User login
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
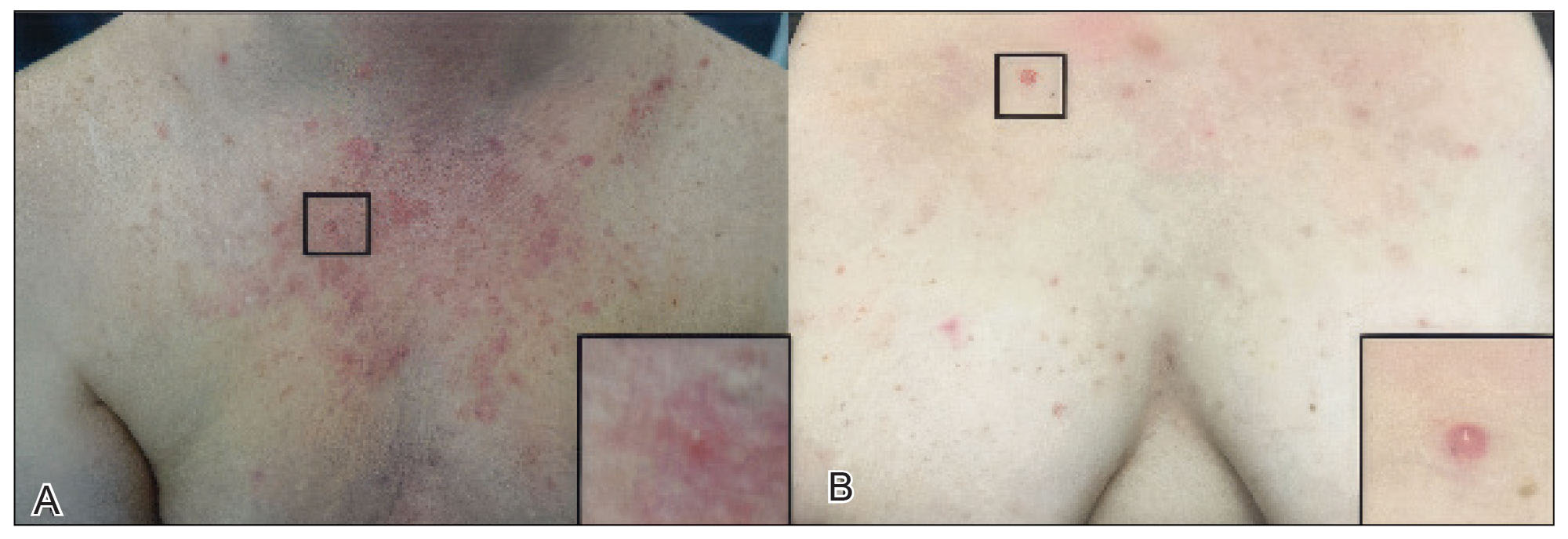
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).

Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
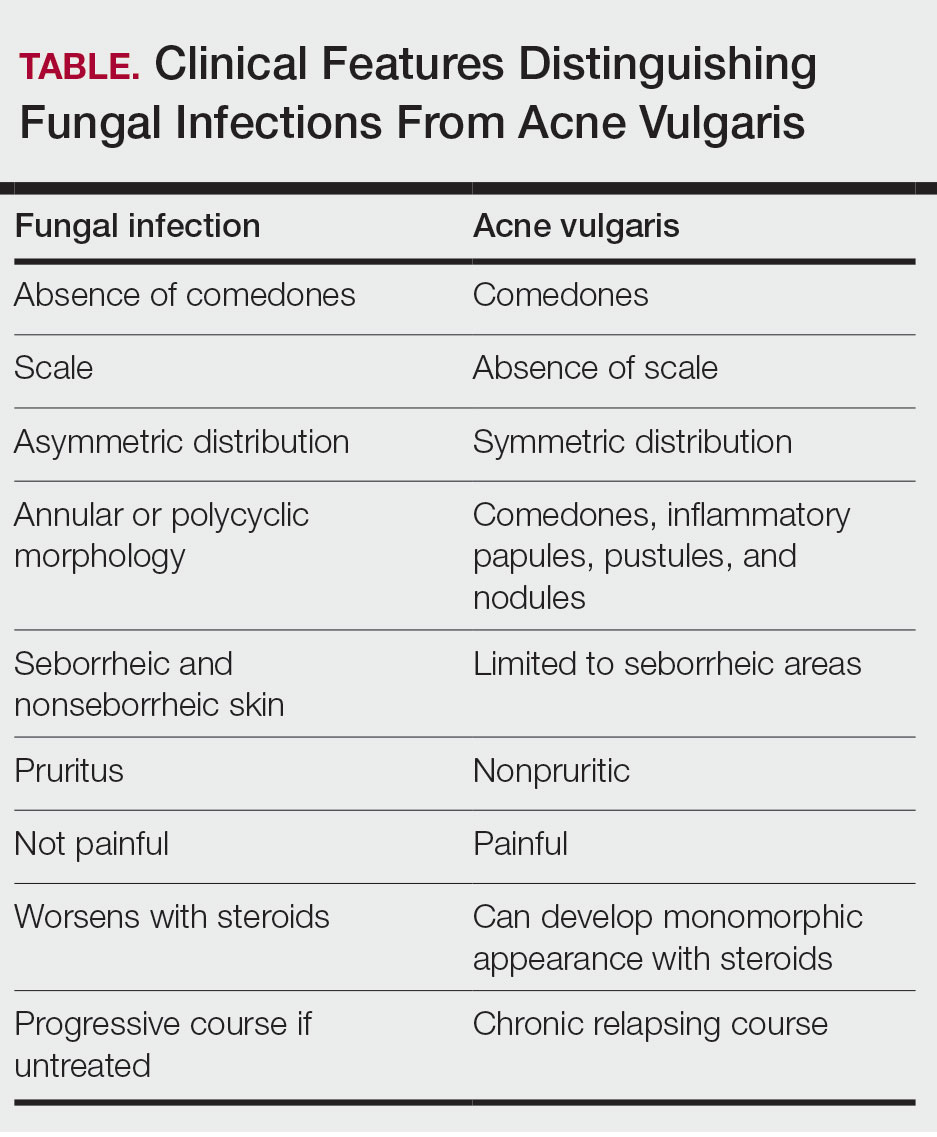
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
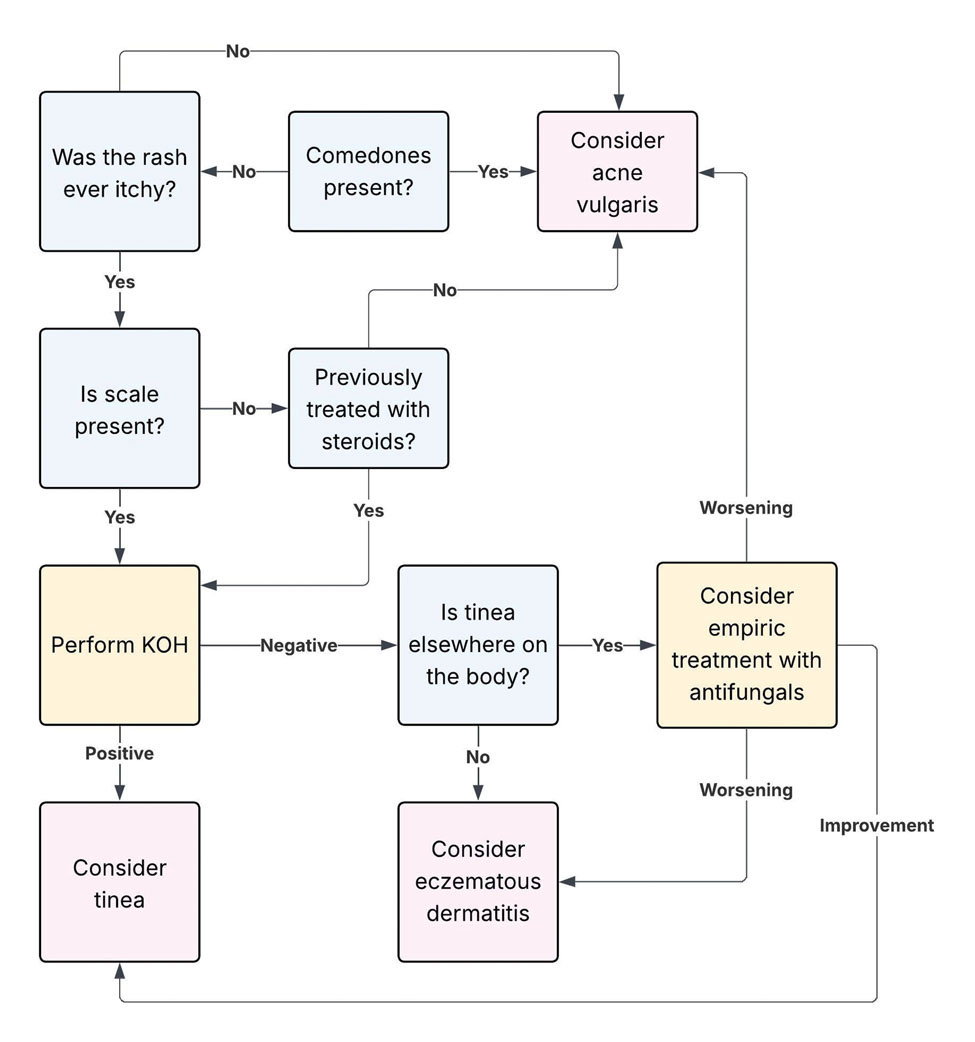
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).
Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).
Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
Practice Points
- Folliculocentric pustules and/or papules from dermatophytes (including tinea incognita and Majocchi granuloma) or Malassezia folliculitis can closely mimic acne, especially following steroid use.
- Key red flags for dermatophyte infection include an absence of comedones, pruritus, and asymmetric or localized lesions in sebum‐rich zones.
- Bedside tools such as dermoscopy, Wood lamp examination, and in-office potassium hydroxide preparation can provide rapid differentiation between dermatophyte infections and acne.
- Prompt antifungal treatment and avoidance of topical steroids can prevent deeper fungal invasion.

Retrospective Analysis of Prevalence and Treatment Patterns of Skin and Nail Candidiasis From US Health Insurance Claims Data
Retrospective Analysis of Prevalence and Treatment Patterns of Skin and Nail Candidiasis From US Health Insurance Claims Data
Candida is a common commensal organism of human skin and mucous membranes. Candidiasis of the skin and nails is caused by overgrowth of Candida species due to excess skin moisture, skin barrier disruption, or immunosuppression. Candidiasis of the skin manifests as red, moist, itchy patches that develop particularly in skin folds. Nail involvement is associated with onycholysis (separation of the nail plate from the nail bed) and subungual debris.1 Data on the prevalence of candidiasis of the skin and nails in the United States are scarce. In this study, we evaluated the prevalence, characteristics, and treatment practices of candidiasis of the skin and nails using data from 2 large US health insurance claims databases.
