportion of variance accounted for by the construct) and uniqueness factors (that determined how well the variables were interpreted by the construct). Factors retained included variables that had uniqueness values of less than 0.7 and factor loadings greater than 0.3. Those associated with uniqueness values greater than 0.7 were left as single items, as were characteristics deemed a priori to be particularly important to antimicrobial stewardship. Factor scales that had only 2 items were converted into indices, while factor scores were generated for those factors that contained 3 or more items.12-15
Data for facility-level antimicrobial utilization measures were obtained from the VA Corporate Data Warehouse from calendar year 2012. The analysis was conducted within the VA Informatics and Computing Infrastructure. All study procedures were approved by the VA Central Institutional Review Board.
Measures
Four utilization measures were defined as dependent measures: overall antimicrobial use; antimicrobial use in patients with non-infectious discharge diagnoses; missed opportunities to convert from parenteral to oral antimicrobial therapy; and missed opportunities to avoid double anaerobic coverage with metronidazole.
Overall antimicrobial use was defined as total acute care (ie, medical/surgical/intensive care) antibacterial use for each facility aggregated as per CDC National Healthcare Safety Network Antimicrobial Use Option guidelines (antimicrobial days per 1000 patient days present). A subanalysis of overall antimicrobial use was restricted to antimicrobial use among patients without an infection-related discharge diagnosis, as we surmised that this measure may capture a greater proportion of potentially unnecessary antimicrobial use. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)16 codes for infectious processes were identified by a combination of those classified previously in the literature,17 and those identified by finding the descendants of all infections named in the Systematized Nomenclature of Medicine--Clinical Terms.18 Next, all remaining codes for principal discharge diagnoses for which antimicrobials were administered were reviewed for potential indications for systemic antibacterial use. Discharges were considered noninfectious if no codes were identified when systemic antimicrobials were or could be indicated. For this measure, antimicrobial days were not counted if administered on or 1 day after the calendar day of surgery warranting antimicrobial prophylaxis.
Missed opportunities for conversion from parenteral to oral (IV to PO) formulations of highly bioavailable oral antimicrobials (ciprofloxacin, levofloxacin, moxifloxacin, azithromycin, clindamycin, linezolid, metronidazole, and fluconazole) were defined as the percentage of days of unnecessary IV therapy that were given when PO therapy could have been used among patients who were not in intensive care units at the time of antimicrobial administration who were receiving other oral medications, using previously described methodology.19Missed opportunities for avoiding redundant anaerobic coverage with metronidazole were defined as the percentage of days in which patients receiving metronidazole also receivedantibiotics with activity against anaerobic bacteria, specifically beta-lactam/beta-lactamase inhibitors, carbapenems, cefotetan/cefoxitin, clindamycin, moxifloxacin, or tigecycline), using previously described methodology.20 Patients for whom C. difficile testing was either ordered or positive within the prior 28 days (indicating potential clinical concern for C. difficile infection) were excluded from this endpoint.
Analysis
The variables derived above were entered into a multivariable model for each of the 4 antimicrobial utilization measures. The least absolute shrinkage and selection operator (LASSO) regression was used to determine significant associations between variables and individual utilization measures.21 LASSO was chosen because it offers advantages over traditional subset selection approaches in large multivariable analyses by assessing covariates simultaneously rather than sequentially, supporting prediction rather than estimation of effect.22P values were not reported as they are not useful in determining statistical significance in this methodology. A tuning parameter of 0.025 was determined for the model based on a cross-validation approach. Significant variables remaining in the model were reported with the percent change in each utilization measure per unit change in the variable of interest. For binary factors, percent change was reported according to whether the variable was present or not. For ordinal variables, percent change was reported according to incremental increase in ordinal score. For continuous variables or variables represented by factor or index scores, percent change was reported per each 25% increase in the range of the score.
RESULTS
Inpatient Facility Antimicrobial Stewardship Characteristics and Antimicrobial Utilization
Frequencies of key facility characteristics that contributed to variable development are included in Table 1. Full survey results across all facilities are included in Appendix B. Factor analysis reduced the total number of variables to 32; however, we also included hospital size and VA complexity score. Thus, 34 variables were evaluated for association with antimicrobial utilization measures: 4 in the evidence domain, 23 in the context domain, and 7 in the facilitation domain (Table 2).
Table 1
Table 1 (continued)
Median facility antimicrobial use was 619 antimicrobial days per 1000 days present (interquartile range [IQR], 554-700; overall range, 346-974). Median facility noninfectious antimicrobial use was 236 per 1000 days present (IQR, 200-286). Missed opportunities for conversion from IV to PO antimicrobial therapy were common, with a median facility value of 40.4% (391/969) of potentially eligible days of therapy (IQR, 32.2-47.8%). Missed opportunities to avoid double anaerobic coverage were less common (median 15.3% (186/1214) of potentially eligible days of therapy (IQR, 11.8%-20.2%; Figure).
Overall Antimicrobial Use
Four variables were associated with decreased overall antimicrobial use, although with small magnitude of change: presence of postgraduate physician/pharmacy training programs (0.03% decrease per quarter increase in factor score; on the order of 0.2 antimicrobial days per 1000 patient days present), presence of pharmacists and/or ID attendings on general medicine ward teams (0.02% decrease per quarter increase in index score), frequency of systematic de-escalation review (0.01% decrease per ordinal increase in score), and degree of involvement of ID physicians and/or fellows in antimicrobial approvals (0.007% decrease per quarter increase in index score). No variables were associated with increased overall antimicrobial use.
Table 2
Table 2 (continued)
Antimicrobial Use among Discharges without Infectious Diagnoses
Six variables were associated with decreased antimicrobial use in patients without infectious discharge diagnoses, while 4 variables were associated with increased use. Variables associated with the greatest magnitude of decreased use included facility educational programs for prudent antimicrobial use (1.8% on the order of 4 antimicrobial days per 1000 patient days present), frequency of systematic de-escalation review (1.5% per incremental increase in score), and whether a facility’s lead antimicrobial stewardship pharmacist had ID training (1.3%). Also significantly associated with decreased use was a factor summarizing the presence of 4 condition-specific stewardship processes (de-escalation policies, policies for addressing antimicrobial use in the context of C. difficile infection, blood culture review, and automatic ID consults for certain conditions) (0.6% per quarter increase in factor score range), the extent to which postgraduate physician/pharmacy training programs were present (0.6% per quarter increase in factor score range), and the number of electronic antimicrobial-specific order sets present (0.4% per order set). The variables associated with increased use of antimicrobials included the presence of antimicrobial stop orders (4.6%), the degree to which non-ID physicians were involved in antimicrobial approvals (0.7% per increase in ordinal score), the level engagement with ASTF online resources (0.6% per quarter increase in factor score range), and hospital size (0.6% per 50-bed increase).
Figure
Missed Opportunities for Parenteral to Oral Antimicrobial Conversion
Missed opportunities for IV to PO antimicrobial conversion had the largest number of significant associations with organizational variables: 14 variables were associated with fewer missed opportunities, while 5 were associated with greater missed opportunities. Variables associated with the largest reductions in missed opportunities for IV to PO conversion included having guidelines for antimicrobial duration (12.8%), participating in regional stewardship collaboratives (8.1%), number of antimicrobial-specific order sets (6.0% per order set), ID training of the ASP pharmacist (4.9%), and VA facility complexity designation (4.2% per quarter increase in score indicating greater complexity).23 Variables associated with more missed opportunities included stop orders (11.7%), overall perceived receptiveness to antimicrobial stewardship among clinical services (9.4%), the degree of engagement with ASTF online resources (6.9% per quarter increase in factor score range), educational programs for prudent antimicrobial use (4.1%), and hospital size (1.0% per 50-bed increase).
Missed Opportunities for Avoidance of Double Anaerobic Coverage
Four variables were associated with more avoidance of double anaerobic coverage: ID training of the lead ASP pharmacist (8.8%), presence of pharmacists and/or ID attendings on acute care ward teams (6.2% per quarter increase in index score), degree of ID pharmacist involvement in antimicrobial approvals, ranging from not at all (score=0) to both weekdays and nights/weekends (score=2; 4.3% per ordinal increase), and the number of antimicrobial-specific order sets (1.5% per order set). No variables were associated with less avoidance of double anaerobic coverage.
Variables Associated with Multiple Favorable or Unfavorable Antimicrobial Utilization Measures
To better assess the consistency of the relationship between organizational variables and measures of antimicrobial use, we tabulated variables that were associated with at least 3 potentially favorable (ie, reduced overall or noninfectious antimicrobial use or fewer missed opportunities) measures. Altogether, 5 variables satisfied this criterion: the presence of postgraduate physician/pharmacy training programs, the number of antimicrobial-specific order sets, frequency of systematic de-escalation review, the presence of pharmacists and/or ID attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist (Table 3). Three other variables were associated with at least 2 unfavorable measures: hospital size, the degree to which the facility engaged with ASTF online resources, and presence of antimicrobial stop orders.
Table 3
DISCUSSION
Variability in ASP implementation across VA allowed us to assess the relationship between ASP and facility elements and baseline patterns of antimicrobial utilization. Hospitalists and hospital policy-makers are becoming more and more engaged in inpatient antimicrobial stewardship. While our results suggest that having pharmacists and/or physicians with formal ID training participate in everyday inpatient activities can favorably improve antimicrobial utilization, considerable input into stewardship can be made by hospitalists and policy makers. In particular, based on this work, the highest yield from an organizational standpoint may be in working to develop order sets within the electronic medical record and systematic efforts to promote de-escalation of broad-spectrum therapy, as well as encouraging hospital administration to devote specific physician and pharmacy salary support to stewardship efforts.
While we noted that finding the ASTF online resources helpful was associated with potentially unfavorable antimicrobial utilization, we speculate that this may represent reverse causality due to facilities recognizing that their antimicrobial usage is suboptimal and thus seeking out sample ASTF policies to implement. The association between the presence of automatic stop orders and potentially unfavorable antimicrobial utilization is less clear since the timeframe was not specified in the survey; it may be that setting stop orders too far in advance may promote an environment in which critical thinking about antimicrobial de-escalation is not encouraged or timely. The larger magnitude of association between ASP characteristics and antimicrobial usage among patients without infectious discharge diagnoses versus overall antimicrobial usage also suggests that clinical situations where infection was of low enough suspicion to not even have the providers eventually list an infectious diagnosis on their discharge summaries may be particularly malleable to ASP interventions, though further exploration is needed in determining how useful this utilization measure may be as a marker for inappropriate antimicrobial use.
Our results complement those of Pakyz et al.24 who surveyed 44 academic medical facilities in March 2013 to develop an ASP intensity score and correlate this score and its specific components to overall and targeted antimicrobial use. This study found that the overall ASP intensity score was not significantly associated with total or targeted antimicrobial use. However, ASP strategies were more associated with decreased total and targeted antimicrobial use than were specific ASP resources. In particular, the presence of a preauthorization strategy was associated with decreased targeted antimicrobial use. Our particular findings that order set establishment and de-escalation efforts are associated with multiple antibiotic outcomes also line up with the findings of Schuts et al,who performed a meta-analysis of the effects of meeting antimicrobial stewardship objectives and found that achieving guideline concordance (such as through establishment of order sets) and successfully de-escalating antimicrobial therapy was associated with reduced mortality.25,26 This meta-analysis, however, was limited by low rigor of its studies and potential for reverse causality. While our study has the advantages of capturing an entire national network of 130 acute care facilities with a 100% response rate, it, too, is limited by a number of issues, most notably by the fact that the survey was not specifically designed for the analysis of antimicrobial utilization measures, patient-level risk stratification was not available, the VA population does not reflect the U.S. population at-large, recall bias, and that antimicrobial prescribing and stewardship practices have evolved in VA since 2012. Furthermore, all of the antimicrobial utilization measures studied are imperfect at capturing inappropriate antibiotic use; in particular, our reliance on principal ICD-9 codes for noninfectious outcomes requires prospective validation. Many survey questions were subjective and subject to misinterpretation; other unmeasured confounders may also be present. Causality cannot be inferred from association. Nevertheless, our findings support many core indicators for hospital ASP recommended by the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,3,4 most notably, having personnel with ID training involved in stewardship and establishing a formal procedure for ASP review for the appropriateness of an antimicrobial at or after 48 hours from the initial order.
In summary, the VA has made efforts to advance the practice of antimicrobial stewardship system-wide, including a 2014 directive that all VA facilities have an ASP,27 since the 2012 HAIG assessment reported considerable variability in antimicrobial utilization and antimicrobial stewardship activities. Our study identifies areas of stewardship that may correlate with, positively or negatively, antimicrobial utilization measures that will require further investigation. A repeat and more detailed antimicrobial stewardship survey was recently completed and will help VA gauge ongoing effects of ASTF activities. We hope to re-evaluate our model with newer data when available.
Acknowledgments
The authors wish to thank Michael Fletcher, Jaime Lopez, and Catherine Loc-Carrillo for their administrative and organizational support of the project and Allison Kelly, MD, for her pivotal role in survey development and distribution. This work was supported by the VA Health Services Research and Development Service Collaborative Research to Enhance and Advance Transformation and Excellence (CREATE) Initiative; Cognitive Support Informatics for Antimicrobial Stewardshipproject (CRE 12-313).
Disclosure
The authors report no financial conflicts of interest.