Methods
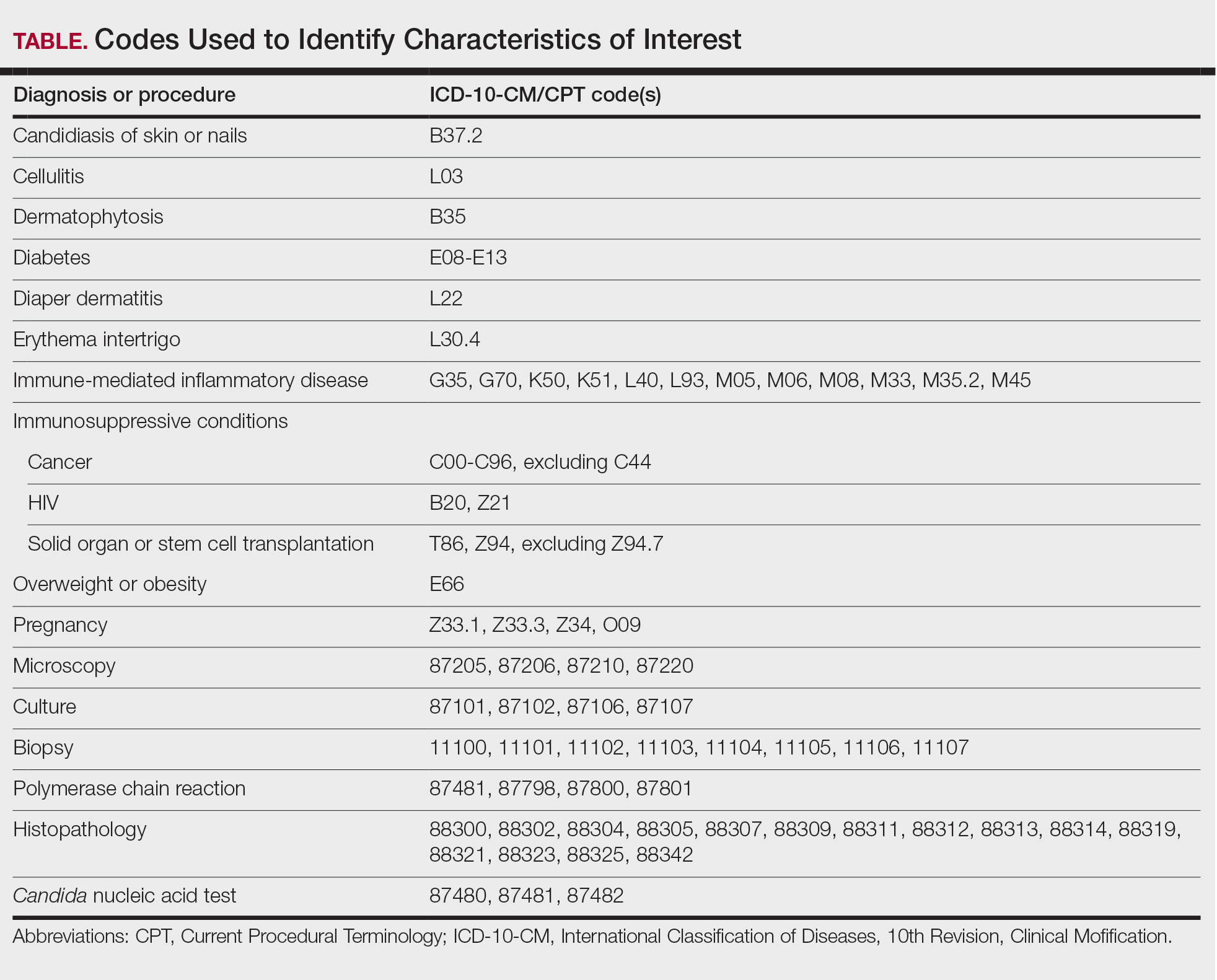
We used the 2023 Merative MarketScan Commercial, Medicare Supplemental, and Multi-State Medicaid Databases (https://www.merative.com/documents/merative-marketscan-research-databases) to identify outpatients with the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) code B37.2 for candidiasis of the skin and nails. The Commercial and Medicare Supplemental databases include health insurance claims data submitted by large employers and health plans for more than 19 million patients throughout the United States, and the Multi-State Medicaid database includes similar data from more than 5 million patients across several geographically dispersed states. The index date for each patient corresponded with their first qualifying diagnosis of skin and nail candidiasis during January 1, 2023, to December 31, 2023. Inclusion in the study required continuous insurance enrollment from 30 days prior to 7 days after the index date, resulting in exclusion of 7% of commercial/Medicare patients and 8% of Medicaid patients. Prevalence per 1000 outpatients was calculated, with stratification by demographic characteristics.
We examined selected diagnoses made on or within 30 days before the index date, diagnostic testing performed within the 7 days before or after the index date after using specific Current Procedural Terminology codes, and outpatient antifungal and combination antifungal-corticosteroid prescriptions made within 7 days before or after the index date (Table). Race/ethnicity data are unavailable in the commercial/Medicare database, and geographic data are unavailable in the Medicaid database.