The deleterious impact of inappropriate and/or excessive antimicrobial usage is well recognized. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that at least 2 million people become infected with antimicrobial-resistant bacteria with 23,000 subsequent deaths and at least $1 billion in excess medical costs per year.1
In response, many healthcare organizations have developed antimicrobial stewardship programs (ASPs). Guidelines co-sponsored by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America, as well as recent statements from the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,all recommend core ASP elements.2-5 The guidelines provide general recommendations on ASP structure, strategies, and activities. The recommended ASP structure is a team of physicians and pharmacists that collaborates with facility governing committees and other stakeholders to optimize antimicrobial use. While personnel with expertise in infectious diseases (ID) often lead ASPs, hospitalists are also recognized as key contributors, especially in quality improvement.6,7 Recommended strategies include prospective audit of antimicrobial use with intervention and feedback and formulary restriction with preauthorization. Recommended activities include education, creation of guidelines, clinical pathways, and order forms, and programs to promote de-escalation and conversion from parenteral (IV) to oral (PO) antimicrobial therapy. However, limited evidence exists regarding the effectiveness of these ASP core elements.8,9 While Cochrane reviews found clear evidence that particular stewardship strategies (eg, audit and feedback, formulary restriction, guidelines implemented with or without feedback, protocols, computerized decision support) can be effective in reducing antimicrobial usage and improving clinical outcomes over the long term, little evidence exists favoring 1 strategy over another.8 Furthermore, most individual studies of ASPs are single-center, making their conclusions less generalizable.
In 2012, the VA National Antimicrobial Stewardship Task Force (ASTF), in conjunction with the VA Healthcare Analysis and Information Group (HAIG) administered a survey on the characteristics of ASPs at all 130 acute care VA facilities (Appendix A). We used these survey results to build an implementation model and then assess associations between facility-level variables and 4 antimicrobial utilization measures.
METHODS
Survey and Data
In 2011, the ASTF was chartered to develop, deploy, and monitor a strategic plan for optimizing antimicrobial therapy management. Monthly educational webinars and sample policies were offered to all facilities, including a sample business plan for stewardship and policies to encourage de-escalation from broad-spectrum antimicrobials, promote conversion from parenteral to oral antimicrobial therapy, avoid unnecessary double anaerobic coverage, and mitigate unnecessary antimicrobial usage in the context of Clostridium difficile infection.10
At the time that ASTF was chartered, the understanding of how ASP structures across VA facilities operated was limited. Hence, to capture baseline institutional characteristics and stewardship activities, ASTF and HAIG developed an inventory assessment of ASPs that was distributed online in November 2012. All 130 VA facilities providing inpatient acute care services responded.
We derived 57 facility characteristics relevant to antimicrobial utilization and conducted a series of factor analyses to simplify the complex dataset, and identify underlying latent constructs. We categorized resulting factors into domains of evidence, context, or facilitation as guided by the Promoting Action on Research Implementation in Health Services framework.11 Briefly, the evidence domain describes how the facility uses codified and noncodified sources of knowledge (eg, research evidence, clinical experience). Organizational context comprises a facility’s characteristics that ensure a more conducive environment to put evidence into practice (eg, supportive leadership, organizational structure, evaluative systems). Facilitation emphasizes a facility personnel’s “state of preparedness” and receptivity to implementation.
Using factor analysis to identify facility factors as correlates of the outcomes, we first examined polychoric correlations among facility characteristics to assess multicollinearity. We performed independent component analysis to create latent constructs of variables that were defined by factor loadings (that indicated the proportion of variance accounted for by the construct) and uniqueness factors (that determined how well the variables were interpreted by the construct). Factors retained included variables that had uniqueness values of less than 0.7 and factor loadings greater than 0.3. Those associated with uniqueness values greater than 0.7 were left as single items, as were characteristics deemed a priori to be particularly important to antimicrobial stewardship. Factor scales that had only 2 items were converted into indices, while factor scores were generated for those factors that contained 3 or more items.12-15
Data for facility-level antimicrobial utilization measures were obtained from the VA Corporate Data Warehouse from calendar year 2012. The analysis was conducted within the VA Informatics and Computing Infrastructure. All study procedures were approved by the VA Central Institutional Review Board.
Measures
Four utilization measures were defined as dependent measures: overall antimicrobial use; antimicrobial use in patients with non-infectious discharge diagnoses; missed opportunities to convert from parenteral to oral antimicrobial therapy; and missed opportunities to avoid double anaerobic coverage with metronidazole.
Overall antimicrobial use was defined as total acute care (ie, medical/surgical/intensive care) antibacterial use for each facility aggregated as per CDC National Healthcare Safety Network Antimicrobial Use Option guidelines (antimicrobial days per 1000 patient days present). A subanalysis of overall antimicrobial use was restricted to antimicrobial use among patients without an infection-related discharge diagnosis, as we surmised that this measure may capture a greater proportion of potentially unnecessary antimicrobial use. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)16 codes for infectious processes were identified by a combination of those classified previously in the literature,17 and those identified by finding the descendants of all infections named in the Systematized Nomenclature of Medicine--Clinical Terms.18 Next, all remaining codes for principal discharge diagnoses for which antimicrobials were administered were reviewed for potential indications for systemic antibacterial use. Discharges were considered noninfectious if no codes were identified when systemic antimicrobials were or could be indicated. For this measure, antimicrobial days were not counted if administered on or 1 day after the calendar day of surgery warranting antimicrobial prophylaxis.
Missed opportunities for conversion from parenteral to oral (IV to PO) formulations of highly bioavailable oral antimicrobials (ciprofloxacin, levofloxacin, moxifloxacin, azithromycin, clindamycin, linezolid, metronidazole, and fluconazole) were defined as the percentage of days of unnecessary IV therapy that were given when PO therapy could have been used among patients who were not in intensive care units at the time of antimicrobial administration who were receiving other oral medications, using previously described methodology.19Missed opportunities for avoiding redundant anaerobic coverage with metronidazole were defined as the percentage of days in which patients receiving metronidazole also receivedantibiotics with activity against anaerobic bacteria, specifically beta-lactam/beta-lactamase inhibitors, carbapenems, cefotetan/cefoxitin, clindamycin, moxifloxacin, or tigecycline), using previously described methodology.20 Patients for whom C. difficile testing was either ordered or positive within the prior 28 days (indicating potential clinical concern for C. difficile infection) were excluded from this endpoint.
Analysis
The variables derived above were entered into a multivariable model for each of the 4 antimicrobial utilization measures. The least absolute shrinkage and selection operator (LASSO) regression was used to determine significant associations between variables and individual utilization measures.21 LASSO was chosen because it offers advantages over traditional subset selection approaches in large multivariable analyses by assessing covariates simultaneously rather than sequentially, supporting prediction rather than estimation of effect.22P values were not reported as they are not useful in determining statistical significance in this methodology. A tuning parameter of 0.025 was determined for the model based on a cross-validation approach. Significant variables remaining in the model were reported with the percent change in each utilization measure per unit change in the variable of interest. For binary factors, percent change was reported according to whether the variable was present or not. For ordinal variables, percent change was reported according to incremental increase in ordinal score. For continuous variables or variables represented by factor or index scores, percent change was reported per each 25% increase in the range of the score.
RESULTS
Inpatient Facility Antimicrobial Stewardship Characteristics and Antimicrobial Utilization
Frequencies of key facility characteristics that contributed to variable development are included in Table 1. Full survey results across all facilities are included in Appendix B. Factor analysis reduced the total number of variables to 32; however, we also included hospital size and VA complexity score. Thus, 34 variables were evaluated for association with antimicrobial utilization measures: 4 in the evidence domain, 23 in the context domain, and 7 in the facilitation domain (Table 2).
Table 1
Table 1 (continued)
Median facility antimicrobial use was 619 antimicrobial days per 1000 days present (interquartile range [IQR], 554-700; overall range, 346-974). Median facility noninfectious antimicrobial use was 236 per 1000 days present (IQR, 200-286). Missed opportunities for conversion from IV to PO antimicrobial therapy were common, with a median facility value of 40.4% (391/969) of potentially eligible days of therapy (IQR, 32.2-47.8%). Missed opportunities to avoid double anaerobic coverage were less common (median 15.3% (186/1214) of potentially eligible days of therapy (IQR, 11.8%-20.2%; Figure).
Overall Antimicrobial Use
Four variables were associated with decreased overall antimicrobial use, although with small magnitude of change: presence of postgraduate physician/pharmacy training programs (0.03% decrease per quarter increase in factor score; on the order of 0.2 antimicrobial days per 1000 patient days present), presence of pharmacists and/or ID attendings on general medicine ward teams (0.02% decrease per quarter increase in index score), frequency of systematic de-escalation review (0.01% decrease per ordinal increase in score), and degree of involvement of ID physicians and/or fellows in antimicrobial approvals (0.007% decrease per quarter increase in index score). No variables were associated with increased overall antimicrobial use.
Table 2
Table 2 (continued)
Antimicrobial Use among Discharges without Infectious Diagnoses
Six variables were associated with decreased antimicrobial use in patients without infectious discharge diagnoses, while 4 variables were associated with increased use. Variables associated with the greatest magnitude of decreased use included facility educational programs for prudent antimicrobial use (1.8% on the order of 4 antimicrobial days per 1000 patient days present), frequency of systematic de-escalation review (1.5% per incremental increase in score), and whether a facility’s lead antimicrobial stewardship pharmacist had ID training (1.3%). Also significantly associated with decreased use was a factor summarizing the presence of 4 condition-specific stewardship processes (de-escalation policies, policies for addressing antimicrobial use in the context of C. difficile infection, blood culture review, and automatic ID consults for certain conditions) (0.6% per quarter increase in factor score range), the extent to which postgraduate physician/pharmacy training programs were present (0.6% per quarter increase in factor score range), and the number of electronic antimicrobial-specific order sets present (0.4% per order set). The variables associated with increased use of antimicrobials included the presence of antimicrobial stop orders (4.6%), the degree to which non-ID physicians were involved in antimicrobial approvals (0.7% per increase in ordinal score), the level engagement with ASTF online resources (0.6% per quarter increase in factor score range), and hospital size (0.6% per 50-bed increase).
Figure
Missed Opportunities for Parenteral to Oral Antimicrobial Conversion
Missed opportunities for IV to PO antimicrobial conversion had the largest number of significant associations with organizational variables: 14 variables were associated with fewer missed opportunities, while 5 were associated with greater missed opportunities. Variables associated with the largest reductions in missed opportunities for IV to PO conversion included having guidelines for antimicrobial duration (12.8%), participating in regional stewardship collaboratives (8.1%), number of antimicrobial-specific order sets (6.0% per order set), ID training of the ASP pharmacist (4.9%), and VA facility complexity designation (4.2% per quarter increase in score indicating greater complexity).23 Variables associated with more missed opportunities included stop orders (11.7%), overall perceived receptiveness to antimicrobial stewardship among clinical services (9.4%), the degree of engagement with ASTF online resources (6.9% per quarter increase in factor score range), educational programs for prudent antimicrobial use (4.1%), and hospital size (1.0% per 50-bed increase).
Missed Opportunities for Avoidance of Double Anaerobic Coverage
Four variables were associated with more avoidance of double anaerobic coverage: ID training of the lead ASP pharmacist (8.8%), presence of pharmacists and/or ID attendings on acute care ward teams (6.2% per quarter increase in index score), degree of ID pharmacist involvement in antimicrobial approvals, ranging from not at all (score=0) to both weekdays and nights/weekends (score=2; 4.3% per ordinal increase), and the number of antimicrobial-specific order sets (1.5% per order set). No variables were associated with less avoidance of double anaerobic coverage.
Variables Associated with Multiple Favorable or Unfavorable Antimicrobial Utilization Measures
To better assess the consistency of the relationship between organizational variables and measures of antimicrobial use, we tabulated variables that were associated with at least 3 potentially favorable (ie, reduced overall or noninfectious antimicrobial use or fewer missed opportunities) measures. Altogether, 5 variables satisfied this criterion: the presence of postgraduate physician/pharmacy training programs, the number of antimicrobial-specific order sets, frequency of systematic de-escalation review, the presence of pharmacists and/or ID attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist (Table 3). Three other variables were associated with at least 2 unfavorable measures: hospital size, the degree to which the facility engaged with ASTF online resources, and presence of antimicrobial stop orders.
Table 3
DISCUSSION
Variability in ASP implementation across VA allowed us to assess the relationship between ASP and facility elements and baseline patterns of antimicrobial utilization. Hospitalists and hospital policy-makers are becoming more and more engaged in inpatient antimicrobial stewardship. While our results suggest that having pharmacists and/or physicians with formal ID training participate in everyday inpatient activities can favorably improve antimicrobial utilization, considerable input into stewardship can be made by hospitalists and policy makers. In particular, based on this work, the highest yield from an organizational standpoint may be in working to develop order sets within the electronic medical record and systematic efforts to promote de-escalation of broad-spectrum therapy, as well as encouraging hospital administration to devote specific physician and pharmacy salary support to stewardship efforts.
While we noted that finding the ASTF online resources helpful was associated with potentially unfavorable antimicrobial utilization, we speculate that this may represent reverse causality due to facilities recognizing that their antimicrobial usage is suboptimal and thus seeking out sample ASTF policies to implement. The association between the presence of automatic stop orders and potentially unfavorable antimicrobial utilization is less clear since the timeframe was not specified in the survey; it may be that setting stop orders too far in advance may promote an environment in which critical thinking about antimicrobial de-escalation is not encouraged or timely. The larger magnitude of association between ASP characteristics and antimicrobial usage among patients without infectious discharge diagnoses versus overall antimicrobial usage also suggests that clinical situations where infection was of low enough suspicion to not even have the providers eventually list an infectious diagnosis on their discharge summaries may be particularly malleable to ASP interventions, though further exploration is needed in determining how useful this utilization measure may be as a marker for inappropriate antimicrobial use.