Results
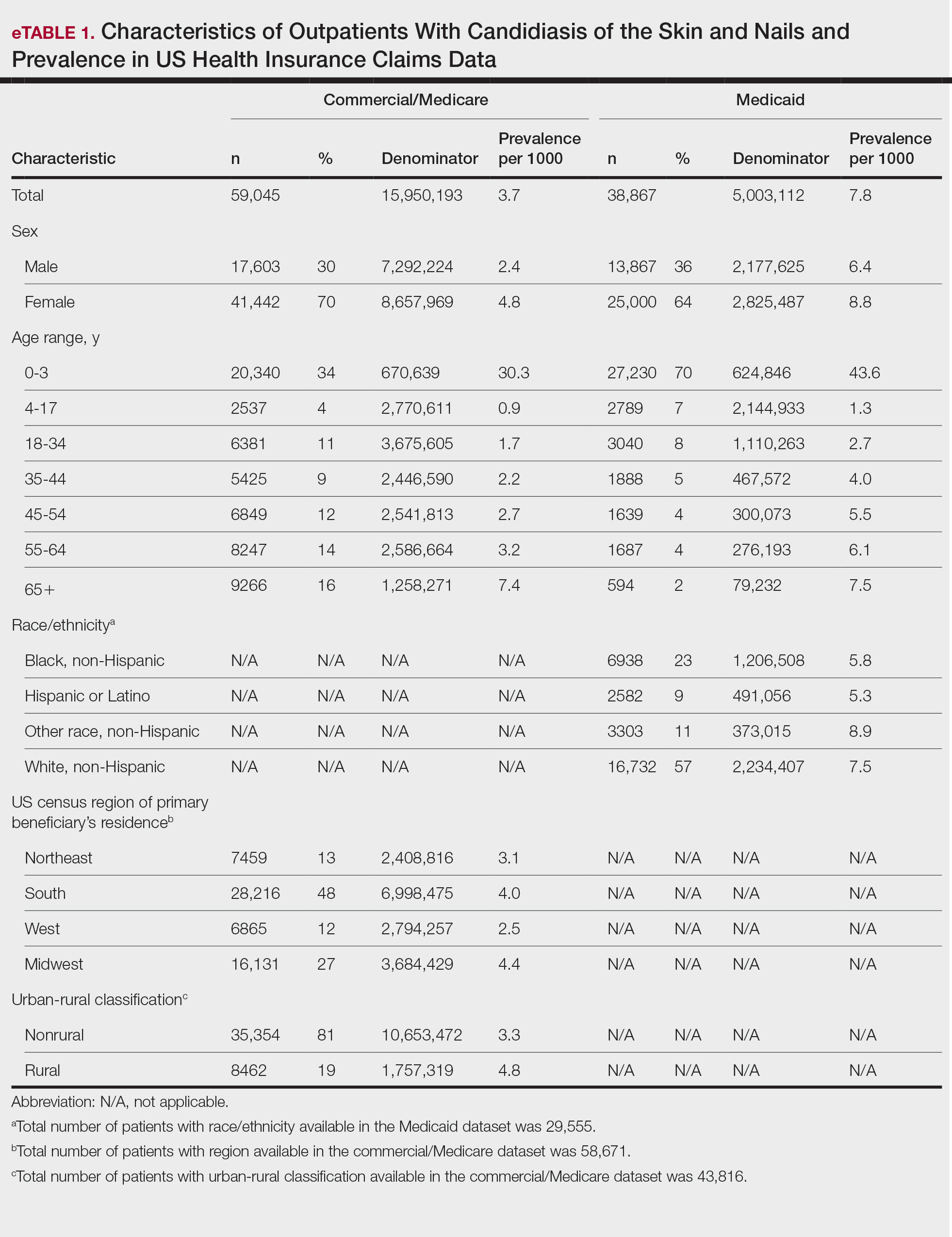
The prevalence of skin and nail candidiasis was 3.7 per 1000 commercial/Medicare outpatients and 7.8 per 1000 Medicaid outpatients (eTable 1). Prevalence was highest among patients aged 0 to 3 years (commercial/Medicare, 30.3 per 1000; Medicaid, 43.6 per 1000), followed by patients 65 years or older (commercial/Medicare, 7.4 per 1000; Medicaid, 7.5 per 1000). Prevalence was higher among females compared with males (commercial/Medicare, 4.8 vs 2.4 per 1000, respectively; Medicaid, 8.8 vs 6.4 per 1000, respectively). Among Medicaid patients, prevalence was highest among those of other race, non-Hispanic (8.9 per 1000) and White non-Hispanic patients (7.5 per 1000). In the commercial/Medicare dataset, prevalence was highest in patients residing in the Midwest (4.4 per 1000) and the South (4.0 per 1000).
Diaper dermatitis was listed as a concurrent diagnosis among 51% of patients aged 0 to 3 years in both datasets (eTable 2). Diabetes (commercial/Medicare, 32%; Medicaid, 36%) and immunosuppressive conditions (commercial/Medicare, 10%; Medicaid, 7%) were most frequent among patients aged 65 years or older. Obesity was most commonly listed as a concurrent diagnosis among patients aged 35 to 64 years (commercial/Medicare, 17%; Medicaid, 23%).

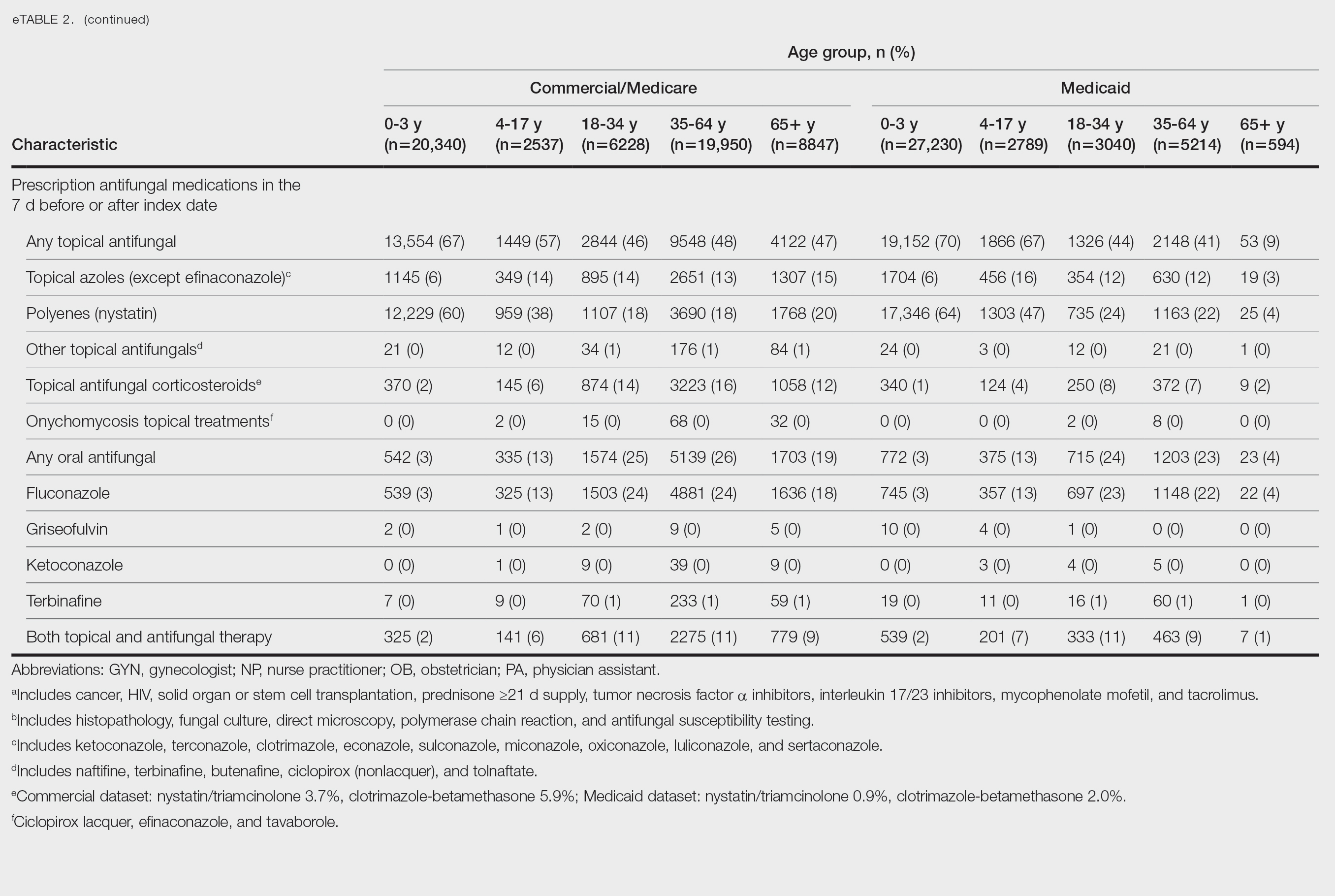
Patients aged 18 to 34 years had the highest rates of diagnostic testing in the 7 days before or after the index date (commercial/Medicare, 9%; Medicaid, 10%). Topical antifungal medications (primarily nystatin) were most frequently prescribed for patients aged 0 to 3 years (commercial/Medicare, 67%; Medicaid, 70%). Topical combination antifungal-corticosteroid medications were most frequently prescribed for patients aged 35 to 64 years in the commercial/Medicare dataset (16%) and for patients aged 18 to 34 years in the Medicaid dataset (8%). Topical onychomycosis treatments were prescribed for fewer than 1% of patients in both datasets. Oral antifungal medications were most frequently prescribed for patients aged 35 to 64 years in the commercial/Medicare dataset (26%) and for patients aged 18 to 34 years in the Medicaid dataset (24%). Fewer than 11% of patients across all age groups in both datasets were prescribed both topical and oral antifungal medications.
Comment
Our analysis provides preliminary insight into the prevalence of skin and nail candidiasis in the United States based on health insurance claims data. Higher prevalence of skin and nail candidiasis among patients with Medicaid compared with those with commercial/Medicare health insurance is consistent with previous studies showing increased rates of other superficial fungal infections (eg, dermatophytosis) among patients of lower socioeconomic status.2 This finding could reflect differences in underlying health status or reduced access to health care, which could delay treatment or follow-up care and potentially lead to prolonged exposure to conditions favoring the development of candidiasis.
In both the commercial/Medicare health insurance and Medicaid datasets, prevalence of diagnosis codes for candidiasis of the skin and nails was highest among infants and toddlers. Diaper dermatitis also was observed in more than half of patients aged 0 to 3 years; this is a well-established risk factor for cutaneous candidiasis, as immature skin barrier function and prolonged exposure to moisture and occlusion facilitate fungal overgrowth.3 In adults, diabetes and obesity were among the most frequent comorbidities observed; both conditions are recognized risk factors for superficial candidiasis due to their impact on immune function and skin integrity.4
In both study cohorts, diagnostic testing in the 7 days before or after the index date was infrequent (≤10%), consistent with most cases being diagnosed clinically.5 Topical antifungals, especially nystatin, were most frequently prescribed for young children, while oral antifungals were more frequently prescribed for adults; nystatin is one of the most well-studied topical treatments for cutaneous candidiasis, and oral fluconazole is the primary systemic treatment for cutaneous candidiasis.1 In our study, the ICD-10-CM code B37.2 appeared to be used primarily for diagnosis of skin rather than nail infections based on the low proportions of patients who received treatment that was onychomycosis specific.
Our study was limited by potential misclassification inherent to data based on diagnosis codes; incomplete capture of underlying conditions given the short continuous enrollment criteria; and lack of information about affected body site(s) and laboratory results, including data identifying the Candida species. A previous study found that Candida parapsilosis and Candida albicans were the most common species involved in candidiasis of the skin and nails and that one-third of isolates exhibited low sensitivity to commonly used antifungals.6 For nails, Candida species are sometimes contaminants rather than pathogens.
Conclusion
Our findings provide a baseline understanding of the epidemiology of candidiasis of the skin and nails in the United States. The growing threat of antifungal resistance, particularly among non-albicans Candida species, underscores the need for appropriate use of antifungals.7 Future epidemiologic studies about laboratory-confirmed candidiasis of the skin and nails to understand causative species and drug resistance would be useful, as would further investigation into disparities.
- Taudorf EH, Jemec GBE, Hay RJ, et al. Cutaneous candidiasis—an evidence-based review of topical and systemic treatments to inform clinical practice. J Eur Acad Dermatol Venereol. 2019;33:1863-1873. doi:10.1111/jdv.15782
- Jenks JD, Prattes J, Wurster S, et al. Social determinants of health as drivers of fungal disease. eClinicalMedicine. 2023;66:102325. doi:10.1016/j.eclinm.2023.102325
- Benitez Ojeda AB, Mendez MD. Diaper dermatitis. StatPearls [Internet]. Updated July 3, 2023. Accessed January 14, 2026. https://www.ncbi.nlm.nih.gov/books/NBK559067/
- Shahabudin S, Azmi NS, Lani MN, et al. Candida albicans skin infection in diabetic patients: an updated review of pathogenesis and management. Mycoses. 2024;67:E13753. doi:10.1111/myc.13753
- Kalra MG, Higgins KE, Kinney BS. Intertrigo and secondary skin infections. Am Fam Physician. 2014;89:569-573.