Our results complement those of Pakyz et al.24 who surveyed 44 academic medical facilities in March 2013 to develop an ASP intensity score and correlate this score and its specific components to overall and targeted antimicrobial use. This study found that the overall ASP intensity score was not significantly associated with total or targeted antimicrobial use. However, ASP strategies were more associated with decreased total and targeted antimicrobial use than were specific ASP resources. In particular, the presence of a preauthorization strategy was associated with decreased targeted antimicrobial use. Our particular findings that order set establishment and de-escalation efforts are associated with multiple antibiotic outcomes also line up with the findings of Schuts et al,who performed a meta-analysis of the effects of meeting antimicrobial stewardship objectives and found that achieving guideline concordance (such as through establishment of order sets) and successfully de-escalating antimicrobial therapy was associated with reduced mortality.25,26 This meta-analysis, however, was limited by low rigor of its studies and potential for reverse causality. While our study has the advantages of capturing an entire national network of 130 acute care facilities with a 100% response rate, it, too, is limited by a number of issues, most notably by the fact that the survey was not specifically designed for the analysis of antimicrobial utilization measures, patient-level risk stratification was not available, the VA population does not reflect the U.S. population at-large, recall bias, and that antimicrobial prescribing and stewardship practices have evolved in VA since 2012. Furthermore, all of the antimicrobial utilization measures studied are imperfect at capturing inappropriate antibiotic use; in particular, our reliance on principal ICD-9 codes for noninfectious outcomes requires prospective validation. Many survey questions were subjective and subject to misinterpretation; other unmeasured confounders may also be present. Causality cannot be inferred from association. Nevertheless, our findings support many core indicators for hospital ASP recommended by the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,3,4 most notably, having personnel with ID training involved in stewardship and establishing a formal procedure for ASP review for the appropriateness of an antimicrobial at or after 48 hours from the initial order.
In summary, the VA has made efforts to advance the practice of antimicrobial stewardship system-wide, including a 2014 directive that all VA facilities have an ASP,27 since the 2012 HAIG assessment reported considerable variability in antimicrobial utilization and antimicrobial stewardship activities. Our study identifies areas of stewardship that may correlate with, positively or negatively, antimicrobial utilization measures that will require further investigation. A repeat and more detailed antimicrobial stewardship survey was recently completed and will help VA gauge ongoing effects of ASTF activities. We hope to re-evaluate our model with newer data when available.
Acknowledgments
The authors wish to thank Michael Fletcher, Jaime Lopez, and Catherine Loc-Carrillo for their administrative and organizational support of the project and Allison Kelly, MD, for her pivotal role in survey development and distribution. This work was supported by the VA Health Services Research and Development Service Collaborative Research to Enhance and Advance Transformation and Excellence (CREATE) Initiative; Cognitive Support Informatics for Antimicrobial Stewardshipproject (CRE 12-313).
Disclosure
The authors report no financial conflicts of interest.
References
1. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/drugresistance/threat-report-2013/. Published 2013. Accessed January 7, 2016. 2. Dellit TH, Owens RC, McGowan JE Jr, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159-177. PubMed 3. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html. Published 2015. Accessed January 7, 2016. 4. Pollack LA, Plachouras D, Gruhler H, Sinkowitz-Cochran R. Transatlantic taskforce on antimicrobial resistance (TATFAR) summary of the modified Delphi process for common structure and process indicators for hospital antimicrobial stewardship programs. http://www.cdc.gov/drugresistance/pdf/summary_of_tatfar_recommendation_1.pdf. Published 2015. Accessed January 7, 2016. 5. Barlam TF, Cosgrove SE, Abbo LM, MacDougal C, Schuetz AN, Septimus EJ, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. PubMed 6. Rohde JM, Jacobsen D, Rosenberg DJ. Role of the hospitalist in antimicrobial stewardship: a review of work completed and description of a multisite collaborative. Clin Ther. 2013;35(6):751-757. PubMed 7. Mack MR, Rohde JM, Jacobsen D, Barron JR, Ko C, Goonewardene M, et al. Engaging hospitalists in antimicrobial stewardship: lessons from a multihosopital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed 8. Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013;4:CD003543. PubMed 9. Filice G, Drekonja D, Wilt TJ, Greer N, Butler M, Wagner B. Antimicrobial stewardship programs in inpatient settings: a systematic review. Washington, DC: Department of Veterans Affairs Health Services Research and Development. http://www.hsrd.research.va.gov/publications/esp/antimicrobial.pdf. Published 2013. Accessed January 7, 2016. 10. Graber CJ, Madaras-Kelly K, Jones MM, Neuhauser MM, Goetz MB. Unnecessary antimicrobial use in the context of Clostridium difficile infection: a call to arms for the Veterans Affairs Antimicrobial Stewardship Task Force. Infect Control Hosp Epidemiol. 2013(6);34:651-653. PubMed 11. Rycroft-Malone J. The PARIHS framework--a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297-304. PubMed 12. Chou AF, Graber CJ, Jones MM, Zhang Y, Goetz MB, Madaras-Kelly K, et al. Specifying an implementation framework for VA antimicrobial stewardship programs. Oral presentation at the VA HSR&D/QUERI National Conference, July 8-9, 2015. Washington, DC: U.S. Department of Veterans Affairs. http://www.hsrd.research.va.gov/meetings/2015/abstract-display.cfm?RecordID=862. Accessed July 5, 2016. 13. Bartholomew DJ. Factor analysis for categorical data. J R Stat Soc. 1980;42:293-321. 14. Flanagan M, Ramanujam R, Sutherland J, Vaughn T, Diekema D, Doebbeling BN. Development and validation of measures to assess prevention and control of AMR in hospitals. Med Care. 2007;45(6): 537-544. PubMed 15. Kline P. An easy guide to factor analysis. New York: Routledge, 1994. 16. Centers for Disease Control and Prevention, National Center for Health Statistics. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Atlanta GA: Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/icd/icd9cm.htm. Published 2013. Accessed January 7, 2016. 17. Huttner B, Jones M, Huttner A, Rubin M, Samore MH. Antibiotic prescription practices for pneumonia, skin and soft tissue infections and urinary tract infections throughout the US Veterans Affairs system. J Antimicrob Chemother. 2013;68(10):2393-2399. PubMed 18. National Institutes of Health. SNOMED Clinical Terms (SNOMED CT). Bethesda, MD: U.S. National Library of Medicine. https://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html. NIH website. Published 2009. Accessed January 7. 2016. 19. Jones M, Huttner B, Madaras-Kelly K, Nechodom K, Nielson C, Bidwell Goetz M, et al. Parenteral to oral conversion of fluoroquinolones: low-hanging fruit for antimicrobial stewardship programs? Infect Control Hosp Epidemiol 2012;33(4): 362-367. PubMed 20. Huttner B, Jones M, Rubin MA, Madaras-Kelly K, Nielson C, Goetz MB, et al. Double trouble: how big a problem is redundant anaerobic antibiotic coverage in Veterans Affairs medical centres? J Antimicrob Chemother. 2012;67(6):1537-1539. PubMed 21. Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc B. 1996;58:267-288. 22. Taylor J, Tibshirani RJ. Statistical learning and selective inference. Proc Natl Acad Sci U S A. 2015;112(25):7629-7634. PubMed 23. VHA Office of Productivity, Efficiency, and Staffing. Facility Complexity Levels. Department of Veterans Affairs website. http://opes.vssc.med.va.gov/FacilityComplexityLevels/Pages/default.aspx. Published 2008. Accessed January 7, 2016. 24. Pakyz AL, Moczygemba LR, Wang H, Stevens MP, Edmond MB. An evaluation of the association between an antimicrobial stewardship score and antimicrobial usage. J Antimicrob Chemother. 2015;70(5):1588-1591. PubMed 25. Schuts EC, Hulscher ME, Mouton JW, Verduin CM, Stuart JW, Overdiek HW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):847-856. PubMed 26. Graber CJ, Goetz MB. Next steps for antimicrobial stewardship. Lancet Infect Dis. 2016;16(7):764-765. PubMed 27. Petzel RA. VHA Directive 1031: Antimicrobial stewardship programs (ASP). Washington, DC: Department of Veterans Affairs.http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2964. Published January 22, 2014. Accessed July 5, 2016.