- Ranđelovic M, Ignjatovic A, Đorđevic M, et al. Superficial candidiasis: cluster analysis of species distribution and their antifungal susceptibility in vitro. J Fungi (Basel). 2025;11:338.
- Hay R. Therapy of skin, hair and nail fungal infections. J Fungi (Basel). 2018;4:99. doi:10.3390/jof4030099
Candida is a common commensal organism of human skin and mucous membranes. Candidiasis of the skin and nails is caused by overgrowth of Candida species due to excess skin moisture, skin barrier disruption, or immunosuppression. Candidiasis of the skin manifests as red, moist, itchy patches that develop particularly in skin folds. Nail involvement is associated with onycholysis (separation of the nail plate from the nail bed) and subungual debris.1 Data on the prevalence of candidiasis of the skin and nails in the United States are scarce. In this study, we evaluated the prevalence, characteristics, and treatment practices of candidiasis of the skin and nails using data from 2 large US health insurance claims databases.
Methods
We used the 2023 Merative MarketScan Commercial, Medicare Supplemental, and Multi-State Medicaid Databases (https://www.merative.com/documents/merative-marketscan-research-databases) to identify outpatients with the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) code B37.2 for candidiasis of the skin and nails. The Commercial and Medicare Supplemental databases include health insurance claims data submitted by large employers and health plans for more than 19 million patients throughout the United States, and the Multi-State Medicaid database includes similar data from more than 5 million patients across several geographically dispersed states. The index date for each patient corresponded with their first qualifying diagnosis of skin and nail candidiasis during January 1, 2023, to December 31, 2023. Inclusion in the study required continuous insurance enrollment from 30 days prior to 7 days after the index date, resulting in exclusion of 7% of commercial/Medicare patients and 8% of Medicaid patients. Prevalence per 1000 outpatients was calculated, with stratification by demographic characteristics.
We examined selected diagnoses made on or within 30 days before the index date, diagnostic testing performed within the 7 days before or after the index date after using specific Current Procedural Terminology codes, and outpatient antifungal and combination antifungal-corticosteroid prescriptions made within 7 days before or after the index date (Table). Race/ethnicity data are unavailable in the commercial/Medicare database, and geographic data are unavailable in the Medicaid database.
Results
The prevalence of skin and nail candidiasis was 3.7 per 1000 commercial/Medicare outpatients and 7.8 per 1000 Medicaid outpatients (eTable 1). Prevalence was highest among patients aged 0 to 3 years (commercial/Medicare, 30.3 per 1000; Medicaid, 43.6 per 1000), followed by patients 65 years or older (commercial/Medicare, 7.4 per 1000; Medicaid, 7.5 per 1000). Prevalence was higher among females compared with males (commercial/Medicare, 4.8 vs 2.4 per 1000, respectively; Medicaid, 8.8 vs 6.4 per 1000, respectively). Among Medicaid patients, prevalence was highest among those of other race, non-Hispanic (8.9 per 1000) and White non-Hispanic patients (7.5 per 1000). In the commercial/Medicare dataset, prevalence was highest in patients residing in the Midwest (4.4 per 1000) and the South (4.0 per 1000).
Diaper dermatitis was listed as a concurrent diagnosis among 51% of patients aged 0 to 3 years in both datasets (eTable 2). Diabetes (commercial/Medicare, 32%; Medicaid, 36%) and immunosuppressive conditions (commercial/Medicare, 10%; Medicaid, 7%) were most frequent among patients aged 65 years or older. Obesity was most commonly listed as a concurrent diagnosis among patients aged 35 to 64 years (commercial/Medicare, 17%; Medicaid, 23%).
Patients aged 18 to 34 years had the highest rates of diagnostic testing in the 7 days before or after the index date (commercial/Medicare, 9%; Medicaid, 10%). Topical antifungal medications (primarily nystatin) were most frequently prescribed for patients aged 0 to 3 years (commercial/Medicare, 67%; Medicaid, 70%). Topical combination antifungal-corticosteroid medications were most frequently prescribed for patients aged 35 to 64 years in the commercial/Medicare dataset (16%) and for patients aged 18 to 34 years in the Medicaid dataset (8%). Topical onychomycosis treatments were prescribed for fewer than 1% of patients in both datasets. Oral antifungal medications were most frequently prescribed for patients aged 35 to 64 years in the commercial/Medicare dataset (26%) and for patients aged 18 to 34 years in the Medicaid dataset (24%). Fewer than 11% of patients across all age groups in both datasets were prescribed both topical and oral antifungal medications.
Comment
Our analysis provides preliminary insight into the prevalence of skin and nail candidiasis in the United States based on health insurance claims data. Higher prevalence of skin and nail candidiasis among patients with Medicaid compared with those with commercial/Medicare health insurance is consistent with previous studies showing increased rates of other superficial fungal infections (eg, dermatophytosis) among patients of lower socioeconomic status.2 This finding could reflect differences in underlying health status or reduced access to health care, which could delay treatment or follow-up care and potentially lead to prolonged exposure to conditions favoring the development of candidiasis.
In both the commercial/Medicare health insurance and Medicaid datasets, prevalence of diagnosis codes for candidiasis of the skin and nails was highest among infants and toddlers. Diaper dermatitis also was observed in more than half of patients aged 0 to 3 years; this is a well-established risk factor for cutaneous candidiasis, as immature skin barrier function and prolonged exposure to moisture and occlusion facilitate fungal overgrowth.3 In adults, diabetes and obesity were among the most frequent comorbidities observed; both conditions are recognized risk factors for superficial candidiasis due to their impact on immune function and skin integrity.4
In both study cohorts, diagnostic testing in the 7 days before or after the index date was infrequent (≤10%), consistent with most cases being diagnosed clinically.5 Topical antifungals, especially nystatin, were most frequently prescribed for young children, while oral antifungals were more frequently prescribed for adults; nystatin is one of the most well-studied topical treatments for cutaneous candidiasis, and oral fluconazole is the primary systemic treatment for cutaneous candidiasis.1 In our study, the ICD-10-CM code B37.2 appeared to be used primarily for diagnosis of skin rather than nail infections based on the low proportions of patients who received treatment that was onychomycosis specific.
Our study was limited by potential misclassification inherent to data based on diagnosis codes; incomplete capture of underlying conditions given the short continuous enrollment criteria; and lack of information about affected body site(s) and laboratory results, including data identifying the Candida species. A previous study found that Candida parapsilosis and Candida albicans were the most common species involved in candidiasis of the skin and nails and that one-third of isolates exhibited low sensitivity to commonly used antifungals.6 For nails, Candida species are sometimes contaminants rather than pathogens.
Conclusion
Our findings provide a baseline understanding of the epidemiology of candidiasis of the skin and nails in the United States. The growing threat of antifungal resistance, particularly among non-albicans Candida species, underscores the need for appropriate use of antifungals.7 Future epidemiologic studies about laboratory-confirmed candidiasis of the skin and nails to understand causative species and drug resistance would be useful, as would further investigation into disparities.
Candida is a common commensal organism of human skin and mucous membranes. Candidiasis of the skin and nails is caused by overgrowth of Candida species due to excess skin moisture, skin barrier disruption, or immunosuppression. Candidiasis of the skin manifests as red, moist, itchy patches that develop particularly in skin folds. Nail involvement is associated with onycholysis (separation of the nail plate from the nail bed) and subungual debris.1 Data on the prevalence of candidiasis of the skin and nails in the United States are scarce. In this study, we evaluated the prevalence, characteristics, and treatment practices of candidiasis of the skin and nails using data from 2 large US health insurance claims databases.
Methods
We used the 2023 Merative MarketScan Commercial, Medicare Supplemental, and Multi-State Medicaid Databases (https://www.merative.com/documents/merative-marketscan-research-databases) to identify outpatients with the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) code B37.2 for candidiasis of the skin and nails. The Commercial and Medicare Supplemental databases include health insurance claims data submitted by large employers and health plans for more than 19 million patients throughout the United States, and the Multi-State Medicaid database includes similar data from more than 5 million patients across several geographically dispersed states. The index date for each patient corresponded with their first qualifying diagnosis of skin and nail candidiasis during January 1, 2023, to December 31, 2023. Inclusion in the study required continuous insurance enrollment from 30 days prior to 7 days after the index date, resulting in exclusion of 7% of commercial/Medicare patients and 8% of Medicaid patients. Prevalence per 1000 outpatients was calculated, with stratification by demographic characteristics.
We examined selected diagnoses made on or within 30 days before the index date, diagnostic testing performed within the 7 days before or after the index date after using specific Current Procedural Terminology codes, and outpatient antifungal and combination antifungal-corticosteroid prescriptions made within 7 days before or after the index date (Table). Race/ethnicity data are unavailable in the commercial/Medicare database, and geographic data are unavailable in the Medicaid database.
Results
The prevalence of skin and nail candidiasis was 3.7 per 1000 commercial/Medicare outpatients and 7.8 per 1000 Medicaid outpatients (eTable 1). Prevalence was highest among patients aged 0 to 3 years (commercial/Medicare, 30.3 per 1000; Medicaid, 43.6 per 1000), followed by patients 65 years or older (commercial/Medicare, 7.4 per 1000; Medicaid, 7.5 per 1000). Prevalence was higher among females compared with males (commercial/Medicare, 4.8 vs 2.4 per 1000, respectively; Medicaid, 8.8 vs 6.4 per 1000, respectively). Among Medicaid patients, prevalence was highest among those of other race, non-Hispanic (8.9 per 1000) and White non-Hispanic patients (7.5 per 1000). In the commercial/Medicare dataset, prevalence was highest in patients residing in the Midwest (4.4 per 1000) and the South (4.0 per 1000).
Diaper dermatitis was listed as a concurrent diagnosis among 51% of patients aged 0 to 3 years in both datasets (eTable 2). Diabetes (commercial/Medicare, 32%; Medicaid, 36%) and immunosuppressive conditions (commercial/Medicare, 10%; Medicaid, 7%) were most frequent among patients aged 65 years or older. Obesity was most commonly listed as a concurrent diagnosis among patients aged 35 to 64 years (commercial/Medicare, 17%; Medicaid, 23%).
Patients aged 18 to 34 years had the highest rates of diagnostic testing in the 7 days before or after the index date (commercial/Medicare, 9%; Medicaid, 10%). Topical antifungal medications (primarily nystatin) were most frequently prescribed for patients aged 0 to 3 years (commercial/Medicare, 67%; Medicaid, 70%). Topical combination antifungal-corticosteroid medications were most frequently prescribed for patients aged 35 to 64 years in the commercial/Medicare dataset (16%) and for patients aged 18 to 34 years in the Medicaid dataset (8%). Topical onychomycosis treatments were prescribed for fewer than 1% of patients in both datasets. Oral antifungal medications were most frequently prescribed for patients aged 35 to 64 years in the commercial/Medicare dataset (26%) and for patients aged 18 to 34 years in the Medicaid dataset (24%). Fewer than 11% of patients across all age groups in both datasets were prescribed both topical and oral antifungal medications.