References
1. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/drugresistance/threat-report-2013/. Published 2013. Accessed January 7, 2016. 2. Dellit TH, Owens RC, McGowan JE Jr, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159-177. PubMed 3. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html. Published 2015. Accessed January 7, 2016. 4. Pollack LA, Plachouras D, Gruhler H, Sinkowitz-Cochran R. Transatlantic taskforce on antimicrobial resistance (TATFAR) summary of the modified Delphi process for common structure and process indicators for hospital antimicrobial stewardship programs. http://www.cdc.gov/drugresistance/pdf/summary_of_tatfar_recommendation_1.pdf. Published 2015. Accessed January 7, 2016. 5. Barlam TF, Cosgrove SE, Abbo LM, MacDougal C, Schuetz AN, Septimus EJ, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. PubMed 6. Rohde JM, Jacobsen D, Rosenberg DJ. Role of the hospitalist in antimicrobial stewardship: a review of work completed and description of a multisite collaborative. Clin Ther. 2013;35(6):751-757. PubMed 7. Mack MR, Rohde JM, Jacobsen D, Barron JR, Ko C, Goonewardene M, et al. Engaging hospitalists in antimicrobial stewardship: lessons from a multihosopital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed 8. Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013;4:CD003543. PubMed 9. Filice G, Drekonja D, Wilt TJ, Greer N, Butler M, Wagner B. Antimicrobial stewardship programs in inpatient settings: a systematic review. Washington, DC: Department of Veterans Affairs Health Services Research and Development. http://www.hsrd.research.va.gov/publications/esp/antimicrobial.pdf. Published 2013. Accessed January 7, 2016. 10. Graber CJ, Madaras-Kelly K, Jones MM, Neuhauser MM, Goetz MB. Unnecessary antimicrobial use in the context of Clostridium difficile infection: a call to arms for the Veterans Affairs Antimicrobial Stewardship Task Force. Infect Control Hosp Epidemiol. 2013(6);34:651-653. PubMed 11. Rycroft-Malone J. The PARIHS framework--a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297-304. PubMed 12. Chou AF, Graber CJ, Jones MM, Zhang Y, Goetz MB, Madaras-Kelly K, et al. Specifying an implementation framework for VA antimicrobial stewardship programs. Oral presentation at the VA HSR&D/QUERI National Conference, July 8-9, 2015. Washington, DC: U.S. Department of Veterans Affairs. http://www.hsrd.research.va.gov/meetings/2015/abstract-display.cfm?RecordID=862. Accessed July 5, 2016. 13. Bartholomew DJ. Factor analysis for categorical data. J R Stat Soc. 1980;42:293-321. 14. Flanagan M, Ramanujam R, Sutherland J, Vaughn T, Diekema D, Doebbeling BN. Development and validation of measures to assess prevention and control of AMR in hospitals. Med Care. 2007;45(6): 537-544. PubMed 15. Kline P. An easy guide to factor analysis. New York: Routledge, 1994. 16. Centers for Disease Control and Prevention, National Center for Health Statistics. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Atlanta GA: Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/icd/icd9cm.htm. Published 2013. Accessed January 7, 2016. 17. Huttner B, Jones M, Huttner A, Rubin M, Samore MH. Antibiotic prescription practices for pneumonia, skin and soft tissue infections and urinary tract infections throughout the US Veterans Affairs system. J Antimicrob Chemother. 2013;68(10):2393-2399. PubMed 18. National Institutes of Health. SNOMED Clinical Terms (SNOMED CT). Bethesda, MD: U.S. National Library of Medicine. https://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html. NIH website. Published 2009. Accessed January 7. 2016. 19. Jones M, Huttner B, Madaras-Kelly K, Nechodom K, Nielson C, Bidwell Goetz M, et al. Parenteral to oral conversion of fluoroquinolones: low-hanging fruit for antimicrobial stewardship programs? Infect Control Hosp Epidemiol 2012;33(4): 362-367. PubMed 20. Huttner B, Jones M, Rubin MA, Madaras-Kelly K, Nielson C, Goetz MB, et al. Double trouble: how big a problem is redundant anaerobic antibiotic coverage in Veterans Affairs medical centres? J Antimicrob Chemother. 2012;67(6):1537-1539. PubMed 21. Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc B. 1996;58:267-288. 22. Taylor J, Tibshirani RJ. Statistical learning and selective inference. Proc Natl Acad Sci U S A. 2015;112(25):7629-7634. PubMed 23. VHA Office of Productivity, Efficiency, and Staffing. Facility Complexity Levels. Department of Veterans Affairs website. http://opes.vssc.med.va.gov/FacilityComplexityLevels/Pages/default.aspx. Published 2008. Accessed January 7, 2016. 24. Pakyz AL, Moczygemba LR, Wang H, Stevens MP, Edmond MB. An evaluation of the association between an antimicrobial stewardship score and antimicrobial usage. J Antimicrob Chemother. 2015;70(5):1588-1591. PubMed 25. Schuts EC, Hulscher ME, Mouton JW, Verduin CM, Stuart JW, Overdiek HW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):847-856. PubMed 26. Graber CJ, Goetz MB. Next steps for antimicrobial stewardship. Lancet Infect Dis. 2016;16(7):764-765. PubMed 27. Petzel RA. VHA Directive 1031: Antimicrobial stewardship programs (ASP). Washington, DC: Department of Veterans Affairs.http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2964. Published January 22, 2014. Accessed July 5, 2016.
Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
Display Headline
Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
Address for correspondence and reprint requests: Christopher J. Graber, MD, MPH, Infectious Diseases Section, VA Greater Los Angeles Healthcare System, 11301 Wilshire Blvd, 111-F, Los Angeles, CA 90073; Telephone: 310-268-3763; Fax: 310 268-4928; E-mail: christopher.graber@va.gov
Content Gating
Open Access (article Unlocked/Open Access)
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo
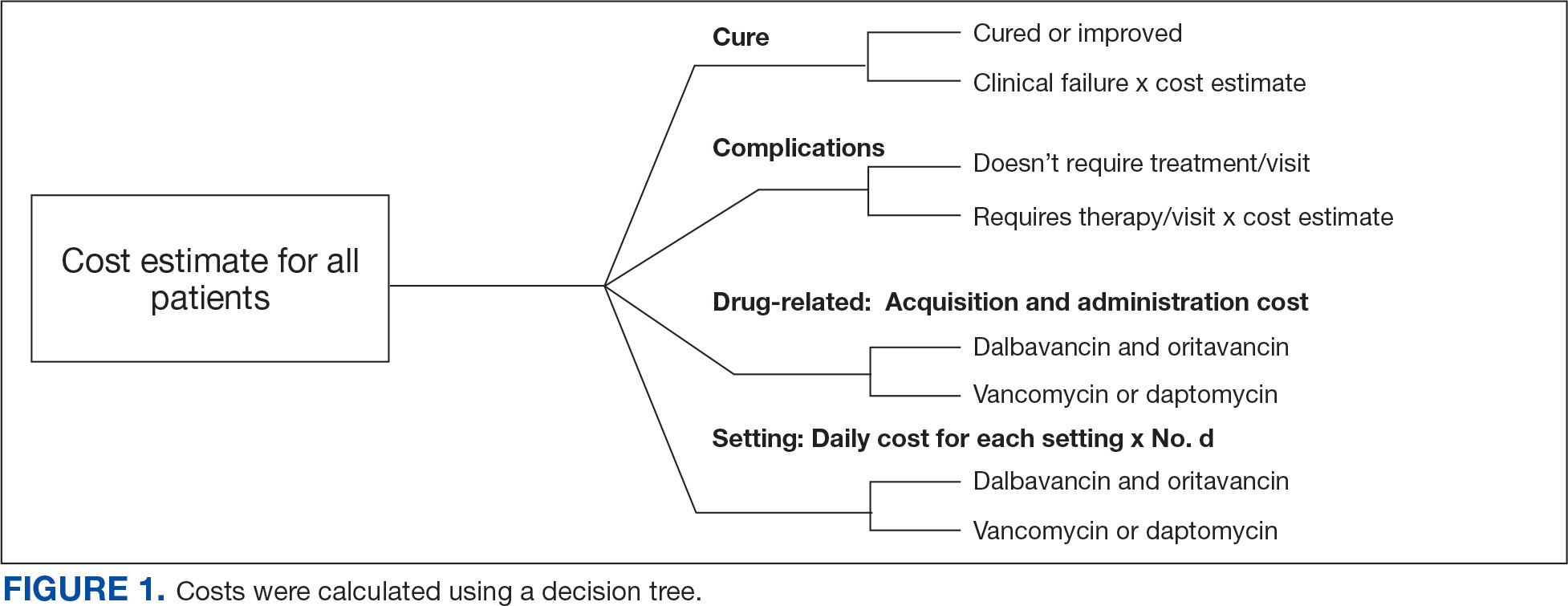
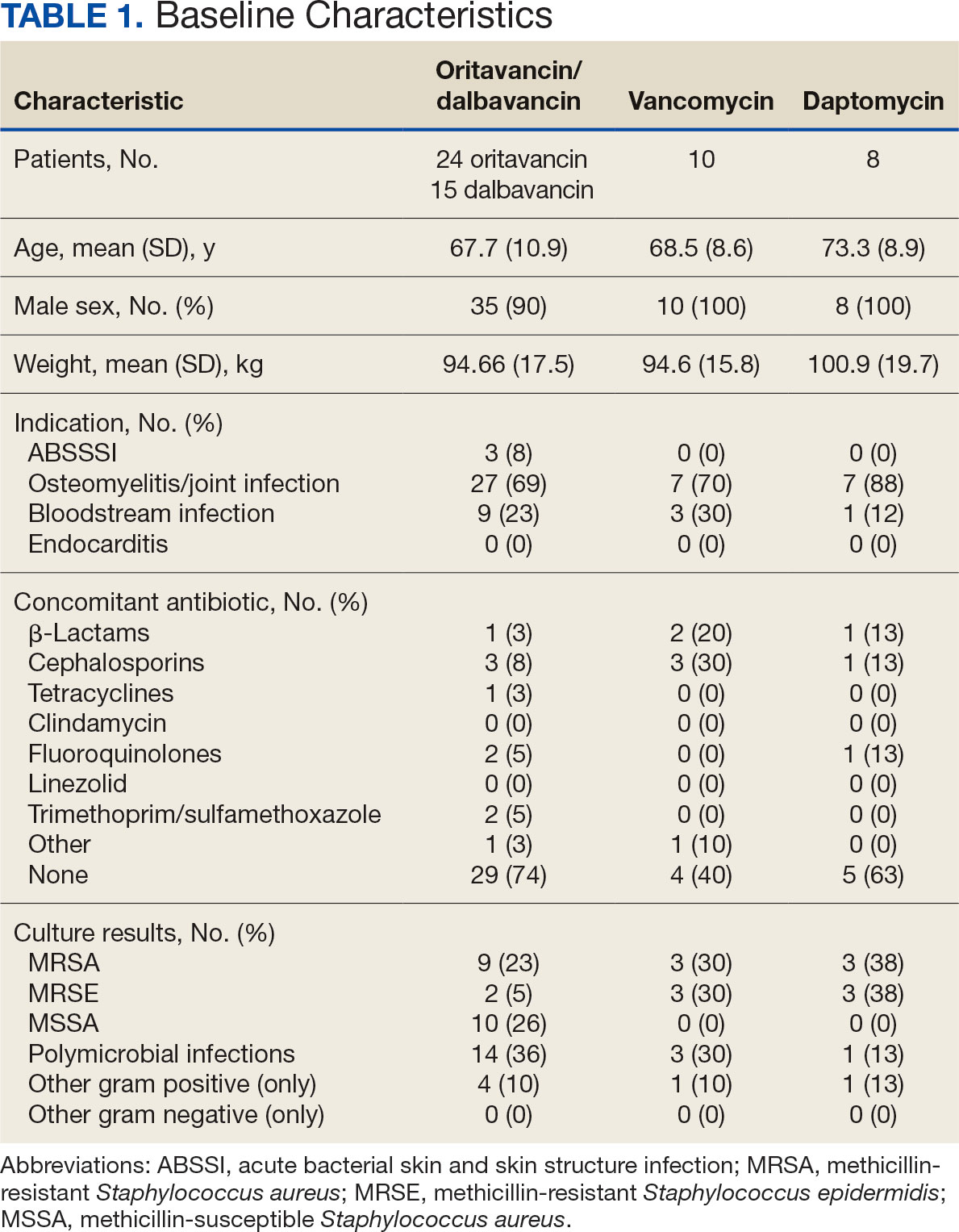

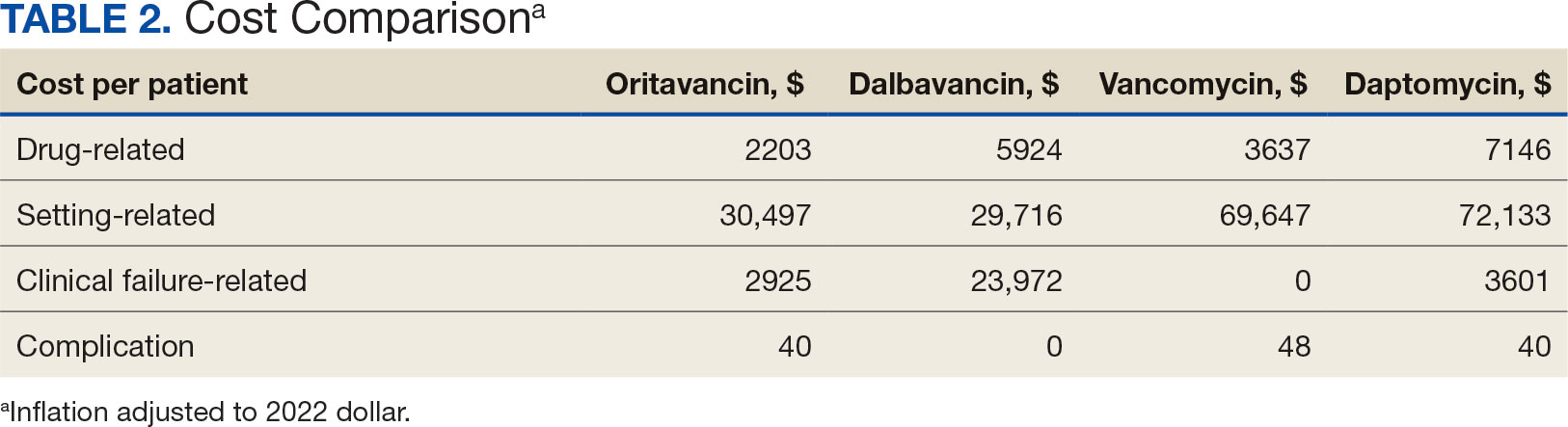
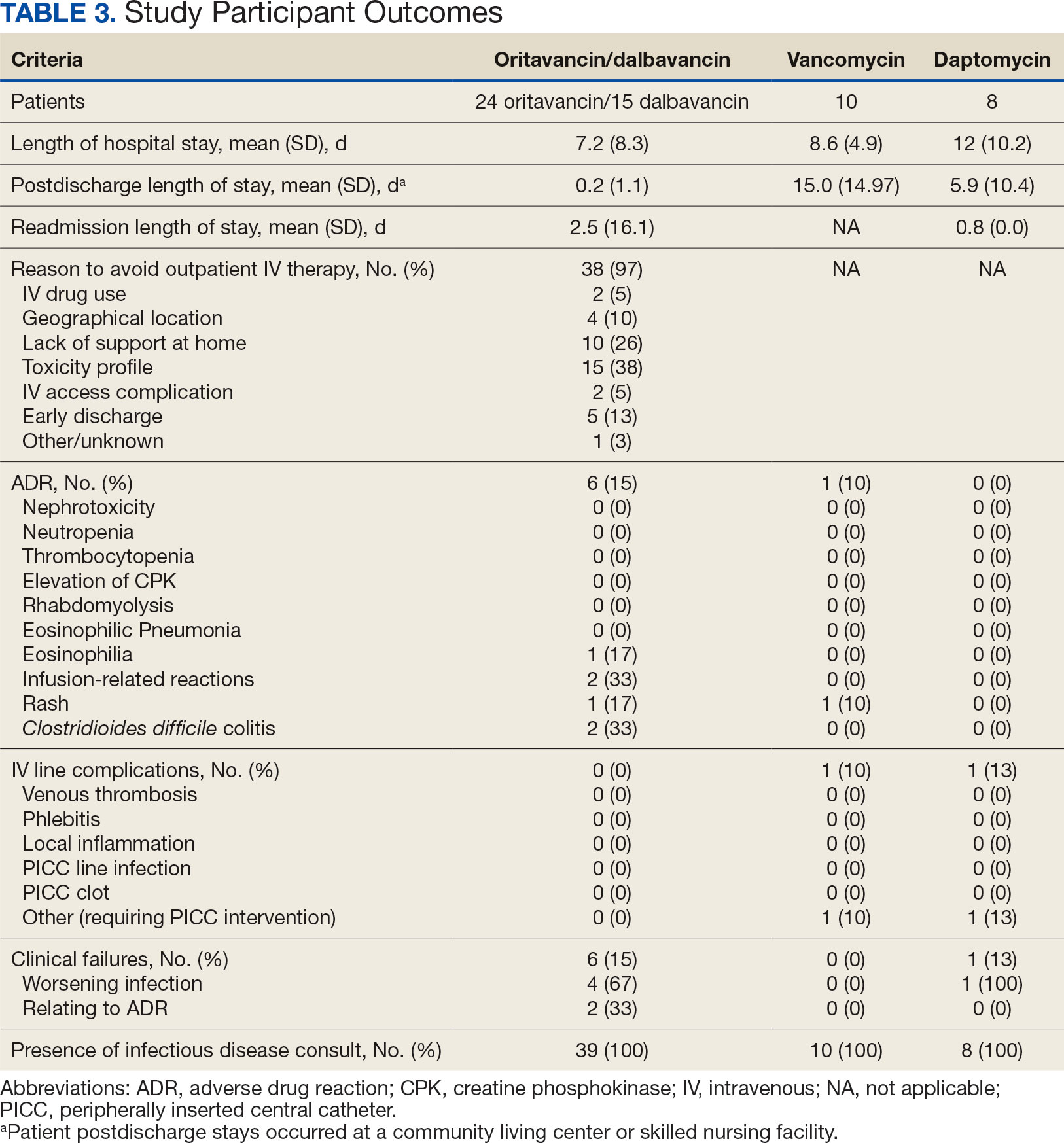


")

")