Comment
Our analysis provides preliminary insight into the prevalence of skin and nail candidiasis in the United States based on health insurance claims data. Higher prevalence of skin and nail candidiasis among patients with Medicaid compared with those with commercial/Medicare health insurance is consistent with previous studies showing increased rates of other superficial fungal infections (eg, dermatophytosis) among patients of lower socioeconomic status.2 This finding could reflect differences in underlying health status or reduced access to health care, which could delay treatment or follow-up care and potentially lead to prolonged exposure to conditions favoring the development of candidiasis.
In both the commercial/Medicare health insurance and Medicaid datasets, prevalence of diagnosis codes for candidiasis of the skin and nails was highest among infants and toddlers. Diaper dermatitis also was observed in more than half of patients aged 0 to 3 years; this is a well-established risk factor for cutaneous candidiasis, as immature skin barrier function and prolonged exposure to moisture and occlusion facilitate fungal overgrowth.3 In adults, diabetes and obesity were among the most frequent comorbidities observed; both conditions are recognized risk factors for superficial candidiasis due to their impact on immune function and skin integrity.4
In both study cohorts, diagnostic testing in the 7 days before or after the index date was infrequent (≤10%), consistent with most cases being diagnosed clinically.5 Topical antifungals, especially nystatin, were most frequently prescribed for young children, while oral antifungals were more frequently prescribed for adults; nystatin is one of the most well-studied topical treatments for cutaneous candidiasis, and oral fluconazole is the primary systemic treatment for cutaneous candidiasis.1 In our study, the ICD-10-CM code B37.2 appeared to be used primarily for diagnosis of skin rather than nail infections based on the low proportions of patients who received treatment that was onychomycosis specific.
Our study was limited by potential misclassification inherent to data based on diagnosis codes; incomplete capture of underlying conditions given the short continuous enrollment criteria; and lack of information about affected body site(s) and laboratory results, including data identifying the Candida species. A previous study found that Candida parapsilosis and Candida albicans were the most common species involved in candidiasis of the skin and nails and that one-third of isolates exhibited low sensitivity to commonly used antifungals.6 For nails, Candida species are sometimes contaminants rather than pathogens.
Conclusion
Our findings provide a baseline understanding of the epidemiology of candidiasis of the skin and nails in the United States. The growing threat of antifungal resistance, particularly among non-albicans Candida species, underscores the need for appropriate use of antifungals.7 Future epidemiologic studies about laboratory-confirmed candidiasis of the skin and nails to understand causative species and drug resistance would be useful, as would further investigation into disparities.
- Taudorf EH, Jemec GBE, Hay RJ, et al. Cutaneous candidiasis—an evidence-based review of topical and systemic treatments to inform clinical practice. J Eur Acad Dermatol Venereol. 2019;33:1863-1873. doi:10.1111/jdv.15782
- Jenks JD, Prattes J, Wurster S, et al. Social determinants of health as drivers of fungal disease. eClinicalMedicine. 2023;66:102325. doi:10.1016/j.eclinm.2023.102325
- Benitez Ojeda AB, Mendez MD. Diaper dermatitis. StatPearls [Internet]. Updated July 3, 2023. Accessed January 14, 2026. https://www.ncbi.nlm.nih.gov/books/NBK559067/
- Shahabudin S, Azmi NS, Lani MN, et al. Candida albicans skin infection in diabetic patients: an updated review of pathogenesis and management. Mycoses. 2024;67:E13753. doi:10.1111/myc.13753
- Kalra MG, Higgins KE, Kinney BS. Intertrigo and secondary skin infections. Am Fam Physician. 2014;89:569-573.
- Ranđelovic M, Ignjatovic A, Đorđevic M, et al. Superficial candidiasis: cluster analysis of species distribution and their antifungal susceptibility in vitro. J Fungi (Basel). 2025;11:338.
- Hay R. Therapy of skin, hair and nail fungal infections. J Fungi (Basel). 2018;4:99. doi:10.3390/jof4030099
- Taudorf EH, Jemec GBE, Hay RJ, et al. Cutaneous candidiasis—an evidence-based review of topical and systemic treatments to inform clinical practice. J Eur Acad Dermatol Venereol. 2019;33:1863-1873. doi:10.1111/jdv.15782
- Jenks JD, Prattes J, Wurster S, et al. Social determinants of health as drivers of fungal disease. eClinicalMedicine. 2023;66:102325. doi:10.1016/j.eclinm.2023.102325
- Benitez Ojeda AB, Mendez MD. Diaper dermatitis. StatPearls [Internet]. Updated July 3, 2023. Accessed January 14, 2026. https://www.ncbi.nlm.nih.gov/books/NBK559067/
- Shahabudin S, Azmi NS, Lani MN, et al. Candida albicans skin infection in diabetic patients: an updated review of pathogenesis and management. Mycoses. 2024;67:E13753. doi:10.1111/myc.13753
- Kalra MG, Higgins KE, Kinney BS. Intertrigo and secondary skin infections. Am Fam Physician. 2014;89:569-573.
- Ranđelovic M, Ignjatovic A, Đorđevic M, et al. Superficial candidiasis: cluster analysis of species distribution and their antifungal susceptibility in vitro. J Fungi (Basel). 2025;11:338.
- Hay R. Therapy of skin, hair and nail fungal infections. J Fungi (Basel). 2018;4:99. doi:10.3390/jof4030099
Retrospective Analysis of Prevalence and Treatment Patterns of Skin and Nail Candidiasis From US Health Insurance Claims Data
Retrospective Analysis of Prevalence and Treatment Patterns of Skin and Nail Candidiasis From US Health Insurance Claims Data
Practice Points
- Candidiasis of the skin or nails is a common outpatient condition that is most frequently diagnosed in infants, toddlers, and adults aged 65 years or older.
- Most cases are diagnosed clinically without diagnostic testing and treated with topical antifungals, but increased attention to formal diagnosis and treatment may be warranted given the emergence of antifungal-resistant Candida species.
